Attached files
| file | filename |
|---|---|
| 8-K - 8-K - ZIOPHARM ONCOLOGY INC | d883170d8k.htm |
| EX-99.1 - EX-99.1 - ZIOPHARM ONCOLOGY INC | d883170dex991.htm |
Exhibit 99.2
In the preliminary prospectus supplement filed pursuant to Rule 424(b)(5) in connection with a public offering of common stock by Ziopharm Oncology, Inc. (the “Company”), the Company provided the following overview of the Company’s business as updates to the information provided in the Company’s previous periodic filings with the Securities and Exchange Commission.
Company Overview
We are a clinical-stage biopharmaceutical company focused on discovering, acquiring, developing and commercializing next generation immunotherapy platforms that leverage cell- and gene-based therapies to treat patients with cancer. We are developing two immuno-oncology platform technologies that utilize the immune system by employing novel, controlled gene expression and innovative cell engineering technologies designed to deliver safe, effective, and scalable non-viral cell- and viral-based gene therapies for the treatment of multiple cancer types. Our first platform is referred to as Sleeping Beauty and is based on the genetic engineering of immune cells using a non-viral transposon/transposase system that is intended to stably reprogram T cells outside of the body for subsequent infusion. Our second platform is termed Controlled IL-12, which is designed to stimulate expression of interleukin 12, or IL-12, a master regulator of the immune system, in a controlled and safe manner to focus the patient’s immune system to attack cancer cells. We believe these two platforms have the potential to provide unique and powerful solutions to address the issues associated with (1) treating solid tumors with heterogeneous and unknown antigens, and (2) providing cost-effective scalable manufacturing solutions for T cell receptor T cell, or TCR+ T, therapies for solid tumors and chimeric antigen receptor, or CAR T cell, or CAR+ T, therapies targeting CD19 on malignant B cells.
Using our Sleeping Beauty platform, we are developing TCR+ T therapies initially to target solid tumors. Our T cell receptor, or TCR, program designs and manufactures T cells that are intended to target tumor-specific antigens, thereby delivering personalized therapy that can attack an individual patient’s cancer. These antigens are referred to as neoantigens as they are only expressed by the tumor, reducing the potential for toxicity upon targeting normal cells. A minority of neoantigens are shared between patients and between classes of tumors and are referred to as “hotspots”. The Sleeping Beauty system uses DNA plasmids to reprogram T cells to express introduced TCRs on a patient-by-patient basis (addressing inter-tumor heterogeneity) and possibly to express more than one TCR for each patient (addressing intra-tumor heterogeneity). The genetic modification using the Sleeping Beauty system of recipient-derived products enables us to target neoantigens in two ways. The first recognizes that most neoantigens are unique to each patient’s tumor and we plan to infuse TCR+ T cells expressing recipient-derived (autologous) TCRs. The second is based on the finding that some neoantigens in hotspots are shared between patients and we plan to administer TCR+ T expressing allogeneic TCRs from a library derived from third parties. We have in-licensed from the National Cancer Institute, or the NCI, multiple allogeneic TCRs derived from third parties that are reactive to mutated KRAS, TP53 and EGFR and we plan to expand our TCR library as part of our commitment to advance clinical development for the treatment of patients whose solid tumors have driver mutations. These TCRs are typically obtained from tumor-infiltrating lymphocytes, or TILs.
Under our Cooperative Research and Development Agreement, the NCI is conducting a Phase 2 clinical trial to evaluate autologous peripheral blood lymphocytes genetically modified with the Sleeping Beauty system to express autologous (personalized) TCRs. The U.S. Food and Drug Administration, or FDA, has cleared the investigational new drug, or IND, application submitted by the NCI for this clinical trial. The trial was initiated in October 2019 and preparations to enable patient enrollment by the NCI are underway. We expect the trial will enroll patients with a broad range of solid tumors over the next several years.
In addition, we are currently planning a clinical program to study our TCR approach with The University of Texas MD Anderson Cancer Center, or MD Anderson. Under this program, we expect to evaluate both our personalized TCR, or autoTCR, approach and our hotspot TCR, or alloTCR, approach. Our autoTCR approach is designed to identify neoantigens and TCRs on a patient-by-patient basis, which we believe should allow it to be broadly applicable to many patients’ solid tumors. The advantage of the alloTCR approach is that a subset of patients with solid tumors may be rapidly treated based on screening them for target neoantigens (e.g., in TP53), identifying human leukocyte antigen, and matching these data to the alloTCRs in the library.
We are also developing CAR+ T therapies using our Sleeping Beauty platform. Our CAR+ T program seeks to solve the complex and costly manufacturing limitations that we believe continue to limit the commercial potential of existing CD19-specific CAR+ T therapies. We believe using DNA plasmids in the Sleeping Beauty system to express a CD19-specific CAR and our proprietary membrane-bound interleukin 15, or mbIL15, in resting T cells obtained from peripheral blood will enable infused T cells to propagate within the patient to target leukemia and lymphoma, thus avoiding the need to numerically expand T cells for weeks in bioreactors before patient administration. The mbIL15 is co-expressed with a “kill switch” or “safety switch” to conditionally eliminate infused T cells. We expect the lower cost of DNA plasmids compared with the virus used by other CAR+ T programs, together with the avoidance of lengthy ex vivo manufacturing, will reduce the cost and complexity of manufacturing CAR+ T cells. These technologies should enable T cells to be infused as soon as the day after gene transfer in a process we refer to as rapid personalized manufacture, or RPM. We are advancing our CAR+ T technology in the United States in collaboration with MD Anderson in a Phase 1 clinical trial in the United States infusing CD19-specific CAR+ T therapies manufactured using our RPM technology. In this trial, we plan to infuse donor-derived T cells after allogeneic bone marrow transplantation, or BMT, for recipients who have relapsed with CD19+ leukemias and lymphomas. We are also advancing our RPM technology including using patient-derived (autologous) T cells in order to treat patients with relapsed or refractory CD19+ leukemias and lymphomas. In a joint venture with TriArm Therapeutics, Ltd., or TriArm, we have formed Eden BioCell, Ltd., or Eden BioCell, to lead the clinical development and commercialization of Sleeping Beauty-generated CD19-specific RPM CAR-T therapies in the People’s Republic of China, Taiwan and Korea. Eden BioCell is focused on advancing our RPM technology using patient-derived (autologous) T cells in order to treat patients with relapsed or refractory CD19+ leukemias and lymphomas. Eden BioCell is owned equally by us and TriArm and the parties share decision-making authority. TriArm has committed up to $35.0 million, of which $10.0 million has been paid as of September 30, 2019, to this joint venture and will also manage all clinical development to execute trials in the designated countries.
Our Controlled IL-12 platform uses virotherapy based on an engineered replication-incompetent adenovirus, referred to as Ad-RTS-hIL-12, plus veledimex as a gene delivery system to conditionally produce IL-12, a potent, naturally occurring anti-cancer protein, to treat patients with solid tumors where a specific target is unknown, including brain cancer. Our Controlled IL-12 platform allows us to deliver IL-12 in a tunable dose as the cytokine is under transcriptional control of the rheoSwitch therapeutic system® (RTS®). We believe the ability regulate production of IL-12 after administration of the virus is critical for the development of this potent cytokine. We are currently studying our Controlled IL-12 Platform as a monotherapy in a Phase 1 clinical trial of patients with recurrent glioblastoma multiforme, or rGBM. Our substudy of this clinical trial is fully enrolled with 36 patients diagnosed with rGBM. The substudy is designed to encourage use of low-dose steroids and 20 mg veledimex to further understand the potential of Controlled IL-12 as a monotherapy. We are also developing our Controlled IL-12 platform in combination with immune checkpoint inhibitors. We are studying Ad-RTS-hIL-12 plus veledimex in combination with OPDIVO® (nivolumab) in a Phase 1 dose-escalation clinical trial of patients with rGBM. We have entered into a clinical supply agreement with Regeneron Pharmaceuticals, Inc., or Regeneron, to evaluate Ad-RTS-hIL-12 plus veledimex in combination with Regeneron’s PD-1antibody Libtayo® (cemiplimab-rwlc) for the treatment of patients with rGBM. We have initiated a Phase 2 clinical trial evaluating Controlled IL-12 (Ad-RTS-hIL-12 plus veledimex, Ad+V), in combination with PD-1 antibody Libtayo® (cemiplimab-rwlc) for the treatment of recurrent or progressive glioblastoma multiforme in adults. In our clinical trials, we have observed that Controlled IL-12 increases T-cell activity in the tumor microenvironment in patients with rGBM and we may conduct trials of Controlled IL-12 in other tumor types as both a monotherapy and in combination with immune checkpoint inhibitors.
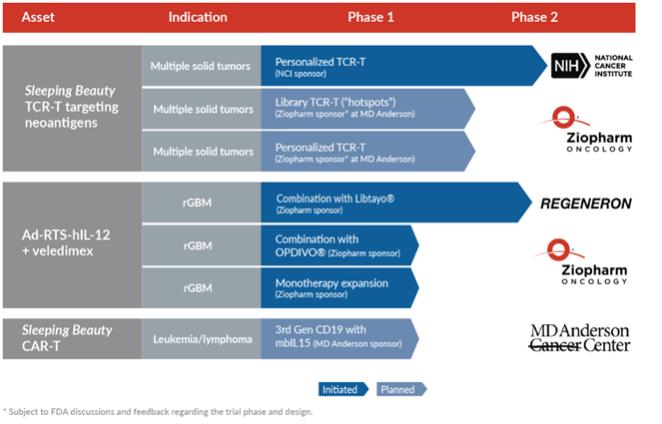
Our Pipeline
Recent Developments
Sleeping Beauty Solid Tumor TCR-T Program
We expect to pursue our TCR+T cell therapy program in collaboration with MD Anderson. In October 2019, we entered into the 2019 Research and Development Agreement with MD Anderson where, we will, among other things, collaborate with MD Anderson on programs to expand our TCR library and conduct clinical trials.
As part of our effort to continue expanding our TCR library, in January 2020, we announced an amendment to our license with the NCI to expand our license to include additional TCRs reactive to mutated KRAS and TP53. We also announced in January 2020 that the journal Clinical Cancer Research published a paper, co-authored by Drew Deniger, Ph.D., who leads our TCR+T cell therapy program. The Clinical Cancer Research publication describes how TCRs with specificity to mutations within TP53 present in tumor cells can be obtained from circulating T cells, which may overcome the need to obtain TILs through surgical resection.
Our third generation CAR+ T program utilizes our proprietary mbIL15, which enables infused T cells to propagate within the patient, thus avoiding the need to numerically expand T cells for weeks in bioreactors before patient administration. At the American Society of Hematology, or ASH, Annual Meeting in December 2019, we presented pre-clinical data of our RPM technology demonstrating that T cells genetically modified using DNA plasmids from the Sleeping Beauty system to express TCRs with mbIL15 exhibit anti-tumor effects.
Controlled IL-12 Platform
In November 2019, we provided an update from two ongoing studies of our Controlled IL-12 platform at the 2019 Society for Neuro-Oncology, or SNO, Annual Meeting.
Monotherapy Expansion Substudy—Interim Results
In a Phase 1 clinical trial of patients with rGBM, referred to as the Main Study, a subset of patients (n=6) with unifocal disease who received single administration of Ad-RTS-hIL-12 with 20 mg daily dosing (15 total planned doses) of veledimex along with low-dose steroids along, achieved 17.8 months median overall survival, or mOS. Thirty-six additional patients with rGBM were recruited into a substudy, referred to as the Expansion Substudy, designed to encourage use of low-dose steroids and 20 mg veledimex to further understand the potential of Controlled IL-12 as a monotherapy. During the 2019 SNO Annual Meeting, we provided an interim update for the Expansion Substudy and announced that:
| • | We observed a decrease in tumor from baseline resulted in a patient’s lesion being too small to measure, assessed as a partial response (per iRANO), with follow up ongoing. |
| • | We provided an analysis of MRI findings of pseudoprogression in subjects with initial increases and subsequent decreases in tumor size, which was consistent with immune-mediated anti-tumor effects. |
| • | We observed that subjects in the Expansion Substudy were comparable to the subjects in the Main Study, except a higher percentage of subjects enrolled in the Expansion Substudy had multifocal disease (as compared with unifocal disease) and fewer previous recurrences of disease. |
| • | Subjects receiving 20 mg of veledimex in both the Main Study and Expansion Substudy (n=20) with unifocal disease at entry, receiving low-dose steroids (defined as <20 mg cumulative dosing of dexamethasone during the time of veledimex dosing) had a mOS of 16.2 months. The mOS for these subjects in the Expansion Substudy alone (n=14) has not been reached at a mean follow up of 9.7 months |
| • | We observed subjects with multifocal disease at initial enrollment that received 20mg of veledimex and low-dose steroids (n=13) had a mOS of 10.1 months. We believe this is consistent with literature, which shows that multifocal glioblastoma is associated with worse prognosis compared to unifocal disease |
| • | Adverse reactions that we observed in the Expansion Substudy as of the data cut-off date were consistent with prior studies of Controlled IL-12 and were predictable, dose-related, and promptly reversible upon discontinuation of veledimex |
Combination Study—Interim Results
We are also studying Ad-RTS-hIL-12 plus veledimex in combination with nivolumab, an immune checkpoint inhibitor, in a Phase 1 dose-escalation trial of patients with rGBM. During the 2019 SNO Annual Meeting, we provided an interim update for this trial and announced that:
| • | We observed a decrease of approximately 64% in a patient’s tumor from baseline resulting in a partial response (per iRANO), with follow up ongoing. |
| • | We provided an analysis of MRI findings of pseudoprogression in subjects, which was consistent with immune-mediated anti-tumor effects. |
| • | Active dosing is ongoing in the trial and mOS has not been reached, with a mean follow up for these subjects of 4.8 months. |
| • | No dose limiting toxicities, no serious adverse events that were considered related to the combination with nivolumab and no clinically significant overlapping toxicities have been observed as of the data cut-off date in the trial. |
| • | Drug-related toxicities we have observed as of the data cut-off date were comparable to the Main Study, and have been predictable, dose-related, and promptly reversible upon discontinuation of veledimex. Further, there were no drug-related deaths reported. |
Sleeping Beauty Solid Tumor CAR+ T Program
In October 2019, we announced the FDA had cleared an IND application submitted by MD Anderson Cancer Center for a Phase 1 clinical trial to evaluate our third generation CD19-specific CAR-T therapies for patients with relapsed CD19+ leukemias and lymphomas. The clinical trial will evaluate CAR-T therapies prepared using our RPM technology.
In January 2020, we announced that a letter published in the Blood, the journal of the American Society of Hematology, discussed long-term outcomes of seven patients with relapsed or refractory B-cell lymphoid malignancies, all of whom had received our second-generation CD19-specific CAR-T cells infused two days following autologous hematopoietic stem-cell transplantation, also referred to as BMT. In this study, four of the seven patients demonstrated sustained persistence of CAR-T (median time of persistence duration was 4.5 years, range 2-5 years). Five-year progression-free survival and overall survival were 71% and 86%, respectively.