Attached files
Table of Contents
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) |
| OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the fiscal year ended December 31, 2011 |
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) |
| OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the transition period to |
Commission File Number 001-33744
TRANS1 INC.
(Exact name of Registrant as specified in its charter)
| DELAWARE | 33-0909022 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. employer identification no.) |
301 GOVERNMENT CENTER DRIVE, WILMINGTON, NC 28403
(Address of principal executive office)(Zip code)
(910) 332-1700
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act
| Title of Each Class: |
Name of Each Exchange on which Registered: | |
| Common Stock, par value $0.0001 per share | The NASDAQ Global Stock Market |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. YES ¨ NO þ
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. YES ¨ NO þ
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. YES þ NO ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulations S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). YES þ NO ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. þ
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See the definitions of “large accelerated filer”, accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer ¨ Accelerated filer ¨ Non-accelerated filer ¨ Smaller reporting company þ
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). YES ¨ NO þ
As of June 30, 2011, the last business day of our most recently completed second fiscal quarter, the aggregate market value of the voting and non-voting stock held by non-affiliates of the registrant was approximately $61.7 million, based on the number of shares held by non-affiliates of the registrant as of that date, which was 13,474,574, and the last reported last sale price of the registrant’s common stock on The NASDAQ Global market on that date, which was $4.58. This calculation does not reflect a determination that persons are affiliates for any other purposes.
The number of shares of the registrant’s common stock outstanding as of March 9, 2012 was 27,246,975 shares.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive Proxy Statement on Schedule 14A to be filed with the Securities and Exchange Commission within 120 days after the close of the fiscal year covered by this annual report, relating to the registrant’s 2012 annual meeting of stockholders, are incorporated by reference into Part III of this annual report. With the exception of the portions of the Proxy Statement specifically incorporated herein by reference, the Proxy Statement is not deemed to be filed as part of this annual report.
Table of Contents
TRANS1 INC.
FORM 10-K FOR THE FISCAL YEAR ENDED DECEMBER 31, 2011
Cautionary Note Regarding Forward-Looking Statements
2
Table of Contents
Cautionary Note Regarding Forward-Looking Statements
In addition to historical financial information, this annual report contains “forward-looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended, or the Securities Act, and Section 21E of the Securities Exchange Act of 1934, as amended, or the Exchange Act, that concern matters that involve risks and uncertainties that could cause actual results to differ materially from those projected in the forward-looking statements. These forward-looking statements are intended to qualify for the safe harbor from liability established by the Private Securities Litigation Reform Act of 1995. All statements other than statements of historical fact contained in this annual report, including statements regarding future events, our future financial performance, our future business strategy and the plans and objectives of management for future operations, are forward-looking statements. We have attempted to identify forward-looking statements by terminology including “anticipates,” “believes,” “can,” “continue,” “could,” “estimates,” “expects,” “intends,” “may,” “plans,” “potential,” “predicts,” “should” or “will” or the negative of these terms or other comparable terminology. Although we do not make forward-looking statements unless we believe we have a reasonable basis for doing so, we cannot guarantee their accuracy. Such forward-looking statements are subject to risks, uncertainties and other factors that could cause actual results and the timing of certain events to differ materially from future results expressed or implied by such forward-looking statements. Such risks, uncertainties and other factors that may cause such differences include, but are not limited to, those discussed in the section entitled “Risk Factors” in Part I, Item 1A of this annual report and in other filings we make with the Securities and Exchange Commission, or the SEC. Furthermore, such forward-looking statements speak only as of the date of this annual report. We expressly disclaim any intent or obligation to update any forward-looking statements after the date hereof to conform such statements to actual results or to changes in our opinions or expectations, except as required by applicable law or the rules of the NASDAQ Stock Market.
References in this annual report to “TranS1”, “we”, “our”, “us”, or the “Company” refer to TranS1 Inc.
3
Table of Contents
PART I
| Item 1. | Business |
Overview
We are a medical device company focused on designing, developing and marketing products that implement our proprietary approaches to treat degenerative conditions of the spine affecting the lower lumbar region. We are committed to delivering minimally invasive surgical technologies that enhance patient clinical care while providing sustained value for our customers. Using our pre-sacral approach, a surgeon can access discs in the lower lumbar region of the spine through an incision adjacent to the tailbone and can perform an entire interbody fusion procedure through instrumentation that provides direct access to the intervertebral space. We developed our pre-sacral approach to allow spine surgeons to access and treat intervertebral spaces without compromising important surrounding soft tissue, nerves and bone structures. We currently market the AxiaLIF® family of products for single and two level lumbar fusion, the VEO™ lateral access and interbody fusion system, the Vectre™ and Avatar™ lumbar posterior fixation systems and Bi-Ostetic™ bone void filler, a biologics product. We also market products that may be used with our AxiaLIF surgical approach, including bowel retractors, a bone graft harvesting system and additional discectomy tools. Our philosophy of continuous improvement is driven by ongoing research and development investment in our core technologies. We support this investment by diligently expanding, maintaining, and protecting our significant patent portfolio.
From our incorporation in 2000 through 2004, we devoted substantially all of our resources to research and development and start-up activities, consisting primarily of product design and development, clinical trials, manufacturing, recruiting qualified personnel and raising capital. We received 510(k) clearance from the U.S. Food and Drug Administration, or FDA, for our AxiaLIF 1L product in the fourth quarter of 2004, and commercially introduced our AxiaLIF 1L product in the United States in the first quarter of 2005. We received a CE mark to market our AxiaLIF 1L product in the European market in the first quarter of 2005 and began commercialization in the first quarter of 2006. We received a CE mark for our AxiaLIF 2L product in the third quarter of 2006 and began commercialization in the European market in the fourth quarter of 2006. We received FDA 510(k) clearance for our AxiaLIF 2L product and began marketing this product in the United States in the second quarter of 2008. The AxiaLIF 2L product was discontinued in 2010 after we launched our AxiaLIF 2L+™ product in July 2010, for which we had received FDA 510(k) clearance in January 2010. We commercially launched our next generation Vectre facet screw system in April 2010. In the first quarter of 2010, we entered into agreements to distribute Avatar, a pedicle screw system, and Bi-Ostetic bone void filler, a biologics product. We commercially launched our AxiaLIF 1L+ product in September 2011, for which we had received FDA 510(k) clearance in March 2011. In 2010, we received 510(k) clearance for our lateral access and interbody fusion system, which was commercially launched in November 2011. We currently sell our products through a direct sales force, independent sales agents and international distributors.
As of December 31, 2011, over 12,000 fusion procedures have been performed globally using our AxiaLIF products. On December 31, 2011, we sold our AxiaLIF products through 30 direct sales personnel and 32 independent sales agents in the United States and 2 direct sales personnel and 19 independent distributors internationally. For the year ended December 31, 2011, our revenues were $19.2 million and our net loss was $18.3 million.
Spine Anatomy
The human spine is the core of the human skeleton and provides important structural support while remaining flexible to allow movement. It consists of 33 separate interlocking bones called vertebrae that are connected by soft tissue and provide stability while facilitating motion. Vertebrae are paired into motion segments that move by means of two facet joints and one disc. The facet joints provide stability and enable the spine to bend and twist while the discs absorb pressures and shocks to the vertebrae. Nerves are contained in the spinal column and run through the foramen openings to the rest of the body.
4
Table of Contents
The vertebrae are categorized into five regions: cervical, thoracic, lumbar, sacral and coccyx. The lumbar region, which is at the bottom of the spine and consists of five vertebrae, is capable of limited movement, and primarily functions as support for the body’s weight. The sacrum consists of five fused vertebrae labeled S1 through S5 directly below the lumbar region and that provide attachment for the hipbones as well as protection to organs in the pelvic area. The coccyx, also known as the tailbone, is at the end of the spine.
Medical Conditions Affecting the Lower Lumbar Spine and Traditional Treatment Alternatives
Degenerative disc disease is a common medical condition affecting the lower lumbar spine and refers to the degeneration of the disc from aging and repetitive stresses resulting in a loss of flexibility, elasticity and shock-absorbing properties. As degenerative disc disease progresses, the space between the vertebrae narrows, which can pinch the nerves exiting the spine and result in back pain, leg pain, numbness and loss of motor function. This lower back pain can be overwhelming for patients as the resulting pain can have significant physical, psychological and financial implications.
Treatment alternatives for lower lumbar spine conditions range from non-operative conservative therapies to highly invasive surgical interventions. Conservative therapies are typically the initial treatments selected by patients and physicians and they include rest, bracing, physical therapy, chiropractics, electrical stimulation and medication. When conservative therapies fail to provide adequate pain relief, surgical interventions, including fusion procedures, may be used to address the pain.
Fusion procedures attempt to alleviate lower back pain by removing problematic disc material and permanently joining together two or more opposing vertebrae. This is done in a manner that restores the appropriate space between the vertebrae surrounding the degenerative disc and eliminates mobility of the affected vertebrae. By restoring disc height and eliminating motion, fusion attempts to both stabilize the spine and prevent the pinching of the nerves exiting the spine, thereby reducing pain.
Traditional fusion procedures typically involve an incision in the skin, and cutting muscle or moving organs to gain access to the spine. The degenerated disc is then removed, a process referred to as a discectomy, and a rigid implant, such as a bone graft or cage, is inserted to stabilize the diseased vertebrae. This process is referred to as fixation. The bone graft or cage is intended to promote the growth of bone between the vertebrae. Surgeons often also affix supplementary rods and screws along the spine to provide additional stabilization while the vertebrae fuse together during the six to eighteen months following surgery. The primary surgical fusion procedures performed in the lower lumbar region include: ALIF, PLIF, TLIF and direct lateral.
Anterior Lumbar Interbody Fusion, or ALIF. To perform an ALIF procedure, surgeons access the spine through an incision on the patient’s abdomen which provides them with direct access to the vertebral space for performing a discectomy and inserting bone grafts for fusion. Supporting soft tissue and nerves are manipulated or removed to accommodate the anterior access required by the ALIF procedure. Surgeons commonly perform ALIF procedures in conjunction with a general or vascular surgeon because critical vasculature and organs must be retracted to gain access to the spine. Complications associated with ALIF procedures include vascular damage to the vena cava and aorta.
Posterior Lumbar Interbody Fusion, or PLIF. To perform a PLIF procedure, surgeons access the spine through an incision on the center of the patient’s back. The surgeon then navigates through muscles and nerves to gain access to the spine. Once at the spine, the surgeon removes bone from the lamina to gain access to the affected disc space where a discectomy is performed and a bone graft is placed. When compared to ALIF procedures, PLIF procedures are generally considered easier to perform and can achieve better nerve root decompression in certain cases. However, the anatomy of the spine prevents surgeons from removing the entire degenerated disc and obtaining optimal access for insertion of an implant or bone graft. Complications associated with PLIF procedures include nerve damage, soft tissue damage and implant migration.
Transforaminal Lumbar Interbody Fusion, or TLIF. TLIF procedures are performed in a similar manner to PLIF procedures, except the surgeon accesses the spine through a small incision slightly to the left or right of the
5
Table of Contents
center of the patient’s back. After reaching the spine, the surgeon removes a portion of the facet joint and navigates through the foramen which provides better visualization and disc removal capabilities than PLIF. Complications associated with TLIF procedures are similar to those found in PLIF procedures including nerve damage, soft tissue damage and implant migration.
Direct Lateral Interbody Fusion. To perform a direct lateral procedure, the surgeon accesses the spine from the patient’s side through one or two small incisions. The direct lateral procedure is not appropriate for fusions in the L5/S1 segment because the pelvis interferes with access. Complications associated with direct lateral procedures are similar to those found in PLIF and TLIF procedures, including nerve damage and implant migration, and also include bowel injury.
360° Lumbar Fusion Procedure. Currently, the most common and structurally rigid lumbar fusion surgery is referred to as a 360° fusion and requires a second surgical procedure immediately following an ALIF, PLIF, TLIF or direct lateral procedure. The additional procedure involves the permanent placement of screws and rods in the back to provide additional support and fusion of the posterior elements while the vertebrae fuse together during the six to eighteen months following surgery.
Limitations of Traditional Lower Lumbar Spine Procedures
While traditional and minimally invasive fusion procedures can be effective at treating medical conditions affecting the lower lumbar spine, common drawbacks of these procedures may include:
| • | Disruption to Soft Tissue and Support Structures. Open lumbar fusion procedures require the creation of a pathway from the skin to the degenerative disc that is large enough to allow direct visualization and work by the surgeon. It is common to cut through healthy muscle or move critical organs, arteries, nerves and soft tissue, which can lead to bleeding, scarring, nerve damage and bowel disruption. |
| • | Significant Blood Loss. As a result of undergoing current lumbar fusion procedures, patients typically experience significant blood loss of between 100 and 1,400 cc of blood. As a result, it is common for patients to use the hospital’s blood supply or donate units of their own blood before a lumbar fusion procedure to replenish any significant blood loss. |
| • | Lengthy Operative Procedure Times. It is common for current lumbar fusion procedures to take between 90 minutes and 4 hours to complete. With some procedures a second surgeon may be required. Long procedure times increase the risks of complications and blood loss. Also, hospital and physician resources are consumed for lengthy periods of time, which can reduce productivity and increase costs. |
| • | Lengthy Patient Hospital Stays. Patients remain in the hospital for an average of three days following a lumbar fusion procedure. |
| • | Significant Patient Recovery Time. Patients typically require three to six months to recover and rehabilitate after undergoing a lumbar fusion procedure before resuming normal activities. |
| • | Unresolved Patient Pain. Patients may continue to experience symptoms after undergoing lumbar fusion procedures even though x-rays show successful fusion has been achieved through the growth of new bone. |
Our Solutions
AxiaLIF Products
We have developed what we believe is a less invasive approach for surgeons to perform fusion and motion preserving surgeries in the L4/L5/S1 region without many of the drawbacks associated with other lumbar fusion procedures. We refer to this proprietary approach as our pre-sacral approach. We have developed and are marketing three fusion products that are delivered using our pre-sacral approach: AxiaLIF 1L, AxiaLIF 1L+ and AxiaLIF 2L+.
6
Table of Contents
To access the spine using our pre-sacral approach, the surgeon creates an incision adjacent to the tailbone while the patient is lying on their stomach. The surgeon then navigates a blunt dissecting tool a short distance along the sacrum using x-ray imaging technologies. As the dissecting tool is advanced, it moves aside soft tissue structures such as fat and loose connective tissue surrounding the anterior sacrum. When the tool reaches an access point near the junction of the S1 and S2 vertebral bodies, a guide pin is inserted through the bone into the disc of the lowest lumbar motion segment (the L5/S1 disc) where the fusion procedure is then performed. A tubular dissector is inserted over the guide pin to create a tissue-protecting working channel between the surgical access site and the L5/S1 disc. This protected working channel provides access to the interior of the disc, where rotating cutters, brushes and rasps are used to remove disc material. This is followed by the introduction of bone graft material with special instrumentation and finally, insertion of our AxiaLIF implants. The implant immediately provides rigid fixation and can provide restoration of disc height based on the clinical pathology of the patient. The AxiaLIF 2L+ procedure uses the same approach to provide access to both the L5/S1 and L4/L5 discs. The AxiaLIF 1L+ and AxiaLIF 2L+ procedures must be supplemented with facet or pedicle screws, which provide fixation for the back of the spine and are supplied by TranS1.
We believe our pre-sacral approach and its associated products provide the following benefits for patients, providers and payors:
| • | Less Invasive Approach Minimizes Complications. Our AxiaLIF products are delivered using our proprietary pre-sacral approach, which we believe is a less invasive solution for delivering fusion products to the L4/L5/S1 region. Procedures performed utilizing our pre-sacral approach have been documented to have favorable clinical safety profiles with low complication rates. In a recently published peer reviewed clinical paper, complication rates from procedures utilizing our pre-sacral approach were shown to be 1.3%. See additional information under the heading “Clinical Experience” below. The most frequent serious complication reported was bowel injury at 0.6% of cases with no reports in this study of permanent injury. |
| • | Spinal Stability. Our approach does not violate or cut through the muscles, ligaments or bones that control the stability of the spine. Thus, the axial approach to the spine does not affect inherent spinal stability, a benefit that cannot be achieved with other approaches to interbody fusion. Moreover, in another recent peer-reviewed retrospective clinical series, the fusion rate associated with procedures utilizing our pre-sacral approach was demonstrated to be 94%. We believe this compares favorably with the fusion rates of 90-95% associated with other fusion procedures. See additional information under the heading “Clinical Experience” below. |
VEO Lateral Access and Interbody Fusion System
Our new VEO Lateral Access and Interbody Fusion System provides for direct visualization during lateral fusion surgery and is indicated for spinal fusion procedures in skeletally mature patients with degenerative disc disease at one or two contiguous levels from L2-S1. Through a combination of direct visualization of the psoas muscle and unrestricted lateral fluoroscopic views, the VEO Lateral System offers visualization of the operative site. The VEO direct visualization approach was designed to help minimize iatrogenic trauma to the psoas muscle and the nerve plexus to help reduce the risk of post-operative complications.
Our VEO Lateral System includes a radiolucent tubular retractor that was designed to prevent soft tissue intrusion. It facilitates the first of two retraction stages, providing direct visualization of the psoas muscle and associated nerves before dissection of the psoas muscle. This intermediary step allows the surgeon to augment neuromonitoring information with direct visualization and was designed to help avoid the nerves when dissecting through the psoas muscle to the operative site.
The VEO’s dual-blade, internal psoas muscle retractor features controlled retraction in the anterior/posterior plane for a muscle-splitting and muscle-sparing approach. The internal retractor reduces muscle disruption and is designed to eliminate muscle creep. The VEO Lateral System offers a comprehensive portfolio of interbody
7
Table of Contents
implants in both parallel and lordotic angles to match each patient’s anatomy. The VEO PEEK interbody implants contain 5 tantalum markers for precise fluoroscopic placement. The large center channel is readily visualized and easily evaluated during and after the procedure.
The VEO Lateral System provides a complete discectomy and endplate preparation instrument set. Designed specifically for a lateral approach, these instruments are dimensionally optimized for operative visualization and controlled surgical manipulations.
Our Strategy
Our goal is to become a global leader in minimally invasive treatments for conditions affecting the lumbar region of the spine. To achieve this goal, we are pursuing the following strategies:
| • | Establish our Pre-Sacral Approach as a Standard of Care for Lower Lumbar Spine Surgery. We believe patients commonly avoid spine fusion surgery due to its invasive nature and other drawbacks associated with other surgical treatment options. We expend significant resources promoting our pre-sacral approach as a less invasive approach to lower back fusion surgery, and we believe the advantages of our technique will enable our AxiaLIF products to become a standard of care for the lower lumbar region of the spine. We also make substantial research and development expenditures to enhance our AxiaLIF products and develop new products to expand our technological advantage in minimally invasive spine surgeries. |
| • | Drive Reimbursement for the AxiaLIF Procedure. We plan to continue to work with our surgeon customers to generate published, peer reviewed clinical literature that demonstrates our procedure’s clinical efficacy and safety. The clinical papers discussed below under the heading “Clinical Experience” are examples of our continued efforts towards the execution of this strategy. We will also continue to work to leverage this data along with our AxiaLIF surgeon advocates, with payors to secure positive coverage decisions for the surgeon reimbursement portion of the AxiaLIF procedure (hospital reimbursement for AxiaLIF already exists). For example, in January 2011, we were informed by Humana Inc., a major health benefits company, that it changed its spinal surgery reimbursement policy to include physician payment coverage for medically necessary interbody fusion procedures when using our pre-sacral AxiaLIF approach. |
| • | Focus our Sales and Marketing Infrastructure to Drive Surgeon Adoption. We intend to continue expending significant resources targeting spine surgeons through our sales and marketing efforts in the United States and internationally in order to drive the adoption of our pre-sacral and lateral approaches. |
| • | Opportunistically Pursue Acquisitions of Complementary Businesses and Technologies. In addition to building our internal product development efforts, we intend to selectively license or acquire complementary products and technologies that we believe will enable us to leverage our growing distribution platform. |
| • | Expand Our Presence in the Direct Lateral Interbody Fusion Market. We intend to support the growing adoption of our VEO Lateral System through focused surgeon training programs, expanded sales representative training and marketing promotion. |
Clinical Experience
As of the date of this annual report, over 12,000 procedures have been performed using our pre-sacral approach by more than 500 surgeons. This amount includes over 10,400 procedures using AxiaLIF 1L or AxiaLIF 1L+ and over 1,800 procedures using AxiaLIF 2L or AxiaLIF 2L+. Our AxiaLIF products have been the subject of a significant number of clinical evaluations and medical publications. We believe that more than 50 articles have now been published about the clinical experience associated with utilizing our AxiaLIF products. The results of two recently published articles are summarized below:
| • | In September 2011, an article was published in the SAS Journal (“Complications with Axial Presacral Lumbar Interbody Fusion: A Five-Year Postmarket Surveillance Experience,” Gundanna, et al) that |
8
Table of Contents
| discusses the outcome of a retrospective clinical study involving 9,152 patients that had previously undergone procedures using our pre-sacral approach. The publication demonstrated that the complication rate arising from lower lumbar fusion utilizing our pre-sacral approach was approximately 1.3%. The most frequent serious complication reported was bowel injury at 0.6% of cases with no reports in this study of permanent injury. |
| • | In September 2011, a separate article was published in Spine (“Minimally-invasive Axial Pre-sacral L5-S1 Interbody Fusion: Two Year Clinical and Radiographic Outcomes,” Tobler, et al) that discusses the outcome of a retrospective clinical series involving 156 patients in four separate medical centers. The publication demonstrated an approximately 63% improvement in patient pain two years after surgery compared to immediately prior to the procedure. In addition, the article discusses that there was a 54% improvement in the Oswestry Disability Index two years after surgery, a commonly used measure for levels of disability in daily living activities, for patients receiving a fusion procedure utilizing our pre-sacral approach. The article also reports that the procedures utilizing our pre-sacral approach demonstrated a 94% fusion rate. We believe this rate compares favorably with the fusion rates of 90-95% associated with other fusion procedures as reported in other studies. The article further concludes that, for the evaluated population, our pre-sacral approach did not result in any vascular or neural injury. In addition, while we have received reports of bowel injury associated with our pre-sacral approach, no bowel injuries were reported in this article. Not all patients have the same experience when treated with AxiaLIF. |
Our Products
We currently market the AxiaLIF family of products for single and two level lumbar fusion, the VEO lateral access and interbody fusion system, the Vectre and Avatar posterior fixation systems and Bi-Ostetic bone void filler, a biologics product. We also market products that may be used with our AxiaLIF surgical approach, including bowel retractors, a bone graft harvesting system and additional discectomy tools.
| • | AxiaLIF Lumbar Fusion Implants. Our AxiaLIF products include surgical instruments designed to create a safe and reproducible access route to the L4/L5/S1 vertebral bodies, fusion implants and supplemental stabilization products. We believe our AxiaLIF implants and instruments, combined with facet screws or pedicle screws, provide surgeons with the tools necessary to perform a lumbar fusion in a less invasive manner. We sell these products to our customers in procedure kits that include all the instruments and implants needed to complete a lumbar fusion. |
| • | Our AxiaLIF 1L+ and AxiaLIF 2L+ implants are threaded titanium rods, that come in varying lengths to enable one-level L5/S1 fusions and two-level L4/L5/S1 fusions. As they are implanted, our proprietary design can allow for the separation of the vertebrae to restore disc height based on the clinical pathology of the patient. The increased disc height relieves pressure on the nerve, while the rod itself provides immediate rigid fixation. |
| • | VEO Lateral Access and Interbody Fusion System. In November 2011, we launched our VEO Lateral Access and Interbody Fusion System. This minimally invasive lateral system features a two-stage retraction method that focuses on nerve visualization followed by controlled retraction. The VEO Lateral System is designed for direct visualization of the psoas muscles and adjacent nerves prior to muscle dissection, and features a full range of PEEK lateral interbody implants and a variety of ergonomic instruments. |
| • | TranS1 Access and Disc Preparation Instruments. Our pre-sacral approach requires the use of a sterile set of surgical instruments that are used to create a working channel and to prepare the disc and vertebrae for our implant. The instrumentation contained in the set includes stainless steel navigation tools and tubular dissectors to create the working channel, as well as nitinol cutters and brushes to cut and remove the degenerated disc material and prepare the disc space for our implant and the bone graft material. |
9
Table of Contents
| • | Vectre Facet Screw System. Our Vectre facet screw system offers a cannulated facet screw inserted over a guidewire to provide stability. The Vectre system features are designed to offer a minimally invasive posterior fixation option in select patients. |
| • | AVATAR Pedicle Screw System. In January 2010, we entered into an agreement to distribute Avatar, a pedicle screw system. Avatar can be used with or without our implants to provide lumbar posterior fixation. The AVATAR MIS System offers cannulated pedicle screws inserted over a guidewire to reduce muscle and tissue trauma. Extended tabs integrated to the screws provide a pathway for secure implantation of the rod while minimizing tissue dissection. Reduction, compression and distraction are achieved with intuitive instrumentation. |
| • | Bi-Ostetic Bone Void Filler. In February 2010, we entered into an agreement to sell Bi-Ostetic, a synthetic, osteoconductive material intended to be used to fill voids and gaps that are not intrinsic to the stability of bone structure. These gaps or voids may be located in the extremities, spine, or pelvis. In spine surgery, it can be used to fill a void in the sacrum or as a substitute or adjunct to autograft or allograft during posterolateral fusion. Bi-ostetic is not indicated for use in the interbody space during interbody fusion procedures or in load bearing applications. |
| • | Iliac Crest Bone Graft Harvesting System. Our Iliac Crest Bone Graft Harvesting System was developed to aid surgeons in harvesting iliac crest autograft via a minimally invasive approach. Fusion success is dependent on a proper disc preparation technique, including a thorough discectomy with removal of the cartilaginous endplate and nuclear material. Use of autograft, which is osteogenic, osteoinductive and osteoconductive, further improves the chances of fusion success. Because it is harvested from the patient, it eliminates risk of disease transmission. It provides structural support as well as scaffolding for new bone growth. |
Product Pipeline
Our product development efforts are currently focused on pursuing improvements to enhance our current product lines and to also pursue products that have a short pathway to regulatory clearance and commercialization. We intend to introduce an AxiaLIF system that offers both the AxiaLIF 1L+ and 2L+ products in a single instrument and implant set, offering manufacturing, distribution and operating room efficiencies, and to refine our VEO Lateral System instruments and implants based on our first year of commercial experience.
In the future, we expect our product offerings will be expanded to address additional clinical applications in the surgical treatment of conditions affecting the lumbar spine with an emphasis on minimally invasive approaches. Such applications could require FDA 510(k) clearance or PMA approval, most likely supported by safety and efficacy data from clinical trials. We also have an active program aimed at developing tools that will improve outcomes and lower complications for our procedures.
Market Opportunity
Our management believes that the current addressable market opportunity for conditions affecting the lower lumbar region of the spine, including conditions such as degenerative disc disease, spondylolisthesis, instability and revision, totals approximately $3.8 billion annually. This amount includes (i) approximately $1.7 billion relating to the implementation of interbody devices such as those utilized in our AxiaLIF 1L+ and AxiaLIF 2L+ procedures, (ii) approximately $1.1 billion relating to the use of ancillary fixation devices, such as Vectre and Avatar, and biologics products, such as Bi-Ostetic, and (iii) approximately $1.0 billion relating to the use of direct lateral systems, such as our VEO Lateral Access and Interbody Fusion System.
Sales and Marketing
Our sales and marketing effort primarily targets spine surgeons. We also market our products at various industry conferences and through industry organized surgical training courses.
10
Table of Contents
In the United States, we market and sell our products through a combination of direct sales representatives and independent sales agents. On December 31, 2011, our U.S. sales team included regional managers, direct sales representatives, case coverage specialists and independent sales agents covering specific geographic regions. Our sales representatives receive a base salary and a percentage of the net sales that they generate. As of December 31, 2011, we had 21 direct sales representatives, 2 case coverage specialists and 7 regional managers. The independent sales agents are compensated based on a percentage of the net sales that they generate. We have agreements with our independent sales agents that provide them with an exclusive right to sell our products in their territories, which are generally terminable upon 90 days’ written notice.
Outside of the United States, we utilize our own direct sales representatives, independent sales agents and third-party distributors. Through December 31, 2011, the majority of our international sales have been in Europe. In 2008, we hired direct sales representatives in Germany, and in 2009 we began direct sales through our own sales representatives and agents in Germany, Switzerland, Netherlands and Belgium. Effective January 1, 2012, we replaced our direct sales representatives in Europe with an independent sales agent, comprised of former employees of our direct sales organization, representing Germany, Netherlands, and Belgium. In 2011, 61.8% of our international revenues were through our direct sales efforts and agents and 38.2% were through third-party distributors.
In 2011, no customer accounted for 10% or more of revenues.
Surgeon Training
We devote significant resources to training and educating surgeons on the specialized skills involved in the proper use of our instruments and implants. We believe that the most effective way to introduce and build market demand for our products is by training spine surgeons in the use of our products. We accomplish our training objectives primarily through cadaver and surrogate models and live case observations with surgeons experienced in our pre-sacral approach. We supplement this training with online didactic tutorials. After this training, surgeons are generally able to perform unsupervised surgeries using our pre-sacral approach. As of December 31, 2011, we had trained over 1,390 U.S. spine surgeons and over 280 surgeons outside of the U.S. in the use of our single-level product. Of the U.S. surgeons trained on our pre-sacral approach, approximately 211 have performed a procedure in the 12 months ended December 31, 2011 using our pre-sacral approach. In addition, we have trained over 470 U.S. spine surgeons in the use of our AxiaLIF 2L and 2L+ products. Through December 31, 2011, we have also trained over 30 U.S. spine surgeons in our VEO lateral access and interbody fusion system. We believe we have the necessary capacity to train a sufficient number of surgeons to meet our current goals.
In February 2012, we opened a new training facility in Raleigh, N.C., which has a state-of-the art operating room unit with a fully equipped surgical suite. The facility provides cadaveric capabilities to allow hands-on training for spine surgeons.
Third-Party Reimbursement
In the United States, healthcare providers generally rely on third-party payors, principally private insurers and governmental payors such as Medicare and Medicaid, to cover and reimburse all or part of the cost of a spine fusion surgery in which our medical device is used. Surgeons are reimbursed for performing the surgical procedure, while hospitals are reimbursed for the cost of the device, all patient care related to the fusion procedure and the overhead associated with maintaining the facility.
Most payors follow Medicare’s Diagnosis-Related Group, or DRG, based payment system for reimbursing facilities. Under this model, hospitals are paid a set amount to cover the costs associated with a fusion patient, including the cost of the device used in the procedure. The most commonly associated DRGs for spinal fusion are 453/454/455 (“Combined Anterior/Posterior Spinal Fusion with major complications and comorbidities (MCC),
11
Table of Contents
with complications and comorbidities (CC) or without MCC/CC”) and 459/460 (“Spinal Fusion Except Cervical with or without MCC”). Private payors typically use Medicare DRGs as a benchmark when setting their own reimbursement rates for facilities but typically pay above Medicare established rates.
Surgeons use the American Medical Association’s (“AMA”) Current Procedural Terminology, or CPT, system to bill payors for their service in performing the AxiaLIF procedures. CPT codes describe the services and procedures provided for patients to third-party payors so that physicians may be reimbursed. Effective January 1, 2009, the AMA implemented a Category III code which describes the work involved in treating AxiaLIF patients. Unlike Category I CPT codes, Category III codes do not have a set value which physicians use as a benchmark for setting their fee. Additionally, some payors view Category III codes as “investigational” or “experimental” and may not reimburse them. However, unlike many new or novel procedures, AxiaLIF is an access variation on the current standard of care (interbody spinal fusion) and has been performed in over 10,000 U.S. procedures. In December 2010, Humana Inc. made a decision to cover the AxiaLIF procedures and reimburse physicians for use of the Category III Code. The reimbursement rates are consistent with reimbursement levels for performing other interbody fusion procedures. In 2011, we received positive reimbursement coverage decisions from Horizon Blue Cross and Blue Shield of New Jersey, and Palmetto GBA, the Medicare Administrator for California, Virginia, North Carolina, South Carolina, Nevada, West Virginia and Hawaii. In 2012, we have received additional positive reimbursement coverage decisions from Health Care Services Corporation, or HCSC, the Blue Cross and Blue Shield provider for Texas, Illinois, New Mexico and Oklahoma, Hawaii Medical Service Association, the Blue Cross and Blue Shield provider for Hawaii, Geisinger, a provider in Pennsylvania, and HealthSpring, a payor in the mid-Atlantic. Following these coverage decisions, we believe that coverage for our AxiaLIF procedure includes approximately 36 million covered lives. However, HCSC has recently issued an updated policy, effective June 1, 2012, that removes coverage for AxiaLIF. We are working diligently to alter this policy prior to its implementation. We intend to pursue further positive reimbursement coverage decisions with other payors in the coming quarters by utilizing published clinical literature and leveraging the support of physicians that perform our procedures. Discussions are normally held with medical directors representing the payors to educate them on the existing published clinical literature.
On March 5, 2012, we announced that the CPT Editorial Panel, or the Panel, has voted to approve an application for a new Category I CPT code, 225XX1, for L5/S1 spinal fusion utilizing our AxiaLIF implant when performing a pre-sacral interbody fusion. In addition, the Panel has voted to establish a new Category III CPT code, 019XXT, as an add-on code to the new Category I code for use when performing L4/5 spinal fusion. The new CPT codes were announced on the AMA’s website on March 2, 2012, and will become effective on January 1, 2013.
Internationally, reimbursement and healthcare payment systems vary substantially from country to country and include single-payor, government-managed systems as well as systems in which private payors and government-managed systems exist side-by-side. Our ability to achieve market acceptance or significant sales volume in international markets we enter will depend in large part on the availability of reimbursement for procedures performed using our products under the healthcare payment systems in such markets. There is favorable reimbursement in Germany for the AxiaLIF 1L procedure. We also received a favorable ruling from the British United Provident Association, the leading provider of private health insurance and healthcare services in the United Kingdom. A small number of countries may require us to gather additional clinical data before recognizing coverage and reimbursement for our products. It is our intent to complete the requisite clinical studies and obtain coverage and reimbursement approval in countries where it makes economic and strategic sense to do so.
We believe that the overall escalating cost of medical products and services has led to, and will continue to lead to, increased pressures on the healthcare industry to reduce the costs of products and services. We cannot assure you that government or other third-party payors will cover and reimburse our procedures in whole or in part in the future or that payment rates will be adequate. In addition, it is possible that future legislation, regulation, or reimbursement policies of third-party payors will adversely affect the demand for our procedures
12
Table of Contents
and products or our ability to sell them on a profitable basis. The unavailability or inadequacy of third-party payor coverage or reimbursement could have a material adverse effect on our business, operating results and financial condition.
Competition
The medical device industry is highly competitive, subject to rapid technological change and significantly affected by new product introductions and market activities of other participants. Our currently marketed products are, and any future products we commercialize will be, subject to intense competition. Our competitors include providers of conservative, non-operative therapies for lower lumbar spine conditions, as well as a number of major medical device companies that have developed or plan to develop products for minimally invasive spine surgery in each of our current and future product categories. We believe that the principal competitive factors in our markets include:
| • | improved outcomes for medical conditions affecting the lower lumbar spine; |
| • | acceptance by spine surgeons; |
| • | ease of use and reliability; |
| • | product price and qualification for reimbursement; |
| • | technical leadership and superiority; |
| • | effective marketing and distribution; and |
| • | speed to market. |
We are aware of several companies that compete or are developing technologies in our current and future product areas. As a result, we expect competition to remain intense. Our most significant competitors are Medtronic Sofamor Danek, Johnson & Johnson DePuy Spine, Stryker Spine, NuVasive, Zimmer Spine, Synthes, Orthofix International, Globus Medical and Alphatec Spine, many of which have substantially greater sales and financial resources than we do. In addition, these companies may have more established distribution networks, entrenched relationships with physicians, and greater experience in launching, marketing, distributing and selling products.
Additional competition also comes from physician-owned spine specific medical device distribution companies, which have expanded in recent years. These companies, which are partially owned or completely owned by spine surgeons, have significant market knowledge and access to the physicians who use our products and the hospitals that purchase our products. These surgeons may have an incentive to direct implant use toward implants that are distributed by these organizations.
Our ability to compete successfully will depend on our ability to develop proprietary products that reach the market in a timely manner, receive adequate reimbursement and demonstrate that they are safer and less invasive than alternatives available for the same purpose. Because of the size of the potential market, we anticipate that companies will dedicate significant resources to developing competing products.
Research and Development
As of December 31, 2011, our research and development team was comprised of 9 employees who have extensive experience in developing products to treat medical conditions affecting the lower lumbar spine. These employees work closely with our clinical advisors and spine surgeon customers to design and enhance our products and approach. Our research and development spending was $5.2 million, $4.2 million and $6.4 million for the years ending December 31, 2011, 2010 and 2009, respectively. Since inception, we have devoted significant resources to develop and enhance our products and expect to continue to do so in the future.
13
Table of Contents
Manufacturing and Supply
We rely on third parties to manufacture all of our products and their components, except for our nitinol nucleus cutter blades, which we manufacture at our facility in Wilmington, North Carolina. Our outsourcing partners are manufacturers that meet FDA, International Organization for Standardization, or ISO, and other internal quality standards, where applicable. We believe these manufacturing relationships allow us to work with suppliers who have the best specific competencies while we minimize our capital investment, control costs and shorten cycle times, all of which we believe allows us to compete with larger-volume manufacturers of spine surgery products.
All of our products and components are assembled, packaged, labeled and sterilized, if applicable, at third-party facilities in the United States under our existing contracts requiring compliance with Good Manufacturing Processes, or GMPs. Following receipt of products or components from our third-party manufacturers, we inspect, warehouse and ship the products and components at our facilities in Wilmington or at a third-party distribution facility in Memphis, Tennessee. We reserve the exclusive right to inspect and assure conformance of each product and component to our specifications. In addition, FDA or other regulatory authorities may inspect our facilities and those of our suppliers to ensure compliance with Quality System Regulations, or QSR.
The majority of our instruments and implants are produced by third-party manufacturers on precision, high-speed machine shop equipment. However, for a certain number of our products, the components and materials used to manufacture such products and the manufacturing operations are performed or supplied by third-party specialty vendors due to their proprietary or non-conventional nature. For example, the blades for our nucleus cutters are made from a metal called nitinol, which is converted into strip form by three manufacturers in the United States known to us. We have sourced nitinol strip from two of these vendors. The nitinol strip is then further converted for us into cutter blanks by a scalpel blade specialty vendor. Other vendors are available to manufacture the cutter blanks, as we may deem desirable or necessary. We convert the cutter blanks into cutter blades at our facilities. Our tissue extractor product is produced for us by a supplier that specializes in wire forming and coiling specifically for the medical device industry. A limited number of similar vendors exist that could be used to produce the tissue extractor product, and we believe we could replace this supplier on reasonable terms without substantial delay, if necessary.
We are currently working with our third-party manufacturers to plan for our future manufacturing requirements. In most cases, we have redundant manufacturing capability with multiple vendors and enjoy the significant capacity this arrangement provides to us. We may consider manufacturing certain products or product components internally, if and when demand or quality requirements make it appropriate to do so. We believe the manufacturing capacity available to us is sufficient to meet our demands into the foreseeable future.
Patents and Proprietary Technology
We rely on a combination of patent, trademark, copyright, trade secret and other intellectual property laws, nondisclosure agreements and other measures to protect our intellectual property rights. We believe that in order to have a competitive advantage, we must develop and maintain the proprietary aspects of our technologies. We require our employees, consultants and advisors to execute confidentiality agreements in connection with their employment, consulting or advisory relationships with us. We also require our employees, consultants and advisors who we expect to work on our products to agree to disclose and assign to us all inventions conceived during the work day, using our property or which relate to our business. We cannot provide any assurance that employees and consultants will abide by the confidentiality or assignment terms of these agreements. Despite any measures taken to protect our intellectual property, unauthorized parties may attempt to copy aspects of our products or to obtain and use information that we regard as proprietary.
14
Table of Contents
Patents
As of December 31, 2011, we had 42 issued United States patents, 15 pending patent applications in the United States, 4 issued European patents, 6 issued Japanese patents and 12 foreign patent application families as counterparts of U.S. cases. The issued and pending patents cover, among other things:
| • | our method for performing trans-sacral procedures in the spine, including diagnostic or therapeutic procedures, and trans-sacral introduction of instrumentation or implants; |
| • | apparatus for conducting these procedures including access, disc preparation and implantation including the current TranS1 instruments individually and in kit form; and |
| • | implants for fusion and motion preservation in the spine. |
Our issued patents begin to expire in 2021 assuming timely payment of all maintenance fees. We have multiple patents covering unique aspects and improvements for many of our methods and products. We do not believe that the expiration of any single patent is likely to significantly affect our business, operating results or prospects.
Trademarks
We own 8 trademark registrations in the United States, 9 trademark registrations in the European Union and 1 registered trademark in Canada. We also own 1 pending trademark application in the United States, 1 pending trademark application in Canada, and 2 pending trademark applications in China.
Government Regulation
Our products are medical devices subject to extensive regulation by the FDA and other U.S. federal and state regulatory bodies and comparable authorities in other countries. To ensure that medical products distributed domestically and internationally are safe and effective for their intended use, FDA and comparable authorities in other countries have imposed regulations that govern, among other things, the following activities that we or our partners perform and will continue to perform:
| • | product design and development; |
| • | registration and listing; |
| • | product testing (preclinical and clinical); |
| • | product manufacturing; |
| • | product labeling; |
| • | product storage; |
| • | premarket clearance or approval; |
| • | advertising and promotion; |
| • | product marketing, sales and distribution; and |
| • | post-market surveillance, including reporting deaths or serious injuries related to products and certain product malfunctions. |
FDA’s Premarket Clearance and Approval Requirements
Unless an exemption applies, each medical device we wish to commercially distribute in the United States will require either prior 510(k) clearance or prior premarket approval from the FDA. The FDA classifies medical devices into one of three classes. Devices deemed to pose lower risk are placed in either class I or II, which in many cases requires the manufacturer to submit to the FDA a premarket notification or 510(k) submission
15
Table of Contents
requesting permission for commercial distribution. This process is known as requesting 510(k) clearance. Some low risk devices are exempt from this requirement. Devices deemed by the FDA to pose the greatest risk, such as many life-sustaining, life-supporting or implantable devices, or devices deemed not substantially equivalent to a legally marketable device, are placed in class III, requiring a PMA. Our current commercial products are class II devices marketed under FDA 510(k) premarket clearance or are Class I and exempt from 510(k) or PMA regulation. Premarket clearance applications are subject to the payment of user fees, paid at the time of submission for FDA review.
510(k) Clearance Pathway
To obtain 510(k) clearance, we must submit a premarket notification demonstrating that the proposed device is substantially equivalent to a legally marketable device not requiring a PMA. Although statutorily mandated to respond to a 510(k) premarket notification within 90 days of submission of the application, FDA’s 510(k) clearance pathway usually takes from three to twelve months, or even longer, depending on the extent of requests for additional information by FDA. Additional information can include clinical data to make a determination regarding substantial equivalence.
After a device receives 510(k) clearance, any modification that could significantly affect its safety or effectiveness, or that would constitute a new or change in its intended use, will require a new 510(k) clearance or, depending on the modification, require a PMA. The FDA requires each manufacturer to determine whether the proposed change requires submission of a 510(k), or a PMA, but the FDA can review any such decision and can disagree with a manufacturer’s determination. If the FDA disagrees with a manufacturer’s determination, the FDA can require the manufacturer to cease marketing and/or recall the modified device until 510(k) clearance or a PMA is obtained. If the FDA requires us to seek 510(k) clearance or a PMA for any modifications to a previously cleared product, we may be required to cease marketing or recall the modified device until we obtain this clearance or approval. Also, in these circumstances, we may be subject to significant regulatory fines or penalties. We have made and plan to continue to make additional product enhancements to our products.
Clinical Trials
Clinical trials are sometimes required for a 510(k) premarket notification. In the U.S., these trials require submission of an application for an investigational device exemption, or IDE, unless the product is deemed a non-significant risk device eligible for more abbreviated IDE requirements. The IDE application must be supported by appropriate data, such as animal and laboratory testing results, showing that it is safe to test the device in humans and that the testing protocol is scientifically sound. The IDE application must be approved in advance by the FDA for a specified number of patients. Clinical trials for a significant risk device may begin once the IDE application is approved by the FDA and the appropriate institutional review boards at the clinical trial sites. Clinical trials must be conducted in accordance with FDA regulations and federal and state regulations concerning human subject protection, including informed consent and healthcare privacy and financial disclosure by clinical investigators. A clinical trial may be suspended by FDA or the investigational review board at any time for various reasons, including a belief that the risks to the study participants outweigh the benefits of participation in the study. Even if a study is completed, the results of our clinical testing may not demonstrate the safety and efficacy of the device, or may be equivocal or otherwise not be sufficient to obtain clearance or approval. Similarly, in Europe the clinical study must be approved by the local ethics committee and in some cases, including studies of high-risk devices, by the Competent Authority in the applicable country.
Pervasive and Continuing FDA Regulation
After a device is placed on the market, numerous FDA and other regulatory requirements continue to apply. These include:
| • | quality system regulation, which requires manufacturers, including third-party contract manufacturers, to follow stringent design, testing, control, documentation, and other quality assurance controls, during all aspects of the manufacturing process; |
16
Table of Contents
| • | establishment registration and listing; |
| • | labeling regulations, and FDA prohibitions against the promotion of products for uncleared or unapproved “off-label” uses; |
| • | medical device reporting obligations, which require that manufacturers submit reports to the FDA if information reasonably suggests that their device (i) may have caused or contributed to a death or serious injury, or (ii) malfunctioned and the device or a similar company device would likely cause or contribute to a death or serious injury if the malfunction were to recur; and |
| • | other post-market surveillance requirements, which apply when necessary to protect the public health or to provide additional safety and effectiveness data for the device. |
We must register and list with FDA as a medical device manufacturer and must obtain all necessary state permits or licenses to operate our business. As manufacturers, we are subject to announced and unannounced inspections by FDA to determine our compliance with quality system regulation and other regulations. We were inspected by the FDA in May 2010 with no Form 483 observations. We believe that we are in substantial compliance with quality system regulation and other regulations.
We are subject to announced and unannounced inspections by the FDA and these inspections may include the manufacturing facilities of our subcontractors.
Fraud and Abuse
We may directly or indirectly be subject to various federal and state laws pertaining to healthcare fraud and abuse, including anti-kickback laws. In particular, the federal healthcare program anti-kickback statute prohibits persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual, or the furnishing, arranging for or recommending a good or service, for which payment may be made in whole or part under federal healthcare programs, such as the Medicare and Medicaid programs. The anti-kickback statute is broad and prohibits many arrangements and practices that are lawful in businesses outside of the healthcare industry. In implementing the statute, the Office of Inspector General, or OIG, has issued a series of regulations, known as the “safe harbors,” which began in July 1991. These safe harbors set forth provisions that, if all their applicable requirements are met, will assure healthcare providers and other parties that they will not be prosecuted under the anti-kickback statute. The failure of a transaction or arrangement to fit precisely within one or more safe harbors does not necessarily mean that it is illegal or that prosecution will be pursued. However, conduct and business arrangements that do not fully satisfy all requirements of an applicable safe harbor may result in increased scrutiny by government enforcement authorities such as the OIG. Penalties for violations of the federal anti-kickback statute include criminal penalties and civil sanctions such as fines, imprisonment and possible exclusion from Medicare, Medicaid and other federal healthcare programs.
The federal False Claims Act prohibits persons from knowingly filing or causing to be filed a false claim to, or the knowing use of false statements to obtain payment from, the federal government. Suits filed under the False Claims Act, known as “qui tam” actions, can be brought by any individual on behalf of the government. These individuals, sometimes known as “relators” or, more commonly, as “whistleblowers,” may share in any amounts paid by the entity to the government in fines or settlement. The number of filings of qui tam actions has increased significantly in recent years, causing more healthcare companies to have to defend a False Claim action. If an entity is determined to have violated the federal False Claims Act, it may be required to pay up to three times the actual damages sustained by the government, plus civil penalties of between $5,500 and $11,000 for each separate false claim. Various states have also enacted similar laws modeled after the federal False Claims Act which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor.
The Health Insurance Portability and Accountability Act of 1996, or HIPAA, created two new federal crimes: healthcare fraud and false statements relating to healthcare matters. The healthcare fraud statute prohibits
17
Table of Contents
knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private payors. A violation of this statute is a felony and may result in fines, imprisonment or exclusion from government sponsored programs. The false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items, or services. A violation of this statute is a felony and may result in fines or imprisonment.
We are also subject to certain state laws that are analogous to each of the federal laws summarized above, such as anti-kickback and false claims laws that may apply to items or services reimbursed by any third-party payor, including commercial insurers, and state laws governing the privacy of certain health information, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
We have adopted policies and procedures designed to comply with the various healthcare laws applicable to our business. However, because of the breadth of these laws and regulations and the sometimes subjective nature of their application, it is possible that some of our business activities could be subject to challenge under one or more of such laws. The risk of being found to have violated such laws is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. In addition, in recent years, we believe that both federal and state regulators have increased regulation, enforcement, inspections and governmental investigations of the medical device industry, which further increases the risk that our business activities could be subject to challenge under certain laws.
In October 2011, we received a subpoena issued by the Department of Health and Human Services, OIG, under the authority of the federal healthcare fraud and false claims laws. The Company is cooperating with the government’s request and is in the process of responding to the subpoena. While no claims have been made against the Company at this time, we cannot predict the ultimate outcome of the matters raised by the OIG, and, if we are found to be in violation of any federal healthcare fraud and false claims laws, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from federal healthcare programs and/or the curtailment or restructuring of our operations.
International
International sales of medical devices are subject to foreign government regulations, which vary substantially from country to country. The time required to obtain approval by a foreign country may be longer or shorter than that required for FDA clearance or approval, and the requirements may differ.
The European Union, which consists of 27 of the major countries in Europe, has adopted numerous directives and standards regulating the design, manufacture, clinical trials, labeling, and adverse event reporting for medical devices. Other countries, such as Switzerland, have voluntarily adopted laws and regulations that mirror those of the European Union with respect to medical devices. Devices that comply with the requirements of a relevant directive will be entitled to bear CE conformity marking and, accordingly, can be commercially distributed throughout the member states of the European Union, and other countries that comply with or mirror these directives. The method of assessing conformity varies depending on the type and class of the product, but normally involves a combination of self-assessment by the manufacturer and a third-party assessment by a “Notified Body,” an independent and neutral institution appointed to conduct conformity assessments. This third-party assessment consists of audits of the manufacturer’s quality system for conformance to applicable quality system standards such as ISO 13485. An assessment by a Notified Body in one country within the European Union is required for each product in order for a manufacturer to commercially distribute the product throughout the European Union. Compliance of the Quality System with ISO 13845 and compliance of each product with the Medical Device Directive (MDD93/42/EEC as amended by directive 2007/47EC) establishes the presumption of conformity with the essential requirements for a CE mark. In August 2004, our quality system was initially certified by Intertek ETL-Semko, a Notified Body, under the European Union Medical Device
18
Table of Contents
Directive to be in compliance with the Canadian Medical Device Conformity Assessment System, or CMDCAS, and ISO standards 9001:2000 and ISO 13485:2003. The system was recertified in September 2010 to CMDCAS, ISO 9001:2008 and ISO 13485:2003 and is due for further recertification in September of 2013.
Employees
As of December 31, 2011, we had 86 employees, most of whom were full-time employees, with 47 employees in U.S. sales, marketing, professional affairs, customer service, and training, 3 employees in international sales, marketing and training, 6 employees in manufacturing, 9 employees in research and development, 16 employees in general and administrative and 5 employees in clinical, regulatory and quality assurance. We believe that our future success will depend in part on our continued ability to attract, hire and retain qualified personnel. None of our employees are represented by a labor union, and we believe that we maintain good relations with our employees. Effective January 1, 2012, we replaced our direct sales representatives in Europe with an independent sales agent, comprised of former employees of our direct sales organization, representing Germany, Netherlands, and Belgium.
General Information
We were incorporated in Delaware in May 2000 under the name “aXiaMed, Inc.” and changed our name to “TranS1 Inc.” in February 2003. Our principal executive office is located at 301 Government Center Drive, Wilmington, North Carolina 28403 and our telephone number is (910) 332-1700. Our website is www.trans1.com. The information on, or that can be accessed through, our website is not incorporated by reference into this annual report and should not be considered to be a part of this annual report.
We make our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to these reports available on our website, at www.trans1.com, free of charge as soon as practicable after filing with the SEC.
All such reports are also available free of charge via EDGAR through the SEC website at www.sec.gov. In addition, the public may read and copy materials filed by us with the SEC at the SEC’s public reference room located at 100 F St., NE, Washington, D.C., 20549. Information regarding operation of the SEC’s public reference room can be obtained by calling the SEC at 1-800-SEC-0330.
19
Table of Contents
| Item 1A. | Risk Factors |
Investing in our common stock involves a high degree of risk. You should carefully consider the following risk factors, as well as the other information contained in this annual report, before deciding whether to invest in shares of our common stock. If any of the following risks actually occur, our business, financial condition, operating results and prospects would suffer. In that case, the trading price of our common stock would likely decline and you might lose all or part of your investment in our common stock. The risks described below are not the only ones we face. Additional risks that we currently do not know about or that we currently believe to be immaterial may also impair our operations and business results.
Risks Related to Our Business
To be commercially successful, spine surgeons must accept that our products are a safe and effective alternative to other surgical treatments of certain spine disorders.
Our revenue is primarily derived from sales of our AxiaLIF products and related surgical instruments. We expect that sales of our AxiaLIF products will continue to account for a substantial portion of our revenues for the foreseeable future. We believe spine surgeons may not widely adopt our products unless they determine, based on experience, long-term clinical data and published peer reviewed journal articles, that our products provide a safe and effective alternative to conventional procedures used to treat certain spine disorders or other non-conventional procedures offered by our competitors. Spine surgeons may be slow to adopt our technology for the following reasons, among others:
| • | lack of long-term clinical data supporting additional patient benefits; |
| • | lack of experience with our products; |
| • | lack of evidence supporting the cost savings, clinical efficacy or safety of our products and procedure over competitive products and medical technologies; |
| • | perceived liability risks generally associated with the use of new products and procedures; |
| • | training time required to use a new product or procedure; and |
| • | availability of adequate coverage and reimbursement for hospitals and surgeons. |
If we are unable to effectively demonstrate to spine surgeons the benefits of our products as compared to other surgical treatments of spine disorders that are available to them and our products fail to achieve market acceptance, our future revenues will be adversely impacted. In addition, we believe recommendations and support of our products by influential spine surgeons are essential for market acceptance and adoption. If we do not receive support from these spine surgeons or do not have favorable long-term clinical data, spine surgeons may not use our products and our future revenues will be harmed, which could result in a decline in the price of our common stock.
The efficacy of our products is not yet supported by long-term clinical data and may therefore prove to be less effective than initially thought.
We obtained 510(k) clearance to manufacture, market and sell all of our currently U.S. marketed products for which FDA clearance is required. In order to obtain 510(k) clearance, a manufacturer must demonstrate to the FDA’s satisfaction that its device is “substantially equivalent” to other legally marketed devices not requiring premarket approval, or PMA. In contrast, certain high-risk and/or new devices require submission of a PMA application to the FDA. Such a PMA application must demonstrate that the device is safe and effective for the proposed indication, and must be supported by extensive data from preclinical studies and human clinical trials. The FDA’s 510(k) clearance process is therefore less costly and rigorous than the PMA process and requires less supporting clinical data. Because our devices were cleared for marketing through the 510(k) process or were exempt from the 510(k) process, we currently lack the breadth of published long-term clinical data supporting the efficacy of our AxiaLIF products and the benefits they offer that might have been generated in connection with the PMA process.
20
Table of Contents
The demand for our products and the prices which customers and patients are willing to pay for our products depend upon the ability of our customers to obtain adequate third-party coverage and reimbursement for their purchases of our products.
Sales of our products depend in part on the availability of adequate coverage and reimbursement from governmental and private payors. In the United States, healthcare providers that purchase our products generally rely on third-party payors, principally Medicare, Medicaid and private health insurance plans, to pay for all or a portion of the costs and fees associated with our AxiaLIF procedures.
Physicians generally use billing codes known as CPT codes to report professional services rendered for reimbursement purposes. The CPT coding system is maintained and updated on an annual basis by the Panel. In 2008, most of the surgeons performing our procedure billed third-party payors using existing ALIF procedure codes. Effective January 1, 2009, the AMA, however, created a new emerging technology CPT code — or Category III code — to facilitate data collection on and assessment of new services and procedures such as the AxiaLIF procedure. This change made it more difficult for physicians to obtain reimbursement for our procedure because many commercial payors view a Category III code as “experimental” or “investigational” and thus will not pre-approve the procedure or will decline to pay for the procedure until they see additional clinical evidence. This uncertainty around the availability and amount of reimbursement has caused some physicians to revert to other fusion surgeries where coverage and reimbursement are more certain. We made a presentation to the Panel at their October 2011 meeting, asking them to consider transitioning the Category III code to a permanent Category I code for our AxiaLIF procedures. On November 8, 2011, the Company received notice from the AMA that the Panel rejected our request to convert Category III codes 0195T and 0196T, used to bill for the service in which the Company’s product is used, to Category I codes. We subsequently presented to the Panel at their February 2012 meeting, again asking them to consider transitioning the Category III code to a permanent Category I code for our AxiaLIF procedures. On March 5, 2012, we announced that the Panel has voted to approve an application for a new Category I CPT code, 225XX1, for L5/S1 spinal fusion utilizing our AxiaLIF implant when performing a pre-sacral interbody fusion. In addition, the Panel has voted to establish a new Category III CPT code, 019XXT, as an add-on code to the new Category I code for use when performing L4/5 spinal fusion. The new CPT codes were announced on the AMA’s website on March 2, 2012, and will become effective on January 1, 2013.
Third-party payors continue to review their coverage policies carefully for existing and new therapies and can, without notice, deny coverage for treatments that include the use of our products. While we have received several positive coverage and reimbursement decisions from payers for the use of our products during the period from January 2011 through March 2012 and are currently engaged in discussions with other payors, it is difficult to predict the timing of receiving any additional positive coverage decisions and there is no guarantee that payors will make any additional positive coverage decisions. Our business would be negatively impacted to the extent any such coverage decisions reduce our customers’ ability to obtain coverage and reimbursement for the procedures using our products. In addition, our stock price could be negatively affected to the extent that coverage decisions by payors do not reflect market expectations for such decisions.
With respect to coverage and reimbursement outside of the United States, reimbursement systems in international markets vary significantly by country, and by region within some countries, and reimbursement approvals must be obtained on a country-by-country basis and can take up to 18 months, or longer. Many international markets have government-managed healthcare systems that govern reimbursement for new devices and procedures. In most markets, there are private insurance systems as well as government-managed systems. Additionally, some foreign reimbursement systems provide for limited payments in a given period and therefore result in extended payment periods. Reimbursement in international markets may require us to undertake country-specific reimbursement activities, including additional clinical studies, which could be time consuming, expensive and may not yield acceptable reimbursement rates.
Furthermore, healthcare costs have risen significantly over the past decade. There have been and may continue to be proposals by legislators, regulators and third-party payors to contain these costs. These
21
Table of Contents
cost-control methods include prospective payment systems, capitated rates, group purchasing, redesign of benefits, pre-authorizations or second opinions prior to major surgery, encouragement of healthier lifestyles and exploration of more cost-effective methods of delivering healthcare. Some healthcare providers in the United States have adopted or are considering a managed care system in which the providers contract to provide comprehensive healthcare for a fixed cost per person. Healthcare providers may also attempt to control costs by authorizing fewer elective surgical procedures or by requiring the use of the least expensive devices possible. These cost-control methods also potentially limit the amount which healthcare providers may be willing to pay for certain types of medical procedures.
In addition, in the United States, no uniform policy of coverage and reimbursement for medical technology exists among payors. Therefore, coverage of and reimbursement for medical technology can differ significantly for each payor. The continuing efforts of third-party payors, whether governmental or commercial, whether inside the United States or outside, to contain or reduce these costs, combined with closer scrutiny of such costs, could restrict our customers’ ability to obtain adequate coverage and reimbursement from these third-party payors. The cost containment measures that healthcare providers are instituting both in the United States and internationally could harm our business by adversely affecting the demand for our products or the price at which we can sell our products.
Reforms to the United States healthcare system may adversely affect our business.
In March 2010, U.S. President Barack Obama signed the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act (collectively, the “PPACA”), which makes a number of substantial changes in the way health care is financed by both governmental and private insurers. Among other things, the PPACA requires medical device manufacturers to pay a sales tax equal to 2.3% of the price for which such manufacturer sells its medical devices, beginning January 1, 2013. A number of states have challenged the constitutionality of certain provisions of PPACA, and many of these challenges are still pending final adjudication in several jurisdictions. Congress has also proposed a number of legislative initiatives, including possible repeal of PPACA. At this time, it remains unclear whether there will be any changes made to PPACA, whether to amend certain provisions or its entirety. We cannot assure you that PPACA, as currently enacted or as amended in the future, will not adversely affect our business and financial results, and we cannot predict how future federal or state legislative or administrative changes relating to healthcare reform will affect our business. The full impact on our business of PPACA is uncertain.
In addition, other legislative changes have been proposed and adopted since PPACA was enacted. Most recently, on August 2, 2011, the President signed into law the Budget Control Act of 2011, which, among other things, created the Joint Select Committee on Deficit Reduction to recommend proposals in spending reductions to Congress. The Joint Select Committee was unable to achieve a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, thereby triggering an automatic reduction in spending programs. These automatic cuts will be made to several government programs and, with respect to Medicare, would include aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, starting in 2013. The full impact on our business of PPACA and the new law is uncertain. Nor is it clear whether other legislative changes will be adopted, if any, or how such changes would affect our industry generally or our ability to successfully commercialize our products or the development of new products.
We have incurred losses since inception and we expect to continue to incur losses for the foreseeable future. We may never achieve or sustain profitability.
We have incurred net losses since our inception in May 2000 and we have an accumulated deficit of $108.9 million through December 31, 2011. To date, we have financed our operations primarily through sales of our equity securities, including the sale of 6,200,000 shares of our common stock for aggregate net proceeds of approximately $18.2 million in September 2011, and have devoted substantially all of our resources to research and development of our products, the commercial launch of our products and the development of a sales team to
22
Table of Contents
market our products. We expect our expenses to increase in connection with our clinical trials and research and development activities, as well as to support our sales and marketing efforts. As a result, we expect to continue to incur operating losses for the foreseeable future. These losses will continue to have an adverse effect on our stockholders’ equity and we may never achieve or sustain profitability.
We are in a highly competitive market segment, which is subject to rapid technological change.
The market for treatment of spine disorders is highly competitive and subject to rapid and profound technological change. Our success depends, in part, upon our ability to maintain a competitive position in the development of technologies and products for use in the treatment of spine disorders. We face competition from both established and development stage companies. Many of these companies have competitive advantages, including:
| • | greater financial and human resources for product development, sales and marketing and patent litigation; |
| • | significantly greater name recognition; |
| • | established relationships with spine surgeons, customers and third-party payors; |
| • | reimbursement codes providing for adequate coverage and reimbursement to hospitals and surgeons; |
| • | additional lines of products, and the ability to offer rebates or bundle products to offer greater discounts or incentives to gain a competitive advantage; |
| • | established sales and marketing, and distribution networks; and |
| • | greater experience in developing new products, conducting clinical trials, preparing regulatory submissions and obtaining regulatory clearance or approval for products and marketing approved products. |
Our failure to continue building effective sales and marketing capabilities for our products could significantly impair our ability to increase sales of our products.
We utilize a hybrid model of independent sales agents and direct sales representatives for product sales in the United States and rely on third-party distributors, direct sales representatives and independent sales agents for international sales. As of December 31, 2011, we employed 30 direct sales representatives in the United States and two direct sales representatives in Europe. Effective January 1, 2012, we converted our direct sales representatives in Europe to an independent sales agent, representing Germany, Netherlands, and Belgium. If we are unable to efficiently manage those individuals, our sales will suffer.
We also rely on marketing arrangements with independent sales agents in the United States and independent distributors in Europe. We do not control, nor monitor the marketing practices of our independent sales agents or distributors and they may not be successful in implementing our marketing plans or complying with applicable laws regarding marketing practices. Independent distributors and sales agents may terminate their relationship with us, or devote insufficient sales efforts to our products, which could have an adverse effect on our operations.
Our future success depends on our ability to develop, receive regulatory clearance or approval for, and introduce new products or product enhancements that will be accepted by the market in a timely manner.
It is important to our business that we continue to build a more complete product offering for treatment of spine disorders. As such, our success will depend in part on our ability to develop and introduce new products and enhancements to our existing products to keep pace with the rapidly changing spine market. However, we may not be able to successfully develop and obtain regulatory clearance or approval for product enhancements, or new products, or these products may not be accepted by spine surgeons or payors who financially support many of the procedures performed with our products.
23
Table of Contents
The success of any new product offering or enhancement to an existing product will depend on several factors, including our ability to:
| • | properly identify and anticipate spine surgeon and patient needs; |
| • | develop and introduce new products or product enhancements in a timely manner; |
| • | avoid infringing upon the intellectual property rights of third parties; |
| • | demonstrate the safety and efficacy of new products with data from preclinical studies and clinical trials; |
| • | obtain the necessary regulatory clearances or approvals for new products or product enhancements; |
| • | be fully FDA-compliant with marketing of new devices or modified products; |
| • | provide adequate training to potential users of our products; |
| • | receive adequate coverage and reimbursement for procedures performed with our products; and |
| • | develop an effective and FDA-compliant, dedicated marketing and distribution network. |
If we do not develop new products or product enhancements in time to meet market demand or if there is insufficient demand for these products or enhancements, our results of operations will suffer.
If clinical trials of our current or future product candidates do not produce results necessary to support regulatory clearance or approval in the United States or elsewhere, we will be unable to commercialize these products.
Clinical failure can occur at any stage of the testing. Our clinical trials may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical and/or non-clinical testing in addition to those we have planned. Our failure to adequately demonstrate the efficacy and safety of any of our devices would prevent or significantly delay receipt of regulatory clearance or approval and, ultimately, the commercialization of that device.
Our international operations subject us to certain operating risks, which could adversely impact our net revenues, results of operations and financial condition.
Sales of our products outside the United States represented 8.8% of our revenue in 2011. The sale and shipment of our products across international borders, as well as the purchase of components and products from international sources, subject us to extensive U.S. and foreign governmental trade, import and export, and customs regulations and laws. Compliance with these regulations is costly and exposes us to penalties for non-compliance. Other laws and regulations that can significantly impact us include various anti-bribery laws, including the U.S. Foreign Corrupt Practices Act and anti-boycott laws. Any failure to comply with applicable legal and regulatory obligations could impact us in a variety of ways that include, but are not limited to, civil and administrative penalties, denial of export privileges, seizure of shipments and restrictions on certain business activities.
Our international operations expose us and our distributors to risks inherent in operating in foreign jurisdictions. These risks include:
| • | the imposition of additional U.S. and foreign governmental controls or regulations; |
| • | the imposition of complicated and costly export licensing requirements; |
| • | the imposition of U.S. or international sanctions against a country, company, person or entity with whom we do business that would restrict or prohibit continued business with the sanctioned country, company, person or entity; |
24
Table of Contents
| • | economic weakness or uncertainty, including the sovereign debt crises affecting several countries in the European Union; |
| • | political instability; |
| • | changes in third-party reimbursement policies that may require some of the patients who receive our products to directly absorb medical costs or that may necessitate the reduction of the selling prices of our products; |
| • | changes in duties and tariffs, license obligations and other non-tariff barriers to trade; |
| • | the imposition of new trade restrictions; |
| • | the imposition of restrictions on the activities of foreign agents, representatives and distributors; |
| • | difficulties in maintaining consistency with our internal guidelines; |
| • | complications arising from enforcing agreements and collecting receivables through certain foreign legal systems; and |
| • | uncertainties surrounding the enforcement or defense of our intellectual property rights. |
We purchase some of the key components of our products from single suppliers. The loss of these suppliers could prevent or delay shipments of our products or delay our clinical trials or otherwise adversely affect our business.
Some of the key components of our products and related services are currently purchased from only single suppliers with which we do not have long-term contracts. Some of these suppliers may be located outside of the United States, which could make us subject to foreign export laws and U.S. import and customs statutes and regulations, thus complicating and delaying shipments of components. If necessary or desirable, we could source our product components and related services from other suppliers. However, establishing additional or replacement suppliers for these components, and obtaining any necessary regulatory clearances or approvals, could take a substantial amount of time and could result in increased costs and impair our ability to produce our products, which would adversely impact our business, operating results and prospects.
If our independent contract manufacturers fail to timely deliver to us sufficient quantities of some of our products and components in a timely manner, our operations may be harmed.
Our reliance on independent contract manufacturers to manufacture most of our products and components involves several risks, including:
| • | inadequate capacity of the manufacturer’s facilities; |
| • | financial difficulties experienced by manufacturers due to the current economic weakness and uncertainty; |
| • | interruptions in access to certain process technologies; and |
| • | reduced control over product availability, quality, delivery schedules, manufacturing yields and costs. |
Shortages of raw materials, production capacity or financial constraints, or delays by our contract manufacturers could negatively affect our ability to meet our production obligations and result in increased prices for affected parts. Any such reduction, constraint or delay may result in delays in shipments of our products or increases in the prices of components, either of which could have a material adverse effect on our business. In addition, we could be forced to secure new or alternative contract manufacturers or suppliers. Securing a replacement contract manufacturer or supplier could be difficult. The introduction of new or alternative manufacturers or suppliers also may require design changes to our devices that are subject to FDA and other regulatory clearances or approvals. We may also be required to assess the new manufacturer’s compliance with
25
Table of Contents
all applicable regulations and guidelines, which could further impede our ability to manufacture our products in a timely manner. As a result, we could incur increased production costs, experience delays in deliveries of our products, suffer damage to our reputation and experience an adverse effect on our business and financial results.
We depend on the specialized knowledge and skills of our officers and other key employees, and if we are unable to retain and motivate them or recruit additional qualified personnel, our business will suffer.
We are highly dependent on our officers and other key employees. Due to the specialized knowledge and skills each of our officers and other key employees possesses with respect to the treatment of spine disorders and our operations, the loss of service of any of our officers and other key employees could delay or prevent the successful completion of our clinical trials, the growth of revenue from existing products and the commercialization of our new products. This risk may be exacerbated by the fact that our principal offices are not located in a large, metropolitan area, which could make it more difficult for us to retain employees or attract new employees with the required set of skills. Each of our officers and key employees may terminate his or her employment without notice and without cause or good reason.
We may need to raise additional capital in the future and, if we are unable to raise capital, it could force us to delay, reduce, eliminate or abandon our commercialization efforts or product development programs.
We completed a public offering of our common stock in September 2011 and we believe that our existing cash and cash equivalent balances and cash receipts generated from sales of our products will be sufficient to meet our anticipated cash requirements for at least the next twelve months. However, our future funding requirements will depend on many factors, including:
| • | market acceptance of our products and the revenues we are able to generate as a result; |
| • | the availability of adequate coverage and reimbursement for hospitals and surgeons; |
| • | the scope, rate of progress and cost of our clinical trials; |
| • | the cost of our research and development activities; |
| • | the cost of defending, in litigation or otherwise, any claims that we infringe third-party patent or other intellectual property rights; |
| • | the cost and timing of additional regulatory clearances or approvals; and |
| • | the cost and timing of establishing additional sales, marketing and distribution capabilities. |
As a result of the recent economic recession, and the continuing economic uncertainty, it has been difficult for companies, particularly small, medical device companies, to obtain equity or debt financing. If we raise additional funds by issuing equity or convertible debt securities, our stockholders may experience dilution and the securities may contain terms that are preferential to the new investors as compared to the holders of our common stock. If we raise additional funds by issuing debt securities, the securities may have rights senior to those associated with our common stock and contain covenants restricting our operations, our ability to pay dividends, the amount of capital expenditures we can make, or our ability to incur additional debt. Any debt financing or additional equity that we raise may contain terms that are not favorable to us or our stockholders. In addition, if we raise additional funds through collaboration and licensing arrangements with third parties, it may be necessary to relinquish some rights to our technologies or our products, or grant licenses on terms that are not favorable to us. If we are unable to raise adequate funds, we may have to delay, reduce the scope of or eliminate some or all of our planned product development and marketing efforts. Additionally, if we do not have, or are not able to obtain, sufficient funds, we may have to delay development or commercialization of our products or license to third parties the rights to commercialize products or technologies that we would otherwise seek to commercialize. We also may have to reduce marketing, customer support or other resources devoted to our products or cease operations.
26
Table of Contents
Pricing pressures in the healthcare industry could lead to further demands for price concessions and restricted access to spinal fusions, which could have an adverse effect on our business, financial condition or results of operations.
Because healthcare costs have risen significantly over the past decade, numerous initiatives and reforms initiated by legislators, regulators and third-party payors to curb these costs have resulted in difficulty in raising or maintaining prices and procedure volumes. The increase in pricing pressure is driven by the competitive environment in the spine market as many larger companies cut prices as they struggle to retain market share as total spine volume growth has begun to subside. Decreasing healthcare utilization as a result of the economic downturn, high unemployment rates, a reduction in the ranks of the full-time employed and the expiration of COBRA benefits has limited the number of patients that are covered for procedures and patients with coverage are faced with increasing deductibles. Additionally, potential patients are increasingly concerned about an extended absence from work, which would be typical of major surgery like lumbar fusion. The spine market generally, and lumbar fusion market in particular, has seen increasing push back from payors with regard to coverage. Spine surgery is a major cost area for payors, and from 2001 to 2008, lumbar fusions for lower back pain grew more than twice as fast as other lumbar fusions. As a result, private payors have increased the criteria that a patient must meet in order to be pre-authorized for lumbar fusion procedures and have put more effort into the preauthorization process. Payors have specifically stopped covering lumbar spine procedures involving degenerative disc disease patients that have no other symptoms such as leg pain or general spinal instability. We expect that market demand, government regulation, third-party reimbursement policies and societal pressures will continue to exert downward pressure on the prices of our products and may adversely impact our business, financial condition or results of operations.
We face the risk of product liability or other claims and may not be able to obtain sufficient insurance coverage, if at all.
Our business exposes us to the risk of product liability claims that is inherent in the testing, manufacturing and marketing of implantable medical devices. We may be subject to product liability claims if our products cause, or merely appear to have caused, an injury or death. Claims may be made by patients, consumers or healthcare providers. Although we have product liability and clinical trial liability insurance that we believe is appropriate for our current level of operations, this insurance is subject to deductibles and coverage limitations. Our current product liability insurance may not continue to be available to us on acceptable terms, if at all, and, if available, these coverages may not be adequate to protect us against any future product liability claims.
Further, we may be subject to claims against us even if the apparent injury is due to the actions of others. For example, we rely on the expertise of spine surgeons, nurses and other associated medical personnel to perform the medical procedure and related processes for our products. If these medical personnel are not properly trained or are negligent in their provision of care, the therapeutic effect of our products may be diminished or the patient may suffer critical injury, which may subject us to liability. In addition, an injury that is caused by the activities of our suppliers may be the basis for a claim against us.
These liabilities could prevent, delay or otherwise adversely interfere with our product commercialization efforts, and result in judgments, fines, damages and other financial liabilities which have adverse effects on our business, operating results and prospects.
We operate primarily at a single location. Any disruption in this facility could adversely affect our business and results of operations.
Our main office is located in Wilmington, North Carolina. In addition, we recently began operating a training facility in Raleigh, North Carolina. Our facilities may be affected by man-made or natural disasters, such as a hurricane. Our facilities, if damaged or destroyed, could require substantial lead-time to repair or replace. Although we believe we possess adequate insurance for damage to our property and the disruption of our business from casualties, this insurance may not be sufficient to cover all of our potential losses and may not continue to be available to us on acceptable terms, or at all.
27
Table of Contents
Risks Related to the Regulatory Environment
If we fail to maintain regulatory approvals and clearances, or are unable to obtain, or experience significant delays in obtaining, FDA clearances or approvals for our future products or product modifications, our ability to commercially distribute and market our products could suffer.
Our products are subject to rigorous regulation by the FDA and numerous other federal, state and foreign governmental authorities. The process of obtaining regulatory clearances or approvals to market a medical device can be costly and time consuming, and we may not be able to obtain these clearances or approvals on a timely basis, if at all. In particular, the FDA permits commercial distribution of most new medical devices only after the device has received clearance under Section 510(k) of the Federal Food, Drug and Cosmetic Act, or is the subject of an approved PMA. The FDA will clear marketing of a non-exempt lower risk medical device through the 510(k) process if the manufacturer demonstrates that the new product is substantially equivalent to other legally marketed products not requiring PMA approval. Our currently commercialized products that are not exempt have been cleared through the 510(k) process. However, we may need to submit a PMA for future products we develop. The PMA process is more costly, lengthy and uncertain than the 510(k) clearance process. A PMA application must be supported by extensive data, including, but not limited to, technical, preclinical, clinical trial, manufacturing and labeling data, to demonstrate to the FDA’s satisfaction the safety and efficacy of the device for its intended use.
Some of our new products will require FDA clearance of a 510(k). Other products may require the approval of a PMA. In addition some of our new products may require clinical trials to support regulatory approval and we may not successfully complete these clinical trials. The FDA may not approve or clear these products for the indications that are necessary or desirable for successful commercialization. The FDA may refuse our requests for 510(k) clearance or premarket approval of new products. Failure to receive clearance or approval for our new products would have an adverse effect on our ability to expand our business.
Any modification to our currently marketed 510(k)-cleared devices that could significantly affect their safety or efficacy, or that would constitute a change in their intended use, requires a new 510(k) clearance or, possibly, a PMA. The FDA requires every manufacturer to make this determination in the first instance, but the FDA may review the manufacturer’s decision. The FDA may not agree with our decisions regarding whether new clearances or approvals are necessary. If the FDA requires us to seek 510(k) clearance or a PMA for any modification to a previously cleared product, we may be required to cease marketing and distributing, or to recall the modified product until we obtain such clearance or approval, and we may be subject to significant regulatory fines or penalties. If the FDA disagrees and requires new clearances or approvals for the modifications, we may be required to recall and stop marketing our products as modified, which could require us to redesign our products and harm our operating results. In these circumstances, we may be subject to significant enforcement actions.
Where we determine that modifications to our products require a new 510(k) clearance or premarket approval application, we may not be able to obtain those additional clearances or approvals for the modifications or additional indications in a timely manner, or at all. For those products sold in the European Union, or E.U., we must notify our E.U. Notified Body if significant changes are made to the products or if there are substantial changes to our quality assurance systems affecting those products. Obtaining clearances and approvals can be a time consuming process, and delays in obtaining required future clearances or approvals would adversely affect our ability to introduce new or enhanced products in a timely manner, which in turn would harm our future growth.
The failure by us or one of our suppliers to comply with U.S. federal, state, and foreign governmental regulations could lead to the imposition of injunctions, suspensions or loss of regulatory clearance or approvals, product recalls, termination of distribution, product seizures or civil penalties, among other things. In the most extreme cases, criminal sanctions or closure of our manufacturing facility are possible. To the extent one of our suppliers fails to comply with applicable U.S. federal, state and foreign regulations, it may affect our ability
28
Table of Contents
either to obtain components and/or finished products or to have our finished products manufactured. In addition, changes in governmental policies or regulations may impose additional regulatory requirements on us, which could delay our ability to obtain new clearances or approvals and increase the costs of compliance. For instance, in response to concerns both within and outside FDA regarding the transparency and robustness of the 510(k) clearance process, in early 2011 FDA announced many action items it intends to take in efforts to improve the 510(k) program. The reforms, which will be implemented through a series of draft guidance documents and regulations issued over the coming months and years, may impose additional or different regulatory requirements on us and make it more difficult for us to obtain 510(k) clearances for our new devices and to commercialize modifications to our existing devices. Similarly, FDA is in the process of revising its manufacturer guidance for the validation of cleaning and sterilization instructions. FDA published a draft guidance for industry in May 2011 that when finalized may impose additional regulatory expectations on us and make it more difficult for us to obtain 510(k) clearances for our new devices or may require us to develop more robust validations for our currently marketed devices. Additionally, the Food and Drug Administration Amendments Act of 2007 (the “Amendments”) require, among other things, that FDA propose, and ultimately implement, regulations that will require manufacturers to label medical devices with unique identifiers unless a waiver is received from FDA. Once implemented, compliance with those regulations may require us to take additional steps in the manufacture of our products and labeling. These steps may require additional resources and could be costly.
Further, foreign governmental authorities that regulate the manufacture and sale of medical devices have become increasingly stringent and, to the extent we market and sell our products internationally, we may be subject to rigorous international regulation in the future. In these circumstances, we rely significantly on our foreign independent distributors to comply with the varying regulations, and any failures on their part could result in restrictions on the sale of our products in foreign countries. Approval or clearance by the FDA does not ensure approval by regulatory authorities in other jurisdictions, and approval by one foreign regulatory authority does not ensure approval by regulatory authorities in other foreign jurisdictions or by the FDA. The foreign regulatory approval process may include all of the risks associated with obtaining FDA approval in addition to other risks. In addition, the time required to obtain foreign approval may differ from that required to obtain FDA approval and we may not obtain foreign regulatory approvals on a timely basis, if at all. We may not be able to file for regulatory approvals and may not receive necessary approvals to commercialize our products in any foreign market
Conducting successful clinical studies may require the enrollment of large numbers of patients, and suitable patients may be difficult to identify and recruit. Patient enrollment in clinical trials and completion of patient participation and follow-up depends on many factors, including the size of the patient population, the nature of the trial protocol, the attractiveness of, or the discomforts and risks associated with, the treatments received by enrolled subjects, the attractiveness of, or the discomforts and risks associated with, the treatments received by enrolled subjects, the availability of appropriate clinical trial investigators and support staff, the proximity of patients to clinical sites and the ability of those patients to comply with the eligibility and exclusion criteria for participation in the clinical trial and meet study compliance requirements.
Development of sufficient and appropriate clinical protocols and data to demonstrate safety and efficacy are required and we may not adequately develop such protocols to support clearance and approval. Further, the FDA may require us to submit data on a greater number of patients than we originally anticipated and/or for a longer follow-up period or change the data collection requirements or data analysis applicable to our clinical trials. Delays in patient enrollment or failure of patients or clinical investigators to continue to participate in a clinical trial may cause an increase in costs and delays in the clearance or approval and attempted commercialization of our products or result in the failure of the clinical trial. In addition, despite considerable time and expense invested in our clinical trials, FDA may not consider our data adequate to demonstrate safety and efficacy. Such increased costs and delays or failures could adversely affect our business, operating results and prospects.
29
Table of Contents
Even if our products are approved by regulatory authorities, if we or our suppliers fail to comply with ongoing FDA or other foreign regulatory authority requirements, or if we experience unanticipated problems with our products, these products could be subject to restrictions or withdrawal from the market.
Any product for which we obtain clearance or approval, and the manufacturing processes, reporting requirements, post-approval clinical data and labeling and promotional activities for such product, will be subject to continued regulatory review, oversight and periodic inspections by the FDA and other domestic and foreign regulatory bodies. In particular, we and our suppliers are required to comply with QSR and Medical Device Directive regulations, which may include ISO standards, for the manufacture of our products and other regulations which cover the methods and documentation of the design, testing, production, control, quality assurance, labeling, packaging, storage and shipping of any product for which we obtain clearance or approval. Regulatory bodies enforce the QSR and ISO regulations through inspections. The failure by us or one of our suppliers to comply with applicable statutes and regulations administered by the FDA and other regulatory bodies, or the failure to timely and adequately respond to any adverse inspectional observations or product safety issues, could result in, among other things, warning letters, fines and civil penalties, delays in approving products, withdrawal or suspension of the approval of products, product recalls, operating restrictions, or unanticipated expenditures to address or defend regulatory actions. If any of these actions were to occur, it would harm our reputation and cause our product sales and profitability to suffer and may prevent us from generating revenue. Furthermore, our key suppliers may not currently be or may not continue to be in compliance with all applicable regulatory requirements which could result in our failure to produce our products on a timely basis and in the required quantities, if at all.
Even if regulatory clearance or approval of a product is granted, such clearance or approval may be subject to limitations on the intended uses for which the product may be marketed and reduce our potential to successfully commercialize the product and generate revenue from the product. If the FDA determines that our promotional materials, labeling, training or other marketing or educational activities constitute promotion of an unapproved use, it could request that we cease or modify our training educational, labeling or promotional materials or subject us to regulatory enforcement actions. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our training educational, labeling or other promotional materials to constitute promotion of an unapproved use, which could result in significant fines or penalties under other statutory authorities, such as laws prohibiting false claims for reimbursement.
We are subject to extensive regulation by the FDA. Our failure to meet strict regulatory requirements could require us to pay fines, incur other costs or even close our facilities.
Our facilities and manufacturing techniques generally must conform to standards that are established by the FDA and other government agencies, including those of European and other foreign governments. These regulatory agencies may conduct periodic audits or inspections of our facilities or our processes to monitor our compliance with applicable regulatory standards. If a regulatory agency finds that we have failed to comply with the appropriate regulatory standards, it may impose fines on us, delay or withdraw pre-market clearances or other regulatory approvals or, if such a regulatory agency determines that our non-compliance is severe, it may close our facilities. Any adverse action by an applicable regulatory agency could impair our ability to produce our products in a cost-effective and timely manner in order to meet our customers’ demands. We may also be required to bear other costs or take other actions that may have a negative impact on our future sales and our ability to generate profits.
Our products may in the future be subject to product recalls that could harm our reputation, business and financial results.
The FDA and similar foreign governmental authorities have the authority to require the recall of commercialized products in the event of material deficiencies or defects in design or manufacture. In the case of the FDA, the authority to require a recall must be based on an FDA finding that there is a reasonable probability
30
Table of Contents
that the device would cause serious injury or death. In addition, foreign governmental bodies have the authority to require the recall of our products in the event of material deficiencies or defects in design or manufacture. Manufacturers may, under their own initiative, recall a product if any material deficiency in a device is found. A government-mandated or voluntary recall by us or one of our distributors could occur as a result of component failures, manufacturing errors, design or labeling defects or other deficiencies and issues. Recalls of any of our products would divert managerial and financial resources and have an adverse effect on our financial condition and results of operations. The FDA requires that certain classifications of recalls be reported to FDA within 10 working days after the recall is initiated. Companies are required to maintain certain records of recalls, even if they are not reportable to the FDA. We may initiate voluntary recalls involving our products in the future that we determine do not require notification of the FDA. If the FDA disagrees with our determinations, they could require us to report those actions as recalls. A future recall announcement could harm our reputation with customers and negatively affect our sales. In addition, the FDA could take enforcement action for failing to report the recalls when they were conducted. Any recall or FDA requirement that we seek additional approvals or clearances could result in significant delays, fines, increased costs associated with modification of a product, loss of revenue and potential operating restrictions imposed by the FDA.
If our products, or malfunction of our products, cause or contribute to a death or a serious injury, we will be subject to medical device reporting regulations, which can result in voluntary corrective actions or agency enforcement actions.
Under the FDA medical device reporting regulations, medical device manufacturers are required to report to the FDA information that a device has or may have caused or contributed to a death or serious injury or has malfunctioned in a way that would likely cause or contribute to death or serious injury if the malfunction of the device or one of our similar devices were to recur. All manufacturers placing medical devices in the market in the European Union are legally bound to report any serious or potentially serious incidents involving devices they produce or sell to the Competent Authority in whose jurisdiction the incident occurred. Were this to happen to us, the relevant Competent Authority would file an initial report, and there would then be a further inspection or assessment if there are particular issues. This would be carried out either by the Competent Authority or it could require that the Notified Body, carry out the inspection or assessment.
Any such adverse event involving our products could result in future voluntary corrective actions, such as recalls or customer notifications, or agency action, such as inspection or enforcement action. Adverse events involving our products have been reported to us in the past, and we cannot guarantee that they will not occur in the future. Any corrective action, whether voluntary or involuntary, as well as defending ourselves in a lawsuit, will require the dedication of our time and capital, distract management from operating our business, and may harm our reputation and financial results.
We are subject to complex and evolving federal and state healthcare laws, including laws relating to fraud and abuse and health information privacy and security, and could be subjected to governmental investigations into our compliance with such laws and substantial penalties if we are shown to have failed to comply with such laws.
Although we do not provide healthcare services, submit claims for third-party reimbursement, or receive payments directly from Medicare, Medicaid, or other third-party payors for our products or the procedures in which our products are used, we are subject to healthcare fraud and abuse regulation and enforcement by both the federal government and the states in which we conduct our business. These healthcare laws and regulations include, for example:
| • | the federal Anti-kickback Statute, which prohibits, among other things, persons or entities from soliciting, receiving, offering or providing remuneration, directly or indirectly, in return for or to induce either the referral of an individual for, or the purchase order or recommendation of, any item or services for which payment may be made under a federal healthcare program such as the Medicare and Medicaid programs; |
31
Table of Contents
| • | the federal Health Insurance Portability and Accountability Act of 1996, which established federal crimes for knowingly and willfully executing a scheme to defraud any healthcare benefit program or making false statements in connection with the delivery of or payment for healthcare benefits, items or services; |
| • | federal false claims laws, which, prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent, and which may apply to entities like us to the extent that our interactions with customers may affect their billing or coding practices; and |
| • | state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws, which may apply to items or services reimbursed by any third-party payor, including commercial insurers. |
We have adopted policies and procedures designed to comply with the various healthcare laws applicable to our business. However, because of the breadth of these laws and regulations and the sometimes subjective nature of their application, it is possible that some of our business activities could be subject to challenge under one or more of such laws. The risk of being found to have violated such laws is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. In addition, in recent years, we believe that both federal and state regulators have increased regulation, enforcement, inspections and governmental investigations of the medical device industry, which further increases the risk that our business activities could be subject to challenge under certain laws. The PPACA, among other things, also amends the intent requirement of the federal anti-kickback and criminal healthcare fraud laws such that a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it, which further expands the breadth of the applicable laws. Furthermore, it is also possible that the government may assert that a claim including items or services resulting from a violation of the federal anti-kickback statute constitutes a false or fraudulent claim for purposes of the false claims statutes.
As discussed in more detail in the risk factor entitled “We are involved in an ongoing governmental investigation, the existence and results of which may adversely impact our business and results of operations”, in October 2011, we received a subpoena issued by the Department of Health and Human Services, Office of Inspector General, under the authority of the federal healthcare fraud and false claims laws. We are cooperating with the government’s request and are in the process of responding to the subpoena. No claims have been made against the Company at this time.
If our past or present operations, or those of our independent sales agents and distributors, are found to be in violation of any federal healthcare fraud and false claims laws, or any other applicable governmental regulations, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from federal healthcare programs and/or the curtailment or restructuring of our operations.
If the healthcare providers or entities with whom we do business are found to be non-compliant with applicable laws, they may be subject to sanctions, which could also have a negative impact on us. Any action against us for violation of these laws, even if we successfully defend against them, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business.
The PPACA imposes new reporting and disclosure requirements on device manufacturers for any “transfer of value” made or distributed to prescribers and other healthcare providers, effective March 30, 2013. Such information will be made publicly available in a searchable format beginning September 30, 2013. In addition, device manufacturers will also be required to report and disclose any investment interests held by physicians and their immediate family members during the preceding calendar year. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $150,000 per year (and up to an aggregate of $1 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests not reported in an annual submission.
32
Table of Contents
In addition, there has been a recent trend of increased federal and state regulation of payments made to physicians for marketing. Some states, such as California, Massachusetts and Vermont, mandate implementation of corporate compliance programs, along with the tracking and reporting of gifts, compensation, and other remuneration to physicians. The shifting commercial compliance environment and the need to build and maintain robust and expandable systems to comply with multiple jurisdictions with different compliance and/or reporting requirements increases the possibility that a healthcare company may run afoul of one or more of the requirements.
We are involved in an ongoing governmental investigation, the existence and results of which may adversely impact our business and results of operations.
In October 2011, we received a subpoena issued by the Department of Health and Human Services, Office of Inspector General, under the authority of the federal healthcare fraud and false claims laws. The subpoena seeks documents for the period January 1, 2008 through October 6, 2011. The Company is cooperating with the government’s request and is in the process of responding to the subpoena. While no claims have been made against the Company at this time, we cannot predict the ultimate outcome of the matters raised by the Office of Inspector General, and, if we are found to be in violation of any federal healthcare fraud and false claims laws, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from federal healthcare programs and/or the curtailment or restructuring of our operations. We are also unable to predict what impact, if any, the outcome of the matters raised by the Office of Inspector General will have on the willingness of surgeons to accept our products, our ability to hire or retain sales representatives and other employees, potential future reimbursement decisions by payors or other significant aspects of our business.
Any of the foregoing potential adverse developments related to the government investigation could have a material adverse effect on our business, financial position and results of operations. In addition, whether or not any claims are brought against the Company, the costs and expenses of responding to the government subpoena could be significant and could have a material adverse effect on our business, financial position and results of operations.
The use, misuse or off-label use of our products may harm our image in the marketplace or result in injuries that lead to product liability suits, which could be costly to our business or result in FDA sanctions if we are deemed to have engaged in such promotion.
Our currently marketed products have been cleared by the FDA’s 510(k) clearance process (or were exempt from the 510(k) process) for use under specific circumstances for the treatment of certain lower lumbar spine conditions. We cannot, however, prevent a physician from using our products or procedure outside of those indications cleared for use, known as off-label use. There may be increased risk of injury if physicians attempt to use our products off-label. We train our sales force not to promote our products for off-label uses. Furthermore, the use of our products for indications other than those indications for which our products have been cleared by the FDA may not effectively treat such conditions, which could harm our reputation in the marketplace among physicians and patients. Physicians may also misuse our products or use improper techniques, potentially leading to injury and an increased risk of product liability. If our products are misused or used with improper technique, we may become subject to costly litigation by our customers or their patients. Product liability claims could divert management’s attention from our core business, be expensive to defend and result in sizable damage awards against us that may not be covered by insurance. If we are deemed by the FDA to have engaged in the promotion of any our products for off-label use, it could request that we modify our training or promotional materials or we could be subject to FDA enforcement action, including significant fines and penalties, and the imposition of these sanctions could also affect our reputation and position within the industry. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our promotional or training materials to constitute promotion of an unapproved use, which could result in significant fines or penalties under other statutory authorities, such as laws prohibiting false claims for reimbursement. Any of these events could harm our business and results of operations and cause our stock price to decline.
33
Table of Contents
Risks Related to Our Intellectual Property
Our ability to protect our intellectual property and proprietary technology through patents and other means is uncertain.
Our success depends significantly on our ability to protect our proprietary rights to the procedures created with, and the technologies used in, our products. We rely on patent protection, as well as a combination of copyright, trade secret and trademark laws, and nondisclosure, confidentiality and other contractual restrictions to protect our proprietary technology. However, these legal means afford only limited protection and may not adequately protect our rights or permit us to gain or keep any competitive advantage. For example, our pending United States and foreign patent applications may not be approved, may not issue as patents in a form that will be advantageous to us, or may issue patents which may be subsequently successfully challenged by others and invalidated. In addition, our pending patent applications include claims to material aspects of our products and procedures that are not currently protected by issued patents. Both the patent application process and the process of managing patent disputes can be time consuming and expensive. The patents we own may not be of sufficient scope or strength to provide us with any meaningful protection or commercial advantage, and competitors may be able to design around our patents or develop products which provide outcomes which are comparable to ours. Although we have taken steps to protect our intellectual property and proprietary technology, including entering into confidentiality agreements and intellectual property assignment agreements with our officers, employees, consultants and advisors, such agreements may not be enforceable or may not provide meaningful protection for our trade secrets or other proprietary information in the event of unauthorized use or disclosure or other breaches of such agreements. Furthermore, the laws of some foreign countries do not protect our intellectual property rights to the same extent as do the laws of the United States.
We rely on our trademarks, trade names, and brand names to distinguish our products from the products of our competitors, and have registered or applied to register many of these trademarks. However, our trademark applications may not be approved. Third parties may also oppose our trademark applications, or otherwise challenge our use of the trademarks. In the event that our trademarks are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition, and could require us to devote resources to advertising and marketing new brands. Further, our competitors may infringe our trademarks, or we may not have adequate resources to enforce our trademarks.
In the event a competitor infringes upon our intellectual property rights, enforcing our rights may be costly, difficult and time consuming and we may not have sufficient resources to enforce such rights.
Any lawsuit, whether initiated by us to enforce our intellectual property rights or by a third party against us alleging infringement, may cause us to expend significant financial and other resources, and may divert our attention from our business and adversely affect our business, operating results and prospects.
The medical device industry is characterized by the existence of a large number of patents and frequent litigation based on allegations of patent infringement. Patent litigation can involve complex factual and legal questions and its outcome is uncertain. Any claim relating to infringement of patents that is successfully asserted against us may require us to pay substantial damages. Even if we were to prevail, any litigation could be costly and time-consuming and would divert the attention of our management and key personnel from our business operations.
Our success will also depend in part on our not infringing patents issued to others, including our competitors and potential competitors. If our products are found to infringe the patents of others, our development, manufacture and sale of such products could be severely restricted or prohibited. In addition, our competitors may independently develop similar technologies. Because of the importance of our patent portfolio and unpatented proprietary technology to our business, we may lose market share to our competitors if we fail to protect our patent rights.
34
Table of Contents
A patent infringement suit or other infringement or misappropriation claim brought against us or any of our strategic partners or licensees may force us or any of our strategic partners or licensees to stop or delay developing, manufacturing or selling potential products that are claimed to infringe a third party’s intellectual property, unless that party grants us or any strategic partners or licensees rights to use its intellectual property. In such cases, we may be required to obtain licenses to patents or proprietary rights of others in order to continue to commercialize our products. However, even if we, our strategic partners or our licensees are able to obtain rights to the third party’s intellectual property, these rights may be non-exclusive, thereby giving our competitors access to the same intellectual property. Also, there is the possibility that we may not be able to obtain any licenses required under any patents or proprietary rights of third parties on acceptable terms. Ultimately, we may be unable to commercialize some of our potential products or may have to cease some of our business operations as a result of patent infringement claims, which could severely harm our business.
Risks Related to our Common Stock
Our directors, officers and principal stockholders have significant voting power and may take actions that may not be in the best interests of our other stockholders.
Entities affiliated with Delphi Ventures and Advanced Technology Ventures, which are each principal stockholders of TranS1 Inc., purchased an aggregate of 2,538,461 shares of common stock in our September 2011 common stock financing at the public offering price. Additionally, David Simpson, one of our directors, and Joseph Slattery, our Chief Financial Officer, purchased 50,000 shares and 15,000 shares, respectively, in the offering at the public offering price. As a result, as of December 31, 2011, our officers, directors and principal stockholders, collectively held approximately 49.4% of our outstanding common stock. These stockholders, if they act together, could potentially exercise their significant voting power and influence the management and affairs of our company and most matters requiring stockholder approval, including the election of directors and approval of significant corporate transactions. This concentration of ownership may not be in the best interests of our other stockholders.
We may be unable to utilize our net operating loss carryforwards to reduce our income taxes.
As of December 31, 2011, we have federal net operating loss carryforwards (“NOL”) of approximately $83.5 million. In general, if there is an “ownership change” with respect to the Company, as defined under Section 382 of the Internal Revenue Code of 1986, as amended (“Code”), the utilization of our NOL carryfowards may be subject to substantial limitations imposed by the Code, and similar state provisions. As a result of prior offerings of our common stock, the utilization of the NOL carryfowards may be subject to the substantial limitations imposed by Section 382 of the Code, and similar state provisions.
The price of our common stock has been, and may continue to be, volatile and our stockholders may not be able to resell shares of our common stock at or above the price paid for such shares.
The price for shares of our common stock on the Nasdaq Global Market has exhibited high levels of volatility with significant price fluctuations, which makes our common stock unsuitable for many investors. For example, for the three years ended December 31, 2011, the closing price of our common stock ranged from a high of $8.60 per share to a low of $1.50 per share. At times, the fluctuations in the price of our common stock may have been unrelated to our operating performance. These broad fluctuations may negatively impact the market price of shares of our common stock.
Trading in our stock has historically been limited, so investors may not be able to sell as much stock as they want at prevailing prices.
The average daily trading volume in our common stock for the year ended December 31, 2011 was approximately 167,000 shares. If limited trading in our stock continues, it may be difficult for investors to sell
35
Table of Contents
their shares in the public market at any given time at prevailing prices. Moreover, the market price for shares of our common stock may be made more volatile because of the relatively low volume of trading in our common stock. When trading volume is low, significant price movement can be caused by the trading in a relatively small number of shares. Volatility in our common stock could cause stockholders to incur substantial losses.
Our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law contain provisions that could have the effect of deterring or delaying changes in incumbent management, proxy contests or changes in control.
Anti-takeover provisions of our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law may have the effect of deterring or delaying attempts by our stockholders to remove or replace management, engage in proxy contests and effect changes in control. The provisions of our charter documents include:
| • | a classified board so that only one of the three classes of directors on our board of directors is elected each year; |
| • | procedures for advance notification of stockholder director nominations and proposals; |
| • | the ability of our board of directors to amend our bylaws without stockholder approval; |
| • | a supermajority stockholder vote requirement for amending certain provisions of our amended and restated certificate of incorporation and our amended and restated bylaws; and |
| • | the ability of our board of directors to issue up to 5,000,000 shares of preferred stock without stockholder approval upon the terms and conditions and with the rights, privileges and preferences as our board of directors may determine. |
In addition, as a Delaware corporation, we are subject to Delaware law, including Section 203 of the Delaware General Corporation Law, or DGCL. In general, Section 203 prohibits a Delaware corporation from engaging in any business combination with any interested stockholder for a period of three years following the date that the stockholder became an interested stockholder unless certain specific requirements are met as set forth in Section 203. These provisions, alone or together, could have the effect of deterring or delaying changes in incumbent management, proxy contests or changes in control.
Item 1B. Unresolved Staff Comments.
None.
In February 2010, we moved into a new facility of approximately 31,000 square feet, located in Wilmington, North Carolina. Of that amount, approximately 5,000 square feet is used for manufacturing and warehousing, 19,000 square feet for office space and 7,000 square feet for research and development activities. This lease expires in December 2014, with an option to extend the lease through December 2019. We believe that our current facility will be sufficient to meet our needs through that time. In October 2011, we entered into a lease for a surgeon training facility of approximately 4,375 square feet, located in Raleigh, North Carolina. Of that amount, approximately 2,200 square feet is used for training activities and 2,175 square feet is used for office space.
We are subject to legal proceedings and claims in the ordinary course of our business. These claims potentially cover a variety of allegations spanning our entire business. The following is a brief discussion of the
36
Table of Contents
most significant claims that have been brought against us in the operation of our business. See Note 5 of Notes to Consolidated Financial Statements included in Item 8 of this annual report for additional discussion of legal matters.
In October 2011, we received a subpoena issued by the Department of Health and Human Services, Office of Inspector General, under the authority of the federal healthcare fraud and false claims statutes. The subpoena seeks documents for the period January 1, 2008 through October 6, 2011. We are cooperating with the government’s request and are in the process of responding to the subpoena. We are unable to predict what action, if any, might be taken in the future by the Department of Health and Human Services, Office of Inspector General or other governmental authorities as a result of the matters related to this subpoena or what impact, if any, the outcome of these matters might have on our consolidated financial position, results of operations, or cash flows. No claims have been made against us at this time.
On January 24, 2012, we received notice that a class action lawsuit had been filed in the U.S. District Court Eastern District, North Carolina, on behalf of a class consisting of all persons other than the defendants who purchased TranS1 securities between February 21, 2008 and October 17, 2011. We are in the process of responding to this lawsuit. We are unable to predict what impact, if any, the outcome of this matter might have on our consolidated financial position, results of operations, or cash flows.
Item 4. Mine Safety Disclosures
Not Applicable
37
Table of Contents
PART II
| Item 5. | Market for the Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Price of Common Stock
Our common stock is traded on the NASDAQ Global Market under the symbol “TSON.” The following table sets forth the high and low sales prices of our common stock as quoted on the NASDAQ Global Market for the periods indicated.
| Price Range | ||||||||
| High | Low | |||||||
| Fiscal 2011: |
||||||||
| Fourth quarter |
$ | 3.33 | $ | 1.39 | ||||
| Third quarter |
5.22 | 2.58 | ||||||
| Second quarter |
5.42 | 4.08 | ||||||
| First quarter |
5.20 | 2.00 | ||||||
| Fiscal 2010: |
||||||||
| Fourth quarter |
$ | 2.63 | $ | 1.76 | ||||
| Third quarter |
2.98 | 2.21 | ||||||
| Second quarter |
3.93 | 2.55 | ||||||
| First quarter |
4.11 | 3.01 | ||||||
The closing price for our common stock as reported by the NASDAQ Global Market on March 9, 2012 was $3.45 per share.
As of March 9, 2012, we had approximately 28 stockholders of record based upon the records of our transfer agent, which does not include beneficial owners of our common stock whose shares are held in the names of various securities brokers, dealers and registered clearing agencies.
Uses of Proceeds from Sale of Registered Securities
On October 22, 2007, we completed our initial public offering of 6,325,000 shares of common stock at the initial public offering price of $15.00 per share. We effected the offering through a Registration Statement on Form S-1 (Registration No. 333-144802), which was declared effective by the SEC on October 16, 2007, and through a Registration Statement on Form S-1 filed pursuant to Rule 462(b) under the Securities Act (Registration No. 333-146753), which became effective upon filing on October 17, 2007 pursuant to Rule 462(b).
In May 2011, we filed a “universal shelf” Registration Statement on Form S-3 (Filing No. 333-174255) with the SEC, which became effective on August 1, 2011 (the “Shelf Registration Statement”). Depending on our non-affiliated public equity float during the time period prior to consummating a financing transaction, and during the time period following effectiveness of the Shelf Registration Statement, the Shelf Registration Statement allows us to raise up to $50 million through the sale of debt securities, common stock, preferred stock, or warrants, or any combination thereof.
On September 21, 2011, we entered into a purchase agreement with Piper Jaffray & Co., as the lead underwriter, to sell 6,200,000 shares of our common stock in a public offering. The shares were offered and sold pursuant to a prospectus supplement dated September 21, 2011 and an accompanying base prospectus dated August 1, 2011, in connection with a “takedown” offering pursuant to the Shelf Registration Statement. On September 26, 2011, the shares were sold to the public at a price of $3.25 per share. The net proceeds, after deducting underwriting discounts, commissions and offering expenses, were $18.2 million. The timing and terms of any additional financing transactions pursuant to the Shelf Registration Statement have not yet been determined.
38
Table of Contents
Dividend Policy
We have never declared or paid any cash dividends on our capital stock. We currently intend to retain future earnings, if any, for development of our business and do not anticipate that we will declare or pay cash dividends on our capital stock in the foreseeable future.
Securities Authorized For Issuance Under Equity Compensation Plans
The information regarding securities authorized for issuance under our equity compensation plans is set forth in Item 12 of this annual report and is incorporated herein by reference.
Stock Price Performance Graph
The following graph compares the cumulative total stockholder return on our common stock from October 17, 2007 (the date our common stock began trading on the NASDAQ Global Market) through December 31, 2011 to that of the cumulative return over such period for (i) The NASDAQ Stock Market Composite Index, and (ii) NASDAQ Medical Equipment Index. Total stockholder return assumes $100.00 invested at the beginning of the period in our common stock and in each of the comparative indices. The graph further assumes that such amount was initially invested in our common stock at the closing market price on the first day of trading, and that any dividends have been reinvested. We have not paid any dividends on our common stock. The stock price performance on the following graph is not necessarily indicative of future stock price performance.
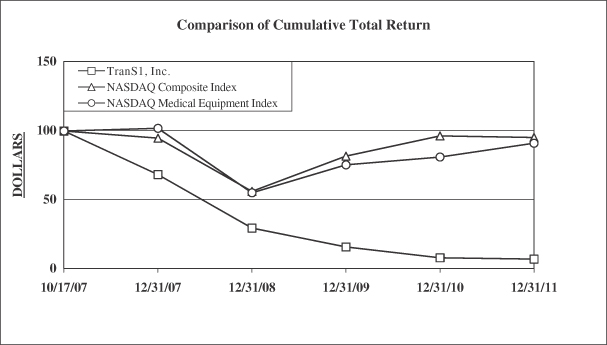
The material in the above performance graph does not constitute soliciting material and should not be deemed filed or incorporated by reference into any other Company filing, whether under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, whether made on, before or after the date of this annual report and irrespective of any general incorporation language in such filing, except to the extent we specifically incorporate this performance graph by reference therein.
39
Table of Contents
| Item 6. | Selected Financial Data. |
The following selected financial data has been derived from our audited consolidated financial statements. You should read the following financial information together with the information under “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our consolidated financial statements and the related notes included elsewhere in this annual report.
| Years Ended December 31, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| (in thousands, except share data) | ||||||||||||||||||||
| Consolidated Statements of Operations Data: |
||||||||||||||||||||
| Revenue |
$ | 19,153 | $ | 26,154 | $ | 29,807 | $ | 25,304 | $ | 16,473 | ||||||||||
| Cost of revenue |
4,555 | 7,104 | 5,687 | 4,315 | 3,042 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Gross profit |
14,598 | 19,050 | 24,120 | 20,989 | 13,431 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Operating expenses |
||||||||||||||||||||
| Research and development |
5,191 | 4,223 | 6,439 | 4,081 | 3,885 | |||||||||||||||
| Sales and marketing |
21,561 | 26,275 | 34,098 | 29,375 | 15,706 | |||||||||||||||
| General and administrative |
6,125 | 8,565 | 7,184 | 7,116 | 3,801 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total operating expenses |
32,877 | 39,063 | 47,721 | 40,572 | 23,392 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Operating loss |
(18,279 | ) | (20,013 | ) | (23,601 | ) | (19,583 | ) | (9,961 | ) | ||||||||||
| Other income, net |
6 | 486 | 405 | 2,548 | 1,384 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net loss |
$ | (18,273 | ) | $ | (19,527 | ) | $ | (23,196 | ) | $ | (17,035 | ) | $ | (8,577 | ) | |||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net loss per common share — basic and diluted |
$ | (0.81 | ) | $ | (0.94 | ) | $ | (1.13 | ) | $ | (0.84 | ) | $ | (1.46 | ) | |||||
| Weighted average common shares outstanding — basic and diluted |
22,587,749 | 20,738,433 | 20,603,600 | 20,288,711 | 5,872,008 | |||||||||||||||
| December 31, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Consolidated Balance Sheet Data: |
||||||||||||||||||||
| Cash, cash equivalents and short-term investments |
$ | 44,751 | $ | 42,536 | $ | 55,251 | $ | 77,266 | $ | 93,921 | ||||||||||
| Working capital |
47,972 | 46,166 | 63,467 | 84,174 | 98,351 | |||||||||||||||
| Total assets |
54,032 | 52,019 | 68,991 | 90,491 | 102,856 | |||||||||||||||
| Noncurrent liabilities |
26 | — | — | — | — | |||||||||||||||
| Common stock |
3 | 2 | 2 | 2 | 2 | |||||||||||||||
| Additional paid in capital |
158,403 | 138,401 | 136,402 | 133,507 | 103,325 | |||||||||||||||
| Total stockholders’ equity |
49,500 | 47,728 | 65,280 | 85,586 | 99,439 | |||||||||||||||
40
Table of Contents
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
The following discussion of our financial condition and results of operations should be read in conjunction with our “Risk Factors” and our consolidated financial statements and the related notes to our consolidated financial statements included in this annual report. The following discussion contains forward-looking statements. See “Cautionary Note Regarding Forward-Looking Statements” at the beginning of this annual report.
Overview
We are a medical device company focused on designing, developing and marketing products that implement our proprietary approach to treat degenerative conditions of the spine affecting the lower lumbar region. We are committed to delivering minimally invasive surgical technologies that enhance patient clinical care while providing sustained value for our customers. Using our pre-sacral approach, a surgeon can access discs in the lower lumbar region of the spine through an incision adjacent to the tailbone and can perform an entire interbody fusion procedure through instrumentation that provides direct access to the intervertebral space. We developed our pre-sacral approach to allow spine surgeons to access and treat intervertebral spaces without compromising important surrounding soft tissue, nerves and bone structures. We believe this approach enables fusion procedures to be performed with potentially lower complication rates, lower blood loss, shorter hospital stays, faster recovery times and reduced pain. We currently market our AxiaLIF® family of products for single and two level lumbar fusion, the VEO™ lateral access and interbody fusion system, the Vectre™ and Avatar™ lumbar posterior fixation systems and Bi-Ostetic™ bone void filler, a biologics product. We also market products that may be used with our AxiaLIF surgical approach, including bowel retractors, a bone graft harvesting system and additional discectomy tools.
From our incorporation in 2000 through 2004, we devoted substantially all of our resources to research and development and start-up activities, consisting primarily of product design and development, clinical trials, manufacturing, recruiting qualified personnel and raising capital. We received 510(k) clearance from the FDA for our AxiaLIF 1L product in the fourth quarter of 2004, and commercially introduced our AxiaLIF 1L product in the United States in the first quarter of 2005. We received a CE mark to market our AxiaLIF 1L product in the European market in the first quarter of 2005 and began commercialization in the first quarter of 2006. We received a CE mark for our AxiaLIF 2L product in the third quarter of 2006 and began commercialization in the European market in the fourth quarter of 2006. We received FDA 510(k) clearance for our AxiaLIF 2L product and began marketing this product in the United States in the second quarter of 2008. The AxiaLIF 2L product was discontinued in 2010 after we launched our AxiaLIF 2L+™ product in July 2010, for which we had received FDA 510(k) clearance in January 2010. We commercially launched our next generation Vectre facet screw system in April 2010. In the first quarter of 2010, we entered into agreements to distribute Avatar, a pedicle screw system, and Bi-Ostetic bone void filler, a biologics product. We commercially launched our AxiaLIF 1L+ product in September 2011, for which we had received FDA 510(k) clearance in March 2011. In 2010, we received 510(k) clearance for our VEO lateral access and interbody fusion system, which was officially launched in November 2011. We currently sell our products through a direct sales force, independent sales agents and international distributors.
We rely on third parties to manufacture all of our products and their components, except for our nitinol nucleus cutter blades, which we manufacture at our facility in Wilmington, North Carolina. Our outsourcing partners are manufacturers that meet FDA, ISO or other internal quality standards, where applicable. We believe these manufacturing relationships allow us to work with suppliers who have the best specific competencies while we minimize our capital investment, control costs and shorten cycle times, all of which we believe allows us to compete with larger-volume manufacturers of spine surgery products.
Since inception, we have been unprofitable. As of December 31, 2011, we had an accumulated deficit of $108.9 million.
41
Table of Contents
We expect to continue to invest in creating a sales and marketing infrastructure for our AxiaLIF family of products in order to gain wider acceptance for them. We also expect to continue to invest in research and development and related clinical trials, and increase general and administrative expenses as we grow. As a result, we will need to generate significant revenue in order to achieve profitability.
In 2011, we received positive reimbursement coverage decisions from Horizon Blue Cross and Blue Shield of New Jersey, and Palmetto GBA, the Medicare Administrator for California, Virginia, North Carolina, South Carolina, Nevada, West Virginia and Hawaii. In 2012, we have received additional positive reimbursement coverage decisions from Health Care Services Corporation, or HCSC, the Blue Cross and Blue Shield provider for Texas, Illinois, New Mexico and Oklahoma, Hawaii Medical Service Association, the Blue Cross and Blue Shield provider for Hawaii, Geisinger, a provider in Pennsylvania, and HealthSpring, a payor in the mid-Atlantic. Following these coverage decisions, we believe that coverage for our AxiaLIF procedure includes approximately 36 million covered lives. However, HCSC has recently issued an updated policy, effective June 1, 2012, that removes coverage for AxiaLIF. We are working diligently to alter this policy prior to its implementation. We intend to pursue further positive reimbursement coverage decisions with other payors in the coming quarters by utilizing published clinical literature and leveraging the support of physicians that perform our procedures. Discussions are normally held with medical directors representing the payors to educate them on the existing published clinical literature.
On March 5, 2012, we announced that the CPT Editorial Panel, or the Panel, has voted to approve an application for a new Category I CPT code, 225XX1, for L5/S1 spinal fusion utilizing our AxiaLIF implant when performing a pre-sacral interbody fusion. In addition, the Panel has voted to establish a new Category III CPT code, 019XXT, as an add-on code to the new Category I code for L4/5 spinal fusion. The new CPT codes were announced on the AMA’s website on March 2, 2012, and will become effective on January 1, 2013.
On September 26, 2011, we completed a public offering of 6,200,000 shares of our common stock at an offering price of $3.25 per share. The offering resulted in aggregate proceeds to us of approximately $18.2 million, net of underwriting discounts, commissions and offering expenses.
Results of Operations
| Years Ended December 31, | ||||||||||||||||||||
| 2011 | 2010 | % change | 2009 | % change | ||||||||||||||||
| (in thousands, except gross margin percentage) | ||||||||||||||||||||
| Revenue |
$ | 19,153 | $ | 26,154 | (26.8 | )% | $ | 29,807 | (12.3 | )% | ||||||||||
| Cost of revenue |
4,555 | 7,104 | (35.9 | )% | 5,687 | 24.9 | % | |||||||||||||
| Gross margin % |
76.2 | % | 72.8 | % | 4.6 | % | 80.9 | % | (10.0 | )% | ||||||||||
| Total operating expenses |
32,877 | 39,063 | (15.8 | )% | 47,721 | (18.1 | )% | |||||||||||||
| Net loss |
(18,273 | ) | (19,527 | ) | 6.4 | % | (23,196 | ) | 15.8 | % | ||||||||||
Revenue
We generate revenue from the sales of our implants and disposable surgical instruments. We have two distinct sales methods. The first method is when implants and/or disposable surgical instruments are sold directly to hospitals or surgical centers for the purpose of conducting a scheduled surgery. Our sales representatives or independent sales agents hand deliver the products to the customer on or before the day of the surgery. The sales representative or independent agent is then responsible for reporting the delivery of the products and the date of the operation to the corporate office for proper revenue recognition. We recognize revenue upon the confirmation that the products have been used in a surgical procedure. The other sales method is for sales to distributors outside the United States. These transactions require the customer to send in a purchase order before shipment will be made and the customer only has the right of return for defective products. We recognize revenue upon the shipment of the product to distributors outside the United States. We expect that a substantial amount of our revenues will continue to be generated in the United States in future periods.
42
Table of Contents
Cost of Revenue
Cost of revenue consists primarily of material and overhead costs related to our products and product royalties. Overhead costs include facilities-related costs, such as rent, utilities and depreciation.
Research and Development
Research and development expenses consist primarily of personnel costs within our product development, regulatory and clinical functions and the costs of clinical studies, product development projects and technology licensing costs. In future periods, we expect research and development expenses to grow as we continue to invest in basic research, clinical trials, product development and intellectual property.
Sales and Marketing
Sales and marketing expenses consist of personnel costs, sales commissions paid to our direct sales representatives and independent sales agents, and costs associated with physician training programs, promotional activities and participation in medical and trade conferences.
General and Administrative
General and administrative expenses consist of personnel costs related to the executive, finance, business development, and human resource functions, as well as professional service fees, legal fees, accounting fees, insurance costs and general corporate expenses.
Other Income, Net
Other income, net is composed of government grants, interest earned on our cash, cash equivalents and available-for-sale securities and the gain or loss on disposal of fixed assets. In 2010, we received grants of $0.5 million from the U.S. Treasury under the Qualifying Therapeutic Discovery Program.
Comparison of the Years Ended December 31, 2011, 2010 and 2009
Revenue. Revenue was $19.2 million in 2011, $26.2 million in 2010 and $29.8 million in 2009. The $7.0 million decrease in revenue from 2010 to 2011 and the $3.6 million decrease in revenue from 2009 to 2010 was primarily a result of a lower number of AxiaLIF cases performed in each subsequent year, which was due primarily to physician reimbursement limitations and insurance denials for lumbar fusion surgery due to the lack of medical necessity. These decreases were partially offset by price increases in April 2011 and April 2010 and increased revenues from the introduction of new or enhanced products, including our new lateral product and the AxiaLIF 1L+ in 2011, and the AxiaLIF 2L+ and bone void filler in 2010. Domestically, sales of our AxiaLIF single level products decreased to $9.4 million in 2011 from $12.9 million in 2010 and $17.1 million in 2009. Sales of our AxiaLIF 2L products were $5.1 million in 2011, $7.8 million in 2010 and $7.8 million in 2009. Sales of our Bi-Ostetic bone void filler, which was introduced in February 2010, increased from $0.6 million in 2010 to $1.0 million in 2011. In 2011, we also generated $0.4 million in revenue from our VEO lateral access and interbody fusion system, which began its limited market release in June 2011 and was commercially launched in November 2011. Additionally, during 2011, 2010 and 2009, we generated $1.0 million, $1.9 million and $3.1 million, respectively, in revenues from sales of our facet and Vectre screw systems. Sales of our pedicle screw system, which was introduced in the first quarter of 2010, decreased from $0.6 million in 2010 to $0.3 million in 2011. In 2011, average revenue per AxiaLIF case continued to increase from 2010 and 2009, due to a price increase effective April 1, 2011, the release of our new AxiaLIF and lateral products and penetration into existing cases by our other products. In 2011, 2010 and 2009, we recorded 1,298, 1,985 and 2,578 domestic AxiaLIF cases, respectively, including 343 AxiaLIF 2L+ cases in 2011, 555 AxiaLIF 2L and 2L+ cases in 2010 and 596 AxiaLIF 2L cases in 2009. Revenue generated outside the United States decreased to $1.7 million in 2011 from $2.4 million in 2010, which was an increase from $1.8 million in 2009. In 2011, 2010 and 2009, initial stocking shipments to new distributors were $47,000, $110,000 and $122,000, respectively. In 2009, we began direct sales
43
Table of Contents
through our own sales representatives and independent sales agents in Europe and generated revenue of $1.0 million in 2011, $1.3 million in 2010 and $543,000 in 2009. In 2011 and 2010, 91% of our revenues were generated in the United States compared to 94% in 2009.
Cost of Revenue. Cost of revenue decreased to $4.6 million in 2011 from $7.1 million in 2010 and $5.7 million in 2009. The $2.5 million decrease from 2010 to 2011 was primarily related to inventory obsolescence reserves of $2.0 million taken in 2010 for products that were being replaced, or were obsolete and excess, compared to $0.5 million in obsolescence reserves taken in 2011, and lower material and overhead costs associated with decreased sales volume for our products. The $1.4 million increase from 2009 to 2010 was primarily related to inventory obsolescence reserves of $2.0 million taken in 2010 as discussed above, partially offset by lower material and overhead costs associated with decreased sales volume for our products. Gross margin increased to 76.2% in 2011, from 72.8% in 2010 which was a decrease from 80.9% in 2009. The increase in gross margin from 2010 to 2011 was primarily related to the additional inventory reserves that were taken in 2010, as discussed above, partially offset by changes in product sales mix and pricing pressures from customers. The decrease in gross margin from 2009 to 2010 was primarily related to the inventory reserves of $2.0 million taken in 2010.
Research and Development. Research and development expenses increased to $5.2 million in 2011 from $4.2 million in 2010, which was a decrease from $6.4 million in 2009. The $1.0 million increase in expense from 2010 to 2011 was primarily the result of a $0.5 million expense in 2011 to acquire the exclusive license of our new VEO lateral access and interbody fusion system and an increase in clinical project-related spending. The $2.2 million decrease in expense from 2009 to 2010 was primarily the result of a $1.0 million expense in 2009 to acquire certain technology development rights and a decrease in project spending in 2010.
Sales and Marketing. Sales and marketing expenses decreased to $21.6 million in 2011 from $26.3 million in 2010 and $34.1 million in 2009. The decrease in expense from 2010 to 2011 of $4.7 million was primarily due to lower personnel-related costs of $3.6 million, including lower commissions of $1.7 million, as we reduced our direct sales headcount, decreased promotional costs by $0.9 million, decreased travel and entertainment expenses by $0.7 million and decreased surgeon training costs by $0.3 million. These lower expenses were partially offset by an increase in consulting costs of $0.4 million related to our reimbursement efforts and $0.2 million related to the closing costs for our international office. The decrease in expense from 2009 to 2010 of $7.8 million was primarily due to decreased personnel related costs of $2.6 million as we reduced our U.S. sales force, decreased travel and entertainment expenses of $2.2 million, lower commissions of $1.7 million related to the lower revenue, decreased surgeon training costs of $1.6 million and a decrease in promotional costs of $0.4 million. These lower expenses were partially offset by severance costs of $0.5 million for employees affected by the sales force reduction.
General and Administrative. General and administrative expenses decreased to $6.1 million in 2011 from $8.6 million in 2010 and $7.2 million in 2009. The decrease in expenses from 2010 to 2011 of $2.5 million was primarily attributable to a decrease in personnel-related costs related to the management transition that incurred in 2010, including severance, recruiting and other personnel-related expenses of $1.1 million, a decrease in employee and related costs of $0.9 million, decreased legal costs of $0.2 million, a decrease in bad debt expense of $0.2 million and a decrease in consulting expense of $0.1 million, offset by an increase in directors and officers insurance of $0.3 million. The increase in expenses from 2009 to 2010 of $1.4 million was primarily attributable to an increase in personnel-related costs related to the management transition that incurred in 2010, including severance, recruiting and other personnel-related expenses of $1.1 million.
Other Income, Net. Other income, net, decreased to $6,000 in 2011 from $0.5 million in 2010, which was an increase from $0.4 million in 2009. The decrease of $0.5 million from 2010 to 2011 was primarily the result of a grant we received from the U.S. Treasury under the Qualifying Therapeutic Discovery Program in 2010 for $0.5 million. The increase of $0.1 million from 2009 to 2010 was primarily the result of the $0.5 million grant discussed above, partially offset by a decrease of $0.3 million in interest income due to our lower cash on hand and lower interest rates on our investments and the loss on disposal of fixed assets of $0.1 million.
44
Table of Contents
Liquidity and Capital Resources
Sources of Liquidity
Since our inception in 2000, we have incurred significant losses and, as of December 31, 2011, we had an accumulated deficit of $108.9 million. We have not yet achieved profitability, and anticipate that we will continue to incur losses in the near term. We expect to continue to fund research and development, sales and marketing and general and administrative expenses at similar to current levels or higher and, as a result, we will need to generate significant revenues to achieve profitability. Prior to our October 2007 initial public offering, our operations were funded primarily with the gross proceeds from the sale of preferred stock of $40.5 million. The net proceeds from our October 2007 initial public offering of $86.7 million and the net proceeds of our September 2011 stock offering of $18.2 million have funded our operations since then.
In May 2011, we filed the Shelf Registration Statement with the SEC, which became effective on August 1, 2011. Depending on our non-affiliated public equity float during the time period prior to consummating a financing transaction, the Shelf Registration Statement allows us to raise up to an additional $29.85 million through the sale of debt securities, common stock, preferred stock, or warrants, or any combination thereof.
On September 21, 2011, we entered into a purchase agreement with Piper Jaffray & Co. as the lead underwriter, to sell 6,200,000 shares of our common stock in a public offering. The shares were offered and sold pursuant to a prospectus supplement dated September 21, 2011 and an accompanying base prospectus dated August 1, 2011, in connection with a “takedown” offering pursuant to the Shelf Registration Statement. On September 26, 2011, the shares were sold to the public at a price of $3.25 per share. The net proceeds, after deducting underwriting discounts, commissions and offering expenses, were $18.2 million. The timing and terms of any additional financing transactions pursuant to the Shelf Registration Statement or otherwise, have not yet been determined.
As of December 31, 2011, we did not have any significant outstanding debt financing arrangements, we had working capital of $48.0 million and our primary source of liquidity was $44.8 million in cash, cash equivalents and short-term investments. We currently invest our cash and cash equivalents primarily in money market treasury funds and our short-term investments primarily in U.S. agency backed debt instruments.
Cash, cash equivalents and short-term investments increased from $42.5 million at December 31, 2010 to $44.8 million at December 31, 2011. The increase of $2.3 million was primarily the result of net cash provided of $18.2 million from the sale of our common stock in the September 2011 public offering, common stock issued under our employee stock purchase plan of $0.2 million and from the exercise of stock options of $0.1 million, offset by net cash used in operating activities of $15.6 million and purchases of property and equipment of $0.7 million.
Cash, cash equivalents and short-term investments decreased from $55.3 million at December 31, 2009 to $42.5 million at December 31, 2010. The decrease of $12.8 million was primarily the result of net cash used in operating activities of $12.3 million and purchases of property and equipment of $0.6 million offset by net cash provided from the issuance of our common stock upon the exercise of stock options of $0.1 million.
Cash Flows
Net Cash Used in Operating Activities. Net cash used in operating activities was $15.6 million in 2011, $12.3 million in 2010 and $20.8 million in 2009. For each of these periods, net cash used in operating activities was attributable primarily to net losses after adjustment for non-cash items, such as depreciation, stock-based compensation expense, inventory reserves, bad debt reserves, and the loss on sale of fixed assets, combined with changes in working capital requirements to support the market acceptance of our products.
45
Table of Contents
Net Cash Provided by Investing Activities. Net cash provided by investing activities was $11.3 million in 2011, $7.3 million in 2010 and $8.0 million in 2009. For each of these periods, this amount reflected purchases or sales and maturities of investments and purchases of property and equipment, primarily for reusable instrument kits used in the field and information technology needs.
Net Cash Provided by Financing Activities. Net cash provided by financing activities was $18.4 million in 2011 and $0.1 million in 2010 and 2009. Net cash provided by financing activities which represented the net proceeds from the issuance of shares of common stock in the September 2011 public offering of $18.2 million, shares issued related to the employee stock purchase plan of $0.2 million, and shares issued upon the exercise of stock options of $0.1 million.
Operating Capital and Capital Expenditure Requirements
We believe that our existing cash and cash equivalents and short-term investments, together with cash received from sales of our products, will be sufficient to meet our anticipated cash needs for at least the next twelve months. We intend to spend substantial amounts on sales and marketing initiatives to support the ongoing commercialization of our products and on research and development activities, including product development, regulatory and compliance, clinical studies in support of our currently marketed products and future product offerings, and the enhancement and protection of our intellectual property. We may need to obtain additional financing to pursue our business strategy, to respond to new competitive pressures or to take advantage of opportunities that may arise.
Under the Shelf Registration Statement, we have the ability to issue debt securities, common stock, preferred stock, or warrants, or any combination thereof. The sale of additional equity or convertible debt securities could result in dilution to our stockholders. In addition, any debt securities we issue could have rights senior to those associated with our common stock and could contain covenants that would restrict our operations. Furthermore, any preferred equity securities we issue could have rights senior to those associated with our common stock. Depending on our non-affiliated public equity float during the time period prior to consummating another financing transaction, the Shelf Registration Statement will allow us to raise up to an additional $29.85 million of securities. The timing and terms of any additional financing transactions, whether pursuant to the Shelf Registration Statement or otherwise, have not yet been determined. Any additional financing may not be available in amounts or on terms acceptable to us, if at all. If we are unable to obtain this additional financing, we may be required to reduce the scope of our planned product development and marketing efforts.
In October 2011, we received a subpoena issued by the Department of Health and Human Services, Office of Inspector General, under the authority of the federal healthcare fraud and false claims statutes. We are cooperating with the government’s request and are in the process of responding to the subpoena. Although we cannot predict whether or when proceedings might be initiated by the federal government or when these matters may be resolved, it is not unusual for investigations such as these to continue for a considerable period of time. Responding to the subpoena will continue to require management’s attention and significant legal expense. Any negative findings could result in substantial financial penalties against us. To our knowledge, no proceedings have been initiated against the Company at this time. We are currently unable to predict what impact, if any, the outcome of this matter might have on our consolidated financial position, results of operations, or cash flows.
In January 2012, we received notice that a class action lawsuit had been filed in the U.S. District Court Eastern District, North Carolina, on behalf of a class consisting of all persons other than the defendants who purchased our common stock between February 21, 2008 and October 17, 2011. Responding to the lawsuit will require management’s attention and significant legal expense. We are currently unable to predict what impact, if any, the outcome of this matter might have on our consolidated financial position, results of operations, or cash flows.
46
Table of Contents
Contractual Obligations and Commitments
The following table discloses information about our contractual obligations by the year in which payments are due as of December 31, 2011:
| Payments Due by Year | ||||||||||||||||||||
| Contractual Obligations and Commitments |
Total | Less Than 1 Year |
1-3 Years | 3-5 Years | After 5 Years |
|||||||||||||||
| ( in thousands) | ||||||||||||||||||||
| Operating leases(1) |
$ | 1,495 | $ | 418 | $ | 864 | $ | 169 | $ | 44 | ||||||||||
| (1) | We rent office space under an operating lease which expires in 2014, with an option to extend the lease through 2019. We also rent space for a training facility which expires in 2017, with an option to extend the lease through 2022. |
Reserves for uncertain tax positions — The table above does not include $1.0 million of total gross unrecognized tax benefits as of December 31, 2011. Due to the high degree of uncertainty regarding the timing of potential cash flows, we cannot reasonably estimate the settlement periods, if any, for these amounts.
Off-Balance Sheet Arrangements
As of December 31, 2011, we did not have any outstanding debt or available debt financing arrangements or off-balance sheet liabilities.
Critical Accounting Policies and Estimates
Our discussion and analysis of our financial condition and results of operations is based upon our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of financial statements requires management to make estimates and judgments that affect the reported amounts of assets and liabilities, revenue and expenses, and disclosures of contingent assets and liabilities at the date of the financial statements. On an on-going basis, we evaluate our estimates, including those related to revenue recognition, accounts receivable reserves, inventory reserves, accrued expenses, income tax valuations and stock-based compensation. We base our estimates on historical experience and various other assumptions that we believe to be reasonable, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not apparent from other sources. Actual results could differ from those estimates under different assumptions or conditions.
We believe the following critical accounting policies affect our more significant judgments and estimates used in the preparation of our consolidated financial statements.
Revenue Recognition. We recognize revenue based on the following criteria: (i) persuasive evidence that an arrangement exists with the customer; (ii) delivery of the products and/or services has occurred; (iii) the selling price has been fixed for the products or services delivered; and (iv) collection is reasonably assured. Revenue is generated from the sale of our implants and disposable surgical instruments. We have two distinct sales methods. The first method is when implants and/or disposable surgical instruments are sold directly to hospitals or surgical centers for the purpose of conducting a scheduled surgery. Our sales representatives or independent sales agents hand deliver the procedure kit to the customer on or before the day of the surgery. The sales representative or independent agent is then responsible for reporting the delivery of the products and the date of the surgery to our corporate office for proper revenue recognition. We recognize revenue upon the confirmation that the products have been used in a surgical procedure. The other sales method is for sales to distributors outside the United States. These distributors order multiple procedure kits at one time to have on hand. These transactions require the customer to send in a purchase order before shipment will be made to the customer. Under the distributor agreements currently in place, a distributor only has the right of return for defective products. We recognize revenue upon the shipment of the product to distributors outside the United States.
47
Table of Contents
Accounts Receivable and Allowances. We monitor collections and payments from our customers and maintain an allowance for doubtful accounts based upon our historical experience and any specific customer collection issues that we have identified. While our credit losses have historically been within our expectations and the allowance established, we may not continue to experience the same credit loss rates that we have in the past. We make estimates on the collectability of customer accounts based primarily on analysis of historical trends and experience and changes in customers’ financial condition. Management uses its best judgment, based on the best available facts and circumstances, and records a reserve against the amounts due to reduce the receivable to the amount that is expected to be collected. These reserves are reevaluated and adjusted as additional information is received that impacts the amount reserved.
Inventory. We state our inventories at the lower of cost or market, computed on a standard cost basis, which approximates actual cost on a first-in, first-out basis and market being determined as the lower of replacement cost or net realizable value. Costs are monitored on an annual basis and updated as necessary to reflect changes in supplier costs and the rate of our overhead absorption is adjusted based on projections of our manufacturing costs and production plan. The components of inventory are reviewed on a periodic basis for excess, obsolete and impaired inventory, and a reserve is recorded for the identified items. An inventory reserve is calculated for estimated excess and obsolete inventory based upon historical turnover and assumptions about future demand for the products and market conditions.
Accounting for Income Taxes. Significant management judgment is required in determining our provision for income taxes, our deferred tax assets and liabilities and any valuation allowance recorded against our net deferred tax assets. We account for income taxes using the liability method which requires the recognition of deferred tax assets or liabilities for the temporary differences between financial reporting and tax bases of the Company’s assets and liabilities and for tax carryforwards at enacted statutory tax rates in effect for the years in which the differences are expected to reverse. The effect on deferred taxes of a change in tax rates is recognized in the period that includes the enactment date. In addition, valuation allowances are established when necessary to reduce deferred tax assets to the amounts expected to be realized. We have recorded a full valuation allowance on our net deferred tax assets as of December 31, 2011 due to uncertainties related to our ability to utilize our deferred tax assets in the foreseeable future.
Stock-Based Compensation. The fair value of stock options is estimated using a Black-Scholes option pricing model. This model requires the input of subjective assumptions, including expected stock price volatility, expected life and estimated forfeitures of each award. All options granted after January 1, 2006 are expensed on a straight-line basis over the vesting period. Due to the limited amount of historical data available to us, particularly with respect to stock-price volatility, employee exercise patterns and forfeitures, actual results could differ materially from our expectations.
Recent Accounting Pronouncements
In May 2011, the FASB issued new authoritative guidance to provide a consistent definition of fair value and ensure that fair value measurements and disclosure requirements are similar between GAAP and International Financial Reporting Standards. This guidance changes certain fair value measurement principles and enhances the disclosure requirements for fair value measurements. This guidance is effective for interim and annual periods beginning after December 15, 2011 and is applied prospectively. We do not expect that the adoption of this guidance will have a material impact on our financial statements.
In June 2011, the FASB issued a standard on the presentation of other comprehensive income. This guidance eliminates the option to present the components of other comprehensive income as part of the statement of changes in stockholders’ equity and requires the presentation of other comprehensive income in a single continuous statement, or in two separate, but consecutive, statements. This guidance is effective for fiscal years and interim periods beginning after December 15, 2011. In December 2011, the FASB issued an amendment to indefinitely defer one of the requirements contained in the June 2011 standard. That requirement called for
48
Table of Contents
reclassification adjustments from accumulated other comprehensive income to be measured and presented by income statement line item in net income and also in other comprehensive income. We do not expect that the adoption of this standard will have a material effect on our financial statements.
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk |
We are filing this annual report as a “Smaller Reporting Company” and, as a result, are not required to provide disclosure in this Item 7A of Part II of Form 10-K.
| Item 8. | Financial Statements and Supplementary Data. |
The consolidated financial statements and supplementary data required by this item are set forth under Item 15 of this annual report.
| Item 9. | Changes in and Disagreements With Accountants on Accounting and Financial Disclosure. |
None.
| Item 9A. | Controls and Procedures |
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our principal executive officer and principal financial officer, evaluated the effectiveness of our disclosure controls and procedures (as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended, or the Exchange Act) as of December 31, 2011. We maintain disclosure controls and procedures that are designed to provide a reasonable assurance level that information required to be disclosed in our reports filed or submitted under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms and that such information is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate, to allow for timely decisions regarding required disclosure. Our management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on the evaluation of our disclosure controls and procedures as of December 31, 2011, our principal executive officer and principal financial officer concluded that, as of such date, our disclosure controls and procedures were effective at the reasonable assurance level.
Internal Control Over Financial Reporting
Management’s annual report on internal control over financial reporting. Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Our internal control system was designed to provide reasonable assurance to our management and board of directors regarding the preparation and fair presentation of published financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness for future periods are subject to the risk that internal control may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management assessed the effectiveness of internal controls over financial reporting as of December 31, 2011. In making this assessment, we used the criteria set forth in Internal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on management’s
49
Table of Contents
assessment, we concluded that, as of December 31, 2011, our internal control over financial reporting was effective based on those criteria.
This annual report does not include an attestation report of our independent registered public accounting firm regarding internal control over financial reporting. Management’s report was not subject to attestation by our independent registered public accounting firm pursuant to rules of the SEC that permit us to provide only management’s report in this annual report.
Changes in Internal Control over Financial Reporting. There has been no change in our internal control over financial reporting (as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) during our most recent fiscal quarter that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Reporting Status
Effective July 1, 2010, we became a “Smaller Reporting Company” under Rule 12b-2 of the Exchange Act and we continue to qualify as a “Smaller Reporting Company” for purposes of filing this annual report. Prior to that date, we were an “Accelerated Filer” under Rule 12b-2. This classification is based on the aggregate market value of our voting and non-voting stock held by non-affiliates as of the last business day of our second fiscal quarter of any particular fiscal year.
| Item 9B. | Other Information. |
None.
50
Table of Contents
PART III
| Item 10. | Directors, Executive Officers and Corporate Governance. |
The information required by this Item is incorporated herein by reference to our definitive Proxy Statement on Schedule 14A, which will be filed within 120 days of December 31, 2011 and delivered to our stockholders in connection with our 2012 annual meeting of stockholders.
| Item 11. | Executive Compensation. |
The information required by this Item is incorporated herein by reference to our definitive Proxy Statement on Schedule 14A, which will be filed within 120 days of December 31, 2011, and delivered to our stockholders in connection with our 2012 annual meeting of stockholders.
The material incorporated herein by reference to the material under the caption “Compensation Committee Report” in the Proxy Statement shall be deemed furnished, and not filed, in this annual report and shall not be deemed incorporated by reference into any filing under the Securities Act or the Exchange Act as a result of this furnishing, except to the extent that we specifically incorporate it by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters. |
| Plan category |
(a) Number of securities to be issued upon exercise of outstanding options, warrants and rights |
(b) Weighted- average exercise price of outstanding options, warrants and rights |
(c) Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a)) |
|||||||||
| Equity compensation plans approved by security holders |
2,729,885 | $ | 4.92 | 1,551,882 | ||||||||
| Equity compensation plans not approved by security holders |
— | — | ||||||||||
|
|
|
|
|
|||||||||
| Total |
2,729,885 | $ | 4.92 | 1,551,882 | ||||||||
|
|
|
|
|
|||||||||
The number of securities remaining available for future issuance includes 187,610 shares available for purchase under the Company’s 2007 Employee Stock Purchase Plan. The number of shares subject to purchase under this plan during the current six-month purchase period ending May 31, 2012 is approximately 39,000.
With the exception of the information regarding securities authorized for issuance under our equity compensation plans set forth above, the information required by this Item is incorporated herein by reference to our definitive Proxy Statement on Schedule 14A, which will be filed within 120 days of December 31, 2011 and delivered to stockholders in connection with our 2012 annual meeting of our stockholders.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence. |
The information required by this Item is incorporated herein by reference to our definitive Proxy Statement on Schedule 14A, which will be filed within 120 days of December 31, 2011, and delivered to our stockholders in connection with our 2012 annual meeting of stockholders.
| Item 14. | Principal Accountant Fees and Services. |
The information required by this Item is incorporated herein by reference to our definitive Proxy Statement on Schedule 14A, which will be filed within 120 days of December 31, 2011, and delivered to our stockholders in connection with our 2012 annual meeting of stockholders.
51
Table of Contents
PART IV
| Item 15. | Exhibits, Financial Statement Schedules. |
| (a) | Financial Statements |
| (1) | Index to Financial Statements |
| Page | ||||
| 55 | ||||
| 56 | ||||
| 57 | ||||
| 58 | ||||
| 59 | ||||
| 60 | ||||
| (2) Financial Statement Schedule: Schedule II — Valuation Accounts |
74 | |||
All other financial statement schedules have been omitted because they are not applicable, not required or the information required is shown in the financial statements or the notes thereto.
| (3) Exhibits |
75 |
The exhibits filed with this annual report on Form 10-K are listed in the Exhibit Index immediately following the financial statement schedules, which Exhibit Index is incorporated herein by reference.
52
Table of Contents
Pursuant to the requirements of Section 13(a) or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this annual report to be signed on its behalf by the undersigned thereunto duly authorized.
| TranS1 Inc. | ||
| By: | /s/ Ken Reali | |
| Ken Reali | ||
| President and Chief Executive Officer | ||
| (Principal Executive Officer) | ||
Date: March 16, 2012
POWER OF ATTORNEY
We, the undersigned directors and officers of TranS1 Inc., do hereby constitute and appoint Ken Reali and Joseph Slattery, and each of them, as our true and lawful attorneys-in-fact and agents with power of substitution, to do any and all acts and things in our name and behalf in our capacities as directors and officers and to execute any and all instruments for us and in our names in the capacities indicated below, which said attorney-in-fact and agent may deem necessary or advisable to enable said corporation to comply with the Securities Exchange Act of 1934, as amended, and any rules, regulations and requirements of the Securities and Exchange Commission, in connection with this Annual Report on Form 10-K, including specifically but without limitation, power and authority to sign for us or any of us in our names in the capacities indicated below, any and all amendments hereto; and we do hereby ratify and confirm all that said attorney-in-fact and agent, shall do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this Annual Report on Form 10-K has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
| /s/ Ken Reali Ken Reali |
President, Chief Executive Officer and Director (Principal Executive Officer) | March 16, 2012 | ||
| /s/ Joseph Slattery Joseph Slattery |
Executive Vice President and Chief Financial Officer (Principal Financial and Accounting Officer) |
March 16, 2012 | ||
| /s/ Michael Carusi Michael Carusi |
Director | March 16, 2012 | ||
| /s/ Paul LaViolette Paul LaViolette |
Lead Director | March 16, 2012 | ||
| /s/ Jonathan Osgood Jonathan Osgood |
Director | March 16, 2012 | ||
| /s/ Richard Randall Richard Randall |
Chairman of the Board | March 16, 2012 | ||
| /s/ James Shapiro James Shapiro |
Director | March 16, 2012 | ||
| /s/ David Simpson David Simpson |
Director | March 16, 2012 | ||
53
Table of Contents
Index to Consolidated Financial Statements
| Page | ||||
| 55 | ||||
| 56 | ||||
| 57 | ||||
| 58 | ||||
| 59 | ||||
| 60 | ||||
54
Table of Contents
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of TranS1 Inc.
In our opinion, the consolidated financial statements listed in the index appearing under Item 15(a)(1) present fairly, in all material respects, the financial position of TranS1, Inc. and its subsidiaries at December 31, 2011 and 2010, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2011 in conformity with accounting principles generally accepted in the United States of America. In addition, in our opinion, the financial statement schedule listed in the index appearing under Item 15(a)(2) presents fairly, in all material respects, the information set forth therein when read in conjunction with the related consolidated financial statements. These financial statements and financial statement schedule are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements and financial statement schedule based on our audits. We conducted our audits of these statements in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
| /s/ PricewaterhouseCoopers LLP |
| Raleigh, NC |
| March 16, 2012 |
55
Table of Contents
Consolidated Balance Sheets
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (In thousands, except share amounts) |
||||||||
| Assets | ||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 38,724 | $ | 24,461 | ||||
| Short-term investments |
6,027 | 18,075 | ||||||
| Accounts receivable, net |
2,522 | 3,654 | ||||||
| Inventory |
4,525 | 3,878 | ||||||
| Prepaid expenses and other assets |
680 | 389 | ||||||
|
|
|
|
|
|||||
| Total current assets |
52,478 | 50,457 | ||||||
| Property and equipment, net |
1,554 | 1,562 | ||||||
|
|
|
|
|
|||||
| Total assets |
$ | 54,032 | $ | 52,019 | ||||
|
|
|
|
|
|||||
| Liabilities and Stockholders’ Equity | ||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 3,303 | $ | 2,214 | ||||
| Accrued expenses |
1,203 | 2,077 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
4,506 | 4,291 | ||||||
|
|
|
|
|
|||||
| Noncurrent liabilities: Commitments and contingencies (Note 5) |
26 | — | ||||||
| Stockholders’ equity: |
||||||||
| Preferred stock, $0.0001 par value; 5,000,000 shares authorized, none issued and outstanding at December 31, 2011 and 2010. |
— | — | ||||||
| Common stock, $0.0001 par value; 75,000,000 shares authorized, 27,244,059 and 20,877,171 shares issued and outstanding at December 31, 2011 and 2010, respectively |
3 | 2 | ||||||
| Additional paid-in capital |
158,403 | 138,401 | ||||||
| Accumulated other comprehensive income (loss) |
13 | (29 | ) | |||||
| Accumulated deficit |
(108,919 | ) | (90,646 | ) | ||||
|
|
|
|
|
|||||
| Total stockholders’ equity |
49,500 | 47,728 | ||||||
|
|
|
|
|
|||||
| Total liabilities and stockholders’ equity |
$ | 54,032 | $ | 52,019 | ||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of these consolidated financial statements.
56
Table of Contents
Consolidated Statements of Operations
(in thousands, except per share amounts)
| Year Ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Revenue |
$ | 19,153 | $ | 26,154 | $ | 29,807 | ||||||
| Cost of revenue |
4,555 | 7,104 | 5,687 | |||||||||
|
|
|
|
|
|
|
|||||||
| Gross profit |
14,598 | 19,050 | 24,120 | |||||||||
|
|
|
|
|
|
|
|||||||
| Operating expenses: |
||||||||||||
| Research and development |
5,191 | 4,223 | 6,439 | |||||||||
| Sales and marketing |
21,561 | 26,275 | 34,098 | |||||||||
| General and administrative |
6,125 | 8,565 | 7,184 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total operating expenses |
32,877 | 39,063 | 47,721 | |||||||||
|
|
|
|
|
|
|
|||||||
| Operating loss |
(18,279 | ) | (20,013 | ) | (23,601 | ) | ||||||
| Other income, net |
6 | 486 | 405 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net loss |
$ | (18,273 | ) | $ | (19,527 | ) | $ | (23,196 | ) | |||
|
|
|
|
|
|
|
|||||||
| Net loss per common share — basic and diluted |
$ | (0.81 | ) | $ | (0.94 | ) | $ | (1.13 | ) | |||
|
|
|
|
|
|
|
|||||||
| Weighted average common shares outstanding — basic and diluted |
22,588 | 20,738 | 20,604 | |||||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
57
Table of Contents
Consolidated Statements of Stockholders’ Equity
| Common Stock | Additional Paid - In Capital |
Accumulated Other Comprehensive Income (Loss) |
Accumulated Deficit |
Total Stockholders’ Equity |
||||||||||||||||||||
| Number | Amount | |||||||||||||||||||||||
| (in thousands, except share data) | ||||||||||||||||||||||||
| Balance at December 31, 2008 |
20,538,333 | $ | 2 | $ | 133,507 | $ | — | $ | (47,923 | ) | $ | 85,586 | ||||||||||||
| Issuance of common stock from exercised options |
110,114 | 96 | 96 | |||||||||||||||||||||
| Stock based compensation |
2,799 | 2,799 | ||||||||||||||||||||||
| Other comprehensive loss |
(5 | ) | (5 | ) | ||||||||||||||||||||
| Net loss |
(23,196 | ) | (23,196 | ) | ||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Balance at December 31, 2009 |
20,648,447 | 2 | 136,402 | (5 | ) | (71,119 | ) | 65,280 | ||||||||||||||||
| Issuance of common stock from exercised options |
228,724 | 148 | 148 | |||||||||||||||||||||
| Stock based compensation |
1,851 | 1,851 | ||||||||||||||||||||||
| Other comprehensive loss |
(24 | ) | (24 | ) | ||||||||||||||||||||
| Net loss |
(19,527 | ) | (19,527 | ) | ||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Balance at December 31, 2010 |
20,877,171 | 2 | 138,401 | (29 | ) | (90,646 | ) | 47,728 | ||||||||||||||||
| Issuance of common stock from exercised options |
104,498 | 111 | 111 | |||||||||||||||||||||
| Issuance of common stock from equity financing |
6,200,000 | 1 | 18,175 | 18,176 | ||||||||||||||||||||
| Issuance of common stock from employee stock purchase plan |
62,390 | 158 | 158 | |||||||||||||||||||||
| Stock based compensation |
1,558 | 1,558 | ||||||||||||||||||||||
| Other comprehensive income |
42 | 42 | ||||||||||||||||||||||
| Net loss |
(18,273 | ) | (18,273 | ) | ||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Balance at December 31, 2011 |
27,244,059 | $ | 3 | $ | 158,403 | $ | 13 | $ | (108,919 | ) | $ | 49,500 | ||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
58
Table of Contents
Consolidated Statements of Cash Flows
| Year Ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| (in thousands) | ||||||||||||
| Cash flows from operating activities: |
||||||||||||
| Net loss |
$ | (18,273 | ) | $ | (19,527 | ) | $ | (23,196 | ) | |||
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||||||
| Depreciation |
662 | 746 | 909 | |||||||||
| Stock-based compensation |
1,558 | 1,851 | 2,799 | |||||||||
| Allowance for excess and obsolete inventory |
521 | 2,004 | 505 | |||||||||
| Provision for bad debts |
31 | 226 | 80 | |||||||||
| Loss on sale of fixed assets |
54 | 70 | — | |||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Decrease in accounts receivable |
1,101 | 46 | 806 | |||||||||
| (Increase) decrease in inventory |
(1,168 | ) | 1,443 | (1,461 | ) | |||||||
| (Increase) decrease in prepaid expenses |
(291 | ) | 287 | (44 | ) | |||||||
| Increase (decrease) in accounts payable |
1,089 | (228 | ) | (454 | ) | |||||||
| Increase (decrease) in accrued expenses |
(848 | ) | 808 | (745 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in operating activities |
(15,564 | ) | (12,274 | ) | (20,801 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Cash flows from investing activities: |
||||||||||||
| Purchases of property and equipment |
(708 | ) | (565 | ) | (1,310 | ) | ||||||
| Purchases of investments |
(16,102 | ) | (18,050 | ) | (50,872 | ) | ||||||
| Sales and maturities of investments |
28,150 | 25,928 | 60,134 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by investing activities |
11,340 | 7,313 | 7,952 | |||||||||
|
|
|
|
|
|
|
|||||||
| Cash flows from financing activities: |
||||||||||||
| Net proceeds from issuance of common stock |
18,334 | 148 | 96 | |||||||||
| Proceeds from exercise of stock options |
111 | — | — | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by financing activities |
18,445 | 148 | 96 | |||||||||
|
|
|
|
|
|
|
|||||||
| Effect of exchange rate changes on cash and cash equivalents |
42 | (24 | ) | — | ||||||||
|
|
|
|
|
|
|
|||||||
| Net increase (decrease) in cash and cash equivalents |
14,263 | (4,837 | ) | (12,753 | ) | |||||||
| Cash and cash equivalents, beginning of period |
24,461 | 29,298 | 42,051 | |||||||||
|
|
|
|
|
|
|
|||||||
| Cash and cash equivalents, end of period |
$ | 38,724 | $ | 24,461 | $ | 29,298 | ||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
59
Table of Contents
Notes to Consolidated Financial Statements
| 1. | Organization |
TranS1 Inc., a Delaware corporation (the “Company”), was incorporated in May 2000 and is headquartered in Wilmington, North Carolina. The Company is a medical device company focused on designing, developing and marketing products to treat degenerative conditions of the spine affecting the lower lumbar region. The Company operates in one business segment. The Company currently markets the AxiaLIF® family of products for single and two level lumbar fusion, the VEO™ lateral access and interbody fusion system, the Vectre™ and Avatar™ posterior fixation systems and Bi-Ostetic™ bone void filler, a biologics product. All of the Company’s AxiaLIF products are delivered using its pre-sacral approach. The Company also markets products that may be used with its surgical approach, including bowel retractors, a bone graft harvesting system and additional discectomy tools. The AxiaLIF 1L product was commercially released in January 2005. The AxiaLIF 2L™ product was commercially released in Europe in the fourth quarter of 2006 and in the United States in the second quarter of 2008. The AxiaLIF 2L product was discontinued in 2010 after the Company launched its AxiaLIF 2L+™ product in July 2010. The Company commercially launched its next generation Vectre facet screw system in April 2010. In the first quarter of 2010, the Company entered into agreements to distribute Avatar, a pedicle screw system, and Bi-Ostetic bone void filler, a biologics product. The Company commercially launched its AxiaLIF 1L+ product in September 2011, for which it had received Food and Drug Administration, or FDA, 510(k) clearance in March 2011. In 2010, the Company received 510(k) clearance for its lateral access and interbody fusion system, which was commercially launched in November 2011. The Company sells its products directly to hospitals and surgical centers in the United States and certain European countries, and to independent distributors elsewhere.
On September 26, 2011, the Company completed a public offering of 6,200,000 shares of its common stock at an offering price of $3.25 per share. The offering resulted in aggregate proceeds to the Company of approximately $18.2 million, net of underwriting discounts, commissions and offering expenses, and has been included in Stockholders’ Equity as common stock and additional paid-in capital. At December 31, 2011 and December 31, 2010, there were 27,244,059 and 20,877,171 shares of common stock issued and outstanding, respectively, and there were no shares of preferred stock issued and outstanding.
The Company is subject to a number of risks similar to other similarly-sized companies in the medical device industry. These risks include, without limitation, acceptance and continued use of the Company’s products by surgeons, the lack of clinical data about the efficacy of these products, uncertainty of reimbursement from third-party payors, cost pressures in the healthcare industry, competitive pressures from substitute products and larger companies, the historical lack of profitability, the dependence on key employees, regulatory approval and market acceptance for new products, compliance with complex and evolving healthcare laws and regulations, uncertainty surrounding the outcome of the matters relating to the subpoena issued to the Company by the Department of Health and Human Services, Office of Inspector General, stockholder class action lawsuits, the reliance on a limited number of suppliers to provide these products, changes in economic conditions, the ability to effectively manage a sales force to meet the Company’s objectives and the ability to conduct successful clinical studies.
| 2. | Summary of Significant Accounting Policies |
Basis of Presentation
The Company has prepared the accompanying consolidated financial statements in conformity with accounting principles generally accepted in the United States of America. The Company’s fiscal year ends on December 31.
60
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Principles of Consolidation
These consolidated financial statements include the accounts of the Company and its subsidiaries. All intercompany transactions and accounts have been eliminated in consolidation.
For the Company’s international operations, local currencies have been determined to be the functional currencies. We translate the financial statements of international subsidiaries to their U.S. dollar equivalents at end-of-period currency exchange rates for assets and liabilities and at average exchange rates for revenues and expenses. We record these translation adjustments as a component of other comprehensive loss within stockholders’ equity. The Company recognizes transaction gains and losses arising from fluctuations in currency exchange rates on transactions denominated in currencies other than the functional currency in the consolidated income statements. The Company incurred a foreign currency exchange gain of $42,000 in 2011 and foreign currency exchange losses of $24,000 and $5,000 in the years ended December 31, 2010 and 2009, respectively.
Use of Estimates
The consolidated financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America. These principles require management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the dates of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting periods. Actual results could differ from those estimates. The principal estimates relate to accounts receivable reserves, inventory reserves, stock-based compensation, accrued expenses and income tax valuations.
Cash and Cash Equivalents
The Company considers all highly liquid investments with an original maturity of three months or less at the date of purchase to be cash equivalents. Cash and cash equivalents include money market treasury funds. Cash equivalents are carried at fair market value. Related unrealized gains and losses were not material as of December 31, 2011 and 2010.
Investments
All marketable investments are classified as available-for-sale and therefore are carried at fair market value. Related unrealized gains and losses were not material as of December 31, 2011 and 2010. Realized gains and losses on the sale of all such investments are reported in earnings and computed using the specific identification cost method and were not material for the years ended December 31, 2011 and 2010. All of the Company’s investments as of December 31, 2011 have maturities of one year or less. Short-term investments at December 31, 2011 and 2010 consisted of U.S. agency backed debt instruments.
Fair Value of Financial Instruments
The carrying values of cash equivalents, short-term investments, accounts receivable, and accounts payable at December 31, 2011 and 2010 approximated their fair values due to the short-term nature of these items.
At December 31, 2011, the Company held certain assets that are required to be measured at fair value on a recurring basis. These assets included available for sale securities classified as cash equivalents and short-term investments. Accounting Standards Codification (“ASC”) 820-10 requires the valuation of investments using a three-tiered approach, which requires that fair value measurements be classified and disclosed in one of three
61
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
tiers. These tiers are: Level 1, defined as quoted prices in active markets for identical assets or liabilities; Level 2, defined as valuations based on observable inputs other than those included in Level 1, such as quoted prices for similar assets and liabilities in active markets, or other inputs that are observable or can be corroborated by observable input data; and Level 3, defined as valuations based on unobservable inputs reflecting the Company’s own assumptions, consistent with reasonably available assumptions made by other market participants.
At December 31, 2011, all available for sale securities are classified as Level 1 assets with a fair value of $44.4 million, which included money market funds of $38.4 million and short-term investments of $6.0 million. At December 31, 2010, all available for sale securities are classified as Level 1 assets with a fair value of $42.1 million, which included money market funds of $24.0 million and short-term investments of $18.1 million. The Company had no Level 2 or Level 3 assets or liabilities at December 31, 2011 or 2010.
Available for sale securities classified as Level 1 assets were:
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (In thousands) | ||||||||
| Cash and cash equivalents |
$ | 38,340 | $ | 24,070 | ||||
| Short-term investments |
6,027 | 18,075 | ||||||
|
|
|
|
|
|||||
| Total available for sale securities |
$ | 44,367 | $ | 42,145 | ||||
|
|
|
|
|
|||||
Accounts Receivable
Accounts receivable are presented net of an allowance for uncollectible accounts. Estimates on the collectability of customer accounts are based primarily on analysis of historical trends and experience and changes in customers’ financial condition. The following table presents the components of accounts receivable:
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (in thousands) | ||||||||
| Gross accounts receivable |
$ | 2,871 | $ | 4,001 | ||||
| Allowance for uncollectible accounts |
(349 | ) | (347 | ) | ||||
|
|
|
|
|
|||||
| Total accounts receivable, net |
$ | 2,522 | $ | 3,654 | ||||
|
|
|
|
|
|||||
Concentration of Credit Risk and Significant Customers
Financial instruments which potentially subject the Company to concentrations of credit risk consist principally of cash and cash equivalents.
The Company places cash deposits with a federally insured financial institution, in amounts that at times exceed the federally insured limit, which was $250,000 at December 31, 2011 and 2010. The total amount of deposits in excess of federally insured limits was $133,342 and $179,335 at December 31, 2011 and 2010, respectively.
In 2011, 2010 and 2009 no customer accounted for 10% or more of revenues. As of December 31, 2011 and 2010, no single customer accounted for 10% or more of the accounts receivable balance.
62
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Inventories
Inventories consist of the following:
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (in thousands) | ||||||||
| Work-in-process |
$ | 2,515 | $ | 2,005 | ||||
| Finished goods |
1,771 | 1,727 | ||||||
| Raw materials |
239 | 146 | ||||||
|
|
|
|
|
|||||
| Total inventories, net |
$ | 4,525 | $ | 3,878 | ||||
|
|
|
|
|
|||||
Inventories are stated at the lower of cost or market, computed on a standard cost basis, which approximates actual cost on a first-in, first-out basis and market being determined as the lower of replacement cost or net realizable value. Costs are monitored on an annual basis and updated as necessary to reflect changes in supplier costs and the rate of our overhead absorption is adjusted based on projections of our manufacturing costs and production plan. The components of inventory are reviewed on a periodic basis for excess, obsolete and impaired inventory, and a reserve is recorded for the identified items. An inventory reserve is calculated for estimated excess and obsolete inventory based upon historical turnover and assumptions about future demand for the products and market conditions. At December 31, 2011 and 2010, the allowance for excess and obsolete inventory was $2.6 million and $2.2 million, respectively.
Property and Equipment
Property and equipment are recorded at cost and depreciated over their estimated useful lives primarily using the straight-line method. Leasehold improvements are amortized over the shorter of the lease term or the estimated useful life of the related asset. Maintenance and repairs are charged to expense as incurred. Upon retirement or sale, the cost of assets disposed of and the related accumulated depreciation and amortization are removed from the accounts and any resulting gain or loss is credited or charged to income.
The estimated useful lives are:
| Furniture and fixtures |
5-10 years | |||
| Equipment |
3-10 years | |||
| Other depreciable assets |
2-10 years | |||
| Leasehold improvements |
Lesser of estimated useful life or lease term |
Revenue Recognition
Revenue is recognized based on the following criteria: (i) persuasive evidence that an arrangement exists with the customer; (ii) delivery of the products and/or services has occurred; (iii) the selling price has been fixed for the products or services delivered; and (iv) collection is reasonably assured. Revenue is generated from the sale of implants and disposable surgical instruments. The Company has two distinct sales methods. The first method is when implants and/or disposable surgical instruments are sold directly to hospitals or surgical centers for the purpose of conducting a scheduled surgery. The Company’s sales representatives or independent sales agents hand deliver the products to the customer on or before the day of the surgery. The sales representative or independent agent is then responsible for reporting the delivery of the products and the date of the surgery to the corporate office for proper revenue recognition. The Company recognizes revenue upon the confirmation that the products have been used in a surgical procedure. The other sales method is for sales to distributors outside the
63
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
United States. These transactions require the customer to send in a purchase order before shipment will be made to the customer. Under the distributor agreements currently in place, a distributor only has the right of return for defective products. The Company recognizes revenue upon the shipment of product to distributors outside the United States.
Cost of Revenue
Cost of revenue consists primarily of material and overhead costs related to the Company’s products and product royalties. Overhead costs include facilities-related costs, such as rent, utilities and depreciation.
Shipping and Handling Costs
Shipping and handling costs in the United States are expensed as incurred and are included in the cost of revenue. These costs are generally not reimbursed by the Company’s customers. Shipping costs relating to sales to distributors outside the United States are either paid directly by the distributor to the freight carrier or charged to the distributor and reimbursed to the Company.
Sales and Marketing Expenses
Sales and marketing expenses consist primarily of personnel costs, sales commissions paid to the Company’s direct sales representatives and independent sales agents, and costs associated with physician training programs, promotional activities, and participation in medical and trade conferences. All costs of advertising and promotional activities are expensed as incurred. Advertising expenses were $0.4 million, $0.7 million and $0.8 million for the years ending December 31, 2011, 2010 and 2009, respectively.
Research and Development Expenses
Research and development expenses consist primarily of personnel costs within the Company’s product development, regulatory and clinical functions, and the costs of clinical studies, product development projects and technology licensing costs. Research and development expenses are expensed as incurred.
General and Administrative Expenses
General and administrative expenses consist of personnel costs related to the executive, finance, business development and human resource functions, as well as professional service fees, legal fees, accounting fees, insurance costs and general corporate expenses.
Patent Costs
Costs associated with the submission of a patent application are expensed as incurred given the uncertainty of the patents resulting in probable future economic benefits to the Company.
Other Income, Net
Other income, net, is composed of government grants, interest earned on our cash, cash equivalents and available-for-sale securities and the gain or loss on disposal of fixed assets. In November 2010, the Company received grants of $0.5 million from the U.S. Treasury under the Qualifying Therapeutic Discovery Program. These grants have been included in other income, net, for the year ended December 31, 2010.
64
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Income Taxes
The Company accounts for income taxes using the liability method which requires the recognition of deferred tax assets or liabilities for the temporary differences between financial reporting and tax bases of the Company’s assets and liabilities and for tax carryforwards at enacted statutory tax rates in effect for the years in which the differences are expected to reverse. The effect on deferred taxes of a change in tax rates is recognized in the period that includes the enactment date. In addition, valuation allowances are established when necessary to reduce deferred tax assets to the amounts expected to be realized.
Stock-Based Compensation
The Company accounts for stock-based compensation under the fair value provisions of ASC 718. ASC 718 requires the recognition of compensation expense, using a fair-value-based method, for costs related to all share-based payments including stock options. ASC 718 requires companies to estimate the fair value of share-based payment awards on the date of grant using an option-pricing model. All options granted after January 1, 2006 are expensed on a straight-line basis over the vesting period.
The Company accounts for stock-based compensation arrangements with nonemployees in accordance with ASC 505-50. The Company records the expense of such services based on the estimated fair value of the equity instrument using the Black-Scholes pricing model. The value of the equity instruments is charged to earnings over the term of the service agreement.
Net Loss Per Common Share
Basic net loss per common share (“Basic EPS”) is computed by dividing net loss by the weighted average number of common shares outstanding. Diluted net loss available to common stockholders per common share (“Diluted EPS”) is computed by dividing net loss by the weighted average number of common shares and dilutive potential common share equivalents then outstanding. The Company’s potential dilutive common shares, which consist of shares issuable upon the exercise of stock options, have not been included in the computation of diluted net loss per share for all periods as the result would be anti-dilutive.
The following table sets forth the potential shares of common stock that are not included in the calculation of diluted net loss per share as the result would be anti-dilutive as of the end of each period presented:
| Year Ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Weighted average stock options outstanding |
2,506,630 | 2,166,657 | 2,110,689 | |||||||||
|
|
|
|
|
|
|
|||||||
Segment and Geographic Reporting
The Company applies ASC 280 which establishes standards for the reporting by business enterprises of information about operating segments, products and services, geographic areas, and major customers. The Company has determined that it did not have any separately reportable segments as of December 31, 2011, 2010 or 2009.
65
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Revenue by geographic area was:
| Year Ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| (in thousands) | ||||||||||||
| United States |
$ | 17,466 | $ | 23,798 | $ | 28,045 | ||||||
| Europe |
1,457 | 2,138 | 1,602 | |||||||||
| Other |
230 | 218 | 160 | |||||||||
|
|
|
|
|
|
|
|||||||
| $ | 19,153 | $ | 26,154 | $ | 29,807 | |||||||
|
|
|
|
|
|
|
|||||||
Long-lived assets are primarily located in the United States.
Recently Issued Accounting Standards
In May 2011, the Financial Accounting Standard Board (“FASB”) issued new authoritative guidance to provide a consistent definition of fair value and ensure that fair value measurements and disclosure requirements are similar between GAAP and International Financial Reporting Standards. This guidance changes certain fair value measurement principles and enhances the disclosure requirements for fair value measurements. This guidance is effective for interim and annual periods beginning after December 15, 2011 and is applied prospectively. The Company does not expect that the adoption of this guidance will have a material impact on its financial statements.
In June 2011, the FASB issued a standard on the presentation of other comprehensive income. This standard eliminates the option to present the components of other comprehensive income as part of the statement of changes in stockholders’ equity and requires the presentation of other comprehensive income in a single continuous statement, or in two separate, but consecutive, statements. This standard is effective for fiscal years and interim periods beginning after December 15, 2011. In December 2011, the FASB issued an amendment to indefinitely defer one of the requirements contained in the June 2011 standard. That requirement called for reclassification adjustments from accumulated other comprehensive income to be measured and presented by income statement line item in net income and also in other comprehensive income. This standard is not expected to have a material effect on the Company’s financial statements.
| 3. | Property and Equipment |
Property and equipment consist of the following:
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (in thousands) | ||||||||
| Furniture and fixtures |
$ | 245 | $ | 241 | ||||
| Equipment |
3,497 | 2,955 | ||||||
| Computer software |
444 | 481 | ||||||
| Leasehold improvements |
682 | 682 | ||||||
| Construction in process |
55 | — | ||||||
|
|
|
|
|
|||||
| 4,923 | 4,359 | |||||||
| Less: accumulated depreciation and amortization |
(3,369 | ) | (2,797 | ) | ||||
|
|
|
|
|
|||||
| $ | 1,554 | $ | 1,562 | |||||
|
|
|
|
|
|||||
Depreciation and amortization expense for the years ended December 31, 2011, 2010 and 2009 was $662,000, $746,000 and $909,000, respectively.
66
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
| 4. | Accrued Expenses |
Accrued expenses consist of the following:
| December 31, | ||||||||
| 2011 | 2010 | |||||||
| (in thousands) | ||||||||
| Commissions |
$ | 365 | $ | 589 | ||||
| Bonus |
351 | 770 | ||||||
| Legal and professional fees |
175 | 300 | ||||||
| Vacation |
136 | 175 | ||||||
| Franchise taxes |
91 | 116 | ||||||
| Travel and entertainment |
23 | 53 | ||||||
| Consulting |
— | 5 | ||||||
| Other |
62 | 69 | ||||||
|
|
|
|
|
|||||
| Total accrued expenses |
$ | 1,203 | $ | 2,077 | ||||
|
|
|
|
|
|||||
| 5. | Commitments and Contingencies |
The Company rents office space under the terms of an operating lease, which expires in 2014, with an option to extend the lease through 2019. The Company also entered into another operating lease agreement in 2011 for a training facility which expires in 2017, with an option to extend the lease through 2022. The Company issued an irrevocable standby letter of credit for $200,000 as security for the training facility lease, which is reduced ratably over the initial lease term.
Future minimum lease payments under operating lease obligations at December 31, 2011 are as follows (in thousands):
| Year ending December 31, |
||||
| 2012 |
$ | 418 | ||
| 2013 |
450 | |||
| 2014 |
414 | |||
| 2015 |
83 | |||
| 2016 and after |
130 | |||
|
|
|
|||
| $ | 1,495 | |||
|
|
|
Rent expense related to operating leases for the years ended December 31, 2011, 2010 and 2009 was $405,000, $401,000 and $204,000, respectively.
In October 2011, the Company received a subpoena issued by the Department of Health and Human Services, Office of Inspector General, under the authority of the federal healthcare fraud and false claims statutes. The subpoena seeks documents for the period January 1, 2008 through October 6, 2011. The Company is cooperating with the government’s request and is in the process of responding to the subpoena. The Company is unable to predict what action, if any, might be taken in the future by the Department of Health and Human Services, Office of Inspector General or other governmental authorities as a result of the matters related to this subpoena or what impact, if any, the outcome of these matters might have on the Company’s consolidated financial position, results of operations, or cash flows. No claims have been made against the Company at this time.
67
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
In January 2012, the Company received notice that a class action lawsuit had been filed in the U.S. District Court Eastern District, North Carolina, on behalf of a class consisting of all persons other than the defendants who purchased TranS1 securities between February 21, 2008 and October 17, 2011. The Company is in the process of responding to this lawsuit. The Company is unable to predict what impact, if any, the outcome of this matter might have on the Company’s consolidated financial position, results of operations, or cash flows.
| 6. | Stockholders’ Equity |
At December 31, 2011 and 2010, the Company’s Amended and Restated Certificate of Incorporation, which was adopted in connection with the Company’s initial public offering, authorized up to 80,000,000 shares of capital stock, of which 75,000,000 shares were designated as common stock with a par value of $0.0001 and up to 5,000,000 shares were designated as preferred stock with a par value of $0.0001. At December 31, 2011 and 2010, there were 27,244,059 and 20,877,171 shares of common stock issued and outstanding, respectively, and there were no shares of preferred stock issued and outstanding.
In 2011, the Company issued 6,200,000 shares of common stock under the September 2011 stock offering for $18.2 million, 104,498 shares of common stock to employees and consultants for $111,000 pursuant to the exercise of stock options, and 62,390 shares of common stock under the employee stock purchase plan for $158,000. In 2010, the Company issued 228,724 shares of common stock to employees and consultants for $148,000 pursuant to the exercise of stock options. In 2009, the Company issued 110,114 shares of common stock to employees and consultants for $96,000 pursuant to the exercise of stock options.
| 7. | Stock Incentive Plans and Stock-Based Compensation |
2007 Employee Stock Purchase Plan
The Company’s board of directors adopted the 2007 Employee Stock Purchase Plan (as amended, the “ESPP”) in July 2007. The ESPP became effective upon the completion of the Company’s initial public offering. A total of 250,000 shares of common stock are available for sale. In addition, the ESPP provides for annual increases in the number of shares available for issuance under the ESPP on the first day of each fiscal year beginning in 2008, equal to the lesser of (i) 2.0% of the outstanding shares of common stock on the first day of such fiscal year or (ii) an amount determined by the administrator of the ESPP. The Company’s Compensation Committee administers the ESPP.
Shares shall be offered pursuant to the ESPP in six-month periods commencing on the first trading day on or after June 1 and December 1 of each year, or on such other date as the administrator may determine.
Our ESPP permits participants to purchase common stock through payroll deductions of up to 10% of their eligible compensation, which includes a participant’s base straight time gross earnings, certain commissions, overtime and shift premium, but exclusive of payments for incentive compensation, bonuses and other compensation. A participant may purchase no more than 10,000 shares during a six- month purchase period. Amounts deducted and accumulated by the participant are used to purchase shares of the Company’s common stock at the end of each six-month purchase period. The purchase price of the shares will be 85% of the fair market value of Company common stock on the exercise date. Participants may end their participation at any time during an offering period, and will be paid their accrued payroll deductions that have not yet been used to purchase shares of common stock. Participation ends automatically upon termination of employment with the Company. Pursuant to ASC 718, the Company is required to recognize compensation expense in connection with purchases under the ESPP.
During the fiscal year ended December 31, 2011, 62,390 shares were issued to participants under the ESPP and no shares were issued during the fiscal years ended December 31, 2010 or 2009 to participants under the ESPP.
68
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
2000 and 2007 Stock Incentive Plans
The Company established the TranS1 Inc. Stock Incentive Plan in 2000, (as amended, the “2000 Plan”) and the 2007 Stock Incentive Plan (the “2007 Plan”) in October 2007 (collectively, the “Plans”) . Under the 2000 Plan, the Company could have granted options to employees, directors or service providers and contractors for a maximum of 3,159,108 shares of the Company’s common stock. The 2000 Plan remains active, but no new options may be granted. Under the 2007 Plan, the Company may grant options to employees, directors or service providers and contractors for a maximum of 2,000,000 shares of the Company’s common stock. As of December 31, 2011, there were 1,551,882 shares available for future issuance under the 2007 Plan. Options granted under the Plans may be incentive stock options or non-qualified stock options. Incentive stock options may only be granted to employees. The exercise periods may not exceed ten years for options. However, in the case of an incentive stock option granted to an optionee who, at the time of the option grant owns stock representing more than 10% of the outstanding shares, the term of the option shall be five years from the date of the grant. The exercise price of incentive stock options cannot be less than 100% of the fair market value per share of the Company’s common stock on the grant date. The exercise price of a nonqualified option under the 2000 Plan and the 2007 Plan shall not be less than 85% and 100%, respectively, of the fair market value per share on the date the option is granted. If an optionee owns more than 10% of the outstanding shares, the exercise price cannot be less than 110% of the fair market value of the stock on the date of the grant. Options granted under the Plans generally vest over periods ranging from three to four years.
The following table summarizes the activity of the Company’s 2000 Plan and 2007 Plan, including the number of shares under options (“Number”) and the weighted average exercise price (“Price”):
| Number | Price | |||||||
| Outstanding as of December 31, 2010 |
2,491,799 | $ | 5.43 | |||||
| Options granted |
888,000 | 3.96 | ||||||
| Options exercised |
(119,823 | ) | 1.56 | |||||
| Options forfeited |
(530,091 | ) | 6.45 | |||||
|
|
|
|
|
|||||
| Outstanding as of December 31, 2011 |
2,729,885 | $ | 4.92 | |||||
|
|
|
|
|
|||||
| Options vested or expected to vest as of December 31, 2011 |
2,522,872 | $ | 4.80 | |||||
|
|
|
|
|
|||||
The following table summarizes information about the Company’s stock options at December 31, 2011:
| Range of Exercise Prices |
Number Outstanding |
Weighted Average Contractual Life (Years) |
Weighted Average Exercise Price |
Number of Options Exercisable |
||||||||||||
| $ 0.11 - $2.00 |
284,357 | 5.5 | $ | 1.21 | 236,857 | |||||||||||
| $ 2.01 - $3.50 |
534,000 | 8.2 | 3.11 | 255,640 | ||||||||||||
| $ 3.51 - $6.00 |
1,430,362 | 8.3 | 4.17 | 478,861 | ||||||||||||
| $ 6.01 - $10.00 |
232,208 | 4.6 | 8.31 | 213,039 | ||||||||||||
| $12.00 - $20.00 |
248,958 | 6.0 | 14.16 | 240,724 | ||||||||||||
|
|
|
|
|
|||||||||||||
| 2,729,885 | 7.5 | 4.92 | 1,425,121 | |||||||||||||
|
|
|
|
|
|||||||||||||
The aggregate intrinsic value of outstanding stock options at December 31, 2011 was $0.2 million. At December 31, 2011, exercisable stock options had an aggregate intrinsic value of $0.2 million, a weighted average contractual life of 6.3 years and a weighted average exercise price of $5.92. At December 31, 2011, options vested or expected to vest had an aggregate intrinsic value of $0.1 million and a weighted average contractual life of 7.9 years.
69
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Stock-Based Compensation for Non-employees
During 2011 and 2010, the Company did not issue any options to purchase common stock to consultants. During 2009, the Company issued options to purchase 2,500 shares of common stock with an exercise price of $6.00 per share to consultants. These options vest over 3 years and expire 10 years from the date of issuance. The Company determined the estimated fair value of the options issued to the consultants using the Black-Scholes pricing model. The Company used the following assumptions in the Black-Scholes pricing model for 2009 grants: 60% volatility, 0% dividend yield, 2.65% risk-free rate and a 6 year expected legal life.
There was no stock-based compensation expense charged to operations on options granted to non-employees for the year ended December 31, 2011 and December 31, 2010. Stock-based compensation expense charged to operations on options granted to non-employees for years ended December 31, 2009 was $8,000. As of December 31, 2011, there was no unrecognized compensation costs related to non-vested stock option awards.
Employee Stock-Based Compensation
Under ASC 718, compensation cost for employee stock-based awards is based on the estimated grant-date fair value and is recognized over the vesting period of the applicable award on a straight-line basis. For the period from January 1, 2006 to December 31, 2011, the Company issued employee stock-based awards in the form of stock options. The Company recorded stock-based compensation expense of $1.6 million, $1.9 million and $2.8 million for the years ended December 31, 2011, 2010 and 2009, respectively. The weighted average grant-date fair value of the employee stock options granted for the years ended December 31, 2011, 2010 and 2009 was $3.96, $3.31 and $6.53 per share, respectively. The aggregate intrinsic value of stock options (the amount by which the market price of the stock on the date of exercise exceeded the exercise price of the option) exercised for the years ended December 31, 2011, 2010 and 2009, was $0.3 million, $0.5 million, and $0.6 million, respectively.
The Company uses the Black-Scholes pricing model to determine the fair value of stock options. The determination of the fair value of stock-based payment awards on the date of grant is affected by our stock price as well as assumptions regarding a number of complex and subjective variables. These variables include our expected stock price volatility over the term of the awards, actual and projected employee stock option exercise behaviors, risk-free interest rates and expected dividends. Prior to the Company’s initial public offering, the Board of Directors, with the assistance of management, performed contemporaneous fair value analyses to determine the fair value of the common stock at the time of the stock option grants. The estimated grant-date fair values of the employee stock options were calculated using the Black-Scholes valuation model, based on the following assumptions for the years ended December 31, 2011, 2010 and 2009:
Expected Life. The expected life of six years is based on the “simplified” method described in the SEC Staff Accounting Bulletin No. 110, which provides guidance regarding the application of ASC 718.
Volatility. Prior to 2008, the Company was a private entity with no historical data regarding the volatility of its common stock. Accordingly, the expected volatility was based on a weighted average of the actual volatility of the Company and the volatility of similar entities for prior periods. In evaluating similarity, the Company considered factors such as industry, stage of life cycle and size. The Company utilized an expected volatility range of 62.0% to 66.7% for 2011, 59.5% to 62.0% for 2010 and 54% to 58% for 2009.
70
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
Risk-Free Interest Rate. The risk-free rate is based on U.S. Treasury zero-coupon issues with remaining terms similar to the expected term on the options. The risk-free rates were:
| Option Grant Year |
Risk-Free Rate Range | |
| 2011 |
1.08% to 2.14% | |
| 2010 |
1.26% to 2.61% | |
| 2009 |
1.79% to 2.52% |
Dividend Yield. The Company has never declared or paid any cash dividends and does not plan to pay cash dividends in the foreseeable future, and, therefore, used an expected dividend yield of zero in the valuation model.
Forfeitures. ASC 718 also requires the Company to estimate forfeitures at the time of grant, and revise those estimates in subsequent periods if actual forfeitures differ from those estimates. The Company uses historical data to estimate pre-vesting option forfeitures and record stock-based compensation expense only for those awards that are expected to vest. All stock-based payment awards are amortized on a straight-line basis over the requisite service periods of the awards, which are generally the vesting periods.
As of December 31, 2011, there was $2.5 million of total unrecognized compensation cost related to non-vested employee stock option awards granted after January 1, 2006, which is expected to be recognized over a weighted-average period of 1.7 years.
| 8. | Income Taxes |
No provision for federal or state income taxes has been recorded as the Company has incurred net operating losses since inception.
Significant components of the Company’s deferred tax assets and liabilities consist of the following:
| 2011 | 2010 | |||||||
| (in thousands) | ||||||||
| Deferred tax assets |
||||||||
| Domestic net operating loss carryforwards |
$ | 31,391 | $ | 25,417 | ||||
| Inventory |
1,016 | 839 | ||||||
| Fixed assets |
450 | 592 | ||||||
| Other |
1,952 | 1,437 | ||||||
| Research and development credit |
1,219 | 1,207 | ||||||
|
|
|
|
|
|||||
| Total deferred tax assets |
36,028 | 29,492 | ||||||
| Valuation allowance for deferred assets |
(36,028 | ) | (29,492 | ) | ||||
|
|
|
|
|
|||||
| Deferred tax assets |
— | — | ||||||
|
|
|
|
|
|||||
| Deferred tax liabilities |
||||||||
| Fixed assets |
— | — | ||||||
|
|
|
|
|
|||||
| Total deferred tax liabilities |
— | — | ||||||
|
|
|
|
|
|||||
| Net deferred tax assets (liabilities) |
$ | — | $ | — | ||||
|
|
|
|
|
|||||
The Company provided a full valuation allowance against its net deferred tax assets. A valuation allowance must be established for deferred tax assets when it is more likely than not (a probability level of more than
71
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
50 percent) that they will not be realized. The increase in valuation allowance resulted primarily from the additional net operating loss carryforward generated. Included in the Company’s deferred tax assets is a foreign net operating loss carryforward of $1 million that is fully offset by a valuation allowance. The Germany subsidiary is in the process of being dissolved. In conjunction with this dissolution, it is likely that the foreign net operating losses will not be utilized and may be written off, along with the corresponding valuation allowance. This will have no effect on the Company’s deferred tax assets or income tax expense.
As of December 31, 2011, the Company had federal and state net operating loss carryforwards of approximately $83.5 million and $79.9 million, respectively. These net operating loss carryforwards begin to expire in 2021 and 2016 for federal and state tax purposes, respectively. Additionally, as of December 31, 2011, the Company had research credit carryforwards of $1.2 million for federal tax purposes. These credit carryforwards begin to expire in 2021. The utilization of the federal net operating loss carryforwards may be subject to limitations under the rules regarding a change in stock ownership as determined by the Internal Revenue Code.
A reconciliation of differences between the U.S. federal income tax rate and the Company’s effective tax rate for the years ended December 31 is as follows:
| 2011 | 2010 | 2009 | ||||||||||||||||||||||
| Amount | % of net loss |
Amount | % of net loss |
Amount | % of net loss |
|||||||||||||||||||
| (in thousands) | ||||||||||||||||||||||||
| Tax at statutory rate |
$ | (6,396 | ) | 35.0 | % | $ | (6,834 | ) | 35.0 | % | $ | (8,119 | ) | 35.0 | % | |||||||||
| State taxes |
(434 | ) | 2.4 | % | (303 | ) | 1.5 | % | (59 | ) | 0.3 | % | ||||||||||||
| Non deductible items |
692 | -3.8 | % | 746 | -3.8 | % | 1,129 | -4.9 | % | |||||||||||||||
| Other |
(130 | ) | 0.7 | % | 330 | -1.7 | % | 348 | -1.5 | % | ||||||||||||||
| R&D credits |
(268 | ) | 1.5 | % | (251 | ) | 1.3 | % | (486 | ) | 2.1 | % | ||||||||||||
| Change in valuation allowance |
6,536 | -35.8 | % | 6,312 | -32.3 | % | 7,187 | -31.0 | % | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Total |
$ | — | 0.0 | % | $ | — | 0.0 | % | $ | — | 0.0 | % | ||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
As of January 1, 2007, the Company adopted the provisions of ASC 740, which clarifies the accounting for uncertainty in tax positions. As of that date, the Company had $1.1 million of unrecognized tax benefits related to the adoption of ASC 740. This would be recorded as a component of income tax expense once the valuation allowance is released. For the year ended December 31, 2011, the Company increased its unrecognized tax benefits by $6,000. The change was recorded as a reduction to the respective deferred tax asset which was reflected as an increase in the valuation allowance. As of December 31, 2011, the Company had $1.0 million of unrecognized tax benefits which, if recognized, would be recorded as a component of income tax expense. The Company’s policy is to record estimated interest and penalties related to the underpayment of income taxes as a component of its income tax provision. As of December 31, 2009, 2010 and 2011, the Company had no accrued interest or tax penalties recorded. A reconciliation of the beginning and ending uncertain tax positions is as follows (in thousands):
| Balance at December 31, 2009 |
$ | 900 | ||
| Gross increases related to current period tax positions |
75 | |||
|
|
|
|||
| Balance at December 31, 2010 |
975 | |||
| Gross increases related to current period tax positions |
6 | |||
|
|
|
|||
| Balance at December 31, 2011 |
$ | 981 | ||
|
|
|
72
Table of Contents
TranS1 Inc.
Notes to Consolidated Financial Statements — (Continued)
In many cases, uncertain tax positions are related to tax years that remain subject to examination by the relevant tax authorities. Given the losses accumulated to date, periods open for examination are 2004 to 2011 for the primary taxing jurisdictions of the United States and North Carolina. The Company currently does not expect a significant change in the liability for uncertain tax provisions in the next 12 months.
| 9. | Comprehensive Loss |
The following table presents the components of other comprehensive income (loss):
| Year Ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| (in thousands) | ||||||||||||
| Net loss |
$ | (18,273 | ) | $ | (19,527 | ) | $ | (23,196 | ) | |||
| Other comprehensive income (loss): |
||||||||||||
| Translation adjustments |
42 | (24 | ) | (5 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Total comprehensive loss |
$ | (18,231 | ) | $ | (19,551 | ) | $ | (23,201 | ) | |||
|
|
|
|
|
|
|
|||||||
| 10. | Quarterly Data (Unaudited) |
The following unaudited quarterly financial data, in the opinion of management, reflects all adjustments, consisting of normal recurring adjustments, necessary to a fair statement of the results for the periods presented (in thousands, except per share data):
| Year Ended December 31, 2011 | ||||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
|||||||||||||
| Total revenues |
$ | 5,130 | $ | 5,337 | $ | 4,696 | $ | 3,990 | ||||||||
| Gross profit |
3,834 | 4,164 | 3,652 | 2,948 | ||||||||||||
| Total operating expenses |
9,578 | 8,493 | 6,947 | 7,859 | ||||||||||||
| Net loss |
$ | (5,726 | ) | $ | (4,309 | ) | $ | (3,327 | ) | $ | (4,911 | ) | ||||
| Basic and diluted net loss per common share |
$ | (0.27 | ) | $ | (0.21 | ) | $ | (0.16 | ) | $ | (0.18 | ) | ||||
| Year Ended December 31, 2010 | ||||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
|||||||||||||
| Total revenues |
$ | 6,713 | $ | 7,244 | $ | 6,339 | $ | 5,858 | ||||||||
| Gross profit |
5,284 | 5,880 | 5,134 | 2,752 | ||||||||||||
| Total operating expenses |
11,591 | 9,541 | 8,945 | 8,986 | ||||||||||||
| Net loss |
$ | (6,356 | ) | $ | (3,646 | ) | $ | (3,791 | ) | $ | (5,734 | ) | ||||
| Basic and diluted net loss per common share |
$ | (0.31 | ) | $ | (0.18 | ) | $ | (0.18 | ) | $ | (0.27 | ) | ||||
73
Table of Contents
SCHEDULE VALUATION AND QUALIFYING ACCOUNTS
SCHEDULE II
VALUATION AND QUALIFYING ACCOUNTS
FOR THE YEARS ENDED DECEMBER 31, 2011, 2010 AND 2009
| Balance at Beginning of Period |
Additions(1) | Deductions(2) | Balance at End of Period |
|||||||||||||
| (in thousands) | ||||||||||||||||
| Accounts Receivable Reserve: |
||||||||||||||||
| Year ended December 31, 2011 |
$ | 347 | $ | 31 | $ | 29 | $ | 349 | ||||||||
| Year ended December 31, 2010 |
193 | 226 | 72 | 347 | ||||||||||||
| Year ended December 31, 2009 |
193 | 80 | 80 | 193 | ||||||||||||
| Balance at Beginning of Period |
Additions(3) | Deductions(4) | Balance at End of Period |
|||||||||||||
| Inventory Reserve: |
||||||||||||||||
| Year ended December 31, 2011 |
$ | 2,155 | $ | 521 | $ | 85 | $ | 2,591 | ||||||||
| Year ended December 31, 2010 |
581 | 2,004 | 430 | 2,155 | ||||||||||||
| Year ended December 31, 2009 |
397 | 505 | 321 | 581 | ||||||||||||
| Balance at Beginning of Period |
Additions | Deductions | Balance at End of Period |
|||||||||||||
| Valuation Allowance for Deferred Tax Assets: |
||||||||||||||||
| Year ended December 31, 2011 |
$ | 29,492 | $ | 6,536 | $ | — | $ | 36,028 | ||||||||
| Year ended December 31, 2010 |
23,180 | 6,354 | 42 | 29,492 | ||||||||||||
| Year ended December 31, 2009 |
15,993 | 7,559 | 372 | 23,180 | ||||||||||||
| (1) | Amount represents customer balances deemed uncollectible. |
| (2) | Uncollectible accounts written-off. |
| (3) | Amount represents excess and obsolete reserve recorded to cost of sales. |
| (4) | Excess and obsolete inventory written-off against reserve. |
74
Table of Contents
| Exhibit |
Description | |
| 3.1 | Amended and Restated Certificate of Incorporation of TranS1 Inc. (incorporated by reference to Exhibit 3.2 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007). | |
| 3.2 | Amended and Restated Bylaws of TranS1 Inc. (incorporated by reference to Exhibit 3.4 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007). | |
| 4.1 | Specimen Common Stock Certificate (incorporated by reference to Exhibit 4.1 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007). | |
| 10.1 | Amended and Restated 2000 Stock Incentive Plan (incorporated by reference to Exhibit 10.1 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007).* | |
| 10.2 | Form of Stock Option Agreement under Amended and Restated 2000 Stock Incentive Plan (incorporated by reference to Exhibit 10.2 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007).* | |
| 10.3 | 2007 Stock Incentive Plan, as amended (incorporated by reference to Appendix A to the Definitive Proxy Statement on Schedule 14A, as filed with the Commission on April 30, 2009).* | |
| 10.4 | Form of Stock Option Agreement under 2007 Stock Incentive Plan (incorporated by reference to Exhibit 10.4 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007).* | |
| 10.5 | 2007 Employee Stock Purchase Plan, as amended on December 16, 2010 and as declared effective on October 16, 2007.** | |
| 10.6 | Lease, dated July 30, 2009, between TranS1 Inc. and Market Place Group, LLC (incorporated by reference to Exhibit 99.1 of TranS1’s Current Report on Form 8-K filed with the Commission on March 11, 2010). | |
| 10.7 | Form of Indemnification Agreement (incorporated by reference to Exhibit 10.7 to the Registration Statement on Form S-1, as amended (File No. 333-144802), and as declared effective on October 16, 2007). | |
| 10.7.1 | Schedule of Parties to Indemnification Agreement.** | |
| 10.8 | Offer Letter, dated December 11, 2009, between TranS1 Inc. and Kenneth Reali (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on January 12, 2010).* | |
| 10.9 | Offer Letter, dated February 22, 2010, between TranS1 Inc. and Dwayne Montgomery (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on March 18, 2010).* | |
| 10.10 | Offer Letter, dated April 13, 2010, between TranS1 Inc. and Joseph Slattery (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on April 21, 2010).* | |
| 10.11 | Offer Letter, dated July 30, 2010, between TranS1 Inc. and Rick Feiler (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on August 4, 2010).* | |
75
Table of Contents
| 7Exhibit |
Description | |
| 10.12 | Offer Letter, dated September 28, 2010, between TranS1 Inc. and Steve Ainsworth (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on October 4, 2010).* | |
| 10.13 | Purchase Agreement, dated September 21, 2011, between TranS1 Inc. and Piper Jaffray & Co. (incorporated by reference to Exhibit 1.1 of TranS1’s Current Report on Form 8-K filed with the Commission on September 26, 2011). | |
| 10.14 | Form of Severance Agreement (incorporated by reference to Exhibit 10.1 of TranS1’s Current Report on Form 8-K filed with the Commission on November 9, 2011).* | |
| 10.14.1 | Schedule of Parties to Severance Agreement.** | |
| 23.1 | Consent of Independent Registered Public Accounting Firm.** | |
| 24.1 | Power of Attorney (included in the signature page). | |
| 31.1 | Certification of Chief Executive Officer Pursuant to Rule 13a-14(a) / 15d-14(a) of the Securities Exchange Act of 1934.** | |
| 31.2 | Certification of Chief Financial Officer Pursuant to Rule 13a-14(a) / 15d-14(a) of the Securities Exchange Act of 1934.** | |
| 32.1 | Certification of Chief Executive Officer Pursuant to Rule 13a-14(b) / 15d-14(b) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350.*** | |
| 32.2 | Certification of Chief Financial Officer Pursuant to Rule 13a-14(b) / 15d-14(b) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350.*** | |
| 101.INS | XBRL Instance Document**** | |
| 101.SCH | XBRL Schema Document**** | |
| 101.CAL | XBRL Calculation Linkbase Document**** | |
| 101.DEF | XBRL Definition Linkbase Document**** | |
| 101.LAB | XBRL Label Linkbase Document**** | |
| 101.PRE | XBRL Presentation Linkbase Document**** | |
| * | These exhibits are identified as management contracts or compensatory plans or arrangements of the Registrant pursuant to Item 15 of Form 10-K. |
| ** | Filed herewith. |
| *** | Furnished herewith. |
| **** | Pursuant to Rule 406T of Regulation S-T, this XBRL information will not be deemed “filed” for the purposes of Section 18 of the Securities and Exchange Act of 1934 or otherwise subject to the liability of that section, nor will it be deemed filed or made a part of a registration statement or prospectus for purposes of Sections 11 and 12 of the Securities Act of 1933, or otherwise subject to liability under those sections. |
76