Attached files
| file | filename |
|---|---|
| EX-31.1 - EXHIBIT 31.1 - POZEN INC /NC | exhibit31_1.htm |
| EX-23.1 - EXHIBIT 23.1 - POZEN INC /NC | exhibit23_1.htm |
| EX-32.1 - EXHIBIT 32.1 - POZEN INC /NC | exhibit32_1.htm |
| EX-31.2 - EXHIBIT 31.2 - POZEN INC /NC | exhibit31_2.htm |
| EX-32.2 - EXHIBIT 32.2 - POZEN INC /NC | exhibit32_2.htm |
| EX-21.1 - EXHIBIT 21.1 - POZEN INC /NC | exhibit21_1.htm |
| EX-10.37 - EXHIBIT 10.37 - POZEN INC /NC | exhibit10_37.htm |
UNITED
STATES
SECURITIES
AND EXCHANGE COMMISSION
WASHINGTON,
D.C. 20549
FORM
10-K
|
x
|
ANNUAL
REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF
1934
|
FOR THE
FISCAL YEAR ENDED DECEMBER 31, 2009
OR
|
¨
|
TRANSITION
REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES EXCHANGE ACT OF
1934
|
FOR THE
TRANSITION PERIOD FROM TO .
Commission
file number 000-31719
POZEN
INC.
(Exact
name of registrant as specified in its charter)
|
Delaware
|
|
62-1657552
|
|
(State
or other jurisdiction of
incorporation
or organization)
|
|
(I.R.S.
Employer
Identification
No.)
|
1414
Raleigh Rd, Suite 400, Chapel Hill, NC 27517
(Address
of principal executive offices including zip code)
(919)
913-1030
(Registrant’s
telephone number, including area code)
Securities
registered pursuant to Section 12(b) of the Act:
|
Title
of each class
|
Name
of each exchange on which registered
|
|
|
Common
Stock, $0.001 par value
|
NASDAQ
Stock Market LLC
|
Securities
registered pursuant to Section 12(g) of the Act:
Preferred
Share Purchase Right
___________________________________________
Indicate
by check mark if the registrant is a well-known seasoned issuer, as defined in
Rule 405 of the Securities Act. Yes ¨ No x.
Indicate
by check mark if the registrant is not required to file reports pursuant to
Section 13 or Section 15(d) of the Act. Yes ¨ No x.
Indicate
by check mark whether the registrant (1) has filed all reports required to be
filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the
preceding 12 months (or for such shorter period that the registrant was required
to file such reports), and (2) has been subject to such filing requirements for
the past 90 days. Yes x No ¨.
Indicate
by check mark whether the registrant has submitted electronically and posted on
its corporate website, if any, every Interactive Data File required to be
submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this
chapter)
during the preceding 12 months (or for such shorter period that the registrant
was required to submit and post such files). Yes ¨ No ¨
Indicate
by check mark if disclosure of delinquent filers pursuant to Item 405 of
Regulation S-K (§229.405 of this chapter) is not contained herein, and will not
be contained, to the best of registrant’s knowledge, in definitive proxy or
information statements incorporated by reference in Part III of this Form 10-K
or any amendment to this Form 10-K. x.
Indicate
by check mark whether the registrant is a large accelerated filer, an
accelerated filer, or a non-accelerated filer. See definition of “large
accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule
12b-2 of the Exchange Act (Check one):
Large accelerated filer ¨ Accelerated
filer x
Non-accelerated filer ¨ Smaller
reporting company ¨
Indicate
by check mark whether the registrant is a shell company (as defined in 12b-2 of
the Act). Yes ¨ No
x.
The
aggregate market value of the common stock held by non-affiliates computed by
reference to the last reported sale price on June 30, 2009 was approximately
$202,522,000. As of February 20, 2010, there were outstanding 29,834,808 shares
of common stock.
DOCUMENTS
INCORPORATED BY REFERENCE:
Portions
of the POZEN Inc. definitive proxy statement to be filed pursuant to Regulation
14A within 120 days after the end of the fiscal year are incorporated by
reference into Part III of this Form 10-K and certain documents are incorporated
by reference into Part IV.
POZEN
INC.
ANNUAL
REPORT ON FORM 10-K
This report includes “forward-looking
statements” within the meaning of the safe harbor provisions of the Private
Securities Litigation Reform Act of 1995. These forward-looking statements
include, but are not limited to, statements about our plans, objectives,
representations and contentions and are not historical facts and typically are
identified by use of terms such as “may,” “will,” “should,” “could,” “expect,”
“plan,” “anticipate,” “believe,” “estimate,” “predict,” “potential,” “continue”
and similar words, although some forward-looking statements are expressed
differently. You should be aware that the forward-looking statements included
herein represent management’s current judgment and expectations, but our actual
results, events and performance could differ materially from those in the
forward-looking statements. The forward-looking statements are subject to a
number of risks and uncertainties which are discussed below in the section
entitled “Item 1A --Risk Factors.” We do not intend to update any of these
factors or to publicly announce the results of any revisions to these
forward-looking statements, other than as is required under the federal
securities laws.
Overview
We are a pharmaceutical company focused
on transforming medicine that can transform lives. We operate a business model
that focuses on the following:
|
·
|
Developing
innovative products that address unmet medical needs in the
marketplace;
|
|
·
|
obtaining
patents for those innovative ideas which we believe have value in the
marketplace;
|
|
·
|
utilizing
a small group of talented employees to develop those ideas by working with
strategic outsource partners;
|
|
·
|
developing
a regulatory pathway with the appropriate agency;
and
|
|
·
|
determining
how best to commercialize our
products.
|
We hire experts with strong project
management skills in the specific disciplines we believe are important to
maintain within our company. We contract with and manage strong outsource
partners as we complete the necessary development work, permitting us to avoid
incurring the cost of buying or building laboratories, manufacturing facilities
or clinical research operation sites. This allows us to control our annual
expenses, but to utilize “best in class” resources as required. We have decided
to retain ownership of our PA product candidates which contain a combination of
a proton pump inhibitor and enteric coated aspirin in a single tablet and have
hired a chief commercial officer who is responsible for developing the
commercialization strategy for these products and conducting all the required
pre-commercialization activities. In the United States, we intend to lead all
commercialization efforts, which may or may not include co-promotion partners.
Outside the United States, we intend to secure relationships with one or more
strong commercial partners with relevant expertise to commercialize our future
products globally. As we commercialize in the United States, we intend to
continue utilizing our outsource model to develop a 21st
century commercial organization, which would include hiring an internal
commercial team to develop strategy and to direct strategic outsource partners
in the implementation of such strategy.
The success of our business is highly
dependent on the marketplace value of our ideas and the related patents we
obtain, our ability to obtain from the required regulatory agencies approval to
sell the developed products and our ability to find strong commercial partners
to successfully commercialize the products or to successfully commercialize the
products ourselves.
Treximet
We have
developed Treximet® in
collaboration with GlaxoSmithKline, or GSK. Treximet is the brand name for the
product combining sumatriptan 85 mg, formulated with RT Technology™ and naproxen
sodium 500 mg in a single tablet designed for the acute treatment of migraine.
On April 15, 2008, the U.S. Food and Drug Administration, or FDA, approved
Treximet for the acute treatment of migraine attacks with or without aura in
adults. Upon receipt of FDA approval, GSK notified us of its intention to launch
the product and Treximet was available in pharmacies in May
2008.
Treximet
incorporates our MT 400 technology, which refers to our proprietary combinations
of a triptan (5-HT1B/1D
agonist) and a non-steroidal anti-inflammatory drug, or NSAID. Under our MT 400
technology, we sought to develop product candidates that provide acute migraine
therapy by combining the activity of two drugs that act by different mechanisms
to reduce the pain and associated symptoms of migraine. We filed the new drug
application, or NDA, for Treximet with the FDA in August 2005, and in June 2006
we received an approvable letter requiring us to provide certain additional
safety information relating to Treximet, some of which required new studies. An
approvable letter is an official notification from the FDA that contains
conditions that must be satisfied prior to obtaining final U.S. marketing
approval. In early January 2007, we delivered a full response to this approvable
letter that provided additional data and analyses and supporting information
addressing the FDA’s safety concerns, including cardiovascular safety. On August
1, 2007, we received a second approvable letter from the FDA for Treximet in
which the FDA requested that we further address the FDA’s concern about the
product’s potential for genotoxicity. In response to this approvable letter, we
submitted the results of three non-clinical (in vitro) studies that provided
clarifying information about the Chinese Hamster Ovary, or CHO, assay and data
from a clinical evaluation of the genotoxic potential of Treximet in human
volunteers which indicated that no chromosomal aberrations were induced in
peripheral blood lymphocytes when Treximet was administered to volunteers for
seven days. On April 15, 2008, the FDA approved Treximet for the acute treatment
of migraine attacks with or without aura in adults.
Our
Principal Product Candidates
We are
also developing product candidates that combine a type of acid inhibitor, a
proton pump inhibitor, or PPI, with an NSAID (our PN program). These product
candidates are intended to provide management of pain and inflammation
associated with conditions such as osteoarthritis, with fewer gastrointestinal
complications compared to an NSAID taken alone.
In August 2006, we entered into an
exclusive global collaboration and license agreement with AstraZeneca AB, or
AstraZeneca, to co-develop and commercialize VIMOVO™ (formerly referred to as PN
400), the brand name for a proprietary fixed dose combinations of the PPI
esomeprazole magnesium with the NSAID naproxen in a single tablet using our PN
formulation technology, which agreement was amended in September 2007 and
October 2008. We began the Phase 3 program in September 2007. As part of the
program, we conducted two Phase 3 pivotal trials of VIMOVO in patients who are
at risk for developing NSAID-associated gastric ulcers, the primary endpoint for
which was the reduction in endoscopic gastric ulcers. In October 2008, the FDA
informed us that it was conducting an internal review of the acceptability of
using endoscopic gastric ulcers as a primary endpoint in clinical trials. In
late January 2009, the FDA informed us that it had completed its internal
discussions and that there was no change to previous agreements that gastric
ulcer incidence was an acceptable primary endpoint for POZEN’s clinical
programs. The two pivotal trials have been completed and met their primary
endpoints. In both trials, patients taking VIMOVO experienced significantly
(p<0.001) fewer endoscopically confirmed gastric ulcers compared to subjects
receiving enteric-coated naproxen during the six-month treatment period with
gastric ulcer incidence rates of 4.1 and 7.1% for VIMOVO and 23.1 and 24.3% for
enteric-coated naproxen in studies 301 and 302, respectively. Data combined from
both studies showed that in patients taking low dose aspirin (n=201), the
incidence of gastric ulcers in the VIMOVO arm was 3.0% compared to 28.4% for
those taking EC naproxen (p<0.001) and patients taking VIMOVO who were not
taking low dose aspirin (n=653) experienced a 6.4% incidence of gastric ulcers
compared to 22.2% among those taking EC naproxen (p<0.001). Additional
analyses examined the incidence of endoscopically confirmed duodenal ulcers
among patients taking VIMOVO. In study 301, patients taking VIMOVO experienced a
0.5% incidence of duodenal ulcers compared to 5.1% taking EC naproxen (p=0.003),
and in study 302, patients taking VIMOVO experienced a 1.0% incidence of
duodenal ulcers, compared to 5.7% incidence among patients taking EC naproxen
(p=0.007). The most frequently reported adverse events among patients taking
both VIMOVO and enteric coated naproxen in the pivotal trials were GI disorders,
including dyspepsia, erosive esophagitis and erosive duodenitis. In addition to
the Phase 3 pivotal trials, we have completed a long-term, open label safety
study. In 2008 we terminated a non-pivotal smaller study in patients at high
risk of gastrointestinal related events from NSAIDs which we believe is not
required for approval. We also conducted additional studies at AstraZeneca’s
expense. The NDA for VIMOVO was submitted on June 30, 2009 and was accepted for
filing by FDA in August 2009. POZEN received a $10.0 million milestone payment
from AstraZeneca in September 2009 for the achievement of such milestone. In
October 2009, AstraZeneca submitted a Marketing Authorization Application, or
MAA, for VIMOVO in the European Union via the Decentralized Procedure and plans
to file for approval in a number of other countries which are not covered by the
Decentralized Procedure.
Our PA product candidates, containing a
combination of a PPI and aspirin, are currently in formulation and clinical
development testing. Our PA product candidates are excluded from our agreement
with AstraZeneca. We have met with the FDA to discuss the overall development
program requirements for PA32540 for the secondary prevention of cardiovascular
disease in patients at risk for gastric ulcers. An investigational new drug
application, or IND, was filed in the fourth quarter of 2007. We have completed
a study which demonstrated the bioequivalence of the salicylic acid component of
PA32540 as compared to 325 mg of enteric-coated aspirin which we believe will
satisfy the FDA’s bioequivalence requirement. We filed a Special Protocol
Assessment, or SPA, with the FDA for the design of the Phase 3 studies for the
product, the primary endpoint for which is the reduction in endoscopic gastric
ulcers. The SPA is a process by which the FDA and a company
reach
agreement
on the Phase 3 pivotal trial protocol design, clinical endpoints and statistical
analyses that are acceptable to support regulatory approval. In October 2008,
the FDA informed us that it was conducting an internal review of the
acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. In late January 2009, the FDA informed us that it had completed
its internal discussions and that there was no change to previous agreements
that gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs. In February 2009, we received written confirmation from the FDA that
endoscopic gastric ulcer incidence was an acceptable primary endpoint for the
Phase 3 clinical studies we proposed in our SPA for PA32540. In October 2009, we
began two pivotal phase 3 and one long-term safety study for PA32540 for the
cardiovascular indication. The primary endpoint of the pivotal studies, which
will include approximately 500 subjects per study, is the cumulative incidence
of gastric ulcers over the six-month treatment period. The duration of the
long-term safety study will be one year and will include approximately 400
subjects.
We are
aware of publications that contain data regarding a possible drug-drug
interaction between clopidogrel (Plavix®), a
widely prescribed anti-platelet agent, and certain enteric-coated proton pump
inhibitors when platelet aggregation is assessed in ex-vivo tests. On November
11, 2009, the FDA issued new drug safety information to healthcare professionals
through a publication entitled “Information for Healthcare Professionals: Update
to the labeling of Clopidogrel Bisulfate (marketed as Plavix) to alert
healthcare professions about a drug interaction with enteric-coated omeprazole
(marketed as Prilosec® and Prilosec® OTC).” The publication stated
that the effect of clopidogrel on platelets was reduced by as much as 47% in
people receiving clopidogrel and omeprazole together. The FDA’s action was
based, in part, on two crossover clinical studies of 72 healthy subjects
administered Plavix alone and with 80 mg EC omeprazole, either together or
administered 12 hours apart.
To assess
whether a similar interaction occurs between clopidogrel and PA32540, which
contains immediate release omeprazole, we have completed a Phase 1 drug-drug
interaction study to evaluate the ex-vivo platelet aggregation effects of
PA32540 plus clopidogrel dosed at the same time or dosed 10 hours apart compared
to aspirin 325mg plus clopidogrel dosed together. When PA32540 and clopidogrel
were dosed together, data from the study showed a mean 36.7% platelet inhibition
compared to a mean 44.0% platelet inhibition when aspirin and clopidogrel were
dosed together suggesting a drug-drug interaction based on the study’s
pre-specified primary analysis. When PA32540 and clopidogrel were dosed 10 hours
apart, data from the study suggested no ex-vivo drug-drug interaction based on
the study’s pre-specified primary analysis. The relevance of these ex vivo
platelet data on cardiovascular events is not known. Published data
on a clinical interaction between PPIs and Plavix from several randomized
controlled trials in cardiovascular patients have reported no clinical impact on
cardiovascular outcomes [Bhatt et al (COGENT 1 2009) and O’Donoghue et al (TIMI
38 2009)]. FDA assessment of these data and the implication to a
future PA32540 label are not known at this time.
We are also continuing to evaluate how
best to commercialize the PA product candidates and programs and have hired a
chief commercial officer to evaluate he commercial opportunities for these
product candidates. We are also conducting both formulation development and
early stage clinical studies with other PA product candidates for indications in
addition to secondary prevention of cardiovascular events. We are evaluating the
regulatory requirements to obtain an indication for PA for the secondary
prevention of colorectal neoplasia. In January 2010, we received input from FDA
to discuss with respect to the development requirements for a possible
indication in colorectal neoplasia. Further discussions are
planned.
We are
also conducting both formulation development and early stage clinical studies
with new product concepts that are currently in the exploratory stage. If
warranted, we may file U.S. and international patent applications with claims
directed toward these novel combinations and formulations.
Overview
of Our Results of Operations
We have incurred significant losses
since our inception and have not yet generated significant revenue from product
sales. As of December 31, 2009, our accumulated deficit was approximately $140.0
million. We record revenue under two categories: licensing revenues and
development revenues. Our licensing revenues include upfront payments upon
contract signing, additional payments if and when certain milestones in the
product’s development or commercialization are reached, and the royalty payments
based on product sales. Additionally, our development revenues include the
billings for the direct costs and certain personnel-related time incurred in
performing additional development activities described under our collaboration
agreements. Our historical operating losses have resulted principally from our
research and development activities, including clinical trial activities for our
product candidates and general and administrative expenses. Research and
development expenses include salaries and benefits for personnel involved in our
research and development activities and direct development costs, which include
costs relating to the formulation and manufacturing of our product candidates,
costs relating to preclinical studies, including toxicology studies, and
clinical trials, and costs relating to compliance with regulatory requirements
applicable to the development of our product candidates. Since inception, our
research and development expenses have represented approximately 72% of our
total operating expenses. For the fiscal year ended December 31, 2009, our
research and development expenses represented approximately 56% of our total
operating expenses.
Operating
losses may be incurred over the next several years as we complete the
development and seek regulatory approval for our product candidates, develop
other product candidates, conduct pre-commercialization activities, and acquire
and/or develop product portfolios in other therapeutic areas. Our results may
vary depending on many factors, including:
|
·
|
The
progress of VIMOVO, our PA product candidates and our other product
candidates in the clinical and regulatory process;
|
|
·
|
The
ability of GSK to successfully commercialize Treximet in the U.S. For
example, Treximet was available in pharmacies within one month from the
date of its approval, but promotional and professional materials for the
product, including direct to consumer advertising, were not approved on a
timely basis by the FDA. The lack of approved materials and delayed
advertising launch may have had an adverse impact on uptake of the
product, thus negatively impacting our royalty revenue;
|
|
·
|
The
establishment of new collaborations and progress and/or maintenance of our
existing collaborations for the development and commercialization of any
of our product candidates;
|
|
·
|
Our
ability to successfully defend our patents against generic
challenges;
|
|
·
|
Our
ability to commercialize our products either by ourselves or with
commercial partners in a highly regulated and extremely competitive
marketplace; and
|
|
·
|
The
acquisition and/or in-licensing, and development of our therapeutic
product candidates.
|
We do not currently have
commercialization or manufacturing capabilities. We have entered into
collaborations and may continue to enter into additional collaborations with
established pharmaceutical or pharmaceutical services companies to commercialize
and manufacture our product candidates once approved. We have decided to retain
control of our PA product candidates. To that end, we have hired a chief
commercial officer to evaluate the commercial opportunities for these product
candidates and to develop a worldwide commercial strategy, which will include
developing internal commercialization capabilities to enable us to commercialize
our products ourselves. Our ability to generate revenue in the near term is
dependent upon our ability, alone or with collaborators, to achieve the
milestones set forth in our collaboration agreements, to enter into additional
collaboration agreements, to successfully develop product candidates, to obtain
regulatory approvals and to successfully manufacture and commercialize our
future products. These milestones are earned when we have satisfied the criteria
set out in our revenue recognition footnote accompanying the financial
statements included elsewhere in this Annual Report on Form 10-K. These payments
generate large non-recurring revenue that will cause large fluctuations in
quarterly and annual profit and loss.
Our
Business Strategy
Our goal is to become a leading
pharmaceutical company focused on developing and commercializing medicines that
can transform lives. The principal elements of our business strategy are
to:
|
·
|
Utilize
expected cash flow from licensed products to fund new product
ideas. We expect to
utilize the cash flows from Treximet and VIMOVO to support the funding of
development and pre-commercialization activities for our PA franchise of
product candidates, as well as other new product concepts now in the
exploratory stage.
|
|
·
|
Develop and
commercialize our portfolio of product candidates. We expect to
focus a substantial portion of our efforts over the next few years on the
further development, approval and commercialization of our existing
portfolio of product candidates and potential product candidates. Our
primary focus in the near-term is on the clinical development of our PA
product candidates. We have hired a chief commercial officer who is
responsible for all pre-commercialization activities as well as developing
the commercialization strategy for the product
candidates.
|
|
·
|
Build a
product pipeline through innovation supplemented, if necessary, by
in-licensing and acquisition. We intend to build our product
pipeline primarily through innovation, but we will also evaluate
in-licensing and/or acquisition opportunities of select proprietary
product candidates. These will include novel products that exhibit
distinct advantages over currently marketed products, as well as
innovative combinations of products in convenient, therapeutically
appropriate formulations.
|
|
·
|
Leverage
development and commercialization efforts through strategic outsourcing.
While maintaining
overall control of the planning, development and regulatory processes, we
seek to enter into strategic outsourcing relationships to develop and
manufacture our product candidates in as cost-effective a manner as
possible. We have contracted and plan to continue to contract with third
parties for product candidate testing, development, and manufacturing and
commercialization
activities.
|
Migraine Market Overview
Migraine
is characterized by recurring attacks of throbbing headache pain, often
associated with visual, auditory or gastrointestinal disturbances. Attacks range
from mild to severe and can last from 4 hours to 72 hours. In the most severe
attacks, migraine sufferers are unable to pursue basic daily activities.
According to the American Council for Headache Education, migraines afflict 25
million to 30 million people in the U.S. alone. As many as 6% of all men and up
to 18% of all women experience a migraine headache at some time in their life.
While the precise mechanism of migraine is unknown, researchers believe migraine
attacks are caused by acute inflammation surrounding selected blood vessels in
the head. The average migraine sufferer experiences the first attack during the
early teen years, and the attacks generally continue throughout
adulthood.
Not all
migraine attacks are of the same severity. Consequently, a variety of oral,
injectable, and intranasal therapies are used to treat different types of
migraine attacks. Many patients use a personal, individually developed,
step-care approach to treat their attacks. Attacks are often treated initially
with simple over-the-counter analgesics, particularly if the patient is unable
to determine if the attack is a migraine or some other type of headache. If
over-the-counter remedies are unsuccessful, patients often turn to more potent
prescription drugs, including narcotics, analgesic/narcotic drug combinations
and triptans.
Triptans
are the family of drugs most commonly prescribed for the treatment of migraine
attacks. Triptans have demonstrated the ability to treat migraines by
constricting blood vessels in the brain. Although triptans can be effective in
treating migraine symptoms, they are often associated with significant side
effects and other disadvantages that include:
|
·
|
the
occurrence of cardiovascular related events, including chest
pain/discomfort, throat discomfort and warm/cold
sensations;
|
|
·
|
the
potential for other serious cardiovascular events, including
death;
|
|
·
|
difficulty
in producing sustained benefits with a single dose in a majority of
patients;
|
|
·
|
the
occurrence of nausea and dizziness during treatment;
and
|
|
·
|
the
need for cardiovascular evaluations from physicians before initially
prescribing triptans to patients with cardiovascular disease risk
factors.
|
Despite
these shortcomings, according to IMS Health’s IMS National Sales
PerspectiveTM, or
IMS, in 2009 total triptan sales in the U.S. were approximately $2.1 billion.
Sumatriptan is the leading triptan product. There are currently three types of
sumatriptan formulations commercially available: oral, intranasal and
injectable. According to IMS, U.S. sales for generic sumatriptan in all dosage
forms totaled approximately $620 million in 2009, while sales of Imitrex®,
marketed by GlaxoSmithKline, in all dosage forms totaled approximately $230
million in 2009. An oral triptan is often the physician’s first choice as a
prescription treatment for migraine pain. Intranasal triptans are often
prescribed for patients requiring faster relief than oral drugs can provide or
who cannot take oral medications. For the most severe attacks, patients
sometimes use an injectable form of a triptan.
MT
400/Treximet
On April
15, 2008, the FDA approved Treximet for the acute treatment of migraine attacks
with or without aura in adults. GSK notified us of its intention to launch the
product and was available in pharmacies in May 2008. As part of our NDA program
for Treximet, we conducted five Phase 1 trials, two Phase 3 pivotal trials, and
one 12-month open label safety trial using a formulation of Treximet developed
by GSK. The Phase 3 pivotal trials, including the endpoints required to evaluate
Treximet, were designed to demonstrate superiority to placebo for relief of pain
and the associated symptoms of migraine (nausea, photophobia and phonophobia) at
two hours. Additionally, the program was designed to demonstrate that each
component makes a contribution to the efficacy of Treximet (the “combination
drug rule” that the FDA requires of all combination products). The efficacy
endpoint for the combination was sustained pain free, which is defined as
improvement
from
moderate or severe pain to no pain at two hours and remaining at no pain through
twenty four hours without the use of rescue medicine. Further, GSK continues to
conduct market support studies for Treximet, including evaluations in a
pediatric population. As required by the terms of our agreement with GSK, we
transferred ownership of the NDA and other regulatory filings for Treximet to
GSK on May 14, 2008, and GSK now has responsibility for all ongoing regulatory
obligations for the product, including post marketing clinical trial
requirements.
We incurred direct development costs
associated with the development of MT 400 and Treximet programs of $0.2 million
for the fiscal year ended December 31, 2009. We incurred total direct
development costs of $26.0 million associated with the development of our MT 400
and Treximet programs. We recorded in the twelve months ended December 31, 2009,
$4.3 million of Treximet royalty revenue, of which $1.1 million is in accounts
receivable at December 31, 2009. Our direct development costs do not include the
cost of research and development personnel or any allocation of our overhead
expenses.
We, along
with GSK, have received Paragraph IV Notice Letters from Par, Alphapharm, and
Alphapharm’s designated agent, Mylan, Teva, and Dr. Reddy’s informing us that
each company had filed an ANDA with the FDA seeking approval to market
sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr.
Reddy’s have each indicated in their respective Notice Letters that they intend
to market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008; Alphapharm and Mylan on January 2, 2009, Teva on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. Our filing of these patent infringement lawsuits
within forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm, Teva and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s, Teva’s and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
Status
of Our Product Candidates and Exploratory Programs
Arthritis
Market Overview
Arthritis
means joint inflammation and the term is used to describe the pain, stiffness
and/or swelling in the joints of the body where one or more bones are joined by
tendons and muscles. An arthritic joint is one that may have varying degrees of
inflammation and possibly destruction of the joint cartilage, which normally
provides a smooth surface enabling adjacent bones to move and glide on each
other during normal motion.
The most
common type of arthritis is called osteoarthritis and is more common with
advancing age. Osteoarthritis is one of the most frequent causes of physical
disability among adults. It is estimated that by 2030, 20% of Americans who are
over the age of 65 years, or approximately 70 million people, will be at risk
for osteoarthritis. People with osteoarthritis usually have joint pain and
limited movement. Unlike some other forms of arthritis, osteoarthritis affects
only the joints. This condition is also sometimes called degenerative joint
disease. Osteoarthritis primarily affects the joint cartilage. Healthy cartilage
allows bones to glide over one another and absorbs energy from the shock of
physical movement. However, with osteoarthritis, the surface layer of cartilage
breaks down and wears away. This allows the bony surface under the cartilage to
rub together, causing, pain, swelling, and loss of motion of the joint. Over
time, affected joints may lose their normal shape. Also, bone spurs, small
growths called osteophytes, may grow on the edges of the joint. Thus bits of
bone or cartilage can break off and float inside the joint space, causing more
pain and possible damage.
The
second most common form of arthritis, rheumatoid arthritis, may affect not only
the joints, but organs of the body as well. Rheumatoid arthritis is recognized
as a systemic disease that involves responses of the immune system that play a
role in the inflammation that affects joints and other organs. Rheumatoid
arthritis may begin at a younger age than does osteoarthritis. Often patients
with rheumatoid arthritis will require medications not only to treat the pain of
arthritis, but drugs which modulate the immune system to control inflammation in
other parts of the body.
Non-steroidal
anti-inflammatory drugs, or NSAIDs, both over-the-counter and prescription, are
commonly taken to manage the pain of backache, osteoarthritis, rheumatoid
arthritis, headache and other painful conditions. In 2009, approximately 89
million anti-arthritis NSAID prescriptions were dispensed for the management of
pain. Of these prescriptions, an estimated 60% of uses were for chronic therapy.
Prescription sales of anti-arthritis NSAIDs in the U.S. in 2009 were $2.8
billion. In spite of their widespread use and apparent safety, according to the
Agency for Healthcare Research and Quality Statistical Brief released in
December 2008, in 2006, there were approximately 16,300 deaths and 246,000
hospitalizations with a primary diagnosis of upper gastrointestinal, or GI,
bleeding. The most common underlying conditions of
GI
bleeding were gastric, duodenal, peptic, or gastrojeujunal ulcers or
perforations, conditions frequently associated with NSAID use. We are responding
to this unmet medical need to provide a “safer NSAID” through development of our
PN product candidates for the treatment of conditions such as osteoarthritis in
patients who are at risk for developing NSAID-associated gastric
ulcers.
PN/VIMOVO
Program
Under our PN program, we have completed
formulation development and clinical studies for several combinations of a PPI
and a NSAID in a single tablet intended to provide effective management of pain
and inflammation associated with chronic conditions such as osteoarthritis, and
intended to have fewer gastrointestinal complications compared to a NSAID taken
alone in patients at risk for developing NSAID associated gastric ulcers. We
initially conducted studies with two PN product formulations in this program -
PN 100, a combination of the PPI lansoprazole and the NSAID naproxen, and PN
200, a combination of the PPI omeprazole and naproxen, prior to entering into
our collaboration with AstraZeneca. Our present development and
commercialization efforts under the PN program are covered under our exclusive
collaboration agreement with AstraZeneca, which we entered into on August 1,
2006 and which was amended in September 2007 and October 2008. Under our
agreement with AstraZeneca, we are co-developing with AstraZeneca, and
AstraZeneca will commercialize, proprietary fixed dose combinations of the PPI
esomeprazole magnesium with the NSAID naproxen in a single tablet. The initial
product to be developed under the agreement, VIMOVO®
(formerly PN 400), is being studied for the treatment of the signs and symptoms
of osteoarthritis, rheumatoid arthritis and ankylosing spondylitis in patients
at risk of developing NSAID-associated gastric ulcers. On March 2, 2007, we
filed an IND with the FDA for VIMOVO and in April 2007, the first Phase 1 study
was initiated.
In
discussions with the FDA during 2005 regarding our development plans for studies
to pursue FDA approval of PN 100 and PN 200, the FDA agreed that by including
naproxen as the NSAID within the PN formulation, we could expect that all
indications for chronic use of naproxen in adults would accrue to the PN
product, if clinical trials successfully demonstrated improved safety (lower
incidence of gastric ulcers) of the PN product compared with naproxen alone and
the PN formulation was shown to be bioequivalent to marketed formulations of
enteric-coated, or EC, naproxen. Prior to entering into our collaboration
agreement with AstraZeneca, we completed a study designed to demonstrate the
bioequivalence of the naproxen component of our PN 200 product candidate
development formulation to EC naproxen. This study demonstrated that the PN 200
product was bioequivalent to the reference drug, EC Naprosyn®, with
respect to the naproxen component.
In early
2006, we submitted a Special Protocol Assessment, or SPA, to the FDA for our
pivotal Phase 3 clinical trials for PN 200. The SPA is a process in which the
FDA provides evaluations and guidance on clinical trial protocols for pivotal
Phase 3 clinical trials. In April 2006, we announced that we had reached an
agreement with the FDA on the Phase 3 pivotal clinical trials for PN 200 for the
treatment of the signs and symptoms of osteoarthritis, rheumatoid arthritis and
ankylosing spondylitis in patients at risk of developing NSAID-associated
gastric ulcers. We also reached agreement with the FDA that the development
program and study design proposed for PN 200 would be applicable to a product
that contained an isomer of omeprazole combined with naproxen. In light of our
collaboration agreement with AstraZeneca, we, along with AstraZeneca have met
with the FDA and confirmed the core development program and the principles in
the SPA already agreed upon do apply to the new product consisting of
proprietary fixed dose combinations of esomeprazole magnesium with
naproxen.
In the third quarter of 2006, we began
recruiting subjects for a six month comparative trial of PN 200 as compared to
EC naproxen in patients requiring chronic NSAID therapy. The primary endpoint
for the trial was the cumulative incidence of gastric ulcers over six months of
treatment. Because we did not have final results until the fourth quarter of
2007, we, together with AstraZeneca reviewed the interim results of this trial
prior to commencing Phase 3 studies of VIMOVO in September 2007. This study has
now been completed and the results which have been presented publicly, indicated
significantly fewer endoscopically confirmed gastric ulcers during the six month
treatment period in subjects on PN 200 compared to subjects receiving
enteric-coated naproxen alone. We conducted two Phase 3 pivotal trials of VIMOVO
in patients who are at risk for developing NSAID-associated gastric ulcers, the
primary endpoint for which is the reduction in endoscopic gastric ulcers. In
October 2008, the FDA informed us that it was conducting an internal review of
the acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. In late January 2009, the FDA informed us that it had completed
its internal discussions and that there was no change to previous agreements
that gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs. The two pivotal trials have been completed and met their primary
endpoints. In both trials, patients taking VIMOVO experienced significantly
(p<0.001) fewer endoscopically confirmed gastric ulcers compared to subjects
receiving enteric-coated naproxen during the six-month treatment period, with
gastric ulcer incidence rates of 4.1 and 7.1% for VIMOVO and 23.1 and 24.3% for
enteric-coated naproxen in studies 301 and 302, respectively. Data combined from
both studies showed that in patients taking low dose aspirin (n=201), the
incidence of gastric ulcers in the VIMOVO arm was 3.0% compared to 28.4% for
those taking EC naproxen (p<0.001) and patients taking VIMOVO who were not
taking low dose aspirin (n=653) experienced a 6.4% incidence of gastric ulcers
compared to 22.2% among those taking EC naproxen (p<0.001). Additional
analyses examined the incidence of endoscopically confirmed duodenal ulcers
among patients taking
VIMOVO.
In study 301, patients taking VIMOVO experienced a 0.5% incidence of duodenal
ulcers compared to 5.1% taking EC naproxen (p=0.003), and in study 302, patients
taking VIMOVO experienced a 1.0% incidence of duodenal ulcers, compared to 5.7%
incidence among patients taking EC naproxen (p=0.007). The most frequently
reported adverse events among patients taking both VIMOVO and enteric coated
naproxen in the pivotal trials were GI disorders, including dyspepsia, erosive
esophagitis and erosive duodenitis. In addition, we are conducting a long-term,
open label safety study for VIMOVO. We have terminated a non-pivotal smaller
study in patients at high risk (i.e., previous bleeding from a gastric ulcer) of
gastrointestinal related events from NSAIDs which is not required for approval.
We have conducted additional studies at AstraZeneca’s expense. The NDA for
VIMOVO was submitted on June 30, 2009 and was accepted for filing in August
2009. POZEN received a $10.0 million milestone payment from AstraZeneca in
September 2009 for the achievement of such milestone.
In 2005,
we also had discussions with the FDA concerning the implications of the FDA’s
guidance issued in June 2005 concerning labeling of NSAID-containing products,
which resulted from an FDA advisory committee meeting held in February 2005. The
advisory committee addressed the safety of NSAIDs, and, in particular, the
cardiovascular risks of COX-2 selective NSAIDs. Based on our discussions with
the FDA reviewing division for PN products, we believe that, unless new
information about naproxen safety concerns becomes available, long-term
cardiovascular safety studies will not be required at this time for FDA approval
of our PN product candidates containing naproxen. However, we cannot guarantee
that such studies will not be required. We will continue to evaluate and review
with the FDA its expectations and recommendations regarding the efficacy and
safety requirements and study design necessary to support approval of NDAs for
our PN product candidates.
Additionally,
we have met with four national European regulatory agencies to discuss the
proposed development program for PN. Under our agreement with AstraZeneca,
AstraZeneca has responsibility for the development program for PN products
outside the U.S., including interactions with regulatory agencies. In October
2009, AstraZeneca submitted a MAA for VIMOVO in the European Union via the
Decentralized Procedure and plans to file for approval in a number of other
countries which are not covered by the Decentralized Procedure.
We cannot
reasonably estimate or know the amount or timing of the costs necessary to
obtain regulatory approval of VIMOVO. Nor can we reasonably estimate or know the
amount or timing of the costs necessary to continue exploratory development
and/or complete the development of any PN product candidates we may seek to
develop or when, if and to what extent we will receive cash inflows from any PN
products. The additional costs that may be incurred include expenses relating to
clinical trials and other research and development activities and activities
necessary to obtain regulatory approvals.
We incurred direct development costs
associated with the development of our PN program of $7.2 million for the fiscal
year ended December 31, 2009, of which, $5.5 million was funded by development
revenue from AstraZeneca. We incurred total direct development cost of $95.7
million associated with the development of our PN program. Our direct
development costs do not include the cost of research and development personnel
or any allocation of our overhead expenses.
PA
Program
As part of our PA program, we are
exploring the development of a combination of a PPI and aspirin in a single
tablet. Similar to the PN program, our PA product candidate is intended to
induce fewer gastrointestinal complications compared to an aspirin taken alone
in patients at risk for developing aspirin associated gastric ulcers. Our PA
product candidates are covered under the same patent as PN, but we have retained
all rights to this program.
Our initial PA product candidate,
PA32540, is currently in clinical development. We completed a Phase 1 proof of
concept study in Canada of an earlier formulation of PA containing 325 mg of
aspirin and 20 mg of omeprazole (PA32520) in the first quarter of 2007. The
primary endpoint was gastrointestinal damage as measured by the Lanza scoring
system used in our previous PN studies. The results were highly significant
(p<0.001) with 10% of the PA group having Lanza 3 or 4 gastrointestinal
damage, whereas 57.5% of the EC aspirin group had this level of gastrointestinal
damage during the 28 day study. We also completed a second proof of concept
study with PA32520 as compared to 81 mg of EC aspirin. These results confirmed
the earlier levels of gastric damage as measured by Lanza scoring at about 10%
for PA32520. While these results in the second study were numerically different
between treatment groups, they did not achieve statistical significance from the
results obtained with 81mg EC aspirin (21%). After reviewing these data, we
decided to increase the dose of omeprazole to 40 mg per tablet and conduct an
additional 28 day Phase 1 study using the formulation containing 40 mg of
immediate release of omeprazole and 325 mg of aspirin (PA32540) compared to 325
mg EC aspirin. Topline results from this study indicate a highly significant
(P=0.003) reduction in gastrointestinal damage with the higher strength PA32540
tablet as compared with 325 mg EC aspirin (2.5% vs. 27.5% grade 3 or 4 Lanza
scores, respectively). In this last study, 75% of subjects treated with the
PA32540 tablet showed no gastrointestinal damage at all as compared to < 50%
with the PA32520 tablet. An IND for the product was filed in the fourth quarter
of 2007 and we met with the FDA in July 2007 to discuss the overall development
program requirements. We completed a study which demonstrated that the salicylic
acid component of PA32540 was
bioequivalent
to the reference drug, EC aspirin, with respect to the aspirin component, and
which we believe will allow our PA product to receive all the cardio- and
cerebrovascular secondary prevention claims of aspirin. In June 2008, we filed
an SPA with the FDA for our pivotal Phase 3 trials for PA32540, the primary
endpoint for which is the reduction in endoscopic gastric ulcers. In October
2008, the FDA informed us that it was conducting an internal review of the
acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. In late January 2009, the FDA informed us that it had completed
its internal discussions and that there was no change to previous agreements
that gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs and in February 2009, we received written confirmation from the FDA
that endoscopic gastric ulcer incidence was an acceptable endpoint for the Phase
3 clinical studies we proposed in our SPA for PA32540. In October 2009, we began
two pivotal phase 3 and one long-term safety study for PA32540 for the
cardiovascular indication. The primary endpoint of the pivotal studies, which
will include approximately 500 subjects per study, is the cumulative incidence
of gastric ulcers over the six-month treatment period. The duration of the
long-term safety study will be one year and will include approximately 400
subjects.
We are
aware of publications that contain data regarding a possible drug-drug
interaction between clopidogrel (Plavix®), a
widely prescribed anti-platelet agent, and certain enteric-coated proton pump
inhibitors when platelet aggregation is assessed in ex-vivo tests. On November
11, 2009, the FDA issued new drug safety information to healthcare professionals
through a publication entitled “Information for Healthcare Professionals: Update
to the labeling of Clopidogrel Bisulfate (marketed as Plavix) to alert
healthcare professions about a drug interaction with enteric-coated omeprazole
(marketed as Prilosec® and Prilosec® OTC).” The publication stated
that the effect of clopidogrel on platelets was reduced by as much as 47% in
people receiving clopidogrel and omeprazole together. The FDA’s action was
based, in part, on two crossover clinical studies of 72 healthy subjects
administered Plavix alone and with 80 mg EC omeprazole, either together or
administered 12 hours apart.
To assess
whether a similar interaction occurs between clopidogrel and PA32540, which
contains immediate release omeprazole, we have completed a Phase 1 drug-drug
interaction study to evaluate the ex-vivo platelet aggregation effects of
PA32540 plus clopidogrel dosed at the same time or dosed 10 hours apart compared
to aspirin 325mg plus clopidogrel dosed together. When PA32540 and clopidogrel
were dosed together, data from the study showed a mean 36.7% platelet inhibition
compared to a mean 44.0% platelet inhibition when aspirin and clopidogrel were
dosed together suggesting a drug-drug interaction based on the study’s
pre-specified primary analysis. When PA32540 and clopidogrel were dosed 10 hours
apart, data from the study suggested no ex-vivo drug-drug interaction based on
the study’s pre-specified primary analysis. The relevance of these ex vivo
platelet data on cardiovascular events is not known. Published data
on a clinical interaction between PPIs and Plavix from several randomized
controlled trials in cardiovascular patients have reported no clinical impact on
cardiovascular outcomes [Bhatt et al (COGENT 1 2009) and O’Donoghue et al (TIMI
38 2009)]. FDA assessment of these data and the implication to a
future PA32540 label are not known at this time.
We are also continuing to evaluate how
best to commercialize the PA product candidates and programs and have hired a
chief commercial officer to evaluate he commercial opportunities for these
product candidates. We are also conducting both formulation development and
early stage clinical studies with other PA product candidates for indications in
addition to secondary prevention of cardiovascular events. We are evaluating the
regulatory requirements to obtain an indication for PA for the secondary
prevention of colorectal neoplasia. In January 2010, we received input from FDA
to discuss with respect to the development requirements for a possible
indication in colorectal neoplasia. Further discussions are
planned.
Additionally, we have met with three
national European regulatory agencies to discuss the proposed development
program for PA. Each of these regulatory agencies has indicated that reduction
in gastric ulcers is an appropriate endpoint for the pivotal trials, along with
demonstrating bioequivalence to the reference drug, EC aspirin, with respect to
the aspirin component. Dose ranging studies may also be required.
We cannot
reasonably estimate or know the amount or timing of the costs necessary to
continue exploratory development and/or complete the development of any PA
product candidates we may seek to develop or when, if and to what extent we will
receive cash inflows from any PA products. The additional costs that may be
incurred include expenses relating to clinical trials and other research and
development activities and activities necessary to obtain regulatory approvals.
We have decided to retain control of our PA product candidates and currently do
not intend to out-license the PA program in the United States. To that end, we
have hired a chief commercial officer to evaluate the commercial opportunities
for these product candidates. We believe value can be added to the PA
product candidates as progress is made through clinical development and, if we
ultimately chose to partner the products later in the development program or
after approval, either outside the United States or on a global basis, we
believe it would be under economic terms more favorable to us.
We are
conducting market research on the PA product candidates, to support our
evaluation of how best to commercialize the PA product candidates and programs,
which may include commercializing the products ourselves in certain territories.
Changing from a commercialization strategy in which the PA product candidates
are out-licensed, in exchange for milestone
and royalty payments, will depend on our available financial resources, the
associated risks of such a change and its overall impact on the PA product
candidates’ value.
We incurred direct development costs
associated with the development of our PA program of $7.7 million during the
fiscal year ended December 31, 2009. We incurred total direct development cost
of $20.2 million associated with the development of our PA program. Our direct
development costs do not include the cost of research and development personnel
or any allocation of our overhead expenses.
Collaborative
Arrangements
We have entered into and may continue
to enter into collaborations with established pharmaceutical or pharmaceutical
services companies to develop, commercialize and/or manufacture our product
candidates. Our existing collaborations are described below.
GlaxoSmithKline
(GSK)
In June 2003, we signed an agreement
with GSK for the development and commercialization of proprietary combinations
of a triptan (5-HT1B/1D
agonist) and a long-acting NSAID. The combinations covered by the agreement are
among the combinations of MT 400. Under the terms of the agreement, GSK has
exclusive rights in the U.S. to commercialize all combinations which combine
GSK’s triptans, including Imitrex®
(sumatriptan succinate) or Amerge®
(naratriptan hydrochloride), with a long-acting NSAID. We were responsible for
development of the first combination product, while GSK provided formulation
development and manufacturing. Pursuant to the terms of the agreement, we
received $25.0 million in initial payments from GSK following termination of the
waiting period under the Hart-Scott-Rodino notification program and the issuance
of a specified patent. In May 2004, we received a $15.0 million milestone
payment as a result of our commencement of Phase 3 clinical trial activities. In
October 2005, we received a $20.0 million milestone payment upon the FDA’s
acceptance for review of the NDA for Treximet, the trade name for the product.
On April 26, 2008, we received, from GSK, $20.0 million in milestone payments
which were associated with the approval of, and GSK’s intent to commercialize,
Treximet. In addition, GSK will pay us two sales performance milestones totaling
$80.0 million if certain sales thresholds are achieved. Up to an additional
$10.0 million per product is payable upon achievement of milestones relating to
other products. On December 31, 2009, we accrued $1.1 million of Treximet
royalty revenue and GSK will also pay us royalties on all net sales of marketed
products until at least the expiration of the last to expire issued applicable
patent (October 2, 2025) based upon the scheduled expiration of currently issued
patents. GSK may reduce, but not eliminate, the royalty payable to us if generic
competitors attain a pre-determined share of the market for the combination
product, or if GSK owes a royalty to one or more third parties for rights it
licenses from such third parties to commercialize the product. The agreement
terminates on the date of expiration of all royalty obligations unless earlier
terminated by either party for a material breach or by GSK at any time upon
ninety (90) days’ written notice to us for any reason or no reason. Among the
contract breaches that would entitle us to terminate the agreement is GSK’s
determination not to further develop or to launch the combination product under
certain circumstances. GSK has the right, but not the obligation, to bring, at
its own expense, an action for infringement of certain patents by third parties.
If GSK does not bring any such action within a certain time frame, we have the
right, at our own expense, to bring the appropriate action. With regard to
certain other patent infringements, we have the sole right to bring an action
against the infringing third party. Each party generally has the duty to
indemnify the other for damages arising from breaches of each party’s
representations, warranties and obligations under the agreement, as well as for
gross negligence or intentional misconduct. We also have a duty to indemnify GSK
for damages arising from our development and manufacture of MT 400 prior to the
effective date of the agreement, and each party must indemnify the other for
damages arising from the development and manufacture of any combination product
after the effective date.
We, along
with GSK, have received Paragraph IV Notice Letters from Par, Alphapharm,
Alphapharm’s designated agent, Mylan, Teva and Dr. Reddy’s informing us that
each company had filed an ANDA with the FDA seeking approval to market
sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr.
Reddy’s have each indicated in their respective Notice Letters that they intend
to market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008, Alphapharm and Mylan on January 2, 2009, Teva on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. Our filing of these patent infringement lawsuits
within forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm Teva, and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s Teva’s, and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
AstraZeneca
AB (AstraZeneca)
In August 2006, we entered into a
collaboration and license agreement dated as of August 1, 2006 and effective
September 7, 2006 with AstraZeneca, a Swedish corporation, regarding the
development and commercialization of proprietary fixed dose
combinations of the PPI esomeprazole magnesium with the NSAID naproxen, in a
single tablet for the management of pain and inflammation associated with
conditions such as osteoarthritis and rheumatoid arthritis in patients who are
at risk for developing NSAID associated gastric ulcers. Under the terms of the
agreement, we granted to AstraZeneca an exclusive, fee-bearing license, in all
countries of the world except Japan, under our patents and know-how relating to
combinations of gastroprotective agents and NSAIDs (other than aspirin and its
derivatives). AstraZeneca had the right, which has now expired, to elect to
include Japan in the licensed territory within two years after the effective
date of the agreement. Pursuant to the terms of the agreement, we received an
upfront license fee of $40.0 million from AstraZeneca following termination of
the waiting period under the Hart-Scott-Rodino notification
program.
In
September 2007, we agreed with AstraZeneca to amend our collaboration and
license agreement effective as of September 6, 2007. Under the terms of the
amendment, AstraZeneca has agreed to pay us up to $345.0 million, in the
aggregate, in milestone payments upon the achievement of certain development,
regulatory and sales events. In September 2007 we received a $10.0 million
payment upon execution of the amendment and a $20.0 million payment in
recognition of the achievement of the primary endpoints for the PN400-104 study,
a study which compared acid suppression of different doses of VIMOVO (formerly
PN 400), and achievement of the interim results of the PN200-301 study, a six
month comparative trial of PN 200 as compared to EC naproxen in patients
requiring chronic NSAID therapy, meeting mutually agreed success criteria. An
additional $55.0 million will be paid upon achievement of certain development
and regulatory milestones, and $260.0 million will be paid as sales performance
milestones if certain aggregate sales thresholds are achieved. Under the
original agreement, we were to have received development and regulatory
milestones totaling $160.0 million, of which $20.0 million was to be paid upon
the successful completion of the proof of concept studies, and sales performance
milestones totaling $175.0 million.
In
addition, the amendment revised the royalty rates we were to have received under
the original agreement. Under the original agreement, we were to receive a
royalty based on annual net sales by AstraZeneca, its affiliates or sublicensees
during the royalty term. The royalty rate varied based on the level of annual
net sales of products made by AstraZeneca, its affiliates and sublicensees,
ranging from the mid-single digits to the mid-teens. Under the amendment, we
will now receive a flat, low double digit royalty rate during the royalty term
on annual net sales of products made by AstraZeneca, its affiliates and
sublicensees, in the U.S. and royalties ranging from the mid-single digits to
the high-teens on annual net sales of products made by AstraZeneca, its
affiliates and sublicensees outside of the U.S. The amendment also revises the
rate of reduction to the royalty rate based upon loss of market share due to
generic competition inside and outside of the U.S. to account for the new
royalty structure.
Our right
to receive royalties from AstraZeneca for the sale of such products under the
collaboration and license agreement, as amended, expires on a country-by-country
basis upon the later of (a) expiration of the last-to-expire of certain patent
rights relating to such products in that country, and (b) ten years after the
first commercial sale of such products in such country.
We
further amended the collaboration and license agreement effective October 1,
2008 to shorten the timing of AstraZeneca’s reimbursement obligation for certain
development expenses incurred by us under the agreement and to update the
description of the target product profile studies (as defined in the agreement)
for VIMOVO.
We retain responsibility for the
development and filing of the NDA for the product in the U.S. AstraZeneca is
responsible for all development activities outside the U.S., as well as for all
manufacturing, marketing, sales and distribution activities worldwide. We have
agreed to bear all expenses related to certain specified U.S. development
activities. All other development expenses, including all manufacturing-related
expenses, will be paid by AstraZeneca. The agreement established joint
committees with representation of both us and AstraZeneca to manage the
development and commercialization of the product. The committees operate by
consensus, but if consensus cannot be reached, we generally will have the
deciding vote with respect to development activities required for marketing
approval of the product in the U.S. and AstraZeneca generally will have the
deciding vote with respect to any other matters.
The agreement, unless earlier
terminated, will expire upon the payment of all applicable royalties for the
products commercialized under the agreement. Either party has the right to
terminate the agreement by notice in writing to the other party upon or after
any material breach of the agreement by the other party, if the other party has
not cured the breach within 90 days after written notice to cure has been given,
with certain exceptions. The parties also can terminate the agreement for cause
under certain defined conditions. In addition, AstraZeneca can terminate the
agreement, at any time, at will, for any reason or
no
reason, in its entirety or with respect to countries outside the U.S., upon 90
days’ notice. If terminated at will, AstraZeneca will owe us a specified
termination payment or, if termination occurs after the product is launched,
AstraZeneca may, at its option, under and subject to the satisfaction of
conditions specified in the agreement, elect to transfer the product and all
rights to us.
Valeant
Pharmaceuticals North America (Valeant NA) (formerly Xcel Pharmaceuticals
Inc.)
In September 2003, we signed an
agreement with Valeant NA for the further development and commercialization of
MT 300. In March 2005, Valeant Pharmaceuticals International (Valeant
International) acquired Valeant NA. Under the terms of the agreement, Valeant NA
would have exclusive rights in the United States to commercialize MT 300 subject
to certain minimum commercialization obligations.
Under the
agreement, if we determine that additional studies or data that are required by
the FDA for approval of the NDA for MT 300 would jeopardize the commercial
viability of MT 300 or exceed our financial resources available for MT 300, we
may elect to withdraw the NDA. If we notify Valeant NA of this situation and
Valeant NA does not assume control of efforts to seek approval of the NDA, then,
under the conditions outlined in the agreement, upon notice from Valeant NA the
agreement will terminate and we would be required to pay Valeant NA a withdrawal
fee of $1.0 million. If Valeant NA decides to assume development, it would be
credited $1.0 million in development expense. Based upon our understandings from
our most recent communications with the FDA and our understanding of the FDA’s
current standards for approval of migraine drugs, we believe it is not possible
to reverse the not approvable status of the NDA for MT 300. In July 2005, we
received a letter from Valeant NA seeking payment of the $1.0 million withdrawal
fee. We do not believe that the withdrawal fee is payable based on our receipt
of a not-approvable letter from the FDA with respect to our NDA for MT 300. The
agreement requires that unresolved disputes by the parties be referred to the
respective chief executive officers for resolution. If still unresolved, the
agreement provides for binding arbitration. Valeant NA has disputed our
conclusion that the withdrawal fee is not payable and has indicated its
intention to pursue the dispute resolution provisions provided for in the
agreement. We intend to vigorously defend our position under the agreement,
although the last written communication from Valeant NA was received in March,
2006. At this time, it is not possible to determine if any withdrawal fee will
be required to be paid to Valeant NA upon the ultimate resolution of this
dispute.
Based upon the delays related to
commercialization of MT 300 due to our receipt of the not-approvable letter for
MT 300 and our efforts to address with the FDA the issues raised in that letter,
we and Valeant NA had previously agreed to extend the time for certain
activities under our agreement with Valeant NA that are dependent on the FDA’s
actions with respect to MT 300. In the event of termination of the agreement,
these obligations will not be relevant. We can give no assurance that Valeant NA
or Valeant International will agree to termination terms acceptable to us or
that we will not be required to pay Valeant NA the withdrawal fee of $1.0
million described above. The $1.0 million upfront fee was taken into revenue as
of December 31, 2008, so any required payment to Valeant NA in the future would
have an impact on our statements of operations.
Manufacturing
We
currently have no manufacturing capability and we do not intend to establish
internal manufacturing capabilities.
To date,
we have entered into arrangements with third-party manufacturers for the supply
of formulated and packaged clinical trial materials. We believe our current
supplier agreements should be sufficient to complete our planned clinical
trials. Under our agreements with GSK and AstraZeneca, it is the obligation of
our partners to supply clinical trial material required to conduct clinical
trials, as well as commercial supplies of products developed under those
agreements. Use of third-party manufacturers enables us to focus on our clinical
development activities, minimize fixed costs and capital expenditures and gain
access to advanced manufacturing process capabilities and expertise. We also
intend to enter into agreements with third-party manufacturers for the
commercial scale manufacturing of our products.
Competition
Competition
for our migraine products that receive regulatory approval will come from
several different sources. Because not all migraine attacks are of the same
severity, a variety of oral, injectable and intranasal therapies are used to
treat different types of migraine attacks. Attacks are often treated initially
with simple over-the-counter analgesics, particularly if the patient is unable
to determine if the attack is a migraine or some other type of headache. These
analgesics include Excedrin Migraine®, which is approved for the pain associated
with migraine. If over-the-counter remedies are unsuccessful, patients often
turn to more potent prescription drugs, including triptans. According to IMS, in
2009, total triptan sales in the U.S. were approximately $2.3 billion. Imitrex,
a triptan product marketed by GSK, had total U.S. sales of approximately $230
million in 2009, according to IMS.
Narcotics
such as codeine and drugs containing analgesic/narcotic combinations, along with
other non-narcotic pain medications, are also used for the treatment of
migraine. If approved, our migraine product candidates will most likely compete
with one or more of these existing migraine therapeutics, as well as any
therapies developed in the future. Based upon their current migraine portfolios,
GSK, Merck & Co., AstraZeneca, Johnson & Johnson, Pfizer, Inc. and Endo
Pharmaceuticals will be our principal competitors for our migraine product
candidates.
The
competition for our PN products that receive regulatory approval will come from
the oral anti-arthritic market, or more specifically the traditional
non-selective NSAIDs (such as naproxen and diclofenac), traditional
NSAID/gastroprotective agent combination products or combination product
packages (such as Arthrotec® and
Prevacid®
NapraPACTM )
and the only remaining COX-2 inhibitor, Celebrex®. The
U.S. prescription market for oral solid NSAIDs was approximately $2.6 billion in
2009, of which 72% was accounted for by Celebrex, according to IMS. This market
is continuing to undergo significant change, due to the voluntary withdrawal of
Vioxx® by
Merck & Co. in September 2004, the FDA-ordered withdrawal of Bextra® by
Pfizer in April 2005 and the issuance of a Public Health Advisory by the FDA in
April 2005 stating that it would require that manufacturers of all prescription
products containing NSAIDs provide warnings regarding the potential for adverse
cardiovascular events as well as life-threatening gastrointestinal events
associated with the use of NSAIDs. Moreover, subsequent to the FDA advisory
committee meeting in February 2005 that addressed the safety of NSAIDs, and, in
particular, the cardiovascular risks of COX-2 selective NSAIDs, the FDA has
indicated that long-term studies evaluating cardiovascular risk will be required
for approval of new NSAID products that may be used on an intermittent or
chronic basis. However, based on a meeting with the FDA in September 2005, we
believe, although we cannot guarantee, that long-term cardiovascular safety
studies may not be required at this time for FDA approval of our PN product
candidates containing naproxen.
The
pharmaceutical and biopharmaceutical industries are intensely competitive and
are characterized by rapid technological progress. Certain pharmaceutical and
biopharmaceutical companies and academic and research organizations currently
engage in, or have engaged in, efforts related to the discovery and development
of new medicines for the treatment of migraine symptoms. Significant levels of
research in chemistry and biotechnology occur in universities and other
nonprofit research institutions. These entities have become increasingly active
in seeking patent protection and licensing revenues for their research results.
They also compete with us in recruiting skilled scientific talent.
Our
ability to compete successfully will be based on our ability to create and
maintain scientifically advanced technology, develop proprietary products,
attract and retain scientific personnel, obtain patent or other protection for
our products, obtain required regulatory approvals and manufacture and
successfully market our products either alone or through outside parties. Some
of our competitors have substantially greater financial, research and
development, manufacturing, marketing and human resources and greater experience
than we do in product discovery, development, clinical trial management, FDA
regulatory review, manufacturing and marketing, which may enable them to compete
more effectively than we can.
Patents
and Proprietary Information
We have
obtained and intend to actively seek to obtain, when appropriate, protection for
our products and proprietary technology by means of U.S. and foreign patents,
trademarks and contractual arrangements. In addition, we rely upon trade secrets
and contractual agreements to protect certain of our proprietary technology and
products.
We have
ten issued U.S. patents and three pending U.S. patent applications, as well as
pending foreign patent applications or issued foreign patents, relating to our
product candidates. We also have U.S. and foreign patent applications pending
relating to novel product concepts. There can be no assurance that our patent
applications will issue as patents or, with respect to our issued patents, that
they will provide us with significant protection. The following provides a
general description of our patent portfolio and is not intended to represent an
assessment of claim limitations or claim scope.
MT
400/Treximet
We have three issued U.S. patents and
one pending U.S. application with claims relating to methods, compositions and
therapeutic packages involving the use of certain NSAIDs and 5-HT receptor
agonists in treating patients with migraine. Outside of the U.S., we have issued
patents in Australia, Canada, Europe, Hong Kong and Japan. The expected
expiration date of the issued patents relating to MT 400 is August 17,
2017.
Oppositions were filed against the
issued European patent in October 2005 by Merck & Co., Inc. and Almirall
Prodesfarma asserting that the European patent should not have been granted. We
filed a response to these oppositions in May 2006, and in March 2007, the
Opposition Division of the European Patent Office called for oral proceedings.
During the oral proceedings and in the written opinion subsequently provided,
the European Patent Office found that claims relating to
combinations
of sumatriptan and naproxen for the treatment of migraine were valid. However,
broader claims relating to certain other 5-HT1B/1D
agonists and long-acting NSAIDs were held to be insufficiently supported by the
presently available technical evidence.
We also have an issued U.S. patent with
claims relating to formulations of MT 400 which, we expect to expire in October
2025. We have additional pending U.S. and foreign patent applications with
claims directed to formulations of MT 400 which, if issued, we expect to expire
between December 2023 and March 2027.
We, along
with GSK, have received Paragraph IV Notice Letters from Par, Alphapharm, and
Alphapharm’s designated agent, Mylan, Teva, and Dr. Reddy’s informing us that
each company had filed an ANDA with the FDA seeking approval to market
sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr.
Reddy’s have each indicated in their respective Notice Letters that they intend
to market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008, Alphapharm and Mylan on January 2, 2009, Teva on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. Our filing of these patent infringement lawsuits
within forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm, Teva and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s, Teva’s and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
PN/PA
We have
issued patents in the U.S., Australia, Mexico and Eurasia, with claims directed
to certain compositions containing a combination of acid inhibitors, including
PPIs, and NSAIDs. The issued patents also have claims to treatment methods
involving the use of such compositions. We have pending U.S. and foreign patent
applications that also have claims to compositions containing acid inhibitors
and NSAIDs and to various treatment methods involving such compositions. The
issued U.S. patent and related U.S. patent applications will expire on February
28, 2023. We expect the foreign patents, as well as additional patents which
issue from the pending foreign patent applications, to expire on May 31,
2022.
We,
together with AstraZeneca, have filed joint patent applications relating to PN.
We expect any patents which issue from these applications to expire in 2029 and
2030.
We have
filed an additional patent application related to PA. We expect any patents
which issue from this application to expire in 2029.
MT
300
With
respect to MT 300, we received U.S., as well as European, Australian and other
foreign patents relating to a high potency formulation of DHE and formulations
of DHE in a pre-filled syringe. The expected expiration date of all of the U.S.
and foreign patents relating to MT 300 is March 15, 2020. We began abandoning
our foreign issued patents and our pending foreign patent applications relating
to MT 300 during 2006 and expect to abandon all foreign patents and patent
applications relating to MT300.
Exploratory
Programs
We have
filed U.S. and international patent applications with claims directed to novel
compositions and formulations for new product concepts that are currently in the
exploratory stage. Any patents which issue from these applications would be
expected to expire between 2027 and 2029.
Government
Regulation
The FDA
and comparable regulatory agencies in foreign countries impose substantial
requirements on the clinical development, manufacture and marketing of
pharmaceutical product candidates. These agencies and other federal, state and
local entities regulate research and development activities and the testing,
manufacture, quality control, safety, effectiveness, labeling, storage,
record-keeping, approval and promotion of our product candidates. All of our
product candidates will require regulatory approval before commercialization. In
particular, therapeutic product candidates for human use are subject to rigorous
preclinical and clinical testing and other requirements of the Federal Food,
Drug and Cosmetic Act, or FFDCA, implemented by the FDA, as well as similar
statutory and regulatory requirements of foreign countries. Obtaining these
marketing approvals and subsequently complying with ongoing statutory and
regulatory requirements is costly and time-consuming. Any failure by us or our
collaborators, licensors or licensees to obtain, or any delay in obtaining,
regulatory approvals or in complying with other regulatory requirements could
adversely affect the commercialization of product candidates then being
developed by us and our ability to receive product or royalty
revenues.
The steps
required before a new drug product candidate may be distributed commercially in
the U.S. generally include:
|
·
|
conducting
appropriate preclinical laboratory evaluations of the product candidate’s
chemistry, formulation and stability and preclinical studies in animals to
assess the potential safety and efficacy of the product
candidate;
|
|
·
|
submitting
the results of these evaluations and tests to the FDA, along with
manufacturing information and analytical data, in an
IND;
|
|
·
|
initiating
clinical trials under the IND and addressing any safety or regulatory
concerns of the FDA;
|
|
·
|
obtaining
approval of Institutional Review Boards, or IRBs, to introduce the drug
into humans in clinical studies;
|
|
·
|
conducting
adequate and well-controlled human clinical trials that establish the
safety and efficacy of the product candidate for the intended use,
typically in the following three sequential, or slightly overlapping
stages:
|
Phase 1:
The product is initially introduced into human subjects or patients and tested
for safety, dose tolerance, absorption, metabolism, distribution and
excretion;
Phase 2:
The product candidate is studied in patients to identify possible adverse
effects and safety risks, to determine dosage tolerance and the optimal dosage,
and to collect some efficacy data;
Phase 3:
The product candidate is studied in an expanded patient population at multiple
clinical study sites, to confirm efficacy and safety at the optimized dose, by
measuring primary and secondary endpoints established at the outset of the
study;
|
·
|
submitting
the results of preclinical studies, and clinical trials as well as
chemistry, manufacturing and control information on the product candidate
to the FDA in a NDA; and
|
|
·
|
obtaining
FDA approval of the NDA prior to any commercial sale or shipment of the
product candidate.
|
This
process can take a number of years and require substantial financial resources.
Each NDA must be accompanied by a user fee, pursuant to the requirements of the
Prescription Drug User Fee Act, or PDUFA, and its amendments. The FDA adjusts
the PDUFA user fees on an annual basis. According to the FDA’s fee schedule,
effective on October 1, 2009 for the fiscal year 2010, the user fee for an
application requiring clinical data, such as an NDA, is $1,405,500. PDUFA also
imposes an annual product fee for each marketed prescription drug ($79,720), and
an annual establishment fee ($457,200) on facilities used to manufacture
prescription drugs and biologics. Fee waivers or reductions are available in
certain circumstances, including a waiver of the application fee for the first
application filed by a small business. However, there are no waivers for product
or establishment fees.
The
results of preclinical studies and initial clinical trials are not necessarily
predictive of the results from large-scale clinical trials, and clinical trials
may be subject to additional costs, delays or modifications due to a number of
factors, including the difficulty in obtaining enough patients, clinical
investigators, product candidate supply and financial support.
Even
after FDA approval has been obtained, further studies, including post-marketing
studies, may be required. Results of post-marketing studies may limit or expand
the further marketing of the products. If we propose any modifications to a
product, including changes in indication, manufacturing process, manufacturing
facility or labeling, a supplement to our NDA may be required to be submitted to
the FDA and approved.
The FDA
may also require testing and surveillance programs to monitor the effect of
approved product candidates that have been commercialized, and the agency has
the power to prevent or limit further marketing of a product candidate based on
the results of these post-marketing programs. Upon approval, a product candidate
may be marketed only in those dosage forms and for those indications approved in
the NDA.
The status of the NDAs we have
submitted to the FDA for Treximet, and VIMOVO is discussed above in
“MT400/Treximet” and “Status of Our Product Candidates and Exploratory Programs
- PN/VIMOVO Program"
In
addition to obtaining FDA approval for each indication to be treated with each
product candidate, each domestic product candidate manufacturing establishment
must register with the FDA, list its product with the FDA, comply with the
applicable FDA current Good Manufacturing Practices, or cGMP, regulations, which
include requirements relating to quality control and quality assurance, as well
as the corresponding maintenance of records and documentation, and permit and
pass manufacturing plant inspections by the FDA. Moreover, the submission of
applications for approval may require additional time to complete manufacturing
stability studies. Foreign establishments manufacturing product for distribution
in the U.S. also must list their product candidates with the FDA and comply with
cGMP regulations. They are also subject to periodic inspection by the FDA or by
local authorities under agreement with the FDA.
Any
product candidates manufactured or distributed by us pursuant to FDA approvals
are subject to extensive continuing regulation by the FDA, including
record-keeping requirements and reporting of adverse experiences with the
product candidate. In addition to continued compliance with standard regulatory
requirements, the FDA may also require post-marketing testing and surveillance
to monitor the safety and efficacy of the marketed product. Adverse experiences
with the product candidate must be reported to the FDA. Product approvals may be
affected and even withdrawn if compliance with regulatory requirements is not
maintained or if problems concerning safety or efficacy of the product are
discovered following approval.
The FFDCA
also mandates that products be manufactured consistent with cGMP regulations. In
complying with the cGMP regulations, manufacturers must continue to spend time,
money and effort in production, record keeping, quality control, and auditing to
ensure that the marketed product meets applicable specifications and other
requirements. The FDA periodically inspects manufacturing facilities to ensure
compliance with cGMP regulations. Failure to comply subjects the manufacturer to
possible FDA action, such as warning letters, suspension of manufacturing,
seizure of the product, voluntary recall of a product or injunctive action, as
well as possible civil penalties. We currently rely on, and intend to continue
to rely on, third parties to manufacture our compounds and product candidates.
These third parties will be required to comply with cGMP
regulations.
Products
manufactured in the U.S. for distribution abroad will be subject to FDA
regulations regarding export, as well as to the requirements of the country to
which they are shipped. These latter requirements are likely to cover the
conduct of clinical trials, the submission of marketing applications, and all
aspects of manufacturing and marketing. Such requirements can vary significantly
from country to country.
We and
our contractors are also subject to various federal, state and local laws,
rules, regulations and policies relating to safe working conditions, laboratory
and manufacturing practices, the experimental use of animals and the use of and
disposal of hazardous or potentially hazardous substances used in connection
with our research work. Although we believe that safety procedures employed for
handling and disposing of such materials comply with current federal, state and
local laws, rules, regulations and policies, the risk of accidental injury or
contamination from these materials cannot be entirely eliminated.
Before a
medicinal product can be supplied in the European Union, or EU, it must first be
granted a marketing authorization. There are three routes by which this may be
achieved: the centralized procedure whereby a single European license is granted
by the European Commission permits the supply of the product in question
throughout the EU or the decentralized, or DC, or mutual recognition procedures,
or MRP, through which the views of one national authority (Reference Member
State, or RMS) are “recognized” by other authorities (Concerned Member States,
or CMS) when conducting their reviews; the DC applies if the medicinal product
in question has not yet received a marketing authorization in any member state
at the time of the application whereas the MRP applies to a currently approved
medicinal product. These latter two processes lead to individual licenses in
each member state for the supply of products in that country only. The
centralized route is compulsory for biotechnology products and is optional for
certain so-called “high technology” products and products containing entirely
new active substances. All products which are not authorized by the centralized
route must be authorized by the DC or MRP unless the product is designed for use
in a single country in which case a National Application can be
made.
In making
an application for a new medicinal product not governed compulsorily by the
centralized procedure, typically use will be made of the DC although the MRP
would be used if a marketing authorization were first secured in an RMS. The
procedural steps for the DC and the MRP are governed by Directive 2001/83/EC, as
amended, and are described in the Notice to Applicants, Volume 2A Chapter 2 -
Mutual Recognition (updated version - November 2005). The procedures provide for
set time periods for each process (DC - 120 days; MRP – 90 days) but if
consensus is not reached between all the CMS and the RMS in that time, the
application is referred to arbitration through the Co-ordination Group for
Mutual Recognition and Decentralized Procedures, or CMD, with referral to the
Committee for Human Medicinal Products, or CHMP. If a referral is made, the
procedure is suspended; marketing of the product would only be possible in the
RMS in the case of an MRP. The
opinion of the CMD/CHMP, which is binding, could support or reject the
objections or alternatively reach a compromise position acceptable to all EU
countries concerned. The arbitration procedure may require the delivery of
additional data. Once granted, any MAA remains subject to pharmacovigilance and
all competent authorities have the power to vary, suspend or revoke an MAA on
grounds of safety.
The
extent of U.S. and foreign government regulation which might result from future
legislation or administrative action cannot be accurately predicted. For
example, in the U.S., although the Food and Drug Administration Modernization
Act of 1997, or FDAMA, modified and created requirements and standards under the
FFDCA with the intent of facilitating product development and marketing, the FDA
is still in the process of developing regulations implementing FDAMA and the
more recent Food and Drug Administration Amendments Act of 2007, or FDAAA. FDA
has been actively implementing drug safety plans called Risk Evaluation and
Mitigation Strategies, or REMS, as authorized by FDAAA, as a condition of drug
approval, or after initial marketing, if FDA becomes aware of new safety data
about the drug. These and other legislative initiatives may impose additional
regulatory requirements on us, and may impact approval of our drugs or our
marketing plans. The actual effect of these and other developments on our own
business is uncertain and unpredictable.
Corporate
Information
We were
incorporated in Delaware on September 25, 1996. Our principal offices are
located in the Exchange Office Building at 1414 Raleigh Road, Suite 400, Chapel
Hill, NC 27517. Our telephone number is (919) 913-1030. We maintain a
website at www.pozen.com and make available free of charge through this website
our Annual Reports on Form 10-K, our Quarterly Reports on Form 10-Q, our Current
Reports on Form 8-K and amendments to those reports filed or furnished pursuant
to Section 13(a) or 15(d) of the Exchange Act as soon as reasonably practicable
after we electronically file such material with, or furnish it to, the SEC. We
also similarly make available, free of charge on our website, the reports filed
with the SEC by our executive officers, directors and 10% stockholders pursuant
to Section 16 under the Exchange Act as soon as reasonably practicable after
copies of those filings are provided to us by those persons. We are not
including the information contained at www.pozen.com, or at any other Internet
address as part of, or incorporating it by reference into, this Annual Report on
Form 10-K.
In
addition, we make available on our website (i) the charters for the
committees of our Board of Directors, including the Audit Committee,
Compensation Committee and Nominating/Corporate Governance Committee, and
(ii) our Code of Business Conduct and Ethics governing our directors,
officers and employees. We intend to disclose on our website any amendments to,
or waivers from, our Code of Business Conduct and Ethics that are required to be
disclosed pursuant to the rules of the Securities and Exchange Commission and
the NASDAQ Stock Market.
Employees
As of
January 31, 2010, we had a total of 31 full-time employees. All of our current
employees are based at our headquarters in Chapel Hill, North Carolina. Of our 31 employees, 16 hold
advanced degrees, including seven with M.D., Pharm.D. or Ph.D.
degrees.
Officers
and Key Employees
Our
current officers and key employees, and their ages as of February 1, 2010, are
as follows:
|
Name
|
|
Age
|
|
Position
|
|
John
R. Plachetka, Pharm.D.
|
|
56
|
|
Chairman,
President and Chief Executive Officer
|
|
William
L. Hodges, CPA
|
|
55
|
|
Senior
Vice President, Finance and Administration, Chief Financial
Officer
|
|
Elizabeth
A. Cermak, MBA
|
52
|
Executive
Vice President, Chief Commercial Officer
|
||
|
Gilda
M. Thomas, JD
|
|
55
|
|
Senior
Vice President, General Counsel
|
|
John
E. Barnhardt, CPA
|
|
60
|
|
Vice
President, Finance & Administration
|
|
Everardus
Orlemans, Ph.D.
|
|
53
|
|
Senior
Vice President, Product Development
|
|
John
G. Fort, MD, MBA
|
|
55
|
|
Chief
Medical Officer
|
John R. Plachetka, Pharm.D. is Chairman
of the Board of Directors, a co-founder, President and Chief Executive Officer
of POZEN and has held such positions since our inception in 1996. Prior to
founding POZEN, Dr. Plachetka was Vice President of Development at Texas
Biotechnology Corporation from 1993 to 1995 and was President and Chief
Executive Officer of Clinical Research Foundation-America, a leading clinical
research organization, from 1990 to 1992. From 1981 to 1990, he was employed at
Glaxo Inc. Dr. Plachetka received his B.S. in Pharmacy from the University of
Illinois College of Pharmacy and his Doctor of Pharmacy from the University of
Missouri-Kansas City.
William
L. Hodges joined POZEN in August 2004 as Senior Vice President of Finance and
Administration and Chief Financial Officer. Mr. Hodges began his career in the
pharmaceutical industry with Burroughs Wellcome Co. in 1985. In 1991, he moved
to London and worked in Group Finance for the Wellcome Foundation, Ltd. Mr.
Hodges worked on mergers and acquisitions and was Regional Controller for
Northern Europe and Japan. In 1993, he returned to Burroughs Wellcome in North
Carolina as Director of Procurement. Mr. Hodges was Vice President, Corporate
Planning and Business Support at GlaxoWellcome before being appointed acting
Senior Vice President and CFO for the fifteen months leading up to the merger
between GlaxoWellcome plc and SmithKline Beecham plc which was completed in
December of 2000. Prior to joining POZEN, Mr. Hodges was Senior Vice President
and CFO of Pergo, Inc. located in Raleigh, North Carolina. Mr. Hodges received
his B.S. from the University of North Carolina at Chapel Hill and is a Certified
Public Accountant.
Elizabeth A. Cermak joined POZEN in
September 2009 as Executive Vice President and Chief Commercial Officer. Prior
to joining POZEN, Ms. Cermak was Worldwide Vice President in the Consumer Health
Division of Johnson and Johnson from 2006. From 2005, she was Vice President
Business Development for McNeil Consumer and Specialty, Inc. and from 2003 to
2005 was Vice President, Women’s Health Franchise at Ortho-McNeil
Pharmaceuticals, Inc. She has spent over 25 years in the healthcare industry and
has led a number of marketing and sales organizations. Ms. Cermak holds an MBA
in Finance from Drexel University in Philadelphia, PA, and a BA Cum Laude in
Accounting and Spanish from Franklin and Marshall College in Lancaster,
PA.
Gilda M.
Thomas joined POZEN in January 2007 as Senior Vice President and General
Counsel. Prior to joining POZEN, Ms. Thomas was Vice President, General Counsel
and company secretary at EMD Pharmaceuticals, Inc., an affiliate of Merck KGaA,
Darmstadt, Germany from July 2001 to December 2006. Prior to joining EMD, she
spent 14 years at Burroughs Wellcome Co., which merged into Glaxo Welcome, Inc.
At Glaxo Wellcome Ms. Thomas was Associate General Counsel responsible for the
13 member corporate section of the legal department. Ms. Thomas received her
J.D. from Harvard Law School, a M.S. from Simmons College and a B.S. degree from
Wellesley College.
John E.
Barnhardt joined POZEN in 1997 as Vice President, Finance and Administration and
Principal Accounting Officer. Prior to joining POZEN, Mr. Barnhardt held finance
and accounting positions with publicly traded companies beginning in 1988. These
positions included Chief Financial Officer of Medco Research, Inc., engaged in
the research and development of pharmaceutical products primarily for the
diagnosis and treatment of cardiovascular disease, and Principal Accounting
Officer of Microwave Laboratories, Inc., a defense contractor developing and
manufacturing traveling wave tubes for electronic countermeasure systems. Mr.
Barnhardt received his B.S. in Zoology from North Carolina State University, and
while employed at Ernst & Ernst (now Ernst & Young LLP), became a
Certified Public Accountant.
Everardus
Orlemans, Ph.D. joined POZEN in November 2005 as Vice President, Clinical
Research and was promoted to Senior Vice President, Product Development in
January 2009. Dr. Orlemans began his professional career with Organon NV, a
pharmaceutical company based in the Netherlands, before transferring to its U.S.
subsidiary, Organon Pharmaceuticals USA, Inc., where his most recent position
was Executive Director of the Clinical Development Unit. Dr. Orlemans was an
employee of Organon NV and/or its U.S. Subsidiary from October 1988 to March
2005. He received a M.S. in Chemistry from Catholic University of Nijmegen in
the Netherlands and his Ph.D. degree from the University of Twente, also located
in the Netherlands.
John G. Fort, M.D. joined POZEN in July
2007 as Chief Medical Officer. Prior to joining POZEN, Dr. Fort was Vice
President, Medical Affairs at Adolor Corporation from 2004 until 2007. Dr. Fort
held positions with Pfizer Inc., including Vice President, Medical Affairs, and
was Vice President, Arthritis and Pain at G.D. Searle & Co., Monsanto
Corporation from September 1994 to December 2003. Prior to joining the
pharmaceutical industry, he was an Associate Professor of Medicine at Thomas
Jefferson University, Division of Rheumatology. Dr. Fort received his M.D. from
the University of Valencia Faculty of Medicine and is board certified in
internal medicine with a subspecialty certification in
rheumatology.
Described below are various risks and
uncertainties that may affect our business. These risks and uncertainties are
not the only ones we face. You should recognize that other significant risks and
uncertainties may arise in the future, which we cannot foresee at this time.
Also, the risks that we now foresee might affect us to a greater or different
degree than expected. Certain risks and uncertainties, including ones that we
currently deem immaterial or that are similar to those faced by other companies
in our industry or business in general, may also affect our business. If any of
the risks described below actually occur, our business, financial condition or
results of operations could be materially and adversely affected.
Risks
Related to Our Business
We
have incurred losses since inception and we may continue to incur losses for the
foreseeable future. Product revenue for products which we license out is
dependent upon the commercialization efforts of our partners, including the
sales and marketing efforts of GSK relating to Treximet.
We have
incurred significant losses since our inception. As of December 31, 2009, we had
an accumulated deficit of approximately $140.0 million. Our ability to receive
product revenue from the sale of products is dependent on a number of factors,
principally the development, regulatory approval and successful
commercialization of our product candidates. We expect that the amount of our
operating losses will fluctuate significantly from quarter to quarter
principally as a result of increases and decreases in our development efforts
and the timing and amount of payments that we may receive from others. We expect
to continue to incur significant operating losses associated with our research
and development efforts and do not know the amount or timing of product revenue
we will receive as a result of sales of Treximet by GlaxoSmithKline, or GSK, or
future sales of other product candidates by commercial partners. For example,
GSK’s inability to launch Treximet with approved promotional and professional
materials, including direct to consumer advertising, may have had an adverse
impact on uptake of the product, thus affecting our royalty
revenue.
Our only
current potential sources of revenue are the payments that we may receive
pursuant to our collaboration agreements with GSK and AstraZeneca. We received
the remaining regulatory milestone payments under our collaboration agreement
with GSK related to Treximet payable upon approval by the U.S. Food and Drug
Administration, or FDA, and notification of GSK’s intent to commercialize
Treximet, receipt of which were delayed as a result of our receipt of a
second approvable letter for the product on August 1, 2007.
We
depend heavily on the success of our product candidates, which may never be
approved for commercial use. If we are unable to develop, gain approval of or
commercialize those product candidates, we will never receive revenues from the
sale of our product candidates.
We
anticipate that for the foreseeable future our ability to achieve profitability
will be dependent on the successful commercialization of Treximet, along with
the successful development, approval and commercialization of our current
product candidates. If we fail to gain timely approval to commercialize our
products from the FDA and other foreign regulatory bodies, we will be unable to
generate the revenue we will need to build our business. These approvals may not
be granted on a timely basis, if at all, and even if and when they are granted,
they may not cover all of the indications for which we seek approval. Many
factors could negatively affect our ability to obtain regulatory approval for
our product candidates. For example, approval of Treximet for commercial use was
significantly delayed by our receipt of two approvable letters, the first of
which we received in June 2006 in which the FDA requested additional safety
information on Treximet, some of which required new studies. On August 1, 2007,
we received a second approvable letter from the FDA for Treximet in which the
FDA requested that we further address the FDA’s concern about the product’s
potential for genotoxicity.
In
October 2008, the FDA informed us that it was conducting an internal review of
the acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. Reduction of endoscopic gastric ulcers was the primary endpoint
in our Phase 3 trials for VIMOVO and the proposed primary endpoint in the
current study design of the Phase 3 trials for our PA32540 product. In late
January 2009, the FDA informed us that it had completed its internal discussions
and that there was no change to previous agreements that gastric ulcer incidence
was an acceptable primary endpoint for our clinical programs. If the FDA had
determined that endoscopic gastric ulcers were no longer an acceptable endpoint
in clinical trials, we might have been required to conduct additional trials and
provide additional data which would have required additional expenses and
delayed filing of the new drug application, or NDA, for VIMOVO.
In
addition to the inability to obtain regulatory approval, many other factors
could negatively affect the success of our efforts to develop and commercialize
our product candidates, including those discussed in the risk factors that
follow as well as negative, inconclusive or otherwise unfavorable results from
any studies or clinical trials, such as those that we obtained with respect to
MT 500, which led to our decision to discontinue development of that product
candidate in 2002.
Changes
in regulatory approval policy or statutory or regulatory requirements, or in the
regulatory environment, during the development period of any of our product
candidates may result in delays in the approval, or rejection, of the
application for approval of one or more of our product candidates. If we fail to
obtain approval, or are delayed in obtaining approval, of our product
candidates, our ability to generate revenue will be severely
impaired.
The
process of drug development and regulatory approval for product candidates takes
many years, during which time the FDA’s interpretations of the standards against
which drugs are judged for approval may evolve or change. The FDA can also
change its approval policies based upon changes in laws and regulations. In
addition, the FDA can decide, based on its then current approval policies, any
changes in those policies and its broad discretion in the approval process, to
weigh the benefits and the risks of every drug candidate. As a result of any of
the foregoing, the FDA may decide that the data we submit in support of an
application for approval of a drug candidate are insufficient for approval. For
example, in October 2008, the FDA has informed us that it was conducting an
internal review of the acceptability of using endoscopic gastric ulcers as a
primary endpoint in clinical trials. Reduction of endoscopic gastric ulcers was
the primary endpoint in our Phase 3 trials for VIMOVO (formerly referred to as
PN 400). In late January 2009, FDA informed us that it had completed its
internal discussions and that there was no change to previous agreements that
gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs. In the event the FDA had determined that endoscopic gastric ulcers
were no longer an acceptable endpoint, we might have been required to conduct
additional trials and provide additional data which would have required
additional expenses and delayed NDA approval of VIMOVO. Further, changes in
policy or interpretation may not be the subject of published guidelines and may
therefore be difficult to evaluate. For example, the FDA has not recently
published guidelines for the approval of new migraine therapies, and we have had
to rely on periodic guidance from the FDA obtained (in conversations) informally
and in other meetings, the content of which may be subject to significant
modification over the period of a drug’s development program. There is also the
risk that we and the FDA may interpret such guidance differently.
Further,
additional information about the potential risks of marketed drugs may affect
the regulatory approval environment, or the FDA’s approval policies, for new
product candidates. For example, in February 2005 an advisory committee convened
by the FDA met to address the potential cardiovascular risks of COX-2 selective
NSAIDs and related drugs in response to disclosures made about possible adverse
effects from the use of some of these drugs. On April 7, 2005, the FDA issued a
Public Health Advisory, or the Advisory, based, in part, upon the
recommendations of the advisory committee. The Advisory stated that it would
require that manufacturers of all prescription products containing NSAIDs
provide warnings regarding the potential for adverse cardiovascular events as
well as life-threatening gastrointestinal events associated with the use of
NSAIDs. Moreover, subsequent to the FDA advisory committee meeting in February
2005, the FDA has indicated that long-term studies evaluating cardiovascular
risk will be required for approval of new NSAID products that may be used on an
intermittent or chronic basis. Based on our discussions with the FDA reviewing
division for PN products, we believe that, unless new information about naproxen
safety concerns becomes available, long-term cardiovascular safety studies will
not be required at this time for FDA approval of our PN product candidates
containing naproxen. However, we cannot guarantee that such studies will not be
required. We will continue to evaluate and review with the FDA its expectations
and recommendations regarding the efficacy and safety requirements and study
design necessary to support approval of NDAs for our PN product candidates and
other product candidates that contain NSAIDs.
If
we, or our current or future collaborators, do not obtain and maintain required
regulatory approvals for one or more of our product candidates, we will be
unable to commercialize those product candidates. Further, if we are delayed in
obtaining or unable to obtain, any required approvals, our collaborators may
terminate, or be entitled to terminate, their agreements with us or reduce or
eliminate their payments to us under these agreements or we may be required to
pay termination payments under these agreements.
Our
product candidates under development are subject to extensive domestic and
foreign regulation. The FDA regulates, among other things, the development,
testing, manufacture, safety, efficacy, record keeping, labeling, storage,
approval, advertisement, promotion, sale and distribution of pharmaceutical
products in the U.S. In order to market our products abroad, we must comply with
extensive regulation by foreign governments. If we are unable to obtain and
maintain FDA and foreign government approvals for our product candidates, we,
alone or through our collaborators, will not be permitted to sell them. Failure
to obtain regulatory approval for a product candidate will prevent us from
commercializing that product candidate. Except for Treximet, which was approved
for commercial sale in the U.S. on April 15, 2008, none of our other product
candidates are approved for sale in the U.S. or any foreign market and they may
never be approved. For example, we received two approvable letters relating to
our NDA for Treximet which communicated the FDA’s concerns that delayed
marketing approval. An approvable letter is an official notification from the
FDA that contains conditions that must be satisfied prior to obtaining final
U.S. marketing approval. In June 2006, we received the first approvable letter
in which the FDA requested additional safety information on Treximet, and in
August 2007, we received a second approvable letter in which the FDA requested
that we address their concern about the potential implications from one
preclinical in vitro chromosomal aberration study in which a signal for
genotoxicity was seen for the combination of naproxen sodium and sumatriptan. We
have also previously received not-approvable letters from the FDA relating to
our NDAs for MT 100 and MT 300.
In the
U.S., a separate NDA or supplement must be filed with respect to each indication
for which marketing approval of a product is sought. Each NDA, in turn, requires
the successful completion of preclinical, toxicology, genotoxicity and
carcinogenicity studies, as well as clinical trials demonstrating the safety and
efficacy of the product for that particular indication. We may not receive
regulatory approval of any of the NDAs that we file with the FDA or of any
approval applications we may seek in the future outside the U.S.
Further,
our current or future collaboration agreements may terminate, or require us to
make certain payments to our collaborators, or our collaborators may have the
right to terminate their agreements with us or reduce or eliminate their
payments to us under these agreements, based on our inability to obtain, or
delays in obtaining, regulatory approval for our product candidates. For
example, under our PN collaboration agreement with AstraZeneca, AstraZeneca has
the right to terminate the agreement if certain delays occur or specified
development and regulatory objectives are not met. For example, this termination
right could have been triggered by AstraZeneca if the FDA had determined that
endoscopic gastric ulcers were no longer an acceptable endpoint and we had been
required to conduct additional trials which would have delayed NDA approval for
VIMOVO. Both AstraZeneca and GSK have the right to terminate their respective
agreement with us upon 90 days notice for any reason. If we or our contract
manufacturers do not maintain required regulatory approvals, we may not be able
to commercialize our products. Approval of a product candidate may be
conditioned upon certain limitations and restrictions as to the drug’s use, or
upon the conduct of further studies, and is subject to continuous review. The
FDA may also require us to conduct additional post-approval studies. These
post-approval studies may include carcinogenicity studies in animals or further
human clinical trials. The later discovery of previously unknown problems with
the product, manufacturer or manufacturing facility may result in criminal
prosecution, civil penalties, recall or seizure of products, or total or partial
suspension of production, as well as other regulatory action against our product
candidates or us. If approvals are withdrawn for a product, or if a product is
seized or recalled, we would be unable to sell that product and therefore would
not receive any revenues from that product.
We and
our contract manufacturers are required to comply with the applicable FDA
current Good Manufacturing Practices, or cGMP, regulations, which include
requirements relating to quality control and quality assurance, as well as the
corresponding maintenance of records and documentation. Further, manufacturing
facilities must be approved by the FDA before they can be used to manufacture
our product candidates, and are subject to additional FDA inspection. We, or our
third-party manufacturers, may not be able to comply with cGMP regulations or
other FDA regulatory requirements, which could result in a delay or an inability
to manufacture the products. If we or our partners wish or need to identify an
alternative manufacturer, delays in obtaining FDA approval of the alternative
manufacturing facility could cause an interruption in the supply of our
products.
Labeling
and promotional activities are subject to scrutiny by the FDA and state
regulatory agencies and, in some circumstances, the Federal Trade Commission.
FDA enforcement policy prohibits the marketing of unapproved products as well as
the marketing of approved products for unapproved, or off-label, uses. These
regulations and the FDA’s interpretation of them may limit our or our partners’
ability to market products for which we gain approval. Failure to comply with
these requirements can result in federal and state regulatory enforcement
action. Further, we may not obtain the labeling claims we or our partners
believe are necessary or desirable for the promotion of our product
candidates.
If
third parties challenge the validity of the patents or proprietary rights of our
marketed products or assert that we have infringed their patents or proprietary
rights, we may become involved in intellectual property disputes and litigation
that would be costly and time consuming and could negatively impact the
commercialization of Treximet and/or any of our products that we develop or
acquire. We have received notice of paragraph IV certifications notifying
us of the filing of ANDAs with the FDA for approval to market a generic version
of Treximet. We filed patent infringement lawsuits in response to these
ANDAs that could lead to costly and time consuming patent
litigation.
The intellectual property rights of
pharmaceutical companies, including us, are generally uncertain and involve
complex legal, scientific and factual questions. Our success in developing and
commercializing pharmaceutical products may depend, in part, on our ability to
operate without infringing on the intellectual property rights of others and to
prevent others from infringing on our intellectual property rights. There has
been substantial litigation regarding patents and other intellectual property
rights in the pharmaceutical industry. For example, third parties seeking to
market generic versions of branded pharmaceutical products often file ANDAs with
the FDA, containing a certifications stating that the ANDA applicant believes
that the patents protecting the branded pharmaceutical product are invalid,
unenforceable and/or not infringed. Such certifications are commonly
referred to as paragraph IV certifications.
We and
GSK have received Paragraph IV Notice Letters from Par, Alphapharm, Alphapharm’s
designated agent, Mylan, Teva and Dr. Reddy’s informing us that each company had
filed an Abbreviated New Drug Application, or ANDA, with the FDA, seeking
approval to market sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par,
Alphapharm, Teva and Dr. Reddy’s have each indicated in their respective Notice
Letters that they intend to market a generic version of Treximet tablets before
the expiration of U.S. Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK
advised us that it has elected not to exercise its first right to bring
infringement suits against Par, Alphapharm, Teva and Dr. Reddy’s. Accordingly,
we filed suit against Par on November 14, 2008, Alphapharm and Mylan on January
2, 2009, Teva on April 14, 2009 and Dr. Reddy’s on August 21, 2009, all in the
United States District Court for the Eastern District of Texas. All four actions
have since been consolidated into one suit. The Company’s filing of these patent
infringement lawsuits within forty-five days of our receipt of the respective
Notice Letters from Par, Alphapharm, Teva and Dr. Reddy’s resulted in the FDA
automatically instituting a stay, or bar, of approval of Par’s, Alphapharm’s,
Teva’s and Dr. Reddy’s respective ANDAs for up to 30 months or until a final
court decision is entered in the infringement suit in favor of the ANDA
applicant, whichever occurs first. Treximet currently has regulatory exclusivity
through April 15, 2011. Treximet may be eligible for an additional six months of
exclusivity upon the completion of certain pediatric studies. Written and
document discovery are in progress. The cases are set for trial in the fourth
quarter of 2010.
Litigation can be time consuming and
costly and we cannot predict with certainty the outcome. If we are
unsuccessful in such a proceeding and the FDA approved a generic version of our
product, such an outcome would have a material adverse effect on sales of
Treximet and our business.
Our
reliance on collaborations with third parties to develop and commercialize our
products is subject to inherent risks and may result in delays in product
development and lost or reduced revenues, restricting our ability to
commercialize our products and adversely affecting our
profitability.
With respect to the products we have
licensed, we depend upon collaborations with third parties to develop these
product candidates and we depend substantially upon third parties to
commercialize these products. As a result, our ability to develop, obtain
regulatory approval of, manufacture and commercialize our existing and possibly
future product candidates depends upon our ability to maintain existing, and
enter into and maintain new, contractual and collaborative arrangements with
others. For those future products we commercialize ourselves, we will continue
to depend substantially upon third parties to implement our commercial strategy.
We also engage, and intend in the future to continue to engage, contract
manufacturers and clinical trial investigators.
In
addition, although not a primary component of our current strategy, the
identification of new compounds or product candidates for development has led
us, and may continue to require us, to enter into license or other collaborative
agreements with others, including pharmaceutical companies and research
institutions. Such collaborative agreements for the acquisition of new compounds
or product candidates would typically require us to pay license fees, make
milestone payments and/or pay royalties. Furthermore, these agreements may
result in our revenues being lower than if we developed our product candidates
ourselves and in our loss of control over the development of our product
candidates.
Contractors
or collaborators may have the right to terminate their agreements with us or
reduce their payments to us under those agreements on limited or no notice and
for no reason or reasons outside of our control. We currently have a
collaboration with GSK for the development and commercialization of
certain triptan combinations using our MT 400 technology, including Treximet, in
the U.S., a global collaboration with AstraZeneca for the development and
commercialization of proprietary combinations of gastroprotective agents and
naproxen, and a collaboration with Valeant NA in the U.S. for the development
and commercialization of MT 300. In these collaboration agreements, our
collaborators have the right to terminate the agreement upon a default by us. In
addition, GSK and AstraZeneca are entitled to terminate their respective
agreements with us upon 90 days’ notice for any reason. Additionally, both GSK
and AstraZeneca have the right to reduce the royalties on net sales of products
payable to us under their respective agreements if generic competitors attain a
pre-determined share of the market for products marketed under the agreements,
or if either GSK or AstraZeneca must pay a royalty to one or more third parties
for rights it licenses from those third parties to commercialize products
marketed under the agreements. AstraZeneca is also entitled to terminate its
agreement with us if certain delays occur or specified development or regulatory
objectives are not met. This termination could have been triggered by
AstraZeneca if the FDA had determined that endoscopic gastric ulcers were no
longer an acceptable endpoint and we had been required to conduct additional
trials which would have delayed NDA approval for VIMOVO. Valeant NA is entitled
to terminate its agreement with us and a $1.0 million withdrawal fee would be
payable by us in the event we choose to withdraw the NDA if we determine that
additional studies or data that are required by the FDA for approval of the NDA
would jeopardize the commercial viability of MT 300 or exceed our financial
resources available for MT 300. Due to our belief that the FDA will not approve
the NDA for MT 300 and there are no additional required studies, we began
discussions with Valeant NA regarding termination of our agreement. Valeant NA
has demanded payment of the $1.0 million withdrawal fee, which we are
disputing.
If our
current or future licensees exercise termination rights they may have, or if
these license agreements terminate because of delays in obtaining regulatory
approvals, or for other reasons, and we are not able to establish replacement or
additional research and development collaborations or licensing arrangements, we
may not be able to develop and/or commercialize our product candidates.
Moreover, any future collaborations or license arrangements we may enter into
may not be on terms favorable to us.
A further
risk we face with our collaborations is that business combinations and changes
in the collaborator or their business strategy may adversely affect their
willingness or ability to complete their obligations to us.
Our
current or any future collaborations or license arrangements ultimately may not
be successful. Our agreements with collaborators typically allow them discretion
in electing whether to pursue various regulatory, commercialization and other
activities or with respect to the timing of the development, such as our
agreement with GSK under which GSK determined, among other things, the exact
formulation and composition of the product candidates using our MT 400
technology for use in the Treximet clinical trials. Similarly, under our
agreement with AstraZeneca, AstraZeneca has the right to manufacture clinical
trial material itself or through a third party. If any collaborator were to
breach its agreement with us or otherwise fail to conduct collaborative
activities in a timely or successful manner, the pre-clinical or clinical
development or commercialization of the affected product candidate or research
program would be delayed or terminated. Any delay or termination of clinical
development or commercialization, such as the delay in FDA approval we
experienced as a result of approvable letters we received from the FDA in June
2006 and August 2007 related to our Treximet NDA, or a delay in FDA approval of
VIMOVO which could have occurred if the FDA determined that
endoscopic gastric ulcers were no longer an acceptable primary endpoint in
clinical trials and we were required to conduct additional clinical trials for
the product, would delay or possibly eliminate our potential product revenues.
Further, our collaborators may be able to exercise control, under certain
circumstances, over our ability to protect our patent rights under patents
covered by the applicable collaboration agreement. For example, under our
collaboration agreements with GSK and AstraZeneca, GSK and AstraZeneca each has
the first right to enforce our patents under their respective agreements and
would have exclusive control over such enforcement litigation. GSK advised us
that it has elected not to exercise its first right to bring infringement suits
against Par, Alphapharm, Teva, and Dr. Reddy’s which have submitted ANDAs to the
FDA for approval to market a generic version of Treximet tablets and we have
filed suit against the four companies in the federal court of the United State
District Court for the Eastern District of Texas.
Other
risks associated with our collaborative and contractual arrangements with others
include the following:
|
·
|
we
may not have day-to-day control over the activities of our contractors or
collaborators;
|
|
·
|
our
collaborators may fail to defend or enforce patents they own on compounds
or technologies that are incorporated into the products we develop with
them;
|
|
·
|
third
parties may not fulfill their regulatory or other
obligations;
|
|
·
|
we
may not realize the contemplated or expected benefits from collaborative
or other arrangements; and
|
|
·
|
disagreements
may arise regarding a breach of the arrangement, the interpretation of the
agreement, ownership of proprietary rights, clinical results or regulatory
approvals.
|
These factors could lead to delays in the development of our product candidates
and/or the commercialization of our products or reduction in the milestone
payments we receive from our collaborators, or could result in our not being
able to commercialize our products. Further, disagreements with our contractors
or collaborators could require or result in litigation or arbitration, which
would be time-consuming and expensive. Our ultimate success may depend upon the
success and performance on the part of these third parties. If we fail to
maintain these relationships or establish new relationships as required,
development of our product candidates and/or the commercialization of our
products will be delayed or may never be realized.
A
collaborator may withdraw support or cease to perform work on our product
candidates if the collaborator determines to develop its own competing product
candidate or other product candidates instead.
We have
entered into collaboration and license agreements, and may continue to enter
into such agreements, with companies that have products and are developing new
product candidates that compete or may compete with our product candidates or
which have greater commercial potential. If one of our collaborators should
decide that the product or a product candidate that the collaborator is
developing would be more profitable for the collaborator than our product
candidate covered by the collaboration or license agreement, the collaborator
may withdraw support for our product candidate or may cease to perform under our
agreement. In the event of a termination of the collaborator’s agreement upon
such cessation of performance, we would need to negotiate an agreement with
another collaborator in order to continue the development and commercialization
efforts for the product candidate. If we were unsuccessful in negotiating
another agreement, we might have to cease development activities of the
particular product candidate. For example, our development and commercialization
agreements with GSK and AstraZeneca are subject to this risk. GSK has publicly
disclosed that it is exploring the development of compounds for the treatment of
migraine. If GSK decides to focus its development and commercialization efforts
on its own products rather than continuing to commercialize Treximet or work
with us on any other product candidates that may be developed under the
agreement, it has the ability to terminate our agreement upon 90 days’ written
notice. And under the terms of our agreement with AstraZeneca, either party has
the right to terminate the agreement by notice in writing to the other party
upon or after any material breach of the agreement by the other party, if the
other party has not cured the breach within 90 days after written notice to cure
has been given, with certain exceptions. The parties also can terminate the
agreement for cause under certain defined conditions. In addition, AstraZeneca
can terminate the agreement, at any time, at will, for any reason or no reason,
in its entirety or with respect to countries outside the U.S., upon 90 days’
notice. If terminated at will, AstraZeneca will owe us a specified termination
payment or, if termination occurs after the product is launched, AstraZeneca
may, at its option, under and subject to the satisfaction of conditions
specified in the agreement, elect to transfer the product and all rights to us.
However, under the circumstance above, or similar circumstance, we may need to
enter into a new development and commercialization agreement and may need to
start the development process all over again. If we were able to negotiate a new
development and commercialization agreement to develop our technology, which is
not certain, or if we decide to commercialize the products previously partnered
by ourselves, we would face delays and redundant expenses in that
development.
We
need to maintain current agreements and enter into additional agreements with
third parties that possess sales, marketing and distribution capabilities, or
establish internally the capability to perform these functions, in order to
successfully market and sell our future drug products.
We have
no sales or distribution personnel or capabilities at the present time. If we
are unable to maintain current collaborations or enter into additional
collaborations with established pharmaceutical or pharmaceutical services
companies to provide those capabilities, or, alternatively, we are unable to
develop sales and distribution capabilities, either internally or through the
use of third parties, we will not be able to successfully commercialize our
products. To the extent that we enter into marketing and sales agreements with
third parties, such as our agreement with GSK which gives GSK responsibility for
marketing and selling Treximet in the United States, our revenues, if any, will
be affected by the sales and marketing efforts of those third parties. We have
decided to retain control of our PA product candidates. We have hired a chief
commercial officer to evaluate the commercial opportunities for our product
candidates and develop a worldwide commercial strategy, which will include
developing internal commercialization capabilities to enable us to commercialize
future products ourselves. We cannot guarantee that, should we elect to develop
our own internal sales and distribution capabilities, we would have sufficient
resources to do so, or would be able to hire the qualified sales and marketing
personnel we would need.
We
need to conduct preclinical, toxicology, genotoxicity and carcinogenicity and
other safety studies, and clinical trials for our product candidates. Any
negative or unanticipated results, unforeseen costs or delays in the conduct of
these studies or trials, or the need to conduct additional studies or trials or
to seek to persuade the FDA to evaluate the results of a study or trial in a
different manner, could cause us to discontinue development of a product
candidate or reduce, delay or eliminate our receipt of potential revenues for
one or more of our product candidates and adversely affect our ability to
achieve profitability.
Generally, we must demonstrate the efficacy and safety of our product candidates
before approval to market can be obtained from the FDA or the regulatory
authorities in other countries. Our existing and future product candidates are
and will be in various stages of clinical development. Depending upon the type
of product candidate and the stage of the development process of a product
candidate, we will need to complete preclinical, toxicology, genotoxicity and
carcinogenicity and other safety studies, as well as clinical trials, on these
product candidates before we submit marketing applications in the United States
and abroad. These studies and trials can be very costly and time-consuming. For
example, long-term cardiovascular safety studies, such as those the FDA has
indicated will be required for approval of certain product candidates containing
NSAIDs, typically take approximately three years. In addition, we rely on third
parties to perform significant aspects of our studies and clinical trials,
introducing additional sources of risk into our development
programs.
It should
be noted that the results of any of our preclinical and clinical trial testing
are not necessarily predictive of results we will obtain in subsequent or more
extensive clinical trials or testing. This may occur for many reasons,
including, among others, differences in study design, including
inclusion/exclusion criteria, the variability of patient characteristics,
including patient symptoms at the time of study treatment, the larger scale
testing of patients in later trials, or differences in formulation or doses of
the product candidate used in later trials. For example, our results from the
first of our two Phase 3 pivotal clinical trials of Treximet differed from the
results of our second Phase 3 clinical trial and from the Phase 2
proof-of-concept trial of MT 400 that we conducted prior to entering into our
collaboration with GSK. Whereas in the Phase 2 trial statistical significance
was reached at two hours over placebo in the relief of all associated symptoms
of migraine (nausea, photophobia and phonophobia), in the first Phase 3 study
Treximet failed to achieve statistical significance at two hours compared to
placebo in the relief of nausea. In the second Phase 3 pivotal clinical trial,
Treximet demonstrated superiority over the individual components measured by
sustained pain-free response (p<0.001 vs. naproxen; p=0.009 vs. sumatriptan)
and met all other regulatory endpoints versus placebo.
The
successful completion of any of our clinical trials depends upon many factors,
including the rate of enrollment of patients. If we are unable to recruit
sufficient clinical patients during the appropriate period, we may need to delay
our clinical trials and incur significant additional costs. We also rely on the
compliance of our clinical trial investigators with FDA regulatory requirements
and noncompliance can result in disqualification of a clinical trial
investigator and data that are unusable. In addition, the FDA or Institutional
Review Boards may require us to conduct additional trials or delay, restrict or
discontinue our clinical trials, including our pivotal trials for PA32540, on
various grounds, including a finding that the subjects or patients are being
exposed to an unacceptable health risk.
Further,
even though we may have completed all clinical trials for a product candidate
that were planned for submission in support of a marketing application, we may
be required to conduct additional clinical trials, studies or investigations or
to submit additional data to support our marketing applications. In addition, we
and/or our marketing or development partners may determine that pre-approval
marketing support studies should be conducted. Unanticipated adverse outcomes of
such studies, including recognition of certain risks to human subjects, could a
have material impact on the approval of filed or planned market applications or
could result in limits placed on the marketing of the product. We may also
determine from time to time that it would be necessary to seek to provide
justification to the FDA or other regulatory agency that would result in
evaluation of the results of a study or clinical trial in a manner that differs
from the way the regulatory agency initially or customarily evaluated the
results. In addition, we may have unexpected results in our preclinical or
clinical trials or other studies that require us to reconsider the need for
certain studies or trials or cause us to discontinue development of a product
candidate. For example, in reviewing our NDA for Treximet, the FDA expressed
concern about the potential implications from one preclinical in vitro
chromosomal aberration study, one of four standard genotoxicity assays, in which
a possible genotoxicity signal was seen for the combination of naproxen sodium
and sumatriptan. Further, additional information about potential drug-drug
interactions may restrict the patient population for our products, thus limiting
the potential market and our potential revenue. For example, recent scientific
publications contain conflicting data regarding a possible interaction between
clopidogrel (Plavix®), a
widely prescribed anti-platelet agent, and proton pump inhibitor products, and
its impact on cardiovascular outcomes. If the clinical relevance of the possible
interaction is unresolved by the time PA 32540 enters the marketplace, even if
the interaction is later proven definitively to have no clinical impact on
cardiovascular outcomes, the market potential of the product may be
reduced.
Once
submitted, an NDA requires FDA approval before the product described in the
application can be distributed or commercialized. Even if we determine that data
from our clinical trials, toxicology, genotoxicity and carcinogenicity studies
are positive, we cannot assure you that the FDA, after completing its analysis,
will not determine that the trials or studies should have been conducted or
analyzed differently, and thus reach a different conclusion from that reached by
us, or request that further trials, studies or analyses be conducted. For
example, the FDA requested additional safety information on Treximet in the
approvable letter we received in June 2006 relating to our NDA for Treximet,
which required conduct of additional studies, and in August 2007, we
received a second approvable letter in which the FDA raised an additional
concern about the potential implications from one preclinical in vitro
chromosomal aberration study, one of four standard genotoxicity assays, in which
a genotoxicity signal was seen for the combination of naproxen sodium and
sumatriptan.
Further,
although we believed that we provided the necessary data to support approval of
the NDAs for MT 100, our proprietary combination of metoclopramide hydrochloride
and naproxen sodium, and MT 300, the FDA issued not-approvable letters for the
MT 100 and MT 300 NDAs in May 2004 and October 2003, respectively, and based
upon our understandings from our most recent communication with the FDA and our
understanding of the FDA’s current standards for approval of migraine drugs, we
do not believe it is possible to reverse the not approvable status of the NDA
for MT 300. In addition, based upon our receipt of the not approvable letter for
MT 100 and the outcome of an August 2005 FDA Advisory Committee meeting relating
to the potential risk of tardive dyskinesia associated with the use of
metacloprimide, one of the components of MT 100, we made the decision to
discontinue further development of MT 100 and we have withdrawn the MAA for the
product in the U.K.
The FDA
may also require data in certain subpopulations, such as pediatric use, or, if
such studies were not previously completed, may require long-term
carcinogenicity studies, prior to NDA approval, unless we can obtain a waiver of
such a requirement. We face similar regulatory hurdles in other countries to
those that we face in the U.S.
Our costs
associated with our human clinical trials vary based on a number of factors,
including:
|
·
|
the
order and timing of clinical indications pursued;
|
|
·
|
the
extent of development and financial support from collaborative parties, if
any;
|
|
·
|
the
need to conduct additional clinical trials or studies;
|
|
·
|
the
number of patients required for enrollment;
|
|
·
|
the
difficulty of obtaining sufficient patient populations and
clinicians;
|
|
·
|
the
difficulty of obtaining clinical supplies of our product candidates;
and
|
|
·
|
governmental
and regulatory delays.
|
We
currently depend and will in the future depend on third parties to manufacture
our product candidates. If these manufacturers fail to meet our requirements or
any regulatory requirements, the product development and commercialization of
our product candidates will be delayed.
We do not
have, and have no plans to develop, the internal capability to manufacture
either clinical trial or commercial quantities of products that we may develop
or have under development. We rely upon third-party manufacturers and our
partners to supply us with our product candidates. We also need supply contracts
to sell our products commercially. There is no guarantee that manufacturers that
enter into commercial supply contracts with us will be financially viable
entities going forward, or will not otherwise breach or terminate their
agreements with us. If we do not have the necessary commercial supply contracts,
or if our current manufacturer is, or any of our future manufacturers are,
unable to satisfy our requirements or meet any regulatory requirements, and we
are required to find alternative sources of supply, there may be additional
costs and delays in product development and commercialization of our product
candidates or we may be required to comply with additional regulatory
requirements.
If
our competitors develop and commercialize products faster than we do or if their
products are superior to ours, our commercial opportunities will be reduced or
eliminated.
Our
product candidates will have to compete with existing and any newly developed
migraine therapies or therapies for any newly developed product candidates for
the treatment of other diseases. There are also likely to be numerous
competitors developing new products to treat migraine and the other diseases and
conditions for which we may seek to develop products in the future, which could
render our product candidates or technologies obsolete or non-competitive. For
example, our primary competitors will likely include large pharmaceutical
companies (including, based upon their current migraine portfolios, GSK, Merck
& Co., AstraZeneca, Johnson & Johnson, Pfizer, Inc. and Endo
Pharmaceuticals), biotechnology companies, universities and public and private
research institutions. The competition for our PN products that receive
regulatory approval will come from the oral NSAID market, or more specifically
the traditional non-selective NSAIDs (such as naproxen and diclofenac),
traditional NSAID/gastroprotective agent combination products or combination
product packages (such as Arthrotec® and
Prevacid®
NapraPACTM),
combinations of NSAIDs and PPIs taken as separate pills and the only remaining
COX-2 inhibitor, Celebrex®. The
competition for our PA product candidates for which we are conducting studies
for secondary prevention of cardiovascular events will come from aspirin itself
as well as other products used for secondary prevention. AstraZeneca, with whom
we are collaborating in the development of VIMOVO, has publicly announced that
it has filed a NDA for a combination product containing aspirin and esomeprazole
which, if approved, will enter the market before and may compete with our
PA32540 product candidates.
Based upon their drug product and pipeline portfolios and the overall
competitiveness of our industry, we believe that we face, and will continue to
face, intense competition from other companies for securing collaborations with
pharmaceutical companies, establishing relationships with academic and research
institutions, and acquiring licenses to proprietary technology. Our competitors,
either alone or with collaborative parties, may also succeed with technologies
or products that are more effective than any of our current or future
technologies or products. Many of our actual or potential competitors, either
alone or together with collaborative parties, have substantially greater
financial resources, and almost all of our competitors have larger numbers of
scientific and administrative personnel than we do.
Many of
these competitors, either alone or together with their collaborative parties,
also have significantly greater experience than we do in:
|
·
|
developing
product candidates;
|
|
·
|
undertaking
preclinical testing and human clinical trials;
|
|
·
|
obtaining
FDA and other regulatory approvals of product candidates;
and
|
|
·
|
manufacturing
and marketing products.
|
Accordingly,
our actual or potential competitors may succeed in obtaining patent protection,
receiving FDA or other regulatory approval or commercializing products where we
cannot or before we do. Any delays we encounter in obtaining regulatory
approvals for our product candidates, such as we experienced as a result of the
approvable letters we received from the FDA in June 2006 and August 2007
relating to the Treximet NDA, and as a result of the not-approvable letters we
received from the FDA on MT 100 and MT 300 increase this risk. Our competitors
may also develop products or technologies that are superior to those that we are
developing, and render our product candidates or technologies obsolete or
non-competitive. If we cannot successfully compete with new or existing
products, our marketing and sales will suffer and we may not ever receive any
revenues from sales of products or may not receive sufficient revenues to
achieve profitability.
If
we are unable to defend our patents in patent infringement lawsuits against
generic companies filing ANDAs for our products, our business may be materially
harmed. Further, defending against these lawsuits may be expensive and will
divert the attention of our management.
We and GSK have received Paragraph IV
Notice Letters from Par, Alphapharm, and Alphapharm’s designated agent, Mylan,
Teva and Dr. Reddy’s informing us that each company had filed an Abbreviated New
Drug Application, or ANDA, with the FDA, seeking approval to market sumatriptan
85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr. Reddy’s have
each indicated in their respective Notice Letters that they intend to market a
generic version of Treximet tablets before the expiration of U.S. Patent Nos.
6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has elected not to
exercise its first right to bring infringement suits against Par, Alphapharm,
Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on November 14,
2008, Alphapharm and Mylan on January 2, 2009, Teva on April 14, 2009, and Dr.
Reddy’s on August 21, 2009, all in the United States District Court for the
Eastern District of Texas. All four actions have since been consolidated into
one suit. Our filing of these patent infringement lawsuits within forty-five
days of our receipt of the respective Notice Letters from Par, Alphapharm and
Teva resulted in the FDA automatically instituting a stay, or bar, of approval
of Par’s, Alphapharm’s, Teva’s, and Dr. Reddy’s respective ANDAs for up to 30
months or until a final court decision is entered in the infringement suit in
favor of the ANDA applicant, whichever occurs first. Treximet currently has
regulatory exclusivity through April 15, 2011. Treximet may be eligible for an
additional six months of exclusivity upon the completion of certain pediatric
studies. Written and document discovery are in progress. The cases are set for
trial in the fourth quarter of 2010.
As with
any litigation proceeding, we cannot predict with certainty the eventual outcome
of the patent infringement lawsuits against Par, Alphapharm, Teva and Dr.
Reddy’s. Furthermore, we will have to continue to incur expenses in connection
with these lawsuits, which may likely be substantial. In the event of an adverse
outcome or outcomes, our business could be materially harmed. Moreover,
responding to and defending pending litigation will result in a significant
diversion of management’s attention and resources and an increase in
professional fees.
If
we are unable to protect our patents or proprietary rights, or if we are unable
to operate our business without infringing the patents and proprietary rights of
others, we may be unable to develop our product candidates or compete
effectively.
The
pharmaceutical industry places considerable importance on obtaining patent and
trade secret protection for new technologies, products and processes. Our
success will depend, in part, on our ability, and the ability of our licensors,
to obtain and to keep protection for our products and technologies under the
patent laws of the United States and other countries, so that we can stop others
from using our inventions. Our success also will depend on our ability to
prevent others from using our trade
secrets. In addition, we must operate in a way that does not infringe, or
violate, the patent, trade secret and other intellectual property rights of
other parties.
We cannot
know how much protection, if any, our patents will provide or whether our patent
applications will issue as patents. The breadth of claims that will be allowed
in patent applications cannot be predicted and neither the validity nor
enforceability of claims in issued patents can be assured. If, for any reason, we are
unable to obtain and enforce valid claims covering our products and technology,
we may be unable to prevent competitors from using the same or similar
technology or to prevent competitors from marketing identical products. For
example, if we are unsuccessful in litigation against Par, Alphapharm, Teva, Dr.
Reddy’s, and other companies who may file ANDAs for Treximet, such companies
could market a generic version of the product after marketing exclusivity
expires. In addition, due to the extensive time needed to develop, test and
obtain regulatory approval for our products, any patents that protect our
product candidates may expire early during commercialization. This may reduce or
eliminate any market advantages that such patents may give us.
In
certain territories outside the U.S., our issued patents may be subject to
opposition by competitors within a certain time after the patent is issued. Such
opposition proceedings and related appeals may not be resolved for several
years, and may result in the partial or total revocation of the issued patent.
For example, in October 2005 oppositions were filed against our issued European
patent for MT 400 by Merck & Co., Inc. and Almirall Prodesfarma asserting
that the European patent should not have been granted. As a result of these
oppositions and subsequent proceedings, the European Patent Office found that
claims relating to combinations of sumatriptan and naproxen for the treatment of
migraine were valid. However, broader claims relating to certain other 5-HT
1B/1D agonists and long-acting NSAIDs were held to be insufficiently supported
by the presently available technical evidence.
We may
need to submit our issued patents for amendment or reissue if we determine that
any claims within our patents should not have been issued. While such a
submission may be based on our view that only specified claims should not have
been granted to us, there can be no assurance that a patent examiner will not
determine that additional claims should not have been granted to us. Such was
the case with one of our patents covering MT 100, which we submitted for reissue
after determining that certain specified claims that are not central to our
protection of MT 100 should not have been issued. In April 2006, we received an
office action on the reissue application and, consistent with our decision not
to devote further resources to the development of this product in the U.S., the
reissue application was abandoned in January 2007.
We may
need to license rights to third party patents and intellectual property to
continue the development and marketing of our product candidates. If we are
unable to acquire such rights on acceptable terms, our development activities
may be blocked and we may be unable to bring our product candidates to
market.
We may
enter into litigation to defend ourselves against claims of infringement, assert
claims that a third party is infringing one or more of our patents, protect our
trade secrets or know-how, or determine the scope and validity of others’ patent
or proprietary rights. For example, we filed patent infringement lawsuits
against Par, Alphapharm and Teva in the federal court in the Eastern District of
Texas in connection with their respective ANDA submissions to the FDA containing
paragraph IV certifications for approval to market sumatriptan 85 mg/naproxen
sodium 500 mg tablets, a generic version of Treximet tablets, before the
expiration of our patents. With respect to some of our product candidates, under
certain circumstances, our development or commercialization collaborators have
the first right to enforce our patents and would have exclusive control over
such enforcement litigation. For example, under our collaboration agreements
with GSK and AstraZeneca, GSK and AstraZeneca each has the first right to
enforce our patents under their respective agreements. GSK advised us that it
has elected not to exercise its first right to bring an infringement suit
against Par, Alphapharm, Teva, and Dr. Reddy’s, each of which have submitted
ANDAs to the FDA for approval to market a generic version of Treximet
tablets.
If we are
found to infringe the patent rights of others, then we may be forced to pay
damages in an amount that might irreparably harm our business and/or be
prevented from continuing our product development and marketing activities.
Additionally, if we or our development or commercialization collaborator seek to
enforce our patents and are unsuccessful, we may be subject to claims for
bringing a failed enforcement action, including claims alleging various forms of
antitrust violations (both state and federal) and unfair competition. If we are
found to be liable for such claims, then we may be forced to pay damages in an
amount that might irreparably harm our business and/or be prevented from
continuing our product development and commercialization activities. Even if we
are successful in defending any such claims of infringement or in asserting
claims against third parties, such litigation is expensive, may have a material
effect on our operations, and may distract management from our business
operations. Regardless of its eventual outcome, any lawsuit that we enter into
may consume time and resources that would impair our ability to develop and
market our product candidates.
We have
entered into confidentiality agreements with our employees, consultants,
advisors and collaborators. However, these parties may not honor these
agreements and, as a result, we may not be able to protect our rights to
unpatented trade secrets and know-how. Others may independently develop
substantially equivalent proprietary information and techniques
or otherwise gain access to our trade secrets and know-how. Also, many of our
scientific and management personnel were previously employed by competing
companies. As a result, such companies may allege trade secret violations and
similar claims against us.
If
we fail to develop, acquire and commercialize additional products or product
candidates, or fail to successfully promote or market approved products, we may
never achieve profitability.
As part
of our business strategy, we plan to identify, self-invent and/or acquire
product candidates or approved products in areas in which we possess particular
knowledge. Because we do not directly engage in basic research or drug
discovery, we may rely upon third parties to sell or license product
opportunities to us. Other companies, including some with substantially greater
financial, marketing and sales resources, are competing with us to acquire such
products and product candidates. We may not be able to acquire rights to
additional products or product candidates on acceptable terms, if at all. In
addition, if we acquire new products or product candidates with different
marketing strategies, distribution channels and bases of competition than those
of our current product candidates, we may not be able to compete favorably in
those product categories.
None
of our products may be accepted by the market.
The
commercial success of our product candidates depends upon the acceptance of
these products in the marketplace. Even if a product displays a favorable
efficacy and safety profile in clinical trials, market acceptance of a product
will not be known until after it is launched and a product may not generate the
revenues that we anticipate. The degree of market acceptance will depend upon a
number of factors, including:
|
·
|
the
acceptance by physicians and third-party payors of Treximet as an
alternative to Imitrex, generic sumatriptan, and other
therapies;
|
|
·
|
the
receipt and timing of regulatory approvals;
|
|
·
|
the
availability of third-party reimbursement;
|
|
·
|
the
indications for which the product is approved;
|
|
·
|
the
rate of adoption by healthcare providers;
|
|
·
|
the
rate of product acceptance by target patient
populations;
|
|
·
|
the
price of the product relative to alternative therapies;
|
|
·
|
the
availability of alternative therapies;
|
|
·
|
the
extent and effectiveness of marketing efforts by our collaborators, and
third-party distributors and agents;
|
|
·
|
the
existence of adverse publicity regarding our products or similar products;
and
|
|
·
|
the
extent and severity of side effects as compared to alternative
therapies.
|
If
we do not receive adequate third-party reimbursements for our future products,
our revenues and profitability will be reduced.
Our
ability to commercialize our product candidates successfully will depend, in
part, on the extent to which reimbursement for the costs of such products and
related treatments will be available from government health administration
authorities, such as Medicare and Medicaid in the U.S., private health insurers
and other organizations. Significant uncertainty exists as to the reimbursement
status of a newly approved healthcare product. Adequate third-party coverage may
not be available to enable us to maintain price levels sufficient to realize an
appropriate return on our investment in product research and development. If
adequate coverage and reimbursement levels are not provided by government and
third-party payors for use of our products, our products may fail to achieve
market acceptance.
Our
future revenues, profitability and access to capital will be affected by the
continuing efforts of governmental and private third-party payors to contain or
reduce the costs of healthcare through various means. We expect that a number of
federal, state and foreign proposals will seek to control the cost of drugs
through governmental regulation. We are unsure of the form that any healthcare
reform legislation may take or what actions federal, state, foreign and private
payors may take in response to any proposed reforms. Therefore, we cannot
predict the effect of any implemented reform on our business.
If
product liability lawsuits are successfully brought against us, we may incur
substantial liabilities and may be required to limit commercialization of our
product candidates.
The
testing and marketing of pharmaceutical products entail an inherent risk of
product liability. Product liability claims might be brought against us by
consumers, healthcare providers, pharmaceutical companies or others selling our
future products. If we cannot successfully defend ourselves against such claims,
we may incur substantial liabilities or be required to limit the
commercialization of our product candidates. We have product liability insurance
that covers our commercialized product and human clinical trials in an amount
equal to up to $10 million annual aggregate limit with a $0.1 million deductible
per claim. The amount of insurance that we currently hold may not be adequate to
cover all liabilities that may occur. However, insurance coverage is becoming
increasingly expensive, and no assurance can be given that we will be able to
maintain insurance coverage at a reasonable cost or in sufficient amounts to
protect us against losses due to liability. We will explore, on an on-going
basis, expanding our insurance coverage related to the sale of Treximet and for
the inclusion of future marketed products when we obtain marketing approval for
such products and commercial sales of such products begin. However, we may not
be able to obtain commercially reasonable product liability insurance for any
products approved for marketing. If a plaintiff brings a successful product
liability claim against us in excess of our insurance coverage, if any, we may
incur substantial liabilities and our business may be harmed or
fail.
We
may need additional funding and may not have access to capital. If we are unable
to raise capital when needed, we may need to delay, reduce or eliminate our
product development or commercialization efforts.
In the
future, we may need to raise additional funds to execute our business strategy.
We have incurred losses from operations since inception and we may continue to
incur additional operating losses. Our actual capital requirements will depend
upon numerous factors, including:
|
·
|
the
progress of our research and development programs;
|
|
·
|
the
progress of preclinical studies, clinical and other testing or the need
conduct additional trials, studies or other testing;
|
|
·
|
the
time and cost involved in obtaining any regulatory
approvals;
|
|
·
|
the
costs of filing, prosecuting, defending and enforcing any patent claims
and other intellectual property rights;
|
|
·
|
the
effect of competing technological and market
developments;
|
|
·
|
the
timing of our receipt, if any, of milestone payments and royalties under
collaborative agreements;
|
|
·
|
the
effect of changes and developments in, or termination of, our
collaborative, license and other relationships;
|
|
·
|
the
terms and timing of any additional collaborative, license and other
arrangements that we may establish; and
|
|
·
|
our
ability to commercialize or arrange for the commercialization of our
product candidates.
|
Our operating expenses for the fiscal
year ended December 31, 2009 totaled $40.2 million, ($34.7 million net of
development revenue received from AstraZeneca for development activities
performed under the agreement) including non-cash compensation expense of $5.1
million related to stock options and other stock-based awards, primarily
associated with our adoption of SFAS No. 123(R) on January 1, 2006. For fiscal
years 2007 through 2009, our average annual operating expenses (including
average non-cash deferred compensation of $5.2 million) were $55.3 million
($37.9 million net of development revenue received from AstraZeneca for
development activities performed under the agreement). As of December 31, 2009,
we had an aggregate of $46.7 million in cash, cash equivalents and short-term
investments. Our operating expenses for 2010 and 2011 may exceed the net level
of our operating expenses in 2009, should we decide to conduct
pre-commercialization activities as a result of our decision to retain control
of our PA product candidate. We believe that we will have sufficient cash
reserves and cash flow to maintain that level of business activities through
2011. However, our anticipated cash flow includes continued receipt of royalty
revenue from GSK’s sale of Treximet, an assumption of additional, new royalty
revenue from AstraZeneca’s sale of VIMOVO and an assumption that we will receive
milestone payments upon VIMOVO’s regulatory approvals, including a $20.0 million
milestone payment upon FDA approval of VIMOVO. In addition, our expenses might
increase during that period beyond currently expected levels if we decide to, or
any regulatory agency requires us to, conduct additional clinical trials,
studies or investigations for any of our product candidates, including in
connection with the agency’s consideration, or reconsideration, of our
regulatory filings for our product candidates. In the event FDA approval of the
market launch of VIMOVO is materially delayed, royalty revenue and cash receipts
from sales of the product would also be delayed. If our projected revenues
decrease, if our projected expenses increase for product candidates currently in
development, or if we pursue additional indications for our PA product
candidate, then, as a result of these or other factors, we may need to raise
additional capital.
We may be
unable to raise additional equity funds when we desire to do so due to
unfavorable market conditions in our industry or generally, or other unforeseen
developments in our business. Further, we may not be able to find sufficient
debt or equity funding, if at all, on acceptable terms. If we cannot, we may
need to delay, reduce or eliminate research and development programs and
therefore may not be able to execute our business strategy. Further, to the
extent that we obtain additional funding through collaboration and licensing
arrangements, it may be necessary for us to give up valuable rights to our
development programs or technologies or grant licenses on terms that may not be
favorable to us.
The sale
by us of additional equity securities or the expectation that we will sell
additional equity securities may have an adverse effect on the price of our
common stock.
We
depend on key personnel and may not be able to retain these employees or recruit
additional qualified personnel, which would harm our research and development
efforts.
We are highly dependent on the efforts
of our key management and scientific personnel, especially John R. Plachetka,
Pharm.D., our Chairman, President and Chief Executive Officer. Dr. Plachetka
signed an amended and restated employment agreement with us on March 14, 2006,
which was amended on September 28, 2007, for a three-year term with automatic
one-year renewal terms. We have also entered into employment agreements with
certain of our other key management personnel, which provide for one or two-year
terms with automatic one-year renewal terms which were amended on September 28,
2007. If we should lose the services of Dr. Plachetka, or are unable to replace
the services of our other key personnel who may leave the Company, such as Dr.
Everardus Orlemans, Ph.D., Senior Vice President, Product Development, John G.
Fort, M.D., Chief Medical Officer, William L. Hodges, Senior Vice President
Finance and Administration and Chief Financial Officer, or Elizabeth A. Cermak,
Executive Vice President and Chief Commercial Officer, or if we fail to recruit
other key scientific personnel, we may be unable to achieve our business
objectives. There is intense competition for qualified scientific personnel.
Since our business is very science-oriented, we need to continue to attract and
retain such people. We may not be able to continue to attract and retain the
qualified personnel necessary for developing our business. Furthermore, our
future success may also depend in part on the continued service of our other key
management personnel and our ability to recruit and retain additional personnel,
as required by our business.
Risks
Related to Potential Commercialization of our Product Candidates
We
are currently evaluating the commercial opportunities for our current product
candidates in connection with our development of a worldwide commercialization
strategy. If we decide to pursue the commercial opportunities for our future
products ourselves and we are unable to develop sales and marketing capabilities
on our own, or through contract sales forces or acquisition, we will not be able
to fully exploit the commercial potential of our future products and the costs
of pursuing such a strategy may have a material adverse impact on our results of
operations.
Although we do not have sales and
marketing experience, we are currently evaluating the commercial opportunities
for our product candidates in connection with our development of a worldwide
commercialization strategy. If we decide to pursue commercialization
opportunities for our future products ourselves, we anticipate making
significant expenditures to grow a sales force to sell such products and expand
our marketing capabilities to support such growth. In order to successfully
exploit our future products, we must successfully market and sell our products
and establish or develop the needed third party contracts to market and
distribute these products. Any failure or extended delay in the expansion of our
sales and marketing capabilities or inability to effectively operate in the
marketplace could adversely impact our business. There can be no assurance that
if we decide to pursue commercialization opportunities ourselves that our sales
and marketing efforts will generate significant revenues and costs of pursuing
such a strategy may have a material adverse impact on our results of operations.
Events or factors that may inhibit or hinder our commercialization efforts
include:
|
●
·
|
developing
our own commercial team will be expensive and time-consuming and could
result in high cash burn or reduced profitability;
|
|
●
·
|
failure
to acquire sufficient or suitable personnel to establish, oversee, or
implement our commercialization strategy;
|
|
●
·
|
failure
to recruit, train, oversee and retain adequate numbers of effective sales
and marketing personnel;
|
|
●
·
|
failure
to acquire sales personnel that can effectively obtain access to or
persuade adequate numbers of physicians to prescribe our
products;
|
|
●
·
|
unforeseen
costs and expenses associated with creating or acquiring and sustaining an
independent sales and marketing organization;
|
|
●
·
|
incurrence
of costs in advance of anticipated revenues and subsequent failure to
generate sufficient revenue to offset additional costs;
and
|
|
●
·
|
our
ability to fund our commercialization efforts on terms acceptable to us,
if at all.
|
If
we decide to pursue commercialization opportunities for our future products
ourselves, failure to comply with the laws governing the marketing and sale of
such future products may result in regulatory agencies taking action against us,
which could significantly harm our business.
If we decide to pursue commercial
opportunities for our future products ourselves, we will be subject to a large
body of legal and regulatory requirements. In particular, there are many
federal, state and local laws that we will need to comply with if we become
engaged in the marketing, promoting, distribution and sale of pharmaceutical
products. The FDA extensively regulates, among other things, promotions and
advertising of prescription drugs. In addition, the marketing and
sale
of
prescription drugs must comply with the Federal fraud and abuse laws, which are
enforced by the Office of the Inspector General of the Division, or OIG, of the
Department of Health and Human Services. These laws make it illegal for anyone
to give or receive anything of value in exchange for a referral for a product or
service that is paid for, in whole or in part, by any federal health program.
The federal government can pursue fines and penalties under the Federal False
Claims Act which makes it illegal to file, or induce or assist another person in
filing, a fraudulent claim for payment to any governmental agency. Because, as
part of our commercialization efforts, we may provide physicians with samples we
will be required to comply with the Prescription Drug Marketing Act, or PDMA,
which governs the distribution of prescription drug samples to healthcare
practitioners. Among other things, the PDMA prohibits the sale, purchase or
trade of prescription drug samples. It also sets out record keeping and other
requirements for distributing samples to licensed healthcare
providers.
In addition, we will need to comply
with the body of laws comprised of the Medicaid Rebate Program, the Veterans’
Health Care Act of 1992 and the Deficit Reduction Act of 2005. This body of law
governs product pricing for government reimbursement and sets forth detailed
formulas for how we must calculate and report the pricing of our products so as
to ensure that the federally funded programs will get the best price. Moreover,
many states have enacted laws dealing with fraud and abuse, false claims, the
distribution of prescription drug samples and gifts and the calculation of best
price. These laws typically mirror the federal laws but in some cases, the state
laws are more stringent than the federal laws and often differ from state to
state, making compliance more difficult. We expect more states to enact similar
laws, thus increasing the number and complexity of requirements with which we
would need to comply.
Compliance with this body of laws is
complicated, time consuming and expensive. Because we do not have experience in
developing, managing and training our employees regarding, a comprehensive
healthcare compliance program, we cannot assure you that we will be in
compliance with all potentially applicable laws and regulations. Even minor,
inadvertent irregularities can potentially give rise to claims that the law has
been violated. Failure to comply with all potentially applicable laws and
regulations could lead to penalties such as the imposition of significant fines,
debarment from participating in drug development and marketing and the exclusion
from government-funded healthcare programs. The imposition of one or more of
these penalties could adversely affect our revenues and our ability to conduct
our business as planned.
In addition, the Federal False Claims
Act, which allows any person to bring suit alleging the false or fraudulent
submission of claims for payment under federal programs and other violations of
the statute and to share in any amounts paid by the entity to the government in
fines or settlement. Such suits, known as qui tam actions, have increased
significantly in recent years and have increased the risk that companies like us
may have to defend a false claim action. We could also become subject to similar
false claims litigation under state statutes. If we are unsuccessful in
defending any such action, such action may have a material adverse effect on our
business, financial condition and results of operations.
Factors
That May Affect Our Stockholders
Our
stock price is volatile, which may result in significant losses to
stockholders.
There has
been significant volatility in the market prices of biotechnology companies’
securities. Various factors and events may have a significant impact on the
market price of our common stock. These factors include:
|
·
|
fluctuations
in our operating results;
|
|
·
|
announcements
of technological innovations, acquisitions or licensing of therapeutic
products or product candidates by us or our
competitors;
|
|
·
|
published
reports by securities analysts;
|
|
·
|
positive
or negative progress with our clinical trials or with regulatory approvals
of our product candidates;
|
|
·
|
commercial
success of Treximet and our other products in the marketplace once
approved;
|
|
·
|
governmental
regulation, including reimbursement
policies;
|
|
·
|
developments
in patent or other proprietary
rights;
|
|
·
|
developments
in our relationships with collaborative
partners;
|
|
·
|
announcements
by our collaborative partners regarding our products or product
candidates;
|
|
·
|
developments
in new or pending litigation;
|
|
·
|
public
concern as to the safety and efficacy of our products;
and
|
|
·
|
general
market conditions.
|
The
trading price of our common stock has been, and could continue to be, subject to
wide fluctuations in response to these factors, including the sale or attempted
sale of a large amount of our common stock into the market. From October 16,
2000, when our common stock began trading on The NASDAQ National Market (now
known as The NASDAQ Global Market), through February 20, 2009, the high and low
sales prices of our common stock ranged from $2.25 to $21.75. Broad market
fluctuations may also adversely affect the market price of our common
stock.
Sales
of substantial amounts of our common stock in the public market by us or our
largest stockholders could depress our stock price.
We have
not sold shares of common stock in a public offering since our initial public
offering in October 2000. Accordingly, we have a relatively small number of
shares that are traded in the market. Approximately 14% of our outstanding
shares are beneficially held by John Plachetka, our President and Chief
Executive Officer. Additionally, we believe, based upon our review of public
filings by certain stockholders and other publicly available information, an
aggregate of approximately 25% of our outstanding share are held by four other
stockholders, with no one stockholder beneficially owning greater than 9% of our
outstanding shares. Any sales of substantial amounts of our common stock in the
public market, including sales or distributions of shares by our large
stockholders, or the perception that such sales or distributions might occur,
could harm the market price of our common stock and could impair our ability to
raise capital through the sale of additional equity securities. For example, our
executive officers may sell shares pursuant to a Rule 10b5-1 trading plans.
Further, stockholders’ ownership will be diluted if we raise additional capital
by issuing equity securities. We filed with the Securities and Exchange
Commission a shelf registration statement on Form S-3, which became effective
January 15, 2009, for an offering under which we may register up to 8,540,000
shares of our common stock for sale to the public in one or more public
offerings. Certain selling stockholders named in the prospectus for the
registration statement may offer up to 540,000 of such shares, and we would not
receive any of the proceeds from sales of those shares. Purchasers of our common
stock in any future offerings by us will incur immediate dilution to the extent
of the difference between our net tangible book value per share after the
offering and the price paid per share by new investors.
Anti-takeover
provisions in our charter documents and under Delaware law could prevent or
delay transactions that our stockholders may favor and may prevent stockholders
from changing the direction of our business or our management.
Provisions
of our charter and bylaws may discourage, delay or prevent a merger or
acquisition that our stockholders may consider favorable, including transactions
in which you might otherwise receive a premium for your shares, and may also
frustrate or prevent any attempt by stockholders to change the direction or
management of POZEN. For example, these provisions:
|
·
|
authorize
the issuance of “blank check” preferred stock without any need for action
by stockholders;
|
|
·
|
provide
for a classified board of directors with staggered three-year
terms;
|
|
·
|
require
supermajority stockholder approval to effect various amendments to our
charter and bylaws;
|
|
·
|
eliminate
the ability of stockholders to call special meetings of
stockholders;
|
|
·
|
prohibit
stockholder action by written consent;
and
|
|
·
|
establish
advance notice requirements for nominations for election to the board of
directors or for proposing matters that can be acted on by stockholders at
stockholder meetings.
|
Further,
in January 2005 our board of directors adopted a stockholder rights plan,
similar to plans adopted by many other publicly-traded companies. The
stockholder rights plan is intended to deter an attempt to acquire us in a
manner or on terms not approved by our board of directors.
Sales
of substantial amounts of our common stock in the public market by us or our
largest stockholders could depress our stock price.
We have
not sold shares of common stock in a public offering since our initial public
offering in October 2000. Accordingly, we have a relatively small number of
shares that are traded in the market. Approximately 14% of our outstanding
shares are beneficially held by John Plachetka, our President and Chief
Executive Officer. Additionally, we believe, based upon our review of public
filings by certain stockholders and other publicly available information, an
aggregate of approximately 25% of our outstanding share are held by four other
stockholders, with no one stockholder beneficially owning greater than 9% of our
outstanding shares. Any sales of substantial amounts of our common stock in the
public market, including sales or distributions of shares by our large
stockholders, or the perception that such sales or distributions might occur,
could harm the market price of our common stock and could impair our ability to
raise capital through the sale of additional equity securities. For example, our
executive officers may sell shares pursuant to a Rule 10b5-1 trading plans.
Further, stockholders’ ownership will be diluted if we raise additional capital
by issuing equity securities. We filed with the Securities and Exchange
Commission a shelf registration statement on Form S-3, which became effective
January 15, 2009, for an offering under which we may register up to 8,540,000
shares of our common stock for sale to the public in one or more public
offerings. Certain selling stockholders named in the prospectus for the
registration statement may offer up to 540,000 of such shares, and we would not
receive any of the proceeds from sales of those shares. Purchasers of our common
stock in any future offerings by us will incur immediate dilution to the extent
of the difference between our net tangible book value per share after the
offering and the price paid per share by new investors.
Anti-takeover
provisions in our charter documents and under Delaware law could prevent or
delay transactions that our stockholders may favor and may prevent stockholders
from changing the direction of our business or our management.
Provisions
of our charter and bylaws may discourage, delay or prevent a merger or
acquisition that our stockholders may consider favorable, including transactions
in which you might otherwise receive a premium for your shares, and may also
frustrate or prevent any attempt by stockholders to change the direction or
management of POZEN. For example, these provisions:
|
·
|
authorize
the issuance of “blank check” preferred stock without any need for action
by stockholders;
|
|
·
|
provide
for a classified board of directors with staggered three-year
terms;
|
|
·
|
require
supermajority stockholder approval to effect various amendments to our
charter and bylaws;
|
|
·
|
eliminate
the ability of stockholders to call special meetings of
stockholders;
|
|
·
|
prohibit
stockholder action by written consent;
and
|
|
·
|
establish
advance notice requirements for nominations for election to the board of
directors or for proposing matters that can be acted on by stockholders at
stockholder meetings.
|
Further,
in January 2005 our board of directors adopted a stockholder rights plan,
similar to plans adopted by many other publicly-traded companies. The
stockholder rights plan is intended to deter an attempt to acquire us in a
manner or on terms not approved by our board of directors.
None.
Since
March 2002, our corporate facilities have been located in 17,000 square feet in
the Exchange Office Building in Chapel Hill, North Carolina under a lease
commencing in March 2002 and expiring in 2010. We have exercised our option to
renew this lease for an additional five year and seven month term, terminating
on September 30, 2015, and we have an additional option to renew the extended
term for one additional three year period. We believe that the Exchange Office
Building facility is adequate for our current needs and that suitable additional
or alternative space will be available in the future on commercially reasonable
terms.
A purported class action lawsuit
claiming violations of securities laws was filed on August
10, 2007 in the U.S. District Court for the Middle District of North
Carolina by a holder of its securities against the Company, its chairman
and chief executive officer and one of its directors. The complaint alleges,
among other claims, violations of Section 10(b), Rule 10b-5, and Section 20(a)
of the Exchange Act arising out of allegedly false and misleading statements
made by the Company concerning its migraine drug candidate, Treximet, during the
purported class period, July 31, 2006 through August 1, 2007. By order dated
February 15, 2008, the Court appointed joint co-lead plaintiffs. On April
25, 2008, the Company received the plaintiffs’ amended and consolidated
complaint which added two current officers of the Company as additional
defendants. The Company and individual defendants filed a motion to dismiss the
amended and consolidated complaint with the Court on June 26, 2008. On August
27, 2008, the plaintiffs voluntarily dismissed their claims against one of the
Company's directors. On February 19, 2009, Magistrate Judge Dixon, to whom
the Court had referred the motion to dismiss, issued a Recommendation that the
Court grant the Company and individual defendants' motion to dismiss without
leave for plaintiffs to file another amended complaint. Plaintiffs filed
objections to the recommendation on March 23, 2009 and a corrected version of
the objections on March 26, 2009. Defendants’ response to these objections was
filed on April 20, 2009. On September 29, 2009, the Court granted the Company’s
and individual defendants’ motion to dismiss and dismissed the claims in their
entirety with prejudice. The plaintiffs have chosen not to appeal the
case.
The
Company and GSK have received Paragraph IV Notice Letters from Par, Alphapharm,
Alphapharm’s designated agent, Mylan, Teva and Dr. Reddy’s, informing us that
each company had filed an Abbreviated New Drug Application, or ANDA, with
the Food and Drug Administration, or FDA, seeking approval to market sumatriptan
85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr. Reddy’s have
each indicated in their respective Notice Letters that they intend to market a
generic version of Treximet tablets before the expiration of U.S. Patent Nos.
6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has elected not to
exercise its first right to bring infringement suits against Par, Alphapharm,
Teva and Dr. Reddy’s. Accordingly, we filed suit against Par on November 14,
2008, Alphapharm and Mylan on January 2, 2009, Teva on April 14, 2009, and Dr.
Reddy’s on August 21, 2009, all in the United States District Court for the
Eastern District of Texas. All four actions have since been consolidated into
one suit. The Company’s filing of these patent infringement lawsuits within
forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm, Teva and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s, Teva’s and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
As with any litigation proceeding, we
cannot predict with certainty the eventual outcome of the class action lawsuit
described above if appealed or the patent infringement lawsuits against Par,
Alphapharm, Teva and Dr. Reddy’s. Furthermore, we will have to incur expenses in
connection with these lawsuits, which may be substantial. In the event of an
adverse outcome or outcomes, our business could be materially harmed. Moreover,
responding to and defending pending litigation will result in a significant
diversion of management’s attention and resources and an increase in
professional fees.
None
Market
Price of and Dividends on the Registrant’s Common Equity
Our
common stock began trading on the NASDAQ National Market (now known as the
NASDAQ Global Market) under the symbol “POZN” on October 11, 2000. As of
February 5, 2010, we estimate that we had approximately 100 stockholders of
record and approximately 5,370 beneficial holders of the common
stock.
The
following table details the high and low sales prices for the common stock as
reported by The NASDAQ Global Market for the periods indicated.
|
Price
Range
|
||||||||
|
2009 Fiscal Year
|
High
|
Low
|
||||||
|
First
Quarter
|
$ | 8.39 | $ | 4.50 | ||||
|
Second
Quarter
|
$ | 8.42 | $ | 5.76 | ||||
|
Third
Quarter
|
$ | 8.19 | $ | 5.85 | ||||
|
Fourth
Quarter
|
$ | 8.00 | $ | 5.16 | ||||
|
Price
Range
|
||||||||
|
2008 Fiscal Year
|
High
|
Low
|
||||||
|
First
Quarter
|
$ | 13.63 | $ | 9.61 | ||||
|
Second
Quarter
|
$ | 14.85 | $ | 9.81 | ||||
|
Third
Quarter
|
$ | 13.48 | $ | 9.50 | ||||
|
Fourth
Quarter
|
$ | 10.91 | $ | 4.61 | ||||
On
February 5, 2010, the closing price for our common stock as reported by the
NASDAQ Global Market was $5.84. We paid no cash dividends in 2009 or 2008. We
currently intend to retain all of our future earnings to finance the growth and
development of our business and do not anticipate paying any cash dividends in
the foreseeable future.
Equity
Compensation Plans
The
following table provides information with respect to our compensation plans
under which equity compensation is authorized as of December 31,
2009.
|
Plan
Category
|
Number of securities to
be
issued upon exercise
of
outstanding options,
warrants
and rights
|
Weighted-average
exercise
price of
outstanding options,
warrants
and rights
|
Number of securities
remaining
available
for
future issuance
under
equity
compensation
plans
|
|||||||||
|
Equity
compensation plans approved by security holders(1)
|
4,093,068 | $ | 9.25 | 1,298,505 | ||||||||
|
Equity
compensation plans not approved by security holders
|
— | — | — | |||||||||
|
Total
|
4,093,068 | $ | 9.25 | 1,298,505 | ||||||||
________
|
(1)
|
Excludes
113,785 restricted stock units issued under our 2000 Equity Compensation
Plan, as amended and restated, to our president and chief executive
officer along with our board of directors
members.
|
Stock
Performance Graph
The
following graph compares the yearly change in the total stockholder return on
our common stock during the period from December 31, 2004 through December
31, 2009 with the total return on the NASDAQ Composite Index, the NASDAQ
Biotechnology Index and the NASDAQ Pharmaceutical Index. The comparison assumes
that $100 was invested on December 31, 2004 in our common stock and in each of
the foregoing indices and assumes reinvestment of dividends, if
any.
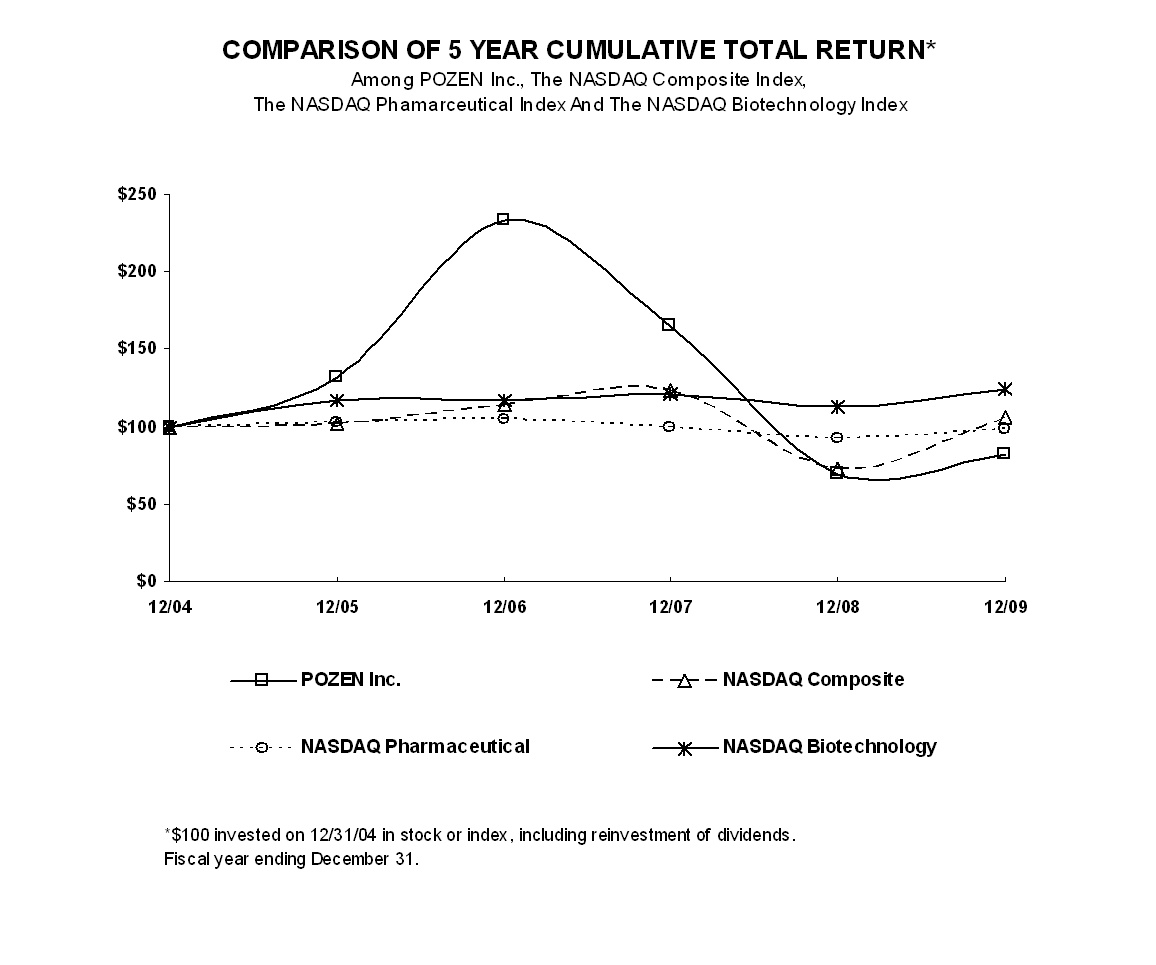
The
following selected financial data are derived from the financial statements of
POZEN Inc., which have been audited by Ernst & Young LLP, independent
registered public accounting firm. The data should be read in conjunction with
the financial statements, related notes and other financial information included
(and incorporated by reference) herein.
|
For
the Year Ended December 31,
|
||||||||||||||||||||
|
2005
|
2006
|
2007
|
2008
|
2009
|
||||||||||||||||
|
|
(in
thousands, except per share data)
|
|
||||||||||||||||||
|
Statement
of Operations Data:
|
|
|
|
|
|
|||||||||||||||
|
Revenue:
|
||||||||||||||||||||
|
Licensing
revenue
|
$
|
28,419
|
$
|
8,682
|
$
|
34,459
|
$
|
37,221
|
$
|
26,651
|
||||||||||
|
Development
revenue
|
228
|
4,835
|
18,985
|
28,912
|
5,536
|
|||||||||||||||
|
Total
revenue
|
28,647
|
13,517
|
53,444
|
66,133
|
32,187
|
|||||||||||||||
|
Operating
expenses:
|
|
|
|
|
|
|||||||||||||||
|
General
and administrative
|
|
|
9,185
|
|
|
|
12,822
|
|
|
|
11,474
|
|
|
|
12,315
|
|
|
|
17,767
|
|
|
Research
and development
|
|
|
18,769
|
|
|
|
22,359
|
|
|
|
39,963
|
|
|
|
61,934
|
|
|
|
22,448
|
|
|
Total
operating expenses
|
|
|
27,954
|
|
|
|
35,181
|
|
|
|
51,437
|
|
|
|
74,249
|
|
|
|
40,215
|
|
|
Interest
and other income
|
|
|
1,266
|
|
|
|
2,354
|
|
|
|
3,326
|
|
|
|
2,140
|
|
|
|
535
|
|
|
Income
(loss) before income tax (expense) benefit
|
1,959
|
(19,310)
|
5,333
|
(5,976
|
)
|
(7,493
|
)
|
|||||||||||||
|
Income
tax (expense) benefit
|
—
|
—
|
(667
|
)
|
—
|
634
|
||||||||||||||
|
Net
income (loss) attributable to common stockholders
|
|
$
|
1,959
|
|
$
|
(19,310
|
)
|
|
$
|
4,666
|
|
$
|
(5,976
|
)
|
|
$
|
(6,859
|
)
|
||
|
Basic
net income (loss) per common share
|
|
$
|
0.07
|
|
$
|
(0.66
|
)
|
|
$
|
0.16
|
|
$
|
(0.20
|
)
|
|
$
|
(0.23
|
)
|
||
|
Shares
used in computing basic net income (loss) per common share
|
|
|
28,939
|
|
|
|
29,225
|
|
|
|
29,593
|
|
|
|
29,762
|
|
|
|
29,814
|
|
|
Diluted
net income per common share
|
|
$
|
0.07
|
|
$
|
(0.66
|
)
|
|
$
|
0.15
|
|
$
|
(0.20
|
)
|
|
$
|
(0.23
|
)
|
||
|
Shares
used in computing diluted net income per common share
|
|
|
29,623
|
|
|
|
29,225
|
|
|
30,581
|
|
|
29,762
|
|
|
29,814
|
||||
|
December
31,
|
||||||||||||||||||||
|
2005
|
2006
|
2007
|
2008
|
2009
|
||||||||||||||||
|
(in
thousands)
|
||||||||||||||||||||
|
Balance
Sheet Data:
|
|
|
|
|
|
|||||||||||||||
|
Cash,
cash equivalents and short-term investments
|
|
$
|
45,838
|
|
|
$
|
62,582
|
|
|
$
|
73,942
|
|
|
$
|
61,682
|
|
|
$
|
46,710
|
|
|
Total
assets
|
|
|
46,687
|
|
|
|
67,141
|
|
|
|
77,387
|
|
|
|
70,436
|
|
|
|
49,160
|
|
|
Total
liabilities
|
|
|
12,788
|
|
|
|
43,027
|
|
|
|
42,136
|
|
|
|
34,784
|
|
|
|
15,402
|
|
|
Accumulated
deficit
|
|
|
(112,521
|
)
|
|
|
(131,831
|
)
|
|
|
(127,165
|
)
|
|
|
(133,140
|
)
|
|
|
(139,999
|
)
|
|
Total
stockholders’ equity
|
|
|
33,899
|
|
|
|
24,114
|
|
|
|
35,251
|
|
|
|
35,652
|
|
|
|
33,758
|
|
Overview
We are a pharmaceutical company
focused on transforming medicine that can transform lives. We operate a business
model that focuses on the following:
|
·
|
developing
innovative product candidates that address unmet needs in the
marketplace;
|
|
·
|
obtaining
patents for those innovative ideas which we believe have value in the
marketplace;
|
|
·
|
utilizing
a small group of talented employees to develop those ideas by working with
strategic outsource partners;
|
|
·
|
developing
a regulatory pathway with the appropriate agency;
and
|
|
·
|
determining
how best to commercialize our products. In the United States, we intend to
lead all commercialization efforts, which may or may not include a
co-promotion partner. Outside the United States, we presently intend to
secure one or more strong commercial partners with relevant expertise
through which we will commercialize our future products
globally.
|
We hire experts with seasoned project
management skills in the specific disciplines we believe are important to
maintain within our company. We contract with and manage experienced outsource
partners as we complete the necessary development work, permitting us to avoid
incurring the cost of buying or building laboratories, manufacturing facilities
or clinical research operation sites. This allows us to control our annual
expenses, but to utilize “best in class” resources as required. We have decided
to retain ownership of our PA product candidates which contain a combination of
a proton pump inhibitor and enteric coated aspirin in a single tablet and have
hired a chief commercial officer who is responsible for developing the
commercialization strategy for these products and conducting all the required
pre-commercialization activities. As we commercialize in the United States, we
intend to continue utilizing our outsource model to develop a 21st
century commercial organization, which would include hiring an internal
commercial team to develop strategy and to direct strategic outsource partners
in the implementation of such strategy.
The success of our business is highly
dependent on the marketplace value of our ideas and the related patents we
obtain, our ability to obtain from the required regulatory agencies approval to
sell the developed products and our ability to find strong commercial partners
to successfully commercialize the products or to successfully commercialize the
products ourselves.
We have
developed Treximet® in
collaboration with GlaxoSmithKline, or GSK. Treximet is the brand name for the
product combining sumatriptan 85 mg, formulated with RT Technology™ and naproxen
sodium 500 mg in a single tablet designed for the acute treatment of migraine.
On April 15, 2008, the FDA approved Treximet for the acute treatment of migraine
attacks with or without aura in adults. Upon receipt of FDA approval, GSK
notified us of its intention to launch the product and Treximet was available in
pharmacies in May 2008.
Treximet
incorporates our MT 400 technology, which refers to our proprietary combinations
of a triptan (5-HT1B/1D
agonist) and a non-steroidal anti-inflammatory drug, or NSAID. Under our MT 400
technology, we sought to develop product candidates that provide acute migraine
therapy by combining the activity of two drugs that act by different mechanisms
to reduce the pain and associated symptoms of migraine. We filed the NDA for
Treximet with the FDA in August 2005, and in June 2006 we received an approvable
letter requiring us to provide certain additional safety information relating to
Treximet, some of which required new studies. An approvable letter is an
official notification from the FDA that contains conditions that must be
satisfied prior to obtaining final U.S. marketing approval. In early January
2007, we delivered a full response to this approvable letter that provided
additional data and analyses and supporting information addressing the FDA’s
safety concerns, including cardiovascular safety. On August 1, 2007, we received
a second approvable letter from the FDA for Treximet in which the FDA requested
that we further address the FDA’s concern about the product’s potential for
genotoxicity. In response to this approvable letter, we submitted the results of
three non-clinical (in vitro) studies that provided clarifying information about
the Chinese Hamster Ovary, or CHO, assay and data from a clinical evaluation of
the genotoxic potential of Treximet in human volunteers which indicated that no
chromosomal aberrations were induced in peripheral blood lymphocytes when
Treximet was administered to volunteers for seven days. On April 15, 2008, the
FDA approved Treximet for the acute treatment of migraine attacks with or
without aura in adults.
We are
also developing product candidates that combine a type of acid inhibitor, a
proton pump inhibitor, or PPI, with an NSAID (our PN program). These product
candidates are intended to provide management of pain and inflammation
associated with conditions such as osteoarthritis, and are intended to have
fewer gastrointestinal complications compared to an NSAID taken
alone.
In August 2006, we entered into an
exclusive global collaboration and license agreement with AstraZeneca AB, or
AstraZeneca, to co-develop and commercialize proprietary fixed dose combinations
of the PPI esomeprazole magnesium with the NSAID naproxen in a single tablet
using our PN formulation technology, which agreement was amended in September
2007 and October 2008. We began the Phase 3 program in September 2007. As part
of the program, we conducted two Phase 3 pivotal trials of VIMOVO™ (formerly
referred to as PN 400) in patients who are at risk for developing
NSAID-associated gastric ulcers, the primary endpoint for which was the
reduction in endoscopic gastric ulcers. In October 2008, the FDA informed us
that it was conducting an internal review of the acceptability of using
endoscopic gastric ulcers as a primary endpoint in clinical trials. In late
January 2009, the FDA informed us that it had completed its internal discussions
and that there was no change to previous agreements that gastric ulcer incidence
was an acceptable primary endpoint for POZEN’s clinical programs. The two
pivotal trials have been completed and met their primary endpoints. In both
trials, patients taking VIMOVO experienced significantly (p<0.001) fewer
endoscopically confirmed gastric ulcers compared to subjects
receiving
enteric-coated
naproxen during the six-month treatment period with gastric ulcer incidence
rates of 4.1 and 7.1% for VIMOVO and 23.1 and 24.3% for enteric-coated naproxen
in studies 301 and 302, respectively. Data combined from both studies showed
that in patients taking low dose aspirin (n=201), the incidence of gastric
ulcers in the VIMOVO arm was 3.0% compared to 28.4% for those taking EC naproxen
(p<0.001) and patients taking VIMOVO who were not taking low dose aspirin
(n=653) experienced a 6.4% incidence of gastric ulcers compared to 22.2% among
those taking EC naproxen (p<0.001). Additional analyses examined the
incidence of endoscopically confirmed duodenal ulcers among patients taking
VIMOVO. In study 301, patients taking VIMOVO experienced a 0.5% incidence of
duodenal ulcers compared to 5.1% taking EC naproxen (p=0.003), and in study 302,
patients taking VIMOVO experienced a 1.0% incidence of duodenal ulcers, compared
to 5.7% incidence among patients taking EC naproxen (p=0.007). The most
frequently reported adverse events among patients taking both VIMOVO and enteric
coated naproxen in the pivotal trials were GI disorders, including dyspepsia,
erosive esophagitis and erosive duodenitis. In addition to the Phase 3 pivotal
trials, we have completed a long-term, open label safety study. We terminated a
non-pivotal smaller study in patients at high risk of gastrointestinal related
events from NSAIDs which we believe is not required for approval. We also
conducted additional studies at AstraZeneca’s expense. The NDA for VIMOVO was
submitted on June 30, 2009 and was accepted for filing in August 2009. POZEN
received a $10 million milestone payment from AstraZeneca in September 2009 for
the achievement of such milestone. On October 15, 2009, AstraZeneca submitted a
Marketing Authorization Application (MAA) for VIMOVO in the European Union via
the Decentralized Procedure.
Our other product candidate, PA, a
combination of a PPI and aspirin, is currently in formulation and clinical
development testing. Our PA product candidates are excluded from our agreement
with AstraZeneca. We have met with the FDA to discuss the overall development
program requirements. An investigational new drug application, or IND, was filed
in the fourth quarter of 2007. We have completed a study which demonstrated the
bioequivalence of the salicylic acid component of PA32540 as compared to 325 mg
of enteric-coated aspirin which we believe will satisfy the FDA’s bioequivalence
requirement. We filed a Special Protocol Assessment, or SPA, with the FDA for
the design of the Phase 3 studies for the product, the primary endpoint for
which is the reduction in endoscopic gastric ulcers. The SPA is a process by
which the FDA and a company reach agreement on the Phase 3 pivotal trial
protocol design, clinical endpoints and statistical analyses that are acceptable
to support regulatory approval. In October 2008, the FDA informed us that it was
conducting an internal review of the acceptability of using endoscopic gastric
ulcers as a primary endpoint in clinical trials. In late January 2009, the FDA
informed us that it had completed its internal discussions and that there was no
change to previous agreements that gastric ulcer incidence was an acceptable
primary endpoint for our clinical programs. In February 2009, we received
written confirmation from the FDA that endoscopic gastric ulcer incidence was an
acceptable primary endpoint for the Phase 3 clinical studies we proposed in our
SPA for PA32540.
We are
aware of publications that contain data regarding a possible drug-drug
interaction between clopidogrel (Plavix®), a
widely prescribed anti-platelet agent, and certain enteric-coated proton pump
inhibitors when platelet aggregation is assessed in ex-vivo tests. On November
11, 2009, the FDA issued new drug safety information to healthcare professionals
through a publication entitled “Information for Healthcare Professionals: Update
to the labeling of Clopidogrel Bisulfate (marketed as Plavix) to alert
healthcare professions about a drug interaction with enteric-coated omeprazole
(marketed as Prilosec® and Prilosec® OTC).” The publication stated
that the effect of clopidogrel on platelets was reduced by as much as 47% in
people receiving clopidogrel and omeprazole together. The FDA’s action was
based, in part, on two crossover clinical studies of 72 healthy subjects
administered Plavix alone and with 80 mg EC omeprazole, either together or
administered 12 hours apart.
To assess
whether a similar interaction occurs between clopidogrel and PA32540, which
contains immediate release omeprazole, we have completed a Phase 1 drug-drug
interaction study to evaluate the ex-vivo platelet aggregation effects of
PA32540 plus clopidogrel dosed at the same time or dosed 10 hours apart compared
to aspirin 325mg plus clopidogrel dosed together. When PA32540 and clopidogrel
were dosed together, data from the study showed a mean 36.7% platelet inhibition
compared to a mean 44.0% platelet inhibition when aspirin and clopidogrel were
dosed together suggesting a drug-drug interaction based on the study’s
pre-specified primary analysis. When PA32540 and clopidogrel were dosed 10 hours
apart, data from the study suggested no ex-vivo drug-drug interaction based on
the study’s pre-specified primary analysis. The relevance of these ex vivo
platelet data on cardiovascular events is not known. Published data
on a clinical interaction between PPIs and Plavix from several randomized
controlled trials in cardiovascular patients have reported no clinical impact on
cardiovascular outcomes [Bhatt et al (COGENT 1 2009) and O’Donoghue et al (TIMI
38 2009)]. FDA assessment of these data and the implication to a
future PA32540 label are not known at this time.
We began Phase 3 studies for PA32540 in
the October 2009. We have decided to retain control of our PA product candidates
and, to that end, have hired a chief commercial officer to evaluate how best to
commercialize these product candidates. We are also conducting both
formulation development and early stage clinical studies with new product
concepts that are currently in the exploratory stage. If warranted, we may file
U.S. and international patent applications with claims directed toward these
novel combinations and formulations.
We have incurred significant losses
since our inception and have not yet generated significant revenue from product
sales. As of December 31, 2009, our accumulated deficit was approximately $140.0
million. We record revenue under two categories: licensing revenues and
development revenues. Our licensing revenues include upfront payments upon
contract signing, additional payments if and when certain milestones in the
product’s development or commercialization are reached, and the royalty payments
based on product sales. Additionally, our development revenues include the
billings for the direct costs and certain personnel-related time incurred in
performing additional development activities described under our collaboration
agreements. Our historical operating losses have resulted principally from our
research and development activities, including clinical trial activities for our
product candidates and general and administrative expenses. Research and
development expenses include salaries and benefits for personnel involved in our
research and development activities and direct development costs, which include
costs relating to the formulation and manufacturing of our product candidates,
costs relating to preclinical studies, including toxicology studies, and
clinical trials, and costs relating to compliance with regulatory requirements
applicable to the development of our product candidates. Since inception, our
research and development expenses have represented approximately 72% of our
total operating expenses. For the twelve months ended December 31, 2009, our
research and development expenses represented approximately 56% of our total
operating expenses.
Operating
losses may be incurred over the next several years as we complete the
development and seek regulatory approval for our product candidates, develop
other product candidates and acquire and develop product portfolios in other
therapeutic areas. Our results may vary depending on many factors,
including:
|
·
|
The
progress of VIMOVO and our PA product candidates and our other product
candidates in the clinical and regulatory process;
|
|
·
|
The
ability of GSK to successfully commercialize Treximet in the U.S. For
example, Treximet was available in pharmacies within one month from the
date of its approval, but promotional and professional materials for the
product, including direct to consumer advertising, were not approved on a
timely basis by the FDA. The lack of approved materials and delayed
advertising launch may have had an adverse impact on uptake of the
product, thus negatively impacting our royalty revenue;
|
|
·
|
The
establishment of new collaborations and progress and/or maintenance of our
existing collaborations for the development and commercialization of any
of our product candidates;
|
|
·
|
Our
ability to successfully defend our patents against generic
challenges;
|
|
·
|
Our
ability to commercialize our products either by ourselves or with
commercial partners in a highly regulated and extremely competitive
marketplace; and
|
|
·
|
The
acquisition and/or in-licensing, and development of our therapeutic
product candidates.
|
We do not currently have
commercialization or manufacturing capabilities. We have entered into
collaborations and may continue to enter into additional collaborations with
established pharmaceutical or pharmaceutical services companies to commercialize
and manufacture our product candidates once approved. We have decided to retain
control of our PA product candidates. To that end, we have hired a chief
commercial officer to evaluate the commercial opportunities for these product
candidates and to develop a worldwide commercial strategy, which will include
developing internal commercialization capabilities to enable us to commercialize
our products ourselves. Our ability to generate revenue in the near term is
dependent upon our ability, alone or with collaborators, to achieve the
milestones set forth in our collaboration agreements, to enter into additional
collaboration agreements, and to successfully develop product candidates, to
obtain regulatory approvals and to successfully manufacture and commercialize
our future products. These milestones are earned when we have satisfied the
criteria set out in our revenue recognition footnote accompanying the financial
statements included elsewhere in this Annual Report on Form 10-K. These payments
generate large non-recurring revenue that will cause large fluctuations in
quarterly and annual profit and loss.
Status
and Expenses Related to Our Product Candidates
There follows a brief discussion of the
status of the development of our product candidates, as well as the costs
relating to our development activities. Our direct research and development
expenses were $16.0 million for the fiscal year ended December 31, 2009, $53.9
million for the fiscal year ended December 31, 2008, and $33.7 million for the
fiscal year ended December 31, 2007. Our research and development expenses that
are not direct development costs consist of personnel and other research and
development departmental costs and are not allocated by product candidate. We
generally do not maintain an allocation of the costs with regard to our
employees’ time by the projects on which they work and, therefore,
are
unable to
identify costs related to the time that employees spend on research and
development by product candidate. Total compensation and benefit costs for our
personnel involved in research and development were $6.2 million for the fiscal
year ended December 31, 2009, $7.6 million for the fiscal year ended December
31, 2008, and $5.9 million for the fiscal year ended December 31, 2007. Total
compensation for the fiscal year ended December 31, 2009 included a $1.7 million
charge for non-cash compensation for stock option expense, a $2.2 million charge
for non-cash compensation for stock option expense for the fiscal year ended
December 31, 2008, and a $1.2 million charge for non-cash compensation for stock
option expense for the fiscal year ended December 31, 2007. Other research and
development department costs were $0.2 million for the fiscal year ended
December 31, 2009, $0.5 million for the fiscal year ended December 31, 2008, and
$0.4 million for the fiscal year ended December 31, 2007.
Treximet.
On April 15, 2008, the FDA approved Treximet for the acute treatment of migraine
attacks with or without aura in adults. GSK notified us of its intention to
launch the product and was available in pharmacies in May 2008. As part of our
NDA program for Treximet, we conducted five Phase 1 trials, two Phase 3 pivotal
trials, and one 12-month open label safety trial using a formulation of Treximet
developed by GSK. The Phase 3 pivotal trials, including the endpoints required
to evaluate Treximet, were designed to demonstrate superiority to placebo for
relief of pain and the associated symptoms of migraine (nausea, photophobia and
phonophobia) at two hours. Additionally, the program was designed to demonstrate
that each component makes a contribution to the efficacy of Treximet (the
“combination drug rule” that the FDA requires of all combination products). The
efficacy endpoint for the combination was sustained pain free, which is defined
as improvement from moderate or severe pain to no pain at two hours and
remaining at no pain through twenty four hours without the use of rescue
medicine. Further, GSK continues to conduct market support studies for Treximet.
As required by the terms of our agreement with GSK, we transferred ownership of
the NDA and other regulatory filings for Treximet to GSK on May 14, 2008, and
GSK now has responsibility for all ongoing regulatory obligations for the
product, including post marketing clinical trial requirements.
We incurred direct development costs associated with the development of MT 400 and Treximet programs of $0.2 million for the fiscal year ended December 31, 2009. We recorded in the fiscal year ended December 31, 2009, $4.3 million of Treximet royalty revenue, of which $1.1 million is in accounts receivable at December 31, 2009. Our direct development costs do not include the cost of research and development personnel or any allocation of our overhead expenses.
We, along
with GSK, have received Paragraph IV Notice Letters from Par, Alphapharm, and
Alphapharm’s designated agent, Mylan, Teva and Dr. Reddy’s informing us that
each company had filed an ANDA with the FDA seeking approval to market
sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva and Dr.
Reddy’s have each indicated in their respective Notice Letters that they intend
to market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008; Alphapharm and Mylan on January 2, 2009, Teva on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. Our filing of these patent infringement lawsuits
within forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm, Teva and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s, Teva’s and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
PN/VIMOVO
Program. Under our PN program, we have completed formulation development
and clinical studies for several combinations of a PPI and a NSAID in a single
tablet intended to provide effective management of pain and inflammation
associated with chronic conditions such as osteoarthritis, and intended to have
fewer gastrointestinal complications compared to a NSAID taken alone in patients
at risk for developing NSAID associated gastric ulcers. We initially conducted
studies with two PN product formulations in this program - PN 100, a combination
of the PPI lansoprazole and the NSAID naproxen, and PN 200, a combination of the
PPI omeprazole and naproxen, prior to entering into our collaboration with
AstraZeneca. Our present development and commercialization efforts under the PN
program are covered under our exclusive collaboration agreement with
AstraZeneca, which we entered into on August 1, 2006 and which was amended in
September 2007 and October 2008. Under our agreement with AstraZeneca, we are
co-developing with AstraZeneca, and AstraZeneca will commercialize, proprietary
fixed dose combinations of the PPI esomeprazole magnesium with the NSAID
naproxen in a single tablet. The initial product to be developed under the
agreement, VIMOVO (formerly PN 400), is being studied for the treatment of the
signs and symptoms of osteoarthritis, rheumatoid arthritis and ankylosing
spondylitis in patients at risk of developing NSAID-associated gastric ulcers.
On March 2, 2007, we filed an IND with the FDA for VIMOVO and in April 2007, the
first Phase 1 study was initiated.
In discussions with the FDA during 2005
regarding our development plans for studies to pursue FDA approval of PN 100 and
PN 200, the FDA agreed that by including naproxen as the NSAID within the PN
formulation, we could expect that all indications for chronic use of naproxen in
adults would accrue to the PN product, if clinical trials successfully
demonstrated improved safety (lower incidence of gastric ulcers) of the PN
product compared with naproxen alone and the PN formulation was shown to be
bioequivalent to marketed formulations of enteric-coated, or EC, naproxen. Prior
to entering into our collaboration agreement with AstraZeneca, we completed a
study designed to demonstrate the bioequivalence of the naproxen component of
our PN 200 product candidate development formulation to EC naproxen. This study
demonstrated that the PN 200 product was bioequivalent to the reference drug, EC
Naprosyn®, with
respect to the naproxen component.
In early
2006, we submitted a SPA to the FDA for our pivotal Phase 3 clinical trials for
PN 200. The SPA is a process in which the FDA provides evaluations and guidance
on clinical trial protocols for pivotal Phase 3 clinical trials. In April 2006,
we announced that we had reached an agreement with the FDA on the Phase 3
pivotal clinical trials for PN 200 for the treatment of the signs and symptoms
of osteoarthritis, rheumatoid arthritis and ankylosing spondylitis in patients
at risk of developing NSAID-associated gastric ulcers. We also reached agreement
with the FDA that the development program and study design proposed for PN 200
would be applicable to a product that contained an isomer of omeprazole combined
with naproxen. In light of our collaboration agreement with AstraZeneca, we,
along with AstraZeneca have met with the FDA and confirmed the core development
program and the principles in the SPA already agreed upon do apply to the new
product consisting of proprietary fixed dose combinations of esomeprazole
magnesium with naproxen.
In the third quarter of 2006, we began
recruiting subjects for a six month comparative trial of PN 200 as compared to
EC naproxen in patients requiring chronic NSAID therapy. The primary endpoint
for the trial was the cumulative incidence of gastric ulcers over six months of
treatment. Because we did not have final results until the fourth quarter of
2007, we, together with AstraZeneca reviewed the interim results of this trial
prior to commencing Phase 3 studies of VIMOVO in September 2007. This study has
now been completed and the results which have been presented publicly, indicated
significantly fewer endoscopically confirmed gastric ulcers during the six month
treatment period in subjects on PN 200 compared to subjects receiving
enteric-coated naproxen alone. We conducted two Phase 3 pivotal trials of VIMOVO
in patients who are at risk for developing NSAID-associated gastric ulcers, the
primary endpoint for which is the reduction in endoscopic gastric ulcers. In
October 2008, the FDA informed us that it was conducting an internal review of
the acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. In late January 2009, the FDA informed us that it had completed
its internal discussions and that there was no change to previous agreements
that gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs. The two pivotal trials have been completed and met their primary
endpoints. In both trials, patients taking VIMOVO experienced significantly
(p<0.001) fewer endoscopically confirmed gastric ulcers compared to subjects
receiving enteric-coated naproxen during the six-month treatment period, with
gastric ulcer incidence rates of 4.1 and 7.1% for VIMOVO and 23.1 and 24.3% for
enteric-coated naproxen in studies 301 and 302, respectively. Data combined from
both studies showed that in patients taking low dose aspirin (n=201), the
incidence of gastric ulcers in the VIMOVO arm was 3.0% compared to 28.4% for
those taking EC naproxen (p<0.001) and patients taking VIMOVO who were not
taking low dose aspirin (n=653) experienced a 6.4% incidence of gastric ulcers
compared to 22.2% among those taking EC naproxen (p<0.001). Additional
analyses examined the incidence of endoscopically confirmed duodenal ulcers
among patients taking VIMOVO. In study 301, patients taking VIMOVO experienced a
0.5% incidence of duodenal ulcers compared to 5.1% taking EC naproxen (p=0.003),
and in study 302, patients taking VIMOVO experienced a 1.0% incidence of
duodenal ulcers, compared to 5.7% incidence among patients taking EC naproxen
(p=0.007). The most frequently reported adverse events among patients taking
both VIMOVO and enteric coated naproxen in the pivotal trials were GI disorders,
including dyspepsia, erosive esophagitis and erosive duodenitis. In addition, we
are conducting a long-term, open label safety study for VIMOVO. We have
terminated a non-pivotal smaller study in patients at high risk (i.e., previous
bleeding from a gastric ulcer) of gastrointestinal related events from NSAIDs
which is not required for approval. We have conducted additional studies at
AstraZeneca’s expense. The NDA for VIMOVO was submitted on June 30, 2009 and was
accepted for filing in August 2009. POZEN received a $10.0 million milestone
payment from AstraZeneca in September 2009 for the achievement of such
milestone.
In 2005,
we also had discussions with the FDA concerning the implications of the FDA’s
guidance issued in June 2005 concerning labeling of NSAID-containing products,
which resulted from an FDA advisory committee meeting held in February 2005. The
advisory committee addressed the safety of NSAIDs, and, in particular, the
cardiovascular risks of COX-2 selective NSAIDs. Based on our discussions with
the FDA reviewing division for PN products, we believe that, unless new
information about naproxen safety concerns becomes available, long-term
cardiovascular safety studies will not be required at this time for FDA approval
of our PN product candidates containing naproxen. However, we cannot guarantee
that such studies will not be required. We will continue to evaluate and review
with the FDA its expectations and recommendations regarding the efficacy and
safety requirements and study design necessary to support approval of NDAs for
our PN product candidates.
Additionally,
we have met with four national European regulatory agencies to discuss the
proposed development program for PN. Under our agreement with AstraZeneca,
AstraZeneca has responsibility for the development program for PN products
outside the U.S., including interactions with regulatory agencies. In October
2009, AstraZeneca submitted a MAA for VIMOVO in the European Union via the
Decentralized Procedure.
We cannot
reasonably estimate or know the amount or timing of the costs necessary to
obtain regulatory approval of VIMOVO. Nor can we reasonably estimate or know the
amount or timing of the costs necessary to continue exploratory development
and/or complete the development of any PN product candidates we may seek to
develop or when, if and to what extent we will receive cash inflows from any PN
products. The additional costs that may be incurred include expenses relating to
clinical trials and other research and development activities and activities
necessary to obtain regulatory approvals.
We incurred direct development costs
associated with the development of our PN program of $7.2 million for the fiscal
year ended December 31, 2009, of which, $5.5 million was funded by development
revenue from AstraZeneca. Our direct development costs do not include the cost
of research and development personnel or any allocation of our overhead
expenses.
PA Program.
As part of our PA program, we are exploring the development of a
combination of a PPI and aspirin in a single tablet. Similar to the PN program,
our PA product candidate is intended to induce fewer gastrointestinal
complications compared to an aspirin taken alone in patients at risk for
developing aspirin associated gastric ulcers. Our PA product candidates are
covered under the same patent as PN, but we have retained all rights to this
program.
Our initial PA product candidate,
PA32540, is currently in clinical development. We completed a Phase 1 proof of
concept study in Canada of an earlier formulation of PA containing 325 mg of
aspirin and 20 mg of omeprazole (PA32520) in the first quarter of 2007. The
primary endpoint was gastrointestinal damage as measured by the Lanza scoring
system used in our previous PN studies. The results were highly significant
(p<0.001) with 10% of the PA group having Lanza 3 or 4 gastrointestinal
damage, whereas 57.5% of the EC aspirin group had this level of gastrointestinal
damage during the 28 day study. We also completed a second proof of concept
study with PA32520 as compared to 81 mg of EC aspirin. These results confirmed
the earlier levels of gastric damage as measured by Lanza scoring at about 10%
for PA32520. While these results in the second study were numerically different
between treatment groups, they did not achieve statistical significance from the
results obtained with 81mg EC aspirin (21%). After reviewing these data, we
decided to increase the dose of omeprazole to 40 mg per tablet and conduct an
additional 28 day Phase 1 study using the formulation containing 40 mg of
immediate release of omeprazole and 325 mg of aspirin (PA32540) compared to 325
mg EC aspirin. Topline results from this study indicate a highly significant
(P=0.003) reduction in gastrointestinal damage with the higher strength PA32540
tablet as compared with 325 mg EC aspirin (2.5% vs. 27.5% grade 3 or 4 Lanza
scores, respectively). In this last study, 75% of subjects treated with the
PA32540 tablet showed no gastrointestinal damage at all as compared to < 50%
with the PA32520 tablet. An IND for the product was filed in the fourth quarter
of 2007 and we met with the FDA in July 2007 to discuss the overall development
program requirements. We completed a study which demonstrated that the salicylic
acid component of PA32540 was bioequivalent to the reference drug, EC aspirin,
with respect to the aspirin component, and which we believe will allow our PA
product to receive all the cardio- and cerebrovascular secondary prevention
claims of aspirin. In June 2008, we filed an SPA with the FDA for our pivotal
Phase 3 trials for PA32540, the primary endpoint for which is the reduction in
endoscopic gastric ulcers. The SPA is a process by which the FDA and a company
reach agreement on the Phase 3 pivotal trial protocol design, clinical endpoints
and statistical analyses that are acceptable to support regulatory approval. In
October 2008, the FDA informed us that it was conducting an internal review of
the acceptability of using endoscopic gastric ulcers as a primary endpoint in
clinical trials. In late January 2009, the FDA informed us that it had completed
its internal discussions and that there was no change to previous agreements
that gastric ulcer incidence was an acceptable primary endpoint for our clinical
programs and in February 2009, we received written confirmation from the FDA
that endoscopic gastric ulcer incidence was an acceptable endpoint for the Phase
3 clinical studies we proposed in our SPA for PA32540.
We are
aware of publications that contain data regarding a possible drug-drug
interaction between clopidogrel (Plavix®), a
widely prescribed anti-platelet agent, and certain enteric-coated proton pump
inhibitors when platelet aggregation is assessed in ex-vivo tests. On November
11, 2009, the FDA issued new drug safety information to healthcare professionals
through a publication entitled “Information for Healthcare Professionals: Update
to the labeling of Clopidogrel Bisulfate (marketed as Plavix) to alert
healthcare professions about a drug interaction with enteric-coated omeprazole
(marketed as Prilosec® and Prilosec® OTC).” The publication stated
that the effect of clopidogrel on platelets was reduced by as much as 47% in
people receiving clopidogrel and omeprazole together. The FDA’s action was
based, in part, on two crossover clinical studies of 72 healthy subjects
administered Plavix alone and with 80 mg EC omeprazole, either together or
administered 12 hours apart.
To assess
whether a similar interaction occurs between clopidogrel and PA32540, which
contains immediate release omeprazole, we have completed a Phase 1 drug-drug
interaction study to evaluate the ex-vivo platelet aggregation effects of
PA32540 plus clopidogrel dosed at the same time or dosed 10 hours apart compared
to aspirin 325mg plus clopidogrel dosed together. When PA32540 and clopidogrel
were dosed together, data from the study showed a mean 36.7% platelet inhibition
compared to a mean 44.0% platelet inhibition when aspirin and clopidogrel were
dosed together suggesting a drug-drug interaction based on the study’s
pre-specified primary analysis. When PA32540 and clopidogrel were dosed 10 hours
apart, data from the study suggested no ex-vivo drug-drug interaction based on
the study’s pre-specified primary analysis. The relevance of these ex vivo
platelet data on cardiovascular events is not known. Published data
on a clinical interaction between PPIs and Plavix from several randomized
controlled trials in cardiovascular patients have reported no clinical impact on
cardiovascular outcomes [Bhatt et al (COGENT 1 2009) and O’Donoghue et al (TIMI
38 2009)]. FDA assessment of these data and the implication to a
future PA32540 label are not known at this time.
We are also continuing to evaluate how
best to commercialize the PA product candidates and programs and have hired a
chief commercial officer to evaluate he commercial opportunities for these
product candidates. We are also conducting both formulation development and
early stage clinical studies with other PA product candidates for indications in
addition to secondary prevention of cardiovascular events. We are evaluating the
regulatory requirements to obtain an indication for PA for the secondary
prevention of colorectal neoplasia. In January 2010, we received input from FDA
to discuss with respect to the development requirements for a possible
indication in colorectal neoplasia. Further discussions are
planned.
Additionally,
we have met with three national European regulatory agencies to discuss the
proposed development program for PA. Each of these regulatory agencies has
indicated that reduction in gastric ulcers is an appropriate endpoint for the
pivotal trials, along with demonstrating bioequivalence to the reference drug,
EC aspirin, with respect to the aspirin component. Dose ranging studies may also
be required.
We cannot
reasonably estimate or know the amount or timing of the costs necessary to
continue exploratory development and/or complete the development of any PA
product candidates we may seek to develop or when, if and to what extent we will
receive cash inflows from any PA products. The additional costs that may be
incurred include expenses relating to clinical trials and other research and
development activities and activities necessary to obtain regulatory approvals.
We have decided to retain control of our PA product candidates and currently do
not intend to partner the PA program. To that end, we have hired a chief
commercial officer to evaluate the commercial opportunities for these product
candidates. We believe value can be added to the PA product candidates as
progress is made through clinical development and, if we ultimately chose to
partner the products later in the development program or after approval, we
believe it would be under economic terms more favorable to us.
We are
conducting market research on the PA product concepts, to support our evaluation
of how best to commercialize the PA product candidates and programs, which may
include commercializing the products ourselves in certain territories. Changing
from a commercialization strategy in which the PA product candidates are
out-licensed, in exchange for milestone and royalty payments, will depend on our
available financial resources, the associated risks of such a change and its
overall impact on the PA product candidates’ value.
We incurred direct development costs
associated with the development of our PA program of $7.7 million during the
fiscal year ended December 31, 2009. Our direct development costs do not include
the cost of research and development personnel or any allocation of our overhead
expenses.
MT
300. In October
2003, we received a not-approvable letter from the FDA related to our NDA for MT
300, which we had submitted in December 2002. We are not currently conducting
any clinical trials for MT 300 and do not expect to incur any additional
significant development costs related to MT 300, nor do we believe that we will
receive any future cash inflows from MT 300. We incurred $0.1 million direct
development costs associated with the development of MT 300 for the fiscal year
ended December 31, 2008. Our direct development costs do not include the cost of
research and development personnel or any allocation of our overhead
expenses.
In July 2005, we received a letter from
Valeant NA, seeking payment of a $1.0 million withdrawal fee required under
certain conditions under the agreement. We do not believe that the withdrawal
fee is payable under the circumstances of receipt of the not-approvable letter
from the FDA. The agreement requires that unresolved disputes by the parties be
referred to the respective chief executive officers for resolution. If still
unresolved, the agreement provides for binding arbitration. Valeant NA has
disputed our conclusion that the withdrawal fee is not payable and has indicated
its intention to pursue the dispute resolution provisions provided for under the
agreement, although the last written communication from Valeant NA was received
in March 2006. In 2008, based upon our evaluation of the facts and
circumstances, we recognized the remaining $1.0 million licensing fee for MT
300. We can give no assurance that Valeant NA will agree to termination terms
acceptable to us, or that we will not be required to pay Valeant NA the
withdrawal fee described above.
Critical
Accounting Policies and Estimates
Management makes certain judgments and
uses certain estimates and assumptions when applying accounting principles
generally accepted in the U.S. in the preparation of our financial statements.
The development and selection of the critical accounting policies, and the
related disclosure about these policies, have been reviewed by the audit
committee of our board of directors. We evaluate our estimates and judgments on
an ongoing basis and base our estimates on historical experience and on
assumptions that we believe to be reasonable under the circumstances. Our
experience and assumptions form the basis for our judgments about the carrying
value of assets and liabilities that are not readily apparent from other
sources. Actual results may vary from what we anticipate and different
assumptions or estimates about the future could change our reported results. We
have critical accounting estimates in the following policy areas: revenue
recognition, accrued expenses, stock-based compensation, fair value measurements
and income taxes.
Revenue Recognition
We record revenue under two categories:
licensing revenues and development revenues. With regard to the licensing
revenues, the licensing and other collaborative agreements have terms that
include up-front payments upon contract signing, additional payments if and when
certain milestones in the product’s development are reached, royalty payments
based on future product sales and withdrawal fees if certain conditions are
met.
Recognition of revenue from
non-refundable up-front payments is deferred by us upon receipt and recognized
over the period ending on the anticipated dates of regulatory approvals, as
specified in the agreements relating to the product candidates. If regulatory
approvals or other events relating to our product candidates are accelerated,
delayed or not ultimately obtained, then the amortization of revenues for these
products would prospectively be accelerated or reduced accordingly.
Milestone payments are recognized as
licensing revenue upon the achievement of specified milestones if (i) the
milestone is substantive in nature and the achievement of the milestone was not
reasonably assured at the inception of the agreement; and (ii) the fees are
non-refundable. Any milestone payments received prior to satisfying these
revenue recognition criteria are recorded as deferred revenue. During the third
quarter of 2009, we received a $10 million milestone payment which was recorded
as licensing revenue in the accompanying statement of operations.
Treximet royalty revenue is recognized
when earned as will any future royalty revenues with respect to the manufacture,
sale or use of our products or technology. For Treximet or those future
arrangements where royalties are reasonably estimable, we recognize revenue
based on estimates of royalties earned during the applicable period and reflect
in future revenue any differences between the estimated and actual royalties.
During the fiscal years ended December 31, 2009 and 2008, we recognized $4.3 and
$2.4 million, respectively, of royalty revenue which is included within
licensing revenue in the accompanying statements of operations. GSK revised
their previous estimate of Medicaid and other rebates which had a $0.1 million
favorable impact on royalties in the third quarter of 2009.
With regards to the development
revenues, our licensing agreements may include payment for development services
provided by us on an hourly rate and direct expense basis. We record such
payments as revenue in accordance with the agreements because we act as
principal in the transaction. Under the collaboration agreements with
AstraZeneca and GSK, we recognize as development revenue the billings for the
direct costs and certain personnel-related time incurred in performing
additional development activities described within the related agreements. The
collaboration agreements establish the rates for billing personnel-related time
incurred and consequently, the associated costs incurred to perform the
additional development activities are not separately captured from ongoing
personnel costs.
Management believes that its current
assumptions and other considerations used to estimate the periods for revenue
recognition described above are appropriate, and historical changes in our
estimates of these periods have not resulted in material changes in the revenue
we recognized. However, we continually review these estimates, which could
result in a change in the deferral period and might impact the timing and amount
of revenue recognition. Further, if regulatory approval for Treximet is
accelerated, delayed or not ultimately obtained, then the amortization of
revenues for this product would prospectively be accelerated or reduced
accordingly.
Development revenue and direct billed
costs for the years ended December 31, 2009, 2008 and 2007 were the
following:
|
Year
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Development
Revenue
|
$ | 5,536,053 | $ | 28,912,399 | $ | 18,985,344 | ||||||
|
Direct
Costs
|
$ | 3,855,552 | $ | 25,934,849 | $ | 16,128,985 | ||||||
As of December 31, 2009, we had
deferred revenue on our balance sheet totaling $7.2 million. We recognized
licensing revenue of $26.7 million for the fiscal year ended December 31, 2009;
$37.2 million for the fiscal year ended December 31, 2008, and $34.4 million for
the fiscal year ended December 31, 2007. Licensing revenue for the fiscal year
ended December 31, 2009 included $10.0 million in milestone revenue related to
the NDA acceptance of VIMOVO and $4.3 million in royalty revenue for Treximet.
Of the licensing revenue during the fiscal year ended 2008, we recognized $20.0
million in milestone revenue related to the approval of, and GSK’s intent to
commercialize Treximet, and $2.4 million in Treximet royalty revenue. A $20.0
million milestone payment from AstraZeneca for the PN 400 program was recognized
in the fiscal year ended December 31, 2007.
Accrued expenses, including contracted
costs
Significant management judgments and
estimates must be made and used in connection with accrued expenses, including
those related to contract costs, such as costs associated with our clinical
trials. Specifically, our management must make estimates of costs incurred to
date but not yet invoiced in relation to contracted, external costs. Management
analyses the progress of product development, clinical trial and toxicology and
related activities, invoices received and budgeted costs when evaluating the
adequacy of the accrued liability for these related costs. Material differences
in the amount and timing of the accrued liability for any period may result if
management made different judgments or utilized different
estimates.
Our management believes that its
current assumptions and other considerations used to estimate accrued expenses
for the period are appropriate. However, determining the date on which certain
contract services commence, the extent of services performed on or before a
given date and the cost of such services involves subjective judgments and
estimates and often must be based upon information provided by third parties. In
the event that we do not identify certain contract costs which have begun to be
incurred or we under- or over-estimate the extent of services performed or the
costs of such services, we adjust our annuals during the period in which the
information becomes available.
Accrued costs related to product
development and operating activities, including clinical trials, based upon the
progress of these activities covered by the related contracts, invoices received
and estimated costs totaled $3.5 million at December 31, 2009 and $5.7 million
at December 31, 2008. The variance, at each of these ending periods, between the
actual expenses incurred and the estimated expenses accrued has been less than
$125,000.
Stock-based compensation
Stock-based compensation cost is
estimated at the grant date based on the fair value of the award and is
recognized as expense over the requisite service period of the award. The fair
value of restricted stock awards is determined by reference to the fair market
value of our common stock on the date of grant. We use the Black-Scholes model
to value service condition and performance condition option awards. For awards
with only service conditions and graded-vesting features, we recognize
compensation cost on a straight-line basis over the requisite service period.
For awards with performance or market conditions, we recognize compensation cost
over the expected period to achieve the performance or market condition,
provided achievement of the performance condition is deemed
probable.
Determining the appropriate fair value
model and related assumptions requires judgment, including estimating stock
price volatility, forfeiture rates, and expected terms. Our expected volatility
rate was estimated based on an equal weighting of the historical volatility of
our common stock over a six year period. The expected term we use was estimated
based on average historical terms to exercise. The risk-free interest rate is
based on seven year U.S. Treasury securities. The pre-vesting forfeiture rate
used for the year ended December 31, 2009 was based on actual historical
rates.
Determining the appropriate amount to
expense for performance-based awards based on the achievement of stated goals
requires judgment, including forecasting future performance results. The
estimate of expense is revised periodically based on the probability of
achieving the required performance targets and adjustments are made as
appropriate. The cumulative impact of any revisions is reflected in the period
of change. If any applicable financial performance goals are not met, no
compensation cost is recognized and any previously recognized compensation cost
is reversed.
Fair
Value Measurement
On
January 1, 2008, we adopted the provisions of FASB ASC 820, Fair Value
Measurement and Disclosure ("FASB ASC 820"). FASB ASC 820 was issued in
September 2006 and is effective for financial statements issued for fiscal years
beginning after November 15, 2007. In February 2008, the Financial Accounting
Standards Board ("FASB") FASB ASC 820 deferred the effective date of FASB ASC
820 for one year for nonfinancial assets and nonfinancial liabilities. It did
not defer recognition and disclosure requirements for financial assets and
financial liabilities or for nonfinancial assets and nonfinancial liabilities
that are remeasured at least annually. Accordingly, as of January 1, 2008, we
have applied the provisions of FASB ASC 820 only to financial assets and
liabilities as discussed below. Our adoption of FASB ASC 820 did not result in
our recording any cumulative effect adjustments to retained
earnings.
Under
FASB ASC 820, fair value is defined as the price that would be received to sell
an asset or paid to transfer a liability (i.e. "the exit price") in an orderly
transaction between market participants at the measurement date. In determining
fair value, we use various valuation approaches, including quoted market prices
and discounted cash flows. FASB ASC 820 also establishes a hierarchy for inputs
used in measuring fair value that maximizes the use of observable inputs and
minimizes the use of unobservable inputs by requiring that the most observable
inputs be used when available. Observable inputs are inputs that market
participants would use in pricing the asset or liability developed based on
market data obtained from independent sources. Unobservable inputs are inputs
that reflect a company's judgment concerning the assumptions that market
participants would use in pricing the asset or liability developed based on the
best information available under the circumstances. The fair value hierarchy is
broken down into three levels based on the reliability of inputs as
follows:
|
·
|
Level
1 - Valuations based on quoted prices in active markets for identical instruments
that the Company is able to access. Since valuations are based on quoted
prices that are readily and regularly available in an active market,
valuation of these products does not entail a significant degree of
judgment.
|
|
·
|
Level
2 - Valuations based on quoted prices in active markets for instruments
that are similar,
or quoted prices in markets that are not active for identical or similar
instruments, and model-derived valuations in which all significant inputs
and significant value drivers are observable in active
markets.
|
|
·
|
Level
3 - Valuations based on inputs that are unobservable and significant to
the overall fair value measurement.
|
The
financial assets for which we perform recurring remeasurements are cash
equivalents and short-term investments. As of December 31, 2009, financial
assets utilizing Level 1 inputs included cash equivalents and short-term
investments. Financial assets utilizing Level 2 inputs included short-term
investments in government agency obligations and corporate fixed income
securities.
Fair
value is a market-based measure considered from the perspective of a market
participant who holds the asset or owes the liability rather than an
entity-specific measure. Therefore, even when market assumptions are not readily
available, our own assumptions are set to reflect those that market participants
would use in pricing the asset or liability at the measurement date. We use
prices and inputs that are current as of the measurement date, including during
periods of market dislocation, such as the recent illiquidity in the auction
rate securities market. In periods of market dislocation, the observability of
prices and inputs may be reduced for many instruments. This condition has
caused, and in the future may cause, our financial instruments to be
reclassified from Level 1 to Level 2 or from Level 2 to Level 3.
FASB ASC
820 requires that the valuation techniques used by us are consistent with at
least one of the three possible approaches: the market approach, income
approach, and/or cost approach. Our Level 1 valuations are based on the market
approach and consist primarily of quoted prices for identical items on active
securities exchanges. Our Level 2 valuations also use the market approach and
are based on significant other observable inputs such as quoted prices for
financial instruments not traded on a daily basis. We did not rely on Level 3
input for valuation of our securities at December 31, 2009.
Income Taxes
We
estimate an annual effective tax rate of negative 8.6% for the year ended
December 31, 2009. Our effective tax rate was negative 8.6% for the twelve month
period ended December 31, 2009. However, the actual effective rate may vary
depending upon actual licensing fees and milestone payments received,
specifically the pre-tax book income for the year, and other factors. Income
taxes have been accounted for using the liability method in accordance with FASB
ASC 740, Income Taxes. Since our inception, we have incurred substantial losses
and may incur substantial and recurring losses in future periods. The Tax Reform
Act of 1986 (the “Act”) provides for a limitation on the annual use of net
operating loss and research and development tax credit carry-forwards (following
certain ownership changes, as defined by the Act) that could limit our ability
to utilize these carry-forwards. We have experienced various ownership changes,
as defined by the Act, as a result of, among other reasons, past financings.
Accordingly, our ability to utilize the aforementioned carry-forwards may be
limited. Additionally, because tax laws limit the time during which these
carry-forwards may be applied against future taxes, we may not be able to take
full advantage of these carry-forwards for federal and state income tax
purposes.
We
currently file income tax returns in the U.S. federal jurisdiction, and the
state of North Carolina. We are no longer subject to federal or North Carolina
income tax examinations by tax authorities for years before 2006. However, the
loss carryforwards generated prior to 2006 may still be subject to change, if we
subsequently begin utilizing these losses in a year that is open under statute
and subject to federal or North Carolina income tax examinations by tax
authorities.
We
adopted the provisions of FASB ASC 740-10, Uncertainty in Income Taxes, on
January 1, 2007 and as a result, there were no material impacts to the financial
statements.
We
recognize any interest and penalties accrued related to unrecognized tax
benefits as income tax expense. During the fiscal years ended December 31, 2009
and 2008, there were no such interest and penalties.
Historical
Results of Operations
Year
ended December 31, 2009 compared to the year ended December 31,
2008
Net income (loss) per share:
Net loss attributable to common stockholders for the fiscal year ended December
31, 2009 was $(6.9) million or $(0.23) per share, on a basic and diluted basis,
as compared to a net loss of $(6.0) million, or $(0.20) per share, on a diluted
basis, for the fiscal year ended December 31, 2008. The net loss for the fiscal
year ended December 31, 2009 included a $(5.1) million or $(0.17) per share
charge for non-cash stock-based compensation expense as compared to $(6.0)
million or $(0.20) per share for the same period of 2008. Additionally, the net
loss before income tax benefit for the fiscal year ended December 31, 2009 was
reduced by a tax benefit decrease of $0.6 million which, based upon recently
enacted legislation, represents the carryback claim that the Company plans to
file for AMT taxes paid in 2007.
Revenue: We recognized total
revenue of $32.2 million for the fiscal year ended December 31, 2009 as compared
to total revenue of $66.1 million for the fiscal year ended December 31, 2008.
The decrease in revenue was primarily due to $23.4 million less developmental
revenue in 2009 and $10.0 million less in milestone payments in 2009. Licensing
revenue for the fiscal year ended December 31, 2009 was $26.7 million compared
to $37.2 million for 2008. Development revenue was $5.5 million for the fiscal
year ended December 31, 2009 compared to $28.9 million for 2008. Our licensing
and collaboration agreements have terms that include upfront payments upon
contract signing and additional payments if and when certain milestones in the
product development or related milestones are achieved. All upfront payments
were deferred and the non-refundable portions are being amortized over the
periods ending on the anticipated dates of regulatory approvals, as specified in
the agreements relating to the product candidates, or the conclusion of any
obligation on our part. Approximately $7.2 million remains in deferred revenue
at December 31, 2009. Substantive milestone payments are recognized as revenue
upon completion of the contractual events. Additionally, our development
revenues include the billings for the direct costs and certain personnel-related
time incurred in performing additional development activities described under
our collaboration agreements. Our costs associated with the billed direct costs
totaled $3.9 million and $25.9 million for the fiscal year ended December 31,
2009 and 2008, respectively. All costs associated with our development revenues
are included in research and development expenses in our Statements of
Operations. The collaboration agreements establish the rates for billing
personnel-related time incurred and consequently, the associated costs incurred
to perform the additional development activities are not separately captured
from ongoing personnel costs.
Research and development:
Research and development expenses decreased by $39.5 million to $22.4 million
for the fiscal year ended December 31, 2009, as compared to the same period of
2008. The decrease was due primarily to a decrease in direct development costs
for our PN program and exploratory programs. Direct development costs for the PN
program decreased by $38.2 million to $7.2 million, primarily due to clinical
trial activities and other product development activities during the fiscal year
ended December 31, 2009, as compared to the same period of 2008. Direct
development costs for the PA program increased by $2.7 million to $7.7 million.
Direct development costs for the exploratory programs decreased by $2.4 million
to $0.5 million, as compared to the same period of 2008. Other departmental
expenses decreased by $1.6 million primarily due to decreased personnel costs,
as compared to the same period of 2008. We have included in our research and
development total expenses the departmental personnel costs associated with our
research and development activities and direct costs associated with
pharmaceutical development, clinical trials, toxicology activities and
regulatory matters.
General and administrative:
General and administrative expenses increased by $5.5 million to $17.8 million
for the fiscal year ended December 31, 2009, as compared to the same period of
2008. The increase was due primarily to increased legal costs for patent defense
and marketing research expenses, which increased $4.5 million and $0.7 million,
respectively, as compared to the same period of 2008. General and administrative
expenses consisted primarily of the costs of administrative personnel, facility
infrastructure, legal expenses, market research, and public company
activities.
Other income: Interest income
was $0.2 million and $1.2 million for the fiscal year ended December 31, 2009
and 2008, respectively. Investment income from bond amortization for the fiscal
year ended December 31, 2009 totaled $0.4 million as compared to $0.9 million
during the same period of 2008. Investment income decreased primarily due to
declining short term interest rates.
Year
ended December 31, 2008 compared to the year ended December 31,
2007
Net (loss) / income per
share: Net loss attributable to common stockholders for the fiscal year
ended December 31, 2008 was $(6.0) million or $(0.20) per share, on a basic and
diluted basis, as compared to a net income of $4.7 million, or $0.15 per share,
on a diluted basis, for the fiscal year ended December 31, 2007. The net loss
for the fiscal year ended December 31, 2008 included a $(6.0) million or $(0.20)
per share charge for non-cash stock-based compensation expense as compared to
$4.3 million or $0.15 per share for the same period of 2007.
Revenue: We recognized total
revenue of $66.1 million for the fiscal year ended December 31, 2008 as compared
to total revenue of $53.4 million for the fiscal year ended December 31, 2007.
The increase in revenue was primarily due to $2.4 million of Treximet royalty
revenue and an increase of $9.9 million in development revenue for the fiscal
year ended December 31, 2008 compared to 2007. Licensing revenue for the fiscal
year ended December 31, 2008 was $37.2 million compared to $34.4 million for
2007. Development revenue was $28.9 million for the fiscal year ended December
31, 2008 compared to $19.0 million for 2007. Our licensing and collaboration
agreements have terms that include upfront payments upon contract signing and
additional payments if and when certain milestones in the product development or
related milestones are achieved. All upfront payments were deferred and the
non-refundable portions are being amortized over the periods ending on the
anticipated dates of regulatory approvals, as specified in the agreements
relating to the product candidates, or the conclusion of any obligation on our
part. Approximately $19.5 million remains in deferred revenue at December 31,
2008. Substantive milestone payments are recognized as revenue upon completion
of the contractual events. Additionally, our development revenues include the
billings for the direct costs and certain personnel-related time incurred in
performing additional development activities described under our collaboration
agreements. Our costs
associated with the billed direct costs totaled $25.9 million and $16.1 million
for the fiscal year ended December 31, 2008 and 2007, respectively. All costs
associated with our development revenues are included in research and
development expenses in our Statements of Operations. The collaboration
agreements establish the rates for billing personnel-related time incurred and
consequently, the associated costs incurred to perform the additional
development activities are not separately captured from ongoing personnel
costs.
Research and development:
Research and development expenses increased by $22.0 million to $61.9 million
for the fiscal year ended December 31, 2008, as compared to the same period of
2007. The increase was due primarily to an increase in direct development costs
for our PN program and exploratory programs, partially offset by a decrease in
direct development costs for our PA program, as compared to the same period of
2007. Direct development costs for the PN program increased by $20.2 million to
$45.4 million, primarily due to clinical trial activities and other product
development activities during the fiscal year ended December 31, 2008, as
compared to the same period of 2007. Direct development costs for the
exploratory programs increased by $1.4 million to $3.1 million, offset by a
decrease of $0.7 million in the PA program, as compared to the same period of
2007. Other direct development costs and departmental expenses increased by $1.0
million primarily due to increased personnel costs, as compared to the same
period of 2007. We have included in our research and development total expenses
the departmental personnel costs associated with our research and development
activities and direct costs associated with pharmaceutical development, clinical
trials, toxicology activities and regulatory matters.
General and administrative:
General and administrative expenses increased by $0.8 million to $12.3 million
for the fiscal year ended December 31, 2008, as compared to the same period of
2007. The increase was due primarily to increased personnel costs and marketing
research expenses, as compared to the same period of 2007. General and
administrative expenses consisted primarily of the costs of administrative
personnel, facility infrastructure, business development expenses and public
company activities.
Other income: Interest income
was $1.2 and $1.5 million for the fiscal years ended December 31, 2008 and 2007,
respectively. Investment income from bond amortization for the fiscal year ended
December 31, 2008 totaled $0.9 million as compared to $1.8 million during the
same period of 2007.
Income
Taxes
At December 31, 2009 and 2008, we
had federal net operating loss carryforwards of approximately $95.1 million and
$81.6 million respectively, state net economic loss carryforwards of
approximately $73.0 million and $68.8 million respectively, and research
and development credit carryforwards of approximately $12.4 million and $11.8
million, respectively. The amount of the NOL related to excess tax based stock
compensation is $4.8 million at December 31, 2009 and 2008. The federal and
state net operating loss carryforwards begin to expire in 2021 and 2014,
respectively, and the research and development credit carryforwards begin to
expire in 2017. For financial reporting purposes, a valuation allowance has been
recognized to offset the deferred tax assets related to the carryforwards. Of
the total increase in valuation allowance of $1.6 million, an increase of $2.5
million was allocable to current operating activities, a decrease of $0.3
million was allocable to a change in the state tax rate, and, as a result of
recently enacted legislation, a decrease of $0.6 million was related to the
carryback claim that the Company plans to file for AMT taxes paid for 2007. When
the valuation allowance is realized, a portion related to excess stock option
compensation will be realized as an increase in additional paid-in capital. Our
effective tax rate was a negative 8.6% for the year ended December 31, 2009.
Based upon our historic losses, management has recorded a valuation allowance on
the net deferred tax assets. Accordingly, we have not recognized a deferred tax
benefit in the current year associated with the projected NOL generated. The
actual effective rate may vary depending upon actual licensing fees and
milestone payments received, specifically the pre-tax book income for the year,
and other factors. Income taxes are computed using the asset and liability
approach, which requires the recognition of deferred tax assets and liabilities
for the expected future tax consequences of events that have been recognized in
our financial statements or tax returns, in accordance with SFAS 109,
“Accounting for Income Taxes.” Since our inception, we have incurred substantial
losses and may incur substantial and recurring losses in future periods. The Tax
Reform Act of 1986 (the “Tax Reform Act”) limits the annual use of net operating
loss and research and development tax credit carry-forwards following certain
ownership changes, as defined by the Tax Reform Act. We have experienced various
ownership changes, as defined by the Tax Reform Act, as a result of, among other
reasons, past financings. Accordingly, our ability to utilize the aforementioned
carry-forwards may be limited. Additionally, because U.S. tax laws limit the
time during which these carry-forwards may be applied against future taxes, we
may not be able to take full advantage of these carry-forwards for federal
income tax purposes.
Liquidity
and Capital Resources
At December 31, 2009, cash and cash
equivalents, along with short-term investments, totaled $46.7 million, a
decrease of $15.0 million compared to December 31, 2008. The decrease in cash
was primarily due to the operating loss for the period and the reduction of
accounts payable and accrued expenses offset in part by cash receipts for
development activities and royalty payments received pursuant to the terms of
our agreements with AstraZeneca and GSK. Our cash is invested in money market
funds that invest primarily in short-term, highly rated investments, including
U.S. Government securities, commercial paper and certificates of deposit
guaranteed by banks and short-term corporate fixed income obligations and U.S.
Government agency obligations.
Short-term investments are held in a
managed investment account designed to increase the return on our cash. This
account, which is invested as described above, is managed within our Board
approved investment policy, which restricts investments to maturities of less
than twelve months, limits concentration to 5% or less and requires minimum
credit ratings of A1/P1, among other requirements. We have considered the impact
of the current economic environment in evaluating the fair value of our
investments. We believe we are adhering to a conservative investment policy.
Nonetheless, given the current credit crisis and other market risks, a downgrade
in any of our A1/P1 investments could result in required action under our
investment policy, and may result in an investment loss.
Because certain holdings in the managed
account have maturities longer than three months, we have classified these
holdings as short-term investments in our balance sheet and accounting
principles require reporting such investments at market value. Any difference
between market value and cost is reported in the stockholders’ equity section of
our financial statements as comprehensive income or loss.
We received $27.3 million in operating
cash during the fiscal year ended December 31, 2009 pursuant to the terms of our
collaboration agreements with AstraZeneca and GSK. In addition, our balance
sheet included a $1.1 million accounts receivable for royalties under the terms
of the AstraZeneca and GSK agreements. Cash received from financing activities
during the period totaled $32.7 thousand reflecting net proceeds from the
exercise of stock options.
Based upon the indirect method of
presenting cash flow, cash used in operating activities totaled $15.1 million
for the fiscal year ended December 31, 2009. Cash used in operating activities
was $13.5 million for the fiscal year ended December 31, 2008. Net cash provided
by investing activities during the fiscal year ended December 31, 2009 totaled
$12.3 million, and $1.8 million for the fiscal year ended December 31, 2008
reflecting investing activities associated with the purchase and sale of
short-term securities. Cash required for our operating activities during 2010 is
projected to increase from our 2009 requirements as a result of increased
development activities. During the fiscal years ended December 31, 2009 and
December 31, 2008 we recorded non-cash stock-based compensation expense of $5.1
million and $6.0 million, respectively, associated with the grant of stock
options and restricted stock.
As of December 31, 2009, we had $23.3
million in cash and cash equivalents and $23.4 million in short-term
investments. Our cash operating expenses for 2010 may exceed those of 2009,
should we decide to conduct pre-commercialization activities, as a result of our
decision to retain control of our PA product candidate. We believe that we will
have sufficient cash reserves and cash flow to maintain our planned level of
business activities through 2011. However, our anticipated cash flow includes
continued receipt of royalty revenue from GSK’s sale of Treximet, an assumption
of additional, new royalty revenue from AstraZeneca’s sale of VIMOVO and an
assumption that we will receive milestone payments upon VIMOVO’s regulatory
approvals, including a $20.0 million milestone payment upon FDA approval of
VIMOVO. In addition, our expenses might increase during that period beyond
currently expected levels if we decide to, or any regulatory agency requires us
to, conduct additional clinical trials, studies or investigations for any of our
product candidates, including in connection with the agency’s consideration, or
reconsideration, of our regulatory filings for our product candidates. In the
event FDA approval of the market launch of VIMOVO is materially delayed, royalty
revenue and cash receipts from sales of the product would also be delayed. If
our projected revenues decrease, our projected expenses increase for our product
candidates current in development, or if we pursue additional indications for
our PA product candidate, then, as a result of these or other factors, we may
need to raise additional capital.
Therefore, as part of our ongoing
assessment of our business and liquidity needs, we regularly assess available
funding options and will consider available funding opportunities as they arise.
We may sell shares of common stock in the future to fund additional development
activities and increase our working capital. We have filed with the Securities
and Exchange Commission, or SEC, and the SEC has declared effective, a shelf
registration statement on Form S-3 under which we have registered up to
8,540,000 shares of our common stock for sale in one or more public offerings.
Certain selling stockholders named in the prospectus for the registration
statement may offer up to an aggregate of 540,000 of such shares, and we will
not receive any of the proceeds from the sales of shares made by the selling
stockholders. Any additional equity financing may be dilutive to stockholders,
and debt financing, if available, may involve restrictive
covenants.
Our
forecast of the period of time through which we expect that our financial
resources will be adequate to support our operations is a forward-looking
statement that involves risks and uncertainties, and actual results could vary
as a result of a number of factors. Our future capital requirements will depend
on many factors, including:
|
·
|
the
number and progress of our clinical trials and other trials and
studies;
|
|
·
|
our
success, or any delays, in obtaining, regulatory approval of our product
candidates and success in, and manner of, commercializing our
products;
|
|
·
|
the
success of our existing collaborations and our ability to establish
additional collaborations;
|
|
·
|
costs
incurred to commercialize our products ourselves should we decide to
retain control of the products or technology and not to enter into
additional collaborations;
|
|
·
|
the
extent to which we acquire or invest in businesses, technologies or
products;
|
|
·
|
costs
incurred to enforce and defend our patent claims and other intellectual
rights;
|
|
·
|
our
ability to negotiate favorable terms with various contractors assisting in
our trials and studies; and
|
|
·
|
costs
incurred in the defense of our Treximet patents against generic companies
that have filed ANDAs with the FDA to market the product prior to the
expiration of our patents.
|
Obligations
and Commitments
The following summarizes our
contractual obligations as of December 31, 2009, and the expected timing of
maturities of those contractual obligations. This table should be read in
conjunction with the notes accompanying our financial statements included
elsewhere in this Annual Report on Form 10-K.
|
Payments
Due by Period
|
||||||||||||||||
|
Contractual
Obligations
|
Total
|
2010
|
2011-2012 |
2013-after
|
||||||||||||
|
($
in thousands)
|
||||||||||||||||
|
Operating
leases1
|
$ | 2,460 | $ | 220 | $ | 934 | $ | 1,306 | ||||||||
|
Product
development agreements2
|
4,440 | 3,323 | 1,117 | — | ||||||||||||
|
Total
contractual obligations
|
$ | 6,900 | $ | 3,543 | $ | 2,051 | $ | 1,306 | ||||||||
|
1
|
These
commitments are associated with operating leases. Payments due reflect
fixed rent expense.
|
|
2
|
Amounts
represent open purchase orders for ongoing pharmaceutical development
activities for our product candidates as of December 31, 2009. These
agreements may be terminated by us at any time without incurring a
termination fee.
|
Recent
Accounting Pronouncements
In June 2009, the Financial Accounting
Standards Board (“FASB”) issued FASB Statement No. 168, The FASB Accounting Standards
Codification™ and the
Hierarchy of Generally Accepted Accounting Principles, which replaces
FASB Statement No. 162, Hierarchy of Generally Accepted
Accounting Principles. Statement No. 168 is effective for financial
statements issued for interim and annual periods ending after September 15,
2009. The FASB Accounting Standards Codification™ (ASC) is a single source of
authoritative US accounting and reporting standards applicable for all
nongovernmental entities, other than guidance issued by the SEC and its staff,
it supersedes current US GAAP including FASB, AICPA, EITF and related literature
and reorganizes thousands of US GAAP pronouncements into approximately 90
accounting topics. The Company adopted Statement 168 effective in its quarter
ending September 30, 2009.
The proceeds from revenue from our
collaboration agreements have been invested in money market funds that invest
primarily in short-term, highly-rated investments, including U.S. Government
securities, commercial paper and certificates of deposit guaranteed by banks and
short-term corporate fixed income obligations and U.S. Government and Government
agency obligations. Under our current policies, we do not use interest rate
derivative instruments to manage our exposure to interest rate changes. Because
of the short-term maturities of our investments, we do not believe that a
decrease in market rates would have a significant negative impact on the value
of our investment portfolio.
Our financial statements and notes
thereto are included elsewhere in this Annual Report on Form 10-K and
incorporated herein by reference. See Item 15 of Part IV.
None.
Our management, with the participation
of our chief executive officer and chief financial officer, evaluated the
effectiveness of our disclosure controls and procedures (as defined in Rules
13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934) as of the end
of the period covered by this report. Based on that evaluation, our chief
executive officer and chief financial officer concluded that our disclosure
controls and procedures as of the end of the period covered by this report are
functioning effectively to provide reasonable assurance that the information
required to be disclosed by us in reports filed under the Securities Exchange
Act of 1934 is (i) recorded, processed, summarized and reported within the time
periods specified in the SEC’s rules and forms and (ii) accumulated and
communicated to our management, including our chief executive officer and chief
financial officer, as appropriate to allow timely decisions regarding
disclosures. A controls system, no matter how well designed and operated, cannot
provide absolute assurance that the objectives of the controls system are met,
and no evaluation of controls can provide absolute assurance that all control
issues and instances of fraud, if any, within a company have been
detected.
Our management’s report on internal
control over financial reporting procedures (as defined in Rules 13a-15(f) and
15d-15(f) under the Securities Exchange Act of 1934) is included with the
financial statements reflected in Item 8 of this Annual Report on Form 10-K and
is incorporated herein by reference.
No change in our internal control over
financial reporting occurred during the third fiscal quarter that has materially
affected, or is reasonably likely to materially affect, our internal control
over financial reporting.
None.
Information required to be disclosed by
this Item with respect to our executive officers is set forth under the caption
“Officers and Key Employees” contained in Part I, Item 1of this annual report on
Form 10-K.
Information required to be disclosed by
this Item about our board of directors is incorporated in this Annual Report on
Form 10-K by reference from the section entitled “Nomination and Election of
Directors” contained in our definitive proxy statement for our 2010 annual
meeting of stockholders scheduled to be held on June 10, 2010, which we intend
to file within 120 days of the end of our fiscal year.
Information required to be disclosed by
this Item about the Section 16(a) compliance of our directors and executive
officers is incorporated in this annual report on Form 10-K by reference from
the section entitled “Section 16(a) Beneficial Ownership Reporting Compliance”
contained in our definitive proxy statement for our 2010 annual meeting of
stockholders scheduled to be held on June 10, 2010, which we intend to file
within 120 days of the end of our fiscal year.
Information required to be disclosed by
this Item about our board of directors, the audit committee of our board of
directors, our audit committee financial expert, our Code of Business Conduct
and Ethics, and other corporate governance matters is incorporated in this
Annual Report on Form 10-K by reference from the section entitled “Board of
Directors and Corporate Governance Matters” contained in our definitive proxy
statement related to our 2010 annual meeting of stockholders scheduled to be
held on June 10, 2010, which we intend to file within 120 days of the end of our
fiscal year.
The text of our Code of Business
Conduct and Ethics, which applies to our directors and employees (including our
principal executive officer, principal financial officer, principal accounting
officer or controller, or persons performing similar functions) is posted in the
“Corporate Governance” section of our website, www.pozen.com. A copy of the Code
of Business Conduct and Ethics can be obtained free of charge on our website. We
intend to disclose on our website any amendments to, or waivers from, our Code
of Business Conduct and Ethics that are required to be disclosed pursuant to the
rules of the Securities and Exchange Commission and The NASDAQ Stock
Market.
Information required to be disclosed by
this Item is incorporated in this Annual Report on Form 10-K by reference from
the sections entitled “Compensation for Executive Officers and Directors” and
“Board of Directors and Corporate Governance Matters” contained in our
definitive proxy statement for our 2010 annual meeting of stockholders scheduled
to be held on June 10, 2010, which we intend to file within 120 days of the end
of our fiscal year.
Information required to be disclosed by
this Item is incorporated in this Annual Report on Form 10-K by reference from
the sections entitled “Principal Stockholders,” “Stock Ownership of Directors,
Nominees for Director, and Executive Officers” and “Compensation for Executive
Officers and Directors” contained in our definitive proxy statement for our 2010
annual meeting of stockholders scheduled to be held on June 10, 2010, which we
intend to file within 120 days of the end of our fiscal year.
The information required to be
disclosed by this Item is incorporated in this Annual Report on Form 10-K by
reference from the section(s) entitled “Certain Relationships and Related Party
Transactions” and “Board of Directors and Corporate Governance Matters,”
“Compensation for Executive Officers and Directors, “Compensation Committee
Interlocks and Insider Participation” and “Compensation Committee Report”
contained in our definitive proxy statement for our 2010 annual meeting of
stockholders scheduled to be held on June 10, 2010, which we intend to file
within 120 days of the end of our fiscal year.
This information required to be
disclosed by this Item is incorporated in this Annual Report on Form 10-K by
reference from the section entitled “Audit and Other Fees” contained in our
definitive proxy statement for our 2010 annual meeting of stockholders scheduled
to be held on June 10, 2010, which we intend to file within 120 days of the end
of our fiscal year.
(a) Financial
Statements and Schedules:
|
1.
|
Financial
Statements
|
The
following financial statements and reports of independent registered public
accounting firm are included herein:
|
Reports
of Independent Registered Public Accounting Firm
|
F-3
|
|
Balance
Sheets
|
F-5
|
|
Statements
of Operations
|
F-6
|
|
Statements
of Stockholders’ Equity
|
F-7
|
|
Statements
of Cash Flows
|
F-8
|
|
Notes
to Financial Statements
|
F-9
|
|
2.
|
Financial
Statement Schedules
|
Not applicable.
|
3.
|
List
of Exhibits
|
|
Exhibit
No.
|
Description
|
||
|
3.1
|
Amended
and Restated Certificate of Incorporation of the
Registrant.*
|
||
|
3.2
|
Second
Amended and Restated Bylaws of POZEN Inc., approved September 19, 2007
(filed as Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed
on September 20, 2007).
|
||
|
3.3
|
Certificate
of Designations of Series A Junior Participating Preferred Stock (filed as
Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed January
12, 2005).
|
||
|
4.1
|
See
Exhibits 3.1, 3.2 and 3.3 for provisions of the Amended and Restated
Certificate of Incorporation and Second Amended and Restated Bylaws of the
Registrant defining rights of the holders of Common Stock and Series A
Junior Participating Preferred Stock of the Registrant.
|
||
|
4.2
|
Rights
Agreement dated January 12, 2005 between Registrant and StockTrans, Inc.
(filed as Exhibit 4.1 to the Registrant’s Current Report on Form 8-K filed
January 12, 2005).
|
||
|
10.1
|
Stock
Option Plan of the Registrant.*
|
||
|
10.2
|
First
Amendment to Stock Option Plan dated February 14,
1997.*
|
||
|
10.3
|
Second
Amended and Restated 2000 Equity Compensation Plan of the Registrant
(filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q
filed August 7, 2007).***
|
||
|
10.4
|
Form
of Incentive Stock Option Agreement under Registrant’s Second Amended and
Restated Equity Compensation Plan (filed as Exhibit 10.2 to the
Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.5
|
Form
of Nonqualified Stock Option Agreement under Registrant’s Second Amended
and Restated Equity Compensation Plan (filed as Exhibit 10.3 to the
Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.6
|
Form
of Non-Employee Director Nonqualified Stock Option Agreement under Second
Amended and Restated Equity Compensation Plan (filed as Exhibit 10.4 to
the Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***.
|
||
|
10.7
|
Form
of Non-Employee Director Restricted Stock Unit Agreement under Second
Amended and Restated Equity Compensation Plan (filed as Exhibit 10.5 to
the Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.8
|
Second
Amended and Restated Executive Employment Agreement with John R. Plachetka
dated March 14, 2006 (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K filed March 16,
2006).***
|
||
|
10.9
|
First
Amendment to Second Amended and Restated Executive Employment Agreement
with John R. Plachetka dated March 14, 2006 (filed as Exhibit 10.1 to the
Registrant’s Quarterly Report on Form 10-Q filed November 5,
2007).***
|
||
|
10.10
|
Executive
Employment Agreement with John E. Barnhardt dated July 25, 2001 (filed as
Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q filed
October 31, 2001).***
|
||
|
10.11
|
First
Amendment to Executive Employment Agreement with John E. Barnhardt, dated
September 28, 2007 (filed as Exhibit 10.7 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007).***
|
||
|
10.12
|
Executive
Employment Agreement with William L. Hodges dated August 3, 2004 (filed as
Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed
October 27, 2004).***
|
||
|
10.13
|
First
Amendment to Executive Employment Agreement with William L. Hodges, dated
September 28, 2007 (filed as Exhibit 10.5 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007).***
|
||
|
10.14
|
POZEN
Inc. 2001 Long Term Incentive Plan (filed as Exhibit 10.6 to the
Registrant’s Quarterly Report on Form 10-Q filed October 31,
2001).***
|
||
|
10.15
|
Certificate
of Award dated August 1, 2001 issued to John R. Plachetka pursuant to
POZEN Inc. 2001 Long Term Incentive Plan (filed as Exhibit 10.7 to the
Registrant’s Quarterly Report on Form 10-Q filed October 31,
2001).***
|
||
|
10.16
|
Summary
of Non-Employee Director Compensation (filed as Exhibit 10.16 to the
Registrant’s Annual Report on Form 10-K filed March 8,
2007).***
|
||
|
10.17
|
Lease
Agreement between The Exchange at Meadowmont LLC and the Registrant dated
as of November 21, 2001 (filed as Exhibit 10.21 to the Registrant’s Annual
Report on Form 10-K filed April 1, 2002).
|
||
|
10.18
|
Product
Development and Commercialization Agreement dated June 11, 2003 between
the Registrant and Glaxo Group Ltd. (filed as Exhibit 10.1 to the
Registrant’s Quarterly Report on Form 10-Q filed August 12, 2003 and Form
10-Q/A filed November 8. 2004).†
|
||
|
10.19
|
License
Agreement dated June 11, 2003 between the Registrant and Glaxo Group Ltd.
(filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q
filed August 12, 2003 and Quarterly Report on Form 10-Q/A filed November
8. 2004).†
|
||
|
10.20
|
Collaboration
and License Agreement dated September 3, 2003 between the Registrant and
Valeant Pharmaceuticals NA (formerly Xcel Pharmaceuticals, Inc.) (filed as
Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed
November 6, 2003 and Quarterly Report on Form 10-Q/A filed November 8.
2004).†
|
||
|
10.21
|
Restricted
Stock Unit Agreement dated May 4, 2004 between Registrant and John R.
Plachetka (filed as Exhibit 10.4 to the Registrant’s Quarterly Report on
Form 10-Q filed July 30, 2004).***
|
||
|
10.22
|
First
Amendment, dated September 28, 2007, to Restricted Stock Unit Agreement,
dated May 4, 2004, between Registrant and John R. Plachetka (filed as
Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed
November 5, 2007).***
|
||
|
10.23
|
Form
of Non-Qualified Stock Option Agreement for Trexima grants issued pursuant
Registrant’s Equity Compensation Plan, as amended and restated (filed as
Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed January
7, 2005).***
|
||
|
10.24
|
Development,
Option and License Agreement dated May 15, 2003 between the Registrant and
Nycomed Danmark ApS (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K filed July 28, 2005, and Current Report on Form 8-K/A
filed January 10, 2006).†
|
||
|
10.25
|
Collaboration
and License Agreement dated August 1, 2006 between the Registrant and
AstraZeneca AB (filed as Exhibit 10.1 to the Registrant’s Quarterly Report
on From 10-Q filed November 3, 2006).†
|
||
|
10.26
|
Amendment
No. 1 to the Collaboration and License Agreement, dated September 6, 2007,
between the Registrant and AstraZeneca AB (filed as Exhibit 10.8 to the
Registrant’s Quarterly Report on Form 10-Q filed November 5, 2007).
†
|
||
|
10.27
|
Side
Letter dated September 19, 2006 Re: Collaboration and License Agreement
dated as of August 1, 2006 by and between the Registrant and AstraZeneca
AB (filed as 10.2 to the Registrant’s Quarterly Report on From 10-Q filed
November 3, 2006).†
|
||
|
10.28
|
Side
Letter Agreement, dated October 1, 2007, between the Registrant and
AstraZeneca, AB (filed as Exhibit 10.9 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007). †
|
||
|
10.29
|
Long-Term
Cash Incentive Award Agreement between the Registrant and John R.
Plachetka dated February 14, 2007 (filed as Exhibit 10.4 to the
Registrant’s Quarterly Report on Form 10-Q filed May 3,
2007).***
|
||
|
10.30
|
First
Amendment to Long Term Incentive Cash Award Agreement, dated September 28,
2007, between the Registrant and John R. Plachetka (filed as Exhibit 10.4
to the Registrant’s Quarterly Report on Form 10-Q filed November 5,
2007).***
|
||
|
10.31
|
Restricted
Stock Unit Agreement with John R. Plachetka dated February 14, 2007 under
Registrant’s 2000 Equity Compensation Plan as Amended and Restated (filed
as Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed
May 3, 2007).***
|
||
|
10.32
|
First
Amendment, dated September 28, 2007, to Restricted Stock Unit Agreement,
dated February 14, 2007, between the Registrant and John R. Plachetka
(filed as Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q
filed November 5, 2007).***
|
||
|
10.33
|
Nonqualified
Stock Option Grant issued to John R. Plachetka dated February 14, 2007
under Registrant’s 2000 Equity Compensation Plan as Amended and Restated
(filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q
filed May 3, 2007).***
|
||
|
10.34
|
Form
of Nonqualified Stock Option Agreement for PN 400 Incentive Program under
Second Amended and Restated 200 Equity Compensation Plan (filed as Exhibit
10.1 to the Registrant’s Current Report on Form 8-K filed on May 8,
2008).***
|
||
|
10.35
|
Amendment
No. 2 to the Collaboration and License Agreement, dated October 1, 2008,
between the registrant and AstraZeneca, AB (filed as Exhibit 10.1 to the
registrant’s Quarterly Report on Form 10-Q filed November 4, 2008).
†
|
||
|
10.36
|
Lease
Modification Agreement No. 1, dated as of February 16, 2009, by and
between the Registrant and The Exchange at Meadowmont LLC (filed as
Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on
February 17, 2009).
|
||
|
10.37
|
Executive
Employment Agreement, dated as of March 25, 2009, between the Company and
Everardus Orlemans, Ph.D.**
|
||
|
10.38
|
Executive
Employment Agreement, dated as of September 14, 2009, between the Company
and Elizabeth Cermak (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K, filed on September 14, 2009).***
|
||
|
10.39
|
Executive
Employment Agreement, dated as of December 10, 2009, between the Company
and John G. Fort, M.D. (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K, filed on December 11, 2009).***
|
||
|
21.1
|
List
of subsidiaries of the Registrant.**
|
||
|
23.1
|
Consent
of Ernst & Young LLP, Independent Registered Public Accounting
Firm.**
|
||
|
31.1
|
Certification
of the Chief Executive Officer pursuant to Rule 13a-14(a) under the
Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the
Sarbanes-Oxley Act of 2002.**
|
||
|
31.2
|
Certification
of the Chief Financial Officer pursuant to Rule 13a-14(a) under the
Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the
Sarbanes-Oxley Act of 2002.**
|
||
|
32.1
|
Certification
of the Chief Executive Officer pursuant to 18 U.S.C. 1350, as adopted
pursuant to Section 906 of the Sarbanes-Oxley Act of
2002.**
|
||
|
32.2
|
Certification
of the Chief Financial Officer pursuant to 18 U.S.C. 1350, as adopted
pursuant to Section 906 of the Sarbanes-Oxley Act of
2002.**
|
||
|
*
|
Incorporated
by reference to the same-numbered exhibit of the Registrant’s Registration
Statement on Form S-1, No. 333-35930.
|
||
|
**
|
Filed
herewith.
|
||
|
***
|
Compensation
Related Contract.
|
||
|
†
|
Confidential
treatment requested. Confidential materials omitted and filed separately
with the Securities and Exchange
Commission.
|
||
(b) Exhibits.
See Item
15(a)(3) above.
(c) Financial
Statement Schedules.
See
Item 15(a)(2) above.
Pursuant
to the requirements of Section 13 or 15(d) of the Securities Exchange Act of
1934, the Registrant has duly caused this Report to be signed on its behalf by
the undersigned, thereunto duly authorized.
|
Registrant:
|
|||||
|
POZEN
Inc.
|
|||||
|
Date:
|
March
9, 2010
|
By:
|
/s/
John R. Plachetka
|
||
|
John
R. Plachetka
|
|||||
|
Chief
Executive Officer
|
|||||
Pursuant to the requirements of the
Securities Exchange Act of 1934, this Report has been signed below by the
following persons on behalf of the registrant and in the capacities and on the
dates indicated.
|
Signature
|
Title
|
Date
|
||
|
/s/
John R. Plachetka
|
Chairman
of the Board, President
|
March
9, 2010
|
||
|
John
R. Plachetka
|
and
Chief Executive Officer
|
|||
|
(Principal
Executive Officer)
|
||||
|
/s/
William L. Hodges
|
Senior
Vice President, Finance and
|
March
9, 2010
|
||
|
William
L. Hodges
|
Administration
and Chief Financial
|
|||
|
Officer
(Principal Financial Officer)
|
||||
|
/s/
John E. Barnhardt
|
Vice
President, Finance and
|
March
9, 2010
|
||
|
John
E. Barnhardt
|
Administration
(Principal
|
|||
|
Accounting
Officer)
|
||||
|
/s/
Arthur S. Kirsch
|
Director
|
March
9, 2010
|
||
|
Arthur
S. Kirsch
|
||||
|
/s/
Angela M. Larson
|
Director
|
March
9, 2010
|
||
|
Angela
M. Larson
|
||||
|
/s/
Kenneth B. Lee, Jr.
|
Director
|
March
9, 2010
|
||
|
Kenneth
B. Lee Jr.
|
||||
|
/s/
James J. Mauzey
|
Director
|
March
9, 2010
|
||
|
James
J. Mauzey
|
||||
|
/s/
Jacques F. Rejeange
|
Director
|
March
9, 2010
|
||
|
Jacques
F. Rejeange
|
||||
|
/s/
Paul J. Rizzo
|
Director
|
March
9, 2010
|
||
|
Paul
J. Rizzo
|
POZEN
Inc.
Audited
Financial Statements
|
Management’s
Report on Internal Control Over Financial Reporting
|
F-2
|
|
Report
of Independent Registered Public Accounting Firm
|
F-3
|
|
Report
of Independent Registered Public Accounting Firm
|
F-4
|
|
Audited
Financial Statements
|
|
|
Balance
Sheets
|
F-5
|
|
Statements
of Operations
|
F-6
|
|
Statements
of Stockholders’ Equity
|
F-7
|
|
Statements
of Cash Flows
|
F-8
|
|
Notes
to Financial Statements
|
F-9
|
Management’s
Report on Internal Control Over Financial Reporting
Management of POZEN Inc. (the
“Company”) is responsible for establishing and maintaining adequate internal
control over financial reporting. Internal control over financial reporting, as
defined in Rule 13a-15(f) or 15d-15(f) promulgated under the Securities Exchange
Act of 1934, is a process designed to provide reasonable assurance regarding the
reliability of financial reporting and the preparation of financial statements
for external purposes in accordance with generally accepted accounting
principles. A company’s internal control over financial reporting includes those
policies and procedures that pertain to the maintenance of records that, in
reasonable detail, accurately and fairly reflect the transactions and
dispositions of the assets of the company; provide reasonable assurance that
transactions are recorded as necessary to permit preparation of financial
statements in accordance with generally accepted accounting principles, and that
receipts and expenditures of the company are being made only in accordance with
authorizations of management and directors of the company; and provide
reasonable assurance regarding prevention or timely detection of unauthorized
acquisition, use, or disposition of the company’s assets that could have a
material effect on the financial statements.
Because of its inherent limitations,
internal control over financial reporting may not prevent or detect
misstatements. Also, projections of any evaluation of effectiveness to future
periods are subject to the risk that controls may become inadequate because of
changes in conditions, or that the degree of compliance with the policies or
procedures may deteriorate. Management evaluated the Company’s internal control
over financial reporting as of December 31, 2009. In making this assessment,
management used the criteria set forth by the Committee of Sponsoring
Organizations of the Treadway Commission in Internal Control-Integrated
Framework (COSO). As a result of this assessment and based on the
criteria in the COSO framework, management has concluded that, as of December
31, 2009, the Company’s internal control over financial reporting was
effective.
The registered public accounting firm
that audited the financial statements included in this report has issued an
attestation report on our internal controls over financial
reporting.
|
/s/
John R. Plachetka
|
/s/
William L. Hodges
|
|||
|
Chairman,
Chief Executive Officer
|
Chief
Financial Officer
|
|||
|
March
9, 2010
|
|
Report
of Independent Registered Public Accounting
Firm
|
/s/ Ernst
& Young LLP
Raleigh,
North Carolina
March 9,
2010
Report of
Independent Registered Public Accounting Firm
The Board
of Directors and Stockholders of POZEN Inc.
We have
audited POZEN Inc.’s internal control over financial reporting as of December
31, 2009, based on criteria established in Internal Control—Integrated Framework
issued by the Committee of Sponsoring Organizations of the Treadway Commission
(the COSO criteria). POZEN Inc.’s management is responsible for maintaining
effective internal control over financial reporting, and for its assessment of
the effectiveness of internal control over financial reporting included in the
accompanying Management’s Report on Internal Control Over Financial Reporting.
Our responsibility is to express an opinion on the company’s internal control
over financial reporting based on our audit.
We
conducted our audit in accordance with the standards of the Public Company
Accounting Oversight Board (United States). Those standards require that we plan
and perform the audit to obtain reasonable assurance about whether effective
internal control over financial reporting was maintained in all material
respects. Our audit included obtaining an understanding of internal control over
financial reporting, assessing the risk that a material weakness exists, testing
and evaluating the design and operating effectiveness of internal control based
on the assessed risk, and performing such other procedures as we considered
necessary in the circumstances. We believe that our audit provides a reasonable
basis for our opinion.
A
company’s internal control over financial reporting is a process designed to
provide reasonable assurance regarding the reliability of financial reporting
and the preparation of financial statements for external purposes in accordance
with generally accepted accounting principles. A company’s internal control over
financial reporting includes those policies and procedures that (1) pertain to
the maintenance of records that, in reasonable detail, accurately and fairly
reflect the transactions and dispositions of the assets of the company; (2)
provide reasonable assurance that transactions are recorded as necessary to
permit preparation of financial statements in accordance with generally accepted
accounting principles, and that receipts and expenditures of the company are
being made only in accordance with authorizations of management and directors of
the company; and (3) provide reasonable assurance regarding prevention or timely
detection of unauthorized acquisition, use or disposition of the company’s
assets that could have a material effect on the financial
statements.
Because
of its inherent limitations, internal control over financial reporting may not
prevent or detect misstatements. Also, projections of any evaluation of
effectiveness to future periods are subject to the risk that controls may become
inadequate because of changes in conditions, or that the degree of compliance
with the policies or procedures may deteriorate.
In our
opinion, POZEN Inc. maintained, in all material respects, effective internal
control over financial reporting as of December 31, 2009, based on the COSO
criteria.
We also
have audited, in accordance with the standards of the Public Company Accounting
Oversight Board (United States), the balance sheets of POZEN Inc. as of December
31, 2009 and 2008 and the related statements of operations, stockholders’ equity
and cash flows for each of the three years in the period ended December 31, 2009
and our report dated March 9, 2010 expressed an unqualified opinion
thereon.
/s/ Ernst
& Young LLP
Raleigh,
North Carolina
March 9,
2010
|
|
POZEN
Inc.
|
|
|
Balance
Sheets
|
|
December
31,
|
||||||||
|
2009
|
2008
|
|||||||
|
ASSETS
|
|
|
||||||
|
Current
assets:
|
|
|
||||||
|
Cash
and cash equivalents
|
|
$
|
23,278,353
|
|
|
$
|
26,119,249
|
|
|
Short-term
investments
|
23,432,100
|
35,562,723
|
||||||
|
Accounts
receivable
|
1,146,072
|
8,119,435
|
||||||
|
Prepaid
expenses and other current assets
|
|
1,259,255
|
|
|
|
562,161
|
|
|
|
Total
current assets
|
|
49,115,780
|
|
|
|
70,363,568
|
|
|
|
Property
and equipment, net of accumulated depreciation
|
|
43,830
|
|
|
|
72,563
|
|
|
|
Total
assets
|
|
$
|
49,159,610
|
|
|
$
|
70,436,131
|
|
|
LIABILITIES
AND STOCKHOLDERS’ EQUITY
|
|
|
||||||
|
Current
liabilities:
|
|
|
||||||
|
Accounts
payable
|
|
$
|
2,412,335
|
|
|
$
|
7,328,428
|
|
|
Accrued
compensation
|
2,287,200
|
2,172,314
|
||||||
|
Accrued
expenses
|
|
3,501,262
|
|
|
|
5,737,254
|
|
|
|
Deferred
revenue
|
7,201,080
|
12,344,708
|
||||||
|
Total
current liabilities
|
|
15,401,877
|
|
|
|
27,582,704
|
|
|
|
Long-term
liabilities:
|
|
|
||||||
|
Deferred
revenue
|
|
—
|
|
|
|
7,201,080
|
|
|
|
Total
liabilities
|
|
15,401,877
|
|
|
|
34,783,784
|
|
|
|
Preferred
stock, $0.001 par value; 10,000,000 shares authorized, issuable in series,
of which 90,000 shares are designated Series A Junior Participating
Preferred Stock, none outstanding
|
—
|
—
|
||||||
|
Common
stock, $0.001 par value, 90,000,000 shares authorized; 29,825,365 and
29,778,310 shares issued and outstanding at December 31, 2009 and December
31, 2008, respectively
|
|
29,825
|
|
|
|
29,778
|
|
|
|
Additional
paid-in capital
|
|
173,715,127
|
|
|
|
168,541,451
|
|
|
|
Accumulated
other comprehensive income
|
11,918
|
221,520
|
||||||
|
Accumulated
deficit
|
|
(139,999,137
|
)
|
|
|
(133,140,402
|
)
|
|
|
Total
stockholders’ equity
|
|
33,757,733
|
|
|
|
35,652,347
|
|
|
|
Total
liabilities and stockholders’ equity
|
|
$
|
49,159,610
|
|
|
$
|
70,436,131
|
|
See
accompanying Notes to Financial Statements.
|
|
POZEN
Inc.
|
|
|
Statements
of Operations
|
|
Year
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
|
|
|
||||||||||
|
Revenue:
|
|
|||||||||||
|
Licensing
revenue
|
$
|
26,651,353
|
$
|
37,221,242
|
$
|
34,459,001
|
||||||
|
Development
revenue
|
5,536,053
|
28,912,399
|
18,985,344
|
|||||||||
|
Total
revenue
|
32,187,406
|
|
|
66,133,641
|
|
|
53,444,345
|
|
||||
|
Operating
expenses:
|
|
|
|
|||||||||
|
General
and administrative
|
|
|
17,767,048
|
|
|
|
12,314,574
|
|
|
|
11,474,608
|
|
|
Research
and development
|
|
|
22,447,833
|
|
|
|
61,934,337
|
|
|
|
39,962,688
|
|
|
Total
operating expenses
|
|
|
40,214,881
|
|
|
|
74,248,911
|
|
|
|
51,437,296
|
|
|
Interest
and other income
|
|
|
535,226
|
|
|
2,139,741
|
|
|
3,326,043
|
|
||
|
Income
(loss) before income tax benefit (expense)
|
|
|
(7,492,249
|
)
|
|
|
(5,975,529
|
)
|
|
|
5,333,092
|
|
|
Income
tax benefit (expense)
|
633,514
|
—
|
(667,000
|
)
|
||||||||
|
Net
income (loss) attributable to common stockholders
|
|
$
|
(6,858,735
|
)
|
|
$
|
(5,975,529
|
)
|
|
$
|
4,666,092
|
|
|
Basic
net income (loss) per common share
|
|
$
|
(0.23
|
)
|
|
$
|
(0.20
|
)
|
|
$
|
0.16
|
|
|
Shares
used in computing basic net income (loss) per common share
|
|
|
29,813,690
|
|
|
|
29,761,847
|
|
|
|
29,592,890
|
|
|
Diluted
net income (loss) per common share
|
$
|
(0.23
|
)
|
$
|
(0.20
|
)
|
|
$
|
0.15
|
|||
|
Shares
used in computing diluted net income (loss) per common
share
|
29,813,690
|
29,761,847
|
30,581,326
|
|||||||||
See
accompanying Notes to Financial Statements.
|
|
POZEN
Inc.
|
|
|
|
Statements
of Stockholders’ Equity
|
|
Accumulated
other
|
Total
|
|||||||||||||||||||
|
Common
|
Additional
|
Comprehensive
|
Accumulated
|
Stockholders'
|
||||||||||||||||
|
Stock
|
Paid-In
Capital
|
Income
(Loss)
|
Deficit
|
Equity
|
||||||||||||||||
|
Balance
at December 31, 2006
|
$ | 29,448 | $ | 155,920,068 | $ | (4,092 | ) | $ | (131,830,965 | ) | $ | 24,114,459 | ||||||||
|
Exercise
of common stock options
|
257 | 2,138,995 | - | - | 2,139,252 | |||||||||||||||
|
Increase
in unrealized gain on investments
|
- | - | 18,632 | - | 18,632 | |||||||||||||||
|
Stock-based
compensation
|
- | 4,312,374 | - | - | 4,312,374 | |||||||||||||||
|
Net
Income
|
- | - | - | 4,666,092 | 4,666,092 | |||||||||||||||
|
Balance
at December 31, 2007
|
29,705 | 162,371,437 | 14,540 | (127,164,873 | ) | 35,250,809 | ||||||||||||||
|
Exercise
of common stock options
|
73 | 166,815 | - | - | 166,888 | |||||||||||||||
|
Increase
in unrealized gain on investments
|
- | - | 206,980 | - | 206,980 | |||||||||||||||
|
Stock-based
compensation
|
- | 6,003,199 | - | - | 6,003,199 | |||||||||||||||
|
Net
Loss
|
- | - | - | (5,975,529 | ) | (5,975,529 | ) | |||||||||||||
|
Balance
at December 31, 2008
|
29,778 | 168,541,451 | 221,520 | (133,140,402 | ) | 35,652,347 | ||||||||||||||
|
Exercise
of common stock options
|
47 | 32,654 | - | - | 32,701 | |||||||||||||||
|
Decrease
in unrealized gain on investments
|
- | - | (209,602 | ) | - | (209,602 | ) | |||||||||||||
|
Stock-based
compensation
|
- | 5,141,022 | - | - | 5,141,022 | |||||||||||||||
|
Net
Loss
|
- | - | - | (6,858,735 | ) | (6,858,735 | ) | |||||||||||||
|
Balance
at December 31, 2009
|
$ | 29,825 | $ | 173,715,127 | $ | 11,918 | $ | (139,999,137 | ) | $ | 33,757,733 | |||||||||
|
See
accompanying Notes to Financial
Statements.
|
|
|
POZEN
Inc.
|
|
|
Statements
of Cash Flows
|
|
Year
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Operating
activities
|
|
|
|
|||||||||
|
Net
(loss) income
|
|
$
|
(6,858,735
|
)
|
|
$
|
(5,975,529
|
)
|
|
$
|
4,666,092
|
|
|
Adjustments
to reconcile net income (loss) to net cash (used in) provided by operating
activities:
|
|
|
|
|||||||||
|
Depreciation
|
|
|
36,744
|
|
|
81,665
|
|
|
89,678
|
|||
|
Loss
on disposal of fixed assets
|
1,051
|
—
|
—
|
|||||||||
|
Bond
amortization income
|
(350,950
|
)
|
(910,839
|
)
|
(1,850,403
|
)
|
||||||
|
Noncash
compensation expense
|
|
|
5,141,022
|
|
|
6,003,199
|
|
|
4,312,374
|
|||
|
Changes
in operating assets and liabilities:
|
|
|
|
|||||||||
|
Accounts
receivable
|
6,973,363
|
(5,990,432
|
)
|
1,138,150
|
||||||||
|
Prepaid
expenses and other current assets
|
|
|
(697,094
|
)
|
|
|
636,236
|
|
|
(89,891
|
)
|
|
|
Accounts
payable and accrued expenses
|
|
|
(7,037,199
|
)
|
|
|
7,512,943
|
|
|
3,568,599
|
||
|
Deferred
revenue
|
|
|
(12,344,708
|
)
|
|
|
(14,865,411
|
)
|
|
|
(4,459,001
|
)
|
|
Net
cash (used in) provided by operating activities
|
|
|
(15,136,506
|
)
|
|
|
(13,508,168
|
)
|
|
|
7,375,598
|
|
|
Investing
activities
|
|
|
|
|||||||||
|
Purchase
of equipment
|
|
|
(9,062
|
)
|
|
|
(36,744
|
)
|
|
|
(23,695
|
)
|
|
Purchase
of investments
|
(25,342,045
|
)
|
(64,382,222
|
)
|
(72,301,799
|
)
|
||||||
|
Sale
of investments
|
37,614,016
|
66,219,427
|
74,173,828
|
|||||||||
|
Net
cash provided by investing activities
|
|
|
12,262,909
|
|
|
1,800,461
|
|
|
1,848,334
|
|||
|
Financing
activities
|
|
|
|
|||||||||
|
Proceeds
from issuance of common stock
|
|
|
32,701
|
|
|
166,888
|
|
|
2,139,252
|
|||
|
Net
cash provided by financing activities
|
|
|
32,701
|
|
|
166,888
|
|
|
2,139,252
|
|||
|
Net
(decrease) increase in cash and cash equivalents
|
|
|
(2,840,896
|
)
|
|
|
(11,540,819
|
)
|
|
|
11,363,184
|
|
|
Cash
and cash equivalents at beginning of year
|
|
|
26,119,249
|
|
|
37,660,068
|
|
|
26,296,884
|
|||
|
Cash
and cash equivalents at end of year
|
|
$
|
23,278,353
|
|
$
|
26,119,249
|
|
$
|
37,660,068
|
|||
See
accompanying Notes to Financial Statements.
POZEN
Inc.
Notes to
Financial Statements
1. Significant
Accounting Policies
General
POZEN Inc. (“we” or “POZEN” or the
“Company”) was incorporated in the State of Delaware on September 25, 1996 and
is operating in a single reportable segment. The Company is a pharmaceutical
company focused primarily on products for the treatment of acute and chronic
pain and other pain-related conditions. Since inception, the Company has focused
its efforts on developing products which can provide improved efficacy, safety
or patient convenience in the treatment of acute and chronic pain and pain
related conditions. The Company has entered into collaboration agreements to
commercialize its product candidates and may continue to enter into such
collaborations. The Company has decided to retain control of certain of its
product candidates and is evaluating how best to commercialize such product
candidates. The Company’s licensing revenues include upfront payments upon
contract signing, additional payments if and when certain milestones in the
product’s development or commercialization are reached, and the eventual royalty
payments based on product sales. Additionally, the Company’s development
revenues include the billings for the direct costs and certain personnel-related
time incurred in performing additional development activities described under
its collaboration agreements. If we elect to commercialize future products
ourselves, we would record sales of such products as revenue.
Use
of Estimates
The preparation of financial statements
in conformity with accounting principles generally accepted in the United States
requires management to make estimates and assumptions that affect the reported
amounts in the financial statements and accompanying notes. Actual results could
differ from the estimates and assumptions used.
Revenue
Recognition
The Company records revenue under two categories: licensing revenues and
development revenues. With regard to the licensing revenues, the Company’s
licensing agreements have terms that include upfront payments upon contract
signing, additional payments if and when certain milestones in the product’s
development or commercialization are reached, and royalty payments based on
product sales. The non-refundable portion of upfront payments received under the
Company’s existing agreements is deferred by the Company upon receipt and
recognized on a straight-line basis over the period ending on the anticipated
date of regulatory approvals, as specified in the agreements relating to the
product candidates, or the conclusion of any obligation on the part of the
Company. For the Company’s current agreements, these periods are estimated to be
as follows:
|
·
|
The
September 2006 $40.0 million licensing fee received from AstraZeneca AB,
or AstraZeneca, related to the August 2006 Collaboration and License
Agreement with AstraZeneca has been deferred and was initially being
amortized over 40 months. The AstraZeneca licensing fee relates to the
Company’s proprietary fixed dose combinations of the proton pump
inhibitor, or PPI, esomeprazole magnesium with the non-steroidal
anti-inflammatory drug, or NSAID, naproxen, in a single tablet. As a
result of the revised development timeline agreed upon in the September
2007 amendment to the AstraZeneca agreement, we extended the amortization
period by 3 months. The September 2007 amendment included a $10.0 million
payment in connection with execution of the amendment. This payment was
deferred to be amortized over 31 months. In 2008, we subsequently extended
the amortization periods by 4 months, as a result of revisions to the
development timeline. We recognized $12.3 million and $13.7 million of
licensing revenue from the amortization of the AstraZeneca licensing fee
and September 2007 amendment for the fiscal years ended December 31, 2009
and 2008, respectively.
|
In
reviewing the terms of the executed agreement and considering the provisions of
FASB ASC 605-25, Multiple Element Arrangements, we concluded that our
involvement in the Global Product Team and the Joint Steering Committee during
the development phase of the collaboration represents a substantive performance
obligation or deliverable as defined in FASB ASC 605-25. Following FDA approval
of the NDA, we believe that participation on the Global Product Team and the
Joint Steering Committee represents a right and a governance role only, rather
than a substantive performance obligation. Given that the participation on the
Global Product Team and Joint Steering Committee during the development phase do
not meet criteria in FASB ASC 605-25 for separation (e.g., no separate
identifiable fair value), we concluded that this deliverable would be combined
with the upfront
payments
received and treated as a single unit-of-accounting for purposes of revenue
recognition. We recognize the combined unit of accounting over the estimated
period of obligation, involvement and responsibility – through the estimated NDA
approval / transfer date, which coincides with our substantive obligation to
serve on the Global Product Team and the Joint Steering Committee.
|
·
|
The
June 2003 initial licensing and patent-issuance milestone payments
totaling $25.0 million for MT 400 received from GlaxoSmithKline, or GSK,
have been deferred and were amortized over the expected period of
development. During 2005 the amortization period was decreased to 39
months based upon the August 2005 submission to the U.S. Food and Drug
Administration (“FDA”) of the Treximet®
new drug application (“NDA”) which occurred earlier than previously
anticipated. The 2005 change in the amortization period resulted in a $0.7
million increase in the 2005 full-year amortization. During 2006, based
upon the June 2006 receipt of an approvable letter from the FDA related to
the Treximet NDA and the December 2006 receipt of a notice from the FDA
that it had requested additional analyses and supporting information
relating to submitted data, $1.9 million of the $25 million initial
licensing and patent-issuance milestone payments was deferred to 2007.
With the receipt of a second approvable letter in August 2007, unamortized
deferred revenue was amortized through March 2008. We recognized $1.2
million of licensing revenue from the amortization of GSK milestone
payments during the fiscal year ended December 31, 2008 and no revenue was
recognized during the fiscal year ended December 31, 2009. The GSK upfront
payments were fully amortized in
2008.
|
Milestone payments are recognized as licensing revenue upon the achievement of
specified milestones if (i) the milestone is substantive in nature and the
achievement of the milestone was not reasonably assured at the inception of the
agreement; and (ii) the fees are non-refundable. Any milestone payments received
prior to satisfying these revenue recognition criteria are recorded as deferred
revenue. During the third quarter of 2009, we received a $10.0 million milestone
payment which was recorded as licensing revenue in the accompanying statement of
operations.
Treximet royalty revenue is recognized
when earned as will any future royalty revenues with respect to the manufacture,
sale or use of the Company’s products or technology. For Treximet or those
future arrangements where royalties are reasonably estimable, the Company
recognizes revenue based on estimates of royalties earned during the applicable
period and reflect in future revenue any differences between the estimated and
actual royalties. During the fiscal year ended December 31, 2009, the Company
recognized $4.3 and $2.4 million, respectively, of royalty revenue which is
included within licensing revenue in the accompanying statements of
operations.
With regards to the development
revenues, the Company’s licensing agreements may include payment for development
services provided by the Company on an hourly rate and direct expense basis. The
Company records such payments as revenue in accordance with the agreements
because we act as principal in the transaction. Under the collaboration
agreements with AstraZeneca and GSK, the Company recognizes as development
revenue the billings for the direct costs and certain personnel-related time
incurred in performing additional development activities described within the
related agreements. The collaboration agreements establish the rates for billing
personnel-related time incurred and consequently, the associated costs incurred
to perform the additional development activities are not separately captured
from ongoing personnel costs.
Development revenue and direct billed
costs for the years ended December 31, 2009, 2008 and 2007 were the
following:
|
2009
|
2008
|
2007
|
||||||||||
|
Development
Revenue
|
$ | 5,536,053 | $ | 28,912,399 | $ | 18,985,344 | ||||||
|
Direct
Costs
|
3,855,552 | 25,934,849 | 16,128,985 | |||||||||
Investments
Investments consist primarily of United States government and government agency
obligations, and corporate fixed income securities. The Company invests in
high-credit quality investments in accordance with its investment policy, which
minimizes the possibility of loss; however, given the recent disruption in the
credit markets and the downgrades of previous high-credit companies, the
possibility of a loss is increased. Under the Company’s investment policy,
investments that have a maturity of greater than three months and less than one
year are classified as short-term, are considered to be available-for-sale and
are carried at fair value with unrealized gains and losses recognized in other
comprehensive income (loss). Realized gains and losses are determined using the
specific identification method and transactions are recorded on a settlement
date basis. Marketable and non-marketable equity investments are evaluated, on
an on-going basis, for market impairment. If it is determined that a decline of
any investment is other-than-temporary, the investment would be written down to
fair value. For
the years
ended December 31, 2009, 2008 and 2007, the Company had $0.2 million, $1.2
million and $1.5 million, respectively, of interest income and $0.4 million,
$0.9 million and $1.8 million, respectively, of bond amortization income
included in other income for the period. As of December 31, 2009 and 2008, there
were no investments in a significant unrealized loss position.
Short-term investments consisted of the
following as of December 31, 2009:
|
Amortized
Cost
|
Unrealized
Gain
|
Unrealized
Loss
|
Fair
Value
|
|||||||||||||
|
Short-term
investments:
|
||||||||||||||||
|
U.S.
treasury and agency securities
|
$ | 20,679,695 | $ | 13,065 | $ | - | $ | 20,692,760 | ||||||||
|
Corporate
notes
|
2,740,487 | 1,623 | (2,770 | ) | 2,739,340 | |||||||||||
|
Total
short-term investments
|
$ | 23,420,182 | $ | 14,688 | $ | (2,770 | ) | $ | 23,432,100 | |||||||
Short-term investments consisted of the
following as of December 31, 2008:
|
Amortized
Cost
|
Unrealized
Gain
|
Unrealized
Loss
|
Fair
Value
|
|||||||||||||
|
Short-term
investments:
|
||||||||||||||||
|
U.S.
treasury and agency securities
|
$ | 30,429,208 | $ | 213,830 | $ | - | $ | 30,643,038 | ||||||||
|
Corporate
notes
|
4,911,995 | 12,584 | (4,894 | ) | 4,919,685 | |||||||||||
|
Total
short-term investments
|
$ | 35,341,203 | $ | 226,414 | $ | (4,894 | ) | $ | 35,562,723 | |||||||
Cash
and Cash Equivalents and Concentration of Credit Risk
The Company considers all highly liquid
investments with a maturity of three months or less when purchased to be cash
equivalents. Cash is invested in interest-bearing investment-grade securities.
Cash is restricted to the extent of a $94,684 letter of credit, maintained in
compliance with the terms of the Company’s office lease.
Cash and cash equivalents include
financial instruments that potentially subject the Company to a concentration of
credit risk. Cash and cash equivalents are of a highly liquid nature and are
insured by the respective financial institutions up to $250,000 per account. Any
excess amounts are uninsured. Cash and cash equivalents are deposited with high
credit quality financial institutions which invest primarily in U.S. Government
securities, highly rated commercial paper and certificates of deposit guaranteed
by banks which are members of the FDIC. The counterparties to the agreements
relating to the Company’s investments consist primarily of the U.S. Government
and various major corporations with high credit standings.
Fair
Value Measurement
Under
FASB ASC 820, fair value is defined as the price that would be received to sell
an asset or paid to transfer a liability (i.e. "the exit price") in an orderly
transaction between market participants at the measurement date. In determining
fair value, we use various valuation approaches, including quoted market prices
and discounted cash flows. FASB ASC 820 also establishes a hierarchy for inputs
used in measuring fair value that maximizes the use of observable inputs and
minimizes the use of unobservable inputs by requiring that the most observable
inputs be used when available. Observable inputs are inputs that market
participants would use in pricing the asset or liability developed based on
market data obtained from independent sources. Unobservable inputs are inputs
that reflect a company's judgment concerning the assumptions that market
participants would use in pricing the asset or liability developed based on the
best information available under the circumstances. The fair value hierarchy is
broken down into three levels based on the reliability of inputs as
follows:
|
·
|
Level
1 - Valuations based on quoted prices in active markets for identical instruments
that the Company is able to access. Since valuations are based on quoted
prices that are readily and regularly available in an active market,
valuation of these products does not entail a significant degree of
judgment.
|
|
·
|
Level
2 - Valuations based on quoted prices in active markets for instruments
that are similar,
or quoted prices in markets that are not active for identical or similar
instruments, and model-derived valuations in which all significant inputs
and significant value drivers are observable in active
markets.
|
|
·
|
Level
3 - Valuations based on inputs that are unobservable and significant to
the overall fair value measurement.
|
The
financial assets for which we perform recurring remeasurements are cash
equivalents and short-term investments. As of December 31, 2009, financial
assets utilizing Level 1 inputs included cash equivalents and short-term
investments. Financial assets utilizing Level 2 inputs included short-term
investments in government agency obligations and corporate fixed income
securities.
Fair
value is a market-based measure considered from the perspective of a market
participant who holds the asset or owes the liability rather than an
entity-specific measure. Therefore, even when market assumptions are not readily
available, our own assumptions are set to reflect those that market participants
would use in pricing the asset or liability at the measurement date. We use
prices and inputs that are current as of the measurement date, including during
periods of market dislocation, such as the recent illiquidity in the auction
rate securities market. In periods of market dislocation, the observability of
prices and inputs may be reduced for many instruments. This condition has
caused, and in the future may cause, our financial instruments to be
reclassified from Level 1 to Level 2 or from Level 2 to Level 3.
FASB ASC
820 requires that the valuation techniques used by us are consistent with at
least one of the three possible approaches: the market approach, income
approach, and/or cost approach. Our Level 1 valuations are based on the market
approach and consist primarily of quoted prices for identical items on active
securities exchanges. Our Level 2 valuations also use the market approach and
are based on significant other observable inputs such as quoted prices for
financial instruments not traded on a daily basis. We did not rely on Level 3
input for valuation of our securities at December 31, 2009.
The following table sets forth our
financial instruments carried at fair value as of December 31, 2009 and December
31, 2008:
|
Financial
Instruments
|
||||||||
|
Carried
at Fair Value
|
||||||||
|
December
31,
2009
|
December
31, 2008
|
|||||||
|
Assets:
|
||||||||
|
Cash
and cash equivalents
|
$ | 23,278,353 | $ | 26,119,249 | ||||
|
Short-term
investments
|
23,432,100 | 35,562,723 | ||||||
|
Total
cash and investments
|
$ | 46,710,453 | $ | 61,681,972 | ||||
The following table sets forth our
financial instruments carried at fair value within the SFAS 157 hierarchy and
using the lowest level of input as of December 31, 2009:
|
Financial
Instruments
|
||||||||||||||||
|
Carried
at Fair Value
|
||||||||||||||||
|
Quoted
prices
|
Significant
other
|
Significant
|
||||||||||||||
|
in
active Markets
|
observable
|
unobservable
|
||||||||||||||
|
for
identical items
|
inputs
|
inputs
|
||||||||||||||
|
(Level
1)
|
(Level
2)
|
(Level
3)
|
Total
|
|||||||||||||
|
Assets:
|
||||||||||||||||
|
Cash
and cash equivalents
|
$ | 23,278,353 | $ | — | $ | — | $ | 23,278,353 | ||||||||
|
Short-term
investments
|
— | 23,432,100 | — | 23,432,100 | ||||||||||||
|
Total
cash and investments
|
$ | 23,278,353 | $ | 23,432,100 | $ | — | $ | 46,710,453 | ||||||||
Realized gains and losses from sales of
our investments are included in “Interest and other income” and unrealized gains
and losses are included as a separate component of equity unless the loss is
determined to be “other-than-temporary.”
In determining whether a decline in
fair value below the original cost is other-than-temporary, we use
a systematic methodology that considers
all available evidence, including the credit rating of the relevant trust, the
parity score (a measure of the trust's ability to meet its obligations as they
come due), general market conditions, and industry and sector performance, among
other factors. We also consider the duration and extent to which the fair value
is less than cost, as well as our intent and ability to hold the investment
until recovery or, if necessary, to the instrument's maturity.
When determining whether an impairment
is other-than-temporary we also consider the following information: (i) if the
market value of the investment is below its current carrying value for an
extended period, which we generally define as nine to twelve months; (ii) if the
issuer has experienced significant financial declines; or (iii) if the issuer
has experienced significant changes in its credit quality, among other factors.
The Company did not have any other-than-temporary impairments during the periods
presented.
Accumulated
Other Comprehensive Income(Loss)
Accumulated other comprehensive income (loss) is comprised of unrealized gains
and losses on marketable securities and is disclosed as a component of
stockholders’ equity. The Company had $11,918 of unrealized gains on its
investments at December 31, 2009 and $221,520 of unrealized gains at December
31, 2008.
Comprehensive income (loss) consists of
the following components for the years ended December 31, 2009, 2008 and
2007:
|
Year
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Net
(loss) income
|
$ | (6,858,735 | ) | $ | (5,975,529 | ) | $ | 4,666,092 | ||||
|
Change
in unrealized (loss) gain on short-term investments
|
(209,602 | ) | 206,980 | 18,632 | ||||||||
|
Total
comprehensive (loss) income
|
$ | (7,068,337 | ) | $ | (5,768,549 | ) | $ | 4,684,724 | ||||
Equipment
Equipment consists primarily of
computer hardware and software and furniture and fixtures and is recorded at
cost. Depreciation is computed using an accelerated method over the estimated
useful lives of the assets ranging from five to seven years. Accumulated
depreciation at December 31, 2009 and 2008 totaled $0.7 million.
Research
and Development Costs, Including Clinical Trial Expenses
Research and development costs are
charged to operations as incurred. The Company has included in research and
development expenses the personnel costs associated with research and
development activities and costs associated with pharmaceutical development,
clinical trials, toxicology activities, and regulatory matters.
Income
Taxes
Income taxes are computed using the
asset and liability approach, which requires the recognition of deferred tax
assets and liabilities for the expected future tax consequences of events that
have been recognized in the Company’s financial statements or tax returns. In
estimating future tax consequences, the Company generally considers all expected
future events other than enactment of changes in tax law or rates. If it is more
likely than not that some or all of a deferred tax asset will not be realized,
the Company records a valuation allowance.
Net
Income (Loss) Per Share
Basic and
diluted net income or loss per common share amounts have been computed using the
weighted-average number of shares of common stock outstanding for the fiscal
years ended December 31, 2009, 2008 and 2007. During the fiscal years ended
December 31, 2009, 2008 and 2007, the Company had potential common stock
equivalents related to its outstanding stock options. These potential common
stock equivalents were not included in diluted loss per share, for the fiscal
years ended 2009 and 2008 because the effect would have been antidilutive.
Accordingly, basic and diluted net loss per share is the same for the fiscal
years 2009 and 2008. The Company has excluded the impact of any shares which
might be issued under the Rights Plan, detailed below, from the earnings per
share calculation because the Rights are not exercisable since the specified
contingent future event has not occurred.
Reconciliation
of denominators for basic and diluted earnings per share
computations:
|
Years
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Weighted-average
shares used in computing
basic
net income (loss) per share
|
29,813,690 | 29,761,847 | 29,592,890 | |||||||||
|
Effect
of dilutive securities
|
— | — | 988,436 | |||||||||
|
Weighted-average
shares used in computing
diluted
net income (loss) per share
|
29,813,690 | 29,761,847 | 30,581,326 | |||||||||
Fair
Value of Financial Instruments
Financial instruments consist of cash
and cash equivalents, short-term investments, accounts receivable and accounts
payable. The carrying values of these amounts approximate the fair value due to
the short-term nature of such instruments.
Patent
Costs
The Company expenses patent costs,
including legal expenses, in the period in which they are incurred. Patent
expenses are included in general and administrative expenses in the Company’s
statements of operations.
Stock-Based
Compensation
On January 1, 2006, we adopted
Statement of Financial Accounting Standards (“SFAS”) No. 123(R), “Share-Based
Payment,” which requires us to account for share-based payment transactions
using a fair value-based method and recognize the related expense in our results
of operations.
Under the fair value recognition
provisions of SFAS No. 123(R), stock-based compensation cost is estimated at the
grant date based on the fair value of the award and is recognized as expense
over the requisite service period of the award. The fair value of restricted
stock awards is determined by reference to the fair market value of our common
stock on the date of grant. Consistent with the valuation method we used for
disclosure-only purposes under the provisions of SFAS No. 123, we use the
Black-Scholes model to value service condition and performance condition option
awards under SFAS No. 123(R). For awards with only service conditions and
graded-vesting features, we recognize compensation cost on a straight-line basis
over the requisite service period. For awards with performance conditions
granted subsequent to our adoption of SFAS No. 123(R), we recognize compensation
cost over the expected period to achieve the performance conditions, provided
achievement of the performance conditions are deemed probable.
Contingencies
A purported class action lawsuit
claiming violations of securities laws was filed on August
10, 2007 in the U.S. District Court for the Middle District of North
Carolina by a holder of its securities against the Company, its chairman
and chief executive officer and one of its directors. The complaint alleges,
among other claims, violations of Section 10(b), Rule 10b-5, and Section 20(a)
of the Exchange Act arising out of allegedly false and misleading statements
made by the Company concerning its migraine drug candidate, Treximet, during the
purported class period, July 31, 2006 through August 1, 2007. By order dated
February 15, 2008, the Court appointed joint co-lead plaintiffs. On April 25,
2008, the Company received the plaintiffs’ amended and consolidated complaint
which added two current officers of the Company as additional defendants. The
Company and individual defendants filed motions to dismiss the amended and
consolidated complaint with the Court on June 26, 2008. On August 27, 2008, the
plaintiffs voluntarily dismissed their claims against one of the Company’s
directors. On February 19, 2009, Magistrate Judge Dixon, to whom the Court
had referred the motion to dismiss, issued a Recommendation that the Court grant
the Company and individual defendants' motion to dismiss without leave for
plaintiffs to file another amended complaint. Plaintiffs filed objections to the
recommendation on March 23, 2009 and a corrected version of the objections on
March 26, 2009. Defendants’ response to these objections was filed on April 20,
2009. On September 29, 2009, the Court granted the Company’s and individual
defendants’ motion to dismiss and dismissed the claims in their entirety with
prejudice. The plaintiffs have chosen not to appeal the case.
The
Company and GSK have received Paragraph IV Notice Letters from Par
Pharmaceuticals Inc., or Par, and Alphapharm Pty Ltd., or Alphapharm, and
Alphapharm’s designated agent, Mylan Pharmaceuticals Inc., Teva Pharmaceuticals
USA, or Teva, and Dr. Reddy’s Laboratories, Inc., or Dr. Reddy’s, informing us
that each company had filed an Abbreviated New Drug Application, or ANDA, with
the Food and Drug Administration, or FDA, seeking approval to market sumatriptan
85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm, Teva, and Dr. Reddy’s
have each indicated in their respective Notice Letters that they intend to
market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008, Alphapharm and Mylan on January 2, 2009 Teva, on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. The Company’s filing of these patent infringement
lawsuits within forty-five days of our receipt of the respective Notice Letters
from Par, Alphapharm, Teva, and Dr. Reddy’s resulted in the FDA automatically
instituting a stay, or bar, of approval of Par’s, Alphapharm’s Teva’s, and Dr.
Reddy’s respective ANDAs for up to 30 months or until a final court decision is
entered in the infringement suit in favor of the ANDA applicant, whichever
occurs first. Treximet currently has regulatory exclusivity through April 15,
2011. Treximet may be eligible for an additional six months of exclusivity upon
the completion of certain pediatric studies. Written and document discovery are
in progress. The cases are set for trial in the fourth quarter of
2010.
As with any litigation proceeding, we
cannot predict with certainty the eventual outcome of the class action lawsuit
described above if appealed or a patent infringement lawsuit against Par,
Alphapharm, Teva, and Dr. Reddy’s. We have incurred $5.1 million in legal fees
through the end of 2009. Furthermore, we will have to incur additional expenses
in connection with these lawsuits, which may be substantial. In the event of an
adverse outcome or outcomes, our business could be materially harmed. Moreover,
responding to and defending pending litigation will result in a significant
diversion of management’s attention and resources and an increase in
professional fees.
Under its 2003 commercialization
collaboration with Valeant NA, related to MT 300, if the Company chooses to
withdraw the MT 300 NDA for commercial or financial reasons under the conditions
specified in the agreement, it could be required to pay a withdrawal fee of $1.0
million. As a result of this contingency, $1.0 million of the $2.0 million
upfront payment received by the Company from Valeant NA pursuant to the
agreement was not initially recognized as revenue.
In July 2005, we received a letter from
Valeant NA, seeking payment of a $1.0 million withdrawal fee required under
certain conditions under the agreement. We do not believe that the withdrawal
fee is payable under the circumstances of receipt of the not-approvable letter
from the FDA. The agreement requires that unresolved disputes by the parties be
referred to the respective chief executive officers for resolution. If still
unresolved, the agreement provides for binding arbitration. Valeant NA has
disputed our conclusion that the withdrawal fee is not payable and has indicated
its intention to pursue the dispute resolution provisions provided for under the
agreement although the last written communication from Valeant NA was received
in March 2006. In 2008, based upon our evaluation of the facts and
circumstances, we recognized the remaining $1.0 million licensing fee for MT
300. We can give no assurance that Valeant NA will agree to termination terms
acceptable to us, or that we will not be required to pay Valeant NA the
withdrawal fee described above.
New
Accounting Pronouncements
In June 2009, the Financial Accounting
Standards Board (“FASB”) issued FASB Statement No. 168, The FASB Accounting Standards
Codification™ and the
Hierarchy of Generally Accepted Accounting Principles, which replaces
FASB Statement No. 162, Hierarchy of Generally Accepted
Accounting Principles. Statement No. 168 is effective for financial
statements issued for interim and annual periods ending after September 15,
2009. The FASB Accounting Standards Codification™ (ASC) is a single source of
authoritative US accounting and reporting standards applicable for all
nongovernmental entities, other than guidance issued by the SEC and its staff,
it supersedes current US GAAP including FASB, AICPA, EITF and related literature
and reorganizes thousands of US GAAP pronouncements into approximately 90
accounting topics. The Company adopted Statement 168 effective in its quarter
ending September 30, 2009.
2. License
Agreements
We have entered into and may continue
to enter into collaborations with established pharmaceutical or pharmaceutical
services companies to develop, commercialize and/or manufacture our product
candidates. Our existing collaborations are described below.
GlaxoSmithKline
(GSK)
In June 2003, we signed an agreement
with GSK for the development and commercialization of proprietary combinations
of a triptan (5-HT1B/1D
agonist) and a long-acting NSAID. The combinations covered by the agreement are
among the combinations of MT 400. Under the terms of the agreement, GSK has
exclusive rights in the U.S. to commercialize all combinations which combine
GSK’s triptans, including Imitrex®
(sumatriptan succinate) or Amerge®
(naratriptan hydrochloride), with a long-acting NSAID. We were responsible for
development of the first combination product, while GSK provided formulation
development and manufacturing. Pursuant to the terms of the agreement, we
received $25.0 million in initial payments from GSK following termination of the
waiting period under the Hart-Scott-Rodino notification program and the issuance
of a specified patent. In May 2004, we received a $15.0 million milestone
payment as a result of our commencement of Phase 3 clinical trial activities. In
October 2005, we received a $20.0 million milestone payment upon the FDA’s
acceptance for review of the NDA for Treximet, the trade name for the product.
On April 26, 2008 the Company received, from GSK, $20.0 million in milestone
payments which were associated with the approval of, and GSK’s intent to
commercialize, Treximet. In addition, GSK will pay us two sales performance
milestones totaling $80.0 million if certain sales thresholds are achieved. Up
to an additional $10.0 million per product is payable upon achievement of
milestones relating to other products. On December 31, 2009, the Company accrued
$1.1 million of Treximet royalty revenue and GSK will also pay us royalties on
all net sales of marketed products until at least the expiration of the last to
expire issued applicable patent (October 2, 2025) based upon the scheduled
expiration of currently issued patents. GSK may reduce, but not eliminate, the
royalty payable to us if generic competitors attain a pre-determined share of
the market for the combination product, or if GSK owes a royalty to one or more
third parties for rights it licenses from such third parties to commercialize
the product. The
agreement
terminates on the date of expiration of all royalty obligations unless earlier
terminated by either party for a material breach or by GSK at any time upon
ninety (90) days’ written notice to us for any reason or no reason. Among the
contract breaches that would entitle us to terminate the agreement is GSK’s
determination not to further develop or to launch the combination product under
certain circumstances. GSK has the right, but not the obligation, to bring, at
its own expense, an action for infringement of certain patents by third parties.
If GSK does not bring any such action within a certain time frame, we have the
right, at our own expense, to bring the appropriate action. With regard to
certain other patent infringements, we have the sole right to bring an action
against the infringing third party. Each party generally has the duty to
indemnify the other for damages arising from breaches of each party’s
representations, warranties and obligations under the agreement, as well as for
gross negligence or intentional misconduct. We also have a duty to indemnify GSK
for damages arising from our development and manufacture of MT 400 prior to the
effective date of the agreement, and each party must indemnify the other for
damages arising from the development and manufacture of any combination product
after the effective date.
We, along
with GSK, have received Paragraph IV Notice Letters from Par, Alphapharm,
Alphapharm’s designated agent, Mylan, Teva, and Dr. Reddy’s informing us that
each company had filed an ANDA with the FDA seeking approval to market
sumatriptan 85 mg/naproxen sodium 500 mg tablets. Par, Alphapharm Teva, and Dr.
Reddy’s have each indicated in their respective Notice Letters that they intend
to market a generic version of Treximet tablets before the expiration of U.S.
Patent Nos. 6,060,499, 6,586,458 and 7,332,183. GSK advised us that it has
elected not to exercise its first right to bring infringement suits against Par,
Alphapharm, Teva, and Dr. Reddy’s. Accordingly, we filed suit against Par on
November 14, 2008, Alphapharm and Mylan on January 2, 2009, Teva on April 14,
2009, and Dr. Reddy’s on August 21, 2009, all in the United States District
Court for the Eastern District of Texas. All four actions have since been
consolidated into one suit. Our filing of these patent infringement lawsuits
within forty-five days of our receipt of the respective Notice Letters from Par,
Alphapharm Teva, and Dr. Reddy’s resulted in the FDA automatically instituting a
stay, or bar, of approval of Par’s, Alphapharm’s Teva’s, and Dr. Reddy’s
respective ANDAs for up to 30 months or until a final court decision is entered
in the infringement suit in favor of the ANDA applicant, whichever occurs first.
Treximet currently has regulatory exclusivity through April 15, 2011. Treximet
may be eligible for an additional six months of exclusivity upon the completion
of certain pediatric studies. Written and document discovery are in progress.
The cases are set for trial in the fourth quarter of 2010.
AstraZeneca
AB (AstraZeneca)
In August 2006, we entered into a
collaboration and license agreement dated as of August 1, 2006 and effective
September 7, 2006 with AstraZeneca, a Swedish corporation, regarding the
development and commercialization of proprietary fixed dose
combinations of the PPI esomeprazole magnesium with the NSAID naproxen, in a
single tablet for the management of pain and inflammation associated with
conditions such as osteoarthritis and rheumatoid arthritis in patients who are
at risk for developing NSAID associated gastric ulcers. Under the terms of the
agreement, we granted to AstraZeneca an exclusive, fee-bearing license, in all
countries of the world except Japan, under our patents and know-how relating to
combinations of gastroprotective agents and NSAIDs (other than aspirin and its
derivatives). AstraZeneca had the right, which has now expired, to elect to
include Japan in the licensed territory within two years after the effective
date of the agreement. Pursuant to the terms of the agreement, we received an
upfront license fee of $40.0 million from AstraZeneca following termination of
the waiting period under the Hart-Scott-Rodino notification
program.
In
September 2007, we agreed with AstraZeneca to amend our collaboration and
license agreement effective as of September 6, 2007. Under the terms of the
amendment, AstraZeneca has agreed to pay us up to $345.0 million, in the
aggregate, in milestone payments upon the achievement of certain development,
regulatory and sales events. In September 2007 we received a $10.0 million
payment upon execution of the amendment and a $20.0 million payment in
recognition of the achievement of the primary endpoints for the PN400-104 study,
a study which compared acid suppression of different doses of VIMOVO (formerly
PN 400), and achievement of the interim results of the PN200-301 study, a six
month comparative trial of PN 200 as compared to EC naproxen in patients
requiring chronic NSAID therapy, meeting mutually agreed success criteria. An
additional $55.0 million will be paid upon achievement of certain development
and regulatory milestones, and $260.0 million will be paid as sales performance
milestones if certain aggregate sales thresholds are achieved. Under the
original agreement, we were to have received development and regulatory
milestones totaling $160.0 million, of which $20.0 million was to be paid upon
the successful completion of the proof of concept studies, and sales performance
milestones totaling $175.0 million.
In
addition, the amendment revised the royalty rates we were to have received under
the original agreement. Under the original agreement, we were to receive a
royalty based on annual net sales by AstraZeneca, its affiliates or sublicensees
during the royalty term. The royalty rate varied based on the level of annual
net sales of products made by AstraZeneca, its affiliates and sublicensees,
ranging from the mid-single digits to the mid-teens. Under the amendment, we
will now receive a flat, low double digit royalty rate during the royalty term
on annual net sales of products made by AstraZeneca, its affiliates and
sublicensees, in the U.S. and royalties ranging from the mid-single digits to
the high-teens on annual net sales of products made by AstraZeneca, its
affiliates and sublicensees outside of the U.S. The amendment also revises the
rate of reduction to the royalty rate based upon loss of market share due to
generic competition inside and outside of the U.S. to account for the new
royalty structure.
Our right
to receive royalties from AstraZeneca for the sale of such products under the
collaboration and license agreement, as amended, expires on a country-by-country
basis upon the later of (a) expiration of the last-to-expire of certain patent
rights relating to such products in that country, and (b) ten years after the
first commercial sale of such products in such country.
We
further amended the collaboration and license agreement effective October 1,
2008 to shorten the timing of AstraZeneca’s reimbursement obligation for certain
development expenses incurred by us under the agreement and to update the
description of the target product profile studies (as defined in the agreement)
for VIMOVO.
We retain responsibility for the
development and filing of the NDA for the product in the U.S. AstraZeneca is
responsible for all development activities outside the U.S., as well as for all
manufacturing, marketing, sales and distribution activities worldwide. We have
agreed to bear all expenses related to certain specified U.S. development
activities. All other development expenses, including all manufacturing-related
expenses, will be paid by AstraZeneca. The agreement established joint
committees with representation of both us and AstraZeneca to manage the
development and commercialization of the product. The committees operate by
consensus, but if consensus cannot be reached, we generally will have the
deciding vote with respect to development activities required for marketing
approval of the product in the U.S. and AstraZeneca generally will have the
deciding vote with respect to any other matters.
The agreement, unless earlier
terminated, will expire upon the payment of all applicable royalties for the
products commercialized under the agreement. Either party has the right to
terminate the agreement by notice in writing to the other party upon or after
any material breach of the agreement by the other party, if the other party has
not cured the breach within 90 days after written notice to cure has been given,
with certain exceptions. The parties also can terminate the agreement for cause
under certain defined conditions. In addition, AstraZeneca can terminate the
agreement, at any time, at will, for any reason or no reason, in its entirety or
with respect to countries outside the U.S., upon 90 days’ notice. If terminated
at will, AstraZeneca will owe us a specified termination payment or, if
termination occurs after the product is launched, AstraZeneca may, at its
option, under and subject to the satisfaction of conditions specified in the
agreement, elect to transfer the product and all rights to us.
Valeant
Pharmaceuticals North American (Valeant NA) (formerly Xcel Pharmaceuticals
Inc.)
In September 2003, we signed an
agreement with Valeant NA for the further development and commercialization of
MT 300. In March 2005, Valeant Pharmaceuticals International (Valeant
International) acquired Valeant NA. Under the terms of the agreement, Valeant NA
would have exclusive rights in the United States to commercialize MT 300 subject
to certain minimum commercialization obligations. Pursuant to the terms of the
agreement, Valeant NA paid us an upfront fee of $2.0 million. Upon certain
future regulatory approvals, including the FDA’s approvals relating to MT 300,
and the achievement of a predetermined sales threshold on MT 300, potential
milestone payments of up to $8.0 million would be due. Valeant NA is also
obligated to pay us royalties on all combined net sales of MT 300 and Valeant
NA’s D.H.E. 45®
(dihydroergotamine mesylate) Injection, upon commercialization of MT 300, until
at least the expiration of the last to expire issued applicable patent (2020,
based upon the scheduled expiration of the last to expire currently issued
applicable patent), subject to reduction in certain instances of generic
competition, or in the event that Valeant NA pays royalties to one or more third
parties to license rights from such third parties to commercialize MT 300. The
agreement terminates on the date of expiration of all royalty obligations (2020,
based upon the scheduled expiration of the last to expire currently issued
applicable patent) unless earlier terminated by either party for a material
breach or in the event that either party determines not to pursue approval of MT
300, under the conditions described below. Under certain circumstances, the
agreement provides for the terminating party to facilitate the assumption of its
responsibilities by the non-terminating party. Generally, each party must
indemnify the other for damages arising from such party’s breach of its
representations, warranties and obligations under the agreement, as well as for
the gross negligence or willful misconduct by either party. Additionally,
Valeant NA must indemnify us for damages arising from the development,
manufacture or use of any product after the effective date of the agreement,
while we must indemnify Valeant NA for any damages arising from such
development, manufacture or use prior to the effective date. We must also
indemnify Valeant NA for any use by us or any sub licensee of certain technology
owned by Valeant NA.
Under the
agreement, if we determine that additional studies or data that are required by
the FDA for approval of the NDA for MT 300 would jeopardize the commercial
viability of MT 300 or exceed our financial resources available for MT 300, we
may elect to withdraw the NDA. If we notify Valeant of this situation and
Valeant NA does not assume control of efforts to seek approval of the NDA, then,
under the conditions outlined in the agreement, upon notice from Valeant NA the
agreement will terminate and we would be required to pay Valeant NA a withdrawal
fee of $1.0 million. If Valeant decides to assume development, it would be
credited $1.0 million in development expense. Based upon our understandings from
our most recent communications with the FDA and our understanding of the FDA’s
current standards for approval of migraine drugs, we believe it is not possible
to reverse the not approvable status of the NDA for MT 300. In July 2005, we
received a letter from Valeant NA seeking payment of the $1.0 million withdrawal
fee. We do not believe that the withdrawal fee is payable based on our receipt
of a not-approvable letter from the FDA with respect to our NDA for MT 300. The
agreement requires that unresolved disputes by the parties be referred to the
respective chief executive officers for resolution. If still unresolved, the
agreement provides for binding arbitration.
Based upon the delays related to
commercialization of MT 300 due to our receipt of the not-approvable letter for
MT 300 and our efforts to address with the FDA the issues raised in that letter,
we and Valeant NA had previously agreed to extend the time for certain
activities under our agreement with Valeant NA that are dependent on the FDA’s
actions with respect to MT 300. In the event of termination of the agreement,
these obligations will not be relevant. Valeant NA has disputed our conclusion
that the withdrawal fee is not payable and has indicated its intention to pursue
the dispute resolution provisions provided for under the agreement although the
last written communication from Valeant NA was received in March 2006. In 2008,
based upon our evaluation of the facts and circumstances, we recognized the
remaining $1.0 million licensing fee for MT 300. We can give no assurance that
Valeant NA will agree to termination terms acceptable to us, or that we will not
be required to pay Valeant NA the withdrawal fee described above.
3. Stockholders’
Equity
Shares
Reserved for Future Issuance
In January 2005, the Company approved a
stockholder rights plan (the “Rights Plan”), pursuant to which the Company
entered into a Rights Agreement dated January 12, 2005 with StockTrans, Inc., as
Rights Agent, and the Company declared a dividend of a right to acquire one
preferred share purchase right (a “Right”) for each outstanding share of the
Company’s Common Stock, $0.001 par value per share, to stockholders of record at
the close of business on January 28, 2005. Generally, the Rights only are
triggered and become exercisable if a person or group acquires beneficial
ownership of 15 percent or more of the Company’s common stock or announces a
tender offer for 15 percent or more of the Company’s common stock. The Rights
Plan is similar to plans adopted by many other publicly-traded companies. The
effect of the Rights Plan is to discourage any potential acquirer from
triggering the Rights without first convincing POZEN’s Board of Directors that
the proposed acquisition is fair to, and in the best interest of, the
shareholders and the Company. The provisions of the Plan will substantially
dilute the equity and voting interest of any potential acquirer unless the Board
of Directors determines that the proposed acquisition is in the best interest of
the shareholders. In connection with the Plan, the Company designated 90,000
shares of its authorized Preferred Stock as Series A Junior Participating
Preferred Stock. Each Right, if and when exercisable, will entitle the
registered holder to purchase from the Company one one-thousandth of a share of
Series A Junior Participating Preferred Stock, $0.001 par value per share, at a
purchase price of $80.00 for each one one-thousandth of a share, subject to
adjustment. Each holder of a Right (except for the Acquiring Person (as defined
in the Rights Plan), whose Rights will be null and void upon such event) shall
thereafter have the right to receive, upon exercise, that number of shares of
Common Stock of the Company (or, in certain circumstances, cash, property or
other securities of the Company) which equals the exercise price of the Right
divided by 50% of the current market price (as defined in the Rights Agreement)
per share of Common Stock at the date of the occurrence of such event. The
Rights can be terminated by POZEN’s Board of Directors and are subject to
optional redemption by the Company at $0.001 per Right. The Rights Plan has a
10-year term and contains provisions requiring a periodic review and evaluation
by the Board of Directors.
At December 31, 2009, shares of our
common stock reserved for future issuance are as follows:
|
|
||||
|
Common
shares available for grant under stock option plans
|
1,298,505 | |||
|
Common
shares issuable pursuant to options and restricted stock units granted
under equity compensations plans
|
4,206,853 | |||
|
Rights
Plan shares issuable as Series A Junior Participating Preferred
Stock
|
90,000 | |||
|
Total
reserved
|
5,595,358 | |||
4. Accrued
Expenses
Accrued expenses consist of the
following at December 31:
|
2009
|
2008
|
|||||||
|
Research
and development costs
|
$ | 2,710,533 | $ | 5,481,698 | ||||
|
Other
|
790,729 | 255,556 | ||||||
| $ | 3,501,262 | $ | 5,737,254 | |||||
5. Income
Taxes
At December 31, 2009 and 2008, we
had federal net operating loss carryforwards of approximately $95.1 million and
$81.6 million respectively, state net economic loss carryforwards of
approximately $73.1 million and $68.8 million respectively, and research and
development credit carryforwards of approximately $12.4 million and $11.8
million, respectively. The amount of the NOL related to excess tax based stock
compensation is $4.8 million and $4.8 million at December 31, 2009 and 2008,
respectively. The federal and state net operating loss carryforwards begin to
expire in 2021 and 2014, respectively, and the research and development credit
carryforwards begin to expire in 2017. For financial reporting purposes, a
valuation allowance has been recognized to offset the deferred tax assets
related to the carryforwards. Of the total increase in valuation allowance of
$1.6 million, an increase of $2.5 million was allocable to current operating
activities, a decrease of $0.3 million was allocable to a change in the state
tax rate, and a decrease of $.6 million was related to the carryback claim that
the Company plans to file for AMT taxes paid in 2007. When the valuation
allowance is realized, a portion related to excess stock option compensation
will be realized as an increase in additional paid-in capital. The utilization
of the loss carryforwards to reduce future income taxes will depend on the
Company’s ability to generate sufficient taxable income prior to the expiration
of the loss carryforwards. In addition, the maximum annual use of net operating
loss and research credit carryforwards is limited in certain situations where
changes occur in stock ownership.
Deferred income taxes reflect the net
tax effects of temporary differences between the carrying amount of assets and
liabilities for financial reporting purposes and the amounts used for income tax
purposes. Significant components of the Company’s deferred tax assets are as
follows at December 31:
|
($
in thousands)
|
||||||||
|
2009
|
2008
|
|||||||
|
Deferred
tax assets:
|
|
|
||||||
|
Net
operating loss carryforwards
|
|
$
|
36,569
|
|
|
$
|
31,371
|
|
|
Research
and development credits
|
|
|
12,363
|
|
|
11,781
|
||
|
Revenue
recognition
|
|
|
2,618
|
|
|
7,279
|
||
|
Equity
compensation and other
|
|
|
6,298
|
|
|
5,802
|
||
|
Total
deferred tax assets
|
|
|
57,848
|
|
|
56,233
|
||
|
Valuation
allowance
|
|
|
(57,848
|
)
|
|
|
(56,233
|
)
|
|
Net
deferred tax asset
|
|
$
|
—
|
|
|
$
|
—
|
|
The components for the income tax
benefit (expense) were as follows:
|
($
in thousands)
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
State
income taxes
|
|
|||||||||||
|
Current
|
|
$
|
—
|
|
$
|
—
|
|
$
|
—
|
|||
|
Deferred
|
|
—
|
|
|
—
|
|
|
—
|
||||
|
Federal
income taxes
|
||||||||||||
|
Current
|
634
|
—
|
(667)
|
|||||||||
|
Deferred
|
—
|
—
|
—
|
|||||||||
|
Income
tax benefit (expense)
|
$
|
634
|
$
|
—
|
$
|
(667)
|
||||||
The actual income tax benefit (expense)
for the years ended December 31, 2009, 2008 and 2007, differed from the
amounts computed by applying the U.S. federal tax rate of 35% to loss (income)
before taxes as a result of the following:
|
($
in thousands)
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Loss
(income) before income tax
|
|
$
|
7,492
|
|
$
|
5,976
|
|
$
|
(5,333
|
)
|
||
|
Federal
tax rate
|
|
|
35
|
%
|
|
|
35
|
%
|
|
|
35
|
%
|
|
Federal
income tax provision at statutory rate
|
|
|
2,622
|
|
|
2,091
|
|
|
(1,867
|
)
|
||
|
State
tax provision
|
|
|
102
|
|
|
36
|
|
|
405
|
|||
|
2,724
|
2,127
|
(1,462
|
)
|
|||||||||
|
Increase
(decrease) in income tax benefit resulting from:
|
|
|
|
|||||||||
|
Research
and development credits
|
|
|
582
|
|
|
1,461
|
|
|
1,551
|
|||
|
Non-deductible
expenses and other
|
|
|
(811
|
)
|
|
|
(847
|
)
|
|
|
(705
|
)
|
|
Change
in state tax rate
|
(246
|
)
|
—
|
90
|
||||||||
|
Change
in valuation allowance
|
|
|
(1,615
|
)
|
|
|
(2,741
|
)
|
|
|
(141
|
)
|
|
Income
tax benefit (expense)
|
|
$
|
634
|
|
|
$
|
—
|
|
|
$
|
(667
|
)
|
The Company adopted the provisions of
FASB ASC 740-10, Uncertainty in Income Taxes, on January 1, 2007. As of December
31, 2006, the Company had not recorded a contingent tax liability.
The Company had gross unrecognized tax
benefits of approximately $0.1 million as of January 1, 2009. As of December 31,
2009, the total gross unrecognized tax benefits were approximately $0.2 million
and of this total, none would reduce the Company’s effective tax rate if
recognized. The Company does not anticipate a significant change in total
unrecognized tax benefits or the Company’s effective tax rate due to the
settlement of audits or the expiration of statutes of limitations within the
next 12 months.
The Company’s policy for recording
interest and penalties associated with tax audits is to record them as a
component of provision for income taxes. The Company has not recorded any
interest or penalty since the adpotion of FASB ASC 740-10.
The Company has analyzed its filing
positions in all significant federal, state and foreign jurisdictions where it
is required to file income tax returns, as well as open tax years in these
jurisdictions. With few exceptions, the Company is no longer subject to US
Federal and state and local tax examinations by tax authorities for years before
2006, although carryforward attributes that were generated prior to 2006 may
still be adjusted upon examination by the IRS if they either have been or will
be used in a future period. No income tax returns are under examination by
taxing authorities.
|
|
Rollforward
of gross unrecognized tax
positions:
|
|
Gross
tax liability at January 1, 2009
|
$ | 136,400 | ||
|
Additions
for tax positions of the current year
|
103,600 | |||
|
Reductions
for tax positions of the prior years
|
(21,400 | ) | ||
|
Gross
tax liability at December 31, 2009
|
$ | 218,600 | ||
6. Equity
Compensation Plans
On November 20, 1996, the Company
established a Stock Option Plan (the “Option Plan”) and authorized the issuance
of options for up to 1,605,310 shares of common stock to attract and retain
quality employees and to allow such employees to participate in the growth of
the Company. In May 2000, the Board of Directors adopted, and in June 2000 the
stockholders approved, the POZEN Inc. 2000 Equity Compensation Plan (the “Plan”)
which authorized up to 3,000,000 shares of common stock for issuance under the
terms of the Plan. In May 2004 an award of 98,135 restricted stock units was
made to the Company’s chief executive officer under the Plan. Those restricted
stock units are not reflected as stock options in the charts below. In 2004, the
Board of Directors adopted and the stockholders approved an amendment to and
restatement of the Plan which provided for an increase in the number of shares
of common stock authorized for issuance under the Plan, from 3,000,000 to
5,500,000, or an increase of 2,500,000 shares. On June 13, 2007, the
stockholders approved the amendment and restatement of the Plan to, among other
things, increase the number of shares authorized for issuance under the 2000
Plan from 5,500,000 to 6,500,000 shares and continue the various performance
criteria for use in establishing specific vesting targets for certain awards
under the Plan so as to qualify the compensation attributable to any such awards
as performance-based compensation under Section 162(m) of the Internal Revenue
Code.
A summary of the Company’s stock option
activity and related information is as follows:
|
Number
of Shares
|
Weighted-Average
Exercise Price
|
|||||||
|
Balance
at December 31, 2008
|
3,732,179 | $ | 9.86 | |||||
|
Options
granted
|
606,285 | 5.99 | ||||||
|
Exercised
|
(35,055 | ) | 0.93 | |||||
|
Forfeited
|
(467,399 | ) | 10.38 | |||||
|
Balance
at December 31, 2009
|
3,836,010 | $ | 9.29 | |||||
The adoption of SFAS No. 123(R) had a
significant impact on our results of operations. Our statements of operations
for the years ended December 31, 2009, 2008 and 2007 include the following
stock-based compensation expense:
|
Years
ended December 31,
|
||||||||||||
|
2009
|
2008
|
2007
|
||||||||||
|
Research
and development
|
$ | 1,734,488 | $ | 2,180,018 | $ | 1,217,264 | ||||||
|
General
and administrative
|
3,406,534 | 3,823,181 | 3,095,110 | |||||||||
|
Total
expenses
|
$ | 5,141,022 | $ | 6,003,199 | $ | 4,312,374 | ||||||
Unrecognized stock-based compensation
expense, including time-based options, performance-based options and restricted
stock awards, expected to be recognized over an estimated weighted-average
amortization period of 1.53 years, was $4.1 million at December 31,
2009.
Time-Based Stock
Awards
The fair value of each time-based award
is estimated on the date of grant using the Black-Scholes option valuation
model, which uses the assumptions described below. Our weighted-average
assumptions used in the Black-Scholes valuation model for equity awards with
time-based vesting provisions granted for the years ended December 31, 2009,
2008 and 2007 are shown in the following table:
|
2009
|
2008
|
2007
|
||||||||||
|
Expected
volatility
|
72.5 – 77.8 | % | 71.3 – 74.5 | % | 76.0 – 79.2 | % | ||||||
|
Expected
dividends
|
0 | % | 0 | % | 0 | % | ||||||
|
Expected
terms
|
6.0
Years
|
5.0
– 6.25 Years
|
6.25
Years
|
|||||||||
|
Risk-free
interest rate
|
2.2 – 2.95 | % | 2.6 – 4.4 | % | 4.4 – 5.1 | % | ||||||
For the years ended December 31, 2009,
2008 and 2007, the expected volatility rate was estimated based on historical
volatility of POZEN common stock over approximately a six year period. For the
years ended December 31, 2009 and 2008, the expected term was based upon average
historical terms to exercise. For the year ended December 31, 2007, the expected
term was estimated based on a simplified method, as allowed under SEC Staff
Accounting Bulletin No. 107, “Share-Based Payment”, averaging the vesting term
and original contractual term. The risk-free interest rate is based on seven
year U.S. Treasury securities. The pre-vesting forfeiture rate used for the
years ended December 31, 2009, 2008 and 2007 was based on historical rates. We
adjust the estimated forfeiture rate based upon actual experience.
A summary of the time-based stock
awards as of December 31, 2009, and changes during the year ended December 31,
2009, are as follows:
|
Time-Based
Stock Awards
|
Underlying
Shares
(000s)
|
Weighted-Average
Exercise Price
|
Average
Remaining Contractual Term
(years)
|
Aggregate
Intrinsic Value
(000s)
|
||||||||||||
|
Outstanding
at December 31, 2008
|
3,732 | $ | 9.86 | 5.2 | $ | 197 | ||||||||||
|
Granted
|
606 | 5.99 | ||||||||||||||
|
Exercised
|
(35 | ) | 0.93 | |||||||||||||
|
Forfeited
or expired
|
(467 | ) | 10.38 | |||||||||||||
|
Outstanding
at December 31, 2009
|
3,836 | 9.29 | 5.0 | $ | 662 | |||||||||||
|
Exercisable
at December 31, 2009
|
2,612 | $ | 9.04 | 4.2 | $ | 520 | ||||||||||
The aggregate intrinsic value of
options outstanding represents the pretax value (the period’s closing market
price, less the exercise price, times the number of in-the-money options) that
would have been received by all option holders had they exercised their options
at the end of the period. The exercise price of stock options granted during the
years ended December 31, 2009, 2008 and 2007 was equal to the market price of
the underlying common stock on the grant date. The total intrinsic value of
stock options exercised during the years ended December 31, 2009, 2008 and 2007
was $0.2 million, $0.6 million and $2.3 million, respectively.
Restricted Stock and
Restricted Stock Units
For the years ended December 31, 2009,
2008 and 2007, the Company recognized $0.1 million, $0.2 million and $0.2
million, respectively, in compensation expense related to restricted stock
units. As of December 31, 2009, there was an aggregate $0.1 million of
unrecognized compensation expense related to unvested restricted stock units. Of
the aggregate amount, $26,000 unrecognized compensation expense related to
unvested restricted stock units under the 2007 award of 20,200 restricted stock
units with a grant-date per-share fair value of $16.89 and $36,000 unrecognized
compensation expense related to unvested restricted stock units under the June
3, 2009 award of 11,000 restricted stock units with a grant-date per-share fair
value of $7.75. As of December 31, 2009, there was no unrecognized compensation
expense related to the May 2004 award of 98,135 restricted stock units. There
were 14,487 unvested restricted stock units outstanding at December 31,
2009.
Performance-Based
Awards
On May 6,
2008, pursuant to an incentive program (the “PN incentive program”) approved by
the Compensation Committee of the Board of Directors of the Company, stock
options were granted to all of the Company’s employees, including its executive
officers, to purchase an aggregate of 281,433 shares of common stock. On
September 10, 2008, additional stock options were granted under the PN incentive
program, to purchase 11,700 shares of common stock. Twenty-five percent (25%) of
the PN incentive program options granted vested during September 2009, upon the
acceptance by the FDA of the NDA for VIMOVOTM
(enteric-coated naproxen / immediate release esomeprazole magnesium,
formerly referred to as PN 400). The remaining seventy-five percent (75%) of the
options granted will vest upon the receipt by the Company of an action letter
from the FDA indicating approval of the NDA for VIMOVO. The options have a
ten-year term. The May 6, 2008 and September 10, 2008 option grants have
exercise prices of $14.45 and $10.82, respectively, which was equal to the
NASDAQ reported market closing price of the Company’s common stock on the date
of grant. The weighted average grant-date fair value of these
performance-based options was $9.66 and $7.08 per share for the May 6, 2008 and
September 1, 2008 option grants, respectively. The fair value of the
performance-based options granted under the PN Incentive Program was estimated
as of the grant date using the Black-Scholes option valuation model without
consideration of the performance measures. The options also include provisions
that require satisfactory employee performance prior to vesting. Additionally,
20,000 options were granted to an executive officer on May 6, 2008 under the PN
incentive plan, with identical grant and exercise terms except that 100% of the
options granted vested during September 2009, upon acceptance by the FDA of the
NDA for VIMOVO. The Company is recognizing compensation costs for these awards
over the expected service period. Total expense related to these awards for the
years ended December 31, 2009 and 2008 were $1.1 million and $0.9 million,
respectively.
As of December 31, 2009, there was $0.4
million in unrecognized compensation expense related to performance-based awards
granted under the PN incentive program. The December 31, 2009 amount is expected
to be recognized over the period ending July 31, 2010. There were 177,794
unvested performance-based options outstanding at December 31, 2009. There were
56,075 awards forfeited during the year ended December 31, 2009. There were no
awards forfeited during the year ended December 31, 2008. No performance-based
awards were exercised during the years ended December 31, 2009 and December 31,
2008. At December 31, 2009, the performance-based options had no intrinsic value
and a remaining contractual life of 8.3 years.
7. Leases
The Company leases its office space and
certain equipment under cancellable and noncancellable operating lease
agreements. Rent expense incurred by the Company was approximately $442,000,
$431,000 and $412,000, for the fiscal years ended December 31, 2009, 2008, and
2007, respectively. The following is a schedule of noncancellable future minimum
lease payments for operating leases at December 31, 2009:
|
($
in thousands)
|
||||
|
2010
|
$ | 220 | ||
|
2011
|
462 | |||
|
2012
|
471 | |||
|
2013
|
441 | |||
|
2014
– there after
|
866 | |||
| $ | 2,460 | |||
On February 16, 2009, the Company
modified certain terms to our existing lease agreement, dated November 21, 2001,
relating to approximately 17,009 square feet of office space located at Exchange
Office Building, Chapel Hill, North Carolina. Under the terms of the
modification, the lease term was extended for an additional 5 years and 7
months, terminating on September 30, 2015. The modification also provides the
Company with a reduced notice period of 7 months for renewals of the lease. The
Company is also entitled to a 3-year lease extension option available at the end
of the term and a first offer right on available space located within the
Exchange Office Building property. As a result of entering into the
modification, the Company’s noncancellable future minimum lease payments for
operating leases increased by approximately $2.7 million over the lease term.
The Company is recognizing rent expense on a straight-line basis over the term
of the lease which resulted in a defered rent balance of $66.5 thousand at
December 31, 2009.
8. Retirement
Savings Plan
In July 1997, the Company adopted a
defined contribution 401(k) plan (the “Plan”) covering substantially all
employees who are at least 21 years of age. Based upon management’s discretion,
the Company may elect to make contributions to the Plan. During the years ended
December 31, 2009, 2008, and 2007, the Company made contributions of $235,581,
$256,690, and $242,358, respectively, to the Plan.
9. Summary
of Operations by Quarter (Unadited)
|
2009
|
||||||||||||||||
|
1st
Quarter
|
2nd
Quarter
|
3rd
Quarter
|
4th
Quarter
|
|||||||||||||
|
Revenue
|
||||||||||||||||
|
Licensed revenue
|
$ | 4,103,620 | $ | 4,034,689 | $ | 14,290,273 | $ | 4,222,771 | ||||||||
|
Development
revenue
|
4,654,762 | 881,290 | — | — | ||||||||||||
|
Total
revenue
|
8,758,382 | 4,915,979 | 14,290,273 | 4,222,771 | ||||||||||||
|
Operating
expenses
|
12,453,348 | 9,342,424 | 7,717,077 | 10,702,031 | ||||||||||||
|
Income
(loss) before income tax benefit (expense)
|
(3,463,259 | ) | (4,270,420 | ) | 6,657,586 | (6,416,156 | ) | |||||||||
|
Income
tax benefit
|
- | - | - | 633,514 | ||||||||||||
|
Net
income (loss) attributable to common stockholders
|
$ | (3,463,259 | ) | (4,270,420 | ) | 6,657,586 | (5,782,642 | ) | ||||||||
|
Basic
net income (loss) per common share
|
$ | (0.12 | ) | (0.14 | ) | 0.22 | (0.19 | ) | ||||||||
|
Diluted
net income (loss) per common share
|
$ | (0.12 | ) | (0.14 | ) | 0.22 | (0.19 | ) | ||||||||
|
Shares
used in computing basic net income (loss) per common share
|
29,778,310 | 29,815,228 | 29,825,365 | 29,825,365 | ||||||||||||
|
Shares
used in computing diluted net income (loss) per common
share
|
29,778,310 | 29,815,228 | 30,023,987 | 29,825,365 | ||||||||||||
|
2008
|
||||||||||||||||
|
1st
Quarter
|
2nd
Quarter
|
3rd
Quarter
|
4th
Quarter
|
|||||||||||||
|
Revenue
|
||||||||||||||||
|
Licensed revenue
|
$ | 3,851,082 | $ | 24,519,015 | $ | 3,603,100 | $ | 5,248,046 | ||||||||
|
Development
revenue
|
3,977,908 | 8,605,038 | 7,542,097 | 8,787,355 | ||||||||||||
|
Total
revenue
|
7,828,990 | 33,124,053 | 11,145,197 | 14,035,401 | ||||||||||||
|
Operating
expenses
|
15,961,507 | 20,287,090 | 19,456,674 | 18,543,640 | ||||||||||||
|
Net
income (loss) attributable to common stockholders
|
$ | (7,371,253 | ) | $ | 13,334,103 | $ | (7,854,980 | ) | $ | (4,083,399 | ) | |||||
|
Basic
net income (loss) per common share
|
$ | (0.25 | ) | $ | 0.45 | $ | (0.26 | ) | $ | (0.14 | ) | |||||
|
Diluted
net income (loss) per common share
|
$ | (0.25 | ) | $ | 0.43 | $ | (0.26 | ) | $ | (0.14 | ) | |||||
|
Shares
used in computing basic net income (loss) per common share
|
29,723,563 | 29,759,250 | 29,786,264 | 29,778,310 | ||||||||||||
|
Shares
used in computing diluted net income (loss) per common
share
|
29,723,563 | 30,707,710 | 29,786,264 | 29,778,310 | ||||||||||||
Because of the method used in
calculating per share data, the quarterly per share data will not necessarily
add to the per share data as computed for the year.
EXHIBIT
INDEX
|
Exhibit
No.
|
Description
|
||
|
3.1
|
Amended
and Restated Certificate of Incorporation of the
Registrant.*
|
||
|
3.2
|
Second
Amended and Restated Bylaws of POZEN Inc., approved September 19, 2007
(filed as Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed
on September 20, 2007).
|
||
|
3.3
|
Certificate
of Designations of Series A Junior Participating Preferred Stock (filed as
Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed January
12, 2005).
|
||
|
4.1
|
See
Exhibits 3.1, 3.2 and 3.3 for provisions of the Amended and Restated
Certificate of Incorporation and Second Amended and Restated Bylaws of the
Registrant defining rights of the holders of Common Stock and Series A
Junior Participating Preferred Stock of the Registrant.
|
||
|
4.2
|
Rights
Agreement dated January 12, 2005 between Registrant and StockTrans, Inc.
(filed as Exhibit 4.1 to the Registrant’s Current Report on Form 8-K filed
January 12, 2005).
|
||
|
10.1
|
Stock
Option Plan of the Registrant.*
|
||
|
10.2
|
First
Amendment to Stock Option Plan dated February 14,
1997.*
|
||
|
10.3
|
Second
Amended and Restated 2000 Equity Compensation Plan of the Registrant
(filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q
filed August 7, 2007).***
|
||
|
10.4
|
Form
of Incentive Stock Option Agreement under Registrant’s Second Amended and
Restated Equity Compensation Plan (filed as Exhibit 10.2 to the
Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.5
|
Form
of Nonqualified Stock Option Agreement under Registrant’s Second Amended
and Restated Equity Compensation Plan (filed as Exhibit 10.3 to the
Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.6
|
Form
of Non-Employee Director Nonqualified Stock Option Agreement under Second
Amended and Restated Equity Compensation Plan (filed as Exhibit 10.4 to
the Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***.
|
||
|
10.7
|
Form
of Non-Employee Director Restricted Stock Unit Agreement under Second
Amended and Restated Equity Compensation Plan (filed as Exhibit 10.5 to
the Registrant’s Quarterly Report on Form 10-Q filed August 7,
2007).***
|
||
|
10.8
|
Second
Amended and Restated Executive Employment Agreement with John R. Plachetka
dated March 14, 2006 (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K filed March 16, 2006).***
|
||
|
10.9
|
First
Amendment to Second Amended and Restated Executive Employment Agreement
with John R. Plachetka dated March 14, 2006 (filed as Exhibit 10.1 to the
Registrant’s Quarterly Report on Form 10-Q filed November 5,
2007).***
|
||
|
10.10
|
Executive
Employment Agreement with John E. Barnhardt dated July 25, 2001 (filed as
Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q filed
October 31, 2001).***
|
||
|
10.11
|
First
Amendment to Executive Employment Agreement with John E. Barnhardt, dated
September 28, 2007 (filed as Exhibit 10.7 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007).***
|
||
|
10.12
|
Executive
Employment Agreement with William L. Hodges dated August 3, 2004 (filed as
Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed
October 27, 2004).***
|
||
|
10.13
|
First
Amendment to Executive Employment Agreement with William L. Hodges, dated
September 28, 2007 (filed as Exhibit 10.5 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007).***
|
||
|
10.14
|
POZEN
Inc. 2001 Long Term Incentive Plan (filed as Exhibit 10.6 to the
Registrant’s Quarterly Report on Form 10-Q filed October 31,
2001).***
|
||
|
10.15
|
Certificate
of Award dated August 1, 2001 issued to John R. Plachetka pursuant to
POZEN Inc. 2001 Long Term Incentive Plan (filed as Exhibit 10.7 to the
Registrant’s Quarterly Report on Form 10-Q filed October 31,
2001).***
|
||
|
10.16
|
Summary
of Non-Employee Director Compensation (filed as Exhibit 10.16 to the
Registrant’s Annual Report on Form 10-K filed March 8,
2007).***
|
||
|
10.17
|
Lease
Agreement between The Exchange at Meadowmont LLC and the Registrant dated
as of November 21, 2001 (filed as Exhibit 10.21 to the Registrant’s Annual
Report on Form 10-K filed April 1, 2002).
|
||
|
10.18
|
Product
Development and Commercialization Agreement dated June 11, 2003 between
the Registrant and Glaxo Group Ltd. (filed as Exhibit 10.1 to the
Registrant’s Quarterly Report on Form 10-Q filed August 12, 2003 and Form
10-Q/A filed November 8. 2004).†
|
||
|
10.19
|
License
Agreement dated June 11, 2003 between the Registrant and Glaxo Group Ltd.
(filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q
filed August 12, 2003 and Quarterly Report on Form 10-Q/A filed November
8. 2004).†
|
||
|
10.20
|
Collaboration
and License Agreement dated September 3, 2003 between the Registrant and
Valeant Pharmaceuticals NA (formerly Xcel Pharmaceuticals, Inc.) (filed as
Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed
November 6, 2003 and Quarterly Report on Form 10-Q/A filed November 8.
2004).†
|
||
|
10.21
|
Restricted
Stock Unit Agreement dated May 4, 2004 between Registrant and John R.
Plachetka (filed as Exhibit 10.4 to the Registrant’s Quarterly Report on
Form 10-Q filed July 30, 2004).***
|
||
|
10.22
|
First
Amendment, dated September 28, 2007, to Restricted Stock Unit Agreement,
dated May 4, 2004, between Registrant and John R. Plachetka (filed as
Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed
November 5, 2007).***
|
||
|
10.23
|
Form
of Non-Qualified Stock Option Agreement for Trexima grants issued pursuant
Registrant’s Equity Compensation Plan, as amended and restated (filed as
Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed January
7, 2005).***
|
||
|
10.24
|
Development,
Option and License Agreement dated May 15, 2003 between the Registrant and
Nycomed Danmark ApS (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K filed July 28, 2005, and Current Report on Form 8-K/A
filed January 10, 2006).†
|
||
|
10.25
|
Collaboration
and License Agreement dated August 1, 2006 between the Registrant and
AstraZeneca AB (filed as Exhibit 10.1 to the Registrant’s Quarterly Report
on From 10-Q filed November 3, 2006).†
|
||
|
10.26
|
Amendment
No. 1 to the Collaboration and License Agreement, dated September 6, 2007,
between the Registrant and AstraZeneca AB (filed as Exhibit 10.8 to the
Registrant’s Quarterly Report on Form 10-Q filed November 5, 2007).
†
|
||
|
10.27
|
Side
Letter dated September 19, 2006 Re: Collaboration and License Agreement
dated as of August 1, 2006 by and between the Registrant and AstraZeneca
AB (filed as 10.2 to the Registrant’s Quarterly Report on From 10-Q filed
November 3, 2006).†
|
||
|
10.28
|
Side
Letter Agreement, dated October 1, 2007, between the Registrant and
AstraZeneca, AB (filed as Exhibit 10.9 to the Registrant’s Quarterly
Report on Form 10-Q filed November 5, 2007). †
|
||
|
10.29
|
Long-Term
Cash Incentive Award Agreement between the Registrant and John R.
Plachetka dated February 14, 2007 (filed as Exhibit 10.4 to the
Registrant’s Quarterly Report on Form 10-Q filed May 3,
2007).***
|
||
|
10.30
|
First
Amendment to Long Term Incentive Cash Award Agreement, dated September 28,
2007, between the Registrant and John R. Plachetka (filed as Exhibit 10.4
to the Registrant’s Quarterly Report on Form 10-Q filed November 5,
2007).***
|
||
|
10.31
|
Restricted
Stock Unit Agreement with John R. Plachetka dated February 14, 2007 under
Registrant’s 2000 Equity Compensation Plan as Amended and Restated (filed
as Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed
May 3, 2007).***
|
||
|
10.32
|
First
Amendment, dated September 28, 2007, to Restricted Stock Unit Agreement,
dated February 14, 2007, between the Registrant and John R. Plachetka
(filed as Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q
filed November 5, 2007).***
|
||
|
10.33
|
Nonqualified
Stock Option Grant issued to John R. Plachetka dated February 14, 2007
under Registrant’s 2000 Equity Compensation Plan as Amended and Restated
(filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q
filed May 3, 2007).***
|
||
|
10.34
|
Form
of Nonqualified Stock Option Agreement for PN 400 Incentive Program under
Second Amended and Restated 200 Equity Compensation Plan (filed as Exhibit
10.1 to the Registrant’s Current Report on Form 8-K filed on May 8,
2008).***
|
||
|
10.35
|
Amendment
No. 2 to the Collaboration and License Agreement, dated October 1, 2008,
between the registrant and AstraZeneca, AB (filed as Exhibit 10.1 to the
registrant’s Quarterly Report on Form 10-Q filed November 4, 2008).
†
|
||
|
10.36
|
Lease
Modification Agreement No. 1, dated as of February 16, 2009, by and
between the Registrant and The Exchange at Meadowmont LLC (filed as
Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on
February 17, 2009).
|
||
|
10.37
|
Executive
Employment Agreement, dated as of March 25, 2009, between the Company and
Everardus Orlemans, Ph.D.**
|
||
|
10.38
|
Executive
Employment Agreement, dated as of September 14, 2009, between the Company
and Elizabeth Cermak (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K, filed on September 14, 2009).***
|
||
|
10.39
|
Executive
Employment Agreement, dated as of December 10, 2009, between the Company
and John G. Fort, M.D. (filed as Exhibit 10.1 to the Registrant’s Current
Report on Form 8-K, filed on December 11, 2009).***
|
||
|
21.1
|
List
of subsidiaries of the Registrant.**
|
||
|
23.1
|
Consent
of Ernst & Young LLP, Independent Registered Public Accounting
Firm.**
|
||
|
31.1
|
Certification
of the Chief Executive Officer pursuant to Rule 13a-14(a) under the
Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the
Sarbanes-Oxley Act of 2002.**
|
||
|
31.2
|
Certification
of the Chief Financial Officer pursuant to Rule 13a-14(a) under the
Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the
Sarbanes-Oxley Act of 2002.**
|
||
|
32.1
|
Certification
of the Chief Executive Officer pursuant to 18 U.S.C. 1350, as adopted
pursuant to Section 906 of the Sarbanes-Oxley Act of
2002.**
|
||
|
32.2
|
Certification
of the Chief Financial Officer pursuant to 18 U.S.C. 1350, as adopted
pursuant to Section 906 of the Sarbanes-Oxley Act of
2002.**
|
||
|
*
|
Incorporated
by reference to the same-numbered exhibit of the Registrant’s Registration
Statement on Form S-1, No. 333-35930.
|
||
|
**
|
Filed
herewith.
|
||
|
***
|
Compensation
Related Contract.
|
||
|
†
|
Confidential
treatment requested. Confidential materials omitted and filed separately
with the Securities and Exchange
Commission.
|
||
(b) Exhibits.
See Item
15(a)(3) above.
(c) Financial
Statement Schedules.
See
Item 15(a)(2) above.
- F-27
-