Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - Adeptus Health Inc. | Financial_Report.xls |
| EX-10.20 - EX-10.20 - Adeptus Health Inc. | adpt-20141231ex1020ebd80.htm |
| EX-31.1 - EX-31.1 - Adeptus Health Inc. | adpt-20141231ex3113a3331.htm |
| EX-23.1 - EX-23.1 - Adeptus Health Inc. | adpt-20141231ex2314f6100.htm |
| EX-32.1 - EX-32.1 - Adeptus Health Inc. | adpt-20141231ex32128a78e.htm |
| EX-10.21 - EX-10.21 - Adeptus Health Inc. | adpt-20141231ex1021cc1f1.htm |
| EX-31.2 - EX-31.2 - Adeptus Health Inc. | adpt-20141231ex31264b617.htm |
| EX-32.2 - EX-32.2 - Adeptus Health Inc. | adpt-20141231ex32261be5d.htm |
| EX-21.1 - EX-21.1 - Adeptus Health Inc. | adpt-20141231ex21134eec4.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-K
(Mark One)
|
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2014
Or
|
◻ |
TRANSITION REPORT PURSUANT TO SECTION 13 or 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number 001-36520
ADEPTUS HEALTH INC.
(Exact name of registrant as specified in its charter)
|
|
|
|
|
Delaware |
|
46-5037387 |
|
(State or other jurisdiction of |
|
(I.R.S. Employer Identification No.) |
2941 Lake Vista Drive
Lewisville, TX 75067
(Address of principal executive offices) (Zip Code)
(972) 899-6666
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
(Title of Class) |
(Name of each exchange which registered) |
|
Class A Common Stock, $0.01 par value per share |
New York Stock Exchange |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ◻ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Securities Act. Yes ◻ No ☒
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ◻
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ◻
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☒
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
|
|
|
|
|
Large accelerated filer |
◻ |
Accelerated filer |
◻ |
|
Non-accelerated filer |
☒ (Do not check if a smaller reporting company) |
Smaller reporting company |
◻ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Securities Exchange Act of 1934). Yes ◻ No ☒
As of June 30, 2014, the aggregate market value of Class A common stock held by non-affiliates was approximately $143.0 million based upon a total of 5,635,000 shares of Class A common stock held by non-affiliates and a closing price of $25.37 per share for the Class A as reported on the New York Stock Exchange on such date.
As of February 15, 2015, 9,861,930 shares of Class A common stock, par value $0.01 per share, and 10,741,839 shares of Class B common stock, par value $0.01 per share, were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Items 10, 11, 12, 13 and 14 of Part III of this Annual Report on Form 10-K incorporate information by reference from the registrant’s definitive proxy statement relating to its 2015 annual meeting of stockholders to be filed with the Securities and Exchange Commission within 120 days after the close of the registrant’s fiscal year.
ADEPTUS HEALTH INC. and SUBSIDIARIES
FORM 10-K
|
|
|
|
|
Page |
|
|
|
|
|
|
|
|
|
|
|
4 |
|
||
|
|
|
26 |
|
||
|
|
|
51 |
|
||
|
|
|
51 |
|
||
|
|
|
51 |
|
||
|
|
|
51 |
|
||
|
|
|
|
|
|
|
|
|
|
51 |
|
||
|
|
|
54 |
|
||
|
|
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
|
56 |
|
|
|
|
|
76 |
|
||
|
|
|
77 |
|
||
|
|
Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
|
105 |
|
|
|
|
|
105 |
|
||
|
|
|
105 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
106 |
|
||
|
|
|
106 |
|
||
|
|
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
|
106 |
|
|
|
|
Certain Relationships and Related Transactions, and Director Independence |
|
106 |
|
|
|
|
|
106 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
107 |
|
||
|
|
|
|
|
|
|
|
|
|
|
108 |
|
|
|
|
|
|
|
|
|
|
|
|
|
109 |
|
2
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
In addition to historical information, this Annual Report on Form 10-K may contain “forward-looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), which are subject to the “safe harbor” created by those sections. All statements, other than statements of historical facts included in this Annual Report on Form 10-K, including statements concerning our plans, objectives, goals, beliefs, business strategies, future events, business conditions, our results of operations, financial position and our business outlook, business trends and other information, may be forward-looking statements. Words such as “estimates,” “expects,” “contemplates,” “will,” “anticipates,” “projects,” “plans,” “intends,” “believes,” “forecasts,” “may,” “should” and variations of such words or similar expressions are intended to identify forward-looking statements. The forward-looking statements are not historical facts, and are based upon our current expectations, beliefs, estimates and projections, and various assumptions, many of which, by their nature, are inherently uncertain and beyond our control. Our expectations, beliefs, estimates and projections are expressed in good faith and we believe there is a reasonable basis for them. However, there can be no assurance that management’s expectations, beliefs, estimates and projections will be achieved and actual results may vary materially from what is expressed in or indicated by the forward-looking statements.
There are a number of risks, uncertainties and other important factors, many of which are beyond our control, that could cause our actual results to differ materially from the forward-looking statements contained in this Annual Report on Form 10-K. Such risks, uncertainties and other important factors that could cause actual results to differ include, among others, the risks, uncertainties and factors set forth under “Risk Factors” in this Annual Report on Form 10-K, as such risk factors may be updated from time to time in our periodic filings with the SEC, and are accessible on the SEC’s website at www.sec.gov, and also include the following:
|
· |
Our ability to implement our growth strategy; |
|
· |
Our ability to maintain sufficient levels of cash flow to meet growth expectations; |
|
· |
Our ability to protect our brand; |
|
· |
Federal and state laws and regulations relating to our facilities, which could lead to the incurrence of significant penalties by us or require us to make significant changes to our operations; |
|
· |
Our ability to locate available facility sites on terms acceptable to us; |
|
· |
Competition from hospitals, clinics and other emergency care providers; |
|
· |
Our dependence on payments from third-party payors; |
|
· |
Our ability to source and procure new products and equipment to meet patient preferences; |
|
· |
Our reliance on Medical Properties Trust (“MPT”) and the MPT Master Funding and Development Agreements; |
|
· |
Disruptions in the global financial markets leading to difficulty in borrowing sufficient amounts of capital to finance the carrying costs of inventory, to pay for capital expenditures and operating costs; |
|
· |
Our ability or the ability of our healthcare system partners to negotiate favorable contracts or renew existing contracts with third-party payors on favorable terms; |
|
· |
Significant changes in our payor mix or case mix resulting from fluctuations in the types of cases treated at our facilities; |
3
|
· |
Significant changes in rules, regulations and systems governing Medicare and Medicaid reimbursements; |
|
· |
Material changes in IRS revenue rulings, case law or the interpretation of such rulings; |
|
· |
Shortages of, or quality control issues with, emergency care-related products, equipment and medical supplies that could result in a disruption of our operations; |
|
· |
The intense competition we face for patients, physician use of our facilities, strategic relationships and commercial payor contracts; |
|
· |
The fact that we are subject to significant malpractice and related legal claims; |
|
· |
The growth of patient receivables or the deterioration in the ability to collect on those accounts; |
|
· |
The impact on us of PPACA, which represents a significant change to the healthcare industry; |
|
· |
Ensuring our continued compliance with HIPAA, which could require us to expend significant resources and capital; and |
|
· |
The factors discussed in Part I, Item 1A. “Risk Factors” |
We caution you that the risks, uncertainties and other factors referenced above may not contain all of the risks, uncertainties and other factors that are important to you. In addition, we cannot assure you that we will realize the results, benefits or developments that we expect or anticipate or, even if substantially realized, that they will result in the consequences or affect us or our business in the way expected. There can be no assurance that (i) we have correctly measured or identified all of the factors affecting our business or the extent of these factors’ likely impact, (ii) the available information with respect to these factors on which such analysis is based is complete or accurate, (iii) such analysis is correct or (iv) our strategy, which is based in part on this analysis, will be successful. All forward-looking statements in this report apply only as of the date of this report or as the date they were made and, except as required by applicable law, we undertake no obligation to publicly update any forward-looking statement, whether as a result of new information, future developments or otherwise.
Unless the context otherwise indicates or requires, references in this Annual Report on Form 10-K to the “Company,” “we,” “us” and “our” refer to Adeptus Health Inc. and its consolidated subsidiaries after giving effect to the Reorganization Transactions (“Reorganization”) described herein and the initial public offering described herein and to Adeptus Health LLC and its consolidated subsidiaries prior to the Reorganization and initial public offering.
We own and operate First Choice Emergency Rooms, the largest network of independent freestanding emergency rooms in the United States. We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. Our facilities are currently located in the Houston, Dallas/Fort Worth, San Antonio and Austin, Texas markets; Colorado Springs and Denver, Colorado; and Phoenix, Arizona. Each of our facilities opened in 2014 were newly constructed.
Since our founding in 2002, our mission has been to address the need within our local communities for immediate and convenient access to quality emergency care in a patient‑friendly, cost‑effective setting. We believe we are transforming the emergency care experience with a differentiated and convenient care delivery model which improves access, reduces wait times and provides high‑quality clinical and diagnostic services on‑site. Our facilities are
4
fully licensed and provide comprehensive, emergency care with an acuity mix that we believe is comparable to hospital‑based emergency rooms.
Emergency care is a significantly underserved market in the United States today and the current system is overburdened.
|
· |
Demand has grown dramatically, with emergency room visits increasing 46.7%, from 90.8 million in 1992 to 133.2 million in 2012, while the number of emergency room departments decreased by 11.4% over the same period, from approximately 5,035 in 1992 to approximately 4,460 in 2012, according to the American Hospital Association. |
|
· |
In their 2014 National Report Card on America’s emergency care environment, the American College of Emergency Physicians assigned an overall grade of “D‑” for the category of access to emergency care, reflecting too few emergency departments to meet the needs of a growing, aging population and the projected increase in the number of insured individuals as a result of the Patient Protection and Affordable Care Act. |
We believe freestanding emergency rooms are an essential part of the solution, providing access to quality care and offering a significantly improved patient experience relative to traditional hospital emergency departments.
What We Do and Why We Are Different
We focus on providing emergency care through our freestanding emergency rooms with the goal of improving the quality of care and enhancing the overall experience for patients and physicians. We have developed an innovative facility design and infrastructure specifically tailored to the emergency care delivery system that combines staff, equipment and physical layout to deliver high‑quality, cost‑effective care. We design, equip, staff and operate our facilities to deliver coordinated patient‑focused care. This approach limits the need to move patients and provides ease of access to all necessary medical services we provide, allowing us to enhance the overall experience of the patient. Our facility design also allows physicians and nursing staff to provide all levels of care required for our patients during their visit. Our philosophy is to center care around the patient, rather than expect the patient to adapt to our facilities and staff. We believe our focused approach increases patient, physician and staff satisfaction. Innovative characteristics of our emergency facilities include:
|
· |
24 / 7 Emergency Care. Freestanding emergency room facilities, which typically range from approximately 6,000 to 7,000 square feet and are located in a convenient, local community setting and open 24 hours a day, seven days a week with on‑site emergency staff, including a physician, at all times; |
|
· |
Board‑Certified Physicians. Staffed with experienced healthcare professionals capable of handling all emergency issues. As of December 31, 2014, we contracted with approximately 434 Board‑certified physicians with an average of 15 years of medical experience who have treated more than 400,000 patients at our facilities; |
|
· |
Streamlined. Streamlined check‑in process designed to have patients seen by a physician within minutes; |
|
· |
Focused Capability. Typically six to nine emergency exam rooms, which include two high‑acuity suites, one child‑friendly pediatric room and a specialized obstetrics/gynecology room; |
|
· |
Coordinated Care. Centralized nurses’ station that serves as a command center to coordinate care; |
|
· |
Full Radiology Suite. In‑house diagnostic imaging technology, including CT scanners, digital x‑rays and ultrasounds, with final reads from on‑call radiologists; and |
5
|
· |
On‑Site Laboratory. On‑site laboratories, which provide results within approximately 20 minutes and are certified by CLIA and accredited by COLA. |
We operate at the higher end of the acuity and emergency care spectrum. Our capabilities and offerings differ from other care models as outlined below:
Spectrum of Primary and Emergency Care Services
Market Opportunity
In their 2014 National Report Card on America’s emergency care environment, ACEP assigned an overall grade of “D‑” for the category of access to emergency care, reflecting too few emergency departments to meet the needs of a growing, aging population and the projected increase in the number of insured individuals as a result of PPACA. We believe freestanding emergency rooms are an essential part of the solution.
Freestanding emergency rooms remain the least penetrated alternate site provider segment in the U.S. healthcare sector. As of 2012, there were approximately 400 freestanding emergency rooms in the United States as compared to approximately 1,400 retail clinics, 6,000 ambulatory surgery centers and 9,300 urgent care centers. We believe this represents a significant opportunity to deliver quality care in the freestanding emergency room setting and transform this underpenetrated market. We have developed a highly scalable business model for establishing new freestanding emergency rooms that include attractive unit economics, sophisticated data analytics to support our site‑selection process, proven real estate development practices and innovative marketing programs. Using this model, we have grown to become more than three times the size of our next largest independent freestanding emergency room competitor and are expanding rapidly. We seek to transform the emergency care delivery model by offering high‑quality, efficient and consumer‑oriented healthcare in our local communities.
We also believe that we offer a dramatically improved patient experience relative to traditional hospital emergency departments by significantly reducing wait times and providing rapid access to Board‑certified physicians on‑site. We also provide convenient access to critical, high‑acuity care as compared with urgent care centers and are open 24 hours a day, seven days a week. Based on patient feedback collected by Press Ganey, First Choice Emergency Room received the prestigious Guardian of Excellence Award in 2013 and 2014 for exceeding the 95th percentile in patient satisfaction nationwide.
Industry Trends
The emergency room remains a critical access point for millions of Americans who experience sudden serious illness or injury in the United States each year. The availability of that care is under pressure and threatened by a wide range of factors, including shrinking capacity and an increasing demand for services. According to AHA, from 1992 to 2012, the number of emergency room visits increased by 46.7%, while the number of emergency departments decreased by 11.4%.
We believe freestanding emergency rooms are an essential part of the solution, providing access to high‑quality emergency care and offering a significantly improved patient experience relative to traditional hospital emergency departments.
6
The chart below sets forth the number of emergency departments and emergency department visits from 1992 to 2012 according to AHA:
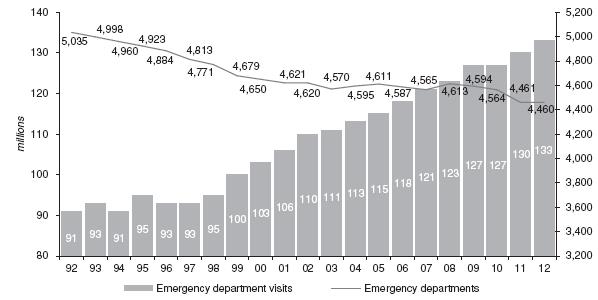
The number of emergency room visits exceeded 130 million in 2012, or approximately 247 visits per minute, and care previously provided in inpatient settings is now increasingly being provided in emergency departments. Factors affecting access to emergency care include availability of emergency departments, capacity of emergency departments, and availability of staffing in emergency departments. As the largest operator of freestanding emergency rooms, we offer a solution that addresses the following trends currently affecting the healthcare services market:
Poor Access to Emergency Care Including a Shortage of Emergency Rooms
According to ACEP, between 1997 and 2007, emergency visit rates increased at two times the rate of growth of the U.S. population, causing a shortage of emergency rooms and persistent emergency department overcrowding with expanding wait times. This emergency room shortage is making it increasingly challenging to meet the rising demand for emergency care. According to ACEP’s National Report Card on America’s emergency care environment, only 4.2% of active physicians are emergency room physicians, yet they are responsible for 28% of all acute care visits and 11% of all outpatient care in the United States. The shortage of emergency rooms has created an acute need for more access and convenient emergency room care.
Emergence of Innovative Care Delivery Settings and Access Points
Healthcare industry trends, including the increasing demand for care, an aging population and the projected increase in the number of people now insured as a result of PPACA, combined with a shortage of access points, is driving the emergence of innovative care delivery models to meet patient needs for emergency care. Increasing demand for emergency care necessitates new healthcare access points such as freestanding emergency rooms for patients to receive timely and high‑quality care. The emergence of freestanding emergency rooms will fill a public need in underserved markets and provide connectivity across the patient care continuum from patient referrals to post‑emergency care. Freestanding emergency rooms remain the least penetrated alternate site segment with strong unit growth. This growth is expected to shift the delivery of healthcare services away from traditional inpatient hospitals to more effective and convenient solutions, such as freestanding emergency rooms and other alternate‑site settings such as urgent care centers and primary care access points.
7
Increasing Healthcare Consumerism
We believe patients will increasingly seek high‑quality and efficient care in cost‑effective settings. As self‑insured employers look to reduce their overall healthcare costs, they are rapidly shifting financial responsibility to patients through higher co‑payments and deductibles. These changes to health plan design, coupled with increased pricing transparency, are encouraging patients to take more control of their healthcare spending and seek out more cost‑effective and efficient options for their healthcare consumption. As consumers take on a larger share of their healthcare costs and spend more on healthcare services, they want a greater say in how and where they receive care, demanding higher quality care, increased convenience and more service for their dollars spent. This trend of increasing consumerism will benefit freestanding emergency room operators as they offer attractive and convenient neighborhood‑based, physician‑focused care at significantly reduced wait times. We believe that, given the choice, consumers will choose freestanding emergency rooms for both their convenience and high‑quality care and outcomes.
Opportunities Created by Healthcare Legislation
The expected increase in the number of people now insured as a result of PPACA may put additional pressure on an already overburdened emergency room system that lacks capacity and access points. This expected influx of newly insured patients creates opportunities for providers of emergency care with attractive and convenient locations capable of delivering high‑quality care. Additionally, we expect PPACA to create greater opportunities for cost‑effective providers of healthcare services as healthcare reform activities are expected to promote the transition from traditional fee‑for‑service payment models to more “at risk” or “capitated” models in which providers receive a flat fee per member per month from payors, regardless of the cost of care. These changes will be reflected through the creation of accountable care organizations or other payment model reforms. We believe this shift will create financial incentives to transition many types of medical procedures out of the hospital and into more convenient settings such as freestanding emergency rooms.
Our Value Proposition
Value Proposition for Patients
As healthcare has evolved, the consumer has taken greater control of healthcare expenditures and demands more convenient access to healthcare, better value and an improved overall patient experience. Our philosophy is to center care around the patient, rather than expect the patient to adapt to our facilities and staff. We offer patients an attractive value proposition:
|
· |
Access to Care. Our facilities are located in a convenient, local community setting and are open 24 hours a day, seven days a week with on‑site emergency staff, including a Board‑certified physician at all times. |
|
· |
Immediate Care. A streamlined check‑in process designed to have patients seen by a physician within minutes. |
|
· |
Physician Focus. Our physicians are focused on the patient, spending more time on patient care than on administrative tasks, providing high‑quality service, prompt diagnoses and the appropriate medical treatment. |
|
· |
Technology. Facilities equipped with full radiology suites, including CT scanners, digital x‑rays and ultrasounds, as well as on‑site laboratories certified by CLIA and accredited by COLA that provide test results within approximately 20 minutes. |
|
· |
Superior Experience. An overall enhanced patient experience. |
8
As a result, based on patient feedback collected by Press Ganey, First Choice Emergency Room received the prestigious Guardian of Excellence Award in 2013 and 2014 for exceeding the 95th percentile in patient satisfaction nationwide.
Value Proposition for Communities
Community providers, including physician’s offices and hospital emergency rooms, serve a critical and valuable purpose in delivering healthcare. However, the shortage of emergency rooms makes it increasingly challenging to meet the rising demand for emergency care. This has led to an overburdened emergency room network that is often poorly aligned with care consumption trends.
We seek to transform the emergency delivery model and fill a public need by offering high‑quality, efficient and consumer‑oriented healthcare in our local communities. We offer communities an attractive value proposition:
|
· |
Access to Care. Facilities located in convenient, local community settings. Approximately 60% of each facility’s patients come from a three‑mile radius, with approximately 80% coming from a five‑mile radius. |
|
· |
24 / 7. Access to Board‑certified physicians at all times, including outside normal business hours. |
|
· |
Partnership. Key partner for health systems seeking to enhance their local community presence through direct admissions relationships and new innovative partnerships. |
|
· |
Care Continuum. Connectivity across the patient‑care continuum from patient referrals to post‑emergency care. |
Value Proposition for Physicians
The evolving healthcare delivery environment, reflected by significant regulatory changes, increasing administrative burdens, shifting competitive provider landscape and a transition to new reimbursement models, is increasing pressure on physicians. We offer an attractive working environment:
|
· |
Team‑Based Care. Team‑based environment, supported by dedicated staff. |
|
· |
Patient Centric. Our model allows physicians to spend more time with each patient, which enables them to focus their attention on the patient in order to deliver high‑quality care. |
|
· |
Dedicated Support. Rapid delivery of lab and diagnostic results through on‑site capabilities. |
|
· |
Physician Friendly. Scheduling flexibility and a well‑defined compensation program. Payment of malpractice insurance coverage premiums for physicians practicing at our facilities. |
Value Proposition for Payors
We believe that our emergency room facilities reduce overall costs for payors by reducing unnecessary tests and patient admittances. According to the National Hospital Ambulatory Medical Care Survey, the national average emergency room inpatient admittance rate was approximately 11.6% in 2011, while our average inpatient admittance rate was approximately 3.8% for the year ended December 31, 2014. We believe our facilities provide comprehensive emergency care with an acuity mix that is comparable to hospital‑based emergency rooms.
Value Proposition for Hospitals
We have an attractive business model that provides communities direct access to emergency care, helping to relieve the overburdened hospital emergency room system. Our facilities provide high‑quality emergency care for a wide variety of conditions, including heart attacks, severe abdominal pain and respiratory distress similar to the care provided in traditional hospital emergency rooms. When hospital‑based services such as surgery or cardiac catheterization are needed, patients are stabilized at our facilities before being transferred to nearby hospitals via ambulance. Transfer agreements are in place with local hospitals that often facilitate direct admission.
9
Competitive Strengths
We believe the following strengths differentiate us from our competitors and will enable us to capitalize on favorable industry dynamics:
Leader in the Rapidly Expanding Freestanding Emergency Room Market
First Choice Emergency Room is the largest freestanding emergency room provider in the United States with 55 facilities as of December 31, 2014, of which 29 were opened in 2014. We are more than three times the size of our next largest independent freestanding emergency room competitor. We believe our innovative facility model enables us to offer our customers comprehensive emergency services with individualized attention and local convenience. We believe that our scale and scope, when combined with our comprehensive service offerings and tailored best practices, differentiate us from our local and regional competitors. Given our market positions in the highly fragmented and rapidly expanding markets in which we provide our services, we believe there continue to be opportunities to build more facilities in existing and new markets, which will result in further expanding our leadership in the freestanding emergency room market.
Superior Patient Experience
We strive to consistently offer a superior patient experience through both our medical staff and facility capabilities. Our emergency rooms are staffed with Board‑certified physicians and emergency‑trained registered nurses capable of handling all emergency room issues with a physician on‑site at all times. Each of our facilities is equipped with a full radiology suite, including CT scanners, digital x‑ray and ultrasound, as well as on‑site laboratories certified by CLIA and accredited by COLA. Our patients are typically face‑to‑face with a medical professional within minutes of arrival, and our patient satisfaction ratings exceed the vast majority of hospital emergency rooms nationally. Based on patient feedback collected by Press Ganey, we exceeded the 95th percentile in the nation for patient satisfaction and received the Guardian of Excellence Award in 2013 and 2014, the highest award bestowed by the organization.
Scalable Service Model Well‑Positioned for Growth
We maintain the highest standards of clinical excellence, led by our 434 contracted Board‑certified physicians who have an average of 15 years of medical experience. We have standardized, highly scalable clinical and operational infrastructure that we believe will support significant continued growth. Our highly trained staff is complemented by our managed care contracting and revenue cycle management expertise. Moreover, our innovative sales and marketing programs combine active outreach and awareness campaigns with patient‑centric marketing programs in order to most effectively reach our target populations. We endeavor to continue to develop multiple sites because we believe regional density creates value through leverage in managed care contracting and greater brand awareness.
Distinctive Real Estate Development Strategy Supports Attractive Unit Growth and Economics
We have built an internal team with significant experience in multi‑unit retail expansion strategy and execution. As a result, our approach to real estate planning is highly consumer‑centric with a discipline traditionally utilized by sophisticated retail businesses. Our proprietary site selection model is a key to the success of our business, allowing us to identify and fill critical voids in community healthcare delivery systems. When combined with our scalable operating structure and attractive new facility model, our real estate development strategy allows us to maximize performance and quickly grow our facility base. Our seasoned real estate planning and development team follows a proven and disciplined strategy that leverages advanced data analytics to identify opportunities to provide underserved communities with high‑quality emergency care.
This development model has also proven commercially successful in highly competitive markets and is currently supporting growth outside of our home state of Texas. Our sophisticated selection guidelines and scalable procedures allow us to open a new facility within 14 to 21 months of site selection, enabling us to quickly capitalize on emerging opportunities. We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. We have a robust pipeline under development designed to support the addition of a similar number of facilities in 2015. Moreover, we have access to a
10
variety of capital sources, including the Medical Properties Trust leasing facility, allowing us to fund the typical $5 million to $6 million build‑out cost of most facilities, inclusive of land acquisition costs. Given our expertise and the scale of our operations, we anticipate these new facilities will be profitable within their first year of operation, generating additional capital to continue capturing significant growth opportunities.
Ability to Attract and Retain High‑Quality Physicians and Clinicians
Through our differentiated recruiting and development programs, we are able to identify and target high‑quality physicians and clinicians to optimally match the needs of our facilities. Each of our facilities is staffed with Board‑certified physicians, who have an average of 15 years of medical experience. Compared to a traditional hospital setting, our physicians have a significantly reduced administrative workload, which allows them to spend more time focusing on patient care. Additionally, we offer our physicians extensive flexibility in managing their work schedules. Due to our customized staffing model, physicians can schedule their own work hours, practice at multiple sites, and take advantage of a wide variety of career development opportunities, including maintaining their own practice or affiliations with other healthcare facilities or hospitals. Consequently, our facilities offer a positive work environment that leads to high retention rates and strong customer and provider relationships. We believe these programs will allow us to continue to effectively recruit physicians and clinicians to support our robust pipeline of new facilities.
Management Team with Significant Public Company Experience
We have an experienced management team that leverages expertise across the healthcare, retail and hospitality sectors. The members of our executive management team with healthcare backgrounds have an average of 11 years of experience in that industry and have proven and extensive knowledge of healthcare operations and facility expansion. Additionally, our management has significant experience with high‑growth, multi‑state customer‑focused operations through involvement in the retail and hospitality sectors. The three most senior members of the executive team have substantial experience in leading publicly traded companies. Over their respective tenures, members of our team have been instrumental in establishing a successful, scalable operating model, consistently generating strong financial results and developing an effective site selection and build‑out process. They have also developed proven recruiting and staffing capabilities to identify, hire and retain high‑quality physicians. We believe the breadth of management’s background and the depth of its expertise will continue to drive our dynamic growth and continued success.
Growth Strategies
We believe we have significant growth potential in both new and existing markets because of our leading market position in the freestanding emergency room sector, high‑quality care delivery, strong unit economics, disciplined development strategy and significant management experience. We plan to pursue the following growth strategies:
Grow our Presence in Existing Markets
We believe there is a significant opportunity to expand in our existing markets including Dallas/Fort Worth, Houston, San Antonio and Austin, Texas as well as Colorado Springs and Denver, Colorado. Our scale, scope and leading market position, combined with our sophisticated, proven site selection and development processes provide us with competitive advantages to continue to expand our facility base in these markets. We endeavor to continue to develop multiple sites because we believe regional density creates value through leverage in managed care contracting and greater brand awareness. We anticipate that as we further build our brand and increase the visibility of our facilities in our existing markets these efforts will increase patient awareness, and drive patient volume and same‑store growth.
Build Strategic Alliances with Leading Health Systems
Development of our existing and new health system alliances is an important part of our continued growth. We expect to be a key partner for health systems seeking to enhance their local community presence through direct admissions relationships and new innovative partnerships. Our alliance with HCA in North Texas provides an example of one such innovative partnership, giving our patients direct access to HCA’s approximately 5,500 physicians and 11 hospitals in North Texas and approximately 3,300 physicians and 9 hospitals in the Houston area. In addition, we have a
11
relationship with the Concentra urgent care clinics in the Dallas/Fort Worth market, whereby we are able to refer workers’ compensation patients to Concentra when follow‑up, non‑emergent, care is needed. We also recently announced our expansion into Arizona through a joint venture with Dignity Health, one of the nation’s largest health systems, with the opening of a full-service healthcare hospital facility and includes plans for additional access to emergency medical care in Phoenix through freestanding emergency departments of the hospital. We believe our ability to alleviate hospital emergency room over‑crowding, while providing a new access point to patients, enhances our value proposition as a partner of choice for health systems.
Pursue a Disciplined Development Strategy in New States and Markets
We intend to continue expanding our facility base through new facility openings in new states and markets by leveraging our core capabilities in site selection, development and efficient facility openings. We view expansion as a core competency and see a significant opportunity to replicate the regional platform model established in Texas in new geographic markets. We entered the Colorado market in 2013. We also entered the Arizona market in 2015, through our partnership with Dignity Health, with a full‑service general hospital in the Phoenix area that has 16 inpatient rooms, two operating rooms, a nine‑room emergency department, a high‑complexity laboratory and a full radiology suite. We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. We have a robust pipeline under development designed to support the addition of a similar number of facilities in 2015. As we expand into new markets, particularly in states with complex regulatory requirements, we believe there is a potential to implement different operating models, such as innovative hospital partnership models, including a hospital hub and freestanding emergency room satellite model.
Operations
Our operations consist primarily of our ownership and management of freestanding emergency care facilities. We provide patients prompt access to high‑quality, Board‑certified physicians and emergency trained registered nurses capable of handling all emergency issues and a wide array of treatments on‑site. We believe our acuity mix is comparable to hospital‑based emergency rooms. Our facilities provide the space and equipment necessary to enable our staff to provide quality emergency care. Each of our facilities is equipped with a full radiology suite, including CT scanners, digital x‑ray and ultrasound, as well as on‑site laboratories certified by CLIA and accredited by COLA. Every facility has transfer agreements in place with local hospitals for patients that need to be transferred to a hospital. In North Texas and the Houston area, we have entered into alliances with HCA to enhance the continuum of care for our patients by streamlining clinical protocols for transfers to hospitals and providing direct access to approximately 5,500 physicians and 11 hospitals in North Texas and approximately 3,300 physicians and 9 hospitals in the Houston area, for follow‑up care.
Facilities
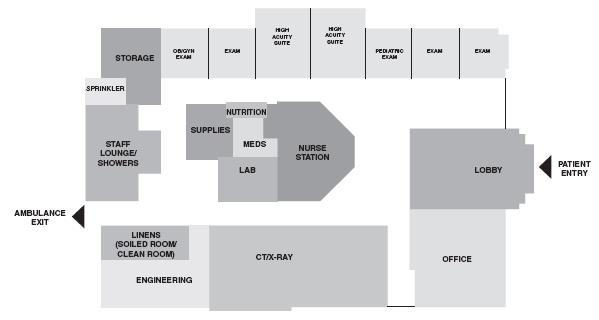
As of December 31, 2014, we had 55 facilities in markets throughout Texas and Colorado. Our facilities are open 24 hours a day, seven days a week, and are designed to ensure that our patients receive high‑quality, rapid, comfortable and convenient emergency medical care. Each facility typically has six to nine emergency exam rooms. These include two high‑acuity suites, one “child‑friendly” pediatric room intended to create a comfortable environment for children, and a specialized obstetrics/gynecology room. All of our facilities have a centralized nurses’ station that acts as the command center providing easy access to our laboratory, radiology suite, supply rooms and secured narcotics area, in addition to being placed so that it maximizes the staff’s line of sight to our suites and exam rooms. If a patient needs to be transported to a hospital, our facilities have ambulance bays that that are located near the emergency suites, providing for rapid and efficient access for emergency medical services personnel.
12
Each facility is designed to be a calm and comfortable setting for patients. There is a lobby and check‑in desk where patients are greeted and welcomed into the facility. As patients are escorted back to their exam room, they see neutrally painted walls with carefully selected artwork, creating a comforting environment, seamless floors designed to minimize and prevent infection, and, in many facilities, a view of the CT scanner. Every pediatric room has a unique, hand‑painted mural and all exam rooms are equipped with flat‑screen televisions. Our facilities are also designed to be a comfortable environment for our clinicians. Our physicians have a private office where they can review notes or make follow‑up calls to patients. In addition, there is a dedicated employee break room and a special employee lounge complete with showers.
Each of our emergency rooms contains a laboratory that is certified by CLIA and accredited by COLA. CLIA defines our laboratories as “moderate complexity labs,” which can perform “waived” and automated tests. The CLIA‑waived tests that we most commonly perform include, but not are limited to, rapid strep, influenza, and respiratory syncytial virus and blood glucose levels. Additionally, there are moderate complexity automated tests that include chemistries, cardiac enzymes, complete blood counts, clotting studies, and a variety of other pertinent diagnostic assessments. All in‑house testing provides results within approximately 20 minutes and those results are immediately provided to the physician for a more efficient diagnostic process. Additional testing which would require pathologist review, such as cultures and sub‑specialty samples, are managed through our relationships with accredited third‑party laboratories. Each laboratory department is supervised by a facility medical director, who acts as the dedicated laboratory director, overseeing all policies, testing, and ongoing operations.
Our facilities are equipped with full radiology suites, including CT scanners, digital x‑rays and ultrasounds. Staffed around the clock with a licensed radiology technologist, our radiology suites are a critical component to the high‑quality care that we provide. Each radiology technologist has a minimum of two years of experience on both the CT and x‑ray modalities in a hospital setting. Our ultrasound machines are operated by certified on‑call ultrasound technologists that provide around‑the‑clock coverage for all of our facilities. All imaging studies are then interpreted off‑site by a contracted group of Board‑certified radiologists that are required to provide final reads within 30 minutes, 24 hours a day, seven days a week.
In addition to our carefully planned layout, laboratories and radiology suites, our facilities are also generally equipped with other features comparable to hospital emergency rooms. Our facilities are equipped with life‑safety code air systems with specialized ventilation and central oxygen with back‑up generators to ensure uninterrupted operations.
13
The below image depicts the typical layout of one of our facilities which range in size from approximately 6,000 to 7,000 square feet:
Staffing
We employ a base “1‑1‑1‑1” model for our staffing needs at each facility, meaning that we have a minimum of one Board‑certified physician, one emergency trained registered nurse, one radiology technologist and one front office staff member on‑site at all times. This is a fixed cost labor model as all facilities are open 24 hours a day, seven days a week. This base staffing can be augmented during periods of high‑patient volume. We operate using two 12‑hour shifts per day, beginning at 7:00 a.m. and 7:00 p.m. Each facility utilizes approximately 35 staff members, made up of four full‑time and five part‑time employees per function. Our full‑time employees work three 12‑hour shifts per week. Each of our facilities also has a facility administrator, who is also the nurse manager. The facility administrator is in charge of all operating aspects of the facility and the coordination of care to patients.
Our physicians are contracted through National Medical Professionals of Texas and National Medical Professionals of Colorado, affiliated professional limited liability companies owned by our Executive Medical Director that handles our physician‑staffing needs in each of the markets where we operate. We currently utilize over 434 accredited Board‑certified physicians. We provide physicians with a unique and attractive opportunity to practice emergency medicine in a work environment with a reduced administrative workload, scheduling flexibility and a covered cost of malpractice insurance, which allows our physicians to focus on providing high‑quality care. Our model allows physicians to spend more time with each patient and thus the ability to focus their attention on the patient in order to deliver quality care.
Our physician recruiters identify and source talent through a variety of methods, including networking, targeted job postings and employee referrals. Once a candidate has been identified, we invite them on‑site to tour our facility and meet with the facility medical director. If the candidate is a fit, a rigorous credentialing process is initiated that verifies the candidate’s education, training, state licensing, experience, current health status and clinical competence.
All of our physicians sign a physician services agreement, which sets forth their duties and responsibilities, assigns each physician to a home facility, outlines shift commitments and guarantees and contains a 90‑day notice of
14
termination provision for both parties. Each facility has a facility medical director, who is the physician responsible for providing clinical guidance and oversight, performing chart reviews, ensuring compliance with infection control protocols and acting as the laboratory director for the facility.
Patients
First Choice Emergency Rooms provide access to high‑quality emergency care in the neighborhoods near each site. Typically, approximately 60% of each facility’s patients come from a three‑mile radius, with approximately 80% coming from a five‑mile radius. Our facilities treat a wide array of emergency patient problems, such as heart attacks, severe abdominal pain and respiratory distress.
Patient satisfaction for First Choice Emergency Room care is among the highest in the nation. First Choice Emergency Room was named a Guardian of Excellence Award winner in 2013 and 2014 by Press Ganey. This award recognizes top‑performing facilities from among participating member hospital emergency rooms that are in the 95th percentile of performance in patient satisfaction nationwide, and is a healthcare industry symbol of achievement.
Illustrative Patient Experiences at First Choice Emergency Rooms
We believe we are transforming the emergency care experience with a differentiated care delivery model, as demonstrated by the below sampling of experiences our patients have had at First Choice Emergency Rooms:
|
· |
Cardiac Event. A man came to the nearby First Choice Emergency Room after experiencing chest pain and shortness of breath for over a day. Within minutes of his arrival he was given an electrocardiogram, which indicated a possible heart attack. While getting his chest x‑ray, his heart stopped beating. The clinical team administered CPR and the patient had a near immediate return of spontaneous circulation. The CT scan showed a large “saddle emboli” (a large blood clot straddling the blood vessels) in his heart and more in his pulmonary vasculature (blood vessels of the lungs). He was anti‑coagulated and transferred to the hospital catheterization laboratory. |
|
· |
Premature Delivery Complication. A 34‑week pregnant woman was rushed into a First Choice Emergency Room in active labor. The baby had already begun to crown and both mother and baby appeared to be in distress. Within four minutes of the patient’s arrival, the baby was delivered. The delivery was complicated by the umbilical cord being wrapped around the baby’s neck, a life‑threatening complication. Our physician properly handled the delivery and as a result both the mother and baby were healthy. |
|
· |
Respiratory Distress. A nearby family practice physician was experiencing shortness of breath and came into a First Choice Emergency Room. Within minutes, her shortness of breath became very severe. Our physician had to intubate (placing a breathing tube into the trachea to allow for mechanical ventilation) the patient to ensure adequate ventilation and oxygenation—a life‑saving measure. The patient was then transported to a nearby hospital to see a thoracic specialist. She has now recovered and regularly refers her patients, as well as her family, to First Choice Emergency Rooms for emergency care. |
|
· |
Accidental Poisoning. A one‑year‑old girl was brought to a First Choice Emergency Room after accidentally drinking toxic cleaning solution. During the three‑minute drive, the young girl elevated from having no symptoms to an almost complete inability to breathe. The First Choice Emergency Room staff immediately treated the patient and the child fully recovered. |
Licensing and Accreditation
All of our facilities are licensed pursuant to state‑specific licensing requirements. Our Texas facilities are licensed as “Freestanding Emergency Medical Care Facilities” by the Texas Department of State Health Services Regulatory Licensing Unit on a bi‑annual basis. Our facilities in Colorado are licensed as “Community Clinics with Emergency Centers” under the administration of the Colorado Department of Public Health and Environment, Health
15
Facilities and Emergency Medical Services Division on an annual basis. Our hospital facility in Arizona in partnership with Dignity Health is licensed as a “General Hospital” under the administration of the Arizona Department of Health Services.
First Choice Emergency Rooms are accredited as an Ambulatory System by the Joint Commission. An independent, not‑for‑profit organization, the Joint Commission is the nation’s oldest and largest standards‑setting and accrediting body in healthcare. Since 1975, the Joint Commission has developed state‑of‑the‑art standards for outpatient ambulatory care organizations. By demonstrating compliance with the Joint Commission’s national standards for healthcare quality and safety, First Choice Emergency Room has earned the Joint Commission’s Gold Seal of Approval. The accreditation award recognizes First Choice Emergency Room’s dedication to continuously comply with the Joint Commission’s state‑of‑the‑art standards.
Risk Management
We have various committees comprised of physicians and clinical personnel that discuss and set internal policies regarding various risk management issues including safety and environment of care, infection control, pharmacy and therapeutics, quality assessment and performance improvement, peer review and chart review. The policies we establish comply with relevant state, federal and regulatory and Joint Commission requirements.
Billing and Payment
We obtain patient service revenues by collecting fees from patients, insurance companies, and other third‑party payors for the professional and technical services provided in our facilities. All billing and coding is done by a centralized team. Claims are typically coded and filed within 72 hours of a patient visit. We manage the entire collections cycle up until the point that an account is written off and transferred to a third‑party collection service. Our general practice, where possible, is to collect estimated co‑payments at the facility. Claims are submitted electronically if the payor accepts electronic claims. We require claims submitted to third‑party payors be paid within timeframes that are generally consistent with industry standard practices, which vary based upon payor type.
We receive payment for patient services from a variety of third‑party payors, such as:
|
· |
health maintenance organizations, preferred provider organizations and private commercial insurance providers; and |
|
· |
out‑of‑pocket payments from patients. |
Charges for all services provided to insured patients are initially billed to and processed by the patients’ insurance provider. We have agreements with insurance companies that provide for payments at amounts different from our established rates. Differences between established rates and those set by insurance programs, as well as charity care, employee and prompt pay adjustments, are recorded as adjustments directly to patient service revenue. Estimated uncollectible amounts from insured patients are recorded as bad debt expense in the period the services are provided. Collection of payment for services provided to patients without insurance coverage is done at the time of service.
We write off as bad debt expense uncollectible accounts receivable arising from insured patient responsibility after all collection efforts have been exhausted and we have determined such accounts will not be collected. We believe that the collections process is another opportunity to differentiate ourselves in our patient’s minds. Our staff is trained to educate our patients on how the insurance company has determined the amount to pay on the claim.
Reimbursement
First Choice Emergency Rooms are full‑service emergency rooms. As such, we collect the emergency room benefits based on a patient’s specific insurance plan. Consistent with billing practices at all emergency rooms and in light of the fact our facilities are open 24 hours a day, seven days a week and staffed with Board‑certified physicians, we bill payors a facility fee, a professional services fee and other related fees.
16
Four major third‑party commercial payors accounted for approximately 84.8% of our patient service revenue for the year ended December 31, 2014. The remaining 13.3% of our patient service revenue comes from other smaller third‑ party commercial payors, self‑pay patients and workers’ compensation. Commercial third‑party payors include private health insurance as well as related payments from patients for deductibles and co‑payments. We enter into contracts with private health insurance and other health benefit groups by granting discounts to such organizations in return for the patient volume they provide. We do not currently bill Medicare or Medicaid for the care we provide.
Our contracts are structured as either case‑rate contracts or as discounts to billed charges. In a case rate contract, a set fee is assigned to visits based on acuity level. We also enter into contracts with payors based on a discount of our billed charges. There are contracted rates for both the professional component and the technical component, as well as a facility fee. Each portion of the claim is billed separately and paid based on the patient’s emergency room benefits.
Self‑pay consists of out‑of‑pocket payments for treatments by patients not otherwise covered by third‑party payors.
Real Estate Development Activities
General Strategy
We own and operate First Choice Emergency Rooms, the largest network of independent freestanding emergency rooms in the United States. We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. We have a robust pipeline under development designed to support the addition of a similar number of facilities in 2015. We have built an internal eight person team with over 150 years of combined experience in multi‑unit retail expansion strategy.
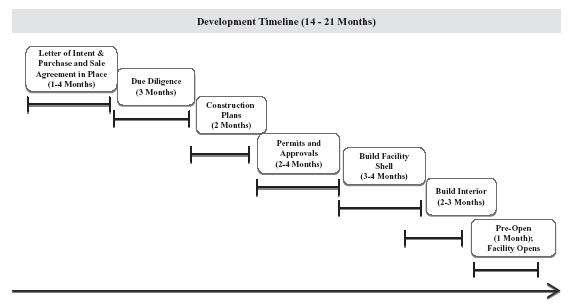
This team has developed a highly scalable business model for establishing new freestanding emergency rooms that include attractive unit economics, sophisticated data analytics to support our site‑selection process, proven real estate development practices and innovative marketing programs. We have developed, and continue to refine, the databases, geographic information systems, and proprietary predictive models that enable us to evaluate the competitive landscape in a market as part of our site‑selection process. This allows us to quantify and qualify the potential for new emergency room facilities within a market, and create a plan for the number and location of emergency room facilities to be developed in a given market. Our proprietary site‑selection model specifically analyzes consumer preferences and habits, anticipated requirements for access to emergency care, and geographic alternatives to competing emergency care providers. The typical cost involved in opening a new freestanding facility is between $5.0 million and $6.0 million, with a typical opening timeline between 14 and 21 months, from the site‑selection phase to the opening of a new facility.
17
The image below depicts our typical development timeline, beginning with sites for which we have already entered into a letter of intent and/or purchase agreement:
Real Estate Financing Sources
We seek to finance each facility on a stand‑alone basis using various sources of financing, including cash generated by our operations, Senior Secured Credit Facility, MPT Agreements and other outside sources.
In June 2013, we entered into an initial MPT Agreement (the “Initial MPT Agreement”) to fund future facility development and construction and in July 2014 we entered into an additional MPT Agreement (the “Additional MPT Agreement” and, together with the Initial MPT Agreement, the “MPT Agreements”) to fund future facilities. The Additional MPT Agreement is separate from and in addition to our Initial MPT Agreement. The Additional MPT Agreement allows a maximum aggregate funding of $150.0 million, of which $89.4 million remained available as of December 31, 2014. All other material terms remain consistent with the Initial MPT Agreement. Under the terms of the MPT Agreements, MPT will acquire parcels of land selected by us, fund the ground‑up construction of new freestanding emergency room facilities and lease the facilities to us upon completion of construction. MPT is required to fund all hard and soft costs, including the project purchase price, closing costs and pursuit costs for the assets relating to the construction of up to 25 facilities with a maximum aggregate funding of $100.0 million. Each completed project will be leased for an initial term of 15 years, with three five‑year renewal options. The MPT Agreements have provided the funding for 19 facilities that opened in 2014, as well 22 facilities under different phases of development.
Marketing
The evolving healthcare environment has motivated consumers to take a much more active role in how and where they receive care. Therefore, our marketing strategies focus on educating local communities on the access and patient care available at First Choice Emergency Room as a key option within the continuum of care. We have a dedicated field marketing team to foster relevant relationships within the community as well as engaged physicians to support medical community outreach. We sponsor and host community activities, including school fundraisers, street parties and sporting events to deepen our local involvement and encourage tours of our facilities and to deliver first‑hand education of our capabilities. Additionally, we have targeted marketing campaigns for each site comprised of direct mail, television, radio, outdoor advertising, digital and social media.
18
As we open new facilities as part of our expansion strategy, our opportunity to strengthen the public’s awareness of our brand and unique services will also increase. For example, our increased penetration in the Dallas/Fort Worth and Houston markets has, and will continue to, enable us to gain both local and market‑wide awareness. We plan to continue these aggressive marketing plans to build community familiarity and acceptance of the services we provide.
Consumer research has helped us refine our innovative facility model to communicate emergency care and ensure an optimal patient experience. From the introductory message of a new facility, to the personalized follow‑up from the staff, the marketing programs highlight the convenient access and high‑ quality care that differentiates First Choice Emergency Rooms. These carefully designed efforts are not only structured to increase patient volume, but also to firmly establish the First Choice Emergency Room brand and experience as an integral part of each community we serve.
Competition
We compete with other emergency care providers on the basis of proximity to the facility, quality of patient care and awareness. In each of our markets we face competition from traditional and evolving medical providers, including other freestanding emergency rooms, both independent and hospital affiliated. Independent freestanding emergency room competitors include: Elite Care, ER Centers of America, Neighbors Emergency Center, PhysiciansER and Texas Emergency Care Center. Given our 24/7 operating hours and ability to handle high‑acuity needs, instead of competing with community medical practices and urgent care clinics, we believe we complement them. Many of our sites work closely with nearby urgent care facilities to ensure the most appropriate patient care for the community. In February 2013 we formed a relationship with the Concentra urgent care clinics in the Dallas/Fort Worth market, whereby we are able to refer workers’ compensation patients to Concentra when follow‑up, non‑emergent, care is needed. We are more than three times the size of our next largest independent freestanding emergency room competitor. While the competition is typically defined by the patient’s proximity to each site, we are gaining an advantage through our expanding scope and resultant brand awareness. In addition to our size, we believe the quality of our care, the clinical staff and the patient word‑of‑mouth will allow us to effectively compete with new entrants into the category.
Government Regulation
The healthcare industry is subject to extensive regulation by federal, state and local governments. Government regulation affects our business by controlling growth, requiring licensing or certification of facilities, regulating how facilities are used and controlling payment for services provided. Our ability to conduct our business and to operate profitably will depend in part upon obtaining and maintaining all necessary licenses and other approvals, and complying with applicable healthcare laws and regulations. See “Risk Factors—Risks Related To Healthcare Regulation.”
State Laws Regarding Prohibition of Corporate Practice of Medicine and Fee Splitting Arrangements
The laws and regulations relating to our operations vary from state to state and approximately 30 states prohibit general business corporations from practicing medicine or controlling physicians’ medical decisions. We believe that we and our physician practice management service relationships with professional entities are in substantial compliance with state laws prohibiting the corporate practice of medicine including Colorado, Arizona and Texas. However, regulatory authorities or other parties, including our affiliated physicians, may attempt to assert that, despite these arrangements, we are impermissibly engaged in the practice of medicine or that our contractual arrangements with affiliated physician groups constitute unlawful fee‑splitting. In this event, we could be subject to adverse judicial or administrative interpretations, to civil or criminal penalties, our contracts could be found legally invalid and unenforceable or we could be required to restructure our contractual arrangements with our affiliated physicians and physician groups.
Of note, the vast majority of our freestanding emergency room facilities are located in Texas. Texas has a fairly robust corporate practice of medicine doctrine. Texas prohibits corporations from employing physicians and receiving money for professional services rendered by the physicians. However, professional associations and professional limited liability companies may employ physicians so long as the owners of such entities are physicians licensed under Texas law. Similarly, there are certain organizations organized under the Texas Non‑Profit Corporation Act that receive
19
certification from the Texas State Board of Medical Examiners to allow ownership in physician organizations by non‑physicians. We believe that we are in compliance with the corporate practice of medicine restrictions in Texas, Colorado and Arizona. The physicians who provide services at our Texas facilities are employed by National Medical Professionals of Texas PLLC, a professional limited liability company owned and operated by our Executive Medical Director. National Medical Professionals of Texas PLLC makes certain payments to us for billing, collection, administrative and other services through a management services agreement. Other private individuals, the Texas Medical Board, the Texas Attorney General or other healthcare providers may attempt to assert that, despite these arrangements, we are impermissibly engaged in the practice of medicine or that our contractual arrangements with affiliated physician groups constitute unlawful fee‑splitting. In this event, we could be subject to adverse judicial or administrative interpretations, to civil or criminal penalties, our contracts could be found legally invalid and unenforceable or we could be required to restructure our contractual arrangements with our affiliated physicians and physician groups.
State Statutes and Regulations Regarding our Operations
Our operating freestanding emergency room facilities in Texas and Colorado, and our hospital facility in Arizona, are subject to many laws and regulations, particularly at the state and local government levels. These laws and regulations require our freestanding emergency rooms and hospital facility to meet various licensing, certification and other requirements. See “Risk Factors—Risks Related To Healthcare Regulation.”
New regulation of our facilities is also possible, which could force us to change our operational approach or lead to a finding by governmental actors that our facilities are out of legal compliance.
State Law Regulation of Construction, Acquisition or Expansion of Emergency Rooms
Thirty‑six states have certificate of need programs that require some level of prior approval for the construction of a new facility, acquisition or expansion of an existing facility, or the addition of new services for various healthcare facilities. One of the most common categories of healthcare services reviewed under certificate of need laws is hospital services, which may include the emergency services we provide at our freestanding emergency rooms. While the states where our facilities are currently operational (Texas, Colorado and Arizona) do not require a certificate of need, other states where we seek to expand our operations may require certificates of need under circumstances not currently applicable to our facilities. See “Risk Factors—Risks Related To Healthcare Regulation.”
In addition, additional state legislation restricting our ability to obtain licensure for new facilities may be enacted. Such licensure challenges may have a material impact on our growth projections and expansion plans.
Laws and Rules Regarding Billing
The majority of our services are paid for by private third‑party payors. These third‑party payors typically have differing and complex billing and documentation requirements that we must meet in order to receive payment for our services. See “Risk Factors—Risks Related To Healthcare Regulation.”
We must also comply with numerous other state and federal laws applicable to our documentation and the claims we submit for payment. Private third‑party payors carefully audit and monitor our compliance with these and other applicable rules. Our failure to comply with the billing and other rules applicable to us could result in non‑payment for services rendered or refunds of amounts previously paid for such services. In addition, non‑compliance with these rules may cause us to incur civil and criminal penalties, including fines, imprisonment and exclusion from government healthcare programs, under a number of state and federal laws. See “Risk Factors—Risks Related to Healthcare Regulation.”
Privacy and Security Laws
HIPAA required HHS to adopt standards to protect the privacy and security of certain health‑related information. The HIPAA privacy regulations contain detailed requirements concerning the use and disclosure of
20
individually identifiable health information and the grant of certain rights to patients with respect to such information by “covered entities.” As a provider of healthcare who conducts certain electronic transactions, each of our facilities is considered a covered entity under HIPAA. In addition to the privacy requirements, HIPAA covered entities must implement certain administrative, physical, and technical security standards to protect the integrity, confidentiality and availability of certain electronic health information received, maintained, or transmitted by covered entities or their business associates. We have taken actions in an effort to be in compliance with these privacy and security regulations and believe that we are in substantial compliance. Ongoing implementation and oversight of privacy security measures involves significant time, effort and expense. A security incident that bypasses our information security systems causing an information security breach, loss of protected health information or other data subject to privacy laws or a material disruption of our operational systems could result in a material adverse impact on our business, along with fines.
States may impose more protective privacy restrictions in laws related to health information and may afford individuals a private right of action with respect to the violation of such laws. We are subject to any federal or state privacy‑related laws that are more restrictive than the privacy regulations issued under HIPAA. In addition, states may also impose restrictions related to the confidentiality of personal information that is not considered “protected health information” under HIPAA. If we fail to comply with HIPAA or similar state laws, we could incur substantial monetary penalties. See “Risk Factors—Risks Related to Healthcare Regulation.”
Licensing, Certification, Accreditation and Related Laws and Guidelines
We and our affiliated physicians are subject to various federal, state and local licensing and certification laws and regulations and accreditation standards and other laws relating to, among other things, the adequacy of medical care, equipment, personnel, operating policies and procedures and state mandated services and service limitations. We are also subject to periodic inspection by governmental and other authorities to assure continued compliance with the various standards necessary for licensing and accreditations. We must be in compliance in order to maintain authorization to provide, or receive payment for, our services. Compliance with these requirements is complicated by the fact that they differ from jurisdiction to jurisdiction, and in some cases are not uniformly applied or interpreted even within the same jurisdiction. Failure to comply with these requirements can lead not only to delays in payment and refund requests, but in extreme cases can give rise to civil or criminal penalties.
In certain jurisdictions, changes in our ownership structure require pre‑ or post‑notification to governmental licensing and certification agencies, or agencies with which we have contracts. Relevant laws in some jurisdictions may also require re‑application or re‑enrollment and approval to maintain or renew our licensure, certification, contracts or other operating authority. Our changes in corporate structure and ownership involving changes in our beneficial ownership required us in some instances to give notice, re‑enroll or make other applications for authority to continue operating in various jurisdictions or to begin to receive payment from government payment programs. The extent of such notices and filings may vary in each jurisdiction in which we operate, although those regulatory entities requiring notification generally request factual information regarding the new corporate structure and new ownership composition of the operating entities that hold the applicable licensing and certification.
We have made consistent efforts to substantially comply with these requirements, yet the agencies that administer these programs or have awarded us contracts may find that we have failed to comply in some material respects. A finding of non‑compliance and any resulting payment delays, refund demands or other sanctions could have a material adverse effect on our business, financial condition or results of operations.
Further, if we pursued any expansion in new states or participation in the Medicare or Medicaid programs for any of our facilities in the future, we would face additional certification requirements and a survey process to be classified as a hospital. Our current accreditation from the Joint Commission as freestanding emergency room facilities does not guarantee that our facilities would meet the Joint Commission hospital standards or Medicare conditions of participation or Medicaid requirements for hospitals.
Health Reform Initiatives
There have been numerous legislative and regulatory initiatives on the federal and state levels for comprehensive reforms affecting the payment for and availability of healthcare services. In March 2010, the President
21
signed PPACA into law, which made major changes in how healthcare is delivered and reimbursed, and increased access to health insurance benefits to the uninsured and underinsured population of the United States. As part of healthcare reform legislation, the Reconciliation Act was signed into law on March 30, 2010, making some limited but important changes to PPACA. PPACA includes a number of provisions that will directly affect our facilities. See “Risk Factors—Risks Related to Healthcare Regulation.”
PPACA represents significant change to the healthcare industry. PPACA includes provisions designed to change how healthcare services are covered, delivered and reimbursed through, among other things, expanded coverage of uninsured individuals, reduced growth in Medicare program spending and the establishment of programs where reimbursement is tied to quality. PPACA also reforms certain aspects of health insurance, expands existing efforts to tie Medicare and Medicaid payments to performance and quality, and contains provisions intended to strengthen fraud and abuse enforcement.
PPACA and other changes in the healthcare industry may adversely affect our business model and revenue. However, because of the continued uncertainty about the implementation of PPACA, we cannot quantify or predict with any certainty the likely impact of PPACA on our business model, financial condition or results of operation.
In each market where we operate, there are hospitals and health systems that compete with us. These hospitals and health systems have powerful and effective lobbying groups to help effectuate changes to state and federal legislation that would otherwise have a negative impact on their operations. As competitors of these entities, we may not receive the benefit of their lobbying efforts and in some circumstances may be negatively impacted by their efforts.
Federal False Claims Act
The Federal government is authorized to impose criminal, civil and administrative penalties on any person or entity that files a false claim for payment from the Medicare or Medicaid programs. False claims filed with private insurers can also lead to criminal and civil penalties. While the criminal statutes are generally reserved for instances of fraudulent intent, the government applies criminal, civil and administrative penalty statutes to a range of circumstances, including coding errors, billing for services not provided, submitting false cost reports, submitting claims resulting from arrangements prohibited by the Stark Law or the Anti‑Kickback Statute, billing for services not rendered in compliance with complex Medicare and Medicaid regulations and guidance, misrepresenting services rendered (e.g., miscoding, upcoding, etc.) and application for duplicate reimbursement. See “Risk Factors—Risks Related to Healthcare Regulation.”
Fair Debt Collection Practices Act
Some of our operations may be subject to compliance with certain provisions of the Fair Debt Collection Practices Act and comparable statutes in many states. Under the Fair Debt Collection Practices Act, a third party collection company is restricted in the methods it uses to contact consumer debtors and elicit payments with respect to placed accounts. Requirements under state collection agency statutes vary, with most requiring compliance similar to that required under the Fair Debt Collection Practices Act. We believe we are in substantial compliance with the Fair Debt Collection Practices Act and comparable state statutes where applicable.
Healthcare Fraud and Abuse Laws
In the event we choose to participate in the Medicare, Medicaid or Tricare program, we would become directly subject to certain federal laws, including without limitation, the Anti‑Kickback Statute and the Stark Law.
The Anti‑Kickback Statute prohibits the knowing and willful offer, payment, solicitation or receipt of remuneration, directly or indirectly, in return for the referral of patients or arranging for the referral of patients, or in return for the recommendation, arrangement, purchase, lease or order of items or services that are covered, in whole or in part, by a federal healthcare program such as Medicare or Medicaid. Many states such as Texas and Arizona have adopted similar prohibitions against kickbacks as the Anti‑Kickback Statute. See “Risk Factors—Risks Related to Healthcare Regulation.”
22
The Stark Law prohibits a physician from referring a patient to a healthcare provider for certain designated health services reimbursable by Medicare if the physician (or close family members) has a financial relationship with that provider, including an investment interest, a loan or debt relationship or a compensation relationship. Some states, including Texas and Colorado, have self‑referral laws similar to Stark Law for Medicaid claims (and commercial claims). Some states also have other healthcare fraud and abuse laws with various reasons for violations. See “Risk Factors—Risks Related to Healthcare Regulation.”
HIPAA Transactions and Code Sets Standards
HIPAA and its implementing regulations establish electronic data transmission standards that all healthcare providers must use for certain electronic healthcare transactions, such as submitting claims for payment for medical services. PPACA requires the adoption of standards for additional electronic transactions and provides for the creation of operating rules to promote uniformity in the implementation of each standardized electronic transaction. Under HIPAA, HHS has also published a final rule requiring the use or updated standard code sets for certain diagnoses and procedures known as ICD‑10 code sets. Use of the ICD‑10 code sets is required beginning October 1, 2015. It is possible that our facilities could experience disruptions or delays in payment due to the implementation of new electronic data transmission standards and the transition to ICD‑10 code sets. We may also experience increased costs in training and operations during the transition from the prior ICD-9 codes, especially if additional delays occur before use of ICD-10 is required.
Regulatory Compliance Program
It is our policy to conduct our business with integrity and in compliance with the law. We have in place, and continue to enhance, a company‑wide compliance program, entitled “Remedy”, that focuses on all areas of regulatory compliance including billing, reimbursement, cost reporting practices and contractual arrangements with referral sources. We have specific corporate policies relating to sexual harassment, ethics, diversity and HIPAA, among others. We have structured our health and welfare plans to be ERISA‑compliant.
We have mechanisms in place to ensure compliance across every aspect of our organization including, but not limited to, the following:
Human Resources
All prospective employees that are offered employment must pass a rigorous background check and drug screen. New employee training and orientation focuses on compliance with company policies related to HIPAA, ethical conduct, sexual harassment and diversity. We mandate that all employees sign our Code of Conduct on an annual basis. All employees are encouraged to report any compliance concerns of any nature to the Chief Compliance Officer through our confidential toll‑free hotline or web portal. We mandate that all reported concerns be investigated by the Chief Compliance Officer and reported to the board of directors on a quarterly basis.
Billing
We have a third party that conducts quarterly audits of a random selection of our patient charts. We also employ a certified hospital outpatient coder to comply with ACEP guidelines. In addition, we conduct a thorough overview of all charges to match vendor charges to claims. When we discover an improper claim or overpayment to a third‑party vendor, it is our practice to disclose the issue to the affected third‑party payor and to refund any resulting overpayments. See “Risk Factors—Risks Related to Healthcare Regulation—Our facilities, billing practices, relationships with healthcare providers and third parties, and our marketing practices may become subject to the Anti‑Kickback Statute, Stark Law, False Claims Act and similar state laws.”
23
Occupational Safety
Our corporate radiation safety officers are hired to ensure that all radiology equipment meets applicable regulatory requirements. All of our radiology technologists are required to wear badges that monitor their exposure to radiology, and these results are sent to applicable authorities.
Properties
Our executive and administrative offices are located in Lewisville, Texas. These offices contain approximately 80,000 square feet of space. We believe these offices are adequate for our current primary needs.
Our emergency care facilities typically range in size from approximately 6,000 to 7,000 square feet. As of December 31, 2014, we provided emergency care in 46 facilities in Texas and 9 facilities in Colorado. We own the real estate on which one of our facilities is located. We lease land and space at 50 locations. These leases expire at various dates between March 31, 2015 and December 31, 2029 and all but three of these leases have one or more renewal options of between five and seven years. We consider all of our offices and facilities to be well‑suited to our present requirements. However, as we expand to additional facilities, or where additional capacity is necessary in a facility, additional space will be obtained where feasible.
The following list summarizes the number of freestanding emergency room facilities operated in each city’s metropolitan area as of December 31, 2014:
|
|
|
|
|
|
Location |
|
Number of |
|
|
Dallas/Fort Worth |
|
19 |
|
|
Houston |
|
20 |
|
|
Austin |
|
4 |
|
|
San Antonio |
|
3 |
|
|
Texas |
|
46 |
|
|
Colorado Springs |
|
3 |
|
|
Denver |
|
6 |
|
|
Colorado |
|
9 |
|
|
Total |
|
55 |
|
In addition, we have one hospital facility located in Phoenix, Arizona
Seasonality
Our patient volumes are sensitive to seasonal fluctuations in emergency activity. Typically, winter months see a higher occurrence of influenza, bronchitis, pneumonia and similar illnesses; however the timing and severity of these outbreaks can vary dramatically. Additionally, as consumers shift towards high deductible insurance plans, they are responsible for a greater percentage of their bill, particularly in the early months of the year before other healthcare spending has occurred, which may lead to an increase in bad debt expense during that period. Our quarterly operating results may fluctuate significantly in the future depending on these and other factors.
Intellectual Property
Some of our service marks and logos may be subject to intellectual property rights. We do not hold any patents. To date, we have not relied heavily on patents or other intellectual property in operating our business. Nevertheless, some of the information technology purchased or used by us may be patented or subject to other intellectual property rights. As a result, we may be found to be, or actions may be brought against us alleging that we are, infringing on the trademark, patent or other intellectual property rights of others, which could give rise to substantial claims against us. In the future, we may wish to obtain or develop trademarks, patents or other intellectual property. However, other practices and public entities, including universities, may have filed applications for (or have been issued) trademarks, patents or
24
other intellectual property rights that may be the same as or similar to those developed or otherwise obtained by us or that we may need in the development of our own intellectual property. The scope and validity of such trademark, patent and other intellectual property rights, the extent to which we may wish or need to acquire such rights and the cost or availability of such rights are presently unknown. In addition, we cannot provide assurance that others will not obtain access to our intellectual property or independently develop the same or similar intellectual property to that developed or otherwise obtained by us.
Employees
As of December 31, 2014, we had 1,869 employees, of which 562 are nurses, and 488 are radiology technologists. Further, we reimburse our employees for the cost of certification exams, which promotes professional development. We believe that our relations with our employees are good. None of our employees are subject to any collective bargaining agreement. We enter into direct independent contractor agreements with our physicians and they do not hold ownership interests in our operations.
Insurance
We maintain liability insurance in amounts that we believe are appropriate for our operations. Currently, we maintain professional and general liability insurance coverage for us and our facilities on a claims‑made basis of $1.0 million per occurrence and $3.0 million in annual aggregate coverage per facility. We also maintain umbrella liability insurance in the aggregate amount of $10.0 million. We also currently maintain property damage insurance with a maximum coverage of $60 million and other types of insurance coverage we believe to be consistent with industry practice. Coverage under certain of these policies is contingent upon the policy being in effect when a claim is made regardless of when the events that caused the claim occurred. The cost and availability of such coverage has varied widely in recent years.
We are insured for worker’s compensation claims up to $1.0 million per claim and per employee with a policy limit of $1.0 million. We submit periodic payments to our insurance broker based upon estimated payroll. We believe that our insurance policies are adequate in amount and coverage for our current and anticipated operations based on both management judgment and external benchmarks.
As of December 31, 2014, our professional liability insurance coverage was $20 million.
History and Corporate Structure
First Choice ER, LLC was founded in 2002. In 2011, funds affiliated with Sterling Partners (our “Sponsor”) acquired a 75% share in First Choice ER, LLC and, in 2013, Adeptus Health LLC was created as a holding company to own and operate First Choice Emergency Rooms.
Adeptus Health Inc. was incorporated as a Delaware corporation on March 7, 2014 for the purpose of conducting our initial public offering, which was completed on June 30, 2014. In connection with the initial public offering, we completed the Reorganization, which among other things, resulted in Adeptus Health Inc. becoming a holding company with its sole material asset being a controlling equity interest in Adeptus Health LLC. As the sole managing member of Adeptus Health LLC, Adeptus Health Inc. operates and controls all of the business and affairs of Adeptus Health LLC and, through Adeptus Health LLC and its subsidiaries, conducts our business. Adeptus Health Inc. owns 100% of the voting rights of Adeptus Health LLC, and therefore has control over Adeptus Health LLC.
Recent Events
In December 2014, we entered the Arizona market through our partnership with Dignity Health with a full-service general hospital. In December, the facility began its training and certification phase of operation and received its CMS certification from the Joint Commission on January 30, 2015. CMS certification allows us to receive reimbursement for services provided to Medicare and Medicaid patients of the hospital as of January 30, 2015.
25
Available Information
We maintain an Internet website under the name www.adhc.com. We make available, free of charge, on our website, our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports, as soon as reasonably practicable after providing such reports to the SEC.
We file annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, proxy statements and other documents with the SEC under the Securities Exchange Act, as amended. The public may read and copy any materials that we file with the SEC at the SEC’s Public Reference Room at 100 F Street, N.E., Washington DC 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. Also, the SEC maintains an Internet website that contains reports, proxy and information statements and other information regarding issuers, including Adeptus Health Inc., that file electronically with the SEC. The public can obtain any document we file with the SEC at www.sec.gov. Information contained on, or connected to, our website is not incorporated by reference into this Annual Report on Form 10-K and should not be considered part of this Annual Report on Form 10-K or any other filing that we make with the SEC.
You should carefully read the risks and uncertainties described below, together with the other information included in this Annual Report on Form 10-K. Any of the following risks could materially affect our business, financial condition or results of operations. The risks described below are not the only risks we face. Additional risks and uncertainties we are not presently aware of or that we currently believe are immaterial could also materially and adversely affect our business, financial condition or results of operations.
Risks Related to Our Business and Our Industry
We may not be able to successfully implement our growth strategy on a timely basis or at all, which could harm our growth and results of operations.
Our growth depends on our ability to open profitable new facilities. Our growth strategy is to substantially grow the number of our freestanding emergency care facilities in 2015 and beyond. Our ability to open profitable facilities depends on many factors, including our ability to:
|
· |
open facilities and achieve brand awareness in new markets; |
|
· |
access capital to fund construction costs and preopening expenses; |
|
· |
manage increases in costs, which could give rise to delays or cost overruns; |
|
· |
recruit and train physicians, nurses and technicians in our local markets; |
|
· |
obtain all required governmental licenses and permits, including state facility licenses, on a timely basis; |
|
· |
compete for appropriate sites in new markets, including against emergency care competitors and against traditional retailers; and |
|
· |
maintain adequate information systems and other operational system capabilities. |
Delays in the opening of new facilities, delays or costs resulting from a decrease in commercial development due to capital constraints, difficulties resulting from commercial, residential and infrastructure development (or lack thereof) near our new facilities, difficulties in staffing and operating new locations or lack of acceptance in new market areas may negatively impact our new facility growth and the costs or the profitability associated with new facilities. Further, additional federal or state legislative or regulatory restrictions or licensure requirements could negatively impact our ability to operate both new and existing facilities.
26
Accordingly, we may not be able to achieve our planned growth or, even if we are able to grow our facility base as planned, any new facilities may not be profitable or otherwise perform as planned. In addition, to the extent we have misjudged the nature and extent of industry trends or our competition, we may have difficulty in achieving our strategic objectives. Failure to successfully implement our growth strategy would likely have an adverse impact on the price of our Class A common stock.
Our expansion into new markets presents increased risks and may require us to develop new business models.
Our continued growth and profitability depend on our ability to successfully realize our growth strategy by expanding the number of facilities we operate in both new and existing markets. We cannot assure you our efforts to expand into new markets, particularly in states where we do not currently operate, will succeed. In order to operate in new markets, we may need to modify our existing business model and cost structure to comply with local regulatory or other requirements, which may expose us to new operational, regulatory or legal risks. In addition, expanding into new states, including our joint venture with Dignity Health and the opening of full‑service general hospitals in Arizona and Texas (planned) in 2015, may subject us to unfamiliar or uncertain local regulations that may adversely affect our operations, for example, by impacting our insurance reimbursement practices or our ability to operate facilities as licensed or unlicensed freestanding emergency rooms or hospitals. See “—Risks Related to Healthcare Regulation” below. Facilities we open in new markets may also take longer to reach expected revenue and profit levels on a consistent basis and may have higher construction, occupancy or operating costs than facilities we open in existing markets, thereby affecting our overall profitability. New markets may have competitive conditions, consumer preferences and healthcare spending patterns that are more difficult to predict or satisfy than our existing markets.
We may need to make greater investments than we originally planned in advertising and promotional activity in new markets to build brand awareness. We may find it more difficult in new markets to hire, motivate and keep qualified physicians, nurses, technicians and other personnel. We may need to augment our labor model to meet regulatory requirements and the overall cost of labor may be higher. As a result, these new facilities may be less successful and may not achieve target facility level profit margins at the same rate or at all. If any steps taken to expand our existing business model into new markets are unsuccessful, we may not be able to achieve our growth strategy and our business, financial condition or results of operations could be adversely affected.
Our long‑term success is highly dependent on our ability to successfully identify and secure appropriate sites for our facilities and develop and expand our operations in existing and new markets.
One of the key means of achieving our growth strategy will be through opening new facilities and operating those facilities on a profitable basis. We expect this to be the case for the foreseeable future. We identify target markets where we can enter or expand, taking into account numerous factors such as the location of our current facilities, demographics, traffic patterns and other factors that support our site‑selection process. As we operate more facilities, our rate of expansion relative to the size of our current facility base will eventually decline. As of December 31, 2014, we had 55 facilities in operation. We have 12 locations currently under construction, including a regional hospital in Texas and 15 locations in the building permit process. Based on our typical development timeline we believe that at least 24 of these facilities will be completed and operational by December 31, 2015. We currently expect that 19 of the facilities will be funded by MPT under the MPT Agreements and the remaining facilities will be funded by other third party capital funding sources. Even though our 2015 expansion strategy is under way, the number and timing of new facilities opened during any given period may be negatively impacted by a number of factors including, without limitation:
|
· |
the cost and availability of capital to fund construction costs and preopening expenses; |
|
· |
the identification and availability of attractive sites for new facilities and the ability to negotiate suitable lease terms; |
|
· |
anticipated commercial, residential and infrastructure development near our new facilities; |
|
· |
the proximity of potential sites to an existing facility; |
|
· |
construction delays or cost overruns that may increase project costs; |
27
|
· |
our ability to obtain zoning, occupancy and other required governmental permits and authorizations on a timely basis; |
|
· |
our ability to control construction and development costs incurred for projects, including those that are not pursued to completion; |
|
· |
hurricanes, floods, fires or other natural disasters that could adversely affect a project; |
|
· |
defects in design or construction that may result in additional costs to remedy or require all or a portion of a property to be closed during the period required to rectify the situation; and |
|
· |
governmental restrictions on the nature and size of a project or timing of completion. |
If we are unable to find and secure attractive locations to expand in existing markets or penetrate new markets, this may harm our ability to increase our revenues and profitability and realize our growth strategy and our financial results may be negatively affected.
New facilities, once opened, may not be profitable, and the increases in comparable facility revenue that we have experienced in the past may not be indicative of future results.
Our results have been, and in the future may continue to be, significantly impacted by a number of factors, including factors outside of our control, related to the opening of new facilities, including the timing of new facility openings, associated facility preopening costs and operating inefficiencies, as well as changes in our geographic concentration due to the opening of new facilities. We typically incur the most significant portion of opening expenses associated with a given facility within the first few months immediately preceding and following the opening of the facility. A new facility generally takes up to 12 months to achieve a level of operating performance comparable to our similar existing facilities due to lack of market awareness and other factors. We also may incur additional costs in new markets, particularly for contracting, real estate, labor, marketing and regional support, which may impact the profitability of those facilities. Accordingly, the volume and timing of new facility openings may have a meaningful impact on our profitability.
Although we target specified operating and financial metrics, new facilities may not meet these targets or may take longer than anticipated to do so. Any new facilities we open may not be profitable or achieve operating results similar to those of our existing facilities. If our new facilities do not perform as planned, our business and future prospects could be harmed. In addition, if we are unable to achieve expected comparable facility revenues, our business, financial condition or results of operations could be adversely affected.
Opening new facilities in existing markets may negatively affect revenue at our existing facilities.
The target area of our facilities varies by location and depends on a number of factors, including population density, other available emergency medical services, area demographics and geography. As a result, the opening of a new facility in or near markets in which we already have facilities could adversely affect the revenues of those existing facilities. Existing facilities could also make it more difficult to build our patient base for a new facility in the same market. Our business strategy does not entail opening new facilities that we believe will materially affect revenue at our existing facilities, but we may selectively open new facilities in and around areas of existing facilities that are operating at or near capacity to effectively serve our patients. Revenue cannibalization between our facilities may become significant in the future as we continue to expand our operations and could affect our revenue growth, which could, in turn, adversely affect our business, financial condition or results of operations.
We are required to make capital expenditures, particularly to implement our growth strategy, in order to remain competitive.
Our capital expenditure requirements primarily relate to identifying expansion opportunities for our facilities, the costs associated to establish such new facilities in existing and new markets and maintaining and upgrading our medical equipment to serve our customers and remain competitive. Our capital expenditures totaled $47.4 million , $46.0 million and $11.5 million, for the years ended December 31, 2014, 2013 and 2012, respectively. In addition,
28
changing competitive conditions or the emergence of any significant advances in medical technology could require us to invest significant capital in additional equipment or capacity in order to remain competitive. If we are unable to fund any such investment or otherwise fail to invest in new medical equipment, our business, financial condition or results of operations could be materially and adversely affected.
We currently rely on our Master Funding and Development Agreements with Medical Properties Trust to execute our expansion strategy.
We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. We have a robust pipeline under development designed to support the addition of a similar number of facilities in 2015. A major source of financing we have and employ to open new facilities is derived from our MPT Agreements. Under the terms of the MPT Agreements, MPT acquires parcels of land, funds the ground‑up construction of new freestanding emergency room facilities and leases the facilities to us upon completion of construction. MPT is also required to fund all hard and soft costs, including the project purchase price, closing costs and pursuit costs for the assets relating to the construction of up to a maximum aggregate funding of $250.0 million, of which 89.4 million remained available under our Additional MPT Agreement as of December 31, 2014. An inability to rely on our relationship with MPT or to obtain alternate funding sources to fund our expansion strategies may require us to delay, scale back or eliminate some or all of the expansion of our current pipeline and future projects, which may have a material adverse effect on our business, operating results, financial condition or prospects.
We may require additional capital to fund our expansion, and our inability to obtain such capital could harm our business.
To support our expansion strategy, we must have sufficient capital to continue to make significant investments in our new and existing facilities. Funding from outside financing or cash generated by our operations may not be sufficient to allow us to sustain our expansion efforts. If funding from outside financing sources or cash flows from operations are not sufficient, we may need additional equity or debt financing to provide the funds required to expand our business. If such financing is not available on satisfactory terms or at all, we may be unable to expand our business or to develop new business at the rate desired and our operating results may suffer. Debt financing increases expenses and must be repaid regardless of operating results, and the documents governing indebtedness may contain covenants that restrict the operation of our business. Equity financing, or debt financing that is convertible into equity, could result in additional dilution to our existing stockholders. Furthermore, our inability to obtain adequate capital resources, whether in the form of equity or debt, to fund our business and growth strategies may require us to delay, scale back or eliminate some or all of our operations or the expansion of our business, which may have a material adverse effect on our business, operating results, financial condition or prospects.
Damage to our reputation or our brand in existing or new markets could negatively impact our business, financial condition and results of operations.
We believe we have built our reputation on the high quality of our emergency medical services, physicians and operating personnel, as well as on our unique culture and the experience of our patients in our facilities, and we must protect and grow the value of our brand to continue to be successful in the future. Our brand may be diminished if we do not continue to make investments in areas such as marketing and advertising, as well as the day‑to‑day investments required for facility operations, equipment upgrades and staff training. Any incident, real or perceived, regardless of merit or outcome, that erodes our brand, such as, but not limited to, patient disability or death due to medical malpractice or allegations of medical malpractice, failure to comply with federal, state or local regulations including allegations or perceptions of non‑compliance or failure to comply with ethical and operating standards, could significantly reduce the value of our brand, expose us to adverse publicity and damage our overall business and reputation. Further, our brand value could suffer and our business could be adversely affected if patients perceive a reduction in the quality of service or staff, or an adverse change in our culture, or otherwise believe we have failed to deliver a consistently positive patient experience.
29
We may be unable to maintain or improve our operating margins, which could adversely affect our financial condition and ability to grow.
If we are unable to successfully manage the potential difficulties associated with growth, we may not be able to capture the efficiencies and opportunities that we expect from our expansion strategy. If we are not able to capture expected efficiencies of scale, maintain patient volumes, improve our systems and equipment, continue our cost discipline and retain appropriate physician and overall labor levels, our operating margins may stagnate or decline, which could have a material adverse effect on our business, financial condition and results of operations and adversely affect the price of our Class A common stock.
Our marketing programs may not be successful.
We incur costs and expend other resources in our marketing efforts to attract and retain patients. Our total marketing initiatives for the years ended December 31, 2014, 2013 and 2012 resulted in costs of approximately $9.3 million, $5.9 million and $2.8 million, respectively. Our marketing activities are principally focused on increasing brand awareness and awareness of our service capabilities and our marketing team is responsible for implementing our marketing efforts through activating field marketing teams, underscoring leadership through brand‑wide program initiatives, participating in trade show sponsorship, white paper publication, arranging for speaking engagements for our senior executives and formal training about our products and services. We also sponsor and host local community activities including fundraisers, street parties and sporting events to bolster our overall community involvement. As we open new facilities, we undertake aggressive marketing campaigns to increase community awareness about our growing presence. We plan to utilize targeted marketing efforts within local neighborhoods, through channels such as direct mail, mobile billboards, radio advertisements, television, community sponsorships and a robust online/social media presence. These initiatives may not be successful, resulting in expenses incurred without the benefit of higher revenue. Our ability to market our services may be restricted or limited by federal or state law.
We face intense competition in the emergency care market, including competition for patients, strategic relationships and commercial payor contracts which could adversely affect our contract and revenue base.
The market for providing emergency care services is highly competitive and each of the individual geographic areas in which we operate has a different competitive landscape. We compete with national, regional and local enterprises, some of which may have greater financial and other resources available to them, greater access to physicians or greater access to potential customers. We may also compete with urgent care centers and physician‑owned facilities for lower‑acuity cases and with hospitals for higher acuity cases. Such competition could adversely affect our ability to obtain new contracts, retain existing contracts and increase or maintain profit margins.
In each of our markets we compete with other healthcare providers for patients and in contracting with commercial payors. We are also in competition with other emergency care providers, hospitals, urgent care centers, clinics and healthcare systems in the communities we serve to attract patients and provide them with the care they need. There are hospitals and health systems that compete with us in each market in which we operate, and many of them have more established relationships with physicians and payors than we do. In addition, other companies are currently in the same or similar business of developing, acquiring and operating emergency care facilities, or may decide to enter this business. We also compete with some of these companies for entry into strategic relationships with health systems. As a result of the differing competitive factors within the markets in which we operate, the individual results of our facilities may be volatile. If we are unable to compete effectively with any of these entities or groups we may be unable to implement our business strategies successfully, which could have a material adverse effect on our business, prospects, results of operations and financial condition.
We may not be able to successfully recruit and retain physicians and other healthcare professionals with the qualifications and attributes we and our patients’ desire.
Our success depends upon our continuing ability to recruit and retain qualified physicians, nurses, technologists and other operating staff. There is currently a national shortage of certain of these healthcare professionals. To the extent that a significant number of physicians within an individual community or market decide to partner with competing
30
emergency care providers, hospitals or health systems and not with us, we may not be able to operate our facilities in such community. We face competition for such personnel from emergency care providers and other organizations. This competition may require us to enhance wages and benefits to recruit and retain qualified personnel. In the event we are unable to recruit and retain these professionals, such shortages could have a material adverse effect on our ability to grow or be profitable.
If we are unable to negotiate and enter into favorable contracts or maintain satisfactory relationships and renew existing contracts on favorable terms with third‑party payors, our revenue and profitability may decrease.
We estimate that 97.8%, 98.8% and 98.1%, of our net patient service revenue for the years ended December 31, 2014, 2013 and 2012, respectively, was derived from third‑party payors such as managed care organizations, commercial insurance providers and employer‑sponsored healthcare plans. We receive most of these payments from third‑party payors that have contracts or other arrangements in place with us in Texas and Colorado. We currently have a contract in place with one significant commercial insurance provider and an arrangement with another organization that enables us to access third‑party payors at in‑network rates. These third‑party payors use a variety of methods for reimbursement depending on the arrangement involved. These arrangements include fee‑for‑service, preferred provider organizations, health maintenance organizations, as well as prepaid and discounted medical service packages and capitated (fixed fee) contracts. Rates for health maintenance organization benefit plans are typically lower than those for preferred provider organization or other benefit plans that offer broader provider access.
There is often pressure to renegotiate our reimbursement levels, including, in particular, in connection with changes to Medicare. Typically, third‑party commercial payors reimburse us based upon contracted discounts to our established base rates. In 2012, we entered into a contract with another large third‑party payor and implemented a price increase in May 2013 and May 2014 under that contract. To date, we have not experienced a shift toward payors who base reimbursement levels on Medicare rates. During the past three years, we have experienced a trend towards increasing reimbursement by third‑party commercial payors. If managed care organizations and other third‑party payors reduce their rates or we were to experience a significant shift in our revenue mix toward Medicare or Medicaid reimbursements, which we currently do not accept, but may accept in the future, then our revenue and profitability may decline and our operating margins will be reduced. Third‑party payors continue to demand discounted fee structures, and the trend toward consolidation among third‑party payors tends to increase their bargaining power over fee structures. Because some third‑party payors rely on all or portions of Medicare payment systems to determine payment rates, changes to government healthcare programs that reduce payments under these programs may negatively impact payments from third‑party payors. Other healthcare providers may impact our ability to negotiate increases and other favorable terms in our reimbursement arrangements with third‑party payors. For example, some of our competitors may negotiate exclusivity provisions with third‑party payors or otherwise restrict the ability of third‑party payors to contract with us or our health system partners. Our results of operations will depend, in part, on our and our health system partners, ability to retain and renew our managed care contracts as well as enter into new managed care contracts on terms favorable to us. Our inability to maintain suitable financial arrangements with third‑party payors could have a material adverse impact on our business.
As various provisions of PPACA are implemented, including the establishment of health insurance exchanges, quality‑based reimbursement and bundled payments, third‑party payors may increasingly demand reduced fees. In addition, there is a growing trend for third‑party payors to take steps to shift the primary cost of care to the plan participant by increasing co‑payments, co‑insurance and deductibles, and these actions could discourage such patients from seeking treatment at our facilities. Patient volumes could decrease if we or our health system partners are unable to enter into acceptable contracts with such third‑party payors, which could have a material adverse effect on our business, prospects, results of operations and financial condition.
We depend on payments from a variety of third‑party payors. If these payments are significantly delayed, are reduced or eliminated our revenue and profitability could decrease.
We depend upon compensation from third‑party payors for the services provided to patients in our facilities. The amount that our facilities receive in payment for their services may be adversely affected by factors we do not control, including state regulatory changes, cost‑containment decisions and changes in reimbursement schedules of
31
third‑party payors and legislative changes. Any reduction or elimination of these payments could have a material adverse effect on our business, prospects, results of operations and financial condition.
Additionally, the reimbursement process is complex and can involve lengthy delays. While we recognize revenue when healthcare services are provided, there can be delays before we receive payment. In addition, third‑party payors may disallow, in whole or in part, requests for reimbursement based on determinations that certain amounts are not reimbursable under plan coverage, that services provided were not medically necessary, that services rendered in our facilities did not require emergency level care or that additional supporting documentation is necessary. Retroactive adjustments may change amounts realized from third‑party payors. Delays and uncertainties in the reimbursement process may adversely affect accounts receivable, increase the overall costs of collection and cause us to incur additional borrowing costs.
Significant changes in our payor mix or acuity mix resulting from fluctuations in the types of patients seen at our facilities could have a material adverse effect on our business, prospects, results of operations and financial condition.
Our results may change from period to period due to fluctuations in payor mix or acuity mix or other factors relating to the type of treatment performed by physicians at our facilities. Payor mix refers to the relative share of total cases provided to patients with, respectively, no insurance, commercial insurance and other coverage. Since, generally speaking, we receive relatively higher payment rates from third‑party payors than self‑pay patients, a significant shift in our payor mix toward a higher percentage of self‑pay or Medicare, Medicaid or other government reimbursement program patients, which we do not currently accept, but may accept in the future, which could occur for reasons beyond our control, could result in a material adverse effect on our business, prospects, results of operations and financial condition. Acuity mix refers to the relative share of total visits by acuity level, which affects the costs of the services we provide as well as the related revenue. Generally speaking, we derive relatively higher revenue from more complex treatments and patient encounters. Therefore, a significant shift in our acuity mix toward a higher percentage of lower revenue treatments could result in a material adverse effect on our business, prospects, results of operations and financial condition.
Failure to timely or accurately bill for our services could have a negative impact on our net revenues, bad debt expense and cash flow.
Billing for our services is complex. The practice of providing medical services in advance of payment or prior to assessing a patient’s ability to pay for such services may have a significant negative impact on our patient service revenue, bad debt expense and cash flow. We bill numerous and varied payors, including self‑pay patients and various forms of commercial insurance providers. Different payors typically have differing forms of billing requirements that must be met prior to receiving payment for services rendered. Self‑pay patients and third‑party payors may fail to pay for services even if they have been properly billed. Reimbursement to us is typically conditioned, among other things, on our providing the proper procedure and diagnosis codes. Incorrect or incomplete documentation and billing information could result in non‑payment for services rendered.
Additional factors that could complicate our billing include:
|
· |
disputes between payors as to which party is responsible for payment; |
|
· |
variation in coverage for similar services among various payors; |
|
· |
the difficulty of adherence to specific compliance requirements, coding and various other procedures mandated by responsible parties; |
|
· |
the fact that we bill payors a facility fee, a professional services fee and other related fees; |
32
|
· |
the transition to new coding standards, which will require significantly more information than the codes currently used for medical coding and will require covered entities to code with much greater detail and specificity; and |
|
· |
failure to obtain proper physician enrollment and documentation in order to bill various payors. |
To the extent the complexity associated with billing for our services causes delays in our cash collections, we assume the financial risk of increased carrying costs associated with the aging of our accounts receivable as well as the increased potential for bad debt expense.
Our relationships with health systems are important to our growth strategy. If we fail to maintain good relationships with these health systems or to enter into new relationships, we may be unable to implement our growth strategy successfully and our reputation could be adversely affected.
Our business depends in part upon the success of our health system partners and the strength of our relationships with those health systems. Our business could be adversely affected by any damage to those health systems’ reputation or to our relationships with them, or as a result of an irreconcilable dispute with a health system partner. Additionally, our reputation in the communities we serve is bolstered by our relationships with our partners. If we are unable to maintain such partnerships, our own reputation could be adversely affected. We may enter into affiliation agreements or have informal arrangements with health systems in which we agree to transfer certain patients to affiliated hospitals in a defined geographic area. We expect to focus on the creation of additional partnerships with health systems, and others, as part of expansion strategy. For example, we have arrangements with HCA to ensure bed availability for our patients in need of acute care services at nearby HCA hospitals in both the North Texas and Houston areas. In addition, we have a relationship with the Concentra urgent care clinics in the Dallas/Fort Worth market, whereby we are able to refer workers’ compensation patients to Concentra when follow‑up, non‑emergent, care is needed. If we are unable to develop and maintain good relationships with such health systems, maintain our existing agreements on terms and conditions favorable to us or enter into relationships with additional health systems on favorable terms, or at all, we may be unable to implement our growth strategies successfully.
We may enter into partnerships with healthcare providers. If this strategy is not successful, our financial performance could be adversely affected.
In recent years, we have entered into strategic business partnerships with hospital systems and other large providers to take advantage of commercial opportunities in our facility based business. For example, and as discussed above, we have agreements with HCA and Concentra to ensure that patients have direct access to nearby hospitals and urgent care centers, as necessary. However, there can be no assurance that our efforts in these areas will continue to be successful.
Moreover, this strategic partnership model exposes us to commercial risks that may be different from our own business model, including that the success of such partnerships is only partially under our operational and legal control, the potential for opportunity costs in not being able to pursue other partnerships should we enter into exclusive arrangements, and the risk that our partners may enter into additional arrangements with our competitors if these arrangements are not exclusive. Furthermore, partnership arrangements may raise fraud and abuse issues. For example, the Office of Inspector General of the Department of Health and Human Services, or the OIG, has taken the position that certain contractual arrangements between a party that receives remuneration for making referrals and a party that receives referrals for a specific type of service may violate the federal Anti‑Kickback Statute, or the Anti‑Kickback Statute, if one purpose of the arrangement is to encourage referrals. Our strategic partnership agreements do not involve the payment of any compensation. We believe our strategic partnership arrangements comply with the Anti‑Kickback Statute; however, other regulatory bodies or a court may interpret these agreements differently and there is a risk that we may be found non‑compliant and subject to government investigation, private and public lawsuits, civil penalties and criminal sanctions. See “Business—Government Regulation—Anti‑Kickback Statute and—State Laws Regarding Prohibition of Corporate Practice of Medicine and Fee Splitting Arrangements.”
33
Proposed changes to financial accounting standards could require our operating leases to be recognized on the balance sheet.
In addition to our significant level of indebtedness, we have considerable obligations relating to our current capital and operating leases. Proposed changes to financial accounting standards could require such leases to be recognized on our balance sheet. All of our existing facilities are subject to leases. All facilities under the MPT Agreements have initial terms of 15 years, with three five‑year renewal options. The terms of our non‑MPT facilities vary, but typically have initial terms of between five and seven years with three‑year to five‑year renewal options. As of December 31, 2014 and 2013, we had 54 and 25 leased facilities, 53 and 24 of which were classified as operating leases and one of which was classified as a capital lease, respectively. The accounting treatment of these leases is described in Note 11 to our consolidated financial statements. For the years ended December 31, 2014, 2013 and 2012, our operating lease expense was approximately $14.6 million, 4.5 million and $2.1 million, respectively.
In May 2013, the Financial Accounting Standards Board, or FASB, and the International Accounting Standards Board issued a revised joint discussion paper highlighting proposed changes to financial accounting standards for leases. The proposed changes would require that substantially all operating leases be recognized as assets and liabilities on our balance sheet, which would be a significant departure from the current standard, which classifies operating leases as off‑balance sheet transactions and accounts for only the current year operating lease expense in the statement of operations. The right to use the leased property would be capitalized as an asset and the expected lease payments over the life of the lease would be accounted for as a liability. The effective date, which has not been determined, could be as early as 2016 and may require retrospective adoption. While we have not quantified the impact this proposed standard would have on our financial statements, if our current operating leases are instead recognized on the balance sheet, it will result in a significant increase in the liabilities reflected on our balance sheet and in the interest expense and depreciation and amortization expense reflected in our statement of operations, while reducing the amount of rent expense. This could potentially decrease our reported net income.
A successful challenge by tax authorities to our treatment of certain physicians as independent contractors or the elimination of an existing safe harbor could materially increase our costs relating to these physicians.
As of December 31, 2014, through National Medical Professionals of Texas PLLC, National Medical Professionals of Colorado, P.C. and National Medical Professionals of Arizona LLC, affiliated professional limited liability companies owned and operated by our Executive Medical Director, we contracted with approximately 434 physicians and other medical staff as independent contractors to fulfill our contractual obligations to customers. Because these staff members are treated as independent contractors rather than as employees, National Medical Professionals of Texas PLLC, National Medical Professionals of Colorado, P.C. and National Medical Professionals of Arizona LLC do not (i) withhold federal or state income or other employment related taxes from their compensation, (ii) make federal or state unemployment tax or Federal Insurance Contributions Act payments with respect to them, (iii) provide workers compensation insurance with respect to them (except in states where they are required to do so for independent contractors), or (iv) allow them to participate in benefits and retirement programs available to employees. The contracts in place with these physicians obligate them to pay these taxes and other costs. Whether these physicians are properly classified as independent contractors generally depends upon the facts and circumstances of our relationship with them. If a challenge to our treatment of these physicians as independent contractors by federal or state authorities were successful and these physicians were treated as employees instead of independent contractors, we and/or National Medical Professionals of Texas PLLC, National Medical Professionals of Colorado, P.C. and National Medical Professionals of Arizona LLC could be liable for taxes, penalties and interest. In addition, there are currently, and have been in the past, proposals made to eliminate an existing safe harbor that would potentially protect us from the imposition of taxes in these circumstances, and similar proposals could be made in the future. If such a challenge were successful or if the safe harbor were eliminated, this could cause a material increase in our costs relating to these physicians and, therefore, a material adverse effect on our business, financial condition and results of operations.
We have experienced net losses and may not achieve or sustain profitability in the future.
We have experienced periods of net losses, including net losses of approximately $17.3 million and $3.0 million for the years ended December 31, 2014 and 2013, respectively. Our revenue may not grow and we may not
34
achieve or maintain profitability in the future. Even if we do achieve profitability, we may not sustain or increase profitability on a quarterly or annual basis in the future. Our ability to achieve profitability will be affected by the other risks and uncertainties described in this section and in “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” If we are not able to achieve, sustain or increase profitability, our business will be materially adversely affected and the price of our Class A common stock may decline.
We depend on our senior management and may not be able to retain those employees or recruit additional qualified personnel.
We depend on our senior management, including Thomas Hall, our Chairman and Chief Executive Officer, Timothy Fielding, our Chief Financial Officer, and Graham Cherrington, our President and Chief Operating Officer. We rely on the extensive experience of our management team across the healthcare, retail and hospitality sectors as well as extensive knowledge of healthcare operations and facility expansion. The loss of services of any of these or any other members of our senior management could adversely affect our business until a suitable replacement can be found. There may be a limited number of persons with the requisite skills to serve in these positions, and we cannot assure you that we would be able to identify or employ such qualified personnel on acceptable terms.
Our business depends on numerous complex information systems, and any failure to successfully maintain these systems or implement new systems could materially harm our operations.
We depend on complex, integrated information systems and standardized procedures for operational and financial information and our billing operations. We may not have the necessary resources to enhance existing information systems or implement new systems where necessary to handle our increased patient volume and changing needs. Furthermore, we may experience unanticipated delays, complications and expenses in implementing, integrating and operating our systems. Any interruptions in operations during periods of implementation would adversely affect our ability to properly allocate resources and process billing information in a timely manner, which could result in customer dissatisfaction and delayed cash flow. In addition, our technology systems, or a disruption in the operation of such systems, could be subject to physical or electronic break‑ins, and similar disruptions from unauthorized tampering. The failure to successfully implement and maintain operational, financial and billing information systems could have an adverse effect on our ability to obtain new business, retain existing business and maintain or increase our profit margins.
Our facilities currently located in Texas, Colorado and Arizona make us particularly sensitive to regulatory, economic and other conditions in those states.
Our facilities are currently located in Texas, Colorado and Arizona. If there were an adverse regulatory, economic or other development in any of these states, our patient volume could decline, our ability to operate our facilities under our existing business model could be impacted, or there could be other unanticipated adverse impacts on our business that could have a material adverse effect on our business, prospects, results of operations and financial condition. See “Risk Factors—Risks Related To Healthcare Regulation—Changes in the rates or methods of third‑party reimbursements, including due to political discord in the budgeting process outside our control, may adversely affect our revenue and operations.”
Our patient volumes are sensitive to seasonal fluctuations and patient concerns over outbreaks and other infectious diseases, which impact our results of operations.
Our patient volumes are sensitive to seasonal fluctuations in emergency activity. Typically, winter months see a higher occurrence of influenza, bronchitis, pneumonia and similar illnesses; however the timing and severity of these outbreaks can vary dramatically. Our patient volumes are influenced by fluctuations in the demand for our healthcare services and are sensitive to patient concerns over pandemic outbreaks such as Ebola and other infectious diseases, including patient concerns over the possibility of acquiring or communicating such diseases in a medical care environment. Additionally, as consumers shift towards high deductible insurance plans, they are responsible for a greater percentage of their bill, particularly in the early months of the year before other healthcare spending has occurred, which may lead to an increase in bad debt expense during that period. Our quarterly operating results may fluctuate significantly in the future depending on these and other factors.
35
Our ability to open and operate facilities may be impacted by weather conditions.
Our construction timelines may be delayed due to weather conditions. This may prevent us from opening facilities on time and increase our preopening expense burden. Additionally, extreme weather or natural disasters could also severely hinder our ability to operate existing facilities, delay capital improvements or cause us to close facilities. For example, in 2014, 38.5% of our patient service revenue was generated from facilities in the Houston market. If a hurricane, or other severe weather, were to affect this market, it could impact our ability to operate these facilities.
Disruptions in our disaster recovery systems or management continuity planning could limit our ability to operate our business effectively.
While we have disaster recovery systems and business continuity plans in place, any disruptions in our disaster recovery systems or the failure of these systems to operate as expected could, depending on the magnitude of the problem, adversely affect our operating results by limiting our capacity to effectively monitor and control our operations. In addition, in the event that a significant number of our management personnel were unavailable in the event of a disaster, our ability to effectively conduct business could be adversely affected.
We could be subject to lawsuits for which we are not fully reserved.
Physicians, hospitals, clinics and other participants in the healthcare industry have become subject to an increasing number of lawsuits alleging medical malpractice and related legal theories such as negligent hiring, supervision and credentialing. Some of these lawsuits may involve large claim amounts and substantial defense costs. We generally procure professional liability insurance coverage for our affiliated medical professionals and professional and corporate entities. As of December 31, 2014, our professional liability insurance coverage was $20 million. This insurance coverage may not cover all claims against us, and insurance coverage may not continue to be available at a cost satisfactory to us to allow for the maintenance of adequate levels of insurance. If one or more successful claims against us were not covered by or exceeded the coverage of our insurance, it could have a material adverse effect on our business, prospects, results of operations and financial condition. Moreover, in the normal course of our business, we are involved in lawsuits, claims, audits and investigations, including those arising out of our billing and marketing practices, employment disputes, contractual claims and other business disputes for which we may have no insurance coverage, and which are not subject to actuarial estimates. The outcome of these matters could have a material effect on our results of operations in the period when we identify the matter, and the ultimate outcome could have a material adverse effect on our financial position, results of operations, or cash flows.
The reserves we establish with respect to our losses not covered under our insurance programs are subject to inherent uncertainties.
In connection with our insurance programs, we establish reserves for losses and related expenses, which represent estimates involving actuarial and statistical projections, at a given point in time, of our expectations of the ultimate resolution and administration costs of losses we have incurred in respect of our liability risks. Insurance reserves are inherently subject to uncertainty. Our reserves are based on historical claims, demographic factors, industry trends, severity and exposure factors and other actuarial assumptions calculated by an independent actuary firm. The independent actuary firm performs studies of projected ultimate losses on an annual basis and provides quarterly updates to those projections. We use these actuarial estimates to determine appropriate reserves. Our reserves could be significantly affected if current and future occurrences differ from historical claim trends and expectations. While we monitor claims closely when we estimate reserves, the complexity of the claims and the wide range of potential outcomes may hamper timely adjustments to the assumptions we use in these estimates. Actual losses and related expenses may deviate, individually and in the aggregate, from the reserve estimates reflected in our consolidated financial statements. As of December 31, 2014 and 2013, we had a reserve of approximately $0.7 million and $0.7 million for incurred but unreported health claims, respectively. If we determine that our estimated reserves are inadequate, we will be required to increase reserves at the time of the determination, which would result in a reduction in our net income in the period in which the deficiency is determined.
36
Insurance coverage for some of our losses may be inadequate and may be subject to the credit risk of commercial insurance providers.
Our insurance coverage is through various third‑party insurers. To the extent we hold policies to cover certain groups of claims or rely on insurance coverage obtained by third parties to cover such claims, but either we or such third parties did not obtain sufficient insurance limits, did not buy an extended reporting period policy, where applicable, or the issuing insurance company is unable or unwilling to pay such claims, we may be responsible for those losses. Furthermore, for our losses that are insured or reinsured through commercial insurance providers, we are subject to the “credit risk” of those insurance companies. While we believe our commercial insurance providers are currently creditworthy, they may not remain so in the future.
We may not be able to adequately protect our intellectual property and other proprietary rights that are material to our business, or to defend successfully against intellectual property infringement claims by third parties.
Our ability to compete effectively depends in part upon our intellectual property rights, including but not limited to our trademarks. Our use of contractual provisions, confidentiality procedures and agreements, and trademark, copyright, unfair competition, trade secret and other laws to protect our intellectual property rights may not be adequate. Litigation may be necessary to enforce our intellectual property rights, or to defend against claims by third parties that the conduct of our businesses or our use of intellectual property infringes upon such third party’s intellectual property rights. Any intellectual property litigation or claims brought against us, whether or not meritorious, could result in substantial costs and diversion of our resources, and there can be no assurances that favorable final outcomes will be obtained in all cases. The terms of any settlement or judgment may require us to pay substantial amounts to the other party or cease exercising our rights in such intellectual property, including ceasing the use of certain trademarks used by us to distinguish our services from those of others or ceasing the exercise of our rights in copyrightable works. In addition, we may have to seek a license to continue practices found to be in violation of a third party’s rights, which may not be available on reasonable terms, or at all. Our business, financial condition or results of operations could be adversely affected as a result.
Risks Related to Healthcare Regulation
We conduct business in a heavily regulated industry and, if we fail to comply with these laws and government regulations, we could incur penalties or be required to make significant changes to our operations.
The healthcare industry is heavily regulated and closely scrutinized by federal, state and local governments. Comprehensive statutes and regulations govern the manner in which we provide and bill for services, our contractual relationships with our physicians, vendors and customers, our marketing activities and other aspects of our operations. Failure to comply with these laws can result in civil and criminal penalties such as fines, damages, overpayment recoupment loss of enrollment status and exclusion from government healthcare programs. The risk of our being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by regulatory authorities or the courts, and their provisions are sometimes open to multiple interpretations. Any action against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our managements’ attention from the operation of our business.
Our physicians, nurses and technicians, as well as the third‑party payors with which we have a relationship are also subject to ethical guidelines and operating standards of professional and trade associations and private accreditation agencies. Compliance with these guidelines and standards is often required by our contracts with our customers or to maintain our reputation.
The laws, regulations and standards governing the provision of healthcare services may change significantly in the future. New or changed healthcare laws, regulations or standards may materially and adversely affect our business. In addition, a review of our business by judicial, law enforcement, regulatory or accreditation authorities could result in a determination that could adversely affect our operations.
37
Our current facilities are subject to state statutes and regulations that govern our operations, and the failure to comply with these laws and regulations can result in civil or criminal sanctions.
Our operating freestanding emergency room facilities in Texas and Colorado, and our hospital in Arizona, are subject to many laws and regulations, particularly at the state and local government levels. These laws and regulations require our freestanding emergency rooms and our hospital in Arizona to meet various licensing, certification and other requirements, including those relating to:
|
· |
building and construction codes, fire codes and life safety standards for our facilities; |
|
· |
the qualifications of medical and support personnel in our facilities; |
|
· |
the adequacy of medical care, equipment, personnel, operating policies and procedures; |
|
· |
required governance boards and organizational plans to oversee the facility; |
|
· |
required services and treatment lines, particularly in the hospital setting; |
|
· |
facility licensure; |
|
· |
maintenance and protection of medical records; |
|
· |
environmental protection, health and safety, including the handling and disposal of medical waste; |
|
· |
development of infection control and quality improvement policies and procedures; |
|
· |
required operating hours; |
|
· |
requirements to treat our emergent patients regardless of ability to pay; |
|
· |
restrictions on advertising and billing with respect to patients to make clear the facility is operating as an emergency room; and |
|
· |
patient transfer agreements and patient transfer plans to care for patients of an acuity beyond the capability of the facility. |
We may be subject to regulatory fines, penalties or other sanctions if our operations or facilities are found to not comply with applicable laws and regulations. Further, these laws and regulations are subject to change. New regulation of such facilities is also possible, which could force us to change our operational approach or lead to a finding by regulators that our facilities do not meet legal requirements.
State law regulation of construction or expansion of emergency rooms could prevent us from developing additional freestanding emergency rooms or other facilities.
Thirty‑six states have certificate of need programs that require some level of prior approval for the construction of a new facility, acquisition or expansion of an existing facility, or the addition of new services for various healthcare facilities. One of the most common categories of healthcare services reviewed under certificate of need laws is hospital services, which may include the emergency services we provide at our freestanding emergency rooms. While the states where our facilities are currently operational (Texas, Colorado and Arizona) do not require a certificate of need, other states where we seek to expand our operations may require certificates of need under circumstances not currently applicable to our facilities. If these states require such a certificate, they may examine any proposed facility for the cost of adding additional services compared with other treatment models, the impact of our proposed facility on existing providers, the need for additional or expanded healthcare services in the relevant market and other analysis that may
38
require changes to our business model. In such case, we may not be able to obtain the necessary certificates of need or other required approvals to meet our expansion plans. In addition, if we seek to acquire other facilities, in certificate of need states, we may be required to obtain a certificate of need before the acquisition, before we replace the equipment or before we expand the acquired facility. If we are unable to obtain such approvals, we may not be able to move forward with a planned acquisition, expand the acquired facility, add additional services to the facility or replace its equipment.
In addition, there is a significant risk of additional state legislation restricting our ability to obtain licensure for new facilities. Only a few states, including Texas and Colorado, currently license the freestanding emergency room facilities that we operate. The lack of a specific licensure process for freestanding emergency facilities may lead state legislators or regulators to aggressively regulate the growth of such facilities, potentially seeking to treat our freestanding emergency room facilities in a manner similar to hospitals. In other states, the growing number of freestanding emergency departments may lead state legislatures to pass legislation requiring us to substantially change our operations or cease our operations in that state entirely. Any such licensure challenges could materially impact our prospects and growth strategy.
Alternatively, without current state licensure of freestanding emergency room facilities, we may need to develop new models or form partnerships with existing facilities to expand to new states. Such challenges were one reason we entered into a joint venture with Dignity Health announced in October 2014. The new partnership has started with Dignity Health Arizona General Hospital, which is licensed as a general hospital by the Arizona Department of Health Services. These alternative models or partnerships may not be as profitable as our current freestanding facilities, and such development may materially impact our prospects or our growth strategy.
We are subject to comprehensive and complex laws and rules that govern the manner in which we bill and are paid for our services by third‑party payors, and the failure to comply with these rules, or allegations that we have failed to do so, can result in civil or criminal sanctions, including exclusion from federal and state healthcare programs.
Substantially all of our services are paid for by third‑party commercial payors. These third‑party payors typically have differing and complex billing and documentation requirements that we must meet in order to receive payment for our services. Reimbursement is typically conditioned on our providing the correct procedure and diagnostic codes and properly documenting the services themselves, including the level of service provided, the medical necessity for the services, the site of service, and the identity of the physician, nurse or technician who provided the service.
We must also comply with numerous other state and federal laws applicable to our documentation and the claims we submit for payment, including but not limited to (i) “coordination of benefits” rules that dictate which payor we must bill first when a patient has potential coverage from multiple payors, (ii) requirements that we obtain the signature of the patient or patient representative, or, in certain cases, alternative documentation, prior to submitting a claim, (iii) requirements that we make repayment within a specified period of time to any payor which pays us more than the amount to which we are entitled, (iv) “reassignment” rules governing our ability to bill and collect professional fees on behalf of our physicians, (v) requirements that our electronic claims for payment be submitted using certain standardized transaction codes and formats and (vi) laws requiring us to handle all health and financial information of our patients in a manner that complies with specified security and privacy standards.
Private third‑party payors carefully audit and monitor our compliance with these and other applicable rules. Our failure to comply with the billing and other rules applicable to us could result in non‑payment for services rendered or refunds of amounts previously paid for such services.
Additionally, on January 16, 2009, the United States Department of Health and Human Services, or HHS, released the final rule mandating that everyone covered by the Administrative Simplification Provisions of the Health Insurance Portability and Accountability Act of 1996, or HIPAA, which includes our facilities must implement the International Classification of Diseases (10th Edition), or ICD‑10, for medical coding on October 1, 2013. HHS subsequently postponed the deadline for implementation of ICD‑10 codes until October 1, 2014, which Congress extended until October 1, 2015, as part of the Protecting Access to Medicare Act of 2014. ICD‑10 codes contain significantly more information than the ICD‑9 codes currently used for medical coding and will require covered entities to code with much greater detail and specificity than ICD‑9 codes. However, the transition to ICD‑10 does not affect
39
Current Procedural Terminology coding for physician services or outpatient procedures. We may incur additional costs for computer system updates, training, and other resources required to implement these changes. We may also incur additional costs from further delays in training staff on both the ICD-9 and ICD-10 codes and maintaining software that can operate under both systems through the inherent uncertainty from ongoing delays it ICD-10 implementation.
If our operations are found to be in violation of these or any of the other laws which govern our activities, any resulting penalties, damages, fines or other sanctions could adversely affect our ability to operate our business and our financial results.
Changes in the rates or methods of third‑party reimbursements, including due to political discord in the budgeting process outside our control, may adversely affect our revenue and operations.
We derive a majority of our revenue from direct billings to patients and third‑party payors. As a result, any changes in the rates or methods of reimbursement for the services we provide could have a significant adverse impact on our revenue and financial results. Reimbursement rates can vary depending on whether the facility provider is an in‑network or out‑of‑network provider. Each of our facilities will be out‑of‑network for some patients. Some facilities, as an out‑of‑network provider, may have issues billing appropriately with certain third‑party payors. In some states, we may rely on state law that requires reimbursement of our services at in‑network rates. A change in state law where the majority of our facilities are operated could have a material effect on our revenue or force us to negotiate lower rates with third‑party payors who may or may not be willing to enter into agreements with us. In the last legislative session, members of the Colorado legislature proposed but did not pass a bill which would have significantly reduced reimbursement rates for our facilities within the state by making it a violation of the state insurance code to bill insurers or their beneficiaries for facility fees. We cannot predict the outcome of any legislation and cannot assure you that the Colorado legislature or another state where we operate would not pass another law that damages our ability to operate under our current model.
Additionally, PPACA could ultimately result in substantial changes in coverage and reimbursement, including changes in coverage or amounts paid by private payors, which could have an adverse impact on our revenue from those sources.
Recent healthcare reform legislation and other changes in the healthcare industry and in healthcare spending could adversely affect our business model, financial condition or results of operations.
Our results of operations and financial condition could be affected by changes in healthcare spending and policy. The healthcare industry is subject to changing political, regulatory and other influences. In March 2010, the President signed PPACA into law, which made major changes in how healthcare is delivered and reimbursed, and increased access to health insurance benefits to the uninsured and underinsured population of the United States. However, certain provisions in PPACA, such as the establishment of the Independent Payment Advisory Board, could cause us to face negative reimbursement rates that would adversely affect our business model.
PPACA may also adversely affect payors by increasing their medical cost trends, which could have an effect on the industry and potentially impact our business and revenue as payors seek to offset these increases by reducing costs in other areas, although the extent of this impact is currently unknown.
Because of the continued uncertainty about the implementation of PPACA, including litigation pending before the U.S. Supreme Court, we cannot quantify or predict with any certainty the likely impact of PPACA on our business model, prospects, financial condition or results of operations. We also anticipate that Congress and state legislatures may continue to review and assess alternative healthcare delivery and payment systems and may in the future propose and adopt legislation effecting additional fundamental changes in the healthcare delivery system. We cannot assure you as to the ultimate content, timing, or effect of changes, nor is it possible at this time to estimate the impact of potential legislation.
40
If current or future laws or regulations force us to restructure our arrangements with physicians, professional corporations and hospitals, we may incur additional costs, lose contracts and suffer a reduction in net revenue under existing contracts, and we may need to refinance our debt or obtain debt holder consent.
A number of laws bear on our relationships with our physicians. State authorities in some jurisdictions could find that our contractual relationships with our physicians violate laws prohibiting the corporate practice of medicine or fee‑splitting. These laws are generally intended to prevent unlicensed persons or entities from interfering with or inappropriately influencing the physician’s professional judgment, but they may also prevent the sharing of professional services income with non‑professional or business interests. Approximately 30 states have some form of corporate practice of medicine restrictions and as we continue to expand into new markets, our current business model may implicate these restrictions. The states in which we currently operate (Colorado, Texas and Arizona) have some level of corporate practice of medicine restrictions. In each of these states, a business corporation may not employ physicians or provide medical services. While we believe we are currently in material compliance with applicable state laws relating to the corporate practice of medicine and fee‑splitting, regulatory authorities or other parties, including our affiliated physicians, may assert that, despite these arrangements, we are impermissibly engaged in the practice of medicine or that our contractual arrangements with affiliated physician groups constitute unlawful fee‑splitting. In this event, we could be subject to adverse judicial or administrative interpretations, to civil or criminal penalties, our contracts could be found legally invalid and unenforceable or we could be required to restructure our contractual arrangements with our affiliated physicians and physician groups.
Our physician contracts include contracts with individual physicians and with physicians organized as separate legal professional entities (e.g., professional medical corporations). Antitrust laws may deem each such physician/entity to be separate, both from us and from each other, and, accordingly, each such physician/practice would be subject to a wide range of laws that prohibit anti‑competitive conduct between or among separate legal entities or individuals. A review or action by regulatory authorities or the courts could force us to terminate or modify our contractual relationships with physicians and affiliated medical groups, or to revise them in a manner that could be materially adverse to our business.
Various licensing and certification laws, regulations and standards apply to us, our affiliated physicians and our relationships with our affiliated physicians. Failure to comply with these laws and regulations could result in our services being found to be non‑reimbursable or prior payments being subject to recoupment, and can give rise to civil or criminal penalties, including loss of licensure for the facility. We routinely take actions we believe are necessary to retain or obtain all requisite licensure and operating authorities, including all building codes, state licensure rules and all state‑mandated services. While we have made reasonable efforts to substantially comply with federal, state and local licensing and certification laws and regulations and standards as we interpret them, agencies that administer these programs may find that we have failed to comply in some material respects. Further, any expansion in new states or participation in the Medicare or Medicaid programs may add additional licensing and certification requirements with which we may not be in full compliance today.
Adverse judicial or administrative interpretations could result in a finding that we are not in compliance with one or more of these laws and rules that affect our relationships with our physicians.
These laws and rules, and their interpretations, may also change in the future. Any adverse interpretations or changes could force us to restructure our relationships with physicians, professional corporations or our hospital systems, or to restructure our operations. This could cause our operating costs to increase significantly. A restructuring could also result in a loss of contracts or a reduction in revenue under existing contracts. Moreover, if we are required to modify our structure and organization to comply with these laws and rules, our financing agreements may prohibit such modifications and require us to obtain the consent of the holders of such debt or require the refinancing of such debt.
41
We are subject to the data privacy, security and breach notification requirements of HIPAA and other data privacy and security laws, and the failure to comply with these rules, or allegations that we have failed to do so, can result in civil or criminal sanctions.
HIPAA required HHS to adopt standards to protect the privacy and security of certain health‑related information. The HIPAA privacy regulations contain detailed requirements concerning the use and disclosure of individually identifiable health information and the grant of certain rights to patients with respect to such information by “covered entities.” As a provider of healthcare who conducts certain electronic transactions, each of our facilities is considered a covered entity under HIPAA. We have taken actions to comply with the HIPAA privacy regulations and believe that we are in substantial compliance with those regulations. These actions include the creation and implementation of policies and procedures, staff training, execution of HIPAA‑compliant contractual arrangements with certain service providers and various other measures. Ongoing implementation and oversight of these measures involves significant time, effort and expense.
In addition to the privacy requirements, HIPAA covered entities must implement certain administrative, physical, and technical security standards to protect the integrity, confidentiality and availability of certain electronic health‑related information received, maintained, or transmitted by covered entities or their business associates. We have taken actions in an effort to be in compliance with these security regulations and believe that we are in substantial compliance, however, a security incident that bypasses our information security systems causing an information security breach, loss of protected health information or other data subject to privacy laws or a material disruption of our operational systems could result in a material adverse impact on our business, along with fines. Ongoing implementation and oversight of these security measures involves significant time, effort and expense.
The Health Information Technology for Economic and Clinical Health Act, or HITECH, as implemented in part by an omnibus final rule published in the Federal Register on January 25, 2013, further requires that patients be notified of any unauthorized acquisition, access, use, or disclosure of their unsecured protected health information, or PHI, that compromises the privacy or security of such information. HHS has established the presumption that all unauthorized uses or disclosures of unsecured protected health information constitute breaches unless the covered entity or business associate establishes that there is a low probability the information has been compromised. HITECH and implementing regulations specify that such notifications must be made without unreasonable delay and in no case later than 60 calendar days after discovery of the breach. If a breach affects 500 patients or more, it must be reported immediately to HHS, which will post the name of the breaching entity on its public website. Breaches affecting 500 patients or more in the same state or jurisdiction must also be reported to the local media. If a breach involves fewer than 500 people, the covered entity must record it in a log and notify HHS of such breaches at least annually. These breach notification requirements apply not only to unauthorized disclosures of unsecured PHI to outside third parties, but also to unauthorized internal access to or use of such PHI.
HITECH significantly expanded the scope of the privacy and security requirements under HIPAA and increased penalties for violations. Currently, violations of the HIPAA privacy, security and breach notification standards may result in civil penalties ranging from $100 to $50,000 per violation, subject to a cap of $1.5 million in the aggregate for violations of the same standard in a single calendar year. The amount of penalty that may be assessed depends, in part, upon the culpability of the applicable covered entity or business associate in committing the violation. Some penalties for certain violations that were not due to “willful neglect” may be waived by the Secretary of HHS in whole or in part, to the extent that the payment of the penalty would be excessive relative to the violation. HITECH also authorized state attorneys general to file suit on behalf of residents of their states. Applicable courts may able to award damages, costs and attorneys’ fees related to violations of HIPAA in such cases. HITECH also mandates that the Secretary of HHS conduct periodic compliance audits of a cross‑section of HIPAA covered entities and business associates. Every covered entity and business associate is subject to being audited, regardless of the entity’s compliance record.
States may impose more protective privacy restrictions in laws related to health information and may afford individuals a private right of action with respect to the violation of such laws. Both state and federal laws are subject to modification or enhancement of privacy protection at any time. We are subject to any federal or state privacy-related laws that are more restrictive than the privacy regulations issued under HIPAA. These statutes vary and could impose additional requirements on us and more severe penalties for disclosures of health information. Texas, Colorado and Arizona each have privacy regulations that impose requirements and restrictions in addition to those under HIPAA. If we
42
fail to comply with HIPAA or similar state laws, including laws addressing data confidentiality, security or breach notification, we could incur substantial monetary penalties and our reputation.
In addition, states may also impose restrictions related to the confidentiality of personal information that is not considered “protected health information” under HIPAA. Such information may include certain identifying information and financial information of our patients. Theses state laws may impose additional notification requirements in the event of a breach of such personal information. Failure to comply with such data confidentiality, security and breach notification laws may result in substantial monetary penalties.
In January 2015, we submitted an enrollment application for our Arizona general hospital to participate in the federal Medicare program and the Arizona Medicaid program. As a result of participating in these programs, we will be required to comply with a number of additional federal and state regulatory schemes.
While the majority of our facilities do not currently participate as providers in the federal Medicare, Medicaid or Tricare programs, our hospital in Arizona recently submitted enrollment applications to participate in these programs. Our Arizona hospital received confirmation of its enrollment in Medicare or Medicaid as of January 30, 2015. By enrolling in these programs, we will face certain federal and state regulatory schemes for the first time. For example, the federal physician self‑referral law (or the Stark Law) and the Anti‑Kickback Statute apply to the provision of healthcare services and supplies to Medicare and Medicaid patients. While we have sought to organize our operations—both at our freestanding emergency rooms that do not participate in these programs and at our newly-opened hospital in Arizona—to comply with both the Stark Law and Anti‑Kickback Statute, we cannot assure you that our enrollment in these government programs will not require some reorganization of our existing relationships with our physicians, referral sources and other partners, or that we will not be subject to government investigation for failure to comply with these laws.
By not participating in these programs at our freestanding emergency rooms, many potential consumers of our services in our target markets may choose to receive services from other providers. To participate in these programs at our freestanding emergency room facilities we would need to significantly modify our current operational model. Such programs, particularly Medicare, have substantial statutory and regulatory requirements to participate. For example, the Medicare program does not currently allow the participation of independent freestanding emergency room facilities. To participate as a Medicare provider in states where we operate only freestanding emergency rooms, we would need to open a central‑hospital facility that owns and operates the satellite freestanding emergency rooms as “provider‑based facilities” under a unified organization. Under Medicare, establishing such a central‑hospital facility with satellite freestanding emergency rooms structure requires a hospital to be “primarily engaged in the provision of services to inpatients.” This requirement could limit our ability to grow by restricting the number of additional freestanding facilities associated with each Medicare‑certified hospital to ensure compliance with the inpatient service requirements. This and other Medicare conditions of participation could be costly and limit our expansion plans. Our current accreditation from The Joint Commission as freestanding emergency room facilities does not guarantee that our facilities would meet The Joint Commission hospital standards, Medicare conditions of participation or Medicaid requirements for hospitals.
Furthermore, the Medicare and Medicaid programs are particularly susceptible to statutory and regulatory changes, retroactive and prospective rate adjustments, spending freezes, federal and state funding reductions and administrative rulings and interpretations concerning, without limitation, patient eligibility requirements, funding levels and the method of calculating payments or reimbursements, all of which we now face for the first time at our Arizona hospital. PPACA reduces annual payment updates for certain providers, including hospitals, and reduces Medicare payments for certain procedures, such as readmissions and hospital‑acquired infections. Furthermore, the Budget Control Act of 2011 requires automatic spending reductions for each fiscal year through 2021. We are unable to predict how these spending reductions will be structured, what other deficit reduction initiatives may be adopted by the U.S. Congress or how these changes will impact our Arizona general hospital or would impact our freestanding emergency room facilities if we enrolled those facilities in the Medicare program.
43
Enrolling as a Medicaid provider also subjects a portion of our revenue to fluctuations and limitations in state budgets. Many state legislatures, including Arizona, Colorado and Texas, are required by their state constitution or laws to balance the state’s budgets annually and the Medicaid program is often the largest budget expenditure for many states. In recent years, as economic forces put pressure on state budgets, many states decreased spending or decreased spending growth for their Medicaid programs. States also continually review and revise their Medicaid programs and request waivers from the Centers for Medicare & Medicaid Services from otherwise national requirements, which could result in certain payments being reduced or eliminated. Such spending changes could have a material impact on the performance of our Arizona general hospital and our freestanding emergency rooms, if such facilities participate in state Medicaid programs.
While our hospital in Arizona operates as a licensed general hospital under Arizona law and has received Joint Commission accreditation, until we receive our Medicare and Medicaid provider agreements we cannot guarantee that this hospital will participate in either program. Such an outcome could have a negative effect on the profitability of this facility since it was designed with the intent for the hospital to be Medicare-certified and participate in government programs.
State regulation of healthcare marketing in our current or target markets could impact our marketing efforts, which may in turn hamper our ability to increase patient volume, increase same store sales, or build awareness of our care model, particularly if we choose to participate in Medicaid in the future.
Some states regulate healthcare providers’ marketing efforts to persons enrolled in governmental healthcare programs, such as Medicaid and the Children’s Health Insurance Program (“CHIP”). These marketing restrictions may impact our future marketing efforts. In particular, some state laws prohibit direct and/or indirect marketing and outreach efforts to enrollees of state-funded governmental healthcare programs. Some states restrict the direct marketing activities of providers by prohibiting providers from engaging in unsolicited personal contact or promotions of their practices to enrollees. In states that restrict providers’ marketing efforts directly, regulations sometimes prohibit provider marketing materials from containing any false, misleading, or inaccurate statements relating to the providers’ services, benefits or costs. A number of states also prohibit provider marketing materials from containing any state-owned logos or making any statement of endorsement by federal or state governmental entities.
Other states, including Arizona, restrict providers’ marketing efforts indirectly by regulating the activities of health plans that contract with state-funded governmental healthcare programs. Some states require state-contracted health plans to report their marketing costs to state regulatory agencies and submit all marketing materials for prior regulatory approval. We are not classified as a health plan, but we may contract with state-contracted health plans as a subcontracted provider subject to such restrictions in the future. In such case, some states’ state-contracted health plans may restrict our marketing activities, in order to ensure the health plans’ compliance with state-funded governmental healthcare programs’ marketing restrictions. For example, a number of state-contracted health plans require their subcontracted providers to submit all marketing materials to the health plan. If the health plan deems it necessary, the health plan may then submit the subcontracted providers’ marketing materials to the appropriate state regulatory agency. To our knowledge, we are currently in compliance with state healthcare marketing laws in the states in which we operate. However, these restrictions are rapidly evolving and we may be required to change our practices in the future. This risk is more pronounced in Arizona where we are enrolling our hospital in the state’s Medicaid program, and such risks may increase in other states if we choose to enroll our facilities in those state’s Medicaid programs.
Our facilities, billing practices, relationships with healthcare providers and third parties, and our marketing practices are (at least in part) subject to the Anti‑Kickback Statute, Stark Law, False Claims Act and similar state laws.
In enrolling in the federal Medicare, Medicaid, or Tricare programs, our Arizona hospital (and any other of our facilities that enroll in such programs in the future) is directly subject to additional federal laws, including, but not limited to, those discussed below.
44
Anti-Kickback Statute
Provisions in Title XI of the Social Security Act, commonly referred to as the Anti‑Kickback Statute, prohibit the knowing and willful offer, payment, solicitation or receipt of remuneration, directly or indirectly, in return for the referral of patients or arranging for the referral of patients, or in return for the recommendation, arrangement, purchase, lease or order of items or services that are covered, in whole or in part, by a federal healthcare program such as Medicare or Medicaid. The definition of “remuneration” has been broadly interpreted to include anything of value such as gifts, discounts, rebates, waiver of payments or providing anything at less than its fair market value. Many states such as Texas and Arizona have adopted similar prohibitions against kickbacks and other practices that are intended to influence the purchase, lease or ordering of healthcare items and services reimbursed by a governmental health program or state Medicaid. Some of these state prohibitions apply to remuneration for referrals of healthcare items or services reimbursed by any payor, including private payors.
Even at facilities where we do not currently accept Medicare, Medicaid or Tricare reimbursement, we could still be subject to the Anti‑Kickback Statute to the extent we have referral or financial relationships with other parties that do participate in those programs.
Violations of the Anti‑Kickback Statute can result in exclusion from Medicare, Medicaid or other governmental programs as well as civil and criminal penalties, such as $25,000 per violation and up to three times the remuneration involved. We may be required to enter into settlement agreements with the government to avoid such sanctions. Typically, such settlement agreements require substantial payments to the government in exchange for the government to release its claims, and may also require us to enter into a Corporate Integrity Agreement, or CIA. The obligations contained in such CIA could have a material adverse effect on our business, financial condition and results of operations.
Stark Law
The Stark Law prohibits a physician from referring a patient to a healthcare provider for certain designated health services reimbursable by Medicare if the physician (or close family members) has a financial relationship with that provider, including an investment interest, a loan or debt relationship or a compensation relationship. The designated health services covered by the law include, among others, hospital inpatient, hospital outpatient, laboratory and imaging services. Some states, including Texas and Colorado, have self‑referral laws similar to Stark Law for Medicaid claims (and commercial claims). States such as Arizona and Texas also require physicians to disclose to their patients that they have a direct financial relationship in a separate diagnostic or treatment agency or in services and goods being prescribed.
Violation of the Stark Law may result in prohibition of payment for services rendered, a refund of any Medicare payments for services that resulted from an unlawful referral, $15,000 civil monetary penalties for specified infractions, criminal penalties, exclusion from Medicare and Medicaid programs, and potential false claims liability. The repayment provisions in the Stark Law are not dependent on the parties having an improper intent; rather, the Stark Law is a strict liability statute and any violation is subject to repayment of all tainted referrals. If physician self‑referral laws are interpreted differently or if other legislative restrictions are issued, we could incur significant sanctions and loss of revenues, or we could have to change our arrangements and operations in a way that could have a material adverse effect on our business, prospects, results of operations and financial condition.
False Claims Act
The federal government is authorized to impose criminal, civil and administrative penalties on any person or entity that files a false claim for payment from the Medicare or Medicaid programs. False claims filed with private insurers can also lead to criminal and civil penalties under state law. While the criminal statutes are generally reserved for instances of fraudulent intent, the government applies criminal, civil and administrative penalty statutes to a range of circumstances, including coding errors, billing for services not provided, submitting false cost reports, submitting claims resulting from arrangements prohibited by the Stark Law or the Anti‑Kickback Statute, billing for services not rendered in compliance with complex Medicare and Medicaid regulations and guidance, misrepresenting services rendered
45
(e.g., miscoding, upcoding, etc.) and application for duplicate reimbursement. Additionally, the federal government has taken the position that claiming reimbursement for unnecessary or substandard services violates these statutes if the claimant should have known that the services were unnecessary or substandard. Criminal penalties also are available in the case of claims filed with private insurers if the federal government shows that the claims constitute mail fraud or wire fraud or violate a number of federal criminal healthcare fraud statutes.
Under the “qui tam” provisions of the Federal False Claims Act, private parties (“relators” or “whistleblowers”) may bring actions against providers on behalf of the federal government. Such private parties are entitled to share in any amounts recovered by the government through trial or settlement. Qui tam cases are sealed by the court at the time of filing. The only parties privy to the information contained in the complaint are the relator, the federal government and the presiding court. In recent years, the number of suits brought by private individuals has increased dramatically.
Both direct enforcement activity by the government and whistleblower lawsuits under the Federal False Claims Act have increased significantly in recent years and have increased the risk of healthcare companies like us having to defend a false claims action, repay claims paid by the government, pay fines or be excluded from the Medicare and Medicaid programs. In addition, under PPACA, providers must report and refund the overpayments before the later of 60 days after the overpayment was identified or the date any corresponding cost report is due, if applicable. Any overpayment that is retained after this deadline is considered an obligation subject to an action under the Federal False Claims Act.
A number of states have enacted false claims acts that are applicable to claims submitted to state Medicaid programs and are similar to the Federal False Claims Act. Section 6031 of the Deficit Reduction Act of 2005 as amended, or DRA, amended federal law to encourage these types of state laws, along with a corresponding increase in state initiated false claims enforcement efforts. Currently, most states and the District of Columbia have some form of state false claims act. As of January 16, 2015, the OIG has reviewed 28 of these laws and determined that 18 of these laws satisfy the DRA standards, including Texas, Arizona and Colorado. Several states were given a grace period to amend their false claims acts to come into compliance with recent amendments to the Federal False Claims Act. We anticipate this figure will continue to increase.
Recovery Audit Program of the Centers for Medicare & Medicaid Services
We believe that the Centers for Medicare & Medicaid Services will continue to operate its Recovery Audit Program, which could randomly audit our Arizona hospital and any other facilities that enroll in the Medicare, Medicaid, or Tricare programs in the future. The Recovery Audit Program’s mission is to identify and correct Medicare improper payments through the efficient detection and collection of overpayments made on claims of healthcare services provided to Medicare beneficiaries, and the identification of underpayments to providers so that the Centers for Medicare & Medicaid Services can implement actions that will prevent future improper payments. Federal law also requires states to create Recovery Audit Programs for their state Medicaid programs. Enrollment in Arizona’s and other states’ Medicaid programs may mean additional state scrutiny of potential overpayments.
The Emergency Medical Treatment and Labor Act
Our participation in Medicare, Medicaid and Tricare at our Arizona hospital subjects the hospital to certain requirements of the Emergency Medical Treatment and Labor Act, or EMTALA. Under EMTALA, all participating hospitals with emergency departments are required to provide an appropriate medical screening examination upon request by any individual to determine whether an emergency medical condition exists or if the patient is in active labor. If the hospital determines that there is an emergency medical condition, then the hospital must stabilize the individual. Violations of these EMTALA obligations (if applicable) could subject us to civil penalties. Furthermore, individuals have a private right of enforcement if they suffer harm that is a direct result of a violation of EMTALA.
Our facilities are subject to state requirements similar to those of EMTALA, regardless of whether our facilities are enrolled in Medicare, Medicaid or Tricare. For example, in Texas, as freestanding emergency room facilities, we are required by state law to provide appropriate screening and examinations to individuals to determine if an emergency
46
medical condition exists. The facilities are also required to provide the necessary stabilizing treatment without assessing the individual’s ability to pay. Violations of these requirements could lead to administrative and criminal penalties.
Changes in our ownership structure and operations may require us to comply with numerous notification and reapplication requirements in order to maintain our licenses, certifications or other authorizations to operate, and failure to do so, or an allegation that we have failed to do so, could result in payment delays, forfeiture of payment or civil and criminal penalties.
We and our contracted physicians are subject to various federal, state and local licensing and certification laws with which we must comply in order to maintain authorization to provide, or receive payment for, our services. Compliance with these requirements is complicated by the fact that they differ from jurisdiction to jurisdiction, and in some cases are not uniformly applied or interpreted even within the same jurisdiction. Failure to comply with these requirements can lead not only to delays in payment and refund requests, but in extreme cases can give rise to civil or criminal penalties.
In certain jurisdictions, changes in our ownership structure require pre‑ or post‑notification to state governmental licensing and certification agencies, or agencies with which we have contracts. Relevant laws in some jurisdictions may also require re‑application or re‑enrollment and approval to maintain or renew our licensure, certification, contracts or other operating authority. Our changes in corporate structure and ownership involving changes in our beneficial ownership required us in some instances to give notice, re‑enroll or make other applications for authority to continue operating in various jurisdictions or to begin to receive payment from government payment programs. The extent of such notices and filings may vary in each jurisdiction in which we operate, although those regulatory entities requiring notification generally request factual information regarding the new corporate structure and new ownership composition of the operating entities that hold the applicable licensing and certification.
While we have made consistent efforts to substantially comply with these requirements, we cannot assure you that the agencies that administer these programs or have awarded us contracts will not find that we have failed to comply in some material respects. A finding of non‑compliance and any resulting payment delays, refund demands or other sanctions could have a material adverse effect on our business, financial condition or results of operations.
Federal law does not mandate coverage or reimbursement amounts by private payors for services provided in our facilities.
PPACA requires all non‑grandfathered insurance plans covering emergency services to cover treatment of a “prudent layperson” who reasonably believes his or her health is in jeopardy at emergency departments of a hospital without regard to whether that hospital is in‑network. PPACA further prohibits insurance providers from requiring pre‑approval authorization or other administrative limits on such services in out‑of‑network hospitals, and has certain minimum payment provisions for emergency care in a hospital emergency department that meet this prudent layperson standard. Our Arizona hospital should be eligible to receive certain payment protections from these provisions for services provided in the hospital’s emergency room. There is no guaranty that these payment protections will continue to be available to us (or any provider) in the future.
These provisions do not currently apply to our freestanding emergency room facilities since these facilities are not hospital emergency departments. Without PPACA’s protections, there is risk that insurance providers may respond to the costs of these new federal mandates by reducing payment to non‑covered freestanding emergency departments, such as our operating facilities. Further, many states previously enacted prudent layperson standards that may benefit our facilities. For instance, Texas requires insurers to reimburse services that meet its prudent layperson standard in all out‑of‑network emergency rooms, including our freestanding emergency room facilities. With the federal changes, states may be less willing to protect non‑hospital emergency room services or to maintain their own prudent layperson standard laws. We cannot guarantee that such changes caused by PPACA will not disadvantage our facilities in a way that materially changes our revenue or operations.
47
Risks Related to Our Organizational Structure
We are an “emerging growth company” as defined in the Securities Act and we cannot be certain if the reduced disclosure requirements applicable to emerging growth companies will make our Class A common stock less attractive to investors.
We are an “emerging growth company” as defined in Section 2(a) of the Securities Act, as modified by the JOBS Act, and we may take advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not “emerging growth companies” including, among other things, not being required to comply with the auditor attestation requirements of Section 404, reduced financial disclosure requirements, which include being permitted to provide only two years of audited financial statements, with correspondingly reduced “Management’s Discussion and Analysis of Financial Condition and Results of Operations” disclosure, reduced disclosure obligations regarding executive compensation and exemptions from the requirements of holding a non‑binding stockholder advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. As a result, our stockholders may not have access to certain information that they may deem important. In addition, Section 107 of the JOBS Act also provides that an emerging growth company can take advantage of the extended transition period provided in Section 7(a)(2) of the Securities Act for complying with new or revised accounting standards. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, will be subject to the same new or revised accounting standards as other public companies that are not emerging growth companies.
We could be an emerging growth company for up to five years following June 24, 2014, the date of our initial public offering, although circumstances could cause us to lose that status earlier, including if our total annual gross revenue exceeds $1.0 billion, if we issue more than $1.0 billion in non‑convertible debt securities during any three‑year period, or if the market value of our Class A common stock held by non‑affiliates exceeds $700.0 million as of any June 30 before that time. Investors may find our Class A common stock less attractive because we may rely on these exemptions. If some investors find our Class A common stock less attractive as a result, there may be a less active trading market for our Class A common stock and our stock price may be more volatile.
Pursuant to the JOBS Act, our independent registered public accounting firm will not be required to attest to the effectiveness of our internal control over financial reporting pursuant to Section 404 for so long as we are an “emerging growth company.”
Section 404 of the Sarbanes‑Oxley Act of 2002, as amended, or the Sarbanes‑Oxley Act, requires annual management assessments of the effectiveness of our internal control over financial reporting, starting with the second annual report that we file with the SEC as a public company, and generally requires in the same report a report by our independent registered public accounting firm on the effectiveness of our internal control over financial reporting. However, under the JOBS Act, our independent registered public accounting firm will not be required to attest to the effectiveness of our internal control over financial reporting pursuant to Section 404 until we are no longer an “emerging growth company.” We could be an “emerging growth company” for up to five years following June 24, 2014, the date of our initial public offering.
Furthermore, we may identify material weaknesses that we may not be able to remediate in time to meet the applicable deadline imposed upon us for compliance with the requirements of Section 404 of the Sarbanes‑Oxley Act. In addition, if we fail to achieve and maintain the adequacy of our internal controls, as such standards are modified, supplemented or amended from time to time, we may not be able to conclude that we have effective internal controls over financial reporting in accordance with Section 404 of the Sarbanes‑Oxley Act. If we are not able to implement the requirements of Section 404 of the Sarbanes‑Oxley Act in a timely manner or with adequate compliance, our independent registered public accounting firm may issue an adverse opinion due to ineffective internal controls over financial reporting and we may be subject to sanctions or investigation by regulatory authorities, such as the SEC. As a result, there could be a negative reaction in the financial markets due to a loss of confidence in the reliability of our financial statements. In addition, we may be required to incur costs in improving our internal control system and the hiring of additional personnel. Any such action could have a material adverse effect on our business, prospects, results of operations and financial condition.
48
Adeptus Health Inc.’s only material asset is its interest in Adeptus Health LLC, and it is accordingly dependent upon distributions from Adeptus Health LLC to pay taxes and pay dividends.
Adeptus Health Inc. is a holding company that was formed in connection with our initial public offering and has no material assets other than its ownership of the limited liability company units of Adeptus Health LLC (the “LLC Units”). Adeptus Health Inc. has no independent means of generating revenue. Adeptus Health Inc. intends to cause Adeptus Health LLC to make distributions to its unitholders in an amount sufficient to cover all applicable taxes at assumed tax rates and dividends, if any. Deterioration in the financial condition, earnings or cash flow of Adeptus Health LLC and its subsidiaries for any reason could limit or impair their ability to pay such distributions. Additionally, to the extent Adeptus Health Inc. needs funds, and Adeptus Health LLC is restricted from making such distributions under applicable law or regulation or under the terms of our financing arrangements, or is otherwise unable to provide such funds, it could materially adversely affect our business, prospects, results of operations or financial condition.
Payments of dividends, if any, will be at the discretion of our board of directors after taking into account various factors, including general and economic conditions, our financial condition and operating results, our available cash and current and anticipated cash needs, capital requirements, contractual, legal, tax and regulatory restrictions and implications of the payment of dividends by us to our stockholders or by our subsidiaries (including Adeptus Health LLC) to us, and such other factors as our board of directors may deem relevant. First Choice ER, LLC and its subsidiaries are currently subject to certain restrictions and covenants under our Senior Secured Credit Facility, including limits on amounts of leverage, interest charges and capital expenditures. These restrictions and covenants may restrict the ability of those entities to make distributions to Adeptus Health Inc. Any additional financing arrangement we enter into in the future may include restrictive covenants that limit our ability to pay dividends. In addition, Adeptus Health LLC is generally prohibited under Delaware law from making a distribution to a member to the extent that, at the time of the distribution, after giving effect to the distribution, liabilities of Adeptus Health LLC (with certain exceptions) exceed the fair value of its assets. Subsidiaries of Adeptus Health LLC are generally subject to similar legal limitations on their ability to make distributions to Adeptus Health LLC.
Adeptus Health Inc. is required to pay the Post‑IPO Unit Holders and the Merged Owner certain tax benefits they may claim arising in connection with subsequent exchanges in the future, and the amounts it may pay could be significant.
In connection with our initial public offering, we entered into a tax receivable agreement with funds affiliated with our Sponsor, funds affiliated with our founders and certain members of management and our board of directors (the “Post‑IPO Unit Holders”) and an affiliate of our Sponsor (the “Merged Owner”) providing for the payment by Adeptus Health Inc. to the Post‑IPO Unit Holders of 85% of the benefits, if any, that Adeptus Health Inc. is deemed to realize as a result of increases in tax basis and certain other tax benefits.
We expect the payments that Adeptus Health Inc. may make under the tax receivable agreement will be substantial. There may be a material negative effect on our liquidity if, as a result of timing discrepancies or otherwise or if distributions to Adeptus Health Inc. by Adeptus Health LLC are not sufficient to permit Adeptus Health Inc. to make payments under the tax receivable agreement after it has paid taxes. The payments under the tax receivable agreement are not conditioned upon the Post‑IPO Unit Holders’ or Merged Owner’s continued ownership of us.
Estimating the amount of payments that may be made under the tax receivable agreement is by its nature imprecise, insofar as the calculation of amounts payable depends on a variety of factors. The actual increase in tax basis, as well as the amount and timing of any payments under the tax receivable agreement, will vary depending upon a number of factors, including the timing of exchanges, the relative value of our assets at the time of the exchange, the price of shares of our common stock at the time of the exchange, the extent to which such exchanges are taxable, the amount and timing of the taxable income we realize in the future and the tax rate then applicable, our use of loss carryovers and the portion of our payments under the tax receivable agreement constituting imputed interest or depreciable or amortizable basis.
49
We are not aware of any issue that would cause the IRS to challenge a tax basis increase; however, if the IRS were successful in making such a challenge, we would not be reimbursed for any payments that may previously have been made under the tax receivable agreement if it is later determined that we did not receive the anticipated corresponding tax benefit. As a result, in certain circumstances we could make payments under the tax receivable agreement in excess of our cash tax savings.
Our corporate structure may result in conflicts of interest between our stockholders and the holders of LLC Units.
We hold our assets and conduct substantially all of our operations through Adeptus Health LLC, which may in the future issue additional LLC Units to third parties. Persons holding LLC Units would have the right to vote on certain amendments to the limited liability company agreement of Adeptus Health LLC, as well as on certain other matters. Persons holding these voting rights may exercise them in a manner that conflicts with the interests of our stockholders. Circumstances may arise in the future when the interests of members in Adeptus Health LLC conflict with the interests of our stockholders. As we are the managing member of Adeptus Health LLC, we have fiduciary duties to the other members of Adeptus Health LLC that may conflict with fiduciary duties our officers and directors owe to our stockholders. These conflicts may result in decisions that are not in the best interests of stockholders.
Our Sponsor has significant influence over us in connection with decisions that require the approval of stockholders, which could limit your ability to influence the outcome of key transactions, including a change of control.
As of December 31, 2014, our Sponsor held approximately 47.5% of the voting power of our outstanding capital stock. As a result of our Sponsor’s ownership, our Sponsor may have, through our board of directors, the ability to control decision‑making with respect to our business direction and policies. We have in recent years depended on our relationship with our Sponsor to help guide our business plan. In addition, our Sponsor has the right to designate certain of the members of our board of directors, as well as members of our nominating and corporate governance committee and compensation committee. Our Sponsor also has consent rights with respect to certain significant corporate actions, including the hiring and firing of our chief executive officer, any change in control and any significant acquisitions, divestitures and equity issuances. As a result, our Sponsor potentially has the ability to influence or effectively control our decisions to enter into any corporate transaction (and the terms thereof) and the ability to prevent any change in the composition of our board of directors and certain transactions that require stockholder approval regardless of whether others believe that such change or transaction is in our best interests. Conversely, our Sponsor may elect to reduce its ownership in our company or reduce its involvement on our board of directors, which could reduce or eliminate the benefits we have historically achieved through our relationship with it. Additionally, our Sponsor is in the business of making investments in companies and may from time to time acquire and hold interests in businesses that compete directly or indirectly with us. Our Sponsor’s interests may differ from yours.
Anti‑takeover provisions in our charter documents and Delaware law might discourage or delay acquisition attempts for us that you might consider favorable.
Our amended and restated certificate of incorporation and amended and restated by‑laws contain provisions that may make the acquisition of our company more difficult without the approval of our board of directors. Among other things, these provisions:
|
· |
authorize the issuance of undesignated preferred stock, the terms of which may be established and the shares of which may be issued without stockholder approval, and which may include super voting, special approval, dividend or other rights or preferences superior to the rights of the holders of Class A common stock; |
|
· |
expressly authorize the board of directors to make, alter or repeal our by‑laws by majority vote; and |
|
· |
establish advance notice requirements for nominations for elections to our board of directors or for proposing matters that can be acted upon by stockholders at stockholder meetings. |
These anti‑takeover provisions and other provisions under Delaware law could discourage, delay or prevent a transaction involving a change in control of our company, including actions that our stockholders may deem advantageous, or negatively affect the trading price of our Class A common stock. These provisions could also
50
discourage proxy contests and make it more difficult for you and other stockholders to elect directors of your choosing and to cause us to take other corporate actions you desire.
Item 1B. Unresolved Staff Comments
None.
Our executive and administrative offices are located in Lewisville, Texas. These offices contain approximately 80,000 square feet of space. We believe these offices are adequate for our current primary needs.
We are involved from time to time in legal and regulatory proceedings concerning matters that arise in the ordinary course of our business. An adverse result in governmental investigations, private lawsuits or other legal proceedings could have a material adverse effect on our financial position. To the best of our knowledge, we are not currently the subject of any material investigation, private lawsuit or other legal proceeding.
Item 4. Mine Safety Disclosures
Not applicable.
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
Our Class A common stock began trading on the New York Stock Exchange under the symbol “ADPT” on June 25, 2014. Prior to that time, there was no market for our common stock. The following table sets forth, for the periods indicated, the high and low sales prices for our Class A common stock from June 25, 2014 through December 31, 2014, as reported by the New York Stock Exchange.
|
Fiscal 2014 |
|
High |
|
Low |
|
||
|
June 25, 2014 through June 30, 2014 |
|
$ |
26.75 |
|
$ |
25.00 |
|
|
Quarter ended September 30, 2014 |
|
$ |
29.33 |
|
$ |
23.35 |
|
|
Quarter ended December 31, 2014 |
|
$ |
38.78 |
|
$ |
24.22 |
|
There is no trading market for shares of our Class B common stock.
Holders
As of February 15, 2015, there were approximately 220 stockholders of record of our Class A common stock and 20 stockholders of record of our Class B common stock. The number of record holders does not reflect the beneficial ownership of shares held in nominee name, nor do they include holders of any restricted stock.
Dividends
We do not currently pay a dividend on our common stock. The declaration, amount and payment of any future dividends on shares of Class A common stock will be at the sole discretion of our board of directors and will depend on, among other things, our results of operations, cash requirements, financial condition, contractual restrictions and other factors that our board of directors may deem relevant. We did not pay any dividends on our common stock from the date
51
our Class A common stock began trading on the New York Stock Exchange on June 25, 2014 through December 31, 2014.
Adeptus Health Inc. is a holding company and has no material assets other than its ownership of LLC Units in Adeptus Health LLC. In the event that we do pay a dividend, we intend to cause Adeptus Health LLC to make distributions to us in an amount sufficient to cover such dividend. If Adeptus Health LLC makes such distributions to us, the other holders of LLC Units will also be entitled to receive distributions pro rata in accordance with the percentages of their respective LLC Units. In addition, the Senior Secured Credit Facility limits the ability of Adeptus Health LLC to pay distributions to us. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations — Liquidity and Capital Resources — Contractual Obligations — Senior Secured Credit Facility.”
Any financing arrangements that we enter into in the future may include restrictive covenants that limit our ability to pay dividends. In addition, Adeptus Health LLC is generally prohibited under Delaware law from making a distribution to a member to the extent that, at the time of the distribution, after giving effect to the distribution, liabilities of Adeptus Health LLC (with certain exceptions) exceed the fair value of its assets. Subsidiaries of Adeptus Health LLC are generally subject to similar legal limitations on their ability to make distributions to Adeptus Health LLC.
Issuer Purchases of Equity Securities
During the quarter ended December 31, 2014, we did not purchase any of our equity securities that are registered under Section 12(b) of the Exchange Act.
52
Performance Graph
The following graph compares the relative performance of our common stock, the S&P 500 Index and the S&P 500 Healthcare Index. This graph covers the period from June 25, 2014 (the date our Class A common stock first began trading on the New York Stock Exchange), through December 31, 2014. In each case, this graph assumes a $100 investment in the Company’s Class A common stock and on each index on June 25, and the reinvestment of all dividends, if any.
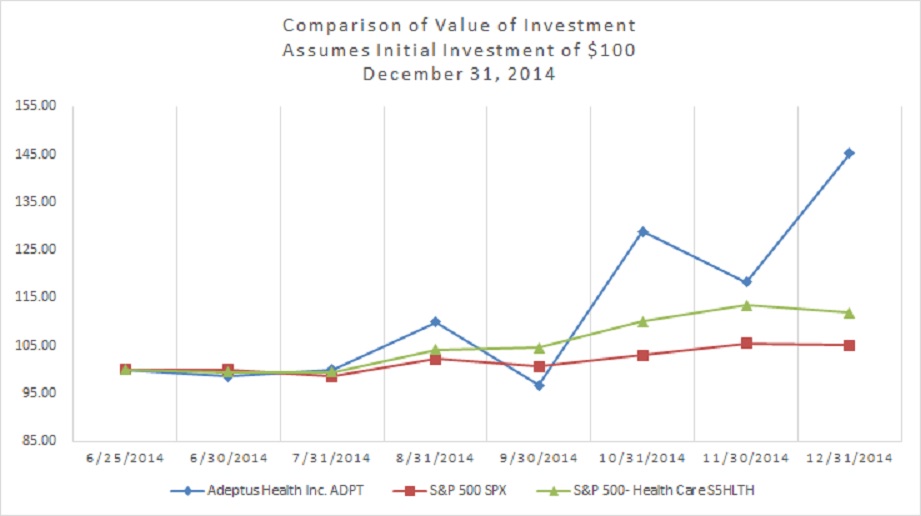
|
Name |
|
June 25, |
|
June 30, |
|
July 31, |
|
August 31, |
|
September 30, |
|
October 31, |
|
November 31, |
|
December 31, |
|
||||||||
|
Adeptus Health Inc. |
|
$ |
100 |
|
$ |
98.52 |
|
$ |
99.96 |
|
$ |
109.86 |
|
$ |
96.70 |
|
$ |
128.85 |
|
$ |
118.21 |
|
$ |
145.24 |
|
|
S&P 500 |
|
|
100 |
|
|
100.04 |
|
|
98.53 |
|
|
102.24 |
|
|
100.65 |
|
|
102.99 |
|
|
105.51 |
|
|
105.07 |
|
|
S&P 500- Health Care |
|
|
100 |
|
|
99.49 |
|
|
99.47 |
|
|
104.16 |
|
|
104.49 |
|
|
109.98 |
|
|
113.49 |
|
|
111.84 |
|
53
Item 6. Selected Financial Data
The following table sets forth the selected historical consolidated financial and other data for the Company as of the dates and for the periods indicated. The selected consolidated statements of operations data presented below for the fiscal years ended December 31, 2014, 2013 and 2012 and the consolidated balance sheet data presented below as of December 31, 2014, 2013 and 2012 have been derived from our audited consolidated financial statements, included in this Annual Report on Form 10-K. You should read the information contained in this table in conjunction with our audited consolidated financial statements, the related notes to the financial statements and the information in Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” included elsewhere in this Annual Report on Form 10-K. Our historical results are not necessarily indicative of our future results.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Statement of Operations Data: |
|
(in thousands, except per share data) |
||||||||
|
Revenue: |
|
|
|
|
|
|
|
|
|
|
|
Patient service revenue |
|
$ |
243,298 |
|
$ |
114,960 |
|
$ |
80,977 |
|
|
Provision for bad debt |
|
|
(32,624) |
|
|
(12,077) |
|
|
(8,376) |
|
|
Net patient service revenue |
|
|
210,674 |
|
|
102,883 |
|
|
72,601 |
|
|
Management and contract services revenue |
|
|
20 |
|
|
— |
|
|
— |
|
|
Total net operating revenue |
|
|
210,694 |
|
|
102,883 |
|
|
72,601 |
|
|
Equity in net loss of unconsolidated joint venture |
|
|
(900) |
|
|
— |
|
|
— |
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
Salaries, wages and benefits |
|
|
136,498 |
|
|
65,244 |
|
|
41,754 |
|
|
General and administrative |
|
|
37,604 |
|
|
17,436 |
|
|
12,805 |
|
|
Other operating expenses |
|
|
27,329 |
|
|
11,185 |
|
|
7,493 |
|
|
(Gain) loss from the disposal or impairment of assets |
|
|
(42) |
|
|
207 |
|
|
652 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
4,640 |
|
|
Total operating expenses |
|
|
216,426 |
|
|
101,992 |
|
|
67,344 |
|
|
(Loss) income from operations |
|
|
(6,632) |
|
|
891 |
|
|
5,257 |
|
|
Other (expense) income: |
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(11,966) |
|
|
(2,827) |
|
|
(1,056) |
|
|
Change in fair market value of derivatives |
|
|
— |
|
|
112 |
|
|
(533) |
|
|
Write-off of deferred loan costs |
|
|
— |
|
|
(440) |
|
|
— |
|
|
Total other (expense) |
|
|
(11,966) |
|
|
(3,155) |
|
|
(1,589) |
|
|
(Loss) income before (benefit) provision for income taxes |
|
|
(18,598) |
|
|
(2,264) |
|
|
3,668 |
|
|
(Benefit) provision for income taxes |
|
|
(1,326) |
|
|
720 |
|
|
467 |
|
|
Net (loss) income |
|
|
(17,272) |
|
|
(2,984) |
|
|
3,201 |
|
|
Less: Net (loss) income attributable to non-controlling interest |
|
|
(13,921) |
|
|
(2,984) |
|
|
3,201 |
|
|
Net loss attributable to Adeptus Health Inc. |
|
$ |
(3,351) |
|
$ |
— |
|
$ |
— |
|
|
Net loss per share of Class A common stock: |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
|
Diluted |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
|
Weighted average shares of Class A common stock: |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
|
Diluted |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
|
Consolidated Balance Sheet Data: |
|
|
|
|
|
|
|
|
|
|
|
Cash |
|
$ |
2,002 |
|
$ |
11,495 |
|
$ |
3,455 |
|
|
Total assets |
|
|
282,818 |
|
|
183,292 |
|
|
120,367 |
|
|
Total debt and capital lease obligations |
|
|
110,935 |
|
|
79,411 |
|
|
23,604 |
|
|
Owners' equity |
|
|
99,880 |
|
|
78,651 |
|
|
82,734 |
|
|
Cash Flow Data: |
|
|
|
|
|
|
|
|
|
|
|
Cash flows provided by (used in): |
|
|
|
|
|
|
|
|
|
|
|
Operating activities |
|
$ |
(24,698) |
|
$ |
6,872 |
|
$ |
11,408 |
|
|
Investing activities |
|
|
(49,448) |
|
|
(44,647) |
|
|
(15,537) |
|
|
Financing activities |
|
|
64,653 |
|
|
45,815 |
|
|
2,820 |
|
|
Other Financial Data: |
|
|
|
|
|
|
|
|
|
|
|
Adjusted EBITDA(1) |
|
$ |
28,200 |
|
$ |
16,010 |
|
$ |
13,689 |
|
|
Same-store revenue(2) |
|
|
85,629 |
|
|
70,641 |
|
|
64,506 |
|
|
Capital expenditures |
|
|
47,429 |
|
|
46,048 |
|
|
11,504 |
|
|
Other Operational Data: |
|
|
|
|
|
|
|
|
|
|
|
Patient volume (number of patient visits) |
|
|
146,058 |
|
|
77,044 |
|
|
58,434 |
|
|
Number of facilities |
|
|
55 |
|
|
26 |
|
|
14 |
|
54
|
(1) |
We define Adjusted EBITDA as net income before interest, taxes, depreciation and amortization, further adjusted to eliminate the impact of certain additional items, including advisory services paid to our Sponsor, facility preopening expenses, management recruiting expenses, stock compensation expense, costs associated with our public offerings and other non-recurring costs. Adjusted EBITDA is included in this Annual Report on Form 10-K because it is a key metric used by management to assess our financial performance. We use Adjusted EBITDA to supplement GAAP measures of performance in order to evaluate the effectiveness of our business strategies, to make budgeting decisions and to compare our performance against that of other peer companies using similar measures. Adjusted EBITDA is also frequently used by analysts, investors and other interested parties to evaluate companies in our industry. |
Adjusted EBITDA is a non‑GAAP measure of our financial performance and should not be considered as an alternative to net income (loss) as a measure of financial performance, or any other performance measure derived in accordance with GAAP, nor should it be construed as an inference that our future results will be unaffected by unusual or other items. In evaluating Adjusted EBITDA, you should be aware that in the future we will incur expenses that are the same as or similar to some of the adjustments in this presentation, such as preopening expenses, stock compensation expense, and other adjustments. Additionally, Adjusted EBITDA is not intended to be a measure of free cash flow for management’s discretionary use, as it does not reflect certain cash requirements such as tax payments, debt service requirements, capital expenditures, facility openings and certain other cash costs that may recur in the future. Adjusted EBITDA contains certain other limitations, including the failure to reflect our cash expenditures, cash requirements for working capital needs and cash costs to replace assets being depreciated and amortized. Management compensates for these limitations by supplementally relying on our GAAP results in addition to using Adjusted EBITDA. Our presentation of Adjusted EBITDA is not necessarily comparable to other similarly titled captions of other companies due to different methods of calculation.
The following table sets forth a reconciliation of our Adjusted EBITDA to net income (loss) using data derived from our consolidated financial statements for the periods indicated:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(dollars in thousands) |
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Net (loss) income |
|
$ |
(17,272) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
4,640 |
|
|
Interest expense(a) |
|
|
11,966 |
|
|
3,155 |
|
|
1,589 |
|
|
(Benefit) provision for income taxes |
|
|
(1,326) |
|
|
720 |
|
|
467 |
|
|
Advisory Services Agreement fees and expenses(b) |
|
|
293 |
|
|
559 |
|
|
553 |
|
|
Preopening expenses(c) |
|
|
10,550 |
|
|
3,977 |
|
|
497 |
|
|
Management recruiting expenses(d) |
|
|
376 |
|
|
719 |
|
|
970 |
|
|
Stock compensation expense(e) |
|
|
1,015 |
|
|
586 |
|
|
253 |
|
|
Initial public offering costs (f) |
|
|
5,157 |
|
|
- |
|
|
- |
|
|
Other(g) |
|
|
2,404 |
|
|
1,358 |
|
|
1,519 |
|
|
Total adjustments |
|
|
45,472 |
|
|
18,994 |
|
|
10,488 |
|
|
Adjusted EBITDA |
|
$ |
28,200 |
|
$ |
16,010 |
|
$ |
13,689 |
|
|
(a) |
Consists of interest expense and fees of $11.9 million, $2.8 million, and $1.1 million for the years ended December 31, 2014, 2013 and 2012, respectively, a gain in fair market value of derivatives of $0.1 million for the year ended December 31, 2013, a loss in fair market value of derivatives of $0.5 million for the year ended December 31, 2012, and a write-off of deferred loan costs of $0.4 million for the year ended December 31, 2013. |
|
(b) |
Consists of management fees and expenses paid to a significant shareholder under our Advisory Services Agreement. The Advisory Services Agreement was terminated in connection with the consummation of our initial public offering in June 2014. |
|
(c) |
Includes labor, marketing costs and occupancy costs prior to opening a facility and the equity in loss of our unconsolidated joint venture in 2014. |
|
(d) |
Third-party costs and fees involved in recruiting our management team. |
|
(e) |
Stock compensation expense associated with grants of management incentive units. |
|
(f) |
Consists of costs incurred in conjunction with our initial public offering, including $2.4 million in bonuses for certain members of management, $2.3 million in costs related to the termination of our Advisory Services Agreement and $0.5 million of other offering costs. |
55
|
(g) |
For the year ended December 31, 2014, we incurred costs to develop long-term strategic goals and objectives totaling $1.7 million, real-estate development costs associated with potential real estate projects that were terminated totaling $0.6 million and board fees and travel expenses paid to members of the board of directors totaling $0.1 million. For the year ended December 31, 2013, we incurred costs to develop long-term strategic goals and objectives totaling approximately $0.5 million, real-estate development costs associated with potential real estate projects that were terminated totaling $0.4 million, board fees and travel expenses paid to members of the board of directors totaling $0.2 million and $0.25 million of termination costs paid to the former CEO. For the year ended December 31, 2012, we incurred terminated real-estate development costs totaling $0.5 million, legal costs primarily associated with real estate development and litigation for violation of our trademark totaling $0.8 million and board fees and travel expenses paid to members of the board of directors totaling approximately $0.2 million. |
|
(2) |
We begin including revenue for a new facility as same‑store revenue from the first day of the 16th full fiscal month following the facility’s opening, which is when we believe same‑store comparison becomes meaningful. When a facility is relocated, we continue to include revenue from that facility in same‑store revenue. Same‑store revenue allows us to evaluate how our facility base is performing by measuring the change in period‑over‑period net revenue in facilities that have been open for 15 months or more. Various factors affect same‑store revenue, including outbreaks of illnesses, changes in marketing and competition. |
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion and analysis of our financial condition should be read together with “Selected Financial Data” and our audited consolidated financial statements and accompanying notes included elsewhere in this filing. This discussion contains forward-looking statements that are subject to known and unknown risks and uncertainties. Actual results and the timing of events may differ significantly from those expressed or implied in such forward-looking statements due to a number of factors, including those set forth under “Risk Factors,” “Special Note Regarding Forward-Looking Statements” and elsewhere in this filing.
Overview
We own and operate First Choice Emergency Rooms, the largest network of independent freestanding emergency rooms in the United States. We have experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013 and to 55 facilities as of December 31, 2014. Our facilities are currently located in the Houston, Dallas/Fort Worth, San Antonio and Austin, Texas markets, as well as in Colorado Springs and Denver, Colorado. In addition, we have one hospital facility located in Phoenix, Arizona.
Since our founding in 2002, our mission has been to address the need within our local communities for immediate and convenient access to quality emergency care in a patient-friendly, cost-effective setting. We believe we are transforming the emergency care experience with a differentiated and convenient care delivery model which improves access, reduces wait times and provides high-quality clinical and diagnostic services on-site. Our facilities are fully licensed and provide comprehensive, emergency care with an acuity mix that we believe is comparable to hospital-based emergency rooms.
Initial Public Offering and Reorganization
On June 30, 2014, we completed our initial public offering of 4,900,000 shares of our Class A common stock at a price to the public of $22.00 per share and received net proceeds of approximately $96.2 million, after deducting underwriting discounts and commissions and offering expenses. An additional 735,000 shares were sold to the public, of which 313,586 shares were sold by a significant stockholder and 421,414 shares were sold by the Company with the proceeds received by the Company used to purchase an equivalent number of LLC Units from such significant stockholder. Adeptus Health LLC used the proceeds it received as a result of our purchase of LLC Units to reduce outstanding borrowings under its credit agreement and for general corporate purposes.
In connection with the initial public offering, we completed the Reorganization, which among other things, resulted in Adeptus Health Inc. becoming a holding company with its sole material asset being a controlling equity interest in Adeptus Health LLC. As the sole managing member of Adeptus Health LLC, Adeptus Health Inc. operates
56
and controls all of the business and affairs of Adeptus Health LLC and, through Adeptus Health LLC and its subsidiaries, conducts our business. Adeptus Health Inc. owns 100% of the voting rights of Adeptus Health LLC, and therefore has control over Adeptus Health LLC. Adeptus Health Inc. consolidates Adeptus Health LLC and its subsidiaries in its consolidated financial statements.
Joint Venture with Dignity Health
On October 22, 2014, we announced our expansion into Arizona through a joint venture with Dignity Health, one of the nation’s largest health systems. The new partnership has started with Dignity Health Arizona General Hospital, a full-service healthcare hospital facility, which was in its training and certification phase until January 30, 2015, when we received our CMS certification from the Joint Commission. This partnership includes plans for additional access to emergency medical care in Phoenix through freestanding emergency departments associated with the hospital. Dignity Health Arizona General Hospital will be a full-service healthcare hospital facility, licensed by the state as a general hospital. The construction of Dignity Health Arizona General Hospital has been recently completed.
We will not consolidate the financial results of the operations of this joint venture. While revenues from this unconsolidated facility are not recorded as revenues by us for GAAP reporting purposes, equity in earnings of joint venture could be a significant portion of our overall earnings.
Industry Trends
The emergency room remains a critical access point for millions of Americans who experience sudden serious illness or injury in the United States each year. The availability of that care is under pressure and threatened by a wide range of factors, including shrinking capacity and an increasing demand for services. According to AHA, from 1992 to 2012, the number of emergency room visits increased by 46.7%, while the number of emergency departments decreased by 11.4%. The number of emergency room visits exceeded 130 million in 2012, or approximately 247 visits per minute, and care previously provided in inpatient settings is now increasingly being provided in emergency departments.
Factors affecting access to emergency care include availability of emergency departments, capacity of emergency departments, and availability of staffing in emergency departments. ACEP's National Report Card on U.S. emergency care rates the access to emergency care category with a near-failing grade of "D-" and a grade of "D+" for the overall emergency room system. As the largest operator of freestanding emergency rooms, we believe we are an essential part of the solution, providing access to high-quality emergency care and offering a significantly improved patient experience relative to traditional hospital emergency departments.
Key Revenue Drivers
Our revenue growth is primarily driven by facility expansion, increasing patient volumes and reimbursement rates.
Facility Expansion
We add new facilities based on capacity, location, demographics and competitive considerations. We expect the new facilities we open to be the primary driver of our revenue growth. Our results of operations have been and will continue to be materially affected by the timing and number of new facility openings and the amount of new facility opening costs incurred. A new facility builds its patient volumes over time and, as a result, generally has lower revenue than our more mature facilities. A new facility generally takes up to 12 months to achieve a level of operating performance comparable to our similar existing facilities.
Patient Volume
We generate revenue by providing emergency care to patients based upon the estimated amounts due from commercial insurance providers, patients and other third-party payors. Revenue per treatment is sensitive to the mix of services used in treating a patient. Our patient volumes are directly correlated to our new facility openings, our targeted
57
marketing efforts and external factors such as severity of annually recurring viruses that lead to increases in patient visits. Revenue is recognized when services are rendered to patients.
Patient volume is supported through marketing programs focused on educating communities about the convenient and high-quality emergency care we provide. Through our targeted marketing campaigns, which include direct mail, radio, television, outdoor advertising, digital and social media, we aim to increase our patient volumes by reaching a broad base of potential patients in order to increase brand awareness. We also have a dedicated field marketing team that works to educate local communities in which we operate about the access and care available at our facilities. Our dedicated field marketing team targets specific audiences by attending local chamber of commerce meetings, meeting with primary care physicians and visiting with school nurses and athletic directors, in order to increase patient volumes within a facility's local community.
Our patient volume is also influenced by conditions that may be beyond our direct control, some of which are seasonal. These conditions include the timing, location and severity of influenza, allergens and other annually recurring viruses, which at times leads to severe upper respiratory concerns.
Reimbursement Rates and Acuity Mix
The majority of our revenue is derived from patients with commercial health insurance coverage. The reimbursement rates set by third-party payors tend to be higher for higher acuity visits, reflecting their higher complexity. Consistent with billing practices at all emergency rooms and in light of the fact our facilities are open 24 hours a day, seven days a week and staffed with Board-certified physicians, we bill payors a facility fee, a professional services fee and other related fees. The reimbursement rates we have been able to negotiate have held relatively stable; however, the mix of both acuity and payors can vary period to period, changing the overall blended reimbursement rate. With select payors, we have the ability to make annual increases in our billed amounts. Although we may begin to do so in the near term, as of December 31, 2014, we did not bill Medicare or Medicaid for the care we provided.
Seasonality
Our patient volumes are sensitive to seasonal fluctuations in emergency activity. Typically, winter months see a higher occurrence of influenza, bronchitis, pneumonia and similar illnesses; however, the timing and severity of these outbreaks can vary dramatically. Additionally, as consumers shift towards high deductible insurance plans, they are responsible for a greater percentage of their bill, particularly in the early months of the year before other healthcare spending has occurred, which may lead to an increase in bad debt expense during that period. Our quarterly operating results may fluctuate significantly in the future depending on these and other factors.
Sources of Revenue by Payor
We receive payments for services rendered to patients from third-party payors or from our patients directly, as described in more detail below. Generally, our revenue is determined by a number of factors, including the payor mix, the number and nature of procedures performed and the rate of payment for the procedures.
58
Patient service revenue before the provision for bad debt by major payor source for the periods indicated is as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
||||||||||
|
December 31, |
||||||||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Third-party payors, including patient portion(1) |
|
$ |
237,972 |
|
$ |
113,603 |
|
$ |
79,408 |
|
|
Self-pay |
|
|
5,326 |
|
|
1,357 |
|
|
1,569 |
|
|
Total all payors |
|
$ |
243,298 |
|
$ |
114,960 |
|
$ |
80,977 |
|
|
(1) |
Patient portion includes deductibles and co-payments. |
Four major third-party payors accounted for 84.8%, 86.7%, and 88.2%, of our patient service revenue for the years ended December 31, 2014, 2013 and 2012, respectively. These same payors also accounted for 80.0%, 79.0% of our accounts receivable as of December 31, 2014 and 2013, respectively. The following table sets forth the percentage of patient service revenue earned by major payor source for the periods indicated:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
|
Payor: |
|
|
|
|
|
|
|
|
Blue Cross Blue Shield |
|
27.6 |
% |
28.0 |
% |
29.1 |
% |
|
United HealthCare |
|
23.6 |
|
26.5 |
|
26.0 |
|
|
Aetna |
|
19.3 |
|
21.0 |
|
22.1 |
|
|
Cigna |
|
14.3 |
|
11.2 |
|
11.0 |
|
|
Other |
|
15.2 |
|
13.3 |
|
11.8 |
|
|
|
|
100.0 |
% |
100.0 |
% |
100.0 |
% |
Third-Party Payors
Third-party payors include health insurance companies as well as related payments from patients for deductibles and co-payments and have historically comprised the vast majority of our patient service revenue. We enter into contracts with health insurance companies and other health benefit groups by granting discounts to such organizations in return for the patient volume they provide.
Most of our commercial revenue is attributable to contracts where a fee is negotiated relative to the service provided at our facilities. Our contracts are structured as either case-rate contracts or as discounts to billed charges. In a case rate contract, a set fee is assigned to visits based on acuity level. We also enter into contracts with payors based on a discount of our billed charges. There are contracted rates for both the professional component and the technical component. Each portion of the claim is billed separately and paid based on the patient's emergency room benefits received.
First Choice Emergency Rooms, like hospital emergency rooms, are full-service emergency rooms licensed by the states of Texas and Colorado. As such, we collect the emergency room benefits based on a patient's specific insurance plan. Additionally, Texas insurance law provides that all fully funded insurance plans should pay all emergency claims at the in-network benefit rate, regardless of the provider's contract status.
Self-Pay
Self-pay consists of out-of-pocket payments for treatments by patients not otherwise covered by third-party payors. For the years ended December 31, 2014, 2013 and 2012, self-pay payments accounted for 2.2%, 1.2%, and 1.9% of our patient service revenue, respectively.
59
Charity Care
Charity care consists of the write-off of all charges associated with patients who are treated but do not have commercial insurance or the ability to self-pay. This includes all charges associated with care provided to patients covered by Medicare and/or Medicaid, as we do not currently receive reimbursements under those programs. For the years ended December 31, 2014, 2013 and 2012, charity care write-offs represented 8.6%, 7.0%, and 7.0%, of our patient service revenue, respectively.
Key Performance Measures
The key performance measures we use to evaluate our business focus on the number of patient visits, or patient volume, same-store revenue and Adjusted EBITDA.
Patient Volume
We utilize patient volume to forecast our expected net revenue and as a basis by which to measure certain costs of the business. We track patient volume at the facility level. The number of patients we treat is influenced by factors we control and also by conditions that may be beyond our direct control. See "—Key Revenue Drivers."
Same-Store Revenue
We begin comparing same-store revenue for a new facility on the first day of the 16th full fiscal month following the facility's opening, which is when we believe same-store comparison becomes meaningful. When a facility is relocated, we continue to include revenue from that facility in same-store revenue. Same-store revenue allows us to evaluate how our facility base is performing by measuring the change in period-over-period net revenue in facilities that have been open for 15 months or more. Various factors affect same-store revenue, including outbreaks of illnesses, changes in marketing and competition. Opening new facilities is an important part of our growth strategy. These new facilities, within 15 months after opening, generally have historically generated between approximately $4.5 million to $5.5 million in annual net revenue and on average have historically incurred approximately $3.5 million in annual operating expenses. On that basis, our average annual estimated operating income, excluding depreciation and amortization, for such facilities has historically been between $1.0 million and $2.0 million, which would represent a facility operating margin, excluding depreciation and amortization, of between approximately 20% and 35%. As we continue to pursue our growth strategy, we anticipate that a significant percentage of our revenue will come from stores not yet included in our same-store revenue calculation.
Adjusted EBITDA
We define Adjusted EBITDA as net income before interest, taxes, depreciation, and amortization, further adjusted to eliminate the impact of certain additional items, including advisory services paid to a significant shareholder, facility pre-opening expenses, management recruiting expenses, stock compensation expense, costs associated with our initial public offering and other non-recurring costs. Adjusted EBITDA is included in this Annual Report on Form 10-K because it is a key metric used by management to assess our financial performance. We use Adjusted EBITDA to supplement GAAP measures of performance in order to evaluate the effectiveness of our business strategies, to make budgeting decisions and to compare our performance against that of other peer companies using similar measures. Adjusted EBITDA is also frequently used by analysts, investors and other interested parties to evaluate companies in our industry.
Adjusted EBITDA is a non-GAAP measure of our financial performance and should not be considered as an alternative to net income (loss) as a measure of financial performance, or any other performance measure derived in accordance with GAAP, nor should it be construed as an inference that our future results will be unaffected by unusual or other items. In evaluating Adjusted EBITDA, you should be aware that in the future we will incur expenses that are the same as or similar to some of the adjustments in this presentation, such as preopening expenses, stock compensation expense, and other adjustments. Additionally, Adjusted EBITDA is not intended to be a measure of free cash flow for management's discretionary use, as it does not reflect certain cash requirements such as tax payments, debt service
60
requirements, capital expenditures, facility openings and certain other cash costs that may recur in the future. Adjusted EBITDA contains certain other limitations, including the failure to reflect our cash expenditures, cash requirements for working capital needs and cash costs to replace assets being depreciated and amortized. Management compensates for these limitations by supplementally relying on our GAAP results in addition to using Adjusted EBITDA. Our presentation of Adjusted EBITDA is not necessarily comparable to other similarly titled captions of other companies due to different methods of calculation.
The following table sets forth a reconciliation of our Adjusted EBITDA to net (loss) income using data derived from our consolidated financial statements for the periods indicated:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(dollars in thousands) |
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Net (loss) income |
|
$ |
(17,272) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
4,640 |
|
|
Interest expense(a) |
|
|
11,966 |
|
|
3,155 |
|
|
1,589 |
|
|
(Benefit) provision for income taxes |
|
|
(1,326) |
|
|
720 |
|
|
467 |
|
|
Advisory Services Agreement fees and expenses(b) |
|
|
293 |
|
|
559 |
|
|
553 |
|
|
Preopening expenses(c) |
|
|
10,550 |
|
|
3,977 |
|
|
497 |
|
|
Management recruiting expenses(d) |
|
|
376 |
|
|
719 |
|
|
970 |
|
|
Stock compensation expense(e) |
|
|
1,015 |
|
|
586 |
|
|
253 |
|
|
Initial public offering costs (f) |
|
|
5,157 |
|
|
- |
|
|
- |
|
|
Other(g) |
|
|
2,404 |
|
|
1,358 |
|
|
1,519 |
|
|
Total adjustments |
|
|
45,472 |
|
|
18,994 |
|
|
10,488 |
|
|
Adjusted EBITDA |
|
$ |
28,200 |
|
$ |
16,010 |
|
$ |
13,689 |
|
|
(a) |
Consists of interest expense and fees of $11.9 million, $2.8 million, and $1.1 million for the years ended December 31, 2014, 2013 and 2012, respectively, a gain in fair market value of derivatives of $0.1 million for the year ended December 31, 2013, a loss in fair market value of derivatives of $0.5 million for the year ended December 31, 2012, and a write-off of deferred loan costs of $0.4 million for the year ended December 31, 2013. |
|
(b) |
Consists of management fees and expenses paid to a significant shareholder under our Advisory Services Agreement. The Advisory Services Agreement was terminated in connection with the consummation of our initial public offering in June 2014. |
|
(c) |
Includes labor, marketing costs and occupancy costs prior to opening a facility and the equity in loss of our unconsolidated joint venture in 2014. |
|
(d) |
Third-party costs and fees involved in recruiting our management team. |
|
(e) |
Stock compensation expense associated with grants of management incentive units. |
|
(f) |
Consists of costs incurred in conjunction with our initial public offering, including $2.4 million in bonuses for certain members of management, $2.3 million in costs related to the termination of our Advisory Services Agreement and $0.5 million of other offering costs. |
|
(g) |
For the year ended December 31, 2014, we incurred costs to develop long-term strategic goals and objectives totaling $1.7 million, real-estate development costs associated with potential real estate projects that were terminated totaling $0.6 million and board fees and travel expenses paid to members of the board of directors totaling $0.1 million. For the year ended December 31, 2013, we incurred costs to develop long-term strategic goals and objectives totaling approximately $0.5 million, real-estate development costs associated with potential real estate projects that were terminated totaling $0.4 million, board fees and travel expenses paid to members of the board of directors totaling $0.2 million and $0.25 million of termination costs paid to the former CEO. For the year ended December 31, 2012, we incurred terminated real-estate development costs totaling $0.5 million, legal costs primarily associated with real estate development and litigation for violation of our trademark totaling $0.8 million and board fees and travel expenses paid to members of the board of directors totaling approximately $0.2 million. |
61
Components of Results of Operations
Revenue
Patient Service Revenue
Patient service revenue primarily consists of charges for the professional and technical services provided to patients, net of contractual allowance, charity care write‑offs, and self‑pay discounts. Revenue is recognized when services are rendered to patients. Charges for all services provided to insured patients are initially billed to and processed by the patients’ insurance provider. Allowed amounts not covered by the insurance companies are then billed to the patients. Collection of payment for services provided to patients without insurance coverage is done at the time of service.
Provision for Bad Debt
Provision for bad debt primarily consists of the estimated uncollectible amounts from insured patients. Provision for bad debt is taken in the quarter the services are provided.
Management and Contract Services Revenue
Management and contract services revenue consists of income we earn in exchange for managing the day-to-day operations of our joint venture; and is calculated as a percentage of the joint venture’s net revenues.
Equity in Loss of Unconsolidated Joint Venture
Equity in the loss of unconsolidated joint venture consists of our share of the net loss of our joint venture, which is based on the hospital’s net loss and the percentage of the hospital’s outstanding equity interests owned by us.
Operating Expenses
Salaries, Wages and Benefits
Salaries, wages and benefits primarily consist of contract payments to our physicians and compensation and benefits to our staff at our facilities and corporate office, including non‑cash stock compensation related to restricted units with time‑ or performance‑based vesting schedules. Salaries, wages and benefits also includes certain labor costs associated with the opening of new facilities. We typically incur higher than normal employee costs at the time of a new store opening associated with set‑up and other opening costs. We employ a base “1‑1‑1‑1” model for our staffing needs at each facility, meaning that we have a minimum of one Board‑certified physician, one emergency trained registered nurse, one radiology technologist and one front office staff member on‑site at all times. This is a fixed cost labor model as all facilities are open 24 hours a day, seven days a week.
General and Administrative
General and administrative expenses primarily consist of marketing, utilities, medical malpractice and other insurance, professional fees, training and development, travel, office and computer, certain preopening costs incurred in connection with the opening of a facility and Advisory Services Agreement fees and expenses. Our marketing activities are principally focused on building awareness in the community to drive patient volume. We utilize targeted marketing efforts within local neighborhoods, through channels such as direct mail, mobile billboards, radio advertisements, television, community sponsorships and a robust online/social media presence.
62
Other Operating Expenses
Other operating expenses primarily consist of facility and equipment lease costs, medical and laboratory supplies, radiology fees and facility maintenance. We lease the majority of our facilities under operating leases with terms ranging from five to 15 years. These leases typically have renewal options. We also lease certain medical equipment under various non‑cancelable operating leases. With the exception of medical and laboratory supplies and radiology fees the facility expenses are fixed in nature.
Loss from the Disposal or Impairment of Assets
Loss from the disposal or impairment of assets primarily consists of the write‑off of assets at closed facilities, leasehold improvements at our former corporate office and other disposal of equipment in the normal course of business.
Depreciation and Amortization
Depreciation and amortization is related to buildings, equipment and leasehold improvements whose cost is depreciated or amortized over the shorter of the non‑cancellable lease term or the estimated useful life of the asset.
Other (Expense) Income
Interest Expense
Interest expense primarily consists of interest on our Senior Secured Credit Facility and on one facility treated as a capital lease.
Change in Fair Market Value of Derivatives
Change in fair market value of derivatives consists of the fair value adjustment of an interest rate swap that was terminated in 2013.
Write‑Off of Deferred Loan Costs
Write‑off of deferred loan costs consists of loan origination costs associated with the credit facility that was refinanced in 2013, which has since been terminated.
Provision for Income Taxes
As of December 31, 2014 we had a net operating loss carryforward of approximately $5.0 million. If not utilized, our federal operating loss carryforward will expire in 2034. A cumulative change in ownership among material shareholders, as defined in Section 382 of the Internal Revenue Code, during a three-year period may limit utilization of the federal net operating loss carryforwards.
63
Results of Operations
Year Ended December 31, 2014 Compared to Year Ended December 31, 2013
The following table summarizes our results of operations for the years ended December 31, 2014 and 2013:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended December 31, |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Percentage of |
|
||
|
|
|
|
|
|
|
|
|
Change from prior |
|
net patient |
|
|||||
|
|
|
|
|
|
|
|
|
period |
|
service revenue |
|
|||||
|
(dollars in thousands) |
|
2014 |
|
2013 |
|
$ |
|
% |
|
2014 |
|
2013 |
|
|||
|
Statement of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenue |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient service revenue |
|
$ |
243,298 |
|
$ |
114,960 |
|
$ |
128,338 |
|
111.6 |
% |
|
|
|
|
|
Provision for bad debt |
|
|
(32,624) |
|
|
(12,077) |
|
|
(20,547) |
|
170.1 |
|
|
|
|
|
|
Net patient service revenue |
|
|
210,674 |
|
|
102,883 |
|
|
107,791 |
|
104.8 |
|
100.0 |
% |
100.0 |
% |
|
Management and contract services revenue |
|
|
20 |
|
|
— |
|
|
20 |
|
— |
|
|
|
|
|
|
Total net operating revenue |
|
|
210,694 |
|
|
102,883 |
|
|
107,811 |
|
104.8 |
|
|
|
|
|
|
Equity in loss of unconsolidated joint venture |
|
|
(900) |
|
|
— |
|
|
(900) |
|
— |
|
|
|
|
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Salaries, wages and benefits |
|
|
136,498 |
|
|
65,244 |
|
|
71,254 |
|
109.2 |
|
64.8 |
|
63.4 |
|
|
General and administrative |
|
|
37,604 |
|
|
17,436 |
|
|
20,168 |
|
115.7 |
|
17.8 |
|
16.9 |
|
|
Other operating expenses |
|
|
27,329 |
|
|
11,185 |
|
|
16,144 |
|
144.3 |
|
13.0 |
|
10.9 |
|
|
(Gain) loss from the disposal or impairment of assets |
|
|
(42) |
|
|
207 |
|
|
(249) |
|
(120.3) |
|
- |
|
0.2 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
7,117 |
|
89.9 |
|
7.1 |
|
7.7 |
|
|
Total operating expenses |
|
|
216,426 |
|
|
101,992 |
|
|
114,434 |
|
112.2 |
|
102.7 |
|
99.1 |
|
|
(Loss) income from operations |
|
|
(6,632) |
|
|
891 |
|
|
(7,523) |
|
(844.3) |
|
(3.1) |
|
0.9 |
|
|
Other (expense) income: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(11,966) |
|
|
(2,827) |
|
|
(9,139) |
|
(323.3) |
|
(5.7) |
|
(2.7) |
|
|
Change in fair market value of derivatives |
|
|
— |
|
|
112 |
|
|
(112) |
|
(100.0) |
|
- |
|
0.1 |
|
|
Write-off of deferred loan costs |
|
|
— |
|
|
(440) |
|
|
440 |
|
(100.0) |
|
- |
|
(0.4) |
|
|
Total other expense |
|
|
(11,966) |
|
|
(3,155) |
|
|
(8,811) |
|
279.3 |
|
(5.7) |
|
(3.1) |
|
|
Loss before (benefit) provision for income taxes |
|
|
(18,598) |
|
|
(2,264) |
|
|
(16,334) |
|
721.5 |
|
(8.8) |
|
(2.2) |
|
|
(Benefit) provision for income taxes |
|
|
(1,326) |
|
|
720 |
|
|
(2,046) |
|
(284.2) |
|
(0.6) |
|
0.7 |
|
|
Net loss |
|
$ |
(17,272) |
|
$ |
(2,984) |
|
$ |
(14,288) |
|
478.8 |
% |
(8.2) |
% |
(2.9) |
% |
Overall
Our results for the year ended December 31, 2014 reflect a 104.8% increase in net patient service revenue of $107.8 million. We recorded a net loss of $17.3 million compared to a net loss of $3.0 million for the year ended December 31, 2013. The net loss was attributable to preopening expenses associated with 29 new facility openings and 2 relocations, interest expense associated with our long-term debt, additional depreciation and amortization expense and costs associated with our initial public offering and other public company costs, partially offset by an increase in net patient service revenue resulting from our growth.
Revenue
Patient Service Revenue
Patient service revenue increased by $128.3 million, or 111.6%, to $243.3 million for the year ended December 31, 2014, from $115.0 million for the year ended December 31, 2013. This increase was primarily attributable to a 20.9% increase in patient volumes generated from new facilities, a 2.4% increase in the number of high acuity patients and a 5.0% overall increase in rates for certain third-party payors beginning in May 2014.
64
Provision for Bad Debt
Our provision for bad debt increased by $20.5 million to $32.6 million for the year ended December 31, 2014, from $12.1 million for the year ended December 31, 2013. Of this increase, $18.5 million was attributable to bad debt associated with revenue generated from new facilities and the remainder was attributable to an increase in patient volume coupled with a shift in payor mix from third party payors to patients.
Net Patient Service Revenue
As a result of the factors described above, our net patient service revenue increased by $107.8 million, or 104.8%, to $210.7 million for the year ended December 31, 2014, from $102.9 million for the year ended December 31, 2013.
Management and Contract Services Revenue
Management and contract services revenue was approximately $20,000 for the year ended December 31, 2014 as a result of our management and contract services agreement associated with our joint venture agreement entered into in November 2014.
Equity in loss of joint venture
Equity in loss of joint venture consists of our 49.9% share of losses generated from our non-controlling equity investment in a hospital facility located in Phoenix, Arizona. Our equity in loss of unconsolidated joint venture was approximately $0.9 million for the year ended December 31, 2014.
Operating Expenses
Salaries, Wages and Benefits
Salaries, wages and benefits increased by $71.3 million to $136.5 million for the year ended December 31, 2014, from $65.2 million for the year ended December 31, 2013. This increase was primarily attributable to an increase in new facilities, which contributed $63.0 million in facility compensation. The remaining $8.3 million increase was primarily attributable to our continued efforts to add staff to support new facility growth.
General and Administrative
General and administrative expenses increased by $20.2 million to $37.6 million for the year ended December 31, 2014, from $17.4 million for the year ended December 31, 2013. This increase was primarily attributable to $5.2 million in costs associated with our initial public offering, $3.4 million in additional marketing costs associated with opening new facilities and our consumer awareness program, $3.5 million in additional facility utilities and insurance expenses, $1.2 million in property taxes, $1.8 million in legal and accounting expenses associated with opening new facilities, $1.3 million in travel expenses associated with increased headcount and the opening of new facilities outside of the Dallas/Fort Worth market and $3.8 million in employee recruiting, development and other corporate expenses.
Other Operating Expenses
Other operating expenses increased by $16.1 million to $27.3 million for the year ended December 31, 2014, from $11.2 million for the year ended December 31, 2013. This increase was primarily attributable to $10.8 million in additional lease costs for buildings and medical equipment at facilities, $0.7 million increase in lease costs for corporate office space and $1.6 million in property insurance and building maintenance for new and existing facilities. Patient care and supply costs at new facilities contributed $4.0 million in additional expenses, offset by a decrease of $1.0 million at legacy facilities.
65
Depreciation and Amortization
Depreciation and amortization expenses increased by $7.1 million to $15.0 million for the year ended December 31, 2014, from $7.9 million for the year ended December 31, 2013. This increase was primarily attributable to the construction of new facilities that opened during 2014 and 2013, as well as new equipment at those facilities.
Other (Expense) Income
Interest Expense
Interest expense primarily consists of interest on our Senior Secured Credit Facility and on one facility treated as a capital lease. Our interest expense increased by $9.1 million to $12.0 million for the year ended December 31, 2014, compared to $2.8 million for the year ended December 31, 2013. This increase was primarily attributable to refinancing our Senior Secured Credit Facility in 2013 at higher interest rates, coupled with an increase in borrowings to fund construction of new facilities.
Loss Before (Benefit) Provision for Income Taxes
As a result of the factors described above, we recorded a loss before (benefit) provision for income taxes of $18.6 million for the year ended December 31, 2014, compared to a net loss of $2.3 million for the year ended December 31, 2013.
(Benefit) Provision for Income Taxes
For the year ended December 21, 2014, we recorded income tax benefit of $1.3 million, which consists of $2.8 million of federal income tax benefit offset by Texas margin tax of $1.5 million. Prior to the Reorganization, we were not a federal taxpayer. The Company’s effective tax rate for the period subsequent to the Reorganization differs from the statutory rate due primarily to state taxes that are not based on pre-tax income/(loss) but on gross margin resulting in state tax expense even in periods of pretax losses.
Net Loss
As a result of the factors described above, we recorded a net loss of $17.3 million for the year ended December 31, 2014, compared to a net loss of $3.0 million for the year ended December 31, 2013.
66
Year Ended December 31, 2013 Compared to Year Ended December 31, 2012
The following table summarizes our results of operations for the years ended December 31, 2013 and 2012:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended December 31, |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Percentage of |
|
||
|
|
|
|
|
|
|
|
|
Change from prior |
|
net patient |
|
|||||
|
|
|
|
|
|
|
|
|
period |
|
service revenue |
|
|||||
|
(dollars in thousands) |
|
2013 |
|
2012 |
|
$ |
|
% |
|
2013 |
|
2012 |
|
|||
|
Statement of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenue |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient service revenue |
|
$ |
114,960 |
|
$ |
80,977 |
|
$ |
33,983 |
|
42.0 |
% |
|
|
|
|
|
Provision for bad debt |
|
|
(12,077) |
|
|
(8,376) |
|
|
(3,701) |
|
44.2 |
|
|
|
|
|
|
Net patient service revenue |
|
|
102,883 |
|
|
72,601 |
|
|
30,282 |
|
41.7 |
|
100 |
% |
100 |
% |
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Salaries, wages and benefits |
|
|
65,244 |
|
|
41,754 |
|
|
23,490 |
|
56.3 |
|
63.4 |
|
57.5 |
|
|
General and administrative |
|
|
17,436 |
|
|
12,805 |
|
|
4,631 |
|
36.2 |
|
16.9 |
|
17.6 |
|
|
Other operating expenses |
|
|
11,185 |
|
|
7,493 |
|
|
3,692 |
|
49.3 |
|
10.9 |
|
10.3 |
|
|
Loss from the disposal or impairment of assets |
|
|
207 |
|
|
652 |
|
|
(445) |
|
(68.3) |
|
0.2 |
|
0.9 |
|
|
Depreciation and amortization |
|
|
7,920 |
|
|
4,640 |
|
|
3,280 |
|
70.7 |
|
7.7 |
|
6.4 |
|
|
Total operating expenses |
|
|
101,992 |
|
|
67,344 |
|
|
34,648 |
|
51.4 |
|
99.1 |
|
92.8 |
|
|
Income from operations |
|
|
891 |
|
|
5,257 |
|
|
(4,366) |
|
(83.1) |
|
0.9 |
|
7.2 |
|
|
Other (expense) income: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(2,827) |
|
|
(1,056) |
|
|
(1,771) |
|
167.7 |
|
(2.7) |
|
(1.5) |
|
|
Change in fair market value of derivatives |
|
|
112 |
|
|
(533) |
|
|
645 |
|
(121.0) |
|
0.1 |
|
(0.7) |
|
|
Write-off of deferred loan costs |
|
|
(440) |
|
|
— |
|
|
(440) |
|
- |
|
(0.4) |
|
- |
|
|
Total other expense |
(3,155) | (1,589) | (1,566) | 98.6 | (3.1) | (2.2) | ||||||||||
|
(Loss) income before provision for income taxes |
|
|
(2,264) |
|
|
3,668 |
|
|
(5,932) |
|
(161.7) |
|
(2.2) |
|
5.1 |
% |
|
Provision for income taxes |
|
|
720 |
|
|
467 |
|
|
253 |
|
54.2 |
|
0.7 |
|
0.6 |
|
|
Net (loss) income |
|
$ |
(2,984) |
|
$ |
3,201 |
|
$ |
(6,185) |
|
(193.2) |
% |
(2.9) |
% |
4.4 |
% |
Overall
Our results for the year ended December 31, 2013 reflect a 41.7% increase in net patient service revenue of $30.3 million, although we recorded a net loss of $3.0 million compared to a net income of $3.2 million for the year ended December 31, 2012. The change from net income to a net loss was attributable primarily to increased expenses incurred in connection with opening new facilities (including, in particular, increases in salaries, wages and benefits), expanding the management team in anticipation of new facility growth, and higher interest expense associated with our refinanced Senior Secured Credit Facility to provide financing for that growth.
Revenue
Patient Service Revenue
Patient service revenue increased by $34.0 million, or 42.0%, to $115.0 million for the year ended December 31, 2013, from $81.0 million for the year ended December 31, 2012. This increase was primarily attributable to a 46.5% increase in patient volumes generated from new facilities, a 4.3% increase in high level acuity patients and a 5% increase in our rates under a large third‑party payor contract in May 2013. New facilities that opened in 2012 and 2013 accounted for an increase in patient service revenue of $33.4 million. Patient service revenue in facilities opened prior to 2012 increased by $2.2 million; however, $1.6 million of this was offset by the closure of our Georgetown, Texas facility in 2012.
67
Provision for Bad Debt
Our provision for bad debt increased by $3.7 million, or 44.2%, to $12.1 million for the year ended December 31, 2013, from $8.4 million for the year ended December 31, 2012. Of this increase, $2.7 million was attributable to revenue generated from facilities that opened in 2013. An additional $1.0 million was a result of the full year of revenue for facilities that opened in 2012. For facilities opened prior to January 1, 2012, bad debt increased by $0.4 million, or 6%, as a result of continued revenue growth. This increase was offset by a reduction in bad debt expense due to the closure of our Georgetown, Texas facility.
Net Patient Service Revenue
As a result of the factors described above, our net patient service revenue increased by $30.3 million, or 41.7%, to $102.9 million for the year ended December 31, 2013, from $72.6 million for the year ended December 31, 2012.
Operating Expenses and Income from Operations
Salaries, Wages and Benefits
Salaries, wages and benefits increased by $23.4 million, or 56.3%, to $65.2 million for the year ended December 31, 2013, from $41.8 million for the year ended December 31, 2012. This increase was primarily attributable to an increase in new facilities, which contributed $16.6 million in facility compensation. In addition, a full year of 24/7 operations in all facilities opened prior to January 1, 2012 contributed $3.2 million. Staff compensation and benefits increased by $4.6 million, which was primarily attributable to annualized costs associated with hiring executives in 2012 and our continued efforts to add staff to support new facility growth.
General and Administrative
General and administrative expenses increased by $4.6 million, or 36.2%, to $17.4 million for the year ended December 31, 2013, from $12.8 million for the year ended December 31, 2012. This increase was primarily attributable to $2.8 million in additional marketing costs associated with opening new facilities and our consumer awareness program, $1.0 million in additional facility utilities and insurance expenses, and $0.4 million in travel expenses associated with increased headcount and the opening of new facilities outside of the Dallas/Fort Worth market.
Other Operating Expenses
Other operating expenses increased by $3.7 million, or 49.3%, to $11.2 million for the year ended December 31, 2013, from $7.5 million for the year ended December 31, 2012. Additional lease costs for building and medical equipment at new facilities contributed $1.6 million to this change. Patient care and supply costs at new facilities contributed $1.4 million in expenses. Existing facilities contributed an increase of $0.7 million in patient care and supply costs, primarily driven by an increase in radiology procedures.
Loss from the Disposal or Impairment of Assets
Loss from the disposal or impairment of assets decreased by $0.4 million, or 68.3%, to $0.2 million for the year ended December 31, 2013, from $0.6 million for the year ended December 31, 2012. This decrease was primarily attributable to an absence of prior‑year costs associated with our former corporate office, which was relocated in 2012.
Depreciation and Amortization
Depreciation and amortization expenses increased by $3.3 million, or 70.7%, to $7.9 million for the year ended December 31, 2013, from $4.6 million for the year ended December 31, 2012. This increase was primarily attributable to the construction of new facilities that opened during 2012 and 2013, as well as new equipment at those facilities.
68
Other (Expense) Income
Interest Expense
Interest expense primarily consists of interest on our Senior Secured Credit Facility and on one facility treated as a capital lease. Our interest expense increased by $1.7 million to $2.8 million for the year ended December 31, 2013, compared to $1.1 million for the year ended December 31, 2012. This increase was primarily attributable to refinancing our Senior Secured Credit Facility in 2013 at higher interest rates and an increase in borrowings to fund construction of new facilities.
Change in Fair Market Value of Derivatives
Our change in fair market value of derivatives was a gain of $0.1 million for the year ended December 31, 2013, compared to a loss of $0.5 million for the year ended December 31, 2012. This improvement was primarily attributable to the change in the fair market value of derivatives related to an interest rate swap not accounted for as a hedge. This interest rate swap was terminated as part of the refinancing of the Senior Secured Credit Facility in 2013.
Write‑Off of Deferred Loan Costs
Our write‑off of deferred loan costs of $0.4 million was associated with the refinancing of the Senior Secured Credit Facility in 2013.
Income (Loss) Before Provision for Income Taxes
As a result of the factors described above, we recorded a loss of $2.3 million for the year ended December 31, 2013, compared to income of $3.7 million for the year ended December 31, 2012, in our income (loss) before provision for income taxes.
Provision for Income Taxes
No provision was made for federal income taxes since we were taxed as a partnership for federal income tax purposes. Provision for income taxes primarily consists of the Texas margin tax. Our provision for income taxes increased by $0.2 million, or 54.2%, to $0.7 million for the year ended December 31, 2013, from $0.5 million for the year ended December 31, 2012. This increase was primarily attributable to increased revenue and increased payroll expenses on which the Texas margin tax is based.
Net Income (Loss)
As a result of the factors described above, we recorded a net loss of $3.0 million for the year ended December 31, 2013, compared to recording net income of $3.2 million for the year ended December 31, 2012.
Liquidity and Capital Resources
We rely on cash flows from operations, the Senior Secured Credit Facility and the MPT Agreement (each as described below) as our primary sources of liquidity. In June 2014, we sold 4,900,000 shares of Class A common stock in an initial public this offering, resulting in proceeds, net of transaction expenses, of $96.2 million. We used part of the net proceeds from the initial public offering to reduce outstanding borrowings under our senior secured credit facility. An additional 735,000 shares of Class A common stock were sold to the public, of which 313,586 shares were sold by a significant stockholder and 421,414 shares were sold by the Company with the proceeds received by the Company used to purchase an equivalent number of LLC Units from such significant stockholder.
Upon the consummation of our initial public offering, we entered into a tax receivable agreement with the Unit holders of Adeptus Health LLC, which provides for the payment from time to time by us to the Unit holders of Adeptus Health LLC of 85% of the amount of the benefits, if any, that we deemed to realize as a result of increases in tax basis and certain other tax benefits related to exchanges of LLC Units pursuant to the exchange agreement, including tax benefits attributable to payments under the tax receivable agreement. These payment obligations are obligations of Adeptus Health Inc. For purposes of the tax receivable agreement, the benefit deemed realized by
69
Adeptus Health Inc. will be computed by comparing its actual income tax liability (calculated with certain assumptions) to the amount of such taxes that we would have been required to pay had there been no increase to the tax basis of the assets of Adeptus Health LLC as a result of the exchanges and had Adeptus Health Inc. not entered into the tax receivable agreement.
Our primary cash needs are construction costs for our new facilities, compensation of our personnel, purchases of medical supplies, facility leases, equipment rentals, marketing initiatives, service of long-term debt and any payments made under the tax receivable agreement. We believe that cash we expect to generate from operations, the availability of borrowings under the Senior Secured Credit Facility and funds available under the MPT Agreement will be sufficient to meet liquidity requirements, including any payments made under the tax receivable agreement, anticipated capital expenditures and payments due under our Senior Secured Credit Facility and MPT Agreement for at least 12 months.
As of December 31, 2014, our principal sources of liquidity included cash of $2.0 million, funds available under our Senior Secured Credit Facility line of credit of $10.0 million, net of $5.5 million and $0.5 million of outstanding borrowing and letters of credit, respectively, and $80.2 million in funds available under our delayed draw term loan, subject to meeting certain debt covenants. As of December 31, 2014, we also had $89.4 million available under the MPT Agreements.
Cash Flows
The following table summarizes our cash flows for the periods indicated:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(dollars in thousands) |
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Net cash (used in) provided by operating activities |
|
$ |
(24,698) |
|
$ |
6,872 |
|
$ |
11,408 |
|
|
Net cash used in investing activities |
|
|
(49,448) |
|
|
(44,647) |
|
|
(15,537) |
|
|
Net cash provided by financing activities |
|
|
64,653 |
|
|
45,815 |
|
|
2,820 |
|
|
Net increase (decrease) in cash |
|
$ |
(9,493) |
|
$ |
8,040 |
|
$ |
(1,309) |
|
Net Cash from Operating Activities
Net cash used in operating activities increased by $31.6 million to $24.7 million for the year ended December 31, 2014, from $6.9 million provided by operating activities for the same period in 2013. This increase was primarily attributable to labor costs on new facilities where revenue is ramping up, corporate labor cost associated with expanding our management team in anticipation of new facility growth, equipment lease costs associated with the new facilities, new facility preopening expenses, marketing expenses, increases in accounts receivable balances due to increased revenues, restricted cash requirements related to the MPT Agreements and interest payments.
Net cash provided by operating activities decreased by $4.5 million, or 39.5%, to $6.9 million for the year ended December 31, 2013, from $11.4 million for the same period in 2012. This decrease was primarily attributable to labor costs on new facilities where revenue is ramping, corporate labor cost associated with expanding our management team in anticipation of new facility growth, equipment lease costs associated with the new facilities, new facility preopening expenses, marketing expenses and interest payments.
Net Cash from Investing Activities
Net cash used in investing activities increased by $4.8 million to $49.4 million for the year ended December 31, 2014, from $44.6 million for the same period in 2013. This increase was primarily attributable to capital expenditures for construction of new facilities.
70
Net cash used in investing activities increased by $29.1 million, or 187.7%, to $44.6 million for the year ended December 31, 2013, from $15.5 million for the same period in 2012. This increase was primarily attributable to capital expenditures for construction of new facilities.
Net Cash from Financing Activities
Net cash provided by financing activities increased by $18.8 million to $64.7 million for the year ended December 31, 2014, from $45.8 million for the same period in 2013. This increase was primarily attributable to proceeds from the initial public offering, net of transaction expenses of $96.2 million, offset by $60.0 million for the payment of a dividend to our then-existing owners prior to our initial public offering, a decrease of $22.1 million over the same period in prior year in borrowings under our Senior Secured Credit Facility to finance construction of new facilities, a decrease of $4.0 million in payments related to deferred loan costs that did not recur in 2014 and an increase of $0.5 million in payments to terminate an interest rate swap agreement in 2013.
Net cash provided by financing activities increased by $43.0 million to $45.8 million for the year ended December 31, 2013, from $2.8 million for the same period in 2012. This increase was primarily attributable to increased borrowing under our original credit facility of $27.0 million and refinancing our Senior Secured Credit Facility and thereby increasing our funded indebtedness by an additional $25.0 million to finance construction of new facilities. This increase was partially offset by a capital contribution of $4.1 million that did not recur in 2013 and loan origination fees of $5.0 million.
Off Balance Sheet Arrangements
During the periods presented, we did not have any relationships with unconsolidated entities or financial partnerships, such as entities often referred to as structured finance or special purpose entities, which would have been established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purpose arrangements. We lease certain medical facilities and equipment under various non-cancelable operating leases. See "—Obligations and Commitments—Operating Lease Obligations."
As a result of our strategy of partnering with Dignity Health for Dignity Health Arizona General Hospital, we do not own a controlling interest in this facility. At December 31, 2014, we accounted for this joint venture under the equity method. Similar to our consolidated facilities, this joint venture has debts. With respect to this joint venture, these debts are not included in our consolidated financial statements. At December 31, 2014, the total debt on the balance sheet of the joint venture was approximately $0.3 million. Our ownership in this joint venture was 49.9% at December 31, 2014.
As described above, our unconsolidated joint venture is structured as an LLC. This joint venture does not provide financing, liquidity, or market or credit risk support for us
Contractual Obligations and Commitments
The following is a summary of our contractual obligations as of December 31, 2014:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(dollars in thousands) |
|
Total |
|
Less than |
|
1 - 3 years |
|
3 - 5 years |
|
More than |
|
|||||
|
Long-term debt obligations |
|
$ |
106,798 |
|
$ |
1,191 |
|
$ |
7,138 |
|
$ |
98,469 |
|
$ |
- |
|
|
Interest on debt obligations(1) |
|
|
33,828 |
|
|
8,377 |
|
|
17,804 |
|
|
7,647 |
|
|
- |
|
|
Capital lease obligations(2) |
|
|
8,230 |
|
|
522 |
|
|
1,077 |
|
|
1,119 |
|
|
5,512 |
|
|
Operating lease obligations |
|
|
248,627 |
|
|
26,318 |
|
|
48,242 |
|
|
34,883 |
|
|
139,184 |
|
|
Total |
|
$ |
397,483 |
|
$ |
36,408 |
|
$ |
74,261 |
|
$ |
142,118 |
|
$ |
144,696 |
|
|
(1) |
The amount of interest on debt obligations represents current obligations using rates in effect as of December 31, 2014. |
|
(2) |
Includes amounts representing interest. |
71
Senior Secured Credit Facility
On October 31, 2013, we entered into a Senior Secured Credit Facility (the “Facility”) for a $75.0 million term loan, which matures on October 31, 2018. The Facility includes an additional $165.0 million delayed draw term loan commitment, which, if unused, expires eighteen months after the closing date, and a $10.0 million revolving commitment that matures on October 31, 2018. All of our assets are pledged as collateral under the Senior Secured Credit Facility. Borrowings under the Facility are used by us to provide financing for working capital and capital expenditures for new facility expansion and replaced our original credit facility.
On March 31, 2014, we amended the Facility to, among other things, increase the maximum aggregate amount permitted to be funded by Medical Properties Trust (“MPT”) under the Master Funding and Development Agreement (the “MPT Agreement”) to $255.0 million.
On June 11, 2014, we entered into a second amendment to the Facility to, among other things, provide for a delayed draw term loan in an aggregate principal amount of up to $75.0 million, up to $60.0 million of which will be used to make specified distributions and up to $10.0 million to repay certain revolving loans. On June 11, 2014, we drew $75.0 million and made the $60.0 million dividend distribution on June 24, 2014.
Borrowings under the Facility bear interest, at our option, at a rate equal to an applicable margin over (a) a base rate determined by reference to the highest of (1) the prime rate, (2) the federal funds effective rate plus 0.50% and (3) LIBOR for an interest period of one month plus 1%, or (b) LIBOR for the applicable interest period. The margin for the Senior Secured Credit Facility is 6.50% in the case of base rate loans and 7.50% in the case of LIBOR loans. The Facility includes an unused line fee of 0.50% per annum on the revolving commitment and delayed draw term loan commitment, a draw fee of 1.0% of the principal amount of each borrowing on the delayed draw term loan and an annual Agency fee of $0.1 million. As of December 31, 2014, we had $80.2 million and approximately $4.0 million available under the delayed draw term commitment and the revolving commitment, respectively, subject to certain debt covenants.
The original principal amount of the term loan will be repaid in consecutive quarterly installments of $0.5 million on the last day of each fiscal quarter commencing with the fiscal quarter ending December 31, 2015 and escalating to $0.9 million for each fiscal quarter ending after December 31, 2016. If drawn, the delayed draw term loan will be repaid in consecutive quarterly installments in an amount based on the repayment calculation contained in the Facility on the last day of each fiscal quarter commencing with the fiscal quarter ending December 31, 2015. We will repay the aggregate principal amount of all revolving loans outstanding on the maturity date, October 31, 2018.
The Facility contains a number of significant negative covenants. Such negative covenants, among other things and subject to certain exceptions, restrict First Choice ER, LLC and its subsidiaries’ ability to incur additional indebtedness, make guarantees and enter into hedging agreements; create liens on assets; enter into sale and leaseback transactions; engage in mergers or consolidations; transfer assets; pay dividends and distributions; change the nature of our business; make investments, loans and advances, including acquisitions; engage in certain transactions with affiliates; amend certain material agreements, including the MPT Agreements and organizational documents; enter into certain joint ventures; enter into certain restrictive agreements; and make certain changes to our accounting practices. In addition, the Facility contains financial covenants that, among other things, require us to maintain a consolidated leverage ratio of at most 7.00 to 1.00 (decreasing to 3.50 to 1.00 as of December 31, 2016 and thereafter); a consolidated interest charge coverage ratio of at least 2.00 to 1.00 (increasing to 2.75 to 1.00 as of June 30, 2015 and thereafter); and a consolidated capital expenditures amount ranging from $30.0 million (for the fiscal year ended December 31, 2014) to $15.0 million (for the fiscal year ended December 31, 2015 and thereafter). The financial covenant calculations are based on First Choice ER, LLC and its subsidiaries as a consolidated group. In addition, the Facility includes certain limitations on intercompany indebtedness. The affirmative covenants, negative covenants, and financial covenants, are measured on a quarterly basis and, as of December 31, 2014, we were in compliance with all covenant requirements.
72
Capital Lease Obligations
Assets under capital leases totaled approximately $4.2 million as of December 31, 2014, and were included within the buildings component of net property and equipment. Accumulated amortization associated with these capital lease assets totaled approximately $0.3 million for the year ended December 31, 2014.
Assets under capital leases totaled approximately $3.9 million as of December 31, 2013, and were included within buildings, computer equipment, medical equipment, office equipment and automobiles. Accumulated amortization associated with these capital lease assets totaled approximately $23,000 for the year ended December 31, 2013.
Operating Lease Obligations
We lease certain medical facilities and equipment under various non-cancelable operating leases. In June 2013, we entered into the Initial Master Funding and Development Agreement (the “MPT Agreement”) with an affiliate of Medical Properties Trust (“MPT) to fund future facilities and in July 2014, we entered into the Additional MPT Agreement.
Pursuant to the MPT Agreements, MPT will acquire parcels of land, fund the ground-up construction of new freestanding emergency room facilities and lease the facilities to us upon completion of construction. Under the terms of the Initial MPT Agreement, MPT was required to fund all hard and soft costs, including the project purchase price, closing costs and pursuit costs for the assets relating to the construction of up to 25 facilities with a maximum aggregate funding of $100.0 million. The maximum aggregate funding under that agreement has been met. The Additional MPT Agreement allows a maximum aggregate funding of $150.0 million, of which $ 89.4 million remained available as of December 31, 2014. All other material terms remain consistent with the Initial MPT Agreement. Each completed project will be leased for an initial term of 15 years, with three five-year renewal options. We follow the guidance in Accounting Standards Codification, or ASC, 840, Leases, and ASC 810, Consolidation, in evaluating the lease as a build-to-suit lease transaction to determine whether we would be considered the accounting owner of the facilities during the construction period. In applying the accounting guidance, we concluded that one facility completed in 2013 under this arrangement qualified for capitalization.
In addition to the MPT Agreements, the Company has entered into similar agreements with certain developers to fund and lead the development efforts on the construction of future facilities. As of December 31, 2014, the Company had total receivables of $13.4 million from the lessor to the MPT Agreements and certain developers for soft costs incurred for facilities currently under development.
We lease approximately 80,000 square feet for our corporate headquarters. Lease expense associated with this lease was $1.4 million for the year ended December 31, 2014.
Capital Expenditures
Our current plans for our business contemplate capital expenditures to expand our operations. The MPT Agreements will be used to fund a significant portion of our new facilities. We typically incur approximately $0.2 million in capital expenditures related to each MPT-funded facility. Facilities funded under the MPT Agreement will be operating leases and thus not considered a capital expenditure.
73
The table below provides our total capital expenditures for the period (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
Year ended |
|
Year ended |
|
||
|
|
|
December 31, 2014 |
|
December 31, 2013 |
|
||
|
Leasehold improvements |
|
$ |
32,076 |
|
$ |
38,786 |
|
|
Computer equipment |
|
|
2,117 |
|
|
1,481 |
|
|
Medical equipment |
|
|
1,656 |
|
|
1,813 |
|
|
Office equipment |
|
|
3,615 |
|
|
707 |
|
|
Automobiles |
|
|
— |
|
|
27 |
|
|
Land |
|
|
7,849 |
|
|
3,234 |
|
|
Buildings |
|
|
116 |
|
|
— |
|
|
|
|
$ |
47,429 |
|
$ |
46,048 |
|
New Accounting Pronouncements
In May 2014, the FASB issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606), which requires an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. The ASU will replace most existing revenue recognition guidance in U.S. GAAP when it becomes effective. The new standard is effective for the Company on January 1, 2017. Early application is not permitted. The standard permits the use of either the retrospective or cumulative effect transition method. The Company is evaluating the effect that ASU 2014-09 will have on its consolidated financial statements and related disclosures. The Company has not yet selected a transition method nor has it determined the effect of the standard on its ongoing financial reporting.
In August 2014, the FASB issued new guidance related to the disclosures around going concern. The new standard update provides guidance around management's responsibility to evaluate whether there is substantial doubt about an entity's ability to continue as a going concern and to provide related footnote disclosures. The new guidance is effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2016. Early adoption is permitted. The Company does not believe the adoption of this guidance will have a material impact on its consolidated financial statements
Critical Accounting Policies
The following is a discussion of our application of critical accounting policies that require our management to make certain assumptions about matters that are uncertain at the time the accounting estimate is made, where our management could reasonably use different estimates, or where accounting changes may reasonably occur from period to period, and in each case would have a material effect on our financial statements.
Patient Revenue and Accounts Receivable
Revenue is recognized when services are rendered to patients. Charges for all services provided to insured patients are initially billed and processed by the patients’ insurance provider. We have agreements with certain insurance companies that provide for in‑network payments that may differ from our established rates or as determined by the patient’s out of network benefits. Differences between established rates and those set by insurance programs, as well as charity care, employee and prompt pay adjustments, are recorded as adjustments directly to patient service revenue. Fee adjustments of approximately $137.1 million, $62.5 million, and $44.5 million were recorded for the years ended December 31, 2014, 2013 and 2012, respectively. Allowable amounts not covered by the insurance companies are then billed to the patients. Estimated uncollectible amounts from insured patients are recorded as bad debt expense in the period in which the services are provided. Collection of payment for services provided to patients without insurance coverage is done at the time of service.
Accounts receivable are reduced by an allowance for doubtful accounts. In establishing our allowance for doubtful accounts, management considers historical collection experience, the aging of the account, the payor
74
classification, and patient payment patterns. Amounts due directly from patients represent our highest collectability risk. There were not any significant changes in the estimates or assumptions underlying the calculation of the allowance for doubtful accounts for the years ended December 31, 2014, 2013 and 2012.
We write off as bad debt expense uncollectible accounts receivable arising from patient responsibility after all collection efforts have been exhausted and it has been determined such accounts will not be collected. Bad debt write‑offs of approximately $24.8 million, $10.1 million and $7.7 million were recorded for the years ended December 31, 2014, 2013 and 2012, respectively.
We treat any patient that is emergent, including patients that may be eligible for Medicare or Medicaid and patients without medical insurance. These services are provided at no charge to the patient. Total charity care was approximately 8.6%, 7.0%, and 2.0% of patient revenue for the years ended December 31, 2014, 2013 and 2012, respectively.
Impairment of Long‑Lived Assets
Long‑lived assets are reviewed for impairment whenever events or circumstances indicate that the carrying amount of an asset or group of assets might not be recoverable. We do not perform a periodic assessment of assets for impairment in the absence of such information or indicators. Conditions that would indicate a potential impairment include a significant decline in the observable market value of an asset or a significant change in the extent or manner in which an asset is used. The impairment review includes a comparison of future projected cash flows generated by the asset or group of assets with its associated net carrying value. If the net carrying value of the asset or group of assets exceeds expected cash flows (undiscounted and without interest charges), an impairment loss is recognized to the extent the carrying amount of the asset exceeds its fair value. There were no impairments recorded for the years ended December 31, 2014 and 2013. We recorded long lived asset impairment charges of $0.3 million for the year ended December 31, 2012, associated with the closing of our former corporate headquarters.
Goodwill
In accordance with the FASB ASC 805, Business Combinations, the purchase method of accounting requires that the excess of purchase price paid over the estimated fair value of identifiable tangible and intangible net assets of acquired businesses be recorded as goodwill. In accordance with the provisions of ASC 350, Intangibles—Goodwill and Other, goodwill is tested for impairment annually, and interim impairment tests are performed whenever an event occurs or circumstances change that indicate an impairment has more likely than not occurred. We have one reporting unit and goodwill is evaluated at that level. We evaluate impairment of goodwill by first performing a qualitative assessment to determine whether it is more likely than not that the fair value of the reporting unit is less than the carrying value. If it is concluded that this is the case, it is necessary to perform a two‑ step impairment test. The first step involves a comparison of the fair value of a reporting unit with its carrying amount. If the carrying value of the reporting unit exceeds its fair value, the second step involves a comparison of the implied fair value and the carrying amount of the goodwill of that reporting unit to determine the impairment charge, if necessary. We have established October 31 as the date for our annual impairment review.
We estimate the fair value of our total invested capital using an income and market approach, reduced by interest bearing debt as of the valuation date. These valuations require management to make estimates and assumptions regarding industry economic factors and prospective financial information. There were no goodwill impairment charges recorded for the years ended December 31, 2014, 2013 and 2012.
Intangible Assets
Intangible assets are recorded at their estimated fair values as of the date of acquisition. Intangible assets consist of trade and domain names and non‑compete agreements. In accordance with ASC 350, Intangibles—Goodwill and Other, we review the intangible assets with indefinite lives, which include trade and domain names, at least annually for impairment, or more often if triggering events exist. Intangible assets with definite lives are reviewed for impairment if an indicator of impairment exists similar to long‑lived assets. An impairment loss is recognized if the carrying amount of
75
an intangible asset is not recoverable and its carrying amount exceeds its fair value. There were no impairment charges recorded on intangible assets for the years ended December 31, 2014, 2013 and 2012. Intangible assets with finite useful lives are amortized over their estimated useful life.
Lease Accounting
We determine whether to account for our facility leases as operating or capital leases depending on the underlying terms of the lease agreement. This determination of classification is complex and requires significant judgment relating to certain information including the estimated fair value and remaining economic life of the facilities, our cost of funds, minimum lease payments and other lease terms. The lease rates under our lease agreements are subject to certain conditional escalation clauses which are recognized when probable or incurred and are based on changes in the consumer price index or certain operational performance measures. As of December 31, 2014 and 2013, we leased 54 and 25 facilities, respectively, 53 and 24 of which we classified as operating leases and one of which we classified as a capital lease, respectively.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
We are exposed to market risks related to changes in variable interest rates. As of December 31, 2014, we had $105.5 million of indebtedness (excluding capital leases) which is at variable interest rates. In seeking to reduce the risks and costs associated with such activities, we manage exposure to changes in interest rates primarily through the use of derivatives. As of December 31, 2014, we have hedged the variable interest rate risk with an interest rate cap covering approximately 40% of our indebtedness. We do not use financial instruments for trading or other speculative purposes, nor do we use leveraged financial instruments.
76
Item 8. Financial Statements and Supplementary Data
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
|
|
|
|
Adeptus Health Inc. and Subsidiaries |
|
|
78 |
|
|
79 |
|
|
80 |
|
|
81 |
|
|
Consolidated Statements of Changes in Shareholders’/Owners’ Equity |
82 |
|
83 |
|
|
84 |
77
Report of Independent Registered Public Accounting Firm
The Board of Directors and Owners
Adeptus Health Inc. and Subsidiaries:
We have audited the accompanying consolidated balance sheets of Adeptus Health Inc. and Subsidiaries (the Company) as of December 31, 2014 and 2013, and the related consolidated statements of operations, comprehensive (loss) income, changes in shareholders’/owners’ equity, and cash flows for each of the years in the three‑year period ended December 31, 2014. These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Adeptus Health Inc. and Subsidiaries as of December 31, 2014 and 2013, and the results of their operations and their cash flows for each of the years in the three‑year period ended December 31, 2014, in conformity with U.S. generally accepted accounting principles.
/s/ KPMG LLP
Dallas, Texas
February 27, 2015
78
Adeptus Health Inc. and Subsidiaries
December 31, 2014 and 2013
(In thousands, except share data)
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
||
|
ASSETS |
|
|
|
|
|
|
|
|
Current assets |
|
|
|
|
|
|
|
|
Cash |
|
$ |
2,002 |
|
$ |
11,495 |
|
|
Restricted cash |
|
|
4,795 |
|
|
294 |
|
|
Accounts receivable, less allowance for doubtful accounts of $13,068 and $5,295, respectively |
|
|
37,422 |
|
|
15,887 |
|
|
Other receivables and current assets |
|
|
17,137 |
|
|
3,901 |
|
|
Medical supplies inventory |
|
|
4,287 |
|
|
1,494 |
|
|
Total current assets |
|
|
65,643 |
|
|
33,071 |
|
|
Property and equipment, net |
|
|
93,892 |
|
|
62,087 |
|
|
Investment in unconsolidated joint venture |
|
|
2,100 |
|
|
— |
|
|
Deposits |
|
|
1,772 |
|
|
750 |
|
|
Deferred tax assets |
|
|
34,084 |
|
|
— |
|
|
Intangibles, net |
|
|
20,015 |
|
|
21,795 |
|
|
Goodwill |
|
|
61,009 |
|
|
61,009 |
|
|
Other long-term assets |
|
|
4,303 |
|
|
4,580 |
|
|
Total assets |
|
$ |
282,818 |
|
$ |
183,292 |
|
|
LIABILITIES AND SHAREHOLDERS'/OWNERS' EQUITY |
|
|
|
|
|
|
|
|
Current liabilities |
|
|
|
|
|
|
|
|
Accounts payable and accrued expenses |
|
$ |
25,420 |
|
$ |
15,207 |
|
|
Accrued compensation |
|
|
13,521 |
|
|
9,158 |
|
|
Current maturities of long-term debt |
|
|
1,816 |
|
|
504 |
|
|
Current maturities of capital lease obligations |
|
|
81 |
|
|
58 |
|
|
Deferred rent |
|
|
607 |
|
|
497 |
|
|
Total current liabilities |
|
|
41,445 |
|
|
25,424 |
|
|
Long-term debt, less current maturities |
|
|
104,982 |
|
|
75,000 |
|
|
Payable to related parties pursuant to tax receivable agreement |
|
|
30,039 |
|
|
— |
|
|
Capital lease obligations, less current maturities |
|
|
4,056 |
|
|
3,849 |
|
|
Deferred rent |
|
|
2,416 |
|
|
368 |
|
|
Total liabilities |
|
|
182,938 |
|
|
104,641 |
|
|
Commitments and contingencies |
|
|
|
|
|
|
|
|
Shareholders'/owners' equity |
|
|
|
|
|
|
|
|
Owners' equity |
|
|
— |
|
|
78,651 |
|
|
Preferred stock, par value $0.01 per share; 10,000,000 shares authorized and zero shares issued and outstanding at December 31, 2014 |
|
|
— |
|
|
— |
|
|
Class A common stock, par value $0.01 per share; 50,000,000 shares authorized, 9,845,016 shares issued and outstanding at December 31, 2014 |
|
|
98 |
|
|
— |
|
|
Class B common stock, par value $0.01 per share; 20,000,000 shares authorized 10,781,153 shares issued and outstanding at December 31, 2014 |
|
|
108 |
|
|
— |
|
|
Additional paid-in capital |
|
|
51,238 |
|
|
— |
|
|
Accumulated other comprehensive loss |
|
|
(74) |
|
|
— |
|
|
Accumulated deficit |
|
|
(3,351) |
|
|
— |
|
|
Non-controlling interest |
|
|
51,861 |
|
|
— |
|
|
Total shareholders'/owners' equity |
|
|
99,880 |
|
|
78,651 |
|
|
Total liabilities and shareholders'/owners' equity |
|
$ |
282,818 |
|
$ |
183,292 |
|
The accompanying notes are an integral part of these consolidated financial statements.
79
Adeptus Health Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF OPERATIONS
Years Ended December 31, 2014, 2013 and 2012
(In thousands, except share data)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|||||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Revenue: |
|
|
|
|
|
|
|
|
|
|
|
Patient service revenue |
|
$ |
243,298 |
|
$ |
114,960 |
|
$ |
80,977 |
|
|
Provision for bad debt |
|
|
(32,624) |
|
|
(12,077) |
|
|
(8,376) |
|
|
Net patient service revenue |
|
|
210,674 |
|
|
102,883 |
|
|
72,601 |
|
|
Management and contract services revenue |
|
|
20 |
|
|
— |
|
|
— |
|
|
Total net operating revenue |
|
|
210,694 |
|
|
102,883 |
|
|
72,601 |
|
|
Equity in net loss of unconsolidated joint venture |
|
|
(900) |
|
|
— |
|
|
— |
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
Salaries, wages and benefits |
|
|
136,498 |
|
|
65,244 |
|
|
41,754 |
|
|
General and administrative |
|
|
37,604 |
|
|
17,436 |
|
|
12,805 |
|
|
Other operating expenses |
|
|
27,329 |
|
|
11,185 |
|
|
7,493 |
|
|
(Gain) loss from the disposal or impairment of assets |
|
|
(42) |
|
|
207 |
|
|
652 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
4,640 |
|
|
Total operating expenses |
|
|
216,426 |
|
|
101,992 |
|
|
67,344 |
|
|
(Loss) income from operations |
|
|
(6,632) |
|
|
891 |
|
|
5,257 |
|
|
Other (expense) income: |
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(11,966) |
|
|
(2,827) |
|
|
(1,056) |
|
|
Change in fair market value of derivatives |
|
|
— |
|
|
112 |
|
|
(533) |
|
|
Write-off of deferred loan costs |
|
|
— |
|
|
(440) |
|
|
— |
|
|
Total other (expense) |
|
|
(11,966) |
|
|
(3,155) |
|
|
(1,589) |
|
|
(Loss) income before (benefit) provision for income taxes |
|
|
(18,598) |
|
|
(2,264) |
|
|
3,668 |
|
|
(Benefit) provision for income taxes |
|
|
(1,326) |
|
|
720 |
|
|
467 |
|
|
Net (loss) income |
|
|
(17,272) |
|
|
(2,984) |
|
|
3,201 |
|
|
Less: Net (loss) income attributable to non-controlling interest |
|
|
(13,921) |
|
|
(2,984) |
|
|
3,201 |
|
|
Net loss attributable to Adeptus Health Inc. |
|
$ |
(3,351) |
|
$ |
— |
|
$ |
— |
|
|
Net loss per share of Class A common stock: |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
|
Diluted |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
|
Weighted average shares of Class A common stock: |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
|
Diluted |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
The accompanying notes are an integral part of these consolidated financial statements.
80
Adeptus Health Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF COMPREHENSIVE (LOSS) INCOME
Years ended December 31, 2014, 2013 and 2012
(in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adeptus Health Inc. |
|
Non-controlling Interest |
|
Total |
|
|||||||||||||||||||||
|
|
|
Year ended December 31, |
|
Year ended December 31, |
|
Year ended December 31, |
|
|||||||||||||||||||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
2014 |
|
2013 |
|
2012 |
|
2014 |
|
2013 |
|
2012 |
|
|||||||||
|
Net (loss) income |
|
$ |
(3,351) |
|
$ |
— |
|
$ |
— |
|
$ |
(13,921) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
$ |
(17,272) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
|
Other comprehensive loss, net of tax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unrealized loss on interest rate contract |
|
|
(74) |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(74) |
|
|
— |
|
|
— |
|
|
Comprehensive (loss) income |
|
$ |
(3,425) |
|
$ |
— |
|
$ |
— |
|
$ |
(13,921) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
$ |
(17,346) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
The accompanying notes are an integral part of these consolidated financial statements.
81
Adeptus Health Inc. and Subsidiaries
CONSOLIDATED STATEMENT OF CHANGES IN SHAREHOLDERS’/OWNERS' EQUITY
Years Ended December 31, 2014, 2013 and 2012
(in thousands, except share data)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adeptus Health LLC |
|
Adeptus Health Inc. |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
Total |
|
|||
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
|
|
Other |
|
Total |
|
Non- |
|
Shareholders/ |
|
|||||||
|
|
|
Owners' |
|
Class A shares |
|
Class B shares |
|
Paid-in |
|
Accumulated |
|
Comprehensive |
|
Shareholders' |
|
Controlling |
|
Owners' |
|
|||||||||||||
|
|
|
Equity |
|
Shares |
|
Amount |
|
Shares |
|
Amount |
|
Capital |
|
Deficit |
|
Loss |
|
Equity |
|
Interest |
|
Equity |
|
|||||||||
|
Balance, December 31, 2011 |
|
$ |
76,969 |
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
76,969 |
|
|
Issuance of units - Class A |
|
|
1,120 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
1,120 |
|
|
Stock Subscription |
|
|
(250) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(250) |
|
|
Additional capital contribution |
|
|
4,114 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
4,114 |
|
|
Stock-based compensation |
|
|
253 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
253 |
|
|
Net income |
|
|
3,201 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
3,201 |
|
|
Distributions |
|
|
(2,673) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(2,673) |
|
|
Balance, December 31, 2012 |
|
|
82,734 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
82,734 |
|
|
Stock Subscription |
|
|
83 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
83 |
|
|
Stock-based compensation |
|
|
586 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
586 |
|
|
Net loss |
|
|
(2,984) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(2,984) |
|
|
Distributions |
|
|
(1,768) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(1,768) |
|
|
Balance, December 31, 2013 |
|
|
78,651 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
78,651 |
|
|
Capital contribution |
|
|
167 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
167 |
|
|
Distributions to existing owners |
|
|
(483) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(483) |
|
|
Stock-based compensation prior to reorganization |
|
|
316 |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
316 |
|
|
Net loss prior to reorganization |
|
|
(7,093) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(7,093) |
|
|
Dividends paid to existing owners |
|
|
(60,000) |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(60,000) |
|
|
Class A common stock |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Issuance of Class A shares in Initial Public Offering, net of issuance costs |
|
|
(311) |
|
5,321,414 |
|
|
53 |
|
— |
|
|
— |
|
|
96,483 |
|
|
— |
|
|
— |
|
|
96,536 |
|
|
— |
|
|
96,225 |
|
|
Investment of merged entity into Class A shares |
|
|
(3,307) |
|
4,474,107 |
|
|
45 |
|
— |
|
|
— |
|
|
3,262 |
|
|
— |
|
|
— |
|
|
3,307 |
|
|
— |
|
|
— |
|
|
Issuance of Class A shares to directors |
|
|
— |
|
13,639 |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Issuance of Class A shares to employees |
|
|
— |
|
35,856 |
|
|
— |
|
39,314 |
|
|
1 |
|
|
(1) |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Class B common stock |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Issuance of Class B shares in Reorganization and Offering |
|
|
(7,940) |
|
— |
|
|
— |
|
10,741,839 |
|
|
107 |
|
|
7,833 |
|
|
— |
|
|
— |
|
|
7,940 |
|
|
— |
|
|
— |
|
|
Recording of non-controlling interest upon reorganization |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
(58,687) |
|
|
— |
|
|
— |
|
|
(58,687) |
|
|
58,687 |
|
|
— |
|
|
Effects of Tax Receivable Agreement (See Note 12) |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
1,992 |
|
|
— |
|
|
— |
|
|
1,992 |
|
|
— |
|
|
1,992 |
|
|
Adjustment to true up tax effects of merger and reorganization |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
(343) |
|
|
— |
|
|
— |
|
|
(343) |
|
|
— |
|
|
(343) |
|
|
Stock-based compensation subsequent to initial public offering |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
699 |
|
|
— |
|
|
— |
|
|
699 |
|
|
— |
|
|
699 |
|
|
Unrealized loss on interest rate contract |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(74) |
|
|
(74) |
|
|
— |
|
|
(74) |
|
|
Net loss subsequent to initial public offering |
|
|
— |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
(3,351) |
|
|
— |
|
|
(3,351) |
|
|
(6,826) |
|
|
(10,177) |
|
|
Balance, December 31, 2014 |
|
$ |
— |
|
9,845,016 |
|
$ |
98 |
|
10,781,153 |
|
$ |
108 |
|
$ |
51,238 |
|
$ |
(3,351) |
|
$ |
(74) |
|
$ |
48,019 |
|
$ |
51,861 |
|
$ |
99,880 |
|
The accompanying notes are an integral part of these consolidated financial statements
82
Adeptus Health Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF CASH FLOWS
Years ended December 31, 2014, 2013 and 2012
(In thousands)
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Cash flows from operating activities: |
||||||||||
|
Net (loss) income |
|
$ |
(17,272) |
|
$ |
(2,984) |
|
$ |
3,201 |
|
|
Adjustments to reconcile net (loss) income to net cash (used in) provided by operating activities: |
|
|
|
|
|
|
|
|
|
|
|
(Gain) loss from the disposal or impairment of assets |
|
|
(42) |
|
|
207 |
|
|
652 |
|
|
Change in fair market value of derivatives |
|
|
— |
|
|
(112) |
|
|
533 |
|
|
Depreciation and amortization |
|
|
15,037 |
|
|
7,920 |
|
|
4,640 |
|
|
Deferred tax benefit |
|
|
(2,147) |
|
|
— |
|
|
— |
|
|
Amortization of deferred loan costs |
|
|
891 |
|
|
293 |
|
|
73 |
|
|
Provision for bad debts |
|
|
32,624 |
|
|
12,077 |
|
|
8,376 |
|
|
Write-off of deferred loan costs |
|
|
— |
|
|
440 |
|
|
— |
|
|
Equity in loss of unconsolidated joint venture |
|
|
900 |
|
|
— |
|
|
— |
|
|
Stock-based compensation |
|
|
1,015 |
|
|
586 |
|
|
253 |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
|
Restricted cash |
|
|
(4,501) |
|
|
(294) |
|
|
— |
|
|
Accounts receivable |
|
|
(54,159) |
|
|
(18,107) |
|
|
(9,867) |
|
|
Other receivables and current assets |
|
|
(8,248) |
|
|
(1,757) |
|
|
(234) |
|
|
Medical supplies inventory |
|
|
(2,793) |
|
|
(850) |
|
|
(73) |
|
|
Other long-term assets |
|
|
63 |
|
|
(79) |
|
|
— |
|
|
Accounts payable and accrued expenses |
|
|
7,413 |
|
|
5,632 |
|
|
180 |
|
|
Accrued compensation |
|
|
4,363 |
|
|
3,883 |
|
|
3,166 |
|
|
Deferred rent |
|
|
2,158 |
|
|
17 |
|
|
508 |
|
|
Net cash (used in) provided by operating activities |
|
|
(24,698) |
|
|
6,872 |
|
|
11,408 |
|
|
Cash flows from investing activities: |
|
|
|
|
|
|
|
|
|
|
|
Cash paid for acquisition (net of cash acquired) |
|
|
— |
|
|
— |
|
|
(3,848) |
|
|
Investment in unconsolidated joint venture |
|
|
(3,000) |
|
|
— |
|
|
— |
|
|
Deposits |
|
|
(1,022) |
|
|
(413) |
|
|
(185) |
|
|
Proceeds from sale of property and equipment |
|
|
2,003 |
|
|
1,814 |
|
|
— |
|
|
Capital expenditures |
|
|
(47,429) |
|
|
(46,048) |
|
|
(11,504) |
|
|
Net cash used in investing activities |
|
|
(49,448) |
|
|
(44,647) |
|
|
(15,537) |
|
|
Cash flows from financing activities: |
|
|
|
|
|
|
|
|
|
|
|
Proceeds from initial public offering, net of underwriters fees and expenses |
|
|
96,226 |
|
|
— |
|
|
— |
|
|
Proceeds from long-term borrowings |
|
|
99,457 |
|
|
102,000 |
|
|
25,700 |
|
|
Payment of deferred loan costs |
|
|
(751) |
|
|
(4,954) |
|
|
(354) |
|
|
Payments on borrowings |
|
|
(70,380) |
|
|
(50,855) |
|
|
(26,776) |
|
|
Payment of capital lease obligations |
|
|
(57) |
|
|
(5) |
|
|
(103) |
|
|
Payment to terminate interest rate swap |
|
|
— |
|
|
(421) |
|
|
— |
|
|
Payment of dividends |
|
|
(60,000) |
|
|
— |
|
|
— |
|
|
Distributions to owners |
|
|
(9) |
|
|
(33) |
|
|
(631) |
|
|
Capital contribution |
|
|
— |
|
|
— |
|
|
4,114 |
|
|
Contribution from original owner |
|
|
167 |
|
|
83 |
|
|
870 |
|
|
Net cash provided by financing activities |
|
|
64,653 |
|
|
45,815 |
|
|
2,820 |
|
|
Net (decrease) increase in cash |
|
|
(9,493) |
|
|
8,040 |
|
|
(1,309) |
|
|
Cash, beginning of period |
|
|
11,495 |
|
|
3,455 |
|
|
4,764 |
|
|
Cash, end of period |
|
$ |
2,002 |
|
$ |
11,495 |
|
$ |
3,455 |
|
See Note 12 for Supplemental Cash Flow Information and Supplemental Noncash Activities
The accompanying notes are an integral part of these consolidated financial statements.
83
Adeptus Health Inc. (the "Company") was incorporated as a Delaware corporation on March 7, 2014 for the purpose of facilitating an initial public offering of common equity. The Company is a holding company with its sole material asset being a controlling equity interest in Adeptus Health LLC. As the sole managing member of Adeptus Health LLC, the Company operates and controls all of the business and affairs of Adeptus Health LLC and, through Adeptus Health LLC and its subsidiaries, conducts its business. Prior to the initial public offering, the Company had not engaged in any business or other activities except in connection with its formation and the initial public offering.
Adeptus Health LLC or its predecessors began operations in 2002 and owns and operates First Choice Emergency Rooms, the largest network of independent freestanding emergency rooms in the United States, delivering both major and minor emergency medical services for adult and pediatric patients. First Choice Emergency Rooms has experienced rapid growth in recent periods, growing from 14 facilities at the end of 2012 to 26 facilities at the end of 2013, and to 55 facilities as of December 31, 2014. The Company’s facilities are currently located in the Houston, Dallas/Fort Worth, San Antonio and Austin, Texas markets; as well as in Colorado Springs and Denver, Colorado; and Phoenix, Arizona.
On June 24, 2014, the Company’s registration statement on Form S-1 (File No. 33-196142) relating to its initial public offering of Class A common stock was declared effective by the Securities and Exchange Commission (“SEC”). The Company sold 4,900,000 shares of Class A common stock in its public offering. An additional 735,000 shares were sold to the public, of which 313,586 shares were sold by a significant stockholder and 421,414 shares were sold by the Company with the proceeds received by the Company used to purchase an equivalent number of LLC Units from such significant stockholder. The Company’s stock began trading on the New York Stock Exchange on June 25, 2014 under the symbol “ADPT,” and the initial public offering closed on June 30, 2014.
In connection with the initial public offering, the limited liability company agreement of Adeptus Health LLC was amended and restated to, among other things, modify its capital structure by replacing the different classes of interests previously held by the Adeptus Health LLC owners to a single new class of units called “LLC Units.” In addition, each LLC Unit holder received on a one-for-one basis one share of the Company’s Class B common stock, which entitles the holder to vote on all matters of Adeptus Health Inc. but has no economic rights. One of the then-existing owners converted a portion of its interest into 4,895,521 shares of the Company’s Class A common stock, which is referred to as the merged entity. The Company and its then-existing owners also entered into an exchange agreement under which they have the right to exchange their LLC Units and shares of Class B common stock for shares of Class A common stock on a one-for-one basis, subject to customary conversion rate adjustments for stock splits, stock dividends and reclassifications. These transactions are collectively referred to as the “Reorganization Transactions.”
The Company consolidates the financial results of Adeptus Health LLC and its subsidiaries and records non-controlling interest for the economic interest in Adeptus Health LLC held by the non-controlling unit holders. The non-controlling interest ownership percentage as of December 31, 2014 was 52.3%.
Prior to the initial public offering, the Company borrowed under the Senior Secured Credit Facility (See Note 8 Debt for further information) to fund a dividend of $60.0 million to the then-existing owners which was paid in connection with the consummation of the initial public offering. The Company used proceeds from the initial public offering to repay indebtedness under the Senior Secured Credit Facility from this borrowing.
84
NOTE 2—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Basis of Presentation
The accompanying consolidated balance sheets as of December 31, 2014 and 2013 and the accompanying consolidated statements of operations and cash flows for each of the three years ended December 31, 2014, 2013 and 2012 represent our financial position, results of operations and cash flows as of and for the years then ended. The consolidated financial statements include the accounts of Adeptus Health Inc. and our wholly owned subsidiaries. All material intercompany accounts and transactions have been eliminated in consolidation.
Accounting Policies and Use of Estimates
The preparation of financial statements in conformity with GAAP requires our management to make certain estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements, and the reported amounts of revenues and expenses during the reporting periods. Significant accounting policies and estimates include: the useful lives of fixed assets, revenue recognition, allowances for doubtful accounts, leases, reserves for employee health benefit obligations, stock-based compensation, and other contingencies. Actual results could differ from these estimates.
Segment and Geographic Information
The Company’s chief operating decision maker is our Chief Executive Officer, who reviews financial information presented on a company-wide basis. As a result, the Company determined that it has a single reporting segment and operating unit structure.
All of the Company’s revenue for the years ended December 31, 2014, 2013 and 2012 was in the United States.
Cash and Cash Equivalents and Concentrations of Risk
The Company includes all securities with a maturity date of three months or less at date of purchase as cash equivalents. The Company currently has no cash equivalents. The Company maintains its cash in bank deposit accounts, which, at times, may exceed federally insured limits. The Company has not experienced any losses in such accounts and does not believe it is exposed to any significant risk related to uninsured bank deposits.
Restricted Cash
Beginning in October 2013, the Company is required to restrict cash for letters of credit related to the Master Funding and Development Agreement. See Note 11 Commitments and Contingencies for more information. Each letter of credit is issued in an amount equal to approximately 50% of one year's base rent relating to completed facilities. As of December 31, 2014 and 2013, restricted cash was $4.8 million and $0.3 million, respectively.
Patient Revenue and Accounts Receivable
Revenues consist primarily of net patient service revenues, which are based on the facilities’ established billing rates less allowances and discounts, principally for patients covered under contractual programs with private insurance companies. Revenue is recognized when services are rendered to patients. Charges for all services provided to insured patients are initially billed and processed by the patients' insurance provider. The Company has agreements with insurance companies that provide for payments to the Company at amounts different from its established rates or as determined by the patient's out of network benefits. Differences between established rates and those set by insurance
85
programs, as well as charity care, employee and prompt pay adjustments, are recorded as adjustments directly to patient service revenue. Fee adjustments of approximately $137.1 million, $62.5 million and $44.5 million were recorded for the years ended December 31, 2014, 2013 and 2012, respectively. Amounts not covered by the insurance companies are then billed to the patients. Estimated uncollectible amounts from insured patients are recorded as bad debt expense in the period the services are provided. Collection of payment for services provided to patients without insurance coverage is done at the time of service.
With respect to management and contract service revenues, amounts are recognized as services are provided. The Company is party to an agreement with a full-service healthcare hospital facility to provide management services. As compensation for these services, the Company charges the managed entity a management fee based on a fixed percentage of the entity’s net revenue. The Company also holds minority ownership in this entity.
Patient service revenue before the provision for bad debts by major payor source for the years ended December 31, 2014, 2013 and 2012 were as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|||||||
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Third-party payors, including patient portion |
|
$ |
237,972 |
|
$ |
113,603 |
|
$ |
79,408 |
|
|
Self-pay |
|
|
5,326 |
|
|
1,357 |
|
|
1,569 |
|
|
Total all payors |
|
$ |
243,298 |
|
$ |
114,960 |
|
$ |
80,977 |
|
The Company receives payments from third-party payors that have contracts with the Company in Texas and Colorado. As of December 31, 2014, the Company has a contract with Blue Cross Blue Shield of Texas and two MultiPlan arrangements whereby the Company accesses a number of third-party payors at in-network rates. Four major third-party payors accounted for 84.8%, 86.7% and 88.2% of patient service revenue for the years ended December 31, 2014, 2013 and 2012, respectively. These same payors also accounted for 80% and 79% of accounts receivable as of December 31, 2014 and 2013, respectively. The following table sets forth the percentage of patient service revenue earned by major payor source for the years ended December 31, 2014, 2013 and 2012:
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
||||
|
|
2014 |
|
2013 |
|
2012 |
|
|
Payor: |
|
|
|
|
|
|
|
Blue Cross Blue Shield |
27.6 |
% |
28.0 |
% |
29.1 |
% |
|
United HealthCare |
23.6 |
|
26.5 |
|
26.0 |
|
|
Aetna |
19.3 |
|
21.0 |
|
22.1 |
|
|
Cigna |
14.3 |
|
11.2 |
|
11.0 |
|
|
Other |
15.2 |
|
13.3 |
|
11.8 |
|
|
|
100.0 |
% |
100.0 |
% |
100.0 |
% |
Accounts receivable are reduced by an allowance for doubtful accounts. In establishing the Company's allowance for doubtful accounts, management considers historical collection experience, the aging of the account, the payor classification, and patient payment patterns. Amounts due directly from patients represent the Company's highest collectability risk. There were not any significant changes in the estimates or assumptions underlying the calculation of the allowance for doubtful accounts for the years ended December 31, 2014 and 2013.
The Company writes off as bad debt expense uncollectible accounts receivable arising from patient responsibility after all collection efforts have been exhausted and it has been determined such accounts will not be
86
collected. Bad debt write-offs of approximately $24.8 million, $10.1 million and $7.7 million were recorded for the years ended December 31, 2014, 2013 and 2012, respectively.
The Company treats anyone that is emergent, including patients that may be eligible for Medicare or Medicaid. These services are provided at no charge to the patient. Total charity care was approximately 8.6%, 7.0% and 2.0% of patient service revenue for the years ended December 31, 2014, 2013 and 2012, respectively.
Advertising Costs
Advertising costs are expensed as incurred. Advertising expense for the years ended December 31, 2014, 2013 and 2012, was approximately $5.4 million, $2.1 million and $1.0 million, respectively, and is included as a component of general and administrative expenses within the consolidated statements of operations.
Medical Supplies Inventory
Inventory is carried at the lower of cost or market using the first-in, first-out method and consists of a standard set of medical supplies held in stock at all facilities.
Property and Equipment
Property and equipment are stated at cost, less accumulated depreciation and amortization computed using the straight-line method over the estimated useful life of each asset. Leasehold improvements are amortized over the shorter of the noncancelable lease term or the estimated useful life of the improvements. When assets are retired, the cost and applicable accumulated depreciation are removed from the respective accounts, and the resulting gain or loss is recognized. Expenditures for normal repairs and maintenance are expensed as incurred. Material expenditures that increase the life of an asset are capitalized and depreciated over the estimated remaining useful life of the asset. The estimated useful lives of depreciable fixed assets are as follows:
|
|
|
|
|
|
|
|
|
Estimated useful life |
|
|
|
|
|
(in years) |
|
|
|
Computer equipment |
|
|
3 |
|
|
Automobiles |
|
|
5 |
|
|
Office equipment |
|
|
5 |
|
|
Medical equipment |
|
|
5 to 7 |
|
|
Leasehold improvement |
|
|
4 to 10 |
|
|
Buildings |
|
|
15 to 20 |
|
Amortization of assets acquired under capital leases is included as a component of depreciation and amortization expense in the accompanying consolidated statements of operations. Amortization is calculated using the straight-line method over the shorter of the useful lives or the term of the underlying lease agreements.
Impairment of Long-Lived Assets
Long-lived assets are reviewed for impairment whenever events or circumstances indicate that the carrying amount of an asset or group of assets might not be recoverable. The Company does not perform a periodic assessment of assets for impairment in the absence of such information or indicators. Conditions that would indicate a potential impairment include a significant decline in the observable market value of an asset or a significant change in the extent or manner in which an asset is used. The impairment review includes a comparison of future projected cash flows generated by the asset or group of assets with its associated net carrying value. If the net carrying value of the asset or group of assets exceeds expected cash flows (undiscounted and without interest charges), an impairment loss is
87
recognized to the extent the carrying amount of the asset exceeds its fair value. The Company recorded long-lived asset impairment charges of $0.3 million for the year ending December 31, 2012, associated with the closing of the former corporate headquarters. There were no impairments recorded for the years ending December 31, 2014 or 2013.
Goodwill
In accordance with the FASB ASC 805, Business Combinations, the purchase method of accounting requires that the excess of purchase price paid over the estimated fair value of identifiable tangible and intangible net assets of acquired businesses be recorded as goodwill. In accordance with the provisions of ASC 350, Intangibles—Goodwill and Other, goodwill is tested for impairment annually, and interim impairment tests are performed whenever an event occurs or circumstances change that indicate an impairment has more likely than not occurred. We have one reporting unit and goodwill is evaluated at that level. We evaluate impairment of goodwill by first performing a qualitative assessment to determine whether it is more likely than not that the fair value of the reporting unit is less than the carrying value. If it is concluded that this is the case, it is necessary to perform a two‑ step impairment test. The first step involves a comparison of the fair value of a reporting unit with its carrying amount. If the carrying value of the reporting unit exceeds its fair value, the second step involves a comparison of the implied fair value and the carrying amount of the goodwill of that reporting unit to determine the impairment charge, if necessary. We have established October 31 as the date for our annual impairment review.
The Company estimates the fair value of its total invested capital using an income and market approach, reduced by interest bearing debt as of the valuation date. These valuations require management to make estimates and assumptions regarding industry economic factors and prospective financial information. There were no goodwill impairment charges recorded for the years ended December 31, 2014, 2013 and 2012.
Intangible Assets
Intangible assets are recorded at their estimated fair values as of the date of acquisition. Intangible assets consist of trade and domain names and noncompete agreements. In accordance with ASC 350, Intangibles—Goodwill and Other , the Company reviews the intangible assets with indefinite lives, which include trade and domain names, at least annually for impairment, or more often if triggering events exist. Intangible assets with definite lives are reviewed for impairment if an indicator of impairment exists similar to long-lived assets. An impairment loss is recognized if the carrying amount of an intangible asset is not recoverable and its carrying amount exceeds its fair value. There were no impairment charges recorded on intangible assets for the years ended December 31, 2014, 2013 or 2012. Intangible assets with finite useful lives are amortized over their estimated useful life.
Fair Value of Financial Instruments
The carrying amounts of the Company's financial instruments, including cash, receivables, accounts payable and accrued liabilities approximate their fair value due to their relatively short maturities. At December 31, 2014 and 2013, the carrying value of the Company's long-term debt was based on the current interest rates and approximates its fair value.
Derivative Instruments and Hedging Activities
The Company recognizes all derivative instruments as either assets or liabilities in the balance sheet at their respective fair values. For derivatives not designated as a hedging instrument, changes in the fair value are recorded in net earnings immediately. For derivatives designated in hedging relationships, changes in the fair value are either offset through earnings against the change in fair value of the hedged item attributable to the risk being hedged or recognized in
88
accumulated other comprehensive income, to the extent the derivative is effective at offsetting the changes in cash flows being hedged until the hedged item affects earnings.
For the year ended December 31, 2012 and continuing through October 31, 2013, the Company maintained one derivative instrument that it did not designate as a hedge. As a result, changes in the fair value were recorded in earnings for this period. Beginning in November 2013, the Company only enters into derivative contracts that it intends to designate as a hedge of a forecasted transaction or the variability of cash flows to be received or paid related to a recognized asset or liability (cash flow hedge). For all hedging relationships, the Company formally documents the hedging relationship and its risk-management objective and strategy for undertaking the hedge, the hedging instrument, the hedged transaction, the nature of the risk being hedged, how the hedging instrument's effectiveness in offsetting the hedged risk will be assessed prospectively and retrospectively, and a description of the method used to measure ineffectiveness. The Company also formally assesses, both at the inception of the hedging relationship and on an ongoing basis, whether the derivatives that are used in hedging relationships are highly effective in offsetting changes in cash flows of hedged transactions. For derivative instruments that are designated and qualify as part of a cash flow hedging relationship, the effective portion of the gain or loss on the derivative is reported as a component of other comprehensive income and reclassified into earnings in the same period or years during which the hedged transaction affects earnings. Gains and losses on the derivative representing either hedge ineffectiveness or hedge components excluded from the assessment of effectiveness are recognized in current earnings.
The Company discontinues hedge accounting prospectively when it determines that the derivative is no longer effective in offsetting cash flows attributable to the hedged risk, the derivative expires or is sold, terminated, or exercised or the cash flow hedge is redesignated because a forecasted transaction is not probable of occurring.
In all situations in which hedge accounting is discontinued and the derivative remains outstanding, the Company continues to carry the derivative at its fair value on the balance sheet and recognizes any subsequent changes in its fair value in earnings. When it is probable that a forecasted transaction will not occur, the Company discontinues hedge accounting and recognizes immediately in earnings gains and losses that were accumulated in other comprehensive income related to the hedging relationship.
Lease Accounting
The Company determines whether to account for its facility leases as operating or capital leases depending on the underlying terms of the lease agreement. This determination of classification is complex and requires significant judgment relating to certain information including the estimated fair value and remaining economic life of the facilities, the Company's cost of funds, minimum lease payments and other lease terms. The lease rates under the Company's lease agreements are subject to certain conditional escalation clauses that are recognized when probable or incurred and are based on changes in the consumer price index or certain operational performance measures. As of December 31, 2014, the Company leased 54 facilities, 53 of which the Company classified as operating leases and one of which the Company classified as a capital lease.
Income Taxes
We provide for income taxes using the asset and liability method. This approach recognizes the amount of federal, state and local taxes payable or refundable for the current year, as well as deferred tax assets and liabilities for the future tax consequence of events recognized in the consolidated financial statements and income tax returns. Deferred income tax assets and liabilities are adjusted to recognize the effects of changes in tax laws or enacted tax rates.
A valuation allowance is required when it is more-likely-than-not that some portion of the deferred tax assets will not be realized. Realization is dependent on generating sufficient future taxable income.
89
We file a consolidated federal income tax return. State income tax returns are filed on a separate, combined or consolidated basis in accordance with relevant state laws and regulations. LPs, LLPs, LLCs and other pass-through entities that we consolidate file separate federal and state income tax returns. We include the allocable portion of each pass-through entity’s income or loss in our federal income tax return. We allocate the remaining income or loss of each pass-through entity to the other partners or members who are responsible for their portion of the taxes.
The (benefit) provision for income taxes totaled $(1.3) million, $0.7 million and $0.5 million for the years ended December 31, 2014, 2013 and 2012, respectively. The Company's estimate of the potential outcome of any uncertain tax positions is subject to management's assessment of relevant risks, facts, and circumstances existing at that time. The Company uses a more likely than not threshold for financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return.
To the extent that the Company's assessment of such tax position changes, the change in estimate is recorded in the period in which the determination is made. The Company reports tax related interest and penalties as a component of the provision for income tax and operating expenses, respectively, if applicable. The Company has not recognized any uncertain tax positions.
Deferred Rent
The Company records rent expense for operating leases on a straight-line basis over the life of the related leases. The Company has certain facility and equipment leases that allow for leasehold improvements allowances, free rent, and escalating rental payments. Straight-line expenses that are greater than the actual amount paid are recorded as deferred rent and amortized over the life of the lease.
Investment in Unconsolidated Joint Venture
Investments in unconsolidated companies in which the Company exerts significant influence but does not control or otherwise consolidate are accounted for using the equity method. The Company has one such investment with an ownership interest of 49.9%.
This investment is included as investment in unconsolidated joint venture in the accompanying consolidated balance sheets.
Equity in net loss of unconsolidated joint venture consists of the Company’s share of the losses generated from its noncontrolling equity investment in one full-service healthcare hospital facility. Because these operations are central to the Company’s business strategy, equity in earnings of unconsolidated affiliates is classified as a component of operating income in the accompanying consolidated statements of operations. The Company has contracts to manage these facilities, which results in the Company having an active role in the operations of these facilities and devoting a significant portion of its corporate resources to the fulfillment of these management responsibilities.
Recent Accounting Pronouncements
In May 2014, the FASB issued ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606), which requires an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. The ASU will replace most existing revenue recognition guidance in U.S. GAAP when it becomes effective. The new standard will become effective for the Company on January 1, 2017. Early application is not permitted. The standard permits the use of either the retrospective or cumulative effect transition method. The Company is evaluating the effect that ASU 2014-09 will have on its consolidated financial statements and related disclosures. The Company has not yet selected a transition method nor has it determined the effect of the standard on its ongoing financial reporting.
90
In August 2014, the FASB issued new guidance related to the disclosures around going concern. The new standard update provides guidance around management's responsibility to evaluate whether there is substantial doubt about an entity's ability to continue as a going concern and to provide related footnote disclosures. The new guidance is effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2016. Early adoption is permitted. The Company does not believe the adoption of this guidance will have a material impact on its consolidated financial statements.
NOTE 3—PROPERTY AND EQUIPMENT
Property and equipment consisted of the following, as of December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
2014 |
|
2013 |
|
||
|
Leasehold improvements |
|
$ |
77,354 |
|
$ |
37,626 |
|
|
Computer equipment |
|
|
3,700 |
|
|
1,583 |
|
|
Medical equipment |
|
|
4,213 |
|
|
2,970 |
|
|
Office equipment |
|
|
4,307 |
|
|
760 |
|
|
Automobiles |
|
|
243 |
|
|
243 |
|
|
Land |
|
|
8,276 |
|
|
2,430 |
|
|
Construction in progress |
|
|
8,835 |
|
|
17,788 |
|
|
Buildings |
|
|
4,667 |
|
|
4,551 |
|
|
|
|
|
111,595 |
|
|
67,951 |
|
|
Less accumulated depreciation |
|
|
(17,703) |
|
|
(5,864) |
|
|
Property and equipment, net |
|
$ |
93,892 |
|
$ |
62,087 |
|
Assets under capital leases totaled approximately $4.2 million and $3.9 million as of December 31, 2014 and 2013, respectively, and were included within the buildings component of net property and equipment. Accumulated depreciation associated with these capital lease assets totaled approximately $0.3 million and $23,000 as of December 31, 2014 and 2013, respectively.
NOTE 4—INVESTMENT IN UNCONSOLIDATED JOINT VENTURE
On October 22, 2014, the Company announced its expansion into Arizona through a joint venture with Dignity Health, one of the nation’s largest health systems. The new partnership has started with Dignity Health Arizona General Hospital, a full-service healthcare hospital facility in Phoenix, Arizona, and includes providing for additional access to emergency medical care in Phoenix. As of December 31, 2014, this facility was in its training and certification phase until such time as it received CMS certification from the Joint Commission. The joint venture received CMS certification on January 30, 2015. Dignity Health Arizona General Hospital is a full-service healthcare hospital facility, licensed by the state as a general hospital. Spanning 39,000 square-feet, the hospital has 16 inpatient rooms, two operating rooms for inpatient and outpatient surgical procedures, an emergency department, a high-complexity laboratory and a full radiology suite. Patients have full access to the Dignity Health area facilities and physicians, and the hospital will provide Phoenix-area residents with 24/7 access to emergency medical care.
The Company accounts for this under the equity method of accounting as an investment in unconsolidated joint venture, as the Company’s level of influence is significant but does not reach the threshold of controlling the entity.
91
Summarized unaudited financial information for the Company’s equity method investee is as follows (in thousands):
|
|
|
|
|
|
|
|
|
Year ended |
|
|
|
|
|
December 31, |
|
|
|
|
|
2014 |
|
|
|
Net patient service revenue |
|
$ |
247 |
|
|
Operating expenses: |
|
|
|
|
|
Salaries, wages and benefits |
|
|
880 |
|
|
General and administrative |
|
|
469 |
|
|
Other operating expenses |
|
|
688 |
|
|
Depreciation and amortization |
|
|
12 |
|
|
Total operating expenses |
|
|
2,049 |
|
|
Loss from operations |
|
|
(1,802) |
|
|
Other (expense) income: |
|
|
|
|
|
Interest expense |
|
|
(1) |
|
|
Total other (expense) |
|
|
(1) |
|
|
Net loss |
|
$ |
(1,803) |
|
|
Balance sheet information (as of December 31, 2014): |
|
|
|
|
|
Current assets |
|
$ |
1 |
|
|
Noncurrent assets |
|
|
5 |
|
|
Current liabilities |
|
|
2 |
|
|
Noncurrent liabilities |
|
|
0.1 |
|
NOTE 5—GOODWILL AND OTHER INTANGIBLE ASSETS
The following table summarizes the change in goodwill during the years ended December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
||
|
Balance at beginning of year |
|
$ |
61,009 |
|
|
61,009 |
|
|
Adjustments |
|
|
— |
|
|
— |
|
|
Balance at end of year |
|
$ |
61,009 |
|
$ |
61,009 |
|
The following table summarizes the change in intangible assets during the years ended December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Noncompete |
|
Trade |
|
Domain |
|
|
|
|
|||
|
|
|
Agreements |
|
Names |
|
Names |
|
Total |
|
||||
|
Balance at December 31, 2012 |
|
$ |
6,675 |
|
$ |
9,300 |
|
$ |
7,600 |
|
$ |
23,575 |
|
|
Additions |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Amortization |
|
|
(1,780) |
|
|
— |
|
|
— |
|
|
(1,780) |
|
|
Balance at December 31, 2013 |
|
$ |
4,895 |
|
$ |
9,300 |
|
$ |
7,600 |
|
$ |
21,795 |
|
|
Additions |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Amortization |
|
|
(1,780) |
|
|
— |
|
|
— |
|
|
(1,780) |
|
|
Balance at December 31, 2014 |
|
$ |
3,115 |
|
$ |
9,300 |
|
$ |
7,600 |
|
$ |
20,015 |
|
92
As of December 31, 2014, the following table sets forth the estimated amortization of the noncompete agreements for the years ending December 31 (in thousands):
|
|
|
|
|
|
2015 |
|
$ |
1,780 |
|
2016 |
|
|
1,335 |
NOTE 6—DERIVATIVE INSTRUMENTS AND HEDGING ACTIVITIES
The Company uses interest-rate-related derivative instruments to manage its exposure related to changes in interest rates on its variable-rate debt instruments. The Company does not enter into derivative instruments for any purpose other than cash flow hedging. The Company does not speculate using derivative instruments.
By using derivative financial instruments to hedge exposures to changes in interest rates, the Company exposes itself to credit risk and market risk. Credit risk is the failure of the counterparty to perform under the terms of the derivative contract. When the fair value of a derivative contract is positive, the counterparty owes the Company, which creates credit risk for the Company. When the fair value of a derivative contract is negative, the Company owes the counterparty, and therefore, the Company is not exposed to the counterparty's credit risk in those circumstances. The Company minimizes counterparty credit risk in derivative instruments by entering into transactions with high-quality counterparties whose credit rating is higher than Aa. The derivative instruments entered into by the Company do not contain credit-risk-related contingent features.
Market risk is the adverse effect on the value of a derivative instrument that results from a change in interest rates, currency exchange rates, or commodity prices. The market risk associated with interest-rate contracts is managed by establishing and monitoring parameters that limit the types and degree of market risk that may be undertaken.
The Company assesses interest rate risk by continually identifying and monitoring changes in interest rate exposures that may adversely impact expected future cash flows and by evaluating hedging opportunities. The Company maintains risk management control systems to monitor interest rate risk attributable to both the Company's outstanding or forecasted debt obligations as well as the Company's offsetting hedge positions. The risk management control systems involve the use of analytical techniques, including cash flow sensitivity analysis, to estimate the expected impact of changes in interest rates on the Company's future cash flows.
Changes in the fair value of interest rate swaps and cap agreements designated as hedging instruments that effectively offset the variability of cash flows associated with variable-rate, long-term debt obligations are reported in accumulated other comprehensive income. These amounts subsequently are reclassified into interest expense as a yield adjustment of the hedged interest payments in the same period in which the related interest affects earnings.
In May 2012, the Company entered into a forward interest rate swap agreement with a notional amount of $24.0 million to manage exposure to changes in interest rates associated with its variable interest rate debt. This agreement had the economic effect of modifying the LIBOR variable component of the Company's interest rate on an equivalent amount of the Company's Term Loan to a fixed rate of 1.20%. This swap agreement was not designated by the Company as a hedge as of December 31, 2013. The Company did not utilize the swap agreement until April 30, 2013. The Company recognized a loss of approximately $0.1 million for the year ended December 31, 2013 and a gain of approximately $0.5 million for the year ended December 31, 2012 on the change in fair value of the swap agreement, which is included as a component of other (expense) income within the consolidated statements of operations.
93
As of December 31, 2014, the Company maintained one interest rate cap agreement with notional amount totaling $37.5 million. This agreement has the economic effect of capping the LIBOR variable component of the Company's interest rate at a maximum of 3.00% on an equivalent amount of the Company's Term Loan debt. The cap agreement was entered into in November 2013 at a cost of $0.09 million and expires on November 30, 2016. This cap agreement is designated as a cash flow hedge and, as a result, changes in the fair values of this cap agreement are reported in other comprehensive income. As of December 31, 2014, approximately $74,000 of deferred losses on derivative instruments are included in other comprehensive income. The cap agreement does not contain credit-risk contingent features.
The following table summarizes the Company's derivative instruments as of December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
||
|
|
|
Balance Sheet Location |
|
Fair Value |
|
Fair Value |
|
||
|
Derivative designated as hedging instruments |
|
|
|
|
|
|
|
|
|
|
Interest rate contracts |
|
Other long-term assets |
|
$ |
19 |
|
$ |
92 |
|
NOTE 7—ACCOUNTS PAYABLE AND ACCRUED EXPENSES
Accounts payable and accrued expenses consisted of the following as of December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
||
|
Accounts payable |
|
$ |
14,133 |
|
$ |
9,405 |
|
|
Accrued expenses |
|
|
4,431 |
|
|
1,267 |
|
|
Accrued tax distribution to LLC Unit holders |
|
|
4,246 |
|
|
3,772 |
|
|
Other |
|
|
2,610 |
|
|
763 |
|
|
Total accounts payable and accrued expenses |
|
$ |
25,420 |
|
$ |
15,207 |
|
94
NOTE 8—DEBT
The components of debt consisted of the following as of December 31, 2014 and 2013 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
2014 |
|
2013 |
|
||
|
Term loan |
|
$ |
75,000 |
|
$ |
75,000 |
|
|
Delayed draw term loan |
|
|
25,000 |
|
|
— |
|
|
Revolving credit |
|
|
5,500 |
|
|
|
|
|
Other financing agreements |
|
|
1,298 |
|
|
504 |
|
|
|
|
|
106,798 |
|
|
75,504 |
|
|
Less current maturities |
|
|
(1,816) |
|
|
(504) |
|
|
|
|
$ |
104,982 |
|
$ |
75,000 |
|
On October 31, 2013, the Company entered into a Senior Secured Credit Facility (the “Facility”) for a $75.0 million term loan which matures on October 31, 2018. The Facility includes an additional $165.0 million delayed draw term loan commitment, which, if unused, expires eighteen months after the closing date, and a $10.0 million revolving commitment that matures on October 31, 2018. All of the Company's assets are pledged as collateral under the Facility. The borrowing under the Facility is used by the Company to provide financing for working capital, capital expenditures and for new facility expansion and replaced the Company's existing credit facility.
On March 31, 2014, the Company amended the Facility to, among other things, increase the maximum aggregate amount permitted to be funded by Medical Properties Trust (“MPT”) under the Master Funding and Development Agreement (the “MPT Agreement”) to $255.0 million.
On June 11, 2014, the Company entered into a second amendment to the Facility to, among other things, provide for a borrowing under the delayed draw term loan in an aggregate principal amount of up to $75.0 million, up to $60.0 million in principal amount of which will be used to make specified distributions and up to $10.0 million in principal amount of which will be used to repay certain revolving loans. On June 11, 2014, the Company drew $75.0 million and made the $60.0 million dividend distribution on June 24, 2014.
Borrowings under the Facility bear interest, at our option, at a rate equal to an applicable margin over (a) a base rate determined by reference to the highest of (1) the prime rate, (2) the federal funds effective rate plus 0.50% and (3) LIBOR of at least 1%, or (b) LIBOR for the applicable interest period. The margin for the Facility is 6.50% in the case of base rate loans and 7.50% in the case of LIBOR loans. The Facility includes an unused line fee of 0.50% per annum on the revolving commitment and delayed draw term loan commitment, a draw fee of 1.0% of the principal amount of each borrowing on the delayed draw term loan and an annual Agency fee of $0.1 million. At December 31, 2014 and 2013, the Company had $80.2 million and $165.0 million available under the delayed draw term commitment, respectively. At December 31, 2014 and 2013, the Company had approximately $4.0 million and $9.5 million available under the revolving commitment, respectively.
The original principal amount of the term loan will be repaid in consecutive quarterly installments of $0.5 million on the last day of each fiscal quarter commencing with the fiscal quarter ending December 31, 2015 and escalating to $0.9 million for each fiscal quarter ending after December 31, 2016. The delayed draw term loans will be repaid in consecutive quarterly installments in an amount based on the repayment calculation contained in the Facility on the last day of each fiscal quarter commencing with the fiscal quarter ending December 31, 2015. The aggregate principal amount of all revolving loans outstanding are due on the maturity date, October 31, 2018.
95
The Facility contains certain affirmative covenants, negative covenants, and financial covenants which are measured on a quarterly basis. As of December 31, 2014, the Company was in compliance with all covenant requirements.
In 2014, the Company entered into finance agreements totaling approximately $1.9 million to finance the renewal of certain insurance policies. The finance agreements have fixed interest rates ranging between 2.49% and 3.25% with principal being repaid over 9 to 11 months. In October 2013, the Company renewed certain insurance policies and entered into a finance agreement totaling approximately $0.8 million. The finance agreement has a fixed interest rate of 1.93% with principal being repaid over 9 months. In October 2012, the Company renewed certain insurance policies and entered into a finance agreement totaling approximately $0.4 million. The finance agreement has a fixed interest rate of 3.48% with principal being repaid over 11 months.
Future Maturities
Scheduled future aggregate maturities of principal of long-term debt are as follows: (in thousands):
|
|
|
|
|
|
Years ending December 31, |
|
Amount |
|
|
2015 |
|
$ |
1,816 |
|
2016 |
|
|
2,763 |
|
2017 |
|
|
5,000 |
|
2018 |
|
|
97,219 |
|
|
|
$ |
106,798 |
NOTE 9—TRANSACTIONS WITH RELATED PARTIES
The Company made payments to a significant shareholder of the Company for management services and reimbursement of certain expenses related to an advisory services agreement. The total amount paid to this related party was approximately $0.8 million, $0.6 million and $0.6 million for the years ended December 31, 2014, 2013 and 2012, respectively. In connection with the consummation of the initial public offering, the advisory services agreement was terminated and the Company paid a $2.0 million termination fee which was paid in July 2014.
The Company made payments for contractor services to various related-party vendors, which totaled approximately $0.06 million, $0.06 million and $0.1 million for the years ended December 31, 2014, 2013 and 2012, respectively.
96
We entered into a license and master services agreement with IO Phoenix One, LLC, or IO, an affiliate of a significant shareholder on November 22, 2013, pursuant to which IO stores and maintains our data centers and modules at its Phoenix, Arizona location. We pay approximately $4,000 per month in license fees with an initial term of 36 months. The total amount payable under the agreement is approximately $148,000, with payments beginning on February 15, 2014.
NOTE 10—EMPLOYEE BENEFIT PLANS
The Company provides a 401(k) savings plan to all employees who have met certain eligibility requirements, including performing one month of service with the Company. The 401(k) plan permits matching and discretionary employer contributions. During the years ended December 31, 2014 and 2013, the Company contributed approximately $0.5 million and $0.3 million to the 401(k) Plan for 2013 and 2012 matching contributions, respectively. The board of directors approved a contribution of $0.9 million for the year ended December 31, 2014, which will be paid during 2015.
NOTE 11—COMMITMENTS AND CONTINGENCIES
Litigation and Asserted Claims
The Company is a defendant in various legal proceedings arising in the ordinary course of business. While, management believes the outcome of pending litigation and claims will not have a material adverse effect on the Company's consolidated financial condition, operations, or cash flows, litigation is subject to inherent uncertainties.
Insurance Arrangements
The Company is self-insured for employee health benefits. Accruals for losses are provided based upon claims experience and actuarial assumptions, including provisions for incurred but not reported losses. At December 31, 2014 and 2013, the Company has an accrual of approximately $0.7 million and $0.7 million, respectively for incurred but not reported claims, which is included in accrued compensation within the consolidated balance sheets.
The Company is insured for worker's compensation claims up to $1.0 million per accident and per employee with a policy limit of $1.0 million. The Company submits periodic payments to its insurance broker based upon estimated payroll. Worker's compensation expense for the years ended December 31, 2014, 2013 and 2012 was approximately $0.3 million, $0.07 million and $ 0.03 million, respectively. The Company is insured for professional liability claims up to $1.0 million per incident and $3.0 million per facility with an aggregate policy limit of $20.0 million.
Leases
The Company leases certain medical facilities and equipment under various noncancelable operating leases. In June 2013, the Company entered into the MPT Agreement with MPT to fund future facilities. The lessor to the MPT Agreement will acquire parcels of land, fund the ground-up construction of new freestanding emergency room facilities and lease the facilities to the Company upon completion of construction. Under the terms of the agreement, the lessor is to fund all hard and soft costs, including the project purchase price, closing costs and pursuit costs for the assets relating to the construction of up to twenty-five facilities with a maximum aggregate funding of $100.0 million. Each completed project will be leased for an initial term of 15 years, with three 5-year renewal options. The Company follows the guidance in ASC 840, Leases, and ASC 810, Consolidation, in evaluating the lease as a build-to-suit lease transaction to determine whether the Company would be considered the accounting owner of the facilities during the construction period.
97
In July 2014, the Company entered into an additional Master Funding and Development Agreement with MPT to fund future facilities. This agreement is separate from and in addition to the Company’s existing MPT Agreement. The new agreement allows for an additional maximum aggregate funding of $150.0 million. All other material terms remain consistent with the existing MPT Agreement.
The Company leases approximately 80,000 square feet for its corporate headquarters. Lease expense associated with this lease was $1.4 million, $0.7 million and $0.1 million for the years ended December 31, 2014, 2013 and 2012, respectively.
Future minimum lease payments required under noncancelable operating leases and future minimum, capital lease payments as of December 31, 2014 were as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
Capital |
|
Operating |
|
||
|
Years ending December 31, |
|
leases |
|
leases |
|
||
|
2015 |
|
$ |
522 |
|
$ |
26,318 |
|
|
2016 |
|
|
533 |
|
|
25,249 |
|
|
2017 |
|
|
544 |
|
|
22,993 |
|
|
2018 |
|
|
554 |
|
|
18,984 |
|
|
2019 |
|
|
565 |
|
|
15,899 |
|
|
Thereafter |
|
|
5,512 |
|
|
139,184 |
|
|
Total future minimum lease payments |
|
$ |
8,230 |
|
$ |
248,627 |
|
|
Less: Amounts representing interest |
|
|
(4,093) |
|
|
|
|
|
Present value of minimum lease payments |
|
|
4,137 |
|
|
|
|
|
Current portion of capital lease obligations |
|
|
81 |
|
|
|
|
|
Long-term portion of capital lease payments |
|
$ |
4,056 |
|
|
|
|
Rent expense totaled approximately $15.2 million, $4.5 million and $2.1 million for the years ended December 31, 2014, 2013 and 2012, respectively and is included as a component of other operating expenses within the Consolidated Statements of Operations.
In January 2013, the Company entered into a termination agreement with the landlord of the leased facility in Georgetown, Texas. Under the termination agreement, the landlord and the Company mutually released the other from any further obligations under the lease and any liability, cause of action, claim, or loss arising out of or connected with the lease. In accordance with the termination agreement, the Company paid the landlord a lease termination fee of $0.2 million.
98
NOTE 12— SUPPLEMENTAL CASH FLOW INFORMATION
Supplemental cash flow information and supplemental noncash activities consisted of the following for the years ended December 31, 2014, 2013 and 2012 (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Supplemental cash flow information: |
|
|
|
|
|
|
|
|
|
|
|
Interest paid |
|
$ |
9,294 |
|
$ |
2,486 |
|
$ |
1,091 |
|
|
Franchise taxes paid |
|
|
680 |
|
|
530 |
|
|
296 |
|
|
Supplemental noncash activities: |
|
|
|
|
|
|
|
|
|
|
|
Acquisition of property and equipment in accounts payable and accrued expenses |
|
$ |
2,239 |
|
$ |
467 |
|
$ |
2,341 |
|
|
Assets acquired through capital lease |
|
|
287 |
|
|
3,911 |
|
|
— |
|
|
Note payable for other financing agreements |
|
|
2,056 |
|
|
757 |
|
|
390 |
|
|
Accrual of owner distributions |
|
|
474 |
|
|
1,735 |
|
|
2,042 |
|
NOTE 13—STOCK BASED COMPENSATION
In connection with the initial public offering, the Company’s Board of Directors adopted the Adeptus Health Inc. 2014 Omnibus Incentive Plan (the “Omnibus Incentive Plan”). The Omnibus Incentive Plan provides for the granting of stock options, restricted stock and other stock-based or performance-based awards to directors, officers, employees, consultants and advisors of the Company and its affiliates. The total number of shares of Class A common stock that may be issued under the Omnibus Incentive Plan is 1,033,500. On June 24, 2014, the Company granted 11,934 restricted Class A shares to its non-employee directors under the Omnibus Incentive Plan, representing the prorated amount of the directors’ annual equity award for fiscal 2014. These restricted shares will vest on January 1, 2015. In July 2014, the Company granted to certain employees 35,856 restricted Class A shares, which vest over 4 years. The fair value of each restricted share award is based on the closing common stock price on the date of grant. The weighted average price of restricted shares granted in 2014 is $24.33 per share. Compensation expense for time-based restricted share awards is recognized over the vesting period on a straight-line basis, adjusted for estimated forfeitures. All outstanding restricted Class A shares were unvested as of December 31, 2014. As of December 31, 2014, there was $0.3 million of unrecognized compensation cost related to time-based restricted share awards. That cost is expected to be recognized over a weighted average period of 2 years. The aggregate intrinsic value of time-based share awards was $0.9 million as of December 31, 2014.
The Company also has one legacy equity-compensation plan, under which it has issued agreements awarding incentive units (restricted units) in the Company to certain employees and non-employee directors. In conjunction with the Reorganization Transactions, these restricted units were replaced with LLC Units with consistent restrictive terms. The restricted units are subject to such conditions as continued employment, passage of time and/or satisfaction of performance criteria as specified in the agreements. The restricted units vest over 3 to 4 years from the date of grant. The Company used a waterfall calculation, based on the capital structure and payout of each class of debt and equity, and a present value pricing model less marketability discount to determine the fair values of the restricted units. The assumptions used in the price simulation model for units granted during 2013 include risk-free interest rates of 0.93%, volatility of 25.0% and a dividend rate of 0%. The weighted average fair value of incentive units granted during the year ended December 31, 2013 was $1,262 and $384 for the time-based and performance based units, respectively. The assumptions used for the 2012 incentive units included a risk-free interest rate of 0.72%, volatility of 30.0% and a dividend yield of 0%. The weighted average fair value of incentive units granted during 2012 was $204 and $37 for the time-based and performance based units, respectively. The Company did not issue any incentive units under the legacy plan during the year ended December 31, 2014.
99
The Company recorded compensation expense of $1.0 million, $0.6 million, and $0.3 million, adjusted for forfeitures, during the years ended December 31, 2014, 2013 and 2012, respectively, related to restricted units with time-based vesting schedules. Compensation expense for the value of the portion of the time-based restricted unit that is ultimately expected to vest is recognized using a straight-line method over the vesting period, adjusted for forfeitures. No compensation expense was recorded during the years ended December 31, 2014 and 2013 related to restricted units with performance-based vesting criteria. If, and when, the Company determines it is probable that the performance condition will be achieved, compensation expense will be recognized cumulatively in such period. Total unrecognized compensation expense related to performance based restricted units was $0.1 million as of December 31, 2014
NOTE 14— INCOME TAXES
The components of our (benefit) provision for income taxes were as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
|
2013 |
|
|
2012 |
|
|
|
|||||||
|
Current: |
|
|
|
|
|
|
|
|
|
Federal |
$ |
- |
|
$ |
- |
|
$ |
- |
|
State |
|
821 |
|
|
720 |
|
|
467 |
|
Total Current Taxes |
|
821 |
|
|
720 |
|
|
467 |
|
Deferred: |
|
|
|
|
|
|
|
|
|
Federal |
|
(2,123) |
|
|
- |
|
|
- |
|
State |
|
(24) |
|
|
- |
|
|
- |
|
Total Deferred Taxes |
|
(2,147) |
|
|
- |
|
|
- |
|
Total Income tax (benefit) provision |
$ |
(1,326) |
|
$ |
720 |
|
$ |
467 |
The reconciliation of our income tax (benefit) expense computed at the U.S. federal statutory tax rate to the actual income tax (benefit) expense is as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
|
2013 |
|
|
2012 |
|
Expense derived by applying the Federal Income tax rate to income (loss) before taxes |
$ |
(6,509) |
|
$ |
(792) |
|
$ |
1,284 |
|
Tax applicable to pass-through entities |
|
4,631 |
|
|
792 |
|
|
(1,284) |
|
State Income Tax, net of federal benefit |
|
534 |
|
|
- |
|
|
- |
|
Investment in Partnership (Nondeductible expenses) |
|
18 |
|
|
- |
|
|
- |
|
|
$ |
(1,326) |
|
$ |
- |
|
$ |
- |
100
Deferred income taxes reflect the net tax effect of temporary differences between the carrying amounts of the assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of our deferred tax assets and liabilities are as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
|
2013 |
|
|
2012 |
|
Deferred Tax Assets |
|
|
|
|
|
|
|
|
|
TRA Liability |
$ |
8,125 |
|
$ |
- |
|
$ |
- |
|
Investment in Partnership |
|
20,940 |
|
|
- |
|
|
- |
|
Net Operating Loss Carryforwards |
|
4,957 |
|
|
- |
|
|
- |
|
State Net Operating Loss Carryforwards |
|
62 |
|
|
- |
|
|
- |
|
Total Deferred Tax Assets |
$ |
34,084 |
|
$ |
- |
|
$ |
- |
Prior to the Reorganization, we were not a federal taxpayer. Due to the timing of the Company’s initial public offering, taxes were calculated based on activity from June 25, 2014 through the end of the period. The Company’s effective tax rate for the period subsequent to June 25, 2014 differs from the statutory rates due primarily to state taxes that are not based on pre-tax income/(loss) but on gross margin resulting in state tax expense even in periods of pretax losses.
Our management evaluates the realizability of the deferred tax assets and determines whether it is more likely than not that the deferred tax assets are realizable. We consider whether a valuation allowance is needed on our deferred tax assets by evaluating all positive and negative evidence relative to our ability to recover deferred tax assets, including scheduled reversals of deferred tax liabilities, projected future taxable income, tax planning strategies and recent financial operations. During 2014, we were able to conclude that given our performance, the forecast of future income, the realization of our deferred tax asset was more likely than not and did not record a valuation allowance for the period. This determination is based on an estimated forecast of future taxable income which includes many judgments and assumptions. Accordingly, it is at least reasonably possible for future changes in one or more assumptions may lead to a change in judgment regarding the necessity of a valuation allowance required in future periods.
Our largest deferred tax asset is related to our investment in partnership of $21.0 million. This deferred tax asset is a result of the differences between the book and tax basis in Adeptus Health LLC, which is the partnership that operates our facilities.
A second component of the deferred tax asset is related to the Tax Receivable Agreement (noted below) liability of $8.1 million. As the Company becomes profitable, the deferred tax asset related to this liability will be reduced.
The final component of the deferred tax asset is the federal net operating loss carryforwards of $5.0 million. The federal net operating losses will begin to expire in 2034. The net operating loss carryforward is primarily related to depreciation and amortization deductions as well as change in accounting method for tax purposes related to bad debts.
A cumulative change in ownership among material shareholders, as defined in Section 382 of the Internal Revenue Code, during a three-year period may limit the utilization of the federal net operating loss carryforwards. At this time, the Company is not subject to the Section 382 limitation; however the Company may be subject to this limitation depending on the extent and timing of change in ownership in the future.
101
Uncertain Tax Positions
At December 31, 2014, the Company has not identified or accrued for any uncertain tax positions. Our policy is to include interest and penalties related to uncertain tax positions, and as of December 31, 2014, there were no accrued interest and penalties. We file tax returns in the U.S. federal jurisdiction and state jurisdictions where we have facilities and operations. We are not currently under audit for federal or any state jurisdictions.
Tax Receivable Agreement
Upon the consummation of the Company’s initial public offering, the Company entered into a tax receivable agreement with the LLC Unit holders after the closing of the offering that provides for the payment from time to time by the Company to the LLC Unit holders of 85% of the amount of the benefits, if any, that the Company is deemed to realize as a result of increases in tax basis and certain other tax benefits related to exchanges of LLC Units pursuant to the exchange agreement, including tax benefits attributable to payments under the tax receivable agreement. These payment obligations are obligations of the Company. For purposes of the tax receivable agreement, the benefit deemed realized by the Company was computed by comparing its actual income tax liability (calculated with certain assumptions) to the amount of such taxes that the Company would have been required to pay had there been no increase to the tax basis of the assets of Adeptus Health LLC as a result of the exchanges and had the Company not entered into the tax receivable agreement. The step-up in basis will depend on the fair value of the LLC Units at conversion.
As of December 31, 2014, the Company has recorded an estimated payable pursuant to the tax receivable agreement of $30.0 million related to certain transactions in conjunction with the initial public offering that are expected to give rise to certain tax benefits in the future.
NOTE 15— NET LOSS PER SHARE
Prior to the consummation of the Company’s initial public offering, the Company did not have outstanding common stock. However, in conjunction with the closing of the initial public offering, an existing owner exchanged their LLC Units for shares of the Company’s Class A common stock. The Company has assumed that 4,895,521 shares of Class A common stock were outstanding during the entire periods subsequent to the Company’s initial public offering for purposes of calculating net loss per share. Additional shares included in the calculation include 4,900,000 Class A common shares issued to the public, 11,934 restricted shares of Class A common stock that were issued to our directors and 38,856 restricted shares of Class A common stock that were issued to certain employees.
102
The following table sets forth the computation of basic and diluted net loss per common share for the years ended December 31, 2014, 2013 and 2012 (in thousands, except share and per share data):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 |
|
2013 |
|
2012 |
|
|||
|
Numerator |
|
|
|
|
|
|
|
|
|
|
|
Net loss attributable to Adeptus Health Inc. |
|
$ |
(3,351) |
|
$ |
— |
|
$ |
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Denominator: |
|
|
|
|
|
|
|
|
|
|
|
Class A common share-weighted average shares |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Effect of dilutive securities: |
|
|
|
|
|
|
|
|
|
|
|
Restricted shares |
|
|
— |
|
|
— |
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Denominator for diluted net loss per Class A common share-weighted average shares |
|
|
9,845,016 |
|
|
— |
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss attributable to Adeptus Health Inc. per Class A common share - Basic |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss attributable to Adeptus Health Inc. per Class A common share - Diluted |
|
$ |
(0.34) |
|
$ |
— |
|
$ |
— |
|
Earnings (loss) per share information is not applicable for reporting periods prior to the initial public offering. The shares of Class B common stock do not share in the earnings or losses of Adeptus Health Inc. and are therefore not participating securities. Accordingly, basic and diluted net loss per share of Class B common stock has not been presented.
NOTE 16—SUBSEQUENT EVENTS
The Company has evaluated subsequent events from the balance sheet date through the date at which the consolidated financial statements were available to be issued, and determined that there were no other items to disclose.
103
NOTE 17—SELECTED QUARTERLY FINANCIAL DATA (UNAUDITED)
The following table presents certain unaudited quarterly statement of operations data for the years ended December 31, 2014 and 2013. Results of operations for any particular quarter are not necessarily indicative of results of operations for a full year or predictive of future periods.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Three months ended |
|
||||||||||||||||||||||
|
|
|
December 31, |
|
September 30, |
|
June 30, |
|
March 31, |
|
December 31, |
|
September 30, |
|
June 30, |
|
March 31, |
|
||||||||
|
|
|
2014 |
|
2014 |
|
2014 |
|
2014 |
|
2013 |
|
2013 |
|
2013 |
|
2013 |
|
||||||||
|
|
|
(in thousands, except per share data) |
|
||||||||||||||||||||||
|
Patient service revenue |
|
$ |
80,290 |
|
$ |
66,533 |
|
$ |
51,946 |
|
$ |
44,529 |
|
$ |
38,885 |
|
$ |
25,947 |
|
$ |
26,831 |
|
$ |
23,297 |
|
|
Provision for bad debt |
|
|
(10,234) |
|
|
(8,934) |
|
|
(7,708) |
|
|
(5,748) |
|
|
(5,173) |
|
|
(2,310) |
|
|
(2,333) |
|
|
(2,261) |
|
|
Net patient service revenue |
|
|
70,056 |
|
|
57,599 |
|
|
44,238 |
|
|
38,781 |
|
|
33,712 |
|
|
23,637 |
|
|
24,498 |
|
|
21,036 |
|
|
Management and contract services revenue |
|
|
20 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Total net operating revenue |
|
|
70,076 |
|
|
57,599 |
|
|
44,238 |
|
|
38,781 |
|
|
33,712 |
|
|
23,637 |
|
|
24,498 |
|
|
21,036 |
|
|
(Loss) income from operations |
|
|
(139) |
|
|
(1,079) |
|
|
(5,072) |
|
|
(341) |
|
|
504 |
|
|
(599) |
|
|
1,401 |
|
|
(415) |
|
|
Net (loss) income |
|
|
(1,477) |
|
|
(3,598) |
|
|
(9,429) |
|
|
(2,767) |
|
|
(1,974) |
|
|
(1,511) |
|
|
1,336 |
|
|
(835) |
|
|
Less: Net (loss) income attributable to non-controlling interest |
|
|
(1,739) |
|
|
(2,001) |
|
|
(7,413) |
|
|
(2,767) |
|
|
(1,974) |
|
|
(1,511) |
|
|
1,336 |
|
|
(835) |
|
|
Net income (loss) attributable to Adeptus Health Inc. |
|
$ |
262 |
|
$ |
(1,597) |
|
$ |
(2,016) |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
|
Net loss per share of Class A common stock: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Basic and Diluted |
|
$ |
0.03 |
|
$ |
(0.16) |
|
$ |
(0.21) |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
104
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
The Company maintains a set of disclosure controls and procedures as that term is defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act that are designed to ensure that information required to be disclosed by the Company in reports that it files or submits under the Exchange Act, is recorded, processed, summarized and reported within the time periods specified in SEC rules and forms, and that such information is accumulated and communicated to the Company's management, including its Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosures. The design of any disclosure controls and procedures is based in part upon certain assumptions about the likelihood of future events, and there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions. Any controls and procedures, no matter how well designed and operated, can provide only reasonable, not absolute, assurance of achieving the desired control objectives. In accordance with Rule 13a-15(b) of the Exchange Act, as of the end of the period covered by this Annual Report on Form 10-K, an evaluation was carried out under the supervision and with the participation of the Company’s management, including its Chief Executive Officer and Chief Financial Officer, of the effectiveness of its disclosure controls and procedures. Based on that evaluation, the Company’s Chief Executive Officer and Chief Financial Officer concluded that the Company’s disclosure controls and procedures, as of the end of the period covered by this Annual Report on Form 10-K, were effective to provide reasonable assurance that information required to be disclosed by the Company in reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in SEC rules and forms and is accumulated and communicated to the Company’s management, including the Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure.
Management’s Annual Report on Internal Control over Financial Reporting
This Annual Report on Form 10-K does not include a report of management’s assessment regarding internal control over financial reporting or an attestation report of our registered public accounting firm due to a transition period established by the rules of the SEC for newly public companies. In addition, under the JOBS Act, we are not required to comply with the auditor attestation requirement of Section 404 as long as we are an “emerging growth company.” See “Risk Factors—Risks Related to Our Organizational Structure”—Pursuant to the JOBS Act, our independent registered public accounting firm will not be required to attest to the effectiveness of our internal control over financial reporting pursuant to Section 404 for so long as we are an ‘emerging growth company’.
Changes in Internal Control Over Financial Reporting
There has been no change in our internal control over financial reporting (as that term is defined in Rules 13a-15(f) under the Exchange Act) during the quarter ended December 31, 2014, that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
On February 24, 2015, the Company approved amendments to each of Messrs. Hall’s, Fielding’s and Cherrington’s Amended and Restated Restricted Units Agreements whereby each of such executive’s performance -vesting LLC Units were confirmed to be fully vested as of such date, and Messrs. Hall, Fielding and Cherrington became fully vested in 137,812, 30,214 and 34,453 LLC Units, respectively.
105
Item 10. Directors, Executive Officers and Corporate Governance
Securities Authorized for Issuance Under Equity Compensation Plans
The following table sets forth, as of December 31, 2014, certain information related to our compensation plans under which our Class A common stock may be issued.
|
|
|
Number of |
|
Weighted-average |
|
Number of |
|
|
Equity compensation plans approved by stockholders(1) |
|
N/A |
|
N/A |
|
984,005 |
|
|
Equity compensation plans not approved by stockholders |
|
— |
|
N/A |
|
— |
|
|
(1) |
Relates to the Adeptus Health Inc. 2014 Omnibus Incentive Plan. |
|
(2) |
The weighted average exercise price does not include outstanding equity awards that are received or exercised for no consideration. |
The additional information required by this item is incorporated by reference to our definitive Proxy Statements for the 2015 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2014.
Item 11. Executive Compensation
The information required by this item is incorporated by reference to our definitive Proxy Statements for the 2015 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2014.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this item is incorporated by reference to our definitive Proxy Statements for the 2015 Annual Meetin of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2014.
Item 13. Certain Relationships and Related Transactions, and Director Independence
The information required by this item is incorporated by reference to our definitive Proxy Statements for the 2015 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2014.
Item 14. Principal Accounting Fees and Services
The information required by this item is incorporated by reference to our definitive Proxy Statements for the 2015 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2014.
106
Item 15. Exhibits and Financial Statement Schedules
|
(a) |
Financial Statements |
|
(1) |
The financial statements filed as a part of this Annual Report on Form 10-K are listed on the index to financial statements. |
|
(b) |
Exhibits |
See Exhibit Index at the end of this Annual Report on Form 10-K, which is incorporated by reference.
107
Signatures
Pursuant to the requirements of Section 13 or 15(d) of the Securities and Exchange Act of 1934, the registrant has duly caused this Annual Report on Form 10-K to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Lewisville, State of Texas, on this 27 day of February 2015.
|
|
|
Adeptus Health Inc. |
|
|
|
|
|
|
By: |
/s/ Thomas S. Hall |
|
|
|
Thomas S. Hall |
|
|
|
Chairman of the Board, President, Chief Executive Officer and Director |
Pursuant to the requirements of the Securities and Exchange Act of 1934, this Annual Report and Form 10-K has been signed by the following persons on behalf of the registrant and in the capacities and on the dates indicated:
|
|
|
|
|
|
|
Signature |
|
Title |
|
Date |
|
|
|
|
|
|
|
/s/ Thomas S. Hall |
|
Chairman of the Board, President, Chief Executive |
|
|
|
Thomas S. Hall |
|
Officer and Director (Principal Executive Officer) |
|
February 27, 2015 |
|
|
|
|
|
|
|
/s/ Timothy L. Fielding |
|
Chief Financial Officer (Principal Financial Officer |
|
|
|
Timothy L. Fielding |
|
and Principal Accounting Officer |
|
February 27, 2015 |
|
|
|
|
|
|
|
/s/ Richard Covert |
|
Vice-Chairman of the Board, Director |
|
February 27, 2015 |
|
Richard Covert |
|
|
|
|
|
|
|
|
|
|
|
/s/ Daniel W. Rosenberg |
|
Director |
|
February 27, 2015 |
|
Daniel W. Rosenberg |
|
|
|
|
|
|
|
|
|
|
|
/s/ Gregory W. Scott |
|
Director |
|
February 27, 2015 |
|
Gregory W. Scott |
|
|
|
|
|
|
|
|
|
|
|
/s/ Ronald L. Taylor |
|
Director |
|
February 27, 2015 |
|
Ronald L. Taylor |
|
|
|
|
|
|
|
|
|
|
|
/s/ Jeffery S. Vender |
|
Director |
|
February 27, 2015 |
|
Jeffery S. Vender |
|
|
|
|
|
|
|
|
|
|
|
/s/ Daniel J. Hosler |
|
Director |
|
February 27, 2015 |
|
Daniel J. Hosler |
|
|
|
|
|
|
|
|
|
|
|
/s/ Steven V. Napolitano |
|
Director |
|
February 27, 2015 |
|
Steven V. Napolitano |
|
|
|
|
108
|
Exhibit No. |
|
Description |
|
|
|
|
|
3.1 |
|
Amended and Restated Certificate of Incorporation of Adeptus Health Inc. (incorporated by reference to Exhibit 3.1 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
3.2 |
|
Amended and Restated By‑laws of Adeptus Health Inc., dated June 25, 2014 (incorporated by reference to Exhibit 3.2 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
4.1 |
|
Stockholders’ Agreement, dated as of June 25, 2014, among Adeptus Health Inc. and the other stockholders named therein (incorporated by reference to Exhibit 4.1 filed with the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.1 |
|
Amended and Restated Limited Liability Company Agreement of Adeptus Health LLC, dated June 24, 2014 (incorporated by reference to Exhibit 10.1 filed with the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.2 |
|
Registration Rights Agreement, dated as of June 25, 2014, by and among the Company and the stockholders named therein (incorporated by reference to Exhibit 10.2 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.3 |
|
Tax Receivable Agreement, dated as of June 25, 2014, among Adeptus Health Inc. and the other parties named therein (incorporated by reference to Exhibit 10.3 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.4 |
|
Agreement and Plan of Merger, dated as of June 24, 2014, by and among Adeptus Health Inc., SCP III AIV THREE‑FCER Blocker, Inc. and SCP III AIV THREE‑FCER Conduit, L.P. (incorporated by reference to Exhibit 10.5 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.5 |
|
Senior Secured Credit Facility, dated as of October 31, 2013, among First Choice ER, LLC, the subsidiaries identified therein, Fifth Street Finance Corp., as Administrative Agent and L/C Arranger, and the other lenders party thereto. (incorporated by reference to Exhibit 10.3 of the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on May 21, 2014. |
|
10.6 |
|
Amendment to Credit Agreement, dated as of March 31, 2014, among First Choice ER, LLC and Fifth Street Finance Corp. (incorporated by reference to Exhibit 10.18 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014. |
|
10.7 |
|
Second Amendment to Credit Agreement and First Amendment to Security and Pledge Agreement, dated as of June 11, 2014, among First Choice ER, LLC and Fifth Street Finance Corp. (incorporated by reference to Exhibit 10.19 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014. |
|
10.8 |
|
Master Funding and Development Agreement, dated as of June 11, 2013, between MPT Operating Partnership, L.P. and First Choice ER, LLC. (portions of this exhibit have been omitted pursuant to a request for confidential treatment) (incorporated by reference to Exhibit 10.4 of the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014. |
109
|
10.9 |
|
Master Funding and Development Agreement, dated as of July 29, 2014, between MPT Operating Partnership, L.P. and First Choice ER, LLC. (portions of this exhibit have been omitted pursuant to a request for confidential treatment) (incorporated by reference to Exhibit 10.13 of the Registrant’s Quarterly Report on From 10-Q (File No. 001-36520) filed with the Commission on August 8, 2014). |
|
10.10 |
|
Advisory Services Agreement, dated as of September 30, 2011, between Sterling Fund Management, LLC and First Choice ER, LLC. (incorporated by reference to Exhibit 10.5 of the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on May 21, 2014. |
|
10.11 |
|
Termination Agreement with respect to the Advisory Services Agreement, dated as of June 24, 2014, between Sterling Fund Management, LLC and First Choice ER, LLC. (incorporated by reference to Exhibit 10.4 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014) |
|
10.12† |
|
Employment Agreement by and between First Choice ER, LLC and Thomas Hall, dated March 12, 2012 (incorporated by reference to Exhibit 10.8 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014). |
|
10.13† |
|
Amendment to Employment Agreement by and between First Choice ER, LLC and Thomas Hall, dated June 24, 2014. (incorporated by reference to Exhibit 10.6 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014) |
|
10.14† |
|
Employment Agreement by and between First Choice ER, LLC and Timothy Fielding, dated January 16, 2013 incorporated by reference to Exhibit 10.9 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014). |
|
10.15† |
|
Amendment to Employment Agreement by and between First Choice ER, LLC and Timothy Fielding, dated June 24, 2014 (incorporated by reference to Exhibit 10.7 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014) |
|
10.16† |
|
Employment Agreement by and between First Choice ER, LLC and Graham Cherrington, dated May 29, 2012 incorporated by reference to Exhibit 10.10 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014). |
|
10.17† |
|
Amendment to Employment Agreement by and between First Choice ER, LLC and Graham Cherrington, dated June 24, 2014 (incorporated by reference to Exhibit 10.8 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014) |
|
10.18† |
|
Form of Amended and Restated Restricted Units Agreement (incorporated by reference to Exhibit 10.14 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014). |
|
10.19† |
|
Adeptus Health Inc. 2014 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.9 of the Registrant’s Current Report on Form 8-K (File No. 001-36520) filed with the Commission on June 30, 2014). |
|
10.20†* |
|
Form of Restricted Stock Grant Notice and Restricted Stock Agreement for Executives. |
|
10.21†* |
|
Form of Restricted Stock Grant Notice and Restricted Stock Agreement for Non-Employee Directors. |
|
10.22† |
|
Form of Chairman of the Board Agreement between Adeptus Health Inc. and Richard Covert (incorporated by reference to Exhibit 10.17 of Amendment No. 1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-196142) filed with the Commission on June 12, 2014). |
|
21.1* |
|
Subsidiaries of the Registrant. |
110
|
23.1* |
|
Consent of KPMG LLP. |
|
31.1* |
|
Certification of Chief Executive Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 |
|
31.2* |
|
Certification of Chief Financial Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 |
|
32.1* |
|
Certification by Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
|
32.2* |
|
Certification of Chief Financial Officer Pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
|
101.INS* |
|
XBRL Instance Document |
|
101.SCH* |
|
XBRL Taxonomy Extension Schema Document |
|
101.CAL* |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
101.DEF* |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
101.LAB* |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
101.PRE* |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
† Management compensatory plan or arrangement.
* Filed herewith.
The agreements and other documents filed as exhibits to this report are not intended to provide factual information or other disclosure other than with respect to the terms of the agreements or other documents themselves, and you should not rely on them for that purpose. In particular, any representations and warranties made by us in these agreements or other documents were made solely within the specific context of the relevant agreement or document and may not describe the actual state of affairs as of the date they were made or at any other time.
111