Attached files
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2010
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
001-33071
(Commission File Number)
EHEALTH, INC.
(Exact name of registrant as specified in its charter)
| Delaware | 56-2357876 | |
| (State of incorporation) | (I.R.S. Employer Identification No.) |
440 EAST MIDDLEFIELD ROAD
MOUNTAIN VIEW, CALIFORNIA 94043
(Address of principal executive offices, including zip code)
(650) 584-2700
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class |
Name of Each Exchange on Which Registered | |
| Common Stock, par value $0.001 per share | The NASDAQ Stock Market LLC | |
| (NASDAQ Global Select Market) |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. YES ¨ NO x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. YES ¨ NO x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. YES x NO ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulations S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). YES ¨ NO ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer ¨ | Accelerated filer x | Non-accelerated filer ¨ | Smaller reporting company ¨ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). YES ¨ NO x
Based on the closing price of the registrant’s common stock on the last business day of the registrant’s most recently completed second fiscal quarter, which was June 30, 2010, the aggregate market value of its shares (based on a closing price of $11.37 per share) held by non-affiliates was $178,350,741. Shares of the registrant’s common stock held by each executive officer and director and by each entity or person that owned 5 percent or more of the registrant’s outstanding common stock were excluded in that such persons may be deemed to be affiliates. This determination of affiliate status is not necessarily a conclusive determination for other purposes.
As of February 28, 2011, 21,349,017 shares of the registrant’s common stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s Definitive Proxy Statement for the 2011 Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010, are incorporated by reference into Part III of this Annual Report on Form 10-K to the extent stated herein.
Table of Contents
TABLE OF CONTENTS
Table of Contents
| ITEM 1. | BUSINESS |
In addition to historical information, this Annual Report on Form 10-K contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. These statements include, among other things, statements concerning impact of the PlanPrescriber acquisition on our growth in the Medicare market; plans to market and license our ecommerce technology to state exchanges and our competitors in this business; timing and impact of medical loss ratio regulations and commission rate changes; elements of our strategy; the impact of health care reform laws on the health insurance industry and on our business; expenditures related to the development of our business; our projections relating to future revenue growth and earnings per share; factors impacting the success of our Medicare business; our expectation that our marketing and advertising expenses will decrease in absolute dollars in 2011; reduction of our cost of acquiring new members; our continuing to enter into relationships with marketing partners in China; expansion into new business areas and additional geographic regions; our utilization of certain tax benefits and the related impact on our financial statements and our cash outlay for taxes for 2011; our expectations and projections relating to our commission rates and other carrier supported programs; our expectation that commission revenue will decrease in absolute dollars and as a percentage of revenue in 2011; our expectation that other revenue will increase in absolute dollars and as a percentage of revenue in 2011; our expectation that our cost of revenue will increase in absolute dollars; our expectation that our customer care and enrollment, technology and content and general and administrative expenses will increase in absolute dollars in 2011; estimates relating to critical accounting policies and related impact on our financial statements; our expectation that stock based compensation will increase; the sufficiency of our cash, cash equivalents and marketable securities; future capital requirements; our potential for collection issues with any of our customers; expectations regarding our future effective tax rate; as well as other statements regarding our future operations, financial condition, prospects and business strategies. These forward-looking statements are subject to certain risks and uncertainties that could cause our actual results to differ materially from those reflected in the forward-looking statements. Factors that could cause or contribute to such differences include, but are not limited to, those discussed in this report, and in particular, the risks discussed under the heading “Risk Factors” in Part I, Item 1A of this report and those discussed in our other Securities and Exchange Commission filings. The following discussion should be read in conjunction with our audited consolidated financial statements and related notes contained therein that appear elsewhere in this report. We undertake no obligation to revise or publicly release the results of any revision to these forward-looking statements. Given these risks and uncertainties, you are cautioned not to place undue reliance on such forward-looking statements.
General
We are the leading online source of health insurance for individuals, families and small businesses. Through our website addresses (www.eHealth.com, www.eHealthInsurance.com, www.eHealthMedicare.com and www.PlanPrescriber.com), consumers can get quotes from leading health insurance carriers, compare plans side by side, and apply for and purchase individual and family, small business, short-term, ancillary and Medicare-related health insurance plans. Our ecommerce technology also enables us to deliver consumers’ health insurance applications electronically to health insurance carriers. As a result, we simplify and streamline the complex and traditionally paper-intensive health insurance sales and purchasing process.
We have invested heavily in technology and content related to our ecommerce platform. We have also invested significant time and resources in obtaining licenses to sell health insurance in all 50 states and the District of Columbia, developing diverse member acquisition programs and establishing relationships with over 180 leading insurance carriers, enabling us to offer thousands of health insurance plans online. Our ecommerce platform can be accessed directly through our website as well as through our network of marketing partners.
In April 2010, we acquired PlanPrescriber, Inc. (“PlanPrescriber,” formerly Experion Systems, Inc.), a privately-held company. PlanPrescriber is a leading provider of online tools to help seniors navigate Medicare health insurance options.
1
Table of Contents
We were incorporated in Delaware in November 1997. Our headquarters are located at 440 East Middlefield Road, Mountain View, California 94043, and our telephone number is (650) 584-2700. Our corporate internet website addresses are www.ehealth.com and www.ehealthinsurance.com. We make our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and amendments to those reports, available free of charge on the Investor Relations page of our web site as soon as reasonably practicable after we file these reports with the Securities and Exchange Commission. The information on or that can be accessed through our websites is not part of this Annual Report on Form 10-K. Further, a copy of this Annual Report on Form 10-K is located at the SEC’s Public Reference Room at 100 F Street, NE, Room 1580, Washington, D.C. 20549. Information on the operation of the Public Reference Room can be obtained by calling the SEC at 1-800-SEC-0330. The SEC maintains an Internet site that contains reports, proxy and information statements and other information regarding our filings at http://www.sec.gov.
Our Business Model
Individual, Family and Small Business Health Insurance Plans
We generate revenue primarily from commissions we receive from health insurance carriers whose individual, family and small business policies are purchased through our ecommerce platform. The commission payments we receive are typically a percentage of the premium on an individual, family or small business health insurance policy that we sold and are made to us on a monthly basis for as long as a policy remains active with us. As a result, much of our revenue for a given financial reporting period relates to policies that we sold prior to the beginning of the period and is recurring in nature. Additionally, health insurance pricing, which is set by the health insurance carrier and approved by state regulators, is not subject to negotiation or discounting by health insurance carriers or our competitors.
Medicare Health Insurance Plans
We began actively marketing the availability of Medicare related insurance plans during 2010 through our online Medicare plan platforms (www.eHealthMedicare.com and www.PlanPrescriber.com). These platforms enable consumers to research and compare Medicare-related insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. The revenue we have generated in our Medicare plan business is primarily referral fees paid to us based on leads generated by our online platforms that are delivered and sold to third parties. In 2010 we also launched online application capabilities for certain Medicare plans, and telephonic enrollment capabilities through our new customer care center in Salt Lake City, Utah. To the extent that we assist in the sale of Medicare-related insurance plans as a health insurance agent, we generate revenue from commissions we receive from health insurance carriers.
Technology Licensing
We also derive revenue from licensing the use of our health insurance ecommerce technology. Our technology platform enables health insurance carriers and agents to market and distribute health insurance plans online. Health insurance carriers or agents that license our technology typically pay us implementation fees and performance-based fees that are based on metrics such as submitted health insurance applications. We also recently began to license our ecommerce technology for use by government agencies and intend to market it to states implementing health insurance exchanges as a result of health care reform legislation. In our government technology licensing business, we may earn a combination of fixed license fees and time- and materials-based fees or we may be paid performance-based fees.
Online Sponsorship and Advertising
We also derive revenue from our online sponsorship advertising program that allows carriers to purchase advertising space in specific markets in a sponsorship area on our website. In return, we are typically paid a monthly fee and a performance-based fee based on metrics such as submitted health insurance applications.
2
Table of Contents
Industry Background
The purchase and sale of health insurance has historically been a complex, time-consuming and paper-intensive process. This complexity can make it difficult to make informed health insurance decisions. In addition, the human error that arises from traditional paper-intensive distribution has historically resulted in a high number of incomplete and inaccurate applications being submitted to health insurance carriers. Incomplete and inaccurate paper applications often result in back-and-forth communications, delay and additional cost. The Internet’s convenient, information-rich and interactive nature offers the opportunity to provide consumers with more organized information, a broader choice of plans and a more efficient process than have typically been available from traditional health insurance distribution channels.
Individual, family and small business health insurance has historically been sold by independent insurance agents and, to a lesser degree, directly by insurance companies. Most of these agents are self-employed or part of small agencies, and they typically service only their local communities. In addition, many of these agents sell health insurance from a limited number of insurance carriers (in some cases only one), resulting in a reduced selection of plans for the consumer.
Medicare is a federal program that provides persons sixty-five years of age and over, and some persons under the age of sixty-five with certain conditions, with hospital and medical insurance benefits. The Centers for Medicare and Medicaid Services, or CMS, an agency of the United States Department of Health and Human Services, administers this original Medicare program. CMS also contracts with private health insurance carriers under the Medicare Advantage and Medicare Part D prescription drug programs for these health insurance carriers to provide health insurance and prescription drug benefits to Medicare eligible individuals. Medicare Advantage plans replace original Medicare. Medicare Part D prescription drug plans provide prescription drug coverage that original Medicare does not provide. In addition, health insurance carriers offer Medicare Supplement health insurance plans, which help to pay health care costs not covered through original Medicare. Medicare-related insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans, are typically marketed and sold by insurance carriers, also known as plan sponsors, through a combination of dedicated internal sales representatives and licensed independent brokers and agents. CMS also offers plan information, comparison tools, call centers and online enrollment for Medicare Advantage and Medicare Part D prescription drug plans.
Recent Developments
In March 2010, the federal Patient Protection and Affordable Care Act and related amendments in the Health Care and Education Reconciliation Act were signed into law. These health care reform laws contain provisions that have and will continue to change the health insurance industry in substantial ways. Among several other provisions, they include a mandate requiring individuals to be insured or face tax penalties; a mandate that certain employers offer their employees group health insurance coverage or face tax penalties; prohibitions against insurance companies using pre-existing health conditions as a reason to deny an application for health insurance; medical loss ratio requirements that require each health insurance carrier to spend a certain percentage of their premium revenue on reimbursement for clinical services and activities that improve health care quality; establishment of state and/or federal health insurance exchanges to facilitate access to, and the purchase of, health insurance; and subsidies and cost-sharing credits to make health insurance more affordable for those below certain income levels.
While many aspects of health care reform do not become effective until 2014, health insurance carriers are required to maintain medical loss ratios of eighty percent in their individual and family health insurance business beginning in 2011. The implementation of the medical loss ratio requirements by insurance carriers has resulted in a reduction in the commission rates that we are paid as a result of our selling individual and family health insurance plans. These reductions will begin to impact our individual and family health insurance plan commission-based revenue starting in 2011.
3
Table of Contents
Our Strategy
Our objective is to continue to strengthen our position as the leading online distribution platform for health insurance sold to individuals, families and small businesses and to enter new business areas where this platform may be leveraged.
Key elements of our strategy are to:
Increase Our Brand Awareness. We believe that building greater awareness of our brand is critical for our continued growth. A significant percentage of our website traffic is direct, and we intend to attempt to grow our direct website traffic by strengthening our brand awareness through a variety of marketing and public relations efforts.
Offer the Best Consumer Experience. We believe that providing the best consumer experience increases market adoption of our services, builds our brand awareness, drives word-of-mouth referrals and improves our visitor-to-member conversion rates. We intend to continue to further develop an online experience that empowers consumers with the knowledge, choice and services they need to select and purchase health insurance plans that best meet their needs.
Extend Our Technology Leadership. We believe that our technology infrastructure and online platform give us a significant competitive advantage for the distribution of individual, family and small business health insurance. To extend our leadership position, we plan to continue to enhance our platform and its key capabilities to increase functionality, reliability, scalability and performance.
Broaden Our Carrier Network and Product Portfolio. Our goal is to continue to add new health insurance carriers and health insurance plans to our ecommerce platform, including plans for Medicare eligible individuals and plans for those who are not eligible for Medicare. We also seek to deepen our technology integration with health insurance carriers, allowing us to further streamline the sales, underwriting and member fulfillment processes and increase revenue opportunities for us and health insurance carriers.
Grow Our Medicare Plan Business. We believe that our technology can be used to streamline and simplify the Medicare plan purchasing process. We seek to enhance the technology behind our online Medicare platforms and further develop demand generation programs in the Medicare market. We plan to continue selling Medicare leads that we generate to third parties and to sell Medicare plans ourselves both online and through our call centers.
Expand Our Technology Licensing Business. Our technology licensing business allows health insurance carriers to use our ecommerce platform to market and sell their own health insurance plans on their websites. It also allows their agents to utilize our technology to power online quoting, content and application submission processes. We intend to attempt to further penetrate the market for online sales solutions for health insurance carriers and their agents. Growth in this business will allow us to enter new markets and participate in business transacted in the traditional agent distribution channel.
Compete in the Government Exchange Market. The recently enacted federal Patient Protection and Affordable Care Act and related amendments in the Health Care and Education Reconciliation Act require the establishment of state health insurance exchanges by 2014 to, among other things, facilitate online access to and the purchase of health insurance. We intend to compete for opportunities to license our technology platform that are presented by these requirements.
Diversify Our Revenue. We plan to continue to diversify our revenue by entering into new business areas where our technology, experience and relationships can be leveraged.
4
Table of Contents
Our Platform and Technology
Our ecommerce platforms organize and present voluminous and complex health insurance information in an objective format and empowers individuals, families and small businesses to research, analyze, compare and purchase a wide variety of health insurance plans. The plans we offer include major medical health insurance coverage such as preferred provider organization, health maintenance organization and indemnity plans, Medicare plans, short-term medical insurance, student health insurance, health savings account eligible health insurance plans and ancillary plans such as dental, vision and life insurance.
Elements of our platform include:
Online Rate Quoting and Comprehensive Plan Information. Our ecommerce platform instantly provides consumers online rate quotes and comprehensive plan benefit information from a large number of health insurance carriers. After entering a minimal amount of relevant information on our website, such as zip code, gender, age, date of birth, smoker or non-smoker and student status, our platform allows consumers to instantly receive a list of applicable health insurance plans and rate and benefit information in an easy-to-understand format. The consumer can sort through the quoted plans based on price, health insurance carrier, deductible amount, or search the list of quoted plans to obtain a subset based on certain consumer preferences.
Plan Comparison and Recommendations. We offer online comparison and recommendation tools that distill voluminous health insurance information. Our ecommerce platform enables consumers to compare and contrast health insurance plans in a side-by-side format based on plan characteristics such as price, plan type, deductible amount, co-payment amount and in-network and out-of-network benefits. To further assist consumers, our automated recommendation capability presents a short series of questions and recommends up to four health insurance plans based on the consumer’s input.
Online Application and Enrollment Forms. Health insurance applications vary widely by carrier and state. Our proprietary graphical Application Designer Tool allows us to capture each application’s unique business rules and build a corresponding online application in XML format. Our online application process offers our consumers significant improvements over the traditional, paper-intensive application process. It employs dynamic business logic to help individuals and families complete application and enrollment forms correctly in real-time. This reduces delay resulting from application rework, a significant problem with traditional health insurance distribution, where incomplete applications are mailed back and forth between the consumer, the traditional agent and the carrier. We further simplify the enrollment process by accepting electronic signature and electronic payment from our consumers.
Electronic Processing Interchange. Our Electronic Processing Interchange (“EPI”) technology integrates our online application process with health insurance carriers’ technology systems, enabling us to electronically deliver our consumers’ applications to health insurance carriers. This expedites the application process by eliminating manual delivery and reducing the need for data entry and human review. Through EPI, we also receive alerts and data from carriers, such as notification of underwriting approval or a request from a carrier for a consumer’s medical records for underwriting purposes, which we then relay electronically to the consumer. These features of our service help prevent applications from becoming delayed or rejected through inactivity of the consumer or the carrier.
Back Office Systems. Our proprietary back office customer relationship management system enables us to provide a full range of customer service tasks in an efficient, highly scalable and personalized manner. Using these tools, we can track each consumer throughout the application process, obtain real-time updates from the carrier, generate automated emails specific to each consumer and access a cross-sell engine and dashboard to identify and track cross-sell opportunities. Our auto-email system is feature-rich with HTML capability, customizable merge tags, granular segmentation and tracking capability.
5
Table of Contents
Carrier Relationships
We have developed partnerships with leading health insurance carriers in the United States, enabling us to offer thousands of health insurance plans online. As of December 31, 2010, we had relationships with over 180 individual, family and small business health insurance carriers, including large national carriers and well-established regional carriers. We typically enter into contractual agency relationships with health insurance carriers that are non-exclusive and terminable on short notice by either party for any reason. In addition, health insurance carriers often have the ability to amend our agreements unilaterally on short notice, including provisions in our agreements relating to our commission rates. In some cases, the amendment or termination of the agreements we have with health insurance carriers may impact the commissions we are paid on health insurance plans that we have already sold. Revenue derived from Aetna represented approximately 16% and 17% of our total revenue in 2009 and 2010, respectively. Revenue derived from carriers owned by WellPoint represented approximately 15% and 12% of our total revenue in 2009 and 2010, respectively. Revenue derived from carriers owned by UnitedHealthcare represented approximately 14% of our total revenue in both 2009 and 2010. Each of these health insurance carriers may terminate our agreements with them and, in some cases, as a result of the termination we may lose our right to receive commissions. In addition, many of our agreements with each of these health insurance carriers are generally amendable on short notice, including the provisions relating to our commission rates.
Marketing
We focus on building brand awareness, increasing website visitors and converting visitors into buyers. Our marketing initiatives are varied and numerous. They include:
Direct Marketing. Our direct member acquisition channel consists of consumers who access our website addresses (www.eHealth.com, www.eHealthInsurance.com, www.PlanPrescriber.com and eHealthMedicare.com) either directly or through algorithmic search listings on Internet search engines and directories.
Online Advertising. Our online advertising member acquisition channel consists of consumers who access our website through paid keyword search advertising from search engines such as Google, MSN and Yahoo!, as well as various Internet marketing programs such as banner advertising and email marketing.
Marketing Partners. Our marketing partner member acquisition channel consists of consumers who access our website through a network of affiliate partners and financial services and other companies. We have established a pay-for-performance network, comprised of hundreds of partners that drive consumers to our ecommerce platform. These partners fall into three general categories:
| • | Financial and online services partners in industries such as banking, insurance, mortgage and association partners. |
| • | Affiliate programs, including our marketing programs managed through Commission Junction. |
| • | Online advertisers and content providers that are specialists in paid and unpaid (algorithmic) search, as well as specialists in other types of Internet marketing. |
We generally compensate our marketing partners for their individual, family and small business health insurance referrals based on the consumer submitting a health insurance application to us. If a marketing partner is licensed to sell health insurance, we may share a percentage of the commission revenue we earn from the health insurance carrier for each member referred by that partner.
Technology and Content
We have a technology and content team consisting of 213 full-time employees as of December 31, 2010, of which 64 are located domestically and 149 are located at our subsidiary in Xiamen, China. Our technology and content team is responsible for ongoing enhancements to the features and functionality of our ecommerce platform, which we believe are critical to maintaining our technology leadership position in the industry.
6
Table of Contents
Government Regulation and Compliance
We distribute health insurance plans in all 50 states and in the District of Columbia. The health insurance industry is heavily regulated. Each of these jurisdictions has its own rules and regulations pertaining to the offer and sale of health insurance plans, typically administered by a department of insurance. State insurance departments have administrative powers relating to, among other things: regulating premium prices; granting and revoking licenses to transact insurance business; approving individuals and entities to which, and circumstances under which, commissions can be paid; regulating advertising, marketing and trade practices; monitoring broker and agent conduct; and imposing continuing education requirements. We are required to maintain valid life and/or health agency and/or agent licenses in each jurisdiction in which we transact health insurance business.
In addition to state regulations, we also are subject to regulations and guidelines issued by CMS that place a number of requirements on health insurance carriers and agents and brokers in connection with the marketing and sale of Medicare Advantage and Medicare Part D prescription drug plans. We are subject to similar requirements of state insurance departments with respect to our marketing and sale of Medicare Supplement plans. CMS and state insurance department regulations and guidelines include a number of prohibitions regarding the ability to contact Medicare eligible individuals and place many restrictions on the marketing of Medicare plans. For example, our health insurance carrier partners are required to obtain CMS or state department of insurance approval of certain aspects of our platforms, call center scripts and other marketing materials used to market Medicare plans. In addition, the laws and regulations applicable to the marketing and sale of Medicare plans are ambiguous, complex and, particularly with respect to regulations and guidance issued by CMS for Medicare Advantage and Medicare Part D prescription drug plans, change frequently.
Intellectual Property
We rely on a combination of trademark, copyright and trade secret laws in the United States and other jurisdictions as well as confidentiality procedures and contractual provisions to protect our proprietary technology and our brand. Our eHealth and eHealthInsurance trademarks have reached incontestability status with the U.S. Patent and Trademark Office, which means the marks have been in use for over five years and, subject to certain limited exceptions, no third party can contest the validity of the marks or our ownership of them. We also have filed patent applications that relate to certain of our technology and business processes.
Competition
The market for selling health insurance plans is highly competitive. We compete with entities and individuals that offer and sell health insurance plans utilizing traditional distribution channels as well as the Internet. Our current or potential competitors include the tens of thousands of local insurance agents across the United States who sell health insurance plans in their communities. There are a number of agents that operate websites and provide an online shopping experience for consumers interested in purchasing health insurance. Some local agents use “lead aggregator” services that use the Internet to find consumers interested in purchasing health insurance and are compensated for referring those consumers to the traditional agent. Most online agents operate in only one or very few states, and some represent only one or a limited number of health insurance carriers. In addition to health insurance brokers and agents, many health insurance carriers directly market and sell their plans to consumers through call centers and their own websites. Although we offer health insurance plans for many of these carriers, they also compete with us by offering their plans directly to consumers. In connection with our marketing of Medicare plans, we compete with the original Medicare program. In addition, CMS offers plan information, comparison tools, call centers and online enrollment for Medicare Advantage and Medicare Part D prescription drug plans.
In licensing our health insurance purchasing platform, we compete with companies providing technology that automates premium quoting, research and analysis of health insurance plans, member enrollment and other tools that support online sales efforts by health insurance carriers and their agents and brokers. We anticipate that in licensing our technology to government entities we will compete with these entities as well as system integrators, software companies, employee benefit service providers, technology consulting companies and others that have experience providing technology and services to federal or state governments.
7
Table of Contents
Seasonality
The number of individual and family health insurance applications submitted through our ecommerce platform has generally increased in our first quarter compared to our fourth quarter and in our third quarter compared to our second quarter. Conversely, we have generally experienced a decline or flattening of individual and family submitted applications in our second quarter compared to our first quarter and in our fourth quarter compared to our third quarter. The reasons for these seasonal patterns are not entirely clear. Since a significant portion of our marketing and advertising expenses are driven by the number of health insurance applications submitted on our ecommerce platform, those expenses are influenced by these seasonal patterns.
In our Medicare plan business, we generate the majority of leads and the majority of referral fees that we are paid for selling these leads during the fourth quarter. We also incur a significant portion of our Medicare plan related marketing expenses during the fourth quarter. We may not be paid for a considerable portion of the referral fees owed to us until the first quarter. This seasonality pattern results from the timing of the annual enrollment period when Medicare-eligible individuals can make changes to their Medicare Advantage or Medicare Part D prescription drug coverage for the following year.
As our business matures, other seasonality trends may develop and the existing seasonality and consumer behavior that we experience may change.
Employees
As of December 31, 2010, we had 641 full-time employees, of which 55 were in marketing and advertising, 242 were in customer care and enrollment, 213 were in technology and content and 131 were in general and administrative. None of our employees are represented by a labor union. We have not experienced any work stoppages and consider our employee relations to be good.
| ITEM 1A. | RISK FACTORS |
In addition to other information in this Annual Report on Form 10-K and in other filings we make with the Securities and Exchange Commission, the following risk factors should be carefully considered in evaluating our business as they may have a significant impact on our business, operating results and financial condition. If any of the following risks actually occurs, our business, financial condition, results of operations and future prospects could be materially and adversely affected. Because of the following factors, as well as other variables affecting our operating results, past financial performance should not be considered as a reliable indicator of future performance and investors should not use historical trends to anticipate results or trends in future periods.
Risks Related to Our Business
Changes and developments in the structure of the health insurance system in the United States could harm our business.
Our business depends upon the private sector of the United States health insurance system, its relative role in financing health care delivery and health insurance carriers’ use of, and payment of commissions to, agents and brokers to market individual and family health insurance plans. In March 2010, the federal Patient Protection and Affordable Care Act and related amendments in the Health Care and Education Reconciliation Act were signed into law. These health care reform laws contain provisions that have and will continue to change the industry in which we operate in substantial ways. Among several other provisions, they include a mandate requiring individuals to be insured or face tax penalties; a mandate that certain employers offer their employees group health insurance coverage or face tax penalties; requirements relating to employer contribution to employee health coverage; prohibitions against insurance companies using pre-existing health conditions as a reason to deny an application for health insurance; prohibitions on rescission of health insurance; prohibitions on lifetime limits; requirements for guaranteed renewability of health insurance plans; health insurance premium setting guidelines; limitations on deductibles and cost-sharing; medical loss ratio requirements that require each health insurance carrier to spend a certain percentage of their premium revenue on reimbursement for clinical
8
Table of Contents
services and activities that improve health care quality; minimum benefit levels for health insurance plans; establishment of state and/or federal health insurance exchanges to facilitate access to, and the purchase of, health insurance; optional open enrollment periods for individual health insurance; assistance for member run health insurance issuers; creation of multi-state health insurance plans to be offered on the exchanges and with oversight from the Office of Personnel Management; requirements for uniform disclosure relating to the costs and benefits of health insurance; government subsidized high risk pools; and subsidies and cost-sharing credits to make health insurance more affordable for those below certain income levels. Many aspects of health care reform do not go into effect until 2014, although certain provisions currently are effective, such as medical loss ratio requirements for individual, family and small business health insurance and a prohibition against insurance companies using pre-existing health conditions as a reason to deny the application of children for health insurance. Healthcare reform legislation requires various departments of the executive branch to adopt regulations implementing its provisions. In addition, state governments have adopted, and will continue to adopt, changes to their existing laws and regulations in light of federal healthcare reform legislation and regulations.
Challenges to the constitutionality of health care reform legislation have been initiated in the federal courts. The challenges center upon the constitutionality of the mandate to purchase health insurance. Decisions on the issue have been inconsistent. These decisions will be appealed and it is impossible to predict the outcome of them.
The implementation of health care reform could increase our competition; reduce or eliminate the need for health insurance agents or demand for the health insurance for individuals, families or small businesses that we sell; decrease the number of health insurance plans that we sell as well as the number of health insurance carriers offering them; cause health insurance carriers to apply more rigorous underwriting standards (until provisions in health care reform legislation limiting underwriting go into effect in 2014) or change the benefits and/or premiums for the plans they sell; or cause health insurance carriers to reduce the amount they pay for our services or change our relationship with them in other ways, any of which could materially harm our business, operating results and financial condition. For instance, the manner in which the federal government and the states implement health insurance exchanges and the process for receiving subsidies and cost-sharing credits could substantially increase our competition and member turnover and substantially reduce the number of individuals, families and small businesses that purchase insurance through us, which would materially harm our business, operating results and financial condition. Various aspects of health care reform could cause health insurance carriers to determine to limit the type of health insurance plans we sell and the geographies in which we sell them. It also could cause health insurance carriers to exit the business of selling insurance plans in a particular jurisdiction, eliminate certain categories of products or attempt to move members into new plans for which we receive lower commissions. If health insurance carriers determine to limit our ability to sell their plans or determine not to sell individual health insurance plans altogether, our business, operating results and financial condition would be materially harmed.
We believe that consumer anticipation of health care reform and confusion regarding its impact has already impacted demand for the health insurance plans we sell and that consumers have deferred applying for health insurance until the substance of health care reform becomes clearer to them. Should consumers continue to do so, our business, operating results and financial condition would be harmed.
The medical loss ratio requirements that are a part of health care reform could harm our business.
The federal Patient Protection and Affordable Care Act enacted in March 2010 and related amendments in the Health Care and Education Reconciliation Act of 2010 contain provisions requiring health insurance carriers to maintain specified medical loss ratios. The medical loss ratio requirements for both individual and family and small business health insurance are effective for calendar year 2011 and later years and, among other things, require health insurance companies to spend 80% of their premium revenue in each of their individual and small group businesses on reimbursement for clinical services and activities that improve health care quality. The medical loss ratio requirement for Medicare Advantage plans is 85% and goes into effect in 2014. Carrier reaction to the individual and family medical loss ratio requirements has been to significantly reduce the
9
Table of Contents
commissions we receive in connection with the sale of these plans. These reductions will significantly impact our business and operating results beginning in 2011. If health insurance carriers reduce or further reduce our commissions, including base commission rates or override commissions, in response to medical loss ratio requirements, or as a result of any other aspect of health care reform, our business, operating results and financial condition would be harmed. In addition, the medical loss ratio requirements may cause certain health insurance carriers to limit the geographies in which they sell health insurance or exit certain markets altogether, place less reliance on agents to distribute their plans, apply stricter underwriting standards (until provisions in health care reform registration limiting underwriting go into effect in 2014) or limit their health insurance offerings in any number of other ways, each of which would harm our business, operating results and financial condition. The implementation of medical loss ratio requirements also could cause health insurance carriers to reduce the amount they are willing to spend in connection with our sponsorship and technology licensing businesses, which also could harm our business, operating results and financial condition.
Our business may be harmed if we lose our relationship with health insurance carriers or our relationship with health insurance carriers is modified.
We typically enter into contractual agency relationships with health insurance carriers that are non-exclusive and terminable on short notice by either party for any reason. In many cases, health insurance carriers also may amend the terms of our agreements unilaterally on short notice. Carriers may be unwilling to allow us to sell their existing or new health insurance plans, or desire to amend our agreements with them, for a variety of reasons, including for competitive or regulatory reasons, as a result of health care reform, as a result of a reluctance to distribute their plans over the Internet or because they do not want to be associated with our brand. In the future, and as a result of health care reform or for other reasons, an increasing number of health insurance carriers may decide to rely on their own internal distribution channels, including traditional in-house agents and carrier websites, to sell their own plans and, in turn, could limit or prohibit us from selling their plans on our ecommerce platform. For instance, carriers may choose to exclude us from their most profitable or popular plans or may determine not to distribute insurance plans in the individual, family and small business markets in certain geographies or altogether. The termination or amendment of our relationship with a carrier could reduce the variety of health insurance plans we offer, which could harm our business, operating results and financial condition. We also could lose a source of or be paid reduced commissions for future sales and for past sales, which would materially harm our business, operating results and financial condition. Our business could also be harmed if in the future we fail to develop new carrier relationships and are unable to offer consumers a wide variety of health insurance plans.
The health insurance industry in the United States has experienced a substantial amount of consolidation over the past several years, resulting in a decrease in the number of health insurance carriers. In the future, we may be forced to offer insurance policies from a reduced number of insurance carriers or to derive a greater portion of our revenue from a more concentrated number of carriers as our business and the health insurance industry evolve. We derived 16% and 17% of our total revenue in 2009 and 2010, respectively, from Aetna. We derived 14% of our total revenue in 2009 and 2010 from carriers owned by UnitedHealthcare. We derived 15% and 12% of our total revenue in 2009 and 2010, respectively, from carriers owned by WellPoint. We have many agreements that govern our sale of individual health insurance plans with these health insurance carriers. Many of these agreements may be unilaterally amended or terminated on short notice by the carrier and the amendment or termination could adversely impact the commission payments that we receive from these health insurance carriers. Notwithstanding our separate agreements with various carriers directly or indirectly owned by the same entity, certain carriers have attempted and may continue to attempt to consolidate our relationship with them, which could increase the impact of carrier concentration on us, decrease the commission rates we receive and adversely affect our financial results, particularly in states where we offer health insurance from a relatively smaller number of carriers or where a small number of carriers dominates the market. The termination, amendment or consolidation of our relationship with these and other health insurance carriers could harm our business, operating results and financial condition.
10
Table of Contents
Our rate of growth will likely decline.
We have recently experienced a significant reduction in the commission rates that our health insurance carriers pay us on the individual and family health insurance plans that we sell. We also have in the past and may in the future continue to make significant expenditures related to the development of our business, including expenditures relating to marketing, website technology development, the expansion of our technology licensing business to governmental entities and the development of our business selling Medicare related health insurance plans. Although we have experienced revenue growth in prior periods, we do not project that we will grow our revenue in 2011 compared to 2010, and we also expect our earnings per share to be substantially lower in 2011 than 2010. Our ability to resume revenue and earnings per share growth thereafter will be dependent upon a number of factors, including the success of our Medicare business, our ability to attract individuals, families and small businesses to purchase health insurance through our ecommerce platform, our maintaining our relationships with health insurance carriers and the commission rates we receive for our sale of health insurance plans, our ability to maintain our relationship with existing members within historical levels and our success in entering into relationships with government entities to perform services and license our technology for use in the implementation of health insurance exchanges and other health care reform related endeavors. If we are not successful in these areas, our business, operating results and financial condition will be harmed.
The number of members approved through us for the purchase of health insurance was less in 2010 than in 2009. Our revenue will be adversely impacted if our membership does not grow. The commission rates that we receive are typically higher in the first twelve months of a policy. After the first twelve months, they generally decline significantly. Accordingly, to the extent that our addition of net new members slows or we experience a reduction in the number of our members, our revenue would be adversely impacted due to a decline in commissions we receive for members whose policies have been active for more than twelve months in addition to the reduction in revenue growth that would occur solely as a result of a decline in our membership growth rate. The commission rates we receive are impacted by a variety of other factors, including the particular health insurance policies chosen by our members, the carriers offering those policies, our members’ states of residence, the laws and regulations in those jurisdictions and health care reform. Our commission rate per member could decrease as a result of either reductions in contractual commission rates or unfavorable changes in health insurance carrier override commission programs, each of which may be beyond our control and may occur on short notice. To the extent these and other factors cause our commission rate per member to decline, our rate of revenue growth may decline and our business, operating results and financial condition would be harmed.
We may not be successful in our efforts to market and sell Medicare-related health insurance plans.
We recently determined to market Medicare-related health insurance plans using our ecommerce platforms, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. We refer to these plans as Medicare plans. We market Medicare plans to Medicare eligible individuals, who are predominately senior citizens over the age of 65. The sale of Medicare Advantage and Medicare Part D prescription drug plans are subject to an annual enrollment period during the fourth quarter of each year, when a substantial percentage of the annual sales of these plans occur. We do not have significant experience in marketing Medicare plans. The revenue we have generated in our Medicare plan business is primarily referral fees paid to us based on leads generated by our online platforms that are delivered and sold to third parties. We also began selling these products directly through our websites and customer care center.
The success of our entry into the market for Medicare plans as a health insurance agent will depend upon our ability to enter into and maintain relationships with health insurance carriers on favorable economic terms to market these plans on our ecommerce platform. If we are not successful in maintaining relationships with health insurance carriers to market their Medicare plans, or if we are unable to enter into a sufficient number of these relationships to offer Medicare eligible individuals the ability to choose from a number of plans from different health insurance carriers in a particular jurisdiction, we may not be successful in marketing Medicare plans, and our business, operating results and financial condition would be harmed.
11
Table of Contents
Our success in expanding into the Medicare plan market as a health insurance agent will also depend upon a number of additional factors, including:
| • | our ability to continue to adapt our ecommerce platform to market Medicare plans, including our development or acquisition of marketing tools and features important in the sale of Medicare plans online and the modification of our existing user experience for new plans targeted at a different demographic; |
| • | United States Department of Health and Human Services, Centers for Medicare and Medicaid Services, or CMS, state department of insurance and health insurance carrier approval of the use of our platforms and other marketing material for the marketing of the Medicare plans we sell; |
| • | our success in marketing our ecommerce platform to Medicare eligible individuals and in entering into business development relationships to drive Medicare eligible individuals to our ecommerce platform; |
| • | our effectiveness in entering into and maintaining relationships with marketing partners, including existing pharmacy chain partners that refer Medicare eligible individuals to us; |
| • | our ability to hire and retain additional employees with experience in Medicare, including our ability to timely implement Medicare sales expertise into our new customer care center in the state of Utah; |
| • | our ability to comply with the numerous, complex and changing laws and regulations and CMS guidelines relating to the marketing and sale of Medicare plans, including conforming our online and offline sales processes to those laws and regulations; and |
| • | the effectiveness with which our competitors market the availability of Medicare plans from sources other than our ecommerce platform. |
As a result of these factors, we may prove unsuccessful in marketing Medicare plans and acting as a health insurance agent in connection with their sale, which would harm our business, operating results and financial condition. In addition, if our efforts to market Medicare plans during any annual enrollment period were impeded due to lack of health insurance carrier or CMS approval, or for other reasons, the impact on our business, operating results and financial condition would be more pronounced given the seasonality of the Medicare plan business and the fact that much of the sales of Medicare plans occur during this period.
Our success in generating Medicare plan lead referral revenue is dependent upon the same factors that could impact our ability to generate Medicare plan commission revenue and is also subject to other risks and uncertainties, including our ability to generate Medicare plan leads. We depend upon CMS to permit us to use Medicare plan data collected by CMS for significant aspects of our PlanPrescriber platform, which has generated the majority of our Medicare plan related lead referral revenue. Most of our Medicare plan lead referral revenue in 2010 came from a single purchaser of leads. We also generate a significant number of Medicare plan leads through a limited number of marketing partner relationships with pharmacy chains. If we do not reduce our dependence upon a limited number of lead purchasers or sources for Medicare plan leads, our business, operating results and financial condition could be harmed as a result of termination of these relationships or the inability of the purchasers to pay us for the number of leads that we generate.
Factors beyond our control may negatively impact our ability to market and sell Medicare plans.
We determined to enter into the Medicare plan market because we believe there is an increasing number of individuals becoming eligible for Medicare, and that Medicare eligible individuals are increasingly using the Internet to shop for health insurance plans that supplement Medicare. We also believe that on average member retention rates and the commissions that health insurance carriers pay in connection with the sale of Medicare plans compare favorably to the member retention rates and commissions we receive in connection with our sale of individual and family health insurance. Should we prove to be wrong, or should these circumstances reverse, our success in marketing Medicare plans would be materially and adversely impacted, which could harm our
12
Table of Contents
business, operating results and financial condition. For instance, portions of health care reform impose significant changes to original Medicare and the Medicare Advantage program by, among other things, increasing the benefits original Medicare provides, reducing payments to Medicare Advantage plans and imposing medical loss ratio requirements for Medicare Advantage plans. In the event health care reform or other circumstances decrease the demand for Medicare Advantage plans or other alternatives to original Medicare, or cause a reduction in the amount paid to agents in connection with the sale of these plans, our business operating results and financial condition could be harmed.
The marketing and sale of Medicare plans are subject to numerous, complex and frequently changing laws and regulations, and any noncompliance with them could harm our business, operating results and financial condition.
The marketing and sale of Medicare plans are subject to numerous laws, regulations and guidelines at the federal and state level. The marketing and sale of Medicare Advantage and Medicare Part D plans are principally regulated by CMS. The marketing and sale of Medicare Supplement plans are principally regulated on a state-by-state basis by state departments of insurance. The laws and regulations applicable to the marketing and sale of Medicare plans are numerous, ambiguous and complex, and, particularly with respect to regulations and guidance issued by CMS for Medicare Advantage and Medicare Part D plans, change frequently. As a result of these laws, regulations and guidelines, we have, and will have to continue to, alter our websites and sales process to comply with several requirements that are not applicable to our sale of non-Medicare-related health insurance plans. For instance, many aspects of our online platforms and our marketing material and processes, as well as changes to these platforms, materials and processes, including call center scripts, must be approved by CMS and by health insurance carriers in light of CMS requirements. In addition, certain aspects of our Medicare plan marketing partner relationships with pharmacy chains have in the past and will in the future been subjected to CMS and health insurance carrier review. Changes to the laws, regulations and guidelines relating to Medicare plans, their interpretation or the manner in which they are enforced could be incompatible with our Medicare plan business model. Due to changes in CMS guidance or enforcement of existing guidance, or as a result of new regulations and guidelines, CMS, state departments of insurance or health insurance carriers may determine not to approve aspects of our online platforms or marketing material and processes and may determine that certain existing aspects of our Medicare related business are not in compliance. As a result, the progress of our Medicare plan business could be slowed or we could be prevented from operating aspects of our Medicare plan business altogether, which would harm our business, operating results and financial condition, particularly if it occurred during the Medicare annual enrollment period. It could also result in the write-down of the value of assets acquired in our PlanPrescriber acquisition.
The impact that health care reform legislation will have on the market for Medicare plans is unclear, but it could change demand for Medicare plans, the way these plans are delivered, the commissions that carriers pay to health insurance agents in connection with their sale or adversely impact us in other ways. In the event that laws and regulations adversely impact our ability to market the availability of any type of Medicare plan on our ecommerce platform, or the amounts that health insurance agents are paid for selling these plans, our business, operating results and financial condition would be harmed.
We expect to reduce our cost of acquisition and other expenses in connection with the sale of our individual and family health insurance plans, which may harm our operating results.
As a result of the reduction in the commission rates we receive for selling individual and family health insurance plans, we expect to reduce our marketing and advertising and other expenses in this area of our business. This reduction will result in fewer individual and family health insurance plan approved members for which we would receive commission revenue, particularly in the event our competitors do not similarly reduce their marketing and advertising and other expenses. The reduction of our cost of acquisition depends significantly on improving the rate at which visitors to our website submit health insurance applications, particularly with respect to paid search advertising, as our paid search costs are incurred on the referral of a potential member
13
Table of Contents
rather than on the submission of a health insurance application. As a result, we may not be successful in reducing our individual and family health insurance cost of acquisition in the event the rate at which visitors to our platform submit individual and family health insurance declines, which would harm our business, operating results and financial condition.
Our future operating results are likely to fluctuate and could fall short of expectations.
Our operating results are likely to fluctuate as a result of a variety of factors, including the factors described elsewhere in this “Risk Factors” section, many of which are outside of our control. As a result, comparing our operating results on a period-to-period basis may not be meaningful and you should not rely on our past results as an indication of our future performance, particularly as a result of the commission rate reductions that we have experienced in our individual and family health insurance business, which will begin to have an impact on our financial results in 2011. If our revenue or operating results fall below the expectations of investors or securities analysts, the price of our common stock could decline substantially.
Our business model is characterized primarily by revenue based on commissions we receive from insurance carriers whose policies are purchased by our members. Although our services are complete upon the approval of a member’s application, we receive commissions and record related revenue, typically on a monthly basis, until the health insurance policy is cancelled or we otherwise do not remain the agent on the policy. A significant component of our marketing and advertising expenses consists of expenses incurred in search engine advertising at the time a consumer clicks on an advertisement and payments owed to our marketing partners in connection with applications submitted on our ecommerce platform by potential members referred to us by our marketing partners. As a result of this timing difference between expense and associated revenue recognition, our operating results and cash flows may be adversely affected in periods where we experience a significant increase in new applicants. In addition, if we incur other unanticipated or one-time expenses in a particular quarter or if we lose a significant amount of our member base for any reason, we would likely be unable to offset these expenses by increasing sales within that quarter or to replace lost revenue in the quarter with revenue from new members. As a result, our quarterly results may suffer due to unanticipated expenses, one-time charges or significant member turnover.
Current economic conditions and other factors beyond our control may negatively impact our business, operating results and financial condition.
Our revenue depends upon demand for health insurance in the individual, family and small business markets, which can be influenced by a variety of factors beyond our control. For instance, an increased number of individuals have become self-employed or unemployed. In addition, as a result of substantial health insurance premium inflation in recent years, we believe that many employers have sought to reduce the costs associated with providing health insurance to their employees, including offering fewer benefits to employees, reducing or eliminating dependent coverage, increasing employee health insurance premium contributions and eliminating health insurance benefits altogether. We have no control over the economic and other factors that influence these trends, and they may reverse, including as a result of health care reform legislation. If economic or other factors beyond our control negatively impact our business, our business, operating results and financial condition could be harmed.
We believe that demand for the health insurance and services we offer has been adversely impacted by recent economic conditions. We cannot be certain of the future impact that the recent recession will have on our business. A further softening of demand for health insurance and services offered by us, whether caused by changes in customer preferences or a weak U.S. economy, including as a result of recent disruptions in the global financial markets or a decrease in general consumer confidence, will result in decreased revenue and growth. Consumers may attempt to reduce expenses by cancelling existing health insurance purchased through us, determine not to purchase new health insurance through us, or purchase health insurance plans with lower premiums for which we receive lower commissions. To the extent the economy or other factors adversely impact
14
Table of Contents
our membership retention or the number or type of health insurance applications submitted through us and that are approved by health insurance carriers, our rate of growth will decline and our business and operating results will be harmed. A continuing negative economic environment could also adversely impact the health insurance carriers whose plans are offered on our ecommerce platform, and they may, among other things, determine to reduce their commission rates, increase premiums or reduce benefits, change their underwriting practices so that fewer health insurance applications are approved or decrease the amount they are willing to spend for marketing purposes, all of which would negatively impact our sale of health insurance as well as our sponsorship and technology licensing businesses.
Economic conditions have caused interest rates to decline. We have experienced a significant reduction in the rate of return on our investments both as a result of the decline in interest rates and as a result of our implementation of more conservative investment policies. Economic conditions could materially and adversely impact our investments in the future, including loss of our principal investment, despite our implementation of more conservative investment policies.
Our business may not grow if consumers are not informed about the availability and accessibility of affordable health insurance.
Numerous health insurance plans are available to consumers in any given market. Most of these plans vary by price, benefits and other policy features. Health insurance terminology and provisions are often confusing and difficult to understand. As a result, researching, selecting and purchasing health insurance can be a complex process. We believe that this complexity has contributed to a perception held by many consumers that individual health insurance is prohibitively expensive and difficult to obtain. We attempt to make the health insurance research and application process on our website understandable and user-friendly. We also attempt to use our website and other means to educate consumers about the accessibility and affordability of health insurance. If consumers are not informed about the availability and accessibility of affordable health insurance or our ecommerce platform is difficult to navigate, our business may not grow and our operating results and financial condition would be harmed.
If we are not successful in cost-effectively converting visitors to our website into members, our business and operating results would be harmed.
Our growth depends in large part upon growth in our membership. The rate at which consumers visiting our ecommerce platform and seeking to purchase health insurance are converted into members is a significant factor in the growth of our membership. A number of factors have influenced, and could in the future influence, the conversion rate for any given period, some of which are outside of our control. These factors include:
| • | changes in consumer shopping behavior due to circumstances outside of our control, such as economic conditions, consumers’ ability or willingness to pay for health insurance, extension of unemployment benefits or proposed or enacted legislative or regulatory changes impacting our business; |
| • | the quality of and changes to the consumer experience on our ecommerce platform or with our customer care center; |
| • | regulatory requirements, including those that make the experience on our online platforms cumbersome or difficult to navigate; |
| • | the variety and affordability of the health insurance plans that we offer; |
| • | system failures or interruptions in the operation of our ecommerce platform or call center operations; |
| • | changes in the mix of consumers who are referred to us through our direct, marketing partner and online advertising member acquisition channels; |
| • | the health insurance carriers offering the health insurance plans for which consumers have expressed interest, and the degree to which our technology is integrated with those carriers; |
15
Table of Contents
| • | health insurance carrier underwriting practices and guidelines applicable to applications submitted by consumers and the amount of time a carrier takes to make a decision on that application; and |
| • | competitive offerings. |
Our conversion rates can be impacted by changes in the mix of consumers referred to us through our member acquisition channels. For example, our conversion rates have historically been lower with respect to consumers referred to us by Internet lead aggregators and relatively higher with respect to consumers coming to us through our direct member acquisition channel. In addition, we may make changes to our ecommerce platform or undertake other initiatives in an attempt to improve consumer experience or for other reasons. These changes in the past, and may in the future, have the unintended consequence of adversely impacting our conversion rates. A decline in the percentage of consumers who submit health insurance applications on our ecommerce platform and are converted into members could cause an increase in our cost of acquiring members on a per member basis. To the extent the rate at which we convert consumers visiting our ecommerce platform into members suffers, our membership growth rate may decline, which would harm our business, operating results and financial condition.
If we are unable to retain our members, our business and operating results would be harmed.
We receive revenue from commissions health insurance carriers pay to us for health insurance policies sold through our ecommerce platform. When one of these policies is cancelled, or if we otherwise do not remain the agent on the policy, we no longer receive the related commission revenue. Individuals, families and small businesses may choose to discontinue their health insurance policies for a variety of reasons. For example, individuals and families may replace a health insurance policy purchased through us with a health insurance policy provided by a new or existing employer or may determine that they cannot afford health insurance. In addition, our members may choose to purchase new policies using a different agent if, for example, they are not satisfied with our customer service or the health insurance plans that we offer. Health insurance carriers may also terminate health insurance plans purchased and held by our members. If we are not successful in transferring members covered under a terminated plan to another policy that we offer, we will lose these members. Our cost in acquiring a new member is substantially greater than the cost involved in maintaining our relationship with an existing member. If we are not able to successfully retain existing members and limit member turnover, our revenue and operating margins could be adversely impacted and our business, operating results and financial condition would be harmed.
Changes in the quality and affordability of the health insurance plans that carriers offer on our ecommerce platform could harm our business and operating results.
The demand for health insurance marketed through our ecommerce platform is impacted by, among other things, the variety, quality and price of the health insurance plans we offer. If health insurance carriers do not continue to provide us with a variety of high-quality, affordable health insurance plans in the individual, family and small business markets, or if their offerings are limited as a result of consolidation in the health insurance industry, health care reform legislation or otherwise, our sales may decrease and our business, operating results and financial condition could be harmed.
Health insurance carriers could determine to reduce the commissions paid to us or change their underwriting practices in ways that reduce the number of insurance policies sold through our ecommerce platform, which could harm our business and operating results.
Our commission rates, and the commission override payments we receive from health insurance carriers for achieving sales volume thresholds or other objectives, are either set by each carrier or negotiated between us and each carrier. Carriers have altered, and may in the future alter, the contractual relationships we have with them on short notice, either by renegotiation or unilateral action. If these contractual changes result in reduced commissions, our business may suffer and our operating results and financial condition could be harmed. In
16
Table of Contents
addition, carriers periodically change the criteria they use for determining whether they are willing to insure individuals as well as other underwriting practices. At various times, carriers have applied more stringent underwriting criteria and practices to applications for health insurance. These practices result in a decrease in the rate at which insurance policies submitted through our ecommerce platform are approved. Changes in carrier underwriting criteria or practices could negatively impact sales of insurance policies on our ecommerce platform and could harm our business, operating results and financial condition.
If we are not able to maintain and enhance our brand, our business and operating results will be harmed.
We believe that maintaining and enhancing our brand identity is critical to our relationships with existing members, marketing partners and health insurance carriers and to our ability to attract new members, marketing partners and health insurance carriers. The promotion of our brand in these and other ways may require us to make substantial investments and we anticipate that, as our market becomes increasingly competitive, these branding initiatives may become increasingly difficult and expensive. Our brand promotion activities may not be successful or yield increased revenue, and to the extent that these activities yield increased revenue, the increased revenue may not offset the expenses we incur and our operating results could be harmed. If we do not successfully maintain and enhance our brand, our business may not grow and we could lose our relationships with health insurance carriers, marketing partners and/or members, which would harm our business, operating results and financial condition.
In addition, we have historically received media attention in connection with our public relations efforts. While we cannot be certain of the impact of media coverage on our business, if it were to be reduced, the number of consumers visiting our platform could decrease, and our cost of acquiring members could increase as a result of a reduction in the number of members coming from our direct member acquisition channel, both of which could harm our business, operating results and financial condition.
System failures or capacity constraints could harm our business and operating results.
The performance, reliability and availability of our ecommerce platforms and underlying network infrastructures are critical to our financial results, our brand and our relationship with members, marketing partners and health insurance carriers. Although we regularly attempt to enhance our ecommerce platform and system infrastructure, system failures and interruptions may occur if we are unsuccessful in these efforts, if we are unable to accurately project the rate or timing of increases in our website traffic or for other reasons, some of which are completely outside our control. Although we have experienced only minor system failures and interruptions to date, we could experience significant failures and interruptions in the future, which would harm our business, operating results and financial condition.
We rely in part upon third-party vendors, including data center and bandwidth providers, to operate our ecommerce platforms. We cannot predict whether additional network capacity will be available from these vendors as we need it, and our network or our suppliers’ networks might be unable to achieve or maintain a sufficiently high capacity of data transmission to allow us to process health insurance applications in a timely manner or effectively download data, especially if our website traffic increases. Any system failure that causes an interruption in or decreases the responsiveness of our services would impair our revenue-generating capabilities and harm our business and operating results and damage our reputation. In addition, any loss of data could result in loss of customers and subject us to potential liability. Our database and systems are vulnerable to damage or interruption from human error, earthquakes, fire, floods, power loss, telecommunications failures, physical or electronic break-ins, computer viruses, acts of terrorism, other attempts to harm our systems and similar events. In addition, our operations are vulnerable to earthquakes in the San Francisco Bay Area and elsewhere in Northern California.
Consumers may access our customer care centers for assistance in connection with submitting health insurance applications after using our ecommerce platform. We depend upon third parties, including telephone service providers and third party software providers, to operate our customer care centers. Any failure of the
17
Table of Contents
systems that we rely upon in the operation of our customer care center could negatively impact sales as well as our relationship with consumers and members, which could harm our business, operating results and financial condition.
If consumers or carriers opt for more traditional or alternative channels for the purchase and sale of health insurance, our business will be harmed.
Our success depends in part upon widespread consumer and health insurance carrier acceptance of the Internet as a marketplace for the purchase and sale of health insurance. Consumers and health insurance carriers may choose to depend more on traditional sources, such as individual agents, or alternative sources may develop, including as a result of health care reform legislation. Our future growth, if any, will depend in part upon:
| • | the growth of the Internet as a commerce medium generally, and as a market for consumer financial plans and services specifically; |
| • | consumers’ willingness to conduct their own health insurance research; |
| • | our ability to make the process of purchasing health insurance online an attractive alternative to traditional and new means of purchasing health insurance; |
| • | our ability to successfully and cost-effectively market our services as superior to traditional or alternative sources for health insurance to a sufficiently large number of consumers; and |
| • | health insurance carriers’ willingness to use us and the Internet as a distribution channel for health insurance plans. |
If consumers and health insurance carriers determine that other sources for health insurance and health insurance applications are superior, our business will not grow and our operating results and financial condition would be harmed.
We depend upon Internet search engines to attract a significant portion of the consumers who visit our website, and if we are unable to effectively advertise on search engines on a cost-effective basis, our business and operating results would be harmed.
We derive a significant portion of our website traffic from consumers who search for health insurance through Internet search engines, such as Google, MSN and Yahoo!. A critical factor in attracting consumers to our website is whether we are prominently displayed in response to an Internet search relating to health insurance. Search engines typically provide two types of search results, algorithmic listings and paid advertisements. We rely on both algorithmic listings and paid advertisements to attract consumers to our website.
Algorithmic search result listings are determined and displayed in accordance with a set of formulas or algorithms developed by the particular Internet search engine. The algorithms determine the order of the listing of results in response to the consumer’s Internet search. From time to time, search engines revise these algorithms. In some instances, these modifications have caused our website to be listed less prominently in algorithmic search results, which has resulted in decreased traffic to our website. We may also be listed less prominently as a result of new websites or changes to existing websites that result in these websites receiving higher algorithmic rankings with the search engine. Our website may become listed less prominently in algorithmic search results for other reasons, such as search engine technical difficulties, search engine technical changes and changes we make to our website. In addition, search engines have deemed the practices of some companies to be inconsistent with search engine guidelines and decided not to list their website in search result listings at all. If we are listed less prominently in, or removed altogether from, search result listings for any reason, the traffic to our website likely would decline and we may not be able to replace this traffic, which in turn would harm our operating results. If we decide to attempt to replace this traffic, we may be required to increase
18
Table of Contents
our marketing expenditures, which would also increase our cost of member acquisition and harm our operating results.
We purchase paid advertisements on search engines in order to attract consumers to our website. We typically pay a search engine for prominent placement of our name and website when particular health insurance-related terms are searched for on the search engine, regardless of the algorithmic search result listings. In some circumstances, the prominence of the placement of our advertisement is determined by a combination of factors, including the amount we are willing to pay and algorithms designed to determine the relevance of our paid advertisement to a particular search term. As with algorithmic search result listings, search engines may revise the algorithms relevant to paid advertisements and websites other than our ecommerce platform may become more optimized for the algorithms. These changes may result in our having to pay increased amounts to maintain our paid advertisement placement in response to a particular search term. We could also have to pay increased amounts should the market share of major search engines continue to become more concentrated with a single search engine. Additionally, we bid against our competitors and others for the display of these paid search engine advertisements. Many of our competitors, including many health insurance carriers, have greater resources with which to bid and better brand recognition than we do. We have experienced increased competition from health insurance carriers and some of our marketing partners for both algorithmic search result listings and for paid advertisements, which has increased our marketing and advertising expenses. If this competition increases further, or if the fees associated with paid search advertisements increase as a result of algorithm changes or other factors, our advertising expenses could rise significantly or we could reduce or discontinue our paid search advertisements, either of which could harm our business, operating results and financial condition. In addition, we believe that the medical loss ratio requirements of health care reform legislation and the reduction in commission rates in the individual and family health insurance market will cause a reduction in the amounts that our competitors, including health insurance carriers, are willing to pay for paid search engine advertisements. Should this not occur, or should it last for a limited period of time, our cost of acquiring members could increase significantly and our operating margins could be reduced, which would harm our business, operating results and financial condition. Additionally, we could experience a reduction in the number of applications for the individual and family health insurance plans, which also would harm our business, operating results and financial condition.
We rely significantly on marketing partners for the sale of health insurance on our ecommerce platforms and our business and operating results would be harmed if we are unable to maintain effective relationships with our existing marketing partners or if we do not establish successful relationships with new marketing partners.
In addition to marketing through Internet search engines, we frequently enter into contractual marketing relationships with other online and offline businesses that promote us to their customers. These marketing partners include financial and online service companies, affiliate programs and online advertisers and content providers. Our subsidiary PlanPrescriber also has relationships with marketing partners, including pharmacy chains that promote our platform to their customers. We compensate many of our marketing partners for their referrals on a submitted health insurance application basis and, if they are licensed to sell health insurance, may share a percentage of the commission we earn from the health insurance carrier for each member referred by the marketing partner.
Many factors influence the success of our relationship with our marketing partners, including:
| • | the continued positive market presence, reputation and growth of the marketing partner; |
| • | the effectiveness of the marketing partner in marketing our website and services, including whether the marketing partner is successful in maintaining the prominence of its website in algorithmic search result listings and paid Internet advertisements; |
| • | the compliance of our marketing partners, and of the manner marketing partners refer consumers to our platforms, with applicable laws, regulations and guidelines; |
19
Table of Contents
| • | the interest of the marketing partner’s customers in the health insurance plans that we offer on our ecommerce platform; |
| • | the contractual terms we negotiate with the marketing partner, including the marketing fees we agree to pay a marketing partner; |
| • | the percentage of the marketing partner’s customers that submit applications or purchase health insurance policies through our ecommerce platform; |
| • | the ability of a marketing partner to maintain efficient and uninterrupted operation of its website; and |
| • | our ability to work with the marketing partner to implement website changes, launch marketing campaigns and pursue other initiatives necessary to maintain positive consumer experiences and acceptable traffic volumes. |
For instance, we partner with Internet lead aggregators who refer a significant number of consumers to our online platforms. Major search engines have in the past and may in the future determine not to list lead aggregator websites prominently in search result listings for various reasons, which would cause a significant reduction in the number of consumers referred to us through our marketing partner channel. If we are unable to maintain successful relationships with our existing marketing partners or fail to establish successful relationships with new marketing partners, our business, operating results and financial condition will be harmed.
The impact that health care reform will have on our relationships with marketing partners is unclear. To the extent that health care reform makes it less profitable or desirable for marketing partners to promote us to their customers, we may lose relationships with existing marketing partners and may have difficulty entering into relationships with new marketing partners. We may also need to reduce the compensation that we pay to marketing partners to the extent that health care reform has the effect of reducing commissions for individual and family health insurance. There is no guarantee that we will be able to amend our agreements to reduce the compensation that we pay to acceptable levels in light of the commission rates that we receive. If we are not able to do so, our business, operating results and financial condition could be harmed. In addition, the promulgation of laws, regulations or guidelines, or the interpretation of existing guidelines, by state departments of insurance or by CMS, could cause our relationships with our marketing partners to be in noncompliance with those laws, regulations and guidelines. For instance, as a result of our acquisition of PlanPrescriber, we have marketing partner relationships with pharmacy chains that utilize aspects of our platform and tools. Our relationships with these pharmacy chains results in the referral of a significant number of individuals to us who are interested in purchasing Medicare plans. If CMS or state departments of insurance were to change existing laws, regulations or guidelines, or interpret existing laws, regulations or guidelines, to prohibit these arrangements, we would experience a significant decline in the number of Medicare eligible individuals who are referred to our platforms and call center, which would harm our business, operating results and financial condition and could result in a write-down of the value of assets acquired in our PlanPrescriber acquisition.
We rely on health insurance carriers to accurately and regularly prepare commission reports, and if these reports are inaccurate or not sent to us in a timely manner, our business and operating results could be harmed. We also may not recognize trends in our membership as a result of a lack of information from health insurance carriers.
Health insurance carriers typically pay us a specified percentage of the premium amount on a health insurance policy that we have sold during the period that a member maintains coverage under the policy. We rely on health insurance carriers to timely and accurately report the amount of commissions earned by us, and we calculate our commission revenue, prepare our financial reports, projections and budgets and direct our marketing and other operating efforts based on the reports we receive from health insurance carriers. It is often difficult for us to independently determine whether or not carriers are accurately reporting commissions due to us. To the extent that health insurance carriers understate or fail to accurately report the amount of commissions
20
Table of Contents
due to us in a timely manner or at all, we will not recognize revenue to which we are entitled, which would harm our business, operating results and financial condition.
We also are dependent on health insurance carriers and others for data related to our membership. For instance, with respect to health insurance plans other than small business group health insurance, health insurance carriers do not directly report member cancellations to us, resulting in the need for us to determine cancellations using payment data that carriers provide. We infer cancellations from this payment data by analyzing whether payments from members have ceased for a period of time, and we may not learn of a cancellation for several months, given that some of our members pay on a schedule less frequently than monthly (e.g., quarterly). With respect to our small business group membership, many groups notify the carrier directly with respect to increases or decreases in group size and policy cancellations. Our insurance carrier partners often do not communicate this information to us, and it often takes a significant amount of time for us to learn about small business group cancellations and changes in our membership within the group itself. We often are not made aware of policy cancellations until the time of the group’s annual renewal.
After we have estimated membership for a period, we may receive information from health insurance carriers that would have impacted the estimate if we had received the information prior to the date of estimation. We may receive commission payments or other information that indicates that a member who was not included in our estimates for a prior period was in fact an active member at that time, or that a member who was included in our estimates was in fact not an active member of ours. We also reconcile information health insurance carriers provide to us and may determine that we were not historically paid commissions owed to us, which would cause us to have underestimated our membership. Additionally, health insurance carriers may require us to return commission payments paid in a prior period due to policy cancellations for members we previously estimated as being active. For these and other reasons, including if current trends in membership cancellation are inconsistent with past cancellation trends that we use to estimate our membership or if carriers subsequently report changes to the commission payments that they previously reported to us, our actual membership could be different from our estimates, perhaps materially. Total revenue per estimated member for the period would also change if our estimated membership changed. Our estimate regarding the average amount of time our members maintain their health insurance plans also could be inaccurate as it is dependent upon the accuracy of our membership estimates.
Our operating results fluctuate depending upon health insurance carrier payment practices and the timing of our receipt of commission reports from health insurance carriers.
The timing of our revenue depends upon the timing of our receipt of commission reports and associated payments from health insurance carriers. Although health insurance carriers typically report and pay commissions to us on a monthly basis, there have been instances where their report of commissions and payment have been delayed, such as during holiday periods. Any delay could materially impact our financial results for a given quarter as we would not be able to recognize the related commission revenue in that quarter. In addition, much of our commission override revenue is not reported and paid to us in accordance with a scheduled pattern, and some is only reported and paid to us once per year. This could result in a large amount of commission revenue from a carrier being recorded in a given quarter that is not indicative of the amount of revenue we may receive from that carrier in subsequent quarters, causing fluctuations in our operating results. We could report revenue below the expectations of our investors or securities analysts in any particular period if a material report or payment from a health insurance carrier were delayed or not received within the time frame required for revenue recognition.
We may be unsuccessful in competing effectively against current and future competitors.
The market for selling health insurance plans is highly competitive. We compete with entities and individuals that offer and sell health insurance plans utilizing traditional distribution channels as well as the Internet. Our current or potential competitors include the tens of thousands of local insurance agents across the
21
Table of Contents
United States who sell health insurance plans in their communities. There are a number of agents that operate websites and provide an online shopping experience for consumers interested in purchasing health insurance. Some local agents use “lead aggregator” services that use the Internet to find consumers interested in purchasing health insurance and are compensated for referring those consumers to the traditional agent. In addition to health insurance brokers and agents, many health insurance carriers directly market and sell their plans to consumers through call centers and their own websites. Although we offer health insurance plans for many of these carriers, they also compete with us by offering their plans directly to consumers. In connection with our marketing of Medicare plans, we compete with the original Medicare program. In addition, CMS offers plan information, comparison tools, call centers and online enrollment for Medicare Advantage and Medicare Part D prescription drug plans.
In licensing our health insurance purchasing platform, we compete with companies providing technology that automates premium quoting, research and analysis of health insurance plans, member enrollment and other tools that support online sales efforts by health insurance carriers and their agents and brokers. We anticipate that in licensing our technology to government entities for health insurance exchange and other purposes, we will compete with these entities as well as system integrators, software companies, employee benefit service providers, technology consulting companies and others that have experience providing technology and services to the federal or state governments.
We may not be able to compete successfully against our current or future competitors. Some of our current and potential competitors have longer operating histories, larger customer bases, greater brand recognition and significantly greater financial, technical, marketing and other resources than we do. As compared to us, our current and future competitors may be able to:
| • | undertake more extensive marketing campaigns for their brands and services; |
| • | devote more resources to website and systems development; |
| • | negotiate more favorable commission rates and commission override payments; and |
| • | make more attractive offers to potential employees, marketing partners and third-party service providers. |
In addition, CMS has the ability to regulate our marketing and sale of Medicare Advantage and Medicare Part D prescription drug plans. Competitive pressures may result in our experiencing increased marketing costs, decreased traffic to our website and loss of market share, or may otherwise harm our business, operating results and financial condition.
There are many risks associated with our operations in China.
A portion of our operations is conducted in China. Among other things, we use employees in China to maintain and update our ecommerce platform. This and other information is delivered to us through secured communications over the Internet. Our business would be harmed if this connection temporarily failed, and we were prevented from promptly updating our software or implementing other changes to our database and systems. Our operations in China also expose us to different and unfamiliar laws, rules and regulations, including different intellectual property laws, which are not as protective of our intellectual property as the laws in the United States, and different labor and tax laws. United States and Chinese trade laws may impose restrictions on the importation of programming or technology to or from the United States. These risks could cause us to incur increased expenses and could harm our ability to effectively and successfully manage our operations in China, which in turn could cause our business, operating results and financial condition to suffer.
In addition, our subsidiary in China has a subsidiary business insurance agency license in the Fujian province in China pursuant to which we are selling health, accident and life insurance in the Fujian province. Our license is up for renewal at the end of 2011. We also have entered into a relationship with a local insurance
22
Table of Contents
agency outside the Fujian province in Shanghai, China, pursuant to which we offer the local insurance agency’s insurance products in Shanghai on our website in our capacity as a technology service provider. We have similar relationships with insurance companies to offer certain of those companies’ products throughout China. Additionally, we have recently entered, and may in the future continue to enter, into relationships with marketing partners to refer additional consumers to our website. We have no prior experience marketing or selling insurance in China or in adapting our business and ecommerce platform to Chinese markets and cultures, legal and regulatory regimes or business customs. For instance, the laws and regulations applicable to our marketing and selling insurance online and assisting others in those efforts in China are unclear, and our operations may be in violation of them. In addition, the laws and regulations may change to prohibit our marketing insurance online. The consequences of violating insurance and other applicable laws and regulations in China are unclear, but they could result in the termination of our license and our ability to host insurance products on our technology platform, payment of fines and damages and could harm our business as a whole. For various reasons, we may not expand in China, and even if we do, there can be no assurance that our ecommerce platform in China would ever generate a significant amount of revenue or otherwise be successful. Our success in establishing an insurance-related business in China is dependent upon many of the factors that influence the success of our business in the United States, including, but not limited to, our receiving regulatory approvals (including the renewal of our license), acceptance of the Internet and our ecommerce platform as a marketplace for the purchase of insurance, our success in marketing our ecommerce platform and in retaining members who purchase insurance through that platform, our ability to enter into and maintain relationships with insurance carriers, commission rates, the affordability of the insurance products offered, insurance carrier business practices, the effectiveness with which we establish a brand identity, performance, reliability and availability of our ecommerce platform, competition, the regulatory environment and the manner in which health care delivery is financed and changes to such environment or manner, our ability to attract qualified personnel and network security.
Our participation and success in the China market may be impacted by additional factors given that outside of Xiamen city, the insurance products offered on our website are offered directly by insurance carriers or through another insurance agent, including our dependence on insurance carriers or the insurance agent for the products on our website, the agent’s relationship with insurance carriers and consumers, our relationship with the insurance carriers and agent, each of the agent’s and the insurance carriers’ ability to maintain licenses and regulatory approvals, and the number, quality and attractiveness of the insurance products offered by the agent and the insurance carrier through our platform. While there is no certainty that we would be able to expand our presence in the insurance industry in China, we may attempt to do so. If we decide to do so, we may need to receive additional government licenses and approvals or enter into additional relationships and may face disadvantages in doing so as a result of our subsidiary in China being wholly foreign owned.
Our sponsorship advertising business may not be successful.
We sell advertising space to health insurance carriers on our website through our sponsorship advertising program. Our sponsorship advertising program allows carriers to purchase advertising space in specific markets in a sponsorship area on our website. Health insurance carriers may determine to eliminate or reduce spending on our sponsorship advertising program as a result of various aspects of health care reform, including the medical loss ratio requirements that became effective in 2011. As a result, our business, operating results and financial condition could be harmed. To the extent that economic conditions, health care reform or other factors impact the amount health insurance carriers are willing to pay for advertising on our ecommerce platform, our sponsorship advertising program will be adversely impacted. The success of our sponsorship advertising program is dependent upon a number of other factors, including the effectiveness of the sponsorship advertising program as a cost-effective method for carriers to obtain additional members, consumer and health insurance carrier adoption of the Internet and our ecommerce platform as a medium for the purchase and sale of health insurance, our ability to attract consumers visiting our ecommerce platform and convert those consumers into members, the existence of a relationship between us and a diverse group of carriers that offer a number of health insurance plans in the markets in which we attempt to sell sponsorship advertising, the cost and other features of the health insurance
23
Table of Contents
plan that is the subject of the sponsorship advertising, the impact the sponsorship advertising has on the sale of the health insurance plan that is the subject of the advertising and the effectiveness of the carrier’s other means of advertising. In addition, while our practice of selling sponsorship advertising is described on our ecommerce platform, it could cause consumers to perceive us as not objective, which could harm our brand and result in a decline in our health insurance sales. It also could adversely impact our relationship with health insurance carriers that do not purchase our sponsorship advertising. As a result, our business, operating results and financial condition could be harmed.
We may not be successful in licensing the use of our ecommerce technology to health insurance carriers and other third parties.
We license the use of our ecommerce technology to health insurance carriers and agents. Carriers use our platform to offer their own health insurance policies on their websites, and agents use it to power their quoting and online content. If we do not grow our revenue from the license of our technology, or if the rate of growth declines, our business, operating results and financial condition may be harmed. The impact that health care reform may have on our technology licensing business is unclear. Health care reform could reduce health insurance carrier and agent demand for our technology licensing platform as a result of the medical loss ratio requirements that became effective in 2011 or for other reasons, and health insurance carriers who currently use the platform could determine to cease using it, reduce the number and type of plans offered on the platform or renegotiate the fees that they pay, any of which would reduce the revenue we receive from our technology licensing business.
The business of licensing the use of our technology to others could facilitate carrier, health insurance agent and other third party competition with us in the sale of health insurance over the Internet and is subject to a number of additional risks and uncertainties, including consumer and health insurance carrier adoption of our ecommerce platform as a medium for the purchase and sale of health insurance, our ability to establish relationships with new health insurance carriers, the reliability and performance of our ecommerce platform and the relative cost of developing competing technology. If we are not able to offer health insurance carriers and other third parties a reliable platform to cost-efficiently offer their plans over the Internet, our technology licensing business will be unsuccessful.
We may not be successful in licensing the use of our technology or performing services pursuant to federal or state government contracts.
An element of our strategy is to license the use of our technology and provide services to government entities in connection with health care reform and its requirement that states establish health insurance exchanges. While we are involved in a small number of government contracts as a prime contractor or as a subcontractor, we are new to government contracting. Generally, government contracts are offered through a competitive bidding process. A number of entities may compete for the award of any particular government contract or related subcontract, and we may not be able to outbid our competitors. Even if we are awarded a contract, unsuccessful bidders may protest or challenge the contract award, which could result in our losing the contract. Complicated rules apply to doing business with the federal and state governments, including without limitation the Federal Acquisition Regulation (FAR), special FAR agency supplements and state procurement laws and regulations. In addition, socio-economic obligations, including various restrictions relating to those of our employees that may perform under the government contract, may accompany government contracts. These requirements may require us to restructure aspects of our operations to perform under a contract, which may be difficult or impossible. As a government contractor, we are subject to audits, cost reviews and investigations by oversight agencies. We may not be successful in our effort to enter into government contracts, and even if we are, we may face difficulty and unanticipated expense in complying with applicable laws, regulations and contractual requirements. If we are not successful in our government contracting efforts, our business, operating results and financial condition could be harmed. In addition, if we fail to comply with the terms of one or more of our government contracts or applicable laws and regulations, we could be suspended or barred from future government projects for a significant period of time, as well as face civil or criminal fines and penalties, which would harm our business, operating results and financial condition.
24
Table of Contents
Government contracts that we have entered into for the use of our services or licensing of our technology have short terms. For instance, our contract with the federal government to provide certain software and information services relating to the federal government’s healthcare reform website has a term of one year. This contract is renewable at the option of the federal government annually for up to three years. Our government contracts may not be renewed for any reason, including as a result of performance of the contract, competing solutions or a change in the governmental entity’s preferences. Furthermore, the contracts may be terminated as a result of our performance or as a result of the performance or actions of third parties involved in the contracts, such as a subcontractor or the prime contractor where we are a subcontractor. The termination or nonrenewal of any of our government contracts could harm our business, operating results and financial condition and make it more difficult to successfully bid on future government contracting opportunities.
We may not be able to adequately protect our intellectual property, which could harm our business and operating results.
We believe that our intellectual property is an essential asset of our business and that our technology infrastructure currently gives us a competitive advantage in the distribution of individual, family and small business health insurance. We rely on a combination of copyright, trademark and trade secret laws as well as confidentiality procedures and contractual provisions to establish and protect our intellectual property rights in the United States. Although we have applied for patents in the United States, they may not result in issued patents. We have not filed for protection of our intellectual property in any foreign jurisdiction other than China. We have Chinese-registered computer software copyrights for an internally-developed software system and a project management tool and have filed certain trademark applications in China. We have not filed any patent applications in China. The efforts we have taken to protect our intellectual property may not be sufficient or effective, and our trademarks, copyrights and patents if issued, may be held invalid or unenforceable. Moreover, the law relating to intellectual property is not as developed in China, and our intellectual property rights may not be as respected in China as they are in the United States. Any United States or other patents issued to us may not be sufficiently broad to protect our proprietary technologies, and given the costs of obtaining patent protection, we may choose not to seek patent protection for certain of our proprietary technologies. We may not be effective in policing unauthorized use of our intellectual property, trade secrets and other confidential information, and even if we do detect violations, litigation may be necessary to enforce our intellectual property rights. Any enforcement efforts we undertake, including litigation, could be time-consuming and expensive, could divert our management’s attention and may result in a court determining that our intellectual property or other rights are unenforceable. If we are not successful in cost-effectively protecting our intellectual property rights, trade secrets and confidential information, our business, operating results and financial condition could be harmed.
We may in the future be subject to intellectual property rights claims, which are extremely costly to defend, could require us to pay significant damages and could limit our ability to use certain technologies in the future.
Companies in the Internet and technology industries own large numbers of patents, copyrights, trademarks and trade secrets and frequently enter into litigation based on allegations of infringement or other violations of intellectual property rights. We have received, and may in the future receive, notices that claim we have misappropriated or misused other parties’ intellectual property rights, and, to the extent we gain greater visibility, we face a higher risk of being the subject of intellectual property infringement claims. There may be third-party intellectual property rights, including issued or pending patents that cover significant aspects of our technologies or business methods. Any intellectual property claim against us, with or without merit, could be time consuming, expensive to settle or litigate and could divert our management’s attention and other resources. These claims also could subject us to significant liability for damages and could result in our having to stop using technology found to be in violation of a third party’s rights. We might be required to seek a license for third-party intellectual property, which may not be available on reasonable terms or at all. Even if a license is available, we could be required to pay significant royalties, which would increase our operating expenses. We may also be required to develop alternative non-infringing technology, which could require significant effort and expense. If we cannot
25
Table of Contents
license or develop technology for any infringing aspect of our business, we would be forced to limit our services and may be unable to compete effectively. Any of these results would harm our business, operating results and financial condition.
Any legal liability, regulatory penalties, or negative publicity for the information on our website or that we distribute will likely harm our business and operating results.
We provide information on our website, through our customer care centers and in other ways regarding health insurance in general and the health insurance plans we market and sell, including information relating to insurance premiums, coverage, benefits, exclusions, limitations, availability, plan comparisons and insurance company ratings. A significant amount of both automated and manual effort is required to maintain the considerable amount of insurance plan information on our website. Separately, from time to time, we use the information provided on our website and otherwise collected by us to publish reports designed to educate consumers, facilitate public debate, and facilitate reform at the state and federal level relating to the accessibility and affordability of health insurance. If the information we provide on our website, through our customer care center or otherwise is not accurate or is construed as misleading, or if we do not properly assist individuals and businesses in purchasing health insurance, members, health insurance carriers and others could attempt to hold us liable for damages, and regulators could attempt to subject us to penalties, revoke our license to transact health insurance business in a particular jurisdiction, and/or compromise the status of our licenses to transact health insurance business in other jurisdictions. In the ordinary course of operating our business, we have received complaints that the information we provided was not accurate or was misleading. Although in the past we have resolved these complaints without significant financial cost, we cannot guarantee that we will be able to do so in the future. In addition, these types of claims could be time-consuming and expensive to defend, could divert our management’s attention and other resources, and could cause a loss of confidence in our services. As a result, whether or not we are able to successfully resolve these claims, they could harm our business, operating results and financial condition.
In the ordinary course of our business, we have received and may continue to receive inquiries from state regulators relating to various matters. We have become, and may in the future become, involved in litigation in the ordinary course of our business. If we are found to have violated laws or regulations, we could be subject to various fines and penalties, including revocation of our licenses to sell insurance, and our business, operating results and financial condition would be harmed. We would also be harmed to the extent that related publicity damages our reputation as a trusted source of information relating to health insurance and its affordability. It could also be costly to defend ourselves regardless of the outcome.
Our ability to attract and retain qualified personnel is critical to our success.
Our success is dependent upon the performance of our senior management and key personnel. Our management and employees can terminate their employment at any time, and the loss of the services of any of our executive officers or key employees could harm our business. For example, we appoint a single writing agent with each insurance carrier. If we lose the service of our appointed writing agent, the duties of writing agent will need to be transitioned to other company personnel. Due to our national reach and the large number of carrier partners whose policies are purchased by our members, this transition may be difficult and requires a significant period of time to complete. If the transition is not successful or takes too long to complete, our agency relationship with particular insurance carriers may be terminated, our commission payments could be discontinued or delayed and, as a result, our business, operating results and financial condition would be harmed. Our success is also dependent upon our ability to attract additional personnel for all areas of our organization. We may not be successful in attracting and retaining personnel on a timely basis, on competitive terms or at all. If we are unable to attract and retain the necessary personnel, our business would be harmed.
Most of our senior management and key employees have sold shares of our common stock in the open market, and some have sold a significant portion of their vested holdings. These employees may be more likely to leave us given that they have liquidated some or a substantial percentage of their holdings. Our senior management and key employees work for us on an at-will basis and our business could be harmed if we lose their services.
26
Table of Contents
If we fail to manage the expansion of our business, our business and operating results would be harmed.
We have expanded our operations significantly and are in the process of entering into the business of selling Medicare plans and providing the use of our technology and services to governmental entities. Our entering into these new areas of business places increasing and significant demands on our management, our operational and financial systems and infrastructure and our other resources. If we do not effectively manage this expansion, the quality of our services could suffer, which could harm our business, operating results and financial condition. In order to successfully expand our business, we need to hire, integrate and retain highly skilled and motivated employees. We also need to continue to improve our existing systems for operational and financial management, including our reporting systems, procedures and controls. These improvements could require significant capital expenditures and place increasing demands on our management. We may not be successful in managing or expanding our operations or in maintaining adequate financial and operating systems and controls. If we do not successfully implement improvements in these areas, our business, operating results and financial condition will be harmed.
Seasonality may cause fluctuations in our financial results.
The number of individual and family health insurance applications submitted through our ecommerce platform has generally increased in our first quarter compared to our fourth quarter and in our third quarter compared to our second quarter. Conversely, we have generally experienced a decline or flattening of individual and family submitted applications in our second quarter compared to our first quarter and in our fourth quarter compared to our third quarter. Since a significant portion of our marketing and advertising expenses are driven by the number of health insurance applications submitted on our ecommerce platform, those expenses are influenced by these patterns. The reasons for these seasonal patterns are not entirely clear. As the use of the Internet for the purchase and sale of health insurance becomes more widely accepted and our business matures, other seasonality trends may develop and the existing seasonality and consumer behavior that we experience may change. Any seasonality that we experience may cause fluctuations in our financial results.
Our business of marketing Medicare plans is very seasonal. The vast majority of Medicare plans are sold in the fourth quarter each year during the Medicare annual enrollment period. We also incur a significant portion of our Medicare plan related marketing expenses during the fourth quarter. We may not be paid for a considerable portion of the referral fees owed to us until the first quarter. This seasonality pattern results from the timing of the annual enrollment period when Medicare-eligible individuals can make changes to their Medicare Advantage or Medicare Part D prescription drug coverage for the following year.
Acquisitions could disrupt our business and harm our financial condition and operating results.
We may decide to acquire businesses, products and technologies. Our ability as an organization to successfully make and integrate acquisitions is unproven. Acquisitions could require significant capital infusions and could involve many risks, including the following:
| • | an acquisition may negatively impact our results of operations because it may require us to incur charges and substantial debt or liabilities, may require the amortization, write down or impairment of amounts related to deferred compensation, goodwill and other intangible assets, or may cause adverse tax consequences, substantial depreciation or deferred compensation charges; |
| • | an acquisition undertaken for strategic business purposes may negatively impact our results of operations; |
| • | we may encounter difficulties in assimilating and integrating the business, technologies, products, personnel or operations of companies that we acquire, particularly if key personnel of the acquired company decide not to work for us; |
| • | an acquisition may disrupt our ongoing business, divert resources, increase our expenses and distract our management; |
27
Table of Contents
| • | we may be required to implement or improve internal controls, procedures and policies appropriate for a public company at a business that prior to the acquisition lacked these controls, procedures and policies; |
| • | the acquired businesses, products or technologies may not generate sufficient revenue to offset acquisition costs or to maintain our financial results; |
| • | we may have to issue equity securities to complete an acquisition, which would dilute our stockholders’ ownership and could adversely affect the market price of our common stock; and |
| • | acquisitions may involve the entry into geographic or business markets in which we have little or no prior experience. |
We cannot assure you that we will be able to identify or consummate any future acquisition on favorable terms, or at all. If we do pursue an acquisition, it is possible that we may not realize the anticipated benefits from the acquisition or that the financial markets or investors will negatively view the acquisition. Even if we successfully complete an acquisition, it could harm our business, operating results and financial condition.
As a part of our initiative to enter into the Medicare plan business, we acquired PlanPrescriber, Inc. in April 2010. PlanPrescriber is a provider of online tools to help seniors navigate Medicare health insurance options. PlanPrescriber has derived its Medicare plan related revenue through the referral of Medicare plan leads to third parties. We may not be able to realize anticipated synergies and opportunities as a result of the acquisition, and the business may not perform as planned as a result of many of the risks and uncertainties that apply to the rest of our business and the marketing of Medicare plans. If anticipated synergies and opportunities are not realized, our business, operating results and financial condition would be harmed.
Issues arising from the implementation of an enterprise data management system could affect our operating results and ability to manage our business effectively.
We believe an enterprise data management system will be important to our accounting, financial and operating functions, and the implementation of a system raises costs and risks associated with the conversion to a new system, including disruption to our normal accounting procedures and problems achieving accuracy in the conversion of electronic data. Failure to properly or adequately address these issues could result in increased costs and the diversion of management’s attention and resources and could harm our operating results and ability to manage our business effectively.
If we fail to maintain proper and effective internal controls, our ability to produce accurate financial statements could be impaired, which could adversely affect our operating results, our ability to operate our business and our stock price.
We have a complex business organization, and we are in the process of expanding our business operations into the areas of the sale of Medicare plans and government contracting. Ensuring that we have adequate internal financial and accounting controls and procedures in place to help ensure that we can produce accurate financial statements on a timely basis is a costly and time-consuming effort that needs to be re-evaluated frequently and is complicated by the expansion of our business operations. Our management, including our chief executive officer and chief financial officer, does not expect that our internal control over financial reporting will prevent all errors or all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Controls can be circumvented by the individual acts of some persons, by collusion of two or more people, or by management override of the controls. Over time, controls may become inadequate because changes in conditions or deterioration in the degree of compliance with policies or procedures may occur. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected.
28
Table of Contents
As a result, we cannot assure that significant deficiencies or material weaknesses in our internal control over financial reporting will not be identified in the future. Any failure to maintain or implement required new or improved controls, or any difficulties we encounter in their implementation, could result in significant deficiencies or material weaknesses, cause us to fail to timely meet our periodic reporting obligations, or result in material misstatements in our financial statements. Any such failure could also adversely affect the results of periodic management evaluations and annual auditor attestation reports regarding disclosure controls and the effectiveness of our internal control over financial reporting required under Section 404 of the Sarbanes-Oxley Act of 2002 and the rules promulgated thereunder. The existence of a material weakness could result in errors in our financial statements that could result in a restatement of financial statements, cause us to fail to timely meet our reporting obligations and cause investors to lose confidence in our reported financial information, leading to a decline in our stock price and potential lawsuits against us.
Changes in our provision for income taxes or adverse outcomes resulting from examination of our income or other tax returns could adversely affect our results.
Our provision for income taxes is subject to volatility and could be adversely affected by earnings differing materially from our projections; by changes in the valuation of our deferred tax assets and liabilities; by expiration of or lapses in the research and development tax credit laws; by tax effects of share-based compensation; or by changes in tax laws, regulations, accounting principles, including accounting for uncertain tax positions, or interpretations thereof. For instance, in October 2010, the state of California approved budget legislation which substantially limits the utilization of net operating losses. The new law did not affect the amount of net operating losses and tax credits that we expect to ultimately use to offset future California taxes, but limited the amount we could utilize in 2010 and will be able to utilize in 2011. Since the majority of our state taxes are in California, where our headquarters are located, our cash outlay for federal and state taxes increased for the year ended December 31, 2010 and is expected to increase for the year ending December 31, 2011.
Significant judgment is required to determine the recognition and measurement attribute prescribed in U.S. generally accepted accounting principles (“U.S. GAAP”) relating to accounting for income taxes. In addition, U.S. GAAP applies to all income tax positions, including the potential recovery of previously paid taxes, which if settled unfavorably could adversely impact our provision for income taxes or additional paid-in capital. In addition, we are subject to examinations of our income tax returns by the Internal Revenue Service and other tax authorities. We assess the likelihood of adverse outcomes resulting from these examinations to determine the adequacy of our provision for income taxes. There may be exposure that the outcomes from these examinations will have an adverse effect on our operating results and financial condition.
Any expansion of our business into foreign countries involves significant risks.
We currently do not sell health insurance or license our technology platform outside the United States other than in China. We may attempt to expand aspects of our business to additional geographic regions. We face significant challenges in connection with expanding our business into any foreign country, since we have no prior experience marketing or selling insurance in any foreign jurisdiction. Additionally, demand for private health insurance is not significant in many foreign countries as a result of government-sponsored health care systems. In addition to facing many of the same challenges we face domestically, we also would have to overcome other obstacles such as:
| • | legal, political or systemic restrictions on the ability of United States companies to market insurance or otherwise do business in foreign countries; |
| • | varied, unfamiliar and unclear legal and regulatory restrictions; |
| • | less extensive adoption of the Internet as a commerce medium or information source and increased restriction on the content of websites; and |
| • | the adaptation of our website and distribution model to fit the particular foreign country. |
29
Table of Contents
As a result of these obstacles, we may find it impossible or prohibitively expensive to expand our services internationally or we may be unsuccessful should we attempt to do so, either of which could harm our business, operating results and financial condition.
Risks Related to Insurance Regulation
Regulation of the sale of health insurance is subject to change, and future regulations could harm our business and operating results.
The laws and regulations governing the offer, sale and purchase of health insurance are subject to change, and future changes may be adverse to our business. For example, a long standing provision in each state’s law that we believe is advantageous to our business is that once health insurance premiums are set by the carrier and approved by state regulators, they are fixed and not generally subject to negotiation or discounting by insurance companies or agents. Additionally, state regulations generally prohibit carriers, agents and brokers from providing financial incentives, such as rebates, to their members in connection with the sale of health insurance. As a result, we do not currently compete with carriers or other agents and brokers on the price of the health insurance plans offered on our website. If these regulations change, we could be forced to reduce prices or provide rebates or other incentives for the health insurance plans sold through our ecommerce platform, which would harm our business, operating results and financial condition.
States have, and will continue, to adopt new laws and regulations in response to health care reform legislation. It is too early to predict how these new laws and regulations will impact our business, but in some cases such laws and regulations could amplify the adverse impacts of health care reform, or may adopt new requirements that adversely impact our business, operating results and financial condition.
We are also subject to additional insurance regulatory risks, because we use the Internet as our distribution platform. In many cases, it is not clear how existing insurance laws and regulations apply to Internet-related health insurance advertisements and transactions. To the extent that new laws or regulations are adopted that conflict with the way we conduct our business, or to the extent that existing laws and regulations are interpreted adversely to us, our business, operating results and financial condition would be harmed.
If we fail to comply with the numerous laws and regulations that are applicable to our individual, family and small business health insurance business, our business and operating results would be harmed.
The individual, family and small business health insurance industry is heavily regulated by each state in the United States. For instance, state regulators require us to maintain a valid license in each state in which we transact health insurance business and further require that we adhere to sales, documentation and administration practices specific to that state. In addition, each employee who transacts health insurance business on our behalf must maintain a valid license in one or more states. Because we do business in all 50 states and the District of Columbia, compliance with health insurance-related laws, rules and regulations is difficult and imposes significant costs on our business. Each jurisdiction’s insurance department typically has the power, among other things, to:
| • | grant and revoke licenses to transact insurance business; |
| • | conduct inquiries into the insurance-related activities and conduct of agents and agencies; |
| • | require and regulate disclosure in connection with the sale and solicitation of health insurance; |
| • | authorize how, by which personnel and under what circumstances insurance premiums can be quoted and published and an insurance policy sold; |
| • | approve which entities can be paid commissions from carriers and the circumstances under which they may be paid; |
30
Table of Contents
| • | regulate the content of insurance-related advertisements, including web pages, and other marketing practices; |
| • | approve policy forms, require specific benefits and benefit levels and regulate premium rates; |
| • | impose fines and other penalties; and |
| • | impose continuing education requirements. |
Due to the complexity, periodic modification and differing interpretations of insurance laws and regulations, we may not have always been, and we may not always be, in compliance with them. New insurance laws, regulations and guidelines also may not be compatible with the sale of health insurance over the Internet or with various aspects of our platform or manner of marketing or selling health insurance plans. Failure to comply with insurance laws, regulations and guidelines or other laws and regulations applicable to our business could result in significant liability, additional department of insurance licensing requirements, the revocation of licenses in a particular jurisdiction and/or our inability to sell health insurance plans, which could significantly increase our operating expenses and otherwise harm our business, operating results and financial condition. Moreover, an adverse regulatory action in one jurisdiction could result in penalties and adversely affect our license status or reputation in other jurisdictions due to the requirement that adverse regulatory actions in one jurisdiction be reported to other jurisdictions. We also are required to maintain health insurance licenses to sell Medicare products. Even if the allegations in any regulatory or other action against us are proven false, any surrounding negative publicity could harm consumer, marketing partner or health insurance carrier confidence in us, which could significantly damage our brand. Because some consumers, marketing partners and health insurance carriers may not be comfortable with the concept of purchasing health insurance using the Internet, any negative publicity may affect us more than it would others in the health insurance industry and would harm our business, operating results and financial condition. Changes in insurance laws, regulations and guidelines may also be incompatible with various aspects of our business and require that we make significant modifications to our existing technology or practices, which may be costly and time-consuming to implement and could also harm our business, operating results and financial condition.
In addition, we have received, and may in the future receive, inquiries from regulators regarding our marketing and business practices. We typically respond by explaining how we believe we are in compliance with relevant regulations or may modify our practices in connection with the inquiry. Any modification of our marketing or business practices in response to future regulatory inquiries could harm our business, operating results or financial condition.
Risks Related to the Internet and Electronic Commerce
Our business is subject to online commerce security risks and, if we are unable to safeguard the security and privacy of confidential data, our business will be harmed.
Our services involve the collection and storage of confidential information of consumers and the transmission of this information to their chosen health insurance carriers. For example, we collect names, addresses, Social Security and credit card numbers, and information regarding the medical history of consumers in connection with their applications for health insurance. We cannot guarantee that we will be free of security breaches. We may be required to expend significant capital and other resources to protect against security breaches or to alleviate problems caused by security breaches. Despite our implementation of security measures, techniques used to obtain unauthorized access or to sabotage systems change frequently. As a result, we may be unable to anticipate these techniques or to implement adequate preventative measures. Any compromise or perceived compromise of our security could damage our reputation and our relationship with our members, marketing partners and health insurance carriers, could reduce demand for our services and could subject us to significant liability as well as regulatory action, which would harm our business, operating results and financial condition. In addition, in the event that data security laws are implemented, or our health insurance carrier or
31
Table of Contents
other partners determine to impose new requirements on us relating to data security, we may not be able to timely comply with such requirements or such requirements may not be compatible with our current processes. Changing our processes could be time consuming and expensive, and failure to timely implement required changes could result in our inability to sell health insurance plans in a particular jurisdiction or for a particular health insurance carrier or subject us to liability for non-compliance, any of which would damage our business, operating results and financial condition.
Government regulation of the Internet could adversely affect our business.
The laws governing general commerce on the Internet remain unsettled and it may take years to fully determine whether and how existing laws such as those governing intellectual property, privacy and taxation apply to the Internet. In addition, the growth and development of the market for electronic commerce may prompt calls for more stringent consumer protection laws that may impose additional burdens on companies conducting business over the Internet. Any new laws or regulations or new interpretations of existing laws or regulations relating to the Internet could harm our business and we could be forced to incur substantial costs in order to comply with them, which would harm our business, operating results and financial condition.
Our business could be harmed if we are unable to correspond with our consumers or market the availability of our ecommerce platform by email.
We use email to market our services to potential members and as the primary means of communicating with our existing members. The laws and regulations governing the use of email for marketing purposes continue to evolve and the growth and development of the market for commerce over the Internet may lead to the adoption of additional legislation. If new laws or regulations are adopted, or existing laws and regulations are interpreted, to impose additional restrictions on our ability to send email to our members or potential members, we may not be able to communicate with them in a cost-effective manner. In addition to legal restrictions on the use of email, Internet service providers and others attempt to block the transmission of unsolicited email, commonly known as “spam.” If an Internet service provider or software program identifies email from us as “spam,” we can be placed on a restricted list that will block our email to members or potential members who maintain email accounts with these Internet service providers or who use these software programs. If we are unable to communicate by email with our members and potential members as a result of legislation, blockage or otherwise, our business, operating results and financial condition would be harmed.
Consumers depend upon third-party service providers to access our website, and our business and operating results could be harmed as a result of technical difficulties experienced by these service providers.
Consumers using our website depend upon Internet, online and other service providers for access to our website. Many of these service providers have experienced significant outages, delays and other difficulties in the past and could experience them in the future. Any significant interruption in access to our website or increase in our website’s response time as a result of these difficulties could damage our relationship with insurance carriers, marketing partners and existing and potential members and could harm our business, operating results and financial condition.
Risks Related to the Ownership of Our Common Stock
The trading price of our common stock may be subject to significant fluctuations and volatility, and our stockholders may be unable to resell their shares at a profit.
The stock markets, in general, and the markets for high technology stocks in particular, have historically experienced high levels of volatility. The market for technology stocks has been extremely volatile and frequently reaches levels that bear no relationship to the past or present operating performance of those companies. These broad market fluctuations may adversely affect the trading price of our common stock. In addition, the trading price of our common stock has been subject to significant fluctuations and may continue to fluctuate or decline, particularly as a result of developments relating to health care reform legislation. Factors that could cause fluctuations in the trading price of our common stock include, but are not limited to, the following:
32
Table of Contents
| • | price and volume fluctuations in the overall stock market from time to time; |
| • | significant volatility in the market price and trading volume of technology companies in general, and companies in our industry; |
| • | actual or anticipated changes in our results of operations or fluctuations in our operating results; |
| • | actual or anticipated changes in the expectations of investors or securities analysts, including changes in financial estimates or investment recommendations by securities analysts who follow our business and changes in perceptions relating to the economy; |
| • | speculation in the press or investment community; |
| • | technological advances or introduction of new products by us or our competitors; |
| • | actual or anticipated developments in our competitors’ businesses or the competitive landscape generally; |
| • | litigation involving us, our industry or both; |
| • | actual or anticipated regulatory developments in the United States or foreign countries, including health care reform legislation in the United States; |
| • | major catastrophic events; |
| • | announcements or developments relating to the economy; |
| • | our sale of common stock or other securities in the future; |
| • | the trading volume of our common stock, as well as sales of large blocks of our stock; or |
| • | departures of key personnel. |
These factors, as well as general economic and political conditions and the announcement of proposed and completed acquisitions or other significant transactions, or any difficulties associated with such transactions, by us or our strategic partners, customers or our current competitors, may materially adversely affect the market price of our common stock in the future. In the past, following periods of volatility in the market price of a company’s securities, securities class action litigation has often been instituted against that company. Such litigation could result in substantial cost and a diversion of management’s attention and resources. In addition, volatility, lack of positive performance in our stock price or changes to our overall compensation program, including our equity incentive program, may adversely affect our ability to retain key employees.
A limited number of stockholders have the ability to influence the outcome of director elections and other matters requiring stockholder approval.
A small number of greater than 5% stockholders and their affiliated entities beneficially owned approximately sixty percent of our outstanding common stock as of December 31, 2010. These stockholders, if they act together, could exert substantial influence over matters requiring approval by our stockholders, including the election of directors, the amendment of our certificate of incorporation and bylaws and the approval of mergers or other business combination transactions. This concentration of ownership may discourage, delay or prevent a change in control of our company, which could deprive our stockholders of an opportunity to receive a premium for their stock as part of a sale of our company and might reduce our stock price. These actions may be taken even if they are opposed by other stockholders.
Certain provisions in our charter documents and Delaware law could discourage takeover attempts and lead to management entrenchment.
Our certificate of incorporation and bylaws contain provisions that could have the effect of delaying or preventing changes in control or changes in our management without the consent of our board of directors. These provisions include:
33
Table of Contents
| • | a classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors; |
| • | cumulative voting in the election of directors is prohibited, which limits the ability of minority stockholders to elect director candidates; |
| • | the exclusive right of our board of directors to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors; |
| • | the ability of our board of directors to determine to issue shares of preferred stock and to determine the price and other terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquiror; |
| • | a prohibition on stockholder action by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders; |
| • | the requirement that a special meeting of stockholders may be called only by the chairman of the board of directors, the chief executive officer or the board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors; and |
| • | advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquiror from conducting a solicitation of proxies to elect the acquiror’s own slate of directors or otherwise attempting to obtain control of us. |
We are also subject to certain anti-takeover provisions under Delaware law. Under Delaware law, a corporation may, in general, not engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other things, the board of directors has approved the transaction.
| ITEM 1B. | UNRESOLVED STAFF COMMENTS |
None.
34
Table of Contents
| ITEM 2. | PROPERTIES |
The following table sets forth the location, approximate square footage and primary use of each of the principal properties we occupied at December 31, 2010:
| Location |
Approximate Square Footage |
Primary Use | ||||
| Mountain View, California – East Middlefield Road |
17,740 | Corporate headquarters, marketing and advertising, technology and content and general and administrative | ||||
| Mountain View, California – North Whisman Road |
7,744 | General and administrative | ||||
| Gold River, California |
38,897 | Customer care and enrollment, technology and content and general and administrative | ||||
| San Francisco, California |
6,500 | Marketing and advertising and general and administrative | ||||
| Salt Lake City, Utah |
12,980 | Customer care and enrollment | ||||
| Maynard, Massachusetts |
11,174 | Marketing and advertising and technology and content | ||||
| Xiamen, China |
48,873 | Technology and content, customer care and enrollment, marketing and advertising and general and administrative | ||||
We lease or sublease all of these properties. We believe our existing facilities will be adequate to meet our needs for the next twelve months.
| ITEM 3. | LEGAL PROCEEDINGS |
In the ordinary course of our business, we have received and may continue to receive inquiries from regulators relating to various matters. We have also become, and may in the future become, involved in litigation in the ordinary course of our business.
| ITEM 4. | RESERVED |
35
Table of Contents
| ITEM 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Our common stock has been quoted on The NASDAQ Global Market under the symbol “EHTH” since our initial public offering on October 13, 2006. Prior to that time, there was no public market for our stock. As of February 28, 2011, there were 67 stockholders of record of our common stock (which does not include the number of stockholders holding shares of our common stock in “street name”) and the closing price of our common stock was $12.54 per share on February 28, 2011 as reported by The NASDAQ Global Market.
The following table sets forth for the indicated period the closing high and low sales prices for our common stock as reported on The NASDAQ Global Market.
| High | Low | |||||||
| First Quarter 2010 |
$ | 18.88 | $ | 15.75 | ||||
| Second Quarter 2010 |
$ | 15.75 | $ | 11.14 | ||||
| Third Quarter 2010 |
$ | 12.91 | $ | 9.54 | ||||
| Fourth Quarter 2010 |
$ | 15.93 | $ | 12.62 | ||||
| Year 2010 |
$ | 18.88 | $ | 9.54 | ||||
| High | Low | |||||||
| First Quarter 2009 |
$ | 16.44 | $ | 11.67 | ||||
| Second Quarter 2009 |
$ | 19.19 | $ | 14.05 | ||||
| Third Quarter 2009 |
$ | 18.90 | $ | 14.20 | ||||
| Fourth Quarter 2009 |
$ | 16.65 | $ | 13.07 | ||||
| Year 2009 |
$ | 19.19 | $ | 11.67 | ||||
Dividend Policy
We have never declared or paid any cash dividend on our common stock. We currently do not expect to pay any dividends in the foreseeable future.
Unregistered Sales of Equity Securities
During the quarter ended December 31, 2010, we did not issue or sell any shares of our common stock or other equity securities pursuant to unregistered transactions in reliance upon an exemption from the registration requirements of the Securities Act of 1933, as amended.
Issuer Purchases of Equity Securities
On November 12, 2008, we announced that our board of directors authorized a stock repurchase program, pursuant to which up to 2,507,950 shares could be repurchased, for a total cost not to exceed $30 million. This stock repurchase program was completed in September 2009 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. On July 27, 2010, we announced that our board of directors approved a stock repurchase program authorizing us to purchase up to $30 million of our common stock. This stock repurchase program was completed in January 2011 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. The cost of the repurchased shares was funded from available working capital for these stock repurchase programs. Share repurchases under these programs complied with Rule 10b-18 under the Securities Exchange Act of 1934, as amended. All shares repurchased under the programs were returned to the status of authorized but unissued shares of common stock. For accounting purposes, common stock repurchased under the programs was recorded
36
Table of Contents
based upon the settlement date of the applicable trade. Such repurchased shares are held in treasury and are presented using the cost method.
The stock repurchase activity under our stock repurchase programs during the years ended December 31, 2009 and 2010 is summarized as follows (in thousands, except share and per share amounts):
| Total Number of Shares Purchased |
Average Price Paid per Share (1) |
Amount of Repurchase |
||||||||||
| Cumulative balance at December 31, 2008 |
50,657 | $ | 12.61 | $ | 639 | |||||||
| Repurchases of common stock during 2009 |
1,827,193 | $ | 16.07 | 29,360 | ||||||||
| Cumulative balance at December 31, 2009 |
1,877,850 | $ | 15.97 | 29,999 | ||||||||
| Repurchases of common stock during 2010 |
2,026,802 | $ | 12.93 | 26,204 | ||||||||
| Cumulative balance at December 31, 2010 |
3,904,652 | $ | 14.39 | $ | 56,203 | |||||||
| (1) | Average price paid per share includes commissions |
In addition to the 3,904,652 shares repurchased under our repurchase programs as of December 31, 2010, we have in treasury 51,476 shares that were surrendered by employees to satisfy tax withholdings due in connection with the vesting of certain restricted stock units. As of December 31, 2010 and 2009, we had a total of 3,956,128 shares and 1,894,355 shares, respectively, held in treasury.
The following table summarizes the stock repurchase activity for the three months ended December 31, 2010 and the approximate dollar value of shares that may yet be purchased pursuant to our stock repurchase program:
| Total Number of Shares Purchased |
Average Price Paid per Share |
Total Number of Shares Purchased as Part of Publicly Announced Program |
Approximate Dollar Amount of Shares that May Yet Be Repurchased |
|||||||||||||
| (in thousands) | ||||||||||||||||
| October 1, 2010 – October 31, 2010 |
605,258 | $ | 13.04 | 605,258 | $ | 13,381 | ||||||||||
| November 1, 2010 – November 30, 2010 |
398,499 | $ | 14.19 | 398,499 | $ | 7,726 | ||||||||||
| December 1, 2010 – December 31, 2010 |
271,807 | $ | 14.46 | 271,807 | $ | 3,796 | ||||||||||
| Total |
1,275,564 | $ | 13.70 | 1,275,564 | ||||||||||||
37
Table of Contents
STOCK PERFORMANCE GRAPH
The following information relating to the price performance of our common stock shall not be deemed “filed” with the Securities and Exchange Commission or “soliciting material” under the Securities Exchange Act of 1934, as amended, or subject to Regulation 14A or 14C, or to liabilities under Section 18 of the Exchange Act, except to the extent that we specifically request that such information be treated as soliciting material or to the extent that we specifically incorporate this information by reference.
The graph below compares the cumulative total stockholder return on our common stock with the cumulative total returns on the NASDAQ Composite index and the Research Data Group (“RDG”) Internet Composite index for the period between our initial public offering on October 13, 2006 and December 31, 2010, assuming an investment of $100 at the beginning of such period and the reinvestment of any dividends. Pursuant to Securities and Exchange Commission rules, the starting value of the investment in our common stock is based on the closing price of our common stock on October 13, 2006, or $22.90 per share. It is not based on our $14.00 per share initial public offering price.
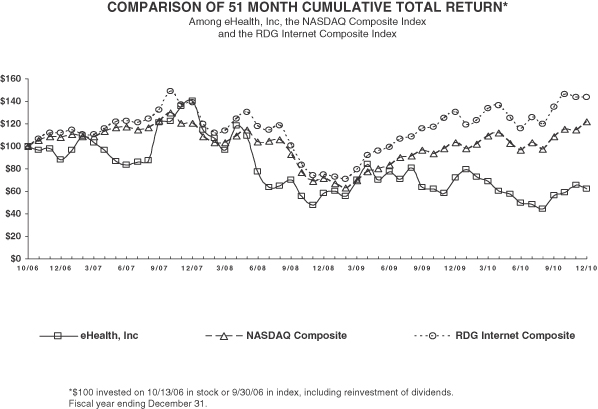
| 10/13/06 | 12/29/06 | 12/31/07 | 12/31/08 | 12/31/09 | 12/31/10 | |||||||||||||||||||
| eHealth, Inc. |
100.00 | 87.82 | 140.22 | 57.99 | 71.75 | 61.97 | ||||||||||||||||||
| NASDAQ Composite |
100.00 | 107.65 | 117.62 | 68.58 | 99.98 | 121.53 | ||||||||||||||||||
| RDG Internet Composite |
100.00 | 111.66 | 136.46 | 73.99 | 138.60 | 143.35 | ||||||||||||||||||
The stock price performance included in this graph is not necessarily indicative of future stock price performance.
38
Table of Contents
| ITEM 6. | SELECTED CONSOLIDATED FINANCIAL DATA |
The following selected consolidated financial data should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and with our consolidated financial statements and accompanying notes included in this Annual Report on Form 10-K.
| Year Ended December 31, | ||||||||||||||||||||
| 2006 | 2007 | 2008 | 2009 | 2010 | ||||||||||||||||
| (in thousands, except per share amounts) | ||||||||||||||||||||
| Consolidated Statements of Income Data: |
||||||||||||||||||||
| Revenue: |
||||||||||||||||||||
| Commission |
$ | 58,943 | $ | 81,502 | $ | 100,839 | $ | 119,259 | $ | 135,366 | ||||||||||
| Other |
2,367 | 6,289 | 10,872 | 15,631 | 25,038 | |||||||||||||||
| Total revenue |
61,310 | 87,791 | 111,711 | 134,890 | 160,404 | |||||||||||||||
| Operating costs and expenses: |
||||||||||||||||||||
| Cost of revenue |
1,305 | 1,702 | 1,746 | 4,581 | 5,499 | |||||||||||||||
| Marketing and advertising* |
21,405 | 29,497 | 42,161 | 53,987 | 60,102 | |||||||||||||||
| Customer care and enrollment* |
10,991 | 12,137 | 14,379 | 14,769 | 17,810 | |||||||||||||||
| Technology and content* |
10,137 | 12,393 | 14,182 | 15,685 | 19,241 | |||||||||||||||
| General and administrative* |
9,482 | 16,046 | 17,983 | 20,028 | 24,055 | |||||||||||||||
| Amortization of acquired intangible assets |
— | — | — | — | 1,138 | |||||||||||||||
| Total operating costs and expenses |
53,320 | 71,775 | 90,451 | 109,050 | 127,845 | |||||||||||||||
| Income from operations |
7,990 | 16,016 | 21,260 | 25,840 | 32,559 | |||||||||||||||
| Interest and other income, net |
1,326 | 5,287 | 3,714 | 938 | 9 | |||||||||||||||
| Income before income taxes |
9,316 | 21,303 | 24,974 | 26,778 | 32,568 | |||||||||||||||
| Provision (benefit) for income taxes |
(7,161 | ) | (10,292 | ) | 10,806 | 11,431 | 15,086 | |||||||||||||
| Net income |
$ | 16,477 | $ | 31,595 | $ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||||||
| Net income per share: |
||||||||||||||||||||
| Basic—common stock |
$ | 1.91 | $ | 1.37 | $ | 0.57 | $ | 0.63 | $ | 0.76 | ||||||||||
| Basic—Class A nonvoting common stock |
$ | 1.91 | $ | — | — | — | — | |||||||||||||
| Diluted—common stock |
$ | 0.80 | $ | 1.22 | $ | 0.55 | $ | 0.61 | $ | 0.73 | ||||||||||
| Diluted—Class A nonvoting common stock |
$ | 0.80 | $ | — | — | — | — | |||||||||||||
| Net income: |
||||||||||||||||||||
| Allocated to common stock |
$ | 16,391 | $ | 31,595 | $ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||||||
| Allocated to Class A nonvoting common stock |
86 | — | — | — | — | |||||||||||||||
| Net income |
$ | 16,477 | $ | 31,595 | $ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||||||
| Weighted average number of shares used in per share amounts: |
||||||||||||||||||||
| Basic—common stock |
8,590 | 23,092 | 24,963 | 24,309 | 23,118 | |||||||||||||||
| Basic—Class A nonvoting common stock |
45 | — | — | — | — | |||||||||||||||
| Diluted—common stock |
20,572 | 25,797 | 25,954 | 25,201 | 23,873 | |||||||||||||||
| Diluted—Class A nonvoting common stock |
45 | — | — | — | — | |||||||||||||||
|
* Includes stock-based compensation as follows: |
||||||||||||||||||||
| Marketing and advertising |
$ | 47 | $ | 218 | $ | 644 | $ | 803 | $ | 808 | ||||||||||
| Customer care and enrollment |
42 | 138 | 266 | 325 | 384 | |||||||||||||||
| Technology and content |
226 | 611 | 898 | 1,194 | 1,622 | |||||||||||||||
| General and administrative |
139 | 539 | 1,686 | 2,513 | 3,581 | |||||||||||||||
| Total |
$ | 454 | $ | 1,506 | $ | 3,494 | $ | 4,835 | $ | 6,395 | ||||||||||
39
Table of Contents
| As of December 31, | ||||||||||||||||||||
| 2006 | 2007 | 2008 | 2009 | 2010 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Consolidated Balance Sheet Data: |
||||||||||||||||||||
| Cash, cash equivalents and marketable securities |
$ | 90,474 | $ | 121,514 | $ | 150,635 | $ | 153,523 | $ | 128,074 | ||||||||||
| Working capital |
86,503 | 126,845 | 148,946 | 148,891 | 128,395 | |||||||||||||||
| Total assets |
104,928 | 147,453 | 168,755 | 169,708 | 185,845 | |||||||||||||||
| Other non-current liabilities |
317 | 252 | 628 | 2,997 | 3,451 | |||||||||||||||
| Retained earnings (accumulated deficit) |
(63,655 | ) | (32,060 | ) | (17,892 | ) | (2,545 | ) | 14,937 | |||||||||||
| Total stockholders’ equity |
95,740 | 135,894 | 154,979 | 151,451 | 162,197 | |||||||||||||||
40
Table of Contents
| ITEM 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
Overview
We are the leading online source of health insurance for individuals, families and small businesses. Through our website addresses (www.eHealth.com, www.eHealthInsurance.com, www.eHealthMedicare.com and www.PlanPrescriber.com), consumers can get quotes from leading health insurance carriers, compare plans side by side, and apply for and purchase individual and family, small business, short-term, ancillary and Medicare-related health insurance plans. Our ecommerce technology also enables us to deliver consumers’ health insurance applications electronically to health insurance carriers. As a result, we simplify and streamline the complex and traditionally paper-intensive health insurance sales and purchasing process.
We have invested heavily in technology and content related to our ecommerce platform. We have also invested significant time and resources in obtaining licenses to sell health insurance in all 50 states and the District of Columbia, developing diverse member acquisition programs and establishing relationships with over 180 leading insurance carriers, enabling us to offer thousands of health insurance plans online. Our ecommerce platform can be accessed directly through our website as well as through our network of marketing partners.
We generate revenue primarily from commissions we receive from health insurance carriers whose individual, family and small business policies are purchased through our ecommerce platform. The commission payments we receive are typically a percentage of the premium on an individual, family or small business health insurance policy that we sold and are made to us on a monthly basis for as long as a policy remains active with us. As a result, much of our revenue for a given financial reporting period relates to policies that we sold prior to the beginning of the period and is recurring in nature. Additionally, health insurance pricing, which is set by the health insurance carrier and approved by state regulators, is not subject to negotiation or discounting by health insurance carriers or our competitors.
In April 2010, we acquired PlanPrescriber, Inc. (“PlanPrescriber,” formerly Experion Systems, Inc.), a privately-held company. PlanPrescriber is a leading provider of online tools to help seniors navigate Medicare health insurance options.
We began actively marketing the availability of Medicare-related health insurance plans during 2010 through our online Medicare plan platforms (www.eHealthMedicare.com and www.PlanPrescriber.com). These platforms enable consumers to research and compare Medicare-related health insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. The revenue we have generated in our Medicare plan business is primarily referral fees paid to us based on leads generated by our online platforms that are delivered and sold to third parties. In 2010 we also launched online application capabilities for certain Medicare plans, and telephonic enrollment capabilities through our new customer care center in Salt Lake City, Utah. To the extent that we assist in the sale of Medicare-related insurance plans as a health insurance agent, we generate revenue from commissions we receive from health insurance carriers.
We also derive revenue from licensing the use of our health insurance ecommerce technology. Our technology platform enables health insurance carriers and agents to market and distribute health insurance plans online. Health insurance carriers or agents that license our technology typically pay us implementation fees and performance-based fees that are based on metrics such as submitted health insurance applications. We also recently began to license our ecommerce technology for use by government agencies and intend to market it to states implementing health insurance exchanges as a result of health care reform legislation. In our government technology licensing business, we may earn a combination of fixed license fees and time- and materials-based fees or we may be paid performance-based fees.
In March 2010, the federal Patient Protection and Affordable Care Act and related amendments in the Health Care and Education Reconciliation Act were signed into law. These health care reform laws contain
41
Table of Contents
provisions that have and will continue to change the health insurance industry in substantial ways. Among several other provisions, they include a mandate requiring individuals to be insured or face tax penalties; a mandate that certain employers offer their employees group health insurance coverage or face tax penalties; prohibitions against insurance companies using pre-existing health conditions as a reason to deny an application for health insurance; medical loss ratio requirements that require each health insurance carrier to spend a certain percentage of their premium revenue on reimbursement for clinical services and activities that improve health care quality; establishment of state and/or federal health insurance exchanges to facilitate access to, and the purchase of, health insurance; and subsidies and cost-sharing credits to make health insurance more affordable for those below certain income levels.
While many aspects of health care reform do not become effective until 2014, health insurance carriers are required to maintain medical loss ratios of eighty percent in their individual and family health insurance business beginning in 2011. The implementation of the medical loss ratio requirements by insurance carriers has resulted in a reduction in the commission rates that we are paid as a result of our selling individual and family health insurance plans. These reductions will begin to impact our individual and family health insurance plan commission-based revenue starting in 2011.
Sources of Revenue
Commission Revenue
We generate most of our revenue from commissions paid to us by health insurance carriers whose health insurance policies we have sold. Commission revenue represented 90%, 88% and 84% of our total revenue for the years ended December 31, 2008, 2009 and 2010, respectively.
Our commission revenue generally represents a percentage of the insurance premium and, to a much lesser extent, commission override payments that insurance carriers pay us for achieving sales volume thresholds or other objectives. Commission rates vary by carrier and by the type of plan purchased by a member. Commission rates also can vary based upon the amount of time that the policy has been active, with commission rates for individual and family policies typically being higher in the first twelve months of the policy. After the first twelve months, commission rates generally decline significantly. As a result, if we do not add a sufficient number of members on new policies, our revenue growth will be negatively impacted. Individuals, families and small businesses purchasing health insurance through us typically pay their premiums on a monthly basis. Insurance carriers typically pay us our commissions monthly, after they receive the premium payment from the member. For certain Medicare health insurance policies, we receive an annual commission payment at the beginning of the policy year. We generally continue to receive the commission payment from the relevant insurance carrier until the health insurance policy is cancelled or we otherwise do not remain the agent on the policy. As a result, the majority of our revenue is recurring in nature and has grown in correlation with the growth we have experienced in our membership base.
Our commission revenue has grown principally as a result of our penetration of the individual and family health insurance market and corresponding growth in our membership. We estimate that as of December 31, 2010 we had approximately 778,300 members compared to an estimated 728,000 members at December 31, 2009. We define a member as an individual covered by an insurance plan for which we are entitled to receive compensation. During the year ended December 31, 2010, we experienced a 2% decrease in the number of applications submitted through us for individual and family health insurance, compared to the year ended December 31, 2009. During the year ended December 31, 2010, the number of individuals approved for individual and family major medical health insurance plans decreased 3% over the number of individuals that were approved during the year ended December 31, 2009. We believe the decrease in the number of applications submitted through us for individual and family health insurance and in the number of individuals approved for individual and family major medical health insurance plans during 2010 was impacted by a number of factors, including consumer confusion related to the timing and impact of the federal health care reform legislation, weak
42
Table of Contents
macro-economic conditions and the federal subsidy for health benefits under the Consolidated Omnibus Budget Reconciliation Act of 1985 (“COBRA”). During the fourth quarter of 2010, we believe that the number of individual and family submitted health insurance applications was further impacted by our decision to reduce our marketing and advertising spending in our online advertising channel relating to those plans and to redirect a portion of this expense to our Medicare plan business. Individual and family health insurance submitted application volumes during the fourth quarter of 2010 were also impacted by several provisions of the federal Patient Protection and Affordable Care Act that became effective in September 2010, including certain minimum benefit requirements and prohibitions against insurance companies using pre-existing health conditions as a reason to deny a health insurance application of a child under the age of 19. As a result, health insurance carriers were making changes to their plans during the fourth quarter of 2010, which decreased available plan inventory on our ecommerce platform. We also believe our health insurance carrier partners adopted more stringent underwriting practices during 2010.
We recognize commission revenue when commissions are reported to us by a health insurance carrier, net of an allowance for future forfeiture amounts payable to carriers due to policy cancellations. Commissions are reported to us by a cash payment and commission statement. We generally receive these communications simultaneously. In instances when we receive the cash payment and commission statement separately and in different accounting periods, we recognize revenue in the period that we receive the earliest communication, provided we receive the second corroborating communication within ten business days following the end of the accounting period. If the second corroborating communication is not received within ten business days following the end of the accounting period, we recognize revenue in the period the second communication is received. We use the data in the commission statements to help identify the members for which we are receiving a commission payment and the amount received for each member, and to estimate our allowance for forfeitures payable to carriers. As a result, we recognize the net amount of compensation earned as the agent in the transaction. Commission override revenue, which we recognize on the same basis as premium commissions, is generally reported to us in a more irregular pattern than premium commissions. As a result, our revenue for a particular quarter could be higher or lower than expectations due to the timing of the reporting of commission override revenue to us.
We began actively marketing the availability of Medicare-related health insurance plans during 2010 through our online Medicare plan platforms (www.eHealthMedicare.com and www.PlanPrescriber.com). These platforms enable consumers to research and compare Medicare-related health insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. While the revenue we have generated in our Medicare plan business has been primarily referral fees paid to us based on leads generated by our online platforms, we also launched in 2010 online application capabilities for certain Medicare plans and telephonic enrollment capabilities through our new customer care center in Salt Lake City, Utah. To the extent that we assist in the sale of Medicare-related insurance plans as a health insurance agent, we generate revenue from commissions we receive from health insurance carriers, and these Medicare commissions are included in commission revenue.
Revenue attributable to major medical individual and family health insurance plans represented approximately 88%, 91% and 91% of our commission revenue in the years ended December 31, 2008, 2009 and 2010, respectively. Revenue attributable to major medical individual and family health insurance plans in the year ended December 31, 2010 included a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided. Major medical individual and family health insurance plans do not include small business, short-term, stand-alone dental, life, student and Medicare-related health insurance plans.
In March 2010, the federal Patient Protection and Affordable Care Act and related amendments in the Health Care and Education Reconciliation Act were signed into law. Among the many provisions included in these health care reform laws are medical loss ratio requirements that require each health insurance carrier to spend a certain percentage of their premium revenue on reimbursement for clinical services and activities that
43
Table of Contents
improve health care quality beginning in 2011. The implementation of the medical loss ratio requirements by insurance carriers has resulted in a reduction in the commission rates that we are paid as a result of our selling individual and family health insurance plans. These reductions will begin to impact our individual and family health insurance plan commission-based revenue starting in 2011.
Using data from the third quarter of 2010, we estimate the amount by which our average individual and family plan base commission rate has changed to be a decline from just over 10% of premium to just below 7%. The estimate of the change in the average rate is calculated by applying the changes in the first and subsequent year commission rates to our membership as of the end of the third quarter of 2010, as if all changes were effective immediately for all individual and family health insurance plan members. Our estimate is revenue-weighted so that a rate reduction implemented by a health insurance carrier with a larger member base with us had a larger impact on the resulting average rate than a change by a carrier with a smaller member base. We also estimated changes for a minority of health insurance carriers which we believe had not completed a review of their commission rates. The commission rate changes apply prospectively to applicable commissions earned on or after January 1, 2011 and the majority of the changes apply only to commissions earned on new members approved in 2011 and thereafter. For the majority of members that were approved prior to the effective date of the commission rate changes, we will continue to be paid commissions at the rates in effect prior to the changes. As a result, the new estimated average base commission rate computed above will phase in over time. Since the calculation is an estimate of the magnitude of the commission changes using our membership composition as of the end of the third quarter of 2010, including the mix by health insurance carrier and plan for past sales, as well as the current mix of members between first year and renewal year, our actual future base commission rate will differ from the estimated rate. The actual commission rate will depend on the mix of future approved members by state, health insurance carrier and plan and the mix between members approved prior to the commission rate changes and those approved after the changes, among other factors. We also expect that in addition to the base commission rate changes, other programs that health insurance carriers have supported, such as commission overrides and sponsorship advertising programs, may be reduced as carriers work to comply with the new medical loss ratio requirements. Based on information currently available to us, we expect commission revenue to decrease in absolute dollars and as a percentage of total revenue in 2011 compared to 2010.
Other Revenue
In addition to the commission revenue we derive from the sale of health insurance plans, we derive revenue from generating and delivering leads, primarily for Medicare plans, from licensing the use of our ecommerce technology and from our online sponsorship and advertising program.
Medicare Lead Referral. Our online Medicare plan platforms (www.eHealthMedicare.com and www.PlanPrescriber.com), enable consumers to research and compare Medicare-related insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. The revenue we have generated in our Medicare plan business is primarily referral fees paid to us based on leads generated by our online platforms that are delivered and sold to third parties. The majority of our lead referral revenue occurs during the Medicare annual enrollment period, which occurs during the fourth quarter of the calendar year.
Technology Licensing. We derive revenue from licensing the use of our health insurance ecommerce technology. Our technology platform enables health insurance carriers and agents to market and distribute health insurance plans online. In our technology licensing business, we are paid implementation fees and performance-based fees that are based on metrics such as submitted health insurance applications. Typically, we are paid a one-time implementation fee, which we recognize on a straight-line basis over the estimated term of the customer relationship (generally the initial term of the agreement), commencing once the technology is available for use by the third party. In addition, we typically generate revenue based on performance criteria that are either measured based on data tracked by us, or based on data tracked by the third party. In instances where the performance criteria data are tracked by us, we recognize revenue in the period of performance. In instances where the performance criteria data are tracked by the third party, we recognize revenue when the amounts earned are both
44
Table of Contents
fixed and determinable and collection is reasonably assured. Typically, this occurs through our receipt of a cash payment from the third party along with a detailed statement containing the data that is tracked by the third party.
We recently began to license our ecommerce technology for use by government agencies and intend to market it to states implementing health insurance exchanges as a result of health care reform legislation. In our government technology licensing business, we may earn a combination of fixed license fees and time- and materials-based fees or we may be paid performance-based fees. We were recently awarded a contract from the federal government to provide technology and information services relating to the federal government’s healthcare reform website. Revenue from this contract is being recognized on a straight-line basis from the date our technology was available for use by the federal government to the end of the initial one-year term of the contract. The contract is renewable annually for up to three years, at the option of the federal government.
Online Sponsorship and Advertising. We derive revenue from our online sponsorship advertising program that allows carriers to purchase advertising space in specific markets in a sponsorship area on our website. In return, we are typically paid a monthly fee and a performance-based fee based on metrics such as submitted health insurance applications.
Based on information currently available to us, we expect other revenue to increase in absolute dollars and as a percentage of total revenue in 2011 compared to 2010 as a result of growth in our technology licensing business, as well as growth in revenue derived from fees paid to us through the generation and delivery of leads, primarily for Medicare-related insurance plans.
Member Acquisition
An important factor in our revenue growth is the growth of our member base. Our marketing initiatives are an important component of our strategy to grow our member base and are focused on three primary member acquisition channels: direct, marketing partners and online advertising. Our marketing initiatives are primarily designed to encourage consumers to complete an online application for health insurance on our ecommerce platform. In addition, we may refer Medicare eligible individuals to third parties who may assist them in enrolling in a Medicare plan. Our marketing channels are as follows:
Direct. Our direct member acquisition channel consists of consumers who access our website addresses (www.eHealth.com, www.eHealthInsurance.com, www.eHealthMedicare.com and www.PlanPrescriber.com) either directly or through algorithmic natural search listings on Internet search engines and directories. For each of the years ended December 31, 2008, 2009 and 2010, applications submitted through us for individual and family health insurance from our direct channel constituted 39%, 42% and 43%, respectively, of all individual and family health insurance applications submitted on our website.
Marketing Partners. Our marketing partner member acquisition channel consists of consumers who access our websites through a network of affiliate partners and financial services and other companies. Growth in our marketing partner channel depends upon our expanding marketing programs with existing partners and adding new partners to our network. For the years ended December 31, 2008, 2009 and 2010, applications submitted through us for individual and family health insurance plans from our marketing partner member acquisition channel constituted approximately 33%, 32% and 29%, respectively, of all individual and family health insurance applications submitted on our website.
Online Advertising. Our online advertising member acquisition channel consists of consumers who access our websites through paid keyword search advertising from search engines such as Google, MSN and Yahoo!, as well as various Internet marketing programs such as banner advertising and email marketing. For the years ended December 31, 2008, 2009 and 2010, applications submitted through us for individual and family health insurance plans from our online advertising channel constituted approximately 28%, 26% and 28%, respectively, of all individual and family health insurance applications submitted on our website.
45
Table of Contents
Operating Costs and Expenses
Cost of Revenue
Cost of revenue consists of payments related to health insurance policies sold to members who were referred to our website by marketing partners with whom we have revenue-sharing arrangements. Cost of revenue also includes direct labor and other direct costs incurred in connection with our contract with the federal government, as well as the amortization of consideration we paid to certain brokers in connection with the transfer of their health insurance members to us as the new broker of record on the underlying policies. In order to enter into a revenue-sharing arrangement, marketing partners must be licensed to sell health insurance in the state where the policy is sold. Costs related to revenue-sharing arrangements are expensed as the related revenue is recognized. Initial direct labor and other direct costs incurred in connection with our contract with the federal government, but prior to the availability of our technology for use by the federal government, were deferred and included in prepaid expenses and other current assets in our consolidated balance sheet as of December 31, 2010 and are being amortized to cost of revenue from the date our technology was available for use by the federal government to the end of the initial one-year term of the contract.
In February 2009, we entered into customer transition and marketing agreements with Health Benefits Direct Corporation (“HBDC”). Pursuant to the agreements, HBDC agreed to transfer to us certain of its existing health insurance members, all of which were members on individual and family major medical policies, as the new broker of record on the underlying policies and agreed to refer future health insurance prospects to us. We paid HBDC initial consideration of $1.3 million, which is being amortized to cost of revenue as we recognize commission revenue related to the transferred members. In addition, we agreed to pay HBDC a percentage of the commission revenue we receive on the transferred policies, as well as a percentage of the future commission revenue we receive on health insurance policies we sell to prospects HBDC refers to us. The ongoing revenue-sharing payments are recorded as cost of revenue expense when we recognize the related revenue.
In November 2010, we entered into an agreement with a partner, whereby the partner transferred certain of its existing Medicare insurance members to us as the broker of record on the underlying policies. Total consideration of $3.3 million is being amortized to cost of revenue as we recognize commission revenue related to the transferred members over a period of up to five years. Of the $3.3 million total consideration, $2.5 million was paid to the partner in November 2010 and $0.8 million is payable in February 2011 and is recorded in accounts payable in the consolidated balance sheets as of December 31, 2010.
We expect cost of revenue to increase in absolute dollars in 2011 compared to 2010 due to a full year of direct labor and other direct costs incurred in connection with our performance under our contract with the federal government and an expected increase in the amount of revenue-sharing expense related to partners.
Marketing and Advertising
Marketing and advertising expenses consist primarily of member acquisition expenses associated with our direct, marketing partner and online advertising member acquisition channels, in addition to compensation and other expenses related to marketing, business development, partner management, public relations and carrier relations personnel who support our offerings. Our direct channel expenses primarily consist of costs for television advertising, radio advertising, print advertising, direct mail and email marketing.
Our marketing partner channel expenses consist primarily of fees paid to marketing partners with which we have a relationship. We compensate a significant number of our marketing partners by paying a fee each time a consumer referral from a partner results in a submitted health insurance application on our ecommerce platform, regardless of whether the consumer’s application is approved by the health insurance carrier. Many of our marketing partners have tiered arrangements in which the amount of the fee increases as the volume of submitted applications we receive from the marketing partner increases over a particular period. We recognize these expenditures in the period when a marketing partner’s referral results in the submission of a health insurance application on our website. The number of individual and family health insurance applications submitted through
46
Table of Contents
our ecommerce platform has generally increased in our first quarter compared to our fourth quarter and in our third quarter compared to our second quarter. Conversely, we have generally experienced a decline or flattening in individual and family submitted applications in our second quarter compared to our first quarter and in our fourth quarter compared to our third quarter. Since a significant portion of our marketing and advertising expenses are driven by the number of health insurance applications submitted on our website, those expenses are influenced by these patterns. In addition, because the total volume of submitted applications that we receive from our marketing partners is largely outside of our control, particularly during any short-term period, and because of our tiered marketing partner arrangements, we could incur expenses in excess of, or below, the amounts we had planned in periods of rapid change in the volume of submitted applications from marketing partner referrals. An unanticipated increase in submitted applications resulting from marketing partner referrals could cause our net income to be lower than our expectation, since the revenue to be derived from submitted applications that are approved by health insurance carriers will not be recognized until future periods.
Paid keyword search advertising on search engines represents the majority of expenses in our online advertising channel. We incur expenses associated with search engine advertising in the period in which the consumer clicks on the advertisement. Similar to our marketing partner channel, expenses in our online advertising channel will increase or decrease in relation to any increase or decrease in consumers referred to our website as a result of such search engine advertising. For example, due to the substantial increase in the number of consumers referred to our website from paid keyword search advertising performed during the Medicare annual enrollment period, we experienced a significant increase in our Medicare online marketing expenses during our fourth quarter of 2010.
We expect our marketing and advertising expenses to decrease in absolute dollars in 2011 compared to 2010 primarily due to an expected decline in costs related to paid keyword search advertising during 2011 as a result of the lower lifetime value of an individual and family health insurance member. The decline in paid search advertising is expected to be partially offset by increased marketing and advertising expenses related to our Medicare plan and government system businesses.
Customer Care and Enrollment
Customer care and enrollment expenses primarily consist of compensation and benefits costs for personnel engaged in pre-sales assistance to applicants who call our customer care center and for enrollment personnel who assist applicants during the underwriting process. We expect customer care and enrollment expenses to increase in absolute dollars in 2011 compared to 2010 as a result of additional personnel and expenditures necessary to develop future Medicare plan sales capabilities, as well as costs related to our new customer care center in Salt Lake City, Utah.
Technology and Content
Technology and content expenses consist primarily of compensation and benefits costs for personnel associated with developing and enhancing our website technology as well as maintaining our website. A majority of our technology and content group is located at our wholly owned subsidiary in China, where technology development costs are generally lower than in the United States. We expect technology and content expenses to increase in absolute dollars in 2011 compared to 2010 due to our continued focus on technology development, technology licensing implementations, an increase in technology and content employees and the enhancement of our current ecommerce platform for Medicare-related insurance plans.
General and Administrative
General and administrative expenses include compensation and benefits costs for staff working in our executive, finance, corporate development, investor relations, government relations, legal, human resources, internal audit, facilities and internal information technology departments. These expenses also include fees paid
47
Table of Contents
for outside professional services, including audit, tax, legal and information technology fees. We expect our general and administrative expenses to increase in absolute dollars in 2011 compared to 2010 due to the increased costs necessary to support the future growth of our business.
Amortization of Acquired Intangible Assets
Acquired intangible assets with finite useful lives, which include purchased technology, pharmacy and customer relationships, trade names, trademarks and website addresses, are amortized over their estimated useful lives and are reviewed for impairment annually or whenever facts or circumstances suggest that the carrying value of these assets may not be recoverable.
48
Table of Contents
Summary of Selected Metrics
The following table shows certain selected quarterly metrics for 2009 and 2010:
| Key Metrics: |
Three Months Ended | |||||||||||||||||||||||||||||||
| March 31, 2009 |
June 30, 2009 |
September 30, 2009 |
December 31, 2009 |
March 31, 2010 |
June 30, 2010 |
September 30, 2010 |
December 31, 2010 |
|||||||||||||||||||||||||
| Operating cash flows (1) |
$ | 4,722,000 | $ | 8,311,000 | $ | 7,649,000 | $ | 9,404,000 | $ | 3,093,000 | $ | 8,164,000 | $ | 5,611,000 | $ | 3,641,000 | ||||||||||||||||
| IFP submitted applications (2) |
141,200 | 121,100 | 131,200 | 122,300 | 135,600 | 117,200 | 143,200 | 111,200 | ||||||||||||||||||||||||
| IFP approved members (3) |
120,900 | 103,400 | 111,100 | 96,100 | 114,200 | 93,400 | 117,300 | 94,200 | ||||||||||||||||||||||||
| Total approved members (4) |
157,700 | 135,800 | 146,900 | 124,400 | 144,400 | 122,700 | 152,800 | 128,300 | ||||||||||||||||||||||||
| Commission revenue (5) |
$ | 28,204,000 | $ | 29,939,000 | $ | 31,086,000 | $ | 30,030,000 | $ | 31,773,000 | $ | 31,872,000 | $ | 32,040,000 | $ | 39,681,000 | ||||||||||||||||
| Commission revenue per estimated member for the period (6) |
$ | 43.35 | $ | 43.16 | $ | 43.36 | $ | 41.29 | $ | 42.84 | $ | 42.21 | $ | 41.78 | $ | 50.97 | ||||||||||||||||
| Total revenue (7) |
$ | 31,917,000 | $ | 33,439,000 | $ | 35,123,000 | $ | 34,411,000 | $ | 35,989,000 | $ | 36,256,000 | $ | 37,451,000 | $ | 50,708,000 | ||||||||||||||||
| Total revenue per estimated member for the period (8) |
$ | 49.24 | $ | 48.21 | $ | 49.00 | $ | 47.31 | $ | 48.53 | $ | 48.02 | $ | 48.84 | $ | 65.13 | ||||||||||||||||
| As of March 31, 2009 |
As of June 30, 2009 |
As of September 30, 2009 |
As of December 31, 2009 |
As of March 31, 2010 |
As of June 30, 2010 |
As of September 30, 2010 |
As of December 31, 2010 |
|||||||||||||||||||||||||
| IFP estimated membership (9) |
585,100 | 614,800 | 630,900 | 636,200 | 661,000 | 660,500 | 679,500 | 680,900 | ||||||||||||||||||||||||
| Total estimated membership (10) |
680,100 | 707,100 | 726,600 | 728,000 | 755,200 | 754,900 | 778,800 | 778,300 | ||||||||||||||||||||||||
| Three Months Ended | ||||||||||||||||||||||||||||||||
| March 31, 2009 |
June 30, 2009 |
September 30, 2009 |
December 31, 2009 |
March 31, 2010 |
June 30, 2010 |
September 30, 2010 |
December 31, 2010 |
|||||||||||||||||||||||||
| Marketing and advertising expenses (11) |
$ | 13,420,000 | $ | 12,945,000 | $ | 14,266,000 | $ | 13,356,000 | $ | 14,818,000 | $ | 13,883,000 | $ | 16,094,000 | $ | 15,307,000 | ||||||||||||||||
| Marketing and advertising as a percentage of total revenue (12) |
42 | % | 39 | % | 41 | % | 39 | % | 41 | % | 38 | % | 43 | % | 30 | % | ||||||||||||||||
| Other Metrics: |
||||||||||||||||||||||||||||||||
| Source of IFP submitted applications (as a percentage of |
||||||||||||||||||||||||||||||||
| Direct (13) |
41 | % | 43 | % | 43 | % | 44 | % | 43 | % | 44 | % | 43 | % | 45 | % | ||||||||||||||||
| Marketing partners (14) |
34 | % | 33 | % | 31 | % | 29 | % | 27 | % | 28 | % | 30 | % | 29 | % | ||||||||||||||||
| Online advertising (15) |
25 | % | 24 | % | 26 | % | 27 | % | 30 | % | 28 | % | 27 | % | 26 | % | ||||||||||||||||
| Total |
100 | % | 100 | % | 100 | % | 100 | % | 100 | % | 100 | % | 100 | % | 100 | % | ||||||||||||||||
| Acquisition cost per individual on IFP submitted |
$ | 62.95 | $ | 73.45 | $ | 74.73 | $ | 73.38 | $ | 73.68 | $ | 79.51 | $ | 75.38 | $ | 88.79 | ||||||||||||||||
49
Table of Contents
Notes:
| (1) | Net cash provided by operating activities for the period from the consolidated statements of cash flows. |
| (2) | IFP applications submitted on eHealth’s website during the period. Applications are counted as submitted when the applicant completes the application, provides a method for payment and clicks the submit button on our website and submits the application to us. The applicant generally has additional actions to take before the application will be reviewed by the insurance carrier, such as providing additional information and providing an electronic signature. In addition, an applicant may submit more than one application. We include applications for IFP plans for which we receive commissions as well as other forms of payment. We define our “IFP” offerings as major medical individual and family health insurance plans, which does not include small business, short-term, stand-alone dental, life, student or Medicare-related health insurance plans. |
| (3) | New IFP members reported to eHealth as approved during the period. Some members that are approved by a carrier do not accept the approval and therefore do not become paying members. Does not include members transferred from Health Benefits Direct Corporation during 2009. |
| (4) | New members for all plans reported to eHealth as approved during the period. Some members that are approved by a carrier do not accept the approval and therefore do not become paying members. Does not include members transferred from Health Benefits Direct Corporation during 2009. |
| (5) | Commission revenue (from all sources) recognized during the period from the consolidated statements of income. Commission revenue for the three months ended December 31, 2010 includes a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided. |
| (6) | Calculated as commission revenue recognized during the period (see note (5) above) divided by average estimated membership for the period (calculated as beginning and ending estimated membership for all plans for the period, divided by two). Commission revenue per estimated member for the three months ended December 31, 2010 increased primarily due to a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided. Ending membership as of December 31, 2009 and 2010 include an estimated 20,000 and 10,000 members, respectively, transferred from Health Benefits Direct Corporation as of each date, net of estimated cancelations since their transfer. |
| (7) | Total revenue (from all sources) recognized during the period from the consolidated statements of income. |
| (8) | Calculated as total revenue recognized during the period (see note (7) above) divided by average estimated membership for the period (calculated as beginning and ending estimated membership for all plans for the period, divided by two). Commission revenue per estimated member for the three months ended December 31, 2010 increased primarily due to a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided. Ending membership as of December 31, 2009 and 2010 include an estimated 20,000 and 10,000 members, respectively, transferred from Health Benefits Direct Corporation as of each date, net of estimated cancelations since their transfer. |
| (9) | Estimated number of members active on IFP insurance policies as of the date indicated. Ending membership as of December 31, 2009 and 2010 include an estimated 20,000 and 10,000 members, respectively, transferred from Health Benefits Direct Corporation as of each date, net of estimated cancelations since their transfer. |
| (10) | Estimated number of members active on all insurance policies as of the date indicated. Ending membership as of December 31, 2009 and 2010 include an estimated 20,000 and 10,000 members, respectively, transferred from Health Benefits Direct Corporation as of each date, net of estimated cancelations since their transfer. |
| (11) | Marketing and advertising expenses for the period from the consolidated statements of income. |
| (12) | Calculated as marketing and advertising expenses for the period (see note (11) above) divided by total revenue for the period (see note (7) above). |
| (13) | Percentage of IFP submitted applications from applicants who came directly to the eHealth website through algorithmic search engine results or otherwise. See note (2) above for further information as to what constitutes a submitted application. |
50
Table of Contents
| (14) | Percentage of IFP submitted applications from applicants sourced through eHealth’s network of marketing partners. See note (2) above for further information as to what constitutes a submitted application. |
| (15) | Percentage of IFP submitted applications from applicants sourced through paid search and other online advertising activities. See note (2) above for further information as to what constitutes a submitted application. |
| (16) | Calculated as marketing and advertising expenses for the period (see note (11) above) divided by the number of individuals on IFP applications submitted on eHealth’s website during the period. This metric may not reflect the true acquisition cost. For the three month periods ended June 30, September 30 and December 31, 2010, the metric includes marketing and advertising expense for Medicare plans in the numerator. |
Our insurance carrier partners bill and collect insurance premiums paid by our members. Carrier partners do not report to us the number of members that we have as of a given date. The majority of our members who terminate their policies do so by discontinuing their premium payments to the carrier and do not inform us of the cancellation. Also, some of our members pay their premiums less frequently than monthly. Given the number of months required to observe non-payment of commissions in order to confirm cancellations, we estimate the number of members who are active on insurance policies as of a specified date. We estimate the number of continuing members on non-small business insurance policies as of a specific date by taking the sum of (i) the number of members for whom we have received a commission payment for the month that is six months (or three months in the case of short-term, student and dental insurance) prior to the date of estimation (after reducing that number using historical experience for assumed member cancellations over, as applicable, the three-month or six-month period); and (ii) the number of approved members over the six-month period (or three months in the case of short-term, student and dental insurance) prior to the date of estimation (after reducing that number using historical experience for an assumed number of members who do not accept their approved policy and for estimated member cancellations through the date of the estimate). We estimate the number of small business group members using the number of initial members at the time the group is approved, and we update this number for changes in membership if such changes are reported to us by the group or carrier in the period it is reported. However, groups generally notify the carrier directly of policy cancellations and increases or decreases in group size without informing us. Additionally, our carrier partners often do not communicate this information to us. We often are made aware of policy cancellations at the time of annual renewal and update our membership statistics accordingly in the period they are reported.
After we have estimated membership for a period, we may receive information from health insurance carriers that would have impacted the estimate if we had received the information prior to the date of estimation. We may receive commission payments or other information that indicates that a member who was not included in our estimates for a prior period was in fact an active member at that time, or that a member who was included in our estimates was in fact not an active member of ours. For instance, we reconcile information carriers provide to us and may determine that we were not historically paid commissions owed to us, which would cause us to have underestimated our membership. Conversely, carriers may require us to return commission payments paid in a prior period due to policy cancellations for members we previously estimated as being active. We reflect updated information regarding our membership in the membership estimate for the current period that we are estimating, if applicable. As a result of the delay in our receipt of information from insurance carriers, actual trends in our membership are most discernable over periods longer than from one quarter to the next. In addition, and as a result of the delay we experience in receiving information about our membership, it is difficult for us to determine with any certainty the impact of current economic and other conditions on our membership retention.
Critical Accounting Policies and Estimates
The discussion and analysis of our consolidated financial condition and results of operations is based upon our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates, judgments and assumptions that affect the reported amount of assets, liabilities, revenues and expenses and related disclosure of
51
Table of Contents
contingent assets and liabilities. On an ongoing basis, we evaluate our estimates, including those related to, but not limited to, allowances for commission forfeitures payable to carriers, the assumptions used in determining stock-based compensation, the useful lives of long-lived assets including property and equipment and intangible assets, fair value of intangible assets, valuation allowance for deferred income taxes, provision for income taxes and fair value of investments. We base our estimates of the carrying value of certain assets and liabilities on historical experience and on various other assumptions that we believe to be reasonable. In many cases, we could reasonably have used different accounting policies and estimates. In some cases, changes in the accounting estimates are reasonably likely to occur from period to period. Accordingly, actual results may differ materially from these estimates.
We believe the following critical accounting policies affect our more significant judgments used in the preparation of our consolidated financial statements.
Revenue Recognition
Commission Revenue. We recognize commission revenue when our commission is reported to us by a health insurance carrier, net of an allowance for future forfeiture amounts payable to carriers due to policy cancellations. Commissions are reported to us by a cash payment and commission statement. We generally receive these communications simultaneously. In instances when we receive the cash payment and commission statement separately and in different accounting periods, we recognize revenue in the period that we receive the earliest communication, provided we receive the second corroborating communication within ten business days following the end of the accounting period. If the second corroborating communication is not received within ten business days following the end of the accounting period, we recognize revenue in the period the second communication is received. We use the data in the commission statements to help identify the members for which we are receiving a commission payment and the amount received for each member, and to estimate our allowance for forfeitures payable to carriers. As a result, we recognize the net amount of compensation earned as the agent in the transaction.
Our insurance carrier partners bill and collect insurance premiums that our members pay. We rely on health insurance carriers to report accurately and in a timely manner the amount of commissions earned by us, and we calculate our commission revenues, prepare our financial reports, projections and budgets, and direct our marketing and other operating efforts based on the reports we receive from them. Each month we analyze the reports we receive from health insurance carriers by comparing them to the database we maintain on our members. It is often difficult for us to independently determine whether or not carriers are reporting all commissions due to us, primarily because the majority of our members who terminate their policies do so by discontinuing their premium payments to the carrier instead of by informing us of the cancellation. Also, some of our members pay their premiums less frequently than monthly. This results in our having to identify underpayment or non-payment of commissions on a policy and follow up with a carrier to obtain an explanation and/or request correction of the amount of commissions paid to us. To the extent that carriers understate or fail to timely and accurately report or pay the amount of commissions due to us, we will not collect and recognize revenue to which we are entitled, which, if material in amount, would adversely affect our operating results and financial condition.
Commission override revenue, which we recognize on the same basis as premium commissions, is generally reported to us in a more irregular pattern than premium commissions. As a result, our revenues for a particular quarter could be higher or lower than expectations due to the timing of the reporting of commission override revenue to us.
Certain commission amounts are subject to forfeiture in circumstances where a member has prepaid his or her premium for a future period of coverage and subsequently cancels his or her policy before the completion of that period. We estimate and record an allowance for these forfeitures based on historical cancellation experience using data provided on commission statements. The forfeitures are typically reported to us by health insurance
52
Table of Contents
carriers one to two months after the commission is reported and paid to us by the carrier. Our estimate of the allowance for forfeitures includes an estimate of both the reporting time lag and the forfeiture amount. Changes in our historical trends would result in changes to our estimated forfeitures in future periods. There were no changes in our average forfeiture rates or reporting time lag during the years ended December 31, 2008, 2009 and 2010 which had a material impact on our allowance for forfeitures.
Other Revenue. We recognize lead referral revenue when persuasive evidence of an arrangement exists, delivery of a lead has occurred, the fee is fixed or determinable and collectability is reasonably assured. Delivery is deemed to have occurred at the time a lead is delivered to the customer.
Our commercial technology licensing business allows carriers the use of our ecommerce platform to offer their own health insurance policies on their websites and agents to utilize our technology to power their online quoting, content and application submission processes. Typically, we are paid a one-time implementation fee, which we recognize on a straight-line basis over the estimated term of the customer relationship (generally the initial term of the agreement), commencing once the technology is available for use by the third party, and a performance fee based on metrics such as submitted health insurance applications. The metrics used to calculate performance fees for both sponsorship advertising and technology licensing are based on performance criteria that are either measured based on data tracked by us, or based on data tracked by the third party. In instances where the performance criteria data is tracked by us, we recognize revenue in the period of performance. In instances where the performance criteria data is tracked by the third party, we recognize revenue when the amounts earned are both fixed and determinable and collection is reasonably assured. Typically, this occurs through our receipt of a cash payment from the third party along with a detailed statement containing the data that is tracked by the third party. In addition, we have begun to license our technology to government agency customers and we were recently awarded a contract from the federal government to provide technology and information services relating to the federal government’s healthcare reform website.
Our contract with the federal government to provide technology and information services relating to the federal government’s healthcare reform website is a multiple element arrangement. We were not able to establish fair value for each element within the contract and, therefore, accounted for the entire contract as one unit of accounting. We deferred all revenue related to the contract until our technology was available for use by the federal government. Revenue is being recognized on a straight-line basis from the date our technology was available for use by the federal government to the end of the initial one-year term of the contract. The contract is renewable annually for up to three additional years, at the option of the federal government.
Our sponsorship advertising program allows carriers to purchase advertising space in specific markets in a sponsorship area on our website. In return, we are typically paid a monthly fee, which is recognized over the period that advertising is displayed, and often a performance fee based on metrics such as submitted health insurance applications.
Deferred revenue consists of deferred technology licensing implementation fees as well as amounts billed or collected from sponsorship or technology licensing customers in advance of our performing our service for such customers. It also includes the amount by which both unbilled and billed services provided under our federal government contract exceed the straight-line revenue recognized to date. We defer commission amounts that have been paid to us related to transactions where our services are complete, but where we cannot currently estimate the allowance for future forfeitures related to those amounts.
53
Table of Contents
Stock-Based Compensation
We recognize stock-based compensation expense in the accompanying consolidated statements of income and comprehensive income based on the fair value of our stock-based awards over their respective vesting periods, which is generally four years. The estimated grant date fair value of our stock-based awards is determined using the Black-Scholes-Merton pricing model and a single option award approach. The weighted-average expected term for stock options granted is calculated using the simplified method, as we do not have sufficient historical option exercise behavior on which to estimate expected terms. The simplified method defines the expected term as the average of the contractual term and the vesting period of the stock option. We have estimated the volatility used as an input to the model based on an analysis of our stock price since our initial public offering in October 2006, as well as an analysis of similar public companies for which we have data. We estimate our expected volatility using the weighted-average of: our implied volatility; our mean reversion volatility; and the mean reversion volatility of similar public companies for which we have data. We have used judgment in selecting these companies, as well as evaluating the available historical and implied volatility data for these companies. The dividend yield is determined by dividing the expected per share dividend during the coming year by the grant date stock price. Through December 31, 2010, we had not declared or paid any cash dividends, and we do not expect to pay any in the foreseeable future. We base the risk-free interest rate on the implied yield currently available on U.S. Treasury zero-coupon issues with a remaining term equal to the expected term of our stock options. The assumptions used in calculating the fair value of stock-based payment awards represent our best estimates, but these estimates involve inherent uncertainties and the application of management judgment. We will continue to use judgment in evaluating the expected term and volatility related to our own stock-based awards on a prospective basis, and incorporating these factors into the model. Changes in key assumptions will significantly impact the valuation of such instruments.
Future stock-based compensation expense is dependent upon the fair value of each option at the date each option is granted and the number of awards issued and outstanding during each period. We expect stock-based compensation expense will increase in the future to the extent the number of equity awards issued and outstanding increases.
Goodwill and Acquired Intangible Assets
Goodwill represents the excess of the consideration paid over the estimated fair value of assets acquired and liabilities assumed in a business acquisition. We do not amortize goodwill but test for impairment on an annual basis on or about November 30 of each year and whenever we become aware of any events occurring or changes in circumstances that would indicate a reduction in its fair value below its carrying amount.
Acquired intangible assets with finite useful lives, which include purchased technology, pharmacy and customer relationships, trade names, trademarks and website addresses, are amortized over their estimated useful lives and are reviewed for impairment annually on or about November 30 of each year or when facts or circumstances suggest that the carrying value of these assets may not be recoverable.
We assess the impairment of goodwill and acquired intangible assets when events or changes in circumstances indicate that the carrying value of the assets or the asset grouping may not be recoverable. Factors that we consider in deciding when to perform an impairment review include significant negative industry or economic trends or significant changes or planned changes in our use of the assets. We measure the recoverability of assets that will continue to be used in our operations by comparing the carrying value of the asset grouping to our estimate of the related total future undiscounted net cash flows. If an asset grouping’s carrying value is not recoverable through the related undiscounted cash flows, the asset grouping is considered to be impaired. The impairment is measured by comparing the difference between the asset grouping’s carrying value and its fair value. Fair value is the price that would be received from selling an asset in an orderly transaction between market participants at the measurement date. Goodwill and intangible assets are considered non-financial assets, and are recorded at fair value only when an impairment charge is recognized.
54
Table of Contents
We must make subjective judgments in determining the independent cash flows that can be related to specific asset groupings. In addition, we must make subjective judgments regarding the remaining useful lives of assets with finite useful lives. When we determine that the useful life of an asset is shorter than we had originally estimated, we accelerate the rate of amortization over the assets’ new, remaining useful life.
Accounting for Income Taxes
We account for income taxes using the liability method. Deferred income taxes are determined based on the differences between the financial reporting and tax bases of assets and liabilities, using enacted statutory tax rates in effect for the year in which the differences are expected to reverse.
Since tax laws and financial accounting standards differ in their recognition and measurement of assets, liabilities, equity, revenues, expenses, gains and losses, differences arise between the amount of taxable income and pretax financial income for a year and between the tax bases of assets or liabilities and their reported amounts in our financial statements. Because we assume that the reported amounts of assets and liabilities will be recovered and settled, respectively, a difference between the tax basis of an asset or a liability and its reported amount in the balance sheet will result in a taxable or a deductible amount in some future years when the related liabilities are settled or the reported amounts of the assets are recovered, which gives rise to a deferred tax asset or liability. We must then assess the likelihood that our deferred tax assets will be recovered from future taxable income and to the extent we believe that recovery does not meet the more likely than not criteria, we must establish a valuation allowance. Management judgment is required in determining any valuation allowance recorded against our net deferred tax assets.
As part of the process of preparing our consolidated financial statements, we are required to estimate our income taxes. This process involves estimating our actual current tax expense together with assessing temporary differences that may result in deferred tax assets, as well as discrete tax items during the period, such as excess tax benefits related to share-based payments.
Assessing the realizability of our deferred tax assets is dependent upon several factors, including the likelihood and amount, if any, of future taxable income in relevant jurisdictions during the periods in which those temporary differences become deductible. We forecast taxable income by considering all available positive and negative evidence, including our history of operating income and losses and our financial plans and estimates that we use to manage the business. These assumptions require significant judgment about future taxable income. As a result, the amount of deferred tax assets considered realizable is subject to adjustment in future periods if estimates of future taxable income change.
Future changes in various factors, such as the amount of stock-based compensation we record during the period and the related tax benefit we realize upon the exercise of employee stock options, potential limitations on the use of our federal and state net operating loss credit carry forwards, pending or future tax law changes including rate changes and the tax benefit from or limitations on our ability to utilize research and development credits, the amount of non-deductible lobbying and acquisition-related costs, changes in our valuation allowance and state and foreign taxes, would impact our estimates, and as a result, could affect our effective tax rate and the amount of income tax expense we record, and pay, in future periods.
55
Table of Contents
Results of Operations
The following table sets forth our operating results and the related percentage of total revenues for the years ended December 31, 2008, 2009 and 2010 (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||
| 2008 | 2009 | 2010 | ||||||||||||||||||||||
| Revenue: |
||||||||||||||||||||||||
| Commission |
$ | 100,839 | 90 | % | $ | 119,259 | 88 | % | $ | 135,366 | 84 | % | ||||||||||||
| Other |
10,872 | 10 | 15,631 | 12 | 25,038 | 16 | ||||||||||||||||||
| Total revenue |
111,711 | 100 | 134,890 | 100 | 160,404 | 100 | ||||||||||||||||||
| Operating costs and expenses: |
||||||||||||||||||||||||
| Cost of revenue |
1,746 | 2 | 4,581 | 3 | 5,499 | 3 | ||||||||||||||||||
| Marketing and advertising |
42,161 | 38 | 53,987 | 40 | 60,102 | 37 | ||||||||||||||||||
| Customer care and enrollment |
14,379 | 13 | 14,769 | 11 | 17,810 | 11 | ||||||||||||||||||
| Technology and content |
14,182 | 13 | 15,685 | 12 | 19,241 | 12 | ||||||||||||||||||
| General and administrative |
17,983 | 16 | 20,028 | 15 | 24,055 | 15 | ||||||||||||||||||
| Amortization of acquired intangible assets |
— | — | — | — | 1,138 | 1 | ||||||||||||||||||
| Total operating costs and expenses |
90,451 | 81 | 109,050 | 81 | 127,845 | 80 | ||||||||||||||||||
| Income from operations |
21,260 | 19 | 25,840 | 19 | 32,559 | 20 | ||||||||||||||||||
| Interest and other income, net |
3,714 | 3 | 938 | 1 | 9 | 0 | ||||||||||||||||||
| Income before income taxes |
24,974 | 22 | 26,778 | 20 | 32,568 | 20 | ||||||||||||||||||
| Provision for income taxes |
10,806 | 10 | 11,431 | 8 | 15,086 | 9 | ||||||||||||||||||
| Net income |
$ | 14,168 | 13 | % | $ | 15,347 | 11 | % | $ | 17,482 | 11 | % | ||||||||||||
Operating costs and expenses include the following amounts related to stock-based compensation (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Marketing and advertising |
$ | 644 | $ | 803 | $ | 808 | ||||||
| Customer care and enrollment |
266 | 325 | 384 | |||||||||
| Technology and content |
898 | 1,194 | 1,622 | |||||||||
| General and administrative |
1,686 | 2,513 | 3,581 | |||||||||
| Total |
$ | 3,494 | $ | 4,835 | $ | 6,395 | ||||||
Years Ended December 31, 2008, 2009 and 2010
Revenue
The following table presents our commission revenue, other revenue and total revenue for the years ended December 31, 2008, 2009 and 2010 and the dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Commission |
$ | 100,839 | $ | 18,420 | 18 | % | $ | 119,259 | $ | 16,107 | 14 | % | $ | 135,366 | ||||||||||||||
| Percentage of total revenue |
90 | % | 88 | % | 84 | % | ||||||||||||||||||||||
| Other |
10,872 | 4,759 | 44 | % | 15,631 | 9,407 | 60 | % | 25,038 | |||||||||||||||||||
| Percentage of total revenue |
10 | % | 12 | % | 16 | % | ||||||||||||||||||||||
| Total revenue |
$ | 111,711 | $ | 23,179 | 21 | % | $ | 134,890 | $ | 25,514 | 19 | % | $ | 160,404 | ||||||||||||||
56
Table of Contents
2010 compared to 2009—Commission revenue increased $16.1 million, or 14%, in 2010 compared to 2009, primarily due to an increase in our membership. Our estimated membership increased approximately 7% to 778,300 at December 31, 2010 from 728,000 at December 31, 2009. Commission revenue also increased as a result of a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided. Other revenue increased $9.4 million, or 60%, in 2010 compared to 2009, primarily due to an increase in Medicare lead referral revenue and, to a lesser extent, revenues related to our technology licensing contract with the federal government.
2009 compared to 2008—Commission revenue increased $18.4 million, or 18%, in 2009 compared to 2008, primarily due to an increase in our membership. Our estimated membership increased approximately 17% to 728,000 at December 31, 2009 from 621,100 at December 31, 2008. Other revenue increased $4.8 million, or 44%, in 2009 compared to 2008, primarily due to an increase of $2.6 million from licensing arrangements related to our technology and an increase of $1.7 million related to sales of carrier sponsorship advertising on our website.
Operating Costs and Expenses
Cost of Revenue
The following table presents our cost of revenue for the years ended December 31, 2008, 2009 and 2010 and the dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Cost of revenue |
$ | 1,746 | $ | 2,835 | 162 | % | $ | 4,581 | $ | 918 | 20 | % | $ | 5,499 | ||||||||||||||
| Percentage of total revenue |
2 | % | 3 | % | 3 | % | ||||||||||||||||||||||
2010 compared to 2009—Cost of revenue increased $0.9 million, or 20%, in 2010 compared to 2009, primarily as a result of the recognition of $1.9 million of deferred and on-going direct labor and other direct costs related to the agreement we entered into in July 2010 with the federal government whereby we provide technology and information services relating to the federal government’s healthcare reform website. Partially offsetting this increase was a decrease of $0.6 million in the amortization of the initial consideration paid to HBDC and a decrease of $0.5 million in revenue-sharing expense related to HBDC due to a decrease in the commission revenue we received in 2010 related to certain health insurance members that were transferred to us. As a percentage of total revenue, cost of revenue was 3% in both 2010 and 2009.
2009 compared to 2008—Cost of revenue increased $2.8 million, or 162%, in 2009 compared to 2008, primarily as a result of our revenue-sharing expense paid to HBDC based on a percentage of commission revenue we received in 2009 related to certain health insurance members transferred to us. Additionally, cost of revenue increased due to the amortization of the initial consideration paid to HBDC in the first quarter of 2009. To a lesser extent, cost of revenue increased as a result of an increase in the number of health insurance policies sold to members who were referred to our website by marketing partners with whom we have revenue-sharing arrangements. As a percentage of total revenue, cost of revenue increased to 3% in 2009 from 2% in 2008.
Marketing and Advertising
The following table presents our marketing and advertising expenses for the years ended December 31, 2008, 2009 and 2010 and the dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Marketing and advertising |
$ | 42,161 | $ | 11,826 | 28 | % | $ | 53,987 | $ | 6,115 | 11 | % | $ | 60,102 | ||||||||||||||
| Percentage of total revenue |
38 | % | 40 | % | 37 | % | ||||||||||||||||||||||
57
Table of Contents
2010 compared to 2009—Marketing and advertising expenses increased $6.1 million, or 11%, in 2010 compared to 2009. This was primarily due to an increase in online advertising expenses of $7.4 million, of which $3.8 million was Medicare plan related. Online advertising costs increased as a result of an increase in paid keyword search advertising costs on Internet search engines, as both the cost per click-through and the number of click-throughs from our online advertising channel increased. Partially offsetting the increase in online advertising expenses was a decrease of $1.1 million in fees we pay to marketing partners for referrals that result in the submission of a health insurance application on our website, due to a decrease in the number of applications submitted on our website through the marketing partner channel during 2010 compared to 2009. As a percentage of total revenue, total marketing and advertising expenses decreased to 37% in 2010 from 40% in 2009 primarily due to growth in total revenue, as well as the receipt in the fourth quarter of 2010 of a one-time commission payment of $6.0 million from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided.
2009 compared to 2008—Marketing and advertising expenses increased $11.8 million, or 28%, in 2009 compared to 2008. This was primarily due to an increase in our online advertising expenses of $7.1 million resulting from an increase in paid keyword search advertising costs on Internet search engines, as the cost and number of click-throughs from the online advertising channel increased. Marketing partner expenses increased $1.9 million due to an increase in the costs per application and the growth in the number of applications submitted on our website through the marketing partner channel during 2009 compared to 2008. Additionally, compensation and benefits costs attributable to marketing and advertising personnel increased $1.6 million associated with an increase in marketing and advertising personnel. We also experienced a decline in the average number of individuals applying for health insurance per application submitted through the direct, marketing partner and online advertising member acquisition channels. As a percentage of total revenue, total marketing and advertising expenses increased to 40% in 2009 from 38% in 2008.
Customer Care and Enrollment
The following table presents our customer care and enrollment expenses for the years ended December 31, 2008, 2009 and 2010 and dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Customer care and enrollment |
$ | 14,379 | $ | 390 | 3 | % | $ | 14,769 | $ | 3,041 | 21 | % | $ | 17,810 | ||||||||||||||
| Percentage of total revenue |
13 | % | 11 | % | 11 | % | ||||||||||||||||||||||
2010 compared to 2009—Customer care and enrollment expenses increased $3.0 million, or 21%, in 2010 compared to 2009, primarily due to incremental compensation and benefits costs associated with the new customer care center we established in Salt Lake City, Utah and, to a lesser extent, with an increase in personnel servicing individual and family health insurance applications submitted through our website. As a result, compensation and benefits increased $2.5 million and facility and operating costs increased $0.3 million in 2010. As a percentage of total revenue, customer care and enrollment expenses were 11% in both 2010 and 2009.
2009 compared to 2008—Customer care and enrollment expenses increased $0.4 million, or 3%, in 2009 compared to 2008, primarily due to an increase in compensation and benefits costs associated with an increase in personnel servicing health insurance applications submitted through our website. As a percentage of total revenue, customer care and enrollment expenses decreased to 11% in 2009 from 13% in 2008 as a result of economies of scale achieved by our customer care and enrollment operations.
58
Table of Contents
Technology and Content
The following table presents our technology and content expenses for the years ended December 31, 2008, 2009 and 2010 and dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Technology and content |
$ | 14,182 | $ | 1,503 | 11 | % | $ | 15,685 | $ | 3,556 | 23 | % | $ | 19,241 | ||||||||||||||
| Percentage of total revenue |
13 | % | 12 | % | 12 | % | ||||||||||||||||||||||
2010 compared to 2009—Technology and content expenses increased $3.6 million, or 23%, for 2010 compared to 2009. This increase was primarily due to an increase of $2.4 million in compensation and benefits and other personnel costs associated with an increase in technology and content personnel, an increase of $0.5 million in annual maintenance fees related to our hardware and software and an increase of $0.4 million in stock-based compensation expense due to additional equity grants to employees in our technology and content departments. As a percentage of total revenue, technology and content expenses were 12% in both 2010 and 2009.
2009 compared to 2008—Technology and content expenses increased $1.5 million, or 11%, in 2009 compared to 2008. This increase was primarily due to an increase of $0.9 million in compensation and benefits costs associated with an increase in technology and content personnel. Additionally, depreciation expense increased $0.3 million due to purchases of computer hardware and software related to our website and stock-based compensation costs increased $0.3 million due to additional equity grants to employees in our technology and content departments. As a percentage of total revenue, technology and content expenses decreased to 12% in 2009 from 13% in 2008 as a result of economies of scale achieved by our technology and content operations.
General and Administrative
The following table presents our general and administrative expenses for the years ended December 31, 2008, 2009 and 2010 and dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| General and administrative |
$ | 17,983 | $ | 2,045 | 11 | % | $ | 20,028 | $ | 4,027 | 20 | % | $ | 24,055 | ||||||||||||||
| Percentage of total revenue |
16 | % | 15 | % | 15 | % | ||||||||||||||||||||||
2010 compared to 2009—General and administrative expenses increased $4.0 million, or 20%, in 2010 compared to 2009, primarily due to a $1.5 million increase in professional fees associated with consulting services, a $1.1 million increase in stock-based compensation expense due to additional equity grants to employees in our general and administrative departments and to members of our board of directors, a $0.8 million increase in compensation and benefits costs due to an increase in general and administrative personnel, primarily as a result of our acquisition of PlanPrescriber, and $0.6 million of acquisition-related costs related to our purchase of PlanPrescriber. As a percentage of total revenue, general and administrative expenses were 15% in both 2010 and 2009.
2009 compared to 2008—General and administrative expenses increased $2.0 million, or 11%, in 2009 compared to 2008, primarily due to an increase in compensation and benefits costs of $1.3 million associated with an increase in our general and administrative personnel. Additionally, stock-based compensation expense increased $0.8 million due to additional equity grants to employees in our general and administrative departments and to board members. Partially offsetting these increases were decreases in recruiting costs and project consultant fees. As a percentage of total revenue, general and administrative expenses decreased to 15% in 2009 from 16% in 2008 as a result of economies of scale achieved by our general and administrative operations.
59
Table of Contents
Amortization of Acquired Intangible Assets
Amortization expense related to intangible assets purchased through our acquisition of PlanPrescriber in April 2010 was $1.1 million for the year ended December 31, 2010.
Interest and Other Income, Net
The following table presents our interest and other income, net, for the years ended December 31, 2008, 2009 and 2010 and the dollar and percentage change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||||||||||
| $ | % | $ | % | |||||||||||||||||||||||||
| Interest and other income, net |
$ | 3,714 | $ | (2,776 | ) | (75 | )% | $ | 938 | $ | (929 | ) | (99 | )% | $ | 9 | ||||||||||||
| Percentage of total revenue |
3 | % | 1 | % | 0 | % | ||||||||||||||||||||||
Interest and other income, net, primarily consists of interest income earned on our invested cash, cash equivalents and marketable securities balances, partially offset by administrative bank fees and investment management fees.
2010 compared to 2009—Interest and other income, net, decreased in 2010 compared to 2009, primarily due to a decline in the average yield earned on our invested cash, cash equivalents and marketable securities. The decline in the average yield we earned our investments was primarily due to a general market decline in interest rates and was also impacted by the mix of investments we held during 2010. During 2010, we reduced our investments in higher-yielding marketable securities. Administrative bank fees, investment management fees and interest expense on our capital lease obligations offset interest earned on our cash, cash equivalents and marketable securities in 2010. Cash, cash equivalents and marketable securities decreased to $128.1 million at December 31, 2010 from $153.5 million at December 31, 2009 primarily due to $27.2 million of net cash used for the acquisition of PlanPrescriber in April 2010 and $26.2 million used to repurchase 2,026,802 shares of eHealth’s common stock during 2010, partially offset by $20.5 million of cash generated from operations. As a percentage of total revenue, interest and other income, net decreased to 0% in 2010 from 1% in 2009.
2009 compared to 2008—Interest and other income, net, decreased $2.8 million, or 75%, in 2009 compared to 2008, primarily due to a decline in the average yield earned on our invested cash, cash equivalents and marketable securities during the year ended December 31, 2009 compared to the year ended December 31, 2008. Interest income totaled $1.0 million and $3.9 million for the years ended December 31, 2009 and 2008, respectively. Cash, cash equivalents and marketable securities increased from $150.6 million at December 31, 2008 to $153.5 million at December 31, 2009 primarily due to cash generated from operations of $30.1 million and net proceeds from the exercise of common stock options of $0.9 million, partially offset by $29.4 million used to repurchase 1,827,193 shares of our common stock, capital expenditures of $1.4 million and initial consideration of $1.3 million paid to HBDC in connection with customer transition and marketing agreements during 2009. As a percentage of total revenue, interest and other income, net decreased to 1% in 2009 from 3% in 2008.
Provision for Income Taxes
The following table presents our provision for income taxes for the year ended December 31, 2008, 2009 and 2010 and the dollar change from the prior year (dollars in thousands):
| Year Ended December 31, 2008 |
Change | Year Ended December 31, 2009 |
Change | Year Ended December 31, 2010 |
||||||||||||||||
| $ | $ | |||||||||||||||||||
| Provision for income taxes |
$ | 10,806 | $ | 626 | $ | 11,431 | $ | 3,655 | $ | 15,086 | ||||||||||
| Percentage of total revenue |
10 | % | 8 | % | 9 | % | ||||||||||||||
60
Table of Contents
2010—In 2010, we recorded a provision for income taxes of $15.1 million, representing an effective tax rate of 46.3%. Our effective tax rate in 2010 was higher than statutory federal and state tax rates due primarily to non-deductible lobbying expenses, tax shortfalls related to share-based payments, non-deductible acquisition-related costs incurred as a result of our purchase of PlanPrescriber and additional state tax expense resulting from adjusting state deferred tax assets for a reduction in California apportionment.
2009—In 2009, we recorded a provision for income taxes of $11.4 million, representing an effective tax rate of 42.7% for 2009. Our effective tax rate in 2009 was higher than statutory federal and state tax rates primarily due to non-deductible lobbying expenses and tax shortfalls related to share-based payments, partially offset by an income tax benefit adjustment related to an increase in our deferred income tax assets resulting from a reduction in estimated limitations on both our federal and California net operating loss carry forwards.
2008—We recorded a provision for income taxes in 2008 of $10.8 million, representing an effective tax rate of 43.3% for 2008. Our effective tax rate in 2008 was higher than statutory federal and state tax rates primarily due to tax shortfalls related to share-based payments.
New California tax legislation in 2008 and again in 2010 limited our ability to utilize net operating loss and tax credit carry forwards to reduce our state income taxes payable in the years ended December 31, 2008, 2009 and 2010. Our cash outlay for federal and state taxes was $0.1 million, $3.0 million and $2.6 million in the years ended December 31, 2008, 2009 and 2010, respectively. Our cash outlay increased in the years 2009 and 2010, compared to 2008 due to the inability to use our net operating loss carry forwards in California to reduce our current tax liability.
Liquidity and Capital Resources
At December 31, 2010, our cash and cash equivalents totaled $128.1 million. Cash equivalents are comprised of financial instruments with an original maturity of 90 days or less from the date of purchase, primarily money market funds. At December 31, 2010 we held no marketable securities. At December 31, 2009, our cash, cash equivalents and marketable securities totaled $153.5 million. Marketable securities were comprised primarily of available-for-sale financial instruments with original maturities of more than 90 days but less than two years from the date of purchase. Marketable securities that are available for use in current operations are classified as current assets in the accompanying consolidated balance sheets regardless of the remaining time to maturity.
On November 12, 2008, we announced that our board of directors authorized a stock repurchase program, pursuant to which up to 2,507,950 shares could be repurchased, for a total cost not to exceed $30 million. This stock repurchase program was completed in September 2009 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. On July 27, 2010, we announced that our board of directors approved a stock repurchase program authorizing us to purchase up to $30 million of our common stock. This stock repurchase program was completed in January 2011 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. The cost of the repurchased shares was funded from available working capital for these stock repurchase programs. Share repurchases under these programs complied with Rule 10b-18 under the Securities Exchange Act of 1934, as amended. All shares repurchased under the programs were returned to the status of authorized but unissued shares of common stock. For accounting purposes, common stock repurchased under the programs was recorded based upon the settlement date of the applicable trade. Such repurchased shares are held in treasury and are presented using the cost method.
61
Table of Contents
The stock repurchase activity under our stock repurchase programs during the years ended December 31, 2009 and 2010 is summarized as follows (in thousands, except share and per share amounts):
| Total Number of Shares Purchased |
Average Price Paid per Share (1) |
Amount of Repurchase |
||||||||||
| Cumulative balance at December 31, 2008 |
50,657 | $ | 12.61 | $ | 639 | |||||||
| Repurchases of common stock during 2009 |
1,827,193 | $ | 16.07 | 29,360 | ||||||||
| Cumulative balance at December 31, 2009 |
1,877,850 | $ | 15.97 | 29,999 | ||||||||
| Repurchases of common stock during 2010 |
2,026,802 | $ | 12.93 | 26,204 | ||||||||
| Cumulative balance at December 31, 2010 |
3,904,652 | $ | 14.39 | $ | 56,203 | |||||||
| (1) | Average price paid per share includes commissions |
The following table presents a summary of our cash flows for the years ended December 31, 2008, 2009 and 2010 (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Net cash provided by (used in): |
||||||||||||
| Operating activities |
$ | 30,194 | $ | 30,086 | $ | 20,509 | ||||||
| Investing activities |
(18,706 | ) | 30,675 | (10,601 | ) | |||||||
| Financing activities |
1,206 | (23,562 | ) | (13,166 | ) | |||||||
The cash flow statement for 2010 includes a $27.1 million cash flow benefit from deferred income taxes, of which approximately $14.3 million of tax benefit, primarily from the utilization of net operating loss carry forwards, is included in cash flow from operations and $12.8 million of net operating loss carry forwards, from the utilization of excess tax benefits related to share-based payments. The utilization of excess tax benefits related to share-based payments is also shown in the cash flow statements for 2010 as both a decrease in cash flow from operating activities and an increase in cash flow from financing activities.
The cash flow statement for 2009 includes a $14.3 million cash flow benefit from taxes, of which approximately $9.3 million of tax benefit, primarily from the utilization of net operating loss carry forwards, is included in cash flow from operations and $5.0 million of net operating loss carry forwards, from the utilization of excess tax benefits related to share-based payments. The utilization of excess tax benefits related to share-based payments is also shown in the cash flow statements for 2009 as both a decrease in cash flow from operating activities and an increase in cash flow from financing activities.
The cash flow statement for 2008 includes a $9.7 million cash flow benefit from taxes, of which approximately $9.4 million of tax benefit, primarily from the utilization of net operating loss carry forwards, is included in cash flow from operations and $0.3 million of net operating loss carry forwards, from the utilization of excess tax benefits related to share-based payments. The utilization of excess tax benefits related to share-based payments is also shown in the cash flow statements for 2008 as both a decrease in cash flow from operating activities and an increase in cash flow from financing activities.
Operating Activities
Cash provided by operating activities primarily consists of net income, adjusted for certain non-cash items including deferred income taxes, depreciation and amortization, amortization and accretion on marketable securities, net, stock-based compensation expense, excess tax benefits from stock-based compensation, and the effect of changes in working capital and other activities.
62
Table of Contents
2010—Our operating activities generated cash of $20.5 million during the year ended December 31, 2010 and consisted of net income of $17.5 million, increased by non-cash items of $11.2 million and partially offset by cash used for working capital and other activities of $8.2 million. Adjustments for non-cash items primarily consisted of $14.3 million of deferred income taxes, $6.4 million of stock-based compensation expense and $2.2 million of depreciation and amortization and $1.1 million of amortization of acquired intangible assets, partially offset by $12.8 million of excess tax benefits from stock-based compensation. Cash used for working capital and other activities primarily consisted of an increase of $8.1 million in accounts receivable primarily due to the seasonality of our Medicare business, a decrease of $3.0 million in other current liabilities, an increase of $1.1 million in prepaid expenses and other current assets and a decrease of $0.5 million in accounts payable, partially offset by an increase of $2.4 million in deferred revenue and an increase of $2.3 million in accrued compensation and benefits.
2009—Our operating activities generated cash of $30.1 million during the year ended December 31, 2009 and consisted of net income of $15.3 million adjusted by non-cash items of $12.1 million and cash provided by working capital and other activities of $2.6 million. Adjustments for non-cash items primarily consisted of $9.4 million of deferred income taxes, $4.8 million of stock-based compensation expense, $2.2 million of depreciation and amortization and $0.7 million of amortization and accretion on marketable securities, net, partially offset by $5.0 million of excess tax benefits from stock-based compensation. Cash provided by working capital and other activities primarily consisted of an increase of $1.1 million in accounts payable and an increase of $0.7 million in accrued marketing expenses.
2008—Our operating activities generated cash of $30.2 million during the year ended December 31, 2008 and consisted of net income of $14.2 million adjusted by non-cash items of $14.5 million and cash provided by working capital and other activities of $1.5 million. Adjustments for non-cash items primarily consisted of $9.5 million of deferred income taxes, $3.5 million of stock-based compensation expense and $1.9 million of depreciation and amortization. Cash provided by working capital and other activities primarily consisted of an increase of $0.7 million in accrued marketing expenses, an increase of $0.7 million in accounts payable and an increase of $0.6 million in other current liabilities, partially offset by an increase of $0.7 million in accounts receivable.
The timing of the recognition of our commission revenue depends upon the timing of our receipt of commission reports and associated commission payments from health insurance carriers. If we were to experience a delay in receiving a commission payment from a health insurance carrier at the end of a quarter, our operating cash flows for that quarter could be negatively impacted. Additionally, commission override payments are reported to us in a more irregular pattern than premium commissions. For example, a carrier may make a commission override payment to us on an annual basis, which would positively impact our cash flows in the quarter the payment is received. The majority of our annual commission override payments are typically received during the first quarter of the year.
Historically, we have experienced a reduction in operating cash flows during the first quarter of the year due to the payment of annual performance bonuses to employees. In addition, a significant portion of our marketing and advertising expenses are driven by the number of health insurance applications submitted on our ecommerce platform. Since our marketing and advertising costs are expensed as incurred and the revenue from approved applications is recognized as commissions are subsequently reported to us, our operating cash flows could be negatively impacted by a substantial increase in the volume of applications submitted during a quarter or positively impacted by a substantial decline in the volume of applications submitted during a quarter. Starting with the fourth quarter of 2010 we began to experience seasonality impacting the timing of our cash flow resulting from our Medicare plan-related activities. In our Medicare plan business, we generate the majority of referral fees during the fourth quarter. We also incur a significant portion of our Medicare plan related marketing expenses during the fourth quarter. We may not be paid for a considerable portion of the referral fees owed to us until the first quarter. This seasonality pattern results from the timing of the annual enrollment period when
63
Table of Contents
Medicare-eligible individuals can make changes to their Medicare Advantage or Medicare Part D prescription drug coverage for the following year.
Investing Activities
Our investing activities primarily consist of purchases, sales and maturities of marketable securities and purchases of computer hardware and software to enhance our website and to support our growth. It also included cash paid in connection with an acquisition in 2010, as well as consideration paid in connection with the transfer to us of certain Medicare plan members for whom we expect to earn future commissions. Marketable securities have generally consisted of investment grade corporate and U.S. government-sponsored enterprise debt securities, commercial paper and certificates of deposit that have a maturity of more than 90 days but less than two years from the date of purchase and are available for use in current operations. These investments are carried at fair value with unrealized gains and losses, net of taxes, reported as a component of stockholders’ equity in the consolidated balance sheets and in comprehensive income on the consolidated statements of income and comprehensive income.
2010—Net cash used in investing activities of $10.6 million during 2010 was attributable to net cash paid of $27.2 million in connection with the acquisition of PlanPrescriber, capital expenditures of $2.9 million and initial consideration of $2.5 million paid to a partner in connection with a customer transition agreements, partially offset by maturities of marketable securities of $22.1 million.
2009—Net cash provided by investing activities of $30.7 million during 2009 was attributable to maturities and sales of marketable securities of $73.9 million, partially offset by purchases of marketable securities of $40.6 million, capital expenditures of $1.4 million and initial consideration of $1.3 million paid to HBDC in connection with customer transition and marketing agreements.
2008—Net cash used in investing activities of $18.7 million during 2008 was attributable to purchases of marketable securities of $85.7 million and capital expenditures of $2.5 million, partially offset by sales and maturities of marketable securities of $10.1 million and $59.3 million, respectively. Capital expenditures in 2008 were impacted by a project relating to the expansion of our data center operations.
Financing Activities
2010— Net cash used in financing activities of $13.2 million during 2010 was due to $26.2 million used to repurchase 2,026,802 shares of our common stock and $0.6 million used to net share settle equity awards, partially offset by $12.8 million of excess tax benefits from stock-based compensation and $0.8 million of proceeds received from the issuance of common stock pursuant to stock option exercises.
2009—Net cash used in financing activities of $23.6 million during 2009 was due to $29.4 million used to repurchase 1,827,193 shares of our common stock, partially offset by $5.0 million of non-cash excess tax benefits from stock-based compensation and $0.9 million of net proceeds received from the issuance of common stock pursuant to stock option exercises.
2008—Cash provided by financing activities of $1.2 million during 2008 was due to $1.5 million of net proceeds received from the issuance of common stock pursuant to stock option exercises, partially offset by $0.6 million utilized to repurchase 50,657 shares of our common stock.
Future Needs
We believe that cash generated from operations and our current cash, cash equivalents and marketable securities will be sufficient to fund our operations for at least the next twelve months. Our future capital requirements will depend on many factors, including our level of investment in technology and advertising
64
Table of Contents
initiatives. We currently do not have any bank debt, line of credit facilities or other borrowing arrangements. To the extent that available funds are insufficient to fund our future activities, we may need to raise additional capital through public or private equity or debt financing to the extent such funding sources are available.
Contractual Obligations and Commitments
The following table presents a summary of our future minimum payments under non-cancellable operating lease agreements and certain contractual service and licensing obligations as of December 31, 2010 (in thousands):
| Years Ending December 31, |
Operating Lease Obligations |
Service and Licensing Obligations |
Total Obligations |
|||||||||
| 2011 |
$ | 3,789 | $ | 357 | $ | 4,146 | ||||||
| 2012 |
2,675 | — | 2,675 | |||||||||
| 2013 |
494 | — | 494 | |||||||||
| 2014 |
213 | — | 213 | |||||||||
| Total |
$ | 7,171 | $ | 357 | $ | 7,528 | ||||||
Operating Lease Obligations
We lease certain of our office, operating facilities, equipment and furniture and fixtures under various operating leases, the latest of which expires in October 2014. Certain of these leases have free or escalating rent payment provisions. We recognize rent expense on our operating leases on a straight-line basis over the terms of the leases, although actual cash payment obligations under certain of these agreements fluctuate over the terms of the agreements.
During 2009, we extended the operating lease for our facility in San Francisco, California for an additional five years, expiring in October 2014, and expanded the operating lease for our facility in China to include additional office space. In April 2010 we acquired an operating lease for our PlanPrescriber facility in Maynard, Massachusetts, which expires in May 2013, and in September 2010 we entered into an operating lease for our new customer care center facility in Salt Lake City, Utah, which expires in February 2012.
Service and Licensing Obligations
We have entered into service and licensing agreements with third party vendors to provide various services, including network access, equipment maintenance and software licensing. The terms of these services and licensing agreements are generally up to three years, the latest of which expires in June 2011. We record the related service and licensing expenses on a straight-line basis, although actual cash payment obligations under certain of these agreements fluctuate over the terms of the agreements.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements, investments in special purpose entities or undisclosed borrowings or debt. Additionally, we are not a party to any derivative contracts or synthetic leases.
Recent Accounting Pronouncements
See Note 1 of Notes to Consolidated Financial Statements for recently issued accounting standards that could have an effect on us.
65
Table of Contents
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
Credit Risk
Our financial instruments that are exposed to concentrations of credit risk principally consist of cash, cash equivalents, marketable securities and accounts receivable. As of December 31, 2009 and 2010, our cash, cash equivalents and marketable securities were invested as follows (in thousands):
| December 31, 2009 |
December 31, 2010 |
|||||||
| Cash (1) |
$ | 7,085 | $ | 11,663 | ||||
| Money market funds (2) |
124,254 | 116,411 | ||||||
| Bonds, commercial paper and certificates of deposit: |
||||||||
| Government sector |
17,891 | — | ||||||
| Financial sector |
3,054 | — | ||||||
| Industrial sector |
1,239 | — | ||||||
| Total cash, cash equivalents and marketable securities |
$ | 153,523 | $ | 128,074 | ||||
| (1) | We deposit our cash, cash equivalents and marketable securities in accounts with major banks and financial institutions and such deposits are in excess of federally insured limits. |
| (2) | At December 31, 2009 and 2010 money market funds consisted of U.S. government-sponsored enterprise bonds and discount notes, U.S. government treasury bills and notes and repurchase agreements collateralized by U.S. government obligations. |
During the years ended December 31, 2008, 2009 and 2010, net unrealized gains and losses incurred on our marketable securities were not significant, and we did not realize any losses on our marketable securities during the years ended December 31, 2008, 2009 and 2010.
We do not require collateral or other security for our accounts receivable. As of December 31, 2010, two customers represented 40% and 24%, respectively, for a total of 64% of our $10.8 million outstanding accounts receivable. No other customers represented 10% or more of our total accounts receivable. We believe the potential for collection issues with any of our customers is minimal as of December 31, 2010. Accordingly, our allowance for uncollectible amounts at December 31, 2010 was not material.
Significant Customers
Substantially all revenue for the years ended December 31, 2008, 2009 and 2010 was generated from customers located in the United States. The following carriers (including carriers owned by them) represented 10% or more of our total revenue for the years ended December 31, 2008, 2009 and 2010:
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Aetna |
14 | % | 16 | % | 17 | % | ||||||
| UnitedHealthcare |
17 | % | 14 | % | 14 | % | ||||||
| WellPoint |
16 | % | 15 | % | 12 | % | ||||||
66
Table of Contents
Foreign Currency Exchange Risk
To date, substantially all of our revenue has been derived from transactions denominated in United States Dollars. We have exposure to adverse changes in exchange rates associated with operating expenses of our foreign operations, which are denominated in Chinese Yuan Renminbi. Foreign currency fluctuations have not had a material impact historically on our results of operations; however, there can be no assurance that future fluctuations will not have material adverse effects on our results of operations. We have not engaged in any foreign currency hedging or other derivative transactions to date.
67
Table of Contents
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
Index to the Consolidated Financial Statements
| 69 | ||||
| 70 | ||||
| 71 | ||||
| 72 | ||||
| 74 | ||||
| 75 | ||||
68
Table of Contents
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders of eHealth, Inc.
We have audited the accompanying consolidated balance sheets of eHealth, Inc. as of December 31, 2010 and 2009, and the related consolidated statements of income and comprehensive income, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2010. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of eHealth, Inc. at December 31, 2010 and 2009, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2010, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), eHealth, Inc.’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated March 15, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Palo Alto, California
March 15, 2011
69
Table of Contents
CONSOLIDATED BALANCE SHEETS
(In thousands, except share and per share information)
| December 31, 2009 |
December 31, 2010 |
|||||||
| Assets | ||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 131,339 | $ | 128,074 | ||||
| Marketable securities |
22,184 | — | ||||||
| Accounts receivable |
2,295 | 10,810 | ||||||
| Deferred income taxes |
6,009 | 5,347 | ||||||
| Prepaid expenses and other current assets |
2,324 | 4,361 | ||||||
| Total current assets |
164,151 | 148,592 | ||||||
| Property and equipment, net |
3,775 | 4,528 | ||||||
| Deferred income taxes |
919 | 3,119 | ||||||
| Other assets |
863 | 3,248 | ||||||
| Acquired intangible assets, net |
— | 12,262 | ||||||
| Goodwill |
— | 14,096 | ||||||
| Total assets |
$ | 169,708 | $ | 185,845 | ||||
| Liabilities and stockholders’ equity | ||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 3,252 | $ | 3,573 | ||||
| Accrued compensation and benefits |
5,051 | 7,523 | ||||||
| Accrued marketing expenses |
3,879 | 3,644 | ||||||
| Deferred revenue |
401 | 2,785 | ||||||
| Other current liabilities |
2,677 | 2,672 | ||||||
| Total current liabilities |
15,260 | 20,197 | ||||||
| Other non-current liabilities |
2,997 | 3,451 | ||||||
| Commitments and contingencies (see Note 9) |
||||||||
| Stockholders’ equity: |
||||||||
| Preferred stock: $0.001 par value; Authorized shares: 10,000,000; Issued and outstanding shares: none |
— | — | ||||||
| Common stock: $0.001 par value; Authorized shares: 100,000,000; 25,311,085 and 25,530,856 shares issued at December 31, 2009 and 2010, respectively; and 23,416,730 and 21,574,728 shares outstanding at December 31, 2009 and 2010, respectively |
25 | 26 | ||||||
| Additional paid-in capital |
183,747 | 203,231 | ||||||
| Treasury stock, at cost: 1,894,355 and 3,956,128 shares at December 31, 2009 and 2010, respectively |
(29,999 | ) | (56,202 | ) | ||||
| Retained earnings (accumulated deficit) |
(2,545 | ) | 14,937 | |||||
| Accumulated other comprehensive income |
223 | 205 | ||||||
| Total stockholders’ equity |
151,451 | 162,197 | ||||||
| Total liabilities and stockholders’ equity |
$ | 169,708 | $ | 185,845 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
70
Table of Contents
CONSOLIDATED STATEMENTS OF INCOME AND COMPREHENSIVE INCOME
(In thousands, except per share amounts)
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Revenue: |
||||||||||||
| Commission |
$ | 100,839 | $ | 119,259 | $ | 135,366 | ||||||
| Other |
10,872 | 15,631 | 25,038 | |||||||||
| Total revenue |
111,711 | 134,890 | 160,404 | |||||||||
| Operating costs and expenses: |
||||||||||||
| Cost of revenue |
1,746 | 4,581 | 5,499 | |||||||||
| Marketing and advertising |
42,161 | 53,987 | 60,102 | |||||||||
| Customer care and enrollment |
14,379 | 14,769 | 17,810 | |||||||||
| Technology and content |
14,182 | 15,685 | 19,241 | |||||||||
| General and administrative |
17,983 | 20,028 | 24,055 | |||||||||
| Amortization of acquired intangible assets |
— | — | 1,138 | |||||||||
| Total operating costs and expenses |
90,451 | 109,050 | 127,845 | |||||||||
| Income from operations |
21,260 | 25,840 | 32,559 | |||||||||
| Interest and other income, net |
3,714 | 938 | 9 | |||||||||
| Income before income taxes |
24,974 | 26,778 | 32,568 | |||||||||
| Provision for income taxes |
10,806 | 11,431 | 15,086 | |||||||||
| Net income |
$ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||
| Comprehensive income: |
||||||||||||
| Net income |
$ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||
| Change in unrealized gain on marketable securities, net of taxes |
156 | (192 | ) | (20 | ) | |||||||
| Foreign currency translation adjustment |
70 | 3 | 2 | |||||||||
| Total comprehensive income |
$ | 14,394 | $ | 15,158 | $ | 17,464 | ||||||
| Net income per share: |
||||||||||||
| Basic |
$ | 0.57 | $ | 0.63 | $ | 0.76 | ||||||
| Diluted |
$ | 0.55 | $ | 0.61 | $ | 0.73 | ||||||
| Weighted average number of shares used in per share amounts: |
||||||||||||
| Basic—common stock |
24,963 | 24,309 | 23,118 | |||||||||
| Diluted—common stock |
25,954 | 25,201 | 23,873 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
71
Table of Contents
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY
(In thousands)
| Common Stock | Additional Paid-in Capital |
Treasury Stock | Deferred Stock-Based Compensation |
Retained Earnings (Accumulated Deficit) |
Accumulated Other Comprehensive Income |
Total Stockholders’ Equity |
||||||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||||||
| Balance at December 31, 2007 |
24,687 | $ | 25 | $ | 167,847 | — | $ | — | $ | (104 | ) | $ | (32,060 | ) | $ | 186 | $ | 135,894 | ||||||||||||||||||
| Issuance of common stock in connection with exercise of common stock options and release of vested restricted stock units |
408 | — | 1,538 | — | — | — | — | — | 1,538 | |||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | 3,425 | — | — | — | — | — | 3,425 | |||||||||||||||||||||||||||
| Amortization of deferred stock-based compensation, net of adjustments for terminated employees |
— | — | (13 | ) | — | — | 82 | — | — | 69 | ||||||||||||||||||||||||||
| Excess tax benefits from stock-based compensation |
— | — | 298 | — | — | — | — | — | 298 | |||||||||||||||||||||||||||
| Change in unrealized gain on investments, net of taxes |
— | — | — | — | — | — | — | 156 | 156 | |||||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | — | — | 70 | 70 | |||||||||||||||||||||||||||
| Repurchase of common stock |
— | — | — | (54 | ) | (639 | ) | — | — | — | (639 | ) | ||||||||||||||||||||||||
| Net income |
— | — | — | — | — | — | 14,168 | — | 14,168 | |||||||||||||||||||||||||||
| Balance at December 31, 2008 |
25,095 | 25 | 173,095 | (54 | ) | (639 | ) | (22 | ) | (17,892 | ) | 412 | 154,979 | |||||||||||||||||||||||
| Issuance of common stock in connection with exercise of common stock options and release of vested restricted stock units |
216 | — | 858 | — | — | — | — | — | 858 | |||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | 4,815 | — | — | — | — | — | 4,815 | |||||||||||||||||||||||||||
| Amortization of deferred stock-based compensation, net of adjustments for terminated employees |
— | — | — | — | — | 22 | — | — | 22 | |||||||||||||||||||||||||||
| Excess tax benefits from stock-based compensation |
— | — | 4,979 | — | — | — | — | — | 4,979 | |||||||||||||||||||||||||||
| Change in unrealized gain on investments, net of taxes |
— | — | — | — | — | — | — | (192 | ) | (192 | ) | |||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | — | — | 3 | 3 | |||||||||||||||||||||||||||
| Repurchase of common stock |
— | — | — | (1,840 | ) | (29,360 | ) | — | — | — | (29,360 | ) | ||||||||||||||||||||||||
| Net income |
— | — | — | — | — | — | 15,347 | — | 15,347 | |||||||||||||||||||||||||||
| Balance at December 31, 2009 |
25,311 | $ | 25 | $ | 183,747 | (1,894 | ) | $ | (29,999 | ) | $ | — | $ | (2,545 | ) | $ | 223 | $ | 151,451 | |||||||||||||||||
72
Table of Contents
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY—(Continued)
(In thousands)
| Common Stock | Additional Paid-in Capital |
Treasury Stock | Deferred Stock-Based Compensation |
Retained Earnings (Accumulated Deficit) |
Accumulated Other Comprehensive Income |
Total Stockholders’ Equity |
||||||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||||||
| Balance at December 31, 2009 |
25,311 | $ | 25 | $ | 183,747 | (1,894 | ) | $ | (29,999 | ) | $ | — | $ | (2,545 | ) | $ | 223 | $ | 151,451 | |||||||||||||||||
| Issuance of common stock in connection with exercise of common stock options and release of vested restricted stock units |
220 | 1 | 227 | — | — | — | — | — | 228 | |||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | 6,395 | — | — | — | — | — | 6,395 | |||||||||||||||||||||||||||
| Excess tax benefits from stock-based compensation |
— | — | 12,853 | — | — | — | — | — | 12,853 | |||||||||||||||||||||||||||
| Change in unrealized gain on investments, net of taxes |
— | — | 9 | — | — | — | — | (20 | ) | (11 | ) | |||||||||||||||||||||||||
| Foreign currency translation adjustment |
— | — | — | — | — | — | — | 2 | 2 | |||||||||||||||||||||||||||
| Repurchase of common stock |
— | — | — | (2,062 | ) | (26,203 | ) | — | — | — | (26,203 | ) | ||||||||||||||||||||||||
| Net income |
— | — | — | — | — | — | 17,482 | — | 17,482 | |||||||||||||||||||||||||||
| Balance at December 31, 2010 |
25,531 | $ | 26 | $ | 203,231 | (3,956 | ) | $ | (56,202 | ) | $ | — | $ | 14,937 | $ | 205 | $ | 162,197 | ||||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
73
Table of Contents
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Operating activities |
||||||||||||
| Net income |
$ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||
| Adjustments to reconcile net income to net cash provided by operating activities: |
||||||||||||
| Deferred income taxes |
9,451 | 9,352 | 14,274 | |||||||||
| Depreciation and amortization |
1,863 | 2,211 | 2,209 | |||||||||
| Amortization of acquired intangible assets |
— | — | 1,138 | |||||||||
| Amortization and accretion on marketable securities, net |
— | 749 | 50 | |||||||||
| Stock-based compensation expense |
3,494 | 4,835 | 6,395 | |||||||||
| Excess tax benefits from stock-based compensation |
(298 | ) | (4,979 | ) | (12,853 | ) | ||||||
| Deferred rent |
(51 | ) | (45 | ) | (11 | ) | ||||||
| Loss on disposal of property and equipment |
45 | 16 | 9 | |||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Accounts receivable |
(705 | ) | (290 | ) | (8,146 | ) | ||||||
| Prepaid expenses and other current assets |
64 | 389 | (1,062 | ) | ||||||||
| Other assets |
196 | 358 | 43 | |||||||||
| Accounts payable |
693 | 1,060 | (459 | ) | ||||||||
| Accrued compensation and benefits |
(41 | ) | 388 | 2,311 | ||||||||
| Accrued marketing expenses |
708 | 717 | (235 | ) | ||||||||
| Deferred revenue |
(9 | ) | (26 | ) | 2,356 | |||||||
| Other current liabilities |
616 | 4 | (2,992 | ) | ||||||||
| Net cash provided by operating activities |
30,194 | 30,086 | 20,509 | |||||||||
| Investing activities |
||||||||||||
| Purchases of property and equipment |
(2,482 | ) | (1,433 | ) | (2,948 | ) | ||||||
| Acquisition of PlanPrescriber, net of cash acquired |
— | — | (27,203 | ) | ||||||||
| Purchase of other assets |
— | (1,280 | ) | (2,550 | ) | |||||||
| Purchases of marketable securities |
(85,653 | ) | (40,550 | ) | — | |||||||
| Sales of marketable securities |
10,120 | 5,006 | — | |||||||||
| Maturities of marketable securities |
59,309 | 68,932 | 22,100 | |||||||||
| Net cash provided by (used in) investing activities |
(18,706 | ) | 30,675 | (10,601 | ) | |||||||
| Financing activities |
||||||||||||
| Net proceeds from exercise of common stock options |
1,618 | 1,031 | 814 | |||||||||
| Cash used to net settle equity awards |
(71 | ) | (171 | ) | (586 | ) | ||||||
| Repurchase of common stock |
(639 | ) | (29,360 | ) | (26,203 | ) | ||||||
| Excess tax benefits from stock-based compensation |
298 | 4,979 | ) | 12,853 | ||||||||
| Principal payments in connection with capital leases |
— | (41 | ) | (44 | ) | |||||||
| Net cash provided by (used in) financing activities |
1,206 | (23,562 | ) | (13,166 | ) | |||||||
| Effect of exchange rate changes on cash and cash equivalents |
47 | 4 | (7 | ) | ||||||||
| Net increase (decrease) in cash and cash equivalents |
12,741 | 37,203 | (3,265 | ) | ||||||||
| Cash and cash equivalents at beginning of period |
81,395 | 94,136 | 131,339 | |||||||||
| Cash and cash equivalents at end of period |
$ | 94,136 | $ | 131,339 | $ | 128,074 | ||||||
| Supplemental disclosure of non-cash activities |
||||||||||||
| Capital lease obligations incurred |
$ | 164 | $ | — | $ | — | ||||||
| Supplemental disclosure of cash flows |
||||||||||||
| Cash paid for interest |
$ | — | $ | 20 | $ | 15 | ||||||
| Cash paid for income taxes |
$ | 133 | $ | 2,999 | $ | 2,577 | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
74
Table of Contents
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1—Summary of Business and Significant Accounting Policies
Description of Business—eHealth, Inc. (the “Company,” “eHealth,” “we” or “us”) offers Internet-based health insurance agency services for individuals, families and small businesses in the United States, as well as technology licensing and Internet advertising services. Our services and technology enable individuals, families and small businesses to compare and purchase health insurance plans from health insurance carriers across the nation. We began actively marketing the availability of Medicare related insurance plans during 2010 and we offer Medicare plan comparison tools and educational materials for Medicare-related insurance plans, including Medicare Advantage, Medicare Supplement and Medicare Part D prescription drug plans. The revenue we have generated in our Medicare plan business is primarily referral fees paid to us based on leads generated by our online platforms that are delivered and sold to third parties. We are licensed to market and sell health insurance in all 50 states and the District of Columbia.
Principles of Consolidation—The consolidated financial statements include the accounts of eHealth, Inc. and its wholly-owned subsidiaries. All intercompany accounts and transactions have been eliminated in consolidation. The consolidated financial statements have been prepared in accordance with U.S. generally accepted accounting principles (“U.S. GAAP”).
Segments—We operate in one business segment. See Note 10—Operating Segments, Geographic Information and Significant Customers for additional information regarding our business segment.
Use of Estimates—The preparation of consolidated financial statements and related disclosures in conformity with U.S. GAAP requires management to make estimates, judgments and assumptions that affect the amounts reported and disclosed in the consolidated financial statements and accompanying notes. On an ongoing basis, we evaluate our estimates, including those related to, but not limited to, the useful lives of long-lived assets including property and equipment and intangible assets, fair value of investments, fair value of intangible assets, allowances for commission forfeitures payable to carriers, valuation allowance for deferred income taxes, provision for income taxes, our assessment whether internal use software and website development costs will result in additional functionality and the assumptions used in determining stock-based compensation. We base our estimates of the carrying value of certain assets and liabilities on historical experience and on various other assumptions that we believe to be reasonable. Actual results may differ from these estimates.
Cash Equivalents—We consider all investments with an original maturity of three months or less from the date of purchase to be cash equivalents. We classify all of our cash equivalents as available-for-sale. Cash and cash equivalents are stated at fair value.
Marketable Securities—We invest in accordance with a policy that seeks to preserve principal while maximizing income without significantly increasing risk. The policy limits investments to certain types of securities issued by institutions with investment-grade credit ratings and places restrictions on maturities and concentration by type and issue. The policy also prohibits investing in certain types of instruments including asset-backed securities, mortgage-backed securities, collateralized bond, debt and mortgage obligations, tax exempt securities, auction rate securities and derivatives. It is our policy to review our marketable securities on at least a quarterly basis to determine if any security is not in compliance with our policy. Additionally, our investment managers are required to inform us within three business days of any credit rating downgrade resulting in non-compliance with our investment policy.
All of our marketable securities are classified as available-for-sale. Marketable securities are carried at their fair value, based on quoted market prices or other available information, with unrealized gains and losses, net of taxes, reported as a component of accumulated other comprehensive income in the accompanying consolidated
75
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
balance sheets. Realized gains and losses on marketable securities are recognized in earnings as a component of interest and other income, net in the consolidated statements of income and comprehensive income. The cost of investments sold is based on the specific identification method.
We determine the appropriate classification of our investments in marketable securities at the time of purchase and reevaluate such designation at each balance sheet date. In response to changes in the availability of and the yield on alternative investments, we may sell certain securities prior to their stated maturities. Marketable securities that are available for use in current operations are classified as current assets in the accompanying consolidated balance sheets regardless of the remaining time to maturity.
It is our policy to review our marketable securities on a regular basis to evaluate whether or not any security has experienced an other-than-temporary decline in fair value. Our policy includes, but is not limited to, reviewing the length of time and extent to which the fair value has been less than the cost, the financial condition and near-term prospects of the issuer, and our intent and ability to retain our investment in the issuer for a period of time sufficient to allow for recovery of fair value. If an investment’s decline in fair value is caused by factors other than changes in interest rates and is deemed to be other-than-temporary, we would reduce the investment’s carrying value to its estimated fair value, as determined based on quoted market prices or other market indicators. No declines in the values of our marketable securities were judged to be other-than-temporary during the years ended December 31, 2008, 2009 and 2010. We did not hold any marketable securities at December 31, 2010.
See Note 3—Balance Sheet Accounts for additional information regarding our marketable securities.
Property and Equipment—Property and equipment are stated at cost, less accumulated depreciation and amortization. Capital lease amortization expenses are included in depreciation expense in our consolidated statements of income and comprehensive income. Depreciation and amortization is computed using the straight-line method based on estimated useful lives as follows:
| Computer equipment and software | 3 to 5 years | |
| Office equipment and furniture | 5 years | |
| Leasehold improvements | Lesser of useful life (typically 5 to 7 years) or related lease term |
Maintenance and minor replacements are expensed as incurred.
See Note 3—Balance Sheet Accounts for additional information regarding our property and equipment.
Goodwill and Acquired Intangible Assets—Goodwill represents the excess of the consideration paid over the estimated fair value of assets acquired and liabilities assumed in a business acquisition. We do not amortize goodwill but test for impairment on an annual basis on or about November 30 of each year and whenever we become aware of any events occurring or changes in circumstances that would indicate a reduction in its fair value below its carrying amount.
Acquired intangible assets with finite useful lives, which include purchased technology, pharmacy and customer relationships, trade names, trademarks and website addresses, are amortized over their estimated useful lives and are reviewed for impairment annually on or about November 30 of each year or when facts or circumstances suggest that the carrying value of these assets may not be recoverable.
We assess the impairment of goodwill and acquired intangible assets when events or changes in circumstances indicate that the carrying value of the assets or the asset grouping may not be recoverable. Factors
76
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
that we consider in deciding when to perform an impairment review include significant negative industry or economic trends or significant changes or planned changes in our use of the assets. We measure the recoverability of assets that will continue to be used in our operations by comparing the carrying value of the asset grouping to our estimate of the related total future undiscounted net cash flows. If an asset grouping’s carrying value is not recoverable through the related undiscounted cash flows, the asset grouping is considered to be impaired. The impairment is measured by comparing the difference between the asset grouping’s carrying value and its fair value. Fair value is the price that would be received from selling an asset in an orderly transaction between market participants at the measurement date. Goodwill and intangible assets are considered non-financial assets, and are recorded at fair value only when an impairment charge is recognized. We assessed the impairment of goodwill and acquired intangible assets on November 30, 2010 and determined that these assets were not considered to be impaired.
We must make subjective judgments in determining the independent cash flows that can be related to specific asset groupings. In addition, we must make subjective judgments regarding the remaining useful lives of assets with finite useful lives. When we determine that the useful life of an asset is shorter than we had originally estimated, we accelerate the rate of amortization over the assets’ new, remaining useful life. We evaluated the remaining useful lives of our assets with finite lives as of November 30, 2010 and determined no adjustments to the remaining lives were required.
Other Long-Lived Assets—We evaluate long-lived assets for impairment annually in the fourth quarter of each year or whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If such assets are considered to be impaired, the impairment to be recognized is measured by the amount by which the carrying amount of the asset exceeds its fair value. No long-lived assets were deemed impaired during the three-year period ended December 31, 2010.
Fair Value of Financial Instruments—The carrying amounts of our financial instruments, including cash and cash equivalents, marketable securities, accounts receivable, accounts payable and accrued liabilities (including accrued compensation and benefits, accrued marketing expenses and other current liabilities), approximate fair value because of their short maturities.
Seasonality—The number of individual and family health insurance applications submitted through our ecommerce platform has generally increased in our first quarter compared to our fourth quarter and in our third quarter compared to our second quarter. Conversely, we have generally experienced a decline or flattening of individual and family submitted applications in our second quarter compared to our first quarter and in our fourth quarter compared to our third quarter. The reasons for these seasonal patterns are not entirely clear. Since a significant portion of our marketing and advertising expenses are driven by the number of health insurance applications submitted on our ecommerce platforms, those expenses are influenced by these seasonal patterns.
In our Medicare plan business, we generate the majority of referral fees during the fourth quarter. We also incur a significant portion of our Medicare plan related marketing expenses during the fourth quarter. We may not be paid for a considerable portion of the referral fees owed to us until the first quarter. This seasonality pattern results from the timing of the annual enrollment period when Medicare-eligible individuals can make changes to their Medicare Advantage or Medicare Part D prescription drug coverage for the following year.
Revenue Recognition—We recognize revenue for our services when each of the following four criteria is met: persuasive evidence of an arrangement exists; delivery has occurred or services have been rendered; the seller’s price to the buyer is fixed or determinable; and collectibility is reasonably assured.
77
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Our revenue is primarily comprised of compensation paid to us by health insurance carriers related to insurance policies that have been purchased by a member who used our service. We define a member as an individual currently covered by an insurance product for which we are entitled to receive compensation from an insurance carrier. Our compensation generally represents a percentage of the premium amount collected by the carrier during the period that a member maintains coverage under a policy (commissions) and, to a much lesser extent, override commissions that health insurance carriers pay us for achieving certain objectives. Premium-based commissions are reported to us after the premiums are collected by the carrier, generally on a monthly basis. We generally continue to receive the commission payment from the relevant insurance carrier until the health insurance policy is cancelled or we otherwise do not remain the agent on the policy. We determine that there is persuasive evidence of an arrangement when we have a commission agreement with a health insurance carrier, a carrier reports to us that it has approved an application submitted through our ecommerce platform and the applicant starts making payments on the policy. Our services are complete when a carrier has approved an application. Collectibility is reasonably assured when commission amounts have been reported to us by a carrier. We recognize commission override revenue when reported to us by a carrier based on the actual attainment of predetermined target sales levels or other objectives as determined by the carrier.
Commissions are reported to us by a cash payment and commission statement. We generally receive these communications simultaneously. In instances when we receive the cash payment and commission statement separately and in different accounting periods, we recognize revenue in the period that we receive the earliest communication, provided we receive the second corroborating communication within ten business days following the end of the accounting period. If the second corroborating communication is not received within ten business days following the end of the accounting period, we recognize revenue in the period the second communication is received. We use the data in the commission statements to help identify the members for which we are receiving a commission payment and the amount received for each member, and to estimate our allowance for forfeitures payable to carriers. As a result, we recognize the net amount of compensation earned as the agent in the transaction.
We rely on health insurance carriers to report accurately and in a timely manner the amount of commissions earned by us, and we calculate our commission revenues, prepare our financial reports, projections and budgets, and direct our marketing and other operating efforts based on the reports we receive from them. Each month we analyze the reports we receive from health insurance carriers by comparing such data to the database we maintain on our members. It is often difficult for us to independently determine whether or not carriers are reporting all commissions due to us, primarily because the majority of our members who terminate their policies do so by discontinuing their premium payments to the carrier instead of by informing us of the cancellation. Also, some of our members pay their premiums less frequently than monthly. This results in our having to identify underpayment or non-payment of commissions on a policy and follow up with a carrier to obtain an explanation and/or request correction of the amount of commissions paid to us. To the extent that carriers understate or fail to timely and accurately report or pay the amount of commissions due to us, we will not collect and recognize revenue to which we are entitled, which, if material in amount, would adversely affect our operating results and financial condition.
Commission override revenue, which we recognize on the same basis as premium commissions, is generally reported to us in a more irregular pattern than premium commissions. As a result, our revenues for a particular quarter could be higher or lower than expectations due to the timing of the reporting of commission override revenue to us.
Certain commission amounts are subject to forfeiture in circumstances where a member has prepaid his or her premium for a future period of coverage and subsequently cancels his or her policy before the completion of
78
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
that period. We estimate and record an allowance for these forfeitures based on historical cancellation experience using data provided on commission statements. The forfeitures are typically reported to us by health insurance carriers one to two months after the commission is reported and paid to us by the carrier. Our estimate of the allowance for forfeitures includes an estimate of both the reporting time lag and the forfeiture amount. Changes in our historical trends would result in changes to our estimated forfeitures in future periods. There were no changes in our average forfeiture rates or reporting time lag during the years ended December 31, 2009 and 2010 which had a material impact on our allowance for forfeitures.
We recognize lead referral revenue when persuasive evidence of an arrangement exists, delivery of a lead has occurred, the fee is fixed or determinable and collectability is reasonably assured. Delivery is deemed to have occurred at the time a lead is delivered to the customer.
Our commercial technology licensing business allows carriers the use of our ecommerce platform to offer their own health insurance policies on their websites and agents to utilize our technology to power their online quoting, content and application submission processes. Typically, we are paid a one-time implementation fee, which we recognize on a straight-line basis over the estimated term of the customer relationship (generally the initial term of the agreement), commencing once the technology is available for use by the third party, and a performance fee based on metrics such as submitted health insurance applications. The metrics used to calculate performance fees for both sponsorship advertising and technology licensing are based on performance criteria that are either measured based on data tracked by us, or based on data tracked by the third party. In instances where the performance criteria data is tracked by us, we recognize revenue in the period of performance. In instances where the performance criteria data is tracked by the third party, we recognize revenue when the amounts earned are both fixed and determinable and collection is reasonably assured. Typically, this occurs through our receipt of a cash payment from the third party along with a detailed statement containing the data that is tracked by the third party. In addition, we have begun to license our technology to government agency customers and we were recently awarded a contract from the federal government to provide technology and information services relating to the federal government’s healthcare reform website.
Our contract with the federal government to provide technology and information services relating to the federal government’s healthcare reform website is a multiple element arrangement. We were not able to establish fair value for each element within the contract and, therefore, accounted for the entire contract as one unit of accounting. We deferred all revenue related to the contract until our technology was available for use by the federal government. Revenue is being recognized on a straight-line basis from the date our technology was available for use by federal government to the end of the initial one-year term of the contract. The contract is renewable annually for up to three additional years, at the option of the federal government.
Our sponsorship advertising program allows carriers to purchase advertising space in specific markets in a sponsorship area on our website. In return, we are typically paid a monthly fee, which is recognized over the period that advertising is displayed, and a performance-based fee based on metrics such as submitted health insurance applications.
In October 2009, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update No. 2009-13—Revenue Recognition (Topic 605): Multiple-Deliverable Revenue Arrangements—a consensus of the FASB Emerging Issues Task Force (“ASU 2009-13”). ASU 2009-13 addresses how to measure and allocate arrangement consideration to one or more units of accounting within certain multiple-deliverable arrangements. ASU 2009-13 modifies the requirements for determining whether a deliverable can be treated as a separate unit of accounting by removing the criterion that objective evidence of fair value must exist for the undelivered
79
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
elements. ASU 2009-13 is effective for us prospectively for revenue arrangements entered into or materially modified beginning January 1, 2011. We are currently evaluating the impact adoption will have on our consolidated financial position, results of operations and cash flows.
Deferred revenue consists of deferred technology licensing implementation fees as well as amounts billed or collected from sponsorship or technology licensing customers in advance of our performing our service for such customers. It also includes the amount by which both unbilled and billed services provided under our federal government contract exceed the straight-line revenue recognized to date. We defer commission amounts that have been paid to us related to transactions where our services are complete, but where we cannot currently estimate the allowance for future forfeitures related to those amounts.
Cost of Revenue—Cost of revenue consists of payments related to health insurance policies sold to members who were referred to our website by marketing partners with whom we have revenue-sharing arrangements Cost of revenue also includes direct labor and other direct costs incurred in connection with our contract with the federal government, as well as the amortization of consideration we paid to certain brokers in connection with the transfer of their health insurance members to us as the new broker of record on the underlying policies. In order to enter into a revenue-sharing arrangement, marketing partners must be licensed to sell health insurance in the state where the policy is sold. Costs related to revenue-sharing arrangements are expensed as the related revenue is recognized. Initial direct labor and other direct costs incurred in connection with our contract with the federal government, but prior to the availability of our technology for use by the federal government, were deferred and included in prepaid expenses and other current assets in our consolidated balance sheet as of December 31, 2010 and are being amortized to cost of revenue from the date our technology was available for use by the federal government to the end of the initial one-year term of the contract.
Costs associated with revenue-sharing of commissions with a health insurance carrier have been offset against commission revenue in the accompanying consolidated statements of income and comprehensive income, while costs associated with revenue-sharing of commissions with partners have been included in cost of revenue.
Marketing and Advertising—Marketing and advertising expenses consist primarily of member acquisition expenses associated with our direct, marketing partner and online advertising member acquisition channels, in addition to compensation and other expenses related to marketing, business development, partner management, public relations and carrier relations personnel who support our offerings. Our direct channel expenses primarily consist of costs for television advertising, radio advertising, print advertising, direct mail and email marketing. We report the cost of advertising as expense in the period in which costs are incurred. Advertising costs incurred in the years ended December 31, 2008, 2009 and 2010 totaled $37.8 million, $49.3 million and $53.9 million, respectively.
Research and Development—Research and development expenses consist primarily of compensation and related expenses incurred for enhancements to the functionality of our website. Research and development costs, which totaled $4.5 million, $5.2 million and $6.4 million for the years ended December 31, 2008, 2009 and 2010, respectively, are included in technology and content expense in the accompanying consolidated statements of income and comprehensive income.
Internal-Use Software and Website Development Costs—We capitalize costs of materials, consultants and compensation and benefits costs of employees who devote time to the development of internal-use software; however, we usually expense as incurred website development costs for new features and functionalities because it is not probable that they will result in additional functionality until they are both developed and tested with confirmation that they are more effective than the current set of features and functionalities on our website. Our judgment is required in determining the point at which various projects enter the states at which costs may be
80
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
capitalized, in assessing the ongoing value of the capitalized costs and in determining the estimated useful lives over which the costs are amortized, which is generally three years. To the extent that we change the manner in which we develop and test new features and functionalities related to our website, assess the ongoing value of capitalized assets or determine the estimated useful lives over which the costs are amortized, the amount of website development costs we capitalize and amortize in future periods would be impacted. Through December 31, 2010, the majority of our internal-use software and website development costs have been expensed as incurred.
Stock-Based Compensation—We recognize stock-based compensation expense in the accompanying consolidated statements of income and comprehensive income based on the fair value of our stock-based awards over their respective vesting periods, which is generally four years. The estimated grant date fair value of our stock-based awards is determined using the Black-Scholes-Merton pricing model and a single option award approach. The weighted-average expected term for stock options granted is calculated using the simplified method, as we do not have sufficient historical option exercise behavior on which to estimate expected terms. The simplified method defines the expected term as the average of the contractual term and the vesting period of the stock option. We have estimated the volatility used as an input to the model based on an analysis of our stock price since our initial public offering, as well as an analysis of similar public companies for which we have data. We estimate our expected volatility using the weighted-average of: our implied volatility; our mean reversion volatility; and the mean reversion volatility of similar public companies for which we have data. We have used judgment in selecting these companies, as well as evaluating the available historical and implied volatility data for these companies. The dividend yield is determined by dividing the expected per share dividend during the coming year by the grant date stock price. Through December 31, 2010, we had not declared or paid any cash dividends, and we do not expect to pay any in the foreseeable future. We base the risk-free interest rate on the implied yield currently available on U.S. Treasury zero-coupon issues with a remaining term equal to the expected term of our stock options. The assumptions used in calculating the fair value of stock-based payment awards represent our best estimates, but these estimates involve inherent uncertainties and the application of management judgment. We will continue to use judgment in evaluating the expected term and volatility related to our own stock-based awards on a prospective basis, and incorporating these factors into the model. Changes in key assumptions will significantly impact the valuation of such instruments.
Income Taxes—We account for income taxes using the liability method. Deferred income taxes are determined based on the differences between the financial reporting and tax bases of assets and liabilities, using enacted statutory tax rates in effect for the year in which the differences are expected to reverse.
FASB ASC Topic 740 prescribes a recognition threshold and measurement approach for uncertain tax positions taken or expected to be taken in a company’s income tax return, and also provides guidance on derecognition, classification, interest and penalties, accounting in interim periods, disclosure, and transition. FASB ASC Topic 740 utilizes a two-step approach for evaluating uncertain tax positions. Step one, Recognition, requires a company to determine if the weight of available evidence indicates that a tax position is more likely than not to be sustained upon audit, including resolution of related appeals or litigation processes, if any. Step two, Measurement, is based on the largest amount of benefit, which is more likely than not to be realized on ultimate settlement.
We consider stock option deduction benefits in excess of book compensation charges realized when we obtain an incremental benefit determined by the “With and Without” calculation method. Under the “With and Without” approach, excess tax benefits related to share-based payments are not deemed to be realized until after the utilization of all other tax benefits available to us. For example, net operating loss and tax credit carry forwards from prior years are used to reduce taxes currently payable prior to deductions from stock option exercises for purposes of financial reporting, while for tax return purposes, current year stock compensation
81
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
deductions are generally used before net operating loss carry forwards. Indirect effects of excess tax benefits, such as the effect on research and development tax credits, are not considered.
Note 2—Acquisition
On April 30, 2010, we acquired 100% of the outstanding common shares and voting interest of PlanPrescriber, Inc. (“PlanPrescriber,” formerly Experion Systems, Inc.), a privately-held company. The purchase price totaled $28.0 million and was primarily paid in cash. PlanPrescriber is a leading provider of online and pharmacy-based tools to help seniors navigate Medicare health insurance options. The acquisition of PlanPrescriber is expected to accelerate our growth in the large and expanding senior market for Medicare insurance. PlanPrescriber is now a wholly-owned subsidiary of eHealth. We recorded the purchase of PlanPrescriber using the acquisition method of accounting and we recognized the assets acquired and liabilities assumed at their fair values as of the date of acquisition. Under the acquisition method, the total purchase price was allocated to PlanPrescriber’s net tangible and intangible assets based upon their estimated fair values as of April 30, 2010. The excess purchase price over the value of the net tangible and identifiable intangible assets was recorded as goodwill. The results of operations are included in our consolidated results of operations beginning with the date of the acquisition. Pro forma results of operations have not been presented because the effects of the acquisition of PlanPrescriber were not material to our consolidated results of operations.
The following table summarizes the final allocation of the purchase price, including the estimated fair values of the assets acquired and liabilities assumed at the acquisition date of April 30, 2010 (in thousands):
| As of April 30, 2010 |
||||
| Cash |
$ | 776 | ||
| Accounts receivable |
369 | |||
| Other acquired assets |
86 | |||
| Acquired intangible assets |
13,400 | |||
| Total identifiable assets acquired |
14,631 | |||
| Deferred tax liabilities |
(180 | ) | ||
| Assumed liabilities |
(568 | ) | ||
| Net identifiable assets acquired |
13,883 | |||
| Goodwill |
14,096 | |||
| Purchase price |
$ | 27,979 | ||
The fair value of acquired accounts receivable approximates the contractual amount. We recognized $0.6 million of acquisition-related costs that were expensed as incurred during the year ended December 31, 2010. These costs are included in general and administrative expenses on the consolidated statements of income and comprehensive income.
82
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following table sets forth the components of intangible assets acquired in connection with the PlanPrescriber acquisition on April 30, 2010, which are subject to amortization (dollars in thousands):
| Fair Value |
Weighted Average Useful Life as of April 30, 2010 |
|||||||
| Purchased technology |
$ | 1,800 | 5.1 years | |||||
| Pharmacy and customer relationships |
10,700 | 8.5 years | ||||||
| Trade names, trademarks and website addresses |
900 | 10.0 years | ||||||
| Acquired intangible assets |
$ | 13,400 | ||||||
The carrying amounts, accumulated amortization and weighted average remaining life of acquired intangible assets subject to amortization as of December 31, 2010 is presented in the table below (dollars in thousands):
| Gross Carrying Amount |
Accumulated Amortization |
Net Carrying Amount |
Weighted Average Remaining Life |
|||||||||||||
| Purchased technology |
$ | 1,800 | $ | (235 | ) | $ | 1,565 | 4.4 years | ||||||||
| Pharmacy and customer relationships |
10,700 | (843 | ) | 9,857 | 7.8 years | |||||||||||
| Trade names, trademarks and website addresses |
900 | (60 | ) | 840 | 9.3 years | |||||||||||
| Acquired intangible assets |
$ | 13,400 | $ | (1,138 | ) | $ | 12,262 | 7.2 years | ||||||||
During the year ended December 31, 2010, amortization expense related to acquired intangible assets totaled $1.1 million.
As of December 31, 2010, expected amortization expense in future periods is as follows (in thousands):
| Years Ending December 31, |
Purchased Technology |
Pharmacy and Customer Relationships |
Trade Names, Trademarks and Website Addresses |
Total | ||||||||||||
| 2011 |
$ | 353 | $ | 1,265 | $ | 90 | $ | 1,708 | ||||||||
| 2012 |
353 | 1,225 | 90 | 1,668 | ||||||||||||
| 2013 |
352 | 1,025 | 90 | 1,467 | ||||||||||||
| 2014 |
352 | 1,025 | 90 | 1,467 | ||||||||||||
| Thereafter |
155 | 5,317 | 480 | 5,952 | ||||||||||||
| Total |
$ | 1,565 | $ | 9,857 | $ | 840 | $ | 12,262 | ||||||||
Note 3—Balance Sheet Accounts
Cash and Cash Equivalents—As of December 31, 2009 and 2010, our cash equivalents consisted of money market accounts that invested in U.S. government-sponsored enterprise bonds and discount notes, U.S. government treasury bills and notes and repurchase agreements collateralized by U.S. government obligations. At December 31, 2009 and 2010, our cash equivalents carried no unrealized gains or losses and we did not realize any significant gains or losses on sales of cash equivalents during the years ended December 31, 2008, 2009 and 2010.
83
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Marketable Securities—As of December 31, 2010, we did not hold any marketable securities. As of December 31, 2009, marketable securities were comprised of available-for-sale financial instruments with original maturities of more than 90 days from the date of purchase. Marketable securities that are available for use in current operations are classified as current assets in the accompanying consolidated balance sheets regardless of the remaining time to maturity. The cost, unrealized gains and losses, net of taxes, and estimated fair value of our marketable securities consisted of the following as of December 31, 2009 (in thousands):
| December 31, 2009 |
Cost | Unrealized Gains |
Unrealized Losses (1) |
Estimated Fair Value |
||||||||||||
| U.S. government-sponsored enterprise bonds |
$ | 17,877 | $ | 15 | $ | (1 | ) | $ | 17,891 | |||||||
| Corporate bonds |
3,053 | 1 | — | 3,054 | ||||||||||||
| U.S. government-sponsored enterprise discount notes |
1,221 | 18 | — | 1,239 | ||||||||||||
| Total marketable securities |
$ | 22,151 | $ | 34 | $ | (1 | ) | $ | 22,184 | |||||||
| (1) | No marketable security had been in a continuous unrealized loss position for more than twelve months as of December 31, 2009. |
We did not realize any significant gains or losses on sales of marketable securities during the years ended December 31, 2009 and 2010.
During the years ended December 31, 2009 and 2010, we recorded immaterial amounts of unrealized gains and losses on our investments in marketable securities. Unrealized gains and losses are the result of the change in fair value of our investments in marketable securities, specifically corporate bonds, at the beginning and end of the period. Unrealized gains and losses are excluded from earnings and reported as a component of stockholders’ equity in the consolidated balance sheets and in comprehensive income on the consolidated statements of income and comprehensive income.
Concentration of Credit Risk—Our financial instruments that are exposed to concentrations of credit risk principally consist of cash, cash equivalents, marketable securities and accounts receivable. We invest our cash, cash equivalents and marketable securities with major banks and financial institutions and, at times, such investments may be in excess of federally insured limits. As of December 31, 2009 and 2010, our cash, cash equivalent and marketable securities balances were invested in securities issued by institutions in the following industries (in thousands):
| Industry |
December 31, 2009 |
December 31, 2010 |
||||||
| Cash |
$ | 7,085 | $ | 11,663 | ||||
| Money market funds (1) |
124,254 | 116,411 | ||||||
| Bonds, commercial paper and certificates of deposit: |
||||||||
| Government sector |
17,891 | — | ||||||
| Financial sector |
3,054 | — | ||||||
| Industrial sector |
1,239 | — | ||||||
| Total cash, cash equivalents and marketable securities |
$ | 153,523 | $ | 128,074 | ||||
| (1) | At December 31, 2009 and 2010, money market accounts invested primarily in U.S. government-sponsored enterprise bonds and discount notes, U.S. government treasury bills and notes and repurchase agreements collateralized by U.S. government obligations. |
84
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets consisted of the following (in thousands):
| As of December 31, | ||||||||
| 2009 | 2010 | |||||||
| Deferred contract costs, net |
$ | — | $ | 1,773 | ||||
| Initial consideration related to book of business transfers, net |
369 | 1,009 | ||||||
| Prepaid insurance |
675 | 464 | ||||||
| Prepaid maintenance contracts |
380 | 464 | ||||||
| Interest receivable |
272 | — | ||||||
| Other |
628 | 651 | ||||||
| Prepaid expenses and other current assets |
$ | 2,324 | $ | 4,361 | ||||
Book of Business Transfers—In February 2009, we entered into customer transition and marketing agreements with Health Benefits Direct Corporation (“HBDC”). Pursuant to the agreements, HBDC agreed to transfer to us certain of its existing health insurance members, all of which were members on individual and family major medical policies, as the new broker of record on the underlying policies and agreed to refer future health insurance prospects to us. We paid HBDC initial consideration of $1.3 million, which is being amortized to cost of revenue as we recognize commission revenue related to the transferred members. In addition, we agreed to pay HBDC a percentage of the commission revenue we receive on the transferred policies, as well as a percentage of the future commission revenue we receive on health insurance policies we sell to prospects HBDC refers to us. The ongoing revenue-sharing payments are recorded as cost of revenue expense when we recognize the related revenue.
In November 2010, we entered into an agreement with a partner, whereby the partner transferred certain of its existing Medicare insurance members to us as the broker of record on the underlying policies. Total consideration of $3.3 million is being amortized to cost of revenue in the consolidated statements of income and comprehensive income as we recognize commission revenue related to the transferred members over a period of up to five years. Of the $3.3 million total consideration, $2.5 million was paid to the partner in November 2010 and $0.8 million is payable in February 2011 and is recorded in accounts payable in the consolidated balance sheets as of December 31, 2010.
Property and Equipment
Property and equipment consisted of the following (in thousands):
| As of December 31, | ||||||||
| 2009 | 2010 | |||||||
| Computer equipment and software |
$ | 8,643 | $ | 11,134 | ||||
| Office equipment and furniture |
1,255 | 1,462 | ||||||
| Leasehold improvements |
779 | 863 | ||||||
| 10,677 | 13,459 | |||||||
| Less accumulated depreciation and amortization |
(6,902 | ) | (8,931 | ) | ||||
| Property and equipment, net |
$ | 3,775 | $ | 4,528 | ||||
85
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Depreciation and amortization expense related to property and equipment totaled $1.8 million, $2.2 million and $2.2 million in the years ended December 31, 2008, 2009 and 2010, respectively.
Other Current Liabilities
Other current liabilities consisted of the following (in thousands):
| As of December 31, | ||||||||
| 2009 | 2010 | |||||||
| Payable to carriers—allowance for forfeitures |
$ | 1,140 | $ | 873 | ||||
| Income taxes payable |
— | 802 | ||||||
| Professional fees |
1,253 | 671 | ||||||
| Other accrued expenses |
284 | 326 | ||||||
| Other current liabilities |
$ | 2,677 | $ | 2,672 | ||||
Note 4—Fair Value Measurements
We define fair value as the price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques we use to measure fair value maximize the use of observable inputs and minimize the use of unobservable inputs. We classify the inputs used to measure fair value into the following hierarchy:
| Level 1 |
Unadjusted quoted prices in active markets for identical assets or liabilities | |
| Level 2 |
Unadjusted quoted prices in active markets for similar assets or liabilities, or | |
| Unadjusted quoted prices for identical or similar assets or liabilities in markets that are not active, or | ||
| Inputs other than quoted prices that are observable for the asset or liability | ||
| Level 3 |
Unobservable inputs for the asset or liability | |
As of December 31, 2010, our cash equivalents were invested in money market funds and were classified as Level 1. We endeavor to utilize the best available information in measuring fair value. We used observable prices in active markets in determining the classification of our money market funds as Level 1.
86
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following table presents information about our financial assets (cash equivalents and marketable securities) that are re-measured and reported at fair value on a recurring basis as of December 31, 2009, and indicates the fair value hierarchy of the valuation techniques we utilized to determine such fair value (in thousands):
| As of December 31, 2009 | ||||||||||||
| Quoted Prices In Active Markets for Identical Assets (Level 1) |
Significant Observable Inputs (Level 2) |
Total | ||||||||||
| Cash equivalents: |
||||||||||||
| Money market funds |
$ | 124,254 | $ | — | $ | 124,254 | ||||||
| Marketable securities: |
||||||||||||
| U.S. government-sponsored enterprise bonds |
— | 17,891 | 17,891 | |||||||||
| Corporate bonds |
— | 3,054 | 3,054 | |||||||||
| U.S. government-sponsored enterprise discount notes |
— | 1,239 | 1,239 | |||||||||
| — | 22,184 | 22,184 | ||||||||||
| Total cash equivalents and marketable securities |
$ | 124,254 | $ | 22,184 | $ | 146,438 | ||||||
We used observable prices in active markets in determining the classification of our money market funds as Level 1. For our other cash equivalents and marketable securities classified as Level 2, we primarily relied on observable quotes in active markets; however if we concluded the market was non-active, we relied on independent market pricing data. We did not hold any financial assets as of December 31, 2009 whereby the fair value measurements were estimated using significant unobservable inputs (Level 3).
Note 5—Stockholders’ Equity and Stock-Based Compensation
Stockholders’ Equity
Preferred Stock—Our board of directors has the authority, without any further action by our stockholders, to issue up to 110,000,000 shares, par value $0.001 per share, of which 10,000,000 shares are designated as preferred stock. As of December 31, 2008, 2009 and 2010, there were no shares of preferred stock outstanding.
Common Stock—On all matters submitted to our stockholders for vote, our common stockholders are entitled to one vote per share, voting together as a single class, and do not have cumulative voting rights. Accordingly, the holders of a majority of the shares of common stock entitled to vote in any election of directors can elect all of the directors standing for election, if they so choose. Subject to preferences that may apply to any shares of preferred stock outstanding, the holders of common stock are entitled to share equally in any dividends, when and if declared by our board of directors. Upon our liquidation, dissolution or winding-up, the holders of common stock are entitled to share equally in all assets remaining after the payment of any liabilities and the liquidation preferences on any outstanding preferred stock. Holders of common stock have no preemptive or conversion rights or other subscription rights and there are no redemption or sinking funds provisions applicable to the common stock.
87
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Shares Reserved—We issue common stock upon the exercise of stock options, the vesting of restricted stock units and upon granting of restricted common stock awards. Shares of authorized but unissued common stock reserved for future issuance were as follows (in thousands):
| As of December 31, | ||||||||
| 2009 | 2010 | |||||||
| Common stock: |
||||||||
| Stock options issued and outstanding |
2,899 | 3,491 | ||||||
| Restricted stock units issued and outstanding |
383 | 370 | ||||||
| Stock options and awards available for future grants |
3,164 | 3,283 | ||||||
| 6,446 | 7,144 | |||||||
Stock Plans—Our 2006 Equity Incentive Plan (the “2006 Plan”) became effective in October 2006. As of December 31, 2010, we had 3,282,655 shares of our common stock available for future grants under the 2006 Plan. In general, if options or shares awarded under the 2006 Plan are forfeited or repurchased, those options or shares will again become available for grant under the 2006 Plan. In addition, on January 1 of each year, the number of shares available for future grant under the 2006 Plan will automatically increase by the lowest of (a) 1,500,000 shares, (b) 4% of the total number of shares of our common stock then outstanding or (c) a lower number determined by our board of directors or its compensation committee. Employees, non-employee members of our board of directors and consultants of our company are eligible to participate in our 2006 Plan. The 2006 Plan requires that the exercise price of stock options and stock appreciation rights awarded shall in no event be less than 100% of the fair market value of a share of common stock on the date of grant.
We also maintain the 1998 Stock Plan and the 2005 Stock Plan, under which we previously granted options to purchase shares of our common stock and restricted common stock. The 1998 and 2005 Stock Plans were terminated with respect to the grant of additional awards upon the effective date of the registration statement related to our initial public offering in October 2006, although we will continue to issue new shares of common stock upon the exercise of stock options previously granted under the 1998 and 2005 Stock Plans.
Our stock options and restricted stock awards granted under the 2006 Plan and the 1998 and 2005 Stock Plans (collectively, the “Stock Plans”) generally vest over four years at a rate of 25% after one year and 1/48th per month thereafter. Our stock options granted prior to December 31, 2007 generally expire after ten years from the date of grant. Stock options granted subsequent to December 31, 2007 generally expire after seven years from the date of grant. As of December 31, 2010, no shares were subject to repurchase. Our restricted stock unit awards granted under the 2006 Plan generally vest over four years at a rate of 25% after one year and 25% annually thereafter.
88
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following table summarizes option activity under the Stock Plans (in thousands, except per share amounts and weighted average remaining contractual life data):
| Shares Available for Grant (1) |
Number of Stock Options |
Weighted Average Exercise Price |
Weighted Average Remaining Contractual Life (years) |
Aggregate Intrinsic Value (2) |
||||||||||||||||
| Balance at December 31, 2007 |
2,464 | 2,626 | $ | 7.44 | 6.41 | $ | 64,787 | |||||||||||||
| Reduction in number of authorized shares (3) |
(28 | ) | — | — | ||||||||||||||||
| Additional shares authorized (4) |
987 | — | — | |||||||||||||||||
| Restricted stock units granted |
(224 | ) | — | — | ||||||||||||||||
| Options granted |
(683 | ) | 683 | $ | 19.39 | |||||||||||||||
| Options exercised |
— | (397 | ) | $ | 4.05 | |||||||||||||||
| Options cancelled |
187 | (187 | ) | $ | 23.17 | |||||||||||||||
| Restricted stock units and awards cancelled |
11 | — | — | |||||||||||||||||
| Balance at December 31, 2008 |
2,714 | 2,725 | $ | 9.85 | 5.91 | $ | 15,878 | |||||||||||||
| Reduction in number of authorized shares (3) |
(17 | ) | — | — | ||||||||||||||||
| Additional shares authorized (4) |
1,002 | — | — | |||||||||||||||||
| Restricted stock units granted |
(215 | ) | — | — | ||||||||||||||||
| Options granted |
(407 | ) | 407 | $ | 15.89 | |||||||||||||||
| Options exercised |
— | (159 | ) | $ | 6.49 | |||||||||||||||
| Options cancelled |
74 | (74 | ) | $ | 22.49 | |||||||||||||||
| Restricted stock units and awards cancelled |
13 | — | — | |||||||||||||||||
| Balance at December 31, 2009 |
3,164 | 2,899 | $ | 10.56 | 5.16 | $ | 20,895 | |||||||||||||
| Reduction in number of authorized shares (3) |
(19 | ) | — | — | ||||||||||||||||
| Additional shares authorized (4) |
937 | — | — | |||||||||||||||||
| Restricted stock units granted |
(132 | ) | — | — | ||||||||||||||||
| Options granted |
(836 | ) | 836 | $ | 15.47 | |||||||||||||||
| Options exercised |
— | (105 | ) | $ | 7.76 | |||||||||||||||
| Options cancelled |
139 | (139 | ) | $ | 15.60 | |||||||||||||||
| Restricted stock units and awards cancelled |
30 | — | — | |||||||||||||||||
| Balance at December 31, 2010 |
3,283 | 3,491 | $ | 11.62 | 4.69 | $ | 16,349 | |||||||||||||
| Vested and expected to vest at December 31, 2010 |
3,419 | $ | 11.53 | 4.65 | $ | 16,302 | ||||||||||||||
| Exercisable at December 31, 2010 |
2,297 | $ | 9.28 | 3.94 | $ | 15,617 | ||||||||||||||
| (1) | Shares available for grant exclude treasury stock of 1,894,355 shares and 3,956,128 shares at December 31, 2009 and 2010, respectively, that could be granted if eHealth determined to do so. |
| (2) | The aggregate intrinsic value is calculated as the difference between the exercise price of the underlying stock options and the fair value of our common stock as of December 31st of each year presented above. |
| (3) | The 1998 and 2005 Stock Plans were terminated with respect to the grant of additional shares upon the effective date of the registration statement related to our initial public offering in October 2006, resulting in reductions in the total number of shares authorized for issuance. |
| (4) | On January 1, 2008, 2009 and 2010, the number of shares authorized for issuance under the 2006 Plan was automatically increased pursuant to the terms of the 2006 Plan by 987,473 shares, 1,001,637 shares and 936,669 shares, respectively. |
89
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Total intrinsic value of stock options exercised during the years ended December 31, 2008, 2009 and 2010 was $7.9 million, $1.4 million and $0.8 million, respectively.
The following table presents total unrecognized stock-based compensation expense as of December 31, 2010 related to stock options and restricted stock units granted to employees under our stock plans (in thousands):
| As of December 31, 2010 |
Stock Options |
Restricted Stock Units |
Total | |||||||||
| Unrecognized stock-based compensation expense |
$ | 7,942 | $ | 4,816 | $ | 12,758 | ||||||
| Estimated forfeitures |
(458 | ) | (283 | ) | (741 | ) | ||||||
| Unrecognized stock-based compensation expense, net of estimated forfeitures |
$ | 7,484 | $ | 4,533 | $ | 12,017 | ||||||
Unrecognized stock-based compensation expense, net of estimated forfeitures, was $12.0 million as of December 31, 2010 and will be amortized on a straight-line basis over the remaining weighted average vesting term of the underlying equity awards which was approximately 2.4 years as of December 31, 2010. Unrecognized stock-based compensation will be adjusted for subsequent changes in estimated forfeitures.
The fair value of stock options granted to employees for the years ended December 31, 2008, 2009 and 2010 was estimated using the following weighted average assumptions:
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Expected term |
4.8 years | 4.6 years | 4.6 years | |||||||||
| Expected volatility |
55.7 | % | 59.8 | % | 52.5 | % | ||||||
| Expected dividend yield |
0 | % | 0 | % | 0 | % | ||||||
| Risk-free interest rate |
3.04 | % | 1.64 | % | 2.25 | % | ||||||
| Weighted average grant-date fair value |
$ | 9.55 | $ | 7.93 | $ | 7.09 | ||||||
The following table summarizes information about stock options outstanding as of December 31, 2010 (in thousands, except per share amounts and weighted average remaining contractual life data):
| Outstanding | Vested and Exercisable | |||||||||||||||
| Exercise |
Number of Shares of Subject to Options |
Weighted Average Remaining Contractual |
Number of Shares of Common Stock Subject to Options |
Weighted Average Exercise Price |
||||||||||||
| $1.00 - $2.00 |
1,045 | 2.40 | 1,045 | $ | 2.00 | |||||||||||
| $4.00 - $6.50 |
22 | 4.04 | 22 | $ | 5.62 | |||||||||||
| $8.00 - $12.20 |
748 | 5.68 | 460 | $ | 8.68 | |||||||||||
| $12.40 - $19.05 |
1,120 | 5.92 | 330 | $ | 15.22 | |||||||||||
| $19.25 - $31.08 |
556 | 5.15 | 440 | $ | 22.90 | |||||||||||
| $1.00 - $31.08 |
3,491 | 4.69 | 2,297 | $ | 9.28 | |||||||||||
90
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The fair value of the restricted stock units is based on eHealth’s stock price on the date of grant, and compensation expense is recognized on a straight-line basis over the vesting period. The following table summarizes restricted stock unit activity under the Stock Plans (in thousands, except weighted average remaining contractual life data):
| Number Outstanding |
Weighted Average Remaining Contractual Life (years) |
Aggregate Intrinsic Value (1) |
||||||||||
| Balance as of December 31, 2007 |
23 | 1.32 | $ | 727 | ||||||||
| Granted |
228 | |||||||||||
| Vested |
(12 | ) | ||||||||||
| Cancelled |
(8 | ) | ||||||||||
| Balance as of December 31, 2008 |
231 | 1.73 | $ | 3,070 | ||||||||
| Granted |
215 | |||||||||||
| Vested |
(60 | ) | ||||||||||
| Cancelled |
(3 | ) | ||||||||||
| Balance as of December 31, 2009 |
383 | 1.47 | $ | 6,289 | ||||||||
| Granted |
132 | |||||||||||
| Vested |
(115 | ) | ||||||||||
| Cancelled |
(30 | ) | ||||||||||
| Balance as of December 31, 2010 |
370 | 2.22 | $ | 4,816 | ||||||||
| Expected to vest at December 31, 2010 |
349 | 2.20 | $ | 4,533 | ||||||||
| (1) | The aggregate intrinsic value is calculated as the fair value of the underlying common stock outstanding and vested and expected to vest as of December 31st of each year presented above. |
Stock Repurchase Programs
On November 12, 2008, we announced that our board of directors authorized a stock repurchase program, pursuant to which up to 2,507,950 shares could be repurchased, for a total cost not to exceed $30 million. This stock repurchase program was completed in September 2009 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. On July 27, 2010, we announced that our board of directors approved a stock repurchase program authorizing us to purchase up to $30 million of our common stock. This stock repurchase program was completed in January 2011 when a cumulative balance of approximately $30 million of common stock, including commissions, had been repurchased. The cost of the repurchased shares was funded from available working capital for these stock repurchase programs. Share repurchases under these programs complied with Rule 10b-18 under the Securities Exchange Act of 1934, as amended. All shares repurchased under the programs were returned to the status of authorized but unissued shares of common stock. For accounting purposes, common stock repurchased under the programs was recorded based upon the settlement date of the applicable trade. Such repurchased shares are held in treasury and are presented using the cost method.
91
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The stock repurchase activity under our stock repurchase programs during the years ended December 31, 2009 and 2010 is summarized as follows (in thousands, except share and per share amounts):
| Total Number of Shares Purchased |
Average Price Paid per Share (1) |
Amount of Repurchase |
||||||||||
| Cumulative balance at December 31, 2008 |
50,657 | $ | 12.61 | $ | 639 | |||||||
| Repurchases of common stock during 2009 |
1,827,193 | $ | 16.07 | 29,360 | ||||||||
| Cumulative balance at December 31, 2009 |
1,877,850 | $ | 15.97 | 29,999 | ||||||||
| Repurchases of common stock during 2010 |
2,026,802 | $ | 12.93 | 26,204 | ||||||||
| Cumulative balance at December 31, 2010 |
3,904,652 | $ | 14.39 | $ | 56,203 | |||||||
| (1) | Average price paid per share includes commissions |
In addition to the 3,904,652 shares repurchased under our repurchase programs as of December 31, 2010, we have in treasury 51,476 shares that were surrendered by employees to satisfy tax withholdings due in connection with the vesting of certain restricted stock units. As of December 31, 2009 and 2010, we had a total of 1,894,355 shares and 3,956,128 shares, respectively, held in treasury.
Stock-Based Compensation
The following table summarizes stock-based compensation expense recorded during the years ended December 31, 2008, 2009 and 2010 (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Common stock options |
$ | 2,481 | $ | 3,055 | $ | 3,936 | ||||||
| Restricted stock units |
931 | 1,756 | 2,459 | |||||||||
| Restricted common stock |
82 | 24 | — | |||||||||
| Total stock-based compensation expense |
$ | 3,494 | $ | 4,835 | $ | 6,395 | ||||||
The following table summarizes stock-based compensation expense by operating function included in the consolidated statements of income and comprehensive income for the years ended December 31, 2008, 2009 and 2010 (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Marketing and advertising |
$ | 644 | $ | 803 | $ | 808 | ||||||
| Customer care and enrollment |
266 | 325 | 384 | |||||||||
| Technology and content |
898 | 1,194 | 1,622 | |||||||||
| General and administrative |
1,686 | 2,513 | 3,581 | |||||||||
| Total stock-based compensation expense |
$ | 3,494 | $ | 4,835 | $ | 6,395 | ||||||
92
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 6—401(k) Plan
In September 1998, our board of directors adopted a defined contribution retirement plan (401(k) Plan), which qualifies under Section 401(k) of the Internal Revenue Code of 1986. Participation in the 401(k) Plan is available to substantially all employees in the United States. Employees can contribute up to 25% of their salary, up to the federal maximum allowable limit, on a before-tax basis to the 401(k) Plan. Employee contributions are fully vested when contributed. Company contributions to the 401(k) Plan are discretionary and are expensed when incurred. In April 2006, we began matching employee contributions to our 401(k) Plan at 25% of an employee’s contribution each pay period, up to a maximum of 1% of the employee’s salary during such pay period. Our matching contributions are expensed as incurred and vest one-third for each of the first three years of the recipient’s service. The recipient is fully vested in all 401(k) Plan matching contributions after three years of service.
Note 7—Income Taxes
The components of our income before income taxes were as follows (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| United States |
$ | 25,318 | $ | 27,262 | $ | 33,226 | ||||||
| Foreign |
(344 | ) | (484 | ) | (658 | ) | ||||||
| Total |
$ | 24,974 | $ | 26,778 | $ | 32,568 | ||||||
The provision for income taxes consisted of the following (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Current: |
||||||||||||
| Federal |
$ | 367 | $ | 6,732 | $ | 13,529 | ||||||
| State |
1,557 | 2,746 | 3,259 | |||||||||
| Foreign |
— | — | 2 | |||||||||
| Total current |
1,924 | 9,478 | 16,790 | |||||||||
| Deferred: |
||||||||||||
| Federal |
8,178 | 2,634 | (1,917 | ) | ||||||||
| State |
704 | (681 | ) | 213 | ||||||||
| Total deferred |
8,882 | 1,953 | (1,704 | ) | ||||||||
| Provision for income taxes |
$ | 10,806 | $ | 11,431 | $ | 15,086 | ||||||
93
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following table provides a reconciliation of the federal statutory income tax rate to our effective tax rate for the years ended December 31, 2008, 2009 and 2010:
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Federal statutory rate |
35.0 | % | 35.0 | % | 35.0 | % | ||||||
| State income taxes |
6.7 | 5.0 | 5.7 | |||||||||
| California apportionment change |
— | — | 2.0 | |||||||||
| Foreign income and withholding taxes |
0.5 | 0.6 | 0.7 | |||||||||
| Research and development tax credits |
(0.2 | ) | (0.2 | ) | (0.1 | ) | ||||||
| Stock-based compensation |
0.7 | 0.6 | 0.6 | |||||||||
| Other |
0.6 | 1.7 | 2.4 | |||||||||
| Effective tax rate |
43.3 | % | 42.7 | % | 46.3 | % | ||||||
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes, together with net operating loss and tax credit carry forwards. Significant components of our deferred tax assets were as follows (in thousands):
| As of December 31, | ||||||||
| 2009 | 2010 | |||||||
| Deferred tax assets: |
||||||||
| Federal, state and foreign net operating loss carry forwards |
$ | 1,083 | $ | 5,159 | ||||
| Federal and state tax credit carry forwards |
712 | 1,231 | ||||||
| Stock-based compensation |
2,356 | 3,365 | ||||||
| Accruals and reserves |
1,423 | 1,983 | ||||||
| Other |
1,602 | 1,846 | ||||||
| Gross deferred tax assets |
7,176 | 13,584 | ||||||
| Valuation allowance |
(248 | ) | (694 | ) | ||||
| Total deferred tax assets |
6,928 | 12,890 | ||||||
| Deferred tax liabilities—acquired intangible assets amortization |
— | (4,424 | ) | |||||
| Total net deferred tax assets |
$ | 6,928 | $ | 8,466 | ||||
| Net deferred tax assets—current |
$ | 6,009 | $ | 5,347 | ||||
| Net deferred tax assets—non-current |
919 | 3,119 | ||||||
| Total net deferred tax assets |
$ | 6,928 | $ | 8,466 | ||||
Assessing the realizability of our deferred tax assets is dependent upon several factors, including the likelihood and amount, if any, of future taxable income in relevant jurisdictions during the periods in which those temporary differences become deductible. We forecast taxable income by considering all available positive and negative evidence, including our history of operating income and losses and our financial plans and estimates that we use to manage the business. These assumptions require significant judgment about future taxable income. As a result, the amount of deferred tax assets considered realizable is subject to adjustment in future periods if estimates of future taxable income change.
94
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The net valuation allowance increased $0.1 million, $0.1 million and $0.4 million in each of the years ended December 31, 2008, 2009 and 2010, respectively, related to net operating carry forwards in China and, beginning in 2010, state net operating losses related to our PlanPrescriber subsidiary.
Our effective tax rate in 2010 was higher than statutory federal and state tax rates primarily due to non-deductible lobbying expenses, tax shortfalls related to share-based payments, non-deductible acquisition-related costs incurred as a result of the purchase of PlanPrescriber and additional state tax expense resulting from adjusting state deferred assets for a reduction in California apportionment. Our effective tax rate in 2009 was higher than statutory federal and state tax rates primarily due to non-deductible lobbying expenses and tax shortfalls related to share-based payments, partially offset by an income tax adjustment related to an increase in our deferred income tax assets resulting from a reduction in estimated limitations on both our federal and California net operating loss carry forwards. Our effective tax rate in 2008 was higher than statutory federal and state tax rates primarily due to tax shortfalls related to share-based payments, as well as penalties and interest associated with our unrecognized tax benefits.
Our federal net operating losses and tax credit carry forwards were available without annual limitations as of December 31, 2010. For tax return purposes, we had net operating loss carry forwards at December 31, 2010 of approximately $18.2 million and $73.9 million for federal income tax and state income tax purposes, respectively. Included in these amounts are unrealized federal and state net operating loss deductions resulting from stock option exercises of approximately $7.9 million and $55.4 million, respectively. The benefit of these unrealized stock option-related deductions has not been included in the deferred tax assets table above and will be recognized as a credit to additional paid-in capital when realized. Federal and state net operating loss carry forwards begin expiring in 2021 and 2012, respectively.
In September 2008, the state of California approved its budget for fiscal year ending June 30, 2009, which contained changes to the California tax law which substantially limited our ability to utilize available state net operating loss and tax credit carry forwards to reduce our state income taxes payable. In October 2010, the state of California approved its budget for fiscal year ending June 30, 2011, which again contained changes to the California tax law which substantially limited our ability to utilize available state net operating loss carry forwards to reduce our state income taxes payable. The changes in the California tax law did not impact our effective tax rates for 2008, 2009 and 2010, and are not expected to impact our effective tax rate for 2011, nor will they affect the amount of net operating loss or tax credit carry forwards that we expect to ultimately use to offset future California taxes, but they did limit the amount of net operating loss carry forwards we were be able to utilize to reduce our taxes payable during 2008, 2009 and 2010, and are expected to limit the amount of net operating loss carry forwards we will be able to utilize to reduce our taxes payable in 2011. As a result of the changes to the California tax law, we experienced an increase in cash taxes payable to the state of California during the years ended December 31, 2008, 2009 and 2010, and are expected to do so for the year ending December 31, 2011.
During the years ended December 31, 2008, 2009 and 2010, primarily due to the restriction on our ability to utilize net operating loss carry forwards to reduce taxes currently payable in California, we utilized excess tax benefits related to share-based payments, which resulted in a decrease in cash generated from operating activities and a corresponding increase in cash generated from financing activities of $0.3 million, $5.0 million and $12.8 million for the years ended December 31, 2008, 2009 and 2010, respectively.
At December 31, 2010, we had tax credit carry forwards of approximately $4.5 million and $0.2 million for federal income tax and state income tax purposes, respectively. Federal tax credit carry forwards begin expiring in 2020 and state tax credits carry forward indefinitely.
95
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
A reconciliation of the beginning and ending amount of our unrecognized tax benefits is as follows (in thousands):
| Unrecognized Tax Benefits |
||||
| Balance at December 31, 2007 |
$ | 2,427 | ||
| Additions based on tax positions related to the current year |
256 | |||
| Additions based on tax positions related to the prior year |
76 | |||
| Settlements |
— | |||
| Balance at December 31, 2008 |
2,759 | |||
| Decreases based on tax positions related to the prior year |
(26 | ) | ||
| Additions based on tax positions related to the current year |
277 | |||
| Settlements |
— | |||
| Balance at December 31, 2009 |
3,010 | |||
| Decreases based on tax positions related to the prior year |
(6 | ) | ||
| Additions based on tax positions related to the current year |
283 | |||
| Settlements |
— | |||
| Balance at December 31, 2010 |
$ | 3,287 | ||
As of December 31, 2009 and 2010, there were $2.4 million and $2.6 million, respectively, of unrecognized tax benefits, that, if recognized, would impact the effective tax rate.
We have elected to record interest and penalties related to uncertain tax positions as income tax expense in the consolidated financial statements. All tax years after 1998 are open to examination and adjustment due to our net operating losses.
Note 8—Net Income Per Share
Basic net income per share is computed by dividing net income by the weighted-average number of common shares outstanding for the period (excluding shares subject to repurchase). Diluted net income per share is computed by dividing the net income for the period by the weighted average number of common and common equivalent shares outstanding during the period. Diluted net income per share is computed giving effect to all potential dilutive common stock, including options, restricted stock and restricted stock units. The dilutive effect of outstanding awards is reflected in diluted earnings per share by application of the treasury stock method.
96
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following table sets forth the computation of basic and diluted net income per share (in thousands, except per share amounts):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Basic: |
||||||||||||
| Numerator: |
||||||||||||
| Net income allocated to common stock |
$ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||
| Denominator: |
||||||||||||
| Weighted average number of common stock shares |
24,964 | 25,130 | 23,525 | |||||||||
| Weighted average number of common stock shares held in treasury |
(1 | ) | (821 | ) | (407 | ) | ||||||
| Net weighted average common stock shares outstanding |
24,963 | 24,309 | 23,118 | |||||||||
| Net income per share—basic: |
$ | 0.57 | $ | 0.63 | $ | 0.76 | ||||||
| Diluted: |
||||||||||||
| Numerator: |
||||||||||||
| Net income allocated to common stock |
$ | 14,168 | $ | 15,347 | $ | 17,482 | ||||||
| Denominator: |
||||||||||||
| Net, weighted average number of common stock shares |
24,963 | 24,309 | 23,118 | |||||||||
| Weighted average number of options |
977 | 838 | 733 | |||||||||
| Weighted average number of restricted stock and restricted stock units |
14 | 54 | 22 | |||||||||
| Total common stock shares used in per share calculation |
25,954 | 25,201 | 23,873 | |||||||||
| Net income per share—diluted: |
$ | 0.55 | $ | 0.61 | $ | 0.73 | ||||||
For each of the years ended December 31, 2008, 2009 and 2010, we had securities outstanding that could potentially dilute earnings per share, but the shares from the assumed conversion or exercise of these securities were excluded in the computation of diluted net income per share as their effect would have been anti-dilutive.
The number of outstanding weighted average anti-dilutive shares that were excluded from the computation of diluted net income per share consisted of the following (in thousands):
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Common stock options |
673 | 1,122 | 1,602 | |||||||||
| Restricted stock units |
9 | 6 | 186 | |||||||||
| Total |
682 | 1,128 | 1,788 | |||||||||
Note 9—Commitments and Contingencies
Leases—We lease certain of our office, operating facilities, equipment and furniture and fixtures under various operating leases, the latest of which expires in October 2014. Certain of these leases have free or escalating rent payment provisions. We recognize rent expense on our operating leases on a straight-line basis over the terms of the leases, although actual cash payment obligations under certain of these agreements fluctuate over the terms of the agreements.
97
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
During 2009, we extended the operating lease for our facility in San Francisco, California for an additional five years, expiring in October 2014, and expanded the operating lease for our facility in China to include additional office space. In April 2010 we assumed an operating lease for our PlanPrescriber facility in Maynard, Massachusetts, which expires in May 2013, and in September 2010 we entered into an operating lease for our new customer care center facility in Salt Lake City, Utah, which expires in February 2012. Total rent expense under all operating leases was approximately $3.3 million, $3.4 million and $3.5 million for the years ended December 31, 2008, 2009 and 2010, respectively.
Future minimum lease payments under non-cancellable operating leases at December 31, 2010 were as follows (in thousands):
| Years Ending December 31, |
Operating Lease Obligations |
|||
| 2011 |
$ | 3,789 | ||
| 2012 |
2,675 | |||
| 2013 |
494 | |||
| 2014 |
213 | |||
| Total minimum lease payments |
$ | 7,171 | ||
Legal Proceedings—In the ordinary course of our business, we have received and may continue to receive inquiries from state regulators relating to various matters. We have become, and may in the future become, involved in litigation in the ordinary course of our business. If we are found to have violated laws or regulations in any of the states, we could be subject to various fines and penalties, including revocation of our license to sell insurance in those states, and our business and financial results would be harmed. We would also be harmed to the extent that related publicity damages our reputation as a trusted source of objective information relating to health insurance and its affordability. It could also be costly to defend ourselves regardless of the outcome.
Guarantees and Indemnifications—We have agreed to indemnify members of our board of directors and our executive officers for fees, expenses, judgments, fines and settlement amounts incurred in any action or proceeding, including actions or proceedings by or in the right of the Company, to which any of them is, or is threatened to be, made a party by reason of their service as a director or officer of the Company or service provided to another company or enterprise at our request. The term of the director and officer indemnification is perpetual as to events or occurrences that take place while the director or officer is, or was, serving at our request. As such, the maximum potential amount of future payment we could be required to make under these indemnification arrangements is unlimited. We, however, maintain directors and officers insurance coverage that limits our exposure under certain circumstances and that may allow us to recover a portion of future amounts paid. Accordingly, we have not recorded any liabilities for these agreements as of December 31, 2009 or 2010.
While we have made various guarantees included in contracts in the normal course of business, primarily in the form of indemnity obligations under certain circumstances, these guarantees do not represent significant commitments or contingent liabilities of the indebtedness of others. Accordingly, we have not recorded a liability related to these indemnification provisions.
98
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 10—Operating Segments, Geographic Information and Significant Customers
Operating Segments—Operating segments are defined as components of an enterprise about which separate financial information is available that is evaluated regularly by the chief operating decision maker, or decision making group, in deciding how to allocate resources and in assessing performance of the Company. Our chief operating decision maker is considered to be our chief executive officer. Our chief executive officer reviews our financial information presented on a consolidated basis in a manner substantially similar to the accompanying consolidated financial statements. Therefore, we have concluded that we operate in one segment, and accordingly we have provided only the required enterprise-wide disclosures.
Geographic Information—Substantially all revenue for all years presented was generated from customers located in the United States. As of December 31, 2009 and 2010, our long-lived assets consisted primarily of property and equipment, goodwill and other indefinite-lived intangible assets and finite-lived intangible assets. Our long-lived assets are attributed to the geographic location in which they are located. Long-lived assets by geographical area were as follows (in thousands):
| As of December 31, 2009 |
As of December 31, 2010 |
|||||||
| United States |
$ | 4,101 | $ | 33,495 | ||||
| China |
537 | 639 | ||||||
| Total |
$ | 4,638 | $ | 34,134 | ||||
Significant Customers—Substantially all revenue for all years presented was generated from customers located in the United States. The following carriers (or carriers owned by them) represented 10% or more of our total revenue for the years ended December 31, 2008, 2009 and 2010:
| Year Ended December 31, | ||||||||||||
| 2008 | 2009 | 2010 | ||||||||||
| Aetna |
14 | % | 16 | % | 17 | % | ||||||
| UnitedHealthcare |
17 | % | 14 | % | 14 | % | ||||||
| WellPoint |
16 | % | 15 | % | 12 | % | ||||||
Revenue attributable to individual and family health insurance plans was approximately 88%, 91% and 91% of our commission revenue in the years ended December 31, 2008, 2009 and 2010, respectively. We define individual and family plan offerings as major medical individual and family health insurance plans, which does not include small business, short-term major medical, stand-alone dental, life, student and Medicare-related health insurance plan offerings.
We do not require collateral or other security for our accounts receivable. As of December 31, 2010, two customers represented 40% and 24%, respectively, for a total of 64% of our $10.8 million outstanding accounts receivable. No other customers represented 10% or more of our total accounts receivable. We believe the potential for collection issues with any of our customers is minimal as of December 31, 2010. Accordingly, our allowance for uncollectible amounts at December 31, 2010 was not material.
99
Table of Contents
EHEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 11—Selected Quarterly Financial Data (Unaudited)
Selected summarized quarterly financial information for 2010 and 2009 is as follows (in thousands, except per share amounts):
| 2010 |
1ST Quarter | 2ND Quarter | 3RD Quarter | 4TH Quarter | Year | |||||||||||||||
| Revenue |
$ | 35,989 | $ | 36,256 | $ | 37,451 | $ | 50,708 | $ | 160,404 | ||||||||||
| Income from operations |
5,899 | 5,752 | 4,842 | 16,066 | 32,559 | |||||||||||||||
| Net income |
3,233 | 3,041 | 2,598 | 8,610 | 17,482 | |||||||||||||||
| Net income per share: |
||||||||||||||||||||
| Basic |
$ | 0.14 | $ | 0.13 | $ | 0.11 | $ | 0.39 | $ | 0.76 | ||||||||||
| Diluted |
$ | 0.13 | $ | 0.13 | $ | 0.11 | $ | 0.38 | $ | 0.73 | ||||||||||
| 2009 |
1ST Quarter | 2ND Quarter | 3RD Quarter | 4TH Quarter | Year | |||||||||||||||
| Revenue |
$ | 31,917 | $ | 33,439 | $ | 35,123 | $ | 34,411 | $ | 134,890 | ||||||||||
| Income from operations |
5,589 | 6,870 | 6,491 | 6,890 | 25,840 | |||||||||||||||
| Net income |
3,143 | 3,994 | 3,452 | 4,758 | 15,347 | |||||||||||||||
| Net income per share: |
||||||||||||||||||||
| Basic |
$ | 0.13 | $ | 0.16 | $ | 0.14 | $ | 0.20 | $ | 0.63 | ||||||||||
| Diluted |
$ | 0.12 | $ | 0.16 | $ | 0.14 | $ | 0.20 | $ | 0.61 | ||||||||||
Revenue for the three months ended December 31, 2010 included a one-time commission payment of $6.0 million which we received from one of our health insurance carrier partners on a number of existing policies, in which all substantial services had been provided.
100
Table of Contents
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
| ITEM 9A. | CONTROLS AND PROCEDURES |
Evaluation of Our Disclosure Controls and Procedures
Our management, with the participation of our chief executive officer and chief financial officer, evaluated the effectiveness of our disclosure controls and procedures pursuant to Rules 13a-15(f) and 15d-15(f) under the Securities Exchange Act of 1934, as amended, as of the end of the period covered by this Annual Report on Form 10-K.
Based on management’s evaluation, our chief executive officer and chief financial officer concluded that our disclosure controls and procedures are effective to provide reasonable assurance that information we are required to disclose in reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in Securities and Exchange Commission rules and forms, and that such information is accumulated and communicated to our management, including our chief executive officer and chief financial officer, as appropriate, to allow timely decisions regarding required disclosure.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Securities Exchange Act of 1934, as amended. Under the supervision and with the participation of our management, including our chief executive officer and chief financial officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2010 based on the guidelines established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Our internal control over financial reporting includes policies and procedures that provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external reporting purposes in accordance with U.S. generally accepted accounting principles.
Based on the results of our evaluation, our management concluded that our internal control over financial reporting was effective as of December 31, 2010. We reviewed the results of management’s assessment with our Audit Committee.
Ernst & Young LLP, an independent registered public accounting firm, has issued a report on internal control over financial reporting, which is presented below.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during the three months ended December 31, 2010 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Inherent Limitations on Effectiveness of Controls
Our management, including our chief executive officer and chief financial officer, do not expect that our disclosure controls or our internal control over financial reporting will prevent all errors and all fraud. A control system, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the
101
Table of Contents
inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, within the Company have been detected. These inherent limitations include the realities that judgments in decision-making can be faulty, and that breakdowns can occur because of a simple error or mistake. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by management override of the controls. The design of any system of controls also is based in part upon certain assumptions about the likelihood of future events, and there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions; over time, controls may become inadequate because of changes in conditions, or the degree of compliance with policies or procedures may deteriorate. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected.
102
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders of
eHealth, Inc.
We have audited eHealth, Inc.’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). eHealth, Inc.’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, eHealth, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2010, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of eHealth, Inc. as of December 31, 2010 and 2009, and the related consolidated statements of income and comprehensive income, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2010 of eHealth, Inc. and our report dated March 15, 2011 expressed an unqualified opinion thereon.
/s/ ERNST & YOUNG LLP
Palo Alto, California
March 15, 2011
103
Table of Contents
| ITEM 9B. | OTHER INFORMATION |
None.
104
Table of Contents
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
The information concerning our directors, executive officers, compliance with Section 16(a) of the Securities Exchange Act of 1934, as amended, and corporate governance required by this Item 10 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010.
We have adopted a code of ethics that applies to all employees, including our principal executive officer, Gary Lauer, principal financial and accounting officer, Stuart Huizinga, and all other executive officers. The code of ethics is available on the investor relations/corporate governance page of our website at www.eHealthInsurance.com. A copy may also be obtained without charge by contacting investor relations, attention Director of Investor Relations, 440 East Middlefield Road, Mountain View, CA 94043 or by calling (650) 210-3111.
We plan to post on our website at the address described above any future amendments or waivers of our Code of Conduct.
| ITEM 11. | EXECUTIVE COMPENSATION |
The information required by Item 11 of Form 10-K is incorporated herein by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
As of December 31, 2010, four of our executive officers are parties to individual Rule 10b5-1 trading plans pursuant to which shares of our common stock will be sold for their account from time to time in accordance with the provisions of the plans without any further action or involvement by the officers.
Additional information required by Item 12 of Form 10-K is incorporated herein by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
The information required by Item 13 of Form 10-K is incorporated herein by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES |
The information required by Item 14 of Form 10-K is incorporated herein by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the Company’s fiscal year ended December 31, 2010.
105
Table of Contents
| ITEM 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES |
| (a) | We have filed the following documents as part of this Annual Report on Form 10-K: |
1. Consolidated Financial Statements
Information in response to this Item is included in Item 8 of Part II of this Annual Report on Form 10-K.
2. Financial Statement Schedules
None.
3. Exhibits
See Item 15(b) below.
(b) Exhibits—We have filed, or incorporated into this Annual Report on Form 10-K by reference, the exhibits listed on the accompanying Index to Exhibits of this Annual Report on Form 10-K.
(c) Financial Statement Schedule—See Item 15(a) above.
106
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
March 15, 2011
eHealth, Inc.
| /S/ GARY L. LAUER |
/S/ STUART M. HUIZINGA | |
| Gary L. Lauer | Stuart M. Huizinga | |
| Chief Executive Officer and Chairman of the Board of Directors |
Chief Financial Officer (Principal Financial and Accounting Officer) |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities indicated on the 15th day of March, 2011.
| Signature |
Title | |
| /S/ STEVEN M. CAKEBREAD Steven M. Cakebread |
Director | |
| /S/ SCOTT N. FLANDERS Scott N. Flanders |
Director | |
| /S/ MICHAEL D. GOLDBERG Michael D. Goldberg |
Director | |
| /S/ LAWRENCE M. HIGBY Lawrence M. Higby |
Director | |
| /S/ RANDALL S. LIVINGSTON Randall S. Livingston |
Director | |
| /S/ JACK L. OLIVER III Jack L. Oliver III |
Director | |
107
Table of Contents
| Description of Exhibit |
Incorporation by Reference Herein | |||||||||
| Exhibit Number |
Form |
Date | ||||||||
| 3.1 | Amended and Restated Certificate of Incorporation of the Registrant | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 3.2 | Amended and Restated Bylaws of the Registrant | Current Report on Form 8-K (File No. 001-33071) | November 17, 2008 | |||||||
| 4.1 | Form of the Registrant’s Common Stock Certificate | Registration Statement on Form S-l, as amended (File No. 333-133526) | June 28, 2006 | |||||||
| 10.1 | Form of Indemnification Agreement entered into between the Registrant and its directors and officers | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.2* | 1998 Stock Plan of the Registrant | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.3 | 2004 Stock Plan for eHealth China | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.4* | 2005 Stock Plan of the Registrant | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.5* | 2006 Equity Incentive Plan of the Registrant, as amended and restated June 15, 2010 | Current Report on Form 8-K (File No. 001-33071) | June 21, 2010 | |||||||
| 10.5.1* | Form of Notice of Stock Option Grant and Stock Option Agreement under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 21, 2007 | |||||||
| 10.5.2* | Form of Notice of Stock Option Grant and Stock Option Agreement (Initial Director Grant) under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 21, 2007 | |||||||
| 10.5.3* | Form of Notice of Stock Option Grant and Stock Option Agreement (Annual Director Grant) under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 21, 2007 | |||||||
| 10.5.4* | Form of Notice of Stock Unit Grant and Stock Unit Agreement under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 21, 2007 | |||||||
| 10.5.5* | Form of Notice of Initial Outside Director Stock Unit Grant Under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 13, 2009 | |||||||
| 10.5.6* | Form of Notice of Annual Outside Director Stock Unit Grant Under the 2006 Equity Incentive Plan of the Registrant | Annual Report on Form 10-K (File No. 001-33071) | March 13, 2009 | |||||||
| 10.5.7* | Form of Outside Director Stock Unit Agreement | Annual Report on Form 10-K (File No. 001-33071) | March 13, 2009 | |||||||
108
Table of Contents
| Description of Exhibit |
Incorporation by Reference Herein | |||||||||
| Exhibit Number |
Form |
Date | ||||||||
| 10.9* | Employment Agreement, dated November 30, 1999, between Gary Lauer and eHealthInsurance Services, Inc. | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.9.1* | Letter Amendment, dated November 2007, amending Offer Letter dated November 30, 1999, between Gary Lauer and eHealthInsurance Services, Inc. | Quarterly Report on Form 10-Q (File No. 001-33071) | November 14, 2007 | |||||||
| 10.9.2* | Second Amendment to Offer Letter, dated December 27, 2008, amending Offer Letter dated November 30, 1999, as amended, between Gary Lauer and eHealthInsurance Services, Inc. | Annual Report on Form 10-K (File No. 001-33071) | March 13, 2009 | |||||||
| 10.9.3* | Management Retention Agreement, effective as of March 4, 2010, between eHealth, Inc. and Gary L. Lauer | Quarterly Report on Form 10-Q (File No. 001-33071) | May 10, 2010 | |||||||
| 10.10* | Employment Agreement, dated May 4, 2000, between Stuart Huizinga and eHealthInsurance Services, Inc., as amended on August 22, 2000 | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.11* | Supplemental Employment Agreement, dated August 24, 2000, between Sheldon Wang and eHealthInsurance Services, Inc. | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.11.1* | Management Retention Agreement, dated January 14, 2010, between Sheldon Wang and eHealth, Inc. | Annual Report on Form 10-K (File No. 001-33071) | March 5, 2010 | |||||||
| 10.12* | Supplemental Employment Agreement, dated August 7, 2000, between Bruce Telkamp and eHealthInsurance Services, Inc. | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.12.1* | Letter Amendment, dated September 2007, amending Offer Letter dated April 6, 2000 and Offer Letter Supplement dated August 7, 2000, between Bruce Telkamp and eHealthInsurance Services, Inc. | Quarterly Report on Form 10-Q (File No. 001-33071) | November 14, 2007 | |||||||
| 10.12.2* | Second Amendment to Offer Letter and Offer Letter Supplement, effective December 29, 2008, amending Offer Letter dated April 6, 2000, as amended, between Bruce Telkamp and eHealthInsurance Services, Inc. | Annual Report on Form 10-K (File No. 001-33071) | March 13, 2009 | |||||||
109
Table of Contents
| Description of Exhibit |
Incorporation by Reference Herein | |||||||||
| Exhibit Number |
Form |
Date | ||||||||
| 10.12.3* | Management Retention Agreement, dated January 14, 2010, between Bruce Telkamp and eHealth, Inc. | Annual Report on Form 10-K (File No. 001-33071) | March 5, 2010 | |||||||
| 10.13* | Letter Agreement, dated November 17, 2005, between Jack L. Oliver III and the Registrant | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.14 | Lease Agreement, dated May 2004, between eHealthInsurance Services, Inc. and Brian Avery, Trustee of the 1983 Avery Investments Trust, as amended | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.14.1 | First Amendment to Lease Agreement, effective as of May 15, 2009, between eHealthInsurance Services, Inc. and Brian Avery, Trustee of the 1983 Avery Investments Trust | Current Report on Form 8-K (File No. 001-33071) | May 21, 2009 | |||||||
| 10.14.2 | Second Amendment to Lease Agreement, effective as of August 5, 2010 between eHealth Insurance Services, Inc. and Brian Avery, Trustee of the 1983 Avery Investments Trust | Current Report on Form 8-K (File No. 001-33071) | August 18, 2010 | |||||||
| 10.15 | Standard Lease Agreement, dated June 10, 2004, between eHealthInsurance Services, Inc. and Gold Pointe E LLC, as amended | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
| 10.15.1 | Fourth Amendment to Standard Lease Agreement (Office), effective as of November 6, 2007, between eHealthInsurance Services, Inc. and Carlsen Investments, LLC | Current Report on Form 8-K (File No. 001-33071) | November 7, 2007 | |||||||
| 10.16 | Office Lease Contract, dated March 31, 2006, among Xiamen Torch Hi-tech Industrial Development Zone Finance Services Center, Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd.; Appendix 1 to Office Lease Contract; and Property Management Service Contract, dated April 4, 2006, between Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Registration Statement on Form S-l, as amended (File No. 333-133526) | April 25, 2006 | |||||||
110
Table of Contents
| Description of Exhibit |
Incorporation by Reference Herein | |||||||||
| Exhibit Number |
Form |
Date | ||||||||
| 10.16.1 | Appendix 3 to Office Lease Contract, dated November 25, 2007, among Xiamen Torch Hi-tech Industrial Development Zone Finance Services Center, Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Annual Report on Form 10-K (File No. 001-33071) | March 17, 2008 | |||||||
| 10.16.2 | Amendment Two to Property Management Service Contract, effective January 16, 2008, between Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Annual Report on Form 10-K (File No. 001-33071) | March 17, 2008 | |||||||
| 10.16.3 | Appendix 4 to Office Lease Contract, dated March 27, 2008, among Xiamen Torch Hi-tech Industrial Development Zone Finance Services Center, Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Quarterly Report on Form 10-Q (File No. 001-33071) | May 12, 2008 | |||||||
| 10.16.4 | Appendix 5 to Office Lease Contract, dated May 19, 2009, among Xiamen Torch Hi-tech Industrial Development Zone Finance Services Center, Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Current Report on Form 8-K (File No. 001-33071) | May 21, 2009 | |||||||
| 10.16.5 | Office Lease Contract, dated September 23, 2009, among Xiamen Torch Hi-tech Industrial Development Zone Finance Services Center, Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Quarter Report on Form 10-Q (File No. 001-33071) | November 9, 2009 | |||||||
| 10.16.6 | Property Management Service Contract, effective September 24, 2009, between Xiamen Software Industry Investment & Development Co., Ltd. and eHealth China (Xiamen) Technology Co., Ltd. | Quarter Report on Form 10-Q (File No. 001-33071) | November 9, 2009 | |||||||
| 10.17* | Executive Bonus Plan | Quarterly Report on Form 10-Q (File No. 001-33071) | May 10, 2010 | |||||||
111
Table of Contents
| Description of Exhibit |
Incorporation by Reference Herein | |||||||||
| Exhibit Number |
Form |
Date | ||||||||
| 10.18* | eHealth, Inc. Performance Bonus Plan | Definitive Proxy Statement on Schedule 14A (File No. 001-33071) | April 21, 2009 | |||||||
| 21.1 | † List of Subsidiaries | |||||||||
| 23.1 | † Consent of Independent Registered Public Accounting Firm | |||||||||
| 31.1 | † Certification of Gary L. Lauer, Chief Executive Officer of eHealth, Inc., pursuant to Exchange Act Rule 13a-14(a) and 15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |||||||||
| 31.2 | † Certification of Stuart M. Huizinga, Chief Financial Officer of eHealth, Inc., pursuant to Exchange Act Rule 13a-14(a) and 15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |||||||||
| 32.1 | ‡ Certification of Gary L. Lauer, Chief Executive Officer of eHealth, Inc., pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |||||||||
| 32.2 | ‡ Certification of Stuart M. Huizinga, Chief Financial Officer of eHealth, Inc., pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |||||||||
| † | Filed herewith. |
| ‡ | Furnished herewith. |
| * | Indicates a management contract or compensatory plan or arrangement. |
112