Attached files
| file | filename |
|---|---|
| EX-31.2 - EX-31.2 - PLx Pharma Inc. | a2227816zex-31_2.htm |
| EX-31.1 - EX-31.1 - PLx Pharma Inc. | a2227816zex-31_1.htm |
| EX-23.1 - EX-23.1 - PLx Pharma Inc. | a2227816zex-23_1.htm |
| EX-32.2 - EX-32.2 - PLx Pharma Inc. | a2227816zex-32_2.htm |
| EX-10.39 - EX-10.39 - PLx Pharma Inc. | a2227816zex-10_39.htm |
| EX-32.1 - EX-32.1 - PLx Pharma Inc. | a2227816zex-32_1.htm |
Use these links to rapidly review the document
Table of Contents
DIPEXIUM PHARMACEUTICALS, INC. FINANCIAL STATEMENTS TABLE OF CONTENTS
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| (Mark One) | ||
ý |
Annual Report Under Section 13 Or 15(d) Of The Securities Exchange Act Of 1934 |
|
For the fiscal year ended December 31, 2015 |
||
or |
||
o |
Transition Report Under Section 13 Or 15(d) Of The Securities Exchange Act Of 1934 |
|
For the transition period from to |
||
COMMISSION FILE NUMBER: 001-36351
DIPEXIUM PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
| Delaware (State or other jurisdiction of incorporation or organization) |
46-4995704 (I.R.S. Employer Identification No.) |
14 Wall Street, 3rd Floor
New York, NY, 10005
(Address of principal executive offices)(Zip Code)
(212) 269-2834
Registrant's telephone number, including area code
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No ý
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes o No ý
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate website, if any, every Interactive Date File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (Section 232.405 of the chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ý No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ý
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer o | Accelerated filer o | Non-accelerated filer o (Do not check if a smaller reporting company) |
Smaller reporting company ý |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 126-2 of the act): Yes o No ý
The aggregate market value of voting stock held by nonaffiliates of the registrant as of June 30, 2015, the last business day of the registrant's most recently completed second fiscal quarter, based on the closing price of the common stock on the NASDAQ stock exchange on June 30, 2015 was $77,568,188.
As of March 21, 2016, 10,351,613 shares of common stock, $0.001 par value per share, were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE:
Portions of our Proxy Statement for the Annual Meeting of Shareholders to be held on May 24, 2016, are incorporated by reference in Items 10, 11, 12, 13 and 14 of Part III.
1
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
We are including the following cautionary statement in this Annual Report on Form 10-K to make applicable and take advantage of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 for any forward-looking statements made by, or on behalf of us. With the exception of historical matters, the matters discussed in this Annual Report on Form 10-K are forward-looking statements (as defined in Section 21E of the Exchange Act) that involve risks and uncertainties that could cause actual results to differ materially from projected results. Accordingly, investors should not place undue reliance on forward-looking statements as a prediction of actual results. The forward-looking statements may include projections and estimates concerning the timing and success of specific projects and our future production, revenues, income and capital spending. When we use the words "believe," "intend," "expect," "may," "should," "anticipate," "could," "estimate," "plan," "predict," "project," or their negatives, or other similar expressions, the statements which include those words are usually forward-looking statements. When we describe strategy that involves risks or uncertainties, we are making forward-looking statements. The forward-looking statements in this Annual Report on Form 10-K speak only as of the date of this Annual Report on Form 10-K; we disclaim any obligation to update these statements unless required by securities law, and we caution you not to rely on them unduly. We have based these forward-looking statements on our current expectations and assumptions about future events. While our management considers these expectations and assumptions to be reasonable, they are inherently subject to significant business, economic, competitive, regulatory and other risks, contingencies and uncertainties, most of which are difficult to predict and many of which are beyond our control. These risks, contingencies and uncertainties relate to, among other matters, the following:
- •
- risks and uncertainties associated with our research and development activities, including our clinical trials;
- •
- our dependence on Locilex® as our only product;
- •
- our ability to raise capital when needed;
- •
- the timing of and our ability to achieve U.S. or international regulatory approvals for Locilex® or any other product
candidates we may develop;
- •
- our dependence on others to conduct clinical research of, and to manufacture and market, Locilex®;
- •
- the terms of future licensing arrangements, and whether we can enter into such arrangements at all;
- •
- risks associated with the timing and receipt of licensing and milestone revenues, if any;
- •
- our ability to gain market acceptance for Locilex® or any other product candidates we may develop;
- •
- our ability to maintain or protect the validity of our patents and other intellectual property, including in connection with pending
or future litigation against us;
- •
- our ability to secure registration for our current and future patent applications;
- •
- our ability to extend our licensed composition of matter patent No. 5,912,231 under the Hatch-Waxman Act with the cooperation
of Scripps;
- •
- our estimates of the size of the prospective markets in which we may offer Locilex®;
- •
- our ability to continue as a going concern;
- •
- our expectations regarding minimizing our development risk;
- •
- our ability to establish new relationships and maintain current relationships;
- •
- our ability to attract and retain key personnel; and
- •
- acceptance of our business model by investors.
2
Overview
We are a late stage pharmaceutical company focused on the development and commercialization of Locilex® (pexiganan cream 0.8%), a novel, first-in-class, broad spectrum, topical antibiotic. Locilex® is a chemically synthesized, 22-amino acid peptide isolated from the skin of the African Clawed Frog. Its novel mechanism of action kills microbial targets by disrupting the bacterial cell membrane; a process known as cell membrane permeability. Locilex® is initially being targeted for the treatment of mild infections of diabetic foot ulcers (or Mild DFI). In 2011, the market for diabetic foot infection therapeutics worldwide was approximately $1.46 billion. Our primary objective is to establish Locilex® as the standard of care for the treatment of patients with Mild DFI. Thereafter, our growth strategy includes potentially expanding the indications for Locilex® to include moderate infections of diabetic foot ulcers (or Moderate DFI) and certain other mild or moderate skin and skin structure infections in superficial wounds.
We believe that we have a clear clinical and regulatory pathway with the potential for United States Food and Drug Administration (or FDA) approval of Locilex® by the second half of 2017. We are conducting two pivotal Phase 3 clinical trials in the United States under the auspicies of our special protocol assessment (or SPA) agreement with the FDA on our Phase 3 program. We intend to complete enrollment in these two pivotal Phase 3, double blind, placebo-controlled superiority studies in the first half of 2016. We successfully conducted two separate Phase 1 skin irritation and skin sensitization studies and we reported data on the first of these two Phase 1 studies in Q3 2014 and reported data on the second Phase 1 study in Q1 2015. If the data from our Phase 3 studies are sufficient to meet the primary endpoint, we expect to submit a new drug application (or NDA) amendment for Locilex® to the FDA and European Medicines Agency (EMA) soon thereafter. We expect to receive a response from the FDA within six months of our NDA amendment submission. In Europe, we anticipate receiving a response from EMA within ten months of submitting a marketing authorization application to the EMA under the centralized process.
According to the Infectious Disease Society of America (or IDSA), diabetic foot infections (or DFI) may be classified by their clinical severity as mild, moderate, or severe. 47% of DFI patients first present to a treating physician in the mild stage of infection, 34% of DFI patients first present at the moderate stage and 18% of DFI patients first present at the severe stage. At the mild stage, patients can typically be treated on an outpatient basis and amputation risk is minimal (2% to 3% in Mild DFI). When not managed effectively, the potential for Mild DFI to progress to a limb- or life-threatening infection increases dramatically. Published research suggests amputation rates increase in Moderate DFI and severe infections of diabetic foot ulcers (or Severe DFI) to approximately 45% and 75%, respectively. Similarly, the hospitalization rate for Mild DFI patients is approximately 10%, increasing in Moderate DFI and Severe DFI to approximately 55% and 85%, respectively. Thus, DFIs are a major cause of patient morbidity, a substantial burden to the healthcare system, and a source of high financial costs.
Systemic antibiotics currently prescribed off-label to treat Mild DFI generate resistant pathogens which create infections that are more difficult to treat. Such antibiotics are also associated with toxic side effects in patients who typically have some degree of compromised liver and kidney function. We believe that a topical preparation like Locilex®, which is locally administered on the open wound and skin, offers significant advantages over systemic treatments. As a topical antibiotic, Locilex® affects only the area to which it is applied, and unlike most systemic antibiotics, it does not spread to the entire body through the bloodstream, which is host to a number of different bacteria other than bacteria causing the skin infection. Topical antibiotics are also delivered to the infected area at a higher concentration than those antibiotics that are delivered systemically. As a result, we believe that topical
3
antibiotics are less likely to develop bacterial resistance, both because the higher antibiotic concentration more effectively kills the infection-causing bacteria before they develop resistance, and because other bacteria in the bloodstream are not exposed to the Locilex® topical cream. Currently, there are no products, including no antibiotics, specifically approved by the FDA for the treatment of Mild DFI, nor are there any topical antibiotics currently approved for any severity of DFI. As such, we believe that Locilex® has the potential to be the first topical antibiotic approved for the treatment of DFI, as well as the first product of any kind to be labeled specifically for the treatment of Mild DFI.
We believe that the key attributes of Locilex® are: (i) it has not generated resistant bacteria systemically; (ii) it has not generated cross resistance with other antibiotics; (iii) it has demonstrated activity against a broad spectrum of pathogens, including difficult to treat gram negative, and anaerobic bacteria; (iv) it has not been systemically absorbed; and (v) it has not caused any significant safety or tolerability issues in over 500 patients treated (all data being that from studies prior to the current double blind Phase 3 studies); and (vi) it has demonstrated significant success treating multi-drug resistant bacteria in several laboratory tests and clinical trials performed to date. These attributes lead us to believe that Locilex® has the potential to be positioned as the standard of care to treat patients with Mild DFI. In addition, data generated to date support the potential use of Locilex® to treat a broad array of mild or moderate skin and skin structure infections in superficial wounds.
As reported in published research, Locilex® has previously demonstrated statistical non-inferiority to a systemic antibiotic in a large-scale, randomized, active-controlled double blind, multi-center clinical study in patients with Mild or Moderate DFI. We have conducted microbiology studies that highlight the sensitivity of resistant bacteria, including methicillin-resistant staphylococcus aureus (or MRSA), vancomycin-resistant enterococcus (or VRE), extended-spectrum b-lactamase (or ESBL) and multi-drug resistant (or MDR) bacteria, to pexiganan, the active pharmaceutical ingredient (or API) in Locilex®. Due to the increased global prevalence of resistant bacteria in all types of skin infections, Locilex® may provide an important therapeutic advance.
We have contracted with third party vendors with respect to all key elements of our clinical and regulatory program, including vendors to: (i) conduct the Phase 3 and Phase 1 clinical trials for Locilex®; (ii) manufacture the API; (iii) formulate the finished product; and (iv) label and package the product. We believe these key relationships will help drive our clinical, regulatory and commercialization program for Locilex® in a timely and efficient manner.
Locilex® was originally sponsored by Magainin Pharmaceuticals, Inc. (or Magainin), which engaged in the FDA review process during 1998 and 1999, ultimately receiving a non-approvable letter based upon two manufacturing issues. We acquired the worldwide rights to pexiganan, the API in Locilex®, from a third party in April 2010. These rights included the prior formulation and all of the clinical and preclinical data generated by Magainin in its FDA review process. This includes data from over 1,000 evaluable patients, including 835 in large-scale, randomized, active-controlled, double blind, multi-center clinical studies as compared to a systemic quinolone standard of care as more fully described below. We believe we have corrected the manufacturing problems encountered by the prior sponsor. See "History of Locilex®" below.
Corporate Conversion
We were organized originally as a limited liability company under the laws of the State of Delaware in January 2010. On March 12, 2014, we converted Dipexium Pharmaceuticals, LLC from a Delaware limited liability company to a Delaware corporation. As a result of the corporate conversion:
- •
- the Class A Membership Interests of Dipexium Pharmaceuticals, LLC became shares of common stock of Dipexium Pharmaceuticals, Inc. pursuant to a conversion ratio of seven shares of common stock of Dipexium Pharmaceuticals, Inc. for each Class A membership interest of Dipexium Pharmaceuticals, LLC previously held. Accordingly, 767,911 Class A Membership
4
- •
- all of the outstanding warrants to purchase Class A Membership Interests of Dipexium Pharmaceuticals, LLC became
warrants to purchase shares of common stock of Dipexium Pharmaceuticals, Inc. in a ratio of seven shares of common stock of Dipexium Pharmaceuticals, Inc. for each Class A
membership interest of Dipexium Pharmaceuticals, LLC underlying such warrants, with the effect that warrants to purchase 4,900 Class A Membership Interests of Dipexium
Pharmaceuticals, LLC outstanding immediately prior to the corporate conversion automatically converted into warrants to purchase 34,300 shares of Dipexium Pharmaceuticals, Inc. upon
consummation of the corporate conversion; and
- •
- the exercise price of all of the outstanding warrants was adjusted in the same ratio as the seven-for-one conversion ratio noted above such that all of our outstanding warrants to purchase Class A Membership Interests of Dipexium Pharmaceuticals, LLC which were exercisable at $60 per Class A membership interest were automatically adjusted such that the new exercise price for the outstanding warrants upon consummating the corporate conversion was $8.57 per share, subject to certain adjustments noted in each of the warrants.
Interests of Dipexium Pharmaceuticals, LLC issued and outstanding immediately prior to the corporate conversion were converted automatically into 5,375,377 shares of Dipexium Pharmaceuticals, Inc.; and
In connection with the corporate conversion, Dipexium Pharmaceuticals, Inc. continued to hold all property of Dipexium Pharmaceuticals, LLC and assumed all of the debts and obligations of Dipexium Pharmaceuticals, LLC. Dipexium Pharmaceuticals, Inc. is governed by a certificate of incorporation filed with the Delaware Secretary of State and bylaws. On the effective date of the corporate conversion, the members of the board of directors of Dipexium Pharmaceuticals, LLC became the members of the board of directors of Dipexium Pharmaceuticals, Inc. and the officers of Dipexium Pharmaceuticals, LLC became the officers of Dipexium Pharmaceuticals, Inc. The purpose of the corporate conversion was to reorganize our corporate structure so that our company would continue as a corporation rather than a limited liability company, and so that our existing investors would own our common stock rather than equity interests in a limited liability company. In order to consummate the corporate conversion, a certificate of conversion was filed with the Secretary of State of the State of Delaware on March 12, 2014.
Our Strategy
Our primary objective is to establish Locilex® as the standard of care to treat patients with Mild DFI. The key elements of our strategy are as follows:
- •
- Complete the Phase 3 program for
Locilex®. As a result of our SPA for Locilex®, we believe the clinical pathway for Locilex® is
clear. Working with our key third party vendors, we commenced our Phase 3 program in the third quarter of 2014 and we anticipate completing enrollment in the first half of 2016.
- •
- Obtain FDA approval of Locilex® for Mild
DFI. If our Phase 3 trials meet their primary endpoints, we plan to submit an NDA amendment for Locilex®. We believe
that Locilex® may be approved by the FDA within 6 months of submitting our NDA amendment.
- •
- Commercially launch Locilex® in the U.S. We
plan to utilize a small specialty sales force to launch Locilex®, if it is approved, in the U.S., initially targeting podiatrists and potentially expanding to other specialty healthcare
providers.
- •
- Expand Locilex®'s FDA-approved uses. If we are able to obtain FDA approval in Mild DFI, we will consider obtaining additional FDA approvals that will enable us to expand the Locilex® label to include patients with Moderate DFI and certain other mild or moderate skin and skin structure infections in superficial wounds.
5
- •
- Commercially launch Locilex® in Europe. Based upon regulatory advice received to date, if our pivotal Phase 3 clinical trials are completed successfully, we plan to file our marketing authorization application (or MAA) in the E.U. under the centralized process promptly following the completion of our Phase 3 program in the U.S.
We will rely on our strong management team, board of directors and scientific advisors to execute our strategy. The individuals on our management team, board of directors and scientific advisors will contribute their significant business development, finance, and regulatory experience to the development and commercialization of Locilex®.
The Antibiotics Market
The widespread use of antibiotics has led to the development of resistant strains of bacteria, which limits the effectiveness of existing drugs, leading the World Health Organization to state in 2011 that antibiotic resistance is one of the greatest threats to human health.
Antibiotic resistance is primarily caused by genetic mutations in bacteria or when bacteria acquire resistance genes from other bacteria. In addition to mutated bacteria being resistant to the drug used for treatment, many bacterial strains can also be cross-resistant, meaning that the use of a particular treatment to address one kind of bacteria can result in resistance to other types of antibiotics. As a result, the effectiveness of many antibiotics has declined, limiting physicians' options to treat serious infections and creating a global health issue. According to the U.S. Centers for Disease Control and Prevention (or CDC), each year in the U.S., at least two million people acquire serious infections with bacteria that are resistant to one or more of the antibiotics designed to treat those infections. Antibiotic resistance has a significant impact on mortality and contributes heavily to healthcare system costs worldwide. In a 2013 report, the CDC estimates antibiotic resistance contributes to as much as $20 billion in direct healthcare costs and $35 billion in indirect costs (lost productivity) to the U.S. economy.
In addition to resistance issues, current antibiotic therapies have other limitations, including serious side effects. These side effects may include: severe allergic reaction, decreased blood pressure, nausea and vomiting, suppression of platelets, pain and inflammation at the site of injection, muscle, renal and oto-toxicities, optic and peripheral neuropathies and headaches. Some of these side effects may be significant enough to require that therapy be discontinued or not used. Furthermore, some systemic treatments require clinicians to closely monitor diabetic patients' blood glucose levels and other parameters, increasing the expense and inconvenience of treatment. As such, we believe that there is a need for new antibiotics that have improved potency and pharmacokinetics, effectiveness against resistant bacterial strains, improved side effect profiles and more flexible administration formulations. Topical formulations having no systemic absorption can complement systemic antibiotics with no drug-drug interaction in patients with localized skin infections.
Market Opportunity for Diabetic Foot Infection
Based upon our analysis of data from industry sources, the markets for DFI therapeutics in the U.S. and worldwide were $1.01 billion and $1.46 billion, respectively. According to the American Medical Association, approximately 12-14% of the U.S. population has diabetes. Based on long-term trends, the number of newly diagnosed cases is expected to increase annually. In published data, results of a meta-analysis of studies that followed patients with diabetes for periods of time between 12 weeks and four years, researchers reported that the incidence of foot ulceration in diabetics was between 8% and 17%. In another three-year study of patients with diabetes, the cumulative incidence of diabetic foot ulcers (or DFUs) was approximately 6%. The majority (approximately 61%) of DFUs are clinically infected at the time the patient initially presents to a treating physician. In addition, another study shows that the incidence of infection recurrence after complete healing approaches 32%.
6
Foot infection is the most frequent diabetic complication requiring hospitalization and the most common precipitating event leading to lower limb amputation. Approximately 1.35 million patients are diagnosed with DFI each year in the U.S., of which approximately 650,000 patients are diagnosed with Mild DFI and approximately 470,000 patients are diagnosed with Moderate DFI. According to published research, 47% of DFI patients present at the mild stage, 34% of DFI patients present at the moderate stage and 18% of DFI patients present at the severe stage. At the mild stage, patients can typically be treated on an outpatient basis and amputation risk is minimal (from 2 to 3% in Mild DFI). When not managed effectively, the potential for Mild DFI to progress to a limb- or life-threatening infection increases dramatically. Published research suggests amputation rates increase in Moderate and Severe DFI to approximately 45% and 75%, respectively. Similarly, the hospitalization rate for Mild DFI patients is approximately 10%, increasing in Moderate and Severe DFI to approximately 55% and 85%, respectively. Thus, DFI are a major cause of patient morbidity, a substantial burden to the healthcare system, and a source of high financial costs.
The goal of any antibiotic regimen is to treat patients with the least invasive therapy for the shortest amount of time, such that infection control can be achieved while minimizing the risk of antibiotic resistance. According to published research, there has long been interest in treating Mild DFI, the extent of which are confined to superficial skin and skin structures, with topical antibacterial agents. In Mild DFI, assuming equivalent or greater efficacy, we believe that a topical treatment such as Locilex® could hold significant advantages over intravenous and oral therapies by avoiding systemic adverse events, providing increased target site concentration, and most importantly, avoiding patient exposure to systemic antibiotic resistance.
While various systemic antibiotics have been approved to treat more severe levels of DFI, according to the 2012 IDSA Clinical Practice Guidelines for the Diagnosis and Treatment of Diabetic Foot Infections, there is no FDA approved antibiotic standard of care for the treatment of Mild DFI. In the absence of any approved treatment for Mild DFI, oral antibiotics, such as quinolones, cephalosporins, or penicillins, are considered to be acceptable for off-label use. We are not aware of any ongoing clinical trials evaluating the use of these oral antibiotics for the treatment of Mild DFI. The IDSA does not recommend the use of any currently FDA approved topical antibiotics for the treatment of Mild DFI. In infected DFUs, currently available prescription wound healing products are either contraindicated, indicated for use only after establishing infection control, or indicated for use as an adjunct, and not a substitute for, antibiotics.
All classes of systemic antibiotics are associated with antibiotic resistance. Furthermore, side effects associated with a variety of systemic therapies include: gastrointestinal infections, liver and renal side effects, serious and sometimes fatal hypersensitivity reactions, central nervous system effects, QT interval prolongation (effects on heartbeat), myelosuppression (effects on bone marrow), and black box warnings for tendinopathy and tendon rupture. Some of these side effects can be exacerbated by drug-drug interactions in diabetic patients who often are on concurrent medications. Diabetics taking a hypoglycemic agent or insulin must be particularly mindful of blood glucose disturbances that can occur with systemic quinolone antibiotic therapy.
In addition to the absence of FDA-approved antibiotics or antimicrobials labeled for the treatment of Mild DFI, research published in 2012 stated that no approved topical antibiotic products had demonstrated sufficient activity to recommend for off-label treatment in DFI of any level of severity. However, in a large-scale, randomized, active-controlled, double blind, multi-center clinical trial, topical Locilex® was noted to be as effective as an oral quinolone in treating Mild or Moderate DFI.
7
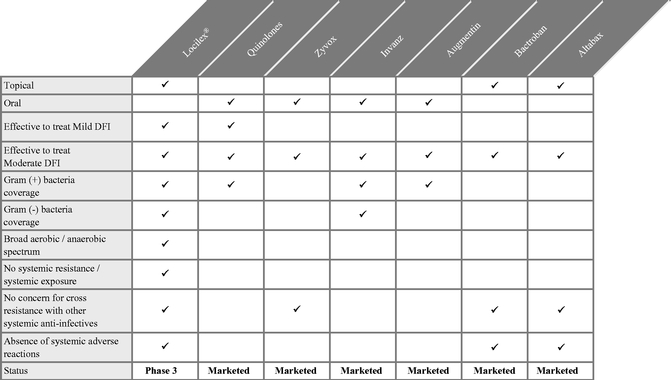
Based upon discussions with our scientific advisors, the following chart highlights the key attributes of products which we believe are the most commonly used products to treat Mild or Moderate DFI:
Mechanism of Action
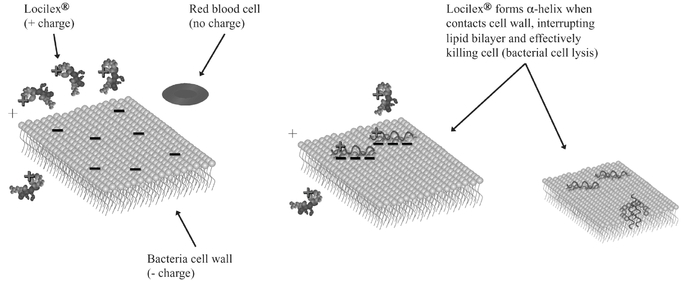
We believe that the particular chemical attributes of Locilex® will differentiate it from other antibiotic agents. Our API, pexiganan acetate, is a new chemical entity that is a chemically synthesized 22-amino acid analog of Magainin II, a natural host defense peptide isolated from skin secretions of the African Clawed Frog. Magainin II is one of a group of peptides that are considered to be the first line of defense against microbial invasion in this host. The peptides are simple linear structures that have a common feature of being basic peptides, which are able to form an amphipathic a-helical structure. This basic a-helical structure is the basis for the peptides' antimicrobial activity as inferred by studies in artificial lipid bilayers. Our API binds to artificial membranes, assumes an a-helical structure, and induces membrane lysis similar to Magainin II. In models of membrane interactions, the peptides exist as a random conformation in aqueous solution and an amphipathic a-helical structure is induced upon an initial ionic interaction with the microbial membrane. This interaction is not mediated by any membrane linked receptor. After ionic interaction, it is postulated that the hydrophobic side of the amphipathic a-helix of the lytic peptide is incorporated into the bilayer. The peptides could interact to form a raft-like structure in the membrane ultimately leading to the disruption of the membrane. In the model, the peptide raft will then realign perpendicular to the membrane surface to form a discrete pore structure with the helical peptides forming the sides of the pore like staves in a barrel. Although membrane disruption as a proposed mechanism of action is shared by other antimicrobial agents (e.g. polymyxin and amphotericin), the distinguishing characteristic of our API is its ability to cause
8
membrane disruption in a broad spectrum of microbes including gram-negative bacteria, gram-positive bacteria, and fungi.
Clinical Development Strategy
Drug Development Strategy
We are conducting two Phase 3 clinical trials of Locilex® for the treatment of Mild DFI (DPX-305 and DPX-306) and the clinical trials are being conducted concurrently. We have an SPA with the FDA relating to the trial design for our Phase 3 studies. The SPA calls for us to conduct two placebo-controlled Phase 3 studies, but does not require us to demonstrate equivalence to oral antibiotics. We began enrollment in these studies in the third quarter of 2014 and we anticipate completing enrollment in the first half of 2016. Both trials are large-scale, randomized, active-controlled double blind, multi-center trials designed to establish the superiority of Locilex® over placebo-cream in the treatment of Mild DFI. We are conducting DPX-305 and DPX-306 at up to 74 clinical sites in the U.S. Each trial will be comprised of 180 patients randomized 1:1 (statistical power 90%; P=0.05) to receive standard wound care (off-loading, debridement) plus twice-daily Locilex® cream or placebo-cream for 14 days. The primary endpoint of the trial will be clinical success, defined as resolution of infection per the clinical judgment of each treating physician using the 2012 DFI treatment guidelines. Microbiological success, defined as complete microbiological response, will be assessed as a secondary endpoint. A second secondary endpoint in the Phase 3 studies compares wound measurement at baseline to wound measurement at Day 28. The primary and secondary endpoints will be assessed for each patient at day 28. Furthermore, the FDA agreed that data from the Locilex® arm of the two prior studies conducted by Locilex®'s prior sponsor can be used to supplement our safety database.
We successfully completed a Phase 1 skin irritation study and a Phase 1 skin sensitization study in 2014. We reported top-line data on the Phase 1 skin irritation study in July 2014 and reported top-line data from the Phase 1 skin sensitization study in February 2015. The first Phase 1 study, for skin irritation, evaluated 30 healthy volunteers, and the second Phase 1 study, for skin sensitization, evaluated 203 healthy volunteers.
We continue to work with Research Pharmaceutical Services, Inc. as the contract research organization to conduct our Phase 3 studies for Locilex®. This work is being performed under the auspices of RRD International, LLC, which has continued to manage all aspects of our scientific, clinical and regulatory development.
9
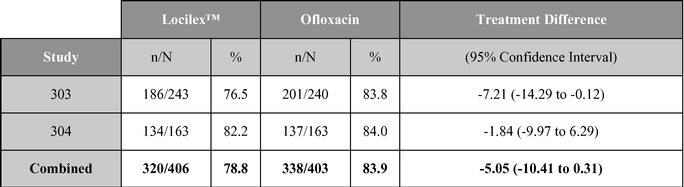
Previous Phase 3 Clinical Trial Results: Studies 303 and 304
Locilex® was previously investigated in two Phase 3 clinical trials in patients with DFI, referred to as Studies 303 and 304, conducted by the prior sponsor. Each trial was a large-scale, randomized, active-controlled, double blind, multi-center, non-inferiority trial designed to establish equivalence of Locilex® to systemic ofloxacin. Across both trials, 835 patients received twice-daily Locilex® cream plus placebo pill or twice-daily oral ofloxacin plus placebo cream for 14 to 28 days. The primary endpoint was the resolution of infection or clinical improvement of infection in response to antimicrobial treatment. Secondary endpoints included eradication of the wound pathogens, healing of the ulcer, development of antibiotic resistance to a study drug, and safety.
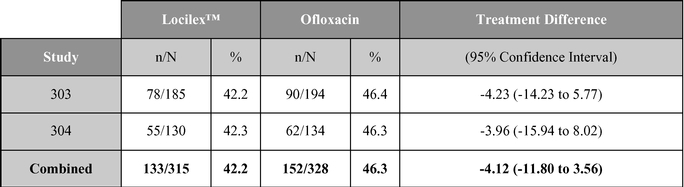
Although one study (Study 303) did not demonstrate equivalence, the second study (Study 304) and the combined data for the two trials did demonstrate equivalent results for topical Locilex® and oral ofloxacin in clinical improvement rates and overall microbiological eradication rates. Guidelines for establishing equivalence for these results were a 95% confidence interval with a lower bound delta of –15%, for clinical effectiveness, and a lower bound delta of –20%, for overall microbiological effectiveness. In each case, the confidence interval must cross zero to establish a statistically significant result. Additionally, there were no statistically significant differences in wound assessment scores between patients treated with Locilex® and ofloxacin. Wound assessment scores decreased at the end of treatment visit in both studies for both treatment arms, and they decreased further at the follow-up visit. No serious adverse events were determined to have been related to either Locilex® or ofloxacin. Moreover, the overall incidence of serious adverse events unrelated to the study medication (12% Locilex® to 9% ofloxacin), including worsening cellulitis (2% to 4%) and amputation (2% to 3%), did not differ significantly between treatment arms. Bacterial resistance to ofloxacin emerged in some patients in the control arm, but no significant resistance to Locilex® emerged among patients in the treatment arm.
A summary table of the primary clinical outcome, secondary microbiological outcome and wound assessment scores are shown below:
Clinical outcome (% cure or improved)
10
Microbiological outcome (% responders)
| |
Locilex® | Ofloxacin | |
|
|||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
|
Change from baseline |
|
Change from baseline |
|
|
|||||||||||||||||||
| |
|
|
P | ||||||||||||||||||||||
| |
Baseline value |
Baseline value |
|||||||||||||||||||||||
Study(s) and variable
|
EOT | Follow-up | EOT | Follow-up | EOT | Follow-up | |||||||||||||||||||
303 |
|||||||||||||||||||||||||
Total wound score, mean value |
25.5 | –7.6 | –8.5 | 24.2 | –8.0 | –8.7 | .61 | .78 | |||||||||||||||||
Wound infection score, mean value |
7.1 | –4.5 | –5.1 | 6.9 | –5.0 | –5.3 | .13 | .55 | |||||||||||||||||
Wound area, median mm2 |
131.5 | –61.9 | 67.8 | 117.3 | –58.3 | –64.4 | .53 | .57 | |||||||||||||||||
Wound depth, median mm |
3.0 | –1.0 | –1.5 | 3.0 | –1.0 | –1.5 | .30 | .48 | |||||||||||||||||
304 |
|||||||||||||||||||||||||
Total wound score, mean value |
26.2 | –8.6 | –9.0 | 25.7 | –8.5 | –8.9 | .92 | .87 | |||||||||||||||||
Wound infection score, mean value |
6.9 | –4.5 | –4.7 | 7.5 | –5.1 | –5.2 | .11 | .24 | |||||||||||||||||
Wound area, median mm2 |
146.9 | –63.0 | –64.7 | 160.8 | –70.2 | –86.4 | .17 | .03 | |||||||||||||||||
Wound depth, median mm |
3.0 | –1.0 | –1.5 | 3.0 | –1.0 | –2.0 | .42 | .58 | |||||||||||||||||
303 and 304 |
|||||||||||||||||||||||||
Total wound score, mean value |
25.8 | –8.0 | –8.7 | 24.8 | –8.2 | –8.7 | .75 | .91 | |||||||||||||||||
Wound infection score, mean value |
7.0 | –4.5 | –5.0 | 7.2 | –5.1 | –5.3 | .03 | .22 | |||||||||||||||||
Wound area, median mm2 |
138.0 | –62.6 | 67.1 | 138.7 | –65.8 | –72.1 | .17 | .07 | |||||||||||||||||
Wound depth, median mm |
3.0 | –1.0 | –1.0 | 3.0 | –1.0 | –2.0 | .20 | .36 | |||||||||||||||||
Source: Lipsky, et al. Clinical Infectious Disease. 2008; 47(12): 1537-45.
Microbiology Study Results
JMI Laboratories, an independent microbiology testing laboratory, has conducted several microbiology studies on our behalf, including a minimum inhibitory concentration (or MIC) study and a minimum bactericidal concentration (or MBC) study on our behalf, in part, to respond to the FDA's request for information on the sensitivity of certain resistant bacteria to Locilex®. The results demonstrate that resistant bacteria, including MRSA, multi-drug resistant pathogens and VRE, are particularly sensitive to the API in Locilex®. These results were deemed satisfactory by the FDA in February 2012.
Most if not all of resistant bacteria tested in the MIC and MBC studies are commonly involved with mild or moderate skin and skin structure infections in superficial wounds. Therefore, we believe these data suggest that Locilex® has potential as a standard of care for mild or moderate skin and skin structure infections in superficial wounds.
11
In addition, we have finalized protocols for 5 new microbiology studies to be conducted on our behalf by outside vendors including JMI Laboratories, in 2016. These microbiology studies are intended to strengthen our planned regulatory submissions with the FDA and European Medicines Agency and will test the activity of pexiganan against a broad range of contemporary microorganisms to provide supportive information for inclusion in the clinical and in vitro list for proposed US drug labelling and for the planned Marketing Authorization Application to be filed in the EU. We anticipate that these 5 studies will be completed on our behalf in the first half of 2016.
Manufacturing and Supply
We utilize three contract manufacturers (or CMOs) to produce Locilex®. Our manufacturing supply chain for Locilex® starts with PolyPeptide Laboratories, Inc. which manufactures pexiganan, the API in Locilex®. At our direction, Polypeptide Laboratories delivers the API to DPT Laboratories, Inc., which formulates the API into a cream formulation on our behalf. DPT Laboratories then delivers the formulated product to Almac Group Limited, which labels, packages, and delivers the finished goods for clinical trials as we request.
In the late 1990s, the prior sponsor engaged in an FDA review process for a prior formulation of Locilex®. In its 1999 non-approvable letter, the FDA identified two cGMP manufacturing issues. The first issue concerned the stability of the formulated product. Examination of the formulated product over time showed evidence of water separation from the cream matrix. The second issue related to the purity level of the API in the product. The prior source of the API yielded a purity level as low as 95%.
After acquiring the rights to Locilex®, we developed a detailed product development plan to arrive at an optimized formulation to address these issues to the satisfaction of the FDA. We believe that the changes we made to the formulation have resolved the previously observed product separation.
PolyPeptide Laboratories, our API manufacturer, has now completed the manufacture of the first of three validation lots of API that we will need for our planned submission of a NDA amendment in the U.S. and marketing authorization application in Europe. We are planning to initiate the manufacture of additional validation lots per regulatory guidelines, and these tasks will be performed starting in the first quarter and second quarter of 2016, respectively.
We have also scaled up the size of our API lots and have completed successfully our scale-up of the first formulated batch of Locilex cream at the 140 kg batch size. The scale-up was achieved successfully in the view of our manufacturing advisors. We have incorporated this commercial-scale batch in the OneStep Phase 3 trials to support our anticipated regulatory submissions.
As previously reported, we continue to anticipate that we will have adequate stability data on 3 cGMP registration batches of product supply well ahead of completion of the OneStep Phase 3 clinical trials. These 3 cGMP registration batches of product supply currently are subject to ongoing stability testing. Our stability testing is conducted in compliance with the ICH Guideline Q1A(R2): International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, ICH Harmonised Tripartate Guideline, Stability Testing of New Drug Substances and Products, Current Step 4 version, Dated 6 February 2003. The purpose of the stability testing is to provide evidence on how the quality of a drug substance or drug product varies with time under the influence of a variety of environmental factors such as temperature, humidity, and light, and to establish a re-test period for the drug substance or a shelf life for the drug product and recommended storage conditions. We believe and our CROs have confirmed that we will have sufficient stability data on the three cGMP batches of commercial supply by mid-2016; to support a new drug application amendment which we anticipate filing soon after receiving top line Phase 3 data. At the present time, the stability data supports a shelf life of at least 24 months for Locilex®.
12
We also believe our peptide is highly purified. The impurity levels of the API used in our commercial scale batch of Locilex® has been confirmed to be 99.4% pure for the API used in our cGMP batches.
In October 2013, we submitted our manufacturing data, including data from the first 30 kg cGMP batch as well as 18-month stability data on our 30 kg non-cGMP batch, to the FDA, and in December 2013 the FDA indicated in written communications with us that Locilex®'s stability and purity levels were acceptable for use in our Phase 3 studies. As a result of the aforementioned activities, we believe we have resolved the stability and purity concerns previously articulated by the FDA.
Commercial Plans
We intend to market and sell Locilex®, if approved, through a small, specialty sales force primarily to podiatrists at extended care facilities, wound care clinics, high volume group podiatry practices, and other treatment centers that specialize in the care of patients with DFI. Initially, we intend to hire a senior national sales officer, a senior marketing officer, and either directly or through a contract sales organization, a small team of fully dedicated Locilex® sales representatives. Based on current data from the Bureau of Labor Statistics, we estimate that there are approximately 13,700 podiatrists in the U.S. Our marketing efforts may also include other specialty healthcare providers.
Intellectual Property
We hold rights to a U.S. patent covering our proprietary formulation of Locilex® and the method of using it for the treatment of skin and wound infections (U.S. Patent Number 8,530,409). This patent was granted in September 2013 and expires in the U.S. in June 2032. The patent incorporates discoveries made by Dow Pharmaceutical Sciences, Inc. (later acquired by Valeant Pharmaceuticals International, Inc.). The application which gave rise to U.S. Patent No. 8,520,409 was assigned to us in June 2013. In addition, we have filed a Patent Cooperation Treaty (or PCT) application claiming priority to U.S. Patent No. 8,520,409 that will allow us to seek corresponding protection outside of the U.S., including in Europe, Japan, China, Australia, and Korea, as well as in other PCT jurisdictions. We commenced national stage patent prosecutions internationally in the fourth quarter of 2014 and will continue to prosecute such patent claims throughout 2015 and potentially 2016. We announced in February 2016 that patents were granted by patent offices in Australia and New Zealand which extend out to 2033 in each of these territories. We anticipate completing the national stage patent prosecutions in other international regions throughout 2016 and potentially 2017.
In addition to this patent, we hold an exclusive sublicense to the composition-of-matter patent covering the pexiganan technology (U.S. Patent No. 5,912,231) which expires in June 2016, not including any patent term extension that we expect to seek under the Drug Price Competition and Patent Term Restoration Act of 1984 (or the Hatch-Waxman Act). We acquired this sublicense when we acquired the rights to Locilex® in April 2010. Our rights to practice the pexiganan technology are originally derived through a license agreement between Scripps Research Institute (or Scripps), the inventor of the pexiganan technology, and Multiple Peptide Systems, Inc. (or MPS). MPS then sublicensed the pexiganan technology to the prior sponsor of the pexiganan program. In October 1996, both of the license and sublicense agreements were amended by Scripps, MPS and the prior sponsor of Locilex® to confirm that the license and sublicense were fully-paid, royalty free and of indefinite duration, with no further economic obligations for the practice of the pexiganan technology.
Although U.S. Patent 5,912,231 supplements our existing intellectual property portfolio, we are chiefly reliant on our U.S. Patent 8,530,409, which covers the novel formulation and method of use for Locilex® and provides for substantially longer patent coverage than U.S. Patent 5,912,231, and that U.S. Patent 8,530,409's attributes as a topical formulation, its potentially broader scope of coverage and opportunity for foreign patent protection offer greater benefits to us than U.S. Patent 5,912,231. As
13
such, we have not yet engaged in any discussions with Scripps regarding a possible patent term extension for U.S. Patent No. 5,912,231. If and when we decide to apply for an extension, we will we will need to work with Scripps throughout the application process to facilitate its approval.
Competition
The pharmaceutical and biotechnology industry is characterized by intense competition, rapid product development and technological change. Competition is intense among manufacturers of prescription pharmaceuticals and other product areas where we may develop and market products in the future. Most of our competitors are large, well established pharmaceutical or healthcare companies with considerably greater financial, marketing, sales and technical resources than are available to us. Additionally, many of our competitors have research and development capabilities that may allow such competitors to develop new or improved products that may compete with Locilex®. Our product could be rendered obsolete or made uneconomical by the development of new products to treat Mild DFI or other acute bacterial skin infections.
Our business, financial condition and results of operation could be materially adversely affected by any one or more of such developments. We cannot assure you that we will be able to compete successfully against current or future competitors or that competition will not have a material adverse effect on our business, financial condition and results of operations. Academic institutions, governmental agencies and other public and private research organizations are also conducting research activities and seeking patent protection and may commercialize products on their own or with the assistance of major healthcare companies for indications for which we are developing Locilex®. We are aware of certain development projects for products to treat or prevent certain diseases targeted by us. The existence of these potential products or other products or treatments of which we are not aware, or products or treatments that may be developed in the future, may adversely affect the marketability of Locilex®.
Even if Locilex® receives regulatory approval, of which there can be no assurance, our competitors' drugs may be more effective, more effectively marketed and sold, or less costly than Locilex®, and may render our product obsolete or non-competitive before we can recover the expenses of developing and commercializing Locilex®.
Although there are currently no products approved specifically to treat Mild DFI, we anticipate that, if approved, Locilex® will compete with other anti-infective products that are marketed for the general treatment of diabetic foot ulcers. These include systemic products that have been generally accepted by the ISDA to treat DFI at other levels of severity such as linezolid (marketed by Pfizer, Inc. as Zyvox), piperacillin/tazobactam (marketed by Pfizer, Inc. as Zosyn), ertapenam (marketed by Merck & Co. as Invanz); generic products recommended by the IDSA for off-label use in the treatment of all severity levels of DFI such as dicloxacillin, clindamycin, cephalexin, ofloxacin, trimethoprim, amoxicillin-clavulanate, and others; as well as antimicrobial wound care dressings such as medicinal grade honey and antiseptics such as silver and iodine. Furthermore, we are aware of other development stage topical or systemic products that may represent significant competition if approved. These include, but are not limited to nemonoxacin/TG-873870 (under development by TaiGen Biotechnology Co., Ltd.), Dermacyn (under development by Oculus Innovative Sciences, Inc.), SR-0379 (under development by Shionigi & Co., Ltd) and Cogenzia (under development by Innocoll, Inc.).
In addition, some of our competitors have greater experience than we do in conducting preclinical and clinical trials and obtaining FDA and other regulatory approvals. Accordingly, our competitors may succeed in obtaining FDA or other regulatory approvals for drug candidates more rapidly than we do. Companies that complete clinical trials, obtain required regulatory agency approvals and commence commercial sale of their drugs before their competitors may achieve a significant competitive advantage. Locilex® therefore may not be commercially competitive with existing products or products
14
under development. With respect to Mild, Moderate or Severe DFI specifically, such competitors include very large international organizations such as Pfizer, Inc., Eli Lilly and Company, Johnson & Johnson, Merck & Co., and GlaxoSmithKline plc.
History of Locilex®
In August 1992, the prior sponsor of Locilex®, Magainin, submitted an initial IND for the prior formulation of Locilex® to study broad spectrum anti-infective activity for the treatment of superficial and complicated dermatological infections. Another IND was submitted in November 1993 to cover a new indication for the treatment of DFI. In the late 1990s, the prior sponsor tested the prior formulation of Locilex®, with over 1,000 human subjects exposed without safety concerns, to such prior formulation of Locilex®, including 835 evaluable patients in two Phase 3 clinical trials. The Phase 3 trial results showed that such prior formulation of topical Locilex® had an approximate 80% response rate measured as resolution or improvement in infection in patients who under today's standards would be considered to have Mild or Moderate DFI. See "—Clinical Development Strategy—Phase 3 Clinical Trial Results: Studies 303 and 304" above.
The FDA Advisory Committee reviewing Locilex® at the time unanimously approved the safety of the product, but did not approve its efficacy and recommended an additional Phase 3 placebo controlled trial. In its 1999 non-approvable letter, the FDA identified certain cGMP manufacturing deficiencies, namely stability and quality control issues, and questions regarding the comparability of the product used in the Phase 3 program versus that which was produced at commercial scale. We believe that these hurdles and a lack of financing ultimately caused Magainin (later renamed Genaera Corporation) to deprioritize the product within their product pipeline. MacroChem Corporation (or MacroChem) licensed the technology in late 2007, after several years of attempting to remediate the manufacturing deficiencies. In February 2009, MacroChem was acquired by Access Pharmaceuticals, Inc. (or Access), which focused on oncology and oncology supportive care product candidates. Rights to Locilex® reverted to Genaera Liquidating Trust (established to sell the drug related assets of Genaera Corporation in liquidation) when Access failed to start a Phase 3 trial by the two-year anniversary of the effective date of the license agreement, triggering a termination right for Genaera Liquidating Trust in December 2009.
In April 2010, we acquired the worldwide rights to pexiganan, the API in Locilex®, and the prior formulation of the product and all related assets after participating in a public auction for our product conducted by Genaera Liquidating Trust. During the period between the FDA non-approval letter received in July 1999 and the second half of 2006, SmithKline Beecham Corporation (now part of GlaxoSmithKline plc) held the exclusive distribution rights to Locilex® in the U.S.
In March 2011, we exercised our exclusive option to buy out the downstream, success-based milestones and royalty obligations related to Locilex® and currently own 100% of our product candidate.
Government Regulation and Product Approval
Governmental authorities in the U.S., at the federal, state and local level, and other countries extensively regulate, among other things, the research, development, testing, manufacture, labeling, packaging, promotion, storage, advertising, distribution, marketing and export and import of products such as those we are developing. Our product candidates must be approved by the FDA through the NDA process before they may be legally marketed in the U.S. and by the European Medicines Agency (or EMA) through the Marketing Authorisation Application (or MAA) process before they may be legally marketed in Europe. Our product candidates will be subject to similar requirements in other countries prior to marketing in those countries. The process of obtaining regulatory approvals and the
15
subsequent compliance with applicable federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources.
U.S. Government Regulation
NDA Approval Processes
In the U.S., the FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act (or FDCA) and implementing regulations. Failure to comply with the applicable U.S. requirements at any time during the product development process or approval process, or after approval, may subject an applicant to administrative or judicial sanctions, any of which could have a material adverse effect on us. These sanctions could include:
- •
- refusal to approve pending applications;
- •
- withdrawal of an approval;
- •
- imposition of a clinical hold;
- •
- warning letters;
- •
- product seizures;
- •
- total or partial suspension of production or distribution; or
- •
- injunctions, fines, disgorgement, or civil or criminal penalties.
The process required by the FDA before a drug may be marketed in the U.S. generally involves the following:
- •
- completion of nonclinical laboratory tests, animal studies and formulation studies conducted according to Good Laboratory Practices
(or GLPs) or other applicable regulations;
- •
- submission to the FDA of an investigational new drug application (or IND), which must become effective before human clinical trials
may begin;
- •
- performance of adequate and well-controlled human clinical trials according to Good Clinical Practices (or GCPs) to establish the
safety and efficacy of the proposed drug for its intended use;
- •
- submission to the FDA of an NDA;
- •
- satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the product is produced to assess
compliance with current cGMPs to assure that the facilities, methods and controls are adequate to preserve the drug's identity, strength, quality and purity; and
- •
- FDA review and approval of the NDA.
Once a pharmaceutical candidate is identified for development, it enters the preclinical or nonclinical testing stage. Nonclinical tests include laboratory evaluations of product chemistry, toxicity and formulation, as well as animal studies. An IND sponsor must submit the results of the nonclinical tests, together with manufacturing information and analytical data, to the FDA as part of the IND. Some nonclinical testing may continue even after the IND is submitted. In addition to including the results of the nonclinical studies, the IND will also include a protocol detailing, among other things, the objectives of the clinical trial, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated if the first phase lends itself to an efficacy determination. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day time period, places the IND on clinical hold. In such a case, the IND sponsor and the FDA must
16
resolve any outstanding concerns before clinical trials can begin. A clinical hold may occur at any time during the life of an IND, and may affect one or more specific studies or all studies conducted under the IND.
All clinical trials must be conducted under the supervision of one or more qualified investigators in accordance with GCPs. They must be conducted under protocols detailing the objectives of the trial, dosing procedures, research subject selection and exclusion criteria and the safety and effectiveness criteria to be evaluated. Each protocol must be submitted to the FDA as part of the IND, and progress reports detailing the status of the clinical trials must be submitted to the FDA annually. Sponsors also must timely report to FDA serious and unexpected adverse reactions, any clinically important increase in the rate of a serious suspected adverse reaction over that listed in the protocol or investigation brochure, or any findings from other studies or animal or in vitro testing that suggest a significant risk in humans exposed to the drug. An institutional review board, or IRB, at each institution participating in the clinical trial must review and approve the protocol before a clinical trial commences at that institution and must also approve the information regarding the trial and the consent form that must be provided to each research subject or the subject's legal representative, monitor the study until completed and otherwise comply with IRB regulations.
Human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
- •
- Phase 1. The drug is initially introduced into
healthy human subjects and tested for safety, dosage tolerance, absorption, metabolism, distribution and elimination. In the case of some products for severe or life-threatening diseases, such as
cancer, especially when the product may be inherently too toxic to ethically administer to healthy volunteers, the initial human testing is often conducted in patients.
- •
- Phase 2. Clinical trials are performed on a
limited patient population intended to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage
tolerance and optimal dosage.
- •
- Phase 3. Clinical trials are undertaken to further evaluate dosage, clinical efficacy and safety in an expanded patient population at geographically dispersed clinical study sites. These studies are intended to establish the overall risk-benefit ratio of the product and provide an adequate basis for product labeling.
Human clinical trials are inherently uncertain and Phase 1, Phase 2 and Phase 3 testing may not be successfully completed. The FDA or the sponsor may suspend a clinical trial at any time for a variety of reasons, including a finding that the research subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB's requirements or if the drug has been associated with unexpected serious harm to patients.
During the development of a new drug, sponsors are given opportunities to meet with the FDA at certain points. These points may be prior to the submission of an IND, at the end of Phase 2 and before an NDA is submitted. Meetings at other times may be requested. These meetings can provide an opportunity for the sponsor to share information about the data gathered to date and for the FDA to provide advice on the next phase of development. Sponsors typically use the meeting at the end of Phase 2 to discuss their Phase 2 clinical results and present their plans for the pivotal Phase 3 clinical trial that they believe will support the approval of the new drug. If a Phase 2 clinical trial is the subject of discussion at the end of Phase 2 meeting with the FDA, a sponsor may be able to request a SPA, the purpose of which is to reach agreement with the FDA on the Phase 3 clinical trial protocol design and analysis that will form the primary basis of an efficacy claim.
17
According to published guidance on the SPA process, a sponsor which meets the prerequisites may make a specific request for a SPA and provide information regarding the design and size of the proposed clinical trial. The FDA is supposed to evaluate the protocol within 45 days of the request to assess whether the proposed trial is adequate, and that evaluation may result in discussions and a request for additional information. A SPA request must be made before the proposed trial begins, and all open issues must be resolved before the trial begins. If a written agreement is reached, it will be documented and made part of the record. The agreement will be binding on the FDA and may not be changed by the sponsor or the FDA after the trial begins except with the written agreement of the sponsor and the FDA or if the FDA determines that a substantial scientific issue essential to determining the safety or efficacy of the drug was identified after the testing began.
Concurrent with clinical trials, sponsors usually complete additional animal safety studies and also develop additional information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing commercial quantities of the product in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the drug and the manufacturer must develop methods for testing the quality, purity and potency of the drug. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the drug candidate does not undergo unacceptable deterioration over its proposed shelf-life.
The results of product development, nonclinical studies and clinical trials, along with descriptions of the manufacturing process, analytical tests and other control mechanisms, proposed labeling and other relevant information are submitted to the FDA as part of an NDA requesting approval to market the product. The submission of an NDA is subject to the payment of user fees, but a waiver of such fees may be obtained under specified circumstances. The FDA reviews all NDAs submitted to ensure that they are sufficiently complete for substantive review before it accepts them for filing. It may request additional information rather than accept an NDA for filing. In this event, the NDA must be resubmitted with the additional information. The resubmitted application also is subject to review before the FDA accepts it for filing.
Once the submission is accepted for filing, the FDA begins an in-depth review. NDAs receive either standard or priority review. A drug representing a significant improvement in treatment, prevention or diagnosis of disease may receive priority review. The FDA may refuse to approve an NDA if the applicable regulatory criteria are not satisfied or may require additional clinical or other data. Even if such data are submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. The FDA reviews an NDA to determine, among other things, whether a product is safe and effective for its intended use and whether its manufacturing is cGMP-compliant. The FDA may refer the NDA to an advisory committee for review and recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendation of an advisory committee, but it generally follows such recommendations. Before approving an NDA, the FDA will inspect the facility or facilities where the product is manufactured and tested. We anticipate that our NDA submission, which may technically be classified as an amended NDA (a so-called Class II resubmission), will address the manufacturing concerns previously articulated by the FDA regarding the prior formulation of Locilex®. Should our NDA be accepted for review, the FDA is supposed to respond within six months of submission.
Recent Changes to the Regulatory Landscape for Anti-Infective Drugs
The analytic approach of the FDA's Anti-Infective Drugs Division has undergone evolution in recent years, primarily driven by concerns that increasingly less effective antibiotics may have been approved in the last 10 to 15 years. The impact of these changes was a rethinking of how antibiotic efficacy is measured in clinical trials, and a review of the statistical tools used to analyze the data. In March 2009, the FDA published a draft guidance entitled "Guidance for Industry Community-Acquired
18
Bacterial Pneumonia: Developing Drugs for Treatment" and in August 2010, it published draft guidance (subsequently published as final guidance in October 2013) entitled "Guidance for Industry Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for Treatment" (or 2010 Guidance). The purpose of this guidance was to address many of the uncertainties regarding what the FDA expected from sponsors and clinical trials for the indications of acute bacterial skin and skin structure infections and community-acquired bacterial pneumonia.
The FDA asked sponsors to include additional measurements in their evaluation of efficacy that the FDA believes are more objective and less susceptible to interpretation by investigators. Non-inferiority comparisons of drugs are the standards for antibiotics, and non-inferiority margins are the margins used in the statistical analysis comparing two treatment arms in a study. These are the statistical margins or rules used to distinguish the degree of potential difference between two antibiotics in a study. In September 2010, one month after issuing the 2010 Guidance, the FDA approved the first antibiotic NDA reviewed pursuant to these new endpoints and non-inferiority margins. The clinical protocol that was reviewed by the FDA in support of our SPA with the FDA includes provisions that are consistent with the 2010 Guidance, as well as the FDA's final guidance published in October 2013.
Expedited Review and Approval
The FDA has various programs, including Fast Track, priority review, and accelerated approval, which are intended to expedite or simplify the process for reviewing drugs, and/or provide for the approval of a drug on the basis of a surrogate endpoint. Even if a drug qualifies for one or more of these programs, the FDA may later decide that the drug no longer meets the conditions for qualification or that the time period for FDA review or approval will be shortened. Generally, drugs that are eligible for these programs are those for serious or life-threatening conditions, those with the potential to address unmet medical needs and those that offer meaningful benefits over existing treatments. For example, Fast Track is a process designed to facilitate the development and expedite the review of drugs to treat serious or life-threatening diseases or conditions and fill unmet medical needs. Priority review is designed to give drugs that offer major advances in treatment or provide a treatment where no adequate therapy exists an initial review within six months as compared to a standard review time of ten months.
Although Fast Track and priority review do not affect the standards for approval, the FDA will attempt to facilitate early and frequent meetings with a sponsor of a Fast Track designated drug and expedite review of the application for a drug designated for priority review. Accelerated approval, which is described in Subpart H of 21 CFR Part 314, provides for an earlier approval for a new drug that is intended to treat a serious or life-threatening disease or condition and that fills an unmet medical need based on a surrogate endpoint. A surrogate endpoint is a laboratory measurement or physical sign used as an indirect or substitute measurement representing a clinically meaningful outcome. As a condition of approval, the FDA may require that a sponsor of a product candidate receiving accelerated approval perform post-marketing clinical trials.
In the Food and Drug Administration Safety and Innovation Act (or FDASIA), which was signed into law in July 2012, Congress encouraged the FDA to utilize innovative and flexible approaches to the assessment of products under accelerated approval. The law required the FDA to issue related draft guidance within a year after the law's enactment and also promulgate confirming regulatory changes. In June 2013, the FDA published a draft Guidance for Industry entitled, "Expedited Programs for Serious Conditions—Drugs and Biologics" which provides guidance on FDA programs that are intended to facilitate and expedite development and review of new drugs as well as threshold criteria generally applicable to concluding that a drug is a candidate for these expedited development and review programs. In addition to the Fast Track, accelerated approval and priority review programs discussed above, the FDA also provided guidance on a new program for Breakthrough Therapy designation. A request for Breakthrough Therapy designation should be submitted concurrently with, or
19
as an amendment to an IND. FDA has already granted this designation to around 30 new drugs and recently approved a couple of Breakthrough Therapy designated drug.
Patent Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of FDA approval of the use of our drug candidates, some of our U.S. patents may be eligible for limited patent term extension under the Hatch-Waxman Act. The Hatch-Waxman Act permits a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product's approval date. The patent term restoration period is generally one-half the time between the effective date of an IND, and the submission date of an NDA, plus the time between the submission date of an NDA and the approval of that application. Only one patent applicable to an approved drug is eligible for the extension and the application for extension must be made prior to expiration of the patent. The United States Patent and Trademark Office, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, we intend to apply for restorations of patent term for some of our currently owned or licensed patents to add patent life beyond their current expiration date, depending on the expected length of clinical trials and other factors involved in the submission of the relevant NDA.
Market exclusivity provisions under the FDCA also can delay the submission or the approval of certain applications. The FDCA provides a five-year period of non-patent marketing exclusivity within the U.S. to the first applicant to gain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety, which is the molecule or ion responsible for the action of the drug substance. During the exclusivity period, the FDA may not accept for review an abbreviated new drug application (or ANDA) or a 505(b)(2) NDA submitted by another company for another version of such drug where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The FDCA also provides three years of marketing exclusivity for an NDA, 505(b)(2) NDA or supplement to an approved NDA if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by the FDA to be essential to the approval of the application, for example, for new indications, dosages or strengths of an existing drug. This three-year exclusivity covers only the conditions associated with the new clinical investigations and does not prohibit the FDA from approving ANDAs for drugs containing the original active agent. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA; however, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness.
FDASIA includes the Generating Antibiotic Incentives Now Act (or GAIN Act), which is intended to provide incentives for the development of new qualified infectious disease products. A new drug that is designated as a qualified infectious disease product after a request by the sponsor that is made before an NDA is submitted will be eligible, if approved, for an additional five years of exclusivity beyond any period of exclusivity to which it would have previously been eligible. In addition, a qualified infectious disease product will receive priority review and Fast Track designation. Qualified infectious disease products are defined as antibacterial or antifungal drugs intended to treat serious or life-threatening infections that are resistant to treatment, or that treat qualifying resistant pathogens identified by the FDA. Examples of pathogens that may be designated as a qualifying pathogen include MRSA, VRE and multi-drug resistant gram-negative bacteria. We believe that Locilex® will qualify for this designation because it has already shown promising results in treating several qualifying pathogens in preclinical studies and clinical trials, and we have applied for "qualified infectious disease product"
20
status under the GAIN Act. On January 14, 2014, we received notification from the FDA that it had denied our request for such status, primarily because there is no clinical evidence that Mild DFI is a serious condition. The FDA invited us to reapply either now if such evidence exists or in the future if such evidence becomes available or if we would like to target another clinical indication. Accordingly, we intend to re-apply for "qualified infectious disease product" status in the first quarter of 2014 based on clinical evidence from the prior Studies 303 and 304 that demonstrates that Locilex® successfully treats resistant bacteria, including MRSA, multi-drug resistant bacteria and VRE, in patients with Moderate DFI, which we believe is widely accepted as a serious condition.
Post-approval Requirements
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory requirements is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval. In addition, the FDA may require testing and surveillance programs to monitor the effect of approved products that have been commercialized, and the FDA has the power to prevent or limit further marketing of a product based on the results of these post-marketing programs.
Any drug products manufactured or distributed by us pursuant to FDA approvals are subject to continuing regulation by the FDA, including, among other things:
- •
- record-keeping requirements;
- •
- reporting of adverse experiences with the drug;
- •
- providing the FDA with updated safety and efficacy information;
- •
- drug sampling and distribution requirements;
- •
- notifying the FDA and gaining its approval of specified manufacturing or labeling changes; and
- •
- complying with FDA promotion and advertising requirements.
Drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and some state agencies for compliance with cGMP and other laws.
We rely, and expect to continue to rely, on third parties for the production of clinical and commercial quantities of our products. Future FDA and state inspections may identify compliance issues at the facilities of our contract manufacturers that may disrupt production or distribution, or require substantial resources to correct.
From time to time, legislation is drafted, introduced and passed in Congress that could significantly change the statutory provisions governing the approval, manufacturing and marketing of products regulated by the FDA. In addition, FDA regulations and guidance are often revised or reinterpreted by the agency in ways that may significantly affect our business and our products. It is impossible to predict whether legislative changes will be enacted, or FDA regulations, guidance or interpretations changed or what the impact of such changes, if any, may be.
21
Regulation Outside of the U.S.
In addition to regulations in the U.S., we will be subject to regulations of other countries governing clinical trials and commercial sales and distribution of our products. Whether or not we obtain FDA approval for a product, we must obtain approval by the comparable regulatory authorities of countries outside of the U.S. before we can commence clinical trials in such countries and approval of the regulators of such countries or economic areas, such as the E.U., before we may market products in those countries or areas. The approval process and requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from place to place, and the time may be longer or shorter than that required for FDA approval.
Under E.U. regulatory systems, a company may submit marketing authorization applications either under a centralized or decentralized procedure. The centralized procedure, which is compulsory for medicines produced by biotechnology or those medicines intended to treat AIDS, cancer, neurodegenerative disorders or diabetes and optional for those medicines which are highly innovative, provides for the grant of a single marketing authorization that is valid for all E.U. member states. The decentralized procedure provides for mutual recognition of national approval decisions. Under this procedure, the holder of a national marketing authorization may submit an application to the remaining member states. Within 90 days of receiving the applications and assessments report, each member state must decide whether to recognize approval. If a member state does not recognize the marketing authorization, the disputed points are eventually referred to the European Commission, whose decision is binding on all member states.
Reimbursement
Sales of our products will depend, in part, on the extent to which the costs of our products will be covered by third-party payors, such as government health programs, commercial insurance and managed healthcare organizations. These third-party payors are increasingly challenging the prices charged for medical products and services. Additionally, the containment of healthcare costs has become a priority of federal and state governments and the prices of drugs have been a focus in this effort. The U.S. government, state legislatures and foreign governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit our net revenue and results. If these third-party payors do not consider our products to be cost-effective compared to other therapies, they may not cover our products after approved as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow us to sell our products on a profitable basis.
The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (or MMA) imposed new requirements for the distribution and pricing of prescription drugs for Medicare beneficiaries. Under Part D, Medicare beneficiaries may enroll in prescription drug plans offered by private entities which will provide coverage of outpatient prescription drugs. Part D plans include both stand-alone prescription drug benefit plans and prescription drug coverage as a supplement to Medicare Advantage plans. Unlike Medicare Part A and B, Part D coverage is not standardized. Part D prescription drug plan sponsors are not required to pay for all covered Part D drugs, and each drug plan can develop its own drug formulary that identifies which drugs it will cover and at what tier or level. However, Part D prescription drug formularies must include drugs within each therapeutic category and class of covered Part D drugs, though not necessarily all the drugs in each category or class. Any formulary used by a Part D prescription drug plan must be developed and reviewed by a pharmacy and therapeutic committee. Government payment for some of the costs of prescription drugs may increase demand for our products for which we receive marketing approval. However, any negotiated prices for our products covered by a Part D prescription drug plan will likely be lower than
22
the prices we might otherwise obtain. Moreover, while the MMA applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own payment rates. Any reduction in payment that results from the MMA may result in a similar reduction in payments from non-governmental payors.
The American Recovery and Reinvestment Act of 2009 provides funding for the federal government to compare the effectiveness of different treatments for the same illness. A plan for the research will be developed by the Department of Health and Human Services, the Agency for Healthcare Research and Quality and the National Institutes for Health, and periodic reports on the status of the research and related expenditures will be made to Congress. Although the results of the comparative effectiveness studies are not intended to mandate coverage policies for public or private payors, it is not clear what effect, if any, the research will have on the sales of any product, if any such product or the condition that it is intended to treat is the subject of a study. It is also possible that comparative effectiveness research demonstrating benefits in a competitor's product could adversely affect the sales of our product candidates. If third-party payors do not consider our products to be cost-effective compared to other available therapies, they may not cover our products as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow us to sell our products on a profitable basis.
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act of 2010 (or collectively, the ACA), enacted in March 2010, is expected to have a significant impact on the health care industry. ACA is expected to expand coverage for the uninsured while at the same time containing overall healthcare costs. With regard to pharmaceutical products, among other things, the ACA is expected to expand and increase industry rebates for drugs covered under Medicaid programs and make changes to the coverage requirements under the Medicare Part D program. We cannot predict the impact of the ACA on pharmaceutical companies, as many of the ACA reforms require the promulgation of detailed regulations implementing the statutory provisions which has not yet occurred. In addition, some members of the U.S. Congress have been seeking to overturn at least portions of the legislation and we expect they will continue to review and assess this legislation and alternative health care reform proposals. Any legal challenges to the ACA, as well as Congressional efforts to repeal the ACA, add to the uncertainty of the legislative changes enacted as part of the ACA.
In addition, in some non-U.S. jurisdictions, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the E.U. provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products. Historically, products launched in the E.U. do not follow price structures of the U.S. and generally tend to be significantly lower.
Scientific Advisory Board
In December 2013, we formally established a Scientific Advisory Board to advise our management regarding our clinical and regulatory development programs and other customary matters. Our scientific advisors are experts in various areas of medicine including DFI, mild and moderate skin and skin structure infections in superficial wounds and podiatry. We believe the advice of our scientific advisors
23
was integral to the quality of our clinical trial protocol for our Phase 3 program and the resulting SPA. Our Scientific Advisory Board is comprised of the following individuals:
- •
- Dr. Jonathan Wilkin. Founding Director (retired)
of the Division of Dermatology and Dental Products at the FDA. Remains active in regulatory matters after over 12 years of FDA service, which included membership on the FDA's Dermatology Drugs
Advisory Committee.
- •
- Dr. Benjamin Lipsky. Emeritus Professor of
Medicine, University of Washington; Visiting Professor, Infectious Diseases, University of Geneva. Teaching Associate, Green Templeton College, University of Oxford. Head of the International Working
Group on the Diabetic Foot (or IWGDF) and lead author of the Diabetic Foot Infection Treatment Guidelines, published in June 2012.
- •
- Dr. David Armstrong. Professor of Surgery and
Director, Southern Arizona Limb Salvage Alliance (or SALSA), University of Arizona College of Medicine. Co-Sponsor of annual Diabetic Foot Global Conference (or DFCon).
- •
- Dr. Warren Joseph. Adjunct Clinical Associate
Professor, Dr. William Scholl College of Podiatric Medicine, Rosland Franklin University of Medicine and Science. Managing Editor of the Journal of the American Podiatric Medical Association.
- •
- Dr. Michael Zasloff. Original inventor of the "magainin peptides" which include pexiganan, while he was a research scientist at the National Institutes of Health (or NIH) in 1987. Co-Founder of Magainin, the original owner of Locilex®. Current Professor, Departments of Surgery & Pediatrics; and Director, Surgical Immunology, Georgetown University School of Medicine.
We will continue to rely upon our scientific advisors in various aspects of our product development program including, without limitation, assisting with the publication in the future of the clinical data generated in our Phase 3 program in coordination with us.
Our Management
Our management team has extensive experience in leading the development of innovative therapeutics and significant expertise in operational, financial and corporate development functions. Our co-founder, President and Chief Executive Officer, David P. Luci, Esq., has managed multiple drug development companies including Bioenvision, Inc. (sold to Genzyme Corporation for $345 million in 2007), MacroChem (sold to Access in 2009), Access and our company. Our co-founder and Executive Chairman, Robert J. DeLuccia, has extensive product development, sales and marketing experience as well as senior level experience in management and operation of pharmaceutical and biotechnology companies of various sizes, including Pifzer, Inc. and Sanofi. Collectively, Messrs. Luci and DeLuccia have over 60 years of combined experience in the pharmaceutical and biotechnology sectors.
Employees
As of March 20, 2016, we have a total of eight employees and consultants, of which five are full-time employees and three are part-time employees or consultants. We believe our relationships with our employees and consultants are satisfactory. We have never experienced employment-related work stoppages and consider that we maintain good relations with our personnel. In addition, to complement our internal expertise, we have contracts with medical and scientific consultants, manufacturers, laboratories, and contract research organizations that specialize in various aspects of drug development including clinical development, preclinical development, manufacturing and regulatory affairs.
24
Available Information
Our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to reports filed pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended (which we refer to herein as the Exchange Act), are filed with the SEC. Such reports and other information that we file with the SEC are available free of charge on our website at http://dipexiumpharmaceuticals.com_and such filings also are available on the SEC website. The public may read and copy any materials that we file with the SEC at the SEC's Public Reference Room at 100 F Street, NE, Room 1580, Washington, DC 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. The SEC maintains an Internet site that contains reports, proxy and information statements and other information regarding issuers that file electronically with the SEC at http://www.sec.gov. The contents of these websites are not incorporated into this filing. Further, the foregoing references to the URLs for these websites are intended to be inactive textual references only.
An investment in our common stock involves a high degree of risk. You should carefully consider the risks described below, together with all of the other information included in this Report, before making an investment decision. If any of the following risks actually occurs, our business, financial condition or results of operations could suffer. In that case, the trading price of our shares of common stock could decline and you may lose all or part of your investment. See "Cautionary Note Regarding Forward Looking Statements" above for a discussion of forward-looking statements and the significance of such statements in the context of this Report.
Risks Relating to Our Business and Industry
We have a very limited operating history and are expected to incur significant operating losses during the early stage of our corporate development.
We were organized on January 14, 2010 and we acquired the rights to our product candidate Locilex® in April 2010. Accordingly, we have a limited operating history. We have not sold our product candidate because it is currently investigational in nature and requires completion of additional clinical and nonclinical trials and studies in order to obtain regulatory approval in the U.S. and abroad. Therefore, our historical financial information consists only of an audit of our financial results at and for the years ended December 31, 2012, 2013, 2014 and 2015. This is very limited historical financial information upon which to base an evaluation of our performance. We are an emerging company, and thus our prospects must be considered in light of the uncertainties, risks, expenses, and difficulties frequently encountered by companies in their early stages of operation, particularly in the pharmaceutical industry. We have generated cumulative losses of approximately $41.1 million since inception, and we expect to continue to incur losses until Locilex® is approved by the FDA and foreign regulatory authorities. Even if regulatory approval is obtained, there is a risk that we will not be able to generate material sales of Locilex®, which would cause us to continue to incur losses. We thus expect to incur substantial operating expenses over the next several years as our product development and marketing activities increase. The amount of future losses and when, if ever, we will achieve profitability are uncertain.
We have never generated revenue, may never generate revenue, are not profitable and may never become profitable.
We expect to incur substantial losses and negative operating cash flow for the foreseeable future, and we may never achieve or maintain profitability. Even if we are able to launch Locilex®, we expect to incur substantial losses for the foreseeable future and may never become profitable.
25
As we have no operating revenue, we also expect to experience negative cash flow for the foreseeable future as we continue to fund our operating losses and capital expenditures. As a result, we will need to generate significant revenues in order to achieve and maintain profitability. We may not be able to generate these revenues or achieve profitability in the future. Our failure to achieve or maintain profitability would negatively impact the value of your securities and potentially require us to shut down our business, which would result in the loss of your investment.
Given our lack of revenue and cash flow, we may need to raise additional capital, which may be unavailable to us or, even if consummated, may cause dilution or place significant restrictions on our ability to operate.
Since we will be unable to generate sufficient, if any, revenue or cash flow to fund our operations for the foreseeable future, we may need to seek additional equity or debt financing to provide the capital required to maintain or expand our operations. We may also need additional funding to continue the development of Locilex®, increase our sales and marketing capabilities, promote brand identity, or develop or acquire complementary companies, technologies and assets, as well as for working capital requirements and other operating and general corporate purposes. Moreover, the regulatory compliance arising out of being a publicly registered company has dramatically increased our costs. Our cash and short-term investments as of December 31, 2015 was approximately $32.2 million. Throughout the year ended December 31, 2015, we raised total net proceeds of approximately $19.7 million from the completion of public offerings of common stock. We expect that we will need approximately $14.5 to $16.5 million over the next 12 months to finance research and development and to cover our ongoing working capital needs.
We do not currently have any arrangements or credit facilities in place as a source of funds, and there can be no assurance that we will be able to raise sufficient additional capital if needed on acceptable terms, or at all. If such financing is not available on satisfactory terms, or is not available at all, we may be required to delay, scale back or eliminate the development of business opportunities and our ability to achieve our business objectives, our competitiveness, and our operations and financial condition may be materially adversely affected. Our inability to fund our business could thus lead to the loss of your investment.
If we raise additional capital by issuing equity securities, the percentage ownership of our existing stockholders may be reduced, and accordingly these stockholders may experience substantial dilution. We may also issue equity securities that provide for rights, preferences and privileges senior to those of our common stock. Given our need for cash and that equity issuance is the most common type of fundraising for companies like ours, the risk of dilution is particularly significant for stockholders of our company.
Debt financing, if obtained, may involve agreements that include liens on our assets and covenants limiting or restricting our ability to take specific actions, such as incurring additional debt. Debt financing would also be required to be repaid regardless of our operating results.
If we raise additional funds through collaborations and licensing arrangements, we may be required to relinquish some rights to Locilex®, or to grant licenses on terms that are not favorable to us.
We have no experience as a company in obtaining regulatory approval for, or commercializing, any product candidate.
As a company, we have never obtained regulatory approval for, or commercialized, any product candidate. It is possible that the FDA may refuse to accept our planned NDA for Locilex® for substantive review, or may conclude after review of our data that our application is insufficient to obtain regulatory approval of Locilex® or any future product candidates. If the FDA does not accept or approve our planned NDA for Locilex®, it may require that we conduct additional clinical, preclinical or manufacturing validation studies, which may be costly, and submit that data before it will reconsider
26
our applications. Depending on the extent of these or any other FDA required studies, approval of any NDA or application that we submit may be significantly delayed, possibly for several years, or may require us to expend more resources than we have available. Any delay in obtaining, or an inability to obtain, regulatory approvals would prevent us from commercializing Locilex®, generating revenues and achieving and sustaining profitability. It is also possible that additional studies, if performed and completed, may not be considered sufficient by the FDA to approve any NDA we submit. If any of these outcomes occur, we may be forced to abandon our planned NDA for Locilex®, which would materially adversely affect our business and could potentially cause us to cease operations. We face similar risks for any approval in a foreign jurisdiction.
Our current and future operations substantially depend on our management team and our ability to hire other key personnel, the loss of any of whom could disrupt our business operations.
Our business depends and will continue to depend in substantial part on the continued service of David P. Luci and Robert J. DeLuccia. Messrs. Luci and DeLuccia are parties to employment agreements for a three year term of service ending in March 2017, subject to automatic one year renewals absent termination with at least six months' notice. Such agreements may also be terminated by us with or without Cause (as defined in the employment agreements) and by each of Messrs. Luci or DeLuccia voluntarily or with Good Reason (as defined in the employment agreements). The loss of the services of either of these individuals would significantly impede implementation and execution of our business strategy and may result in the failure to reach our goals. We do not carry key person life insurance on any of our management, which would leave our company uncompensated for the loss of any of our management.
Our future viability and ability to achieve sales and profit will also depend on our ability to attract, retain and motivate highly qualified personnel in the diverse areas required for continuing our operations. There is a risk that we will be unable to attract, train or retain qualified personnel, both near term or in the future, and our failure to do so may severely damage our prospects.
There is a risk that Locilex® will not receive regulatory approval, and without regulatory approval we will not be able to market Locilex®.
Our business currently depends entirely on the successful development and commercialization of Locilex®. Our ability to generate revenue related to product sales, if ever, will depend on the successful development and regulatory approval of Locilex® for the treatment of Mild DFI.
We currently have no products approved for sale and we cannot guarantee that we will ever have marketable products. The development of a product candidate and issues relating to its approval and marketing are subject to extensive regulation by the FDA in the U.S., the European Medicines Agency (or EMA) in Europe and regulatory authorities in other countries, with regulations differing from country to country. We are not permitted to market our product candidates in the U.S. or Europe until we receive approval of a NDA from the FDA or a Marketing Authorisation Application (or MAA) from the EMA, respectively.
NDAs and MAAs must include extensive data and supporting information to establish the product candidate's safety and effectiveness for each desired indication. NDAs and MAAs must also include significant information regarding the chemistry, manufacturing and controls for the product. Obtaining approval of a NDA or a MAA is a lengthy, expensive and uncertain process, and we may not be successful in obtaining approval. The FDA and the EMA review processes can take years to complete and approval is never guaranteed. If we submit a NDA to the FDA, the FDA must decide whether to accept or reject the submission for filing. We cannot be certain that any submissions will be accepted for filing and review by the FDA. Regulators of other jurisdictions, such as the EMA, have their own procedures for approval of product candidates.
27
Even if a product is approved, the FDA or the EMA, as the case may be, may limit the indications for which the product may be marketed, require extensive warnings on the product labeling or require expensive and time-consuming clinical trials or reporting as conditions of approval. Regulatory authorities in countries outside of the U.S. and Europe also have requirements for approval of drug candidates with which we must comply prior to marketing in those countries. Obtaining regulatory approval for marketing of a product candidate in one country does not ensure that we will be able to obtain regulatory approval in any other country.
In addition, delays in approvals or rejections of marketing applications in the U.S., Europe or other countries may be based upon many factors, including regulatory requests for additional analyses, reports, data, preclinical studies and clinical trials, regulatory questions regarding different interpretations of data and results, changes in regulatory policy during the period of product development and the emergence of new information regarding Locilex® or other product candidates we may develop or acquire in the future. Also, regulatory approval for Locilex® or other product candidates we may develop or acquire in the future may be withdrawn.
Before we submit a NDA to the FDA or a MAA to the EMA for Locilex® , we must successfully complete two Phase 3 trials. We cannot predict whether our future trials and studies will be successful or whether regulators will agree with our conclusions regarding the preclinical studies and clinical trials we have conducted to date.
If we are unable to obtain approval from the FDA, the EMA or other regulatory agencies for Locilex® and any other product candidates we may develop or acquire in the future, or if, subsequent to approval, we are unable to successfully commercialize Locilex® or our other product candidates we may develop or acquire in the future, we will not be able to generate sufficient revenue to become profitable or to continue our operations.
Locilex®'s prior sponsor encountered certain difficulties in manufacturing Locilex® on a commercial scale, and there is a risk that we will continue to experience manufacturing issues that may prevent Locilex® from receiving regulatory approval.
In the late 1990s, a prior formulation of Locilex® was tested by Magainin, Locilex®'s prior sponsor, with over 1,000 human subjects exposed to such prior formulation of Locilex®, including 835 evaluable patients in two Phase 3 clinical trials. The FDA Advisory Committee reviewing Locilex® at the time unanimously approved the safety of the product, but did not recommend approval based upon its efficacy and recommended an additional Phase 3 placebo controlled trial. In its 1999 non-approvable letter, the FDA identified certain cGMP manufacturing deficiencies, namely stability and quality control issues, and raised questions regarding the comparability of the product used in the Phase 3 program versus that which was produced at commercial scale.
Since we acquired rights to Locilex®, we have worked with our third-party vendors to address the stability and purity concerns previously articulated by the FDA. However, we cannot guarantee that such deficiencies will be deemed resolved to the FDA's satisfaction, that the FDA or other regulatory agencies will not identify new manufacturing concerns, or that, once regulatory approval is granted, our manufacturers will be able to comply with applicable regulations to maintain the quality of our product. If we are unable to resolve any outstanding manufacturing issues, the cost and timing for achieving regulatory approval could materially increase and could prevent us from meeting the developmental milestones necessary to maintain the viability of our business.
28
Even if Locilex® gains regulatory approval, it may never achieve market acceptance or any level of commercial success. Our failure to achieve market acceptance will prevent or delay our ability to generate material revenues.
Our future financial performance will depend, to a large extent, upon the introduction and physician and patient acceptance of our product candidate, Locilex®. Even if approved for marketing by the necessary regulatory authorities, Locilex® may not achieve market acceptance or reimbursement by Medicare, Medicaid or third party payors.
The degree of market acceptance for Locilex® will depend upon a number of factors, including:
- •
- regulatory clearance of marketing claims for the uses that we are developing;
- •
- demonstration of the advantages, safety and efficacy for Locilex®;
- •
- pricing and reimbursement policies of government and third-party payors such as insurance companies, health maintenance organizations
and other health plan administrators;
- •
- our ability to attract corporate partners, including pharmaceutical companies, to assist in commercializing our formulation of
Locilex®; and
- •
- our ability to timely and effectively manufacture and market Locilex®, either on our own or through third parties.
Physicians, various other healthcare providers, patients, payors or the medical community in general may be unwilling to accept, utilize or recommend Locilex®. If we are unable to obtain regulatory approval, or are unable (either on our own or through third parties) to manufacture, commercialize and market Locilex® or any future product candidates we may develop or acquire when planned, we may not achieve any market acceptance or generate revenue, which could cause our business to fail.
If we are unable to convince physicians as to the benefits of our products or product candidates, we may incur delays or additional expense in our attempt to establish market acceptance.
Use of our products and, if approved, our product candidates will require physicians to be informed regarding the intended benefits of our products and product candidates. The time and cost of such an educational process may be substantial. Inability to carry out this physician education process may adversely affect market acceptance of our proposed formulations or products. We may be unable to timely educate physicians regarding our intended pharmaceutical formulations or products in sufficient numbers to achieve our marketing plans or to achieve product acceptance. Any delay in physician education may materially delay or reduce demand for our formulations or products. In addition, we may expend significant funds toward physician education before any acceptance or demand for our products or product candidates is created, if at all. Nonetheless, even with our best efforts, certain physicians may never prescribe our product.
Our failure to complete or meet key milestones relating to the development of Locilex® or other product candidates we may develop or acquire in the future would significantly impair the viability of our company.
In order to be commercially viable, we must successfully research, develop, obtain regulatory approval for, manufacture, introduce, market and distribute Locilex® and, if applicable, any future product candidates we may develop. With respect to Locilex® in particular, we must meet a number of critical developmental milestones, including:
- •
- demonstration, through clinical trials, that Locilex® is safe and effective; and
- •
- establishment of a viable Good Manufacturing Process capable of potential scale-up.
29
The estimated required capital and time-frames necessary to achieve these developmental milestones as described in this report or as we may state from time to time is subject to inherent risks, many of which may be beyond our control. As such, we may not be able to achieve these or similar milestones for Locilex® or any product candidate we may develop or acquire in the future. Our failure to meet these or other critical milestones would adversely affect the viability of our company.
Conducting and completing the clinical trials necessary for FDA approval is costly and subject to intense regulatory scrutiny as well as the risk of failing to meet the primary endpoints of such trials. We will not be able to commercialize and sell Locilex® without completing such trials.
In order to conduct clinical trials that are necessary to obtain approval by the FDA to market Locilex® or any other product candidate we may develop or acquire in the future, it is necessary to receive clearance from the FDA to conduct such clinical trials. We must conduct two Phase 3 clinical trials for Locilex®. We commenced both Phase 3 trials in the third quarter of 2014. We may not be able to commence, enroll sufficient patients in, properly conduct or complete such trials. If we cannot achieve all of these goals, our viability will be materially impaired.
In addition, the FDA can halt clinical trials at any time during the conduct of clinical trials for safety reasons or because we or our clinical investigators did not follow the FDA's requirements for conducting clinical trials. If our trials are permanently halted by the FDA, we would not be able to achieve any revenue from such product as it is illegal to sell any drug for human consumption or use without FDA approval. If our trials are temporarily halted by the FDA, the cost and timing for potentially achieving regulatory approval could be materially increased.
Moreover, there is a risk that our clinical trials will fail to meet their primary endpoint, which would make them unacceptable in having Locilex® approved by the FDA. If this were to occur, the announcement of such an event would very likely cause our public stock price to decrease, perhaps significantly, and such event would otherwise materially and adversely affect our business, results of operations and viability.
Locilex® may have undesirable side effects which may delay or prevent marketing approval, or, if approval is received, require it to be taken off the market, require it to include safety warnings or otherwise limit sales of the product.
Unforeseen side effects from Locilex® could arise either during clinical development or, if approved, after Locilex® has been marketed. This could cause regulatory approvals for, or market acceptance of, Locilex® more difficult and more costly to obtain.
To date, no serious adverse events have been attributed to Locilex®, though approximately 12% of patients in prior clinical trials experienced serious adverse events unrelated to Locilex®. The results of our planned or any future clinical trials may show that Locilex® causes undesirable or unacceptable side effects, which could interrupt, delay or halt clinical trials, and result in delay of,or failure to obtain, marketing approval from the FDA and other regulatory authorities, or result in marketing approval from the FDA and other regulatory authorities with restrictive label warnings.
If Locilex® receives marketing approval and we or others later identify undesirable or unacceptable side effects caused by the use of Locilex®:
- •
- regulatory authorities may withdraw their approval of the product, which would force us to remove Locilex® from the
market;
- •
- regulatory authorities may require the addition of labeling statements, specific warnings, a contraindication or field alerts to physicians and pharmacies;
30
- •
- we may be required to change instructions regarding the way the product is administered, conduct additional clinical trials or change
the labeling of the product;
- •
- we may be subject to limitations on how we may promote the product;
- •
- sales of the product may decrease significantly;
- •
- we may be subject to litigation or product liability claims; and
- •
- our reputation may suffer.
Any of these events could prevent us or our potential future collaborators from achieving or maintaining market acceptance of Locilex® or could substantially increase commercialization costs and expenses, which in turn could delay or prevent us from generating significant revenues from the sale of Locilex®.
We currently have no marketing and sales organization and have no experience as a company in marketing pharmaceutical products. If we are unable to establish our own marketing and sales capabilities, or enter into agreements with third parties to market and sell our products after they are approved, we may not be able to generate product revenues.
We do not have a sales organization for the marketing, sales and distribution of any pharmaceutical products. In order to commercialize Locilex® or any other product candidate we may develop or acquire in the future, we must develop these capabilities on our own or make arrangements with third parties for the marketing, sales and distribution of our products. The establishment and development of our own sales force would be expensive and time consuming and could delay any product launch, and we cannot be certain that we would be able to successfully develop this capability. As a result, we may seek one or more partners to handle some or all of the sales and marketing of Locilex® in the U.S. and elsewhere. There also may be certain markets within the U.S. for Locilex® for which we may seek a co-promotion arrangement. However, we may not be able to enter into arrangements with third parties to sell Locilex® on favorable terms or at all. In the event we are unable to develop our own marketing and sales force or collaborate with a third-party marketing and sales organization, we would not be able to commercialize Locilex® or any other product candidates that we develop, which would negatively impact our ability to generate product revenues. Furthermore, whether we commercialize products on our own or rely on a third party to do so, our ability to generate revenue will be dependent on the effectiveness of the sales force. In addition, to the extent we rely on third parties to commercialize our approved products, we will likely receive less revenues than if we commercialized these products ourselves.
We rely heavily on third parties for conducting clinical trials, marketing and distributing Locilex®.
We presently are party to, and expect that we will be required to enter into, agreements with commercial partners to perform clinical trials for us and to engage in sales, marketing and distribution efforts for Locilex® or other product candidates we may acquire in the future. We may be unable to establish or maintain third-party relationships on a commercially reasonable basis, if at all. In addition, these third parties may have similar or more established relationships with our competitors or other larger customers. Moreover, the loss for any reason of one or more of these key partners could have a significant and adverse impact on our business. If we are unable to obtain or retain third party sales and marketing vendors on commercially acceptable terms, we may not be able to commercialize Locilex® as planned and we may experience delays in or suspension of our marketing launch of Locilex®. The same could apply to other product candidates we may develop or acquire in the future. Our dependence upon third parties may adversely affect our ability to generate profits or acceptable profit margins and our ability to develop and deliver such products on a timely and competitive basis.
31
We rely on single source third-party contract manufacturing organizations to manufacture and supply Locilex® for us. If one of our suppliers or manufacturers fails to perform adequately or fulfill our needs, or if these agreements are terminated by the third parties, we may be required to incur significant costs and devote significant efforts to find new suppliers or manufacturers. We may also face delays in the development and commercialization of Locilex® or other product candidates that we may develop or acquire in the future.
We currently have limited experience in, and we do not own facilities for, manufacturing Locilex® or any other product candidate we may develop or acquire in the future. We rely upon single source third-party contract manufacturing organizations to manufacture and supply large quantities of our product candidates. We currently utilize PolyPeptide Laboratories, Inc. for the bulk manufacturing of Locilex® and DPT Laboratories, Inc. for the formulation of Locilex®. In addition, we are using Almac Group Limited to label the 15 gram tubes of Locilex® and distribute as we direct.
The manufacture of pharmaceutical products in compliance with current good manufacturing practice (or cGMP) regulations requires significant expertise and capital investment, including the development of advanced manufacturing techniques and process controls. Manufacturers of pharmaceutical products often encounter difficulties in production, including difficulties with production costs and yields, quality control, including stability of the product candidate and quality assurance testing, or shortages of qualified personnel. If our manufacturers were to encounter any of these difficulties or otherwise fail to comply with their obligations to us or under applicable regulations, our ability to provide study materials in our preclinical studies and clinical trials would be jeopardized. Any delay or interruption in the supply of clinical trial materials could delay the completion of our clinical trials, increase the costs associated with maintaining our clinical trial programs and, depending upon the period of delay, require us to commence new trials at significant additional expense or terminate the studies and trials completely.
Our suppliers and manufacturers for Locilex® must comply with cGMP requirements enforced by the FDA through its facilities inspection program. These requirements include, among other things, quality control, quality assurance and the maintenance of records and documentation. Manufacturers of our component materials may be unable to comply with these cGMP requirements and with other FDA, state and foreign regulatory requirements. The FDA or similar foreign regulatory agencies at any time may also implement new standards, or change their interpretation and enforcement of existing standards for manufacture, packaging or testing of products. We have little control over our manufacturers' compliance with these regulations and standards. A failure to comply with these requirements may result in fines and civil penalties, suspension of production, suspension or delay in product approval, product seizure or recall, or withdrawal of product approval. If the safety of any product supplied is compromised due to our manufacturers' failure to adhere to applicable laws or for other reasons, we may not be able to obtain regulatory approval for or successfully commercialize our products, and we may be held liable for any injuries sustained as a result. Any of these factors could cause a delay of clinical trials, regulatory submissions, approvals or commercialization of Locilex® or any product candidates we may develop or acquire in the future or entail higher costs or impair our reputation.
Our current agreements with our suppliers do not provide for the entire supply of the bulk drug necessary for full-scale commercialization. In the event that we and our suppliers cannot agree to the terms and conditions for them to provide some or all of our bulk drug clinical and commercial supply needs, or if any single-source supplier terminates the agreement in response to a breach by us, we would not be able to manufacture the bulk drug on a commercial scale until a qualified alternative supplier is identified, which could also delay the development of, and impair our ability to commercialize, Locilex® or any product candidates we may develop or acquire in the future.
32
The number of third-party suppliers with the necessary manufacturing and regulatory expertise and facilities for our company is limited, and it could be expensive and take a significant amount of time to arrange for alternative suppliers, which could have a material adverse effect on our business. New suppliers of any bulk drug would be required to qualify under applicable regulatory requirements and would need to have sufficient rights under applicable intellectual property laws to the method of manufacturing such ingredients. Obtaining the necessary FDA approvals or other qualifications under applicable regulatory requirements and ensuring non-infringement of third-party intellectual property rights could result in a significant interruption of supply and could require the new manufacturer to bear significant additional costs which may be passed on to us.
Failure to obtain marketing approval in foreign jurisdictions would prevent our products from being marketed in such jurisdictions.
In order to market and sell our products in the European Union and many other jurisdictions, we or our collaborators must obtain separate marketing approvals and comply with numerous and varying regulatory requirements. The approval procedure varies among countries and can involve additional testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval. The regulatory approval process outside the United States generally includes all of the risks associated with obtaining FDA approval. In addition, in many countries outside the United States, a product cannot be approved for reimbursement before the product can be approved for sale in that country. We or our collaborators may not obtain approvals from regulatory authorities outside the United States on a timely basis, if at all. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA. We may not be able to file for marketing approvals and may not receive necessary approvals to commercialize our product in any market.
We will need to increase the size of our organization, and we may experience difficulties in managing growth.
As of March 20, 2016, we had eight employees and consultants, of which five are full-time employees and three are part-time employees or consultants. We will need to expand our managerial, operational, financial and other resources in order to manage our operations and clinical trials, continue our development activities and commercialize Locilex® and any other product candidates we may develop or acquire in the future. Our management and personnel, systems and facilities currently in place are not adequate to support this future growth. Our need to effectively execute our business strategy requires that we:
- •
- manage our clinical trials effectively, including two Phase 3 clinical trials for Locilex®. The Phase 3
clinical trials are expected to be conducted at up to 60 trial sites in the U.S. and are expected to be managed on our behalf by RRD International, LLC;
- •
- manage our internal development efforts effectively while carrying out our contractual obligations to licensors, contractors,
collaborators, government agencies and other third parties;
- •
- continue to improve our operational, financial and management controls, reporting systems and procedures; and
- •
- identify, recruit, maintain, motivate and integrate additional employees in several vocational areas.
If we are unable to expand our managerial, operational, financial and other resources to the extent required to manage our development and commercialization activities, our business will be materially adversely affected.
33
We are exposed to product liability, nonclinical and clinical liability risks which could place a substantial financial burden upon us, should lawsuits be filed against us.
Our business exposes us to potential product liability and other liability risks that are inherent in the testing, manufacturing and marketing of pharmaceutical formulations and products. We expect that such claims are likely to be asserted against us at some point. In addition, the use in our clinical trials of pharmaceutical formulations and products and the subsequent sale of these formulations or products by us or our potential collaborators may cause us to bear a portion of or all product liability risks. We currently have $3 million in insurance coverage relating to personal injury, product liability, medical expenses, and office premises. However, any claim under such insurance policies may be subject to certain exceptions, and may not be honored fully, in part, in a timely manner, or at all, and may not cover the full extent of liability we may actually face. Therefore, a successful liability claim or series of claims brought against us could have a material adverse effect on our business, financial condition and results of operations.
Government and other efforts to reform the healthcare industry could have adverse effects on our company, including the inability of users of our current and future approved products to obtain adequate reimbursement from third-party payers, which could lead to diminished market acceptance of, and revenues from, such products.
On March 23, 2010, President Obama signed into law the Patient Protection and Affordable Care Act (or the PPACA). The Healthcare and Education Reconciliation Act of 2010 (or the Reconciliation Act), which contains a number of amendments to the PPACA, was signed into law on March 30, 2010. Two primary goals of the PPACA, combined with the Reconciliation Act (which we collectively refer to as the Healthcare Reform Legislation), are to provide for increased access to coverage for healthcare and to reduce healthcare-related expenses. On June 28, 2012, the United States Supreme Court upheld the constitutionality of the requirement in PPACA that individuals maintain health insurance or pay a penalty.
The Healthcare Reform Legislation contains a number of provisions that are expected to impact our business and operations or those of our commercial partners, including provisions governing enrollment in federal healthcare programs, reimbursement and discount programs and fraud and abuse prevention and control. The impact of these programs on our business is presently uncertain and may have unexpected consequences for our company. For example, expansion of health insurance coverage under the Healthcare Reform Legislation may result in a reduction in uninsured patients and increase in the number of patients with access to healthcare that have either private or public program coverage, and subsequently prescription drug coverage, including coverage for those products currently approved or in development by us or our partners. However, this outcome, along with any other potential benefits of the Healthcare Reform Legislation which could prove a benefit for us or our commercial partners, is uncertain and may not occur.
In addition to the Healthcare Reform Legislation, we expect that there will continue to be proposals by legislators or new laws, rules and regulations at both the federal and state levels, as well as actions by healthcare and insurance regulators, insurance companies, health maintenance organizations and other payers of healthcare costs aimed at keeping healthcare costs down while expanding individual healthcare benefits. Certain of these changes (including, without limitation, those enacted in connection with the federal or state implementation of the Healthcare Reform Legislation) could impose limitations on the prices we or our commercial partners will be able to charge for any of our approved products or the amounts of reimbursement available for these products from governmental agencies or third-party payors, or may increase the tax obligations on life sciences companies such as ours. Any or all of these changes (which are presently unclear and subject to potential modification on an ongoing basis) could impact the ability of users of our approved products to obtain insurance reimbursement for the use of such products or the ability of healthcare
34
professionals to prescribe such products, any of which could have a material adverse effect on our revenues (royalty or otherwise), potential profitability and results of operations.
Furthermore, the ability of our company to commercialize our products will depend in part on the extent to which appropriate reimbursement levels for the cost of our proposed formulations and products and related treatments are obtained by governmental authorities, private health insurers, managed care, and other organizations and may all result in lower prices for or rejection of our products, which could further have a material adverse effect on our revenues (royalty or otherwise) and results of operations.
We may also be subject to healthcare laws, regulation and enforcement; our failure to comply with those laws could have a material adverse effect on our results of operations and financial conditions.
Although we currently do not directly market or promote any of our products, we may also be subject to several healthcare regulations and enforcement by the federal government and the states and foreign governments in which we conduct our business. The laws that may affect our ability to operate include:
- •
- the federal Health Insurance Portability and Accountability Act of 1996 (or HIPAA), as amended by the Health Information Technology
for Economic and Clinical Health Act, which governs the conduct of certain electronic healthcare transactions and protects the security and privacy of protected health information;
- •
- the federal healthcare programs' Anti-Kickback Law, which prohibits, among other things, persons from knowingly and willfully
soliciting, receiving, offering or paying remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual for, or the purchase, order or recommendation of, any
good or service for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs;
- •
- federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be
presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent;
- •
- federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating
to healthcare matters; and
- •
- state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers.
If our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, the curtailment or restructuring of our operations, the exclusion from participation in federal and state healthcare programs and imprisonment, any of which could adversely affect our ability to operate our business and our financial results.
We and our management are parties to a lawsuit which, if adversely decided against, could impact our rights to Locilex®.
In April 2010, we acquired the worldwide rights to develop pexiganan, the active pharmaceutical ingredient in Locilex®, from Genaera Liquidating Trust, which was put in place to liquidate the assets of Genaera Corporation. In June 2012, we, along with our two senior executives and several other unrelated defendants, were sued in the Federal District Court for the Eastern District of Pennsylvania by a former shareholder of Genaera Corporation and purported to be on behalf of other Genaera Corporation shareholders, alleging, in pertinent part, that our company's acquisition of the rights to
35
pexiganan (the active ingredient in Locilex®, and which rights included the rights to the prior formulation of Locilex®) was for what was alleged to be inadequate consideration, and as a result, it was alleged that we and our senior executives aided and abetted a breach of fiduciary duty by Genaera Corporation and the Genaera Liquidating Trust to the former shareholders of Genaera Corporation. It was also alleged that we and our senior executives aided and abetted a breach of the duty of the trustee at common law and under a certain trust agreement which was alleged to exist and which was executed by Argyce LLC (or Argyce), as trustee. The agreement called for Argyce to create the Genaera Liquidating Trust pursuant to which Argyce apparently was appointed to liquidate the assets formerly held by Genaera Corporation. One of these assets was pexiganan, which we acquired via public auction conducted by Argyce on behalf of the Genaera Liquidating Trust.
The case against our company and our senior executives was dismissed with prejudice by the Federal District Court, without leave to refile, on August 12, 2013 based on the argument that Plaintiff's claims were time barred, and a subsequent motion to reconsider such dismissal was denied by the Federal District Court. Prior to the dismissal there was no request or action to seek class certification by the plaintiff though it was purportedly filed on behalf of other former Genaera Corporation shareholders. Plaintiff appealed the dismissal of the suit as well as the denial of the motion to reconsider to the Third Circuit Appellate Court, which granted Plaintiff's appeal.
On October 17, 2014, the Third Circuit Appellate Court, in a 2-1 decision with a strong dissenting opinion, reversed the trial court's dismissal of Plaintiff's claims based on the expiration of the applicable statutes of limitation and remanded the case to the Federal District Court. In a 2-1 decision, the Third Circuit held that more information was necessary to determine when Plaintiff should have been on notice of his claims to determine the applicability of the discovery rule, which could serve to extend the time frame in which Plaintiff could bring his claims. Due to the strong dissent, all Defendants filed the necessary documents requesting a petition for rehearing en banc, by the majority of the Third Circuit justices who are in active service. The Third Circuit denied the request for en banc hearing and remanded this case to District Court.
Upon remand to the Federal District Court, all Defendants moved to dismiss the complaint for reasons other than being time barred. The Company and the executives moved for dismissal based on Plaintiff's inability to make a case for aiding and abetting a breach of fiduciary duty because there was no underlying breach and such an aiding and abetting claim requires an element of knowing participation in the fiduciary breach which cannot be established by Plaintiff.
The District Court held a hearing on this in September 2015 and the District Court delivered an Order on November 10, 2015 pursuant to which the District Court granted the Motion to Dismiss filed by each and every defendant including the Company and its executives. In December 2015, Plaintiff appealed the Federal District Court's decision to the Third Circuit Appellate Court and we anticipate a decision on whether to grant Plaintiff's appeal by the Third Circuit Appellate Court in 2016. The Company will continue to vigorously defend Plaintiff's claims on the factual record, which it believes will prove that the Company is not liable to the Plaintiff in any regard.
If we were to lose such case, our rights to the prior formulation of Locilex® could be lost, which may impair the commercial viability of our product or the timeline to potential regulatory approval. If we were required to settle the case, we may lose certain rights to Locilex® or be required to pay damages, which could have a material adverse effect on our company, our business plans and results of operations.
We may form strategic alliances in the future with respect to our Locilex® development program and we may not realize the benefits of such alliances.
We may form one or more strategic alliances, create joint ventures or collaborations or enter into licensing arrangements with one or more third parties with respect to our Locilex® drug development
36
program that we believe will complement or augment our existing business. For example, we may attempt to find a partner for licensing, development and/or commercialization of Locilex® in one or more Asian territories, or other unpartnered areas of the world. We routinely engage, and are engaged, in partnering discussions with a range of pharmaceutical and biotechnology companies and could enter into new collaborations at any time. We face significant competition in seeking appropriate strategic partners, and the negotiation process to secure appropriate terms is time-consuming and complex. Any delays in identifying suitable development partners and entering into agreements to develop our product candidates could also delay the commercialization of our product candidates, which may reduce their competitiveness even if they reach the market.
In addition, we may be unable to establish such a strategic partnership for any future product candidates and programs on terms that are acceptable to us, or at all. This may be because our product candidates and programs may be deemed to be at too early of a stage of development for collaborative effort, our research and development pipeline may be viewed as insufficient, and/or third parties may not view our product candidates and programs as having sufficient potential for commercialization for several reasons including, but not limited to, lack of patent protections outside the U.S. Even if we are able to enter into a strategic alliance or license arrangement with one or more third parties, there is a risk that the collaboration will not achieve any measure of success, or that any future partner will commit sufficient resources to the development, regulatory approval, and commercialization effort for such products, or that such alliances will result in us achieving revenues that justify such transactions.
Trends toward managed healthcare and downward price pressures on medical products and services may limit our ability to profitably sell Locilex® or other product candidates we may develop or acquire in the future.
Lower prices for pharmaceutical products may result from:
- •
- third-party payors' increasing challenges to the prices charged for medical products and services;
- •
- the trend toward managed healthcare in the U.S. and the concurrent growth of HMOs and similar organizations that can control or
significantly influence the purchase of healthcare services and products; and
- •
- legislative proposals to reform healthcare or reduce government insurance programs.
The cost containment measures that healthcare providers are instituting, including practice protocols and guidelines and clinical pathways, and the effect of any healthcare reform, could limit our ability to profitably sell Locilex® or any other products that we may develop or acquire which obtain FDA approval. Moreover, any future legislation or regulation, if any, relating to the healthcare industry or third-party coverage and reimbursement, may adverse impact our ability to generate sales revenue and cause our business to suffer.
We will compete with larger and better capitalized companies, and competitors in the drug development or pharmaceutical industries may develop competing products which outperform or supplant Locilex®.
Competition in the worldwide pharmaceutical industry, including the sector for antibiotic agents that we will operate in, is intense. Pharmaceutical companies and/or other technology companies have developed (and are currently marketing in competition with us), have sought to develop and may in the future seek to develop or acquire and market other products that may successfully treat skin or wound infections in superficial wounds which do and may compete with Locilex®. Competitors have developed and may in the future develop similar or different products which may become more accepted by the marketplace or which may supplant Locilex® entirely. In addition, many of our current competitors are, and future competitors may be, significantly larger and better financed than we are, thus giving them a significant advantage. With respect to Mild, Moderate or Severe DFI specifically, such competitors include very large international organizations such as Pfizer, Inc., Eli Lilly and Company, Johnson &
37
Johnson and GlaxoSmithKline plc. We may be unable to respond to competitive forces presently in the marketplace (including competition from larger companies), which would severely impact our business.
If ultimate users of Locilex® or any other product candidates we may develop or acquire in the future are unable to obtain adequate reimbursement from third-party payors, or if new restrictive legislation is adopted, market acceptance of our proposed products may be limited and we may not achieve material revenues.
The continuing efforts of government and insurance companies, health maintenance organizations and other payors of healthcare costs to contain or reduce costs of healthcare may affect our future revenues and profitability, and the future revenues and profitability of our potential customers, suppliers and collaborative partners and the availability of capital. For example, in the U.S., given recent federal and state government initiatives directed at lowering the total cost of healthcare, the U.S. Congress and state legislatures will likely continue to focus on healthcare reform, the cost of prescription pharmaceuticals and on the reform of the Medicare and Medicaid systems. While we cannot predict whether any such legislative or regulatory proposals will be adopted, the announcement or adoption of such proposals and related laws, rules and regulations could materially harm our business, financial conditions results of operations or stock price. Moreover, the passage of the Patient Protection and Affordable Care Act in 2010, and efforts to amend or repeal such law, has created significant uncertainty relating to the scope of government regulation of healthcare and related legal and regulatory requirements, which could have an adverse impact on sales of our products.
In addition, our ability to commercialize Locilex® or any future product candidates will depend in part on the extent to which appropriate reimbursement levels for the cost of such products and related treatments are adopted by third party payors, such as by governmental health programs, private health insurers and other organizations, such as HMOs. Consumers and third-party payors are increasingly challenging the prices charged for drugs and healthcare services.
Even if we obtain FDA approval of Locilex®, or any other product candidate we may develop or acquire in the future, we may never obtain approval or commercialize our products outside of the U.S., which would limit our ability to realize their full market potential. If foreign approval is obtained, there are risks in conducting business in international markets.
In order to market Locilex® or any other products we may develop or acquire outside of the U.S., we must establish and comply with numerous and varying regulatory requirements of other countries regarding safety and efficacy. Clinical trials conducted in one country may not be accepted by regulatory authorities in other countries, and regulatory approval in one country does not mean that regulatory approval will be obtained in any other country. Approval procedures vary among countries and can involve additional product testing and validation and additional administrative review periods. Seeking foreign regulatory approvals could result in significant delays, difficulties and costs for us and require additional preclinical studies or clinical trials which would be costly and time consuming. Regulatory requirements can vary widely from country to country and could delay or prevent the introduction of Locilex® or any future products in those countries. Satisfying these and other regulatory requirements is costly, time consuming, uncertain and subject to unanticipated delays. In addition, our failure to obtain regulatory approval in the U.S. or any foreign country may delay or have negative effects on the process for regulatory approval in other countries. We do not have any product candidates approved for sale in the U.S. or any foreign country and we do not have experience as a company in obtaining regulatory approval in international markets. If we fail to comply with regulatory requirements in a foreign country or to obtain and maintain required approvals, our potential market for Locilex® or other products will be reduced and our ability to realize the full market potential of our products will be harmed.
If approved for commercialization in a foreign country, we intend to enter into agreements with third parties to market Locilex® whenever it may be approved and wherever we have the right to
38
market it. Consequently, we expect that we will be subject to additional risks relating to entering into international business relationships, including:
- •
- lack of adequate protection from intellectual property rights in foreign countries, which could occur if we do not have issued patents
in force in such foreign countries covering our products, their methods of use and methods of manufacture;
- •
- the potential for so-called parallel importing, which is what happens when a local seller, faced with high or higher local prices (for
instance, because the goods have patent protection in such country), opts to import goods from a foreign market (with low or lower prices) rather than buy them locally;
- •
- unexpected changes in tariffs, trade barriers and regulatory requirements;
- •
- economic weakness, including inflation, or political instability in particular foreign economies and markets;
- •
- compliance with laws for employees traveling abroad;
- •
- foreign taxes, including withholding of payroll taxes;
- •
- foreign currency fluctuations, which could result in increased operating expenses and reduced revenues;
- •
- workforce uncertainty in countries where labor unrest is more common than in the U.S.;
- •
- production shortages resulting from any events affecting the API and/or finished drug product supply or manufacturing capabilities
abroad;
- •
- business interruptions resulting from geo-political actions, including war and terrorism, or natural disasters including earthquakes,
typhoons, floods and fires; and
- •
- failure to comply with Office of Foreign Asset Control rules and regulations and the Foreign Corrupt Practices Act.
These and other risks may materially adversely affect our ability to attain or sustain revenue from international markets.
Failure to achieve and maintain effective internal controls could have a material adverse effect on our business.
Effective internal controls are necessary for us to safeguard our assets and provide reliable financial reports. If we cannot provide reliable financial reports, our operating results could be harmed. All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation.
While we continue to evaluate and improve our internal controls, we are a small company with limited staff, and we cannot be certain that the measures we implement will ensure that we design, undertake and maintain adequate controls over our financial processes and reporting in the future. Any failure to implement required new or improved controls, or difficulties encountered in their implementation, could harm our operating results or cause us to fail to meet our reporting obligations.
Failure to achieve and maintain an effective internal control environment could cause investors to lose confidence in our reported financial information, which could have a material adverse effect on our stock price. In addition, if our efforts to comply with new or changed laws, regulations, and standards differ from the activities intended by regulatory or governing bodies due to ambiguities
39
related to practice, regulatory authorities may initiate legal proceedings against us and our business may be harmed.
Our internal computer systems, or those of our contract research organization and other key vendors or consultants, may fail or suffer security breaches, which could result in a material disruption of our product development program.
Our internal computer systems and those of our contract research organization and other key vendors and consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. While we have not experienced any such system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our programs. For example, the loss of clinical trial data from completed or ongoing clinical trials for Locilex® could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach results in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development of Locilex® could be delayed.
Our employees and consultants may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements.
We are exposed to the risk of employee or consultant fraud or other misconduct. Misconduct by our employees or consultants could include intentional failures to comply with FDA regulations, provide accurate information to the FDA, comply with manufacturing standards, comply with federal and state healthcare fraud and abuse laws and regulations, report financial information or data accurately or disclose unauthorized activities to us. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Employee and consultant misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter such misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant fines or other sanctions.
Business disruptions could seriously harm our future revenues and financial condition and increase our costs and expenses.
Our operations could be subject to earthquakes, power shortages, telecommunications failures, floods, hurricanes, typhoons, fires, extreme weather conditions, medical epidemics and other natural or manmade disasters or business interruptions. The occurrence of any of these business disruptions could seriously harm our operations and financial condition and increase our costs and expenses.
We may engage in strategic transactions that could impact our liquidity, increase our expenses and present significant distractions to our management.
From time to time, we may consider strategic transactions, such as acquisitions of companies, asset purchases, and out-licensing or in-licensing of products, product candidates or technologies. Additional potential transactions that we may consider include a variety of different business arrangements,
40
including spin-offs, strategic partnerships, joint ventures, restructurings, divestitures, business combinations and investments. Any such transaction may require us to incur non-recurring or other charges, may increase our near- and long-term expenditures and may pose significant integration challenges or disrupt our management or business, which could adversely affect our operations and financial results. For example, these transactions may entail numerous operational and financial risks, including:
- •
- exposure to unknown liabilities;
- •
- disruption of our business and diversion of our management's time and attention in order to develop acquired products, product
candidates or technologies;
- •
- incurrence of substantial debt or dilutive issuances of equity securities to pay for acquisitions;
- •
- higher-than-expected acquisition and integration costs;
- •
- write-downs of assets or goodwill or impairment charges;
- •
- increased amortization expenses;
- •
- difficulty and cost in combining the operations and personnel of any acquired businesses with our operations and personnel;
- •
- impairment of relationships with key suppliers or customers of any acquired businesses due to changes in management and ownership; and
- •
- inability to retain key employees of any acquired businesses.
Accordingly, although there can be no assurance that we will undertake or successfully complete any transactions of the nature described above, any transactions that we do complete may be subject to the foregoing or other risks, could have a material adverse effect on our business, results of operations, financial condition and prospects.
Risks Relating to Our Intellectual Property
Our ability to achieve commercial success depends to a material extent on our ability to maintain adequate intellectual property protection for our products and technology. If we are unable to obtain and maintain adequate intellectual property rights for Locilex®, it may materially and adversely affect our ability to market and generate sales of the product.
Due to the exclusivity that intellectual property protection can afford, our commercial success depends to a material extent on our ability to obtain and maintain adequate intellectual property protection for Locilex® (and any other products we may develop in the future) in the U.S. and other countries.
As of February 8, 2016, our patent estate included a U.S. patent (U.S. Patent No. 8,530,409), corresponding granted patents in Australia and New Zealand, and corresponding applications pending in Brazil, Canada, China, Eurasia, Europe, Indonesia, Israel, Japan, Korea, Mexico, Singapore and South Africa. We also have an exclusive sublicense from Scripps Research Institute (or Scripps) , the inventor of the pexiganan technology, to a U.S. patent (U.S. Patent No. 5,912,231), directed to pexiganan, the API used in Locilex®. We consider our U.S. Patent No. 8,530,409, which relates to our new, proprietary formulation of Locilex® and methods of using it to treat skin or wound infection, to be particularly important to our company primarily due to its substantially longer patent term coverage, its novel attributes as a topical formulation, its potentially broader scope of coverage and its opportunity for foreign patent protection. While we currently have pending applications in foreign jurisdictions corresponding to U.S. Patent No. 8,530,409, no assurance can be given that any foreign patents will issue, or that even if any such patents were to issue, such patents would provide meaningful protection for Locilex®.
41
Our patent estate related to Locilex® is critical to our commercial viability. There is a risk that our pending patent applications may not result in issued patents, and that any of our issued patents will not include claims that are sufficiently broad to provide adequate protection for Locilex®, including meaningful protection from our competitors. Additionally, the success of an application for the patent term extension of our licensed patent will require the cooperation of the licensor, which cooperation cannot be guaranteed. We will be able to protect our proprietary rights from unauthorized use by third parties only to the extent that Locilex® (and any other products we may develop in the future) is covered by valid and enforceable patents that are of sufficient scope to effectively prevent competitive products or are effectively maintained as trade secrets within our organization. If third parties disclose or misappropriate or design around our proprietary rights, it may materially and adversely impact our position in the market.
We apply for patents covering both our technologies and product candidates, as we deem appropriate. However, we may fail to apply for patents on important technologies or improvements in our technologies in a timely fashion, or at all. Our existing patents and any future patents we obtain may not be sufficiently broad to prevent others from using our technologies or from developing competing products and technologies. Moreover, the patent positions of numerous biotechnology and pharmaceutical companies are highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. As a result, the validity and enforceability of our patents cannot be predicted with certainty. In addition, no assurances can be given that:
- •
- we were the first to make the inventions covered by each of our issued patents and pending patent applications;
- •
- we were the first to file patent applications for these inventions;
- •
- others will not independently develop similar or alternative technologies or duplicate any of our technologies by inventing around our
claims;
- •
- a third party will not challenge our proprietary rights, and if challenged that a court will hold that our patents are valid and
enforceable;
- •
- any patents issued to us or our collaboration partners will cover our product as ultimately developed, or provide us with any
competitive advantages, or will not be challenged by third parties;
- •
- we will develop additional proprietary technologies that are patentable; or
- •
- the patents of others will not have an adverse effect on our business.
In addition, there are numerous recent changes to the patent laws and proposed changes to the rules of the USPTO which may have a significant impact on our ability to protect our technology and enforce our intellectual property rights. For example, on September 16, 2011, President Obama signed the Leahy-Smith America Invents Act which codifies several significant changes to the U.S. patent laws, including, among other things, changing from a "first to invent' to a "first inventor to file" system, limiting where a patentee may file a patent suit, eventually eliminating interference proceedings while maintaining derivation actions, and creating a set of procedures to challenge patents in the USPTO after they have issued. The effects of these changes are currently uncertain as the USPTO has just implemented regulations related to these changes and the courts have yet to address many of these provisions in the context of a dispute. Furthermore, we have not assessed the applicability of the act and new regulations on the specific patents discussed herein. The U.S. Supreme Court has also issued decisions, the full impact of which is not yet known. For example, on March 20, 2012 in Mayo Collaborative Services, DBA Mayo Medical Laboratories, et al. v. Prometheus Laboratories, Inc., the Court held that several claims drawn to measuring drug metabolite levels from patient samples and correlating them to drug doses were not patentable subject matter. The decision appears to impact
42
diagnostics patents that merely apply a law of nature via a series of routine steps and it has created uncertainty around the ability to patent certain biomarker-related method claims. Additionally, on June 13, 2013 in Association for Molecular Pathology v. Myriad Genetics, Inc., the Court held that claims to isolated genomic DNA are not patentable, but claims to complementary DNA (or cDNA) molecules were held to be valid. The effect of the decision on patents for other isolated natural products is uncertain.
We are dependent on a third party to maintain the patent exclusivity for the API in Locilex®
We hold an exclusive, worldwide sublicense to the composition-of-matter patent, U.S. Patent No. 5,912,231, which expires in June 2016, excluding any patent term restoration that we may seek under the Hatch-Waxman Act. Our rights to practice the pexiganan technology are derived through a license agreement between Scripps and Multiple Peptide Systems Inc. (or MPS). MPS subsequently sublicensed the pexiganan technology to the prior sponsor of the pexiganan clinical and regulatory program. On October 1, 1996, both the license agreement and sublicense agreement were amended by the parties to confirm that the license and sublicense were fully-paid and royalty-free with no further economic obligations for the practice of the pexiganan technology.
We will need to enlist the cooperation of Scripps should we decide to apply for a five-year patent term extension of U.S. Patent No. 5,912,231 under the Hatch Waxman Act, and such cooperation is not guaranteed. Although U.S. Patent 5,912,231 supplements our existing intellectual property portfolio, we are chiefly reliant on our U.S. Patent 8,530,409, which covers the novel formulation and method of use for Locilex® and provides for substantially longer patent coverage (until June 2032) than U.S. Patent 5,912,231. As such, we have not yet engaged in any discussions with Scripps regarding a possible patent term extension for U.S. Patent No. 5,912,231 and a patent term extension is filed only after regulatory approval. If and when we decide to apply for an extension, we will bear the costs of preparing and filing the application, but Scripps, as the owner of U.S. Patent No. 5,912,231, will submit the application. Accordingly, we will need to work with Scripps throughout the application process to facilitate its approval. An inability to extend the patent past 2016 may impair our competitive position if other companies use pexiganan as an API to develop a product that, once approved by the FDA, competes with Locilex®.
We may become subject to third parties' claims alleging infringement of their patents and proprietary rights or seeking to invalidate our patents or proprietary rights, or we may need to become involved in lawsuits to protect or enforce our patents, which could be costly, time consuming, delay or prevent the development and commercialization of our product candidates, or put our patents and other proprietary rights at risk.
Litigation relating to infringement or misappropriation of patent and other intellectual property rights in the pharmaceutical and biotechnology industries is common. We may become subject to third-party claims in the future relating to our technologies, processes, formulations, methods, or products that would cause us to incur substantial expenses and which, if successful, could cause us to pay substantial damages and attorney's fees, if we are found to be infringing a third party's patent rights. We may also become subject to claims that we have misappropriated the trade secrets of others. These risk are exacerbated by the fact that the validity and breadth of claims covered in pharmaceutical patents is, in most instances, uncertain and highly complex. We would be particularly at risk if any such claims relate to our key U.S. Patent No. 8,530,409 covering our particular formulation of and method of use for Locilex®.
Furthermore, if a patent infringement suit is brought against us relating to Locilex® (or any other products we may develop or acquire in the future), our research, development, manufacturing or sales activities relating to Locilex® or the product candidate that is the subject of the suit may be delayed or terminated. As a result of patent infringement claims, or in order to avoid potential infringement claims, we or our collaborators may choose to seek, or be required to seek, a license from the third
43
party, which would be likely to include a requirement to pay license fees or royalties or both. These licenses may not be available on acceptable terms, or at all. Even if a license can be obtained on acceptable terms, the rights may be nonexclusive, which would give our competitors access to the same intellectual property rights. If we are unable to enter into a license on acceptable terms, we or our collaborators could be prevented from commercializing Locilex® (or any other products we may develop or acquire in the future), or forced to modify such product candidates, or to cease some aspect of our business operations, which could harm our business significantly.
In addition, competitors may infringe our patents, or misappropriate or violate our other intellectual property rights. To counter infringement or unauthorized use, we may find it necessary to file infringement or other claims to protect our intellectual property rights. In addition, in any infringement proceeding brought by us against a third party to enforce our rights, a court may decide that a patent of ours is invalid or unenforceable, or may refuse to stop the other party from using the technology at issue on the basis that our patents do not cover the technology in question. An adverse result in any such litigation proceeding could put one or more of our patents at risk of being invalidated or interpreted narrowly, which could open us up to additional competition and have a material adverse effect on our business.
The cost to us of any patent litigation or other proceedings, even if resolved in our favor, could be substantial. Such litigation or proceedings could substantially increase our operating losses and reduce our resources available for development activities. We may not have sufficient financial or other resources to adequately conduct such litigation or proceedings, and such litigation could impair our ability to raise funding for our company. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their substantially greater financial resources. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments, and, if securities analysts or investors perceive these results to be negative, there could be a substantial adverse effect on the price of our common stock. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace. Patent litigation and other proceedings may also require significant time and attention of management and technical staff, which may materially and adversely impact our financial position and results of operations. Furthermore, because of the substantial amount of discovery required in connection with any intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation.
As a result of any such litigation, we may also be required to: (i) cease selling, making, importing, incorporating or using one or more or all of our products that incorporate intellectual property of others, which would adversely affect our revenue; or (ii) redesign our products, which would be costly and time-consuming.
Restrictions on our patent rights relating to Locilex® may limit our ability to prevent third parties from competing against us.
Assuming FDA approval, our ability to market and sell Locilex® will depend, in part, on our ability to obtain and maintain patent protection for Locilex® (or any products we may develop in the future), preserve our trade secrets, prevent third parties from infringing upon our proprietary rights and operate without infringing upon the proprietary rights of others. The U.S. patent that we sublicense from Scripps (U.S. Patent No. 5,912,231), which is directed to the composition of matter of pexiganan, expires on June 15, 2016 without any term extension. The foreign patents corresponding to U.S. Patent No. 5,912,231 expired in 2009. As a result, we have no foreign patent protection for the pexiganan API. We have recently been issued a U.S. patent, U.S. Patent No. 8,530,409, covering our new formulation of Locilex® as well as a method of using this new formulation to treat skin or wound infections. The U.S. Patent No. 8,530,409 claims are directed to very specific formulations of the pexiganan API, and
44
their methods of use to treat skin or wound infections. As a result, U.S. Patent No. 8,530,409 would not prevent third party competitors from creating, making and marketing alternative formulations of pexiganan, including topical formulations, that fall outside the scope of the U.S. Patent No. 8,530,409 claims. There can be no assurance that any such alternative formulations will not be equally effective as Locilex®. Introduction of any such competitive product could have a material adverse effect on sales of Locilex®. Moreover, even if these competitors do not actively promote their product for our targeted indication, physicians may prescribe these products "off-label." Although off-label prescriptions may infringe or contribute to the infringement of method-of-use patents, the practice is common and such infringement is difficult to prevent or prosecute.
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on Locilex® or any product candidates we may develop or acquire in the future throughout the world would be prohibitively expensive. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and furthermore, may export otherwise infringing products to territories where we have patent protection, but where enforcement is not as strong as that in the U.S. These products may compete with our future products in jurisdictions where we do not have any issued patents and our patent claims or other intellectual property rights may not be effective or sufficient to prevent them from so competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property protection, particularly those relating to biopharmaceuticals, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial cost and divert our efforts and attention from other aspects of our business.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other provisions during the patent process. There are situations in which noncompliance can result in abandonment or lapse of a patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, competitors might be able to enter the market earlier than would otherwise have been the case.
If our Locilex® trademark is not adequately protected, then we may not be able to build name recognition in our markets of interest and our business may be adversely affected.
Our registered trademark, Locilex®, may be challenged, infringed, circumvented or declared generic or determined to be infringing on other marks. We may not be able to protect our rights to this trademark, which we need to build name recognition by potential partners or customers in our markets of interest. Over the long term, if we are unable to establish name recognition based on our trademark, then we may not be able to compete effectively and our business may be adversely affected.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition to seeking patent protection for Locilex®, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive
45
position. We seek to protect these trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, corporate collaborators, outside scientific collaborators, contract manufacturers, consultants, advisors and other third parties. We also enter into confidentiality and invention or patent assignment agreements with our employees and consultants that obligate them to assign their inventions to us. Despite these efforts, any of these parties may breach the agreements and disclose our proprietary information, including our trade secrets, and we may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the U.S., including in foreign jurisdictions, are less willing or unwilling to protect trade secrets. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by competitor, our competitive position would be harmed.
Risks Related to Ownership of Our Common Stock
The market price of our common stock may be highly volatile, and you could lose all or part of your investment.
The trading price of our common stock is likely to be volatile. This volatility may prevent you from being able to sell your shares at or above the price you paid for your shares. Our stock price could be subject to wide fluctuations in response to a variety of factors, which include:
- •
- any adverse results or delays in commencement or completion of our planned Phase 3 clinical trials for Locilex®;
- •
- any adverse results or delays in the commencement or completion of our planned Phase 1 clinical trials for
Locilex®;
- •
- any delay in preparing or filing our NDA for Locilex® and any adverse development or perceived adverse development with
respect to the FDA's review of the NDA, including without limitation the FDA's issuance of a "refusal to file" letter or a request for additional information;
- •
- changes in laws or regulations applicable to Locilex® or any future product candidates, including but not limited to
clinical trial requirements for approvals;
- •
- unanticipated serious safety concerns related to the use of Locilex® or any future product candidates;
- •
- a decision to initiate a clinical trial, not to initiate a clinical trial or to terminate an existing clinical trial;
- •
- our inability to obtain adequate product supply for Locilex® or any future product candidate, or the inability to do so at
acceptable prices;
- •
- adverse regulatory decisions;
- •
- the introduction of new products or technologies offered by us or our competitors;
- •
- the effectiveness of our or our potential partners' commercialization efforts;
- •
- the inability to effectively manage our growth;
- •
- actual or anticipated variations in quarterly operating results;
- •
- our failure to meet or exceed the estimates and projections of the investment community;
46
- •
- the perception of the pharmaceutical industry by the public, legislatures, regulators and the investment community;
- •
- the overall performance of the U.S. equity markets and general political and economic conditions;
- •
- developments concerning our sources of manufacturing supply and any commercialization partners;
- •
- announcements of significant acquisitions, strategic partnerships, joint ventures or capital commitments by us or our competitors;
- •
- disputes or other developments relating to proprietary rights, including patents, litigation matters and our ability to obtain patent
protection for our technologies;
- •
- additions or departures of key scientific or other consultants or management personnel;
- •
- adverse market reaction to any indebtedness we may incur or securities we may issue in the future;
- •
- sales of our common stock by our stockholders in the future;
- •
- significant lawsuits, including patent or stockholder litigation;
- •
- changes in the market valuations of similar companies;
- •
- the trading volume of our common stock;
- •
- effects of natural or man-made catastrophic events or other business interruptions; and
- •
- other events or factors, many of which are beyond our control.
In addition, the stock market in general, and the stock of biotechnology companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies. Broad market and industry factors may negatively affect the market price of our common stock, regardless of our actual operating performance.
Our failure to meet the continued listing requirements of The NASDAQ Capital Market could result in a de-listing of our stock, which could limit investors' ability to make transactions in our securities and subject us to additional trading restrictions.
Our common stock is listed on The NASDAQ Capital Market, a national securities exchange. If we fail to satisfy the continued listing requirements of The NASDAQ Capital Market, such as the corporate governance requirements or the minimum closing bid price requirement, the NASDAQ Stock Market (or NASDAQ) may take steps to de-list our common stock. Such a de-listing would likely have a negative effect on the price of our common stock and would impair your ability to sell or purchase our common stock when you wish to do so. In the event of a de-listing, we would take actions to restore our compliance with NASDAQ's listing requirements, but we can provide no assurance that any such action taken by us would allow our common stock to become listed again, stabilize the market price or improve the liquidity of our common stock, prevent our common stock from dropping below the NASDAQ minimum bid price requirement or prevent future non-compliance with NASDAQ's listing requirements.
If The NASDAQ Capital Market does not maintain the listing of our securities for trading on its exchange, we could face significant material adverse consequences, including:
- •
- a limited availability of market quotations for our securities;
47
- •
- reduced liquidity with respect to our securities;
- •
- a determination that our shares of common stock are "penny stock" which will require brokers trading in our shares of common stock to
adhere to more stringent rules, possibly resulting in a reduced level of trading activity in the secondary trading market for our shares of common stock;
- •
- a limited amount of news and analyst coverage for our company; and
- •
- a decreased ability to issue additional securities or obtain additional financing in the future.
The National Securities Markets Improvement Act of 1996, which is a federal statute, prevents or preempts the states from regulating the sale of certain securities, which are referred to as "covered securities." For as long as our common stock is listed on The NASDAQ Capital Market, our common stock will be covered securities. Although the states are preempted from regulating the sale of our securities, the federal statute does allow the states to investigate companies if there is a suspicion of fraud, and, if there is a finding of fraudulent activity, then the states can regulate or bar the sale of covered securities in a particular case. Furthermore, if we were no longer listed on The NASDAQ Capital Market, our common stock would not be covered securities and we would be subject to regulation in each state in which we offer our securities.
If our shares become subject to the penny stock rules, it would become more difficult to trade our shares.
The Commission has adopted rules that regulate broker-dealer practices in connection with transactions in penny stocks. Penny stocks are generally equity securities with a price of less than $5.00, other than securities registered on certain national securities exchanges or authorized for quotation on certain automated quotation systems, provided that current price and volume information with respect to transactions in such securities is provided by the exchange or system. If we do not retain a listing on The NASDAQ Capital Market and if the price of our common stock is less than $5.00, our common stock will be deemed a penny stock. The penny stock rules require a broker-dealer, before a transaction in a penny stock not otherwise exempt from those rules, to deliver a standardized risk disclosure document containing specified information. In addition, the penny stock rules require that before effecting any transaction in a penny stock not otherwise exempt from those rules, a broker-dealer must make a special written determination that the penny stock is a suitable investment for the purchaser and receive (i) the purchaser's written acknowledgment of the receipt of a risk disclosure statement; (ii) a written agreement to transactions involving penny stocks; and (iii) a signed and dated copy of a written suitability statement. These disclosure requirements may have the effect of reducing the trading activity in the secondary market for our common stock, and therefore stockholders may have difficulty selling their shares.
There can be no assurance that we will ever provide liquidity to our investors through a sale of our company.
While acquisitions of pharmaceutical companies like ours are not uncommon, potential investors are cautioned that no assurances can be given that any form of merger, combination, or sale of our company will take place, or that any merger, combination, or sale, even if consummated, would provide liquidity or a profit for our investors. You should not invest in our company with the expectation that we will be able to sell the business in order to provide liquidity or a profit for our investors.
The financial and operational projections that we may make from time to time are subject to inherent risks.
The projections that we provide herein or our management may provide from time to time (including, but not limited to, those relating to potential peak sales amounts, clinical and regulatory timelines, production and supply matters, commercial launch dates, and other financial or operational matters) reflect numerous assumptions made by management, including assumptions with respect to our
48
specific as well as general business, regulatory, economic, market and financial conditions and other matters, all of which are difficult to predict and many of which are beyond our control. Accordingly, there is a risk that the assumptions made in preparing the projections, or the projections themselves, will prove inaccurate. There may be differences between actual and projected results, and actual results may be materially different from those contained in the projections. The inclusion of the projections in this report should not be regarded as an indication that we, our management, the underwriters or their respective representatives considered or consider the projections to be a guaranteed prediction of future events, and the projections should not be relied upon as such.
Messrs. Luci and DeLuccia hold a significant concentration of our common stock, which could limit the ability of our other stockholders to influence the direction of our company.
As calculated by the Commision rules of beneficial ownership, David P. Luci and Robert J. DeLuccia, each executive officers and directors of our company, each own approximately 18.7% of our outstanding common stock as of March 19, 2016. Accordingly, they collectively may have the ability to significantly influence or determine the election of all of our directors or the outcome of most corporate actions requiring stockholder approval such as: (i) a merger or a sale of our company, (ii) a sale of all or substantially all of our assets, and (iii) amendments to our articles of incorporation and bylaws. This concentration of voting power and control could have a significant effect in delaying, deferring or preventing an action that might otherwise be beneficial to our other stockholders and be disadvantageous to our stockholders with interests different from those individuals. These individuals also have significant control over our business as officers and directors of our company. There is a risk that they may exercise this ability in a manner that advances their best interests and not necessarily those of our other stockholders.
We incur significant increased costs as a result of operating as a public company and our management is required to devote substantial time to new compliance initiatives.
As a public company, we incur significant legal, accounting and other expenses that we did not incur as a private company. The Sarbanes-Oxley Act, as well as rules subsequently implemented by the Commission and NASDAQ, has imposed various requirements on public companies. Our management and other personnel devote a substantial amount of time to these compliance initiatives. Moreover, compliance with these rules and regulations have increased our legal, accounting and financial compliance costs substantially. In addition, these rules and regulations may make our activities related to legal, accounting and financial compliance more difficult, time-consuming and costly and may also place undue strain on our personnel, systems and resources. If these requirements divert the attention of our management and personnel from other business concerns, they could have a material adverse effect on our business, financial condition and results of operations. For example, we expect these rules and regulations to make it more difficult and more expensive for us to obtain director and officer liability insurance, and we may be required to incur substantial costs to maintain our current levels of such coverage. We estimate the additional costs we may incur to respond to these requirements to range from $500,000 to $1.0 million annually, although unforeseen circumstances could increase actual costs.
An investment in our company may involve tax implications, and you are encouraged to consult your own advisors as neither we nor any related party is offering any tax assurances or guidance regarding our company or your investment.
The formation of our company and our financings, as well as an investment in our company generally, involves complex federal, state and local income tax considerations. Neither the Internal Revenue Service nor any State or local taxing authority has reviewed the transactions described herein, and may take different positions than the ones contemplated by management. You are strongly urged
49
to consult your own tax and other advisors prior to investing, as neither we nor any of our officers, directors or related parties is offering you tax or similar advice, nor are any such persons making any representations and warrants regarding such matters.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
Under Section 382 of the Internal Revenue Code of 1986, as amended, referred to as the Internal Revenue Code, if a corporation undergoes an "ownership change" (generally defined as a greater than 50% change (by value) in its equity ownership over a three-year period), the corporation's ability to use its pre-change net operating loss carryforwards and other pre-change tax attributes (such as research tax credits) to offset its post-change income may be limited. We believe that, with our recent IPO, taken together with our private placements within a three-year period and other transactions that have occurred over the past three years, we may have triggered an "ownership change" limitation. We may also experience ownership changes in the future as a result of subsequent shifts in our stock ownership, including as a result of the completion of our recent IPO when it is taken together with other transactions we may consummate in the succeeding three-year period. As a result, if we earn net taxable income, our ability to use our pre-change net operating loss carryforwards to offset U.S. federal taxable income may be subject to limitations, which potentially could result in increased future tax liability to us.
As an "emerging growth company" under applicable law, we will be subject to lessened disclosure requirements, which could leave our stockholders without information or rights available to stockholders of more mature companies.
For as long as we remain an "emerging growth company" as defined in the Jumpstart Our Business Startups Act of 2012 (which we refer to herein as the JOBS Act), we have elected to take advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not "emerging growth companies" including, but not limited to:
- •
- not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act;
- •
- taking advantage of an extension of time to comply with new or revised financial accounting standards;
- •
- reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements; and
- •
- exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved.
We expect to take advantage of these reporting exemptions until we are no longer an "emerging growth company." Because of these lessened regulatory requirements, our stockholders would be left without information or rights available to stockholders of more mature companies.
Because we have elected to use the extended transition period for complying with new or revised accounting standards for an "emerging growth company" our financial statements may not be comparable to companies that comply with public company effective dates.
We have elected to use the extended transition period for complying with new or revised accounting standards under Section 102(b)(1) of the JOBS Act. This election allows us to delay the adoption of new or revised accounting standards that have different effective dates for public and private companies until those standards apply to private companies. As a result of this election, our financial statements may not be comparable to companies that comply with public company effective
50
dates, and thus investors may have difficulty evaluating or comparing our business, performance or prospects in comparison to other public companies, which may have a negative impact on the value and liquidity of our common stock.
If securities or industry analysts do not publish or cease publishing research or reports about us, our business or our market, or if they change their recommendations regarding our common stock adversely, the price of our common stock and trading volume could decline.
The trading market for our common stock may be influenced by the research and reports that securities or industry analysts may publish about us, our business, our market or our competitors. If any of the analysts who may cover us change their recommendation regarding our common stock adversely, or provide more favorable relative recommendations about our competitors, the price of our common stock would likely decline. If any analyst who may cover us was to cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which in turn could cause the price of our common stock or trading volume to decline.
Anti-takeover provisions in our charter documents and Delaware law could discourage, delay or prevent a change in control of our company and may affect the trading price of our common stock.
As of the completion of our corporate conversion on March 12, 2014, we are a Delaware corporation. The anti-takeover provisions of the Delaware General Corporation Law may discourage, delay or prevent a change in control by prohibiting us from engaging in a business combination with an interested stockholder for a period of three years after the person becomes an interested stockholder, even if a change in control would be beneficial to our existing stockholders. In addition, our certificate of incorporation and bylaws may discourage, delay or prevent a change in our management or control over us that stockholders may consider favorable. Our certificate of incorporation and bylaws:
- •
- provide that vacancies on our board of directors, including newly created directorships, may be filled only by a majority vote of
directors then in office;
- •
- not provide stockholders with the ability to take action by written consent;
- •
- provide that special meetings of stockholders may only be called by our Chairman and/or President, our board of directors or a
super-majority (662/3%) of our stockholders;
- •
- place restrictive requirements (including advance notification of stockholder nominations and proposals) on how special meetings of
stockholders may be called by our stockholders;
- •
- not provide stockholders with the ability to cumulate their votes; and
- •
- provide that only a super-majority of our stockholders (662/3%) may amend our bylaws.
We do not expect to pay dividends for the foreseeable future.
We do not expect to pay dividends on our common stock offered in this transaction for the foreseeable future. Accordingly, any potential investor who anticipates the need for current dividends should not purchase our securities.
ITEM 1B. UNRESOLVED STAFF COMMENTS.
None.
Effective May 2014, the Company entered into a sublease agreement for office space with monthly payments of $13,098 with inflationary escalations in 2015 and the first three months of 2016. The term of the sublease ends on March 30, 2016. Total minimum sublease payments for the remaining term of the sublease from December 31, 2015 to March 30, 2016 are $39,294.
51
In January 2016, the Company entered into a lease for office space commencing in March 2016 with current monthly payments of $18,857, subject to inflationary escalations and adjustments thereafter. The term of the lease is for five years and five months. We believe this space is adequate as our principal executive office location.
From time to time, we may become involved in various lawsuits and legal proceedings, which arise in the ordinary course of business. Litigation is subject to inherent uncertainties, and an adverse result in these or other matters may arise from time to time that may harm business.
The Company and its two original executives were three of some 30 defendants in a lawsuit filed by a former stockholder of Genaera Corporation, which was the predecessor of the Genaera Liquidating Trust, the party from which the Company purchased the worldwide rights to pexiganan, the active ingredient of the Product Locilex® on April 8, 2010. The complaint was filed on June 8, 2012 in the United States District Court for the Eastern District of Pennsylvania (Civil Action No. 12-3265) by Alan W. Schmidt, individually and on behalf of former Genaera Corporation shareholders. Among others, the suit was filed against the Company, as well as John A. Skolas and Argyce, LLC, who were responsible for the administration of the Trust and who sold pexiganan to the Company via a public auction. The defendants listed in the complaint included several individuals and companies formerly associated with Genaera Corporation, the Trust and/or Argyce, LLC. Also included in the defendant group were several other pharmaceutical companies that were involved in acquiring the former drug-related assets of the Genaera Corporation.
The complaint alleged, among other things, the Company and its two executives aided and abetted a breach of fiduciary duty alleged to have been committed by the former director and officers of Genaera Corporation before it was approved for dissolution by its shareholders and also Argyce, LLC, the trustee of the Liquidating Trust. Plaintiff claims that the Company, and its executives, aided and abetted a breach of the duties of the board of directors and the trustee under common law and under a certain trust agreement allegedly signed between Argyce, LLC, as the trustee, and the Liquidating Trust. With regard to the claims made against the Company and two executives, the plaintiff alleged, in pertinent part, that the Company's acquisition of the pexiganan rights was for alleged inadequate consideration, and that the Company and its management aided and abetted a breach of fiduciary duty by the Genaera Corporation defendants who were formerly associated with Genaera Corporation and/or the Trust.
The Company and its two executives filed a motion to dismiss the complaint within the prescribed time period. All of the other defendants in this litigation also filed motions to dismiss, and a court order by the Federal District Court granted each and every motion to dismiss, with prejudice, without leave to refile, on August 12, 2013 based on the argument that Plaintiff's claims were time barred. A subsequent motion to reconsider such dismissal was denied by the Federal District Court. Plaintiff appealed the dismissal to the United States Third Circuit Court of Appeals seeking reversal of the dismissal and the Third Circuit Court granted Plaintiff's appeal. On October 17, 2014, the Third Circuit Appellate Court, in a 2-1 decision with a strong dissenting opinion, reversed the trial court's dismissal of Plaintiff's claims based on the expiration of the applicable statutes of limitation. In a 2-1 decision, the Third Circuit held that more information was necessary to determine when Plaintiff should have been on notice of his claims to determine the applicability of the discovery rule, which could serve to extend the time frame in which Plaintiff could bring his claims. Due to the strong dissent, all Defendants filed the necessary documents requesting a petition for rehearing en banc, by the majority of the Third Circuit justices who are in active service. The Third Circuit denied the request for en banc hearing and remanded this case to District Court.
52
Upon remand to the Federal District Court, all Defendants moved to dismiss the complaint for reasons other than being time barred. The Company and the executives moved for dismissal based on Plaintiff's inability to make a case for aiding and abetting a breach of fiduciary duty because there was no underlying breach and such an aiding and abetting claim requires an element of knowing participation in the fiduciary breach which cannot be established by Plaintiff.
The District Court held a hearing on this in September 2015 and the District Court delivered an Order on November 10, 2015 pursuant to which the District Court granted the Motion to Dismiss filed by each and every defendant including the Company and its executives. In December 2015, Plaintiff appealed the Federal District Court's decision to the Third Circuit Appellate Court and we anticipate a decision on whether to grant Plaintiff's appeal by the Third Circuit Appellate Court in 2016. The Company will continue to vigorously defend Plaintiff's claims on the factual record, which it believes will prove that the Company is not liable to the Plaintiff in any regard.
ITEM 4. MINE SAFETY DISCLOSURES.
Not Applicable.
ITEM 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS, AND ISSUER PURCHASES OF EQUITY SECURITIES.
Market Information
Our Common Stock is listed the NASDAQ Capital Market, under the symbol "DPRX".
The following table shows, for the periods indicated, the high and low sales prices per share of our common stock as reported by the NASDAQ Capital Market.
| |
High | Low | |||||
|---|---|---|---|---|---|---|---|
2016 |
|||||||
Quarter ended March 31, 2016 (as of March 21, 2016) |
10.04 | 6.15 | |||||
2015 |
|||||||
Quarter ended March 31, 2015 |
$ | 14.23 | $ | 10.71 | |||
Quarter ended June 30, 2015 |
$ | 14.99 | $ | 11.50 | |||
Quarter ended September 30, 2015 |
$ | 16.89 | $ | 11.95 | |||
Quarter ended December 31, 2015 |
$ | 14.07 | $ | 10.57 | |||
2014 |
|||||||
Quarter ended March 31, 2014 |
$ | 14.04 | $ | 9.95 | |||
Quarter ended June 30, 2014 |
$ | 11.29 | $ | 8.61 | |||
Quarter ended September 30, 2014 |
$ | 10.30 | $ | 8.63 | |||
Quarter ended December 31, 2014 |
$ | 11.67 | $ | 9.80 | |||
Holders
As of December 31, 2015, there were 83 holders of record of our common stock.
Registration Rights
Each of our investors in our previous private placements is party to an Investor Rights Agreement affording them certain "piggy back" registration rights with respect to their Class A Membership Interests in our company and Class A Membership Interests underlying warrants held by such investors. These rights remain in effect notwithstanding the conversion that was consummated converting
53
Dipexium LLC into Dipexium, Inc. that was consummated in March 2014. These pre-IPO holders currently have the right to certain "piggy back" registration rights with respect to 402,248 shares of our common stock and shares of common stock underlying warrants to purchase 24,500 shares.
Dividends
We have never declared or paid any cash dividends on our equity interests and we do not anticipate paying any cash dividends in the foreseeable future. The payment of dividends, if any, in the future is within the discretion of our board of directors and will depend on our earnings, capital requirements and financial condition and other relevant facts. We currently intend to retain all future earnings, if any, to finance the development and growth of our business.
Securities Authorized for Issuance under Equity Compensation Plans
Securities Authorized for Issuance Under Equity Compensation Plans
The following table indicates shares of common stock authorized for issuance under our 2013 Equity Incentive Plan as of December 31, 2015:
Plan category
|
Number of securities to be issued upon exercise of outstanding options, warrants and unvested common shares |
Weighted-average exercise price of outstanding options, warrants and unvested |
Number of securities remaining available for future issuance |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
Equity compensation plans approved by security holders |
1,164,787 | $ | 12.90 | 1,028,881 | ||||||
Equity compensation plans not approved by security holders |
||||||||||
Total |
1,164,787 | $ | 12.90 | 1,028,881 | ||||||
ITEM 6. SELECTED FINANCIAL DATA.
We are a smaller reporting company as defined by Rule 12b-2 of the Exchange Act and are not required to provide the information under this item.
ITEM 7. MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS.
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and related notes appearing elsewhere in this Report. This discussion and analysis contains forward-looking statements that involve risks, uncertainties and assumptions. The actual results may differ materially from those anticipated in these forward-looking statements as a result of certain factors, including, but not limited to, those which are not within our control.
Description of Business
We are a late stage pharmaceutical company focused on the development and commercialization of Locilex® (pexiganan cream 0.8%), a novel, first-in-class, broad spectrum, topical antibiotic. Locilex® is a chemically synthesized, 22-amino acid peptide isolated from the skin of the African Clawed Frog. Its novel mechanism of action kills microbial targets by disrupting the bacterial cell membrane; a process known as cell membrane permeability. Locilex® is initially being targeted for the treatment of mild infections of diabetic foot ulcers (or Mild DFI). In 2011, the market for diabetic foot infection therapeutics worldwide was approximately $1.46 billion. Our primary objective is to establish Locilex® as the standard of care for the treatment of patients with Mild DFI. Thereafter, our growth strategy
54
includes potentially expanding the indications for Locilex® to include moderate infections of diabetic foot ulcers (or Moderate DFI) and certain other mild or moderate skin and skin structure infections in superficial wounds.
We believe that we have a clear clinical and regulatory pathway with the potential for United States Food and Drug Administration (or FDA) approval of Locilex® by the second half of 2017. We are conducting two pivotal Phase 3 clinical trials in the United States under the auspicies of our special protocol assessment (or SPA) agreement with the FDA on our Phase 3 program. We intend to complete enrollment in these two pivotal Phase 3, double blind, placebo-controlled superiority studies in the first half of 2016. We successfully conducted two separate Phase 1 skin irritation and skin sensitization studies and we reported data on the first of these two Phase 1 studies in Q3 2014 and reported data on the second Phase 1 study in Q1 2015. If the data from our Phase 3 studies are sufficient to meet the primary endpoint, we expect to submit a new drug application (or NDA) amendment for Locilex® to the FDA soon thereafter. We expect to receive a response from the FDA within six months of our NDA submission.
According to the Infectious Disease Society of America (or IDSA), diabetic foot infections (or DFI) may be classified by their clinical severity as mild, moderate, or severe. 47% of DFI patients first present to a treating physician in the mild stage of infection, 34% of DFI patients first present at the moderate stage and 18% of DFI patients first present at the severe stage. At the mild stage, patients can typically be treated on an outpatient basis and amputation risk is minimal (2% to 3% in Mild DFI). When not managed effectively, the potential for Mild DFI to progress to a limb- or life-threatening infection increases dramatically. Published research suggests amputation rates increase in Moderate DFI and severe infections of diabetic foot ulcers (or Severe DFI) to approximately 45% and 75%, respectively. Similarly, the hospitalization rate for Mild DFI patients is approximately 10%, increasing in Moderate DFI and Severe DFI to approximately 55% and 85%, respectively. Thus, DFIs are a major cause of patient morbidity, a substantial burden to the healthcare system, and a source of high financial costs.
Systemic antibiotics currently prescribed off-label to treat Mild DFI generate resistant pathogens which create infections that are more difficult to treat. Such antibiotics are also associated with toxic side effects in patients who typically have some degree of compromised liver and kidney function. We believe that a topical preparation like Locilex®, which is locally administered on the open wound and skin, offers significant advantages over systemic treatments. As a topical antibiotic, Locilex® affects only the area to which it is applied, and unlike most systemic antibiotics, it does not spread to the entire body through the bloodstream, which is host to a number of different bacteria other than bacteria causing the skin infection. Topical antibiotics are also delivered to the infected area at a higher concentration than those antibiotics that are delivered systemically. As a result, we believe that topical antibiotics are less likely to develop bacterial resistance, both because the higher antibiotic concentration more effectively kills the infection-causing bacteria before they develop resistance, and because other bacteria in the bloodstream are not exposed to the Locilex® topical cream. Currently, there are no products, including no antibiotics, specifically approved by the FDA for the treatment of Mild DFI, nor are there any topical antibiotics currently approved for any severity of DFI. As such, we believe that Locilex® has the potential to be the first topical antibiotic approved for the treatment of DFI, as well as the first product of any kind to be labeled specifically for the treatment of Mild DFI.
We believe that the key attributes of Locilex® are: (i) it has not generated resistant bacteria systemically; (ii) it has not generated cross resistance with other antibiotics; (iii) it has demonstrated activity against a broad spectrum of pathogens, including difficult to treat gram negative, and anaerobic bacteria; (iv) it has not been systemically absorbed; and (v) it has not caused any significant safety or tolerability issues in over 500 patients treated (all data being that from studies prior to the current double blind Phase 3 studies); and (vi) it has demonstrated significant success treating multi-drug resistant bacteria in several laboratory tests and clinical trials performed to date. These attributes lead
55
us to believe that Locilex® has the potential to be positioned as the standard of care to treat patients with Mild DFI. In addition, data generated to date support the potential use of Locilex® to treat a broad array of mild or moderate skin and skin structure infections in superficial wounds.
As reported in published research, Locilex® has previously demonstrated statistical non-inferiority to a systemic antibiotic in a large-scale, randomized, active-controlled double blind, multi-center clinical study in patients with Mild or Moderate DFI. We have conducted microbiology studies that highlight the sensitivity of resistant bacteria, including methicillin-resistant staphylococcus aureus (or MRSA), vancomycin-resistant enterococcus (or VRE), extended-spectrum b-lactamase (or ESBL) and multi-drug resistant (or MDR) bacteria, to pexiganan, the active pharmaceutical ingredient (or API) in Locilex®. Due to the increased global prevalence of resistant bacteria in all types of skin infections, Locilex® may provide an important therapeutic advance.
We have contracted with third party vendors with respect to all key elements of our clinical and regulatory program, including vendors to: (i) conduct the Phase 3 and Phase 1 clinical trials for Locilex®; (ii) manufacture the API; (iii) formulate the finished product; and (iv) label and package the product. We believe these key relationships will help drive our clinical and regulatory program for Locilex® in a timely and efficient manner.
Locilex® was originally sponsored by Magainin Pharmaceuticals, Inc. (or Magainin), which engaged in the FDA review process during 1998 and 1999, ultimately receiving a non-approvable letter based upon two manufacturing issues. We acquired the worldwide rights to pexiganan, the API in Locilex®, from a third party in April 2010. These rights included the prior formulation and all of the clinical and preclinical data generated by Magainin in its FDA review process. This includes data from over 1,000 evaluable patients, including 835 in large-scale, randomized, active-controlled, double blind, multi-center clinical studies as compared to a systemic quinolone standard of care as more fully described below. We believe we have corrected the manufacturing problems encountered by the prior sponsor. See "History of Locilex®" below.
Dipexium Pharmaceuticals, LLC ("Dipexium LLC") was organized under the laws of the State of Delaware in January 2010. In March 2014, we effected a corporate conversion pursuant to which we succeeded to the business of Dipexium LLC and the holders of Membership Interests of Dipexium LLC became stockholders of Dipexium Pharmaceuticals, Inc.
Plan of Operation
Our primary objective is to establish Locilex® as the standard of care to treat patients with Mild DFI. The key elements of our strategy are as follows:
- •
- Complete the Phase 3 program for
Locilex®. As a result of our SPA for Locilex®, we believe the clinical pathway for Locilex® is
clear. Working with our key third party vendors, we commenced our Phase 3 program in the third quarter of 2014 and expect to complete enrollment in the first half of 2016;
- •
- Obtain FDA approval of Locilex® for Mild
DFI. If our Phase 3 trials meet their primary endpoint, we plan to submit our NDA for Locilex®. We believe that
Locilex® may be approved by the FDA within 6 months of filing a NDA amendment with the FDA;
- •
- Commercially launch Locilex® in the U.S. If
FDA approved, we plan to utilize a small specialty sales force to launch Locilex® in the U.S., initially targeting podiatrists and potentially expanding to other specialty healthcare
providers;
- •
- Expand Locilex®'s FDA-approved uses. If we are able to obtain FDA approval in Mild DFI, we will consider obtaining additional FDA approvals that will enable us to expand the Locilex®
56
- •
- Commence clinical and regulatory activities in Europe. Based upon regulatory advice received to date, if our pivotal Phase 3 clinical trials are completed successfully, we plan to file our marketing authorization application (or MAA) in the E.U. under the centralized process promptly following the completion of our Phase 3 program in the U.S.;
label to include patients with Moderate DFI and certain other mild or moderate skin and skin structure infections in superficial wounds;
We will rely on our strong management team, board of directors and scientific advisors to execute our strategy. The individuals on our management team, board of directors and scientific advisors will contribute their significant business development, regulatory, finance and commercial experiences to the development and commercialization of Locilex®.
Drug Development Strategy
We are conducting concurrently two pivotal Phase 3 clinical trials of Locilex® for the treatment of Mild DFI. The trials are referred to as DPX-305 and DPX-306, or OneStep-1 and OneStep-2.
We have an SPA with the FDA relating to the trial design for our Phase 3 studies. The SPA calls for us to conduct two placebo-controlled pivotal Phase 3 studies, but does not require us to demonstrate equivalence to oral antibiotics. DPX-305 and DPX-306 are between 65-70% enrolled as of December 31, 2015 and are tracking closely with one another in terms of enrollment. We expect to complete enrollment in the first half of 2016. Both trials are randomized, placebo-controlled, double blind, multi-center superiority studies in 180 evaluable patients in each trial. These trials are designed to establish the superiority of Locilex® over placebo-cream in the treatment of Mild DFI.
We are conducting the OneStep-1 and OneStep-2 trials at up to 74 clinical sites in the U.S. The primary endpoint of the trials will be clinical success, defined as resolution of infection in the clinical judgment of each treating physician using the objective standards articulated in the 2012 DFI treatment guidelines. Microbiological success, defined as complete microbiological response, will be assessed as one of the secondary endpoints. All of the primary and secondary endpoints will be assessed for each patient on the 28th day following entry into the study. Furthermore, the FDA has agreed that data from the Locilex® arm of the two prior studies conducted by Locilex®'s prior sponsor can be used to supplement our safety database.
We also have completed enrollment in DPX-110, our Phase 1 skin irritation study and announced top-line data in July 2014 and we completed enrollment in DPX-120, a Phase 1 skin sensitization study, in Q3 2014 and reported top line data in February 2015.
Research Pharmaceutical Services, Inc. (a division of PRA International) is the contract research organization conducting our Phase 3 studies for Locilex®. This work is being performed under the auspices of RRD International, LLC, which is managing all aspects of our scientific, clinical and regulatory development.
Research Pharmaceutical Services, Inc. also is working with us on our European clinical and regulatory strategy in coordination with RRD International, LLC.
Opportunities, Challenges and Risks
We are a late-stage pharmaceutical company and have never generated revenue. Currently we do not have a stable recurring source of revenues sufficient to cover our operating costs. We incurred net losses of $18.7 million and $13.6 million for the years ended December 31, 2015 and 2014, respectively.
57
Our business and ability to execute our business strategy are subject to a number of risks and challenges:
- •
- We are heavily dependent on attaining regulatory approval for and, if approved, successfully commercializing
Locilex®. Locilex® is our only product candidate. As such, all of our resources and efforts have been and are
expected for the foreseeable future to be dedicated to the development and commercialization of Locilex®. As such, we are subject to the risk of dependency on this sole product, and if we
fail to gain FDA or other regulatory approvals for Locilex® (for example, for use in treating mild or moderate skin and skin structure infections in superficial wounds), our viability
would be materially impacted unless we were able to develop or acquire other product candidates.
- •
- The clinical and regulatory approval process for Locilex® may be lengthy and is inherently
unpredictable. Although we anticipate certain time frames for our clinical and regulatory pathway for Locilex®, the
enrollment and/or approval process of the FDA and comparable foreign regulatory authorities may be lengthy and time consuming. These processes are inherently unpredictable, and if we are ultimately
unable to obtain regulatory approval for Locilex®, our business will be substantially harmed.
- •
- Manufacturing issues may prevent Locilex® from receiving regulatory
approval. Although we believe that we have successfully worked with our third-party vendors to resolve the manufacturing issues
encountered by Locilex®'s prior sponsor and previously identified by the FDA, to the extent that such issues are not resolved, regulatory approval for Locilex® may be delayed
or withheld, and we may not be able to meet the developmental milestones necessary to continue our business.
- •
- Even if Locilex® is approved, the market may not accept it as a viable treatment option. Even if Locilex® is approved, there is a risk that it may not be accepted in the marketplace for a variety of reasons. If we are unable to generate revenue from sales of Locilex®, our business will be substantially harmed.
Results of Operations
Year Ended December 31, 2015 Compared to the Year Ended December 31, 2014
Summary Table
The following table presents a summary of the changes in our results of operations for the year ended December 31, 2015, compared with the year ended December 31, 2014:
| |
Years Ended December 31, |
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
Percentage Increase |
|||||||||
| |
2015 | 2014 | ||||||||
| |
(in thousands) |
|
||||||||
Research and Development Expenses |
$ | 11,286 | $ | 8,898 | 27 | % | ||||
Selling, General, and Administrative Expenses |
$ | 7,479 | $ | 4,685 | 60 | % | ||||
Total Operating Expenses |
$ | 18,765 | $ | 13,583 | 38 | % | ||||
Interest Income |
$ | 22 | $ | 2 | 1,000 | % | ||||
Net Loss |
$ | 18,743 | $ | 13,581 | 38 | % | ||||
Research and Development Expenses
Research and development expenses were $11.3 million for the year ended December 31, 2015, and $8.9 million for the year ended December 31, 2014, an increase of $2.4 million. Research and
58
development expenses increased primarily due to the increased enrollment in Phase 3 clinical trials and the related trial expenses.
Selling, General, and Administrative Expenses
Selling, general, and administrative expenses were $7.5 million for the year ended December 31, 2015, and $4.7 million for the year ended December 31, 2014, an increase of $2.8 million. The increase in general and administrative expenses is primarily attributable to an increase of $1.9 million for noncash share-based compensation related expenses, an increase of $0.3 million of increased compensation expenses due to a full twelve months of salary activity, an increase of $0.3 million in marketing expenses, and an increase of $0.3 million in legal, insurance, and office related expenses.
Net Loss
Net loss was $18.7 million for the year ended December 31, 2015, and $13.6 million for the year ended December 31,2014, an increase of $5.1 million. This was due to the increase in research and development expenses of $2.4 million and an increase in general and administrative expenses of $2.8 million for the reasons stated above.
Liquidity and Capital Resources
Overview
We have generated no revenue from operations and we have incurred cumulative losses of approximately $41.1 million since inception. We have funded our operations primarily from equity issuances. We received net cash proceeds of approximately $9.7 million from equity financings closed between July 2010 and November 2013. All of our equity financings were consummated at $50 per Class A membership interest ($7.14 on a post-conversion basis) with 50% warrant coverage at 120% of the issue price or $60 per interest ($8.57 on a post-conversion basis). On March 18, 2014, we closed an initial public offering of 3,162,500 shares of our common stock at a public offering price of $12.00 per share. Gross proceeds raised by us in the offering were approximately $38.0 million, and net proceeds to us were approximately $34.5 million.
On June 30, 2015, the Company completed a stock offering issuing 1,702,000 shares of common stock at a price of $12.50 per share, resulting in net proceeds of approximately $19.7 million after deducting underwriting discounts of $1.3 million and offering costs of approximately $0.3 million.
We believe that we have sufficient cash to fund our operations through 2017.
As of December 31, 2015, we had working capital of approximately $30.8 million, consisting primarily of $32.2 million of cash and short-term investments, offset by $1.6 million of accounts payable and accrued expenses.
The following table sets forth selected cash flow information for the periods indicated (in thousands):
| |
For years ended December 31, |
||||||
|---|---|---|---|---|---|---|---|
| |
2015 | 2014 | |||||
Net cash used in operating activities |
$ | (14,592 | ) | $ | (11,277 | ) | |
Net cash used in investing activities |
(26,957 | ) | — | ||||
Net cash provided by financing activities |
19,744 | 34,456 | |||||
| | | | | | | | |
Net increase (decrease) in cash |
$ | (21,805 | ) | $ | 23,179 | ||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
59
Net Cash Used in Operating Activities
Net cash used in operating activities was $14.6 million for the year ended December 31, 2015. The net loss for this period was greater than the net cash used in operating activities by $4.1 million, which was primarily attributable to $3.8 million of share-based compensation and a $0.3 million increase in accounts payable.
Net cash used in operating activities was $11.3 million for the year ended December 31, 2014. The net loss for this period was greater than the net cash used in operating activities by $2.3 million, which was primarily attributable to $1.9 million of share-based compensation, a $0.5 million increase in accounts payable, partially offset by a $0.1 million increase in prepaid expenses.
Net Cash Used in Investing Activities
Net cash used in investing activities for the year ended December 31, 2015 was $27.0 million, which is attributable to the $31.0 million investment in United States Treasury bonds offset by $4.0 million in bond maturities.
Net Cash Provided by Financing Activities
Net cash provided by financing activities for the year ended December 31, 2015 was $19.8 million, which was attributable to the net proceeds from the Company's secondary stock offering.
Net cash provided by financing activities for the year ended December 31, 2014 was $34.5 million, which was attributable to the net proceeds from the Company's initial public offering.
Contractual Obligations
Effective May 2014, the Company entered into a sublease agreement for office space with current monthly payments of $13,098. The term of the sublease ends on March 30, 2016 with inflationary escalations in 2015 and the first three months of 2016. Total minimum sublease payments for the remaining term of the sublease from December 31, 2015 to March 30, 2016 are $39,294.
In January 2016, the Company entered into a lease for office space commencing in March 2016 with current monthly payments of $18,857, subject to inflationary escalations and adjustments thereafter. The term of the lease is for five years and five months. We believe this space is adequate as our principal executive office location.
Recent Accounting Pronouncements
In August 2014, the Financial Accounting Standards Board, (FASB), issued Accounting Standards Update, or ASU, No. 2014-15, Presentation of Financial Statements-Going Concern (Subtopic 205-40): Disclosure of Uncertainties about an Entity's Ability to Continue as a Going Concern, which defines management's responsibility to assess an entity's ability to continue as a going concern, and to provide related footnote disclosures if there is substantial doubt about its ability to continue as a going concern. The pronouncement is effective for annual reporting periods ending after December 15, 2016 with early adoption permitted. The adoption of this guidance is not expected to have a material impact on our financial statements.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740), which requires that all deferred income tax assets and liabilities be presented as noncurrent in the statement of financial position. The pronouncement is effective for financial statements issued for annual periods beginning after December 15, 2018 with early application permitted. The adoption of this guidance is not expected to have a material impact on our financial statements.
60
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842), which includes amendments that require lessees to recognize a lease liability for all long-term leases (lease terms more than 12 months) at the commencement date. The lease liability is a lessee's obligation to make lease payments arising from a lease, measured on a discounted basis. The amendments also require lessees to recognize a right-of-use asset for all long-term leases. The right-of-use asset is an asset that represents the lessee's right to use, or control the use of, a specified asset for the lease term. For leases with a term of 12 months or less, a lessee is permitted to make an accounting policy election by class of underlying asset not to recognize lease assets and lease liabilities. If a lessee makes this election, it should recognize lease expense for such leases generally on a straight-line basis over the lease term. The amendments in this ASU require qualitative disclosures along with specific quantitative disclosures. The amendments in this ASU are effective for fiscal years beginning after December 15, 2018, and interim periods within those fiscal years. Early application is permitted. Lessees (for capital and operating leases) and lessors (for sales-type, direct financing, and operating leases) must apply a modified retrospective transition approach for leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements. The modified retrospective approach would not require any transition accounting for leases that expired before the earliest comparative period presented. The Company is currently evaluating the provisions of this amendment.
Critical Accounting Policies and Estimates
Basis of Presentation
On April 5, 2012, the JOBS Act was signed into law. The JOBS Act contains provisions that, among other things, reduce certain reporting requirements for qualifying public companies. As an "emerging growth company," we may, under Section 7(a)(2)(B) of the Securities Act of 1933 (or Securities Act), delay adoption of new or revised accounting standards applicable to public companies until such standards would otherwise apply to private companies. We may take advantage of this extended transition period until the first to occur of the date that we (i) are no longer an "emerging growth company" or (ii) affirmatively and irrevocably opt out of this extended transition period. We have elected to take advantage of the benefits of this extended transition period. Our financial statements may therefore not be comparable to those of companies that comply with such new or revised accounting standards. Until the date that we are no longer an "emerging growth company" or affirmatively and irrevocably opt out of the exemption provided by Securities Act Section 7(a)(2)(B), upon issuance of a new or revised accounting standard that applies to our financial statements and that has a different effective date for public and private companies, we will disclose the date on which adoption is required for non-emerging growth companies and the date on which we will adopt the recently issued accounting standard. Our management's discussion and analysis of our financial condition and results of operations is based on our financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States, or GAAP. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities and expenses. On an ongoing basis, we evaluate these estimates and judgments, including those described below. We base our estimates on our historical experience and on various other assumptions that we believe to be reasonable under the circumstances. These estimates and assumptions form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results and experiences may differ materially from these estimates.
Share-Based Compensation
We account for the cost of services performed by directors received in exchange for an award of Class A Membership Interests, common stock, or stock options, based upon the grant date fair value of the award. In accordance with the Accounting Standards Codification, we recognize compensation expense, net of estimated forfeitures, on a straight-line basis over the vesting period.
61
We account for the cost of services performed by vendors in exchange for an award of membership interests or common stock based upon the grant date fair value of the award or fair value of the services rendered, whichever is more readily determinable. In accordance with the Accounting Standards Codification, we recognize the expense in the same period and in the same manner as if we had paid cash for the services.
Research and Development Expenses
Although the Company manages the conduct of our own clinical trials, we rely on third parties to conduct our preclinical studies and to provide services, including data management, statistical analysis and electronic compilation for our clinical trials, as well as for the manufacture of our clinical trial supplies. At the end of each reporting period, the Company compares the payments made to each service provider to the estimated progress towards completion of the related project. Factors that are considered in preparing these estimates include the number of subjects enrolled in studies, milestones achieved and other criteria related to the efforts of our vendors. These estimates are subject to change as additional information becomes available. Depending on the timing of payments to vendors and estimated services provided, the Company records net prepaid or accrued expenses related to these costs.
Off-Balance Sheet Arrangements
We did not have, during the periods presented, and we are currently not party to, any off-balance sheet arrangements.
Seasonality
We do not have a seasonal business cycle. Our operating results are generally derived evenly throughout the calendar year.
Subsequent Events
In December 2015, the Paediatric Committee of the European Medicines Agency issued its opinion granting a product specific waiver for paediatric clinical studies of Locilex® under applicable European Guidelines and, in January 2016, the EMA adopted a decision granting the paediatric waiver in accordance with the opinion of the Paediatric Committee.
In February 2016, FDA delivered formal agreement with the Company's initial pediatric study plan, pursuant to which the regulatory authority agrees that pediatric studies are not required to be performed by the Company at this time.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK.
We are a smaller reporting company as defined by Rule 12b-2 of the Exchange Act and are not required to provide the information under this item.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA.
Our financial statements required to be filed pursuant to this Item 8 appear in a separate section of this report beginning on page F-1.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE.
None.
62
ITEM 9A. CONTROLS AND PROCEDURES.
Disclosure Controls and Procedures
Our management is responsible for establishing and maintaining adequate controls over financial reporting (as that term is defined in Rules 13a-15(f) and 15d-15(f) under the Securities Exchange Act of 1934, as amended (the "Exchange Act")). Our management, with the participation of our principal executive officer and principal financial and accounting officer, conducted an evaluation of the effectiveness of our disclosure controls and procedures (as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act), as of the end of the period covered by this report. Based on this evaluation, our principal executive officer and principal financial and accounting officer each concluded that, as of the end of such period, our disclosure controls and procedures were effective in ensuring that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized, and reported on a timely basis, and is accumulated and communicated to our management, including our principal executive officer and principal financial and accounting officer, as appropriate to allow timely decisions regarding required disclosure.
Changes in Internal Controls Over Financial Reporting
Our management, including our principal executive officer, and principal financial and accounting officer, conducted an evaluation of any changes in our internal control over financial reporting (as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) that occurred during our most recently completed fiscal quarter. Based on that evaluation, our principal executive officer, and principal financial and accounting officer concluded that there has not been any change in our internal control over financial reporting during that quarter that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Internal Control Over Financial Reporting
This annual report does not include an attestation report of the Company's registered public accounting firm regarding internal control over financial reporting. Management's report was not subject to attestation by the Company's registered public accounting firm pursuant to the rules of the Securities Exchange Commission that permit the Company to provide only management's report in this annual report.
Management assessed the effectiveness of our internal control over financial reporting as of December 31, 2015. In making this assessment, management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control—Integrated Framework issued in 2013. Based upon the assessments, management has concluded that as of December 31, 2015 our internal control over financial reporting was effective to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements in accordance with U.S. GAAP.
None.
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE.
The information required by this Item is incorporated herein by reference from the information under the captions "PROPOSAL NO. 1—ELECTION OF DIRECTORS—Biographies of Nominees," "CORPORATE GOVERNANCE—"Board of Directors," "Board of Directors Meetings and Attendance," "Compliance with Section 16(a) of the Exchange Act," "BOARD COMMITTEES,"
63
"DIRECTOR COMPENSATION," "DIRECTORS AND EXECUTIVE OFFICERS" in the Proxy Statement for the annual meeting of shareholders to be held on May 24, 2016 (the "Proxy Statement").
Executive Officers of Dipexium Pharmaceuticals
The following table, as of March 15, 2016, sets forth the names of our executive officers along with their respective ages and positions:
Name
|
Age | Title | |||
|---|---|---|---|---|---|
Robert J. DeLuccia |
70 | Executive Chairman and Director | |||
David P. Luci, Esq. |
49 | President, Chief Executive Officer, Secretary and Director | |||
David Garrett |
40 | Vice President, Finance and Corporate Development | |||
Robert G. Shawah |
49 | Chief Accounting Officer and Treasurer | |||
Robert J. DeLuccia. Mr. DeLuccia serves as Executive Chairman of our company and is one of the two co-founders and managing partners of our company, which was formed in 2010. Mr. DeLucia has served as our Executive Chairman since March 2014. From 2004 to 2009, Mr. DeLuccia served in several capacities at MacroChem, a development-stage, publicly traded pharmaceutical company using topical drug delivery technology for products in dermatology, podiatry, urology and cancer, including as Chairman, President and Chief Executive Officer, and as director. Mr. DeLuccia currently serves as a member of the board of directors of IBEX Technologies Inc., which manufactures and markets proprietary enzymes (heparinases and chondroitinases) for use in pharmaceutical research and Heparinase I, used in many leading hemostasis monitoring devices.
David P. Luci. Since March 2014, Mr. Luci has served as President, Chief Executive Officer, and Secretary of our company, is a member of the board of directors and is one of the two co-founders and managing partners of our company, which predecessor was formed in 2010. Prior to co-founding our company, from June 2006 to January 2010, Mr. Luci served as a member of the board of directors of Access Pharmaceuticals, where he also served as Chairman of the Audit Committee and Chairman of the Compensation Committee, as well as serving in a consulting capacity following the disposition of MacroChem to Access Pharmaceuticals. From December 2007 through February 2009, Mr. Luci served as a member of the board of directors and President of MacroChem. Prior to that, Mr. Luci served as Executive Vice President, Chief Financial Officer, General Counsel and Corporate Secretary of Bioenvision, Inc. (or Bioenvision), an international biopharmaceutical company focused upon the development, marketing and commercialization of oncology products and product candidates. Mr. Luci created and managed Bioenvision's principal executive offices located in New York as well as its satellite office located in Tokyo, Japan. Mr. Luci was instrumental in creating Bioenvision's international commercial enterprise; managed the worldwide development of Evoltra (clofarabine) as a member of the product's Joint Steering Committee in conjunction with senior executives of Bioenvision's partner, Genzyme Corporation; and orchestrated, structured and negotiated the sale of Bioenvision in 2007 to Genzyme Corporation for $345 million. Mr. Luci began his career with Ernst & Whinney LLP (now Ernst &Young LLP) in New York as a certified public accountant working in the Healthcare Practice Group. He later practiced corporate law at Paul Hastings LLP in New York, where his practice encompassed all aspects of public and private mergers and acquisitions, corporate finance, restructurings and private equity transactions, with a core focus in the healthcare industry. Mr. Luci graduated from Bucknell University with a degree as a Bachelor of Science in Business Administration with a concentration in Accounting and graduated from Albany Law School of Union University (Cum Laude: 1994) where he served as Managing Editor of the Journal of Science & Technology. Mr. Luci became a certified public accountant in the State of Pennsylvania in 1990 (inactive) and is a member of the New York State Bar Association.
64
David Garrett. Since March 2014 Mr. Garrett has served as our Vice President, Finance and Corporate Development. Beginning in January 2012 and presently, Mr. Garrett serves as Managing Partner of Aumoe Partners, LLC (or Aumoe Partners), a financial advisory firm which he founded. He will join our company as a full time employee upon the completion of this offering. Aumoe Partners has served as a financial and business development consultant to our company. Prior to founding Aumoe Partners, Mr. Garrett served as Director, Healthcare Equity Sales and Capital Markets at Canaccord Genuity, Inc. from July 2008 to November 2011. From 1999 to 2008, Mr. Garrett served as an equity analyst covering the biotechnology and specialty pharmaceuticals industries at Scudder Kemper Investments, Wachovia Securities, UBS Securities, and Fortis Securities. Over the course of his career, Mr. Garrett has assisted over 45 emerging biotechnology and medical technology companies in initial public offerings, secondary public offerings and private placements of public equity that collectively have raised over $2.9 billion. Mr. Garrett received a Bachelor's Degree in Economics from the University of Wisconsin, Madison.
Robert G. Shawah. Since March 2014 Mr. Shawah has served as our Chief Accounting Officer and Treasurer. From 2005 to 2013, Mr. Shawah served as a Vice President of Baldwin Pearson & Co., Inc. focusing on structuring transactions in the commercial and industrial real estate market in Fairfield County, Connecticut, as well as financial reporting responsibility. From 1997 to 2005, he served Sales and Financial Engineer for CC1 Inc., a private New Hampshire firm that designed and manufactured camera-based technical equipment for the printing industry. Prior to 1997, Mr. Shawah held financial management positions at Victorinox/Swiss Army Brands and Grace Cocoa, a division of W.R. Grace. His responsibilities at these firms included accounting, financial reporting, and foreign currency transactions. Mr. Shawah is a certified public accountant in the Commonwealth of Pennsylvania (inactive) and spent the first five years of his career in the audit division of Arthur Andersen LLP. Mr. Shawah received his Bachelor's Degree in Business Administration from Bucknell University.
We have a written Code of Business Conduct that applies to our Chief Executive Officer (Principal Executive Officer), Chief Financial Officer (Principal Financial and Accounting Officer) and others. The Code of Business Conduct is available on our website at www.dipexiumpharmaceuticals.com. Any amendments to, or waivers from, a provision of our code of employee business conduct and ethics that applies to our principal executive officer, our principal financial and accounting officer and that relates to any element of the code of ethics enumerated in paragraph (b) of Item 406 of Regulation S-K shall be disclosed by posting such information on our website.
ITEM 11. EXECUTIVE COMPENSATION.
The information required on executive compensation is incorporated by reference from the discussion under the headings "Executive Compensation", "Outstanding Equity Awards at fiscal year end 2015", and "Compensation Pursuant To Agreements and Plans", as well as all footnote information to the various tables, of the Company's Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
The required information on director compensation is incorporated by reference from the discussion under the "Director Compensation" table of the Company's Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS.
The information required by this Item is incorporated by reference from the information under the caption "BENEFICIAL OWNERSHIP OF SECURITIES" and "SECURITIES AUTHORIZED FOR
65
ISSUANCE UNDER DIPEXIUM PHARMACEUTICALS COMPENSATION PLAN" in the Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS AND DIRECTOR INDEPENDENCE.
The required information on transactions with related persons is incorporated by reference from the discussion under the heading "Transactions with Related Persons" of the Company's Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
The required information on director independence is incorporated by reference from the discussion under the heading "Independence of Directors" of the Company's Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
ITEM 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES.
The information required for this item is incorporated by reference from the discussion under "Audit Committee Report" beginning with the caption "Pre-Approval Policy for Services of Independent Registered Public Accounting Firm" through "Fees for Services provided by Independent Registered Public Accounting Firm" of the Company's Proxy Statement for the Annual Meeting of Shareholders to be held May 24, 2016.
ITEM 15. FINANCIAL STATEMENT SCHEDULES, EXHIBITS.
| Exhibit Number |
Description of Document | ||
|---|---|---|---|
| 1.1 | Underwriting Agreement (incorporated by reference to Exhibit 1.1 to Form 8-K filed on March 18, 2014). | ||
| 1.2 | Underwriting Agreement (incorporated by reference to Exhibit 1.1 to Form 8-K filed on June 25, 2015). | ||
| 2.1 | Asset Purchase Agreement, dated April 8, 2010, by and between the registrant and Genaera Liquidating Trust (incorporated by reference to Exhibit 2.1 to Form S-1 filed on February 6, 2014). | ||
| 2.2 | Form of Certificate of Conversion pursuant to which the registrant will be reorganized into a corporation. (incorporated by reference to Exhibit 2.2 to Form S-1 filed on February 6, 2014). | ||
| 3.1 | Certificate of Formation of Dipexium Pharmaceuticals, LLC. (incorporated by reference to Exhibit 3.1 to Form S-1 filed on March 18, 2014). | ||
| 3.2 | Certificate of Incorporation of Dipexium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 3.2 to Form S-1 filed on February 6, 2014). | ||
| 3.3 | (a) Bylaws of Dipexium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 3.3 to Form S-1 filed on February 6, 2014). | ||
(b) Amended and Restated Bylaws of Dipexium Pharmaceuticals, Inc (incorporated by reference to Exhibit 3.1 to Form 8-K filed on June 18, 2014). |
|||
| 3.4 | Amended Bylaws of Dipexium Pharmaceuticals, Inc (incorporated by reference to Exhibit 3.1 to Form 8-K filed on July 20, 2015). | ||
66
| Exhibit Number |
Description of Document | ||
|---|---|---|---|
| 10.1 | 2013 Equity Incentive Plan. (incorporated by reference to Exhibit 10.1 to Form S-1 filed on February 6, 2014). | ||
| 10.2 | Form of Director Indemnification Agreement (incorporated by reference to Exhibit 10.2 to Form S-1 filed on February 6, 2014). | ||
| 10.3 | Amended and Restated Employment Agreement, dated February 3, 2014, between Dipexium Pharmaceuticals, Inc. and David P. Luci (incorporated by reference to Exhibit 10.3 to Form S-1 filed on February 6, 2014). | ||
| 10.4 | Amended and Restated Employment Agreement, dated February 3, 2014, between Dipexium Pharmaceuticals, Inc. and Robert J. DeLuccia (incorporated by reference to Exhibit 10.4 to Form S-1 filed on February 6, 2014). | ||
| 10.5 | Employment Agreement, dated February 3, 2014, between Dipexium Pharmaceuticals, Inc. and David Garrett (incorporated by reference to Exhibit 10.5 to Form S-1 filed on February 6, 2014). | ||
| 10.6 | Employment Agreement, dated February 3, 2014, between Dipexium Pharmaceuticals, Inc. and Robert G. Shawah (incorporated by reference to Exhibit 10.6 to Form S-1 filed on February 6, 2014). | ||
| 10.7 | Form of Securities Purchase Agreement, dated July 23, 2010, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.7 to Form S-1 filed on February 6, 2014). | ||
| 10.8 | Form of Securities Purchase Agreement, dated March 11, 2011, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.8 to Form S-1 filed on February 6, 2014). | ||
| 10.9 | Form of Securities Purchase Agreement, dated October 14, 2011, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.9 to Form S-1 filed on February 6, 2014). | ||
| 10.10 | Form of Securities Purchase Agreement, dated March 30, 2012, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.10 to Form S-1 filed on February 6, 2014). | ||
| 10.11 | Form of Securities Purchase Agreement, dated November 21, 2012, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.11 to Form S-1 filed on February 6, 2014). | ||
| 10.12 | Form of Securities Purchase Agreement, dated February 13, 2013, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.12 to Form S-1 filed on February 6, 2014). | ||
| 10.13 | Form of Securities Purchase Agreement, dated July 12, 2013, by and between the registrant and each of the named purchasers (incorporated by reference to Exhibit 10.13 to Form S-1 filed on February 6, 2014). | ||
| 10.14 | Form of Warrant, dated July 23, 2010, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.14 to Form S-1 filed on February 6, 2014). | ||
| 10.15 | Form of Warrant, dated March 11, 2011, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.15 to Form S-1 filed on February 6, 2014). | ||
| 10.16 | Form of Warrant, dated October 14, 2011, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.16 to Form S-1 filed on February 6, 2014). | ||
67
| Exhibit Number |
Description of Document | ||
|---|---|---|---|
| 10.17 | Form of Warrant, dated March 30, 2012, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.17 to Form S-1 filed on February 6, 2014). | ||
| 10.18 | Form of Warrant, dated November 21, 2012, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.18 to Form S-1 filed on February 6, 2014). | ||
| 10.19 | Form of Warrant, dated February 13, 2013, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.19 to Form S-1 filed on February 6, 2014). | ||
| 10.20 | Form of Warrant, dated July 12, 2013, issued by the registrant to certain purchasers (incorporated by reference to Exhibit 10.20 to Form S-1 filed on February 6, 2014). | ||
| 10.21 | Form of Investor Rights Agreement, dated July 23, 2010, between the registrant and certain purchasers (incorporated by reference to Exhibit 10.21 to Form S-1 filed on February 6, 2014). | ||
| 10.22 | Form of Investor Rights Agreement Joinder, between the registrant and certain purchasers (incorporated by reference to Exhibit 10.22 to Form S-1 filed on February 6, 2014). | ||
| 10.23 | Master Services Agreement, dated August 23, 2010, between the registrant and RRD International, LLC (incorporated by reference to Exhibit 10.23 to Form S-1 filed on February 6, 2014). | ||
| 10.24 | Bill of Sale and Assignment Agreement, dated March 21, 2011, between the registrant and Genaera Liquidating Trust (incorporated by reference to Exhibit 10.24 to Form S-1 filed on February 6, 2014). | ||
| 10.25 | Research and Development Agreement, dated December 8, 2011, between the registrant and DPT Laboratories, Inc. (incorporated by reference to Exhibit 10.25 to Form S-1 filed on February 6, 2014). | ||
| 10.26 | Laboratory Services Agreement, dated May 22, 2012, between the registrant and Covance Laboratories Inc. (incorporated by reference to Exhibit 10.26 to Form S-1 filed on February 6, 2014). | ||
| 10.27 | Master Services Agreement, dated September 3, 2013, between the registrant and PolyPeptide Laboratories, Inc. (incorporated by reference to Exhibit 10.27 to Form S-1 filed on February 6, 2014). | ||
| 10.28 | Quality Agreement, dated September 3, 2013, between registrant and PolyPeptide Laboratories, Inc. (incorporated by reference to Exhibit 10.28 to Form S-1 filed on February 6, 2014). | ||
| 10.29 | Master Agreement for the Provision of Pharmaceutical Support Services, dated October 9, 2013, between registrant and Almac Group Limited (incorporated by reference to Exhibit 10.29 to Form S-1 filed on February 6, 2014). | ||
| 10.30 | Master Services Agreement, dated October 25, 2013, between the registrant and Research Pharmaceutical Sciences, Inc. (incorporated by reference to Exhibit 10.30 to Form S-1 filed on February 6, 2014). | ||
| 10.31 | License Agreement, dated October 20, 1988, by and between Scripps Research and Clinic Foundation and Multiple Peptide Systems (incorporated by reference to Exhibit 10.31 to Form S-1 filed on February 6, 2014). | ||
| 10.32 | Second Amendment to License Agreement, dated September 24, 1996, by and between Scripps Research and Clinic Foundation and Multiple Peptide Systems (incorporated by reference to Exhibit 10.32 to Form S-1 filed on February 6, 2014). | ||
68
| Exhibit Number |
Description of Document | ||
|---|---|---|---|
| 10.33 | Agreement, dated November 4, 1988, by and between Multiple Peptide Systems and Magainin Sciences Inc. (incorporated by reference to Exhibit 10.33 to Form S-1 filed on February 6, 2014). | ||
| 10.34 | Second Amendment to Agreement, dated September 24, 1996, by and between Multiple Peptide Systems and Magainin Pharmaceuticals Inc. (incorporated by reference to Exhibit 10.34 to Form S-1 filed on February 6, 2014). | ||
| 10.35 | Product Development Agreement, dated January 1, 2014, between the registrant and RRD International, LLC (incorporated by reference to Exhibit 10.35 to Form S-1 filed on February 6, 2014). | ||
| 10.36 | Sublease, effective May 5, 2014 (incorporated by reference to Exhibit 10.1 to Form 8-K filed on May 13, 2014). | ||
| 10.37 | Product Development Agreement, dated May 22, 2014 by and between RRD International, LLC and Dipexium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 10.1 to Form 8-K filed on May 29, 2014). | ||
| 10.38 | Consulting Agreement, dated June 4, 2014 by and between Drug Development Advisors and Dipexium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 10.1 to Form 8-K filed on June 9, 2014). | ||
| 10.39 | Amendment No. 1 to the 2013 Equity Incentive Plan, dated March 24, 2015. | ||
| 14.1 | Code of Ethics (incorporated by reference to Exhibit 24.1 to Form 10-K filed on March 23, 2015). | ||
| 21.1 | List of Subsidiaries (incorporated by reference to Exhibit 21.1 to Form 10-K filed on March 23, 2015). | ||
| 23.1 | Consent of Independent Registered Public Accounting Firm | ||
| 31.1 | Certification of Principal Executive Officer, pursuant to 18 U.S.C. Section 1350 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. | ||
| 31.2 | Certification of Principal Financial and Accounting Officer, pursuant to 18 U.S.C. Section 1350 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. | ||
| 32.1 | * | Certification of Principal Executive Officer, pursuant to 18 U.S.C. Section 1350 as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | |
| 32.2 | * | Certification of Principal Financial and Accounting Officer, pursuant to 18 U.S.C. Section 1350 as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | |
| 101.INS | XBRL Instance Document | ||
| 101.SCH | XBRL Taxonomy Schema | ||
| 101.CAL | XBRL Taxonomy Calculation Linkbase | ||
| 101.DEF | XBRL Taxonomy Definition Linkbase | ||
| 101.LAB | XBRL Taxonomy Label Linkbase | ||
| 101.PRE | XBRL Taxonomy Presentation Linkbase | ||
- *
- In accordance with SEC Release 33-8238, Exhibits 32.1 and 32.2 are being furnished and not filed.
69
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following person on behalf of the Registrant.
Dated: March 22, 2016 |
DIPEXIUM PHARMACEUTICALS, INC. | |||
|
By: |
/s/ DAVID P. LUCI |
||
|
By: |
/s/ ROBERT G. SHAWAH |
||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following person on behalf of the Registrant and in the capacities and on the dates indicated.
Person
|
Capacity
|
Date
|
||||
|---|---|---|---|---|---|---|
| /s/ ROBERT J. DELUCCIA Robert J. DeLuccia |
Executive Chairman and Director | March 22, 2016 | ||||
/s/ DAVID P. LUCI David P. Luci, Esq. |
President, Chief Executive Officer, Director (Principal Executive Officer) |
March 22, 2016 |
||||
/s/ ROBERT G. SHAWAH Robert G. Shawah |
Chief Accounting Officer and Treasurer (Principal Financial and Accounting Officer) |
March 22, 2016 |
||||
/s/ JACK H. DEAN Dr. Jack H. Dean |
Director |
March 22, 2016 |
||||
/s/ MICHAEL DUFFY Michael Duffy, Esq. |
Director |
March 22, 2016 |
||||
/s/ THOMAS HARRISON Thomas Harrison |
Director |
March 22, 2016 |
||||
70
Person
|
Capacity
|
Date
|
||||
|---|---|---|---|---|---|---|
| /s/ WILLIAM J. MCSHERRY William J. McSherry, Jr., Esq. |
Director | March 22, 2016 | ||||
/s/ BARRY KAGAN Barry Kagan |
Director |
March 22, 2016 |
||||
71
DIPEXIUM PHARMACEUTICALS, INC.
FINANCIAL STATEMENTS
TABLE OF CONTENTS
F-1
Report of Independent Registered Public Accounting Firm
The
Board of Directors and Members
Dipexium Pharmaceuticals, Inc.
We have audited the accompanying balance sheets of Dipexium Pharmaceuticals, Inc. as of December 31, 2015 and 2014, and the related statements of operations, changes in members' and shareholders' equity and cash flows for each of the years in the two-year period ended December 31, 2015. Dipexium Pharmaceuticals, Inc.'s management is responsible for these financial statements. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of Dipexium Pharmaceuticals, Inc. as of December 31, 2015 and 2014, and the results of its operations and its cash flows for each of the years in the two-year period ended December 31, 2015, in conformity with accounting principles generally accepted in the United States of America.
/s/
CohnReznick LLP
Roseland, New Jersey
March 22, 2016
F-2
DIPEXIUM PHARMACEUTICALS, INC.
BALANCE SHEETS
December 31, 2015 and 2014
| |
2015 | 2014 | |||||
|---|---|---|---|---|---|---|---|
ASSETS |
|||||||
CURRENT ASSETS |
|||||||
Cash |
$ | 5,234,953 | $ | 27,040,325 | |||
Short-term Investments |
26,977,362 | — | |||||
Prepaid Expenses |
146,145 | 120,128 | |||||
| | | | | | | | |
TOTAL CURRENT ASSETS |
32,358,460 | 27,160,453 | |||||
| | | | | | | | |
OTHER ASSETS |
|||||||
Security Deposit |
49,385 | 49,385 | |||||
| | | | | | | | |
TOTAL OTHER ASSETS |
49,385 | 49,385 | |||||
| | | | | | | | |
TOTAL ASSETS |
$ | 32,407,845 | $ | 27,209,838 | |||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
LIABILITIES AND SHAREHOLDERS' EQUITY |
|||||||
CURRENT LIABILITIES |
|||||||
Accounts Payable and Accrued Expenses |
$ | 1,606,307 | $ | 1,260,598 | |||
| | | | | | | | |
TOTAL LIABILITIES |
1,606,307 | 1,260,598 | |||||
| | | | | | | | |
COMMITMENTS AND CONTINGENCIES |
|||||||
SHAREHOLDERS' EQUITY |
|||||||
Common Stock: $.001 par value, 30,000,000 shares authorized, 10,301,114 and 8,538,329 shares issued and outstanding at December 31, 2015 and December 31, 2014, respectively |
10,301 | 8,538 | |||||
Additional paid-in capital |
71,852,692 | 48,259,451 | |||||
Accumulated deficit |
(41,061,455 | ) | (22,318,749 | ) | |||
| | | | | | | | |
TOTAL SHAREHOLDERS' EQUITY |
30,801,538 | 25,949,240 | |||||
| | | | | | | | |
TOTAL LIABILITIES AND SHAREHOLDERS' EQUITY |
$ | 32,407,845 | $ | 27,209,838 | |||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
See notes to financial statements.
F-3
DIPEXIUM PHARMACEUTICALS, INC.
STATEMENTS OF OPERATIONS
Years Ended December 31, 2015 and 2014
| |
2015 | 2014 | |||||
|---|---|---|---|---|---|---|---|
REVENUES |
$ | — | $ | — | |||
| | | | | | | | |
EXPENSES |
|||||||
OPERATING EXPENSES |
|||||||
Research and Development Expenses |
11,286,236 | 8,898,280 | |||||
Selling, General and Administrative Expenses |
7,478,527 | 4,684,497 | |||||
| | | | | | | | |
TOTAL OPERATING EXPENSES |
18,764,763 | 13,582,777 | |||||
| | | | | | | | |
LOSS FROM OPERATIONS |
(18,764,763 | ) | (13,582,777 | ) | |||
Interest Income |
22,057 | 1,793 | |||||
| | | | | | | | |
NET LOSS |
$ | (18,742,706 | ) | $ | (13,580,984 | ) | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
LOSS PER SHARE |
|||||||
Basic and diluted net loss per common share |
$ | (1.99 | ) | $ | (1.73 | ) | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
Weighted average common shares/units outstanding basic and diluted |
9,432,705 | 7,850,350 | |||||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
See notes to financial statements.
F-4
DIPEXIUM PHARMACEUTICALS, INC.
STATEMENTS OF CHANGES IN MEMBERS' AND SHAREHOLDERS' EQUITY
Years Ended December 31, 2015 and 2014
| |
|
|
|
|
|
|
Total Members' and Shareholders' Equity |
|||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
|
|
Common Stock | |
|
|||||||||||||||||
| |
Class A Membership Interests |
Membership Interests Amount |
Additional Paid-In Capital |
Accumulated Deficit |
||||||||||||||||||
| |
Shares | Amount | ||||||||||||||||||||
Balance at January 1, 2014 |
735,588 | $ | 3,206,231 | $ | 3,206,231 | |||||||||||||||||
Issuance of Restricted Membership Interest Awards |
1,000 | |||||||||||||||||||||
Issuance of Restricted Membership Interest to Vendors |
7,604 | 380,200 | $ | 69,812 | 450,012 | |||||||||||||||||
Issuance of Membership Interest for Warrant Conversion |
23,719 | |||||||||||||||||||||
Corporate Conversion |
(767,911 | ) | (3,586,431 | ) | 5,375,377 | $ | 5,375 | 12,318,821 | $ | (8,737,765 | ) | — | ||||||||||
Initial Public Offering, Net of Issuance Costs |
3,162,500 | 3,163 | 34,452,506 | 34,455,669 | ||||||||||||||||||
Share-Based Compensation |
1,418,312 | 1,418,312 | ||||||||||||||||||||
Cashless Exercise of Warrants |
452 | |||||||||||||||||||||
Net Loss |
(13,580,984 | ) | (13,580,984 | ) | ||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | |
Balance at December 31, 2014 |
— | — | 8,538,329 | 8,538 | 48,259,451 | (22,318,749 | ) | 25,949,240 | ||||||||||||||
Share-Based payments to vendors |
43,953 | 44 | 575,167 | 575,211 | ||||||||||||||||||
Share-Based compensation |
14,000 | 14 | 3,275,894 | 3,275,908 | ||||||||||||||||||
Cashless Exercise of Warrants |
2,832 | 3 | (3 | ) | — | |||||||||||||||||
Issuance of Common Stock, net of issuance costs |
1,702,000 | 1,702 | 19,742,183 | 19,743,885 | ||||||||||||||||||
Net Loss |
(18,742,706 | ) | (18,742,706 | ) | ||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | |
Balance at December 31, 2015 |
— | $ | — | 10,301,114 | $ | 10,301 | $ | 71,852,692 | $ | (41,061,455 | ) | $ | 30,801,538 | |||||||||
| | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | |
See notes to financial statements.
F-5
DIPEXIUM PHARMACEUTICALS, INC.
STATEMENTS OF CASH FLOWS
Years Ended December 31, 2015 and 2014
| |
2015 | 2014 | |||||
|---|---|---|---|---|---|---|---|
Operating Activities: |
|||||||
Net Loss |
$ | (18,742,706 | ) | $ | (13,580,984 | ) | |
Adjustments to reconcile net loss to net cash used in operating activities: |
|||||||
Share-Based Compensation |
3,275,908 | 1,418,312 | |||||
Share-Based Payments to Vendors |
575,211 | 450,012 | |||||
Amortization of short-term investment interest income |
(20,621 | ) | |||||
(Increase) / Decrease In: |
|||||||
Prepaid Expenses |
(26,017 | ) | (74,034 | ) | |||
Security Deposit |
— | (49,385 | ) | ||||
Accounts Payable and Accrued Expenses |
345,708 | 559,590 | |||||
| | | | | | | | |
Net Cash Used In Operating Activities |
(14,592,517 | ) | (11,276,489 | ) | |||
| | | | | | | | |
Investing Activities: |
|||||||
Proceeds of Short-term Investments |
4,000,000 | ||||||
Purchase of Short-term Investments |
(30,956,740 | ) | — | ||||
| | | | | | | | |
Net Cash Used In Investing Activities |
(26,956,740 | ) | — | ||||
| | | | | | | | |
Financing Activities: |
|||||||
Proceeds from issuance of Common Stock, net of issuance costs |
19,743,885 | 34,455,669 | |||||
| | | | | | | | |
Net Cash Provided By Financing Activities |
19,743,885 | 34,455,669 | |||||
| | | | | | | | |
Net Increase (Decrease) In Cash |
(21,805,372 | ) | 23,179,180 | ||||
Cash at Beginning of Year |
27,040,325 | 3,861,145 | |||||
| | | | | | | | |
Cash at End of Year |
$ | 5,234,953 | $ | 27,040,325 | |||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
See notes to financial statements.
F-6
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS
NOTE 1—NATURE OF OPERATIONS
Business
Dipexium Pharmaceuticals, Inc. (the "Company"), a Delaware corporation, is a late stage pharmaceutical company focused on the development and commercialization of Locilex® (pexiganan cream 0.8%). The Company was formed on January 14, 2010.
On March 12, 2014, the Company completed a corporate conversion from a limited liability company to a corporation in conjunction with an initial public offering ("IPO") of common stock. As a result of the corporate conversion, holders of the Class A Membership Interests and warrants in Dipexium Pharmaceuticals, LLC, became holders of common stock and warrants of Dipexium Pharmaceuticals, Inc.
The Company has experienced net losses and negative cash flows from operations since inception and expects these conditions to continue for the foreseeable future. The Company has needed to raise capital from sales of its securities to sustain operations. In March 2014, the Company completed an IPO of common stock with proceeds, net of issuance costs, of approximately $34.5 million. In June 2015, the Company completed an additional public offering of common stock with net proceeds of approximately $19.7 million. As of December 31, 2015, the Company had cash and short-term investments totaling approximately $32.2 million. Based on the Company's projected expenditures for 2016 and 2017, management currently believes that its current cash balances should be sufficient to fund the Company's operations through 2017. However, if the Company's assumptions underlying its estimated expenses prove to be wrong, it may have to raise additional capital sooner than anticipated.
There can be no assurance that the Company's research and development will be successfully completed or that any Company product will be approved or commercially viable. The Company is subject to risks common to companies in the biopharmaceutical industry including, but not limited to, dependence on collaborative arrangements, development by the Company or its competitors of new technological innovations, dependence on key personnel, protection of proprietary technology, development of sales and marketing infrastructure and compliance with Food and Drug Administration ("FDA") and other governmental regulations and approval requirements.
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Use of Estimates
The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of expenses during the reporting period. Actual results could differ from those estimates.
Cash, Cash Equivalents, and Short-Term Investments
The Company considers all highly-liquid instruments purchased with a maturity of three months or less to be cash equivalents. Instruments with maturities greater than three months, but less than twelve months are included in short-term investments. The Company purchases United States Treasury bills with maturities ranging from six to twelve months which are classified as being held to maturity and are carried at amortized cost. Securities classified as held to maturity securities are those securities that management has the intent and ability to hold to maturity.
F-7
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
The Company maintains its cash balance in one financial institution. The balance is insured up to the maximum allowable by the Federal Deposit Insurance Company ("FDIC"). The Company has not experienced any losses in such accounts and does not believe it is exposed to any significant risk of loss on cash. At times, the cash balance may exceed the maximum limit of the FDIC.
Guaranteed Payments to Members
Guaranteed payments to members of the Company prior to the March 2014 corporate conversion, that were designated to represent reasonable compensation for services rendered, were accounted for as Company expenses rather than an allocation of the Company's net income.
Research and Development
In accordance with Accounting Standards Codification ("ASC") 730, Accounting for Research and Development Costs, the Company expenses research and development costs when incurred. At times, the Company may make cash advances for research and development services. These amounts are capitalized and expensed in the period the service is provided. The Company incurred net research and development expenses in the amounts of $11,286,236 and $8,898,280 for the years ended December 31, 2015 and 2014, respectively.
Although the Company manages the conduct of its clinical trials, it relies on third parties to conduct its clinical and preclinical studies and to provide services, including data management, statistical analysis and electronic compilation for clinical trials, as well as for the manufacture of clinical trial supplies. At the end of each reporting period, the Company compares the payments made to each service provider to the estimated progress towards completion of the related project. Factors that are considered in preparing these estimates include the number of subjects enrolled in studies, milestones achieved and other criteria related to the efforts of the vendors. These estimates are subject to change as additional information becomes available. Depending on the timing of payments to vendors and estimated services provided, the Company records net prepaid or accrued expenses related to these costs.
Share-Based Compensation
The Company accounts for the cost of services performed by officers and directors received in exchange for an award of Company membership interests, common stock, or stock options, based on the grant-date fair value of the award. In accordance with ASC 718, Stock Compensation, the Company recognizes compensation expense, net of estimated forfeitures, on a straight-line basis over the service period.
Share-Based Payments to Vendors
The Company accounts for the cost of services performed by vendors in exchange for an award of Company membership interests or common stock based on the grant-date fair value of the award or fair value of the services rendered, whichever is more readily determinable and adjusted to fair value at each reporting date. Such fair value is measured as of the earlier of the date the other party becomes committed to provide goods or services or the date performance by the other party is complete. The Company recognizes the expense in the same period and in the same manner as if the Company had paid cash for the services.
F-8
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Income Taxes
Prior to the Company's corporate conversion in March 2014, the Company was organized as a limited liability company. As such, the Company was not a tax paying entity for Federal income tax purposes and, therefore, no income tax expense had been recorded in the financial statements. Income or loss of the Company was passed through to members for inclusion in their respective income tax returns.
Subsequent to the corporate conversion in March 2014, the Company became a taxable entity. As such, the Company recognizes deferred tax assets and liabilities for temporary differences between the financial reporting basis and the tax basis of the Company's assets and liabilities and the expected benefits of net operating loss carryforwards. The impact of changes in tax rates and laws on deferred taxes, if any, applied during the years in which temporary differences are expected to be settled, is reflected in the financial statements in the period of enactment. The measurement of deferred tax assets is reduced, if necessary, if, based on weight of the evidence, it is more likely than not that some, or all, of the deferred tax assets will not be realized. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in the period that such tax rate changes are enacted. The Company had no material amounts recorded for uncertain tax positions, interest or penalties in the accompanying financial statements. The Company currently estimates an annual effective tax rate of 0% as the Company incurred losses for the years ended December 31, 2015and 2014 for both financial statement and tax purposes. Therefore, no Federal or state income tax expense has been recorded in the financial statements.
Based on the Company's history of generating operating losses and its anticipation of operating losses continuing in the foreseeable future, the Company has determined that it is more likely than not that the tax benefits from these net operating losses would not be realized and a full valuation allowance against all deferred tax assets has been recorded at December 31, 2015 and 2014, respectively. In the event the Company becomes profitable for a period of two or more years, with future expectations at that time of profitability for future years prior to any significant change in its equity capitalization, the Company would have an opportunity to realize benefit from the deferred tax asset at such time in the future.
Fair value of financial instruments
The carrying amount of certain of the Company's financial instruments, including cash and accounts payable, is shown at cost, which approximates fair value. Short-term investments with maturities ranging from six to twelve months are classified as being held to maturity and are carried at amortized cost. The age of gross unrealized gains and the fair value of related securities at December 31, 2015 were as follows:
| |
Total (maturities within 12 months) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
Cost | Unrealized Gain |
Fair Value | |||||||
Held to Maturity: |
||||||||||
Debt Securities: |
||||||||||
United States Government sponsored bonds |
$ | 26,958,214 | $ | 4,646 | $ | 26,962,860 | ||||
F-9
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
For the year ended December 31, 2015, the amount of total amortized interest income was $20,621. The carrying value of $26,977,362 as of December 31, 2015, is equal to the amortized cost plus the amortized interest income of $19,148 on the remaining bonds held at December 31, 2015.
NOTE 3—ACCOUNTS PAYABLE AND ACCRUED EXPENSES
Accounts payable and accrued expenses at December 31, 2015 and 2014 are as follows:
| |
December 31, 2015 | December 31, 2014 | |||||
|---|---|---|---|---|---|---|---|
Accrued compensation expense |
$ | 663,404 | $ | 511,769 | |||
Accrued research and development |
859,053 | 641,997 | |||||
Accrued professional fees |
55,787 | 23,901 | |||||
Other accounts payable and accrued expenses |
28,063 | 82,931 | |||||
| | | | | | | | |
Totals |
$ | 1,606,307 | $ | 1,260,598 | |||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
NOTE 4—ISSUANCE OF MEMBERSHIP INTERESTS and COMMON STOCK
On March 18, 2014, the Company completed an IPO issuing 3,162,500 shares of common stock at a price of $12 per share, resulting in net proceeds of $34,455,669 after deducting underwriting discounts of $2,656,500 and offering costs $837,831. The then outstanding Class A Membership Interests were converted to shares of common stock using a conversion ratio of 7 to 1, resulting in the conversion of 767,911 Class A Membership Interests into an aggregate of 5,375,377 shares of common stock.
On June 30, 2015, the Company completed a stock offering issuing 1,702,000 shares of common stock at a price of $12.50 per share, resulting in net proceeds of approximately $19.7 million after deducting underwriting discounts of $1.3 million and offering costs of approximately $0.3 million.
NOTE 5—SHARE-BASED COMPENSATION and STOCK OPTIONS
Prior to the corporate conversion in March 2014, the Company granted awards of restricted Class A Membership Interests to board members in exchange for services. These membership interests awards were originally scheduled to vest over a period of either 3 or 4 years, with the first year beginning on the date the member joined the board. In each case, these membership interests involved accelerated vesting upon a change of control or other business combination. The fair value of the membership interests granted was equal to the per-membership interest value of the most recent private placement ($50 per membership interest). Total compensation expense in the amount of $100,000 and $125,000 has been recognized as director fees for the years ended December 31, 2015 and 2014, respectively.
F-10
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 5—SHARE-BASED COMPENSATION and STOCK OPTIONS (Continued)
The following table summarizes the non-vested Class A Membership Interests at December 31, 2015 giving effect to the corporate conversion and the associated activity:
| |
Class A Membership Interests converted to Common Stock 7:1 ratio |
|||
|---|---|---|---|---|
Nonvested at January 1, 2014 |
77,000 | |||
Granted |
— | |||
Forfeited |
(21,000 | ) | ||
Vested |
(14,000 | ) | ||
| | | | | |
Nonvested at December 31, 2014 |
42,000 | |||
Granted |
— | |||
Forfeited |
— | |||
Vested |
(14,000 | ) | ||
| | | | | |
Nonvested at December 31, 2015 |
28,000 | |||
| | | | | |
| | | | | |
| | | | | |
In December 2013, 1,000 Membership Interests were issued to a member of the board of directors and vested in February 2014.
As of December 31, 2015, there was $120,833 of total unrecognized compensation cost related to these awards. That cost is expected to be recognized over a weighted average period of 1.25 years.
In November 2013, the board of directors adopted the 2013 Equity Incentive Plan. The plan became effective as of the completion of the corporate conversion and the closing of the IPO. The 2013 Equity Incentive Plan currently reserves 2,141,169 common shares available for issuance. The purpose of the plan is to attract and retain directors, officers, and employees whose services are considered valuable to the Company.
In March 2014, effective at the closing of the Company's IPO, the Company granted stock options to purchase 853,787 common shares (10% of the common stock outstanding) to its four executives. The options were issued pursuant to the 2013 Equity Incentive Plan at an exercise price of $13.93 and vest over thirty-six (36) equal monthly installments. In April 2014, a new employee received 7,500 stock options at an exercise price of $10.46 vesting over a three (3) year period.
In January 2015, the Company granted stock options to purchase 251,000 common shares to its five employees, outside directors, and certain non-employee consultants. The options were issued pursuant to the 2013 Equity Incentive Plan at an exercise price of $11.35, with one-half of the options vesting upon issuance and the balance vesting evenly over the subsequent 24 months. A portion of the January stock option grant, 35,000 options, was granted to non-employees for services rendered. As such, the Company expensed $353,150, the entire portion of those non-employee grants, at the grant date.
Compensation expense associated with these awards is recognized over the vesting period based on the fair value of the option at the grant date determined based on the Black-Scholes model. Option valuation models require the input of highly subjective assumptions including the expected price volatility. The Company's employee stock options have characteristics significantly different from those of traded options, and changes in the subjective input assumptions can materially affect the fair value estimate.
F-11
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 5—SHARE-BASED COMPENSATION and STOCK OPTIONS (Continued)
Because there is no public market for the Company's stock options and very little historical experience with the Company's stock, similar public companies were used for comparison and expectations as to the price volatility assumptions required for fair value computation using the Black-Scholes methodology.
The Company determined the fair value of the option awards using the Black-Scholes option pricing model and the following weighted average assumptions:
| |
Year Ended December 31, 2015 |
Year Ended December 31, 2014 |
||
|---|---|---|---|---|
Expected term |
5.65 years | 4.3 years | ||
Volatility |
62.1% | 59.6% | ||
Dividend yield |
0% | 0% | ||
Risk free interest rate |
1.58% | 1.23% |
ASC 718 requires stock compensation expense to be recorded net of estimated forfeitures. The Company currently estimates there will be no forfeitures of options.
A summary of the Company's stock option activity is as follows:
| |
Number of Options |
Weighted Average Exercise Price |
|||||
|---|---|---|---|---|---|---|---|
Outstanding at January 1, 2014 |
— | ||||||
Granted |
861,287 | $ | 13.90 | ||||
Forfeited |
— | ||||||
| | | | | | | | |
Outstanding at December 31, 2014 |
861,287 | $ | 13.90 | ||||
Granted |
251,000 | $ | 11.35 | ||||
Forfeited |
— | ||||||
| | | | | | | | |
Outstanding and expected to vest at December 31, 2015 |
1,112,287 | $ | 13.32 | ||||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
Compensation expense relating to options for the years ended December 31, 2015 and 2014 was $3,175,908 and $1,322,479, respectively. The total compensation expense not yet recognized as of December 31, 2015 was $2,473,027. The weighted average vesting period over which the total compensation expense will be recorded related to unvested options not yet recognized as of December 31, 2015 was approximately 1.2 years. The weighted average grant date fair values were $7.61 and $5.88 for 2015 and 2014, respectively. The intrinsic value of the stock options was $0 as of December 31, 2015 and 2014, with a remaining weighted average contractual life of 5.4 years and 5.74 years as of December 31, 2015 and 2014, respectively. Total options excercisable at December 31, 2015 were 657,314.
NOTE 6—SHARE-BASED PAYMENTS TO VENDORS
In January 2014, the Company entered into a Product Development Agreement with RRD International, LLC ("RRD"), pursuant to which RRD provides certain strategic product development services to the Company during the term of the agreement which was calendar year 2014. These product development services include the management of the Company's ongoing Phase 3 clinical trials, developing, planning and execution of a fully integrated product development strategy and
F-12
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 6—SHARE-BASED PAYMENTS TO VENDORS (Continued)
implementation of that strategy either directly or with third party vendors. As consideration for services rendered, the Company agreed to pay RRD partially in cash and by issuing 7,604 of the Company's Class A Membership Interests. The Company expensed the fair value of the Class A Membership Interests, $50 per Class A Membership Interest, based on the most recent private placement.
In January 2015, the Company entered into a new amendment to the Product Development Agreement with RRD dated January 2014, pursuant to which RRD will continue to provide certain strategic product development services to the Company for an additional six-month term. As consideration for services rendered, the Company has agreed to pay RRD a total of $600,000, consisting of $450,000 in cash and $150,000 in restricted shares of the Company's common stock (12,346 shares). The Company recorded research and development expense relating to this six-month agreement of $608,495, including the cash payments and stock issuance.
In July 2015, the Company entered into two new amendments to the Product Development Agreement with RRD dated January 2014, pursuant to which RRD will continue to provide certain strategic product development services to the Company for an additional six-month term. These services include management of the Company's ongoing Phase 3 clinical trials, developing, planning, and execution of a fully integrated product development strategy and implementation of that strategy either directly or with third party vendors. The services also include activities to support the initiation and the preparation of the New Drug Application ("NDA") Amendment. As consideration for the services rendered, the Company has agreed to pay RRD approximately $1.7 million, consisting of approximately $1.27 million in cash and approximately $423,000 in restricted common stock (31,607 shares). Terms of the services to be provided after December 2015, if any, will be negotiated at a later date. The Company recognizes the costs incurred in connection with this agreement as research and development expenses as services are rendered. The Company recorded research and development expense relating to this agreement of $1,686,965, including cash and stock issuance, for the year ended December 31, 2015.
In January 2016, the Company entered into two new amendments to the Product Development Agreement with RRD dated January 2014, pursuant to which RRD will continue to provide certain strategic product development services to the Company for an additional six-month term.
NOTE 7—INCOME TAXES
The Company has $25.5 million of net operating loss carryforwards and $1.2 million of research tax credit carryforwards as of December 31, 2015. The net operating loss carryforwards and research tax credit carryforwards begin to expire in 2034 and will be utilized for tax purposes at such time the Company generates taxable income. The utilization of these net operating loss carryforwards may also be limited to the extent the Company has certain ownership changes pursuant to section 382 of the Internal Revenue Code.
F-13
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 7—INCOME TAXES (Continued)
The components of the net deferred income tax asset at December 31, 2015 and 2014 are as follows:
| |
2015 | 2014 | |||||
|---|---|---|---|---|---|---|---|
Deferred tax assets: |
|||||||
Net operating loss carryforwards |
$ | 11,353,162 | $ | 4,797,498 | |||
Share-based compensation |
2,023,572 | 588,860 | |||||
Research and development credit carryforwards |
1,205,464 | 506,325 | |||||
| | | | | | | | |
Gross deferred tax assets |
14,582,198 | 5,892,683 | |||||
Less valuation allowance |
(14,582,198 | ) | (5,892,683 | ) | |||
| | | | | | | | |
Net deferred tax asset |
$ | — | $ | — | |||
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
In assessing the realizability of deferred tax assets, the Company considers whether it is more-likely-than-not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income during the periods in which the temporary differences representing net future deductible amounts become deductible. After consideration of all the evidence, both positive and negative, the Company has recorded a full valuation allowance against their net deferred tax assets at December 31, 2015 because the Company has determine that it is more-likely-than-not that these assets will not be fully realized.
The Company reserves 100% of the deferred tax asset pursuant to applicable GAAP accounting rules. In the event the Company becomes profitable for a period of two or more years, with future expectations at that time of profitability for future years prior to any significant change in its equity capitalization, the Company would have an opportunity to realize benefit from the deferred tax asset at such time in the future.
The Company did not have unrecognized tax benefits as of December 31, 2015, and does not expect this to change significantly over the next twelve months. The Company recognizes interest and penalties accrued on any unrecognized tax benefits as a component of income tax expense. As of December 31, 2015, the Company has not accrued interest or penalties related to any uncertain tax positions.
A reconciliation of income tax expense (benefit) at the statutory Federal income tax rate and income taxes as reflected in the financial statements for both years ending December 31, 2015 and 2014 is as follows:
Federal income tax expense at statutory rate |
(34.0 | )% | ||
State income tax, net of federal benefit |
— | |||
Permanent differences |
0.1 | |||
Change in valuation allowance |
33.9 | |||
| | | | | |
Effective income tax rate |
— | % | ||
| | | | | |
| | | | | |
| | | | | |
The Company has generated research credits but has not conducted a study to document the qualified activities. This study may result in an adjustment to research and development credit carryforwards; however, until a study is completed and any adjustment is known, no amounts are being
F-14
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 7—INCOME TAXES (Continued)
presented as an uncertain tax position for these years. A full valuation allowance has been provided against research and development credits and, if an adjustment is required, this adjustment to the deferred tax asset established for the research and development credit carryforwards would be offset by an adjustment to the valuation allowance.
The Company files income tax returns in the U.S. Federal jurisdiction, and various state and local jurisdictions.
NOTE 8—LEASE OF OFFICE SPACE
Effective May 2014, the Company entered into a sublease agreement for office space with current monthly payments of $13,098. The term of the sublease ends on March 30, 2016 with inflationary escalations in 2015 and the first three months of 2016. Total minimum sublease payments for the remaining term of the sublease from December 31, 2015 to March 30, 2016 are $39,294.
In January 2016, the Company entered into a lease for office space commencing in March 2016 with current monthly payments of $18,857 subject to inflationary escalations and adjustments thereafter. The term of the lease is for five years and five months with total minimum lease payments of approximately $1.28 million. The future minimum lease payments under this lease are as follows:
Year ending December 31: |
||||
2016 |
$ | 169,713 | ||
2017 |
$ | 231,534 | ||
2018 |
$ | 238,004 | ||
2019 |
$ | 244,658 | ||
2020 |
$ | 251,522 | ||
Thereafter |
$ | 150,347 | ||
| | | | | |
Total |
$ | 1,285,778 | ||
| | | | | |
| | | | | |
| | | | | |
NOTE 9—LEGAL MATTERS
The Company and its two original executives were three of some 30 defendants in a lawsuit filed by a former stockholder of Genaera Corporation, which was the predecessor of the Genaera Liquidating Trust, the party from which the Company purchased the worldwide rights to pexiganan, the active ingredient of the Product Locilex® on April 8, 2010. The complaint was filed on June 8, 2012 in the United States District Court for the Eastern District of Pennsylvania (Civil Action No. 12-3265) by Alan W. Schmidt, individually and on behalf of former Genaera Corporation shareholders. Among others, the suit was filed against the Company, as well as John A. Skolas and Argyce, LLC, who were responsible for the administration of the Trust and who sold pexiganan to the Company via a public auction. The defendants listed in the complaint included several individuals and companies formerly associated with Genaera Corporation, the Trust and/or Argyce, LLC. Also included in the defendant group were several other pharmaceutical companies that were involved in acquiring the former drug-related assets of the Genaera Corporation.
The complaint alleged, among other things, the Company and its two executives aided and abetted a breach of fiduciary duty alleged to have been committed by the former director and officers of Genaera Corporation before it was approved for dissolution by its shareholders and also Argyce, LLC,
F-15
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 9—LEGAL MATTERS (Continued)
the trustee of the Liquidating Trust. Plaintiff claims that the Company, and its executives, aided and abetted a breach of the duties of the board of directors and the trustee under common law and under a certain trust agreement allegedly signed between Argyce, LLC, as the trustee, and the Liquidating Trust. With regard to the claims made against the Company and two executives, the plaintiff alleged, in pertinent part, that the Company's acquisition of the pexiganan rights was for alleged inadequate consideration, and that the Company and its management aided and abetted a breach of fiduciary duty by the Genaera Corporation defendants who were formerly associated with Genaera Corporation and/or the Trust.
The Company and its two executives filed a motion to dismiss the complaint within the prescribed time period. All of the other defendants in this litigation also filed motions to dismiss, and a court order by the Federal District Court granted each and every motion to dismiss, with prejudice, without leave to refile, on August 12, 2013 based on the argument that Plaintiff's claims were time barred. A subsequent motion to reconsider such dismissal was denied by the Federal District Court. Plaintiff appealed the dismissal to the United States Third Circuit Court of Appeals seeking reversal of the dismissal and the Third Circuit Court granted Plaintiff's appeal. On October 17, 2014, the Third Circuit Appellate Court, in a 2-1 decision with a strong dissenting opinion, reversed the trial court's dismissal of Plaintiff's claims based on the expiration of the applicable statutes of limitation. In a 2-1 decision, the Third Circuit held that more information was necessary to determine when Plaintiff should have been on notice of his claims to determine the applicability of the discovery rule, which could serve to extend the time frame in which Plaintiff could bring his claims. Due to the strong dissent, all Defendants filed the necessary documents requesting a petition for rehearing en banc, by the majority of the Third Circuit justices who are in active service. The Third Circuit denied the request for en banc hearing and remanded this case to District Court.
Upon remand to the Federal District Court, all Defendants moved to dismiss the complaint for reasons other than being time barred. The Company and the executives moved for dismissal based on Plaintiff's inability to make a case for aiding and abetting a breach of fiduciary duty because there was no underlying breach and such an aiding and abetting claim requires an element of knowing participation in the fiduciary breach which cannot be established by Plaintiff.
The District Court held a hearing on this in September 2015 and the District Court delivered an Order on November 10, 2015 pursuant to which the District Court granted the Motion to Dismiss filed by each and every defendant including the Company and its executives. In December 2015, Plaintiff appealed the Federal District Court's decision to the Third Circuit Appellate Court and the Company anticipates a decision on whether to grant Plaintiff's appeal by the Third Circuit Appellate Court in 2016. The Company will continue to vigorously defend against Plaintiff's claims on the factual record, which it believes will prove that the Company is not liable to the Plaintiff in any regard.
NOTE 10—RELATED PARTY TRANSACTIONS
The individual employed as the Company's Vice President, Finance and Corporate Development as of the closing of the initial public offering, is the owner of Aumoe Partners, LLC ("Aumoe"), which was engaged in January 2012 to perform certain financial advisory services. The Company incurred $0 and $22,500 in fees to Aumoe for the years ended December 31, 2015 and 2014, respectively, which were recorded in general and administrative expenses.
F-16
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 10—RELATED PARTY TRANSACTIONS (Continued)
The Company engaged the consulting services of Drug Development Advisors ("DDA") pursuant to which DDA performed detailed analysis on a number of the Company's preclinical studies in connection with the NDA process. DDA is owned and operated by a member of the Company's board of directors. The Company incurred expenses for services provided by DDA in the amounts of $24,550 and $30,734 for the years ended December 31, 2015 and 2014, respectively, which were recorded in research and development expenses.
NOTE 11—NET LOSS PER SHARE
Basic and diluted net loss per common share for the years ended December 31, 2015 and 2014, respectively, were determined by dividing net loss by the weighted average common shares outstanding during the period. The Company's potentially dilutive shares, which include 1,112,287 of stock options, 28,000 unvested common shares, and 24,500 warrants, have not been included in the computation of diluted net loss per share for all periods as the result would be antidilutive. On March 12, 2014, the Company completed a corporate conversion from a limited liability company to a corporation (the "Conversion"). Accordingly, the outstanding Class A Membership Interests were converted to shares of common stock using a conversion ratio of 7 to 1, resulting in the conversion of its 767,911 Class A Membership Interests into an aggregate of 5,375,377 shares of common stock. The effects of this Conversion on the Company's net loss per share have been reflected for all periods presented retroactively.
NOTE 12—RECENT ACCOUNTING PRONOUNCEMENTS
In August 2014, the Financial Accounting Standards Board issued Accounting Standards Update ("ASU") 2014-15, Presentation of Financial Statements—Going Concern, which requires management of an entity to evaluate whether there are conditions or events, considered in the aggregate, that raise substantial doubt about the entity's ability to continue as a going concern within one year after the date that the financial statements are issued or available to be issued. This update will become effective beginning January 1, 2017, with early adoption permitted. The Company is currently evaluating the provisions of this amendment.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740), which requires that all deferred income tax assets and liabilities be presented as noncurrent in the statement of financial position. The pronoucement is effective for financial statements issued for annual periods beginning after December 15, 2018 with early application permitted. The adoption of this guidance is not expected to have a material impact on the Company's financial statements.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842), which includes amendments that require lessees to recognize a lease liability for all long-term leases (lease terms more than 12 months) at the commencement date. The lease liability is a lessee's obligation to make lease payments arising from a lease, measured on a discounted basis. The amendments also require lessees to recognize a right-of-use asset for all long-term leases. The right-of-use asset is an asset that represents the lessee's right to use, or control the use of, a specified asset for the lease term. For leases with a term of 12 months or less, a lessee is permitted to make an accounting policy election by class of underlying asset to not recognize lease assets and lease liabilities. If a lessee makes this election, it should recognize lease expense for such leases generally on a straight-line basis over the lease term. The amendments in this ASU require qualitative disclosures along with specific quantitative disclosures.
F-17
DIPEXIUM PHARMACEUTICALS, INC.
NOTES TO THE FINANCIAL STATEMENTS (Continued)
NOTE 12—RECENT ACCOUNTING PRONOUNCEMENTS (Continued)
The amendments in this ASU are effective for fiscal years beginning after December 15, 2018, and interim periods within those fiscal years. Early application is permitted. Lessees (for capital and operating leases) and lessors (for sales-type, direct financing, and operating leases) must apply a modified retrospective transition approach for leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements. The modified retrospective approach would not require any transition accounting for leases that expired before the earliest comparative period presented. The Company is currently evaluating the provisions of this amendment.
F-18