Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - UNITED SURGICAL PARTNERS INTERNATIONAL INC | d422817d8k.htm |
 October 2012
Exhibit 99.1 |
 2
SAFE HARBOR STATEMENT
This presentation contains forward-looking statements,
including those regarding United Surgical Partners
International, Inc. and the services it provides. Investors
are cautioned not to place an undue reliance on these
forward-looking statements, which will speak only as of
the date of this presentation. United Surgical Partners
International, Inc. undertakes no obligation to publicly
revise these forward-looking statements. |
 3
NON-GAAP MEASUREMENT
We
have
used
the
non-GAAP
financial
measurement
term
“EBITDA.”
EBITDA
is calculated as operating income plus net gain (loss) on deconsolidations,
disposals, impairments and depreciation and amortization. USPI uses EBITDA
and EBITDA less noncontrolling interests as analytical indicators for
purposes of allocating resources and assessing performance. EBITDA is
commonly used as an analytical indicator within the health care industry and
also serves as a measure of leverage
capacity
and
debt
service
ability.
EBITDA
should
not
be
considered
as
a
measure of financial performance under generally accepted accounting principles,
and the items excluded from EBITDA could be significant components in
understanding and assessing financial performance.
Because EBITDA is not a measurement determined in accordance with
generally
accepted
accounting
principles
and
is
thus
susceptible
to
varying
calculation methods, EBITDA as presented by USPI may not be comparable to
similarly titled measures of other companies. |
 4
$2.0+bn
of
revenues
under
management
–
200+
facilities
that
will
perform
over
900,000
cases
by over 8,800 physician utilizers
High quality, low cost provider of surgical services
Leading operator
in an attractive
industry segment
Proven management
team
Attractive business
and payor mix
KEY HIGHLIGHTS
High margin, elective procedures with over half of revenue from orthopedic
specialties 75% private insurance; operating discipline yields bad debt
expense of ~2% of revenues Two-thirds of our facilities are owned in a
partnership with and partially owned by various not- for-profit
healthcare systems (hospital partners) Provides long-term strategic
stability in the market place with strong brand reputation and
stability
Working
with
existing
partners
(physician
and
hospitals)
to
grow
market
share
and
enhance
strategic
positioning
Adjusted EBITDA CAGR of 10% from 2007 to 2011
Cumulative Free Cash Flow of $229 million from 2009 to 2011
June YTD 2012 EBITDA up 9% to $96m from $89m in 2011
Majority of USPI’s senior management has been with the Company over 10
years Consistent financial
performance
Focused on key
strategic markets with
significant share
Unique JV
partnership
strategy
1.
Consolidated
Adjusted
EBITDA
less
noncontrolling
interest
2.
Consolidated FCF calculated as adjusted EBITDA less capital expenditures, cash
interest, cash taxes and change in working capital (defined as increases
(decreases) in cash from changes in operating assets and liabilities, net effects from purchases of new businesses)
1
2 |
 5
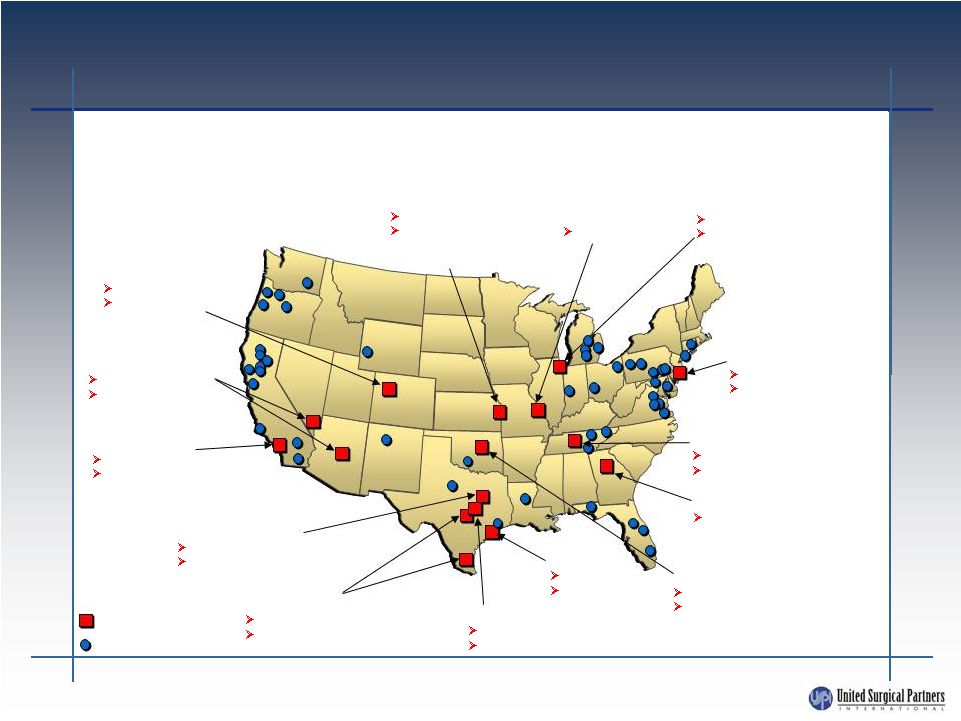
KEY MARKETS
Major Market
Facilities
USPI operates 204 facilities in 25 states
Denver
6 facilities
Centura Health
Partnership
Oklahoma City
1 facility
INTEGRIS Health
Partnership
St. Louis
18 facilities
New Jersey
10 facilities
Meridian Health
Partnership
Nashville
22 facilities
St. Thomas Partnership
Atlanta
6 facilities
Houston
19 facilities
Memorial
Hermann
Partnership
Austin
4 facilities
Seton Partnership
San Antonio/Corpus Christi
3 facilities
CHRISTUS Health Partnership
Dallas/Ft. Worth
30 facilities
Baylor Health Care
System Partnership
Phoenix/Las Vegas
11 facilities
Dignity Health
Partnership
Los Angeles
6 facilities
Dignity Health
Partnership
Kansas City
6 facilities
North Kansas City
Hospital Ascension
Partnership
Chicago
5 facilities
NorthShore University
HealthSystem, Adventist
Partnership |
 6
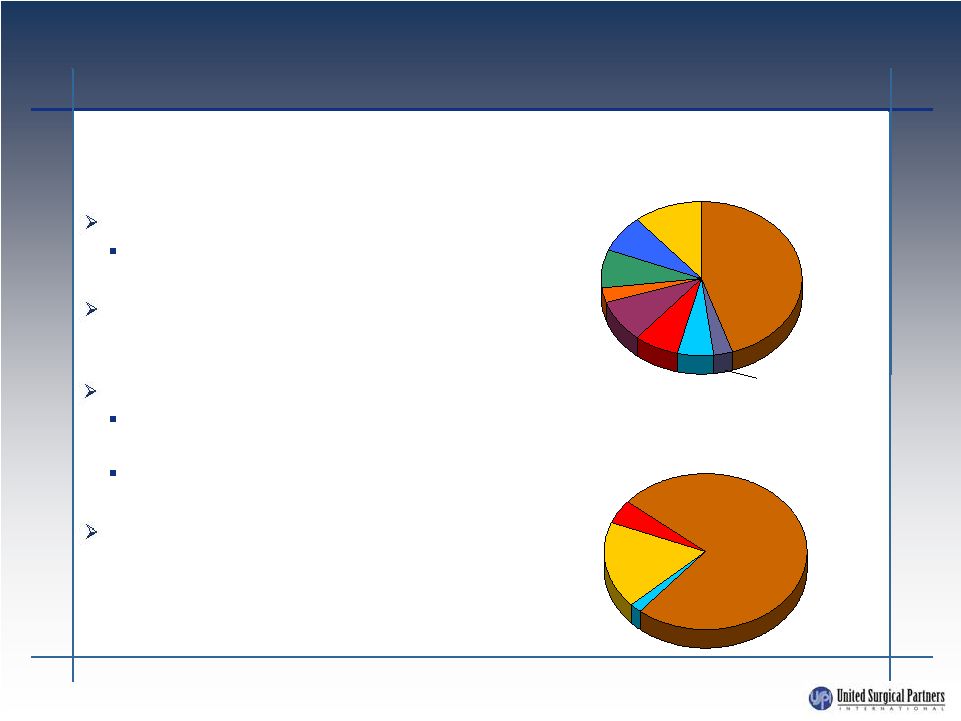
FAVORABLE REVENUE AND PAYOR
MIX
High margin, elective procedures
56% of revenue mix from orthopedic
and pain management
Diversification of specialties insulates USPI
from negative utilization and specialty pricing
changes
75% private insurance
Insurance companies favor low cost
providers
Modest exposure to government
reimbursement fluctuations
Reliable payors and operating discipline yields
bad debt expense of ~2% of revenues and
receivable days outstanding is under 35 days
Low risk cash flows from high margin
specialties and reliable payors:
Orthopedic
Gynecology
ENT
GI
Cosmetic
Ophthalmology
Medical/Other
Pain Mgmt
11%
11%
45%
45%
3%
3%
6%
6%
7%
7%
9%
9%
8%
8%
3%
3%
8%
8%
2011 U.S. Revenue Mix
Private
Insurance
Self-pay
18%
18%
75%
75%
2%
2%
2011 U.S. Payor Mix
Government
General
5%
5%
Other |
 7
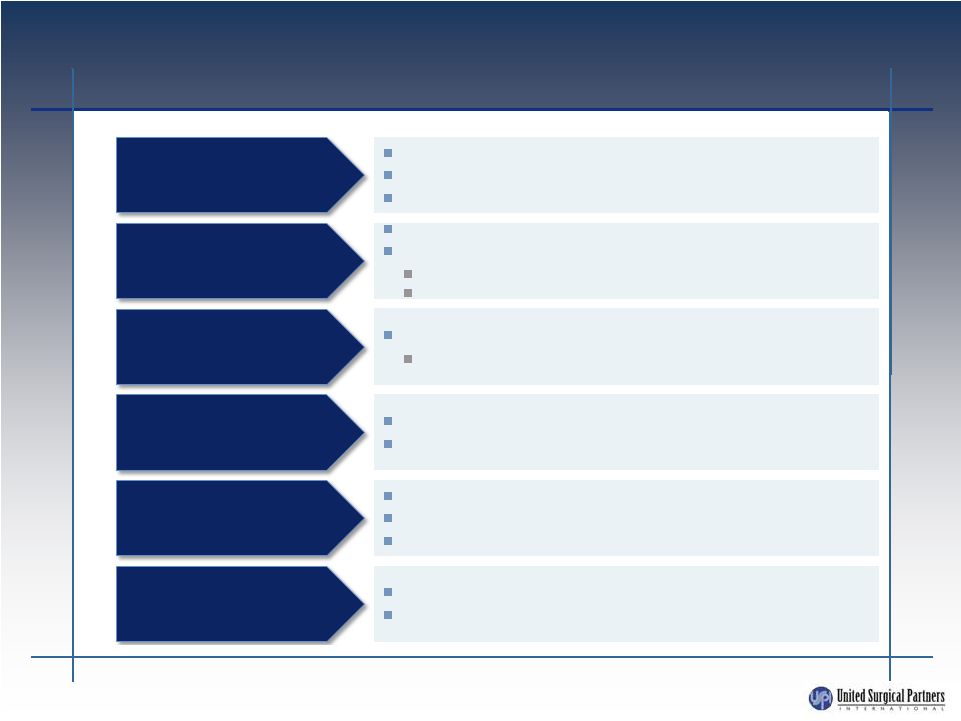
STRONG FINANCIAL AND OPERATING
PERFORMANCE POST LBO
72 acquisitions
20 de novo facility development
15 new Health System Partners
Facility revenue CAGR of 15% from 2006 to 2011
Positive each of the past 5 years
Same facility revenue + 6% for 2011
Same facility revenue +6% for first half of 2012
Facility EBITDA CAGR of 14% from 2006 to 2011
Same facility margin increased 34 bps to 31.6% in 2011
25% SWB as a % of revenue
3% G&A as a % of system-wide revenue
Installed decision support system
Improved quality management system
EHR Investment
30 facilities divested
75% of revenue from top 10 markets
Expansion
Facility revenue growth
Facility EBITDA margin
Cost management
System enhancements
Portfolio management |
 8
U.S. INDUSTRY OVERVIEW
ASCs have been widely successful and are a significant presence in
the U.S. healthcare delivery system
Advantages in patient safety and physician efficiency are meaningful
Significant savings to patients, government and commercial payors
Typically a savings to commercial insurers
Medicare savings >40%
Medicare beneficiary savings >50%
Able to reduce overall healthcare costs and manage need for surgical
services in an integrated care environment
Industry poised for consolidation
Top ten companies own less than 20%
Growth of new facilities has slowed in recent years |
 9
FRAGMENTED MARKET
Further consolidation likely within the industry and USPI is well-positioned
to capitalize
There are over 375 surgery center chains that own 2 or more ASCs.
Top ten companies still own less than 20%
Some ASCs and ASC companies choosing to sell in face of current headwinds
From
2000
–
2009,
the
percentage
of
ASCs
owned
by
a
multi-facility
chain
increased from 22% to 35%
Source: SDI’s Outpatient Surgery Center Profiling Solution
Multi-facility
Independent
USPI facilities
2009
6,181
2,170
(35%)
4,011
(65%)
2008
5,876
2,136
(36%)
3,740
(64%)
2006
5,349
1,341
(25%)
4,008
(75%)
2004
3,957
984
(25%)
2,973
(75%)
2002
3,570
787
(22%)
2,783
(78%)
2000
3,172
704
(22%)
2,468
(78%)
49
64
87
141
161
165 |
 POSITIONED FOR REFORM
OPPORTUNITIES
Post-reform, positioned to play an important role in managing increased need
for surgical services due to coverage of previously uninsured lives
Health System Partnerships
Physician
Partners
Professional Management
USPI is proven,
trusted partner
USPI involvement
can alleviate
historical distrust of
hospitals
USPI can help
provide targeted
solutions for
strategic
positioning
JV model in place
Commitment to highest level of quality service
Comfort regarding proper utilization of brand
Ability to assist with out-of-hospital strategies
Proven ability to execute and operate low
cost, high quality facilities
Proven ability in managing professional
partnerships
Opportunities
for USPI to
assist with
enhancement
of strategic
network
capabilities
Access to
Capital
In a rapidly
changing
environment,
ability to enhance
speed to market
with new models
where there are
capital
constraints
10 |
 11
HEALTHCARE SYSTEM PARTNERS
Benefits
to
Healthcare
Systems
Leverage USPI’s operational expertise
and singular focus
Provides a strategy to promote
physician alignment and strategic
network capabilities
Provides defensive mechanism to
maintain short-stay surgical business
Provides capital and spreads risk
through USPI and physicians’
investment
Provides an opportunity to expand in
new markets at lower capital outlay
than a hospital
Benefits to USPI
Provides long-term strategic
stability in the marketplace
Provides brand, image,
reputation and credibility
Accelerates growth
Enhances relationships with
managed care payors
143 facilities are in a partnership with a healthcare system
|
 12
HEALTHCARE SYSTEM PARTNERS
USPI’s strategy of partnering with not-for-profit healthcare
systems aligns the Company’s facilities with strong
networks of physicians and hospitals that are prominent in their
communities and known for providing high quality care
|
 13
GROWTH STRATEGY
Work with existing partners (physicians and hospitals) to grow market
share and enhance strategic positioning
Poised to react to current economic conditions and legislative
changes
Acquisition of troubled facilities
Selective acquisition of strong facilities
Selective de novo development
Selective acquisition of multi-facility companies
Selectively enter new markets with existing or new partners
Attractive demographics and/or payor characteristics
Prominent health system that embraces physician
alignment
strategy
Prominent physicians who are influential in the market
|
 14
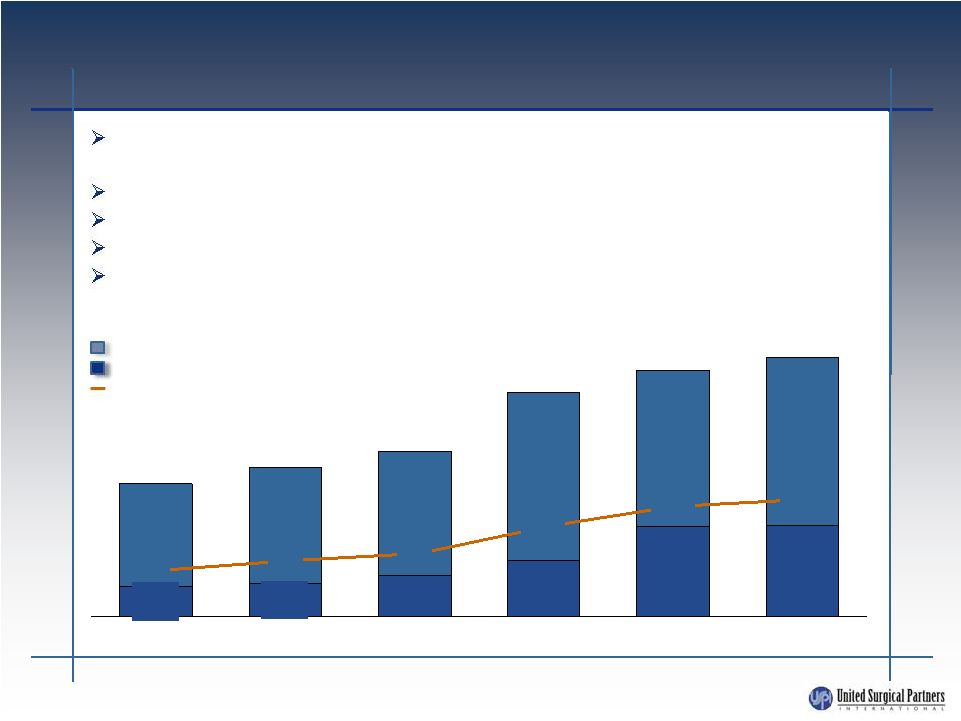
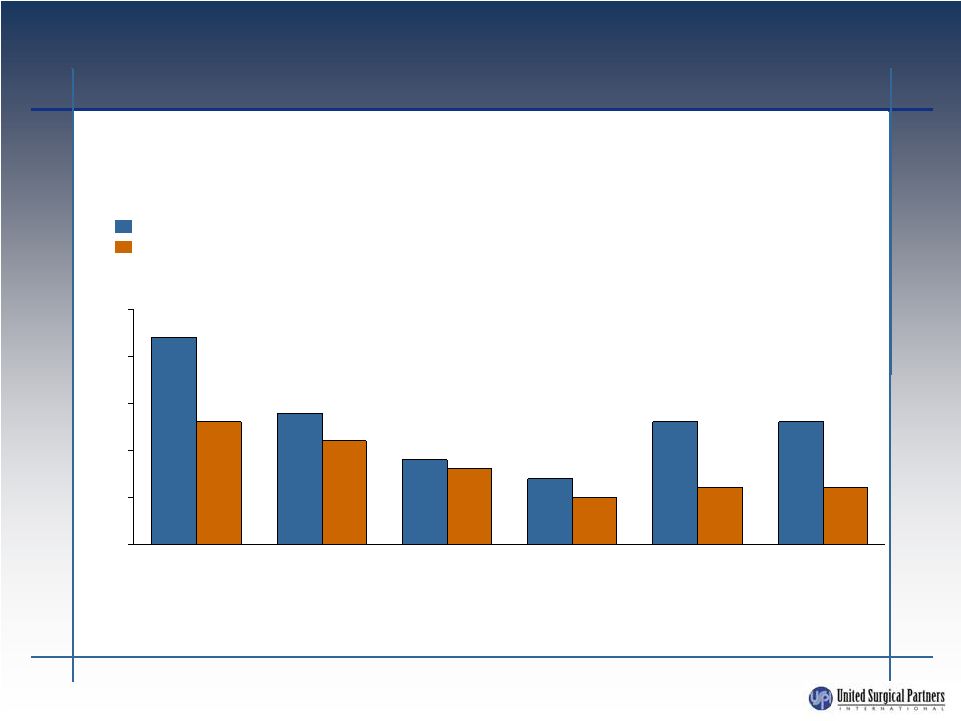
SUSTAINED REVENUE GROWTH
Systemwide revenue growth and U.S. same facility revenue growth
U.S.
Facilities
operated
152
161
165
185
200
202
13%
13%
7%
9%
14%
22%
6%
6%
5%
8%
11%
13%
0%
5%
10%
15%
20%
25%
2007
2008
2009
2010
2012
YTD
2011
U.S. same facility revenue growth
Systemwide revenue growth |
 15
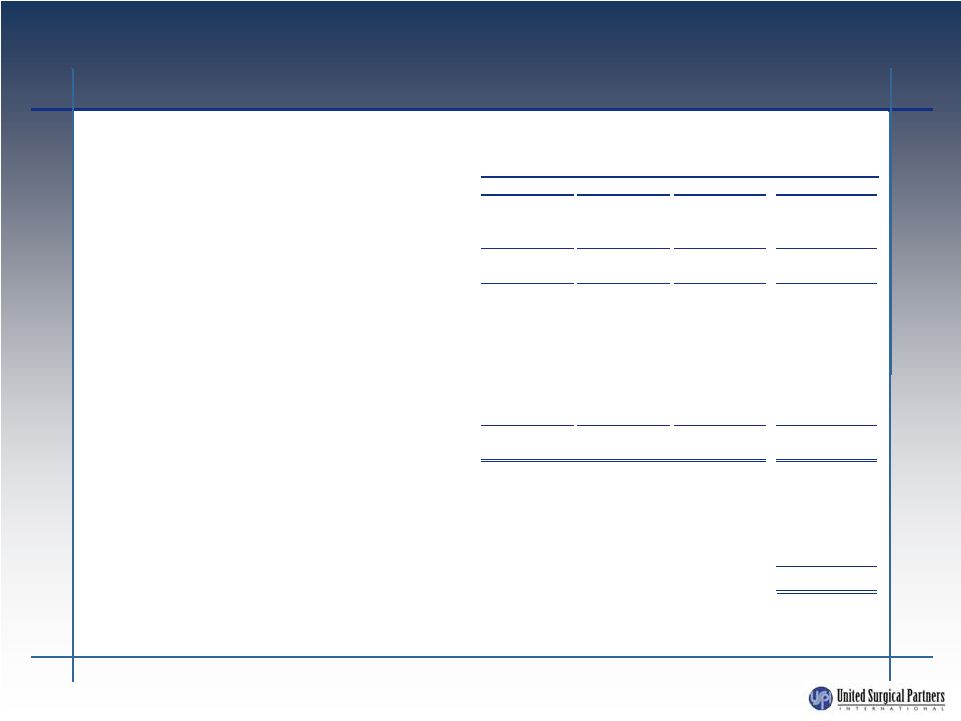
U.S. ADJUSTED EBITDA BRIDGE
Note: See last page for Footnotes to U.S. Adjusted EBITDA Bridge
Unaudited Pro Forma
Years Ended December 31,
($ in thousands)
2009
2010
2011
2011 As Adjusted
Operating Income
178,176
$
194,611
$
233,659
$
233,659
$
Depreciation and Amortization
24,432
22,493
21,177
21,177
EBITDA
202,608
$
217,104
$
254,836
$
254,836
$
Net income attributable to noncontrolling interests
(65,313)
(60,240)
(69,779)
(69,779)
EBITDA less noncontrolling interests
137,295
$
156,864
$
185,057
$
185,057
$
Net (gain) loss on deconsolidations, disposals and impairments
29,162
6,378
(1,529)
(1,529)
Impairment of unconsolidated affiliate
-
3,676
-
-
De novo start-up losses
a
-
136
4,009
4,009
Acquisition costs
b
-
2,857
3,314
3,314
Expense related to prior acquisition
c
-
6,000
-
-
Equity compensation
1,951
2,168
1,237
1,237
Management fee
d
2,000
2,000
2,000
2,000
Adjusted EBITDA,
excluding the pro forma effect of recent and pending acquisitions
170,408
$
180,079
$
194,088
$
194,088
$
Titan acquisition (14 facilities)
e
6,239
Acquisition of facility in Hackensack, New Jersey
3,549
Acquisition of facility in San Diego, California
g
599
Acquisition of facility in Midland, Texas
h
546
Acquisition of facility in Phoenix, Arizona
i
518
Titan buy-up (one facility)
4,434
Adjusted EBITDA
k
209,973
$
j
f |
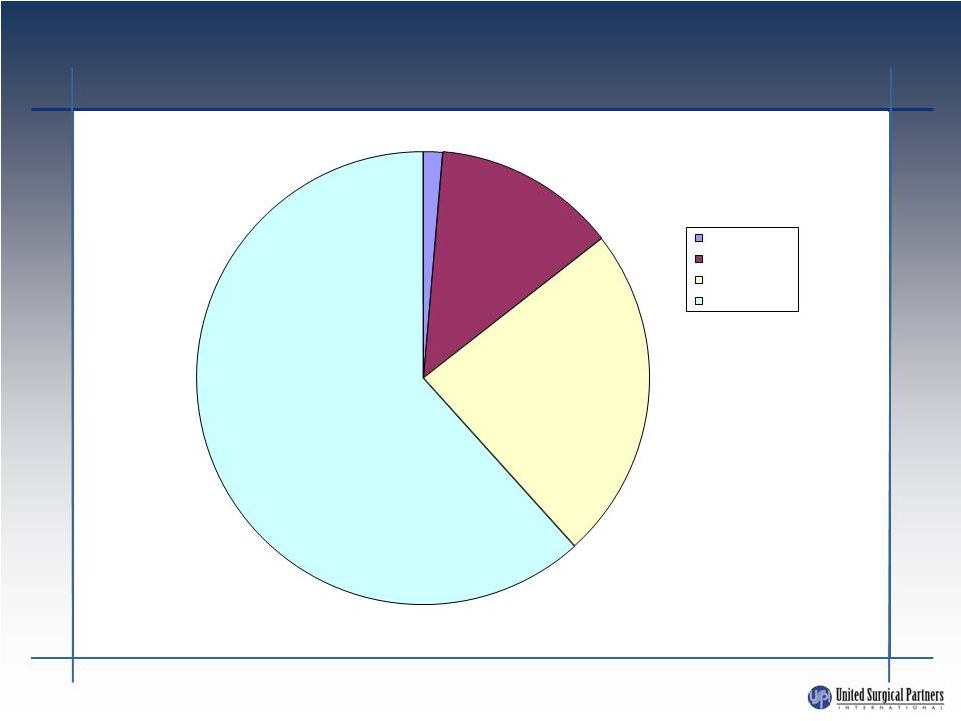 DEBT
MATURITIES Total debt $1.3 billion as of June 30, 2012
16
2%
13%
24%
61%
Next 12 Months
Months 13-36
Months 37-60
Beyond 5 years
$322.8M
$834.6M |
 17
SUMMARY
USPI is well positioned: low cost, high quality, high customer
satisfaction provider
Partner with key local not-for-profit hospital systems
Strong partnering capabilities will continue to provide opportunities
for growth, even in difficult times
Focused on key strategic markets with significant market share
Stable revenue growth
Strong equity sponsor in WCAS
Capitalized for growth and flexibility |
 18
FOOTNOTES TO U.S. ADJUSTED
EBITDA BRIDGE
a.
Represents the share of operating losses incurred primarily by a hospital located in Phoenix,
Arizona. The hospital opened in June 2010. The Company owns 50% of the hospital and the
remaining 50% is owned by a local not-for-profit hospital partner. This hospital has no physician ownership as it opened after the
Patient Protection and Affordable Care Act was enacted on March 23, 2010, which disallowed physician
ownership in this hospital.
b.
Represents transaction expenses and related costs incurred related to our acquisitions of HealthMark
Partners, Inc. in 2010 and Titan Health Corporation primarily in 2011.
c.
Represents payment of fee related to the settlement of a dispute regarding an acquisition of a
facility in 2003.
d.
Represents annual management fees paid to Welsh Carson Anderson & Stowe.
e.
Effective September 1, 2011, we acquired 100% of the equity interests in Titan Health Corporation, or
Titan. We paid cash totaling $43.4 million, net of $5.0 million of cash acquired. Titan has an
equity investment in 14 ambulatory surgery centers. In addition, we paid approximately $14.3 million in cash to
physicians in order to obtain additional ownership in six of these centers. Adjusted EBITDA has been
increased to reflect this acquisition as though it were effective January 1, 2011, by applying
our ownership percentage and management contract earnings formula to the historical financial statements of the
acquiree for the months of 2011 that preceded our acquisition.
f.
Effective December 1, 2011, we paid cash of approximately $23.7 million to acquire a noncontrolling
equity interest and right to manage a facility in Hackensack, New Jersey. Adjusted EBITDA has
been increased to reflect this acquisition as though it were effective January 1, 2011, by applying our
ownership percentage and management contract earnings formula to the historical financial statements
of the acquiree for the months of 2011 that preceded our acquisition.
g.
Effective December 31, 2011, we paid cash of approximately $3.3 million to acquire a controlling
equity interest and right to manage a facility in San Diego, California. Adjusted EBITDA has
been increased to reflect this acquisition as though it were effective January 1, 2011, by applying our ownership percentage
and management contract earnings formula to the historical financial statements of the acquiree for
2011.
h.
Effective February 1, 2012, we paid cash of approximately $3.1 million to acquire a noncontrolling
equity interest and right to manage a facility in Midland, Texas. Adjusted EBITDA has been
increased to reflect this acquisition as though it were effective January 1, 2011, by applying our ownership percentage and
management contract earnings formula to the historical financial statements of the acquiree for
2011.
i.
Effective March 1, 2012, we paid cash of approximately $3.0 million to acquire a noncontrolling
equity interest and right to manage a facility in Phoenix, Arizona. Adjusted EBITDA has been
increased to reflect this acquisition as though it were effective January 1, 2011, by applying our ownership percentage
and management contract earnings formula to the historical financial statements of the acquiree for
2011.
j.
Represents a pending acquisition of additional ownership in a Titan facility in Cherry Hill, New
Jersey. We currently have a minority interest in such facility and have reached an agreement
in principle to acquire a controlling interest for $18.0 million in cash. At this time, we have completed our due diligence and
believe we have completed negotiation of the definitive documentation for the acquisition, but such
documentation remains subject to the approval of certain physicians at the facility and
therefore has not yet been signed. We expect to sign the definitive documentation and close the acquisition by March 31, 2012,
however, we can provide no assurance that acquisition will close by such date, if at all. For
purposes of this offering memorandum, we have assumed such acquisition will be completed, and
therefore Adjusted EBITDA has been increased to reflect this acquisition as though it were effective January 1, 2011, by
applying our ownership percentage and management contract earnings formula to the historical
financial statements of the acquiree for 2011.
k.
Adjusted EBITDA does not reflect two additional acquisition opportunities that are currently pending.
We have substantially completed our due diligence with respect to such acquisitions and are in
active negotiations with the existing owners of such businesses, but have not reached a definitive agreement with the
existing owners. At this time, the Company expects to pay approximately $24.4 million in cash to
complete such acquisitions. Based on diligence completed to date, if such acquisitions were
completed as of January 1, 2011, we estimate that the Adjusted EBITDA contribution from such acquisitions would have been
approximately $2.6 million. However, this estimate is subject to our ongoing diligence review. While
we expect to complete such acquisitions within a few months of the consummation of this
offering, we can provide no assurance that such acquisitions will close during that time, if at all. |