Attached files
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K |
(Mark One) | |||
ý | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 | ||
For the fiscal year ended December 31, 2017 | |||
OR | |||
¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 | ||
For the transition period from __________ to __________ | |||
Commission File Number: 0-19034 | ||
REGENERON PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
New York | 13-3444607 | |
(State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) | |
777 Old Saw Mill River Road, Tarrytown, New York | 10591-6707 | |
(Address of principal executive offices) | (Zip Code) | |
(914) 847-7000
(Registrant's telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
Title of each class | Name of each exchange on which registered | |
Common Stock - par value $.001 per share | NASDAQ Global Select Market | |
Securities registered pursuant to section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. | Yes | ý | No | ¨ |
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. | Yes | ¨ | No | ý |
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. | Yes | ý | No | ¨ |
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). | Yes | ý | No | ¨ |
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§232.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this form 10-K. | ý | |||
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer”, “accelerated filer”, “smaller reporting company” and "emerging growth company" in Rule 12b-2 of the Exchange Act. | ||||
Large accelerated filer | ý | Accelerated filer | ¨ | Non-accelerated filer | ¨ | Smaller reporting company | ¨ | Emerging growth company | ¨ | ||||||
(Do not check if a smaller reporting company) | |||||||||||||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. | ¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). | Yes | ¨ | No | ý |
The aggregate market value of the voting and non-voting common stock held by non-affiliates of the registrant was approximately $50,337,000,000, computed by reference to the closing sales price of the stock on NASDAQ on June 30, 2017, the last trading day of the registrant's most recently completed second fiscal quarter. For purposes of this calculation only, the registrant has assumed that all of its directors and executive officers, and no other persons, are its affiliates. This determination of affiliate status is not necessarily a determination for other purposes. | ||||
The number of shares outstanding of each of the registrant's classes of common stock as of February 1, 2018: | ||||
Class of Common Stock | Number of Shares | |
Class A Stock, $.001 par value | 1,911,354 | |
Common Stock, $.001 par value | 105,785,444 | |
DOCUMENTS INCORPORATED BY REFERENCE |
Specified portions of the Registrant's definitive proxy statement to be filed in connection with solicitation of proxies for its 2018 Annual Meeting of Shareholders are incorporated by reference into Part III of this Form 10-K. Exhibit index is located on pages 88 to 95 of this filing. |
REGENERON PHARMACEUTICALS, INC.
ANNUAL REPORT ON FORM 10-K
TABLE OF CONTENTS
Page Numbers | ||||
"ARCALYST®", "EYLEA®", "ZALTRAP®", "VelocImmune®", "VelociGene®", "VelociMouse®", "VelociMab®", "VelociSuite®", and "Regeneron Genetics Center®" are trademarks of Regeneron Pharmaceuticals, Inc. Trademarks and trade names of other companies appearing in this report are, to the knowledge of Regeneron Pharmaceuticals, Inc., the property of their respective owners. |
PART I
ITEM 1. BUSINESS
This Annual Report on Form 10-K contains forward-looking statements that involve risks and uncertainties relating to future events and the future performance of Regeneron Pharmaceuticals, Inc. (where applicable, together with its subsidiaries, "Regeneron," "Company," "we," "us," and "our"), and actual events or results may differ materially from these forward-looking statements. Words such as "anticipate," "expect," "intend," "plan," "believe," "seek," "estimate," variations of such words, and similar expressions are intended to identify such forward-looking statements, although not all forward-looking statements contain these identifying words. These statements concern, and these risks and uncertainties include, among others, the nature, timing, and possible success and therapeutic applications of our products, product candidates, and research and clinical programs now underway or planned, including without limitation EYLEA® (aflibercept) Injection, Dupixent® (dupilumab) Injection, Praluent® (alirocumab) Injection, Kevzara® (sarilumab) Injection, cemiplimab, fasinumab, and evinacumab; the likelihood and timing of achieving any of our anticipated clinical development milestones; unforeseen safety issues resulting from the administration of products and product candidates in patients, including serious complications or side effects in connection with the use of our product candidates in clinical trials; the likelihood and timing of possible regulatory approval and commercial launch of our late-stage product candidates and new indications for marketed products, including without limitation EYLEA, Dupixent, Praluent, Kevzara, cemiplimab, fasinumab, and evinacumab; the extent to which the results from the research and development programs conducted by us or our collaborators may be replicated in other studies and lead to therapeutic applications; ongoing regulatory obligations and oversight impacting our marketed products (such as EYLEA, Dupixent, Praluent, and Kevzara), research and clinical programs, and business, including those relating to patient privacy; determinations by regulatory and administrative governmental authorities which may delay or restrict our ability to continue to develop or commercialize our products and product candidates; competing drugs and product candidates that may be superior to our products and product candidates; uncertainty of market acceptance and commercial success of our products and product candidates; our ability to manufacture and manage supply chains for multiple products and product candidates; the ability of our collaborators, suppliers, or other third parties to perform filling, finishing, packaging, labeling, distribution, and other steps related to our products and product candidates; coverage and reimbursement determinations by third-party payers, including Medicare and Medicaid; unanticipated expenses; the costs of developing, producing, and selling products; our ability to meet any of our financial projections or guidance, including without limitation capital expenditures, and changes to the assumptions underlying those projections or guidance; the potential for any license or collaboration agreement, including our agreements with Sanofi, Bayer, and Teva Pharmaceutical Industries Ltd. (or their respective affiliated companies, as applicable), to be cancelled or terminated without any further product success; and risks associated with intellectual property of other parties and pending or future litigation relating thereto, including without limitation the patent litigation proceedings relating to Dupixent and Praluent described further in Note 17 to our Consolidated Financial Statements included in this report. These statements are made based on management's current beliefs and judgment, and the reader is cautioned not to rely on any such statements. In evaluating such statements, shareholders and potential investors should specifically consider the various factors identified under Part I, Item 1A. "Risk Factors," which could cause actual events and results to differ materially from those indicated by such forward-looking statements. We do not undertake any obligation to update publicly any forward-looking statement, whether as a result of new information, future events, or otherwise.
General
Regeneron Pharmaceuticals, Inc. is a fully integrated biotechnology company that discovers, invents, develops, manufactures, and commercializes medicines for the treatment of serious diseases. Our commercialized medicines and product candidates in development are designed to help patients with eye disease, allergic and inflammatory diseases, heart disease, pain, cancer, and infectious and other serious medical conditions.
Our significant 2017 business highlights include:
• | EYLEA (aflibercept) Injection, which is approved by the U.S. Food and Drug Administration (FDA), European Union (EU), Japan, and certain other countries for use in retinal indications, delivered net sales growth of 11.4% over 2016 in the United States and net sales growth of 18.9% outside the United States. In December 2017, the supplemental Biologics License Application (sBLA) for a 12-week dosing interval of EYLEA in patients with neovascular age-related macular degeneration (wet AMD) was filed with the FDA, with a target action date of August 11, 2018. A Phase 3 study for the treatment of non-proliferative diabetic retinopathy (NPDR) in patients without diabetic macular edema (DME) completed enrollment. |
• | Dupixent (dupilumab) for the treatment of adults with moderate-to-severe atopic dermatitis received regulatory approval in the United States and EU. We also reported positive results from two additional pivotal Phase 3 studies of dupilumab for the treatment of asthma, and recently submitted an sBLA with the FDA. We reported positive results in the Phase 2 study in eosinophilic esophagitis (EoE). Phase 3 studies in patients (12-17 years of age and 6-11 years of age) with atopic dermatitis and pediatric patients (6-11 years of age) with asthma were initiated. |
2
• | The Phase 3 cardiovascular outcomes study of Praluent has recently been completed, and a Phase 3 study for the treatment of homozygous familial hypercholesterolemia (HoFH) was initiated. The U.S. Court of Appeals for the Federal Circuit ordered a new trial on the issues of written description and enablement and vacated the permanent injunction in the ongoing PCSK9 litigation. The sBLA for use of Praluent with apheresis was filed with the FDA, with a target action date of August 24, 2018. |
• | Kevzara for the treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) received regulatory approval in the United States, EU, and Japan. |
• | We reported positive top-line results from a pivotal Phase 2 study of cemiplimab in advanced cutaneous squamous cell carcinoma (CSCC). We have commenced a rolling BLA submission to the FDA and expect to complete the submission in the first quarter of 2018. The FDA granted Breakthrough Therapy designation to cemiplimab for the treatment of adults with metastatic CSCC and adults with locally advanced and unresectable CSCC. A Phase 3 study as a first-line treatment for non-small cell lung cancer (NSCLC) and a Phase 3 study in cervical cancer were initiated. A potentially pivotal Phase 2 study in basal cell carcinoma (BCC) was also initiated. |
• | Phase 3 efficacy studies of fasinumab in osteoarthritis of the knee or hip were initiated, while the Phase 3 long-term safety study in osteoarthritis continued patient enrollment. A Phase 3 study in chronic low back pain in patients with concomitant osteoarthritis of the knee and hip was also initiated. |
• | The FDA granted Breakthrough Therapy designation for evinacumab for the treatment of hypercholesterolemia in patients with HoFH. |
• | We advanced one new product candidate (REGN3918, an antibody to complement 5 (C5)) into Phase 1 clinical development. |
• | We entered into significant new research and development license and collaboration arrangements, including agreements with the Biomedical Advanced Research Development Authority (BARDA) of the U.S. Department of Health and Human Services (HHS) to develop new treatments to combat infectious diseases; Decibel Therapeutics, Inc. to discover and develop new potential therapeutics to protect, repair, and restore hearing; and ISA Pharmaceuticals B.V. to develop ISA101, an immunotherapy targeting human papillomavirus type 16 (HPV16)-induced cancer, in combination with cemiplimab. |
• | From a growth perspective, we hired our 6,000th employee, completed a new lease financing for our laboratory and office facilities in Tarrytown, New York, continued to expand our bulk drug product manufacturing operations in Rensselaer, New York, and continued build-out and validation activities at our Limerick, Ireland commercial manufacturing facility. |
• | We were named the top employer in the global biotech and pharmaceutical industry by Science magazine. We have been ranked first for five of the past seven years, with second-place rankings in 2015 and 2011. |
Our total revenues were $5,872.2 million in 2017, compared to $4,860.4 million in 2016 and $4,103.7 million in 2015. Our net income was $1,198.5 million, or $10.34 per diluted share, in 2017, compared to $895.5 million, or $7.70 per diluted share, in 2016, and $636.1 million, or $5.52 per diluted share, in 2015. Refer to Part II, Item 7. "Management's Discussion and Analysis of Financial Condition and Results of Operations - Results of Operations" below for further details of our financial results, including amounts incurred related to research and development activities.
We currently have six products that have received marketing approval:
• | EYLEA (aflibercept) Injection, known in the scientific literature as VEGF Trap-Eye, is available in the United States, EU, Japan, and certain other countries outside the United States for the treatment of wet AMD, DME, macular edema following retinal vein occlusion (RVO), which includes macular edema following central retinal vein occlusion (CRVO) and macular edema following branch retinal vein occlusion (BRVO). EYLEA is also available in the EU, Japan, and certain other countries outside the United States for the treatment of myopic choroidal neovascularization (mCNV) and in the United States for the treatment of diabetic retinopathy in patients with DME. |
We are collaborating with Bayer on the global development and commercialization of EYLEA outside the United States. Bayer markets, and records revenue from sales of EYLEA outside the United States, where, for countries other than Japan, the companies share equally the profits and losses from sales of EYLEA. In Japan, we are entitled to receive a percentage of the sales of EYLEA. We maintain exclusive rights to EYLEA in the United States and are entitled to all profits from such sales.
• | Dupixent (dupilumab) Injection. On March 28, 2017, the FDA approved Dupixent for the treatment of adult patients with moderate-to-severe atopic dermatitis whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The launch of Dupixent commenced in March following the FDA approval. In September 2017, the European Commission granted marketing authorization for Dupixent for use in adults with moderate-to-severe atopic dermatitis who are candidates for systemic therapy and in January 2018, the Ministry of Health, Labor and Welfare (MHLW) in Japan approved Dupixent for the treatment of atopic dermatitis in adults not adequately controlled with existing therapies. |
3
We are collaborating with Sanofi on the global development and commercialization of Dupixent. Sanofi records product sales for Dupixent, and we and Sanofi share profits and losses from sales of Dupixent. We have exercised our option to co-promote Dupixent in the United States and thus far have not exercised any of our options to co-promote Dupixent outside the United States.
• | Praluent (alirocumab) Injection is available in the United States where it is indicated as an adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease (ASCVD), who require additional lowering of high low-density lipoprotein (LDL) cholesterol. Praluent is also available in certain European countries and in Japan. In April 2017, the FDA approved the sBLA for a once-monthly (every four weeks), 300 mg dose of Praluent. In July 2017, the FDA approved the sBLA for Praluent's time out of refrigeration, which was increased from 24 hours to 30 days. The effect of Praluent on cardiovascular morbidity and mortality has not been determined. |
Sanofi records product sales for Praluent, and we and Sanofi share profits and losses from sales of Praluent. We have exercised our option to co-promote Praluent in the United States and thus far have not exercised any of our options to co-promote Praluent outside the United States.
See Note 17 to our Consolidated Financial Statements for information regarding the patent infringement proceedings relating to Praluent, which may impact Praluent's commercial availability in certain jurisdictions.
• | Kevzara (sarilumab) Solution for Subcutaneous Injection. In January 2017, Health Canada approved Kevzara for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have an inadequate response to or intolerance to one or more biologic or non-biologic disease modifying anti-rheumatic drugs (DMARDs). This was the first approval of Kevzara worldwide. On May 22, 2017, the FDA approved Kevzara for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have an inadequate response or intolerance to one or more DMARDs. In June 2017, the European Commission granted marketing authorization for Kevzara in combination with methotrexate (MTX) for the treatment of moderately to severely active rheumatoid arthritis in adult patients who have responded inadequately to, or who are intolerant to one or more DMARDs; Kevzara may be used as monotherapy in case of intolerance to MTX or when treatment with MTX is inappropriate. In September 2017, the MHLW in Japan approved Kevzara for the treatment of adult patients with rheumatoid arthritis who have had an inadequate response to conventional treatments. |
Sanofi records product sales for Kevzara, and we and Sanofi share profits and losses from sales of Kevzara. We have exercised our option to co-promote Kevzara in the United States and thus far have not exercised any of our options to co-promote Kevzara outside the United States.
• | ARCALYST® (rilonacept) Injection for Subcutaneous Use is available in the United States for the treatment of Cryopyrin-Associated Periodic Syndromes (CAPS), including Familial Cold Auto-inflammatory Syndrome (FCAS) and Muckle-Wells Syndrome (MWS), in adults and children 12 years and older. CAPS are a group of rare, inherited, auto-inflammatory conditions characterized by life-long, recurrent symptoms of rash, fever/chills, joint pain, eye redness/pain, and fatigue. Intermittent, disruptive exacerbations or flares can be triggered at any time by exposure to cooling temperatures, stress, exercise, or other unknown stimuli. |
• | ZALTRAP® (ziv-aflibercept) Injection for Intravenous Infusion, known in the scientific literature as VEGF Trap, is available in the United States, EU, and certain other countries for treatment, in combination with 5-fluorouracil, leucovorin, irinotecan (FOLFIRI), of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen. Pursuant to a 2015 amended and restated ZALTRAP agreement, Sanofi is solely responsible for the development and commercialization of ZALTRAP, and Sanofi pays us a percentage of aggregate net sales of ZALTRAP. |
4
Marketed Products
Net Product Sales of Regeneron-Discovered Products(1) | Year Ended December 31, | |||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
EYLEA in the United States | $ | 3,701.9 | $ | 3,323.1 | $ | 2,676.0 | ||||||
ARCALYST | 16.5 | 15.3 | 13.5 | |||||||||
Net product sales recorded by Regeneron | $ | 3,718.4 | $ | 3,338.4 | $ | 2,689.5 | ||||||
EYLEA outside of the United States(1) | $ | 2,226.9 | $ | 1,872.3 | $ | 1,413.3 | ||||||
EYLEA global | $ | 5,928.8 | $ | 5,195.4 | $ | 4,089.3 | ||||||
Global net product sales recorded by Sanofi(1): | ||||||||||||
Praluent in the United States | $ | 131.4 | $ | 94.4 | $ | 9.5 | ||||||
Praluent outside of the United States | 63.3 | 21.9 | 1.0 | |||||||||
Praluent global | 194.7 | 116.3 | 10.5 | |||||||||
Dupixent | 256.5 | — | — | |||||||||
Kevzara | 13.3 | — | — | |||||||||
ZALTRAP | 83.8 | 72.3 | 85.7 | |||||||||
Net product sales recorded by Sanofi | $ | 548.3 | $ | 188.6 | $ | 96.2 | ||||||
(1) As described in the "General" section above, Bayer records net product sales of EYLEA outside the United States and Sanofi records global net product sales of Praluent, Dupixent, Kevzara, and ZALTRAP. | ||||||||||||
Programs in Clinical Development
All 15 of our product candidates in clinical development were discovered in our research laboratories and are summarized below. We used our VelocImmune® technology to generate each of the antibodies in the table below. There are numerous uncertainties associated with drug development, including uncertainties related to safety and efficacy data from each phase of drug development (including any post-approval studies), uncertainties related to the enrollment and performance of clinical trials, changes in regulatory requirements, and changes in the competitive landscape affecting a product candidate. Refer to Part I, Item 1A, "Risk Factors" for a description of these and other risks and uncertainties that may affect our clinical programs.
5
Phase 1 | Phase 2 | Phase 3 | |||||
Cemiplimab (REGN2810)(a) | Dupilumab(a) | EYLEA | |||||
Antibody to programmed cell death protein 1 (PD-1)(h) | Antibody to the interleukin-4 receptor (IL-4R) alpha subunit | Ÿ | NPDR in patients without DME | ||||
Ÿ | Solid tumors and advanced hematologic malignancies | Ÿ | EoE(c) | Dupilumab(a) | |||
REGN3767(a) | Sarilumab(a) | Ÿ | Atopic dermatitis in adolescents and pediatrics (6–17 years of age) | ||||
Antibody to Lymphocyte Activation Gene 3 (LAG-3) protein | Antibody to the interleukin-6 receptor (IL-6R) | Ÿ | Atopic dermatitis in pediatrics (6 months–5 years of age) (Phase 2/3) | ||||
Ÿ | Advanced malignancies (administered alone or in combination with cemiplimab) | Ÿ | Polyarticular-course juvenile idiopathic arthritis (pcJIA) | Ÿ | Asthma in adults and adolescents | ||
Ÿ | Asthma in pediatrics (6–11 years of age) | ||||||
REGN1979 | Cemiplimab(a) | Ÿ | Nasal polyps | ||||
Bispecific antibody against CD20 and CD3 | Ÿ | Metastatic or locally advanced and unresectable CSCC (pivotal study)(d) | Praluent(a) | ||||
Ÿ | Certain B-cell malignancies (monotherapy and in combination cemiplimab)(c) | Ÿ | BCC (potentially pivotal study) | Antibody to PCSK9 | |||
Evinacumab (REGN1500)(f) | Ÿ | LDL cholesterol reduction and prevention of cardiovascular events | |||||
REGN3470-3471-3479(g) | Antibody to angiopoietin-like protein 3 (ANGPTL3) | Ÿ | HoFH(c) | ||||
Multi-antibody therapy to Ebola virus | Ÿ | HoFH(c)(d) | Cemiplimab(a) | ||||
Ÿ | Ebola virus infection(c) | Ÿ | Refractory hypercholesterolemia (both HeFH and non-FH) | Ÿ | First-line treatment for NSCLC | ||
REGN1908-1909(f) | Ÿ | Cervical cancer | |||||
Multi-antibody therapy to Feld1 | Fasinumab (REGN475)(b)(f) | ||||||
Ÿ | Allergic disease | Ÿ | Osteoarthritis of knee and hip | ||||
REGN3500(a) | Ÿ | Chronic low back pain in patients with concomitant osteoarthritis of the knee and hip | |||||
Antibody to interleukin-33 (IL-33). Studied as monotherapy and in combination with dupilumab. | |||||||
Evinacumab (REGN1500)(f) | |||||||
Ÿ | Asthma | Ÿ | HoFH(c)(d) | ||||
Trevogrumab (REGN1033)(f) | |||||||
Antibody to myostatin (GDF8) | |||||||
Ÿ | Muscle wasting diseases (in combination with REGN2477) | ||||||
REGN2477(f) | |||||||
Antibody to Activin A | |||||||
Ÿ | Fibrodysplasia ossificans progressiva (FOP)(c)(e) | ||||||
Ÿ | Muscle-wasting diseases (in combination with trevogrumab) | ||||||
REGN3918(f) | |||||||
Antibody to complement 5 (C5) | |||||||
Ÿ | Paroxysmal nocturnal hemoglobinuria (PNH) | ||||||
6
(a) In collaboration with Sanofi | ||||
(b) In collaboration with Teva and Mitsubishi Tanabe Pharma | ||||
(c) FDA granted orphan drug designation | ||||
(d) FDA granted Breakthrough Therapy designation | ||||
(e) FDA granted Fast Track designation | ||||
(f) Sanofi did not opt-in to or elected not to continue to co-develop the product candidate. Under the terms of our agreement, Sanofi is entitled to receive royalties on any future global sales of the product candidate. | ||||
(g) Sanofi did not opt-in to the product candidate. Under the terms of our agreement, Sanofi is entitled to receive royalties on any future sales of the product candidate. We and BARDA of the HHS are parties to agreements (including an agreement executed in September 2017 - see "Other Programs" below for further information) whereby HHS provides certain funding to support research, development, and manufacturing of an antibody therapy for the treatment of Ebola virus infection. | ||||
(h) Studied as monotherapy and in combination with other antibodies and treatments | ||||
In the third quarter of 2017, we reported that a Phase 3 study evaluating suptavumab (REGN2222), an antibody to the Respiratory Syncytial Virus-F (RSV-F) protein, did not meet its primary endpoint of preventing medically-attended RSV infections in infants. Suptavumab did show signs of efficacy in a subgroup of patients. Adverse events were generally balanced between suptavumab and placebo. We have discontinued further clinical development of suptavumab.
In the fourth quarter of 2017, we reported that results from two Phase 2 studies that added the angiopoietin2 (Ang2) antibody nesvacumab to EYLEA did not provide sufficient differentiation to warrant Phase 3 development. The RUBY study evaluated patients with DME and the ONYX study evaluated patients with wet AMD. EYLEA results were consistent with findings in previous clinical studies, and there were no new safety signals in these studies. Results from RUBY and ONYX will be further analyzed and will be submitted for presentation at a future medical congress.
Our core business strategy is to maintain a strong foundation in basic scientific research and discovery-enabling technologies, and to build on that foundation with our clinical development, manufacturing, and commercial capabilities. Our objective is to continue to be an integrated, multi-product biopharmaceutical company that provides patients and medical professionals with important options for preventing and treating human diseases.
We believe that our ability to develop product candidates is enhanced by the application of our VelociSuite® technology platforms. Our discovery platforms are designed to identify specific proteins of therapeutic interest for a particular disease or cell type and validate these targets through high-throughput production of genetically modified mice using our VelociGene® technology to understand the role of these proteins in normal physiology, as well as in models of disease. Our human antibody technology (VelocImmune) and cell line expression technologies (VelociMab®) may then be utilized to discover and produce new product candidates directed against the disease target. Our antibody product candidates currently in clinical trials were developed using VelocImmune. We continue to invest in the development of enabling technologies to assist in our efforts to identify, develop, manufacture, and commercialize new product candidates.
Trap-based Clinical Program - Ophthalmologic Diseases
EYLEA (aflibercept) - Ophthalmologic Diseases
Overview
EYLEA is a recombinant fusion protein, consisting of portions of human VEGF receptors 1 and 2 extracellular domains fused to the Fc portion of human IgG1 and formulated as an iso-osmotic solution for intravitreal administration. EYLEA acts as a soluble decoy receptor that binds VEGF-A and placental growth factor (PlGF) and thereby can inhibit the binding and activation of these cognate VEGF receptors. EYLEA is specially purified and contains iso-osmotic buffer concentrations, which optimizes it for injection into the eye.
Diabetic Retinopathy
Diabetic retinopathy is a complication of diabetes mellitus characterized by microvascular damage to the blood vessels in the retina. It can progress to proliferative diabetic retinopathy (PDR), where new, abnormal vessels that are susceptible to hemorrhage grow initially from the retina and/or optic disc and extend beyond the internal limiting membrane. PDR can subsequently lead to various vision-threatening complications such as vitreous hemorrhage, traction macular detachment, and Neovascular Glaucoma (NVG). Patients are often observed until disease progresses sufficiently to warrant intraocular surgery (vitrectomy) or, more commonly, extensive laser treatment (panretinal photocoagulation (PRP)). PRP is utilized with the intent of preserving function of the central retina, but is inherently destructive to the peripheral retina and may result in loss of peripheral vision.
A Phase 3 study (PANORAMA) to assess the efficacy and safety of intravitreal aflibercept in patients with moderately severe to severe NPDR without DME has completed enrollment.
7
Late-Stage Antibody-based Clinical Programs
Dupixent (dupilumab; IL-4R Antibody) for allergic and inflammatory conditions
Overview
IL-4R is required for signaling by the cytokines IL-4 and IL-13. Both of these cytokines are critical mediators of Type 2 inflammation, which drives the formation of Immunoglobulin E (IgE) antibodies and allergic diseases like atopic dermatitis (eczema), asthma, nasal polyps, and eosinophilic esophagitis. Dupilumab is a fully human monoclonal antibody generated using our VelocImmune technology and is designed to bind to IL-4R alpha subunit to block signaling from both IL-4 and IL-13.
Atopic Dermatitis
Phase 3 Studies in Adolescent and Pediatric Patients. In the first quarter of 2017, a Phase 3 study in adolescent patients (12–17 years of age) with moderate-to-severe atopic dermatitis was initiated, and in the fourth quarter of 2017, a Phase 3 study in pediatric patients (from six years to 11 years of age) with severe atopic dermatitis was also initiated. Additionally, in the first quarter of 2018, we initiated a Phase 2/3 study in younger pediatric patients (from six months to five years of age) with severe atopic dermatitis.
In 2016, the FDA granted Breakthrough Therapy designation for dupilumab for the treatment of moderate-to-severe (12 to less than 18 years of age) and severe (6 months to less than 12 years of age) atopic dermatitis in patients who are not adequately controlled with, or who are intolerant to, topical medication.
Other Phase 3 Studies. The Phase 3 LIBERTY AD CAFÉ study of Dupixent investigated two dose regimens of Dupixent (300 mg weekly and 300 mg every two weeks) with concomitant topical corticosteroids in adult patients with moderate-to-severe atopic dermatitis who are inadequately controlled with or intolerant to the broad immunosuppressant drug cyclosporine A (CSA), or when this treatment is medically inadvisable. The primary endpoint of this study was the proportion of patients with a 75% or greater improvement from baseline in their Eczema Area and Severity Index (EASI-75) score at 16 weeks. In April 2017, we and Sanofi announced that the results of the LIBERTY AD CAFÉ study were positive and demonstrated an acceptable safety profile. These results were submitted to the EMA and in September 2017, we and Sanofi presented the results at the European Academy of Dermatology and Venereology (EADV) Congress.
In March 2017, at the Annual Meeting of the American Academy of Dermatology, we and Sanofi presented additional detailed results from the Phase 3 LIBERTY AD CHRONOS study. This study met its primary and secondary endpoints, with patients receiving Dupixent along with topical corticosteroids (TCS) achieving significantly improved measures of overall disease severity at 16 and 52 weeks, compared to TCS alone in adults with uncontrolled moderate-to-severe atopic dermatitis.
Asthma
Phase 3 Program. LIBERTY ASTHMA QUEST is a Phase 3 study that evaluated dupilumab in adult and adolescent patients with uncontrolled persistent asthma. It is a global, placebo-controlled Phase 3 study that enrolled more than 1,900 patients. Patients were randomized into four groups: dupilumab 200 mg every other week with a loading dose of 400 mg, dupilumab 300 mg every other week with a loading dose of 600 mg, and two separate placebo groups. Patients were randomized in a 2:1 fashion to active drug versus placebo. The two primary endpoints of the study were the annualized rate of severe exacerbation events at 52 weeks and the absolute change from baseline in a standard measure of lung function known as pre-bronchodilator forced expiratory volume over one second (FEV1) at 12 weeks. The pre-specified primary analysis included hierarchical evaluation of these endpoints in the overall population, in patients with 150 eosinophilic cells/microliter or greater, and in patients with 300 eosinophilic cells/microliter or greater. In the study, approximately 50% of patients had 300 eosinophilic cells/microliter or greater and approximately 70% of patients had 150 eosinophilic cells/microliter or greater. Higher eosinophil counts are generally thought to be associated with poorer asthma control and higher rates of exacerbations, as was observed in the placebo patients in this study.
In the third quarter of 2017, we and Sanofi announced that the LIBERTY ASTHMA QUEST study met its two primary endpoints. Dupilumab, when added to standard therapies, reduced severe asthma attacks (exacerbations) and improved lung function. At 52 weeks, in the 300 mg dose group, dupilumab reduced severe asthma attacks by 46% in the overall population, 60% in patients with 150 eosinophilic cells/microliter or greater, and 67% in patients with 300 eosinophilic cells/microliter or greater (p<0.001 for all groups). At 12 weeks, in the 300 mg dupilumab dose group, mean improvement in lung function over placebo as assessed by FEV1 was 130 mL (9%) in the overall population, 150 mL (11%) in patients with 150 eosinophilic cells/microliter or greater, and 240 mL (18%) in patients with 300 eosinophilic cells/microliter or greater (p<0.001 for all groups). Changes in FEV1 of 100 to 200 mL are considered clinically relevant.
In the LIBERTY ASTHMA QUEST study, the exacerbations and FEV1 results for the 200 mg and 300 mg dupilumab dose groups were generally comparable. The extent of patient response correlated with allergic or atopic status as reflected by blood eosinophils and other markers. Less activity was observed in patients with less than 150 eosinophilic cells/microliter. The overall
8
rates of adverse events, deaths, infections, conjunctivitis, herpes, and discontinuations were comparable between the dupilumab and placebo groups. Injection site reactions were more common in the dupilumab groups (17%) compared to placebo (8%). All patients continued throughout the study on a medium or high dose inhaled corticosteroid (ICS) and up to two additional controller medicines. Eosinophil subgroups were classified based on baseline levels. Detailed results from this study will be submitted for presentation at a future medical congress.
In the fourth quarter of 2017, we and Sanofi announced that LIBERTY ASTHMA VENTURE, a randomized Phase 3 study examining the ability of dupilumab to reduce oral corticosteroid use in adults and adolescents with severe steroid-dependent asthma, met its primary endpoint and key secondary endpoints. Patients with severe chronic asthma have compromised lung function. In VENTURE, baseline FEV1 was approximately 52% of predicted normal. Oral corticosteriods (OCS) are typically prescribed to improve lung function and reduce asthma attacks in these severe patients. The VENTURE study enrolled 210 patients (103 in the dupilumab group and 107 in the placebo group) with severe asthma and regular use of OCS in the six months prior to enrollment. This Phase 3 trial enrolled severe steroid-dependent asthma patients without regard to baseline eosinophil levels or other biomarkers. The results showed improvements compared to placebo on lung function and exacerbations across patient subgroups - those with baseline eosinophil counts above 300 cells/microliter, above 150 cells/microliter, and below 150 cells/microliter.
For the primary endpoint, at 24 weeks in the overall population, dupilumab added to standard therapies significantly reduced the use of maintenance OCS by 70% on average (median reduction of 100%) compared to 42% with placebo (median reduction of 50%) (p<0.0001). In prespecified analyses of patients with baseline eosinophil counts greater than or equal to 300 cells/microliter, adding dupilumab significantly reduced OCS use by 80% on average (median reduction of 100%) compared to 43% for placebo (median reduction of 50%) (nominal p=0.0001). At 24 weeks, despite the reduced use of OCS, patients treated with dupilumab had 59% fewer attacks (exacerbations) in the overall population (p<0.0001) and 71% fewer attacks in patients with eosinophil counts greater than or equal to 300 cells/microliter. In addition to reducing exacerbations while reducing oral steroid dependence, dupilumab also improved lung function. At 24 weeks, the placebo-adjusted improvement in FEV1 on dupilumab was 220 mL (15%) in the overall population (p=0.0007) and 320 mL (25%) in patients with eosinophil counts greater than or equal to 300 cells/microliter (nominal p=0.0049).
The safety and tolerability profile of dupilumab in the LIBERTY ASTHMA VENTURE study was consistent with previous studies. There were more injection-site reactions reported with dupilumab (9%) vs. placebo (4%). There were more dupilumab-treated patients with an increase in eosinophil counts (14% dupilumab vs. 1% placebo), most of which were mild and the vast majority of which resolved. Overall rates of adverse events, including infections, conjunctivitis, and herpes, were comparable between the dupilumab and placebo groups.
Based on discussions with the FDA, our previously reported and published Phase 2b LIBERTY ASTHMA QUEST study served as the second required pivotal efficacy study for the sBLA for asthma. The results from the LIBERTY ASTHMA VENTURE study were also included in the sBLA for asthma, which was submitted with the FDA in the fourth quarter of 2017.
The TRAVERSE study, a long-term safety extension study, is also included in the LIBERTY ASTHMA clinical development program.
Phase 3 Study in Pediatric Patients. In the second quarter of 2017, a Phase 3 study in pediatric patients (from six to 11 years of age) with uncontrolled persistent asthma was initiated.
Nasal Polyps
Phase 3 Study. In 2017, we completed enrollment in two Phase 3 studies, as part of the LIBERTY NP SINUS program, in adult patients with bilateral nasal polyps on a background therapy with intranasal corticosteroids.
Eosinophilic Esophagitis
Phase 2 Study. EoE is a chronic allergic inflammatory disease manifested by tissue injury and pain and difficulty swallowing. People with EoE may also have allergies, asthma, atopic dermatitis, and chronic respiratory disease.
In the second quarter of 2017, we and Sanofi announced positive results from a 12-week Phase 2 proof-of-concept study of dupilumab in patients with active, moderate-to-severe EoE. In the fourth quarter of 2017, we and Sanofi presented these results at the World Congress of Gastroenterology. The study showed that compared to placebo, patients who received dupilumab weekly reported a significant improvement in the ability to swallow. The primary endpoint of the study was the change from baseline to week 10 in the Straumann Dysphagia Instrument (SDI) score, a 0–9 point patient-reported measure of swallowing difficulty, with 9 indicating more severe symptoms. A total of 47 patients were randomized to dupilumab 300 mg weekly following a 600 mg loading dose or placebo. Mean baseline SDI score was 6.4 in each group. At week 10, patients who received dupilumab reported a significant improvement in the ability to swallow with a three point reduction in their SDI score (45% improvement) compared to 1.3 points (19% improvement) for those patients who received placebo (p=0.0304).
9
Secondary endpoints of the study included endoscopic and histopathologic measures of disease severity, as well as other symptoms. The results include:
• | The mean change in the Eosinophilic Esophagitis Endoscopic Reference Score (EoE-EREFS) at 12 weeks was significantly reduced by 1.9 points from baseline (48% improvement) in patients who received dupilumab compared to 0.3 points (7% improvement) for those who received placebo (p=0.0006). EoE-EREFS is a visual measure of disease severity (inflammation and fibrosis in the esophagus) on a 0–8 point scale, with 8 indicating more severe disease. The mean baseline score was 3.9 for dupilumab and 4.3 for placebo. |
• | The mean percent change in overall peak intraepithelial eosinophil count from baseline to 12 weeks was significantly reduced by 93% in patients who received dupilumab compared to an increase of 14% in those who received placebo (p<0.0001). |
• | The mean percent change in a composite measure of symptoms and quality of life, as measured by Eosinophilic Esophagitis Symptom Activity Index (EEsAI), was numerically improved at 10 weeks (although not statistically significant) by 35% in patients who received dupilumab compared to an 11% improvement for those who received placebo (p=0.085). |
There were no new significant safety concerns in this study. Compared to placebo, higher rates of injection site reactions were observed on dupilumab.
In the third quarter of 2017, the FDA granted orphan drug designation to dupilumab for the treatment of EoE.
Praluent for LDL cholesterol reduction
Overview
Elevated LDL cholesterol ("bad cholesterol") level is a validated risk factor leading to cardiovascular disease. Statins are a class of drugs that lower LDL cholesterol (LDL-C) through inhibition of HMG-CoA, an enzyme regulating the early and rate-limiting step in cholesterol biosynthesis that ultimately results in an increase in LDL receptors to increase the uptake of plasma LDL lipoproteins. Similar to statins, PCSK9 impacts the number of available LDL receptors and therefore plays a key role in modulating LDL-C levels in the body. PCSK9 is a secreted protein that binds to and induces the destruction of the LDL receptor, thereby interfering with cellular uptake and increasing circulating levels of LDL cholesterol. In a landmark study published in The New England Journal of Medicine in March 2006, patients with lower than normal PCSK9 levels due to a genetic abnormality not only had significantly lower levels of LDL-C, but also a significant reduction in the risk of coronary heart disease (CHD). We used our VelocImmune technology to generate a fully human monoclonal antibody inhibitor of PCSK9, called Praluent, which lowers LDL cholesterol.
Clinical Program
The potential of Praluent to reduce cardiovascular events is being prospectively assessed in the 18,000-patient ODYSSEY OUTCOMES study (with data expected in the first quarter of 2018). To be entered into the ODYSSEY OUTCOMES study, patients had to have had a heart attack or unstable angina requiring hospitalization within the previous year, and inadequately controlled LDL cholesterol despite receiving maximally-tolerated statins and potentially other lipid-lowering therapies.
A Phase 4 randomized, placebo-controlled, long-term study that prospectively evaluates the effect of Praluent on neurocognitive function remains ongoing. This is a post-marketing commitment we made to the FDA.
In the second quarter of 2017, we and Sanofi presented positive results from two Phase 3b/4 studies (ODYSSEY-INSULIN and ODYSSEY-DYSLIPIDEMIA) that evaluated Praluent in patients with diabetes. A majority of patients in both trials reached their lipid goals on Praluent 75 mg administered every two weeks. The overall safety profile was consistent with observations in the ODYSSEY Phase 3 program.
The sBLA for use of Praluent with apheresis has been filed with the FDA, with a target action date of August 24, 2018.
In the fourth quarter of 2017, a Phase 3 study in HoFH was initiated.
Kevzara (sarilumab; IL-6R Antibody) for inflammatory diseases
Overview
IL-6 is a key cytokine driving inflammation and joint destruction in RA. Sarilumab, generated using our VelocImmune technology, is a fully human monoclonal antibody to IL-6R.
10
Polyarticular-course Juvenile Idiopathic Arthritis (pcJIA)
A Phase 2 study of sarilumab in pcJIA was initiated in 2016.
Cemiplimab (REGN2810; PD-1 Antibody) for cancer
Overview
The PD-1 immune checkpoint pathway has emerged as a major mechanism by which cancers evade immune destruction. Several drugs blocking either PD-1 or PD-L1 (one of the two ligands bound by PD-1) have been approved. Cemiplimab is a fully-human high-affinity anti-PD-1 antibody that was generated using the Velocimmune platform. We are developing cemiplimab as a foundation for a diverse and comprehensive immuno-oncology portfolio. Our initial approval strategy is focused on monotherapy in selected indications. Subsequent development activities are expected to include combinations with other anti-cancer agents.
Clinical Program
Cemiplimab is in Phase 1 clinical development in a variety of malignancies, both as monotherapy and in combination with other antibodies or treatments. In 2016, we initiated a pivotal Phase 2 study for the treatment of metastatic or locally advanced and unresectable CSCC. In the second quarter of 2017, we initiated a Phase 3 study in first-line treatment for NSCLC and a potentially pivotal Phase 2 study in BCC. In the third quarter of 2017, we also initiated a Phase 3 study in cervical cancer.
In June 2017, we and Sanofi announced positive preliminary results in patients with advanced CSCC. We presented data at the 2017 American Society of Clinical Oncology (ASCO) Annual Meeting from 26 patients pooled from two expansion cohorts of the cemiplimab Phase 1 study. Ten patients with distantly metastatic CSCC were enrolled in one expansion cohort and 16 patients with inoperable (unresectable) locally or regionally advanced CSCC were enrolled in a second expansion cohort. Treatment with cemiplimab led to an investigator-assessed overall response rate (ORR) of 46.2% and a disease control rate (DCR) of 69.2%. The median progression-free survival and overall survival were not reached at the data cutoff date with a median follow up of 6.9 months (range: 1.1 to 13.8 months; ongoing). One patient experienced progressive disease following an initial response to cemiplimab, and two patients were not evaluable for response due to death, which was considered unrelated to cemiplimab. The most common treatment-related adverse event of any grade was fatigue (23.1%). Grade 3 or higher adverse events included arthralgia (3.8%), maculopapular rash (3.8%), asthenia (3.8%), aspartate aminotransferase (AST) elevation (3.8%), and alanine aminotransferase (ALT) elevation (3.8%). We found no apparent association between the treatment response and level of PD-L1 (programmed death ligand 1) expression.
In the third quarter of 2017, the FDA granted cemiplimab Breakthrough Therapy designation for the treatment of adults with metastatic CSCC and adults with locally advanced and unresectable CSCC.
In December 2017, we and Sanofi announced positive top-line results from the pivotal Phase 2 EMPOWER-CSCC 1 study of cemiplimab in 82 patients with advanced CSCC. Cemiplimab demonstrated an ORR of 46.3%, determined by independent review. The median duration of response (DOR) had not yet been reached at the data cut-off point (32 of 38 responses were ongoing). At the time of this analysis, all patients had a minimum follow up of 6 months. The safety profile in the study was generally consistent with approved anti-PD-1 agents. These pivotal data will form the basis of a rolling BLA submission to the FDA, which we have initiated.
Cemiplimab is also being studied by other companies in combination with their proprietary assets. For example, in the second quarter of 2017, we and Inovio Pharmaceuticals, Inc. entered into a clinical and supply agreement for a Phase 1b/2a immuno-oncology study that will be conducted by Inovio in patients with newly-diagnosed glioblastoma multiforme (GBM) and will evaluate cemiplimab in combination with Inovio's INO-5401 T cell activating immunotherapy encoding multiple antigens and INO-9012, an immune activator encoding IL-12. Also in the second quarter of 2017, we and SillaJen, Inc. entered into a clinical and supply agreement for a Phase 1b dose-escalation study in renal cell carcinoma (RCC), or kidney cancer. The study will evaluate cemiplimab in combination with SillaJen's oncolytic vaccinia virus, Pexa-Vec, in patients with previously treated metastatic or unresectable renal cell carcinoma.
In the fourth quarter of 2017, we and ISA Pharmaceuticals entered into a collaboration agreement to develop ISA101, an immunotherapy targeting HPV16-induced cancer, in combination with cemiplimab. We and ISA will jointly fund and conduct clinical trials of the combination treatment in cervical cancer and head-and-neck cancer.
11
Fasinumab (REGN475; NGF Antibody) for pain due to osteoarthritis and chronic low back pain
Overview
Pain is among the most common reasons people see the doctor and why analgesics, including opioids, are among the most commonly prescribed drugs. Pain is a major cause of work disability and impaired quality of life. Targeting NGF is a potential new way to manage pain without resorting to opiods. NGF expression is elevated in many acute and chronic painful conditions and NGF blockade has demonstrated efficacy in clinical trials. Fasinumab is a fully human monoclonal antibody to NGF, generated using our VelocImmune technology.
The fasinumab clinical development program is expected to comprise approximately 10,000 patients treated with fasinumab.
Osteoarthritis
We initiated a Phase 3 long-term safety study in patients with pain due to osteoarthritis of the knee or hip in 2016 and a Phase 3 efficacy study in patients with pain due to osteoarthritis of the knee or hip in the second quarter of 2017. In the third quarter of 2017, we initiated a Phase 3 efficacy study of fasinumab compared to placebo or naproxen in patients with pain due to osteoarthritis of the knee or hip and in the fourth quarter of 2017 we initiated a Phase 3 efficacy study with multiple nonsteroidal anti-inflammatory drugs (NSAIDs) in patients with pain due to osteoarthritis.
As previously reported, in our Phase 2/3 clinical study in osteoarthritis, the incidence of adjudicated arthropathies in patients on fasinumab was found to be potentially dose-dependent. The ongoing fasinumab osteoarthritis pain pivotal Phase 3 program excludes higher doses associated with a higher incidence of arthropathy.
Chronic Low Back Pain
A Phase 3 study in chronic low back pain in patients with concomitant osteoarthritis was initiated in the fourth quarter of 2017.
Evinacumab (REGN1500; Antibody to ANGPTL3) for cardiovascular and metabolic disease
Overview
ANGPTL3 is a protein secreted by the liver. ANGPTL3 inhibition lowers plasma levels of triglycerides, LDL-C, and high-density lipoprotein cholesterol (HDL-C). Evinacumab is a fully human monoclonal antibody and a specific inhibitor of ANGPTL3. We are investigating the use of evinacumab in patients with dyslipidemias.
HoFH
A Phase 2 study for the treatment of HoFH is fully enrolled and ongoing. A Phase 3 study in HoFH was initiated in the first quarter of 2018.
Refractory Hypercholesterolemia
A Phase 2 study in refractory hypercholesterolemia (both HeFH and non-FH) was initiated in the fourth quarter of 2017 .
Other Programs
Our preclinical research programs include the areas of oncology and immuno-oncology, angiogenesis, ophthalmology, metabolic and related diseases, muscle diseases and disorders, inflammation and immune diseases, bone and cartilage, pain and neurobiology, cardiovascular diseases, and infectious diseases.
In 2015, we and BARDA of the HHS entered into an agreement to develop, test, and manufacture an antibody therapy (REGN3470-3471-3479) for the treatment of Ebola virus infection. Under the terms of the agreement, HHS provides funding to support our preclinical development, antibody manufacturing, and for a Phase 1 study in healthy volunteers, and has the option to provide additional funding for further manufacturing and development studies. In September 2017, we and BARDA entered into an additional agreement whereby HHS provides additional funding for the continued development of REGN3470-3471-3479, a potential BLA filing, and initial procurement of the therapy for national security preparedness. In addition, in 2016, we and BARDA entered into an agreement whereby HHS will provide certain funding to manufacture and study two antibody therapies for the potential treatment of Middle East Respiratory Syndrome (MERS).
In September 2017, we and BARDA also entered into an agreement to discover, research, develop, and manufacture a portfolio of antibodies targeting up to 10 pathogens, starting with Influenza virus, that pose significant risk to public health. The emerging pathogens treatment portfolio will be pursued using an Other Transaction Agreement (OTA), which provides a funding and collaboration vehicle for HHS to promote innovation in technology for advanced research and development. Under the OTA,
12
which has a term of 10 years, HHS will fund 80% of our costs for research, development, and manufacturing activities for antibodies that are selected to move forward.
Research and Development Technologies
Many proteins that play an important role in biology and disease are secreted by cells or located on the cell surface. Moreover, cells communicate through secreted factors and surface molecules. Our scientists have developed two different technologies to make protein therapeutics that potently and specifically block, activate, or inhibit the action of specific cell surface or secreted molecules. The first technology fuses receptor components to the constant region of an antibody molecule to make a class of drugs we call "Traps". EYLEA, ZALTRAP, and ARCALYST are drugs generated using our Trap technology. VelociSuite is our second technology platform. It is used for discovering, developing, and producing fully human antibodies that can address both secreted and cell-surface targets.
VelociSuite. VelociSuite consists of VelocImmune, VelociGene, VelociMouse®, VelociMab, and other related technologies. The VelocImmune mouse platform is utilized to produce fully human antibodies. VelocImmune was generated by exploiting our VelociGene technology (see below), in a process in which six megabases of mouse immune gene loci were replaced, or "humanized," with corresponding human immune gene loci. VelocImmune mice can be used efficiently to generate fully human antibodies to targets of therapeutic interest. VelocImmune and our entire VelociSuite offer the potential to increase the speed and efficiency through which human antibody therapeutics may be discovered and validated, thereby improving the overall efficiency of our early stage drug development activities. We are utilizing the VelocImmune technology to produce our next generation of drug candidates for preclinical and clinical development.
Our VelociGene platform allows custom and precise manipulation of very large sequences of DNA to produce highly customized alterations of a specified target gene, or genes, and accelerates the production of knock-out and transgenic expression models without using either positive/negative selection or isogenic DNA. In producing knock-out models, a color or fluorescent marker may be substituted in place of the actual gene sequence, allowing for high-resolution visualization of precisely where the gene is active in the body during normal body functioning as well as in disease processes. For the optimization of preclinical development and pharmacology programs, VelociGene offers the opportunity to humanize targets by replacing the mouse gene with the human homolog. Thus, VelociGene allows scientists to rapidly identify the physical and biological effects of deleting or over-expressing the target gene, as well as to characterize and test potential therapeutic molecules.
Our VelociMouse technology platform allows for the direct and immediate generation of genetically altered mice from embryonic stem cells (ES cells), thereby avoiding the lengthy process involved in generating and breeding knockout mice from chimeras. Mice generated through this method are normal and healthy and exhibit a 100% germ-line transmission. Furthermore, mice developed using our VelociMouse technology are suitable for direct phenotyping or other studies. We have also developed our VelociMab platform for the rapid screening of antibodies and rapid generation of expression cell lines for our Traps and our VelocImmune human antibodies.
We have utilized our VelociSuite technologies to develop a class of potential drug candidates, known as bi-specific antibodies. In the area of immunotherapies in oncology, we are exploring the use of bi-specific antibodies that target tumor antigens and the CD3 receptor on T-cells to harness the oncolytic properties of T-cells. Our first such bi-specific antibody, REGN1979, targets CD20 and CD3. We are exploring additional indications and applications for our bi-specific technologies, such as bi-specific antibodies to mucin 16 (MUC16) and B-cell maturation antigen (BCMA).
Regeneron Genetics Center®. In 2014, we launched a new human genetics initiative via a wholly owned subsidiary, Regeneron Genetics Center LLC (RGC). RGC leverages de-identified clinical, genomic, and molecular data from human volunteers to identify medically relevant associations in a blinded fashion designed to preserve patients' privacy. The objective of RGC is to expand the use of human genetics for discovering and validating genetic factors that cause or influence a range of diseases where there are major unmet medical needs, with the prospect of improving the drug discovery and development process. RGC is undertaking multiple approaches, including large population-based efforts as well as family- and founder-based approaches. RGC utilizes laboratory automation and innovative approaches to cloud computing to achieve high-quality throughput.
Central to the work of RGC is a collaboration with the Geisinger Health System of Pennsylvania. Geisinger collects samples from consented patient volunteers, while RGC performs sequencing and genotyping to generate de-identified genomic data. In addition, RGC has expanded on its foundational population-based collaboration with Geisinger with a growing number of other organizations worldwide.
In January 2018, we, along with AbbVie Inc., Alnylam Pharmaceuticals Inc., AstraZeneca PLC, Biogen Inc., and Pfizer Inc., announced the formation of a consortium to fund the generation of genetic exome sequence data from 500,000 volunteer participants who make up the UK Biobank health resource. The other companies will each commit up to $10.0 million in funding for Regeneron to sequence the UK Biobank's samples, which will be performed at the RGC facility. Consortium members will have a limited period of exclusive access to the sequencing data, before the data will be made available to other health researchers by UK Biobank.
13
License Agreements
In September 2017, we entered into a license agreement with a third party, which grants the third party the right to develop and commercialize new indications for ARCALYST in certain jurisdictions, including the United States. We currently maintain exclusive rights to ARCALYST in the United States for existing indications, and are entitled to all profits from such sales. Commencing with the receipt of marketing approval by the third party for the first new indication in the United States, we will grant commercial rights to ARCALYST for our existing indications to the third party.
Collaboration Agreements
Collaborations with Sanofi
Antibodies. Our Discovery and Preclinical Development Agreement (Antibody Discovery Agreement) with Sanofi ended on December 31, 2017 without any extension. Praluent, Dupixent, Kevzara, cemiplimab, REGN3500, and REGN3767 were discovered and initially developed under the Antibody Discovery Agreement. Praluent, Dupixent, Kevzara, and REGN3500 will continue to be developed, and commercialized as applicable, with Sanofi under the Antibody License and Collaboration Agreement (LCA). Cemiplimab and REGN3767 will continue to be developed with Sanofi under the immuno-oncology collaboration. We have the right to develop or continue to develop other product candidates discovered under the Antibody Discovery Agreement independently or with other collaborators.
Under the terms of the LCA, development costs for the drug candidate are shared between the companies, with Sanofi generally funding these costs as they are incurred by us, except that following receipt of the first positive Phase 3 trial results for a co-developed drug candidate, subsequent Phase 3 trial-related costs for that drug candidate are shared 80% by Sanofi and 20% by us. We are generally responsible for reimbursing Sanofi for half of the total development costs for all collaboration antibody products from our share of profits from commercialization of collaboration products to the extent they are sufficient for this purpose. We are obligated to use commercially reasonable efforts to supply clinical requirements of each drug candidate under the collaboration until commercial supplies of that drug candidate are being manufactured.
Effective January 7, 2018, we and Sanofi entered into a letter agreement (Letter Agreement) amending the LCA in connection with, among other matters, the allocation of additional funds to certain proposed activities relating to the development of dupilumab and REGN3500 and non-approval trials of dupilumab (collectively, the Dupilumab/REGN3500 Eligible Investments). Pursuant to the Letter Agreement, we have agreed to allow Sanofi to satisfy in whole or in part its funding obligations with respect to the Dupilumab/REGN3500 Eligible Investments for the quarterly periods commencing on January 1, 2018 and ending on September 30, 2020 by selling up to 600,000 shares of our Common Stock directly or indirectly owned by Sanofi. Refer to the "Immuno-Oncology" section below for further details regarding the Letter Agreement.
Under our collaboration agreement, Sanofi records product sales for commercialized products, and Regeneron has the right to co-promote such products on a country-by-country basis. We have exercised our option to co-promote Dupixent, Praluent, and Kevzara in the United States. We have not exercised any of our options to co-promote these antibodies outside the United States; however, we retain the right to do so at a future date subject to the terms of the collaboration agreement. We and Sanofi will equally share profits and losses from sales within the United States. We and Sanofi share profits outside the United States on a sliding scale based on sales starting at 65% (Sanofi)/35% (us) and ending at 55% (Sanofi)/45% (us), and share losses outside the United States at 55% (Sanofi)/45% (us). In addition to profit sharing, we are entitled to receive up to $250.0 million in sales milestone payments, with milestone payments commencing after aggregate annual sales outside the United States exceed $1.0 billion on a rolling 12-month basis.
Immuno-Oncology. In July 2015, we and Sanofi entered into a global strategic collaboration to discover, develop, and commercialize antibody-based cancer treatments in the field of immuno-oncology (the IO Collaboration). The IO Collaboration is governed by an Immuno-oncology Discovery and Development Agreement (IO Discovery Agreement), and an Immuno-oncology License and Collaboration Agreement (IO License and Collaboration Agreement). In connection with the IO Discovery Agreement, Sanofi made a $265.0 million non-refundable up-front payment to us. Pursuant to the IO Discovery Agreement, we will spend up to $1,090.0 million (IO Discovery Budget) to identify and validate potential immuno-oncology targets and develop therapeutic antibodies against such targets through clinical proof-of-concept. Sanofi will reimburse us for up to $825.0 million (IO Discovery Funding) of these costs, subject to certain annual limits. The term of the IO Discovery Agreement will continue through the later of five years from the effective date of the IO Collaboration or the date the IO Discovery Budget is exhausted, subject to Sanofi's option to extend it for up to an additional three years for the continued development (and funding) of selected ongoing programs. Pursuant to the IO Discovery Agreement, we will be primarily responsible for the design and conduct of all research activities, including target identification and validation, antibody development, preclinical activities, toxicology studies, manufacture of preclinical and clinical supplies, filing of Investigational New Drug Applications (INDs), and clinical development through proof-of-concept. We will reimburse Sanofi for half of the development costs they funded that are attributable to clinical development of antibody product candidates under the IO Discovery Agreement from our share of future profits, if any, from commercialized
14
IO Collaboration products to the extent they are sufficient for this purpose. With regard to product candidates for which proof-of-concept is established, Sanofi will have the option to license rights to the product candidate pursuant to the IO License and Collaboration Agreement (as further described below).
In connection with the IO License and Collaboration Agreement, Sanofi made a $375.0 million non-refundable up-front payment to us. If Sanofi exercises its option to license rights to a product candidate thereunder, it will co-develop the drug candidate with us through product approval. Principal control of development of each product candidate that enters development under the IO License and Collaboration Agreement will alternate between us and Sanofi on a candidate-by-candidate basis. Sanofi will fund drug candidate development costs up front for the candidates for which it is the principal controlling party and we will reimburse half of the total development costs for all such candidates from our share of future IO Collaboration profits to the extent they are sufficient for this purpose. In addition, we and Sanofi will share equally, on an ongoing basis, the development costs for the drug candidates for which we are the principal controlling party. The party having principal control over the development of a product candidate will also lead the commercialization activities for such product candidate in the United States. We are obligated to use commercially reasonable efforts to supply clinical requirements of each drug candidate under the IO License and Collaboration Agreement until commercial supplies of that IO drug candidate are being manufactured. For all products commercialized under the IO License and Collaboration Agreement, Sanofi will lead commercialization activities outside of the United States. Each party will have the right to co-promote licensed products in countries where it is not the lead commercialization party. The parties will share equally in profits and losses in connection with the commercialization of collaboration products.
Under the terms of the IO License and Collaboration Agreement, the parties will also co-develop our antibody product candidate targeting PD-1 (cemiplimab). We have principal control over the development of cemiplimab, and the parties share equally, on an ongoing basis, development expenses for cemiplimab. Pursuant to the January 7, 2018 Letter Agreement with Sanofi, the cemiplimab development budget has been increased to a total of $1.640 billion, $990.0 million over the budget originally set forth in the IO License and Collaboration Agreement. Under the Letter Agreement, we have also agreed to allow Sanofi to satisfy in whole or in part its funding obligation with respect to cemiplimab development costs for the quarterly periods commencing on October 1, 2017 and ending on September 30, 2020 by selling up to 800,000 shares of our Common Stock directly or indirectly owned by Sanofi.
If Sanofi desires to sell shares of our Common Stock during the term of the Letter Agreement to satisfy a portion or all of its funding obligations for the cemiplimab development and/or, as noted above, Dupilumab/REGN3500 Eligible Investments, we may elect to purchase, in whole or in part, such shares from Sanofi. If we do not elect to purchase such shares, Sanofi may sell the applicable number of shares (subject to certain daily and quarterly limits) in one or more open-market transactions.
With regard to cemiplimab, we will lead commercialization activities in the United States, while Sanofi will lead commercialization activities outside of the United States and the parties will equally share profits from worldwide sales. Sanofi has exercised its option to co-promote cemiplimab in the United States. We will be entitled to a milestone payment of $375.0 million in the event that global sales of certain licensed products targeting PD-1 (including cemiplimab), together with sales of any other products licensed under the IO License and Collaboration Agreement and sold for use in combination with any of such licensed products targeting PD-1, equal or exceed $2.0 billion in any consecutive twelve-month period.
Collaborations with Bayer
EYLEA outside the United States. Since October 2006, we and Bayer have been parties to a license and collaboration agreement for the global development and commercialization outside the United States of EYLEA. Under the agreement, we and Bayer collaborate on, and share the costs of, the development of EYLEA. Bayer markets EYLEA outside the United States, where, for countries other than Japan, the companies share equally in profits and losses from sales of EYLEA. In Japan, we are entitled to receive a tiered percentage of between 33.5% and 40.0% of EYLEA net sales.
Commencing with the first commercial sale of EYLEA in a major market country outside the United States, we became obligated to reimburse Bayer for 50% of the development costs that it has incurred under the agreement from our share of the collaboration profits (including payments to us based on sales in Japan). The reimbursement payment in any quarter will equal 5% of the then outstanding repayment obligation, but never more than our share of the collaboration profits in the quarter unless we elect to reimburse Bayer at a faster rate. As a result, we expect that a portion of our share of EYLEA profits outside the United States will be used to reimburse Bayer for this repayment obligation.
Within the United States, we retain exclusive commercialization rights to EYLEA and are entitled to all profits from any such sales.
15
Ang2 antibody outside the United States. In March 2016, we entered into an agreement with Bayer governing the joint development and commercialization outside the United States of nesvacumab, an antibody product candidate to Ang2, including REGN910-3 (nesvacumab in combination with aflibercept), for the treatment of ocular diseases or disorders. In connection with the agreement, Bayer made a $50.0 million non-refundable up-front payment to us and is obligated to pay 25% of global development costs and 50% of development costs exclusively for the territory outside the United States.
In the fourth quarter of 2017, we reported that results from two Phase 2 studies that added nesvacumab to EYLEA did not provide sufficient differentiation to warrant Phase 3 development.
Collaboration with Mitsubishi Tanabe Pharma
Fasinumab. In September 2015, we entered into a collaboration agreement with Mitsubishi Tanabe Pharma Corporation (MTPC) providing MTPC with development and commercial rights to fasinumab in Japan, South Korea, Taiwan, Indonesia, Thailand, the Philippines, Malaysia, Singapore, Vietnam, Myanmar, and Sri Lanka (the MTPC Territories). In connection with the agreement, MTPC made a $10.0 million non-refundable up-front payment in 2015, and in 2016, MTPC made additional payments totaling $60.0 million to us. In the second quarter of 2017, we earned a $30.0 million development milestone from MTPC, and in the fourth quarter of 2017, MTPC made additional payments totaling $25.0 million to us related to development milestones achieved by MTPC. We are entitled to receive up to an aggregate of $100.0 million in additional development milestone and other contingent payments.
Under the agreement, we are obligated to manufacture and supply MTPC with clinical and commercial supplies of fasinumab. If fasinumab is commercialized in the MTPC Territories, we will supply the product to MTPC at a tiered purchase price, which ranges from 30% to 50% of net sales of the product (subject to adjustment in certain circumstances), and are eligible for additional payments up to an aggregate of $100.0 million upon the achievement of specified annual net sales amounts starting at $200.0 million.
Collaboration with Teva
Fasinumab. In September 2016, we entered into a collaboration agreement with Teva to develop and commercialize fasinumab globally, excluding certain Asian countries that are subject to our collaboration agreement with MTPC (as described above). In connection with the agreement, Teva made a $250.0 million non-refundable up-front payment in 2016. We will lead global development activities, and the parties will share equally, on an ongoing basis, development costs under a global development plan. During 2017, we earned $25.0 million and $35.0 million development milestones from Teva, and we are entitled to receive up to an aggregate of $400.0 million in additional development milestones and up to an aggregate of $1,890.0 million in contingent payments upon achievement of specified annual net sales amounts. We are responsible for the manufacture and supply of fasinumab globally.
Within the United States, we will lead commercialization activities, and the parties will share equally in any profits or losses in connection with commercialization of fasinumab. In the territory outside of the United States, Teva will lead commercialization activities and we will supply product to Teva at a tiered purchase price, which is calculated as a percentage of net sales of the product (subject to adjustment in certain circumstances).
Manufacturing
We currently manufacture bulk drug materials at our manufacturing facilities in Rensselaer, New York, which consists of approximately 565,000 square feet of owned research, manufacturing, office, and warehouse space. We currently have approximately 101,000 liters of cell culture capacity, and are approved by the FDA and other regulatory agencies to manufacture our marketed products at these facilities.
We also own an approximately 445,000 square foot facility in Limerick, Ireland, which we acquired in 2014 and subsequently renovated to accommodate and support our growth and expand our manufacturing capacity. The facility has received certain manufacturing approvals by regulatory agencies, including the FDA, and is in the process of further validation, as required by regulatory authorities, for the manufacture of our bulk drug products.
Certain raw materials or other products necessary for the manufacture and formulation of our products and product candidates are provided by single-source unaffiliated third-party suppliers. In addition, we rely on certain third parties to perform packaging, filling, finishing, labeling, distribution, laboratory testing, and other services related to the manufacture of our products and product candidates, and to supply various raw materials and other products. See Part I, Item 1A. "Risk Factors - Risks Related to Manufacturing and Supply" for further information.
Among the conditions for regulatory marketing approval of a medicine is the requirement that the prospective manufacturer's quality control and manufacturing procedures conform to the good manufacturing practice (GMP) regulations of the health authority. In complying with standards set forth in these regulations, manufacturers must continue to expend time, money, and effort in the
16
areas of production and quality control to ensure full technical compliance. Manufacturing establishments, both foreign and domestic, are also subject to inspections by or under the authority of the FDA and by other national, federal, state, and local agencies.
Sales and Marketing
We have a New Products Marketing and Planning group, a Market Research group, and a Market Access group to evaluate commercial opportunities for our targets and drug candidates, assess the competitive environment, and analyze the commercial potential of our product portfolio, and prepare for market launch of new products. These groups are fully functional to support our product and product candidates that we are independently developing and/or commercializing, and also work closely with our collaborators for co-developed products to develop marketing plans and forecasts and to develop and execute pre-launch market development programs.
We also have a full-service commercialization group to handle various aspects of our commercial programs. The group includes experienced professionals in the fields of marketing, communications, professional education, patient education and advocacy, reimbursement and market access, trade and distribution, commercial operations, commercial analytics, market research, and forecasting. Moreover, for our marketed products, we have hired, trained, and deployed a field-based organization including regional directors, medical specialists, and reimbursement managers, each typically with a number of years of experience in the biopharmaceutical industry in a variety of therapeutic areas including oncology, ophthalmology, immunology, and inflammation. We have approximately 600 field-based employees in the United States.
Customers
We sell EYLEA in the United States to several distributors and specialty pharmacies. We sell ARCALYST in the United States to two specialty pharmacies. Under these distribution models, the distributors and specialty pharmacies generally take physical delivery of product. For EYLEA, the distributors and specialty pharmacies generally sell the product directly to healthcare providers, whereas for ARCALYST, the specialty pharmacies sell the product directly to patients. We had sales to three customers (Besse Medical, a subsidiary of AmerisourceBergen Corporation; McKesson Corporation; and Curascript SD Specialty Distribution, a subsidiary of Express Scripts) that each accounted for more than 10% of total gross product revenue for the year ended December 31, 2017. On a combined basis, our product sales to these customers accounted for approximately 99% of our gross product revenue for the year ended December 31, 2017. We are also a party to collaboration agreements with Bayer and Sanofi, whereby our collaborator is responsible for recording product sales of EYLEA outside the United States and global sales of Dupixent, Praluent, and Kevzara, respectively.
Competition
We face substantial competition from pharmaceutical, biotechnology, and chemical companies. Many of our competitors have substantially greater research, preclinical, and clinical product development, manufacturing capabilities, and financial, marketing, and human resources than we do. Competition from smaller competitors may also be or become more significant if those competitors acquire or discover patentable inventions, form collaborative arrangements, or merge with large pharmaceutical companies. Even if we are able to commercialize additional product candidates, one or more of our competitors may have brought a competitive product to market earlier than us or may have obtained or obtain patent protection that dominates or adversely affects our activities or products. Our ability to compete depends, to a great extent, on how fast we can develop safe and effective product candidates, complete clinical testing and approval processes, and supply commercial quantities of the product to the market. Competition among product candidates approved for sale is based on efficacy, safety, reliability, availability, price, patent position, and other factors.
17
EYLEA. The following table provides an overview of the competitive landscape for EYLEA:
Competitor Product/Product Candidate | Commercial or Development Status | Competitor | Indication | Territory | ||||
Lucentis® (ranibizumab) | Approved | Novartis AG and Genentech/Roche | Wet AMD, DME, macular edema following RVO (including CRVO and BRVO), diabetic retinopathy in patients with DME, and mCNV | Worldwide | ||||
Avastin® (bevacizumab) (off-label) | Used to treat wet AMD, DME, and macular edema following RVO | Genentech/Roche | Wet AMD, DME, and macular edema following RVO | Worldwide | ||||
Ozurdex® (dexamethasone intravitreal implant) | Approved | Allergan, PLC | DME, RVO | Worldwide | ||||
Iluvien® (fluocinolone acetonide intravitreal implant) | Approved | Alimera Sciences, Inc. | DME | United States, EU | ||||
Conbercept | Approved in China for wet AMD In development for other eye indications | Chengdu Kanghong Pharmaceutical Group | Wet AMD | China | ||||
Brolucizumab (RTH258), a single chain antibody fragment directed against VEGF-A | In development (two non-inferiority Phase 3 trials comparing RTH258 and EYLEA met their primary endpoint in June 2017) | Novartis | Wet AMD | — | ||||
Abicipar pegol (anti-VEGF-A-DARPin®) | In development (non-inferiority Phase 3 trial initiated in 2015 comparing dosing regimens of abicipar pegol and Lucentis) | Allergan | Wet AMD and related conditions | — | ||||
RG7716, a bi-specific antibody targeting anti-VEGF and Ang2 | In development (Phase 2) | Genentech/Roche | Wet AMD, DME | — | ||||
Lucentis port delivery system | In development (Phase 2) | Genentech/Roche | Wet AMD and related conditions | — | ||||
X-82, an orally administered small molecule tyrosine kinase inhibitor in development for use in combination with EYLEA or Lucentis | In development (Phase 2) | Tyrogenex | Wet AMD and related conditions | — | ||||
DE-122, an anti-endoglin antibody in development for use in combination with EYLEA or Lucentis | In development (Phase 2) | Santen Pharmaceuticals Co. Ltd./ TRACON Pharmaceuticals, Inc. | Wet AMD and related conditions | — | ||||
GB-102, an intravitreally administered depot formulation of the small molecule tyrosine kinase inhibitor, sunitinib | In development (Phase 2) | Graybug Vision, Inc. | Wet AMD and related conditions | — | ||||
18
EYLEA (continued): | ||||||||
Competitor Product/Product Candidate | Commercial or Development Status | Competitor | Indication | Territory | ||||
OPT-302, a VEGFR-3 large molecule trap in development for use in combination with EYLEA or Lucentis | In development (Phase 2b) | Opthea Limited | Wet AMD and related conditions | — | ||||
M710, a biosimilar to EYLEA | In development (Phase 3) | Momenta Pharmaceuticals, Inc. (in partnership with Mylan N.V.) | Wet AMD and related conditions | — | ||||
CHS-3351, a biosimilar to Lucentis | In development (Phase 1) | Coherus BioSciences, Inc. | Wet AMD and related conditions | — | ||||
PF582, a biosimilar to Lucentis | In development (Phase 1/2 completed in August 2016) | Pfenex Inc. | Wet AMD and related conditions | — | ||||
FYB201, a biosimilar to Lucentis | In development (Phase 3) | Formycon AG (in collaboration with Bioeq GmbH) | Wet AMD and related conditions | — | ||||
SB11, a biosimilar to Lucentis | In development (Phase 3) | Samsung Bioepis Co., Ltd. | Wet AMD and related conditions | — | ||||
Razumab, a biosimilar to Lucentis | Approved in India for wet AMD and related conditions | Intas Phamaceuticals Limited | Wet AMD and related conditions | India | ||||
The table above is not exhaustive. For additional information regarding the substantial competition EYLEA faces, see also Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of EYLEA - The commercial success of EYLEA is subject to strong competition" and Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of Products - Our product candidates or new indications for our marketed products, if any are approved for marketing, may face significant competition."
19
Dupixent. The following table provides an overview of the competitive landscape for Dupixent:
Competitor Product/Product Candidate | Commercial or Development Status | Competitor | Indication | Territory | ||||
Eucrisa® (crisaborole) | Approved | Pfizer | Mild-to-moderate atopic dermatitis | United States | ||||
Xolair® (omalizumab) | Approved | Roche/Novartis | Asthma | Worldwide | ||||
Nucala® (mepolizumab) | Approved for asthma In development (Phase 2) for atopic dermatitis | GlaxoSmithKline (GSK) | Asthma and atopic dermatitis | Worldwide | ||||
Cinqair® (reslizumab) | Approved | Teva | Asthma | Worldwide | ||||
Fasenra® (benralizumab) | Approved | AstraZeneca | Asthma | United States, EU | ||||
Tralokinumab, an anti-IL-13 antibody | In development (Phase 3) | AstraZeneca/ LEO Pharma Inc. | Atopic dermatitis | — | ||||
Baricitinib, an orally administered JAK inhibitor | In development (Phase 3) | Eli Lilly and Company/Incyte Corporation | Atopic dermatitis | — | ||||
PF-04965842, an orally administered JAK inhibitor | In development (Phase 3) | Pfizer | Atopic dermatitis | — | ||||
Upadacitinib, an orally administered JAK inhibitor | In development (Phase 3) | AbbVie | Atopic dermatitis | — | ||||
Fevipiprant, an orally administered CRTH2 antagonist | In development (Phase 3) | Novartis | Asthma | — | ||||
Tezepelumab, an anti-TSLP antibody | In development (Phase 3) | Amgen Inc./AstraZeneca | Asthma | — | ||||
ANB-020, an anti-IL-33 antibody | In development (Phase 2) | AnaptysBio, Inc. | Asthma and atopic dermatitis | — | ||||
Lebrikizumab, an anti-IL-13 antibody | In development (Phase 2) | Dermira, Inc./Roche | Atopic dermatitis | — | ||||
Nemolizumab, an anti-IL-31R antibody | In development (Phase 2) | Galderma S.A. | Atopic dermatitis | — | ||||
CNTO7610, an anti-ST2 antibody | In development (Phase 2 for asthma and Phase 1 for atopic dermatitis) | Johnson & Johnson | Asthma and atopic dermatitis | — | ||||
RG6149, an anti-ST2 antibody | In development (Phase 2) | Roche | Asthma | — | ||||
MEDI-9314, an anti-IL-4R antibody | In development (Phase 1) | AstraZeneca | Atopic dermatitis | — | ||||
PRS-060, an inhaled anticalin targeting IL-4R | In development (Phase 1) | AstraZeneca/ Pieris Pharmaceuticals, Inc. | Asthma | — | ||||
The table above is not exhaustive. For additional information regarding the substantial competition Dupixent faces, see also Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara) - The commercial success of Dupixent, Praluent, and Kevzara is subject to strong competition."
20
Praluent. The following table provides an overview of the competitive landscape for Praluent:
Competitor Product/Product Candidate | Commercial or Development Status | Competitor | Indication | Territory | ||||
Repatha® (evolocumab) | Approved | Amgen | (1) Reduce the risk of myocardial infarction, stroke, and coronary revascularization in adults with established cardiovascular disease, (2) primary hyperlipidemia, and (3) HoFH | Worldwide | ||||
Inclisiran (ALN-PCSsc) | In development (Phase 2) | Alnylam Pharmaceuticals (in collaboration with The Medicines Company) | RNAi molecule against PCSK9 (injectable, small molecule) | — | ||||
ETC-1002 (bempedoic acid) | In development (Phase 3) | Esperion Therapeutics, Inc. | ACL-inhibitor (oral, small molecule) | — | ||||
Gemcabene | In development (Phase 2) | Gemphire Therapeutics Inc. | Cholesterol synthesis inhibitor (oral, small molecule) | — | ||||
The table above is not exhaustive. For additional information regarding the substantial competition Praluent faces, see also Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara) - The commercial success of Dupixent, Praluent, and Kevzara is subject to strong competition."
21
Kevzara. The following table provides an overview of the competitive landscape for Kevzara:
Competitor Product/Product Candidate | Commercial or Development Status | Competitor | Indication | Territory | ||||
Actemra® (tocilizumab) | Approved | Roche | Rheumatoid arthritis | Worldwide | ||||
Orencia® (abatacept) | Approved | Bristol-Myers Squibb Company | Rheumatoid arthritis | Worldwide | ||||
Xeljanz® (tofacitinib) | Approved | Pfizer | Rheumatoid arthritis | Worldwide | ||||
Olumiant® (baricitinib) | Approved | Eli Lilly/Incyte | Rheumatoid arthritis | EU | ||||
Olokizumab, an anti-IL-6 antibody | In development (Phase 3) | R-Pharm | Rheumatoid arthritis | — | ||||
Upadacitinib, an orally administered JAK inhibitor | In development (Phase 3) | AbbVie | Rheumatoid arthritis | — | ||||
Filgotinib, an orally administered JAK inhibitor | In development (Phase 3) | Gilead Sciences, Inc./ Galapagos NV | Rheumatoid arthritis | — | ||||
Peficitinib, an orally administered JAK inhibitor | In development (Phase 3) | Astellas Pharma Inc. | Rheumatoid arthritis | — | ||||
Clazakizumab, an anti-IL-6 antibody | In development (Phase 2) | Vitaeris Inc. | Rheumatoid arthritis | — | ||||
Vobarilizumab, an anti-IL-6R antibody fragment | In development (Phase 2) | Ablynx NV | Rheumatoid arthritis | — | ||||
Gerilimzumab, an anti-IL-6 antibody | In development (Phase 1) | Bird Rock Bio, Inc. | Rheumatoid arthritis | — | ||||
The table above is not exhaustive. For additional information regarding the substantial competition Kevzara faces, see also Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara) - The commercial success of Dupixent, Praluent, and Kevzara is subject to strong competition."
22
Antibodies in Development. Our clinical candidates in development are all fully human antibodies which were generated using our VelocImmune technology. Our antibody generation technologies and clinical candidates face competition from many pharmaceutical and biotechnology companies using various technologies. Numerous other companies are developing therapeutic antibody products. Companies have generated therapeutic products that are currently in development or on the market that are derived from recombinant DNA that comprise human antibody sequences. Astellas has licensed our VelocImmune technology to use it as part of their internal antibody development programs.
The following table provides an overview of the competitive landscape for our antibody programs that are in late-stage clinical development:
Regeneron Antibody Program | Competitor | Competitor Product/Product Candidate | Commercial or Development Status | Target | ||||
Cemiplimab (Phase 2/3) Target: PD-1 | Bristol-Myers Squibb | Opdivo® (nivolumab) | Approved | Antibody against PD-1 | ||||
Merck & Co., Inc. | Keytruda® (pembrolizumab) | Approved | Antibody against PD-1 | |||||
Pfizer/ Merck | Bavencio® (avelumab) | Approved | Antibody against PDL-1 | |||||
Roche | Tecentriq® (atezolizumab) | Approved | Antibody against PDL-1 | |||||
AstraZeneca | Imfinzi® (durvalumab) | Approved | Antibody against PDL-1 | |||||
Novartis | PDR001 | In development (Phase 3) | Antibody against PD-1 | |||||
Celgene Corporation/ BeiGene Ltd. | BGB-A317 | In development (Phase 3) | Antibody against PD-1 | |||||
Agenus Inc. | AGEN2034 | In development (Phase 1) | Antibody against PD-1 | |||||
TESARO, Inc./AnaptysBio | TSR-042 | In development (Phase 1) | Antibody against PD-1 | |||||
Pfizer | PFE-06801591 | In development (Phase 1) | Antibody against PD-1 (Subcutaneous Formulation) | |||||
Fasinumab (Phase 3) Target: NGF | Pfizer/Eli Lilly | Tanezumab | In development (Phase 3) | Antibody against NGF | ||||
Evinacumab (Phase 3) Target: ANGPTL3 | Ionis Pharmaceuticals, Inc./Akcea Therapeutics, Inc. | AKCEA-ANGPTL3-LRx | In development (Phase 2) | Ligand conjugated antisense drug against ANGPTL3 | ||||
The table above is not exhaustive and focuses on antibody competitors. We are also aware of several companies developing or marketing small molecules that may compete with our antibody product candidates in various indications, if such product candidates obtain regulatory approval in those indications.
For additional information regarding our antibody programs and the substantial competition they face, see Part I, Item 1A. "Risk Factors - Risks Related to Commercialization of Products - Our product candidates or new indications for our marketed products, if any are approved for marketing, may face significant competition."
Other Areas. Many pharmaceutical and biotechnology companies are attempting to discover new therapeutics for indications in which we invest substantial time and resources. In these and related areas, intellectual property rights have been sought and certain rights have been granted to competitors and potential competitors of ours, and we may be at a substantial competitive disadvantage in such areas as a result of, among other things, our lack of experience, trained personnel, and expertise. A number of corporate and academic competitors are involved in the discovery and development of novel therapeutics that are the focus of other research or development programs we are now conducting. Some of these competitors are currently conducting advanced preclinical and clinical research programs in these areas. These and other competitors may have established substantial intellectual property and other competitive advantages.
23
If any of these or other competitors announces a successful clinical study involving a product that may be competitive with one of our product candidates or the grant of marketing approval by a regulatory agency for a competitive product, such developments may have an adverse effect on our business, operating results, financial condition, cash flows, or future prospects.
We also compete with academic institutions, governmental agencies, and other public or private research organizations, which conduct research, seek patent protection, and establish collaborative arrangements for the development and marketing of products that would provide royalties or other consideration for use of their technology. These institutions are becoming more active in seeking patent protection and licensing arrangements to collect royalties or other consideration for use of the technology they have developed. Products developed in this manner may compete directly with products we develop. We also compete with others in acquiring technology from these institutions, agencies, and organizations.
Patents, Trademarks, and Trade Secrets
Our success depends, in part, on our ability to obtain patents, maintain trade secret protection, and operate without infringing on the proprietary rights of third parties (see Part I, Item 1A. "Risk Factors - Risks Related to Intellectual Property and Market Exclusivity - We may be restricted in our development, manufacturing, and/or commercialization activities by patents or other proprietary rights of others, and could be subject to damage awards if we are found to have infringed such patents or rights"; and Note 17 to our Consolidated Financial Statements). Our policy is to file patent applications to protect technology, inventions, and improvements that we consider important to our business and operations. We hold an ownership interest in a number of issued patents in the United States and foreign countries with respect to our products and technologies. In addition, we hold an ownership interest in hundreds of patent applications in the United States and foreign countries.
Our patent portfolio includes granted patents and pending patent applications covering our VelociSuite technologies, including our VelocImmune mouse platform which produces fully human antibodies. Our issued patents covering these technologies generally expire between 2020 and 2030. However, we continue to file patent applications directed to improvements to these technology platforms.
Our patent portfolio also includes issued patents and pending applications relating to commercialized products and our product candidates in clinical development. These patents cover the proteins and DNA encoding the proteins, manufacturing patents, method of use patents, and pharmaceutical compositions.
The following table describes our U.S. patents and European patents (EP) that we currently consider of primary importance to our marketed products, including the territory, patent number, general subject matter class, and expected expiration dates. The noted expiration dates include any patent term adjustments. Certain of these patents may also be entitled to term extensions. We continue to pursue additional patents and patent term extensions in the United States and other jurisdictions covering various aspects of our products that may, if issued, extend exclusivity beyond the expiration of the patents listed in the table below. One or more patents with the same or earlier expiry date may fall under the same "general subject matter class" for certain products and are not separately listed.
24
Product | Molecule | Territory | Patent No. | General Subject Matter Class | Expiration | |||||
EYLEA | aflibercept | US | 7,070,959 | Composition of Matter | June 16, 2023* | |||||
US | 8,092,803 | Formulation | June 21, 2027 | |||||||
US | 9,254,338 | Methods of Treatment | May 22, 2032 | |||||||
EP | 1183353 | Composition of Matter | May 23, 2025** | |||||||
EP | 2364691 | Formulation | June 14, 2027 | |||||||
EP | 1544299 | Methods of Treatment | May 23, 2020 | |||||||
Dupixent | dupilumab | US | 7,608,693 | Composition of Matter | October 2, 2027 | |||||
US | 8,945,559 | Formulation | October 17, 2032 | |||||||
US | 8,075,887 | Methods of Treatment | April 17, 2028 | |||||||
US | 8,337,839 | Methods of Treatment | October 2, 2027 | |||||||
US | 9,290,574 | Methods of Treatment | July 10, 2034 | |||||||
US | 9,574,004 | Methods of Treatment | December 22, 2033 | |||||||
EP | 2356151 | Composition of Matter | October 27, 2029 | |||||||
Praluent*** | alirocumab | US | 8,062,640 | Composition of Matter | December 15, 2029 | |||||
US | 8,795,669 | Formulation | July 27, 2032 | |||||||
US | 8,357,371 | Methods of Treatment | December 21, 2029 | |||||||
US | 9,550,837 | Methods of Treatment | December 15, 2029 | |||||||
US | 9,724,411 | Methods of Treatment | January 15, 2031 | |||||||
EP | 2358756 | Composition of Matter | December 15, 2029 | |||||||
Kevzara | sarilumab | US | 7,582,298 | Composition of Matter | January 4, 2028 | |||||
US | 9,173,880 | Formulation | December 6, 2031 | |||||||
US | 8,080,248 | Methods of Treatment | June 1, 2027 | |||||||
EP | 2041177 | Composition of Matter | June 1, 2027 | |||||||
EP | 2766039 | Methods of Treatment | October 10, 2032 | |||||||
* A patent term extension has been granted by the U.S. Patent and Trademark Office, extending the original patent term (May 23, 2020), insofar as it covers EYLEA, to June 16, 2023. | ||||||||||
** Supplementary protection certificates have been granted in 14 European countries, extending the original patent term (May 23, 2020) in those countries to May 23, 2025, and are pending in nine additional European countries. | ||||||||||
*** See Note 17 to our Consolidated Financial Statements for information regarding the patent infringement proceedings relating to Praluent, which may impact Praluent's commercial availability in the United States and other jurisdictions. | ||||||||||
In addition, in the United States and certain other countries, our competitive position may be enhanced due to the availability of market exclusivity under relevant law (for additional information regarding market exclusivity, see Part I, Item 1A. "Risk Factors - Risks Related to Intellectual Property and Market Exclusivity - Loss or limitation of patent rights, and new regulatory pathways for biosimilar competition, could reduce the duration of market exclusivity for our products"). The effect of expiration of a patent relating to a particular product also depends upon other factors, such as the nature of the market and the position of the product in it, the growth of the market, the complexities and economics of the process for manufacture of the active ingredient of the product, and the requirements of new drug provisions of the Federal Food, Drug and Cosmetic Act or similar laws and regulations in other countries.
We also are the nonexclusive licensee of a number of additional patents and patent applications. These include fully paid-up and royalty-free licenses to certain patents relating to VEGF receptor proteins, known as the Davis-Smyth patents, and other related technology patents for the prevention or treatment of human eye diseases and eye disorders through administration of EYLEA to the eye.
Patent law relating to the patentability and scope of claims in the biotechnology field is evolving and our patent rights are subject to this additional uncertainty. The degree of patent protection that will be afforded to our products in the United States and other important commercial markets is uncertain and is dependent upon the scope of protection decided upon by the patent offices, courts, and governments in these countries. There is no certainty that our existing patents or others, if obtained, will provide us protection from competition or provide commercial benefit.
25
Others may independently develop similar products or processes to those developed by us, duplicate any of our products or processes or, if patents are issued to us, design around any products and processes covered by our patents. We expect to continue, when appropriate, to file product and process applications with respect to our inventions. However, we may not file any such applications or, if filed, the patents may not be issued. Patents issued to or licensed by us may be infringed by the products or processes of others.
Defense and enforcement of our intellectual property rights is expensive and time consuming, even if the outcome is favorable to us. It is possible that patents issued or licensed to us will be successfully challenged, that a court may find that we are infringing validly issued patents of third parties, or that we may have to alter or discontinue the development of our products or pay licensing fees to take into account patent rights of third parties (see Part I, Item 1A. "Risk Factors - Risks Related to Intellectual Property and Market Exclusivity - We may be restricted in our development, manufacturing, and/or commercialization activities by patents or other proprietary rights of others, and could be subject to damage awards if we are found to have infringed such patents or rights"; and Note 17 to our Consolidated Financial Statements).
Government Regulation
Regulation by government authorities in the United States and foreign countries is a significant factor in the research, development, manufacture, and marketing of our products and our product candidates. A summary of regulatory requirements that are relevant to our business is provided below. These include (i) preclinical requirements; (ii) product approval requirements; (iii) post-approval regulation; (iv) pricing and reimbursement requirements; and (v) other applicable requirements. For a description of material regulatory risks we face, please also refer to Part I, Item 1A. "Risk Factors."
Preclinical Requirements
The activities required before a product candidate may be marketed in the United States begin with preclinical tests. Preclinical tests include laboratory evaluations and animal studies to assess the potential safety and efficacy of the product candidate and its formulations. Preclinical trials must comply with the FDA's Good Laboratory Practices (GLPs) and the U.S. Department of Agriculture's Animal Welfare Act. The results of these studies must be submitted to the FDA as part of an IND, which must be reviewed by the FDA before proposed clinical testing can begin. In other countries, the data are reviewed by regulatory authorities as part of our clinical trial applications. The FDA or other regulatory authorities may ask for additional data in order to begin a clinical study. In addition, based on safety data that emerge from our studies, such regulatory authorities may put a study or an entire clinical development program on hold pending receipt of additional data. These actions by the FDA or other regulatory authorities can result in a delay or termination of a clinical development program.
Product Approval
All of our product candidates will require regulatory approval before they can be commercialized. In particular, human therapeutic products are subject to rigorous preclinical and clinical trials and other pre-market approval requirements by the FDA and foreign authorities. The structure and substance of the FDA and foreign pharmaceutical regulatory practices evolve over time as government priorities change. The ultimate outcome and impact of such developments cannot be predicted.
Typically, clinical testing involves a three-phase process. In Phase 1, trials are typically conducted with a small number of healthy volunteers to determine the early safety profile of the product candidate for treatment of the relevant disease. In Phase 2, clinical trials are conducted with subjects afflicted with a specific disease or disorder to provide enough data to evaluate the preliminary safety, tolerability, and efficacy of different potential doses of the product candidate. In Phase 3, large-scale clinical trials are conducted with patients afflicted with the specific disease or disorder in order to provide enough data to understand the efficacy and safety profile of the product candidate, as required by the FDA. If concerns arise about the safety of the product candidate, the FDA can stop clinical trials by placing them on a "clinical hold." The results of the preclinical and clinical testing of a biologic product candidate are then submitted to the FDA in the form of a BLA for evaluation to determine whether the product candidate may be approved for commercial sale under the Public Health Service Act. Under the Prescription Drug User Fee Act, we must pay fees to the FDA for review of any BLA, which can exceed $2 million. In responding to a BLA, the FDA may grant marketing approval, request additional information, or deny the application. Before approving a new drug or biologic product, the FDA also requires that the facilities at which the product will be manufactured or advanced through the supply chain be in compliance with current Good Manufacturing Practices, or cGMP, requirements and regulations governing the manufacture, shipment, and storage of the product. The FDA also can audit the sponsor of the BLA to determine if the clinical studies were conducted in compliance with current Good Clinical Practice, or cGCP, requirements.
Any approval required by the FDA for any of our product candidates may not be obtained on a timely basis, or at all. The designation of a clinical trial as being of a particular phase is not necessarily indicative that such a trial will be sufficient to satisfy the parameters of a particular phase, and a clinical trial may contain elements of more than one phase notwithstanding the designation of the trial as being of a particular phase. The results of preclinical studies or early stage clinical trials may not predict long-term safety or efficacy of our compounds when they are tested or used more broadly in humans.
26
Approval of a product candidate by comparable regulatory authorities in foreign countries is generally required prior to commencement of marketing of the product in those countries. The approval procedure varies among countries and may involve additional testing, and the time required to obtain such approval may differ from that required for FDA approval. Approval by a regulatory authority in one jurisdiction does not guarantee approval by comparable regulatory authorities in other jurisdictions.
Various federal, state, and foreign statutes and regulations also govern or influence the research, manufacture, safety, labeling, storage, record keeping, marketing, transport, and other aspects of pharmaceutical product candidates. The lengthy process of seeking these approvals and the compliance with applicable statutes and regulations require the expenditure of substantial resources. Any failure by us or our collaborators or licensees to obtain, or any delay in obtaining, regulatory approvals could adversely affect the manufacturing or marketing of our products and our ability to receive product or royalty revenue.
For additional information regarding U.S. and foreign regulatory approval processes and requirements, see Part I, Item 1A, "Risk Factors - Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products - Obtaining and maintaining regulatory approval for drug products is costly, time-consuming, and highly uncertain."
Post-Approval Regulation
The FDA and comparable regulatory authorities in other jurisdictions may also require us to conduct additional clinical trials after granting approval of a product. The FDA has the explicit authority to require postmarketing studies (also referred to as post-approval or Phase 4 studies), labeling changes based on new safety information, and compliance with FDA-approved risk evaluation and mitigation strategies.
Following approval, the FDA regulates the marketing and promotion of our products, which must comply with the Food, Drug, and Cosmetic Act and applicable FDA implementing standards. The FDA's review of promotional activities includes healthcare provider-directed and direct-to-consumer advertising as well as sales representatives' communications. The FDA may take enforcement action for promoting unapproved uses of a product or other violations of its advertising and promotion laws and regulations. See Part I, Item 1A, "Risk Factors - Regulatory and Litigation Risks - If we market and sell approved products in a way that violates federal or state healthcare laws, we may be subject to civil or criminal penalties."
Adverse-event reporting and submission of periodic reports is required following marketing approval. We may be subject to audits by the FDA and other regulatory authorities to ensure that we are complying with the applicable requirements. In addition, we and our third-party providers are required to maintain compliance with cGMPs, and are subject to inspections by the FDA or comparable regulatory authorities in other jurisdictions to confirm such compliance. Changes of suppliers or modifications of methods of manufacturing may require amending our application(s) to the FDA or such comparable foreign regulatory authorities and acceptance of the change by the FDA or such comparable foreign regulatory authorities prior to release of product(s). Prescription drug manufacturers in the U.S. must comply with applicable provisions of the Drug Supply Chain Security Act and provide and receive product tracing information, maintain appropriate licenses, ensure they only work with other properly licensed entities, and have procedures in place to identify and properly handle suspect and illegitimate products. We may also be subject to state regulations related to the manufacturing and distribution of our products.
Failure to comply with these laws and regulations may lead the FDA and comparable regulatory authorities in other jurisdictions to take regulatory action, including suspending manufacturing or withdrawing their approval of a product.
Pricing and Reimbursement
Sales in the United States of our marketed products are dependent, in large part, on the availability and extent of reimbursement from third-party payers, including private payer healthcare and insurance programs, health maintenance organizations, pharmacy benefit management companies, and government programs such as Medicare and Medicaid. Sales of our marketed products in other countries are dependent, in large part, on coverage and reimbursement mechanisms and programs administered by health authorities in those countries. See Part I, Item 1A, "Risk Factors - Risks Related to Commercialization of Products - The successful commercialization of our marketed products, as well as our late-stage product candidates or new indications for our marketed products, if approved, will depend on obtaining and maintaining coverage and reimbursement for use of these products from third-party payers, including Medicare and Medicaid in the United States, and these payers may not cover or adequately reimburse for use of our products or may do so at levels that make our products uncompetitive and/or unprofitable, which would materially harm our business, prospects, operating results, and financial condition."
Medicaid is a joint federal and state program that is administered by the states for low income and disabled beneficiaries. Under the Medicaid Drug Rebate Program, we are required to pay a rebate for each unit of product reimbursed by the state Medicaid programs. The amount of the rebate is established by law and is adjusted upward if average manufacture price (AMP) increases more than inflation (measured by the Consumer Price Index - Urban). The rebate amount is calculated each quarter based on our report of current AMP and best price for each of our products to CMS. The requirements for calculating AMP and best price are
27
complex. We are required to report any revisions to AMP or best price previously reported within a certain period, which revisions could affect our rebate liability for prior quarters. In addition, if we fail to provide information timely or we are found to have knowingly submitted false information to the government, the statute governing the Medicaid Drug Rebate Program provides for civil monetary penalties.
Medicare is a federal program that is administered by the federal government that covers individuals age 65 and over as well as those with certain disabilities. Medicare Part B generally covers drugs that must be administered by physicians or other health care practitioners; are provided in connection with certain durable medical equipment; or are certain oral anti-cancer drugs and certain oral immunosuppressive drugs. Medicare Part B pays for such drugs under a payment methodology based on the average sales price (ASP) of the drugs. Manufacturers, including us, are required to provide ASP information to CMS on a quarterly basis. The manufacturer-submitted information is used to calculate Medicare payment rates. If a manufacturer is found to have made a misrepresentation in the reporting of ASP, the governing statute provides for civil monetary penalties. Medicare Part D provides coverage to enrolled Medicare patients for self-administered drugs (i.e., drugs that are not administered by a physician). Medicare Part D is administered by private prescription drug plans approved by the U.S. government and, subject to detailed program rules and government oversight, each drug plan establishes its own Medicare Part D formulary for prescription drug coverage and pricing, which the drug plan may modify from time to time. The prescription drug plans negotiate pricing with manufacturers and pharmacies, and may condition formulary placement on the availability of manufacturer discounts. In addition, manufacturers, including us, are required to provide to CMS a 50% discount on brand name prescription drugs utilized by Medicare Part D beneficiaries when those beneficiaries are in the coverage gap phase of the Part D benefit design.
Our products are subject to discounted pricing when purchased by federal agencies via the Federal Supply Schedule (FSS). FSS participation is required for our products to be covered and reimbursed by the Veterans Administration (VA), Department of Defense, Coast Guard, and Public Health Service (PHS). Coverage under Medicaid, Medicare, and the PHS pharmaceutical pricing program is also conditioned upon FSS participation. FSS pricing is intended not to exceed the price that we charge our most-favored non-federal customer for a product. In addition, prices for drugs purchased by the VA, Department of Defense (including drugs purchased by military personnel and dependents through the TriCare retail pharmacy program), Coast Guard, and PHS are subject to a cap on pricing equal to 76% of the non-federal average manufacturer price (non-FAMP). An additional discount applies if non-FAMP increases more than inflation (measured by the Consumer Price Index - Urban). In addition, if we fail to provide information timely or we are found to have knowingly submitted false information to the government, the governing statute provides for civil monetary penalties.
To maintain coverage of our products under the Medicaid Drug Rebate Program and Medicare Part B, we are required to extend significant discounts to certain covered entities that purchase products under Section 340B of the PHS pharmaceutical pricing program. Purchasers eligible for discounts include hospitals that serve a disproportionate share of financially needy patients, community health clinics, and other entities that receive certain types of grants under the Public Health Service Act. For all of our products, we must agree to charge a price that will not exceed the amount determined under statute (the "ceiling price") when we sell outpatient drugs to these covered entities. In addition, we may, but are not required to, offer these covered entities a price lower than the 340B ceiling price. The 340B discount formula is based on AMP and is generally similar to the level of rebates calculated under the Medicaid Drug Rebate Program.
Private payor healthcare and insurance providers, health maintenance organizations, and pharmacy benefit managers in the United States are adopting more aggressive utilization management techniques and are increasingly requiring significant discounts and rebates from manufacturers as a condition to including products on formulary with favorable coverage and copayment/coinsurance. As a consequence, these payers may not cover or adequately reimburse for use of our products or may do so at levels that disadvantage them relative to competitive products.
Outside the United States, within the EU, our products are paid for by a variety of payors, with governments being the primary source of payment. Government health authorities in the EU determine or influence reimbursement of products, and set prices or otherwise regulate pricing. Negotiating prices with governmental authorities can delay commercialization of our products. Governments may use a variety of cost-containment measures to control the cost of products, including price cuts, mandatory rebates, value-based pricing, and reference pricing (i.e., referencing prices in other countries or prices of competitive products and using those reference prices to set a price). Budgetary pressures in many EU countries are continuing to cause governments to consider or implement various cost-containment measures, such as price freezes, increased price cuts and rebates, and expanded generic substitution and patient cost-sharing.
28
Other Regulatory Requirements
We are subject to health care "fraud and abuse" laws, such as the federal False Claims Act, the anti-kickback provisions of the federal Social Security Act, and other state and federal laws and regulations. Federal and state anti-kickback laws prohibit, among other things, payments or other remuneration to induce or reward someone to purchase, prescribe, endorse, or recommend a product that is reimbursed under federal or state healthcare programs. Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government, or knowingly making, or causing to be made, a false statement to get a false claim paid. See Part I, Item 1A, "Risk Factors - Regulatory and Litigation Risks - If we market and sell approved products in a way that violates federal or state healthcare laws, we may be subject to civil or criminal penalties."
Our business activities outside of the United States are subject to the Foreign Corrupt Practices Act, or FCPA, and similar anti-bribery or anti-corruption laws, regulations or rules of other countries in which we operate, including the U.K. Bribery Act. See Part I, Item 1A, "Risk Factors - Regulatory and Litigation Risks - Risks from the improper conduct of employees, agents, contractors, or collaborators could adversely affect our reputation and our business, prospects, operating results, and financial condition."
Numerous federal and state laws, including state security breach notification laws, state health information privacy laws, and federal and state consumer protection laws, govern the collection, use, and disclosure of personal information. In addition, most health care providers, including research institutions from which we or our collaborators obtain patient health information, are subject to privacy and security regulations promulgated under the Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act. Although we are not directly subject to HIPAA other than with respect to providing certain employee benefits, we could potentially be subject to criminal penalties if we, our affiliates, or our agents knowingly obtain or disclose individually identifiable health information maintained by a HIPAA-covered entity in a manner that is not authorized or permitted by HIPAA. Outside the United States, our clinical trial programs and research collaborations may implicate international data protection laws, including the EU Data Protection Directive and the General Data Protection Regulation (GDPR) that is replacing it. See Part I, Item 1A, "Risk Factors - Regulatory and Litigation Risks - We face potential liability related to the privacy of health information we obtain from clinical trials sponsored by us or our collaborators, from research institutions and our collaborators, and directly from individuals."
In addition to the foregoing, our present business is, and our future business will be, subject to regulation under the United States Atomic Energy Act, the Clean Air Act, the Clean Water Act, the Comprehensive Environmental Response, Compensation and Liability Act, the National Environmental Policy Act, the Toxic Substances Control Act, the Resource Conservation and Recovery Act, national restrictions, and other current and potential future local, state, federal, and foreign regulations.
Business Segments
We manage our business as one segment which includes all activities related to the discovery, development, and commercialization of medicines for the treatment of serious medical conditions. For financial information related to our one segment, see Part II, Item 6. "Selected Financial Data" and our Consolidated Financial Statements and related notes.
Employees
As of December 31, 2017, we had approximately 6,200 full-time employees. We believe that we have been successful in attracting skilled and experienced personnel in a highly competitive environment; however, competition for these personnel is intense. None of our personnel are covered by collective bargaining agreements and our management considers its relations with our employees to be good.
Corporate Information
We were incorporated in the State of New York in 1988 and publicly listed in 1991. Our principal executive offices are located at 777 Old Saw Mill River Road, Tarrytown, New York 10591, and our telephone number at that address is (914) 847-7000.
We make available free of charge on or through our Internet website (http://www.regeneron.com) our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and, if applicable, amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act, as soon as reasonably practicable after we electronically file such material with, or furnish it to, the Securities and Exchange Commission (SEC).
Investors and other interested parties should note that we use our media and investor relations website (http://newsroom.regeneron.com) and our social media channels to publish important information about Regeneron, including information that may be deemed material to investors. We encourage investors and other interested parties to review the information we may publish through our media and investor relations website and the social media channels listed on our media and investor relations website, in addition to our SEC filings, press releases, conference calls, and webcasts.
29
ITEM 1A. RISK FACTORS
We operate in an environment that involves a number of significant risks and uncertainties. We caution you to read the following risk factors, which have affected, and/or in the future could affect, our business, prospects, operating results, and financial condition. The risks described below include forward-looking statements, and actual events and our actual results may differ materially from these forward-looking statements. Additional risks and uncertainties not currently known to us or that we currently deem immaterial may also impair our business, prospects, operating results, and financial condition. Furthermore, additional risks and uncertainties are described under other captions in this report and should also be considered by our investors.
Risks Related to Commercialization of EYLEA
We are substantially dependent on the success of EYLEA. If we or Bayer are unable to continue to successfully commercialize EYLEA, our business, prospects, operating results, and financial condition will be materially harmed.
EYLEA net sales represent a substantial portion of our revenues and this concentration of our net sales in a single product makes us substantially dependent on that product. For the years ended December 31, 2017 and 2016, EYLEA net sales in the United States represented 63% and 68% of our total revenues, respectively. If we were to experience difficulty with the commercialization of EYLEA in the United States, if Bayer were to experience any difficulty with the commercialization of EYLEA outside the United States, or if we and Bayer are unable to maintain current marketing approvals of EYLEA, we may experience a reduction in revenue and may not be able to sustain profitability, and our business, prospects, operating results, and financial condition would be materially harmed.
We expect that the continued commercial success of EYLEA will depend on many factors, including the following:
• | effectiveness of the commercial strategy in and outside the United States for the marketing of EYLEA, including pricing strategy and the continued effectiveness of efforts to obtain, and the timing of obtaining, adequate third-party reimbursements; |
• | maintaining and successfully monitoring commercial manufacturing arrangements for EYLEA with third parties who perform fill/finish or other steps in the manufacture of EYLEA to ensure that they meet our standards and those of regulatory authorities, including the FDA, which extensively regulate and monitor pharmaceutical manufacturing facilities; |
• | our ability to meet the demand for commercial supplies of EYLEA; |
• | our ability to differentiate EYLEA from Lucentis and other competitive products, and the willingness of retinal specialists and patients to switch from Lucentis or off-label use of repackaged Avastin to EYLEA or to start treatment with EYLEA; |
• | sufficient coverage of, and reimbursement for, EYLEA by third-party payers, including Medicare and Medicaid in the United States and other government and private payers in the United States and foreign jurisdictions; |
• | our ability to maintain sales of EYLEA in the face of competitive products, including those currently in clinical development; |
• | the results of post-approval studies of EYLEA (whether conducted by us or by others and whether mandated by regulatory agencies or voluntary), and studies of other products that could implicate VEGF inhibitors as a class or are perceived to do so; |
• | the effect of existing and new health care laws and regulations currently being considered or implemented in the United States, including reporting and disclosure requirements of such laws and regulations and the potential impact of such requirements on physician prescription practices; and |
• | risks associated with intellectual property of other parties and pending or future litigation relating thereto, as discussed under "Risks Related to Intellectual Property and Market Exclusivity" below. |
More detailed information about the risks related to the commercialization of EYLEA is provided in the risk factors below.
30
We and Bayer are subject to significant ongoing regulatory obligations and oversight with respect to EYLEA. If we or Bayer fail to maintain regulatory compliance for EYLEA, EYLEA marketing approval may be withdrawn, which would materially harm our business, prospects, operating results, and financial condition.
We and Bayer are subject to significant ongoing regulatory obligations and oversight with respect to EYLEA for its currently approved indications in the United States, EU, and other countries where the product is approved. If we or Bayer fail to maintain regulatory compliance for EYLEA for its currently approved indications (including for any of the reasons discussed below under "Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products - Obtaining and maintaining regulatory approval for drug products is costly, time-consuming, and highly uncertain"), EYLEA marketing approval may be withdrawn, which would materially harm our business, prospects, operating results, and financial condition. Failure to comply may also subject us to sanctions, product recalls, or withdrawals of previously approved marketing applications. See also "Risks Related to Manufacturing and Supply - If we fail to meet the stringent requirements of governmental regulation in the manufacture of drug products or product candidates, we could incur substantial remedial costs, delays in the development or approval of our product candidates or new indications for our marketed products and/or in their commercial launch if they obtain regulatory approval, and a reduction in sales" below.
Serious complications or side effects in connection with the use of EYLEA could materially harm our business, prospects, operating results, and financial condition.
Serious complications or serious, unexpected side effects in connection with the use of EYLEA could materially harm our business, prospects, operating results, and financial condition. For additional information about some of these risks, see "Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products - Serious complications or side effects in connection with the use of our products and in clinical trials for our product candidates and new indications for our marketed products could cause our regulatory approvals to be revoked or limited or lead to delay or discontinuation of development of our product candidates or new indications for our marketed products, which could severely harm our business, prospects, operating results, and financial condition" below.
Sales of EYLEA are dependent on the availability and extent of reimbursement from third-party payers, and changes to such reimbursement may materially harm our business, prospects, operating results, and financial condition.
Our sales in the United States of EYLEA are dependent, in large part, on the availability and extent of reimbursement from third-party payers, including private payer healthcare and insurance programs, health maintenance organizations, pharmacy benefit management companies, and government programs such as Medicare and Medicaid. Sales of EYLEA in other countries are dependent, in large part, on similar programs in those countries. In the United States, there is an increased focus from the federal government and others on analyzing the impact of various regulatory programs on the federal deficit, which could result in increased pressure on federal programs to reduce costs, including limiting federal healthcare expenditures. For example, in September 2011 the Office of Inspector General (OIG) of the Department of Health and Human Services issued a report entitled "Review of Medicare Part B Avastin and Lucentis Treatments for Age-Related Macular Degeneration" in which the OIG details possible savings to the Medicare program by using off-label, repackaged Avastin rather than Lucentis for the treatment of wet AMD. A reduction in the availability or extent of reimbursement from U.S. government programs could have a material adverse effect on the sales of EYLEA. Economic pressure on state budgets may also have a similar impact. In addition, other third-party payers (including pharmacy benefit management companies) are challenging the prices charged for healthcare products and increasingly limiting, and attempting to limit, both coverage and level of reimbursement for prescription drugs. Since EYLEA is too expensive for most patients to afford without health insurance coverage, if adequate coverage and reimbursement by third-party payers, including Medicare and Medicaid in the United States, is not available, our ability to successfully commercialize EYLEA will be materially adversely impacted. Our sales and potential profits and our business, prospects, operating results, and financial condition would be materially harmed. See also "Risks Related to Commercialization of Products - The successful commercialization of our marketed products, as well as our late-stage product candidates or new indications for our marketed products, if approved, will depend on obtaining and maintaining coverage and reimbursement for use of these products from third-party payers, including Medicare and Medicaid in the United States, and these payers may not cover or adequately reimburse for use of our products or may do so at levels that make our products uncompetitive and/or unprofitable, which would materially harm our business, prospects, operating results, and financial condition" below.
31
The commercial success of EYLEA is subject to strong competition.
The market for eye disease products is very competitive. For example, Novartis and Genentech/Roche are collaborating on the commercialization and further development of a VEGF antibody fragment, Lucentis, for the treatment of various eye indications. Lucentis is approved in one or more jurisdictions for the treatment of wet AMD, macular edema following RVO (including CRVO and BRVO), DME, diabetic retinopathy, and mCNV. In addition, we are aware of several companies developing biosimilar versions of EYLEA. For example, Momenta Pharmaceuticals (in partnership with Mylan) is developing M710 (currently in a Phase 3 trial in patients with wet AMD). Competitors are also exploring the development of a biosimilar version of Lucentis; in particular, Pfenex is developing PF582 (a Phase 1b/2a trial in patients with wet AMD has been completed), Formycon (in collaboration with Bioeq) is developing FYB201 (currently in a Phase 3 trial in patients with wet AMD), and Samsung Bioepis is developing SB11 (currently in a Phase 3 trial in patients with wet AMD).
Other competitive or potentially competitive products include Allergan's Ozurdex (approved by the FDA for the treatment of macular edema following RVO and for the treatment of DME) and Alimera Sciences' Iluvien (approved by the FDA for the treatment of DME in patients who have been previously treated with a course of corticosteroids and did not have a clinically significant rise in intraocular pressure), both of which are intravitreal implants of corticosteroids. Many other companies are working on the development of product candidates and extended delivery devices for the potential treatment of wet AMD, DME, and RVO, including those that act by blocking VEGF and VEGF receptors, as well as small interfering ribonucleic acids (siRNAs) that modulate gene expression. For example, Genentech/Roche is developing a Lucentis port delivery system implant (currently in a Phase 2 study in patients with wet AMD). Novartis is developing RTH258 (ESBA1008), a humanized monoclonal single-chain FV (scFv) antibody fragment targeting VEGF-A for wet AMD, and announced in June 2017 that two Phase 3 studies of RTH258 met their primary endpoint of non-inferiority to EYLEA. Allergan is developing abicipar pegol for wet AMD and related conditions (currently studied in Phase 3 trials against Lucentis as a comparator drug). Additionally, companies are developing products (or combinations of products) to treat wet AMD that act by blocking VEGF and VEGF receptors, as well as other targets (for example, Ang2). Genentech/Roche is developing a bi-specific antibody (RG7716) targeting both VEGF and Ang2 for wet AMD and DME (currently in Phase 2 trials for both indications). Products that are being developed for use in combination with EYLEA and/or Lucentis may also pose a competitive threat. Opthea is developing OPT-302, a VEGFR-3 large molecule trap in combination with Lucentis in a Phase 2 trial for wet AMD. Santen (in partnership with TRACON) is developing DE-122, an anti-endoglin antibody in combination with Lucentis in a Phase 2 trial for wet AMD. Small-molecule tyrosine kinase inhibitors that have activity against VEGF may also compete against EYLEA, if approved for wet AMD and/or related conditions. Graybug is developing GB-102, an intravitreally administered depot formulation of the small molecule tyrosine kinase inhibitor, sunitinib, in a Phase 1/2 trial for wet AMD. Tyrogenex is developing X-82, an orally administered small-molecule tyrosine kinase inhibitor, in a Phase 2 trial in combination with an anti-VEGF. Competitors are also developing other eye-drop formulations, devices, oral therapies, and gene/cell therapies for various indications that, if approved, would compete with EYLEA in one or more of its currently approved indications.
In addition, ophthalmologists are using off-label, third-party repackaged versions of Genentech/Roche's approved VEGF antagonist, Avastin, for the treatment of wet AMD, DME, and RVO. The relatively low cost of therapy with repackaged Avastin presents a significant competitive challenge in these indications. Avastin is also being evaluated in eye diseases in clinical trials in certain countries. Furthermore, Lucentis and off-label use of repackaged Avastin present significant competitive challenges as doctors and patients have had significant experience using these medicines. The relatively low cost of repackaged Avastin in treating patients may exacerbate the competitive challenge which EYLEA faces in the eye indications for which it is approved. Amgen (in collaboration with Allergan) has obtained regulatory approval of a biosimilar version of Avastin in the United States and the EU, and other competitors are also developing a biosimilar version of Avastin. Off-label use of any such biosimilar in one or more of the eye indications for which EYLEA is approved may put further pressure on the commercialization of EYLEA.
Finally, ZALTRAP has not been manufactured and formulated for use in intravitreal injections, and there is a risk that third parties may attempt to repackage ZALTRAP for off-label use and sale for the treatment of wet AMD and other diseases of the eye, which would present a potential low-cost competitive threat to EYLEA for its approved indications. We are aware of claims by third parties, including those based on published clinical data, that ZALTRAP (ziv-aflibercept) may be safely administered to the eye.
See also "Risks Related to Commercialization of Products - We may be unsuccessful in continuing the commercialization of our marketed products or in commercializing our product candidates or new indications for our marketed products, if approved, which would materially and adversely affect our business, profitability, and future prospects" below and Part I. Item 1. "Business - Competition" of this report.
We rely on our collaboration with Bayer for commercializing EYLEA.
While we have established our own sales and marketing organization for EYLEA in the United States for its currently approved indications, we have no sales, marketing, commercial, or distribution capabilities for EYLEA outside the United States.
32
Under the terms of our license and collaboration agreement with Bayer (which is terminable by Bayer at any time upon six or twelve months' advance notice, depending on the circumstances giving rise to termination), we rely on Bayer for sales, marketing, and distribution of EYLEA in countries outside the United States. If we and Bayer are unsuccessful in continuing to commercialize EYLEA, our ability to sustain profitability would be materially impaired. We have limited commercial capabilities outside the United States and would have to develop or outsource these capabilities. Therefore, termination of the Bayer collaboration agreement would create substantial new and additional risks to the successful commercialization of EYLEA, particularly outside the United States. For additional information regarding our collaboration with Bayer, see "Risks Related to Our Reliance on Third Parties - If our collaboration with Bayer for EYLEA is terminated, or Bayer materially breaches its obligations thereunder, our business, prospects, operating results, and financial condition, and our ability to continue to develop EYLEA and commercialize EYLEA outside the United States in the time expected, or at all, would be materially harmed" below.
Sales of EYLEA recorded by us and Bayer could be reduced by imports from countries where EYLEA may be available at lower prices.
Our sales of EYLEA in the United States and Bayer's sales of EYLEA in other countries may be reduced if EYLEA is imported into those countries from lower priced markets, whether legally or illegally (a practice known as parallel trading or reimportation). Parallel traders (who may repackage or otherwise alter the original product or sell it through alternative channels such as mail order or the Internet) take advantage of the price differentials between markets arising from factors including sales costs, market conditions (such as intermediate trading stages), tax rates, or national regulation of prices. Under our arrangement with Bayer, pricing and reimbursement for EYLEA outside the United States is the responsibility of Bayer. Prices for EYLEA in jurisdictions outside the United States are based on local market economics and competition and are likely to differ from country to country. In the United States, prices for pharmaceuticals are generally higher than in the bordering nations of Canada and Mexico and our sales of EYLEA in the United States may be reduced if EYLEA marketed in those nations is imported into the United States. Parallel-trading practices also are of particular relevance to the EU, where they have been encouraged by the current regulatory framework. These types of imports may exert pressure on the pricing of EYLEA in a particular market or reduce our or Bayer's sales, thereby adversely affecting our results of operations. In addition, there are proposals to legalize the import of pharmaceuticals from outside the United States into the United States. If such proposals were implemented, our future revenues derived from EYLEA sales could be reduced.
33
Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara)
If we or Sanofi are unable to successfully commercialize Dupixent, Praluent, or Kevzara, our business, prospects, operating results, and financial condition may be materially harmed.
We expect that the commercial success of Dupixent, Praluent, and Kevzara will depend on many factors, including the following (as applicable):
• | effectiveness of the commercial strategy in and outside the United States for the marketing of these products, including pricing strategy and the effectiveness of efforts to obtain, and the timing of obtaining, adequate third-party reimbursements; |
• | our and Sanofi's ability to differentiate these products from competitive products (including, in the case of Dupixent, Pfizer's Xeljanz and Eli Lilly's Olumiant; in the case of Praluent, Amgen's Repatha; and, in the case of Kevzara, Genentech/Roche's Actemra), as well as product candidates currently in clinical development (such as, in the case of Dupixent, the antibody product candidates being developed by Roche, LEO Pharma, AstraZeneca, Galderma, AnaptysBio, and Amgen); |
• | the outcome of the pending patent infringement proceedings relating to Dupixent (described further in Note 17 to our Consolidated Financial Statements), and other risks relating to Dupixent associated with intellectual property of other parties and pending or future litigation relating thereto, as discussed under "Risks Related to Intellectual Property and Market Exclusivity" below; |
• | the outcome of the pending patent infringement proceedings relating to Praluent initiated by Amgen against us and Sanofi (described further in Note 17 to our Consolidated Financial Statements), and other risks relating to Praluent associated with intellectual property of other parties and pending or future litigation relating thereto, as discussed under "Risks Related to Intellectual Property and Market Exclusivity" below; |
• | sufficient coverage of, and reimbursement for, these products by third-party payers, including Medicare and Medicaid in the United States and other government and private payers in the United States and foreign jurisdictions; |
• | payer restrictions on eligible patient populations and the reimbursement process, both in the United States and abroad; |
• | the results of post-approval studies, whether conducted by us or by others and whether mandated by regulatory agencies or voluntary (including, in the case of Praluent, the ODYSSEY OUTCOMES trial prospectively assessing the potential of Praluent to demonstrate cardiovascular benefit), and studies of other products that could implicate an entire class of products or are perceived to do so; |
• | our ability to meet the demand for commercial supplies of these products; |
• | the effect of existing and new health care laws and regulations currently being considered or implemented in the United States, including reporting and disclosure requirements of such laws and regulations and the potential impact of such requirements on physician prescription practices; and |
• | maintaining and successfully monitoring commercial manufacturing arrangements for these products with parties who perform fill/finish or other steps in the manufacture of these products to ensure that they meet our standards and those of regulatory authorities, including the FDA, which extensively regulate and monitor pharmaceutical manufacturing facilities. |
More detailed information about the risks related to the commercialization of Dupixent, Praluent, and Kevzara is provided in the risk factors below.
We and Sanofi are subject to significant ongoing regulatory obligations and oversight with respect to Dupixent, Praluent, and Kevzara. If we or Sanofi fail to maintain regulatory compliance for Dupixent, Praluent, or Kevzara, the applicable marketing approval may be withdrawn, which would materially harm our business, prospects, operating results, and financial condition.
We and Sanofi are subject to significant ongoing regulatory obligations and oversight with respect to Dupixent, Praluent, and Kevzara for their currently approved indications in the United States, EU, and other countries. If we or Sanofi fail to maintain regulatory compliance for Dupixent, Praluent, or Kevzara for the currently approved indications (including because the product does not meet the relevant endpoints of any required post-approval studies, such as, in the case of Praluent, the ODYSSEY OUTCOMES trial, or for any of the other reasons discussed below under "Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products - Obtaining and maintaining regulatory approval for drug products is costly, time-consuming, and highly uncertain"), the applicable marketing approval may be withdrawn, which would materially harm our business, prospects, operating results, and financial condition. Failure to comply may also subject us to sanctions, product recalls, or withdrawals of previously approved marketing applications. See also "Risks Related to Manufacturing and Supply - If we fail to meet the stringent requirements of governmental regulation in the manufacture of drug products or product candidates, we could incur substantial remedial costs, delays in the development or approval of our product candidates or new indications for our marketed products and/or in their commercial launch if they obtain regulatory approval, and a reduction in sales" below.
Serious complications or side effects in connection with the use of Dupixent, Praluent, or Kevzara could materially harm our business, prospects, operating results, and financial condition.
34
Serious complications or serious, unexpected side effects in connection with the use of Dupixent, Praluent, or Kevzara could materially harm our business, prospects, operating results, and financial condition. For additional information about some of these risks, see "Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products - Serious complications or side effects in connection with the use of our products and in clinical trials for our product candidates and new indications for our marketed products could cause our regulatory approvals to be revoked or limited or lead to delay or discontinuation of development of our product candidates or new indications for our marketed products, which could severely harm our business, prospects, operating results, and financial condition" below.
Sales of Dupixent, Praluent, and Kevzara are dependent on the availability and extent of reimbursement from third-party payers in the United States and other countries, and changes to such reimbursement may materially harm our business, prospects, operating results, and financial condition.
Sales in the United States of Dupixent, Praluent, and Kevzara are dependent, in large part, on the availability and extent of reimbursement from third-party payers, including private payer healthcare and insurance programs, health maintenance organizations, pharmacy benefit management companies, and government programs such as Medicare and Medicaid. Sales of Dupixent, Praluent, and Kevzara in other countries are dependent, in large part, on similar reimbursement mechanisms and programs in those countries.
Government and other third-party payers (including pharmacy benefit management companies) are challenging the prices charged for healthcare products and increasingly limiting, and attempting to limit, both coverage and level of reimbursement for prescription drugs, such as by requiring outcomes-based or other pay-for-performance pricing arrangements. They are also imposing restrictions on eligible patient populations and the reimbursement process, including by means of required prior authorizations and utilization management criteria. For example, pharmacy benefit management companies often develop formularies to reduce their cost for medications. The breadth of the products covered by formularies varies considerably from one pharmacy benefit management company to another. Failure to be included in such formularies or to achieve favorable formulary status may negatively impact the utilization and market share of Dupixent, Praluent, and Kevzara. If Dupixent, Praluent, or Kevzara is not included within an adequate number of formularies, adequate reimbursement levels are not provided, the eligible insured patient population for Dupixent, Praluent, or Kevzara is limited, or a key payer refuses to provide reimbursement for Dupixent, Praluent, or Kevzara in a particular jurisdiction altogether, this could have a material adverse effect on our and Sanofi's ability to commercialize the applicable product.
In the United States, there also is an increased focus from the federal government and others on analyzing the impact of various regulatory programs on the federal deficit, which could result in increased pressure on federal programs to reduce costs, including limiting federal healthcare expenditures. Economic pressure on state budgets may also have a similar impact. A reduction in the availability or extent of reimbursement from U.S. government programs could have a material adverse effect on the sales of Dupixent, Praluent, and Kevzara. Since Dupixent, Praluent, and Kevzara are too expensive for most patients to afford without health insurance coverage, if adequate coverage and reimbursement by third-party payers in the United States and other countries, including Medicare and Medicaid in the United States, is not available, our ability to successfully commercialize the applicable product will be materially adversely impacted. Our sales and potential profits and our business, prospects, operating results, and financial condition would be materially harmed. See also "Risks Related to Commercialization of Products - The successful commercialization of our marketed products, as well as our late-stage product candidates or new indications for our marketed products, if approved, will depend on obtaining and maintaining coverage and reimbursement for use of these products from third-party payers, including Medicare and Medicaid in the United States, and these payers may not cover or adequately reimburse for use of our products or may do so at levels that make our products uncompetitive and/or unprofitable, which would materially harm our business, prospects, operating results, and financial condition" below.
The commercial success of Dupixent, Praluent, and Kevzara is subject to strong competition.
There is significant actual and potential future competition for Dupixent. A number of companies are developing antibodies that, if approved, may compete with Dupixent in its current or potential future indications, including Roche (in collaboration with Dermira) (an antibody against IL-13); LEO Pharma (in collaboration with AstraZeneca ) (IL-13 antibody tralokinumab being developed in the atopic dermatitis indication); AstraZeneca (antibodies against IL-4R and IL-5R, as well as IL-13 antibody tralokinumab being developed in the asthma indication); Galderma (an antibody against IL-31R); AnaptysBio (an antibody against IL-33); and Amgen (in collaboration with AstraZeneca) (an antibody against thymic stromal lymphopoietin, or TSLP). GSK's Nucala and Teva's Cinqair, both of which are antibodies against IL-5, may also compete with Dupixent in its current or potential future indications. We are also aware of companies developing or marketing small molecules that may compete with Dupixent in its current or potential future indications. These include Pfizer's Eucrisa, a topical ointment that competes with Dupixent in the atopic dermatitis indication; and JAK inhibitors, such as AbbVie's upadacitinib, Pfizer's PF-04965842, and Eli Lilly's Olumiant.
35
There also is significant actual and potential future competition for Praluent. Amgen's Repatha has already received regulatory approvals in jurisdictions including the U.S., the EU, and Japan. Amgen may obtain marketing approval for Repatha in one or more additional countries before Praluent is approved in those countries. Amgen may also receive approval for additional indications, such as cardiovascular risk reduction, before Praluent. Other companies with development programs for injectables against PCSK9 include Alnylam Pharmaceuticals (in collaboration with The Medicines Company), which has a clinical program underway with inclisiran, an RNAi molecule against PCSK9. In addition, there are therapeutic products targeting PCSK9 operating through other mechanisms of action in development, including oral products and vaccines. Oral products that lower LDL-C, if approved, may also be competitive with PCSK9 inhibitors, including Praluent. These include bempedoic acid, which is being developed by Esperion Therapeutics, and gemcabene, which is being developed by Gemphire Therapeutics.
Kevzara also faces competition from actual and potential future products. Genentech/Roche is marketing an antibody against IL-6R (Actemra) for the treatment of rheumatoid arthritis that competes with Kevzara. In addition, several other companies, including Alder Biopharmaceuticals, Inc. (in collaboration with Vitaeris), Ablynx, R-Pharm, CJSC, and Bird Rock Bio have antibodies against IL-6 or IL-6R in clinical development. Further, oral, small-molecule JAK inhibitors such as Pfizer's Xeljanz, Eli Lilly's Olumiant, and AbbVie's upadacitinib may pose a competitive threat for Kevzara.
We rely on our Antibody Collaboration with Sanofi for commercializing Dupixent, Praluent, and Kevzara.
In accordance with the terms of our Antibody Collaboration with Sanofi, we have elected to co-promote Dupixent, Kevzara, and Praluent with Sanofi in the United States. As such, we continue to rely in part on Sanofi's sales and marketing organization in the United States. If we and Sanofi fail to coordinate our United States sales and marketing efforts effectively, sales of Dupixent, Praluent, or Kevzara (as applicable) may be materially affected. Sanofi also maintains other important responsibilities relating to Dupixent, Praluent, and Kevzara in the United States. For example, Sanofi records product sales for Dupixent, Praluent, and Kevzara in the United States, serves as the lead regulatory party for certain products and product candidates included in the Antibody Collaboration (e.g., is responsible for regulatory filings and negotiations relating to such products and product candidates) in the United States, and may lead negotiations with payors relating to such products and product candidates. We also rely on Sanofi for sales, marketing, and distribution of Dupixent, Praluent, and Kevzara in countries outside the United States. If we or Sanofi are unsuccessful in commercializing Dupixent, Praluent, or Kevzara, or if Sanofi terminates the Antibody Collaboration with us, our business, prospects, operating results, and financial condition may be materially impaired. We have limited commercial capabilities outside the United States and would have to develop or outsource these capabilities for Dupixent, Praluent, and Kevzara. Therefore, termination of our Antibody Collaboration would create substantial new and additional risks to the successful commercialization of Dupixent, Praluent, and Kevzara, particularly outside the United States. For additional information regarding our Antibody Collaboration with Sanofi, see "Risks Related to Our Reliance on Third Parties - If any of our collaborations with Sanofi is terminated, our business, prospects, operating results, and financial condition, and our ability to discover, develop, manufacture, and commercialize our pipeline of product candidates in the time expected, or at all, would be materially harmed" below.
Sales of Dupixent, Praluent, and Kevzara recorded by Sanofi could be reduced by imports from countries where these products may be available at lower prices.
Sales of Dupixent, Praluent, and Kevzara recorded by Sanofi in the United States and other countries (which impact our share of any profits or losses from the commercialization of these products under our Antibody Collaboration with Sanofi and, therefore, our results of operations) may be reduced if the applicable product is imported into those countries from lower priced markets, whether legally or illegally (a practice known as parallel trading or reimportation). Parallel traders (who may repackage or otherwise alter the original product or sell it through alternative channels such as mail order or the Internet) take advantage of the price differentials between markets arising from factors including sales costs, market conditions (such as intermediate trading stages), tax rates, or national regulation of prices. Under our Antibody Collaboration with Sanofi, pricing and reimbursement for Dupixent, Praluent, and Kevzara outside the United States is the responsibility of Sanofi. Prices for Dupixent, Praluent, and Kevzara in jurisdictions outside the United States are based on local market economics and competition and are likely to differ from country to country. In the United States, prices for pharmaceuticals are generally higher than in the bordering nations of Canada and Mexico and sales of Dupixent, Praluent, and Kevzara in the United States that are recorded by Sanofi may be reduced if the applicable product marketed in those bordering nations is imported into the United States. Parallel-trading practices also are of particular relevance to the EU, where they have been encouraged by the current regulatory framework. These types of imports may exert pressure on the pricing of Dupixent, Praluent, and Kevzara in a particular market or the sales recorded by Sanofi, thereby adversely affecting our results of operations. In addition, there are proposals to legalize the import of pharmaceuticals from outside the United States into the United States. If such proposals were implemented, our future revenues derived from Dupixent, Praluent, or Kevzara sales could be reduced.
36
Risks Related to Maintaining Approval of Our Marketed Products and the Development and Obtaining Approval of Our Product Candidates and New Indications for Our Marketed Products
If we do not maintain regulatory approval for our marketed products, and obtain regulatory approval for our product candidates or new indications for our marketed products, we will not be able to market or sell them, which would materially and negatively impact our business, prospects, operating results, and financial condition.
We cannot sell or market products without regulatory approval. If we do not maintain regulatory approval for our marketed products, and obtain regulatory approval for our product candidates or new indications of our marketed products, the value of our Company and our business, prospects, operating results, and financial condition will be materially harmed. If we are unable to obtain regulatory approval for our product candidates, or if we are materially delayed in doing so, our business, prospects, operating results, and financial condition may be materially harmed.
Obtaining and maintaining regulatory approval for drug products is costly, time-consuming, and highly uncertain.
In the United States, we must obtain and maintain approval from the FDA for each drug we intend to sell. Obtaining FDA approval is typically a lengthy and expensive process, and approval is highly uncertain. We cannot predict with certainty if or when we might submit for regulatory approval any of our product candidates currently under development. Any approvals we may obtain may not cover all of the clinical indications for which we are seeking approval. Also, an approval might contain significant limitations in the form of narrow indications, warnings, precautions, or contra-indications with respect to conditions of use. The FDA has substantial discretion in the approval process (including with respect to setting specific conditions for submission) and may either refuse to accept an application for substantive review or may form the opinion after review of an application that the application is insufficient to allow approval of a product candidate. If the FDA does not accept our application for review or approve our application, it may require that we conduct additional clinical, preclinical, or manufacturing validation studies and submit the data before it will reconsider our application. Depending on the extent of these or any other studies that might be required, approval of any applications that we submit may be delayed significantly, or we may be required to expend more resources. It is also possible that any such additional studies, if performed and completed, may not be considered sufficient by the FDA to make our applications approvable. If any of these outcomes occur, we may be forced to delay or abandon our applications for approval.
In certain instances (such as when we use a biomarker-based test to identify and enroll specific patients in a clinical trial), regulatory approval of a companion diagnostic to our therapeutic product candidate may be required as a condition to regulatory approval of the therapeutic product candidate. We may need to rely on third parties to provide companion diagnostics for use with our product candidates. Such third parties may be unable or unwilling on terms acceptable to us to provide such companion diagnostics or to obtain timely regulatory approval of such companion diagnostics, which could negatively impact regulatory approval of our product candidates or may result in increased development costs or delays.
The FDA may also require us to conduct additional clinical trials after granting approval of a product. Its ability to do so has been enhanced by the Food and Drug Administration Amendments Act of 2007, pursuant to which the FDA has the explicit authority to require postmarketing studies (also referred to as post-approval or Phase 4 studies), labeling changes based on new safety information, and compliance with FDA-approved risk evaluation and mitigation strategies. Post-approval studies, whether conducted by us or by others and whether mandated by regulatory agencies or voluntary, and other data about our marketed products (or data about products similar to our marketed products that implicate an entire class of products or are perceived to do so) may result in changes in product labeling, restrictions on use, product withdrawal or recall, loss of approval, or lower sales of our products.
According to the FDA policies under the Prescription Drug User Fee Act, the FDA system of review times for new drugs includes standard review and priority review. Standard review can be accomplished in a ten-month time frame from the time the application is filed by the FDA (filing date), which typically occurs approximately 60 days following submission of the application by the applicant. The FDA has stated the goal to act on 90% of standard new molecular entity (NME) New Drug Application (NDA) and original BLA submissions within 10 months of the filing date. A priority review designation is given to drugs that treat a serious condition and offer major advances in treatment, or provide a treatment where no adequate therapy exists, and may also be afforded to a human drug application based on a priority review voucher. The FDA has stated the goal to act on 90% of priority NME NDA and original BLA submissions within six months of the filing date. However, the FDA's review goals are subject to change and the duration of the FDA's review depends on a number of factors, including the number and types of other applications that are submitted to the FDA around the same time period or are pending. Even if any of our applications receives a priority review designation, we may not ultimately be able to obtain approval of our application within a time frame consistent with the FDA's stated review goals or at all, and such designation may not actually lead to a faster development or regulatory review or approval process.
37
The FDA enforces Good Clinical Practices (GCPs) and other regulations through periodic inspections of trial sponsors, clinical research organizations (CROs), principal investigators, and trial sites. If we or any of the third parties conducting our clinical studies are determined to have failed to fully comply with GCPs, the study protocol or applicable regulations, the clinical data generated in those studies may be deemed unreliable. This could result in non-approval of our product candidates by the FDA, or we or the FDA may decide to conduct additional inspections or require additional clinical studies, which would delay our development programs, require us to incur additional costs, and could substantially harm our business, prospects, operating results, and financial condition.
Before approving a new drug or biologic product, the FDA requires that the facilities at which the product will be manufactured or advanced through the supply chain be in compliance with current Good Manufacturing Practices, or cGMP, requirements and regulations governing the manufacture, shipment, and storage of the product. These cGMP requirements and regulations are not prescriptive instructions on how to manufacture products, but rather a series of principles that must be observed during manufacturing; as a result, their implementation may not be clearly delineated and may present a challenging task. Manufacturing product candidates in compliance with these regulatory requirements is complex, time-consuming, and expensive. To be successful, our products must be manufactured in compliance with regulatory requirements, and at competitive costs. If we or any of our product collaborators, or third-party manufacturers, product packagers, labelers, or other parties performing steps in the supply chain are unable to maintain regulatory compliance, the FDA can impose regulatory sanctions, including, among other things, refusal to approve a pending application for a new drug or biologic product, or revocation of a pre-existing approval. For example, on October 28, 2016, the FDA issued a Complete Response Letter relating to the BLA for Kevzara, which referred to certain deficiencies identified during a routine cGMP inspection of the Sanofi facility in Le Trait, France where Kevzara is filled and finished; while the BLA for Kevzara has since been approved by the FDA, this delayed the FDA approval of Kevzara. For additional information, see "Risks Related to Manufacturing and Supply - If we fail to meet the stringent requirements of governmental regulation in the manufacture of drug products or product candidates, we could incur substantial remedial costs, delays in the development or approval of our product candidates or new indications for our marketed products and/or in their commercial launch if they obtain regulatory approval, and a reduction in sales." Our business, prospects, operating results, and financial condition may be materially harmed as a result of noncompliance with the requirements and regulations described in this paragraph.
In addition to the FDA and other regulatory agency regulations in the United States, we are subject to a variety of foreign regulatory requirements governing human clinical trials, manufacturing, marketing and approval of drugs, and commercial sale and distribution of drugs in foreign countries. The foreign regulatory approval process is similarly likely to be a lengthy and expensive process, the result of which is highly uncertain, and foreign regulatory requirements include all of the risks associated with FDA approval as well as country specific regulations. In addition, actions by a regulatory agency in a country or region with respect to a product candidate may have an impact on the approval process for that product candidate in another country or region. Foreign regulatory authorities often also have the authority to require post-approval studies, which involve various risks similar to those described above. Whether or not we obtain FDA approval for a product in the United States, we must obtain approval of the product by the comparable regulatory authorities in foreign countries before we can conduct clinical trials of or market that product or any other product in those countries.
Preclinical and clinical studies required for our product candidates and new indications of our marketed products are expensive and time-consuming, and their outcome is highly uncertain. If any such studies are delayed or yield unfavorable results, regulatory approval for our product candidates or new indications of our marketed products may be delayed or become unobtainable.
As described above, we must conduct extensive testing of our product candidates and new indications of our marketed products before we can obtain regulatory approval to market and sell them. We need to conduct both preclinical animal testing and human clinical trials. Conducting such studies is a lengthy, time-consuming, and expensive process. These tests and trials may not achieve favorable results for many reasons, including, among others, failure of the product candidate to demonstrate safety or efficacy, the development of serious or life-threatening adverse events (or side effects) caused by or connected with exposure to the product candidate (or prior or concurrent exposure to other products or product candidates), difficulty in enrolling and maintaining subjects in a clinical trial, lack of sufficient supplies of the product candidate or comparator drug, and the failure of clinical investigators, trial monitors, contractors, consultants, or trial subjects to comply with the trial plan, protocol, or applicable regulations related to GLPs or GCPs. A clinical trial may fail because it did not include and retain a sufficient number of patients to detect the endpoint being measured or reach statistical significance. A clinical trial may also fail because the dose(s) of the investigational drug included in the trial were either too low or too high to determine the optimal effect of the investigational drug in the disease setting.
We will need to reevaluate any drug candidate that does not test favorably and either conduct new studies, which are expensive and time consuming, or abandon that drug development program. If preclinical testing yields unfavorable results, product candidates may not advance to clinical trials. The failure of clinical trials to demonstrate the safety and effectiveness of our clinical candidates for the desired indication(s) would preclude the successful development of those candidates for such indication(s), in which event our business, prospects, operating results, and financial condition may be materially harmed.
38
Furthermore, some of our product candidates (such as cemiplimab) are studied in combination with agents and treatments developed by us or our collaborators. There may be additional risks and unforeseen safety issues resulting from such combined administration, any of which may materially adversely impact clinical development of these product candidates and our ability to obtain regulatory approval.
Successful development of our current and future product candidates is uncertain.
Only a small minority of all research and development programs ultimately result in commercially successful drugs. Clinical trials may not demonstrate statistically sufficient effectiveness and safety to obtain the requisite regulatory approvals for these product candidates in these indications. Many companies in the biopharmaceutical industry, including our Company, have suffered significant setbacks in clinical trials, even after promising results have been obtained in earlier trials. In a number of instances, we have terminated the development of product candidates due to a lack of or only modest effectiveness, and clinical trials evaluating our product candidates failed to meet the relevant endpoints. For example, in August 2017, we reported that the Phase 3 study evaluating suptavumab, an antibody to RSV, did not meet its primary endpoint of preventing medically-attended RSV infections in infants; as a result, we have discontinued further clinical development of this antibody.
Moreover, even if we obtain positive results from preclinical testing or clinical trials, we may not achieve the same success in future trials, or the FDA and analogous foreign regulatory authorities may deem the results insufficient for an approval. For instance, based on the results of three Phase 3 studies, we submitted a supplemental BLA filing to the FDA seeking approval of ARCALYST for the prevention of gout flares in patients initiating uric acid-lowering drug therapy. In May 2012, the Arthritis Advisory Committee of the FDA voted to recommend against approval of ARCALYST for the prevention of gout flares in patients initiating uric acid-lowering drug therapy and, in July 2012, we received a Complete Response Letter from the FDA requesting additional information, including clinical data, as well as additional CMC information related to a proposed new dosage form. We have discontinued development of ARCALYST for gout.
Many of our clinical trials are conducted under the oversight of Independent Data Monitoring Committees (IDMCs). These independent oversight bodies are made up of external experts who review the progress of ongoing clinical trials, including available safety and efficacy data, and make recommendations concerning a trial's continuation, modification, or termination based on interim, unblinded data. Any of our ongoing clinical trials may be discontinued or amended in response to recommendations made by responsible IDMCs based on their review of such interim trial results. For example, in September 2009, a Phase 3 trial that was evaluating ZALTRAP as a first-line treatment for metastatic pancreatic cancer in combination with gemcitabine was discontinued at the recommendation of an IDMC after a planned analysis of interim efficacy data determined that the trial would not meet its efficacy endpoint. The recommended termination of any of our ongoing late-stage clinical trials by an IDMC could negatively impact the future development of our product candidate(s), and our business, prospects, operating results, and financial condition may be materially harmed.
We are studying our antibody-based product candidates in a wide variety of indications in clinical trials. Many of these trials are exploratory studies designed to evaluate the safety profile of these compounds and to identify what diseases and uses, if any, are best suited for these product candidates. These product candidates may not demonstrate the requisite efficacy and/or safety profile to support continued development for some or all of the indications that are being, or are planned to be, studied, which would diminish our clinical "pipeline" and could negatively affect our future prospects and the value of our Company.
39
Serious complications or side effects in connection with the use of our products and in clinical trials for our product candidates and new indications for our marketed products could cause our regulatory approvals to be revoked or limited or lead to delay or discontinuation of development of our product candidates or new indications for our marketed products, which could severely harm our business, prospects, operating results, and financial condition.
During the conduct of clinical trials, patients report changes in their health, including illnesses, injuries, and discomforts, to their study doctor. Often, it is not possible to determine whether or not the drug candidate being studied caused these conditions. Various illnesses, injuries, and discomforts have been reported from time-to-time during clinical trials of our product candidates and new indications for our marketed products. It is possible that as we test our drug candidates or new indications in larger, longer, and more extensive clinical programs, or as use of these drugs becomes more widespread if they receive regulatory approval, illnesses, injuries, and discomforts that were observed in earlier trials, as well as conditions that did not occur or went undetected in previous trials, will be reported by patients. Many times, side effects are only detectable after investigational drugs are tested in large-scale, Phase 3 clinical trials or, in some cases, after they are made available to patients after approval. If additional clinical experience indicates that any of our product candidates or new indications for our marketed products has many side effects or causes serious or life-threatening side effects, the development of the product candidate may be delayed or fail, or, if the product candidate has received regulatory approval, such approval may be revoked, which would severely harm our business, prospects, operating results, and financial condition.
With respect to EYLEA, there are many potential safety concerns associated with significant blockade of VEGF that may limit our ability to further successfully develop and/or commercialize aflibercept. These serious and potentially life-threatening risks, based on clinical and preclinical experience of VEGF inhibitors, include bleeding, intestinal perforation, hypertension, proteinuria, congestive heart failure, heart attack, and stroke. Other VEGF blockers have reported side effects that became evident only after large-scale trials or after marketing approval when large numbers of patients were treated. There are risks inherent in the intravitreal administration of drugs like aflibercept (such as intraocular inflammation, sterile and culture positive endophthalmitis, corneal decomposition, retinal detachment, and retinal tear), which can cause injury to the eye and other complications. The side effects previously reported for EYLEA include conjunctival hemorrhage, macular degeneration, eye pain, retinal hemorrhage, and vitreous floaters. These and other complications or side effects could harm further development and/or commercialization of aflibercept.
Dupilumab is being studied in additional indications, including atopic dermatitis in adolescent and pediatric patients, asthma in adults and adolescents, nasal polyps, and eosinophilic esophagitis. There is no guarantee that marketing approval of dupilumab in any of these indications will be successfully obtained. The side effects previously reported for dupilumab include hypersensitivity reactions, conjunctivitis and keratitis, injection-site reactions, eye and eyelid inflammation, and cold sores. These and other complications or side effects could harm further development and/or commercialization of dupilumab.
The potential of Praluent to demonstrate cardiovascular benefit is being prospectively assessed in the ODYSSEY OUTCOMES trial. There is no guarantee that Praluent will meet the relevant endpoints of this trial. In addition, there are side effects associated with PCSK9 inhibitor antibodies such as Praluent that may limit our ability to further successfully develop and/or commercialize Praluent, such as new-onset diabetes mellitus, injection-site reactions, hypersensitivity reactions, immunogenicity, demyelination, and changes in neurocognitive function.
There also are risks inherent in subcutaneous injections (which are used for administering our antibody-based products and product candidates, including Dupixent, Praluent, and Kevzara), such as injection-site reactions (including redness, itching, swelling, pain, and tenderness) and other side effects. These and other complications or side effects could harm further development and/or commercialization of our antibody-based products and product candidates, including Dupixent, Praluent, or Kevzara.
Our product candidates in development are recombinant proteins that could cause an immune response, resulting in the creation of harmful or neutralizing antibodies against the therapeutic protein.
In addition to the safety, efficacy, manufacturing, and regulatory hurdles faced by our product candidates, the administration of recombinant proteins frequently causes an immune response, resulting in the creation of antibodies against the therapeutic protein. The antibodies can have no effect or can totally neutralize the effectiveness of the protein, or require that higher doses be used to obtain a therapeutic effect. In some cases, the antibody can cross-react with the patient's own proteins, resulting in an "auto-immune" type disease. Whether antibodies will be created can often not be predicted from preclinical or clinical experiments, and their detection or appearance is often delayed, so neutralizing antibodies may be detected at a later date, in some cases even after pivotal clinical trials have been completed.
40
We may be unable to formulate or manufacture our product candidates in a way that is suitable for clinical or commercial use, which would delay or prevent continued development of such candidates and/or receipt of regulatory approval or commercial sale, which could materially harm our business, prospects, operating results, and financial condition.
If we are unable to continue to develop suitable product formulations or manufacturing processes to support large-scale clinical testing of our product candidates, including our antibody-based product candidates, we may be unable to supply necessary materials for our clinical trials, which would delay or prevent the development of our product candidates. Similarly, if we are unable, directly or through our collaborators or third parties, to supply sufficient quantities of our products or develop formulations of our product candidates suitable for commercial use, we will be unable to obtain regulatory approval for those product candidates.
Many of our products are intended to be used and, if approved, our product candidates may be used in combination with drug-delivery devices, which may result in additional regulatory and other risks.
Many of our products (including Dupixent, Praluent, and Kevzara) are used and, if approved, some of our product candidates may be used in combination with a drug-delivery device, including a pre-filled syringe, patch pump, auto-injector, or other delivery system. The success of our product candidates may depend to a significant extent on the performance of such devices, some of which may be novel or comprised of complex components. Given the increased complexity of the review process when approval of the product and device is sought under a single marketing application and the additional risks resulting from a product candidate's designation as a combination product discussed below, our product candidates used with such drug-delivery devices may be substantially delayed in receiving regulatory approval or may not be approved at all. The FDA review process and criteria for such applications is not a well-established area, which could also lead to delays in the approval process. In addition, some of these drug-delivery devices may be provided by single-source, third-party providers or our collaborators. In any such case, we may be dependent on the sustained cooperation of those third-party providers or collaborators to supply the devices; to conduct the studies required for approval or clearance by the applicable regulatory agencies; and to continue to meet the applicable regulatory and other requirements to maintain approval or clearance once it has been received. Failure to successfully develop or supply the devices, delays in or failure of the studies conducted by us, our collaborators, or third-party providers, or failure of our Company, our collaborators, or the third-party providers to obtain or maintain regulatory approval or clearance of the devices could result in increased development costs, delays in or failure to obtain regulatory approval, and associated delays in a product candidate reaching the market. Loss of regulatory approval or clearance of a device that is used with our product may also result in the removal of our product from the market. Further, failure to successfully develop or supply these devices, or to gain or maintain their approval, could adversely affect sales of the related products.
In the United States, each component of a combination product is subject to the requirements established by the FDA for that type of component, whether a drug, biologic, or device. The determination whether a product is a combination product or two separately regulated products is made by the FDA on a case-by-case basis. Although a single marketing application is generally sufficient for the approval, clearance, or licensure of a combination product, the FDA may determine that separate marketing applications are necessary. In addition, submitting separate marketing applications may be necessary to receive some benefit that accrues only from approval under a particular type of application. This could significantly increase the resources and time required to bring a particular combination product to market.
41
Risks Related to Intellectual Property and Market Exclusivity
If we cannot protect the confidentiality of our trade secrets or our patents are insufficient to protect our proprietary rights, our business and competitive position will be harmed.
Our business requires using sensitive and proprietary technology and other information that we protect as trade secrets. We seek to prevent improper disclosure of these trade secrets through confidentiality agreements. If our trade secrets are improperly disclosed, by our current or former employees, our collaborators, or otherwise, it would help our competitors and adversely affect our business. We will be able to protect our proprietary rights only to the extent that our proprietary technologies and other information are covered by valid and enforceable patents or are effectively maintained as trade secrets. The patent position of biotechnology companies, including our Company, involves complex legal and factual questions and, therefore, enforceability cannot be predicted with certainty. Our patents may be challenged, invalidated, held to be unenforceable, or circumvented. Patent applications filed outside the United States may be challenged by other parties, for example, by filing third-party observations that argue against patentability or an opposition. Such opposition proceedings are increasingly common in the EU and are costly to defend. For example, our European Patent No. 1,360,287 was, and our European Patent No. 2,264,163 is, the subject of opposition proceedings in the EPO, as described in Part I, Item 3. "Legal Proceedings" of our Annual Report on Form 10-K for the year ended December 31, 2016 and in Note 17 to our Consolidated Financial Statements included in this report, respectively. We have pending patent applications in the USPTO, the EPO, and the patent offices of other foreign jurisdictions, and it is likely that we will need to defend patents from challenges by others from time to time in the future. Certain of our U.S. patents may also be challenged by parties who file a request for post-grant review or inter partes reexamination under the America Invents Act of 2011 or ex parte reexamination. Post-grant proceedings are increasingly common in the United States and are costly to defend. Our patent rights may not provide us with a proprietary position or competitive advantages against competitors. Furthermore, even if the outcome is favorable to us, the enforcement of our intellectual property rights can be extremely expensive and time consuming.
We may be restricted in our development, manufacturing, and/or commercialization activities by patents or other proprietary rights of others, and could be subject to damage awards if we are found to have infringed such patents or rights.
Our commercial success depends significantly on our ability to operate without infringing the patents and other proprietary rights of others. Other parties may allege that they own blocking patents to our products in clinical development or even to products that have received regulatory approval and are being or have been commercialized, either because they claim to hold proprietary rights to the composition of a product or the way it is manufactured or the way it is used. Moreover, other parties may allege that they have blocking patents to antibody-based products made using our VelocImmune technology, or any other of our technologies, either because of the way the antibodies are discovered or produced or because of a proprietary composition covering an antibody or the antibody's target.
We have been in the past, are currently, and may in the future be involved in patent litigation and other proceedings involving patents and other intellectual property. For example, we are currently party to patent infringement proceedings initiated by Amgen against us and Sanofi relating to Praluent and patent infringement proceedings relating to Dupixent, as described in Note 17 to our Consolidated Financial Statements. In addition, we are currently party to patent infringement proceedings initiated by us relating to our European Patent No. 1,360,287, our European Patent No. 2,264,163, and our U.S. Patent No. 8,502,018, all of which concern genetically altered mice capable of producing chimeric antibodies that are part human and part mouse, as described in Note 17 to our Consolidated Financial Statements.
We are aware of patents and pending patent applications owned by others that respectively claim antibodies to IL-4R and methods of treating conditions including atopic dermatitis and asthma with such antibodies; antibodies to IL-6R and methods of treating conditions including rheumatoid arthritis with such antibodies; antibodies to PCSK9 and methods of treating hypercholesterolemia with such antibodies; and antibodies to PD-1 and methods of treating cancer with such antibodies. In addition to Dupixent (dupilumab), Praluent (alirocumab), and Kevzara (sarilumab), our late-stage antibody-based pipeline includes fasinumab, an antibody to NGF; cemiplimab, an antibody to PD-1, intended for the treatment of certain cancer indications including advanced CSCC; and evinacumab, an antibody to ANGPTL3. With respect to Dupixent, we are aware of certain patents owned by Immunex Corporation, a wholly owned subsidiary of Amgen. These patents include U.S. Patent No. 8,679,487 (currently subject to the patent infringement proceedings described in Note 17 to our Consolidated Financial Statements) and European Patent No. 2,292,665 (the '665 Patent) and are generally directed to antibodies that bind to IL-4R. On September 30, 2016, Sanofi initiated a revocation proceeding to invalidate the U.K. counterpart of the '665 Patent in the United Kingdom. At the joint request of the parties to the revocation proceeding, the U.K. Patents Court ordered on January 30, 2017 that the revocation action be stayed pending the final determination of the currently pending EPO opposition proceedings initiated by us and Sanofi in relation to the '665 Patent. The oral hearing before the EPO on the oppositions occurred on November 20, 2017, at which the claims of the '665 Patent were found invalid and the patent was revoked. A final written decision of revocation of the '665 Patent was issued by the EPO on January 4, 2018 (subject to appeal). On September 20, 2017 and September 21, 2017, respectively, we and Sanofi initiated opposition proceedings in the EPO against Immunex's European Patent No. 2,990,420 (the '420 Patent), a divisional patent of the
42
'665 Patent (i.e., a patent that shares the same priority date, disclosure, and patent term of the parent '665 Patent but contains claims to a different invention). The original patent term of the Immunex patents is set to expire in 2021.
Although we do not believe that any of our late-stage antibody-based product candidates infringes any valid claim in these patents or patent applications, these other parties could initiate lawsuits for patent infringement and assert that their patents are valid and cover our late-stage antibody-based product candidates, similar to the patent infringement proceedings referred to above. Further, we are aware of a number of patent applications of others that, if granted with claims as currently drafted, may cover our current or planned activities. It could be determined that our products and/or actions in manufacturing or selling our products or product candidates infringe such patents.
Patent holders could assert claims against us for damages and seek to prevent us from manufacturing, selling, or developing our products or product candidates, and a court may find that we are infringing validly issued patents of others. In the event that the manufacture, use, or sale of any of our products or product candidates infringes on the patents or violates other proprietary rights of others, we may be prevented from pursuing product development, manufacturing, and commercialization of those drugs and may be required to pay costly damages. In addition, in the event that we assert our patent rights against other parties that we believe are infringing our patent rights, such parties may challenge the validity of our patents and we may become the target of litigation, which may result in an outcome that is unfavorable to us. Any of these adverse developments may materially harm our business, prospects, operating results, and financial condition. In any event, legal disputes are likely to be costly and time consuming to defend.
We seek to obtain licenses to patents when, in our judgment, such licenses are needed or advisable. If any licenses are required, we may not be able to obtain such licenses on commercially reasonable terms, if at all. The failure to obtain any such license could prevent us from developing or commercializing any one or more of our products or product candidates, which could severely harm our business.
Loss or limitation of patent rights, and new regulatory pathways for biosimilar competition, could reduce the duration of market exclusivity for our products.
In the pharmaceutical and biotechnology industries, the majority of an innovative product's commercial value is usually realized during the period in which it has market exclusivity. In the United States and some other countries, when market exclusivity expires and generic versions of a product are approved and marketed, there usually are very substantial and rapid declines in the product's sales.
If our late-stage product candidates or other clinical candidates are approved for marketing in the United States or elsewhere, market exclusivity for those products will generally be based upon patent rights and/or certain regulatory forms of exclusivity. As described above under "If we cannot protect the confidentiality of our trade secrets or our patents are insufficient to protect our proprietary rights, our business and competitive position will be harmed," the scope and enforceability of our patent rights may vary from country to country. The failure to obtain patent and other intellectual property rights, or limitations on the use, or the loss, of such rights could materially harm us. Absent patent protection or regulatory exclusivity for our products, it is possible, both in the United States and elsewhere, that generic, biosimilar, and/or interchangeable versions of those products may be approved and marketed, which would likely result in substantial and rapid reductions in revenues from sales of those products.
Under the federal Patient Protection and Affordable Care Act (PPACA), enacted in 2010, there is an abbreviated path in the United States for regulatory approval of products that are demonstrated to be "biosimilar" or "interchangeable" with an FDA-approved biological product. The PPACA provides a regulatory mechanism that allows for FDA approval of biologic drugs that are similar to (but not generic copies of) innovative drugs on the basis of less extensive data than is required by a full BLA. Under this regulation, an application for approval of a biosimilar may be filed four years after approval of the innovator product. However, qualified innovative biological products will receive 12 years of regulatory exclusivity, meaning that the FDA may not approve a biosimilar version until 12 years after the innovative biological product was first approved by the FDA. However, the term of regulatory exclusivity may not remain at 12 years in the United States and could be shortened.
A number of jurisdictions outside of the United States have also established abbreviated pathways for regulatory approval of biological products that are biosimilar to earlier versions of biological products. For example, the EU has had an established regulatory pathway for biosimilars since 2005.
The increased likelihood of biosimilar competition has increased the risk of loss of innovators' market exclusivity. Due to this risk, and uncertainties regarding patent protection, if our late-stage product candidates or other clinical candidates are approved for marketing, it is not possible to predict the length of market exclusivity for any particular product with certainty based solely on the expiration of the relevant patent(s) or the current forms of regulatory exclusivity. It is also not possible to predict changes in United States regulatory law that might reduce biological product regulatory exclusivity. The loss of market exclusivity for a product would likely materially and negatively affect revenues from product sales of that product and thus our financial results and condition.
43
Risks Related to Manufacturing and Supply
We rely on limited internal and contracted manufacturing and supply chain capacity, which could result in our being unable to continue to successfully commercialize EYLEA, to successfully commercialize Dupixent, Praluent, and Kevzara and, if approved, our product candidates or other indications for our marketed products, and to advance our clinical pipeline.
Our manufacturing facilities would be inadequate to produce the active pharmaceutical ingredients of (a) our current marketed products, including EYLEA, Dupixent, Praluent, and Kevzara, and (b) our antibody-based product candidates in sufficient clinical quantities if our clinical pipeline advances as planned. In addition to expanding our internal capacity, we intend to rely on our collaborators, as well as contract manufacturers, to produce commercial quantities of drug material needed for commercialization of our products to the extent such quantities are not manufactured at our own facility. As we increase our production in anticipation of potential regulatory approval for our late-stage antibody-based product candidates, our current manufacturing capacity will likely not be sufficient, and we may depend on our collaborators or contract manufacturers, to produce adequate quantities of drug material for both commercial and clinical purposes. We rely entirely on other parties and our collaborators for filling and finishing services. Generally, in order for other parties to perform any step in the manufacturing and supply chain, we must transfer technology to the other party, which can be time consuming and may not be successfully accomplished without considerable cost and expense, or at all. We will have to depend on these other parties to perform effectively on a timely basis and to comply with regulatory requirements. If for any reason they are unable to do so, and as a result we are unable to directly or through other parties manufacture and supply sufficient commercial and clinical quantities of our products on acceptable terms, or if we should encounter delays or other difficulties in our relationships with our collaborators, contract manufacturers, or other parties involved in our supply chain which adversely affect the timely manufacture and supply of our products or product candidates, our business, prospects, operating results, and financial condition may be materially harmed.
Expanding our manufacturing capacity will be costly and we may be unsuccessful in doing so in a timely manner, which could delay or prevent the launch and successful commercialization of our marketed products and late-stage product candidates or other indications for our marketed products if they are approved for marketing and could jeopardize our current and future clinical development programs.
We own an approximately 445,000-square-foot facility in Limerick, Ireland, which we purchased and subsequently renovated to expand our manufacturing capacity and support our global supply chain. In the future, we may lease, operate, purchase, or construct additional facilities to conduct expanded manufacturing activities. Expanding our manufacturing capacity to supply commercial quantities of the active pharmaceutical ingredients for our marketed products and our late-stage product candidates if they are approved for marketing, and to supply clinical drug material to support the continued growth of our clinical programs, will require substantial additional expenditures and various regulatory approvals and permits. In addition, while the Limerick, Ireland facility has received certain manufacturing approvals by regulatory agencies, including the FDA, the facility remains subject to securing certain other governmental permits, and there is no guarantee that we will be able to obtain the remaining required permits in the contemplated timeframe, or at all. Further, we will need to hire and train significant numbers of employees and managerial personnel to staff our expanding manufacturing and supply chain operations. Start-up costs can be large, and scale-up entails significant risks related to process development and manufacturing yields. In addition, we may face difficulties or delays in developing or acquiring the necessary production equipment and technology to manufacture sufficient quantities of our product candidates at reasonable costs and in compliance with applicable regulatory requirements. The FDA and analogous foreign regulatory authorities must determine that our existing and any expanded manufacturing facilities comply, or continue to comply, with cGMP requirements for both clinical and commercial production and license them, or continue to license them, accordingly, and such facilities must also comply with applicable environmental, safety, and other governmental permitting requirements. We may not successfully expand or establish sufficient manufacturing capabilities or manufacture our products economically or in compliance with cGMPs and other regulatory requirements, and we and our collaborators may not be able to build or procure additional capacity in the required timeframe to meet commercial demand for our late-stage product candidates if they receive regulatory approval, and to continue to meet the requirements of our clinical programs. This would interfere with our efforts to successfully commercialize our marketed products, including EYLEA, Dupixent, Praluent, and Kevzara, and could also delay or require us to discontinue one or more of our clinical development programs. As a result, our business, prospects, operating results, and financial condition could be materially harmed.
44
Our ability to manufacture products may be impaired if any of our manufacturing activities, or the activities of third parties involved in our manufacture and supply chain, are found to infringe patents of others.
Our ability to continue to manufacture products in our Rensselaer, New York and Limerick, Ireland facilities and at additional facilities (if any) in the future, or to utilize third parties to produce our products, to supply raw materials or other products, or to perform fill/finish services or other steps in our manufacture and supply chain, depends on our and their ability to operate without infringing the patents or other intellectual property rights of others. Other parties may allege that our manufacturing activities, or the activities of third parties involved in our manufacture and supply chain (which may be located in jurisdictions outside the United States), infringe patents or other intellectual property rights. A judicial or regulatory decision in favor of one or more parties making such allegations could directly or indirectly preclude the manufacture of our products to which those intellectual property rights apply on a temporary or permanent basis, which could materially harm our business, prospects, operating results, and financial condition.
If sales of EYLEA, Dupixent, Praluent, or Kevzara do not meet the levels currently expected, or if the launch of any of our product candidates is delayed or unsuccessful, we may face costs related to excess inventory or unused capacity at our manufacturing facilities and at the facilities of third parties or our collaborators.
We have large-scale manufacturing operations in Rensselaer, New York and Limerick, Ireland. We use our manufacturing facilities primarily to produce bulk product for commercial supply of our marketed products and clinical and preclinical candidates for ourselves and our collaborations. We also plan to use such facilities to produce bulk product for commercial supply of new indications of our marketed products and new product candidates if they are approved for marketing. If our clinical candidates are discontinued or their clinical development is delayed, if the launch of new indications for our marketed products or new product candidates is delayed or does not occur, or if such products are launched and the launch is unsuccessful or the product is subsequently recalled or marketing approval is rescinded, we may have to absorb one hundred percent of related overhead costs and inefficiencies, as well as similar costs of third-party contract manufacturers performing services for us. In addition, if we or our collaborators experience excess inventory, it may be necessary to write down or even write off such excess inventory, which could adversely affect our operating results.
Third-party service or supply failures, or other failures, business interruptions, or other disasters affecting our manufacturing facilities in Rensselaer, New York and Limerick, Ireland or the facilities of any other party participating in the supply chain, would adversely affect our ability to supply our products.
We currently manufacture all of our bulk drug materials at our manufacturing facilities in Rensselaer, New York and Limerick, Ireland. We would be unable to manufacture these materials if our Rensselaer and Limerick facilities were to cease production due to regulatory requirements or actions, business interruptions, labor shortages or disputes, contaminations, fire, natural disasters, acts of war or terrorism, or other problems.
Many of our products and product candidates are very difficult to manufacture. As our products and product candidates are biologics, they require processing steps that are more difficult than those required for most chemical pharmaceuticals. Accordingly, multiple steps are needed to control the manufacturing processes. Problems with these manufacturing processes, even minor deviations from the normal process or from the materials used in the manufacturing process (which may not be detectable by us in a timely manner), could lead to product defects or manufacturing failures, resulting in lot failures, product recalls, product liability claims, and insufficient inventory. Also, the complexity of our manufacturing process may make it difficult, time-consuming, and expensive to transfer our technology to our collaborators or contract manufacturers.
Also, certain raw materials or other products necessary for the manufacture and formulation of our marketed products and product candidates, some of which are difficult to source, are provided by single-source unaffiliated third-party suppliers. In addition, we rely on certain third parties or our collaborators to perform filling, finishing, distribution, laboratory testing, and other services related to the manufacture of our marketed products and product candidates, and to supply various raw materials and other products. We would be unable to obtain these raw materials, other products, or services for an indeterminate period of time if any of these third parties were to cease or interrupt production or otherwise fail to supply these materials, products, or services to us for any reason, including due to regulatory requirements or actions (including recalls), adverse financial developments at or affecting the supplier, failure by the supplier to comply with cGMPs, contaminations, business interruptions, or labor shortages or disputes. In any such circumstances, we may not be able to engage a backup or alternative supplier or service provider in a timely manner or at all. This, in turn, could materially and adversely affect our ability to manufacture or supply marketed products and product candidates, which could materially and adversely affect our business and future prospects.
Certain of the raw materials required in the manufacture and the formulation of our product candidates may be derived from biological sources, including mammalian tissues, bovine serum, and human serum albumin. There are certain European regulatory restrictions on using these biological source materials. If we are required to substitute for these sources to comply with European regulatory requirements, our clinical development or commercial activities may be delayed or interrupted.
45
If we fail to meet the stringent requirements of governmental regulation in the manufacture of drug products or product candidates, we could incur substantial remedial costs, delays in the development or approval of our product candidates or new indications for our marketed products and/or in their commercial launch if they obtain regulatory approval, and a reduction in sales.
We and our third-party providers are required to maintain compliance with cGMPs, and are subject to inspections by the FDA or comparable agencies in other jurisdictions to confirm such compliance. Changes of suppliers or modifications of methods of manufacturing may require amending our application(s) to the FDA or such comparable foreign agencies and acceptance of the change by the FDA or such comparable foreign agencies prior to release of product(s). Because we produce multiple products and product candidates at our facility in Rensselaer, New York, including EYLEA, Dupixent, Praluent, Kevzara, ZALTRAP, and ARCALYST, there are increased risks associated with cGMP compliance. Our inability, or the inability of our third-party fill/finish or other service providers, to demonstrate ongoing cGMP compliance could require us to engage in lengthy and expensive remediation efforts, withdraw or recall product, halt or interrupt clinical trials, and/or interrupt commercial supply of any marketed products, and could also delay or prevent our obtaining regulatory approval for our late-stage product candidates or new indications for our marketed products. For example, on October 28, 2016, the FDA issued a Complete Response Letter relating to the BLA for Kevzara, which referred to certain deficiencies identified during a routine cGMP inspection of the Sanofi fill-and-finish facility in Le Trait, France. While the BLA for Kevzara has since been approved by the FDA, this delayed the FDA approval of Kevzara. Any delay, interruption, or other issue that arises in the manufacture, fill/finish, packaging, or storage of any drug product or product candidate as a result of a failure of our facilities or the facilities or operations of third parties to pass any regulatory agency inspection or maintain cGMP compliance could significantly impair our ability to develop, obtain approval for, and successfully commercialize our products, which would substantially harm our business, prospects, operating results, and financial condition. Any finding of non-compliance could also increase our costs, cause us to delay the development of our product candidates, result in delay in our obtaining, or our not obtaining, regulatory approval of product candidates or new indications for our marketed products, and cause us to lose revenue from any marketed products, which could be seriously detrimental to our business, prospects, operating results, and financial condition.
Risks Related to Commercialization of Products
We may be unsuccessful in continuing the commercialization of our marketed products or in commercializing our product candidates or new indications for our marketed products, if approved, which would materially and adversely affect our business, profitability, and future prospects.
Even if clinical trials demonstrate the safety and effectiveness of any of our product candidates for a specific disease and the necessary regulatory approvals are obtained, the commercial success of any of our product candidates or new indications for our marketed products will depend upon, among other things, their acceptance by patients, the medical community, and third-party payers and on our and our collaborators' ability to successfully manufacture, market and distribute those products in substantial commercial quantities or to establish and manage the required infrastructure to do so, including large-scale information technology systems and a large-scale distribution network. Establishing and maintaining sales, marketing, and distribution capabilities are expensive and time-consuming. Even if we obtain regulatory approval for our product candidates or new indications, if they are not successfully commercialized, we will not be able to recover the significant investment we have made in developing such products and our business, prospects, operating results, and financial condition would be severely harmed.
The commercial success of our products may also be adversely affected by guidelines or recommendations to healthcare providers, administrators, payers, and patient communities that result in decreased use of our products. Such guidelines or recommendations may be published not only by governmental agencies, but also professional societies, practice management groups, private foundations, and other interested parties.
Our product candidates are delivered either by intravenous infusion or by intravitreal or subcutaneous injections, which are generally less well received by patients than tablet or capsule delivery and this could adversely affect the commercial success of those products if they receive marketing approval.
For a description of additional risks relating specifically to the commercialization of EYLEA, Dupixent, Praluent, and Kevzara, see above under "Risks Related to Commercialization of EYLEA" and "Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara)" (as applicable).
46
Our product candidates or new indications for our marketed products, if any are approved for marketing, may face significant competition.
There is substantial competition in the biotechnology and pharmaceutical industries from biotechnology, pharmaceutical, and chemical companies. Many of our competitors have substantially greater research, preclinical and clinical product development and manufacturing capabilities, as well as financial, marketing, and human resources, than we do. Our smaller competitors may also enhance their competitive position if they acquire or discover patentable inventions, form collaborative arrangements, or merge with large pharmaceutical companies. Even if we achieve commercialization of our product candidates, our competitors have achieved, and may continue to achieve, product commercialization before our products are approved for marketing and sale.
Our earlier-stage clinical candidates in development are all fully human antibodies, which were generated using our VelocImmune technology. Our antibody generation technologies and earlier-stage clinical candidates face competition from many pharmaceutical and biotechnology companies using various technologies.
We are aware of several pharmaceutical and biotechnology companies actively engaged in the research and development of antibody-based products against targets that are also the targets of our early- and late-stage product candidates. For example, Pfizer (in collaboration with Eli Lilly) is developing an antibody-based product candidate against NGF. For cemiplimab, there are several competitors that are marketing or developing antibodies against PD-1 and/or PDL-1, including Bristol-Myers Squibb's Opdivo, Merck's Keytruda, Roche's Tecentriq, AstraZeneca's Imfinzi, Pfizer's Bavencio, Novartis's PDR001, and Celgene/BeiGene's BGB-A317. Competitors to evinacumab include Ionis Pharmaceuticals/Akcea Therapeutics’ AKCEA-ANGPTL3-LRx, a ligand conjugated antisense drug against ANGPTL3. We are also aware of several companies developing or marketing small molecules that may compete with our antibody-based product candidates in various indications, if such product candidates obtain regulatory approval in those indications.
If any of these or other competitors announces a successful clinical study involving a product that may be competitive with one of our product candidates or the grant of marketing approval by a regulatory agency for a competitive product, such developments may have an adverse effect on our business or future prospects. In addition, the first product to reach the market in a therapeutic area is often at a significant competitive advantage relative to later entrants to the market. Accordingly, the relative speed with which we, or our collaborators, can develop our products candidates, complete the clinical trials and approval processes, and, if such product candidates are approved for marketing and sale, supply commercial quantities to the market is expected to continue to be an important competitive factor. Due to the uncertainties associated with developing biopharmaceutical products, we may not be the first to obtain marketing approval for a product against any particular target, which may have a material adverse effect on our business or future prospects.
The successful commercialization of our marketed products, as well as our late-stage product candidates or new indications for our marketed products, if approved, will depend on obtaining and maintaining coverage and reimbursement for use of these products from third-party payers, including Medicare and Medicaid in the United States, and these payers may not cover or adequately reimburse for use of our products or may do so at levels that make our products uncompetitive and/or unprofitable, which would materially harm our business, prospects, operating results, and financial condition.
Our future revenues and profitability will be adversely affected in a material manner if United States and foreign governmental payers, private third-party insurers and payers (such as health maintenance organizations and pharmacy benefit management companies), and other third-party payers, including Medicare and Medicaid, do not adequately defray or reimburse the cost of our products to the patients. If these entities do not provide coverage and reimbursement with respect to our products or provide an insufficient level of coverage and reimbursement, our products may be too costly for many patients to afford them, and physicians may not prescribe them. Many third-party payers cover only selected drugs, or may prefer selected drugs, making drugs that are not covered or preferred by such payers more expensive for patients. Third-party payers may also require prior authorization for reimbursement, or require failure on another type of treatment before covering a particular drug, particularly with respect to higher-priced drugs. As our currently marketed products and product candidates are biologics, bringing them to market may cost more than bringing traditional, small-molecule drugs to market due to the complexity associated with the research, development, production, supply and regulatory review of such products. Given cost sensitivities in many health care systems, our currently marketed products and product candidates are likely to be subject to continued pricing pressures, which may have an adverse impact on our business, prospects, operating results, and financial condition.
In addition, in order for private insurance and governmental payers (such as Medicare and Medicaid in the United States) to reimburse the cost of our products, we must, among other things, maintain our FDA registration and our National Drug Code, maintain formulary approval by pharmacy benefits managers, and maintain recognition by insurance companies and the Centers for Medicare & Medicaid Services (CMS). There is no certainty that we will be able to obtain or maintain the applicable requirements for reimbursement (including relevant formulary coverage) of our current and future products, which may have a material adverse effect on our business.
47
Government and other third-party payers (including pharmacy benefit management companies) are challenging the prices charged for healthcare products and increasingly limiting, and attempting to limit, both coverage and level of reimbursement for prescription drugs, such as by requiring outcomes-based or other pay-for-performance pricing arrangements. They are also imposing restrictions on eligible patient populations and the reimbursement process (including by means of required prior authorizations and utilization management criteria). In March 2010, the PPACA and a related reconciliation bill were enacted in the United States. This legislation imposes cost-containment and other measures that are likely to adversely affect the amount of reimbursement for our current and future products. The full effects of this legislation depend on a number of factors, many of which are beyond our control, including new regulations and guidance issued by CMS and other federal and state agencies. Some states are also considering legislation that would control the prices and reimbursement of prescription drugs, and state Medicaid programs are increasingly requesting manufacturers to pay supplemental rebates and requiring prior authorization by the state program for use of any prescription drug for which supplemental rebates are not being paid. It is likely that federal and state legislatures and health agencies will continue to focus on additional health care reform measures in the future that will impose additional constraints on prices and reimbursements for our products.
There is a risk that third-party payers, including Medicare and Medicaid in the United States, may not cover and/or reimburse our current and future products at levels required for us to successfully commercialize these products. Any limitation imposed by third-party payers on the use of our products if they are approved for marketing, or any action or decision by CMS or analogous foreign agencies or authorities which for any reason denies coverage or reimbursement for our products or provides coverage or reimbursement at levels that harm our products' competitiveness or leads to lower prices for those products, will have a material negative effect on our ability to sustain profitability. In certain foreign countries, pricing, coverage, and level of reimbursement of prescription drugs are subject to governmental control, and we and our collaborators may be unable to obtain coverage, pricing, and/or reimbursement on terms that are favorable to us or necessary for us or our collaborators to successfully commercialize our products in those countries. In some foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing and reimbursement vary widely from country to country, and may take into account the clinical effectiveness, cost, and service impact of existing, new, and emerging drugs and treatments. For example, the EU provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. Our results of operations may suffer if we or our collaborators are unable to market our products in foreign countries or if coverage and reimbursement for our products in foreign countries is limited or delayed.
We are dependent upon a small number of customers for a significant portion of our revenue, and the loss of or significant reduction in sales to these customers would adversely affect our results of operations.
We sell EYLEA in the United States to several distributors and specialty pharmacies. Under this distribution model, the distributors and specialty pharmacies generally take physical delivery of product and generally sell the product directly to healthcare providers. For the year ended December 31, 2017, product sales to three customers accounted on a combined basis for 99% of our total gross product revenue. We expect this significant customer concentration to continue for the foreseeable future. Our ability to generate and grow sales of EYLEA will depend, in part, on the extent to which our distributors and specialty pharmacies are able to provide adequate distribution of EYLEA to healthcare providers. Although we believe we can find additional distributors, if necessary, our revenue during any period of disruption could suffer and we might incur additional costs. In addition, these customers are responsible for a significant portion of our net trade accounts receivable balances. The loss of any large customer, a significant reduction in sales we make to them, any cancellation of orders they have made with us, or any failure to pay for the products we have shipped to them could adversely affect our results of operations.
If we need to establish commercial capabilities outside the United States and are unable to do so, our business, prospects, operating results, and financial condition may be adversely affected.
We have limited commercial capabilities outside the United States and do not currently have an organization for the sales, marketing, and distribution of marketed products outside the United States. There may be circumstances in which we need to establish commercial capabilities outside the United States, including because we decide to exercise our option to co-promote a product outside the United States or commercialize a particular product independently; we are unable to find an appropriate collaborator; or our existing collaborator decides not to opt in, decides to opt out, or breaches its obligations to us with respect to a particular product.
In order to commercialize any products outside the United States, we must build our sales, marketing, distribution, managerial, and other non-technical capabilities in the relevant markets or make arrangements with third parties to perform these services, which would likely be expensive and time consuming and could delay product launch in one or more markets outside the United States. We cannot be certain that we will be able to successfully develop commercial capabilities outside the United States within
48
an acceptable time frame or at all. These and other difficulties relating to commercializing our products outside the United States may severely harm our business, prospects, operating results, and financial condition.
For additional risks relating to commercialization of EYLEA, Dupixent, Praluent, and Kevzara outside the United States, see also "Risks Related to Commercialization of EYLEA - We rely on our collaboration with Bayer for commercializing EYLEA" and "Risks Related to Commercialization of Our Antibody-based Products (Dupixent, Praluent, and Kevzara) - We rely on our Antibody Collaboration with Sanofi for commercializing Dupixent, Praluent, and Kevzara" (as applicable).
Regulatory and Litigation Risks
If the testing or use of our products harms people, or is perceived to harm them even when such harm is unrelated to our products, we could be subject to costly and damaging product liability claims.
The testing, manufacturing, marketing, and sale of drugs for use in people expose us to product liability risk. Any informed consent or waivers obtained from people who enroll in our clinical trials may not protect us from liability or the cost of litigation. We may also be subject to claims by patients who use our approved products, or our product candidates if those product candidates receive regulatory approval and become commercially available, that they have been injured by a side effect associated with the drug. Even in a circumstance in which we do not believe that an adverse event is related to our products or product candidates, the related investigation may be time consuming or inconclusive and may have a negative impact on our reputation or business. We may face product liability claims and be found responsible even if injury arises from the acts or omissions of third parties who provide fill/finish or other services. To the extent we maintain product liability insurance in relevant periods, such insurance may not cover all potential liabilities or may not completely cover any liability arising from any such litigation. Moreover, in the future we may not have access to liability insurance or be able to maintain our insurance on acceptable terms.
If we market and sell approved products in a way that violates federal or state healthcare laws, we may be subject to civil or criminal penalties.
The FDA regulates the marketing and promotion of our products, which must comply with the Food, Drug, and Cosmetic Act and applicable FDA implementing standards. The FDA's review of promotional activities includes healthcare provider-directed and direct-to-consumer advertising as well as sales representatives' communications. The FDA may take enforcement action for promoting unapproved uses of a product or other violations of its advertising laws and regulations.
In addition to FDA and related regulatory requirements, we are subject to health care "fraud and abuse" laws, such as the federal False Claims Act, the anti-kickback provisions of the federal Social Security Act, and other state and federal laws and regulations. Federal and state anti-kickback laws prohibit, among other things, payments or other remuneration to induce or reward someone to purchase, prescribe, endorse, or recommend a product that is reimbursed under federal or state healthcare programs. If we provide payments or other remuneration to a healthcare professional to induce the prescribing of our products, we could face liability under state and federal anti-kickback laws.
Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government, or knowingly making, or causing to be made, a false statement to get a false claim paid. Pharmaceutical companies have been prosecuted under these laws for a variety of alleged promotional and marketing activities, such as allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product; reporting to pricing services inflated average wholesale prices that were then used by federal programs to set reimbursement rates; engaging in promotion for uses that the FDA has not approved, known as off-label uses, that caused claims to be submitted to Medicaid for non-covered off-label uses; and submitting inflated best price information to the Medicaid Rebate program. The majority of states also have statutes or regulations similar to the federal anti-kickback law and false claims laws, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payer. Sanctions under these federal and state laws may include civil monetary penalties, exclusion of a manufacturer's products from reimbursement under government programs, criminal fines, and imprisonment. Even if it is determined that we have not violated these laws, government investigations into these issues typically require the expenditure of significant resources and generate negative publicity, which would harm our business, prospects, operating results, and financial condition. Because of the breadth of these laws and the narrowness of the safe harbors, it is possible that some of our business activities could be challenged under one or more of such laws.
49
As part of the PPACA, the federal government requires that pharmaceutical manufacturers record any "transfers of value" made to U.S. prescribers and certain other healthcare providers and teaching hospitals. Information provided by companies is aggregated and posted annually on an "Open Payments" website, which is managed by CMS, the agency responsible for implementing these disclosure requirements. We will need to continue to dedicate significant resources to comply with these requirements and to be prepared to comply with additional reporting obligations outside of the United States that may apply in the future. The PPACA also includes various provisions designed to strengthen fraud-and-abuse enforcement, such as increased funding for enforcement efforts and the lowering of the intent requirement of the federal anti-kickback statute and criminal health care fraud statute such that a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, several states have legislation requiring pharmaceutical companies to establish marketing compliance programs, file periodic reports with the state or make periodic public disclosures on sales, marketing, pricing, clinical trials, and other activities. Many of these requirements and standards are new or uncertain, and the penalties for failure to comply with these requirements may be unclear. If we are found not to be in full compliance with these laws, we could face enforcement actions, fines, and other penalties, and could receive adverse publicity, which would harm our business, prospects, operating results, and financial condition. Additionally, access to such data by fraud-and-abuse investigators and industry critics may draw scrutiny to our collaborations with reported entities.
Risks from the improper conduct of employees, agents, contractors, or collaborators could adversely affect our reputation and our business, prospects, operating results, and financial condition.
We cannot ensure that our compliance controls, policies, and procedures will in every instance protect us from acts committed by our employees, agents, contractors, or collaborators that would violate the laws or regulations of the jurisdictions in which we operate, including, without limitation, healthcare, employment, foreign corrupt practices, trade restrictions and sanctions, environmental, competition, and patient privacy and other privacy laws and regulations. Such improper actions could subject us to civil or criminal investigations, and monetary and injunctive penalties, and could adversely impact our ability to conduct business, operating results, and reputation.
In particular, our business activities outside of the United States are subject to the Foreign Corrupt Practices Act, or FCPA, and similar anti-bribery or anti-corruption laws, regulations or rules of other countries in which we operate, including the U.K. Bribery Act. The FCPA generally prohibits offering, promising, giving, or authorizing others to give anything of value, either directly or indirectly, to a non-U.S. government official in order to influence official action, or otherwise obtain or retain business. The FCPA also requires public companies to make and keep books and records that accurately and fairly reflect the transactions of the corporation and to devise and maintain an adequate system of internal accounting controls. Our business is heavily regulated and therefore involves significant interaction with public officials, including officials of non-U.S. governments. Additionally, in many other countries, the health care providers who prescribe pharmaceuticals are employed by their government, and the purchasers of pharmaceuticals are government entities; therefore, our dealings with these prescribers and purchasers are subject to regulation under the FCPA. Recently the Securities and Exchange Commission, or SEC, and Department of Justice have increased their FCPA enforcement activities with respect to pharmaceutical companies. There is no certainty that all of our employees, agents, contractors, or collaborators, or those of our affiliates, will comply with all applicable laws and regulations, particularly given the high level of complexity of these laws. Violations of these laws and regulations could result in fines, criminal sanctions against us, our officers, or our employees, requirements to obtain export licenses, cessation of business activities in sanctioned countries, implementation of compliance programs, and prohibitions on the conduct of our business. Any such violations could include prohibitions on our ability to offer our products in one or more countries and could materially damage our reputation, our brand, our international expansion efforts, our ability to attract and retain employees, and our business, prospects, operating results, and financial condition.
Our operations may involve hazardous materials and are subject to environmental, health, and safety laws and regulations. Compliance with these laws and regulations is costly, and we may incur substantial liability arising from our activities involving the use of hazardous materials.
As a biopharmaceutical company with significant research and development and manufacturing operations, we are subject to extensive environmental, health, and safety laws and regulations, including those governing the use of hazardous materials. Our research and development and manufacturing activities involve the controlled use of chemicals, infectious agents (such as viruses, bacteria, and fungi), radioactive compounds, and other hazardous materials. The cost of compliance with environmental, health, and safety regulations is substantial. If an accident involving these materials or an environmental discharge were to occur, we could be held liable for any resulting damages, or face regulatory actions, which could exceed our resources or insurance coverage.
50
Our business is subject to increasingly complex corporate governance, public disclosure, and accounting requirements and regulations that could adversely affect our business, operating results, and financial condition.
We are subject to changing rules and regulations of various federal and state governmental authorities as well as the stock exchange on which our Common Stock is listed. These entities, including the SEC and The NASDAQ Stock Market LLC, have issued a significant number of new and increasingly complex requirements and regulations over the course of the last several years and continue to develop additional requirements and regulations in response to laws enacted by Congress, including the Sarbanes-Oxley Act of 2002 and, most recently, the Dodd-Frank Wall Street Reform and Protection Act, or the Dodd-Frank Act. There are significant corporate governance and executive compensation-related provisions in the Dodd-Frank Act that expressly authorized or required the SEC to adopt additional rules in these areas, a number of which have yet to be fully implemented. Our efforts to comply with these requirements and regulations have resulted in, and are likely to continue to result in, an increase in expenses and a diversion of management's time from other business activities.
Changes in laws and regulations affecting the healthcare industry could adversely affect our business.
All aspects of our business, including research and development, manufacturing, marketing, pricing, sales, litigation, and intellectual property rights, are subject to extensive legislation and regulation. Changes in applicable federal and state laws and agency regulations could have a materially negative impact on our business. These include:
• | changes in the FDA and foreign regulatory processes for new therapeutics that may delay or prevent the approval of any of our current or future product candidates; |
• | new laws, regulations, or judicial decisions related to healthcare availability or the payment for healthcare products and services, including prescription drugs, that would make it more difficult for us to market and sell products once they are approved by the FDA or foreign regulatory agencies; |
• | changes in FDA and foreign regulations that may require additional safety monitoring prior to or after the introduction of new products to market, which could materially increase our costs of doing business; and |
• | changes in FDA and foreign cGMPs that may make it more difficult and costly for us to maintain regulatory compliance and/or manufacture our marketed product and product candidates in accordance with cGMPs. |
As described above, the PPACA and potential regulations thereunder easing the entry of competing follow-on biologics into the marketplace, other new legislation or implementation of existing statutory provisions on importation of lower-cost competing drugs from other jurisdictions, and legislation on comparative effectiveness research are examples of previously enacted and possible future changes in laws that could adversely affect our business.
The current U.S. administration and Congress could carry out significant changes in legislation, regulation, and government policy (including with respect to the possible repeal of all or portions of the PPACA, possible government reimbursement changes, and possible changes in the existing treaty and trade relationships with other countries), as evidenced by statements and recent actions of the current president and certain members of Congress. While it is not possible to predict whether and when any such changes will occur, changes in the laws, regulations, and policies governing the development and approval of our product candidates and the commercialization, importation, and reimbursement of our products could adversely affect our business. In addition, our development and commercialization activities could be harmed or delayed by a shutdown of the U.S. government, including the FDA.
Risks associated with our operations outside of the United States could adversely affect our business.
We have operations and conduct business outside the United States and we plan to expand these activities. Consequently, we are, and will continue to be, subject to risks related to operating in foreign countries, which include:
• | unfamiliar foreign laws or regulatory requirements or unexpected changes to those laws or requirements; |
• | other laws and regulatory requirements to which our business activities abroad are subject, such as the FCPA and the U.K. Bribery Act (discussed in greater detail above under "Risks from the improper conduct of employees, agents, contractors, or collaborators could adversely affect our reputation and our business, prospects, operating results, and financial condition"); |
• | changes in the political or economic condition of a specific country or region; |
• | fluctuations in the value of foreign currency versus the U.S. dollar; |
• | our ability to deploy overseas funds in an efficient manner; |
• | tariffs, trade protection measures, import or export licensing requirements, trade embargoes, and sanctions (including those administered by the Office of Foreign Assets Control of the U.S. Department of the Treasury), and other trade barriers; |
• | difficulties in attracting and retaining qualified personnel; and |
• | cultural differences in the conduct of business. |
51
For example, on June 23, 2016, the United Kingdom held a referendum in which voters approved an exit from the EU, commonly referred to as "Brexit." As a result of the referendum, the British government has begun negotiating the terms of the United Kingdom's future relationship with the EU. We do not know to what extent Brexit will impact the business and regulatory environment in the United Kingdom, the rest of the EU, or other countries. Changes impacting our ability to conduct business in the United Kingdom or other EU countries, or changes to the regulatory regime applicable to our operations in those countries (such as with respect to the approval of our product candidates), may materially and adversely impact our business, prospects, operating results, and financial condition.
We may incur additional tax liabilities related to our operations.
We are subject to income tax in the United States and various foreign jurisdictions. Significant judgment is required in determining our worldwide tax liabilities, and our effective tax rate is derived from a combination of the applicable statutory rates in the various jurisdictions in which we operate. We record liabilities that involve significant management judgment for uncertain tax positions. The Internal Revenue Service or other domestic or foreign taxing authorities may disagree with our interpretation of tax law as applied to the operations of Regeneron and its subsidiaries or with the positions we may take with respect to particular tax issues on our tax returns. Consequently, our reported effective tax rate and our after-tax cash flows may be materially and adversely affected by tax assessments or judgments in excess of accrued amounts we have estimated in preparing our financial statements. Further, our effective tax rate may also be adversely affected by numerous other factors, including changes in the mix of our profitability from country to country and changes in tax laws and regulations. Changes in tax laws of various jurisdictions in which we do business could also result from the base erosion and profits shifting, or BEPS, recommendations by the Organization for Economic Co-operation and Development. If these recommendations (or other changes in law) were adopted by the countries in which we do business, it could adversely affect our provision for income tax and our current rate.
On December 22, 2017, President Trump signed into law H.R.1., "An Act to provide for reconciliation pursuant to titles II and V of the concurrent resolution on the budget for fiscal year 2018" (also known as the "Tax Cuts and Jobs Act") (the Act). Most of the provisions of the Act went into effect on January 1, 2018. The Act includes a number of provisions that are expected to impact our operating results, cash flows, and financial condition, including reducing the U.S. federal corporate tax rate from 35% to 21%, changing the taxation of foreign earnings (including taxation of certain global intangible low-taxed income), allowing for immediate expensing of qualified assets, repealing the deduction for domestic manufacturing, and imposing further limitations on the deductibility of executive compensation.
We face potential liability related to the privacy of health information we obtain from clinical trials sponsored by us or our collaborators, from research institutions and our collaborators, and directly from individuals.
Most health care providers, including research institutions from which we or our collaborators obtain patient health information, are subject to privacy and security regulations promulgated under the Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act. For example, as part of our human genetics initiative, our wholly-owned subsidiary, Regeneron Genetics Center LLC, has entered into collaborations with research institutions, including the Geisinger Health System, which are subject to such regulations. Regeneron is not currently classified as a covered entity or business associate under HIPAA and thus is not subject to its requirements or penalties. However, any person may be prosecuted under HIPAA's criminal provisions either directly or under aiding-and-abetting or conspiracy principles. Consequently, depending on the facts and circumstances, we could face substantial criminal penalties if we knowingly receive individually identifiable health information from a HIPAA-covered health care provider or research institution that has not satisfied HIPAA's requirements for disclosure of individually identifiable health information. In addition, we may maintain sensitive personally identifiable information, including health information, that we receive throughout the clinical trial process, in the course of our research collaborations, and directly from individuals (or their healthcare providers) who enroll in our patient assistance programs. As such, we may be subject to state laws requiring notification of affected individuals and state regulators in the event of a breach of personal information, which is a broader class of information than the health information protected by HIPAA. Our clinical trial programs and research collaborations outside the U.S. (such as our consortium with AbbVie, Alnylam Pharmaceuticals, AstraZeneca, Biogen, and Pfizer to fund the generation of genetic exome sequence data from the UK Biobank health resource) may implicate international data protection laws, including the EU Data Protection Directive and the General Data Protection Regulation (GDPR) that is replacing it. Our activities outside the U.S. impose additional compliance requirements and generate additional risks of enforcement for noncompliance, including the new risk of substantial financial penalties for data breach or improper processing of personal data under the GDPR. Failure by our collaborators to comply with the strict rules on the transfer of personal data outside of the EU into the U.S. may result in the imposition of criminal and administrative sanctions on such collaborators, which could adversely affect our business and could create liability for us. Furthermore, certain health privacy laws, data breach notification laws, consumer protection laws, and genetic testing laws may apply directly to our operations and/or those of our collaborators and may impose restrictions on our collection, use, and dissemination of individuals' health information. Moreover, patients about whom we or our collaborators obtain health information, as well as the providers who share this information with us, may have statutory or contractual rights that limit our ability to use and disclose the information. We are
52
likely to be required to expend significant capital and other resources to ensure ongoing compliance with applicable privacy and data security laws both inside and outside the United States. Claims that we have violated individuals' privacy rights or breached our contractual obligations, even if we are not found liable, could be expensive and time-consuming to defend and could result in adverse publicity that could harm our business.
If we or any collaborators fail to comply with applicable federal, state, or local regulatory requirements, we could be subject to a range of regulatory actions that could affect our or any collaborators' ability to commercialize our products and could harm or prevent sales of any affected products that we are able to commercialize, or could substantially increase the costs and expenses of commercializing and marketing our products. Any threatened or actual government enforcement action could also generate adverse publicity and require that we devote substantial resources that could otherwise be used in other aspects of our business.
Increasing use of social media could give rise to liability, breaches of data security, or reputational damage.
We and our employees are increasingly utilizing social media tools as a means of communication both internally and externally. Despite our efforts to monitor evolving social media communication guidelines and comply with applicable rules, there is risk that the use of social media by us or our employees to communicate about our products or business may cause us to be found in violation of applicable requirements. In addition, our employees may knowingly or inadvertently make use of social media in ways that may not comply with our social media policy or other legal or contractual requirements, which may give rise to liability, lead to the loss of trade secrets or other intellectual property, or result in public exposure of personal information of our employees, clinical trial patients, customers, and others. Furthermore, negative posts or comments about us or our products in social media could seriously damage our reputation, brand image, and goodwill. Any of these events could have a material adverse effect on our business, prospects, operating results, and financial condition and could adversely affect the price of our Common Stock.
Risks Related to Our Reliance on Third Parties
If any of our collaborations with Sanofi is terminated, our business, prospects, operating results, and financial condition, and our ability to discover, develop, manufacture, and commercialize our pipeline of product candidates in the time expected, or at all, would be materially harmed.
We rely heavily on funding from Sanofi to support certain research and development programs, including our immuno-oncology research and development programs. Sanofi has committed to reimburse us for up to $825.0 million of the costs of our efforts to identify and validate potential immuno-oncology targets and develop fully-human therapeutic antibodies against such targets under the IO Discovery and Development Agreement over the term of the IO Discovery and Development Agreement. Sanofi also initially funds almost all of the development expenses incurred in connection with the clinical development of product candidates for which Sanofi is the principal controlling party under our IO Collaboration. In addition, Sanofi initially funds half of the development expenses incurred in connection with the clinical development of product candidates for which we are the principal controlling party under our IO Collaboration. We rely on Sanofi to fund these activities. In addition, with respect to Dupixent, Praluent, Kevzara, and REGN3500, which Sanofi co-develops with us under our Antibody Collaboration, or for products or product candidates for which Sanofi is the principal controlling party under our IO Collaboration, we rely on Sanofi to lead much of the clinical development efforts and assist with obtaining and maintaining regulatory approval. Following regulatory approval, we also rely on Sanofi to lead (i) the commercialization efforts of Dupixent, Praluent, Kevzara, and REGN3500 under our Antibody Collaboration and (ii) the commercialization efforts outside the Unites States to support all products that are co-developed by Sanofi and us under our IO Collaboration (as well as the commercialization efforts in the United States to support all products for which Sanofi is the principal controlling party under our IO Collaboration).
If Sanofi does not elect to co-develop the product candidates discovered under our IO Collaboration or opts out of their development, unless we enter into a collaboration agreement with another party, we would be required to fund and conduct on our own the clinical trials, regulatory activities, and the ensuing commercialization efforts to support those antibody-based products. For example, under our Antibody Collaboration, Sanofi elected not to continue co-development of fasinumab and trevogrumab, and decided not to opt in to the evinacumab and other programs. In addition, as previously reported, we will now be required to fund all of our antibody discovery activities and the research and preclinical development activities of our drug candidates, as Sanofi’s funding obligations under the Antibody Discovery Agreement have ceased.
53
If Sanofi terminates the License and Collaboration Agreement or the IO Collaboration or fails to comply with its payment obligations under any of our collaborations, our business, prospects, operating results, and financial condition would be materially harmed. We would be required to either expend substantially more resources than we have anticipated to support our research and development efforts, which could require us to seek additional funding that might not be available on favorable terms or at all, or materially cut back on such activities. If Sanofi does not perform its obligations with respect to the product candidates that it elects to co-develop, our ability to develop, manufacture, and commercialize these product candidates will be significantly adversely affected. We have limited commercial capabilities outside the United States and would have to develop or outsource these capabilities for products commercialized under our Antibody Collaboration, such as Dupixent, Praluent, and Kevzara (see also "Risks Related to Commercialization of Products - If we need to establish commercial capabilities outside the United States and are unable to do so, our business, prospects, operating results, and financial condition may be adversely affected" above). Termination of the License and Collaboration Agreement would create substantial new and additional risks to the successful development and commercialization of Dupixent, Praluent, and Kevzara, particularly outside the United States.
If our collaboration with Bayer for EYLEA is terminated, or Bayer materially breaches its obligations thereunder, our business, prospects, operating results, and financial condition, and our ability to continue to commercialize EYLEA outside the United States would be materially harmed.
We rely heavily on Bayer to assist with the commercialization of EYLEA outside the United States. We continue to rely on Bayer to obtain and maintain regulatory approval outside the United States and provide all sales, marketing, and commercial support for the product outside the United States. In particular, Bayer has responsibility for selling EYLEA outside the United States using its sales force and, in Japan, in cooperation with Santen pursuant to a Co-Promotion and Distribution Agreement with Bayer's Japanese affiliate. If Bayer and, in Japan, Santen do not perform their obligations in a timely manner, or at all, our ability to commercialize EYLEA outside the United States will be significantly adversely affected. Bayer has the right to terminate its collaboration agreement with us at any time upon six or twelve months' advance notice, depending on the circumstances giving rise to termination. If Bayer were to terminate its collaboration agreement with us, we may not have the resources or skills to replace those of our collaborator, which could require us to seek another collaboration that might not be available on favorable terms or at all, and could cause significant delays in the commercialization of EYLEA outside the United States and result in substantial additional costs to us. We have limited commercial capabilities outside the United States and would have to develop or outsource these capabilities (see also "Risks Related to Commercialization of Products - If we need to establish commercial capabilities outside the United States and are unable to do so, our business, prospects, operating results, and financial condition may be adversely affected" above). Termination of the Bayer collaboration agreement would create substantial new and additional risks to the successful commercialization of EYLEA outside the United States.
Our collaborators and service providers may fail to perform adequately in their efforts to support the development, manufacture, and commercialization of our drug candidates and current and future products.
We depend upon third-party collaborators, including Sanofi, Bayer, and service providers such as CROs, outside testing laboratories, clinical investigator sites, and third-party manufacturers, fill/finish, and product packagers and labelers, to assist us in the manufacture and preclinical and clinical development of our product candidates. We also depend, or will depend, on some of these third parties in connection with the commercialization of our marketed products and our late-stage product candidates and new indications for our marketed products if they are approved for marketing. If any of our existing collaborators or service providers breaches or terminates its agreement with us or does not perform its development or manufacturing services under an agreement in a timely manner (including as a result of its inability to perform due to financial or other relevant constraints) or in compliance with applicable GMPs, GLPs, or GCP standards, we could experience additional costs, delays, and difficulties in the manufacture or development of, or in obtaining approval by regulatory authorities for, or successfully commercializing our product candidates.
We and our collaborators rely on third-party service providers to support the distribution of our marketed products and for many other related activities in connection with the commercialization of these marketed products. Despite our or our collaborators' arrangements with them, these third parties may not perform adequately. If these service providers do not perform their services adequately, sales of our marketed products will suffer.
54
Risk Related to Employees
We are dependent on our key personnel and if we cannot recruit and retain leaders in our research, development, manufacturing, and commercial organizations, our business will be harmed.
We are highly dependent on certain of our executive officers, other key members of our senior management team, and our Chairman. If we are not able to retain (or for any other reason lose the services of) any of these persons, our business may suffer. In particular, we depend on the services of P. Roy Vagelos, M.D., the Chairman of our board of directors; Leonard S. Schleifer, M.D., Ph.D., our President and Chief Executive Officer; George D. Yancopoulos, M.D., Ph.D., our President and Chief Scientific Officer; and Neil Stahl, Ph.D., our Executive Vice President, Research and Development. As we continue to commercialize EYLEA, Dupixent, Praluent, and Kevzara and, assuming the receipt of required regulatory approvals, other products, we are also highly dependent on the expertise and services of members of our senior management leading these commercialization efforts. There is intense competition in the biotechnology industry for qualified scientists and managerial personnel in the development, manufacture, and commercialization of drugs. We may not be able to continue to attract and retain the qualified personnel necessary to continue to advance our business and achieve our strategic objectives.
Information Technology Risks
Significant disruptions of information technology systems or breaches of data security could adversely affect our business.
Our business is increasingly dependent on critical, complex, and interdependent information technology systems, including Internet-based systems, to support business processes as well as internal and external communications. The size and complexity of our computer systems make us potentially vulnerable to IT system breakdowns, internal and external malicious intrusion, and computer viruses, which may impact product production and key business processes. We also have outsourced significant elements of our information technology infrastructure and operations to third parties, which may allow them to access our confidential information and may also make our systems vulnerable to service interruptions or to security breaches from inadvertent or intentional actions by such third parties or others.
In addition, our systems are potentially vulnerable to data security breaches - whether by employees or others - which may expose sensitive data to unauthorized persons. Data security breaches could lead to the loss of trade secrets or other intellectual property, result in demands for ransom or other forms of blackmail, or lead to the public exposure of personal information (including sensitive personal information) of our employees, clinical trial patients, customers, and others. Such attacks are of ever-increasing levels of sophistication and are made by groups and individuals with a wide range of motives (including industrial espionage) and expertise, including by organized criminal groups, “hacktivists,” nation states, and others. As a company with an increasingly global presence, our systems are subject to frequent attacks. Due to the nature of some of these attacks, there is a risk that an attack may remain undetected for a period of time. While we continue to make investments to improve the protection of data and information technology, there can be no assurance that our efforts will prevent service interruptions or security breaches.
Such disruptions and breaches of security could result in legal proceedings, liability under laws that protect the privacy of personal information, disruptions to our operations, and damage to our reputation, which could have a material adverse effect on our business, prospects, operating results, and financial condition.
Risks Related to Our Financial Results, Liquidity, and Need for Additional Financing
If we cannot sustain profitability, our business, prospects, operating results, and financial condition would be materially harmed.
Beginning in 2012, we reported profitability; prior to that, we generally incurred net losses. If we cannot sustain profitability, we may be unable to continue our operations. In the absence of substantial revenue from the sale of products on an ongoing basis, including our sales of EYLEA, and our share of the profits from Bayer's sales of EYLEA outside the United States, or from other sources, the amount, timing, nature, or source of which cannot be predicted, we may incur substantial losses again as we conduct our research and development activities, commercialize our approved products, and prepare for possible commercialization of our other product candidates and new indications of our marketed products.
55
We may need additional funding in the future, which may not be available to us, and which may force us to delay, reduce or eliminate our product development programs or commercialization efforts.
We expend substantial resources for research and development, including costs associated with clinical testing of our product candidates and new indications of our marketed products, the commercialization of products, and capital expenditures. We believe our existing capital resources and borrowing availability under our revolving credit facility, together with funds generated by current and anticipated EYLEA net product sales and funding we are entitled to receive under our collaboration agreements, will enable us to meet our anticipated operating needs for the foreseeable future. However, one or more of our collaboration agreements may terminate, our revenues may fall short of our projections or be delayed, or our expenses may increase, any of which could result in our capital being consumed significantly faster than anticipated. In addition, our expenses may increase for many reasons, including expenses in connection with the commercialization of our marketed products and the potential commercial launches of our product candidates and new indications for our marketed products, manufacturing scale-up, expenses related to clinical trials testing of antibody-based product candidates we are developing on our own (without a collaborator), and expenses for which we are responsible in accordance with the terms of our collaboration agreements.
We cannot be certain that our existing capital resources and our current and anticipated revenues will be sufficient to meet our operating needs. We may require additional financing in the future and we may not be able to raise additional funds on acceptable terms or at all. For example, in March 2017, we completed $720.0 million lease financing for our existing corporate headquarters and other rentable area consisting of approximately 170 acres of predominately office buildings and laboratory space located in the towns of Mount Pleasant and Greenburgh, NY, which will become due and payable in full on the five-year anniversary of the closing date unless extended with the consent of all the participants and subject to certain other conditions. Our ability to refinance or to obtain additional financing could be adversely affected if there is a significant decline in the demand for our products or other significantly unfavorable changes in economic conditions. Volatility in the financial markets could increase borrowing costs or affect our ability to raise capital. If additional financing is necessary and we obtain it through the sale of equity securities, such sales will likely be dilutive to our shareholders. Debt financing arrangements may require us to pledge certain assets or enter into covenants that would restrict our business activities or our ability to incur further indebtedness and may be at interest rates and contain other terms that are not favorable to our shareholders. Should we require and be unable to raise sufficient funds (i) to complete the development of our product candidates, (ii) to successfully commercialize our late-stage product candidates or new indications for our marketed products if they obtain regulatory approval, and (iii) to continue our manufacturing and marketing of our marketed products, we may face delay, reduction, or elimination of our research and development or preclinical or clinical programs and our commercialization activities, which would significantly limit our potential to generate revenue.
Changes in foreign currency exchange rates could have a material adverse effect on our operating results.
Our revenue from outside of the United States will increase as our products, whether marketed by us or our collaborators, gain marketing approval in such jurisdictions. Our primary foreign currency exposure relates to movements in the Japanese yen, euro, British pound sterling, and Australian dollar. If the U.S. dollar weakens against a specific foreign currency, our revenues will increase, having a positive impact on net income, but our overall expenses will increase, having a negative impact. Likewise, if the U.S. dollar strengthens against a specific foreign currency, our revenues will decrease, having a negative impact on net income, but our overall expenses will decrease, having a positive impact. Therefore, significant changes in foreign exchange rates can impact our operating results and the financial condition of our Company.
Our investments are subject to risks and other external factors that may result in losses or affect the liquidity of these investments.
As of December 31, 2017, we had $812.7 million in cash and cash equivalents and $2,083.3 million in marketable securities (including $62.8 million in equity securities). Our investments consist primarily of fixed-income securities, including investment-grade corporate bonds. These fixed-income investments are subject to external factors that may adversely affect their market value or liquidity, such as interest rate, liquidity, market, and issuer credit risks, including actual or anticipated changes in credit ratings. The equity securities we hold may experience significant volatility and may decline in value or become worthless if the issuer experiences an adverse development. Furthermore, our equity investments could be subject to dilution (and decline in value) as a result of the issuance of additional equity interests. If any of our investments suffer market price declines that are other than temporary, their value could be impaired, which may have an adverse effect on our financial condition and operating results.
56
Risks Related to Our Common Stock
Our stock price is extremely volatile.
There has been significant volatility in our stock price and generally in the market prices of biotechnology companies' securities. Various factors and events may have a significant impact on the market price of our Common Stock. These factors include, by way of example:
• | net product sales of our marketed products, in particular EYLEA and Dupixent, as well as our overall operating results; |
• | if any of our product candidates or our new indications for our marketed products receive regulatory approval, net product sales of, and profits from, these product candidates and new indications; |
• | market acceptance of, and the market share for, our marketed products, especially EYLEA and Dupixent; |
• | whether our net products sales and net profits underperform, meet, or exceed the expectations of investors or analysts; |
• | announcement of actions by the FDA or foreign regulatory authorities or their respective advisory committees regarding our, or our collaborators', or our competitors', currently pending or future application(s) for regulatory approval of product candidate(s) or new indications for marketed products; |
• | announcement of submission of an application for regulatory approval of one or more of our, or our competitors', product candidates or new indications for marketed products; |
• | progress, delays, or results in clinical trials of our or our competitors' product candidates or new indications for marketed products; |
• | announcement of technological innovations or product candidates by us or competitors; |
• | claims by others that our products or technologies infringe their patents; |
• | challenges by others to our patents in the EPO and in the USPTO; |
• | public concern as to the safety or effectiveness of any of our marketed products or product candidates or new indications for our marketed products; |
• | pricing or reimbursement actions, decisions, or recommendations by government authorities, insurers, or other organizations (such as health maintenance organizations and pharmacy benefit management companies) affecting the coverage, reimbursement, or use of any of our marketed products or competitors' products; |
• | our ability to raise additional capital as needed on favorable terms; |
• | developments in our relationships with collaborators or key customers; |
• | developments in the biotechnology industry or in government regulation of healthcare, including those relating to compounding; |
• | large sales of our Common Stock by our executive officers, directors, or significant shareholders; |
• | changes in tax rates, laws, or interpretation of tax laws; |
• | arrivals and departures of key personnel; |
• | general market conditions; |
• | trading activity that results from the rebalancing of stock indices in which our Common Stock is included, or the inclusion or exclusion of our Common Stock from such indices; |
• | other factors identified in these "Risk Factors"; and |
• | the perception by the investment community or our shareholders of any of the foregoing factors. |
The trading price of our Common Stock has been, and could continue to be, subject to wide fluctuations in response to these and other factors, including the sale or attempted sale of a large amount of our Common Stock in the market. As discussed in greater detail under "Future sales of our Common Stock by our significant shareholders or us may depress our stock price and impair our ability to raise funds in new share offerings" below, a large percentage of our Common Stock is owned by a small number of our principal shareholders, and our largest shareholder, Sanofi, has been maintaining its percentage ownership of our Common Stock but has previously publicly disclosed that it may opportunistically increase its percentage ownership of our Common Stock (note, however, that we have agreed to grant a limited waiver of the requirement that Sanofi maintain the Highest Percentage Threshold (as defined below) as a condition to its director designation right during the term of the letter agreement with Sanofi described below under "Our existing shareholders may be able to exert significant influence over matters requiring shareholder approval and over our management"). As a result, the public float of our Common Stock (i.e., the portion of our Common Stock held by public investors, as opposed to the Common Stock held by our directors, officers, and principal shareholders) is low relative to many large public companies. As our Common Stock is less liquid than the stock of companies with broader public ownership, its trading price may fluctuate significantly more than the stock market as a whole. These factors may exacerbate the volatility in the trading price of our Common Stock and may negatively impact your ability to liquidate your investment in Regeneron at the time you wish at a price you consider satisfactory. Broad market fluctuations may also adversely affect the market price of our Common Stock. In the past, securities class action litigation has often been initiated against companies following periods of volatility in their stock price. This type of litigation could result in substantial costs and divert our management's attention and resources, and could also require us to make substantial payments to satisfy judgments or to settle litigation, which may harm our business, prospects, operating results, and financial condition.
57
Future sales of our Common Stock by our significant shareholders or us may depress our stock price and impair our ability to raise funds in new share offerings.
A small number of our shareholders beneficially own a substantial amount of our Common Stock. As of December 31, 2017, our five largest shareholders plus Dr. Schleifer, our Chief Executive Officer, beneficially owned approximately 47.2% of our outstanding shares of Common Stock, assuming, in the case of our Chief Executive Officer, the conversion of his Class A Stock into Common Stock and the exercise of all options held by him which are exercisable within 60 days of December 31, 2017. As of December 31, 2017, Sanofi beneficially owned 23,880,537 shares of our Common Stock, representing approximately 22.6% of the shares of Common Stock then outstanding. Under our January 2014 amended and restated investor agreement with Sanofi, Sanofi has three demand rights to require us to use all reasonable efforts to conduct a registered underwritten offering with respect to shares of our Common Stock held by Sanofi from time to time; however, shares of our Common Stock held by Sanofi from time to time are subject to a "lock-up" and may not be sold until December 20, 2020 (other than with respect to an aggregate of up to 1,400,000 shares, as to which we have agreed to waive the lock-up during the term of the letter agreement with Sanofi described below under "Our existing shareholders may be able to exert significant influence over matters requiring shareholder approval and over our management"). These restrictions on dispositions are subject to earlier termination upon the occurrence of certain events, such as the consummation of a change-of-control transaction involving us or a dissolution or liquidation of our Company. In December 2015, Sanofi disclosed in an amendment to its Schedule 13D filed with the SEC its intention to purchase (subject to market conditions, including the price and availability of shares of our Common Stock, and legal and regulatory requirements) additional shares of our Common Stock to maintain and opportunistically increase its beneficial ownership on a percentage basis up to the maximum allowed under the "standstill" provisions of our amended and restated investor agreement with Sanofi, or 30% of our Class A Stock and Common Stock (taken together). If Sanofi, our other significant shareholders, or we sell substantial amounts of our Common Stock in the public market (including, in the case of Sanofi, as a result of the lock-up waiver referred to above), or there is a perception that such sales may occur, the market price of our Common Stock could fall. Sales of Common Stock by our significant shareholders, including Sanofi, also might make it more difficult for us to raise funds by selling equity or equity-related securities in the future at a time and price that we deem appropriate.
Our existing shareholders may be able to exert significant influence over matters requiring shareholder approval and over our management.
Holders of Class A Stock, who are generally the shareholders who purchased their stock from us before our initial public offering, are entitled to ten votes per share, while holders of Common Stock are entitled to one vote per share. As of December 31, 2017, holders of Class A Stock held 15.3% of the combined voting power of all shares of Common Stock and Class A Stock then outstanding. These shareholders, if acting together, would be in a position to significantly influence the election of our directors and the vote on certain corporate transactions that require majority or supermajority approval of the combined classes, including mergers and other business combinations. This may result in our taking corporate actions that other shareholders may not consider to be in their best interest and may affect the price of our Common Stock. As of December 31, 2017:
• | our current executive officers and directors beneficially owned 10.4% of our outstanding shares of Common Stock, assuming conversion of their Class A Stock into Common Stock and the exercise of all options held by such persons which are exercisable within 60 days of December 31, 2017, and 21.5% of the combined voting power of our outstanding shares of Common Stock and Class A Stock, assuming the exercise of all options held by such persons which are exercisable within 60 days of December 31, 2017; and |
• | our five largest shareholders plus Dr. Schleifer, our Chief Executive Officer, beneficially owned approximately 47.2% of our outstanding shares of Common Stock, assuming, in the case of our Chief Executive Officer, the conversion of his Class A Stock into Common Stock and the exercise of all options held by him which are exercisable within 60 days of December 31, 2017. In addition, these five shareholders plus our Chief Executive Officer held approximately 53.0% of the combined voting power of our outstanding shares of Common Stock and Class A Stock, assuming the exercise of all options held by our Chief Executive Officer which are exercisable within 60 days of December 31, 2017. |
Pursuant to the January 2014 amended and restated investor agreement with us, Sanofi has agreed to vote its shares as recommended by our board of directors, except that it may elect to vote proportionally with the votes cast by all of our other shareholders with respect to certain change-of-control transactions and to vote in its sole discretion with respect to liquidation or dissolution of our Company, stock issuances equal to or exceeding 20% of the outstanding shares or voting rights of Common Stock and Class A Stock (taken together), and new equity compensation plans or amendments if not materially consistent with our historical equity compensation practices.
In addition, we are required under the amended and restated investor agreement to appoint an individual agreed upon by us and Sanofi to our board of directors. Subject to certain exceptions, we are required to use our reasonable efforts (including recommending that our shareholders vote in favor) to cause the election of this designee at our annual shareholder meetings for so long as (other than during the term of the letter agreement described below) Sanofi maintains an equity interest in us that is the lower of (i) the highest percentage ownership Sanofi attains following its acquisition of 20% of our outstanding shares of Class
58
A Stock and Common Stock (taken together) (which occurred in April 2014), and (ii) 25% of our outstanding shares of Class A Stock and Common Stock (taken together) (Highest Percentage Threshold). This designee is required to be "independent" of our Company, as determined under NASDAQ rules, and not to be a current or former officer, director, employee, or paid consultant of Sanofi. The current Sanofi designee, N. Anthony Coles, M.D., is a Class II director whose current term expires at the 2020 annual shareholder meeting.
Effective January 7, 2018, we and Sanofi and certain of Sanofi's direct and indirect subsidiaries entered into a letter agreement in connection with (a) the increase of the development budget amount for cemiplimab set forth in the IO License and Collaboration Agreement and (b) the allocation of additional funds to certain proposed activities relating to the development of dupilumab and REGN3500 and non-approval trials of dupilumab (the Dupilumab/REGN3500 Eligible Investments). Pursuant to the letter agreement, we have agreed, among other things, to grant a limited waiver of Sanofi's obligation to maintain the Highest Percentage Threshold during the term of the letter agreement in order to allow Sanofi to satisfy in whole or in part (a) its funding obligations with respect to the cemiplimab development costs under the IO License and Collaboration Agreement for the quarterly periods commencing on October 1, 2017 and ending on September 30, 2020 by selling up to 800,000 shares of our Common Stock directly or indirectly owned by Sanofi and (b) its funding obligations with respect to the costs incurred by or on behalf of the parties to the Antibody License and Collaboration Agreement with respect to the Dupilumab/REGN3500 Eligible Investments for the quarterly periods commencing on January 1, 2018 and ending on September 30, 2020 by selling up to 600,000 shares of our Common Stock directly or indirectly owned by Sanofi. In addition, we and Sanofi have agreed that, upon termination of the letter agreement, the amended and restated investor agreement will be amended to define "Highest Percentage Threshold" as the lower of (i) 25% of our outstanding shares of Class A Stock and Common Stock (taken together) and (ii) the higher of (a) Sanofi's percentage ownership of Class A Stock and Common Stock (taken together) on such termination date and (b) the highest percentage ownership of our outstanding shares of Class A Stock and Common Stock (taken together) Sanofi attains following such termination date.
The anti-takeover effects of provisions of our charter, by-laws, and of New York corporate law, as well as the contractual provisions in our investor and collaboration agreements and certain provisions of our compensation plans and agreements, could deter, delay, or prevent an acquisition or other "change in control" of us and could adversely affect the price of our Common Stock.
Our certificate of incorporation, our by-laws, and the New York Business Corporation Law contain various provisions that could have the effect of delaying or preventing a change in control of our Company or our management that shareholders may consider favorable or beneficial. Some of these provisions could discourage proxy contests and make it more difficult for shareholders to elect directors and take other corporate actions. These provisions could also limit the price that investors might be willing to pay in the future for shares of our Common Stock. These provisions include:
• | authorization to issue "blank check" preferred stock, which is preferred stock that can be created and issued by the board of directors without prior shareholder approval, with rights senior to those of our Common Stock and Class A Stock; |
• | a staggered board of directors, so that it would take three successive annual shareholder meetings to replace all of our directors; |
• | a requirement that removal of directors may only be effected for cause and only upon the affirmative vote of at least eighty percent (80%) of the outstanding shares entitled to vote for directors, as well as a requirement that any vacancy on the board of directors may be filled only by the remaining directors; |
• | a provision whereby any action required or permitted to be taken at any meeting of shareholders may be taken without a meeting, only if, prior to such action, all of our shareholders consent, the effect of which is to require that shareholder action may only be taken at a duly convened meeting; |
• | a requirement that any shareholder seeking to bring business before an annual meeting of shareholders must provide timely notice of this intention in writing and meet various other requirements; and |
• | under the New York Business Corporation Law, in addition to certain restrictions which may apply to "business combinations" involving our Company and an "interested shareholder," a plan of merger or consolidation of our Company must be approved by two-thirds of the votes of all outstanding shares entitled to vote thereon. See the risk factor above captioned "Our existing shareholders may be able to exert significant influence over matters requiring shareholder approval and over our management." |
Pursuant to the January 2014 amended and restated investor agreement between us and Sanofi, Sanofi is bound by certain "standstill" provisions, which contractually prohibit Sanofi from seeking to directly or indirectly exert control of our Company or acquiring more than 30% of our Class A Stock and Common Stock (taken together). This prohibition will remain in place until the earliest of (i) the later of the fifth anniversaries of the expiration or earlier termination of our License and Collaboration Agreement with Sanofi relating to our Antibody Collaboration or our ZALTRAP collaboration agreement with Sanofi, each as amended; (ii) our announcement recommending acceptance by our shareholders of a tender offer or exchange offer that, if consummated, would constitute a change of control involving us; (iii) the public announcement of any definitive agreement
59
providing for a change of control involving us; (iv) the date of any issuance of shares of Common Stock by us that would result in another party having more than 10% of the voting power of our outstanding Class A Stock and Common Stock (taken together) unless such party enters into a standstill agreement containing certain terms substantially similar to the standstill obligations of Sanofi; or (v) other specified events, such as a liquidation or dissolution of our Company.
Similarly, under our 2016 ANG2 license and collaboration agreement with Bayer, Bayer is bound by certain "standstill" provisions, which contractually prohibit Bayer from seeking to influence the control of our Company or acquiring more than 20% of our outstanding Class A Stock and Common Stock (taken together). This prohibition will remain in place until the earliest of (i) the fifth anniversary of the expiration or earlier termination of the agreement; (ii) the public announcement of a tender offer, exchange offer, or other proposal that would constitute a change of control of our Company; (iii) the acquisition by a third party or a group of third parties (other than by Dr. Schleifer or his affiliates) of more than 20% of the voting power of our outstanding Class A Stock and Common Stock (taken together); (iv) the issuance of shares of capital stock to another party (other than to an underwriter in a public offering) that would result in such party's having more than 7% of the voting power of our outstanding Class A Stock and Common Stock (taken together) unless such third party enters into a standstill agreement containing terms substantially similar to the standstill obligations of Bayer; or (v) other specified events, such as a liquidation or dissolution of our Company.
Further, pursuant to the 2016 collaboration agreement between us and Teva, Teva and its affiliates are bound by certain "standstill" provisions, which contractually prohibit them from seeking to directly or indirectly exert control of our Company or acquiring more than 5% of our Class A Stock and Common Stock (taken together). This prohibition will remain in place until the earliest of (i) the fifth anniversary of the expiration or earlier termination of the agreement; (ii) our announcement recommending acceptance by our shareholders of a tender offer or exchange offer that, if consummated, would constitute a change of control involving us; (iii) the public announcement of any definitive agreement providing for a change of control involving us; (iv) the acquisition by a third party or a group of third parties of more than 30% of the voting power of our outstanding Class A Stock and Common Stock (taken together); (v) the date of any issuance of shares of capital stock by us that would result in another party having more than 10% of the voting power of our outstanding Class A Stock and Common Stock (taken together) unless such party enters into a standstill agreement containing certain terms substantially similar to the standstill obligations of Teva; or (vi) other specified events, such as a liquidation or dissolution of our Company.
In addition, our Change in Control Severance Plan and the employment agreement with our Chief Executive Officer, each as amended and restated, provide for severance benefits in the event of termination as a result of a change in control of our Company. Also, stock option awards issued under our Second Amended and Restated 2000 Long-Term Incentive Plan, our 2014 Long-Term Incentive Plan, and our Amended and Restated 2014 Long-Term Incentive Plan may become fully vested in connection with a "change in control" of our Company, as defined in the plans. Further, under the amended and restated investor agreement between us and Sanofi, we are required to appoint an individual agreed upon by us and Sanofi to our board of directors and to use our reasonable efforts to cause the election of this designee at our annual shareholder meetings for so long as Sanofi maintains a specified equity interest in us. As described above under "Our existing shareholders may be able to exert significant influence over matters requiring shareholder approval and over our management," a Sanofi designee currently serves on our board of directors. These contractual provisions may also have the effect of deterring, delaying, or preventing an acquisition or other change in control.
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 2. PROPERTIES
We conduct our research, development, manufacturing, and administrative activities at our owned and leased facilities. A summary of our significant owned and leased properties is provided below.
Tarrytown, New York
At our Tarrytown, New York location, we lease approximately 1,467,000 square feet of laboratory and office space, of which approximately 1,180,000 square feet is occupied by Regeneron. Refer to Part II, Item 7. "Management's Discussion and Analysis of Financial Condition and Results of Operations - Liquidity and Capital Resources - Tarrytown, New York Leases" for further details. We also own an approximate 100-acre parcel of undeveloped land adjacent to our Tarrytown, New York location; we intend to develop this property to accommodate and support our growth, primarily in connection with expanding our existing research and development and office space.
60
Sleepy Hollow, New York
We own an office building in Sleepy Hollow, New York, consisting of approximately 383,000 square feet, which is partially occupied by Regeneron. We intend to occupy the entire building and use it as additional office space to support the growth of our existing Tarrytown facilities.
Rensselaer, New York
We own facilities in Rensselaer, New York totaling approximately 565,000 square feet of research, manufacturing, office, and warehouse space. We also lease approximately 75,000 square feet of additional laboratory and office space. We also own approximately 130 acres of land near our Rensselaer, New York location, and began to develop this property in connection with expanding our existing manufacturing and warehouse space.
Troy, New York
We own an office building in Troy, New York, consisting of approximately 217,000 square feet, which we are utilizing as additional office space to support the growth of our existing Rensselaer facilities.
Limerick, Ireland
We own a manufacturing facility in Limerick Ireland, consisting of approximately 445,000 square feet, which was purchased and subsequently renovated to accommodate and support our growth and expand our manufacturing capacity. The facility has received certain manufacturing approvals by regulatory agencies, including the FDA, and is in the process of further validation for the manufacture of our bulk drug products.
ITEM 3. LEGAL PROCEEDINGS
The information called for by this item is incorporated herein by reference to the information set forth in Note 17 to our Consolidated Financial Statements included in this report.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
61
PART II
ITEM 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS, AND ISSUER PURCHASES OF EQUITY SECURITIES
Market for Registrant's Common Equity
Our Common Stock, par value $.001 per share, is quoted on The NASDAQ Global Select Market under the symbol "REGN." Our Class A Stock, par value $.001 per share, is not publicly quoted or traded.
The following table sets forth, for the periods indicated, the range of high and low sales prices for our Common Stock as reported by The NASDAQ Global Select Market:
High | Low | |||||||
2017 | ||||||||
First Quarter | $ | 401.21 | $ | 340.09 | ||||
Second Quarter | 543.55 | 360.00 | ||||||
Third Quarter | 526.12 | 426.47 | ||||||
Fourth Quarter | 477.00 | 353.14 | ||||||
2016 | ||||||||
First Quarter | $ | 532.91 | $ | 348.96 | ||||
Second Quarter | 433.93 | 329.09 | ||||||
Third Quarter | 443.99 | 348.43 | ||||||
Fourth Quarter | 452.96 | 325.35 | ||||||
As of February 1, 2018, there were 177 shareholders of record of our Common Stock and 17 shareholders of record of our Class A Stock.
We have never paid cash dividends on our Common Stock or Class A Stock and do not anticipate paying any in the foreseeable future.
62
STOCK PERFORMANCE GRAPH
Set forth below is a line graph comparing the cumulative total shareholder return on Regeneron's Common Stock with the cumulative total return of (i) The NQ US Benchmark Pharma TR Index, and (ii) Standard & Poor's 500 Stock Index (S&P 500) for the period from December 31, 2012 through December 31, 2017. The comparison assumes that $100 was invested on December 31, 2012 in our Common Stock and in both of the foregoing indices. All values assume reinvestment of the pre-tax value of dividends paid by companies included in these indices. The historical stock price performance of our Common Stock shown in the graph below is not necessarily indicative of future stock price performance.
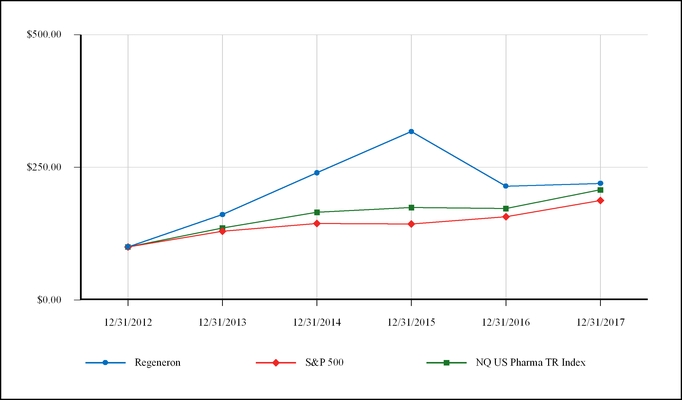
12/31/2012 | 12/31/2013 | 12/31/2014 | 12/31/2015 | 12/31/2016 | 12/31/2017 | ||||||||||||||||||
Regeneron | $ | 100.00 | $ | 160.89 | $ | 239.81 | $ | 317.34 | $ | 214.58 | $ | 219.77 | |||||||||||
S&P 500 | $ | 100.00 | $ | 129.60 | $ | 144.36 | $ | 143.31 | $ | 156.98 | $ | 187.47 | |||||||||||
NQ US Pharma TR Index | $ | 100.00 | $ | 135.68 | $ | 165.28 | $ | 174.27 | $ | 172.37 | $ | 207.54 | |||||||||||
This performance graph shall not be deemed "filed" for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or incorporated by reference into any filing of ours under the Securities Act of 1933, as amended, or the Securities Exchange Act, except as shall be expressly set forth by specific reference to such filing.
Issuer Purchases of Equity Securities
The following table reflects shares of Common Stock withheld by us for employees to satisfy their tax withholding obligations arising upon the vesting of restricted equity awards granted under one of our long-term incentive plans in the fourth quarter of 2017.
63
Period | Total Number of Shares (or Units) Purchased | Average Price Paid per Share (or Unit) | Total Number of Shares (or Units) Purchased as Part of Publicly Announced Plans or Programs | Maximum Number (or Approximate Dollar Value) of Shares (or Units) that May Yet Be Purchased Under the Plans or Programs | |||||||||
10/1/2017-10/31/2017 | 184 | $ | 440.50 | — | — | ||||||||
11/1/2017-11/30/2017 | 515 | $ | 405.27 | — | — | ||||||||
12/1/2017-12/31/2017 | 257,850 | $ | 386.90 | — | — | ||||||||
Total | 258,549 | $ | 386.97 | — | — | ||||||||
64
Item 6. Selected Financial Data
The selected financial data set forth below for the years ended December 31, 2017, 2016, and 2015 and as of December 31, 2017 and 2016 are derived from and should be read in conjunction with our audited financial statements, including the notes thereto, included elsewhere in this report. The selected financial data for the years ended December 31, 2014 and 2013 and as of December 31, 2015, 2014, and 2013 are derived from our audited financial statements not included in this report. Certain prior year amounts have been reclassified to conform to the current year's presentation.
Year Ended December 31, | ||||||||||||||||||||
(In thousands, except per share data) | 2017 | 2016 | 2015 | 2014 | 2013 | |||||||||||||||
Statement of Operations Data: | ||||||||||||||||||||
Revenues: | ||||||||||||||||||||
Net product sales | $ | 3,718,463 | $ | 3,338,390 | $ | 2,689,478 | $ | 1,750,762 | $ | 1,425,839 | ||||||||||
Sanofi and Bayer collaboration revenue | 1,815,245 | 1,402,935 | 1,339,361 | 1,036,854 | 650,400 | |||||||||||||||
Other revenue | 338,519 | 119,102 | 74,889 | 31,941 | 28,506 | |||||||||||||||
5,872,227 | 4,860,427 | 4,103,728 | 2,819,557 | 2,104,745 | ||||||||||||||||
Expenses: | ||||||||||||||||||||
Research and development | 2,075,142 | 2,052,295 | 1,620,577 | 1,271,353 | 859,947 | |||||||||||||||
Selling, general, and administrative | 1,320,433 | 1,177,697 | 838,526 | 519,267 | 346,393 | |||||||||||||||
Cost of goods sold | 202,507 | 194,624 | 241,702 | 129,030 | 118,048 | |||||||||||||||
Cost of collaboration and contract manufacturing | 194,554 | 105,070 | 151,007 | 75,988 | 37,307 | |||||||||||||||
3,792,636 | 3,529,686 | 2,851,812 | 1,995,638 | 1,361,695 | ||||||||||||||||
Income from operations | 2,079,591 | 1,330,741 | 1,251,916 | 823,919 | 743,050 | |||||||||||||||
Other income (expense), net | (1,080 | ) | (926 | ) | (26,819 | ) | (62,684 | ) | (46,668 | ) | ||||||||||
Income before income taxes | 2,078,511 | 1,329,815 | 1,225,097 | 761,235 | 696,382 | |||||||||||||||
Income tax expense (1) | (880,000 | ) | (434,293 | ) | (589,041 | ) | (423,109 | ) | (282,644 | ) | ||||||||||
Net income | $ | 1,198,511 | $ | 895,522 | $ | 636,056 | $ | 338,126 | $ | 413,738 | ||||||||||
Net income per share - basic | $ | 11.27 | $ | 8.55 | $ | 6.17 | $ | 3.36 | $ | 4.23 | ||||||||||
Net income per share - diluted | $ | 10.34 | $ | 7.70 | $ | 5.52 | $ | 2.98 | $ | 3.72 | ||||||||||
As of December 31, | ||||||||||||||||||||
(In thousands) | 2017 | 2016 | 2015 | 2014 | 2013 | |||||||||||||||
Balance Sheet Data: | ||||||||||||||||||||
Cash, cash equivalents, and marketable securities (current and non-current) | $ | 2,896,074 | $ | 1,902,944 | $ | 1,677,385 | $ | 1,360,634 | $ | 1,083,875 | ||||||||||
Total assets | 8,764,286 | 6,973,466 | 5,609,132 | 3,837,672 | 2,950,130 | |||||||||||||||
Convertible senior notes (current and non-current) | — | — | 10,802 | 146,773 | 320,315 | |||||||||||||||
Capital and facility lease obligations (current and non-current) | 703,453 | 481,126 | 364,708 | 312,291 | 185,323 | |||||||||||||||
Stockholders' equity | 6,144,078 | 4,449,245 | 3,654,837 | 2,550,251 | 1,964,716 | |||||||||||||||
(1) As a result of the Tax Cuts and Jobs Act being signed into law in December 2017, income taxes for the year ended December 31, 2017 included a charge of $326.2 million related to the re-measurement of our U.S. net deferred tax assets at the lower enacted corporate tax rate. Refer to Item 7. "Management's Discussion and Analysis of Financial Condition and Results of Operations - Results of Operations - Income Taxes" below for further details.
65
ITEM 7. | MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
The following discussion should be read in conjunction with the consolidated financial statements and related notes included elsewhere in this report.
Overview
We are a fully integrated biotechnology company that discovers, invents, develops, manufactures, and commercializes medicines for the treatment of serious diseases. Our commercialized medicines and product candidates in development are designed to help patients with eye disease, allergic and inflammatory diseases, heart disease, pain, cancer, and infectious and other serious medical conditions.
As described in Part I, Item 1. "Business - General," and "Business - Marketed Products," we currently have six products that have received marketing approval: EYLEA (aflibercept) Injection, Dupixent (dupilumab) Injection, Praluent (alirocumab) Injection, Kevzara (sarilumab) Solution for Subcutaneous Injection, ARCALYST (rilonacept) Injection for Subcutaneous Use, and ZALTRAP (ziv-aflibercept) Injection for Intravenous Infusion. We also have 15 product candidates in clinical development, all of which were discovered in our research laboratories. These consist of a Trap-based clinical program and 14 fully human antibody product candidates, as summarized in Part I, Item 1. "Business - General."
The planning, execution, and results of our clinical programs are significant factors that can affect our operating and financial results. In our clinical programs, key events in 2017 and 2018 to date were, and plans for the remainder of 2018 are, as follows:
Trap-based Clinical Program: | ||||
2017 and 2018 Events to Date | 2018 Plans | |||
EYLEA | Ÿ | Bayer received regulatory approval for EYLEA for various indications and continued to pursue regulatory applications for marketing approval in additional countries | Ÿ | FDA decision on sBLA for every 12-week dosing interval in wet AMD |
Ÿ | Submit sBLA for pre-filled syringe | |||
Ÿ | Completed patient enrollment in Phase 3 study for the treatment of NPDR in patients without DME | Ÿ | Bayer to submit for additional regulatory approvals outside the United States for various indications | |
Ÿ | sBLA for every 12-week dosing interval in wet AMD filed with FDA, with a target action date of August 11, 2018 | Ÿ | Regulatory agency decisions on applications outside the United States for various indications, including wet AMD and DME in China | |
Ÿ | Report data from Phase 3 PANORAMA study for the treatment of NPDR in patients without DME, and submit sBLA | |||
66
Antibody-based Clinical Programs: | ||||
2017 and 2018 Events to Date | 2018 Plans | |||
Dupixent (dupilumab; IL-4R Antibody) | Ÿ | Presented detailed results from one-year Phase 3 CHRONOS study at the Annual Meeting of the American Academy of Dermatology | Ÿ | Submit for additional regulatory approvals in atopic dermatitis outside the United States |
Ÿ | FDA approved Dupixent for the treatment of adults with moderate-to-severe atopic dermatitis | Ÿ | Regulatory agency decisions on atopic dermatitis applications outside the United States | |
Ÿ | Initiated Phase 3 studies in adolescent patients (12–17 years of age) and pediatric patients (6–11 years of age) with atopic dermatitis | Ÿ | Report data from Phase 3 study in adolescent patients (12–17 years of age) with atopic dermatitis | |
Ÿ | Initiated Phase 2/3 study in pediatric patients (6 months–5 years of age) with severe atopic dermatitis | Ÿ | FDA filing and decision on sBLA for asthma in adult/adolescent patients | |
Ÿ | Regulatory applications submitted for atopic dermatitis in various jurisdictions outside the United States | Ÿ | Submit for EU and Japan regulatory approval in asthma in adult/adolescent patients | |
Ÿ | Reported positive results from the LIBERTY AD CAFÉ study in atopic dermatitis | Ÿ | Report data from Phase 3 studies in nasal polyps | |
Ÿ | European Commission granted marketing approval for Dupixent for the treatment of adults with moderate-to-severe atopic dermatitis | Ÿ | Initiate Phase 3 study in eosinophilic esophagitis | |
Ÿ | Initiate Phase 2 study in peanut allergy | |||
Ÿ | MHLW in Japan approved Dupixent for the treatment of atopic dermatitis in adults not adequately controlled with existing therapies | Ÿ | Initiate Phase 2 study as an adjunct to immunotherapy for grass allergy | |
Ÿ | Initiated Phase 3 study in pediatric patients (6–11 years of age) with asthma | Ÿ | Initiate Phase 3 program in chronic obstructive pulmonary disease (COPD) | |
Ÿ | Reported positive top-line results from Phase 3 LIBERTY ASTHMA QUEST study | Ÿ | Initiate clinical program evaluating co-morbid allergic conditions | |
Ÿ | Reported positive top-line results from Phase 3 LIBERTY ASTHMA VENTURE study | |||
Ÿ | Submitted sBLA for asthma for patients aged 12 and over | |||
Ÿ | Reported positive results from Phase 2 study in EoE | |||
Ÿ | FDA granted orphan drug designation for the treatment of EoE | |||
Ÿ | Completed patient enrollment in Phase 3 study in nasal polyps | |||
Praluent (PCSK9 Antibody) | Ÿ | Permanent injunction barring commercialization of Praluent in the United States suspended on February 8, 2017 and vacated on October 5, 2017 | Ÿ | Report results from ODYSSEY OUTCOMES study |
Ÿ | Submit for additional regulatory approvals outside the United States | |||
Ÿ | FDA approved sBLA for monthly dosing regimen | Ÿ | Regulatory agency decisions on applications outside the United States | |
Ÿ | FDA granted orphan drug designation for treatment of HoFH | Ÿ | FDA decision on sBLA for use with apheresis | |
Ÿ | Reported positive results from two Phase 3b/4 studies in patients with diabetes | Ÿ | Initiate Phase 3 pediatric studies in HoFH and HeFH | |
67
Antibody-based Clinical Programs (continued): | ||||
2017 and 2018 Events to Date | 2018 Plans | |||
Ÿ | ODYSSEY study data presented at the European Society of Cardiology (ESC) Congress | |||
Ÿ | Initiated Phase 3 study in HoFH | |||
Ÿ | sBLA for use with apheresis filed with FDA, with a target action date of August 24, 2018 | |||
Kevzara (sarilumab; IL-6R Antibody) | Ÿ | Regulatory applications submitted in various jurisdictions outside the United States | Ÿ | Submit for additional regulatory approvals outside of the United States |
Ÿ | Health Canada approved Kevzara for the treatment of adult patients with RA | Ÿ | Regulatory agency decisions on applications outside the United States | |
Ÿ | Resubmitted BLA and FDA accepted for review | Ÿ | Continue patient enrollment in Phase 2 study in pcJIA | |
Ÿ | FDA approved Kevzara for the treatment of adult patients with RA | Ÿ | Initiate Phase 3 study in giant cell arteritis | |
Ÿ | European Commission granted marketing authorization for Kevzara for the treatment of adult patients with RA | Ÿ | Initiate Phase 3 study in polymyalgia rheumatica | |
Ÿ | MHLW in Japan approved Kevzara for the treatment of adult patients with RA | |||
Suptavumab (RSV-F Antibody) | Ÿ | Completed patient enrollment in Phase 3 study | ||
Ÿ | Reported results from Phase 3 study, and discontinued further clinical development | |||
Cemiplimab (REGN2810; PD-1 Antibody) | Ÿ | Continued patient enrollment in Phase 1 and Phase 2 studies | Ÿ | Complete rolling submission of BLA for CSCC and FDA decision on BLA |
Ÿ | Reported positive preliminary results from Phase 1 study in patients with advanced CSCC | Ÿ | Submit for regulatory approval in CSCC in the EU | |
Ÿ | FDA granted Breakthrough Therapy designation for the treatment of adults with metastatic CSCC and adults with locally advanced and unresectable CSCC | Ÿ | Initiate additional studies in non-small cell lung cancer and various other indications | |
Ÿ | Continue patient enrollment in various studies | |||
Ÿ | Reported positive top-line results from pivotal Phase 2 CSCC study | |||
Ÿ | Commenced rolling submission of BLA for CSCC | |||
Ÿ | Initiated Phase 3 study in first-line treatment for non-small cell lung cancer | |||
Ÿ | Initiated potentially pivotal Phase 2 study in BCC | |||
Ÿ | Initiated Phase 3 study in cervical cancer | |||
Fasinumab (NGF Antibody) | Ÿ | Continued patient enrollment in Phase 3 long-term safety study in osteoarthritis | Ÿ | Continue patient enrollment in Phase 3 osteoarthritis studies |
Ÿ | Initiated Phase 3 efficacy studies in osteoarthritis | Ÿ | Report data from first Phase 3 efficacy study in osteoarthritis | |
Ÿ | Initiated Phase 3 study in chronic low back pain in patients with concomitant osteoarthritis of the knee and hip | Ÿ | Advance Phase 3 program in chronic low back pain | |
68
Antibody-based Clinical Programs (continued): | ||||
2017 and 2018 Events to Date | 2018 Plans | |||
Evinacumab (ANGPTL3 Antibody) | Ÿ | FDA granted Breakthrough Therapy designation for the treatment of hypercholesterolemia in patients with HoFH | Ÿ | Initiate Phase 2 study in severe hypertriglyceridemia |
Ÿ | Reported positive Phase 2 results at medical conferences | |||
Ÿ | Data and analysis from genetics, preclinical, and clinical study published in the New England Journal of Medicine | |||
Ÿ | Initiated Phase 2 study in refractory hypercholesterolemia (both HeFH and non-FH) | |||
Ÿ | Initiated Phase 3 study in HoFH | |||
Nesvacumab/aflibercept (Ang2 Antibody co-formulated with aflibercept) | Ÿ | Completed patient enrollment in Phase 2 ONYX study in wet AMD | ||
Ÿ | Reported results from Phase 2 ONYX and RUBY studies, which did not provide sufficient differentiation to warrant Phase 3 studies | |||
Trevogrumab (GDF8 Antibody) | Ÿ | Initiated Phase 1 combination therapy study with REGN2477 | Ÿ | Complete Phase 1 combination study and report results |
Ÿ | Completed patient enrollment in Phase 1 combination therapy study | |||
REGN1908-1909 (Feld1 Antibody) | Ÿ | Continue early stage development | ||
REGN1979 (CD20 and CD3 Antibody) | Ÿ | Continued patient enrollment in Phase 1 study | Ÿ | Continue evaluation in non-Hodgkin lymphomas |
Ÿ | FDA granted orphan drug designation in diffuse large B-cell lymphoma | |||
REGN3470-3471-3479 (Multi-antibody therapy to Ebola virus) | Ÿ | Completed Phase 1 study in healthy volunteers | Ÿ | Initiate additional healthy volunteer study |
REGN2477 (Activin A Antibody) | Ÿ | FDA granted orphan drug designation for the treatment of FOP | Ÿ | Initiate Phase 2 study in patients with FOP |
Ÿ | FDA granted Fast Track designation for the prevention and treatment of heterotopic ossification in patients with FOP | |||
REGN3500 (IL-33 Antibody) | Ÿ | Initiated Phase 1 studies in patients with asthma | Ÿ | Initiate Phase 2 programs in asthma, COPD, and atopic dermatitis |
Ÿ | Completed Phase 1 study in healthy volunteers | |||
REGN3767 (LAG-3 Antibody) | Ÿ | Continued patient enrollment in Phase 1 study | Ÿ | Open monotherapy expansion cohorts as well as in combination with cemiplimab in multiple indications |
REGN3918 (C5 Antibody) | Ÿ | Initiated Phase 1 study in healthy volunteers | Ÿ | Complete Phase 1 study in healthy volunteers |
Developing and commercializing new medicines entails significant risk and expense. Before significant revenues from the commercialization of our antibody candidates or new indications for our marketed products can be realized, we (or our collaborators) must overcome a number of hurdles which include successfully completing research and development and obtaining regulatory approval from the FDA and regulatory authorities in other countries. In addition, the biotechnology and pharmaceutical industries are rapidly evolving and highly competitive, and new developments may render our products and technologies uncompetitive or obsolete.
69
Our ability to continue to generate profits and to generate positive cash flow from operations over the next several years depends significantly on our continued success in commercializing EYLEA. We expect to continue to incur substantial expenses related to our research and development activities, a significant portion of which we expect to be reimbursed by our collaborators. Also, our research and development activities outside our collaborations, the costs of which are not reimbursed, are expected to expand and require additional resources. We also expect to incur substantial costs related to the commercialization of EYLEA, Dupixent, Praluent, and Kevzara, as well as preparation for potential commercialization of cemiplimab and other indications of dupilumab. Our financial results may fluctuate from quarter to quarter and will depend on, among other factors, the net sales of our marketed products, the scope and progress of our research and development efforts, the timing of certain expenses, the continuation of our collaborations, in particular with Sanofi and Bayer, including our share of collaboration profits or losses from sales of commercialized products and the amount of reimbursement of our research and development expenses that we receive from collaborators, and the amount of income tax expense we incur, which is partly dependent on the profits or losses we earn in each of the countries in which we operate. We cannot predict whether or when new products or new indications for marketed products will receive regulatory approval or, if any such approval is received, whether we will be able to successfully commercialize such product(s) and whether or when they may become profitable.
Critical Accounting Policies and Use of Estimates
A summary of the significant accounting policies that impact us is provided in Note 1 to our Consolidated Financial Statements. The preparation of financial statements in accordance with accounting principles generally accepted in the United States of America (GAAP) requires management to make estimates and assumptions that affect reported amounts and related disclosures in the financial statements. Management considers an accounting estimate to be critical if:
• | it requires an assumption (or assumptions) regarding a future outcome; and |
• | changes in the estimate or the use of different assumptions to prepare the estimate could have a material effect on our results of operations or financial condition. |
Management believes the current assumptions used to estimate amounts reflected in our Consolidated Financial Statements are appropriate. However, if actual experience differs from the assumptions used in estimating amounts reflected in our Consolidated Financial Statements, the resulting changes could have a material adverse effect on our results of operations, and in certain situations, could have a material adverse effect on our liquidity and financial condition. The critical accounting estimates that impact our Consolidated Financial Statements are described below.
Revenue Recognition
Product Revenue
Product sales consist of U.S. sales of EYLEA and ARCALYST. Revenue from product sales is recognized when persuasive evidence of an arrangement exists, title to product and associated risk of loss have passed to the customer, the price is fixed or determinable, collection from the customer is reasonably assured, we have no further performance obligations, and returns can be reasonably estimated. We record revenue from product sales upon delivery to our distributors and specialty pharmacies (collectively, our customers).
Revenue from product sales is recorded net of applicable provisions for rebates and chargebacks under governmental and other programs, such as Medicaid and Veterans' Administration (VA), distribution-related fees, and other sales-related deductions. We estimate reductions to product sales based upon contracts with customers and government agencies, statutorily-defined discounts applicable to government-funded programs, historical experience, estimated payer mix, inventory levels in the distribution channel, shelf life of the product, and other relevant factors. Calculating these provisions involves estimates and judgments. We review our estimates of rebates, chargebacks, and other applicable provisions each period and record any necessary adjustments in the current period's net product sales. The following table summarizes the provisions, and credits/payments, for sales-related deductions.
70
(In millions) | Rebates & Chargebacks | Distribution- Related Fees | Other Sales- Related Deductions | Total | |||||||||||
Balance as of December 31, 2014 | $ | 3.1 | $ | 21.2 | $ | 0.5 | $ | 24.8 | |||||||
Provisions | 61.1 | 122.5 | 9.6 | 193.2 | |||||||||||
Credits/payments | (57.8 | ) | (95.3 | ) | (9.6 | ) | (162.7 | ) | |||||||
Balance as of December 31, 2015 | 6.4 | 48.4 | 0.5 | 55.3 | |||||||||||
Provisions | 93.4 | 154.4 | 30.4 | 278.2 | |||||||||||
Credits/payments | (87.1 | ) | (173.3 | ) | (27.3 | ) | (287.7 | ) | |||||||
Balance as of December 31, 2016 | 12.7 | 29.5 | 3.6 | 45.8 | |||||||||||
Provisions | 167.8 | 194.1 | 46.4 | 408.3 | |||||||||||
Credits/payments | (150.6 | ) | (189.5 | ) | (28.7 | ) | (368.8 | ) | |||||||
Balance as of December 31, 2017 | $ | 29.9 | $ | 34.1 | $ | 21.3 | $ | 85.3 | |||||||
Collaboration Revenue
We earn collaboration revenue in connection with collaboration agreements to develop and commercialize product candidates and utilize our technology platforms. These arrangements may require us to deliver various rights, services, and/or goods across the entire life cycle of a product or product candidate. The terms of these agreements typically include that consideration be provided to us in the form of non-refundable up-front payments, research progress (milestone) payments, payments for development and commercialization activities, and sharing of profits or losses arising from the commercialization of products. In arrangements involving multiple deliverables, we must determine whether each deliverable qualifies as a separate unit of accounting, whether the deliverables have value to the collaborator on a standalone basis, and how the consideration should be allocated to each separate unit of accounting based on the relative selling price of each deliverable. Payments which are based on achieving a specific substantive performance milestone, involving a degree of risk, are recognized as revenue when the milestone is achieved and the related payment is due and non-refundable, provided there is no future service obligation associated with that milestone. In determining whether a payment is deemed to be a substantive performance milestone, we take into consideration (i) the enhancement in value to the related development product candidate, (ii) our performance and the relative level of effort required to achieve the milestone, (iii) whether the milestone relates solely to past performance, and (iv) whether the milestone payment is considered reasonable relative to all of the deliverables and payment terms. Payments for achieving milestones which are not considered substantive are deferred and recognized over the related performance period.
In connection with non-refundable licensing payments, our performance period estimates are principally based on projections of the scope, progress, and results of our research and development activities. Due to the variability in the scope of activities and length of time necessary to develop a drug product, changes to development plans as programs progress, and uncertainty in the ultimate requirements to obtain governmental approval for commercialization, revisions to performance period estimates are likely to occur periodically, and could result in material changes to the amount of revenue recognized each year in the future. In addition, our estimated performance periods may change if development programs encounter delays, or we and our collaborators decide to expand or contract our clinical plans for a drug candidate in various disease indications.
When we are entitled to reimbursement of all or a portion of the research and development expenses that we incur under a collaboration, we record those reimbursable amounts as collaboration revenue proportionately as we recognize our expenses. If the collaboration is a cost-sharing arrangement in which both we and our collaborator perform development work and share costs, we also recognize, as research and development expense in the period when our collaborator incurs development expenses, the portion of the collaborator's development expenses that we are obligated to reimburse. Our collaborators provide us with estimated development expenses for the most recent fiscal quarter. Our collaborators' estimates are reconciled to their actual expenses for such quarter in the subsequent fiscal quarter, and our portion of our collaborators' development expenses that we are obligated to reimburse is adjusted on a prospective basis accordingly, as necessary.
Under our collaboration agreements, product sales and cost of sales for products which are currently approved are recorded by our collaborators. We share in any profits or losses arising from the commercialization of such products. Our collaborator provides us with our estimated share of the profits or losses from commercialization of such products for the most recent fiscal quarter. Our collaborators' estimates of profits or losses for such quarter are reconciled to actual profits or losses in the subsequent fiscal quarter, and our share of the profit or loss is adjusted on a prospective basis accordingly, as necessary.
71
Clinical Trial Expenses
Clinical trial costs are a significant component of research and development expenses and include costs associated with third-party contractors. We outsource a substantial portion of our clinical trial activities, utilizing external entities such as CROs, independent clinical investigators, and other third-party service providers to assist us with the execution of our clinical studies. For each clinical trial that we conduct, certain clinical trial costs are expensed immediately, while others are expensed over time based on the expected total number of patients in the trial, the rate at which patients enter the trial, and/or the period over which clinical investigators or CROs are expected to provide services.
Clinical activities which relate principally to clinical sites and other administrative functions to manage our clinical trials are performed primarily by CROs. CROs typically perform most of the start-up activities for our trials, including document preparation, site identification, screening and preparation, pre-study visits, training, and program management. On a budgeted basis, these start-up costs are typically 10% to 20% of the total contract value. On an actual basis, this percentage range can be significantly wider, as many of our contracts with CROs are either expanded or reduced in scope compared to the original budget, while start-up costs for the particular trial may not change materially. These start-up costs usually occur within a few months after the contract has been executed and are event-driven in nature. The remaining activities and related costs, such as patient monitoring and administration, generally occur ratably throughout the life of the individual contract or study. In the event of early termination of a clinical trial, we accrue and recognize expenses in an amount based on our estimate of the remaining non-cancelable obligations associated with the winding down of the clinical trial and/or penalties.
For clinical study sites, where payments are made periodically on a per-patient basis to the institutions performing the clinical study, we accrue expenses on an estimated cost-per-patient basis, based on subject enrollment and activity in each quarter. The amount of clinical study expense recognized in a quarter may vary from period to period based on the duration and progress of the study, the activities to be performed by the sites each quarter, the required level of patient enrollment, the rate at which patients actually enroll in and drop-out of the clinical study, and the number of sites involved in the study. Clinical trials that bear the greatest risk of change in estimates are typically those that have a significant number of sites, require a large number of patients, have complex patient screening requirements, and span multiple years. During the course of a trial, we adjust our rate of clinical expense recognition if actual results differ from our estimates. Our estimates and assumptions for clinical expense recognition could differ significantly from our actual results, which could cause material increases or decreases in research and development expenses in future periods when the actual results become known.
Stock-based Compensation
We recognize stock-based compensation expense for grants of stock option and restricted stock awards under our long-term incentive plans to employees and non-employee members of our board of directors based on the grant-date fair value of those awards. The grant-date fair value of an award is generally recognized as compensation expense over the award's requisite service period.
We use the Black-Scholes model to compute the estimated fair value of stock option awards. Using this model, fair value is calculated based on assumptions with respect to (i) expected volatility of our Common Stock price, (ii) the periods of time over which employees and members of our board of directors are expected to hold their options prior to exercise (expected lives), (iii) expected dividend yield on our Common Stock, and (iv) risk-free interest rates, which are based on quoted U.S. Treasury rates for securities with maturities approximating the options' expected lives. Expected volatility has been estimated based on actual movements in our stock price over the most recent historical periods equivalent to the options' expected lives. Expected lives are principally based on our historical exercise experience with previously issued employee and board of directors option grants. The expected dividend yield is zero as we have never paid dividends and do not currently anticipate paying any in the foreseeable future. Stock-based compensation expense also includes an estimate, which is made at the time of grant, of the number of awards that are expected to be forfeited. This estimate is revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates.
The assumptions used in computing the fair value of stock option awards reflect our best estimates but involve uncertainties related to market and other conditions, many of which are outside of our control. Changes in any of these assumptions may materially affect the fair value of stock option awards granted and the amount of stock-based compensation recognized in future periods.
72
Income Taxes
We recognize deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements or tax returns. Under this method, deferred tax assets and liabilities are determined on the basis of the difference between the tax basis of assets and liabilities and their respective financial reporting amounts ("temporary differences") at enacted tax rates in effect for the years in which the differences are expected to reverse. A valuation allowance is established for deferred tax assets for which it is more likely than not that some portion or all of the deferred tax assets will not be realized. We periodically re-assess the need for a valuation allowance against our deferred tax assets based on various factors including our historical earnings experience by taxing jurisdiction, forecasts of future operating results, and utilization of net operating losses and tax credits prior to their expiration. Significant judgment is required in making this assessment.
Uncertain tax positions, for which management's assessment is that there is more than a 50% probability of sustaining the position upon challenge by a taxing authority based upon its technical merits, are subjected to certain recognition and measurement criteria. Significant judgment is required in making this assessment, and, therefore, we re-evaluate uncertain tax positions and consider various factors, including, but not limited to, changes in tax law, the measurement of tax positions taken or expected to be taken in tax returns, and changes in facts or circumstances related to a tax position. We adjust the level of the liability to reflect any subsequent changes in the relevant facts and circumstances surrounding the uncertain positions.
Inventories
We capitalize inventory costs associated with our products prior to regulatory approval when, based on management's judgment, future commercialization is considered probable and the future economic benefit is expected to be realized; otherwise, such costs are expensed as research and development. The determination to capitalize inventory costs is based on various factors, including status and expectations of the regulatory approval process, any known safety or efficacy concerns, potential labeling restrictions, and any other impediments to obtaining regulatory approval.
We periodically analyze our inventory levels to identify inventory that may expire prior to expected sale or has a cost basis in excess of its estimated realizable value, and write-down such inventories as appropriate. In addition, our products are subject to strict quality control and monitoring which we perform throughout the manufacturing process. If certain batches or units of product no longer meet quality specifications or become obsolete due to expiration, we record a charge to cost of goods sold to write down such unmarketable inventory to its estimated realizable value.
Contingencies
We accrue, based on management's judgment, for an estimated loss when the potential loss from claims or legal proceedings is considered probable and the amount can be reasonably estimated. As additional information becomes available, or based on specific events such as the outcome of litigation or settlement of claims, we reassess the potential liability related to pending claims and litigation, and may change our estimates.
73
Results of Operations
Net Income
Net Income | Year Ended December 31, | ||||||||||
(In millions) | 2017 | 2016 | 2015 | ||||||||
Revenues | $ | 5,872.2 | $ | 4,860.4 | $ | 4,103.7 | |||||
Operating expenses | (3,792.6 | ) | (3,529.7 | ) | (2,851.8 | ) | |||||
Other income (expense), net | (1.1 | ) | (0.9 | ) | (26.8 | ) | |||||
Income before income taxes | 2,078.5 | 1,329.8 | 1,225.1 | ||||||||
Income tax expense | (880.0 | ) | (434.3 | ) | (589.0 | ) | |||||
Net income | $ | 1,198.5 | $ | 895.5 | $ | 636.1 | |||||
Net income per share - diluted | $ | 10.34 | $ | 7.70 | $ | 5.52 | |||||
Revenues
Revenues | Year Ended December 31, | ||||||||||
(In millions) | 2017 | 2016 | 2015 | ||||||||
Net product sales in the United States: | |||||||||||
EYLEA | $ | 3,701.9 | $ | 3,323.1 | $ | 2,676.0 | |||||
ARCALYST | 16.5 | 15.3 | 13.5 | ||||||||
Sanofi and Bayer collaboration revenue: | |||||||||||
Sanofi | 877.2 | 658.7 | 758.9 | ||||||||
Bayer | 938.1 | 744.3 | 580.5 | ||||||||
Other revenue | 338.5 | 119.0 | 74.8 | ||||||||
Total revenues | $ | 5,872.2 | $ | 4,860.4 | $ | 4,103.7 | |||||
Net Product Sales
Net product sales of EYLEA in the United States increased in 2017 compared to 2016 and 2015 due to higher sales volume, partly offset by an increase in sales-related deductions primarily due to payer sales mix and new rebate programs.
74
Sanofi Collaboration Revenue
Sanofi Collaboration Revenue | Year Ended December 31, | |||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
Antibody: | ||||||||||||
Reimbursement of Regeneron research and development expenses - Discovery Agreement | $ | 130.0 | $ | 130.0 | $ | 145.0 | ||||||
Reimbursement of Regeneron research and development expenses - License and Collaboration Agreement | 378.4 | 434.9 | 590.4 | |||||||||
Reimbursement of Regeneron commercialization-related expenses | 368.8 | 305.9 | 155.3 | |||||||||
Regeneron's share of losses in connection with commercialization of antibodies | (442.6 | ) | (459.0 | ) | (240.0 | ) | ||||||
Other | 119.1 | 28.4 | 12.3 | |||||||||
Total Antibody | 553.7 | 440.2 | 663.0 | |||||||||
Immuno-oncology: | ||||||||||||
Reimbursement of Regeneron research and development expenses - Discovery Agreement | 138.8 | 86.5 | 29.2 | |||||||||
Reimbursement of Regeneron research and development expenses - License and Collaboration Agreement | 101.2 | 52.0 | 10.8 | |||||||||
Other | 83.5 | 80.0 | 40.0 | |||||||||
Total Immuno-oncology | 323.5 | 218.5 | 80.0 | |||||||||
ZALTRAP: | ||||||||||||
Reimbursement of Regeneron research and development expenses | — | — | 0.7 | |||||||||
Other | — | — | 15.2 | |||||||||
Total ZALTRAP | — | — | 15.9 | |||||||||
Total Sanofi collaboration revenue | $ | 877.2 | $ | 658.7 | $ | 758.9 | ||||||
The lower reimbursement of antibody research and development costs under our License and Collaboration Agreement in 2017 compared to 2016 was primarily due to decreased reimbursement levels for Dupixent (dupilumab) subsequent to the receipt of the first positive Phase 3 trial results, and U.S. regulatory approval for, atopic dermatitis, in accordance with the terms of our collaboration agreement. The lower reimbursement of research and development costs under our License and Collaboration Agreement in 2016 compared to 2015 was primarily due to decreased collaboration development activities for Praluent, dupilumab, and REGN2222.
Reimbursement of Regeneron commercialization-related expenses represents reimbursement of internal and external costs in connection with commercializing Praluent, Kevzara, and Dupixent.
In accordance with the companies' License and Collaboration Agreement, we and Sanofi began sharing commercial expenses related to Praluent and Kevzara in 2014 and Dupixent in 2016. As such, during the same periods in which we recorded reimbursements from Sanofi related to our commercialization expenses, we also recorded our share of losses in connection with the companies commercializing Praluent, Kevzara, and Dupixent within Sanofi collaboration revenue. In 2017, Sanofi collaboration revenues in connection with commercialization of antibodies were positively impacted, compared to 2016, by higher sales of collaboration antibody products (see table below), higher reimbursements of Dupixent commercialization-related expenses, and a decrease in the collaborations' Praluent commercialization expenses, which were partially offset by an increase in the collaborations' Kevzara commercialization expenses. In 2016, Sanofi collaboration revenues were negatively impacted, compared to 2015, by higher commercialization expenses in connection with the launch of Praluent, and higher expenses in connection with preparing to commercialize Kevzara and Dupixent.
The following table summarizes global net product sales recorded by Sanofi:
75
Year Ended December 31, | ||||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
Praluent in the United States | $ | 131.4 | $ | 94.4 | $ | 9.5 | ||||||
Praluent outside of the United States | 63.3 | 21.9 | 1.0 | |||||||||
Praluent global | 194.7 | 116.3 | 10.5 | |||||||||
Dupixent | 256.5 | — | — | |||||||||
Kevzara | 13.3 | — | — | |||||||||
In March 2017, the FDA approved Dupixent for the treatment of adult patients with moderate-to-severe atopic dermatitis, and in September 2017, the European Commission granted marketing authorization for Dupixent for use in adults with moderate-to-severe atopic dermatitis who are candidates for systemic therapy. In May 2017, the FDA approved Kevzara for the treatment of rheumatoid arthritis in adult patients, and in June 2017, the European Commission granted marketing authorization for Kevzara for the treatment of rheumatoid arthritis in adult patients. The sales of Dupixent and Kevzara in 2017 primarily consist of U.S. sales.
During 2017, other Sanofi antibody revenue included (i) reimbursements by Sanofi in connection with commercial manufacturing activities under the terms of our collaboration agreement and (ii) an acceleration of the recognition of deferred revenue from an $85.0 million up-front payment and other payments in connection with Sanofi's decision to end our Antibody Discovery Agreement on December 31, 2017 without any extension.
In July 2015, we and Sanofi entered into a global strategic collaboration to discover, develop, and commercialize antibody-based cancer treatments in the field of immuno-oncology. Sanofi's reimbursement of immuno-oncology research and development costs under our IO Discovery Agreement increased in 2017, compared to 2016 and 2015, primarily due to an increase in pre-clinical research activities for additional product candidates. Sanofi's reimbursement of immuno-oncology research and development costs under our IO License and Collaboration Agreement increased in 2017, compared to 2016 and 2015, as we advanced the cemiplimab clinical program into late-stage clinical development.
Other Sanofi immuno-oncology revenue includes recognition of deferred revenue from $640.0 million of up-front payments received in 2015 in connection with the execution of the IO Collaboration agreements.
In February 2015, we entered into an Amended ZALTRAP Agreement with Sanofi which amended and restated the ZALTRAP Collaboration Agreement. Under the Amended ZALTRAP Agreement, Sanofi is solely responsible for the development and commercialization of ZALTRAP. As a result, in the first quarter of 2015, we recognized $14.9 million of collaboration revenue, which was previously recorded as deferred revenue under the original ZALTRAP collaboration agreement, related to (i) amounts that were previously reimbursed by Sanofi for manufacturing commercial supplies of ZALTRAP since our risk of inventory loss no longer existed, and (ii) the unamortized portion of up-front payments from Sanofi as we had no further performance obligations.
Bayer Collaboration Revenue
Bayer Collaboration Revenue | Year Ended December 31, | |||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
EYLEA: | ||||||||||||
Regeneron's net profit in connection with commercialization of EYLEA outside the United States | $ | 802.3 | $ | 649.2 | $ | 466.7 | ||||||
Sales milestones | — | — | 15.0 | |||||||||
Reimbursement of Regeneron EYLEA development expenses | 13.3 | 9.0 | 8.9 | |||||||||
Other | 58.7 | 52.6 | 69.4 | |||||||||
Total EYLEA | 874.3 | 710.8 | 560.0 | |||||||||
Ang2 antibody and PDGFR-beta antibody: | ||||||||||||
Reimbursement of development expenses | 17.8 | 18.3 | 10.1 | |||||||||
Other | 46.0 | 15.2 | 10.4 | |||||||||
Total Ang2 antibody and PDGFR-beta antibody | 63.8 | 33.5 | 20.5 | |||||||||
Total Bayer collaboration revenue | $ | 938.1 | $ | 744.3 | $ | 580.5 | ||||||
76
Bayer records revenue from sales of EYLEA outside the United States. Regeneron's net profit in connection with commercialization of EYLEA outside the United States is summarized below.
Regeneron's Net Profit from EYLEA Sales Outside the United States | Year Ended December 31, | |||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
Net product sales outside the United States | $ | 2,226.9 | $ | 1,872.3 | $ | 1,413.3 | ||||||
Regeneron's share of collaboration profit from sales outside the United States | 856.1 | 703.3 | 521.8 | |||||||||
Reimbursement of EYLEA development expenses incurred by Bayer in accordance with Regeneron's payment obligation | (53.8 | ) | (54.1 | ) | (55.1 | ) | ||||||
Regeneron's net profit in connection with commercialization of EYLEA outside the United States | $ | 802.3 | $ | 649.2 | $ | 466.7 | ||||||
In 2015, we earned our final $15.0 million sales milestone from Bayer, upon total aggregate net sales of specific commercial supplies of EYLEA outside the United States exceeding $200.0 million over a twelve-month period.
Other EYLEA revenue primarily consists of reimbursement of other Regeneron EYLEA expenses, including reimbursements for producing EYLEA commercial supplies for Bayer. In addition, other EYLEA revenue in the first five months of 2016 and for the full year 2015 includes Bayer's share of royalties payable to Genentech pursuant to a license and settlement agreement in connection with sales of EYLEA outside the United States; the obligation to pay Genentech royalties on such sales ended in May 2016. Other EYLEA revenue also includes recognition of deferred revenue related to the 2006 EYLEA up-front and 2007 non-substantive milestone payments from Bayer.
In March 2016, we entered into an agreement with Bayer governing the joint development and commercialization outside the United States of nesvacumab, an antibody product candidate to Ang2, including in combination with aflibercept, for the treatment of ocular diseases or disorders. In connection with the agreement, Bayer made a $50.0 million non-refundable up-front payment to us, which was recorded as deferred revenue and was being recognized as revenue over the related performance period. Bayer is also obligated to pay 25% of global development costs and 50% of development costs exclusively for the territory outside the United States. In the fourth quarter of 2017, we reported that results from two nesvacumab Phase 2 studies did not provide sufficient differentiation to warrant Phase 3 development; therefore, we recognized $37.4 million of revenue related to the acceleration of the recognition of deferred revenue from the up-front payment received from Bayer.
In 2014, we entered into a PDGFR-beta antibody collaboration agreement with Bayer. Bayer collaboration revenue also includes reimbursement of PDGFR-beta antibody development expenses related to Bayer's obligation to pay 25% of global development costs and 50% of development costs exclusively for the territory outside the United States. We discontinued clinical development of PDGFR-beta antibody in the first quarter of 2017.
Other Revenue
Other Revenue | Year Ended December 31, | |||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
Teva collaboration revenue: | ||||||||||||
Reimbursement of Regeneron research and development expenses | $ | 115.1 | $ | 24.2 | — | |||||||
Substantive development milestones | 60.0 | — | — | |||||||||
Other | 46.4 | 13.7 | — | |||||||||
Total Teva collaboration revenue | 221.5 | 37.9 | — | |||||||||
Other revenue | 117.0 | 81.2 | $ | 74.9 | ||||||||
Total other revenue | $ | 338.5 | $ | 119.1 | $ | 74.9 | ||||||
In September 2016, we and Teva entered into a collaboration agreement to develop and commercialize fasinumab. In 2017, we earned, and recognized as revenue, development milestones of $25.0 million and $35.0 million from Teva. Other Teva collaboration revenue includes recognition of a portion of deferred revenue from a $250.0 million up-front payment.
77
In 2017, we earned, and recognized as revenue, a $30.0 million development milestone from MTPC. In addition, in 2017, MTPC made additional payments totaling $25.0 million related to development milestones achieved by MTPC, which were recorded as deferred revenue and are being recognized as revenue over the same performance period as the up-front payment. The revenue recognized in connection with the MTPC milestones are included in Other revenue in the table above.
In addition to revenues earned in connection with our agreement with MTPC, "Other revenue" in the table above includes:
• | Under the terms of the Amended ZALTRAP Agreement, Sanofi's reimbursement for manufacturing commercial supplies of ZALTRAP and a percentage of aggregate net sales of ZALTRAP. |
• | Recognition of revenue related to amortization of the $165.0 million up-front payment we received in August 2010, which was deferred upon receipt and is being recognized as revenue through mid-2018, in connection with the VelocImmune license agreement with Astellas. In addition, Astellas will make a $130.0 million second payment to us in June 2018 unless the license agreement has been terminated prior to that date. Astellas has the right to terminate the agreement at any time by providing 90 days' advance written notice. |
• | Royalties in connection with a June 2009 agreement with Novartis, under which we receive royalties on worldwide sales of Novartis' Ilaris® (canakinumab). The royalty rates in the agreement start at 4% and reach 15% when annual sales exceed $1.5 billion, and we are entitled to royalties until Novartis ceases sale of products subject to royalty. |
Expenses
Year Ended December 31, | Increase (Decrease) | |||||||||||||||||||
(In millions) | 2017 | 2016 | 2015 | 2017 vs. 2016 | 2016 vs. 2015 | |||||||||||||||
Research and development | $ | 2,075.1 | $ | 2,052.3 | $ | 1,620.6 | $ | 22.8 | $ | 431.7 | ||||||||||
Selling, general, and administrative | 1,320.4 | 1,177.7 | 838.5 | 142.7 | 339.2 | |||||||||||||||
Cost of goods sold | 202.5 | 194.6 | 241.7 | 7.9 | (47.1 | ) | ||||||||||||||
Cost of collaboration and contract manufacturing | 194.6 | 105.1 | 151.0 | 89.5 | (45.9 | ) | ||||||||||||||
Total operating expenses | $ | 3,792.6 | $ | 3,529.7 | $ | 2,851.8 | $ | 262.9 | $ | 677.9 | ||||||||||
Average headcount | 5,780 | 4,927 | 3,713 | 853 | 1,214 | |||||||||||||||
Our average headcount in 2017 increased compared to 2016 principally in connection with expanding our manufacturing activities. Average headcount in 2016 increased compared to 2015 principally in connection with expanding our research and development, manufacturing, and commercialization activities.
Operating expenses in 2017, 2016, and 2015 included a total of $507.3 million, $559.9 million, and $459.0 million, respectively, of non-cash compensation expense related to employee stock options and restricted stock. As of December 31, 2017, unrecognized non-cash compensation expense related to outstanding stock options and unvested restricted stock was $816.6 million and $34.9 million, respectively. We expect to recognize this non-cash compensation expense related to stock options and restricted stock over weighted-average periods of 1.9 years and 4.0 years, respectively.
Research and Development Expenses
The following table summarizes our estimates of direct research and development expenses by clinical development program and other significant categories of research and development expenses. Direct research and development expenses are comprised primarily of costs paid to third parties for clinical and product development activities, including costs related to preclinical research activities, clinical trials, drug filling, packaging, and labeling, and the portion of research and development expenses incurred by our collaborators that we are obligated to reimburse. Indirect research and development expenses have not been allocated directly to each program, and primarily consist of costs to compensate personnel, overhead and infrastructure costs to maintain our facilities, costs to manufacture bulk drug product (including pre-launch commercial supplies which were not capitalized as inventory) at our manufacturing facilities, and other costs related to activities that benefit multiple projects.
78
Research and Development Expenses | Year Ended December 31, | Increase (Decrease) | ||||||||||||||||||
(In millions) | 2017 | 2016* | 2015* | 2017 vs. 2016 | 2016 vs. 2015 | |||||||||||||||
Direct research and development expenses: | ||||||||||||||||||||
Dupilumab | $ | 199.9 | $ | 221.6 | $ | 227.8 | $ | (21.7 | ) | $ | (6.2 | ) | ||||||||
Cemiplimab | 114.2 | 40.5 | 11.5 | 73.7 | 29.0 | |||||||||||||||
Fasinumab | 153.8 | 110.4 | 31.2 | 43.4 | 79.2 | |||||||||||||||
Praluent | 84.9 | 85.6 | 108.9 | (0.7 | ) | (23.3 | ) | |||||||||||||
Suptavumab | 27.7 | 25.9 | 16.8 | 1.8 | 9.1 | |||||||||||||||
Sarilumab | 9.4 | 20.5 | 31.4 | (11.1 | ) | (10.9 | ) | |||||||||||||
Other product candidates in clinical development and other research programs | 251.5 | 344.9 | 223.3 | (93.4 | ) | 121.6 | ||||||||||||||
Total direct research and development expenses | 841.4 | 849.4 | 650.9 | (8.0 | ) | 198.5 | ||||||||||||||
Indirect research and development expenses: | ||||||||||||||||||||
Payroll and benefits | 578.5 | 556.1 | 463.4 | 22.4 | 92.7 | |||||||||||||||
Clinical manufacturing costs | 388.2 | 404.9 | 327.1 | (16.7 | ) | 77.8 | ||||||||||||||
Research, licensing, and other development costs | 62.9 | 51.6 | 35.0 | 11.3 | 16.6 | |||||||||||||||
Occupancy and other operating costs | 204.1 | 190.3 | 144.2 | 13.8 | 46.1 | |||||||||||||||
Total indirect research and development expenses | 1,233.7 | 1,202.9 | 969.7 | 30.8 | 233.2 | |||||||||||||||
Total research and development expenses | $ | 2,075.1 | $ | 2,052.3 | $ | 1,620.6 | $ | 22.8 | $ | 431.7 | ||||||||||
* Certain prior year amounts have been reclassified to conform to the current year's presentation. | ||||||||||||||||||||
"Direct research and development expenses - Other product candidates in clinical development and other research programs" in 2017 included a $25.0 million up-front payment made in connection with a November 2017 agreement with Decibel Therapeutics, and in 2016 included the $75.0 million and $25.0 million up-front payments made in connection with the license and collaboration agreements with Intellia and Adicet, respectively. Clinical manufacturing costs increased in 2016, compared to 2015, primarily due to costs related to manufacturing additional drug supplies of dupilumab, fasinumab, and cemiplimab, partly offset by lower costs related to manufacturing less clinical supplies of Praluent. Research and development expenses included Non-Cash Compensation Expense of $271.9 million in 2017, $313.0 million in 2016, and $255.7 million in 2015.
There are numerous uncertainties associated with drug development, including uncertainties related to safety and efficacy data from each phase of drug development, uncertainties related to the enrollment and performance of clinical trials, changes in regulatory requirements, changes in the competitive landscape affecting a product candidate, and other risks and uncertainties described in Part I, Item 1A, "Risk Factors." The lengthy process of seeking FDA approvals, and subsequent compliance with applicable statutes and regulations, require the expenditure of substantial resources. Any failure by us to obtain, or delay in obtaining, regulatory approvals could materially adversely affect our business. As a result of the variability in the duration and costs necessary to develop a pharmaceutical product, potential opportunities and/or uncertainties related to future indications to be studied, the estimated cost and scope of the projects, and our ultimate ability to obtain governmental approval for commercialization, we have not provided estimates of the total cost to bring our product candidates to market. Similarly, we are unable to reasonably estimate if our product candidates in clinical development will generate material product revenues and net cash inflows.
79
Selling, General, and Administrative Expenses
Selling, general, and administrative expenses increased in 2017, compared to 2016, primarily due to (i) an increase in commercialization-related expenses associated with Dupixent and EYLEA, and, to a lesser extent, Kevzara and cemiplimab, partly offset by lower commercialization-related expenses associated with Praluent, and (ii) higher headcount and headcount-related costs. Selling, general, and administrative expenses increased in 2016 compared to 2015 primarily due to (i) higher commercialization-related expenses associated with Praluent and higher commercialization-related expenses in connection with preparing to launch sarilumab and dupilumab, (ii) higher contributions to not-for-profit organizations, including donations to independent not-for-profit patient assistance organizations, and (iii) higher headcount and headcount-related costs. Selling, general, and administrative expenses also included $208.4 million, $231.2 million, and $193.0 million of Non-cash Compensation Expense in 2017, 2016, and 2015, respectively.
Cost of Goods Sold
Cost of goods sold increased slightly in 2017, compared to 2016, principally due to an increase in start-up costs for our Limerick manufacturing facility, offset due to the fact that, effective May 2016, we were no longer obligated to pay royalties to Genentech based on U.S. sales of EYLEA. Cost of goods sold decreased in 2016, compared to 2015, principally due to the fact that, effective May 2016, we are no longer obligated to pay royalties to Genentech based on U.S. sales of EYLEA; this decrease was partly offset by an increase in Limerick start-up costs and an increase in U.S. EYLEA net sales.
Cost of Collaboration and Contract Manufacturing
Cost of collaboration and contract manufacturing increased in 2017, compared to 2016, primarily due to costs we incurred in connection with validating our Limerick manufacturing commercial facility related to products that are in collaboration with Sanofi, partly offset by the fact that 2016 included royalties payable to Genentech based on sales of EYLEA outside the United States (which ended in May 2016). Cost of collaboration and contract manufacturing was also adversely impacted by inventory write-offs and reserves totaling $57.2 million in 2017 primarily related to product that no longer met quality specifications, compared to $11.2 million and $23.5 million in 2016 and 2015, respectively.
Cost of collaboration and contract manufacturing decreased in 2016, compared to 2015, primarily due to lower royalties since our obligation to pay Genentech based on sales of EYLEA outside the United States ended in May 2016.
Other Income and Expense
Other expenses in 2017 include the recognition of a $30.1 million loss on debt extinguishment related to the 2017 Tarrytown lease transaction. See Note 12 to our Consolidated Financial Statements. This expense was largely offset by investment income earned from our marketable securities in 2017.
Other expenses in 2016 and 2015 included the recognition of a $0.5 million and $18.9 million loss, respectively, in connection with convertible notes which were surrendered for conversion during the respective periods. Other expenses in 2016 also included a $9.8 million other-than-temporary impairment charge related to an investment in an equity security.
80
Income Taxes
Year Ended December 31, | ||||||||||||
(In millions) | 2017 | 2016 | 2015 | |||||||||
Income tax expense | $ | 880.0 | $ | 434.3 | $ | 589.0 | ||||||
Effective tax rate | 42.3 | % | 32.7 | % | 48.1 | % | ||||||
On December 22, 2017, the bill known as the "Tax Cuts and Jobs Act" (the Act) was signed into law. The Act, which became effective with respect to most of its provisions as of January 1, 2018, includes a number of provisions that are expected to impact us, including reducing the U.S. federal corporate income tax rate from 35% to 21%, changing the taxation of foreign earnings (including taxation of certain global intangible low-taxed income), allowing immediate expensing of the cost for qualified assets, repealing the deduction for domestic manufacturing, and imposing further limitations on the deductibility of executive compensation. Changes in tax rates and tax laws are accounted for in the period of enactment. Therefore, as a result of the Act being signed into law, we recognized a provisional charge of $326.2 million in the fourth quarter of 2017 related to the re-measurement of our U.S. net deferred tax assets at the lower enacted corporate tax rates. The 2017 effective tax rate was negatively impacted by this charge, and was partly offset by the tax benefit associated with stock-based compensation. The provisional charge recorded in the fourth quarter of 2017 is an estimate and subject to further analysis, interpretation, and clarification of the Act, which could result in changes to this estimate during 2018.
The 2016 effective tax rate was positively impacted, compared to the U.S. federal statutory rate, by the tax benefit associated with stock-based compensation, partly offset by the negative impact of losses incurred in foreign jurisdictions with rates lower than the U.S. federal statutory rate. As described in Note 1 and Note 16 of our Consolidated Financial Statements, during 2016 we adopted Accounting Standards Update 2016-09, which requires an entity to recognize all excess tax benefits and tax deficiencies in connection with stock-based compensation as income tax expense or benefit in the income statement (previously, excess tax benefits were recognized in additional paid-in capital).
The 2015 effective tax rate was negatively impacted, compared to the U.S. federal statutory rate, by losses incurred in foreign jurisdictions with rates lower than the U.S. federal statutory rate, partly offset by the positive impact of the domestic manufacturing deduction.
Liquidity and Capital Resources
Our financial condition is summarized as follows:
As of December 31, | Increase | ||||||||||
(In millions) | 2017 | 2016 | (Decrease) | ||||||||
Financial assets: | |||||||||||
Cash and cash equivalents | $ | 812.7 | $ | 535.2 | $ | 277.5 | |||||
Marketable securities - current | 596.8 | 503.5 | 93.3 | ||||||||
Marketable securities - non-current | 1,486.5 | 864.2 | 622.3 | ||||||||
$ | 2,896.0 | $ | 1,902.9 | $ | 993.1 | ||||||
Working capital: | |||||||||||
Current assets | $ | 4,335.0 | $ | 3,180.2 | $ | 1,154.8 | |||||
Current liabilities | 1,135.5 | 1,241.5 | (106.0 | ) | |||||||
$ | 3,199.5 | $ | 1,938.7 | $ | 1,260.8 | ||||||
Additionally, as of December 31, 2017, we had borrowing availability of $750.0 million under a revolving credit facility (see further description under "Credit Facility" below).
81
Sources and Uses of Cash for the Years Ended December 31, 2017, 2016, and 2015
Year Ended December 31, | Increase (Decrease) | |||||||||||||||||||
(In millions) | 2017 | 2016 | 2015 | 2017 vs. 2016 | 2016 vs. 2015 | |||||||||||||||
Cash flows provided by operating activities | $ | 1,307.1 | $ | 1,473.4 | $ | 1,330.8 | $ | (166.3 | ) | $ | 142.6 | |||||||||
Cash flows used in investing activities | (1,005.2 | ) | (1,046.9 | ) | (907.6 | ) | 41.7 | $ | (139.3 | ) | ||||||||||
Cash flows used in financing activities | (24.4 | ) | (700.4 | ) | (262.8 | ) | 676.0 | $ | (437.6 | ) | ||||||||||
Cash Flows from Operating Activities
2017. Our net income in 2017 included Non-cash Compensation Expense of $507.3 million. Deferred tax assets as of December 31, 2017 decreased by $318.8 million, compared to December 31, 2016, primarily due to the re-measurement of our U.S. net deferred tax assets at the lower enacted corporate tax rates pursuant to the Act (as described above) and additional tax depreciation, partly offset by an increase in deferred tax assets related to share-based compensation. Cash flows from operating activities for the year ended December 31, 2017 were negatively impacted by $926.5 million in connection with changes in other assets and liabilities. Included in such change was a decrease in deferred revenue by $113.1 million compared to December 31, 2016, partly due to the acceleration of the recognition of deferred revenue in connection with the Sanofi Antibody Discovery Agreement and the Bayer nesvacumab agreement; see "Results of Operations" section above for further details.
2016. Our net income in 2016 included Non-cash Compensation Expense of $559.9 million. Deferred tax assets as of December 31, 2016 increased by $360.1 million, compared to December 31, 2015, primarily due to an increase in share-based compensation, the tax basis of intangible assets, and deferred revenue. Deferred revenue increased by $244.3 million as of December 31, 2016, compared to December 31, 2015, primarily due to $250.0 million and $60.0 million of payments received during 2016 from Teva and Mitsubishi, respectively, in connection with the companies' respective fasinumab collaborations, and the $50.0 million up-front payment from Bayer in connection with the companies' Ang2 collaboration, partly offset primarily by the amortization of these 2016 payments and past up-front payments from Sanofi. Accounts payable, accrued expenses, and other liabilities increased by $254.0 million as of December 31, 2016, compared to December 31, 2015, primarily due to higher tax related liabilities.
2015. Our net income in 2015 included Non-cash Compensation Expense of $459.0 million. Deferred tax assets as of December 31, 2015 increased by $121.6 million, compared to December 31, 2014, primarily due to an increase in share-based compensation, partly offset by a reduction in our deferred tax assets related to fixed assets and deferred revenue. Deferred revenue increased by $608.9 million as of December 31, 2015, compared to December 31, 2014, primarily due to $640.0 million of up-front payments received from Sanofi in connection with the companies' IO Collaboration, partly offset by related amortization which commenced in the third quarter of 2015.
Cash Flows from Investing Activities
Capital expenditures were $272.6 million, $511.9 million, and $677.9 million in 2017, 2016, and 2015, respectively. Capital expenditures decreased in 2017, compared to 2016, in part due to less capital expenditures in connection with renovations and additions at our Limerick, Ireland and Rensselaer, New York manufacturing facilities. Capital expenditures decreased in 2016, compared to 2015, primarily due to less capital expenditures in connection with renovations of our Limerick, Ireland manufacturing facility and 2015 included the acquisition of an approximate 100-acre parcel of undeveloped land adjacent to our current Tarrytown, New York location for an aggregate purchase price of $73.0 million.
82
We expect to incur capital expenditures of $420 million to $500 million in 2018 primarily in connection with expanding a portion of our manufacturing facilities at our Rensselaer, New York facility, continued renovations and expansion of our Limerick, Ireland facility, and laboratory expansion and renovations at our Tarrytown, New York facilities.
Cash Flows from Financing Activities
In 2017, proceeds in connection with capital and facility lease obligations relate to our receipt of $57.0 million in connection with the March 2017 lease transaction as described below under "Tarrytown, New York Leases". In 2016 and 2015, $12.9 million and $166.5 million principal amount of our Notes, respectively, that was previously surrendered for conversion was settled in cash. Also during 2016 and 2015, we paid an aggregate amount of $643.4 million and $573.5 million, respectively, to warrant holders to reduce the maximum number of shares of Common Stock issuable upon exercise of the warrants. In 2015, cash flows from financing activities included $405.3 million due to utilization of excess tax benefits in connection with stock option exercises, which offset cash tax obligations. In 2016, we elected to adopt Accounting Standards Update 2016-09, Compensation - Stock Compensation, Improvements to Employee Share-Based Payment Accounting; consequently, we began to record excess tax benefits as an operating activity in the statement of cash flows.
Credit Facility
In March 2015, we entered into an agreement with a syndicate of lenders (the Credit Agreement) which provides for a $750.0 million senior unsecured five-year revolving credit facility (the Credit Facility). The Credit Agreement includes an option for us to elect to increase the commitments under the Credit Facility and/or to enter into one or more tranches of term loans in the aggregate principal amount of up to $250.0 million subject to the consent of the lenders providing the additional commitments or term loans, as applicable, and certain other conditions. Proceeds of the loans under the Credit Facility may be used to finance working capital needs, and for general corporate or other lawful purposes, of Regeneron and its subsidiaries. The Credit Agreement also provides a $100.0 million sublimit for letters of credit. The Credit Agreement includes an option for us to elect to extend the maturity date of the Credit Facility beyond March 2020, subject to the consent of the extending lenders and certain other conditions. Amounts borrowed under the Credit Facility may be prepaid, and the commitments under the Credit Facility may be terminated, at any time without premium or penalty. We had no borrowings outstanding under the Credit Facility as of December 31, 2017.
The Credit Agreement contains financial and operating covenants. Financial covenants include a maximum total leverage ratio and a minimum interest expense coverage ratio. We were in compliance with all covenants of the Credit Facility as of December 31, 2017.
Sanofi Funding of Certain Development Costs
As described in Part 1, Item 1. "Business - Collaborations - Collaborations with Sanofi," effective January 7, 2018, we and Sanofi entered into a Letter Agreement in connection with, among other matters, increasing the development budget amount for cemiplimab and allocating additional funds to certain proposed activities relating to the development of dupilumab and REGN3500 and non-approval trials of dupilumab. Pursuant to the Letter Agreement, we have agreed to allow Sanofi to satisfy in whole or in part its funding obligations with respect to cemiplimab development and/or Dupilumab/REGN3500 Eligible Investments by selling up to 1,400,000 shares of our Common Stock directly or indirectly owned by Sanofi through September 30, 2020. If Sanofi desires to sell shares of our Common Stock during the term of the Letter Agreement to satisfy a portion or all of its funding obligations for the cemiplimab development and/or Dupilumab/REGN3500 Eligible Investments, we may elect to purchase, in whole or in part, such shares from Sanofi. If we do not elect to purchase such shares, Sanofi may sell the applicable number of shares (subject to certain daily and quarterly limits) in one or more open-market transactions.
Tarrytown, New York Leases
We lease laboratory and office facilities in Tarrytown, New York. On December 30, 2016, we entered into a Purchase Agreement with BMR-Landmark at Eastview LLC and BMR-Landmark at Eastview IV LLC (collectively, BMR), pursuant to which we agreed to purchase BMR's Tarrytown, New York facilities (the Facility) for a purchase price of $720.0 million. We occupy a significant portion of the Facility, with the remaining rentable area under leases to third-party tenants. In accordance with the terms of the Purchase Agreement, we paid $57.0 million toward the purchase price to BMR in December 2016.
On March 3, 2017, we entered into a Participation Agreement with Banc of America Leasing & Capital LLC (BAL), as lessor, and a syndicate of lenders (collectively, the Participants). The Participation Agreement provided for lease financing in connection with the acquisition by BAL of the Facility and our lease of the Facility from BAL. On March 3, 2017, we assigned our right to take title to the Facility under the Purchase Agreement to BAL, and the Participants advanced $720.0 million, which was used by BAL to finance the purchase price for the Facility and to reimburse us for the $57.0 million payment we made to BMR in December 2016.
83
On March 3, 2017, we also entered into a lease agreement (the Lease) with BAL, pursuant to which we have leased the Facility from BAL for a five-year term. As a result of entering into the lease agreement, certain parts of the Facility became subleased from us by existing third-party tenants. The Lease requires us to pay all maintenance, insurance, taxes, and other costs arising out of the use of the Facility. We are also required to make monthly payments of basic rent during the term of the Lease in an amount equal to a variable rate per annum based on the one-month London Interbank Offered Rate (LIBOR), plus an applicable margin that varies with our debt rating and total leverage ratio.
The Participation Agreement and the Lease include an option for us to elect to extend the maturity date of the Participation Agreement and the term of the Lease for an additional five-year period, subject to the consent of all the Participants and certain other conditions. We also have the option prior to the end of the term of the Lease to (a) purchase the Facility by paying an amount equal to the outstanding principal amount of the Participants' advances under the Participation Agreement, all accrued and unpaid interest and yield thereon, and all other outstanding amounts under the Participation Agreement, the Lease, and certain related documents or (b) sell the Facility to a third party on behalf of BAL. The advances under the Participation Agreement mature, and all amounts outstanding thereunder will become due and payable in full at the end of the term of the Lease.
The Participation Agreement and the Lease contain financial and operating covenants, which are substantially similar to the covenants set forth in our Credit Facility. We were in compliance with all covenants of the Participation Agreement and the Lease as of December 31, 2017.
Funding Requirements
The amount required to fund operations will depend on various factors, including revenues from net product sales, the potential regulatory approval and commercialization of our product candidates and the timing thereof, the status of competitive products, the success of our research and development programs, the potential future need to expand our professional and support staff and facilities, the status of patents and other intellectual property rights (and future litigation related thereto), the delay or failure of a clinical trial of any of our potential drug candidates, and the continuation, extent, and success of our collaborations (in particular those with Sanofi and Bayer). We believe that our existing capital resources, borrowing availability under our revolving credit facility, funds generated by anticipated EYLEA net product sales, and, as described above under Part 1, Item 1. "Business - Collaborations," funding for reimbursement of research and development costs that we are entitled to receive under our collaboration agreements, will enable us to meet our projected operating needs for the foreseeable future.
The following table summarizes our contractual obligations as of December 31, 2017.
Payments Due by Period | ||||||||||||||||||||
(In millions) | Total | Less than one year | 1 to 3 years | 3 to 5 years | Greater than 5 years | |||||||||||||||
Purchase and other obligations (1) | $ | 1,404.3 | $ | 816.9 | $ | 485.9 | $ | 62.8 | $ | 38.7 | ||||||||||
Capital and facility lease obligations (2) | 105.7 | 21.1 | 50.1 | 34.5 | — | |||||||||||||||
Operating leases | 21.9 | 9.0 | 7.0 | 4.4 | 1.5 | |||||||||||||||
Total contractual obligations | $ | 1,531.9 | $ | 847.0 | $ | 543.0 | $ | 101.7 | $ | 40.2 | ||||||||||
(1) | Purchase and other obligations primarily relate to research and development commitments, including those related to clinical trials, and capital expenditures. Our obligation to pay certain of these amounts may increase or be reduced based on relevant future events. |
(2) | Represents rent payments with respect to capital lease and facility lease obligations in connection with our property leases in Tarrytown, New York, as described under "Tarrytown, New York Leases" above and Note 12 to our Consolidated Financial Statements. Amounts in the table above exclude the purchase price we would be obligated to pay if we were to exercise our option to purchase the Facility. |
Liabilities for unrecognized tax benefits, totaling $146.2 million at December 31, 2017, are not included in the table of contractual obligations above as, due to their nature, there is a high degree of uncertainty regarding the period of potential future cash settlement with taxing authorities. See Note 16 to our Consolidated Financial Statements.
We expect continued increases in our expenditures, particularly in connection with our research and development activities (including preclinical and clinical programs). The amount of funding that will be required for our clinical programs depends upon the results of our research and preclinical programs and early-stage clinical trials, regulatory requirements, the duration and results of clinical trials underway and of additional clinical trials that we decide to initiate, and the various factors that affect the cost of each trial. Under certain collaboration agreements, the amount of funding for reimbursement of research and development costs that we are entitled to receive is capped at a specified amount; therefore, we may elect to independently fund certain research and development costs in excess of such capped amounts. Pursuant to the Antibody Discovery Agreement, as amended, Sanofi was
84
responsible for funding up to $130.0 million of our antibody discovery activities in 2017. Our Antibody Discovery Agreement with Sanofi ended on December 31, 2017 and, therefore, there will be no funding from Sanofi under the Antibody Discovery Agreement beyond 2017.
Clinical trial costs are dependent, among other things, on the size and duration of trials (for example, we have several ongoing late-stage clinical trials which are large and for which we expect to incur significant costs), fees charged for services provided by clinical trial investigators and other third parties, the costs for manufacturing the product candidate for use in the trials, and for supplies, laboratory tests, and other expenses.
We anticipate continuing to incur substantial commercialization costs for EYLEA, Dupixent, Praluent, and Kevzara, as well as in connection with our late-stage antibody product candidates, including cemiplimab. Commercialization costs over the next few years will depend on, among other things, the market potential for product candidates, whether commercialization costs are shared with a collaborator, regulatory approval of additional product candidates, and whether we may be required to pay additional royalties or share the profits from sales of products pursuant to our license or collaboration agreements or otherwise.
We expect that expenses related to the filing, prosecution, defense, and enforcement of patents and other intellectual property will be substantial.
We enter into research collaboration and licensing agreements that may require us to pay (i) amounts upon the achievement of various development and commercial milestones, which, in the aggregate, could be significant, and/or (ii) royalties calculated based on a percentage of net product sales. The payment of these amounts, however, is contingent upon the occurrence of various future events, which have a high degree of uncertainty of occurring and for which the specific timing cannot be predicted. Because of these factors, such payments are not included in the table of contractual obligations above. See Note 3 and Note 12 to our Consolidated Financial Statements.
Under our Antibody and IO Collaborations with Sanofi and our collaboration with Bayer for EYLEA outside the United States, we and our collaborator share profits and losses in connection with commercialization of drug products. Profits or losses under each collaboration are measured by calculating net sales less cost of goods sold and shared commercialization and other expenses. If the applicable collaboration is profitable, we have contingent contractual obligations to reimburse Sanofi and Bayer for a defined percentage (generally 50%) of agreed-upon development expenses funded by Sanofi and Bayer. These reimbursements would be deducted each quarter, in accordance with a formula, from our share of the collaboration profits (and, for our EYLEA collaboration with Bayer, inclusive of our percentage on product sales in Japan) otherwise payable to us, unless, in the case of EYLEA, we elect to reimburse these expenses at a faster rate. As of December 31, 2017, our contingent reimbursement obligation to Bayer for EYLEA was approximately $251 million and our contingent reimbursement obligation to Sanofi in connection with the companies' Antibody Collaboration and IO Collaboration was approximately $2,558 million and $22 million, respectively. Therefore, we expect that, for the foreseeable future, a portion of our share of profits from sales of EYLEA outside the United States and a portion of our share of profits, if any, from sales of Dupixent, Praluent, Kevzara, and cemiplimab (if approved) will be used to reimburse our collaborator for these obligations.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements that are currently material or reasonably likely to be material to our consolidated financial position or results of operations.
Future Impact of Recently Issued Accounting Standards
See Note 1 to our Consolidated Financial Statements for a summary of recently issued accounting standards.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
Our earnings and cash flows are subject to fluctuations due to changes in interest rates, principally in connection with our investments in marketable securities, which consist primarily of corporate bonds, direct obligations of the U.S. government and its agencies and other debt securities guaranteed by the U.S. government, and municipal bonds. We do not believe we are materially exposed to changes in interest rates related to our investments, and we do not currently use interest rate derivative instruments to manage exposure to interest rate changes of our investments. We estimate that a 100 basis point, or 1%, unfavorable change in interest rates would have resulted in approximately a $23.2 million and $20.9 million decrease in the fair value of our investment portfolio as of December 31, 2017 and 2016, respectively.
85
We have exposure to market risk for changes in interest rates, including the interest rate risk relating to our March 2017 variable rate Tarrytown, New York lease (as described in Item 7. "Management's Discussion and Analysis of Financial Condition and Results of Operations - Liquidity and Capital Resources - Tarrytown, New York Leases"). Our interest rate exposure is primarily offset by our investments in marketable securities. In addition, beginning in the second quarter of 2017, we began to further manage our interest rate exposure through the use of derivative instruments. All of our derivative instruments are utilized for risk management purposes, and are not used for trading or speculative purposes. We continue to monitor our interest rate risk and may utilize additional derivative instruments and/or other strategies in the future to further mitigate our interest rate exposure.
We have hedged a portion of our floating interest rate exposure using interest rate swap and interest rate cap contracts (see Note 6 to our Consolidated Financial Statements). We estimate that a 100 basis point, or 1%, unfavorable change in interest rates would not have a material impact on the fair value of our interest rate swap or interest rate cap contracts. The following table summarizes the notional amounts of our outstanding interest rate swap and cap contracts as of December 31, 2017:
(In millions) | Notional Amount | |||
Interest rate swap contracts | $ | 75.0 | ||
Interest rate cap contracts | $ | 75.0 | ||
Credit Quality Risk
We have an investment policy that includes guidelines on acceptable investment securities, minimum credit quality, maturity parameters, and concentration and diversification. Nonetheless, deterioration of the credit quality of an investment security subsequent to purchase may subject us to the risk of not being able to recover the full principal value of the security. In 2017 and 2015, we recorded no charges for other-than-temporary impairments of our marketable securities, and in 2016, we recorded an other-than-temporary impairment charge of $9.8 million related to our investment in an equity security.
We are subject to credit risk associated with the receivables due from our collaborators Bayer, Sanofi, and Teva. We are also subject to credit risk in connection with accounts receivable from our product sales of EYLEA and ARCALYST. These accounts receivable are due from several distributors and specialty pharmacies, who are our customers. We have contractual payment terms with each of our customers, and we monitor our customers' financial performance and credit worthiness so that we can properly assess and respond to any changes in their credit profile. In addition, we may insure a portion of our accounts receivables within our overall risk management practices. During 2017, 2016, and 2015, we did not recognize any charges for write-offs of accounts receivable related to our marketed products. As of December 31, 2017 and 2016, three customers accounted on a combined basis for 99% of our net trade accounts receivables.
Foreign Exchange Risk
As discussed further above, Bayer markets EYLEA outside the United States and Sanofi markets Dupixent, Praluent, and Kevzara worldwide, and we share in profits and losses with these collaborators from commercialization of products (including the receipt of a percentage of EYLEA sales in Japan). In addition, pursuant to the applicable terms of the agreements with our collaborators, we also share in certain worldwide development expenses incurred by our collaborators. We also incur worldwide development expenses for clinical products we are developing independently, in addition to incurring expenses outside of the United States in connection with our international operations. Therefore, significant changes in foreign exchange rates of the countries outside the United States where our product is sold, where development expenses are incurred by us or our collaborators, or where we incur operating expenses can impact our operating results and financial condition. As sales outside the United States continue to grow, and as we expand our international operations, we will continue to assess potential steps, including foreign currency hedging and other strategies, to mitigate our foreign exchange risk.
Item 8. Financial Statements and Supplementary Data
The financial statements required by this Item are included on pages F-1 through F-46 of this report. The supplementary financial information required by this Item is included at page F-46 of this report.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None.
86
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our principal executive officer and principal financial officer, conducted an evaluation of the effectiveness of our disclosure controls and procedures (as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934 (the "Exchange Act")) as of the end of the period covered by this Annual Report on Form 10-K. Based on this evaluation, our principal executive officer and principal financial officer each concluded that, as of the end of such period, our disclosure controls and procedures were effective in ensuring that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized, and reported on a timely basis, and is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate to allow timely decisions regarding required disclosures.
Management Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Our management conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2017 using the framework in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on that evaluation, our management has concluded that our internal control over financial reporting was effective as of December 31, 2017. The effectiveness of the Company's internal control over financial reporting as of December 31, 2017 has been audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm, as stated in their report which appears under Item 15.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Changes in Internal Control over Financial Reporting
There has been no change in our internal control over financial reporting (as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) during the quarter ended December 31, 2017 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Our management, including our principal executive officer and principal financial officer, does not expect that our disclosure controls and procedures or internal controls over financial reporting will prevent all errors and all fraud. A control system, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the system are met and cannot detect all deviations. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud or deviations, if any, within the company have been detected. Projections of any evaluation of effectiveness to future periods are subject to the risks that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Item 9B. Other Information
None.
87
PART III
Item 10. Directors, Executive Officers and Corporate Governance
The information required by this item (other than the information set forth in the next paragraph in this Item 10) will be included in our definitive proxy statement with respect to our 2018 Annual Meeting of Shareholders to be filed with the SEC, and is incorporated herein by reference.
We have adopted a code of business conduct and ethics that applies to our officers, directors, and employees. The full text of our code of business conduct and ethics can be found on our website (http://www.regeneron.com) under the "Investors & Media" heading on the "Corporate Governance" page. We may satisfy the disclosure requirements under Item 5.05 of Form 8-K regarding an amendment to, or a waiver from, a provision of our code of business conduct and ethics that applies to our principal executive officer, principal financial officer, principal accounting officer, or controller, or persons performing similar functions, by posting such information on our website where it is accessible through the same link noted above.
Item 11. Executive Compensation
The information called for by this item will be included in our definitive proxy statement with respect to our 2018 Annual Meeting of Shareholders to be filed with the SEC, and is incorporated herein by reference.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information called for by this item will be included in our definitive proxy statement with respect to our 2018 Annual Meeting of Shareholders to be filed with the SEC, and is incorporated herein by reference.
Item 13. Certain Relationships and Related Transactions, and Director Independence
The information required by this item will be included in our definitive proxy statement with respect to our 2018 Annual Meeting of Shareholders to be filed with the SEC, and is incorporated herein by reference.
Item 14. Principal Accountant Fees and Services
The information called for by this item will be included in our definitive proxy statement with respect to our 2018 Annual Meeting of Shareholders to be filed with the SEC, and is incorporated herein by reference.
PART IV
Item 15. Exhibits and Financial Statement Schedules
(a) 1. Financial Statements
The consolidated financial statements filed as part of this report are listed on the Index to Financial Statements on page F-1.
2. Financial Statement Schedules
All schedules for which provision is made in the applicable accounting regulations of the Securities and Exchange Commission are not required under the related instructions or are inapplicable and, therefore, have been omitted.
3. Exhibits
Exhibit Number | Description |
3.1 | |
3.2 | |
4.1 | |
4.2 | |
88
10.1 + | |
10.1.1 + | |
10.1.2 + | |
10.1.3 + | |
10.1.5 + | |
10.1.6 + | |
10.1.7 + | |
10.1.8 + | |
10.1.9 + | |
10.1.10 + | |
10.2 + | |
10.2.1 + | |
10.2.2 + | |
10.2.3 + | |
10.2.4 + | |
89
10.2.5 + | |
10.2.6 + | |
10.2.7 + | |
10.2.8 + | |
10.2.9 + | |
10.2.10 + | |
10.2.11 + | |
10.2.12 + | |
10.2.13 + | |
10.2.14 + | |
10.2.15 + | |
10.2.16 + | |
10.3 + | |
10.4* + | |
10.5 + | |
10.6 + | |
10.7 + | |
10.8* | |
90
10.9* | |
10.10* | |
10.10.1* | |
10.11 | |
10.12 | |
10.12.1* | |
10.12.2 | |
10.12.3 | |
10.12.4 | |
10.12.5 | |
10.12.6 | |
10.12.7 | |
10.12.8 | |
10.12.9 | |
10.12.10 | |
10.12.11 | |
10.12.12 | |
10.12.13 | |
10.12.14 | |
10.12.15 | |
91
10.12.16 | |
10.12.17 | |
10.13 | |
10.13.1 | |
10.14* | |
10.14.1* | |
10.15* | |
10.15.1* | |
10.16* | |
10.16.1* | |
10.16.2* | |
10.17 | |
10.18 | |
10.19 | |
10.20 | |
10.20.1 | |
10.20.2 | |
92
10.20.3 | |
10.20.4 | |
10.21 | |
10.22 | |
10.22.1 | |
10.22.2 | |
10.22.3 | |
10.22.4 | |
10.23 | |
10.24 | |
10.24.1 | |
10.24.2 | |
10.24.3 | |
10.24.4 | |
10.24.5 | |
10.25 | |
10.26 | |
93
10.26.1 | |
10.26.2 | |
10.26.3 | |
10.27* | |
10.27.1* | |
10.27.2* | |
10.27.3 | |
10.28* | |
10.29 | |
10.29.1 | |
10.30* | |
10.31* | |
10.32* | |
10.33* | |
10.34* | |
94
10.35* | |
10.36 | |
10.37 | |
10.38 | |
21.1 | |
23.1 | |
24.1 | |
31.1 | |
31.2 | |
32 | |
101 | Interactive Data File |
101.INS | XBRL Instance Document |
101.SCH | XBRL Taxonomy Extension Schema |
101.CAL | XBRL Taxonomy Extension Calculation Linkbase |
101.DEF | XBRL Taxonomy Extension Definition Document |
101.LAB | XBRL Taxonomy Extension Label Linkbase |
101.PRE | XBRL Taxonomy Extension Presentation Linkbase |
_______ | |
* | Portions of this document have been omitted and filed separately with the Commission pursuant to requests for confidential treatment pursuant to Rule 24b-2. | |
+ | Indicates a management contract or compensatory plan or arrangement. | |
Item 16. Form 10-K Summary
None.
95
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
REGENERON PHARMACEUTICALS, INC. | |||||
Date: | February 8, 2018 | By: | /s/ LEONARD S. SCHLEIFER | ||
Leonard S. Schleifer, M.D., Ph.D. | |||||
President and Chief Executive Officer | |||||
96
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Leonard S. Schleifer, President and Chief Executive Officer, and Robert E. Landry, Senior Vice President, Finance and Chief Financial Officer, and each of them, his or her true and lawful attorney-in-fact and agent, with the full power of substitution and resubstitution, for him or her and in his or her name, place, and stead, in any and all capacities therewith, to sign any and all amendments to this Annual Report on Form 10-K, and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto each said attorney-in-fact and agent full power and authority to do and perform each and every act and thing requisite and necessary to be done, as fully to all intents and purposes as such person might or could do in person, hereby ratifying and confirming all that each said attorney-in-fact and agent, or either of them, or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated:
Signature | Title | Date | ||
/s/ LEONARD S. SCHLEIFER | President, Chief Executive Officer, and Director (Principal Executive Officer) | February 8, 2018 | ||
Leonard S. Schleifer, M.D., Ph.D. | ||||
/s/ ROBERT E. LANDRY | Senior Vice President, Finance and Chief Financial Officer (Principal Financial Officer) | February 8, 2018 | ||
Robert E. Landry | ||||
/s/ CHRISTOPHER R. FENIMORE | Vice President, Controller (Principal Accounting Officer) | February 8, 2018 | ||
Christopher R. Fenimore | ||||
/s/ GEORGE D. YANCOPOULOS | President, Chief Scientific Officer, and Director | February 8, 2018 | ||
George D. Yancopoulos, M.D., Ph.D. | ||||
/s/ P. ROY VAGELOS | Chairman of the Board | February 8, 2018 | ||
P. Roy Vagelos, M.D. | ||||
/s/ CHARLES A. BAKER | Director | February 8, 2018 | ||
Charles A. Baker | ||||
/s/ BONNIE L. BASSLER | Director | February 8, 2018 | ||
Bonnie L. Bassler, Ph.D. | ||||
/s/ MICHAEL S. BROWN | Director | February 8, 2018 | ||
Michael S. Brown, M.D. | ||||
/s/ N. ANTHONY COLES | Director | February 8, 2018 | ||
N. Anthony Coles, M.D. | ||||
/s/ JOSEPH L. GOLDSTEIN | Director | February 8, 2018 | ||
Joseph L. Goldstein, M.D. | ||||
/s/ CHRISTINE A. POON | Director | February 8, 2018 | ||
Christine A. Poon | ||||
/s/ ARTHUR F. RYAN | Director | February 8, 2018 | ||
Arthur F. Ryan | ||||
/s/ GEORGE L. SING | Director | February 8, 2018 | ||
George L. Sing | ||||
/s/ MARC TESSIER-LAVIGNE | Director | February 8, 2018 | ||
Marc Tessier-Lavigne, Ph.D. | ||||
/s/ HUDA Y. ZOGHBI | Director | February 8, 2018 | ||
Huda Y. Zoghbi, M.D. | ||||
97
REGENERON PHARMACEUTICALS, INC.
INDEX TO FINANCIAL STATEMENTS
Page Numbers | ||
F- 1
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of
Regeneron Pharmaceuticals, Inc.:
Opinions on the Financial Statements and Internal Control over Financial Reporting
We have audited the accompanying consolidated balance sheets of Regeneron Pharmaceuticals, Inc. and its subsidiaries as of December 31, 2017 and 2016, and the related consolidated statements of operations and comprehensive income; stockholders' equity and cash flows for each of the three years in the period ended December 31, 2017, including the related notes (collectively referred to as the “consolidated financial statements”). We also have audited the Company's internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2017 and 2016, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2017 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the COSO.
Basis for Opinions
The Company's management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in Management's Report on Internal Control Over Financial Reporting under Item 9A. Our responsibility is to express opinions on the Company's consolidated financial statements and on the Company's internal control over financial reporting based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) ("PCAOB") and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud, and whether effective internal control over financial reporting was maintained in all material respects.
Our audits of the consolidated financial statements included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
Definition and Limitations of Internal Control over Financial Reporting
A company's internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company's internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company's assets that could have a material effect on the financial statements.
F- 2
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
Florham Park, New Jersey
February 8, 2018
We have served as the Company’s auditor since 1989.
F- 3
REGENERON PHARMACEUTICALS, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share data)
December 31, | |||||||
2017 | 2016 | ||||||
ASSETS | |||||||
Current assets: | |||||||
Cash and cash equivalents | $ | 812,733 | $ | 535,203 | |||
Marketable securities | 596,847 | 503,481 | |||||
Accounts receivable - trade, net | 1,538,642 | 1,343,368 | |||||
Accounts receivable from Sanofi | 193,684 | 92,989 | |||||
Accounts receivable from Bayer | 242,014 | 175,263 | |||||
Inventories | 726,138 | 399,356 | |||||
Prepaid expenses and other current assets | 224,972 | 130,528 | |||||
Total current assets | 4,335,030 | 3,180,188 | |||||
Marketable securities | 1,486,494 | 864,260 | |||||
Property, plant, and equipment, net | 2,358,605 | 2,083,421 | |||||
Deferred tax assets | 506,291 | 825,303 | |||||
Other assets | 77,866 | 20,294 | |||||
Total assets | $ | 8,764,286 | $ | 6,973,466 | |||
LIABILITIES AND STOCKHOLDERS' EQUITY | |||||||
Current liabilities: | |||||||
Accounts payable and accrued expenses | $ | 815,078 | $ | 879,096 | |||
Capital and facility lease obligations | — | 129,557 | |||||
Deferred revenue from Sanofi, current portion | 177,746 | 115,267 | |||||
Deferred revenue - other, current portion | 142,392 | 116,397 | |||||
Other current liabilities | 267 | 1,178 | |||||
Total current liabilities | 1,135,483 | 1,241,495 | |||||
Capital and facility lease obligations | 703,453 | 351,569 | |||||
Deferred revenue from Sanofi | 379,936 | 503,474 | |||||
Deferred revenue - other | 249,263 | 327,298 | |||||
Other long-term liabilities | 152,073 | 100,385 | |||||
Total liabilities | 2,620,208 | 2,524,221 | |||||
Commitments and contingencies (Note 12) | |||||||
Stockholders' equity: | |||||||
Preferred Stock, $.01 par value; 30,000,000 shares authorized; issued and outstanding - none | — | — | |||||
Class A Stock, convertible, $.001 par value; 40,000,000 shares authorized; shares issued and outstanding - 1,911,354 in 2017 and 1,911,456 in 2016 | 2 | 2 | |||||
Common Stock, $.001 par value; 320,000,000 shares authorized; shares issued - 109,477,222 in 2017 and 107,860,567 in 2016 | 110 | 108 | |||||
Additional paid-in capital | 3,512,833 | 3,029,993 | |||||
Retained earnings | 2,946,733 | 1,748,222 | |||||
Accumulated other comprehensive income (loss) | 640 | (12,840 | ) | ||||
Treasury Stock, at cost; 3,763,868 shares in 2017 and 2016 | (316,240 | ) | (316,240 | ) | |||
Total stockholders' equity | 6,144,078 | 4,449,245 | |||||
Total liabilities and stockholders' equity | $ | 8,764,286 | $ | 6,973,466 | |||
The accompanying notes are an integral part of the financial statements. | |||||||
F- 4
REGENERON PHARMACEUTICALS, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE INCOME
(In thousands, except per share data)
Year Ended December 31, | ||||||||||||
2017 | 2016 | 2015 | ||||||||||
Statements of Operations | ||||||||||||
Revenues: | ||||||||||||
Net product sales | $ | 3,718,463 | $ | 3,338,390 | $ | 2,689,478 | ||||||
Sanofi collaboration revenue | 877,193 | 658,665 | 758,873 | |||||||||
Bayer collaboration revenue | 938,052 | 744,270 | 580,488 | |||||||||
Other revenue | 338,519 | 119,102 | 74,889 | |||||||||
5,872,227 | 4,860,427 | 4,103,728 | ||||||||||
Expenses: | ||||||||||||
Research and development | 2,075,142 | 2,052,295 | 1,620,577 | |||||||||
Selling, general, and administrative | 1,320,433 | 1,177,697 | 838,526 | |||||||||
Cost of goods sold | 202,507 | 194,624 | 241,702 | |||||||||
Cost of collaboration and contract manufacturing | 194,554 | 105,070 | 151,007 | |||||||||
3,792,636 | 3,529,686 | 2,851,812 | ||||||||||
Income from operations | 2,079,591 | 1,330,741 | 1,251,916 | |||||||||
Other income (expense): | ||||||||||||
Other income (expense), net | 24,039 | 6,269 | (12,578 | ) | ||||||||
Interest expense | (25,119 | ) | (7,195 | ) | (14,241 | ) | ||||||
(1,080 | ) | (926 | ) | (26,819 | ) | |||||||
Income before income taxes | 2,078,511 | 1,329,815 | 1,225,097 | |||||||||
Income tax expense | (880,000 | ) | (434,293 | ) | (589,041 | ) | ||||||
Net income | $ | 1,198,511 | $ | 895,522 | $ | 636,056 | ||||||
Net income per share - basic | $ | 11.27 | $ | 8.55 | $ | 6.17 | ||||||
Net income per share - diluted | $ | 10.34 | $ | 7.70 | $ | 5.52 | ||||||
Weighted average shares outstanding - basic | 106,338 | 104,719 | 103,061 | |||||||||
Weighted average shares outstanding - diluted | 115,954 | 116,367 | 115,230 | |||||||||
Statements of Comprehensive Income | ||||||||||||
Net income | $ | 1,198,511 | $ | 895,522 | $ | 636,056 | ||||||
Other comprehensive income (loss), net of tax: | ||||||||||||
Unrealized gain (loss) on marketable securities | 12,715 | (21,412 | ) | (43,679 | ) | |||||||
Unrealized gain on cash flow hedges | 765 | — | — | |||||||||
Comprehensive income | $ | 1,211,991 | $ | 874,110 | $ | 592,377 | ||||||
The accompanying notes are an integral part of the financial statements. | ||||||||||||
F- 5
REGENERON PHARMACEUTICALS, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
For the Years Ended December 31, 2017, 2016, and 2015
(In thousands)
Class A Stock | Common Stock | Additional Paid-in Capital | Retained Earnings | Accumulated Other Comprehensive Income (Loss) | Treasury Stock | Total Stockholders' Equity | |||||||||||||||||||||||||||||||
Shares | Amount | Shares | Amount | Shares | Amount | ||||||||||||||||||||||||||||||||
Balance, December 31, 2014 | 1,973 | $ | 2 | 102,475 | $ | 102 | $ | 2,450,782 | $ | 216,644 | $ | 52,251 | (2,018 | ) | $ | (169,530 | ) | $ | 2,550,251 | ||||||||||||||||||
Issuance of Common Stock in connection with exercise of stock options | — | — | 2,457 | 2 | 215,460 | — | — | — | — | 215,462 | |||||||||||||||||||||||||||
Common Stock tendered upon exercise of stock options and vesting of restricted stock in connection with employee tax obligations | — | — | (298 | ) | — | (160,538 | ) | — | — | — | — | (160,538 | ) | ||||||||||||||||||||||||
Issuance of Common Stock in connection with conversion of convertible notes | — | — | 1,625 | 2 | 818,358 | — | — | — | — | 818,360 | |||||||||||||||||||||||||||
Issuance of Common Stock in connection with Company 401(k) Savings Plan | — | — | 31 | — | 15,382 | — | — | — | — | 15,382 | |||||||||||||||||||||||||||
Issuance of restricted stock under Long-Term Incentive Plan | — | — | 28 | — | — | — | — | — | — | — | |||||||||||||||||||||||||||
Class A Stock converted to Common Stock | (60 | ) | — | 60 | — | — | — | — | — | — | — | ||||||||||||||||||||||||||
Stock-based compensation charges | — | — | — | — | 464,022 | — | — | — | — | 464,022 | |||||||||||||||||||||||||||
Excess tax benefit from stock-based compensation | — | — | — | — | 405,317 | — | — | — | — | 405,317 | |||||||||||||||||||||||||||
Acquisition of Common Stock in connection with exercise of convertible note hedges | — | — | — | — | 136,539 | — | — | (1,625 | ) | (136,539 | ) | — | |||||||||||||||||||||||||
Reduction of warrants | — | — | — | — | (449,456 | ) | — | — | — | — | (449,456 | ) | |||||||||||||||||||||||||
Reclassification of warrant liability | — | — | — | — | 23,317 | — | — | — | — | 23,317 | |||||||||||||||||||||||||||
Reduction of equity component of convertible notes | — | — | — | — | (819,657 | ) | — | — | — | — | (819,657 | ) | |||||||||||||||||||||||||
Net income | — | — | — | — | — | 636,056 | — | — | — | 636,056 | |||||||||||||||||||||||||||
Other comprehensive loss, net of tax | — | — | — | — | — | — | (43,679 | ) | — | — | (43,679 | ) | |||||||||||||||||||||||||
Balance, December 31, 2015 | 1,913 | 2 | 106,378 | 106 | 3,099,526 | 852,700 | 8,572 | (3,643 | ) | (306,069 | ) | 3,654,837 | |||||||||||||||||||||||||
Issuance of Common Stock in connection with exercise of stock options | — | — | 1,697 | 2 | 115,180 | — | — | — | — | 115,182 | |||||||||||||||||||||||||||
Common Stock tendered upon exercise of stock options and vesting of restricted stock in connection with employee tax obligations | — | — | (382 | ) | — | (143,182 | ) | — | — | — | — | (143,182 | ) | ||||||||||||||||||||||||
Issuance of Common Stock in connection with conversion of convertible notes | — | — | 121 | — | 48,004 | — | — | — | — | 48,004 | |||||||||||||||||||||||||||
F- 6
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY (continued) | |||||||||||||||||||||||||||||||||||||
Class A Stock | Common Stock | Additional Paid-in Capital | Retained Earnings | Accumulated Other Comprehensive Income (Loss) | Treasury Stock | Total Stockholders' Equity | |||||||||||||||||||||||||||||||
Shares | Amount | Shares | Amount | Shares | Amount | ||||||||||||||||||||||||||||||||
Issuance of Common Stock in connection with Company 401(k) Savings Plan | — | — | 27 | — | 16,561 | — | — | — | — | 16,561 | |||||||||||||||||||||||||||
Issuance of restricted stock under Long-Term Incentive Plan | — | — | 17 | — | — | — | — | — | — | — | |||||||||||||||||||||||||||
Class A Stock converted to Common Stock | (2 | ) | — | 2 | — | — | — | — | — | — | — | ||||||||||||||||||||||||||
Stock-based compensation charges | — | — | — | — | 574,887 | — | — | — | — | 574,887 | |||||||||||||||||||||||||||
Acquisition of Common Stock in connection with exercise of convertible note hedges | — | — | — | — | 10,171 | — | — | (121 | ) | (10,171 | ) | — | |||||||||||||||||||||||||
Reduction of warrants | — | — | — | — | (643,365 | ) | — | — | — | — | (643,365 | ) | |||||||||||||||||||||||||
Reduction of equity component of convertible notes | — | — | — | — | (47,789 | ) | — | — | — | — | (47,789 | ) | |||||||||||||||||||||||||
Net income | — | — | — | — | — | 895,522 | — | — | — | 895,522 | |||||||||||||||||||||||||||
Other comprehensive loss, net of tax | — | — | — | — | — | — | (21,412 | ) | — | — | (21,412 | ) | |||||||||||||||||||||||||
Balance, December 31, 2016 | 1,911 | 2 | 107,860 | 108 | 3,029,993 | 1,748,222 | (12,840 | ) | (3,764 | ) | (316,240 | ) | 4,449,245 | ||||||||||||||||||||||||
Issuance of Common Stock in connection with exercise of stock options | — | — | 2,249 | 2 | 240,578 | — | — | — | — | 240,580 | |||||||||||||||||||||||||||
Common Stock tendered upon exercise of stock options in connection with employee tax obligations | — | — | (481 | ) | — | (201,621 | ) | — | — | — | — | (201,621 | ) | ||||||||||||||||||||||||
Issuance of restricted stock under Long-Term Incentive Plan | — | — | 63 | — | — | — | — | — | — | — | |||||||||||||||||||||||||||
Common Stock tendered upon vesting of restricted stock in connection with employee tax obligations | — | — | (259 | ) | — | (100,067 | ) | — | — | — | — | (100,067 | ) | ||||||||||||||||||||||||
Issuance of Common Stock in connection with Company 401(k) Savings Plan | — | — | 45 | — | 19,416 | — | — | — | — | 19,416 | |||||||||||||||||||||||||||
Stock-based compensation charges | — | — | — | — | 524,534 | — | — | — | — | 524,534 | |||||||||||||||||||||||||||
Net income | — | — | — | — | — | 1,198,511 | — | — | — | 1,198,511 | |||||||||||||||||||||||||||
Other comprehensive income, net of tax | — | — | — | — | — | — | 13,480 | — | — | 13,480 | |||||||||||||||||||||||||||
Balance, December 31, 2017 | 1,911 | $ | 2 | 109,477 | $ | 110 | $ | 3,512,833 | $ | 2,946,733 | $ | 640 | (3,764 | ) | $ | (316,240 | ) | $ | 6,144,078 | ||||||||||||||||||
The accompanying notes are an integral part of the financial statements. | |||||||||||||||||||||||||||||||||||||
F- 7
REGENERON PHARMACEUTICALS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
Year Ended December 31, | ||||||||||||
2017 | 2016 | 2015 | ||||||||||
Cash flows from operating activities: | ||||||||||||
Net income | $ | 1,198,511 | $ | 895,522 | $ | 636,056 | ||||||
Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||||
Depreciation and amortization | 145,467 | 104,745 | 74,909 | |||||||||
Non-cash compensation expense | 507,277 | 559,878 | 459,049 | |||||||||
Other non-cash charges and expenses, net | 63,581 | 45,139 | 52,562 | |||||||||
Deferred taxes | 318,809 | (360,078 | ) | (121,623 | ) | |||||||
Changes in assets and liabilities: | ||||||||||||
Increase in Sanofi, Bayer, and trade accounts receivable | (362,720 | ) | (143,827 | ) | (491,421 | ) | ||||||
Increase in inventories | (314,195 | ) | (149,776 | ) | (111,825 | ) | ||||||
(Increase) decrease in prepaid expenses and other assets | (113,331 | ) | 23,543 | (79,476 | ) | |||||||
(Decrease) increase in deferred revenue | (113,099 | ) | 244,270 | 608,892 | ||||||||
(Decrease) increase in accounts payable, accrued expenses, and other liabilities | (23,188 | ) | 253,980 | 303,657 | ||||||||
Total adjustments | 108,601 | 577,874 | 694,724 | |||||||||
Net cash provided by operating activities | 1,307,112 | 1,473,396 | 1,330,780 | |||||||||
Cash flows from investing activities: | ||||||||||||
Purchases of marketable and other securities | (1,277,140 | ) | (809,419 | ) | (557,105 | ) | ||||||
Sales or maturities of marketable securities | 544,584 | 274,456 | 327,437 | |||||||||
Capital expenditures | (272,626 | ) | (511,941 | ) | (677,933 | ) | ||||||
Net cash used in investing activities | (1,005,182 | ) | (1,046,904 | ) | (907,601 | ) | ||||||
Cash flows from financing activities: | ||||||||||||
Proceeds in connection with capital and facility lease obligations | 57,000 | 5,085 | 27,373 | |||||||||
Payments in connection with capital and facility lease obligations | (19,925 | ) | (32,774 | ) | (1,353 | ) | ||||||
Repayments of convertible senior notes | — | (12,894 | ) | (166,467 | ) | |||||||
Payments in connection with reduction of outstanding warrants | — | (643,365 | ) | (573,487 | ) | |||||||
Proceeds from issuance of Common Stock | 240,213 | 126,739 | 206,358 | |||||||||
Payments in connection with Common Stock tendered for employee tax obligations | (301,688 | ) | (143,182 | ) | (160,537 | ) | ||||||
Excess tax benefit from stock-based compensation | — | — | 405,317 | |||||||||
Net cash used in financing activities | (24,400 | ) | (700,391 | ) | (262,796 | ) | ||||||
Net increase (decrease) in cash and cash equivalents | 277,530 | (273,899 | ) | 160,383 | ||||||||
Cash and cash equivalents at beginning of period | 535,203 | 809,102 | 648,719 | |||||||||
Cash and cash equivalents at end of period | $ | 812,733 | $ | 535,203 | $ | 809,102 | ||||||
Supplemental disclosure of cash flow information | ||||||||||||
Cash paid for interest (net of amounts capitalized) | $ | 18,678 | $ | 5,454 | $ | 10,582 | ||||||
Cash paid for income taxes | $ | 754,843 | $ | 481,360 | $ | 276,092 | ||||||
The accompanying notes are an integral part of the financial statements. | ||||||||||||
F- 8
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
(Unless otherwise noted, dollars in thousands, except per share data)
1. Business Overview and Summary of Significant Accounting Policies
Organization and Business
Regeneron Pharmaceuticals, Inc. and its subsidiaries (collectively, the "Company" or "Regeneron") is a fully integrated biopharmaceutical company that discovers, invents, develops, manufactures, and commercializes medicines for the treatment of serious diseases. The Company's commercialized medicines and product candidates in development are designed to help patients with eye disease, allergic and inflammatory diseases, heart disease, pain, cancer, and infectious and other serious medical conditions. The Company's products that have received marketing approval consist of EYLEA® (aflibercept), Dupixent® (dupilumab), Praluent® (alirocumab), Kevzara® (sarilumab), ARCALYST® (rilonacept), and ZALTRAP® (ziv-aflibercept). The Company is a party to collaboration agreements to develop and commercialize, as applicable, certain products and product candidates (see Note 3).
The Company operates in one business segment, which includes all activities related to the discovery, development, and commercialization of pharmaceutical products for the treatment of serious medical conditions. The Company's business is subject to certain risks including, but not limited to, uncertainties relating to conducting pharmaceutical research, product development, obtaining regulatory approvals, market acceptance, competition, and obtaining and enforcing patents.
Basis of Presentation
The consolidated financial statements include the accounts of Regeneron and its wholly-owned subsidiaries. Intercompany balances and transactions are eliminated in consolidation. Certain reclassifications have been made to prior period amounts to conform with the current period's presentation.
Use of Estimates
The preparation of financial statements in conformity with generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Actual results could differ from those estimates. Estimates which could have a significant impact on the Company's financial statements include provisions related to product sales, such as rebates, chargebacks, and distribution-related fees; periods over which payments, including non-refundable up-front, license, and milestone payments, are recognized as revenue in connection with collaboration and other agreements; periods over which certain clinical trial costs are recognized; fair value of stock options; inventory that may expire prior to expected sale or has a cost basis in excess of its estimated realizable value; capitalization of inventory costs associated with the Company's products prior to regulatory approval; provisions for loss contingencies; deferred tax asset valuation allowances; the assessment of uncertain tax positions; and the provisional amount recorded in connection with the enactment of tax laws (see Note 16).
With respect to the Company's collaborations with Sanofi and Bayer:
• | Included in Sanofi collaboration revenue is the Company's share of profits or losses from commercialization of antibodies, which is provided by Sanofi, and includes an estimate of the Company's share of profits or losses for the most recent fiscal quarter. |
• | Included in Bayer collaboration revenue is the Company's share of profits or losses from commercialization of EYLEA outside the United States, which is provided by Bayer, and includes an estimate of the Company's share of profits or losses for the most recent fiscal quarter. |
• | Included in research and development expenses is the Company's share of development expenses incurred by Bayer and Sanofi, including the Company's share of Bayer and Sanofi estimated development expenses for the most recent fiscal quarter. |
These estimates for the most recent period are adjusted on a prospective basis, if necessary, in the subsequent period to reflect actual amounts.
Cash and Cash Equivalents
The Company considers all highly liquid debt instruments with a maturity of three months or less when purchased to be cash equivalents. The carrying amount reported in the Consolidated Balance Sheet for cash and cash equivalents approximates its fair value.
F- 9
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Marketable Securities
The Company has an investment policy that includes guidelines on acceptable investment securities, minimum credit quality, maturity parameters, and concentration and diversification. The Company invests its excess cash primarily in marketable securities issued by investment grade institutions. The Company considers its marketable securities to be "available-for-sale," as defined by authoritative guidance issued by the Financial Accounting Standards Board ("FASB"). These assets are carried at fair value and the unrealized gains and losses are included in accumulated other comprehensive income (loss). Realized gains and losses on marketable securities are included as a component of other income (expense), net. The Company reviews its portfolio of marketable securities, using both quantitative and qualitative factors, to determine if declines in fair value below cost are other-than-temporary. If a decline in the fair value of a marketable security in the Company's investment portfolio is deemed to be other-than-temporary, the Company writes down the cost basis of the security to its current fair value and recognizes a loss as a charge against income.
Accounts Receivable - Trade
The Company's trade accounts receivable arise from product sales and represent amounts due from its distributors and specialty pharmacies (collectively, the Company's "customers"), which are all located in the United States. The Company monitors the financial performance and credit worthiness of its large customers so that it can properly assess and respond to changes in their credit profile. The Company provides reserves against trade receivables for estimated losses, if any, that may result from a customer's inability to pay. Amounts determined to be uncollectible are written-off against the reserve.
Inventories
Inventories are stated at the lower of cost or estimated realizable value. The Company determines the cost of inventory using the first-in, first-out, or FIFO, method.
The Company capitalizes inventory costs associated with the Company's products prior to regulatory approval when, based on management's judgment, future commercialization is considered probable and the future economic benefit is expected to be realized; otherwise, such costs are expensed as research and development. The determination to capitalize inventory costs is based on various factors, including status and expectations of the regulatory approval process, any known safety or efficacy concerns, potential labeling restrictions, and any other impediments to obtaining regulatory approval.
The Company periodically analyzes its inventory levels to identify inventory that may expire prior to expected sale or has a cost basis in excess of its estimated realizable value, and writes-down such inventories as appropriate. In addition, the Company's products are subject to strict quality control and monitoring which the Company performs throughout the manufacturing process. If certain batches or units of product no longer meet quality specifications or become obsolete due to expiration, the Company records a charge to write down such unmarketable inventory to its estimated realizable value.
Property, Plant, and Equipment
Property, plant, and equipment are stated at cost, net of accumulated depreciation. Depreciation is provided on a straight-line basis over the estimated useful lives of the assets. Leasehold improvements are amortized over the shorter of the estimated useful lives of the assets or the lease term. Costs of construction of certain long-lived assets include capitalized interest, which is amortized over the estimated useful life of the related asset. Expenditures for maintenance and repairs which do not materially extend the useful lives of the assets are charged to expense as incurred. The cost and accumulated depreciation or amortization of assets retired or sold are removed from the respective accounts, and any gain or loss is recognized in operations. The estimated useful lives of property, plant, and equipment are as follows:
Building and improvements | 10–50 years | |
Laboratory and other equipment | 3–10 years | |
Furniture and fixtures | 5 years | |
The Company periodically assesses the recoverability of long-lived assets, such as property, plant, and equipment, and evaluates such assets for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable.
F- 10
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Revenue Recognition
a. Product Revenue
Product revenue consists of U.S. sales of EYLEA and ARCALYST. Revenue from product sales is recognized when persuasive evidence of an arrangement exists, title to product and associated risk of loss have passed to the customer, the price is fixed or determinable, collection from the customer is reasonably assured, the Company has no further performance obligations, and returns can be reasonably estimated. The Company's written contracts with its customers stipulate product is shipped freight on board destination (FOB destination). The Company records revenue from product sales upon delivery to its customers.
The Company sells EYLEA in the United States to several distributors and specialty pharmacies. The Company sells ARCALYST in the United States to specialty pharmacies. Under these distribution models, the distributors and specialty pharmacies generally take physical delivery of product. For EYLEA, the distributors and specialty pharmacies generally sell the product directly to healthcare providers, whereas for ARCALYST, the specialty pharmacies sell the product directly to patients.
Revenue from product sales is recorded net of applicable provisions for rebates and chargebacks under governmental and other programs, distribution-related fees, and other sales-related deductions. Calculating these provisions involves estimates and judgments. The Company reviews its estimates of rebates, chargebacks, and other applicable provisions each period and records any necessary adjustments in the current period's net product sales.
Government Rebates and Chargebacks: The Company estimates reductions to product sales for Medicaid and Veterans' Administration ("VA") programs, and for certain other qualifying federal and state government programs. Based upon the Company's contracts with government agencies, statutorily-defined discounts applicable to government-funded programs, historical experience, and estimated payer mix, the Company estimates and records an allowance for rebates and chargebacks. The Company's liability for Medicaid rebates consists of estimates for claims that a state will make for a current quarter, claims for prior quarters that have been estimated for which an invoice has not been received, and invoices received for claims from prior quarters that have not been paid. The Company's reserves related to discounted pricing to VA, Public Health Services ("PHS"), and other institutions (collectively "qualified healthcare providers") represent the Company's estimated obligations resulting from contractual commitments to sell products to qualified healthcare providers at prices lower than the list prices the Company charges to its customers (i.e., distributors and specialty pharmacies). The Company's customers charge the Company for the difference between what they pay for the products and the ultimate selling price to the qualified healthcare providers. The Company's reserve for this discounted pricing is based on expected sales to qualified healthcare providers and the chargebacks that customers have already claimed.
Distribution-Related Fees: The Company has written contracts with its customers that include terms for distribution-related fees. The Company estimates and records distribution and related fees due to its customers generally based on gross sales.
Product Returns: Consistent with industry practice, the Company offers its customers a limited right to return product purchased directly from the Company, which is principally based upon the product's expiration date. The Company will accept returns for three months prior to and up to six months after the product expiration date. Product returned is generally not resalable given the nature of the Company's products and method of administration. The Company develops estimates for product returns based upon historical experience, inventory levels in the distribution channel, shelf life of the product, and other relevant factors. The Company monitors product supply levels in the distribution channel, as well as sales by its customers of EYLEA to healthcare providers and ARCALYST to patients using product-specific data provided by its customers. If necessary, the Company's estimates of product returns may be adjusted in the future based on actual returns experience, known or expected changes in the marketplace, or other factors.
b. Collaboration Revenue
The Company earns collaboration revenue in connection with collaboration agreements to develop and commercialize product candidates and utilize the Company's technology platforms. These arrangements may require the Company to deliver various rights, services, and/or goods across the entire life cycle of a product or product candidate. The terms of these agreements typically include that consideration be provided to the Company in the form of non-refundable up-front payments, milestone payments, payments for development and commercialization activities, and sharing of profits or losses arising from the commercialization of products.
In connection with non-refundable up-front payments, the Company's performance period estimates are principally based on projections of the scope, progress, and results of its research and development activities. Due to the variability in the scope of
F- 11
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
activities and length of time necessary to develop a drug product, changes to development plans as programs progress, and uncertainty in the ultimate requirements to obtain regulatory approval for commercialization, revisions to performance period estimates are likely to occur periodically, and could result in material changes to the amount of revenue recognized each year. In addition, estimated performance periods may change if development programs encounter delays, or the Company and its collaborators decide to expand or contract the clinical plans for a drug candidate in various disease indications.
In arrangements involving multiple deliverables, each required deliverable is evaluated to determine whether it qualifies as a separate unit of accounting. This determination is generally based on whether the deliverables in the arrangement meet certain criteria, including whether the delivered item or items has value to the collaborator on a standalone basis. The arrangement's consideration that is fixed and determinable is allocated to each separate unit of accounting based on the relative selling price of each deliverable. If multiple collaboration activities or rights do not require separation, they are combined into a single unit of accounting and recognized over the performance period, which is the period over which the Company is obligated to deliver goods or services. The Company estimates its performance period based on the specific terms of each agreement, and adjusts the performance periods, if appropriate, based on the applicable facts and circumstances.
Payments which are based on achieving a specific substantive performance milestone, involving a degree of risk, are recognized as revenue when the milestone is achieved and the related payment is due and non-refundable, provided there is no future service obligation associated with that milestone. Substantive performance milestones typically consist of significant achievements in the development life-cycle of the related product candidate, such as completion of clinical trials, filing for approval with regulatory agencies, and receipt of approvals by regulatory agencies. In determining whether a payment is deemed to be a substantive performance milestone, the Company takes into consideration (i) the enhancement in value to the related development product candidate, (ii) the Company's performance and the relative level of effort required to achieve the milestone, (iii) whether the milestone relates solely to past performance, and (iv) whether the milestone payment is considered reasonable relative to all of the deliverables and payment terms. Payments for achieving milestones which are not considered substantive are deferred and recognized over the related performance period.
The Company enters into collaboration agreements that include varying arrangements regarding which parties perform and bear the costs of research and development activities. The Company may share the costs of research and development activities with a collaborator, or the Company may be reimbursed for all or a significant portion of the costs of the Company's research and development activities. The Company records its internal and third-party development costs associated with these collaborations as research and development expenses. When the Company is entitled to reimbursement of all or a portion of the research and development expenses that it incurs under a collaboration, the Company records those reimbursable amounts as collaboration revenue proportionately as the Company recognizes its expenses. If the collaboration is a cost-sharing arrangement in which both the Company and its collaborator perform development work and share costs, the Company also recognizes, as research and development expense in the period when its collaborator incurs development expenses, the portion of the collaborator's development expenses that the Company is obligated to reimburse. The Company may also be obligated to use commercially reasonable efforts to supply commercial bulk product to its collaborators. In such cases, the Company is reimbursed for its manufacturing costs as commercial product is shipped to its collaborators; however, recognition of such cost reimbursements as collaboration revenue is deferred until the product is sold by the Company's collaborators to third-party customers, at which time the Company's risk of inventory loss no longer exists. In addition, at that time, the related manufacturing costs for the sold product, which had been capitalized into inventory, are recognized by the Company.
Under the Company's collaboration agreements, product sales and cost of sales for products which are currently approved are recorded by the Company's collaborators as they are deemed to be the principal in the transaction. The Company shares in any profits or losses arising from the commercialization of such products. The Company records its share of the profits or losses from commercialization of such products as collaboration revenue, representing net product sales less cost of goods sold and shared commercialization and other expenses.
Research and Development Expenses
Research and development expenses include costs directly attributable to the conduct of research and development programs, including the cost of salaries, payroll taxes, employee benefits, materials, supplies, depreciation on and maintenance of research equipment, costs related to research collaboration and licensing agreements, the cost of services provided by outside contractors, including services related to the Company's clinical trials, clinical trial expenses, the full cost of manufacturing drug for use in research, preclinical development, and clinical trials, amounts that the Company is obligated to reimburse to collaborators for research and development expenses that they incur, and the allocable portions of facility costs, such as rent, utilities, insurance, repairs and maintenance, depreciation, and general support services. Costs associated with research and development are expensed.
F- 12
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Clinical trial costs are a significant component of research and development expenses and include costs associated with third-party contractors. The Company outsources a substantial portion of its clinical trial activities, utilizing external entities such as contract research organizations ("CROs"), independent clinical investigators, and other third-party service providers to assist the Company with the execution of its clinical studies. For each clinical trial that the Company conducts, certain clinical trial costs are expensed immediately, while others are expensed over time based on the expected total number of patients in the trial, the rate at which patients enter the trial, and/or the period over which clinical investigators or CROs are expected to provide services.
Clinical activities which relate principally to clinical sites and other administrative functions to manage the Company's clinical trials are performed primarily by CROs. CROs typically perform most of the start-up activities for the Company's trials, including document preparation, site identification, screening and preparation, pre-study visits, training, and program management. These start-up costs usually occur within a few months after the contract has been executed and are event-driven in nature. The remaining activities and related costs, such as patient monitoring and administration, generally occur ratably throughout the life of the individual contract or study. In the event of early termination of a clinical trial, the Company accrues and recognizes expenses in an amount based on its estimate of the remaining non-cancelable obligations associated with the winding down of the clinical trial and/or penalties.
For clinical study sites, where payments are made periodically on a per-patient basis to the institutions performing the clinical study, the Company accrues expenses on an estimated cost-per-patient basis, based on subject enrollment and activity in each quarter. The amount of clinical study expense recognized in a quarter may vary from period to period based on the duration and progress of the study, the activities to be performed by the sites each quarter, the required level of patient enrollment, the rate at which patients actually enroll in and drop-out of the clinical study, and the number of sites involved in the study. Clinical trials that bear the greatest risk of change in estimates are typically those that have a significant number of sites, require a large number of patients, have complex patient screening requirements, and span multiple years. During the course of a trial, the Company adjusts its rate of clinical expense recognition if actual results differ from the Company's estimates. The Company's estimates and assumptions for clinical expense recognition could differ significantly from its actual results, which could cause material increases or decreases in research and development expenses in future periods when the actual results become known.
Stock-based Compensation
The Company recognizes stock-based compensation expense for grants of stock option and restricted stock awards under the Company's Long-Term Incentive Plans to employees and non-employee members of the Company's board of directors based on the grant-date fair value of those awards. The grant-date fair value of an award is generally recognized as compensation expense over the award's requisite service period.
The Company uses the Black-Scholes model to compute the estimated fair value of stock option awards. Using this model, fair value is calculated based on assumptions with respect to (i) expected volatility of the Company's Common Stock price, (ii) the periods of time over which employees and members of the board of directors are expected to hold their options prior to exercise (expected lives), (iii) expected dividend yield on the Common Stock, and (iv) risk-free interest rates. Stock-based compensation expense also includes an estimate, which is made at the time of grant, of the number of awards that are expected to be forfeited. This estimate is revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates.
Income Taxes
The Company recognizes deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements or tax returns. Under this method, deferred tax assets and liabilities are determined on the basis of the difference between the tax basis of assets and liabilities and their respective financial reporting amounts ("temporary differences") at enacted tax rates in effect for the years in which the differences are expected to reverse. A valuation allowance is established for deferred tax assets for which it is more likely than not that some portion or all of the deferred tax assets will not be realized.
Uncertain tax positions, for which management's assessment is that there is more than a 50% probability of sustaining the position upon challenge by a taxing authority based upon its technical merits, are subjected to certain recognition and measurement criteria. The Company re-evaluates uncertain tax positions and consider various factors, including, but not limited to, changes in tax law, the measurement of tax positions taken or expected to be taken in tax returns, and changes in facts or circumstances related to a tax position. The Company adjusts the level of the liability to reflect any subsequent changes in the relevant facts and circumstances surrounding the uncertain positions. The Company recognizes interest and penalties related to income tax matters in income tax expense.
F- 13
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Per Share Data
Basic net income per share is computed by dividing net income by the weighted average number of shares of Common Stock and Class A Stock outstanding. Net income per share is presented on a combined basis, inclusive of Common Stock and Class A Stock outstanding, as each class of stock has equivalent economic rights. Basic net income per share excludes restricted stock awards until vested. Diluted net income per share includes the potential dilutive effect of common stock equivalents as if such securities were converted or exercised during the period, when the effect is dilutive. Common stock equivalents include: (i) outstanding stock options and restricted stock under the Company's Long-Term Incentive Plans, which are included under the "treasury stock method" when dilutive, (ii) if applicable, Common Stock to be issued upon the assumed conversion of the Company's convertible senior notes, which are included under the "if-converted method" when dilutive, and (iii) if applicable, Common Stock to be issued upon the exercise of outstanding warrants, which are included under the "treasury stock method" when dilutive.
Concentration of Credit Risk
Financial instruments which potentially expose the Company to concentrations of credit risk consist of cash, cash equivalents, certain financial instruments, and accounts receivable. A large portion of the Company's cash is held by a few major financial institutions. In accordance with the Company's policies, the Company mandates asset diversification and monitors exposure with its counterparties.
Concentrations of credit risk with respect to accounts receivable are significant. The Company has a concentration of credit risk associated with the receivables due from its collaborators Bayer, Sanofi, and Teva. The Company is also subject to credit risk with accounts receivable from its product sales of EYLEA and ARCALYST, which are due from several distributors and specialty pharmacies (the Company's customers). As of December 31, 2017 and 2016, three individual customers accounted for 99% of the Company's net trade accounts receivable balances. The Company has contractual payment terms with each of its customers, and the Company monitors its customers' financial performance and credit worthiness so that it can properly assess and respond to any changes in their credit profile. In addition, the Company may insure a portion of its accounts receivables within its overall risk management practices. As of December 31, 2017 and 2016, there were no reserves against trade accounts receivable. In addition, during the years ended December 31, 2017, 2016, and 2015, the Company did not recognize any charges for write-offs of trade accounts receivable.
Recently Issued Accounting Standards
In May 2014, the FASB issued Accounting Standards Update 2014-09 ("ASU 2014-09"), Revenue from Contracts with Customers, which, along with subsequent amendments to ASU 2014-09 issued by the FASB, will replace existing revenue recognition guidance. The new standard requires an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. To achieve that core principle, an entity must identify the contract(s) with a customer, identify the performance obligations in the contract, determine the transaction price, allocate the transaction price to the performance obligations in the contract, and recognize revenue when (or as) the entity satisfies the performance obligation. The new standard will be effective for annual and interim reporting periods beginning after December 15, 2017. The standard allows for two transition methods - retrospectively to each prior reporting period presented (full retrospective method) or retrospectively with the cumulative effect of initially applying the standard recognized at the date of initial adoption (modified retrospective method). The Company will adopt the standard using the modified retrospective method. The Company does not currently expect the new standard to have a material impact on total revenues. However, the adoption of the new standard may result in changes to the timing of revenue recognition related to collaboration agreements where the Company has concluded that bundled goods or services are not distinct. As a result, substantive development milestones, which were previously recognized in the period when the milestone was achieved, will be recognized over the remaining performance period under the new standard. The Company has substantially completed its impact assessment, and expects that the adoption of the new standard will require a cumulative-effect adjustment to reduce retained earnings on January 1, 2018 by approximately $140 million, net of tax. In connection with adopting the new standard, the Company does not anticipate implementing significant changes to its internal controls or systems. The Company continues to evaluate the impact of the new guidance on its financial statement disclosures.
In January 2016, the FASB issued Accounting Standards Update 2016-01, Recognition and Measurement of Financial Assets and Financial Liabilities. The amendments require equity investments (except those accounted for under the equity method of accounting or those that result in consolidation of the investee) to be measured at fair value with changes in fair value recognized in net income. In addition, the amendments allow companies to measure equity investments that do not have readily determinable fair values at cost minus impairment, if any, and adjusted for observable price changes in orderly transactions for identical or similar investments of the same issuer. The Company has elected this measurement method for the equity investments it holds as
F- 14
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
of January 1, 2018 that do not have readily determinable fair values. The amendments are effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2017. As of December 31, 2017, the Company's unrealized gain from equity securities was $6.6 million, which was recorded within accumulated other comprehensive income (loss). The Company will record a cumulative-effect adjustment to opening retained earnings for this unrealized gain as of the beginning of the year ending December 31, 2018. The amendments related to equity investments without readily determinable fair values shall be applied prospectively to equity investments that exist as of the date of adoption. The implementation of the amendments is expected to increase the volatility of the Company's net income.
In February 2016, the FASB issued Accounting Standards Update 2016-02, Leases. The new standard requires a lessee to recognize in its balance sheet (for both finance and operating leases) a liability to make lease payments and a right-of-use asset representing its right to use the underlying asset for the lease term. The amendments are effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2018. Early adoption is permitted; however, the Company expects to adopt this standard in the first quarter of 2019. The Company is evaluating the impact that this guidance will have on the Company's financial statements, including related disclosures, and expects the new standard to have a significant impact on its internal controls, systems, and processes.
2. Product Sales
Net product sales consist of the following:
Year Ended December 31, | ||||||||||||
Net Product Sales in the United States | 2017 | 2016 | 2015 | |||||||||
EYLEA | $ | 3,701,917 | $ | 3,323,081 | $ | 2,676,040 | ||||||
ARCALYST | 16,546 | 15,309 | 13,438 | |||||||||
Net Product Sales | $ | 3,718,463 | $ | 3,338,390 | $ | 2,689,478 | ||||||
The Company had product sales to certain customers that accounted for more than 10% of total gross product revenue for each of the years ended December 31, 2017, 2016, and 2015. Sales to each of these customers as a percentage of the Company's total gross product revenue are as follows:
Year Ended December 31, | ||||||||
2017 | 2016 | 2015 | ||||||
Besse Medical, a subsidiary of AmerisourceBergen Corporation | 51 | % | 55 | % | 67 | % | ||
McKesson Corporation | 29 | % | 28 | % | 26 | % | ||
Curascript SD Specialty Distribution, a subsidiary of Express Scripts | 19 | % | 16 | % | ** | |||
** For the year ended December 31, 2015, sales to Curascript SD Specialty Distribution represented less than 10% of total gross product revenue.
F- 15
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Revenue from product sales is recorded net of applicable provisions for rebates and chargebacks, distribution-related fees, and other sales-related deductions. Accruals for chargebacks are recorded as a direct reduction to accounts receivable and accruals for rebates and distribution-related fees are recorded within accrued liabilities. The following table summarizes the provisions, and credits/payments, for these sales-related deductions for the years ended December 31, 2017, 2016, and 2015.
Rebates & Chargebacks | Distribution- Related Fees | Other Sales- Related Deductions | Total | ||||||||||||
Balance as of December 31, 2014 | $ | 3,083 | $ | 21,166 | $ | 532 | $ | 24,781 | |||||||
Provisions | 61,124 | 122,466 | 9,600 | 193,190 | |||||||||||
Credits/payments | (57,788 | ) | (95,319 | ) | (9,615 | ) | (162,722 | ) | |||||||
Balance as of December 31, 2015 | 6,419 | 48,313 | 517 | 55,249 | |||||||||||
Provisions | 93,385 | 154,477 | 30,442 | 278,304 | |||||||||||
Credits/payments | (87,092 | ) | (173,325 | ) | (27,285 | ) | (287,702 | ) | |||||||
Balance as of December 31, 2016 | 12,712 | 29,465 | 3,674 | 45,851 | |||||||||||
Provisions | 167,755 | 194,132 | 46,383 | 408,270 | |||||||||||
Credits/payments | (150,627 | ) | (189,455 | ) | (28,737 | ) | (368,819 | ) | |||||||
Balance as of December 31, 2017 | $ | 29,840 | $ | 34,142 | $ | 21,320 | $ | 85,302 | |||||||
3. Collaboration and License Agreements
The Company has entered into various agreements related to its activities to research, develop, manufacture, and commercialize product candidates and utilize its technology platforms. Significant agreements of this kind are described below.
a. Sanofi
Sanofi owned a total of 23,880,537 shares of the Company's Common Stock as of December 31, 2017, a portion of which was purchased in connection with the companies' ZALTRAP and antibody collaborations described below. See Note 13 for a description of the investor agreement between Sanofi and the Company.
F- 16
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
The collaboration revenue the Company earned from Sanofi is detailed below:
Year Ended December 31, | ||||||||||||
Sanofi Collaboration Revenue | 2017 | 2016 | 2015 | |||||||||
Antibody: | ||||||||||||
Reimbursement of Regeneron research and development expenses | $ | 508,364 | $ | 564,900 | $ | 735,439 | ||||||
Reimbursement of Regeneron commercialization-related expenses | 368,859 | 305,947 | 155,271 | |||||||||
Regeneron's share of losses in connection with commercialization of antibodies | (442,610 | ) | (459,058 | ) | (240,042 | ) | ||||||
Other | 119,076 | 28,379 | 12,322 | |||||||||
Total Antibody | 553,689 | 440,168 | 662,990 | |||||||||
Immuno-oncology: | ||||||||||||
Reimbursement of Regeneron research and development expenses | 239,981 | 138,497 | 39,961 | |||||||||
Other | 83,523 | 80,000 | 40,000 | |||||||||
Total Immuno-oncology | 323,504 | 218,497 | 79,961 | |||||||||
ZALTRAP: | ||||||||||||
Reimbursement of Regeneron research and development expenses | — | — | 686 | |||||||||
Other | — | — | 15,236 | |||||||||
Total ZALTRAP | — | — | 15,922 | |||||||||
$ | 877,193 | $ | 658,665 | $ | 758,873 | |||||||
Other selected financial information in connection with the Company's collaboration agreements with Sanofi is as follows:
As of December 31, | ||||||||
2017 | 2016 | |||||||
Antibody: | ||||||||
Accounts receivable, net | $ | 121,001 | $ | 47,268 | ||||
Deferred revenue | $ | 117,682 | $ | 98,741 | ||||
Immuno-oncology: | ||||||||
Accounts receivable, net | $ | 59,274 | $ | 40,647 | ||||
Deferred revenue | $ | 440,000 | $ | 520,000 | ||||
F- 17
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Antibodies
In November 2007, the Company entered into a global, strategic collaboration with Sanofi to discover, develop, and commercialize fully human monoclonal antibodies (the "Antibody Collaboration"). The Antibody Collaboration was governed by the companies' Discovery and Preclinical Development Agreement ("Antibody Discovery Agreement") and a License and Collaboration Agreement (each as amended). In connection with the execution of the Antibody Discovery Agreement in 2007, the Company received a non-refundable up-front payment of $85.0 million from Sanofi. In addition, under the Antibody Discovery Agreement, Sanofi funded the Company's research to identify and validate potential drug discovery targets and develop fully human monoclonal antibodies against these targets. Pursuant to the Antibody Discovery Agreement, as amended, Sanofi agreed to fund the Company's research activities up to $145.0 million in 2015, and up to $130.0 million in both 2016 and 2017. The Company's Antibody Discovery Agreement with Sanofi ended on December 31, 2017 without any extension and, therefore, funding from Sanofi under the Antibody Discovery Agreement ceased after 2017. The Company accelerated the recognition of deferred revenue from the $85.0 million up-front payment and other payments in connection with Sanofi's decision to end the Antibody Discovery Agreement between the Company and Sanofi on December 31, 2017. The Company has the right to develop or continue to develop product candidates discovered under the Antibody Discovery Agreement, with the exception of those that are being developed (and commercialized, as applicable) under the Antibody License and Collaboration Agreement, independently or with other collaborators.
Under the License and Collaboration Agreement, agreed-upon worldwide development expenses incurred by both companies are funded by Sanofi, except that following receipt of the first positive Phase 3 trial results for a co-developed drug candidate, subsequent Phase 3 trial-related costs for that drug candidate ("Shared Phase 3 Trial Costs") are shared 80% by Sanofi and 20% by Regeneron. Consequently, the Company recognized as research and development expense $91.8 million, $108.6 million, and $92.6 million in 2017, 2016, and 2015, respectively, its share of antibody development expenses that Sanofi incurred related to Praluent, Kevzara (sarilumab), and, commencing in 2016, Dupixent (dupilumab). If the Antibody Collaboration becomes profitable, Regeneron will be obligated to reimburse Sanofi for 50% of worldwide development expenses that were fully funded by Sanofi and 30% of Shared Phase 3 Trial Costs, in accordance with a defined formula based on the amounts of these expenses and the Company's share of collaboration profits from commercialization of collaboration products. However, the Company is only required to apply 10% of its share of the profits from the Antibody Collaboration in any calendar quarter to reimburse Sanofi for these development costs. The Company's contingent reimbursement obligation to Sanofi under the Antibody Collaboration was approximately $2,558 million as of December 31, 2017.
Effective January 7, 2018, the Company and Sanofi entered into a letter agreement (the "Letter Agreement") in connection with, among other matters, the allocation of additional funds to certain activities relating to the development of dupilumab and REGN3500 and non-approval trials of dupilumab (collectively, the "Dupilumab/REGN3500 Eligible Investments"). Refer to the "Immuno-Oncology" section below for further details regarding the Letter Agreement.
Regeneron is obligated to use commercially reasonable efforts to supply clinical requirements of each drug candidate under the Antibody Collaboration until commercial supplies of that drug candidate are being manufactured. Sanofi leads commercialization activities for products developed under the License and Collaboration Agreement, subject to the Company's right to co-promote such products. The Company has exercised its option to co-promote Praluent, Kevzara, and Dupixent in the United States and thus far has not exercised any of its options to co-promote Praluent, Kevzara, and Dupixent outside the United States. The parties equally share profits and losses from sales within the United States. The parties share profits outside the United States on a sliding scale based on sales starting at 65% (Sanofi)/35% (Regeneron) and ending at 55% (Sanofi)/45% (Regeneron), and losses outside the United States at 55% (Sanofi)/45% (Regeneron). In addition to profit sharing, the Company is entitled to receive up to $250.0 million in sales milestone payments, with milestone payments commencing only if and after aggregate annual sales outside the United States exceed $1.0 billion on a rolling twelve-month basis.
"Reimbursement of Regeneron commercialization-related expenses" in the table above represents reimbursement of internal and external costs in connection with commercializing Praluent, Kevzara, and, effective in 2016, Dupixent. During the same periods that the Company recorded reimbursements from Sanofi related to the Company's commercialization expenses, the Company also recorded its share of losses in connection with the companies commercializing Praluent, Kevzara, and Dupixent within Sanofi collaboration revenue. In March 2017, the U.S. Food and Drug Administration ("FDA") approved Dupixent for the treatment of adult patients with moderate-to-severe atopic dermatitis, and in September 2017, the European Commission granted marketing authorization for Dupixent for use in adults with moderate-to-severe atopic dermatitis who are candidates for systemic therapy. In May 2017, the FDA approved Kevzara for the treatment of adult patients with moderately to severely active rheumatoid
F- 18
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
arthritis, and in June 2017, the European Commission granted marketing authorization for Kevzara for the treatment of rheumatoid arthritis in adult patients.
With respect to each antibody product in development under the License and Collaboration Agreement, Sanofi or the Company may, by giving twelve months' notice, opt-out of further development and/or commercialization of the product, in which event the other party retains exclusive rights to continue the development and/or commercialization of the product. The License and Collaboration Agreement contains other termination provisions, including for material breach by the other party. Upon termination of the collaboration in its entirety, the Company's obligation to reimburse Sanofi for development costs out of any future profits from collaboration products will terminate.
Immuno-Oncology
In July 2015, the Company and Sanofi entered into a collaboration to discover, develop, and commercialize antibody-based cancer treatments in the field of immuno-oncology (the "IO Collaboration"). The IO Collaboration is governed by an Immuno-oncology Discovery and Development Agreement ("IO Discovery Agreement"), and an Immuno-oncology License and Collaboration Agreement ("IO License and Collaboration Agreement"). In connection with the IO Discovery Agreement, Sanofi made a $265.0 million non-refundable up-front payment to the Company. Pursuant to the IO Discovery Agreement, the Company will spend up to $1,090.0 million ("IO Discovery Budget") to identify and validate potential immuno-oncology targets and develop therapeutic antibodies against such targets through clinical proof-of-concept. Sanofi will reimburse the Company for up to $825.0 million ("IO Discovery Funding") of these costs, subject to certain annual limits. The term of the IO Discovery Agreement will continue through the later of five years from the effective date of the IO Collaboration or the date the IO Discovery Budget is exhausted, subject to Sanofi’s option to extend it for up to an additional three years for the continued development (and funding) of selected ongoing programs. Pursuant to the IO Discovery Agreement, the Company is primarily responsible for the design and conduct of all research activities, including target identification and validation, antibody development, preclinical activities, toxicology studies, manufacture of preclinical and clinical supplies, filing of Investigational New Drug ("IND") Applications, and clinical development through proof-of-concept. The Company will reimburse Sanofi for half of the development costs they funded that are attributable to clinical development of antibody product candidates under the IO Discovery Agreement from Regeneron's share of future profits, if any, from commercialized IO Collaboration products to the extent they are sufficient for this purpose. However, the Company is only required to apply 10% of its share of the profits from IO Collaboration products in any calendar quarter towards reimbursing Sanofi for these development costs. The Company's contingent reimbursement obligation to Sanofi under the IO Collaboration was approximately $22 million as of December 31, 2017. With regard to product candidates for which proof-of-concept is established, Sanofi has the option to license rights to the product candidate pursuant to the IO License and Collaboration Agreement (as further described below). If Sanofi does not exercise its option to license rights to a product candidate, the Company will retain the exclusive right to develop and commercialize such product candidate and Sanofi will be entitled to receive a royalty on sales.
In connection with the IO License and Collaboration Agreement, Sanofi made a $375.0 million non-refundable up-front payment to the Company. If Sanofi exercises its option to license rights to a product candidate thereunder, it will co-develop the drug candidate with the Company through product approval. Principal control of development of each product candidate that enters development under the IO License and Collaboration Agreement alternates between the Company and Sanofi on a candidate-by-candidate basis. Sanofi funds drug candidate development costs up front for the candidates for which it is the principal controlling party and the Company will reimburse half of the total development costs for all such candidates from its share of future IO Collaboration profits to the extent they are sufficient for this purpose, subject to the same 10% reimbursement provision described above. In addition, Sanofi and the Company share equally, on an ongoing basis, the development costs for the drug candidates for which the Company is the principal controlling party. The party having principal control over the development of a product candidate also leads the commercialization activities for such product candidate in the United States. For all products commercialized under the IO License and Collaboration Agreement, Sanofi will lead commercialization activities outside of the United States. Each party will have the right to co-promote licensed products in countries where it is not the lead commercialization party. The parties will share equally in profits and losses in connection with the commercialization of collaboration products. The Company is obligated to use commercially reasonable efforts to supply clinical requirements of each drug candidate under the IO License and Collaboration Agreement until commercial supplies of that IO drug candidate are being manufactured.
Under the terms of the IO License and Collaboration Agreement, the parties are co-developing the Company’s antibody product candidate (cemiplimab) targeting the receptor known as programmed cell death protein 1 (PD-1). The parties share equally, on an ongoing basis, development expenses for cemiplimab up to a total of $1.640 billion, an increase of $990.0 million over the budget set forth in the original IO License and Collaboration Agreement. The cemiplimab development budget has been increased pursuant
F- 19
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
to the Letter Agreement. Pursuant to the Letter Agreement, the Company has agreed to allow Sanofi to satisfy in whole or in part its funding obligations with respect to cemiplimab development and Dupilumab/REGN3500 Eligible Investments by selling up to 1,400,000 shares of the Company's Common Stock directly or indirectly owned by Sanofi through September 30, 2020. If Sanofi desires to sell shares of the Company's Common Stock during the term of the Letter Agreement to satisfy a portion or all of its funding obligations for the cemiplimab development and/or Dupilumab/REGN3500 Eligible Investments, the Company may elect to purchase, in whole or in part, such shares from Sanofi. If the Company does not elect to purchase such shares, Sanofi may sell the applicable number of shares (subject to certain daily and quarterly limits) in one or more open-market transactions.
The Company has principal control over the development of cemiplimab and will lead commercialization activities in the United States, subject to Sanofi’s right to co-promote, while Sanofi will lead commercialization activities outside of the United States and the parties will equally share profits from worldwide sales. The Company will be entitled to a milestone payment of $375.0 million in the event that global sales of certain licensed products targeting PD-1 (including cemiplimab), together with sales of any other products licensed under the IO License and Collaboration Agreement and sold for use in combination with any of such licensed products targeting PD-1, equal or exceed $2.0 billion in any consecutive twelve-month period.
With respect to each product candidate that enters development under the IO License and Collaboration Agreement, Sanofi or the Company may, by giving twelve months’ notice, opt-out of further development and/or commercialization of the product, in which event the other party will retain exclusive rights to continue the development and/or commercialization of such product.
At the inception of the IO Collaboration, the Company's significant deliverables consisted of (i) license to certain rights and intellectual property, (ii) providing research and development services, and (iii) manufacturing clinical supplies. The Company concluded that the license did not have standalone value, primarily due to the fact that such rights were not sold separately by the Company, nor could Sanofi receive any benefit from the license without the fulfillment of other ongoing obligations by the Company, including the clinical supply arrangement. Therefore, the deliverables were considered a single unit of accounting. Consequently, the $640.0 million in aggregate up-front payments made by Sanofi during 2015 in connection with the execution of the IO Collaboration has been recorded as deferred revenue, and is being recognized as revenue over the related performance period.
ZALTRAP
In September 2003, the Company entered into a collaboration agreement ("ZALTRAP Collaboration Agreement") with Aventis Pharmaceuticals Inc. (predecessor to Sanofi U.S.) to jointly develop and commercialize ZALTRAP. In February 2015, the Company and Sanofi entered into an amended and restated ZALTRAP agreement ("Amended ZALTRAP Agreement"), pursuant to which Sanofi is solely responsible for the development and commercialization of ZALTRAP for cancer indications worldwide. Sanofi bears the cost of all development and commercialization activities and reimburses Regeneron for its costs for any such activities. Sanofi pays the Company a percentage of aggregate net sales of ZALTRAP during each calendar year, which percentage shall be from 15% to 30%, depending on the aggregate net sales of ZALTRAP in such calendar year.
As a result of entering into the Amended ZALTRAP Agreement, in the first quarter of 2015, the Company recognized $14.9 million of collaboration revenue, which was previously recorded as deferred revenue under the ZALTRAP Collaboration Agreement. In addition, during the years ended December 31, 2017, 2016 and 2015, the Company recorded $24.8 million, $26.2 million, and $38.8 million, respectively, in other revenue, primarily related to a percentage of net sales of ZALTRAP and manufacturing ZALTRAP commercial supplies for Sanofi.
F- 20
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
b. Bayer
The collaboration revenue the Company earned from Bayer is detailed below:
Year Ended December 31, | ||||||||||||
Bayer Collaboration Revenue | 2017 | 2016 | 2015 | |||||||||
EYLEA: | ||||||||||||
Regeneron's net profit in connection with commercialization of EYLEA outside the United States | $ | 802,298 | $ | 649,232 | $ | 466,667 | ||||||
Sales milestones | — | — | 15,000 | |||||||||
Reimbursement of Regeneron EYLEA development expenses | 13,325 | 9,010 | 8,887 | |||||||||
Other | 58,634 | 52,527 | 69,466 | |||||||||
Total EYLEA | 874,257 | 710,769 | 560,020 | |||||||||
Ang2 antibody and PDGFR-beta antibody: | ||||||||||||
Reimbursement of development expenses | 17,841 | 18,327 | 10,075 | |||||||||
Other | 45,954 | 15,174 | 10,393 | |||||||||
Total Ang2 antibody and PDGFR-beta antibody | 63,795 | 33,501 | 20,468 | |||||||||
$ | 938,052 | $ | 744,270 | $ | 580,488 | |||||||
Deferred revenue in connection with the Company's collaboration agreements with Bayer is as follows:
As of December 31, | ||||||||
2017 | 2016 | |||||||
EYLEA | $ | 68,734 | $ | 62,373 | ||||
Ang2 antibody | — | $ | 45,739 | |||||
EYLEA outside the United States
In October 2006, the Company entered into a license and collaboration agreement with Bayer for the global development and commercialization outside the United States of EYLEA. Under the terms of the agreement, Bayer made a non-refundable up-front payment to the Company of $75.0 million. The Company also received from Bayer a $20.0 million development milestone payment in 2007 (which, for the purpose of revenue recognition, was not considered substantive). The $75.0 million up-front payment and the $20.0 million milestone payment are being recognized as collaboration revenue over the related estimated performance period.
All agreed-upon EYLEA development expenses incurred by the Company and Bayer, under a global development plan, are shared equally. The Company is also obligated to use commercially reasonable efforts to supply clinical and commercial bulk product of EYLEA. Bayer has the right to terminate the license and collaboration agreement without cause with at least six months' or twelve months' advance notice depending on defined circumstances at the time of termination. In the event of termination of the agreement for any reason, the Company retains all rights to EYLEA.
Bayer markets EYLEA outside the United States, where, for countries other than Japan, the companies share equally in profits and losses from sales of EYLEA. In Japan, the Company is entitled to receive a tiered percentage of between 33.5% and 40.0% of EYLEA net sales. Within the United States, the Company is responsible for commercialization of EYLEA and retains exclusive rights to all profits from such commercialization in the United States. The Company is obligated to reimburse Bayer out of its share of the collaboration profits (including the Company's percentage of sales of EYLEA in Japan) for 50% of the agreed-upon development expenses that Bayer has incurred in accordance with a formula based on the amount of development expenses that Bayer has incurred and the Company's share of the collaboration profits, or at a faster rate at the Company's option. The Company's contingent reimbursement obligation to Bayer was approximately $251 million as of December 31, 2017.
F- 21
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
In 2015, the Company earned, and recorded as revenue, the final sales milestone payment from Bayer, in the amount of $15.0 million, upon total aggregate net sales of specific commercial supplies of EYLEA outside the United States exceeding $200.0 million over a twelve-month period.
In periods when Bayer incurs agreed-upon EYLEA development expenses that benefit the collaboration and Regeneron, the Company recognizes, as additional research and development expense, the portion of Bayer's EYLEA development expenses that the Company is obligated to reimburse. In 2015, the Company recognized as research and development expense $13.7 million of EYLEA development expenses that the Company was obligated to reimburse to Bayer. Such expenses were not material in 2017 and 2016.
Ang2 antibody outside the United States
In March 2016, the Company entered into an agreement with Bayer governing the joint development and commercialization outside the United States of nesvacumab, an antibody product candidate to angiopoietin-2 (Ang2), including REGN910-3 (Ang2 in combination with aflibercept), for the treatment of ocular diseases or disorders. In connection with the agreement, Bayer made a $50.0 million non-refundable up-front payment to the Company and is obligated to pay 25% of global development costs and 50% of development costs exclusively for the territory outside the United States.
At the inception of the agreement, the Company's significant deliverables consisted of (i) a license to certain rights and intellectual property, (ii) providing research and development services, and (iii) manufacturing clinical supplies. The Company concluded that the license did not have standalone value, as such right was not sold separately by the Company, nor could Bayer receive any benefit from the license without the fulfillment of other ongoing obligations by the Company, including the clinical supply arrangement. Therefore, the deliverables were considered a single unit of accounting. Consequently, the $50.0 million up-front payment was initially recorded as deferred revenue, and was being recognized as revenue over the related performance period.
In the fourth quarter of 2017, the Company reported that results from two Phase 2 studies that added nesvacumab to EYLEA did not provide sufficient differentiation to warrant Phase 3 development. Therefore, during the fourth quarter of 2017, the Company recognized $37.4 million of revenue related to the acceleration of the recognition of deferred revenue from the up-front payment received from Bayer.
PDGFR-beta antibody outside the United States
In January 2014, the Company entered into a license and collaboration agreement with Bayer governing the joint development and commercialization outside the United States of an antibody product candidate to Platelet Derived Growth Factor Receptor Beta (PDGFR-beta), including REGN2176-3, a combination product candidate comprised of an antibody to PDGFR-beta co-formulated with aflibercept. The agreement provided that the Company would conduct the initial development of the PDGFR-beta antibody through completion of the first proof-of-concept study, upon which Bayer would have a right to opt-in to license and collaborate on further development and commercialization outside the United States. In connection with the agreement, Bayer made a $25.5 million non-refundable up-front payment to the Company, and was obligated to pay 25% of global development costs and 50% of development costs exclusively for the territory outside the United States under the initial development plan.
From inception of the agreement until Bayer had the right to opt-in to the collaboration, the Company's sole significant deliverable was research and development services provided in accordance with the agreement. Therefore, the up-front payment was allocated to this deliverable, initially recorded as deferred revenue, and was recognized as revenue over the related performance period.
Effective in the first quarter of 2017, the Company discontinued clinical development of REGN2176-3, and on July 31, 2017, the Company and Bayer agreed to terminate this collaboration agreement.
c. Mitsubishi Tanabe Pharma
In September 2015, the Company and Mitsubishi Tanabe Pharma Corporation ("MTPC") entered into a collaboration agreement (the "MTPC Collaboration Agreement") providing MTPC with development and commercial rights to fasinumab, the Company's nerve growth factor antibody in late-stage clinical development, in certain Asian countries (the "MTPC Territories"). In connection with the agreement, MTPC made a $10.0 million non-refundable up-front payment. In 2016, MTPC made additional payments totaling $60.0 million to the Company, which were recorded as deferred revenue and are being recognized as revenue over the same performance period as the up-front payment.
F- 22
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
In 2017, the Company earned, and recognized as a substantive milestone, a $30.0 million development milestone from MTPC upon initiation of a Phase 3 trial. In addition, in 2017, MTPC made additional payments totaling $25.0 million related to development milestones achieved by MTPC, which were recorded as deferred revenue and are being recognized as revenue over the same performance period as the up-front payment. The Company is entitled to receive up to an aggregate of $20.0 million in development milestones if achieved by the Company and $80.0 million in other contingent payments, primarily related to development milestones achieved by MTPC.
Under the MTPC Collaboration Agreement, the Company is obligated to manufacture and supply MTPC with clinical and commercial supplies of fasinumab. If fasinumab is commercialized in the MTPC Territories, the Company will supply the product to MTPC at a tiered purchase price, which ranges from 30% to 50% of net sales of the product (subject to adjustment in certain circumstances), and is eligible for additional payments up to an aggregate of $100.0 million upon the achievement of specified annual net sales amounts starting at $200.0 million. Unless terminated earlier in accordance with its provisions, the MTPC Collaboration Agreement will continue to be in effect until such time as MTPC has ceased developing or commercializing fasinumab in the MTPC Territories.
At the inception of the MTPC Collaboration Agreement, the Company's significant deliverables consisted of (i) exclusive rights to develop and commercialize fasinumab in the MTPC Territories, and (ii) manufacturing clinical supplies. The Company concluded that the license did not have standalone value, as such right was not sold separately by the Company, nor could MTPC receive any benefit from the license without the manufacturing services to be rendered by the Company. Therefore, the deliverables were considered a single unit of accounting. Consequently, the $10.0 million up-front payment was initially recorded as deferred revenue, and is being recognized as revenue over the related performance period.
The Company recognized $40.6 million and $14.4 million of revenue in 2017 and 2016, respectively, in connection with the MTPC Collaboration Agreement. Revenue recognized in connection with this agreement was not material in 2015.
d. Teva
In September 2016, the Company and Teva entered into a collaboration agreement (the "Teva Collaboration Agreement") to develop and commercialize fasinumab globally, excluding the MTPC Territories (as described above). In connection with the Teva Collaboration Agreement, Teva made a $250.0 million non-refundable up-front payment in September 2016. The Company leads global development activities, and the parties share development costs equally, on an ongoing basis, under a global development plan.
In 2017, the Company earned, and recognized as substantive milestones, development milestones of $25.0 million and $35.0 million, respectively, from Teva upon initiation of two Phase 3 trials. In addition, the Company is entitled to receive up to an aggregate of $400.0 million in development milestones and up to an aggregate of $1,890.0 million in contingent payments upon achievement of specified annual net sales amounts. The Company is responsible for the manufacture and supply of fasinumab globally.
Within the United States, the Company will lead commercialization activities, and the parties will share equally in any profits and losses in connection with commercialization of fasinumab. In the territory outside the United States, Teva will lead commercialization activities and the Company will supply product to Teva at a tiered purchase price, which is calculated as a percentage of net sales of the product (subject to adjustment in certain circumstances). Unless terminated earlier in accordance with its provisions, the Teva Collaboration Agreement will continue to be in effect until such time as neither party is developing or commercializing fasinumab.
At the inception of the Teva Collaboration Agreement, the Company's significant deliverables consisted of (i) a license to certain rights and intellectual property, (ii) providing research and development services, and (iii) manufacturing clinical supplies. The Company concluded that the license did not have standalone value, primarily due to the fact that such rights were not sold separately by the Company, nor could Teva receive any benefit from the license without the fulfillment of the other ongoing obligations by the Company, including the clinical supply arrangement. Therefore, the deliverables were considered a single unit of accounting. Consequently, the $250.0 million up-front payment was initially recorded as deferred revenue, and is being recognized as revenue over the related performance period.
The Company recognized $221.5 million and $37.9 million of revenue in 2017 and 2016, respectively, in connection with the Teva Collaboration Agreement.
F- 23
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
e. Intellia Therapeutics
In April 2016, the Company entered into a license and collaboration agreement with Intellia Therapeutics, Inc. to advance CRISPR/Cas gene-editing technology for in vivo therapeutic development. The Company collaborates with Intellia to conduct research for the discovery, development, and commercialization of new therapies, in addition to the research and technology development of the CRISPR/Cas platform. In connection with the execution of the agreement, the Company made a $75.0 million up-front payment, which was recorded as research and development expense in the second quarter of 2016. In May 2016, Intellia completed an initial public offering ("IPO") of its common stock; as part of a concurrent private placement, the Company purchased $50.0 million of Intellia common stock (see Note 5).
f. Adicet Bio
In July 2016, the Company entered into a license and collaboration agreement with Adicet Bio, Inc., a privately held company, to develop next-generation engineered immune-cell therapeutics with fully human chimeric antigen receptors ("CARs") and T-cell receptors ("TCRs") directed to disease-specific cell surface antigens in order to enable the precise engagement and killing of tumor cells. In connection with the execution of the agreement, the Company made a $25.0 million up-front payment to Adicet, which was recorded as research and development expense in the third quarter of 2016, and is obligated to provide Adicet with research funding over the course of a five-year research term.
g. Decibel Therapeutics
In November 2017, the Company entered into an agreement with Decibel Therapeutics, Inc., a privately held company, to discover and develop new potential therapeutics to protect, repair, and restore hearing. In connection with the execution of the agreement, the Company made a $25.0 million up-front payment to Decibel, which was recorded as research and development expense in the fourth quarter of 2017. Simultaneous with the execution of the agreement, the Company also purchased an aggregate of $25.0 million of Decibel preferred stock, which was recorded within other assets (non-current) as of December 31, 2017.
Under the terms of the agreement, Decibel will lead development and commercialization activities and retains worldwide development and commercialization rights to any products developed under the agreement. The parties will equally share Decibel's development costs for products developed under the agreement, provided that the Company has the option to elect to cease funding the development of products at pre-determined development periods, and the Company may be required to pay additional amounts based upon potential development milestones achieved. The Company is entitled to tiered royalties on any future net sales of products developed and commercialized under the agreement.
h. Astellas
In March 2007, the Company entered into a six-year, non-exclusive license agreement with Astellas Pharma Inc. to allow Astellas to utilize the Company's VelocImmune® technology in its internal research programs to discover human monoclonal antibodies. In July 2010, the license agreement with Astellas was amended and extended through June 2023. Under the terms of the amended agreement, Astellas made a $165.0 million up-front payment to the Company in 2010, which was deferred upon receipt and is being recognized as revenue ratably over a seven-year period beginning in mid-2011. In addition, Astellas will make a $130.0 million second payment to the Company in June 2018 unless the license agreement has been terminated prior to that date. Astellas has the right to terminate the agreement at any time by providing 90 days' advance written notice. Under certain limited circumstances, such as a material breach of the agreement by the Company, Astellas may terminate the agreement and receive a refund of a portion of its up-front payment or, if such termination occurs after June 2018, a portion of its second payment, to the Company under the July 2010 amendment to the agreement. The Company is entitled to receive a mid-single digit royalty on any future sales of antibody products discovered by Astellas using the Company's VelocImmune technology.
i. Other
In addition to the collaboration agreements discussed above, the Company has various other collaboration agreements that are not individually, or in the aggregate, significant to its operating results or financial condition at this time. Pursuant to the terms of those agreements, the Company may be required to pay, or it may receive, additional amounts upon the achievement of various development and commercial milestones which in the aggregate could be significant. The Company may also incur, or get reimbursed for, significant research and development costs if the related product candidate(s) were to advance to late stage clinical trials. In addition, if any products related to these collaborations are approved for sale, the Company may be required to pay, or it
F- 24
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
may receive, royalties on future sales. The payment or receipt of these amounts, however, is contingent upon the occurrence of various future events.
4. Marketable Securities
Marketable securities as of December 31, 2017 and 2016 consist of both debt securities of investment grade issuers as well as equity securities of publicly traded companies.
The following tables summarize the Company's investments in marketable securities:
Amortized | Unrealized | Fair | ||||||||||||||
As of December 31, 2017 | Cost Basis | Gains | Losses | Value | ||||||||||||
Corporate bonds | $ | 1,717,976 | $ | 2,176 | $ | (7,672 | ) | $ | 1,712,480 | |||||||
U.S. government and government agency obligations | 186,699 | 34 | (1,241 | ) | 185,492 | |||||||||||
Municipal bonds | 4,600 | — | (13 | ) | 4,587 | |||||||||||
Commercial paper | 106,973 | — | — | 106,973 | ||||||||||||
Certificates of deposit | 11,024 | — | — | 11,024 | ||||||||||||
Equity securities | 56,191 | 6,594 | — | 62,785 | ||||||||||||
$ | 2,083,463 | $ | 8,804 | $ | (8,926 | ) | $ | 2,083,341 | ||||||||
As of December 31, 2016 | ||||||||||||||||
Corporate bonds | $ | 1,076,964 | $ | 630 | $ | (4,743 | ) | $ | 1,072,851 | |||||||
U.S. government and government agency obligations | 132,923 | 58 | (641 | ) | 132,340 | |||||||||||
Municipal bonds | 7,663 | 1 | (20 | ) | 7,644 | |||||||||||
Commercial paper | 63,074 | 1 | — | 63,075 | ||||||||||||
Certificates of deposit | 42,612 | — | — | 42,612 | ||||||||||||
Equity securities | 57,251 | 5,551 | (13,583 | ) | 49,219 | |||||||||||
$ | 1,380,487 | $ | 6,241 | $ | (18,987 | ) | $ | 1,367,741 | ||||||||
The Company classifies its debt security investments based on their contractual maturity dates. The debt securities listed as of December 31, 2017 mature at various dates through October 2022. The fair values of debt security investments by contractual maturity consist of the following:
As of December 31, | ||||||||
2017 | 2016 | |||||||
Maturities within one year | $ | 593,783 | $ | 503,481 | ||||
Maturities after one year through five years | 1,426,773 | 815,041 | ||||||
$ | 2,020,556 | $ | 1,318,522 | |||||
F- 25
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
The following table shows the fair value of the Company's marketable securities that have unrealized losses and that are deemed to be only temporarily impaired, aggregated by investment category and length of time that the individual securities have been in a continuous unrealized loss position.
Less than 12 Months | 12 Months or Greater | Total | |||||||||||||||||||||
As of December 31, 2017 | Fair Value | Unrealized Loss | Fair Value | Unrealized Loss | Fair Value | Unrealized Loss | |||||||||||||||||
Corporate bonds | $ | 930,970 | $ | (4,924 | ) | $ | 256,750 | $ | (2,748 | ) | $ | 1,187,720 | $ | (7,672 | ) | ||||||||
U.S. government and government agency obligations | 110,532 | (409 | ) | 67,921 | (832 | ) | 178,453 | (1,241 | ) | ||||||||||||||
Municipal bonds | 2,582 | (10 | ) | 2,005 | (3 | ) | 4,587 | (13 | ) | ||||||||||||||
$ | 1,044,084 | $ | (5,343 | ) | $ | 326,676 | $ | (3,583 | ) | $ | 1,370,760 | $ | (8,926 | ) | |||||||||
As of December 31, 2016 | |||||||||||||||||||||||
Corporate bonds | $ | 759,222 | $ | (4,685 | ) | $ | 36,407 | $ | (58 | ) | $ | 795,629 | $ | (4,743 | ) | ||||||||
U.S. government and government agency obligations | 81,170 | (641 | ) | — | — | 81,170 | (641 | ) | |||||||||||||||
Municipal bonds | 7,141 | (20 | ) | — | — | 7,141 | (20 | ) | |||||||||||||||
Equity securities | 36,417 | (13,583 | ) | — | — | 36,417 | (13,583 | ) | |||||||||||||||
$ | 883,950 | $ | (18,929 | ) | $ | 36,407 | $ | (58 | ) | $ | 920,357 | $ | (18,987 | ) | |||||||||
During the year ended December 31, 2016, the Company recorded an other-than-temporary impairment charge of $9.8 million related to its investment in an equity security. There were no other-than-temporary impairment charges recorded on the Company's investments during 2017 or 2015. During the year ended December 31, 2017, the Company recorded realized gains of $8.3 million and realized losses were not material. Realized gains and losses on sales of marketable securities were not material for the years ended December 31, 2016 and 2015.
With respect to marketable securities, for the years ended December 31, 2017, 2016, and 2015, amounts reclassified from accumulated other comprehensive income (loss) into other income (expense), net were related to the 2016 impairment charge on the equity security and realized gains and losses on sales described above.
F- 26
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
5. Fair Value Measurements
The Company's assets that are measured at fair value on a recurring basis consist of the following:
Fair Value Measurements at Reporting Date Using | |||||||||||
As of December 31, 2017 | Fair Value | Quoted Prices in Active Markets for Identical Assets (Level 1) | Significant Other Observable Inputs (Level 2) | ||||||||
Available-for-sale marketable securities: | |||||||||||
Corporate bonds | $ | 1,712,480 | — | $ | 1,712,480 | ||||||
U.S. government and government agency obligations | 185,492 | — | 185,492 | ||||||||
Municipal bonds | 4,587 | — | 4,587 | ||||||||
Commercial paper | 106,973 | — | 106,973 | ||||||||
Certificates of deposit | 11,024 | — | 11,024 | ||||||||
Equity securities | 62,785 | $ | 62,785 | — | |||||||
$ | 2,083,341 | $ | 62,785 | $ | 2,020,556 | ||||||
As of December 31, 2016 | |||||||||||
Available-for-sale marketable securities: | |||||||||||
Corporate bonds | $ | 1,072,851 | — | $ | 1,072,851 | ||||||
U.S. government and government agency obligations | 132,340 | — | 132,340 | ||||||||
Municipal bonds | 7,644 | — | 7,644 | ||||||||
Commercial paper | 63,075 | — | 63,075 | ||||||||
Certificates of deposit | 42,612 | — | 42,612 | ||||||||
Equity securities | 49,219 | $ | 49,219 | — | |||||||
$ | 1,367,741 | $ | 49,219 | $ | 1,318,522 | ||||||
Marketable securities included in Level 2 are valued using quoted market prices for similar instruments in active markets, quoted prices for identical or similar instruments in markets that are not active, or model-based valuations in which significant inputs used are observable. The Company considers market liquidity in determining the fair value for these securities. The Company did not record any charges for other-than-temporary impairment of its Level 2 marketable securities in 2017, 2016, and 2015.
There were no purchases, sales, or maturities of Level 3 marketable securities and no unrealized gains or losses related to Level 3 marketable securities for the years ended December 31, 2017 and 2016. During 2016, transfers of marketable securities from Level 2 to Level 1 were $44.1 million in connection with the lapse of transfer restrictions in November 2016 on the Company's investment in Intellia common shares (see Note 3). The Company's policy for recognition of transfers between levels of the fair value hierarchy is to recognize any transfer at the beginning of the fiscal quarter in which the determination to transfer was made. There were no other transfers of marketable securities between Levels 1, 2, or 3 classifications during the years ended December 31, 2017 and 2016.
The fair value of interest rate swap and interest rate cap contracts, which were recorded within other assets (non-current), was not material as of December 31, 2017 (see Note 6). The fair value of these contracts was determined based on Level 2 inputs, using significant inputs that are observable either directly or indirectly, including London Interbank Offered Rate ("LIBOR") and interest rate swap rates.
F- 27
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
6. Derivative Instruments and Hedging Activities
The Company is exposed to market fluctuations in interest rates, including those in connection with its March 2017 lease agreement (see Note 12). During 2017, the Company entered into interest rate swap and interest rate cap agreements to manage a portion of such interest rate risk. All of the Company’s derivative instruments are utilized for risk management purposes, and are not used for trading or speculative purposes.
The Company's derivative instruments are designated as cash flow hedges for accounting purposes. Since the specific terms of the derivative instruments match those of the item being hedged, the derivative instruments are deemed to be highly effective in offsetting the changes in cash flows of the hedged item. As such, changes in the fair value of these derivatives are recorded in accumulated other comprehensive income (loss) until the underlying transaction affects earnings, and are then reclassified to earnings in the same account as the hedged transaction. The Company would record any gain or loss related to the ineffectiveness directly to earnings.
The Company assesses, both at inception and on an ongoing basis, whether derivatives used continue to be highly effective in offsetting changes in cash flows of the hedged items. The Company does not exclude any portion of the cash flow hedge contracts from the assessment of hedge effectiveness. If and when a derivative is no longer expected to be highly effective, hedge accounting is discontinued.
The following table summarizes the notional amounts of the Company's outstanding interest rate swap and cap agreements as of December 31, 2017:
Notional Amount | |||
Interest rate swap contracts | $ | 75,000 | |
Interest rate cap contracts | $ | 75,000 | |
As it relates to cash flow hedges, for the year ended December 31, 2017, amounts of gains and losses recognized in other comprehensive income (loss), and amounts reclassified from accumulated other comprehensive income (loss) into interest expense were not material. As of December 31, 2017, the amounts expected to be reclassified out of accumulated other comprehensive income into interest expense over the next 12 months are not expected to be material. For the year ended December 31, 2017, there were no gains or losses recorded related to the ineffective portion of the derivative instruments.
7. Inventories
Inventories consist of the following:
As of December 31, | |||||||
2017 | 2016 | ||||||
Raw materials | $ | 190,045 | $ | 92,287 | |||
Work-in-process | 302,042 | 202,301 | |||||
Finished goods | 21,791 | 13,334 | |||||
Deferred costs | 212,260 | 91,434 | |||||
$ | 726,138 | $ | 399,356 | ||||
Deferred costs represent the costs of product manufactured and shipped to the Company's collaborators for which recognition of revenue has been deferred (see Note 1).
F- 28
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
8. Property, Plant, and Equipment
Property, plant, and equipment consists of the following:
As of December 31, | |||||||
2017 | 2016 | ||||||
Land | $ | 192,757 | $ | 103,906 | |||
Building and improvements | 1,441,565 | 1,278,283 | |||||
Leasehold improvements | 102,599 | 101,101 | |||||
Construction-in-progress | 408,857 | 318,929 | |||||
Laboratory and other equipment | 599,153 | 554,181 | |||||
Furniture, computer and office equipment, and other | 179,968 | 152,525 | |||||
2,924,899 | 2,508,925 | ||||||
Less, accumulated depreciation and amortization | (566,294 | ) | (425,504 | ) | |||
$ | 2,358,605 | $ | 2,083,421 | ||||
As of December 31, 2017 and 2016, $1,692.9 million and $1,441.2 million, respectively, of the Company's net property, plant, and equipment was located in the United States and $665.7 million and $642.2 million, respectively, was located in Europe (primarily in Ireland).
Depreciation and amortization expense (including amortization expense related to capital and facility leases) on property, plant, and equipment amounted to $142.2 million, $104.7 million, and $74.9 million for the years ended December 31, 2017, 2016, and 2015, respectively.
Property, plant, and equipment, at cost, as of December 31, 2017 and 2016 included $724.1 million and $407.1 million, respectively, of leased property under the Company's capital and facility leases at its Tarrytown, New York facility. See Note 12. Accumulated amortization related to these assets amounted to $47.9 million and $44.0 million as of December 31, 2017 and 2016, respectively.
9. Accounts Payable and Accrued Expenses
Accounts payable and accrued expenses consist of the following:
As of December 31, | |||||||
2017 | 2016 | ||||||
Accounts payable | $ | 178,183 | $ | 134,984 | |||
Accrued payroll and related costs | 191,825 | 153,086 | |||||
Accrued clinical trial expense | 120,891 | 91,753 | |||||
Accrued sales-related charges, deductions, and royalties | 194,542 | 159,985 | |||||
Income taxes payable | 227 | 235,776 | |||||
Other accrued expenses and liabilities | 129,410 | 103,512 | |||||
$ | 815,078 | $ | 879,096 | ||||
F- 29
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
10. Deferred Revenue
Deferred revenue consists of the following:
As of December 31, | |||||||
2017 | 2016 | ||||||
Current portion: | |||||||
Received or receivable from Sanofi (see Note 3a) | $ | 177,746 | $ | 115,267 | |||
Received or receivable from Bayer (see Note 3b) | 39,000 | 31,084 | |||||
Received or receivable from MTPC (see Note 3c) | 14,027 | 9,188 | |||||
Received or receivable from Teva (see Note 3d) | 43,535 | 43,122 | |||||
Received for technology license agreement (see Note 3h) | 10,280 | 23,572 | |||||
Other | 35,550 | 9,431 | |||||
$ | 320,138 | $ | 231,664 | ||||
Long-term portion: | |||||||
Received or receivable from Sanofi (see Note 3a) | $ | 379,936 | $ | 503,474 | |||
Received or receivable from Bayer (see Note 3b) | 29,734 | 77,028 | |||||
Received or receivable from MTPC (see Note 3c) | 56,106 | 45,940 | |||||
Received or receivable from Teva (see Note 3d) | 153,823 | 194,050 | |||||
Received for technology license agreement (see Note 3h) | — | 10,280 | |||||
Other | 9,600 | — | |||||
$ | 629,199 | $ | 830,772 | ||||
11. Debt
a. Convertible Debt
In October 2011, the Company issued $400.0 million aggregate principal amount of 1.875% convertible senior notes (the "Notes") in a private placement, and the Notes matured on October 1, 2016. The Notes were convertible, subject to certain conditions, into cash, shares of the Company's Common Stock, or a combination of cash and shares of Common Stock, at the Company's option. The Notes initial conversion price was $84.02 per share. In connection with the offering of the Notes, the Company entered into convertible note hedge ("call option") and warrant transactions with multiple counterparties, including an affiliate of the initial purchaser of the Notes. The convertible note hedge covered, subject to customary anti-dilution adjustments, the number of shares of the Company's Common Stock that initially underlie the Notes, and were intended to reduce the potential dilutive impact of the conversion feature of the Notes.
During 2015, the Company settled conversion obligations for $166.5 million principal amount of the Company's Notes that was previously surrendered for conversion, and consequently paid $166.5 million in cash and issued 1,625,113 shares of Common Stock. In addition, in 2015, the Company allocated $819.7 million of the settlement consideration provided to the Note holders to the reacquisition of the equity component of the Notes, and recognized such amount as a reduction of stockholders' equity. In 2015, the Company also recognized an $18.9 million loss on the debt extinguishment. In connection with the Note conversions in 2015, the Company also exercised a proportionate amount of its convertible note hedges, for which the Company received 1,625,088 shares of Common Stock, which was approximately equal to the number of shares the Company was required to issue to settle the non-cash portion of the related Note conversions. The Company recorded the cost of the shares received, or $136.5 million, as Treasury Stock during 2015.
During 2016, the Company settled conversion obligations for $12.9 million principal amount of the Company's Notes. Consequently, in 2016, the Company paid $12.9 million in cash and issued 121,058 shares of Common Stock. In addition, the Company allocated $47.8 million of the settlement consideration provided to the Note holders to the reacquisition of the equity component of the Notes, and recognized such amount as a reduction of stockholders' equity. The loss on the debt extinguishment in connection with the Notes that were surrendered for conversion during 2016 was not material. As a result of these Note
F- 30
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
conversions, the Company also exercised a proportionate amount of its convertible note hedges during 2016, for which the Company received 121,048 shares of Common Stock, which was approximately equal to the number of shares the Company was required to issue to settle the non-cash portion of the related Note conversions. The Company recorded the cost of the shares received, or $10.2 million, as Treasury Stock during 2016.
Total interest expense associated with the Notes, net of capitalized interest as applicable, was not material in 2016 and 2015.
Warrant Transactions
In November 2015, the Company entered into an amendment agreement with a warrant holder whereby the parties agreed to reduce a portion of the number of warrants held by the warrant holder. The Company was able to settle, at its option, any payments due under the amendment agreement in cash or by delivering shares of Common Stock. As a result of the warrant holder closing out a portion of its hedge position prior to December 31, 2015, the Company paid a total of $50.0 million in 2015 to reduce the number of warrants it held by 115,970. Additionally, during January 2016, the warrant holder closed out additional portions of its hedge position, and, as a result, the Company paid a total of $135.3 million in the first quarter of 2016 to further reduce the number of warrants held by such warrant holder by 360,406.
In addition to the warrant transactions described above, during 2015, the Company entered into other agreements to reduce the number of warrants held by warrant holders. The Company was able to settle, at its option, any payments due under the amendment agreement in cash or by delivering shares of Common Stock. Pursuant to the agreements, the Company paid an aggregate amount of $399.5 million to the warrant holders during 2015 to reduce the number of shares of Common Stock issuable upon exercise of the warrant by 898,547 in the aggregate.
In February 2016, the Company entered into an amendment agreement with a warrant holder whereby the parties agreed to reduce a portion of the number of warrants held by the warrant holder. The Company was able to settle, at its option, any payments due under the amendment agreement in cash or by delivering shares of Common Stock. As a result of the warrant holder closing out a portion of its hedge position during 2016, the Company paid a total of $106.9 million to reduce the number of warrants held by such warrant holder by 403,665.
In November 2016, the Company and warrant holders entered into warrant termination agreements whereby the parties agreed to cancel the remaining warrants held by the warrant holders and to terminate the respective warrant agreements in consideration for payments by the Company of $401.2 million in the aggregate. The Company made the termination payments in the fourth quarter of 2016, and, as a result, no warrants remained outstanding as of December 31, 2016.
b. Credit Facility
In March 2015, the Company entered into an agreement with a syndicate of lenders (the "Credit Agreement") which provides for a $750.0 million senior unsecured five-year revolving credit facility (the "Credit Facility"). The Credit Agreement includes an option for the Company to elect to increase the commitments under the Credit Facility and/or to enter into one or more tranches of term loans in the aggregate principal amount of up to $250.0 million subject to the consent of the lenders providing the additional commitments or term loans, as applicable, and certain other conditions. Proceeds of the loans under the Credit Facility may be used to finance working capital needs, and for general corporate or other lawful purposes, of Regeneron and its subsidiaries. The Credit Agreement also provides a $100.0 million sublimit for letters of credit. The Credit Agreement includes an option for the Company to elect to extend the maturity date of the Credit Facility beyond March 2020, subject to the consent of the extending lenders and certain other conditions. Amounts borrowed under the Credit Facility may be prepaid, and the commitments under the Credit Facility may be terminated, at any time without premium or penalty.
Any loans under the Credit Facility have a variable interest rate based on either LIBOR or an alternate base rate, plus an applicable margin that varies with the Company's debt rating and total leverage ratio. The Company had no borrowings outstanding under the Credit Facility as of December 31, 2017.
The Credit Agreement contains financial and operating covenants. Financial covenants include a maximum total leverage ratio and a minimum interest expense coverage ratio. The Company was in compliance with all covenants of the Credit Facility as of December 31, 2017.
F- 31
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
12. Commitments and Contingencies
a. Leases
The Company leases laboratory and office facilities in Tarrytown, New York (the "Tarrytown Leases"). Prior to December 30, 2016, certain of the premises under the Tarrytown Leases had been accounted for as operating leases, while for certain other buildings the Company leased, the Company was deemed, in substance, to be the owner of the landlord's buildings (collectively, the "Build-to-Suit Buildings") in accordance with the application of FASB authoritative guidance. On December 30, 2016, the Company entered into a Purchase Agreement with BMR-Landmark at Eastview LLC and BMR-Landmark at Eastview IV LLC (collectively, "BMR"), pursuant to which the Company agreed to purchase BMR's Tarrytown, New York facilities (the "Facility") for a purchase price of $720.0 million. The Company occupies a significant portion of the Facility, with the remaining rentable area under leases to third-party tenants. In accordance with the terms of the Purchase Agreement, the Company paid $57.0 million toward the purchase price to BMR in December 2016.
Upon entering into the December 30, 2016 Purchase Agreement with BMR, the premises under the Company's Tarrytown Leases that were historically accounted for as operating leases were deemed to be modified, as the Company now had the option to purchase the Facility under terms that made it reasonably assured to be exercised. Consequently, the leases for such premises were re-classified as a capital lease upon execution of the Purchase Agreement, and a proportionate amount of the $57.0 million payment was recorded as reduction of the initial capital lease liability. The execution of the Purchase Agreement did not impact the balance sheet classification for the Build-to-Suit Buildings; however, a proportionate amount of the $57.0 million payment was recorded as a reduction to the related facility lease obligation.
On March 3, 2017, the Company also entered into a Participation Agreement with Banc of America Leasing & Capital LLC ("BAL"), as lessor, and a syndicate of lenders (collectively, the "Participants"). The Participation Agreement provided for lease financing in connection with the acquisition by BAL of the Facility and the Company's lease of the Facility from BAL. On March 3, 2017, the right to take title to the Facility under the Purchase Agreement was assigned by the Company to BAL, and the Participants advanced $720.0 million, which was used by BAL to finance the purchase price for the Facility and to reimburse the Company for the $57.0 million payment made to BMR in December 2016. The $57.0 million reimbursement was recorded by the Company in March 2017 as an increase to capital and facility lease obligations in amounts equal to those initially recorded as reductions upon making such payment to BMR in December 2016.
On March 3, 2017, the Company entered into a lease agreement (the "Lease") with BAL, pursuant to which the Company has leased the Facility from BAL for a five-year term. As a result of entering into the Lease, certain parts of the Facility became subleased from the Company by existing third-party tenants. The Lease requires the Company to pay all maintenance, insurance, taxes, and other costs arising out of the use of the Facility. The Company is also required to make monthly payments of basic rent during the term of the Lease in an amount equal to a variable rate per annum based on the one-month LIBOR, plus an applicable margin that varies with the Company’s debt rating and total leverage ratio.
The Participation Agreement and the Lease include an option for the Company to elect to extend the maturity date of the Participation Agreement and the term of the Lease for an additional five-year period, subject to the consent of all the Participants and certain other conditions. The Company also has the option prior to the end of the term of the Lease to (a) purchase the Facility by paying an amount equal to the outstanding principal amount of the Participants' advances under the Participation Agreement, all accrued and unpaid interest and yield thereon, and all other outstanding amounts under the Participation Agreement, the Lease, and certain related documents or (b) sell the Facility to a third party on behalf of BAL. The advances under the Participation Agreement mature, and all amounts outstanding thereunder will become due and payable in full at the end of the term of the Lease.
As a result of entering into the Lease, the premises that were classified as a capital lease as of December 31, 2016 were reassessed. As described above, the Company has the option to purchase the Facility, and as a result, the Company is deemed to have continuing involvement in such premises. Accordingly, these premises continue to be classified as a capital lease, with the related property, plant, and equipment and capital lease liability remaining on the Company's Consolidated Balance Sheet. In addition, as described above, upon entering into the Lease, the Company began to lease space occupied by third-party tenants. The lease of such premises is also classified as a capital lease. The execution of the Lease did not impact the balance sheet classification for the Build-to-Suit Buildings. However, in 2017, the Company recorded a $30.1 million loss on extinguishment of debt associated with the Build-to-Suit Buildings. In the aggregate, the Company recorded $720.0 million of capital and facility lease obligations upon execution of the Lease for the Facility.
F- 32
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
The Participation Agreement and the Lease contain financial and operating covenants, which are substantially similar to the covenants set forth in the Company's credit facility (see Note 11). The Company was in compliance with all covenants of the Participation Agreement and the Lease as of December 31, 2017.
Commitments under Operating Leases
The estimated future minimum noncancelable lease commitments under operating leases, as of December 31, 2017, are as follows:
Facilities | Equipment | Total | ||||||||||
2018 | $ | 2,866 | $ | 6,097 | $ | 8,963 | ||||||
2019 | 3,095 | 817 | 3,912 | |||||||||
2020 | 2,713 | 426 | 3,139 | |||||||||
2021 | 2,386 | 45 | 2,431 | |||||||||
2022 | 1,901 | 26 | 1,927 | |||||||||
Thereafter | 1,498 | 8 | 1,506 | |||||||||
$ | 14,459 | $ | 7,419 | $ | 21,878 | |||||||
Rent expense under operating leases was:
Year Ended December 31, | Facilities | Equipment | Total | |||||||||
2017 | $ | 3,138 | $ | 1,151 | $ | 4,289 | ||||||
2016 | $ | 15,861 | $ | 852 | $ | 16,713 | ||||||
2015 | $ | 14,659 | $ | 543 | $ | 15,202 | ||||||
Capital and Facility Lease Obligations
In 2017, 2016, and 2015, the Company recognized $19.5 million, $5.4 million, and $9.7 million, respectively, of interest expense in connection with the Company's capital and facility lease obligations.
As of December 31, 2017, the estimated future minimum noncancelable commitments under the Company's capital and facility lease obligations, excluding the purchase price the Company would be obligated to pay if the Company were to exercise its option to purchase the Facility (as described above), are as follows:
Capital and Facility Lease Obligations | ||||
2018 | $ | 21,085 | ||
2019 | 23,838 | |||
2020 | 26,257 | |||
2021 | 27,650 | |||
2022 | 6,837 | |||
Thereafter | — | |||
$ | 105,667 | |||
F- 33
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
b. Research Collaboration and Licensing Agreements
As part of the Company's research and development efforts, the Company enters into research collaboration and licensing agreements with other companies, universities, and other organizations. These agreements contain varying terms and provisions which include fees to be paid by the Company, services to be provided, and license rights to certain proprietary technology developed under the agreements. Some of these agreements may require the Company to pay additional amounts upon the achievement of various development and commercial milestones, contingent upon the occurrence of various future events. Additionally, some of the agreements contain provisions which require the Company to pay royalties, as defined, at rates that range from 0.5% to 15.0%, in the event the Company sells or licenses any proprietary products developed under the respective agreements. The Company also has contingent reimbursement obligations to its collaborators Sanofi and Bayer once the applicable collaboration becomes profitable. See Note 3.
The Company and Genentech, a member of the Roche Group, entered into a Non-Exclusive License and Partial Settlement Agreement, as amended (the "Genentech Agreement"), that covered making, using, and selling EYLEA for the prevention of human eye diseases and disorders, and ended the litigation relating to those matters. Pursuant to the Genentech Agreement, the Company received a non-exclusive license to certain patents relating to VEGF receptor proteins, known as the Davis-Smyth patents, and other technology patents. The Genentech Agreement obligated the Company to make payments to Genentech based on worldwide sales of EYLEA through May 7, 2016, when the licenses granted to the Company thereunder became fully paid up and royalty free for the duration of the remaining term of the underlying patents. All payments to Genentech under the Genentech Agreement were made by the Company, and Bayer shared in all such payments based on the proportion of EYLEA sales outside the United States to worldwide EYLEA sales.
For the years ended December 31, 2017, 2016, and 2015, the Company recorded royalty expense of $30.8 million, $125.3 million, and $247.9 million, respectively, based on product sales of commercial products under various licensing agreements (including the Genentech Agreement described above).
13. Stockholders' Equity
The Company's Restated Certificate of Incorporation, as amended, provides for the issuance of up to 40 million shares of Class A Stock, par value $0.001 per share, and 320 million shares of Common Stock, par value $0.001 per share. Shares of Class A Stock are convertible, at any time, at the option of the holder into shares of Common Stock on a share-for-share basis. Holders of Class A Stock have rights and privileges identical to Common Stockholders except that each share of Class A is entitled to ten votes per share, while each share of Common Stock is entitled to one vote per share. Class A Stock may only be transferred to specified Permitted Transferees, as defined. Under the Company's Restated Certificate of Incorporation, the Company's board of directors is authorized to issue up to 30 million shares of Preferred Stock, in series, with rights, privileges, and qualifications of each series determined by the board of directors.
In December 2007, Sanofi purchased 12 million newly issued, unregistered shares of the Company's Common Stock. As a condition to the closing of this transaction, Sanofi entered into an investor agreement, as amended and restated, with the Company. Under the terms of the amended and restated investor agreement, Sanofi has three demand rights to require the Company to use all reasonable efforts to conduct a registered underwritten public offering with respect to shares of the Company's Common Stock held by Sanofi from time to time. Under the amended and restated investor agreement, Sanofi has also agreed not to dispose of any shares of the Company's Common Stock beneficially owned by Sanofi from time to time until December 20, 2020 (subject to the limited waiver described below). These restrictions on dispositions are subject to earlier termination upon the occurrence of certain events, such as the consummation of a change-of-control transaction involving the Company or the Company's dissolution or liquidation, and certain restrictions have been imposed on the manner of sales thereafter.
As described in Note 3, effective January 7, 2018, the Company and Sanofi entered into a Letter Agreement, which, among other things, has amended certain provisions of the amended and restated investor agreement. Pursuant to the Letter Agreement, the Company has granted Sanofi a limited waiver of the lock-up obligations under the investor agreement to allow Sanofi to sell up to an aggregate of 1,400,000 shares of the Company's Common Stock held by Sanofi for the quarterly periods through September 30, 2020.
Further, pursuant to the amended and restated investor agreement, Sanofi is bound by certain "standstill" provisions, which contractually prohibit Sanofi from seeking to directly or indirectly exert control of the Company or acquiring more than 30% of the outstanding shares of the Company's Class A Stock and Common Stock (taken together). This prohibition will remain in place until the earliest of (i) the later of the fifth anniversaries of the expiration or earlier termination of the Company's License and
F- 34
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Collaboration Agreement with Sanofi and the Company's ZALTRAP Agreement with Sanofi, each as amended, and (ii) other specified events. Sanofi has also agreed to vote as recommended by the Company's board of directors, except that it may elect to vote proportionally with the votes cast by all of the Company's other shareholders with respect to certain change-of-control transactions, and to vote in its sole discretion with respect to liquidation or dissolution, stock issuances equal to or exceeding 20% of the outstanding shares or voting rights of the Company's Class A Stock and Common Stock (taken together), and new equity compensation plans or amendments if not materially consistent with the Company's historical equity compensation practices. The rights and restrictions under the investor agreement are subject to termination upon the occurrence of certain events.
In addition, upon Sanofi reaching 20% ownership of the Company's outstanding shares of Class A Stock and Common Stock (taken together) during 2014, the Company was required to appoint an individual agreed upon by the Company and Sanofi to the Company's board of directors. This individual is required to be independent of the Company, and not to be a current or former officer, director, employee, or paid consultant of Sanofi. Subject to certain exceptions, the Company is required to use its reasonable efforts (including recommending that its shareholders vote in favor) to cause the election of this designee at the Company's annual shareholder meetings for so long as (other than during the term of the Letter Agreement) Sanofi maintains a specified equity interest in the Company.
In connection with the Company's license and collaboration agreements with Bayer for the joint development and commercialization outside the United States of antibody product candidates to PDGFR-beta and Ang2 (see Note 3b), Bayer is bound by certain "standstill" provisions, which contractually prohibit Bayer from seeking to influence the control of the Company or acquiring more than 20% of the Company's outstanding shares of Class A Stock and Common Stock (taken together). With respect to each of these agreements, this prohibition will remain in place until the earliest of (i) the fifth anniversary of the expiration or earlier termination of the agreement (which, in the case of the PDGFR-beta license and collaboration agreement, occurred on July 31, 2017) or (ii) other specified events.
Further, pursuant to the 2016 Teva Collaboration Agreement, Teva and its affiliates are bound by certain "standstill" provisions, which contractually prohibit them from seeking to directly or indirectly exert control of the Company or acquiring more than 5% of the Company's Class A Stock and Common Stock (taken together). This prohibition will remain in place until the earliest of (i) the fifth anniversary of the expiration or earlier termination of the agreement or (ii) other specified events.
As described in Note 11, during 2016 and 2015, the Company elected to settle Notes that which were surrendered for conversion through a combination of cash and shares of the Company's Common Stock; exercised convertible note hedges, for which the Company received shares of Common Stock; and made payments to reduce the number of warrants and/or cancel the remaining number of warrants held by warrant holders.
14. Long-Term Incentive Plans
In 2000, the Company established the Regeneron Pharmaceuticals, Inc. 2000 Long-Term Incentive Plan which, as amended and restated and approved by the Company's shareholders (the "2000 Incentive Plan"), provided for the issuance of up to 35,397,043 shares of Common Stock in respect of awards, in addition to any shares subject to awards that were returned to the 2000 Incentive Plan upon expiration, forfeiture, surrender, exchange, cancellation, or termination of previously granted awards.
In 2014, the Company established, and the Company's shareholders approved, the Regeneron Pharmaceuticals, Inc. 2014 Long-Term Incentive Plan (the "Original 2014 Incentive Plan"). In 2017, the Company adopted the Amended and Restated Regeneron Pharmaceuticals, Inc. 2014 Long-Term Incentive Plan (the "Amended and Restated 2014 Incentive Plan") and registered an additional 12,000,000 shares of Common Stock issuable under the Amended and Restated 2014 Incentive Plan. As of the shareholder approval date, the Amended and Restated 2014 Incentive Plan provided for the issuance of up to 18,559,431 shares of Common Stock in respect of awards. In addition, upon the expiration, forfeiture, surrender, exchange, cancellation, or termination of any award previously granted under the 2000 Incentive Plan, the Original 2014 Incentive Plan, or the Amended and Restated 2014 Incentive Plan, any shares subject to such award are added to the pool of shares available for grant under the Amended and Restated 2014 Incentive Plan. Employees of the Company, including officers, and nonemployees, including consultants and nonemployee members of the Company's board of directors (collectively, "Participants"), may receive awards as determined by a committee of independent directors ("Committee"), subject to certain limitations set forth in the Amended and Restated 2014 Incentive Plan.
The awards that may be made under the Amended and Restated 2014 Incentive Plan include: (a) incentive stock options and nonqualified stock options, (b) shares of restricted stock, (c) shares of phantom stock, (d) stock appreciation rights (“SARs”), (e) stock bonuses, and (f) other awards.
F- 35
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Stock option awards grant Participants the right to purchase shares of Common Stock at prices determined by the Committee, with exercise prices that are equal to or greater than the average of the high and low market prices of the Company's Common Stock on the date of grant (the "Market Price"). Options vest over a period of time determined by the Committee, generally on a pro rata basis over a three- to four-year period. The Committee also determines the expiration date of each option. The maximum term of options that have been awarded under the 2000 Incentive Plan, the Original 2014 Incentive Plan, and the Amended and Restated 2014 Incentive Plan (collectively, the "Incentive Plans") is ten years.
Restricted stock awards grant Participants shares of restricted Common Stock or allow Participants to purchase such shares at a price determined by the Committee. Such shares are nontransferable for a period determined by the Committee ("vesting period"). Should employment terminate, as specified in the Incentive Plans, except as determined by the Committee in its discretion and subject to the applicable Incentive Plan documents, the ownership of any unvested restricted stock will be transferred to the Company.
Phantom stock awards provide the Participant the right to receive, within 30 days of the date on which the share vests, an amount, in cash and/or shares of Common Stock as determined by the Committee, equal to the sum of the fair market value of a share of Common Stock on the date such share of phantom stock vests and the aggregate amount of cash dividends paid with respect to a share of Common Stock during the period from the grant date of the share of phantom stock to the date on which the share vests.
SARs entitle the Participant to a payment (in cash or shares) equal to the appreciation in the value of the Common Stock during a specified period above the base price specified by the Committee, which may not be less than 100% of the Market Price of the Common Stock on the day the SARs are granted. SARs granted under the Amended and Restated 2014 Incentive Plan are exercisable for a maximum period of 10 years from the date of grant (subject to early termination such as upon a termination of employment), or such lesser period as the Committee shall determine, and the vesting schedule is determined by the Committee.
Stock bonus awards are bonuses payable in shares of Common Stock which are granted at the discretion of the Committee. Other awards are other forms of awards which are valued based on the Common Stock. Subject to the provisions of the Amended and Restated 2014 Incentive Plan, the terms and provisions of such other awards are determined solely on the authority of the Committee.
The Incentive Plans contain provisions that allow for the Committee to provide for the immediate vesting of awards upon a change in control of the Company, as defined in the Incentive Plans.
As of December 31, 2017, there were 15,768,378 shares available for future grants under the Amended and Restated 2014 Incentive Plan. No additional awards may be made under the 2000 Incentive Plan or the Original 2014 Incentive Plan.
F- 36
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
a. | Stock Options |
Transactions involving stock option awards during 2017 under the Company's Incentive Plans are summarized in the table below.
Number of Shares | Weighted-Average Exercise Price | Weighted-Average Remaining Contractual Term (in years) | Intrinsic Value | |||||||||||
Outstanding as of December 31, 2016 | 25,136,027 | $ | 269.69 | |||||||||||
2017: | Granted | 4,235,015 | $ | 383.56 | ||||||||||
Forfeited | (704,136 | ) | $ | 434.25 | ||||||||||
Expired | (100,727 | ) | $ | 505.96 | ||||||||||
Exercised | (2,360,806 | ) | $ | 122.92 | ||||||||||
Outstanding as of December 31, 2017 | 26,205,373 | $ | 295.98 | 6.52 | $ | 2,904,974 | ||||||||
Vested and expected to vest as of December 31, 2017 | 24,667,723 | $ | 293.65 | 6.46 | $ | 2,904,723 | ||||||||
Exercisable as of December 31, 2017 | 16,263,766 | $ | 223.00 | 5.08 | $ | 2,894,474 | ||||||||
The Company satisfies stock option exercises with newly issued shares of the Company's Common Stock. The total intrinsic value of stock options exercised during 2017, 2016, and 2015 was $735.6 million, $550.4 million, and $1,031.6 million, respectively. The intrinsic value represents the amount by which the market price of the underlying stock exceeds the exercise price of an option.
The table below summarizes the weighted-average exercise prices and weighted-average grant-date fair values of options issued during the years ended December 31, 2017, 2016, and 2015. The fair value of each option granted under the Company's Incentive Plans during these periods was estimated on the date of grant using the Black-Scholes option-pricing model.
Number of Options Granted | Weighted-Average Exercise Price | Weighted-Average Fair Value | |||||||||
2017: | |||||||||||
Exercise price equal to Market Price | 4,235,015 | $ | 383.56 | $ | 118.70 | ||||||
2016: | |||||||||||
Exercise price equal to Market Price | 4,201,978 | $ | 386.44 | $ | 126.68 | ||||||
2015: | |||||||||||
Exercise price equal to Market Price | 4,495,487 | $ | 537.29 | $ | 181.65 | ||||||
For the years ended December 31, 2017, 2016, and 2015, the Company recognized $492.8 million, $546.0 million, and $443.7 million, respectively, of non-cash stock-based compensation expense related to stock option awards (net of amounts capitalized to inventory of $16.8 million, $14.6 million, and $4.8 million, respectively). As of December 31, 2017, there was $816.6 million of stock-based compensation cost related to outstanding stock options, net of estimated forfeitures, which had not yet been recognized. The Company expects to recognize this compensation cost over a weighted-average period of 1.9 years.
F- 37
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Fair Value Assumptions:
The following table summarizes the weighted average values of the assumptions used in computing the fair value of option grants during 2017, 2016, and 2015.
2017 | 2016 | 2015 | |||||||
Expected volatility | 31 | % | 34 | % | 35 | % | |||
Expected lives from grant date | 5.1 years | 5.1 years | 5.1 years | ||||||
Expected dividend yield | 0 | % | 0 | % | 0 | % | |||
Risk-free interest rate | 2.16 | % | 1.84 | % | 1.68 | % | |||
Expected volatility has been estimated based on actual movements in the Company's stock price over the most recent historical periods equivalent to the options' expected lives. Expected lives are principally based on the Company's historical exercise experience with previously issued employee and board of directors' option grants. The expected dividend yield is zero as the Company has never paid dividends and does not currently anticipate paying any in the foreseeable future. The risk-free interest rates are based on quoted U.S. Treasury rates for securities with maturities approximating the options' expected lives.
b. | Restricted Stock |
A summary of the Company's activity related to restricted stock awards during 2017 is summarized below:
Number of Shares | Weighted-Average Grant Date Fair Value | |||||||
Outstanding as of December 31, 2016 | 546,820 | $ | 141.85 | |||||
2017: | Granted | 63,030 | $ | 379.60 | ||||
Vested | (501,590 | ) | $ | 115.07 | ||||
Forfeited | (2,000 | ) | $ | 381.92 | ||||
Outstanding as of December 31, 2017 | 106,260 | $ | 404.72 | |||||
The Company recognized non-cash stock-based compensation expense from restricted stock awards of $14.5 million, $13.9 million, and $15.3 million in 2017, 2016, and 2015, respectively (net of amounts capitalized to inventory, which were not material for each of the three years). As of December 31, 2017, there was $34.9 million of stock-based compensation cost related to unvested shares of restricted stock which had not yet been recognized. The Company expects to recognize this compensation cost over a weighted-average period of 4.0 years.
15. Employee Savings Plans
The Company maintains the Regeneron Pharmaceuticals, Inc. 401(k) Savings Plan, as amended and restated (the "Savings Plan"). The terms of the Savings Plan allow U.S. employees (as defined by the Savings Plan) to contribute to the Savings Plan a percentage of their compensation. In addition, the Company may make discretionary contributions ("Contribution"), as defined, to the accounts of participants under the Savings Plan. The Company recognized $19.6 million, $17.7 million, and $15.4 million of Contribution expense in 2017, 2016, and 2015, respectively.
The Company also maintains the Regeneron Ireland Pension Plan (the "Ireland Plan"), a defined contribution occupational pension plan which covers all eligible Ireland-based employees (as defined by the Ireland Plan). Contributions to the Ireland Plan are comprised of two components: (i) a minimum mandatory employee and employer contribution rate, and (ii) a matching feature, whereby the Company will match employee contributions up to a certain percentage. Employees can make additional voluntary contributions to the Ireland Plan. Expenses recognized by the Company related to contributions to the Ireland Plan were not material during 2017, 2016, and 2015.
F- 38
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
16. Income Taxes
The Company is subject to U.S. federal, state, and foreign income taxes. Components of income before income taxes consist of the following:
Year Ended December 31, | ||||||||||||
2017 | 2016 | 2015 | ||||||||||
United States | $ | 1,964,759 | $ | 1,650,959 | $ | 1,665,087 | ||||||
Foreign | 113,752 | (321,144 | ) | (439,990 | ) | |||||||
$ | 2,078,511 | $ | 1,329,815 | $ | 1,225,097 | |||||||
Components of income tax expense consist of the following:
Year Ended December 31, | ||||||||||||
2017 | 2016 | 2015 | ||||||||||
Current: | ||||||||||||
Federal | $ | 560,250 | $ | 786,964 | $ | 686,561 | ||||||
State | (4,086 | ) | 8,769 | 28,568 | ||||||||
Foreign | 4,827 | (1,362 | ) | 4,004 | ||||||||
Total current tax expense | 560,991 | 794,371 | 719,133 | |||||||||
Deferred: | ||||||||||||
Federal | 317,064 | (377,368 | ) | (119,849 | ) | |||||||
State | (1,258 | ) | 13,431 | (3,768 | ) | |||||||
Foreign | 3,203 | 3,859 | (6,475 | ) | ||||||||
Total deferred tax expense (benefit) | 319,009 | (360,078 | ) | (130,092 | ) | |||||||
$ | 880,000 | $ | 434,293 | $ | 589,041 | |||||||
On December 22, 2017, the bill known as the "Tax Cuts and Jobs Act" (the "Act") was signed into law. The Act, which became effective with respect to most of its provisions as of January 1, 2018, significantly revises U.S. corporate income tax laws by, among other things, reducing the U.S. federal corporate income tax rate from 35% to 21%, changing the taxation of foreign earnings (including taxation of certain global intangible low-taxed income ("GILTI")), allowing immediate expensing for qualified assets, repealing the deduction for domestic manufacturing, and imposing further limitations on the deductibility of executive compensation. As a result of the Act being signed into law, the Company recognized a provisional charge of $326.2 million in the fourth quarter of 2017 related to the re-measurement of its U.S. net deferred tax assets at the lower enacted corporate tax rates. The provisional charge recorded in the fourth quarter of 2017 is an estimate, and the measurement of deferred tax assets is subject to further analysis, such as developing interpretations and clarifications of the provisions of the Act, which could result in changes to this estimate during 2018. In addition, the Company has not yet elected an accounting method regarding whether to record deferred tax assets and liabilities for expected amounts of GILTI inclusions or whether to treat such amounts as a period cost.
The Company elected to early adopt Accounting Standards Update 2016-09, Compensation -Stock Compensation, Improvements to Employee Share-Based Payment Accounting, during the second quarter of 2016. Consequently, in 2017 and 2016, the Company recorded excess tax benefits of $191.0 million and $144.8 million, respectively, within income tax expense. In 2015, the Company utilized $405.3 million of excess tax benefits in connection with stock option exercises, which were credited to additional paid-in capital as realized.
The Company also recorded an income tax provision in its Statement of Comprehensive Income of $24.9 million during the year ended December 31, 2015, primarily related to unrealized gains on available-for-sale marketable securities. Such amounts were not material for the years ended December 31, 2017 and 2016.
F- 39
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
A reconciliation of the U.S. statutory income tax rate to the Company's effective income tax rate is as follows:
Year Ended December 31, | ||||||||
2017 | 2016 | 2015 | ||||||
U.S. federal statutory tax rate | 35.0 | % | 35.0 | % | 35.0 | % | ||
Impact of change in U.S. corporate tax rate (the Act) | 15.7 | — | — | |||||
Stock-based compensation | (9.0 | ) | (10.9 | ) | — | |||
State and local income taxes | 0.1 | 1.3 | 0.9 | |||||
Taxation of non-U.S. operations | 0.7 | 8.8 | 12.2 | |||||
Income tax credits | (1.3 | ) | (1.2 | ) | (1.6 | ) | ||
Non-deductible Branded Prescription Drug Fee | 1.7 | 1.9 | 2.0 | |||||
Domestic production activities deduction | (2.6 | ) | (2.8 | ) | (3.2 | ) | ||
Other permanent differences | 2.0 | 0.6 | 2.8 | |||||
Effective income tax rate | 42.3 | % | 32.7 | % | 48.1 | % | ||
In 2017, the difference between the U.S. federal statutory rate of 35% and the Company's effective tax rate of 42.3% was primarily attributable to the negative impact of the charge related to the re-measurement of the Company's U.S. net deferred tax assets upon the enactment of the Act (see above), partly offset by the tax benefit associated with stock-based compensation. In 2016, the difference between the U.S. federal statutory rate of 35% and the Company's effective tax rate of 32.7% was primarily attributable to the tax benefit associated with stock-based compensation, partly offset by the negative impact of losses incurred in foreign jurisdictions with rates lower than the U.S. federal statutory rate. In 2015, the difference between the U.S. federal statutory rate of 35% and the Company's effective tax rate of 48.1% was primarily attributable to losses incurred in foreign jurisdictions with rates lower than the U.S. federal statutory rate, partly offset by the positive impact of the domestic manufacturing deduction.
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of the Company's deferred tax assets and liabilities are as follows:
As of December 31, | ||||||||
2017 | 2016 | |||||||
Deferred tax assets: | ||||||||
Deferred revenue | $ | 102,441 | $ | 214,587 | ||||
Deferred compensation | 391,034 | 515,984 | ||||||
Fixed assets and intangible assets | — | 21,139 | ||||||
Accrued expenses | 38,312 | 37,188 | ||||||
Other | 26,387 | 49,100 | ||||||
558,174 | 837,998 | |||||||
Valuation allowance | (4,187 | ) | (3,420 | ) | ||||
Total deferred tax assets | 553,987 | 834,578 | ||||||
Deferred tax liabilities: | ||||||||
Fixed assets and intangible assets | (44,629 | ) | — | |||||
Other | (3,067 | ) | (9,275 | ) | ||||
Total deferred tax liabilities | (47,696 | ) | (9,275 | ) | ||||
Net deferred tax assets | $ | 506,291 | $ | 825,303 | ||||
F- 40
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
The Company's 2012 through 2016 federal income tax returns remain open to examination by the IRS. The Company's 2012 and 2013 federal income tax returns are currently under audit by the IRS. The Company's state income tax returns from 2013 to 2016 remain open to examination. The United States and many states generally have statutes of limitation ranging from 3 to 5 years; however, those statutes could be extended due to the Company's net operating loss and tax credit carryforward positions in a number of the Company's tax jurisdictions. In general, tax authorities have the ability to review income tax returns for loss periods in which the statute of limitation has previously expired to adjust the net operating loss carryforward or tax credits generated in those years.
The following table summarizes the gross amounts of unrecognized tax benefits. The amount of unrecognized tax benefits that, if settled, would impact the effective tax rate is $146.2 million, $107.2 million, and $102.1 million as of December 31, 2017, 2016, and 2015, respectively.
2017 | 2016 | 2015 | ||||||||||
Balance as of January 1 | $ | 117,166 | $ | 116,572 | $ | 57,615 | ||||||
Gross increases related to current year tax positions | 49,028 | 45,575 | 59,909 | |||||||||
Gross decreases related to prior year tax positions | (5,606 | ) | (42,284 | ) | (952 | ) | ||||||
Gross decrease due to settlements, recapture, filed returns, and lapse of statutes of limitation | (14,430 | ) | (2,697 | ) | — | |||||||
Balance as of December 31 | $ | 146,158 | $ | 117,166 | $ | 116,572 | ||||||
In 2017, 2016 and 2015, the increases in unrecognized tax benefits related primarily to the Company's calculation of certain tax credits and other items related to the Company's international operations. In addition, in 2017 and 2016, there was a decrease in unrecognized tax benefits related to a settlement in connection with a disputed state tax matter. In 2017, 2016, and 2015, accrued interest related to unrecognized tax benefits recorded by the Company was not material. The Company does not believe that it is reasonably possible that its unrecognized tax benefits as of December 31, 2017 will decrease within the next twelve months as a result of the resolution of tax exposures.
17. Legal Matters
From time to time, the Company is a party to legal proceedings in the course of the Company's business. Costs associated with the Company's involvement in legal proceedings are expensed as incurred. The outcome of any such proceedings, regardless of the merits, is inherently uncertain. If the Company were unable to prevail in any such proceedings, its consolidated financial position, results of operations, and future cash flows may be materially impacted.
Proceedings Relating to '287 Patent, '163 Patent, and '018 Patent
The Company is a party to patent infringement litigation initiated by the Company involving its European Patent No. 1,360,287 (the "'287 Patent"), its European Patent No. 2,264,163 (the "'163 Patent"), and its U.S. Patent No. 8,502,018 (the "'018 Patent"). Each of these patents concerns genetically engineered mice capable of producing chimeric antibodies that are part human and part mouse. Chimeric antibody sequences can be used to produce high-affinity fully human monoclonal antibodies. In these proceedings, the Company claims infringement of several claims of the '287 Patent, the '163 Patent, and the '018 Patent (as applicable), and seeks, among other types of relief, an injunction and an account of profits in connection with the defendants' infringing acts, which may include, among other things, the making, use, keeping, sale, or offer for sale of genetically engineered mice (or certain cells from which they are derived) that infringe one or more claims of the '287 Patent, the '163 Patent, and the '018 Patent (as applicable).
On September 25, 2013, the Company commenced patent infringement litigation against Kymab Ltd in the English High Court of Justice, Chancery Division, Patents Court, in London, asserting the '287 Patent and '163 Patent. A trial to adjudicate the claims of infringement and counterclaims of invalidity of the '287 Patent and the '163 Patent was held from November 16, 2015 through December 8, 2015. On February 1, 2016, the court issued a final judgment, finding that the asserted claims of the '287 and '163 Patents are novel, not obvious, and infringed by Kymab's genetically engineered mice. However, the court invalidated the '287 and '163 Patents on the ground of insufficiency. The hearing for the Company's appeal and Kymab's cross-appeal was held on October 17–20, 2017.
F- 41
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
On March 11, 2014, the Company commenced '287 Patent infringement litigation and '018 Patent infringement litigation against Merus B.V., a company based in Utrecht, The Netherlands, in the District Court of The Hague (currently stayed by agreement of the parties) and the United States District Court for the Southern District of New York, respectively. On November 21, 2014, the United States District Court for the Southern District of New York issued its Opinion and Order on Claim Construction in the '018 Patent infringement litigation, in which it held the '018 Patent invalid and not infringed. On November 2, 2015, the United States District Court for the Southern District of New York issued an opinion and order finding that the '018 Patent was procured by inequitable conduct, thus rendering it unenforceable. On July 27, 2017, the United States Court of Appeals for the Federal Circuit (the "Federal Circuit") affirmed the District Court's decision regarding inequitable conduct without deciding the issues of validity and infringement. On September 12, 2017, the Company filed a petition for panel rehearing and/or rehearing en banc in the Federal Circuit. On December 26, 2017, the Federal Circuit issued an order denying the Company's petition for panel rehearing and rehearing en banc.
On July 8 and July 13, 2016, notices of opposition against the '163 Patent were filed in the European Patent Office (the "EPO") by Merus N.V. and Kymab and Novo Nordisk A/S, respectively. The notices assert, as applicable, lack of novelty, lack of inventive step, and insufficiency. The Company's response to the oppositions was filed on December 30, 2016. Following an oral hearing before the Opposition Division of the EPO on February 5–7, 2018, the Opposition Division upheld the '163 Patent without amendments.
With respect to the '287 Patent infringement and '018 Patent infringement litigation against Merus B.V., Merus has filed a motion seeking the payment of attorney's fees it incurred by the Company; if the Company is ultimately required to pay such fees, such payment is not expected to have a material impact on the Company's financial statements. Other than as noted in the preceding sentence, the Company is not at this time able to predict the outcome of, or estimate possible gain or a range of possible loss, if any, related to, the '287 Patent, '163 Patent, and '018 Patent proceedings.
Proceedings Relating to Praluent (alirocumab) Injection
As described in greater detail below, the Company is currently a party to patent infringement actions initiated by Amgen Inc. against the Company and Sanofi (and/or the Company's and Sanofi's respective affiliated entities) in a number of jurisdictions relating to Praluent, which the Company is jointly developing and commercializing with Sanofi.
In the United States, Amgen has asserted a number of U.S. patents, which were subsequently narrowed to U.S. Patent Nos. 8,829,165 (the "'165 Patent") and 8,859,741 (the "'741 Patent"), and seeks a permanent injunction to prevent the Company and the Sanofi defendants from commercial manufacturing, using, offering to sell, or selling within the United States (as well as importing into the United States) (collectively, "Commercializing") Praluent. Amgen also seeks a judgment of patent infringement of the asserted patents, monetary damages (together with interest), costs and expenses of the lawsuits, and attorneys' fees. A jury trial in this litigation was held in the United States District Court for the District of Delaware (the "District Court") from March 8 to March 16, 2016. During the course of the trial, the District Court ruled as a matter of law in favor of Amgen that the asserted patent claims were not obvious, and in favor of the Company and the Sanofi defendants that there was no willful infringement of the asserted patent claims by the Company or the Sanofi defendants. On March 16, 2016, the jury returned a verdict in favor of Amgen, finding that the asserted claims of the '165 and '741 Patents were not invalid based on either a lack of written description or a lack of enablement. On January 3, 2017, the District Court issued a final opinion and judgment, denying the Company and the Sanofi defendants' motions for new trial and judgment as a matter of law. The District Court also denied as moot Amgen's motion to strike the Company and the Sanofi defendants' request to obtain a judgment as a matter of law, which allowed the Federal Circuit to address the Company and the Sanofi defendants' patent invalidity arguments on appeal. On January 12, 2017, the Company and the Sanofi defendants filed a notice of appeal with the Federal Circuit. On April 19, 2017, the District Court granted Amgen's motion to amend the judgment on an accounting of supplemental damages and enhancement of such damages if deemed appropriate, but deferred the order until after the Federal Circuit issued a decision on the appeal. Oral argument on the appeal was held on June 6, 2017. On October 5, 2017, the Federal Circuit reversed in part the District Court's decision, remanded for a new trial on the issues of written description and enablement, and, as discussed below, vacated the District Court's permanent injunction. In addition, it affirmed the District Court's ruling that Amgen's patents were not obvious. The Federal Circuit further concluded the Company and the Sanofi defendants were not entitled to judgment as a matter of law on the issues of written description and enablement on this record. On December 6, 2017, Amgen filed a petition for rehearing en banc in the Federal Circuit; and, on February 6, 2018, the Company and the Sanofi defendants filed their response.
On January 5, 2017, the District Court granted a permanent injunction prohibiting Regeneron and the Sanofi defendants from Commercializing Praluent in the United States but subsequently delayed its imposition until February 21, 2017. The Federal Circuit stayed the injunction pending appeal on February 8, 2017 and vacated it on October 5, 2017.
F- 42
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
On July 25, 2016, Amgen filed a lawsuit against Regeneron, Sanofi-Aventis Groupe S.A., Sanofi-Synthelabo Limited, Aventis Pharma Limited, Sanofi Winthrop Industrie S.A., and Sanofi-Aventis Deutschland GmbH in the English High Court of Justice, Chancery Division, Patents Court, in London, seeking a declaration of infringement of Amgen's European Patent No. 2,215,124 (the "'124 Patent"), which pertains to PCSK9 monoclonal antibodies, by Praluent. The lawsuit also seeks a permanent injunction, damages, an accounting of profits, and costs and interest. On February 8, 2017, the court temporarily stayed this litigation on terms mutually agreed by the parties.
Also on July 25, 2016, Amgen filed a lawsuit for infringement of the '124 Patent against Regeneron, Sanofi-Aventis Groupe S.A., Sanofi Winthrop Industrie S.A., and Sanofi-Aventis Deutschland GmbH in the Regional Court of Düsseldorf, Germany (the "Düsseldorf Regional Court"), seeking a permanent injunction, an accounting of marketing activities, a recall of Praluent and its removal from distribution channels, and damages. On November 14, 2017, the Düsseldorf Regional Court issued a decision staying the infringement proceedings until a decision of the Opposition Division of the EPO concerning the pending opposition filed by the Company, Sanofi, and several other opponents against the '124 Patent (as discussed below). Following Amgen's request to reopen the proceedings in light of the issuance of the Preliminary Opinion (as defined below), the Düsseldorf Regional Court has scheduled an oral hearing for September 11, 2018.
On September 26, 2016, Amgen filed a lawsuit for infringement of the '124 Patent in the Tribunal de grande instance in Paris, France against Regeneron, Sanofi-Aventis Groupe S.A., Sanofi Winthrop Industrie, and Sanofi Chimie (subsequently added as a defendant). Amgen is seeking the prohibition of allegedly infringing activities with a €10,000 penalty per drug unit of Praluent produced in violation of the court order sought by Amgen; an appointment of an expert for the assessment of damages; disclosure of technical (including supply-chain) and accounting information to the expert and the court; provisional damages of €10.0 million (which would be awarded on an interim basis pending final determination); reimbursement of costs; publication of the ruling in three newspapers; and provisional enforcement of the decision to be issued, which would ensure enforcement of the decision (including any provisional damages) pending appeal. Amgen is not seeking a preliminary injunction in this proceeding at this time. On April 10, 2017, the Company and the Sanofi parties filed briefs seeking invalidation of certain of the claims of the '124 Patent, and Amgen filed a response on July 28, 2017. Oral hearing on this infringement lawsuit is currently scheduled for June 29, 2018.
The '124 Patent is also subject to opposition proceedings in the EPO seeking to invalidate certain of its claims, which were initiated by Sanofi on February 24, 2016 and, separately, by the Company, Sanofi, and several other opponents on November 24, 2016. On December 13, 2017, the Opposition Division of the EPO issued a preliminary, non-binding opinion (the "Preliminary Opinion") regarding the validity of the '124 Patent, indicating that it currently considers the claims of a new request filed by Amgen in response to the opposition to satisfy the requirements for patentability. The Preliminary Opinion was accompanied by a summons to oral hearing to be held on November 28–30, 2018.
On May 19, 2017, Amgen filed a lawsuit for infringement of Amgen's Japanese Patent Nos. 5,906,333 (the "'333 Patent") and 5,705,288 (the "'288 Patent") in the Tokyo District Court Civil Division against Sanofi K.K. Amgen's complaint alleges that manufacturing, selling or otherwise transferring, and offering to sell or otherwise transfer Praluent (alirocumab) in Japan (as well as importing Praluent (alirocumab) into Japan) infringe the '333 and '288 Patents. The complaint further seeks a permanent injunction, disposal of product, and court costs. The Company has not been named as a defendant in this litigation.
At this time, the Company is not able to predict the outcome of, or estimate a range of possible loss, if any, related to these proceedings.
Proceedings Relating to Dupixent (dupilumab) Injection
On March 20, 2017, the Company, Sanofi-Aventis U.S. LLC, and Genzyme Corporation filed a complaint against Amgen and Immunex Corporation, a wholly owned subsidiary of Amgen, in the United States District Court for the District of Massachusetts seeking a declaratory judgment that the Company's and the other plaintiffs' Commercializing of Dupixent does not directly or indirectly infringe U.S. Patent No. 8,679,487 (the "'487 Patent") owned by Immunex Corporation relating to antibodies that bind the human interleukin-4 receptor. On May 1, 2017, the Company and the other plaintiffs filed a notice of voluntary dismissal of this action without prejudice.
On March 23, 2017, the Company, Sanofi-Aventis U.S. LLC, and Genzyme Corporation initiated an inter partes review ("IPR") in the United States Patent and Trademark Office ("USPTO") seeking a declaration of invalidity of the '487 Patent. On July 28 and 31, 2017, the same parties filed two additional IPR petitions in the USPTO seeking declarations of invalidity of the '487 Patent based on different grounds (the "Additional IPR Petitions"). On October 4, 2017, the Patent Trial and Appeal Board of the USPTO
F- 43
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
issued a decision on the first IPR petition and declined to institute an IPR proceeding to review the validity of the '487 Patent. The Additional IPR Petitions are still pending.
On April 5, 2017, Immunex Corporation filed a complaint against the Company, Sanofi, Sanofi-Aventis U.S. LLC, Genzyme Corporation, and Aventisub LLC in the United States District Court for the Central District of California seeking a judgment of patent infringement of the '487 Patent and a declaratory judgment of infringement of the '487 Patent, in each case by the Company's and the other defendants' Commercializing of Dupixent; monetary damages (together with interest); an order of willful infringement of the '487 Patent, which would allow the court in its discretion to award damages up to three times the amount assessed; costs and expenses of the lawsuit; and attorneys' fees. Immunex is not seeking an injunction in this proceeding at this time. On June 21, 2017, the court denied a motion to dismiss Immunex's complaint previously filed by the Company and the Sanofi parties. On June 28, 2017, the Company and the Sanofi parties filed an answer to Immunex's complaint and counterclaims against Immunex and Amgen (which was amended on October 31, 2017 to, among other things, add an inequitable conduct allegation), and Immunex and Amgen filed an answer to the counterclaims on July 28, 2017. A combined hearing on the construction of certain disputed claim terms of the '487 Patent and summary judgment on the issue of indefiniteness of the '487 Patent claims has been scheduled for March 12, 2018. A jury trial has been scheduled to start on March 19, 2019.
At this time, the Company is not able to predict the outcome of, or estimate a range of possible loss, if any, related to these proceedings.
Proceedings Relating to Shareholder Derivative Claims
On December 30, 2015, an alleged shareholder filed a shareholder derivative complaint in the New York Supreme Court, naming the then current and certain former non-employee members of the Company's board of directors, the Chairman of the board of directors, the Company's Chief Executive Officer, and the Company's Chief Scientific Officer as defendants and Regeneron as a nominal defendant. The complaint asserts that the individual defendants breached their fiduciary duties and were unjustly enriched when they approved and/or received allegedly excessive compensation in 2013 and 2014. The complaint seeks damages in favor of the Company for the alleged breaches of fiduciary duties and unjust enrichment; changes to Regeneron's corporate governance and internal procedures; invalidation of the Regeneron Pharmaceuticals, Inc. 2014 Long-Term Incentive Plan with respect to the individual defendants' compensation and a shareholder vote regarding the individual defendants' equity compensation; equitable relief, including an equitable accounting with disgorgement; and award of the costs of the action, including attorneys' fees. On June 28, 2017, the court dismissed the plaintiff's claims with respect to certain compensation awarded in 2013 but denied the defendants' motion to dismiss the other claims set forth in the complaint. On November 8, 2017, another alleged shareholder filed a second shareholder derivative complaint in the New York Supreme Court, naming the then current and certain former non-employee members of the Company's board of directors, the Chairman of the board of directors, the Company's Chief Executive Officer, the Company's Chief Scientific Officer, and Regeneron as defendants. The complaint asserts that the individual defendants breached their fiduciary duties and were unjustly enriched when they approved and/or received allegedly excessive compensation in 2014, 2015, and 2016. The complaint seeks damages in favor of Regeneron for the alleged breaches of fiduciary duties and unjust enrichment; changes to Regeneron's corporate governance and internal procedures; invalidation of Regeneron's 2014 Long-Term Incentive Plan with respect to the individual defendants' compensation and the imposition of meaningful limits on the amount of equity payable to the individual defendants; a shareholder vote regarding the individual defendants' equity compensation; equitable relief, including an equitable accounting with disgorgement; and award of the costs of the action, including attorneys' fees. On December 4, 2017, the plaintiff in the second action moved to consolidate both actions, to be appointed lead plaintiff, and to have its counsel be appointed lead counsel in the proposed consolidated action. The court scheduled a hearing on the motion on March 7, 2018. The parties in both the first derivative action and the second derivative action have agreed to a schedule for document discovery and the filing of defendants' appeal of the court's June 28, 2017 decision, as well as a stay of all non-document discovery pending a decision on defendants' appeal. Pursuant to the Company's By-Laws and the New York Business Corporation Law, expenses in connection with the foregoing are being advanced by the Company for the individual defendants.
On or about December 15, 2015, the Company received a shareholder litigation demand upon the Company's board of directors made by a purported Regeneron shareholder. On or about November 3, 2017, the Company received a second shareholder litigation demand upon the Company's board of directors made by another purported Regeneron shareholder, which is substantially similar to the December 15, 2015 shareholder litigation demand. The demands assert that the then current and certain former non-employee members of the board of directors and the Chairman of the board of directors excessively compensated themselves in 2013 and 2014. The demands request that the board of directors investigate and bring legal action against these directors for breach of fiduciary duty, unjust enrichment, and corporate waste, and implement internal controls and systems designed to prohibit and prevent similar actions in the future. On December 20, 2017, the parties to the shareholder derivative action filed on December
F- 44
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
30, 2015, entered into a stipulation with the second demanding shareholder. The stipulation provides that the purported shareholder will intervene as a plaintiff in the action, and that the purported shareholder's litigation demand will be withdrawn and deemed null and void. The stipulation was approved by the court on January 18, 2018. The first shareholder litigation demand has also since been withdrawn.
At this time, the Company is not able to predict the outcome of, or estimate a range of possible loss, if any, relating to these matters.
Department of Justice Investigation
In January 2017, the Company received a subpoena from the U.S. Attorney's Office for the District of Massachusetts requesting documents relating to its support of 501(c)(3) organizations that provide financial assistance to patients; documents concerning its provision of financial assistance to patients with respect to products sold or developed by Regeneron (including EYLEA, Praluent, ARCALYST, and ZALTRAP); and certain other related documents and communications. The Company is cooperating with this investigation. The Company cannot predict the outcome or duration of this investigation or any other legal proceedings or any enforcement actions or other remedies that may be imposed on the Company arising out of this investigation.
18. Net Income Per Share
The Company's basic net income per share amounts have been computed by dividing net income by the weighted average number of shares of Common Stock and Class A Stock outstanding. Net income per share is presented on a combined basis, inclusive of Common Stock and Class A Stock outstanding, as each class of stock has equivalent economic rights. Diluted net income per share includes the potential dilutive effect of other securities as if such securities were converted or exercised during the period, when the effect is dilutive. The calculations of basic and diluted net income per share are as follows:
Year Ended December 31, | ||||||||||||
2017 | 2016 | 2015 | ||||||||||
Net income - basic | $ | 1,198,511 | $ | 895,522 | $ | 636,056 | ||||||
Effect of dilutive securities: | ||||||||||||
Convertible senior notes - interest expense and amortization of discount and note issuance costs | — | 397 | — | |||||||||
Net income - diluted | $ | 1,198,511 | $ | 895,919 | $ | 636,056 | ||||||
(Shares in thousands) | ||||||||||||
Weighted average shares - basic | 106,338 | 104,719 | 103,061 | |||||||||
Effect of dilutive securities: | ||||||||||||
Stock options | 9,132 | 10,177 | 9,446 | |||||||||
Restricted stock | 484 | 474 | 477 | |||||||||
Convertible senior notes | — | 61 | — | |||||||||
Warrants | — | 936 | 2,246 | |||||||||
Dilutive potential shares | 9,616 | 11,648 | 12,169 | |||||||||
Weighted average shares - diluted | 115,954 | 116,367 | 115,230 | |||||||||
Net income per share - basic | $ | 11.27 | $ | 8.55 | $ | 6.17 | ||||||
Net income per share - diluted | $ | 10.34 | $ | 7.70 | $ | 5.52 | ||||||
F- 45
REGENERON PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(Unless otherwise noted, dollars in thousands, except per share data)
Shares which have been excluded from diluted per share amounts because their effect would have been antidilutive, include the following:
Year Ended December 31, | |||||||||
(Shares in thousands) | 2017 | 2016 | 2015 | ||||||
Stock options | 9,161 | 8,041 | 1,343 | ||||||
Restricted stock | — | 19 | — | ||||||
Convertible senior notes | — | — | 994 | ||||||
19. Statement of Cash Flows
Supplemental disclosure of non-cash investing and financing activities
Included in accounts payable and accrued expenses as of December 31, 2017, 2016, and 2015 were $41.8 million, $28.2 million, and $50.7 million, respectively, of accrued capital expenditures.
The Company recognized additional capital and facility lease obligations of $201.2 million, $154.9 million, and $26.0 million during 2017, 2016 and 2015, respectively, in connection with the Company's Tarrytown Leases (see Note 12).
20. Unaudited Quarterly Results
Summarized quarterly financial data (unaudited) for the years ended December 31, 2017 and 2016 are set forth in the following tables.
First Quarter Ended March 31, 2017 | Second Quarter Ended June 30, 2017* | Third Quarter Ended September 30, 2017 | Fourth Quarter Ended December 31, 2017** | |||||||||||||
Revenues | $ | 1,318,991 | $ | 1,470,116 | $ | 1,500,673 | $ | 1,582,447 | ||||||||
Net income | $ | 248,931 | $ | 387,744 | $ | 388,317 | $ | 173,519 | ||||||||
Net income per share - basic | $ | 2.36 | $ | 3.66 | $ | 3.64 | $ | 1.62 | ||||||||
Net income per share - diluted | $ | 2.16 | $ | 3.34 | $ | 3.32 | $ | 1.50 | ||||||||
First Quarter Ended March 31, 2016*** | Second Quarter Ended June 30, 2016 | Third Quarter Ended September 30, 2016 | Fourth Quarter Ended December 31, 2016 | |||||||||||||
Revenues | $ | 1,200,849 | $ | 1,212,629 | $ | 1,220,122 | $ | 1,226,827 | ||||||||
Net income | $ | 181,385 | $ | 196,218 | $ | 264,804 | $ | 253,115 | ||||||||
Net income per share - basic | $ | 1.74 | $ | 1.88 | $ | 2.53 | $ | 2.41 | ||||||||
Net income per share - diluted | $ | 1.59 | $ | 1.69 | $ | 2.27 | $ | 2.19 | ||||||||
* During the quarterly period ended June 30, 2017, the Company recorded an out-of-period adjustment to reflect a correction in the Company's accounting for its lease of its Tarrytown, New York facility. The adjustment, which was related to the March 3, 2017 lease transaction, resulted in the recognition of a non-cash loss on debt extinguishment of $30.1 million.
** As a result of the Act being signed into law on December 22, 2017, the Company recognized a charge of $326.2 million in the fourth quarter of 2017 related to the re-measurement of its U.S. net deferred tax assets at the lower enacted corporate tax rate (see Note 16).
*** Due to the adoption of ASU 2016-09 in the second quarter of 2016, the Company revised its net income from the amounts originally reported for the quarterly period ended March 31, 2016 to include a $15.6 million income tax benefit, which was originally recorded as additional paid-in capital.
F- 46