Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - NOVAVAX INC | Financial_Report.xls |
| EX-10.4 - EXHIBIT 10.4 - NOVAVAX INC | v401319_ex10-4.htm |
| EX-32.2 - EXHIBIT 32.2 - NOVAVAX INC | v401319_ex32-2.htm |
| EX-23.1 - EXHIBIT 23.1 - NOVAVAX INC | v401319_ex23-1.htm |
| EX-10.5 - EXHIBIT 10.5 - NOVAVAX INC | v401319_ex10-5.htm |
| EX-31.2 - EXHIBIT 31.2 - NOVAVAX INC | v401319_ex31-2.htm |
| EX-10.6 - EXHIBIT 10.6 - NOVAVAX INC | v401319_ex10-6.htm |
| EX-32.1 - EXHIBIT 32.1 - NOVAVAX INC | v401319_ex32-1.htm |
| EX-23.2 - EXHIBIT 23.2 - NOVAVAX INC | v401319_ex23-2.htm |
| EX-21.1 - EXHIBIT 21.1 - NOVAVAX INC | v401319_ex21-1.htm |
| EX-31.1 - EXHIBIT 31.1 - NOVAVAX INC | v401319_ex31-1.htm |
| EX-10.35 - EXHIBIT 10.35 - NOVAVAX INC | v401319_ex10-35.htm |
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2014
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to .
Commission File No. 0-26770
NOVAVAX, INC.
(Exact name of Registrant as specified in its charter)
|
Delaware (State of incorporation) |
20 Firstfield Road (Address of principal executive offices) |
22-2816046 (I.R.S. Employer Identification No.) |
Registrant’s telephone number, including area code: (240) 268-2000
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Name of each exchange on which registered | |
| Common Stock, Par Value $0.01 per share | The NASDAQ Global Select Market |
Securities registered pursuant to Section 12(g) of the Act: Not Applicable
Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨
Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the Registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the Registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the Registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer x | Accelerated filer ¨ | Non-accelerated filer ¨ (Do not check if a smaller reporting company) |
Smaller reporting company ¨ |
Indicate by check mark whether the Registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the voting and non-voting common equity held by non-affiliates of the Registrant (based on the last reported sale price of Registrants common stock on June 30, 2014 on the NASDAQ Global Select Market) was approximately $934,600,000.
As of February 23, 2015, there were 239,379,766 shares of the Registrant’s common stock outstanding.
Documents incorporated by reference: Portions of the Registrant’s Definitive Proxy Statement to be filed no later than 120 days after the fiscal year ended December 31, 2014 in connection with the Registrant’s 2015 Annual Meeting of Stockholders are incorporated by reference into Part III of this Annual Report on Form 10-K to the extent indicated herein.
NOVAVAX, INC.
TABLE OF CONTENTS
| i |
CERTAIN DEFINITIONS
All references in this Annual Report on Form 10-K to “Novavax,” the “Company,” “we,” “us,” and “our” refer to Novavax, Inc. and its consolidated subsidiary, Novavax AB (unless the context otherwise indicates).
NOTE REGARDING TRADEMARKS
Matrix-M™ and Matrix™ are trademarks of Novavax. Any other trademarks referred to in this Annual Report on Form 10-K are the property of their owners. All rights reserved. We do not intend our use or display of other companies’ trade names or trademarks to imply an endorsement or sponsorship of us by such companies, or any relationship with any of these companies.
FORWARD-LOOKING INFORMATION
This Annual Report on Form 10-K contains forward-looking statements, within the meaning of the Private Securities Litigation Reform Act that involve risks and uncertainties. In some cases, forward-looking statements are identified by words such as “believe,” “anticipate,” “intend,” “plan,” “will,” “may” “expect” and similar expressions. All of these forward-looking statements are based on information available to us at this time, speak only as of the date of this Annual Report on Form 10-K, and we assume no obligation to update any of these statements. Actual results could differ from those projected in these forward-looking statements as a result of many factors, including those identified in the section titled “Risk Factors,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere. We urge you to review and consider the various disclosures made by us in this report, and those detailed from time to time in our filings with the Securities and Exchange Commission (“SEC”), that attempt to advise you of the risks and factors that may affect our future results. Given these risks and uncertainties, readers are cautioned not to place undue reliance on such forward-looking statements.
| i |
Overview
Novavax, Inc., together with its wholly-owned subsidiary, Novavax AB, is a clinical-stage vaccine company focused on the discovery, development and commercialization of recombinant nanoparticle vaccines and adjuvants. Using innovative proprietary recombinant nanoparticle vaccine technology, we produce vaccine candidates to efficiently and effectively respond to both known and newly emerging diseases.
We were incorporated in 1987 under the laws of the State of Delaware. Our principal executive offices are located at 20 Firstfield Road, Gaithersburg, Maryland, 20878, and our telephone number is (240) 268-2000. Our common stock is currently listed on the Nasdaq Global Select Market under the symbol “NVAX.”
Our vaccine candidates are genetically engineered three-dimensional nanostructures that incorporate immunologically important proteins. Our product pipeline targets a variety of infectious diseases with vaccine candidates currently in clinical development for respiratory syncytial virus (“RSV”), seasonal influenza, pandemic influenza, and the Ebola virus (“EBOV”). We have additional pre-clinical stage programs in a variety of infectious diseases, including the Middle East respiratory syndrome coronavirus (“MERS”). Further, CPL Biologics Private Limited (“CPLB”), our joint venture company in India, is actively developing a number of vaccine candidates that were genetically engineered by Novavax, including a seasonal influenza VLP vaccine candidate that completed enrollment of its Phase 3 clinical trial in India in 2014, and its rabies vaccine that completed its Phase 1/2 clinical trial in India in 2014.
We are also developing proprietary technology for the production of immune stimulating saponin-based adjuvants, through our Swedish wholly-owned subsidiary, Novavax AB. Our Matrix™ adjuvant technology utilizes selected quillaja fractions that, through our manufacturing process form separate matrix structures, to develop modern, multi-purpose immune-modulating adjuvant products for a broad range of potential vaccine applications. Our lead adjuvant for human applications, Matrix-M™, has been successfully tested in a Phase 1/2 clinical trial for our pandemic influenza H7N9 vaccine candidate, conducted under our contract with the U.S. Department of Health and Human Services, Biomedical Advanced Research and Development Authority (“HHS BARDA”) and we are currently testing Matrix-M in conjunction with our EBOV vaccine candidate in a Phase 1 clinical trial. Genocea Biosciences, Inc. has licensed rights to our Matrix technology and is conducting clinical trials with its herpes simplex 2 vaccine candidate using Matrix-M.
Our joint venture with Cadila Pharmaceuticals Limited (“Cadila”), CPLB, is developing and manufacturing vaccines, biological therapeutics and diagnostics in India. CPLB is owned 20% by us and 80% by Cadila. CPLB operates a manufacturing facility in India for the production of vaccines and is actively developing a number of vaccine candidates that were genetically engineered by us.
| 1 |
Clinical Product Pipeline
A current summary of our significant research and development programs and status of related products in development follows:
| Program | Development Stage | Funding Collaborator | ||
| Respiratory Syncytial Virus (RSV) | ||||
| · Elderly | Phase 2 | |||
| · Maternal Immunization | Phase 2 | PATH | ||
| · Pediatric | Phase 1 | |||
| Influenza | ||||
| · Seasonal Quadrivalent | Phase 2 | HHS BARDA | ||
| · Pandemic H7N9 | Phase 2 | HHS BARDA | ||
| Other | ||||
| · Ebola Virus (EBOV) | Phase 1 | |||
| · Combination (Influenza/RSV) | Pre-Clinical | |||
| CPLB Programs (India) | ||||
| · Seasonal Influenza | Phase 3 | |||
| · Rabies | Phase 1/2 |
Respiratory Syncytial Virus (RSV)
RSV is a major respiratory pathogen with a significant burden of disease in the very young and in the elderly. In healthy adults, RSV infections are generally mild to moderate in severity, but are typically more severe in infants and young children as well as adults over the age of 601. Globally, RSV is a common cause of childhood respiratory infection, with a disease burden of 64 million cases and approximately 160,000 deaths annually2. Severe RSV disease results in 3.4 million hospital admissions per year globally3 and disproportionately affects infants below six months of age. In infants, toddlers and young pre-school and school-age children, RSV infections result in the need for frequent medical care, including emergency room and office visits and are associated with increased recurrent wheezing that can persist for years. In the U.S., nearly all children become infected with RSV before they are two years of age; it has been associated with 20% of hospitalizations and 15% of office visits for acute respiratory infection in young children4. It is also estimated that between 11,000 and 17,000 elderly and high risk adults die of RSV infection or its complications annually in the U.S., and up to 180,000 are hospitalized for serious respiratory symptoms.5 Currently, there is no approved RSV vaccine available for any of these populations, so an RSV vaccine has the potential to protect millions of persons from this far-reaching unmet medical need.
We are developing our respiratory syncytial virus fusion (F) protein nanoparticle vaccine candidate (“RSV F vaccine candidate”) for the benefit of three susceptible target populations: the elderly, infants (receiving protection through antibodies transferred from their mothers who would be immunized during the last trimester of pregnancy) and pediatrics.
1 Dawson-Caswell, D, et al., (2011) Am Fam Physician. 83:143 - 146
2 Nair, H., et al., (2010) Lancet. 375:1545 - 1555
3 WHO, (2014) “RSV Vaccine Status;” www.who.int/immunization/research/meetings_workshops/WHO_PDVAC_RSV.pdf
4 Hall, CB, et al., (2009) N Engl J Med. 360(6):588-98
5Falsey, A., et al., (2014) Infectious Disorders. 12(2): 98-102
| 2 |
RSV Elderly Program
In October 2014, we initiated enrollment in a Phase 2 dose-confirmation clinical trial of our RSV F vaccine candidate in 1,600 older adults (>60 years of age). Recruitment was completed in November, and the preliminary data from this trial are expected in the third quarter of 2015. We believe these data will inform the next steps in the development of our RSV elderly program. Data from our earlier Phase 1 clinical trial in the elderly, initiated in October 2012, corroborates our previous clinical experiences with our RSV F vaccine candidate. In May 2014, we released one-year follow-up data from that Phase 1 clinical trial demonstrating that, for the group receiving the 90μg antigen dose without adjuvant, anti-F levels and palivizumab competing antibodies were significantly elevated over baseline at day 180, with neutralizing antibody levels that were considered protective for both the RSV A and RSV B strains. We believe these findings support the development of an annual RSV F vaccine candidate dose that can provide protection over the four to five month period of a typical RSV season.
RSV Maternal Immunization Program
In September 2014, we initiated a Phase 2 clinical trial of our RSV F vaccine candidate in healthy women in their third trimester of pregnancy. This trial, which is designed to enroll fifty (50) pregnant women, will evaluate the safety and immunogenicity of our RSV F vaccine candidate in pregnant women and assesses the impact of maternal immunization on RSV-specific antibody levels through the baby’s first six months of life and infant safety through the first year of life. The preliminary data from this trial are expected in the third quarter of 2015 and will inform the next steps in the development of our RSV maternal program. In November 2014, we announced that the U.S. Food and Drug Administration, Center for Biologics Evaluation and Research (“FDA”) had granted Fast Track Designation to our RSV F vaccine candidate for protection of infants via maternal immunization. The Fast Track Designation, established by the FDA Modernization Act of 1997, is intended for products that treat serious or life-threatening diseases or conditions, and that demonstrate the potential to address unmet medical needs for such diseases or conditions. The program is intended to facilitate development and expedite review of drugs to treat serious and life-threatening conditions so that an approved product can reach the market expeditiously. Fast Track Designation specifically facilitates meetings to discuss all aspects of development to support licensure and it provides the opportunity to submit sections of a Biologics License Application (“BLA”) on a rolling basis as data become available, which permits the FDA to review modules of the BLA as they are received instead of waiting for the entire BLA submission.
In April 2014, we announced positive top-line safety and immunogenicity data from a Phase 2 clinical trial in women of childbearing age that were similar to, or exceeded, immune responses seen in our previous clinical trials. This Phase 2 clinical trial evaluated the safety and immunogenicity of two dose levels of our RSV vaccine candidate, in one or two injections, with and without an aluminum phosphate adjuvant, in 720 healthy women of childbearing age. These positive data supported Novavax’ decision to progress to the previously discussed Phase 2 clinical trial in pregnant women.
PATH Vaccine Solutions (“PATH”) Clinical Development Agreement for RSV Maternal Program
In conjunction with our development of our RSV F vaccine candidate for maternal immunization, in 2012 we entered into a clinical development agreement with PATH to develop our RSV F vaccine candidate in certain low-resource countries. We refer to this as our RSV Collaboration Program. We were awarded approximately $2.0 million by PATH for initial funding under the agreement to partially support our Phase 2 dose-ranging clinical trial in women of childbearing age described above. In October 2013, the funding under this agreement was increased by $0.4 million to support reproductive toxicology studies, which was necessary before we began conducting clinical trials in pregnant women. In December 2013, we entered into an amendment with PATH providing an additional $3.5 million in funding to support the Phase 2 dose-confirmation clinical trial in 720 women of childbearing age. In October 2014, we entered into an amendment with PATH providing an additional $1.0 million towards the development of a strategy for approaching a Phase 3 clinical trial in our RSV maternal immunization program and are in ongoing discussion with PATH for additional funding. We retain global rights to commercialize the product and will support PATH in its goal to make an RSV maternal vaccine product affordable and available in low-resource countries. To the extent PATH elects to continue to fund 50% of our external clinical development costs for the RSV Collaboration Program, but we do not continue development, we would then grant PATH a fully-paid license to our RSV F vaccine candidate technology for use in pregnant women in certain contractually defined low-resource countries.
| 3 |
RSV Pediatric Program
While the burden of RSV disease falls heavily on newborn infants, RSV is also a prevalent and currently unaddressed problem in pediatrics. This third market segment for our RSV vaccine candidate remains an important opportunity. In November 2014, we initiated a Phase 1 clinical trial of our RSV F vaccine candidate in 150 healthy children two to six years of age. This trial is designed to evaluate the safety and immunogenicity of our RSV F vaccine candidate in children. The data from this trial are expected in late 2015 or in the first half of 2016 and will inform the next steps in the development of our RSV pediatric program.
Influenza
Influenza is a world-wide infectious disease that causes illness in humans with symptoms ranging from mild to life-threatening; serious illness occurs not only in susceptible populations such as pediatrics and the elderly, but also in the general population when unique strains of influenza arise, for which most humans have not developed protective antibodies. Influenza is a major burden on public health worldwide; estimates of one million deaths each year are attributed to influenza.6 It is further estimated that, each year, influenza attacks 5%-10% of adults and 20%-30% of children, causing significant levels of illness, hospitalization and death.7
Although a number of licensed seasonal influenza vaccines are currently commercially available in most geographies, and these manufacturers have capabilities to develop influenza vaccines that are responsive to unique and emerging influenza strains, we believe our influenza virus-like particle (“VLP”) vaccine candidates have immunological advantages over currently available vaccines. These advantages stem from the fact that our influenza VLPs contain three of the major structural virus proteins that are important for fighting influenza: hemagglutinin (“HA”) and neuraminidase (“NA”), both of which stimulate the body to produce antibodies that neutralize the influenza virus and prevent its spread through the cells in the respiratory tract, and the matrix 1 protein (“M1”), which stimulates cytotoxic T lymphocytes to kill cells that may already be infected. Our VLPs are not made from live viruses and have no influenza genetic nucleic material in their inner core, which render them incapable of replicating and causing the disease.
Seasonal Quadrivalent Influenza Vaccine
Developing and commercializing a seasonal influenza vaccine is an important business opportunity and strategic goal for Novavax. The Advisory Committee for Immunization Practices of the Center for Disease Control and Prevention (“CDC”) recommends that all persons aged six months and older should be vaccinated annually against seasonal influenza. In conjunction with these universal recommendations, attention from the 2009 influenza H1N1 pandemic, along with reports of cases of avian-based influenza strains, has increased public health awareness of the importance of seasonal influenza vaccination, the market for which is expected to continue to grow worldwide in both developed and developing global markets.
In recent years, trivalent influenza vaccines (three influenza strains: two influenza A strains and one influenza B strain) have been made generally available on a worldwide basis. With two distinct lineages of influenza B viruses circulating, public health authorities have advocated for the addition of a second influenza B strain to provide additional protection. Vaccine manufacturers have responded through the development and licensure of quadrivalent (i.e., four influenza strains: two influenza A strains and two influenza B strains) influenza vaccines. It is expected that quadrivalent seasonal influenza vaccines will ultimately replace trivalent seasonal influenza vaccines in the global market. There are currently four quadrivalent influenza vaccines licensed in the U.S., although additional quadrivalent seasonal influenza vaccines are expected to be licensed over the next several years. Current estimates for seasonal influenza vaccine growth in the top seven markets (U.S., Japan, France, Germany, Italy, Spain and UK), show potential growth from approximately $3.2 billion in the 2012/13 season to $5.3 billion by the 2021/2022 season.8 Recombinant seasonal influenza vaccines, like the candidate we are developing, have an important advantage: once licensed for commercial sale, large quantities of vaccines can be quickly and cost-effectively manufactured without the use of either the live influenza virus or eggs.
6 Resolution of the World Health Assembly. Prevention and control of influenza pandemics and annual epidemics. WHA56.19. 28 May 2003
7 WHO. Vaccines against influenza. WHO position paper – November 2012 Weekly Epidemiol Record 2012;87(47):461–76.
8 Influenza Vaccines Forecasts. Datamonitor (2013)
| 4 |
In November 2014, under our contract with HHS-BARDA, we initiated a Phase 2 clinical trial of our quadrivalent seasonal influenza VLP vaccine candidate in 400 healthy adults. The primary outcomes of the trial will assess safety and tolerability of the seasonal influenza VLP vaccine candidate and quantify immune responses to each of the four influenza strains based on hemagglutination-inhibiting antibody titers. In addition, secondary outcomes will evaluate neuraminidase-inhibition antibody titers for all four influenza strains. The preliminary data from this trial are expected in the second quarter of 2015 and will inform the next steps in the development of our quadrivalent seasonal influenza VLP vaccine candidate. Data from our previous Phase 2 clinical trial, announced in July 2012, showed that our quadrivalent seasonal influenza VLP vaccine candidate demonstrated immunogenicity against all four viral strains based on hemagglutination inhibition responses at day 21, was well-tolerated, and met the FDA accelerated approval seroprotection rates criterion for all four viral strains, although the potential to fulfill the seroconversion rates criterion was demonstrated in just three of the four viral strains. Following that Phase 2 clinical trial, we focused our activities on manufacturing processes that will better ensure consistent, enhanced immune responses for all four strains.
Pandemic H7N9 Influenza Vaccine
In the aftermath of the 2009 pandemic of the A(H1N1) influenza strain, prevention of the potential devastation of a human influenza pandemic remains a key priority with both governmental health authorities and influenza vaccine manufacturers. In the U.S. alone, the 2009 H1N1 influenza pandemic led to the production of approximately 126 million doses of monovalent (single strain) vaccine. Public health awareness and government preparedness for the next potential influenza pandemic are driving development of vaccines that can be manufactured quickly against a potentially threatening influenza strain. Until the spring of 2013, industry and health experts focused attention on developing a monovalent H5N1 influenza vaccine as a potential key defense against a future pandemic threat; however, a significant number of reported cases in China of an avian-based influenza strain, known as A(H7N9), has shifted attention to the potential development of a monovalent H7N9 influenza vaccine.
In collaboration with HHS BARDA, we have now developed and delivered compelling safety and immunogenicity data on two pandemic vaccine candidates, H5N1 and H7N9, which provide the U.S. government with alternatives for dealing with future potential threats. In September 2014, we announced positive results from a Phase 1/2 clinical trial of our pandemic H7N9 influenza VLP vaccine candidate adjuvanted with Matrix-M in 610 healthy adults. Under our contract with HHS BARDA, the Phase 1/2 clinical trial was designed as a dose-ranging, randomized, observer-blinded, placebo-controlled clinical trial, to determine the contribution of Matrix-M to potential antigen dose sparing regimens. Our pandemic H7N9 influenza VLP vaccine candidate, with and without Matrix-M, was well tolerated and demonstrated a safety profile similar to the company’s prior experience with another saponin-based adjuvant. Matrix-M adjuvanted formulations demonstrated immunogenicity and dose-sparing benefits relative to unadjuvanted antigen. Hemagglutination-inhibiting antibody titers were generally comparable to those reported in prior studies with another saponin adjuvant and the vaccine also elicited significant anti-neuraminidase antibodies. In October 2014, we announced that the FDA had granted Fast Track Designation to our pandemic H7N9 influenza VLP vaccine candidate with Matrix-M.
Potential Accelerated Approval Pathway for Influenza
In the past, we have referenced attainment of accelerated approval immunogenicity endpoints for seroprotection and seroconversion as a potential pathway for licensure of our influenza vaccines. The criteria for granting such accelerated approval of a BLA, the biologic equivalent to a New Drug Application or “NDA,” for new seasonal and pandemic influenza vaccines was published by the FDA. Under FDA guidance, developers that can demonstrate results that meet or exceed certain specified immunogenicity endpoint criteria in their clinical trials may, at the FDA’s discretion, be granted a license to market a product prior to submission of traditional clinical endpoint efficacy trial data. It should be noted that FDA licensure based on accelerated approval nevertheless requires sponsors to conduct a post-licensure efficacy study to demonstrate the clinical benefit of the vaccine, which would thereby support traditional approval of the vaccine. Because it is not possible to conduct a clinical endpoint efficacy study for a pandemic vaccine in advance of a declared pandemic, FDA’s pandemic guidance allows for submission of seasonal influenza clinical efficacy data for the purpose of confirming clinical benefit of a pandemic vaccine manufactured by the same process. Thus, the demonstration of efficacy with a seasonal vaccine provides a key link between the seasonal and pandemic programs. Accelerated approval further necessitates a shortage of influenza vaccine relative to the total population recommended to receive such vaccine, a situation that persists with seasonal influenza vaccines.
| 5 |
Although we have not ruled out this accelerated approval approach, particularly for our pandemic influenza program or certain populations within our seasonal influenza program, we do not expect to pursue accelerated approval of our quadrivalent seasonal influenza VLP vaccine candidate, largely because of the uncertainty as to whether the accelerated approval pathway will be available to us at the time of our BLA submissions and the unknown ability of current and new influenza strains to meet such accelerated approval criteria. We are planning, therefore, to pursue traditional licensure of our quadrivalent seasonal influenza VLP vaccine candidate by conducting a clinical endpoint efficacy study for the purpose of submitting the data within the original BLA. These efficacy data will also support the requirement for clinical efficacy data for our pandemic influenza program. We plan to discuss with the FDA our licensure pathways (both the traditional pathway for seasonal and possible accelerated pathways for pandemic and certain populations within the seasonal influenza program) during future formal meetings. The likely impact of such an efficacy trial would be an additional year or more before the FDA grants licensure to our quadrivalent seasonal influenza VLP vaccine candidate.
HHS BARDA Contract for Recombinant Influenza Vaccines
HHS BARDA awarded us a contract in 2011 that funds the development of both our multivalent seasonal influenza and monovalent pandemic influenza VLP vaccine candidates. Our contract with HHS BARDA is a cost-plus-fixed-fee contract, which reimburses us for allowable direct contract costs incurred plus allowable indirect costs and a fixed-fee earned in the ongoing clinical development and product scale-up of our multivalent seasonal and monovalent pandemic influenza vaccines. In September 2014, we announced that HHS BARDA had exercised and initiated a two-year option to our contract, which not only extended the contract until September 2016, but also added scope to support our development activities leading up to planned Phase 3 clinical studies and $70 million of funding on top of the remainder of the $97 million base period funding. During 2014, we recognized revenue of $26.0 million and have recognized approximately $78 million in revenue since the inception of the contract.
Ebola virus (EBOV)
Recent news reports have centered around EBOV, formerly known as Ebola hemorrhagic fever, which is a severe, often fatal illness in humans. Multiple strains of EBOV have been identified, the most recent of which, the 2014 Makona strain (previously referred to as the Guinea strain), is associated with a case fatality rate of between 50% and 90%. There are currently no licensed treatments proven to neutralize the virus, but a range of blood, immunological and drug therapies are under development. It should be noted, however, that recent vaccine approaches target either a previous strain of the virus or were initially developed to be delivered by genetic vectors. Our EBOV glycoprotein (GP) vaccine candidate, which was modeled using the 2014 Makona strain, has been successfully tested in rodent, rabbit, and non-human primate pre-clinical models. We have also tested the vaccine with our Matrix-M adjuvant, which appears to significantly contribute to enhanced immunogenicity and dose-sparing.
We initiated production under good manufacturing practices (“GMP”) of our EBOV GP vaccine in the fourth quarter of 2014 and in February 2015, we announced the initiation of enrollment in a Phase 1 clinical trial of our EBOV GP vaccine candidate in 150 healthy adults to evaluate the safety and immunogenicity of this vaccine candidate in ascending doses, with and without our Matrix-M adjuvant. We expect preliminary data from this trial to be available in mid-2015. In addition, we announced successful preliminary data from a non-human primate challenge study of our EBOV GP vaccine candidate in which the challenge was lethal for the control animal, whereas 100% of the immunized animals were protected. Plans for the subsequent clinical trial(s) will be developed based on the results of our Phase 1 clinical trial and in collaboration with global regulatory authorities and world health agencies.
Combination Respiratory (Influenza and RSV)
Given the ongoing development of our quadrivalent seasonal influenza VLP vaccine candidate and our RSV F vaccine candidate, we see an important opportunity to develop a combination respiratory vaccine candidate. This opportunity presents itself most evidently in the elderly, although we have not ruled out developing a combination respiratory vaccine for the non-elderly. Early pre-clinical development efforts have given us confidence that such a combination vaccine is viable and in animal models, provides acceptable immunogenicity. We intend to explore this development opportunity by conducting a Phase 1 clinical trial in such a combination vaccine in 2015.
| 6 |
CPLB Programs (India)
Seasonal Influenza
CPLB completed enrollment of an on-going Phase 3 clinical trial of its seasonal influenza VLP vaccine candidate in the second half of 2014. Assuming positive safety and immunogenicity data from this Phase 3 clinical trial, CPLB would expect to seek regulatory market authorization, the Indian equivalent of a BLA, for its seasonal influenza VLP vaccine candidate.
Rabies
CPLB is developing a rabies G protein vaccine candidate that we genetically engineered and completed enrollment of an ongoing Phase 1/2 clinical trial in India in 2014. The objective is to develop a recombinant vaccine that can be administered both as a pre-exposure prophylaxis for residents of certain higher-risk geographies and travelers to such locations, and as a post-exposure prophylaxis using fewer doses than the current standard of care. In October 2014, CPLB presented clinical results from Stage I of the Phase 1/2 clinical trial, demonstrating that all vaccine recipients, at various doses levels and schedules, showed seroprotective antibody levels at day 14 that were sustained through day 180. The vaccine candidate, which was found to be safe and well-tolerated, also induced seroprotective levels with two-dose and three-dose regimens. Assuming positive clinical data from Stage II of the Phase 1/2 clinical trial, CPLB would plan to initiate a Phase 3 clinical trial.
Discovery Programs
Our vaccine platform technology provides an efficient system to rapidly develop antigens to selected targets, refine manufacturing processes and optimize development across multiple vaccine candidates. We pay close attention to global reports of emerging diseases for which there do not appear to be immediate cures and where a vaccine protocol could offer potential protection. In addition to our response to the A(H7N9) influenza strain (as previously discussed), we have been monitoring reports concerning MERS, a novel coronavirus first identified in September 2012 by an Egyptian virologist. MERS became an emerging threat in 2013, with the WHO currently reporting more than 850 confirmed cases of infection and more than 350 deaths. The MERS virus is a part of the coronavirus family that includes the severe acute respiratory syndrome coronavirus (“SARS”). Because of the public health priority given to MERS, within weeks of getting the virus’ sequence, we successfully produced a vaccine candidate designed to provide protection against MERS. This vaccine candidate, which was made using our recombinant nanoparticle vaccine technology, is based on the major surface spike protein, which we had earlier identified as the antigen of choice in our work with a SARS vaccine candidate. In April 2014, in collaboration with the University of Maryland, School of Medicine, we published results that showed our investigational vaccine candidates against both MERS and SARS blocked infection in laboratory studies. Although the development of a MERS vaccine candidate currently remains a pre-clinical program, we believe that our MERS vaccine candidate offers a viable option to interested global public health authorities.
Vaccine Platform Technologies
We believe that our platform technology offers time-saving advantages both in terms of production time against traditional egg-based vaccine manufacturing, and in terms of establishing a vaccine production facility (either as a new green-field project or through a retrofit of an existing facility). For example, currently approved influenza vaccines are typically produced by growing virus in chicken eggs, from which the virus is extracted and further processed. This 50-year-old egg-based production method requires four to six months of lead time for production of a new strain of virus and significant investment in fixed production facilities. Moreover, there can be additional delays because manufacturers must modify the selected influenza virus strain in order for it to be produced efficiently in the egg. The vaccine shortage during the 2004 influenza season (caused in part by a contamination issue at a facility in the United Kingdom) highlighted the limitations of current production methods and the need for increased vaccine manufacturing capacity. It also heightened concerns regarding manufacturers’ capacity to respond to a pandemic, when the number of vaccine doses required will be higher than the number required for seasonal influenza vaccines and manufacturing lead times will be even shorter. This concern was borne out again in the 2009 H1N1 influenza pandemic as, “despite an intensive effort to develop a pandemic vaccine, the 2009 H1N1 vaccine arrived too late to have a significant effect on the dynamics of the fall disease wave.”9 Compared with traditional vaccine production, we believe our processes allow for faster production of vaccine. Because our process uses genetic information and not the virus itself, we can quickly construct clones of the virus as soon as the genetic information is available. This factor alone can shorten the time for creating new vaccine by several weeks compared to traditional vaccine manufacturing.
| 7 |
Importantly, we also believe that a manufacturing facility that produces our vaccines can be implemented and validated in significantly less time than traditional cell-based vaccine manufacturing facilities and without the costly containment features associated with handling live viruses. We produce our vaccine candidates using a baculovirus expression system in insect cells with lower-cost equipment that can be readily deployed both nationally and internationally. By not requiring significant production batch sizes, production capacity can be employed quickly. We estimate the time to qualify a facility that utilizes our processes can be months faster than a fixed-pipe bioreactor facility used in cell-based manufacturing.
Virus-Like Particles (VLPs)
Our VLP vaccine technology platform is based on protein structures that visually resemble viruses. However, these are non-infectious particles that, for many viral diseases, have been shown in animal studies and clinical trials to make effective vaccines. VLPs closely mimic natural virus particles with repeating protein structures that can elicit broad and strong antibody and cellular immune responses, but lack the genetic material required for replication. VLP technology is a proven technology that is employed in currently marketed products. Our proprietary VLPs include multiple proteins and lipids that can be tailored to induce robust and broad immune responses similar to natural infections. Our advanced VLP technology has the potential to develop vaccines for a wide range of human infectious diseases where there are significant unmet medical needs, some of which have not been addressed by other technologies. We have used formal criteria based upon medical need, technical feasibility and commercial value to select vaccine candidates for development.
We believe that our influenza vaccines are designed to address many of the significant unmet needs related to seasonal and pandemic influenza. There are several points of differentiation of our influenza vaccines when compared to traditional egg-based, or new mammalian-based approaches that form the basis to address unmet medical needs and capitalize on commercial opportunities. Our influenza VLPs contain components that provide a broad and robust immune response. Specifically, the VLPs contain the viral components HA, NA and M1. Traditional egg-based vaccines contain meaningful levels of HA, but not of NA or M1. The HA sequence in our VLPs is the same as in the wild-type virus and could prove to be more effective or immunogenic than influenza vaccines produced using egg or mammalian cell-lines, which alter HA. In addition, the NA and M1 in our VLPs may play a role in reducing the severity of the disease by inducing antibody responses and cell mediated immunity. NA and M1 are both highly conserved, and immunity to these viral components may help provide additional protection throughout an entire influenza season, even as strains mutate. Data from our seasonal influenza Phase 2a clinical trial in healthy adults showed that 50% to 73% of the volunteers immunized with our VLP vaccine had a four-fold increase in the antibody that blocks NA activity. Finally, because of the VLP structure and components, they may have greater immunogenicity in two vulnerable populations –pediatrics and the elderly.
9 BARDA Strategic Plan 2011-2016 (2010)
| 8 |
Recombinant Protein Nanoparticle Vaccines
Our recombinant protein nanoparticle vaccine technology is based on self-assembling protein structures, which differ from traditional VLPs in that these particles do not generally occur in nature and can be made from key antigenic proteins from pathogenic organisms, including viruses, bacteria, parasites or even cancer cells. Protein nanoparticles closely resemble the natural structure of surface antigens of disease organisms, but lack the genetic material required for replication and therefore are not infectious. An advantage of this technology is that the formation of nanoparticles is done in vitro thereby making it possible to assemble nanoparticles from one or more highly purified proteins. This results in high purity vaccines with certain manufacturing advantages over more traditional products. Potential immunological advantages of protein nanoparticle vaccines are presentation of epitopes (antibody binding sites) in a more native configuration for improved efficacy, efficient recognition by the immune system’s antigen presenting cells (“APCs”) and triggering robust immune responses. Recognition of the nanoparticle vaccine’s repeating protein patterns by the APCs toll-like receptors to stimulate innate immunity and the high purity and lack of synthetic material adds to the potential safety of recombinant nanoparticle vaccines. Protein nanoparticle vaccine technology has expanded our early-stage vaccines in development to include both virus and non-virus disease targets. Our most advanced protein nanoparticle vaccine candidate is our RSV F vaccine candidate, which is manufactured from highly purified F protein.
Matrix Adjuvants
Adjuvants are mostly used as an additional component in various vaccines in order to enable the vaccine to induce a strong immune response for protection against microbial infections. Novavax AB has developed a number of adjuvant formulations, all based on our proprietary Matrix™ technology. These adjuvant formulations possess excellent immunostimulatory features with the ability to increase and prolong the protective benefits of vaccines. Our research and development over the years have resulted in a range of high-quality products on both the human vaccine and international veterinary vaccine markets.
The goals of our adjuvant technology are strong antibody and cell-mediated immune responses induced by low antigen doses, long-duration immune responses, with low risk for allergic reactions or other adverse events. We believe these qualities give our Matrix adjuvants a number of important advantages over many other types of adjuvants, where novel, less well-characterized substances are often hampered by safety concerns or limited efficacy. Our Matrix-M adjuvant provides a potent adjuvant effect that has been well tolerated in clinical trials. We also believe that the strong immune response and opportunity to reduce the quantity of antigen dose can significantly reduce the production cost of our vaccines. This means that our Matrix-M adjuvant has the potential to be of immense value when there is inadequate vaccine manufacturing capacity during an emerging threat such as an influenza pandemic.
Competition in RSV, Influenza and Ebola Vaccines
The biopharmaceutical industry and the vaccine market are intensely competitive and are characterized by rapid technological progress. Our technology is based upon utilizing the baculovirus expression system in insect cells to make VLPs and protein nanoparticle vaccines. We believe this system offers many advantages when compared to other technologies and is uniquely suited for developing an RSV vaccine, seasonal and pandemic influenza vaccines, as well as vaccines against other infectious diseases.
There is currently no approved RSV vaccine for sale in the world; however, a number of vaccine manufacturers, academic institutions and other organizations currently have, or have had, programs to develop such a vaccine. In addition, many other companies are developing products to prevent disease caused by RSV using a variety of technology platforms, including various viral vector technologies and competitive VLP technologies. We believe that our RSV vaccine candidates, utilizing recombinant F-protein antigens, are more effective than RSV vaccine candidates in development by our competitors; however, such efficaciousness cannot be guaranteed. Although we are not aware of all our competitors’ efforts, we believe that MedImmune LLC, a subsidiary of AstraZeneca PLC, may have the second most advanced RSV vaccine program after Novavax, as it has reported testing in Phase 1 and Phase 1/2 clinical trials, in an intranasal, recombinant, live attenuated, RSV vaccine for the prevention of lower respiratory tract disease caused by RSV, as well as a combination intranasal vaccine for the prevention of several infant respiratory illnesses, including RSV. Additional entities have also entered into early clinical trials including GlaxoSmithKline and the National Institute of Allergy and Infectious Diseases, an institute under the U.S. National Institutes of Health.
Unlike the comparatively low amount of competition developing RSV vaccines, there are a number of companies developing and selling vaccines for seasonal and pandemic influenza employing historic vaccine technology, as well as new technologies. The table below provides a list of major vaccine competitors and corresponding licensed influenza vaccine technologies.
| 9 |
| Company | Competing Technology Description | |
| Sanofi Pasteur, SA | Inactivated sub-unit (egg-based) | |
| MedImmune, LLC (a subsidiary of AstraZeneca PLC) | Nasal, live attenuated (egg-based) | |
| GlaxoSmithKline plc | Inactivated split-vaccine (egg-based) | |
| CSL Ltd (formerly Novartis, Inc.) | Inactivated sub-unit (cell and egg-based) | |
| Protein Sciences Corporation | Recombinant HA trivalent (insect cell-based) |
There are many seasonal influenza vaccines currently approved and marketed, and most of these are marketed by major pharmaceutical companies that have significantly greater financial and technical resources, experience and expertise than we have. Competition in the sale of these seasonal influenza vaccines is intense. Therefore, newly developed and approved products must be differentiated from existing vaccines in order to have commercial success. In order to show differentiation in the seasonal influenza market, a product should be more efficacious and/or be less expensive and quicker to manufacture. Many of our competitors are working on new products and new generations of current products, some by adding an adjuvant that is used to increase the immunogenicity of that product, each of which is intended to be more efficacious than currently marketed products. Another differentiating factor is recombinant manufacturing, which we believe can be quicker and less-expensive than traditional egg-based manufacturing. The FDA approved the first recombinant seasonal influenza vaccine called “Flublok” manufactured by Protein Sciences Corporation in 2013.
Despite the significant competition and advancing technologies, some of which are similar to our own, we believe that our seasonal influenza product will be as efficacious as, or more so than, current products or products being developed by our competitors, and that our manufacturing system provides savings in both time and money; however, there can be no guarantee that our seasonal influenza vaccine will prove to be efficacious or that our manufacturing system will prove to be sufficiently effective and differentiated to ensure commercial success.
Vaccine candidates against Ebola virus have been in development for more than a decade; however, with the recent epidemic in West Africa, focus on viable vaccine candidates has intensified. In addition to the Phase 1 clinical trial that we recently initiated in February 2015, WHO reports two other vaccine candidates that are currently being tested in humans: one by GlaxoSmithKline in collaboration with the United States National Institute of Allergy and Infectious Diseases, and the other by a collaboration of NewLink Genetics, Merck Vaccines USA and the Public Health Agency of Canada. While these other vaccine candidates offer promise, we believe there are accompanying challenges, including: high-dose level requirements; utilization of glycoprotein from older strains that have a significant number of amino acid changes when compared to the 2014 Makona strain; difficult storage requirements at temperatures below –60°C; and difficulties associated with immune response to the viral vectors which could limit their multi-dose vaccine potential. In contrast, we have developed a Phase 1 vaccine candidate that has performed well with low doses utilizing our Matrix-M adjuvant; was derived from the 2014 Makona strain; appears to be stable at 2–8°C; and appears to provide enhanced immunogenicity as a multi-dose vaccine.
In general, competition among pharmaceutical products is based in part on product efficacy, safety, reliability, availability, price and patent position. An important factor is the relative timing of the market introduction of our products and our competitors’ products. Accordingly, the speed with which we can develop products, complete the clinical trials and approval processes and supply commercial quantities of the products to the market is an important competitive factor. Our competitive position also depends upon our ability to show differentiation with a product that is more efficacious, particularly in the relevant target populations and/or be less expensive and quicker to manufacture. It also depends upon our ability to attract and retain qualified personnel, obtain patent protection or otherwise develop proprietary products or processes and secure sufficient capital resources for the often substantial period between technological conception and commercial sale.
Patents and Proprietary Rights
We generally seek patent protection for our technology and product candidates in the U.S. and abroad. The patent position of biopharmaceutical firms generally is highly uncertain and involves complex legal and factual questions. Our success will depend, in part, on whether we can:
| 10 |
| · | obtain patents to protect our own technologies and product candidates; |
| · | obtain licenses to use the technologies of third-parties, which may be protected by patents; |
| · | protect our trade secrets and know-how; and |
| · | operate without infringing the intellectual property and proprietary rights of others. |
Patent rights; licenses. We have intellectual property (patents, licenses, know-how) related to our vaccines, manufacturing process and other technologies. Currently, we have or have rights to over 100 U.S. patents and corresponding foreign patents and patent applications relating to vaccines and biologics. Our core vaccine-related intellectual property extends beyond the year 2025.
In 2007, we entered into a non-exclusive license agreement with Wyeth Holdings Corporation, a subsidiary of Pfizer Inc. (Wyeth), to obtain rights to a family of patents and patent applications covering VLP technology for use in human vaccines in certain fields, with expected patent expiration in early 2022.
In July 2010, U.S. Patent No. 7,763,450 for Functional Influenza Virus-Like Particles was issued by the U.S. Patent & Trademark Office. The patent covers, in part, the use of influenza gene sequences for high-yield production of consistent influenza VLP vaccines to protect against current and future seasonal and pandemic strains of influenza viruses. In December 2011, European Patent No. 1644037 was issued by the European Patent Office covering this technology.
In December 2011, U.S. Patent No. 8,080,255 for Functional Influenza Virus-Like Particles was issued by the U.S. Patent & Trademark Office. The patent covers, in part, methods of inducing substantial immunity to an influenza virus infection in a human and administering to the human a VLP comprising M1, HA and NA proteins. The M1 protein is derived from a particular avian influenza strain, A/Indonesia/5/05.
In April 2013, European Patent No. 2343084 for Functional Influenza Virus-Like Particles was issued by the European Patent Office. The patent covers, in part, vaccine compositions containing VLPs that contain M1, HA, and NA proteins. The VLPs are self-assembled from host cells.
In August 2013, U.S Patent No. 8,506,967 for Functional Influenza Virus-Like Particles was issued by the U.S. Patent & Trademark Office. The patent covers, in part, methods of inducing substantial immunity to an influenza virus infection in a human and administering to the human a VLP comprising M1, HA and NA proteins. The M1 protein is from an avian influenza M1 protein from a different strain of influenza virus than the influenza HA protein and the influenza NA protein.
In October 2013, U.S Patent No. 8,551,756 for Avian influenza chimeric VLPs was issued by the U.S. Patent & Trademark Office. The patent covers, in part, methods of increasing the efficiency of VLP production using M1 proteins derived from strain A/Indonesia/5/05.
In November 2013, U.S Patent No. 8,592,197 for Functional Influenza Virus-Like Particles was issued by the U.S. Patent & Trademark Office. The patent covers, in part, influenza VLP vaccines containing M1, HA, and NA proteins where the M1 protein is from a different stain than the HA and NA proteins.
In April 2014, U.S Patent No. 8,697,088 for Novel VLPs Derived From Cells That do not Express a Viral Matrix or Core Protein was issued by the U.S. Patent & Trademark Office. The patent covers, in part, methods of making influenza VLP that contain HA and NA proteins but lack any viral matrix or core protein.
In May 2014, U.S Patent No. 8,715,692 for Modified RSV F Proteins and Methods of Their Use was issued by the U.S. Patent & Trademark Office. The patent covers, in part, RSV F vaccines.
In February 2015, U.S Patent No. 8,951,537 for Functional Influenza Virus-Like Particles (VLPS) was issued by the U.S. Patent & Trademark Office. The patent covers, in part, methods of making influenza VLP vaccines that contain M1 from a particular influenza strain and HA and NA proteins from a different strain.
| 11 |
The Federal Technology Transfer Act of 1986 and related statutory guidance encourages the dissemination of science and technology innovation. While our recent contract with HHS BARDA provides us with the right to retain ownership in our inventions that may arise during performance of that contract, with respect to certain other collaborative research efforts with the U.S. government, certain developments and results that may have commercial potential are to be freely published, not treated as confidential and we may be required to negotiate a license to developments and results in order to commercialize products. There can be no assurance that we will be able to successfully obtain any such license at a reasonable cost, or that such development and results will not be made available to our competitors on an exclusive or non-exclusive basis.
Trade secrets. To a more limited extent, we rely on trade secret protection and confidentiality agreements to protect our interests. It is our policy to require employees, consultants, contractors, manufacturers, collaborators and other advisors to execute confidentiality agreements upon the commencement of employment, consulting or collaborative relationships with us. We also require confidentiality agreements from any entity that is to receive confidential information from us. With respect to employees, consultants and contractors, the agreements generally provide that all inventions made by the individual while rendering services to us shall be assigned to us as our property.
Government Regulations
The development, production and marketing of biological products, which included the vaccine candidates being developed by Novavax or our collaborators, are subject to regulation for safety, efficacy and quality by numerous governmental authorities in the U.S. and other countries. As a U.S. based company, we focus on the U.S. regulatory process and the standards imposed by the FDA, International Conference on Harmonisation (ICH) and other agencies because we believe, for the most part, meeting U.S. and ICH standards will allow us to satisfy regulatory agencies in other countries where we intend to do business. We are aware that expectations in some venues, notably in the European Union, differ to some degree and we are taking proactive steps to address such differences. In the U.S., the development, manufacturing and marketing of human pharmaceuticals and vaccines are subject to extensive regulation under the Federal Food, Drug, and Cosmetic Act, and biological products are subject to regulation under provisions of that Act and the Public Health Service Act. The FDA not only assesses the safety and efficacy of these products but it also regulates, among other things, the testing, manufacture, labeling, storage, record-keeping, advertising and promotion of such products. The process of obtaining FDA licensure for a new vaccine is costly and time-consuming.
Vaccine clinical development follows the same general regulatory pathway as drugs and other biologics. Before applying for FDA licensure to market any new vaccine candidate, we must first submit an investigational new drug application (“IND”) that explains to the FDA, among other things, the results of pre-clinical testing conducted in laboratory animals, the method of manufacture, quality control tests for release and what we propose to do for human testing. At this stage, the FDA decides whether it is reasonably safe to move forward with testing the vaccine in humans. We must then conduct Phase 1 clinical trials and larger-scale Phase 2 and 3 clinical trials that demonstrate the safety and efficacy of our vaccine candidate to the satisfaction of the FDA. Once these trials are complete, a BLA can be submitted to the FDA requesting licensure of the vaccine for marketing based on the vaccine’s safety and efficacy.
During the FDA’s review of a BLA, the proposed manufacturing facility undergoes a pre-approval inspection during which the FDA examines in detail the production of the vaccine as it is in progress. Vaccine licensure also requires the provision of adequate product labeling to allow health care providers to understand the vaccine’s proper use, including its potential benefits and risks, to communicate with patients and parents, and to safely deliver the vaccine to the public. Until a vaccine is given to the general population, all potential adverse events cannot be anticipated. Thus, the FDA may require Phase 4 post-marketing clinical trials for vaccines after licensure to continue gathering safety, and sometimes effectiveness/efficacy data in the indicated and additional populations.
In order to ensure continuing safety, the FDA continues to oversee the production of vaccines even after the vaccine and manufacturing processes are approved. For example, monitoring of the vaccine and of production activities, including periodic facility inspections, must continue as long as the manufacturer holds a license for the product. Manufacturers may also be required to submit to the FDA the results of their own tests for potency, safety and purity for each vaccine lot, if requested by the FDA. They may also be required to submit samples of each vaccine lot to the FDA for testing.
| 12 |
In addition to obtaining FDA licensure for each product, each domestic manufacturing establishment must be registered with the FDA, is subject to FDA inspection and must comply with GMP regulations. To supply products for use either in the U.S. or outside the U.S., including clinical trials, U.S. and foreign manufacturing establishments, including third-party facilities, must comply with GMP regulations and are subject to periodic inspection by the FDA or by corresponding regulatory agencies in their home country.
The development process for a biological product, such as a vaccine, typically takes a long period of time to complete. Pre-clinical studies may take several years to complete and there is no guarantee that the FDA will permit an IND to become effective and allow the investigational product to advance to clinical testing. Clinical trials may take several years to complete. After the completion of the required phases of clinical trials, if the data indicate that the vaccine is safe and effective, a BLA is submitted to the FDA to approve the marketing and commercial shipment of the vaccine. This process takes substantial time and effort and the FDA may not accept the BLA for filing. Even if accepted, the FDA might not grant licensure. The FDA license process may take up to two years and may take longer if substantial questions about the submission arise. The FDA may require post-marketing testing and surveillance to monitor the safety of the applicable products.
In 1992, the FDA instituted regulations that allow approval of certain products that treat serious or life-threatening illnesses and provide meaningful therapeutic benefit over existing treatments based on a surrogate endpoint, versus a clinical outcome, which can take many more years to demonstrate. Surrogate endpoints, generally a laboratory measurement or other physical sign shown to have some correlation with clinical benefit, can considerably shorten the time development time leading up to FDA licensure. The FDA bases its decision on whether to accept a proposed surrogate endpoint on the scientific support for that endpoint. The company developing the product is required to conduct further studies to confirm it’s the clinical benefit in Phase 4 confirmatory efficacy trials. We plan to seek traditional approval for our quadrivalent seasonal influenza vaccine, but have not ruled out the potential use of accelerated approval for specific populations and for our pandemic influenza vaccine candidates.
In addition to regulatory approvals that must be obtained in the U.S., an investigational product is also subject to regulatory approval in other countries in which it is intended to be marketed. No such product can be marketed in a country until the regulatory authorities of that country have approved an appropriate marketing application. FDA licensure does not assure approval by other regulatory authorities. In addition, in many countries, the government is involved in the pricing of the product. In such cases, the pricing review period often begins after market approval is granted.
We are also subject to regulation under the Occupational Safety and Health Act, the Environmental Protection Act, the Toxic Substances Control Act, the Resource Conservation and Recovery Act and other present and potential federal, state or local regulations, including national and local regulations that govern our facility in Sweden. These and other laws govern our use, handling and disposal of various biological and chemical substances used in, and waste generated by our operations. Our research and development involves the controlled use of hazardous materials, chemicals and viruses. Although we believe that our safety procedures for handling and disposing of such materials comply with the standards prescribed by state and federal regulations, the risk of accidental contamination or injury from these materials cannot be completely eliminated. In the event of such an accident, we could be held liable for any damages that result and any such liability could exceed our resources. Additionally, for formulations containing controlled substances, we are subject to Drug Enforcement Act regulations.
There have been a number of federal and state legislative changes made over the last few years regarding the pricing of pharmaceutical and biological products, government control and other changes to the healthcare system of the U.S. It is uncertain how such legislative changes will be adopted or what actions federal, state or private payers for medical goods and services may take in response to such legislation. We cannot predict the effect such healthcare changes will have on our business, and no assurance can be given that any such reforms will not have a material adverse effect.
Manufacturing
Our primary manufacturing facility is located at our corporate headquarters at 20 Firstfield Road in Gaithersburg, Maryland. The facility is our late-stage clinical and commercial-scale manufacturing facility for production of our vaccines. The facility has 53,000 square feet of combined GMP manufacturing, laboratory and office space. Our Rockville, Maryland facility houses our 10,000 square foot GMP pilot manufacturing facility that produces clinical trial material. Novavax AB, located in Uppsala, Sweden, produces our Matrix adjuvants in an approximately 15,000 square foot facility comprised of GMP manufacturing, laboratory and office space.
| 13 |
Sources of Supply
Most of the raw materials and other supplies required in our business are generally available from various vendors in quantities adequate to meet our needs. In some cases, we have only qualified one vendor for certain of our manufacturing components. Prior to the initiation of commercial production, we plan, where feasible, to qualify multiple vendors of critical raw materials. One key vendor is GE Healthcare Company (“GEHC”), which supplies disposable components, resins, media and buffers used in our manufacturing process. GEHC and other vendors that supply our key manufacturing materials are or will be audited for compliance with GMP standards.
An important component of our Matrix adjuvant technology is extracted from a species of soap-bark tree (Quillaja saponaria) that grows mainly in Chile, and while we have been able to acquire quillaja extract as needed from our current suppliers, we are focused on establishing appropriate alternative supply arrangements for high-quality quillaja extract.
Business Development
We believe our proprietary vaccine technology affords us a range of traditional and non-traditional commercialization options that are broader than those of existing vaccine companies. We strive to create sustainable value by working to obtain non-dilutive funding, similar to our agreements with HHS BARDA or PATH, to fund future trials in our seasonal and pandemic influenza programs and our RSV program, to continue development of our vaccine candidates until such vaccines can be licensed on a regional basis, to retain commercial rights in major markets and generate product sales revenue and, in certain markets, to commercialize our products through partners and other strategic relationships.
In addition to our aforementioned contracts with HHS BARDA and PATH, some examples of our strategic relationships are our collaboration with GEHC, the joint venture we established with Cadila, and a licensing agreement with LG Life Sciences, Ltd. (“LGLS”).
Our relationship with GEHC started in 2007, when we entered a co-marketing agreement for a pandemic influenza vaccine solution for select international countries. More recently, our collaboration uses GEHC’s bioprocessing and manufacturing solutions and design expertise in conjunction with Novavax’ manufacturing platform.
CPLB is owned 20% by us and 80% by Cadila. It was established in 2009 to develop and manufacture certain vaccine candidates, biogeneric products and diagnostic products for the territory of India. CPLB operates a manufacturing facility in India for the production of vaccines and is actively developing a number of vaccine candidates that were genetically engineered by us. CPLB’s seasonal VLP influenza vaccine candidate completed enrollment of its Phase 3 clinical trial in India in 2014, and CPLB’s rabies vaccine candidate began its Phase 1/2 clinical trial in India in 2014.
Employees
As of February 23, 2015, we had 308 full-time employees, of whom 62 hold M.D. or Ph.D. degrees and 72 of whom hold other advanced degrees. Of our total workforce, 251 are engaged primarily in research, development and manufacturing activities and 57 are engaged primarily in executive, business development, finance and accounting, legal and administrative functions. None of our U.S. employees are represented by labor unions or covered by collective bargaining agreements; 29 of our 30 Swedish employees are covered by typical collective bargaining agreements. We consider our relations with our employees to be good.
| 14 |
Availability of Information
Our website address is www.novavax.com. We make available, free of charge and through our website, our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and any amendments to any such reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended, as soon as reasonably practicable after filed with or furnished to the SEC. Further, a copy of this Annual Report on Form 10-K is located at the SEC’s Public Reference Room at 100 F Street, NE, Washington, D.C. 20549. Information on the operation of the Public Reference Room can be obtained by calling the SEC at 1-800-SEC-0330. The SEC maintains an Internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC at www.sec.gov.
We use our website (www.novavax.com) as a means of disclosing material non-public information and for complying with our disclosure obligations under Regulation Fair Disclosure promulgated by the SEC. These disclosures are included on our website (www.novavax.com) in the “Investor Info” or “Newsroom” sections. Accordingly, investors should monitor these portions of our website (www.novavax.com), in addition to following our press releases, SEC filings and public conference calls and webcasts.
We webcast our earnings calls and certain events we participate in or host with members of the investment community on the investor relations section of our website. Additionally, we provide notifications of news or announcements regarding press and earnings releases as part of the investor relations section of our website. The contents of our website are not part of this Annual Report on Form 10-K, or any other report we file with, or furnish to, the SEC.
| 15 |
You should carefully consider the following risk factors in evaluating our business. There are a number of risk factors that could cause our actual results to differ materially from those that are indicated by forward-looking statements. Some of the risks described relate principally to our business and the industry in which we operate. Others relate principally to the securities market and ownership of our common stock. The risks and uncertainties described below are not the only ones facing us. Additional risks and uncertainties that we are unaware of, or that we currently deem immaterial, also may become important factors that affect us. If any of the following risks occur, our business, financial condition or results of operations could be materially and adversely affected. You should also consider the other information included in this Annual Report on Form 10-K.
RISKS RELATED TO OUR BUSINESS AND INDUSTRY
We have a history of losses and our future profitability is uncertain.
Our expenses have exceeded our revenue since our formation in 1987, and our accumulated deficit at December 31, 2014 was $493.1 million. Our revenue for the last three fiscal years was $30.7 million in 2014, $20.9 million in 2013, and $22.1 million in 2012. Prior to 2011, we recorded limited revenue from research contracts, licenses and agreements to provide vaccine candidates, services and technologies. We cannot be certain that we will be successful in entering into strategic alliances or collaborative arrangements with other companies and government agencies that will result in significant revenue to offset our expenses. Our net losses for the last three fiscal years were $82.9 million in 2014, $52.0 million in 2013, and $28.5 million in 2012.
Our recent historical losses have predominantly resulted from research and development expenses for our vaccine candidates, manufacturing-related expenses, costs related to protection of our intellectual property and for other general operating expenses. Our expenses have exceeded our revenue since inception. We believe our expenses will continue to increase, as a result of higher research and development efforts to support the development of our vaccine candidates.
Although certain specified costs associated with the development of our influenza vaccines may be reimbursed under our contract with HHS BARDA, and to a more limited extent, certain outside costs associated with the development of our RSV maternal vaccine may be reimbursed under our contract with PATH, nevertheless we expect to continue to incur significant operating expenses and anticipate that our losses will increase in the foreseeable future as we seek to:
| · | conduct clinical trials for RSV, Ebola and an RSV-influenza combination respiratory vaccine candidate; |
| · | conduct pre-clinical studies for other early-stage vaccine candidates; |
| · | comply with the FDA’s manufacturing facility and compliance requirements; |
| · | invest in our manufacturing process for commercial-scale and cost-efficiency; and |
| · | maintain, expand and protect our intellectual property portfolio. |
As a result, we expect our cumulative operating losses to increase until such time, if ever, that product sales, licensing fees, royalties, milestones, contract research and other sources generate sufficient revenue to fund our operations. We cannot predict when, if ever, we might achieve profitability and cannot be certain that we will be able to sustain profitability, if achieved.
| 16 |
We have limited financial resources and we are not certain that we will be able to maintain our current level of operations or be able to fund the further development of our vaccine candidates.
We do not expect to generate revenue from product sales, licensing fees, royalties, milestones, contract research or other sources in an amount sufficient to fully fund our operations for the foreseeable future, and we will therefore use our cash resources and expect to require additional funds to maintain our operations, continue our research and development programs, commence future pre-clinical studies and clinical trials, seek regulatory approvals and manufacture and market our products. We will seek such additional funds through public or private equity or debt financings, collaborative licensing and development arrangements, non-dilutive government contracts and grants and other sources. While we continue to apply for contracts or grants from academic institutions, non-profits and governmental entities, there are no assurances that we would be successful. We cannot be certain that adequate additional funding will be available to us on acceptable terms, if at all. If we cannot raise the additional funds required for our anticipated operations, we may be required to delay significantly, reduce the scope of or eliminate one or more of our research or development programs, downsize our general and administrative infrastructure, or seek alternative measures to avoid insolvency, including arrangements with collaborative partners or others that may require us to relinquish rights to certain of our technologies or vaccine candidates. If we raise additional funds through future offerings of shares of our common stock or other securities, such offerings would cause dilution of current stockholders’ percentage ownership in the Company, which could be substantial. Future offerings also could have a material and adverse effect on the price of our common stock.
Economic uncertainty may adversely affect our access to capital, cost of capital and ability to execute our business plan as scheduled.
Generally, worldwide economic conditions remain uncertain. Access to capital markets is critical to our ability to operate. Traditionally, biopharmaceutical companies have funded their research and development expenditures through raising capital in the equity markets. Declines and uncertainties in these markets in the past have severely restricted raising new capital and have affected companies’ ability to continue to expand or fund existing research and development efforts. We require significant capital for research and development for our vaccine candidates and clinical trials. The general economic and capital market conditions, both in the U.S. and worldwide, have been volatile in the past and at times have adversely affected our access to capital and increased the cost of capital. There is no certainty that the capital and credit markets will be available to raise additional capital on favorable terms. If economic conditions become worse, our future cost of equity or debt capital and access to the capital markets could be adversely affected. In addition, if we are unable to access the capital markets on favorable terms, this could affect our ability to execute our business plan as scheduled. Moreover, we rely and intend to rely on third-parties, including our clinical research organizations and certain other important vendors and consultants. As a result of the global economic situation, there may be a disruption or delay in the performance of our third-party contractors and suppliers. If such third-parties are unable to adequately satisfy their contractual commitments to us in a timely manner, our business could be adversely affected.
Even with the HHS BARDA contract award and the exercise of the contract option period, we may not be able to fully fund our influenza programs.
The HHS BARDA contract is a cost-plus-fixed-fee contract that only reimburses certain specified activities that have been previously authorized by HHS BARDA. There is no guarantee that additional activities will not be needed and, if so, that HHS BARDA will reimburse us for these activities. Additionally, there are significant requirements associated with operating as a federal government contractor, which includes having appropriate accounting, project tracking and earned-value management systems implemented and operational, and we may not be able to consistently meet these requirements. Performance under the HHS BARDA contract requires that we comply with appropriate regulations and operational mandates, which require us to engage internal and external expertise for compliance. Our ability to be regularly and fully reimbursed for our activities will depend on our ability to comply and demonstrate compliance with such requirements.
The HHS BARDA contract award does not guarantee that we will be successful in future clinical trials, that the vaccine candidates will be licensed by the FDA, or that the contract award will continue to be available throughout the contract period.
The HHS BARDA contract provides a cost-plus-fixed-fee reimbursement opportunity for certain specified clinical and development activities, but we remain fully responsible for conducting these approved activities. The award of the HHS BARDA contract does not guarantee that any of these activities will be successful. Our inability to be successful with certain key clinical or development activities could jeopardize our ability to obtain FDA licensure to sell our vaccines.
| 17 |
HHS BARDA could decide to potentially delay certain of our activities, and we may elect to move forward with certain activities at our own risk and without HHS BARDA reimbursement.
Under the HHS BARDA contract, HHS BARDA regularly reviews our development efforts and clinical activities. Under certain circumstances, HHS BARDA may advise us to delay certain activities and invest additional time and resources before proceeding. If we follow such HHS BARDA advice, overall program delays and costs associated with additional resources for which we had not planned may result. Also, the costs associated with following such advice may or may not be reimbursed by HHS BARDA under our contract. Finally, we may decide not to follow the advice provided by HHS BARDA and instead pursue activities that we believe are in the best interest of the program and of the Company, even if HHS BARDA would not reimburse us under our contract.
HHS BARDA may decide not to extend our contract beyond the recently exercised option period.
The HHS BARDA contract has recently been extended by an additional two years through the option period for a total performance period of approximately five and a half years. Depending on how we perform during the option period, HHS BARDA may decide whether or not to extend the contract to include additional periods of time to complete the contract deliverables. For example, the HHS BARDA contract anticipates that we file BLAs for licensure of both our seasonal influenza vaccine and our pandemic influenza vaccine; however, there is no guarantee that we will successfully complete all of the tasks required to file BLAs during this period. Although we believe that, based on our progress to date and the activities that we have planned in the future, HHS BARDA will want to extend the contract, there can be no guarantee that HHS BARDA will decide to extend our contract beyond September 2016.
Because of changes to the influenza vaccine industry and regulatory environment, accelerated approval by the FDA of our seasonal influenza vaccine candidate may not be available.
FDA regulations allow for the accelerated approval of a seasonal influenza vaccine based on a surrogate endpoint (i.e., HAI data) when there is a shortage of vaccine because influenza is a serious and sometimes, life-threatening disease. This may allow developers to obtain licensure well ahead of the timeline for demonstrating clinical efficacy, which is necessary for traditional approval. Because the seasonal influenza vaccine industry has made significant steps to provide sufficient supply to the recommended population in the U.S, the FDA may no longer view the development of our seasonal influenza vaccine as meeting an unmet medical need.
Our expectation that our pandemic influenza vaccine candidate will be granted accelerated approval by the FDA is not guaranteed.
As is the case with seasonal influenza, the FDA has articulated the immunogenicity criteria for accelerated approval of vaccines that address potential pandemic influenza strains. Because a controlled efficacy clinical trial of a pandemic vaccine candidate is not logistically or ethically possible, accelerated approval will require evidence that a seasonal vaccine made by the same manufacturing process as the pandemic vaccine is efficacious. There is no guarantee the FDA will grant accelerated approval of our pandemic vaccine before we provide seasonal influenza efficacy data. Also, because we currently anticipate that our seasonal influenza vaccine would not get accelerated approval from the FDA, it is likely that we would need to conduct larger and more expensive efficacy clinical trials and that licensure of our seasonal vaccine will be materially delayed for a year or more, assuming such licensure occurs at all, which may, in turn, delay the FDA approval of our pandemic vaccine.
Our wholly-owned subsidiary Novavax AB, collaborations with regional partners, such as Cadila, LGLS, and PATH, as well as contracts with international providers, expose us to additional risks associated with doing business outside the U.S., and any adverse event could have a material negative impact on our operations.
Swedish-based Novavax AB is a wholly-owned subsidiary of Novavax, Inc. We have also formed a joint venture with Cadila in India, entered into a license agreement with LGLS in South Korea, a clinical development agreement with PATH and have entered into other agreements and arrangements with companies in other countries. We plan to continue to enter into collaborations or partnerships with companies, non-profit organizations and local governments in other parts of the world. Risks of conducting business outside the U.S. include:
| 18 |
| · | multiple regulatory requirements could affect our ability to develop, manufacture and sell products in such local markets; |
| · | compliance with anti-bribery laws such as the United States Foreign Corrupt Practices Act and similar anti-bribery laws in other jurisdictions; |
| · | trade protections measures and import and export licensing requirements; |
| · | difficulties in and costs of staffing, managing and operating our international operations; |
| · | changes in environmental, health and safety laws; |
| · | fluctuations in foreign currency exchange rates; |
| · | potentially negative consequences from changes in or interpretations of tax laws; |
| · | political instability and actual or anticipated military or potential conflicts; |
| · | economic instability, inflation, recession and interest rate fluctuations; |
| · | minimal or diminished protection of intellectual property; and |
| · | possible nationalization and expropriation. |
These risks, individually or in the aggregate, could have a material adverse effect on our business, financial conditions, results of operations and cash flows.
Current or future regional relationships may hinder our ability to engage in larger transactions.
We have entered into regional collaborations to develop our vaccine candidates in certain parts of the world, and we may enter into additional regional collaborations. Our relationships with Cadila, LGLS, and PATH are examples of these regional relationships. These relationships are likely to involve the licensing of our technology to our partner or entering into a distribution agreement, frequently on an exclusive basis. Generally, these exclusive agreements are restricted to certain territories. Because we have entered into exclusive license and distribution agreements, larger companies may not be interested, or able, to enter into collaborations with us on a worldwide-scale. Also, these regional relationships may make us an unattractive target for an acquisition.
We are a biopharmaceutical company and face significant risk in developing, manufacturing and commercializing our products.
We focus our research and development activities on vaccines, an area in which we have particular strengths and a technology that appears promising. The outcome of any research and development program is highly uncertain. Only a small fraction of biopharmaceutical development programs ultimately result in commercial products or even product candidates and a number of events could delay our development efforts and negatively impact our ability to obtain regulatory approval for, and to manufacture, market and sell, a vaccine. Vaccine candidates that initially appear promising often fail to yield successful products. In many cases, pre-clinical studies or clinical trials will show that a product candidate is not efficacious or that it raises safety concerns or has other side effects that outweigh its intended benefit. Success in pre-clinical or early clinical trials may not translate into success in large-scale clinical trials. Further, success in clinical trials will likely lead to increased investment, accelerating cumulative losses to bring such products to market. Even if clinical trial results appear positive, regulatory approval may not be obtained if the FDA does not agree with our interpretation of the results and we may face challenges when scaling-up the production process to commercial levels. Even after a product is approved and launched, general usage or post-marketing clinical trials may identify safety or other previously unknown problems with the product, which may result in regulatory approvals being suspended, limited to narrow indications or revoked, which may otherwise prevent successful commercialization. Intense competition in the vaccine industry could also limit the successful commercialization of our products.
Many of our competitors have significantly greater resources and experience, which may negatively impact our commercial opportunities and those of our current and future licensees.
The biotechnology and pharmaceutical industries are subject to intense competition and rapid and significant technological change. We have many potential competitors, including major pharmaceutical companies, specialized biotechnology firms, academic institutions, government agencies and private and public research institutions. Many of our competitors have significantly greater financial and technical resources, experience and expertise in:
| 19 |
| · | research and development; |
| · | pre-clinical testing; |
| · | designing and implementing clinical trials; |
| · | regulatory processes and approvals; |
| · | production and manufacturing; and |
| · | sales and marketing of approved products. |
Principal competitive factors in our industry include:
| · | the quality and breadth of an organization’s technology; |
| · | management of the organization and the execution of the organization’s strategy; |
| · | the skill and experience of an organization’s employees and its ability to recruit and retain skilled and experienced employees; |
| · | an organization’s intellectual property portfolio; |
| · | the range of capabilities, from target identification and validation to drug discovery and development to manufacturing and marketing; and |
| · | the availability of substantial capital resources to fund discovery, development and commercialization activities. |
Large and established companies, such as Merck & Co., Inc., GlaxoSmithKline plc, CSL Ltd, Sanofi Pasteur, SA, Pfizer Inc. and MedImmune, LLC (a subsidiary of AstraZeneca PLC), among others, compete in the vaccine market. In particular, these companies have greater experience and expertise in securing government contracts and grants to support their research and development efforts, conducting testing and clinical trials, obtaining regulatory approvals to market products, manufacturing such products on a broad scale and marketing approved products.
There are many seasonal influenza vaccines currently approved and marketed. Competition in the sale of these seasonal influenza vaccines is intense. Therefore, newly developed and approved products must be differentiated from existing vaccines in order to have commercial success. In order to show differentiation in the seasonal influenza market, a product must be more efficacious, particularly in older adults, and/or be less expensive and quicker to manufacture. Many of our competitors are working on new products and new generations of current products, each of which is intended to be more efficacious than products currently being marketed. Our seasonal influenza vaccine candidate may not prove to be more efficacious than current products or products under development by our competitors. Further, our manufacturing system may not provide enough savings of time or money to provide the required differentiation for commercial success.
We are also aware that there are multiple companies with active RSV vaccine programs at various stages of development. Thus, while there is no RSV vaccine currently on the market, there is likely to be significant and consistent competition as these active programs mature. Different RSV vaccines may work better for different segments of the population, so it may be difficult for a single RSV vaccine manufacturer to provide vaccines that are marketable to multiple population segments. Geographic markets are also likely to vary significantly, which may make it difficult to market a single RSV vaccine worldwide. Even if a manufacturer brings an RSV vaccine to license, it is likely that competitors will continue to work on new products that could be more efficacious and/or less expensive. Our RSV vaccine candidate may not be as far along in development as other active RSV vaccine programs about which we are not aware, nor as efficacious as products under development by competing companies.
We believe that there are at least two EBOV vaccine candidates that are currently being tested in humans: one by GlaxoSmithKline in collaboration with the United States National Institute of Allergy and Infectious Diseases, and the other by a collaboration of NewLink Genetics, Merck Vaccines USA and the Public Health Agency of Canada. Vaccine candidates against EBOV have been in development for more than a decade by large pharmaceutical companies, smaller biotech companies, government agencies and academic labs worldwide, and with the high visibility of the recent West Africa epidemic, continued development activities are likely to continue and potentially increase.
| 20 |
Regardless of the disease, smaller or early-stage companies and research institutions may also prove to be significant competitors, particularly through collaborative arrangements with large and established pharmaceutical companies. As these companies develop their technologies, they may develop proprietary positions, which may prevent or limit our product development and commercialization efforts. We will also face competition from these parties in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and subject registration for clinical trials and in acquiring and in-licensing technologies and products complementary to our programs or potentially advantageous to our business. If any of our competitors succeed in obtaining approval from the FDA or other regulatory authorities for their products sooner than we do or for products that are more effective or less costly than ours, our commercial opportunity could be significantly reduced.
In order to effectively compete, we will have to make substantial investments in development, testing, manufacturing and sales and marketing or partner with one or more established companies. There is no assurance that we will be successful in gaining significant market share for any vaccine. Our technologies and vaccines also may be rendered obsolete or non-competitive as a result of products introduced by our competitors to the marketplace more rapidly and at a lower cost.
If we are unable to attract or retain key management or other personnel, our business, operating results and financial condition could be materially adversely affected.
We depend on our senior executive officers, as well as key scientific and other personnel. The loss of these individuals could harm our business and significantly delay or prevent the achievement of research, development or business objectives. We have had turnover situations in key executive positions and the lack of management continuity and resulting lack of long-term history with our Company along with the learning curve that executives experience when they join our management team could result in operational and administrative inefficiencies and added costs. If we were to experience additional turnover at the executive level, these risks could be exacerbated.
We may not be able to attract qualified individuals for other key management or other personnel positions on terms acceptable to us. Competition for qualified employees is intense among pharmaceutical and biotechnology companies, and the loss of qualified employees, or an inability to attract, retain and motivate additional highly skilled employees required for the expansion of our activities, could hinder our ability to complete clinical trials successfully and develop marketable products.
We also rely from time to time on outside advisors who assist us in formulating our research and development and clinical strategy. We may not be able to attract and retain these individuals on acceptable terms, which could have a material adverse effect on our business, financial condition and results of operations.
We may have product liability exposure.
The administration of drugs or vaccines to humans, whether in clinical trials or after marketing clearances are obtained, can result in product liability claims. We maintain product liability insurance coverage in the total amount of $20 million aggregate for all claims arising from the use of products in clinical trials prior to FDA approval. Coverage is relatively expensive, and the market pricing can significantly fluctuate. Therefore, we may not be able to maintain insurance at a reasonable cost. There can be no assurance that we will be able to maintain our existing insurance coverage or obtain coverage for the use of our other products in the future. This insurance coverage and our resources may not be sufficient to satisfy all liabilities resulting from product liability claims. A successful claim may prevent us from obtaining adequate product liability insurance in the future on commercially desirable items, if at all. Even if a claim is not successful, defending such a claim would be time-consuming and expensive, may damage our reputation in the marketplace and would likely divert management’s attention.
Regardless of merit or eventual outcome, liability claims may result in:
| · | decreased demand for our products; |
| · | impairment of our business reputation; |
| · | withdrawal of clinical trial participants; |
| · | costs of related litigation; |
| 21 |
| · | substantial monetary awards to subjects or other claimants; |
| · | loss of revenue; and |
| · | inability to commercialize our vaccine candidates. |
We may not be able to win government, academic institution or non-profit contracts or grants.
From time to time, we may apply for contracts or grants from government agencies, academic institutions, and non-profit entities. Such contracts or grants can be highly attractive because they provide capital to fund the ongoing development of our technologies and vaccine candidates without diluting our stockholders. However, there is often significant competition for these contracts or grants. Entities offering contracts or grants may have requirements to apply for or to otherwise be eligible to receive certain contracts or grants that our competitors may be able to satisfy that we cannot. In addition, such entities may make arbitrary decisions as to whether to offer contracts or make grants, to whom the contracts or grants will be awarded and the size of the contracts or grants to each awardee. Even if we are able to satisfy the award requirements, there is no guarantee that we will be a successful awardee. Therefore, we may not be able to win any contracts or grants in a timely manner, if at all.
Raising additional capital by issuing securities or through collaboration and licensing arrangements may cause dilution to existing stockholders or require us to relinquish rights to our technologies or vaccine candidates.
If we are unable to partner with a third-party to advance the development of one or more of our vaccine candidates, we will need to raise money through additional debt or equity financings. To the extent that we raise additional capital by issuing equity securities, our stockholders will experience immediate dilution, which may be significant. There is also a risk that such equity issuances may cause an ownership change under the Internal Revenue Code of 1986, as amended, and similar state provisions, thus limiting our ability to use our net operating loss carryforwards and credits. To the extent that we raise additional capital through licensing arrangements or arrangements with collaborative partners, we may be required to relinquish, on terms that may not be favorable to us, rights to some of our technologies or vaccine candidates that we would otherwise seek to develop or commercialize ourselves. In addition, current economic conditions may also negatively affect the desire or ability of potential collaborators to enter into transactions with us. They may also have to delay or cancel research and development projects or reduce their overall budgets.
Our business may be adversely affected if we do not successfully execute our business development initiatives.
We anticipate growing through both internal development projects, as well as external opportunities, which include the acquisition, partnering and in-licensing of products, technologies and companies or the entry into strategic alliances and collaborations. The availability of high quality opportunities is limited, and we may fail to identify candidates that we and our stockholders consider suitable or complete transactions on terms that prove advantageous. In order to pursue such opportunities, we may require significant additional financing, which may not be available to us on favorable terms, if at all. Even if we are able to successfully identify and complete acquisitions, like our business combination with Novavax AB, we may not be able to integrate the assets or take full advantage of the opportunities and, consequently, may not realize the benefits that we expect.
To effectively manage our current and future potential growth, we will need to continue to enhance our operational, financial and management processes and to effectively expand, train and manage our employee base. Supporting our growth initiatives will require significant expenditures and management resources, including investments in research and development, manufacturing and other areas of our business. If we do not successfully manage our growth and do not successfully execute our growth initiatives, then our business and financial results may be adversely impacted, and we may incur asset impairment or restructuring charges.
| 22 |
Litigation could have a material adverse impact on our results of operation and financial condition.
In addition to intellectual property litigation, from time to time, we may be subject to other litigation. Regardless of the merits of any claims that may be brought against us, litigation could result in a diversion of management’s attention and resources and we may be required to incur significant expenses defending against these claims. If we are unable to prevail in litigation, we could incur substantial liabilities. Where we can make a reasonable estimate of the liability relating to pending litigation and determine that it is probable, we record a related liability. As additional information becomes available, we assess the potential liability and revise estimates as appropriate. However, because of uncertainties relating to litigation, the amount of our estimates could be wrong.
PRODUCT DEVELOPMENT RISKS
Because our vaccine product development efforts depend on new and rapidly evolving technologies, we cannot be certain that our efforts will be successful.
Our vaccine development efforts depend on new, rapidly evolving technologies and on the marketability and profitability of our products. Our development efforts and, if those are successful, commercialization of our vaccines could fail for a variety of reasons, and include the possibility that:
| · | our recombinant nanoparticle vaccine technologies, any or all of the products based on such technologies or our proprietary manufacturing process will be ineffective or unsafe, or otherwise fail to receive necessary regulatory clearances or commercial viability; |
| · | we are unable to scale-up our manufacturing capabilities in a cost-effective manner; |
| · | the products, if safe and effective, will be difficult to manufacture on a large-scale or uneconomical to market; |
| · | our manufacturing facility will fail to continue to pass regulatory inspections; |
| · | proprietary rights of third-parties will prevent us or our collaborators from exploiting technologies, and manufacturing or marketing products; and |
| · | third-party competitors will gain greater market share due to superior products or marketing capabilities. |
We have not completed the development of vaccine products and we may not succeed in obtaining the FDA licensure necessary to sell such vaccine products.
The development, manufacture and marketing of our pharmaceutical and biological products are subject to government regulation in the U.S. and other countries, including the European Medicines Agency and the Swedish Medical Products Agency with respect to our adjuvant product being developed in Sweden. In the U.S. and most foreign countries, we must complete rigorous pre-clinical testing and extensive clinical trials that demonstrate the safety and efficacy of a product in order to apply for regulatory approval to market the product. None of our vaccine candidates have yet gained regulatory approval in the U.S. or elsewhere. We also have vaccine candidates in clinical trials and pre-clinical laboratory or animal studies.
The steps generally required by the FDA before our proposed investigational products may be marketed in the U.S. include:
| · | performance of pre-clinical (animal and laboratory) tests; |
| · | submissions to the FDA of an IND, which must become effective before clinical trials may commence; |
| · | performance of adequate and well-controlled clinical trials to establish the safety and efficacy of the investigational product in the intended target population; |
| · | performance of a consistent and reproducible manufacturing process intended for commercial use, including appropriate manufacturing data and regulatory inspections; |
| · | submission to the FDA of a BLA or a NDA; and |
| Ÿ | FDA approval of the BLA or NDA before any commercial sale or shipment of the product. |
| 23 |
The processes are expensive and can take many years to complete, and we may not be able to demonstrate the safety and efficacy of our vaccine candidates to the satisfaction of regulatory authorities. The start of clinical trials can be delayed or take longer than anticipated for many and varied reasons, many of which are out of our control. Safety concerns may emerge that could lengthen the ongoing clinical trials or require additional clinical trials to be conducted. Promising results in early clinical trials may not be replicated in subsequent clinical trials. Regulatory authorities may also require additional testing, and we may be required to demonstrate that our proposed products represent an improved form of treatment over existing therapies, which we may be unable to do without conducting further clinical trials. Moreover, if the FDA or a foreign regulatory body grants regulatory approval of a product, the approval may be limited to specific indications or limited with respect to its distribution. Expanded or additional indications for approved products may not be approved, which could limit our revenue. Foreign regulatory authorities may apply similar limitations or may refuse to grant any approval. Consequently, even if we believe that pre-clinical and clinical data are sufficient to support regulatory approval for our vaccine candidates, the FDA and foreign regulatory authorities may not ultimately grant approval for commercial sale in any jurisdiction. If our vaccine candidates are not approved, our ability to generate revenue will be limited and our business will be adversely affected.
If we are unable to manufacture our vaccines in sufficient quantities, at sufficient yields or are unable to obtain regulatory approvals for a manufacturing facility for our vaccines, we may experience delays in product development, clinical trials, regulatory approval and commercial distribution.
Completion of our clinical trials and commercialization of our vaccine candidates require access to, or development of, facilities to manufacture our vaccine candidates at sufficient yields and at commercial-scale. We have limited experience manufacturing any of our vaccine candidates in the volumes that will be necessary to support large-scale clinical trials or commercial sales. Efforts to establish these capabilities may not meet initial expectations as to scheduling, scale-up, reproducibility, yield, purity, cost, potency or quality.
Manufacturing our vaccines candidates involves a complicated process with which we have limited experience. If we are unable to manufacture our vaccine candidates in clinical quantities or, when necessary, in commercial quantities and at sufficient yields, then we must rely on third-parties. Other third-party manufacturers must also receive FDA approval before they can produce clinical material or commercial products. Our vaccines may be in competition with other products for access to these facilities and may be subject to delays in manufacture if third-parties give other products greater priority. We may not be able to enter into any necessary third-party manufacturing arrangements on acceptable terms, or on a timely basis. In addition, we have to enter into technical transfer agreements and share our know-how with the third-party manufacturers, which can be time-consuming and may result in delays.
Influenza vaccines are seasonal in nature. If a vaccine is not available early enough in the influenza season, we would likely have difficulty selling the vaccine. Further, pandemic outbreaks present only short-term opportunities for us. There is no way to predict when there will be a pandemic outbreak, the strain of the influenza or how long the pandemic will last. For these reasons, any delay in the delivery of an influenza vaccine could result in lower sales volumes, lower sale prices, or no sales. Because the strain of the seasonal influenza changes annually, inventory of seasonal vaccine cannot be sold during a subsequent influenza season. Any delay in the manufacture of our influenza vaccines could adversely affect our ability to sell the vaccines.
Our reliance on contract manufacturers may adversely affect our operations or result in unforeseen delays or other problems beyond our control. Because of contractual restraints and the limited number of third-party manufacturers with the expertise, required regulatory approvals and facilities to manufacture our bulk vaccines on a commercial-scale, replacement of a manufacturer may be expensive and time-consuming and may cause interruptions in the production of our vaccine. A third-party manufacturer may also encounter difficulties in production. These problems may include:
| · | difficulties with production costs, scale-up and yields; |
| · | availability of raw materials and supplies; |
| · | quality control and assurance; |
| · | shortages of qualified personnel; |
| · | compliance with strictly enforced federal, state and foreign regulations that vary in each country where product might be sold; and |
| · | lack of capital funding. |
| 24 |
As a result, any delay or interruption could have a material adverse effect on our business, financial condition, results of operations and cash flows.
Our manufacturing facilities may not be “Phase 3 ready” during 2015, which may impede or delay our ability to manufacture one or more vaccine candidates for subsequent clinical trials or obtain BLA for such vaccines.
Our manufacturing facility in Gaithersburg, Maryland, which is designed to manufacture Phase 3 vaccine candidates, has completed refurbishment and relocation of equipment from our Belward facility, as well as installation of new equipment, and although validation to begin manufacturing has been largely completed, additional equipment and validation work is ongoing, and there are risks associated with bringing the facility to “Phase 3 readiness.” These risks include but are not limited to contractor issues and delays, licensing and permitting delays or rejections, limitations and delays on the installation of new or custom-ordered equipment, issues associated with validating equipment, processes or other aspects of ensuring GMP manufacturing. There are many aspects of the project that rely on third party contractors and subcontractors, and delays are frequently encountered.
We must identify vaccines for development with our technologies and establish successful third-party relationships.
The near and long-term viability of our vaccine candidates will depend in part on our ability to successfully establish new strategic collaborations with pharmaceutical and biotechnology companies, non-profit organizations and government agencies. Establishing strategic collaborations and obtaining government funding is difficult and time-consuming. Potential collaborators may reject collaborations based upon their assessment of our financial, regulatory or intellectual property position or based on their internal pipeline; government agencies may reject contract or grant applications based on their assessment of public need, the public interest, our products’ ability to address these areas, or other reasons beyond our expectations or control. If we fail to establish a sufficient number of collaborations or government relationships on acceptable terms, we may not be able to commercialize our vaccine candidates or generate sufficient revenue to fund further research and development efforts.
Even if we establish new collaborations or obtain government funding, these relationships may never result in the successful development or commercialization of any vaccine candidates for several reasons, including the fact that:
| · | we may not have the ability to control the activities of our partners and cannot provide assurance that they will fulfill their obligations to us, including with respect to the license, development and commercialization of vaccine candidates, in a timely manner or at all; |
| · | such partners may not devote sufficient resources to our vaccine candidates or properly maintain or defend our intellectual property rights; |
| · | any failure on the part of our partners to perform or satisfy their obligations to us could lead to delays in the development or commercialization of our vaccine candidates and affect our ability to realize product revenue; and |
| · | disagreements, including disputes over the ownership of technology developed with such collaborators, could result in litigation, which would be time-consuming and expensive, and may delay or terminate research and development efforts, regulatory approvals and commercialization activities. |
Our collaborators will be subject to the same regulatory approval of their manufacturing facility and process as Novavax. Before we could begin commercial manufacturing of any of our vaccine candidates, we and our collaborators must pass a pre-approval inspection before FDA approval and comply with the FDA’s GMP regulations. If our collaborators fail to comply with these requirements, our vaccine candidates would not be approved. If our collaborators fail to comply with these requirements after approval, we could be subject to possible regulatory action and may be limited in the jurisdictions in which we are permitted to sell our products.
If we or our collaborators fail to maintain our existing agreements or in the event we fail to establish agreements as necessary, we could be required to undertake research, development, manufacturing and commercialization activities solely at our own expense. These activities would significantly increase our capital requirements and, given our lack of sales, marketing and distribution capabilities, significantly delay the commercialization of our vaccine candidates.
| 25 |
Because we depend on third-parties to conduct some of our laboratory testing, clinical trials, and manufacturing, we may encounter delays in or lose some control over our efforts to develop products.
We are dependent on third-party research organizations to conduct some of our laboratory testing, clinical trials and manufacturing activities. If we are unable to obtain any necessary services on acceptable terms, we may not complete our product development efforts in a timely manner. We may lose some control over these activities and become too dependent upon these parties. These third-parties may not complete testing or manufacturing activities on schedule, within budget, or when we request. We may not be able to secure and maintain suitable research organizations to conduct our laboratory testing, clinical trials and manufacturing activities. We have not manufactured any of our vaccine candidates at a commercial level and may need to identify additional third-party manufacturers to scale-up and manufacture our products.
We are responsible for confirming that each of our clinical trials is conducted in accordance with its general investigational plan and protocol. Moreover, the FDA and foreign regulatory agencies require us to comply with regulations and standards, commonly referred to as good clinical practices, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the clinical trial participants are adequately protected. The FDA and foreign regulatory agencies also require us to comply with good manufacturing practices. Our reliance on third-parties does not relieve us of these responsibilities and requirements. These third-parties may not successfully carry out their contractual duties or regulatory obligations or meet expected deadlines. In addition, these third-parties may need to be replaced or the quality or accuracy of the data they obtain may be compromised or the product they manufacture may be contaminated due to the failure to adhere to our clinical and manufacturing protocols, regulatory requirements or for other reasons. In any such event, our pre-clinical development activities or clinical trials may be extended, delayed, suspended or terminated, and we may not be able to obtain regulatory approval of, or commercially manufacture, our vaccine candidates.
Our collaborations may not be profitable.
We have formed CPLB with Cadila in India and, in connection with it, entered into a master services agreement pursuant to which we may request certain services from Cadila in the areas of biologics research, pre-clinical development, clinical development, process development, manufacturing scale-up and general manufacturing related services in India. We and Cadila amended the master services agreement first in July 2011, and subsequently in March 2013, March 2014 and February 2015, in each case to extend the term by one year for which services can be provided by Cadila under this agreement. Under the revised terms, if, by March 2016, the amount of services provided by Cadila under the master services agreement is less than $7.5 million, we will pay Cadila the portion of the shortfall amount that is less than or equal to $2.0 million and 50% of the portion of the shortfall amount that exceeds $2.0 million. We and Cadila also agreed to an amendment that allows CPLB, as of the beginning of 2013, to provide services on behalf of Cadila. Through December 31, 2014, we have purchased $5.7 million in services from Cadila pursuant to this agreement, including amounts in which CPLB provided the services on behalf of Cadila.
We have entered into a license agreement with LGLS that allows them to use our manufacturing and production technology to develop and sell our influenza vaccines. We have also entered into a clinical development agreement with PATH related to our RSV vaccine for maternal immunization in low-resource countries. To the extent PATH continues to fund 50% of the Company’s external clinical development costs, but the Company does not continue development, the Company would grant PATH a fully-paid license to its RSV F vaccine technology for use in pregnant women in such low-resource countries at terms that may not be favorable to the Company.
We cannot predict when, if at all, these relationships will lead to approved products, sales, or otherwise provide revenue to the Company or become profitable.
| 26 |
We have limited marketing capabilities, and if we are unable to enter into collaborations with marketing partners or develop our own sales and marketing capability, we may not be successful in commercializing any approved products.
Although we have initiated preliminary activities in anticipation of commercialization of our vaccine candidates, we currently have no dedicated sales, marketing or distribution capabilities. As a result, we will depend on collaborations with third-parties that have established distribution systems and sales forces. To the extent that we enter into co-promotion or other licensing arrangements, our revenue will depend upon the efforts of third-parties, over which we may have little or no control. If we are unable to reach and maintain agreements with one or more pharmaceutical companies or collaborators, we may be required to market our products directly. Developing a marketing and sales force is expensive and time-consuming and could delay a product launch. We cannot be certain that we will be able to attract and retain qualified sales personnel or otherwise develop this capability.
Our vaccine candidates may never achieve market acceptance even if we obtain regulatory approvals.
Even if we receive regulatory approvals for the commercial sale of our vaccine candidates, the commercial success of these vaccine candidates will depend on, among other things, their acceptance by physicians, patients, third-party payers, such as health insurance companies and other members of the medical community, as a vaccine and cost-effective alternative to competing products. If our vaccine candidates fail to gain market acceptance, we may be unable to earn sufficient revenue to continue our business. Market acceptance of, and demand for, any product that we may develop and commercialize will depend on many factors, including:
| · | our ability to provide acceptable evidence of safety and efficacy; |
| · | the prevalence and severity of adverse side effects; |
| · | whether our vaccines are differentiated from other vaccines based on immunogenicity; |
| · | availability, relative cost and relative efficacy of alternative and competing treatments; |
| · | the effectiveness of our marketing and distribution strategy; |
| · | publicity concerning our products or competing products and treatments; and |
| · | our ability to obtain sufficient third-party insurance coverage or reimbursement. |
In particular, there are significant challenges to market acceptance for seasonal influenza vaccines. For our seasonal vaccine to be accepted in the market, we must demonstrate differentiation from other seasonal vaccines that are currently approved and marketed. This can mean that the vaccine is more effective in certain populations, such as in older adults, or cheaper and quicker to produce. There are no assurances that our vaccine will be more efficacious than other vaccines.
If our vaccine candidates do not become widely accepted by physicians, patients, third-party payers and other members of the medical community, our business, financial condition and results of operations could be materially and adversely affected.
We may not be able to secure sufficient supplies of a key component of our adjuvant technology.
Because an important component of our adjuvant technology is extracted from a species of soap-bark tree (Quillaja saponaria) grown in Chile, we need long term access to quillaja extract with a consistent and sufficiently high quality. We need a secure supply of raw material, as well as back-up suppliers, or our adjuvant products may be delayed.
If reforms in the health care industry make reimbursement for our potential products less likely, the market for our potential products will be reduced, and we could lose potential sources of revenue.
Our success may depend, in part, on the extent to which reimbursement for the costs of vaccines will be available from third-party payers, such as government health administration authorities, private health insurers, managed care programs and other organizations. Over the past decade, the cost of health care has risen significantly, and there have been numerous proposals by legislators, regulators and third-party health care payers to curb these costs. Some of these proposals have involved limitations on the amount of reimbursement for certain products. Similar federal or state health care legislation may be adopted in the future and any products that we or our collaborators seek to commercialize may not be considered cost-effective. Adequate third-party insurance coverage may not be available for us to establish and maintain price levels that are sufficient for realization of an appropriate return on our investment in product development. Moreover, the existence or threat of cost control measures could cause our corporate collaborators to be less willing or able to pursue research and development programs related to our vaccine candidates.
| 27 |
REGULATORY RISKS
We may fail to obtain regulatory approval for our products on a timely basis or comply with our continuing regulatory obligations after approval is obtained.
Delays in obtaining regulatory approval can be extremely costly in terms of lost sales opportunities, loss of any potential marketing advantage of being early to market and increased clinical trial costs. The speed with which we begin and complete our pre-clinical studies necessary to begin clinical trials, clinical trials and our applications for marketing approval will depend on several factors, including the following:
| · | our ability to manufacture or obtain sufficient quantities of materials for use in necessary pre-clinical studies and clinical trials; |
| · | prior regulatory agency review and approval; |
| · | approval of the protocol and the informed consent form by the review board of the institution conducting the clinical trial; |
| · | the rate of subject or patient enrollment and retention, which is a function of many factors, including the size of the subject or patient population, the proximity of subjects and patients to clinical sites, the eligibility criteria for the clinical trial and the nature of the protocol; |
| · | negative test results or side effects experienced by clinical trial participants; |
| · | analysis of data obtained from pre-clinical and clinical activities, which are susceptible to varying interpretations and which interpretations could delay, limit or prevent further studies or regulatory approval; |
| · | the availability of skilled and experienced staff to conduct and monitor clinical trials and to prepare the appropriate regulatory applications; and |
| · | changes in the policies of regulatory authorities for drug or vaccine approval during the period of product development. |
We have limited experience in conducting and managing the pre-clinical studies and clinical trials necessary to obtain regulatory marketing approvals. We may not be permitted to continue or commence additional clinical trials. We also face the risk that the results of our clinical trials may be inconsistent with the results obtained in pre-clinical studies or clinical trials of similar products or that the results obtained in later phases of clinical trials may be inconsistent with those obtained in earlier phases. A number of companies in the biopharmaceutical and product development industry have suffered significant setbacks in advanced clinical trials, even after experiencing promising results in early animal and human testing.
Regulatory agencies may require us or our collaborators to delay, restrict or discontinue clinical trials on various grounds, including a finding that the subjects or patients are being exposed to an unacceptable health risk. In addition, we or our collaborators may be unable to submit applications to regulatory agencies within the time frame we currently expect. Once submitted, applications must be approved by various regulatory agencies before we or our collaborators can commercialize the product described in the application. All statutes and regulations governing the conduct of clinical trials are subject to change in the future, which could affect the cost of such clinical trials. Any unanticipated costs or delays in our clinical trials could delay our ability to generate revenue and harm our financial condition and results of operations.
| 28 |
Failure to obtain regulatory approval in foreign jurisdictions would prevent us from marketing our products internationally.
We intend to have our vaccine candidates marketed outside the U.S. In furtherance of this objective, we have entered into relationships with Cadila in India, LGLS in South Korea and PATH. In order to market our products in the European Union, India, Asia and many other non-U.S. jurisdictions, we must obtain separate regulatory approvals and comply with numerous and varying regulatory requirements. The approval procedure varies among countries and can involve additional testing and data review. The time required to obtain foreign regulatory approval may differ from that required to obtain FDA approval. The foreign regulatory approval process may include all of the risks associated with obtaining FDA approval. We may not obtain foreign regulatory approvals on a timely basis, if at all. Approval by a regulatory agency, such as the FDA, does not ensure approval by any other regulatory agencies, for example in other foreign countries. However, a failure or delay in obtaining regulatory approval in one jurisdiction may have a negative effect on the regulatory approval process in other jurisdictions, including approval by the FDA. The failure to obtain regulatory approval in foreign jurisdictions could harm our business.
Even if regulatory approval is received for our vaccine candidates, the later discovery of previously unknown problems with a product, manufacturer or facility may result in restrictions, including withdrawal of the product from the market.
Even if a product gains regulatory approval, such approval is likely to limit the indicated uses for which it may be marketed, and the product and the manufacturer of the product will be subject to continuing regulatory review, including adverse event reporting requirements and the FDA’s general prohibition against promoting products for unapproved uses. Failure to comply with any post-approval requirements can, among other things, result in warning letters, product seizures, recalls, substantial fines, injunctions, suspensions or revocations of marketing licenses, operating restrictions and criminal prosecutions. Any of these enforcement actions, any unanticipated changes in existing regulatory requirements or the adoption of new requirements, or any safety issues that arise with any approved products, could adversely affect our ability to market products and generate revenue and thus adversely affect our ability to continue our business.
We also may be restricted or prohibited from marketing or manufacturing a product, even after obtaining product approval, if previously unknown problems with the product or its manufacture are subsequently discovered and we cannot provide assurance that newly discovered or developed safety issues will not arise following any regulatory approval. With the use of any vaccine by a wide patient population, serious adverse events may occur from time to time that initially do not appear to relate to the vaccine itself, and only if the specific event occurs with some regularity over a period of time does the vaccine become suspect as having a causal relationship to the adverse event. Any safety issues could cause us to suspend or cease marketing of our approved products, possibly subject us to substantial liabilities, and adversely affect our ability to generate revenue and our financial condition.
Because we are subject to environmental, health and safety laws, we may be unable to conduct our business in the most advantageous manner.
We are subject to various laws and regulations relating to safe working conditions, laboratory and manufacturing practices, the experimental use of animals, emissions and wastewater discharges, and the use and disposal of hazardous or potentially hazardous substances used in connection with our research, including infectious disease agents. We also cannot accurately predict the extent of regulations that might result from any future legislative or administrative action. Any of these laws or regulations could cause us to incur additional expense or restrict our operations.
Our facilities in Maryland are subject to various local, state and federal laws and regulations relating to safe working conditions, laboratory and manufacturing practices, the experimental use of animals and the use and disposal of hazardous or potentially hazardous substances, including chemicals, microorganisms and various hazardous compounds used in connection with our research and development activities. In the U.S., these laws include the Occupational Safety and Health Act, the Toxic Test Substances Control Act and the Resource Conservation and Recovery Act. Similar national and local regulations govern our facility in Sweden. We cannot eliminate the risk of accidental contamination or discharge or injury from these materials. Federal, state, and local laws and regulations govern the use, manufacture, storage, handling and disposal of these materials. We could be subject to civil damages in the event of an improper or unauthorized release of, or exposure of individuals to, these hazardous materials. In addition, claimants may sue us for injury or contamination that results from our use or the use by third-parties of these materials, and our liability may exceed our total assets. Compliance with environmental laws and regulations may be expensive, and current or future environmental regulations may impair our research, development or production efforts.
| 29 |
Although we have general liability insurance, these policies contain exclusions from insurance against claims arising from pollution from chemicals or pollution from conditions arising from our operations. Our collaborators are working with these types of hazardous materials in connection with our collaborations. In the event of a lawsuit or investigation, we could be held responsible for any injury we or our collaborators cause to persons or property by exposure to, or release of, any hazardous materials. However, we believe that we are currently in compliance with all applicable environmental and occupational health and safety regulations.
Even if we successfully commercialize any of our vaccine candidates, either alone or in collaboration, we face uncertainty with respect to pricing, third-party reimbursement and healthcare reform, all of which could adversely affect any commercial success of our vaccine candidates.
Our ability to collect revenue from the commercial sale of our vaccines may depend on our ability, and that of any current or potential future collaboration partners or customers, to obtain adequate levels of coverage and reimbursement for such products from third-party payers such as:
| · | government health administration authorities; |
| · | private health insurers; |
| · | health maintenance organizations; |
| · | pharmacy benefit management companies; and |
| · | other healthcare-related organizations. |
Third-party payers are increasingly challenging the prices charged for medical products and may deny coverage or offer inadequate levels of reimbursement if they determine that a prescribed product has not received appropriate clearances from the FDA, or foreign equivalent, or other government regulators, is not used in accordance with cost-effective treatment methods as determined by the third-party payer, or is experimental, unnecessary or inappropriate. Prices could also be driven down by health maintenance organizations that control or significantly influence purchases of healthcare products.
In both the U.S. and some foreign jurisdictions, there have been a number of legislative and regulatory proposals and initiatives to change the health care system in ways that could affect our ability to sell vaccines. Some of these proposed and implemented reforms could result in reduced reimbursement rates for medical products, and while we have no current vaccines available for commercial sale, the impact of such reform could nevertheless adversely affect our business strategy, operations and financial results. In March 2010, President Obama signed into law a legislative overhaul of the U.S. healthcare system, known as the Patient Protection and Affordable Care Act of 2010, as amended by the Healthcare and Education Affordability Reconciliation Act of 2010 (PPACA). As a result of this new legislation, substantial changes could be made to the current system for paying for healthcare in the United States, including changes made in order to extend medical benefits to those who currently lack insurance coverage. The long-term ramifications of PPACA remain unclear and many details regarding implementation of PPACA are yet to be determined, however, the cost-containment measures that healthcare providers are instituting and the results of healthcare reforms may negatively impact the commercial prospects of one or more of our vaccine candidates currently in development.
INTELLECTUAL PROPERTY RISKS
Our success depends on our ability to maintain the proprietary nature of our technology.
Our success in large part depends on our ability to maintain the proprietary nature of our technology and other trade secrets. To do so, we must prosecute and maintain existing patents, obtain new patents and pursue trade secret and other intellectual property protection. We also must operate without infringing the proprietary rights of third-parties or allowing third-parties to infringe our rights. We currently have or have rights to over 100 U.S. patents and corresponding foreign patents and patent applications covering our technologies. However, patent issues relating to pharmaceuticals and biologics involve complex legal, scientific and factual questions. To date, no consistent policy has emerged regarding the breadth of biotechnology patent claims that are granted by the U.S. Patent and Trademark Office or enforced by the federal courts. Therefore, we do not know whether our patent applications will result in the issuance of patents, or that any patents issued to us will provide us with any competitive advantage. We also cannot be sure that we will develop additional proprietary products that are patentable. Furthermore, there is a risk that others will independently develop or duplicate similar technology or products or circumvent the patents issued to us.
| 30 |
There is a risk that third-parties may challenge our existing patents or claim that we are infringing their patents or proprietary rights. We could incur substantial costs in defending patent infringement suits or in filing suits against others to have their patents declared invalid or claim infringement. It is also possible that we may be required to obtain licenses from third-parties to avoid infringing third-party patents or other proprietary rights. We cannot be sure that such third-party licenses would be available to us on acceptable terms, if at all. If we are unable to obtain required third-party licenses, we may be delayed in or prohibited from developing, manufacturing or selling products requiring such licenses.
Although our patent filings include claims covering various features of our vaccine candidates, including composition, methods of manufacture and use, our patents do not provide us with complete protection against the development of competing products. Some of our know-how and technology is not patentable. To protect our proprietary rights in unpatentable intellectual property and trade secrets, we require employees, consultants, advisors and collaborators to enter into confidentiality agreements. These agreements may not provide meaningful protection for our trade secrets, know-how or other proprietary information.
Third parties may claim we infringe their intellectual property rights.
Our research, development and commercialization activities, including any vaccine candidates resulting from these activities, may infringe or be claimed to infringe patents owned by third-parties and to which we do not hold licenses or other rights. There may be rights we are not aware of, including applications that have been filed, but not published that, when issued, could be asserted against us. These third-parties could bring claims against us, and that would cause us to incur substantial expenses and, if successful against us, could cause us to pay substantial damages. Further, if a patent infringement suit were brought against us, we could be forced to stop or delay research, development, manufacturing or sales of the product or biologic drug candidate that is the subject of the suit.
As a result of patent infringement claims, or in order to avoid potential claims, we may choose or be required to seek a license from the third-party. These licenses may not be available on acceptable terms, or at all. Even if we are able to obtain a license, the license would likely obligate us to pay license fees or royalties or both, and the rights granted to us might be non-exclusive, which could result in our competitors gaining access to the same intellectual property. Ultimately, we could be prevented from commercializing a product, or be forced to cease some aspect of our business operations, if, as a result of actual or threatened patent infringement claims, we are unable to enter into licenses on acceptable terms. All of the issues described above could also impact our collaborators, which would also impact the success of the collaboration and therefore us.
There has been substantial litigation and other proceedings regarding patent and other intellectual property rights in the pharmaceutical and biotechnology industries. In addition to infringement claims against us, we may become a party to other patent litigation and other proceedings, including interference proceedings declared by the U.S. Patent and Trademark Office and opposition proceedings in the European Patent Office, regarding intellectual property rights with respect to our products and technology.
We may become involved in litigation to protect or enforce our patents or the patents of our collaborators or licensors, which could be expensive and time-consuming.
Competitors may infringe our patents or the patents of our collaborators or licensors. As a result, we may be required to file infringement claims to counter infringement for unauthorized use. This can be expensive, particularly for a company of our size, and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours is not valid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover its technology. An adverse determination of any litigation or defense proceeding could put one or more of our patents at risk of being invalidated or interpreted narrowly and could put our patent applications at the risk of not issuing.
| 31 |
Interference proceedings brought by the U.S. Patent and Trademark Office may be necessary to determine the priority of inventions with respect to our patent applications or those of our collaborators or licensors. Litigation or interference proceedings may fail and, even if successful, may result in substantial costs and distraction to our management. We may not be able, alone or with our collaborators and licensors, to prevent misappropriation of our proprietary rights, particularly in countries where the laws may not protect such rights as fully as in the U.S.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. In addition, during the course of this kind of litigation, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If investors perceive these results to be negative, the market price for our common stock could be significantly harmed.
We may need to license intellectual property from third-parties and, if our right to use the intellectual property we license is affected, our ability to develop and commercialize our vaccine candidates may be harmed.
We expect that we will need to license intellectual property from third-parties in the future and that these licenses will be material to our business. We will not own the patents or patent applications that underlie these licenses, and we will not control the enforcement of the patents. We will rely upon our licensors to properly prosecute and file those patent applications and prevent infringement of those patents.
Our license agreement with Wyeth, which gives us rights to a family of patents and patent applications that are expected to expire in early 2022, covering VLP technology for use in human vaccines in certain fields of use, is non-exclusive. These applications are very significant to our business. If each milestone is achieved for any particular vaccine candidate, we would likely be obligated to pay an aggregate of $14 million to Wyeth for each vaccine candidate developed and commercialized under the agreement. Achievement of each milestone is subject to many risks, including those described in these Risk Factors. Annual license fees under the Wyeth agreement aggregate to $0.2 million per year. We are currently in discussion with Wyeth to potentially amend the agreement and restructure a $3 million milestone payment owed as a result of CPLB’s initiation of a Phase 3 clinical trial for its seasonal influenza VLP vaccine candidate in the third quarter of 2014; however, there is no guarantee that Wyeth will agree to such an amendment in which case Novavax would be obligated to promptly pay the milestone payment. An additional milestone payment associated with commercialization may also be triggered by CPLB activities and there is no guarantee that Wyeth would agree to restructure such milestone payment through another amendment.
While many of the licenses under which we have rights provide us with rights in specified fields, the scope of our rights under these and other licenses may be subject to dispute by our licensors or third-parties. In addition, our rights to use these technologies and practice the inventions claimed in the licensed patents and patent applications are subject to our licensors abiding by the terms of those licenses and not terminating them. Any of our licenses may be terminated by the licensor if we are in breach of a term or condition of the license agreement, or in certain other circumstances.
Our vaccine candidates and potential vaccine candidates will require several components that may each be the subject of a license agreement. The cumulative license fees and royalties for these components may make the commercialization of these vaccine candidates uneconomical.
If patent laws or the interpretation of patent laws change, our competitors may be able to develop and commercialize our discoveries.
Important legal issues remain to be resolved as to the extent and scope of available patent protection for biopharmaceutical products and processes in the U.S. and other important markets outside the U.S., such as Europe and Japan. In addition, foreign markets may not provide the same level of patent protection as provided under the U.S. patent system. Litigation or administrative proceedings may be necessary to determine the validity and scope of certain of our and others’ proprietary rights. Any such litigation or proceeding may result in a significant commitment of resources in the future and could force us to do one or more of the following: cease selling or using any of our products that incorporate the challenged intellectual property, which would adversely affect our revenue; obtain a license from the holder of the intellectual property right alleged to have been infringed, which license may not be available on reasonable terms, if at all; and redesign our products to avoid infringing the intellectual property rights of third-parties, which may be time-consuming or impossible to do. In addition, changes in, or different interpretations of, patent laws in the U.S. and other countries may result in patent laws that allow others to use our discoveries or develop and commercialize our products. We cannot provide assurance that the patents we obtain or the unpatented technology we hold will afford us significant commercial protection.
| 32 |
RISKS RELATED TO OUR COMMON STOCK AND ORGANIZATIONAL STRUCTURE
Because our stock price has been and will likely continue to be highly volatile, the market price of our common stock may be lower or more volatile than expected.
Our stock price has been highly volatile. The stock market in general and the market for biopharmaceutical companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. From January 1, 2014 through December 31, 2014, the closing sale price of our common stock has been as low as $3.69 per share and as high as $6.65 per share. The market price of our common stock may be influenced by many factors, including:
| · | future announcements about us or our collaborators or competitors, including the results of testing, technological innovations or new commercial products; |
| · | clinical trial results; |
| · | depletion of our cash reserves; |
| · | sale of equity securities or issuance of additional debt; |
| · | announcement by us of significant strategic partnerships, collaborations, joint ventures, capital commitments or acquisitions; |
| · | changes in government regulations; |
| · | impact of competitor successes and in particular development success of vaccine candidates that compete with our own vaccine candidates; |
| · | developments in our relationships with our collaboration partners; |
| · | announcements relating to health care reform and reimbursement levels for new vaccines and other matters affecting our business and results, regardless of accuracy; |
| · | sales of substantial amounts of our stock by existing stockholders (including stock by insiders or 5% stockholders); |
| · | development, spread or new announcements related to pandemic influenza; |
| · | litigation; |
| · | public concern as to the safety of our products; |
| · | significant set-backs or concerns with the industry or the market as a whole; |
| · | regulatory inquiries, reviews and potential action, including from the FDA or the SEC; |
| · | recommendations by securities analysts or changes in earnings estimates; and |
| · | the other factors described in this Risk Factors section. |
In addition, the stock market in general, and the market for emerging and biopharmaceutical companies in particular, have experienced extreme price and volume fluctuations that have particularly affected the market price for many of those companies. These fluctuations have often been unrelated to the operating performance of these companies. These broad market fluctuations may cause the market price of our common stock to be lower or more volatile than expected.
Provisions of our Certificate of Incorporation and By-laws and Delaware law could delay or prevent the acquisition of the Company, even if such acquisition would be beneficial to stockholders, and could impede changes in our Board.
Provisions in our organizational documents could hamper a third-party’s attempt to acquire, or discourage a third-party from attempting to acquire control of, the Company. Stockholders who wish to participate in these transactions may not have the opportunity to do so. Our organizational documents also could limit the price investors are willing to pay in the future for our securities and make it more difficult to change the composition of our Board in any one year. Certain provisions include the right of the existence of a staggered board with three classes of directors serving staggered three-year terms and advance notice requirements for stockholders to nominate directors and make proposals.
| 33 |
As a Delaware corporation, we are also afforded the protections of Section 203 of the Delaware General Corporation Law, which will prevent us from engaging in a business combination with a person who acquires at least 15% of our common stock for a period of three years from the date such person acquired such common stock, unless advance board or stockholder approval was obtained.
Any delay or prevention of a change of control transaction or changes in our board or management could deter potential acquirers or prevent the completion of a transaction in which our stockholders could receive a substantial premium over the then current market price for their shares.
We have never paid dividends on our capital stock, and we do not anticipate paying any such dividends in the foreseeable future.
We have never paid cash dividends on our common stock. We currently anticipate that we will retain all of our earnings for use in the development of our business and do not anticipate paying any cash dividends in the foreseeable future. As a result, capital appreciation, if any, of our common stock would be the only source of gain for stockholders until dividends are paid, if at all.
| Item 1B. | UNRESOLVED STAFF COMMENTS |
None.
| Item 2. | PROPERTIES |
We lease three facilities in Gaithersburg, Maryland and one in Rockville, Maryland. In conjunction with our acquisition of Novavax AB in 2013, we acquired a facility lease in Uppsala, Sweden. A summary of our current facilities is set forth below.
| Property | Approximate | |||
| Location | Square Footage | |||
| Rockville, MD |
51,200 | Vaccine research and development and manufacturing facility | ||
| 20FF Gaithersburg, MD | 53,000 | Corporate headquarters, vaccine research and development and manufacturing facility | ||
| 21FF Gaithersburg, MD | 19,400 | Research and development laboratory facility and offices | ||
| 22FF Gaithersburg, MD | 21,000 | Administrative, clinical and regulatory offices | ||
| Uppsala, Sweden | 15,400 | Adjuvant manufacturing facility and research and development and administrative offices | ||
| Total square footage | 160,000 |
| Item 3. | LEGAL PROCEEDINGS |
We currently have no material pending legal proceedings.
| Item 4. | MINE SAFETY DISCLOSURES |
Not applicable.
| 34 |
| Item 5. | MARKET FOR REGISTRANT’S COMMON EQUITY AND RELATED STOCKHOLDER MATTERS |
Our common stock trades on The NASDAQ Global Select Market under the symbol “NVAX.” The following table sets forth the range of high and low closing sale prices for our common stock as reported on The NASDAQ Global Select Market for each quarter in the two most recent years:
| Quarter Ended | High | Low | ||||||
| December 31, 2014 | $ | 5.98 | $ | 4.05 | ||||
| September 30, 2014 | $ | 5.01 | $ | 4.08 | ||||
| June 30, 2014 | $ | 5.13 | $ | 3.69 | ||||
| March 31, 2014 | $ | 6.65 | $ | 4.13 | ||||
| December 31, 2013 | $ | 5.16 | $ | 2.76 | ||||
| September 30, 2013 | $ | 3.38 | $ | 2.11 | ||||
| June 30, 2013 | $ | 2.69 | $ | 1.79 | ||||
| March 31, 2013 | $ | 2.28 | $ | 1.75 | ||||
On February 23, 2015, the last sale price reported on The NASDAQ Global Select Market for our common stock was $9.49. Our common stock was held by approximately 433 stockholders of record as of February 23, 2015, one of which is Cede & Co., a nominee for Depository Trust Company (or DTC). All of the shares of common stock held by brokerage firms, banks and other financial institutions as nominees for beneficial owners are deposited into participant accounts at DTC, and are therefore considered to be held of record by Cede & Co. as one stockholder. We have not paid any cash dividends on our common stock since our inception. We do not anticipate declaring or paying any cash dividends in the foreseeable future.
Securities Authorized for Issuance under our Equity Compensation Plans
Information regarding our equity compensation plans, including both stockholder approved plans and non-stockholder approved plans, is included in Item 12 of this Annual Report on Form 10-K (Annual Report).
| 35 |
Performance Graph
The graph below compares the cumulative total stockholders return on our common stock for the last five fiscal years with the cumulative total return on the NASDAQ Composite Index and the Russell 2000 Growth Biotechnology Index (which includes Novavax) over the same period, assuming the investment of $100 in our common stock, the NASDAQ Composite Index and the Russell 2000 Growth Biotechnology Index on December 31, 2009, and reinvestments of all dividends.
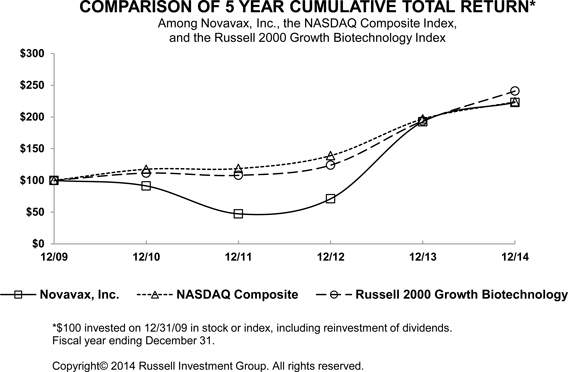
Value of $100 invested on December 31, 2009 in stock or index, including reinvestment of dividends, for fiscal years ended December 31:
| 12/31/09 | 12/31/10 | 12/31/11 | 12/31/12 | 12/31/13 | 12/31/14 | |||||||||||||||||||
| Novavax, Inc. | $ | 100.00 | $ | 91.35 | $ | 47.37 | $ | 71.05 | $ | 192.48 | $ | 222.93 | ||||||||||||
| NASDAQ Composite Index | $ | 100.00 | $ | 117.61 | $ | 118.70 | $ | 139.00 | $ | 196.83 | $ | 223.74 | ||||||||||||
| RUSSELL 2000 Growth Biotechnology Index | $ | 100.00 | $ | 111.52 | $ | 108.02 | $ | 124.06 | $ | 193.76 | $ | 240.78 |
This graph is not “soliciting material,” is not deemed “filed” with the SEC and is not to be incorporated by reference in any filing of the Company under the Securities Act of 1933, as amended, or the Exchange Act, whether made before or after the date hereof and irrespective of any general incorporation language in any such filing.
| 36 |
| Item 6. | SELECTED FINANCIAL DATA |
The following table sets forth selected financial data for each of the years in the five-year period ended December 31, 2014, which has been derived from our audited financial statements. The information below should be read in conjunction with our financial statements and notes thereto and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” included elsewhere in this Annual Report. These historical results are not necessarily indicative of results that may be expected for future periods.
| For The Years Ended December 31, | ||||||||||||||||||||
| 2014(1) | 2013(2) | 2012 | 2011 | 2010 | ||||||||||||||||
| (in thousands, except per share amounts) | ||||||||||||||||||||
| Statements of Operations Data: | ||||||||||||||||||||
| Revenue | $ | 30,659 | $ | 20,915 | $ | 22,076 | $ | 14,688 | $ | 343 | ||||||||||
| Net loss | (82,947 | ) | (51,983 | ) | (28,507 | ) | (19,364 | ) | (35,708 | ) | ||||||||||
| Basic and diluted net loss per share | (0.37 | ) | (0.31 | ) | (0.22 | ) | (0.17 | ) | (0.34 | ) | ||||||||||
| Weighted average shares used in computing basic and diluted net loss per share | 225,848 | 169,658 | 131,726 | 113,610 | 104,768 | |||||||||||||||
| As of December 31, | ||||||||||||||||||||
| 2014(1) | 2013(2) | 2012 | 2011 | 2010 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Balance Sheet Data: | ||||||||||||||||||||
| Cash and marketable securities(3) | $ | 168,056 | $ | 133,068 | $ | 50,344 | $ | 18,309 | $ | 31,676 | ||||||||||
| Total current assets | 188,158 | 145,001 | 50,408 | 26,109 | 33,337 | |||||||||||||||
| Working capital(4) | 154,042 | 126,879 | 38,733 | 18,530 | 23,071 | |||||||||||||||
| Total assets | 276,002 | 235,125 | 102,345 | 66,576 | 74,844 | |||||||||||||||
| Long-term debt, less current portion(5) | 503 | 1,199 | 990 | 300 | 320 | |||||||||||||||
| Accumulated deficit | (493,093 | ) | (410,146 | ) | (358,163 | ) | (329,656 | ) | (310,292 | ) | ||||||||||
| Total stockholders’ equity | 229,618 | 203,234 | 80,240 | 53,849 | 59,050 | |||||||||||||||
____________________
| (1) | In 2014, we completed a public offering of 28,750,000 shares of common stock resulting in net proceeds of approximately $108 million. |
| (2) | In 2013, we completed the acquisition of Novavax AB (see Note 4 to consolidated financial statements in Item 8) and a public offering of 31,846,950 shares of common stock resulting in net proceeds of approximately $95 million. |
| (3) | Includes non-current marketable securities of $6,233 at December 31, 2012. |
| (4) | Working capital is computed as the excess of current assets over current liabilities. |
| (5) | Includes non-current portion of capital leases. |
| 37 |
| Item 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
Any statements in the discussion below and elsewhere in this report, about the expectations, beliefs, plans, objectives, assumptions or future events or performance of Novavax, Inc. (“Novavax,” and together with its wholly-owned subsidiary, Novavax AB, the “Company,” “we” or “us”) are not historical facts and are forward-looking statements. Such forward-looking statements include, without limitation, statements with respect to our capabilities; goals; expectations regarding future revenue and expense levels; potential market sizes and demand for our product candidates; the efficacy, safety and intended utilization of our product candidates; the development of our clinical-stage product candidates and our recombinant vaccine and adjuvant technologies; the development of our pre-clinical product candidates; the conduct, timing and potential results from clinical and other trials; plans regarding regulatory filings; the expected timing and content of regulatory actions; reimbursement by the Department of Health and Human Services, Biomedical Advanced Research and Development Authority (“HHS BARDA”); the potential modification to our license agreement with Wyeth Holdings Corporation, a subsidiary of Pfizer Inc. (“Wyeth”); our available cash resources and the availability of financing generally; plans regarding partnering activities, business development initiatives and the adoption of stock incentive plans, and other factors referenced herein. You can identify these forward-looking statements by the use of words or phrases such as “believe,” “may,” “could,” “will,” “would,” “possible,” “can,” “estimate,” “continue,” “ongoing,” “consider,” “anticipate,” “intend,” “seek,” “plan,” “project,” “expect,” “should,” “would,” or “assume” or the negative of these terms, or other comparable terminology, although not all forward-looking statements contain these words. Accordingly, these statements involve estimates, assumptions and uncertainties that could cause actual results to differ materially from those expressed or implied in them. Any or all of our forward-looking statements in this Annual Report may turn out to be inaccurate or materially different than actual results.
Because the risk factors discussed in this Annual Report, and other risk factors of which we are not aware, could cause actual results or outcomes to differ materially from those expressed in any forward-looking statements made by or on behalf of us, you should not place undue reliance on any such forward-looking statements. These statements are subject to risks and uncertainties, known and unknown, which could cause actual results and developments to differ materially from those expressed or implied in such statements. We have included important factors in the cautionary statements included in this Annual Report, particularly those identified in Part I, Item 1A, “Risk Factors” of this Annual Report, that we believe could cause actual results or events to differ materially from the forward-looking statements that we make. These and other risks may also be detailed and modified or updated in our reports and other documents filed with the Securities and Exchange Commission (SEC) from time to time under the Securities Act and/or the Exchange Act. You are encouraged to read these filings as they are made.
Although we believe that the expectations reflected in our forward-looking statements are reasonable, we cannot guarantee future results, events, levels of activity, performance or achievement. Further, any forward-looking statements speak only as of the date on which it is made, and we undertake no obligation to update or revise any forward-looking statements, whether as a result of new information, future events or otherwise, unless required by law. New factors emerge from time to time, and it is not possible for us to predict which factors will arise. In addition, we cannot assess the impact of each factor on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements.
Overview
We are a clinical-stage vaccine company focused on the discovery, development and commercialization of recombinant nanoparticle vaccines and adjuvants. Using innovative proprietary recombinant nanoparticle vaccine technology, we produce vaccine candidates to efficiently and effectively respond to both known and newly emerging diseases. Our vaccine candidates are genetically engineered three-dimensional nanostructures that incorporate immunologically important proteins. Our product pipeline targets a variety of infectious diseases with vaccine candidates currently in clinical development for respiratory syncytial virus (“RSV”), seasonal influenza, pandemic influenza and the Ebola virus (“EBOV”). We have additional pre-clinical stage programs in a variety of infectious diseases, including Middle East Respiratory Syndrome (“MERS”). Further, CPL Biologics Private Limited (“CPLB”), our joint venture company with Cadila Pharmaceuticals Limited (“Cadila”) in India, is actively developing a number of vaccine candidates that were genetically engineered by Novavax, including its seasonal VLP influenza vaccine candidate that completed enrollment of a Phase 3 clinical trial in India in 2014, and its rabies vaccine that completed its Phase 1/2 clinical trial in India in 2014. CPLB is owned 20% by us and 80% by Cadila. CPLB operates a manufacturing facility in India for the production of vaccines
| 38 |
We are also developing proprietary technology for the production of immune stimulating saponin-based adjuvants, through our Swedish wholly-owned subsidiary, Novavax AB. Our Matrix adjuvant technology utilizes selected quillaja fractions, which form separate matrix structures, to develop modern, multi-purpose immune-modulating adjuvant products for a broad range of potential vaccine applications. Our lead adjuvant for human applications, Matrix-M™, has been successfully tested in a Phase 1/2 clinical trial for our pandemic influenza H7N9 vaccine candidate, conducted under our contract with HHS BARDA, and we are currently testing Matrix-M in conjunction with our EBOV vaccine candidate in a Phase 1 clinical trial. Genocea Biosciences, Inc. (“Genocea”) has licensed rights to our Matrix technology and is conducting clinical trials with its herpes simplex 2 vaccine candidate using Matrix-M.
Clinical Product Pipeline
A current summary of our significant research and development programs and status of related products in development follows:
| Program | Development Stage | Funding Collaborator | ||
| Respiratory Syncytial Virus (RSV) | ||||
| · Elderly | Phase 2 | |||
| · Maternal Immunization | Phase 2 | PATH | ||
| · Pediatric | Phase 1 | |||
| Influenza | ||||
| · Seasonal Quadrivalent | Phase 2 | HHS BARDA | ||
| · Pandemic H7N9 | Phase 2 | HHS BARDA | ||
| Other | ||||
| · Ebola Virus (EBOV) | Phase 1 | |||
| · Combination (Influenza/RSV) | Pre-Clinical | |||
| CPLB Programs (India) | ||||
| · Seasonal Influenza | Phase 3 | |||
| · Rabies | Phase 1/2 |
Respiratory Syncytial Virus (RSV)
RSV is a major respiratory pathogen with a significant burden of disease in the very young and in the elderly. In healthy adults, RSV infections are generally mild to moderate in severity, but are typically more severe in infants and young children, as well as adults over the age of 60.10 Globally, RSV is a common cause of childhood respiratory infection, with a disease burden of 64 million cases and approximately 160,000 deaths annually.11 Severe RSV disease results in 3.4 million hospital admissions per year globally12 and disproportionately affects infants below six months of age. In infants, toddlers and young pre-school and school-age children, RSV infections result in the need for frequent medical care, including emergency room and office visits and are associated with increased recurrent wheezing that can persist for years. In the U.S., nearly all children become infected with RSV before they are two years of age, and it has been associated with 20% of hospitalizations and 15% of office visits for acute respiratory infection in young children13. It is also estimated that between 11,000 and 17,000 elderly and high risk adults die of RSV infection or its complications annually in the U.S., and up to 180,000 are hospitalized for serious respiratory symptoms.14 Currently, there is no approved RSV vaccine available for any of these populations, so an RSV vaccine has the potential to protect millions of persons from this far-reaching unmet medical need.
10 Dawson-Caswell, D, et al., (2011) Am Fam Physician. 83:143 - 146
11 Nair, H., et al., (2010) Lancet. 375:1545 - 1555
12 WHO, (2014) “RSV Vaccine Status;” www.who.int/immunization/research/meetings_workshops/WHO_PDVAC_RSV.pdf
| 39 |
We are developing our respiratory syncytial virus fusion (F) protein nanoparticle vaccine candidate (“RSV F Vaccine”) for the benefit of three susceptible target populations: the elderly, infants (receiving protection through antibodies transferred from their mothers who would be immunized during the last trimester of pregnancy) and pediatrics.
RSV Elderly Program
In October 2014, we initiated enrollment in a Phase 2 dose-confirmation clinical trial of our RSV F Vaccine in 1,600 elderly adults (>60 years of age). Recruitment was completed in November, and the preliminary data from this trial are expected in the third quarter of 2015. We believe these data will inform the next steps in the development of our RSV elderly program. Data from our earlier Phase 1 clinical trial in the elderly, initiated in October 2012, corroborates our previous clinical experiences with our RSV F vaccine candidate. In May 2014, we released one-year follow up data from that Phase 1 clinical trial demonstrating that, for the group receiving the 90μg antigen dose without adjuvant, anti-F levels and palivizumab competing antibodies were significantly elevated over baseline at day 180, with neutralizing antibody levels that were considered protective for both the RSV A and RSV B strains. We believe these findings support the development of an annual RSV F vaccine candidate dose that can provide protection over the four-to-five month period of a typical RSV season.
RSV Maternal Immunization Program
In September 2014, we initiated a Phase 2 clinical trial of our RSV F Vaccine in fifty (50) healthy women in their third trimester of pregnancy. This trial is designed to evaluate the safety and immunogenicity of our RSV F Vaccine in pregnant women and assesses the impact of maternal immunization on RSV-specific antibody levels through the baby’s first six months of life and infant safety through the first year of life. The preliminary data from this trial are anticipated in the third quarter of 2015 and will inform the next steps in the development of our RSV maternal program. In November 2014, we announced that the U.S. Food and Drug Administration, Center for Biologics Evaluation and Research (“FDA”) had granted Fast Track Designation to our RSV F Vaccine for protection of infants via maternal immunization. The Fast Track designation, established by the FDA Modernization Act of 1997, is intended for products that treat serious or life-threatening diseases or conditions, and that demonstrate the potential to address unmet medical needs for such diseases or conditions. The program is intended to facilitate development and expedite review of drugs to treat serious and life-threatening conditions so that an approved product can reach the market expeditiously. Fast Track designation specifically facilitates meetings to discuss all aspects of development to support licensure and it provides the opportunity to submit sections of a Biologics License Application (“BLA”) on a rolling basis as data become available, which permits the FDA to review modules of the BLA as they are received instead of waiting for the entire BLA submission.
In April 2014, we announced positive top-line safety and immunogenicity data from a Phase 2 clinical trial in women of childbearing age that were similar to, or exceeded, immune responses seen in our previous clinical trials. This Phase 2 clinical trial evaluated the safety and immunogenicity of two dose levels of our RSV F vaccine candidate, in one or two injections, with and without an aluminum phosphate adjuvant, in 720 healthy women of childbearing age. These positive data supported Novavax’ decision to progress to the previously discussed Phase 2 clinical trial in pregnant women.
13 Hall, CB, et al., (2009) N Engl J Med. 360(6):588-98
14 Falsey, A., et al., (2014) Infectious Disorders. 12(2): 98-102
| 40 |
PATH Vaccine Solutions (“PATH”) Clinical Development Agreement for RSV Maternal Program
In conjunction with our development of our RSV F vaccine candidate for maternal immunization, in 2012 we entered into a clinical development agreement with PATH to develop our RSV F vaccine candidate in certain low-resource countries. We refer to this as our RSV Collaboration Program. We were awarded approximately $2.0 million by PATH for initial funding under the agreement to partially support our Phase 2 dose-ranging clinical trial in women of childbearing age described above. In October 2013, the funding under this agreement was increased by $0.4 million to support reproductive toxicology studies, which was necessary before we began conducting clinical trials in pregnant women. In December 2013, we entered into an amendment with PATH providing an additional $3.5 million in funding to support the Phase 2 dose-confirmation clinical trial in 720 women of childbearing age. In October 2014, we entered into an amendment with PATH providing an additional $1.0 million towards the development of a strategy for approaching Phase 3 clinical trials of our RSV maternal immunization program and are in ongoing discussion with PATH for additional funding. We retain global rights to commercialize the product and will support PATH in its goal to make an RSV maternal vaccine product affordable and available in low-resource countries. To the extent PATH elects to continue to fund 50% of our external clinical development costs for the RSV Collaboration Program, but we do not continue development, we would then grant PATH a fully-paid license to our RSV F vaccine candidate technology for use in pregnant women in certain contractually defined, low-resource countries.
RSV Pediatric Program
While the burden of RSV disease falls heavily on newborn infants, RSV is also a prevalent and currently unaddressed problem in pediatrics. This third market segment for our RSV vaccine candidate remains an important opportunity. In November 2014, we initiated a Phase 1 clinical trial of our RSV F Vaccine in 150 healthy children two to six years old. This trial is designed to evaluate the safety and immunogenicity of our RSV F Vaccine in children. The preliminary data from this trial are expected in late 2015 or in the first half of 2016 and will inform the next steps in the development of our RSV pediatric program.
Influenza
Influenza is a world-wide infectious disease that causes illness in humans with symptoms ranging from mild to life-threatening; serious illness occurs not only in susceptible populations such as pediatrics and the elderly, but also in the general population because of unique strains of influenza for which most humans have not developed protective antibodies. Influenza is a major burden on public health worldwide: estimates of one million deaths each year are attributed to influenza.15 It is further estimated that, each year, influenza attacks between five and ten percent of adults and 20% to 30% of children, causing significant levels of illness, hospitalization and death.16
Although a number of licensed seasonal influenza vaccines are currently commercially available in most geographies, and these manufacturers have capabilities to develop influenza vaccines that are responsive to unique and emerging influenza strains, we believe our influenza virus-like particle (“VLP”) vaccine candidates have immunological advantages over currently available vaccines. These immunological advantages stem from the fact that our influenza VLPs contain three of the major structural virus proteins that are important for fighting influenza: hemagglutinin (“HA”) and neuraminidase (“NA”), both of which stimulate the body to produce antibodies that neutralize the influenza virus and prevent its spread through the cells in the respiratory tract, and matrix 1 (“M1”), which stimulates cytotoxic T lymphocytes to kill cells that may already be infected. Our VLPs are not made from live viruses and have no genetic nucleic material in their inner core, which render them incapable of replicating and causing disease.
15 Resolution of the World Health Assembly. Prevention and control of influenza pandemics and annual epidemics. WHA56.19. 28 May 2003
16 WHO. Vaccines against influenza. WHO position paper – November 2012 Weekly Epidemiol Record 2012;87(47):461–76.
| 41 |
Seasonal Quadrivalent Influenza Vaccine
Developing and commercializing a seasonal influenza vaccine is an important business opportunity and strategic goal for Novavax. The Advisory Committee for Immunization Practices of the Center for Disease Control and Prevention (“CDC”) recommends that all persons aged six months and older should be vaccinated annually against seasonal influenza. In conjunction with these universal recommendations, attention from the 2009 influenza H1N1 pandemic, along with reports of other cases of avian-based influenza strains, has increased public health awareness of the importance of seasonal influenza vaccination, the market for which is expected to continue to grow worldwide in both developed and developing global markets.
In recent years, trivalent influenza vaccines (three influenza strains: two influenza A strains and one influenza B strain) have been made generally available on a worldwide basis. With two distinct lineages of influenza B viruses circulating, public health authorities have advocated for the addition of a second influenza B strain to provide additional protection. Vaccine manufacturers have responded through the development and licensure of quadrivalent (i.e., four influenza strains: two influenza A strains and two influenza B strains) influenza vaccines. It is expected that quadrivalent seasonal influenza vaccines will ultimately replace trivalent seasonal influenza vaccines in the global market. There are currently four quadrivalent influenza vaccines licensed in the U.S., although additional quadrivalent seasonal influenza vaccines are expected to be licensed over the next several years. Current estimates for seasonal influenza vaccine growth in the top seven markets (U.S., Japan, France, Germany, Italy, Spain and UK), show potential growth from approximately $3.2 billion in the 2012/13 season to $5.3 billion by the 2021/2022 season.17 Recombinant seasonal influenza vaccines, like the candidate we are developing, have an important advantage: once licensed for commercial sale, large quantities of vaccines can be quickly and cost-effectively manufactured without the use of either the live influenza virus or eggs.
In November 2014, under our contract with HHS BARDA, we initiated a Phase 2 clinical trial of our quadrivalent seasonal influenza VLP vaccine candidate in 400 healthy adults. The primary outcomes of the trial will assess safety and tolerability of the seasonal influenza VLP vaccine candidate and quantify immune responses to each of the four influenza strains based on hemagglutination-inhibiting antibody titers. In addition, secondary outcomes will evaluate neuraminidase-inhibition antibody titers for all four influenza strains. The preliminary data from this trial are expected in the second quarter of 2015 and will inform the next steps in the development of our quadrivalent seasonal influenza VLP vaccine candidate. Data from our previous Phase 2 clinical trial, announced in July 2012, showed that our quadrivalent seasonal influenza VLP vaccine candidate demonstrated immunogenicity against all four viral strains based on hemagglutination inhibition responses at day 21, was well-tolerated, and met the FDA accelerated approval seroprotection rates criterion for all four viral strains, although the potential to fulfill the seroconversion rates criterion was demonstrated in just three of the four viral strains. Following that Phase 2 clinical trial, we focused our activities on manufacturing processes that will better ensure consistent, enhanced immune responses in all four strains.
Pandemic H7N9 Influenza Vaccine
In the aftermath of the 2009 pandemic of the A(H1N1) influenza strain, prevention of the potential devastation of a human influenza pandemic remains a key priority with both governmental health authorities and influenza vaccine manufacturers. In the U.S. alone, the 2009 H1N1 influenza pandemic led to the production of approximately 126 million doses of monovalent (single strain) vaccine. Public health awareness and government preparedness for the next potential influenza pandemic are driving development of vaccines that can be manufactured quickly against a potentially threatening influenza strain. Until the spring of 2013, industry and health experts focused attention on developing a monovalent H5N1 influenza vaccine as a potential key defense against a future pandemic threat; however, a significant number of reported cases in China of an avian-based influenza strain, known as A(H7N9), has shifted attention to the potential development of a monovalent H7N9 influenza vaccine.
In collaboration with HHS BARDA, we have now developed and delivered compelling safety and immunogenicity data on two pandemic vaccine candidates, H5N1 and H7N9, which provide the U.S. government with alternatives for dealing with future potential threats. In September 2014, we announced positive results from a Phase 1/2 clinical trial of our H7N9 influenza VLP vaccine candidate adjuvanted with Matrix-M in 610 healthy adults. Under our contract with HHS BARDA, the Phase 1/2 clinical trial was designed as a dose-ranging, randomized, observer-blinded, placebo-controlled clinical trial, to determine the contribution of Matrix-M to potential antigen dose sparing regimens. Our H7N9 influenza VLP vaccine candidate, with and without Matrix-M, was well tolerated and demonstrated a safety profile similar to the company’s prior experience with another saponin-based adjuvant. Matrix-M adjuvanted formulations demonstrated immunogenicity and dose-sparing benefits relative to unadjuvanted antigen. Hemagglutination-inhibiting antibody titers were generally comparable to those reported in prior studies with another saponin adjuvant and the vaccine also elicited significant anti-neuraminidase antibodies. In October 2014, we announced that the FDA had granted fast track designation to our H7N9 influenza VLP vaccine candidate with Matrix-M.
17 Influenza Vaccines Forecasts. Datamonitor (2013)
| 42 |
Potential Accelerated Approval Pathway for Influenza
In the past, we have referenced attainment of accelerated approval immunogenicity endpoints for seroprotection and seroconversion as a potential pathway for licensure of our influenza vaccines. The criteria for granting such accelerated approval of a BLA (the biologic equivalent to a New Drug Application or “NDA”) for new seasonal and pandemic influenza vaccines was published by the FDA. Under FDA guidance, developers that can demonstrate results that meet or exceed certain specified immunogenicity endpoint criteria in their clinical trials may, at the FDA’s discretion, be granted a license to market a product prior to submission of traditional clinical endpoint efficacy trial data. It should be noted that FDA licensure based on accelerated approval nevertheless requires sponsors to conduct a post-licensure efficacy study to demonstrate the clinical benefit of the vaccine, which would thereby support traditional approval of the vaccine. Because it is not possible to conduct a clinical endpoint efficacy study for a pandemic vaccine in advance of a declared pandemic, FDA’s pandemic guidance allows for submission of seasonal influenza clinical efficacy data for the purpose of confirming clinical benefit of a pandemic vaccine manufactured by the same process. Thus, the demonstration of efficacy with a seasonal vaccine provides a key link between the seasonal and pandemic programs. Accelerated approval further necessitates a shortage of influenza vaccine relative to the total population recommended to receive such vaccine, a situation that persists with seasonal influenza vaccines.
Although we have not ruled out this accelerated approval approach, particularly for our pandemic influenza program or certain populations within our seasonal influenza program, we do not expect to pursue accelerated approval of our quadrivalent seasonal influenza VLP vaccine candidate, largely because of the uncertainty as to whether the accelerated approval pathway will be available to us at the time of our BLA submission and the unknown ability of current and new influenza strains to meet such accelerated approval criteria. We are planning, therefore, to pursue traditional licensure of our quadrivalent seasonal influenza VLP vaccine candidate by conducting a clinical endpoint efficacy study for the purpose of submitting the data within the original BLA. These efficacy data will also support the requirement for clinical efficacy data for our pandemic vaccine program. We plan to discuss with the FDA our licensure pathways (both the traditional pathway for seasonal and possible accelerated pathways for pandemic and certain populations within the seasonal program) during future formal meetings. The likely impact of such an efficacy trial would be an additional year or more before the FDA grants licensure to our quadrivalent seasonal influenza VLP vaccine candidate.
HHS BARDA Contract for Recombinant Influenza Vaccines
HHS BARDA awarded us a contract in 2011, which funds the development of both our multivalent seasonal influenza and pandemic influenza VLP vaccine candidates. Our contract with HHS BARDA is a cost-plus-fixed-fee contract, which reimburses us for allowable direct contract costs incurred plus allowable indirect costs and a fixed-fee earned in the ongoing clinical development and product scale-up of our multivalent seasonal and monovalent pandemic influenza vaccines. In September 2014, we announced that HHS BARDA had exercised and initiated a two-year option to our contract, which not only extended the contract until September 2016, but also added scope to support our development activities leading up to planned Phase 3 clinical studies and $70 million of funding on top of the remainder of the $97 million base period funding. During 2014, we recognized revenue of $26.0 million and have recognized approximately $78 million in revenue since the inception of the contract.
| 43 |
Ebola Virus (EBOV)
Recent news reports have centered around EBOV, formerly known as Ebola hemorrhagic fever, which is a severe, often fatal illness in humans. Five strains of EBOV have been identified, the most recent of which, the 2014 Guinea-based EBOV strain, is associated with a case fatality rate of 50% to 90%. There are currently no licensed treatments proven to neutralize the virus, but a range of blood, immunological and drug therapies are under development. Despite the development of such therapies, current vaccine approaches target either a previous strain of the virus or were initially developed to be delivered by genetic vectors. Our EBOV glycoprotein (“GP”) vaccine candidate, which was modeled using the 2014 Guinea-based EBOV strain, has been successfully tested in rodent, rabbit, and non-human primate pre-clinical models. We have also tested the vaccine with our Matrix-M adjuvant, which appears to significantly contribute to enhanced immunogenicity and dose-sparing.
We initiated large-scale GMP production of our EBOV GP vaccine candidate in the fourth quarter of 2014. In February 2015, we announced the initiation of enrollment in a Phase 1 clinical trial of our EBOV GP vaccine candidate in 150 healthy adults to evaluate the safety and immunogenicity of this vaccine candidate in ascending doses, with and without our Matrix-M adjuvant. We expect preliminary data from this trial to be available in mid-2015. In addition, we announced successful preliminary data from a non-human primate challenge study of our EBOV GP vaccine candidate in which the challenge was lethal for the control animal, whereas 100% of the immunized animals were protected. Plans to demonstrate the safety and efficacy in a large-scale global clinical trial will be developed based on the results of our Phase 1 clinical trial and in collaboration with global regulatory authorities and world health agencies.
Combination Respiratory (Influenza and RSV)
Given the ongoing development of our quadrivalent seasonal influenza VLP vaccine candidate and our RSV F vaccine candidate, we see an important opportunity to develop a combination respiratory vaccine candidate. This opportunity presents itself most evidently in the elderly, although we have not ruled out developing a combination respiratory vaccine for the non-elderly. Early pre-clinical development efforts have given us confidence that such a combination vaccine is viable and in animal models, provides acceptable immunogenicity. We intend to explore this development opportunity by conducting a Phase 1 clinical trial in such a combination vaccine in 2015.
CPLB Programs (India)
Seasonal Influenza
CPLB completed enrollment of its on-going Phase 3 clinical trial of its seasonal VLP influenza vaccine candidate in the second half of 2014. Assuming positive safety and immunogenicity data from this Phase 3 clinical trial, CPLB plans to file for regulatory market authorization, the Indian equivalent of a BLA, for its seasonal VLP vaccine candidate.
Rabies
CPLB is developing a rabies G protein vaccine candidate that we genetically engineered and completed enrollment of an ongoing Phase 1/2 clinical trial in India in 2014. The objective is to develop a recombinant vaccine that can be administered both as a pre-exposure prophylaxis for residents of certain higher-risk geographies and travelers to such locations, and as a post-exposure prophylaxis using fewer doses than the current standard of care. In October 2014, CPLB presented clinical results from Stage I of the Phase 1/2 clinical trial, demonstrating that all vaccine recipients, at various doses levels and schedules, showed seroprotective antibody levels at day 14 that were sustained through day 180. The vaccine candidate, which was found to be safe and well-tolerated, also induced seroprotective levels with two-dose and three-dose regimens. Assuming positive clinical data from Stage II of the Phase 1/2 clinical trial, CPLB would plan to initiate a Phase 3 clinical trial.
| 44 |
Discovery Programs
Our vaccine platform technology provides an efficient system to rapidly develop antigens to selected targets, refine manufacturing processes and optimize development across multiple vaccine candidates. We pay close attention to global reports of emerging diseases for which there do not appear to be immediate cures and where a vaccine protocol could offer potential protection. In addition to our response to the A(H7N9) influenza strain (as previously discussed), we have been monitoring reports concerning MERS, a novel coronavirus first identified in September 2012 by an Egyptian virologist. MERS became an emerging threat in 2013, with the WHO currently reporting more than 850 confirmed cases of infection and more than 350 deaths. The MERS virus is a part of the coronavirus family that includes the severe acute respiratory syndrome coronavirus (“SARS”). Because of the public health priority given to MERS, within weeks of getting the virus’ sequence, we successfully produced a vaccine candidate designed to provide protection against MERS. This vaccine candidate, which was made using our recombinant nanoparticle vaccine technology, is based on the major surface spike protein, which we had earlier identified as the antigen of choice in our work with a SARS vaccine candidate. In April 2014, in collaboration with the University of Maryland, School of Medicine, we published results that showed our investigational vaccine candidates against both MERS and SARS blocked infection in laboratory studies. Although the development of a MERS vaccine candidate currently remains a pre-clinical program, we believe that our MERS vaccine candidate offers a viable option to interested global public health authorities.
Sales of Common Stock
In June 2014, we completed a public offering of 28,750,000 shares of our common stock, including 3,750,000 shares of common stock that were issued upon the exercise in full of the option to purchase additional shares granted to the underwriters, at a price of $4.00 per share resulting in net proceeds of approximately $108 million.
In September 2013, we completed a public offering of 31,846,950 shares of our common stock, including 4,153,950 shares of common stock that were issued upon the exercise in full of the option to purchase additional shares granted to the underwriters, at a price of $3.14 per share resulting in net proceeds of approximately $95 million.
In 2012, we entered into an At Market Issuance Sales Agreement (“Sales Agreement”), under which our Board of Directors (the “Board”) approved the sale of up to an aggregate of $50 million in gross proceeds of our common stock. The shares of common stock are being offered pursuant to a shelf registration statement filed with the SEC in March 2013, which replaced the previous shelf registration statement filed in 2010. The Board’s standing Finance Committee (the “Committee”) assists with its responsibilities to monitor, provide advice to our senior management and approve all capital raising activities. The Committee has been authorized by the Board, absent any action by the Board to the contrary, to take any additional actions necessary to carry out the Board’s authorization of the issuance and sale of the common stock sold pursuant to the Sales Agreement. In doing so, the Committee is authorized to set the amount of shares to be sold, the period of time during which such sales may occur and the minimum sales price per share. During 2013, we sold 12.6 million shares at sales prices ranging from $2.06 to $3.38 per share, resulting in approximately $34.0 million in net proceeds. The most recent sales to occur under the Sales Agreement were in September 2013. As of December 31, 2014, we have approximately $15 million available under the Sales Agreement.
Critical Accounting Policies and Use of Estimates
The discussion and analysis of our financial condition and results of operations are based upon our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States.
The preparation of our consolidated financial statements requires us to make estimates, assumptions and judgments that affect the reported amounts of assets, liabilities and equity and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. These estimates, particularly estimates relating to accounting for revenue, the valuation of our marketable securities, stock-based compensation, long-lived assets, goodwill and estimated recovery of our net deferred tax assets have a material impact on our consolidated financial statements and are discussed in detail throughout our analysis of the results of operations discussed below.
We base our estimates on historical experience and various other assumptions that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets, liabilities and equity that are not readily apparent from other sources. Actual results and outcomes could differ from these estimates and assumptions.
| 45 |
Revenue
We recognize revenue under research contracts when a contract has been executed, the contract price is fixed or determinable, delivery of services or products has occurred and collection of the contract price is reasonably assured. Payments received in advance of work performed are recorded as deferred revenue and losses on contracts, if any, are recognized in the period in which they become known.
We are currently performing a research and development contract for a U.S. Government agency under a cost reimbursable fixed price contract. Under such cost reimbursable contracts, we are reimbursed and recognize revenue as allowable costs are incurred plus a portion of the fixed-fee earned. We consider fixed-fees under cost reimbursable contracts to be earned in proportion to the allowable costs incurred in performance of the work as compared to total estimated contract costs, with such costs incurred representing a reasonable measurement of the proportional performance of the work completed. Under our HHS BARDA contract, certain activities must be pre-approved by HHS BARDA in order for their costs to be deemed allowable direct costs. Direct costs incurred under cost reimbursable contracts are recorded as cost of government contracts revenue. Our HHS BARDA contract provides the U.S. government the ability to terminate the contract for convenience or to terminate for default if the Company fails to meet its obligations as set forth in the statement of work. We believe that if the government were to terminate the HHS BARDA contract for convenience, the costs incurred through the effective date of such termination and any settlement costs resulting from such termination would be allowable costs. Payments to us under cost reimbursable contracts, such as the HHS BARDA contract, are provisional payments subject to adjustment upon annual audit by the government. An audit by the U.S government of fiscal years 2011 and 2012 was completed in the first quarter of 2014, which resulted in no significant adjustments. An audit of fiscal year 2013 has been initiated, but has not been completed as of the date of this filing. Management believes that revenue for periods not yet audited has been recorded in amounts that are expected to be realized upon final audit and settlement. When the final determination of the allowable costs for any year has been made, revenue and billings may be adjusted accordingly in the period that the adjustment is known.
Our collaborative research and development agreements may include an upfront payment, payments for research and development services, milestone payments and royalties. Agreements with multiple deliverables are evaluated to determine if the deliverables can be divided into more than one unit of accounting. A deliverable can generally be considered a separate unit of accounting if both of the following criteria are met: (1) the delivered item(s) has value to the customer on a stand-alone basis; and (2) if the arrangement includes a general right of return relative to the delivered item(s), delivery or performance of the undelivered item(s) is considered probable and substantially in our control. Deliverables that cannot be divided into separate units are combined and treated as one unit of accounting. Consideration received is allocated among the separate units of accounting based on the relative selling price method. Deliverables under these arrangements typically include rights to intellectual property, research and development services and involvement by the parties in steering committees. Historically, deliverables under our collaborative research and development agreements have been deemed to have no stand-alone value and as a result have been treated as a single unit of accounting. In addition, we analyze our contracts and collaborative agreements to determine whether the payments received should be recorded as revenue or as a reduction to research and development expenses. In reaching this determination, management considers a number of factors, including whether we are the principal under the arrangement, and whether the arrangement is significant to, and part of, our core operations. Historically, payments received under its contracts and collaborative agreements have been recognized as revenue since we act as a principal in the arrangement and the activities are core to our operations.
When the performance under a fixed price contract can be reasonably estimated, revenue for fixed price contracts is recognized under the proportional performance method and earned in proportion to the contract costs incurred in performance of the work as compared to total estimated contract costs. Costs incurred under fixed price contracts represent a reasonable measurement of proportional performance of the work. Direct costs incurred under collaborative research and development agreements are recorded as research and development expenses. If the performance under a fixed price contract cannot be reasonably estimated, we recognize the revenue on a straight-line basis over the contract term.
Revenue associated with upfront payments under arrangements is recognized over the contract term or when all obligations associated with the upfront payment have been satisfied.
| 46 |
Revenue from the achievement of research and development milestones, if deemed substantive, is recognized as revenue when the milestones are achieved and the milestone payments are due and collectible. If not deemed substantive, we would recognize such milestone as revenue upon its achievement on a straight-line basis over the remaining expected term of the research and development period. Milestones are considered substantive if all of the following conditions are met: (1) the milestone is non-refundable; (2) there is substantive uncertainty of achievement of the milestone at the inception of the arrangement; (3) substantive effort is involved to achieve the milestone and such achievement relates to past performance; and (4) the amount of the milestone appears reasonable in relation to the effort expended and all of the deliverables and payment terms in the arrangement.
Marketable Securities
Our marketable securities are classified as available-for-sale securities and are carried at fair value. Unrealized gains and losses on these securities, if determined not to be “other-than-temporary,” are included in accumulated other comprehensive income (loss) in stockholders’ equity. Investments are evaluated periodically to determine whether a decline in value is other-than-temporary. Management reviews criteria, such as the magnitude and duration of the decline, as well as the Company’s ability to hold the securities until market recovery, to predict whether the loss in value is other-than-temporary. If a decline in value is determined to be other-than-temporary, the value of the security is reduced and the impairment is recorded in the statements of operations. For marketable securities carried at fair value, we disclose the level within the fair value hierarchy as prescribed by Accounting Standard Codification (“ASC”) 820, Fair Value Measurements and Disclosures. We evaluate the types of securities in our investment portfolio to determine the proper classification in the fair value hierarchy based on trading activity and market inputs. We generally obtain information from an independent third-party to help us determine the fair value of securities in Level 2 of the fair value hierarchy. Investment income is recorded when earned and included in investment income.
Stock-Based Compensation
We account for our stock-based compensation under our equity compensation plans in accordance with ASC 718, Compensation-Stock Compensation. This standard requires us to measure the cost of employee services received in exchange for equity awards based on the grant-date fair value of the award. Employee stock-based compensation is estimated at the date of grant based on the award’s fair value using the Black-Scholes option-pricing model and is recognized as an expense on a straight-line basis over the requisite service period for those awards expected to vest. The Black-Scholes option-pricing model requires the use of certain assumptions, the most significant of which are our estimates of the expected volatility of the market price of our common stock and the expected term of the award. Our estimate of the expected volatility is based on historical volatility over the look-back period corresponding to the expected term. The expected term represents the period during which our stock-based awards are expected to be outstanding. We estimate this amount based on historical experience of similar awards, giving consideration to the contractual terms of the awards, vesting requirements and expectation of future employee behavior, including post-vesting exercise and forfeiture history. We review our valuation assumptions at each grant date and, as a result, our assumptions in future periods may change. Also, the accounting estimate of stock-based compensation expense is reasonably likely to change from period to period as further equity awards are made and adjusted for cancellations.
Impairments of Long-Lived Assets
We account for the impairment of long-lived assets (including finite-lived intangible assets) by performing an evaluation of the recoverability of the carrying value of long-lived assets whenever events or changes in circumstances indicate that the carrying value of the asset may not be recoverable. Examples of events or changes in circumstances that indicate that the recoverability of the carrying value of an asset should be assessed include, but are not limited to, the following: a significant decrease in the market value of an asset, a significant change in the extent or manner in which an asset is used, a significant physical change in an asset, a significant adverse change in legal factors or in the business climate that could affect the value of an asset, an adverse action or assessment by a regulator, an accumulation of costs significantly in excess of the amount originally expected to acquire or construct an asset, a current period operating or cash flow loss combined with a history of operating or cash flow losses and/or a projection or forecast that demonstrates continuing losses associated with an asset used for the purpose of producing revenue. We consider historical performance and anticipated future results in our evaluation of potential impairment. Accordingly, when indicators of impairment are present, we evaluate the carrying value of these assets in relation to the operating performance of the business and future undiscounted cash flows expected to result from the use of these assets. Impairment losses are recognized when the sum of expected future cash flows is less than the assets’ carrying value.
| 47 |
Goodwill
Goodwill was generated from two business acquisitions. Our goodwill is not amortized, but is subject to impairment tests annually, or more frequently should indicators of impairment arise. Because the Company’s only business is the development of recombinant vaccines, the Company operates as a single operating segment and reporting unit. We utilize the market approach and, if considered necessary, the income approach to determine if we have an impairment of our goodwill. The market approach serves as the primary approach and is based on market value of invested capital. To ensure that our capital stock is the appropriate measurement of fair value, we have considered factors such as, our trading volume, diversity of investors and analyst coverage. The concluded fair value of our reporting unit significantly exceeded the carrying value at December 31, 2014 and 2013. The income approach is used as a confirming look to the market approach, if considered necessary. Goodwill impairment may exist if the carrying value of a reporting unit exceeds its estimated fair value, which we test annually at December 31. If the carrying value of the reporting unit exceeds its fair value, step two of the impairment analysis is performed. In step two of the analysis, an impairment loss is recorded equal to the excess of the carrying value of the reporting unit’s goodwill over its implied fair value should such a circumstance arise.
Given the current economic conditions and the uncertainties regarding their impact on us, there can be no assurance that the estimates and assumptions made for purposes of our goodwill impairment testing will prove to be accurate predictions of the future, or that any change in the assumptions or the current economic conditions will not trigger more frequently than on an annual basis. If our assumptions are not achieved or economic conditions deteriorate further, we may be required to record goodwill impairment charges in future periods.
Income Taxes
We recognize deferred tax assets and liabilities for expected future tax consequences of temporary differences between the carrying amounts and tax basis of assets and liabilities. Under the liability method, deferred income taxes are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax basis and operating loss carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the year in which those temporary differences are expected to be recovered or settled. The effect of changes in tax rates on deferred tax assets and liabilities is recognized in income in the period such changes are enacted.
Developing our provision for income taxes and analyzing our tax position requires significant judgment and knowledge of federal and state income tax laws, regulations and strategies, including the determination of deferred tax assets and liabilities and any valuation allowances that may be required for deferred tax assets.
We assess the likelihood of realizing our deferred tax assets to determine whether an income tax valuation allowance is required. Based on such evidence that can be objectively verified, we determine whether it is more likely than not that all or a portion of the deferred tax assets will be realized. The main factors that we consider include: cumulative losses in recent years; income/losses expected in future years; the applicable statute of limitations; and potential limitations on available net operating loss and tax credit carryforwards.
Tax benefits associated with uncertain tax positions are recognized in the period in which one of the following conditions is satisfied: (1) the more likely than not recognition threshold is satisfied; (2) the position is ultimately settled through negotiation or litigation; or (3) the statute of limitations for the taxing authority to examine and challenge the position has expired. Tax benefits associated with an uncertain tax position are reversed in the period in which the more likely than not recognition threshold is no longer satisfied.
| 48 |
A valuation allowance is established when necessary to reduce net deferred tax assets to the amount expected to be realized. We concluded that the realization of deferred tax assets is dependent upon future earnings, if any, the timing and amount of which are uncertain. Accordingly, our net deferred tax assets have been fully offset by a valuation allowance.
Recent Accounting Guidance Not Yet Adopted
For detailed information regarding recently issued accounting pronouncements and the expected impact on our consolidated financial statements, see Note 3, “Summary of Significant Accounting Policies” in the accompanying Notes to Consolidated Financial Statements included in this Annual Report.
Results of Operations for Fiscal Years 2014, 2013 and 2012 (amounts in tables are presented in thousands, except per share information)
The following is a discussion of the historical financial condition and results of operations of Novavax, Inc., which includes Novavax AB’s operations since the acquisition date of July 31, 2013, and should be read in conjunction with the consolidated financial statements and notes thereto set forth in this Annual Report. Additional information concerning factors that could cause actual results to differ materially from those in our forward-looking statements is described under Part I, Item 1A, “Risk Factors” of this Annual Report.
Revenue:
| 2014 | 2013 | 2012 | Change
2013 to 2014 | Change
2012 to 2013 | ||||||||||||||||
| Revenue: | ||||||||||||||||||||
| Total revenue | $ | 30,659 | $ | 20,915 | $ | 22,076 | $ | 9,744 | $ | (1,161 | ) | |||||||||
Revenue for 2014 was $30.7 million as compared to $20.9 million for 2013, an increase of $9.7 million, or 47%. Revenue for 2014 and 2013 was primarily comprised of services performed under the HHS BARDA contract, and to a much lesser extent, the PATH clinical development agreement and revenue from Novavax AB. The increase in revenue is primarily due to the higher level of activity in 2014 associated with our Phase 1/2 clinical trial of our H7N9 pandemic VLP vaccine candidate and manufacturing work for our Phase 2 seasonal influenza clinical trial under the HHS BARDA contract, as compared to 2013. We also had increased revenue in 2014 associated with Novavax AB resulting from twelve months of activity in 2014 as compared to only five months in 2013.
Revenue for 2013 was $20.9 million as compared to $22.1 million for 2012, a decrease of $1.2 million, or 5%. Revenue for 2013 and 2012 was primarily comprised of services performed under the HHS BARDA contract and, to a much lesser extent, the PATH clinical development agreement and in 2013, revenue of $0.7 million from Novavax AB. The decrease in revenue is primarily due to the higher level of activity in 2012 associated with our influenza clinical trials under the HHS BARDA contract as compared to 2013 when no similar clinical trials were initiated. In connection with the February 2014 amendment of the HHS BARDA contract, we recorded revenue of $2.7 million in the fourth quarter of 2013 relating to manufacturing and other activities that support the Phase 1 clinical trial of our H7N9 influenza VLP candidate and Matrix-M adjuvant, which was conducted in the first half of 2014.
For 2015, we expect a significant increase in revenue associated with our increased clinical trial and product development activities under the HHS BARDA contract to support the initiation of later-stage clinical trials of our quadrivalent seasonal influenza and pandemic H7N9 influenza VLP vaccine candidates.
| 49 |
Costs and Expenses:
| 2014 | 2013 | 2012 | Change
2013 to 2014 | Change
2012 to 2013 | ||||||||||||||||
| Costs and Expenses: | ||||||||||||||||||||
| Cost of government contracts revenue. | $ | 14,987 | $ | 8,222 | $ | 14,692 | $ | 6,765 | $ | (6,470 | ) | |||||||||
| Research and development | 79,435 | 50,308 | 26,907 | 29,127 | 23,401 | |||||||||||||||
| General and administrative | 19,928 | 14,819 | 10,142 | 5,109 | 4,677 | |||||||||||||||
| Total costs and expenses | $ | 114,350 | $ | 73,349 | $ | 51,741 | $ | 41,001 | $ | 21,608 | ||||||||||
Cost of Government Contracts Revenue
Cost of government contracts revenue includes direct costs of salaries, laboratory supplies, consultants and subcontractors and other direct costs associated with our process development, manufacturing, clinical, regulatory and quality assurance activities under research contracts. Cost of government contracts revenue increased to $15.0 million for 2014 from $8.2 million for 2013, an increase of $6.8 million, or 82%. The increase in cost of government contracts revenue is primarily related to the costs of our Phase 1/2 clinical trial using our pandemic H7N9 influenza VLP vaccine candidate and Matrix-M adjuvant and manufacturing work for our Phase 2 quadrivalent seasonal VLP influenza clinical trial, as compared to 2013. For 2015, we expect a significant increase in cost of government contracts revenue associated with our increased clinical trial and product development activities under the HHS BARDA contract to support the initiation of later-stage clinical trials of our quadrivalent seasonal influenza and pandemic H7N9 influenza VLP vaccine candidates.
Cost of government contracts revenue decreased to $8.2 million for 2013 from $14.7 million for 2012, a decrease of $6.5 million, or 44%. The decrease in cost of government contracts revenue is primarily related to the levels of activity associated with our influenza clinical trials previously mentioned, including the 205 Trial (see discussion of the 205 Trial in Note 8 to the financial statements included herewith).
Research and Development Expenses
Research and development expenses include salaries, laboratory supplies, consultants and subcontractors and other expenses associated with our process development, manufacturing, clinical, regulatory and quality assurance activities for internally funded programs. In addition, indirect costs such as, fringe benefits and overhead expenses, are also included in research and development expenses. Research and development expenses increased to $79.4 million for 2014 from $50.3 million for 2013, an increase of $29.1 million, or 58%. Excluding the increase in research and development expenses of $3.6 million from Novavax AB resulting from twelve months of activity in 2014 as compared to only five months in 2013, the increase in research and development expenses was primarily due to higher employee-related costs, the preparation and initiation of three RSV F vaccine candidate clinical trials in 2014, the initiation of our EBOV GP vaccine candidate program and a $3.0 million milestone payment accrued under the Wyeth agreement, as compared to 2013. For 2015, we expect a significant increase in research and development expenses primarily due to additional RSV F vaccine candidate clinical trials and employee-related and facility costs to support product development of our RSV F vaccine candidate and other potential vaccine candidates.
Research and development expenses increased to $50.3 million for 2013 from $26.9 million for 2012, an increase of $23.4 million, or 87%. Excluding the increase in research and development expenses of approximately $3.0 million from Novavax AB, the increase in research and development expenses was primarily due to increased costs relating to our clinical trials of our RSV F vaccine candidate and pandemic H7N9 influenza VLP vaccine candidate (internally funded programs at the time) and higher employee-related costs.
| 50 |
Costs and Expenses by Functional Area
We track our cost of government contracts revenue and research and development expenses by the type of costs incurred in identifying, developing, manufacturing and testing vaccine candidates. We evaluate and prioritize our activities according to functional area and therefore believe that project-by-project information would not form a reasonable basis for disclosure to our investors. At December 31, 2014, we had 258 employees dedicated to our research and development programs versus 175 employees as of December 31, 2013. Historically, we did not account for internal research and development expenses by project, since our employees work time is spread across multiple programs and our internal manufacturing clean-room facility produces multiple vaccine candidates.
The following summarizes our cost of government contracts revenue and research and development expenses by functional area for the year ended December 31 (in millions).
| 2014 | 2013 | |||||||
| Manufacturing | $ | 53.5 | $ | 31.0 | ||||
| Vaccine Discovery | 6.2 | 5.6 | ||||||
| Clinical and Regulatory | 34.7 | 21.9 | ||||||
| Total cost of government contracts revenue and research and development expenses | $ | 94.4 | $ | 58.5 | ||||
We do not provide forward-looking estimates of costs and time to complete our research programs due to the many uncertainties associated with vaccine development. As we obtain data from pre-clinical studies and clinical trials, we may elect to discontinue or delay clinical trials in order to focus our resources on more promising vaccine candidates. Completion of clinical trials may take several years or more, but the length of time can vary substantially depending upon the phase, size of clinical trial, primary and secondary endpoints and the intended use of the vaccine candidate. The cost of clinical trials may vary significantly over the life of a project as a result of a variety of factors, including:
| · | the number of patients who participate in the clinical trials; |
| · | the number of sites included in the clinical trials; |
| · | if clinical trial locations are domestic, international or both; |
| · | the time to enroll patients; |
| · | the duration of treatment and follow-up; |
| · | the safety and efficacy profile of the vaccine candidate; and |
| · | the cost and timing of, and the ability to secure, regulatory approvals. |
As a result of these uncertainties, we are unable to determine with any significant degree of certainty the duration and completion costs of our research and development projects or when, and to what extent, we will generate future cash flows from our research projects.
General and Administrative Expenses
General and administrative expenses increased to $19.9 million for 2014 from $14.8 million for 2013, an increase of $5.1 million, or 34%. Excluding the increase in general and administrative expenses of approximately $0.7 million from Novavax AB resulting from twelve months of activity in 2014 as compared to only five months in 2013, the increase was primarily due to higher employee-related costs, as compared to 2013. For 2015, we expect general and administrative expenses to increase primarily due to increased employee costs and pre-commercialization activities.
General and administrative expenses increased to $14.8 million for 2013 from $10.1 million for 2012, an increase of $4.7 million, or 46%. Excluding the increase in general and administrative expenses of approximately $1.0 million from Novavax AB, the increase was primarily due to higher professional fees, including those associated with our acquisition of Novavax AB.
| 51 |
Other Income (Expense):
| 2014 | 2013 | 2012 | Change
2013 to 2014 | Change
2012 to 2013 | ||||||||||||||||
| Other Income (Expense): | ||||||||||||||||||||
| Investment income | $ | 286 | $ | 187 | $ | 165 | $ | 99 | $ | 22 | ||||||||||
| Interest expense | (157 | ) | (160 | ) | (32 | ) | 3 | (128 | ) | |||||||||||
| Other income, net | — | 182 | 45 | (182 | ) | 137 | ||||||||||||||
| Realized gains on marketable securities | 615 | — | 879 | 615 | (879 | ) | ||||||||||||||
| Change in fair value of warrant liability | — | 267 | 101 | (267 | ) | 166 | ||||||||||||||
| Total other income (expense) | $ | 744 | $ | 476 | $ | 1,158 | $ | 268 | $ | (682 | ) | |||||||||
We had total other income, net of $0.7 million for 2014 compared to total other income, net of $0.5 million for the same period in 2013. The change in fair value of our warrant liability resulted in a $0.3 million decrease in total other income, net for 2014, as compared to 2013. The warrants expired unexercised on July 31, 2013. For 2014, we sold our auction rate security and received proceeds of $1.8 million resulting in a realized gain of $0.6 million.
We had total other income, net of $0.5 million for 2013 compared to total other income, net of $1.2 million for 2012, a decrease of $0.7 million. In 2012, two of our auction rate securities were redeemed at approximately par value and resulted in $0.9 million in realized gains as we had recorded other-than-temporary impairments on these securities in previous periods.
Net Loss:
| 2014 | 2013 | 2012 | Change
2013 to 2014 | Change
2012 to 2013 | ||||||||||||||||
| Net Loss: | ||||||||||||||||||||
| Net loss | $ | (82,947 | ) | $ | (51,983 | ) | $ | (28,507 | ) | $ | (30,964 | ) | $ | (23,476 | ) | |||||
| Net loss per share | $ | (0.37 | ) | $ | (0.31 | ) | $ | (0.22 | ) | $ | (0.06 | ) | $ | (0.09 | ) | |||||
| Weighted average shares outstanding | 225,848 | 169,658 | 131,726 | 56,190 | 37,932 | |||||||||||||||
Net loss for 2014 was $82.9 million, or $0.37 per share, as compared to $52.0 million, or $0.31 per share, for 2013, an increased net loss of $31.0 million. The increased net loss was primarily due to higher research and development spending, including increased costs relating to our RSV F vaccine candidate and higher employee-related costs.
Net loss for 2013 was $52.0 million, or $0.31 per share, as compared to $28.5 million, or $0.22 per share, for 2012, an increased net loss of $23.5 million. The increased net loss was primarily due to higher research and development spending, including increased costs relating to clinical trials of our RSV F vaccine candidate and pandemic H7N9 influenza VLP vaccine candidate and higher employee-related costs.
The increase in weighted average shares outstanding for 2014 and 2013 is primarily a result of sales of our common stock in 2014 and 2013.
Liquidity Matters and Capital Resources
Our future capital requirements depend on numerous factors including, but not limited to, the commitments and progress of our research and development programs, the progress of pre-clinical and clinical testing, the time and costs involved in obtaining regulatory approvals, the costs of filing, prosecuting, defending and enforcing patent claims and other intellectual property rights and manufacturing costs. We plan to continue to have multiple vaccines and products in various stages of development, and we believe our operating expenses and capital requirements will fluctuate depending upon the timing of certain events, such as the scope, initiation, rate and progress of our pre-clinical studies and clinical trials and other research and development activities.
| 52 |
As of December 31, 2014, we had $168.1 million in cash and cash equivalents and marketable securities as compared to $133.1 million as of December 31, 2013. These amounts consisted of $32.3 million in cash and cash equivalents and $135.7 million in marketable securities as of December 31, 2014 as compared to $119.5 million in cash and cash equivalents and $13.6 million in marketable securities at December 31, 2013.
The following table summarizes cash flows for 2014 and 2013 (in thousands):
| 2014 | 2013 | Change
2013 to 2014 | ||||||||||
| Summary of Cash Flows: | ||||||||||||
| Net cash (used in) provided by: | ||||||||||||
| Operating activities | $ | (67,014 | ) | $ | (45,359 | ) | $ | (21,655 | ) | |||
| Investing activities | (129,833 | ) | 16,392 | (146,225 | ) | |||||||
| Financing activities | 109,717 | 131,035 | (21,318 | ) | ||||||||
| Effect on exchange rate on cash and cash equivalents | (6 | ) | 4 | (10 | ) | |||||||
| Net increase (decrease) in cash and cash equivalents | (87,136 | ) | 102,072 | (189,208 | ) | |||||||
| Cash and cash equivalents at beginning of year | 119,471 | 17,399 | 102,072 | |||||||||
| Cash and cash equivalents at end of year | $ | 32,335 | $ | 119,471 | $ | (87,136 | ) | |||||
Net cash used in operating activities increased to $67.0 million for 2014 as compared to $45.4 million for 2013. The increase in cash usage was primarily due to increased costs relating to our RSV F vaccine candidate, higher employee-related costs and timing of vendor payments.
During 2014 and 2013, our investing activities consisted primarily of purchases and sales, maturities and redemptions of marketable securities and capital expenditures. In 2014, we primarily purchased marketable securities to increase our rate of return on our marketable securities relative to returns available to money market funds. Capital expenditures for 2014 and 2013 were $7.3 million and $5.8 million, respectively. The increase in capital expenditures was primarily due to the purchase of laboratory equipment for process development, analytical development and manufacturing scale-up required to support our maturing product portfolio. In 2015, we expect our level of capital expenditures to be significantly higher than our 2014 spending as we continue to scale up our capacity in anticipation of Phase 3 clinical trials and related regulatory obligations in the upcoming years.
Our financing activities consisted primarily of sales of our common stock, and to a lesser extent, stock option exercises and purchases under our employee stock purchase plan in 2014. In 2014, we received net proceeds of approximately $108 million through our public offering at $4.00 per share. In 2013, we received net proceeds of $94.7 million through our public offering at a sales price of $3.14 per share and $34.0 million through our Sales Agreement at an average sales price of $2.76 per share.
In November 2011, we entered into lease agreements under which we lease our manufacturing, laboratory and office space in Gaithersburg, Maryland with rent payments for such space to the landlord that commenced April 1, 2014. Under the terms of the arrangement, the landlord provided us with a tenant improvement allowance of $2.5 million and an additional tenant improvement allowance of $3.0 million (collectively, the Improvement Allowance). The additional tenant improvement allowance is to be paid back to the landlord over the remaining term of the lease agreement through additional rent payments. We were funded $0.5 million and $0.7 million in 2014 and 2013, respectively, and have been funded $5.5 million in total under the Improvement Allowance.
| 53 |
In 2007, we entered into an agreement to license certain rights from Wyeth. The Wyeth license is a non-exclusive, worldwide license to a family of patents and patent applications covering VLP technology for use in human vaccines in certain fields, with expected patent expiration in early 2022. The Wyeth license provides for us to make an upfront payment (previously made), ongoing annual license fees, sublicense payments, milestone payments on certain development activities and royalties on any product sales. The milestone payments are one-time only payments applicable to each related vaccine program. At present, our seasonal influenza VLP vaccine program (including CPLB’s seasonal influenza program) and our pandemic influenza VLP vaccine program are the only two programs to which the Wyeth license applies. The license may be terminated by Wyeth only for cause and may be terminated by us only after we have provided ninety (90) days’ notice that we have absolutely and finally ceased activity, including through any affiliate or sublicense, related to the manufacturing, development, marketing or sale of products covered by the license. Payments under the agreement to Wyeth from 2007 through 2014 totaled $6.4 million. We are currently in discussion with Wyeth to potentially amend the agreement and restructure the milestone payment owed as a result of CPLB’s initiation of a Phase 3 clinical trial for its seasonal influenza VLP vaccine candidate in the third quarter of 2014. Such milestone payment is only owed once for our seasonal influenza VLP vaccine program and we would not be required to pay again if we or any of our affiliates initiate an additional Phase 3 clinical trial in a seasonal influenza VLP vaccine candidate. The $3.0 million milestone has been recorded in accrued expenses on the consolidated balance sheet at December 31, 2014 and as a research and development expense in 2014.
In connection with CPLB, we entered into a master services agreement with Cadila, which we and Cadila amended in July 2011, and subsequently in March 2013, March 2014 and February 2015, in each case to extend the term by one year for which services can be provided by Cadila under this agreement. Under the revised terms, if, by March 2016, the amount of services provided by Cadila under the master services agreement is less than $7.5 million, we will pay Cadila the portion of the shortfall amount that is less than or equal to $2.0 million and 50% of the portion of the shortfall amount that exceeds $2.0 million. The Company and Cadila also agreed to an amendment that allows CPLB, as of the beginning of 2013, to provide services on behalf of Cadila. Through December 31, 2014, we have purchased $5.7 million in services from Cadila pursuant to this agreement, including amounts in which CPLB provided the services on behalf of Cadila.
Based on our December 31, 2014 cash and cash equivalents, marketable securities balances, the anticipated revenue under the contract with HHS BARDA and other resources, we believe we have adequate capital to fund our operating plans at least for the next twelve months. Additional capital may be required in the future to develop our vaccine candidates through clinical development, manufacturing and commercialization. Our ability to obtain such additional capital will likely be subject to various factors, including our ability to perform and thus generate revenue under the HHS BARDA contract, our overall business performance and market conditions.
Any capital raised by an equity offering will likely be substantially dilutive to the existing stockholders and any licensing or development arrangement may require us to give up rights to a product or technology at less than its full potential value. We cannot provide any assurance that new financing will be available on commercially acceptable terms, if at all. If we are unable to perform under the HHS BARDA contract or obtain additional capital, we will assess our capital resources and may be required to delay, reduce the scope of, or eliminate one or more of our product research and development programs, and/or downsize our organization, including our general and administrative infrastructure.
Contractual Obligations
The following table summarizes our contractual obligations as of December 31, 2014 (in thousands):
| Contractual Obligations: | Total | Less
than One Year | 1 - 3 Years | 3 - 5 Years | More than 5 Years | |||||||||||||||
| Operating leases | $ | 28,250 | $ | 4,903 | $ | 7,845 | $ | 5,063 | $ | 10,439 | ||||||||||
| Capital lease | 175 | 67 | 108 | — | — | |||||||||||||||
| Notes payable | 998 | 603 | 395 | — | — | |||||||||||||||
| Purchase obligation | 1,800 | 1,800 | — | — | — | |||||||||||||||
| Research funding payment | 1,531 | — | 1,531 | — | — | |||||||||||||||
| Accrued milestone payment | 3,000 | 3,000 | — | — | — | |||||||||||||||
| Total contractual obligations | $ | 35,754 | $ | 10,373 | $ | 9,879 | $ | 5,063 | $ | 10,439 | ||||||||||
Our purchase obligation consists of our anticipated timing of future purchases for services pursuant to the master services agreement with Cadila. We are required to purchase from Cadila, through March 2016, services for biologic research, pre-clinical development, clinical development, process development, manufacturing scale-up and general manufacturing related services. As of December 31, 2014, our remaining obligation to Cadila under the master services agreement was $1.8 million. Our research funding payment includes the research funding received under the Genocea agreement (see Note 4 to consolidated financial statements in Item 8). Our accrued milestone payment includes the milestone payment incurred in 2014 under the Wyeth agreement (see above for further discussion).
| 54 |
Off-Balance Sheet Arrangements
We are not involved in any off-balance sheet agreements that have or are reasonably likely to have a material future effect on our financial condition, changes in financial condition, revenue or expenses, results of operations, liquidity, capital expenditures or capital resources.
| Item 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
The primary objective of our investment activities is preservation of capital, with the secondary objective of maximizing income. As of December 31, 2014, we had cash and cash equivalents of $32.3 million, marketable securities of $135.7 million, all of which are short-term, and working capital of $154.0 million.
Our exposure to market risk is primarily confined to our investment portfolio. As of December 31, 2014, our investments were classified as available-for-sale. We do not believe that a change in the market rates of interest would have any significant impact on the realizable value of our investment portfolio. Changes in interest rates may affect the investment income we earn on our marketable securities when they mature and the proceeds are reinvested into new marketable securities and, therefore, could impact our cash flows and results of operations.
Interest and dividend income is recorded when earned and included in investment income. Premiums and discounts, if any, on marketable securities are amortized or accreted to maturity and included in investment income. The specific identification method is used in computing realized gains and losses on the sale of our securities.
We are headquartered in the U.S. where we conduct the vast majority of our business activities. We have one foreign consolidated subsidiary, Novavax AB, which is located in Sweden. A 10% decline in the exchange rate between the U.S. dollar and Swedish Krona would result in a reduction of stockholders’ equity of approximately $3.1 million at December 31, 2014.
We do not have material debt and, as such, do not believe that we are exposed to any material interest rate risk as a result of our borrowing activities.
| Item 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
The information required by this item is set forth on pages F-1 to F-28.
| Item 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
| Item 9A. | CONTROLS AND PROCEDURES |
Evaluation of Disclosure Controls and Procedures
The term “disclosure controls and procedures” (defined in SEC Rule 13a-15(e)) refers to the controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files under the Securities Exchange Act of 1934 (the “Exchange Act”) is recorded, processed, summarized and reported, within time periods specified in the rules and forms of the Securities and Exchange Commission. “Disclosure controls and procedures” include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure.
| 55 |
The Company’s management, with the participation of the chief executive officer and the chief financial officer, has evaluated the effectiveness of the Company’s disclosure controls and procedures as of the end of the period covered by this annual report (the “Evaluation Date”). Based on that evaluation, the Company’s chief executive officer and chief financial officer have concluded that, as of the Evaluation Date, such controls and procedures were effective.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is defined in Rules 13a-15(f) and 15d-15(f) promulgated under the Exchange Act, as a process designed by, or under the supervision of, the Company’s principal executive officer and principal financial officer and effected by the Company’s board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with accounting principles generally accepted in the United States (“GAAP”). Such internal control includes those policies and procedures that:
| · | pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of the assets of the Company; |
| · | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with GAAP, and that receipts and expenditures of the Company are being made only in accordance with authorizations of management and directors of the Company; and |
| · | provide reasonable assurance regarding prevention or timely detection of an unauthorized acquisition, use or disposition of the Company’s assets that could have a material effect on the financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2014. In making this assessment, our management used the criteria set forth in the 2013 Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on its assessment, our management has determined that, as of December 31, 2014, our internal controls over financial reporting are effective based on those criteria.
Ernst & Young LLP has issued an attestation report on our internal control over financial reporting. This report is included in the Reports of Independent Registered Public Accounting Firm in Item 15.
Changes in Internal Control over Financial Reporting
Our management, including our chief executive officer and chief financial officer, has evaluated any changes in our internal control over financial reporting that occurred during the quarterly period ended December 31, 2014, and has concluded that there was no change that occurred during the quarterly period ended December 31, 2014 that materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
| Item 9B. | OTHER INFORMATION |
None.
| 56 |
| Item 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
The information required by this item is incorporated by reference from our definitive Proxy Statement for our 2015 Annual Meeting of Stockholders scheduled to be held in June 2015 (the “2015 Proxy Statement”). We expect to file the 2015 Proxy Statement within 120 days after the close of the fiscal year ended December 31, 2014.
| Item 11. | EXECUTIVE COMPENSATION |
We incorporate herein by reference the information required by this item concerning executive compensation to be contained in the 2015 Proxy Statement.
| Item 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
We incorporate herein by reference the information required by this item concerning security ownership of certain beneficial owners and management and related stockholder matters to be contained in the 2015 Proxy Statement.
The following table provides our equity compensation plan information as of December 31, 2014. Under these plans, our common stock may be issued upon the exercise of options and purchases under our Employee Stock Purchase Plan (“ESPP”). See also the information regarding our stock options and ESPP in Note 13 to the financial statements included herewith.
Equity Compensation Plan Information
| Plan Category | Number
of Securities (a) | Weighted-Average
Exercise Price of Outstanding Options, Warrants and Rights (b) | Number
of Securities (c) | |||||||||
| Equity compensation plans approved by security holders(1) | 16,963,098 | $ | 3.23 | 6,150,571 | ||||||||
| Equity compensation plans not approved by security holders | N/A | N/A | N/A | |||||||||
| (1) | Includes our 2005 Stock Incentive Plan, 1995 Stock Option Plan and ESPP. |
| Item 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
We incorporate herein by reference the information required by this item concerning certain related party transactions set forth in Note 17 to our financial statements included herewith. We incorporate herein by reference other information required by this item concerning certain other relationships and related transactions and director independence to be contained in the 2015 Proxy Statement.
| Item 14. | PRINCIPAL ACCOUNTING FEES AND SERVICES |
We incorporate herein by reference the information required by this item concerning principal accountant fees and services to be contained in the 2015 Proxy Statement.
| 57 |
| Item 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES |
| (a) | The following documents are filed as part of the Annual Report: |
| (1) | Index to Financial Statements |
| Reports of Independent Registered Public Accounting Firms | F-2 |
| Consolidated Balance Sheets as of December 31, 2014 and 2013 | F-5 |
| Consolidated Statements of Operations and Statements of Comprehensive Loss for the years ended December 31, 2014, 2013 and 2012 | F-6 |
| Consolidated Statements of Stockholders’ Equity for the years ended December 31, 2014, 2013 and 2012 | F-7 |
| Consolidated Statements of Cash Flows for the years ended December 31, 2014, 2013 and 2012 | F-8 |
| Notes to Consolidated Financial Statements | F-9 |
| (2) | Financial Statement Schedules |
Financial statement schedules are omitted because they are not applicable, not required under the instructions or all the information required is set forth in the financial statements or notes thereto.
| (3) | Exhibits |
Exhibits marked with a single asterisk (*) are filed herewith.
Exhibits marked with a double plus sign (††) refer to management contracts, compensatory plans or arrangements.
Confidential treatment has been granted for portions of exhibits marked with a double asterisk (**).
All other exhibits listed have previously been filed with the Commission and are incorporated herein by reference.
| 58 |
| Exhibit | ||
| Number | Description | |
| 3.1 | Amended and Restated Certificate of Incorporation of the Registrant (Incorporated by reference to Exhibit 3.1 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 1996, filed March 21, 1997), as amended by the Certificate of Amendment dated December 18, 2000 (Incorporated by reference to Exhibit 3.4 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2000, filed March 29, 2001), as further amended by the Certificate of Amendment dated July 8, 2004 (Incorporated by reference to Exhibit 3.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2004, filed August 9, 2004), as further amended by the Certificate of Amendment dated May 13, 2009 (Incorporated by reference to Exhibit 3.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed August 10, 2009), as further amended by the Certificate of Amendment dated June 13, 2013 (Incorporated by reference to Exhibit 3.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2013, filed on August 8, 2013) | |
| 3.2 | Amended and Restated By-Laws of the Registrant (Incorporated by reference to Exhibit 3.2 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2012, filed on March 12, 2013) | |
| 4.1 | Specimen stock certificate for shares of common stock of the Registrant, par value $.01 per share (Incorporated by reference to Exhibit 4.1 to the Registrant’s Registration Statement on Form 10, File No. 0-26770, filed September 14, 1995) | |
| 4.2 | Registration Rights Agreement between Novavax, Inc. and Satellite Overseas (Holdings) Limited, dated March 31, 2009 (Incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2009, filed on May 11, 2009) | |
| 10.1†† | Novavax, Inc. 1995 Stock Option Plan, as amended (Incorporated by reference to Appendix A of the Registrant’s Definitive Proxy Statement filed on March 31, 2003 in connection with the Annual Meeting held on May 7, 2003) | |
| 10.2†† | Novavax, Inc. Amended and Restated 2005 Stock Incentive Plan (Incorporated by reference to Exhibit 10.2 to the Company’s Annual Report for the year ended December 31, 2012, filed March 12, 2013) | |
| 10.3†† | Amendment to Amended and Restated 2005 Stock Incentive Plan (Incorporated by reference to Appendix 1 of the Registrant’s Definitive Proxy Statement filed April 30, 2014 in connection with the Annual Meeting held on June 12, 2014) | |
| 10.4††* | Form of Non-Statutory Stock Option Award Agreement granted under the Novavax, Inc. Amended and Restated 2005 Stock Incentive Plan | |
| 10.5††* | Form of Incentive Stock Option Award Agreement granted under the Novavax, Inc. Amended and Restated 2005 Stock Incentive Plan | |
| 10.6††* | Form of Restricted Stock Award Agreement granted under the Novavax, Inc. Amended and Restated 2005 Stock Incentive Plan | |
| 10.7†† | 2013 Employee Stock Purchase Plan (Incorporated by reference to Appendix C to the Registrant’s Definitive Proxy Statement filed on April 30, 2013 in connection with the Annual Meeting held on June 13, 2013) | |
| 10.8†† | Employment Agreement between Novavax, Inc. and Stanley C. Erck, dated as of February 15, 2010 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K, filed on June 1, 2010) |
| 59 |
| 10.9†† | Employment Agreement between Novavax, Inc. and Stanley C. Erck, dated as of June 22, 2011 (Incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report for the quarter ended June 30, 2011, filed on August 9, 2011) | |
| 10.10†† | Employment Agreement between Novavax, Inc. and Gregory M. Glenn dated July 1, 2010 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K, filed on July 6, 2010) | |
| 10.11†† | Employment Agreement between Novavax, Inc. and Russell P. Wilson dated November 7, 2011 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K, filed on November 14, 2011) | |
| 10.12†† | Employment Agreement between Novavax, Inc. and Timothy J. Hahn dated June 22, 2011 (Incorporated by reference to Exhibit 10.12 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2011, filed on March 14, 2012) | |
| 10.13†† | Employment agreement between Novavax, Inc. and Barclay A. Phillips dated June 24, 2013 (Incorporated by reference to Exhibit 99.2 to the Registrant’s Current Report on Form 8-K, filed on June 28, 2013) | |
| 10.14†† | Novavax, Inc. Amended and Restated Change in Control Severance Benefit Plan, (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K, filed on January 5, 2009) | |
| 10.15†† | Form of Indemnification Agreement entered into between the Registrant and its directors and officers (Incorporated by reference to Exhibit 10.19 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2009, filed on March 16, 2010) | |
| 10.16 | Lease Agreement between GP Rock One, LLC and Novavax, Inc., dated as of May 7, 2007 (Incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report for the quarter ended June 30, 2008, filed on August 11, 2008) | |
| 10.17 | First Amendment to Lease Agreement between GP Rock One, LLC and Novavax, Inc., dated as of May 30, 2008 (Incorporated by reference to Exhibit 10.5 to the Registrant’s Quarterly Report for the quarter ended June 30, 2008, filed on August 11, 2008) | |
| 10.18 | Second Amendment to Lease Agreement between BMR-9920 Belward Campus Q, LLC (formerly GP Rock One, LLC) and Novavax, Inc., dated as of June 26, 2008 (Incorporated by reference to Exhibit 10.6 to the Registrant’s Quarterly Report for the quarter ended June 30, 2008, filed on August 11, 2008) | |
| 10.19 | Lease Agreement for space at 20 Firstfield between ARE-20/22/1300 Firstfield Quince Orchard, LLC and Novavax, Inc., dated as of November 18, 2011 (Incorporated by reference to Exhibit 10.23 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2011, filed on March 14, 2012) | |
| 10.20 | Lease Agreement for space at 22 Firstfield between ARE-20/22/1300 Firstfield Quince Orchard, LLC and Novavax, Inc., dated as of November 18, 2011 (Incorporated by reference to Exhibit 10.25 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2011, filed on March 14, 2012) | |
| 10.21** | Contract, effective as of February 24, 2011, between Novavax, Inc. and HHS/OS/ASPR/BARDA (Incorporated by reference to Exhibit 10.1 to the Registrant’s Amendment No. 1 to its Quarterly Report on Form 10-Q/A for the quarter ended on March 31, 2011, filed November 4, 2011) |
| 60 |
| 10.22** | Contract Amendment/Modification No. 5 between Novavax, Inc. and HHS/OS/ASPR/BARDA, dated February 21, 2014 (Incorporated by reference to Exhibit 10.25 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2013, filed on March 12, 2014) | |
| 10.23** | Contract Amendment/Modification No. 6 between Novavax, Inc. and HHS/OS/ASPR/BARDA, dated September 22, 2014 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2014, filed on November 6, 2014) | |
| 10.24** | License Agreement, entered in February 25, 2011, effective as of December 9, 2010, between Novavax, Inc. and LG Life Sciences, Ltd. (Incorporated by reference to Exhibit 10.2 to the Registrant’s Amendment No. 1 to its Quarterly Report on Form 10-Q/A for the quarter ended March 31, 2011, filed on November 4, 2011) | |
| 10.25** | License Agreement, dated July 5, 2007, between Novavax, Inc. and Wyeth Holdings Corporation (Incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2007, filed on August 9, 2007) | |
| 10.26** | Amendment No. 1 to License Agreement, effective as of March 17, 2010, between Novavax, Inc. and Wyeth Holdings Corporation (Incorporated by reference to Exhibit 10.49 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2010, filed on August 6, 2010) | |
| 10.27 | At Market Issuance Sales Agreement, dated October 1, 2012, between Novavax, Inc. and MLV & Co. LLC (Incorporated by reference to Exhibit 1.1 to the Registrant’s Current Report on Form 8-K, filed on October 2, 2012) | |
| 10.28 | Stock Purchase Agreement between Novavax, Inc. and Satellite Overseas (Holdings) Limited, dated March 31, 2009 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2009, filed on May 11, 2009) | |
| 10.29** | Amended and Restated Joint Venture Agreement between Novavax, Inc. and Cadila Pharmaceuticals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.30** | Amended and Restated Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.31 | Amendment No. 1 to Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Limited dated July 27, 2011 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2011, filed on November 8, 2011) | |
| 10.32 | Amendment No. 2 to Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Limited dated March 7, 2013 (Incorporated by reference to Exhibit 10.32 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2012, filed on March 12, 2013) | |
| 10.33 | Amendment No. 3 to Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Ltd. dated October 29, 2013 (Incorporated by reference to Exhibit 10.1 to the Registrant’s Report on Form 8-K, filled on October 30, 2013) | |
| 10.34 | Amendment No. 4 to Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Ltd. dated March 5, 2014 (Incorporated by reference to Exhibit 10.37 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2013, filled on March 12, 2014) | |
| 10.35* | Amendment No. 5 to Master Services Agreement between Novavax, Inc. and Cadila Pharmaceuticals Ltd. dated February 25, 2015 |
| 61 |
| 10.36** | Amended and Restated Supply Agreement between Novavax, Inc. and CPL Biologicals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.6 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.37** | Amended and Restated Technical Services Agreement between Novavax, Inc. and CPL Biologicals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.7 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.38** | Amended and Restated Seasonal / Other License Agreement between Novavax, Inc. and CPL Biologicals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.8 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.39** | Amended and Restated Option to Obtain License between Novavax, Inc. and CPL Biologicals Limited, dated as of June 29, 2009 (Incorporated by reference to Exhibit 10.9 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2009, filed on August 10, 2009) | |
| 10.40** | H1N1 License to Agreement between Novavax, Inc. and CPL Biologicals Private Limited, dated October 6, 2009 (Incorporated by reference to Exhibit 10.45 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2009, filed on March 16, 2010) | |
| 14 | Code of Business Conduct and Ethics (Incorporated by reference to Exhibit 14 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2011, filed on August 9, 2011) | |
| 21.1* | Subsidiaries of the Registrant | |
| 23.1* | Consent of Ernst & Young LLP, Independent Registered Public Accounting Firm | |
| 23.2* | Consent of Grant Thornton LLP, Independent Registered Public Accounting Firm | |
| 31.1* | Certification of chief executive officer pursuant to Rule 13a-14(a) or 15d-14(e) of the Securities Exchange Act | |
| 31.2* | Certification of chief financial officer pursuant to Rule 13a-14(a) or 15d-14(e) of the Securities Exchange Act | |
| 32.1* | Certification of chief executive officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
| 32.2* | Certification of chief financial officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
| 62 |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| NOVAVAX, INC. | ||
| By: | /s/ Stanley C. Erck | |
| President, Chief Executive Officer | ||
| and Director | ||
Date: February 27, 2015
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the Registrant and in the capacities and on the dates indicated:
| Name | Title | Date | ||
| /s/ Stanley C. Erck | President and Chief Executive Officer and | February 27, 2015 | ||
| Stanley C. Erck | Director (Principal Executive Officer) | |||
| /s/ Barclay A. Phillips | Senior Vice President, Chief Financial | February 27, 2015 | ||
| Barclay A. Phillips | Officer and Treasurer (Principal Financial | |||
| and Principal Accounting Officer) | ||||
| /s/ James F. Young | Chairman of the Board of Directors | February 27, 2015 | ||
| James F. Young | ||||
| /s/ Richard H. Douglas | Director | February 27, 2015 | ||
| Richard H. Douglas | ||||
| /s/ Gary C. Evans | Director | February 27, 2015 | ||
| Gary C. Evans | ||||
| /s/ Michael A. McManus | Director | February 27, 2015 | ||
| Michael A. McManus | ||||
| /s/ Rajiv I. Modi | Director | February 27, 2015 | ||
| Rajiv I. Modi |
| 63 |
INDEX TO FINANCIAL STATEMENTS
Years ended December 31, 2014, 2013 and 2012
Contents
| F-1 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders of
Novavax, Inc.
We have audited the accompanying consolidated balance sheet of Novavax, Inc. as of December 31, 2014, and the related consolidated statements of operations, comprehensive loss, stockholders’ equity, and cash flows for the year then ended. These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these financial statements based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audit provides a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Novavax, Inc. at December 31, 2014, and the consolidated results of its operations and its cash flows for the year then ended in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), Novavax, Inc.’s internal control over financial reporting as of December 31, 2014, based on criteria established in the Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) and our report dated February 26, 2015 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Baltimore, MD
February 26, 2015
| F-2 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders of
Novavax, Inc.
We have audited Novavax, Inc.’s internal control over financial reporting as of December 31, 2014, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the COSO criteria). Novavax Inc.’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in Item 9A, Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, Novavax, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2014, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance of Novavax Inc. as of December 31, 2014 and the related consolidated statements of operations, comprehensive loss, changes in stockholders’ equity, and cash flows for the period then ended of Novavax Inc. and our report dated February 26, 2015 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Baltimore, MD
February 26, 2015
| F-3 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Stockholders of
Novavax, Inc.
We have audited the accompanying consolidated balance sheet of Novavax, Inc. (a Delaware corporation) and subsidiary (the “Company”) as of December 31, 2013, and the related consolidated statements of operations, comprehensive loss, changes in stockholders’ equity, and cash flows for each of the two years in the period ended December 31, 2013. These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Novavax, Inc. and subsidiary as of December 31, 2013, and the results of their operations and their cash flows for each of the two years in the period ended December 31, 2013 in conformity with accounting principles generally accepted in the United States of America.
/s/ Grant Thornton LLP
McLean, Virginia
March 12, 2014
| F-4 |
NOVAVAX, INC.
| December 31, | ||||||||
| 2014 | 2013 | |||||||
| (in thousands, except share and per share information) | ||||||||
| ASSETS | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | 32,335 | $ | 119,471 | ||||
| Marketable securities | 135,721 | 13,597 | ||||||
| Restricted cash | 297 | 1,417 | ||||||
| Accounts receivable – billed | 7,510 | 1,911 | ||||||
| Accounts receivable – unbilled | 3,100 | 4,988 | ||||||
| Prepaid expenses and other current assets | 9,195 | 3,617 | ||||||
| Total current assets | 188,158 | 145,001 | ||||||
| Property and equipment, net | 19,737 | 14,251 | ||||||
| Intangible assets, net | 12,577 | 16,250 | ||||||
| Goodwill | 54,612 | 58,707 | ||||||
| Other non-current assets | 918 | 916 | ||||||
| Total assets | $ | 276,002 | $ | 235,125 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||
| Current liabilities: | ||||||||
| Accounts payable | $ | 12,908 | $ | 5,985 | ||||
| Accrued expenses | 19,397 | 10,411 | ||||||
| Current portion of notes payable | 603 | 877 | ||||||
| Deferred rent | 1,138 | 470 | ||||||
| Other current liabilities | 70 | 379 | ||||||
| Total current liabilities | 34,116 | 18,122 | ||||||
| Deferred revenue | 2,500 | 2,500 | ||||||
| Non-current portion of notes payable | 395 | 1,004 | ||||||
| Deferred rent | 7,734 | 8,502 | ||||||
| Other non-current liabilities | 1,639 | 1,763 | ||||||
| Total liabilities | 46,384 | 31,891 | ||||||
| Commitments and contingencies | — | — | ||||||
| Stockholders’ equity: | ||||||||
| Preferred stock, $0.01 par value, 2,000,000 shares authorized; no shares issued and outstanding | — | — | ||||||
| Common stock, $0.01 par value, 300,000,000 shares authorized at December 31, 2014 and 2013; and 239,287,294 shares issued and 238,831,864 shares outstanding at December 31, 2014 and 209,110,744 shares issued and 208,655,314 shares outstanding at December 31, 2013 | 2,393 | 2,091 | ||||||
| Additional paid-in capital | 729,373 | 612,900 | ||||||
| Accumulated deficit | (493,093 | ) | (410,146 | ) | ||||
| Treasury stock, 455,430 shares, cost basis | (2,450 | ) | (2,450 | ) | ||||
| Accumulated other comprehensive income (loss) | (6,605 | ) | 839 | |||||
| Total stockholders’ equity | 229,618 | 203,234 | ||||||
| Total liabilities and stockholders’ equity | $ | 276,002 | $ | 235,125 | ||||
The accompanying notes are an integral part of these financial statements.
| F-5 |
NOVAVAX, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
| For the Years ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| (in thousands, except per share information) | ||||||||||||
| Revenue: | ||||||||||||
| Government contracts | $ | 26,213 | $ | 17,708 | $ | 20,671 | ||||||
| Research and development collaborations | 4,446 | 3,207 | 1,405 | |||||||||
| Total revenue | 30,659 | 20,915 | 22,076 | |||||||||
| Costs and expenses: | ||||||||||||
| Cost of government contracts revenue | 14,987 | 8,222 | 14,692 | |||||||||
| Research and development | 79,435 | 50,308 | 26,907 | |||||||||
| General and administrative | 19,928 | 14,819 | 10,142 | |||||||||
| Total costs and expenses | 114,350 | 73,349 | 51,741 | |||||||||
| Loss from operations | (83,691 | ) | (52,434 | ) | (29,665 | ) | ||||||
| Other income (expense): | ||||||||||||
| Investment income | 286 | 187 | 165 | |||||||||
| Interest expense | (157 | ) | (160 | ) | (32 | ) | ||||||
| Other income, net | — | 182 | 45 | |||||||||
| Realized gains on marketable securities | 615 | — | 879 | |||||||||
| Change in fair value of warrant liability | — | 267 | 101 | |||||||||
| Loss from operations before income tax expense | (82,947 | ) | (51,958 | ) | (28,507 | ) | ||||||
| Income tax expense | — | 25 | — | |||||||||
| Net loss | $ | (82,947 | ) | $ | (51,983 | ) | $ | (28,507 | ) | |||
| Basic and diluted net loss per share | $ | (0.37 | ) | $ | (0.31 | ) | $ | (0.22 | ) | |||
| Basic and diluted weighted average number of common shares outstanding | 225,848 | 169,658 | 131,726 | |||||||||
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
| For the Years ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| (in thousands) | ||||||||||||
| Net loss | $ | (82,947 | ) | $ | (51,983 | ) | $ | (28,507 | ) | |||
| Other comprehensive income (loss): | ||||||||||||
| Net unrealized gains (losses) on investments available-for-sale | (65 | ) | 186 | (402 | ) | |||||||
| Reclassification adjustment for gains included in net loss | (615 | ) | — | — | ||||||||
| Foreign currency translation adjustment | (6,764 | ) | 223 | — | ||||||||
| Other comprehensive income (loss) | (7,444 | ) | 409 | (402 | ) | |||||||
| Comprehensive loss | $ | (90,391 | ) | $ | (51,574 | ) | $ | (28,909 | ) | |||
The accompanying notes are an integral part of these financial statements.
| F-6 |
NOVAVAX, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’
EQUITY
For the Years ended December 31, 2014, 2013 and 2012
| Accumulated | ||||||||||||||||||||||||||||
| Additional | Other | Total | ||||||||||||||||||||||||||
| Common Stock | Paid-in | Accumulated | Treasury | Comprehensive | Stockholders’ | |||||||||||||||||||||||
| Shares | Amount | Capital | Deficit | Stock | Income (Loss) | Equity | ||||||||||||||||||||||
| (in thousands, except share information) | ||||||||||||||||||||||||||||
| Balance at December 31, 2011 | 117,480,867 | $ | 1,175 | $ | 383,948 | $ | (329,656 | ) | $ | (2,450 | ) | $ | 832 | $ | 53,849 | |||||||||||||
| Non-cash compensation cost for stock options and restricted stock | — | — | 2,091 | — | — | — | 2,091 | |||||||||||||||||||||
| Exercise of stock options | 90,534 | 1 | 53 | — | — | — | 54 | |||||||||||||||||||||
| Issuance of common stock, net of issuance costs of $365 | 30,827,346 | 308 | 52,847 | — | — | — | 53,155 | |||||||||||||||||||||
| Unrealized gain (loss) on marketable securities | — | — | — | — | — | (402 | ) | (402 | ) | |||||||||||||||||||
| Net loss | — | — | — | (28,507 | ) | — | — | (28,507 | ) | |||||||||||||||||||
| Balance at December 31, 2012 | 148,398,747 | 1,484 | 438,939 | (358,163 | ) | (2,450 | ) | 430 | 80,240 | |||||||||||||||||||
| Non-cash compensation cost for stock options, ESPP and restricted stock | — | — | 2,480 | — | — | — | 2,480 | |||||||||||||||||||||
| Exercise of stock options | 667,867 | 7 | 1,491 | — | — | — | 1,498 | |||||||||||||||||||||
| Issuance of common stock, net of issuance costs of $6,067 | 60,044,130 | 600 | 169,990 | — | — | — | 170,590 | |||||||||||||||||||||
| Unrealized gain (loss) on marketable securities | — | — | — | — | — | 186 | 186 | |||||||||||||||||||||
| Foreign currency translation adjustment | — | — | — | — | — | 223 | 223 | |||||||||||||||||||||
| Net loss | — | — | — | (51,983 | ) | — | — | (51,983 | ) | |||||||||||||||||||
| Balance at December 31, 2013 | 209,110,744 | 2,091 | 612,900 | (410,146 | ) | (2,450 | ) | 839 | 203,234 | |||||||||||||||||||
| Non-cash compensation cost for stock options, ESPP and restricted stock | — | — | 6,090 | — | — | — | 6,090 | |||||||||||||||||||||
| Exercise of stock options/Purchase under ESPP | 1,411,550 | 14 | 2,776 | — | — | — | 2,790 | |||||||||||||||||||||
| Restricted stock issued as compensation | 15,000 | — | — | — | — | — | — | |||||||||||||||||||||
| Issuance of common stock, net of issuance costs of $7,105 | 28,750,000 | 288 | 107,607 | — | — | — | 107,895 | |||||||||||||||||||||
| Unrealized gain (loss) on marketable securities | — | — | — | — | — | (680 | ) | (680 | ) | |||||||||||||||||||
| Foreign currency translation adjustment | — | — | — | — | — | (6,764 | ) | (6,764 | ) | |||||||||||||||||||
| Net loss | — | — | — | (82,947 | ) | — | — | (82,947 | ) | |||||||||||||||||||
| Balance at December 31, 2014 | 239,287,294 | $ | 2,393 | $ | 729,373 | $ | (493,093 | ) | $ | (2,450 | ) | $ | (6,605 | ) | $ | 229,618 | ||||||||||||
The accompanying notes are an integral part of these financial statements.
| F-7 |
NOVAVAX, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
| For the Years ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| (in thousands) | ||||||||||||
| Operating Activities: | ||||||||||||
| Net loss | $ | (82,947 | ) | $ | (51,983 | ) | $ | (28,507 | ) | |||
| Reconciliation of net loss to net cash used in operating activities: | ||||||||||||
| Change in fair value of warrant liability | ― | (267 | ) | (101 | ) | |||||||
| Depreciation and amortization | 4,424 | 2,591 | 1,666 | |||||||||
| Loss (Gain) on disposal of property and equipment | 534 | (32 | ) | (28 | ) | |||||||
| Amortization of net premiums (discounts) on marketable securities | 415 | 507 | (18 | ) | ||||||||
| Deferred rent | (552 | ) | 897 | 660 | ||||||||
| Non-cash stock-based compensation | 6,090 | 2,480 | 2,091 | |||||||||
| Realized gains on marketable securities | (615 | ) | ― | (879 | ) | |||||||
| Other | 60 | (200 | ) | ― | ||||||||
| Changes in operating assets and liabilities: | ||||||||||||
| Restricted cash | 1,120 | (431 | ) | (986 | ) | |||||||
| Accounts receivable – billed | (5,705 | ) | (451 | ) | 954 | |||||||
| Accounts receivable – unbilled | 1,888 | (3,418 | ) | 266 | ||||||||
| Prepaid expenses and other assets | (5,904 | ) | 402 | 40 | ||||||||
| Accounts payable and accrued expenses | 13,979 | 4,184 | 2,009 | |||||||||
| Deferred revenue | (253 | ) | (341 | ) | 258 | |||||||
| Lease incentives received | 452 | 703 | 4,346 | |||||||||
| Net cash used in operating activities | (67,014 | ) | (45,359 | ) | (18,229 | ) | ||||||
| Investing Activities: | ||||||||||||
| Capital expenditures | (7,268 | ) | (5,785 | ) | (4,341 | ) | ||||||
| Proceeds from disposal of property and equipment | 39 | 116 | 324 | |||||||||
| Net cash received from acquisition | ― | 3,034 | ― | |||||||||
| Purchases of marketable securities | (176,469 | ) | (14,754 | ) | (48,652 | ) | ||||||
| Proceeds from sales, maturities and redemptions of marketable securities | 53,865 | 33,781 | 20,407 | |||||||||
| Net cash provided by (used in) investing activities | (129,833 | ) | 16,392 | (32,262 | ) | |||||||
| Financing Activities: | ||||||||||||
| Principal payments of capital leases | (124 | ) | (87 | ) | (104 | ) | ||||||
| Principal payments of notes payable | (671 | ) | (473 | ) | (60 | ) | ||||||
| Proceeds from notes payable | ― | 1,450 | 650 | |||||||||
| Changes in restricted cash | (2 | ) | (1 | ) | (756 | ) | ||||||
| Cash paid with acquisition | (171 | ) | ― | ― | ||||||||
| Net proceeds from sales of common stock, net of offering costs of $7.1 million, $6.1 million and $0.4 million, respectively |
107,896 | 128,648 | 54,002 | |||||||||
| Proceeds from the exercise of stock options and employee stock purchases | 2,789 | 1,498 | 54 | |||||||||
| Net cash provided by financing activities | 109,717 | 131,035 | 53,786 | |||||||||
| Effect of exchange rate on cash and cash equivalents | (6 | ) | 4 | ― | ||||||||
| Net increase (decrease) in cash and cash equivalents | (87,136 | ) | 102,072 | 3,295 | ||||||||
| Cash and cash equivalents at beginning of year | 119,471 | 17,399 | 14,104 | |||||||||
| Cash and cash equivalents at end of year | $ | 32,335 | $ | 119,471 | $ | 17,399 | ||||||
| Supplemental disclosure of non-cash activities: | ||||||||||||
| Common stock issued in connection with acquisition | $ | ― | $ | 41,942 | $ | ― | ||||||
| Capital expenditures included in accounts payable and accrued expenses | $ | 2,615 | $ | 379 | $ | 1,321 | ||||||
| Deposit applied towards the purchase of equipment | $ | ― | $ | ― | $ | 500 | ||||||
| Equipment acquired under a capital lease | $ | ― | $ | ― | $ | 399 | ||||||
| Supplemental disclosure of cash flow information: | ||||||||||||
| Cash interest payments | $ | 179 | $ | 177 | $ | 20 | ||||||
The accompanying notes are an integral part of these financial statements.
| F-8 |
NOVAVAX, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2014, 2013 and 2012
Note 1 – Organization
Novavax, Inc. (“Novavax,” and together with its wholly-owned subsidiary, “Novavax AB,” the “Company”) is a clinical-stage vaccine company focused on the discovery, development and commercialization of recombinant nanoparticle vaccines and adjuvants. The Company’s product pipeline targets a variety of infectious diseases with vaccine candidates currently in clinical development for respiratory syncytial virus (“RSV”), seasonal influenza, pandemic influenza and Ebola virus (“EBOV”). The Company has additional pre-clinical stage programs in a variety of infectious diseases, including Middle East Respiratory Syndrome (“MERS”).
Note 2 – Operations
The Company’s vaccine candidates currently under development, some of which include adjuvants, will require significant additional research and development efforts that include extensive pre-clinical and clinical testing, and regulatory approval prior to commercial use.
As a clinical-stage vaccine company, the Company has primarily funded its operations from proceeds through the sale of its common stock in equity offerings and revenue under its contract with the Department of Health and Human Services, Biomedical Advanced Research and Development Authority (“HHS BARDA”) and, to a lesser degree, revenue under its contract with Path Vaccine Solutions (“PATH”). Management regularly reviews the Company’s cash and cash equivalents and marketable securities against its operating budget and forecast to monitor the sufficiency of the Company’s working capital, and anticipates continuing to draw upon available sources of capital to meet its product development activities.
Note 3 – Summary of Significant Accounting Policies
Basis of Presentation
The accompanying consolidated financial statements include the accounts of Novavax, Inc. and its wholly-owned subsidiary, Novavax AB, since July 31, 2013, the date Novavax AB was acquired. All intercompany accounts and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of the consolidated financial statements in conformity with accounting principles generally accepted in the United States, requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenue and expenses during the reporting period. Actual results could differ materially from those estimates.
| F-9 |
Cash and Cash Equivalents
Cash and cash equivalents consist of highly liquid investments with maturities of three months or less from the date of purchase. Cash and cash equivalents consist of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Cash | $ | 4,481 | $ | 4,251 | ||||
| Money market funds | 20,354 | 100,049 | ||||||
| Government-backed security | 7,500 | ― | ||||||
| Corporate debt securities | ― | 15,171 | ||||||
| Cash and cash equivalents | $ | 32,335 | $ | 119,471 | ||||
Cash equivalents are recorded at cost plus accrued interest, which approximate fair value due to their short-term nature.
Marketable Securities
Marketable securities consist primarily of commercial paper, asset-backed securities and corporate notes. Classification of marketable securities between current and non-current is dependent upon the maturity date at the balance sheet date taking into consideration the Company’s ability and intent to hold the investment to maturity.
Interest and dividend income is recorded when earned and included in investment income in the consolidated statements of operations. Premiums and discounts, if any, on marketable securities are amortized or accreted to maturity and included in investment income in the consolidated statements of operations. The specific identification method is used in computing realized gains and losses on the sale of the Company’s securities.
The Company classifies its marketable securities with readily determinable fair values as “available-for-sale.” Investments in securities that are classified as available-for-sale are measured at fair market value in the consolidated balance sheets, and unrealized holding gains and losses on marketable securities are reported as a separate component of stockholders’ equity until realized. Marketable securities are evaluated periodically to determine whether a decline in value is “other-than-temporary.” The term “other-than-temporary” is not intended to indicate a permanent decline in value. Rather, it means that the prospects for a near term recovery of value are not necessarily favorable, or that there is a lack of evidence to support fair values equal to, or greater than, the carrying value of the security. Management reviews criteria, such as the magnitude and duration of the decline, as well as the Company’s ability to hold the securities until market recovery, to predict whether the loss in value is other-than-temporary. If a decline in value is determined to be other-than-temporary, the value of the security is reduced and the impairment is recorded as other income, net in the consolidated statements of operations.
Concentration of Credit Risk
Financial instruments, which possibly expose the Company to concentration of credit risk, consist primarily of cash and cash equivalents and marketable securities. The Company’s investment policy limits investments to certain types of instruments, including auction rate securities, high-grade corporate debt securities and money market instruments, places restrictions on maturities and concentrations in certain industries and requires the Company to maintain a certain level of liquidity. At times, the Company maintains cash balances in financial institutions, which may exceed federally insured limits. The Company has not experienced any losses relating to such accounts and believes it is not exposed to a significant credit risk on its cash and cash equivalents.
Fair Value Measurements
The Company applies Accounting Standards Codification (“ASC”) Topic 820, Fair Value Measurements and Disclosures, for financial and non-financial assets and liabilities.
ASC 820 discusses valuation techniques, such as the market approach (comparable market prices), the income approach (present value of future income or cash flow) and the cost approach (cost to replace the service capacity of an asset or replacement cost). The statement utilizes a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value into three broad levels. The following is a brief description of those three levels:
| F-10 |
- Level 1: Observable inputs such as quoted prices (unadjusted) in active markets for identical assets or liabilities.
- Level 2: Inputs other than quoted prices that are observable for the asset or liability, either directly or indirectly. These include quoted prices for similar assets or liabilities in active markets and quoted prices for identical or similar assets or liabilities in markets that are not active.
- Level 3: Unobservable inputs that reflect the reporting entity’s own assumptions.
Restricted Cash
The Company’s restricted cash includes payments received under the PATH agreement (See Note 8) until such time as the Company has paid for the outside services performed under the agreement. In addition, the Company’s non-current restricted cash with respect to its manufacturing, laboratory and office space in Gaithersburg, Maryland functions as collateral for letters of credit, which serve as security deposits for the duration of the leases. At December 31, 2014 and 2013, non-current restricted cash is $0.8 million and is recorded as other non-current assets on the consolidated balance sheets.
Accounts Receivable – Billed
Accounts receivable – billed arise primarily from the Company’s contract with HHS BARDA and are reported at amounts expected to be collected in future periods. No allowance for doubtful accounts is deemed necessary.
Accounts Receivable – Unbilled
Accounts receivable – unbilled relate to service contracts and agreements for which work has been performed, though invoicing has not yet occurred. All of the Accounts receivable – unbilled are expected to be billed and collected within the next 12 months.
Property and Equipment
Property and equipment are stated at cost and are depreciated using the straight-line method over the estimated useful lives of the assets, generally three to seven years. Amortization of leasehold improvements is computed using the straight-line method over the shorter of the estimated useful lives of the improvements or the remaining term of the lease. Repairs and maintenance costs are expensed as incurred.
Impairment of Long-Lived Assets
Long-lived assets are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable based on the criteria for accounting for the impairment or disposal of long-lived assets under FASB ASC Topic 360, Property, Plant and Equipment.
Impairment of Goodwill
Goodwill is subject to impairment tests annually or more frequently should indicators of impairment arise.
The Company has determined since its only business is the development of recombinant vaccines that it operates as a single operating segment and reporting unit. The Company utilizes primarily the market approach and, if considered necessary, the income approach to determine if it has an impairment of its goodwill. The market approach is based on market value of invested capital. To ensure that the Company’s capital stock is the appropriate measurement of fair value, the Company considers factors such as its trading volume, diversity of investors and analyst coverage. When utilized, the income approach is used as a confirming look to the market approach, if considered necessary. Goodwill impairment may exist if the carrying value of the reporting unit exceeds its estimated fair value. If the carrying value of the reporting unit exceeds its fair value, step two of the impairment analysis is performed. In step two of the analysis, an impairment loss is recorded equal to the excess of the carrying value of the reporting unit’s goodwill over its implied fair value should such a circumstance arise.
| F-11 |
At December 31, 2014 and 2013, the Company used the market approach to determine if the Company had an impairment of its goodwill. Step one of the impairment test states that if the fair value of a reporting unit exceeds its carrying amount, goodwill is considered not to be impaired. The fair value of the Company’s reporting unit was substantially higher than the carrying value, resulting in no impairment to goodwill at December 31, 2014 and 2013.
Equity Method Investment
The Company has an equity investment in CPL Biologicals Private Limited (“CPLB”). The Company accounts for this investment using the equity method (see Note 8). Under the equity method of accounting, investments are stated at initial cost and are adjusted for subsequent additional investments and the Company’s proportionate share of earnings or losses and distributions up to the amount initially invested or advanced.
Revenue Recognition
The Company performs research and development for U.S. Government agencies and other collaborators under cost reimbursable and fixed price contracts, including license and clinical development agreements. The Company recognizes revenue under research contracts when a contract has been executed, the contract price is fixed or determinable, delivery of services or products has occurred and collection of the contract price is reasonably assured. Payments received in advance of work performed are recorded as deferred revenue and losses on contracts, if any, are recognized in the period in which they become known.
Under cost reimbursable contracts, the Company is reimbursed and recognizes revenue as allowable costs are incurred plus a portion of the fixed-fee earned. The Company considers fixed-fees under cost reimbursable contracts to be earned in proportion to the allowable costs incurred in performance of the work as compared to total estimated contract costs, with such costs incurred representing a reasonable measurement of the proportional performance of the work completed. Under its HHS BARDA contract, certain activities must be pre-approved by HHS BARDA in order for their costs to be deemed allowable direct costs. Direct costs incurred under cost reimbursable contracts are recorded as cost of government contracts revenue. The Company’s HHS BARDA contract provides the U.S. government the ability to terminate the contract for convenience or to terminate for default if the Company fails to meet its obligations as set forth in the statement of work. The Company believes that if the government were to terminate the HHS BARDA contract for convenience, the costs incurred through the effective date of such termination and any settlement costs resulting from such termination would be allowable costs. Payments to the Company under cost reimbursable contracts with agencies of the U.S. Government, such as the HHS BARDA contract, are provisional payments subject to adjustment upon annual audit by the government. An audit by the U.S government of fiscal years 2011 and 2012 was completed in the first quarter of 2014, which resulted in no significant adjustments. An audit of fiscal year 2013 has been initiated, but has not been completed as of the date of this filing. Management believes that revenue for periods not yet audited has been recorded in amounts that are expected to be realized upon final audit and settlement. When the final determination of the allowable costs for any year has been made, revenue and billings may be adjusted accordingly in the period that the adjustments are known.
The Company’s collaborative research and development agreements may include an upfront payment, payments for research and development services, milestone payments and royalties. Agreements with multiple deliverables are evaluated to determine if the deliverables can be divided into more than one unit of accounting. A deliverable can generally be considered a separate unit of accounting if both of the following criteria are met: (1) the delivered item(s) has value to the customer on a stand-alone basis; and (2) if the arrangement includes a general right of return relative to the delivered item(s), delivery or performance of the undelivered item(s) is considered probable and substantially in control of the Company. Deliverables that cannot be divided into separate units are combined and treated as one unit of accounting. Consideration received is allocated among the separate units of accounting based on the relative selling price method. Deliverables under these arrangements typically include rights to intellectual property, research and development services and involvement by the parties in steering committees. Historically, deliverables under the Company’s collaborative research and development agreements have been deemed to have no stand-alone value and as a result have been treated as a single unit of accounting. In addition, the Company analyzes its contracts and collaborative agreements to determine whether the payments received should be recorded as revenue or as a reduction to research and development expenses. In reaching this determination, management considers a number of factors, including whether the Company is principal under the arrangement, and whether the arrangement is significant to, and part of, the Company’s core operations. Historically, payments received under its contracts and collaborative agreements have been recognized as revenue since the Company acts as a principal in the arrangement and the activities are core to its operations.
| F-12 |
When the performance under a fixed price contract can be reasonably estimated, revenue for fixed price contracts is recognized under the proportional performance method and earned in proportion to the contract costs incurred in performance of the work as compared to total estimated contract costs. Costs incurred under fixed price contracts represent a reasonable measurement of proportional performance of the work. Direct costs incurred under collaborative research and development agreements are recorded as research and development expenses. If the performance under a fixed price contract cannot be reasonably estimated, the Company recognizes the revenue on a straight-line basis over the contract term.
Revenue associated with upfront payments under arrangements is recognized over the contract term or when all obligations associated with the upfront payment have been satisfied.
Revenue from the achievement of research and development milestones, if deemed substantive, is recognized as revenue when the milestones are achieved and the milestone payments are due and collectible. If not deemed substantive, the Company would recognize such milestone as revenue upon its achievement on a straight-line basis over the remaining expected term of the research and development period. Milestones are considered substantive if all of the following conditions are met: (1) the milestone is non-refundable; (2) there is substantive uncertainty of achievement of the milestone at the inception of the arrangement; (3) substantive effort is involved to achieve the milestone and such achievement relates to past performance; and (4) the amount of the milestone appears reasonable in relation to the effort expended and all of the deliverables and payment terms in the arrangement.
Cost of Government Contracts Revenue
Cost of government contracts revenue includes direct costs of salaries, laboratory supplies, consultants and subcontractors and other direct costs associated with the Company’s process development, manufacturing, clinical, regulatory and quality assurance activities under research contracts. Cost of government contracts revenue does not include allocations of indirect costs.
Stock-Based Compensation
The Company accounts for stock-based compensation related to grants of stock options, restricted stock awards and purchases under its Employee Stock Purchase Plan (the “ESPP”) at fair value. The Company recognizes compensation expense related to such awards on a straight-line basis over the requisite service period (generally the vesting period) of the equity awards that are expected to vest, which typically occurs ratably over periods ranging from six months to four years. See Note 13 for a further discussion on stock-based compensation.
The expected term of stock options granted was based on the Company’s historical option exercise experience and post-vesting forfeiture experience using the historical expected term from the vesting date, whereas the expected term for purchases under the ESPP was based on the purchase periods included in the offering. The expected volatility was determined using historical volatilities based on stock prices over a look-back period corresponding to the expected term. The risk-free interest rate was determined using the yield available for zero-coupon U.S. government issues with a remaining term equal to the expected term. The forfeiture rate was determined using historical pre-vesting forfeiture rates since the inception of the plans. The Company has never paid a dividend, and as such, the dividend yield is zero, and the Company does not intend to pay dividends in the foreseeable future.
Restricted stock awards have been recorded as compensation expense over the expected vesting period based on the fair value at the award date and the number of shares ultimately expected to vest using the straight-line method of amortization.
The Company accounts for share-based awards issued to non-employees by determining the fair value of equity awards given as consideration for services rendered to be recognized as compensation expense over the shorter of the vesting or service periods. In cases where an equity award is not fully vested, such equity award is revalued on each subsequent reporting date until vesting is complete with a cumulative catch-up adjustment recognized for any changes in its estimated fair value.
| F-13 |
Research and Development Expenses
Research and development expenses include salaries, laboratory supplies, consultants and subcontractors and other expenses associated with the Company’s process development, manufacturing, clinical, regulatory and quality assurance activities for internally funded programs. In addition, indirect costs such as, fringe benefits and overhead expenses, are also included in research and development expenses. These expenses exclude costs associated with cost of government contracts revenue.
Warrant Accounting
The Company accounted for the warrants to purchase 0.5 shares of Common Stock (the “Warrants”) at a price of $2.68 per unit in accordance with applicable accounting guidance in ASC 815, Derivatives and Hedging, as derivative liabilities, and the Warrants had been classified as such in the Company’s balance sheet. In compliance with applicable accounting standards, registered warrants that require the issuance of registered shares upon exercise and do not sufficiently preclude an implied right to cash settlement are accounted for as derivative liabilities. The Company used the Monte Carlo Simulation model to determine the fair value of the Warrants, which required the input of subjective assumptions, including the expected stock price volatility and probability of a fundamental transaction (a strategic merger or sale). All Warrants subject to this accounting treatment expired unexercised on July 31, 2013.
Income Taxes
The Company accounts for income taxes in accordance with ASC Topic 740, Income Taxes. Under the liability method, deferred income taxes are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax basis and operating loss carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the year in which those temporary differences are expected to be recovered or settled. The effect of changes in tax rates on deferred tax assets and liabilities is recognized in income in the period such changes are enacted. A valuation allowance is established when necessary to reduce net deferred tax assets to the amount expected to be realized.
Tax benefits associated with uncertain tax positions are recognized in the period in which one of the following conditions is satisfied: (1) the more likely than not recognition threshold is satisfied; (2) the position is ultimately settled through negotiation or litigation; or (3) the statute of limitations for the taxing authority to examine and challenge the position has expired. Tax benefits associated with an uncertain tax position are reversed in the period in which the more likely than not recognition threshold is no longer satisfied.
Interest and penalties related to income tax matters are recorded as income tax expense. At December 31, 2014 and 2013, the Company had no accruals for interest or penalties related to income tax matters.
Net Loss per Share
Net loss per share is computed using the weighted average number of shares of common stock outstanding. All outstanding warrants, stock options and unvested restricted stock awards totaling 16,978,098, 11,992,918 and 12,732,383 shares at December 31, 2014, 2013 and 2012, respectively, are excluded from the computation for 2014, 2013 and 2012, as their effect is anti-dilutive.
Foreign Currency
The accompanying consolidated financial statements are presented in U.S. dollars. The functional currency of the Company’s wholly-owned subsidiary is the local currency in which the subsidiary is located (Swedish Krona). The translation of assets and liabilities of Novavax AB to U.S. dollars is made at the exchange rate in effect at the consolidated balance sheet date, while equity accounts are translated at historical rates. The translation of statement of operations data is made at the average exchange rate in effect for the period. The translation of operating cash flow data is made at the average exchange rate in effect for the period, and investing and financing cash flow data is translated at the exchange rate in effect at the date of the underlying transaction. Translation gains and losses are recognized as a component of accumulated other comprehensive income (loss) in the accompanying consolidated balance sheets. The foreign currency translation adjustment balance included in accumulated other comprehensive income (loss) was ($6.5) million and $0.2 million at December 31, 2014 and 2013, respectively.
| F-14 |
Segment Information
The Company manages its business as one operating segment: developing recombinant vaccines. The Company does not operate separate lines of business with respect to its vaccine candidates. Accordingly, the Company does not have separately reportable segments as defined by ASC 280, Segment Reporting.
Recent Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board issued ASU 2014-09, Revenue from Contracts with Customers (Topic 606) (“ASU 2014-09”), which supersedes nearly all existing revenue recognition guidance under Topic 605, Revenue Recognition. The new standard requires a company to recognize revenue when it transfers goods and services to customers in an amount that reflects the consideration that the company expects to receive for those goods or services. ASU 2014-09 defines a five-step process that includes identifying the contract with the customer, identifying the performance obligations in the contract, determining the transaction price, allocating the transaction prices to the performance obligations in the contract and recognizing revenue when (or as) the entity satisfies the performance obligations. ASU 2014-09 will be effective for the Company on January 1, 2017. The Company is evaluating the potential impact that ASU 2014-09 will have on its consolidated financial position and results of operations.
Reclassifications
Due to new information obtained in the first quarter of 2014 about facts and circumstances that existed on July 31, 2013 (the “Acquisition Date”) regarding certain accrued contingencies related to its pre-existing contractual rights and obligations, the Company reduced at December 31, 2013 such accrued expenses and the carrying value of its goodwill retrospectively as of the Acquisition Date related to the acquisition by $0.8 million from $11.2 million to $10.4 million and from $26.2 million to $25.4 million, respectively.
Note 4 – Acquisition
In 2013, Novavax acquired 99.5% of all of the outstanding shares, warrants and stock options of Isconova AB through the issuance of approximately 15.6 million shares of its Common Stock valued at $41.9 million (based on the closing price of Novavax’ Common Stock on the Acquisition Date) and cash of approximately $22,000. Upon the acquisition, Isconova AB was renamed Novavax AB. During the second quarter of 2014, the Company completed its purchase of the remaining 0.5% shares outstanding from the holders of such securities of Novavax AB. This transaction has been accounted for using the purchase method of accounting, with Novavax as the acquirer. The results of Novavax AB’s operations have been included in the consolidated financial statements since the Acquisition Date.
The table below summarizes the final allocation of the purchase price based upon the fair values of assets acquired and liabilities assumed at the Acquisition Date.
| (in thousands) | ||||
| Cash and cash equivalents | $ | 3,056 | ||
| Accounts receivable – billed | 447 | |||
| Prepaid expenses and other assets | 1,092 | |||
| Property and equipment | 165 | |||
| Intangible assets | 16,620 | |||
| Goodwill | 25,424 | |||
| Accounts payable and other current liabilities | (2,994 | ) | ||
| Capital leases | (94 | ) | ||
| Notes payable | (193 | ) | ||
| Other non-current liabilities | (1,559 | ) | ||
| Total purchase price | $ | 41,964 | ||
| F-15 |
A substantial portion of the assets acquired consisted of intangible assets relating to its proprietary adjuvant technology and collaboration agreements. The fair values of the proprietary technology and agreements were determined based on estimates of expected future discounted net cash flows. The fair value measurements are based on significant unobservable inputs that were developed by the Company using publicly available information, market participant assumptions, cost and development assumptions, expected synergies and other cost savings that a market participant would be expected to realize as a result of the combination and certain other high-level assumptions. Amortization expense for intangible assets is being recorded on a straight-line basis over the expected useful lives of the assets, ranging from seven to 20 years. The weighted average useful lives for the proprietary adjuvant technology and collaboration agreements are 20 years and 12 years, respectively. The weighted average useful life for all acquired intangible assets is 17 years.
The Company incurred approximately $1.3 million in transaction costs related to the acquisition, which is included in general and administrative expenses in the Company’s consolidated statement of operations for the year ended December 31, 2013.
The following unaudited consolidated pro forma financial information is presented as if the acquisition occurred on January 1, 2012. The unaudited pro forma financial information has been presented for comparative purposes only and is not necessarily indicative of results of operations that would have been achieved had the Company completed the acquisition during the periods presented, or the future consolidated results of operations of the combined company. The unaudited pro forma financial information combines the historical results of operations of Novavax and Isconova AB for the periods presented below:
|
Year Ended December 31, |
||||||||
| 2013 | 2012 | |||||||
| (in thousands) | ||||||||
| Revenue | $ | 22,785 | $ | 24,810 | ||||
| Net loss | $ | (55,594 | ) | $ | (35,042 | ) | ||
| Basic and diluted net loss per share | $ | (0.31 | ) | $ | (0.24 | ) | ||
Novavax AB entered into a license and collaboration agreement and received research funding prior to the acquisition that is required to be repaid upon notice in the first quarter of 2016. At December 31, 2014, such research funding liability is $1.5 million and is included in other non-current liabilities in the consolidated balance sheet.
Note 5 – Fair Value Measurements
The following table represents the Company’s fair value hierarchy for its financial assets and liabilities measured at fair value on a recurring basis:
| Fair Value at December 31, 2014 | Fair Value at December 31, 2013 | |||||||||||||||||||||||
| Assets | Level 1 | Level 2 | Level 3 | Level 1 | Level 2 | Level 3 | ||||||||||||||||||
| Auction rate security | $ | ― | $ | ― | $ | — | $ | 1,790 | $ | ― | $ | — | ||||||||||||
| Money market funds | 20,354 | ― | — | 100,049 | — | — | ||||||||||||||||||
| Government-backed security | — | 7,500 | — | ― | — | — | ||||||||||||||||||
| Asset-backed securities | — | 46,624 | — | — | — | — | ||||||||||||||||||
| Corporate debt securities | — | 89,097 | — | — | 26,978 | — | ||||||||||||||||||
| Total cash equivalents and marketable securities | $ | 20,354 | $ | 143,221 | $ | — | $ | 101,839 | $ | 26,978 | $ | — | ||||||||||||
During the years ended December 31, 2014 and 2013, the Company did not have any transfers between levels.
The amounts in the Company’s consolidated balance sheet for accounts receivable – billed, accounts receivable – unbilled and accounts payable approximate fair value due to their short-term nature. Based on borrowing rates available to the Company, the fair value of capital lease and notes payable approximates their carrying value.
| F-16 |
Note 6 – Marketable Securities
Marketable securities classified as available-for-sale as of December 31, 2014 and 2013 were comprised of (in thousands):
| December 31, 2014 | December 31, 2013 | |||||||||||||||||||||||||||||||
Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Fair Value | Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Fair Value | |||||||||||||||||||||||||
| Auction rate security | $ | — | $ | — | $ | — | $ | — | $ | 1,175 | $ | 615 | $ | — | $ | 1,790 | ||||||||||||||||
| Asset-backed securities | 46,660 | — | (36 | ) | 46,624 | — | — | — | — | |||||||||||||||||||||||
| Corporate debt securities | 89,126 | 8 | (37 | ) | 89,097 | 11,806 | 1 | — | 11,807 | |||||||||||||||||||||||
| Total | $ | 135,786 | $ | 8 | $ | (73 | ) | $ | 135,721 | $ | 12,981 | $ | 616 | $ | — | $ | 13,597 | |||||||||||||||
In 2014, the Company sold its remaining auction rate security and received proceeds of $1.8 million resulting in a realized gain of $0.6 million, all of which resulted from reclassification adjustments out of accumulated other comprehensive income (loss) in 2014.
Marketable Securities – Unrealized Losses
The Company owned 41 available-for-sale securities as of December 31, 2014. Of these 41 securities, 38 had unrealized losses of less than $0.1 million as of December 31, 2014. The Company did not have any investments in a loss position for greater than 12 months as of December 31, 2014. The Company has evaluated its marketable securities and has determined that none of these investments has an other-than-temporary impairment, as it has no intent to sell securities with unrealized losses and it is not more likely than not that the Company will be required to sell any securities with unrealized losses, given the Company’s current and anticipated financial position.
Note 7 – Goodwill and Intangible Assets
Goodwill
The changes in the carrying amounts of goodwill for the year ended December 31, 2014 and 2013 were as following (in thousands):
Year Ended December 31, | ||||||||
| 2014 | 2013 | |||||||
| Beginning balance | $ | 58,707 | $ | 33,141 | ||||
| Goodwill resulting from acquisition of business | — | 25,424 | ||||||
| Currency translation | (4,095 | ) | 142 | |||||
| Ending balance | $ | 54,612 | $ | 58,707 | ||||
| F-17 |
Intangible Assets
Purchased intangible assets consisted of the following as of December 31, 2014 and 2013 (in thousands):
| December 31, 2014 | December 31, 2013 | |||||||||||||||||||||||
Gross Carrying Amount | Accumulated Amortization | Intangible Assets, Net | Gross Carrying Amount | Accumulated Amortization | Intangible Assets, Net | |||||||||||||||||||
| Finite-lived intangible assets: | ||||||||||||||||||||||||
| Proprietary adjuvant technology | $ | 9,565 | $ | (678 | ) | $ | 8,887 | $ | 11,514 | $ | (240 | ) | $ | 11,274 | ||||||||||
| Collaboration agreements | 4,319 | (629 | ) | 3,690 | 5,199 | (223 | ) | 4,976 | ||||||||||||||||
| Total identifiable intangible assets | $ | 13,884 | $ | (1,307 | ) | $ | 12,577 | $ | 16,713 | $ | (463 | ) | $ | 16,250 | ||||||||||
Amortization expense for the years ended December 2014 December 31, 2013 was $1.1 million and $0.5 million, respectively. Estimated amortization expense for existing intangible assets for each of the five succeeding years ending December 31, is as follows (in thousands):
| Year | Amount | |||
| 2015 | $ | 923 | ||
| 2016 | 923 | |||
| 2017 | 923 | |||
| 2018 | 923 | |||
| 2019 | 923 | |||
Note 8 – U.S. Government Agreement, Joint Venture and Collaborations
HHS BARDA Contract for Recombinant Influenza Vaccines
HHS BARDA initially awarded the Company a contract in 2011, which funds the development of both the Company’s seasonal and pandemic influenza VLP vaccine candidates. The contract with HHS BARDA is a cost-plus-fixed-fee contract, which reimburses the Company for allowable direct contract costs incurred plus allowable indirect costs and a fixed-fee earned in the ongoing clinical development and product scale-up of its multivalent seasonal and monovalent pandemic H7N9 influenza VLP vaccine candidates. In September 2014, HHS BARDA exercised and initiated a two-year option to the contract, which included scope to support development activities leading up to planned Phase 3 clinical studies, added $70 million of funding on top of the remainder of the $97 million base period funding, and extended the contract until September 2016. During 2014, the Company recognized revenue of $26.0 million and has recognized approximately $78 million in revenue since the inception of the contract. Billings under the contract are based on approved provisional indirect billing rates, which permit recovery of fringe benefits, overhead and general and administrative expenses. These indirect rates are subject to audit by HHS BARDA on an annual basis. An audit by the U.S government of fiscal years 2011 and 2012 was completed in the first quarter of 2014, which resulted in no significant adjustments. An audit of fiscal year 2013 has been initiated, but has not been completed as of the date of this filing. Management believes that revenue for periods not yet audited has been recorded in amounts that are expected to be realized upon final audit and settlement. When the final determination of the allowable costs for any year has been made, revenue and billings may be adjusted accordingly in the period that the adjustments are known.
In 2012, the Company decided to conduct a Phase 2 clinical trial of its quadrivalent seasonal influenza VLP vaccine candidate in Australia (“205 Trial”) under appropriate local regulatory authorization. Based on the Company’s discussions with HHS BARDA in 2012, the outside clinical trial costs for the 205 Trial were withheld and may only be submitted for consideration of reimbursement to HHS BARDA and recorded as revenue by the Company after it submits the 205 Trial data in a quadrivalent investigational new drug application (“Quadrivalent IND”), and those costs are approved by HHS BARDA. The outside clinical trial costs of the 205 Trial conducted in 2012 totaled $2.9 million. These costs were recorded as an expense in the period incurred as a cost of government contracts revenue. The FDA accepted the Quadrivalent IND in the fourth quarter of 2014, prior to the Company’s initiation of its Phase 2 dose-confirmatory clinical trial; however, despite ongoing discussions with HHS BARDA, the Company is still awaiting HHS BARDA’s approval for the reimbursement of its 205 Trial costs, thus no revenue has been recorded in 2014.
| F-18 |
CPLB Joint Venture
The Company is party to a Joint Venture Agreement with Cadila Pharmaceuticals Limited (“Cadila”) pursuant to which the Company and Cadila formed CPLB, of which 20% is owned by the Company and 80% is owned by Cadila. CPLB was established to develop and manufacture certain of the Company’s vaccine candidates and certain of Cadila’s biogeneric and diagnostic products for the territory of India. CPLB has the right to negotiate definitive license arrangements in India to certain of the Company’s future vaccine products and certain of Cadila’s future biogeneric and diagnostic products, prior to the Company or Cadila licensing such rights to third-parties. The Company has the right to negotiate definitive license arrangements for vaccines developed by CPLB using Company technology for commercialization in every country except India and for vaccines developed by CPLB using Cadila technology for commercialization in certain other countries, including the U.S. Cadila has supported and continues to support CPLB’s operations. CPLB is actively developing a number of vaccine candidates that were genetically engineered by Novavax. CPLB’s lead vaccine candidates are its seasonal influenza vaccine candidate, which completed enrollment of its Phase 3 clinical trial in India in 2014, and its rabies vaccine, which completed enrollment of its Phase 1/2 clinical trial in India in 2014. In connection with the Joint Venture Agreement, in 2009, the Company also entered into additional agreements, including a master services agreement with Cadila (see Note 16). Because CPLB’s activities and operations are controlled and funded by Cadila, the Company accounts for its investment using the equity method. Since the carrying value of the Company’s initial investment was nominal and there is no guarantee or commitment to provide future funding, the Company has not recorded nor expects to record losses related to this investment in the foreseeable future.
LG Life Sciences, Ltd. (“LGLS”) License Agreement
In 2011, the Company entered into a license agreement with LGLS that allows LGLS to use the Company’s technology to develop and commercially sell influenza vaccines exclusively in South Korea and non-exclusively in certain other specified countries. At its own cost, LGLS is responsible for funding both its clinical development of the influenza VLP vaccines and a manufacturing facility to produce such vaccines in South Korea. Under the license agreement, the Company is obligated to provide LGLS with information and materials related to the manufacture of the licensed products, provide on-going project management and regulatory support and conduct clinical trials of its influenza vaccines in order to obtain FDA approval in the U.S. The term of the license agreement is expected to terminate in 2027. Payments to the Company under the license agreement include an upfront payment of $2.5 million, reimbursements of certain development and product costs, payments related to the achievement of certain milestones and royalty payments in the high single digits from LGLS’s future commercial sales of influenza VLP vaccines. The upfront payment has been deferred and recorded in deferred revenue in the consolidated balance sheets and will be recognized when the previously mentioned obligations in the agreement are satisfied, which may not occur until the end of the term of the agreement. Payments for milestones under the agreement will be recognized on a straight-line basis over the remaining term of the research and development period upon achievement of such milestone. Any royalties under the agreement will be recognized as earned.
PATH Vaccine Solutions (“PATH”) Clinical Development Agreement
In 2012, the Company entered into a clinical development agreement with PATH (the “RSV Collaboration Program”) to develop its RSV F vaccine candidate in certain low-resource countries. The Company was awarded approximately $2.0 million by PATH for initial funding under the agreement to partially support its Phase 2 dose-ranging clinical trial in women of childbearing age. In October 2013, the funding under this agreement was increased by $0.4 million to support reproductive toxicology studies, which was necessary before we began conducting clinical trials in pregnant women. In December 2013, the Company entered into an amendment with PATH providing an additional $3.5 million in funding to support the Phase 2 dose-confirmation clinical trial in women of childbearing age. In October 2014, the Company entered into an amendment with PATH providing an additional $1.0 million towards the development of a strategy for approaching Phase 3 clinical trials of our RSV maternal immunization program and is in ongoing discussion with PATH for additional funding. The Company retains global rights to commercialize the product and will support PATH in its goal to make an RSV maternal vaccine product affordable and available in low-resource countries. To the extent PATH elects to continue to fund 50% of the Company’s external clinical development costs for the RSV Collaboration Program, but the Company does not continue development, the Company would then grant PATH a fully-paid license to the Company’s RSV F vaccine candidate technology for use in pregnant women in certain contractually defined, low-resource countries. The term of the agreement has been extended to April 2015. The Company recognized revenue of approximately $2.6 million in 2014, and has recognized approximately $6.4 million in revenue since the inception of the agreement. Revenue under this arrangement is being recognized under the proportional performance method and earned in proportion to the contract costs incurred in performance of the work as compared to total estimated contract costs. Costs incurred under this agreement represent a reasonable measurement of proportional performance of the services being performed.
| F-19 |
Note 9 – Other Financial Information
Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets consist of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Laboratory supplies | $ | 7,564 | $ | 1,754 | ||||
| Other prepaid expenses and other current assets | 1,631 | 1,863 | ||||||
| Prepaid expenses and other current assets | $ | 9,195 | $ | 3,617 | ||||
Property and Equipment, net
Property and equipment is comprised of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Machinery and equipment | $ | 16,712 | $ | 11,951 | ||||
| Leasehold improvements | 8,843 | 8,192 | ||||||
| Computer software and hardware | 1,733 | 1,200 | ||||||
| Construction in progress | 3,719 | 2,328 | ||||||
| 31,007 | 23,671 | |||||||
| Less ― accumulated depreciation and amortization | (11,270 | ) | (9,420 | ) | ||||
| Property and equipment, net | $ | 19,737 | $ | 14,251 | ||||
Depreciation and amortization expense was approximately $4.4 million, $2.6 million and $1.7 million for the years ended December 31, 2014, 2013 and 2012, respectively. Machinery and equipment included $0.4 million and $0.6 million of equipment acquired under a capital leases with accumulated depreciation of $0.2 million as of December 31, 2014 and 2013, respectively.
Accrued Expenses
Accrued expenses consist of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Employee benefits and compensation | $ | 8,597 | $ | 5,323 | ||||
| Research and development accruals | 9,826 | 3,657 | ||||||
| Other accrued expenses | 974 | 1,431 | ||||||
| Accrued expenses | $ | 19,397 | $ | 10,411 | ||||
| F-20 |
Note 10 – Long-Term Debt
Notes Payable
Notes payable consist of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Equipment loan; 12.1%, principal payments due in monthly installments totaling $48 through December 2016 | $ | 967 | $ | 1,538 | ||||
| Loan agreement; bearing interest at 3% per annum; repayment is conditional | — | 200 | ||||||
| Bank loans; 7.50%-8.50%, principal payments due quarterly totaling $22 through May 2015 | 31 | 143 | ||||||
| Total | 998 | 1,881 | ||||||
| Less ― current portion | (603 | ) | (877 | ) | ||||
| Long-term portion | $ | 395 | $ | 1,004 |
Equipment Loan
In September 2012, the Company entered into a master security agreement with General Electric Capital Corporation (“GE”), whereby the Company could borrow up to $2.0 million to finance the purchases of equipment (each, an “Equipment Loan”). Each Equipment Loan bears interest at the three-year U.S. Government treasury rate plus 11.68%, provided that the rate shall not be less than 12.1%, and is to be repaid over forty-two (42) months. GE will maintain a security interest in all equipment financed under the Equipment Loan. Interest accrues on the outstanding balance until paid in full. As of December 31, 2013, the Company financed $2.0 million in total under the Equipment Loans.
Loan Agreements
In May 2008, the Company entered into a loan agreement with the State of Maryland. The repayment of loan amount and accrued interest was conditioned upon the Company meeting the capital investment and employment requirements during the term of the loan. In 2014, the loan agreement with State of Maryland was forgiven as the Company met the capital investment and employment requirements and is recorded as other income, net in the Company’s consolidated statements of operations.
Aggregate future minimum principal payments on long-term debt at December 31, 2013 are as follows (in thousands):
| Year | Amount | |||
| 2015 | $ | 603 | ||
| 2016 | 395 | |||
| Total minimum principal payments | $ | 998 | ||
Note 11 – Warrant Liability
In July 2008, the Company completed a registered direct offering of 6,686,650 units, raising approximately $17.5 million in net proceeds. Each unit consisted of one share of Common Stock and one Warrant. The Warrants represented the right to acquire an aggregate of 3,343,325 shares of common stock at an exercise price of $3.62 per share and expired unexercised on July 31, 2013.
During 2013 and 2012, the Company recorded as other income in its statements of operations a change in fair value of warrant liability of $0.3 million and $0.1 million, respectively.
Note 12 – Stockholders’ Equity
In June 2014, the Company completed a public offering of 28,750,000 shares of its common stock, including 3,750,000 shares of common stock that were issued upon the exercise in full of an option to purchase additional shares granted to the underwriters, at a price of $4.00 per share resulting in net proceeds of approximately $108 million.
| F-21 |
In September 2013, the Company completed a public offering of 31,846,950 shares of its common stock, including 4,153,950 shares of common stock that were issued upon the exercise in full of an option to purchase additional shares granted to the underwriters, at a price of $3.14 per share resulting in net proceeds of approximately $95 million.
In 2012, the Company entered into an At Market Issuance Sales Agreement (“Sales Agreement”), under which the Board of Directors of the Company (the “Board”) approved the Company’s sale of up to an aggregate of $50 million in gross proceeds of its common stock. The shares of common stock are being offered pursuant to a shelf registration statement filed with the SEC in March 2013, which replaced the previous shelf registration statement filed in 2010. The Board’s standing Finance Committee (the “Committee”) assists with its responsibilities to monitor, provide advice to the Company’s senior management and approve all capital raising activities. The Committee has been authorized by the Board, absent any action by the Board to the contrary, to take any additional actions necessary to carry out the Board’s authorization of the issuance and sale of the common stock pursuant to the Sales Agreement. In doing so, the Committee is authorized to set the amount of shares to be sold, the period of time during which such sales may occur and the minimum sales price per share. During 2013, the Company sold 12.6 million shares at sales prices ranging from $2.06 to $3.38 per share, resulting in $34.0 million in net proceeds. The most recent sales that occurred under the Sales Agreement were in September 2013. As of December 31, 2014, the Company had approximately $15 million available under the Sales Agreement.
Note 13 – Stock-Based Compensation
Stock Options
The Company has granted equity awards under several plans, two of which remain active. Under the Amended and Restated 2005 Stock Incentive Plan (the “2005 Plan”), equity awards may be granted to officers, directors, employees, consultants and advisors to the Company and any present or future subsidiary. The 2005 Plan, approved in May 2005 and amended most recently in June 2014 by the Company’s stockholders, currently authorizes the grant of equity awards for up to 26,312,192 shares of common stock, which included, at the time of approval of the 2005 Plan, a maximum 5,746,468 shares of common stock subject to stock options outstanding under the Company’s 1995 Stock Option Plan (the “1995 Plan”) that may revert to and become issuable under the 2005 Plan if such options expire or otherwise terminate unexercised. The Company received approval at its 2014 annual meeting of stockholders to increase the number of shares of common stock available for issuance under the 2005 Plan by 4,000,000 shares. The term of the Company’s 1995 Plan has expired and no new awards will be made under the 1995 Plan; however, outstanding stock options remain in existence in accordance with their terms.
Under the 2005 Plan and the 1995 Plan, incentive stock options, having a maximum term of 10 years, can be or were granted at no less than 100% of the fair value of the Company’s common stock at the time of grant. Grants of stock options are generally exercisable over periods ranging from six months to four years.
Because the 2005 Plan expired in the first quarter of 2015, the Company intends to adopt a 2015 stock incentive plan and submit it for approval to its stockholders at the 2015 annual meeting of stockholders.
| F-22 |
Stock Options Awards
The following is a summary of option activity under the 2005 Plan and the 1995 Plan for the year ended December 31, 2014:
| 2005 Stock Incentive Plan | 1995 Stock Option Plan | |||||||||||||||
| Stock Options | Weighted-Average Exercise Price |
Stock Options | Weighted-Average Exercise Price |
|||||||||||||
| Outstanding at January 1, 2014 | 11,788,100 | $ | 1.87 | 188,150 | $ | 5.04 | ||||||||||
| Granted | 6,418,000 | $ | 5.50 | — | $ | — | ||||||||||
| Exercised | (898,302 | ) | $ | 1.67 | (32,450 | ) | $ | 4.81 | ||||||||
| Forfeited | (378,450 | ) | $ | 2.79 | — | $ | — | |||||||||
| Expired | (1,250 | ) | $ | 1.57 | (120,700 | ) | $ | 5.76 | ||||||||
| Outstanding at December 31, 2014 | 16,928,098 | $ | 3.24 | 35,000 | $ | 2.21 | ||||||||||
| Vested and expected to vest at December 31, 2014 | 15,445,657 | $ | 3.09 | 35,000 | $ | 2.21 | ||||||||||
| Shares exercisable at December 31, 2014 | 6,069,997 | $ | 2.07 | 35,000 | $ | 2.21 | ||||||||||
| Shares available for grant at December 31, 2014 | 4,531,369 | |||||||||||||||
The fair value of the stock options granted for the years ended December 31, 2014, 2013 and 2012, was estimated at the date of grant using the Black-Scholes option-pricing model with the following assumptions:
| 2014 | 2013 | 2012 | ||||||||
| Weighted average fair value of options granted | $2.39 | $1.07 | $0.71 | |||||||
| Risk-free interest rate | 1.24%-2.22% | 0.54%-1.36% | 0.55%-1.54% | |||||||
| Dividend yield | 0% | 0% | 0% | |||||||
| Volatility | 52.47%-67.93% | 51.55%-73.72% | 75.5%-78.6% | |||||||
| Expected term (in years) | 4.04-6.96 | 3.91-7.05 | 3.34-7.09 | |||||||
| Expected forfeiture rate | 0%-23.15% | 0%-23.15% | 0%-23.15% | |||||||
The aggregate intrinsic value and weighted average remaining contractual term of stock options exercisable as of December 31, 2014 was approximately $23.6 million and 6.3 years, respectively. The aggregate intrinsic value and weighted average remaining contractual term of options vested and expected to vest as of December 31, 2014 was $44.3 million and 7.6 years, respectively. The aggregate intrinsic value represents the total intrinsic value (the difference between the Company’s closing stock price on the last trading day of 2014 and the exercise price, multiplied by the number of in-the-money options) that would have been received by the option holders had all option holders exercised their options on December 31, 2014. This amount is subject to change based on changes to the fair market value of the Company’s common stock. The aggregate intrinsic value of options exercised for 2014, 2013 and 2012 was $3.4 million, $0.6 million and $0.1 million, respectively.
Stock options issued to non-employees are measured at their estimated fair value. Stock-based compensation expense is recognized when services are rendered; however, the expense may fluctuate with changes in the fair value of the underlying common stock, until the award is vested. The Company recorded $0.3 million and $0.1 million in stock-based compensation expense related to stock options granted to non-employees in 2014 and 2013, respectively.
Employee Stock Purchase Plan
In 2013, the Company adopted an Employee Stock Purchase Plan (the “ESPP”), which authorized an aggregate of 2,000,000 shares of common stock to be purchased, which will increase 5% on each anniversary of its adoption up to a maximum of 3,000,000 shares. The ESPP allows employees to purchase shares of common stock of the Company at each purchase date through payroll deductions of up to a maximum of 15% of their compensation, at 85% of the lesser of the market price of the shares at the time of purchase or the market price on the beginning date of an option period (or, if later, the date during the option period when the employee was first eligible to participate). At December 31, 2014, there were 1,619,202 shares available for issuance under the ESPP.
| F-23 |
The ESPP is considered compensatory for financial reporting purposes. As such, the fair value of ESPP shares was estimated at the date of grant using the Black-Scholes option-pricing model with the following assumptions:
| Year Ended December 31, | Year Ended December 31, | |||||||
| 2014 | 2013 | |||||||
| Range of Black-Scholes fair value of ESPP shares granted | $0.78-$2.08 | $0.78 | ||||||
| Risk-free interest rate | 0.04%-0.24% | 0.04% | ||||||
| Dividend yield | 0% | 0% | ||||||
| Volatility | 50.80%-67.57% | 50.80% | ||||||
| Expected term (in years) | 0.5-1.5 | 0.5 | ||||||
| Expected forfeiture rate | 5% | 5% | ||||||
Stock-based compensation related to the ESPP for 2014 and 2013 was $0.7 million and $0.1 million, respectively.
Restricted Stock Awards
The following is a summary of restricted stock awards activity for the year ended December 31, 2014:
|
Number of Shares |
Per Share Weighted-Average Grant-Date Fair Value |
|||||||
| Outstanding at January 1, 2014 | 16,667 | $ | 1.39 | |||||
| Restricted stock granted | 15,000 | $ | 4.48 | |||||
| Restricted stock vested | (16,667 | ) | $ | 1.39 | ||||
| Restricted stock forfeited | — | $ | — | |||||
| Outstanding at December 31, 2014 | 15,000 | $ | 4.48 | |||||
The Company recorded stock-based compensation expense for awards issued under the above mentioned plans in the statements of operations as follows (in thousands):
| Years ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Research and development | $ | 2,843 | $ | 1,262 | $ | 873 | ||||||
| General and administrative | 3,247 | 1,218 | 1,218 | |||||||||
| Total stock-based compensation expense | $ | 6,090 | $ | 2,480 | $ | 2,091 | ||||||
As of December 31, 2014, there was approximately $13.3 million of total unrecognized compensation expense (net of estimated forfeitures) related to unvested options and restricted stock awards. This unrecognized compensation expense is expected to be recognized over a weighted average period of 1.3 years.
Note 14 – Employee Benefits
The Company maintains a defined contribution 401(k) retirement plan, pursuant to which employees who have completed 90 days of service may elect to contribute up to 100% of their compensation on a tax deferred basis up to the maximum amount permitted by the Internal Revenue Code of 1986, as amended.
During 2012, the Company increased its match from 25% to 50% of the first 6% of the participants’ deferral. Contributions to the 401(k) plan vest equally over a three-year period. The Company has recorded expense, net of forfeitures, of approximately $0.5 million, $0.4 million and $0.1 million in 2014, 2013 and 2012, respectively.
| F-24 |
The Company’s foreign subsidiary has a pension plan under local tax and labor laws and is obligated to make contributions to this plan. Contributions and other expenses related to this plan were approximately $0.4 million and $0.2 million in 2014 and 2013, respectively.
Note 15 – Income Taxes
The Company losses by jurisdiction are as follows (in thousands):
| 2014 | 2013 | 2012 | ||||||||||
| Domestic | $ | (76,742 | ) | $ | (48,691 | ) | $ | (28,507 | ) | |||
| Foreign | (6,205 | ) | (3,292 | ) | — | |||||||
| Total net loss | $ | (82,947 | ) | $ | (51,983 | ) | $ | (28,507 | ) | |||
The components of the income tax provision are as follows (in thousands):
| 2014 | 2013 | 2012 | ||||||||||
| Current U.S. | $ | — | $ | — | $ | — | ||||||
| Current foreign | — | 25 | — | |||||||||
| Deferred | — | — | ― | |||||||||
| Net provision | $ | — | $ | 25 | $ | — | ||||||
Deferred tax assets (liabilities) consist of the following at December 31 (in thousands):
| 2014 | 2013 | |||||||
| Net operating losses U.S. | $ | 148,451 | $ | 123,907 | ||||
| Net operating losses foreign | 6,535 | 6,405 | ||||||
| Research tax credits | 11,068 | 9,175 | ||||||
| Other | 9,963 | 6,844 | ||||||
| Total deferred tax assets | 176,017 | 146,331 | ||||||
| Intangibles | (2,773 | ) | (3,573 | ) | ||||
| Other | (321 | ) | (227 | ) | ||||
| Total deferred tax liabilities | (3,094 | ) | (3,800 | ) | ||||
| Net deferred tax assets | 172,923 | 142,531 | ||||||
| Less valuation allowance | (172,923 | ) | (142,531 | ) | ||||
| Deferred tax assets, net | $ | — | $ | — | ||||
The valuation allowance increased by $30.4 million, $7.1 million and $9.4 million for the years ended December 31, 2014, 2013 and 2012, respectively, due to increases in net deferred tax assets.
The differences between the U.S. federal statutory tax rate and the Company’s effective tax rate are as follows:
| 2014 | 2013 | 2012 | ||||||||||
| Statutory federal tax rate | (34 | )% | (34 | )% | (34 | )% | ||||||
| State income taxes, net of federal benefit | (3 | )% | (3 | )% | (8 | )% | ||||||
| Research and development and other tax credits | (2 | )% | (7 | )% | 0 | % | ||||||
| Expiration of net operating losses | 0 | % | 0 | % | 6 | % | ||||||
| Other | 2 | % | 3 | % | 3 | % | ||||||
| Change in valuation allowance | 37 | % | 41 | % | 33 | % | ||||||
| 0 | % | 0 | % | 0 | % | |||||||
Realization of net deferred tax assets is dependent on the Company’s ability to generate future taxable income, which is uncertain. Accordingly, a full valuation allowance was recorded against these assets as of December 31, 2014 and 2013 as management believes it is more likely than not that the assets will not be realizable. The increase in the valuation allowance was due to increased continued losses and credits in the current year.
| F-25 |
As of December 31, 2014, the Company had tax return reported federal net operating losses and tax credits available as follows (in thousands):
| Amount | ||||
| Federal net operating losses expiring through the year 2034 | $ | 402,192 | ||
| Foreign net operating losses (no expiration) | 29,705 | |||
| Research tax credits expiring through the year 2034 | 10,975 | |||
| Alternative-minimum tax credit (no expiration) | 94 | |||
Utilization of the net operating loss carryforwards and credits may be subject to an annual limitation due to prior ownership change of the Company. The Company does not expect such limitation, if any, to impact the use of the net operating losses.
Beginning in 2006, the windfall equity-based compensation deductions are tracked, but will not be recorded to the balance sheet until management determines more likely than not that such amounts will be utilized. As of December 31, 2014 and 2013, the Company had $5.0 million and $2.4 million of windfall stock compensation deductions, respectively. If and when realized, the tax benefit associated with these deductions will be credited to additional paid-in capital. These excess benefit deductions are included in the total federal and state net operating losses disclosed above.
Tabular Reconciliation of Unrecognized Tax Benefits (in thousands):
| Amount | ||||
| Unrecognized tax benefits as of January 1, 2013 | $ | 4,801 | ||
| Gross increases — tax positions in prior period | ― | |||
| Gross decreases — tax positions in prior period | ― | |||
| Gross increases — current-period tax positions | — | |||
| Increases (decreases) from settlements | — | |||
| Unrecognized tax benefits as of December 31, 2013 | $ | 4,801 | ||
| Gross increases — tax positions in prior period | — | |||
| Gross decreases — tax positions in prior period | — | |||
| Gross increases — current-period tax positions | — | |||
| Increases (decreases) from settlements | — | |||
| Unrecognized tax benefits as of December 31, 2014 | $ | 4,801 | ||
To the extent these unrecognized tax benefits are ultimately recognized, it would affect the annual effective income tax rate unless otherwise offset by a corresponding change in the valuation allowance. The Company does not expect that the amounts of unrecognized tax benefits will change significantly within the next twelve months.
The Company files income tax returns in the U.S. federal jurisdiction and in various states, as well as in Sweden. The Company has U.S. tax net operating losses and credit carryforwards that are subject to examination from 1998 through 2014. The statute extends for a number of years beyond the year in which the losses were generated for tax purposes. Since a portion of these carryforwards may be utilized in the future, many of these attribute carryforwards remain subject to examination. The returns in Sweden are subject to examination from 2009 through 2014.
The Company’s policy is to recognize interest and penalties related to income tax matters in income tax expense. As of December 31, 2014 and 2013, the Company had no accruals for interest or penalties related to income tax matters.
Note 16 – Commitments and Contingencies
Operating Leases
The Company conducts its operations from leased facilities, under operating leases with terms expiring in 2017 for its Rockville, Maryland facility, 2023 for its Gaithersburg, Maryland facilities and 2017 for its Uppsala, Sweden facility. The leases contain provisions for future rent increases and periods in which rent payments are reduced (abated). Also, the leases obligate the Company to pay building operating costs. Under the terms of one lease agreement, the landlord provided the Company with a tenant improvement allowance of $2.5 million and an additional tenant improvement allowance of $3 million, such additional tenant improvement allowance is to be paid back to the landlord during the remainder of the term of such lease agreement through additional rent payments (collectively, the “Improvement Allowance”). The Company has been funded $0.5 million and $0.7 million in 2014 and 2013, respectively, and has been funded $5.5 million in total under the Improvement Allowance. The Company records a deferred rent liability to account for the funding under the Improvement Allowance and to record rent expense on a straight-line basis for these operating leases.
| F-26 |
Future minimum rental commitments under non-cancelable leases as of December 31, 2014 are as follows (in thousands):
| Year | Operating Leases | |||
| 2015 | $ | 4,903 | ||
| 2016 | 4,934 | |||
| 2017 | 2,911 | |||
| 2018 | 2,500 | |||
| 2019 | 2,563 | |||
| Thereafter | 10,439 | |||
| Total minimum lease payments | $ | 28,250 | ||
Total rent expenses approximated $3.6 million, $3.4 million and $3.2 million for the years ended December 31, 2014, 2013 and 2012, respectively.
Purchase Obligations
The Company and Cadila entered into a master services agreement pursuant to which the Company may request services from Cadila in the areas of biologics research, pre-clinical development, clinical development, process development, manufacturing scale-up and general manufacturing related services in India. In July 2011, and subsequently in March 2013, March 2014 and February 2015, the Company and Cadila amended the master services agreement to extend the term by one year for which services can be provided by Cadila under this agreement. Under the revised terms, if, by March 31, 2016, the amount of services provided by Cadila is less than $7.5 million, the Company will pay Cadila the portion of the shortfall amount that is less than or equal to $2.0 million and 50% of the portion of the shortfall amount that exceeds $2.0 million. When calculating the shortfall, the amount of services provided by Cadila includes amounts that have been paid under all project plans, the amounts that will be paid under ongoing executed project plans and amounts for services that had been offered to Cadila, that Cadila was capable of performing, but exercised its right not to accept such project. The term of the master services agreement is seven years, but may be terminated by either party if there is a material breach that is not cured within 30 days of notice or, at any time after three years, provided that 90 days prior notice is given to the other party. Through December 31, 2014, the Company has purchased $5.7 million in services from Cadila pursuant to this agreement, which includes services provided, since the beginning of 2013, by CPLB to the Company on behalf of Cadila pursuant to an October 2013 amendment authorizing such CPLB services. During 2014, the Company purchased $2.7 million in services from Cadila pursuant to this agreement, $1.0 million of which were provided by CPLB on behalf of Cadila. As of December 31, 2014, the Company’s remaining obligation to Cadila under the master services agreement is $1.8 million. The Company has recognized as expense the entire amount related to CPLB as the Company has not recorded any equity income (loss) of CPLB (see Note 8).
Contingencies
License Agreement with Wyeth Holdings Corporation
In 2007, the Company entered into an agreement to license certain rights from Wyeth Holding Corporation, a subsidiary of Pfizer Inc. (“Wyeth”). The Wyeth license is a non-exclusive, worldwide license to a family of patents and patent applications covering VLP technology for use in human vaccines in certain fields, with expected patent expiration in early 2022. The Wyeth license provides for the Company to make an upfront payment (previously made), ongoing annual license fees, sublicense payments, milestone payments on certain development activities and royalties on any product sales. The milestone payments are one-time only payments applicable to each related vaccine program. At present, the Company’s seasonal influenza VLP vaccine program (including CPLB’s seasonal influenza program) and its pandemic influenza VLP vaccine program are the only two programs to which the Wyeth license applies. The license may be terminated by Wyeth only for cause and may be terminated by the Company only after it has provided ninety (90) days’ notice that the Company has absolutely and finally ceased activity, including through any affiliate or sublicense, related to the manufacturing, development, marketing or sale of products covered by the license. If each milestone is achieved for any particular vaccine candidate, the Company would likely be obligated to pay an aggregate of $14 million to Wyeth for each product developed and commercialized under the agreement. Annual license fees under the agreement total $0.2 million per annum. The royalty to be paid by the Company under the agreement, if a product is approved by the FDA for commercialization, will be based on a single digit percentage of net sales. Payments under the agreement to Wyeth as of December 31, 2014 aggregated $6.4 million, of which the Company paid the annual license fees during each of the three years ended December 31, 2014 and a $0.3 million sublicense payment in 2014. The Company is currently in discussions with Wyeth to potentially amend the agreement and restructure the milestone payment owed as a result of CPLB’s initiation of a Phase 3 clinical trial for its seasonal influenza VLP vaccine candidate in the third quarter of 2014. Such milestone payment is only owed once for the Company’s seasonal influenza VLP vaccine program and it would not be required to make another payment if it or any of its affiliates initiate an additional Phase 3 clinical trial in a seasonal influenza VLP vaccine candidate. The $3.0 million milestone has been accrued for on the consolidated balance sheet at December 31, 2014 and recorded as a research and development expense in 2014.
Litigation
There are currently no asserted claims against the Company. Management has determined that a material loss resulting from either asserted claims or unasserted claims (situations where claims may be reasonably anticipated even if not yet asserted) is not reasonably possible.
Note 17 – Related Party Transactions
Dr. Rajiv Modi, a director of Novavax, is also the managing director of Cadila. The Company and Cadila have formed the CPLB joint venture (see Note 8). The Company and Cadila also have entered into a master services agreement, pursuant to which Cadila may perform certain research, development and manufacturing services for the Company up to $7.5 million. A subsidiary of Cadila owns 7.5 million shares of the Company’s outstanding common stock as of December 31, 2014. Since entering into the master services agreement and through December 31, 2014, the Company has incurred $5.7 million under the agreement. The amount due and unpaid for services performed under the master services agreement at both December 31, 2014 and 2013 was $0.4 million.
| F-27 |
Note 18 – Quarterly Financial Information (Unaudited)
The Company’s unaudited quarterly information for the years ended December 31, 2014 and 2013 is as follows:
| Quarter Ended | ||||||||||||||||
| March 31 | June 30 | September 30 | December 31 | |||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| 2014: | ||||||||||||||||
| Revenue | $ | 7,462 | $ | 8,259 | $ | 8,214 | $ | 6,724 | ||||||||
| Net loss | $ | (13,810 | ) | $ | (17,864 | ) | $ | (19,727 | ) | $ | (31,546 | ) | ||||
| Net loss per share | $ | (0.07 | ) | $ | (0.08 | ) | $ | (0.08 | ) | $ | (0.13 | ) | ||||
| Quarter Ended | ||||||||||||||||
| March 31 | June 30 | September 30 | December 31 | |||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| 2013: | ||||||||||||||||
| Revenue | $ | 3,833 | $ | 3,531 | $ | 4,802 | $ | 8,748 | ||||||||
| Net loss | $ | (9,996 | ) | $ | (12,633 | ) | $ | (15,300 | ) | $ | (14,054 | ) | ||||
| Net loss per share | $ | (0.07 | ) | $ | (0.08 | ) | $ | (0.09 | ) | $ | (0.07 | ) | ||||
The net loss per share was calculated for each three-month period on a stand-alone basis. As a result, the sum of the net loss per share for the four quarters may not equal the net loss per share for the respective twelve-month period.
| F-28 |