Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - CONTINUCARE CORP | dex322.htm |
| EX-32.1 - EX-32.1 - CONTINUCARE CORP | dex321.htm |
| EX-31.1 - EX-31.1 - CONTINUCARE CORP | dex311.htm |
| EX-23.1 - EX-23.1 - CONTINUCARE CORP | dex231.htm |
| EX-31.2 - EX-31.2 - CONTINUCARE CORP | dex312.htm |
| EX-21.1 - EX-21.1 - CONTINUCARE CORP | dex211.htm |
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended: June 30, 2011
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number: 001-12115
CONTINUCARE CORPORATION
(Exact Name of Registrant as Specified in Its Charter)
| Florida | 59-2716023 | |
| (State or Other Jurisdiction of Incorporation or Organization) |
(I.R.S. Employer Identification No.) | |
| 7200 Corporate Center Drive Suite 600 Miami, Florida |
33126 | |
| (Address of Principal Executive Offices) | (Zip Code) | |
Registrant’s Telephone Number, Including Area Code (305) 500-2000
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of Each Exchange On Which Registered | |
| COMMON STOCK | NYSE | |
| $.0001 PAR VALUE |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ¨ No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. Check one:
| Large accelerated filer | ¨ | Accelerated filer | x | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | ¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ¨ No x
The aggregate market value of the voting common stock held by non-affiliates of the registrant on December 31, 2010 was approximately $151,633,000.
Number of shares outstanding of each of the registrant’s classes of Common Stock at August 31, 2011: 60,838,266 shares of Common Stock, $.0001 par value per share.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the proxy statement for the registrant’s Annual Meeting of Shareholders for the fiscal year ended June 30, 2011 are incorporated by reference into Part III of this Form 10-K.
Table of Contents
CONTINUCARE CORPORATION
ANNUAL REPORT ON FORM 10-K
FOR THE YEAR ENDED JUNE 30, 2011
| PAGE | ||||||
| 3 | ||||||
| Item 1. | 3 | |||||
| Item 1A. | 13 | |||||
| Item 1B. | 20 | |||||
| Item 2. | 20 | |||||
| Item 3. | 20 | |||||
| Item 4. | 20 | |||||
| Item 5. | 20 | |||||
| Item 6. | 22 | |||||
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
23 | ||||
| Item 7A. | 32 | |||||
| Item 8. | 33 | |||||
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
33 | ||||
| Item 9A. | 33 | |||||
| Item 9B. | 34 | |||||
| Item 10. | 35 | |||||
| Item 11. | 35 | |||||
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
35 | ||||
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
35 | ||||
| Item 14. | 35 | |||||
| Item 15. | 35 | |||||
| 38 | ||||||
2
Table of Contents
Unless otherwise indicated or the context otherwise requires, all references in this Annual Report on Form 10-K to “we,” “us,” “our,” “Continucare” or the “Company” refer to Continucare Corporation and its consolidated subsidiaries, and all references to “the MDHC Companies” refer to Miami Dade Health Centers, Inc. and its affiliated companies. All references to a “Fiscal” year refer to our fiscal year which ends June 30.
The following business description should be read in conjunction with the consolidated financial statements and notes thereto appearing elsewhere in this Annual Report on Form 10-K.
Company Overview
We are primarily a provider of primary care physician services. Through our network of 18 medical centers, we provide primary care medical services on an outpatient basis. We also provide medical management services to independent physician affiliates (“IPAs”). All of our medical centers and IPAs are located in Miami-Dade, Broward, Hillsborough and Palm Beach Counties, Florida. Substantially all of our revenues are derived from managed care agreements with three health maintenance organizations (“HMOs”), Humana Medical Plans, Inc. (“Humana”), Vista Healthplan of South Florida, Inc. and its affiliated companies including Summit Health Plan, Inc. (“Vista”), and Wellcare Health Plans, Inc. and its affiliated companies (“Wellcare”). Our managed care agreements with these HMOs are primarily risk agreements under which we receive for our services a monthly capitated fee with respect to the patients assigned to us. The capitated fee is a percentage of the premium that the HMOs receive with respect to those patients. In return, we assume full financial responsibility for the provision of all necessary medical care to our patients even for services we do not provide directly. Revenue generated under contracts with Humana, Vista and Wellcare accounted for approximately 69%, 19% and 5%, respectively, of our total revenue for Fiscal 2011. For Fiscal 2011, approximately 87% and 7% of our revenue was generated by providing services to Medicare-eligible and Medicaid-eligible members, respectively, under such risk arrangements. As of June 30, 2011, we provided services to or for approximately 27,100 patients on a risk basis and approximately 9,800 patients on a limited or non-risk basis. Additionally, during Fiscal 2011 we provided services to over 6,000 patients on a non-risk fee-for-service basis.
We also operate or manage sleep diagnostic centers at over 70 locations in 15 states through Seredor Corporation, our subsidiary established to conduct sleep service activities. The centers conduct sleep studies to determine whether patients suffer from sleep disorders and, if so, the severity of the condition. The clinical staff at the centers are expertly trained in sleep disorders and work with physicians, respiratory therapists, and clinicians utilizing state-of-the-art equipment to effectively diagnose and treat patients.
We began operating as a public company in 1996 as the successor to a Florida corporation originally incorporated in 1986. Our principal place of business is 7200 Corporate Center Drive, Suite 600, Miami, Florida 33126. Our telephone number is 305-500-2000.
Merger Transaction
Merger Agreement
On June 26, 2011, Continucare entered into an Agreement and Plan of Merger (the “Merger Agreement”) with Metropolitan Health Networks, Inc. (“Metropolitan”) and Cab Merger Sub, Inc., a Florida corporation and a wholly owned subsidiary of Metropolitan (“Merger Subsidiary”), providing for the merger of Continucare with Merger Subsidiary. Subject to the terms and conditions of the Merger Agreement, which has been unanimously approved by the boards of directors of the respective parties, Merger Subsidiary will be merged with and into Continucare (the “Merger”), with Continucare surviving the Merger as a wholly owned subsidiary of Metropolitan.
On August 22, 2011, at a Special Meeting of Shareholders, the Merger Agreement and the transactions contemplated thereby were approved by Continucare stockholders. Assuming all conditions to closing are met, Continucare and Metropolitan expect to close the acquisition on or about the end of September 2011. There can be no assurance that the acquisition will close.
At the effective time of the Merger, each share of Continucare common stock outstanding immediately prior to the effective time (other than shares owned by Continucare, Metropolitan, or shareholders who have properly demanded and perfected appraisal rights under Florida law) will be converted into the right to receive $6.25 in cash, without interest, and 0.0414 of a share of Metropolitan common stock (the “Merger Consideration”). No fractional shares of Metropolitan common stock will be issued in the Merger, and Continucare’s stockholders will receive cash in lieu of fractional shares, if any, of Metropolitan common stock. Each share of Metropolitan common stock outstanding immediately prior to the effective time will remain outstanding and will not be
3
Table of Contents
affected by the Merger. Upon completion of the transaction, Continucare stockholders will own approximately 5.8% of Metropolitan’s outstanding common stock. Metropolitan has filed a Registration Statement on Form S-4 relating to the shares of Metropolitan common stock to be issued in the acquisition. The registration statement was declared effective by the Securities and Exchange Commission (“SEC”) on July 22, 2011.
At the effective time of the Merger, each issued and outstanding option to purchase Continucare common stock will become fully vested and be cancelled in exchange for the right to receive an amount of cash equal to $6.45 less the per share exercise price of the option, subject to withholding taxes.
The value of the equity consideration portion of the Merger Consideration is subject to change based upon changes in the market price of Metropolitan’s common stock prior to closing. The total value of the transaction is approximately $416 million, excluding transaction and financing fees.
In the event that a party fails to satisfy its covenants or representations under the Merger Agreement, the agreement provides customary termination rights, and, under certain circumstances, a $12 million termination fee and up to $1.5 million of expense reimbursement. If, under certain circumstances, the Merger Agreement is terminated as a result of the Merger not being consummated on or before November 1, 2011 and if, within 12 months following the date of termination, Continucare enters into a written agreement, arrangement or understanding regarding an alternative acquisition proposal, then Continucare will be required to pay Metropolitan a termination fee of $9 million and up to $1.5 million of expense reimbursement. Upon the termination of the Merger Agreement under specified circumstances, including, among others, Metropolitan’s failure to obtain financing required to complete the acquisition, after all of the other conditions to closing have been met, Metropolitan will be required to pay Continucare a $12 million termination fee and up to $1.5 million of expense reimbursement. If, under certain circumstances, Continucare does not generate a targeted minimum cash amount of $51.7 million by November 1, 2011, the Merger Agreement may be terminated by Metropolitan and neither party will be required to pay the other party a termination fee or an expense reimbursement.
Voting Agreement
In connection with the Merger Agreement, Phillip Frost, M.D., a member of the board of directors of Continucare, and certain entities related to Dr. Frost, who in the aggregate beneficially own approximately 26 million shares of Continucare common stock, representing approximately 43% of the outstanding common stock of Continucare, in their capacities as shareholders of Continucare, executed a voting agreement with Metropolitan, dated June 26, 2011 (the “Voting Agreement”), which requires, among other things, such shareholders to vote their shares of Continucare common stock in favor of the Merger Agreement and the transactions contemplated thereby. The Voting Agreement will terminate on the earliest to occur of (i) the termination of the Merger Agreement in accordance with its terms, (ii) a written agreement of the parties to terminate the Voting Agreement and (iii) the effective time of the Merger.
Change in Control and Separation Agreements
In connection with the Merger Agreement, Richard Pfenniger, Continucare’s Chairman of the Board, Chief Executive Officer and President, and Fernando Fernandez, Continucare’s Senior Vice President – Finance, Chief Financial Officer and Treasurer, each entered into a Change in Control and Separation Agreement with Metropolitan, pursuant to which, upon completion of the Merger (a) Metropolitan will pay to Mr. Pfenniger $475,000 (less applicable taxes) over a twelve month period beginning no later than 30 days after completion of the Merger in accordance with Metropolitan’s normal payroll policies and a lump sum payment of $20,262, which is the value of one year of welfare benefits and (b) Metropolitan will pay to Mr. Fernandez $256,000 (less applicable taxes) over a twelve month period beginning no later than 90 days after completion of the Merger in accordance with Metropolitan’s normal payroll policies and a lump sum payment of $32,886, which is the value of one year of welfare benefits. In addition, if the Merger is completed, Mr. Pfenniger’s and Mr. Fernandez’s employment with Metropolitan (as the parent of Continucare, if the Merger is completed) will terminate, in the case of Mr. Pfenniger, at the effective time of the Merger and, in the case of Mr. Fernandez, on February 15, 2012 (or prior to that date on 30 days’ written notice from one party to the other), and both Mr. Pfenniger and Mr. Fernandez will be paid in one single payment on Metropolitan’s first payroll date after termination of employment an amount equal to: (i) any accrued but unpaid base salary and any bonus payments as of the termination of employment, (ii) any payments with respect to vacations earned but unused through the termination of employment, and (iii) any amount due as reimbursement of expenses incurred before the termination of employment. The Change in Control and Separation Agreements also contain certain covenants regarding confidentiality of information, non-competition and non-solicitation of Continucare employees by each of Mr. Pfenniger and Mr. Fernandez applicable until the first anniversary of the termination of their employment. No payments under the severance agreements will be made and the parties will have no obligations to one another under the severance agreements if the Merger is not completed.
Litigation Related to the Merger
On July 1, 2011, a putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Kathryn Karnell, Trustee and the Aaron and Kathryn Karnell Revocable Trust U/A Dtd 4/9/09 against Continucare, the members of the Continucare Board, individually, Metropolitan, and the merger subsidiary. Also on July 1, 2011, a second putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by
4
Table of Contents
Steven L. Fuller against Continucare, the members of the Continucare Board, individually, Metropolitan, and the merger subsidiary. On July 6, 2011, a third putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Hilary Kramer against Continucare, the members of the Continucare board of directors, individually, Metropolitan, and the merger subsidiary. On July 12, 2011, a fourth putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Jamie Suprina against Continucare, the members of the Continucare board of directors, individually, Metropolitan, and the merger subsidiary. Each of these suits sought to enjoin the proposed transaction between Continucare and Metropolitan, as well as attorneys’ fees. The Fuller, Kramer, and Suprina suits also sought rescissory and other money damages.
On July 28, 2011, an order was granted by the Court to consolidate these actions and appoint the lead plaintiff and the lead plaintiff’s counsel.
On August 12, 2011, the defendants entered into a preliminary settlement agreement ("Memorandum of Understanding") with the lead plaintiff regarding the settlement of the actions. In connection with the Memorandum of Understanding, Continucare agreed to make certain additional disclosures to its shareholders, which are contained in Continucare's Form 8-K filed with the SEC on August 12, 2011. Subject to the completion of certain confirmatory discovery by the lead plaintiff’s counsel, the parties will enter into a definitive stipulation of settlement. The definitive stipulation of settlement will be subject to customary conditions, including consummation of the merger and court approval following notice to Continucare’s shareholders. In the event that the parties enter into a definitive stipulation of settlement, a hearing will be scheduled at which the court will consider the fairness, reasonableness and adequacy of the settlement which, if finally approved by the court, will resolve all of the claims that were or could have been brought in the actions being settled, including all claims relating to the merger transaction, the merger agreement, and any disclosure made in connection therewith. In addition, in connection with the settlement, the parties contemplate that the lead plaintiff’s counsel will petition the court for an award of attorneys’ fees and expenses to be paid by Continucare. There can be no assurance that the parties will ultimately enter into a definitive stipulation of settlement or that the court will approve the settlement. In such event, the litigation would resume.
Continucare, the director defendants, and Metropolitan vigorously deny all liability with respect to the facts and claims alleged in the lawsuits, and specifically deny that supplemental disclosure was required under any applicable rule, statute, regulation or law. However, solely to avoid the risk of delaying or adversely affecting the merger and the related transactions and to minimize the expense of defending the lawsuits, Continucare, its directors, and Metropolitan agreed to the settlement described above.
Acquisitions
In Fiscal 2011, we acquired three operators of sleep diagnostic centers and a related entity that provides continuous positive airway pressure (CPAP) devices and supplies. The aggregate total purchase price for these acquired entities consisted of cash consideration paid of $11.2 million and future contingent cash consideration up to a maximum of $2.0 million subject to the achievement of certain future earnings targets. In April 2011, we paid $0.7 million of the $1.0 million maximum contingent cash consideration pertaining to the earnings of the acquired entities generated for the year ended December 31, 2010. As a result, the remaining maximum contingent cash consideration was $1.0 million as of June 30, 2011. The three acquired operators of sleep diagnostic centers operate a combined 58 sleep diagnostic centers in nine states.
Industry Overview
The United States health care market is large and growing. According to the Centers For Medicare and Medicaid Services (“CMS”), total outlays on health care in the United States were approximately $2.5 trillion in 2009 and were projected to reach approximately $4.6 trillion in 2020, representing an annual rate of increase of approximately 5.8%. The rate of the overall increase of health care outlays in the United States has been greater than the growth of the economy as a whole (measured by gross domestic product, or GDP). For example, in 2009 the rate of growth of total United States medical outlays was approximately 4% as compared to an approximate 2% decline in the GDP. The high growth rate of health care outlays is expected to continue. In 2009, health care outlays represented approximately 17.6% of GDP. CMS projects that this amount will increase to 19.8% of GDP by 2020. In addition, United States health care outlays have increased at a faster rate than the consumer price index. According to CMS, medical outlays in the United States were projected to grow by approximately 3.9% in 2010, as compared to actual increases of 4.0% in 2009, 4.7% in 2008 and 6.1% in 2007.
The Medicare sector of the United States health care market is also large and growing. Medicare provided health care benefits to approximately 47 million elderly and disabled Americans in 2010, or approximately 15% of the population of the United States. With the coming retirement of the “Baby Boom” generation, a significant increase in the number of Medicare beneficiaries is forecast, with the number of Medicare beneficiaries expected to rise to over 75 million, or greater than 20% of the projected population of the United States, by 2030. Medicare outlays have also grown faster than both the GDP and the consumer price index, which growth is forecast to continue. For example, annual Medicare outlays exceeded $500 billion in 2009 and are expected to grow to over $900 billion by 2020.
5
Table of Contents
Medicare was established in 1965 and traditionally provided fee-for-service (indemnity) coverage for its members. Under fee-for-service coverage, Medicare assumes responsibility for paying all or a portion of the member’s covered medical fees, subject, in some cases, to a deductible or coinsurance payment. There are private Medicare managed care programs that provide an alternative to traditional fee-for-service coverage. Through a contract with CMS, private insurers, such as HMOs, may contract with CMS to provide health insurance coverage in exchange for a fixed monthly payment per member per month for Medicare-eligible individuals. Individuals who elect to participate in private Medicare managed care programs typically receive additional benefits not covered by Medicare’s traditional fee-for-service coverage program and are relieved of the obligation to pay some or all deductible or coinsurance amounts due.
Participation in private Medicare managed care programs increased during the 1990s reaching a peak of 6.2 million participants in 1998, or approximately 16% of the Medicare-eligible population. As of November 2003, the number of participants had decreased to 4.6 million, or approximately 11% of the Medicare-eligible population. The number of participating private health plans also decreased during this period going from 346 plans in 1998 to 155 in November 2003. This decline in participation has been attributed to unpredictable and insufficient payments resulting from the alteration of payments to private plans associated with the Balanced Budget Act of 1997.
The Medicare Modernization Act, adopted in December 2003, was intended, in part, to modernize and revitalize private plans under Medicare. The Medicare Modernization Act established the Medicare prescription drug offering that began in 2006, established new tax-advantaged Health Savings Account regulations and made significant changes to the private Medicare managed care programs which were named Medicare Advantage. These changes were a response to the decreased managed care participation in Medicare and the resulting lack of choice for Medicare beneficiaries. The Medicare Modernization Act made favorable changes to the premium rate calculation methodology and generally provides for program rates that we believe will better reflect the increased cost of medical services provided to Medicare beneficiaries.
As a result of the Medicare Modernization Act’s enhanced payment rates and other provisions designed to expand Medicare Advantage offerings and make them more attractive to plan sponsors and beneficiaries, enrollment in Medicare Advantage programs has increased since December 2003 from approximately 5.3 million participants, or approximately 13% of the Medicare-eligible population, to approximately 11.9 million participants, or approximately 25% of the Medicare-eligible population, as of June 2011. The number of participating private health plans also increased dramatically during this period going from 155 plans in November 2003 to 555 plans in June 2011.
In March 2010, the President signed into law The Patient Protection and Affordable Care Act, and The Health Care and Education Reconciliation Act of 2010. The provisions of these new laws include, among other things, limitations on Medicare Advantage payment rates and Medicaid coverage expansion to individuals with incomes under 133% of the poverty level beginning in 2014. Because there is considerable uncertainty regarding the financial impact of these reforms, we cannot currently predict the effect such reforms will have on our business. However, the lowering of future Medicare Advantage payment rates as well as other provisions of these new laws may have a material adverse effect on our business, results of operations, financial position and cash flows.
As a result of the growing increases in health care outlays in the United States, insurers, employers, state and federal governments and other health insurance payors have sought to reduce or control the sustained increases in health care costs. One response to these cost increases has been a shift away from the traditional fee-for-service method of paying for health care to managed health care models, such as HMOs.
HMOs offer a comprehensive health care benefits package in exchange for a fixed prepaid monthly fee or premium per enrollee that does not vary through the contract period regardless of the quantity of medical services required or used. HMOs enroll members by entering into contracts with employer groups or directly with individuals to provide a broad range of health care services for a prepaid charge. HMOs contract directly with medical clinics, independent physicians, hospitals and other health care providers to administer medical care to HMO enrollees. Often the payment to physicians is in the form of a fixed monthly fee per enrollee, which is called a capitation payment. Once negotiated, the total payment is based on the number of enrollees covered, regardless of the actual need for and utilization of covered services.
Physicians, including sole practitioners and small physician groups, find themselves at a competitive disadvantage in the current managed care environment. Physicians are generally not equipped by training or experience to handle all of the functions of a modern medical practice, such as negotiation of contracts with specialists and HMOs, claims administration, financial services, provider relations, member services, medical management including utilization management and quality assurance, data collection and management information systems. Additionally, a proliferation of state and federal regulations has increased the paperwork burden and hampered the application of the traditional controls used by managed care organizations. Physicians increasingly are responding to these pressures within the managed care industry by affiliating with organizations such as ours to assist them in managing their practices.
6
Table of Contents
Our Market and Business Strategy
The population of Florida was approximately 18.8 million in 2010, and approximately 29% of those residents were located in Miami-Dade, Broward and Hillsborough Counties. As of June 2011, approximately 1.1 million residents of Florida were enrolled in Medicare Advantage plans out of a Medicare-eligible population of approximately 3.4 million. The three primary HMOs with which we are affiliated account for approximately 44% of Medicare Advantage participants in the markets we serve.
Our strategy is to:
| • | increase patient volume at our existing medical centers; |
| • | selectively expand our network of medical centers; |
| • | further develop our IPA management activities; and |
| • | selectively expand our operations into other areas in which we believe we can leverage our expertise in order to establish additional sources of revenue. |
Increasing Patient Volume
Our core business is comprised of our established network of medical centers from which we provide primary care services on an outpatient basis. The dominant focus of these medical centers has historically been serving patients enrolled in Medicare Advantage plans sponsored by our HMO affiliates. We seek to increase the number of patients using our medical centers through the general marketing efforts of our affiliated HMOs and on our own through targeted marketing efforts. In addition to building our Medicare Advantage patient base we seek to increase the number of patients we serve in other lines of business. In particular we desire to increase our Medicaid patient base. In furtherance of this objective we have modified our arrangements with certain of our existing HMO affiliates to add Medicaid as a covered line of business and have expanded our Medicaid HMO affiliations.
Selectively Expanding Our Network
We may seek to add additional medical centers or other medical facilities to our network either through acquisition or start up, although no assurance can be given of our ability to establish or acquire any additional locations. To date, we have focused on Miami-Dade, Broward and Hillsborough Counties, Florida. We expect we will identify and select acquisition candidates based in large part on the following broad criteria:
| • | quality of medical professionals and other staff; |
| • | history of profitable operations or a predictable synergy such as opportunities for economies of scale through a consolidation of management functions; |
| • | competitive environment; and |
| • | geographic proximity to our current operations. |
Developing Our IPA Management Activities
We currently provide management services to a network of IPAs. We enhance the operations of our IPA physician practices by providing assistance with medical utilization management, pharmacy management and specialist network development. Additionally, we provide financial reports for our IPA practices to further assist with their operations. We believe that we can leverage our skill at providing medical management services to IPA practices to a larger group of IPA practices and will seek to selectively add new IPA practices to enhance our IPA management activities. We intend to continue affiliating with physicians who are sole practitioners or who operate in small groups to staff and expand our network.
Selectively Expanding Our Operations Into Other Areas
We are actively exploring expansion of our operations into other areas in which we believe we can leverage our expertise in order to establish additional sources of revenue. As part of this strategy, in Fiscal 2010 we acquired two operators of sleep diagnostic centers and in Fiscal 2011 we acquired three operators of sleep diagnostic centers and a related entity that provides continuous positive airway pressure (CPAP) devices and supplies. Through Seredor Corporation, we operate and manage sleep diagnostic centers at over 70 locations in 15 states. The centers conduct sleep studies to determine whether patients suffer from sleep disorders and, if so, the severity of the condition. The most common sleep disorder, obstructive sleep apnea (or OSA), is a serious, though often undiagnosed health condition that afflicts more than 18 million adults in the United States. OSA sufferers stop breathing repeatedly during sleep in intervals that may last 10 seconds to a minute or longer. Key symptoms of OSA include daytime sleepiness, loud snoring, gasping or choking during sleep, and depression and irritability. OSA increases the risk of hypertension, heart disease, mood and memory problems. It also increases the risks of automobile crashes and other accidents. The clinical staff at the centers are expertly trained in sleep disorders and work with physicians, neurologists, respiratory therapists, and clinicians utilizing state-of-the-art equipment to effectively diagnose and treat patients.
7
Table of Contents
Our Medical Centers
At our medical centers, physicians who are our employees or independent contractors act as primary care physicians practicing in the area of general, family and internal medicine with medical specialty services provided in certain of our centers. A typical medical center is operated in an office space that ranges from 5,000 to 8,000 square feet although two of our medical centers comprise approximately 23,000 and 49,000 square feet of space. In addition, certain of our medical centers provide diagnostic imaging services. A medical center is typically staffed with approximately two to three physicians, and is open five days a week. The physicians we employ or with whom we contract are generally retained under written agreements that provide for a rolling one-year term, subject to earlier termination in some circumstances. Under our standard physician agreements we are responsible for providing our physicians with malpractice insurance coverage.
Our IPAs
We provide management assistance to IPAs. Our services include providing assistance with medical utilization management, pharmacy management and specialist network development. Additionally, we provide financial reports for our IPAs to further assist with their practices. These services currently relate primarily to those patients served by the IPAs who are enrolled in health plans primarily offered by Humana and Vista. As of June 30, 2011, these IPAs provided services to over 4,000 patients.
Effective January 1, 2006, we entered into an Independent Practice Association Participation Agreement (the “Risk IPA Agreement”) with Humana under which we agreed to assume certain management responsibilities on a risk basis for Humana’s Medicare and Medicaid members assigned to certain IPAs practicing in Miami-Dade, Broward and Palm Beach Counties, Florida. Under the Risk IPA Agreement, we receive a capitation fee established as a percentage of the premium that the health plan receives for those members who have selected the IPAs as their primary care physicians and assume responsibilities for the cost of substantially all medical services provided to these members, even those we do not provide directly. Effective January 1, 2008, we entered into an agreement with Vista under which we agreed to assume certain management responsibilities on a limited risk basis for Vista’s Medicare members assigned to certain IPAs practicing in Miami-Dade and Broward Counties, Florida. Our IPAs practice primary care medicine on an outpatient basis in facilities similar to our medical centers. Our IPA physicians typically earn a capitated fee for the services they provide and may be entitled to obtain bonus distributions if they operate their practice in accordance with their negotiated contract.
Medicare and Medicaid Considerations
Substantially all of our revenue is generated by providing services to Medicare-eligible patients and Medicaid-eligible patients. The federal government has enacted significant reforms to the U.S. health care system which will have an impact on future revenues that we generate from our Medicare and Medicaid patients. In March 2010, the President signed into law The Patient Protection and Affordable Care Act, and The Health Care and Education Reconciliation Act of 2010. The provisions of these new laws include, among other things, limitations on Medicare Advantage payment rates and Medicaid coverage expansion to individuals with incomes under 133% of the poverty level beginning in 2014. Because there is considerable uncertainty regarding the financial impact of these reforms, we cannot currently predict the effect such reforms will have on our business. However, the lowering of future Medicare Advantage payment rates as well as other provisions of these new laws may have a material adverse effect on our business, results of operations, financial position and cash flows.
The premiums our HMO affiliates receive from CMS for their Medicare Prescription Drug Plans are subject to periodic adjustment, positive or negative, based upon the application of risk corridors that compare their plans’ revenues as estimated in their bids to actual prescription drug costs. Variances exceeding certain thresholds may result in CMS making additional payments to the HMOs or require the HMOs to refund to CMS a portion of the payments they received. Our contracted HMO affiliates estimate and periodically adjust premium revenues related to the risk corridor payment adjustments, and a portion of each such HMO’s estimated premium revenue adjustment is allocated to us. As a result, the revenues recognized under our risk arrangements with these HMOs are net of the portion of the estimated risk corridor adjustment allocated to us. The portion of any such risk corridor adjustment that the HMOs allocate to us may not directly correlate to the historical utilization patterns of our patients or the costs that we may incur in future periods. During Fiscal 2011, 2010 and 2009, our HMO affiliates allocated to us adjustments related to their risk corridor payments which had the effect of reducing our operating income by approximately $0.2 million, $0.4 million and $0.2 million, respectively.
Our HMO Affiliates
We currently have managed care agreements with several HMOs. Our most significant HMO affiliates are Humana, Vista and Wellcare. Under our risk agreements with Humana, Vista and Wellcare, we receive for our services capitated monthly payments per patient at a rate established by the respective contract. In return, we assume full financial responsibility for the provision of all necessary medical care to our patients, even services we do not provide directly. In Fiscal 2011, we generated approximately 69%, 19% and 5% of our revenue from contracts with Humana, Vista and Wellcare, respectively. We continually review and attempt to renegotiate the terms of our managed care agreements in an effort to obtain more favorable terms. We may selectively add new HMO
8
Table of Contents
affiliations, but we can provide no assurance that we will be successful in doing so. The loss of significant HMO contracts and/or the failure to regain or retain such HMO’s patients or the related revenues without entering into new HMO affiliations could have a material adverse effect on our business, results of operations and financial condition.
Humana
We currently have three agreements with Humana under which we provide medical services to members of Humana’s Medicare, Medicaid, commercial and other group health care plans; however, the majority of the revenue that we derive from our relationship with Humana is generated under two agreements, a Physician Practice Management Participation Agreement (the “Humana PPMP Agreement”) and an Integrated Delivery System Participation Agreement (the “IDS Agreement”). Under these agreements we provide or arrange for the provision of covered medical services to each Humana member who selects one of our physicians as his or her primary care physician. We receive a capitated fee with respect to the patients assigned to us. For most of our Humana patients the capitated fee is a percentage of the premium that Humana receives with respect to those patients. These agreements are subject to Humana’s changes to the covered benefits that it elects to provide to its members and other terms and conditions. We must also comply with the terms of Humana’s policies and procedures, including Humana’s policies regarding referrals, approvals and utilization management and quality assessment.
The term of the Humana PPMP Agreement extends through July 31, 2014, unless terminated earlier for cause, and, thereafter, the Humana PPMP Agreement renews for subsequent three-year terms unless either party provides 90-days written notice of its intent not to renew. The IDS Agreement extends through April 1, 2014 with automatic subsequent three-year renewal terms unless either party provides 180-days written notice of its intent not to renew. Each of these agreements provide Humana the right to immediately terminate the agreement, and/or any individual physician credentialed under the agreements, upon written notice, (i) if we and/or any of our physician’s continued participation in the relevant agreement may affect adversely the health, safety or welfare of any Humana member; (ii) if we and/or any of our physician’s continued participation in the relevant agreement may bring Humana or its health care networks into disrepute; (iii) in the event of one of our doctor’s death or incompetence; (iv) if any of our physicians fail to meet Humana’s credentialing criteria; (v) in accordance with Humana’s policies and procedures, (vi) if we engage in or acquiesce to any act of bankruptcy, receivership or reorganization; or (vii) if Humana loses its authority to do business in total or as to any limited segment or business (but only to that segment). We and Humana may also each terminate these agreements upon 90 days’ prior written notice (with an opportunity to cure, if possible) in the event of the other’s material breach of the relevant agreement.
In some cases, Humana may provide 30 days’ notice as to an amendment or modification of these agreements, including but not limited to, renegotiation of rates, covered benefits and other terms and conditions. Such amendments may include changes to the compensation rates. If Humana exercises its right to amend these agreements upon 30 days’ written notice, we may object to such amendment within the 30-day notice period. If we object to such amendment within the requisite time frame, Humana may terminate the relevant agreement upon 90 days’ written notice.
The third agreement we have with Humana is the Risk IPA Agreement. Under the Risk IPA Agreement, we agreed to assume certain management responsibilities on a risk basis for Humana’s Medicare and Medicaid members assigned to selected primary care physicians in Miami-Dade, Broward and Palm Beach Counties, Florida in return for a capitated fee per patient. The capitated fee is based on a percentage of the premium that Humana receives with respect to that patient.
Vista
We provide medical services to members of Vista’s Medicare, Medicaid, commercial and individual health care plans. Under our agreements with Vista, we provide or arrange for the provision of covered medical services to each Vista member who selects one of our physicians as his or her primary care physician. Under our two primary agreements with Vista, we receive a capitated fee with respect to the Vista patients assigned to us. For commercial and individual Vista patients the capitated fee is a fixed monthly payment per member. For Medicare and Medicaid patients the capitated fee is a percentage of the premium that Vista receives with respect to those patients. Our agreements with Vista are subject to Vista’s changes to the covered benefits that Vista elects to provide to its members and other terms and conditions. We must also comply with the terms of Vista’s policies and procedures, including Vista’s policies regarding referrals, approvals and utilization management and quality assessment.
One of our two primary agreements with Vista expires on June 30, 2012 and the other expires on September 1, 2012 and each will automatically renew for successive one year periods unless either party provides the other with 60-days notice of its intent to terminate such agreement. Vista may terminate either of these agreements with us immediately if we materially breach the relevant agreement, provided that we are given an opportunity to cure such breach, and if we experience certain events of bankruptcy or insolvency. In addition, each of these agreements permits Vista to immediately terminate the agreement if Vista determines, in its sole reasonable discretion, that (i) our actions or inactions or those of our health care professionals are causing or may cause imminent danger to the health, safety or welfare of any Vista member; (ii) our or our health care professionals’ licenses, DEA registrations, hospital staff privileges, rights to participate in the Medicare or Medicaid program or other accreditations are restricted, suspended or revoked or if any of our health care professionals voluntarily relinquish any of those credentials and we do not promptly terminate that professional; (iii) our health care professionals’ ability to practice medicine is effectively impaired by an action of the Board of
9
Table of Contents
Medicine or other governmental agency; (iv) we are convicted of a criminal offense related to our involvement in Medicaid, Medicare or social service programs under Title XX of the Social Security Act; or (v) we or our medical professionals engaged in any other behavior or activity that could be hazardous or injurious to any Vista member.
Effective January 1, 2008, we entered into an agreement with Vista under which we agreed to assume certain management responsibilities on a limited risk basis for Vista’s Medicare members assigned to certain IPAs practicing in Miami-Dade and Broward Counties, Florida.
Wellcare
We are a party to two agreements with Wellcare under which we provide or arrange for the provision of medical services to each member of Wellcare’s Medicare plans who selects one of our physicians as his or her primary care physician. One of these agreements, the Physician Provider Agreement, is a risk arrangement under which we receive for our services a capitated fee with respect to the patients assigned to us. The capitated fee is a percentage of the premium that Wellcare receives with respect to those patients. This agreement has a one-year term and automatic subsequent one-year renewal terms, subject to certain termination provisions stipulated in the agreement. Under the risk arrangement we assume financial responsibility for the provision of all necessary medical care to our patients. Our other agreement with Wellcare, which is also a risk arrangement for Wellcare’s Medicare members, expires November 1, 2011 with automatic subsequent one year renewal terms unless either party provides the other with 90-days notice of its intent to terminate.
We also have contracts with Wellcare and its affiliates for the provision of care for members of their Medicaid plans.
Under our agreements with Humana, Vista and Wellcare, there are circumstances under which we could be obligated to continue to provide medical services to patients in our care following a termination of the applicable agreement. In certain cases, this obligation could require us to provide care to patients following the bankruptcy or insolvency of our HMO affiliate. Accordingly, our obligations to provide medical services to our patients (and the associated costs we incur) may not terminate at the time that our agreement with the HMO terminates, and we may not be able to recover our cost of providing those services from the HMO.
Compliance Program
We have implemented a compliance program intended to provide ongoing monitoring and reporting to detect and correct potential regulatory compliance problems but we cannot assure that it will detect or prevent all regulatory problems. The program establishes compliance standards and procedures for employees and agents. The program includes, among other things: written policies, including our Code of Conduct and Ethics; in-service training for our employees on topics such as insider trading, anti-kickback laws, Federal False Claims Act and Anti-Self Referral Act; and a “hot line” for employees to anonymously report violations.
Competition
The health care industry is highly competitive. We compete for patients with many other health care providers, including local physicians and practice groups as well as local, regional and national networks of physicians and health care companies. We believe that competition for patients is generally based upon the reputation of the physician treating the patient, the physician’s expertise, the physician’s demeanor and manner of engagement with the patient, and the HMOs that the physician is affiliated with. We also compete with other local, regional and national networks of physicians and health care companies for the services of physicians and for HMO affiliations. Some of our competitors have greater resources than we do, and we may not be able to continue to compete effectively in this industry. Further, additional competitors may enter our markets, and this increased competition may have an adverse effect on our revenues.
Government Regulation
General. Our business is primarily regulated by the federal government and various states where we operate. The laws and regulations governing our operations are generally intended to benefit and protect health plan members and providers. The government agencies administering these laws and regulations have broad latitude to enforce them. These laws and regulations, along with the terms of our contracts, regulate how we do business, what services we offer, and how we interact with our patients, other providers and the public. We are subject to various governmental reviews, audits and investigations to verify our compliance with our contracts and applicable laws and regulations.
A summary of the material aspects of the government regulations to which we are subject is set forth below. However, there can be no assurance that any such laws will not change or ultimately be interpreted in a manner inconsistent with our practices, and an adverse interpretation could have a material adverse effect on our operations, financial condition or cash flows.
Present and Prospective Federal and State Reimbursement Regulation. Our operations are affected on a day-to-day basis by numerous legislative, regulatory and industry-imposed operational and financial requirements, which are administered by a variety of
10
Table of Contents
federal and state governmental agencies as well as by self-regulatory associations and commercial medical insurance reimbursement programs. Our physicians must reassign their Medicare billing and collection rights to us. Accordingly, we have filed with Medicare the necessary applications for all our physicians to reassign their Medicare billing and collection rights to us.
Federal “Fraud and Abuse” Laws and Regulations. The Anti-Kickback Law makes it a criminal felony offense to knowingly and willfully offer, pay, solicit or receive remuneration in order to induce business for which reimbursement is provided under federal health care programs, including without limitation, the Medicare and Medicaid programs. Violations of these laws are punishable by monetary fines, civil and criminal penalties, exclusion from government health care programs and forfeiture of amounts collected in violation of such laws. The scope of prohibited payments under the Anti-Kickback Law is broad and includes economic arrangements involving hospitals, physicians and other health care providers, including joint ventures, space and equipment rentals, purchases of physician practices and management and personal services contracts. The Anti-Kickback Law provides for certain safe harbors to its prohibitions, however, failure to meet a safe harbor does not necessarily mean that an arrangement violates the Anti-Kickback Law. Rather, each arrangement must be analyzed based on its specific facts and the intent of the parties.
State Fraud and Abuse Laws and Regulations. Various states also have anti-kickback laws applicable to licensed health care professionals and other providers and, in some instances, applicable to any person engaged in the proscribed conduct. For example, the Florida “Patient Brokering Act” imposes criminal penalties for offering, soliciting, receiving or paying any commission, bonus, rebate, kickback, or bribe, directly or indirectly in cash or in kind, or engaging in any split-fee arrangement, in any form whatsoever, in return for the referral of patients or patronage from a health care provider or health care facility or in return for the acceptance or acknowledgement of treatment from a health care provider or health care facility. The Florida statutory provisions regulating the practice of medicine include similar language as grounds for disciplinary action against a physician, a practice commonly known as “fee splitting.” The applicability of such laws is dependent upon the particular state in which we conduct business.
Federal Restrictions on Physician Referrals. Federal laws and regulations also restrict physician referrals to health care entities with which such physicians have financial relationships (commonly referred to as the “Stark Law”). Specifically, the Stark Law prohibits a physician, or an immediate family member, who has a financial relationship with a health care entity, from referring Medicare or Medicaid patients with limited exceptions, to that entity for the following “designated health services”: clinical laboratory services, physical therapy services, occupational therapy services, speech-language pathology services, radiology services, including magnetic resonance imaging, computerized axial tomography scans and ultrasound services, speech-language pathology services, durable medical equipment and supplies, radiation therapy services and supplies, parenteral and enteral nutrients, equipment and supplies, prosthetics, orthotics and prosthetic devices, home health services, outpatient prescription drugs, and inpatient and outpatient hospital services. A financial relationship is defined to include an ownership or investment in, or a compensation relationship with, a health care entity. The Stark Law also prohibits a health care entity receiving a prohibited referral from billing the Medicare or Medicaid programs for any services rendered to a patient as a result of the prohibited referral. The Stark Law contains certain exceptions that protect parties from liability if the parties comply with all of the requirements of the applicable exception. The sanctions under the Stark Law include denial and refund of payments, civil monetary penalties and exclusions from participation in the Medicare and Medicaid programs.
State Restrictions on Physician Referrals. Various states also have laws that restrict physician referrals to health care entities with which such physicians have financial relationships. In Florida, for example, the Florida Patient Self Referral Act of 1992 (“Florida Act”) regulates patient referrals by a health care provider to certain providers of health care services in which the referring provider has an investment interest. Unlike the federal Stark regulations, the Florida act applies only to investment interests and does not affect compensation relationships between the referring provider and the entity to which the provider is referring patients. The penalties for breach of the Florida Act include denial and refund of claims payments and civil monetary penalties. Further, the Florida Act is not limited to referrals for items and services paid for by the Medicare or Medicaid programs, and instead applies to all payors, including health insurers and private pay. The applicability of such state laws is dependent upon the particular state in which we conduct business.
Privacy Laws. The privacy, security and transmission of health information is subject to federal and state laws and regulations, including the Healthcare Insurance Portability and Accountability Act of 1996 (“HIPAA”) and regulations enacted under HIPAA with respect to, among other things, the privacy of certain individually identifiable health information, the transmission of protected health information and standards for the security of electronic health information. Florida state professional licensing statutes also include privacy laws specific to the profession. For example, there are certain privacy laws that apply to physicians and mental health professionals.
Corporate Practice of Medicine Doctrine. Many states prohibit business corporations from providing, or holding themselves out as a provider of medical care. Possible sanctions for violation of any of these restrictions or prohibitions include loss of licensure or eligibility to participate in reimbursement programs (including Medicare and Medicaid), asset forfeitures and civil and criminal penalties. These laws vary from state to state and are subject to interpretation by the courts and regulatory agencies. Florida, the state in which we primarily operate our clinics, does not have a prohibition against the corporate practice of medicine. Our operations in other states are primarily facility-based and not subject to these types of restrictions.
11
Table of Contents
Clinic and Facility Regulation and Licensure. Each state has its own laws regarding the regulation and licensure of clinics and facilities. For example, the Florida Agency for Health Care Administration (“AHCA”) requires us to license each of our medical centers and sleep study laboratories. Each medical center must renew its health care clinic licensure bi-annually. Further, the Florida Health Care Clinic Act requires that clinics have a medical director and prohibits such medical director or any physician affiliated with the medical director's group practice from making referrals to the clinic if the clinic provides certain health care services, such as magnetic resonance imaging, static radiographs, computed tomography, or positron emission tomography. Violation of this prohibition against medical director referrals is a third degree felony. Each state has different requirements and regulations.
Limitations on Contractual Joint Ventures. The Office of Inspector General (“OIG”) has issued various Special Advisory Bulletins raising concerns throughout the healthcare industry about the legality of a variety of provider joint ventures. The suspect arrangements involve a healthcare provider expanding into a related service line by contracting with an existing provider of that service to serve the providers existing patient population. In the OIG’s view, the provider’s share of the profits of the new venture constitutes remuneration for the referral of the provider’s Medicare/Medicaid patients and thus may violate the federal Anti-kickback Statute.
Occupational Safety and Health Administration (“OSHA”). In addition to OSHA regulations applicable to businesses generally, we must comply with, among other things, the OSHA directives on occupational exposure to blood borne pathogens, the federal Needlestick Safety and Prevention Act, OSHA injury and illness recording and reporting requirements, federal regulations relating to proper handling of laboratory specimens, spill procedures and hazardous waste disposal, and patient transport safety requirements.
Environmental Regulations. Our clinics are required to comply with federal and state regulations applicable to the disposal of biomedical waste, the use of radiology and nuclear medicine, and the use of diagnostic imaging equipment.
Medicare Marketing Restrictions. As a health care provider, we are subject to federal marketing rules and regulations that limit, among other things, offering any gift or other inducement to Medicare beneficiaries to encourage them to come to us for their health care.
Sanctioned Parties. The Balanced Budget Act of 1997 (“BBA”) includes provisions that allow for the temporary or permanent exclusion from participation in Medicare or any state health care program of any individual or entity who or which has been convicted of a health care related crime as well as other specified offenses. The BBA also provides for fines against any person that arranges or contracts with an excluded person for the provision of items or services.
Healthcare Reform. The federal government has enacted significant reforms to the U.S. health care system. In March 2010, the President signed into law The Patient Protection and Affordable Care Act, and The Health Care and Education Reconciliation Act of 2010. The provisions of these new laws include, among other things, limiting Medicare Advantage payment rates. While there is considerable uncertainty of the financial impact of these reforms, the lowering of future Medicare Advantage payment rates as well as other provisions of these new laws may have a material adverse effect on our business, results of operations, financial position and cash flows.
Health Care Professional Licensure and Supervision. Our physicians are subject to licensure requirements administered by the applicable state professional licensing boards, including the particular state’s Board of Medicine, Board of Nursing, and other licensing boards. The failure of a health care professional to maintain a license with the applicable board could result in a shortage of health care providers and may trigger termination of one or more of our managed care agreements.
Employees
At June 30, 2011, we employed or contracted with approximately 870 individuals of whom approximately 67 are physicians in our medical centers.
Insurance
We rely on insurance to protect us from many business risks, including medical malpractice and “stop-loss” insurance. Our business entails an inherent risk of claims against physicians for professional services rendered to patients, and we periodically become involved as a defendant in medical malpractice lawsuits. Medical malpractice claims are subject to the attendant risk of substantial damage awards. Although we maintain insurance against these claims, if liability results from any of our pending or any future medical malpractice claims, there can be no assurance that our medical malpractice insurance coverage will be adequate to cover liability arising out of these proceedings. There can be no assurance that pending or future litigation will not have a material adverse affect on us or that liability resulting from litigation will not exceed our insurance coverage.
In most cases, as is the trend in the health care industry, as insurance policies expire we may be required to procure policies
12
Table of Contents
with narrower coverage, more exclusions and higher premiums. In some cases, coverage may not be available at any price. There can be no assurance that the insurance that we maintain and intend to maintain will be adequate, or that the cost of insurance and limitations in coverage will not adversely affect our business, financial position or results of operations.
Available Information
We file annual, quarterly and current reports, proxy statements and other information with the SEC. You may read and copy any document we file at the SEC’s public reference rooms in Washington, D.C., New York, New York, and Chicago, Illinois. Please call the SEC at 1-800-SEC-0330 for further information on the public reference rooms. Our SEC filings are also available to the public from the SEC’s website at http://www.sec.gov.
Our website address is www.continucare.com. We make available free of charge on or through our internet website our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and amendments to those reports, filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934 as soon as reasonably practicable after such material has been filed with, or furnished to, the SEC. Information on our website does not constitute part of this Annual Report on Form 10-K.
Our business, financial condition, results of operations, cash flows and prospects, and the prevailing market price and performance of our common stock, may be adversely affected by a number of factors, including the matters discussed below. Certain statements and information set forth in this Annual Report on Form 10-K, as well as other written or oral statements made from time to time by us or by our authorized officers on our behalf, constitute “forward-looking statements” within the meaning of the Federal Private Securities Litigation Reform Act of 1995. We intend for our forward-looking statements to be covered by the safe harbor provisions for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995. You should note that forward-looking statements in this document speak only as of the date of this Annual Report on Form 10-K and we undertake no duty or obligation to update or revise our forward-looking statements, whether as a result of new information, future events or otherwise. Although we believe that the expectations, plans, intentions and projections reflected in our forward-looking statements are reasonable, such statements are subject to risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. The risks, uncertainties and other factors that our shareholders and prospective investors should consider include the following:
Risks related to our business
Our operations are dependent on three health maintenance organizations.
We derive substantially all of our revenues under our managed care agreements with three HMOs, Humana, Vista and Wellcare. In Fiscal 2011, we generated approximately 69%, 19% and 5% of our revenues from contracts with Humana, Vista and Wellcare, respectively. These agreements have terms ranging from one to three years, with automatic renewal terms unless a party provides prior notice of its intention not to renew. These agreements also provide the HMOs with the right to terminate an agreement prior to the expiration of the term upon the occurrence of specified events. Accordingly, there is no assurance that these agreements will remain in effect. The loss of our managed care agreements with these HMOs, particularly Humana or Vista or significant reductions in payments to us under these contracts could have a material adverse effect on our business, financial condition and results of operations.
Under our most important contracts we are responsible for the cost of medical services to our patients in return for a capitated fee.
Our most important contracts with Humana, Vista and Wellcare are risk agreements under which we receive for our services fixed monthly payments per patient at a rate established by the contract, also called a capitated fee. In return, we assume full financial responsibility for the provision of all necessary medical care to our patients, even services we do not provide directly. Accordingly, we will be unable to adjust the revenues we receive under those contracts and, if medical claims expense exceeds our estimates, our profits may decline. Relatively small changes in the ratio of our health care expenses to capitated revenues we receive can create significant changes in our financial results.
Our revenues will be affected by the Medicare Risk Adjustment program.
The majority of patients to whom we provide care are Medicare-eligible and participate in the Medicare Advantage program. CMS implemented its Medicare Risk Adjustment project whereby it transitioned its premium calculation methodology to a system that takes into account the health status of Medicare Advantage participants in determining premiums paid for each participant, rather than only considering demographic factors, as was historically the case. The premium calculation under the risk adjustment system is
13
Table of Contents
100% based on risk adjustment payments.
We believe the risk adjustment methodology has generally increased our revenues per patient to date but cannot assure what future impact this risk adjustment methodology will continue to have on our business, results of operations, or financial condition. It is also possible that the risk adjustment methodology may result in fluctuations in our revenues from year to year.
CMS is performing audits of selected Medicare Advantage plans to validate the provider coding practices under the risk-adjustment methodology used to reimburse Medicare Advantage plans. These audits involve a review of a sample of medical records for the HMO contracts selected for audit. CMS has selected for audit several of the contracts of our HMO affiliates for the 2007 contract year and we expect that CMS will continue conducting such audits beyond the 2007 contract year. Due to the uncertainties principally related to CMS’ audit payment adjustment methodology, we are unable to determine whether these audits would ultimately result in an unfavorable adjustment to us. Accordingly, we are unable to estimate the financial impact of such adjustment if one occurs as a result of these audits. Although the amount of the adjustment to us, if any, is not reasonably estimable at this time, such adjustment may have a material adverse effect on our results of operations, financial position, and cash flows.
If we are unable to manage medical benefits expense effectively, our profitability will likely be reduced.
We cannot be profitable if our costs of providing the required medical services exceed the revenues that we derive from those services. However, our most important contracts with Humana, Vista and Wellcare require us to assume full financial responsibility for the provision of all necessary medical care in return for a capitated fee per patient at a rate established by the contract. Accordingly, as the costs of providing medical services to our patients under those contracts increases, the profits we receive with respect to those patients decreases. If the cost of providing medical services to our patients under those contracts exceeds our estimates or if we are not able to properly manage our services, our business, results of operations, financial condition and ability to satisfy our obligations could be adversely affected.
A failure to accurately estimate incurred but not reported medical benefits expense will affect our profitability.
Our medical benefits expense includes estimates of medical claims incurred but not reported, or IBNR. We estimate our medical cost liabilities using actuarial methods based on historical data adjusted for payment patterns, cost trends, utilization of health care services and other relevant factors. Actual conditions, however, could differ from those assumed in the estimation process. Due to the inherent uncertainties associated with the factors used in these assumptions, materially different amounts could be reported in our financial statements for a particular period under different possible conditions or using different, but still reasonable, assumptions. Adjustments, if necessary, are made to medical benefits expense when the criteria used to determine IBNR change and when actual claim costs are ultimately determined. Although we believe our past estimates of IBNR have been adequate, they may prove to have been inadequate in the future and our future estimates may not be adequate, any of which would adversely affect our results of operations and cash flows. Further, our inability to estimate IBNR accurately may also affect our ability to take timely corrective actions, further exacerbating the extent of any adverse effect on our results of operations.
We compete with many health care providers for patients and HMO affiliations.
The health care industry is highly competitive. We compete for patients with many other health care providers, including local physicians and practice groups as well as local, regional and national networks of physicians and health care companies. We believe that competition for patients is generally based upon the reputation of the physician treating the patient, the physician’s expertise, and the physician’s demeanor and manner of engagement with the patient, and the HMOs with which the physician is affiliated. We also compete with other local, regional and national networks of physicians and health care companies for the services of physicians and for HMO affiliations. Some of our competitors have greater resources than we do, and we may not be able to continue to compete effectively in this industry. Further, additional competitors may enter our markets, and this increased competition may have an adverse effect on our revenues.
We may not be able to successfully recruit or retain existing relationships with qualified physicians and medical professionals.
We depend on our physicians and other medical professionals to provide medical services to our managed care patients and independent physicians contracting with us to participate in provider networks we develop or manage. We compete with general acute care hospitals and other health care providers for the services of medical professionals. In addition, the reputation, expertise and demeanor of our physicians and other medical professionals are instrumental to our ability to attract patients. Demand for physicians and other medical professionals are high and such professionals often receive competing offers. If we are unable to successfully recruit and retain medical professionals our ability to successfully implement our business strategy could suffer. No assurance can be given that we will be able to continue to recruit and retain a sufficient number of qualified physicians and other medical professionals.
Our business exposes us to the risk of medical malpractice lawsuits.
Our business entails an inherent risk of claims against physicians for professional services rendered to patients, and we
14
Table of Contents
periodically become involved as a defendant in medical malpractice lawsuits. Medical malpractice claims are subject to the attendant risk of substantial damage awards. Although we maintain insurance against these claims, if liability results from any of our pending or any future medical malpractice claims, there can be no assurance that our medical malpractice insurance coverage will be adequate to cover liability arising out of these proceedings or that as a result of such liability we will be able to renew our medical malpractice insurance coverage on acceptable terms, if at all. There can be no assurance that pending or future litigation will not have a material adverse affect on us or that liability resulting from litigation will not exceed our insurance coverage.
We primarily operate in Florida.
Our revenues are primarily derived from our operations in Florida. Adverse economic, regulatory, or other developments in Florida (including hurricanes) could have a material adverse effect on our financial condition or results of operations. In the event that we expand our primary operations into new geographic markets, we will need to establish new relationships with physicians and other health care providers. In addition, we will be required to comply with laws and regulations of states that differ from the ones in which we currently operate, and may face competitors with greater knowledge of such local markets. There can be no assurance that we will be able to establish relationships, realize management efficiencies or otherwise establish a presence in new geographic markets.
A significant portion of our voting power is concentrated.
One of our directors, Dr. Phillip Frost, and entities affiliated with him, beneficially owned approximately 43% of our outstanding common stock as of August 31, 2011. Based on the significant beneficial ownership of our common stock by Dr. Frost, other shareholders have limited ability to influence corporate actions requiring shareholder approval, including the election of directors. Dr. Frost may exert significant influence over any actions requiring shareholder approval. This influence may make us less attractive as a target for a takeover proposal. It may also make it more difficult to discourage a merger proposal that Dr. Frost favors or to wage a proxy contest for the removal of incumbent directors. As a result, this may deprive the holders of our common stock of an opportunity they might otherwise have to sell their shares at a premium over the prevailing market price in connection with a merger or acquisition of us or with or by another company.
We are dependent on our executive officers and other key employees.
Our operations are highly dependent on the efforts of our Chief Executive Officer and our other key employees. Our executive officers and key employees do not have employment agreements with us, but are instead employed on an “at will” basis. While we believe that we could find replacements, the loss of any of their leadership, knowledge and experience could negatively impact our operations. Replacing any of our executive officers or key employees might be difficult or take an extended period of time because a limited number of individuals in the managed care industry have the breadth and depth of skills and experience necessary to operate a business such as ours. Our success is also dependent on our ability to hire and retain qualified management, technical and medical personnel. We may be unsuccessful in recruiting and retaining such personnel, which could negatively impact our operations.
We depend on the management information systems of our affiliated HMOs.
Our operations are dependent on the management information systems of the HMOs with which we contract. Our affiliated HMOs provide us with certain financial and other information, including reports and calculations of costs of services provided and payments to be received by us. Both the software and hardware our HMO affiliates use to provide us with that information have been subject to rapid technological change. Because we rely on this technology but do not own or have direct access to it, we have limited ability to ensure that it is properly maintained, serviced and updated. In addition, information systems such as these may be vulnerable to failure, acts of sabotage such as “hacking”, and obsolescence. If our principal HMO affiliates were to temporarily or permanently lose the use of the information systems that provide us with the information on which we depend or the underlying patient and physician data, our business and results of operations could be materially and adversely affected. Because our HMO affiliates generate certain of the information on which we depend, we have less control over the manner in which that information is generated than we would if we generated the information internally.
We depend on our information processing systems.
Our information processing systems allow us to monitor the medical services we provide to patients. They also enable us to provide our HMO affiliates with information they use to calculate the payments due to us. For example, revenue we are entitled to receive under our HMO agreements is dependent, in part, on the health status of our patients and demographic factors, and we rely on our information processing systems to compile all or a portion of that data. The failure to accurately and timely provide that data to our HMO affiliates could impact the revenue we receive for our patients. These systems are vital to our growth. Although we license most of our information processing systems from third-party vendors we believe to be reliable, we developed certain elements of our information processing systems internally. Our current systems may not perform as expected or provide efficient operational solutions if:
| • | we fail to adequately identify or are unsuccessful in implementing solutions for our information and processing needs; |
15
Table of Contents
| • | our processing or information systems fail; or |
| • | we fail to upgrade systems as necessary. |
Volatility of our stock price could adversely affect you.
The market price of our common stock could fluctuate significantly as a result of many factors, including factors that are beyond our ability to control or foresee. These factors include:
| • | state and federal budget decreases; |
| • | adverse publicity regarding HMOs and other managed care organizations; |
| • | government action regarding eligibility; |
| • | changes in government payment levels; |
| • | changes in state mandatory programs; |
| • | changes in expectations of our future financial performance or changes in financial estimates, if any, of public market analysts; |
| • | announcements relating to our business or the business of our competitors; |
| • | conditions generally affecting the managed care industry or our provider networks; |
| • | the success of our operating strategy; |
| • | the operating and stock price performance of other comparable companies; |
| • | the termination of any of our contracts; |
| • | regulatory or legislative changes; |
| • | acts of war or terrorism or an increase in hostilities in the world; and |
| • | general economic conditions, including inflation and unemployment rates. |
A failure to successfully implement our business strategy could materially and adversely affect our operations and growth opportunities.
Our business strategy is to increase patient volume at our existing medical centers; selectively expand our network to include additional medical centers or other medical facilities and to penetrate new geographic markets; further develop our IPA management activities; and selectively expand our operations into other areas in which we believe we can leverage our expertise in order to establish additional sources of revenue. Our ability to achieve our business strategy is subject to a variety of factors, many of which are beyond our control, and we may not be successful in implementing our strategy. In addition, the implementation of our strategy may not lead to improved operating results. We may decide to alter or discontinue aspects of our business strategy and may adopt alternative or additional strategies due to business or competitive factors or factors not currently expected, such as unforeseen costs and expenses or events beyond our control. Any failure to successfully implement our business strategy could materially and adversely affect our results of operations and growth opportunities.
Our intangible assets represent a substantial portion of our total assets.
Our balance sheet includes intangible assets, including goodwill and other separately identifiable intangible assets, of approximately $85.9 million, which represented approximately 48% of our total assets at June 30, 2011. The most significant component of our intangible assets consists of intangible assets recorded as a result of the acquisition of the MDHC Companies in October 2006, which increased goodwill by approximately $58.9 million and other intangible assets by approximately $8.7 million.
We are required to review our intangible assets, including our goodwill, for impairment on an annual basis or more frequently if certain indicators of impairment arise. The goodwill impairment test is performed annually for each of our two reporting units: Provider Services and Sleep Services. Should we determine that an indicator of impairment has occurred, we would be required to perform an additional impairment test. Indicators of impairment include, among other things:
| • | a significant adverse change in legal factors or the business climate; |
| • | the loss of a key HMO contract; |
| • | an adverse action by a regulator; |
| • | unanticipated competition; |
| • | loss of key personnel; or |
| • | allocation of goodwill to a portion of business that is to be sold. |
If we determine that an impairment of goodwill exists as a result of our annual impairment test or that indicators of impairment exist, there is a risk that a portion of our intangible assets would be considered impaired and must be written-off during that period. Such a write-off could have a material adverse effect on our results of operations.
16
Table of Contents
Competition for acquisition targets and acquisition financing and other factors may impede our ability to acquire other businesses and may inhibit our growth.
We anticipate that a portion of our future growth may be accomplished through acquisitions. The success of this strategy depends upon our ability to identify suitable acquisition candidates, reach agreements to acquire these companies, obtain necessary financing on acceptable terms and successfully integrate the operations of these businesses. In pursuing acquisition and investment opportunities, we may compete with other companies that have similar growth strategies. Some of these competitors are larger and have greater financial and other resources than we have. This competition may prevent us from acquiring businesses that could improve our growth or expand our operations.
Our acquisitions could result in integration difficulties, unexpected expenses, diversion of management’s attention and other negative consequences.
As part of our growth strategy, we plan to continue to evaluate potential business acquisition opportunities that we anticipate will provide new product and market opportunities, benefit from and maximize our existing assets and add critical mass. Any such acquisitions would require us to integrate the technology, products and services, operations, systems and personnel of the acquired businesses with our own and to attempt to grow the acquired businesses as part of our company. The successful integration of businesses we have acquired and may acquire in the future is critical to our future success, and if we are unsuccessful in integrating these businesses, our operations and financial results could suffer. The risks and challenges associated with the acquisition and integration of an acquired business include, but are not limited to, the following:
| • | we may be unable to centralize and consolidate our financial, operational and administrative functions with those of the businesses we acquire; |
| • | our management’s attention may be diverted from other business concerns; |
| • | we may be unable to retain and motivate key employees of an acquired company; |
| • | litigation, indemnification claims and other unforeseen claims and liabilities may arise from the acquisition or operation of acquired businesses; |
| • | the costs necessary to complete integration may exceed our expectations or outweigh some of the intended benefits of the transactions we complete; |
| • | we may be unable to maintain the patients or goodwill of an acquired business; and |
| • | the costs necessary to improve the operating systems and services of an acquired business may exceed our expectations. |
Risks related to our industry
Recently enacted health care reform, including The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of 2010, could have a material adverse effect on our business.
The federal government has enacted significant reforms to the U.S. health care system. In March 2010, the President signed into law The Patient Protection and Affordable Care Act, and The Health Care and Education Reconciliation Act of 2010. The provisions of these new laws include, among other things, limiting Medicare Advantage payment rates. While there is considerable uncertainty of the financial impact of these reforms, the lowering of future Medicare Advantage payment rates as well as other provisions of these new laws may have a material adverse effect on our business, results of operations, financial position and cash flows.
We are subject to government regulation.
Our primary business is regulated by the federal government and the State of Florida. The laws and regulations governing our operations are generally intended to benefit and protect health plan members and providers rather than our shareholders. The government agencies administering these laws and regulations have broad latitude to enforce them. These laws and regulations, along with the terms of our contracts, regulate how we do business, what services we offer, and how we interact with our patients, other providers and the public. We are subject to various governmental reviews, audits and investigations to verify our compliance with our contracts and applicable laws and regulations. Any adverse review, audit or investigation could result in:
| • | forfeiture of amounts we have been paid; |
| • | imposition of civil or criminal penalties, fines or other sanctions on us; |
| • | loss of our right to participate in government-sponsored programs, including Medicare and Medicaid; |
| • | damage to our reputation in various markets; |
| • | increased difficulty in hiring or retaining qualified medical personnel or marketing our products and services; and |
| • | loss of one or more of our licenses to provide health care services. |
17
Table of Contents
Any of these events could reduce our revenues and profitability and otherwise adversely affect our operating results.
The health care industry is subject to continued scrutiny.
The health care industry, generally, and HMOs specifically, have been the subject of increased government and public scrutiny in recent years, which has focused on the appropriateness of the care provided, referral and marketing practices and other matters. Increased media and public attention has focused on the outpatient services industry in particular as a result of allegations of fraudulent practices related to the nature and duration of patient treatments, illegal remuneration and certain marketing, admission and billing practices by certain health care providers. The alleged practices have been the subject of federal and state investigations, as well as other legal proceedings. There can be no assurance that we or our HMO affiliates will not be subject to federal or state review from time to time, and any such investigation could adversely impact our business or results of operations, even if we are not ultimately found to have violated the law.
Our insurance coverage may not be adequate, and rising insurance premiums could negatively affect our profitability.
We rely on insurance to protect us from many business risks, including, “stop loss” insurance. In most cases, as is the trend in the health care industry, as insurance policies expire, we may only be able to procure policies with narrower coverage, more exclusions and higher premiums. In some cases, coverage may not be available at any price. There can be no assurance that the insurance that we maintain and intend to maintain will be adequate, or that the cost of insurance and limitations in coverage will not adversely affect our business, financial position or results of operations.
Deficit spending and economic downturns could negatively impact our results of operations.
Adverse developments in the economy often result in decreases in the federal budget and associated changes in the federal government’s spending priorities. We are presently in a period of deficit spending by the federal government, and those deficits are expected to continue for at least the next several years. Continued deficit spending by the federal government could lead to increased pressure to reduce governmentally funded programs such as Medicare and Medicaid. If governmental funding of the Medicare or Medicaid programs was reduced without a counterbalancing adjustment in the benefits offered to patients, our results of operations could be negatively impacted. In addition, decreases in state budgets and associated changes in state spending could negatively affect our profitability.
Many factors that increase health care costs are largely beyond our ability to control.
Increased utilization or unit cost, competition, government regulations and many other factors may, and often do, cause actual health care costs to increase and these cost increases can adversely impact our profitability. These factors may include, among other things:
| • | increased use of medical facilities and services, including prescription drugs and doctors’ office visits; |
| • | increased cost of such services; |
| • | new benefits to patients added by the HMOs to their covered services, whether as a result of the Medicare Modernization Act or otherwise; |
| • | changes or reductions of our utilization management functions such as preauthorization of services, concurrent review or requirements for physician referrals; |
| • | catastrophes (including hurricanes), epidemics or terrorist attacks; |
| • | the introduction of new or costly treatments, including new technologies; |
| • | new government mandated benefits or other regulatory changes; and |
| • | increases in the cost of “stop loss” or other insurance. |
Many of these factors are beyond our ability to control or predict.
Risks Related to the Merger
There can be no assurance that the merger will be consummated. The pendency of the merger, or the failure of the merger to be consummated, could have an adverse effect on Continucare’s stock price, business, financial condition, results of operations or prospects.
The merger is subject to a number of conditions to closing including, (i) the absence of legal prohibitions on the consummation of the merger; (ii) Metropolitan’s consummation on the terms and conditions set forth, and receipt of an aggregate amount of $355 million from the debt financing described in the debt commitment letter from General Electric Capital Corporation, referred to as “the debt commitment party”, which financing is subject to the satisfaction of a number of closing conditions set forth in the debt commitment letter; (iii) the authorization for listing on the NYSE Amex, subject to official notice of issuance, of the shares of Metropolitan common stock to be issued in the merger; (iv) the absence of any stop order on Metropolitan’s Form S-4 registering the
18
Table of Contents
shares of Metropolitan common stock to be issued in the merger by the SEC, and proceedings of the SEC seeking a stop order, suspending the effectiveness of such registration statement; (v) the accuracy of the representations and warranties of the parties and compliance by the parties with their respective obligations under the merger agreement; and (vi) Continucare’s satisfaction of the minimum cash condition. If the closing conditions set forth in the merger agreement are not met or waived, the companies will not be able to complete the merger.
If the merger agreement is terminated in certain circumstances, Continucare or Metropolitan may be required to pay the other a termination fee of up to $12 million, as well as to reimburse the other party for up to $1.5 million of its out-of-pocket costs and expenses incurred in connection with the merger agreement, but would, in general, have no further obligations to the other party, even if the merger agreement is terminated as a result of an intentional breach by a party.
Further, the pendency of the merger could disrupt Continucare’s businesses, in any of the following ways, among others:
| • | Continucare employees may experience uncertainty about their future roles with the combined company, which might adversely affect the combined companies ability to retain and hire key managers and other employees; and |
| • | the attention of management of Continucare may be directed toward the completion of the merger and transaction-related considerations and may be diverted from the day-to-day business operations of their respective companies. |
Continucare may face additional challenges in competing for new business and retaining or renewing business. These disruptions could be exacerbated by a delay in the completion of the merger or termination of the merger agreement.
For the foregoing reasons, there can be no assurance that the pendency of the merger, or the failure of the merger to be consummated, will not have an adverse effect on Continucare’s stock price, business, financial condition, results of operations or prospectus.
The price of Metropolitan common stock might decline before the completion of the merger, which would decrease the value of the merger consideration to be received by Continucare shareholders in the merger.
Upon completion of the merger, Continucare shareholders will be entitled to receive for each share of Continucare common stock that they own, $6.25 in cash and 0.0414 of a share of Metropolitan common stock. The exchange ratio will not be adjusted to reflect stock price changes prior to the completion of the merger. Because the market price of Metropolitan common stock at the time the merger is completed may vary significantly from the market price on the date of the merger agreement, the market value of the merger consideration received by Continucare shareholders in the merger may be lower than the market value of the merger consideration at the date of the merger agreement. On June 24, 2011, the last full trading day prior to the public announcement of the proposed merger, Metropolitan common stock closed at $4.88 per share as reported on the NYSE Amex.
The condition of the financial markets, including volatility and weakness in the equity, capital and credit markets, could limit the availability and terms of debt and equity financing sources to fund the capital and liquidity requirements of Metropolitan’s businesses, including financing Metropolitan must undertake in connection with the merger.
In connection with the merger, Metropolitan obtained the debt commitment letter from the debt commitment party in an aggregate amount of $355 million. These funds, in addition to existing cash balances, will be sufficient to finance the cash consideration to Continucare shareholders in the merger and to refinance certain existing Metropolitan debt. Subject to certain conditions, Metropolitan expects to have in place approximately $355 million of long-term financing, of which approximately $330 million is expected to be outstanding at the time of consummation of the merger. Metropolitan may not be able to complete the planned financing of the merger on the terms and the timetable that Metropolitan and Continucare anticipate. If Metropolitan were unable to complete these financings, Metropolitan would likely be unable to consummate the merger.
There may be a long delay between Continucare receiving the necessary shareholder approval for the merger and the closing of the merger, during which time Continucare will lose the ability to consider and pursue alternative acquisition proposals, which might otherwise be superior to the merger.
Following the Continucare special meeting held on August 22, 2011, the merger agreement prohibits Continucare from taking any actions to review, consider or recommend any alternative acquisition proposals, including those that could be superior to Continucare’s shareholders when compared to the merger. Given the delay between the shareholder approval and closing, the time during which Continucare could be prevented from reviewing, considering or recommending such proposals could be significant.
19
Table of Contents
If the merger is not consummated on or before November 1, 2011, either Continucare or Metropolitan may choose not to proceed with the merger.
Either Continucare or Metropolitan may terminate the merger agreement if the merger has not been completed on or before November 1, 2011, unless the failure of the merger to be completed on or before November 1, 2011 has resulted from the failure of the party seeking to terminate the merger agreement to fulfill in all material respects all of its obligations under merger agreement.
Continucare shareholders will have a significantly reduced ownership and voting interest after the merger and will exercise less influence over the management and policies of Metropolitan than they do over Continucare.
Continucare shareholders currently have the right to vote in the election of the Continucare Board and on other matters affecting Continucare. When the merger occurs, each Continucare shareholder that receives shares of Metropolitan common stock will become a shareholder of Metropolitan with a percentage ownership of the combined company that is much smaller than the shareholder’s percentage ownership of Continucare. It is expected that the former shareholders of Continucare as a group will own approximately 5.8% of the outstanding shares of Metropolitan immediately after the merger, based on the number of shares of Metropolitan and Continucare common stock issued and outstanding as of June 30, 2011. Because of this, Continucare shareholders will have less influence over the management and policies of Metropolitan than they now have over the management and policies of Continucare.
The rights of Continucare shareholders will change when they become shareholders of Metropolitan upon completion of the merger.
Upon completion of the merger, Continucare shareholders will become Metropolitan shareholders. There are numerous differences between the rights of a shareholder of Continucare and the rights of a shareholder of Metropolitan.
| ITEM 1B. | UNRESOLVED STAFF COMMENTS |
None.
| ITEM 2. | PROPERTIES |
We lease approximately 9,800 square feet of corporate office space in Miami, Florida under a lease expiring in January 2015 with average annual lease payments of approximately $0.2 million.
Of the 18 medical centers that we operated as of June 30, 2011 located in Miami-Dade, Broward and Hillsborough Counties, Florida, five are leased from independent landlords, one is leased from a landlord affiliated with certain of the principal owners of the MDHC Companies, and ten are leased from Humana. The leases with Humana are tied to our managed care arrangement. We also own a facility in Hialeah, Florida, comprising approximately 49,000 square feet of medical office and administrative space and a 7,000 square foot medical facility in Homestead, Florida.
| ITEM 3. | LEGAL PROCEEDINGS |
We are involved in legal proceedings incidental to our business that arise from time to time in the ordinary course of business including, but not limited to, claims related to the alleged malpractice of employed and contracted medical professionals, workers’ compensation claims and other employee-related matters, and minor disputes with equipment lessors and other vendors. We record an accrual for claims related to legal proceedings, which includes amounts for insurance deductibles and projected exposure, based on our estimate of the ultimate outcome of such claims. We do not believe that the ultimate resolution of these matters will have a material adverse effect on our business, results of operations, financial condition, or cash flows. However, the results of these matters cannot be predicted with certainty, and an unfavorable resolution of one or more of these matters could have a material adverse effect on our business, results of operations, financial condition, cash flow, and prospects.
In addition we were involved in litigation regarding our merger with Metropolitan, which is described under “Business – Merger Transaction – Litigation Related to the Merger.”
| ITEM 4. | (REMOVED AND RESERVED) |
| ITEM 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Our common stock began trading on the New York Stock Exchange (“NYSE”) on November 1, 2010 under the symbol
20
Table of Contents
“CNU.” Before that, our common stock traded on NYSE Amex under the same symbol. The following table sets forth the high and low sale prices of our common stock as reported on the appropriate exchange for each of the quarters indicated.
| HIGH | LOW | |||||||
| Fiscal Year 2011: |
||||||||
| Quarter Ended June 30, 2011 |
$ | 6.32 | $ | 4.13 | ||||
| Quarter Ended March 31, 2011 |
5.80 | 3.76 | ||||||
| Quarter Ended December 31, 2010 |
5.09 | 3.85 | ||||||
| Quarter Ended September 30, 2010 |
4.24 | 3.25 | ||||||
| Fiscal Year 2010 |
||||||||
| Quarter Ended June 30, 2010 |
$ | 4.25 | $ | 3.28 | ||||
| Quarter Ended March 31, 2010 |
5.25 | 3.66 | ||||||
| Quarter Ended December 31, 2009 |
4.50 | 2.57 | ||||||
| Quarter Ended September 30, 2009 |
3.29 | 2.31 | ||||||
As of the close of business on August 31, 2011, there were approximately 91 record holders of our common stock. We have not declared or paid dividends on our common stock and do not contemplate declaring or paying dividends in the foreseeable future. In addition, the Merger Agreement prohibits us from paying dividends.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of June 30, 2011, with respect to all of our compensation plans under which equity securities are authorized for issuance:
| Plan Category |
Number of securities to be issued upon exercise of outstanding options, warrants and rights |
Weighted average exercise price of outstanding options, warrants and rights |
Number of securities remaining available for future issuance |
|||||||||
| Equity compensation plans approved by stockholders |
6,690,084 | $ | 2.79 | 3,190,917 | ||||||||
| Equity compensation plans not approved by stockholders |
— | — | — | |||||||||
|
|
|
|
|
|||||||||
| 6,690,084 | 3,190,917 | |||||||||||
|
|
|
|
|
|||||||||
21
Table of Contents
Performance Graph
Set forth below is a line graph comparing the cumulative total shareholder return on Continucare’s common stock against the cumulative total return of the NYSE Amex Composite Index, the NYSE Composite Index, and the NASDAQ Health Services Index for the period from June 30, 2006 to June 30, 2011, based on a $100 investment. We added the NYSE Composite Index for comparative purposes because our stock began trading on the NYSE on November 1, 2010.
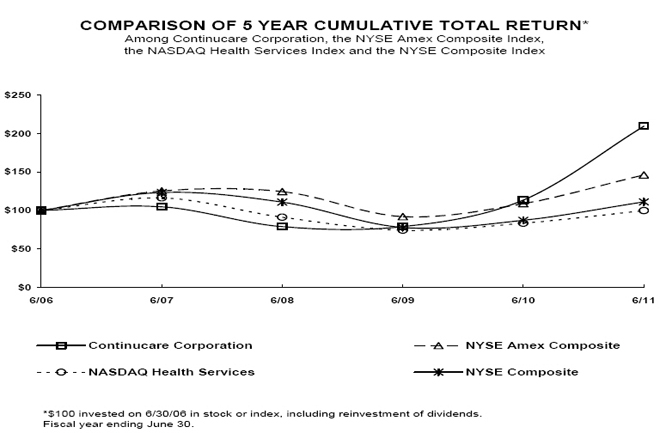
| Cumulative Total Return | ||||||||||||||||||||||||
| 6/06 | 6/07 | 6/08 | 6/09 | 6/10 | 6/11 | |||||||||||||||||||
| Continucare Corporation |
100.00 | 104.75 | 78.98 | 78.98 | 113.56 | 209.49 | ||||||||||||||||||
| NYSE Amex Composite |
100.00 | 125.36 | 124.63 | 92.01 | 108.97 | 146.13 | ||||||||||||||||||
| NASDAQ Health Services |
100.00 | 116.30 | 91.21 | 74.38 | 83.58 | 99.77 | ||||||||||||||||||
| NYSE Composite |
100.00 | 123.47 | 110.83 | 77.89 | 87.34 | 111.18 | ||||||||||||||||||
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
Our Board of Directors approved a previously announced stock repurchase program to authorize the repurchase of 15,000,000 shares of our common stock. Any such repurchases will be made from time to time at the discretion of our management in the open market or in privately negotiated transactions subject to market conditions and other factors. We anticipate that any such repurchases of shares will be funded through cash from operations. The stock repurchase program was originally approved by the Board of Directors in February 2005. There is no expiration date specified for this program. During the three months ended June 30, 2011, we did not repurchase any shares of our common stock.
| ITEM 6. | SELECTED FINANCIAL DATA |
Set forth below is our selected historical consolidated financial data as of and for Fiscal 2011, 2010, 2009, 2008 and 2007 that has been derived from our audited consolidated financial statements. The selected historical consolidated financial data should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and the consolidated financial statements and accompanying notes included elsewhere herein.
22
Table of Contents
CONSOLIDATED STATEMENTS OF OPERATIONS DATA:
| For the Year Ended June 30, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| Revenue |
$ | 333,458,208 | $ | 310,791,463 | $ | 281,270,360 | $ | 254,440,048 | $ | 217,146,287 | ||||||||||
| Operating expenses: |
||||||||||||||||||||
| Medical services: |
||||||||||||||||||||
| Medical claims |
216,226,209 | 208,857,229 | 199,167,856 | 181,097,183 | 161,153,828 | |||||||||||||||
| Other direct costs |
38,892,426 | 31,484,513 | 28,456,121 | 26,942,472 | 22,919,746 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total medical services |
255,118,635 | 240,341,742 | 227,623,977 | 208,039,655 | 184,073,574 | |||||||||||||||
| Administrative payroll and employee benefits |
16,297,890 | 16,308,854 | 12,655,975 | 12,119,139 | 9,192,670 | |||||||||||||||
| General and administrative |
22,140,000 | 18,021,123 | 16,261,750 | 16,413,801 | 13,990,439 | |||||||||||||||
| Merger transaction expenses |
2,487,939 | — | — | — | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total operating expenses |
296,044,464 | 274,671,719 | 256,541,702 | 236,572,595 | 207,256,683 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Income from operations |
37,413,744 | 36,119,744 | 24,728,658 | 17,867,453 | 9,889,604 | |||||||||||||||
| Interest income (expense), net |
199,523 | (50,084 | ) | 152,784 | 534,928 | 306,446 | ||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Income before income tax provision |
37,613,267 | 36,069,660 | 24,881,442 | 18,402,381 | 10,196,050 | |||||||||||||||
| Income tax provision |
13,701,318 | 13,893,353 | 9,600,321 | 7,132,727 | 3,892,605 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net income |
$ | 23,911,949 | $ | 22,176,307 | $ | 15,281,121 | $ | 11,269,654 | $ | 6,303,445 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Net income per common share: |
||||||||||||||||||||
| Basic |
$ | .39 | $ | .37 | $ | .25 | $ | .16 | $ | .10 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Diluted |
$ | .38 | $ | .36 | $ | .24 | $ | .16 | $ | .10 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| CONSOLIDATED BALANCE SHEET DATA: |
|
|||||||||||||||||||
| As of June 30, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| Total assets |
$ | 180,905,008 | $ | 153,865,592 | $ | 125,303,386 | $ | 118,490,304 | $ | 116,937,548 | ||||||||||
| Long-term obligations, including current portion |
$ | 323,481 | $ | 326,309 | $ | 204,985 | $ | 196,379 | $ | 331,319 | ||||||||||
| ITEM 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
General
The following discussion and analysis should be read in conjunction with the consolidated financial statements and notes thereto appearing elsewhere in this Annual Report on Form 10-K. We are primarily a provider of primary care physician services. Through our network of 18 medical centers, we provide primary care medical services on an outpatient basis. We also provide practice management services to IPAs. All of our medical centers and IPAs are located in Miami-Dade, Broward, Hillsborough and Palm Beach Counties, Florida. As of June 30, 2011, we provided services to or for approximately 27,100 patients on a risk basis and approximately 9,800 patients on a limited or non-risk basis. Additionally, during Fiscal 2011 we also provided services to over 6,000 patients on a non-risk fee-for-service basis. In Fiscal 2011, approximately 87% and 7% of our revenue was generated by providing services to Medicare-eligible and Medicaid-eligible members, respectively, under risk agreements that require us to assume responsibility to provide and pay for all of our patients’ medical needs in exchange for a capitated fee, typically a percentage of the premium received by an HMO from various payor sources.
We also operate or manage sleep diagnostic centers at over 70 locations in 15 states through Seredor Corporation, a subsidiary established to conduct sleep service activities. The centers conduct sleep studies to determine whether patients suffer from sleep disorders and, if so, the severity of the condition. The clinical staff at the centers are expertly trained in sleep disorders and work with physicians, respiratory therapists, and clinicians utilizing state-of-the-art equipment to effectively diagnose and treat patients.
Merger Transaction
On June 26, 2011, Continucare entered into an Agreement and Plan of Merger (the “Merger Agreement”) with Metropolitan Health Networks, Inc. (“Metropolitan”) and Cab Merger Sub, Inc., a Florida corporation and a wholly owned subsidiary of Metropolitan (“Merger Subsidiary”), providing for the merger of Continucare with Merger Subsidiary. Subject to the terms and conditions of the Merger Agreement, which has been unanimously approved by the boards of directors of the respective parties, Merger Subsidiary will be merged with and into Continucare (the “Merger”), with Continucare surviving the Merger as a wholly owned subsidiary of Metropolitan.
On August 22, 2011, at a Special Meeting of Shareholders, the Merger Agreement and the transactions contemplated thereby were approved by Continucare stockholders. Assuming all conditions to closing are met, Continucare and Metropolitan expect to close the acquisition on or about the end of September 2011. There can be no assurance that the acquisition will close.
23
Table of Contents
At the effective time of the Merger, each share of Continucare common stock outstanding immediately prior to the effective time (other than shares owned by Continucare, Metropolitan, or shareholders who have properly demanded and perfected appraisal rights under Florida law) will be converted into the right to receive $6.25 in cash, without interest, and 0.0414 of a share of Metropolitan common stock (the “Merger Consideration”). No fractional shares of Metropolitan common stock will be issued in the Merger, and Continucare’s stockholders will receive cash in lieu of fractional shares, if any, of Metropolitan common stock. Each share of Metropolitan common stock outstanding immediately prior to the effective time will remain outstanding and will not be affected by the Merger. Upon completion of the transaction, Continucare stockholders will own approximately 5.8% of Metropolitan’s outstanding common stock.
At the effective time of the Merger, each issued and outstanding option to purchase Continucare common stock will become fully vested and be cancelled in exchange for the right to receive an amount of cash equal to $6.45 less the per share exercise price of the option, subject to withholding taxes.
The value of the equity consideration portion of the Merger Consideration is subject to change based upon changes in the market price of Metropolitan’s common stock prior to closing. The total value of the transaction is approximately $416 million, excluding transaction and financing fees.
Acquisitions
In August 2010 and September 2010, we acquired three operators of sleep diagnostic centers and a related entity that provides continuous positive airway pressure (CPAP) devices and supplies. The three acquired operators of sleep diagnostic centers operate a combined 58 sleep diagnostic centers in nine states. The aggregate total purchase price for these acquired entities consisted of cash consideration paid of $11.2 million and future contingent cash consideration up to a maximum of $2.0 million subject to the achievement of certain future earnings targets. We accrued $1.5 million of the contingent cash consideration based on a preliminary fair value estimate on the acquisition date, which was determined using significant unobservable inputs (Level 3) in a probability-weighted income approach, discounted to present value using a weighted-average cost of capital. In April 2011, we paid $0.7 million of the contingent cash consideration resulting in a remaining maximum contingent cash consideration of $1.0 million and a decrease in the accrued liability to $0.8 million. During the three-month period ended June 30, 2011, we re-measured the estimated fair value of the contingent cash consideration and based on changes in future earnings estimates of the acquired entities, we recorded an adjustment to reduce the related accrued liability by $0.6 million to $0.2 million as of June 30, 2011 and increase income from operations by $0.6 million. We will re-measure the estimated fair value of the contingent cash consideration on a quarterly basis and any subsequent adjustments based on actual payments or revised estimates will be recognized in the condensed consolidated statements of income during the period of adjustment. The revenues, expenses and results of operations of the acquired companies have been included in our condensed consolidated statements of income from the dates of acquisition.
Medicare and Medicaid Considerations
Substantially all of our revenue is generated by providing services to Medicare-eligible patients and Medicaid-eligible patients. The federal government has enacted significant reforms to the U.S. health care system which will have an impact on future revenues that we generate from our Medicare and Medicaid patients. In March 2010, the President signed into law The Patient Protection and Affordable Care Act, and The Health Care and Education Reconciliation Act of 2010. The provisions of these new laws include, among other things, limitations on Medicare Advantage payment rates and Medicaid coverage expansion to individuals with incomes under 133% of the poverty level beginning in 2014. Because there is considerable uncertainty regarding the financial impact of these reforms, we cannot currently predict the effect such reforms will have on our business. However, the lowering of future Medicare Advantage payment rates as well as other provisions of these new laws may have a material adverse effect on our business, results of operations, financial position and cash flows.
As a result of the Medicare Prescription Drug Plan, our HMO affiliates have established or expanded prescription drug benefit plans for their Medicare Advantage members. Under the terms of our risk arrangements, we are financially responsible for a substantial portion of the cost of the prescription drugs our patients receive, and, in exchange, our HMO affiliates have agreed to provide us with an additional per member capitated fee related to prescription drug coverage. However, there can be no assurance that the additional fee that we receive will be sufficient to reimburse us for the additional costs that we may incur under the Medicare Prescription Drug Plan.
In addition, the premiums our HMO affiliates receive from the Centers for Medicare and Medicaid Services (“CMS”) for their Medicare Prescription Drug Plans is subject to periodic adjustment, positive or negative, based upon the application of risk corridors that compare their plans’ revenues targeted in their bids to actual prescription drug costs. Variances exceeding certain thresholds may result in CMS making additional payments to the HMOs or require the HMOs to refund to CMS a portion of the payments they received. Our contracted HMO affiliates estimate and periodically adjust premium revenues related to the risk corridor payment adjustment, and a portion of the HMO’s estimated premium revenue adjustment is allocated to us. As a result, the revenues recognized under our risk arrangements with our HMO affiliates are net of the portion of the estimated risk corridor adjustment allocated to us. The portion of any such risk corridor adjustment that the HMOs allocate to us may not directly correlate to the
24
Table of Contents
historical utilization patterns of our patients or the costs that we may incur in future periods. Our HMO affiliates allocated to us adjustments related to their risk corridor payments which had the effect of reducing our operating income by $0.2 million, $0.4 million and $0.2 million during Fiscal 2011, 2010 and 2009, respectively.
Critical Accounting Policies and Estimates
The discussion and analysis of our financial condition and results of operations is based upon our consolidated financial statements and accompanying notes, which have been prepared in accordance with accounting principles generally accepted in the United States of America. The preparation of these financial statements and accompanying notes requires us to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Certain of the amounts recorded on our financial statements could change materially under different, yet still reasonable, estimates and assumptions. We base our estimates and assumptions on historical experience, knowledge of current events and expectations of future events, and we continuously evaluate and update our estimates and assumptions. However, our estimates and assumptions may ultimately prove to be incorrect or incomplete and, as a result, our actual results may differ materially from those previously reported. We believe the following critical accounting policies involve the most significant judgments and estimates used in the preparation of our consolidated financial statements.
Revenue Recognition
Under our risk contracts with HMOs, we receive a percentage of premium or other capitated fee for each patient that chooses one of our physicians as their primary care physician. Revenue under these agreements is generally recorded in the period we assume responsibility to provide services at the rates then in effect as determined by the respective contract. As part of the Medicare Advantage program, CMS periodically recomputes the premiums to be paid to the HMOs based on updated health status of participants and updated demographic factors. In addition, the premiums paid to the HMOs are subject to periodic adjustment based on CMS’s risk corridor adjustment methodology related to the Medicare Prescription Drug Plan. We record adjustments to revenue at the time that the information necessary to make the determination of the adjustment is received from the HMO or the applicable government body and it is determined that the collectibility of such adjustments is reasonably assured or the likelihood of repayment is probable. The net effect of these premium adjustments included in revenue were favorable retroactive Medicare adjustments of $0.1 million, $0.4 million and $0.9 million for Fiscal 2011, 2010 and 2009, respectively.
Under our risk agreements, we assume responsibility for the cost of all medical services provided to the patient, even those we do not provide directly, in exchange for a percentage of premium or other capitated fee. To the extent that patients require more frequent or expensive care, our revenue under a contract may be insufficient to cover the costs of care provided. When it is probable that expected future health care costs and maintenance costs under a contract or group of existing contracts will exceed anticipated capitated revenue on those contracts, we recognize losses on our prepaid health care services with HMOs. No contracts were considered loss contracts at June 30, 2011 because we have the right to terminate unprofitable physicians and close unprofitable centers under our managed care contracts.
Under our limited risk and non-risk contracts with HMOs, we receive a capitation fee or management fee based on the number of patients for which we are providing services on a monthly basis. Under our limited risk contracts, we also receive a percentage of the surplus generated as determined by the respective contract. The fees and our portion of the surplus generated under these arrangements are recorded as revenue in the period in which services are provided as determined by the respective contract.
Payments under both our risk contracts and our non-risk contracts (for both the Medicare Advantage program as well as Medicaid) are also subject to reconciliation based upon historical patient enrollment data. We record any adjustments to this revenue at the time that the information necessary to make the determination of the adjustment is received from the HMO or the applicable governmental body.
Medical Claims Expense Recognition
The cost of health care services provided or contracted for is accrued in the period in which the services are provided. This cost includes our estimate of the related liability for medical claims incurred in the period but not yet reported, or IBNR. The liability for IBNR is presented in the balance sheet netted against amounts due from HMOs. Changes in this estimate can materially affect, either favorably or unfavorably, our results from operations and overall financial position.
We develop our estimate of IBNR primarily based on historical claims incurred per member per month. We adjust our estimate if we have unusually high or low inpatient utilization or if benefit changes provided under the HMO plans are expected to significantly increase or reduce our claims exposure. We also make adjustments for differences between the estimated claims expense recorded in prior months and actual claims expense as claims are paid by the HMO and reported to us. We use an actuarial analysis as an additional tool to further corroborate our estimate of IBNR.
25
Table of Contents
As medical claims are settled, actual amounts paid for claims incurred in prior periods vary from previously estimated liabilities. During Fiscal 2011, amounts paid related to claims incurred in prior fiscal years were $1.1 million lower than the related liability for IBNR recorded as of June 30, 2010 resulting in a corresponding favorable adjustment to medical claims expense in Fiscal 2011. The favorable adjustment represents 0.5% of medical claims expense recorded in Fiscal 2011.
During Fiscal 2010, amounts paid related to claims incurred in prior fiscal years were $1.0 million lower than the related liability for IBNR recorded as of June 30, 2009 resulting in a corresponding favorable adjustment to medical claims expense in Fiscal 2010. This difference represents 0.5% of medical claims expense recorded in Fiscal 2010.
During Fiscal 2009, amounts paid related to claims incurred in prior fiscal years were $0.3 million higher than the related liability for IBNR recorded as of June 30, 2008 resulting in a corresponding unfavorable adjustment to medical claims expense in Fiscal 2009. This difference represents 0.1% of medical claims expense recorded in Fiscal 2009.
Based on our analysis as of June 30, 2011, we recorded a liability of $23.9 million for IBNR which was relatively unchanged from the liability of $23.4 million recorded as of June 30, 2010. The liability of $23.4 million recorded as of June 30, 2010 was relatively unchanged from the liability of $23.7 million recorded as of June 30, 2009.
Consideration of Impairment Related to Goodwill and Other Intangible Assets
Our balance sheet includes intangible assets, including goodwill and other separately identifiable intangible assets, of approximately $85.9 million, which represented approximately 48% of our total assets at June 30, 2011. The most significant component of the intangible assets consists of the intangible assets recorded in connection with the acquisition of the MDHC Companies. The purchase price, including acquisition costs, of approximately $66.2 million was allocated to the estimated fair value of acquired tangible assets of $13.9 million, identifiable intangible assets of $8.7 million and assumed liabilities of $15.3 million, resulting in goodwill totaling $58.9 million.
We do not amortize goodwill and intangible assets with indefinite useful lives. We review such assets for impairment on an annual basis or more frequently if certain indicators of impairment arise. We amortize intangible assets with definite useful lives over their respective useful lives to their estimated residual values and also review for impairment annually, or more frequently if certain indicators of impairment arise. Indicators of an impairment include, among other things, a significant adverse change in legal factors or the business climate, the loss of a key HMO contract, an adverse action by a regulator, unanticipated competition, and the loss of key personnel or allocation of goodwill to a portion of business that is to be sold.
The goodwill impairment test requires the allocation of goodwill and all other assets and liabilities to reporting units. We have determined that we have two reporting units: Provider Services and Sleep Services. Our goodwill impairment reviews are determined using a two-step process. The first step of the process is to compare the fair value of a reporting unit with its carrying amount, or book value, including goodwill. If the fair value of a reporting unit exceeds its carrying amount, the goodwill of the reporting unit is not impaired and the second step of the impairment review is not necessary. If the carrying amount of a reporting unit exceeds its fair value, the second step of the goodwill impairment review is required to be performed to estimate the implied fair value of the reporting unit’s goodwill. The implied fair value of the reporting unit’s goodwill is compared with the carrying amount of that goodwill. If the carrying amount of the reporting unit’s goodwill exceeds the implied fair value of that goodwill, an impairment loss is recognized in an amount equal to that excess. We completed our annual impairment test as of May 1, 2011, and determined that no impairment existed. In addition, no indicators of impairment were noted and accordingly, no impairment charges were required at June 30, 2011. Should we later determine that an indicator of impairment exists, we would be required to perform an additional impairment test.
Realization of Deferred Income Tax Assets
We recognize deferred income tax assets and liabilities using enacted tax rates for the effect of temporary differences between the book and tax bases of recorded assets and liabilities. We evaluate the realizability of the deferred income tax assets and reduce such assets by a valuation allowance if it is more likely than not that some portion or all of the deferred income tax asset will not be realized.
As part of the process of preparing our consolidated financial statements, we estimate our income taxes based on our actual current tax exposure together with assessing temporary differences resulting from differing treatment of items for tax and accounting purposes. We also recognize as deferred income tax assets the future tax benefits from net operating loss carryforwards. We evaluate the realizability of these deferred income tax assets by assessing their valuation allowances and by adjusting the amount of such allowances, if necessary. Among the factors used to assess the likelihood of realization are our projections of future taxable income streams, the expected timing of the reversals of existing temporary differences, and the impact of tax planning strategies that could be implemented to avoid the potential loss of future tax benefits. However, changes in tax codes, statutory tax rates or future taxable income levels could materially impact our valuation of income tax accruals and assets and could cause our provision for income taxes to vary significantly from period to period. At June 30, 2011, we had deferred income tax liabilities in excess of deferred income tax assets of approximately $4.3 million.
26
Table of Contents
Stock-Based Payment
We recognize compensation costs in our financial statements related to our stock-based payment transactions over the period services are rendered according to the fair value of the stock-based awards issued.
We have elected to calculate the fair value of our employee stock options using the Black-Scholes option pricing model. Using this model we calculated the fair value for employee stock options granted during Fiscal 2011 and 2010 based on the following assumptions: risk-free interest rate ranging from 0.63% to 2.58% and 0.73% to 3.05%, respectively; dividend yield of 0%; weighted-average volatility factor of the expected market price of our common stock of 59.4% and 60.4%, respectively, and weighted-average expected life of the options ranging from 2 to 7 years depending on the vesting provisions of each option. The fair value for employee stock options granted during Fiscal 2009 was calculated based on the following assumptions: risk-free interest rate ranging from 0.66% to 3.19%; dividend yield of 0%; volatility factor of the expected market price of our common stock of 58.6%; and weighted-average expected life of the option ranging from 2 to 7 years depending on the vesting provisions of each option. The expected life of the options is based on the historical exercise behavior of our employees. The expected volatility factor is based on the historical volatility of the market price of our common stock as adjusted for certain events that management deemed to be non-recurring and non-indicative of future events.
We recognized share-based compensation cost of $1.8 million, $1.4 million and $1.2 million, respectively, for Fiscal 2011, 2010 and 2009. For Fiscal 2011, 2010 and 2009, we recognized excess tax benefits resulting from the exercise of stock options of approximately $0.2 million, $1.4 million and $0.1 million, respectively. As of June 30, 2011, there was $1.6 million of total unrecognized compensation cost related to non-vested options, which is expected to be recognized over a weighted average period of 2 years.
Because our stock options have characteristics significantly different from traded options and because changes in the subjective input assumptions can materially affect the fair value estimate, in management’s opinion, it is possible that existing models may not necessarily provide a reliable measure of the fair value of our employee stock options. We selected the Black-Scholes model based on our experience with it, its wide use by issuers comparable to us, and our review of alternate option valuation models.
The effect of applying the fair value method of accounting for stock options on reported net income for any period may not be representative of the effects for future periods because our outstanding options typically vest over a period of several years and additional awards may be made in future periods.
Results of Operations
The following table sets forth, for the periods indicated, selected operating data as a percentage of total revenue.
| Year ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Revenue |
100.0 | % | 100.0 | % | 100.0 | % | ||||||
| Operating expenses: |
||||||||||||
| Medical services: |
||||||||||||
| Medical claims |
64.8 | 67.2 | 70.8 | |||||||||
| Other direct costs |
11.7 | 10.1 | 10.1 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total medical services |
76.5 | 77.3 | 80.9 | |||||||||
| Administrative payroll and employee benefits |
4.9 | 5.3 | 4.5 | |||||||||
| General and administrative |
6.6 | 5.8 | 5.8 | |||||||||
| Merger transaction expenses |
0.8 | — | — | |||||||||
|
|
|
|
|
|
|
|||||||
| Total operating expenses |
88.8 | 88.4 | 91.2 | |||||||||
|
|
|
|
|
|
|
|||||||
| Income from operations |
11.2 | 11.6 | 8.8 | |||||||||
| Interest income (expense), net |
0.1 | — | — | |||||||||
|
|
|
|
|
|
|
|||||||
| Income before income tax provision |
11.3 | 11.6 | 8.8 | |||||||||
| Income tax provision |
4.1 | 4.5 | 3.4 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net income |
7.2 | % | 7.1 | % | 5.4 | % | ||||||
|
|
|
|
|
|
|
|||||||
COMPARISON OF FISCAL YEAR ENDED JUNE 30, 2011 TO FISCAL YEAR ENDED JUNE 30, 2010
Revenue
Revenue increased by $22.7 million, or 7.3%, to $333.5 million for Fiscal 2011 from $310.8 million for Fiscal 2010 due primarily to increases in our Medicare revenue and in our revenue related to the operations of the sleep diagnostic centers.
27
Table of Contents
The most significant component of our revenue is the revenue we generate from Medicare patients under risk arrangements which increased by $11.1 million, or 4.0%, during Fiscal 2011. During Fiscal 2011, revenue generated by our Medicare risk arrangements increased approximately 5.1% on a per patient per month basis and Medicare patient months decreased by approximately 1.1% over Fiscal 2010. The increase in the per member per month Medicare revenue was primarily due to an increase in premiums resulting from the Medicare risk adjustment program.
Effective January 1, 2011, the capitation payments we receive under our percentage of premium arrangements with our HMO affiliates for our Medicare Advantage patients decreased by approximately 2% before taking into account any premium adjustments resulting from changes in Medicare risk adjustment scores. After taking into account our premium adjustments resulting from changes in Medicare risk adjustment scores, revenue generated by our Medicare risk arrangements increased approximately 5.1% on a per patient per month basis for the six-month period ended June 30, 2011.
Under the Medicare risk adjustment program, the health status and demographic factors of Medicare Advantage participants are taken into account in determining premiums paid for each participant. CMS periodically recomputes the premiums to be paid to the HMOs based on the updated health status and demographic factors of the Medicare Advantage participants. In addition, the premiums paid to the HMOs for their Medicare Prescription Drug Plan are subject to periodic adjustment based upon CMS’s risk corridor adjustment methodology. The net effect of these premium adjustments included in revenue for the three-month periods ended June 30, 2011 and 2010 were favorable retroactive Medicare adjustments of $0.6 million and $0.5 million, respectively, and for Fiscal 2011 and 2010 were favorable retroactive Medicare adjustments of $0.1 million and $0.4 million, respectively. Future Medicare risk adjustments may result in reductions of revenue depending on the future health status and demographic factors of our patients as well as the application of CMS’s risk corridor methodology to the HMOs Medicare Prescription Drug Programs.
Revenue generated under contracts with Humana, Vista and Wellcare accounted for approximately 69%, 19% and 5%, respectively, of our total revenue for Fiscal 2011. Revenue generated under contracts with Humana, Vista and Wellcare accounted for approximately 72%, 20% and 6%, respectively, of our total revenue for Fiscal 2010.
Operating Expenses
Medical services expenses are comprised of medical claims expense and other direct costs related to the provision of medical services to our patients. Because our risk contracts with HMOs provide that we are financially responsible for the cost of substantially all medical services provided to our patients under those contracts, our medical claims expense includes the costs of prescription drugs these patients receive as well as medical services provided to patients by providers other than us. Other direct costs consist primarily of salaries, taxes and benefits of our health professionals providing primary care services including a portion of our share-based compensation cost, medical malpractice insurance costs, capitation payments to our IPA physicians and fees paid to independent contractors providing medical services to our patients.
Medical services expenses for Fiscal 2011 increased by $14.8 million, or 6.1%, to $255.1 million from $240.3 million for Fiscal 2010. Medical claims expense, which is the largest component of medical services expense, increased by $7.3 million, or 3.5%, to $216.2 million for Fiscal 2011 from $208.9 million for Fiscal 2010 primarily due to an increase in Medicare claims expense of $6.3 million, or 3.4%. The increase in Medicare claims expense resulted from a 4.5% increase in medical claims expense on a per patient per month basis, partially offset by a 1.1% decrease in Medicare patient months. The increase in Medicare per patient per month medical claims expense is primarily attributable to enhanced benefits offered by our HMO affiliates in 2011 and inflationary trends in the health care industry.
As a percentage of revenue, medical services expenses decreased to 76.5% for Fiscal 2011 as compared to 77.3% for Fiscal 2010. Our claims loss ratio (medical claims expense as a percentage of revenue generated under risk arrangements) decreased to 68.5% for Fiscal 2011 from 68.8% for Fiscal 2010. These decreases were primarily due to an increase in Medicare revenue at a greater rate than the increase in Medicare claims expense on a per patient per month basis. HMOs, however, are under continuous competitive pressure to offer enhanced and possibly more expensive benefits to their Medicare Advantage members. The premiums CMS pays to HMOs for Medicare Advantage members are generally not increased as a result of those benefit enhancements. This could increase our claims loss ratio in future periods, which could reduce our profitability and cash flows.
Other direct costs increased by $7.4 million, or 23.5%, to $38.9 million for Fiscal 2011 from $31.5 million for Fiscal 2010. As a percentage of revenue, other direct costs increased to 11.7% for Fiscal 2011 from 10.1% for Fiscal 2010. The increase in the amount of other direct costs was primarily due to an increase in payroll expense and related benefits related to the operations of the sleep diagnostic centers that were acquired in Fiscal 2011.
Administrative payroll and employee benefits expenses remained relatively unchanged at $16.3 million for Fiscal 2011 and 2010. As a percentage of revenue, administrative payroll and employee benefits expenses decreased to 4.9% for Fiscal 2011 from 5.2% for Fiscal 2010.
General and administrative expenses increased by $4.1 million, or 22.9%, to $22.1 million for Fiscal 2011 from $18.0 million for Fiscal 2010. As a percentage of revenue, general and administrative expenses increased to 6.6% for Fiscal 2011 from 5.8% for
28
Table of Contents
Fiscal 2010. The increase in general and administrative expenses was primarily due to expenses related to the operations of the sleep diagnostic centers that were acquired in Fiscal 2011.
Merger transaction expenses of $2.5 million consisted primarily of investment banking fees and legal fees incurred in Fiscal 2011 in connection with the merger transaction with Metropolitan.
Income from Operations
Income from operations for Fiscal 2011 increased by $1.3 million, or 3.6%, to $37.4 million from $36.1 million for Fiscal 2010.
Taxes
An income tax provision of $13.7 million and $13.9 million was recorded for Fiscal 2011 and 2010, respectively. The effective income tax rates were 36.4% and 38.5% for Fiscal 2011 and 2010, respectively. The decrease in the effective tax rate was primarily due to a decrease in the income tax provision of approximately $0.9 million resulting from a decrease in our liability for unrecognized tax benefits as a result of the lapse of the applicable statute of limitations.
Net Income
Net income for Fiscal 2011 increased by $1.7 million, or 7.8%, to $23.9 million from $22.2 million for Fiscal 2010.
COMPARISON OF FISCAL YEAR ENDED JUNE 30, 2010 TO FISCAL YEAR ENDED JUNE 30, 2009
Revenue
Revenue increased by $29.5 million, or 10.5%, to $310.8 million for Fiscal 2010 from $281.3 million for Fiscal 2009 due primarily to increases in our Medicare revenue.
The most significant component of our revenue is the revenue we generate from Medicare patients under risk arrangements which increased by $24.2 million, or 9.5%, during Fiscal 2010. During Fiscal 2010, revenue generated by our Medicare risk arrangements increased approximately 12.2% on a per patient per month basis and Medicare patient months decreased by approximately 2.4% over Fiscal 2009. The increase in the per member per month Medicare revenue was primarily due to a rate increase in Medicare premiums and an increase in premiums resulting from the Medicare risk adjustment program. The decrease in Medicare patient months was primarily due to the termination of at risk management services related to certain IPA practices.
Effective January 1, 2010, the capitation payments we receive under our percentage of premium arrangements with our HMO affiliates for our Medicare Advantage patients decreased by approximately 5% before taking into account any premium adjustments resulting from changes in Medicare risk adjustment scores. After taking into account our premium adjustments resulting from changes in Medicare risk adjustment scores, revenue generated by our Medicare risk arrangements increased approximately 6.8% on a per patient per month basis for the six-month period ended June 30, 2010.
Included in revenue for the three-month periods ended June 30, 2010 and 2009 were favorable retroactive Medicare adjustments related to Medicare premiums and risk corridor adjustments of $0.5 million and $0.7 million, respectively, and for Fiscal 2010 and 2009 were favorable retroactive Medicare adjustments of $0.4 million and $0.9 million, respectively.
Revenue generated under contracts with Humana, Vista and Wellcare accounted for approximately 72%, 20% and 6%, respectively, of our total revenue for Fiscal 2010. Revenue generated under contracts with Humana, Vista and Wellcare accounted for approximately 72%, 18% and 8%, respectively, of our total revenue for Fiscal 2009.
Operating Expenses
Medical services expenses for Fiscal 2010 increased by $12.7 million, or 5.6%, to $240.3 million from $227.6 million for Fiscal 2009. Medical claims expense, which is the largest component of medical services expense, increased by $9.7 million, or 4.9%, to $208.9 million for Fiscal 2010 from $199.2 million for Fiscal 2009 primarily due to an increase in Medicare claims expense of $6.9 million, or 3.8%. The increase in Medicare claims expense resulted from a 6.4% increase in medical claims expense on a per patient per month basis, partially offset by a 2.4% decrease in Medicare patient months. The increase in Medicare per patient per month medical claims expense is primarily attributable to enhanced benefits offered by our HMO affiliates in 2009 and inflationary trends in the health care industry, partially offset by improved utilization outcomes.
As a percentage of revenue, medical services expenses decreased to 77.3% for Fiscal 2010 as compared to 80.9% for Fiscal 2009. Our claims loss ratio (medical claims expense as a percentage of revenue generated under risk arrangements) decreased to 68.8% for Fiscal 2010 from 72.0% for Fiscal 2009. These decreases were primarily due to an increase in Medicare revenue at a
29
Table of Contents
greater rate than the increase in Medicare claims expense on a per patient per month basis.
Other direct costs increased by $3.0 million, or 10.6%, to $31.5 million for Fiscal 2010 from $28.5 million for Fiscal 2009. As a percentage of revenue, other direct costs remained relatively unchanged at 10.1% for Fiscal 2010 and 2009. The increase in the amount of other direct costs was primarily due to an increase in payroll expense and related benefits related to the operations of the sleep diagnostic centers that we acquired in Fiscal 2010.
Administrative payroll and employee benefits expenses increased by $3.6 million, or 28.9%, to $16.3 million for Fiscal 2010 from $12.7 million for Fiscal 2009. As a percentage of revenue, administrative payroll and employee benefits expenses increased to 5.3% for Fiscal 2010 from 4.5% for Fiscal 2009. The increase in administrative payroll and employee benefits expenses was primarily due to increases in personnel, annual salary increases and increases in incentive plan accruals related to our earnings in Fiscal 2010.
General and administrative expenses increased by $1.7 million, or 10.8%, to $18.0 million for Fiscal 2010 from $16.3 million for Fiscal 2009. As a percentage of revenue, general and administrative expenses remained relatively unchanged at 5.8% for Fiscal 2010 and 2009. The increase in general and administrative expenses was primarily due to expenses related to the operations of the sleep diagnostic centers that we acquired in Fiscal 2010.
Income from Operations
Income from operations for Fiscal 2010 increased by $11.4 million, or 46.1%, to $36.1 million from $24.7 million for Fiscal 2009.
Taxes
An income tax provision of $13.9 million and $9.6 million was recorded for Fiscal 2010 and 2009, respectively. The effective income tax rates remained relatively unchanged at 38.5% and 38.6% for Fiscal 2010 and 2009, respectively.
Net Income
Net income for Fiscal 2010 increased by $6.9 million, or 45.1%, to $22.2 million from $15.3 million for Fiscal 2009.
Liquidity and Capital Resources
At June 30, 2011, working capital was $64.9 million, an increase of $15.4 million from $49.5 million at June 30, 2010. Cash and cash equivalents increased by $13.0 million to $50.5 million at June 30, 2011 compared to $37.5 million at June 30, 2010. The increases in working capital and cash and cash equivalents at June 30, 2011 as compared to June 30, 2010 was primarily due to net income of $23.9 million for Fiscal 2011, partially offset by net cash of $11.5 million used for the acquisition of sleep diagnostic centers. In August 2011, we collected approximately $3.6 million of Medicare premium adjustments which were included in amounts due from HMOs at June 30, 2011. At August 31, 2011, our cash and cash equivalents increased to approximately $56.8 million.
Net cash of $28.1 million was provided by operating activities during Fiscal 2011 compared to $27.0 million in Fiscal 2010 and $17.6 million in Fiscal 2009. The $1.1 million increase in cash provided by operating activities for Fiscal 2011 compared to Fiscal 2010 was primarily due to increases in net income of $1.7 million and depreciation and amortization expenses of $1.2 million and net decreases in due from HMOs of $0.9 million and excess tax benefits related to the exercise of stock options of $1.2 million, partially offset by a net decrease in accrued expenses and other current liabilities of $3.5 million. The $9.4 million increase in cash provided by operating activities for Fiscal 2010 compared to Fiscal 2009 was primarily due to an increase in net income of $6.9 million and an increase in accrued expenses and other current liabilities of $3.3 million relating primarily to incentive plan accruals.
Net cash of $15.2 million was used for investing activities in Fiscal 2011 compared to $4.3 million in Fiscal 2010 and $3.1 million in Fiscal 2009. The $10.9 million increase in net cash used for investing activities for Fiscal 2011 primarily related to an increase in cash used for the acquisition of sleep diagnostic centers. The $1.2 million increase in net cash used for investing activities for Fiscal 2010 compared to Fiscal 2009 primarily related to the net cash used of $1.5 million for the acquisition of sleep diagnostic centers.
Net cash of approximately $0.1 million was provided by financing activities in Fiscal 2011 compared to $1.0 million in Fiscal 2010 and net cash used of $10.6 million in Fiscal 2009. The $0.9 million decrease in cash provided by financing activities for Fiscal 2011 compared to Fiscal 2010 was primarily due a $1.2 million decrease in excess tax benefits related to the exercise of stock options. The $11.6 million increase in cash provided by financing activities for Fiscal 2010 compared to Fiscal 2009 was primarily due to a $10.6 million decrease in cash used for the repurchase our common stock.
In May 2011, we entered into an asset purchase agreement with an entity that provides primary care physician services on an outpatient basis in Broward County, Florida. The purchase price of $3.0 million will be paid in cash at closing, which is expected to
30
Table of Contents
occur during the three-month period ended December 31, 2011.
Pursuant to the terms under our managed care agreements with certain of our HMO affiliates, we posted irrevocable standby letters of credit amounting to $1.3 million to secure our payment obligations to those HMOs. We are required to maintain these letters of credit throughout the term of the managed care agreements.
In December 2009, we entered into a credit facility agreement (the “Credit Facility”) in order to renew and refinance our existing credit facilities. The Credit Facility consists of two revolving credit facilities totaling $10,000,000 with a maturity date of January 31, 2012. Interest on borrowings under the Credit Facility accrues at a per annum rate equal to the sum of 2.40% and the one-month LIBOR (0.19% at June 30, 2011), floating daily. The Credit Facility contains certain customary representations and warranties, and certain financial and other customary covenants including covenants requiring us, on a consolidated basis, to maintain an adjusted tangible net worth of at least $25 million and a fixed charge coverage ratio of not less than 1.50 to 1. Substantially all of our assets serve as collateral for the Credit Facility. At June 30, 2011, there was no outstanding principal balance on the Credit Facility. At June 30, 2011, we had letters of credit outstanding of $1.3 million which reduced the amount available for borrowing under the Credit Facility to $8.7 million.
Our Board of Directors approved a previously announced stock repurchase program to authorize the repurchase of 15,000,000 shares of our common stock. Any such repurchases will be made from time to time at the discretion of our management in the open market or in privately negotiated transactions subject to market conditions and other factors. We anticipate that any such repurchases of shares will be funded through cash from operations. We did not repurchase any shares of our common stock during Fiscal 2011. During Fiscal 2010 and 2009 we repurchased no shares and 5,419,004 shares, respectively, of our common stock for approximately $0 million and $10.6 million, respectively. As of August 31, 2011, we had repurchased a total of 11,907,004 shares of our common stock for approximately $25.0 million pursuant to this stock repurchase program.
We believe that we will be able to fund our capital commitments and our anticipated operating cash requirements for at least the next twelve months and satisfy any remaining obligations from our working capital, anticipated cash flows from operations and our Credit Facility.
Off-Balance Sheet Arrangements
We had no off-balance sheet arrangements as of June 30, 2011, and have not entered into any transactions involving unconsolidated, limited purpose entities or commodity contracts.
Contractual Obligations
The following is a summary of our long-term debt, capital and operating lease obligations, and contractual obligations as of June 30, 2011:
| Payment due by Period | ||||||||||||||||||||
| Total | Less than 1 Year |
1-3 Years | 3-5 Years | More than 5 Years |
||||||||||||||||
| Capital Lease Obligations (1) |
$ | 355,592 | $ | 164,921 | $ | 179,903 | $ | 10,768 | $ | — | ||||||||||
| Operating Lease Obligations (1) |
12,118,746 | 3,360,551 | 5,093,942 | 3,400,060 | 264,193 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total |
$ | 12,474,338 | $ | 3,525,472 | $ | 5,273,845 | $ | 3,410,828 | $ | 264,193 | ||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| (1) | The payments shown above for Capital Lease Obligations and Operating Lease Obligations reflect all payments due under the terms of the respective leases. See Note 4 to our Consolidated Financial Statements appearing elsewhere in this Annual Report on Form 10-K to reconcile the payments shown above to the capital lease obligations recorded in our Consolidated Balance Sheets. |
FORWARD-LOOKING STATEMENTS
Our business, financial condition, results of operations, cash flows and prospects, and the prevailing market price and performance of our common stock, may be adversely affected by a number of factors, including the matters discussed below. Certain statements and information set forth in this Annual Report on Form 10-K, as well as other written or oral statements made from time to time by us or by our authorized executive officers on our behalf, constitute “forward-looking statements” within the meaning of the Federal Private Securities Litigation Reform Act of 1995. We intend for our forward-looking statements to be covered by the safe harbor provisions for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995, and we set forth this statement and these risk factors in order to comply with such safe harbor provisions. You should note that our forward-looking statements speak only as of the date of this Annual Report on Form 10-K or when made and we undertake no duty or obligation to update or revise our forward-looking statements, whether as a result of new information, future events or otherwise. Although we believe that the expectations, plans, intentions and projections reflected in our forward-looking statements are reasonable, such
31
Table of Contents
statements are subject to risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. The risks, uncertainties and other factors that our shareholders and prospective investors should consider include, but are not limited to, the following:
| • | Our operations are dependent on three health maintenance organizations; |
| • | Under our most important contracts we are responsible for the cost of medical services to our patients in return for a capitated fee; |
| • | Our revenues will be affected by the Medicare Risk Adjustment program; |
| • | If we are unable to manage medical benefits expense effectively, our profitability will likely be reduced; |
| • | A failure to accurately estimate incurred but not reported medical benefits expense will affect our profitability; |
| • | We compete with many health care providers for patients and HMO affiliations; |
| • | We may not be able to successfully recruit or retain existing relationships with qualified physicians and medical professionals; |
| • | Our business exposes us to the risk of medical malpractice lawsuits; |
| • | We primarily operate in Florida; |
| • | A significant portion of our voting power is concentrated; |
| • | We are dependent on our executive officers and other key employees; |
| • | We depend on the management information systems of our affiliated HMOs; |
| • | We depend on our information processing systems; |
| • | Volatility of our stock price could adversely affect you; |
| • | A failure to successfully implement our business strategy could materially and adversely affect our operations and growth opportunities; |
| • | Our intangible assets represent a substantial portion of our total assets; |
| • | Competition for acquisition targets and acquisition financing and other factors may impede our ability to acquire other businesses and may inhibit our growth; |
| • | Our acquisitions could result in integration difficulties, unexpected expenses, diversion of management’s attention and other negative consequences; |
| • | Recently enacted health care reform, including The Patient Protection and Affordable Care Act and The Health Care and Education Reconciliation Act of 2010, could have a material adverse effect on our business; |
| • | We are subject to government regulation; |
| • | The health care industry is subject to continued scrutiny; |
| • | Our insurance coverage may not be adequate, and rising insurance premiums could negatively affect our profitability; |
| • | Deficit spending and economic downturns could negatively impact our results of operations; |
| • | Many factors that increase health care costs are largely beyond our ability to control; |
| • | There can be no assurance that the merger will be consummated. The pendency of the merger, or the failure of the merger to be consummated, could have an adverse effect on Continucare’s stock price, business, financial condition, results of operations or prospects; |
| • | The price of Metropolitan common stock might decline before the completion of the merger, which would decrease the value of the merger consideration to be received by Continucare shareholders in the merger; |
| • | The condition of the financial markets, including volatility and weakness in the equity, capital and credit markets, could limit the availability and terms of debt and equity financing sources to fund the capital and liquidity requirements of Metropolitan’s businesses, including financing Metropolitan must undertake in connection with the merger; |
| • | There may be a long delay between Continucare receiving the necessary shareholder approval for the merger and the closing of the merger, during which time Continucare will lose the ability to consider and pursue alternative acquisition proposals, which might otherwise be superior to the merger; |
| • | If the merger is not consummated on or before November 1, 2011, either Continucare or Metropolitan may choose not to proceed with the merger; |
| • | Continucare shareholders will have a significantly reduced ownership and voting interest after the merger and will exercise less influence over the management and policies of Metropolitan than they do over Continucare; and |
| • | The rights of Continucare shareholders will change when they become shareholders of Metropolitan upon completion of the merger. |
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
At June 30, 2011, we held cash equivalent investments in high grade, short-term securities, which are not typically subject to material market risk. At June 30, 2011, we had capital lease obligations outstanding at fixed rates. For loans with fixed interest rates, a hypothetical 10% change in interest rates would have no material impact on our future earnings and cash flows related to these instruments and would have an immaterial impact on the fair value of these instruments. Our Credit Facility has a variable interest rate and is interest rate sensitive, however, we had no amount outstanding under the Credit Facility at June 30, 2011. We have no
32
Table of Contents
material risk associated with foreign currency exchange rates or commodity prices.
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
Our consolidated financial statements and independent registered public accounting firm’s report thereon appear beginning on page F-2. See index to such consolidated financial statements and reports on page F-1.
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
| ITEM 9A. | CONTROLS AND PROCEDURES |
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Exchange Act Rules 13a-15(e) or Rule 15d-15(e)) as of the end of the period covered by this Annual Report. Based on that evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that, as of June 30, 2011, our disclosure controls and procedures were effective to ensure that information required to be disclosed by us in the reports that we file or submit under the Exchange Act (i) is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms and (ii) is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure.
Our Chief Executive Officer’s and Chief Financial Officer’s conclusions regarding the effectiveness of our disclosure controls and procedures should be considered in light of the following limitations on the effectiveness of our disclosure controls and procedures, some of which pertain to most, if not all, business enterprises, and some of which arise as a result of the nature of our business. Our management, including our Chief Executive Officer and our Chief Financial Officer, does not expect that our disclosure controls and procedures will prevent all errors or improper conduct. A control system, no matter how well conceived and operated, can provide only reasonable assurance that the objectives of the control system will be met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of improper conduct, if any, will be detected. These inherent limitations include the realities that judgments in decision-making can be faulty and that breakdowns can occur because of simple error or mistake. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by management override of the controls. Further, the design of any control system is based, in part, upon assumptions about the likelihood of future events, and there can be no assurance that any control system design will succeed in achieving its stated goals under all potential future conditions. Additionally, over time, controls may become inadequate because of changes in conditions or the degree of compliance with the policies or procedures may deteriorate. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected. In addition, we depend on our HMO affiliates for certain financial and other information that we receive concerning the revenue and expenses that we earn and incur. Because our HMO affiliates generate that information for us, we have less control over the manner in which that information is generated.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Exchange Act Rules Rule 13a-15(f) or Rule 15d-15(f)). Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with U.S. generally accepted accounting principles and includes those policies and procedures that (i) pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of our assets, (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with U.S. generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors, and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on our financial statements. Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our internal control over financial reporting as of the end of the period covered by this report based on the Internal Control – Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on that evaluation, our management concluded that our internal control over financial reporting was effective as of June 30, 2011. Ernst & Young LLP, our independent registered public accounting firm, which audited our financial statements included in this report, has issued an attestation report on our internal control over financial reporting. Their report is included herein.
33
Table of Contents
Changes in Internal Control over Financial Reporting
Based on an evaluation, under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, there has been no change in our internal control over financial reporting during our last fiscal quarter that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Section 302 Certifications
Provided with this report are certifications of our Chief Executive Officer and Chief Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 and the SEC’s implementing regulations. This Item 9A contains the information concerning the evaluations referred to in those certifications, and you should read this information in conjunction with those certifications for a more complete understanding of the topics presented.
Report of Independent Registered Public Accounting Firm
The Board of Directors and Shareholders of Continucare Corporation
We have audited Continucare Corporation’s internal control over financial reporting as of June 30, 2011, based on criteria established in Internal Control – Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). Continucare Corporation’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Annual Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, Continucare Corporation maintained, in all material respects, effective internal control over financial reporting as of June 30, 2011, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of Continucare Corporation as of June 30, 2011 and 2010 and the related consolidated statements of income, shareholders’ equity and cash flows for each of the three years in the period ended June 30, 2011 and our report dated September 7, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Certified Public Accountants
Miami, Florida
September 7, 2011
| ITEM 9B. | OTHER INFORMATION |
None.
34
Table of Contents
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
The information required by Item 10 is incorporated by reference to our Proxy Statement for our Annual Meeting of Shareholders for the fiscal year ended June 30, 2011, which will be filed with the Securities and Exchange Commission no later than 120 days after the end of the fiscal year covered by this Form 10-K, or, alternatively, by amendment to this Form 10-K under cover of Form 10-K/A no later than the end of such 120 day period.
| ITEM 11. | EXECUTIVE COMPENSATION |
The information required by Item 11 is incorporated by reference to our Proxy Statement for our Annual Meeting of Shareholders for the fiscal year ended June 30, 2011, which will be filed with the Securities and Exchange Commission no later than 120 days after the end of the fiscal year covered by this Form 10-K, or, alternatively, by amendment to this Form 10-K under cover of Form 10-K/A no later than the end of such 120 day period.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
The information required by Item 12 is incorporated by reference to our Proxy Statement for our Annual Meeting of Shareholders for the fiscal year ended June 30, 2011, which will be filed with the Securities and Exchange Commission no later than 120 days after the end of the fiscal year covered by this Form 10-K, or, alternatively, by amendment to this Form 10-K under cover of Form 10-K/A no later than the end of such 120 day period.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
The information required by Item 13 is incorporated by reference to our Proxy Statement for our Annual Meeting of Shareholders for the fiscal year ended June 30, 2011, which will be filed with the Securities and Exchange Commission no later than 120 days after the end of the fiscal year covered by this Form 10-K, or, alternatively, by amendment to this Form 10-K under cover of Form 10-K/A no later than the end of such 120 day period.
| ITEM 14. | PRINCIPAL ACCOUNTING FEES AND SERVICES |
The information required by Item 14 is incorporated by reference to our Proxy Statement for our Annual Meeting of Shareholders for the fiscal year ended June 30, 2011, which will be filed with the Securities and Exchange Commission no later than 120 days after the end of the fiscal year covered by this Form 10-K, or, alternatively, by amendment to this Form 10-K under cover of Form 10-K/A no later than the end of such 120 day period.
| ITEM 15. | EXHIBITS, FINANCIAL STATEMENT SCHEDULES |
| (a)(1) | Financial Statements | |
| Reference is made to the Index set forth on Page F-1 of this Annual Report on Form 10-K. | ||
| (a)(2) | Financial Statement Schedules | |
All schedules have been omitted because they are inapplicable or the information is provided in the consolidated financial statements, including the notes hereto.
| (a)(3) | Exhibits | |
| 3.1 | Restated Articles of Incorporation, as amended. (1) | |
| 3.2 | Amended and Restated Bylaws. (2) | |
| 3.3 | First Amendment to the Amended and Restated Bylaws. (3) | |
| 4.1 | Form of certificate evidencing shares of Common Stock. (4) | |
| 4.2 | Registration Rights Agreement, dated as of October 30, 1997, by and between Continucare Corporation and Loewenbaum & Company Incorporated. (5) | |
| 10.1 | Continucare Corporation Amended and Restated 1995 Stock Option Plan.** (6) | |
35
Table of Contents
| 10.2 | Amended and Restated 2000 Stock Option Plan (as amended and restated on November 4, 2009). ** (7) | |
| 10.3 | Form of Stock Option Agreement.**(8) | |
| 10.4 | Physician Practice Management Participation Agreement between Continucare Medical Management, Inc., and Humana Medical Plan, Inc. entered into as of the 1st day of August, 1998. (9) | |
| 10.5 | Amended and Restated Primary Care Provider Services dated November 12, 2004, by and between Vista Healthplan of South Florida, Inc., Vista Insurance Plan, Inc. and Continucare Medical Management, Inc. (10) | |
| 10.6 | WCMA Loan and Security Agreement dated March 9, 2000 between Merrill Lynch Business Financial Services, Inc. and Continucare Corporation. (11) | |
| 10.7 | Letter Agreement dated March 18, 2005 between Merrill Lynch Business Financial Services, Inc. and Continucare Corporation. (12) | |
| 10.8 | Form of Promissory Note dated December 29, 2004. (13) | |
| 10.9 | Letter Agreement between Continucare Corporation and Merrill Lynch Business Financial Services, Inc. regarding amendment and extension of Credit Facility. (14) | |
| 10.10 | Asset Purchase Agreement, dated as of May 10, 2006, among Continucare Corporation, a Florida corporation, CNU Blue 1, Inc., a Florida corporation and a wholly-owned subsidiary of CNU, CNU Blue2, LLC, a Florida limited liability company and a wholly-owed subsidiary of Buyer, Miami Dade Health and Rehabilitation Services, Inc., a Florida corporation, Miami Dade Health Centers, Inc., a Florida corporation, West Gables Open MRI Services, Inc., a Florida corporation, Kent Management Systems, Inc., Pelu Properties, Inc., a Florida corporation, Peluca Investments, LLC, a Florida limited liability company owned by the Owners, and Miami Dade Health Centers One, Inc., a Florida corporation, MDHC Red, Inc., a Florida corporation, and each of the shareholders of each Seller identified therein. (15) | |
| 10.11 | Integrated Delivery System Participation Agreement effective as of April 1, 1999 between MDHRS and Humana Medical Plan, Inc., as amended. (16) | |
| 10.12 | Management Services Agreement dated as of September 1, 2004 between MDHC and Vista Healthplan, Inc., as amended. (17) | |
| 10.13 | WCMA Reducing Revolver Loan and Security Agreement dated September 26, 2006, between Continucare MDHC LLC and Merrill Lynch Business Financial Services, Inc. (18) | |
| 10.14 | WCMA Reducing Revolver Loan and Security Agreement dated September 26, 2006, between Continucare MDHC LLC and Merrill Lynch Business Financial Services, Inc. (19) | |
| 10.15 | Amendment of Credit Facility dated September 26, 2006, between Continucare Corporation and Merrill Lynch Business Financial Services, Inc. (20) | |
| 10.16 | Independent Practice Association Participation Agreement dated as of October 11, 2007 by and among Continucare Medical Management, Inc. and Humana Insurance Company, Humana Health Insurance Company of Florida, Inc., Humana Medical Plan, Inc. and their affiliates that underwrite or administer health plans. (21) | |
| 10.17 | Independent Practice Association Participation Agreement dated as of October 11, 2007 by and among Continucare Medical Management, Inc. and Humana Insurance Company, Humana Health Insurance Company of Florida, Inc., Humana Medical Plan, Inc. and their affiliates that underwrite or administer health plans. (22) | |
| 10.18 | Independent Practice Association Participation Agreement dated as of October 11, 2007 by and among Continucare Medical Management, Inc. and Humana Insurance Company, Humana Health Insurance Company of Florida, Inc., Humana Medical Plan, Inc. and their affiliates that underwrite or administer health plans. (23) | |
| 10.19 | Credit Facility Agreement, dated as of December 18, 2009, among Continucare Corporation, as a Borrower, Continucare MDHC, LLC, as a Borrower, and Bank of America, N.A., as Bank. (24) | |
| 10.20 | Agreement and Plan of Merger, dated as of June 26, 2011, by and among Metropolitan Health Networks, Inc., Cab Merger Sub, Inc. and Continucare Corporation.+ | |
| 21.1 | Subsidiaries of the Company.* | |
| 23.1 | Consent of Independent Registered Public Accounting Firm. * | |
| 31.1 | Section 302 Certification of Chief Executive Officer. * | |
| 31.2 | Section 302 Certification of Chief Financial Officer. * | |
| 32.1 | Certification Pursuant to 18 U.S.C. Section 1350, as Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.*** | |
36
Table of Contents
| 32.2 | Certification Pursuant to 18 U.S.C. Section 1350, as Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.*** | |
Documents incorporated by reference to the exhibit number indicated below to the following filings by the Company under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934.
| (1) | Exhibit 3.1 to the Post Effective Amendment No. 1 to the Registration Statement on SB-2 on Form S-3 Registration Statement filed on October 30, 1996. | |
| (2) | Exhibit 3.1 to the Form 8-K dated September 12, 2006, filed September 13, 2006. | |
| (3) | Exhibit 3.2 to the Form 8-K dated November 6, 2007, filed November 7, 2007. | |
| (4) | Exhibit 4.1 to the Post Effective Amendment No. 1 to the Registration Statement on SB-2 on Form S-3 Registration Statement filed on October 30, 1996. | |
| (5) | Exhibit 4.2 to the Form 8-K dated October 30, 1997, filed November 13, 1997. | |
| (6) | Schedule 14A dated December 26, 1997 and filed with the Commission on December 30, 1997. | |
| (7) | Exhibit 10.1 to the Form 8-K dated February 9, 2010, filed February 12, 2010. | |
| (8) | Exhibit 10.1 to the Form 10-Q for the quarterly period ended September 30, 2004. | |
| (9) | Exhibit 10.11 to the Form 10-K for the fiscal year ended June 30, 2000. | |
| (10) | Exhibit 10.1 to the Form 10-Q for the quarterly period ended December 31, 2004. | |
| (11) | Exhibit 4.1 to the Form 10-Q for the quarterly period ended March 31, 2000. | |
| (12) | Exhibit 10.1 to the Form 10-Q for the quarterly period ended March 31, 2005. | |
| (13) | Exhibit 10.1 to the Form 8-K dated December 30, 2004, filed January 5, 2005. | |
| (14) | Exhibit 10.1 to the Form 8-K dated March 8, 2006, filed on March 10, 2006. | |
| (15) | Exhibit 10.1 to the Form 8-K dated May 10, 2006, filed on May 11, 2006. | |
| (16) | Exhibit 10.1 to the Form 10-Q for the quarterly period ended September 30, 2006. | |
| (17) | Exhibit 10.2 to the Form 10-Q for the quarterly period ended September 30, 2006. | |
| (18) | Exhibit 10.3 to the Form 10-Q for the quarterly period ended September 30, 2006. | |
| (19) | Exhibit 10.4 to the Form 10-Q for the quarterly period ended September 30, 2006. | |
| (20) | Exhibit 10.5 to the Form 10-Q for the quarterly period ended September 30, 2006. | |
| (21) | Exhibit 10.1 to the Form 8-K dated October 11, 2007, filed on October 15, 2007. | |
| (22) | Exhibit 10.2 to the Form 8-K dated October 11, 2007, filed on October 15, 2007. | |
| (23) | Exhibit 10.3 to the Form 8-K dated October 11, 2007, filed on October 15, 2007. | |
| (24) | Exhibit 4.1 to the Form 8-K dated December 18, 2009, filed December 23, 2009. | |
| (25) | Exhibit 2.1 to the Form 8-K dated June 26, 2011, filed June 27, 2011. | |
| * | Filed herewith |
| ** | Management contract or compensatory plan or arrangement |
| *** | Furnished herewith |
| + | Schedules to the Agreement and Plan of Merger, dated as of June 26, 2011, by and among Metropolitan Health Networks, Inc., Cab Merger Sub, Inc. and Continucare Corporation have been omitted pursuant to Item 601(b)(2) of Regulation S-K. The registrant hereby undertakes to furnish on a supplemental basis a copy of any omitted schedules to the Securities and Exchange Commission upon request. |
37
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| CONTINUCARE CORPORATION | ||
| By: | /s/ Richard C. Pfenniger, Jr. | |
| RICHARD C. PFENNIGER, JR. | ||
| Chairman of the Board, Chief Executive Officer and President | ||
| (Principal Executive Officer) | ||
Dated: September 7, 2011
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| SIGNATURE | TITLE | DATE | ||
| /s/ Richard C. Pfenniger, Jr. Richard C. Pfenniger, Jr. |
Chairman of the Board, Chief Executive Officer, President and Director (Principal Executive Officer) |
September 7, 2011 | ||
| /s/ Fernando L. Fernandez Fernando L. Fernandez |
Senior Vice President – Finance, Chief Financial Officer, Treasurer and Secretary (Principal Financial and Accounting Officer) |
September 7, 2011 | ||
| /s/ Robert J. Cresci Robert J. Cresci |
Director | September 7, 2011 | ||
| /s/ Neil Flanzraich Neil Flanzraich |
Director | September 7, 2011 | ||
| /s/ Phillip Frost, M.D. Phillip Frost, M.D. |
Director | September 7, 2011 | ||
| /s/ Jacob Nudel, M.D. Jacob Nudel, M.D. |
Director | September 7, 2011 | ||
| /s/ Marvin Sackner, M.D. Marvin Sackner, M.D. |
Director | September 7, 2011 | ||
| /s/ Jacqueline Simkin Jacqueline Simkin |
Director | September 7, 2011 | ||
| /s/ A. Marvin Strait A. Marvin Strait |
Director | September 7, 2011 | ||
38
Table of Contents
INDEX TO FINANCIAL STATEMENTS
F-1
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Shareholders of Continucare Corporation
We have audited the accompanying consolidated balance sheets of Continucare Corporation as of June 30, 2011 and 2010, and the related consolidated statements of income, shareholders' equity, and cash flows for each of the three years in the period ended June 30, 2011. These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Continucare Corporation at June 30, 2011 and 2010, and the consolidated results of its operations and its cash flows for each of the three years in the period ended June 30, 2011, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), Continucare Corporation's internal control over financial reporting as of June 30, 2011, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated September 7, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Certified Public Accountants
Miami, Florida
September 7, 2011
F-2
Table of Contents
CONTINUCARE CORPORATION
| June 30, | ||||||||
| 2011 | 2010 | |||||||
| ASSETS | ||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 50,480,963 | $ | 37,542,445 | ||||
| Certificate of deposit |
— | 668,755 | ||||||
| Due from HMOs, net of a liability for incurred but not reported medical claims expense of approximately $23,889,000 and $23,394,000 at June 30, 2011 and 2010, respectively |
19,575,901 | 18,920,388 | ||||||
| Prepaid expenses and other current assets |
4,870,628 | 2,631,136 | ||||||
| Deferred income tax assets |
642,844 | 140,057 | ||||||
|
|
|
|
|
|||||
| Total current assets |
75,570,336 | 59,902,781 | ||||||
| Property and equipment, net |
16,084,193 | 12,728,184 | ||||||
| Goodwill |
79,625,601 | 73,994,444 | ||||||
| Intangible assets, net of accumulated amortization of approximately $6,602,000 and $4,705,000 at June 30, 2011 and 2010, respectively |
6,307,565 | 4,296,507 | ||||||
| Deferred income tax assets |
3,178,884 | 2,830,929 | ||||||
| Other assets, net |
138,429 | 112,747 | ||||||
|
|
|
|
|
|||||
| Total assets |
$ | 180,905,008 | $ | 153,865,592 | ||||
|
|
|
|
|
|||||
| LIABILITIES AND SHAREHOLDERS’ EQUITY | ||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 1,754,938 | $ | 810,376 | ||||
| Accrued expenses and other current liabilities |
8,608,832 | 9,041,162 | ||||||
| Income taxes payable |
262,261 | 590,673 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
10,626,031 | 10,442,211 | ||||||
| Deferred income tax liabilities |
8,078,793 | 7,145,507 | ||||||
| Other liabilities |
183,382 | 249,248 | ||||||
|
|
|
|
|
|||||
| Total liabilities |
18,888,206 | 17,836,966 | ||||||
| Commitments and contingencies |
||||||||
| Shareholders’ equity: |
||||||||
| Common stock, $0.0001 par value: 100,000,000 shares authorized; 60,663,266 shares issued and outstanding at June 30, 2011 and 60,504,012 shares issued and outstanding at June 30, 2010 |
6,066 | 6,050 | ||||||
| Additional paid-in capital |
109,936,415 | 107,860,204 | ||||||
| Accumulated earnings |
52,074,321 | 28,162,372 | ||||||
|
|
|
|
|
|||||
| Total shareholders’ equity |
162,016,802 | 136,028,626 | ||||||
|
|
|
|
|
|||||
| Total liabilities and shareholders’ equity |
$ | 180,905,008 | $ | 153,865,592 | ||||
|
|
|
|
|
|||||
The accompanying notes are an integral part of these consolidated financial statements.
F-3
Table of Contents
CONTINUCARE CORPORATION
CONSOLIDATED STATEMENTS OF INCOME
| For the Year Ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Revenue |
$ | 333,458,208 | $ | 310,791,463 | $ | 281,270,360 | ||||||
| Operating expenses: |
||||||||||||
| Medical services: |
||||||||||||
| Medical claims |
216,226,209 | 208,857,229 | 199,167,856 | |||||||||
| Other direct costs |
38,892,426 | 31,484,513 | 28,456,121 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total medical services |
255,118,635 | 240,341,742 | 227,623,977 | |||||||||
|
|
|
|
|
|
|
|||||||
| Administrative payroll and employee benefits |
16,297,890 | 16,308,854 | 12,655,975 | |||||||||
| General and administrative |
22,140,000 | 18,021,123 | 16,261,750 | |||||||||
| Merger transaction expenses |
2,487,939 | — | — | |||||||||
|
|
|
|
|
|
|
|||||||
| Total operating expenses |
296,044,464 | 274,671,719 | 256,541,702 | |||||||||
|
|
|
|
|
|
|
|||||||
| Income from operations |
37,413,744 | 36,119,744 | 24,728,658 | |||||||||
| Interest income (expense), net |
199,523 | (50,084 | ) | 152,784 | ||||||||
|
|
|
|
|
|
|
|||||||
| Income before income tax provision |
37,613,267 | 36,069,660 | 24,881,442 | |||||||||
| Income tax provision |
13,701,318 | 13,893,353 | 9,600,321 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net income |
$ | 23,911,949 | $ | 22,176,307 | $ | 15,281,121 | ||||||
|
|
|
|
|
|
|
|||||||
| Net income per common share: |
||||||||||||
| Basic |
$ | .39 | $ | .37 | $ | .25 | ||||||
|
|
|
|
|
|
|
|||||||
| Diluted |
$ | .38 | $ | .36 | $ | .24 | ||||||
|
|
|
|
|
|
|
|||||||
| Weighted average common shares outstanding: |
||||||||||||
| Basic |
60,584,930 | 59,777,789 | 61,405,620 | |||||||||
|
|
|
|
|
|
|
|||||||
| Diluted |
62,439,900 | 61,565,397 | 62,488,340 | |||||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Table of Contents
CONTINUCARE CORPORATION
CONSOLIDATED STATEMENTS OF SHAREHOLDERS’ EQUITY
| Common Stock | Additional Paid-In Capital |
Accumulated Earnings (Deficit) |
Total Shareholders’ Equity |
|||||||||||||||||
| Shares | Amount | |||||||||||||||||||
| Balance at June 30, 2008 |
64,796,303 | $ | 6,480 | $ | 114,514,853 | $ | (9,295,056 | ) | $ | 105,226,277 | ||||||||||
| Recognition of compensation expense related to issuance of stock options |
— | — | 1,163,472 | — | 1,163,472 | |||||||||||||||
| Excess tax benefits related to exercise of stock options |
— | — | 116,593 | — | 116,593 | |||||||||||||||
| Issuance of stock upon exercise of stock options |
13,750 | 1 | 23,374 | — | 23,375 | |||||||||||||||
| Repurchase and retirement of common stock |
(5,419,004 | ) | (542 | ) | (10,607,773 | ) | (10,608,315 | ) | ||||||||||||
| Net income |
— | — | — | 15,281,121 | 15,281,121 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Balance at June 30, 2009 |
59,391,049 | 5,939 | 105,210,519 | 5,986,065 | 111,202,523 | |||||||||||||||
| Recognition of compensation expense related to issuance of stock options |
— | — | 1,391,768 | — | 1,391,768 | |||||||||||||||
| Excess tax benefits related to exercise of stock options |
— | — | 1,374,921 | — | 1,374,921 | |||||||||||||||
| Issuance of stock upon exercise of stock options |
1,448,220 | 145 | 1,417,176 | — | 1,417,321 | |||||||||||||||
| Shares withheld in connection with exercise of stock options |
(335,257 | ) | (34 | ) | (1,408,079 | ) | — | (1,408,113 | ) | |||||||||||
| Purchase of noncontrolling interest in sleep diagnostic centers |
— | — | (126,101 | ) | — | (126,101 | ) | |||||||||||||
| Net income |
— | — | — | 22,176,307 | 22,176,307 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Balance at June 30, 2010 |
60,504,012 | 6,050 | 107,860,204 | 28,162,372 | 136,028,626 | |||||||||||||||
| Recognition of compensation expense related to issuance of stock options |
— | — | 1,823,107 | — | 1,823,107 | |||||||||||||||
| Excess tax benefits related to exercise of stock options |
— | — | 164,411 | — | 164,411 | |||||||||||||||
| Issuance of stock upon exercise of stock options |
255,500 | 26 | 455,174 | — | 455,200 | |||||||||||||||
| Shares withheld in connection with exercise of stock options |
(96,246 | ) | (10 | ) | (366,481 | ) | — | (366,491 | ) | |||||||||||
| Net income |
— | — | — | 23,911,949 | 23,911,949 | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Balance at June 30, 2011 |
60,663,266 | $ | 6,066 | $ | 109,936,415 | $ | 52,074,321 | $ | 162,016,802 | |||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Table of Contents
CONTINUCARE CORPORATION
CONSOLIDATED STATEMENTS OF CASH FLOWS
| For the Year Ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES |
||||||||||||
| Net income |
$ | 23,911,949 | $ | 22,176,307 | $ | 15,281,121 | ||||||
| Adjustments to reconcile net income to net cash provided by operating activities: |
||||||||||||
| Depreciation and amortization |
4,134,437 | 2,895,621 | 2,303,327 | |||||||||
| Change in liability for unrecognized tax benefit |
(899,357 | ) | — | — | ||||||||
| Gain on change in fair value of contingent consideration |
(620,946 | ) | — | — | ||||||||
| Loss on impairment of fixed assets |
— | 96,000 | — | |||||||||
| Loss on disposal of fixed assets |
19,821 | 18,668 | 65,760 | |||||||||
| Provision for bad debts |
392,702 | 118,895 | — | |||||||||
| Compensation expense related to issuance of stock options |
1,823,107 | 1,391,768 | 1,163,472 | |||||||||
| Excess tax benefits related to exercise of stock options |
(164,411 | ) | (1,374,921 | ) | (116,593 | ) | ||||||
| Deferred income tax expense |
82,544 | 675,796 | 230,923 | |||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Due from HMOs, net |
(655,513 | ) | (1,596,789 | ) | (1,997,816 | ) | ||||||
| Prepaid expenses and other current assets |
(60,643 | ) | 88,596 | (104,129 | ) | |||||||
| Other assets, net |
(8,216 | ) | 56,365 | 42,735 | ||||||||
| Accounts payable |
676,841 | 137,270 | 249,587 | |||||||||
| Accrued expenses and other current liabilities |
(229,780 | ) | 3,270,660 | (33,689 | ) | |||||||
| Income taxes payable |
(328,412 | ) | (984,838 | ) | 549,398 | |||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by operating activities |
28,074,123 | 26,969,398 | 17,634,096 | |||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES |
||||||||||||
| Purchases of certificates of deposit |
— | (10,705 | ) | (682,948 | ) | |||||||
| Proceeds from maturities of certificates of deposit |
668,755 | 575,603 | 723,442 | |||||||||
| Acquisition of sleep diagnostic centers, net of cash acquired |
(11,497,530 | ) | (1,507,858 | ) | — | |||||||
| Purchase of property and equipment |
(4,372,181 | ) | (3,337,260 | ) | (3,100,935 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in investing activities |
(15,200,956 | ) | (4,280,220 | ) | (3,060,441 | ) | ||||||
| CASH FLOWS FROM FINANCING ACTIVITIES |
||||||||||||
| Principal repayments under capital lease obligations |
(187,769 | ) | (300,584 | ) | (115,225 | ) | ||||||
| Proceeds from exercise of stock options |
455,200 | 1,417,287 | 23,375 | |||||||||
| Shares withheld in connection with exercise of stock options |
(366,491 | ) | (1,408,079 | ) | — | |||||||
| Excess tax benefits related to exercise of stock options |
164,411 | 1,374,921 | 116,593 | |||||||||
| Purchase of noncontrolling interest in sleep diagnostic centers |
— | (126,101 | ) | — | ||||||||
| Repurchase of common stock |
— | — | (10,608,315 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by (used in) financing activities |
65,351 | 957,444 | (10,583,572 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| Net increase in cash and cash equivalents |
12,938,518 | 23,646,622 | 3,990,083 | |||||||||
| Cash and cash equivalents at beginning of fiscal year |
37,542,445 | 13,895,823 | 9,905,740 | |||||||||
|
|
|
|
|
|
|
|||||||
| Cash and cash equivalents at end of fiscal year |
$ | 50,480,963 | $ | 37,542,445 | $ | 13,895,823 | ||||||
|
|
|
|
|
|
|
|||||||
F-6
Table of Contents
CONTINUCARE CORPORATION
CONSOLIDATED STATEMENTS OF CASH FLOWS (CONTINUED)
| For the Year Ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| SUPPLEMENTAL DISCLOSURE OF NONCASH INVESTING AND FINANCING TRANSACTIONS: |
||||||||||||
| Purchase of equipment, furniture and fixtures with proceeds of capital lease obligations |
$ | 184,941 | $ | 228,413 | $ | 123,831 | ||||||
|
|
|
|
|
|
|
|||||||
| Retirement of treasury stock |
$ | — | $ | — | $ | 10,608,315 | ||||||
|
|
|
|
|
|
|
|||||||
| SUPPLEMENTAL DISCLOSURE OF CASH FLOW INFORMATION: |
||||||||||||
| Cash paid for taxes |
$ | 14,450,184 | $ | 13,870,000 | $ | 8,820,000 | ||||||
|
|
|
|
|
|
|
|||||||
| Cash paid for interest |
$ | 19,675 | $ | 19,041 | $ | 16,255 | ||||||
|
|
|
|
|
|
|
|||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-7
Table of Contents
CONTINUCARE CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
NOTE 1
General
Continucare Corporation (“we”, “us”, “our”, “Continucare” or the “Company”), is primarily a provider of primary care physician services on an outpatient basis in Florida. We provide medical services to patients through employee physicians, advanced registered nurse practitioners and physicians’ assistants. Additionally, we provide medical management services to independent physician affiliates (“IPAs”). Also, through our subsidiary, Seredor Corporation, we operate sleep diagnostic centers in fifteen states. Substantially all of our revenue is derived from managed care agreements with three health maintenance organizations, Humana Medical Plans, Inc. (“Humana”), Vista Healthplan of South Florida, Inc. and its affiliated companies (“Vista”), and Wellcare Health Plans, Inc. and its affiliated companies (“Wellcare”) (collectively, the “HMOs”). We began operating as a public company in 1996 as the successor to a Florida corporation originally incorporated in 1986. All references to a “Fiscal” year refer to our fiscal year which ends June 30.
Merger Transaction
On June 26, 2011, Continucare entered into an Agreement and Plan of Merger (the “Merger Agreement”) with Metropolitan Health Networks, Inc. (“Metropolitan”) and Cab Merger Sub, Inc., a Florida corporation and a wholly owned subsidiary of Metropolitan (“Merger Subsidiary”), providing for the merger of Continucare with Merger Subsidiary. Subject to the terms and conditions of the Merger Agreement, which has been unanimously approved by the boards of directors of the respective parties, Merger Subsidiary will be merged with and into Continucare (the “Merger”), with Continucare surviving the Merger as a wholly owned subsidiary of Metropolitan.
On August 22, 2011, at a Special Meeting of Shareholders, the Merger Agreement and the transactions contemplated thereby were approved by Continucare stockholders. Assuming all conditions to closing are met, Continucare and Metropolitan expect to close the acquisition on or about the end of September 2011. There can be no assurance that the acquisition will close.
At the effective time of the Merger, each share of Continucare common stock outstanding immediately prior to the effective time (other than shares owned by Continucare, Metropolitan, or shareholders who have properly demanded and perfected appraisal rights under Florida law) will be converted into the right to receive $6.25 in cash, without interest, and 0.0414 of a share of Metropolitan common stock (the “Merger Consideration”). No fractional shares of Metropolitan common stock will be issued in the Merger, and Continucare’s stockholders will receive cash in lieu of fractional shares, if any, of Metropolitan common stock. Each share of Metropolitan common stock outstanding immediately prior to the effective time will remain outstanding and will not be affected by the Merger. Upon completion of the transaction, Continucare stockholders will own approximately 5.8% of Metropolitan’s outstanding common stock.
At the effective time of the Merger, each issued and outstanding option to purchase Continucare common stock will become fully vested and be cancelled in exchange for the right to receive an amount of cash equal to $6.45 less the per share exercise price of the option, subject to withholding taxes.
The value of the equity consideration portion of the Merger Consideration is subject to change based upon changes in the market price of Metropolitan’s common stock prior to closing. The total value of the transaction is approximately $416 million, excluding transaction and financing fees.
In the event that a party fails to satisfy its covenants or representations under the Merger Agreement, the agreement provides customary termination rights, and, under certain circumstances, a $12 million termination fee and up to $1.5 million of expense reimbursement. If, under certain circumstances, the Merger Agreement is terminated as a result of the Merger not being consummated on or before November 1, 2011 and if, within 12 months following the date of termination, Continucare enters into a written agreement, arrangement or understanding regarding an alternative acquisition proposal, then Continucare will be required to pay Metropolitan a termination fee of $9 million and up to $1.5 million of expense reimbursement. Upon the termination of the Merger Agreement under specified circumstances, including, among
F-8
Table of Contents
others, Metropolitan’s failure to obtain financing required to complete the acquisition, after all of the other conditions to closing have been met, Metropolitan will be required to pay Continucare a $12 million termination fee and up to $1.5 million of expense reimbursement. If, under certain circumstances, Continucare does not generate a targeted minimum cash amount of $51.7 million by November 1, 2011, the Merger Agreement may be terminated by Metropolitan and neither party will be required to pay the other party a termination fee or an expense reimbursement.
In connection with the Merger Agreement, Phillip Frost, M.D., a member of the board of directors of Continucare, and certain entities related to Dr. Frost, who in the aggregate beneficially own approximately 26 million shares of Continucare common stock, representing approximately 43% of the outstanding common stock of Continucare, in their capacities as shareholders of Continucare, executed a voting agreement with Metropolitan, dated June 26, 2011 (the “Voting Agreement”), which requires, among other things, such shareholders to vote their shares of Continucare common stock in favor of the Merger Agreement and the transactions contemplated thereby. The Voting Agreement will terminate on the earliest to occur of (i) the termination of the Merger Agreement in accordance with its terms, (ii) a written agreement of the parties to terminate the Voting Agreement and (iii) the effective time of the Merger.
In connection with the Merger Agreement, Richard Pfenniger, Continucare’s Chairman of the Board, Chief Executive Officer and President, and Fernando Fernandez, Continucare’s Senior Vice President – Finance, Chief Financial Officer and Treasurer, each entered into a Change in Control and Separation Agreement with Metropolitan, pursuant to which, upon completion of the Merger (a) Metropolitan will pay to Mr. Pfenniger $475,000 (less applicable taxes) over a twelve month period beginning no later than 30 days after completion of the Merger in accordance with Metropolitan’s normal payroll policies and a lump sum payment of $20,262, which is the value of one year of welfare benefits and (b) Metropolitan will pay to Mr. Fernandez $256,000 (less applicable taxes) over a twelve month period beginning no later than 90 days after completion of the Merger in accordance with Metropolitan’s normal payroll policies and a lump sum payment of $32,886, which is the value of one year of welfare benefits. In addition, if the Merger is completed, Mr. Pfenniger’s and Mr. Fernandez’s employment with Metropolitan (as the parent of Continucare, if the Merger is completed) will terminate, in the case of Mr. Pfenniger, at the effective time of the Merger and, in the case of Mr. Fernandez, on February 15, 2012 (or prior to that date on 30 days’ written notice from one party to the other), and both Mr. Pfenniger and Mr. Fernandez will be paid in one single payment on Metropolitan’s first payroll date after termination of employment an amount equal to: (i) any accrued but unpaid base salary and any bonus payments as of the termination of employment, (ii) any payments with respect to vacations earned but unused through the termination of employment, and (iii) any amount due as reimbursement of expenses incurred before the termination of employment. The Change in Control and Separation Agreements also contain certain covenants regarding confidentiality of information, non-competition and non-solicitation of Continucare employees by each of Mr. Pfenniger and Mr. Fernandez applicable until the first anniversary of the termination of their employment. No payments under the severance agreements will be made and the parties will have no obligations to one another under the severance agreements if the Merger is not completed.
Acquisitions
In August 2010 and September 2010, we acquired three operators of sleep diagnostic centers and a related entity that provides continuous positive airway pressure (CPAP) devices and supplies. The three acquired operators of sleep diagnostic centers operate a combined 58 sleep diagnostic centers in nine states. The aggregate total purchase price for these acquired entities consisted of cash consideration paid of $11.2 million and future contingent cash consideration up to a maximum of $2.0 million subject to the achievement of certain future earnings targets. We accrued $1.5 million of the contingent cash consideration based on a preliminary fair value estimate on the acquisition date, which was determined using significant unobservable inputs (Level 3) in a probability-weighted income approach, discounted to present value using a weighted-average cost of capital. In April 2011, we paid $0.7 million of the contingent cash consideration resulting in a remaining maximum contingent cash consideration of $1.0 million and a decrease in the accrued liability to $0.8 million. During the three-month period ended June 30, 2011, we re-measured the estimated fair value of the contingent cash consideration and based on changes in future earnings estimates of the acquired entities, we recorded an adjustment to reduce the related accrued liability by $0.6 million to $0.2 million as of June 30, 2011 and increase income from operations by $0.6 million. We will re-measure the estimated fair value of the contingent cash consideration on a quarterly basis and any subsequent adjustments based on actual payments or revised estimates will be recognized in the condensed consolidated statements of income during the period of adjustment. The revenues, expenses and results of operations of the acquired companies have been included in our condensed consolidated statements of income from the dates of
F-9
Table of Contents
acquisition.
NOTE 2 – SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
A summary of significant accounting policies followed by us is as follows:
Principles of Consolidation
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiaries. All significant intercompany transactions and balances have been eliminated in consolidation.
Accounting Estimates
The preparation of consolidated financial statements in conformity with accounting principles generally accepted in the United States (“generally accepted accounting principles”) requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenues, and expenses. Because of the inherent uncertainties of this process, actual results could differ from those estimates. Such estimates include the recognition of revenue, the recoverability of intangible assets, the collectibility of receivables, the realization of deferred income tax assets and the accrual for incurred but not reported (“IBNR”) claims.
Fair Value of Financial Instruments
Our financial instruments consist mainly of cash and cash equivalents, certificates of deposit, amounts due from HMOs, accounts payable, and capital lease obligations. The carrying amounts of our cash and cash equivalents, certificates of deposit, amounts due from HMOs, accounts payable and accrued expenses approximate fair value due to the short-term nature of these instruments. At June 30, 2011 and 2010, the carrying value of our capital lease obligations approximate fair value based on the terms of the obligations.
Cash and Cash Equivalents
We define cash and cash equivalents as those highly-liquid investments purchased with maturities of three months or less from the date of purchase.
Certificates of Deposit
Certificates of deposit have original maturities of greater than three months. Included in the consolidated balance sheet as of June 30, 2010 was one certificate of deposit for approximately $0.7 million which exceeded the $250,000 Federal Deposit Insurance Corporation limit.
Due from HMOs
Under the terms of our contracts with our HMO affiliates, we have the right to offset amounts due to our HMO affiliates against amounts our respective HMO affiliates owe us and each of our HMO affiliates has a comparable right.
Our HMO affiliates process and pay medical claims and certain other costs on our behalf. Based on the terms of the contracts with our HMO affiliates, we receive a net payment from our HMO affiliates that is calculated by offsetting revenue earned with medical claims expense, which is calculated as claims paid on our behalf plus an amount reserved for claims incurred but not reported. Therefore, the amounts due from the HMOs are presented on the balance sheet net of an estimated liability for claims incurred but not reported, which is calculated based on historical data adjusted for payment patterns, cost trends, utilization of health care services and other relevant factors. In the event medical claims expense exceeds revenue, our HMO affiliates have the right to offset future payments owed to us by the amount of such deficit.
Property and Equipment
Equipment, furniture and leasehold improvements are stated at cost. Depreciation is computed using the straight-line method over the estimated useful lives of the related assets, which range from three to five years. Leasehold improvements are amortized over the underlying assets’ useful lives or the term of the lease, whichever is shorter. The buildings and land purchased in connection with the acquisition of Miami Dade Health Centers, Inc. and its affiliated companies (collectively, the “MDHC Companies”) were recorded at their estimated fair values as of the date of the acquisition. The buildings are depreciated using the straight-line method over their estimated useful lives which approximate forty years. Repairs and maintenance costs are expensed as incurred. Improvements and replacements are capitalized.
F-10
Table of Contents
Goodwill and Other Intangible Assets
We do not amortize goodwill and intangible assets with indefinite useful lives. We review goodwill and intangible assets with indefinite useful lives annually for impairment, or more frequently if certain indicators arise. We amortize intangible assets with definite useful lives over their respective estimated useful lives to their estimated residual values and also review for impairment annually, or more frequently if certain indicators arise. Indicators of an impairment include, among other things, a significant adverse change in legal factors or the business climate, the loss of a key HMO contract, an adverse action by a regulator, unanticipated competition, loss of key personnel or allocation of goodwill to a portion of a business that is to be sold.
The goodwill impairment test requires the allocation of goodwill and all other assets and liabilities to reporting units. We have determined that we have two reporting units: Provider Services and Sleep Diagnostic Services. Our goodwill impairment reviews are determined using a two-step process. The first step of the process is to compare the fair value of a reporting unit with its carrying amount, or book value, including goodwill. If the fair value of a reporting unit exceeds its carrying amount, the goodwill of the reporting unit is not impaired and the second step of the impairment review is not necessary. If the carrying amount of a reporting unit exceeds its fair value, the second step of the goodwill impairment review is required to be performed to estimate the implied fair value of the reporting unit’s goodwill. The implied fair value of the reporting unit’s goodwill is compared with the carrying amount of that goodwill. If the carrying amount of the reporting unit’s goodwill exceeds the implied fair value of that goodwill, an impairment loss is recognized in an amount equal to that excess. We perform the annual impairment test as of May 1st of each year. Should it later be determined that an indicator of impairment has occurred, we would be required to perform an additional impairment test. No impairment charges were required during the fiscal years ended June 30, 2011, 2010 or 2009.
Share-Based Payment
We recognize compensation costs in our financial statements related to our stock-based payment transactions over the period services are rendered according to the fair value of the stock-based awards issued.
Earnings Per Share
Basic earnings per share is computed by dividing net income or loss by the weighted average common shares outstanding for the period. Diluted earnings per share reflects the potential dilution that could occur if securities or other contracts to issue common stock were exercised or converted into common stock or resulted in the issuance of common stock that then shared in our earnings (see Note 6).
Revenue Recognition
We provide services to patients on either a capitated monthly fee arrangement with HMOs or under a fee for service arrangement. The percentage of total revenue relating to Humana approximated 69%, 72% and 72% for Fiscal 2011, 2010 and 2009, respectively. The percentage of total revenue relating to Vista approximated 19%, 20% and 18% for Fiscal 2011, 2010 and 2009, respectively. The percentage of total revenue relating to Wellcare approximated 5%, 6% and 8% for Fiscal 2011, 2010 and 2009, respectively.
Under our risk contracts with HMOs, we receive a percentage of premium or other capitated fee for each patient that chooses one of our physicians as their primary care physician. Revenue under these agreements is generally recorded in the period we assume responsibility to provide services at the rates then in effect as determined by the respective contract. As part of the Medicare Advantage program, CMS periodically recomputes the premiums to be paid to the HMOs based on updated health status of participants and updated demographic factors. In addition, the premiums paid to the HMOs are subject to periodic adjustment based on CMS’s risk corridor adjustment methodology related to the Medicare Prescription Drug Plan. We record adjustments to revenue at the time that the information necessary to make the determination of the adjustment is received from the HMO or the applicable government body and it is determined that the collectibility of such adjustments is reasonably assured or the likelihood of repayment is probable. The net effect of these premium adjustments included in revenue were favorable retroactive Medicare adjustments of $0.1 million, $0.4 million and $0.9 million for Fiscal 2011, 2010 and 2009, respectively.
Under our risk agreements, we assume responsibility for the cost of all medical services provided to the patient, even those we do not provide directly, in exchange for a percentage of premium or other capitated fee. To the extent
F-11
Table of Contents
that patients require more frequent or expensive care, our revenue under a contract may be insufficient to cover the costs of care provided. When it is probable that expected future health care costs and maintenance costs under a contract or group of existing contracts will exceed anticipated capitated revenue on those contracts, we recognize losses on our prepaid health care services with HMOs. No contracts were considered loss contracts at June 30, 2011 and June 30, 2010 because we have the right to terminate unprofitable physicians and close unprofitable centers under our managed care contracts.
Our HMO contracts have various expiration dates ranging from one to three years with automatic renewal terms. Upon negotiation of any of the HMO contracts, the expiration dates may be extended beyond the automatic renewal terms.
Under our limited risk and non-risk contracts with HMOs, we receive a capitation fee or management fee based on the number of patients for which we provide services on a monthly basis. Under our limited risk contracts, we also receive a percentage of the surplus generated as determined by the respective contract. The fees and our portion of the surplus generated under these arrangements are recorded as revenue in the period in which services are provided as determined by the respective contract.
Payments under both our risk contracts and our non-risk contracts (for both the Medicare Advantage program as well as Medicaid) are also subject to reconciliation based upon historical patient enrollment data. We record any adjustments to this revenue at the time that the information necessary to make the determination of the adjustment is received from the HMO or the applicable governmental body.
Medical Service Expense
We contract with or employ various health care providers to provide medical services to our patients. Primary care physicians are compensated on either a salary or capitation basis. For patients enrolled under risk managed care contracts, the cost of specialty services are paid on either a fee for service, per diem or capitation basis.
The cost of health care services provided or contracted for is accrued in the period in which the services are provided. This cost includes an estimate of the related liability for medical claims incurred but not yet reported that is primarily based on historical claims experience and current factors such as unusually high or low utilization and benefit changes provided under HMO plans. Estimates are adjusted as changes in these factors occur and such adjustments are reported in the period of determination. We use an actuarial analysis as an additional tool to further corroborate our estimate of the related liability for medical claims incurred but not yet reported.
Stop-loss Insurance
Our health care costs are limited through agreements with the HMOs. The HMOs charge us a per member per month fee that limits our health care costs for any individual patient. Health care costs in excess of annual limits are generally handled directly by the HMOs and we are not entitled to and do not receive any related insurance recoveries.
Other Comprehensive Income
We had no comprehensive income items other than net income for all years presented.
Subsequent Events
We evaluated subsequent events for recognition or disclosure through the time these financial statements were filed in this Annual Report on Form 10-K.
NOTE 3 – GOODWILL AND OTHER INTANGIBLE ASSETS
The most significant component of the goodwill and other intangible assets included in the accompanying consolidated balance sheets consists of the goodwill and other intangible assets recorded in connection with the acquisition of the MDHC Companies in October 2006. The purchase price, including acquisition costs, of approximately $66.2 million was allocated to the estimated fair value of acquired tangible assets of $13.9 million, identifiable intangible assets of $8.7 million and assumed liabilities of $15.3 million as of October 1, 2006, resulting in goodwill totaling $58.9 million. The identifiable intangible assets of $8.7 million consisted of estimated fair values of $1.6 million assigned to the trade name, $6.2 million to customer relationships and $0.9 million to a
F-12
Table of Contents
noncompete agreement. The trade name was determined to have an estimated useful life of six years and the customer relationships and noncompete agreements were each determined to have estimated useful lives of eight and five years, respectively. The fair values of the customer relationships and other identifiable intangible assets are amortized over their estimated lives using the straight-line method. As of June 30, 2011, accumulated amortization for the trade name, customer relationships, and noncompete agreements was $1.3 million, $3.8 million, and $0.8 million, respectively. The weighted average amortization period for these identifiable intangible assets is 7.1 years. The customer relationships are non-contractual. The fair value of the identifiable intangible assets was determined, with the assistance of an outside valuation firm, based on standard valuation techniques.
In Fiscal 2011, the purchase price related to the acquisition of the three operators of sleep diagnostic centers and a related entity that provides CPAP devices and supplies was allocated, on a preliminary basis, to the estimated fair values of the acquired tangible and intangible assets and the assumed liabilities. Goodwill and other identifiable intangible assets recorded in connection with these acquisitions were $5.6 million and $3.9 million, respectively. The identifiable intangible assets of $3.9 million, which primarily consist of the estimated fair value of customer relationships, have accumulated amortization of $0.7 million and a weighted average amortization period of 5.1 years. The fair value of the identifiable intangible assets was determined based on standard valuation techniques.
The increases in goodwill of $5.6 million and $0.8 million during Fiscal 2011 and 2010, respectively, were related to the goodwill recorded in connection with the acquisition of sleep diagnostic centers.
The change in goodwill for our two reporting units during Fiscal 2011 was as follows:
| Provider Services |
Sleep Services |
Total | ||||||||||
| Balance at June 30, 2010 |
$ | 73,204,582 | $ | 789,862 | $ | 73,994,444 | ||||||
| Acquisition of sleep diagnostic centers |
— | 5,644,530 | 5,644,530 | |||||||||
| Purchase price adjustments |
— | (13,373 | ) | (13,373 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Balance at June 30, 2011 |
$ | 73,204,582 | $ | 6,421,019 | $ | 79,625,601 | ||||||
|
|
|
|
|
|
|
|||||||
Total amortization expense for identifiable intangible assets was $1.9 million, $1.3 million and $1.3 million for Fiscal 2011, 2010 and 2009, respectively. The estimated aggregate amortization expense for intangible assets as of June 30, 2011 will be approximately $1.9 million, $1.7 million, $1.6 million, $0.7 million, and $0.3 million for each of the five succeeding fiscal years, respectively.
NOTE 4 – PROPERTY AND EQUIPMENT
Property and equipment are summarized as follows:
| June 30, | Estimated Useful Lives |
|||||||||||
|
|
|
|||||||||||
| 2011 | 2010 | (in years) | ||||||||||
| Land |
$ | 1,919,746 | $ | 1,919,746 | — | |||||||
| Building and improvements |
5,923,877 | 5,328,851 | 40 | |||||||||
| Construction in progress |
765,772 | 313,411 | — | |||||||||
| Vehicles |
1,496,878 | 1,012,677 | 5 | |||||||||
| Furniture, fixtures and equipment |
10,356,045 | 5,638,814 | 3-5 | |||||||||
| Furniture and equipment under capital lease |
599,599 | 762,293 | 3-5 | |||||||||
| Leasehold improvements |
3,960,148 | 2,920,223 | 5 | |||||||||
|
|
|
|
|
|||||||||
| 25,022,065 | 17,896,015 | |||||||||||
| Less accumulated depreciation and amortization |
(8,937,872 | ) | (5,167,831 | ) | ||||||||
|
|
|
|
|
|||||||||
| $ | 16,084,193 | $ | 12,728,184 | |||||||||
|
|
|
|
|
|||||||||
Depreciation expense for the years ended June 30, 2011, 2010 and 2009 was approximately $2.2 million, $1.6 million and $1.0 million, respectively.
We entered into various noncancellable leases for certain furniture and equipment that are classified as capital leases. The leases are payable over three to five years at incremental borrowing rates ranging from 6% to 8% per
F-13
Table of Contents
annum. Accumulated amortization for assets recorded under capital lease agreements was approximately $0.3 million and $0.5 million at June 30, 2011 and 2010, respectively. Amortization of assets recorded under capital lease agreements was approximately $0.2 million, $0.2 million and $0.1 million for the years ended June 30, 2011, 2010 and 2009, respectively, and is included in depreciation expense for all years presented.
Future minimum lease payments under all capital leases are as follows:
| For the year ending June 30, |
||||
| 2012 |
$ | 164,921 | ||
| 2013 |
114,712 | |||
| 2014 |
65,191 | |||
| 2015 |
10,768 | |||
|
|
|
|||
| 355,592 | ||||
| Less amount representing imputed interest |
32,111 | |||
|
|
|
|||
| Present value of obligations under capital lease |
323,481 | |||
| Less current portion |
140,099 | |||
|
|
|
|||
| Long-term capital lease obligations |
$ | 183,382 | ||
|
|
|
The current and long-term portions of obligations under capital leases are classified within accrued expenses and other current liabilities and other liabilities, respectively, in the accompanying consolidated balance sheets.
NOTE 5 – DEBT
In December 2009, we entered into a credit facility agreement (the “Credit Facility”) in order to renew and refinance our existing credit facilities. The Credit Facility consists of two revolving credit facilities totaling $10,000,000 with a maturity date of January 31, 2012. Interest on borrowings under the Credit Facility accrues at a per annum rate equal to the sum of 2.40% and the one-month LIBOR (0.19% at June 30, 2011), floating daily. The Credit Facility contains certain customary representations and warranties, and certain financial and other customary covenants including covenants requiring us, on a consolidated basis, to maintain an adjusted tangible net worth of at least $25 million and a fixed charge coverage ratio of not less than 1.50 to 1. Substantially all of our assets serve as collateral for the Credit Facility. At June 30, 2011, there was no outstanding principal balance on the Credit Facility. At June 30, 2011, we had letters of credit outstanding of $1.3 million which reduced the amount available for borrowing under the Credit Facility to $8.7 million. Under the Credit Facility, we are no longer required to use certificates of deposit as collateral for outstanding letters of credit.
NOTE 6 – EARNINGS PER SHARE
A reconciliation of the denominator of the basic and diluted earnings per share computation is as follows:
| Year Ended June 30, | ||||||||||||
|
|
|
|||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Basic weighted average number of shares outstanding |
60,584,930 | 59,777,789 | 61,405,620 | |||||||||
| Dilutive effect of stock options |
1,854,970 | 1,787,608 | 1,082,720 | |||||||||
|
|
|
|
|
|
|
|||||||
| Diluted weighted average number of shares outstanding |
62,439,900 | 61,565,397 | 62,488,340 | |||||||||
|
|
|
|
|
|
|
|||||||
| Not included in calculation of dilutive earnings per share as impact is antidilutive: |
||||||||||||
| Stock options outstanding |
280,000 | 267,500 | 3,775,750 | |||||||||
NOTE 7 – SHARE-BASED PAYMENT
The Amended and Restated Continucare Corporation 2000 Stock Incentive Plan (the “2000 Stock Incentive Plan”), which has been approved by our shareholders, permits the grant of stock options and restricted stock awards in respect of up to 13,000,000 shares of common stock to our employees, directors, independent contractors and consultants. In February 2010, our shareholders approved an amendment and extension of the 2000 Stock Incentive Plan to increase the aggregate number of shares of common stock authorized for issuance pursuant to the 2000 Stock Incentive Plan from 9,000,000 to 13,000,000 and to extend the expiration date of the 2000 Stock Incentive Plan
F-14
Table of Contents
from 2010 to 2020. Under the terms of the 2000 Stock Incentive Plan, options are granted at the fair market value of the stock at the date of grant and expire no later than ten years after the date of grant. Options granted under the plan generally vest over four years, but the terms of the 2000 Stock Incentive Plan provide for accelerated vesting if there is a change in control of the Company. Historically, we have issued authorized but previously unissued shares of common stock upon option exercises. However, we do not have a policy regarding the issuance or repurchase of shares upon option exercise or the source of those shares. No restricted stock awards have been issued under the 2000 Stock Incentive Plan.
We recognize the cost relating to stock-based payment transactions in the financial statements over the period services are rendered according to the fair value of the stock-based awards issued.
We calculate the fair value for employee stock options using a Black-Scholes option pricing model at the time the stock options are granted and that amount is amortized over the vesting period of the stock options, which is generally up to four years. The fair value for employee stock options granted during Fiscal 2011 and 2010 was calculated based on the following assumptions: risk-free interest rate ranging from 0.63% to 2.58% and 0.73% to 3.05%, respectively; dividend yield of 0%; weighted-average volatility factor of the expected market price of our common stock of 59.4% and 60.4%, respectively; and weighted-average expected life of the options ranging from 2 to 7 years depending on the vesting provisions of each option. The fair value for employee stock options granted during Fiscal 2009 was calculated based on the following assumptions: risk-free interest rate ranging from 0.66% to 3.19%; dividend yield of 0%; volatility factor of the expected market price of our common stock of 58.6%; and weighted-average expected life of the option ranging from 2 to 7 years depending on the vesting provisions of each option. The expected life of the options is based on the historical exercise behavior of our employees. The expected volatility factor is based on the historical volatility of the market price of our common stock as adjusted for certain events that management deemed to be non-recurring and non-indicative of future events.
We recognized share-based compensation cost of $1.8 million, $1.4 million and $1.2 million for Fiscal 2011, 2010 and Fiscal 2009, respectively. For Fiscal 2011, 2010 and 2009, we recognized excess tax benefits resulting from the exercise of stock options of approximately $0.2 million, $1.4 million and $0.1 million, respectively. The excess tax benefits had a positive effect on cash flow from financing activities with a corresponding reduction in cash flow from operating activities in Fiscal 2011, 2010 and 2009 of $0.2 million, $1.4 million and $0.1 million, respectively. During Fiscal 2011, 2010 and 2009, we issued 159,254 shares, 1,112,963 shares and 13,750 shares, respectively, of common stock, net of shares withheld, in connection with the exercise of stock options.
The following table summarizes information related to our stock option activity for Fiscal 2011:
| Number of Shares |
Weighted Average Exercise Price |
|||||||
| Outstanding at beginning of the year |
5,839,334 | $ | 2.50 | |||||
| Granted |
1,335,000 | 3.90 | ||||||
| Exercised |
(255,500 | ) | 1.78 | |||||
| Forfeited |
(167,500 | ) | 3.23 | |||||
| Expired |
(61,250 | ) | 2.49 | |||||
|
|
|
|||||||
| Outstanding at end of the year |
6,690,084 | $ | 2.79 | |||||
|
|
|
|||||||
| Exercisable at end of the year |
4,428,994 | |||||||
|
|
|
|||||||
| Weighted average fair value per share of options granted during the year |
$ | 2.05 | ||||||
|
|
|
|||||||
The weighted average fair value per share of options granted during Fiscal 2010 and 2009 was $1.59 and $1.04, respectively.
F-15
Table of Contents
The following table summarizes information about options outstanding and exercisable at June 30, 2011:
| Options Outstanding | Options Exercisable | |||||||||||||||||||||
| Range
of |
Number Outstanding |
Weighted Average Exercise Price |
Weighted Average Remaining Contractual Life |
Number Exercisable |
Weighted Average Exercise Price |
Weighted Average Remaining Contractual Life |
||||||||||||||||
| $1.35-$2.59 |
3,549,584 | $ | 2.21 | 4.9 | 3,045,369 | $ | 2.18 | 4.6 | ||||||||||||||
| $2.63-$5.23 |
3,140,500 | $ | 3.45 | 7.8 | 1,383,625 | $ | 3.35 | 6.3 | ||||||||||||||
The total intrinsic value of options outstanding and options exercisable was $22.7 million at June 30, 2011. The total intrinsic value of options exercised during Fiscal 2011, 2010 and 2009 was approximately $0.7 million, $4.4 million and $9,000, respectively. As of June 30, 2011, there was approximately $1.6 million of total unrecognized compensation cost related to non-vested stock options, which is expected to be recognized over a weighted-average period of 2 years.
We had 9.9 million shares of common stock reserved for future issuance related to stock options at June 30, 2011.
NOTE 8 – INCOME TAXES
We recognize deferred income tax assets and liabilities based upon differences between the financial reporting and tax bases of assets and liabilities. We measure such assets and liabilities using the enacted tax rates and laws that will be in effect when the differences are expected to reverse.
We recorded a liability for unrecognized tax benefits of approximately $1.0 million at June 30, 2010 which included accrued interest of approximately $0.1 million, and included such liabilities in accrued expenses and other current liabilities on the accompanying consolidated balance sheets. We recognize interest accrued related to unrecognized tax benefits in interest expense. During the three-month period ended March 31, 2011, our liability for unrecognized tax benefits decreased by approximately $1.0 million and our income tax provision and interest expense decreased by $0.9 million and $0.1 million, respectively, as a result of the lapse of the applicable statute of limitations. We are no longer subject to tax examinations by tax authorities for fiscal years ended on or prior to June 30, 2007.
We recorded an income tax provision of $13.7 million, $13.9 million and $9.6 million for Fiscal 2011, 2010 and 2009, respectively. The income tax provision consisted of the following:
| Year Ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Current: |
||||||||||||
| Federal |
$ | 11,554,447 | $ | 10,847,528 | $ | 8,199,853 | ||||||
| State |
2,064,327 | 2,370,029 | 1,158,154 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
13,618,774 | 13,217,557 | 9,358,007 | |||||||||
|
|
|
|
|
|
|
|||||||
| Deferred: |
||||||||||||
| Federal |
77,042 | 543,787 | 181,483 | |||||||||
| State |
5,502 | 132,009 | 60,831 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
82,544 | 675,796 | 242,314 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total income tax provision |
$ | 13,701,318 | $ | 13,893,353 | $ | 9,600,321 | ||||||
|
|
|
|
|
|
|
|||||||
Deferred income taxes reflect the net effect of temporary differences between the carrying amount of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. The tax effects of temporary differences that give rise to deferred income tax assets and deferred income tax liabilities are as follows:
F-16
Table of Contents
| June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Deferred income tax assets: |
||||||||||||
| Bad debt and notes receivable reserve |
$ | 98,968 | $ | 17,023 | $ | — | ||||||
| Other |
478,028 | 56,873 | 75,573 | |||||||||
| Impairment charge |
487,046 | 742,836 | 999,617 | |||||||||
| Share-based compensation |
2,757,686 | 2,154,254 | 1,861,818 | |||||||||
|
|
|
|
|
|
|
|||||||
| Deferred income tax assets |
3,821,728 | 2,970,986 | 2,937,008 | |||||||||
| Deferred income tax liabilities: |
||||||||||||
| Depreciable/amortizable assets |
(7,549,964 | ) | (6,527,954 | ) | (5,818,179 | ) | ||||||
| Basis difference in tangible assets |
(528,829 | ) | (617,553 | ) | (617,553 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Deferred income tax liabilities |
(8,078,793 | ) | (7,145,507 | ) | (6,435,732 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net deferred income tax liabilities |
$ | (4,257,065 | ) | $ | (4,174,521 | ) | $ | (3,498,724 | ) | |||
|
|
|
|
|
|
|
|||||||
After consideration of all the evidence, both positive and negative (including, among others, our projections of future taxable income and profitability in recent fiscal years), management determined that no valuation allowance was necessary at June 30, 2011, 2010 and 2009 to reduce the deferred income tax assets to the amount that will more likely than not be realized. At June 30, 2011, we did not have any net operating losses available for carryforward.
A reconciliation of the statutory federal income tax rate with our effective income tax rate for the years ended June 30, 2011, 2010 and 2009 is as follows:
| Year Ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Statutory federal rate |
35.00 | % | 35.00 | % | 35.00 | % | ||||||
| State income taxes, net of federal income tax benefit |
3.65 | 3.58 | 3.58 | |||||||||
| Change in liability for unrecognized tax benefit |
(2.39 | ) | — | — | ||||||||
| Other non-deductible items |
0.17 | (0.06 | ) | 0.01 | ||||||||
|
|
|
|
|
|
|
|||||||
| Effective tax rate |
36.43 | % | 38.52 | % | 38.59 | % | ||||||
|
|
|
|
|
|
|
|||||||
NOTE 9 – SHARE REPURCHASE PROGRAM
Our Board of Directors approved a previously announced stock repurchase program to authorize the repurchase of 15,000,000 shares of our common stock. Any such repurchases will be made from time to time at the discretion of our management in the open market or in privately negotiated transactions subject to market conditions and other factors. As of August 31, 2011, we had repurchased 11,907,004 shares of our common stock for approximately $25.0 million.
NOTE 10 – EMPLOYEE BENEFIT PLAN
In January 1997, we adopted a tax qualified employee savings and retirement plan covering our eligible employees. The Continucare Corporation 401(k) Profit Sharing Plan (the “401(k) Plan”) was most recently amended and restated in December 2008. The 401(k) Plan is intended to qualify under Section 401 of the Internal Revenue Code (the “Code”) and contains a feature described in Code Section 401(k) under which a participant may elect to have his or her compensation reduced by up to 75% (subject to IRS limits) and have that amount contributed to the 401(k) Plan. In October 2001, the Internal Revenue Service issued a favorable determination letter for the 401(k) Plan, and the latest amendment and restatement has been timely submitted to the Internal Revenue Service for a new favorable determination letter.
Under the 401(k) Plan, new employees who are at least 18 years of age are eligible to participate in the 401(k) Plan after 90 days of service. Eligible employees may elect to contribute to the 401(k) Plan up to a maximum amount of tax deferred contribution allowed by the Internal Revenue Code. We may, at our discretion, make a matching contribution and a non-elective contribution to the 401(k) Plan. There were no matching contributions for the years ended June 30, 2011, 2010 or 2009. Participants in the 401(k) Plan would not begin to vest in the employer contribution until the end of two years of service, with full vesting achieved after five years of service.
F-17
Table of Contents
NOTE 11—COMMITMENTS AND CONTINGENCIES
Legal Proceedings
We are involved in legal proceedings incidental to our business that arise from time to time in the ordinary course of business including, but not limited to, claims related to the alleged malpractice of employed and contracted medical professionals, workers’ compensation claims and other employee-related matters, and minor disputes with equipment lessors and other vendors. We have recorded an accrual for claims related to legal proceedings, which includes amounts for insurance deductibles and projected exposure, based on management’s estimate of the ultimate outcome of such claims. We do not believe that the ultimate resolution of these matters will have a material adverse effect on our business, results of operations, financial condition, or cash flows. However, the results of these matters cannot be predicted with certainty, and an unfavorable resolution of one or more of these matters could have a material adverse effect on our business, results of operations, financial condition, cash flow, and prospects.
Contingencies
CMS is performing audits of selected Medicare Advantage plans to validate the provider coding practices under the risk-adjustment methodology used to reimburse Medicare Advantage plans. These audits involve a review of a sample of medical records for the HMO contracts selected for audit. CMS has selected for audit several of the contracts of our HMO affiliates for the 2007 contract year and we expect that CMS will continue conducting such audits beyond the 2007 contract year. Due to the uncertainties principally related to CMS’ audit payment adjustment methodology, we are unable to determine whether these audits would ultimately result in an unfavorable adjustment to us. Accordingly, we are unable to estimate the financial impact of such adjustment if one occurs as a result of these audits. Although the amount of the adjustment to us, if any, is not reasonably estimable at this time, such adjustment may have a material adverse effect on our results of operations, financial position, and cash flows.
Leases
We lease office space and equipment under various non-cancelable operating leases. Rent expense under such operating leases was approximately $3.5 million, $2.9 million and $2.7 million for the years ended June 30, 2011, 2010 and 2009, respectively. Future annual minimum payments under such leases as of June 30, 2011 are as follows:
| For the fiscal year ending June 30, |
||||
| 2012 |
$ | 3,360,551 | ||
| 2013 |
2,609,305 | |||
| 2014 |
2,484,637 | |||
| 2015 |
2,232,559 | |||
| 2016 and thereafter |
1,431,694 | |||
|
|
|
|||
| Total |
$ | 12,118,746 | ||
|
|
|
NOTE 12 – VALUATION AND QUALIFYING ACCOUNTS
Activity in our valuation and qualifying accounts consists of the following:
| Year ended June 30, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Allowance for doubtful accounts related to accounts and other receivables: |
||||||||||||
| Balance at beginning of period |
$ | 44,129 | $ | — | $ | 783,741 | ||||||
| Provision for doubtful accounts |
392,702 | 118,895 | — | |||||||||
| Acquisition of sleep diagnostic centers |
407,514 | — | — | |||||||||
| Write-offs of uncollectible accounts receivable |
(519,791 | ) | (74,766 | ) | (783,741 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Balance at end of period |
$ | 324,554 | $ | 44,129 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
NOTE 13 – RELATED PARTY TRANSACTIONS
We became a party to a lease agreement for office space owned by Dr. Luis Cruz, a director of the Company
F-18
Table of Contents
through February 2010. For Fiscal 2011, 2010 and 2009, expenses related to this lease were approximately $0.4 million for each fiscal year. This lease is scheduled to terminate on December 31, 2011 with an option to renew for an additional five years.
Effective November 1, 2007, we entered into agreements with Centers of Medical Excellence, Inc., an entity owned by Dr. Cruz pursuant to which this entity acted as one of our independent physician affiliates in connection with the provision of primary care health services to a limited number of Medicare Advantage members enrolled in plans sponsored by CarePlus Health Plans, Inc. The arrangement was on substantially similar terms to arrangements we have with our other independent physician affiliates under at risk arrangements where we provide medical utilization services and pay a primary care capitation fee to the provider. Under this arrangement, CarePlus paid us a monthly capitation fee based on the number of CarePlus Medicare Advantage members who selected Centers of Medical Excellence as their primary care provider and we in turn paid a monthly primary care capitation fee to Centers of Medical Excellence. Centers of Medical Excellence was also eligible to receive a bonus from us if they operated in a cumulative surplus. For Fiscal 2011, 2010 and 2009, we recognized an operating profit of $0 million, $0.3 million and an operating loss of $0.2 million, respectively, related to this arrangement. Effective December 31, 2009, we terminated our agreements with Centers of Medical Excellence, Inc.
On September 19, 2008, we purchased an aggregate of 400,000 shares of our common stock from certain family trusts of Dr. Cruz. Dr. Cruz does not have a beneficial ownership in the shares of common stock held by these family trusts. Continucare paid $2.14 per share for the shares for an aggregate purchase price of $856,000. The per share purchase price paid by Continucare represented a 10% discount from the closing price of Continucare’s common stock on September 19, 2008.
On September 19, 2008, we purchased an aggregate of 600,000 shares of our common stock from Mr. Garcia. Continucare paid $2.14 per share for the shares for an aggregate purchase price of $1,284,000. The per share purchase price paid by Continucare represented a 10% discount from the closing price of Continucare’s common stock on September 19, 2008.
On October 23, 2008, we entered into a joint venture with Dr. Jacob Nudel, a director of the Company, that sought to establish medical provider networks to provide services on an outpatient basis to patients sustaining injuries related to automobile accidents, which we refer to as special purpose provider networks. Under the revenue and cost sharing provisions of the joint venture, provided that we had a liquidation preference with respect to 100% of our capital contributions, (i) all ordinary cash flow of the joint venture would have been distributed to us and Dr. Nudel, pro rata in accordance with the parties ownership interest, and (ii) all net proceeds from capital transaction or liquidation proceeds would have been distributed, first, to us until such time as we had received aggregate distributions equal to our aggregate capital contributions, and thereafter, to us and Dr. Nudel, pro rata in accordance with the parties ownership interest. The Company and Dr. Nudel each had a 50% ownership interest in the joint venture. For Fiscal 2011, 2010 and 2009, we recorded operating expenses of approximately $0 million, $0.4 million and $0.3 million, respectively, related to the joint venture. In April 2010, we terminated the business activities of the joint venture and recognized a loss on impairment of fixed assets of approximately $0.1 million during Fiscal 2010.
On January 15, 2009, we purchased an aggregate of 1,100,000 shares of its common stock from Mr. Garcia. Continucare paid $1.71 per share for the shares for an aggregate purchase price of $1,881,000. The per share purchase price paid by Continucare was the closing price of Continucare’s common stock on January 15, 2009.
On March 12, 2009, we purchased an aggregate of 350,000 shares of its common stock from certain family trusts of Dr. Cruz. Dr. Cruz does not have a beneficial ownership in the shares of common stock held by these family trusts. Continucare paid $1.69 per share for the shares for an aggregate purchase price of $591,500. The per share purchase price paid by Continucare represented a 5% discount from the closing price of Continucare’s common stock on March 12, 2009.
F-19
Table of Contents
NOTE 14 – QUARTERLY CONSOLIDATED FINANCIAL INFORMATION (UNAUDITED)
| For the Year Ended June 30, 2011 | ||||||||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
Full Year |
||||||||||||||||
| Total revenue |
$ | 78,941,845 | $ | 80,314,998 | $ | 85,651,548 | $ | 88,549,817 | $ | 333,458,208 | ||||||||||
| Net income |
$ | 5,792,754 | $ | 6,198,170 | $ | 7,257,346 | $ | 4,663,679 | $ | 23,911,949 | ||||||||||
| Net income per common share: |
||||||||||||||||||||
| Basic |
$ | .10 | $ | .10 | $ | .12 | $ | .08 | $ | .39 | ||||||||||
| Diluted |
$ | .09 | $ | .10 | $ | .12 | $ | .07 | $ | .38 | ||||||||||
| For the Year Ended June 30, 2010 | ||||||||||||||||||||
| First Quarter |
Second Quarter |
Third Quarter |
Fourth Quarter |
Full Year |
||||||||||||||||
| Total revenue |
$ | 75,972,366 | $ | 75,256,100 | $ | 80,274,545 | $ | 79,288,452 | $ | 310,791,463 | ||||||||||
| Net income |
$ | 5,308,339 | $ | 5,288,679 | $ | 5,900,611 | $ | 5,678,678 | $ | 22,176,307 | ||||||||||
| Net income per common share: |
||||||||||||||||||||
| Basic |
$ | .09 | $ | .09 | $ | .10 | $ | .09 | $ | .37 | ||||||||||
| Diluted |
$ | .09 | $ | .09 | $ | .09 | $ | .09 | $ | .36 | ||||||||||
Basic and diluted net income per common share for each of the quarters presented above are based on the respective weighted average number of common shares outstanding for the quarters. The sum of the quarterly basic and diluted net income per common share amounts may not be equal to the full year basic and diluted net income per common share amounts due to rounding.
NOTE 15 – SUBSEQUENT EVENTS
On July 1, 2011, a putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Kathryn Karnell, Trustee and the Aaron and Kathryn Karnell Revocable Trust U/A Dtd 4/9/09 against Continucare, the members of the Continucare Board, individually, Metropolitan, and the merger subsidiary. Also on July 1, 2011, a second putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Steven L. Fuller against Continucare, the members of the Continucare Board, individually, Metropolitan, and the merger subsidiary. On July 6, 2011, a third putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Hilary Kramer against Continucare, the members of the Continucare board of directors, individually, Metropolitan, and the merger subsidiary. On July 12, 2011, a fourth putative class action was filed in the Circuit Court of the Eleventh Judicial Circuit in and for Miami-Dade County, Florida by Jamie Suprina against Continucare, the members of the Continucare board of directors, individually, Metropolitan, and the merger subsidiary. Each of these suits sought to enjoin the proposed transaction between Continucare and Metropolitan, as well as attorneys’ fees. The Fuller, Kramer, and Suprina suits also sought rescissory and other money damages.
On July 28, 2011, an order was granted by the Court to consolidate these actions and appoint the lead plaintiff and the lead plaintiff’s counsel.
On August 12, 2011, the defendants entered into a preliminary settlement agreement (“Memorandum of Understanding”) with the lead plaintiff regarding the settlement of the actions. In connection with the Memorandum of Understanding, Continucare agreed to make certain additional disclosures to its shareholders, which are contained in Continucare's Form 8-K filed with the SEC on August 12, 2011. Subject to the completion of certain confirmatory discovery by the lead plaintiff’s counsel, the parties will enter into a definitive stipulation of settlement. The definitive stipulation of settlement will be subject to customary conditions, including consummation of the merger and court approval following notice to Continucare’s shareholders. In the event that the parties enter into a definitive stipulation of settlement, a hearing will be scheduled at which the court will consider the fairness, reasonableness
F-20
Table of Contents
and adequacy of the settlement which, if finally approved by the court, will resolve all of the claims that were or could have been brought in the actions being settled, including all claims relating to the merger transaction, the merger agreement, and any disclosure made in connection therewith. In addition, in connection with the settlement, the parties contemplate that the lead plaintiff’s counsel will petition the court for an award of attorneys’ fees and expenses to be paid by Continucare. There can be no assurance that the parties will ultimately enter into a definitive stipulation of settlement or that the court will approve the settlement. In such event, the litigation would resume.
Continucare, the director defendants, and Metropolitan vigorously deny all liability with respect to the facts and claims alleged in the lawsuits, and specifically deny that supplemental disclosure was required under any applicable rule, statute, regulation or law. However, solely to avoid the risk of delaying or adversely affecting the merger and the related transactions and to minimize the expense of defending the lawsuits, Continucare, its directors, and Metropolitan agreed to the settlement described above.
On August 22, 2011, at a Special Meeting of Shareholders, the Merger Agreement and the transactions contemplated thereby were approved by Continucare shareholders. Assuming all conditions to closing are met, Continucare and Metropolitan expect to close the acquisition on or about the end of September 2011. There can be no assurance, however, that the acquisition will close.
F-21
Table of Contents
EXHIBIT INDEX
| Description |
Exhibit Number |
|||
| Subsidiaries of the Company |
21.1 | |||
| Consent of Independent Registered Public Accounting Firm |
23.1 | |||
| Section 302 Certification of Chief Executive Officer |
31.1 | |||
| Section 302 Certification of Chief Financial Officer |
31.2 | |||
| Certification Pursuant to 18 U.S.C. Section 1350, as Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
32.1 | |||
| Certification Pursuant to 18 U.S.C. Section 1350, as Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
32.2 | |||