Attached files
| file | filename |
|---|---|
| EX-32.1 - EXHIBIT 32.1 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex32-1.htm |
| EX-31.3 - EXHIBIT 31.3 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex31-3.htm |
| EX-31.2 - EXHIBIT 31.2 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex31-2.htm |
| EX-31.1 - EXHIBIT 31.1 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex31-1.htm |
| EX-23.1 - EXHIBIT 23.1 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex23-1.htm |
| EX-21.1 - EXHIBIT 21.1 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex21-1.htm |
| EX-4.1 - EXHIBIT 4.1 - U S PHYSICAL THERAPY INC /NV | hc10009190x1_ex4-1.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
(Mark One)
| ☑ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
FOR THE FISCAL YEAR ENDED DECEMBER 31, 2019
OR
| o | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
FOR THE TRANSITION PERIOD FROM TO
COMMISSION FILE NUMBER 1-11151
U.S. PHYSICAL THERAPY, INC.
(EXACT NAME OF REGISTRANT AS SPECIFIED IN ITS CHARTER)
|
NEVADA
|
76-0364866
|
|
(STATE OR OTHER JURISDICTION OF INCORPORATION
OR ORGANIZATION) |
(I.R.S. EMPLOYER IDENTIFICATION NO.)
|
|
1300 WEST SAM HOUSTON PARKWAY SOUTH,
SUITE 300, HOUSTON, TEXAS |
77042
|
|
(ADDRESS OF PRINCIPAL EXECUTIVE OFFICES)
|
(ZIP CODE)
|
REGISTRANT’S TELEPHONE NUMBER, INCLUDING AREA CODE: (713) 297-7000
SECURITIES REGISTERED PURSUANT TO SECTION 12(b) OF THE EXCHANGE ACT:
|
Title of Each Class
|
Trading Symbol
|
Name of Each Exchange on Which Registered
|
|
Common Stock, $.01 par value
|
USPH
|
New York Stock Exchange
|
SECURITIES REGISTERED PURSUANT TO SECTION 12(g) OF THE EXCHANGE ACT: NONE
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No ☑
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes o No ☑
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☑ No o
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☑ No o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer”, “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer
|
☑
|
Accelerated filer
|
o
|
|
Non-accelerated filer
|
o (Do not check if a smaller reporting company)
|
Smaller reporting company
|
o
|
|
|
|
Emerging growth company
|
o
|
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. o
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No ☑
The aggregate market value of the shares of the registrant’s common stock held by non-affiliates of the registrant at June 30, 2019 was $778.6 million based on the closing sale price reported on the NYSE for the registrant’s common stock on June 30, 2019, the last business day of the registrant’s most recently completed second fiscal quarter. For purposes of this computation, all executive officers, directors and 5% or greater beneficial owners of the registrant were deemed to be affiliates. Such determination should not be deemed an admission that such executive officers, directors and beneficial owners are, in fact, affiliates of the registrant.
As of February 28, 2020, the number of shares outstanding of the registrant’s common stock, par value $.01 per share, was: 12,774,600.
DOCUMENTS INCORPORATED BY REFERENCE
|
DOCUMENT
|
PART OF FORM 10-K
|
|
Portions of Definitive Proxy Statement for the 2020 Annual Meeting of Shareholders
|
Part III
|
FORWARD-LOOKING STATEMENTS
We make statements in this report that are considered to be forward-looking statements within the meaning given such term under Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”). These statements contain forward-looking information relating to the financial condition, results of operations, plans, objectives, future performance and business of our Company. These statements (often using words such as “believes”, “expects”, “intends”, “plans”, “appear”, “should” and similar words) involve risks and uncertainties that could cause actual results to differ materially from those we project. Included among such statements are those relating to opening clinics, availability of personnel and the reimbursement environment. The forward-looking statements are based on our current views and assumptions and actual results could differ materially from those anticipated in such forward-looking statements as a result of certain risks, uncertainties, and factors, which include, but are not limited to:
| • | changes as the result of government enacted national healthcare reform; |
| • | changes in Medicare rules and guidelines and reimbursement or failure of our clinics to maintain their Medicare certification and/or enrollment status; |
| • | revenue we receive from Medicare and Medicaid being subject to potential retroactive reduction; |
| • | business and regulatory conditions including federal and state regulations; |
| • | governmental and other third party payor inspections, reviews, investigations and audits, which may result in sanctions or reputational harm and increased costs; |
| • | compliance with federal and state laws and regulations relating to the privacy of individually identifiable patient information, and associated fines and penalties for failure to comply; |
| • | changes in reimbursement rates or payment methods from third party payors including government agencies, and changes in the deductibles and co-pays owed by patients; |
| • | revenue and earnings expectations; |
| • | legal actions, which could subject us to increased operating costs and uninsured liabilities; |
| • | general economic conditions; |
| • | availability and cost of qualified physical therapists; |
| • | personnel productivity and retaining key personnel; |
| • | competitive, economic or reimbursement conditions in our markets which may require us to reorganize or close certain clinics and thereby incur losses and/or closure costs including the possible write-down or write-off of goodwill and other intangible assets; |
| • | competitive environment in the industrial injury prevention business, which could result in the termination or non-renewal of contractual service arrangements and other adverse financial consequences for that service line; |
| • | acquisitions, purchase of non-controlling interests (minority interests) and the successful integration of the operations of the acquired businesses; |
| • | maintaining our information technology systems with adequate safeguards to protect against cyber-attacks; |
| • | a security breach of our or our third party vendors’ information technology systems may subject us to potential legal action and reputational harm and may result in a violation of the Health Insurance Portability and Accountability Act of 1996 of the Health Information Technology for Economic and Clinical Health Act; |
| • | maintaining adequate internal controls; |
| • | maintaining necessary insurance coverage; |
| • | the potential impact of the coronavirus; |
1
| • | availability, terms, and use of capital; and |
| • | weather and other seasonal factors. |
Many factors are beyond our control. Given these uncertainties, you should not place undue reliance on our forward-looking statements. Please see the other sections of this report and our other periodic reports filed with the Securities and Exchange Commission (the “SEC”) for more information on these factors. Our forward-looking statements represent our estimates and assumptions only as of the date of this report. Except as required by law, we are under no obligation to update any forward-looking statement, regardless of the reason the statement may no longer be accurate.
2
PART I
| ITEM 1. | BUSINESS. |
GENERAL
Our company, U.S. Physical Therapy, Inc. (“we”, “us”, “our” or the “Company”), through its subsidiaries, operates outpatient physical therapy clinics that provide pre-and post-operative care for a variety of orthopedic-related disorders and sports-related injuries, treatment for neurological-related injuries and rehabilitation of injured workers. We primarily operate through subsidiary clinic partnerships in which we generally own a 1% general partnership interest and a 24% to 99% limited partnership interest and the managing therapist(s) of the clinics owns the remaining limited partnership interest in the majority of the clinics (hereinafter referred to as “Clinic Partnerships”). To a lesser extent, we operate some clinics through wholly-owned subsidiaries under profit sharing arrangements with therapists (hereinafter referred to as “Wholly-Owned Facilities”). We also have a majority interest in a company, which is a leading provider of industrial injury prevention services. Services provided in this business include onsite injury prevention and rehabilitation, performance optimization, post-offer employment testing, functional capacity evaluations and ergonomic assessments. The majority of these services are contracted with and paid for directly by employers including a number of Fortune 500 companies. Other clients include large insurers and their contractors. These services are performed through Industrial Sports Medicine Professionals, consisting of both physical therapists and specialized certified athletic trainers (ATCs).
Unless the context otherwise requires, references in this Annual Report on Form 10-K to “we”, “our” or “us” includes the Company and all of its subsidiaries.
Our strategy is to acquire single and multi-clinic outpatient physical therapy practices and to develop outpatient physical therapy clinics, primarily to operate as satellites in an existing partnership, on national basis. At December 31, 2019, we operated 583 clinics in 40 states. The average age of the 583 clinics in operation at December 31, 2019 was 10.4 years. Our highest concentration of clinics are in the following states: Texas, Tennessee, Michigan, Virginia, Florida, Oregon, Maryland, Georgia, Pennsylvania and Arizona. In addition to our 583 clinics, at December 31, 2019, we also managed 26 physical therapy practices for unrelated physician groups and hospitals and operated the industrial injury prevention business, as described below.
During the last three years, we completed the following multi-clinic acquisitions:
Acquisition |
Date |
% Interest Acquired |
Number of Clinics |
||||
2019 |
|||||||
September 2019 Acquisition |
September 30, 2019 |
67 | % |
11 | |||
2018 |
|||||||
August 2018 Acquisition |
August 31 |
70 | % |
4 | |||
2017 |
|||||||
January 2017 Acquisition |
January 1 |
70 | % |
17 | |||
May 2017 Acquisition |
May 31 |
70 | % |
4 | |||
June 2017 Acquisition |
June 30 |
60 | % |
9 | |||
October 2017 Acquisition |
October 31 |
70 | % |
9 | |||
In addition to the above multi-clinic acquisitions, in March 2017, we acquired a 55% interest in the initial industrial injury prevention business. On April 30, 2018, we acquired a 65% interest in another business in the industrial injury prevention sector and in connection with the closing we combined the two businesses. After the combination, we owned a 59.45% interest in the combined business, Briotix Health, Limited Partnership (“Briotix Health”). On April 11, 2019, we acquired a third company that is a provider of industrial injury prevention services. The acquired company specializes in delivering injury prevention and care, post offer employment testing, functional capacity evaluations and return-to-work services. It performs these services across a network in 45 states including onsite at eleven client locations. The business was then combined with Briotix Health increasing our ownership position in the partnership to approximately 76.0%.
3
Also during 2019, we purchased the assets and business of one physical therapy clinic in a separate transaction. The clinic operates as a satellite clinic of one of the existing partnerships. Besides the August 2018 multi-clinic acquisition, through several of our majority owned Clinic Partnerships we acquired five separate clinic practices that year. These practices operate as satellites of the respective existing Clinic Partnerships. During 2017, we purchased the assets and business of two physical therapy clinics in separate transactions. One clinic was consolidated with an existing clinic and the other operates as a satellite clinic of one of the existing partnerships.
The results of operations of the acquired clinics have been included in our consolidated financial statements since the date of their respective acquisition.
We continue to seek to attract for employment physical therapists who have established relationships with physicians and other referral sources by offering these therapists a competitive salary and incentives based on the profitability of the clinic that they manage. For multi-site clinic practices in which a controlling interest is acquired by us, the prior owners typically continue on as employees to manage the clinic operations, retaining a non-controlling ownership interest in the clinics and receiving a competitive salary for managing the clinic operations. In addition, we have developed satellite clinic facilities as part of existing Clinic Partnerships and Wholly-Owned facilities, with the result that a substantial number of Clinic Partnerships and Wholly-Owned facilities operate more than one clinic location. In 2020, we intend to continue to acquire clinic practices and continue to focus on developing new clinics and on opening satellite clinics where appropriate along with increasing our patient volume through marketing and new programs.
Therapists at our clinics initially perform a comprehensive evaluation of each patient, which is then followed by a treatment plan specific to the injury as prescribed by the patient’s physician. The treatment plan may include a number of procedures, including therapeutic exercise, manual therapy techniques, ultrasound, electrical stimulation, hot packs, iontophoresis, education on management of daily life skills and home exercise programs. A clinic’s business primarily comes from referrals by local physicians. The principal sources of payment for the clinics’ services are managed care programs, commercial health insurance, Medicare/Medicaid and workers’ compensation insurance.
We were re-incorporated in April 1992 under the laws of the State of Nevada and have operating subsidiaries organized in various states in the form of limited partnerships, limited liability companies and wholly-owned corporations. This description of our business should be read in conjunction with our financial statements and the related notes contained in Item 8 in this Annual Report on Form 10-K. Our principal executive offices are located at 1300 West Sam Houston Parkway South, Suite 300, Houston, Texas 77042. Our telephone number is (713) 297-7000. Our website is www.usph.com.
OUR CLINICS
Most of our clinics are operated as Clinic Partnerships in which we own the general partnership interest and a majority of the limited partnership interests. The managing healthcare practitioner of the clinics usually owns a portion of the limited partnership interests. Generally, the therapist partners have no interest in the net losses of Clinic Partnerships, except to the extent of their capital accounts. Since we also develop satellite clinic facilities of existing clinics, most Clinic Partnerships consist of more than one clinic location. As of December 31, 2019, through wholly-owned subsidiaries, we owned a 1% general partnership interest in all the Clinic Partnerships. Our limited partnership interests range from 24% to 99% in the Clinic Partnerships. For the vast majority of the Clinic Partnerships, the managing healthcare practitioner is a physical therapist who owns the remaining limited partnership interest in the Clinic Partnership.
For our Clinic Partnership agreements related to those that we acquired a majority interest, generally, the prior management continues to own a 10% to 50% interest.
Typically, each therapist partner or director, including those employed by Clinic Partnerships in which we acquired a majority interest, enters into an employment agreement for a term of up to five years with their Clinic Partnership. Each agreement typically provides for a covenant not to compete during the period of his or her employment and for up to two years thereafter. Under each employment agreement, the therapist partner receives a base salary and may receive a bonus based on the net revenues or profits generated by their Clinic Partnership or specific clinic. In the case of Clinic Partnerships, the therapist partner receives earnings distributions based upon their ownership interest. Upon termination of employment, we typically have the right, but not the
4
obligation, to purchase the therapist’s partnership interest in de novo Clinic Partnerships. In connection with most of our acquired clinics, in the event that a limited minority partner’s employment ceases and certain requirements are met as detailed in the respective limited partnership agreements, we have a call right (the “Call Right”) and the selling entity or individual has a put right (the “Put Right”) with respect to the partner’s limited partnership interests. The Put Right and the Call Right do not expire, even upon an individual partner’s death, and contain no mandatory redemption feature. The purchase price of the partner’s limited partnership interest upon exercise of the Put Right or the Call Right is calculated at a predetermined multiple of earnings performance as detailed in the respective agreements.
Each Clinic Partnership maintains an independent local identity, while at the same time enjoying the benefits of national purchasing, negotiated third-party payor contracts, centralized support services and management practices. Under a management agreement, one of our subsidiaries provides a variety of support services to each clinic, including supervision of site selection, construction, clinic design and equipment selection, establishment of accounting systems and billing procedures and training of office support personnel, processing of accounts payable, operational direction, auditing of regulatory compliance, payroll, benefits administration, accounting services, legal services, quality assurance and marketing support.
Our typical clinic occupies approximately 1,000 to 5,000 square feet of leased space in an office building or shopping center. We attempt to lease ground level space for patient ease of access to our clinics.
Typical minimum staff at a clinic consists of a licensed physical therapist and an office manager. As patient visits grow, staffing may also include additional physical therapists, occupational therapists, therapy assistants, aides, exercise physiologists, athletic trainers and office personnel. Therapy services are performed under the supervision of a licensed therapist.
We provide services at our clinics on an outpatient basis. Patients are usually treated for approximately one hour per day, two to three times a week, typically for two to six weeks. We generally charge for treatment on a per procedure basis. Medicare patients are charged based on prescribed time increments and Medicare billing standards. In addition, our clinics will develop, when appropriate, individual maintenance and self-management exercise programs to be continued after treatment. We continually assess the potential for developing new services and expanding the methods of providing our existing services in the most efficient manner while providing high quality patient care.
FACTORS INFLUENCING DEMAND FOR THERAPY SERVICES
We believe that the following factors, among others, influence the growth of outpatient physical therapy services:
Economic Benefits of Therapy Services. Purchasers and providers of healthcare services, such as insurance companies, health maintenance organizations, businesses and industries, continuously seek cost savings for traditional healthcare services. We believe that our therapy services provide a cost-effective way to prevent short-term disabilities from becoming chronic conditions, to help avoid invasive procedures, to speed recovery from surgery and musculoskeletal injuries and eliminate or minimize the need for opioids.
Earlier Hospital Discharge. Changes in health insurance reimbursement, both public and private, have encouraged the earlier discharge of patients to reduce costs. We believe that early hospital discharge practices foster greater demand for outpatient physical therapy services.
Aging Population. In general, the elderly population has a greater incidence of disability compared to the population as a whole. As this segment of the population continues to grow, we believe that demand for rehabilitation services will expand.
Increase in Obesity. Two of every three American men are considered to be overweight or obese and the rate continues to grow. The strain on a person’s body can be significant. Physical therapy services help the obese become more active and fit by teaching them how to move in ways that are pain free.
MARKETING
We focus our marketing efforts primarily on physicians, including orthopedic surgeons, neurosurgeons, physiatrists, internal medicine physicians, podiatrists, occupational medicine physicians and general practitioners. In marketing to the physician community, we emphasize our commitment to quality patient care and regular
5
communication with physicians regarding patient progress. We employ personnel to assist clinic directors in developing and implementing marketing plans for the physician community and to assist in establishing relationships with health maintenance organizations, preferred provider organizations, industry, case managers and insurance companies.
SOURCES OF REVENUE
Payor sources for clinic services are primarily managed care programs, commercial health insurance, Medicare/Medicaid and workers’ compensation insurance. Commercial health insurance, Medicare and managed care programs generally provide coverage to patients utilizing our clinics after payment by the patients of normal deductibles and co-insurance payments. Workers’ compensation laws generally require employers to provide, directly or indirectly through insurance, costs of medical rehabilitation for their employees from work-related injuries and disabilities and, in some jurisdictions, mandatory vocational rehabilitation, usually without any deductibles, co-payments or cost sharing. Treatments for patients who are parties to personal injury cases are generally paid from the proceeds of settlements with insurance companies or from favorable judgments. If an unfavorable judgment is received, collection efforts are generally not pursued against the patient and the patient’s account is written-off against established reserves. Bad debt reserves relating to all receivable types are regularly reviewed and adjusted as appropriate.
The following table shows our payor mix for the years ended:
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
||||||||||||||||
Payor |
Net Patient Revenue |
Percentage |
Net Patient Revenue |
Percentage |
Net Patient Revenue |
Percentage |
||||||||||||
(Net Patient Revenues in Thousands) |
||||||||||||||||||
Managed Care Programs |
$ | 124,516 | 28.7 | % |
$ | 134,748 | 32.3 | % |
$ | 120,773 | 31.0 | % |
||||||
Commercial Health Insurance |
79,535 | 18.4 | % |
72,786 | 17.4 | % |
79,968 | 20.5 | % |
|||||||||
Medicare/Medicaid |
132,611 | 30.6 | % |
117,554 | 28.1 | % |
103,713 | 26.7 | % |
|||||||||
Workers’ Compensation Insurance |
63,542 | 14.7 | % |
59,942 | 14.4 | % |
55,364 | 14.2 | % |
|||||||||
Other |
33,141 | 7.6 | % |
32,673 | 7.8 | % |
29,408 | 7.6 | % |
|||||||||
Total |
$ | 433,345 | 100.0 | % |
$ | 417,703 | 100.0 | % |
$ | 389,226 | 100.0 | % |
||||||
Our business depends to a significant extent on our relationships with commercial health insurers, health maintenance organizations, preferred provider organizations and workers’ compensation insurers. In some geographical areas, our clinics must be approved as providers by key health maintenance organizations and preferred provider plans to obtain payments. Failure to obtain or maintain these approvals would adversely affect financial results.
During the year ended December 31, 2019, approximately 35.1% of our visits and 30.6% of our net patient revenues were from patients with Medicare or Medicaid program coverage. To receive Medicare reimbursement, a facility (Medicare Certified Rehabilitation Agency) or the individual therapist (Physical/Occupational Therapist in Private Practice) must meet applicable participation conditions set by the Department of Health and Human Services (“HHS”) relating to the type of facility, equipment, recordkeeping, personnel and standards of medical care, and also must comply with all state and local laws. HHS, through Centers for Medicare & Medicaid Services (“CMS”) and designated agencies, periodically inspects or surveys clinics/providers for approval and/or compliance. We anticipate that our newly developed and acquired clinics will become certified as Medicare providers or will be enrolled as a group of physical/occupation therapists in a private practice. Failure to obtain or maintain this certification would adversely affect financial results.
The Medicare program reimburses outpatient rehabilitation providers based on the Medicare Physician Fee Schedule (“MPFS”). For services provided in 2018, a 0.5% increase was applied to the fee schedule payment rates; for services provided in 2019, a 0.25% increase was applied to the fee schedule payment rates before applying the mandatory budget neutrality adjustment. For services provided in 2020 through 2025, a 0.0% update will be applied each year to the fee schedule payment rates, before applying the mandatory budget neutrality adjustment. However, in the 2020 MPFS Final Rule, CMS proposed an increase to the code values for office/outpatient evaluation and management (E/M) codes and cuts to other codes to maintain budget neutrality of the MPFS. This change in code valuations would be effective January 1, 2021. Under the proposal,
6
physical/occupational therapy services could see code reductions that may result in an estimated 8% decrease in payment. In announcing this possible reduction in the applicable physical/occupational therapy codes, CMS indicated that it would further consider and address industry and provider concerns before finalizing the 2021 code values.
Beginning in 2021, payments to individual therapists (Physical/Occupational Therapist in Private Practice) paid under the fee schedule may be subject to adjustment based on performance in the Merit Based Incentive Payment System (“MIPS”), which measures performance based on certain quality metrics, resource use, and meaningful use of electronic health records. Under the MIPS requirements, a provider's performance is assessed according to established performance standards each year and then is used to determine an adjustment factor that is applied to the professional's payment for the corresponding payment year. The provider’s MIPS performance in 2019 will determine the payment adjustment in 2021. Each year from 2019 through 2024, professionals who receive a significant share of their revenues through an alternate payment model (“APM”), (such as accountable care organizations or bundled payment arrangements) that involves risk of financial losses and a quality measurement component will receive a 5% bonus in the corresponding payment year. The bonus payment for APM participation is intended to encourage participation and testing of new APMs and to promote the alignment of incentives across payors. The specifics of the MIPS and APM adjustments will be subject to future notice and comment rule-making.
The Budget Control Act of 2011 increased the federal debt ceiling in connection with deficit reductions over the next ten years, and requires automatic reductions in federal spending by approximately $1.2 trillion. Payments to Medicare providers are subject to these automatic spending reductions, subject to a 2% cap. On April 1, 2013, a 2% reduction to Medicare payments was implemented. The Bipartisan Budget Act of 2015, enacted on November 2, 2015, extended the 2% reductions to Medicare payments through fiscal year 2025. The Bipartisan Budget Act of 2018, enacted on February 9, 2018, extends the 2% reductions to Medicare payments through fiscal year 2027.
Historically, the total amount paid by Medicare in any one year for outpatient physical therapy, occupational therapy, and/or speech-language pathology services provided to any Medicare beneficiary was subject to an annual dollar limit (i.e., the “Therapy Cap” or “Limit”). For 2017, the annual Limit on outpatient therapy services was $1,980 for combined Physical Therapy and Speech Language Pathology services and $1,980 for Occupational Therapy services. As a result of Bipartisan Budget Act of 2018, the Therapy Caps have been eliminated, effective as of January 1, 2018.
Under the Middle Class Tax Relief and Job Creation Act of 2012 (“MCTRA”), since October 1, 2012, patients who met or exceeded $3,700 in therapy expenditures during a calendar year have been subject to a manual medical review to determine whether applicable payment criteria are satisfied. The $3,700 threshold is applied to Physical Therapy and Speech Language Pathology Services; a separate $3,700 threshold is applied to the Occupational Therapy. The MACRA directed CMS to modify the manual medical review process such that those reviews will no longer apply to all claims exceeding the $3,700 threshold and instead will be determined on a targeted basis based on a variety of factors that CMS considers appropriate The Bipartisan Budget Act of 2018 extends the targeted medical review indefinitely, but reduces the threshold to $3,000 through December 31, 2027. For 2028, the threshold amount will be increased by the percentage increase in the Medicare Economic Index (“MEI”) for 2028 and in subsequent years the threshold amount will increase based on the corresponding percentage increase in the MEI for such subsequent year.
CMS adopted a multiple procedure payment reduction (“MPPR”) for therapy services in the final update to the MPFS for calendar year 2011. The MPPR applied to all outpatient therapy services paid under Medicare Part B — occupational therapy, physical therapy and speech-language pathology. Under the policy, the Medicare program pays 100% of the practice expense component of the Relative Value Unit (“RVU”) for the therapy procedure with the highest practice expense RVU, then reduces the payment for the practice expense component for the second and subsequent therapy procedures or units of service furnished during the same day for the same patient, regardless of whether those therapy services are furnished in separate sessions. Since 2013, the practice expense component for the second and subsequent therapy service furnished during the same day for the same patient was reduced by 50%. In addition, the MCTRA directed CMS to implement a claims-based data collection program to gather additional data on patient function during the course of therapy in order to better understand patient conditions and outcomes. All practice settings that provide outpatient therapy services are required to
7
include this data on the claim form. Since 2013, therapists have been required to report new codes and modifiers on the claim form that reflect a patient’s functional limitations and goals at initial evaluation, periodically throughout care, and at discharge. Reporting of these functional limitation codes and modifiers are required on the claim for payment.
Medicare claims for outpatient therapy services furnished by therapy assistants on or after January 1, 2020 must include a modifier indicating the service was furnished by a therapy assistant. Outpatient therapy services furnished on or after January 1, 2022 in whole or part by a therapy assistant will be paid at an amount equal to 85% of the payment amount otherwise applicable for the service.
Statutes, regulations, and payment rules governing the delivery of therapy services to Medicare beneficiaries are complex and subject to interpretation. We believe that we are in compliance in all material respects with all applicable laws and regulations and are not aware of any pending or threatened investigations involving allegations of potential wrongdoing that would have a material effect on our financial statements as of December 31, 2019. Compliance with such laws and regulations can be subject to future government review and interpretation, as well as significant regulatory action including fines, penalties, and exclusion from the Medicare program. For 2019, net patient revenue from Medicare accounted for approximately $119.4 million.
REGULATION AND HEALTHCARE REFORM
Numerous federal, state and local regulations regulate healthcare services and those who provide them. Some states into which we may expand have laws requiring facilities employing health professionals and providing health-related services to be licensed and, in some cases, to obtain a certificate of need (that is, demonstrating to a state regulatory authority the need for, and financial feasibility of, new facilities or the commencement of new healthcare services). Only one of the states in which we currently operate requires a certificate of need for the operation of our physical therapy business functions. Our therapists and/or clinics, however, are required to be licensed, as determined by the state in which they provide services. Failure to obtain or maintain any required certificates, approvals or licenses could have a material adverse effect on our business, financial condition and results of operations.
Regulations Controlling Fraud and Abuse. Various federal and state laws regulate financial relationships involving providers of healthcare services. These laws include Section 1128B(b) of the Social Security Act (42 U.S. C. § 1320a-7b[b]) (the “Fraud and Abuse Law”), under which civil and criminal penalties can be imposed upon persons who, among other things, offer, solicit, pay or receive remuneration in return for (i) the referral of patients for the rendering of any item or service for which payment may be made, in whole or in part, by a Federal health care program (including Medicare and Medicaid); or (ii) purchasing, leasing, ordering, or arranging for or recommending purchasing, leasing, ordering any good, facility, service, or item for which payment may be made, in whole or in part, by a Federal health care program (including Medicare and Medicaid). We believe that our business procedures and business arrangements are in compliance with these provisions. However, the provisions are broadly written and the full extent of their specific application to specific facts and arrangements to which we are a party is uncertain and difficult to predict. In addition, several states have enacted state laws similar to the Fraud and Abuse Law, which may be more restrictive than the federal Fraud and Abuse Law.
The Office of the Inspector General (“OIG”) of HHS has issued regulations describing compensation financial arrangements that fall within a “Safe Harbor” and, therefore, are not viewed as illegal remuneration under the Fraud and Abuse Law. Failure to fall within a Safe Harbor does not mean that the Fraud and Abuse Law has been violated; however, the OIG has indicated that failure to fall within a Safe Harbor may subject an arrangement to increased scrutiny under a “facts and circumstances” test.
The OIG also has issued special fraud alerts and special advisory bulletins to remind the provider community of the importance and application of certain aspects of the Fraud and Abuse Law. One of the OIG special fraud alerts related to the rental of space in physician offices by persons or entities to which the physicians refer patients. The OIG’s stated concern in these arrangements is that rental payments may be disguised kickbacks to the physician-landlords to induce referrals. We rent clinic space for some of our clinics from referring physicians and have taken the steps that we believe are necessary to ensure that all leases comply to the extent possible and applicable, with the space rental Safe Harbor to the Fraud and Abuse Law.
8
One of the OIG’s special advisory bulletins addressed certain complex contractual arrangements for the provision of items and services. This special advisory bulletin identified several characteristics commonly exhibited by suspect arrangements, the existence of one or more of which could indicate a prohibited arrangement to the OIG. Generally, the indicia of a suspect contractual joint venture as identified by the special advisory bulletin and an associated OIG advisory opinion include the following:
New Line of Business. A provider in one line of business (“Owner”) expands into a new line of business that can be provided to the Owner’s existing patients, with another party who currently provides the same or similar item or service as the new business (“Manager/Supplier”).
Captive Referral Base. The arrangement predominantly or exclusively serves the Owner’s existing patient base (or patients under the control or influence of the Owner).
Little or No Bona Fide Business Risk. The Owner’s primary contribution to the venture is referrals; it makes little or no financial or other investment in the business, delegating the entire operation to the Manager/Supplier, while retaining profits generated from its captive referral base.
Status of the Manager/Supplier. The Manager/Supplier is a would-be competitor of the Owner’s new line of business and would normally compete for the captive referrals. It has the capacity to provide virtually identical services in its own right and bill insurers and patients for them in its own name.
Scope of Services Provided by the Manager/Supplier. The Manager/Supplier provides all, or many, of the new business’ key services.
Remuneration. The practical effect of the arrangement, viewed in its entirety, is to provide the Owner the opportunity to bill insurers and patients for business otherwise provided by the Manager/Supplier. The remuneration from the venture to the Owner (i.e., the profits of the venture) takes into account the value and volume of business the Owner generates.
Exclusivity. The arrangement bars the Owner from providing items or services to any patients other than those coming from Owner and/or bars the Manager/Supplier from providing services in its own right to the Owner’s patients.
Due to the nature of our business operations, many of our management service arrangements exhibit one or more of these characteristics. However, we believe we have taken steps regarding the structure of such arrangements as necessary to sufficiently distinguish them from these suspect ventures, and to comply with the requirements of the Fraud and Abuse Law. However, if the OIG believes we have entered into a prohibited contractual joint venture, it could have an adverse effect on our business, financial condition and results of operations.
Although the business of managing physician-owned physical therapy facilities is regulated by the Fraud and Abuse Law, the manner in which we contract with such facilities often falls outside the complete scope of available Safe Harbors. We believe our arrangements comply with the Fraud and Abuse Law, even though federal courts provide limited guidance as to the application of the Fraud and Abuse Law to these arrangements. If our management contracts are held to violate the Fraud and Abuse Law, it could have an adverse effect on our business, financial condition and results of operations.
Stark Law. Provisions of the Omnibus Budget Reconciliation Act of 1993 (42 U.S.C. § 1395nn) (the “Stark Law”) prohibit referrals by a physician of “designated health services” which are payable, in whole or in part, by Medicare or Medicaid, to an entity in which the physician or the physician’s immediate family member has an investment interest or other financial relationship, subject to several exceptions. Unlike the Fraud and Abuse Law, the Stark Law is a strict liability statute. Proof of intent to violate the Stark Law is not required. Physical therapy services are among the “designated health services”. Further, the Stark Law has application to our management contracts with individual physicians and physician groups, as well as, any other financial relationship between us and referring physicians, including medical advisor arrangements and any financial transaction resulting from a clinic acquisition. The Stark Law also prohibits billing for services rendered pursuant to a prohibited referral. Several states have enacted laws similar to the Stark Law. These state laws may cover all (not just Medicare and Medicaid) patients. As with the Fraud and Abuse Law, we consider the Stark Law in planning our clinics, establishing contractual and other arrangements with physicians, marketing and other
9
activities, and believe that our operations are in compliance with the Stark Law. If we violate the Stark Law or any similar state laws, our financial results and operations could be adversely affected. Penalties for violations include denial of payment for the services, significant civil monetary penalties, and exclusion from the Medicare and Medicaid programs.
HIPAA. In an effort to further combat healthcare fraud and protect patient confidentially, Congress included several anti-fraud measures in the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”). HIPAA created a source of funding for fraud control to coordinate federal, state and local healthcare law enforcement programs, conduct investigations, provide guidance to the healthcare industry concerning fraudulent healthcare practices, and establish a national data bank to receive and report final adverse actions. HIPAA also criminalized certain forms of health fraud against all public and private payors. Additionally, HIPAA mandates the adoption of standards regarding the exchange of healthcare information in an effort to ensure the privacy and electronic security of patient information and standards relating to the privacy of health information. Sanctions for failing to comply with HIPAA include criminal penalties and civil sanctions. In February of 2009, the American Recovery and Reinvestment Act of 2009 (“ARRA”) was signed into law. Title XIII of ARRA, the Health Information Technology for Economic and Clinical Health Act (“HITECH”), provided for substantial Medicare and Medicaid incentives for providers to adopt electronic health records (“EHRs”) and grants for the development of health information exchange (“HIE”). Recognizing that HIE and EHR systems will not be implemented unless the public can be assured that the privacy and security of patient information in such systems is protected, HITECH also significantly expanded the scope of the privacy and security requirements under HIPAA. Most notable are the mandatory breach notification requirements and a heightened enforcement scheme that includes increased penalties, and which now apply to business associates as well as to covered entities. In addition to HIPAA, a number of states have adopted laws and/or regulations applicable in the use and disclosure of individually identifiable health information that can be more stringent than comparable provisions under HIPAA.
We believe that our operations comply with applicable standards for privacy and security of protected healthcare information. We cannot predict what negative effect, if any, HIPAA/HITECH or any applicable state law or regulation will have on our business.
Other Regulatory Factors. Political, economic and regulatory influences are fundamentally changing the healthcare industry in the United States. Congress, state legislatures and the private sector continue to review and assess alternative healthcare delivery and payment systems. Potential alternative approaches could include mandated basic healthcare benefits, controls on healthcare spending through limitations on the growth of private health insurance premiums and Medicare and Medicaid spending, the creation of large insurance purchasing groups, and price controls. Legislative debate is expected to continue in the future and market forces are expected to demand only modest increases or reduced costs. For instance, managed care entities are demanding lower reimbursement rates from healthcare providers and, in some cases, are requiring or encouraging providers to accept capitated payments that may not allow providers to cover their full costs or realize traditional levels of profitability. We cannot reasonably predict what impact the adoption of federal or state healthcare reform measures or future private sector reform may have on our business.
COMPETITION
The healthcare industry, including the physical therapy business, is highly competitive. The physical therapy business is highly fragmented with no company having a significant market share nationally. We believe that we are one of the third largest national outpatient rehabilitation providers.
Competitive factors affecting our business include quality of care, cost, treatment outcomes, convenience of location, and relationships with, and ability to meet the needs of, referral and payor sources. Our clinics compete, directly or indirectly, with many types of healthcare providers including the physical therapy departments of hospitals, private therapy clinics, physician-owned therapy clinics, and chiropractors. We may face more intense competition if consolidation of the therapy industry continues.
We believe that our strategy of providing key therapists in a community with an opportunity to participate in ownership or clinic profitability provides us with a competitive advantage by helping to ensure the commitment of local management to the success of the clinic.
10
We also believe that our competitive position is enhanced by our strategy of locating our clinics, when possible, on the ground floor of buildings and shopping centers with nearby parking, thereby making the clinics more easily accessible to patients. We offer convenient hours. We also attempt to make the decor in our clinics less institutional and more aesthetically pleasing than traditional hospital clinics.
ENFORCEMENT ENVIRONMENT
In recent years, federal and state governments have launched several initiatives aimed at uncovering behavior that violates the federal civil and criminal laws regarding false claims and fraudulent billing and coding practices. Such laws require providers to adhere to complex reimbursement requirements regarding proper billing and coding in order to be compensated for their services by government payors. Our compliance program requires adherence to applicable law and promotes reimbursement education and training; however, a determination that our clinics’ billing and coding practices are false or fraudulent could have a material adverse effect on us.
As a result of our participation in the Medicare and Medicaid programs, we are subject to various governmental inspections, reviews, audits and investigations to verify our compliance with these programs and applicable laws and regulations. In addition, our Corporate Integrity Agreement requires annual audits to be performed by an independent review organization on a small sample of our clinics, the results of which are reported to the federal government. See “-Compliance Program – Corporate Integrity Agreement”. Managed care payors may also reserve the right to conduct audits. An adverse inspection, review, audit or investigation could result in: refunding amounts we have been paid; fines penalties and/or revocation of billing privileges for the affected clinics; expansion of the scope of our Corporate Integrity Agreement; exclusion from participation in the Medicare or Medicaid programs or one or more managed care payor network; or damage to our reputation.
We and our clinics are subject to federal and state laws prohibiting entities and individuals from knowingly and willfully making claims to Medicare, Medicaid and other governmental programs and third party payors that contain false or fraudulent information. The federal False Claims Act encourages private individuals to file suits on behalf of the government against healthcare providers such as us. As such suits are generally filed under seal with a court to allow the government adequate time to investigate and determine whether it will intervene in the action, the implicated healthcare providers often are unaware of the suit until the government has made its determination and the seal is lifted. Violations or alleged violations of such laws, and any related lawsuits, could result in (i) exclusion from participation in Medicare, Medicaid and other federal healthcare programs, or (ii) significant financial or criminal sanctions, resulting in the possibility of substantial financial penalties for small billing errors that are replicated in a large number of claims, as each individual claim could be deemed a separate violation. In addition, many states also have enacted similar statutes, which may include criminal penalties, substantial fines, and treble damages.
COMPLIANCE PROGRAM
Our Compliance Program. Our ongoing success depends upon our reputation for quality service and ethical business practices. We operate in a highly regulated environment with many federal, state and local laws and regulations. We take a proactive interest in understanding and complying with the laws and regulations that apply to our business.
Our Board of Directors (the “Board”) has adopted a Code of Business Conduct and Ethics and a set of Corporate Governance Guidelines to clarify the ethical standards under which the Board and management carry out their duties. In addition, the Board has created a Compliance Committee of the Board (“Compliance Committee”) whose purpose is to assist the Board in discharging their oversight responsibilities with respect to compliance with federal and state laws and regulations relating to healthcare.
We have issued an Ethics and Compliance Manual and created compliance training materials, hand-outs and an on-line testing program. These tools were prepared to ensure that every employee of our Company and subsidiaries has a clear understanding of our mutual commitment to high standards of professionalism, honesty, fairness and compliance with the law in conducting business. These standards are administered by our Chief Compliance Officer (“CCO”), who has the responsibility for the day-to-day oversight, administration and development of our compliance program. The CCO, internal and external counsel, management and the Compliance Committee review our policies and procedures for our compliance program from time to time in an effort to improve operations and to ensure compliance with requirements of standards, laws and regulations and
11
to reflect the on-going compliance focus areas which have been identified by management, counsel or the Compliance Committee. We also have established systems for reporting potential violations, educating our employees, monitoring and auditing compliance and handling enforcement and discipline.
Committees. Our Compliance Committee, appointed by the Board, consists of four independent directors. The Compliance Committee has general oversight of our Company’s compliance with the legal and regulatory requirements regarding healthcare operations. The Compliance Committee relies on the expertise and knowledge of management, the CCO and other compliance and legal personnel. The CCO regularly communicates with the Chairman of the Compliance Committee. The Compliance Committee meets at least four times a year or more frequently as necessary to carry out its responsibilities and reports regularly to the Board regarding its actions and recommendations.
We also have an Internal Compliance Committee, which is comprised of Company leaders in the areas of operations, clinical services, finance, human resources, legal, information technology and credentialing. The Internal Compliance Committee has the responsibility for evaluating and assessing Company areas of risk relating to compliance with federal and state healthcare laws, and generally to assist the CCO. The Internal Compliance Committee meets at least four times a year or more frequently as necessary to carry out its responsibilities. In addition, management has appointed a team to address our Company’s compliance with HIPAA. The HIPAA team consists of a security officer and employees from our legal, information systems, finance, operations, compliance, business services and human resources departments. The team prepares assessments and makes recommendations regarding operational changes and/or new systems, if needed, to comply with HIPAA.
Each clinic certified as a Medicare Rehabilitation Agency has a formally appointed governing body composed of a member of our management and the director/administrator of the clinic. The governing body retains legal responsibility for the overall conduct of the clinic. The members confer regularly and discuss, among other issues, clinic compliance with applicable laws and regulations. In addition, there are Professional Advisory Committees which serve as Infection Control Committees. These committees meet in the facilities and function as advisors.
We have in place a Risk Management Committee consisting of, among others, the CCO, the Corporate Vice President of Administration, and other legal, compliance and operations personnel. This committee reviews and monitors all employee and patient incident reports and provides clinic personnel with actions to be taken in response to the reports.
Reporting Violations. In order to facilitate our employees’ ability to report in confidence, anonymously and without retaliation any perceived improper work-related activities, accounting irregularities and other violations of our compliance program, we have set up an independent national compliance hotline. The compliance hotline is available to receive confidential reports of wrongdoing Monday through Friday (excluding holidays), 24 hours a day. The compliance hotline is staffed by experienced third party professionals trained to utilize utmost care and discretion in handling sensitive issues and confidential information. The information received is documented and forwarded timely to the CCO, who, together with the Compliance Committee, has the power and resources to investigate and resolve matters of improper conduct.
Educating Our Employees. We utilize numerous methods to train our employees in compliance related issues. All employees complete an initial training program comprised of numerous modules relating to our business and proper practices. The directors/administrators also provide periodic “refresher” training for existing employees and one-on-one comprehensive training with new hires. The corporate compliance group responds to questions from clinic personnel and conducts frequent teleconference meetings, webinars and training sessions on a variety of compliance related topics.
When a clinic opens, we provide a package of compliance materials containing manuals and detailed instructions for meeting Medicare Conditions of Participation Standards and other compliance requirements. During follow up training with the director/administrator of the clinic, compliance department staff explain various details regarding requirements and compliance standards. Compliance staff will remain in contact with the director/administrator while the clinic is implementing compliance standards and will provide any assistance required. All new office managers receive training (including Medicare, regulatory and corporate compliance, insurance billing, charge entry and transaction posting and coding, daily, weekly and monthly accounting reports)
12
from the training staff at the corporate office. The corporate compliance group will assist in continued compliance, including guidance to the clinic staff with regard to Medicare certifications, state survey requirements and responses to any inquiries from regulatory agencies.
Monitoring and Auditing Clinic Operational Compliance. We have in place audit programs and other procedures to monitor and audit clinic operational compliance with applicable policies and procedures. We employ internal auditors who, as part of their job responsibilities, conduct periodic audits of each clinic. Most clinics are audited at least once every 24 months and additional focused audits are performed as deemed necessary. During these audits, particular attention is given to compliance with Medicare and internal policies, Federal and state laws and regulations, third party payor requirements, and patient chart documentation, billing, reporting, record keeping, collections and contract procedures. The audits typically are conducted on site and include interviews with the employees involved in management, operations, billing and accounts receivable.
Formal audit reports are prepared and reviewed with corporate management and the Compliance Committee. Each clinic director/administrator receives a letter instructing them of any corrective measures required. Each clinic director/administrator then works with the compliance team and operations to ensure such corrective measures are achieved.
Handling Enforcement and Discipline. It is our policy that any employee who fails to comply with compliance program requirements or who negligently or deliberately fails to comply with known laws or regulations specifically addressed in our compliance program should be subject to disciplinary action up to and including discharge from employment. The Compliance Committee, compliance staff, human resources staff and management investigate violations of our compliance program and impose disciplinary action as considered appropriate.
Corporate Integrity Agreement. We also perform certain additional compliance related functions pursuant to the Corporate Integrity Agreement (“Corporate Integrity Agreement” or “CIA”) that we entered into with the OIG. The CIA, which became effective as of December 21, 2015, outlines certain specific requirements relating to compliance oversight and program implementation, as well as periodic reporting. In addition, pursuant to the CIA, an independent review organization annually will perform a Medicare billing and coding audit on a small group of randomly selected Company clinics. Our Company Compliance Program has been modified so as to comply with the requirements of the CIA. The term of the CIA is five years.
The CIA was entered into as part of the settlement by one of our Subsidiaries with the U. S. Department of Justice related to certain Medicare billings that occurred between 2007 and 2009 at a single outpatient physical therapy clinic. The settlement resolved claims relating to whether certain physical therapy services provided to a limited number of Medicare patients at the clinic satisfied all of the criteria for payment by the Medicare program, including proper supervision of physical therapist assistants. The Subsidiary paid $718,000 in 2015 to resolve the matter, and we and the Subsidiary entered into the CIA. The Subsidiary no longer conducts any business.
EMPLOYEES
At December 31, 2019, we employed approximately 5,400 people, of which approximately 3,200 were full-time employees. At that date, no Company employees were governed by collective bargaining agreements or were members of a union. We consider our relations with our employees to be good.
In the states in which our current clinics are located, persons performing designated physical therapy services are required to be licensed by the state. Based on standard employee screening systems in place, all persons currently employed by us who are required to be licensed are licensed. We are not aware of any federal licensing requirements applicable to our employees.
AVAILABLE INFORMATION
Our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act are made available free of charge on our internet website at www.usph.com as soon as reasonably practicable after we electronically file such material with, or furnish it to, the SEC.
13
| ITEM 1A. | RISK FACTORS. |
Our business, operations and financial condition are subject to various risks. Some of these risks are described below, and readers of this Annual Report on Form 10-K should take such risks into account in evaluating our Company or making any decision to invest in us. This section does not describe all risks applicable to our Company, our industry or our business, and it is intended only as a summary of material factors affecting our business.
Risks related to our business and operations
Healthcare reform legislation may affect our business.
In recent years, many legislative proposals have been introduced or proposed in Congress and in some state legislatures that would affect major changes in the healthcare system, either nationally or at the state level. At the federal level, Congress has continued to propose or consider healthcare budgets that substantially reduce payments under the Medicare programs. See “Business- Sources of Revenue” in Item 1 for more information. The ultimate content, timing or effect of any healthcare reform legislation and the impact of potential legislation on us is uncertain and difficult, if not impossible, to predict. That impact may be material to our business, financial condition or results of operations.
Our operations are subject to extensive regulation.
The healthcare industry is subject to extensive federal, state and local laws and regulations relating to:
| • | facility and professional licensure/permits, including certificates of need; |
| • | conduct of operations, including financial relationships among healthcare providers, Medicare fraud and abuse, and physician self-referral; |
| • | addition of facilities and services; and |
| • | billing and payment for services. |
In recent years, there have been heightened coordinated civil and criminal enforcement efforts by both federal and state government agencies relating to the healthcare industry. We believe we are in substantial compliance with all laws, but differing interpretations or enforcement of these laws and regulations could subject our current practices to allegations of impropriety or illegality or could require us to make changes in our methods of operations, facilities, equipment, personnel, services and capital expenditure programs and increase our operating expenses. If we fail to comply with these extensive laws and government regulations, we could become ineligible to receive government program reimbursement, suffer civil or criminal penalties or be required to make significant changes to our operations. In addition, we could be forced to expend considerable resources responding to an investigation or other enforcement action under these laws or regulations. For a more complete description of certain of these laws and regulations, see “Business—Regulation and Healthcare Reform” and “Business – Compliance Program” in Item 1.
The healthcare industry is subject to extensive federal, state and local laws and regulations relating to (1) facility and professional licensure, including certificates of need, (2) conduct of operations, including financial relationships among healthcare providers, Medicare fraud and abuse and physician self-referral, (3) addition of facilities and services and enrollment of newly developed facilities in the Medicare program, (4) payment for services and (5) safeguarding protected health information.
Both federal and state regulatory agencies inspect, survey and audit our facilities to review our compliance with these laws and regulations. While our facilities intend to comply with the existing licensing, Medicare certification requirements and accreditation standards, there can be no assurance that these regulatory authorities will determine that all applicable requirements are fully met at any given time. A determination by any of these regulatory authorities that a facility is not in compliance with these requirements could lead to the imposition of requirements that the facility takes corrective action, assessment of fines and penalties, or loss of licensure or Medicare certification of accreditation. These consequences could have an adverse effect on our Company.
The Company’s CIA imposes certain compliance related functions and reporting obligations on us. In addition, the CIA requires us to engage an independent review organization to conduct annual audits of randomly selected Company clinics in order to review compliance with federal requirements relating to the proper billing
14
and coding for claims. While our facilities intend to comply with the federal requirements for properly coding and billing claims for reimbursement, there can be no assurance that these audits will determine that all applicable requirements are fully met at the clinics that are reviewed. In addition, a failure to fully comply with the requirements of the CIA may subject us to the assessment of fines and penalties, or exclusion from participation in the Medicare program. These consequences could have a materially adverse effect on our Company.
Decreases in Medicare reimbursement rates and payment reductions applied to the second and subsequent therapy services may adversely affect our financial results.
The Medicare program reimburses outpatient rehabilitation providers based on the Medicare Physician Fee Schedule (“MPFS”). For services provided in 2018, a 0.5% increase was applied to the fee schedule payment rates; for services provided in 2019, a 0.25% increase was applied to the fee schedule payment rates before applying the mandatory budget neutrality adjustment. For services provided in 2020 through 2025, a 0.0% percent update will be applied each year to the fee schedule payment rates, before applying the mandatory budget neutrality adjustment. However, in the 2020 MPFS Final Rule, CMS proposed an increase to the code values for office/outpatient evaluation and management (E/M) codes and cuts to other codes to maintain budget neutrality of the MPFS. This change in code valuations would be effective January 1, 2021. Under the proposal, physical/occupational therapy services could see code reductions that may result in an estimated 8% decrease in payment. In announcing this possible reduction in the applicable physical/occupational therapy codes, CMS indicated that it would further consider and address industry and provider concerns before finalizing the 2021 code values.
Beginning in 2021, payments to individual therapists (Physical/Occupational Therapist in Private Practice) paid under the fee schedule may be subject to adjustment based on performance in the Merit Based Incentive Payment System (“MIPS”), which measures performance based on certain quality metrics, resource use, and meaningful use of electronic health records. Under the MIPS requirements, a provider's performance is assessed according to established performance standards each year and then is used to determine an adjustment factor that is applied to the professional's payment for the corresponding payment year. The provider’s MIPS performance in 2019 will determine the payment adjustment in 2021. Each year from 2019 through 2024, professionals who receive a significant share of their revenues through an alternate payment model (“APM”), (such as accountable care organizations or bundled payment arrangements) that involves risk of financial losses and a quality measurement component will receive a 5% bonus in the corresponding payment year. The bonus payment for APM participation is intended to encourage participation and testing of new APMs and to promote the alignment of incentives across payors. The specifics of the MIPS and APM adjustments will be subject to future notice and comment rule-making.
The Budget Control Act of 2011 increased the federal debt ceiling in connection with deficit reductions over the next ten years, and requires automatic reductions in federal spending by approximately $1.2 trillion. Payments to Medicare providers are subject to these automatic spending reductions, subject to a 2% cap. On April 1, 2013, a 2% reduction to Medicare payments was implemented. The Bipartisan Budget Act of 2015, enacted on November 2, 2015, extended the 2% reductions to Medicare payments through fiscal year 2025. The Bipartisan Budget Act of 2018, enacted on February 9, 2018, extends the 2% reductions to Medicare payments through fiscal year 2027.
Historically, the total amount paid by Medicare in any one year for outpatient physical therapy, occupational therapy, and/or speech-language pathology services provided to any Medicare beneficiary was subject to an annual dollar limit (i.e., the “Therapy Cap” or “Limit”). For 2017, the annual Limit on outpatient therapy services was $1,980 for combined Physical Therapy and Speech Language Pathology services and $1,980 for Occupational Therapy services. As a result of Bipartisan Budget Act of 2018, the Therapy Caps have been eliminated, effective as of January 1, 2018.
Under the Middle Class Tax Relief and Job Creation Act of 2012 (“MCTRA”), since October 1, 2012, patients who met or exceeded $3,700 in therapy expenditures during a calendar year have been subject to a manual medical review to determine whether applicable payment criteria are satisfied. The $3,700 threshold is applied to Physical Therapy and Speech Language Pathology Services; a separate $3,700 threshold is applied to the Occupational Therapy. The MACRA directed CMS to modify the manual medical review process such that those reviews will no longer apply to all claims exceeding the $3,700 threshold and instead will be determined
15
on a targeted basis based on a variety of factors that CMS considers appropriate The Bipartisan Budget Act of 2018 extends the targeted medical review indefinitely, but reduces the threshold to $3,000 through December 31, 2027. For 2028, the threshold amount will be increased by the percentage increase in the Medicare Economic Index (“MEI”) for 2028 and in subsequent years the threshold amount will increase based on the corresponding percentage increase in the MEI for such subsequent year.
CMS adopted a multiple procedure payment reduction (“MPPR”) for therapy services in the final update to the MPFS for calendar year 2011. The MPPR applied to all outpatient therapy services paid under Medicare Part B — occupational therapy, physical therapy and speech-language pathology. Under the policy, the Medicare program pays 100% of the practice expense component of the Relative Value Unit (“RVU”) for the therapy procedure with the highest practice expense RVU, then reduces the payment for the practice expense component for the second and subsequent therapy procedures or units of service furnished during the same day for the same patient, regardless of whether those therapy services are furnished in separate sessions. Since 2013, the practice expense component for the second and subsequent therapy service furnished during the same day for the same patient was reduced by 50%. In addition, the MCTRA directed CMS to implement a claims-based data collection program to gather additional data on patient function during the course of therapy in order to better understand patient conditions and outcomes. All practice settings that provide outpatient therapy services are required to include this data on the claim form. Since 2013, therapists have been required to report new codes and modifiers on the claim form that reflect a patient’s functional limitations and goals at initial evaluation, periodically throughout care, and at discharge. Reporting of these functional limitation codes and modifiers are required on the claim for payment.
Medicare claims for outpatient therapy services furnished by therapy assistants on or after January 1, 2020 must include a modifier indicating the service was furnished by a therapy assistant. Outpatient therapy services furnished on or after January 1, 2022 in whole or part by a therapy assistant will be paid at an amount equal to 85% of the payment amount otherwise applicable for the service.
Statutes, regulations, and payment rules governing the delivery of therapy services to Medicare beneficiaries are complex and subject to interpretation. We believe that we are in compliance, in all material respects, with all applicable laws and regulations and are not aware of any pending or threatened investigations involving allegations of potential wrongdoing that would have a material effect on the our financial statements as of December 31, 2019. Compliance with such laws and regulations can be subject to future government review and interpretation, as well as significant regulatory action including fines, penalties, and exclusion from the Medicare program. For year ended December 31, 2019, net patient revenues from Medicare were approximately $119.4 million.
Given the history of frequent revisions to the Medicare program and its reimbursement rates and rules, we may not continue to receive reimbursement rates from Medicare that sufficiently compensate us for our services or, in some instances, cover our operating costs. Limits on reimbursement rates or the scope of services being reimbursed could have a material adverse effect on our revenue, financial condition and results of operations. Additionally, any delay or default by the federal or state governments in making Medicare and/or Medicaid reimbursement payments could materially and, adversely, affect our business, financial condition and results of operations.
We expect the federal and state governments to continue their efforts to contain growth in Medicaid expenditures, which could adversely affect our revenue and profitability.
Medicaid spending has increased rapidly in recent years, becoming a significant component of state budgets. This, combined with slower state revenue growth, has led both the federal government and many states to institute measures aimed at controlling the growth of Medicaid spending, and in some instances reducing aggregate Medicaid spending. We expect these state and federal efforts to continue for the foreseeable future. Furthermore, not all of the states in which we operate, most notably Texas, have elected to expand Medicaid as part of federal healthcare reform legislation. There can be no assurance that the program, on the current terms or otherwise, will continue for any particular period of time beyond the foreseeable future. If Medicaid reimbursement rates are reduced or fail to increase as quickly as our costs, or if there are changes in the rules governing the Medicaid program that are disadvantageous to our businesses, our business and results of operations could be materially and adversely affected.
16
Revenue we receive from Medicare and Medicaid is subject to potential retroactive reduction.
Payments we receive from Medicare and Medicaid can be retroactively adjusted after examination during the claims settlement process or as a result of post-payment audits. Payors may disallow our requests for reimbursement, or recoup amounts previously reimbursed, based on determinations by the payors or their third-party audit contractors that certain costs are not reimbursable because either adequate or additional documentation was not provided or because certain services were not covered or deemed to not be medically necessary. Significant adjustments, recoupments or repayments of our Medicare or Medicaid revenue, and the costs associated with complying with investigative audits by regulatory and governmental authorities, could adversely affect our financial condition and results of operations.
Additionally, from time to time we become aware, either based on information provided by third parties and/or the results of internal audits, of payments from payor sources that were either wholly or partially in excess of the amount that we should have been paid for the service provided. Overpayments may result from a variety of factors, including insufficient documentation supporting the services rendered or medical necessity of the services or other failures to document the satisfaction of the necessary conditions of payment. We are required by law in most instances to refund the full amount of the overpayment after becoming aware of it, and failure to do so within requisite time limits imposed by the law could lead to significant fines and penalties being imposed on us. Furthermore, our initial billing of and payments for services that are unsupported by the requisite documentation and satisfaction of any other conditions of payment, regardless of our awareness of the failure at the time of the billing or payment, could expose us to significant fines and penalties. We, and/or certain of our operating companies, could also be subject to exclusion from participation in the Medicare or Medicaid programs in some circumstances as well, in addition to any monetary or other fines, penalties or sanctions that we may incur under applicable federal and/or state law. Our repayment of any such amounts, as well as any fines, penalties or other sanctions that we may incur, could be significant and could have a material and adverse effect on our results of operations and financial condition.
From time to time we are also involved in various external governmental investigations, audits and reviews. Reviews, audits and investigations of this sort can lead to government actions, which can result in the assessment of damages, civil or criminal fines or penalties, or other sanctions, including restrictions or changes in the way we conduct business, loss of licensure or exclusion from participation in government programs. Failure to comply with applicable laws, regulations and rules could have a material and adverse effect on our results of operations and financial condition. Furthermore, becoming subject to these governmental investigations, audits and reviews can also require us to incur significant legal and document production expenses as we cooperate with the government authorities, regardless of whether the particular investigation, audit or review leads to the identification of underlying issues.
As a result of increased post-payment reviews of claims we submit to Medicare for our services, we may incur additional costs and may be required to repay amounts already paid to us.
We are subject to regular post-payment inquiries, investigations and audits of the claims we submit to Medicare for payment for our services. These post-payment reviews have increased as a result of government cost-containment initiatives. These additional post-payment reviews may require us to incur additional costs to respond to requests for records and to pursue the reversal of payment denials, and ultimately may require us to refund amounts paid to us by Medicare that are determined to have been overpaid.
For a further description of this and other laws and regulations involving governmental reimbursements, see “Business—Sources of Revenue” and “—Regulation and Healthcare Reform” in Item 1.
An economic downturn, state budget pressures, sustained unemployment and continued deficit spending by the federal government may result in a reduction in reimbursement and covered services.
An economic downturn, including the consequences of coronavirus, could have a detrimental effect on our revenues. Historically, state budget pressures have translated into reductions in state spending. Given that Medicaid outlays are a significant component of state budgets, we can expect continuing cost containment pressures on Medicaid outlays for our services in the states in which we operate. In addition, an economic downturn, coupled with sustained unemployment, may also impact the number of enrollees in managed care programs as well as the profitability of managed care companies, which could result in reduced reimbursement rates.
17
The existing federal deficit, as well as deficit spending by federal and state governments as the result of adverse developments in the economy or other reasons, can lead to continuing pressure to reduce governmental expenditures for other purposes, including government-funded programs in which we participate, such as Medicare and Medicaid. Such actions in turn may adversely affect our results of operations.
We depend upon reimbursement by third-party payors.
Substantially all of our revenues are derived from private and governmental third-party payors. In 2019, approximately 69.4% of our revenues were derived collectively from managed care plans, commercial health insurers, workers’ compensation payors, and other private pay revenue sources while approximately 30.6% of our revenues were derived from Medicare and Medicaid. Initiatives undertaken by industry and government to contain healthcare costs affect the profitability of our clinics. These payors attempt to control healthcare costs by contracting with healthcare providers to obtain services on a discounted basis. We believe that this trend will continue and may limit reimbursement for healthcare services. If insurers or managed care companies from whom we receive substantial payments were to reduce the amounts they pay for services, our profit margins may decline, or we may lose patients if we choose not to renew our contracts with these insurers at lower rates. In addition, in certain geographical areas, our clinics must be approved as providers by key health maintenance organizations and preferred provider plans. Failure to obtain or maintain these approvals would adversely affect our financial results.
In recent years, through legislative and regulatory actions, the federal government has made substantial changes to various payment systems under the Medicare program. See “Business—Sources of Revenue” in Item 1 for more information including changes to Medicare reimbursement. Additional reforms or other changes to these payment systems may be proposed or adopted, either by the U.S. Congress or by CMS, including bundled payments, outcomes-based payment methodologies and a shift away from traditional fee-for-service reimbursement. If revised regulations are adopted, the availability, methods and rates of Medicare reimbursements for services of the type furnished at our facilities could change. Some of these changes and proposed changes could adversely affect our business strategy, operations and financial results.
We face inspections, reviews, audits and investigations under federal and state government programs and contracts. These audits could have adverse findings that may negatively affect our business.
As a result of our participation in the Medicare and Medicaid programs, we are subject to various governmental inspections, reviews, audits and investigations to verify our compliance with these programs and applicable laws and regulations. Managed care payors may also reserve the right to conduct audits. An adverse inspection, review, audit or investigation could result in:
| • | refunding amounts we have been paid pursuant to the Medicare or Medicaid programs or from managed care payors; |
| • | state or federal agencies imposing fines, penalties and other sanctions on us; |
| • | temporary suspension of payment for new patients to the facility or agency; |
| • | decertification or exclusion from participation in the Medicare or Medicaid programs or one or more managed care payor networks; |
| • | expansion of the scope of our Corporate Integrity Agreement; |
| • | damage to our reputation; |
| • | the revocation of a facility’s or agency’s license; and |
| • | loss of certain rights under, or termination of, our contracts with managed care payors. |
If adverse inspections, reviews, audits or investigations occur and any of the results noted above occur, it could have a material adverse effect on our business and operating results.
18
Our facilities are subject to extensive federal and state laws and regulations relating to the privacy of individually identifiable information.
HIPAA required the HHS to adopt standards to protect the privacy and security of individually identifiable health-related information. The department released final regulations containing privacy standards in 2000 and published revisions to the final regulations in 2002. The privacy regulations extensively regulate the use and disclosure of individually identifiable health-related information. The regulations also provide patients with significant rights related to understanding and controlling how their health information is used or disclosed. The security regulations require healthcare providers to implement administrative, physical and technical practices to protect the security of individually identifiable health information that is maintained or transmitted electronically. HITECH, which was signed into law in 2009, enhanced the privacy, security and enforcement provisions of HIPAA by, among other things establishing security breach notification requirements, allowing enforcement of HIPAA by state attorneys general, and increasing penalties for HIPAA violations. Violations of HIPAA or HITECH could result in civil or criminal penalties.
In addition to HIPAA, there are numerous federal and state laws and regulations addressing patient and consumer privacy concerns, including unauthorized access or theft of personal information. State statutes and regulations vary from state to state. Lawsuits, including class actions and action by state attorneys general, directed at companies that have experienced a privacy or security breach also can occur.
We have established policies and procedures in an effort to ensure compliance with these privacy related requirements. However, if there is a breach, we may be subject to various penalties and damages and may be required to incur costs to mitigate the impact of the breach on affected individuals.
In conducting our business, we are required to comply with applicable laws regarding fee-splitting and the corporate practice of medicine.
Some states prohibit the “corporate practice of therapy” that restricts business corporations from providing physical therapy services through the direct employment of therapist physicians or from exercising control over medical decisions by therapists. The laws relating to corporate practice vary from state to state and are not fully developed in each state in which we have facilities. Typically, however, professional corporations owned and controlled by licensed professionals are exempt from corporate practice restrictions and may employ therapists to furnish professional services. Those professional corporations may be managed by business corporations, such as the Company.
Some states also prohibit entities from engaging in certain financial arrangements, such as fee-splitting, with physicians or therapists. The laws relating to fee-splitting also vary from state to state and are not fully developed. Generally, these laws restrict business arrangements that involve a physician or therapist sharing medical fees with a referral source, but in some states, these laws have been interpreted to extend to management agreements between physicians or therapists and business entities under some circumstances.
We believe that our current and planned activities do not constitute fee-splitting or the unlawful corporate practice of medicine as contemplated by these state laws. However, there can be no assurance that future interpretations of such laws will not require structural and organizational modification of our existing relationships with the practices. If a court or regulatory body determines that we have violated these laws or if new laws are introduced that would render our arrangements illegal, we could be subject to civil or criminal penalties, our contracts could be found legally invalid and unenforceable (in whole or in part), or we could be required to restructure our contractual arrangements with our affiliated physicians and other licensed providers.
Failure to maintain effective internal control over our financial reporting could have an adverse effect on our ability to report our financial results on a timely and accurate basis.
We are required to produce our consolidated financial statements in accordance with the requirements of accounting principles generally accepted in the United States of America. Effective internal control over financial reporting is necessary for us to provide reliable financial reports, to help mitigate the risk of fraud and to operate successfully. We are required by federal securities laws to document and test our internal control procedures in order to satisfy the requirements of the Sarbanes-Oxley Act of 2002, which requires annual management assessments of the effectiveness of our internal control over financial reporting.
19
Testing and maintaining our internal control over financial reporting can be expensive and divert our management’s attention from other matters that are important to our business. We may not be able to conclude on an ongoing basis that we have effective internal control over financial reporting in accordance with applicable law, or our independent registered public accounting firm may not be able to issue an unqualified attestation report if we conclude that our internal control over financial reporting is not effective. If we fail to maintain effective internal control over financial reporting, or our independent registered public accounting firm is unable to provide us with an unqualified attestation report on our internal control, we could be required to take costly and time-consuming corrective measures, be required to restate the affected historical financial statements, be subjected to investigations and/or sanctions by federal and state securities regulators, and be subjected to civil lawsuits by security holders. Any of the foregoing could also cause investors to lose confidence in our reported financial information and in our company and would likely result in a decline in the market price of our stock and in our ability to raise additional financing if needed in the future.
We may be adversely affected by a security breach, such as a cyber-attack, which may cause a violation of HIPAA or HITECH and subject us to potential legal and reputational harm.
In the normal course of business, our information technology systems hold sensitive patient information including patient demographic data and other protected health information, which is subject to HIPAA and HITECH. We also contract with third-party vendors to maintain and store our patient’s individually identifiable health information. Numerous state and federal laws and regulations address privacy and information security concerns resulting from our access to our patient’s and employee’s personal information.
Our information technology systems and those of our vendors that process, maintain, and transmit such data are subject to computer viruses, cyber-attacks, or breaches. We adhere to policies and procedures designed to ensure compliance with HIPAA and other privacy and information security laws and require our third-party vendors to do so as well. If, however, we or our third-party vendors experience a breach, loss, or other compromise of unsecured protected health information or other personal information, such an event could result in significant civil and criminal penalties, lawsuits, reputational harm, and increased costs to us, any of which could have a material adverse effect on our financial condition and results of operations.
Furthermore, while our information technology systems, and those of our third-party vendors, are maintained with safeguards protecting against cyber-attacks. A cyber-attack that bypasses our information technology security systems, or those of our third-party vendors, could result in a material adverse effect on our business, financial condition, results of operations, or cash flows. In addition, our future results could be adversely affected due to the theft, destruction, loss, misappropriation, or release of protected health information, other confidential data or proprietary business information, operational or business delays resulting from the disruption of information technology systems and subsequent mitigation activities, or regulatory action taken as a result of such incident. We provide our employees training and regular reminders on important measures they can take to prevent breaches. We routinely identify attempts to gain unauthorized access to our systems. However, given the rapidly evolving nature and proliferation of cyber threats, there can be no assurance our training and network security measures or other controls will detect, prevent, or remediate security or data breaches in a timely manner or otherwise prevent unauthorized access to, damage to, or interruption of our systems and operations. Accordingly, we may be vulnerable to losses associated with the improper functioning, security breach, or unavailability of our information systems as well as any systems used in acquired operations.
We depend upon the cultivation and maintenance of relationships with the physicians in our markets.
Our success is dependent upon referrals from physicians in the communities our clinics serve and our ability to maintain good relations with these physicians and other referral sources. Physicians referring patients to our clinics are free to refer their patients to other therapy providers or to their own physician owned therapy practice. If we are unable to successfully cultivate and maintain strong relationships with physicians and other referral sources, our business may decrease and our net operating revenues may decline.
We depend upon our ability to recruit and retain experienced physical therapists.
Our revenue generation is dependent upon referrals from physicians in the communities our clinics serve, and our ability to maintain good relations with these physicians. Our therapists are the front line for generating these referrals and we are dependent on their talents and skills to successfully cultivate and maintain strong
20
relationships with these physicians. If we cannot recruit and retain our base of experienced and clinically skilled therapists, our business may decrease and our net operating revenues may decline. Periodically, we have clinics in isolated communities that are temporarily unable to operate due to the unavailability of a therapist who satisfies our standards.
We may also experience increases in our labor costs, primarily due to higher wages and greater benefits required to attract and retain qualified healthcare personnel, and such increases may adversely affect our profitability. Furthermore, while we attempt to manage overall labor costs in the most efficient way, our efforts to manage them may have limited effectiveness and may lead to increased turnover and other challenges.
Our revenues may fluctuate due to weather.
We have a significant number of clinics in states that normally experience snow and ice during the winter months. Also, a significant number of our clinics are located in states along the Gulf Coast and Atlantic Coast which are subject to periodic winter storms, hurricanes and other severe storm systems. Periods of severe weather may cause physical damage to our facilities or prevent our staff or patients from traveling to our clinics, which may cause a decrease in our net operating revenues.
We operate in a highly competitive industry.
We encounter competition from local, regional or national entities, some of which have superior resources or other competitive advantages. Intense competition may adversely affect our business, financial condition or results of operations. For a more complete description of this competitive environment, see “Business—Competition” in Item 1. An adverse effect on our business, financial condition or results of operations may require us to write-down goodwill.
We may incur closure costs and losses.
The competitive, economic or reimbursement conditions in our markets in which we operate may require us to reorganize or to close certain clinics. In the event a clinic is reorganized or closed, we may incur losses and closure costs. The closure costs and losses may include, but are not limited to, lease obligations, severance, and write-down or write-off of goodwill and other intangible assets.
Future acquisitions may use significant resources, may be unsuccessful and could expose us to unforeseen liabilities.
As part of our growth strategy, we intend to continue pursuing acquisitions of outpatient physical therapy clinics. Acquisitions may involve significant cash expenditures, potential debt incurrence and operational losses, dilutive issuances of equity securities and expenses that could have an adverse effect on our financial condition and results of operations. Acquisitions involve numerous risks, including:
| • | the difficulty and expense of integrating acquired personnel into our business; |
| • | the diversion of management’s time from existing operations; |
| • | the potential loss of key employees of acquired companies; |
| • | the difficulty of assignment and/or procurement of managed care contractual arrangements; and |
| • | the assumption of the liabilities and exposure to unforeseen liabilities of acquired companies, including liabilities for failure to comply with healthcare regulations. |
Issuance of shares in connection with financing transactions or under stock incentive plans will dilute current stockholders.
Pursuant to our stock incentive plans, our Compensation Committee of the Board, consisting solely of independent directors, is authorized to grant stock awards to our employees, directors and consultants. Shareholders will incur dilution upon the exercise of any outstanding stock awards or the grant of any restricted stock. In addition, if we raise additional funds by issuing additional common stock, or securities convertible into or exchangeable or exercisable for common stock, further dilution to our existing stockholders will result, and new investors could have rights superior to existing stockholders.
21
The number of shares of our common stock eligible for future sale could adversely affect the market price of our stock.
At December 31, 2019, we had reserved approximately 300,000 shares for future equity grants. We may issue additional restricted securities or register additional shares of common stock under the Securities Act of 1933, as amended (the “Securities Act”), in the future. The issuance of a significant number of shares of common stock upon the exercise of stock options or the availability for sale, or sale, of a substantial number of the shares of common stock eligible for future sale under effective registration statements, under Rule 144 or otherwise, could adversely affect the market price of the common stock.
Provisions in our articles of incorporation and bylaws could delay or prevent a change in control of our company, even if that change would be beneficial to our stockholders.
Certain provisions of our articles of incorporation and bylaws may delay, discourage, prevent or render more difficult an attempt to obtain control of our company, whether through a tender offer, business combination, proxy contest or otherwise. These provisions include the charter authorization of “blank check” preferred stock and a restriction on the ability of stockholders to call a special meeting.
ITEM 1B. UNRESOLVED STAFF COMMENTS.
None
| ITEM 2. | PROPERTIES. |
We lease the properties used for our clinics under non-cancelable operating leases with terms ranging from one to five years, with the exception of the property for one clinic which we own. We intend to lease the premises for any new clinic locations except in rare instances where leasing is not a cost-effective alternative. Our typical clinic occupies 1,000 to 5,000 square feet.
We also lease our executive offices located in Houston, Texas, under a non-cancelable operating lease expiring in February 2028. We currently lease approximately 44,000 square feet of space (including allocations for common areas) at our executive offices.
| ITEM 3. | LEGAL PROCEEDINGS. |
We are a party to various legal actions, proceedings, and claims (some of which are not insured), and regulatory and other governmental audits and investigations in the ordinary course of our business. We cannot predict the ultimate outcome of pending litigation, proceedings, and regulatory and other governmental audits and investigations. These matters could potentially subject us to sanctions, damages, recoupments, fines, and other penalties. The Department of Justice, CMS, or other federal and state enforcement and regulatory agencies may conduct additional investigations related to our businesses in the future that may, either individually or in the aggregate, have a material adverse effect on our business, financial position, results of operations, and liquidity.
Healthcare providers are subject to lawsuits under the qui tam provisions of the federal False Claims Act. Qui tam lawsuits typically remain under seal for some time while the government decides whether or not to intervene on behalf of a private qui tam plaintiff (known as a relator) and take the lead in the litigation. These lawsuits can involve significant monetary damages and penalties and award bounties to private plaintiffs who successfully bring the suits. We are and have been a defendant in these cases in the past, and may be named as a defendant in similar cases from time to time in the future.
Florida Litigation
On August 19, 2019, we received notice of a qui tam lawsuit filed by a relator on behalf of the United States, titled U.S. ex rel. Bonnie Elsdon, v. U.S. Physical Therapy, Inc., U.S. Physical Therapy, Ltd., Rehab Partners #2, Inc., The Hale Hand Center, Limited Partnership (the “Hale Partnership”), and Suzanne Hale. This whistleblower lawsuit was filed in the U.S. District Court for the Southern District of Texas, seeking damages and civil penalties under the federal False Claim Act. This lawsuit was originally filed under seal by a
22
former employee of The Hale Hand Center, Limited Partnership (“Hale Partnership”), a majority-owned subsidiary of the Company, on May 25, 2018. The U.S Government declined to intervene in the case and unsealed the Complaint on July 17, 2019. The plaintiff - relator served the Complaint on us and the other named defendants on August 19, 2019.
The Complaint alleges that the Hale Partnership engaged in conduct to purposely “upcode” its billings for services provided to Medicare patients. The plaintiff - relator points to three dates of service and provides examples of what it alleges are inflated billings by the Hale Partnership; the relator then claims that similar false claims must have occurred on other days and at other Company-owned partnerships.
On October 3, 2019, we filed Motions to Dismiss based on numerous grounds on behalf of each of the named defendants. On October 29, 2019, the plaintiff-relator dismissed three of the named defendants, Rehab Partners #2, Inc., U.S. Physical Therapy, Ltd., and Suzanne Hale. The Motions to Dismiss as to the remaining two defendants has been fully briefed and is pending before the Court for a ruling.
We have engaged counsel and fully investigated the matter, and believe that the allegations in the Complaint have no merit. We intend to vigorously defend this action, but at this time we are unable to predict the timing and outcome of the matter.
| ITEM 4. | MINE SAFETY DISCLOSURES. |
Not Applicable.
PART II
| ITEM 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES. |
Our common stock has traded on the New York Stock Exchange (“NYSE”) since August 14, 2012 under the symbol “USPH.” Prior to that, our common stock was traded on the Nasdaq Global Select Market under the symbol “USPH”. As of February 27, 2020, there were 83 holders of record of our outstanding common stock.
DIVIDENDS
On February 25, 2020, the Board of Directors declared a dividend of $0.32 per share on all shares of common stock issued and outstanding to those shareholders of record on March 13, 2020 payable on April 17, 2020. During 2019, we paid a quarterly dividend of $0.27 for first and second quarter and for third and fourth quarter, $0.30 per share totaling $1.14 per share for the year, which amounted to a total of aggregate cash payments of dividend to holders of our common stock in 2019 of approximately $14.5 million. During 2018, we paid a regular quarterly dividend of $0.23 per share, totaling $0.92 per share, which amounted to a total of aggregate cash payments of dividends to holders of our common stock in 2018 of approximately $11.7 million. During 2017, we paid a quarterly dividend of $0.20 per share totaling $0.80 per share for 2017, which amounted to a total of aggregate cash payments of dividends to holders of our common stock in 2017 of approximately $10.1 million. We are currently restricted from paying dividends in excess of $20,000,000 in any fiscal year on our common stock under the Credit Agreement (as defined in “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations — Liquidity and Capital Resources”).
23
FIVE YEAR PERFORMANCE GRAPH
The performance graph and related description shall not be deemed incorporated by reference into any filing under the Securities Act or under the Exchange Act, except to the extent that we specifically incorporate this information by reference. In addition, the performance graph and the related description shall not be deemed “soliciting material” or “filed” with the SEC or subject to Regulation 14A or 14C.
On August 14, 2012, our common stock began trading on NYSE. The following performance graph compares the cumulative total stockholder return of our common stock to The NYSE Composite Index and the NYSE Health Care Index for the period from December 31, 2014 through December 31, 2019. The graph assumes that $100 was invested in our common stock and the common stock of each of the companies listed on The NYSE Composite Index and The NYSE Health Care Index on December 31, 2014 and that any dividends were reinvested.
Comparison of Five Years Cumulative Total Return for the Year Ended December 31, 2019
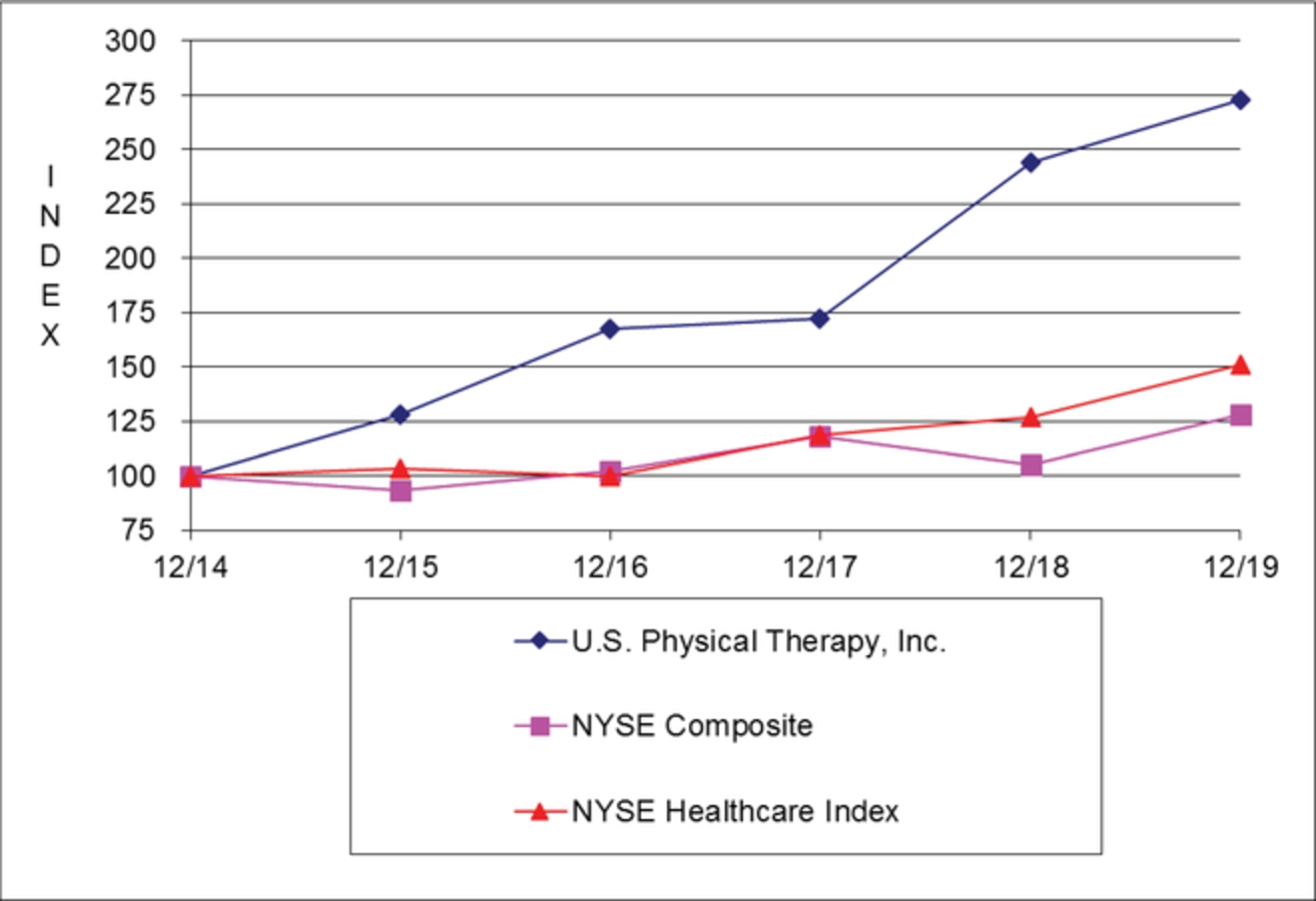
12/14 |
12/15 |
12/16 |
12/17 |
12/18 |
12/19 |
|||||||||||||
U. S. Physical Therapy, Inc. |
100 | 128 | 167 | 172 | 244 | 273 | ||||||||||||
NYSE Composite |
100 | 94 | 102 | 118 | 105 | 128 | ||||||||||||
NYSE Healthcare Index |
100 | 103 | 100 | 119 | 127 | 151 | ||||||||||||
24
| ITEM 6. | SELECTED FINANCIAL DATA. |
The following selected financial data should be read in conjunction with the description of our critical accounting policies set forth in “Management’s Discussion and Analysis of Results of Operations and Financial Condition” and the Consolidated Financial Statements and Notes included herein.
For the Years Ended December 31, |
|||||||||||||||
2019 |
2018 |
2017 |
2016 |
2015 |
|||||||||||
($ in thousands, except per share data) |
|||||||||||||||
Net revenues |
$ | 481,969 | $ | 453,911 | $ | 414,051 | $ | 356,546 | $ | 331,302 | |||||
Operating income |
$ | 67,425 | $ | 60,314 | $ | 54,728 | $ | 49,533 | $ | 47,294 | |||||
Gain on derecognition of debt |
$ | — | $ | 1,846 | $ | — | $ | — | $ | — | |||||
Gain on sale of partnership interest |
$ | 5,514 | $ | — | $ | — | $ | — | $ | — | |||||
Interest expense |
|||||||||||||||
Mandatorily redeemable non-controlling interests - change in redemption value |
$ | — | $ | — | $ | 12,894 | $ | 6,169 | $ | 2,670 | |||||
Mandatorily redeemable non-controlling interests - earnings allocable |
$ | — | $ | — | $ | 6,055 | $ | 4,057 | $ | 3,538 | |||||
Debt and other |
$ | 2,079 | $ | 2,042 | $ | 2,111 | $ | 1,252 | $ | 1,031 | |||||
Total interest expense |
$ | 2,079 | $ | 2,042 | $ | 21,060 | $ | 11,478 | $ | 7,239 | |||||
Net income |
$ | 57,259 | $ | 48,842 | $ | 27,724 | $ | 26,268 | $ | 26,489 | |||||
Net income attributable to non-controlling interests |
$ | 17,220 | $ | 13,969 | $ | 5,468 | $ | 5,717 | $ | 5,874 | |||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | $ | 22,256 | $ | 20,551 | $ | 20,615 | |||||
Per share net income attributable to USPH shareholders: |
|||||||||||||||
Basic and diluted |
$ | 2.45 | $ | 1.31 | $ | 1.76 | $ | 1.64 | $ | 1.66 | |||||
Dividends declared and paid per common share |
$ | 1.14 | $ | 0.92 | $ | 0.80 | $ | 0.68 | $ | 0.60 | |||||
Computation of earnings per share - USPH shareholders: |
|||||||||||||||
Net Income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | $ | 22,256 | $ | 20,551 | $ | 20,615 | |||||
Charges to retained earnings: |
|||||||||||||||
Revaluation of redeemable non-controlling interest |
$ | (11,893 | ) |
$ | (24,770 | ) |
$ | (201 | ) |
$ | — | $ | — | ||
Tax effect at statutory rate (federal and state) of 26.25% |
$ | 3,121 | $ | 6,502 | $ | 75 | $ | — | $ | — | |||||
$ | 31,267 | $ | 16,605 | $ | 22,130 | $ | 20,551 | $ | 20,615 | ||||||
Earnings per share (Basic and diluted) |
$ | 2.45 | $ | 1.31 | $ | 1.76 | $ | 1.64 | $ | 1.66 | |||||
Shares used in computation: |
|||||||||||||||
Basic and diluted earnings per share - weighted-average shares |
12,756 | 12,666 | 12,570 | 12,500 | 12,392 | ||||||||||
On December 31, |
|||||||||||||||
2019 |
2018 |
2017 |
2016 |
2015 |
|||||||||||
($ in thousands) |
|||||||||||||||
Total assets |
$ | 560,845 | $ | 443,166 | $ | 418,982 | $ | 351,231 | $ | 303,757 | |||||
Mandatorily redeemable non-controlling interests |
$ | — | $ | — | $ | 327 | $ | 69,190 | $ | 45,974 | |||||
Long-term debt, less current portion |
$ | 50,361 | $ | 38,402 | $ | 56,728 | $ | 50,596 | $ | 48,335 | |||||
Working capital |
$ | 24,823 | $ | 37,268 | $ | 37,530 | $ | 41,347 | $ | 41,193 | |||||
Current ratio |
1.41 | 1.89 | 1.95 | 2.68 | 3.17 | ||||||||||
25
| ITEM 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS. |
EXECUTIVE SUMMARY
Our Business. We operate outpatient physical therapy clinics that provide pre- and post-operative care and treatment for a variety of orthopedic-related disorders and sports-related injuries, neurologically-related injuries and rehabilitation of injured workers. At December 31, 2019, we operated 583 clinics in 40 states. The average age of our clinics at December 31, 2019 was 10.4 years. In addition to our ownership and operation of outpatient physical therapy clinics, we also manage physical therapy facilities for third parties, such as physicians and hospitals, with 26 such third-party facilities under management as of December 31, 2019.
In March 2017, we acquired a 55% interest in the initial industrial injury prevention business. On April 30, 2018, we made a second acquisition and subsequently combined the two businesses. After the combination, the Company owned a 59.45% interest in the combined business, Briotix Health, Limited Partnership (“Briotix Health”). Services provided include onsite injury and ergonomic assessments. The majority of these services are contracted with and paid for directly by employers, including a number of Fortune 500 companies. Other clients include large insurers and their contractors. We perform these services through Industrial Sports Medicine Professionals, consisting of both physical therapists and specialized certified athletic trainers (ATCs). On April 11, 2019, we acquired a third company that is a provider of industrial injury prevention services. The acquired company specializes in delivering injury prevention and care, post offer employment testing, functional capacity evaluations and return-to-work services. It performs these services across a network in 45 states including onsite at eleven client locations. The acquired business was then combined with Briotix Health increasing our ownership position in the partnership to approximately 76.0%.
In addition to the above acquired interests in the industrial injury prevention businesses, during 2019, 2018 and 2017, we completed the following multi-clinic acquisitions:
Acquisition |
Date |
% Interest Acquired |
Number of Clinics |
||||
2019 |
|||||||
September 2019 Acquisition |
September 30, 2019 |
67 | % |
11 | |||
2018 |
|||||||
August 2018 Acquisition |
August 31 |
70 | % |
4 | |||
2017 |
|||||||
January 2017 Acquisition |
January 1 |
70 | % |
17 | |||
May 2017 Acquisition |
May 31 |
70 | % |
4 | |||
June 2017 Acquisition |
June 30 |
60 | % |
9 | |||
October 2017 Acquisition |
October 31 |
70 | % |
9 | |||
Also during 2019, we purchased the assets and business of one physical therapy clinic in a separate transaction. The clinic operates as a satellite clinic of one of our existing partnerships. Besides the multi-clinic acquisition in 2018, through several of our majority owned Clinic Partnerships, we acquired five separate clinic practices. These practices operate as satellites of the respective existing Clinic Partnerships. Also, during 2017, we purchased the assets and business of two physical therapy clinics in separate transactions. One clinic was consolidated with an existing clinic and the other operates as a satellite clinic of one of our existing partnerships.
The results of operations of the acquired clinics have been included in our consolidated financial statements since the date of their respective acquisition. We intend to continue to pursue additional acquisition opportunities, develop new clinics and open satellite clinics.
26
CRITICAL ACCOUNTING POLICIES
Critical accounting policies are those that have a significant impact on our results of operations and financial position involving significant estimates requiring our judgment. Our critical accounting policies are:
Revenue Recognition.
Revenues are recognized in the period in which services are rendered. Net patient revenues consists of revenues for physical therapy and occupational therapy clinics that provide pre-and post-operative care and treatment for orthopedic related disorders, sports-related injuries, preventative care, rehabilitation of injured workers and neurological-related injuries. Net patient revenues (patient revenues less estimated contractual adjustments) are recognized at the estimated net realizable amounts from third-party payors, patients and others in exchange for services rendered when obligations under the terms of the contract are satisfied. There is an implied contract between us and the patient upon each patient visit. Generally, this occurs as we provide physical and occupational therapy services, as each service provided is distinct and future services rendered are not dependent on previously rendered services. We have agreements with third-party payors that provide for payments to us at amounts different from its established rates. The allowance for estimated contractual adjustments is based on terms of payor contracts and historical collection and write-off experience.
Management contract revenues, which are included in other revenues in the consolidated statements of net income, are derived from contractual arrangements whereby we manage a clinic owned by a third party. We do not have any ownership interest in these clinics. Typically, revenues are determined based on the number of visits conducted at the clinic and recognized at the point in time when services are performed. Costs, typically salaries for our employees, are recorded when incurred.
Revenues from the industrial injury prevention business, which are also included in other revenues in the consolidated statements of net income, are derived from onsite services we provide to clients’ employees including injury prevention, rehabilitation, ergonomic assessments and performance optimization. Revenue from the industrial injury prevention business is recognized when obligations under the terms of the contract are satisfied. Revenues are recognized at an amount equal to the consideration we expect to receive in exchange for providing injury prevention services to its clients. The revenue is determined and recognized based on the number of hours and respective rate for services provided in a given period.
Additionally, other revenues include services we provide on-site, such as schools and industrial worksites, for physical or occupational therapy services, and athletic trainers and gym membership fees. Contract terms and rates are agreed to in advance between us and the third parties. Services are typically performed over the contract period and revenue is recorded at the point of service. If the services are paid in advance, revenue is recorded as a contract liability over the period of the agreement and recognized at the point in time when the services are performed.
In May 2014, March 2016, April 2016, and December 2016, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2014-09, Revenue from Contracts with Customers, ASU 2016-08, Revenue from Contracts with Customers, Principal versus Agent Considerations, ASU 2016-10, Revenue from Contracts with Customers, Identifying Performance Obligations and Licensing, ASU 2016-12, Revenue from Contracts with Customers, Narrow Scope Improvements and Practical Expedients, and ASU 2016-20, Technical Corrections and Improvements to Topic 606, Revenue from Contracts with Customer (collectively the “standards”), respectively, which supersede most of the current revenue recognition requirements (“ASC 606”). The core principle of the new guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services.
We implemented the new standards beginning January 1, 2018 using a modified retrospective transition method. The principal change relates to how the new standard requires healthcare providers to estimate the amount of variable consideration to be included in the transaction price up to an amount which is probable that a significant reversal will not occur. The most common forms of variable consideration we experience are amounts for services provided that are ultimately not realizable from a customer. There were no changes to revenues or other revenues upon implementation. Under the new standards, our estimate for unrealizable amounts will continue to be recognized as a reduction to revenue. The bad debt expense historically reported will not materially change.
27
For ASC 606, there is an implied contract between us and the patient upon each patient visit. Separate contractual arrangements exist between us and third party payors (e.g. insurers, managed care programs, government programs, workers' compensation programs which establish the amounts the third parties pay on behalf of the patients for covered services rendered. While these agreements are not considered contracts with the customer, they are used for determining the transaction price for services provided to the patients covered by the third party payors. The payor contracts do not indicate performance obligations for us, but indicate reimbursement rates for patients who are covered by those payors when the services are provided. At that time, we are obligated to provide services for the reimbursement rates stipulated in the payor contracts. The execution of the contract alone does not indicate a performance obligation. For self-paying customers, the performance obligation exists when we provide the services at established rates. The difference between our established rate and the anticipated reimbursement rate is accounted for as an offset to revenue – contractual allowance.
We determine allowances for doubtful accounts based on the specific agings and payor classifications at each clinic. The provision for doubtful accounts is included in clinic operating costs in the statements of net income. Patient accounts receivable, which are stated at the historical carrying amount net of contractual allowances, write-offs and allowance for doubtful accounts, includes only those amounts we estimate to be collectible.
The following table details the revenue related to the various categories.
Year Ended December 31, |
|||||||||
2019 |
2018 |
2017 |
|||||||
Patient revenues |
$ | 433,345 | $ | 417,703 | $ | 389,226 | |||
Management contract revenues |
8,676 | 8,339 | 6,275 | ||||||
Industrial injury prevention services revenues |
37,462 | 25,466 | 14,908 | ||||||
Other revenues |
2,486 | 2,403 | 3,642 | ||||||
$ | 481,969 | $ | 453,911 | $ | 414,051 | ||||
Contractual Allowances. Contractual allowances result from the differences between the rates charged for services performed and expected reimbursements by both insurance companies and government sponsored healthcare programs for such services. Medicare regulations and the various third party payors and managed care contracts are often complex and may include multiple reimbursement mechanisms payable for the services provided in our clinics. We estimate contractual allowances based on our interpretation of the applicable regulations, payor contracts and historical calculations. Each month we estimate our contractual allowance for each clinic based on payor contracts and the historical collection experience of the clinic and applies an appropriate contractual allowance reserve percentage to the gross accounts receivable balances for each payor of the clinic. Based on our historical experience, calculating the contractual allowance reserve percentage at the payor level is sufficient to allow us to provide the necessary detail and accuracy with our collectability estimates. However, the services authorized and provided and related reimbursement are subject to interpretation that could result in payments that differ from our estimates. Payor terms are periodically revised necessitating continual review and assessment of the estimates made by management. Our billing systems may not capture the exact change in our contractual allowance reserve estimate from period to period. Therefore, in order to assess the accuracy of our revenues and hence our contractual allowance reserves, our management regularly compares its cash collections to corresponding net revenues measured both in the aggregate and on a clinic-by-clinic basis. In the aggregate, the historical difference between net revenues and corresponding cash collections has generally reflected a difference within approximately 1% of net revenues. Additionally, analysis of subsequent period’s contractual write-offs on a payor basis reflects a difference within approximately 1% between the actual aggregate contractual reserve percentage as compared to the estimated contractual allowance reserve percentage associated with the same period end balance. As a result, we believe that a reasonable likely change in the contractual allowance reserve estimate would not be more than 1% at December 31, 2019. For purposes of demonstrating the sensitivity of this estimate on our Company’s financial condition, a one percent increase or decrease in our aggregate contractual allowance reserve percentage would decrease or increase, respectively, net patient revenue by approximately $1.2 million for the year ended December 31, 2019. Management believes the changes in the estimate of the contractual allowance reserve for the periods ended December 31, 2019, 2018 and 2017 have not been material to the statement of income.
28
The following table sets forth information regarding our patient accounts receivable as of the dates indicated (in thousands):
December 31, |
||||||
2019 |
2018 |
|||||
Gross patient accounts receivable |
$ | 124,035 | $ | 108,141 | ||
Less contractual allowances |
75,109 | 60,718 | ||||
Subtotal - accounts receivable |
48,926 | 47,423 | ||||
Less allowance for doubtful accounts |
2,698 | 2,672 | ||||
Net patient accounts receivable |
$ | 46,228 | $ | 44,751 | ||
The following table presents our patient accounts receivable aging by payor class as of the dates indicated (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||||||||||||||
Payor |
Current to 120 Days |
120+ Days |
Total |
Current to 120 Days |
120+ Days |
Total |
||||||||||||
Managed Care/ Commercial Plans |
$ | 14,159 | $ | 1,783 | $ | 15,942 | $ | 14,852 | $ | 2,263 | $ | 17,115 | ||||||
Medicare/Medicaid |
11,408 | 1,491 | 12,899 | 10,026 | 1,736 | 11,762 | ||||||||||||
Workers Compensation* |
6,593 | 1,121 | 7,714 | 7,056 | 1,339 | 8,395 | ||||||||||||
Self-pay |
4,365 | 3,040 | 7,405 | 4,497 | 3,748 | 8,245 | ||||||||||||
Other** |
808 | 1,460 | 2,268 | 945 | 961 | 1,906 | ||||||||||||
Totals |
$ | 37,333 | $ | 8,895 | $ | 46,228 | $ | 37,376 | $ | 10,047 | $ | 47,423 | ||||||
| * | Workers compensation is paid by state administrators or their designated agents. |
| ** | Other includes primarily litigation claims and, to a lesser extent, vehicular insurance claims. |
Reimbursement for Medicare beneficiaries is based upon a fee schedule published by HHS. For a more complete description of our third party revenue sources, see “Business—Sources of Revenue” in Item 1.
Provision for Doubtful Accounts. We determine our provision for doubtful accounts based on the specific agings and payor classifications at each clinic. We review the accounts receivable aging and rely on prior experience with particular payors to determine an appropriate reserve for doubtful accounts. Historically, clinics that have a large number of aged accounts generally have less favorable collection experience, and thus, require a higher provision. Accounts that are ultimately determined to be uncollectible are written off against our bad debt provision. The amount of our aggregate provision for doubtful accounts is regularly reviewed for adequacy in light of current and historical experience.
Accounting for Income Taxes. We account for income taxes under the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases and operating loss and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in income in the period that includes the enactment date. We recognize the financial statement benefit of a tax position only after determining that the relevant tax authority would more likely than not sustain the position following an audit. For tax positions meeting the more-likely-than-not threshold, the amount to be recognized in the financial statements is the largest benefit that has a greater than 50 percent likelihood of being realized upon ultimate settlement with the relevant tax authority.
The Tax Cuts and Jobs Act of 2017 (the “TCJA”) was passed by Congress on December 20, 2017 and signed into law by President Trump on December 22, 2017. The TCJA made significant changes to U.S. corporate income tax laws including a decrease in the corporate income tax rate to 21% effective January 1,
29
2018. As a result, we revalued our deferred tax assets and liabilities. Based on a review and analysis as of December 31, 2017, we recorded a reduction in our net deferred tax liabilities of $4.3 million thereby reducing our provision for income taxes by such amount for the 2017 year.
We do not believe that we have any significant uncertain tax positions at December 31, 2019, nor is this expected to change within the next twelve months due to the settlement and expiration of statutes of limitation.
We did not have any accrued interest or penalties associated with any unrecognized tax benefits nor was any interest expense recognized during the twelve months ended December 31, 2019 and 2018.
Carrying Value of Long-Lived Assets. Our property and equipment, intangible assets and goodwill (collectively, our “long-lived assets”) comprise a significant portion of our total assets. The accounting standards require that we periodically, and upon the occurrence of certain events, assess the recoverability of our long-lived assets. If the carrying value of our property and equipment exceeds their undiscounted cash flows, we are required to write the carrying value down to estimated fair value.
Goodwill. The fair value of goodwill and other intangible assets with indefinite lives are tested for impairment annually and upon the occurrence of certain events, and are written down to fair value if considered impaired. We evaluate goodwill for impairment on at least an annual basis (in the third quarter) by comparing the fair value of its reporting units to the carrying value of each reporting unit including related goodwill. We evaluate indefinite lived tradenames using the relief from royalty method in conjunction with its annual goodwill impairment test. We operate a one segment business which is made up of various clinics within partnerships. The partnerships are components of regions and are aggregated to that operating segment level for the purpose of determining reporting units when performing the annual goodwill impairment test. In 2019, 2018 and 2017, we had six regions. In addition to the six regions, in 2018 and 2019, the impairment test included a separate analysis for the industrial injury prevention business.
An impairment loss generally would be recognized when the carrying amount of the net assets of a reporting unit, inclusive of goodwill and other intangible assets, exceeds the estimated fair value of the reporting unit. The estimated fair value of a reporting unit is determined using two factors: (i) earnings prior to taxes, depreciation and amortization for the reporting unit multiplied by a price/earnings ratio used in the industry and (ii) a discounted cash flow analysis. A weight is assigned to each factor and the sum of each weight times the factor is considered the estimated fair value. For 2019, the factors (i.e., price/earnings ratio, discount rate and residual capitalization rate) were updated to reflect current market conditions. The evaluation of goodwill in 2019, 2018 and 2017 did not result in any goodwill amounts that were deemed impaired. In 2017, we wrote off the goodwill of $0.5 million related to the closure of a single clinic acquired partnership due to the loss of a significant management contract.
Redeemable Non-Controlling Interests. The non-controlling interests that are reflected as redeemable non-controlling interests in our consolidated financial statements consist of those owners, including us, that have certain redemption rights, whether currently exercisable or not, and which currently, or in the future, require that we purchase or the owner sell the non-controlling interest held by the owner, if certain conditions are met and the owners request the purchase (“Put Right”). We also have a call right (“Call Right”). The Put Right or Call Right may be triggered by the owner or us, respectively, at such time as both of the following events have occurred: 1) termination of the owner’s employment, regardless of the reason for such termination, and 2) the passage of specified number of years after the closing of the transaction, typically three to five years, as defined in the limited partnership agreement. The Put Rights and Call Rights are not automatic (even upon death) and require either the owner or us to exercise our rights when the conditions triggering the Put or Call Rights have been satisfied. The purchase price is derived at a predetermined formula based on a multiple of trailing twelve months earnings performance as defined in the respective limited partnership agreements.
On the date we acquire a controlling interest in a partnership and the limited partnership agreement for such partnerships contains redemption rights not under our control, the fair value of the non-controlling interest is recorded in the consolidated balance sheet under the caption – Redeemable non-controlling interests. Then, in each reporting period thereafter until it is purchased by us, the redeemable non-controlling interest is adjusted to the greater of its then current redemption value or initial value, based on the predetermined formula defined in the respective limited partnership agreement. As a result, the value of the non-controlling interest is not adjusted below its initial value. We record any adjustment in the redemption value, net of tax, directly to retained earnings and not in the consolidated statements of income. Although the adjustments are not reflected in the consolidated
30
statements of income, current accounting rules require that we reflect the adjustments, net of tax, in the earnings per share calculation. The amount of net income attributable to redeemable non-controlling interest owners is included in consolidated net income on the face of the consolidated income statement. We believe the redemption value (i.e. the carrying amount) and fair value are the same.
Effective December 31, 2017, we entered into amendments to our limited partnership agreements for our acquired partnerships replacing the mandatory redemption feature. No monetary consideration was paid to the partners to amend the agreements. The amended limited partnership agreements provide that, upon the triggering events, we have a Call Right and the selling entity or individual has a Put Right for the purchase and sale of the limited partnership interest held by the partner. Once triggered, the Put Right and the Call Right do not expire, even upon an individual partner’s death, and contain no mandatory redemption feature. The purchase price of the partner’s limited partnership interest upon the exercise of either the Put Right or the Call Right is calculated per the terms of the respective agreements. We accounted for the amendment of the limited partnership agreements as an extinguishment of the outstanding mandatorily redeemable non-controlling interests, which were classified as liabilities, through the issuance of new redeemable non-controlling interests classified in temporary equity. Pursuant to Accounting Standards Codification (“ASC”) 470-50-40-2, we removed the outstanding liabilities at their carrying amounts, recognized the new temporary equities at their fair value, and recorded no gain or loss on extinguishment as management believes the redemption value (i.e. the carrying amount) and fair value are the same. In summary, the redemption values of the mandatorily redeemable non-controlling interest (previously classified as liabilities) were reclassified as redeemable non-controlling interest (temporary equity) at fair value on the December 31, 2017 consolidated balance sheet.
Non-Controlling Interests – We recognize non-controlling interests, in which we have no obligation but the right to purchase the non-controlling interests, as equity in the consolidated financial statements separate from the parent entity’s equity. The amount of net income attributable to non-controlling interests is included in consolidated net income on the face of the consolidated statements of income. Operating losses are allocated to non-controlling interests even when such allocation creates a deficit balance for the non-controlling interest partner. When we purchase a non-controlling interest and the purchase price exceeds the book value at the time of purchase, any excess or shortfall is recognized as an adjustment to additional paid-in capital.
SELECTED OPERATING AND FINANCIAL DATA
The following table and discussion relates to continuing operations unless otherwise noted. The defined terms with their respective description used in the following discussion are listed below:
|
2019
|
Year ended December 31, 2019
|
|
2018
|
Year ended December 31, 2018
|
|
2017
|
Year ended December 31, 2017
|
|
New Clinics
|
Clinics opened or acquired during the year ended December 31, 2019
|
|
Mature Clinics
|
Clinics opened or acquired prior to January 1, 2019
|
|
2018 New Clinics
|
Clinics opened or acquired during the year ended December 31, 2018
|
|
2018 Mature Clinics
|
Clinics opened or acquired prior to January 1, 2018
|
|
2017 New Clinics
|
Clinics opened or acquired during the year ended December 31, 2017
|
|
2017 Mature Clinics
|
Clinics opened or acquired prior to January 1, 2017
|
|
2016 New Clinics
|
Clinics opened or acquired during the year ended December 31, 2016
|
The following table presents selected operating and financial data, used by management as key indicators of our operating performance:
For the Years Ended December 31, |
|||||||||
2019 |
2018 |
2017 |
|||||||
Number of clinics, at the end of period |
583 | 591 | 578 | ||||||
Working Days |
255 | 255 | 254 | ||||||
Average visits per day per clinic |
27.6 | 26.6 | 25.9 | ||||||
Total patient visits |
4,091,967 | 3,957,534 | 3,705,226 | ||||||
Net patient revenue per visit |
$ | 105.90 | $ | 105.55 | $ | 105.05 | |||
31
RESULTS OF OPERATIONS
FISCAL YEAR 2019 COMPARED TO FISCAL 2018
| • | Net revenues increased $28.1 million, or 6.2%, from $453.9 million in 2018 to $481.9 million in 2019, primarily due to an increase in net patient revenues from physical therapy operations due to internal growth and new clinic development plus an acquisition, and an increase in the revenue from the industrial injury prevention business due to internal growth and acquisitions. |
| • | For the year ended December 31, 2019, our Operating Results (as defined below) increased 7.3% to $36.0 million, or $2.82 per diluted share, as compared to $33.5 million, or $2.65 per diluted share, for 2018. Operating Results, a non-Generally Accepted Accounting Principle (“GAAP”) measure, equals net income attributable to our shareholders per the consolidated statements of net income less the gain on the sale of a partnership interest in 2019 and the gain on the derecognition of debt in 2018, both net of tax, as described below. The earnings per share from Operating Results also excludes the impact of the revaluation of redeemable non-controlling interest. On June 30, 2019, we sold 50% of our interest in one physical therapy partnership to the group’s founders for $11.6 million and recognized a net pre-tax gain of $5.5 million which is not included in Operating Results. See table below for a detailed computation (in thousands, except per share data): |
Year Ended December 31, |
||||||
2019 |
2018 |
|||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | ||
Adjustments: |
||||||
Gain on sale of partnership interest |
(5,514 | ) |
— | |||
Gain on derecognition of debt |
— | (1,846 | ) |
|||
Tax effect at statutory rate (federal and state) of 26.25% |
1,447 | 484 | ||||
Operating Results |
$ | 35,972 | $ | 33,511 | ||
Basic and diluted Operating Results per share |
$ | 2.82 | $ | 2.65 | ||
Shares used in computation - basic and diluted |
12,756 | 12,666 | ||||
| • | For the year ended December 31, 2019, our net income attributable to its shareholders, in accordance with GAAP, was $40.0 million as compared to $34.9 million for the comparable period of 2018. For both periods of 2019, in accordance with current accounting guidance, the revaluation of redeemable non-controlling interest, net of tax, is not included in net income but rather charged directly to retained earnings; however, the chare or credit for this change is included in the earnings per basic and diluted share calculation. See table below (in thousands, except per share data). |
Year Ended December 31, |
||||||
2019 |
2018 |
|||||
Computation of earnings per share - USPH shareholders: |
||||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | ||
Charges to retained earnings: |
||||||
Revaluation of redeemable non-controlling interest |
(11,893 | ) |
(24,770 | ) |
||
Tax effect at statutory rate (federal and state) of 26.25% |
3,121 | 6,502 | ||||
$ | 31,267 | $ | 16,605 | |||
Earnings per share (basic and diluted) |
$ | 2.45 | $ | 1.31 | ||
32
| • | For 2019, our Adjusted EBITDA increased by 8.5% to $67.3 million from $62.1 million in 2018. Adjusted EBITDA is defined as earnings before gain on derecognition of debt, gain on sale of partnership interest, interest income, interest expense – debt and other, taxes, depreciation, amortization and equity-based awards compensation expense. See reconciliation of Adjusted EBITDA to net income attributable to our shareholders in the following table (in thousands): |
Year Ended December 31, |
||||||
2019 |
2018 |
|||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | ||
Adjustments: |
||||||
Depreciation and amortization |
10,095 | 9,755 | ||||
Gain on sale of partnership interest |
(5,514 | ) |
— | |||
Gain on derecognition of debt |
— | (1,846 | ) |
|||
Interest income |
(46 | ) |
(93 | ) |
||
Interest expense - debt and other |
2,079 | 2,042 | ||||
Provision for income taxes |
13,647 | 11,369 | ||||
Equity-based awards compensation expense |
6,985 | 5,939 | ||||
Adjusted EBITDA |
$ | 67,285 | $ | 62,039 | ||
The above tables reconcile net income attributable to our shareholders calculated in accordance with GAAP to Adjusted EBITDA and Operating Results, non-GAAP measures defined above. We believe providing Operating Results and Adjusted EBITDA are useful information to our investors for the purposes of comparing our period-to-period results. In addition, we believe that providing Operating Results, which eliminates certain items described above that can be subject to volatility and unusual costs, as one of the principal measures to evaluate and monitor financial performance period over period. We believe that Operating Results is useful information for investors to use in comparing the Company's period-to-period results as well as for comparing with other similar businesses. We believe reporting Adjusted EBITDA is useful information for investors in comparing the Company’s period-to-period results as well as comparing with similar businesses which report adjusted EBITDA as defined by their company.
Operating Results and Adjusted EBITDA are not measures of financial performance under GAAP. Operating Results and Adjusted EBITDA should not be considered in isolation or as an alternative to, or substitute for, net income attributable to USPH shareholders presented in the consolidated financial statements.
Net Patient Revenues
| • | Net patient revenues from physical therapy operations increased to $433.3 million in 2019 from $417.7 million in 2018, an increase of $15.6 million, or 3.7%, due to an increase in total patient visits of 3.4% (discussed below) and an increase in the average net patient revenue per visit to $105.90 from $105.55. Of the $15.6 million increase in net patient revenues, $10.8 million related to an increase in business of Mature Clinics and $4.8 million related to New Clinics. The net patient revenues related to the 30 clinics sold on June 30, 2019 had the effect of reducing total net revenues by $11.6 million in 2019 (only the first six months included for the 2019 year - $12.2 million) compared to 2018 (twelve months total was $23.8 million). |
| • | Total patient visits increased to 4,092,000 for 2019 from 3,958,000 for 2018. The growth in patient visits was attributable to 43,000 visits in New Clinics and an increase of 91,000 visits for Mature Clinics. |
| • | Net patient revenues are based on established billing rates less allowances and discounts for patients covered by contractual programs and workers’ compensation. Net patient revenues reflect contractual and other adjustments, which we evaluate monthly, relating to patient discounts from certain payors. Payments received under these contractual programs and workers’ compensation are based on predetermined rates and are generally less than the established billing rates of the clinics. |
33
Other Revenues
Other revenues consist of the following (in thousands):
Year Ended December 31, |
||||||
December 31, 2019 |
December 31, 2018 |
|||||
Industrial injury prevention services revenues |
37,462 | 25,466 | ||||
Management contract revenues |
8,676 | 8,339 | ||||
Other revenues |
2,486 | 2,403 | ||||
$ | 48,624 | $ | 36,208 | |||
Other revenues, consisting primarily of industrial injury prevention business and management fees revenue, increased by $12.4 million, from $36.2 million in 2018 to $48.6 million in 2019. Revenues from management contracts were $8.7 million for 2019 as compared to $8.3 million for 2018. Revenue from the industrial injury prevention business increased 47.1% to $37.5 million in 2019 compared to $25.5 million in 2018 due to internal growth and acquisitions. Other miscellaneous revenue was $2.4 million for both 2019 and 2018.
Operating Costs
Total operating costs were $369.5 million in 2019, or 76.7% (a reduction of 90 basis points) of net revenues, as compared to $352.2 million in 2018, or 77.6% of net revenues. The $17.3 million increase was attributable to $10.3 million in operating costs related to New Clinics, an increase of $9.2 million related to Mature Clinics, an increase of $8.8 million related to the industrial injury prevention business and an increase in management contracts costs of $0.1 million offset by a reduction in expenses related to the clinics sold of $11.1 million. See table detailing acquisition dates above under – “Executive Summary”. Each component of clinic operating costs is discussed below:
Operating Costs—Salaries and Related Costs
Salaries and related costs increased to $274.2 million for 2019 from $259.2 million for 2018, an increase of $15.0 million, or 5.8%. Approximately $2.7 million of the increase was attributable to New Clinics, an additional $13.3 million related to Mature Clinics and $7.3 million related to the industrial injury prevention business primarily due to the acquisition in 2019. Salaries and related costs for 2019 as compared to 2018 was reduced by expenses related to the clinics sold of $8.3 million. Salaries and related costs related to management contracts remained consistent. Included in salaries and related costs was approximately $1.4 million in higher employee healthcare costs than planned. Salaries and related costs as a percentage of net revenues was 56.9% for 2019 and 57.1% for 2018.
Operating Costs—Rent, Supplies, Contract Labor and Other
Rent, supplies, contract labor and other costs increased to $90.4 million for 2019 from $88.4 million for 2018, an increase of $2.0 million, or 2.2%. Approximately $3.1 million of the increase was attributable to New Clinics, $0.3 million of the decrease was due to lower costs at various Mature Clinics, $1.8 million increase was due to the industrial injury prevention businesses, $0.1 million related to management contracts and offset by a reduction in expenses related to the clinics sold of $2.7 million. Rent, supplies, contract labor and other costs as a percent of net revenues was 18.8% for 2019 and 19.5% for 2018.
Operating Costs—Provision for Doubtful Accounts
The provision for doubtful accounts for net patient receivables was $4.9 million for 2019 and $4.6 million for 2018. As a percentage of net patient revenues, the provision for doubtful accounts were 1.0% for both 2019 and 2018.
Our provision for doubtful accounts as a percentage of total patient accounts receivable was 5.5% at December 31, 2019 and 5.6% at December 31, 2018. The provision for doubtful accounts at the end of each period is based on a detailed, clinic-by-clinic review of overdue accounts and is regularly reviewed in the aggregate in light of historical experience.
34
The average accounts receivable days outstanding were 33 days at December 31, 2019 and 37 days at December 31, 2018. Net patient receivables in the amount of $4.8 million and $3.9 million were written-off in 2019 and 2018, respectively.
Gross Profit
Gross profit in 2019 grew by 10.6% or $10.8 million to $112.5 million, as compared to $101.7 million in 2018. The gross profit percentage grew to 23.3% of net revenue in the recent year as compared to 22.4% for 2018. The gross profit percentage for our physical therapy clinics was 23.6% for 2019 as compared to 22.7% for 2018. The gross profit percentage on management contracts was 14.8% for 2019 as compared to 12.1% for 2018. The gross profit percentage for the industrial injury prevention business was 22.4% for 2019 as compared to 20.4% for 2018.
Corporate Office Costs
Corporate office costs, consisting primarily of salaries, benefits and equity based compensation of corporate office personnel and directors, rent, insurance costs, depreciation and amortization, travel, legal, compliance, professional, marketing and recruiting fees, were $45.0 million for 2019 and $41.3 million for 2018. The dollar increase is primarily due to increases in salaries, benefits and equity based compensation. Corporate office costs as a percentage of net revenues were 9.3% for 2019 and 9.1% in 2018.
Interest Expense – debt and other
Interest expense – debt and other was $2.1 million for 2019 and $2.0 million for 2018. At December 31, 2019, $46.0 million was outstanding under our Amended Credit Agreement (as defined below under “—Liquidity and Capital Resources”). See “—Liquidity and Capital Resources” below for a discussion of the terms of our Amended Credit Agreement.
Gain on Sale of Partnership Interest
The gain of $5.5 million resulted from a sale of partnership interest. As previously disclosed, on June 30, 2019, we sold a 50% interest in one physical therapy partnership to the group’s founders. The sales proceeds, all of which was in cash, was $11.6 million.
Gain on Derecognition of Debt
In 2018, the gain from derecognition of debt of $1.8 million related to a liability to some former physical therapy partners which was no longer deemed payable.
Provision for Income Taxes
The provision for income tax in 2019 was $13.6 million and $11.4 million in 2018. The provision for income tax as a percentage of income before taxes less net income attributable to non-controlling interest was 25.4% in 2019 and 24.6% in 2018.
Net Income Attributable to Non-controlling Interests
Net income attributable to non-controlling interests was $17.2 million in 2019 and $13.9 million in 2018. Net income attributable to non-controlling interests (permanent equity) was $6.6 million in 2019 as compared to $5.5 million in 2018. Net income attributable to redeemable non-controlling interests (temporary equity) was $10.6 million in 2019 and $8.4 million in 2018.
RESULTS OF OPERATIONS
FISCAL YEAR 2018 COMPARED TO FISCAL 2017
| • | Net revenues increased $39.8 million, or 9.6%, from $414.1 million in 2017 to $453.9 million in 2018, primarily due to an increase in net patient revenues from physical therapy operations from both internal growth and acquisitions, an increase in the revenue from the industrial injury prevention business from a combination of internal growth plus an acquisition and an increase in revenue from acquired management contracts. Our first company in the industrial injury prevention business was acquired in March 2017 and, on April 30, 2018, we made a second acquisition. |
35
| • | For the year ended December 31, 2018, our Operating Results increased 28.1% to $33.5 million, or $2.65 per diluted share, as compared to $26.2 million, or $2.08 per diluted share, for the 2017 year. Operating Results (as defined below), a non-generally accepted accounting principles (“non-GAAP”) measure, for the 2018 fourth quarter and for the 2018 year, equals net income attributable to our shareholders excluding gain on derecognition of debt, net of taxes. For the 2017 fourth quarter and 2017 year, Operating Results is defined as net income attributable to our shareholders prior to the benefit due to the revaluation of deferred tax assets and liabilities due to the 2017 Tax Cuts and Jobs Act (“TCJA”), and prior to charges for interest expense – mandatorily redeemable non-controlling interests – change in redemption value and charges for costs related to restatement of financials – legal and accounting, both charges net of tax. See table below. |
| • | For the year ended December 31, 2018, our net income attributable to its shareholders, in accordance with GAAP, was $34.9 million, $1.31 per share, as compared to $22.3 million, or $1.76 per share, for the 2017 year. For both periods of 2018, in accordance with current accounting guidance, the revaluation of redeemable non-controlling interest, net of tax, is not included in net income but rather charged directly to retained earnings, but is included in the earnings per basic and diluted share calculation. See table below. |
| • | For 2018, our Adjusted EBITDA increased by 7.1% to $62.1 million from $57.9 million in 2017. See definition and reconciliation of Adjusted EBITDA in the following table. |
Year Ended December 31, |
||||||
2018 |
2017 |
|||||
Computation of earnings per share - USPH shareholders |
||||||
Net income attributable to USPH shareholders |
$ | 34,873 | $ | 22,256 | ||
Charges to retained earnings: |
||||||
Revaluation of redeemable non-controlling interest |
(24,770 | ) |
(201 | ) |
||
Tax effect at statutory rate (federal and state) of 26.25% |
6,502 | 75 | ||||
$ | 16,605 | $ | 22,130 | |||
Basic and diluted per share |
$ | 1.31 | $ | 1.76 | ||
Adjustments: |
||||||
Tax benefit - revaluation of deferred tax assets and liabilities |
— | (4,325 | ) |
|||
Gain on derecognition of debt |
(1,846 | ) |
— | |||
Interest expense MRNCI * - change in redemption value |
— | 12,894 | ||||
Cost related to restatement of financials - legal and accounting |
— | 670 | ||||
Revaluation of redeemable non-controlling interest |
24,770 | 201 | ||||
Tax effect at statutory rate (federal and state) of 26.25% and 39.25%, respectively |
(6,018 | ) |
(5,405 | ) |
||
Operating results |
$ | 33,511 | $ | 26,165 | ||
Basic and diluted operating results per share |
$ | 2.65 | $ | 2.08 | ||
Shares used in computation: |
||||||
Basic and diluted |
12,666 | 12,570 | ||||
36
Year Ended December 31, |
||||||
2018 |
2017 |
|||||
Net income attributable to USPH shareholders |
$ | 34,873 | $ | 22,256 | ||
Adjustments: |
||||||
Depreciation and amortization |
9,755 | 9,710 | ||||
Gain on derecognition of debt |
(1,846 | ) |
— | |||
Interest income |
(93 | ) |
(88 | ) |
||
Interest expense MRNCI * - change in redemption value |
— | 12,894 | ||||
Interest expense - debt and other |
2,042 | 2,111 | ||||
Provision for income taxes |
11,369 | 6,032 | ||||
Equity-based awards compensation expense |
5,939 | 5,032 | ||||
Adjusted EBITDA |
$ | 62,039 | $ | 57,947 | ||
| * | Mandatorily redeemable non-controlling interests |
The above table details the calculation of basic and diluted earnings per share attributable to our shareholders and reconciles net income attributable to our shareholders calculated in accordance with GAAP to Adjusted EBITDA and Operating Results, non-GAAP measures defined below. We believe providing Operating Results and Adjusted EBITDA are useful information to our investors for the purposes of comparing our period-to-period results. In addition, we believe that providing Operating Results allows our investors to compare our results with other similar businesses since most do not have redeemable instruments and therefore have different liability and equity structures. We use Operating Results, which eliminates the MRNCI – change in redemption which is a current non-cash item that can be subject to volatility and unusual costs, as one of the principal measures to evaluate and monitor financial performance period over period. Adjusted EBITDA is defined as earnings before gain on derecognition of debt, interest income, interest expense – mandatorily redeemable non-controlling interests – change in redemption value, interest expense – debt and other, taxes, depreciation, amortization and equity-based awards compensation expense.
Operating Results and Adjusted EBITDA are not measures of financial performance under GAAP. Operating Results and Adjusted EBITDA should not be considered in isolation or as an alternative to, or substitute for, net income attributable to USPH shareholders presented in the consolidated financial statements.
Net Patient Revenues
| • | Net patient revenues increased to $417.7 million for 2018 from $389.2 million for 2017, an increase of $28.5 million, or 7.3%. The increase in net patient revenues of $28.5 million consisted of an increase of $4.7 million from New Clinics and $23.8 million from Mature Clinics. During 2018, we acquired one multi-clinic group consisting of four clinics and five other single clinic practices for a total of 9 clinics. The net patient revenues from acquired clinics are included in our results of operations since the respective date of their acquisition. See above table and discussion under “—Executive Summary” detailing our multi-clinic acquisitions. |
| • | Total patient visits increased to 3,958,000 for 2018 from 3,705,000 for 2017. The growth in patient visits was attributable to 43,000 visits in New Clinics and an increase of 210,000 visits for Mature Clinics primarily due to 2017 New Clinics. |
| • | The average net patient revenue per visit slightly increased to $105.55 in 2018 from $105.05 in 2017. |
| • | Net patient revenues are based on established billing rates less allowances and discounts for patients covered by contractual programs and workers’ compensation. Net patient revenues reflect contractual and other adjustments, which we evaluate monthly, relating to patient discounts from certain payors. Payments received under these contractual programs and workers’ compensation are based on predetermined rates and are generally less than the established billing rates of the clinics. |
37
Other Revenues
Other revenues, consisting primarily of our industrial injury prevention business and management fees revenue, increased by $11.4 million, from $24.8 million in 2017 to $36.2 million in 2018. The revenues from the recently acquired industrial injury prevention business were $25.5 million in 2018 and $14.9 million in 2017. Revenues from management contracts were $8.3 million for 2018 as compared to $7.4 million for 2017. Other miscellaneous revenue was $2.4 million for 2018 and $2.5 million for 2017.
Operating Costs
Operating costs were $352.2 million, or 77.6% of net revenues, for 2018 and $323.4 million, or 78.1% of net revenues, for 2017. The dollar increase was attributable to $5.3 million in operating costs for New Clinics, an additional $15.1 million related to a Mature Clinics, $7.4 million related to the addition of the industrial injury prevention business, and an increase of $1.0 million related to management contracts. The 2017 closure costs of $0.6 million, included in operating costs, are primarily due to the closure of a single clinic acquired partnership due to the loss of a significant management contract. (See table detailing acquisition dates above under – “Executive Summary”). Each component of clinic operating costs is discussed below:
Operating Costs—Salaries and Related Costs
Salaries and related costs increased to $259.2 million for 2018 from $237.1 million for 2017, an increase of $22.1 million, or 9.3%. Approximately $3.3 million of the increase was attributable to New Clinics, $12.6 million of the increase was due to higher costs at various Mature Clinics primarily due to an increase in salaries and related costs in 2017 New Clinics which had a full year of activity in 2018, $5.4 million was due to higher salary costs at the industrial injury prevention businesses primarily due to the acquisition in April of 2018 and $0.8 million related to management contracts. Salaries and related costs as a percentage of net revenues was 57.1% for 2018 and 57.3% for 2017.
Operating Costs—Rent, Supplies, Contract Labor and Other
Rent, supplies, contract labor and other costs increased to $88.4 million for 2018 from $82.1 million for 2017, an increase of $6.3 million, or 7.7%. Approximately $1.9 million of the increase was attributable to New Clinics, $1.7 million of the increase was due to higher costs at various Mature Clinics, $1.7 million was due to the industrial injury prevention businesses primarily due to the acquisition in April of 2018 and $1.0 million related to management contracts. For 2018, New Clinics accounted for approximately $1.9 million of the increase, the industrial injury prevention business accounted for approximately $0.7 million and 2017 New Clinics accounted for approximately $3.7 million of the increase due to a full year of activity. Rent, supplies, contract labor and other costs as a percent of net revenues was 19.5% for 2018 and 19.8% for 2017.
Operating Costs—Provision for Doubtful Accounts
The provision for doubtful accounts for net patient receivables was $4.6 million for 2018 and $3.7 million for 2017. As a percentage of net patient revenues, the provision for doubtful accounts was 1.0% for 2018 and 0.9% for 2017.
Our provision for doubtful accounts as a percentage of total patient accounts receivable was 5.6% at December 31, 2018 and 4.9% at December 31, 2017. The provision for doubtful accounts at the end of each period is based on a detailed, clinic-by-clinic review of overdue accounts and is regularly reviewed in the aggregate in light of historical experience.
The average accounts receivable days outstanding were 37 days at December 31, 2018 and 36 days at December 31, 2017. Net patient receivables in the amount of $3.9 million and $3.3 million were written-off in 2018 and 2017, respectively.
Closure Costs
For 2018 and 2017, closure costs amounted to a credit of $9,000 and a charge of $599,000, respectively. As previously mentioned, the 2017 closure costs are primarily due to the closure of a single clinic acquired partnership due to the loss of a significant management contract.
38
Gross Profit
The gross profit in 2018 grew by 12.2% or $11.1 million to $101.7 million, as compared to $90.6 million in 2017. The gross profit percentage grew to 22.4% of net revenue in the recent year as compared to 21.9% for 2017. The gross profit percentage for our physical therapy clinics was 22.7% for 2018 as compared to 22.5% for 2017. The gross profit percentage on management contracts was 12.1% for 2018 as compared to 14.9% for 2017. The gross profit percentage for the industrial injury prevention business was 20.4% for 2018 as compared to 13.3% for 2017.
Corporate Office Costs
Corporate office costs, consisting primarily of salaries, benefits and equity based compensation of corporate office personnel and directors, rent, insurance costs, depreciation and amortization, travel, legal, compliance, professional, marketing and recruiting fees, were $41.3 million for 2018 and $35.9 million for 2017. The dollar increase is primarily due to increases in salaries, benefits and equity based compensation. Corporate office costs as a percentage of net revenues were 9.1% for 2018 and 8.7% in 2017.
Interest Expense – mandatorily redeemable non-controlling interest – change in redemption value.
We no longer have mandatorily redeemable non-controlling interests. As previously mentioned, due to amended partnerships agreements, the redemption values of the mandatorily redeemable non-controlling interests (previously classified as liabilities) were reclassified as redeemable non-controlling interest (temporary equity) at fair value on the December 31, 2017 consolidated balance sheet. For 2017, the earnings and liabilities attributable to mandatorily redeemable non-controlling interests were recorded within the consolidated statements of income line item: Interest expense – mandatorily redeemable non-controlling interests – earnings allocable and in the consolidated balance sheet line item: Mandatorily redeemable non-controlling interests. For 2018, any adjustments in the redemption value, net of tax, are recorded directly to retained earnings and are not reflected in the consolidated statements of income. Although the redemption adjustments are not reflected in the consolidated statements of income, current accounting rules require that we reflect these adjustments, net of tax, in the earnings per share calculation.
Interest Expense mandatorily redeemable non-controlling interest – change in redemption value for the 2017 year was $12.9 million. The change in redemption value for acquired partnerships was based on the redemption amount (which is derived from a formula based on a specified multiple times the underlying business’ trailing twelve months of earnings before interest, taxes, depreciation, amortization and our internal management fee) at the end of the reporting period compared to the end of the previous period. This change is directly related to an increase or decrease in the profitability and underlying value of our partnerships as compared to the prior year.
Interest Expense – mandatorily redeemable non-controlling interest – earnings allocable.
For 2018, the amount of net income attributable to redeemable non-controlling interest owners is included in consolidated net income on the face of the consolidated statement of income in the line item – Net income attributable to non-controlling interests. For 2017, interest expense – mandatorily redeemable non-controlling interest – earnings allocable, which represent the portion of earnings allocable to the holders of mandatorily redeemable non-controlling interests, was $6.1 million.
Interest Expense – debt and other
Interest expense – debt and other was $2.0 million for 2018 and $2.1 million for 2017. At December 31, 2018, $38.0 million was outstanding under our Amended Credit Agreement (as defined below under “—Liquidity and Capital Resources”). See “—Liquidity and Capital Resources” below for a discussion of the terms of our Amended Credit Agreement.
Gain on Derecognition of Debt
Gain on derecognition of debt was $1.8 million for the year 2018 as a liability relating to some former physical therapy partners is no longer deemed payable.
39
Provision for Income Taxes
The provision for income tax in 2018 was $11.4 million, inclusive of a $0.5 million benefit related to the reconciliation of the 2017 federal and state returns to our book provision. Without this benefit, the provision for income taxes as a percentage of income before taxes less net income attributable to non-controlling interest was 25.7%. The income tax expense in 2017 was $6.0 million. Included in 2017 is a tax benefit of $4.3 million due to the revaluation of deferred tax assets and liabilities due to the TCJA. Also, included in 2017 was a charge of $0.3 million related to a detailed reconciliation of the federal and state taxes payable and receivable accounts along with federal and state deferred tax assets and liability accounts at December 31, 2016. Without this reconciliation charge and prior to the $4.3 million tax benefit, the provision for income taxes as a percentage of income before taxes less net income attributable to non-controlling interest was 35.6%. As reported, the provision for income tax as a percentage of income before taxes less net income attributable to non-controlling interest was 24.6% in 2018 and 21.3% in 2017.
Net Income Attributable to Non-controlling Interests
Net income attributable to non-controlling interests was $13.9 million in 2018 and $5.5 million in 2017. Net income attributable to non-controlling interests (permanent equity) was $5.5 million in 2018 as compared to $5.2 million in 2017. Net income attributable to redeemable non-controlling interests (temporary equity) was $8.4 million in 2018 and $0.2 million in 2017.
LIQUIDITY AND CAPITAL RESOURCES
We believe that our business is generating sufficient cash flow from operating activities to allow us to meet our short-term and long-term cash requirements, other than those with respect to future significant acquisitions. At December 31, 2019, we had $23.5 million in cash and cash equivalents compared to $23.4 million at December 31, 2018. Although the start-up costs associated with opening new clinics and our planned capital expenditures are significant, we believe that our cash and cash equivalents and availability under our Amended Credit Agreement are sufficient to fund the working capital needs of our operating subsidiaries, future clinic development and acquisitions and investments through at least December 2020. Significant acquisitions would likely require financing under our Amended Credit Agreement.
Effective December 5, 2013, we entered into an Amended and Restated Credit Agreement with a commitment for a $125.0 million revolving credit facility. This agreement was amended in August 2015, January 2016, March 2017 and November 2017 (hereafter referred to as “Amended Credit Agreement”). The Amended Credit Agreement is unsecured and has loan covenants, including requirements that we comply with a consolidated fixed charge coverage ratio and consolidated leverage ratio. Proceeds from the Amended Credit Agreement may be used for working capital, acquisitions, purchases of our common stock, dividend payments to our common stockholders, capital expenditures and other corporate purposes. The pricing grid is based on our consolidated leverage ratio with the applicable spread over LIBOR ranging from 1.25% to 2.0% or the applicable spread over the Base Rate ranging from 0.1% to 1%. Fees under the Amended Credit Agreement include an unused commitment fee ranging from 0.25% to 0.3% depending on our consolidated leverage ratio and the amount of funds outstanding under the Amended Credit Agreement.
The January 2016 amendment to the Amended Credit Agreement increased the cash and noncash consideration that we could pay with respect to acquisitions permitted under the Amended Credit Agreement to $50,000,000 for any fiscal year, and increased the amount we may pay in cash dividends to our shareholders in an aggregate amount not to exceed $10,000,000 in any fiscal year. The March 2017 amendment, among other items, increased the amount we may pay in cash dividends to our shareholders in an aggregate amount not to exceed $15,000,000 in any fiscal year. The November 2017 amendment, among other items, adjusted the pricing grid as described above, increased the aggregate amount we may pay in cash dividends to $20,000,000 to our shareholders and extended the maturity date to November 30, 2021.
On December 31, 2019, $46.0 million was outstanding on the Amended Credit Agreement resulting in $79.0 million of availability. As of the date of this report, we were in compliance with all of the covenants thereunder.
Cash was provided by operations ($62.4 million), proceeds on sale of partnership interest ($11.6 million) and net proceeds from our Amended Credit Agreement ($8.0 million). The major uses of cash for investing and
40
financing activities included: purchase of interests in businesses ($30.6 million), distributions to non-controlling interests ($16.2 million), payments of cash dividends to our shareholders ($14.6 million), purchases of fixed assets ($10.2 million), purchases of redeemable non-controlling interest, temporary equity ($8.7 million) and payments on notes payable ($1.4 million)
On September 30, 2019, we acquired a 67% interest in an eleven-clinic physical therapy practice. The purchase price for the 67% interest was $12.4 million, of which $12.1 million was paid in cash and $0.3 million in a seller note that is payable in two principal installments totaling $150,000 each, plus accrued interest in September 2020 and September 2021. The note accrues interest at 5.0% per annum.
On April 30, 2018, we purchased a 65% interest in the assets and business of industrial injury prevention services, for an aggregate purchase price of $8.6 million in cash and $400,000 in seller note that is payable, plus accrued interest, on April 30, 2019. The initial industrial injury prevention business was acquired in March 2017 and, on April 30, 2018, we made a second acquisition with the two businesses then combined. After the combination, we owned a 59.45% interest in the combined business, Briotix Health. On April 11, 2019, we acquired a company that is a provider of industrial injury prevention services. The acquired company specializes in delivering injury prevention and care, post offer employment testing, functional capacity evaluations and return-to-work services. It performs these services across a network in 45 states including onsite at eleven client locations. The business was then combined with Briotix Health, increasing our ownership position in the Briotix Health partnership to approximately 76.0%. The purchase price for the acquired company was $22.9 million ($23.6 million less cash acquired of $0.7 million), which consisted of $18.9 million in cash, (of which $0.5 million will be paid to certain shareholders), and a $4.0 million seller note. The note accrues interest at 5.5% and the principal and accrued interest is payable, on April 9, 2021.
On August 31, 2018 we acquired a 70% interest in a four-clinic physical therapy practice. The purchase price for the 70% interest was $7.3 million in cash and $400,000 in a seller note that is payable in two principal installments totaling $200,000 each, plus accrued interest. The first installment was paid in August 2019 and the second installment remains payable in August 2020.
On February 28, 2018, through one of our majority owned partnerships, we acquired the assets and business of two physical therapy clinics, for an aggregate purchase price of $760,000 in cash and $150,000 in a seller note which was paid along with accrued interest on August 31, 2019.
In addition to the multi-clinic acquisitions above in 2018, we through several of our majority owned Clinic Partnerships, acquired five separate clinic practices. These practices will operate as satellites of the respective existing clinic partnership.
Historically, we have generated sufficient cash from operations to fund our development activities and to cover operational needs. We plan to continue developing new clinics and making additional acquisitions. We have from time to time purchased the non-controlling interests of limited partners in our Clinic Partnerships. We may purchase additional non-controlling interests in the future. Generally, any acquisition or purchase of non-controlling interests is expected to be accomplished using a combination of cash and financing. Any large acquisition would likely require financing.
We make reasonable and appropriate efforts to collect accounts receivable, including applicable deductible and co-payment amounts. Claims are submitted to payors daily, weekly or monthly in accordance with our policy or payor’s requirements. When possible, we submit our claims electronically. The collection process is time consuming and typically involves the submission of claims to multiple payors whose payment of claims may be dependent upon the payment of another payor. Claims under litigation and vehicular incidents can take a year or longer to collect. Medicare and other payor claims relating to new clinics awaiting CMS approval initially may not be submitted for six months or more. When all reasonable internal collection efforts have been exhausted, accounts are written off prior to sending them to outside collection firms. With managed care, commercial health plans and self-pay payor type receivables, the write-off generally occurs after the account receivable has been outstanding for 120 days or longer.
41
We have future obligations for debt repayments, employment agreements and future minimum rentals under operating leases. The obligations as of December 31, 2019 are summarized as follows (in thousands):
Total |
2020 |
2021 |
2022 |
2023 |
2024 |
Thereafter |
|||||||||||||||
Credit Agreement |
$ | 46,000 | $ | — | $ | 46,000 | $ | — | $ | — | $ | — | $ | — | |||||||
Notes Payable |
5,089 | 728 | 4,361 | — | — | — | — | ||||||||||||||
Interest Payable |
320 | 253 | 67 | — | — | — | — | ||||||||||||||
Employee Agreements |
74,407 | 50,840 | 20,968 | 1,421 | 1,178 | — | — | ||||||||||||||
Operating Leases |
115,490 | 35,784 | 28,022 | 20,618 | 14,332 | 8,302 | 8,432 | ||||||||||||||
$ | 241,306 | $ | 87,605 | $ | 99,418 | $ | 22,039 | $ | 15,510 | $ | 8,302 | $ | 8,432 | ||||||||
We generally enter into various notes payable as a means of financing our acquisitions. Our present outstanding notes payable primarily relate to the acquisition of a business, acquisition of a majority interest in a business. At December 31, 2019, our remaining outstanding balance on these notes aggregated $5.1 million. The note payable for the acquisition of a business of $4.0 million is payable in April 2021. The other $1.1 million of notes are generally payable in equal annual installments of principal over two years plus any accrued and unpaid interest. See above table for a detail of future principal payments. Interest accrues at various interest rates ranging from 3.75% to 5.00% per annum, subject to adjustment.
In conjunction with acquisitions, we entered into amendments to our limited partnership agreements for our acquired partnerships. The limited partnership agreements, as amended, provide that, upon the triggering events, we have a Call Right and the selling entity or individual has a Put Right for the purchase and sale of the limited partnership interest held by the partner. Once triggered, the Put Right and the Call Right do not expire, even upon an individual partner’s death, and contain no mandatory redemption feature. The purchase price of the partner’s limited partnership interest upon the exercise of either the Put Right or the Call Right is calculated per the terms of the respective agreements and classified as redeemable non-controlling interest (temporary equity) in our consolidated balance sheets. The fair value of the redeemable non-controlling interest at December 31, 2019 was $137.8 million.
As of December 31, 2019, we have accrued $4.3 million related to credit balances and overpayments due to patients and payors. This amount is expected to be paid in 2020.
From September 2001 through December 31, 2008, our Board of Directors (“Board”) authorized us to purchase, in the open market or in privately negotiated transactions, up to 2,250,000 shares of our common stock. In March 2009, the Board authorized the repurchase of up to 10% or approximately 1,200,000 shares of our common stock (“March 2009 Authorization”). Our Amended Credit Agreement permits share repurchases of up to $15,000,000, subject to compliance with covenants. We are required to retire shares purchased under the March 2009 Authorization.
There is no expiration date for the share repurchase program. As of December 31, 2019, there are currently an additional estimated 131,176 shares (based on the closing price of $114.35 on December 31, 2019) that may be purchased from time to time in the open market or private transactions depending on price, availability and our cash position. We did not purchase any shares of our common stock during the year ended December 31, 2019 and 2018.
Off Balance Sheet Arrangements
With the exception of operating leases for our executive offices and clinic facilities discussed in Note 16 to our consolidated financial statements included in Item 8, we have no off-balance sheet debt or other off-balance sheet financing arrangements.
FACTORS AFFECTING FUTURE RESULTS
The risks related to our business and operations include:
| • | changes as the result of government enacted national healthcare reform; |
| • | changes in Medicare rules and guidelines and reimbursement or failure of our clinics to maintain their Medicare certification status; |
42
| • | revenue we receive from Medicare and Medicaid being subject to potential retroactive reduction; |
| • | business and regulatory conditions including federal and state regulations; |
| • | governmental and other third party payor inspections, reviews, investigations and audits; |
| • | compliance with federal and state laws and regulations relating to the privacy of individually identifiable patient information, and associated fines and penalties for failure to comply; |
| • | changes in reimbursement rates or payment methods from third party payors including government agencies and deductibles and co-pays owed by patients; |
| • | revenue and earnings expectations; |
| • | legal actions, which could subject us to increased operating costs and uninsured liabilities; |
| • | general economic conditions; |
| • | availability and cost of qualified physical therapists; |
| • | personnel productivity and retaining key personnel; |
| • | competitive, economic or reimbursement conditions in our markets which may require us to reorganize or close certain clinics and thereby incur losses and/or closure costs including the possible write-down or write-off of goodwill and other intangible assets; |
| • | competitive environment in the industrial injury prevention business, which could result in the termination or non-renewal of contractual service arrangements and other adverse financial consequences for that service line; |
| • | acquisitions, purchase of non-controlling interests (minority interests) and the successful integration of the operations of the acquired businesses; |
| • | maintaining our information technology systems with adequate safeguards to protect against cyber-attacks; |
| • | maintaining adequate internal controls; |
| • | maintaining necessary insurance coverage; |
| • | the potential impact of the coronavirus; |
| • | availability, terms, and use of capital; and |
| • | weather and other seasonal factors. |
See also Risk Factors in Item 1A of this Annual Report on Form 10-K.
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK. |
We do not maintain any derivative instruments such as interest rate swap arrangements, hedging contracts, futures contracts or the like. Our only indebtedness as of December 31, 2019 was the outstanding balance of seller notes of $5.1 million and an outstanding balance on our Amended Credit Agreement of $46.0 million. The outstanding balance under our Amended Credit Agreement is subject to fluctuating interest rates. A 1% change in the interest rate would yield an additional $460,000 of interest expense. See Note 9 to our consolidated financial statements included in Item 8.
43
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA. |
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS AND RELATED INFORMATION
Audited Financial Statements: |
|||
44
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Shareholders
U.S. Physical Therapy, Inc.
Opinion on the financial statements
We have audited the accompanying consolidated balance sheets of U.S. Physical Therapy, Inc. (a Nevada corporation) and subsidiaries (the “Company”) as of December 31, 2019 and 2018, the related consolidated statements of income, changes in equity, and cash flows for each of the three years in the period ended December 31, 2019, and the related notes and financial statement schedule included under Item 15(a) (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2019 and 2018, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2019, in conformity with accounting principles generally accepted in the United States of America.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (“PCAOB”), the Company’s internal control over financial reporting as of December 31, 2019, based on criteria established in the 2013 Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”), and our report dated February 28, 2020 expressed an unqualified opinion.
Change in accounting principle
As discussed in Note 2 to the consolidated financial statements, the Company changed its method of accounting for leases on January 1, 2019 due to the adoption of Accounting Standards Codification (“ASC”) 842, Leases.
Basis for opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical audit matter
The critical audit matter communicated below is a matter arising from the current period audit of the financial statements that was communicated or required to be communicated to the audit committee and that: (1) relates to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of a critical audit matter does not alter in any way our opinion on the financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing separate opinions on the critical audit matter or on the accounts or disclosures to which it relates.
Measurement of Patient Revenue Net of Contractual Adjustments
As discussed in Note 2 to the consolidated financial statements, revenues are recognized in the period in which services are rendered. Net patient revenues (patient revenues less estimated contractual adjustments) are recognized at the estimated net realizable amounts from third-party payors, patients and others in exchange for services rendered when obligations under the terms of the contract are satisfied. The Company has agreements
45
with third-party payors that provides for payments at amounts different from its established rates. Each month the Company estimates its contractual adjustment for each clinic based on the terms of third-party payor contracts and the historical collection and write-off experience of the clinic and applies a contractual adjustment reserve percentage to the gross accounts receivable balances. The Company then performs a comparison of cash collections to corresponding net revenues for the prior twelve months. We identified the measurement of contractual adjustments as a critical audit matter.
The principal consideration for our determination that the measurement of contractual adjustments is a critical audit matter is that the estimate requires a high degree of auditor subjectivity in evaluating management’s assumptions related to developing future collection patterns across the various clinic locations.
Our audit procedures related to the Company’s measurement of contractual adjustments included the following, among others.
| • | We tested the design and operating effectiveness of controls relating to billing and cash collection, net rate trend analysis by clinic and cash collection versus net revenue trend analysis. |
| • | For a sample of patient visits, we inspected and compared underlying documents for each transaction, which included gross billing rates and cash collected (net revenue). |
| • | For a sample of patient visits, we traced gross billings and net revenue to net revenue recorded in the general ledger and to each report used in determining and assessing the contractual adjustment calculation. |
| • | We compared cash collections to recorded net revenue over a twelve month period ending December 31, 2019 and again for the twelve month period ending in the first month subsequent to period end, to identify whether there were unusual trends that would indicate that the usage of historical collection patterns would no longer be reasonable to predict future collection patterns. |
/s/ GRANT THORNTON LLP
We have served as the Company’s auditor since 2004.
Houston, Texas
February 28, 2020
46
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Shareholders
U.S. Physical Therapy, Inc.
Opinion on internal control over financial reporting
We have audited the internal control over financial reporting of U.S. Physical Therapy, Inc. (a Nevada corporation) and subsidiaries (the “Company”) as of December 31, 2019, based on criteria established in the 2013 Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”). In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2019, based on criteria established in the 2013 Internal Control—Integrated Framework issued by COSO.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (“PCAOB”), the consolidated financial statements of the Company as of and for the year ended December 31, 2019, and our report dated February 28, 2020 expressed an unqualified opinion on those financial statements.
Basis for opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and limitations of internal control over financial reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ GRANT THORNTON LLP
Houston, Texas
February 28, 2020
47
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
(In thousands, except share data)
December 31, 2019 |
December 31, 2018 |
|||||
ASSETS |
||||||
Current assets: |
||||||
Cash and cash equivalents |
$ | 23,548 | $ | 23,368 | ||
Patient accounts receivable, less allowance for doubtful accounts of $2,698 and $2,672, respectively |
46,228 | 44,751 | ||||
Accounts receivable - other |
9,823 | 6,742 | ||||
Other current assets |
5,787 | 4,353 | ||||
Total current assets |
85,386 | 79,214 | ||||
Fixed assets: |
||||||
Furniture and equipment |
54,942 | 52,611 | ||||
Leasehold improvements |
33,247 | 31,712 | ||||
Fixed assets, gross |
88,189 | 84,323 | ||||
Less accumulated depreciation and amortization |
66,099 | 64,154 | ||||
Fixed assets, net |
22,090 | 20,169 | ||||
Operating lease right-of-use assets |
81,586 | — | ||||
Goodwill |
317,676 | 293,525 | ||||
Other identifiable intangible assets, net |
52,588 | 48,828 | ||||
Other assets |
1,519 | 1,430 | ||||
Total assets |
$ | 560,845 | $ | 443,166 | ||
LIABILITIES, REDEEMABLE NON-CONTROLLING INTERESTS, USPH SHAREHOLDERS’ EQUITY AND NON-CONTROLLING INTERESTS |
||||||
Current liabilities: |
||||||
Accounts payable - trade |
$ | 2,494 | $ | 2,019 | ||
Accrued expenses |
30,855 | 38,493 | ||||
Current portion of operating lease liabilities |
26,486 | — | ||||
Current portion of notes payable |
728 | 1,434 | ||||
Total current liabilities |
60,563 | 41,946 | ||||
Notes payable, net of current portion |
4,361 | 402 | ||||
Revolving line of credit |
46,000 | 38,000 | ||||
Deferred taxes |
10,071 | 9,012 | ||||
Deferred rent |
— | 2,159 | ||||
Operating lease liabilities, net of current portion |
60,258 | — | ||||
Other long-term liabilities |
141 | 829 | ||||
Total liabilities |
181,394 | 92,348 | ||||
Redeemable non-controlling interests - temporary equity |
137,750 | 133,943 | ||||
Commitments and contingencies (Note 10) |
||||||
U.S. Physical Therapy, Inc. (“USPH”) shareholders’ equity: |
||||||
Preferred stock, $.01 par value, 500,000 shares authorized, no shares issued and outstanding |
— | — | ||||
Common stock, $.01 par value, 20,000,000 shares authorized, 14,989,337 and 14,899,233 shares issued, respectively |
150 | 149 | ||||
Additional paid-in capital |
87,383 | 80,028 | ||||
Retained earnings |
184,352 | 167,396 | ||||
Treasury stock at cost, 2,214,737 shares |
(31,628 | ) |
(31,628 | ) |
||
Total USPH shareholders’ equity |
240,257 | 215,945 | ||||
Non-controlling interests - permanent equity |
1,444 | 930 | ||||
Total USPH shareholders' equity and non-controlling interests |
241,701 | 216,875 | ||||
Total liabilities, redeemable non-controlling interests, USPH shareholders' equity and non-controlling interests |
$ | 560,845 | $ | 443,166 | ||
See notes to consolidated financial statements.
48
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF INCOME
(In thousands, except per share data)
Year Ended |
|||||||||
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
|||||||
Net patient revenues |
$ | 433,345 | $ | 417,703 | $ | 389,226 | |||
Other revenues |
48,624 | 36,208 | 24,825 | ||||||
Net revenues |
481,969 | 453,911 | 414,051 | ||||||
Operating costs: |
|||||||||
Salaries and related costs |
274,233 | 259,228 | 237,067 | ||||||
Rent, supplies, contract labor and other |
90,379 | 88,426 | 82,096 | ||||||
Provision for doubtful accounts |
4,858 | 4,603 | 3,672 | ||||||
Closure costs |
25 | (9 | ) |
599 | |||||
Total operating costs |
369,495 | 352,248 | 323,434 | ||||||
Gross profit |
112,474 | 101,663 | 90,617 | ||||||
Corporate office costs |
45,049 | 41,349 | 35,889 | ||||||
Operating income |
67,425 | 60,314 | 54,728 | ||||||
Gain on sale of partnership interest |
5,514 | — | — | ||||||
Gain on derecognition of debt |
— | 1,846 | — | ||||||
Interest and other income, net |
46 | 93 | 88 | ||||||
Interest expense: |
|||||||||
Mandatorily redeemable non-controlling interests - change in redemption value |
— | — | (12,894 | ) |
|||||
Mandatorily redeemable non-controlling interests - earnings allocable |
— | — | (6,055 | ) |
|||||
Debt and other |
(2,079 | ) |
(2,042 | ) |
(2,111 | ) |
|||
Total interest expense |
(2,079 | ) |
(2,042 | ) |
(21,060 | ) |
|||
Income before taxes |
70,906 | 60,211 | 33,756 | ||||||
Provision for income taxes |
13,647 | 11,369 | 6,032 | ||||||
Net income |
57,259 | 48,842 | 27,724 | ||||||
Less: net income attributable to non-controlling interests: |
|||||||||
Non-controlling interests - permanent equity |
(6,561 | ) |
(5,536 | ) |
(5,224 | ) |
|||
Redeemable non-controlling interests - temporary equity |
(10,659 | ) |
(8,433 | ) |
(244 | ) |
|||
(17,220 | ) |
(13,969 | ) |
(5,468 | ) |
||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | $ | 22,256 | |||
Basic and diluted earnings per share attributable to USPH shareholders |
$ | 2.45 | $ | 1.31 | $ | 1.76 | |||
Shares used in computation - basic and diluted |
12,756 | 12,666 | 12,570 | ||||||
Dividends declared per common share |
$ | 1.14 | $ | 0.92 | $ | 0.80 | |||
See notes to consolidated financial statements.
49
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CHANGES IN EQUITY
(In thousands)
U.S. Physical Therapy, Inc. |
|||||||||||||||||||||||||||
Common Stock |
Additional Paid-In Capital |
Retained Earnings |
Treasury Stock |
Total Shareholders’ Equity |
Non- Controlling Interests |
Total |
|||||||||||||||||||||
Shares |
Amount |
Shares |
Amount |
||||||||||||||||||||||||
Balance January 1, 2017 |
14,733 | $ | 147 | $ | 68,687 | $ | 150,342 | (2,215 | ) |
$ | (31,628 | ) |
$ | 187,548 | $ | 1,140 | $ | 188,688 | |||||||||
Issuance of restricted stock, net of cancellations |
76 | 1 | — | — | — | — | 1 | 1 | |||||||||||||||||||
Revaluation of redeemable non-controlling interest, net of tax |
— | — | — | (126 | ) |
— | — | (126 | ) |
— | (126 | ) |
|||||||||||||||
Compensation expense - equity-based awards |
— | — | 5,032 | — | — | — | 5,032 | — | 5,032 | ||||||||||||||||||
Transfer of compensation liability for certain stock issued pursuant to long-term incentive plans |
— | — | 165 | — | — | — | 165 | — | 165 | ||||||||||||||||||
Sale of non-controlling interest, net of tax and purchases |
— | — | 56 | — | — | — | 56 | (20 | ) |
36 | |||||||||||||||||
Dividends paid to USPT shareholders |
— | — | — | (10,066 | ) |
— | — | (10,066 | ) |
— | (10,066 | ) |
|||||||||||||||
Distributions to non-controlling interest partners |
— | — | — | — | — | — | — | (5,300 | ) |
(5,300 | ) |
||||||||||||||||
Other |
— | — | — | — | — | — | — | 160 | 160 | ||||||||||||||||||
Net income attributable to non-controlling interets - permanent equity |
— | — | — | — | — | — | 5,224 | 5,224 | |||||||||||||||||||
Net income attributable to USPH shareholders |
— | — | — | 22,256 | — | — | 22,256 | — | 22,256 | ||||||||||||||||||
Balance December 31, 2017 |
14,809 | 148 | 73,940 | 162,406 | (2,215 | ) |
(31,628 | ) |
204,866 | 1,204 | 206,070 | ||||||||||||||||
Issuance of restricted stock, net of cancellations |
90 | 1 | — | — | — | — | 1 | — | 1 | ||||||||||||||||||
Revaluation of redeemable non-controlling interest, net of tax |
— | — | — | (18,268 | ) |
— | — | (18,268 | ) |
— | (18,268 | ) |
|||||||||||||||
Compensation expense - equity-based awards |
— | — | 5,939 | — | — | — | 5,939 | — | 5,939 | ||||||||||||||||||
Transfer of compensation liability for certain stock issued pursuant to long-term incentive plans |
— | — | 373 | — | — | — | 373 | — | 373 | ||||||||||||||||||
Sale of non-controlling interest, net of purchases and tax |
— | — | (224 | ) |
— | — | — | (224 | ) |
(48 | ) |
(272 | ) |
||||||||||||||
Dividends paid to USPT shareholders |
— | — | — | (11,664 | ) |
— | — | (11,664 | ) |
— | (11,664 | ) |
|||||||||||||||
Distributions to non-controlling interest partners |
— | — | — | — | — | — | — | (5,812 | ) |
(5,812 | ) |
||||||||||||||||
Other |
— | — | — | 49 | — | — | 49 | 50 | 99 | ||||||||||||||||||
Net income attributable to non-controlling interets - permanent equity |
— | — | — | — | — | — | — | 5,536 | 5,536 | ||||||||||||||||||
Net income attributable to USPH shareholders |
— | — | — | 34,873 | — | — | 34,873 | — | 34,873 | ||||||||||||||||||
Balance December 31, 2018 |
14,899 | 149 | 80,028 | 167,396 | (2,215 | ) |
(31,628 | ) |
215,945 | 930 | 216,875 | ||||||||||||||||
Issuance of restricted stock, net of cancellations |
90 | 1 | — | — | — | — | 1 | — | 1 | ||||||||||||||||||
Revaluation of redeemable non-controlling interest, net of tax |
— | — | — | (8,771 | ) |
— | — | (8,771 | ) |
— | (8,771 | ) |
|||||||||||||||
Compensation expense - equity-based awards |
— | — | 6,985 | — | — | — | 6,985 | — | 6,985 | ||||||||||||||||||
Transfer of compensation liability for certain stock issued pursuant to long-term incentive plans |
— | — | 636 | — | — | — | 636 | — | 636 | ||||||||||||||||||
Purchase of partnership interests - redeemable non-controlling interests |
— | — | (266 | ) |
— | — | — | (266 | ) |
(26 | ) |
(292 | ) |
||||||||||||||
Sale of non-controlling interest, net of purchases and tax |
— | — | — | 196 | — | — | 196 | — | 196 | ||||||||||||||||||
Dividends paid to USPT shareholders |
— | — | — | (14,555 | ) |
— | — | (14,555 | ) |
— | (14,555 | ) |
|||||||||||||||
Distributions to non-controlling interest partners |
— | — | — | — | — | — | — | (6,014 | ) |
(6,014 | ) |
||||||||||||||||
Other |
— | — | — | 47 | — | — | 47 | (7 | ) |
40 | |||||||||||||||||
Net income attributable to non-controlling interest - permanent equity |
— | — | — | — | — | — | — | 6,561 | 6,561 | ||||||||||||||||||
Net income attributable to USPH shareholders |
— | — | — | 40,039 | — | — | 40,039 | — | 40,039 | ||||||||||||||||||
Balance December 31, 2019 |
14,989 | $ | 150 | $ | 87,383 | $ | 184,352 | (2,215 | ) |
$ | (31,628 | ) |
$ | 240,257 | $ | 1,444 | $ | 241,701 | |||||||||
See notes to consolidated financial statements.
50
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
Year Ended |
|||||||||
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
|||||||
OPERATING ACTIVITIES |
|||||||||
Net income including non-controlling interests |
$ | 57,259 | $ | 48,842 | $ | 27,724 | |||
Adjustments to reconcile net income including non-controlling interests to net cash provided by operating activities: |
|||||||||
Depreciation and amortization |
10,095 | 9,755 | 9,710 | ||||||
Provision for doubtful accounts |
4,858 | 4,603 | 3,672 | ||||||
Equity-based awards compensation expense |
6,985 | 5,939 | 5,032 | ||||||
Deferred income taxes |
4,651 | 4,813 | (4,864 | ) |
|||||
Gain on sale of partnership interest |
(5,514 | ) |
— | — | |||||
Gain on derecognition of Debt |
— | (1,846 | ) |
— | |||||
Other |
96 | 167 | 621 | ||||||
Changes in operating assets and liabilities: |
|||||||||
Increase in patient accounts receivable |
(6,376 | ) |
(3,434 | ) |
(3,447 | ) |
|||
Increase in accounts receivable - other |
(2,499 | ) |
(1,087 | ) |
(3,022 | ) |
|||
(Increase) decrease in other assets |
(1,878 | ) |
345 | 2,086 | |||||
(Decrease) increase in accounts payable and accrued expenses |
(4,209 | ) |
4,876 | 6,979 | |||||
Increase in mandatorily redeemable non-controlling interests |
— | — | 11,579 | ||||||
(Decrease) increase in other liabilities |
(1,020 | ) |
32 | 456 | |||||
Net cash provided by operating activities |
62,448 | 73,005 | 56,526 | ||||||
INVESTING ACTIVITIES |
|||||||||
Purchase of fixed assets |
(10,189 | ) |
(7,193 | ) |
(7,095 | ) |
|||
Purchase of majority interest in businesses |
(30,597 | ) |
(16,367 | ) |
(36,682 | ) |
|||
Purchase of redeemable non-controlling interest, temporary equity |
(8,651 | ) |
— | — | |||||
Purchase of non-controlling interest, permanent equity |
(428 | ) |
(350 | ) |
— | ||||
Sales of non-controlling interest-permanent equity |
207 | — | 121 | ||||||
Proceeds on sale of partnership interest, net |
11,601 | — | — | ||||||
Proceeds on sale of fixed assets |
64 | 1 | 81 | ||||||
Net cash used in investing activities |
(37,993 | ) |
(23,909 | ) |
(43,575 | ) |
|||
FINANCING ACTIVITIES |
|||||||||
Distributions to non-controlling interests, permanent and temporary equity |
(16,235 | ) |
(15,646 | ) |
(5,572 | ) |
|||
Cash dividends paid to shareholders |
(14,555 | ) |
(11,664 | ) |
(10,066 | ) |
|||
Proceeds from revolving line of credit |
145,000 | 103,000 | 93,000 | ||||||
Payments on revolving line of credit |
(137,000 | ) |
(119,000 | ) |
(85,000 | ) |
|||
Payments to settle mandatorily redeemable non-controlling interests |
— | (265 | ) |
(2,361 | ) |
||||
Principal payments on notes payable |
(1,433 | ) |
(4,044 | ) |
(1,227 | ) |
|||
Other |
(52 | ) |
(42 | ) |
161 | ||||
Net cash used in financing activities |
(24,275 | ) |
(47,661 | ) |
(11,065 | ) |
|||
Net increase in cash and cash equivalents |
180 | 1,435 | 1,886 | ||||||
Cash and cash equivalents - beginning of period |
23,368 | 21,933 | 20,047 | ||||||
Cash and cash equivalents - end of period |
$ | 23,548 | $ | 23,368 | $ | 21,933 | |||
SUPPLEMENTAL DISCLOSURES OF CASH FLOW INFORMATION |
|||||||||
Cash paid during the period for: |
|||||||||
Income taxes |
$ | 9,856 | $ | 9,183 | $ | 8,543 | |||
Interest |
$ | 1,890 | $ | 2,357 | $ | 2,113 | |||
Non-cash investing and financing transactions during the period: |
|||||||||
Purchase of businesses - seller financing portion |
$ | 4,300 | $ | 950 | $ | 2,150 | |||
Purchase of business - payable to common shareholders of acquired business |
$ | 502 | $ | — | $ | — | |||
Notes payable related to purchase of redeemable non-controlling interest, temporary equity |
$ | 283 | $ | — | $ | — | |||
Notes payable related to purchase of non-controlling interest, permanent equity |
$ | 103 | $ | — | $ | — | |||
Notes receivable related to sale of partnership interest - redeemable non-controlling interest |
$ | 2,870 | $ | — | $ | — | |||
See notes to consolidated financial statements.
51
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
YEARS ENDED DECEMBER 31, 2019, 2018 and 2017
1. Organization, Nature of Operations and Basis of Presentation
U.S. Physical Therapy, Inc. and its subsidiaries (together, the “Company”) operate outpatient physical therapy clinics that provide pre-and post-operative care for a variety of orthopedic-related disorders and sports-related injuries, treatment for neurological-related injuries and rehabilitation of injured workers. As of December 31, 2019, the Company owned and/or operated 583 clinics in 40 states. The clinics’ business primarily originates from physician referrals. The principal sources of payment for the clinics’ services are managed care programs, commercial health insurance, Medicare/Medicaid, workers’ compensation insurance and proceeds from personal injury cases. In addition to the Company’s ownership and operation of outpatient physical therapy clinics, it also manages physical therapy facilities for third parties, such as physicians and hospitals, with 26 such third-party facilities under management as of December 31, 2019.
In March 2017, the Company acquired a 55% interest in the initial industrial injury prevention business. On April 30, 2018, the Company acquired a 65% interest in another business in the industrial injury prevention sector. On April 30, 2018, the Company combined the two businesses. After the combination, the Company owned a 59.45% interest in the combined business, Briotix Health, Limited Partnership (“Briotix Health”), the Company’s industrial injury prevention operation. On April 11, 2019, the Company acquired a third company that is a provider of industrial injury prevention services. The acquired company specializes in delivering injury prevention and care, post offer employment testing, functional capacity evaluations and return-to-work services. It performs these services across a network in 45 states including onsite at eleven client locations. The business was then combined with Briotix Health increasing the Company’s ownership position in the partnership to approximately 76.0%. Services provided include onsite injury prevention and rehabilitation, performance optimization, post-offer employment testing, functional capacity evaluations and ergonomic assessments. The majority of these services are contracted with and paid for directly by employers, including a number of Fortune 500 companies. Other clients include large insurers and their contractors. These services are performed through Industrial Sports Medicine Professionals, consisting of both physical therapists and specialized certified athletic trainers (ATCs).
In addition to the above acquired interests in the industrial injury prevention business, during the last three years, the Company completed the following multi-clinic acquisitions:
Acquisition |
Date |
% Interest Acquired |
Number of Clinics |
||||
2019 |
|||||||
September 2019 Acquisition |
September 30, 2019 |
67 | % |
11 | |||
2018 |
|||||||
August 2018 Acquisition |
August 31 |
70 | % |
4 | |||
2017 |
|||||||
January 2017 Acquisition |
January 1 |
70 | % |
17 | |||
May 2017 Acquisition |
May 31 |
70 | % |
4 | |||
June 2017 Acquisition |
June 30 |
60 | % |
9 | |||
October 2017 Acquisition |
October 31 |
70 | % |
9 | |||
Also during 2019, the Company purchased the assets and business of one physical therapy clinic in a separate transaction. The clinic operates as a satellite clinic of one of the existing partnerships. Besides the multi-clinic acquisition in 2018, the Company, through several of its majority owned Clinic Partnerships, acquired five separate clinic practices. These practices operate as satellites of the respective existing Clinic Partnerships. During 2017, the Company purchased the assets and business of two physical therapy clinics in separate transactions. One clinic was consolidated with an existing clinic and the other operates as a satellite clinic of one of the existing partnerships.
52
The results of operations of the acquired clinics have been included in the Company’s consolidated financial statements since the date of their respective acquisition. The Company intends to continue to pursue additional acquisition opportunities, develop new clinics and open satellite clinics.
The consolidated financial statements include the accounts of U.S. Physical Therapy, Inc. and its subsidiaries. All significant intercompany transactions and balances have been eliminated. The Company primarily operates through subsidiary clinic partnerships, in which the Company generally owns a 1% general partnership interest and a 24% to 99% limited partnership interest. The managing therapist of each clinic owns the remaining limited partnership interest in the majority of the clinics (hereinafter referred to as “Clinic Partnership”). To a lesser extent, the Company operates some clinics through wholly-owned subsidiaries under profit sharing arrangements with therapists (hereinafter referred to as “Wholly-Owned Facilities”).
Clinic Partnerships
For non-acquired Clinic Partnerships, the earnings and liabilities attributable to the non-controlling interests, typically owned by the managing therapist, directly or indirectly, are recorded within the balance sheets and income statements as non-controlling interests – permanent equity. For acquired Clinic Partnerships with redeemable non-controlling interests, the earnings attributable to the redeemable non-controlling interests are recorded within the consolidated statements of income line item – net income attributable to redeemable non-controlling interests – temporary equity and the equity interests are recorded on the consolidated balance sheet as redeemable non-controlling interests – temporary equity.
Prior to 2018, for acquired Clinic Partnerships with mandatorily redeemable non-controlling interests, the earnings and liabilities attributable to the non-controlling interest are recorded within the consolidated statements of income line item: Interest expense – mandatorily redeemable non-controlling interests – earnings allocable.
Effective December 31, 2017, the Company entered into amendments to its acquired limited partnership agreements replacing the mandatory redemption feature. No monetary consideration was paid to the partners to amend the agreements. The amended limited partnership agreements provide that, upon certain events, the Company has a call right (the “Call Right”) and the selling entity has a put right (the “Put Right”) for the purchase and sale of the limited partnership interest held by the partner. Once triggered, the Put Right and the Call Right do not expire, even upon an individual partner’s death, and contain no mandatory redemption feature. The purchase price of the partner’s limited partnership interest upon the exercise of either the Put Right or the Call Right is calculated per the terms of the respective agreements. The Company accounted for the amendment of its limited partnership agreements as an extinguishment of the outstanding Seller Entity Interests, as defined in Note 5, classified as liabilities through the issuance of new Seller Entity Interests classified in temporary equity. Pursuant to ASC 470-50-40-2, the Company removed the outstanding liability-classified Seller Entity Interests at their carrying amounts, recognized the new temporary-equity-classified Seller Entity Interests at their fair value, and recorded no gain or loss on extinguishment as management believes the redemption value (i.e. the carrying amount) and fair value are the same. In summary, the redemption values of the mandatorily redeemable non-controlling interest (previously classified as liabilities) were reclassified as redeemable non-controlling interest (temporary equity) at fair value on the December 31, 2017 consolidated balance sheet. See Note 5 - Redeemable Non-Controlling Interests – for further discussion.
Wholly-Owned Facilities
For Wholly-Owned Facilities with profit sharing arrangements, an appropriate accrual is recorded for the amount of profit sharing due the clinic partners/directors. The amount is expensed as compensation and included in clinic operating costs—salaries and related costs. The respective liability is included in current liabilities—accrued expenses on the consolidated balance sheets.
53
2. Significant Accounting Policies
Cash Equivalents
The Company maintains its cash and cash equivalents at financial institutions. The Company considers all highly liquid investments with a maturity of three months or less when purchased to be cash equivalents. The combined account balances at several institutions typically exceed Federal Deposit Insurance Corporation (“FDIC”) insurance coverage and, as a result, there is a concentration of credit risk related to amounts on deposit in excess of FDIC insurance coverage. Management believes that this risk is not significant.
Long-Lived Assets
Fixed assets are stated at cost. Depreciation is computed on the straight-line method over the estimated useful lives of the related assets. Estimated useful lives for furniture and equipment range from three to eight years and for software purchased from three to seven years. Leasehold improvements are amortized over the shorter of the related lease term or estimated useful lives of the assets, which is generally three to five years.
Impairment of Long-Lived Assets and Long-Lived Assets to Be Disposed Of
The Company reviews property and equipment and intangible assets with finite lives for impairment upon the occurrence of certain events or circumstances that indicate the related amounts may be impaired. Assets to be disposed of are reported at the lower of the carrying amount or fair value less costs to sell.
Goodwill
Goodwill represents the excess of the amount paid and fair value of the non-controlling interests over the fair value of the acquired business assets, which include certain identifiable intangible assets. Historically, goodwill has been derived from acquisitions and, prior to 2009, from the purchase of some or all of a particular local management’s equity interest in an existing clinic. Effective January 1, 2009, if the purchase price of a non-controlling interest by the Company exceeds or is less than the book value at the time of purchase, any excess or shortfall is recognized as an adjustment to additional paid-in capital.
The fair value of goodwill and other identifiable intangible assets with indefinite lives are tested for impairment annually and upon the occurrence of certain events, and are written down to fair value if considered impaired. The Company evaluates goodwill for impairment on at least an annual basis (in its third quarter) by comparing the fair value of its reporting units to the carrying value of each reporting unit including related goodwill. The Company evaluates indefinite lived tradenames using the relief from royalty method in conjunction with its annual goodwill impairment test. The Company operates a one segment business which is made up of various clinics within partnerships. The partnerships are components of regions and are aggregated to the operating segment level for the purpose of determining the Company’s reporting units when performing its annual goodwill impairment test. In 2019, 2018 and 2017, there were six regions. In addition to the six regions, in 2018 and 2019, the impairment test included a separate analysis for the industrial injury prevention business, a separate reporting unit.
An impairment loss generally would be recognized when the carrying amount of the net assets of a reporting unit, inclusive of goodwill and other identifiable intangible assets, exceeds the estimated fair value of the reporting unit. The estimated fair value of a reporting unit is determined using two factors: (i) earnings prior to taxes, depreciation and amortization for the reporting unit multiplied by a price/earnings ratio used in the industry and (ii) a discounted cash flow analysis. A weight is assigned to each factor and the sum of each weight times the factor is considered the estimated fair value. For 2019, the factors (i.e., price/earnings ratio, discount rate and residual capitalization rate) were updated to reflect current market conditions. The evaluation of goodwill in 2019, 2018 and 2017 did not result in any goodwill amounts that were deemed impaired.
The Company has not identified any triggering events occurring after the testing date that would impact the impairment testing results obtained. The Company will continue to monitor for any triggering events or other indicators of impairment.
54
Redeemable Non-Controlling Interests
The non-controlling interests that are reflected as redeemable non-controlling interests in the consolidated financial statements consist of those that the owners and the Company have certain redemption rights, whether currently exercisable or not, and which currently, or in the future, require that the Company purchase or the owner sell the non-controlling interest held by the owner, if certain conditions are met. The purchase price is derived at a predetermined formula based on a multiple of trailing twelve months earnings performance as defined in the respective limited partnership agreements. The redemption rights can be triggered by the owner or the Company at such time as both of the following events have occurred: 1) termination of the owner’s employment, regardless of the reason for such termination, and 2) the passage of specified number of years after the closing of the transaction, typically three to five years, as defined in the limited partnership agreement. The redemption rights are not automatic or mandatory (even upon death) and require either the owner or the Company to exercise its rights when the conditions triggering the redemption rights have been satisfied.
On the date the Company acquires a controlling interest in a partnership, and the limited partnership agreement for such partnership contains redemption rights not under the control of the Company, the fair value of the non-controlling interest is recorded in the consolidated balance sheet under the caption – Redeemable non-controlling interests. Then, in each reporting period thereafter until it is purchased by the Company, the redeemable non-controlling interest is adjusted to the greater of its then current redemption value or initial carrying value, based on the predetermined formula defined in the respective limited partnership agreement. As a result, the value of the non-controlling interest is not adjusted below its initial carrying value. The Company records any adjustment in the redemption value, net of tax, directly to retained earnings and are not reflected in the consolidated statements of income. Although the adjustments are not reflected in the consolidated statements of income, current accounting rules require that the Company reflects the adjustments, net of tax, in the earnings per share calculation. The amount of net income attributable to redeemable non-controlling interest owners is included in consolidated net income on the face of the consolidated statements of net income. Management believes the redemption value (i.e. the carrying amount) and fair value are the same.
Mandatorily Redeemable Non-Controlling Interests
The non-controlling interests that are reflected as mandatorily redeemable non-controlling interests in the consolidated statements of income consist of those owners who have certain redemption rights, whether currently exercisable or not, and which currently, or in the future, require that the Company purchase the non-controlling interest of those owners at a predetermined formula based on a multiple of trailing twelve months earnings performance as defined in the respective limited partnership agreements. The redemption rights are triggered at such time as both of the following events have occurred: 1) termination of the owner’s employment, regardless of the reason for such termination, and 2) the passage of specified number of years after the closing of the transaction, typically three to five years, as defined in the limited partnership agreement.
Prior to September 30th 2017, on the date the Company acquired a controlling interest in a partnership and the limited partnership agreement for such partnership contained mandatory redemption rights, the fair value of the non-controlling interest was recorded in the long-term liabilities section of the consolidated balance sheet under the caption – Mandatorily redeemable non-controlling interests. In each reporting period thereafter until purchased by the Company, the redeemable non-controlling interest was being adjusted to its then current redemption value, based on the predetermined formula defined in the respective partnership agreement. The Company reflected any adjustment in the redemption value and any earnings attributable to the mandatorily redeemable non-controlling interest in its consolidated statements of income by recording the adjustments and earnings to other income and expense in the captions - Interest expense – mandatorily redeemable non-controlling interests – change in redemption value and Interest expense – mandatorily redeemable non-controlling interests – earnings allocable.
As previously mentioned due to amendments of the limited partnership agreements entered into by the Company, the redemption values of the mandatorily redeemable non-controlling interest (previously classified as liabilities) have been amended and are now classified as redeemable non-controlling interest (temporary equity) at fair value on the December 31, 2019 consolidated balance sheet.
55
Non-Controlling Interests
The Company recognizes non-controlling interests, in which the Company has no obligation but the right to purchase the non-controlling interests, as permanent equity in the consolidated financial statements separate from the parent entity’s equity. The amount of net income attributable to non-controlling interests is included in consolidated net income on the face of the statements of net income. Changes in a parent entity’s ownership interest in a subsidiary that do not result in deconsolidation are treated as equity transactions if the parent entity retains its controlling financial interest. The Company recognizes a gain or loss in net income when a subsidiary is deconsolidated. Such gain or loss is measured using the fair value of the non-controlling equity investment on the deconsolidation date.
When the purchase price of a non-controlling interest by the Company exceeds the book value at the time of purchase, any excess or shortfall is recognized as an adjustment to additional paid-in capital. Additionally, operating losses are allocated to non-controlling interests even when such allocation creates a deficit balance for the non-controlling interest partner.
Revenue Recognition
In May 2014, March 2016, April 2016, and December 2016, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2014-09, Revenue from Contracts with Customers, ASU 2016-08, Revenue from Contracts with Customers, Principal versus Agent Considerations, ASU 2016-10, Revenue from Contracts with Customers, Identifying Performance Obligations and Licensing, ASU 2016-12, Revenue from Contracts with Customers, Narrow Scope Improvements and Practical Expedients, and ASU 2016-20, Technical Corrections and Improvements to Topic 606, Revenue from Contracts with Customer (collectively the “standards”), respectively, which supersede most of the current revenue recognition requirements (“ASC 606”). The core principle of the new guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services.
The Company implemented the new standards beginning January 1, 2018 using a modified retrospective transition method. The principal change relates to how the new standard requires healthcare providers to estimate the amount of variable consideration to be included in the transaction price up to an amount which is probable that a significant reversal will not occur. The most common forms of variable consideration the Company experiences are amounts for services provided that are ultimately not realizable from a customer. There were no changes to revenues or other revenues upon implementation. Under the new standards, the Company’s estimate for unrealizable amounts will continue to be recognized as a reduction to revenue. The bad debt expense historically reported will not materially change.
For ASC 606, there is an implied contract between us and the patient upon each patient visit. Separate contractual arrangements exist between us and third party payors (e.g. insurers, managed care programs, government programs, workers' compensation) which establish the amounts the third parties pay on behalf of the patients for covered services rendered. While these agreements are not considered contracts with the customer, they are used for determining the transaction price for services provided to the patients covered by the third party payors. The payor contracts do not indicate performance obligations for us, but indicate reimbursement rates for patients who are covered by those payors when the services are provided. At that time, the Company is obligated to provide services for the reimbursement rates stipulated in the payor contracts. The execution of the contract alone does not indicate a performance obligation. For self-paying customers, the performance obligation exists when we provide the services at established rates. The difference between the Company’s established rate and the anticipated reimbursement rate is accounted for as an offset to revenue – contractual allowance.
The following table details the revenue related to the various categories.
Year Ended December 31, |
|||||||||
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
|||||||
Net patient revenues |
$ | 433,345 | $ | 417,703 | $ | 389,226 | |||
Management contract revenues |
8,676 | 8,339 | 6,275 | ||||||
Industrial injury prevention services revenues |
37,462 | 25,466 | 14,908 | ||||||
Other revenues |
2,486 | 2,403 | 3,642 | ||||||
$ | 481,969 | $ | 453,911 | $ | 414,051 | ||||
56
Patient revenues
Revenues are recognized in the period in which services are rendered. Net patient revenues consists of revenues for physical therapy and occupational therapy clinics that provide pre-and post-operative care and treatment for orthopedic related disorders, sports-related injuries, preventative care, rehabilitation of injured workers and neurological-related injuries. Net patient revenues (patient revenues less estimated contractual adjustments) are recognized at the estimated net realizable amounts from third-party payors, patients and others in exchange for services rendered when obligations under the terms of the contract are satisfied. There is an implied contract between us and the patient upon each patient visit. Generally, this occurs as the Company provides physical and occupational therapy services, as each service provided is distinct and future services rendered are not dependent on previously rendered services. The Company has agreements with third-party payors that provide for payments to the Company at amounts different from its established rates.
Medicare Reimbursement
The Medicare program reimburses outpatient rehabilitation providers based on the Medicare Physician Fee Schedule (“MPFS”). For services provided in 2019, a 0.25% increase has been applied to the fee schedule payment rates before applying the mandatory budget neutrality adjustment. For services provided in 2020 through 2025, a 0.0% percent update will be applied each year to the fee schedule payment rates, before applying the mandatory budget neutrality adjustment. Beginning in 2021, payments to individual therapists (Physical/Occupational Therapist in Private Practice) paid under the fee schedule may be subject to adjustment based on performance in the Merit Based Incentive Payment System (“MIPS”), which measures performance based on certain quality metrics, resource use, and meaningful use of electronic health records. Under the MIPS requirements, a provider's performance is assessed according to established performance standards each year and then is used to determine an adjustment factor that is applied to the professional's payment for the corresponding payment year. The provider’s MIPS performance in 2019 will determine the payment adjustment in 2021. Each year from 2019 through 2024, professionals who receive a significant share of their revenues through an alternate payment model (“APM”), (such as accountable care organizations or bundled payment arrangements) that involves risk of financial losses and a quality measurement component will receive a 5% bonus in the corresponding payment year. The bonus payment for APM participation is intended to encourage participation and testing of new APMs and to promote the alignment of incentives across payors. The specifics of the MIPS and APM adjustments will be subject to future notice and comment rule-making.
The Budget Control Act of 2011 increased the federal debt ceiling in connection with deficit reductions over the next ten years, and requires automatic reductions in federal spending by approximately $1.2 trillion. Payments to Medicare providers are subject to these automatic spending reductions, subject to a 2% cap. On April 1, 2013, a 2% reduction to Medicare payments was implemented. The Bipartisan Budget Act of 2015, enacted on November 2, 2015, extended the 2% reductions to Medicare payments through fiscal year 2025. The Bipartisan Budget Act of 2018, enacted on February 9, 2018, extends the 2% reductions to Medicare payments through fiscal year 2027.
Historically, the total amount paid by Medicare in any one year for outpatient physical therapy, occupational therapy, and/or speech-language pathology services provided to any Medicare beneficiary was subject to an annual dollar limit (i.e., the “Therapy Cap” or “Limit”). For 2017, the annual Limit on outpatient therapy services was $1,980 for combined Physical Therapy and Speech Language Pathology services and $1,980 for Occupational Therapy services. As a result of Bipartisan Budget Act of 2018, the Therapy Caps have been eliminated, effective as of January 1, 2018.
Under the Middle Class Tax Relief and Job Creation Act of 2012 (“MCTRA”), since October 1, 2012, patients who met or exceeded $3,700 in therapy expenditures during a calendar year have been subject to a manual medical review to determine whether applicable payment criteria are satisfied. The $3,700 threshold is applied to Physical Therapy and Speech Language Pathology Services; a separate $3,700 threshold is applied to the Occupational Therapy. The MACRA directed Centers for Medicare and Medicaid Services (“CMS”) to modify the manual medical review process such that those reviews will no longer apply to all claims exceeding the $3,700 threshold and instead will be determined on a targeted basis based on a variety of factors that CMS considers appropriate. The Bipartisan Budget Act of 2018 extended the targeted medical review indefinitely, but
57
reduced the threshold to $3,000 through December 31, 2027. For 2028, the threshold amount will be increased by the percentage increase in the Medicare Economic Index (“MEI”) for 2028. In subsequent years the threshold amount will increase based on the corresponding percentage increase in the MEI for such subsequent year.
CMS adopted a multiple procedure payment reduction (“MPPR”) for therapy services in the final update to the MPFS for calendar year 2011. The MPPR applied to all outpatient therapy services paid under Medicare Part B — occupational therapy, physical therapy and speech-language pathology. Under the policy, the Medicare program pays 100% of the practice expense component of the Relative Value Unit (“RVU”) for the therapy procedure with the highest practice expense RVU, then reduces the payment for the practice expense component for the second and subsequent therapy procedures or units of service furnished during the same day for the same patient, regardless of whether those therapy services are furnished in separate sessions. Since 2013, the practice expense component for the second and subsequent therapy service furnished during the same day for the same patient was reduced by 50%.
Medicare claims for outpatient therapy services furnished by therapy assistants on or after January 1, 2020 must include a modifier indicating the service was furnished by a therapy assistant. Outpatient therapy services furnished on or after January 1, 2022 in whole or part by a therapy assistant will be paid at an amount equal to 85% of the payment amount otherwise applicable for the service.
Statutes, regulations, and payment rules governing the delivery of therapy services to Medicare beneficiaries are complex and subject to interpretation. The Company believes that it is in compliance, in all material respects, with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing that would have a material effect on the Company’s financial statements as of December 31, 2019. Compliance with such laws and regulations can be subject to future government review and interpretation, as well as significant regulatory action including fines, penalties, and exclusion from the Medicare program. Net patient revenue from Medicare were approximately $119.4 million, $103.6 million and $92.6 million, respectively, for 2019, 2018 and 2017.
Management Contract Revenues
Management contract revenues, which are included in other revenues, are derived from contractual arrangements whereby the Company manages a clinic for third party owners. The Company does not have any ownership interest in these clinics. Typically, revenues are determined based on the number of visits conducted at the clinic and recognized at a point in time when services are performed. Costs, typically salaries for the Company’s employees, are recorded when incurred.
Industrial Injury Prevention Services Revenues
Revenue from the industrial injury prevention business, which are also included in other revenues in the consolidated statements of net income, are derived from onsite services we provide to clients’ employees including injury prevention, rehabilitation, ergonomic assessments and performance optimization. Revenue from the Company’s industrial injury prevention business is recognized when obligations under the terms of the contract are satisfied. Revenues are recognized at an amount equal to the consideration the company expects to receive in exchange for providing injury prevention services to its clients. The revenue is determined and recognized based on the number of hours and respective rate for services provided in a given period.
Other Revenues
Additionally, other revenues include services the Company provides on-site, such as schools and industrial worksites, for physical or occupational therapy services, and athletic trainers and gym membership fees. Contract terms and rates are agreed to in advance between the Company and the third parties. Services are typically performed over the contract period and revenue is recorded at the point of service. If the services are paid in advance, revenue is recorded as a contract liability over the period of the agreement and recognized at the point in time, when the services are performed.
58
Contractual Allowances
The allowance for estimated contractual adjustments is based on terms of payor contracts and historical collection and write-off experience. Contractual allowances result from the differences between the rates charged for services performed and expected reimbursements by both insurance companies and government sponsored healthcare programs for such services. Medicare regulations and the various third party payors and managed care contracts are often complex and may include multiple reimbursement mechanisms payable for the services provided in Company clinics. The Company estimates contractual allowances based on its interpretation of the applicable regulations, payor contracts and historical calculations. Each month the Company estimates its contractual allowance for each clinic based on payor contracts and the historical collection experience of the clinic and applies an appropriate contractual allowance reserve percentage to the gross accounts receivable balances for each payor of the clinic. Based on the Company’s historical experience, calculating the contractual allowance reserve percentage at the payor level is sufficient to allow the Company to provide the necessary detail and accuracy with its collectability estimates. However, the services authorized and provided and related reimbursement are subject to interpretation that could result in payments that differ from the Company’s estimates. Payor terms are periodically revised necessitating continual review and assessment of the estimates made by management. The Company’s billing system does not capture the exact change in its contractual allowance reserve estimate from period to period in order to assess the accuracy of its revenues and hence its contractual allowance reserves. Management regularly compares its cash collections to corresponding net revenues measured both in the aggregate and on a clinic-by-clinic basis. In the aggregate, historically the difference between net revenues and corresponding cash collections has generally reflected a difference within approximately 1% of net revenues. Additionally, analysis of subsequent periods’ contractual write-offs on a payor basis reflects a difference within approximately 1% between the actual aggregate contractual reserve percentage as compared to the estimated contractual allowance reserve percentage associated with the same period end balance. As a result, the Company believes that a change in the contractual allowance reserve estimate would not likely be more than 1% at December 31, 2019.
Allowance for Doubtful Accounts
The Company determines allowances for doubtful accounts based on the specific agings and payor classifications at each clinic. The provision for doubtful accounts is included in operating costs in the statements of net income. Patient accounts receivable, which are stated at the historical carrying amount net of contractual allowances, write-offs and allowance for doubtful accounts, includes only those amounts the Company estimates to be collectible.
Income Taxes
Income taxes are accounted for under the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases and operating loss and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in income in the period that includes the enactment date.
The Company recognizes the financial statement benefit of a tax position only after determining that the relevant tax authority would more likely than not sustain the position following an audit. For tax positions meeting the more-likely-than-not threshold, the amount to be recognized in the financial statements is the largest benefit that has a greater than 50 percent likelihood of being realized upon ultimate settlement with the relevant tax authority.
The Tax Cuts and Jobs Act of 2017 (the “TCJA”) was passed by Congress on December 20, 2017 and signed into law by President Trump on December 22, 2017. The TCJA made significant changes to U.S. corporate income tax laws including a decrease in the corporate income tax rate to 21% effective January 1, 2018. As a result, the Company revalued its deferred tax assets and liabilities. Based on a review and analysis as of December 31, 2017, the Company estimated a reduction of its net deferred tax liabilities by $4.3 million thereby reducing its provision for income taxes by such amount for the 2017 year.
59
The Company did not have any accrued interest or penalties associated with any unrecognized tax benefits nor was any interest expense recognized during the twelve months ended December 31, 2019, 2018 and 2017. The Company will book any interest or penalties, if required, in interest and other expense, as appropriate.
Fair Values of Financial Instruments
The carrying amounts reported in the balance sheets for cash and cash equivalents, accounts receivable, accounts payable and notes payable approximate their fair values due to the short-term maturity of these financial instruments. The carrying amount under the Amended Credit Agreement and the redemption value of Redeemable non-controlling interests approximate the respective fair values. The fair value of the Company’s redeemable non-controlling interests is determined based on “Level 3” inputs. The interest rate on the Amended Credit Agreement, which is tied to LIBOR, is set at various short-term intervals, as detailed in the Amended Credit Agreement.
Segment Reporting
Operating segments are components of an enterprise for which separate financial information is available that is evaluated regularly by chief operating decision makers in determining the allocation of resources and in assessing performance. The Company identifies operating segments based on management responsibility and believes it meets the criteria for aggregating its operating segments into a single reportable segment.
Use of Estimates
In preparing the Company’s consolidated financial statements, management makes certain estimates and assumptions, especially in relation to, but not limited to, goodwill impairment, tradenames, allocations of purchase price, allowance for receivables, tax provision and contractual allowances, that affect the amounts reported in the consolidated financial statements and related disclosures. Actual results may differ from these estimates.
Self-Insurance Program
The Company utilizes a self-insurance plan for its employee group health and dental insurance coverage administered by a third party. Predetermined loss limits have been arranged with the insurance company to minimize the Company’s maximum liability and cash outlay. Accrued expenses include the estimated incurred but unreported costs to settle unpaid claims and estimated future claims. Management believes that the current accrued amounts are sufficient to pay claims arising from self-insurance claims incurred through December 31, 2019.
Restricted Stock
Restricted stock issued to employees and directors is subject to continued employment or continued service on the board, respectively. Generally, restrictions on the stock granted to employees lapse in equal annual installments on the following four anniversaries of the date of grant. For those shares granted to directors, the restrictions will lapse in equal quarterly installments during the first year after the date of grant. For those granted to officers, the restriction will lapse in equal quarterly installments during the four years following the date of grant. Compensation expense for grants of restricted stock is recognized based on the fair value per share on the date of grant amortized over the vesting period. The Company recognizes any forfeitures as they occur. The restricted stock issued is included in basic and diluted shares for the earnings per share computation.
Recently Adopted Accounting Guidance
In May 2014, March 2016, April 2016, and December 2016, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2014-09, Revenue from Contracts with Customers, ASU 2016-08, Revenue from Contracts with Customers, Principal versus Agent Considerations, ASU 2016-10, Revenue from Contracts with Customers, Identifying Performance Obligations and Licensing, ASU 2016-12, Revenue from Contracts with Customers, Narrow Scope Improvements and Practical Expedients, and ASU 2016-20, Technical Corrections and Improvements to Topic 606, Revenue from Contracts with Customer (collectively “the standards”), respectively, which supersede most of the current revenue recognition requirements. The core principle of the new guidance is that an entity should recognize revenue to depict the
60
transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. New disclosures about the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers are also required. The original standards were effective for fiscal years beginning after December 15, 2016; However, in July 2015, the FASB approved a one-year deferral of these standards, with a new effective date for fiscal years beginning after December 15, 2017. The standards require the selection of a retrospective or cumulative effect transition method.
The Company implemented the new standards beginning January 1, 2018 using a modified retrospective transition method. Adoption of the new standard did not result in material changes to the presentation of net revenues and bad debt expense in the consolidated statements of income, and the presentation of the amount of income from operations and net income will be unchanged upon adoption of the new standards. The principal change relates to how the new standard requires healthcare providers to estimate the amount of variable consideration to be included in the transaction price up to an amount which is probable that a significant reversal will not occur. The most common forms of variable consideration the Company experiences are amounts for services provided that are ultimately not realizable from a customer. Under the new standards, the Company’s estimate for unrealizable amounts will continue to be recognized as a reduction to revenue. The bad debt expense historically reported will not materially change.
In February 2016, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) No. 2016-02, Leases (Topic 842) (“ASC 842”), which amended prior accounting standards for leases.
The Company implemented the new lease standard, ASC Topic 842 – Leases as of January 1, 2019 using the transition method in ASU 2018-11 issued in July 2018 which allows the Company to initially apply the new leases standard at adoption date and recognize a cumulative-effect adjustment to the opening balance of retained earnings in the period of adoption. There was no adjustment required to retained earnings upon adoption. Accordingly, no retrospective adjustments were made to the comparative periods presented. The Company elected certain of the practical expedients permitted, including the expedient that allows the Company to retain its existing lease assessment and classification.
Adoption of ASC 842 resulted in an increase to total assets and liabilities due to the recording of operating lease right-of-use assets (“ROU”) and operating lease liabilities of approximately $78.0 million and $82.6 million respectively, as of January 1, 2019 for operating leases as a lessee. The adoption did not materially impact the Company’s consolidated statement of income or cash flows. See Footnote 10 - Leases for further discussion of leases.
In August 2018, the Securities Exchange Commission (“SEC”) issued Final Rule 33-10532, Disclosure Update and Simplification, which amends certain disclosure requirements that were redundant, duplicative, overlapping or superseded by other SEC disclosure requirements. The amendments generally eliminated or otherwise reduced certain disclosure requirements of various SEC rules and regulations. However, in some cases, the amendments require additional information to be disclosed, including changes in stockholders’ equity in interim periods. The rule is effective 30 days after its publication in the Federal Register. The rule was posted on October 4, 2018. On September 25, 2018, the SEC released guidance advising it will not object to a registrant adopting the requirement to include changes in stockholders’ equity in the Form 10-Q for the first quarter beginning after the effective date of the rule. The Company adopted this guidance in its Form 10-Q for the period ended March 31, 2019.
In January 2017, the FASB issued ASU 2017-04, Simplifying the Test for Goodwill Impairment (Topic 350), which eliminates the requirement to calculate the implied fair value of goodwill to measure a goodwill impairment change. ASU 2017-04 is effective prospectively for fiscal years, and the interim periods within those years, beginning after December 15, 2019. There was no impact to goodwill from this change.
Recently Issued Accounting Guidance
In June 2016, the FASB issued ASU 2016-13, Financial Instruments – Credit Losses, which added a new impairment model (known as the current expected credit loss (CECL) model) that is based on expected losses rather than incurred losses. Under the new guidance, an entity recognizes as an allowance its estimate of expected credit losses. The CECL model applies to most debt instruments, including trade receivables. The
61
CECL model does not have a minimum threshold for recognition of impairment losses and entities will need to measure expected credit losses on assets that have a low risk of loss. The standard is required to be applied using the modified retrospective approach with a cumulative-effect adjustment to retained earnings, if any, upon adoption.
The Company has completed the adoption of the standard on January 1, 2020. The financial instruments subject to ASU 2016-13 are the Company’s accounts receivable derived from contracts with customers. A significant portion of the Company’s accounts receivable is from highly-solvent, creditworthy payors including governmental programs such as Medicare and Medicaid, and highly regulated commercial insurers. The Company’s estimate of expected credit losses as of January 1, 2020, using its expected credit loss evaluation process, resulted in no adjustments to the allowance for credit losses and no cumulative-effect adjustment to retained earnings on the adoption date of the standard.
Subsequent Event
On February 26, 2020, the Company completed an acquisition of a four clinic physical therapy practice. The clinics are held in four separate partnerships. On the date of purchase, the Company acquired approximately 65% of the equity interests, with the practice’s clinical founders and associates retaining approximately 35%. The aggregate purchase price for the acquisition was approximately $12.2 million.
3. Acquisitions of Businesses
During 2019, 2018 and 2017, the Company acquired a majority interest in the following multi-clinic physical therapy practices:
Acquisition |
Date |
% Interest Acquired |
Number of Clinics |
||||
2019 |
|||||||
September 2019 Acquisition |
September 30, 2019 |
67 | % |
11 | |||
2018 |
|||||||
August 2018 Acquisition |
August 31 |
70 | % |
4 | |||
2017 |
|||||||
January 2017 Acquisition |
January 1 |
70 | % |
17 | |||
May 2017 Acquisition |
May 31 |
70 | % |
4 | |||
June 2017 Acquisition |
June 30 |
60 | % |
9 | |||
October 2017 Acquisition |
October 31 |
70 | % |
9 | |||
On September 30, 2019, the Company acquired a 67% interest in an eleven-clinic physical therapy practice. The purchase price for the 67% interest was $12.4 million, of which $12.1 million was paid in cash and $0.3 million in a seller note that is payable in two principal installments totaling $150,000 each, plus accrued interest in September 2020 and September 2021. The note accrues interest at 5.0% per annum.
On April 11, 2019, the Company acquired a company that is a provider of industrial injury prevention services. The acquired company specializes in delivering injury prevention and care, post offer employment testing, functional capacity evaluations and return-to-work services. It performs these services across a network of 45 states including onsite at eleven client locations. The business was then combined with Briotix Health, the Company’s industrial injury prevention operation, increasing the Company’s ownership position in the Briotix Health partnership to approximately 76.0%. The purchase price for the acquired company was $22.9 million ($23.6 million less cash acquired of $0.7 million), which consisted of $18.9 million in cash, (of which $0.5 million will be paid to certain shareholders), and a $4.0 million seller note. The note accrues interest at 5.5% and the principal and accrued interest is payable, on April 9, 2021.
The results of operations of the acquired clinics have been included in the Company’s consolidated financial statements since the date of their respective acquisition. The Company intends to continue to pursue additional acquisition opportunities, develop new clinics and open satellite clinics.
62
The purchase price for the 2019 acquisitions has been preliminarily allocated as follows (in thousands):
IIPS* |
Clinic Practice |
Total |
|||||||
Cash paid, net of cash acquired ($900) |
$ | 18,427 | $ | 12,170 | $ | 30,597 | |||
Payable to shareholders of seller |
486 | — | 486 | ||||||
Seller note |
4,000 | 300 | 4,300 | ||||||
Total consideration |
$ | 22,913 | $ | 12,470 | $ | 35,383 | |||
Estimated fair value of net tangible assets acquired: |
|||||||||
Total current assets |
$ | 1,907 | $ | 697 | $ | 2,604 | |||
Total non-current assets |
611 | 3,028 | 3,639 | ||||||
Total liabilities |
(1,504 | ) |
(2,846 | ) |
(4,350 | ) |
|||
Net tangible assets acquired |
$ | 1,014 | $ | 879 | $ | 1,893 | |||
Referral relationships |
1,500 | 1,500 | 3,000 | ||||||
Non-compete |
590 | 700 | 1,290 | ||||||
Tradename |
2,500 | 1,600 | 4,100 | ||||||
Goodwill |
17,309 | 14,021 | 31,330 | ||||||
Fair value of non-controlling interest (classified as redeemable non-controlling interests) |
— | (6,230 | ) |
(6,230 | ) |
||||
$ | 22,913 | $ | 12,470 | $ | 35,383 | ||||
| * | Industrial injury prevention services |
On August 31, 2018, the Company acquired a 70% interest in a four-clinic physical therapy practice. The purchase price for the 70% interest was $7.3 million in cash and $0.4 million in a seller note that is payable in two principal installments totaling $200,000 each, plus accrued interest. The first installment was paid in cash in August 2019 and the second installment remains payable in August 2020.
On April 30, 2018, the Company acquired a 65% interest in another business in the industrial injury prevention sector. The aggregate purchase price for the 65% interest was $8.6 million in cash and $400,000 in a seller note that was paid on April 30, 2019. On April 30, 2018, the Company combined its two businesses. After the combination, the Company owned a 59.45% interest in the combined business, Briotix Health. See discussion above regarding an additional acquisition on April 30, 2019 in the industrial injury prevention business.
In addition, during 2018, the Company, through several of its majority owned Clinic Partnerships, acquired five separate clinic practices. These practices operate as satellites of the existing Clinic Partnership. The aggregate purchase price was $1.0 million inclusive of cash of $850,000 and a note payable of $150,000. The note accrued interest at 4.5% and the principal and accrued interest, was paid in cash on August 31, 2019.
The purchase price for the 2018 acquisitions were allocated as follows (in thousands):
Cash paid, net of cash acquired ($372) |
$ | 16,367 | |
Seller notes |
950 | ||
Total consideration |
$ | 17,317 | |
Estimated fair value of net tangible assets acquired: |
|||
Total current assets |
$ | 1,633 | |
Total non-current assets |
305 | ||
Total liabilities |
(525 | ) |
|
Net tangible assets acquired |
$ | 1,413 | |
Referral relationships |
2,926 | ||
Non-compete |
298 | ||
Tradename |
990 | ||
Goodwill |
19,835 | ||
Fair value of non-controlling interest (classified as redeemable non-controlling interests) |
(8,145 | ) |
|
$ | 17,317 |
63
On January 1, 2017, the Company acquired a 70% interest in a seventeen-clinic physical therapy practice. The purchase price for the 70% interest was $10.7 million in cash and $0.5 million in a seller note that was payable in two principal installments totaling $250,000 each, plus accrued interest. The first installment was paid in January 2018 and the second installment in January 2019.
On May 31, 2017, the Company acquired a 70% interest in a four-clinic physical therapy practice. The purchase price for the 70% interest was $2.3 million in cash and $250,000 in a seller note that was payable in two principal installments totaling $125,000 each, plus accrued interest. The first installment was paid in May 2018 and the second installment in May 2019.
On June 30, 2017, the Company acquired a 60% interest in a nine-clinic physical therapy practice. The purchase price for the 60% interest was $15.8 million in cash and $0.5 million in a seller note that was payable in two principal installments totaling $250,000 each, plus accrued interest. The first installment was paid in June 2018 and the second installment in June 2019.
On October 31, 2017, the Company acquired a 70% interest in a nine-clinic physical therapy practice and two management contracts with third party providers. The purchase price for the 70% interest was $4.0 million in cash and $0.5 million in a seller note that was payable in two principal installments totaling $250,000 each, plus accrued interest. The first installment was paid in October 2018 and the second installment in October 2019.
Also, in 2017, the Company purchased the assets and business of two physical therapy clinics in separate transactions. One clinic was consolidated with an existing clinic and the other operates as a satellite clinic of one of the existing partnerships.
The purchase price for the 2017 acquisitions were allocated as follows (in thousands):
Cash paid, net of cash acquired ($2,297) |
$ | 36,682 | |
Seller notes |
2,150 | ||
Total consideration |
$ | 38,832 | |
Estimated fair value of net tangible assets acquired: |
|||
Total current assets |
$ | 5,853 | |
Total non-current assets |
1,527 | ||
Total liabilities |
(2,865 | ) |
|
Net tangible assets acquired |
$ | 4,515 | |
Referral relationships |
4,250 | ||
Non-compete |
660 | ||
Tradename |
6,850 | ||
Goodwill |
46,722 | ||
Fair value of non-controlling interest (classified as redeemable non-controlling interests) |
(13,883 | ) |
|
Fair value of non-controlling interest (originally classified as mandatorily redeemable non-controlling interests) |
(10,282 | ) |
|
$ | 38,832 |
The finalized purchase prices plus the fair value of the non-controlling interests for the acquisition in 2018 and 2017 were allocated to the fair value of the assets acquired, inclusive of identifiable intangible assets, i.e. trade names, referral relationships and non-compete agreements, and liabilities assumed based on the fair values at the acquisition date, with the amount exceeding the fair values being recorded as goodwill. For the acquisitions in 2019, the Company is in the process of completing its formal valuation analysis to identify and determine the fair value of tangible and identifiable intangible assets acquired and the liabilities assumed. Thus, the final allocation of the purchase price may differ from the preliminary estimates used at December 31, 2019 based on additional information obtained and completion of the valuation of the identifiable intangible assets. Changes in the estimated valuation of the tangible assets acquired, the completion of the valuation of identifiable intangible assets and the completion by the Company of the identification of any unrecorded pre-acquisition contingencies, where the liability is probable and the amount can be reasonably estimated, will likely result in adjustments to goodwill. The Company does not expect the adjustments to be material.
64
For the acquisitions in 2019, the values assigned to the referral relationships and non-compete agreements are being amortized to expense equally over the respective estimated lives. For referral relationships, the amortization period is 11.0 years. For non-compete agreements, the amortization period is 6.0 years. The values assigned to tradenames are tested annually for impairment.
For the acquisitions in 2018 and 2017, the values assigned to the referral relationships and non-compete agreements are being amortized to expense equally over the respective estimated lives. For referral relationships, the weighted average amortization period was 10.54 and 10.10 years at December 31, 2018 and December 31, 2017, respectively. For non-compete agreements, the weighted average amortization period was 6.00 and 5.16 years at December 31, 2018 and December 31, 2017, respectively. Generally, the values assigned to tradenames are tested annually for impairment.
For the 2019, 2018 and 2017 acquisitions, total current assets primarily represent patient accounts receivable. Total non-current assets are fixed assets, primarily equipment, used in the practices.
The consideration paid for each of the acquisitions was derived through arm’s length negotiations. Funding for the cash portions was derived from proceeds from the Company’s revolving credit facility. The results of operations of the acquisitions have been included in the Company’s consolidated financial statements since their respective date of acquisition. Unaudited proforma consolidated financial information for the acquisitions in 2019, 2018 and 2017 acquisitions have not been included as the results, individually and in the aggregate.
4. Acquisitions and Sale of Non-Controlling Interests
During 2019, the Company acquired additional interests in four partnerships which are included in non-controlling interest. The additional interests purchased in each of the partnerships ranged from 1% and 55%. Also in 2019, the Company sold a 1% interest in a partnership. The net after-tax difference between the payments and the portion of undistributed earnings of $196,000 was credited to additional paid-in capital.
During 2018, the Company acquired additional interests in three partnerships included in non-controlling interest. The additional interests purchased in each of the partnerships ranged from 5.5% and 35%. The net after-tax difference of $224,000 was credited to additional paid-in capital.
During 2017, the Company acquired additional interests in two partnerships included in non-controlling interest. The additional interests purchased in each of the partnerships was 35%. The net after-tax difference of $56,000 was credited to additional paid-in capital.
5. Redeemable Non-Controlling Interest
Since October 2017, when the Company acquires a majority interest (the “Acquisition”) in a physical therapy clinic business (referred to as “Therapy Practice”), these Acquisitions occur in a series of steps which are described below.
| 1. | Prior to the Acquisition, the Therapy Practice exists as a separate legal entity (the “Seller Entity”). The Seller Entity is owned by one or more individuals (the “Selling Shareholders”) most of whom are physical therapists that work in the Therapy Practice and provide physical therapy services to patients. |
| 2. | In conjunction with the Acquisition, the Seller Entity contributes the Therapy Practice into a newly-formed limited partnership (“NewCo”), in exchange for one hundred percent (100%) of the limited and general partnership interests in NewCo. Therefore, in this step, NewCo becomes a wholly-owned subsidiary of the Seller Entity. |
| 3. | The Company enters into an agreement (the “Purchase Agreement”) to acquire from the Seller Entity a majority (ranges from 50% to 90%) of the limited partnership interest and in all cases 100% of the general partnership interest in NewCo. The Company does not purchase 100% of the limited partnership interest because the Selling Shareholders, through the Seller Entity, want to maintain an ownership percentage. The consideration for the Acquisition is primarily payable in the form of cash at closing and a small two-year note in lieu of an escrow (the “Purchase Price”). The Purchase Agreement does not contain any future earn-out or other contingent consideration that is payable to the Seller Entity or the Selling Shareholders. |
65
| 4. | The Company and the Seller Entity also execute a partnership agreement (the “Partnership Agreement”) for NewCo that sets forth the rights and obligations of the limited and general partners of NewCo. After the Acquisition, the Company is the general partner of NewCo. |
| 5. | As noted above, the Company does not purchase 100% of the limited partnership interests in NewCo and the Seller Entity retains a portion of the limited partnership interest in NewCo (“Seller Entity Interest”). |
| 6. | In most cases, some or all of the Selling Shareholders enter into an employment agreement (the “Employment Agreement”) with NewCo with an initial term that ranges from three to five years (the “Employment Term”), with automatic one-year renewals, unless employment is terminated prior to the end of the Employment Term. As a result, a Selling Shareholder becomes an employee (“Employed Selling Shareholder”) of NewCo. The employment of an Employed Selling Shareholder can be terminated by the Employed Selling Shareholder or NewCo, with or without cause, at any time. In a few situations, a Selling Shareholder does not become employed by NewCo and is not involved with NewCo following the closing; in those situations, such Selling Shareholders sell their entire ownership interest in the Seller Entity as of the closing of the Acquisition. |
| 7. | The compensation of each Employed Selling Shareholder is specified in the Employment Agreement and is customary and commensurate with his or her responsibilities based on other employees in similar capacities within NewCo, the Company and the industry. |
| 8. | The Company and the Selling Shareholder (including both Employed Selling Shareholders and Selling Shareholders not employed by NewCo) execute a non-compete agreement (the “Non-Compete Agreement”) which restricts the Selling Shareholder from engaging in competing business activities for a specified period of time (the “Non-Compete Term”). A Non-Compete Agreement is executed with the Selling Shareholders in all cases. That is, even if the Selling Shareholder does not become an Employed Selling Shareholder, the Selling Shareholder is restricted from engaging in a competing business during the Non-Compete Term. |
| 9. | The Non-Compete Term commences as of the date of the Acquisition and expires on the later of: |
| a. | Two years after the date an Employed Selling Shareholders’ employment is terminated (if the Selling Shareholder becomes an Employed Selling Shareholder) or |
| b. | Five to six years from the date of the Acquisition, as defined in the Non-Compete Agreement, regardless of whether the Selling Shareholder is employed by NewCo. |
| 10. | The Non-Compete Agreement applies to a restricted region which is defined as a 15-mile radius from the Therapy Practice. That is, an Employed Selling Shareholder is permitted to engage in competing businesses or activities outside the 15-mile radius (after such Employed Selling Shareholder no longer is employed by NewCo) and a Selling Shareholder who is not employed by NewCo immediately is permitted to engage in the competing business or activities outside the 15-mile radius. |
The Partnership Agreement contains provisions for the redemption of the Seller Entity Interest, either at the option of the Company (the “Call Right”) or at the option of the Seller Entity (the “Put Right”) as follows:
| 1. | Put Right |
| a. | In the event that any Selling Shareholder’s employment is terminated under certain circumstances prior to the fifth anniversary of the Closing Date, the Seller Entity thereafter may have an irrevocable right to cause the Company to purchase from Seller Entity the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest at the purchase price described in “3” below. |
| b. | In the event that any Selling Shareholder is not employed by NewCo as of the fifth anniversary of the Closing Date and the Company has not exercised its Call Right with respect to the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest, Seller Entity thereafter shall have the Put Right to cause the Company to purchase from Seller Entity the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest at the purchase price described in “3” below. |
66
| c. | In the event that any Selling Shareholder’s employment with NewCo is terminated for any reason on or after the fifth anniversary of the Closing Date, the Seller Entity shall have the Put Right, and upon the exercise of the Put Right, the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest shall be redeemed by the Company at the purchase price described in “3” below. |
| 2. | Call Right |
| a. | If any Selling Shareholder’s employment by NewCo is terminated prior to the fifth anniversary of the Closing Date, the Company thereafter shall have an irrevocable right to purchase from Seller Entity the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest, in each case at the purchase price described in “3” below. |
| b. | In the event that any Selling Shareholder’s employment with NewCo is terminated for any reason on or after the fifth anniversary of the Closing Date, the Company shall have the Call Right, and upon the exercise of the Call Right, the Terminated Selling Shareholder’s Allocable Percentage of Seller Entity’s Interest shall be redeemed by the Company at the purchase price described in “3” below. |
| 3. | For the Put Right and the Call Right, the purchase price is derived from a formula based on a specified multiple of NewCo’s trailing twelve months of earnings before interest, taxes, depreciation, amortization, and the Company’s internal management fee, plus an Allocable Percentage of any undistributed earnings of NewCo (the “Redemption Amount”). NewCo’s earnings are distributed monthly based on available cash within NewCo; therefore, the undistributed earnings amount is small, if any. |
| 4. | The Purchase Price for the initial equity interest purchased by the Company is also based on the same specified multiple of the trailing twelve-month earnings that is used in the Put Right and the Call Right noted above. |
| 5. | The Put Right and the Call Right do not have an expiration date, but the Seller Entity Interest is not required to be purchased by the Company or sold by the Seller Entity. |
| 6. | The Put Right and the Call Right never apply to Selling Shareholders who do not become employed by NewCo, since the Company requires that such Selling Shareholders sell their entire ownership interest in the Seller Entity at the closing of the Acquisition. |
An Employed Selling Shareholder’s ownership of his or her equity interest in the Seller Entity predates the Acquisition and the Company’s purchase of its partnership interest in NewCo. The Employment Agreement and the Non-Compete Agreement do not contain any provision to escrow or “claw back” the equity interest in the Seller Entity held by such Employed Selling Shareholder, nor the Seller Entity Interest in NewCo, in the event of a breach of the employment or non-compete terms. More specifically, even if the Employed Selling Shareholder is terminated for “cause” by NewCo, such Employed Selling Shareholder does not forfeit his or her right to his or her full equity interest in the Seller Entity and the Seller Entity does not forfeit its right to any portion of the Seller Entity Interest. The Company’s only recourse against the Employed Selling Shareholder for breach of either the Employment Agreement or the Non-Compete Agreement is to seek damages and other legal remedies under such agreements. There are no conditions in any of the arrangements with an Employed Selling Shareholder that would result in a forfeiture of the equity interest held in the Seller Entity or of the Seller Entity Interest.
67
For the year ended December 31, 2019 and 2018, the following table details the changes in the carrying amount (fair value) of the redeemable non-controlling interests (in thousands):
Year Ended |
||||||
December 31, 2019 |
December 31, 2018 |
|||||
Beginning balance |
$ | 133,943 | $ | 102,572 | ||
Operating results allocated to redeemable non-controlling interest partners |
10,659 | 8,433 | ||||
Distributions to redeemable non-controlling interest partners |
(10,221 | ) |
(9,835 | ) |
||
Changes in the fair value of redeemable non-controlling interest |
11,893 | 24,770 | ||||
Purchases of redeemable non-controlling interest |
(8,934 | ) |
8,145 | |||
Fair value of redeemable non-controlling interest - amended partnership agreements |
— | — | ||||
Acquired interest |
6,230 | — | ||||
Sales of redeemable non-controlling interest - temporary equity |
3,120 | — | ||||
Reduction of non-controlling interest due to sale of USPh partnership interest |
(6,132 | ) |
— | |||
Notes receivable related to sales of redeemable non-controlling interest - temporary equity |
(2,870 | ) |
(142 | ) |
||
Other |
62 | — | ||||
Ending balance |
$ | 137,750 | $ | 133,943 | ||
The following table categorizes the carrying amount (fair value) of the redeemable non-controlling interests (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||
Contractual time period has lapsed but holder's employment has not been terminated |
$ | 51,921 | $ | 42,624 | ||
Contractual time period has not lapsed and holder's employment has not been terminated |
85,829 | 91,319 | ||||
Holder's employment has terminated and contractual time period has expired |
— | — | ||||
Holder's employment has terminated and contractual time period has not expired |
— | — | ||||
$ | 137,750 | $ | 133,943 | |||
6. Goodwill
The changes in the carrying amount of goodwill as of December 31, 2019 and 2018 consisted of the following (in thousands):
Year Ended December 31, 2019 |
Year Ended December 31, 2018 |
|||||
Beginning balance |
$ | 293,525 | $ | 271,338 | ||
Goodwill acquired |
31,330 | 19,778 | ||||
Goodwill related to partnership interest sold |
(7,325 | ) |
— | |||
Goodwill adjustments for purchase price allocation of businesses acquired in prior year |
146 | 2,409 | ||||
Ending balance |
$ | 317,676 | $ | 293,525 | ||
68
7. Intangible Assets, net
Intangible assets, net as of December 31, 2019 and 2018 consisted of the following (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||
Tradenames |
$ | 32,049 | $ | 30,256 | ||
Referral relationships, net of accumulated amortization of $11,677 and $9,370, respectively |
18,367 | 16,895 | ||||
Non-compete agreements, net of accumulated amortization of $5,424 and $4,716, respectively |
2,172 | 1,677 | ||||
$ | 52,588 | $ | 48,828 | |||
Tradenames, referral relationships and non-compete agreements are related to the businesses acquired. The value assigned to tradenames has an indefinite life and is tested at least annually for impairment using the relief from royalty method in conjunction with the Company’s annual goodwill impairment test. The value assigned to referral relationships is being amortized over their respective estimated useful lives which range from 6 to 16 years. Non-compete agreements are amortized over the respective term of the agreements which range from 5 to 6 years.
The following table details the amount of amortization expense recorded for intangible assets for the years ended December 31, 2019, 2018 and 2017 (in thousands):
Year Ended December 31, 2019 |
Year Ended December 31, 2018 |
Year Ended December 31, 2017 |
|||||||
Referral relationships |
$ | 2,307 | $ | 2,161 | $ | 1,934 | |||
Non-compete agreements |
708 | 616 | 720 | ||||||
$ | 3,015 | $ | 2,777 | $ | 2,654 | ||||
For one acquisition, the value assigned to tradename was being amortized over the term of the six year agreement in which the Company had acquired the right to use the specific tradename.
The remaining balances of the referral relationships and non-compete agreements is expected to be amortized as follows (in thousands):
Referral Relationships |
Non-Compete Agreements |
||||||
Years Ending December 31, |
Annual Amount |
Years Ending December 31, |
Annual Amount |
||||
2020 |
$ | 2,403 | 2020 |
$ | 619 | ||
2021 |
$ | 2,403 | 2021 |
$ | 541 | ||
2022 |
$ | 2,354 | 2022 |
$ | 364 | ||
2023 |
$ | 2,247 | 2023 |
$ | 294 | ||
2024 |
$ | 2,082 | 2024 |
$ | 238 | ||
Thereafter |
$ | 6,878 | Thereafter |
$ | 116 | ||
8. Accrued Expenses
Accrued expenses as of December 31, 2019 and 2018 consisted of the following (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||
Salaries and related costs |
$ | 19,340 | $ | 21,726 | ||
Credit balances due to patients and payors |
4,303 | 7,293 | ||||
Group health insurance claims |
2,277 | 3,124 | ||||
Other |
4,935 | 6,350 | ||||
Total |
$ | 32,066 | $ | 38,493 | ||
69
9. Notes Payable
Notes payable as of December 31, 2019 and 2018 consisted of the following (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||
Credit Agreement average effective interest rate of 3.9% inclusive of unused fee |
$ | 46,000 | $ | 38,000 | ||
Various notes payable with $728 plus accrued interest due in the next year, interest accrues in the range of 4.75% through 5.50% per annum |
5,089 | 1,836 | ||||
$ | 51,089 | $ | 39,836 | |||
Less current portion |
(728 | ) |
(1,434 | ) |
||
Long term portion |
$ | 50,361 | $ | 38,402 | ||
Effective December 5, 2013, the Company entered into an Amended and Restated Credit Agreement with a commitment for a $125.0 million revolving credit facility. This agreement was amended in August 2015, January 2016, March 2017 and November 2017 (hereafter referred to as “Amended Credit Agreement”). The Amended Credit Agreement is unsecured and has loan covenants, including requirements that the Company comply with a consolidated fixed charge coverage ratio and consolidated leverage ratio. Proceeds from the Amended Credit Agreement may be used for working capital, acquisitions, purchases of the Company’s common stock, dividend payments to the Company’s common stockholders, capital expenditures and other corporate purposes. The pricing grid which is based on the Company’s consolidated leverage ratio with the applicable spread over LIBOR ranging from 1.25% to 2.0% or the applicable spread over the Base Rate ranging from 0.1% to 1%. Fees under the Amended Credit Agreement include an unused commitment fee ranging from 0.25% to 0.3% depending on the Company’s consolidated leverage ratio and the amount of funds outstanding under the Amended Credit Agreement.
The January 2016 amendment to the Amended Credit Agreement increased the cash and noncash consideration that the Company could pay with respect to acquisitions permitted under the Amended Credit Agreement to $50,000,000 for any fiscal year, and increased the amount the Company may pay in cash dividends to its shareholders in an aggregate amount not to exceed $10,000,000 in any fiscal year. The March 2017 amendment, among other items, increased the amount the Company may pay in cash dividends to its shareholders in an aggregate amount not to exceed $15,000,000 in any fiscal year. The November 2017 amendment, among other items, adjusted the pricing grid as described above, increased the aggregate amount the Company may pay in cash dividends to its shareholders to an amount not to exceed $20,000,000 and extended the maturity date to November 30, 2021.
On December 31, 2019, $46.0 million was outstanding on the Credit Agreement resulting in $79.0 million of availability. As of December 31, 2019, the Company was in compliance with all of the covenants thereunder.
The Company generally enters into various notes payable as a means of financing a portion of its acquisitions and purchasing of non-controlling interests. In conjunction with the transactions related to these in 2019, the Company entered into notes payable in the aggregate amount of $4.7 million of which an aggregate principal payment of $0.3 million is due in 2020 and $4.4 million is due in 2021. Interest accrues in the range of 4.75% to 5.50% per annum and is payable with each principal installment.
Aggregate annual payments of principal required pursuant to the Credit Agreement and the various notes payable subsequent to December 31, 2019 are as follows (in thousands):
During the twelve months ended December 31, 2020 |
$ | 728 | |
During the twelve months ended December 31, 2021 |
50,361 | ||
$ | 51,089 |
70
10. Leases
The Company has operating leases for its corporate offices and operating facilities. The Company determines if an arrangement is a lease at the inception of a contract. Effective January 1, 2019, right-of-use assets and operating lease liabilities are included in the consolidated balance sheet. Right-of-use assets represent the Company’s right to use an underlying asset during the lease term and operating lease liabilities represent net present value of the Company’s obligation to make lease payments arising from the lease. Right-of-use assets and operating lease liabilities are recognized at commencement date based on the net present value of the fixed lease payments over the lease term. The Company’s operating lease terms are generally five years or less. The Company’s lease terms include options to extend or terminate the lease when it is reasonably certain that the option will be exercised. As most of the Company’s operating leases do not provide an implicit rate, the Company uses its incremental borrowing rate based on the information available at commencement date in determining the present value of lease payments. Operating fixed lease expense is recognized on a straight-line basis over the lease term.
In accordance with ASC 842, the Company records on its consolidated balance sheet leases with a term greater than 12 months. The Company has elected, in compliance with current accounting standards, not to record leases with an initial terms of 12 months or less in the consolidated balance sheet. ASC 842 requires the separation of the fixed lease components from the variable lease components. The Company has elected the practical expedient to account for separate lease components of a contract as a single lease cost thus causing all fixed payments to be capitalized. Non-lease and variable cost components are not included in the measurement of the right-of-use assets or operating lease liabilities. The Company also elected the package of practical expedients permitted within ASC 842, which among other things, allows the Company to carry forward historical lease classification. Variable lease payment amounts that cannot be determined at the commencement of the lease such as increases in lease payments based on changes in index rates or usage are not included in the right-of-use assets or operating lease liabilities. These are expensed as incurred and recorded as variable lease expense.
For the year ended December 31, 2019, the components of lease expense were as follows (in thousands):
Year Ended December 31, 2019 |
|||
Operating lease cost |
$ | 30,225 | |
Short-term lease cost |
1,212 | ||
Variable lease cost |
6,074 | ||
Total lease cost* |
$ | 37,511 | |
| * | Sublease income was immaterial |
Lease cost is reflected in the consolidated statement of net income in the line item – rent, supplies, contract labor and other.
For the year ended December 31, 2019, supplemental cash flow information related to leases was as follows (in thousands):
Year Ended December 31, 2019 |
|||
Cash paid for amounts included in the measurement of operating lease liabilities (in thousands) |
$ | 30,077 | |
Right-of-use assets obtained in exchange for new operating lease liabilities (in thousands)* |
$ | 113,222 | |
| * | Includes the right-of-use assets obtained in exchange for lease liabilities of $82.6 million which were recognized upon adoption of ASC Topic 842 at January 1, 2019. |
71
The aggregate future lease payments for operating leases as of December 31, 2019 were as follows (in thousands):
Year |
Amount |
||
2020 |
$ | 29,279 | |
2021 |
23,369 | ||
2022 |
17,039 | ||
2023 |
11,528 | ||
2024 |
6,453 | ||
Therafter |
6,129 | ||
Total lease payments |
$ | 93,797 | |
Less: imputed interest |
7,053 | ||
Total operating lease liabilities |
$ | 86,744 | |
Average lease terms and discount rates were as follows:
Year Ended December 31, 2019 |
|||
Weighted-average remaining lease term - Operating leases |
4.05 Years |
||
Weighted-average discount rate - Operating leases |
3.9 | % |
|
11. Income Taxes
Significant components of deferred tax assets and liabilities included in the consolidated balance sheets at December 31, 2019 and 2018 were as follows (in thousands):
December 31, 2019 |
December 31, 2018 |
|||||
Deferred tax assets: |
||||||
Compensation |
$ | 1,964 | $ | 1,842 | ||
Allowance for doubtful accounts |
514 | 600 | ||||
Acquired net operating losses |
840 | — | ||||
Lease obligations - including closed clinics |
21,445 | 34 | ||||
Deferred tax assets |
$ | 24,763 | $ | 2,476 | ||
Deferred tax liabilities: |
||||||
Depreciation and amortization |
$ | (13,195 | ) |
$ | (11,309 | ) |
Operating lease right-of-use assets |
(21,416 | ) |
— | |||
Other |
(223 | ) |
(179 | ) |
||
Deferred tax liabilities |
(34,834 | ) |
(11,488 | ) |
||
Net deferred tax liability |
$ | (10,071 | ) |
$ | (9,012 | ) |
The deferred tax assets and liabilities related to purchased interests not yet finalized may result in an immaterial adjustment.
During 2019, the Company recorded deferred tax assets of $3.0 million related to the revaluation of redeemable non-controlling interests and acquisitions of non-controlling interests. In addition, during 2019, the Company recorded an adjustment to the deferred tax assets of $0.3 million as a result of a detailed reconciliation of its federal and state taxes payable and receivable accounts along with its federal and state deferred tax asset and liability accounts with its federal and state tax returns for 2018. The offset of this adjustment was a decrease to the previously reported federal income tax receivable. As of December 31, 2019, the Company has a federal income tax receivable of $1.5 million and state tax receivables of $1.3 million. The tax receivables are included in other current assets on the accompanying consolidated balance sheets.
72
The differences between the federal tax rate and the Company’s effective tax rate for the years ended December 31, 2019, 2018 and 2017 were as follows (in thousands):
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
||||||||||||||||
U. S. tax at statutory rate |
$ | 11,274 | 21.0 | % |
$ | 9,710 | 21.0 | % |
$ | 9,900 | 35.0 | % |
||||||
Tax legislation adjustment |
— | 0.0 | % |
— | 0.0 | % |
(4,325 | ) |
(15.3 | )% |
||||||||
State income taxes, net of federal benefit and tax reform |
2,059 | 3.8 | % |
1,722 | 3.7 | % |
1,060 | 3.7 | % |
|||||||||
Excess equity compensation deduction |
(871 | ) |
(1.6 | )% |
(806 | ) |
(1.7 | )% |
(1,139 | ) |
(4.0 | )% |
||||||
Non-deductible expenses |
1,185 | 2.2 | % |
743 | 1.6 | % |
560 | 2.0 | % |
|||||||||
Other |
— | 0.0 | % |
— | 0.0 | % |
(24 | ) |
(0.1 | )% |
||||||||
$ | 13,647 | 25.4 | % |
$ | 11,369 | 24.6 | % |
$ | 6,032 | 21.3 | % |
|||||||
As a result of TCJA, the Company revalued its deferred tax assets and liabilities as of December 31, 2017. Based on a review and analysis as of December 31, 2017, the Company estimated a reduction of its net deferred tax liabilities by $4.3 million thereby reducing its provision for income taxes by such amount for the 2017 year.
Significant components of the provision for income taxes for the years ended December 31, 2019, 2018 and 2017 were as follows (in thousands):
December 31, 2019 |
December 31, 2018 |
December 31, 2017 |
|||||||
Current: |
|||||||||
Federal |
$ | 6,523 | $ | 5,357 | $ | 9,332 | |||
State |
2,473 | 1,199 | 1,564 | ||||||
Total current |
8,996 | 6,556 | 10,896 | ||||||
Deferred: |
|||||||||
Federal |
3,730 | 3,771 | (5,233 | ) |
|||||
State |
921 | 1,042 | 369 | ||||||
Total deferred |
4,651 | 4,813 | (4,864 | ) |
|||||
Total income tax provision |
$ | 13,647 | $ | 11,369 | $ | 6,032 | |||
For 2019, 2018 and 2017, the Company performed a detailed reconciliation of its federal and state taxes payable and receivable accounts along with its federal and state deferred tax asset and liability accounts. The adjustments were immaterial. The Company considers this reconciliation process to be an annual control.
The Company is required to establish a valuation allowance for deferred tax assets if, based on the weight of available evidence, it is more likely than not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income during the periods in which those temporary differences become deductible. Management considers the projected future taxable income and tax planning strategies in making this assessment. Based upon the level of historical taxable income and projections for future taxable income in the periods which the deferred tax assets are deductible, management believes that a valuation allowance is not required, as it is more likely than not that the results of future operations will generate sufficient taxable income to realize the deferred tax assets.
The Company’s U.S. federal returns remain open to examination for 2016 through 2018 and U.S. state jurisdictions are open for periods ranging from 2015 through 2018.
The Company does not believe that it has any significant uncertain tax positions at December 31, 2019 and December 31, 2018, nor is this expected to change within the next twelve months due to the settlement and expiration of statutes of limitation.
The Company did not have any accrued interest or penalties associated with any unrecognized tax benefits nor was any interest expense recognized during the years ended December 31, 2019, 2018 and 2017.
73
12. Equity Based Plans
The Company has the following equity based plans with outstanding equity grants:
The Amended and Restated 1999 Employee Stock Option Plan (the “Amended 1999 Plan”) permits the Company to grant to non-employee directors and employees of the Company up to 600,000 non-qualified options to purchase shares of common stock and restricted stock (subject to proportionate adjustments in the event of stock dividends, splits, and similar corporate transactions). The exercise prices of options granted under the Amended 1999 Plan are determined by the Compensation Committee. The period within which each option will be exercisable is determined by the Compensation Committee. The Amended 1999 Plan was approved by the shareholders of the Company at the 2008 Shareholders Meeting on May 20, 2008.
The Amended and Restated 2003 Stock Option Plan (the “Amended 2003 Plan”) permits the Company to grant to key employees and outside directors of the Company incentive and non-qualified options and shares of restricted stock covering up to 2,100,000 shares of common stock (subject to proportionate adjustments in the event of stock dividends, splits, and similar corporate transactions). The material terms of the Amended 2003 Plan was reapproved by the shareholders of the Company at the 2015 Shareholders Meeting on May 19, 2015 and an increase in the number of shares authorized for issuance from 1,750,000 to 2,100,000 was approved at the 2016 Shareholders Meeting on March 17, 2016.
A cumulative summary of equity plans as of December 31, 2019 follows:
Authorized |
Restricted Stock Issued |
Outstanding Stock Options |
Stock Options Exercised |
Stock Options Exercisable |
Shares Available for Grant |
|||||||||||||
Equity Plans |
||||||||||||||||||
Amended 1999 Plan |
600,000 | 416,402 | — | 139,791 | — | 7,775 | ||||||||||||
Amended 2003 Plan |
2,100,000 | 1,019,995 | — | 778,300 | — | 301,705 | ||||||||||||
2,700,000 | 1,436,397 | — | 918,091 | — | 309,480 | |||||||||||||
During 2019, 2018 and 2017, the Company granted the following shares of restricted stock to directors, officers and employees pursuant to its equity plans as follows:
Year Granted |
Number of Shares |
Weighted Average Fair Value Per Share |
||||
2019 |
91,682 | $ | 104.85 | |||
2018 |
93,801 | $ | 78.63 | |||
2017 |
79,475 | $ | 62.19 | |||
During 2019, 2018 and 2017, the following shares were cancelled due to employee terminations prior to restrictions lapsing:
Year Cancelled |
Number of Shares |
Weighted Average Fair Value Per Share |
||||
2019 |
1,578 | $ | 87.88 | |||
2018 |
3,867 | $ | 59.51 | |||
2017 |
2,875 | $ | 63.12 | |||
Generally, restrictions on the stock granted to employees lapse in equal annual installments on the following four anniversaries of the date of grant. For those shares granted to directors, the restrictions will lapse in equal quarterly installments during the first year after the date of grant. For those granted to officers, the restriction will lapse in equal quarterly installments during the four years following the date of grant.
There were 150,771 and 152,926 shares outstanding as of December 31, 2019 and December 31, 2018 respectively, for which restrictions had not lapsed. The restrictions will lapse in 2020 through 2023.
Compensation expense for grants of restricted stock is recognized based on the fair value on the date of grant. Compensation expense for restricted stock grants was $7.0 million, $5.9 million, and $5.0 million, respectively, for 2019, 2018 and 2017. As of December 31, 2019, the remaining $9.2 million of compensation expense will be recognized from 2019 through 2022.
74
13. Preferred Stock
The Board is empowered, without approval of the shareholders, to cause shares of preferred stock to be issued in one or more series and to establish the number of shares to be included in each such series and the rights, powers, preferences and limitations of each series. There are no provisions in the Company’s Articles of Incorporation specifying the vote required by the holders of preferred stock to take action. All such provisions would be set out in the designation of any series of preferred stock established by the Board. The bylaws of the Company specify that, when a quorum is present at any meeting, the vote of the holders of at least a majority of the outstanding shares entitled to vote who are present, in person or by proxy, shall decide any question brought before the meeting, unless a different vote is required by law or the Company’s Articles of Incorporation.
Because the Board has the power to establish the preferences and rights of each series, it may afford the holders of any series of preferred stock, preferences, powers, and rights, voting or otherwise, senior to the right of holders of common stock. The issuance of the preferred stock could have the effect of delaying or preventing a change in control of the Company.
14. Common Stock
From September 2001 through December 31, 2008, the Board authorized the Company to purchase, in the open market or in privately negotiated transactions, up to 2,250,000 shares of the Company’s common stock. In March 2009, the Board authorized the repurchase of up to 10% or approximately 1,200,000 shares of its common stock (“March 2009 Authorization”). The Amended Credit Agreement permits share repurchases of up to $15,000,000, subject to compliance with covenants. The Company is required to retire shares purchased under the March 2009 Authorization.
Under the March 2009 Authorization, the Company has purchased a total of 859,499 shares. There is no expiration date for the share repurchase program. There are currently an additional estimated 131,176 shares (based on the closing price of $114.35 on December 31, 2019, the last business day in 2019) that may be purchased from time to time in the open market or private transactions depending on price, availability and the Company’s cash position. The Company did not purchase any shares of its common stock during 2019 or 2018.
15. Defined Contribution Plan
The Company has several 401(k) profit sharing plans covering all employees with three months of service. For certain plans, the Company makes matching contributions. The Company may also make discretionary contributions of up to 50% of employee contributions. The Company did not make any discretionary contributions for the years ended December 31, 2019, 2018 and 2017. The Company matching contributions totaled $2.0 million, $1.8 million and $1.5 million, respectively, for the years ended December 31, 2019, 2018 and 2017.
16. Commitments and Contingencies
Operating Leases
The Company has entered into operating leases for its executive offices and clinic facilities. In connection with these agreements, the Company incurred rent expense of $37.5 million, $37.1 million and $34.8 million for the years ended December 31, 2019, 2018 and 2017, respectively. Several of the leases provide for an annual increase in the rental payment based upon the Consumer Price Index. The majority of the leases provide for renewal periods ranging from one to five years. The agreements to extend the leases typically specify that rental rates would be adjusted to market rates as of each renewal date.
The future minimum operating lease commitments for each of the next five years and thereafter and in the aggregate as of December 31, 2019 are as follows (in thousands):
2020 |
$ | 35,784 | |
2021 |
28,022 | ||
2022 |
20,618 | ||
2023 |
14,332 | ||
2024 |
8,302 | ||
Thereafter |
8,432 | ||
Total |
$ | 115,490 |
75
Employment Agreements
At December 31, 2019, the Company had outstanding employment agreements with four of its executive officers one of which has provided notice of a planned retirement in October 2020. These remaining three agreements, which presently expire on December 31, 2020, provide for automatic two year renewals at the conclusion of each expiring term or renewal term. All of the agreements contain a provision for annual adjustment of salaries.
In addition, the Company has outstanding employment agreements with most of the managing physical therapist partners of the Company’s physical therapy clinics and with certain other clinic employees which obligate subsidiaries of the Company to pay compensation of $39.3 million in 2020 and $8.6 million in the aggregate from 2021 through 2023. In addition, many of the employment agreements with the managing physical therapists provide for monthly bonus payments calculated as a percentage of each clinic’s net revenues (not in excess of operating profits) or operating profits.
17. Earnings Per Share
The computations of basic and diluted earnings per share for the years ended December 31, 2019, 2018 and 2017 are as follows (in thousands, except per share data):
Year Ended December 31, 2019 |
Year Ended December 31, 2018 |
Year Ended December 31, 2017 |
|||||||
Computation of earnings per share - USPH shareholders: |
|||||||||
Net income attributable to USPH shareholders |
$ | 40,039 | $ | 34,873 | $ | 22,256 | |||
Charges to retained earnings: |
|||||||||
Revaluation of redeemable non-controlling interest |
(11,893 | ) |
(24,770 | ) |
(201 | ) |
|||
Tax effect at statutory rate (federal and state) of 26.25% |
3,121 | 6,502 | 75 | ||||||
$ | 31,267 | $ | 16,605 | $ | 22,130 | ||||
Earnings per share (basic and diluted) |
$ | 2.45 | $ | 1.31 | $ | 1.76 | |||
Shares used in computation: |
|||||||||
Basic and diluted earnings per share - weighted-average shares |
12,756 | 12,666 | 12,570 | ||||||
18. Selected Quarterly Financial Data (Unaudited)
Q1 2019 |
Q2 2019 |
Q3 2019 |
Q4 2019 |
|||||||||
Net patient revenues |
$ | 106,650 | $ | 113,363 | $ | 104,392 | $ | 108,940 | ||||
Net revenues |
$ | 116,231 | $ | 126,373 | $ | 117,251 | $ | 122,114 | ||||
Gross profit |
$ | 26,718 | $ | 31,425 | $ | 27,372 | $ | 26,959 | ||||
Operating income |
$ | 15,425 | $ | 19,898 | $ | 16,816 | $ | 15,286 | ||||
Net income |
$ | 12,375 | $ | 19,800 | $ | 13,069 | $ | 12,015 | ||||
Net income attributable to USPH shareholders |
$ | 8,443 | $ | 14,620 | $ | 9,047 | $ | 7,929 | ||||
Basic and diluted earnings per share attributable to common shareholders: |
$ | 0.39 | $ | 0.85 | $ | 0.66 | $ | 0.55 | ||||
Shares used in computation - basic and diluted |
12,707 | 12,767 | 12,774 | 12,774 | ||||||||
76
Q1 2018 |
Q2 2018 |
Q3 2018 |
Q4 2018 |
|||||||||
Net patient revenues |
$ | 100,552 | $ | 105,989 | $ | 103,354 | $ | 107,808 | ||||
Net revenues |
$ | 108,342 | $ | 115,098 | $ | 113,122 | $ | 117,349 | ||||
Gross profit |
$ | 23,214 | $ | 27,154 | $ | 26,076 | $ | 25,219 | ||||
Operating income |
$ | 13,051 | $ | 17,026 | $ | 15,433 | $ | 14,804 | ||||
Net income |
$ | 10,054 | $ | 13,236 | $ | 11,879 | $ | 13,673 | ||||
Net income attributable to USPH shareholders |
$ | 7,117 | $ | 9,246 | $ | 8,102 | $ | 10,408 | ||||
Basic and diluted earnings per share attributable to common shareholders: |
$ | 0.27 | $ | 0.48 | $ | 0.13 | $ | 0.43 | ||||
Shares used in computation - basic and diluted |
12,616 | 12,677 | 12,685 | 12,685 | ||||||||
77
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE. |
Not applicable.
| ITEM 9A. | CONTROLS AND PROCEDURES. |
Evaluation of Disclosure Controls and Procedures
Our management, including our Chief Executive Officer and Chief Financial Officer, has conducted an evaluation of the effectiveness of our disclosure controls and procedures (as defined in Rule 13a-15(e) promulgated under the Exchange Act) as of the end of the fiscal period covered by this report. Based upon that evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that our disclosure controls and procedures are effective in ensuring that the information required to be disclosed in the reports we file or submit under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the rules and forms of the SEC and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding disclosure.
Management’s Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rule 13a-15(f) under the Exchange Act. U.S. Physical Therapy, Inc. and subsidiaries’ (the “Company”) internal control over financial reporting is designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles.
Internal control over financial reporting includes those policies and procedures that:
| • | Pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the Company; |
| • | Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of the Company’s management and directors; and |
| • | Provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the Company’s assets that could have a material effect on the financial statements. |
Internal control over financial reporting cannot provide absolute assurance of achieving financial reporting objectives because of its inherent limitations. Internal control over financial reporting is a process that involves human diligence and compliance and is subject to lapses in judgment and breakdowns resulting from human failures. Internal control over financial reporting can also be circumvented by collusion or improper management override. Because of such limitations, there is a risk that material misstatements may not be prevented or detected on a timely basis by internal control over financial reporting. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. However, these inherent limitations are known features of the financial reporting process. Therefore, it is possible to design into the process safeguards to reduce, though not eliminate, the risk.
Management conducted an assessment of the effectiveness of our internal control over financial reporting as of December 31, 2019. In making this assessment, management used the criteria described in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this assessment, management concluded that our internal control over financial reporting was effective as of December 31, 2019.
The Company’s internal control over financial reporting has been audited by Grant Thornton LLP, an independent registered public accounting firm, as stated in their report included on page 45.
78
Changes in Internal Control over Financial Reporting
There have been no changes in our internal control over financial reporting during the quarter ended December 31, 2019 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
| ITEM 9B. | OTHER INFORMATION. |
Not applicable.
PART III
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE. |
The information required in response to this Item 10 is incorporated herein by reference to our definitive proxy statement relating to our 2020 Annual Meeting of Stockholders to be filed with the SEC pursuant to Regulation 14A, not later than 120 days after the end of our fiscal year covered by this report.
| ITEM 11. | EXECUTIVE COMPENSATION. |
The information required in response to this Item 11 is incorporated herein by reference to our definitive proxy statement relating to our 2020 Annual Meeting of Stockholders to be filed with the SEC pursuant to Regulation 14A, not later than 120 days after the end of our fiscal year covered by this report.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS. |
The information required in response to this Item 12 is incorporated herein by reference to our definitive proxy statement relating to our 2020 Annual Meeting of Stockholders to be filed with the SEC pursuant to Regulation 14A, not later than 120 days after the end of our fiscal year covered by this report.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE. |
The information required in response to this Item 13 is incorporated herein by reference to our definitive proxy statement relating to our 2020 Annual Meeting of Stockholders to be filed with the SEC pursuant to Regulation 14A, not later than 120 days after the end of our fiscal year covered by this report.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES. |
The information required in response to this Item 14 is incorporated herein by reference to our definitive proxy statement relating to our 2020 Annual Meeting of Stockholders to be filed with the SEC pursuant to Regulation 14A, not later than 120 days after the end of our fiscal year covered by this report.
PART IV
| ITEM 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES. |
| (a) | Documents filed as a part of this report: |
| 1. | Financial Statements. Reference is made to the Index to Financial Statements and Related Information under Item 8 in Part II hereof, where these documents are listed. |
| 2. | Financial Statement Schedules. See page 84 for Schedule II — Valuation and Qualifying Accounts. All other schedules are omitted because of the absence of conditions under which they are required or because the required information is shown in the financial statements or notes thereto. |
| 3. | Exhibits. The exhibits listed in List of Exhibits on the next page are filed or incorporated by reference as part of this report. |
| ITEM 16. | Form 10-K Summary – |
None.
79
EXHIBIT INDEX
LIST OF EXHIBITS
|
Number
|
Description
|
|
3.1
|
Articles of Incorporation of the Company [filed as an exhibit to the Company’s Form 10-Q for the quarterly period ended June 30, 2001 and incorporated herein by reference].
|
|
|
|
|
3.2
|
Amendment to the Articles of Incorporation of the Company [filed as an exhibit to the Company’s Form 10-Q for the quarterly period ended June 30, 2001 and incorporated herein by reference].
|
|
|
|
|
3.3
|
Bylaws of the Company, as amended [filed as an exhibit to the Company’s Form 10-KSB for the year ended December 31, 1993 and incorporated herein by reference—Commission File Number—1-11151].
|
|
|
|
|
4.1*
|
Description of Company Securities [filed herewith the Company’s Form 10-K for the year ended December 31, 2019 filed with the SEC on February 28, 2020.]
|
|
|
|
|
10.1+
|
1999 Employee Stock Option Plan (as amended and restated May 20, 2008) [incorporated by reference to Appendix A to the Company’s Definitive Proxy Statement on Schedule 14A, filed with the SEC on April 17, 2008].
|
|
|
|
|
10.2+
|
U.S. Physical Therapy, Inc. 2003 Stock Incentive Plan, (as amended and restated effective March 26, 2016) [incorporated herein by reference to Appendix A to the Company's Definitive Proxy Statement on Schedule 14A filed with the SEC on April 7, 2016.]
|
|
|
|
|
10.3+
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.1 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.4+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.2 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.5+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.3 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.6+
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.1 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.7+
|
U. S. Physical Therapy, Inc. Discretionary Long-Term Incentive Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.2 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.8+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.3 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.9+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.4 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
80
|
Number
|
Description
|
|
10.10+
|
U. S. Physical Therapy, Inc. Long Term Incentive Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
10.11+
|
U. S. Physical Therapy, Inc. Discretionary Long Term Incentive Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
10.12+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
10.13+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
10.14+
|
U. S. Physical Therapy, Inc. Objective Long Term Incentive Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
10.15+
|
U. S. Physical Therapy, Inc. Discretionary Long Term Incentive Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
10.16+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
10.17+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
10.18+
|
Form of Restricted Stock Agreement [incorporated by reference to Exhibit 10.5 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
10.19+
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K/A filed with the SEC on February 9, 2018.]
|
|
|
|
|
10.20+
|
U. S. Physical Therapy, Inc. Discretionary Long –Term Incentive Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
|
10.21+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
|
10.22+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
81
|
Number
|
Description
|
|
10.23+
|
U. S. Physical Therapy, Inc. Objective Long-Term Incentive Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
10.24+
|
U. S. Physical Therapy, Inc. Discretionary Long-Term Incentive Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
10.25+
|
U. S. Physical Therapy, Inc. Objective Cash/RSA Bonus Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
10.26+
|
U. S. Physical Therapy, Inc. Discretionary Cash/RSA Bonus Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
10.27+
|
Second Amended and Restated Credit Agreement dated as of November 10, 2017 among the Company, as Borrower, Bank of America, N.A. as Administrative Agent and the Lenders Patty (incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on November 14, 2017).
|
|
|
|
|
10.28+
|
Second Amended and Restated Employment Agreement by and between the Company and Christopher J. Reading dated effective February 9, 2016 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
10.29+
|
Second Amended and Restated Employment Agreement by and between the Company and Lawrance W. McAfee dated effective February 9, 2016 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
10.30+
|
Amended and Restated Employment Agreement by and between the Company and Glenn D. McDowell dated effective February 9, 2016 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
10.31+
|
Employment Agreement commencing on March 1, 2018 by and between the Company and Graham Reeve [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 7, 2018].
|
|
|
|
|
10.32+
|
Objective Long-Term Incentive Plan for Senior Management [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
10.33+
|
Discretionary Long-Term Incentive Plan for Senior Management [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
10.34+
|
Objective Cash/RSA Bonus Plan for Senior Management [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
10.35+
|
Discretionary Cash/RSA Bonus Plan for Senior Management [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
82
|
Number
|
Description
|
|
10.36+
|
Third Amended and Restated Employment Agreement by and between the Company and Christopher J. Reading dated effective May 21, 2019 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
10.37+
|
Third Amended and Restated Employment Agreement by and between the Company and Lawrance W. McAfee dated effective May 21, 2019 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
10.38+
|
Second Amended and Restated Employment Agreement by and between the Company and Glenn D. McDowell dated effective May 21, 2019 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
10.39+
|
Amended & Restated Employment Agreement commencing by and between the Company and Graham Reeve dated effective May 21, 2019 [incorporated by reference to Exhibit 10.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
10.40+
|
Restricted Stock Agreement [incorporated by reference to Exhibit 10.5 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
21.1*
|
Subsidiaries of the Registrant
|
|
|
|
|
23.1*
|
Consent of Independent Registered Public Accounting Firm—Grant Thornton LLP
|
|
|
|
|
31.1*
|
Certification of Chief Executive Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
31.2*
|
Certification of Chief Financial Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
31.3*
|
Certification of Controller pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
32.1*
|
Certification of Periodic Report of the Chief Executive Officer, Chief Financial Officer and Controller pursuant to Rule 13a-14(b) of the Securities Exchange Act of 1934, as amended, and 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002
|
|
|
|
|
101.INS*
|
XBRL Instance Document
|
|
|
|
|
101.SCH*
|
XBRL Taxonomy Extension Schema Document
|
|
|
|
|
101.CAL*
|
XBRL Taxonomy Extension Calculation Linkbase Document
|
|
|
|
|
101.DEF*
|
XBRL Taxonomy Extension Definition Linkbase Document
|
|
|
|
|
101.LAB*
|
XBRL Taxonomy Extension Label Linkbase Document
|
|
|
|
|
101.PRE*
|
XBRL Taxonomy Extension Presentation Linkbase Document
|
| * | Filed herewith |
| + | Management contract or compensatory plan or arrangement. |
83
FINANCIAL STATEMENT SCHEDULE*
SCHEDULE II — VALUATION AND QUALIFYING ACCOUNTS
U.S. PHYSICAL THERAPY, INC. AND SUBSIDIARIES
Balance at Beginning of Period |
Additions Charged to Costs and Expenses |
Additions Charged to Other Accounts |
Deductions |
Balance at End of Period |
|||||||||||
YEAR ENDED DECEMBER 31, 2019: |
|||||||||||||||
Reserves and allowances deducted from asset accounts: |
|||||||||||||||
Allowance for doubtful accounts(1) |
$ | 2,672 | $ | 4,858 | — | $ | 4,832(2 | ) |
$ | 2,698 | |||||
YEAR ENDED DECEMBER 31, 2018: |
|||||||||||||||
Reserves and allowances deducted from asset accounts: |
|||||||||||||||
Allowance for doubtful accounts |
$ | 2,273 | $ | 4,603 | — | $ | 4,204(2 | ) |
$ | 2,672 | |||||
YEAR ENDED DECEMBER 31, 2017: |
|||||||||||||||
Reserves and allowances deducted from asset accounts: |
|||||||||||||||
Allowance for doubtful accounts |
$ | 1,792 | $ | 3,672 | — | $ | 3,191(2 | ) |
$ | 2,273 | |||||
| (1) | Related to patient accounts receivable and accounts receivable—other. |
| (2) | Uncollectible accounts written off, net of recoveries. |
| * | All other schedules are omitted because of the absence of conditions under which they are required or because the required information is shown in the financial statements or notes thereto. |
84
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
U.S. PHYSICAL THERAPY, INC.
|
|
|
|
|
(Registrant)
|
|
|
|
|
|
|
By:
|
/s/ Lawrance W. McAfee
|
|
|
|
Lawrance W. McAfee
|
|
|
|
Chief Financial Officer
|
|
|
|
|
|
|
By:
|
/s/ Jon C. Bates
|
|
|
|
Jon C. Bates
|
|
|
|
Vice President/Controller
|
Date: February 28, 2020
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities indicated as of the date indicated above.
|
/s/ Chris J. Reading
|
Chief Executive Officer, President and Director
(Principal Executive Officer) |
February 28, 2020
|
|
Chris J. Reading
|
||
|
|
|
|
|
/s/ Lawrance W. McAfee
|
Executive Vice President, Chief Financial Officer and Director (Principal Financial Officer and Principal Accounting Officer)
|
February 28, 2020
|
|
Lawrance W. McAfee
|
||
|
|
|
|
|
/s/ Jerald L. Pullins
|
Chairman of the Board
|
February 28, 2020
|
|
Jerald L. Pullins
|
|
|
|
|
|
|
|
/s/ Mark J. Brookner
|
Director
|
February 28, 2020
|
|
Mark J. Brookner
|
|
|
|
|
|
|
|
/s/ Harry S. Chapman
|
Director
|
February 28, 2020
|
|
Harry S. Chapman
|
|
|
|
|
|
|
|
/s/ Bernard A. Harris
|
Director
|
February 28, 2020
|
|
Dr. Bernard A. Harris, Jr.
|
|
|
|
|
|
|
|
/s/ Kathleen A. Gilmartin
|
Director
|
February 28, 2020
|
|
Kathleen A. Gilmartin
|
|
|
|
|
|
|
|
/s/ Edward L. Kuntz
|
Director
|
February 28, 2020
|
|
Edward L. Kuntz
|
|
|
|
|
|
|
|
/s/ Reginald E. Swanson
|
Director
|
February 28, 2020
|
|
Reginald E. Swanson
|
|
|
|
|
|
|
|
/s/ Clayton K. Trier
|
Director
|
February 28, 2020
|
|
Clayton K. Trier
|
|
|
85
EXHIBIT INDEX (NOT UPDATED)
LIST OF EXHIBITS
|
Number
|
Description
|
|
Articles of Incorporation of the Company [filed as an exhibit to the Company’s Form 10-Q for the quarterly period ended June 30, 2001 and incorporated herein by reference].
|
|
|
|
|
|
Amendment to the Articles of Incorporation of the Company [filed as an exhibit to the Company’s Form 10-Q for the quarterly period ended June 30, 2001 and incorporated herein by reference].
|
|
|
|
|
|
3.3
|
Bylaws of the Company, as amended [filed as an exhibit to the Company’s Form 10-KSB for the year ended December 31, 1993 and incorporated herein by reference—Commission File Number—1-11151].
|
|
|
|
|
Description of Company Securities [filed herewith the Company’s Form 10-K for the year ended December 31, 2019 filed with the SEC on February 28, 2020.]
|
|
|
|
|
|
10.1+
|
1999 Employee Stock Option Plan (as amended and restated May 20, 2008) [incorporated by reference to Appendix A to the Company’s Definitive Proxy Statement on Schedule 14A, filed with the SEC on April 17, 2008].
|
|
|
|
|
10.2+
|
Form of Restricted Stock Agreement [incorporated by reference to Exhibit 10.17 to the Company’s Annual Report on Form 10-K filed with the SEC on March 12, 2013.]
|
|
|
|
|
10.3+
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.1 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.4+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.2 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.5+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for 2013, effective March 27, 2013 [incorporated by reference to Exhibit 99.3 to the Company Current Report on Form 8-K filed with the SEC on April 1, 2013].
|
|
|
|
|
10.6+
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.1 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.7+
|
U. S. Physical Therapy, Inc. Discretionary Long-Term Incentive Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.2 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.8+
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.3 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
10.9+
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2014, effective March 21, 2014 [incorporated by reference to Exhibit 99.4 to the Company Current Report on Form 8-K filed with the SEC on March 27, 2014].
|
|
|
|
|
U. S. Physical Therapy, Inc. Long Term Incentive Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
86
|
Number
|
Description
|
|
U. S. Physical Therapy, Inc. Discretionary Long Term Incentive Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2015, effective March 23, 2015 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 27, 2015.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Objective Long Term Incentive Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Discretionary Long Term Incentive Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2016, effective March 10, 2016 [incorporated by reference to Exhibit 10.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
|
Form of Restricted Stock Agreement [incorporated by reference to Exhibit 10.5 to the Company’s Current Report on Form 8-K filed with the SEC on March 16, 2016].
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Long-Term Incentive Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K/A filed with the SEC on February 9, 2018.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Discretionary Long –Term Incentive Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Objective Cash Bonus Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Discretionary Cash Bonus Plan for Senior Management for 2017, effective March 24, 2017 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 30, 2017.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Objective Long-Term Incentive Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
|
U.S. Physical Therapy, Inc. Discretionary Long-Term Incentive Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
|
U. S. Physical Therapy, Inc. Objective Cash/RSA Bonus Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
87
|
Number
|
Description
|
|
U. S. Physical Therapy, Inc. Discretionary Cash/RSA Bonus Plan for Senior Management for 2018, effective April 9, 2018 [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on April 12, 2018.]
|
|
|
|
|
|
Second Amended and Restated Credit Agreement dated as of November 10, 2017 among the Company, as Borrower, Bank of America, N.A. as Administrative Agent and the Lenders Patty (incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on November 14, 2017).
|
|
|
|
|
|
Second Amended and Restated Employment Agreement by and between the Company and Christopher J. Reading dated effective February 9, 2016 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
|
Second Amended and Restated Employment Agreement by and between the Company and Lawrance W. McAfee dated effective February 9, 2016 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
|
Amended and Restated Employment Agreement by and between the Company and Glenn D. McDowell dated effective February 9, 2016 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K, filed with the SEC on February 12, 2016].
|
|
|
|
|
|
Employment Agreement commencing on March 1, 2018 by and between the Company and Graham Reeve [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 7, 2018].
|
|
|
|
|
|
Objective Long-Term Incentive Plan for Senior Management [incorporated by reference to Exhibit 99.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
|
Discretionary Long-Term Incentive Plan for Senior Management [incorporated by reference to Exhibit 99.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
|
Objective Cash/RSA Bonus Plan for Senior Management [incorporated by reference to Exhibit 99.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
|
Discretionary Cash/RSA Bonus Plan for Senior Management [incorporated by reference to Exhibit 99.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 8, 2019.]
|
|
|
|
|
|
Third Amended and Restated Employment Agreement by and between the Company and Christopher J. Reading dated effective May 21, 2019 [incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
|
Third Amended and Restated Employment Agreement by and between the Company and Lawrance W. McAfee dated effective May 21, 2019 [incorporated by reference to Exhibit 10.2 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
|
Second Amended and Restated Employment Agreement by and between the Company and Glenn D. McDowell dated effective May 21, 2019 [incorporated by reference to Exhibit 10.3 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
88
|
Number
|
Description
|
|
Amended & Restated Employment Agreement commencing by and between the Company and Graham Reeve dated effective May 21, 2019 [incorporated by reference to Exhibit 10.4 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
|
Restricted Stock Agreement [incorporated by reference to Exhibit 10.5 to the Company’s Current Report on Form 8-K filed with the SEC on March 22, 2019]
|
|
|
|
|
|
21.1*
|
Subsidiaries of the Registrant
|
|
|
|
|
23.1*
|
Consent of Independent Registered Public Accounting Firm—Grant Thornton LLP
|
|
|
|
|
Certification of Chief Executive Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
|
Certification of Chief Financial Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
|
Certification of Controller pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as amended
|
|
|
|
|
|
Certification of Periodic Report of the Chief Executive Officer, Chief Financial Officer and Controller pursuant to Rule 13a-14(b) of the Securities Exchange Act of 1934, as amended, and 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002
|
|
|
|
|
|
101.INS*
|
XBRL Instance Document
|
|
|
|
|
101.SCH*
|
XBRL Taxonomy Extension Schema Document
|
|
|
|
|
101.CAL*
|
XBRL Taxonomy Extension Calculation Linkbase Document
|
|
|
|
|
101.DEF*
|
XBRL Taxonomy Extension Definition Linkbase Document
|
|
|
|
|
101.LAB*
|
XBRL Taxonomy Extension Label Linkbase Document
|
|
|
|
|
101.PRE*
|
XBRL Taxonomy Extension Presentation Linkbase Document
|
| * | Filed herewith |
| + | Management contract or compensatory plan or arrangement. |
89