Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - MEDICINOVA INC | d8k.htm |
 ©
MediciNova, Inc. 2010 Exhibit 99.1 Accelerating the global development and commercialization of innovative pharmaceuticals |
 ©
MediciNova, Inc. 2010 Forward-Looking Statements Forward-Looking Statements Statements in this presentation that are not historical in nature constitute forward-looking statements
within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act
of 1995. These forward-looking statements include statements regarding MediciNova’s
clinical trials supporting the safety and efficacy of its product candidates and the potential
novelty of such product candidates as treatments for disease, plans and objectives for clinical trials and product development, strategies, future performance, expectations, assumptions, financial condition,
liquidity and capital resources. These forward-looking statements may be preceded by, followed
by or otherwise include the words "believes," "expects," "anticipates,"
"intends," "estimates," "projects," "can," "could," "may," “will,” "would," or similar expressions. Actual results or events may differ materially from those expressed or implied in any forward-looking
statements due to various factors, including the risks and uncertainties inherent in clinical
trials and product development and commercialization, such as the uncertainty in results of
clinical trials for product candidates, the uncertainty of whether the results of clinical trials
will be predictive of results in later stages of product development, the risk of delays or failure to obtain or maintain regulatory approval, the risk of failure of the third parties upon whom MediciNova relies
to conduct its clinical trials and manufacture its product candidates to perform as expected, the
risk of increased cost and delays due to delays in the commencement, enrollment, completion or
analysis of clinical trials or significant issues regarding the adequacy of clinical trial designs
or the execution of clinical trials and the timing, cost and design of future clinical trials and
research activities; the timing of expected filings with the FDA; MediciNova’s failure to execute strategic plans or strategies successfully; MediciNova’s collaborations with third parties; MediciNova’s ability to
realize the anticipated strategic and financial benefits from its acquisition of Avigen, Inc., to
integrate the two ibudilast development programs and to pursue discussions with potential partners
to secure a strategic collaboration to advance the clinical development of the combined
development program; the availability of funds to complete product development plans and MediciNova’s ability to raise sufficient capital when needed, or at all; intellectual property or contract rights; and the other
risks and uncertainties described in MediciNova’s filings with the Securities and Exchange
Commission, including MediciNova’s annual report on Form 10-K for the year ended December
31, 2008 and its subsequent periodic reports on Forms 10-Q and 8-K. You are cautioned not
to place undue reliance on these forward-looking statements, which speak only as of the date January 11, 2010. MediciNova disclaims any intent or obligation to revise or update these forward-looking
statements. |
 ©
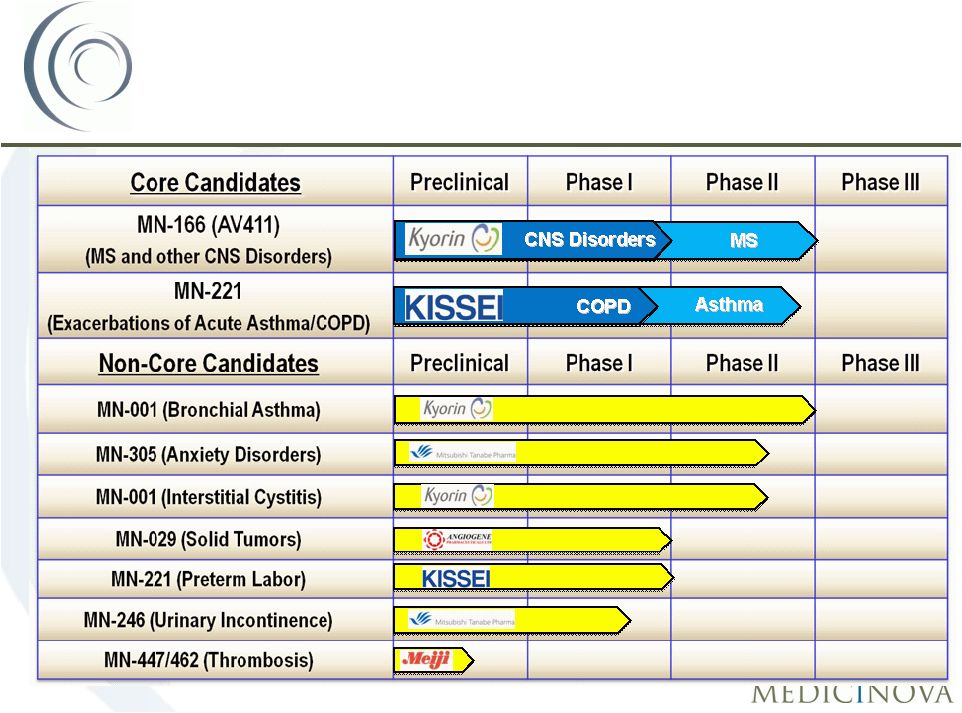
MediciNova, Inc. 2010 3 MediciNova Overview: • Founded in September 2000 • Headquartered in San Diego, CA • Additional office in Tokyo, Japan • Dual-listing on NasdaqGM as MNOV and Osaka Securities Exchange as 4875 • $85.7 million Market Cap (NasdaqGM) as of 12/31/2009 Development Company Focused on Differentiated Product Candidates • Unique access to differentiated, potentially high-value assets primarily from Japanese
alliances (Kyorin, Kissei, Mitsubishi Tanabe Pharma, Meiji) New Approaches to Treat Serious Medical Conditions: • MN-221: Intravenous (IV) acute asthma and COPD candidate • Potential $1 billion+ combined market opportunity worldwide* • MN-166 (AV411): oral multiple sclerosis candidate; additional enabled neurological
conditions • In 2008, over $8 billion in worldwide MS therapeutic sales** Corporate Overview: Corporate Overview: MediciNova, Inc. MediciNova, Inc. **Source: Individual annual reports of leading MS companies, 2008 *Source: Internal MediciNova projections |
 Pro Forma Summary of Securities Ownership Potential Financing from Avigen as of 12/31/2009 Acquisition 4 Pro Forma Stockholder Review Pro Forma Stockholder Review Note: Assumes Second Payment Consideration in the amount of $1.1 million was paid at closing, that all convertible notes, including those issued as part of the Second Payment Consideration, were converted on December 31, 2009 and that no rounding of fractional shares occurred as part of the conversion calculations. Common Stock Equivalents # Shares MediciNova Stockholders 12,172,510 Avigen Stockholders (1st payment consideration) 4,330,268 Avigen Stockholders (2nd payment consideration) 134,325 MediciNova Exercisable Options 1,319,391 Total 17,956,494 Ownership % MediciNova Stockholders 67.8% Avigen Stockholders (both pmt. considerations) 24.9% MediciNova Exercisable Options 7.3% Total 100.0% Potential Cash Available to MediciNova (Conversion price of $6.80 per MNOV share) First Payment Consideration (@ ~$1.19/share) $29,445,824.82 Second Payment Consideration (@ ~$0.04/share) $913,408.56 Total Cash Potentially Available to MediciNova $30,359,233.38 This pro forma ownership table is presented for illustrative purposes only and does not indicate actual ownership of MediciNova shares at any past, present, of future date. Actual ownership of MediciNova shares will depend on a variety of factors, including the actual amount of the Second Payment Consideration, the rounding of fractional shares set
forth in the governing the convertible notes and the number of holders electing to convert their convertible notes into MediciNova
shares. |
 ©
MediciNova, Inc. 2010 5 Definition: • Acute Asthma Exacerbations: Long-lasting and severe asthma episodes that are not responsive to initial bronchodilator or corticosteroid therapies • COPD Exacerbations: Sustained worsening of the patient's condition, from the stable state and beyond normal day-to-day variations, that is acute in onset Market Opportunity: • Potential $1 billion+ combined market opportunity worldwide* (acute asthma & COPD exacerbations) Current Standard of Care (SOC): • Beta agonists - Inhaled • Anticholinergics - Inhaled • Corticosteroids - IV or oral **Source: National Center for Health Statistics / CDC, WHO website, “Core Health indicators” MN-221 for Exacerbations of MN-221 for Exacerbations of Acute Asthma and COPD Acute Asthma and COPD COPD Discharged Hospitalized 72% 28% ~1.9 million Asthma 52% 48% ~1.5 million Hospitalization Rates Amongst Asthma and COPD Patients** *Source: Internal MediciNova projections |
 ©
MediciNova, Inc. 2010 6 MN-221: A New Approach to Treating MN-221: A New Approach to Treating Exacerbations of Acute Asthma & COPD Exacerbations of Acute Asthma & COPD MN-221: A novel, highly selective 2 - adrenergic receptor agonist Three potential advantages over current therapy: 1. Improved Efficacy • Route of Administration (IV v. Inhalation) 2. Improved Safety • Higher selectivity for 2 receptor than 1 • Partial agonist for 1 receptor 3. Reduced Health Care Expenses |
 ©
MediciNova, Inc. 2010 7 Human Human -Adrenergic Receptor -Adrenergic Receptor Selectivity Selectivity Test Drug 1 IC 50 (M) 2 IC 50 (M) 2 -Adrenoceptor Selectivity (IC 50 for 1 / IC 50 for 2 ) Levalbuterol 7.40E-06 1.40E-06 5.3 Albuterol 9.40E-06 1.60E-06 5.9 Terbutaline 6.00E-05 6.50E-06 9.2 MN-221 5.90E-06 1.40E-07 42.4 |
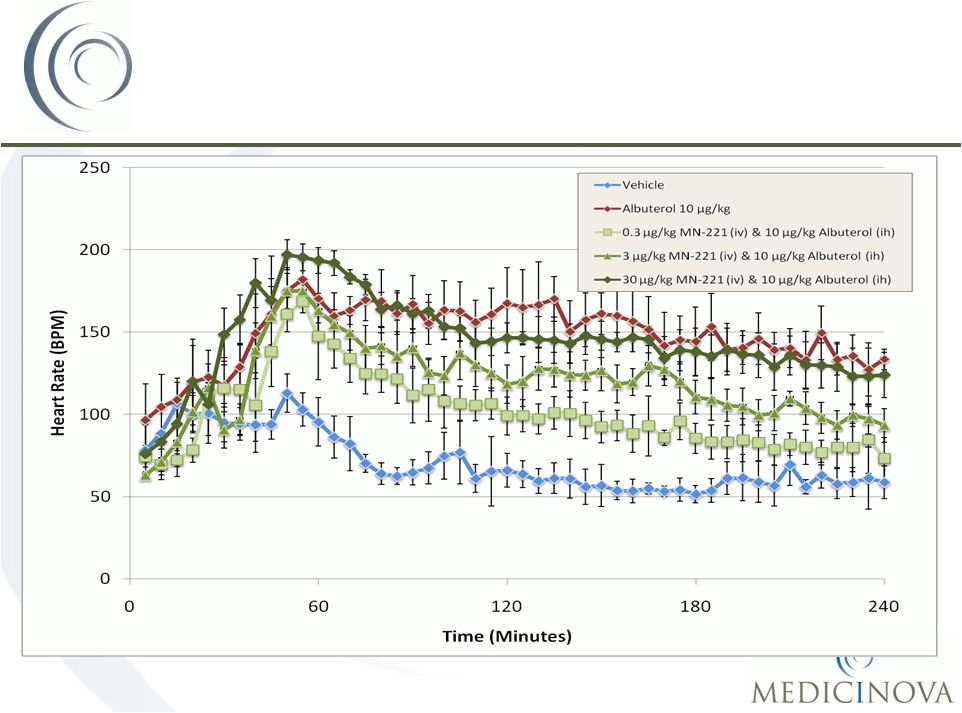 ©
MediciNova, Inc. 2010 Effect on Heart
rate: Effect on Heart
rate: Combination of MN-221 & Albuterol Combination of MN-221 & Albuterol in Dogs in Dogs 8 |
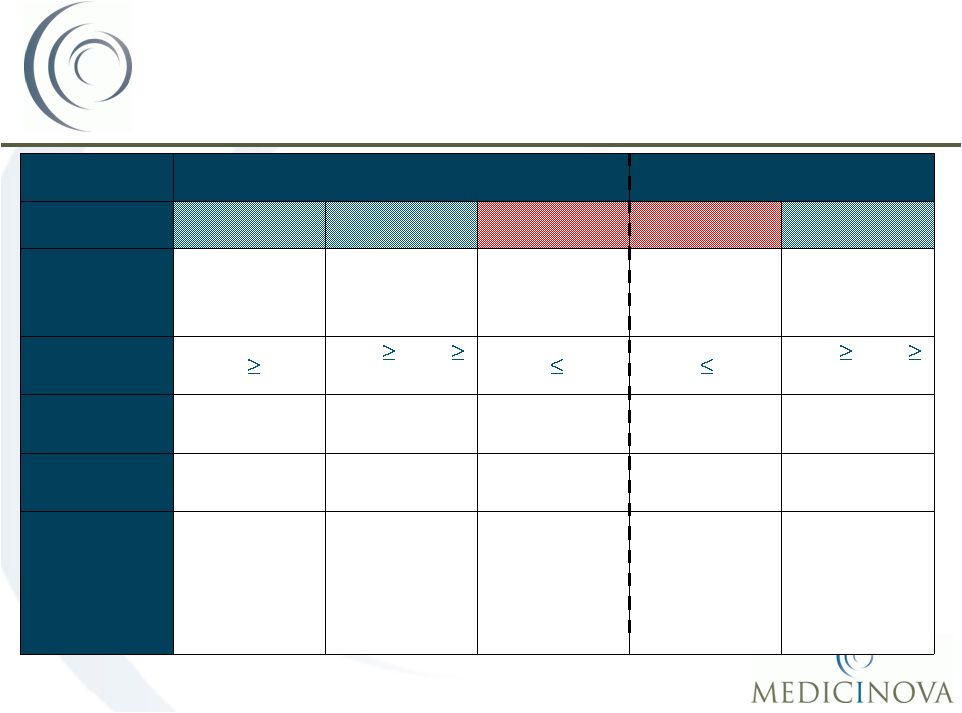 ©
MediciNova, Inc. 2010 MN-221 Clinical Trials MN-221 Clinical Trials 9 Completed Studies Completed Studies Ongoing Studies Ongoing Studies CL-004 CL-005 CL-006 CL-007 CL-010 Indication Indication Mild-to-moderate Asthmatics Moderate-to- Severe Asthmatics Acute Exacerbations of Asthma Acute Exacerbations of Asthma Moderate-to- Severe COPD patients FEV FEV 1 1 (Entry Criteria) (Entry Criteria) FEV 1 60% 75% FEV 1 40% FEV 1 55% FEV 1 50% 80% FEV 1 30% Number of Number of Patients Patients 23 17 29 200 48 Number of Number of Sites Sites 4 4 8 ~45 6 Doses Tested Doses Tested Compared to Compared to Placebo Placebo 5.25, 15, 52.5, 150, 240, 450, 900 µg over 15 min 1080 µg over 2-hr; 1,125 µg over 1-hr 240, 450 µg over 15 min; 1080 µg over 2-hr 1200 µg over 1-hr 300, 600, 1200 µ g over 1-hr Note: CL-004, CL-005, CL-010 located in clinical sites. CL-006,
CL-007 located in emergency departments. |
 ©
MediciNova, Inc. 2010 MN-221-CL-004:
MN-221-CL-004:
Mean Change in FEV Mean Change in FEV 1 1 10 p < 0.05 p < 0.001 p < 0.05 p < 0.001 |
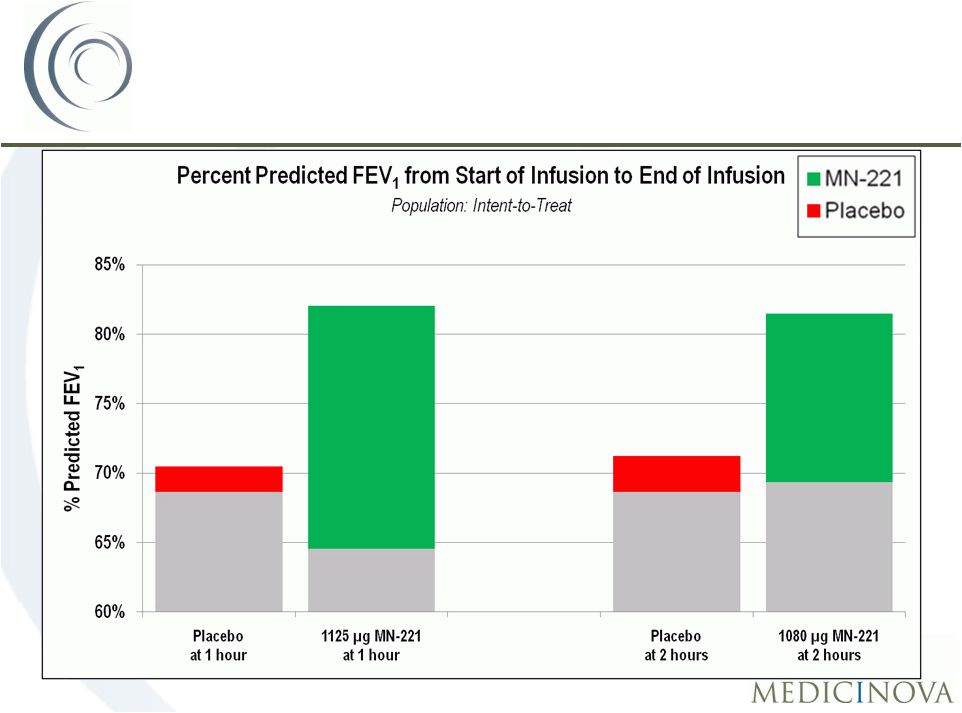 ©
MediciNova, Inc. 2010 MN-221-CL-005:
MN-221-CL-005:
Mean Change in FEV Mean Change in FEV 1 1 11 Baseline: 64.6% Baseline: 69.4% 1 Hour: 82.0% 2 Hours: 81.5% Baseline: 68.6% Baseline: 68.6% 1 Hour: 70.5% 2 Hours: 71.2% |
 ©
MediciNova, Inc. 2010 12 What did we learn from the MN-221-CL-006 clinical trial? • There were no safety concerns with adding MN-221 to the standard of care. • There was a reduction in the hospitalization rate among patients treated with MN-221. • Overall, improvement in FEV 1 was greater for patients receiving MN-221 than placebo. • A dose of 1,200 µ
g of MN-221 administered over one hour was selected for the MN-221-CL-007 clinical trial. MN-221-CL-006:
MN-221-CL-006:
What have we learned? What have we learned? |
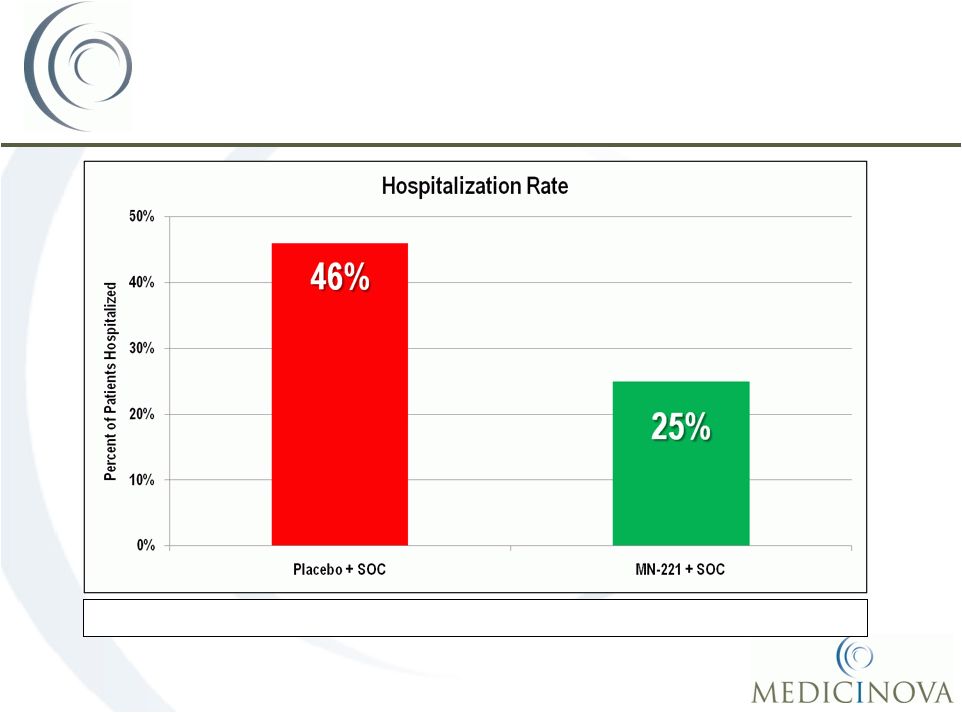 ©
MediciNova, Inc. 2010 MN-221-CL-006: MN-221-CL-006: Hospitalization Rate by Treatment Group Hospitalization Rate by Treatment Group 13 MN-221 reduced the hospitalization rate by 45% Note: SOC means standard of care. |
 ©
MediciNova, Inc. 2010 • Randomized, placebo-controlled, double-blind, multi-center Phase II clinical
trial • 200 patients with severe, acute exacerbations of asthma (FEV 1 50% predicted) at ~35 Emergency Department sites in US, Canada, Australia, and New Zealand • Dose Groups (~100 patients/group): • 1,200 µg MN-221 over 1 hour (600 µg in 15 minutes; 600 µg in 45 minutes) • Placebo • Patients will receive Standard of Care (SOC) treatment in addition to adjunctive
treatment with MN-221 or placebo • Primary efficacy endpoint will be improvement in FEV 1 (% predicted) at 5 hours • The study is designed to have 80% power to detect a treatment difference
of 5 percentage points in FEV1 (% predicted) when comparing MN-221 + SOC to
Placebo + SOC at a two sided -level of 0.05. • Anticipated completion in 2H, 2010* MN-221-CL-007: MN-221-CL-007: Study Design Study Design 14 Note: Development plans / timelines for MN-
221 clinical trials are subject to change *Anticipated completion date based on current projections |
 ©
MediciNova, Inc. 2010 • Randomized, double-blind, placebo-controlled Phase Ib dose escalation study • 48 subjects with stable moderate-to-severe COPD (FEV 1 30% < 80% and FEV 1 /FVC ratio < 0.7) at 6 sites in the US • Doses: • 300 µg MN-221 over 1-hour (150 µg in 15 minutes; 150 µg in 45 minutes)
or placebo • 600 µg MN-221 over 1-hour (300 µg in 15 minutes; 300 µg in 45 minutes)
or placebo • 1,200 µg MN-221 over 1-hour (600 µg in 15 minutes; 600 µg in 45 minutes) or placebo • Outcome measures – descriptive statistics only – FEV 1 , PK, safety • Anticipated completion in 1H, 2010* MN-221-CL-010 (COPD): MN-221-CL-010 (COPD): Study Design Study Design 15 Note: Development plans / timelines for MN-221 clinical trials are subject to change *Anticipated completion date based on current projections |
 ©
MediciNova, Inc. 2010 16 MN-166 for Multiple Sclerosis (MS): • Oral administration • Multiple mechanisms of action, both neuroprotective and anti-inflammatory • MN-166 targets primarily chronic aspects of MS • Benign safety profile Mechanisms of Action: Potentially Neuroprotective • Inhibits nitric oxide and reactive oxygen species production • Stimulates release of neuronal growth factors • Reduces demyelination Anti-inflammatory • Inhibits PDE’s and MIF, leukotriene release, proinflammatory cytokines (TNFa, IL-1b, MCP, IL-6) • Can increase IL-10 release Current Standard of Care: • Beta interferons (Rebif ® , Avonex ® , Betaseron/Betaferon ® ), Copaxone ® , Tysabri ® • Primary focus is on acute treatment of MS symptoms (i.e., relapse rate) MN-166 for the Treatment of MN-166 for the Treatment of Multiple Sclerosis Multiple Sclerosis |
 ©
MediciNova, Inc. 2010 Placebo-controlled, Randomized, Double-blind Phase II Study: • Year 1 - Placebo, 30 mg/day, 60mg/day • Year 2 - 30 mg/day, 60mg/day • 297 patients (~100 patients/group) @ 25 sites in Serbia, Ukraine, Belarus, Bulgaria and Romania Key Inclusion Criteria: • Males or females aged 18 to 55 years, with relapsing remitting (RR) and/or secondary progressive (SP) Multiple Sclerosis with continued relapses; • One MRI scan taken two weeks prior to treatment start using a standardized MRI protocol with at least one Gd-enhancing lesion; • An Expanded Disability Status Scale (EDSS) score of 5.5 or less at the screening
and baseline visits. Safety Profile: • 89% (264 of 297) of subjects completed the first 12 months of the study • 82.5% (245 of 297) of subjects completed the full 24 months of the study • Adverse effects reported more frequently in MN-166-treated than placebo-treated
subjects: GI effects & depression Completed Clinical Study: Completed Clinical Study: MN-166-CL-001 MN-166-CL-001 17 |
       ©
MediciNova, Inc. 2010 18 P-Value: 0.04 P-Value: 0.035 MN-166 Targets Primarily MN-166 Targets Primarily Chronic Aspects of MS Chronic Aspects of MS P-Value: 0.026 P-Value: 0.004 P-Value: 0.09 P-Value: 0.08 Note: P-values listed on this slide compare placebo group to 60mg/day group of
MN-166 Indicative of Potential
Neuroprotective Effect: • Reduced brain volume loss • Reduced conversion of acute lesions to persistent black holes • Sustained disability progression was significantly less likely Acute Clinical Benefit: • Prolong time to relapse (by 127 days.) • Annualized relapse rate Protocol-Defined Primary Endpoint (Surrogate Endpoint): • No significant reduction in the cumulative number of active (gadolinium-enhancing (T1)
and non-enhancing new/enlarging (T2)) lesions on cranial MRI scans over 12
months of treatment was observed • Positive trends were observed in volume of gadolinium-enhancing (T1) lesions |
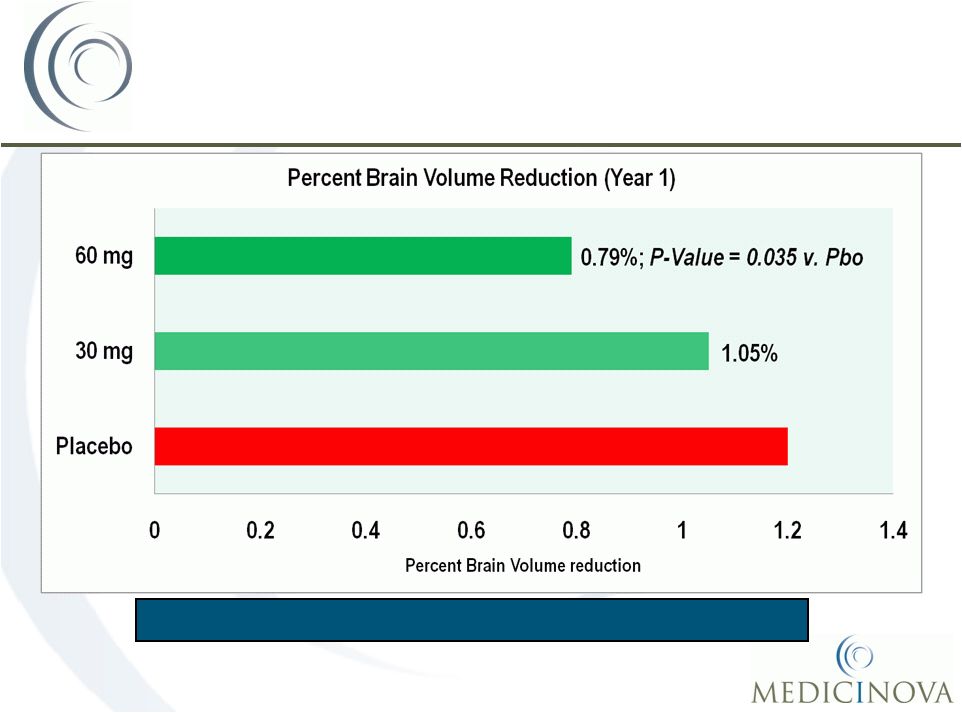 ©
MediciNova, Inc. 2010 Brain volume changes are linked to axonal loss 19 MN-166 - MN-166 - Chronic Efficacy Chronic Efficacy Demonstrated: Effects on Brain Volume Demonstrated: Effects on Brain Volume 1.20% |
 ©
MediciNova, Inc. 2010 Parameter Treatment Groups Placebo 30 mg/day 60 mg/day Number Patients w. New Lesions (NL) at Month 2 72 64 56 Total Number of NLs in all Patients at Month 2 426 338 315 Total Number of Persistent Black Holes (PBH) at Month 10 98 58 47 Percentage of Lesions Evolving to PBHs at Month 10 23% 17% 14% Percent Reduction from Placebo Group - 26% 39% P-Value - 0.036 0.004 New T1 gadolinium-enhancing or new T2 lesions were defined as NL in the first on-study MRI at month 2 Lesions that were hypointense and inactive at month 10 were PBH Relative Risk (RR) of NL evolution to PBH was analyzed using a general linear model with the error term from the Poisson distribution Reduction of Persistent Black Hole Reduction of Persistent Black Hole Formation Formation 20 |
 ©
MediciNova, Inc. 2010 Disability Progression is defined as a sustained increase in EDSS (increase in EDSS 1 maintained for four consecutive months) Sustained Disability Progression Sustained Disability Progression 21 4.1% (49% Reduction) 5.3% (34% Reduction) 8.0% Sustained disability progression was significantly less likely (~50%) in those patients receiving MN-166 at 30 or 60 mg per day for 24 months than in those patients receiving the drug for 12 months (p=0.026). |
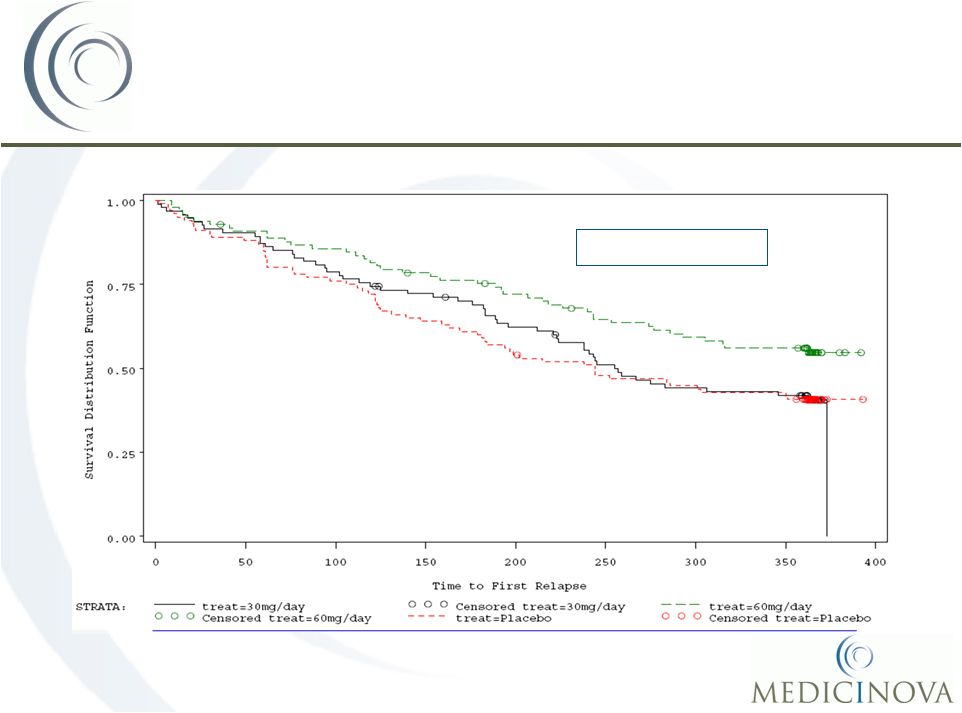 ©
MediciNova, Inc. 2010 22 Acute Efficacy Demonstrated: Acute Efficacy Demonstrated: Time to First Relapse Time to First Relapse Median 401 days Median 244 days P-Value: 0.044 Plot of Time to First Relapse by Treatment (ITT) Core (Year 1)
|
 ©
MediciNova, Inc. 2010 23 AV411: Value to MediciNova • Both AV411 and MN-166 are ibudilast • API and drug product supply • 4 completed Phase I and Ib/IIa clinical trials • Open IND for ibudilast (Analgesia, Addiction) • Clinical & preclinical support for MN-166 dosing up to 100 mg/day • 2 method of use patents issued in 2009; multiple filings in progress • Analog compounds behind ibudilast • First-generation development candidate: AV1013 – composition of matter patent issued • Second-generation dual target leads Opioid Withdrawal & Neuropathic Pain Indications • Ibudilast is a good glial cell attenuator in vitro and in the central nervous system (CNS) in
vivo. • Glial cell activation contributes to reward and withdrawal aspects of opioids and the development and maintenance of neuropathic pain. • AV411 represents a new pharmocotherapy approach for drug addiction and neuropathic pain. Additional Value from Avigen Additional Value from Avigen Deal Deal |
 ©
MediciNova, Inc. 2010 24 AV411: Ongoing clinical trial • Study Objective: Assess AV411 safety/tolerability/PK and preliminary efficacy for opiate
withdrawal in heroin-dependent subjects • Ongoing clinical trial run jointly by the New York State Psychiatric Institute and Columbia
University in NYC (Investigator IND study; MediciNova is not the sponsor) • Trial to enroll ~30 patients (10 completers/cohort) • Anticipated completion in 1H, 2010* AV411: Opioid AV411: Opioid Withdrawal Withdrawal Trial Design/Endpoints Week 1 2 3 Treatment Morphine (30 mg QID) and Placebo BID Morphine (30 mg QID) and Placebo BID or 20 mg BID of Ibudilast or 40 mg BID of Ibudilast Placebo BID or 20 mg BID of Ibudilast or 40 mg BID of Ibudilast Endpoints Safety, Tolerability, PK Safety, Tolerability, PK Withdrawal scores, Safety, Tolerability, PK Note: QID refers to taking the medication four times per day; BID refers to taking the
medication twice a day *Anticipated completion date based on current
projections |
 ©
MediciNova, Inc. 2010 25 Commercially-Attractive Commercially-Attractive Diversified Portfolio Diversified Portfolio |
          ©
MediciNova, Inc. 2010 26 Leadership Years Experience Background Yuichi Iwaki, MD, PhD Yuichi Iwaki, MD, PhD CEO & President 34 Professor at USC, formerly Professor at University of Pittsburgh; Advisor to JAFCO, Tanabe Shintaro Shintaro Asako, Asako, , CPA Chief Financial Officer 12 KPMG USA (Audit), Arthur Andersen USA Masatsune Masatsune Okajima, Okajima,
, CMA VP, Head of Japanese Office 18 Daiwa Securities SMBC, Sumitomo Capital Securities, Sumitomo Bank Management Team with Management Team with Global Experience Global Experience Alan Dunton, MD, PhD Clinical Development Consultant & Board Member 27 CEO of Panacos & Metaphore; President of the Janssen Research Foundation, a J&J company |
 ©
MediciNova, Inc. 2010 27 Near-Term Business Plan: 1. Secure a global partnership for MN-166 (AV411) 2. Secure a regional partnership (ex-US/Japan rights) for MN-221 Clinical Milestones: 1. MN-221-CL-007 Phase II Study for Acute Exacerbations of Asthma • Anticipated completion 2H, 2010* 2. MN-221-CL-010 Phase Ib Study in Moderate-to-Severe COPD Patients • Anticipated completion in 1H, 2010* 3. Ongoing AV411 Study for Opioid Withdrawal • Anticipated completion in 1H, 2010* Investment Highlights Investment Highlights *Anticipated completion dates based on current projections Note: Development plans / timelines for MN-221 clinical trials are subject to
change |