Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - ZIOPHARM ONCOLOGY INC | Financial_Report.xls |
| EX-31.1 - EX-31.1 - ZIOPHARM ONCOLOGY INC | d914910dex311.htm |
| EX-32.1 - EX-32.1 - ZIOPHARM ONCOLOGY INC | d914910dex321.htm |
| EX-31.2 - EX-31.2 - ZIOPHARM ONCOLOGY INC | d914910dex312.htm |
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-Q
(Mark One)
| x | QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the quarterly period ended March 31, 2015
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number 001-33038
ZIOPHARM Oncology, Inc.
(Exact name of registrant as specified in its charter)
| Delaware | 84-1475642 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
One First Avenue, Parris Building 34, Navy Yard Plaza
Boston, Massachusetts 02129
(617) 259-1970
(Address, including zip code, and telephone number, including
area code, of registrant’s principal executive offices)
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes: x No: ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes: x No: ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer | ¨ | Accelerated filer | x | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | ¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes: ¨ No: x
The number of shares of the registrant’s common stock, $.001 par value, outstanding as of May 1, 2015, was 128,232,537 shares.
Table of Contents
ZIOPHARM Oncology, Inc.
NOTE REGARDING FORWARD-LOOKING STATEMENTS
This report contains forward-looking statements that are based on our current beliefs and expectations. These forward-looking statements may be accompanied by such words as “anticipate,” “believe,” “estimate,” “expect,” “forecast,” “intend,” “may,” “plan,” “project,” “target,” “will” and other words and terms of similar meaning. Reference is made in particular to forward-looking statements regarding:
| • | our ability to finance our operations and business initiatives and obtain funding for such activities; |
| • | the sufficiency of our cash, investments and cash flows from operations and our expected uses of cash; |
| • | the costs and timing of the development and commercialization of our pipeline products and services; |
| • | additional planned regulatory filings for and commercialization of our immuno-oncology and synthetic immuno-oncology product candidates; |
| • | whether any of our other therapeutic discovery and development efforts will advance further in pre-clinical research or in the clinical trials process and whether and when, if at all, they will receive final approval from the U.S. Food and Drug Administration or equivalent foreign regulatory agencies and for which indications; |
| • | whether any other therapeutic products we develop will be successfully marketed if approved; |
| • | our ability to achieve the results contemplated by our collaboration agreements; |
| • | competition from other pharmaceutical and biotechnology companies; |
| • | the development of, and our ability to take advantage of, the market for our therapeutic products; contract manufacturing activity; |
| • | the anticipated amount, timing and accounting of deferred revenues, milestone and other payments under licensing, collaboration or acquisition agreements, research and development costs and other expenses; |
| • | the strength and enforceability of our intellectual property rights and the protection afforded by our patent rights; |
| • | our assessment of the potential impact on our future revenues of healthcare reform legislation in the United States; |
| • | the timing and impact of measures worldwide designed to reduce healthcare costs; |
| • | the impact of the deterioration of the credit and economic conditions in certain countries in Europe; and general economic conditions. |
These forward-looking statements involve risks and uncertainties, including those that are described in the “Risk Factors” section of this report and elsewhere within this report that could cause actual results to differ materially from those reflected in such statements. You should not place undue reliance on these statements. Forward-looking statements speak only as of the date of this report. We do not undertake any obligation to publicly update any forward-looking statements.
NOTE REGARDING COMPANY REFERENCES
Throughout this report, “ZIOPHARM,” the “Company,” “we,” “us” and “our” refer to ZIOPHARM Oncology, Inc.
NOTE REGARDING TRADEMARKS
All trademarks, trade names and service marks appearing in this Quarterly Report on Form 10-Q are the property of their respective owners.
2
Table of Contents
ZIOPHARM Oncology, Inc.
3
Table of Contents
ZIOPHARM Oncology, Inc.
(unaudited)
(in thousands, except share and per share data)
| March 31, | December 31, | |||||||
| 2015 | 2014 | |||||||
| ASSETS |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 129,684 | $ | 42,803 | ||||
| Receivables |
62 | 145 | ||||||
| Prepaid expenses and other current assets |
857 | 1,139 | ||||||
|
|
|
|
|
|||||
| Total current assets |
130,603 | 44,087 | ||||||
| Property and equipment, net |
426 | 531 | ||||||
| Deposits |
128 | 128 | ||||||
| Other non-current assets |
491 | 491 | ||||||
|
|
|
|
|
|||||
| Total assets |
$ | 131,648 | $ | 45,237 | ||||
|
|
|
|
|
|||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY |
||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 779 | $ | 2,004 | ||||
| Accrued expenses |
8,220 | 7,182 | ||||||
| Deferred revenue—current portion |
1,088 | 1,360 | ||||||
| Deferred rent—current portion |
405 | 280 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
10,492 | 10,826 | ||||||
| Deferred rent |
553 | 570 | ||||||
|
|
|
|
|
|||||
| Total liabilities |
11,045 | 11,396 | ||||||
|
|
|
|
|
|||||
| Commitments and contingencies (note 6) |
||||||||
| Stockholders’ equity: |
||||||||
| Common stock, $0.001 par value; 250,000,000 shares authorized; 128,232,537 and 104,452,105 shares issued and outstanding at March 31, 2015 and December 31, 2014, respectively |
128 | 104 | ||||||
| Additional paid-in capital—common stock |
571,318 | 406,349 | ||||||
| Accumulated deficit |
(450,843 | ) | (372,612 | ) | ||||
|
|
|
|
|
|||||
| Total stockholders’ equity |
120,603 | 33,841 | ||||||
|
|
|
|
|
|||||
| Total liabilities and stockholders’ equity |
$ | 131,648 | $ | 45,237 | ||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of the unaudited interim financial statements.
4
Table of Contents
ZIOPHARM Oncology, Inc.
(unaudited)
(in thousands, except share and per share data)
| For the Three Months Ended | ||||||||
| March 31, | ||||||||
| 2015 | 2014 | |||||||
| Research contract revenue |
$ | 272 | $ | 200 | ||||
|
|
|
|
|
|||||
| Operating expenses: |
||||||||
| Research and development, including costs of research contracts |
74,249 | 6,542 | ||||||
| General and administrative |
4,250 | 3,442 | ||||||
|
|
|
|
|
|||||
| Total operating expenses |
78,499 | 9,984 | ||||||
|
|
|
|
|
|||||
| Loss from operations |
(78,227 | ) | (9,784 | ) | ||||
| Other income (expense), net |
(4 | ) | (9 | ) | ||||
| Change in fair value of warrants |
— | 82 | ||||||
|
|
|
|
|
|||||
| Net loss |
$ | (78,231 | ) | $ | (9,711 | ) | ||
|
|
|
|
|
|||||
| Net loss per share—basic and diluted |
$ | (0.69 | ) | $ | (0.10 | ) | ||
|
|
|
|
|
|||||
| Weighted average common shares outstanding used to compute net loss per share—basic and diluted |
113,410,250 | 100,229,200 | ||||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of the unaudited interim financial statements.
5
Table of Contents
ZIOPHARM Oncology, Inc.
STATEMENT OF STOCKHOLDERS’ EQUITY
For the Three months Ended March 31, 2015
(unaudited)
(in thousands, except share and per share data)
| Additional | ||||||||||||||||||||
| Common Stock | Paid-in | Total | ||||||||||||||||||
| Capital | Accumulated | Stockholders’ | ||||||||||||||||||
| Shares | Amount | Common | Deficit | Equity | ||||||||||||||||
| Balance at December 31, 2014 |
104,452,105 | $ | 104 | $ | 406,349 | $ | (372,612 | ) | $ | 33,841 | ||||||||||
| Stock-based compensation |
— | — | 1,093 | — | 1,093 | |||||||||||||||
| Exercise of employee stock options |
592,200 | — | 2,541 | — | 2,541 | |||||||||||||||
| Repurchase of restricted common stock |
(33,931 | ) | — | (246 | ) | — | (246 | ) | ||||||||||||
| Issuance of common stock in public offering, net of $267 thousand in issuance expenses |
11,500,000 | 12 | 94,308 | — | 94,320 | |||||||||||||||
| Issuance of common stock in licensing agreement |
11,722,163 | 12 | 67,273 | — | 67,285 | |||||||||||||||
| Net loss |
— | — | — | (78,231 | ) | (78,231 | ) | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Balance at March 31, 2015 |
128,232,537 | $ | 128 | $ | 571,318 | $ | (450,843 | ) | $ | 120,603 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
The accompanying notes are an integral part of the unaudited interim financial statements.
6
Table of Contents
ZIOPHARM Oncology, Inc.
(unaudited)
(in thousands)
| For the Three Months | ||||||||
| Ended March 31, | ||||||||
| 2015 | 2014 | |||||||
| Cash flows from operating activities: |
||||||||
| Net loss |
$ | (78,231 | ) | $ | (9,711 | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||
| Depreciation and amortization |
122 | 124 | ||||||
| Stock-based compensation |
1,093 | 1,223 | ||||||
| Change in fair value of warrants |
— | (82 | ) | |||||
| Common stock issued in exchange for license agreement |
67,285 | — | ||||||
| Change in operating assets and liabilities: |
||||||||
| (Increase) decrease in: |
||||||||
| Receivables |
83 | 118 | ||||||
| Prepaid expenses and other current assets |
282 | 359 | ||||||
| Other noncurrent assets |
— | 11 | ||||||
| Increase (decrease) in: |
||||||||
| Accounts payable |
(1,224 | ) | 156 | |||||
| Accrued expenses |
1,037 | (605 | ) | |||||
| Deferred revenue |
(272 | ) | (200 | ) | ||||
| Deferred rent |
108 | (47 | ) | |||||
|
|
|
|
|
|||||
| Net cash used in operating activities |
(9,717 | ) | (8,654 | ) | ||||
|
|
|
|
|
|||||
| Cash flows from investing activities: |
||||||||
| Purchases of property and equipment |
(17 | ) | (2 | ) | ||||
|
|
|
|
|
|||||
| Net cash used in investing activities |
(17 | ) | (2 | ) | ||||
|
|
|
|
|
|||||
| Cash flows from financing activities: |
||||||||
| Proceeds from exercise of stock options |
2,541 | 969 | ||||||
| Payments to employees for repurchase of common stock |
(246 | ) | (132 | ) | ||||
| Proceeds from the issuance of common stock, net |
94,320 | — | ||||||
|
|
|
|
|
|||||
| Net cash provided by financing activities |
96,615 | 837 | ||||||
|
|
|
|
|
|||||
| Net increase (decrease) in cash and cash equivalents |
86,881 | (7,819 | ) | |||||
| Cash and cash equivalents, beginning of period |
42,803 | 68,204 | ||||||
|
|
|
|
|
|||||
| Cash and cash equivalents, end of period |
$ | 129,684 | $ | 60,385 | ||||
|
|
|
|
|
|||||
| Supplementary disclosure of cash flow information: |
||||||||
| Cash paid for interest |
$ | — | $ | — | ||||
|
|
|
|
|
|||||
| Cash paid for income taxes |
$ | — | $ | — | ||||
|
|
|
|
|
|||||
| Supplementary disclosure of noncash investing and financing activities: |
||||||||
| Issuance of common stock in license agreement |
$ | 67,285 | $ | — | ||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of the unaudited interim financial statements.
7
Table of Contents
ZIOPHARM Oncology, Inc.
(unaudited)
1. Business
Overview
ZIOPHARM Oncology, Inc., which is referred to as “ZIOPHARM” or the “Company”, is a biopharmaceutical company that seeks to acquire, develop and commercialize, on its own or with partners, a diverse portfolio of cancer therapies that can address unmet medical needs.
The Company’s operations to date have consisted primarily of raising capital and conducting research and development. The Company’s fiscal year ends on December 31.
The Company has operated at a loss since its inception in 2003 and has minimal revenues. The Company anticipates that losses will continue for the foreseeable future. At March 31, 2015, the Company’s accumulated deficit was approximately $450.8 million. The Company’s ability to continue operations after its current cash resources are exhausted depends on its ability to obtain additional financing or to achieve profitable operations, as to which no assurances can be given. Cash requirements may vary materially from those now planned because of changes in the Company’s focus and direction of its research and development programs, competitive and technical advances, patent developments, regulatory changes or other developments. Additional financing will be required to continue operations after the Company exhausts its current cash resources and to continue its long-term plans for clinical trials and new product development. There can be no assurance that any such financing can be obtained by the Company, or if obtained, what the terms thereof may be, or that any amount that the Company is able to raise will be adequate to support the Company’s working capital requirements until it achieves profitable operations.
Basis of Presentation
The accompanying unaudited interim financial statements have been prepared in accordance with the instructions to Form 10-Q pursuant to the rules and regulations of the Securities and Exchange Commission. Certain information and note disclosures required by generally accepted accounting principles in the United States have been condensed or omitted pursuant to such rules and regulations.
It is management’s opinion that the accompanying unaudited interim financial statements reflect all adjustments (which are normal and recurring) that are necessary for a fair statement of the results for the interim periods. The unaudited interim financial statements should be read in conjunction with the audited financial statements and the notes thereto for the year ended December 31, 2014, included in the Company’s Form 10-K, for such fiscal year.
The year-end balance sheet data was derived from the audited financial statements but does not include all disclosures required by generally accepted accounting principles in the United States.
The results disclosed in the Statements of Operations for the three months ended March 31, 2015 are not necessarily indicative of the results to be expected for the full fiscal year.
Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Although the Company regularly assesses these estimates, actual results could differ from those estimates. Changes in estimates are recorded in the period in which they become known.
8
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
1. Business—(continued)
The Company’s most significant estimates and judgments used in the preparation of its financial statements are:
| • | Clinical trial expenses; |
| • | Fair value measurements for stock based compensation; and |
| • | Income taxes. |
Subsequent Events
The Company evaluated all events and transactions that occurred after the balance sheet date through the date of this filing. Except as disclosed below and the Ares Trading Agreement in footnote 6, the Company did not have any other material subsequent events that impacted its financial statements or disclosures.
On May 7, 2015, the Company announced the appointment of Laurence J. N. Cooper, M.D., Ph.D., to the position of Chief Executive Officer. Dr. Cooper brings extensive experience in pioneering the development of adoptive cellular therapies in the field of oncology and translating immunology into clinical practice. Jonathan Lewis, M.D., Ph.D., the Company’s former Chief Executive Officer remains a member of its Board of Directors. Prior to becoming the Company’s Chief Executive Officer, Dr. Cooper was a tenured professor at The University of Texas MD Anderson Cancer Center, which he joined in 2006. In addition to being a tenured professor of Pediatrics and Immunology, Dr. Cooper’s other appointments at MD Anderson included Section Chief, Cell Therapy, Children’s Cancer Hospital; and Associate Director, Center for Cancer Immunology Research. He obtained his M.D. and Ph.D. degrees at Case Western Reserve University in Cleveland and then training in Pediatric Oncology and Bone Marrow Transplantation at the Fred Hutchinson Cancer Research Center in Seattle. Dr. Cooper has received numerous awards and honors and in addition to numerous other professional appointments, he has authored more than 140 journal articles, book chapters, and abstracts. Dr. Cooper has been appointed a Visiting Scientist at MD Anderson where he will continue to direct the efforts of the Cooper Lab.
2. Financings
On February 3, 2015, the Company entered into an underwriting agreement with J.P. Morgan Securities LLC, as representative of the several underwriters named therein, relating to the issuance and sale of 10,000,000 shares of its common stock. The price to the public in the offering was $8.75 per share, and the underwriters agreed to purchase the shares from the Company pursuant to the underwriting agreement at a purchase price of $8.225 per share. Under the terms of the underwriting agreement, the Company also granted the underwriters an option, exercisable for 30 days, to purchase up to an additional 1,500,000 shares of common stock at a purchase price of $8.225 per share. The offering was made pursuant to the Company’s effective registration statement on Form S-3 (Registration Statement No. 333-201826) previously filed with the SEC, and a prospectus supplement thereunder. The underwriters purchased the 10,000,000 shares and the additional 1,500,000 shares on February 9 and February 17, 2015, respectively. The net proceeds from the offering were approximately $94.3 million after deducting underwriting discounts and estimated offering expenses payable by the Company.
3. Summary of Significant Accounting Policies
The Company’s significant accounting policies were identified in the Company’s Form 10-K for the fiscal year ended December 31, 2014. There have been no material changes in those policies since the filing of its Form 10-K.
9
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
4. Fair Value Measurements
The Company accounts for its financial assets and liabilities using fair value measurements. The accounting standard defines fair value, establishes a framework for measuring fair value under generally accepted accounting principles and enhances disclosures about fair value measurements. Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value must maximize the use of observable inputs and minimize the use of unobservable inputs. The standard describes a fair value hierarchy based on three levels of inputs, of which the first two are considered observable and the last unobservable, that may be used to measure fair value which are the following:
| • | Level 1—Quoted prices in active markets for identical assets or liabilities. |
| • | Level 2—Inputs other than Level 1 that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities. |
| • | Level 3—Unobservable inputs that are supported by little or no market activity and that are significant to the fair value of the assets or liabilities. |
Assets and liabilities measured at fair value on a recurring basis as of March 31, 2015 and December 31, 2014 are as follows:
| ($ in thousands) | Fair Value Measurements at Reporting Date Using | |||||||||||||||
| Description |
Balance as of March 31, 2015 |
Quoted Prices in Active Markets for Identical Assets/Liabilities (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
||||||||||||
| Cash equivalents |
$ | 119,025 | $ | 119,025 | $ | — | $ | — | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
10
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
4. Fair Value Measurements – (continued)
| ($ in thousands) | Fair Value Measurements at Reporting Date Using | |||||||||||||||
| Description |
Balance as of December 31, 2014 |
Quoted Prices in Active Markets for Identical Assets/Liabilities (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
||||||||||||
| Cash equivalents |
$ | 37,290 | $ | 37,290 | $ | — | $ | — | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
The cash equivalents represent deposits in a short term United States treasury money market mutual fund quoted in an active market and classified as a Level 1 asset.
5. Net Loss per Share
Basic net loss per share is computed by dividing net loss by the weighted average number of shares of common stock outstanding for the period. The Company’s potential dilutive shares, which include outstanding common stock options, unvested restricted stock and warrants, have not been included in the computation of diluted net loss per share for any of the periods presented as the result would be anti-dilutive. Such potential shares of common stock at March 31, 2015 and 2014 consist of the following:
| March 31, | ||||||||
| 2015 | 2014 | |||||||
| Stock options |
5,924,297 | 6,159,828 | ||||||
| Unvested restricted common stock |
96,073 | 296,406 | ||||||
| Warrants |
— | 10,539,767 | ||||||
|
|
|
|
|
|||||
| 6,020,370 | 16,996,001 | |||||||
|
|
|
|
|
|||||
11
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies
Operating Leases
Prior to December 31, 2012, the Company entered into an operating lease in New York, NY, consisting of 6,251 square feet of office space. In accordance with this agreement, the Company entered into a letter of credit in the amount of $388 thousand, naming the Company’s landlord as beneficiary. In January 2012, the Company amended the lease agreement, adding 1,008 square feet of office space. As of December 31, 2012, the Company occupied 7,259 square feet of space in New York, NY, and maintained a $388 thousand letter of credit. The collateral for the letter of credit is recorded in other non-current assets on the balance sheet as of March 31, 2015. The lease for office space in New York, NY expires in October 2018.
On October 17, 2013, the Company entered into a sublease agreement to lease 7,259 square feet in its New York office to a subtenant. The Company remains primarily liable to pay rent on the original lease. The Company recorded a loss on the sublease in the amount of $729 thousand for the year ended December 31, 2013, representing the remaining contractual obligation of $2.3 million, less $1.6 million in payments from its subtenant. The Company retired assets in this subleased area as a result of this sublease with a net book value of $392 thousand, and recorded a loss on disposal of fixed assets for the same amount for the year ended December 31, 2013. The Company continues to maintain a $388 thousand letter of credit. The collateral for the letter of credit is recorded in other non-current assets on the balance sheet as of March 31, 2015. The lease for office space in New York, NY expires in October 2018.
Prior to December 31, 2012, the Company entered into separate operating lease agreements for various spaces in a building in Boston, MA. That space consisted of 5,249 square feet on the first floor, 8,538 square feet on the second floor, and 6,959 square feet on the third floor. In June 2012, the Company re-negotiated a master lease for the entire Boston office space, added 9,800 square feet of office space on the fourth floor, surrendered 4,113 square feet from the second floor, and incorporated all floors’ lease agreements under the same master agreement expiring in August 2016. The Company provided an additional $41 thousand security deposit for the additional space on the fourth floor. As of March 31, 2015, a total security deposit of $127 thousand is included in deposits on the balance sheet.
On August 30, 2013, the Company entered into a sublease agreement to lease 5,249 square feet in our Boston office to a subtenant. The Company remains liable to pay rent on the original lease. This sublease tenant vacated the lease in October 2014. As of December 31, 2014, the Company applied the $20 thousand deposit against outstanding rent. As of March 31, 2015, the company concluded that it was unlikely to locate a sublease tenant for a short period lease and recorded an additional loss on this sublease of $167 thousand representing the remaining contractual obligation.
As of March 31, 2015, the Company occupies 21,184 square feet of space in its Boston, MA office and has paid a total of $127 thousand for security deposits, which are recorded in other non-current assets on the balance sheet.
Total rent expense was approximately $177 thousand and $167 thousand for the three months ended March 31, 2015 and 2014, respectively.
The Company records rent expense on a straight-line basis over the term of the lease. Accordingly, the Company has recorded a liability for deferred rent at March 31, 2015 and 2014 of $958 thousand ($405 thousand current and $553 thousand long-term) and $1.0 million ($224 thousand current and $792 thousand long-term), respectively, which is recorded in deferred rent on the balance sheet.
12
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
License Agreements
Exclusive Channel Partner Agreement with Intrexon Corporation
On January 6, 2011, the Company entered into an Exclusive Channel Partner Agreement, or the Channel Agreement, with Intrexon that governs a “channel partnering” arrangement in which the Company uses Intrexon’s technology directed towards in vivo expression of effectors in connection with the development of Ad-RTS-IL-12 + veledimex and DC-RTS-IL-12 + veledimex and generally to research, develop and commercialize products, in each case in which DNA is administered to humans for expression of anti-cancer effectors for the purpose of treatment or prophylaxis of cancer, which the Company collectively refer to as the Cancer Program. The Channel Agreement establishes committees comprised of representatives of the Company and Intrexon that govern activities related to the Cancer Program in the areas of project establishment, chemistry, manufacturing and controls, clinical and regulatory matters, commercialization efforts and intellectual property.
The Channel Agreement grants the Company a worldwide license to use patents and other intellectual property of Intrexon in connection with the research, development, use, importing, manufacture, sale, and offer for sale of products involving DNA administered to humans for expression of anti-cancer effectors for the purpose of treatment or prophylaxis of cancer, which is collectively referred to as the ZIOPHARM Products. Such license is exclusive with respect to any clinical development, selling, offering for sale or other commercialization of ZIOPHARM Products, and otherwise is non-exclusive. Subject to limited exceptions, the Company may not sublicense the rights described without Intrexon’s written consent.
Under the Channel Agreement, and subject to certain exceptions, the Company is responsible for, among other things, the performance of the Cancer Program, including development, commercialization and certain aspects of manufacturing of ZIOPHARM Products. Intrexon is responsible for the costs of establishing manufacturing capabilities and facilities for the bulk manufacture of products developed under the Cancer Program, certain other aspects of manufacturing and costs of discovery-stage research with respect to platform improvements and costs of filing, prosecution and maintenance of Intrexon’s patents.
Subject to certain expense allocations and other offsets provided in the Channel Agreement, the Company will pay Intrexon on a quarterly basis 50% of net profits derived in that quarter from the sale of ZIOPHARM Products, calculated on a ZIOPHARM Product-by- ZIOPHARM Product basis. The Company has likewise agreed to pay Intrexon on a quarterly basis 50% of revenue obtained in that quarter from a sublicensor in the event of a sublicensing arrangement. In addition, in partial consideration for each party’s execution and delivery of the Channel Agreement, the Company entered into a Stock Purchase Agreement with Intrexon.
Upon termination of the Channel Agreement, the Company may continue to develop and commercialize any ZIOPHARM Product that, at the time of termination:
| • | Is being commercialized by the Company; |
| • | Has received regulatory approval; |
| • | Is a subject of an application for regulatory approval that is pending before the applicable regulatory authority; or |
| • | Is the subject of at least an ongoing Phase 2 clinical trial (in the case of a termination by Intrexon due to an uncured breach or a voluntary termination by the Company), or an ongoing Phase 1 clinical trial in the field (in the case of a termination by the Company due to an uncured breach or a termination by Intrexon following an unconsented assignment by the Company or our election not to pursue development of a Superior Therapy). |
The Company’s obligation to pay 50% of net profits or revenue described above with respect to these “retained” products will survive termination of the Channel Agreement.
13
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
On March 27, 2015, the Company and Intrexon entered into the Exclusive Channel Partner Amendment, or the ECP, amending the Channel Agreement. The ECP Amendment modifies the scope of the parties’ collaboration under the Channel Agreement in connection with the Ares Trading Agreement discussed below. Pursuant to the ECP Amendment, the chimeric antigen receptor T-Cell products to be developed and commercialized pursuant to the Ares Trading Agreement shall be included within the Intrexon/ZIOPHARM collaboration under the Channel Agreement. The ECP Amendment provides that Intrexon will pay to the Company fifty percent of all payments Intrexon receives for upfronts, milestones and royalties under the Ares Trading Agreement.
License Agreement—The University of Texas M. D. Anderson Cancer Center
On January 13, 2015, the Company, together with Intrexon, entered into a License Agreement with MD Anderson. Pursuant to the License, the Company and Intrexon hold an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel chimeric antigen receptor (CAR) T-cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies.
Pursuant to the terms of the License, MD Anderson received consideration of $50 million in shares of the Company’s common stock (or 10,124,561 shares), and $50 million in shares of Intrexon’s common stock in each case based on a trailing 20 day volume weighted average of the closing price of the Company’s and Intrexon’s common stock ending on the date prior to the announcement of the entry into the License, collectively referred to as the License Shares, pursuant to the terms of the License Shares Securities Issuance Agreement described below.
In addition, pursuant to the License, MD Anderson has agreed to transfer to the Company certain existing research programs described in the License and to grant to Intrexon and the Company certain additional technology rights related thereto. In connection with such transfer, the terms of the License also require the Company and Intrexon to enter into a research and development agreement with MD Anderson pursuant to which the Company will provide funding for certain research and development activities of MD Anderson for a period of three years, in an amount between $15 and $20 million per year. The first quarterly payment of $3.75 million due under this arrangement was paid on April 13, 2015.
The term of the License expires on the last to occur of (a) the expiration of all patents licensed thereunder, or (b) the twentieth anniversary of the date of the License; provided, however, that following the expiration of the term, the Company and Intrexon shall then have a fully-paid up, royalty free, perpetual, irrevocable and sublicensable license to use the licensed intellectual property thereunder. After ten years from the date of the License and subject to a 90 day cure period, MD Anderson will have the right to convert the License into a non-exclusive license if the Company and Intrexon are not using commercially reasonable efforts to commercialize the licensed intellectual property on a case-by-case basis. After five years from the date of the License and subject to a 180 day cure period, MD Anderson will have the right to terminate the License with respect to specific technology(ies) funded by the government or subject to a third party contract if the Company and Intrexon are not meeting the diligence requirements in such funding agreement or contract, as applicable. Subject to a 30 day cure period, MD Anderson has the right to terminate the License if the Company and Intrexon fail to timely deliver the shares due in consideration for the License. MD Anderson may also terminate the agreement with written notice upon material breach by the Company and Intrexon, if such breach has not been cured within 60 days of receiving such notice. In addition, the License will terminate upon the occurrence of certain insolvency events for both the Company and Intrexon and may be terminated by the mutual written agreement of the Company, Intrexon and MD Anderson.
14
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
On January 9, 2015, in order to induce MD Anderson to enter into the License on an accelerated schedule, the Company and Intrexon entered into a letter agreement, or the Letter Agreement, pursuant to which MD Anderson received consideration of $7.5 million in shares of common stock (or 1,597,602 shares), and $7.5 million in shares of Intrexon’s common stock in each case based on a trailing 20 day volume weighted average of the closing price of the Company’s and Intrexon’s common stock ending on the date prior to the Letter Agreement, collectively referred to as the Incentive Shares, in the event that the License was entered into on or prior to 8:00 am pacific time on January 14, 2015, referred to as the Accelerated Closing Deadline. The Incentive Shares were issued to MD Anderson on March 11, 2015 pursuant to the terms of the Incentive Shares Securities Issuance Agreement described below.
In connection with the entry into the License, on January 13, 2015, the Company entered into a Securities Issuance Agreement with MD Anderson, or the License Shares Securities Issuance Agreement, pursuant to which the Company agreed to issue and sell the License Shares to MD Anderson in consideration for the License. The closing of the issuance and sale of the License Shares under the License Shares Securities Issuance Agreement occurred on March 11, 2015.
In connection with the entry into the Letter Agreement, on January 13, 2015, the Company entered into a Securities Issuance Agreement with MD Anderson, or the Incentive Shares Securities Issuance Agreement, pursuant to which the Company agreed to issue and sell the Incentive Shares to MD Anderson in consideration for the execution and delivery of the License on or prior to the Accelerated Closing Deadline in connection with the Letter Agreement. The closing of the issuance and sale of the Incentive Shares under the Incentive Shares Securities Issuance Agreement occurred on March 11, 2015.
Also in connection with the License and the issuance of the License Shares and the Incentive Shares, on January 13, 2015, the Company and MD Anderson entered into a Registration Rights Agreement, or the Registration Rights Agreement, pursuant to which the Company agreed to file a “resale” registration statement, or the Registration Statement, registering the resale of the License Shares, the Incentive Shares and any other shares of the Company’s common stock held by MD Anderson on the date that the Registration Statement is filed, within 15 days of the closing under the License Shares Securities Issuance Agreement. Under the Registration Rights Agreement, the Company is obligated to use its reasonable best efforts to cause the Registration Statement to be declared effective as promptly as practicable after filing and in no event later than 120 days of the closing under the License Shares Securities Issuance Agreement and to maintain the effectiveness of the Registration Statement until all securities therein are sold or are otherwise can be sold pursuant to Rule 144, without any restrictions. A prospectus supplement under the Company’s already effective registration statement on Form S-3 (SEC File No. 333-201826), was filed on April 1, 2015 in satisfaction of the Company’s obligations under the Registration Rights Agreement.
The Company has determined that the rights acquired in the License represent in process research and development with no alternative future use. Accordingly, during the three months ended March 31, 2015, the Company recorded a charge of $67.3 million to research and development expense representing the fair value of the 11,722,163 shares of its common stock on the date the license was executed.
Ares Trading License and Collaboration Agreement
On March 27, 2015, the Company and Intrexon entered into the Ares Trading Agreement with Ares Trading, a company within the pharmaceutical business of Merck KGaA, Darmstadt, Germany, through which the parties established a collaboration for the research and development and commercialization of Products (as defined below) for the prophylactic, therapeutic, palliative or diagnostic use for cancer in humans, which we refer to as the Field.
The Ares Trading Agreement provides for the establishment of committees composed of Ares Trading and Intrexon representatives that will govern activities in, among others, the areas of project establishment, research plans and intellectual property.
The Ares Trading Agreement grants Ares Trading an exclusive, worldwide, royalty-bearing, sub-licensable license under the Company’s and Intrexon’s patents, know-how and proprietary platform of research tools and technology necessary for the Company and Intrexon to perform their tasks directed towards the design, identification, culturing, and/or production of genetically modified cells to (a) generate and test Chimeric Antigen Receptor T-Cell Products (as defined in the Ares Trading Agreement) solely for the development, regulatory approval and commercialization of Products containing such Chimeric Antigen Receptor T-Cell Products pursuant to the licenses granted in clauses (b) and (c) of this paragraph; (b) develop and commercialize Products in the Field, worldwide, provided that such Products are not Out-of-Scope Products (as defined below) where Ares Trading has not exercised its Option (as defined below); and (c) commercialize the chimeric antigen receptor for Products.
15
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
Exclusivity
During the term of the Ares Trading Agreement, subject to the change in control provisions described below, neither the Company nor Intrexon may, directly or indirectly, clinically develop or commercialize any chimeric antigen receptor or Chimeric Antigen Receptor T-Cell Products in the Field other than pursuant to the Ares Trading Agreement, or grant any third party the right to research, develop or commercialize any chimeric antigen receptor or Chimeric Antigen Receptor T-Cell Products in the Field, other than pursuant to the Ares Trading Agreement, or, in the case of Intrexon, pursuant to its rights of independent development as described below. In addition, neither the Company nor Intrexon may, directly or indirectly, clinically develop or commercialize any chimeric antigen receptor or Chimeric Antigen Receptor T-Cell Products in the Field against a Target in animal health.
If Ares Trading fails to exercise its Option with respect to an Out-of-Scope Target as described below, Ares Trading may not directly or indirectly, clinically develop or commercialize any Chimeric Antigen Receptor T-Cell Product against such Out-of-Scope Target under the Ares Trading Agreement.
Consideration and Royalties
Ares Trading will pay an upfront fee of $115.0 million to Intrexon as consideration for entry into the Ares Trading Agreement. Intrexon will pay 50% of the fee to the Company in accordance with the ECP Amendment, discussed above. Ares Trading will, pursuant to the terms of the Ares Trading Agreement, pay Intrexon certain fees for the research and development activities related to the Products.
Subject to certain expense allocations, Ares Trading will pay Intrexon royalties ranging from the lower-single digits to the lower-double digits of the net sales derived from the sale of Products developed under the Ares Trading Agreement, on a Product-by-Product and a country-by-country basis, which royalties are subject to increase under the Option, as described below. Royalty amounts are subject to adjustment, and the royalty term will terminate, based upon certain conditions as further described in the Ares Trading Agreement. In accordance with the ECP Amendment, Intrexon will pay to the Company 50% of all royalties that it receives under the Ares Trading Agreement.
The Agreement initially covers two Targets (as defined below) for which Ares Trading must pay a cash fee. Ares Trading may elect additional Targets by paying Intrexon a cash fee.
Milestones
Ares Trading has to make certain payments to Intrexon upon Ares Trading’s achievement of designated milestones. Intrexon will pay 50% of all milestones that it receives under the Ares Trading Agreement to the Company under the ECP Amendment. These payments are payable in cash and are generally due within 30 days of the achievement of the relevant milestone.
Development and commercial milestones. Development milestone payments (not to exceed a capped amount per Product) are payable, on a Product-by-Product basis, upon events further defined in the Ares Trading Agreement with respect to the first four approved indications for the Product. Ares Trading shall also make commercial milestone payments with respect to each Product upon the achievement in a calendar year of tiers of annual worldwide net sales of the Product. In aggregate, the potential payments for development and commercial milestones shall be up to $413 million per Product (or $826 million for the first two Products).
Technical milestones. Ares Trading must pay to Intrexon further cash fees upon certain technical achievements further specified in the Agreement.
16
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
Responsibilities
For each Target selected by Ares Trading, Intrexon is responsible for conducting research and development and the manufacture and supply of Products for use in each Phase 1 clinical trial. Ares Trading is responsible for manufacturing and supplying Products for development use after each Phase 1 clinical trial and for commercialization in the Field.
“Product” means (a) any pharmaceutical product containing a Chimeric Antigen Receptor T-Cell Product developed by Intrexon under a research program for which the joint steering committee established under the Ares Trading Agreement determines to file an investigational new drug application or under a research program for which Ares Trading has exercised the Option (as defined below) or (b) any pharmaceutical product containing a Chimeric Antigen Receptor T-Cell Product developed by or on behalf of Ares Trading that is a derivative of or is otherwise developed from or based upon a Chimeric Antigen Receptor T-Cell Product described in clause (a).
“Target” means a unique molecular species or combination thereof (or naturally occurring allelic variant, glycosylation variant, or mutant thereof) that (a) is chemically distinct from other molecules, (b) is a human peptide, protein, polysaccharide or lipid, and (c) wherein a binding entity derives recognized therapeutic value from binding such molecular species.
Option
Intrexon may suggest a Target to Ares Trading, and if Ares Trading decides not to include such Target in a research program, it would be deemed to be an “Out-of-Scope Target” under the Ares Trading Agreement, Intrexon may, subject to certain conditions, independently exploit Products directed toward such Out-of-Scope Target at its own cost. The Ares Trading Agreement refers to such products as Out-of-Scope Products. Notwithstanding the foregoing, Intrexon may not develop a cell targeting an Out-of-Scope Target in the Field that according to the term defined in the Agreement would qualify as a “Competitive Product”. At the stage of finalization of the Phase 1 clinical trial enrollment of the first Out-of-Scope Product related to the Out-of-Scope Target, Ares Trading may exercise an option, or the Option, to make the Out-of-Scope Product a Product under the Ares Trading Agreement by notifying Intrexon it is doing so and by paying Intrexon a cash fee and paying increased royalties to Intrexon on such Product covered by the exercise of Ares Trading’s Option, subject to the other terms and conditions relating to royalty payments.
If Ares Trading does not exercise the Option related to an Out-of-Scope Target and Out-of Scope Product, Intrexon may further exploit such Out-of-Scope Target and Out-of Scope Product independently from Ares Trading (subject to the restrictions on Intrexon contained in the Ares Trading Agreement, including Intrexon’s obligation not to develop a Competitive Product), in consideration for which (i) Intrexon must pay to Ares Trading a lower double digit percentage of all financial and non-financial consideration received by Intrexon for or in connection with such Out-of-Scope Product, up to a capped amount, which is referred to as the One-Time Intrexon Program Option Fee and (ii) once the One-Time Intrexon Program Option Fee has been paid by Intrexon, Intrexon must provide a credit to Ares Trading under the Ares Trading Agreement, subject to certain conditions, of a mid-single digit percentage of all financial and non-financial consideration received by Intrexon for or in connection with such Out-of-Scope Target or Out-of-Scope Product.
Termination and Change in Control
Ares Trading may voluntarily terminate, on a Product-by-Product and country-by-country basis or in its entirety, the Ares Trading Agreement upon 90 days’ written notice to Intrexon. Intrexon and Ares Trading may each terminate the Ares Trading Agreement if the other party materially breaches the Ares Trading Agreement and fails to cure the breach.
Upon termination of the Ares Trading Agreement, Ares Trading, upon written notice to Intrexon, may continue to develop and commercialize any Product (i) for which a Phase 3 clinical trial has been initiated and of which development has not been terminated by Ares Trading or (ii) that is then being commercialized by Ares Trading. The Option and the payment obligations due to Ares Trading each survive termination of the Ares Trading Agreement with respect to research programs initiated by Intrexon for Out-of-Scope Products started before the effective date of termination.
17
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
If either the Company or Intrexon, which for purposes of this paragraph, is referred to as the Acquiring Party, acquires a third party that has a program competitive to that described under the Ares Trading Agreement, the Acquiring Party may either divest such competitive program within 12 months or include all products under the acquired program as Out-of-Scope Products, which would then become subject to the Option.
If any of the Company, Intrexon, or Ares Trading, which for purposes of this paragraph, is referred to as the Acquired Party, merges with or consolidates with or is acquired by a third party the exclusivity obligations applicable to such person, as described above, will not apply, so long as (i) the competitive program does not use any intellectual property of the Acquired Party or Ares Trading, and (ii) does not utilize services of the personnel of the Acquired Party.
The Ares Trading Agreement is subject review under the Hart-Scott-Rodino Antitrust Improvements Act of 1976 which review is expected to be completed during the second quarter of 2015. Accordingly, the agreement will be accounted for in the second quarter of 2015.
License Agreement with DEKK-Tec, Inc.
On October 15, 2004, the Company entered into a license agreement with DEKK-Tec, Inc., pursuant to which it was granted an exclusive, worldwide license for palifosfamide.
In consideration for the license rights, DEKK-Tec is entitled to receive payments upon achieving certain milestones in varying amounts which on a cumulative basis may total $4.0 million. Of the aggregate milestone payments, most will be creditable against future royalty payments as referenced below. Additionally, the Company issued DEKK-Tec an option to purchase 27,616 shares of the Company’s common stock for $0.02 per share, of which 13,808 options are still outstanding. DEKK-Tec is entitled to receive single digit percentage royalty payments on the sales of palifosfamide should it be approved for commercial sale. The Company’s obligation to pay royalties will terminate on a country-by-country basis upon the expiration of all valid claims of patents in such country covering licensed product, subject to earlier termination in the event of defaults by the parties under the license agreement. No milestones under the license agreement have been reached or expensed since 2010.
License Agreement with Southern Research Institute
On December 22, 2004, the Company entered into an Option Agreement with the Southern Research Institute, or SRI, pursuant to which the Company was granted an exclusive option to obtain an exclusive license to SRI’s interest in certain intellectual property, including exclusive rights related to certain isophosphoramide mustard analogs. On February 5, 2007, the Company exercised its option and entered into the exclusive license agreement. Under the license agreement, the Company is required to remit minimum annual royalty payments of $25 thousand until the first commercial sale of a licensed product. These payments were made for the years ended December 31, 2014, 2013, and 2012. The Company may be required to make payments upon achievement of certain milestones in varying amounts which on a cumulative basis could total up to $775 thousand. In addition, SRI will be entitled to receive single digit percentage royalty payments on the sales of a licensed product in any country until all licensed patents rights in that country which are utilized in the product have expired. No milestones under the license agreement were reached or expensed since the agreement’s inception.
18
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
Patent and Technology License Agreement—The University of Texas M. D. Anderson Cancer Center and the Texas A&M University System.
On August 24, 2004, the Company entered into a patent and technology license agreement with The Board of Regents of the University of Texas System, acting on behalf of The University of Texas M. D. Anderson Cancer Center and the Texas A&M University System, which the Company refers to, collectively, as the Licensors. Under this agreement, the Company was granted an exclusive, worldwide license to rights (including rights to U.S. and foreign patent and patent applications and related improvements and know-how) for the manufacture and commercialization of two classes of organic arsenicals (water- and lipid-based) for human and animal use. The class of water-based organic arsenicals includes darinaparsin.
The Company issued options to purchase 50,222 shares outside the 2003 Stock Option Plan for $0.002 per share following the successful completion of certain clinical milestones, of which 37,666 have vested. The remaining 12,556 shares will vest upon enrollment of the first patient in a multi-center pivotal clinical trial i.e. a human clinical trial intended to provide the substantial evidence of efficacy necessary to support the filing of an approvable New Drug Application, or NDA. In addition, the Licensors are entitled to receive certain milestone payments. The Company may be required to make additional payments upon achievement of certain other milestones in varying amounts which on a cumulative basis could total up to an additional $4.5 million. In addition, the Licensors are entitled to receive single digit percentage royalty payments on sales from a licensed product and will also be entitled to receive a portion of any fees that the Company may receive from a possible sublicense under certain circumstances.
The license agreement also contains other provisions customary and common in similar agreements within the industry, such as the right to sublicense the Company rights under the agreement. On July 31, 2014, the Company amended and restated the License and Collaboration Agreement between the Company and Solasia Pharma K.K. or Solasia, granting to Solasia an exclusive worldwide license to develop and commercialize darinaparsin, and related organoarsenic molecules, in both intravenous and oral forms in all indications for human use. Solasia will be responsible for all costs related to the development, manufacturing and commercialization of darinaparsin. The Licensors will receive a portion of all milestone and royalty payments made by Solasia to the Company in accordance with the terms of the Company’s license agreement with the Licensors.
Collaboration Agreement with Solasia Pharma K.K.
On March 7, 2011, the Company entered into a License and Collaboration Agreement with Solasia Pharma K.K., or Solasia.
Pursuant to the License and Collaboration Agreement, the Company granted Solasia an exclusive license to develop and commercialize darinaparsin in both IV and oral forms and related organic arsenic molecules, in all indications for human use in a pan- Asian/Pacific territory comprised of Japan, China, Hong Kong, Macau, Republic of Korea, Taiwan, Singapore, Australia, New Zealand, Malaysia, Indonesia, Philippines and Thailand.
As consideration for the license, the Company received an upfront payment of $5.0 million to be used exclusively for further clinical development of darinaparsin outside of the pan-Asian/Pacific territory, and will be entitled to receive additional payments of up to $32.5 million in development-based milestones and up to $53.5 million in sales-based milestones. The Company will also be entitled to receive double digit royalty payments from Solasia based upon net sales of licensed products in the applicable territories, once commercialized, and a percentage of sublicense revenues generated by Solasia. Under the License and Collaboration Agreement, the Company provided Solasia with drug product to conduct clinical trials. These transfers were accounted for as a reduction of research and development costs and an increase in collaboration receivables. The agreement provides that Solasia will be responsible for the development and commercialization of darinaparsin in the pan-Asian/Pacific territory.
19
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
On July 31, 2014, the Company entered into an amendment and restatement of the License and Collaboration Agreement granting Solasia an exclusive worldwide license to develop and commercialize darinaparsin, and related organoarsenic molecules, in both intravenous and oral forms in all indications for human use. In exchange, the Company will be eligible to receive from Solasia development-and sales-based milestones, a royalty on net sales of darinaparsin, once commercialized, and a percentage of any sublicense revenues generated by Solasia. Solasia will be responsible for all costs related to the development, manufacturing and commercialization of darinaparsin. The Company’s Licensors will receive a portion of all milestone and royalty payments made by Solasia to the Company in accordance with the terms of the Company’s license agreement with the Licensors.
The $5.0 million upfront payment received in March 2011 is being amortized over the period of the Company’s research and development effort. The Company originally estimated this period to be 75 months. In accordance with the amended and restated License and Collaboration Agreement with Solasia, the Company is no longer obligated to continue their research and development efforts in connection with the upfront payment. However, there are certain deliverables that are included in the amended and restated License and Collaboration Agreement including transfer of intellectual property and prior research and development results, which were originally estimated by management to be completed by March 31, 2015 when the amended and restated License and Collaboration Agreement was signed in July 2014 Management subsequently reassessed the period of performance related to the remaining transitional services to be completed under the agreement and determined that the services are now expected to be completed by March 31, 2016. Accordingly, the Company has recorded $272 thousand in revenue during the three months ended March 31, 2015 while the remaining deferred revenue balance of $1.1 million at March 31, 2015 has been classified as current.
License Agreement with Baxter Healthcare Corporation
On November 3, 2006, the Company entered into a definitive Asset Purchase Agreement for indibulin and a License Agreement to proprietary nanosuspension technology with affiliates of Baxter Healthcare S.A. The purchase included the entire indibulin intellectual property portfolio as well as existing drug substance and capsule inventories. The terms of the Asset Purchase Agreement included an upfront cash payment and an additional payment for existing inventory. During each of the years ended December 31, 2014, 2013, and 2012, the installment payments of $250 thousand were met and expensed.
Collaboration Agreement with Harmon Hill, LLC
On June 27, 2013, the Company signed a collaboration agreement with Harmon Hill to provide consulting and other services for the development and commercialization of oncology therapeutics by ZIOPHARM, effective April 1, 2013. Under the agreement the Company has agreed to pay Harmon Hill $15 thousand per month for the consulting services. Subject to renewal or extension by the parties, the term of the agreement is for a one year period. The Company expensed $45 thousand and $45 thousand for the three months ended March 31, 2014 and 2015, respectively.
20
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
6. Commitments and Contingencies – (continued)
CRO Services Agreement with Novella Clinical, Inc.
On December 4, 2008, the Company entered into a Master Clinical Research Organization Services Agreement with Novella Clinical, Inc., or Novella, under which Novella provides CRO services in support of the Company’s clinical trials. The work order for the newest trial being conducted by Novella was signed on November 2, 2012. Novella was entitled to cumulative payments of up to $790 thousand under these arrangements, which is payable in varying amounts upon Novella achieving specified milestones. During the year ended December 31, 2012, the Company expensed $256 thousand upon the achievement of various milestones. During the year ended December 31, 2013, two database related milestones and one site activation related milestone were met and expensed totaling $136 thousand.
On August 18, 2014 and November 6, 2014, the Company signed two amendments of the Master Clinical Research Organization Services Agreement with Novella. The amendments reflect the removal of data management, statistical and clinical study report services, as well as a change in the timeline and scope of clinical trial support. During the year ended December 31, 2014, three clinical milestones were met and expensed totaling $236 thousand. The remaining milestone of $10 thousand was met and expensed during the quarter ended March 31, 2015.
CRO Services Agreement with MS Clinical Services, LLC.
On July 24, 2014, the Company entered into a Master Clinical Research Organization Services Agreement with MS Clinical Services, LLC, or Medsource, under which Medsource provides CRO services in support of the Company’s clinical trials. There are no milestones associated with this agreement.
CRO Services Agreement with PPD Development, L.P.
The Company was party to a Master Clinical Research Organization Services Agreement with PPD Development, L. P., or PPD, dated January 29, 2010, a related work order dated June 25, 2010 and a related work order dated April 8, 2011 under which PPD provides clinical research organization, or CRO, services in support of the Company’s clinical trials. There are no remaining milestones related to this agreement.
CRO Services Agreement with Pharmaceutical Research Associates, Inc.
On December 13, 2011, the Company entered into a Master Clinical Research Organization Services Agreement with Pharmaceutical Research Associates, Inc., or PRA, under which PRA provides CRO services in support of the Company’s clinical trials. There are no remaining milestones related to this agreement.
21
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
7. Related Party Transactions
On January 6, 2011, the Company entered into an Exclusive Channel Partner Agreement, or Channel Agreement, with Intrexon Corporation, or Intrexon. The Company’s director, Randall J. Kirk, is the CEO, a director, and the largest stockholder of Intrexon.
On March 27, 2015, the Company and Intrexon entered into a Second Amendment to Exclusive Channel Partner Agreement amending the Channel Agreement, which is referred to as the ECP Amendment. The ECP Amendment modified the scope of the parties’ collaboration under the Channel Agreement in connection with the worldwide License and Collaboration Agreement, or the Ares Trading Agreement, which the Company and Intrexon entered into with ARES Trading S.A., or Ares Trading, on March 27, 2015. The ECP Amendment provided that Intrexon will pay to the Company fifty percent of all payments that Intrexon receives for upfronts, milestones and royalties under the Ares Trading Agreement (see Note 6 to the financial statements, Commitments and Contingencies, for additional disclosure relating to the ECP Amendment, the Channel Agreement and the Ares Trading Agreement). The Amendment also reduces Intrexon’s aggregate commitment under a Stock Purchase Agreement that the parties executed in connection with the Existing ECP Agreement to purchase the Company’s common stock from $50.0 million to $43.5 million, which has been satisfied.
During the three months ended March 31, 2014, the Company expensed $1.7 million for services performed by Intrexon, of which $0.5 million was recorded in accrued expenses. During the three months ended March 31, 2015, the Company expensed $3.0 million for services performed by Intrexon, of which the full amount is included in accrued expenses at March 31, 2015.
On February 2, 2015, Intrexon purchased 1,440,000 shares of common stock in the Company’s public offering (see Note 2 to the financial statements, Financings).
Intrexon’s common stock purchases were made on terms that were the same as others participating in the above financing.
On January 13, 2015, the Company, together with Intrexon, entered into a license agreement with The University of Texas M.D. Anderson Cancer Center, or MD Anderson, which is referred to as the License. Pursuant to the License, the Company and Intrexon hold an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel CAR-T cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies. In partial consideration for entering into the MD Anderson License, the Company also entered into a letter agreement with Intrexon and MD Anderson on January 9, 2015, which is referred to as the MD Anderson Letter Agreement, as well as a Securities Issuance Agreement, which is referred to as the License Shares Securities Issuance Agreement, another Securities Issuance Agreement, which is referred to as the Incentive Shares Securities Issuance Agreement, and a Registration Rights Agreement, which is referred to as the MD Anderson Registration Rights Agreement, with MD Anderson on January 13, 2015. As a result of the common stock issued to MD Anderson in connection with these transactions, MD Anderson became a beneficial holder of more than five percent of the Company’s common stock. (See Note 6 to the financial statements, Commitments and Contingencies, for additional disclosure relating to the License and the transactions contemplated thereby).
8. Warrants
The Company has issued both warrants that are accounted for as liabilities and warrants that are accounted for as equity instruments.
The Company follows accounting standards that provide guidance in assessing whether an equity-issued financial instrument is indexed to an entity’s own stock for purposes of determining whether a financial instrument should be treated as a derivative and classified as a liability. Accounting standards require that liability classified warrants be recorded at their fair value at each financial reporting period and the resulting gain or loss be recorded as other income (expense) in the Statements of Operations. Fair value is measured using the binomial valuation model.
There were no warrants outstanding at March 31, 2015 or December 31, 2014.
Liability-Classified Warrants
In connection with the December 2009 public offering, the Company issued warrants to purchase an aggregate of 8,206,520 shares of common stock (including the investor warrants and 464,520 warrants issued to the Underwriters). The investor warrants were exercisable immediately and the underwriter warrants exercisable six months after the date of issuance. The warrants had a 5 year term. Subject to certain exceptions, these warrants provided anti-dilution protection should common stock or common stock equivalents be subsequently issued at a price less than the exercise price of the warrants then in effect.
The Company assessed whether the 2009 Warrants require accounting as derivatives. The Company determined that these warrants were not indexed to the Company’s own stock in accordance with accounting standards codification Topic 815, Derivatives and Hedging. As such, the Company has concluded these warrants did not meet the scope exception for determining whether the instruments require accounting as derivatives and were classified as liabilities.
The Company used the Binomial/Monte Carlo pricing model to estimate the value of the liability-classified warrants. The following assumptions were used in the Binomial/Monte Carlo valuation model at March 31, 2014 (no warrants were outstanding during the three months ended March 31, 2015):
| 2014 | ||||
| Risk-free interest rate |
0.11 | % | ||
| Expected life in years |
0.69 | |||
| Expected volatility |
80 | % | ||
| Expected dividend yield |
0 | |||
| Steps per year |
13 | |||
The change in the fair value of the warrant liability resulted in a gain of $82 thousand for the three months ended March 31, 2014. The change in the fair value of the warrant liability was charged to other income (expense) in the Statements of Operations.
There were no warrant exercises during the three months ended March 31, 2014 and no warrants were outstanding during the three months ended March 31, 2015.
22
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
9. Common Stock
On February 3, 2015, the Company entered into an underwriting agreement with J.P. Morgan Securities LLC, as representative of the several underwriters named therein, relating to the issuance and sale of 10,000,000 shares of the Company’s common stock. The price to the public in the offering was $8.75 per share, and the underwriters agreed to purchase the shares from the Company pursuant to the underwriting agreement at a purchase price of $8.225 per share. Under the terms of the underwriting agreement, the Company also granted the underwriters an option, exercisable for 30 days, to purchase up to an additional 1,500,000 shares of common stock at a purchase price of $8.225 per share. The offering was made pursuant to the Company’s effective registration statement on Form S-3 (Registration Statement No. 333-201826) previously filed with the SEC, and a prospectus supplement thereunder. The underwriters purchased the 10,000,000 shares and the additional 1,500,000 shares on February 9 and 17, 2015, respectively. The net proceeds from the offering were approximately $94.3 million after deducting underwriting discounts and estimated offering expenses payable by the Company.
On January 13, 2015, the Company, together with Intrexon, entered into the License with MD Anderson. Pursuant to the License, the Company and Intrexon hold an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel chimeric antigen receptor (CAR) T-cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies.
Pursuant to the terms of the License, MD Anderson received consideration of $50 million in shares of the Company’s common stock (or 10,124,561 shares), and $50 million in shares of Intrexon’s common stock in each case based on a trailing 20 day volume weighted average of the closing price of the Company’s and Intrexon’s common stock ending on the date prior to the announcement of the entry into the License, collectively referred to as the License Shares, pursuant to the terms of the License Shares Securities Issuance Agreement. The License Shares were issued on March 11, 2015.
On January 9, 2015, in order to induce MD Anderson to enter into the License on an accelerated schedule, the Company and Intrexon entered into a letter agreement, or the Letter Agreement, pursuant to which MD Anderson received consideration of $7.5 million in shares of the Company’s common stock (or 1,597,602 shares), and $7.5 million in shares of Intrexon’s common stock in each case based on a trailing 20 day volume weighted average of the closing price of the Company’s and Intrexon’s common stock ending on the date prior to the Letter Agreement, collectively referred to as the Incentive Shares, in the event that the License was entered into on or prior to 8:00 am pacific time on January 14, 2015, referred to as the Accelerated Closing Deadline. The Incentive Shares were issued on March 11, 2015.
10. Stock-Based Compensation
The Company recognized stock-based compensation expense on all employee and non-employee awards as follows:
| For the three months | ||||||||
| ended March 31, | ||||||||
| (in thousands) | 2015 | 2014 | ||||||
| Research and development |
$ | 295 | $ | 376 | ||||
| General and administrative |
798 | 847 | ||||||
|
|
|
|
|
|||||
| Stock-based employee compensation expense |
$ | 1,093 | $ | 1,223 | ||||
|
|
|
|
|
|||||
The Company granted 50,000 and 80,500 stock options during the three months ended March 31, 2015 and 2014 that had a weighted-average grant date fair value of $6.58 and $3.34 per share, respectively.
23
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
10. Stock-Based Compensation (continued)
At March 31, 2015, total unrecognized compensation costs related to unvested stock options outstanding amounted to $7.7 million. The cost is expected to be recognized over a weighted-average period of 1.63 years.
On March 31, 2014, the Company extended the contractual life of 71,167 fully vested stock options held by one employee by an additional 9 months.
On March 31, 2014, the Company extended the contractual life of 33,333 fully vested stock options and 66,667 unvested stock options held by one employee.
On September 8, 2014, the Company extended the contractual life of 82,834 fully vested stock options and 23,333 unvested stock options held by one employee by an additional 3 months.
On September 15, 2014, the Company extended the contractual life of 39,167 fully vested stock options and 113,333 unvested stock options held by one employee.
For the three months ended March 31, 2015 and 2014, the fair value of stock options was estimated on the date of grant using a Black-Scholes option valuation model with the following assumptions:
| For the three months ended March 31, | ||||
| 2015 | 2014 | |||
| Risk-free interest rate |
1.63 - 1.64% | 1.76 - 2.11% | ||
| Expected life in years |
6 | 6 | ||
| Expected volatility |
85.48 - 86.81% | 94.46 - 94.55% | ||
| Expected dividend yield |
0 | 0 | ||
24
Table of Contents
ZIOPHARM Oncology, Inc.
NOTES TO FINANCIAL STATEMENTS (unaudited)
10. Stock-Based Compensation – (continued)
Stock option activity under the Company’s stock option plan for the three months ended March 31, 2015 is as follows:
| (in thousands, except share and per share data) | Number of Shares |
Weighted- Average Exercise Price |
Weighted- Average Contractual Term (Years) |
Aggregate Intrinsic Value |
||||||||||||
| Outstanding, December 31, 2014 |
6,505,663 | $ | 4.07 | |||||||||||||
| Granted |
50,000 | 9.10 | ||||||||||||||
| Exercised |
(592,200 | ) | 4.29 | |||||||||||||
| Cancelled |
(39,166 | ) | 4.26 | |||||||||||||
|
|
|
|
|
|||||||||||||
| Outstanding, March 31, 2015 |
5,924,297 | $ | 4.09 | 6.36 | $ | 39,564 | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Vested and unvested expected to vest at March 31, 2015 |
5,878,611 | $ | 4.08 | 5.33 | $ | 39,259 | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Options exercisable, March 31, 2015 |
3,185,297 | $ | 4.08 | 5.33 | $ | 21,297 | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Options exercisable, December 31, 2014 |
3,781,162 | $ | 4.10 | 5.80 | $ | 4,130 | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Options available for future grant |
4,572,935 | |||||||||||||||
|
|
|
|||||||||||||||
A summary of the status of unvested restricted stock for the three months ended March 31, 2015 is as follows:
| Number of Shares | Weighted-Average Grant Date Fair Value |
|||||||
| Non-vested, December 31, 2014 |
144,508 | $ | 4.70 | |||||
| Granted |
— | — | ||||||
| Vested |
(48,435 | ) | 4.51 | |||||
| Cancelled |
— | — | ||||||
|
|
|
|
|
|||||
| Non-vested, March 31, 2015 |
96,073 | $ | 4.79 | |||||
|
|
|
|
|
|||||
At March 31, 2015, total unrecognized compensation costs related to unvested restricted stock outstanding amounted to $0.5 million. The cost is expected to be recognized over a weighted-average period of 1.00 years.
25
Table of Contents
Item 2. Management’s Discussion and Analysis of Financial Condition and Results of Operations
Forward Looking Statements
This quarterly report on Form 10-Q contains “forward-looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. In particular, statements contained in this Form 10-Q, including but not limited to, statements regarding the costs and timing of our clinical trials and of the development and commercialization of our pipeline products and services; the sufficiency of our cash, investments and cash flows from operations and our expected uses of cash; our ability to finance our operations and business initiatives and obtain funding for such activities; our future results of operations and financial position, business strategy and plan prospects, projected revenue or costs and objectives of management for future research, development or operations, are forward-looking statements. These statements relate to our future plans, objectives, expectations and intentions and may be identified by words such as “may,” “will,” “should,” “expects,” “plans,” “anticipates,” “intends,” “targets,” “projects,” “contemplates,” “believes,” “seeks,” “goals,” “estimates,” “predicts,” “potential” and “continue” or similar words. Readers are cautioned that these forward-looking statements are only predictions and are subject to risks, uncertainties, and assumptions that are difficult to predict, including those identified below, under Part II, Item 1A. “Risk Factors” and elsewhere herein. Therefore, actual results may differ materially and adversely from those expressed in any forward-looking statements. We undertake no obligation to revise or update any forward-looking statements for any reason.
Company Overview
ZIOPHARM Oncology, Inc. is a biopharmaceutical company that seeks to acquire, develop and commercialize, on its own or with commercial partners, a diverse portfolio of cancer therapies that can address unmet medical needs through synthetic immuno-oncology. Pursuant to an exclusive channel collaboration agreement (or “ECC”) with Intrexon Corporation, or Intrexon, we obtained rights to Intrexon’s synthetic immuno-oncology platform for use in the field of oncology, which included a clinical stage product candidate, Ad-RTS-IL-12 used with the oral activator veledimex. The synthetic immuno-oncology platform is an industrialized engineering approach for molecular and cell biology and gene control. It employs an inducible gene-delivery system that enables controlled in vivo expression of genes that produce therapeutic proteins to treat cancer. Ad-RTS-IL-12 + veledimex uses this gene delivery system to produce Interleukin-12, or IL-12, a potent, naturally occurring anti-cancer protein. We have completed two Phase 2 studies evaluating Ad-RTS-IL-12 + veledimex, the first for the treatment of metastatic melanoma, and the second for the treatment of metastatic breast cancer; data from these Phase 2 studies was presented in December 2014. We are continuing to pursue intratumoral injection of Ad-RTS-IL-12 + veledimex in breast cancer and brain cancer.
In addition to our synthetic immuno-oncology programs, Intrexon (and we, through our ECC agreement with Intrexon) recently obtained an exclusive, worldwide license to certain immuno-oncology technologies owned and licensed by The University of Texas M.D. Anderson Cancer Center, or MD Anderson, including technologies relating to novel chimeric antigen receptors, or CARs, natural killer, or NK cells and T cell receptors, or TCRs. Combining these technologies with Intrexon’s technology suite and clinically tested RheoSwitch Therapeutic System®, or RTS®, IL-12 modules, we plan to develop CAR-T and other immune cells that will target and kill cancer cells. We plan to leverage the synergy between the platforms to accelerate a promising synthetic immuno-oncology pipeline, with up to five CAR-T therapies expected to enter the clinic in 2015 and programs for the development of allogeneic CAR-T therapies that can be used off-the-shelf expected to be initiated in 2016.
We plan to continue to combine Intrexon’s technology suite with our capabilities to translate science to the patient, and to identify and develop additional products to stimulate or inhibit key pathways, including those used by the body’s immune system, to treat cancer.
On March 30, 2015, the Company and Intrexon entered into a global collaboration focused exclusively on chimeric antigen receptor T-cell (CAR-T) products with Merck Serono, a biopharmaceutical division of Merck KGaA, Darmstadt, Germany. Intrexon will share the economic provisions of this collaboration equally with the Company, including an upfront payment of $115 million expected to be received during the second quarter, milestones and royalties. Under the collaboration Aries will elect CAR-T targets, two initially, for which it will provide certain research funding. Through the ECP between Intrexon and the Company, the Company will be responsible for any additional research and development expenditures. Once these candidates reach investigational new drug (IND) stage, the programs will be transferred to Aries for clinical development and commercialization. The Company and Intrexon will also independently conduct research and development on other CAR-T candidates, with Merck having the opportunity during clinical development to opt-in.
Enabling Technology
Synthetic immuno-oncology entails the application of engineering principles to biological systems for the purpose of designing and constructing new biological systems or redesigning/modifying existing biological systems. Biological systems are governed by DNA, the building block of gene programs, which control cellular processes by coding for the production of proteins and other molecules that have a functional purpose and by regulating the activities of these molecules. This regulation occurs via complex biochemical and cellular reactions working through intricate cell signaling pathways, and control over these molecules modifies the output of biological systems. Synthetic immuno-oncology has been enabled by the application of information technology and advanced statistical analysis, also known as bioinformatics, to genetic engineering, as well as by improvements in DNA synthesis. Synthetic immuno-oncology aims to engineer gene-based programs or codes to modify cellular function to achieve a desired biological outcome. Its application is intended to allow more precise control of drug concentration and dose, thereby improving the therapeutic index associated with the resulting drug.
26
Table of Contents
On January 6, 2011, we entered into an Exclusive Channel Partner Agreement with Intrexon, which we refer to as the Channel Agreement, to develop and commercialize novel DNA-based therapeutics in the field of cancer treatment by combining Intrexon’s synthetic immuno-oncology platform with our capabilities to translate science to the patient. As a result, our DNA synthetic immuno-oncology platform employs an inducible gene-delivery system that enables regulated and controlled delivery of genes that produce therapeutic proteins to treat cancer. The first example of this regulated controlled delivery is achieved by producing IL-12, a potent, naturally occurring anti-cancer protein, under the control of Intrexon’s proprietary biological “switch” to turn on and off (and on and off repeatedly) the therapeutic protein expression at the tumor site. We and Intrexon refer to this “switch” as the RheoSwitch Therapeutic System® or RTS® platform. Our initial drug candidate being developed using the synthetic immuno-oncology platform is Ad-RTS-IL-12 + veledimex.
More detailed descriptions of our clinical development for each are set forth below under the caption “Product candidates.”
Immuno-oncology
Immuno-oncology, which utilizes a patient’s own immune system to treat cancer, is one of the most actively pursued areas of research by biotechnology and pharmaceutical companies today. Cancer cells contain mutated proteins and may overexpress other proteins usually found in the body at low levels. The immune system typically recognizes unusual or aberrant cell protein expression and eliminates these cells in a highly efficient process known as immune surveillance. A central player in immune surveillance is a type of white blood cell known as the T cell. In healthy individuals, T cells identify and kill infected or abnormal cells, including cancer cells. Cancer cells develop the ability to evade immune surveillance, which is a key factor in their growth, spread, and persistence. In the last five years, there has been substantial scientific progress in countering these evasion mechanisms using immunotherapies, or therapies that activate the immune system.
On January 13, 2015, we, together with Intrexon, entered into a license agreement with MD Anderson, which we refer to as the MD Anderson License. Pursuant to the MD Anderson License, we and Intrexon hold an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel CAR-T cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies.
Combining the non-viral genetic engineering technologies we licensed from MD Anderson together with Intrexon’s industrialized approach to gene engineering and cell control, we believe we can rapidly and efficiently reprogram T cells to express a particular CAR or TCR construct that will enable the T cell to recognize and target cancer cells. CAR-T cells target cell surface tumor antigens, such as CD-19, that exist on cancer cells and that are independent of human leukocyte antigens, or HLAs, and which we refer to as “public” antigens. TCR+ cells target tumor antigens that are dependent on HLAs and which we refer to as “private” antigens. Natural killer cells target tumors with loss of HLAs, or tumors with no antigens. Most CAR-T cell and TCR products currently being developed by competitors are autologous, or derived from the patient’s own blood, and gene engineered with viral technology. As a result, the patient’s blood must be harvested, shipped to a manufacturing facility where it is modified using a retrovirus to express the CAR or TCR, and then shipped back to be infused into the patient. The process can take several weeks to a month and is very labor intensive and costly. Currently, this complex technique can only be done in very sophisticated laboratories. We believe we will be able to manufacture our CAR-T cells and TCRs using non-viral methods, which we expect will enable a simpler process requiring only days or hours and result in a lower cost of manufacturing. Our non-viral methods could also potentially enable autologous point of care treatment, where a patient’s own T cells would be modified at or near the point of care, for example, utilizing a local blood bank, to express the CAR-T or TCR construct and then infused back into the patient, potentially during the same visit. In addition, we intend to use our non-viral methods to develop allogeneic treatments that can be used off-the-shelf. An allogeneic off-the-shelf treatment would enable a patient to be treated with a CAR-T or TCR construct that is created from a separate healthy donor, personalized for that patient, and then distributed to the point of care. Our non-viral methods, which we believe are nimble, fast and less costly than other approaches, together with our industrialized, scalable engineering approach are expected to enable highly efficient and less costly manufacturing approaches to gene engineered cell-based therapy. In addition, our proprietary RheoSwitch Therapeutic System® may give us the ability to control in vivo gene expression (on-off-on-off etc.) in CAR-T or TCR cells, which we believe could result in significantly lower toxicity compared to other products currently in development.
On March 30, 2015, the Company and Intrexon entered into a global collaboration focused exclusively on chimeric antigen receptor T-cell (CAR-T) products with Merck Serono, a biopharmaceutical division of Merck KGaA, Darmstadt, Germany. Intrexon will share the economic provisions of this collaboration equally with the Company, including an upfront payment of $115 million expected to be received during the second quarter, milestones and royalties. Under the collaboration Aries will elect CAR-T targets, two initially, for which it will provide certain research funding. Through the ECP between Intrexon and the Company, the Company will be responsible for any additional research and development expenditures. Once these candidates reach investigational new drug (IND) stage, the programs will be transferred to Aries for clinical development and commercialization. The Company and Intrexon will also independently conduct research and development on other CAR-T candidates, with Merck having the opportunity during clinical development to opt-in.
27
Table of Contents
Cancer Overview
Cancer is a group of diseases characterized by either the runaway growth of cells or the failure of cells to die normally. Often, cancer cells spread to distant parts of the body, where they can form new tumors. Cancer can arise in any organ of the body and, according to the American Cancer Society, strikes slightly less than one of every two American men and a little more than one of every three American women at some point in their lives.
It is reported that there are more than 100 different varieties of cancer. Carcinomas, the most common type of cancer, originate in tissues that cover a surface or line a cavity of the body. Lymphomas are cancers of the lymph system, which is a circulatory system that bathes and cleanses the body’s cells. Leukemias involve blood-forming tissues and blood cells. As their name indicates, brain tumors are cancers that begin in the brain, skin cancers, including melanomas, originate in the skin, while soft tissue sarcoma, or STS, arises in soft tissue. Cancers are considered metastatic if they spread through the blood or lymphatic system to other parts of the body to form secondary tumors.
Cancer is caused by a series of mutations (alterations) in genes that control cells’ ability to grow and divide. Some mutations are inherited; others arise from environmental factors such as smoking or exposure to chemicals, radiation, or viruses that damage cells’ DNA. The mutations cause cells to divide relentlessly or lose their normal ability to die.
According to the American Cancer Society, it was estimated that about 1,658,370 new cases of cancer are expected to be diagnosed in 2015 and about 589,430 Americans are expected to die from cancer in 2015. The cost of treating cancer is significant. The Agency for Healthcare Research and Quality estimates that the direct medical cost of cancer in 2011 was $88.7 billion.
Cancer Treatments
Major treatments for cancer include surgery, radiotherapy, chemotherapy and immunotherapy. Newer approaches such as anti-angiogenic and targeted therapies are rapidly evolving. Other treatment for cancer may involve supportive care. While there are many experimental treatments under investigation, including DNA and other immunological based therapies, we believe cancer treatment will remain a significant unmet medical need.
Product candidates
The following chart identifies our current synthetic immuno-oncology product candidates and their stage of development, each of which are described in more detail below.
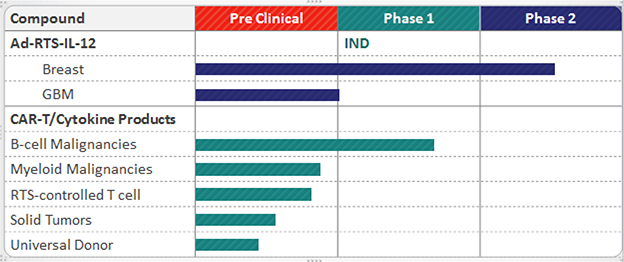
28
Table of Contents
Synthetic immuno-oncology Programs:
Ad-RTS-IL-12 + veledimex
Ad-RTS-IL-12 + veledimex has been evaluated in two Phase 2 studies, the first for the treatment of metastatic melanoma, and the second for the treatment of unresectable recurrent or metastatic breast cancer. Ad-RTS-IL-12 + veledimex is our lead product candidate, which uses our gene delivery system to produce IL-12, a potent, naturally occurring anti-cancer protein.
More specifically, IL-12 is a potent immunostimulatory cytokine which activates and recruits dendritic cells that facilitate the cross-priming of tumor antigen-specific T cells. Intratumoral administration of Ad-RTS-IL-12 + veledimex, which allows for adjustment of IL-12 gene expression upon varying the dose of veledimex, is designed to reduce the toxicity elicited by systemic delivery of IL-12, and increase efficacy through high intratumoral expression.
We reported the controlled local expression of IL-12 as an immunotherapeutic treatment of glioma (brain cancer) in animal models through the use of the RTS® at the October 2013 AACR-NCI-EORTC conference. Veledimex brain penetration was demonstrated in normal mice and monkeys with intact blood brain barriers. Treatment with Ad-RTS-IL-12 + veledimex and DC-RTS-IL-12 + veledimex both demonstrated dose-related increase in survival in the mouse GL-261 glioma model with no adverse clinical signs observed. In December 2013, we announced the unanimous approval of the Recombinant DNA Advisory Committee of the National Institutes of Health, or the RAC/NIH, for the initiation of a Phase 1 study of Ad-RTS-IL-12 + veledimex, in subjects with recurrent or progressive high grade gliomas. The U.S Food and Drug Administration, or FDA, has requested additional nonclinical information to support the Phase 1 study and this data has been generated. Subject to reaching agreement with the FDA, we anticipate initiation of the Phase 1 study during the first half of 2015. Glioblastoma is by far the most frequent malignant brain tumor and is associated with a particularly aggressive course and dismal prognosis. The current standard of care is based on surgical resection to the maximum feasible extent, followed by radiotherapy and concomitant adjuvant temozolomide. Such aggressive treatment, however, is associated with only modest improvements in survival resulting in a very high unmet medical need.
At the American Association for Cancer Research, or AACR, 2014 Annual Meeting, in April 2014, we presented data from a preclinical study conducted jointly by us and Intrexon demonstrating the anti-tumor effects and tolerability of Ad-RTS-mIL-12 in a glioblastoma murine model. Veledimex was found to effectively cross the blood brain barrier, with dose-related increases in plasma and brain tissue exposure, and no accumulation in brain tissue following repeat dosing. The study data demonstrated that administration of Ad-RTS-mIL-12 + veledimex resulted in dose-related increases in survival of four- to five-fold, without exhibiting an adverse safety profile, when compared to median survival in vehicle control groups.
At the 17th Annual Meeting of the American Society of Gene and Cell Therapy, or ASGCT, in May 2014, we presented results demonstrating the potent anti-tumor and anti-cancer stem cell effects of Ad-RTS-IL-12 in a preclinical glioma model. Results from human and laboratory studies of Ad-RTS-IL-12 demonstrated that precise control of IL-12 gene expression levels can be achieved using Intrexon’s RTS®. Rapid, tight modulation of in vivo expression of IL-12 using the activator ligand, veledimex, was demonstrated across these studies. When IL-12 expression was “switched on” it rapidly led to expression and an immune response. This immune response was characterized by an increase in tumor infiltrating lymphocytes with system wide immune activation. The data presented in May 2014 further demonstrated that Ad-RTS-IL-12 has potent anti-cancer effects in a glioma model, showing both a reduction in tumor mass and prolonged survival when compared to existing treatment standards. The data also showed a significant reduction in cancer stem cells, as measured by dramatically reduced nestin levels. Cancer stem cells are thought to play a critical role in recurrence and metastasis.
29
Table of Contents
At the AACR 2014 Immunology and Immunotherapy Meeting in December 2014, together with Intrexon, we presented clinical results from the Ad-RTS-hIL-12 + veledimex studies in patients with advanced breast cancer and melanoma demonstrating local and systemic IL-12-mediated anti-cancer activity, as well as safety and control of both immune- and IL-12-mediated toxicity with use of the RTS® gene switch. In two open-label Phase 2 clinical studies, twelve patients with metastatic advanced stage breast cancer and twenty-six patients with metastatic melanoma were administered Ad-RTS-hIL-12. Following intra-tumoral injection of Ad-RTS-hIL-12, expression of IL-12 within patients was controlled by the RTS® gene switch using the oral activator ligand, veledimex, at doses ranging from 5mg to 160mg. All subjects had heavy tumor burden and disease progression at the time of enrollment, with mean number of prior therapies at 14 and 10 for breast cancer and melanoma patients, respectively. Treatment with Ad-RTS-hIL-12 + veledimex resulted in an increase in the immune cytokine IL-12 and downstream cytokines, IFN- g, IP-10 and IL-10, resulting in a significant increase in the number of CD8+ T-cells. Among seven evaluable subjects in the Phase 2 clinical study of Ad-RTS-IL-12 + veledimex in patients with recurrent or metastatic breast cancer, three had stable disease, including one triple negative breast cancer subject who crossed the primary endpoint of 16 week progression free survival, for a disease control rate (stable disease or better) of 43%. Target lesions and tumor burden were significantly reduced in approximately 40% of patients. In the Phase 1/2 study of Ad-RTS-hIL-12 + veledimex in subjects with unresectable stage III/IV melanoma, of eighteen evaluable subjects, one had a partial response and six had stable disease, for a disease control rate of 39%. In melanoma patients for whom a response was observed, there was evidence of local and systemic anti-cancer activity. The adverse event profile of Ad-RTS-hIL-12 + veledimex in both melanoma and breast cancer was predictable, reversible and characteristic of immune activation. The most common ³ Grade 3 treatment emergent adverse events, or TEAEs, in breast cancer and melanoma included neutropenia and electrolyte abnormalities (21%) each, LFTs increased (16%), leukopenia (13%) and pyrexia, hypotension, lymphopenia, anemia, and cytokine release syndrome (11%) each. Importantly, all TEAEs and SAEs ³ Grade 3 reversed rapidly upon discontinuation of veledimex oral dosing.
Also at the AACR 2014 Immunology and Immunotherapy Meeting in December 2014, together with Intrexon, we presented preclinical data supporting the potential for cytolytic activity against solid tumor targets with allogeneic, genetically-modified stem cells enabled for controlled release of cell-linking moieties, or CLMs, within the tumor micro-environment and preclinical data describing the development of a novel, high-throughput screening technology for rapidly identifying bi-specific antibodies capable of inducing targeted immunologic activity through the activation of T-cells or other immune cells against tumors. CLMs are small bi-specific antibody fragments capable of directing potent T-cell mediated tumor lysis by bridging the immunologic synapses of T-cells and surface targets on tumor cells. Previous studies have shown that the systemic distribution and pharmacokinetic profile of bi-specific antibodies limit their utility for many target/effector combinations. In two preclinical studies, Intrexon and Ziopharm researchers interrogated a large number of CLM-based effectors for their ability to activate white blood cells from peripheral blood and lyse receptor target-positive tumor cells. Allogeneic, tumor targeting stem cells were then genetically modified to express CLMs within the tumor microenvironment using the RTS® platform as a mechanism for providing spatial and temporal control. The first study demonstrated the ability of Intrexon’s proprietary image-based screening systems and rapid DNA assembly to screen a large number of EGFR and HER2 receptor-targeted CLM variants for their ability to recruit CD3+ T-cells and mediate selective cell killing against target positive cells in peripheral blood co-cultures. The image-based screening platform allowed for real time target cell killing information to be obtained, as well as kinetic cell morphologic analyses to understand the dynamics of killing activity, thereby shortening the developmental timeline to lead candidate selection. The second study validated these CLM candidates in scalable, allogeneic endometrial regenerative cells, or ERCs, genetically modified to express an anti-CD3-anti-EGFR CLM under RTS® ligand inducible control. Expression of CLMs under the RTS® inducible promoter provided effective control of CLM secretion and modulation of killing activity, with veledimex-dependent cytotoxicity of greater than 80% against an EGFR+ KRAS mutant lung cancer cell model. CLM-expressing ERCs were found to be effective in co-culture killing assays at cellular doses as low as 1% of target cells. These data supported the feasibility of localized cytolytic activity of CLM-secreting allogeneic cell therapy products against EGFR+ KRAS mutant solid tumor malignancies.
We have completed the Phase 2 monotherapy studies in melanoma and breast cancer using Ad-RTS-IL-12 + veledimex. On April 27, 2015, we announced the initiation of a Phase 1b/2 study of Ad-RTS-hIL-12 + veledimex following standard chemotherapy for the treatment of patients with locally advanced or metastatic breast cancer. The study will be conducted at the Memorial Sloan Kettering Cancer Center in New York. As the treatment of advanced melanoma has undergone and continues to undergo a rapid evolution with the introduction and approval of highly promising new single and combination agents, the standard of care in this indication has become uncertain, resulting in a much more competitive and commercially unpredictable environment. As a result, we are pursuing intratumoral injection of Ad-RTS-IL-12 + veledimex in brain cancer and breast cancer, and will pause further development of Ad-RTS-IL-12 + veledimex in melanoma with intratumoral injection. However, through current strategic initiatives, we expect to utilize RTS-IL-12 + veledimex in cell based immunotherapy of melanoma and other cancers. We plan to initiate a Phase 1 trial to evaluate Ad-RTS-IL-12 + veledimex as a single agent in the treatment of patients with brain cancer in the first half of 2015.
30
Table of Contents
CAR-T, NK and TCR Cells
We are actively pursuing non-viral, genetic engineering technologies to develop novel CAR-T, NK and TCR cells. Combining this technology with Intrexon’s industrialized synthetic biologic engineering and clinically tested and validated RTS IL-12 modules, represents a differentiated approach to genetically modified CAR-T cell and other immune cells. Employing novel cell engineering techniques and multigenic gene programs, we expect to implement next-generation non-viral adoptive cellular therapies based on designer cytokines and CARs under control of RTS® technology targeting both hematologic malignancies and solid tumors. We plan to leverage the synergy between the platforms to accelerate a promising synthetic immuno-oncology pipeline, with up to five CAR-T therapies expected to enter the clinic in 2015 and programs for the development of allogeneic CAR-T therapies that can be used off-the-shelf expected to be initiated in 2016.
Research suggests that T cells can be re-programmed to have a very strong anti-cancer therapeutic effect through the expression of CARs to redirect specificity to tumors without HLA restrictions. The signature event within this field has resulted from the infusion of T cells expressing CARs into patients with B cells leukemias and lymphomas. Many of these patients have responded to these new therapies with a durable and dramatic anti-tumor effect after infusing CD19-specific T cells. Despite the highly promising results that have been demonstrated by early researchers in the field, current technologies and approaches have shown a number of serious drawbacks, including toxicity, manufacturing complexity and expense. A particular problem is that infusions of T cells into patients with large amounts of disease have invariably led to significant issues of toxicity for recipient patients. These toxicities primarily involve three major, potentially catastrophic side-effects:
| • | The rapid killing of tumor cells releases a large number intracellular constituents that are very toxic to various organs and is called “tumor lysis syndrome” that can be fatal, |
| • | the supra-physiologic release of cytokines (“cytokine storm”) that causes fever, instability of blood pressure, mental status changes and on occasion, death, and |
| • | on-target, and off-tissue toxicity represented by the concomitant damage of normal B cells and loss of humoral (antibody) immunity. |
We expect to be able to tightly control expansion and activation of CAR-T cells in the body, which has the potential to alleviate or abrogate these toxicities.
31
Table of Contents
MD Anderson’s platform, which uses the exclusive Sleeping Beauty system, or SB system, generates and characterizes new CAR-T designs, which enables a high throughput approach to evaluate the CAR-T. This “EZ-CAR-T” non-viral system is used to fashion immuno-receptors that differ in specificity and ability to activate T cells. These CAR-T molecules are evaluated in a “go/no go” system based on serial killing and protection of T cells from activation-induced cell death. Non-viral gene transfer using the SB system is unique in the field of oncology. Examples of cell engineering techniques that we expect to employ with the SB system are induced pluripotent stem cell (iPSC) processing technologies combined with Laser-enabled Analysis and Processing, or LEAP®, which consists of computerized image-based selection and laser processing for very rapid cell identification and purification as well as AttSite® Recombinases, which involves stable, targeted gene integration and expression with proprietary serine recombinases. We believe the advanced DNA vectors derived from SB can be used to avoid the expense and manufacturing difficulty associated with creating CAR-T cells using viral vectors. After electroporation, the transposon/transposase improves the efficiency of integration of plasmids used to express CAR and other transgenes in T cells. Propagation of genetically modified T cells on activating and propagating cells, or AaPC, provide a competitive advantage over other non-viral methods of modification. The SB system combined with artificial antigen-presenting cells can selectively propagate and thus retrieve CAR+ T cells suitable for human application. T cells can also be genetically modified using these technologies to target a panel (several) cancer antigen targets. We are on the verge of implementing technology to manufacture “minimally-manipulated” T cells within days of gene transfer by electroporation.
We expect this platform will rapidly integrate with Intrexon’s RTS® and multigenic control gene programs. The programs are also designed and built for rapid transition to universal donor products or minimally manipulated point of care products. Dr. Laurence Cooper and colleagues at MD Anderson recently published research which demonstrated that transformed, primary, and pluripotent stem cells can be permanently modified to eliminate HLA-A expression, demonstrating how to generate a priori cells from one allogeneic donor for infusion into multiple recipients representing a significant step towards our goal of on-demand therapy that can be pre-deployed at multiple sites and infused when needed. The primary factor limiting the development of a universal donor product is the existence of graft-vs-host response, or GVHD. GVHD occurs because the newly transplanted cells regard the recipient’s body as foreign. When this happens, the newly transplanted cells attack the recipient’s body. Additional research from Dr. Cooper and colleagues at MD Anderson suggests that “universal” allogeneic T cells generated from one donor could be administered to multiple recipients. This is achieved by genetically editing CD19-specific CAR+ T cells to eliminate expression of the endogenous a ß TCR, the gene responsible for triggering GVHD, without compromising CAR-dependent effector functions. Genetically modified T cells are generated using the SB system to stably introduce the CD19-specific CAR with subsequent permanent deletion of a or ß TCR chains with nucleases. The translation of the SB system and AaPC for use in clinical trials highlights how a nimble and cost-effective approach to developing genetically modified T cells can be used to implement clinical trials infusing next-generation T cells with improved therapeutic potential. We are expanding our initial trials targeting CD19 and planning to conduct additional trials with re-designed CAR-Ts expanding beyond CD19+ tumor cells.
Anticipated Milestones
We expect the following milestones to occur in 2015 and 2016:
| • | Intra-tumoral IL-12 RheoSwitch® programs: |
| • | Early data is expected in the fourth quarter of 2015 for our Phase 1/2 study in Breast Cancer with standard of care. |
| • | Early data is expected in the fourth quarter of 2015 for our Phase 1 study of Glioblastoma multiforme (GBM). |
| • | CAR-T programs: |
| • | We expect to initiate two Phase 1 studies of next-generation CD19 CARs in the second quarter of 2015. |
| • | We expect to initiate a Phase 1 study of next-generation CAR with an inducible cytokine in the fourth quarter of 2015. |
| • | We expect to initiate a novel CAR for myeloid malignancies in the fourth quarter of 2015. |
| • | We expectinterim data on two Phase 1 CARs studies in advanced leukemia and lymphomas in the fourth quarter of 2015. |
| • | We expect to initiate other leukemia and solid tumor CAR-T cell studies in 2016. |
| • | We expect to initiate allogeneic, off-the-shelf T-cell studies in 2016. |
Data from all programs is expected in 2015 and 2016. We are also evaluating additional potential preclinical candidates and continuing discovery efforts aimed at identifying other potential product candidates under our Channel Agreement with Intrexon. In addition, we may seek to enhance our pipeline in synthetic immuno-oncology through focused strategic transactions, which may include acquisitions, partnerships and in-licensing activities. We are actively seeking to out-license some or all of our small molecule programs to further support our synthetic immuno-oncology efforts.
Small Molecule Programs
In addition to our synthetic immuno-oncology programs discussed above, we have certain rights to three small molecule programs, palifosfamide (or isophosphoramide mustard), darinaparsin and indibulin, all of which we are no longer directly pursuing. With respect to palifosfamide, in March 2013, we announced that the pivotal Phase 3 study, PICASSO 3, did not meet its primary endpoint of progression-free survival, and that we would terminate our development program in metastatic soft tissue sarcoma. In addition, we recently received the overall survival endpoint data from our study of palifosfamide in combination with carboplatin and etoposide chemotherapy versus carboplatin and etoposide alone in chemotherapy naïve patients with metastatic small cell lung cancer, which we refer to as MATISSE. This data will be submitted for presentation at a scientific forum during the first half of 2015.
32
Table of Contents
We are seeking transactions with third parties for the possible out-license of palifosfamide, or we may seek to terminate any further efforts with respect to palifosfamide and cease any further expenditure. With respect to darinaparsin, we have entered into an amended and restated global licensing agreement with Solasia Pharma K.K., or Solasia, on July 31, 2014 granting Solasia an exclusive worldwide license to develop and commercialize darinaparsin, and related organoarsenic molecules, in both intravenous and oral forms in all indications for human use. In exchange, we will be eligible to receive from Solasia development-and sales-based milestones, a royalty on net sales of darinaparsin, once commercialized, and a percentage of any sublicense revenues generated by Solasia. During 2014, we determined to no longer pursue clinical development of indibulin.
33
Table of Contents
Financial Overview
Overview of Results of Operations
Three months ended March 31, 2015 compared to three months ended March 31, 2014
Revenue. Revenue during the three months ended March 31, 2015 and 2014 was as follows:
| Three months ended March 31, |
||||||||||||||||
| 2015 | 2014 | Change | ||||||||||||||
| ($ in thousands) | ||||||||||||||||
| Collaboration revenue |
$ | 272 | $ | 200 | $ | 72 | 36 | % | ||||||||
Revenue for the three months ended March 31, 2015 increased in comparison to the three months ended March 31, 2014. In connection with our March 7, 2011 collaboration agreement with Solasia Pharma K.K., we received $5.0 million in research and development funding which was being earned over the period of effort, originally estimated to be 75 months. In July 2014, we entered into an amended and restated License and Collaboration Agreement with Solasia (see Note 6 to the accompanying unaudited financial statements), resulting in the Company no longer being obligated to continue their research and development efforts in connection with the upfront payment. However, there are certain deliverables that are included in the amended and restated License and Collaboration Agreement which are not separable from the agreement and have no stand-alone value. As a result, the Company has determined that the estimated period for amortizing the upfront payment is now through March 31, 2016. Accordingly, the Company has recorded $272 thousand in revenue during the three months ended March 31, 2015 while the remaining deferred revenue balance of $1.1 million at March 31, 2015 has been classified as current.
Research and development expenses. Research and development expenses during the three months ended March 31, 2015 and 2014 were as follows:
| Three months ended March 31, | ||||||||||||||||
| 2015 | 2014 | Change | ||||||||||||||
| ($ in thousands) | ||||||||||||||||
| Research and development |
$ | 72,249 | $ | 6,542 | $ | 65,707 | 1004 | % | ||||||||
Research and development expenses for the three months ended March 31, 2015 increased by $65.7 million when compared to the three months ended March 31, 2014. The increase is due to the fair value of the common shares issued to M.D. Anderson in consideration for the license in the amount of $67.3 million, increased immunotherapy expenses of $0.9 million, and offset against decreases in employee costs of $0.9 million.
34
Table of Contents
Our research and development expense consists primarily of licensing costs, collaboration costs, salaries and related expenses for personnel, costs of contract manufacturing services, costs of facilities and equipment, fees paid to professional service providers in conjunction with our clinical trials, fees paid to research organizations in conjunction with preclinical animal studies, costs of materials used in research and development, consulting, license and milestone payments and sponsored research fees paid to third parties.
We have not accumulated and tracked our internal historical research and development costs or our personnel and personnel-related costs on a program-by-program basis. Our employee and infrastructure resources are allocated across several projects, and many of our costs are directed to broadly applicable research endeavors. As a result, we cannot state the costs incurred for each of our oncology programs on a program-by-program basis.
Our future research and development expenses in support of our current and future programs will be subject to numerous uncertainties in timing and cost to completion. We test potential products in numerous preclinical studies for safety, toxicology and efficacy. We may conduct multiple clinical trials for each product. As we obtain results from trials, we may elect to discontinue or delay clinical trials for certain products in order to focus our resources on more promising products or indications. Completion of clinical trials may take several years or more, and the length of time generally varies substantially according to the type, complexity, novelty and intended use of a product. It is not unusual for preclinical and clinical development of each of these types of products to require the expenditure of substantial resources.
We estimate that clinical trials of the type generally needed to secure new drug approval are typically completed over the following timelines:
| Clinical Phase |
Estimated Completion Period | |
| Phase 1 |
1 - 2 years | |
| Phase 2 |
2 - 3 years | |
| Phase 3 |
2 - 4 years |
The duration and the cost of clinical trials may vary significantly over the life of a project as a result of differences arising during clinical development, including, among others, the following:
| • | The number of clinical sites included in the trials; |
| • | The length of time required to enroll suitable patents; |
| • | The number of patients that ultimately participate in the trials; |
| • | The duration of patient follow-up to ensure the absence of long-term product-related adverse events; and |
| • | The efficacy and safety profile of the product. |
As a result of the uncertainties discussed above, we are unable to determine the duration and completion costs of our programs or when and to what extent we will receive cash inflows from the commercialization and sale of a product. Our inability to complete our programs in a timely manner or our failure to enter into appropriate collaborative agreements could significantly increase our capital requirements and could adversely impact our liquidity. These uncertainties could force us to seek additional, external sources of financing from time-to-time in order to continue with our product development strategy. Our inability to raise additional capital, or to do so on terms reasonably acceptable to us, would jeopardize the future success of our business.
35
Table of Contents
General and administrative expenses. General and administrative expenses during the three months ended March 31, 2015 and 2014 were as follows:
| Three months ended March 31, |
||||||||||||||||
| 2015 | 2014 | Change | ||||||||||||||
| ($ in thousands) | ||||||||||||||||
| General and administrative |
$ | 4,250 | $ | 3,442 | $ | 808 | 23 | % | ||||||||
General and administrative expenses for the three months ended March 31, 2015 increased by $808 thousand when compared to the three months ended March 31, 2014. The increase was primarily due to costs associated with contracted outside services related to the MD Anderson transaction.
Other income (expense). Other income (expense) for three months ended March 31, 2015 and 2014 were as follows:
| Three months ended March 31, |
||||||||||||||||
| 2015 | 2014 | Change | ||||||||||||||
| ($ in thousands) | ||||||||||||||||
| Other income, net |
$ | (4 | ) | $ | (9 | ) | $ | 5 | (56 | %) | ||||||
| Change in fair value of warrants |
— | 82 | (82 | ) | 100 | % | ||||||||||
|
|
|
|
|
|
|
|||||||||||
| Total |
$ | (4 | ) | $ | 73 | $ | (77 | ) | ||||||||
|
|
|
|
|
|
|
|||||||||||
The increase in other income (expense) from the three months ended March 31, 2015 compared to the three months ended March 31, 2014 was due primarily to the change in the fair value of liability-classified warrants, which expired on December 9, 2014.
36
Table of Contents
Liquidity and Capital Resources
As of March 31, 2015, we had approximately $129.7 million in cash and cash equivalents, compared to $42.8 million in cash and cash equivalents as of December 31, 2014. Excluding the expected receipt in the second quarter of 2015 of $57.5 million from Intrexon related to the Ares Trading Agreement and given our current development plans, we anticipate that our current cash resources will be sufficient to fund our operations into the second quarter of 2017. However, changes may occur that would consume our existing capital prior to that time, including the scope and progress of our research and development efforts and changes in governmental regulation. Actual costs may ultimately vary from our current expectations, which could materially impact our use of capital and our forecast of the period of time through which our financial resources will be adequate to support our operations. We have estimated the sufficiency of our cash resources based in part on the anticipated advancement of our synthetic immuno-oncology product candidates in the clinic under our exclusive channel partnership with Intrexon and our license agreement with The University of Texas M.D. Anderson Cancer Center, and we expect that the costs associated with these and additional product candidates will increase the level of our overall research and development expenses significantly going forward.
Although all human clinical trials are expensive and difficult to design and implement, we believe that due to complexity, costs associated with clinical trials for synthetic immuno-oncology products are greater than the corresponding costs associated with clinical trials for small molecule candidates.
In addition to these factors, our actual cash requirements may vary materially from our current expectations for a number of other factors that may include, but are not limited to, changes in the focus and direction of our development programs, competitive and technical advances, costs associated with the development of our product candidates, our ability to secure partnering arrangements, and costs of filing, prosecuting, defending and enforcing our intellectual property rights. If we exhaust our capital reserves more quickly than anticipated, regardless of the reason, and we are unable to obtain additional financing on terms acceptable to us or at all, we will be unable to proceed with development of some or all of our product candidates on expected timelines and will be forced to prioritize among them.
We expect that we will need additional financing to support our long-term plans for clinical trials and new product development. We expect to finance our cash needs through the sale of equity securities, strategic collaborations and/or debt financings, or through other sources that may be dilutive to existing stockholders. There can be no assurance that we will be able to obtain funding from any of these sources or, if obtained, what the terms of such funding(s) may be, or that any amount that we are able to obtain will be adequate to support our working capital requirements until we achieve profitable operations. We have no current committed sources of additional capital. Recently, capital markets have experienced a period of instability that may severely hinder our ability to raise capital within the time periods needed or on terms we consider acceptable, if at all. If we are unable to raise additional funds when needed, we may not be able to continue development and regulatory approval of our products, or we could be required to delay, scale back or eliminate some or all our research and development programs.
37
Table of Contents
The following table summarizes our net increase (decrease) in cash and cash equivalents for the three months ended March 31, 2015 and 2014:
| Three months ended March 31, |
||||||||
| 2015 | 2014 | |||||||
| ($ in thousands) | ||||||||
| Net cash provided by (used in): |
||||||||
| Operating activities |
$ | (9,717 | ) | $ | (8,654 | ) | ||
| Investing activities |
(17 | ) | (2 | ) | ||||
| Financing activities |
96,615 | 837 | ||||||
|
|
|
|
|
|||||
| Net increase (decrease) in cash and cash equivalents |
$ | 86,881 | $ | (7,819 | ) | |||
|
|
|
|
|
|||||
Net cash used in operating activities was $9.7 million for the three months ended March 31, 2015 compared to $8.7 million for the three months ended March 31, 2014. The increase in cash used in operating activities relates to increased immunotherapy expenses of $0.9 million.
Net cash used in investing activities was $17 thousand for the three months ended March 31, 2015 compared to $2 thousand for the three months ended March 31, 2014. The change was due to increased spending on property, plant, and equipment.
Net cash provided by financing activities was $96.6 million for the three months ended March 31, 2015 compared to $0.9 million for the three months ended March 31, 2014. The change is primarily attributable to financing proceeds of approximately $94.3 million associated with the company’s February 3, 2015 financing (see Note 2) and $2.5 million from stock option exercises.
38
Table of Contents
Operating capital and capital expenditure requirements
We anticipate that losses will continue for the foreseeable future. At March 31, 2015, our accumulated deficit was approximately $450.8 million. Our actual cash requirements may vary materially from those planned because of a number of factors including:
| • | Changes in the focus, direction and pace of our development programs; |
| • | Competitive and technical advances; |
| • | Costs associated with the development of our product candidates; |
| • | Our ability to secure partnering arrangements; |
| • | Costs of filing, prosecuting, defending and enforcing any patent claims and any other intellectual property rights, or other developments, and |
| • | Other matters identified under Part II – Item 1A. “Risk Factors.” |
Working capital as of March 31, 2015 was $120.1 million, consisting of $130.6 million in current assets and $10.5 million in current liabilities. Working capital as of December 31, 2014 was $33.3 million, consisting of $44.1 million in current assets and $10.8 million in current liabilities.
Contractual obligations
The following table summarizes our outstanding obligations as of March 31, 2015 and the effect those obligations are expected to have on our liquidity and cash flows in future periods:
| Less than | More than | |||||||||||||||||||
| ($ in thousands) | Total | 1 year | 2 - 3 years | 4 - 5 years | 5 years | |||||||||||||||
| Operating leases |
$ | 2,854 | $ | 1,244 | $ | 1,313 | $ | 297 | $ | — | ||||||||||
| Royalty and license fees |
46,850 | 12,525 | 30,550 | 3,775 | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total |
$ | 49,704 | $ | 13,769 | $ | 31,863 | $ | 4,072 | $ | — | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Our commitments for operating leases relate to the lease for our corporate headquarters in Boston, MA, and office space in New York, NY. Our commitments for royalty and license fees relate to our royalty agreements with Southern Research Institute, requiring minimum royalty payments, as well as our license agreement with The University of Texas M. D. Anderson Cancer Center, requiring payment upon the first patient treated in a pivotal trial in darinaparsin, currently being developed under the amended and restated License and Collaboration Agreement with Solasia. As part of the amended and restated License and Collaboration agreement with Solasia (see Note 6), we will receive full reimbursement of this license payment. The contract milestone and contract installment payments relate to our agreement with Baxter Healthcare Corporation for the purchase of the assets relating to indibulin, and to our CRO agreements with Novella Clinical, Inc. The remaining contract installment payments to Baxter are comprised of three separate $250 thousand payments on November 3, 2015-2017. However, for the purpose of the above table, we have assumed that the payment of the milestones will occur within five years of March 31, 2015. Included in the above table are obligations for the subleased portion of our New York office as noted in Note 6. We expect to receive a total of $306 thousand in the next year, $640 thousand in the next 2-3 years, and $195 thousand in the next 4-5 years from our subtenant in the New York office.
On January 13, 2015, the Company entered into a license agreement with The University of Texas M.D. Anderson Cancer Center as detailed in Note 6. The agreement includes minimum quarterly payments of $3.75 million included in the above table within “Royalty and License Fees”. The Company’s obligations related to this agreement are payments of $11.25 million in the column “Less than 1 Year”, $30 million in the column “2 – 3 Years” and $3.75 million in the column “4 – 5 Years.”
39
Table of Contents
Off-balance sheet arrangements
During the three months ended March 31, 2015 and 2014, we did not engage in any off-balance sheet arrangements.
Critical Accounting Policies and Estimates
In our Annual Report on Form 10-K, for the fiscal year ended December 31, 2014, our most critical accounting policies and estimates upon which our financial status depends were identified as those relating to stock-based compensation; net operating losses and tax credit carryforwards; and impairment of long-lived assets. We reviewed our policies and determined that those policies remain our most critical accounting policies for the three months ended March 31, 2015.
Item 3. Quantitative and Qualitative Disclosures about Market Risk
Our exposure to market risk is limited to our cash. The goals of our investment policy are preservation of capital, fulfillment of liquidity needs and fiduciary control of cash. We also seek to maximize income from our investments without assuming significant risk. To achieve our goals, we maintain our cash in interest-bearing bank accounts in global banks, United States treasuries and other government-backed investments, which are subject to minimal interest rate risk.
Effect of Currency Exchange Rates and Exchange Rate Risk Management
We conduct clinical studies outside of the United States primarily in Western Europe. These business operations are not material at this time, therefore any currency fluctuations will not have a material impact on our financial position, results of operations or cash flows.
Item 4. Controls and Procedures
Our management, with the participation of our principal executive officer and principal financial officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) or 15d-15(e) under the Securities Exchange Act of 1934, as amended, or the Exchange Act) as of the end of the period covered by this report. Based on such evaluation, our principal executive officer and principal financial officer have concluded that, as of the end of such period, our disclosure controls and procedures were effective in ensuring that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported, on a timely basis, and is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate, to allow timely decisions regarding required disclosure.
No change in our internal control over financial reporting (as defined in Exchange Act Rules 13a-15(f) and 15d-15(f)) occurred during the period covered by this quarterly report that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
40
Table of Contents
In the ordinary course of business, we may periodically become subject to legal proceedings and claims arising in connection with ongoing business activities. The results of litigation and claims cannot be predicted with certainty, and unfavorable resolutions are possible and could materially affect our results of operations, cash flows or financial position. In addition, regardless of the outcome, litigation could have an adverse impact on us because of defense costs, diversion of management resources and other factors.
While the outcome of these proceedings and claims cannot be predicted with certainty, there are no matters, as of March 31, 2015, that, in the opinion of management, might have a material adverse effect on our financial position, results of operations or cash flows.
The following important factors could cause our actual business and financial results to differ materially from those contained in forward-looking statements made in this Quarterly Report on Form 10-Q or elsewhere by management from time to time. The risk factors in this report have been revised to incorporate changes to our risk factors from those included in our Annual Report on Form 10-K for the fiscal year ended December 31, 2014. The risk factors set forth below with an asterisk (*) next to the title are new risk factors or risk factors containing changes, which may be material, from the risk factors previously disclosed in Item 1A of our Annual Report on Form 10-K for the fiscal year ended December 31, 2014, as filed with the Securities and Exchange Commission.
RISKS RELATED TO OUR BUSINESS
Our plans to develop and commercialize, through our License with MD Anderson and Intrexon and our Channel Agreement with Intrexon, nonviral adoptive cellular therapies based on designer cytokines and novel chimeric antigen receptor (CAR) T-cell therapies are new approaches to cancer treatment that present significant challenges in a competitive landscape and the success of our efforts depends in large part on our owned and licensed intellectual property, and our efforts may be affected by litigation and developments in intellectual property law outside of our control.
We intend to employ technologies licensed from MD Anderson pursuant to the MD Anderson License described above in “Summary—Recent developments”, and from Intrexon, pursuant to our existing Channel Agreement with Intrexon, to pursue the development and commercialization of nonviral adoptive cellular therapies based on cytokines and CARs under control of the RTS® technology targeting both hematologic and solid tumor malignancies. Because this is a new approach to cancer immunotherapy and cancer treatment generally, developing and commercializing product candidates subjects us to a number of challenges, including:
| • | obtaining regulatory approval from the FDA and other regulatory authorities that have very limited experience with the commercial development of genetically modified T-cell therapies for cancer; |
| • | developing and deploying consistent and reliable processes for engineering a patient’s T-cells ex vivo and infusing the engineered T-cells back into the patient; |
| • | possibly conditioning patients with chemotherapy in conjunction with delivering each of the potential products, which may increase the risk of adverse side effects of the potential products; |
| • | educating medical personnel regarding the potential side effect profile of each of the potential products, such as the potential adverse side effects related to cytokine release; |
| • | developing processes for the safe administration of these potential products, including long-term follow-up for all patients who receive the potential products; |
| • | sourcing additional clinical and, if approved, commercial supplies for the materials used to manufacture and process the potential products; |
| • | developing a manufacturing process and distribution network with a cost of goods that allows for an attractive return on investment; |
| • | establishing sales and marketing capabilities after obtaining any regulatory approval to gain market acceptance; |
| • | developing therapies for types of cancers beyond those addressed by the current potential products; and |
| • | not infringing the intellectual property rights, in particular, the patent rights, of third parties, including competitors developing alternative CAR T-cell therapies |
41
Table of Contents
We cannot be sure that T-cell immunotherapy technologies that we intend to develop in partnership with MD Anderson and Intrexon will yield satisfactory products that are safe and effective, scalable, or profitable. Moreover, public perception of therapy safety issues, including adoption of new therapeutics or novel approaches to treatment, may adversely influence the willingness of subjects to participate in clinical trials, or if approved, of physicians to subscribe to the novel treatment mechanics. Physicians, hospitals and third-party payors often are slow to adopt new products, technologies and treatment practices that require additional upfront costs and training. Physicians may not be willing to undergo training to adopt this novel and personalized therapy, may decide the therapy is too complex to adopt without appropriate training and may choose not to administer the therapy. Based on these and other factors, hospitals and payors may decide that the benefits of this new therapy do not or will not outweigh its costs.
Our CAR-T product candidates are supported by limited clinical data, all of which has been generated through trials conducted by MD Anderson, not by us. We plan to assume control of the overall clinical and regulatory development of our CAR-T product candidates, and any failure to obtain, or delays in obtaining, sponsorship of investigational new drug applications, or INDs, or in filing new INDs sponsored by us for these or any other product candidates we determine to advance could negatively affect the timing of our potential future clinical trials. Such an impact on timing could increase research and development costs and could delay or prevent obtaining regulatory approval for our product candidates, either of which could have a material adverse effect on our business. Further, we did not control the design or conduct of the previous trials. It is possible that the FDA will not accept these previous trials as providing adequate support for future clinical trials, whether controlled by us or third parties, for any of one or more reasons, including the safety, purity, and potency of the product candidate, the degree of product characterization, elements of the design or execution of the previous trials or safety concerns, or other trial results. We may also be subject to liabilities arising from any treatment-related injuries or adverse effects in patients enrolled in these previous trials. As a result, we may be subject to unforeseen third-party claims and delays in our potential future clinical trials. We may also be required to repeat in whole or in part clinical trials previously conducted by MD Anderson, which will be expensive and delay the submission and licensure or other regulatory approvals with respect to any of our product candidates.
In addition, the results of the limited clinical trials conducted by MD Anderson to date may not be replicated in future clinical trials. Our CAR-T product candidates may fail to show the desired safety and efficacy in clinical development and we cannot assure you that the results of any future trials will demonstrate the value and efficacy of our product candidates. Moreover, there are a number of regulatory requirements that we must satisfy before we can continue clinical trials of CAR-T or other cellular therapy product candidates in the United States. Satisfaction of these requirements will entail substantial time, effort and financial resources. Any time, effort and financial resources we expend on our CAR-T and other early-stage product candidate development programs may adversely affect our ability to continue development and commercialization of our synthetic immuno-oncology product candidates.
The biopharmaceutical industry, and the rapidly evolving market for developing genetically engineered T-cells in particular, is characterized by intense competition and rapid innovation. Genetically engineering T-cells faces significant competition in the CAR technology space from multiple companies and their collaborators, such as Novartis/University of Pennsylvania, Bluebird bio/Celgene/Baylor College of Medicine, Kite Pharma/National Cancer Institute, Juno Therapeutics/Fred Hutchinson Cancer Research Center/Memorial Sloan-Kettering Cancer Center/Seattle Children’s Research Institute, Cellectis/Pfizer and Adaptimmune/GSK. We face competition from non-cell based treatments offered by other companies such as Amgen, AstraZeneca, Bristol-Myers, Incyte, Merck, and Roche. Even if we obtain regulatory approval of potential products, we may not be the first to market and that may affect the price or demand for our potential products. Additionally, the availability and price of our competitors’ products could limit the demand and the price we are able to charge for our potential products. We may not be able to implement our business plan if the acceptance of our potential products is inhibited by price competition or the reluctance of physicians to switch from existing methods of treatment to our potential products, or if physicians switch to other new drug or biologic products or choose to reserve our potential products. Additionally, a competitor could obtain orphan product exclusivity from the FDA with respect to such competitor’s product. If such competitor product is determined to be the same product as one of our potential products, that may prevent us from obtaining approval from the FDA for such potential products for the same indication for seven years, except in limited circumstances.
We are dependent on patents, know-how, and proprietary technology that are licensed from others, particularly MD Anderson and Intrexon. Any termination of these licenses could result in the loss of significant rights and could harm our ability to commercialize our product candidates. Disputes may also arise between us and these licensors regarding intellectual property subject to a license agreement, including those relating to:
| • | the scope of rights granted under the applicable license agreement and other interpretation-related issues; |
| • | whether and the extent to which our technology and processes, and the technology and processes of Intrexon, MD Anderson and our other licensors, infringe on intellectual property of the licensor that is not subject to the applicable license agreement; |
| • | our right to sublicense patent and other rights to third parties pursuant to our relationships with our licensors and partners; |
| • | whether we and/or Intrexon are complying with our diligence obligations with respect to the use of the licensed technology in relation to our development and commercialization of our potential products under the MD Anderson License with MD Anderson; and |
| • | the allocation of ownership of inventions and know-how resulting from the joint creation or use of intellectual property by our licensors and by us. |
42
Table of Contents
If disputes over intellectual property that we have licensed prevent or impair our ability to maintain our current licensing arrangements, particularly with MD Anderson, on acceptable terms, we may be unable to successfully develop and commercialize the affected potential products. We are generally also subject to all of the same risks with respect to protection of intellectual property that we license as we are for intellectual property that we own. If we or our licensors fail to adequately protect this intellectual property, our ability to commercialize potential products under our applicable licenses could suffer.
There is a substantial amount of litigation involving patents and other intellectual property rights in the biotechnology and pharmaceutical industries, as well as administrative proceedings for challenging patents, including interference, derivation, and reexamination proceedings before the United States Patent and Trademark Office, or U.S. PTO, or oppositions and other comparable proceedings in foreign jurisdictions. Recently, due to changes in U.S. law referred to as patent reform, new procedures including inter partes review and post-grant review have been implemented, which adds uncertainty to the possibility of challenge to our or our licensors’ patents in the future.
* We will require additional financial resources in order to continue ongoing development of our product candidates; if we are unable to obtain these additional resources, we may be forced to delay or discontinue clinical testing of our product candidates.
We have not generated significant revenue and have incurred significant net losses in each year since our inception. For the three months ended March 31, 2015, we had a net loss of $78.2 million, and, as of March 31, 2015, we have incurred approximately $450.8 million of cumulative net losses since our inception in 2003. We expect to continue to incur significant operating expenditures and net losses. Further development of our product candidates, including product candidates that we may develop under our Channel Agreement with Intrexon, will likely require substantial increases in our expenses as we:
| • | Continue to undertake clinical trials for product candidates; |
| • | Scale-up the formulation and manufacturing of our product candidates; |
| • | Seek regulatory approvals for product candidates; |
| • | work with regulatory authorities to identify and address program related inquiries; |
| • | Implement additional internal systems and infrastructure; |
| • | Hire additional personnel; |
| • | Begin to advance candidates pursuant to the License with MD Anderson; and |
| • | Commence providing funding for certain research and development activities of MD Anderson pursuant to the terms of the License. |
We continue to seek additional financial resources to fund the further development of our product candidates. If we are unable to obtain sufficient additional capital, one or more of these programs could be placed on hold. Because we are currently devoting a significant portion of our resources to the development of synthetic immuno-oncology, further progress with the development of our other candidates may be significantly delayed and may depend on the licensing of those compounds to third parties.
As of March 31, 2015, we have approximately $129.7 million of cash and cash equivalents. Excluding the expected receipt in the second quarter of 2015 of $57.5 million from Intrexon related to the Ares Trading Agreement and given our current development plans, we anticipate that our current cash resources will be sufficient to fund our operations into the second quarter of 2017. We do not know whether additional financing will be available on terms favorable or acceptable to us when needed, if at all. Our business is highly cash-intensive and our ability to continue operations after our current cash resources are exhausted depends on our ability to obtain additional financing and/or achieve profitable operations, as to which no assurances can be given. If adequate additional funds are not available when required, or if we are unsuccessful in entering into partnership agreements for the further development of our products, we will be required to delay, reduce or eliminate planned preclinical and clinical trials and may be forced to terminate the approval process for our product candidates from the FDA or other regulatory authorities. In addition, we could be forced to discontinue product development, forego attractive business opportunities or pursue merger or divestiture strategies. In the event we are unable to obtain additional financing, we may be forced to cease operations altogether.
43
Table of Contents
*We need to raise additional capital to fund our operations. The manner in which we raise any additional funds may affect the value of your investment in our common stock.
As of March 31, 2015, we had incurred approximately $450.8 million of cumulative net losses and had approximately $129.7 million of cash and cash equivalents. Excluding the expected receipt in the second quarter of 2015 of $57.5 million from Intrexon related to the Ares Trading Agreement and given our current development plans, we anticipate that our current cash resources will be sufficient to fund our operations into the second quarter of 2017. However, changes may occur that would consume our existing capital prior to then, including expansion of the scope of, and/or slower than expected progress of, our research and development efforts and changes in governmental regulation. Actual costs may ultimately vary from our current expectations, which could materially impact our use of capital and our forecast of the period of time through which our financial resources will be adequate to support our operations. We have estimated the sufficiency of our cash resources based in part on the discontinuation of the PICASSO 3 pivotal trial for first-line metastatic STS and our adaptive Phase 3 trial for first-line SCLC for IV palifosfamide. Also our estimates include the advancement of our synthetic immuno-oncology product candidates in the clinic under our Channel Agreement with Intrexon and our increased expenses as we begin to advance candidates pursuant to the MD Anderson License with MD Anderson and commence providing funding for certain research and development activities of MD Anderson pursuant to the terms of the MD Anderson License, and we expect that the costs associated with these and additional product candidates will increase the level of our overall research and development expenses significantly going forward.
In addition to above factors, our actual cash requirements may vary materially from our current expectations for a number of other factors that may include, but are not limited to, changes in the focus and direction of our development programs, competitive and technical advances, costs associated with the development of our product candidates, our ability to secure partnering arrangements, and costs of filing, prosecuting, defending and enforcing our intellectual property rights. If we exhaust our capital reserves more quickly than anticipated, regardless of the reason, and we are unable to obtain additional financing on terms acceptable to us or at all, we will be unable to proceed with development of some or all of our product candidates on expected timelines and will be forced to prioritize among them.
The unpredictability of the capital markets may severely hinder our ability to raise capital within the time periods needed or on terms we consider acceptable, if at all. Moreover, if we fail to advance one or more of our current product candidates to later-stage clinical trials, successfully commercialize one or more of our product candidates, or acquire new product candidates for development, we may have difficulty attracting investors that might otherwise be a source of additional financing.
Our need for additional capital and limited capital resources may force us to accept financing terms that could be significantly dilutive to existing stockholders. To the extent that we raise additional capital by issuing equity securities, our stockholders may experience dilution. In addition, we may grant future investors rights superior to those of our existing stockholders. If we raise additional funds through collaborations and licensing arrangements, it may be necessary to relinquish some rights to our technologies, product candidates or products, or grant licenses on terms that are not favorable to us. If we raise additional funds by incurring debt, we could incur significant interest expense and become subject to covenants in the related transaction documentation that could affect the manner in which we conduct our business.
Clinical trials are very expensive, time-consuming, and difficult to design and implement.
Human clinical trials are very expensive and difficult to design, initiate and implement, in part because they are subject to rigorous regulatory requirements. The clinical trial start up and process itself is also time-consuming and results are inherently uncertain. We estimate that clinical trials of our product candidates will take at least several years to complete. Furthermore, failure can occur at any stage of the trials, and we could encounter problems that cause us to delay the start of, abandon or repeat clinical trials. The commencement and completion of clinical trials may be delayed by several factors, including:
| • | Additional nonclinical data requests by regulatory agencies; |
| • | Unforeseen safety issues; |
| • | Determination of dosing issues; |
| • | Lack of effectiveness during clinical trials; |
| • | Slower than expected rates of patient recruitment and enrollment; |
| • | Inability to monitor patients adequately during or after treatment; |
| • | Inability or unwillingness of medical investigators to follow our clinical protocols; and |
| • | Regulatory determinations to temporarily or permanently cease enrollment for other reasons not related to patient safety. |
44
Table of Contents
Success in preclinical testing and early clinical trials does not ensure that later clinical trials will be successful. For example, despite positive findings in earlier clinical trials, our product candidate palifosfamide failed to meet the primary endpoint of the Phase 3 PICASSO 3 trial. In addition, we or the FDA may suspend our clinical trials at any time if it appears that we are exposing participants to unacceptable health risks or if the FDA finds deficiencies in our Investigational New Drug, or IND, submission or in the conduct of these trials.
See also “Risk Factors— Our product candidates are in various stages of clinical trials, which are very expensive and time-consuming. We cannot be certain when we will be able to file an NDA or BLA, with the FDA and any failure or delay in completing clinical trials for our product candidates could harm our business.”
We may not be able to obtain or maintain orphan drug exclusivity for our product candidates.
We have received Orphan Drug designations for darinaparsin for the treatment of peripheral T-cell lymphoma in both the United States and Europe, and we may be able to receive additional Orphan Drug designation from the FDA and the European Medicines Agency, or EMA, for other product candidates. In the United States, orphan designation is available to drugs intended to treat, diagnose or prevent a rare disease or condition that affects fewer than 200,000 people in the United States at the time of application for orphan designation. Orphan designation qualifies the sponsor of the product for a tax credit and marketing incentives. The first sponsor to receive FDA marketing approval for a drug with an orphan designation is entitled to a seven-year exclusive marketing period in the United States for that product for that indication and, typically, a waiver of the prescription drug user fee for its marketing application. However, a drug that the FDA considers to be clinically superior to, or different from, the approved orphan drug, even though for the same indication, may also obtain approval in the United States during the seven-year exclusive marketing period. Orphan drug exclusive marketing rights may also be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug. There is no guarantee that any of our other product candidates will receive Orphan Drug designation or that, even if such product candidate is granted such status, the product candidate’s clinical development and regulatory approval process will not be delayed or will be successful.
We may not be able to commercialize any products, generate significant revenues, or attain profitability.
To date, none of our product candidates have been approved for commercial sale in any country. The process to develop, obtain regulatory approval for, and commercialize potential drug candidates is long, complex, and costly. Unless and until we receive approval from the FDA and/or other regulatory authorities for our product candidates, we cannot sell our drugs and will not have product revenues. Even if we obtain regulatory approval for one or more of our product candidates, if we are unable to successfully commercialize our products, we may not be able to generate sufficient revenues to achieve or maintain profitability, or to continue our business without raising significant additional capital, which may not be available. Our failure to achieve or maintain profitability could negatively impact the trading price of our common stock.
Ethical, legal and social concerns about synthetic biologically engineered products could limit or prevent the use of our product candidates.
Our products candidates use a synthetic immuno-oncology platform. Public perception about the safety and environmental hazards of, and ethical concerns over, genetically engineered products could influence public acceptance of our product candidates. If we and our collaborators are not able to overcome the ethical, legal and social concerns relating to synthetic biological engineering, our product candidates may not be accepted. These concerns could result in increased expenses, regulatory scrutiny, delays or other impediments to the public acceptance and commercialization of our product candidates. Our ability to develop and commercialize products could be limited by public attitudes and governmental regulation.
The subject of genetically modified organisms has received negative publicity, which has aroused public debate. This adverse publicity could lead to greater regulation and trade restrictions on the development and commercialization of genetically altered products. Further, there is a risk that our product candidates could cause adverse health effects or other adverse events, which could also lead to negative publicity.
The synthetic biological platform that we use may have significantly enhanced characteristics compared to those found in naturally occurring organisms, enzymes or microbes. While we believe we produce synthetic biological technologies only for use in a controlled laboratory and industrial environment, the release of such synthetic biological technologies into uncontrolled environments could have unintended consequences. Any adverse effect resulting from such a release could have a material adverse effect on our business and financial condition, and we may have exposure to liability for any resulting harm.
45
Table of Contents
Our use of synthetic immuno-oncology to develop product candidates may become subject to increasing regulation in the future.
Most of the laws and regulations concerning synthetic immuno-oncology relate to the end products produced using synthetic biology, but that may change. For example, the Presidential Commission for the Study of Bioethical Issues recommended in December 2010 that the federal government oversee, but not regulate, synthetic biology research. The Presidential Commission also recommended that the government lead an ongoing review of developments in the synthetic biology field and that the government conduct a reasonable risk assessment before the field release of synthetic organisms. Other findings and recommendations have been published by the Presidential Commission through 2014. Synthetic immuno-oncology may become subject to additional government regulations as a result of the recommendations, which could require us to incur significant additional capital and operating expenditures and other costs in complying with these laws and regulations.
The technology on which our Channel Agreement with Intrexon Corporation is based in part on early stage technology in the field of human oncologic therapeutics.
Our Channel Agreement with Intrexon contemplates our using Intrexon’s advanced transgene engineering platform for the controlled and precise cellular production of anti-cancer effectors. The synthetic immuno-oncology effector platform in which we have acquired rights represents early-stage technology in the field of human oncology biotherapeutic, with DC-RTS-IL-12 + veledimex having completed a Phase 1 study in melanoma and Ad-RTS-IL-12 + veledimex having completed two Phase 2 studies, in melanoma and breast cancer. The Company is continuing to pursue intratumoral injection of Ad-RTS-IL-12 + veledimex in brain cancer and breast cancer. Although we plan to leverage Intrexon’s synthetic immuno-oncology platform for additional products targeting key pathways used by cancers to grow and metastasize, we may not be successful in developing and commercializing these products for a variety of reasons. The risk factors set forth herein that apply to our small molecule drug candidates, which are in various stages of development, also apply to product candidates that we seek to develop under our Channel Agreement with Intrexon.
We will incur additional expenses in connection with our Channel Agreement with Intrexon Corporation.
The synthetic immuno-oncology platform, in which we have acquired rights for cancer indications from Intrexon, includes two existing product candidates, Ad-RTS-IL-12+ veledimex and DC-RTS-IL-12 + veledimex. Upon entry into the Channel Agreement with Intrexon, we assumed responsibility for the clinical development of these product candidates, which we expect will increase the level of our overall research and development expenses significantly going forward. Although all human clinical trials are expensive and difficult to design and implement, we believe that due to complexity, costs associated with clinical trials for synthetic immuno-oncology products are greater than the corresponding costs associated with clinical trials for small molecule candidates. In addition to increased research and development costs, prior to the adoption of our April 2013 workforce reduction plan, we added headcount in part to support our Channel Agreement endeavors, and we may need to do so again in the future which would add to our general and administrative expenses going forward.
Although our forecasts for expenses and the sufficiency of our capital resources takes into account our plans to develop the Intrexon products, the actual costs associated therewith may be significantly in excess of forecasted amounts. In addition to the amount and timing of expenses related to the clinical trials, our actual cash requirements may vary materially from our current expectations for a number of other factors that may include, but are not limited to, changes in the focus and direction of our development programs, competitive and technical advances, costs associated with the development of our product candidates and costs of filing, prosecuting, defending and enforcing our intellectual property rights. If we exhaust our capital reserves more quickly than anticipated, regardless of the reason, and we are unable to obtain additional financing on terms acceptable to us or at all, we will be unable to proceed with development of some or all of our product candidates on expected timelines and will be forced to prioritize among them.
We may not be able to retain the exclusive rights licensed to us by Intrexon Corporation to develop and commercialize products involving DNA administered to humans for expression of anti-cancer effectors for the purpose of treatment or prophylaxis of cancer.
Under the Channel Agreement, we use Intrexon’s technology directed towards in vivo expression of effectors in connection with the development of Ad-RTS-IL-12+ veledimex and DC-RTS-IL-12 + veledimex and generally to research, develop and commercialize products, in each case in which DNA is administered to humans for expression of anti-cancer effectors for the purpose of treatment or prophylaxis of cancer, which we collectively refer to as the Cancer Program. The Channel Agreement grants us a worldwide license to use patents and other intellectual property of Intrexon in connection with the research, development, use, importing, manufacture, sale, and offer for sale of products involving DNA administered to humans for expression of anti-cancer effectors for the purpose of treatment or prophylaxis of cancer, which we refer to collectively as the ZIOPHARM Products. Such license is exclusive with respect to any clinical development, selling, offering for sale or other commercialization of ZIOPHARM Products, and otherwise is non-exclusive. Subject to limited exceptions, we may not sublicense the rights described without Intrexon’s written consent. Under the Channel Agreement, and subject to certain exceptions, we are responsible for, among other things, the performance of the Cancer Program, including development, commercialization and certain aspects of manufacturing of ZIOPHARM Products.
46
Table of Contents
Intrexon may terminate the Channel Agreement if we fail to use diligent efforts to develop and commercialize ZIOPHARM Products or if we elect not to pursue the development of a Cancer Program identified by Intrexon that is a “Superior Therapy” as defined in the Channel Agreement. We may voluntarily terminate the Channel Agreement upon 90 days written notice to Intrexon. Upon termination of the Channel Agreement, we may continue to develop and commercialize any ZIOPHARM Product that, at the time of termination:
| • | Is being commercialized by us; |
| • | Has received regulatory approval; |
| • | Is a subject of an application for regulatory approval that is pending before the applicable regulatory authority; or |
| • | Is the subject of at least an ongoing Phase 2 clinical trial (in the case of a termination by Intrexon due to an uncured breach or a voluntary termination by us), or an ongoing Phase 1 clinical trial in the field (in the case of a termination by us due to an uncured breach or a termination by Intrexon following an unconsented assignment by us or our election not to pursue development of a Superior Therapy). |
Our obligation to pay 50% of net profits or revenue as described further in our Annual Report on Form 10-K under the heading “Business—License Agreements, Intellectual Property and Other Agreements—Exclusive Channel Partner Agreement with Intrexon Corporation” with respect to these “retained” products will survive termination of the Channel Agreement.
There can be no assurance that we will be able to successfully perform under the Channel Agreement and if the Channel Agreement is terminated it may prevent us from achieving our business objectives.
We will incur additional expenses in connection with our License Agreement with The University of Texas M.D. Anderson Cancer Center
Pursuant to the MD Anderson License with MD Anderson, we, together with Intrexon, obtained an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel CAR-T cell, T-NK and TCR cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies. Pursuant to the MD Anderson License, MD Anderson agreed to transfer to us certain existing research programs described in the MD Anderson License and we, together with Intrexon, agreed to enter into a research and development agreement pursuant to which we will provide funding for certain research and development activities of MD Anderson for a period of three years from the date of the MD Anderson License, in an amount between $15 and $20 million per year. In addition, we also expect to enter into additional collaboration and technology transfer agreements with MD Anderson and Intrexon to accelerate technology and clinical development of these product candidates. We expect to increase the level of our overall research and development expenses significantly going forward as a result of each of these items.
In addition, in light of our entry into the MD Anderson License with MD Anderson, we expect to build a base of operations in Houston, Texas to join and collaborate with the MD Anderson academic and medical community, which may require that we add headcount in the future, and which could add to our general and administrative expenses going forward.
Although our forecasts for expenses and the sufficiency of our capital resources takes into account our plans to develop the technology licensed from MD Anderson and our obligations under the MD Anderson License, the MD Anderson License was entered into on January 13, 2015 and is only beginning to be implemented, therefore the actual costs associated therewith may be significantly in excess of forecasted amounts. In addition to the amount and timing of expenses related to our relationship with MD Anderson, our actual cash requirements may vary materially from our current expectations for a number of other factors that may include, but are not limited to, the final terms and conditions of the research and development agreement contemplated by the MD Anderson License, costs associated with opening a new operational facility in Houston, Texas, changes in the focus and direction of our development programs, competitive and technical advances, costs associated with the development of our product candidates and costs of filing, prosecuting, defending and enforcing our intellectual property rights. If we exhaust our capital reserves more quickly than anticipated, regardless of the reason, and we are unable to obtain additional financing on terms acceptable to us or at all, we will be unable to proceed with development of some or all of our product candidates on expected timelines and will be forced to prioritize among them.
47
Table of Contents
We may not be able to retain the rights licensed to us and Intrexon by The University of Texas M.D. Anderson Cancer Center to technologies relating to novel chimeric antigen receptor (CAR) T-cell therapies and other related technologies.
Under the MD Anderson License, we, together with Intrexon, received an exclusive, worldwide license to certain technologies owned and licensed by MD Anderson including technologies relating to novel CAR-T cell, T-NK and TCR cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson, as well as either co-exclusive or non-exclusive licenses under certain related technologies. When combined with Intrexon’s technology suite and ZIOPHARM’s clinically tested RheoSwitch Therapeutic System® interleukin-12 modules, the resulting proprietary methods and technologies may help realize the promise of genetically modified CAR-T cell and other immune cells by tightly controlling cell expansion and activation in the body, minimizing off-target and unwanted on-target effects and toxicity while maximizing therapeutic efficacy. The term of the MD Anderson License expires on the last to occur of (a) the expiration of all patents licensed thereunder, or (b) the twentieth anniversary of the date of the MD Anderson License; provided, however, that following the expiration of the term, the Company and Intrexon shall then have a fully-paid up, royalty free, perpetual, irrevocable and sublicensable license to use the licensed intellectual property thereunder.
After 10 years from the date of the MD Anderson License and subject to a 90 day cure period, MD Anderson will have the right to convert the MD Anderson License into a non-exclusive license if we and Intrexon are not using commercially reasonable efforts to commercialize the licensed intellectual property on a case-by-case basis. After five years from the date of the MD Anderson License and subject to a 180-day cure period, MD Anderson will have the right to terminate the MD Anderson License with respect to specific technology(ies) funded by the government or subject to a third party contract if we and Intrexon are not meeting the diligence requirements in such funding agreement or contract, as applicable. Subject to a 30-day cure period, MD Anderson has the right to terminate the MD Anderson License if we and Intrexon fail to timely deliver the shares due in consideration for the MD Anderson License. MD Anderson may also terminate the agreement with written notice upon material breach by us or Intrexon, if such breach has not been cured within 60 days of receiving such notice. In addition, the MD Anderson License will terminate upon the occurrence of certain insolvency events for both us or Intrexon and may be terminated by the mutual written agreement of us, Intrexon and MD Anderson.
There can be no assurance that we will be able to successfully perform under the MD Anderson License and if the MD Anderson License is terminated it may prevent us from achieving our business objectives.
We have a limited operating history upon which to base an investment decision.
We have not demonstrated an ability to perform the functions necessary for the successful commercialization of any product candidates. The successful commercialization of any product candidates will require us to perform a variety of functions, including:
| • | Continuing to undertake preclinical development and clinical trials; |
| • | Participating in regulatory approval process; |
| • | Formulating and manufacturing products; and |
| • | Conducting sales and marketing activities. |
Our operations have been limited to organizing and staffing our company, acquiring, developing and securing our proprietary product candidates, and undertaking preclinical and clinical trials of our product candidates. These operations provide a limited basis for you to assess our ability to commercialize our product candidates and the advisability of investing in our securities.
48
Table of Contents
Because we currently neither have nor intend to establish internal research capabilities, we are dependent upon pharmaceutical and biotechnology companies and academic and other researchers to sell or license us their product candidates and technology.
Proposing, negotiating, and implementing an economically viable product acquisition or license is a lengthy and complex process. We compete for partnering arrangements and license agreements with pharmaceutical, biopharmaceutical, and biotechnology companies, many of which have significantly more experience than we do, and have significantly more financial resources. Our competitors may have stronger relationships with certain third parties including academic research institutions, with whom we are interested in collaborating and may have, therefore, a competitive advantage in entering into partnering arrangements with those third parties. We may not be able to acquire rights to additional product candidates on terms that we find acceptable, or at all.
We expect that any product candidate to which we acquire rights will require significant additional development and other efforts prior to commercial sale, including extensive clinical testing and approval by the FDA and applicable foreign regulatory authorities. All drug product candidates are subject to the risks of failure inherent in pharmaceutical product development, including the possibility that the product candidate will not be shown to be sufficiently safe or effective for approval by regulatory authorities. Even if our product candidates are approved, they may not be economically manufactured or produced, or be successfully commercialized.
We actively evaluate additional product candidates to acquire for development. Such additional product candidates, if any, could significantly increase our capital requirements and place further strain on the time of our existing personnel, which may delay or otherwise adversely affect the development of our existing product candidates. We must manage our development efforts and clinical trials effectively, and hire, train and integrate additional management, administrative, and sales and marketing personnel. We may not be able to accomplish these tasks, and our failure to accomplish any of them could prevent us from successfully growing.
We may not be able to successfully manage our growth.
In the future, if we are able to advance our product candidates to the point of, and thereafter through, clinical trials, we will need to expand our development, regulatory, manufacturing, marketing and sales capabilities or contract with third parties to provide for these capabilities. Any future growth will place a significant strain on our management and on our administrative, operational, and financial resources. Therefore, our future financial performance and our ability to commercialize our product candidates and to compete effectively will depend, in part, on our ability to manage any future growth effectively. To manage this growth, we must expand our facilities, augment our operational, financial and management systems, and hire and train additional qualified personnel. If we are unable to manage our growth effectively, our business may be harmed.
Our business will subject us to the risk of liability claims associated with the use of hazardous materials and chemicals.
Our contract research and development activities may involve the controlled use of hazardous materials and chemicals. Although we believe that our safety procedures for using, storing, handling and disposing of these materials comply with federal, state and local laws and regulations, we cannot completely eliminate the risk of accidental injury or contamination from these materials. In the event of such an accident, we could be held liable for any resulting damages and any liability could have a materially adverse effect on our business, financial condition, and results of operations. In addition, the federal, state and local laws and regulations governing the use, manufacture, storage, handling and disposal of hazardous or radioactive materials and waste products may require our contractors to incur substantial compliance costs that could materially adversely affect our business, financial condition, and results of operations.
We rely on key executive officers and scientific and medical advisors, and their knowledge of our business and technical expertise would be difficult to replace.
We are highly dependent on Dr. Laurence J.N. Cooper, our Chief Executive Officer, Caesar J. Belbel, our Executive Vice President and Chief Legal Officer and our principal scientific, regulatory, and medical advisors. Dr. Cooper’s and Mr. Belbel’s employment are governed by a written employment agreement. Dr. Cooper and Mr. Belbel may terminate their employment with us at any time, subject, however, to certain non-compete and non-solicitation covenants. The loss of the technical knowledge and management and industry expertise of Dr. Cooper and Mr. Belbel, or any of our other key personnel, could result in delays in product development, loss of customers and sales, and diversion of management resources, which could adversely affect our operating results. We do not carry “key person” life insurance policies on any of our officers or key employees.
49
Table of Contents
If we are unable to hire additional qualified personnel, our ability to grow our business may be harmed.
We will need to hire additional qualified personnel with expertise in preclinical and clinical research and testing, government regulation, formulation and manufacturing, and eventually, sales and marketing. We compete for qualified individuals with numerous biopharmaceutical companies, universities, and other research institutions. Competition for such individuals is intense and we cannot be certain that our search for such personnel will be successful. Attracting and retaining qualified personnel will be critical to our success. If we are unable to hire additional qualified personnel, our ability to grow our business may be harmed.
We may incur substantial liabilities and may be required to limit commercialization of our products in response to product liability lawsuits.
The testing and marketing of medical products entail an inherent risk of product liability. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our products, if approved. Even a successful defense would require significant financial and management resources. Regardless of the merit or eventual outcome, liability claims may result in:
| • | Decreased demand for our product candidates; |
| • | Injury to our reputation; |
| • | Withdrawal of clinical trial participants; |
| • | Withdrawal of prior governmental approvals; |
| • | Costs of related litigation; |
| • | Substantial monetary awards to patients; |
| • | Product recalls; |
| • | Loss of revenue; and |
| • | The inability to commercialize our product candidates. |
We currently carry clinical trial insurance and product liability insurance. However, an inability to renew our policies or to obtain sufficient insurance at an acceptable cost could prevent or inhibit the commercialization of pharmaceutical products that we develop, alone or with collaborators.
Our business and operations would suffer in the event of system failures.
Despite the implementation of security measures, our internal computer systems and those of our current and future contractors and consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. While we are not aware of any such material system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our development programs and our business operations. For example, the loss of clinical trial data from completed or future clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. Likewise, we rely on third parties to manufacture our drug candidates and conduct clinical trials, and similar events relating to their computer systems could also have a material adverse effect on our business. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development and commercialization of our drug candidates could be delayed.
50
Table of Contents
RISKS RELATED TO THE CLINICAL TESTING, REGULATORY APPROVAL AND MANUFACTURING OF OUR PRODUCT CANDIDATES
If we are unable to obtain the necessary U.S. or worldwide regulatory approvals to commercialize any product candidate, our business will suffer.
We may not be able to obtain the approvals necessary to commercialize our product candidates, or any product candidate that we may acquire or develop in the future for commercial sale. We will need FDA approval to commercialize our product candidates in the United States and approvals from regulatory authorities in foreign jurisdictions equivalent to the FDA to commercialize our product candidates in those jurisdictions. In order to obtain FDA approval of any product candidate, we must submit to the FDA a New Drug Application, or NDA, or Biologics License Application, or BLA, demonstrating that the product candidate is safe for humans and effective for its intended use. This demonstration requires significant research and animal tests, which are referred to as preclinical studies, as well as human tests, which are referred to as clinical trials. Satisfaction of the FDA’s regulatory requirements typically takes many years, depending upon the type, complexity, and novelty of the product candidate, and will require substantial resources for research, development, and testing. We cannot predict whether our research, development, and clinical approaches will result in drugs that the FDA will consider safe for humans and effective for their intended uses. The FDA has substantial discretion in the drug approval process and may require us to conduct additional preclinical and clinical testing or to perform post-marketing studies. The approval process may also be delayed by changes in government regulation, future legislation, or administrative action or changes in FDA policy that occur prior to or during our regulatory review. Delays in obtaining regulatory approvals may:
| • | Delay commercialization of, and our ability to derive product revenues from, our product candidates; |
| • | Impose costly procedures on us; and |
| • | Diminish any competitive advantages that we may otherwise enjoy. |
Even if we comply with all FDA requests, the FDA may ultimately reject one or more of our NDAs or BLAs. We cannot be sure that we will ever obtain regulatory approval for any of our product candidates. Failure to obtain FDA approval for our product candidates will severely undermine our business by leaving us without a saleable product, and therefore without any potential revenue source, until another product candidate can be developed. There is no guarantee that we will ever be able to develop or acquire another product candidate or that we will obtain FDA approval if we are able to do so.
In foreign jurisdictions, we similarly must receive approval from applicable regulatory authorities before we can commercialize any drugs. Foreign regulatory approval processes generally include all of the risks associated with the FDA approval procedures described above.
Our product candidates are in various stages of clinical trials, which are very expensive and time-consuming. We cannot be certain when we will be able to submit an NDA or BLA to the FDA and any failure or delay in completing clinical trials for our product candidates could harm our business.
Our product candidates are in various stages of development and require extensive clinical testing. Notwithstanding our current clinical trial plans for each of our existing product candidates, we may not be able to commence additional trials or see results from these trials within our anticipated timelines. As such, we cannot predict with any certainty if or when we might submit an NDA or BLA for regulatory approval of our product candidates or whether such an NDA or BLA will be accepted. Because we do not anticipate generating revenues unless and until we submit one or more NDAs or BLAs and thereafter obtain requisite FDA approvals, the timing of our NDA or BLA submissions and FDA determinations regarding approval thereof, will directly affect if and when we are able to generate revenues.
Our product candidates may cause undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial profile of an approved label, or result in significant negative consequences following any potential marketing approval.
As with many pharmaceutical and biological products, treatment with our product candidates may produce undesirable side effects or adverse reactions or events. If our product candidates or similar products or product candidates under development by third parties demonstrate unacceptable adverse events, we may be required to halt or delay further clinical development of our product candidates. The FDA, the EMA or other foreign regulatory authorities could order us to cease further development of or deny approval of our product candidates for any or all targeted indications. The product-related side effects could affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition and prospects significantly.
51
Table of Contents
The results of our clinical trials may not support our product candidate claims.
Even if our clinical trials are completed as planned, we cannot be certain that their results will support approval of our product candidates. The FDA normally expects two randomized, well-controlled Phase 3 pivotal studies in support of approval of an NDA or BLA. Success in preclinical testing and early clinical trials does not ensure that later clinical trials will be successful, and we cannot be certain that the results of later clinical trials will replicate the results of prior clinical trials and preclinical testing. For example, despite positive findings in earlier clinical trials, our product candidate palifosfamide failed to meet the primary endpoints of the Phase 3 PICASSO 3 trial, causing us to suspend clinical development of palifosfamide in soft tissue sarcoma. The clinical trial process may fail to demonstrate that our product candidates are safe for humans and effective for the indicated uses. This failure would cause us to abandon a product candidate and may delay development of other product candidates. Any delay in, or termination of, our clinical trials will delay the submission of our NDAs or BLAs with the FDA and, ultimately, our ability to commercialize our product candidates and generate product revenues. In addition, our clinical trials involve small patient populations. Because of the small sample size, the results of these clinical trials may not be indicative of future results.
Our synthetic immuno-oncology product candidates are based on a novel technology, which makes it difficult to predict the time and cost of product candidate development and subsequently obtaining regulatory approval. Currently, no gene therapy products have been approved in the United States and only one product has been approved in Europe.
We have recently focused our product research and development efforts on our synthetic immuno-oncology product candidates under our Channel Agreement with Intrexon. These products, including Ad-RTS-IL-12+ veledimex, are based on gene therapy technology. Due to the novelty of this medical technology, there can be no assurance that any development problems we experience in the future related to our synthetic immuno-oncology platform will not cause significant delays or unanticipated costs, or that such development problems can be solved. We may also experience unanticipated problems or delays in expanding our manufacturing capacity or transferring our manufacturing process to commercial partners, which may prevent us from completing our clinical studies or commercializing our synthetic immuno-oncology product candidates on a timely or profitable basis, if at all.
In addition, the clinical study requirements of the FDA, the EMA and other regulatory agencies and the criteria these regulators use to determine the safety and efficacy of a product candidate vary substantially according to the type, complexity, novelty and intended use and market of the potential products. The regulatory approval process for novel product candidates such as ours can be more expensive and take longer than for other, better known or extensively studied pharmaceutical or other product candidates. Currently, only one gene therapy product, UniQure’s Glybera, which received marketing authorization from the EMA in 2012, has been approved in Europe but has not yet been launched for commercial sale, which makes it difficult to determine how long it will take or how much it will cost to obtain regulatory approvals for our product candidates in either the United States or Europe. Approvals by the EMA may not be indicative of what the FDA may require for approval.
Regulatory requirements governing gene and cell therapy products have changed frequently and may continue to change in the future. For example, the FDA has established the Office of Cellular, Tissue and Gene Therapies within its Center for Biologics Evaluation and Research, or CBER, to consolidate the review of gene therapy and related products, and the Cellular, Tissue and Gene Therapies Advisory Committee to advise CBER on its review. Gene therapy clinical studies conducted at institutions that receive funding for recombinant DNA research from the U.S. National Institutes of Health, or the NIH, are also subject to review by the NIH Office of Biotechnology Activities’ Recombinant DNA Advisory Committee, or the RAC. Although the FDA decides whether individual gene therapy protocols may proceed, the RAC review process can impede the initiation of a clinical trial, even if the FDA has reviewed the trial and approved its initiation. Conversely, the FDA can put an IND on clinical hold even if the RAC has provided a favorable review. For example, our planned Phase 1 clinical trial of Ad-RTS-IL-12 + veledimex, in subjects with recurrent or progressive high grade gliomas (brain cancer) received approval from the NIH RAC in December 2013, but the FDA requested additional nonclinical information prior to permitting clinical study initiation, which we are currently generating. Also, before a clinical trial can begin at an NIH-funded institution, that institution’s institutional review board, or IRB, and its Institutional Biosafety Committee will have to review the proposed clinical trial to assess the safety of the trial. In addition, adverse developments in clinical trials of gene therapy products conducted by others may cause the FDA or other regulatory bodies to change the requirements for approval of any of our product candidates.
These regulatory review committees and advisory groups and the new guidelines they promulgate may lengthen the regulatory review process, require us to perform additional studies, increase our development costs, lead to changes in regulatory positions and interpretations, delay or prevent approval and commercialization of these treatment candidates or lead to significant post-approval limitations or restrictions. As we advance our synthetic immuno-oncology product candidates, we will be required to consult with these regulatory and advisory groups, and comply with applicable guidelines. If we fail to do so, we may be required to delay or discontinue development of our product candidates. These additional processes may result in a review and approval process that is longer than we otherwise would have expected for oncology product candidates. Delay or failure to obtain, or unexpected costs in obtaining, the regulatory approval necessary to bring a potential product to market could decrease our ability to generate sufficient product revenue to maintain our business.
52
Table of Contents
Because we are dependent upon clinical research institutions and other contractors for clinical testing and for research and development activities, the results of our clinical trials and such research activities are, to a certain extent, beyond our control.
We materially rely upon independent investigators and collaborators, such as universities and medical institutions, to conduct our preclinical and clinical trials under agreements with us. These collaborators are not our employees and we cannot control the amount or timing of resources that they devote to our programs. These investigators may not assign as great a priority to our programs or pursue them as diligently as we would if we were undertaking such programs ourselves. If outside collaborators fail to devote sufficient time and resources to our drug development programs, or if their performance is substandard, the approval of our FDA applications, if any, and our introduction of new products, if any, will be delayed. These collaborators may also have relationships with other commercial entities, some of whom may compete with us. If our collaborators assist our competitors to our detriment, our competitive position would be harmed.
Our reliance on third parties to formulate and manufacture our product candidates exposes us to a number of risks that may delay the development, regulatory approval and commercialization of our products or result in higher product costs.
We do not have experience in drug formulation or manufacturing of drugs or biologics and do not intend to establish our own manufacturing facilities. Although we will work closely with and rely upon Intrexon on the manufacturing and scale-up of Intrexon product candidates, we lack the resources and expertise to formulate or manufacture our own product candidates. We currently are contracting for the manufacture of our product candidates. We intend to contract with one or more manufacturers to manufacture, supply, store, and distribute drug supplies for our clinical trials. If a product candidate we develop or acquire in the future receives FDA approval, we will rely on one or more third-party contractors or Intrexon to manufacture our products. Our anticipated future reliance on a limited number of third-party manufacturers exposes us to the following risks:
| • | We may be unable to identify manufacturers on acceptable terms or at all because the number of potential manufacturers is limited and the FDA must approve any replacement contractor. This approval would require new testing and compliance inspections. In addition, a new manufacturer would have to be educated in, or develop substantially equivalent processes for, production of our products after receipt of FDA approval, if any. |
| • | Our third-party manufacturers might be unable to formulate and manufacture our products in the volume and of the quality required to meet our clinical needs and commercial needs, if any. |
| • | Our future contract manufacturers may not perform as agreed or may not remain in the contract manufacturing business for the time required to supply our clinical trials or to successfully produce, store, and distribute our products. |
| • | Drug manufacturers are subject to ongoing periodic unannounced inspection by the FDA, the Drug Enforcement Administration and corresponding state agencies to ensure strict compliance with good manufacturing practices, or cGMP, and other government regulations and corresponding foreign standards. We do not have control over third-party manufacturers’ compliance with these regulations and standards. |
| • | If any third-party manufacturer makes improvements in the manufacturing process for our products, we may not own, or may have to share, the intellectual property rights to the innovation. |
| • | Our third-party manufacturers may not be able to comply with cGMP regulations or similar regulatory requirements outside the United States. Our failure, or the failure of our third-party manufacturers, to comply with applicable regulations could result in sanctions being imposed on us, including clinical holds, fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of drug candidates or products, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect supplies of our products. |
Each of these risks could delay our clinical trials, the approval, if any, of our product candidates by the FDA or the commercialization of our product candidates or result in higher costs or deprive us of potential product revenues.
Any drug candidate for which we obtain marketing approval could be subject to post-marketing restrictions or withdrawal from the market and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with our products, when and if any of them are approved.
Any drug candidate for which we obtain marketing approval, along with the manufacturing processes, post-approval clinical data, labeling, advertising and promotional activities for such product, will be subject to continual requirements of and review by the FDA and other regulatory authorities. These requirements include submissions of safety and other post-marketing information and reports, registration and listing requirements, cGMP requirements relating to manufacturing, quality control, quality assurance and corresponding maintenance of records and documents, requirements regarding the distribution of samples to physicians and recordkeeping. Even if marketing approval of a drug candidate is granted, the approval may be subject to limitations on the indicated uses for which the product may be marketed or to the conditions of approval, including the requirement to implement a risk evaluation and mitigation strategy, or REMS, which could include requirements for a restricted distribution system. If any of our drug candidates receives marketing approval, the accompanying label may limit the approved use of our drug, which could limit sales of the product.
53
Table of Contents
The FDA may also impose requirements for costly post-marketing studies or clinical trials and surveillance to monitor the safety or efficacy of our approved products. The FDA closely regulates the post-approval marketing and promotion of drugs to ensure drugs are marketed only for the approved indications and in accordance with the provisions of the approved labeling. The FDA imposes stringent restrictions on manufacturers’ communications regarding off-label use and if we market our products outside of their approved indications, we may be subject to enforcement action for off-label marketing. Violations of the FDCA relating to the promotion of prescription drugs may lead to investigations alleging violations of federal and state health care fraud and abuse laws, as well as state consumer protection laws.
In addition, later discovery of previously unknown adverse events or other problems with our products, manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may yield various results, including:
| • | Litigation involving patients taking our drug; |
| • | Restrictions on such products, manufacturers or manufacturing processes; |
| • | Restrictions on the labeling or marketing of a product; |
| • | Restrictions on product distribution or use; |
| • | Requirements to conduct post-marketing studies or clinical trials; |
| • | Warning letters; |
| • | Withdrawal of the products from the market; |
| • | Refusal to approve pending applications or supplements to approved applications that we submit; |
| • | Recall of products; |
| • | Fines, restitution or disgorgement of profits or revenues; |
| • | Suspension or withdrawal of marketing approvals; |
| • | Damage to relationships with existing and potential collaborators; |
| • | Unfavorable press coverage and damage to our reputation; |
| • | Refusal to permit the import or export of our products; |
| • | Product seizure; or |
| • | Injunctions or the imposition of civil or criminal penalties. |
Noncompliance with similar European Union requirements regarding safety monitoring or pharmacovigilance can also result in significant financial penalties. Similarly, failure to comply with U.S. and foreign regulatory requirements regarding the development of products for pediatric populations and the protection of personal health information can also lead to significant penalties and sanctions.
RISKS RELATED TO OUR ABILITY TO COMMERCIALIZE OUR PRODUCT CANDIDATES
If we are unable either to create sales, marketing and distribution capabilities or enter into agreements with third parties to perform these functions, we will be unable to commercialize our product candidates successfully.
We currently have no marketing, sales, or distribution capabilities. If and when we become reasonably certain that we will be able to commercialize our current or future product candidates, we anticipate allocating resources to the marketing, sales and distribution of our proposed products in North America and in certain other countries; however, we cannot assure that we will be able to market, sell, and distribute our products successfully. Our future success also may depend, in part, on our ability to enter into and maintain collaborative relationships for such capabilities and to encourage the collaborator’s strategic interest in the products under development, and such collaborator’s ability to successfully market and sell any such products. Although we intend to pursue certain collaborative arrangements regarding the sale and marketing of certain of our product candidates, there are no assurances that we will be able to establish or maintain collaborative arrangements or, if we are able to do so, whether we would be able to conduct our own sales efforts. There can also be no assurance that we will be able to establish or maintain relationships with third-party collaborators or develop in-house sales and distribution capabilities. To the extent that we depend on third parties for marketing and distribution, any revenues we receive will depend upon the efforts of such third parties, and there can be no assurance that such efforts will be successful. In addition, there can also be no assurance that we will be able to market and sell our product candidates in the United States or overseas.
If we are not able to partner with a third party and are not successful in recruiting sales and marketing personnel or in building a sales and marketing infrastructure, we will have difficulty commercializing our product candidates, which would harm our business. If we rely on pharmaceutical or biotechnology companies with established distribution systems to market our products, we will need to establish and maintain partnership arrangements, and we may not be able to enter into these arrangements on acceptable terms or at all. To the extent that we enter into co-promotion or other arrangements, any revenues we receive will depend upon the efforts of third parties that may not be successful and that will be only partially in our control.
54
Table of Contents
If we cannot compete successfully for market share against other drug companies, we may not achieve sufficient product revenues and our business will suffer.
The market for our product candidates is characterized by intense competition and rapid technological advances. If a product candidate receives FDA approval, it will compete with a number of existing and future drugs and therapies developed, manufactured and marketed by others. Existing or future competing products may provide greater therapeutic convenience or clinical or other benefits for a specific indication than our products, or may offer comparable performance at a lower cost. If our products fail to capture and maintain market share, we may not achieve sufficient product revenues and our business will suffer.
We will compete against fully integrated pharmaceutical companies and smaller companies that are collaborating with larger pharmaceutical companies, academic institutions, government agencies and other public and private research organizations. Many of these competitors have products already approved or in development. In addition, many of these competitors, either alone or together with their collaborative partners, operate larger research and development programs or have substantially greater financial resources than we do, as well as significantly greater experience in:
| • | Developing drugs and biopharmaceuticals; |
| • | Undertaking preclinical testing and human clinical trials; |
| • | Obtaining FDA and other regulatory approvals of drugs and biopharmaceuticals; |
| • | Formulating and manufacturing drugs and biopharmaceuticals; and |
| • | Launching, marketing, and selling drugs and biopharmaceuticals. |
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may develop. Our competitors also may obtain FDA or other regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market. In addition, our ability to compete may be affected in many cases by insurers or other third-party payors seeking to encourage the use of generic products.
If physicians and patients do not accept and use our product candidates, our ability to generate revenue from sales of our products will be materially impaired.
Even if the FDA approves our product candidates, physicians and patients may not accept and use them. Acceptance and use of our products will depend upon a number of factors including:
| • | Perceptions by members of the healthcare community, including physicians, about the safety and effectiveness of our drugs; |
| • | Pharmacological benefit and cost-effectiveness of our products relative to competing products; |
| • | Availability of coverage and adequate reimbursement for our products from government or other healthcare payors; |
| • | Effectiveness of marketing and distribution efforts by us and our licensees and distributors, if any; and |
| • | The price at which we sell our products. |
Because we expect sales of our current product candidates, if approved, to generate substantially all of our product revenues for the foreseeable future, the failure of a drug to find market acceptance would harm our business and could require us to seek additional financing in order to fund the development of future product candidates.
Our ability to generate product revenues will be diminished if our drugs do not obtain coverage adequate reimbursement from payors.
Our ability to commercialize our drugs, alone or with collaborators, will depend in part on the extent to which coverage and reimbursement will be available from government and health administration authorities, private health maintenance organizations and health insurers and other third-party payors.
Patients who are prescribed medicine for the treatment of their conditions generally rely on third-party payors to reimburse all or part of the costs associated with their prescription drugs. Adequate coverage and reimbursement from governmental healthcare programs, such as Medicare and Medicaid, and commercial payors is critical to new product acceptance. Coverage decisions may depend upon clinical and economic standards that disfavor new drug products when more established or lower cost therapeutic alternatives are already available or subsequently become available. Even if we obtain coverage for our product candidates, the resulting reimbursement payment rates might not be adequate or may require co-payments that patients find unacceptably high. Patients are unlikely to use our product candidates unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost of our product candidates.
55
Table of Contents
In addition, the market for our product candidates for which we may receive regulatory approval will depend significantly on access to third-party payors’ drug formularies, or lists of medications for which third-party payors provide coverage and reimbursement. The industry competition to be included in such formularies often leads to downward pricing pressures on pharmaceutical companies. Also, third-party payors may refuse to include a particular branded drug in their formularies or otherwise restrict patient access to a branded drug when a less costly generic equivalent or other alternative is available.
Third-party payors, whether foreign or domestic, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In addition, in the United States, no uniform policy of coverage and reimbursement for drug products exists among third-party payors. Therefore, coverage and reimbursement for drug products can differ significantly from payor to payor. As a result, the coverage determination process is often a time-consuming and costly process that requires us to provide scientific and clinical support for the use of our products to each payor separately, with no assurance that approval will be obtained. If we are unable to obtain coverage of and adequate payment levels for our product candidates from third-party payors, physicians may limit how much or under what circumstances they will prescribe or administer them and patients may decline to purchase them. This in turn could affect our ability to successfully commercialize our products and impact our profitability, results of operations, financial condition, and future success.
In addition, in many foreign countries, particularly the countries of the European Union, the pricing of prescription drugs is subject to government control. In some non-U.S. jurisdictions, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the EU provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. We may face competition for our product candidates from lower-priced products in foreign countries that have placed price controls on pharmaceutical products. In addition, there may be importation of foreign products that compete with our own products, which could negatively impact our profitability.
Healthcare legislative reform measures may have a material adverse effect on our business and results of operations.
In both the United States and certain foreign jurisdictions, there have been a number of legislative and regulatory proposals in recent years that change the healthcare system in ways that could impact our future ability to sell our product candidates profitably. For example, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 established a new Part D prescription drug benefit, which became effective January 1, 2006. Under the prescription drug benefit, Medicare beneficiaries can obtain prescription drug coverage from private sector plans that are permitted to limit the number of prescription drugs that are covered in each therapeutic category and class on their formularies. If any of our product candidates that are approved by the FDA are not widely included on the formularies of these plans, our ability to market our products to the Medicare population could suffer.
Furthermore, there have been and continue to be a number of initiatives at the federal and state level that seek to reduce healthcare costs. Most recently, in March 2010, President Obama signed into law the Patient Protection and Affordable Health Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively the PPACA, which includes measures that significantly change the way healthcare is financed by both governmental and private insurers. Among the provisions of the PPACA of importance to the pharmaceutical industry are the following:
| • | An annual, nondeductible fee on any entity that manufactures or imports certain branded prescription drugs and biologic agents, apportioned among these entities according to their market share in certain government healthcare programs, beginning in 2011; |
| • | An increase in the statutory minimum rebates a manufacturer must pay under the Medicaid Drug Rebate Program, retroactive to January 1, 2010, to 23% and 13% of the average manufacturer price for most branded and generic drugs, respectively; |
| • | A new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D, beginning in 2011; |
| • | Extension of manufacturers’ Medicaid rebate liability to covered drugs dispensed to individuals who are enrolled in Medicaid managed care organizations, effective March 23, 2010; |
Expansion of eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to additional individuals beginning in April 2010 and by adding new mandatory eligibility categories for certain individuals with income at or below 133% of the Federal Poverty Level beginning in 2014, thereby potentially increasing both the volume of sales and manufacturers’ Medicaid rebate liability; a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D, beginning in 2011;
56
Table of Contents
| • | Expansion of the entities eligible for discounts under the Public Health Service pharmaceutical pricing program, effective in January 2010; |
| • | A new requirement to annually report drug samples that manufacturers and distributors provide to physicians, effective April 1, 2012; |
| • | Expansion of healthcare fraud and abuse laws, including the False Claims Act and the Anti-Kickback Statute, new government investigative powers, and enhanced penalties for noncompliance; |
| • | A licensure framework for follow-on biologic products; |
| • | A new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; |
| • | Creation of the Independent Payment Advisory Board which, beginning in 2014, will have authority to recommend certain changes to the Medicare program that could result in reduced payments for prescription drugs and those recommendations could have the effect of law even if Congress does not act on the recommendations; and |
| • | Establishment of a Center for Medicare Innovation at CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug spending beginning by January 1, 2011. |
In addition, other legislative changes have been proposed and adopted since the PPACA was enacted. In August 2011, President Obama signed into law the Budget Control Act of 2011, which, among other things, created the Joint Select Committee on Deficit Reduction to recommend proposals in spending reductions to Congress. The Joint Select Committee on Deficit Reduction did not achieve its targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, triggering the legislation’s automatic reductions to several government programs. These reductions include aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, which went into effect on April 1, 2013. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, which, among other things, further reduced Medicare payments to several providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. The full impact of these new laws, as well as laws and other reform and cost containment measures that may be proposed and adopted in the future, remains uncertain, but may result in additional reductions in Medicare and other healthcare funding, which could have a material adverse effect on our future customers and accordingly, our ability to generate revenue, attain profitability, or commercialize our products.
If we fail to comply with federal and state healthcare laws, including fraud and abuse and health information privacy and security laws, we could face substantial penalties and our business, results of operations, financial condition and prospects could be adversely affected.
As a pharmaceutical company, even though we do not and will not control referrals of healthcare services or bill directly to Medicare, Medicaid or other third-party payors, certain federal and state healthcare laws and regulations pertaining to fraud and abuse and patients’ rights are and will be applicable to our business. We could be subject to healthcare fraud and abuse and patient privacy regulation by both the federal government and the states in which we conduct our business. The laws that may affect our ability to operate include:
| • | The federal Anti-Kickback Statute, which constrains our marketing practices, educational programs, pricing policies, and relationships with healthcare providers or other entities, by prohibiting, among other things, soliciting, receiving, offering or paying remuneration, directly or indirectly, to induce, or in return for, either the referral of an individual or the purchase or recommendation of an item or service reimbursable under a federal healthcare program, such as the Medicare and Medicaid programs; |
| • | Federal civil and criminal false claims laws and civil monetary penalty laws, which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent; |
| • | The federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, which created new federal criminal statutes that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; |
| • | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, and its implementing regulations, which imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information; and |
57
Table of Contents
| • | New requirements to report certain financial arrangements with physicians and teaching hospitals, as defined in the PPACA and its implementing regulations, including reporting any “transfer of value” made or distributed to teaching hospitals, prescribers, and other healthcare providers and reporting any ownership and investment interests held by physicians and their immediate family members and applicable group purchasing organizations during the preceding calendar year, with data collection required as of August 1, 2013 and reporting to the Centers for Medicare & Medicaid Services, or CMS, to be required by March 31, 2014 and by the 90th day of each subsequent calendar year; |
| • | State and foreign law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers, and state and foreign laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts. |
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available, it is possible that some of our business activities could be subject to challenge under one or more of such laws. In addition, recent health care reform legislation has further strengthened these laws. For example, the PPACA, among other things, amends the intent requirement of the federal anti-kickback and criminal healthcare fraud statutes. A person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. Moreover, the PPACA provides that the government may assert that a claim including items or services resulting from a violation of the federal anti-kickback statute constitutes a false or fraudulent claim for purposes of the False Claims Act.
To the extent that any of our product candidates is ultimately sold in a foreign country, we may be subject to similar foreign laws and regulations.
If we or our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from participation in United States federal or state health care programs, and the curtailment or restructuring of our operations. Any penalties, damages, fines, curtailment or restructuring of our operations could materially adversely affect our ability to operate our business and our financial results. Although compliance programs can mitigate the risk of investigation and prosecution for violations of these laws, the risks cannot be entirely eliminated. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. Moreover, achieving and sustaining compliance with applicable federal and state privacy, security and fraud laws may prove costly.
Our ability to use net operating loss carryforwards to reduce future tax payments may be limited or restricted.
We have generated significant net operating loss carryforwards, or NOLs, and research and development tax credits, or R&D credits, as a result of our incurrence of losses and our conduct of research activities since inception. We generally are able to carry NOLs and R&D credits forward to reduce our tax liability in future years. However, our ability to utilize the NOLs and R&D credits is subject to the rules of Sections 382 and 383 of the Internal Revenue Code, respectively. Those sections generally restrict the use of NOLs and R&D credits after an “ownership change.” An ownership change occurs if, among other things, the stockholders (or specified groups of stockholders) who own or have owned, directly or indirectly, 5% or more of a corporation’s common stock or are otherwise treated as 5% stockholders under Section 382 and the United States Treasury Department regulations promulgated thereunder increase their aggregate percentage ownership of that corporation’s stock by more than 50 percentage points over the lowest percentage of the stock owned by these stockholders over the applicable testing period. In the event of an ownership change, Section 382 imposes an annual limitation on the amount of taxable income a corporation may offset with NOL carry forwards and Section 383 imposes an annual limitation on the amount of tax a corporation may offset with business credit (including the R&D credit) carry forwards. Any unused annual limitation may be carried over to later years until the applicable expiration date for the respective NOL or R&D credit carry forwards. We may have experienced an “ownership change” within the meaning of Section 382 in the past and there can be no assurance that we have not experienced additional ownership changes, or that we will not experience an ownership change as a result of this offering. As a result, our NOLs and R&D credits may be subject to limitations and we may be required to pay taxes earlier and in larger amounts than would be the case if our NOLs or R&D credits were freely usable.
58
Table of Contents
Our synthetic immuno-oncology product candidates may face competition in the future from follow-on biologics.
With the enactment of the Biologics Price Competition and Innovation Act of 2009, or BPCIA, as part of the Patient Protection and Affordable Care Act, an abbreviated pathway for the approval of follow-on biological products was created. The new abbreviated regulatory pathway establishes legal authority for the FDA to review and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” with an existing brand product. Under the BPCIA, an application for a biosimilar product cannot be approved by the FDA until 12 years after the original branded product was approved under a BLA. This data exclusivity does not prevent another company from developing a product that is highly similar to the original branded product, generating its own data and seeking approval. Data exclusivity only assures that another company cannot rely upon the data within the innovator’s application to support the biosimilar product’s approval.
In his proposed budget for fiscal year 2014, President Obama proposed to cut this 12-year period of exclusivity down to seven years. He also proposed to prohibit additional periods of exclusivity due to minor changes in product formulations, a practice often referred to as “evergreening.” It is possible that Congress may take these or other measures to reduce or eliminate periods of exclusivity.
The new law is complex and is only beginning to be interpreted and implemented by the FDA. As a result, its ultimate impact is subject to uncertainty, and could have a material adverse effect on the future commercial prospects for our biological products. Since enactment of the BCPIA, the FDA has issued several draft guidance documents discussing the biosimilar pathway, but to date, no biosimilar or interchangeable product has been approved. Although it is unclear what final implementation of the BCPIA will entail, such FDA implementation could have a material adverse effect on the future commercial prospects for our product candidates.
RISKS RELATED TO OUR INTELLECTUAL PROPERTY
If we or our licensors fail to adequately protect or enforce our intellectual property rights or secure rights to patents of others, the value of our intellectual property rights would diminish and our ability to successfully commercialize our products may be impaired.
Our success, competitive position, and future revenues will depend in part on our ability and the abilities of our licensors to obtain and maintain patent protection for our products, methods, processes and other technologies, to preserve our trade secrets, to prevent third parties from infringing on our proprietary rights, and to operate without infringing the proprietary rights of third parties.
To date, we have exclusive rights to certain United States and foreign intellectual property with respect to our small molecule product candidates, with respect to the Intrexon technology, including the existing Intrexon product candidates, and with respect to CAR-T, NK and TCR cell therapies arising from the laboratory of Laurence Cooper, M.D., Ph.D., professor of pediatrics at MD Anderson. Under our Channel Agreement with Intrexon, Intrexon has the sole right to conduct and control the filings, prosecution and maintenance of the patents and patent applications licensed to us. Although under the agreement Intrexon has agreed to consider in good faith and consult with us regarding any comments we may have regarding these patents and patent applications, we cannot guarantee that our comments will be solicited or followed. Under the License Agreement with MD Anderson, future filings and applications require the agreement of each of MD Anderson, Intrexon and us, and MD Anderson has the right to control the preparation and filing of additional patent applications unless the parties agree that we or Intrexon may prosecute the application directly. Although under the agreement MD Anderson has agreed to review and incorporate any reasonable comments that we or Intrexon may have regarding these patents and patent applications, we cannot guarantee that our comments will be solicited or followed. Without direct control of the channel program patents and patent applications, we are dependent on Intrexon or MD Anderson, as applicable, to keep us advised of prosecution, particularly in foreign jurisdictions where prosecution information may not be publicly available. We anticipate that we, Intrexon and MD Anderson will file additional patent applications both in the United States and in other countries. However, we cannot predict or guarantee:
| • | The degree and range of protection any patents will afford us against competitors, including whether third parties will find ways to invalidate or otherwise circumvent our patents; |
| • | If and when patents will be issued; |
| • | Whether or not others will obtain patents claiming subject matter related to or relevant to our product candidates; or |
| • | Whether we will need to initiate litigation or administrative proceedings that may be costly whether we win or lose. |
The patent prosecution process is expensive and time-consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost, in a timely manner, or in all jurisdictions. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. Moreover, in some circumstances, we do not have the right to control the preparation, filing and prosecution of patent applications, or to maintain the patents, covering technology that we license from third parties. We may also require the cooperation of our licensors in order to enforce the licensed patent rights, and such cooperation may not be provided. Therefore, these patents and applications may not be prosecuted and enforced in a manner consistent with the best interests of our business.
59
Table of Contents
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions and has in recent years been the subject of much litigation. In addition, the laws of foreign countries may not protect our rights to the same extent as the laws of the United States and we may fail to seek or obtain patent protection in all major markets. For example, European patent law restricts the patentability of methods of treatment of the human body more than United States law does. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after filing, or in some cases not at all.
Changes in patent laws or in interpretations of patent laws in the United States and other countries may diminish the value of our intellectual property or narrow the scope of our patent protection. In September 2011, the Leahy-Smith America Invents Act, or the Leahy-Smith Act, was signed into law, resulting in a number of significant changes to United States patent law. These changes include provisions that affect the way patent applications will be prosecuted and may also affect patent litigation. In addition, the United States Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. This combination of events has created uncertainty with respect to the value of patents, once obtained, and with regard to our ability to obtain patents in the future. As the U.S. PTO continues to implement the Leahy-Smith Act, and as the federal courts have the opportunity to interpret the Leahy-Smith Act, the laws and regulations governing patents, and the rules regarding patent procurement could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future.
Certain technologies utilized in our research and development programs are already in the public domain. Moreover, a number of our competitors have developed technologies, filed patent applications or obtained patents on technologies, compositions and methods of use that are related to our business and may cover or conflict with our owned or licensed patent applications, technologies or product candidates. Such conflicts could limit the scope of the patents that we may be able to obtain or may result in the rejection of claims in our patent applications. Because patent applications in the United States and many foreign jurisdictions are typically not published until eighteen months after filing, or in some cases not at all, and because publications of discoveries in the scientific literature often lag behind actual discoveries, neither we nor our licensors can be certain that others have not filed or maintained patent applications for technology used by us or covered by our pending patent applications without our being aware of these applications. Therefore, we cannot know with certainty whether we were the first to make the inventions claimed in our owned patents or pending patent applications, or that we were the first to file for patent protection of such inventions, nor can we know whether those from whom we license patents were the first to make the inventions claimed or were the first to file. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain. Our pending and future patent applications may not result in patents being issued which protect our technology or products, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products. Changes in either the patent laws or interpretation of the patent laws in the United States and other countries may diminish the value of our patents or narrow the scope of our patent protection. In addition, our own earlier filed patents and applications or those of Intrexon may limit the scope of later patents we obtain or may result in the rejection of claims in our later filed patent applications. If third parties filed patent applications or obtained patents on technologies, compositions and methods of use that are related to our business and that cover or conflict with our owned or licensed patent applications, technologies or product candidates, we may be required to challenge such protection, terminate or modify our programs impacted by such protection or obtain licenses from such third parties, which might not be available on acceptable terms, or at all.
Even if our owned and licensed patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our owned or licensed patents by developing similar or alternative technologies or products in a non-infringing manner.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our owned and licensed patents may be challenged in the courts or patent offices in the United States and abroad. Such challenges may result in loss of exclusivity or freedom to operate or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. Given the amount of time required for the development, testing and regulatory review of new drug candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
60
Table of Contents
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
Our success also depends upon the skills, knowledge, and experience of our scientific and technical personnel, our consultants and advisors, as well as our licensors and contractors. To help protect our proprietary know-how and our inventions for which patents may be unobtainable or difficult to obtain, and to maintain our competitive position, we rely on trade secret protection and confidentiality agreements. To this end, it is our general policy to require our employees, consultants, advisors, and contractors to enter into agreements that prohibit the disclosure of confidential information and, where applicable, require disclosure and assignment to us of the ideas, developments, discoveries, and inventions important to our business. These agreements may not provide adequate protection for our trade secrets, know-how or other proprietary information in the event of any unauthorized use or disclosure or the lawful development by others of such information. Moreover, we may not be able to obtain adequate remedies for any breaches of these agreements. Our trade secrets may also be obtained by third parties by other means, such as breaches of our physical or computer security systems. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the United States are less willing or unwilling to protect trade secrets. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us. If any of our trade secrets, know-how or other proprietary information is disclosed, the value of our trade secrets, know-how and other proprietary rights would be significantly impaired and our business and competitive position would suffer.
Third-party claims of intellectual property infringement would require us to spend significant time and money and could prevent us from developing or commercializing our products.
In order to protect or enforce patent rights, we, or Intrexon, may initiate patent infringement litigation against third parties. Similarly, we may be sued by others for patent infringement. We also may become subject to proceedings conducted in the United States Patent and Trademark Office, including interference proceedings to determine the priority or derivation of inventions, or post-grant review, inter partes review, or reexamination proceedings reviewing the patentability of our patented claims. In addition, any foreign patents that are granted may become subject to opposition, nullity, or revocation proceedings in foreign jurisdictions having such proceedings. The defense and prosecution, if necessary, of intellectual property actions are costly and divert technical and management personnel away from their normal responsibilities.
Our commercial success depends upon our ability, and the ability of our collaborators, to develop, manufacture, market and sell our drug candidates without infringing the proprietary rights of third parties. There is considerable intellectual property litigation in the biotechnology and pharmaceutical industries. While no such litigation has been brought against us and we have not been held by any court to have infringed a third party’s intellectual property rights, we cannot guarantee that our products or use of our products do not infringe third-party patents. It is also possible that we have failed to identify relevant third-party patents or applications. For example, applications filed before November 29, 2000 and certain applications filed after that date that will not be filed outside the United States remain confidential until patents issue. Patent applications in the United States and elsewhere are published approximately 18 months after the earliest filing, which is referred to as the priority date. Therefore, patent applications covering our products or technology could have been filed by others without our knowledge. Additionally, pending patent applications which have been published can, subject to certain limitations, be later amended in a manner that could cover our products or the use of our products.
Our research, development and commercialization activities, as well as any product candidates or products resulting from these activities, may infringe or be claimed to infringe patents or patent applications under which we do not hold licenses or other rights. Patents do not protect its owner from a claim of infringement of another owner’s patent. Therefore, our patent position cannot and does not provide any assurance that we are not infringing the patent rights of another.
The patent landscape in the field of synthetic immuno-oncology, which we are pursuing under our Channel Agreement with Intrexon, is particularly complex. We are aware of numerous United States and foreign patents and pending patent applications of third parties that cover compositions, methods of use and methods of manufacture of synthetic immuno-oncology, including biotherapeutics involving the in vivo expression of human IL-12. In addition, there may be patents and patent applications in the field of which we are not aware. The technology we license from Intrexon is early-stage technology and we are just beginning the process of designing and developing products using this technology. Although we will seek to avoid pursuing the development of products that may infringe any patent claims that we believe to be valid and enforceable, we may fail to do so. Moreover, given the breadth and number of claims in patents and pending patent applications in the field of synthetic immuno-oncology and the complexities and uncertainties associated with them, third parties may allege that we are infringing upon patent claims even if we do not believe such claims to be valid and enforceable.
61
Table of Contents
If a claim for patent infringement is asserted, there can be no assurance that the resolution of the claim would permit us to continue marketing the relevant product on commercially reasonable terms, if at all. We may not have sufficient resources to bring these actions to a successful conclusion. If we do not successfully defend any infringement actions to which we become a party or are unable to have infringed patents declared invalid or unenforceable, we may have to pay substantial monetary damages, which can be tripled if the infringement is deemed willful, or be required to discontinue or significantly delay commercialization and development of the affected products.
Any legal action against us or our collaborators claiming damages and seeking to enjoin developmental or marketing activities relating to affected products could, in addition to subjecting us to potential liability for damages, require us or our collaborators to obtain licenses to continue to develop, manufacture, or market the affected products. Such a license may not be available to us on commercially reasonable terms, if at all.
An adverse determination in a proceeding involving our owned or licensed intellectual property may allow entry of generic substitutes for our products.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for noncompliance with these requirements.
Periodic maintenance fees on any issued patent are due to be paid to the U.S. PTO and foreign patent agencies in several stages over the lifetime of the patent. The U.S. PTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Noncompliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. In such an event, our competitors might be able to enter the market, which would have a material adverse effect on our business.
If we breach any of the agreements under which we license rights to products or technology from others, we could lose license rights that are material to our business or be subject to claims by our licensors.
We license rights to products and technology that are important to our business, and we expect to enter into additional licenses in the future. For instance, we have exclusively licensed patents and patent applications under our Channel Agreement with Intrexon and under our License with MD Anderson. Under these agreements, we are subject to a range of commercialization and development, sublicensing, royalty, patent prosecution and maintenance, insurance and other obligations.
Any failure by us to comply with any of these obligations or any other breach by us of our license agreements could give the licensor the right to terminate the license in whole, terminate the exclusive nature of the license or bring a claim against us for damages. Any such termination or claim could have a material adverse effect on our financial condition, results of operations, liquidity or business. Even if we contest any such termination or claim and are ultimately successful, such dispute could lead to delays in the development or commercialization of potential products and result in time-consuming and expensive litigation or arbitration. On termination we may be required to license to the licensor any related intellectual property that we developed.
In addition, in certain cases, the rights licensed to us are rights of a third party licensed to our licensor. In such instances, if our licensors do not comply with their obligations under such licenses, our rights under our license agreements with our licensor may be adversely affected.
We may be subject to claims by third parties asserting that our employees or we have misappropriated their intellectual property, or claiming ownership of what we regard as our own intellectual property.
Many of our employees were previously employed at universities or other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although we try to ensure that our employees do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that these employees or we have used or disclosed intellectual property, including trade secrets or other proprietary information, of any such employee’s former employer. Litigation may be necessary to defend against these claims.
62
Table of Contents
In addition, while it is our policy to require our employees and contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact develops intellectual property that we regard as our own. Our and their assignment agreements may not be self-executing or may be breached, and we may be forced to bring claims against third parties, or defend claims they may bring against us, to determine the ownership of what we regard as our intellectual property.
If we fail in prosecuting or defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in prosecuting or defending against such claims, litigation could result in substantial costs and be a distraction to management.
OTHER RISKS RELATED TO OUR COMPANY
Our stock price has been, and may continue to be, volatile.
The market price of our common stock has been highly volatile. The stock market from time to time experiences significant price and volume fluctuations unrelated to the operating performance of particular companies. In addition, factors such as fluctuations in our operating results, future sales of our common stock, announcements of the timing and amount of product sales, announcements of the status of development of our products, announcements of technological innovations or new therapeutic products by us or our competitors, announcements regarding collaborative agreements, laboratory or clinical trial results, government regulation, FDA determinations on the approval of a product candidate NDA submission, developments in patent or other proprietary rights, public concern as to the safety of drugs developed by us or others, changes in reimbursement policies, comments made by securities analysts and general market conditions may have a substantial effect on the market price of our common stock.
We are subject to Sarbanes-Oxley and the reporting requirements of federal securities laws, which can be expensive.
As a public reporting company, we are subject to the Sarbanes-Oxley Act of 2002, as well as to the information and reporting requirements of the Securities Exchange Act of 1934, as amended, or the Exchange Act, and other federal securities laws. As a result, we incur significant legal, accounting, and other expenses that we would not incur as a private company, including costs associated with our public company reporting requirements and corporate governance requirements. As an example of public reporting company requirements, we evaluate the effectiveness of disclosure controls and procedures and of our internal control over financing reporting in order to allow management to report on such controls. Sarbanes-Oxley generally requires that a public reporting company’s independent registered public accounting firm attest to the effectiveness of the company’s internal control over financial reporting as of the end of each fiscal year in the company’s Annual Report on Form 10-K. In addition, any updates to our finance and accounting systems, procedures and controls, which may be required as a result of our ongoing analysis of internal controls, or results of testing by our independent auditor, may require significant time and expense. As a company with limited accounting resources, a significant amount of management’s time and attention has been and will continue to be diverted from our business to ensure compliance with these regulatory requirements. This diversion of management’s time and attention may have a material adverse effect on our business, financial condition and results of operations.
Management is working to continuously monitor and improve internal controls and has set in place controls to mitigate the potential segregation of duties risk. In the event significant deficiencies or material weaknesses are identified in our internal control over financial reporting that we cannot remediate in a timely manner, or if we are unable to receive a positive attestation from our independent registered public accounting firm with respect to our internal controls over financial reporting, investors and others may lose confidence in the reliability of our financial statements and the trading price of our common stock and ability to obtain any necessary equity or debt financing could suffer. In addition, in the event that our independent registered public accounting firm is unable to rely on our internal controls over financial reporting in connection with its audit of our financial statements, and in the further event that it is unable to devise alternative procedures in order to satisfy itself as to the material accuracy of our financial statements and related disclosures, we may be unable to file our periodic reports with the United States Securities and Exchange Commission, or SEC. This would likely have an adverse effect on the trading price of our common stock and our ability to secure any necessary additional equity or debt financing, and could result in the delisting of our common stock from the NASDAQ Capital Market, which would severely limit the liquidity of our common stock.
63
Table of Contents
Anti-takeover provisions in our charter documents and under Delaware law may make an acquisition of us, which may be beneficial to our stockholders, more difficult.
Provisions of our amended and restated certificate of incorporation and bylaws, as well as provisions of Delaware law, could make it more difficult for a third party to acquire us, even if doing so would benefit our stockholders. These provisions authorize the issuance of “blank check” preferred stock that could be issued by our board of directors to increase the number of outstanding shares and hinder a takeover attempt, and limit who may call a special meeting of stockholders. In addition, Section 203 of the Delaware General Corporation Law generally prohibits a publicly-held Delaware corporation from engaging in a business combination with a party that owns at least 15% of its common stock unless the business combination is approved by the company’s board of directors before the person acquires the 15% ownership stake or later by its board of directors and two-thirds of its stockholders. Section 203 could have the effect of delaying, deferring or preventing a change in control that our stockholders might consider to be in their best interests.
In connection with our January 2011 issuance of shares of common stock to Intrexon in a private placement transaction, our board of directors waived the Section 203 prohibition with respect to a future business combination with Intrexon.
Because we do not expect to pay dividends, you will not realize any income from an investment in our common stock unless and until you sell your shares at profit.
We have never paid dividends on our capital stock and we do not anticipate that we will pay any dividends for the foreseeable future. Accordingly, any return on an investment in us will be realized, if at all, only when you sell shares of our common stock.
If securities and/or industry analysts fail to continue publishing research about our business, if they change their recommendations adversely or if our results of operations do not meet their expectations, our stock price and trading volume could decline.
The trading market for our common stock will be influenced by the research and reports that industry or securities analysts publish about us or our business. If one or more of these analysts cease coverage of our company or fail to publish reports on us regularly, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline. In addition, it is likely that in some future period our operating results will be below the expectations of securities analysts or investors. If one or more of the analysts who cover us downgrade our stock, or if our results of operations do not meet their expectations, our stock price could decline.
Our stock price is volatile and may decline regardless of our operating performance, and you may not be able to resell your shares at or above the price at which you purchased such shares.
The market price for our common stock is volatile and may fluctuate significantly in response to a number of factors, most of which we cannot control, including:
| • | Price and volume fluctuations in the overall stock market; |
| • | Market conditions or trends in our industry or the economy as a whole; |
| • | Changes in operating performance and stock market valuations of other biopharmaceutical companies generally, or those that develop and commercialize cancer drugs in particular; |
| • | The financial projections we may provide to the public, any changes in these projections or our failure to meet these projections; |
| • | Changes in financial estimates or ratings by any securities analysts who follow our common stock, our failure to meet these estimates or failure of those analysts to initiate or maintain coverage of our common stock; |
| • | The public’s response to press releases or other public announcements by us or third parties, including our filings with the Securities Exchange Commission, or SEC, and announcements relating to product development, litigation and intellectual property impacting us or our business; |
| • | The sustainability of an active trading market for our common stock; |
| • | Future sales of our common stock by our executive officers, directors and significant stockholders; |
| • | Announcements of mergers or acquisition transactions; |
| • | Our inclusion or deletion from certain stock indices; |
| • | Announcements of medical innovations or new products by our competitors; |
| • | Announcements of changes in our senior management; |
| • | Other events or factors, including those resulting from war, incidents of terrorism, natural disasters or responses to these events; and |
| • | Changes in accounting principles. |
64
Table of Contents
In addition, the stock markets, and in particular the NASDAQ Capital Market, have experienced extreme price and volume fluctuations that have affected and continue to affect the market prices of equity securities of many biopharmaceutical companies. Stock prices of many biopharmaceutical companies have fluctuated in a manner unrelated or disproportionate to the operating performance of those companies. In the past, stockholders have instituted securities class action litigation following periods of market volatility. If we were involved in securities litigation, we could incur substantial costs and our resources and the attention of management could be diverted from our business.
*Our principal stockholders, executive officers and directors have substantial control over the company, which may prevent you and other stockholders from influencing significant corporate decisions and may harm the market price of our common stock.
As of March 31, 2015, our executive officers, directors and holders of five percent or more of our outstanding common stock, beneficially owned, in the aggregate, 18.2% of our outstanding common stock. These stockholders may have interests that conflict with our other stockholders and, if acting together, have the ability to influence the outcome of matters submitted to our stockholders for approval, including the election and removal of directors and any merger, consolidation or sale of all or substantially all of our assets. Accordingly, this concentration of ownership may harm the market price of our common stock by:
| • | Delaying, deferring or preventing a change in control; |
| • | Impeding a merger, consolidation, takeover or other business combination involving us; or |
| • | Discouraging a potential acquirer from making a tender offer or otherwise attempting to obtain control of us |
65
Table of Contents
Item 2. Unregistered Sale of Equity Securities and Use of Proceeds
Unregistered Sale of Equity Securities and Use of Proceeds
During the three months ended March 31, 2015, we issued an aggregate of 11,722,163 shares of our common stock, constituting the License Shares and the Incentive Shares, to MD Anderson pursuant to the License, and the License Shares Securities Issuance Agreement and Incentive Shares Securities Issuance Agreement entered into in connection therewith.
The issuance of the License Shares and the Incentive Shares was not registered under the Securities Act of 1933, as amended, or the Securities Act, in reliance on the exemption from federal registration under Section 4(a)(2) of the Securities Act and/or Rule 506 promulgated thereunder, based on the Company’s belief that the offer and sale of the License Shares and the Incentive Shares has not and will not involve a public offering as MD Anderson is an “accredited investor” as defined under Section 501 promulgated under the Securities Act and no general solicitation has been involved in the offer and sale of the License Shares or the Incentive Shares.
Issuer Purchases of Equity Securities
During the three months ended March 31, 2015, we purchased 33,931 shares of common stock in settlement of employee tax withholding obligations due upon the vesting of restricted stock. The following table provides information about these purchases of restricted shares for the three months ended March 31, 2015:
| Period |
Total Number of Shares Purchased |
Average Price Paid Per Share ($) |
||||||
| January 1 to 31, 2015 |
19,330 | $ | 5.13 | |||||
| February 1 to 28, 2015 |
14,601 | $ | 10.06 | |||||
| March 1 to 31, 2015 |
— | $ | — | |||||
|
|
|
|||||||
| Total |
33,931 | |||||||
|
|
|
|||||||
Item 3. Defaults upon Senior Securities
Not applicable.
Item 4. Mine Safety Disclosures
Not applicable.
Not applicable.
The exhibits listed in the Exhibit Index immediately preceding such exhibits are filed as part of this report and such Exhibit Index is incorporated herein by reference.
66
Table of Contents
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
| /s/ Laurence J.N. Cooper |
| Laurence J.N. Cooper, M.D., Ph.D. |
| Chief Executive Officer |
| (Principal Executive Officer) |
Dated: May 7, 2015
| /s/ Kevin G. Lafond |
| Kevin G. Lafond |
| Vice President, Chief Accounting Officer and Treasurer |
| (Principal Financial and Accounting Officer) |
Dated: May 7, 2015
67
Table of Contents
EXHIBIT INDEX
| 10.1 | Letter Agreement by and between ZIOPHARM Oncology, Inc., Intrexon Corporation and The University of Texas System Board of Regents on behalf of The University of Texas M.D. Anderson Cancer Center, dated as of January 9, 2015 (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed January 14, 2015) | |
| 10.2 | Securities Issuance Agreement by and among ZIOPHARM Oncology, Inc., The University of Texas System Board of Regents on behalf of The University of Texas M.D. Anderson Cancer Center dated as of January 13, 2015 (relating to the License Shares, as defined in the Registrant’s Current Report on Form 8-K filed January 14, 2015) (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed January 14, 2015) | |
| 10.3 | Securities Issuance Agreement by and among ZIOPHARM Oncology, Inc., The University of Texas System Board of Regents on behalf of The University of Texas M.D. Anderson Cancer Center dated as of January 13, 2015 (relating to the Incentive Shares, as defined in the Registrant’s Current Report on Form 8-K filed January 14, 2015) (incorporated by reference to Exhibit 10.3 to the Registrant’s Current Report on Form 8-K filed January 14, 2015) | |
| 10.4 | Registration Rights Agreement by and among ZIOPHARM Oncology, Inc., The University of Texas System Board of Regents on behalf of The University of Texas M.D. Anderson Cancer Center dated as of January 13, 2015 (incorporated by reference to Exhibit 10.4 to the Registrant’s Current Report on Form 8-K filed January 14, 2015) | |
| 10.5# | License Agreement by and among ZIOPHARM Oncology, Inc., Intrexon Corporation and The University of Texas System Board of Regents on behalf of The University of Texas M.D. Anderson Cancer Center, dated as of January 13, 2015 (incorporated by reference to Exhibit 10.5 to the Registrant’s Current Report on Form 8-K filed January 28, 2015) | |
| 10.6## | License and Collaboration Agreement by and among Intrexon Corporation, ARES TRADING Trading S.A., and ZIOPHARM Oncology, Inc. dated as of March 27, 2015 (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed April 2, 2015) | |
| 10.7 | Second Amendment to Exclusive Channel Partner Agreement by and between ZIOPHARM Oncology, Inc. and Intrexon Corporation dated as of March 27, 2015 (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed April 2, 2015) | |
| 31.1* | Certification pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 31.2* | Certification pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 32.1* | Certifications pursuant to 18 U.S.C. Section 1350 | |
| 101.INS* | XBRL Instance Document | |
| 101.SCH* | XBRL Taxonomy Extension Schema Document | |
| 101.CAL* | XBRL Taxonomy Extension Calculation Linkbase Document | |
| 101.DEF* | XBRL Taxonomy Definition Linkbase Document | |
| 101.LAB* | XBRL Taxonomy Extension Label Linkbase Document | |
| 101.PRE* | XBRL Taxonomy Extension Presentation Linkbase Document | |
| * | Filed herewith. |
| # | Confidential treatment has been granted as to certain portions of this exhibit pursuant to Rule 24b-2 of the Exchange Act. |
| ## | Confidential treatment has been requested as to certain portions of this exhibit pursuant to Rule 24b-2 of the Exchange Act. |
68