Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - DELCATH SYSTEMS, INC. | d452668d8k.htm |
 Investor Presentation
(NASDAQ: DCTH)
December 2012
Exhibit 99.1 |
 Forward-looking Statements
2
DELCATH SYSTEMS, INC
Private Securities Litigation Reform Act of 1995 provides a safe harbor for
forward-looking statements made by the Company or on its behalf. This
presentation contains forward-looking statements, which are subject to certain risks and uncertainties that can cause
actual results to differ materially from those described. Factors that may cause such
differences include, but are not limited to, uncertainties relating to: timing of
completion of the FDA’s review of our NDA, the extent to which the FDA may request additional
information or data and our ability to provide the same in a timely manner, acceptability of
the Phase 1, 2 and 3 clinical trial data by the FDA, FDA approval of the Company's
NDA for the treatment of metastatic ocular melanoma to the liver, adoption, use and
resulting sales, if any, for the chemosaturation system in the United States, adoption, use
and resulting sales, if any, for the Hepatic CHEMOSAT delivery system in the EEA, our
ability to successfully commercialize the chemosaturation system in various markets
and the potential of the chemosaturation system as a treatment for patients with cancers in
the liver, the timing and our ability to successfully enter into strategic
partnership and distribution arrangements in foreign markets including Australia and key Asian
markets and resulting sales, if any, from the same, patient outcomes using the Generation 2
system, approval of the current or future chemosaturation system for other indications
and/or for use with various chemotherapeutic agents, actions by the FDA or other
foreign regulatory agencies, our ability to obtain reimbursement for the CHEMOSAT system in
various markets, submission and publication of the Phase II and III clinical
trial data, the timing and results of research and development projects, the timing and
results of future clinical trials including the initiation of clinical trials in key Asian
markets with the Hepatic CHEMOSAT Delivery System device for intra-hepatic
arterial delivery and extracorporeal filtration of doxorubicin, approval of the Hepatic CHEMOSAT
Delivery System to delver and filter doxorubicin in key Asian markets and adoption,
sales, if any, and patient outcomes using the same, the timing, price and use, if
any, of the committee equity financing facility with Terrapin, the timing and use, if any, of the line of
credit from SVB and our ability to access this facility and uncertainties regarding our
ability to obtain financial and other resources for any research, development and
commercialization activities. These factors, and others, are discussed from time to time in our filings
with the Securities and Exchange Commission. You should not place undue reliance on these
forward-looking statements, which speak only as of the date they are made. We
undertake no obligation to publicly update or revise these forward-looking statements to
reflect events or circumstances after the date they are made.
|
 Our
Mission Concentrating the Power of Chemotherapy for Disease Control in the
Liver •
We are a cancer therapy company
•
Our technology offers the opportunity to gain control of tumors in
the liver
•
The liver is a site where uncontrolled disease is often life-limiting or
leads to withdrawal of systemic treatments in favor of palliative
care
•
We plan on being a fully-integrated company and are building the
infrastructure to develop and commercialize our products in
Europe and North America, while pursuing opportunities in other
regions.
o
In Europe, CHEMOSAT with Melphalan is approved and is currently being sold
•
We believe that our first product, CHEMOSAT, may extend the
lives of a large number of cancer patients
3
DELCATH SYSTEMS, INC |
 The
Problem •
Metastatic disease to the liver, brain or lungs is often the life-
limiting location of solid tumors
o
In contrast to the brain and lungs, where systemic chemotherapy
and radiation can exert some degree of local control, tumors in the
liver are not particularly responsive to chemotherapy and radiation
therapy
•
Existing treatments to control tumors in the liver include:
Surgical resection
Radioembolization (SIRT)
Chemoembolization (TACE)
Radiofrequency ablation (RFA), Microwave, Cryoablation
Hepatic arterial infusion (HAI)
Systemic chemotherapy
4
DELCATH SYSTEMS, INC
Existing Liver Cancer Treatments Have Significant Limitations
|
 Existing Liver Cancer Treatments Have Limitations
Unmet Medical Need Exists for More Effective Liver Cancer Treatments
Treatment
Advantages
Disadvantages
Systemic
–
Non-invasive
–
Repeatable
–
Systemic toxicities
–
Limited efficacy in liver
Regional
(e.g., Isolated Hepatic Perfusion)
–
Therapeutic effect
–
Targeted
–
Invasive/limited repeatability
–
Multiple treatments are
required but not possible
Focal
(e.g. surgery, radioembolization,
chemoembolization, radio
frequency ablation)
–
Partial removal or
treatment of tumors
–
Only 10% to 20% resectable
–
Invasive and/or limited
repeatability
–
Treatment is limited by tumor
size, number of lesions and
location
–
Tumor revascularization
–
Cannot treat diffuse disease
5
DELCATH SYSTEMS, INC |
 Diffuse
Hepatic
Metastases
from
Melanoma
•
Diffuse disease in the liver is prevalent
•
Effective treatment for patients with liver-limited or dominant cancers
remains a clinical challenge
•
Whole organ therapy creates a new option for patients in the management
of liver dominant disease
6
DELCATH SYSTEMS, INC |
 Concentrating the Power of Chemotherapy for Disease Control in the Liver
Our Solution –
Whole Organ-Focus Disease Control
•
Our proprietary CHEMOSAT system isolates the liver
circulation, delivers an ultra-high concentration of
chemotherapy (melphalan) to the liver and filters most of the
chemotherapy out of the blood prior to returning it to the patient
•
The procedure typically takes approximately two hours to
complete and involves a team including the interventional
radiologist and perfusionist
•
CHEMOSAT (Gen 2) has demonstrated minimal systemic
toxicities and impact to blood components in initial commercial
use and may complement systemic therapy
•
CHEMOSAT has been used on approximately 200 patients
to date through clinical development and early commercial launch
7
DELCATH SYSTEMS, INC |
 1.
ISOLATE
2.
SATURATE
3.
FILTRATE
The Delcath CHEMOSAT System
Minimally Invasive, Repeatable Liver Procedure That Could Complement Systemic
Therapy Chemosaturation
8
DELCATH SYSTEMS, INC
•
Improves disease
control in the liver
•
Treats entire liver
(macro and micro)
•
Controls systemic
toxicities
•
Allows for over 100x
effective dose
escalation at tumor
site |
 Concentrating the Power of Chemotherapy for Disease Control in the Liver
The Data
•
We conducted a randomized Phase 3 study under a Special
Protocol Assessment (“SPA”) using Generation 1 of our
chemosaturation system with melphalan in patients with
melanoma (ocular and cutaneous) metastatic to the liver
•
Melanoma liver metastases are relatively homogeneous
regardless of origin
•
Liver metastases are typically the life-limiting aspect of the
disease
•
Melanoma is notoriously insensitive to systemic chemotherapy
and our study was a great demonstration of our technology’s
potential in a challenging histology
9
DELCATH SYSTEMS, INC |
 Phase
III Clinical Trial Design Randomized to CS
93 patients: ocular
or cutaneous melanoma
Best Alternative Care (BAC)
Investigator and patient decision
(any and all treatments)
CS/Melphalan
Treat every 4 weeks x 4 rounds
(responders
can receive up to 6 rounds)
Cross-over
Primary Trial Endpoint
•
Statistically significant difference in Hepatic Progression
Free Survival (“hPFS”): p < 0.05
(IRC) •
Over 80% of Oncologic drugs approved by FDA between
2005
–
2007
on
endpoints
other
than
overall
survival
Modeled hPFS for Trial Success:
7.73 months (CS)
vs.
4 months (BAC)
Secondary Trial
Endpoints
•
Investigator hPFS
•
Hepatic objective response rate
•
Overall objective response rate
•
Overall
Survival
–
Diluted
by
Cross
Over
•
SAP calls for analysis of various patient subsets
Pre-CS (Baseline)
Post-CS (22+ Months)
Hepatic
Response
–
Metastatic
Melanoma
Fully Powered, 93 Patient, Randomized, Multi-Center NCI Led Study
CS =
ChemoSaturation (CHEMOSAT)
10
DELCATH SYSTEMS, INC |
 INDEPENDENT
REVIEW
COMMITTEE
(IRC)
ASSESSMENT
-
UPDATED ANALYSIS (4 June 2012)
Hepatic progression-free survival (IRC)
Positive Phase III Results –
Primary Endpoint hPFS
CS-PHP Demonstrated 4x or 5.3 months Improvement in Primary Endpoint of hPFS
1.0
0.8
0.6
0.4
0.2
0.0
Proportion of patients surviving
Hazard ratio = 0.50
(95% CI 0.31–0.80)
P=0.0029
Chemosaturation (CS-PHP)
Best alternative care (BAC)
0
5
10 15
20
25
30
Intent-to-treat population
7.0
1.7
5.3 mo
Months
11
DELCATH SYSTEMS, INC |
 INVESTIGATOR
ASSESSMENT
-
Overall progression-free survival (investigator)
Positive Phase III Results –
Overall PFS
CS-PHP also Demonstrated a Highly Statistically Significant Improvement in Overall
PFS Chemosaturation (CS-PHP)
Best alternative care (BAC)
Hazard ratio = 0.42
(95% CI 0.27–0.64)
P<0.0001
1.0
0.8
0.6
0.4
0.2
0.0
5.4
1.6
3.8 mo
0
5 10 15
20
25
30 35 40
45
50 55 UPDATED
ANALYSIS (4 June 2012)
Intent-to-treat population
Months
Proportion of patients surviving
12
DELCATH SYSTEMS, INC |
 TOTOL
CS-PHP vs BAC ONLY Overall Survival –
Exploratory Subset Analysis
Overall Survival Tail For CS-PHP Treated Patients
Proportion of subjects surviving
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
12
36
0
24
48
60
11.4
Total CS-PHP incl.
crossover
BAC only
Months
4.1
Intent-to-treat population
7.3 mo
13
DELCATH SYSTEMS, INC |
 Positive Phase III Results
•
Primary endpoint (hPFS by IRC) exceeded, p value =
0.0029, hazard ratio of 0.50 as of June,
2012 o
CS/PHP
median
hepatic
progression
free
survival
(hPFS)
was
4-fold
of
control,
or
5.3
months
improvement
o
CS/PHP
achieved
a
median
hPFS
of
7.0
months
vs
1.7
months
for
BAC
control
o
75% overall clinical benefit (CR + PR + SD)
•
Secondary endpoints consistent with primary endpoints
o
CS/PHP achieved a median overall PFS of 5.4 months vs. 1.6 months for BAC
o
OS –
No difference demonstrated due to heavy crossover from BAC to CS/PHP
o
Median OS 10.6 months vs. 10.0 months for CS/PHP and BAC
respectively •
OS exploratory analyses supportive of key observations
o
Median overall survival of 11.4 months for all patients treated with melphalan,
including crossover o
BAC patients did not cross-over to CS/PHP had a median survival of 4.1
months o
7 CS/PHP-treated and 3 BAC-only patients still alive as of 6/2012
•
Gen 1 Safety profile –
consistent with currently approved labeling for melphalan
o
30-day deaths on PHP: 3/44 patients (6.8%)
1 Neutropenic Sepsis (2.3%); 1 Hepatic Failure 2.5% (95% tumor burden); 1 gastric
perforation o
30-day deaths on BAC: 3/49 patients (6.1%)
Trial Outcomes Favorable and Consistent with Special Protocol Assessment
14
DELCATH SYSTEMS, INC |
 The
Evidence for Melphalan Melphalan, an established chemotherapy agent, is proven
active at high doses with broad antitumor activity
Authors
Technique
N
Tumor
Drug(s)
ORR,
%
Median OS,
months
Grover et al. 2004
IHP
13
NET
Melphalan ±
TNF
50
48
Noter et al. 2004
IHP
8
Ocular melanoma
Melphalan
50
10
Alexander et al. 2000
IHP
22
Ocular melanoma
Melphalan ±
TNF
62
11
Alexander et al. 2003
IHP
29
Ocular melanoma
Melphalan
62
12
Alexander et al. 2009
IHP
120
Colorectal
Melphalan ±
TNF, TNF
61
17
van Iersel et al. 2008
IHP
154
Colorectal
Melphalan
50
25
van Iersel et al. 2010
IHP
99
Colorectal
Melphalan
–
25
Verhoef et al. 2008
PHP
24
Various
Melphalan
62
–
4. Alexander HR Jr, et al. Clin Cancer Res 2003;9:6343-9
5. Alexander HR Jr, et al. Ann Surg Oncol 2009;16:1852-9
6. Van Iersel LB, et al. Ann Oncol 2008;19:1127-34
7. Van Iersel LB, et al. Ann Oncol 2010;21:1662-7
8. Verhoef C, et al. Ann Surg Oncol 15:1367-74
1. Grover AC, et al. Surgery 2004;136:1176-82
2. Noter SL, et al. Melanoma Res 2004;14:67-72
3. Alexander HR Jr, et al. Clin Cancer Res 2000;6:3062-70
15
DELCATH SYSTEMS, INC |
 Melphalan Sensitivity: In Vitro Tumor Cell Lines Study
We Believe CHEMOSAT Will Be Effective On a Wide Range of Solid Tumors
192 uM
Cancer Origin
(Cell lines)
Thyroid (2)
Ovarian (1)
Melanoma (5)
CNS (4)
Sarcoma (5)
Head and Neck (2)
Bladder (5)
Colon (5)
Cervix (3)
Cholangiocarcinoma
(1)
Prostate (2)
Pancreas (4)
Primary Liver (4)
Lung (5)
Breast (5)
Kidney (5)
Uterus (1)
Apoptosis
Induction
(uM)
2.54
4.31
4.53
6.40
6.68
6.78
9.50
15.12
15.16
16.00
17.55
25.00
25.04
28.60
31.82
44.60
35.30
200
150
100
50
0
Melphalan Sensitivity-
Apoptosis Induction
Tissue
of
Origin
of
Cancer
Cell
Lines
Melphalan Conc. Achieved
16
DELCATH SYSTEMS, INC |
 Our Opportunity
Concentrating the Power of Chemotherapy for Disease Control in the Liver
•
•
•
•
At the concentrations of melphalan we are achieving in the
liver, we believe CHEMOSAT will be effective on a wide variety
of histologies
We believe that physicians are recognizing the broad
applicability of CHEMOSAT, based on early experience and
their interest in testing our technology with melphalan in a
variety of tumor histologies
CE Mark approved broad indication
Large global market opportunity with pharmaceutical-like gross
margin
~
80%
17
DELCATH SYSTEMS, INC |
 CHEMOSAT -
Potential Multi-Billion Dollar Market
$7 Billion Annual Global Opportunity with Pharmaceutical-Like Gross Margins
Sources: LEK Consulting, GLOBOCAN, Company estimates.
EU: Initial target countries of Germany, UK, Italy, France, Spain, Netherlands, Ireland.
APAC: Initial target countries of China, Japan, S. Korea, Taiwan, Australia.
Assumes 2.5 treatments per patient.
Assumes EU ASP of $15K; US ASP of $25K; APAC ASP of $5K.
200,000
175,000
150,000
125,000
100,000
75,000
50,000
25,000
0
USA
EU
APAC
5,585
5,585
7,671
99,749
19,861
33,953
52,143
33,966
33,966
7,202
8,212
8,708
6,563
4,085
55,389
$2.2 B
42,367
$2.6 B
189,943
$2.2 B
HCC
CRC
Melanoma
NET
18
DELCATH SYSTEMS, INC |
 Approved (CE
Mark Device) NDA Filing Accepted by the FDA with PDUFA goal date of June 15, 2013
Application Submitted/ Planned –
Mutual Recognition of European CE Mark
Global Commercialization Status
Addressing A Multi-Billion Dollar Global Market
19
DELCATH SYSTEMS, INC |
 European
Commercialization Strategy Strategy:
•
Focus efforts in 7 Target Countries (EU 5 + Netherlands & Ireland)
•
8-10 leading EU cancer centers as initial training centers
•
Validate business model and demonstrate scalability
•
Push and Pull marketing and selling strategy
Tactics & Execution:
•
Educate medical and surgical oncologists via contract organization
•
Sell to hospital-based oncologists, interventional radiologists, surgeons and C-suite
decision makers with combination of direct sales and distributors
•
Focus on medical and surgical oncologists at referral centers
•
Hospitals procure melphalan from third parties and physicians use at their discretion
•
Establish
European
patient
education
and
awareness
programs
(PR,
website)
•
Leverage interim reimbursement channels, while pursuing permanent procedure reimbursement
•
Focused clinical trial program to generate additional data and build clinical experience across
multiple centers for various tumor types (e.g. HCC, NET and CRC)
Currently In Initial Training and Marketing Phase
Establish EU
Operations
Initial
Training and
Marketing
Full
Commercial
Launch
20
DELCATH SYSTEMS, INC |
 Patient Referral Path
Interventional
Radiologist
Offers chemosaturation
procedure
Patient
Primary
Care
Medical
Oncologist
Offers systemic therapy
Surgical
Oncologist
Offers resection or
other focal therapy
Chemosaturation
Diagnosis
of Cancer
Identification
of
liver
involvement
with no
improvement from systemic
therapy
21
DELCATH SYSTEMS, INC
When
liver
disease
is
controlled,
patients
return
to
the
Medical
Oncologist for additional systemic therapy |
 CHEMOSAT Training and
Marketing Commenced in Europe Continue Training and Marketing Centers
Roll-Out •
Entered training and marketing agreements with leading cancer centers in Europe
o
Milan, Italy –
European Institute of Oncology (IEO)
o
Frankfurt, Germany –
Johann Wolfgang Goethe-Universität (JWG)
o
Kiel,
Germany
–
Universitätsklinikum
Schleswig-Holstein
o
Villejuif, France –
Cancer Institute Gustave Roussy (IGR)
o
Barcelona, Spain –
El Hospital Quiron
o
Naples,
Italy
–
Instituto
Nazionale
Tumori
Fondazione
"G.
Pascale"
o
Amsterdam,
The
Netherlands
–
Netherlands
Cancer
Institute-Antoni
van
Leeuwenhoek
Hospital
o
Erlangen,
Germany
–
University
Hospital
of
Erlangen
o
Pamplona, Spain –
Clinica Universidad de Navarra
o
Bordeaux, France –
Hôpital Saint-André
(St Andre)
o
Galway, Ireland –
University Hospital Galway (UHG)
o
Leiden,
The
Netherlands
–
Leiden
University
Medical
Center
o
Southampton, United Kingdom –
Southampton University Hospital (SUH)
o
Göttingen, Germany -
University Medical Center Göttingen (UMG)
•
Training completed and patients treated at IEO, JWG, IGR, St Andre, UHG, SUH and UMG
o
Liver metastases from cutaneous melanoma, ocular melanoma, gastric cancer, breast cancer,
neuroendocrine tumor (NET), hepatocellular carcinoma (HCC) and
cholangiocarcinoma DELCATH SYSTEMS, INC
22
•
• |
 European Reimbursement
Considerations •
No
centralized
pan-European
medical
device
reimbursement
body
–
reimbursement
mechanisms vary greatly at national and regional levels across our target markets
•
Working
with
reimbursement
specialists
to
execute
plan
in
each
of
our
key
markets
for
both
interim and long term reimbursement
•
Italy
–
Secured
a
pathway
for
reimbursement
using
an
existing
Diagnosis
Related
Group
code
(DRG)
for
use
with
CHEMOSAT.
We
will
continue
to
seek
additional
supplemental
new
technology payments, and potentially pursue a new higher reimbursing DRG for CHEMOSAT
o
A limited number of procedures are currently being covered by private payment and
research funding
•
Apply for funding under existing New Technology Payment programs
o
Italy –
First Regional Application submitted for supplemental (in addition to DRG) new technology
payments.
o
Germany -
Interim reimbursement process is being actively sponsored and driven by the German
Radiology Society –
12 NUB applications filed
o
United Kingdom –
Our lead centers are seeking to gain PCT (Primary Care Trust) approval. This
would allow us to perform CHEMOSAT procedures in 3 to 4 key centers in the UK
Reimbursement
Program Now In Execution Phase
DELCATH SYSTEMS, INC
23
•
•
•
• |
 International Strategy beyond EU and US
•
Leverage CE Mark to obtain reciprocal regulatory approvals for CHEMOSAT
System in other international markets
o
Obtained approval for Gen 2 CHEMOSAT System with melphalan in Austrailia
•
International regulatory submissions status:
Application
submitted
and
expected
approvals
in
Hong Kong
-
2012 (Gen 2 expected in Dec.)
Canada
-
2012 (Gen 2 expected in Dec.)
Singapore
-
2013
Argentina
-
2013
Brazil
-
2014
Intend
to
submit
applications
S. Korea
(CHEMOSAT Doxorubicin)
Mexico
China
(CHEMOSAT Doxorubicin)
Taiwan
Russia
India
Japan
Israel
•
Utilize 3 party melphalan and doxorubicin available to physicians
Combination of Strategic Partnerships and Specialty Distributors
DELCATH SYSTEMS, INC
24
rd |
 U.S.
FDA Regulatory Status •
NDA accepted and under active FDA review since submission in mid
August, 2012. We are working closely with the FDA during the review
process.
•
Based on the FDA’s recommendation, we have decided to focus our
NDA’s initial labeling on unresectable metastatic ocular melanoma in
the liver
•
PDUFA goal date of June 15, 2013 assigned by the FDA
•
FDA advised Oncology Drug Advisory Committee (ODAC) panel to be
expected in May 2013
•
NDA filing included:
o
Comprehensive set of additional data in a new FDA compliant
CDISC database
o
Gen 2 filter as part of the Chemistry, Manufacturing and Control
(CMC) module
•
We
have
also
amended
IND
and
Expanded
Access
Program
(EAP)
and
Gen 2 has been accepted by the FDA for use in EAP, compassionate
use and prospective clinical trials in the US
DELCATH SYSTEMS, INC
25
•
•
•
•
• |
 U.S.
Commercialization Strategy •
Initial focus on centers that participated in the phase III clinical trial
•
Educate Medical Oncologists via Medical Science Liaison (MSL)
•
Direct strategy to sell to Interventional Radiologists and Oncologists
o
Approximately 12 sales territories ultimately expanding to as many as 60
territories as revenues ramp
•
Utilize top centers from Phase III trial as Centers of Excellence for
training and support
•
Intend to seek chemosaturation specific CPT reimbursement code,
based upon value proposition relative to other cancer therapies
Direct Sales Channels with MSL Clinical Support
DELCATH SYSTEMS, INC
26
•
•
•
•
• |
 Clinical Development Program
•
Goals:
Expand US (CS-PHP: MEL) label indications beyond the
current indication we are seeking
Generate robust clinical data to support commercialization
•
FDA has accepted IND Amendment to include Gen 2 device in
Expanded Access Program (EAP), compassionate use (CU),
and all future clinical trials
•
On track to initiate EAP to treat first patient
•
Activate EU Registry to systematically collect data from
commercial experience
Establish CHEMOSAT as the Standard of Care (SOC) for Disease Control in the
Liver DELCATH SYSTEMS, INC
27
•
•
•
• |
 Clinical Development Program
•
Intend
to
initiate
new
pivotal
trials
(first
patient
enrolled
in
2013),
pending
discussion with the FDA:
Hepatocellular carcinoma (HCC)
o
Global Phase 3 Randomized CHEMOSAT Melphalan vs. BSC for
Sorafenib Failure
Advanced colorectal cancer (CRC) with liver dominant metastasis
o
Global Phase 3 Randomized CHEMOSAT Melphalan vs.
Available Alternatives
Neuroendocrine tumor (NET) with liver dominant disease
o
Global Phase 3 Randomized CHEMOSAT Melphalan vs.
Available Alternatives
•
Phase 2 studies in multiple indications: HCC, NET, CRC, melanoma
•
Global
Investigator-initiated
trials
(IITs)
–
opportunity-driven
Establish CHEMOSAT as the Standard of Care (SOC) for Disease Control in the
Liver DELCATH SYSTEMS, INC
28
•
•
• |
 CHEMOSAT System for
Doxorubicin – CE Mark
Satisfied all of the requirements to affix the CE Mark to Hepatic
CHEMOSAT Delivery System device for intra-hepatic arterial delivery
and extracorporeal filtration of doxorubicin in October, 2012
o
Provides a pathway for regulatory approval in China and S. Korea
Provides basis for partnership opportunities in China and S. Korea
where doxorubicin has a broad label for multiple tumor types
Multiple published Phase I/II studies from MD Anderson Cancer Center
and Yale with percutaneous hepatic perfusion (PHP) and Kobe
University using doxorubicin show promising response rates for HCC*
Plan
to
use
CHEMOSAT
Doxorubicin
in
Asia
Phase
III
2L
HCC trials
Addressing the Large HCC Market Opportunity in China
DELCATH SYSTEMS, INC
29
•
•
•
• |
 2012
Milestones •
First patients have been treated with CHEMOSAT Melphalan in Europe -
Done
•
Execute contract for MSL services in EU in 1Q 2012 (Quintiles was selected to
support EU launch of CHEMOSAT) -
Done
•
Secure agreements with 8-10 leading cancer centers in EU -
Done
•
Obtain CE Mark for Gen 2 CHEMOSAT Melphalan -
Done
•
US NDA submission in August 2012 -
Done
•
US NDA acceptance with standard review in October 2012 -
Done
•
Obtain CE Mark for CHEMOSAT Doxorubicin in 2H 2012 -
Done
•
Submission for publications of Phase III data and mNET arm of Phase II data in
Q4 2012
•
First patients enrolled in EAP in Q4 2012
•
Initiate EU Registry in Q4 2012
•
Potential Asia strategic partnership –
dedicated BD with China a top priority
DELCATH SYSTEMS, INC
30 |
 Cash &
Cash Equivalents: $28.3 million at September 30, 2012
Financing:
$21.1 million (net) raised in a follow-on equity
offering in May 2012
ATM Program
$21.5 million remaining as of November 2012
Committed Equity Financing
Facility (CEFF)
Up to $35 million as of December 5, 2012
Working Capital Line of Credit:
$20.0 million credit facility
Debt:
None
Cash Spend:
$14.6 million in 3Q2012
Shares Outstanding:
75.1 million (85.5
million
fully
diluted
Institutional Ownership:
13%
Market Capitalization:
$120 million as of November 30, 2012
Avg. Daily Volume (3 mo.):
1,000,000
1) Fully diluted includes an additional 4.8 million options and 5.6 million warrants
1
)
DELCATH SYSTEMS, INC
31
Financial Update |
 Team
Executive
Title
Prior Affiliation(s)
Years of
Experience
Eamonn Hobbs
President and CEO
AngioDynamics, E-Z-EM
31
Graham Miao, Ph.D.
EVP & CFO
D&B, Pagoda Pharma, Schering-Plough,
Pharmacia, JP Morgan
22
Krishna Kandarpa, M.D.,
Ph.D.
CSO and EVP, R&D
Harvard, MIT(HST), Cornell, UMass
32
Agustin Gago
EVP, Global Sales
AngioDynamics, E-Z-EM
30
Jennifer Simpson, Ph.D.
EVP, Global Marketing
Eli Lilly (ImClone), Johnson & Johnson
(Ortho Biotech)
22
Peter Graham, J.D.
EVP, General Counsel &
Global Human Resources
Bracco, E-Z-EM
17
David McDonald
EVP, Business Development
AngioDynamics, RBC Capital Markets
29
John Purpura
EVP, Regulatory Affairs & Quality
Assurance
E-Z-EM, Sanofi-Aventis
28
Harold Mapes
EVP, Global Operations
AngioDynamics, Mallinkrodt
26
J. Chris Houchins
SVP, Clinical Affairs
Arno, Schering-Plough, Pfizer,
Pharmacia, GD Searle
21
Gloria Lee, M.D., PH.D.
SVP, Global Clinical Development
Hoffmann-La Roche, Syndax
Pharmaceuticals, Inc.
20
Bill Appling
SVP Medical Device R&D
AngioDynamics
26
Dan Johnston, Ph.D.
VP, Pharmaceutical R&D
Pfizer, Wyeth
11
DELCATH SYSTEMS, INC
32 |
 Appendices
33
DELCATH SYSTEMS, INC |
 Appendix I
Intellectual Property
34
DELCATH SYSTEMS, INC |
 Intellectual Property
•
Patent Protection
o
5 U.S. patents in force and 6 U.S. patent applications pending
o
6 foreign patents in force (with patent validity in 22 countries) and 15 foreign
patent applications pending
o
Primary device patent set to expire August 2016
o
Up to 5 years of patent extension post FDA approval
•
Trade Secret Protection
o
Developed improved filter media via new manufacturing processes
•
FDA Protection
o
Orphan Drug Designation granted for melphalan in the treatment of ocular
melanoma, cutaneous melanoma and metastatic neuroendocrine tumors, as well as
for doxorubicin in the treatment of HCC
Provides 7 years of marketing exclusivity post FDA approval
o
Additional Orphan Drug applications to be filed for other drugs and indications,
including melphalan for HCC and CRC
Multiple Levels of Protection
DELCATH SYSTEMS, INC
35 |
 Appendix
II CHEMOSAT Market Opportunity
by Disease and Target Counties
DELCATH SYSTEMS, INC
36 |
 •
Europe
–
Largest
near-term
opportunity
•
CRC
–
Largest opportunity worldwide
•
Melanoma
–
Largest opportunity is in US
•
China-
Largest opportunity for HCC
Market Opportunity by Disease (patients)
Market Opportunity defined as Total Potential
Market (TPM) for CHEMOSAT
®
10000
Melanoma
7500
5000
2500
0
30000
25000
20000
15000
0
10000
5000
NET
CRC
40000
30000
20000
10000
0
100000
80000
60000
40000
20000
0
37
DELCATH SYSTEMS, INC
HCC
1.
Primary cancer incidence
2.
Adjusted for predominant disease in the liver (primary
or metastatic cancer)
3.
Adjusted
for
addressable
patients
via
Delcath
CHEMOSAT
® |
 Europe Market by Disease
– Device Only
Germany
(Direct)
UK
(Direct)
France
(Indirect)
Italy
(Indirect)
Spain
(Indirect)
Netherlands
(Direct)
Ireland
(Direct)
Total
Potential
(patients)
Potential
Market
($ MM)
1,2,3
Total Potential Market #Patients
Ocular
Melanoma
404
297
295
285
197
79
19
1,576
$ 62
Cutaneous
Melanoma
1,625
994
753
801
360
379
73
4,987
$ 206
CRC
9,902
5,300
5,475
7,281
4,016
1,644
335
33,953
$1,339
HCC
(Primary)
1,637
720
1,514
2,597
1,087
82
35
7,671
$277
NET
1,783
1,336
1,353
1,299
974
360
98
7,202
$ 281
TOTAL
15,351
8,647
9,389
12,263
6,634
2,545
560
55,389
$ 2,166
Europe Presents Significant Potential Market Opportunity
Sources: LEK Consulting, GLOBOCAN, Company estimates.
1) Assumes 2.5 treatments per patient.
2) Assumes ASP of ~$15K USD.
3) Assumes mix of direct sales and distributors.
38
DELCATH SYSTEMS, INC |
 US Market by Disease
– Device and Drug Combination
Liver Metastasis
Potential Market
# Patients
Potential Market
# Procedures
Potential Market
($MM)
1,2
Ocular
Melanoma
1,685
4,213
$ 105
Cutaneous
Melanoma
7,023
17,557
$ 439
CRC
19,861
49,653
$ 1,241
HCC (Primary)
5,586
13,964
$ 349
NET
8,212
20,530
$ 513
TOTAL
42,367
105,917
$ 2,648
Sources: LEK Consulting, GLOBOCAN, Company estimates.
1) Assume 2.5 treatments per patient.
2) Estimated ASP of $25K.
39
DELCATH SYSTEMS, INC |
 APAC Market by Disease
China
(Device)
S. Korea
(Device)
Japan
(Device)
Taiwan
(Device)
Australia
(Device)
Total
Potential
(patients)
Potential
Market
($MM)
1,2
Total Potential Market #Patients
HCC
(Primary)
85,780
3,258
8,296
2,152
263
99,749
$ 1,156
Other
CRC
31,127
3,245
14,298
1,441
2,031
52,143
$ 642
NET
29,197
1,048
2,759
500
462
33,966
$ 393
Ocular
Melanoma
1,765
66
175
31
96
2,134
$ 25
Cutaneous
Melanoma
382
43
136
246
1,144
1,951
$ 23
OTHER
TOTAL
62,472
4,403
17,368
2,218
3,733
90,194
$ 1,083
TOTAL
148,104
7,661
25,665
4,370
3,996
189,943
$ 2,239
APAC Target Markets Represent Over $2 Billion Potential Market Opportunity
Sources: LEK Consulting, GLOBOCAN, Company estimates.
1) Assume 2.5 treatments per patient.
2) Estimated ASP of ~$5K.
40
DELCATH SYSTEMS, INC |
 Appendix III
CHEMOSAT Melphalan Phase I and II
41
DELCATH SYSTEMS, INC |
 Melphalan Dosing & Background
•
Well understood, dose dependant, tumor preferential, alkylating cytotoxic agent
that demonstrates little to no hepatic toxicity
•
Manageable systemic toxicities associated with Neutropenia and
Thrombocytopenia
•
Drug dosing 12x higher than FDA-approved dose via systemic IV
chemotherapy •
Dose delivered to tumor is over 100x higher than that of systemic IV
chemotherapy
An Established Drug for Liver Cancer Therapy
Type
Dosing (mg/kg)
Multiple Myeloma (label)
Chemoembolization
Surgical Isolated Hepatic Perfusion (IHP)
Myeloablation
Chemosaturation (PHP)
0.25
0.62
1.50
2.50-3.50
3.00
DELCATH SYSTEMS, INC
42 |
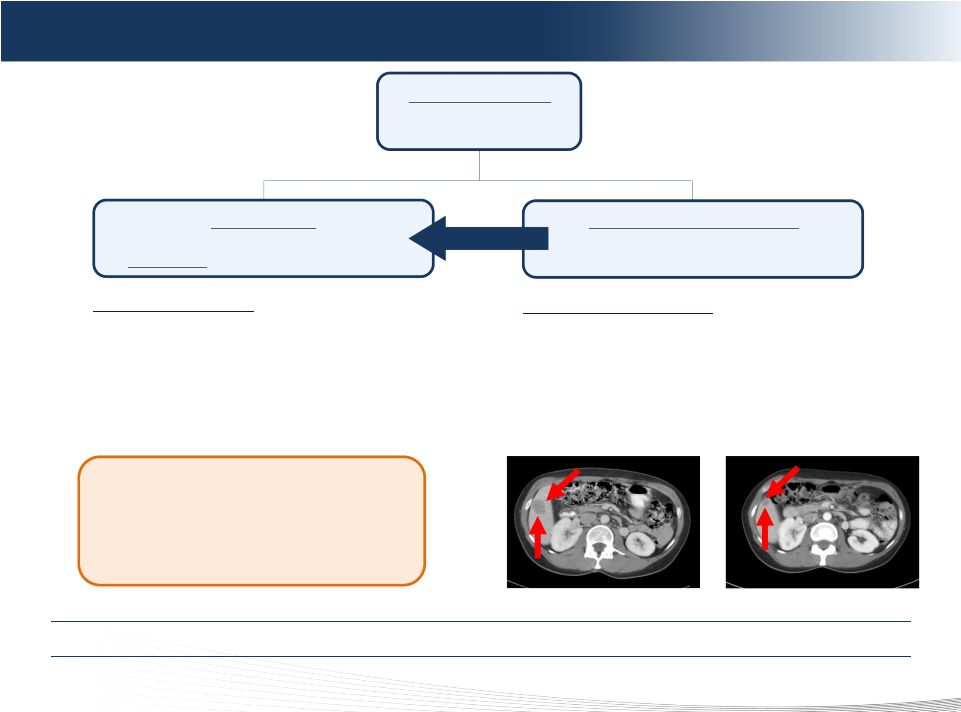
 Phase
II NCI Trial – Metastatic Neuroendocrine Cohort
Pre-CS
(Baseline)
Post-CS #2
(+4 Months)
Post-CS #1
(+6 Weeks)
Compelling Clinical Data in Attractive mNET Market
*Presentation at ECCO/ESMO 2011 annual meeting.
Phase II mNET Tumor Cohort (n=24)*
Number (n)
Primary Tumor Histology
Carcinoid
Pancreatic Islet Cell
Response
Not Evaluable (Toxicity, Incomplete Treatment, Orthotopic Liver
Transplantation
Progressive Disease
Minor Response / Stable Disease
Partial
Response
(30.0%
-
99.0%
Tumor
Reduction)
Complete Response (No Evidence of Disease)
Objective Tumor Response
Objective Tumor Response Rate
Duration (months)
Median Hepatic PFS
Overall Survival After CS
4
20
4
2
4
1
13
14
58%
15.5
30.4
DELCATH SYSTEMS, INC
43 |
 Phase
II NCI Trial – Hepatobilliary carcinoma
•
11 patients with tumors of hepatobiliary origin: 5 HCC, 2 intrahepatic and
3 extrahepatic cholangiocarcinoma,1 mixed histology
•
CHEMOSAT treatment showed encouraging anti-tumor activities in
hepatocellular carcinoma (HCC)
o
1 Confirmed partial response lasting 7 months
o
2 stable disease lasting 8 months, 6 months respectively
•
Safety profile –
consistent with pivotal US Phase III melanoma trial
•
HCC is the most common primary cancer of the liver, with approximately
750,000* new cases diagnosed worldwide annually
•
Intend to invest in new HCC trials with CHEMOSAT
Encouraging Initial Positive Signal for Primary Liver Cancer
*Source: GLOBOCAN
44
DELCATH SYSTEMS, INC |
 •
Substantial clinical evidence of benefit of using melphalan to treat
mCRC via isolated hepatic perfusion (IHP) procedure
o
Over 800 patients treated in 15 studies since 1998
o
Patients treated only once
o
Median
response
rate
of
47%
(range
29%-76%)
¹
•
Delcath
Phase
II
NCI
Chemosaturation
Trial
–
mCRC
Cohort
o
Challenges enrolling at NCI
o
16 patients treated since 2004
o
Inconclusive
efficacy
due
to
advanced
disease
status
(generally
5
or
6
line)
o
Safety profile –
expected and consistent with pivotal FDA Phase III
melanoma trial
•
Intend to invest in new mCRC trials with CHEMOSAT Melphalan
Strong Rationale for Using CHEMOSAT with Melphalan to Treat mCRC
1) van Iersel LB, Koopman M, Van D, V, et al. Ann Oncol. 2010;21:1662-7.
Phase II NCI Trial –
mCRC Cohort
45
DELCATH SYSTEMS, INC
th
th |
 Appendix IV
Published Phase I/II Studies of
Doxorubicin with PHP (percutaneous hepatic
perfusion) for HCC
DELCATH SYSTEMS, INC
46 |
 3
No. of
pts
No. of
PHP/
pt
Disease stage
(tumor diameter)
Treatment
Median survival
(mo)
Response Rates
Reference
HCC
(n=79)
CHM
(n=23)
1–4
1–2
IV A: n=66
IV B: n=13
All multiple bilobar
Extrahepatic disease in 52%
Doxorubicin 60–150 mg/m²
Cisplatin 50–150 mg/m²
Mitomycin C 50–200 mg/m²
16
13
HCC pts
RR 64.5%
5-year survival 20.3%
Kobe
Phase I/II
HCC
(n=11)
1–3
Mean 9.5 cm
Doxorubicin 60–120 mg/m²
6.5
13 (responders)
2 (non-responders)
RR 20%
MDACC
Phase I
HCC
(n=5)
CHM
(n=8)
Other
(n=8)
2–4
Extrahepatic disease in 17%
Doxorubicin 50–120 mg/m²
5-FU 1000–5000 mg/m²
NR
RR 22%
Yale
Phase I
HCC
(n=7)
Other
(n=11)
1–10
NR
Doxorubicin 90–120 mg/m²
23 (responders)
8 (non-responders)
RR 58%
Yale
4
Phase I
Phase I/II Studies of PHP-Doxorubicin For HCC
Delivered Safely in Multiple Studies with Promising Response Rates
1) Ku Y et al. Chir Gastroenterol 2003;19:370–376.
2) Curley SA et al. Ann Surg Oncol 1994;1:389–99.
3) Ravikumar TS et al. J Clin Oncol 1994;12:2723–36.
4) Hwu WJ et al. Oncol Res 1999;11:529–37.
47
DELCATH SYSTEMS, INC
1
2 |
 Appendix V
Product Development Pipeline
48
DELCATH SYSTEMS, INC |
 Product Development Pipeline
•
Melanoma liver mets
•
Proprietary drug-melphalan &
CHEMOSAT
•
All liver cancers –
melphalan
•
Classified as Medical Device
•
3
party melphalan
•
Gen 2 melphalan CE Mark
•
CHEMOSAT for additional drugs
•
CHEMOSAT for other organs (lung
and brain)
•
mCRC and HCC indications
Initial Opportunity
Near Term (< 5 years)
Intermediate Term (> 5 years)
•
Doxorubicin system CE Mark
•
mCRC and HCC clinical trials
•
CHEMOSAT for additional drugs
•
CHEMOSAT for other organs (lung
and brain)
•
CHEMOSAT Melphalan in Taiwan
and Japan
•
CHEMOSAT Doxorubicin in
China and South Korea
•
3
party doxorubicin
•
CHEMOSAT for additional drugs
•
CHEMOSAT for other organs (lung
and brain)
•
CHEMOSAT Melphalan in
Australia and Hong Kong
•
3
party melphalan
Development Aligned to Address Significant Market Opportunity
U
S
E
U
A
S
I
A
rd
rd
rd
49
DELCATH SYSTEMS, INC |
 Appendix VI
European Regulatory Update
50
DELCATH SYSTEMS, INC |
 European Regulatory Update
•
Retained new Notified Body
•
Device reclassified from class III to class IIB, permitting self-certification
in accordance with the same established quality management system
o
The primary difference between Class III and Class IIb is that for Class IIb
medical devices the Notified Body is not required to carry out an
examination of the product’s design dossier as part of its conformity
assessment o
The Company must continue to comply with the essential requirements of the EU
Medical
Devices
Directive
(Directive
93/42
EC)
and
is
subject
to
a
conformity
assessment procedure requiring the intervention of a Notified Body
o
The conformity assessment procedure for Class IIb medical devices requires the
manufacturer to lodge an application for the assessment of its quality
system for the design, manufacture and inspection of its medical devices by
a Notified Body o
The Notified Body will audit the system to determine whether it conforms to the
provisions of the Medical Devices Directive. If the Notified Body’s
assessment is favorable it will issue a Full Quality Assurance Certificate,
which enables the manufacturer to draw a Declaration of Conformity and
affix the CE mark to the medical devices covered by the assessment
o
Thereafter, the Notified Body will carry out periodic audits to ensure that the
approved quality system is applied by the manufacturer.
51
DELCATH SYSTEMS, INC |
 ©
2011 DELCATH SYSTEMS, INC. ALL RIGHTS RESERVED |