Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - Taysha Gene Therapies, Inc. | tsha-ex322_7.htm |
| EX-32.1 - EX-32.1 - Taysha Gene Therapies, Inc. | tsha-ex321_6.htm |
| EX-31.2 - EX-31.2 - Taysha Gene Therapies, Inc. | tsha-ex312_8.htm |
| EX-31.1 - EX-31.1 - Taysha Gene Therapies, Inc. | tsha-ex311_9.htm |
| EX-23.1 - EX-23.1 - Taysha Gene Therapies, Inc. | tsha-ex231_1464.htm |
| EX-10.15 - EX-10.15 - Taysha Gene Therapies, Inc. | tsha-ex1015_1051.htm |
| EX-10.14 - EX-10.14 - Taysha Gene Therapies, Inc. | tsha-ex1014_852.htm |
| EX-10.13 - EX-10.13 - Taysha Gene Therapies, Inc. | tsha-ex1013_851.htm |
| EX-10.5 - EX-10.5 - Taysha Gene Therapies, Inc. | tsha-ex105_792.htm |
| EX-4.2 - EX-4.2 - Taysha Gene Therapies, Inc. | tsha-ex42_791.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-K
(Mark One)
|
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2020
OR
|
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from ___________ to ___________
Commission File Number: 001-39536
Taysha Gene Therapies, Inc.
(Exact Name of Registrant as Specified in its Charter)
|
Delaware |
84-3199512 |
|
( State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer |
|
|
|
|
2280 Inwood Road Dallas, Texas |
75235 |
|
(Address of principal executive offices) |
(Zip Code) |
Registrant’s telephone number, including area code: (214) 612-0000
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
|
Common stock, par value $0.00001 per share |
|
TSHA |
|
The Nasdaq Stock Market LLC |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
|
☐ |
|
Accelerated filer |
|
☐ |
|
|
|
|
|
|||
|
Non-accelerated filer |
|
☒ |
|
Smaller reporting company |
|
☒ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Emerging growth company |
|
☒ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
The registrant was not a public company as of the last business day of its most recently completed second fiscal quarter and therefore cannot calculate the aggregate market value of its voting and non-voting common equity held by non-affiliates as of such date.
As of March 3, 2021, the registrant had 37,761,435 shares of common stock, $0.00001 par value per share, outstanding.
|
|
|
Page |
|
|
|
|
|
Item 1. |
1 |
|
|
Item 1A. |
47 |
|
|
Item 1B. |
90 |
|
|
Item 2. |
90 |
|
|
Item 3. |
90 |
|
|
Item 4. |
90 |
|
|
|
|
|
|
Item 5. |
91 |
|
|
Item 6. |
91 |
|
|
Item 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operation |
92 |
|
Item 7A. |
101 |
|
|
Item 8. |
F-1 |
|
|
Item 9. |
Changes in and Disagreements With Accountants on Accounting and Financial Disclosure |
103 |
|
Item 9A. |
103 |
|
|
Item 9B. |
103 |
|
|
|
|
|
|
Item 10. |
104 |
|
|
Item 11. |
106 |
|
|
Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
111 |
|
Item 13. |
Certain Relationships and Related Transactions, and Director Independence |
113 |
|
Item 14. |
116 |
|
|
|
|
|
|
Item 15. |
117 |
|
|
Item 16. |
118 |
|
|
119 |
||
i
SPECIAL CAUTIONARY NOTICE REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K, or this Annual Report, contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended, or the Exchange Act, that involve substantial risks and uncertainties. The forward-looking statements are contained principally in Part I, Item 1. “Business,” Part I, Item 1A. “Risk Factors,” and Part II, Item 7. “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” but are also contained elsewhere in this Annual Report. In some cases, you can identify forward-looking statements by the words “may,” “might,” “will,” “could,” “would,” “should,” “expect,” “intend,” “plan,” “objective,” “anticipate,” “believe,” “estimate,” “predict,” “project,” “potential,” “continue” and “ongoing,” or the negative of these terms, or other comparable terminology intended to identify statements about the future. These statements involve known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance or achievements to be materially different from the information expressed or implied by these forward-looking statements. Although we believe that we have a reasonable basis for each forward-looking statement contained in this Annual Report, we caution you that these statements are based on a combination of facts and factors currently known by us and our expectations of the future, about which we cannot be certain. Forward-looking statements include statements about:
|
|
• |
the timing, progress and results of our preclinical studies and clinical trials of our product candidates, including statements regarding the timing of initiation and completion of studies or trials and related preparatory work, the period during which the results of the trials will become available and our research and development programs; |
|
|
• |
the timing of our planned Investigational New Drug and Clinical Trial Agreement submissions, initiation of clinical trials and timing of expected clinical results for TSHA-101, TSHA-118, TSHA-102 and TSHA-104 and any other current and future product candidates that we advance; |
|
|
• |
the timing of any submission of filings for regulatory approval of, and our ability to obtain and maintain regulatory approvals for, our current and future product candidates; |
|
|
• |
the outbreak of the novel strain of coronavirus disease, COVID-19, which could adversely impact our business, including our preclinical studies, clinical supply and clinical trials; |
|
|
• |
our ability to identify patients with the diseases treated by our product candidates, and to enroll patients in trials; |
|
|
• |
our expectations regarding the size of the patient populations, market acceptance and opportunity for and clinical utility of our product candidates, if approved for commercial use; |
|
|
• |
our manufacturing capabilities and strategy, including the scalability and commercial viability of our manufacturing methods and processes; |
|
|
• |
our expectations regarding the scope of any approved indication for TSHA-101, TSHA-118, TSHA-102 and TSHA-104 or any other current or future product candidate that we advance; |
|
|
• |
our ability to successfully commercialize our product candidates; |
|
|
• |
our ability to leverage our platform, including our next-generation technologies, to identify and develop future product candidates; |
|
|
• |
our estimates of our expenses, ongoing losses, future revenue, capital requirements and our need for or ability to obtain additional funding before we can expect to generate any revenue from product sales; |
|
|
• |
our ability to establish or maintain collaborations or strategic relationships; |
|
|
• |
our ability to identify, recruit and retain key personnel; |
|
|
• |
our reliance upon intellectual property licensed from third parties and our ability to obtain such licenses on commercially reasonable terms or at all; |
|
|
• |
our ability to protect and enforce our intellectual property position for our product candidates, and the scope of such protection; |
|
|
• |
our financial performance; |
|
|
• |
our competitive position and the development of and projections relating to our competitors or our industry; |
|
|
• |
our estimates regarding future revenue, expenses and needs for additional financing; and |
|
|
• |
our expectations regarding the time during which we will be an emerging growth company under the JOBS Act. |
You should refer to “Item 1A. Risk Factors” in this Annual Report for a discussion of important factors that may cause our actual results to differ materially from those expressed or implied by our forward-looking statements. As a result of these factors, we
cannot assure you that the forward-looking statements in this Annual Report will prove to be accurate. Furthermore, if our forward-looking statements prove to be inaccurate, the inaccuracy may be material. In light of the significant uncertainties in these forward-looking statements, you should not regard these statements as a representation or warranty by us or any other person that we will achieve our objectives and plans in any specified time frame, or at all. The forward-looking statements in this Annual Report represent our views as of the date of this Annual Report. We anticipate that subsequent events and developments may cause our views to change. However, while we may elect to update these forward-looking statements at some point in the future, we undertake no obligation to publicly update any forward-looking statements, whether as a result of new information, future events or otherwise, except as required by law. You should, therefore, not rely on these forward-looking statements as representing our views as of any date subsequent to the date of this Annual Report.
You should read this report and the documents that we reference in this report, completely and with the understanding that our actual future results may be materially different from what we expect. We qualify all of our forward-looking statements by these cautionary statements.
All brand names or trademarks appearing in this Annual Report are the property of their respective owners. Solely for convenience, the trademarks and trade names in this Annual Report are referred to without the symbols ® and TM, but such references should not be construed as any indication that their respective owners will not assert, to the fullest extent under applicable law, their rights thereto.
Unless the context requires otherwise, references in this report to “Taysha,” the “Company,” “we,” “us,” and “our” refer to Taysha Gene Therapies, Inc. together with its consolidated subsidiaries.
Overview
We are a patient-centric gene therapy company focused on developing and commercializing AAV-based gene therapies for the treatment of monogenic diseases of the central nervous system, or CNS, in both rare and large patient populations. We were founded in partnership with The University of Texas Southwestern Medical Center, or UT Southwestern, to develop and commercialize transformative gene therapy treatments. Together with UT Southwestern, we are advancing a deep and sustainable product portfolio of 25 gene therapy product candidates, with exclusive options to acquire four additional development programs at no cost. By combining our management team’s proven experience in gene therapy drug development and commercialization with UT Southwestern’s world-class gene therapy research capabilities, we believe we have created a powerful engine to develop transformative therapies to dramatically improve patients’ lives. A Phase 1/2 clinical trial of TSHA-101 for the treatment of infantile GM2 gangliosidosis was initiated by Queen’s University under an accepted Clinical Trial Application, or CTA, in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We also plan to submit an investigational new drug application, or IND, for TSHA-101 for the treatment of GM2 gangliosidosis to the U.S. Food and Drug Administration, or the FDA, and initiate a Phase 1/2 clinical trial in the United States, each in the second half of 2021. In addition, we plan to submit INDs / CTAs for each of TSHA-102 (Rett syndrome) and TSHA-104 (SURF1-associated Leigh syndrome) in the second half of 2021 and one of the following programs in 2021: TSHA-103 (SLC6A1 haploinsufficiency disorder), TSHA-105 (SLC13A5 deficiency), TSHA-111-LAFORIN (Lafora disease), TSHA-111-MALIN (Lafora disease), TSHA-112 (APBD) or TSHA-119 (GM2 AB variant). We are also developing TSHA-118 for the treatment of CLN1 disease (one of the forms of Batten disease) and intend to initiate a Phase 1/2 clinical trial of TSHA-118 in the second half of 2021 under a currently open IND. Further, we are working to advance four new undisclosed programs focused on neurodevelopmental disorders, genetic epilepsies and neurodegenerative diseases into preclinical development in 2021. In addition to our product pipeline candidates, we are building a platform of next-generation technologies to optimize key components of our AAV-based gene therapies, including redosing, transgene regulation and capsid development.
Our pipeline consists of AAV9-based gene therapies intended to be delivered using the intrathecal route of administration. Our manufacturing process utilizes suspension HEK293 cell culture that is highly scalable from the preclinical stages of development through commercialization. We believe this combination of AAV9, intrathecal delivery and suspension cell culture will accelerate our product development timelines while enhancing our probability of successfully developing and commercializing safe, efficacious therapies for patients.
We use an adeno-associated virus serotype 9, or AAV9, capsid, to deliver therapeutic genes engineered to replace a mutated gene, enhance the expression of a silenced gene or decrease the expression of a gene, depending on the underlying biology of the specific disease. In preclinical studies, the AAV9 capsid has been observed to have significantly higher transduction efficiency in cells of the CNS in comparison to AAV serotypes used in other gene therapy programs. In third-party clinical trials, AAV9 has been shown to be well tolerated, and in 2019, Zolgensma was approved as the first systemic gene therapy utilizing AAV9 for the treatment of spinal muscular atrophy, or SMA, Type 1, a severe neurodegenerative disease.
We use intrathecal administration, which involves direct delivery of our gene therapies to the cerebrospinal fluid, or CSF, to facilitate optimal biodistribution and cell transduction within the CNS. Because the CNS is immune-privileged, intrathecal gene therapy may be administered even in the presence of pre-existing antibodies to AAV. We believe that intrathecal delivery of AAV9-based gene therapies provides the highest likelihood of achieving transformative efficacy for patients suffering from severe, life-threatening neurological diseases.
Our flexible manufacturing processes allow us to produce our gene therapy product candidates efficiently at scale. Through our partnership with UT Southwestern, we have access to a Good Manufacturing Practice-, or GMP-, compliant manufacturing suite that utilizes a suspension HEK293 process to produce AAV9. We believe this capacity will be sufficient to meet the clinical demand for our full pipeline of product candidates. We also are establishing our own commercial-scale, GMP-compliant manufacturing facility in Durham, North Carolina to meet demand in the event that our product candidates receive marketing approval. We expect to initiate construction on this facility in 2021.
1
Our portfolio of gene therapy candidates targets broad neurological indications across three distinct therapeutic categories, which together have the potential to address over 500,000 patients in the United States and the European Union: neurodegenerative diseases, neurodevelopmental disorders and genetic epilepsies. Neurodegenerative diseases refer to conditions characterized by the progressive degeneration of the structures and functions of the CNS. Our neurodegenerative product candidates include TSHA-101 for the treatment of GM2 gangliosidosis, a family of severe neurodegenerative diseases that includes Tay-Sachs disease and Sandhoff disease, TSHA-118 for the treatment of CLN1, a progressive, fatal neurodegenerative disease with early childhood onset, and TSHA-104 for the treatment of SURF1-associated Leigh syndrome, a fatal, early-onset neurodegenerative disease. Neurodevelopmental disorders are a group of conditions with onset during the time when the brain is developing and are a reflection of disabilities associated primarily with the functioning of the neurological system and brain. One of our neurodevelopmental product candidates, TSHA-102, is in development for the treatment of Rett syndrome, which is one of the most common genetic causes of severe intellectual disability. Genetic epilepsies refer to disorders with recurrent seizures associated with abnormal development of the brain. One of our genetic epilepsy product candidates, TSHA-103, is in development for the treatment of SLC6A1 haploinsufficiency disorder, which is one of the most common monogenic causes of epilepsy. A Phase 1/2 clinical trial of TSHA-101 was initiated by Queen’s University under a CTA in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We plan to submit an IND for TSHA-101 for the treatment of GM2 gangliosidosis to the FDA and initiate a Phase 1/2 clinical trial in the United States, each in the second half of 2021. In addition, we plan to submit an IND / CTA for each of TSHA-102 in Rett syndrome and TSHA-104 in SURF1-associated Leigh syndrome in the second half of 2021 and one of the following programs in 2021: TSHA-103 in SLC6A1 haploinsufficiency disorder, TSHA-105 in SLC13A5 deficiency, TSHA-111-LAFORIN in Lafora disease, TSHA-111-MALIN in Lafora disease, TSHA-112 in APBD or TSHA-119 in GM2 AB variant. We also plan to initiate a Phase 1/2 clinical trial of TSHA-118 in CLN1 in the second half of 2021 under a currently open IND. Further, we are working to advance four new undisclosed new programs focused on neurodevelopmental disorders, genetic epilepsies and neurodegenerative diseases into preclinical development in 2021.
We have established an exclusive, differentiated partnership with UT Southwestern, one of the premier academic medical centers in the United States. We hold an exclusive, worldwide royalty-free license from UT Southwestern to discover, develop and commercialize gene therapies for our pipeline. Within the framework of our partnership, UT Southwestern will conduct discovery and preclinical research, lead IND-enabling studies, manufacture GMP vectors for use in preclinical studies and clinical trials and execute natural history studies to support the development of our product candidates. We are responsible for all clinical development, regulatory filings, strategy, commercial manufacturing and commercialization of approved product candidates. UT Southwestern has developed a state-of-the-art GMP viral vector manufacturing facility with the capacity to support the development of our product candidates from the discovery stage through early clinical development. We believe these factors differentiate our partnership with UT Southwestern from traditional collaborations between industry and academia and will enable us to advance our development programs with speed and scale. Our collaboration with UT Southwestern is led by Dr. Steven Gray, an expert in the development of AAV-based gene therapies for CNS disorders, and Dr. Berge Minassian, an expert in the diagnosis, management and treatment of rare pediatric neurological disorders. Drs. Gray and Minassian are also our scientific founders and currently serve as our Chief Scientific Advisor and Chief Medical Advisor, respectively.
We believe that we have established a unique position in advancing the development of gene therapies. Our scientific founders, Drs. Gray and Minassian, have extensive experience in developing gene therapies and conducting clinical trials for complex CNS diseases. Our management team has significant experience in discovering, developing, manufacturing and commercializing gene therapies. The members of our leadership team have specialized expertise developed at companies including Audentes Therapeutics, AveXis, BioMarin, PTC Therapeutics, Rocket Pharmaceuticals, and Sanofi-Genzyme. Our board of directors played an integral role in the formation of our company and is comprised of Sean Nolan, the chairman of our board of directors and former Chief Executive Officer of AveXis, Phillip B. Donenberg, the former Chief Financial Officer of AveXis, Paul B. Manning of PBM Capital, Sukumar Nagendran, M.D., the former Chief Medical Officer of AveXis, Kathleen Reape, M.D., the former Chief Medical Officer of Spark Therapeutics, Laura Sepp-Lorenzino, Ph.D., Chief Scientific Officer of Intellia Therapeutics, and RA Session II, our President, Chief Executive Officer and Founder.
2
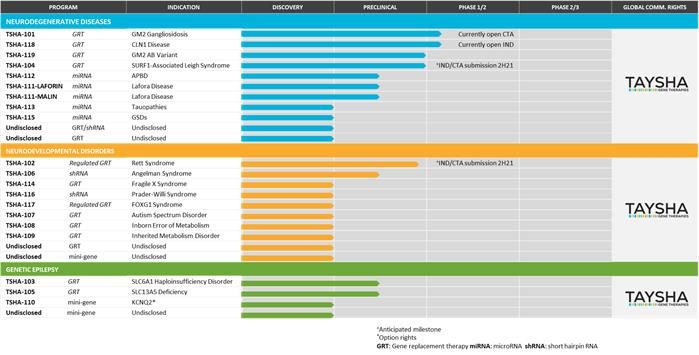
We are advancing a deep and sustainable product portfolio of 25 gene therapy product candidates for monogenic diseases of the CNS in both rare and large patient populations, with exclusive options to acquire four additional development programs at no cost. Our portfolio of gene therapy candidates targets broad neurological indications across three distinct therapeutic categories: neurodegenerative diseases, neurodevelopmental disorders and genetic epilepsies. Our current pipeline, including the stage of development of each of our product candidates, is represented in the table below.
TSHA-101, a neurodegenerative disease product candidate, is being developed for the treatment of GM2 gangliosidosis, including Tay-Sachs disease and Sandhoff disease. GM2 gangliosidosis refers to a group of lysosomal storage disorders resulting from a deficiency in the ß-hexosaminidase A, or Hex A, enzyme, leading to an accumulation of GM2 ganglioside in lysosomes and ultimately neuronal cell death and neurodegeneration. We are developing TSHA-101 as a bicistronic HEXBP2A-HEXA transgene packaged into an AAV9 vector under the control of a CAG promoter. A Phase 1/2 clinical trial of TSHA-101 was initiated by Queen’s University under a CTA in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We plan to submit an IND and initiate a clinical trial in the United States, each in the second half of 2021.
TSHA-118, a neurodegenerative disease product candidate, is being developed for the treatment of CLN1 disease (one of the forms of Batten disease), a lysosomal storage disorder that is a progressive, fatal disease with early childhood onset. TSHA-118 is a self-complementary AAV9 viral vector that expresses human codon-optimized CLN1 complementary deoxyribonucleic acid under control of the chicken ß-actin hybrid promoter. Preclinical studies evaluating safety and biodistribution have been conducted, and we plan to initiate a Phase 1/2 clinical trial of TSHA-118 in the second half of 2021 under a currently open IND.
TSHA-102, a neurodevelopmental disorder product candidate, is being developed for the treatment of Rett syndrome, one of the most common genetic causes of severe intellectual disability, characterized by rapid developmental regression and in many cases caused by heterozygous loss of function mutations in MECP2, a gene essential for neuronal and synaptic function in the brain. We designed TSHA-102 to prevent gene overexpression-related toxicity by inserting microRNA, or miRNA target binding sites into the 3’ untranslated region of viral genomes. This overexpression of MECP2 is seen in the clinic in patients with a condition known as MECP2 duplication syndrome, where elevated levels of MECP2 result in a clinical phenotype similar to Rett syndrome both in terms of symptoms and severity. TSHA-102 is constructed from a neuronal specific promoter, MeP426, coupled with the miniMECP2 transgene, a truncated version of MECP2, and miRNA-Responsive Auto-Regulatory Element, or miRARE, our novel miRNA target panel, packaged in self-complementary AAV9. We plan to submit an IND / CTA for TSHA-102 in the second half of 2021 and initiate a clinical trial by the end of 2021.
TSHA-104, a neurodegenerative disease product candidate, is being developed for the treatment of Surfeit locus 1, or SURF1-associated Leigh syndrome, a fatal, early-onset neurodegenerative disease. TSHA-104 is constructed from a codon-optimized version of the human SURF1 gene packaged within a self-complementary AAV9 viral vector under the control of a modified version of the chicken ß-actin, or CBA, promoter CBA hybrid intron, or CBh. We plan to submit an IND / CTA for TSHA-104 in the second half of 2021 and initiate a Phase 1/2 clinical trial by the end of 2021.
3
We plan to submit an IND / CTA in 2021 for one of the following programs: TSHA-103 in SLC6A1 haploinsufficiency disorder, TSHA-105 in SLC13A5 deficiency, TSHA-111-LAFORIN in Lafora disease, TSHA-111-MALIN in Lafora disease, TSHA-112 in APBD or TSHA-119 in GM2 AB variant.
Our Strategic Partnership with The University of Texas Southwestern Medical Center
We have established a differentiated partnership with UT Southwestern, one of the premier academic medical centers in the United States with a focus on integrating pioneering biomedical research with exceptional clinical care and education. The UT Southwestern Gene Therapy Program is led by Steven Gray, Ph.D., Director of the Viral Vector Core and Associate Professor in the Department of Pediatrics, and Berge Minassian, M.D., Division Chief of Child Neurology.
Dr. Gray serves as our Chief Scientific Advisor. His core expertise is in AAV-based gene therapy vector engineering and optimizing approaches to deliver therapeutic transgene to the CNS. His research also includes the design and execution of preclinical studies to apply these approaches toward the development of treatments for neurological diseases including giant axonal neuropathy, or GAN, Krabbe disease, Batten disease, Tay-Sachs disease, Sandhoff disease and Rett syndrome. He is the lead investigator on the GAN gene therapy project, which was the first clinical development program to deliver AAV9 through intrathecal administration. Dr. Gray has published over 50 peer-reviewed papers in journals such as New England Journal of Medicine, Molecular Therapy, Nature Biotechnology, Gene Therapy and The Proceedings of the National Academy of Sciences. His research has been funded by the National Institute for Neurological Disorders and Stroke, as well as numerous large and small research foundations and patient advocacy organizations. In 2019, Dr. Gray was the recipient of the American Society for Gene and Cell Therapy Outstanding New Investigator Award. He earned his Ph.D. in molecular biology from Vanderbilt University and a B.S. with honors from Auburn University. He performed his postdoctoral fellowship focusing on gene therapy in the laboratory of world-renowned gene therapy expert Jude Samulski at the University of North Carolina, Chapel Hill.
Dr. Minassian serves as our Chief Medical Advisor. He is a Professor in the Departments of Pediatrics, Neurology and Neurotherapeutics and Neuroscience at UT Southwestern. He is the Division Chief of Child Neurology and serves on the faculty of the Children’s Medical Center Research Institute at UT Southwestern. Dr. Minassian is a pediatric neurologist whose clinical specialties are epilepsy, neurodegenerative diseases and neurodevelopmental conditions. In 2004, Dr. Minassian described a new MECP2 isoform, MECP2B and its encoded protein MECP2B. Dr. Minassian is also credited with discovering the EPM2A and EPM2B genes that cause Lafora disease. He has published more than 120 scholarly articles and authored or contributed to 10 books, and his many professional honors include the Jacob’s Ladder 2014 Norman Saunders International Research Prize for Outstanding Scientist, the American Academy of Neurology 2007 Dreifuss-Penry Epilepsy Award, the Canadian Pediatric Society 2008 Sanofi Pasteur Research Award and the American Epilepsy Society 1996 Young Investigator Award. Dr. Minassian is a Fellow (Neurology) of the Royal College of Physicians and Surgeons of Canada.
Our partnership with UT Southwestern is differentiated from traditional collaborations between industry and academia due to our access to UT Southwestern’s faculty, manufacturing facility and integrated research and clinical care approach, which, together, we believe will enable us to advance our development programs with speed and scale. Under the terms of our collaboration and license agreement with UT Southwestern, we have received an exclusive, worldwide royalty-free license to discover, develop and commercialize gene therapies for our pipeline.
Through our partnership, we are able to leverage the collective expertise of UT Southwestern researchers, clinicians and investigators with decades of experience in conducting cutting-edge research and providing clinical care, including in the neurodegenerative disease, neurodevelopmental disorder and genetic epilepsy therapeutic categories. Drs. Gray and Minassian expect significant growth in the number of researchers, clinicians, scientists and experts in gene therapy process development and manufacturing affiliated with the Gene Therapy Program over the next five years.
UT Southwestern’s state-of-the art, GMP viral vector manufacturing facility consists of a full process development laboratory and 500-liter GMP suite with the capacity to support multiple preclinical and early clinical development efforts in parallel.
UT Southwestern is home to a major pediatric neurology residency program. Dr. Minassian has spent more than two decades diagnosing patients with rare, often fatal disorders of the CNS. Dr. Minassian is focused on transforming the practice of clinical neurology through a commitment to integrating patient care and teaching, with the goal of fostering the development of new disease-modifying therapies. This unique integration of research and clinical care provides us with key insights into our patients’ disease and its progression, symptoms and impact on quality of life. We plan to use these insights to design and refine our preclinical studies and clinical trials, understand incidence, prevalence and molecular epidemiology of the diseases and disorders we intend to treat, select the appropriate clinical endpoints for our efficacy studies and identify and characterize serum and imaging biomarkers. We also expect that UT Southwestern will serve as a source of enrollment for our clinical trials, which is critically important for the less prevalent diseases in our pipeline. We collaborate with UT Southwestern to foster relationships with patient advocacy organizations and research foundations, including the National Tay-Sachs & Allied Diseases Association, Cure and Action for Tay-Sachs, SLC6A1 Connect, TESS Research Foundation, Cure Surf1 Foundation, Rett Syndrome Research Trust and FOXG1 Research Foundation.
4
In addition, we have entered into a Sponsored Research Agreement with UT Southwestern to fund the discovery and development of novel gene therapy candidates and next-generation technologies for monogenic diseases of the CNS. This expanded partnership will support UT Southwestern’s discovery efforts. We will pay the actual costs incurred by and reasonable overhead of UT Southwestern in conducting the research under the Sponsored Research Agreement, and we will have an exclusive option on new programs new programs and intellectual property associated with, and arising from, such research.
Our Strategy
We are building a patient-centric business with the goal of developing AAV-based gene therapies for the treatment of monogenic diseases of the CNS in both rare and large patient populations. We are focused on executing the following elements of our strategy:
|
|
• |
Build a sustainable gene therapy company. Our goal is to build a gene therapy company with a sustainable pipeline of product candidates and a consistent stream of new commercial product launches. To that end, we are focused on advancing our current pipeline of AAV9-based gene therapies while actively developing our next-generation platforms to discover and develop additional product candidates. |
|
|
• |
Advance our lead product candidates through clinical trials to commercialization. Our product portfolio currently consists of 25 gene therapy product candidates targeting a diverse set of rare and prevalent CNS indications, with exclusive options to acquire four additional development programs from UT Southwestern at no cost. We intend to develop, seek regulatory approval and commercialize each product candidate in our portfolio. A Phase 1/2 clinical trial of TSHA-101 was initiated by Queen’s University under a CTA in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We plan to submit an IND for TSHA-101 for the treatment of GM2 gangliosidosis to the FDA and initiate a Phase 1/2 clinical trial in the United States, each in the second half of 2021. In addition, we plan to submit an IND / CTA for each of TSHA-102 in Rett syndrome and TSHA-104 in SURF1-associated Leigh syndrome in the second half of 2021 and one of the following programs in 2021: TSHA-103 in SLC6A1 haploinsufficiency disorder, TSHA-105 in SLC13A5 deficiency, TSHA-111-LAFORIN in Lafora disease, TSHA-111-MALIN in Lafora disease, TSHA-112 in APBD or TSHA-119 in GM2 AB variant. We intend to initiate a Phase 1/2 clinical trial of TSHA-118 in CLN1 disease in 2021 under a currently open IND. If our clinical trials are successful, we plan to discuss expedited regulatory approval strategies with regulatory authorities. Further, we intend to advance four undisclosed programs into preclinical development in 2021. |
|
|
• |
Leverage our relationship with UT Southwestern. We are anchored by a differentiated strategic partnership with UT Southwestern that allows us to access a highly experienced team of researchers and clinicians with deep experience in the underlying biology and treatment of monogenic CNS disorders and the patient populations that they treat. We believe that our partnership with UT Southwestern provides us with a significant advantage to discover, develop and commercialize novel gene therapies. |
|
|
• |
Utilize scalable manufacturing technologies. A critical component of the development of any complex biological therapy, including gene therapies, is the ability to manufacture the therapy efficiently at scale. Through our partnerships with UT Southwestern and Catalent, we have access to GMP manufacturing suites designed for a suspension HEK293 process to produce AAV9, which we believe will enable us to produce material suitable for clinical trials in a cost and time-efficient manner. We believe the capacity offered though our partnerships with Catalent and UT Southwestern will be sufficient to meet the clinical demand for our current pipeline of product candidates. Because we currently utilize the AAV9 capsid across our product portfolio, our product candidates differ primarily by their therapeutic transgene, and we believe that minimal changes to our optimized upstream and downstream processes are expected to be required to manufacture each product candidate. Finally, we have entered into a lease agreement to occupy and configure an approximately 187,000-square-foot commercial-scale cGMP manufacturing facility in Durham, North Carolina, which we expect will meet clinical and commercial demand if our product candidates receive marketing approval. We expect to initiate construction on this facility in 2021. |
|
|
• |
Develop our next-generation platform technologies. In addition to our pipeline of AAV9-based gene therapies, we are actively developing three distinct platform technologies to enable the discovery, development, and rapid translation of new gene therapies: a proprietary technology to allow redosing of AAV-based gene therapies, transgene regulation (miRARE) and novel capsid development. |
|
|
• |
Evaluate strategic opportunities to accelerate development timelines and maximize the value of our product candidate pipeline. We intend to evaluate opportunities to maximize the value of our product candidate pipeline. We believe these structures may provide us with the opportunity to leverage the financial and other resources of partners to advance the development of our product candidate pipeline in key geographies. |
Our Approach
Our approach to developing and commercializing gene therapies centers on the use of AAV9 delivered directly to the CSF using intrathecal administration. We manufacture our therapies using a scalable, HEK293 suspension-based process. We believe the combination of AAV9 manufactured in suspension and delivered intrathecally will allow us to advance the development candidates in our product pipeline.
5
Background on AAV9, Intrathecal Administration and Manufacturing
Since its discovery more than 50 years ago, AAV has been one of the most well studied vectors for the delivery of gene therapies, having been studied in over 250 clinical trials. We utilize AAV9, an AAV serotype with a unique ability to cross the blood-brain barrier and transduce cells of the CNS. AAV9 has been widely characterized across numerous preclinical studies and more than 15 ongoing or completed clinical trials and has a well-characterized biodistribution, safety, tolerability and efficacy profile. In 2019, the FDA approved Zolgensma, the first systemic gene therapy that utilizes AAV9, for the treatment of SMA Type 1 in infants.
Intrathecal administration refers to the injection of a therapy directly into the CSF. The procedure is routinely performed in an outpatient setting and is generally well tolerated. We intend to administer our product candidates intrathecally, as we believe that intrathecal administration confers several advantages for the delivery of gene therapies to the CNS. In comparison to intravenous administration, intrathecal administration allows for a lower dose of the therapy, as the vector is confined to the CNS with limited uptake into off-target tissues. Because the CNS is immune-privileged, intrathecal gene therapy may be administered even in the presence of pre-existing antibodies to AAV. Finally, intrathecally delivered gene therapies have limited exposure to peripheral organs, which enables a higher concentration of vector to be delivered to the diseased tissue of interest. A growing body of literature supports the safety and relevance of lumbar intrathecal injection to deliver AAV9 to the CNS and achieve favorable biodistribution and transgene expression profiles. In comparison to other AAV serotypes, AAV9 administration through lumbar intrathecal injection has been shown to result in superior transduction of multiple cells within the CNS.
We believe that intrathecally delivered AAV9-based gene therapies are more likely to achieve clinical and regulatory success than alternative delivery approaches. A third party is conducting a clinical trial of 32 patients to evaluate the efficacy, safety and tolerability of a one-time intrathecal administration of AAV9 delivering a copy of the SMN1 gene for the treatment of SMA Type 2. As of December 2019, a similar tolerability and adverse event profile had been observed in the patients receiving intrathecal delivery as compared to patients receiving intravenous delivery. The same third party has dosed over 600 patients intrathecally or intravenously with this AAV9 therapy and has observed that it has been well tolerated, with durability of up to five years post-dosing. In a third-party clinical trial of patients with CLN6 Batten disease, 12 infant and pediatric patients were dosed with AAV9 delivering CLN6 via intrathecal administration. In this trial, the AAV9 product candidate was well tolerated, with no drug-related adverse events observed. The same third party is currently conducting a clinical trial of an AAV9 product candidate delivering CLN3 via intrathecal administration. Four patients have been dosed to date, with no serious adverse events observed.
We use a scalable production process for our product candidates using a suspension cell culture process in which mammalian HEK293 cells are transiently transfected with plasmid DNA. Our production process, including all process development, product characterization, analytical capabilities and purification techniques, is designed to efficiently scale to support our clinical and commercial development needs. The utilization of the AAV9 capsid across our product portfolio allows us to manufacture each product with minimal changes expected to be required to our optimized upstream and downstream process, since each of our product candidates differ primarily by their therapeutic transgene.
Our Therapeutic Strategy
We design our product candidates based on the underlying biology of the disease target and the characteristics that we believe will result in maximum therapeutic benefit for patients.
Gene replacement therapies. To treat diseases or disorders caused by a missing gene or limited expression of a gene due to loss-of-function mutations, we design our product candidates to replace the gene of interest. In general, these product candidates are comprised of a codon-optimized DNA transgene, or minigene, that encodes the wild type gene of interest, coupled with a promoter selected to ensure expression in the cell or tissue-type of interest.
Regulated gene replacement therapies. In a number of disorders, including Rett syndrome and FOXG1 syndrome, the expression of a therapeutic transgene needs to be regulated. In these disorders, high doses of transgene-expressing vectors may be harmful, while low doses may avoid toxicity but be sub-therapeutic. For disorders that require replacement of dose-sensitive genes, we have combined high-throughput miRNA profiling and genome mining to create miRARE, our novel miRNA target panel. This approach is designed to enable our product candidates to maintain safe transgene expression levels in the brain. Importantly, this built-in regulation system is fully endogenous, and therefore does not require any additional exogenous drug application.
Vectorized miRNA gene therapies. In certain diseases within our pipeline, including Lafora disease, adult polyglucosan body disease or APBD, and tauopathies, the goal of our product candidates is to silence the expression of genes that are involved in or considered to be the root cause of disease onset and progression. To accomplish this, we design transgenes that express miRNA, which are small, non-coding sequences of RNA that result in silencing of gene expression.
Vectorized shRNA gene therapies. In certain diseases such as Prader-Willi syndrome and Angelman syndrome, the goal of our product candidates is to activate a constitutively silenced gene to generate a therapeutic effect under control of the endogenous promoters of the cell. We utilize transgenes that express short-hairpin RNA, or shRNA, which, upon binding to the target of interest, are designed to reactivate a silenced gene.
6
We design our preclinical studies to be highly translational into clinical trials, including to replicate the timing of dosing at points when the disease model has advanced and the phenotype is more pronounced, include relevant immunosuppressive regimes that are the standard of care for the disease target or commonly administered with gene therapies and use animal models that are reflective of the severity of the human disease. Our goal is to evaluate the safety, efficacy and biodistribution of our product candidates and generate dose-response data that inform our selection of the optimal doses for clinical translation. We believe that our stringent approach to evaluating efficacy in preclinical studies, including in studies in non-human primates, or NHPs, will translate into clinical trials and may be predictive of the clinical effect of our product candidates.
Our Next-Generation Platform Technologies
In addition to our pipeline of AAV9 product candidates, we are building a suite of platforms to develop next-generation technologies that can optimize key components of an AAV-based gene therapy.
Novel Route of Administration to Allow Redosing
We are advancing a novel AAV dosing platform with the potential to facilitate redosing by administering AAV-based gene therapies directly to the vagus nerve. In preclinical studies in adult rats, we observed that AAV9 delivery to the vagus nerve resulted in efficient targeting of the vagal neurons. In preclinical studies in dogs, AAV delivery to the vagus nerve was well tolerated at all doses. Post-mortem analysis showed that vagal nerve fibers and neurons were microscopically normal.
We believe that direct administration of our AAV9 therapies to the vagus nerve could be useful to treat the peripheral and autonomic manifestations of the CNS diseases in our pipeline. We plan to further evaluate the safety and feasibility of this approach in NHPs.
Regulated Transgene Expression Using miRARE
In a number of disorders, including Rett syndrome and FOXG1 syndrome, the expression of a therapeutic transgene needs to be regulated. In these disorders, high doses of transgene-expressing vectors may be harmful, while low doses may avoid toxicity but be sub-therapeutic. For disorders that require replacement of dose-sensitive genes, we have combined high-throughput miRNA profiling and genome mining to create miRARE, our novel miRNA target panel. This approach is designed to enable our product candidates to maintain safe transgene expression levels in the brain. Importantly, this built-in regulation system harnesses endogenous systems, and therefore does not require any additional exogenous drug application.
Novel Capsid Identification
We are developing a novel AAV capsid platform that utilizes machine learning, capsid shuffling and directed evolution to improve targeted delivery. Our approach allows us to identify capsids with improved properties in mice and NHPs in parallel to maximize their translational relevance. We are utilizing single-molecule, real-time, or SMRT, sequencing analysis for high throughput characterization of these capsids.
We believe that our approach will allow us to rapidly identify new capsids to drive new product candidates for CNS disorders with novel biodistribution and transduction profiles into our development pipeline.
Our Product Pipeline
Neurodegenerative Diseases
Our neurodegenerative disease programs target diseases that are characterized by the progressive degeneration of the structures and functions of the CNS. Degeneration and death of neuronal cells causes symptoms ranging from cognitive decline, functional impairment and, ultimately, death. Globally, neurodegenerative diseases represent an immense unmet medical need and disease management is complicated by a lack of effective symptomatic and disease-modifying therapies. Progressive neurodegeneration is a hallmark of numerous severe diseases each characterized by distinct etiology. Common neurodegenerative diseases include Alzheimer’s disease, Parkinson’s disease, amyotrophic lateral sclerosis, SMA and GM2 gangliosidosis.
A Phase 1/2 clinical trial of TSHA-101, a neurodegenerative product candidate, for the treatment of GM2 gangliosidosis was initiated by Queen’s University under a CTA in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We are also developing TSHA-118 for the treatment of CLN1 disease (one of the subtypes of Batten disease), for which we intend to initiate a Phase 1/2 clinical trial in the second half of 2021 under a currently open IND. In addition, we plan to submit an IND / CTA for the treatment of SURF1-associated Leigh syndrome in the second half of 2021 and to initiate a Phase 1/2 clinical trial of TSHA-104 by the end of 2021. We are developing additional product candidates for the treatment of prevalent neurodegenerative diseases, including Alzheimer’s disease, Parkinson’s disease and other tauopathies, and rare diseases such as APBD and Lafora disease.
7
TSHA-101 for the Treatment of GM2 Gangliosidosis
Overview of GM2 Gangliosidosis
GM2 gangliosidosis, which comprises Tay-Sachs disease and Sandhoff disease, refers to a group of lysosomal storage disorders caused by accumulation of the GM2 ganglioside in the lysosomes of cells within the CNS. Gangliosides are lipid components of cell membranes particularly abundant in the plasma membranes of neurons. Accumulation of GM2 ganglioside is caused by a deficiency in the Hex A enzyme, which is responsible for hydrolysis, or breakdown, of the GM2 ganglioside. This accumulation results in lysosomal rupture, leading to a poorly understood inflammatory cascade that leads to neuronal cell death and neurodegeneration. The global incidence of GM2 gangliosidosis is approximately one per 150,000 live births. Approximately 80% to 85% of patients are diagnosed with an infantile form of GM2 gangliosidosis, with the remainder diagnosed with a juvenile or early-adulthood form of the disease. There are no approved therapies for the treatment of GM2 gangliosidosis, and care is generally palliative. Children diagnosed with GM2 gangliosidosis appear normal at birth but experience rapid neurodegeneration, culminating in death before the age of four, and patients with juvenile GM2 gangliosidosis rarely survive beyond their mid-teens. The estimated prevalence of GM2 gangliosidosis is 500 patients in the United States and European Union.
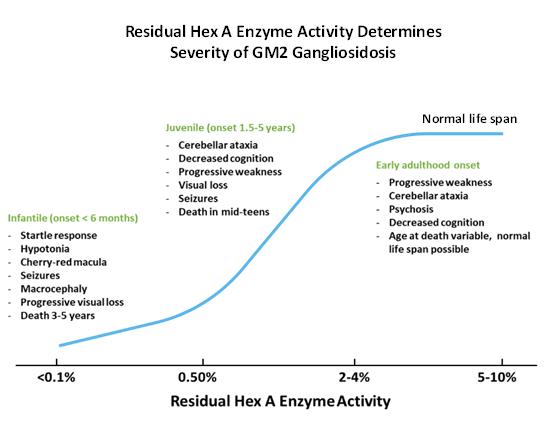
The Hex A enzyme is a heterodimer composed of two subunits: ß-hexosaminidase a (encoded in humans by the HEXA gene) and ß-hexosaminidase ß (encoded in humans by the HEXB gene). GM2 gangliosidosis caused by a mutation of the HEXA gene is termed Tay-Sachs disease, while Sandhoff disease is caused by a mutation of the HEXB gene. Tay-Sachs disease and Sandhoff disease result in clinically indistinguishable phenotypes for which there is no effective treatment. As illustrated in the graphic below, in GM2 gangliosidosis, its most common and severe form, the disease is characterized by a lack of Hex A enzyme activity, while juvenile GM2 gangliosidosis is characterized by Hex A enzyme activity that is 0.5% to less than 2% of normal activity. Adult-onset GM2 gangliosidosis patients have Hex A enzyme activity levels typically in the range of 2% to 4% of normal Hex A activity and may live a normal lifespan. We believe that the “critical threshold” for normal hydrolysis of GM2 ganglioside is estimated to be 5% to 10% of normal Hex A activity.
We believe that successful gene therapy to treat Tay-Sachs disease or Sandhoff disease requires expression of the α and ß subunits in a 1:1 ratio to ensure that Hex A expression confers a therapeutic benefit. An imbalanced expression of either subunit could result in the formation of a dysfunctional homodimer, or identical proteins, which would limit the efficacy of the therapy. Several therapeutic approaches utilize single vectors encoding either the α or ß subunit, while other approaches have utilized multiple vectors carrying the HEXA and HEXB genes separately. However, these approaches either fail to deliver the Hex A subunits in the appropriate ratio or require the simultaneous transduction of cells to achieve efficacy.
Similar to other lysosomal enzymes, Hex A is ubiquitously expressed and therefore concerns related to off-target effects or overexpression are limited. In addition, Hex A is secreted from transduced cells and can be taken up by neighboring cells to correct their phenotype, making it possible to cure these diseases without the need to transduce every cell, a process referred to as cross-correction.
8
Studies suggest that restoring Hex A enzyme levels to approximately 10% of normal may result in complete phenotypic absence of the disease.
Our Solution: TSHA-101
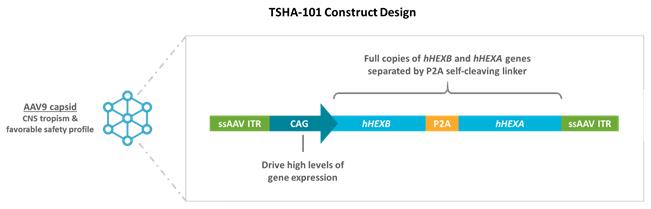
We are developing TSHA-101, a neurodegenerative product candidate, for the treatment of GM2 gangliosidosis. TSHA-101 is a bicistronic, or dual loci of transcription, HEXBP2A- HEXA transgene packaged into an AAV9 vector under the control of the CAG promoter. We have designed TSHA-101 to link the human HEXA and HEXB genes, utilizing a cleavable peptide linker, to ensure that the expression of each the subunit occurs simultaneously at the appropriate 1:1 ratio. This approach is designed to maximize the expression of Hex A enzyme while minimizing the required therapeutic dosage.
Because GM2 gangliosidosis is clinically well defined, we believe we can leverage that knowledge to develop TSHA-101 with a higher probability of clinical and regulatory success. If approved, we believe that TSHA-101 could have a transformational impact on these severely underserved patients and their families. As TSHA-101 is designed to secrete the Hex A enzyme from transduced cells, uptake of the enzyme by neighboring cells via cross-correction has the potential to result in therapeutic benefit independent of their transduction status. In addition, we believe Hex A enzyme activity in the serum and CSF can serve as a potential biomarker to detect and help verify treatment effects on GM2 gangliosidosis during the early stages of clinical development.
We have received orphan drug designation and rare pediatric disease designation from the FDA for TSHA-101 for the treatment of GM2 gangliosidosis.
Preclinical Studies
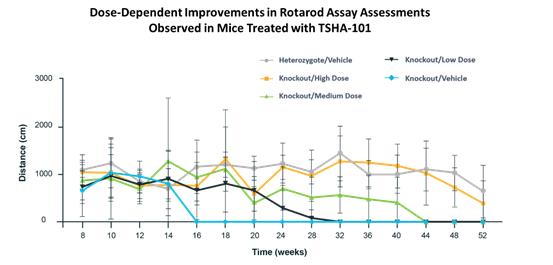
In preclinical studies, we observed evidence of improvements in behavioral assays and GM2 ganglioside accumulation across all dose levels of TSHA-101, which we believe supports continued development of TSHA-101. In these studies, TSHA-101 was administered at three dose levels via intrathecal lumbar puncture to a mouse model of Sandhoff disease, selected for its ability to recapitulate the severity of the human disease: a high dose of 2.5 x 1011 vg/mouse, a medium dose of 1.25 x 1011 vg/mouse and a low dose of 0.625 x 1011 vg/mouse. Mice were dosed at six weeks of age and subjected to a battery of behavioral tests when they reached eight weeks of age. At 16 weeks, a cohort of mice were euthanized, at which time GM2 ganglioside accumulation, Hex A enzyme levels and vector biodistribution were evaluated. An additional cohort was followed to a humane long-term endpoint defined as 15% body weight loss or an absent righting reflex.
9
Across all dose levels, we observed a significant improvement in survival in mice treated with TSHA-101 as compared to mice treated with vehicle alone, as illustrated below. A clear dose-response relationship was observed, with the high dose, medium dose and low dose of TSHA-101 shown to increase survival by 3.4-, 2.3- and 1.5-fold relative to vehicle control, respectively.
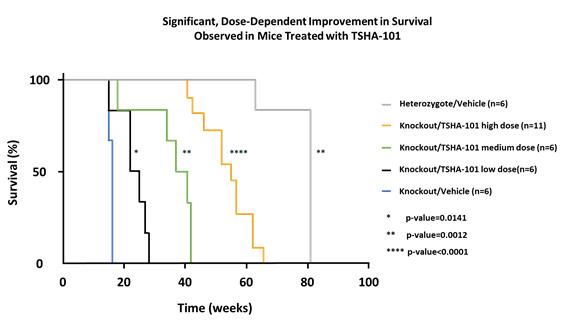
A result is considered to be statistically significant when the probability of the result occurring by random chance, rather than from the efficacy of the treatment, is sufficiently low. The conventional method for determining the statistical significance of a result is known as the “p-value,” which represents the probability that random chance caused the result (e.g., a p-value = 0.01 means that there is a 1% probability that the difference between the control group and the treatment group is purely due to random chance). Generally, a p-value less than 0.05 is considered statistically significant.
We observed similar dose-dependent responses in our behavioral assessments of mice in the open field test and rotarod assays, both of which are commonly used tests to evaluate motor coordination in mice, as illustrated below.
10
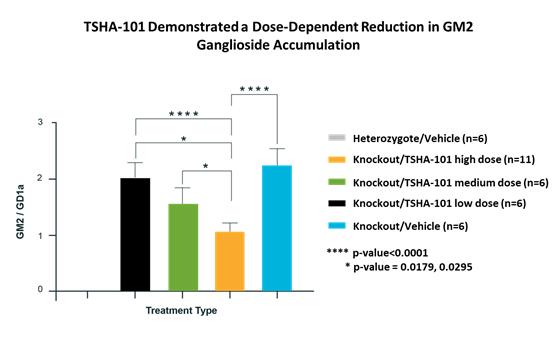
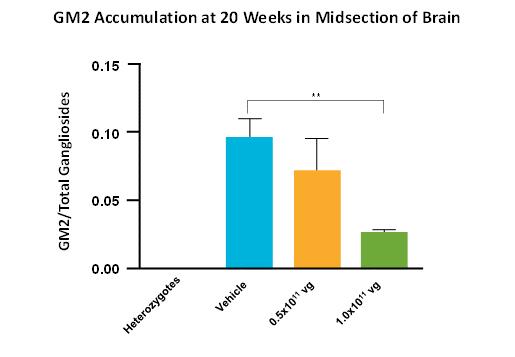
At 16 weeks, we performed a GM2 ganglioside assay on the middle section of the brain of mice in all treatment groups. We observed a dose-dependent decrease in ganglioside accumulation, as illustrated below, suggesting a restoration of Hex A enzyme activity.
In preclinical studies designed to evaluate safety, no adverse findings or evidence of toxicity attributable to TSHA-101 were observed. To characterize the safety profile of TSHA-101, wild type mice were intrathecally administered a low dose of TSHA-101 of 2.5 x 1011 vg/mouse or a high dose of 5 x 1011 vg/mouse. The effect of immunosuppressants were also investigated. Mice received daily administration of prednisone and rapamycin, two immunosuppressants commonly used in combination with gene therapies.
At five weeks of age, a cohort of nine mice were euthanized as baseline controls. These mice did not receive gene therapy or immunosuppression. The experimental mice began receiving daily dosages of either 24 µg prednisone and 100 µg rapamycin or a vehicle gavage that continued for the remainder of the study. At six weeks, the experimental mice were administered either a vehicle treatment or TSHA-101 at either the low dose or high dose. Mice continued daily gavaging until their pre-assigned endpoint. Five male and five female mice from the first, second and third cohorts were euthanized at one week, four weeks and three months post-gene therapy injections, respectively. All mice from the fourth cohort were euthanized at four weeks post-gene therapy administration.
Complete blood cell count and biochemistry analyses were performed on whole blood and serum samples. Enzyme-linked immunospot assays were performed on the mice euthanized at four weeks and three months post-injection to assess the immune response of the mice. The biodistribution of the virus was also determined through quantitative polymerase chain reaction.
Clinical Development
In December 2020, Queen’s University received CTA approval from Health Canada for its investigator-sponsored Phase 1/2 clinical trial of TSHA-101 in patients with a confirmed diagnosis of GM2 gangliosidosis. Patients will be evaluated over one year, followed by a longer-term extension period to monitor ongoing safety, developmental progression, select efficacy measures and biomarkers, consistent with other pediatric gene therapy trials. An independent data safety monitoring board will review data from each patient on an ongoing basis to ensure that stopping criteria are not met and monitor the well-being of the patients in the trial. Patients will receive TSHA-101 in a total dose of 5x1014 vg (modified dependent on age and predicted CSF volume) via intrathecal administration. The trial will measure safety and efficacy (including biomarker activity). Efficacy will be evaluated by motor function scales, assessment of head lag as a reflection of head lag, prevention of developmental regression, control of seizure activity and prevention of loss of milestones, as measured by validated scales. Additional measures of efficacy are expected to include plasma and CSF Hex A enzyme activity, GM2 ganglioside reduction and magnetic resonance imaging. Patient quality of life and caretaker burden using appropriate and accepted scales and observer-reported outcomes are also expected to be measured. Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. Following preliminary results from the Queen’s University Phase 1/2 clinical trial, we plan to submit an IND to the FDA in the second half of 2021 to commence a clinical trial for TSHA-101 in the United States in the second half of 2021, which we believe could serve as a pivotal trial to support registration subject to discussions with the FDA.
11
TSHA-118 (Formerly ABO-202) for the Treatment of CLN1 Disease
Overview of CLN1 Disease
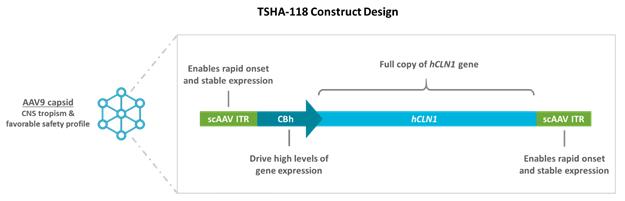
CLN1 disease (one of the forms of Batten disease), a lysosomal storage disorder, is a progressive, fatal neurodegenerative disease with early childhood onset that has an estimated incidence of approximately 1 in 138,000 live births worldwide. The estimated prevalence of CLN1 disease is 900 patients in the United States and European Union. CLN1 disease is caused by loss-of-function mutations in the CLN1 gene that encodes the enzyme palmitoyl-protein thioesterase-1, or PPT1, a small glycoprotein involved in the degradation of certain lipid-modified proteins. Loss of function mutations in the CLN1 gene causes accumulation of these lipid-modified proteins in cells, eventually leading to aggregation, neuronal cellular dysfunction and, ultimately neuronal cell death.
In the infantile-onset form of CLN1 disease, clinical symptoms appear between six to 24 months and include rapid deterioration of speech and motor function, refractory epilepsy, ataxia and visual failure. Infantile-onset CLN1 patients are typically poorly responsive by five years of age and remain noncommunicative until their death, which usually occurs by seven years of age. Late-infantile-onset CLN1 disease begins between two to four years of age with initial visual and cognitive decline followed by the development of ataxia and myoclonus, or quick, involuntary muscle jerks. Juvenile-onset CLN1 disease patients present between the ages of five to ten years old, with vision loss as a first symptom followed by cognitive decline, seizures and motor decline. Approximately 60% of the children diagnosed with CLN1 disease in the United States present with early-onset infantile forms, with the remaining 40% experiencing later-onset childhood forms.
All currently available therapeutic approaches for patients with CLN1 disease are targeted towards the treatment of symptoms, and no disease-modifying therapies have been approved. Gene therapy has shown promise in correcting forms of neuronal ceroid lipofuscinoses, or NCL, diseases that involve mutations in soluble enzymes, in part, due to cross-correction of neighboring non-transduced cells.
Our Solution: TSHA-118
We believe that the introduction of a functional CLN1 gene using an AAV9 vector delivered intrathecally to the CNS exposure offers the potential of a disease-modifying therapeutic approach for this disease. TSHA-118 is a self-complementary AAV9 viral vector that expresses human codon-optimized CLN1 complementary deoxyribonucleic acid under control of the chicken ß-actin hybrid promoter. We acquired exclusive worldwide rights to TSHA-118 (formerly ABO-202) in August 2020 pursuant to a license agreement with Abeona Therapeutics Inc., or Abeona.
TSHA-118 has been granted orphan drug designation, rare pediatric disease designation and fast track designation from the FDA and orphan drug designation from the EMA for the treatment of CLN1 disease.
Preclinical Studies
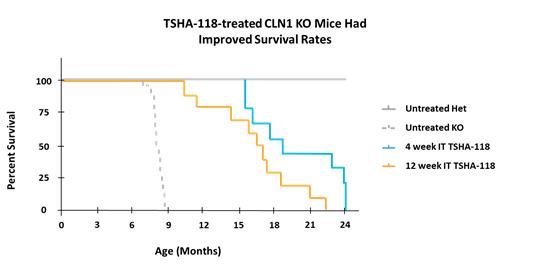
In third-party preclinical studies, evidence of improvements in behavioral outcomes, survival and restoration of PPT1 enzymatic activity was observed, which we believe supports continued development of TSHA-118. In these studies, TSHA-118 was administered at a dose of 7.0 x 1011 vg/mouse via intrathecal lumbar puncture to a mouse model of CLN1 disease, selected for its ability to recapitulate the severity of the human disease. The results from this study showed that intrathecal treatment with TSHA-118 significantly extended survival of CLN1 knockout mice, with enhanced survival and behavioral outcomes correlating with treatment at younger ages and higher doses.
12
As illustrated in the figure below, mice treated with TSHA-118 at four weeks or twelve weeks of age had a mean survival of 18.7 or 16.7 months, respectively, compared to approximately 8 months survival for untreated CLN1 knockout mice.
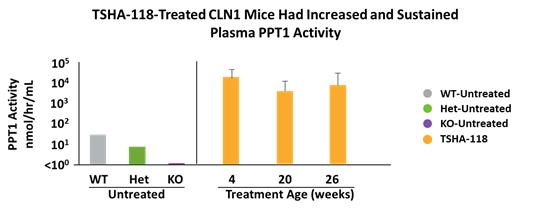
PPT1 enzyme activity in serum was measured at selected timepoints following TSHA-118 delivery by intrathecal administration at four, twenty or twenty-six weeks of age. Serum was collected either at four months post-treatment or at the humane endpoint.
As shown in the figure below, heterozygous mice had roughly 30% of normal serum PPT1 activity compared to wild-type mice. In contrast, treatment of CLN1 knockout mice with TSHA-118 resulted in supraphysiological levels of active PPT1 in the serum in comparison to wild-type and heterozygous mice.
Clinical Development
We expect to initiate a global Phase 1/2 dose-escalation and expansion trial subject to feedback from applicable regulatory agencies in the second half of 2021. The trial is expected to enroll up to 18 patients, including patients with classic infantile onset, late infantile onset and juvenile forms of CLN1 disease. We will conduct the trial in the United States following an amendment to the currently open IND that Abeona transferred to us. A data monitoring committee will review safety information from the first patient dosed in each cohort before the second participant from that cohort can be enrolled and will also be involved in overall safety review and safety management in the trial.
We expect that the key endpoints in the trial will include: safety and tolerability; developmental milestones; PPT1 enzyme activity in the serum and CSF; change in clinical progression as measured by the Unified Batten Disease Rating Scale, Hamburg Scale; changes in a number of other developmental scales, including the Vineland Adaptive Behavior Scales-Third Edition, Bayley Scales of Infant and Toddler Development; seizure frequency, type and medication; ophthalmological assessment; quality of life and caregiver burden; and changes in MRI, including volumetric changes of the brain
13
Additional Neurodegenerative Programs
TSHA-104 for SURF1-Associated Leigh Syndrome
We are developing TSHA-104, a neurodegenerative product candidate, for the treatment of SURF1-associated Leigh syndrome. The SURF1 gene encodes the SURF1 protein, which plays a critical role in mitochondrial translation and is involved in the assembly of the cytochrome c oxidase complex. Mutations in SURF1 lead to SURF1-associated Leigh syndrome, a recessively inherited mitochondrial disease, and are the most frequent cause of Leigh syndrome, a rapidly progressive neurological condition characterized by the degeneration of the CNS. To date over 100 SURF1 mutations, including non-sense, frame shift and missense variants have been described in literature. The incidence of SURF1-associated Leigh syndrome is estimated to be approximately 1 in 100,000 live births. The estimated prevalence of SURF1 deficiency is 300 to 400 patients in the United States and European Union.
SURF1-associated Leigh syndrome can lead to difficulty swallowing in infancy, with subsequent failure to thrive. Severely diseased muscle tone leading to respiratory failure, movement disorders and balance abnormalities are common. According to the literature, only a few patients have been reported to survive beyond 10 years of age. In the majority of SURF1-deficient patients, serum lactate is elevated, and elevated levels of serum lactate have been reported in the CSF as well, indicative of mitochondrial dysfunction. We are pursuing a gene replacement strategy with the goal of restoring mitochondrial function in patients with SURF1-associated Leigh syndrome caused by loss-of-function mutations.
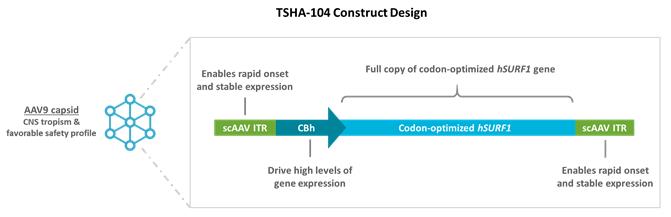
We are constructing TSHA-104 from a codon-optimized version of the human SURF1 gene packaged within a self-complementary AAV9 viral vector under the control of a CBh promoter. We plan to submit an IND / CTA for TSHA-104 in the second half of 2021 and initiate a Phase 1/2 clinical trial by the end of 2021.
We have received orphan drug designation and rare pediatric disease designation from the FDA for TSHA-104 for the treatment of SURF1-associated Leigh Syndrome.
Preclinical Studies
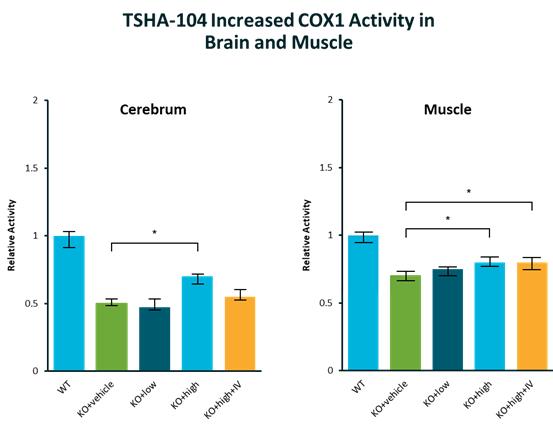
Data from preclinical studies suggest that functional gene replacement strategy could restore mitochondrial functions in SURF1-associated Leigh syndrome caused by SURF1 loss-of-function mutations, which we believe supports continued development of TSHA-104. In these studies, TSHA-104 was administered at two dose levels via intrathecal lumbar puncture to a knock-out mouse model of
14
SURF1-associated Leigh syndrome. Intrathecal treatment with TSHA-104 was observed to be well tolerated. TSHA-104 also induced SURF1 expression in the brain and partially rescued COX activity in a tissue specific manner as shown below.
15
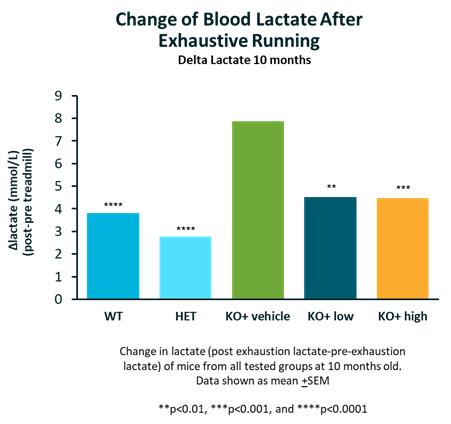
As shown below, TSHA-104 restored elevation of blood lactate on exhaustive exercise in the SURF1 knock-out mice.
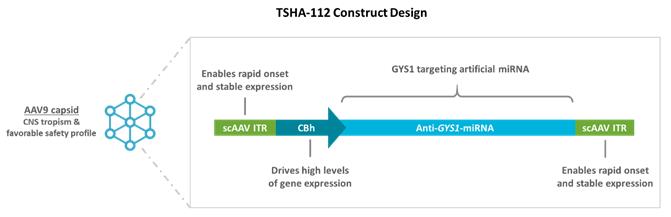
TSHA-112 for Adult Polyglucosan Body Disease
We are developing TSHA-112 for the treatment of APBD. APBD is caused by reduced glycogen branching enzyme, or GBE1, activity. GBE1 is responsible for the creation of branches during glycogen synthesis and reduced GBE1 activity results in elongated glycogen changes that form poorly soluble aggregates (polyglucosan bodies) in the liver, muscle and CNS. Symptoms of APBD include sensory loss in the legs, progressive muscle weakness, gait disturbances, urinary difficulties and mild cognitive impairment. APBD is a late onset, prime of life disease with an age of onset between 40 to 50 years. The prevalence of APBD is unknown, but we estimate it is approximately 10,000 patients in the United States and European Union.
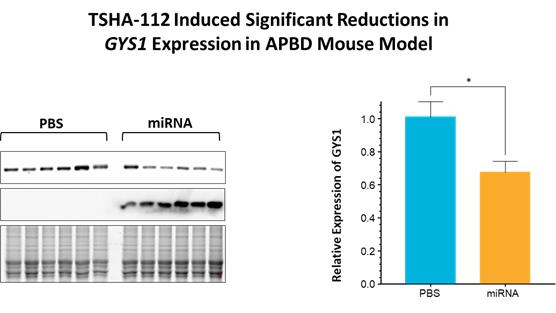
We are developing TSHA-112 as an AAV9 viral vector with miRNA targeting the knockdown of the GYS1 gene to treat APBD.
16
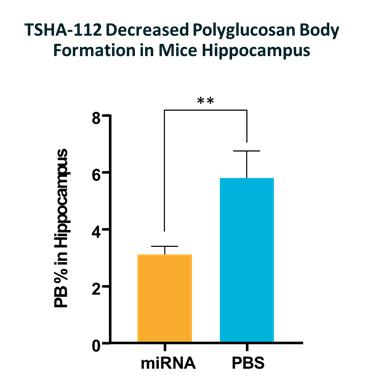
In preclinical studies, miRNA knockdown of GYS1 induced structural reduction of polyglucosan bodies as shown below.
In addition, TSHA-112 demonstrated decreases in polyglucosan body formation in mice hippocampus as shown below.
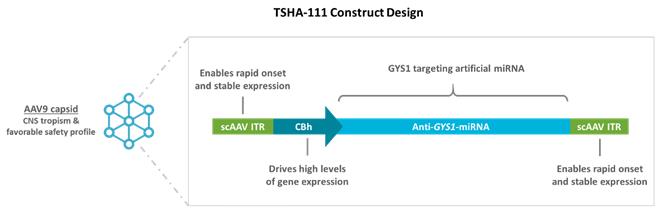
TSHA-111 (TSHA-111-LAFORIN for EPM2A and TSHA-111-MALIN for EPM2B) for Lafora Disease
We are developing TSHA-111-LAFORIN and TSHA-111-MALIN for the treatment of Lafora EPM2A and Lafora EPM2B disease, respectively, which are fatal glycogen storage disorders. Lafora disease starts in adolescents, usually with myoclonus, or involuntary muscle jerks, that rapidly evolve into progressive dementia, refractory epilepsy, cerebellar ataxia and respiratory failure, and generally results in death within about a decade. The epidemiology of Lafora disease is unknown although estimates suggest a prevalence of approximately 1 in 250,000 individuals worldwide. The estimated prevalence of Lafora disease is 700 patients in the United States and European Union. Currently, there is no treatment available for Lafora disease.
17
Lafora disease is caused by loss of function mutations in EPM2A or EPM2B genes, which encode the glycogen phosphatase Laforin or the E3 ubiquitin ligase Malin, respectively. Both Laforin and Malin are involved in the formation of regulating glycogen metabolism and the absence of either protein results in poorly branched cytoplasmic inclusions, known as Lafora bodies. Studies indicate that these inclusions are the primary driver of neurodegeneration and other brain abnormalities associated with Lafora disease.
We are developing TSHA-111-LAFORIN and TSHA-111-MALIN as AAV9 viral vectors with miRNA targeting the knockdown of GYS1.
Preclinical Studies
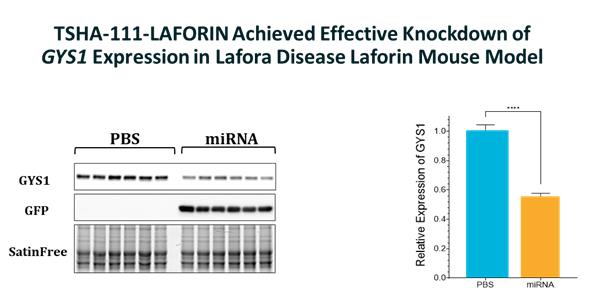
In preclinical studies, TSHA-111-LAFORIN achieved effective knockdown of GYS1 expression in the Lafora disease laforin mouse model. In addition, TSHA-111-LAFORIN reduced insoluble glycogen in ground brain tissue in the laforin mouse model as shown below.
18
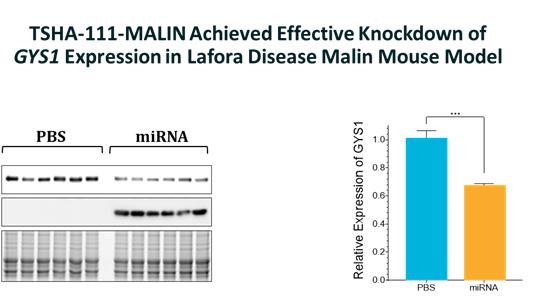
In preclinical studies, TSHA-111-MALIN achieved effective knockdown of GYS1 expression in the Lafora disease malin mouse model. In addition, TSHA-111-MALIN reduced insoluble glycogen in ground brain tissue in the malin mouse model as shown below.
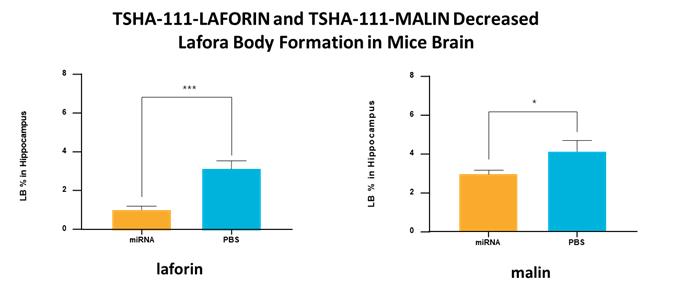
In preclinical studies, TSHA-111-LAFORIN and TSHA-111-MALIN decreased Lafora body formation in mice brain in the laforin and malin mouse models as shown below.
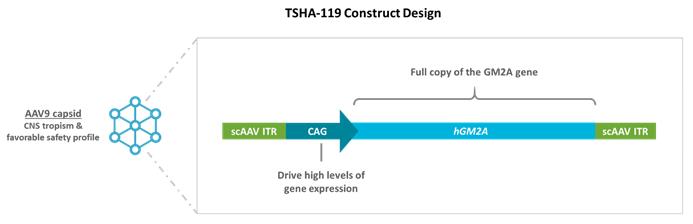
TSHA-119 for GM2 AB Variant
We are developing TSHA-119 for the treatment of GM2 AB variant.
Tay-Sachs and Sandhoff disease are caused by mutations in ß-hexosaminidase α (encoded in humans by the HEXA gene) and ß-hexosaminidase ß (encoded in humans by the HEXB gene), respectively. GM2 AB variant is caused by deficiency of the GM2 activator protein (GM2AP). GM2AP is a protein that works in tandem with the β-hexosaminidase enzyme to degrade and prevent toxic accumulation of GM2 ganglioside in the lysosome of the cell. Loss-of-function mutations result in a deficiency of GM2AP causing intra-lysosomal accumulation of GM2 and other glycolipids in neuronal cells ultimately resulting in cell death. In patients with AB variant, Hex A levels are normal and phenotypically, AB variant is indistinguishable from Tay-Sachs and Sandhoff disease.
In preclinical studies, Gm2a knockout mice, which develop abnormal brain histomorphology as well as slight impaired motor activity, were utilized to evaluate the safety, efficacy, and tolerability of TSHA-119. Mice were treated by intrathecal injection of TSHA-119 at postnatal day 1 (PND 1) or at 6 weeks of age at two different doses; a low dose or a high dose.
19
A significant reduction in GM2 ganglioside was evident in the mid-section of the brain in both the low dose and high dose cohorts, demonstrating a dose-dependent reduction of GM2 gangliosides as shown in the figure below. Long-term follow up studies which include bi-monthly behavioral as well as biochemical and histological analysis are currently underway.
In preclinical studies, TSHA-119 caused a dose-dependent reduction of GM2 accumulation in mice as shown below.
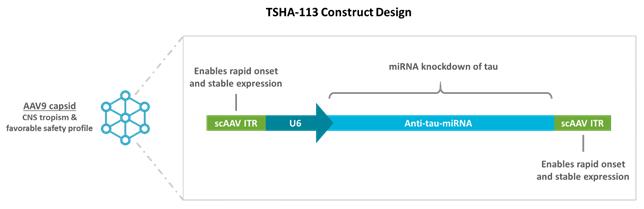
TSHA-113 for Tauopathies
We are developing TSHA-113 for the treatment of tauopathies. Tau accumulation predicts neurodegeneration in Alzheimer’s disease, and the propagation of tau aggregates is thought to mediate the progression of several neurodegenerative diseases, including progressive supranuclear palsy, corticobasal degeneration, behavioral variant frontotemporal degeneration, chronic traumatic encephalopathy, frontotemporal dementia and parkinsonism linked to chromosome 17.
As a result, multiple strategies are currently being tested to reduce tau and ameliorate the effects of these diseases. Preclinical studies testing tau anti-sense oligonucleotides, or ASOs, in the PS19 tauopathy mouse model prevented neuronal loss and showed a reversal of pathological tau deposition and seeding. This treatment in being tested in clinical trials. While promising, ASOs only reduced tau protein levels by approximately 50% in mice, and they required repeated, life-long intrathecal administration to reach this maximum effect.
We are developing TSHA-113 to utilize AAV-mediated gene silencing to deliver life-long reduction of tau protein levels in neurons following administration of a single dose. We are developing tau-specific miRNA shuttles that have been designed to target mRNA for all six isoforms of tau found in the human brain and/or mouse brain. Our preliminary data in cells has shown that our tau
20
miRNA selectively reduced some human and mouse tau expression in vitro and we have packaged our miRNA shuttles in AAV9 capsids for further evaluation in mouse models of human tauopathies.
TSHA-115 for Glycogen Storage Diseases
We are developing TSHA-115 for the treatment of glycogen storage diseases. TSHA-115 is designed to utilize a miRNA approach to knockdown GYS1, thereby inhibiting glycogen synthase in the brain. We believe this approach will provide therapeutic utility in not only Lafora disease or APBD, but potentially other glycogen storage diseases as well.
Our preliminary data show that RNA interference-mediated silencing of GYS1 messenger RNA, or mRNA, provided therapeutic benefit in mouse models of Lafora and APBD by decreasing abnormal glycogen formation in the brain.
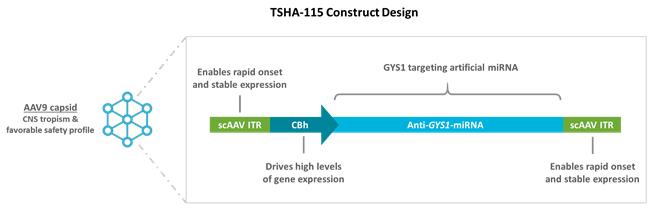
We plan to expand the development of the GYS1 miRNA knockdown approach into additional glycogen storage disorders. TSHA-115 has achieved animal proof-of-concept in three distinct animal models for laforin, malin, and glycogen branching enzyme, or GBE.
Neurodevelopmental Disorders
Neurodevelopmental disorders are a group of conditions whose age of onset occurs during the time when the brain is developing, typically between infancy and adolescence. Neurodevelopmental disorders can manifest as difficulties with language, speech and communication, motor skills, behavior, memory, learning and other neurological functions. The range of developmental deficits varies from very specific limitations of learning or control of executive functions to severe global impairments of social skills, intelligence and motor functioning.
The treatment of neurodevelopmental disorders is tailored towards symptom management and administered by an interdisciplinary team of neurologists, clinical psychologists, cognitive therapists, speech and language experts, behavioral therapists, and other specialists. Pharmacological interventions include but are not limited to typical and atypical antipsychotics, antiepileptic drugs, antidepressants and anti-anxiety medications.
We are developing TSHA-102, a neurodevelopmental product candidate, for the treatment of Rett syndrome. We are also developing product candidates for the treatment of other neurodevelopmental disorders, including Angelman syndrome, Fragile X syndrome, Prader-Willi syndrome and FOXG1 syndrome.
21
TSHA-102 for the Treatment of Rett Syndrome
Overview of Rett Syndrome
Rett syndrome is one of the most common genetic causes of severe intellectual disability worldwide with an incidence rate of one in every 10,000 live female births. The estimated prevalence of Rett syndrome is 25,000 patients in the United States and European Union. After a period of normal development, girls with Rett syndrome experience rapid developmental regression characterized by a loss of speech and motor control. Cognitive and intellectual disabilities are common, as is dysfunction of the autonomic nervous system, or ANS, resulting in breathing, cardiovascular, and gastrointestinal abnormalities. Approximately 95% of Rett syndrome patients are females carrying heterozygous loss-of-function mutations in MECP2, a gene encoding methyl CpG-binding protein that is essential for neuronal and synaptic function in the brain.
Currently, there is no cure for Rett syndrome and available treatments for Rett syndrome are mainly to address symptoms. The primary focus of symptomatic therapy is ensuring that patients have access to the appropriate care specialists along with access to occupational therapy, speech therapy and physiotherapy. Sodium valproate, lamotrigine, levetiracetam, carbamazepine and clobazam are commonly prescribed to control seizures. There is a sudden death rate of 26% in Rett syndrome and patients mainly perish due to cardiac complications, respiratory infection and respiratory failure.
In February 2007, Sir Adrian Bird, Ph.D., a Professor of Genetics at the University of Edinburgh, published a seminal paper demonstrating the reversibility of symptoms associated with Rett syndrome in mice. This work suggested for the first time that neurological damage caused by the absence of MECP2 may be reversible in children and adults with Rett syndrome. To demonstrate the ability to reverse the onset of Rett syndrome, researchers in the Bird lab generated mouse models in which MECP2 expression was conditionally silenced, which resulted in neurological and behavioral deficits that mirrored those seen in patients diagnosed with Rett syndrome. Upon reactivation of the MECP2 gene, behavioral deficits were restored, and electrophysiological function was also returned to levels seen in wild type mice. These findings represented a landmark moment for the field and provided evidence that it may be possible to not only halt the symptoms of Rett syndrome, but to potentially reverse the course of the disease.
Several peer-reviewed publications have subsequently explored the safety and efficacy of AAV-based gene therapy for the treatment of Rett syndrome, including in preclinical studies that showed that delivery of MECP2 and, more recently, miniMECP2, extended the survival of MECP2 knockout mice, a commonly used mouse model that recapitulates the symptoms of Rett syndrome. However, AAV delivery of MECP2 or miniMECP2 resulted in dose-dependent toxicity in wild type and MECP2 knock out mice. Given the underlying biology of the disease, there is consensus among researchers that toxicity in these models is most likely linked to unregulated expression of MECP2 or miniMECP2. This overexpression of MECP2 is seen in the clinic in patients with a condition known as MECP2 duplication syndrome, where elevated levels of MECP2 result in a clinical phenotype similar to Rett syndrome both in terms of symptoms and severity.
Our Solution: TSHA-102
We are developing TSHA-102, a neurodevelopmental product candidate, for the treatment of Rett syndrome. In order to develop an effective therapy for Rett syndrome, MECP2 expression needs to be titrated to correct the MECP2 deficiency while avoiding side effects associated with toxic overexpression.
22
MECP2 is a transcription factor within the cell that regulates many other genes involved in neurodevelopmental function. Levels of MECP2 are regulated within the cell endogenously by a number of different miRNAs. We utilized this natural regulatory phenomenon to develop miRARE, our miRNA target panel. miRARE binds those endogenous miRNA species whose expression levels are upregulated as a result of exogenous MECP2 protein expression. When miRARE is incorporated into the 3’ untranslated region of our expression cassette, it functions as a mechanism to permit therapeutic expression of MECP2 while buffering against toxic overexpression, as shown in the figure below.
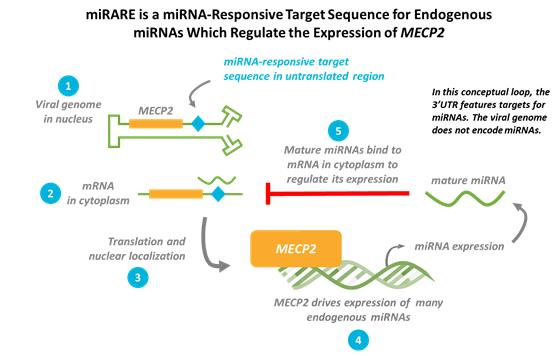
TSHA-102 is constructed from a neuronal specific promoter, MeP426, coupled with the miniMECP2 transgene and our miRARE panel packaged in self-complementary AAV9.
We have received orphan drug designation and rare pediatric disease designation from the FDA for TSHA-102 for the treatment of Rett syndrome.
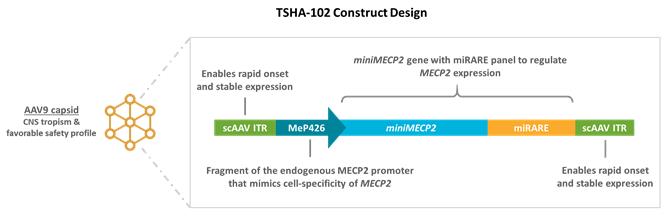
23
In preclinical studies, we observed that TSHA-102 had a favorable tolerability profile and increased survival in a wild type mice model. In these studies, wild type mice were treated with low doses of 1 x 1011 vg or high doses of 1 x 1012 of either unregulated AAV9/MECP2, unregulated AAV9/miniMECP2 or TSHA-102 at four to five weeks of age. Mice treated with the high dose of unregulated constructs experienced early lethality, while the low dose unregulated constructs were similar to vehicle. Mice treated with TSHA-102 had no deaths associated with treatment, as shown in the figure below.
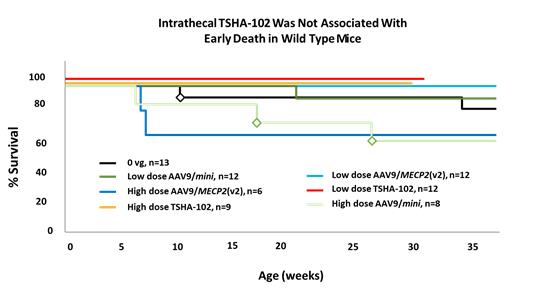
MECP2 dose-dependent side effects, leading to an increase in the aggregate score of a well-recognized, validated Rett behavioral assessment tool used in mice, were observed in the cohorts treated with unregulated AAV9/MECP2 or AAV9/miniMECP2, as shown in the figure below. This increase in aggregate score is a reflection of overexpression of MECP2 causing Rett-like symptoms in these mice, as is seen in MECP2 duplication syndrome. In contrast, TSHA-102 was well tolerated and aggregate scores were similar to those of mice treated with vehicle only. This aggregate scale includes six sub-scales for abnormal mobility, abnormal gait, hindlimb clasping, tremors, abnormal breathing and abnormal general appearance. Sub-scales were each assessed on a scale of 0 to 12, with 12 being the maximum aggregate score attainable. Scorers were blind to treatment and genotype, and lower scores indicate better tolerability.
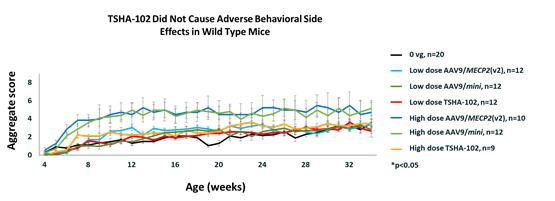
24
In MECP2 knockout mice, unregulated AAV9/miniMECP2 failed to extend survival at either dose tested. In contrast, TSHA-102 dosed at 1x1012 vg/mouse extended survival by 56%. Importantly, although there is a strong trend toward increased survival in mice treated with AAV9/MECP2, studies in wild type mice showed unacceptable toxicity with this vector design at this dose.
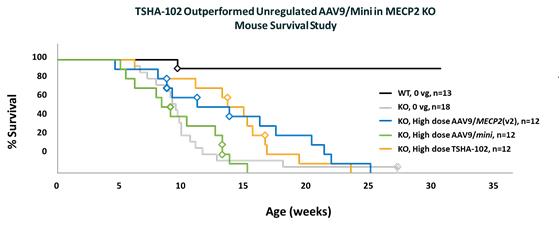
We observed TSHA-102 to be well tolerated, with no behavioral abnormalities or other side effects associated with MECP2 overexpression. We evaluated the safety of TSHA-102 in wild type mice following intrathecal administration. While AAV9/MECP2 and AAV9/miniMECP2 caused dose-responsive reductions in weight, weight reduction was not observed in mice treated with TSHA-102. In addition, no tail lesions were observed among mice treated with TSHA-102. In contrast, lesions were observed in 8% to 17% of wild type mice treated with unregulated AAV9/miniMECP2 and 8% of mice treated with unregulated AAV9/MECP2.
Clinical Development
Following the completion of Good Laboratory Practice, or GLP, toxicology studies in NHPs and the completion of additional preclinical studies, we intend to submit an IND / CTA for TSHA-102 for Rett syndrome in the second half of 2021 and initiate a clinical trial by the end of 2021. In clinical trials, we intend to evaluate safety, tolerability and efficacy utilizing multiple clinical scales and clinical assessments. Breathing disorders are reported in over 66% of patients with Rett syndrome, often leading to sleep disorders. Patients hyperventilate, hold their breath and have apneic episodes, leading to poor sleep quality. Accordingly, we plan to measure both sleep quality and breathing in our clinical trials. In addition, epilepsy is reported in over 60% of patients with Rett syndrome and likely will serve as a secondary efficacy endpoint in our trials.
Additional Neurodevelopmental Programs
TSHA-106 for Angelman Syndrome
We are developing TSHA-106 for the treatment of Angelman syndrome, a neurodevelopmental disorder caused by a maternal deficiency of the UBE3A gene. Angelman syndrome is characterized by profound developmental delay, ataxia and gait disturbance, sleep disorder, seizures, heightened anxiety and aggression and severe speech impairments. Angelman syndrome affects approximately one per 12,000 to 20,000 patients worldwide. The estimated prevalence of Angelman syndrome is 55,000 patients in the United States and European Union.
Angelman syndrome is an imprinting disorder in which the maternal gene is deficient and the paternal copy of UBE3A is intact but silenced by a long non-coding RNA, UBE3A antisense transcript, or UBE3A-ATS. Delivery of an ASO targeting UBE3A-ATS showed promising results in ameliorating Angelman syndrome symptoms in a transgenic mouse model.
25
We are developing TSHA-106 to target the UBE3A-ATS transcript through shRNA knock-down with an AAV-based strategy in order to achieve broad distribution of the shRNA expression cassette across the entire CNS following a single intrathecal dose.
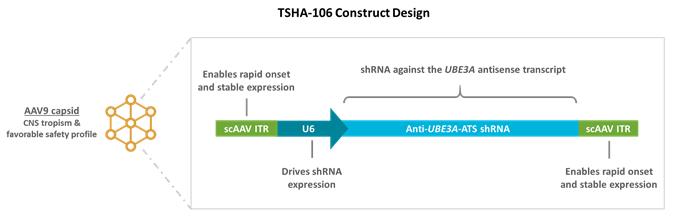
TSHA-114 for Fragile X Syndrome
We are developing TSHA-114 for the treatment of Fragile X syndrome, the most common single gene cause of autism and cognitive impairment, affecting about one in 6,000 individuals worldwide. The estimated prevalence of Fragile X syndrome is 100,000 patients in the United States and European Union. Fragile X syndrome is diagnosed around three years of age and characterized by anxiety, aggression, hyperactivity, attention deficits and sleep and communication disruption.
Fragile X syndrome is caused by a pathological expansion of a CGG triplet repeat in the 5’ untranslated region of the FMR1 gene. Expansion of the triplet above the normal 5–55 repeats to 200 or more causes hypermethylation of the gene promoter, and shutdown of transcription and translation of the encoded protein, fragile X mental retardation protein, or FMRP. The expanded repeat also induces formation of RNA: DNA heteroduplexes that induces epigenetic gene silencing. Although most patients with Fragile X syndrome do not express FMRP, some individuals with the full mutation produce low amounts of the protein (less than 10% of normal levels). FMRP expression in unaffected persons varies greatly from person to person. Current pharmacotherapeutic treatments for Fragile X syndrome are solely directed towards symptom relief.
We are developing TSHA-114 using truncated promoters that mimic the natural developmental expression of FMRP. In addition, we have selected to express a human FMRP isoform to ensure that FMRP expression is appropriately localized to the cytosol, axon, nerve terminals, and nucleus in the proper ratios.
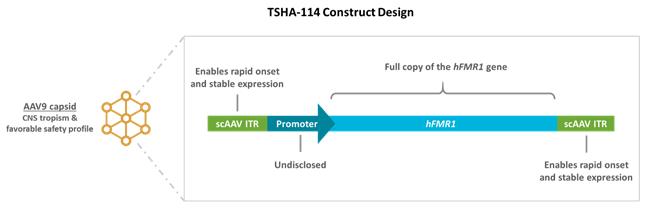
TSHA-116 for Prader-Willi Syndrome
We are developing TSHA-116 for the treatment of Prader-Willi syndrome, a genetic disorder caused by paternal loss-of-function of genes along 15q11-q13 chromosomal region, or PWS genes, due to an imprinting defect. The prevalence of Prader-Willi syndrome is estimated to be approximately one per 10,000 to 30,000 persons. The estimated prevalence of Prader-Willi syndrome is 40,000 patients in the United States and European Union. During infancy, patients with Prader-Willi syndrome have feeding difficulties, poor growth and weak muscle tone. As the patient begins to age, their appetite becomes insatiable, resulting in obesity and type 2 diabetes. In addition, patients typically have mild to moderate intellectual disabilities, behavioral issues and sleep abnormalities.
26
In patients, with Prader-Willi syndrome, the maternal genes are intact but silenced by epigenetic regulation, or the modulation of gene expression. Epigenetic regulation is accomplished by the euchromatic histone lysine N-methyltransferase-2, or EHMT2, gene.
We are developing TSHA-116 to restore gene function through reactivation of the silenced maternal genes. To accomplish this, we are designing vectors to target EHMT2 through shRNA knock-down and reduced levels of EHMT2, which would in turn activate the silenced PWS gene.
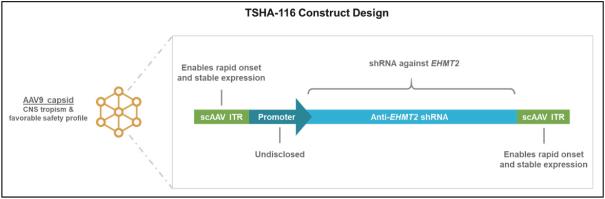
TSHA-117 for FOXG1 Syndrome
We are developing TSHA-117 for the treatment of FOXG1 syndrome. FOXG1 syndrome is a neurodevelopmental disorder caused by pathogenic mutations in the FOXG1 gene. The symptoms of FOXG1 syndrome include severe developmental and intellectual disabilities, growth restriction with microcephaly, epilepsy and hyperkinetic-dyskinetic movement disorder. The incidence rate is estimated to be one per 30,000 live births. The estimated prevalence of FOXG1 is 20,000 patients in the United States and European Union. The number of identified patients is expected to steadily increase as more children are tested for Autism Spectrum Disorder and other genetic disorders. Currently, there are no specific therapies for FOXG1 syndrome and medical management of the disease is largely focused on symptomatic relief.
The literature suggests that dosage of the FOXG1 gene needs to be regulated to avoid off-target expression or overexpression of FOXG1.
We are developing TSHA-117 using our miRARE panel to regulate FOXG1 expression levels.
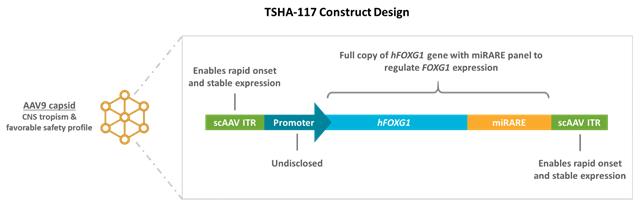
TSHA-107 for an Autism Spectrum Disorder, TSHA-108 for an Inborn Error of Metabolism and TSHA-109 for an Inherited Metabolic Disorder
We are also developing the following product candidates for the treatment of neurodevelopmental disorders. We are developing TSHA-107 for the treatment of an autism spectrum disorder associated with an increased risk of epilepsy, for which there is currently no therapeutic option. We are developing TSHA-108 for the treatment of an inborn error of metabolism associated with intellectual disability, prominent speech and language delay, autistic behaviors and seizures. We are developing TSHA-109 for a rare, inherited metabolic disorder that, if untreated, results in speech deficits, ataxia, learning disabilities and other neurological complications. We are constructing each of these product candidates from a codon-optimized version of the applicable gene packaged within a self-complementary AAV9 viral vector.
27
Our genetic epilepsy category targets disorders with recurrent seizures associated with abnormal development of the brain. In children with early-onset epilepsy, the detrimental effects of uncontrolled seizures are often associated with, and may be responsible for, the neurodevelopmental disabilities that often appear subsequent to the onset of seizures. A number of childhood-onset epilepsies are caused by mutations in a single gene and represent a compelling target for gene therapy. The goal of our product candidates is to target the underlying cause of the disease to simultaneously control seizures and treat any associated developmental comorbidities.
We are developing TSHA-103, a genetic epilepsy product candidate, for the treatment of SLC6A1 haploinsufficiency disorder. We are also developing TSHA-105 for the treatment of SLC13A5 deficiency and TSHA-110 for the treatment of KCNQ2-related disorders.
TSHA-103 for SLC6A1 haploinsufficiency disorder
Overview of SLC6A1 haploinsufficiency disorder
SLC6A1 haploinsufficiency disorder is caused by loss-of-function mutations in the SLC6A1 gene. Loss of-function mutations in the SLC6A1 gene have been identified as one of the most common monogenic causes of epilepsy with myoclonic atonic seizures, or brief and abrupt seizures followed by loss of muscle strength, as well as autism spectrum disorder and intellectual disability.
Patients diagnosed with SLC6A1 haploinsufficiency disorder typically present with developmental delay, varying degrees of intellectual disability, seizures and abnormal EEG characterized by generalized spike-wave discharges. Most patients are refractory to pharmacological seizure control although a portion of patients become seizure free during the course of disease progression. Importantly, seizure control is not associated with improved cognitive outcomes, which highlights the complexity of the disease as well as the need for novel therapies directed at its underlying pathology.
Approximately 81% of patients with SLC6A1 haploinsufficiency disorder have epilepsy, with typical absence seizures, which are abrupt and followed by lack of awareness, being the predominant form observed. In addition, 91% of individuals exhibit developmental delays, with more than 80% characterized as mild or moderate intellectual disability. Ataxia, or tremors, is present in approximately 29% of individuals, while autism or autistic features are observed in approximately 24% of individuals diagnosed with SLC6A1 haploinsufficiency disorder.
The SLC6A1 gene encodes the gamma-aminobutyric acid, or GABA, transporter 1, or GAT1. GAT1 is a voltage-dependent transporter responsible for the reuptake of GABA, a non-protein amino acid that is well characterized for its role as a major inhibitory neurotransmitter within the mammalian CNS. GAT1 plays a critical role in the reuptake of GABA from neuronal synapses and extracellular spaces and as a result, a critical role in balancing neuronal excitations. When GABA transport is disrupted, brain development is negatively impacted resulting in deficits in attention and cognition as well as seizures.
The exact incidence and prevalence of SLC6A1 haploinsufficiency disorder is unknown but we believe the estimated prevalence is 17,000 patients in the United States and European Union. According to recently published data, the incidence of SLC6A1 haploinsufficiency disorder is approximately 1 in 36,000 live births. We believe that SLC6A1 haploinsufficiency disorder is underdiagnosed as the underlying biology was only recently elucidated and the gene had not been part of commercially available genetic epilepsy screening panels. Clinician education and expanded use of genetic screening panels that include SLC6A1 will likely lead to increased identification of individuals with these mutations.
Our Solution: TSHA-103
We are developing TSHA-103, a genetic epilepsy product candidate, for the treatment of SLC6A1 haploinsufficiency disorder. TSHA-103 is a gene replacement therapy constructed from a codon-optimized version of the human SLC6A1 gene packaged within a self-complementary AAV9 viral vector under the control of a JeT promoter. We are currently conducting preclinical studies of TSHA-103.
28
We have received orphan drug designation and rare pediatric disease designation from the FDA for TSHA-103 for the treatment of epilepsy caused by SLC6A1 haploinsufficiency disorder.
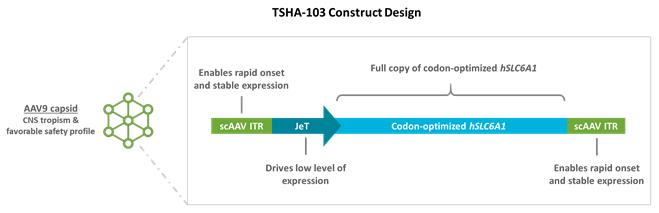
Additional Genetic Epilepsy Programs
TSHA-105 for SLC13A5 Deficiency
We are developing TSHA-105 for the treatment of SLC13A5 deficiency, a rare autosomal recessive epileptic encephalopathy characterized by the onset of seizures within the first few days of life. The estimated prevalence of SLC13A5 deficiency is 1,900 patients in the United States and European Union. Affected children have impairments in gross motor function and speech production with relative preservation of fine motor skills and receptive speech. SLC13A5 deficiency is caused by bi-allelic loss-of function mutations in the SLC13A5 gene, which codes for a sodium dependent citrate transporter, or NaCT, that is largely expressed in the brain and liver. To date, all tested mutations result in no or a greatly reduced amount of the citrate in the cells.
Diminished NaCT function leads to loss of neuronal uptake of citrate and other metabolites such as succinate that are critical to brain energy metabolism and function. Currently, there are no approved therapies for SLC13A5 deficiency, and treatment is largely to address symptoms.
We are developing TSHA-105 as a gene replacement therapy for SLC13A5 deficiency. TSHA-105 is constructed from a codon-optimized human SLC13A5 gene packaged in a self-complementary AAV9 capsid.
We have received orphan drug designation and rare pediatric disease designation from the FDA for TSHA-105 for the treatment of epilepsy caused by caused by SLC13A5 deficiency.
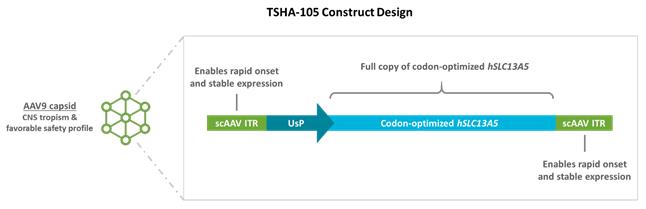
Preclinical Studies
In preliminary safety studies conducted in wildtype mice, vehicle or TSHA-105 was administered via CSF delivery. Weight and survival in the control and treatment group were the same and no overt toxicities were observed for up to one-year post-treatment.
29
Studies to evaluate TSHA-105 were conducted using SLC13A5 knockout mice. In comparison to age-matched, wildtype controls, SLC13A5 knockout mice exhibit altered citrate metabolism along with abnormal EEG activity and increased seizure susceptibility. At 3 months of age, SLC13A5 knockout mice were treated with TSHA-105 via CSF delivery. Administration of TSHA-105 resulted in a significant, sustainable decrease of plasma citrate levels up to 3-months post-injection, as shown below.
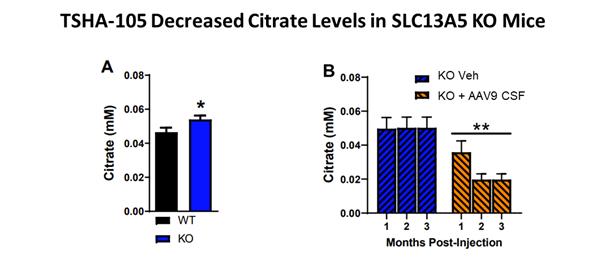
In addition, in ongoing EEG studies, TSHA-105 normalized EEG activity and decreased the number of seizures in knockout mice in comparison vehicle-treated controls as shown below.
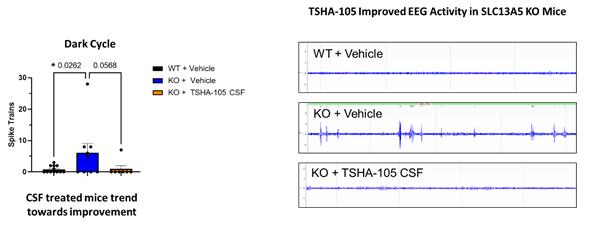
TSHA-110 for KCNQ2 Developmental & Epileptic Encephalopathy
We have an exclusive option from UT Southwestern to develop TSHA-110 for the treatment of KCNQ2 Developmental and Epileptic Encephalopathy, or KCNQ2. Patients with KCNQ2 typically present with seizures in the first week of life. Seizures appear as tonic, or with stiffening of the body, often associated with jerking and changes in breathing or heart rate. These seizures often resolve within months to years but children have some degree of developmental impairment involving one or more domains (motor, social, language, cognition). There is wide variability in the symptoms of patients with a KCNQ2 diagnosis. Some have very limited, or no noticeable seizure activity and the developmental impairment can range from mild to severe, depending on a number of different factors. Some children may also have autistic features or other comorbidities. The incidence of KCNQ2 is approximately 1 in 35,000 live births. The estimated prevalence in KCNQ2 developmental and epileptic encephalopathy is 37,000 patients in the United States and European Union.
30
We plan to exercise the option to acquire rights to TSHA-110 from UT Southwestern, following which we expect to develop TSHA-110 as a KCNQ2 transgene packaged within an AAV9 vector.
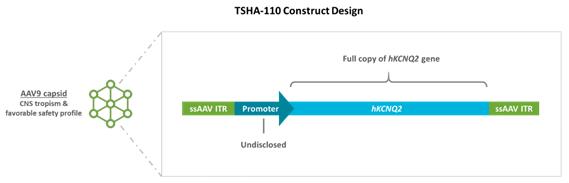
Our Next-Generation Platform Technologies
In addition to our AAV9 candidates, we are building a suite of platforms to develop next-generation technologies that can optimize key components of an AAV-based gene therapy as part of our strategy to develop a sustainable pipeline of product candidates and a consistent stream of new commercial product launches.
Novel Route of Administration to Allow Redosing
We are advancing a novel AAV dosing platform with the potential to facilitate redosing by administering AAV-based gene therapies directly to the vagus nerve. The development of AAV-neutralizing antibodies after administration of an initial dose has historically presented a challenge in the ability to redose patients with gene therapies. In preclinical studies in adult rats, we observed that AAV9 delivery to the vagus nerve resulted in efficient targeting of the vagal neurons in the ANS. We subsequently performed experiments to assess the feasibility of targeting genes to ANS neurons in rats already treated with an intrathecal injection of AAV9. Rats were immunized with AAV9 by an intrathecal injection of AAV9/GAN and then received a direct vagus nerve injection with AAV9/GFP either four or fourteen weeks after the intrathecal injection. AAV9-immunized rats had efficient green fluorescent protein, or GFP, transduction in vagal nerve fibers and neurons. There was no evidence of neuroinflammation or significant chronic inflammatory infiltrates.
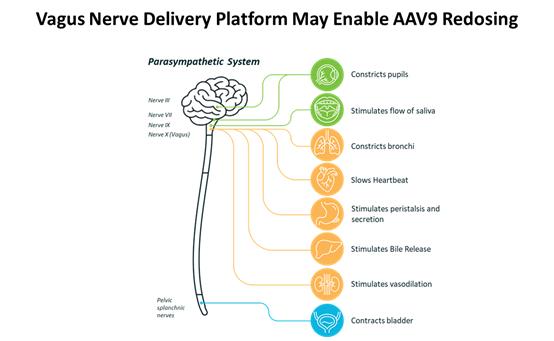
31
In preclinical studies in dogs, adult hounds received a direct vagus nerve injection of increasing volumes of vehicle and were allowed to recover for two weeks. AAV delivery to the vagus nerve was well tolerated at all doses. Vocalization, weight, eating and fecal output were monitored pre- and post-surgery, and post-mortem analysis showed that vagal nerve fibers and neurons were microscopically normal.
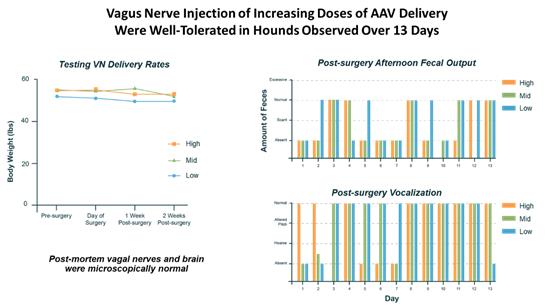
We plan to further evaluate the safety and feasibility of this approach in NHPs.
Regulated Transgene Expression Using miRARE
In a number of disorders, including Rett syndrome and FOXG1 syndrome, the expression of a therapeutic transgene needs to be regulated. In these disorders, high doses of transgene-expressing vectors may be harmful, while low doses may avoid toxicity but be sub-therapeutic. For disorders that require replacement of dose-sensitive genes, we have combined high-throughput miRNA profiling and genome mining to create miRARE, our novel miRNA target panel. This approach is designed to enable our product candidates to maintain safe transgene expression levels in the brain. Importantly, this built-in regulation system is fully endogenous, and therefore does not require any additional exogenous drug application. Instead, the miRARE system utilizes endogenous transgene-responsive miRNA to downregulate transgene expression in the event that overexpression occurs. While our initial intent is to utilize our miRARE panel to develop gene replacement therapies for Rett syndrome and FOXG1 syndrome, we believe the system may be applicable to a number of other dose-sensitive genes.
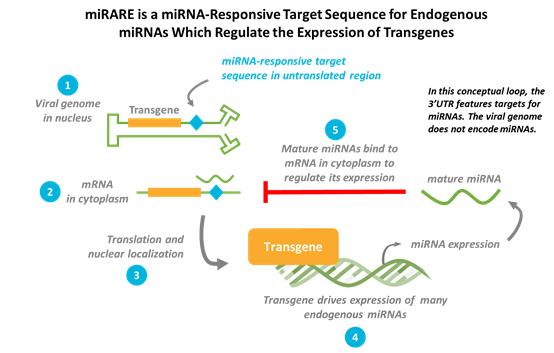
32
Successful clinical translation of gene therapies depends upon efficient transgene delivery and expression across the entire CNS. Directed evolution is a powerful and proven method to develop novel AAV vector capsids that exhibit properties distinct from naturally occurring serotypes. However, to date, most novel capsids have been derived in rodents or in vitro models whose properties may or may not translate to other species, in particular primates.
We have developed a new approach that utilizes AAV whole capsid shuffling and directed evolution, combined with machine learning techniques, to develop novel AAV capsids in mice and NHPs in parallel. We are utilizing SMRT sequencing analysis for a high throughput evaluation of recovered whole AAV capsid genes. SMRT sequencing has the advantage of sequencing the entire capsid gene in a single read with high accuracy, enabling sequencing the entire shuffled capsid rather than only an insert region or barcode.
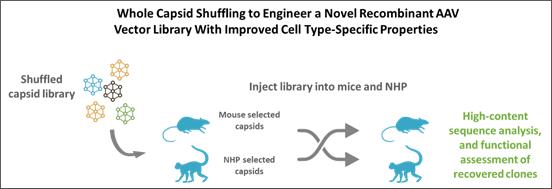
We believe that our approach will allow us to rapidly identify new capsids for the treatment of CNS disorders and drive new product candidates with novel biodistribution and transduction profiles into our development pipeline.
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly changing technologies, significant competition and a strong emphasis on intellectual property. This is also true for the development and commercialization of treatments for neurodegenerative diseases, neurodevelopmental disorders and genetic epilepsies, and broadly across gene therapies. While we believe that our focus, strength of team, expertise in gene therapy, scientific knowledge and intellectual property provide us with competitive advantages, we face competition from several different sources, including large and small biopharmaceutical companies, academic research institutions, government agencies and public and private research institutions. Not only must we compete with other companies that are focused on gene transfer technology, but any product candidates that we successfully develop and commercialize will compete with existing therapies and new therapies that may become available in the future.
Many of our competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, clinical trials, regulatory approvals and product marketing than we do. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
The majority of our programs face limited competition as there are no approved disease-modifying therapies for the treatment of the GM2 gangliosidosis, CLN1 disease, Rett syndrome, SLC6A1 haploinsufficiency disorder, SURF1-associated Leigh syndrome, SLC13A5 disorder, Fragile X syndrome, Angelman syndrome or the other development programs in our pipeline.
Sio Gene Therapies is developing AXO-AAV-GM2 for the treatment of GM2 gangliosidosis. AXO-AAV-GM2 delivers two AAVrh8 vectors, each encoding either HEXA or HEXB genes, directly to the CNS with the intention of producing functioning ß-hexosaminidase.
Amicus, in collaboration with Nationwide Children’s Hospital, is developing a gene therapy candidate for CLN1 disease that is currently in discovery stage.
Novartis, through its acquisition of AveXis, is developing a product candidate for the treatment of Rett syndrome, AVXS-201, a preclinical AAV9 capsid vector that carries AAV ITR sequences and a minimal MECP2 promoter that is designed to be active in the CNS
33
in an unregulated manner. In addition, the Rett Syndrome Research Trust, Amicus Therapeutics and Sarepta have disclosed the existence of discovery-stage gene therapy programs although the development status of these programs is unclear.
Manufacturing
Through our collaboration with the UT Southwestern Gene Therapy Program, we have access to a new, state-of-the-art AAV production facility which includes approximately 2,000 square feet of laboratory space for process development and research-grade AAV vector production, as well as a 1,000 square foot ISO7 cleanroom facility dedicated solely for cGMP AAV vector manufacture.
This facility is outfitted with new equipment purchased in 2018 and 2019 for research-grade and GMP-grade AAV vector production. The process development lab is equipped with two Sartorius Biostat B Controller Stations with four 10 liter glass bioreactors and four 2 liter glass bioreactors, a Sartorius Biostat STR 50 liter bioreactor with controller and a Sartorius AMBR 250 process development bioreactor. Our strategic partnership with UT Southwestern provides us with access to this facility to allow for process development for development programs.
The UT Southwestern GMP facility is equipped with a Sartorius Biostat STR 50 liter bioreactor with controller, a Sartorius Biostat STR 500 liter bioreactor with controller, Sartoflow Smart tangential flow filtration unit, a Sartorius FlexAct UD, two bioprocessing workstations and an automated dispenser to support our AAV9 manufacturing needs for early clinical trials. We believe this capacity will be sufficient to meet the clinical demand for our full pipeline of product candidates.
In addition to our manufacturing capabilities provided by UT Southwestern, we have entered into a lease agreement to occupy and configure an approximately 187,000-square-foot commercial-scale cGMP manufacturing facility in Durham, North Carolina. We are currently engaged with engineering, architectural and construction firms to develop and execute our comprehensive facility build strategy, including pipeline and capacity planning assessment, benchmarking, quality systems and programs, and other strategic efforts related to the design and build out of the new facility to support commercial scale manufacturing of our pipeline programs.
License Agreements
Research, Collaboration and License Agreement with The University of Texas Southwestern Medical Center
In November 2019, we entered into a research, collaboration and license agreement, or the UT Southwestern Agreement, with The Board of Regents of the University of Texas System on behalf of UT Southwestern, as amended in April 2020. Under the UT Southwestern Agreement, UT Southwestern is primarily responsible for preclinical development activities with respect to licensed products for use in certain specified indications (up to IND-enabling studies), and we are responsible for all subsequent clinical development and commercialization activities with respect to licensed products. UT Southwestern will conduct such preclinical activities for a two-year period under mutually agreed upon sponsored research agreements that are funded by us. During the initial research phase, we have the right to expand the scope of specified indications under the UT Southwestern Agreement. We currently have 15 product candidates pursuant to the UT Southwestern Agreement, option rights with respect to KCNQ2 and options for an additional four indications. The research program activities will be overseen by a joint steering committee.
In connection with the UT Southwestern Agreement, we obtained an exclusive, worldwide, royalty-free license under certain patent rights of UT Southwestern and a non-exclusive, worldwide, royalty-free license under certain know-how of UT Southwestern, in each case to make, have made, use, sell, offer for sale and import licensed products for use in certain specified indications. Additionally, we obtained a non-exclusive, worldwide, royalty-free license under certain patents and know-how of UT Southwestern for use in all human uses, with a right of first refusal to obtain an exclusive license under certain of such patent rights and an option to negotiate an exclusive license under other of such patent rights at no cost. We are required to use commercially reasonable efforts to develop, obtain regulatory approval for, and commercialize at least one licensed product.
In connection with the license grant, we issued to UT Southwestern 2,179,000 shares of our common stock. We do not have any future milestone or royalty obligations to UT Southwestern under the UT Southwestern Agreement, other than costs related to the maintenance of patents.
The UT Southwestern Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last valid claim of a licensed patent in such country for such licensed product. After the initial research term, we may terminate the agreement, on an indication-by-indication and licensed product-by-licensed product basis, at any time upon specified written notice to UT Southwestern. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party.
34
License Agreement with Queen’s University at Kingston
In February 2020, we entered into a license agreement, or the Queen’s University Agreement, with Queen’s University at Kingston, or Queen’s University. In connection with the Queen’s University Agreement, we obtained an exclusive, perpetual, worldwide, royalty-bearing license, with the right to grant sublicenses through multiple tiers, under certain patent rights and know-how related to bicistronic vectors, including with respect to TSHA-101, of Queen’s University, including certain improvements to such patent rights and know-how, to develop products in any field which use one or more valid claims of the patents licensed under the Queen’s University Agreement, or the Licensed Patents, or the technology, information and intellectual property related to the patents licensed under the Queen’s University Agreement, or the Licensed Technology and together with the Licensed Patents, the Licensed Products, and to make, have made, use, sell, offer for sale, import and export Licensed Products and otherwise exploit such patents and know-how for use in certain specified indications. We also obtained an exclusive right of first negotiation to license certain next-generation technology and improvements of Queen’s University that do not constitute an already-licensed improvement to the Licensed Technology. The Licensed Patent will expire in 2037, absent any patent term adjustment or extension.
We are required to use commercially reasonable efforts to exploit the Licensed Technology in countries where it is commercially reasonable to develop Licensed Products, including by meeting certain diligence milestones within certain specified periods of time. In addition, we have final decision-making authority on the filing, prosecution or maintenance of Licensed Patents.
In connection with the Queen’s University Agreement, we paid Queen’s University a one-time fee of $3.0 million as an upfront fee and $0.2 million to reimburse Queen’s University for certain plasmid production costs. We are obligated to pay Queen’s University up to $10.0 million in the aggregate upon achievement of certain regulatory milestones, up to $10.0 million in the aggregate upon achievement of commercial milestones, a low single digit royalty on net sales of Licensed Products, subject to certain customary reductions, and a percentage of non-royalty sublicensing revenue ranging in the low double digits. Royalties are payable on a Licensed Product-by-Licensed Product basis and country-by-country basis until expiration of the last valid claim of a Licensed Patent covering such Licensed Product in such country and the expiration of any regulatory exclusivity for such Licensed Product in such country. Additionally, we are obligated to pay Queen’s University a low double-digit portion of any amounts received by us in connection with the sale of a priority review voucher related to a Licensed Product, not to exceed a low eight-figure amount.
The Queen’s University Agreement expires upon the expiration of the last royalty term of a Licensed Product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. We may elect to terminate the agreement upon specified prior written notice to Queen’s University.
We were also obligated under the terms of a separate research grant agreement to reimburse Queen’s University for certain clinical manufacturing production costs of approximately $3.8 million all of which was paid in 2020.
License Agreements with Abeona
CLN1
In August 2020, we entered into a license agreement, or the Abeona CLN1 Agreement, with Abeona. In connection with the Abeona CLN1 Agreement, we obtained an exclusive, worldwide, royalty-bearing license, with the right to grant sublicenses under certain patents, know-how and materials originally developed by the University of North Carolina at Chapel Hill and Abeona to research, develop, manufacture, have manufactured, use, and commercialize licensed products for gene therapy for the prevention, treatment, or diagnosis of CLN1 disease in humans.
Subject to certain obligations of Abeona, we are required to use commercially reasonable efforts to develop at least one licensed product and commercialize at least one licensed product in the United States.
In connection with the license grant, we paid Abeona a one-time upfront license fee of $3.0 million. We are obligated to pay Abeona up to $26.0 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed product and high single-digit royalties on net sales of licensed products. Royalties are payable on a licensed product-by-licensed product and country-by-country basis until the latest of the expiration or revocation or complete rejection of the last licensed patent covering such licensed product in the country where the licensed product is sold, the loss of market exclusivity in such country where the product is sold, or, if no licensed product exists in such country and no market exclusivity exists in such country, ten years from first commercial sale of such licensed product in such country. In addition, concurrent with the Abeona CLN1 Agreement we entered into a purchase and reimbursement agreement with Abeona, pursuant to which we purchased specified inventory from Abeona for total consideration of $4.0 million.
The Abeona CLN1 Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. We may terminate the agreement for convenience upon specified prior written notice to Abeona.
35
In October 2020, we entered into a license agreement, or the Abeona Rett Agreement, with Abeona pursuant to which we obtained an exclusive, worldwide, royalty-bearing license, with the right to grant sublicenses under certain patents, know-how and materials originally developed by the University of North Carolina at Chapel Hill, the University of Edinburgh and Abeona to research, develop, manufacture, have manufactured, use, and commercialize licensed products for gene therapy and the use of related transgenes for Rett syndrome.
Subject to certain obligations of Abeona, we are required to use commercially reasonable efforts to develop at least one licensed product and commercialize at least one licensed product in the United States.
In connection with the Abeona Rett Agreement, we paid Abeona a one-time upfront license fee of $3.0 million. We are obligated to pay Abeona up to $26.5 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed product and high single-digit royalties on net sales of licensed products. Royalties are payable on a licensed product-by-licensed product and country-by-country basis until the latest of the expiration or revocation or complete rejection of the last licensed patent covering such licensed product in the country where the licensed product is sold, the loss of market exclusivity in such country where the product is sold, or, if no licensed product exists in such country and no market exclusivity exists in such country, ten years from first commercial sale of such licensed product in such country.
The Abeona Rett Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. We may terminate the agreement for convenience upon specified prior written notice to Abeona.
Intellectual Property
We actively seek to protect our proprietary technology, inventions, and other intellectual property that is commercially important to the development of our business by a variety of means, for example seeking, maintaining, and defending patent rights, whether developed internally or licensed from third parties. We also may rely on trade secrets and know-how relating to our proprietary technology platform, on continuing technological innovation and on in-licensing opportunities to develop, strengthen and maintain the strength of our position in the field of gene therapy that may be important for the development of our business. We also intend to seek patent protection or rely upon trade secret rights to protect other technologies that may be used to discover and validate targets, and that may be used to manufacture and develop novel gene therapy products. We are a party to license agreements that give us rights to use specific technologies in our gene therapy products and in manufacturing our products. Additional regulatory protection may also be afforded through data exclusivity, market exclusivity and patent term extensions where available.
As of January 26, 2021, we in-license five pending Patent Cooperation Treaty, or PCT, applications, 27 pending foreign patent applications and 13 pending United States patent applications, of which seven are United States utility patent applications, which, if issued, are expected to expire between 2037and 2040, without taking into account any possible patent term adjustment, and six that are United States provisional patent applications, where patent applications claiming priority to these provisional patent applications, if issued, are expected to expire in 2041, without taking into account any possible patent term adjustment. Our policy is to file patent applications to protect technology, inventions and improvements to inventions that may be commercially important to the development of our business.
We in-license one pending PCT application and one United States utility patent application that relate to our TSHA-103 SLC6A1 program. This United States utility patent application, and any foreign patent applications based on this PCT application, if issued, are expected to expire in 2040, without taking into account any possible patent term adjustment. We in-license one PCT patent application and one United States utility patent application that relate to our TSHA-104 SURF1 program. This United States utility patent application, and any foreign patent applications based on this PCT application, if issued, are expected to expire in 2040, without taking into account any possible patent term adjustment. Patent applications directed to our most advanced product candidates are summarized below:
TSHA-101
We in-license a United States utility patent application directed to a bicistronic HEXBP2A-HEXA transgene packaged into an AAV vector, and methods of using that vector to treat GM2 gangliosidosis, such as Tay-Sachs disease or Sandhoff disease, which, if issued, is expected to expire in 2037, without taking into account any possible patent term adjustment. This application has no foreign counterparts.
36
We in-license certain patent rights directed to a palmitoyl-protein thioesterase 1-encoding transgene packaged into an AAV vector, and methods of using that vector to treat CLN1 disease (one of the forms of Batten disease). Specifically, pursuant to our license agreement with Abeona we have in-licensed one PCT patent application assigned to Abeona. Patent applications based on this PCT application, if issued, are expected to expire in 2040, without taking into account any possible patent term adjustment. In addition, pursuant to the Abeona CLN1 agreement, we have sublicensed 15 pending patent applications worldwide assigned to the University of North Carolina at Chapel Hill. These patent applications, if issued, are expected to expire in 2037, without taking into account any possible patent term adjustment.
TSHA-102
We in-license one PCT patent application and one United States utility patent application directed to a minigene encoding MECP2 packaged into an AAV vector, and methods of using that vector to treat Rett syndrome. This United States utility patent application, and any foreign patent applications based on this PCT application, if issued, are expected to expire in 2040, without taking into account any possible patent term adjustment. We also in-license 15 pending patent applications worldwide directed to MECP2 expression cassettes for gene therapy. These patent applications, if issued, are expected to expire in 2038, without taking into account any possible patent term adjustment.
We also rely on trade secrets, know-how, continuing technological innovation and confidential information to develop and maintain our proprietary position and protect aspects of our business that are not amenable to, or that we do not consider appropriate for, patent protection. We seek to protect employees, consultants, scientific advisors, contractors and others who may have access to proprietary information, under which they are bound to assign to us inventions made during the term of their employment or term of service. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems.
Government Regulation
The FDA and other regulatory authorities at federal, state and local levels, as well as in foreign countries, extensively regulate, among other things, the research, development, testing, manufacture, quality control, import, export, safety, effectiveness, labeling, packaging, storage, distribution, record keeping, approval, advertising, promotion, marketing, post-approval monitoring and post-approval reporting of biologics such as those we are developing.
Biological products are subject to regulation under the Food, Drug, and Cosmetic Act, or FDCA, and the Public Health Service Act, or PHSA, and other federal, state, local and foreign statutes and regulations. We, along with third-party contractors, will be required to navigate the various preclinical, clinical and commercial approval requirements of the governing regulatory agencies of the countries in which we wish to conduct studies or seek approval or licensure of our product candidates.
U.S. Biologics Regulation
The process required by the FDA before biological product candidates may be marketed in the United States generally involves the following:
|
|
• |
completion of extensive preclinical laboratory tests and animal studies performed in accordance with applicable regulations, including the GLP regulations; |
|
|
• |
submission to the FDA of an IND, which must become effective before clinical trials may begin; |
|
|
• |
approval by an independent institutional review board, or IRB, or ethics committee at each clinical site before the trial is commenced; |
|
|
• |
performance of adequate and well-controlled human clinical trials to establish the safety, purity and potency of the proposed biological product candidate for its intended purpose; |
|
|
• |
preparation of and submission to the FDA of a biologics license application, or BLA, after completion of all pivotal clinical trials; |
|
|
• |
a determination by the FDA within 60 days of its receipt of a BLA to file the application for review; |
|
|
• |
satisfactory completion of an FDA pre-approval inspection of the manufacturing facility or facilities at which the proposed product is produced to assess compliance with current Good Manufacturing Practice requirements, or cGMPs, and to assure that the facilities, methods and controls are adequate to preserve the biological product’s continued safety, purity and potency, and of selected clinical investigation sites to assess compliance with the FDA’s good clinical practices, or GCPs; |
|
|
• |
satisfactory completion of an FDA Advisory Committee review, if applicable; and |
|
|
• |
FDA review and approval, or licensure, of a BLA to permit commercial marketing of the product for particular indications for use in the United States. |
37
Preclinical and Clinical Development
Prior to beginning the first clinical trial with a product candidate, we must submit an IND to the FDA. An IND is a request for authorization from the FDA to administer an investigational new drug product to humans. The central focus of an IND submission is on the general investigational plan and the protocol or protocols for preclinical studies and clinical trials. The IND also includes results of animal and in vitro studies assessing the toxicology, pharmacokinetics, pharmacology and pharmacodynamic characteristics of the product, chemistry, manufacturing and controls information, and any available human data or literature to support the use of the investigational product. An IND must become effective before human clinical trials may begin. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day period, raises safety concerns or questions about the proposed clinical trial. In such a case, the IND may be placed on clinical hold and the IND sponsor and the FDA must resolve any outstanding concerns or questions before the clinical trial can begin. Submission of an IND therefore may or may not result in FDA authorization to begin a clinical trial.
In addition to the submission of an IND to the FDA before initiation of a clinical trial in the United States, certain human clinical trials involving recombinant or synthetic nucleic acid molecules are subject to oversight at the local level as set forth in the NIH Guidelines. Specifically, under the NIH Guidelines, supervision of human gene transfer trials includes evaluation and assessment by an Institutional Biosafety Committee, or IBC, a local institutional committee that reviews and oversees research utilizing recombinant or synthetic nucleic acid molecules at that institution. The IBC assesses the safety of the research and identifies any potential risk to public health or the environment, and such review may result in some delay before initiation of a clinical trial. While the NIH Guidelines are not mandatory unless the research in question is being conducted at or sponsored by institutions receiving NIH funding of recombinant or synthetic nucleic acid molecule research, many companies and other institutions not otherwise subject to the NIH Guidelines voluntarily follow them.
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCPs, which include the requirement that all research subjects provide their informed consent for their participation in any clinical study. Clinical trials are conducted under protocols detailing, among other things, the objectives of the study, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated. A separate submission to the existing IND must be made for each successive clinical trial conducted during product development and for any subsequent protocol amendments. Furthermore, an independent IRB for each site proposing to conduct the clinical trial must review and approve the plan for any clinical trial and its informed consent form before the clinical trial begins at that site, and must monitor the study until completed. Regulatory authorities, the IRB or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk or that the trial is unlikely to meet its stated objectives. Some studies also include oversight by an independent group of qualified experts organized by the clinical study sponsor, known as a data safety monitoring board, which provides authorization for whether or not a study may move forward at designated check points based on access to certain data from the study and may halt the clinical trial if it determines that there is an unacceptable safety risk for subjects or other grounds, such as no demonstration of efficacy. There are also requirements governing the reporting of ongoing preclinical studies and clinical trials and clinical study results to public registries.
For purposes of BLA approval of a product candidate, human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
|
|
• |
Phase 1. For gene therapies, the investigational product is initially introduced into patients with the target disease or condition. These studies are designed to test the safety, dosage tolerance, absorption, metabolism and distribution of the investigational product in humans, the side effects associated with increasing doses, and, if possible, to gain early evidence on effectiveness. |
|
|
• |
Phase 2. The investigational product is administered to a limited patient population to evaluate the preliminary efficacy, optimal dosages and dosing schedule and to identify possible adverse side effects and safety risks. |
|
|
• |
Phase 3. The investigational product is administered to an expanded patient population to further evaluate dosage, to provide statistically significant evidence of clinical efficacy and to further test for safety, generally at multiple geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall risk/benefit ratio of the investigational product and to provide an adequate basis for product approval. |
When these phases overlap or are combined, the trials may be referred to as Phase 1/2 or Phase 2/3.
In some cases, the FDA may require, or companies may voluntarily pursue, additional clinical trials after a product is approved to gain more information about the product. These so-called Phase 4 studies may be made a condition to approval of the BLA. Concurrent with clinical trials, companies may complete additional animal studies and develop additional information about the characteristics of the product candidate, and must finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, must develop methods for testing the identity, strength, quality and purity of the final product, or for biologics, the safety, purity and potency. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the product candidate does not undergo unacceptable deterioration over its shelf life.
38
During all phases of clinical development, regulatory agencies require extensive monitoring and auditing of all clinical activities, clinical data, and clinical study investigators. The FDA or the sponsor or its data safety monitoring board may suspend a clinical study at any time on various grounds, including a finding that the research patients or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical study at its institution if the clinical study is not being conducted in accordance with the IRB’s requirements or if the biological product candidate has been associated with unexpected serious harm to patients. There are also requirements governing the reporting of ongoing clinical trials and completed clinical trial results to public registries. Sponsors of clinical trials of FDA-regulated products, including biologics, are required to register and disclose certain clinical trial information, which is publicly available at www.clinicaltrials.gov.
BLA Submission and Review
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, the results of product development, nonclinical studies and clinical trials are submitted to the FDA as part of a BLA requesting approval to market the product for one or more indications. The BLA must include all relevant data available from pertinent preclinical studies and clinical trials, including negative or ambiguous results as well as positive findings, together with detailed information relating to the product’s chemistry, manufacturing, controls, and proposed labeling, among other things. The submission of a BLA requires payment of a substantial application user fee to the FDA, unless a waiver or exemption applies. The FDA has sixty days from the applicant’s submission of a BLA to either issue a refusal to file letter or accept the BLA for filing, indicating that it is sufficiently complete to permit substantive review.
Once a BLA has been accepted for filing, the FDA’s goal is to review standard applications within ten months after it accepts the application for filing, or, if the application qualifies for priority review, six months after the FDA accepts the application for filing. In both standard and priority reviews, the review process is often significantly extended by FDA requests for additional information or clarification. The FDA reviews a BLA to determine, among other things, whether a product is safe, pure and potent for its intended use, and whether the facility in which it is manufactured, processed, packed or held meets standards designed to assure and preserve the product’s identity, safety, strength, quality, potency and purity. The FDA may convene an advisory committee to provide clinical insight on application review questions. Before approving a BLA, the FDA will typically inspect the facility or facilities where the product is manufactured. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving a BLA, the FDA will typically inspect one or more clinical sites to assure compliance with GCPs. If the FDA determines that the application, manufacturing process or manufacturing facilities are not acceptable, it will outline the deficiencies in the submission and often will request additional testing or information. Notwithstanding the submission of any requested additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
After the FDA evaluates a BLA and conducts inspections of manufacturing facilities where the investigational product and/or its drug substance will be manufactured, the FDA may issue an approval letter or a Complete Response letter. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A Complete Response letter will describe all of the deficiencies that the FDA has identified in the BLA, except that where the FDA determines that the data supporting the application are inadequate to support approval, the FDA may issue the Complete Response letter without first conducting required inspections, testing submitted product lots and/or reviewing proposed labeling. In issuing the Complete Response letter, the FDA may recommend actions that the applicant might take to place the BLA in condition for approval, including requests for additional information or clarification, which may include the potential requirement for additional clinical studies. The FDA may delay or refuse approval of a BLA if applicable regulatory criteria are not satisfied, require additional testing or information and/or require post-marketing testing and surveillance to monitor safety or efficacy of a product.
If regulatory approval of a product is granted, such approval will be granted for particular indications and may entail limitations on the indicated uses for which such product may be marketed. For example, the FDA may approve the BLA with a Risk Evaluation and Mitigation Strategy, or REMS, to ensure the benefits of the product outweigh its risks. A REMS is a safety strategy to manage a known or potential serious risk associated with a product and to enable patients to have continued access to such medicines by managing their safe use, and could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA also may condition approval on, among other things, changes to proposed labeling or the development of adequate controls and specifications. Once approved, the FDA may withdraw the product approval if compliance with pre- and post-marketing requirements is not maintained or if problems occur after the product reaches the marketplace. The FDA may require one or more Phase 4 post-market studies and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization, and may limit further marketing of the product based on the results of these post-marketing studies.
Expedited Development and Review Programs
The FDA offers a number of expedited development and review programs for qualifying product candidates. The fast track program is intended to expedite or facilitate the process for reviewing new products that meet certain criteria. Specifically, new products are eligible for fast track designation if they are intended to treat a serious or life-threatening disease or condition and demonstrate the potential to address unmet medical needs for the disease or condition. Fast track designation applies to the combination of the product and the specific indication for which it is being studied. The sponsor of a fast track product has opportunities for frequent interactions with the review team during product development and, once a BLA is submitted, the product may be eligible for priority review. A fast track
39
product may also be eligible for rolling review, where the FDA may consider for review sections of the BLA on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the BLA, the FDA agrees to accept sections of the BLA and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the BLA.
A product intended to treat a serious or life-threatening disease or condition may also be eligible for breakthrough therapy designation to expedite its development and review. A product can receive breakthrough therapy designation if preliminary clinical evidence indicates that the product, alone or in combination with one or more other drugs or biologics, may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. The designation includes all of the fast track program features, as well as more intensive FDA interaction and guidance beginning as early as Phase 1 and an organizational commitment to expedite the development and review of the product, including involvement of senior managers.
An RMAT is defined as cell therapies, therapeutic tissue engineering products, human cell and tissue products, and combination products using any such therapies or products. Gene therapies, including genetically modified cells that lead to a durable modification of cells or tissues may meet the definition of a Regenerative Medicine Therapy. The RMAT program is intended to facilitate efficient development and expedite review of RMATs, which are intended to treat, modify, reverse, or cure a serious or life-threatening disease or condition. A new drug application or a BLA for an RMAT may be eligible for priority review or accelerated approval through (1) surrogate or intermediate endpoints reasonably likely to predict long-term clinical benefit or (2) reliance upon data obtained from a meaningful number of sites. Benefits of such designation also include early interactions with FDA to discuss any potential surrogate or intermediate endpoint to be used to support accelerated approval. A Regenerative Medicine Therapy that is granted accelerated approval and is subject to post-approval requirements may fulfill such requirements through the submission of clinical evidence, clinical studies, patient registries, or other sources of real world evidence, such as electronic health records; the collection of larger confirmatory data sets; or post-approval monitoring of all patients treated with such therapy prior to its approval.
Any marketing application for a biologic submitted to the FDA for approval, including a product with a fast track designation and/or breakthrough therapy designation, may be eligible for other types of FDA programs intended to expedite the FDA review and approval process, such as priority review and accelerated approval. A product is eligible for priority review if it has the potential to provide a significant improvement in the treatment, diagnosis or prevention of a serious disease or condition. For original BLAs, priority review designation means the FDA’s goal is to take action on the marketing application within six months of the 60-day filing date.
Additionally, products studied for their safety and effectiveness in treating serious or life-threatening diseases or conditions may receive accelerated approval upon a determination that the product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. As a condition of accelerated approval, the FDA will generally require the sponsor to perform adequate and well-controlled post-marketing clinical studies to verify and describe the anticipated effect on irreversible morbidity or mortality or other clinical benefit. In addition, the FDA currently requires as a condition for accelerated approval pre-approval of promotional materials, which could adversely impact the timing of the commercial launch of the product.
Fast track designation, breakthrough therapy designation, RMAT designation, priority review and accelerated approval do not change the standards for approval but may expedite the development or approval process. Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan designation to a drug or biologic intended to treat a rare disease or condition, which is a disease or condition that affects fewer than 200,000 individuals in the United States, or 200,000 or more than individuals in the United States for which there is no reasonable expectation that the cost of developing and making available in the United States a drug or biologic for this type of disease or condition will be recovered from sales in the United States for that drug or biologic. Orphan drug designation must be requested before submitting a BLA. After the FDA grants orphan drug designation, the generic identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. The orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review or approval process.
If a product that has orphan drug designation subsequently receives the first FDA approval for the disease for which it has such designation, the product is entitled to orphan drug exclusive approval (or exclusivity), which means that the FDA may not approve any other applications, including a full BLA, to market the same biologic for the same indication for seven years, except in limited circumstances, such as a showing of clinical superiority to the product with orphan drug exclusivity or if the holder of the orphan drug exclusivity cannot assure the availability of sufficient quantities of the orphan drug to meet the needs of patients with the disease or condition for which the drug was designated. Orphan drug exclusivity does not prevent the FDA from approving a different drug or
40
biologic for the same disease or condition, or the same drug or biologic for a different disease or condition. Among the other benefits of orphan drug designation are tax credits for certain research and a waiver of the BLA application fee.
A designated orphan drug may not receive orphan drug exclusivity if it is approved for a use that is broader than the indication for which it received orphan designation. In addition, exclusive marketing rights in the United States may be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantities of the product to meet the needs of patients with the rare disease or condition.
Rare Pediatric Disease Designation and Priority Review Vouchers
Under the FDCA, as amended, the FDA incentivizes the development of drugs and biologics that meet the definition of a “rare pediatric disease,” defined to mean a serious or life-threatening disease in which the serious of life-threatening manifestations primarily affect individuals aged from birth to 18 years and the disease affects fewer than 200,000 individuals in the United States or affects 200,000 or more in the United States and for which there is no reasonable expectation that the cost of developing and making in the United States a drug for such disease or condition will be received from sales in the United States of such drug. The sponsor of a product candidate for a rare pediatric disease may be eligible for a voucher that can be used to obtain a priority review for a subsequent human drug or biologic application after the date of approval of the rare pediatric disease drug product, referred to as a priority review voucher, or PRV. A sponsor may request rare pediatric disease designation from the FDA prior to the submission of its NDA or BLA. A rare pediatric disease designation does not guarantee that a sponsor will receive a PRV upon approval of its NDA or BLA. Moreover, a sponsor who chooses not to submit a rare pediatric disease designation request may nonetheless receive a PRV upon approval of their marketing application if they request such a voucher in their original marketing application and meet all of the eligibility criteria. If a PRV is received, it may be sold or transferred an unlimited number of times. Congress has extended the PRV program until September 30, 2024, with the potential for PRVs to be granted until September 30, 2026.
Post-Approval Requirements
Any products manufactured or distributed by us pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to record-keeping, reporting of adverse experiences, periodic reporting, product sampling and distribution, and advertising and promotion of the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims, are subject to prior FDA review and approval. There also are continuing user fee requirements, under which the FDA assesses an annual program fee for each product identified in an approved BLA. Biologic manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMPs, which impose certain procedural and documentation requirements upon us and our third-party manufacturers. Changes to the manufacturing process are strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMPs and impose reporting requirements upon us and any third-party manufacturers that we may decide to use. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain compliance with cGMPs and other aspects of regulatory compliance.
The FDA may withdraw approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical studies to assess new safety risks; or imposition of distribution restrictions or other restrictions under a REMS program. Other potential consequences include, among other things:
|
|
• |
restrictions on the marketing or manufacturing of a product, complete withdrawal of the product from the market or product recalls; |
|
|
• |
fines, warning or untitled letters or holds on post-approval clinical studies; |
|
|
• |
refusal of the FDA to approve pending applications or supplements to approved applications, or suspension or revocation of existing product approvals; |
|
|
• |
product seizure or detention, or refusal of the FDA to permit the import or export of products; |
|
|
• |
consent decrees, corporate integrity agreements, debarment or exclusion from federal healthcare programs; |
|
|
• |
mandated modification of promotional materials and labeling and the issuance of corrective information; |
|
|
• |
the issuance of safety alerts, Dear Healthcare Provider letters, press releases and other communications containing warnings or other safety information about the product; or |
|
|
• |
injunctions or the imposition of civil or criminal penalties. |
41
The FDA closely regulates the marketing, labeling, advertising and promotion of biologics. A company can make only those claims relating to safety and efficacy, purity and potency that are approved by the FDA and in accordance with the provisions of the approved label. However, companies may share truthful and not misleading information that is otherwise consistent with a product’s FDA approved labeling. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses. Failure to comply with these requirements can result in, among other things, adverse publicity, warning letters, corrective advertising and potential civil and criminal penalties. Physicians may prescribe legally available products for uses that are not described in the product’s labeling and that differ from those tested by us and approved by the FDA. Such off-label uses are common across medical specialties. Physicians may believe that such off-label uses are the best treatment for many patients in varied circumstances. The FDA does not regulate the behavior of physicians in their choice of treatments. The FDA does, however, restrict manufacturer’s communications on the subject of off-label use of their products.
Biosimilars and Reference Product Exclusivity
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively the ACA, includes a subtitle called the Biologics Price Competition and Innovation Act, or BPCIA, which created an abbreviated approval pathway for biological products that are biosimilar to or interchangeable with an FDA-approved reference biological product. To date, a number of biosimilars have been licensed under the BPCIA, and numerous biosimilars have been approved in Europe. The FDA has issued several guidance documents outlining an approach to review and approval of biosimilars.
Biosimilarity, which requires that there be no clinically meaningful differences between the biological product and the reference product in terms of safety, purity, and potency, can be shown through analytical studies, animal studies, and a clinical study or studies. Interchangeability requires that a product is biosimilar to the reference product and the product must demonstrate that it can be expected to produce the same clinical results as the reference product in any given patient and, for products that are administered multiple times to an individual, the biologic and the reference biologic may be alternated or switched after one has been previously administered without increasing safety risks or risks of diminished efficacy relative to exclusive use of the reference biologic. Complexities associated with the larger, and often more complex, structures of biological products, as well as the processes by which such products are manufactured, pose significant hurdles to implementation of the abbreviated approval pathway that are still being worked out by the FDA.
Under the BPCIA, an application for a biosimilar product may not be submitted to the FDA until four years following the date that the reference product was first licensed by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until 12 years from the date on which the reference product was first licensed. During this 12-year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing that applicant’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of its product. The BPCIA also created certain exclusivity periods for biosimilars approved as interchangeable products. At this juncture, it is unclear whether products deemed “interchangeable” by the FDA will, in fact, be readily substituted by pharmacies, which are governed by state pharmacy law.
The BPCIA is complex and continues to be interpreted and implemented by the FDA. In addition, government proposals have sought to reduce the 12-year reference product exclusivity period. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. As a result, the ultimate impact, implementation, and impact of the BPCIA is subject to significant uncertainty.
Foreign Regulation
In order to market any product outside of the United States, we would need to comply with numerous and varying regulatory requirements of other countries and jurisdictions regarding quality, safety, and efficacy and governing, among other things, clinical trials, marketing authorization, commercial sales and distribution of our products. Whether or not we obtain FDA approval for a product, we would need to obtain the necessary approvals by the comparable foreign regulatory authorities before we can commence clinical trials or marketing of the product in foreign countries and jurisdictions. Although many of the issues discussed above with respect to the United States apply similarly in the context of the European Union, the approval process varies between countries and jurisdictions and can involve additional product testing and additional administrative review periods. The time required to obtain approval in other countries and jurisdictions might differ from and be longer than that required to obtain FDA approval. Regulatory approval in one country or jurisdiction does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country or jurisdiction may negatively impact the regulatory process in others.
42
Other Healthcare Laws and Compliance Requirements
Pharmaceutical companies are subject to additional healthcare regulation and enforcement by the federal government and by authorities in the states and foreign jurisdictions in which they conduct their business. Such laws include, without limitation: the U.S. federal Anti-Kickback Statute, the civil False Claims Act, the Health Insurance Portability and Accountability Act of 1996, or HIPAA, and similar foreign, federal and state fraud and abuse, transparency and privacy laws.
The U.S. federal Anti-Kickback Statute prohibits, among other things, persons and entities from knowingly and willfully soliciting, receiving, offering or paying remuneration, to induce, or in return for, either the referral of an individual, or the purchase or recommendation of an item or service for which payment may be made under any federal healthcare program. The term remuneration has been interpreted broadly to include anything of value, including stock options. The U.S. federal Anti-Kickback Statute has been interpreted to apply to arrangements between pharmaceutical manufacturers on one hand and prescribers, purchasers, and others on the other hand. There are a number of statutory exceptions and regulatory safe harbors protecting some common activities from prosecution, but they are drawn narrowly, and practices that involve remuneration, such as consulting agreements, that may be alleged to be intended to induce prescribing, purchasing or recommending may be subject to scrutiny if they do not qualify for an exception or safe harbor. Failure to meet all of the requirements of a particular applicable statutory exception or regulatory safe harbor does not make the conduct per se illegal under the U.S. federal Anti-Kickback Statute. Instead, the legality of the arrangement will be evaluated on a case-by-case basis based on a cumulative review of all of its facts and circumstances. Our practices may not in all cases meet all of the criteria for protection under a statutory exception or regulatory safe harbor. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. In addition, a claim including items or services resulting from a violation of the U.S. federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act.
Civil and criminal false claims laws, and civil monetary penalty laws, including the civil False Claims Act, which can be enforced through civil whistleblower or qui tam actions, prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment to the federal government, including federal healthcare programs, that are false or fraudulent. For example, the civil False Claims Act prohibits any person or entity from knowingly presenting, or causing to be presented, a false claim for payment to the federal government or knowingly making, using or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government. A claim includes “any request or demand” for money or property presented to the U.S. government. Several pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product.
HIPAA created additional federal civil and criminal liability for, among other things, knowingly and willfully executing a scheme to defraud any healthcare benefit program, or obtain, by means of false or fraudulent pretenses, representations, or promises, any of the money or property owned by, or under the custody or control of, any healthcare benefit program, regardless of the payor (e.g., public or private) and knowingly and willfully falsifying, concealing, or covering up by any trick or device a material fact or making any materially false statements in connection with the delivery of, or payment for, healthcare benefits, items or services relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity can be found guilty of violating HIPAA without actual knowledge of the statute or specific intent to violate it. In addition, HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, and their respective implementing regulations, impose certain requirements on HIPAA covered entities, which include certain healthcare providers, healthcare clearing houses and health plans, and individuals and entities that provide services on their behalf that involve individually identifiable health information, known as business associates, relating to the privacy, security and transmission of individually identifiable health information, as well as their covered subcontractors. HITECH also created new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorneys’ fees and costs associated with pursuing federal civil actions.
The U.S. federal Physician Payments Sunshine Act requires certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with specific exceptions, to annually report to CMS information related to payments or other transfers of value made to physicians (currently defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. Effective January 1, 2022, these reporting obligations will extend to include transfers of value made during the previous year to physician assistants, nurse practitioners, clinical nurse specialists, anesthesiologist assistants, certified registered nurse anesthetists and certified nurse midwives.
We are also subject to additional similar U.S. state and foreign law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third party payors, including private insurers, or that apply regardless of payor, state laws which require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government, state and local laws which require pharmaceutical companies to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures, state laws which require the reporting of information related to drug pricing, state and local laws requiring the registration of pharmaceutical sales representatives, and state and foreign laws governing the privacy and security of health information which, in some cases, differ from each
43
other in significant ways, and may not have the same effect, thus complicating compliance efforts. If our operations are found to be in violation of any of such laws or any other governmental regulations that apply, we may be subject to penalties, including, without limitation, significant civil, criminal and administrative penalties, imprisonment damages, fines, exclusion from government-funded healthcare programs, such as Medicare and Medicaid or similar programs in other countries or jurisdictions, integrity oversight and reporting obligations to resolve allegations of non-compliance, disgorgement, imprisonment, contractual damages, reputational harm, diminished profits and the curtailment or restructuring of our operations.
Coverage and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any pharmaceutical or biological product for which we obtain regulatory approval. Sales of any product, if approved, depend, in part, on the extent to which such product will be covered by third-party payors, such as federal, state, and foreign government healthcare programs, commercial insurance and managed healthcare organizations, and the level of reimbursement, if any, for such product by third-party payors. Decisions regarding whether to cover any of our product candidates, if approved, the extent of coverage and amount of reimbursement to be provided are made on a plan-by-plan basis. Further, no uniform policy for coverage and reimbursement exists in the United States, and coverage and reimbursement can differ significantly from payor to payor.
Nonetheless, product candidates may not be considered medically necessary or cost effective. A decision by a third-party payor not to cover any product candidates we may develop could reduce physician utilization of such product candidates once approved and have a material adverse effect on our sales, results of operations and financial condition Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement rates, but also have their own methods and approval process apart from Medicare determinations. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our product candidates to each payor separately, with no assurance that coverage and adequate reimbursement will be applied consistently or obtained in the first instance.
For products administered under the supervision of a physician, obtaining coverage and adequate reimbursement may be particularly difficult because of the higher prices often associated with such drugs. Additionally, separate reimbursement for the product itself or the treatment or procedure in which the product is used may not be available, which may impact physician utilization.
In addition, the U.S. government, state legislatures and foreign governments have continued implementing cost-containment programs, including price controls, restrictions on coverage and reimbursement and requirements for substitution of generic products. Third-party payors are increasingly challenging the prices charged for medical products and services, examining the medical necessity and reviewing the cost effectiveness of pharmaceutical or biological products, medical devices and medical services, in addition to questioning safety and efficacy. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit sales of any product that receives approval. Decreases in third-party reimbursement for any product or a decision by a third-party not to cover a product could reduce physician usage and patient demand for the product.
Outside the United States, ensuring adequate coverage and payment for any biological candidates we may develop will face challenges. Pricing of prescription pharmaceuticals is subject to governmental control in many countries. Pricing negotiations with governmental authorities can extend well beyond the receipt of regulatory marketing approval for a product and may require us to conduct a clinical trial that compares the cost effectiveness of any product candidates we may develop to other available therapies. The conduct of such a clinical trial could be expensive and result in delays in our commercialization efforts. In the European Union, pricing and reimbursement schemes vary widely from country to country. Some countries provide that products may be marketed only after a reimbursement price has been agreed. Some countries may require the completion of additional studies that compare the cost-effectiveness of a particular product candidate to currently available therapies (so called health technology assessments) in order to obtain reimbursement or pricing approval. For example, the European Union provides options for its member states to restrict the range of products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. European Union member states may approve a specific price for a product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the product on the market. Other member states allow companies to fix their own prices for products but monitor and control prescription volumes and issue guidance to physicians to limit prescriptions. Recently, many countries in the European Union have increased the amount of discounts required on pharmaceuticals and these efforts could continue as countries attempt to manage healthcare expenditures, especially in light of the severe fiscal and debt crises experienced by many countries in the European Union. The downward pressure on healthcare costs in general, particularly prescription products, has become intense. As a result, increasingly high barriers are being erected to the entry of new products. Political, economic, and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various European Union member states, and parallel trade (arbitrage between low-priced and high-priced member states), can further reduce prices. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products, if approved in those countries.
44
The United States and some foreign jurisdictions are considering or have enacted a number of reform proposals to change the healthcare system. There is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality or expanding access. In the United States, the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by federal and state legislative initiatives, including those designed to limit the pricing, coverage, and reimbursement of pharmaceutical and biopharmaceutical products, especially under government-funded healthcare programs, and increased governmental control of drug pricing.
The ACA, which was enacted in March 2010, substantially changed the way healthcare is financed by both governmental and private insurers in the United States, and significantly affected the pharmaceutical industry. The ACA contains a number of provisions of particular import to the pharmaceutical and biotechnology industries, including, but not limited to, those governing enrollment in federal healthcare programs, a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected, and annual fees based on pharmaceutical companies’ share of sales to federal healthcare programs. Since its enactment, there have been judicial, Congressional and executive branch challenges to certain aspects of the ACA, and we expect there will be additional challenges and amendments to the ACA in the future. For example, Congress has considered legislation that would repeal or repeal and replace all or part of the ACA. While Congress has not passed comprehensive repeal legislation, it has enacted laws that modify certain provisions of the ACA such as removing penalties, which started on January 1, 2019, for not complying with ACA’s individual mandate to carry health insurance, delaying the implementation of certain ACA-mandated fees, and increasing the point-of-sale discount that is owed by pharmaceutical manufacturers who participate in Medicare Part D. On December 14, 2018, a U.S. District Court Judge in Texas ruled that the ACA is unconstitutional in its entirety because the “individual mandate” was repealed by Congress as part of legislation enacted in 2017, informally titled the Tax Cuts and Jobs Act, or the Tax Act. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit ruled that the individual mandate was unconstitutional and remanded the case back to the District Court to determine whether the remaining provisions of the ACA are invalid as well. The United States Supreme Court is currently reviewing this case, although it is unclear when a decision will be made. It is also unclear how such litigation and other efforts to repeal and replace the ACA will impact the ACA and our business.
Other legislative changes have been proposed and adopted since the ACA was enacted, including aggregate reductions of Medicare payments to providers of 2% per fiscal year and reduced payments to several types of Medicare providers. These reductions went into effect in April 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2030 unless additional action is taken by Congress. However, pursuant to COVID-19 pandemic relief legislation, these Medicare sequester reductions have been suspended from May 1, 2020 through March 31, 2021 due to the COVID-19 pandemic.
Moreover, there has recently been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. At the federal level, the Trump administration’s budget proposal for fiscal year 2021 contains includes a $135 billion allowance to support legislative proposals seeking to reduce drug prices, increase competition, lower out-of-pocket drug costs for patients and increase patient access to lower-cost generic and biosimilar drugs. On March 10, 2020, the Trump administration sent “principles” for drug pricing to Congress, calling for legislation that would, among other things, cap Medicare Part D beneficiary out-of-pocket pharmacy expenses, provide an option to cap Medicare Part D beneficiary monthly out-of-pocket expenses and place limits on pharmaceutical price increases. The Trump administration previously released a “Blueprint” to lower drug prices and reduce out of pocket costs of drugs that contains additional proposals to increase manufacturer competition, increase the negotiating power of certain federal healthcare programs, incentivize manufacturers to lower the list price of their products and reduce the out of pocket costs of drug products paid by consumers. On July 24, 2020 and September 13, 2020, the Trump administration announced several executive orders related to prescription drug pricing that seek to implement several of the administration’s proposals. As a result, the FDA released a final rule on September 24, 2020, effective November 30, 2020, providing guidance for states to build and submit importation plans for drugs from Canada. Further, on November 20, 2020, the U.S. Department of Health and Human Services, or HHS, finalized a regulation removing safe harbor protection for price reductions from pharmaceutical manufacturers to plan sponsors under Part D, either directly or through pharmacy benefit managers, unless the price reduction is required by law. The rule also creates a new safe harbor for price reductions reflected at the point-of-sale, as well as a safe harbor for certain fixed fee arrangements between pharmacy benefit managers and manufacturers. On November 20, 2020, CMS issued an interim final rule implementing President Trump’s Most Favored Nation executive order, which would tie Medicare Part B payments for certain physician-administered drugs to the lowest price paid in other economically advanced countries, effective January 1, 2021. On December 28, 2020, the United States District Court in Northern California issued a nationwide preliminary injunction against implementation of the interim final rule. It is unclear whether the Biden administration will work to reverse these measures or pursue similar policy initiatives.
Although a number of these and other proposed measures may require additional authorization to become effective, Congress and the Trump administration have each indicated that it will continue to seek new legislative and/or administrative measures to control drug costs. Additional state and federal healthcare reform measures may be adopted in the future. Further, it is possible that additional governmental action is taken in response to the COVID-19 pandemic. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
45
Our human capital is integral to helping us achieve our mission of eradicating monogenic diseases of the CNS. We have built a culture of high performance based on our core values:
|
|
• |
|
Being an ally to the rare disease community; |
|
|
• |
|
Uncovering never-before-seen scientific discoveries; |
|
|
• |
|
Developing cutting-edge technologies and medicines; |
|
|
• |
|
Having a true sense for the term “partnership”; and |
|
|
• |
|
Exploring uncharted territory, just like the first Texas “wildcatters”. |
Our human capital objectives include, as applicable, identifying, recruiting, retaining, incentivizing and integrating our existing and additional employees. The principal purposes of our equity incentive plans are to attract, retain and motivate selected employees, consultants and directors through the granting of stock-based compensation awards.
As of December 31, 2020, we had 38 employees, all of whom were full-time. All of our employees are located in the United States. None of our employees are represented by a labor union or covered by a collective bargaining agreement. We consider our relationship with our employees to be good.
Corporate Information
We were incorporated under the laws of the State of Texas in September 2019. In February 2020, we converted to a Delaware corporation. Our principal executive offices are located at 2280 Inwood Road, Dallas, Texas 75235 and our telephone number is (214) 612-0000.
Available Information
Our internet website address is www.tayshagtx.com. In addition to the information about us and our subsidiaries contained in this Annual Report, information about us can be found on our website. Our website and information included in or linked to our website are not part of this Annual Report.
Our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended, are available free of charge through our website as soon as reasonably practicable after they are electronically filed with or furnished to the Securities and Exchange Commission, or SEC. Additionally the SEC maintains an internet site that contains reports, proxy and information statements and other information. The address of the SEC's website is www.sec.gov.
46
The following information sets forth risk factors that could cause our actual results to differ materially from those contained in forward-looking statements we have made in this Annual Report on Form 10-K and those we may make from time to time. You should carefully consider the risks described below, in addition to the other information contained in this Annual Report on Form 10-K and our other public filings. Our business, financial condition or results of operations could be harmed by any of these risks. The risks and uncertainties described below are not the only ones we face. Additional risks not presently known to us or other factors not perceived by us to present significant risks to our business at this time also may impair our business operations.
Selected Risks Affecting Our Business Our business is subject to a number of risks of which you should be aware before making a decision to invest in our common stock. These risks are more fully described in this “Risk Factors” section, including the following:
|
|
• |
We have incurred significant losses since our inception. We expect to incur losses over the next several years and may never achieve or maintain profitability. |
|
|
• |
We will need substantial additional funding to meet our financial obligations and to pursue our business objectives. If we are unable to raise capital when needed, we could be forced to curtail our planned operations and the pursuit of our growth strategy. |
|
|
• |
We were founded in 2019. We have a limited operating history and no history of commercializing products, which may make it difficult for an investor to evaluate the success of our business to date and to assess our future viability. |
|
|
• |
We are very early in our development efforts and all of our product candidates are in preclinical or clinical development. If we are unable to successfully develop, receive regulatory approval for and commercialize our product candidates for these or any other indications, or successfully develop any other product candidates, or experience significant delays in doing so, our business will be harmed. |
|
|
• |
Because gene therapy is novel and the regulatory landscape that governs any product candidates we may develop is rigorous, complex, uncertain and subject to change, we cannot predict the time and cost of obtaining regulatory approval, if we receive it at all, for any product candidates we may develop. |
|
|
• |
We intend to identify and develop novel gene therapy product candidates, which makes it difficult to predict the time, cost and potential success of product candidate development. |
|
|
• |
The regulatory approval processes of the FDA, European Medicines Agency, or the EMA, and comparable foreign authorities are lengthy, time consuming and inherently unpredictable. If we are not able to obtain required regulatory approval for our product candidates, our business will be substantially harmed. |
|
|
• |
We have not yet tested any product candidates in clinical trials. Success in preclinical studies or earlier clinical trials may not be indicative of results in future clinical trials. |
|
|
• |
We may not be successful in our efforts to build a pipeline of additional product candidates or our next-generation platform technologies. |
|
|
• |
Our business and operations may be adversely affected by the evolving and ongoing COVID-19 global pandemic. |
|
|
• |
Gene therapies are novel, complex and difficult to manufacture. We could experience manufacturing problems that result in delays in the development or commercialization of our product candidates or otherwise harm our business. |
|
|
• |
We and our contract manufacturers for AAV9 are subject to significant regulation with respect to manufacturing our products. The third-party manufacturing facilities on which we rely, and any manufacturing facility that we may have in the future, including our facility in Durham, North Carolina, may have limited capacity or fail to meet the applicable stringent regulatory requirements. |
|
|
• |
We currently rely exclusively on our collaboration with UT Southwestern for our preclinical research and development programs, including for discovering, preclinically developing and conducting all IND-enabling studies for our lead product candidates and our near-term future pipeline. Failure or delay of UT Southwestern to fulfill all or part of its obligations to us under the agreement, a breakdown in collaboration between the parties or a complete or partial loss of this relationship would materially harm our business. |
|
|
• |
UT Southwestern has entered into collaborations with third parties, including certain of our competitors, addressing targets and disease indications outside the scope of our collaboration. As a result, UT Southwestern may have competing interests with respect to their priorities and resources. |
|
|
• |
Negative public opinion of gene therapy and increased regulatory scrutiny of gene therapy and genetic research may adversely impact the development or commercial success of our current and future product candidates. |
|
|
• |
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively. |
47
|
|
AAV vectors that have an AAV9 capsid serotype. If we commercialize any of our product candidates prior to the expiry of those patents in 2026 without a license, REGENX could bring an action claiming infringement. |
|
|
• |
If we are unable to obtain or protect intellectual property rights related to any of our product candidates, we may not be able to compete effectively in our market. |
Risks Related to our Financial Position and Capital Needs
We have incurred significant losses since our inception. We expect to incur losses over the next several years and may never achieve or maintain profitability.
Since our inception, we have incurred significant net losses, and we expect to continue to incur significant expenses and operating losses for the foreseeable future. Our net losses were $60.0 million for the year ended December 31, 2020 and $1.1 million for the period from September 20, 2019 (the date of our inception) through December 31, 2019, respectively. As of December 31, 2020, we had an accumulated deficit of $61.1 million. We have financed our operations with $307.0 million in gross proceeds from equity financings, including from our initial public offering and private placements of convertible preferred stock. We have no products approved for commercialization and have never generated any revenue from product sales.
All of our product candidates are still in the clinical or preclinical development stage. We expect to continue to incur significant expenses and operating losses over the next several years. We expect that it could be several years, if ever, before we have a commercialized product. Our net losses may fluctuate significantly from quarter to quarter and year to year. We anticipate that our expenses will increase substantially as we:
|
|
• |
continue to advance the preclinical and clinical development of our product candidates and preclinical and discovery programs; |
|
|
• |
conduct our planned clinical trials of TSHA-101 and TSHA-118, as well as initiate and complete additional clinical trials of TSHA-101, TSHA-118, TSHA-102 and TSHA-104 and any other current and future product candidates that we advance; |
|
|
• |
seek regulatory approval for any product candidates that successfully complete clinical trials; |
|
|
• |
continue to develop our gene therapy product candidate pipeline and next-generation platforms; |
|
|
• |
scale up our clinical and regulatory capabilities; |
|
|
• |
manufacture cGMP material for clinical trials or potential commercial sales; |
|
|
• |
establish and validate a commercial-scale cGMP manufacturing facility; |
|
|
• |
establish a commercialization infrastructure and scale up internal and external manufacturing and distribution capabilities to commercialize any product candidates for which we may obtain regulatory approval; |
|
|
• |
adapt our regulatory compliance efforts to incorporate requirements applicable to marketed products; |
|
|
• |
maintain, expand and protect our intellectual property portfolio; |
|
|
• |
hire additional clinical, manufacturing quality control, regulatory, manufacturing and scientific and administrative personnel; |
|
|
• |
add operational, financial and management information systems and personnel, including personnel to support our product development and planned future commercialization efforts; and |
|
|
• |
incur additional legal, accounting and other expenses in operating as a public company. |
To date, we have not generated any revenue. To become and remain profitable, we must succeed in developing and eventually commercializing product candidates that generate significant revenue. This will require us to be successful in a range of challenging activities, including completing preclinical testing and clinical trials of our product candidates, obtaining regulatory approval, and manufacturing, marketing and selling any product candidates for which we may obtain regulatory approval, as well as discovering and developing additional product candidates. We are only in the preliminary stages of most of these activities and all of our product candidates are in clinical or preclinical development. We may never succeed in these activities and, even if we do, may never generate any revenue or revenue that is significant enough to achieve profitability.
Even if we achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would depress the value of our company and could impair our ability to raise capital, expand our business, maintain our development efforts, obtain product approvals, diversify our offerings or continue our operations. A decline in the value of our company could also cause you to lose all or part of your investment.
48
We have a limited operating history and no history of commercializing products, which may make it difficult for an investor to evaluate the success of our business to date and to assess our future viability.
We are a clinical-stage gene therapy company with a limited operating history. We commenced operations in 2019, and our operations to date have been largely focused on organizing and staffing our company, business planning, raising capital and entering into collaboration and license agreements for conducting preclinical research and development activities for our product candidates and gene therapy pipeline. To date, we have not yet demonstrated our ability to successfully complete clinical trials, including pivotal clinical trials, obtain regulatory approvals, manufacture a product on a commercial scale, or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful commercialization. Consequently, any predictions you make about our future success or viability may not be as accurate as they could be if we had a longer operating history or a history of successfully developing and commercializing products.
We may encounter unforeseen expenses, difficulties, complications, delays and other known or unknown factors in achieving our business objectives. We will need to develop commercial capabilities, and we may not be successful in doing so.
We will need substantial additional funding to meet our financial obligations and to pursue our business objectives. If we are unable to raise capital when needed, we could be forced to curtail our planned operations and the pursuit of our growth strategy.
Our operations have consumed substantial amounts of cash since inception. Identifying potential product candidates and conducting preclinical testing and clinical trials is a time-consuming, expensive and uncertain process that takes years to complete, and we may never generate the necessary data or results required to obtain regulatory approval and achieve product sales. We expect to continue to incur significant expenses and operating losses over the next several years as we conduct clinical trials of our product candidates, initiate future clinical trials of our product candidates, advance our preclinical programs, seek marketing approval for any product candidates that successfully complete clinical trials and advance any of our other product candidates we may develop or otherwise acquire. In addition, our product candidates, if approved, may not achieve commercial success. Our revenue, if any, will be derived from sales of products that we do not expect to be commercially available for a number of years, if at all. If we obtain marketing approval for any product candidates that we develop or otherwise acquire, we expect to incur significant commercialization expenses related to product sales, marketing, distribution and manufacturing. We also expect an increase in our expenses associated with creating additional infrastructure to support operations as a public company.
As of December 31, 2020, we had cash and cash equivalents of $251.3 million. We believe that our existing cash and cash equivalents will be sufficient to fund our operating expenses and capital requirements into 2023. This estimate is based on assumptions that may prove to be wrong, and we could use our available capital resources sooner than we expect. Changes may occur beyond our control that would cause us to consume our available capital before that time, including changes in and progress of our development activities, acquisitions of additional product candidates, and changes in regulation. Our future capital requirements will depend on many factors, including:
|
|
• |
the scope, progress, costs and results of discovery, preclinical development, laboratory testing and clinical trials for TSHA-101, TSHA-118, TSHA-102, TSHA-104 and any current and future product candidates that we advance; |
|
|
• |
the extent to which we develop, in-license or acquire other product candidates and technologies in our gene therapy product candidate pipeline; |
|
|
• |
the costs and timing of process development and manufacturing scale-up activities associated with our product candidates and other programs as we advance them through preclinical and clinical development; |
|
|
• |
the number and development requirements of product candidates that we may pursue; |
|
|
• |
the costs, timing and outcome of regulatory review of our product candidates; |
|
|
• |
our headcount growth and associated costs as we expand our research and development capabilities and establish a commercial infrastructure; |
|
|
• |
the costs of establishing and maintaining our own commercial-scale cGMP manufacturing facility; |
|
|
• |
the costs and timing of future commercialization activities, including product manufacturing, marketing, sales, and distribution, for any of our product candidates for which we receive marketing approval; |
|
|
• |
the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending any intellectual property-related claims; |
|
|
• |
the revenue, if any, received from commercial sales of our product candidates for which we receive marketing approval; and |
|
|
• |
the costs of operating as a public company. |
We will require additional capital to achieve our business objectives. Additional funds may not be available on a timely basis, on favorable terms, or at all, and such funds, if raised, may not be sufficient to enable us to continue to implement our long-term business strategy. Further, our ability to raise additional capital may be adversely impacted by potential worsening global economic conditions and
49
the recent disruptions to and volatility in the credit and financial markets in the United States and worldwide resulting from the ongoing COVID-19 pandemic. If we are unable to raise sufficient additional capital, we could be forced to curtail our planned operations and the pursuit of our growth strategy.
Raising additional capital may cause dilution to our stockholders, restrict our operations or require us to relinquish rights to our technologies or product candidates.
Until such time, if ever, as we can generate substantial revenue, we may finance our cash needs through a combination of equity offerings, government or private party grants, debt financings and license and collaboration agreements. We do not currently have any other committed external source of funds. To the extent that we raise additional capital through the sale of equity or convertible debt securities, your ownership interest will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect your rights as a common stockholder. Debt financing and equity financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends.
If we raise additional funds through collaborations, strategic alliances or marketing, distribution or licensing arrangements with third parties, we may be required to relinquish valuable rights to our technologies, future revenue streams or product candidates, grant licenses on terms that may not be favorable to us or commit to future payment streams. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit, reduce or terminate our product development or future commercialization efforts or grant rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves.
Risks Related to the Development of our Product Candidates
We are very early in our development efforts and all of our product candidates are in clinical or preclinical development. If we are unable to successfully develop, receive regulatory approval for and commercialize our product candidates for these or any other indications, or successfully develop any other product candidates, or experience significant delays in doing so, our business will be harmed.
We are very early in our development efforts and all of our product candidates are still in clinical or preclinical development. Queen’s University initiated a Phase 1/2 clinical trial of TSHA-101 under a Clinical Trial Agreement, or CTA, with Health Canada, and we intend to initiate a Phase 1/2 clinical trial of TSHA-118 in 2021 under a currently open IND. Each of our programs and product candidates will require additional preclinical and/or clinical development, regulatory approval, obtaining manufacturing supply, capacity and expertise, building a commercial organization or successfully outsourcing commercialization, substantial investment and significant marketing efforts before we generate any revenue from product sales. We do not have any products that are approved for commercial sale, and we may never be able to develop or commercialize marketable products.
Our ability to generate revenue from our product candidates, which we do not expect will occur for several years, if ever, will depend heavily on the successful development, regulatory approval and eventual commercialization of our product candidates. The success of TSHA-101, TSHA-118, TSHA-102 and TSHA-104, or any other product candidates that we develop or otherwise may acquire will depend on several factors, including:
|
|
• |
effective INDs from the FDA or comparable foreign applications that allow commencement of our planned clinical trials or future clinical trials for our product candidates; |
|
|
• |
successful enrollment and completion of clinical trials, including under the FDA’s current GCPs and current Good Laboratory Practices; |
|
|
• |
timely and successful completion of preclinical studies, including toxicology studies, biodistribution studies and minimally efficacious dose studies in animals, where applicable, and clinical trials; |
|
|
• |
sufficiency of our financial and other resources to complete the necessary preclinical studies and clinical trials; |
|
|
• |
successful development of, or making arrangements with third-party manufacturers for, our commercial manufacturing processes for any of our product candidates that receive regulatory approval; |
|
|
• |
receipt of timely marketing approvals from applicable regulatory authorities; |
|
|
• |
launching commercial sales of products, if approved, whether alone or in collaboration with others; |
|
|
• |
acceptance of the benefits and use of our products, including method of administration, if approved, by patients, the medical community and third-party payors, for their approved indications; |
|
|
• |
the prevalence and severity of adverse events experienced with TSHA-101, TSHA-118, TSHA-102 and TSHA-104 or any other product candidates; |
|
|
• |
the availability, perceived advantages, cost, safety and efficacy of alternative therapies for any product candidate, and any indications for such product candidate, that we develop; |
50
|
|
• |
our ability to produce TSHA-101, TSHA-118, TSHA-102 and TSHA-104 or any other product candidates we develop on a commercial scale; |
|
|
• |
obtaining and maintaining patent, trademark and trade secret protection and regulatory exclusivity for our product candidates and otherwise protecting our rights in our intellectual property portfolio; |
|
|
• |
maintaining compliance with regulatory requirements, including cGMPs, and complying effectively with other procedures; |
|
|
• |
obtaining and maintaining third-party coverage and adequate reimbursement and patients’ willingness to pay out-of-pocket in the absence of such coverage and adequate reimbursement; and |
|
|
• |
maintaining a continued acceptable safety, tolerability and efficacy profile of the products following approval. |
If we are not successful with respect to one or more of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully commercialize the product candidates we develop, which would materially harm our business. If we do not receive marketing approvals for any product candidate we develop, we may not be able to continue our operations.
We intend to identify and develop novel gene therapy product candidates, which makes it difficult to predict the time, cost and potential success of product candidate development.
Our strategy is to identify, develop and commercialize gene therapy product candidates using an AAV9 capsid for intrathecal delivery of therapeutic transgenes to certain kinds of cells. Our future success depends on the successful development of these novel therapeutic approaches. To date, very few products that utilize gene transfer have been approved in the United States or Europe and no gene therapy products that utilize an intrathecal method of administration have been approved. There have been a limited number of clinical trials of gene transduction technologies, with only two product candidates ever approved by the FDA.
Although AAV9 has been tested in numerous clinical trials and is used in two currently approved products, we cannot be certain that our AAV9 product candidates will successfully complete preclinical studies and clinical trials, or that they will not cause significant adverse events or toxicities. We also cannot be certain that we will be able to avoid triggering toxicities in our future preclinical studies or clinical trials or that our intrathecal method of administration will not cause unforeseen side effects or other challenges. Any such results could impact our ability to develop a product candidate, including our ability to enroll patients in our clinical trials. As a result of these factors, it is more difficult for us to predict the time and cost of product candidate development, and we cannot predict whether the application of our approach to gene therapy, or any similar or competitive programs, will result in the identification, development, and regulatory approval of any product candidates, or that other gene therapy programs will not be considered better or more attractive. There can be no assurance that any development problems we experience in the future related to our current gene therapy product candidates or any of our research programs will not cause significant delays or unanticipated costs, or that such development problems can be solved. We may also experience delays and challenges in achieving sustainable, reproducible, and scalable production. Any of these factors may prevent us from completing our preclinical studies or clinical trials or commercializing any product candidates we may develop on a timely or profitable basis, if at all.
Because gene therapy is novel and the regulatory landscape that governs any product candidates we may develop is rigorous, complex, uncertain and subject to change, we cannot predict the time and cost of obtaining regulatory approval, if we receive it at all, for any product candidates we may develop.
The regulatory requirements that will govern any novel gene therapy product candidates we develop are not entirely clear and are subject to change. Within the broader genetic medicine field, very few therapeutic products have received marketing authorization from the FDA or the EMA. Even with respect to more established products that fit into the categories of gene therapies or cell therapies, the regulatory landscape is still developing. Regulatory requirements governing gene therapy products and cell therapy products have changed frequently and will likely continue to change in the future. Moreover, there is substantial overlap in those responsible for regulation of existing gene therapy products and cell therapy products. For example, in the United States, the FDA has established the Office of Tissues and Advanced Therapies within its Center for Biologics Evaluation and Research, or CBER, to consolidate the review of gene therapy and related products, and the Cellular, Tissue and Gene Therapies Advisory Committee to advise CBER on its review.
Our product candidates will need to meet safety and efficacy standards applicable to any new biologic under the regulatory framework administered by the FDA. In addition to FDA oversight and oversight by IRBs, under guidelines promulgated by the National Institutes of Health, or NIH, gene therapy clinical trials are also subject to review and oversight by an IBC, a local institutional committee that reviews and oversees research utilizing recombinant or synthetic nucleic acid molecules at that institution. The IBC assesses the safety of the research and identifies any potential risk to public health or the environment. While the NIH guidelines are not mandatory unless the research in question is being conducted at or sponsored by institutions receiving NIH funding of recombinant or synthetic nucleic acid molecule research, many companies and other institutions not otherwise subject to the NIH Guidelines voluntarily follow them. Although the FDA decides whether individual gene therapy protocols may proceed, the review process and determinations of other reviewing bodies can impede or delay the initiation of a clinical trial, even if the FDA has reviewed the trial and approved its initiation.
51
The same applies in the European Union. The EMA’s Committee for Advanced Therapies, or CAT, is responsible for assessing the quality, safety, and efficacy of advanced-therapy medicinal products. Advanced-therapy medicinal products include gene therapy medicines, somatic-cell therapy medicines and tissue-engineered medicines. The role of the CAT is to prepare a draft opinion on an application for marketing authorization for a gene therapy medicinal candidate that is submitted to the EMA. In the European Union, the development and evaluation of a gene therapy product must be considered in the context of the relevant EU guidelines. The EMA may issue new guidelines concerning the development and marketing authorization for gene therapy products and require that we comply with these new guidelines. As a result, the procedures and standards applied to gene therapy products and cell therapy products may be applied to any gene therapy product candidate we may develop, but that remains uncertain at this point.
Adverse developments in preclinical studies or clinical trials conducted by others in the field of gene therapy and gene regulation products may cause the FDA, the EMA, and other regulatory bodies to revise the requirements for approval of any product candidates we may develop or limit the use of products utilizing gene regulation technologies, either of which could harm our business. In addition, the clinical trial requirements of the FDA, the EMA, and other regulatory authorities and the criteria these regulators use to determine the safety and efficacy of a product candidate vary substantially according to the type, complexity, novelty, and intended use and market of the potential products. The regulatory approval process for product candidates such as ours can be more expensive and take longer than for other, better known, or more extensively studied pharmaceutical or other product candidates. Further, as we are developing novel potential treatments for diseases in which, in some cases, there is little clinical experience with potential new endpoints and methodologies, there is heightened risk that the FDA, the EMA or other regulatory bodies may not consider the clinical trial endpoints to provide clinically meaningful results, and the resulting clinical data and results may be more difficult to analyze. In addition, we may not be able to identify or develop appropriate animal disease models to enable or support planned clinical development. Any natural history studies that we may conduct or rely upon in our clinical development may not be accepted by the FDA, EMA or other regulatory authorities. Regulatory agencies administering existing or future regulations or legislation may not allow production and marketing of products utilizing gene regulation technology in a timely manner or under technically or commercially feasible conditions. In addition, regulatory action or private litigation could result in expenses, delays, or other impediments to our research programs or the commercialization of resulting products. Further, approvals by one regulatory agency may not be indicative of what other regulatory agencies may require for approval.
The regulatory review committees and advisory groups described above and the new guidelines they promulgate may lengthen the regulatory review process, require us to perform additional preclinical studies or clinical trials, increase our development costs, lead to changes in regulatory positions and interpretations, delay or prevent approval and commercialization of these treatment candidates, or lead to significant post-approval limitations or restrictions. As we advance our research programs and develop future product candidates, we will be required to consult with these regulatory and advisory groups and to comply with applicable guidelines. If we fail to do so, we may be required to delay or discontinue development of any product candidates we identify and develop. These additional processes may result in a review and approval process that is longer than we otherwise would have expected. Delays as a result of an increased or lengthier regulatory approval process or further restrictions on the development of our product candidates can be costly and could negatively impact our ability to complete clinical trials and commercialize our current and future product candidates in a timely manner, if at all.
Preclinical studies and clinical trials are expensive, time-consuming, difficult to design and implement and involve an uncertain outcome. Further, we may encounter substantial delays in completing the development of our product candidates.
All of our product candidates are in clinical or preclinical development and their risk of failure is high. The clinical trials and manufacturing of our product candidates are, and the manufacturing and marketing of our products, if approved, will be, subject to extensive and rigorous review and regulation by numerous government authorities in the United States and in other countries where we intend to test and market our product candidates. Before obtaining regulatory approvals for the commercial sale of any of our product candidates, we must demonstrate through lengthy, complex and expensive preclinical testing and clinical trials that our product candidates are both safe and effective for use in each target indication. In particular, because our product candidates are subject to regulation as biological products, we will need to demonstrate that they are safe, pure and potent for use in their target indications. Each product candidate must demonstrate an adequate risk versus benefit profile in its intended patient population and for its intended use.
Clinical testing is expensive and can take many years to complete, and is subject to uncertainty. We cannot guarantee that any clinical trials will be conducted as planned or completed on schedule, if at all. Failure can occur at any time during the clinical trial process. Even if our future clinical trials are completed as planned, we cannot be certain that their results will support the safety and effectiveness of our product candidates for their targeted indications or support continued clinical development of such product candidates. Our future clinical trial results may not be successful.
In addition, even if such trials are successfully completed, we cannot guarantee that the FDA or foreign regulatory authorities will interpret the results as we do, and more trials could be required before we submit our product candidates for approval. This is particularly true for clinical trials in very rare diseases, such as with TSHA-101 for the treatment of GM2 gangliosidosis, TSHA-118 for the treatment of CLN1 disease (one of the forms of Batten disease), and TSHA-102 for the treatment of Rett syndrome, where the very small patient population makes it difficult or impossible to conduct two traditional, adequate and well-controlled studies, and therefore the FDA or comparable foreign regulatory authorities are often required to exercise flexibility in approving therapies for such diseases. Moreover, results acceptable to support approval in one jurisdiction may be deemed inadequate by another regulatory authority to support regulatory approval in that other jurisdiction. To the extent that the results of the trials are not satisfactory to the FDA or foreign regulatory authorities for support of a marketing application, we may be required to expend significant resources, which may not be available to us, to conduct additional trials in support of potential approval of our product candidates.
52
To date, we have not initiated or completed any clinical trials required for the approval of our product candidates. We may experience delays in conducting any clinical trials and we do not know whether our clinical trials will begin on time, need to be redesigned, recruit and enroll patients on time or be completed on schedule, or at all. Events that may prevent successful or timely completion of clinical development include:
|
|
• |
inability to generate sufficient preclinical, toxicology, or other in vivo or in vitro data to support the initiation of clinical trials; |
|
|
• |
delays in sufficiently developing, characterizing or controlling a manufacturing process suitable for advanced clinical trials, including our natural history studies; |
|
|
• |
delays in developing suitable assays for screening patients for eligibility for trials with respect to certain product candidates; |
|
|
• |
delays in reaching agreement with the FDA, EMA or other regulatory authorities as to the design or implementation of our clinical trials; |
|
|
• |
obtaining regulatory approval to commence a clinical trial; |
|
|
• |
reaching an agreement on acceptable terms with clinical trial sites or prospective contract research organizations, or CROs, the terms of which can be subject to extensive negotiation and may vary significantly among different clinical trial sites; |
|
|
• |
obtaining IRB approval at each trial site; |
|
|
• |
recruiting suitable patients to participate in a clinical trial; |
|
|
• |
having patients complete a clinical trial or return for post-treatment follow-up; |
|
|
• |
clinical sites, CROs or other third parties deviating from trial protocol or dropping out of a trial; |
|
|
• |
failure to perform in accordance with the FDA’s GCP requirements, or applicable regulatory guidelines in other countries; |
|
|
• |
addressing patient safety concerns that arise during the course of a trial, including occurrence of adverse events associated with the product candidate that are viewed to outweigh its potential benefits; |
|
|
• |
adding a sufficient number of clinical trial sites; or |
|
|
• |
manufacturing sufficient quantities of product candidate for use in clinical trials. |
We may experience numerous unforeseen events during, or as a result of, clinical trials that could delay or prevent our ability to receive marketing approval or commercialize our product candidates or significantly increase the cost of such trials, including:
|
|
• |
we may experience changes in regulatory requirements or guidance, or receive feedback from regulatory authorities that requires us to modify the design of our clinical trials; |
|
|
• |
clinical trials of our product candidates may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical trials or abandon development programs; |
|
|
• |
the number of patients required for clinical trials of our product candidates may be larger than we anticipate, enrollment in these clinical trials may be slower than we anticipate or participants may drop out of these clinical trials at a higher rate than we anticipate; |
|
|
• |
our third-party contractors may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
|
|
• |
we or our investigators might have to suspend or terminate clinical trials of our product candidates for various reasons, including non-compliance with regulatory requirements, a finding that our product candidates have undesirable side effects or other unexpected characteristics, or a finding that the participants are being exposed to unacceptable health risks; |
|
|
• |
the cost of clinical trials of our product candidates may be greater than we anticipate and we may not have funds to cover the costs; |
|
|
• |
the supply or quality of our product candidates or other materials necessary to conduct clinical trials of our product candidates may be insufficient or inadequate; |
|
|
• |
regulators may revise the requirements for approving our product candidates, or such requirements may not be as we anticipate; and |
|
|
• |
any future collaborators that conduct clinical trials may face any of the above issues, and may conduct clinical trials in ways they view as advantageous to them but that are suboptimal for us. |
53
If we are required to conduct additional clinical trials or other testing of our product candidates beyond those that we currently contemplate, if we are unable to successfully complete clinical trials of our product candidates or other testing, if the results of these trials or tests are not positive or are only modestly positive or if there are safety concerns, we may:
|
|
• |
incur unplanned costs; |
|
|
• |
be delayed in obtaining marketing approval for our product candidates or not obtain marketing approval at all; |
|
|
• |
obtain marketing approval in some countries and not in others; |
|
|
• |
obtain marketing approval for indications or patient populations that are not as broad as intended or desired; |
|
|
• |
obtain marketing approval with labeling that includes significant use or distribution restrictions or safety warnings, including boxed warnings or Risk Evaluation and Mitigation Strategies, or REMS; |
|
|
• |
be subject to additional post-marketing testing requirements; or |
|
|
• |
have the product removed from the market after obtaining marketing approval. |
We could encounter delays if a clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such trials are being conducted, by the Data Safety Monitoring Board for such trial or by the FDA, EMA or other regulatory authorities. Such authorities may impose such a suspension or termination due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA, EMA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial.
All of our product candidates will require extensive clinical testing before we are prepared to submit a BLA or marketing authorization application, or MAA, for regulatory approval. We cannot predict with any certainty if or when we might complete the clinical development for our product candidates and submit a BLA or MAA for regulatory approval of any of our product candidates or whether any such BLA or MAA will be approved. We may also seek feedback from the FDA, EMA or other regulatory authorities on our clinical development program, and the FDA, EMA or such regulatory authorities may not provide such feedback on a timely basis, or such feedback may not be favorable, which could further delay our development programs.
We cannot predict with any certainty whether or when we might complete a given clinical trial. If we experience delays in the commencement or completion of our clinical trials, or if we terminate a clinical trial prior to completion, the commercial prospects of our product candidates could be harmed, and our ability to generate revenues from our product candidates may be delayed or lost. In addition, any delays in our clinical trials could increase our costs, slow down the development and approval process and jeopardize our ability to commence product sales and generate revenues. Any of these occurrences may harm our business, financial condition and results of operations. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of our product candidates.
The regulatory approval processes of the FDA, EMA and comparable foreign authorities are lengthy, time consuming and inherently unpredictable. If we are not able to obtain required regulatory approval for our product candidates, our business will be substantially harmed.
The time required to obtain approval or other marketing authorizations by the FDA, EMA and comparable foreign authorities is unpredictable, and it typically takes many years following the commencement of clinical trials and depends upon numerous factors, including the substantial discretion of the regulatory authorities. In addition, approval policies, regulations, and the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions. We have not obtained regulatory approval for any product candidate, and it is possible that we may never obtain regulatory approval for any product candidates we may seek to develop in the future. Neither we nor any current or future collaborator is permitted to market any drug product candidates in the United States until we receive regulatory approval of a BLA from the FDA, and we cannot market it in the European Union until we receive approval for a MAA from the EMA, or other required regulatory approval in other countries. To date, we have had only limited discussions with the FDA regarding clinical development programs or regulatory approval for any product candidate within the United States. In addition, we have only had limited discussions with Health Canada, and no discussions with the EMA and other comparable foreign authorities, regarding clinical development programs or regulatory approval for any product candidate outside of the United States.
Prior to obtaining approval to commercialize any drug product candidate in the United States or abroad, we must demonstrate with substantial evidence from well-controlled clinical trials, and to the satisfaction of the FDA or foreign regulatory agencies, that such product candidates are safe, pure and effective for their intended uses. Results from preclinical studies and clinical trials can be interpreted in different ways. Even if we believe the preclinical or clinical data for our product candidates are promising, such data may not be sufficient to support approval by the FDA and other regulatory authorities. The FDA may also require us to conduct additional preclinical studies or clinical trials for our product candidates either prior to or after approval, or it may object to elements of our clinical development programs.
54
Of the large number of products in development, only a small percentage successfully complete the FDA or foreign regulatory approval processes and are commercialized. The lengthy approval and marketing authorization process as well as the unpredictability of future clinical trial results may result in our failing to obtain regulatory approval and marketing authorization to market our product candidates, which would significantly harm our business, financial condition, results of operations and prospects.
We have invested a significant portion of our time and financial resources in the development of our preclinical product candidates. Our business is dependent on our ability to successfully complete preclinical and clinical development of, obtain regulatory approval for, and, if approved, successfully commercialize TSHA-101, TSHA-118, TSHA-102 and TSHA-104 and any future product candidates in a timely manner.
Even if we eventually complete clinical testing and receive approval of a BLA or foreign marketing application for TSHA-101, TSHA-118, TSHA-102 and TSHA-104, or any future product candidates, the FDA, EMA or the applicable foreign regulatory agency may grant approval or other marketing authorization contingent on the performance of costly additional clinical trials, including post-marketing clinical trials. The FDA, EMA or the applicable foreign regulatory agency also may approve or authorize for marketing a product candidate for a more limited indication or patient population than we originally request, and the FDA, EMA or applicable foreign regulatory agency may not approve or authorize the labeling that we believe is necessary or desirable for the successful commercialization of a product candidate. Any delay in obtaining, or inability to obtain, applicable regulatory approval or other marketing authorization would delay or prevent commercialization of that product candidate and would materially adversely impact our business and prospects.
In addition, the FDA, EMA and other regulatory authorities may change their policies, issue additional regulations or revise existing regulations, or take other actions, which may prevent or delay approval of our future products under development on a timely basis. Such policy or regulatory changes could impose additional requirements upon us that could delay our ability to obtain approvals, increase the costs of compliance or restrict our ability to maintain any marketing authorizations we may have obtained.
We have not yet completed testing of any product candidate in clinical trials. Success in preclinical studies or earlier clinical trials may not be indicative of results in future clinical trials.
Success in preclinical testing and early clinical trials does not ensure that later clinical trials will generate the same results or otherwise provide adequate data to demonstrate the efficacy and safety of a product candidate. Preclinical tests and Phase 1 and Phase 2 clinical trials are primarily designed to test safety, to study pharmacokinetics and pharmacodynamics and to understand the side effects of product candidates at various doses and schedules. Success in preclinical or animal studies and early clinical trials does not ensure that later large-scale efficacy trials will be successful nor does it predict final results. For example, we may be unable to identify suitable animal disease models for our product candidates, which could delay or frustrate our ability to proceed into clinical trials or obtain marketing approval. Our product candidates may fail to show the desired safety and efficacy in clinical development despite positive results in preclinical studies or having successfully advanced through initial clinical trials. Further, our Phase 1/2 clinical trials of TSHA-101, TSHA-118, TSHA-102 and TSHA-104 will involve small patient populations. Because of the small sample sizes, the results of these trials may not be indicative of results of future clinical trials. Further, although other gene therapy clinical trials conducted by others also utilized AAV9 vectors, these trials should not be relied upon as evidence that our planned clinical trials will succeed.
Many companies in the pharmaceutical and biotechnology industries have suffered significant setbacks in late-stage clinical trials even after achieving promising results in preclinical testing and earlier-stage clinical trials. Data obtained from preclinical and clinical activities are subject to varying interpretations, which may delay, limit or prevent regulatory approval. In addition, we may experience regulatory delays or rejections as a result of many factors, including changes in regulatory policy during the period of our product candidate development. Any such delays could negatively impact our business, financial condition, results of operations and prospects.
Interim “top-line” and preliminary results from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final data.
From time to time, we may publish interim top-line or preliminary results from our clinical trials. Interim results from clinical trials that we may complete are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data become available. Preliminary or top-line results also remain subject to audit and verification procedures that may result in the final data being materially different from the preliminary data we previously published. As a result, interim and preliminary data should be viewed with caution until the final data are available. Differences between preliminary or interim data and final data could significantly harm our business prospects and may cause the trading price of our common stock to fluctuate significantly.
Our preclinical studies and clinical trials may fail to demonstrate the safety and efficacy of our product candidates, or serious adverse or unacceptable side effects may be identified during the development of our product candidates, which could prevent or delay regulatory approval and commercialization, increase our costs or necessitate the abandonment or limitation of the development of some of our product candidates.
Before obtaining regulatory approvals for the commercial sale of our product candidates, we must demonstrate through lengthy, complex and expensive preclinical testing and clinical trials that our product candidates are safe, pure and effective for use in each target indication, and failures can occur at any stage of testing. Preclinical studies and clinical trials often fail to demonstrate safety or efficacy of
55
the product candidate studied for the target indication. Among the risks in any gene therapy product based on viral vectors are the risks of immunogenicity, elevated liver enzymes and insertional oncogenesis, which is the process whereby the insertion of a functional gene near a gene that is important in cell growth or division results in uncontrolled cell division, which could potentially enhance the risk of malignant transformation.
While new AAV vectors have been developed to reduce side effects previously reported in third-party gene therapy treatments, and AAV9 has been generally well tolerated in clinical trials and in approved products, gene therapy is still a relatively new approach to disease treatment and additional adverse side effects could develop. There also is the potential risk of delayed adverse events following exposure to gene therapy products due to persistent biologic activity of the genetic material or other components of products used to carry the genetic material.
Possible adverse side effects that could occur with treatment with gene therapy products include an immunologic reaction early after administration, which, while not necessarily adverse to the patient’s health, could substantially limit the effectiveness of the treatment. For example, in previous third-party clinical trials involving other AAV vectors for gene therapy, some subjects experienced the development of a T-cell antibody response, whereby after the vector is within the target cells, the cellular immune response system triggers the removal of transduced cells by activated T-cells. Other preclinical studies have suggested that high dosages of AAV administration may result in toxicity due to degeneration of the dorsal root ganglia. If our vectors demonstrate a similar effect in other programs, we may decide or be required to perform additional preclinical studies or to halt or delay further clinical development of our product candidates.
In addition to side effects caused by the product candidate, the administration process or related procedures also can cause adverse side effects. Each of our lead product candidates are expected to be administered by intrathecal injection. While this method of administration has been available for decades, its use for therapies is relatively new, no gene therapy is currently approved for intrathecal administration, and it may be perceived as having greater risk than more common methods of administration, such as intravenous injection. If any such adverse events occur, our clinical trials could be suspended or terminated. If we cannot demonstrate that any adverse events were not caused by the drug or administration process or related procedures, the FDA, EMA or foreign regulatory authorities could order us to cease further development of, or deny approval of, our product candidates for any or all targeted indications. Even if we are able to demonstrate that all future serious adverse events are not product-related, such occurrences could affect patient recruitment or the ability of enrolled patients to complete the trial. Moreover, if we elect, or are required, to not initiate, delay, suspend or terminate any future clinical trial of any of our product candidates, the commercial prospects of such product candidates may be harmed and our ability to generate product revenues from any of these product candidates may be delayed or eliminated. Any of these occurrences may harm our ability to develop other product candidates, and may harm our business, financial condition and prospects significantly.
If our product candidates are associated with side effects in clinical trials or have characteristics that are unexpected, we may need to abandon their development or limit development to more narrow uses in which the side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective. The FDA or an IRB may also require that we suspend, discontinue, or limit our clinical trials based on safety information, or that we conduct additional animal or human studies regarding the safety and efficacy of our product candidates which we have not planned or anticipated. Such findings could further result in regulatory authorities failing to provide marketing authorization for our product candidates or limiting the scope of the approved indication, if approved. Many product candidates that initially showed promise in early stage testing have later been found to cause side effects that prevented further development of the product candidate.
Additionally, if one or more of our product candidates receives marketing approval, and we or others identify undesirable side effects caused by such products, a number of potentially significant negative consequences could result, including:
|
|
• |
regulatory authorities may withdraw approvals of such product; |
|
|
• |
regulatory authorities may require additional warnings on the labels; |
|
|
• |
we may be required to create a medication guide outlining the risks of such side effects for distribution to patients or other requirements subject to a REMS; |
|
|
• |
we could be sued and held liable for harm caused to patients; |
|
|
• |
we may not be able to achieve or maintain third-party payor coverage and adequate reimbursement; and |
|
|
• |
our reputation and physician or patient acceptance of our products may suffer. |
There can be no assurance that we will resolve any issues related to any product-related adverse events to the satisfaction of the FDA or foreign regulatory agency in a timely manner or at all. Moreover, any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate, if approved, and could significantly harm our business, results of operations and prospects.
56
As an organization, we have never conducted pivotal clinical trials, and may be unable to do so for any product candidates we may develop, including TSHA-101, TSHA-118, TSHA-102, and TSHA-104.
We will need to successfully complete our ongoing and planned clinical trials, including pivotal clinical trials, in order to obtain FDA approval to market our product candidates. Carrying out later-stage clinical trials and the submission of a successful BLA is a complicated process. As an organization, we have initiated our first Phase 1/2 clinical trial, have not previously conducted any later stage or pivotal clinical trials, have limited experience in preparing, submitting and prosecuting regulatory filings and have not previously submitted a BLA for any product candidate. In addition, we have had limited interactions with the FDA and cannot be certain how many additional clinical trials of our product candidates will be required or how such trials should be designed. Consequently, we may be unable to successfully and efficiently execute and complete necessary clinical trials in a way that leads to BLA submission and approval of any product candidate. We may require more time and incur greater costs than our competitors and may not succeed in obtaining regulatory approvals of product candidates that we develop. Failure to commence or complete, or delays in, our planned clinical trials, could prevent us from or delay us in commercializing our product candidates.
The disorders we seek to treat have low prevalence and it may be difficult to identify and enroll patients with these disorders. If we experience delays or difficulties in the enrollment and/or maintenance of patients in clinical trials, our receipt of necessary regulatory approvals could be delayed or prevented.
Successful and timely completion of clinical trials will require that we enroll a sufficient number of patients. Patient enrollment, a significant factor in the timing of clinical trials, is affected by many factors, including the size and nature of the patient population and competition for patients with other trials. Genetic diseases generally, and especially the rare diseases for which some of our current product candidates are targeted, have low incidence and prevalence. For example, we estimate global incidence of GM2 gangliosidosis, the target indication for TSHA-101, is approximately 1 in 150,000 live births, and accordingly it may be difficult for us to identify and timely recruit a sufficient number of eligible patients to conduct our clinical trials. Further, any natural history studies that we or our collaborators may conduct may fail to provide us with patients for our clinical trials because patients enrolled in the natural history studies may not be good candidates for our clinical trials, or may choose to not enroll in our clinical trials.
Trials may be subject to delays as a result of patient enrollment taking longer than anticipated or patient withdrawal. We may not be able to initiate or continue clinical trials for our product candidates if we are unable to locate and enroll a sufficient number of eligible patients to participate in these trials as required by the FDA, EMA or foreign regulatory authorities. We cannot predict how successful we will be at enrolling subjects in future clinical trials. Subject enrollment is affected by other factors including:
|
|
• |
the eligibility criteria for the trial in question; |
|
|
• |
the size of the patient population and process for identifying patients; |
|
|
• |
the perceived risks and benefits of the product candidate in the trial, including relating to AAV9-based gene therapy approaches and intrathecal delivery systems; |
|
|
• |
the availability of competing commercially available therapies and other competing therapeutic candidates’ clinical trials; |
|
|
• |
the willingness of patients to be enrolled in our clinical trials; |
|
|
• |
the efforts to facilitate timely enrollment in clinical trials; |
|
|
• |
potential disruptions caused by the COVID-19 pandemic, including difficulties in initiating clinical sites, enrolling and retaining participants, diversion of healthcare resources away from clinical trials, travel or quarantine policies that may be implemented, and other factors; |
|
|
• |
the patient referral practices of physicians; |
|
|
• |
the ability to monitor patients adequately during and after treatment; and |
|
|
• |
the proximity and availability of clinical trial sites for prospective patients. |
Our inability to enroll a sufficient number of patients for clinical trials would result in significant delays and could require us to abandon one or more clinical trials altogether. Enrollment delays in these clinical trials may result in increased development costs for our product candidates, which would cause the value of our company to decline and limit our ability to obtain additional financing. Furthermore, we expect to rely on CROs and clinical trial sites to ensure the proper and timely conduct of our clinical trials and we will have limited influence over their performance.
Furthermore, even if we are able to enroll a sufficient number of patients for our clinical trials, we may have difficulty maintaining enrollment of such patients in our clinical trials.
57
We may seek orphan drug designation for some of our product candidates and we may be unsuccessful, or may be unable to maintain the benefits associated with orphan drug designation, including the potential for market exclusivity, for product candidates for which we obtain orphan drug designation.
Regulatory authorities in some jurisdictions, including the United States, may designate drugs or biologics intended to treat relatively small patient populations as orphan drug products. Under the Orphan Drug Act, the FDA may designate a drug or biologic as an orphan drug if it is intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals in the United States, or a patient population of 200,000 or more in the United States where there is no reasonable expectation that the cost of developing the drug will be recovered from sales in the United States.
In the United States, orphan drug designation entitled a party to financial incentives such as tax advantages and user fee waivers. Opportunities for grant funding toward clinical trial costs may also be available for clinical trials of drugs or biologics for rare diseases, regardless of whether the drugs or biologics are designated for the orphan use. In addition, if a drug or biologic with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to a seven year period of marketing exclusivity, which precludes the FDA from approving another marketing application for the same drug and indication for that time period, except in limited circumstances. If our competitors are able to obtain orphan drug exclusivity prior to us, for products that constitute the “same drug” and treat the same indications as our product candidates, we may not be able to have competing products approved by the applicable regulatory authority for a significant period of time.
We have obtained orphan drug designation from the FDA for TSHA-101 for treatment of GM2 gangliosidosis, TSHA-102 for the treatment of Rett syndrome, TSHA-103 for the treatment of SLC6A1 haploinsufficiency disorder, TSHA-104 for the treatment of SURF1-associated Leigh syndrome and TSHA-105 for the treatment of SLC13A5 deficiency. In addition, TSHA-118 has received orphan drug designation for the treatment of CLN1 disease from the FDA and EMA. We may seek orphan designation for certain of our other current and future product candidates. However, we may be unsuccessful in obtaining orphan drug designation for these or other product candidates, and may be unable to maintain the benefits associated with orphan drug designation. Even if we obtain orphan drug exclusivity for any of our product candidates, that exclusivity may not effectively protect those product candidates from competition because different drugs can be approved for the same condition, and orphan drug exclusivity does not prevent the FDA from approving the same or a different drug in another indication. Even after an orphan drug is granted orphan exclusivity and approved, the FDA can subsequently approve a later application for the same drug for the same condition before the expiration of the seven-year exclusivity period if the FDA concludes that the later drug is clinically superior in that it is shown to be safer in a substantial portion of the target populations, more effective or makes a major contribution to patient care. In addition, a designated orphan drug may not receive orphan drug exclusivity if it is approved for a use that is broader than the indication for which it received orphan designation. Moreover, orphan-drug-exclusive marketing rights in the United States may be lost if the FDA later determines that the request for designation was materially defective or if we are unable to manufacture sufficient quantities of the product to meet the needs of patients with the rare disease or condition. Orphan drug designation neither shortens the development time or regulatory review time of a drug nor gives the drug any advantage in the regulatory review or approval process.
We have received rare pediatric disease designation for TSHA-101 for the treatment of GM2 gangliosidosis, TSHA-118 for the treatment of CLN1 disease, TSHA-102 for the treatment of Rett syndrome, TSHA-103 for the treatment of SLC6A1 haploinsufficiency, TSHA-104 for the treatment of SURF1-associated Leigh syndrome and TSHA-105 for the treatment of SLC13A5 deficiency. However, a marketing application for TSHA-101, TSHA-118, TSHA-102, TSHA-103, TSHA-104 and TSHA-105, if approved, may not meet the eligibility criteria for a PRV or the rare pediatric disease designation program may sunset before FDA is able consider us for a voucher.
We have received rare pediatric disease designation for TSHA-101 for the treatment of GM2 gangliosidosis (Tay-Sachs Disease and Sandhoff Disease), TSHA-118 for the treatment of CLN1 disease, TSHA-102 for the treatment of Rett syndrome, TSHA-103 for the treatment of SLC6A1 haploinsufficiency, TSHA-104 for the treatment of SURF1-associated Leigh syndrome and TSHA-105 for the treatment of SLC13A5 deficiency. Designation of a drug or biologic as a product for a rare pediatric disease does not guarantee that a BLA for such drug or biologic will meet the eligibility criteria for a rare pediatric disease PRV at the time the application is approved. Under the FDCA, we will need to request a rare pediatric disease PRV in our original BLA for TSHA-101, TSHA-118, TSHA-102, TSHA-103, TSHA-104, TSHA-105 and any other candidates for which we submit a marketing application. The FDA may determine that a BLA for TSHA-101, TSHA-118, TSHA-102, TSHA-103, TSHA-104 or TSHA-105, if approved, does not meet the eligibility criteria for a PRV, including for the following reasons:
|
|
• |
GM2 gangliosidosis, CLN1 disease, Rett syndrome, SLC6A1 haploinsufficiency, SURF1-associated Leigh syndrome or SLC13A5 deficiency no longer meet the definition of a rare pediatric disease; |
|
|
• |
the BLA contains an active ingredient that has been previously approved in a BLA; |
|
|
• |
the BLA is not deemed eligible for priority review; |
|
|
• |
the BLA does not rely on clinical data derived from studies examining a pediatric population and dosages of the drug intended for that population (that is, if the BLA does not contain sufficient clinical data to allow for adequate labeling for use by the full range of affected pediatric patients); or |
|
|
• |
the BLA is approved for a different adult indication than the rare pediatric disease for which TSHA-101, TSHA-118, TSHA-102, TSHA-103, TSHA-104 or TSHA-105 are designated. |
58
The authority for the FDA to award rare pediatric disease PRVs for drugs that have received rare pediatric disease designation prior to September 30, 2024 currently expires on September 30, 2026. If the BLA for TSHA-101, TSHA-118, TSHA-102, TSHA-103, TSHA-104 or TSHA-105 is not approved prior to September 30, 2026 for any reason, regardless of whether it meets the criteria for a rare pediatric disease PRV, it will not be eligible for a PRV. However, it is also possible the authority for FDA to award rare pediatric disease PRVs will be further extended through federal lawmaking.
We have received fast track designation for TSHA-118 for the treatment of CLN1 disease, and we may seek fast track designation for our other product candidates. Even if received, fast track designation may not actually lead to a faster review or approval process and does not increase the likelihood that our product candidates will receive marketing approval.
We have received fast track designation for TSHA-118 for the treatment of neurocognitive manifestations of the patients with CLN1 disease, and we may seek fast track designation for our other product candidates. If a drug or biologic is intended for the treatment of a serious or life-threatening condition and the product demonstrates the potential to address unmet medical needs for this condition, the sponsor may apply for FDA fast track designation for a particular indication. There is no assurance that the FDA will grant this status to any of our other proposed product candidates. If granted, fast track designation makes a product eligible for more frequent interactions with FDA to discuss the development plan and clinical trial design, as well as rolling review of the application, which means that the company can submit completed sections of its marketing application for review prior to completion of the entire submission. Marketing applications of products candidates with fast track designation may qualify for priority review under the policies and procedures offered by the FDA, but the fast track designation does not assure any such qualification or ultimate marketing approval by the FDA. The FDA has broad discretion whether or not to grant fast track designation, so even if we believe a particular product candidate is eligible for this designation, there can be no assurance that the FDA would decide to grant it. Even if we do receive fast track designation, we may not experience a faster development process, review or approval compared to conventional FDA procedures, and receiving a fast track designation does not provide any assurance of ultimate FDA approval. In addition, the FDA may withdraw fast track designation at any time if it believes that the designation is no longer supported by data from our clinical development program.
We may expend our limited resources to pursue a particular product candidate or indication and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and management resources, we must focus on development programs and product candidates that we identify for specific indications. As such, we are currently primarily focused on the development of the following programs: TSHA-101 (GM2 gangliosidosis), TSHA-118 (CLN1 disease), TSHA-102 (Rett syndrome) and TSHA-104 (SURF1-associated Leigh syndrome), each of which we have advanced into clinical development or intend to advance into clinical development in 2021. In addition, we are evaluating each of TSHA-103 (SLC6A1 haploinsufficiency), TSHA-105 (SLC13A5 deficiency), TSHA-111-LAFORIN (Lafora disease), TSHA-111-MALIN (Lafora disease), TSHA-112 (APBD), and TSHA-119 (GM2 AB variant) in IND/CTA-enabling studies in 2021. As a result, we may forego or delay pursuit of opportunities with other product candidates or for other indications for these product candidates that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on current and future development programs and product candidates for specific indications may not yield any commercially viable products. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such product candidate.
We plan to conduct and may in the future conduct additional clinical trials for our product candidates outside the United States, and the FDA and similar foreign regulatory authorities may not accept data from such trials.
We plan to conduct a clinical trial in Canada and may in the future choose to conduct additional clinical trials outside the United States, including in Australia, Europe or other foreign jurisdictions. The acceptance of trial data from clinical trials conducted outside the United States by the FDA may be subject to certain conditions. In cases where data from clinical trials conducted outside the United States are intended to serve as the sole basis for marketing approval in the United States, the FDA will generally not approve the application on the basis of foreign data alone unless (i) the data are applicable to the United States population and United States medical practice; (ii) the trials were performed by clinical investigators of recognized competence and (iii) the data may be considered valid without the need for an on-site inspection by the FDA or, if the FDA considers such an inspection to be necessary, the FDA is able to validate the data through an on-site inspection or other appropriate means. Additionally, the FDA’s clinical trial requirements, including sufficient size of patient populations and statistical powering, must be met. Many foreign regulatory bodies have similar approval requirements. In addition, such foreign trials would be subject to the applicable local laws of the foreign jurisdictions where the trials are conducted. There can be no assurance that the FDA or any similar foreign regulatory authority will accept data from trials conducted outside of the United States or the applicable jurisdiction. If the FDA or any similar foreign regulatory authority does not accept such data, it would result in the need for additional trials, which would be costly and time-consuming and delay aspects of our business plan, and which may result in our product candidates not receiving approval or clearance for commercialization in the applicable jurisdiction.
We may not be successful in our efforts to build a pipeline of additional product candidates.
Our business model is centered on developing therapies for patients with rare, monogenic CNS disorders by establishing focused selection criteria to select, develop and advance product candidates that we believe will have a high probability of technical and regulatory
59
success through development into commercialization. We may not be able to continue to identify and develop new product candidates, including from our next-generation platform technologies, in addition to the pipeline of product candidates that we have established through our collaboration with UT Southwestern. Even if we are successful in continuing to build our pipeline, the potential product candidates that we identify may not be suitable for clinical development. For example, they may be shown to have harmful side effects or other characteristics that indicate that they are unlikely to be drugs that will receive marketing approval and achieve market acceptance. If we do not successfully develop and commercialize product candidates based upon our approach, we will not be able to obtain product revenue in future periods, which likely would result in significant harm to our financial position and adversely affect our stock price.
If we do not achieve our projected development goals in the time frames we announce and expect, the commercialization of our products may be delayed.
From time to time, we may estimate the timing of the accomplishment of various scientific, clinical, regulatory, manufacturing and other product development goals, which we sometimes refer to as milestones. These milestones may include the commencement or completion of preclinical studies and clinical trials and the submission of regulatory filings, including IND submissions. From time to time, we may publicly announce the expected timing of some of these milestones. All of these milestones are, and will be, based on a variety of assumptions. The actual timing of these milestones can vary significantly compared to our estimates, in some cases for reasons beyond our control. We may experience numerous unforeseen events during, or as a result of, any future clinical trials that we conduct that could delay or prevent our ability to receive marketing approval or commercialize our product candidates.
Our business and operations may be adversely affected by the evolving and ongoing COVID-19 global pandemic.
Our business and operations may be adversely affected by the effects of the recent and evolving COVID-19 virus, which was declared by the World Health Organization as a global pandemic. The COVID-19 pandemic has resulted in travel and other restrictions in order to reduce the spread of the disease, including public health directives and orders in the United States and the European Union that, among other things and for various periods of time, directed individuals to shelter at their places of residence, directed businesses and governmental agencies to cease non-essential operations at physical locations, prohibited certain non-essential gatherings and events and ordered cessation of non-essential travel. Future remote work policies and similar government orders or other restrictions on the conduct of business operations related to the COVID-19 pandemic may negatively impact productivity and may disrupt our ongoing research and development activities and our clinical programs and timelines, the magnitude of which will depend, in part, on the length and severity of the restrictions and other limitations on our ability to conduct our business in the ordinary course. Further, such orders also may impact the availability or cost of materials, which would disrupt our supply chain and manufacturing efforts and could affect our ability to conduct ongoing and planned clinical trials and preparatory activities.
Although our current and planned clinical trials have not been impacted by the COVID-19 pandemic to date, we may experience related disruptions in the future that could severely impact our clinical trials, including:
|
|
• |
delays, difficulties or a suspension in clinical site initiation, including difficulties in recruiting clinical site investigators and clinical site staff; |
|
|
• |
interruptions in our ability to manufacture and deliver drug supply for trials; |
|
|
• |
diversion of healthcare resources away from the conduct of clinical trials, including the diversion of hospitals serving as our clinical trial sites and hospital staff supporting the conduct of our clinical trials; |
|
|
• |
changes in local regulations as part of a response to the COVID-19 outbreak that may require us to change the ways in which our clinical trials are conducted, which may result in unexpected costs, or to discontinue the clinical trials altogether; |
|
|
• |
interruption of key clinical trial activities, such as clinical trial site monitoring, and the ability or willingness of subjects to travel to trial sites due to limitations on travel imposed or recommended by federal or state governments, employers and others; |
|
|
• |
limitations in employee resources that would otherwise be focused on the conduct of our clinical trials, including because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; |
|
|
• |
delays in necessary interactions with local regulators, ethics committees and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; and |
|
|
• |
refusal of the FDA to accept data from clinical trials in these affected geographies. |
The spread of COVID-19, which has caused a broad impact globally, may materially affect us economically. While the potential economic impact brought by, and the duration of, COVID-19 may be difficult to assess or predict, it could result in significant disruption of global financial markets, reducing our ability to access capital, which could in the future negatively affect our liquidity. In addition, a recession or market correction resulting from the spread of COVID-19 could materially affect our business and the value of our common stock.
The global COVID-19 pandemic continues to rapidly evolve. The extent to which the COVID-19 pandemic impacts our business and operations, including our clinical development and regulatory efforts, will depend on future developments that are highly uncertain and
60
cannot be predicted with confidence at the time of this Annual Report on Form 10-K, such as the duration of the outbreak, the duration and effect of business disruptions and the short-term effects and ultimate effectiveness of the travel restrictions, quarantines, social distancing requirements and business closures in the United States and other countries to contain and treat the disease and the availability, timing and effectiveness of a vaccine, both domestically and globally. Accordingly, we do not yet know the full extent of potential delays or impacts on our business, our clinical and regulatory activities, healthcare systems or the global economy as a whole. However, these impacts could adversely affect our business, financial condition, results of operations and growth prospects.
In addition, to the extent the ongoing COVID-19 pandemic adversely affects our business and results of operations, it may also have the effect of heightening many of the other risks and uncertainties described in this “Risk Factors” section.
The United Kingdom’s withdrawal from the European Union may adversely impact our ability to obtain regulatory approvals of our product candidates in the European Union, result in restrictions or imposition of taxes and duties for importing our product candidates into the European Union and require us to incur additional expenses in order to develop, manufacture and commercialize our product candidates in the European Union.
Following the result of a referendum in 2016, the United Kingdom left the European Union on January 31, 2020, commonly referred to as Brexit. Pursuant to the formal withdrawal arrangements agreed to by the United Kingdom and the European Union, the United Kingdom was subject to a transition period until December 31, 2020, or the Transition Period, during which European Union rules continued to apply. A trade and cooperation agreement, or the Trade and Cooperation Agreement, that outlines the future trading relationship between the United Kingdom and the European Union was agreed to in December 2020.
Since a significant proportion of the regulatory framework in the United Kingdom applicable to our business and our product candidates is derived from European Union directives and regulations, Brexit has had, and will continue to have, a material impact on the regulatory regime with respect to the development, manufacture, importation, approval and commercialization of our product candidates in the United Kingdom or the European Union. For example, Great Britain is no longer covered by the centralized procedures for obtaining European Union-wide marketing authorizations from the EMA, and a separate marketing authorization will be required to market our product candidates in Great Britain. It is currently unclear whether the Medicines & Healthcare products Regulatory Agency in the United Kingdom is sufficiently prepared to handle the increased volume of MAAs that it is likely to receive. Any delay in obtaining, or an inability to obtain, any marketing approvals, as a result of Brexit or otherwise, would delay or prevent us from commercializing our product candidates in the United Kingdom or the European Union and limit our ability to generate revenue and achieve and sustain profitability. While the Trade and Cooperation Agreement provides for the tariff-free trade of medicinal products between the United Kingdom and the European Union, there may be additional non-tariff costs to such trade that did not exist prior to the end of the Transition Period. Further, should the United Kingdom diverge from the European Union from a regulatory perspective in relation to medicinal products, tariffs could be put into place in the future. We could therefore, both now and in the future, face significant additional expenses (when compare to prior to the end of the Transition Period) to operate our business, which could significantly and materially harm or delay our ability to generate revenues or achieve profitability of our business. Any further changes in international trade, tariff and import/export regulations as a result of Brexit or otherwise may impose unexpected duty costs or other non-tariff barriers on us. These developments, or the perception that any of them could occur, may significantly reduce global trade and, in particular, trade between the impacted nations and the United Kingdom. It is also possible that Brexit may negatively affect our ability to attract and retain employees, particularly those from the European Union.
Risks Related to the Manufacturing of our Product Candidates
Gene therapies are novel, complex and difficult to manufacture. We could experience manufacturing problems that result in delays in the development or commercialization of our product candidates or otherwise harm our business.
The manufacture of gene therapy products is technically complex and necessitates substantial expertise and capital investment. Production difficulties caused by unforeseen events may delay the availability of material for our clinical studies.
We currently rely on the UT Southwestern Gene Therapy Program to manufacture our product candidates. Although we are establishing our own manufacturing facility to provide clinical and commercial supply of our product candidates, we expect to rely on UT Southwestern for our manufacturing needs for the foreseeable future. To date, UT Southwestern has met our manufacturing requirements and quality standards for our program materials, and we expect that UT Southwestern will be capable of providing sufficient quantities of our program materials to meet anticipated clinical trial scale demands. We believe that there are alternate sources of supply for our program materials that can satisfy our clinical and commercial requirements, although we cannot be certain that identifying and establishing relationships with such sources, if necessary, would not result in significant delay or material additional costs.
The manufacturers of pharmaceutical products must comply with strictly enforced cGMP requirements, state and federal regulations, as well as foreign requirements when applicable. Any failure of us or our contract manufacturing organizations, or CMOs, to adhere to or document compliance to such regulatory requirements could lead to a delay or interruption in the availability of our program materials for clinical trials or enforcement action from the FDA, EMA or foreign regulatory authorities. If we or our manufacturers were to fail to comply with the FDA, EMA or other regulatory authority, it could result in sanctions being imposed on us, including clinical holds, fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of product candidates or products, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect supplies of our product candidates. Our potential future dependence upon others for the manufacture of our product candidates may also adversely affect our future profit margins and our ability to commercialize any product candidates that receive regulatory approval on a timely and competitive basis.
61
Biological products are inherently difficult to manufacture. Although we believe that the manufacture of our product candidates may be simplified due to their shared raw materials and other similarities, we cannot be certain that this will be the case and we may be required to develop manufacturing methods that ultimately differ significantly between product candidates, which would require that we invest substantial time and capital to develop suitable manufacturing methods. Our program materials are manufactured using technically complex processes requiring specialized equipment and facilities, highly specific raw materials, cells, and reagents, and other production constraints. Our production process requires a number of highly specific raw materials, cells and reagents with limited suppliers. Even though we aim to have backup supplies of raw materials, cells and reagents whenever possible, we cannot be certain they will be sufficient if our primary sources are unavailable. A shortage of a critical raw material, cell line, or reagent, or a technical issue during manufacturing may lead to delays in clinical development or commercialization plans. We are particularly susceptible to any shortages, delays or our inability to obtain suitable AAV9 raw materials, given that all of our current and planned product candidates require this starting material. Any changes in the manufacturing of components of the raw materials we use could result in unanticipated or unfavorable effects in our manufacturing processes, resulting in delays.
We and our contract manufacturers for AAV9 are subject to significant regulation with respect to manufacturing our products. The third-party manufacturing facilities on which we rely, and any manufacturing facility that we may have in the future, including our facility in Durham, North Carolina, may have limited capacity or fail to meet the applicable stringent regulatory requirements.
We currently have relationships with a limited number of suppliers for the manufacturing of plasmids and viruses, components of our product candidates. However, if we experience slowdowns or problems with our facility or those of our manufacturing partners and are unable to establish or scale our internal manufacturing capabilities, we will need to continue to contract with manufacturers that can produce the preclinical, clinical and commercial supply of our products. Each supplier may require licenses to manufacture such components if such processes are not owned by the supplier or in the public domain and we may be unable to license such intellectual property rights on reasonable commercial terms or to transfer or sublicense the intellectual property rights we may have with respect to such activities.
All entities involved in the preparation of therapeutics for clinical trials or commercial sale, including our existing CMOs for components of our product candidates, are subject to extensive regulation. Components of a finished therapeutic product approved for commercial sale or used in late-stage clinical trials in the European Union must be manufactured in accordance with cGMP. These regulations govern manufacturing processes and procedures (including record keeping) and the implementation and operation of quality systems to control and assure the quality of investigational products and products approved for sale. Poor control of production processes can lead to the introduction of adventitious agents or other contaminants, or to inadvertent changes in the properties or stability of our product candidates that may not be detectable in final product testing. We are at an increased risk given that our product candidates have been and for the foreseeable future will be produced on the same manufacturing lines, which could, for example, lead to issues with cross-contamination. We or our CMOs must supply all necessary documentation in support of a BLA or MAA on a timely basis. Our facilities and quality systems and the facilities and quality systems of some or all of our third-party contractors must pass a pre-approval inspection for compliance with the applicable regulations as a condition of regulatory approval of our product candidates or any of our other potential products. In addition, the regulatory authorities may, at any time, audit or inspect a manufacturing facility involved with the preparation of our product candidates or our other potential products or the associated quality systems for compliance with the regulations applicable to the activities being conducted, and they could put a hold on one or more of our clinical trials if the facilities of our contract development and manufacturing organizations, or CDMOs, do not pass such audit or inspections. If these facilities do not pass a pre-approval plant inspection, FDA approval of the products will not be granted.
The regulatory authorities also may, at any time following approval of a product for sale, inspect or audit our manufacturing facilities or those of our third-party contractors. If any such inspection or audit identifies a failure to comply with applicable regulations or if a violation of our product specifications or applicable regulations occurs independent of such an inspection or audit, we or the relevant regulatory authority may require remedial measures that may be costly and/or time-consuming for us or a third party to implement and that may include the temporary or permanent suspension of a clinical trial or commercial sales or the temporary or permanent closure of a facility. Any such remedial measures imposed upon us or third parties with whom we contract could harm our business. If we or any of our third-party manufacturers fail to maintain regulatory compliance, the FDA can impose regulatory sanctions including, among other things, refusal to approve a pending application for a new drug product or biologic product, or revocation of a pre-existing approval. As a result, our business, financial condition and results of operations may be harmed. Additionally, if supply from one approved manufacturer is interrupted, there could be a significant disruption in commercial supply. An alternative manufacturer would need to be qualified through a BLA and/or MAA supplement which could result in further delay. The regulatory agencies may also require additional studies if a new manufacturer is relied upon for commercial production. Switching manufacturers may involve substantial costs and is likely to result in a delay in our desired clinical and commercial timelines.
These factors could cause the delay of clinical trials, regulatory submissions, required approvals or commercialization of our product candidates, cause us to incur higher costs and prevent us from commercializing our products successfully, if approved. Furthermore, if our suppliers fail to meet contractual requirements, and we are unable to secure one or more replacement suppliers capable of production at a substantially equivalent cost, our clinical trials may be delayed or we could lose potential revenue.
62
We depend on third-party suppliers for materials used in the manufacture of our product candidates, and the loss of these third-party suppliers or their inability to supply us with adequate materials could harm our business.
We rely on third-party suppliers for certain materials and components required for the production of our product candidates. Our dependence on these third-party suppliers and the challenges we may face in obtaining adequate supplies of materials involve several risks, including limited control over pricing, availability, and quality and delivery schedules. There is substantial demand and limited supply for certain of the raw materials used to manufacture gene therapy products. As a small company, our negotiation leverage is limited and we are likely to get lower priority than our competitors that are larger than we are. We cannot be certain that our suppliers will continue to provide us with the quantities of these raw materials that we require or satisfy our anticipated specifications and quality requirements. Any supply interruption in limited or sole sourced raw materials could materially harm our ability to manufacture our product candidates until a new source of supply, if any, could be identified and qualified. We may be unable to find a sufficient alternative supply channel in a reasonable time or on commercially reasonable terms. Any performance failure on the part of our suppliers could delay the development and potential commercialization of our product candidates, including limiting supplies necessary for clinical trials and regulatory approvals, which would have a material adverse effect on our business.
Any contamination or interruption in our manufacturing process, shortages of raw materials or failure of our suppliers of plasmids and viruses to deliver necessary components could result in delays in our clinical development or marketing schedules.
Given the nature of gene therapy manufacturing, there is a risk of contamination. Any contamination could adversely affect our ability to produce product candidates on schedule and could, therefore, harm our results of operations and cause reputational damage. Some of the raw materials required in our manufacturing process are derived from biologic sources. Such raw materials are difficult to procure and may be subject to contamination or recall. A material shortage, contamination, recall or restriction on the use of biologically derived substances in the manufacture of our product candidates could adversely impact or disrupt the commercial manufacturing or the production of clinical material, which could adversely affect our development timelines and our business, financial condition, results of operations and prospects.
Changes in methods of product candidate manufacturing or formulation may result in additional costs or delay.
As product candidates proceed through preclinical studies to late-stage clinical trials towards potential approval and commercialization, it is common that various aspects of the development program, such as manufacturing methods and formulation, are altered along the way in an effort to optimize processes and product characteristics. Such changes carry the risk that they will not achieve our intended objectives. Any such changes could cause our product candidates to perform differently and affect the results of planned clinical trials or other future clinical trials conducted with the materials manufactured using altered processes. Such changes may also require additional testing, FDA notification or FDA approval. This could delay completion of clinical trials, require the conduct of bridging clinical trials or the repetition of one or more clinical trials, increase clinical trial costs, delay approval of our product candidates and jeopardize our ability to commence sales and generate revenue. In addition, we may be required to make significant changes to our upstream and downstream processes across our pipeline, which could delay the development of our future product candidates.
Risks Related to the Commercialization of our Product Candidates
Even if any of our product candidates receive marketing approval, they may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success.
If any of our product candidates receive marketing approval, they may nonetheless fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. If our product candidates do not achieve an adequate level of acceptance, we may not generate significant revenue and we may not become profitable. The degree of market acceptance of our product candidates, if approved for commercial sale, will depend on a number of factors, including:
|
|
• |
the efficacy, safety and potential advantages compared to alternative treatments; |
|
|
• |
our ability to offer our products for sale at competitive prices; |
|
|
• |
the convenience and ease of administration compared to alternative treatments; |
|
|
• |
product labeling or product insert requirements of the FDA or foreign regulatory authorities, including any limitations or warnings contained in a product’s approved labeling, including any black box warning or REMS; |
|
|
• |
the willingness of the target patient population to try new treatments and of physicians to prescribe these treatments; |
|
|
• |
our ability to hire and retain a sales force in the United States; |
|
|
• |
the strength of marketing and distribution support; |
|
|
• |
the availability of third-party coverage and adequate reimbursement for TSHA-101, TSHA-118, TSHA-102 TSHA-104 and any other product candidates, once approved; |
|
|
• |
the prevalence and severity of any side effects; and |
|
|
• |
any restrictions on the use of our products together with other medications. |
63
Negative public opinion of gene therapy and increased regulatory scrutiny of gene therapy and genetic research may adversely impact the development or commercial success of our current and future product candidates.
Our potential therapeutic products involve introducing genetic material into a patient’s cells via intrathecal administration. The clinical and commercial success of our potential products will depend in part on public acceptance of the use of gene therapy and gene regulation for the prevention or treatment of human diseases. Public attitudes may be influenced by claims that gene therapy and gene regulation are unsafe, unethical or immoral, and consequently, our products may not gain the acceptance of the public or the medical community. Adverse public attitudes may adversely impact our ability to enroll clinical trials. Moreover, our success will depend upon physicians prescribing, and their patients being willing to receive, treatments that involve the use of product candidates we may develop in lieu of, or in addition to, existing treatments with which they are already familiar and for which greater clinical data may be available.
More restrictive government regulations or negative public opinion would have a negative effect on our business or financial condition and may delay or impair the development and commercialization of our product candidates or demand for any products once approved. For example, in 2003, trials using early versions of murine gamma-retroviral vectors, which integrate with, and thereby alter, the host cell’s DNA, have led to several well-publicized adverse events, including reported cases of leukemia. Although none of our current product candidates utilize murine gamma-retroviral vectors, our product candidates use AAV9 viral vectors. Among the risks in any gene therapy product based on viral vectors are the risks of immunogenicity, elevated liver enzymes, and insertional oncogenesis. If any of our vectors demonstrate a similar effect we may decide or be required to halt or delay further clinical development of any product candidates that utilize that vector. Adverse events in our or others’ clinical trials, even if not ultimately attributable to our product candidates, and the resulting publicity could result in increased governmental regulation, unfavorable public perception, potential regulatory delays in the testing or approval of our product candidates, stricter labeling requirements for those product candidates that are approved and a decrease in demand for any such product candidates. The risk of cancer remains a concern for gene therapy and we cannot assure that it will not occur in any of our planned or future clinical trials or in any clinical trials conducted by other companies. In addition, there is the potential risk of delayed adverse events following exposure to gene therapy products due to persistent biological activity of the genetic material or other components of products used to carry the genetic material. In addition, for our regulated gene replacement therapy candidates that require that the expression of a therapeutic transgene be tightly regulated, such as TSHA-104, we may inadvertently cause overexpression, which could lead to numerous issues, including safety and toxicity concerns. Furthermore, these regulatory gene replacement therapy candidates require the insertion of miRNA targets into the viral genome, which is a technology that to our knowledge is not present in any approved gene therapy products. If any such adverse events occur, commercialization of our product candidates or further advancement of our clinical trials could be halted or delayed, which would have a negative impact on our business and operations.
If we are unable to establish sales, marketing and distribution capabilities for TSHA-101, TSHA-118, TSHA-102 TSHA-104 or any other product candidate that may receive regulatory approval, we may not be successful in commercializing those product candidates if and when they are approved.
We do not have sales or marketing infrastructure. To achieve commercial success for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any other product candidate for which we may obtain marketing approval, we will need to establish a sales and marketing organization. In the future, we expect to build a focused sales and marketing infrastructure to market some of our product candidates in the United States, if and when they are approved. There are risks involved with establishing our own sales, marketing and distribution capabilities. For example, recruiting and training a sales force is expensive and time consuming and could delay any product launch. If the commercial launch of a product candidate for which we recruit a sales force and establish marketing capabilities is delayed or does not occur for any reason, we would have prematurely or unnecessarily incurred these commercialization expenses. This may be costly, and our investment would be lost if we cannot retain or reposition our sales and marketing personnel.
Factors that may inhibit our efforts to market our products on our own include:
|
|
• |
our inability to recruit, train and retain adequate numbers of effective sales and marketing personnel; |
|
|
• |
the inability of sales personnel to obtain access to physicians in order to educate physicians about our product candidates, once approved; |
|
|
• |
the lack of complementary products to be offered by sales personnel, which may put us at a competitive disadvantage relative to companies with more extensive product lines; and |
|
|
• |
unforeseen costs and expenses associated with creating an independent sales and marketing organization. |
If we are unable to establish our own sales, marketing and distribution capabilities and are forced to enter into arrangements with, and rely on, third parties to perform these services, our revenue and our profitability, if any, are likely to be lower than if we had developed such capabilities ourselves. In addition, we may not be successful in entering into arrangements with third parties to sell, market and distribute our product candidates or may be unable to do so on terms that are favorable to us. We likely will have little control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our products effectively. If we do not establish sales, marketing and distribution capabilities successfully, either on our own or in collaboration with third parties, we will not be successful in commercializing our product candidates.
64
The affected populations for our other product candidates may be smaller than we or third parties currently project, which may affect the addressable markets for our product candidates.
We currently focus our research and product development on several indications that are orphan diseases. However, our projections of the number of people who have the diseases we are seeking to treat, as well as the subset of people with these diseases who have the potential to benefit from treatment with our product candidates, are estimates based on our knowledge and understanding of these diseases. These estimates may prove to be incorrect and new studies may further reduce the estimated incidence or prevalence of this disease. The number of patients in the United States, the European Union and elsewhere may turn out to be lower than expected, may not be otherwise amenable to treatment with our product candidate or patients may become increasingly difficult to identify and access, all of which would adversely affect our business, financial condition, results of operations and prospects.
The total addressable market opportunity for our product candidates will ultimately depend upon a number of factors including the diagnosis and treatment criteria included in the final label, if approved for sale in specified indications, acceptance by the medical community, patient access and product pricing and reimbursement. Incidence and prevalence estimates are frequently based on information and assumptions that are not exact and may not be appropriate, and the methodology is forward-looking and speculative. The process we have used in developing an estimated incidence and prevalence range for the indications we are targeting has involved collating limited data from multiple sources. Accordingly, the incidence and prevalence estimates included in this Annual Report on Form 10-K should be viewed with caution. Further, the data and statistical information used in this Annual Report on Form 10-K, including estimates derived from them, may differ from information and estimates made by our competitors or from current or future studies conducted by independent sources.
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively.
Drug development, particularly in the gene therapy field, is highly competitive and subject to rapid and significant technological advancements. As a significant unmet medical need exists in the neurology field, particularly for the treatment of neurodegenerative diseases, neurodevelopmental disorders and genetic epilepsies, there are several large and small pharmaceutical companies focused on delivering therapeutics for the treatment of these diseases. Further, it is likely that additional drugs will become available in the future for the treatment of our target indications.
We believe that the majority of our programs will face limited competition as there are no approved disease-modifying therapies for the treatment of the GM2 gangliosidosis, CLN1 disease, Rett syndrome, SLC6A1-related disorder, SURF1-associated Leigh syndrome, SLC13A5 disorder, Fragile X syndrome, Angelman syndrome or the other development programs in our pipeline. However, we are aware that our competitors are developing product candidates for the treatment of diseases that our product candidates will target. With respect to TSHA-101, we are aware that Sio Gene Therapies is developing AXO-AAV-GM2 for the treatment of GM2 gangliosidosis, and with respect to TSHA-102, we are aware that Novartis is developing AVXS-201 for the treatment of Rett syndrome. We are also aware that the Rett Syndrome Research Trust, Amicus Therapeutics, or Amicus, and Sarepta Therapeutics have disclosed the existence of discovery-stage gene therapy programs for the treatment of Rett syndrome. With respect to TSHA-118, we are aware that Amicus, in collaboration with Nationwide Children’s Hospital, is developing a gene therapy product candidate for CLN1 disease.
Many of our existing or potential competitors have substantially greater financial, technical and human resources than we do and significantly greater experience in the discovery and development of product candidates, as well as in obtaining regulatory approvals of those product candidates in the United States and in foreign countries. Our current and potential future competitors may also have significantly more experience commercializing drugs, particularly gene therapy and other biological products, that have been approved for marketing. Mergers and acquisitions in the pharmaceutical and biotechnology industries could result in even more resources being concentrated among a small number of our competitors.
We will face competition from other drugs or from other non-drug products currently approved or that will be approved in the future in the neurology field, including for the treatment of diseases and disorders in the therapeutic categories we intend to target. Therefore, our ability to compete successfully will depend largely on our ability to:
|
|
• |
develop and commercialize drugs that are superior to other products in the market; |
|
|
• |
demonstrate through our clinical trials that our product candidates are differentiated from existing and future therapies; |
|
|
• |
attract qualified scientific, product development and commercial personnel; |
|
|
• |
obtain patent or other proprietary protection for our medicines; |
|
|
• |
obtain required regulatory approvals; |
|
|
• |
obtain coverage and adequate reimbursement from, and negotiate competitive pricing with, third-party payors; and |
|
|
• |
successfully collaborate with pharmaceutical companies in the discovery, development and commercialization of new medicines. |
65
The availability of our competitors’ products could limit the demand, and the price we are able to charge, for any product candidate we develop. The inability to compete with existing or subsequently introduced drugs would have an adverse impact on our business, financial condition and prospects. In addition, the reimbursement structure of approved gene therapies by other companies could impact the anticipated reimbursement structure of our gene therapies, if approved, and our business, financial condition, results of operations and prospects.
Established pharmaceutical companies may invest heavily to accelerate discovery and development of novel compounds or to in-license novel compounds that could make our product candidates less competitive. In addition, any new product that competes with an approved product must demonstrate compelling advantages in efficacy, convenience, tolerability and safety in order to overcome price competition and to be commercially successful. Accordingly, our competitors may succeed in obtaining patent protection, discovering, developing, receiving regulatory and marketing approval for, or commercializing, drugs before we do, which would have an adverse impact on our business and results of operations.
Any product candidates for which we intend to seek approval as biologic products may face competition sooner than anticipated.
The BPCIA created an abbreviated approval pathway for biological products that are biosimilar to or interchangeable with an FDA-licensed reference biological product. Under the BPCIA, an application for a biosimilar product may not be submitted to the FDA until four years following the date that the reference product was first licensed by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until 12 years from the date on which the reference product was first licensed. During this 12-year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing the sponsor’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of their product. The law is complex and is still being interpreted and implemented by the FDA. As a result, its ultimate impact, implementation and meaning are subject to uncertainty. While it is uncertain when such processes intended to implement BPCIA may be fully adopted by the FDA, any such processes could have an adverse effect on the future commercial prospects for our biological products.
There is a risk that any of our product candidates approved as a biological product under a BLA would not qualify for the 12-year period of exclusivity or that this exclusivity could be shortened due to congressional action or otherwise, or that the FDA will not consider our product candidates to be reference products for competing products, potentially creating the opportunity for generic competition sooner than anticipated. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. Moreover, the extent to which a biosimilar, once approved, will be substituted for any one of our reference products in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing. If competitors are able to obtain marketing approval for biosimilars referencing our candidates, if approved, our products may become subject to competition from such biosimilars, with the attendant competitive pressure and potential adverse consequences.
The success of our product candidates will depend significantly on coverage and adequate reimbursement or the willingness of patients to pay for these procedures.
We believe our success depends on obtaining and maintaining coverage and adequate reimbursement for our product candidates, including TSHA-101 for the treatment of GM2 gangliosidosis, TSHA-118 for the treatment of CLN1 disease, TSHA-102 for the treatment of Rett syndrome and TSHA-104 for the treatment of SURF1-associated Leigh syndrome, and the extent to which patients will be willing to pay out-of-pocket for such products, in the absence of reimbursement for all or part of the cost. In the United States and in other countries, patients who are provided medical treatment for their conditions generally rely on third-party payors to reimburse all or part of the costs associated with their treatment. The availability of coverage and adequacy of reimbursement for our products by third-party payors, including government health care programs (e.g., Medicare, Medicaid, TRICARE), managed care providers, private health insurers, health maintenance organizations, and other organizations is essential for most patients to be able to afford medical services and pharmaceutical products such as our product candidates. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own coverage and reimbursement policies. However, decisions regarding the extent of coverage and amount of reimbursement to be provided are made on a payor-by-payor basis. One payor’s determination to provide coverage for a drug product does not assure that other payors will also provide coverage, and adequate reimbursement. The principal decisions about reimbursement for new medicines are typically made by the Centers for Medicare & Medicaid Services, or CMS, an agency within HHS. CMS decides whether and to what extent products will be covered and reimbursed under Medicare and private payors tend to follow CMS to a substantial degree.
Third-party payors determine which products and procedures they will cover and establish reimbursement levels. Even if a third-party payor covers a particular product or procedure, the resulting reimbursement payment rates may not be adequate. Patients who are treated in-office for a medical condition generally rely on third-party payors to reimburse all or part of the costs associated with the procedure, including costs associated with products used during the procedure, and may be unwilling to undergo such procedures in the absence of such coverage and adequate reimbursement. Physicians may be unlikely to offer procedures for such treatment if they are not covered by insurance and may be unlikely to purchase and use our product candidates, if approved, for our stated indications unless coverage is provided and reimbursement is adequate. In addition, for products administered under the supervision of a physician, obtaining coverage and adequate reimbursement may be particularly difficult because of the higher prices often associated with such drugs.
66
Reimbursement by a third-party payor may depend upon a number of factors, including the third-party payor’s determination that a procedure is safe, effective and medically necessary; appropriate for the specific patient; cost-effective; supported by peer-reviewed medical journals; included in clinical practice guidelines; and neither cosmetic, experimental, nor investigational. Further, increasing efforts by third-party payors in the United States and abroad to cap or reduce healthcare costs may cause such organizations to limit both coverage and the level of reimbursement for newly approved products and, as a result, they may not cover or provide adequate payment for our product candidates. In order to secure coverage and reimbursement for any product that might be approved for sale, we may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of our products, in addition to the costs required to obtain FDA or comparable regulatory approvals. Additionally, we may also need to provide discounts to purchasers, private health plans or government healthcare programs. Our product candidates may nonetheless not be considered medically necessary or cost-effective. If third-party payors do not consider a product to be cost-effective compared to other available therapies, they may not cover the product after approval as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow a company to sell its products at a profit. We expect to experience pricing pressures from third-party payors in connection with the potential sale of any of our product candidates.
Foreign governments also have their own healthcare reimbursement systems, which vary significantly by country and region, and we cannot be sure that coverage and adequate reimbursement will be made available with respect to the treatments in which our products are used under any foreign reimbursement system.
There can be no assurance that TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any other product candidate, if approved for sale in the United States or in other countries, will be considered medically reasonable and necessary, that it will be considered cost-effective by third-party payors, that coverage or an adequate level of reimbursement will be available or that reimbursement policies and practices in the United States and in foreign countries where our products are sold will not adversely affect our ability to sell our product candidates profitably, if they are approved for sale.
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any products that we may develop.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical trials and will face an even greater risk if we commercially sell any products that we may develop. If we cannot successfully defend ourselves against claims that our product candidates or drugs caused injuries, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
|
|
• |
decreased demand for any product candidates or drugs that we may develop; |
|
|
• |
injury to our reputation and significant negative media attention; |
|
|
• |
withdrawal of clinical trial participants; |
|
|
• |
significant costs to defend the related litigation; |
|
|
• |
substantial monetary awards paid to trial participants or patients; |
|
|
• |
loss of revenue; |
|
|
• |
reduced resources of our management to pursue our business strategy; and |
|
|
• |
the inability to commercialize any products that we may develop. |
Although we maintain product liability insurance coverage, such insurance may not be adequate to cover all liabilities that we may incur. We may need to increase our insurance coverage as we expand our clinical trials or if we commence commercialization of our product candidates. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
Risks Related to Our Dependence on Third Parties
We currently rely exclusively on our collaboration with UT Southwestern for our preclinical research and development programs, including for discovering, preclinically developing and conducting all IND-enabling studies for our lead product candidates and our near-term future pipeline. Failure or delay of UT Southwestern to fulfill all or part of its obligations to us under the agreement, a breakdown in collaboration between the parties or a complete or partial loss of this relationship would materially harm our business.
Our collaboration with UT Southwestern is critical to our business. We entered into the UT Southwestern Agreement with UT Southwestern to discover and develop certain AAV vector-based therapeutics, and the product candidates developed under such collaboration currently represent all of our pipeline and discovery programs. We currently rely exclusively on UT Southwestern for all of our preclinical research and development capabilities, and in particular the UT Southwestern Gene Therapy Program under the direction of Drs. Steven Gray and Berge Minassian. Pursuant to the UT Southwestern Agreement, UT Southwestern is primarily responsible for discovery, preclinical development activities, including all IND-enabling non-clinical studies and research grade manufacturing, and other collaborative activities set forth in the plan for the funded research including leading interactions with FDA and other regulatory
67
authorities. Although we plan to be the sponsor for each product candidate’s IND, UT Southwestern will be the holder of the Health Canada CTA for TSHA-101. Either party has the right in certain circumstances to terminate the collaboration pursuant to the terms of the UT Southwestern Agreement. If UT Southwestern delays or fails to perform its obligations under the UT Southwestern Agreement, disagrees with our interpretation of the terms of the collaboration or our discovery plan or terminates our existing agreement, our pipeline of product candidates would be significantly adversely affected and our prospects will be materially harmed.
The term of the research funding portion of the UT Southwestern Agreement, under which we have the ability to acquire exclusive rights to additional gene therapy products for rare, monogenic CNS indications, expires in November 2021, subject to mutual agreement to extend research funding pursuant to sponsored research agreements. If we seek to extend the research portion of our collaboration, we will need to negotiate a new or amended agreement, which may not be available to us on equally favorable terms, if at all. UT Southwestern has also entered into collaborations with third parties, including certain of our competitors, addressing targets and disease indications outside the scope of our collaboration. As a result, UT Southwestern may have competing interests with respect to their priorities and resources. We may have disagreements with UT Southwestern with respect to the interpretation of the UT Southwestern Agreement, use of resources or otherwise that could cause our relationship with UT Southwestern to deteriorate. As a result, UT Southwestern may reduce their focus on, and resources allocated to, our programs, potentially delaying or terminating our ability to advance product candidates through preclinical studies. Additionally, if either of Dr. Gray or Dr. Minassian were to leave UT Southwestern or to otherwise no longer be meaningfully involved with us, our preclinical research and development capabilities may be substantially reduced.
Further, under the UT Southwestern Agreement, UT Southwestern is primarily responsible for prosecuting and maintaining our licensed intellectual property, and it may fail to properly prosecute, maintain or defend such intellectual property. In such event, if we are unable to otherwise maintain or defend such intellectual property, we could face the potential invalidation of the intellectual property or be subjected to litigation or arbitration, any of which would be time-consuming and expensive. To enforce the licensed intellectual property rights under the UT Southwestern Agreement, we will need to coordinate with UT Southwestern, which could slow down or hamper our ability to enforce our licensed intellectual property rights. In such event, we could face increased competition that could materially and adversely affect our business.
We intend to rely on third parties to conduct a significant portion of our existing clinical trials and potential future clinical trials for product candidates, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such trials.
We have engaged a CRO for the Phase 1/2 clinical trial of TSHA-101 under a CTA in Canada and intend to engage CROs for our other planned clinical trials. We expect to continue to rely on third parties, including clinical data management organizations, medical institutions and clinical investigators, to conduct those clinical trials. Any of these third parties may terminate their engagements with us, some in the event of an uncured material breach and some at any time for convenience. If any of our relationships with these third parties terminate, we may not be able to timely enter into arrangements with alternative third parties or to do so on commercially reasonable terms, if at all. Switching or adding CROs involves substantial cost and requires management time and focus. In addition, there is a natural transition period when a new CRO commences work. As a result, delays occur, which can materially impact our ability to meet our desired clinical development timelines. Though we intend to carefully manage our relationships with our CROs, there can be no assurance that we will not encounter challenges or delays in the future or that these delays or challenges will not have a material adverse impact on our business, financial condition and prospects. Further, the performance of our CROs may also be interrupted by the ongoing COVID-19 pandemic, including due to travel or quarantine policies, heightened exposure of CRO staff who are healthcare providers to COVID-19 or prioritization of resources toward the pandemic.
In addition, any third parties conducting our clinical trials will not be our employees, and except for remedies available to us under our agreements with such third parties, we cannot control whether or not they devote sufficient time and resources to our clinical programs. If these third parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to obtain regulatory approval for or successfully commercialize our product candidates. Consequently, our results of operations and the commercial prospects for our product candidates would be harmed, our costs could increase substantially and our ability to generate revenue could be delayed significantly.
We rely on these parties for execution of our preclinical studies and clinical trials, and generally do not control their activities. Our reliance on these third parties for research and development activities will reduce our control over these activities but will not relieve us of our responsibilities. For example, we will remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the trial. Moreover, the FDA requires us to comply with standards, commonly referred to as GCPs, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. We also are required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database, ClinicalTrials.gov, within specified timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions. If we or any of our CROs or other third parties, including trial sites, fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA, EMA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our
68
marketing applications. We cannot assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials complies with GCP regulations. In addition, our clinical trials must be conducted with product produced under cGMP conditions. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process.
In addition, principal investigators for our clinical trials may serve as scientific advisors or consultants to us from time to time and receive compensation in connection with such services. Under certain circumstances, we may be required to report some of these relationships to the FDA. The FDA may conclude that a financial relationship between us and a principal investigator has created a conflict of interest or otherwise affected interpretation of the trial. The FDA may therefore question the integrity of the data generated at the applicable clinical trial site and the utility of the clinical trial itself may be jeopardized. This could result in a delay in approval, or rejection, of our marketing applications by the FDA and may ultimately lead to the denial of marketing approval of TSHA-101, TSHA-118, TSHA-102TSHA-104 or any other product candidates.
We also expect to rely on other third parties to store and distribute product supplies for our clinical trials. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidates or commercialization of our products, producing additional losses and depriving us of potential revenue.
We may seek collaborations with third parties for the development or commercialization of our product candidates. If those collaborations are not successful, we may not be able to capitalize on the market potential of these product candidates.
We may seek third-party collaborators for the development and commercialization of our product candidates, including for the commercialization of any of our product candidates that are approved for marketing outside the United States. Our likely collaborators for any such arrangements include regional and national pharmaceutical companies and biotechnology companies. If we enter into any additional such arrangements with any third parties, we will likely have limited control over the amount and timing of resources that our collaborators dedicate to the development or commercialization of our product candidates. Our ability to generate revenue from these arrangements will depend on our collaborators’ abilities to successfully perform the functions assigned to them in these arrangements.
Collaborations involving our product candidates would pose the following risks to us:
|
|
• |
collaborators have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
|
|
• |
collaborators may not perform their obligations as expected; |
|
|
• |
collaborators may not pursue development and commercialization of any product candidates that achieve regulatory approval or may elect not to continue or renew development or commercialization programs based on clinical trial results, changes in the collaborators’ strategic focus or available funding, or external factors, such as an acquisition, that divert resources or create competing priorities; |
|
|
• |
collaborators may delay clinical trials, provide insufficient funding for a clinical trial program, stop a clinical trial or abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
|
|
• |
collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our product candidates if the collaborators believe that competitive products are more likely to be successfully developed or can be commercialized under terms that are more economically attractive than ours; |
|
|
• |
we could grant exclusive rights to our collaborators that would prevent us from collaborating with others; |
|
|
• |
product candidates discovered in collaboration with us may be viewed by our collaborators as competitive with their own product candidates or drugs, which may cause collaborators to cease to devote resources to the commercialization of our product candidates; |
|
|
• |
a collaborator with marketing and distribution rights to one or more of our product candidates that achieve regulatory approval may not commit sufficient resources to the marketing and distribution of such products; |
|
|
• |
disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the preferred course of development, might cause delays or termination of the research, development or commercialization of product candidates, might lead to additional responsibilities for us with respect to product candidates, or might result in litigation or arbitration, any of which would be time-consuming and expensive; |
|
|
• |
collaborators may not properly maintain or defend our or their intellectual property rights or may use our or their proprietary information in such a way as to invite litigation that could jeopardize or invalidate such intellectual property or proprietary information or expose us to potential litigation; |
69
|
|
• |
collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; and |
|
|
• |
collaborations may be terminated for the convenience of the collaborator and, if terminated, we could be required to raise additional capital to pursue further development or commercialization of the applicable product candidates. |
Collaboration agreements may not lead to development or commercialization of product candidates in the most efficient manner or at all. If any future collaborator of ours were to be involved in a business combination, the continued pursuit and emphasis on our product development or commercialization program could be delayed, diminished or terminated.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for any collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include the design or results of clinical trials, the likelihood of approval by the FDA or similar regulatory authorities outside the United States, the potential market for the subject product candidate, the costs and complexities of manufacturing and delivering such product candidate to patients, the potential of competing products, the existence of uncertainty with respect to our ownership of technology, which can exist if there is a challenge to such ownership without regard to the merits of the challenge and industry and market conditions generally. The collaborator may also consider alternative product candidates or technologies for similar indications that may be available to collaborate on and whether such a collaboration could be more attractive than the one with us for our product candidate. Collaborations are complex and time-consuming to negotiate and document. In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators.
We may not be able to negotiate additional collaborations on a timely basis, on acceptable terms, or at all. If we are unable to do so, we may have to curtail the development of such product candidate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms or at all. If we do not have sufficient funds, we may not be able to further develop our product candidates or bring them to market and generate revenue.
Risks Related to our Intellectual Property
If we are unable to obtain or protect intellectual property rights related to any of our product candidates, we may not be able to compete effectively in our market.
We rely upon a combination of patents, trade secret protection and confidentiality agreements to protect the intellectual property related to our product candidates. Our success depends in large part on our ability to obtain and maintain patent and other intellectual property protection in the United States and in other countries with respect to our proprietary technology and product candidates.
As of January 26, 2021, we in-license five pending PCT applications, 27 pending foreign patent applications and 13 pending United States patent applications, of which seven are United States utility patent applications, which, if issued, are expected to expire between 2037 and 2040, without taking into account any possible patent term adjustment, and six are United States provisional patent applications, where patent applications claiming priority to these provisional patent applications, if issued, are expected to expire in 2041, without taking into account any possible patent term adjustment. We cannot offer any assurances about which of our patent applications will issue, the breadth of any resulting patent or whether any of the issued patents will be found invalid and unenforceable or will be threatened by third parties. We cannot offer any assurances that the breadth of our granted patents will be sufficient to stop a competitor from developing and commercializing a product, including a biosimilar product that would be competitive with one or more of our product candidates. Furthermore, any successful challenge to these patents or any other patents owned by or licensed to us after patent issuance could deprive us of rights necessary for the successful commercialization of any of our product candidates. Further, if we encounter delays in regulatory approvals, the period of time during which we could market a product candidate under patent protection could be reduced.
The patent prosecution process is expensive and time-consuming. We may not be able to prepare, file and prosecute all necessary or desirable patent applications at a commercially reasonable cost or in a timely manner or in all jurisdictions. It is also possible that we may fail to identify patentable aspects of inventions made in the course of development and commercialization activities before it is too late to obtain patent protection on them. Moreover, depending on the terms of any future in-licenses to which we may become a party, we may not have the right to control the preparation, filing and prosecution of patent applications, or to maintain the patents, covering technology in-licensed from third parties. Therefore, these patents and patent applications may not be prosecuted and enforced in a manner consistent with the best interests of our business.
In addition to the protection provided by our patent estate, we rely on trade secret protection and confidentiality agreements to protect proprietary know-how that is not amenable to patent protection. Although we generally require all of our employees to assign their inventions to us, and all of our employees, consultants, advisors and any third parties who have access to our proprietary know-how,
70
information, or technology to enter into confidentiality agreements, we cannot provide any assurances that all such agreements have been duly executed, or that our trade secrets and other confidential proprietary information will not be disclosed. Moreover, our competitors may independently develop knowledge, methods and know-how equivalent to our trade secrets. Competitors could purchase our products, if approved, and replicate some or all of the competitive advantages we derive from our development efforts for technologies on which we do not have patent protection. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed.
We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, our agreements or security measures may be breached, and we may not have adequate remedies for any breach. Also, if the steps taken to maintain our trade secrets are deemed inadequate, we may have insufficient recourse against third parties for misappropriating the trade secret. In addition, others may independently discover our trade secrets and proprietary information. For example, the FDA is considering whether to make additional information publicly available on a routine basis, including information that we may consider to be trade secrets or other proprietary information, and it is not clear at the present time how the FDA’s disclosure policies may change in the future. If we are unable to prevent material disclosure of the non-patented intellectual property related to our technologies to third parties, and there is no guarantee that we will have any such enforceable trade secret protection, we may not be able to establish or maintain a competitive advantage in our market, which could materially adversely affect our business, results of operations and financial condition.
Patent terms may be inadequate to protect our competitive position on our products for an adequate amount of time, and if we do not obtain protection under the Hatch-Waxman Amendments and similar non-United States legislation for extending the term of patents covering each of our product candidates, our business may be materially harmed.
Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. Depending upon the timing, duration and conditions of FDA marketing approval of our product candidates, one or more of our United States patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, referred to as the Hatch-Waxman Amendments, and similar legislation in the European Union. The Hatch-Waxman Amendments permit a patent term extension of up to five years for a patent covering an approved product as compensation for effective patent term lost during product development and the FDA regulatory review process. A patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval. Only one patent may be extended, and only those claims covering the approved drug, a method for using it, or a method for manufacturing it may be extended. However, we may not receive an extension if we fail to apply within applicable deadlines, fail to apply prior to expiration of relevant patents or otherwise fail to satisfy applicable requirements. Moreover, the length of the extension could be less than we request. If we are unable to obtain patent term extension or the term of any such extension is less than we request, the period during which we can enforce our patent rights for that product will be shortened and our competitors may obtain approval to market competing products sooner. As a result, our revenue from applicable products could be reduced and could have a material adverse effect on our business.
If we fail to comply with our obligations in our current and future intellectual property licenses with third parties, we could lose rights that are important to our business.
We are heavily reliant upon licenses to certain patent rights and proprietary technology for the development of our product candidates, in particular the UT Southwestern Agreement and our license agreements with Queen’s University and Abeona. These license agreements impose diligence, development and commercialization timelines and milestone payment, royalty, insurance and other obligations on us. If we fail to comply with our obligations, our licensors may have the right to terminate our licenses, in which event we might not be able to develop, manufacture or market any product that is covered by the intellectual property we in-license from such licensor and may face other penalties. Such an occurrence would materially adversely affect our business prospects.
Licenses to additional third-party technology and materials that may be required for our development programs may not be available in the future or may not be available on commercially reasonable terms, or at all, which could have a material adverse effect on our business and financial condition. Although we control the prosecution, maintenance and enforcement of the licensed and sublicensed intellectual property relating to our product candidates, we may require the cooperation of our licensors and any upstream licensor, which may not be forthcoming. Therefore, we cannot be certain that the prosecution, maintenance and enforcement of these patent rights will be in a manner consistent with the best interests of our business. If we or our licensor fail to maintain such patents, or if we or our licensor lose rights to those patents or patent applications, the rights we have licensed may be reduced or eliminated and our right to develop and commercialize any of our product candidates that are the subject of such licensed rights could be adversely affected. In addition to the foregoing, the risks associated with patent rights that we license from third parties will also apply to patent rights we may own in the future. Further, if we fail to comply with our development obligations under our license agreements, we may lose our patent rights with respect to such agreement on a territory-by-territory basis, which would affect our patent rights worldwide.
Termination of our current or any future license agreements would reduce or eliminate our rights under these agreements and may result in our having to negotiate new or reinstated agreements with less favorable terms or cause us to lose our rights under these
71
agreements, including our rights to important intellectual property or technology. Any of the foregoing could prevent us from commercializing our other product candidates, which could have a material adverse effect on our operating results and overall financial condition.
In addition, intellectual property rights that we in-license in the future may be sublicenses under intellectual property owned by third parties, in some cases through multiple tiers. The actions of our licensors may therefore affect our rights to use our sublicensed intellectual property, even if we are in compliance with all of the obligations under our license agreements. Should our licensors or any of the upstream licensors fail to comply with their obligations under the agreements pursuant to which they obtain the rights that are sublicensed to us, or should such agreements be terminated or amended, our ability to develop and commercialize our product candidates may be materially harmed.
Patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our future patents.
Our ability to obtain patents is highly uncertain because, to date, some legal principles remain unresolved, and there has not been a consistent policy regarding the breadth or interpretation of claims allowed in patents in the United States. Furthermore, the specific content of patents and patent applications that are necessary to support and interpret patent claims is highly uncertain due to the complex nature of the relevant legal, scientific, and factual issues. Changes in either patent laws or interpretations of patent laws in the United States and other countries may diminish the value of our intellectual property or narrow the scope of our patent protection.
For example, on September 16, 2011, the Leahy-Smith America Invents Act, or the Leahy-Smith Act, was signed into law. The Leahy-Smith Act included a number of significant changes to United States patent law. These included provisions that affect the way patent applications will be prosecuted and may also affect patent litigation. The United States Patent and Trademark Office, or USPTO, has developed new and untested regulations and procedures to govern the full implementation of the Leahy-Smith Act, and many of the substantive changes to patent law associated with the Leahy-Smith Act, and in particular, the first to file provisions, became effective in March 2013. The Leahy-Smith Act has also introduced procedures making it easier for third parties to challenge issued patents, as well as to intervene in the prosecution of patent applications. Finally, the Leahy-Smith Act contained new statutory provisions that require the USPTO to issue new regulations for their implementation, and it may take the courts years to interpret the provisions of the new statute. It is too early to tell what, if any, impact the Leahy-Smith Act will have on the operation of our business and the protection and enforcement of our intellectual property. However, the Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our future patents. Further, the United States Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on actions by the United States Congress, the federal courts and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce patents that we have owned or licensed or that we might obtain in the future. An inability to obtain, enforce, and defend patents covering our proprietary technologies would materially and adversely affect our business prospects and financial condition.
Similarly, changes in patent laws and regulations in other countries or jurisdictions, changes in the governmental bodies that enforce them or changes in how the relevant governmental authority enforces patent laws or regulations may weaken our ability to obtain new patents or to enforce patents that we may obtain in the future. Further, the laws of some foreign countries do not protect proprietary rights to the same extent or in the same manner as the laws of the United States. As a result, we may encounter significant problems in protecting and defending our intellectual property both in the United States and abroad. For example, if the issuance in a given country of a patent covering an invention is not followed by the issuance in other countries of patents covering the same invention, or if any judicial interpretation of the validity, enforceability or scope of the claims or the written description or enablement, in a patent issued in one country is not similar to the interpretation given to the corresponding patent issued in another country, our ability to protect our intellectual property in those countries may be limited. Changes in either patent laws or in interpretations of patent laws in the United States and other countries may materially diminish the value of our intellectual property or narrow the scope of our patent protection.
We may be involved in lawsuits to protect or enforce our patents, which could be expensive, time consuming and unsuccessful.
Competitors may infringe the patents for which we have applied. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming. If we initiate legal proceedings against a third party to enforce a patent covering one of our product candidates, the defendant could counterclaim that the patent covering our product or product candidate is invalid and/or unenforceable. In patent litigation in the United States, counterclaims alleging invalidity and/or unenforceability are common, and there are numerous grounds upon which a third party can assert invalidity or unenforceability of a patent. In an infringement proceeding, a court may decide that the patent claims we are asserting are invalid and/or unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patent claims do not cover the technology in question. Third parties may also raise similar claims before administrative bodies in the United States or abroad, even outside the context of litigation. Such mechanisms include re-examination, post grant review, inter partes review and equivalent proceedings in foreign jurisdictions (for example, opposition proceedings). Such proceedings could result in revocation of or amendment to our patents in such a way that they no longer cover our product candidates. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With
72
respect to the validity question, for example, we cannot be certain that there is no invalidating prior art, of which we, our patent counsel, and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability, we would lose at least part, and perhaps all, of the patent protection on our product candidates. An adverse result in any litigation or defense proceedings could put one or more of our patents at risk of being invalidated or interpreted narrowly, could put our patent applications at risk of not issuing and could have a material adverse impact on our business.
Interference proceedings provoked by third parties or brought by us may be necessary to determine the priority of inventions with respect to our patent applications. An unfavorable outcome could require us to cease using the related technology or force us to take a license under the patent rights of the prevailing party, if available. Furthermore, our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms. Our defense of litigation or interference proceedings may fail and, even if successful, may result in substantial costs and distract our management and other employees. We may not be able to prevent misappropriation of our intellectual property rights, particularly in countries where the laws may not protect those rights as fully as in the United States.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions, or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock.
We may be unsuccessful in licensing or acquiring intellectual property from third parties that may be required to develop and commercialize our product candidates.
A third party may hold intellectual property, including patent rights that are important or necessary to the development and commercialization of our product candidates. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our product candidates, in which case we would be required to acquire or obtain a license to such intellectual property from these third parties, and we may be unable to do so on commercially reasonable terms or at all. The licensing or acquisition of third-party intellectual property rights is a competitive area, and several more established companies may pursue strategies to license or acquire third-party intellectual property rights that we may consider attractive or necessary. These established companies may have a competitive advantage over us due to their size, capital resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment or at all. If we are unable to successfully obtain rights to required third-party intellectual property rights or maintain the existing intellectual property rights we have, we may have to abandon development of the relevant program or product candidate, which could have a material adverse effect on our business.
Third parties may initiate legal proceedings alleging that we are infringing their intellectual property rights, the outcome of which would be uncertain.
As our current and future product candidates progress toward commercialization, the possibility of a patent infringement claim against us increases. We cannot provide any assurance that our current and future product candidates do not infringe other parties’ patents or other proprietary rights, and competitors or other parties may assert that we infringe their proprietary rights in any event. We may become party to, or threatened with, adversarial proceedings or litigation regarding intellectual property rights with respect to our current and future product candidates, including interference or derivation proceedings before the USPTO. Even if we believe such claims are without merit, a court of competent jurisdiction could hold that these third-party patents are valid, enforceable and infringed, which could have a negative impact on our ability to commercialize TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates. In order to successfully challenge the validity of any such United States patent in federal court, we would need to overcome a presumption of validity. As this burden is high and requires us to present clear and convincing evidence as to the invalidity of any such United States patent claim, there is no assurance that a court of competent jurisdiction would agree with us and invalidate the claims of any such United States patent. Moreover, given the vast number of patents in our field of technology, we cannot be certain that we do not infringe existing patents or that we will not infringe patents that may be granted in the future.
While we may decide to initiate proceedings to challenge the validity of these or other patents in the future, we may be unsuccessful, and courts or patent offices in the United States and abroad could uphold the validity of any such patent. Furthermore, because patent applications can take many years to issue and may be confidential for 18 months or more after filing, and because pending patent claims can be revised before issuance, there may be applications now pending which may later result in issued patents that may be infringed by the manufacture, use or sale of our product candidates. Regardless of when filed, we may fail to identify relevant third-party patents or patent applications, or we may incorrectly conclude that a third-party patent is invalid or not infringed by our product candidates or activities. If a patent holder believes that one of our product candidates infringes its patent, the patent holder may sue us even if we have received patent protection for our technology. Moreover, we may face patent infringement claims from non-practicing entities that have no relevant drug revenue and against whom our own patent portfolio may thus have no deterrent effect. If a patent infringement suit were threatened or brought against us, we could be forced to stop or delay research, development, manufacturing or sales of the drug or product candidate that is the subject of the actual or threatened suit.
73
We are aware of issued patent or patents issued to REGENX that claim AAV vectors that have an AAV9 capsid serotype. If we commercialize any of our product candidates prior to the expiry of those patents in 2026 without a license, the patent owner could bring an action claiming infringement. In August 2020, we received a letter from REGENX that stated REGENX is the owner of or has exclusive licenses to various issued patents or patent applications regarding the use of AAV9 vectors and offered to discuss licensing the applicable patents from them. We intend to review their letter in detail and to take appropriate actions based on our review, which may include, if we deem it appropriate, speaking with REGENX regarding their letter. If we are found to infringe a third party’s valid intellectual property rights, we could be required to obtain a license from such third party to continue commercializing our product candidates. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if a license can be obtained on acceptable terms, the rights may be non-exclusive, which could give our competitors access to the same technology or intellectual property rights licensed to us. If we fail to obtain a required license, we may be unable to effectively market product candidates based on our technology, which could limit our ability to generate revenue or achieve profitability and possibly prevent us from generating revenue sufficient to sustain our operations. Alternatively, we may need to redesign our infringing products, which may be impossible or require substantial time and monetary expenditure. Under certain circumstances, we could be forced, including by court orders, to cease commercializing our product candidates. In addition, in any such proceeding or litigation, we could be found liable for substantial monetary damages, potentially including treble damages and attorneys’ fees, if we are found to have willfully infringed the patent at issue. A finding of infringement could prevent us from commercializing our product candidates or force us to cease some of our business operations, which could harm our business. Any claims by third parties that we have misappropriated their confidential information or trade secrets could have a similar negative impact on our business.
The cost to us in defending or initiating any litigation or other proceeding relating to patent or other proprietary rights, even if resolved in our favor, could be substantial, and litigation would divert our management’s attention. Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could delay our research and development efforts and limit our ability to continue our operations.
We may be subject to claims that our employees, consultants, or independent contractors have wrongfully used or disclosed confidential information of third parties.
We employ individuals who were previously employed at other biotechnology or biopharmaceutical companies. Although we try to ensure that our employees, consultants and advisors do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or our employees, consultants, or independent contractors have inadvertently or otherwise used or disclosed confidential information of our employees’ former employers or other third parties. We may also be subject to claims that former employers or other third parties have an ownership interest in our future patents. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and even if we are successful, litigation could result in substantial cost and be a distraction to our management and other employees.
We may be subject to claims challenging the inventorship or ownership of our future patents and other intellectual property.
We may also be subject to claims that former employees, collaborators, or other third parties have an ownership interest in our patent applications, our future patents, or other intellectual property. We may be subject to ownership disputes in the future arising, for example, from conflicting obligations of consultants or others who are involved in developing our product candidates. Although it is our policy to require our employees and contractors who may be involved in the conception or development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who, in fact, conceives or develops intellectual property that we regard as our own, and we cannot be certain that our agreements with such parties will be upheld in the face of a potential challenge, or that they will not be breached, for which we may not have an adequate remedy. The assignment of intellectual property rights may not be self-executing or the assignment agreements may be breached, and litigation may be necessary to defend against these and other claims challenging inventorship or ownership. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Reliance on third parties requires us to share our trade secrets, which increases the possibility that a competitor will discover them or that our trade secrets will be misappropriated or disclosed.
If we rely on third parties to manufacture or commercialize our product candidates, or if we collaborate with additional third parties for the development of such product candidates, we must, at times, share trade secrets with them. We may also conduct joint research and development programs that may require us to share trade secrets under the terms of our research and development partnerships or similar agreements. We seek to protect our proprietary technology in part by entering into confidentiality agreements and, if applicable, material transfer agreements, consulting agreements or other similar agreements with our advisors, employees, third-party contractors and consultants prior to beginning research or disclosing proprietary information. These agreements typically limit the rights of the third parties to use or disclose our confidential information, including our trade secrets. Despite the contractual provisions employed when working with third parties, the need to share trade secrets and other confidential information increases the risk that such trade secrets become known by our competitors, are inadvertently incorporated into the technology of others, or are disclosed or used in violation of these agreements.
74
Given that our proprietary position is based, in part, on our know-how and trade secrets, a competitor’s discovery of our trade secrets or other unauthorized use or disclosure could have an adverse effect on our business and results of operations.
In addition, these agreements typically restrict the ability of our advisors, employees, third-party contractors and consultants to publish data potentially relating to our trade secrets. Despite our efforts to protect our trade secrets, we may not be able to prevent the unauthorized disclosure or use of our technical know-how or other trade secrets by the parties to these agreements. Moreover, we cannot guarantee that we have entered into such agreements with each party that may have or have had access to our confidential information or proprietary technology and processes. Monitoring unauthorized uses and disclosures is difficult, and we do not know whether the steps we have taken to protect our proprietary technologies will be effective. If any of the collaborators, scientific advisors, employees, contractors and consultants who are parties to these agreements breaches or violates the terms of any of these agreements, we may not have adequate remedies for any such breach or violation, and we could lose our trade secrets as a result. Moreover, if confidential information that is licensed or disclosed to us by our partners, collaborators, or others is inadvertently disclosed or subject to a breach or violation, we may be exposed to liability to the owner of that confidential information. Enforcing a claim that a third party illegally obtained and is using our trade secrets, like patent litigation, is expensive and time consuming, and the outcome is unpredictable. In addition, courts outside the United States are sometimes less willing to protect trade secrets.
We may enjoy only limited geographical protection with respect to certain patents and we may not be able to protect our intellectual property rights throughout the world.
Filing and prosecuting patent applications and defending patents covering our product candidates in all countries throughout the world would be prohibitively expensive. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we have patent protection, but enforcement rights are not as strong as that in the United States or Europe. These products may compete with our product candidates, and our future patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
In addition, we may decide to abandon national and regional patent applications before they are granted. The examination of each national or regional patent application is an independent proceeding. As a result, patent applications in the same family may issue as patents in some jurisdictions, such as in the United States, but may issue as patents with claims of different scope or may even be refused in other jurisdictions. It is also quite common that depending on the country, the scope of patent protection may vary for the same product candidate or technology.
While we intend to protect our intellectual property rights in our expected significant markets, we cannot ensure that we will be able to initiate or maintain similar efforts in all jurisdictions in which we may wish to market our product candidates. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate, which may have an adverse effect on our ability to successfully commercialize our product candidates in all of our expected significant foreign markets. If we encounter difficulties in protecting, or are otherwise precluded from effectively protecting, the intellectual property rights important for our business in such jurisdictions, the value of these rights may be diminished, and we may face additional competition from others in those jurisdictions.
The laws of some jurisdictions do not protect intellectual property rights to the same extent as the laws or rules and regulations in the United States and Europe and many companies have encountered significant difficulties in protecting and defending such rights in such jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents, trade secrets, and other intellectual property rights, which could make it difficult for us to stop the infringement of our future patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in other jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our future patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing as patents, and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
Some countries also have compulsory licensing laws under which a patent owner may be compelled to grant licenses to third parties. In addition, some countries limit the enforceability of patents against government agencies or government contractors. In those countries, the patent owner may have limited remedies, which could materially diminish the value of such patents. If we are forced to grant a license to third parties with respect to any patents relevant to our business, our competitive position may be impaired.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment, and other requirements imposed by government patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other government fees on patents and/or applications will be due to be paid to the USPTO and various government patent agencies outside of the United States over the lifetime of our patents and/or applications and any patent rights we may obtain in the future. Furthermore, the USPTO and various non-United States government patent agencies require compliance with several procedural, documentary, fee payment and other similar provisions during the patent application process. In many cases, an inadvertent lapse of a patent or patent application can be cured by payment of a late fee or by other means in
75
accordance with the applicable rules. There are situations, however, in which non-compliance can result in abandonment or lapse of the patents or patent applications, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, potential competitors might be able to enter the market, which could have a material adverse effect on our business.
Any trademarks we have obtained or may obtain may be infringed or otherwise violated, or successfully challenged, resulting in harm to our business.
We expect to rely on trademarks as one means to distinguish our product candidates, if approved for marketing, from the drugs of our competitors. Once we select new trademarks and apply to register them, our trademark applications may not be approved. Third parties may oppose or attempt to cancel our trademark applications or trademarks, or otherwise challenge our use of the trademarks. In the event that our trademarks are successfully challenged, we could be forced to rebrand our drugs, which could result in loss of brand recognition and could require us to devote resources to advertising and marketing new brands. Our competitors may infringe or otherwise violate our trademarks and we may not have adequate resources to enforce our trademarks. Any of the foregoing events may have a material adverse effect on our business.
Intellectual property rights do not necessarily address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations and may not adequately protect our business or permit us to maintain our competitive advantage. The following examples are illustrative:
|
|
• |
others may be able to make products that are similar to or otherwise competitive with our product candidates but that are not covered by the claims of our current or future patents; |
|
|
• |
an in-license necessary for the manufacture, use, sale, offer for sale or importation of one or more of our product candidates may be terminated by the licensor; |
|
|
• |
we or future collaborators might not have been the first to make the inventions covered by our issued or future issued patents or our pending patent applications; |
|
|
• |
we or future collaborators might not have been the first to file patent applications covering certain of our inventions; |
|
|
• |
others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; |
|
|
• |
it is possible that our pending patent applications will not lead to issued patents; |
|
|
• |
issued patents that we own or in-license may be held invalid or unenforceable as a result of legal challenges by our competitors; |
|
|
• |
issued patents that we own or in-license may not provide coverage for all aspects of our product candidates in all countries; |
|
|
• |
our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; |
|
|
• |
we may not develop additional proprietary technologies that are patentable; and |
|
|
• |
the patents of others may have an adverse effect on our business. |
Should any of these events occur, they could significantly harm our business, results of operations and prospects.
76
Risks Related to Legal and Regulatory Compliance Matters
Our relationships with customers, healthcare providers, including physicians, and third-party payors are subject, directly or indirectly, to federal and state healthcare fraud and abuse laws, false claims laws, health information privacy and security laws, and other healthcare laws and regulations. If we are unable to comply, or have not fully complied, with such laws, we could face substantial penalties.
Healthcare providers, including physicians, and third-party payors in the United States and elsewhere will play a primary role in the recommendation and prescription of any product candidates for which we obtain marketing approval. Our current and future arrangements with healthcare professionals, principal investigators, consultants, customers and third-party payors subject us to various federal and state fraud and abuse laws and other healthcare laws, including, without limitation, the federal Anti-Kickback Statute, the federal civil and criminal false claims laws and the law commonly referred to as the Physician Payments Sunshine Act and regulations promulgated under such laws. These laws will impact, among other things, our clinical research, proposed sales, marketing and educational programs, and other interactions with healthcare professionals. In addition, we may be subject to patient privacy laws by both the federal government and the states in which we conduct or may conduct our business. The laws that will affect our operations include, but are not limited to:
|
|
• |
the federal Anti-Kickback Statute, which prohibits, among other things, individuals or entities from knowingly and willfully soliciting, receiving, offering or paying any remuneration (including any kickback, bribe or rebate), directly or indirectly, overtly or covertly, in cash or in kind in return for, or to induce, either the referral of an individual, or the purchase, lease, order or arrangement for or recommendation of the purchase, lease, order or arrangement for any good, facility, item or service for which payment may be made, in whole or in part, under a federal healthcare program, such as the Medicare and Medicaid programs. The term “remuneration” has been broadly interpreted to include anything of value. Although there are a number of statutory exceptions and regulatory safe harbors protecting some common activities from prosecution, the exceptions and safe harbors are drawn narrowly. Practices that involve remuneration that may be alleged to be intended to induce prescribing, purchases or recommendations may be subject to scrutiny if they do not qualify for an exception or safe harbor. A person does not need to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation. In addition, the ACA signed into law in 2010, provides that the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act; |
|
|
• |
the federal civil and criminal false claims laws, including, without limitation, the federal False Claims Act, which can be enforced by private citizens through civil whistleblower or qui tam actions, and civil monetary penalty laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment or approval from the federal government, including Medicare, Medicaid and other government payors, that are false or fraudulent or knowingly making, using or causing to be made or used a false record or statement material to a false or fraudulent claim or to avoid, decrease or conceal an obligation to pay money to the federal government. A claim includes “any request or demand” for money or property presented to the United States federal government. Several pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. Other companies have been prosecuted for causing false claims to be submitted because of the companies’ marketing of products for unapproved, and thus non-reimbursable, uses; |
|
|
• |
HIPAA, which created additional federal criminal statutes which prohibit, among other things, a person from knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third-party payors and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation; |
|
|
• |
HIPAA, as amended by the HITECH, and their implementing regulations, which imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information on health plans, healthcare clearinghouses and certain healthcare providers, known as “covered entities”, and their respective HIPAA “business associates”, which are independent contractors that perform certain services for or on behalf of covered entities involving the use or disclosure of individually identifiable health information, as well as their covered subcontractors. HITECH also created new tiers of civil monetary penalties, amended HIPAA to make civil and criminal penalties directly applicable to business associates, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce HIPAA and seek attorneys’ fees and costs associated with pursuing federal civil actions; |
|
|
• |
the federal transparency laws, including the federal Physician Payments Sunshine Act, which requires certain manufacturers of drugs, medical devices, biologicals and medical supplies for which payment is available under Medicare, Medicaid or the State Children’s Health Insurance Program, with specific exceptions, to report annually to CMS information related to: (i) payments or other “transfers of value’’ made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and (ii) ownership and investment interests held by physicians and their immediate family members. Effective January 1, 2022, these reporting obligations will extend to include transfers of value made during the previous year to physician assistants, nurse practitioners, clinical nurse specialists, anesthesiologist assistants, certified registered nurse anesthetists and certified nurse midwives; and |
77
Because of the breadth of these laws and the narrowness of the statutory exceptions and regulatory safe harbors available, it is possible that some of our business activities could be subject to challenge under one or more of such laws. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant penalties, including, without limitation, civil, criminal and administrative penalties, damages, fines, disgorgement, imprisonment, exclusion from participating in federal and state funded healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if we become subject to a corporate integrity agreement or similar agreement to resolve allegations of non-compliance with these laws, contractual damages, diminished profits and future earnings, reputational harm and the curtailment or restructuring of our operations, any of which could harm our business.
The risk of our being found in violation of these laws is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. The shifting compliance environment and the need to build and maintain robust and expandable systems to comply with multiple jurisdictions with different compliance and/or reporting requirements increases the possibility that a healthcare company may run afoul of one or more of the requirements.
Even if we obtain regulatory approval for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates, they will remain subject to ongoing regulatory oversight.
Even if we obtain any regulatory approval for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates, such product candidates, once approved, will be subject to ongoing regulatory requirements applicable to manufacturing, labeling, packaging, storage, advertising, promoting, sampling, record-keeping and submitting of safety and other post-market information, among other things. Any regulatory approvals that we receive for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates may also be subject to a REMS, limitations on the approved indicated uses for which the drug may be marketed or to the conditions of approval, or requirements that we conduct potentially costly post-marketing testing, including Phase 4 trials and surveillance to monitor the quality, safety and efficacy of the drug. An unsuccessful post-marketing study or failure to complete such a study could result in the withdrawal of marketing approval. We will further be required to immediately report any serious and unexpected adverse events and certain quality or production problems with our products to regulatory authorities along with other periodic reports.
Any new legislation addressing drug safety issues could result in delays in product development or commercialization, or increased costs to assure compliance. We will also have to comply with requirements concerning advertising and promotion for our products. Promotional communications with respect to prescription drug products are subject to a variety of legal and regulatory restrictions and must be consistent with the information in the product’s approved label. As such, we will not be allowed to promote our products for indications or uses for which they do not have approval, commonly known as off-label promotion. The holder of an approved BLA must submit new or supplemental applications and obtain prior approval for certain changes to the approved product, product labeling, or manufacturing process. A company that is found to have improperly promoted off-label uses of their products may be subject to significant civil, criminal and administrative penalties.
In addition, drug manufacturers are subject to payment of user fees and continual review and periodic inspections by the FDA and other regulatory authorities for compliance with cGMP requirements and adherence to commitments made in the BLA or foreign marketing application. If we, or a regulatory authority, discover previously unknown problems with a drug, such as adverse events of unanticipated severity or frequency, or problems with the facility where the drug is manufactured or if a regulatory authority disagrees with the promotion, marketing or labeling of that drug, a regulatory authority may impose restrictions relative to that drug, the manufacturing facility or us, including requesting a recall or requiring withdrawal of the drug from the market or suspension of manufacturing.
If we fail to comply with applicable regulatory requirements following approval of TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates, a regulatory authority may:
|
|
• |
issue an untitled letter or warning letter asserting that we are in violation of the law; |
|
|
• |
seek an injunction or impose administrative, civil or criminal penalties or monetary fines; |
|
|
• |
suspend or withdraw regulatory approval; |
78
|
|
• |
refuse to approve a pending BLA or comparable foreign marketing application (or any supplements thereto) submitted by us or our strategic partners; |
|
|
• |
restrict the marketing or manufacturing of the drug; |
|
|
• |
seize or detain the drug or otherwise require the withdrawal of the drug from the market; |
|
|
• |
refuse to permit the import or export of product candidates; or |
|
|
• |
refuse to allow us to enter into supply contracts, including government contracts. |
Any government investigation of alleged violations of law could require us to expend significant time and resources in response and could generate negative publicity. The occurrence of any event or penalty described above may inhibit our ability to commercialize TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates and harm our business, financial condition, results of operations and prospects.
Even if we obtain FDA or EMA approval any of our product candidates in the United States or European Union, we may never obtain approval for or commercialize any of them in any other jurisdiction, which would limit our ability to realize their full market potential.
In order to market any products in any particular jurisdiction, we must establish and comply with numerous and varying regulatory requirements on a country-by-country basis regarding safety and efficacy.
Approval by the FDA in the United States or the EMA in the European Union does not ensure approval by regulatory authorities in other countries or jurisdictions. However, the failure to obtain approval in one jurisdiction may negatively impact our ability to obtain approval elsewhere. In addition, clinical trials conducted in one country may not be accepted by regulatory authorities in other countries, and regulatory approval in one country does not guarantee regulatory approval in any other country.
Approval processes vary among countries and can involve additional product testing and validation and additional administrative review periods. Seeking foreign regulatory approval could result in difficulties and increased costs for us and require additional preclinical studies or clinical trials which could be costly and time consuming. Regulatory requirements can vary widely from country to country and could delay or prevent the introduction of our products in those countries. We do not have any product candidates approved for sale in any jurisdiction, including in international markets, and we do not have experience in obtaining regulatory approval in international markets. If we fail to comply with regulatory requirements in international markets or to obtain and maintain required approvals, or if regulatory approvals in international markets are delayed, our target market will be reduced and our ability to realize the full market potential of any product we develop will be unrealized.
Healthcare legislative or regulatory reform measures may have a negative impact on our business and results of operations.
In the United States and some foreign jurisdictions, there have been, and continue to be, several legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval of product candidates, restrict or regulate post-approval activities, and affect our ability to profitably sell any product candidates for which we obtain marketing approval.
Among policy makers and payors in the United States and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and/or expanding access. In the United States, the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by major legislative initiatives. For example, in March 2010, the ACA was passed, which substantially changed the way healthcare is financed by both the government and private insurers, and significantly impacts the United States pharmaceutical industry. The ACA, among other things: (i) established an annual, nondeductible fee on any entity that manufactures or imports certain specified branded prescription drugs and biologic agents apportioned among these entities according to their market share in some government healthcare programs; (ii) expanded the entities eligible for discounts under the 340B drug pricing program; (iii) increased the statutory minimum rebates a manufacturer must pay under the Medicaid Drug Rebate Program to 23.1% and 13% of the average manufacturer price, or AMP, for most branded and generic drugs, respectively, and capped the total rebate amount for innovator drugs at 100% of the AMP; (iv) expanded the eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to additional individuals and by adding new eligibility categories for individuals with income at or below 133% (as calculated, it constitutes 138%) of the federal poverty level, thereby potentially increasing manufacturers’ Medicaid rebate liability; (v) addressed a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for certain drugs and biologics that are inhaled, infused, instilled, implanted or injected; (vi) introduced a new Medicare Part D coverage gap discount program in which manufacturers must now agree to offer 70% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D (increased from 50%, effective January 1, 2019, pursuant to the Bipartisan Budget Act of 2018); (vii) created a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; and (viii) established the Center for Medicare and Medicaid Innovation at CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug.
79
There remain judicial and congressional challenges to certain aspects of the ACA, as well as efforts by the Trump administration to repeal or replace certain aspects of the ACA. While Congress has not passed comprehensive repeal legislation, several bills affecting the implementation of certain taxes under the ACA have been signed into law. The Tax Act includes a provision that repealed, effective January 1, 2019, the tax-based shared responsibility payment imposed by the ACA on certain individuals who fail to maintain qualifying health coverage for all or part of a year that is commonly referred to as the “individual mandate.” In addition, the 2020 federal spending package permanently eliminated, effective January 1, 2020, the ACA-mandated “Cadillac” tax on high-cost employer-sponsored health coverage and medical device tax and, effective January 1, 2021, also eliminated the health insurer tax. On December 14, 2018, a Texas United States District Court Judge ruled that the ACA is unconstitutional in its entirety because the “individual mandate” was repealed by Congress as part of the Tax Act. Additionally, on December 18, 2019, the United States Court of Appeals for the 5th Circuit upheld the District Court ruling that the individual mandate was unconstitutional and remanded the case back to the District Court to determine whether the remaining provisions of the ACA are invalid as well. The United States Supreme Court is currently reviewing this case, although it is unclear when a decision will be made. It is also unclear how such litigation and other efforts to repeal and replace the ACA will impact the ACA and our business.
Other legislative changes have been proposed and adopted since the ACA was enacted. These changes include aggregate reductions to Medicare payments to providers of 2% per fiscal year pursuant to the Budget Control Act of 2011, which began in 2013, and due to subsequent legislative amendments to the statute, including the BBA, will remain in effect through 2030, unless additional congressional action is taken. COVID-19 pandemic relief legislation suspended the 2% Medicare sequester from May 1, 2020 through March 31, 2021. The American Taxpayer Relief Act of 2012, among other things, further reduced Medicare payments to several providers, including hospitals and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. These laws may result in additional reductions in Medicare and other healthcare funding, which could have an adverse effect on customers for our product candidates, if approved, and, accordingly, our financial operations.
Additionally, there has been heightened governmental scrutiny in the United States of pharmaceutical pricing practices in light of the rising cost of prescription drugs and biologics. Such scrutiny has resulted in several recent congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for products. At the federal level, the Trump administration’s budget proposal for fiscal year 2021 includes a $135 billion allowance (over a period of time) to support legislative proposals seeking to reduce drug prices, increase competition, lower out-of-pocket drug costs for patients, and increase patient access to lower-cost generic and biosimilar drugs. On March 10, 2020, the Trump administration sent “principles” for drug pricing to Congress, calling for legislation that would, among other things, cap Medicare Part D beneficiary out-of-pocket pharmacy expenses, provide an option to cap Medicare Part D beneficiary monthly out-of-pocket expenses, and place limits on pharmaceutical price increases. Further, the Trump administration previously released a plan to lower drug prices and reduce out of pocket costs of drugs that contained proposals to increase drug manufacturer competition, increase the negotiating power of certain federal healthcare programs, incentivize manufacturers to lower the list price of their products, and reduce the out of pocket costs of drug products paid by consumers. On July 24, 2020 and September 13, 2020, the Trump administration announced several executive orders related to prescription drug pricing that attempt to implement several of the Administration’s proposals. As a result, the FDA released a final rule, effective November 30, 2020, providing guidance for states to build and submit importation plans for drugs from Canada. Further, on November 20, 2020, HHS finalized a regulation removing safe harbor protection for price reductions from pharmaceutical manufacturers to plan sponsors under Part D, either directly or through pharmacy benefit managers, unless the price reduction is required by law. The rule also creates a new safe harbor for price reductions reflected at the point-of-sale, as well as a safe harbor for certain fixed fee arrangements between pharmacy benefit managers and manufacturers. On November 20, 2020, CMS issued an interim final rule implementing President Trump’s Most Favored Nation executive order, which would tie Medicare Part B payments for certain physician-administered drugs to the lowest price paid in other economically advanced countries, effective January 1, 2021. On December 28, 2020, the United States District Court in Northern California issued a nationwide preliminary injunction against implementation of the interim final rule. It is unclear whether the Biden administration will work to reverse these measures or pursue similar policy initiatives. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
We expect that these and other healthcare reform measures that may be adopted in the future may result in more rigorous coverage criteria and in additional downward pressure on the price that we receive for any approved drug. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability, or commercialize our drugs. It is also possible that additional governmental action is taken in response to the COVID-19 pandemic.
In addition, FDA regulations and guidance may be revised or reinterpreted by the FDA in ways that may significantly affect our business and our products. The Trump administration has also taken several executive actions, including the issuance of a number of Executive Orders, that could impose significant burdens on, or otherwise materially delay, the FDA’s ability to engage in routine oversight activities such as implementing statutes through rulemaking, issuance of guidance, and review and approval of marketing applications. It is difficult to predict how these requirements will be interpreted and implemented and the extent to which they will impact the FDA’s ability to exercise its regulatory authority. If these executive actions impose restrictions on the FDA’s ability to engage in oversight and implementation activities in the normal course, our business may be negatively impacted. Any new regulations or guidance, or revisions or
80
reinterpretations of existing regulations or guidance, may impose additional costs or lengthen FDA review times for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future product candidates. We cannot determine how changes in regulations, statutes, policies, or interpretations when and if issued, enacted or adopted, may affect our business in the future. Such changes could, among other things, require:
|
|
• |
additional clinical trials to be conducted prior to obtaining approval; |
|
|
• |
changes to manufacturing methods; |
|
|
• |
recalls, replacements, or discontinuance of one or more of our products; and |
|
|
• |
additional recordkeeping. |
Such changes would likely require substantial time and impose significant costs, or could reduce the potential commercial value of TSHA-101, TSHA-118, TSHA-102, TSHA-104, or other product candidates, and could materially harm our business and our financial results. In addition, delays in receipt of or failure to receive regulatory clearances or approvals for any other products would harm our business, financial condition, and results of operations.
Disruptions at the FDA, the SEC and other government agencies caused by funding shortages or global health concerns could hinder their ability to hire and retain key leadership and other personnel, prevent new products and services from being developed or commercialized in a timely manner or otherwise prevent those agencies from performing normal business functions on which the operation of our business may rely, which could negatively impact our business.
The ability of the FDA to review and approve new products can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, and statutory, regulatory, and policy changes. Average review times at the agency have fluctuated in recent years as a result. In addition, government funding of the SEC and other government agencies on which our operations may rely, including those that fund research and development activities, is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other agencies may also slow the time necessary for new drugs or biologics to be reviewed and/or approved by necessary government agencies, which would adversely affect our business. For example, over the last several years, including most recently from December 22, 2018 to January 25, 2019, the U.S. government has shut down several times and certain regulatory agencies, such as the FDA and the SEC, have had to furlough critical FDA, SEC and other government employees and stop critical activities. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business.
Separately, in response to the COVID-19 pandemic, on March 10, 2020 the FDA announced its intention to postpone most inspections of foreign manufacturing facilities and products while local, national and international conditions warrant. The FDA has developed a rating system to assist in determining when and where it is safest to conduct prioritized domestic inspections. Regulatory authorities outside the U.S. may adopt similar restrictions or other policy measures in response to the COVID-19 pandemic and may experience delays in their regulatory activities.
Risks Related to Employee Matters and Managing our Growth
Our future success depends on our ability to retain key executives and to attract, retain and motivate qualified personnel.
We are highly dependent on the management, development, clinical, financial and business development expertise of our executive officers, particularly RA Session II, our President and Chief Executive Officer. Each of our executive officers may currently terminate their employment with us at any time. We do not maintain “key person” insurance for any of our executives or employees.
Recruiting and retaining qualified scientific and clinical personnel and, if we progress the development of our product pipeline toward scaling up for commercialization, manufacturing and sales and marketing personnel, will also be critical to our success. The loss of the services of our executive officers or other key employees could impede the achievement of our development and commercialization objectives and seriously harm our ability to successfully implement our business strategy. Furthermore, replacing executive officers and key employees may be difficult and may take an extended period of time because of the limited number of individuals in our industry with the breadth of skills and experience required to successfully develop, gain regulatory approval of and commercialize products. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these key personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. We also experience competition for the hiring of scientific and clinical personnel from universities and research institutions. In addition, we rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us. If we are unable to continue to attract and retain high quality personnel, our ability to pursue our growth strategy will be limited.
81
We expect to expand our clinical development and regulatory capabilities and potentially implement sales, marketing and distribution capabilities, and as a result, we may encounter difficulties in managing our growth, which could disrupt our operations.
As of December 31, 2020, we had 38 employees. As our development progresses, we expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of clinical product development, regulatory affairs and, if any of our product candidates receives marketing approval, sales, marketing and distribution. To manage our anticipated future growth, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel. The expansion of our operations may lead to significant costs and may divert our management and business development resources. Any inability to manage growth could delay the execution of our business plans or disrupt our operations.
Our employees, independent contractors, consultants, collaborators, principal investigators, CROs, suppliers and vendors may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements.
We are exposed to the risk that our employees, independent contractors, consultants, collaborators, principal investigators, CROs, suppliers and vendors may engage in fraudulent conduct or other illegal activity. Misconduct by these parties could include intentional, reckless and/or negligent conduct that violates FDA regulations, including those laws requiring the reporting of true, complete and accurate information to the FDA, manufacturing standards, federal and state healthcare laws and regulations, and laws that require the true, complete and accurate reporting of financial information or data. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Misconduct by these parties could also involve the improper use of individually identifiable information, including, without limitation, information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. We have adopted a code of business conduct and ethics, but it is not always possible to identify and deter misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant civil, criminal and administrative penalties, including, without limitation, damages, fines, disgorgement, imprisonment, exclusion from participation in government healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if we become subject to a corporate integrity agreement or similar agreement to resolve allegations of non-compliance with these laws, and the curtailment or restructuring of our operations.
Risks Related to Ownership of our Common Stock
An active trading market for our common stock may not continue to be developed or sustained.
Prior to our initial public offering, there was no public market for our common stock. Although our common stock is listed on The Nasdaq Global Market, an active trading market for our shares may never develop or be sustained. If an active market for our common stock does not develop or is not sustained, it may be difficult for you to sell shares of our common stock at an attractive price or at all.
The trading price of the shares of our common stock may be volatile, and purchasers of our common stock could incur substantial losses.
Our stock price may be volatile. The stock market in general and the market for biopharmaceutical companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. As a result of this volatility, investors may not be able to sell their common stock at or above the price paid for the shares. The market price for our common stock may be influenced by many factors, including:
|
|
• |
the reporting of unfavorable preclinical results; |
|
|
• |
the commencement, enrollment or results of our clinical trials of TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any future clinical trials we may conduct, or changes in the development status of our product candidates; |
|
|
• |
any delay in our regulatory filings for TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any other product candidate we may develop, and any adverse development or perceived adverse development with respect to the applicable regulatory authority’s review of such filings, including without limitation the FDA’s issuance of a “refusal to file” letter or a request for additional information; |
|
|
• |
adverse results from, delays in or termination of clinical trials; |
|
|
• |
adverse regulatory decisions, including failure to receive regulatory approval of our product candidates; |
82
|
|
• |
unanticipated serious safety concerns related to the use of TSHA-101, TSHA-118, TSHA-102, TSHA-104 or any other product candidate; |
|
|
• |
changes in financial estimates by us or by any equity research analysts who might cover our stock; |
|
|
• |
conditions or trends in our industry; |
|
|
• |
changes in the market valuations of similar companies; |
|
|
• |
stock market price and volume fluctuations of comparable companies and, in particular, those that operate in the biopharmaceutical industry; |
|
|
• |
publication of research reports about us or our industry or positive or negative recommendations or withdrawal of research coverage by securities analysts; |
|
|
• |
announcements by us or our competitors of significant acquisitions, strategic partnerships or divestitures; |
|
|
• |
our relationships with our collaborators; |
|
|
• |
announcements of investigations or regulatory scrutiny of our operations or lawsuits filed against us; |
|
|
• |
investors’ general perception of our company and our business; |
|
|
• |
recruitment or departure of key personnel; |
|
|
• |
overall performance of the equity markets; |
|
|
• |
trading volume of our common stock; |
|
|
• |
disputes or other developments relating to proprietary rights, including patents, litigation matters and our ability to obtain patent protection for our technologies; |
|
|
• |
significant lawsuits, including patent or stockholder litigation; |
|
|
• |
changes in the structure of healthcare payment systems; |
|
|
• |
general political and economic conditions; and |
|
|
• |
other events or factors, many of which are beyond our control. |
The stock market in general, and the Nasdaq Global Market and biotechnology companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies, including very recently in connection with the ongoing COVID-19 pandemic, which has resulted in decreased stock prices for many companies notwithstanding the lack of a fundamental change in their underlying business models or prospects. Broad market and industry factors, including potentially worsening economic conditions and other adverse effects or developments relating to the ongoing COVID-19 pandemic, may negatively affect the market price of our common stock, regardless of our actual operating performance. The realization of any of the above risks or any of a broad range of other risks, including those described in this section, could have a significant and material adverse impact on the market price of our common stock.
In addition, in the past, stockholders have initiated class action lawsuits against pharmaceutical and biotechnology companies following periods of volatility in the market prices of these companies’ stock. Such litigation, if instituted against us, could cause us to incur substantial costs and divert management’s attention and resources from our business.
If equity research analysts do not publish research or reports, or publish unfavorable research or reports, about us, our business or our market, our stock price and trading volume could decline.
The trading market for our common stock will be influenced by the research and reports that equity research analysts publish about us and our business. As a newly public company, we have only limited research coverage by equity research analysts. Equity research analysts may elect not to provide research coverage of our common stock, and such lack of research coverage may adversely affect the market price of our common stock. In the event we do have equity research analyst coverage, we will not have any control over the analysts or the content and opinions included in their reports. The price of our stock could decline if one or more equity research analysts downgrade our stock or issue other unfavorable commentary or research. If one or more equity research analysts ceases coverage of our company or fails to publish reports on us regularly, demand for our stock could decrease, which in turn could cause our stock price or trading volume to decline.
83
A significant portion of our total outstanding shares are restricted from immediate resale but may be sold into the market in the near future. This could cause the market price of our common stock to drop significantly, even if our business is doing well.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. If our stockholders sell, or the market perceives that our stockholders intend to sell, substantial amounts of our common stock in the public market, the market price of our common stock could decline significantly.
As of March 3, 2021, we have outstanding 37,761,435 shares of common stock. Of these shares, 9,050,000 shares are freely tradable.
In addition, we have filed a registration statement on Form S-8 under the Securities Act of 1933, as amended, or the Securities Act, registering the issuance of approximately 7.6 million shares of common stock subject to options or other equity awards issued or reserved for future issuance under our equity incentive plans. Shares registered under this registration statement on Form S-8 will be available for sale in the public market subject to vesting arrangements and exercise of options, the lock-up agreements described above and the restrictions of Rule 144 in the case of our affiliates.
Additionally, the holders of an aggregate of approximately 27.9 million shares of our common stock, or their transferees, will have rights, subject to some conditions, to require us to file one or more registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders. If we were to register the resale of these shares, they could be freely sold in the public market. If these additional shares are sold, or if it is perceived that they will be sold, in the public market, the trading price of our common stock could decline.
Provisions in our corporate charter documents and under Delaware law may prevent or frustrate attempts by our stockholders to change our management and hinder efforts to acquire a controlling interest in us, and the market price of our common stock may be lower as a result.
There are provisions in our certificate of incorporation and bylaws that may make it difficult for a third party to acquire, or attempt to acquire, control of our company, even if a change of control was considered favorable by you and other stockholders. For example, our board of directors has the authority to issue up to 10,000,000 shares of preferred stock. The board of directors can fix the price, rights, preferences, privileges, and restrictions of the preferred stock without any further vote or action by our stockholders. The issuance of shares of preferred stock may delay or prevent a change of control transaction. As a result, the market price of our common stock and the voting and other rights of our stockholders may be adversely affected. An issuance of shares of preferred stock may result in the loss of voting control to other stockholders.
Our charter documents also contain other provisions that could have an anti-takeover effect, including:
|
|
• |
only one of our three classes of directors will be elected each year; |
|
|
• |
stockholders will not be entitled to remove directors other than by a 66 2/3% vote and only for cause; |
|
|
• |
stockholders will not be permitted to take actions by written consent; |
|
|
• |
stockholders cannot call a special meeting of stockholders; and |
|
|
• |
stockholders must give advance notice to nominate directors or submit proposals for consideration at stockholder meetings. |
In addition, we are subject to the anti-takeover provisions of Section 203 of the Delaware General Corporation Law, which regulates corporate acquisitions by prohibiting Delaware corporations from engaging in specified business combinations with particular stockholders of those companies. These provisions could discourage potential acquisition proposals and could delay or prevent a change of control transaction. They could also have the effect of discouraging others from making tender offers for our common stock, including transactions that may be in your best interests. These provisions may also prevent changes in our management or limit the price that investors are willing to pay for our stock.
Concentration of ownership of our common stock among our existing executive officers, directors and principal stockholders may prevent new investors from influencing significant corporate decisions.
Our executive officers, directors and current beneficial owners of 5% or more of our common stock and their respective affiliates beneficially own a majority of our common stock. As a result, these persons, acting together, would be able to significantly influence all matters requiring stockholder approval, including the election and removal of directors, any merger, consolidation, sale of all or substantially all of our assets, or other significant corporate transactions.
84
Some of these persons or entities may have interests different than yours. For example, because many of these stockholders purchased their shares at prices substantially below the current market price of our common stock and have held their shares for a longer period, they may be more interested in selling our company to an acquirer than other investors, or they may want us to pursue strategies that deviate from the interests of other stockholders.
We are an “emerging growth company” and a “smaller reporting company” and, as a result of the reduced disclosure and governance requirements applicable to emerging growth companies and smaller reporting companies, our common stock may be less attractive to investors.
We are an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and we intend to take advantage of some of the exemptions from reporting requirements that are applicable to other public companies that are not emerging growth companies, including:
|
|
• |
not being required to comply with the auditor attestation requirements in the assessment of our internal control over financial reporting; |
|
|
• |
not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements; |
|
|
• |
reduced disclosure obligations regarding executive compensation in our periodic reports, proxy statements and registration statements; and |
|
|
• |
not being required to hold a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. |
We cannot predict if investors will find our common stock less attractive because we will rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile. We may take advantage of these reporting exemptions until we are no longer an emerging growth company. We will remain an emerging growth company until December 31, 2025 or, if earlier, (i) the last day of the fiscal year in which we have total annual gross revenue of at least $1.07 billion, (ii) the date on which we are deemed to be a large accelerated filer, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the prior June 30th, or (iii) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period.
Even after we no longer qualify as an emerging growth company, we may, under certain circumstances, still qualify as a “smaller reporting company,” which would allow us to take advantage of many of the same exemptions from disclosure requirements, including reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements.
We have broad discretion in the use our cash and cash equivalents, including the net proceeds from our initial public offering.
We have broad discretion over the use of our cash and cash equivalents, including the net proceeds from our recent initial public offering. You may not agree with our decisions, and our use of the proceeds may not yield any return on your investment. Our failure to apply our cash and cash equivalents effectively could compromise our ability to pursue our growth strategy and we might not be able to yield a significant return, if any, on our investment of these net proceeds. You will not have the opportunity to influence our decisions on how to use our cash and cash equivalents.
Because we do not anticipate paying any cash dividends on our common stock in the foreseeable future, capital appreciation, if any, will be your sole source of gains and you may never receive a return on your investment.
You should not rely on an investment in our common stock to provide dividend income. We have not declared or paid cash dividends on our common stock to date. We currently intend to retain our future earnings, if any, to fund the development and growth of our business. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future. Investors seeking cash dividends should not purchase our common stock.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware and the federal district courts of the United States of America will be the exclusive forums for substantially all disputes between us and our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us or our directors, officers or employees.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware is the exclusive forum for the following types of actions or proceedings under Delaware statutory or common law:
|
|
• |
any derivative action or proceeding brought on our behalf; |
|
|
• |
any action asserting a breach of fiduciary duty; |
85
|
|
• |
any action asserting a claim against us arising under the Delaware General Corporation Law, our amended and restated certificate of incorporation, or our amended and restated bylaws; |
|
|
• |
any claim or cause of action seeking to interpret, apply, enforce or determine the validity of our restated certificate or our amended and restated bylaws; |
|
|
• |
any claim or cause of action as to which the Delaware General Corporation Law confers jurisdiction on the Court of Chancery of the state of Delaware; and |
|
|
• |
any action asserting a claim against us that is governed by the internal-affairs doctrine. |
This provision would not apply to suits brought to enforce a duty or liability created by the Exchange Act. Furthermore, Section 22 of the Securities Act creates concurrent jurisdiction for federal and state courts over all such Securities Act actions. Accordingly, both state and federal courts have jurisdiction to entertain such claims. To prevent having to litigate claims in multiple jurisdictions and the threat of inconsistent or contrary rulings by different courts, among other considerations, our amended and restated certificate of incorporation further provides that the federal district courts of the United States of America will be the exclusive forum for resolving any complaint asserting a cause of action arising under the Securities Act. While the Delaware courts have determined that such choice of forum provisions are facially valid, a stockholder may nevertheless seek to bring a claim in a venue other than those designated in the exclusive forum provisions. In such instance, we would expect to vigorously assert the validity and enforceability of the exclusive forum provisions of our amended and restated certificate of incorporation. This may require significant additional costs associated with resolving such action in other jurisdictions and there can be no assurance that the provisions will be enforced by a court in those other jurisdictions.
These exclusive forum provisions may limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes with us or our directors, officers, or other employees, which may discourage lawsuits against us and our directors, officers and other employees. If a court were to find either exclusive-forum provision in our amended and restated certificate of incorporation to be inapplicable or unenforceable in an action, we may incur further significant additional costs associated with resolving the dispute in other jurisdictions, all of which could seriously harm our business.
General Risks
We are subject to a variety of stringent and changing privacy and data security laws, contractual obligations, self-regulatory schemes, government regulation, and standards related to data privacy and security. The actual or perceived failure by us, our partners, or vendors to comply with such obligations could harm our reputation, subject us to significant fines and liability, disrupt our clinical trials, or otherwise adversely affect our business.
We collect, receive, store, process, use, generate, transfer, disclose, make accessible, protect and share personal information and other information, including information we collect about patients and healthcare providers in connection with clinical trials in the U.S. and abroad, or Process or Processing, necessary to operate our business, for legal and marketing purposes, and for other business-related purposes.
There are numerous federal, state, local, and international laws, regulations, and guidance regarding privacy, information security and Processing, or Data Protection Laws, the number and scope of which is changing, subject to differing applications and interpretations, and which may be inconsistent among jurisdictions, or in conflict with other rules, laws or Data Protection Obligations.
For example, US States have also begun to introduce more and more comprehensive privacy legislation. The California Consumer Privacy Act of 2018, or CCPA, which went into effect on January 1, 2020, affords consumers expanded privacy protections. Aspects of the CCPA and its interpretation and enforcement remain uncertain. The potential effects of the CCPA are far-reaching and may require us to modify our data processing practices and policies and to incur substantial costs and expenses in an effort to comply. For example, the CCPA gives California residents expanded rights to access and require deletion of their personal information, opt-out of certain personal information sharing, and receive detailed information about how their personal information is used. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches and statutory damages ranging from $100 to $750 per violation, which is expected to increase data breach class action litigation and result in significant exposure to costly legal judgements and settlements. The CCPA will be expanded substantially on January 1, 2023, when the California Privacy Rights Act of 2020, or CPRA becomes fully operative. The CPRA will, among other things, give California residents the ability to limit use of certain sensitive personal information, further restrict the use of cross-contextual advertising, establish restrictions on the retention of personal information, expand the types of data breaches subject to the CCPA’s private right of action, provide for increased penalties for CPRA violations concerning California residents under the age of 16, and establish a new California Privacy Protection Agency to implement and enforce the new.
Our operations may be subject to increased scrutiny or attention from foreign data protection authorities. Our clinical trial programs and research collaborations outside the United States may implicate foreign data protection laws, including in Canada and Europe. European data protection laws, including, without limitation, the EU’s the General Data Protection Regulation, or the GDPR, impose stringent data protection requirements on processing the personally identifiable information of individuals residing in the European Economic Area, or EEA, Switzerland, and United Kingdom, or collectively, Europe. Among other things, the GDPR requires us to give detailed disclosures about how we collect, use and share personal information, contractually commit to data protection measures in our
86
contracts with vendors, maintain adequate data security measures, notify regulators and affected individuals of certain data breaches, meet extensive privacy governance and documentation requirements, and honor individuals’ data protection rights, including their rights to access, correct and delete their personal information. In addition, the GDPR increases the scrutiny of transfers of personal information from clinical trial sites located in Europe to the United States and other jurisdictions that the European Commission does not recognize as having “adequate” data protection laws. Companies that violate the GDPR can face private litigation, prohibitions on data processing, and imposes substantial fines for breaches and violations (up to the greater of €20 million or 4% of our consolidated annual worldwide gross revenue).
European data protection laws also generally prohibit the transfer of personal information from Europe to the United States and most other countries unless the parties to the transfer have implemented specific safeguards to protect the transferred personal information. One of the primary safeguards used for transfers of personal information from the European Union and Switzerland to the United States until recently was the Privacy Shield framework administered by the U.S. Department of Commerce, which was invalidated by a decision of the European Union’s highest court in July 2020. The same decision also cast doubt on the viability of one of the primary alternatives to the Privacy Shield, namely, the European Commission’s Standard Contractual Clauses, as a vehicle for such transfers. Similarly, the Swiss Federal Data Protection and Information Commissioner has opined that the Privacy Shield is inadequate for transfers of data from Switzerland to the U.S. and raised similar questions regarding the Standard Contractual Clauses. At present, there are few, if any, viable alternatives to the Standard Contractual Clauses and, therefore, there is uncertainty regarding how to lawfully transfer personal information from Europe to the U.S. and other countries. Failure to comply with the GDPR’s cross-border data restrictions may increase our exposure to its heightened sanctions, restrict our clinical trial activities in Europe, and limit our ability to collaborate with partners, third-party service providers and other companies subject to European data protection laws.
In addition, it is unclear whether the transfer of personal information from the EEA to the United Kingdom will continue to remain lawful under the GDPR following Brexit. Pursuant to a post-Brexit trade deal between the United Kingdom and the EU, transfers of personal information from the EEA to the United Kingdom are not considered restricted transfers under the GDPR for a period of up to six months starting January 1, 2021. However, unless the EU Commission makes an adequacy finding with respect to the United Kingdom before the end of that period, the United Kingdom will be considered a “third country” under the GDPR and transfers of European personal information to the United Kingdom will require an approved compliance mechanism to render such transfers lawful under the GDPR. Although the United Kingdom’s primary data protection legislation is designed to be consistent with the GDPR, uncertainty remains regarding how data transfers to and from the United Kingdom will be regulated after Brexit. We may incur liabilities, expenses, costs, and other operational losses under the GDPR and applicable EU Member States and the United Kingdom data privacy laws in connection with any measures we take to comply with them. Additionally, other countries outside of Europe have enacted or are considering enacting similar cross-border data transfer restrictions and laws requiring local data residency, which could increase the cost and complexity of delivering our services and operating our business.
We are also subject to the terms of our privacy and security policies, representations, certifications, standards, publications and frameworks, or Privacy Policies, and contractual obligations to third parties related to privacy, information security and Processing, or Data Protection Obligations, including without limitation, operating rules and standards imposed by industry organizations. Data Protection Laws and data protection worldwide are, and are likely to remain, uncertain for the foreseeable future. We strive to comply with applicable Data Protection Laws, Privacy Policies and Data Protection Obligations to the extent possible, but we may at times fail to do so, or may be perceived to have failed to do so. Moreover, despite our efforts, we may not be successful in achieving compliance if our personnel, partners or vendors do not comply with applicable Data Protection Laws, Privacy Policies and Data Protection Obligations.
If we fail, or are perceived to have failed, to address or comply with applicable Data Protection Laws, Privacy Policies and Data Protection Obligations, such failure or perceived failure could: increase our compliance and operational costs; expose us to regulatory scrutiny, actions, fines and penalties; result in reputational harm; interrupt or stop clinical trials; result in litigation and liability; result in an inability to process personal information or to operate in certain jurisdictions; cause a material adverse impact to business operations or financial results, and; otherwise result in other material harm to our business.
With applicable Data Protection Laws, Privacy Policies and Data Protection Obligations imposing complex and burdensome obligations, and with substantial uncertainty over the interpretation and application of these requirements, we have faced and may face additional challenges in addressing and complying with them, and making necessary changes to our Privacy Policies and practices, and may incur material costs and expenses in an effort to do so, any of which could materially adversely affect our business operations and financial results, and may limit the adoption and use of, and reduce the overall demand for, our products, which could have an adverse impact on our business.
If our security measures are compromised now, or in the future, or the security, confidentiality, integrity or availability of, our information technology, software, services, communications or data is compromised, limited or fails, this could result in material harm to our business, including without limitation, a material interruption to our operations, harm to our reputation, significant fines, penalties and liability, breach or triggering of Data Protection Laws, Privacy Policies and Data Protection Obligations, or material disruption of our clinical trials or other business activity.
In the ordinary course of our business, we may collect, process and store proprietary, confidential and sensitive information, including personal information (including health information), intellectual property, trade secrets, and proprietary business information owned or controlled by ourselves or other parties.
87
We may use third-party service providers and subprocessors to help us operate our business and engage in Processing on our behalf. We may also share sensitive information with our partners or other third parties in conjunction with our business. If we, our service providers, partners or other relevant third parties have experienced, or in the future experience, any security incident(s) that result in, any data loss, deletion or destruction, unauthorized access to, loss of, unauthorized acquisition or disclosure of, or inadvertent exposure or disclosure of, sensitive information, or compromise related to the security, confidentiality, integrity or availability of our information technology, software, services, communications or data (or those of our service providers, partners or other relevant third parties), or collectively a Security Breach, it may have a material adverse effect on our business, including without limitation, regulatory investigations or enforcement actions, litigation, indemnity obligations, negative publicity and financial loss. For example, the loss of clinical trial data from completed or ongoing or planned clinical trials could result in delays in our regulatory approval efforts and could require us to incur substantial cost to recover or reproduce such data.
Cyberattacks, malicious internet-based activity and online and offline fraud are prevalent and continue to increase. In addition to traditional computer “hackers,” threat actors, software bugs, malicious code (such as viruses and worms), employee theft or misuse, denial-of-service attacks (such as credential stuffing), and ransomware attacks, sophisticated nation-state and nation-state supported actors now engage in attacks (including advanced persistent threat intrusions). We may also be the subject of phishing attacks, viruses, malware installation, server malfunction, software or hardware failures, loss of data or other computer assets, adware or other similar issues. Moreover, Security Breaches can result in the diversion of funds, and interruptions, delays, or outages in our operations and services, including due to ransomware attacks, which have increased in frequency and severity.
We may be required to expend significant resources, fundamentally change our business activities and practices, or modify our operations, including our clinical trial activities or information technology, in an effort to protect against Security Breaches and to mitigate, detect, and remediate actual and potential vulnerabilities. Applicable Data Protection Laws, Privacy Policies and Data Protection Obligations may require us to implement specific security measures or use industry-standard or reasonable measures to protect against Security Breaches. While we have implemented security measures designed to protect against Security Breaches there can be no assurance that our security measures or those of our service providers, partners and other third parties, will be effective in protecting against all Security Breaches and material adverse impacts that may arise from such breaches. The recovery systems, security protocols, network protection mechanisms and other security measures that we (and our third parties) have integrated into our platform, systems, networks and physical facilities, which are designed to protect against, detect and minimize Security Breaches, may not be adequate to prevent or detect service interruption, system failure or data loss.
We have not always been able in the past and may be unable in the future to detect, anticipate, measure or prevent threats or techniques used to detect or exploit vulnerabilities in our (or our third parties’) information technology, services, communications or software, or cause Security Breaches, because such threats and techniques change frequently, are often sophisticated in nature, and may not be detected until after an incident has occurred. In addition, security researchers and other individuals have in the past and will continue in the future to actively search for and exploit actual and potential vulnerabilities in our (or our third parties’) information technology and communications. We cannot be certain that we will be able to address any such vulnerabilities, in whole or part, and there may be delays in developing and deploying patches and other remedial measures to adequately address vulnerabilities.
Applicable Data Protection Laws, Privacy Policies and Data Protection Obligations may require us to notify relevant stakeholders of Security Breaches, including affected individuals, regulators and credit reporting agencies. Such disclosures are costly, and the disclosures or the failure to comply with such requirements, could lead to material adverse impacts, including without limitation, negative publicity, a loss of confidence in our security measures or breach of contract claims. There can be no assurance that the limitations of liability in our contracts would be enforceable or adequate or would otherwise protect us from liabilities or damages if we fail to comply with Applicable Data Protection Laws, Privacy Policies or Data Protection Obligations related to information security or Security Breaches.
We may not have adequate insurance coverage in the event of a Security Breach. We cannot assure that our existing coverage will be adequate or otherwise protect us from or adequately mitigate liabilities or damages with respect to claims, costs, expenses, litigation, fines, penalties, business loss, data loss, regulatory actions or material adverse impacts arising out of our privacy and security practices, Processing or Security Breaches we may experience, or that such coverage will continue to be available on acceptable terms or at all. The successful assertion of one or more large claims against us that exceeds our available insurance coverage, or results in changes to our insurance policies (including premium increases or the imposition of large deductible or co-insurance requirements), could have an adverse effect on our business. In addition, we cannot be sure that our existing insurance coverage and coverage for errors and omissions will continue to be available on acceptable terms or that our insurers will not deny coverage as to any future claim.
Our business activities will be subject to the Foreign Corrupt Practices Act, or FCPA, and similar anti-bribery and anti-corruption laws.
As we expand our business activities outside of the United States, including our clinical trial efforts, we will be subject to the FCPA and similar anti-bribery or anti-corruption laws, regulations or rules of other countries in which we operate. The FCPA generally prohibits offering, promising, giving, or authorizing others to give anything of value, either directly or indirectly, to a non-United States government official in order to influence official action, or otherwise obtain or retain business. The FCPA also requires public companies to make and keep books and records that accurately and fairly reflect the transactions of the corporation and to devise and maintain an adequate system of internal accounting controls. Our business is heavily regulated and therefore involves significant interaction with public officials, including officials of non-United States governments. Additionally, in many other countries, the healthcare providers who
88
prescribe pharmaceuticals are employed by their government, and the purchasers of pharmaceuticals are government entities; therefore, our dealings with these prescribers and purchasers will be subject to regulation under the FCPA. Recently the SEC and Department of Justice have increased their FCPA enforcement activities with respect to biotechnology and pharmaceutical companies. There is no certainty that all of our employees, agents, suppliers, manufacturers, contractors, or collaborators, or those of our affiliates, will comply with all applicable laws and regulations, particularly given the high level of complexity of these laws. Violations of these laws and regulations could result in fines, criminal sanctions against us, our officers, or our employees, the closing down of facilities, including those of our suppliers and manufacturers, requirements to obtain export licenses, cessation of business activities in sanctioned countries, implementation of compliance programs, and prohibitions on the conduct of our business. Any such violations could include prohibitions on our ability to offer our products in one or more countries as well as difficulties in manufacturing or continuing to develop our products, and could materially damage our reputation, our brand, our international expansion efforts, our ability to attract and retain employees, and our business, prospects, operating results, and financial condition.
If we fail to maintain proper and effective internal controls, our ability to produce accurate financial statements on a timely basis could be impaired.
We are subject to the reporting requirements of the Securities Exchange Act of 1934, the Sarbanes-Oxley Act of 2002, or the Sarbanes-Oxley Act, and the rules and regulations of the stock market on which our common stock is listed. The Sarbanes-Oxley Act requires, among other things, that we maintain effective disclosure controls and procedures and internal control over financial reporting.
Commencing with our fiscal year ending December 31, 2021, we must perform system and process evaluation and testing of our internal control over financial reporting to allow management to report on the effectiveness of our internal control over financial reporting in our Form 10-K filing for that year, as required by Section 404 of the Sarbanes-Oxley Act. This will require that we incur substantial additional professional fees and internal costs to expand our accounting and finance functions and that we expend significant management efforts. Prior to our initial public offering, we have never been required to test our internal control within a specified period, and, as a result, we may experience difficulty in meeting these reporting requirements in a timely manner.
We may identify weaknesses in our system of internal financial and accounting controls and procedures that could result in a material misstatement of our financial statements. Our internal control over financial reporting will not prevent or detect all errors and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that misstatements due to error or fraud will not occur or that all control issues and instances of fraud will be detected.
If we are not able to comply with the requirements of Section 404 of the Sarbanes-Oxley Act in a timely manner, or if we are unable to maintain proper and effective internal controls, we may not be able to produce timely and accurate financial statements. If that were to happen, the market price of our stock could decline and we could be subject to sanctions or investigations by the stock exchange on which our common stock is listed, the SEC or other regulatory authorities.
Our effective tax rate may fluctuate, and we may incur obligations in tax jurisdictions in excess of accrued amounts.
We are subject to taxation in more than one tax jurisdiction. As a result, our effective tax rate is derived from a combination of applicable tax rates in the various places that we operate. In preparing our financial statements, we estimate the amount of tax that will become payable in each such jurisdiction. Nevertheless, our effective tax rate may be different than experienced in the past due to numerous factors, including passage of newly enacted tax legislation, changes in the mix of our profitability from jurisdiction to jurisdiction, the results of examinations and audits of our tax filings, our inability to secure or sustain acceptable agreements with tax authorities, changes in accounting for income taxes and changes in existing tax laws. Any of these factors could cause us to experience an effective tax rate significantly different from previous periods or our current expectations and may result in tax obligations in excess of amounts accrued in our financial statements.
We might not be able to utilize a significant portion of our net operating loss carryforwards.
We expect to generate significant federal and state net operating loss, or NOL, carryforwards in the future. These NOL carryforwards could expire unused and be unavailable to offset future income tax liabilities. Under the Tax Cuts and Jobs, or the Tax Act, as modified by the Coronavirus Aid, Relief, and Economic Security Act, or CARES Act, federal NOLs incurred in taxable years beginning after December 31, 2017 and in future taxable years may be carried forward indefinitely, but the deductibility of such federal NOLs incurred in the taxable year beginning after December 31, 2020 is limited. It is uncertain how various states will respond to the Tax Act and CARES Act. In addition, under Section 382 of the Internal Revenue Code of 1986, as amended, and corresponding provisions of state law, if a corporation undergoes an “ownership change,” which is generally defined as a greater than 50% change, by value, in its equity ownership over a three-year period, the corporation’s ability to use its pre-change NOL carryforwards and other pre-change tax attributes to offset its post-change income or taxes may be limited. The completion of our recent initial public offering, together with private placements and other transactions that have occurred since our inception, may have triggered such an ownership change pursuant to Section 382. We have not yet completed a Section 382 analysis. We may experience ownership changes as a result of subsequent shifts in our stock ownership, some of which may be outside of our control. If an ownership change occurs and our ability to use our NOL carryforwards is materially limited, it would harm our future operating results by effectively increasing our future tax obligations.
89
We will incur increased costs and demands upon management as a result of being a public company.
As a public company listed in the United States, we will incur significant additional legal, accounting and other costs including the cost of director and officer liability insurance. These additional costs could negatively affect our financial results. In addition, changing laws, regulations and standards relating to corporate governance and public disclosure, including regulations implemented by the SEC and the Nasdaq Stock Market, may increase legal and financial compliance costs and make some activities more time-consuming. These laws, regulations and standards are subject to varying interpretations and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. We intend to invest resources to comply with evolving laws, regulations and standards, and this investment may result in increased general and administrative expenses and a diversion of management’s time and attention from revenue-generating activities to compliance activities. If notwithstanding our efforts to comply with new laws, regulations and standards, we fail to comply, regulatory authorities may initiate legal proceedings against us and our business may be harmed.
Failure to comply with these rules might also make it more difficult for us to obtain some types of insurance, including director and officer liability insurance, and we might be forced to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. The impact of these events could also make it more difficult for us to attract and retain qualified persons to serve on our board of directors, on committees of our board of directors or as members of senior management.
Item 1B. Unresolved Staff Comments.
None.
As part of our strategic partnership with UT Southwestern, we are provided with office space at UT Southwestern for administrative activities. In addition, in January 2021, we entered into a lease agreement for 15,000 square feet of administrative space in Dallas, Texas, pursuant to a lease agreement that expires approximately ten years after the date on which certain improvements to the office space have been made and it is tendered to us for possession, which we presently anticipate to be delivered on or about April 15, 2021. In December 2020, we entered into a lease agreement for approximately 187,500 square feet of a manufacturing facility in Durham, North Carolina, pursuant to a lease agreement that expires in September 2036. We have two options to extend the term of that lease, each for a period of an additional five years.
We believe that our facilities are suitable and adequate to meet our needs. We intend to add new facilities or expand existing facilities as we add employees, and we believe that suitable additional or substitute space will be available as needed to accommodate any such expansion of our operations.
We are not subject to any material legal proceedings. From time to time, we may be involved in various claims and legal proceedings relating to claims arising out of our operations. We are not currently a party to any legal proceedings that, in the opinion of our management, are likely to have a material adverse effect on our business. Regardless of outcome, litigation can have an adverse impact on us because of defense and settlement costs, diversion of management resources and other factors.
Item 4. Mine Safety Disclosures.
Not applicable.
90
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Information for Common Stock
Our common stock is listed on The Nasdaq Global Market under the symbol “TSHA.”
Holders of Record
As of March 3, 2021, we had 115 holders of record of our common stock, which excludes stockholders whose shares were held in nominee or street name by brokers. The actual number of common stockholders is greater than the number of record holders, and includes stockholders who are beneficial owners, but whose shares are held in street name by brokers and other nominees. This number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
Dividend Policy
We have never paid cash dividends on any of our capital stock and currently intend to retain our future earnings, if any, to fund the development and growth of our business.
Use of Proceeds from Initial Public Offering
On September 23, 2020, our Registration Statement on Form S-1, as amended (File No. 333-248559), was declared effective in connection with our initial public offering, pursuant to which we sold an aggregate of 9,050,000 shares of our common stock, including the full exercise of the underwriters’ option to purchase additional shares, at a price to the public of $20.00 per share. The joint book-running managers of our initial public offering were Goldman Sachs & Co. LLC, Morgan Stanley & Co. LLC, Jefferies LLC, and Chardan Capital Markets, LLC acted as lead manager. There has been no material change in the planned use of proceeds from our initial public offering as described in our prospectus filed pursuant to Rule 424(b)(4) under the Securities Act with the SEC on September 25, 2020.
Issuer Purchases of Equity Securities
None.
Item 6. Selected Financial Data.
We are a smaller reporting company as defined by Rule 12b-2 of the Exchange Act and are not required to provide the information required under this item.
91
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and related notes.
Overview
We are a patient-centric gene therapy company focused on developing and commercializing AAV-based gene therapies for the treatment of monogenic diseases of the CNS in both rare and large patient populations. We were founded in partnership with UT Southwestern to develop and commercialize transformative gene therapy treatments. Together with UT Southwestern, we are advancing a deep and sustainable product portfolio of 19 gene therapy product candidates, with exclusive options to acquire four additional development programs at no cost. By combining our management team’s proven experience in gene therapy drug development and commercialization with UT Southwestern’s world-class gene therapy research capabilities, we believe we have created a powerful engine to develop transformative therapies to dramatically improve patients’ lives. A Phase 1/2 clinical trial of TSHA-101 was initiated by Queen’s University under a CTA in Canada and Queen’s University expects to report preliminary safety and biomarker data in the second half of 2021 and preliminary clinical data by the end of 2021. We plan to submit an IND for TSHA-101 for the treatment of GM2 gangliosidosis to the FDA and initiate a Phase 1/2 clinical trial in the United States, each in the second half of 2021. In addition, we plan to submit INDs / CTAs for each of TSHA-102 in Rett syndrome and TSHA-104 in SURF1-associated Leigh syndrome in the second half of 2021 and one of the following programs in 2021: TSHA-103 in SLC6A1 haploinsufficiency, TSHA-105 in SLC13A5 deficiency, TSHA-111-LAFORIN in Lafora disease, TSHA-111-MALIN in Lafora disease, TSHA-112 in APBD and TSHA-119 in GM2 AB variant. We are also developing TSHA-118 for the treatment of CLN1 disease (one of the forms of Batten disease) and intend to initiate a Phase 1/2 clinical trial of TSHA-118 in 2021 under a currently open IND. In addition to our product pipeline candidates, we are building a platform of next-generation technologies to optimize key components of our AAV-based gene therapies, including redosing, transgene regulation and capsid development.
We have a limited operating history. Since our inception, our operations have focused on organizing and staffing our company, business planning, raising capital and entering into collaboration agreements for conducting preclinical research and development activities for our product candidates. All of our lead product candidates are still in the clinical or preclinical development stage. We do not have any product candidates approved for sale and have not generated any revenue from product sales. We have funded our operations through the sale of equity, raising an aggregate of $307.0 million of gross proceeds from our initial public offering and private placements of our convertible preferred stock.
Since our inception, we have incurred significant operating losses. Our net losses were $60.0 million for the year ended December 31, 2020 and $1.1 million for the period from September 20, 2019 (date of inception) through December 31, 2019. As of December 31, 2020, we had an accumulated deficit of $61.1 million. We expect to continue to incur significant expenses and operating losses for the foreseeable future. We anticipate that our expenses will increase significantly in connection with our ongoing activities, as we:
|
|
• |
continue to advance the preclinical and clinical development of our product candidates and preclinical and discovery programs; |
|
|
• |
conduct our clinical trial of TSHA-101, as well as initiate and complete additional clinical trials of TSHA-101, TSHA-118, TSHA-102, TSHA-104 and any other current and future product candidates that we advance; |
|
|
• |
seek regulatory approval for any product candidates that successfully complete clinical trials; |
|
|
• |
continue to develop our gene therapy product candidate pipeline and next-generation platforms; |
|
|
• |
scale up our clinical and regulatory capabilities; |
|
|
• |
manufacture cGMP material for clinical trials or potential commercial sales; |
|
|
• |
establish and validate a commercial-scale cGMP manufacturing facility; |
|
|
• |
establish a commercialization infrastructure and scale up internal and external manufacturing and distribution capabilities to commercialize any product candidates for which we may obtain regulatory approval; |
|
|
• |
adapt our regulatory compliance efforts to incorporate requirements applicable to marketed products; |
|
|
• |
maintain, expand and protect our intellectual property portfolio; |
|
|
• |
hire additional clinical, manufacturing quality control, regulatory, manufacturing and scientific and administrative personnel; |
|
|
• |
add operational, financial and management information systems and personnel, including personnel to support our product development and planned future commercialization efforts; and |
|
|
• |
incur additional legal, accounting and other expenses in operating as a public company. |
92
Research, Collaboration and License Agreement with The University of Texas Southwestern Medical Center
In November 2019, we entered into the UT Southwestern Agreement with The Board of Regents of the University of Texas System on behalf of UT Southwestern, as amended in April 2020.
In connection with the UT Southwestern Agreement, we obtained an exclusive, worldwide, royalty-free license under certain patent rights of UT Southwestern and a non-exclusive, worldwide, royalty-free license under certain know-how of UT Southwestern, in each case to make, have made, use, sell, offer for sale and import licensed products for use in certain specified indications. Additionally, we obtained a non-exclusive, worldwide, royalty-free license under certain patents and know-how of UT Southwestern for use in all human uses, with a right of first refusal to obtain an exclusive license under certain of such patent rights and an option to negotiate an exclusive license under other of such patent rights. We are required to use commercially reasonable efforts to develop, obtain regulatory approval for, and commercialize at least one licensed product.
In connection with the entry into the UT Southwestern Agreement, we issued to UT Southwestern 2,179,000 shares of our common stock. We do not have any future milestone or royalty obligations to UT Southwestern under the UT Southwestern Agreement, other than costs related to the maintenance of patents.
License Agreement with Queen’s University
In February 2020, we entered into the Queen’s University Agreement with Queen’s University. In connection with the Queen’s University Agreement, we obtained an exclusive, perpetual, worldwide, royalty-bearing license, with the right to grant sublicenses, under certain patent rights and know-how of Queen’s University, including certain improvements to the foregoing, to make, have made, use, offer for sale, sell and import licensed products and otherwise exploit such patents and know-how for use in certain specified indications. We also obtained an exclusive right of first negotiation to license certain next generation technology and improvements of Queen’s University that do not constitute an already-licensed improvement to the licensed technology.
In connection with the Queen’s University Agreement, we paid Queen’s University a one-time fee of $3.0 million as an upfront fee and approximately $0.2 million to reimburse Queen’s University for certain plasmid production costs. We are obligated to pay Queen’s University up to $10.0 million in the aggregate upon achievement of certain regulatory milestones and up to $10.0 million in the aggregate upon achievement of certain commercial milestones, a low single digit royalty on net sales of licensed products, subject to certain customary reductions, and a percentage of non-royalty sublicensing revenue ranging in the low double digits. Royalties are payable on a licensed product-by-licensed product basis and country-by-country basis until expiration of the last valid claim of a licensed patent covering such licensed product in such country and the expiration of any regulatory exclusivity for such licensed product in such country. Additionally, we are obligated to pay Queen’s University a low double-digit portion of any amounts received by us in connection with the sale of a PRV related to a licensed product, not to exceed a low eight-figure amount.
In connection with a separate research grant agreement with Queen’s University, we reimbursed Queen’s University for certain manufacturing production costs totaling $3.8 million.
License Agreement with Abeona (CLN1 Disease)
In August 2020, we entered into the Abeona CLN1 Agreement with Abeona. In connection with the Abeona CLN1 Agreement, we obtained an exclusive, worldwide, royalty-bearing license, with the right to grant sublicenses under certain patents, know-how and materials originally developed by the University of North Carolina at Chapel Hill and Abeona to research, develop, manufacture, have manufactured, use, and commercialize licensed products for gene therapy for the prevention, treatment, or diagnosis of CLN1 Disease (one of the forms of Batten disease) in humans.
93
In connection with the license grant, we paid Abeona a one-time upfront license fee of $3.0 million. We are obligated to pay Abeona up to $26.0 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed product and high single-digit royalties on net sales of licensed products. Royalties are payable on a licensed product-by-licensed product and country-by-country basis until the latest of the expiration or revocation or complete rejection of the last licensed patent covering such licensed product in the country where the licensed product is sold, the loss of market exclusivity in such country where the product is sold, or, if no licensed product exists in such country and no market exclusivity exists in such country, ten years from first commercial sale of such licensed product in such country. In addition, concurrent with the Abeona CLN1 Agreement we entered into a purchase and reimbursement agreement with Abeona, pursuant to which we purchased specified inventory from Abeona and reimbursed Abeona for certain research and development costs previously incurred for total consideration of $4.0 million.
The Abeona CLN1 Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. We may terminate the agreement for convenience upon specified prior written notice to Abeona.
License Agreement with Abeona (Rett Syndrome)
In October 2020, we entered into the Abeona Rett Agreement with Abeona pursuant to which we obtained an exclusive, worldwide, royalty-bearing license, with the right to grant sublicenses under certain patents, know-how and materials originally developed by the University of North Carolina at Chapel Hill, the University of Edinburgh and Abeona to research, develop, manufacture, have manufactured, use, and commercialize licensed products for gene therapy and the use of related transgenes for Rett syndrome.
Subject to certain obligations of Abeona, we are required to use commercially reasonable efforts to develop at least one licensed product and commercialize at least one licensed product in the United States.
In connection with the Abeona Rett Agreement, we paid Abeona a one-time upfront license fee of $3.0 million. We are obligated to pay Abeona up to $26.5 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed product and high single-digit royalties on net sales of licensed products. Royalties are payable on a licensed product-by-licensed product and country-by-country basis until the latest of the expiration or revocation or complete rejection of the last licensed patent covering such licensed product in the country where the licensed product is sold, the loss of market exclusivity in such country where the product is sold, or, if no licensed product exists in such country and no market exclusivity exists in such country, ten years from first commercial sale of such licensed product in such country.
The Abeona Rett Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. We may terminate the agreement for convenience upon specified prior written notice to Abeona.
Impact of COVID-19 on Our Business
We have been actively monitoring the COVID-19 situation and its impact globally. Our financial results for the year ended December 31, 2020 were not impacted by COVID-19, and we currently do not expect any material impact on our financial results in 2021. We believe the remote working arrangements and travel restrictions imposed by various governmental jurisdictions have had limited impact on our ability to maintain internal operations during the year ended December 31, 2020. The extent to which COVID-19 may impact our business and operations will depend on future developments that are highly uncertain and cannot be predicted with confidence, such as the duration of the outbreak, the effectiveness of actions to contain and treat COVID-19 and the availability, timing and effectiveness of a vaccine, both domestically and globally. We cannot presently predict the scope and severity of any potential business shutdowns or disruptions, including to our planned clinical trials and preclinical studies. Any such shutdowns or other business interruptions could result in material and negative effects to our ability to conduct our business in the manner and on the timelines presently planned, which could have a material adverse impact on our business, results of operation and financial condition.
94
Components of Results of Operations
Revenue
To date, we have not recognized any revenue from any sources, including from product sales, and we do not expect to generate any revenue from the sale of products, if approved, in the foreseeable future. If our development efforts for our product candidates are successful and result in regulatory approval, or license agreements with third parties, we may generate revenue in the future from product sales. However, there can be no assurance as to when we will generate such revenue, if at all.
Operating Expenses
Research and Development Expenses
Research and development expenses primarily consist of preclinical development of our product candidates and discovery efforts, including conducting preclinical studies, manufacturing development efforts, preparing for clinical trials and activities related to regulatory filings for our product candidates. Research and development expenses are recognized as incurred and payments made prior to the receipt of goods or services to be used in research and development are capitalized until the goods or services are received. Costs incurred in obtaining technology licenses through asset acquisitions are charged to research and development expense if the licensed technology has not reached technological feasibility and has no alternative future use. Research and development expenses include or could include:
|
|
• |
employee-related expenses, including salaries, bonuses, benefits, stock-based compensation, other related costs for those employees involved in research and development efforts; |
|
|
• |
external research and development expenses incurred under agreements with consultants, CROs, investigative sites and consultants to conduct our preclinical studies; |
|
|
• |
costs related to manufacturing material for our preclinical studies and clinical trials, including fees paid to CMOs; |
|
|
• |
laboratory supplies and research materials; |
|
|
• |
costs related to compliance with regulatory requirements; and |
|
|
• |
facilities, depreciation and other allocated expenses, which include direct and allocated expenses for rent, maintenance of facilities, insurance and equipment. |
Research and development activities are central to our business model. We have historically not tracked our research and development expenses on a program-by-program basis as such costs are deployed across multiple projects under development. Product candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical development, primarily due to the increased size and duration of later-stage clinical trials. We plan to substantially increase our research and development expenses for the foreseeable future as we continue the development of our product candidates and manufacturing processes and conduct discovery and research activities for our preclinical programs. We cannot determine with certainty the timing of initiation, the duration or the completion costs of current or future preclinical studies and clinical trials of our product candidates due to the inherently unpredictable nature of preclinical and clinical development. Clinical and preclinical development timelines, the probability of success and development costs can differ materially from expectations. We anticipate that we will make determinations as to which product candidates to pursue and how much funding to direct to each product candidate on an ongoing basis in response to the results of ongoing and future preclinical studies and clinical trials, regulatory developments and our ongoing assessments as to each product candidate’s commercial potential. We will need to raise substantial additional capital in the future. Our clinical development costs are expected to increase significantly as we commence clinical trials. Our future expenses may vary significantly each period based on factors such as:
|
|
• |
expenses incurred to conduct preclinical studies required to advance our product candidates into clinical development; |
|
|
• |
per patient trial costs, including based on the number of doses that patients received; |
|
|
• |
the number of patients who enroll in each trial; |
|
|
• |
the number of trials required for approval; |
|
|
• |
the number of sites included in the trials; |
|
|
• |
the countries in which the trials are conducted; |
|
|
• |
the length of time required to enroll eligible patients; |
|
|
• |
the drop-out or discontinuation rates of patients; |
|
|
• |
potential additional safety monitoring requested by regulatory agencies; |
|
|
• |
the duration of patient participation in the trials and follow-up; |
|
|
• |
the phase of development of the product candidate; |
|
|
• |
third-party contractors failing to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
95
|
|
• |
regulators or IRBs requiring that we or our investigators suspend or terminate clinical development for various reasons, including noncompliance with regulatory requirements or a finding that the participants are being exposed to unacceptable health risks; and |
|
|
• |
the efficacy and safety profile of our product candidates. |
General and Administrative Expenses
General and administrative expenses consist or will consist principally of salaries and related costs for personnel in executive and administrative functions, including stock-based compensation, travel expenses and recruiting expenses. Other general and administrative expenses include professional fees for legal, consulting, accounting and audit and tax-related services and insurance costs. We began paying salaries and related costs for personnel during the quarter ended June 30, 2020 and granted equity awards to employees and directors during the year ended December 31, 2020.
We anticipate that our general and administrative expenses will increase in the future as we increase our headcount to support our expanded infrastructure, as well as the initiation and continuation of our preclinical studies and clinical trials for our product candidates. We also anticipate that our general and administrative expenses will increase as a result of payments for accounting, audit, legal, consulting services, as well as costs associated with maintaining compliance with Nasdaq listing rules and SEC requirements, director and officer liability insurance, investor and public relations activities and other expenses associated with operating as a public company. We anticipate the additional costs for these services will increase our general and administrative expenses by between $6.0 million and $7.0 million on an annual basis, including the cost of director and officer liability insurance.
Results of Operations
Results of Operations for the Year Ended December 31, 2020 and the Period from September 20, 2019 (date of inception) through December 31, 2019
The following table summarizes our results of operations for the year ended December 31, 2020 and the period from September 20, 2019 (date of inception) through December 31, 2019 (in thousands):
|
|
|
For the Year Ended December 31, 2020 |
|
|
Period from September 20, 2019 (date of inception) through December 31, 2019 |
|
||
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
31,893 |
|
|
$ |
987 |
|
|
General and administrative |
|
|
11,109 |
|
|
|
128 |
|
|
Total operating expenses |
|
|
43,002 |
|
|
|
1,115 |
|
|
Loss from operations |
|
|
(43,002 |
) |
|
|
(1,115 |
) |
|
Other expense: |
|
|
|
|
|
|
|
|
|
Change in fair value of preferred stock tranche liability |
|
|
(17,030 |
) |
|
|
— |
|
|
Interest income |
|
|
49 |
|
|
|
— |
|
|
Interest expense |
|
|
(28 |
) |
|
|
— |
|
|
Total other expense, net |
|
|
(17,009 |
) |
|
|
— |
|
|
Net loss |
|
$ |
(60,011 |
) |
|
$ |
(1,115 |
) |
Research and Development Expenses
Research and development expenses were $31.9 million for the year ended December 31, 2020, compared to $1.0 million for the period from September 20, 2019 (date of inception) through December 31, 2019. The $30.9 million increase was primarily attributable to $10.0 million of expenses recognized pursuant to the Abeona CLN1 and Rett IP License Agreements, $6.8 million pursuant to the Queen’s University Agreement, which included $3.8 million related to the manufacture of clinical trial materials and a $3.0 million licensing fee. Additionally, we incurred an increase of $3.2 million related to the UT Southwestern Agreement and $1.7 million in other sponsored research agreements for our various product candidates. Additionally, we incurred $2.9 million in research and development manufacturing and other raw material purchases, which included a $1.7 million cell line licensing fee. We also incurred $1.6 million for regulatory and clinical consulting, $1.0 million for all other research and development consulting fees including technical operations support, and employee compensation and benefits expenses of $3.1 million, which included $1.2 million of non-cash stock-based compensation. All other spending for research and development activities totaled $0.6 million.
General and Administrative Expenses
General and administrative expenses were $11.1 million for the year ended December 31, 2020, compared to $0.1 million for the period from September 20, 2019 (date of inception) through December 31, 2019. The increase of approximately $11.0 million was
96
primarily attributable to $5.6 million of compensation and benefits related to new hires, which included $2.2 million of non-cash stock-based compensation. Additionally, we incurred $2.1 million in consulting fees, which included patient advocacy consulting fees and personnel recruiting expenses. We also incurred $1.8 million of professional fees, which included $1.1 million in legal expenses related to general corporate matters and $0.7 million in accounting and auditing fees. Finally, we incurred $1.0 million related to insurance expenses and $0.5 million of marketing expenses and other general administrative expenses.
Other Expense
Change in Fair Value of Preferred Stock Tranche Liability
We determined that our obligation to issue, and the investors’ right to purchase, additional shares of Series A convertible preferred stock pursuant to the milestone closings represented a freestanding financial instrument, or the tranche liability. The tranche liability was initially recorded at fair value. We concluded that the tranche liability met the definition of a freestanding financial instrument, as it was legally detachable and separately exercisable from the initial closing of the Series A convertible preferred stock.
On June 30, 2020, ahead of the anticipated closing of the Series B preferred stock financing at a purchase price of $17.00 per share on July 2, 2020, certain investors elected to exercise in full their options to purchase their pro-rata portion of the milestone shares prior to our achievement of the clinical milestones and purchased 200,000 shares of Series A convertible preferred stock. We remeasured the fair value of the entire tranche liability at June 30, 2020, and recognized a non-cash expense of approximately $17.0 million. The tranche liability was extinguished upon the issuance of the Series A milestone shares on July 1, 2020 and July 2, 2020, and no additional changes in fair value were recorded.
Liquidity and Capital Resources
Overview
Since our inception, we have not generated any revenue and have incurred significant operating losses. As of December 31, 2020, we had cash and cash equivalents of $251.3 million. We have funded our operations through equity financings, raising an aggregate of $307.0 million in gross proceeds from our initial public offering and private placements of convertible preferred stock. Specifically, between March and July 2020, we closed on the sale of an aggregate of 10,000,000 shares of Series A convertible preferred stock for gross proceeds of $30.0 million. In July and August 2020, we closed on the sale of an aggregate of 5,647,048 shares of Series B convertible preferred stock for gross proceeds of $96.0 million. In September 2020, we raised gross proceeds of $181.0 million in our initial public offering.
Funding Requirements
To date, we have not generated any revenues from the commercial sale of approved drug products, and we do not expect to generate substantial revenue for at least the next few years. If we fail to complete the development of our product candidates in a timely manner or fail to obtain their regulatory approval, our ability to generate future revenue will be compromised. We do not know when, or if, we will generate any revenue from our product candidates, and we do not expect to generate significant revenue unless and until we obtain regulatory approval of, and commercialize, our product candidates. We expect our expenses to increase in connection with our ongoing activities, particularly as we continue the research and development of, initiate clinical trials of and seek marketing approval for our product candidates. In addition, if we obtain approval for any of our product candidates, we expect to incur significant commercialization expenses related to sales, marketing, manufacturing and distribution. Furthermore, we expect to incur additional costs associated with operating as a public company. We anticipate that we will need substantial additional funding in connection with our continuing operations. If we are unable to raise capital when needed or on attractive terms, we could be forced to delay, reduce or eliminate our research and development programs or future commercialization efforts.
We believe that our existing cash and cash equivalents will enable us to fund our operating expenses and capital requirements into 2023. We intend to devote our existing cash and cash equivalents to the clinical and preclinical development of our product candidates. We have based this estimate on assumptions that may prove to be imprecise, and we could utilize our available capital resources sooner than we expect.
Because of the numerous risks and uncertainties associated with research, development and commercialization of biological products, we are unable to estimate the exact amount of our operating capital requirements. Our future funding requirements will depend on many factors, including, but not limited to:
|
|
• |
the scope, progress, costs and results of discovery, preclinical development, laboratory testing and clinical trials for TSHA-101, TSHA-118, TSHA-102, TSHA-104 and any current and future product candidates that we advance; |
|
|
• |
the extent to which we develop, in-license or acquire other product candidates and technologies in our gene therapy product candidate pipeline; |
97
|
|
• |
the number and development requirements of product candidates that we may pursue; |
|
|
• |
the costs, timing and outcome of regulatory review of our product candidates; |
|
|
• |
our headcount growth and associated costs as we expand our research and development capabilities and establish a commercial infrastructure; |
|
|
• |
the costs of establishing and maintaining our own commercial-scale cGMP manufacturing facility; |
|
|
• |
the costs and timing of future commercialization activities, including product manufacturing, marketing, sales, and distribution, for any of our product candidates for which we receive marketing approval; |
|
|
• |
the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending any intellectual property-related claims; |
|
|
• |
the revenue, if any, received from commercial sales of our product candidates for which we receive marketing approval; and |
|
|
• |
the costs of operating as a public company. |
Identifying potential product candidates and conducting preclinical studies and clinical trials is a time-consuming, expensive and uncertain process that takes many years to complete, and we may never generate the necessary data or results required to obtain marketing approval and achieve product sales. In addition, our product candidates, if approved, may not achieve commercial success. Our commercial revenues, if any, will be derived from sales of product candidates that we do not expect to be commercially available in the near term, if at all. Accordingly, we will need to continue to rely on additional financing to achieve our business objectives. Adequate additional financing may not be available to us on acceptable terms, or at all. To the extent that we raise additional capital through the sale of equity or convertible debt securities, the terms of these equity securities or this debt may restrict our ability to operate. Any future debt financing and equity financing, if available, may involve agreements that include covenants limiting and restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures, entering into profit-sharing or other arrangements or declaring dividends. If we raise additional funds through collaborations, strategic alliances or marketing, distribution or licensing arrangements with third parties, we may be required to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or to grant licenses on terms that may not be favorable to us.
We are continuing to assess the effect that the COVID-19 pandemic may have on our business and operations. The extent to which COVID-19 may impact our business and operations will depend on future developments that are highly uncertain and cannot be predicted with confidence, such as the duration of the outbreak, the duration and effect of business disruptions and the short-term effects and ultimate effectiveness of the travel restrictions, quarantines, social distancing requirements and business closures in the United States and other countries to contain and treat the disease and the availability, timing and effectiveness of a vaccine, both domestically and globally. While the potential economic impact brought by, and the duration of, COVID-19 may be difficult to assess or predict, a widespread pandemic could result in significant disruption of global financial markets, reducing our ability to access capital, which could in the future negatively affect our liquidity. In addition, a recession or market correction resulting from the spread of COVID-19 could materially affect our business and the value of our common stock.
Cash Flows
The following table shows a summary of our cash flows for the year ended December 31, 2020 and the period from September 20, 2019 (date of inception) through December 31, 2019 (in thousands):
|
|
|
For the Year Ended December 31, 2020 |
|
|
Period from September 20, 2019 (date of inception) through December 31, 2019 |
|
||
|
Net cash used in operating activities |
|
$ |
(30,729 |
) |
|
$ |
— |
|
|
Net cash used in investing activities |
|
|
(9,082 |
) |
|
|
— |
|
|
Net cash provided by financing activities |
|
|
291,064 |
|
|
|
— |
|
|
Net change in cash and cash equivalents |
|
$ |
251,253 |
|
|
$ |
— |
|
Operating Activities
For the year ended December 31, 2020, our net cash used in operating activities of $30.7 million primarily consisted of a net loss of $60.0 million, primarily attributable to our spending on research and development expenses. The net loss of $60.0 million was partially offset by $29.4 million in adjustments for non-cash items, primarily due to the change in the fair value of the preferred stock tranche liability of $17.0 million and stock-based compensation expense of $3.4 million, as well as the upfront payment to acquire the license rights pursuant to the Queen’s University Agreement for $3.0 million, and the upfront payments related to the Abeona CLN1 and Rett Agreements for $3.0 million each, all of which were recorded as a component of research and development expenses and are reported as investing cash outflows.
98
Prior to the issuance and sale of our Series A convertible preferred stock in March 2020, we had no cash. Outstanding accrued expenses of $0.2 million as of December 31, 2019 were paid in 2020 following the receipt of the proceeds from the issuance and sale of our Series A convertible preferred stock.
Investing Activities
During the year ended December 31, 2020, investing activities used $9.1 million of cash primarily attributable to the upfront fees paid pursuant to the Queen’s University Agreement, the Abeona CLN1 Agreement and the Abeona Rett Agreement.
Financing Activities
During the year ended December 31, 2020, financing activities provided $291.1 million of cash, which was primarily attributable to the receipt of $165.9 million in net proceeds from our initial public offering, $95.8 million in net proceeds from the sale of our Series B convertible preferred stock and $29.4 million in net proceeds from the sale of our Series A convertible preferred stock.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined in the rules and regulations of the SEC.
Critical Accounting Policies and Significant Judgments and Estimates
This management’s discussion and analysis of our financial condition and results of operations is based on our financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles, or U.S. GAAP. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, and expenses and the disclosure of contingent assets and liabilities in our financial statements. In accordance with U.S. GAAP, we evaluate our estimates and judgments on an ongoing basis, including those related to research and development expenses, the preferred stock tranche liability and stock-based compensation. We base our estimates on historical experience, known trends and events, and various other factors that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
We define our critical accounting policies as those accounting principles that require us to make subjective estimates and judgments about matters that are uncertain and are likely to have a material impact on our financial condition and results of operations, as well as the specific manner in which we apply those principles. While our significant accounting policies are more fully described in Note 2 to our audited consolidated financial statements located in Part IV, Item 15 of this Annual Report on Form 10-K, we believe the following are the critical accounting policies used in the preparation of our financial statements that require significant estimates and judgments.
Research and Development Costs
We have entered into research and development contracts with research institutions and other companies. These agreements are generally cancelable, and related payments are recorded as research and development expenses as incurred. Payments for these activities are based on the terms of the individual agreements, which may differ from the pattern of costs incurred, and are reflected on the balance sheet as prepaid or accrued expenses. We record accruals for estimated ongoing research costs. When evaluating the adequacy of the accrued liabilities, we analyze progress of the studies, including the phase or completion of events, invoices received and contracted costs.
Research and development costs primarily consist of payroll, stock-based compensation, certain manufacturing costs, laboratory costs and other supplies, and the cost to acquire third-party licenses.
Costs incurred in obtaining technology licenses through asset acquisitions are charged to research and development expense if the licensed technology has not reached technological feasibility and has no alternative future use.
Stock‑Based Compensation
We account for all stock-based payments to employees and non-employees, including grants of stock options, restricted stock awards, or “RSAs” and restricted stock units or, “RSUs” based on their respective grant date fair values. We estimate the fair value of stock option grants using the Black-Scholes option pricing model, which is affected principally by the estimated fair value of shares of our common stock and requires management to make a number of other assumptions, including the expected life of the option, the volatility of the underlying shares, the risk-free interest rate and expected dividends. Expected volatility is based on the historical share volatility of a set of comparable publicly traded companies over a period of time equal to the expected term of the options. Due to the lack of historical exercise history, the expected term of our stock options is determined using the “simplified” method. The risk-free interest rate is
99
determined by reference to the U.S. Treasury yield curve in effect at the time of grant of the award for time periods approximately equal to the expected term of the award. Expected dividend yield is zero based on the fact that we have never paid cash dividends and do not expect to pay any cash dividends in the foreseeable future.
Prior to September 23, 2020, the fair value of common stock underlying our stock options, RSAs and RSUs was estimated by our board of directors considering, among other things, contemporaneous valuations of our common stock prepared by unrelated third-party valuation firms. After the IPO, the fair value of common stock is based on the closing price of our common stock on the Nasdaq Global Select Market as reported on the date of the grant.
The RSAs and RSUs are valued based on the fair value of our common stock on the date of grant. The Company expenses stock-based compensation related to stock options, RSAs and RSUs over the requisite service period using the straight-line method. All stock-based compensation costs are recorded in research and development expense or general and administrative expense in the consolidated statements of operations based upon the respective employee’s roles within our Company. Forfeitures are recorded as they occur.
Preferred Stock Tranche liability
We determined that our obligation to issue, and the investors’ right to purchase, additional shares of Series A convertible preferred stock pursuant to the milestone closings represent a freestanding financial instrument, or the tranche liability. The tranche liability was initially recorded at fair value. The proceeds from the sale of the convertible preferred stock are first allocated to the fair value of the tranche liability, with the remaining proceeds from the sale of the convertible preferred stock allocated to the Series A convertible preferred stock. The tranche liability is remeasured at each reporting period and upon the exercise or expiration of the obligation, with gains and losses arising from subsequent changes in its fair value recognized as a component of other expense in the consolidated statements of operations. At the time of the exercise or expiration of the tranche liability, any remaining value of the tranche liability is reclassified to convertible preferred stock on the consolidated balance sheet. Between June 30, 2020 and July 2, 2020, all of the 4,000,000 Milestone Shares were issued and the related tranche liability was extinguished in its entirety, and we reclassified the entire tranche liability of $18.1 million to convertible preferred stock on the consolidated balance sheets.
We estimated the fair value of the tranche liability using a Monte Carlo simulation at the initial issuance date. As of March 4, 2020, the simulations occurred based on our implied aggregate equity value derived from the Series A convertible preferred stock offering price of $3.00 per share, along with, in part, the following subjective assumptions: risk-free rate of 0.59%, an expected volatility of 80%, the expected term to a liquidity event of one year and a 60% probability of achieving the clinical milestones and timing thereof. Subsequently, we estimated the fair value of the tranche liability using a backsolve approach at June 30, 2020, which was calculated based on our aggregate equity value derived from the Series B convertible preferred stock offering price of $17.00 per share. The subsequent remeasurement also considered, in part, a risk-free rate of 0.17%, an expected volatility of 80% and the expected term to a liquidity event of 0.5 years.
100
Recent Accounting Pronouncements
See Note 2 to our audited consolidated financial statements located in Part IV, Item 15 of this Annual Report on Form 10-K for a description of recent accounting pronouncements applicable to our financial statements.
Emerging Growth Company and Smaller Reporting Company Status
In April 2012, the JOBS Act was enacted. Section 107 of the JOBS Act provides that an “emerging growth company” can take advantage of the extended transition period provided in Section 7(a)(2)(B) of the Securities Act of 1933, as amended, for complying with new or revised accounting standards. Thus, an emerging growth company can delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We elected the extended transition period for complying with new or revised accounting standards, which delays the adoption of these accounting standards until they would apply to private companies. In addition, as an emerging growth company, we may take advantage of specified reduced disclosure and other requirements that are otherwise applicable generally to public companies. These provisions include:
|
|
• |
an exception from compliance with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, as amended; |
|
|
• |
reduced disclosure about our executive compensation arrangements in our periodic reports, proxy statements and registration statements; |
|
|
• |
exemptions from the requirements of holding non-binding advisory votes on executive compensation or golden parachute arrangements; and |
|
|
• |
an exemption from compliance with the requirements of the Public Company Accounting Oversight Board regarding the communication of critical audit matters in the auditor’s report on financial statements. We may take advantage of these provisions until we no longer qualify as an emerging growth company. We will cease to qualify as an emerging growth company on the date that is the earliest of: (i) December 31, 2025, (ii) the last day of the fiscal year in which we have more than $1.07 billion in total annual gross revenues, (iii) the date on which we are deemed to be a “large accelerated filer” under the rules of the SEC, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the prior June 30th, or (iv) the date on which we have issued more than $1.0 billion of non-convertible debt over the prior three-year period. We may choose to take advantage of some but not all of these reduced reporting burdens. We have taken advantage of certain reduced reporting requirements in this Annual Report on Form 10-K and our other filings with the SEC. Accordingly, the information contained herein may be different than you might obtain from other public companies in which you hold equity interests. |
We are also a “smaller reporting company,” meaning that the market value of our shares held by non-affiliates is less than $700 million and our annual revenue was less than $100 million during the most recently completed fiscal year. We may continue to be a smaller reporting company if either (i) the market value of our shares held by non-affiliates is less than $250 million or (ii) our annual revenue was less than $100 million during the most recently completed fiscal year and the market value of our shares held by non-affiliates is less than $700 million. If we are a smaller reporting company at the time we cease to be an emerging growth company, we may continue to rely on exemptions from certain disclosure requirements that are available to smaller reporting companies. Specifically, as a smaller reporting company, we may choose to present only the two most recent fiscal years of audited financial statements in our Annual Report on Form 10-K and, similar to emerging growth companies, smaller reporting companies have reduced disclosure obligations regarding executive compensation.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
We are a smaller reporting company as defined by Rule 12b-2 of the Exchange Act and are not required to provide the information required under this item.
101
Item 8. Financial Statements and Supplementary Data.
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Taysha Gene Therapies, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Taysha Gene Therapies, Inc. (the “Company”) as of December 31, 2020 and 2019, the related consolidated statements of operations, stockholders' equity (deficit), and cash flows, for the year ended December 31, 2020 and for the period from September 20, 2019 (date of inception) through December 31, 2019, and the related notes (collectively referred to as the "financial statements"). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2020 and 2019, and the results of its operations and its cash flows for the year ended December 31, 2020 and for the period from September 20, 2019 (date of inception) through December 31, 2019, in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Deloitte & Touche LLP
Dallas, Texas
March 3, 2021
We have served as the Company's auditor since 2020.
F-1
Consolidated Balance Sheets
(in thousands, except share and per share data)
|
|
|
December 31, |
|
|
December 31, |
|
||
|
|
|
2020 |
|
|
2019 |
|
||
|
ASSETS |
|
|
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
251,253 |
|
|
$ |
— |
|
|
Prepaid expenses and other current assets |
|
|
6,626 |
|
|
|
— |
|
|
Deferred offering costs |
|
|
— |
|
|
|
15 |
|
|
Total current assets |
|
|
257,879 |
|
|
|
15 |
|
|
Deferred lease asset |
|
|
715 |
|
|
|
— |
|
|
Property and equipment, net |
|
|
287 |
|
|
|
— |
|
|
Total assets |
|
$ |
258,881 |
|
|
$ |
15 |
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY (DEFICIT) |
|
|
|
|
|
|
|
|
|
Current liabilities |
|
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
1,994 |
|
|
$ |
— |
|
|
Accrued expenses and other current liabilities |
|
|
5,135 |
|
|
|
150 |
|
|
Total current liabilities |
|
|
7,129 |
|
|
|
150 |
|
|
Other non-current liabilities |
|
|
450 |
|
|
|
— |
|
|
Total liabilities |
|
|
7,579 |
|
|
|
150 |
|
|
Commitments and contingencies - Note 11 |
|
|
|
|
|
|
|
|
|
Stockholders' equity (deficit) |
|
|
|
|
|
|
|
|
|
Preferred stock, $0.00001 par value per share; 10,000,000 shares authorized and no shares issued and outstanding as of December 31, 2020; no shares authorized, issued and outstanding as of December 31, 2019 |
|
|
— |
|
|
|
— |
|
|
Common stock, $0.00001 par value per share; 200,000,000 shares authorized and 37,761,435 issued and outstanding as of December 31, 2020; 10,895,000 shares authorized, 10,894,999 issued and outstanding as of December 31, 2019 |
|
|
— |
|
|
|
— |
|
|
Additional paid-in capital |
|
|
312,428 |
|
|
|
980 |
|
|
Accumulated deficit |
|
|
(61,126 |
) |
|
|
(1,115 |
) |
|
Total stockholders’ equity (deficit) |
|
|
251,302 |
|
|
|
(135 |
) |
|
Total liabilities and stockholders' equity (deficit) |
|
$ |
258,881 |
|
|
$ |
15 |
|
The accompanying notes are an integral part of these consolidated financial statements.
F-2
Consolidated Statements of Operations
(in thousands, except share and per share data)
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
31,893 |
|
|
$ |
987 |
|
|
General and administrative |
|
|
11,109 |
|
|
|
128 |
|
|
Total operating expenses |
|
|
43,002 |
|
|
|
1,115 |
|
|
Loss from operations |
|
|
(43,002 |
) |
|
|
(1,115 |
) |
|
Other expense: |
|
|
|
|
|
|
|
|
|
Change in fair value of preferred stock tranche liability |
|
|
(17,030 |
) |
|
|
— |
|
|
Interest income |
|
|
49 |
|
|
|
— |
|
|
Interest expense |
|
|
(28 |
) |
|
|
— |
|
|
Total other expense, net |
|
|
(17,009 |
) |
|
|
— |
|
|
Net loss |
|
$ |
(60,011 |
) |
|
$ |
(1,115 |
) |
|
Net loss per common share, basic and diluted |
|
$ |
(3.40 |
) |
|
$ |
(0.12 |
) |
|
Weighted average common shares outstanding, basic and diluted |
|
|
17,665,683 |
|
|
|
9,625,679 |
|
The accompanying notes are an integral part of these consolidated financial statements
F-3
Consolidated Statements of Convertible Preferred Stock and Stockholders’ Equity (Deficit)
(in thousands, except share data)
|
|
|
Series A |
|
|
Series B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total |
|
|||||||||||
|
|
|
Convertible |
|
|
Convertible |
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
|
|
|
|
|
Stockholders' |
|
||||||||||||
|
|
|
Preferred Stock |
|
|
Preferred Stock |
|
|
|
Common Stock |
|
|
Paid-in |
|
|
Accumulated |
|
|
Equity |
|
||||||||||||||||||
|
|
|
Shares |
|
|
Amount |
|
|
Shares |
|
|
Amount |
|
|
|
Shares |
|
|
Amount |
|
|
Capital |
|
|
Deficit |
|
|
(Deficit) |
|
|||||||||
|
Balance as of September 20, 2019 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(date of inception) |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
|
|
|
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
$ |
— |
|
|
Issuance of Founders Shares |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
8,715,999 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Issuance of common stock for UT Southwestern license |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
2,179,000 |
|
|
|
— |
|
|
|
980 |
|
|
|
— |
|
|
|
980 |
|
|
Net loss |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
|
|
— |
|
|
|
(1,115 |
) |
|
|
(1,115 |
) |
|
Balance as of December 31, 2019 |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
|
|
|
10,894,999 |
|
|
$ |
— |
|
|
$ |
980 |
|
|
$ |
(1,115 |
) |
|
$ |
(135 |
) |
|
Issuance of Series A convertible preferred stock, net of offering costs of $605 and issuance of preferred stock tranche liability of $1,050 |
|
|
10,000,000 |
|
|
|
28,345 |
|
|
|
— |
|
|
|
— |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Issuance of Series B convertible preferred stock, net of offering costs of $185 |
|
|
|
|
|
|
|
|
|
|
5,647,048 |
|
|
|
95,815 |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Reclassification of preferred stock tranche liability upon issuance of Series A milestone shares |
|
|
— |
|
|
|
18,080 |
|
|
|
— |
|
|
|
— |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Conversion of Series A and Series B convertible preferred stock to common stock |
|
|
(10,000,000 |
) |
|
|
(46,425 |
) |
|
|
(5,647,048 |
) |
|
|
(95,815 |
) |
|
|
|
17,047,378 |
|
|
|
— |
|
|
|
142,240 |
|
|
|
— |
|
|
|
142,240 |
|
|
Issuance of shares of common stock in initial public offering, net of offering costs and underwriting discounts and commissions of $15,145 |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
9,050,000 |
|
|
|
— |
|
|
|
165,854 |
|
|
|
— |
|
|
|
165,854 |
|
|
Issuance of restricted stock award |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
769,058 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stock-based compensation |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
— |
|
|
|
— |
|
|
|
3,354 |
|
|
|
— |
|
|
|
3,354 |
|
|
Net loss |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(60,011 |
) |
|
|
(60,011 |
) |
|
Balance as of December 31, 2020 |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
|
|
|
37,761,435 |
|
|
$ |
— |
|
|
$ |
312,428 |
|
|
$ |
(61,126 |
) |
|
$ |
251,302 |
|
The accompanying notes are an integral part of these consolidated financial statements
F-4
Consolidated Statements of Cash Flows
(in thousands)
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Cash flows from operating activities |
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(60,011 |
) |
|
$ |
(1,115 |
) |
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
Depreciation expense |
|
|
9 |
|
|
|
— |
|
|
Change in fair value of preferred stock tranche liability |
|
|
17,030 |
|
|
|
— |
|
|
Research and development license expense |
|
|
9,000 |
|
|
|
980 |
|
|
Stock-based compensation |
|
|
3,354 |
|
|
|
— |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
Prepaid expenses and other assets |
|
|
(6,585 |
) |
|
|
— |
|
|
Accounts payable |
|
|
1,961 |
|
|
|
— |
|
|
Accrued expenses and other liabilities |
|
|
4,513 |
|
|
|
135 |
|
|
Net cash used in operating activities |
|
|
(30,729 |
) |
|
|
— |
|
|
Cash flows from investing activities |
|
|
|
|
|
|
|
|
|
Purchase of research and development licenses |
|
|
(9,000 |
) |
|
|
— |
|
|
Purchase of property and equipment |
|
|
(82 |
) |
|
|
— |
|
|
Net cash used in investing activities |
|
|
(9,082 |
) |
|
|
— |
|
|
Cash flows from financing activities |
|
|
|
|
|
|
|
|
|
Proceeds from issuance of common stock in initial public offering, net of underwriting discounts and commission and other offering costs |
|
|
165,854 |
|
|
|
— |
|
|
Proceeds from issuances of Series A convertible preferred stock, net of issuance costs |
|
|
29,395 |
|
|
|
— |
|
|
Proceeds from issuance of Series B convertible preferred stock, net of issuance costs |
|
|
95,815 |
|
|
|
— |
|
|
Proceeds from notes payable to related party |
|
|
1,673 |
|
|
|
— |
|
|
Repayment of notes payable to related party |
|
|
(1,673 |
) |
|
|
— |
|
|
Net cash provided by financing activities |
|
|
291,064 |
|
|
|
— |
|
|
Net increase in cash and cash equivalents |
|
|
251,253 |
|
|
|
— |
|
|
Cash at the beginning of the period |
|
|
— |
|
|
|
— |
|
|
Cash at the end of the period |
|
$ |
251,253 |
|
|
$ |
— |
|
|
Supplemental disclosure of cash flow information: |
|
|
|
|
|
|
|
|
|
Cash paid for interest |
|
$ |
28 |
|
|
$ |
— |
|
|
Supplemental disclosure of noncash investing and financing activities: |
|
|
|
|
|
|
|
|
|
Property and equipment in accounts payable and accrued expenses |
|
$ |
214 |
|
|
$ |
— |
|
|
Reclassification of preferred stock tranche liability upon share issuance |
|
$ |
18,080 |
|
|
$ |
— |
|
|
Allocation of preferred stock tranche liability |
|
$ |
1,050 |
|
|
$ |
— |
|
|
Conversion of Series A and Series B convertible preferred stock to common stock |
|
$ |
142,240 |
|
|
$ |
— |
|
|
Deferred offering costs not yet paid |
|
$ |
— |
|
|
$ |
15 |
|
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Notes to Consolidated Financial Statements
Note 1—Organization and Description of Business Operations
Taysha Gene Therapies, Inc. (the “Company” or “Taysha”) was originally formed under the laws of the State of Texas on September 20, 2019 (“Inception”). Taysha converted to a Delaware corporation on February 13, 2020, which had no impact to the Company’s par value or issued and authorized capital structure.
Taysha is a patient-centric gene therapy company focused on developing and commercializing AAV-based gene therapies for the treatment of monogenic diseases of the central nervous system (“CNS”) in both rare and large patient populations.
Stock Split
On September 16, 2020, the Company effected a 1.0895-for-one stock split of its authorized, issued and outstanding shares of common stock and a proportional adjustment to the existing conversion ratios for each series of the Company’s convertible preferred stock as discussed in Note 7. Accordingly, all share and per share amounts for the periods presented in the accompanying consolidated financial statements and notes thereto have been adjusted retroactively, where applicable, to reflect this stock split and adjustment of the convertible preferred stock conversion ratios. On September 16, 2020, the Company also increased the number of shares of common stock authorized for issuance under the 2020 Equity Incentive Plan (the “Existing Plan”) to 3,845,294.
Initial Public Offering
On September 23, 2020, the Company’s registration statement on Form S-1 (File No. 333-248559) related to the initial public offering (“IPO”) of its common stock became effective and on September 28, 2020, the IPO closed. Pursuant to the IPO, the Company issued and sold 9,050,000 shares of common stock at a public offering price of $20.00 per share, which included 1,180,434 shares of common stock issued upon the exercise in full of the underwriters’ option to purchase additional shares. The Company received net proceeds of $165.9 million after deducting underwriting discounts and commissions and other offering costs. The shares began trading on the Nasdaq Global Select Market on September 24, 2020.
On September 28, 2020, in connection with the closing of the IPO, 10,000,000 shares of Series A and 5,647,048 shares of Series B convertible preferred stock automatically converted into an aggregate of 17,047,378 shares of common stock with a conversion ratio of 1.0895 shares of common stock for each share of Series A and Series B convertible preferred stock.
As a result of the IPO, including the underwriters’ exercise in full of their option to purchase additional shares, and the conversions of the Series A and B convertible preferred stock, the Company’s total number of outstanding shares increased by 26,097,378 immediately following the closing of the IPO.
Upon the effectiveness of the Company’s registration statement related to the IPO, the Company’s 2020 Stock Incentive Plan (the “New Plan”) and 2020 Employee Stock Purchase Plan became effective. At that time, all shares reserved for issuance under the Existing Plan ceased to be available for issuance under such plan and became available for issuance under the New Plan.
Liquidity and Capital Resources
The Company has incurred operating losses since Inception and expects to continue to incur significant operating losses for the foreseeable future and may never become profitable. As of December 31, 2020, the Company had an accumulated deficit of $61.1 million.
Prior to the closing of the Company’s IPO, between March and July 2020, the Company closed on the sale of an aggregate of 10,000,000 shares of Series A convertible preferred stock for gross proceeds of $30.0 million. Between July and August 2020, the Company closed on the sale of an aggregate of 5,647,048 shares of Series B convertible preferred stock for gross proceeds of $96.0 million.
Due to the proceeds received from the IPO and the sale of its Series A and Series B convertible preferred stock, management believes that its existing financial resources are sufficient to continue operating activities at least one year past the issuance date of these consolidated financial statements. Future capital requirements will depend on many factors, including the timing and extent of spending on research and development and the market acceptance of the Company’s products. The Company will need to obtain additional financing in order to complete clinical studies and launch and commercialize any product candidates for which it receives regulatory approval. There can be no assurance that such financing will be available or will be on terms acceptable to the Company.
F-6
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
During December 2019, the novel coronavirus (“COVID-19”) emerged and subsequently spread worldwide. The World Health Organization declared COVID-19 a global pandemic in March 2020, resulting in federal, state and local governments and private entities implementing various restrictions, including travel restrictions, restrictions on public gatherings, stay at home orders, and advisories and quarantining people who may have been exposed to the virus. The Company has been actively monitoring COVID-19 and its impact globally. Management believes the financial results for the year ended December 31, 2020 were not significantly impacted by COVID-19. In addition, management believes the remote working arrangements and travel restrictions imposed by various governmental jurisdictions have had limited impact on the Company’s ability to maintain internal operations during the year ended December 31, 2020. The full extent to which the COVID-19 pandemic will directly or indirectly impact the Company’s business, results of operations and financial condition will depend on future developments that are highly uncertain, including as a result of new information that may emerge concerning COVID-19 and the actions taken to contain it or treat COVID-19.
Note 2—Significant Accounting Policies
Basis of Presentation
The Company’s financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America (“U.S. GAAP”) as determined by the Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) and include all adjustments necessary for the fair presentation of the Company’s financial position for the periods presented.
Principles of Consolidation
The accompanying consolidated financial statements include the accounts of Taysha and its inactive wholly owned U.S. subsidiaries that were incorporated during 2020. All intercompany transactions and balances have been eliminated in consolidation.
Emerging Growth Company
From time to time, new accounting pronouncements are issued by FASB, or other standard setting bodies and adopted by the Company as of the specified effective date. Unless otherwise discussed, the impact of recently issued standards that are not yet effective will not have a material impact on the Company’s financial statements upon adoption. Under the Jumpstart Our Business Startups Act of 2012, as amended, the Company meets the definition of an emerging growth company, and has elected the extended transition period for complying with new or revised accounting standards, which delays the adoption of these accounting standards until they would apply to private companies.
Use of Estimates
The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of expenses during the reporting period. The most significant estimates and assumptions in the Company’s financial statements relate to the determination of the fair value of the common stock prior to the IPO (as an input into stock-based compensation), estimating preclinical manufacturing accruals and accrued or prepaid research and development expenses, and the valuation of the preferred stock tranche liability. These estimates and assumptions are based on current facts, historical experience and various other factors believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities and the recording of expenses that are not readily apparent from other sources. Actual results may differ materially from these estimates. To the extent there are material differences between the estimates and actual results, the Company’s future results of operations will be affected.
Risks and Uncertainties
The Company is subject to risks common to companies in the biotechnology industry, including, but not limited to, development by the Company or its competitors of technological innovations, risks of failure of clinical studies, dependence on key personnel, protection of proprietary technology, compliance with government regulations, and ability to transition from preclinical manufacturing to commercial production of products.
The Company’s product candidates require approvals from the FDA and comparable foreign regulatory agencies prior to commercial sales in their respective jurisdictions. There can be no assurance that any product candidates will receive the necessary approvals. If the Company was denied approval, approval was delayed or the Company was unable to maintain approval for any product candidate, it could have a materially adverse impact on the Company.
Segments
Operating segments are identified as components of an enterprise about which separate discrete financial information is available for evaluation by the chief operating decision-maker in making decisions regarding resource allocation and assessing performance. The Company views its operations and manages its business as a single operating segment, which is the business of developing AAV-based gene therapies for the treatment of rare monogenic diseases of the CNS.
F-7
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
As of December 31, 2020 and 2019, the Company did not have assets located outside of the United States.
Cash and Cash Equivalents
Cash and cash equivalents consist of funds held in a standard checking account and a standard savings account. The Company considers all highly liquid investments with an original maturity of three months or less at the date of purchase to be cash equivalents. As of December 31, 2020 and 2019, respectively, the Company had no cash equivalents.
Concentrations of Credit Risk
Financial instruments that potentially subject the Company to significant concentration of credit risk consist primarily of cash and cash equivalents. Periodically, the Company may maintain deposits in financial institutions in excess of government insured limits. Management believes that the Company is not exposed to significant credit risk as the Company’s deposits are held at financial institutions that management believes to be of high credit quality. The Company has not experienced any losses on these deposits.
Fair Value of Financial Instruments
The Company’s financial assets and liabilities are accounted for in accordance with ASC 820, Fair Value Measurements and Disclosures which defines fair value as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. The fair value hierarchy requires an entity to maximize the use of observable inputs when measuring fair value and classifies those inputs into three levels:
Level 1—Observable inputs, such as quoted prices in active markets for identical assets or liabilities.
Level 2—Inputs other than Level 1 inputs that are either directly or indirectly observable, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the instrument’s anticipated life.
Level 3—Unobservable inputs in which there is little or no market data, which require the reporting entity to develop its own assumptions.
To the extent the valuation is based on models or inputs that are less observable or unobservable in the market, the determination of fair values requires more judgement. Accordingly, the degree of judgement exercised by the Company in determining fair value is greatest for instruments categorized as Level 3. A financial instrument’s level within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement.
The carrying values reported in the Company’s consolidated balance sheets for cash and cash equivalents, prepaid expenses and other current assets, accounts payable, accrued expenses and other current liabilities are reasonable estimates of their fair values due to the short-term nature of these items.
Deferred Offering Costs
The Company capitalizes certain legal, professional, accounting and other third-party fees that are directly associated with in-process equity financings as deferred offering costs until such financings are consummated. After consummation of the equity financing, these costs are recorded in stockholders’ deficit as a reduction of additional paid-in capital generated as a result of an equity financing. Should the in-process equity financing be abandoned, the deferred offering costs will be expensed immediately as a charge to operating expenses in the statements of operations. As of December 31, 2020 and 2019, there was $0 and $15,000, respectively, of deferred offering costs capitalized on the consolidated balance sheets. The $15,000 capitalized as of December 31, 2019 related to the Company’s Series A convertible preferred stock financing that closed in March 2020 (see Note 7).
Deferred offering costs, consisting of legal, accounting, and filing fees directly relating to the IPO and the Company’s Series A and Series B preferred stock financings, were capitalized and offset against the related proceeds upon the completion of the offerings in 2020. Upon completion of the IPO in September 2020, approximately $2.5 million of deferred offering costs were offset against the IPO proceeds in additional paid-in capital.
Property and Equipment, net
Property and equipment are stated at cost less accumulated depreciation and consist solely of computer equipment and laboratory equipment. Depreciation expense is recognized using the straight-line method over its estimated useful life of three to five years.
F-8
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
Upon retirement or sale, the cost of assets disposed of and the related accumulated depreciation are removed from the accounts and any resulting gain or loss is included in loss from operations. Expenditures for repairs and maintenance are charged to expense as incurred.
Impairment of Long-Lived Assets
The Company evaluates its long-lived assets, which consist of property and equipment, for impairment whenever events or changes in circumstances indicate that the carrying amount of such assets may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to the future undiscounted net cash flows expected to be generated by the asset. If such assets are considered to be impaired, the impairment to be recognized is measured by the amount by which the carrying amount of the asset exceeds the fair value of the asset. There were no impairment losses recognized during the year ended December 31, 2020 and the period from Inception to December 31, 2019.
Convertible Preferred Stock
The Company recorded shares of its convertible preferred stock at their respective fair values on the dates of issuance, net of issuance costs. The Company applied the guidance in ASC 480-10-S99-3A, SEC Staff Announcement: Classification and Measurement of Redeemable Securities and therefore classified the Series A convertible preferred stock as mezzanine equity. The convertible preferred stock was recorded outside of stockholders’ deficit because, in the event of certain deemed liquidation events considered not solely within the Company’s control, such as a merger, acquisition and sale of all or substantially all of the Company’s assets (a “Deemed Liquidation Event”), the convertible preferred stock would become redeemable at the option of the holders. In the event of a change of control of the Company, proceeds received from the sale of such shares would have been distributed in accordance with the liquidation preferences set forth in the Company’s Amended and Restated Certificate of Incorporation. The Company determined not to adjust the carrying values of the convertible preferred stock to the liquidation preferences of such shares because of the uncertainty of whether or when such an event would occur. All shares of the Company’s previously issued and outstanding convertible preferred stock were converted into shares of common stock upon the closing of the IPO (see Note 7).
Preferred Stock Tranche Liability
The Company determined that its obligation to issue, and the Company’s investors’ right to purchase, additional shares of Series A convertible preferred stock pursuant to the milestone closings (see Note 7) represented a freestanding financial instrument (the “tranche liability”). The tranche liability was initially recorded at fair value. The proceeds from the sale of the convertible preferred stock were first allocated to the fair value of the tranche liability with the remaining proceeds from the sale of the convertible preferred stock allocated to the Series A convertible preferred stock. The tranche liability was remeasured at each reporting period and upon the exercise or expiration of the obligation, with gains and losses arising from subsequent changes in its fair value recognized in other expense in the consolidated statements of operations. At the time of the exercise or expiration of the tranche liability, any remaining value of the tranche liability was reclassified to convertible preferred stock on the consolidated balance sheets.
Research and Development
The Company has entered into research and development contracts with research institutions and other companies. These agreements are generally cancelable, and related payments are recorded as research and development expenses as incurred. Payments for these activities are based on the terms of the individual agreements, which may differ from the pattern of costs incurred, and are reflected on the consolidated balance sheets as prepaid or accrued expenses. The Company records accruals for estimated ongoing research costs. When evaluating the adequacy of the accrued liabilities, the Company analyzes progress of the studies, including the phase or completion of events, invoices received and contracted costs.
Research and development costs primarily consist of payroll, stock-based compensation, certain manufacturing costs, laboratory costs and other supplies, and the cost to acquire licenses.
Costs incurred in obtaining technology licenses through asset acquisitions are charged to research and development expense if the licensed technology has not reached technological feasibility and has no alternative future use.
F-9
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
The Company accounts for all stock-based payments to employees and non-employees, including grants of stock options, restricted stock awards, or RSAs, and restricted stock units, or RSUs, based on their respective grant date fair values. The Company estimates the fair value of stock option grants using the Black-Scholes option pricing model, which is affected principally by the estimated fair value of shares of the Company’s common stock and requires management to make a number of other assumptions, including the expected life of the option, the volatility of the underlying shares, the risk-free interest rate and expected dividends. Expected volatility is based on the historical share volatility of a set of comparable publicly traded companies over a period of time equal to the expected term of the options. Due to the lack of historical exercise history, the expected term of the Company’s stock options is determined using the “simplified” method. The risk-free interest rate is determined by reference to the U.S. Treasury yield curve in effect at the time of grant of the award for time periods approximately equal to the expected term of the award. Expected dividend yield is zero based on the fact that the Company has never paid cash dividends and does not expect to pay any cash dividends in the foreseeable future.
Prior to September 23, 2020, the fair value of common stock underlying the Company’s stock options, RSAs and RSUs was estimated by the Company’s board of directors considering, among other things, contemporaneous valuations of the Company’s common stock prepared by unrelated third-party valuation firms. After the IPO, the fair value of common stock is based on the closing price of the Company’s common stock on the Nasdaq Global Select Market as reported on the date of the grant.
The RSAs and RSUs are valued based on the fair value of the Company’s common stock on the date of grant. The Company expenses stock-based compensation related to stock options, RSAs and RSUs over the requisite service period using the straight-line method. All stock-based compensation costs are recorded in research and development expense or general and administrative expense in the consolidated statements of operations based upon the respective employee’s roles within the Company. Forfeitures are recorded as they occur.
Income Taxes
Income taxes are recorded in accordance with ASC 740, Income Taxes (“ASC 740”), which provides for deferred taxes using an asset and liability approach. The Company recognizes deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements or tax returns. Deferred tax assets and liabilities are determined based on the difference between the financial statement and tax bases of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse, and net operating loss (“NOL”) carryforwards and research and development tax credit (“R&D Credit”) carryforwards. Valuation allowances are provided, if based upon the weight of available evidence, it is more likely than not that some or all of the deferred tax assets will not be realized. The Company has recorded a full valuation allowance to reduce its net deferred income tax assets to zero. In the event the Company were to determine that it would be able to realize some or all its deferred income tax assets in the future, an adjustment to the deferred income tax asset valuation allowance would increase income in the period such determination was made.
The Company accounts for uncertain tax positions in accordance with the provisions of ASC 740. When uncertain tax positions exist, the Company recognizes the tax benefit of tax positions to the extent that the benefit would more likely than not be realized assuming examination by the taxing authority. The determination as to whether the tax benefit will more likely than not be realized is based upon the technical merits of the tax position as well as consideration of the available facts and circumstances. At December 31, 2019, the Company had no liability for income tax associated with uncertain tax positions. During the year ended December 31, 2020, the Company recorded gross unrecognized tax benefits that were not significant. The unrecognized tax benefits, if recognized, would not affect the effective income tax rate due to the valuation allowance that currently offsets deferred tax assets. The Company does not expect the unrecognized tax benefits to change significantly over the next 12 months. The Company would recognize any corresponding interest and penalties associated with its income tax positions in income tax expense. There was no income tax interest or penalties incurred for the year ended December 31, 2020 or for the period from Inception to December 31, 2019.
Comprehensive Loss
Comprehensive loss is equal to net loss as presented in the accompanying consolidated statements of operations, as the Company did not have any other comprehensive income or loss for the periods presented.
Recently Adopted Accounting Pronouncements
In May 2014, the FASB issued ASC 606, Revenue from Contracts with Customers (“ASC 606”). This guidance applies to any entity that either enters into contracts with customers to transfer goods or services or enters into contracts for the transfer of nonfinancial assets unless those contracts are within the scope of other standards. The core principle of this guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. This guidance supersedes existing revenue recognition guidance, including most industry-specific guidance, as well as certain related guidance on accounting for contract costs. The Company early adopted ASC 606 upon its Inception. As the Company does not have any contracts with customers, the adoption of this guidance did not have any impact on the Company’s consolidated financial statements.
F-10
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
In June 2018, the FASB issued Accounting Standards Update (“ASU”) No. 2018-07, Compensation – Stock Compensation (Topic 718) (“ASU 2018-07”). This update is intended to reduce cost and complexity and to improve financial reporting for share-based payments issued to non-employees (for example, service providers, external legal counsel, suppliers, etc.). The ASU expands the scope of Topic 718, Compensation—Stock Compensation, which currently only includes share-based payments issued to employees, to also include share-based payments issued to non-employees for goods and services. Consequently, the accounting for share-based payments to non-employees and employees will be substantially aligned. The Company early adopted ASU 2018-07 upon its Inception. The adoption of this ASU did not have a material effect on the Company’s consolidated financial statements at Inception. The Company applied this accounting pronouncement to the issuance of shares to the Board of Regents of the University of Texas System (see Note 5).
In August 2018, the FASB issued ASU No. 2018-13, Fair Value Measurement (ASC Topic 820) (“ASU 2018-13”), which modifies, removes and adds certain disclosure requirements on fair value measurements based on the FASB Concepts Statement, Conceptual Framework for Financial Reporting—Chapter 8: Notes to Financial Statements. The amendments on changes in unrealized gains and losses, the range and weighted-average of significant unobservable inputs used to develop Level 3 fair value measurements and the narrative description of measurement uncertainty should be applied prospectively for only the most recent interim or annual period presented in the initial fiscal year of adoption. All other amendments should be applied retrospectively to all periods presented upon their effective date. The Company adopted ASU 2018-13 as of January 1, 2020 for the annual period. The adoption of the guidance did not have a material impact on the Company’s consolidated financial statements.
In November 2018, the FASB issued ASU No. 2018-18 – Collaborative Arrangements, which clarifies that certain transactions between collaborative arrangement participants should be accounted for as revenue when the collaborative arrangement participant is a customer in the context of a unit of account and precludes recognizing as revenue consideration received from a collaborative arrangement participant if the participant is not a customer. The Company early adopted this standard as of January 1, 2020 for the annual period and it will be applied to interim periods after December 31, 2020. This ASU requires retrospective adoption to the date the Company adopted ASC 606, which was upon its Inception, by recognizing a cumulative-effect adjustment to the opening balance of retained earnings of the earliest annual period presented. As the Company does not have any contracts with customers or collaborative arrangements, the adoption of this guidance did not have any impact on the Company’s consolidated financial statements.
Recently Issued Accounting Pronouncements
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842), as amended, with guidance regarding the accounting for and disclosure of leases. This update requires lessees to recognize the liabilities related to all leases, including operating leases, with a term greater than 12 months on the balance sheets. This update also requires lessees and lessors to disclose key information about their leasing transactions. This guidance will become effective for the Company for annual reporting periods beginning after December 15, 2021 and interim periods within fiscal years beginning after December 15, 2022. The Company is currently evaluating the impact of this standard on its consolidated financial statements.
In December 2019, the FASB issued ASU No. 2019-12, Income Taxes (Topic 740): Simplifying the Accounting for Income Taxes (“ASU 2019-12”), which is intended to simplify various aspects related to accounting for income taxes. ASU 2019-12 removes certain exceptions to the general principles in ASC 740 and also clarifies and amends existing guidance to improve consistent application. This guidance is effective for fiscal years beginning after December 15, 2021, and interim periods within fiscal years beginning after December 15, 2022, with early adoption permitted. The Company is currently evaluating the impact of this standard on its consolidated financial statements.
Note 3—Property and Equipment
Property and Equipment consisted of the following (in thousands):
|
|
|
December 31, |
|
|
December 31, |
|
||
|
|
|
2020 |
|
|
2019 |
|
||
|
Computer equipment |
|
$ |
95 |
|
|
$ |
— |
|
|
Construction in progress |
|
|
201 |
|
|
|
— |
|
|
|
|
|
296 |
|
|
|
— |
|
|
Accumulated depreciation |
|
|
(9 |
) |
|
|
— |
|
|
Property and equipment, net |
|
$ |
287 |
|
|
$ |
— |
|
Depreciation expense was $9,000 for the year ended December 31, 2020. There was no depreciation expense in prior periods.
F-11
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
Note 4—Supplemental Financial Information
Accrued expenses and other current liabilities consisted of the following (in thousands):
|
|
|
December 31, |
|
|
December 31, |
|
||
|
|
|
2020 |
|
|
2019 |
|
||
|
Accrued research and development |
|
$ |
2,106 |
|
|
$ |
7 |
|
|
Accrued compensation |
|
|
1,766 |
|
|
|
— |
|
|
Accrued professional fees |
|
|
999 |
|
|
|
122 |
|
|
Other |
|
|
264 |
|
|
|
21 |
|
|
Total accrued expenses and other current liabilities |
|
$ |
5,135 |
|
|
$ |
150 |
|
Prepaid expenses and other current assets consisted of the following (in thousands):
|
|
|
December 31, |
|
|
December 31, |
|
||
|
|
|
2020 |
|
|
2019 |
|
||
|
Prepaid insurance |
|
$ |
2,480 |
|
|
$ |
— |
|
|
Prepaid research and development |
|
|
2,462 |
|
|
|
— |
|
|
Prepaid clinical trial |
|
|
944 |
|
|
|
— |
|
|
Other |
|
|
740 |
|
|
|
— |
|
|
Total prepaid expenses and other current assets |
|
$ |
6,626 |
|
|
$ |
— |
|
Note 5—Research, Collaboration, Grant and License Agreements
UT Southwestern Agreement
On November 19, 2019, the Company entered into a research, collaboration and license agreement (“UT Southwestern Agreement”) with the Board of Regents of the University of Texas System (“UT System”) on behalf of The University of Southwestern Medical Center (“UT Southwestern”). Under the UT Southwestern Agreement, UT Southwestern is primarily responsible for preclinical development activities with respect to licensed products for use in certain specified indications (up to IND-enabling studies), and the Company is responsible for all subsequent clinical development and commercialization activities with respect to the licensed products. UT Southwestern will conduct such preclinical activities for a two-year period under mutually agreed upon sponsored research agreements that were entered into beginning in April 2020. During the initial research phase, the Company has the right to expand the scope of specified indications under the UT Southwestern Agreement.
In connection with the UT Southwestern Agreement, the Company obtained an exclusive, worldwide, royalty-free license under certain patent rights of UT Southwestern and a non-exclusive, worldwide, royalty-free license under certain know-how of UT Southwestern, in each case to make, have made, use, sell, offer for sale and import licensed products for use in certain specified indications. Additionally, the Company obtained a non-exclusive, worldwide, royalty-free license under certain patents and know-how of UT Southwestern for use in all human uses, with a right of first refusal to obtain an exclusive license under certain of such patent rights and an option to negotiate an exclusive license under other of such patent rights. The Company is required to use commercially reasonable efforts to develop, obtain regulatory approval for, and commercialize at least one licensed product.
On April 2, 2020, the Company amended the UT Southwestern Agreement to include the addition of another licensed product and certain indications, and a right of first refusal to the Company over certain patient dosing patents. No additional consideration was transferred in connection with this amendment.
The UT Southwestern Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last valid claim of a licensed patent in such country for such licensed product. After the initial research term, the Company may terminate the agreement, on an indication-by-indication and licensed product-by-licensed product basis, at any time upon specified written notice to UT Southwestern. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party.
In November 2019, as partial consideration for the license rights granted under the UT Southwestern Agreement, the Company issued 2,179,000 shares of its common stock, or 20% of its then outstanding fully-diluted common stock, to UT Southwestern. As additional consideration, UT Southwestern was entitled to receive additional shares if their holdings fell below 10% on a fully-diluted basis before or as a result of the completion of a qualified financing. In March 2020, following the initial closing of the Series A convertible preferred stock agreement, which met the definition of such qualified financing, the anti-dilution feature expired and no additional shares were issued. The Company does not have any future milestone or royalty obligations to UT Southwestern under the UT Southwestern Agreement other than costs related to maintenance of patents.
F-12
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
The Company also had the right of first refusal for any shares that UT Southwestern wishes to sell that officially expired upon the closing of the IPO. UT Southwestern did not sell any shares before the closing of the IPO.
The fair value of the shares issued was determined to be $980,000 which was recorded as an increase to common stock and additional paid-in capital and a corresponding research and development expense during the period from Inception through December 31, 2019. The cost to acquire this license is recorded within research and development expense in the consolidated statements of operations because the license relates to specific preclinical research and development activities that do not have an alternative future use. As the acquisition of the license was settled through the issuance of shares of the Company’s common stock, this transaction fell within the scope of ASC Topic 718 since equity was issued in exchange for goods (the license). Specifically, the Company recorded the cost of the license as a non-employee share based payment, measured at the grant date fair value of the common stock of $0.45 per share. The common shares were equity-classified. The anti-dilution provision was concluded to represent a performance condition tied to a future liquidity event, which was not considered probable of occurring at December 31, 2019 since it was deemed outside of the Company’s control.
Since there was an absence of a public trading market for the Company’s common stock during the period from Inception to December 31, 2019, the valuation of the common stock issued to UT System was performed using methodologies, approaches, and assumptions consistent with the American Institute of Certified Public Accountants Audit and Accounting Practice Aid Series: Valuation of Privately-Held-Company Equity Securities Issued as Compensation. The estimated fair value of the Company’s common stock was determined with the assistance of a third-party specialist using an Option-Pricing Method (“OPM”). Under the OPM, the Company used a backsolve method so that the enterprise value equaled the contemplated value of the Company determined by the Series A convertible preferred stock financing transaction which initially closed on March 4, 2020 (see Note 7), and giving consideration to any value-generating events that may have occurred between March 4, 2020 and the date the common shares were issued to UT System on November 19, 2019. A discount for lack of marketability (“DLOM”) of 20% was applied to derive the valuation price. The DLOM used was derived from the then-current estimates of the time to a liquidity event made by the Company’s board of directors, with input from the Company’s senior management. The estimates are based, in part, on subjective assumptions.
Queen’s Agreement
In late December 2019, the Company entered into a research grant agreement (“RGA”) with Queen’s University at Kingston (“Queen’s”), for certain research and development activities related to the generation of AAV9 vector. The Company committed to fund $3.8 million under the RGA with Queen’s. The Company agreed to issue Queen’s a promise-to-pay note whereby any amounts paid directly by Queen’s for the manufacture of the vector for use in the funded research activities, to the extent such amounts have not already been funded by the Company to Queen’s, become a loan obligation for the Company (the “Note”), subject to an interest rate of 6%. Any amounts outstanding under the Note were required to be repaid, along with any accrued interest, by or before June 30, 2020. In the event of default, any amount outstanding shall be deemed immediately payable by RA Session II, the Company’s President and Chief Executive Officer, as a personal guarantor (see Note 6). For the period from Inception through December 31, 2019, the Company did not incur any expenses associated with the Queen’s RGA, and no amounts were due or outstanding under the Note as of December 31, 2019. For the year ended December 31, 2020, the Company paid all expenses associated with the Queen’s RGA, thus no amounts were due or outstanding under the Note as of December 31, 2020, and the promise-to-pay has therefore expired.
On February 21, 2020, the Company entered into a license agreement with Queen’s (the “Queen’s Agreement”) to obtain the exclusive perpetual, royalty-bearing license, with the right to sublicense through multiple tiers, under certain patent rights and know-how of Queen’s, including certain improvements to such patent rights and know-how, to develop products in any field which use one or more valid claims of the patents licensed under the Queen’s Agreement (the “Licensed Patents”), or the technology, information and intellectual property related to the patents licensed under the Queen’s Agreement (together with the Licensed Patents, the “Licensed Products”), and to make, have made, use, sell, offer for sale, import and export Licensed Products and otherwise exploit such patents and know-how for use in certain specified indications. In exchange for the rights granted to the Company, the Company made a cash payment of $3.0 million in April 2020 which is recorded in research and development expenses in the consolidated statements of operations and included as an investing outflow in the consolidated statements of cash flows since the acquired license does not have an alternative future use. The Company is obligated to make aggregate cash payments of up to $10.0 million upon the completion of a combination of regulatory milestones and up to $10.0 million upon the completion of a combination of commercial milestones. In further consideration of the rights granted, beginning with the Company’s first commercial sale of the Licensed Products, the Company will also pay an annual earned royalty in the low single digits on net sales of Licensed Products, subject to certain customary reductions, and a percentage of non-royalty sublicensing revenue ranging in the low double digits. Royalties are payable, on a Licensed Products-by-Licensed Products and a country-by-country basis, until expiration of the last valid claim of a Licensed Patent covering such Licensed Products in such country and the expiration of any regulatory exclusivity for such Licensed Products in such country.
F-13
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
In August 2020, the Company entered into license and inventory purchase agreements with Abeona Therapeutics Inc. (“Abeona”) for worldwide exclusive rights to certain intellectual property rights and know-how relating to the research, development and manufacture of ABO-202, an AAV-based gene therapy for CLN1 disease (one of the forms of Batten disease). Under the terms of the agreements, the Company made initial cash payments to Abeona of $3.0 million for the upfront license fee and $4.0 million for purchase of clinical materials and reimbursement for previously incurred development costs in October 2020. In exchange for the license rights, the Company recorded an aggregate of $7.0 million within research and development expenses in the consolidated statements of operations and included the license fee of $3.0 million as an investing outflow in the consolidated statements of cash flows since the acquired license does not have an alternative future use. The Company is obligated to make up to $26.0 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed CLN1 product. The Company will also pay an annual earned royalty in the high single digits on net sales of any licensed CLN1 products. The license agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. The Company may terminate the license agreement for convenience upon specified prior written notice to Abeona.
Abeona Rett Agreement
On October 29, 2020, the Company entered into a license agreement (the “Abeona Rett Agreement”) with Abeona pursuant to which the Company obtained an exclusive, worldwide, royalty-bearing license, with the right to grant sublicenses under certain patents, know-how and materials originally developed by the University of North Carolina at Chapel Hill, the University of Edinburgh and Abeona to research, develop, manufacture, have manufactured, use, and commercialize licensed products for gene therapy and the use of related transgenes for Rett syndrome.
Subject to certain obligations of Abeona, the Company is required to use commercially reasonable efforts to develop at least one licensed product and commercialize at least one licensed product in the United States.
In connection with the Abeona Rett Agreement, the Company paid Abeona a one-time upfront license fee of $3.0 million which is recorded in research and development expenses in the consolidated statements of operations and included as an investing outflow in the consolidated statements of cash flows since the acquired license does not have an alternative future use. The Company is obligated to pay Abeona up to $26.5 million in regulatory-related milestones and up to $30.0 million in sales-related milestones per licensed Rett product and high single-digit royalties on net sales of licensed Rett products. Royalties are payable on a licensed product-by-licensed product and country-by-country basis until the latest of the expiration or revocation or complete rejection of the last licensed patent covering such licensed product in the country where the licensed product is sold, the loss of market exclusivity in such country where the product is sold, or, if no licensed product exists in such country and no market exclusivity exists in such country, ten years from first commercial sale of such licensed product in such country.
The Abeona Rett Agreement expires on a country-by-country and licensed product-by-licensed product basis upon the expiration of the last royalty term of a licensed product. Either party may terminate the agreement upon an uncured material breach of the agreement or insolvency of the other party. The Company may terminate the agreement for convenience upon specified prior written notice to Abeona.
Catalent Agreements
During October and November 2020, the Company entered into two agreements (the “Catalent Agreements”) with Catalent Maryland, Inc. (“Catalent”) to support the development and manufacturing of the Company’s gene therapies for CLN1 and Rett syndrome at Catalent’s Maryland-based gene therapy facilities. The Company engaged Catalent, which is a Contract Development and Manufacturing Organization (CDMO), to conduct services related to technology transfer, process development, analytical development, qualification, project administration and manufacture of CLN1 and Rett syndrome gene therapies suitable for use in nonclinical, United States and European Union Phase 1/2 clinical trials.
In connection with the Catalent Agreements, the Company paid Catalent an upfront project initiation fee of $2.0 million which is recorded as a prepaid expense in the consolidated balance sheets. The fee will be credited toward fees and expenses incurred under the Catalent Agreements. The Company therefore reduces the prepaid expense concurrently with expenses as they are incurred.
Note 6—Related Party Transactions
RA Session II, President and Chief Executive Officer and a member of the Company’s board of directors, is a guarantor under the Guaranty and Security Agreement between himself, Queen’s and the Company, and in the event of the Company’s failure to fund its obligations under the RGA with Queen’s, has personally guaranteed payments due by the Company to Queen’s.
F-14
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
In addition, the Company entered into two secured promissory notes with Mr. Session in January 2020 for an aggregate of $1.67 million, with 10% interest. The Company secured the notes with a first priority security interest in certain assets of the Company. As of December 31, 2020, the Company has repaid the notes in full. As a result, Mr. Session released his security interest in the collateral. During the year ended December 31, 2020, the Company incurred and paid approximately $28,000 of interest expense related to the notes.
In March 2020, the Company entered into a services agreement with PBM Capital Group, LLC (“PBM”), an affiliate of PBM TGT Holdings, LLC whereby PBM provides accounting and other administrative and management services related to payroll administration, human resources, bookkeeping, preparation of financial statements and tax returns, accounts payable and receivable, and other similar functions for a fee of $2,500 per month. Paul B. Manning, a member of the Company’s board of directors and a holder of more than 5% of the Company’s capital stock, is the Chief Executive Officer of PBM Capital Group, LLC and has sole voting and investment power with respect to the shares held by PBM TGT Holdings, LLC. In September 2020, PBM TGT Holdings, LLC distributed all of the shares of Series A convertible preferred stock it previously held to its beneficial owners, including Mr. Manning and entities controlled by Mr. Manning, for no additional consideration in accordance with the terms of its operating agreement. As of December 31, 2020, inclusive of certain pass-through direct costs, the Company has approximately $9,800 due to PBM, which is included in accounts payable in the consolidated balance sheets.
Note 7— Stockholders’ Equity (Deficit), Convertible Preferred Stock and Tranche Liability
At December 31, 2019, the Company was authorized to issue 10,895,000 shares of common stock with a par value of $0.00001 per share. RA Session II and one other individual were issued 8,661,524 and 54,475 shares of the Company’s common stock (“Founders Shares”), respectively, upon the formation of the Company on September 20, 2019. RA Session II and the other individual had not paid the Company for the aggregate par value, which approximated fair value at Inception, for these Founders Shares as of December 31, 2019. All amounts owed for the issuance of these Founders Shares were settled in July 2020.
On November 19, 2019, the Company issued 2,179,000 shares of the Company’s common stock to UT System in exchange for a license agreement. The fair value of the shares on the date of issuance was $980,000 in the aggregate. Except for the issuance of common stock to UT System in connection with the UT Southwestern Agreement, the Company did not grant any equity-based awards during the period from its Inception through December 31, 2019.
Authorized shares
The Company amended its certificate of incorporation on March 4, 2020, July 2, 2020 and again on July 28, 2020 such that the total number of shares of common stock authorized to be issued was increased to 32,685,000, and the total number of shares of preferred stock authorized to be issued was increased to 15,647,052, of which 10,000,000 preferred shares were designated Series A convertible preferred stock and 5,647,052 were designated Series B convertible preferred stock. On September 28, 2020, the Company amended its certificate of incorporation such that the total number of shares of common stock authorized to be issued was increased to 200,000,000, and the total number of shares of new preferred stock authorized to be issued was 10,000,000. As of December 31, 2020, no shares of preferred stock were issued or outstanding.
IPO
On September 28, 2020, the Company issued an aggregate of 7,869,566 shares of common stock in the IPO, and on September 29, 2020, the Company issued an aggregate of 1,180,434 shares of common stock upon the underwriters’ exercise in full of their option to purchase additional shares, each at the public offering price of $20.00 per share less underwriting discounts and commissions. In connection with the IPO, the Company received gross proceeds of $181.0 million, which was offset by issuance costs, including underwriters’ discounts and commissions, of approximately $15.1 million.
In connection with the closing of the IPO, 10,000,000 shares of Series A convertible preferred stock and 5,647,048 shares of Series B convertible preferred stock automatically converted into an aggregate of 17,047,378 shares of common stock with a conversion ratio of 1.0895 shares of common stock for each share of Series A and Series B convertible preferred stock then outstanding.
As a result of the IPO, the underwriters’ exercise of their option, and the conversions of the Series A and B convertible preferred stock, the Company’s total number of outstanding shares increased by 26,097,378 immediately following the closing of the IPO.
Series A and B convertible preferred stock
On March 4, 2020, the Company entered into a purchase agreement (the “Series A Purchase Agreement”) providing for a private placement of up to 10,000,000 shares of Series A convertible preferred stock at an original issuance price of $3.00 per share, subject to separate closings, including: (1) 6,000,000 shares at the initial closing on March 4, 2020, and (2) 2,000,000 shares at each of two subsequent closings triggered by the achievement of specific clinical milestones. The Series A Purchase Agreement obligated the Company to issue and sell and the Series A investors to purchase up to a total of 4,000,000 additional shares of Series A convertible preferred stock (the “Milestone Shares”) at the same price per share upon the achievement of certain defined clinical milestones (the “tranche liability”). The determination as to whether the milestone events had been met was subject to certification by the Board of Directors. Each Series A
F-15
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
investor had the right, but not the obligation, to purchase all or any portion of the Milestone Shares at any time in its sole option and in its sole and absolute discretion, whether or not the Company had achieved the applicable clinical milestone.
On June 30, 2020, several affiliated Series A investors elected to exercise in full their options to purchase 200,000 shares, representing all of their remaining pro-rata portion of the Milestone Shares, prior to the Company’s achievement of the clinical milestones for gross proceeds of $0.6 million. The remainder of the Series A investors exercised in full their options to purchase 3,800,000 shares, representing all of their remaining pro-rata portion of the Milestone Shares, prior to the Company’s achievement of the clinical milestones, for gross proceeds of $11.4 million between July 1, 2020 and July 2, 2020. As part of this issuance, the Company issued and sold 3,266,667 shares to PBM TGT Holdings, LLC and 400,000 shares to Nolan Capital, LLC, which stockholders are controlled by certain members of the Company’s board of directors.
On July 2, 2020, the Company entered into a purchase agreement (the “Series B Purchase Agreement”), as later amended on July 28, 2020, providing for a private placement of up to 5,647,052 shares of Series B convertible preferred stock. The Company sold 5,647,048 shares of Series B convertible preferred stock at a price of $17.00 per share in multiple closings in July and August 2020 for gross proceeds of $96.0 million. The majority of investors that participated in the Series B Purchase Agreement were new investors.
As described above, in connection with the closing of the IPO, all shares of Series A and Series B convertible preferred stock were automatically converted into an aggregate of 17,047,378 shares of common stock with a conversion ratio, which was adjusted for the stock split, of 1.0895 shares of common stock for each share of Series A and Series B convertible preferred stock then outstanding.
Series A convertible preferred stock tranche liability
The Company concluded that the tranche liability met the definition of a freestanding financial instrument, as it was legally detachable and separately exercisable from the initial closing of the Series A convertible preferred stock.
The estimated fair value of the tranche liability was determined using a Monte Carlo simulation at the initial issuance date. As of March 4, 2020, the simulations occurred based on the implied aggregate equity value of the Company derived from the Series A convertible preferred stock offering price of $3.00 per share, along with, in part, the following subjective assumptions: risk-free rate of 0.59%, an expected volatility of 80%, the expected term to a liquidity event of 1 year, and a 60% probability of achieving the clinical milestones and timing thereof. Subsequently, the estimated fair value of the tranche liability was determined using a backsolve approach at June 30, 2020, immediately prior to the issuance of the Milestone Shares, which was calculated based on the aggregate equity value of the Company derived from the Series B convertible preferred stock offering price of $17.00 per share. The subsequent remeasurement also considered, in part, a risk-free rate of 0.17%, an expected volatility of 80%, and the expected term to a liquidity event of 0.5 years.
Based on the analysis, the Company recorded a preferred stock tranche liability of $1.1 million at the issue date to account for the obligation to issue the Milestone Shares at a predetermined fixed price at a future settlement date.
At June 30, 2020, ahead of the anticipated closing of the Series B Purchase Agreement for $17.00 per share that occurred on July 2, 2020, certain investors elected to exercise in full their options to their pro-rata portion of the Milestone Shares prior to the Company’s achievement of the clinical milestones and purchased 200,000 shares of Series A convertible preferred stock. The Company remeasured the fair value of the entire tranche liability at June 30, 2020 and recognized a non-cash expense of $17.0 million in the consolidated statements of operations. Between June 30, 2020 and July 2, 2020, all of the 4,000,000 Milestone Shares were issued and the related tranche liability was extinguished in its entirety, and the Company reclassified the entire tranche liability of $18.1 million to convertible preferred stock on the consolidated balance sheets.
The Company concluded that no beneficial conversion feature (“BCF”) existed as the effective conversion price of the Series A convertible preferred stock exceeded the fair value of the Company’s common stock at each of the commitment dates. Specifically, at the commitment date of June 30, 2020, when 200,000 Milestone Shares were issued, the deemed proceeds were equal to the cash proceeds received for the shares of Series A convertible preferred stock and the fair value of the tranche liability that related to the Milestone Shares, or $7.52 per share. As the effective conversion price exceeded the fair value of the Company’s common stock at the commitment date, no BCF existed.
F-16
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
The following table provides a reconciliation of the preferred stock tranche liability measured at fair value using Level 3 significant unobservable inputs (in thousands):
|
Balance at December 31, 2019 |
|
$ |
— |
|
|
Fair value at issuance of Series A convertible preferred stock |
|
|
1,050 |
|
|
Change in fair value |
|
|
17,030 |
|
|
Settlement of preferred stock tranche liability due to issuance of Milestone Shares |
|
|
(18,080 |
) |
|
Balance at December 31, 2020 |
|
$ |
— |
|
Note 8—Stock-Based Compensation
On July 1, 2020, the Company’s board of directors approved the Existing Plan which permits the granting of incentive stock options, non-statutory stock options, stock appreciation rights, RSAs, RSUs and other stock-based awards to employees, directors, officers and consultants. On July 1, 2020, 3,529,412 shares of common stock were authorized for issuance under the Existing Plan. On September 16, 2020, the Company increased the number of shares of common stock authorized for issuance under the Existing Plan to 3,845,294.
On September 16, 2020, the Company’s stockholders approved the New Plan, which became effective upon the execution of the underwriting agreement in connection with the IPO. The number of shares available for future issuance under the New Plan is the sum of (1) 3,390,168 new shares of common stock, (2) 209,841 remaining shares of common stock reserved under the Existing Plan that became available for issuance upon the effectiveness of the New Plan and (3) the number of shares of common stock subject to outstanding awards under the Existing Plan when the New Plan became effective that thereafter expire or are forfeited, canceled, withheld to satisfy tax withholding or to purchase or exercise an award, repurchased by the Company or are otherwise terminated. At December 31, 2020, there were 2,941,509, shares available for future grant under the New Plan. The number of shares of common stock reserved for issuance under the New Plan will automatically increase on January 1 of each year, for a period of ten years, from January 1, 2021 continuing through January 1, 2030, by 5% of the total number of shares of common stock outstanding on December 31 of the preceding calendar year, or a lesser number of shares as may be determined by the Company’s board of directors.
Furthermore, on September 16, 2020, the Company’s stockholders approved the Employee Stock Purchase Plan (“ESPP”), which became effective upon the execution of the underwriting agreement in connection with the IPO. The maximum number of shares of common stock that may be issued under the ESPP will not exceed 362,000 shares of common stock, plus the number of shares of common stock that are automatically added on January 1st of each year for a period of up to ten years, commencing on the first January 1 following the IPO Date and ending on (and including) January 1, 2030, in an amount equal to the lesser of (i) one percent (1.0%) of the total number of shares of capital stock outstanding on December 31st of the preceding calendar year, and (ii) 724,000 shares of common stock. No issuances have been made under the ESPP as of December 31, 2020.
Stock Options
On July 1, 2020, options to purchase 2,896,782 shares of common stock under the Existing Plan were awarded to certain employees and consultants of the Company with an exercise price per share of $0.80, which were expected to vest over a four-year period, all of which were subsequently cancelled (the “Cancelled Options”). The grant date fair value of the Cancelled Options was $13.8 million at the original grant date. In exchange, the Company awarded 2,518,932 RSUs on September 2, 2020, which are expected to vest over a four-year term. The Company accounted for the changes in award terms as a modification in accordance with ASC 718 Compensation – Stock Compensation. The modification is accounted for as an exchange of the original award for a new award with total compensation cost equal to the grant-date fair value of the original award plus any incremental value measured on the modification date. The Company determined that there was no incremental value as the fair value of the original award immediately before the modification was greater than the fair value of the new award immediately after the modification. Accordingly, the Company will recognize the remaining compensation cost at the time of the modification of $13.2 million over the vesting period of the RSUs.
The estimated fair value of the Company’s common stock at July 1, 2020 was $5.28 per share, as determined using information derived from the issuance price of the Company’s Series B convertible preferred stock of $17.00 per share on July 2, 2020. The valuation of the common stock was determined using an option-pricing model under which shares are valued by creating a series of call options with exercise prices based on the liquidation preferences and conversion terms of each equity class, adjusted for a discount for the lack of marketability to account for a lack of access to an active public market.
The following assumptions were used to estimate the fair value of the Cancelled Options that were granted on July 1, 2020:
|
Risk-free interest rate |
|
|
0.31 |
% |
|
Expected dividend yield |
|
|
— |
|
|
Expected term in years |
|
|
6.3 |
|
|
Expected volatility |
|
|
80 |
% |
F-17
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
During the year ended December 31, 2020, excluding the Cancelled Options, options to purchase 674,842 shares of common stock were granted with a weighted-average exercise price per share of $20.68. On September 2, 2020, options to purchase 16,342 shares of common stock under the Existing Plan were awarded to certain directors of the Company with an exercise price per share of $14.90, and on various dates beginning at the closing of the IPO through December 31, 2020, 658,500 shares of common stock under the New Plan were awarded with a weighted-average exercise price per share of $20.83. The stock options generally vest over three or four years and have a ten-year contractual term.
The following weighted-average assumptions were used to estimate the fair value of stock options, excluding the Cancelled Options, for the year ended December 31, 2020:
|
Risk-free interest rate |
|
|
0.54 |
% |
|
Expected dividend yield |
|
|
— |
|
|
Expected term in years |
|
|
6.2 |
|
|
Expected volatility |
|
|
77 |
% |
The following table summarizes stock option activity, excluding the Cancelled Options, during the year ended December 31, 2020:
|
|
|
|
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
|
|
|
Weighted |
|
|
Average |
|
|
Aggregate |
|
||||
|
|
|
|
|
|
|
Average |
|
|
Remaining |
|
|
Intrinsic |
|
|||
|
|
|
Stock |
|
|
Exercise |
|
|
Contractual |
|
|
Value |
|
||||
|
|
|
Options |
|
|
Price |
|
|
Life (in years) |
|
|
(in thousands) |
|
||||
|
Outstanding at December 31, 2019 |
|
|
— |
|
|
$ |
— |
|
|
|
— |
|
|
$ |
— |
|
|
Options granted |
|
|
674,842 |
|
|
|
20.68 |
|
|
|
|
|
|
|
|
|
|
Outstanding at December 31, 2020 |
|
|
674,842 |
|
|
$ |
20.68 |
|
|
|
9.8 |
|
|
$ |
3,953 |
|
|
Vested and expected to vest at December 31, 2020 |
|
|
674,842 |
|
|
$ |
20.68 |
|
|
|
9.8 |
|
|
$ |
3,953 |
|
|
Options exercisable at December 31, 2020 |
|
|
12,054 |
|
|
$ |
20.25 |
|
|
|
9.8 |
|
|
$ |
76 |
|
The aggregate intrinsic value in the above table is calculated as the difference between the fair value of the Company’s common stock as of December 31, 2020 and the exercise price of the stock options. The weighted-average grant date fair value per share for the stock option awards, excluding the Cancelled Options, granted during the year ended December 31, 2020 was $13.73. As of December 31, 2020, the total unrecognized compensation related to unvested stock option awards granted was $8.8 million, which the Company expects to recognize over a weighted-average period of approximately 3.6 years.
Restricted Stock Units
On September 2, 2020, the Company issued 331,121 RSUs to an employee under the Existing Plan; 25% of the shares of common stock underlying the RSUs vest at each anniversary over a four-year period. The RSUs are subject to a service-based vesting condition. The RSUs were also subject to a liquidity-based performance vesting condition that was met upon the closing of the IPO. The Company at any time may accelerate the vesting of the RSUs. Such shares are not accounted for as outstanding until they vest. As of December 31, 2020, the total unrecognized compensation related to unvested RSUs granted, including the remaining compensation cost associated with the RSUs granted on September 2, 2020 in exchange for the Cancelled Options, was $16.2 million which is expected to be amortized on a straight-line basis over the weighted-average remaining vesting period of approximately 2.1 years. The Company’s RSU activity for the year ended December 31, 2020 was as follows:
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
Grant Date |
|
|
|
|
|
Number |
|
|
Fair Value |
|
||
|
|
|
of Shares |
|
|
per Share |
|
||
|
Nonvested at January 1, 2020 |
|
|
— |
|
|
$ |
— |
|
|
Replacement restricted units granted |
|
|
2,518,932 |
|
|
|
5.25 |
|
|
Restricted units granted |
|
|
331,121 |
|
|
|
14.90 |
|
|
Vested |
|
|
— |
|
|
|
— |
|
|
Nonvested at December 31, 2020 |
|
|
2,850,053 |
|
|
$ |
6.37 |
|
F-18
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
RA Session II, the Company’s President and Chief Executive Officer, was awarded 769,058 RSAs under the Existing Plan on July 1, 2020, which are expected to vest over a three-year term, subject to continuous employment. As of December 31, 2020, the total unrecognized compensation related to unvested RSAs granted was $3.2 million which is expected to be amortized on a straight-line basis over the weighted-average remaining vesting period of approximately 2.3 years. The fair value of these RSAs at the grant date of July 1, 2020 was $5.28 per share.
The Company’s RSA activity for the year ended December 31, 2020 was as follows:
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
|
|
|
Grant Date |
|
|
|
|
|
Number |
|
|
Fair Value |
|
||
|
|
|
of Shares |
|
|
per Share |
|
||
|
Nonvested at December 31, 2019 |
|
|
— |
|
|
$ |
— |
|
|
Restricted stock granted |
|
|
769,058 |
|
|
|
5.28 |
|
|
Vested |
|
|
— |
|
|
|
— |
|
|
Nonvested at December 31, 2020 |
|
|
769,058 |
|
|
$ |
5.28 |
|
The following table summarizes the total stock-based compensation expense for the stock options, RSAs and RSUs recorded in the consolidated statements of operations for the year ended December 31, 2020 and for the period from Inception to December 31, 2019 (in thousands):
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Research and development expense |
|
$ |
1,167 |
|
|
$ |
— |
|
|
General and administrative expense |
|
|
2,187 |
|
|
|
— |
|
|
Total |
|
$ |
3,354 |
|
|
$ |
— |
|
Note 9—Net Loss Per Common Share
Basic net loss per common share is computed by dividing net loss attributable to common stockholders by the weighted-average number of shares of common stock outstanding for the period. Since the Company had a net loss in the periods presented, basic and diluted net loss per common share are the same.
The following table represents the calculation of basic and diluted net loss per common share for the year ended December 31, 2020 and the period from Inception to December 31, 2019 (in thousands, except share and per share data):
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
|
$ |
(60,011 |
) |
|
$ |
(1,115 |
) |
|
|
Weighted-average shares of common stock outstanding used to compute net loss per common share, basic and diluted |
|
|
17,665,683 |
|
|
|
9,625,679 |
|
|
Net loss per common share, basic and diluted |
|
$ |
(3.40 |
) |
|
$ |
(0.12 |
) |
F-19
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
The following common stock equivalents outstanding as of December 31, 2020 and 2019, respectively, were excluded from the computation of diluted net loss per share attributable to common stockholders for the periods presented because including them would have been anti‑dilutive:
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Unvested RSUs |
|
|
2,850,053 |
|
|
|
— |
|
|
Unvested RSAs |
|
|
769,058 |
|
|
|
— |
|
|
Stock options |
|
|
674,842 |
|
|
|
— |
|
|
Total |
|
|
4,293,953 |
|
|
|
— |
|
Note 10—Income Taxes
Provision for income taxes
There is no provision for income taxes because the Company has incurred operating losses and capitalized certain items for income tax purposes since its inception and maintains a full valuation allowance against its net deferred tax assets. The reported amount of income tax expense for the period differs from the amount that would result from applying the federal statutory tax rate to net loss before taxes primarily because of the change in valuation allowance.
On March 27, 2020, the CARES Act, an economic relief package in response to the COVID-19 pandemic, was signed into law. The CARES Act contains several corporate income tax provisions, including making remaining alternative minimum tax credits immediately refundable; providing a 5-year carryback of NOL carryforwards generated in tax years 2018, 2019, and 2020, and removing the 80% taxable income limitation on utilization of those NOLs if carried back to prior tax years or utilized in tax years beginning before 2021; and temporarily liberalizing the interest deductibility rules under Section 163(j) of the Tax Cuts and Jobs Act, by raising the adjusted taxable income limitation from 30% to 50% for tax years 2019 and 2020 and giving taxpayers the election of using 2019 adjusted taxable income for purposes of computing 2020 interest deductibility. The CARES Act did not have a material effect on the realizability of deferred income tax assets or tax expense in 2020.
The effective tax rate of the Company's provision (benefit) for income taxes differs from the federal statutory rate as follows:
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Statutory rate |
|
|
21.00 |
% |
|
|
21.00 |
% |
|
State tax |
|
|
0.06 |
% |
|
|
— |
|
|
General business credits |
|
|
1.06 |
% |
|
|
— |
|
|
Other permanent differences |
|
|
(0.25 |
)% |
|
|
— |
|
|
Change in valuation allowance |
|
|
(15.91 |
)% |
|
|
(21.00 |
)% |
|
Change in fair value of tranche liability |
|
|
(5.96 |
)% |
|
|
— |
|
|
Income tax provision (benefit) |
|
|
0.00 |
% |
|
|
0.00 |
% |
Deferred tax assets and valuation allowance
Deferred tax assets reflect the tax effects of NOLs, tax credit carryovers, and temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. At December 31, 2020 and December 31, 2019, the significant components of the Company’s net deferred tax asset are as follows (in thousands):
F-20
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
|
|
|
For the Year Ended December 31, 2020 |
|
|
For the Period from September 20, 2019 (date of inception) to December 31, 2019 |
|
||
|
Net operating loss carryforwards |
|
$ |
5,810 |
|
|
$ |
— |
|
|
Tax credit carryforwards |
|
|
672 |
|
|
|
— |
|
|
Accruals and reserves |
|
|
334 |
|
|
|
— |
|
|
Other |
|
|
21 |
|
|
|
— |
|
|
Intangibles |
|
|
2,390 |
|
|
|
206 |
|
|
Organizational and start-up costs |
|
|
— |
|
|
|
28 |
|
|
Non-qualified stock options |
|
|
555 |
|
|
|
— |
|
|
Total deferred tax assets |
|
|
9,782 |
|
|
|
234 |
|
|
Valuation allowance |
|
|
(9,782 |
) |
|
|
(234 |
) |
|
Deferred tax asset, net of allowance |
|
$ |
— |
|
|
$ |
— |
|
There are no deferred tax liabilities as of December 31, 2020 and December 31, 2019, respectively. The valuation allowance is equal to the total deferred tax asset amounts as of December 31, 2020 and December 31, 2019 as there are no deferred tax liabilities in the respective periods. ASC 740 requires that the tax benefit of net operating losses, temporary differences and credit carryforwards be recorded as an asset to the extent that management assesses that realization is "more likely than not." Realization of the future tax benefits is dependent on the Company's ability to generate sufficient taxable income within the carryforward period. Because of the Company's recent history of operating losses, management believes that recognition of the deferred tax assets arising from the above-mentioned future tax benefits is currently not likely to be realized and, accordingly, has provided a valuation allowance.
The valuation allowance increased by $9.5 million during the year ended December 31, 2020 and by $0.2 million for the period from Inception to December 31, 2019.
There were no net operating loss and tax credit carryforwards as of December 31, 2019. As of December 31, 2020, there were net federal operating losses of $27.7 million, federal tax credit carryforward of $0.9 million, and state tax credit carryforward of less than $0.1 million. The net operating losses and state tax credit carryforward do not expire. The federal tax credit carryforward will expire in 2040. The Company files federal and state income tax returns and, in the normal course of business, the Company is subject to examination by these taxing authorities.
Pursuant to Section 382 of the Internal Revenue Code, certain substantial changes in the Company's ownership may result in a limitation on the amount of NOL carryforwards and tax credit carryforwards that may be used in future years. Utilization of the NOL and tax credit carryforwards may be subject to a substantial annual limitation under Section 382 of the Internal Revenue Code of 1986 due to ownership change limitations that have occurred previously or that could occur in the future. These ownership changes may limit the amount of NOL and tax credit carryforwards that can be utilized annually to offset future taxable income and tax, respectively. The Company has not completed a study to assess whether an ownership change has occurred, or whether there have been multiple ownership changes since its formation. There could also be additional ownership changes in the future which may result in additional limitations on the utilization of NOL carryforwards and credits.
Note 11—Commitments and Contingencies
Litigation
The Company is not a party to any material legal proceedings and is not aware of any pending or threatened claims. From time to time, the Company may be subject to various legal proceedings and claims that arise in the ordinary course of its business activities.
Commitments
In the normal course of business, the Company enters into contracts that contain a variety of indemnifications with its employees, licensors, suppliers and service providers. The Company’s maximum exposure under these arrangements is unknown at December 31, 2020. The Company does not anticipate recognizing any significant losses relating to these arrangements.
As of December 31, 2019, the Company was not a party to any leasing agreements. On December 17, 2020, the Company entered into a lease agreement (the “Durham Lease”) with Patriot Park Partners II, LLC, a Delaware limited liability company (the “Landlord”), pursuant to which the Company agreed to lease approximately 187,500 square feet of a manufacturing facility located at 5 National Way, Durham, North Carolina (the “Facility”). The Durham Lease commences on April 1, 2021 and is expected to have a term of approximately fifteen years and six months. The Company has two options to extend the term of the Durham Lease, each for a period of an additional five years.
F-21
Taysha Gene Therapies, Inc.
Notes to Consolidated Financial Statements
The Company was not required to provide a security deposit in connection with its entry into the Durham Lease. The Company will be responsible for constructing interior improvements within the Facility. The Company also has a one-time right of first offer during the term of the Durham Lease to purchase the Facility. The Landlord has the right to terminate the Durham Lease upon specified events of default, including the Company’s failure to pay rent in a timely manner and upon the occurrence of certain events of insolvency with respect to the Company.
The Company may terminate the Durham Lease if construction of the base building shell of the Facility is not complete by May 16, 2021.
As of December 31, 2020, the Company incurred initial direct costs to enter into the Durham Lease of approximately $0.8 million. The costs have been recorded on the consolidated balance sheets as a deferred lease asset and will be amortized into earnings over the term of the Durham Lease.
The following table summarizes lease commitments as of December 31, 2020 (in thousands):
|
Year Ending December 31, |
|
|
|
|
|
2021 |
|
$ |
314 |
|
|
2022 |
|
|
1,282 |
|
|
2023 |
|
|
1,317 |
|
|
2024 |
|
|
1,354 |
|
|
2025 |
|
|
1,391 |
|
|
Thereafter |
|
|
17,599 |
|
|
Total Lease Commitments |
|
$ |
23,257 |
|
Note 12—Subsequent Events
Lease Agreement
On January 11, 2021, the Company entered into a lease agreement (the “Dallas Lease”) with Pegasus Park, LLC, a Delaware limited liability company (the “Dallas Landlord”), pursuant to which the Company will lease approximately 15,000 square feet of office space at 3000 Pegasus Park Drive, Dallas, Texas 75247 (the “Office Space”). The Dallas Lease commences on the date on which certain improvements to the Office Space have been made and the Office Space is tendered to the Company for possession, which the Company and the Dallas Landlord presently anticipate to be delivered on or about April 15, 2021, and will have a term of approximately ten years. The Company has an option to extend the term of the Dallas Lease for one additional period of five years. Total future minimum lease payments under the Dallas Lease over the initial 10 year term are approximately $4.9 million. The Company may terminate the Dallas Lease if the Office Space is not delivered with all improvements to be made by the Dallas Landlord pursuant to the Dallas Lease if not substantially completed by May 31, 2021.
Equity Grants
In January, February, and March 2021, the Company granted options to purchase an aggregate of 1,621,900 shares of its common stock at a weighted-average exercise price of $28.81 per share.
F-22
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
We maintain “disclosure controls and procedures,” as defined in Rule 13a-15(e) and Rule 15d-15(e) under the Exchange Act that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to our management, including our principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure.
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act ), as of the end of the period covered by this Form 10-K. Based on such evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that as of December 31, 2020, our disclosure controls and procedures were effective to provide reasonable assurance that the information required to be disclosed by us in this Form 10-K was (a) reported within the time periods specified by SEC rules and regulations, and (b) communicated to our management, including our Chief Executive Officer and Chief Financial Officer, to allow timely decisions regarding any required disclosure.
Management's Report on Internal Control Over Financial Reporting
This Annual Report on Form 10-K does not include a report of management’s assessment regarding internal control over financial reporting or an attestation report of our independent registered public accounting firm as allowed by the SEC during the transition period for newly public companies.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting identified in management’s evaluation pursuant to Rules 13a-15(d) or 15d-15(d) of the Exchange Act during the quarter ended December 31, 2020 that materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Inherent Limitations on Effectiveness of Internal Controls
In designing and evaluating the disclosure controls and procedures, management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable, not absolute, assurance of achieving the desired control objectives. In addition, the design of disclosure controls and procedures must reflect the fact that there are resource constraints and that management is required to apply judgment in evaluating the benefits of possible controls and procedures relative to their costs. Our management, including our Chief Executive Officer and Chief Financial Officer, believes that our disclosure controls and procedures and internal control over financial reporting are designed to provide reasonable assurance of achieving their objectives and are effective at the reasonable assurance level. However, our management does not expect that our disclosure controls and procedures or our internal control over financial reporting will prevent all errors and all fraud.
None.
103
Item 10. Directors, Executive Officers and Corporate Governance.
The names of our directors and executive officers, their ages as of March 1, 2021 and certain other information about them are set forth below. There are no family relationships among any of our directors or executive officers.
Executive Officers
RA Session II, age 42, has served as our President and Chief Executive Officer and a member of our board of directors since our founding in September 2019. In addition to serving as our President and Chief Executive Officer, Mr. Session currently serves as Entrepreneur-in-Residence of the University of Texas Southwestern Medical Center. He has served on the board of directors of Chardan Healthcare Acquisition 2 Corp. since April 2020. Mr. Session previously served as Chief Business Officer of the gene therapy subsidiaries of BridgeBio Pharma, Inc., a biopharmaceutical company, from January 2019 to April 2020; Senior Vice President, Corporate Strategy and Project Management of AveXis, Inc., a gene therapy company, from March 2017 to May 2018; and in various roles for PTC Therapeutics, Inc., a biopharmaceutical company, from June 2013 to March 2017, most recently as the Vice President of Commercial Development. Mr. Session has also served as an advisor to multiple biotechnology companies, including Alcyone Lifesciences, Inc. from January 2019 to December 2019, 4D Molecular Therapeutics, Inc. from August 2018 to December 2019 and Celenex from June 2018 to September 2018. Mr. Session earned a B.S.B.A. in finance from the University of North Carolina at Charlotte, an M.S.F. in finance from Texas A&M University-Commerce and an M.B.A. from Texas A&M University-Commerce. Our board of directors believes that Mr. Session is qualified to serve as a director based on his role as our Chief Executive Officer and his extensive management experience in the biotechnology industry.
Kamran Alam, age 43, has served as our Chief Financial Officer since August 2020. Mr. Alam previously served as Senior Vice President, Finance and Principal Financial Officer of Rocket Pharmaceuticals, Inc., a biopharmaceutical company, from October 2019 to July 2020 and as Vice President, Finance at AveXis, Inc., a gene therapy company, from April 2016 to October 2019. From 2013 to April 2016, he held positions of increasing responsibility at Aptinyx Inc., a biopharmaceutical company, where at the time of his departure he was a Senior Director, Finance and Accounting. Mr. Alam is a Certified Public Accountant and earned a B.B.A. from the Ross School of Business at University of Michigan and an M.B.A. in finance from the Kelley School of Business at Indiana University.
Suyash Prasad, M.B.B.S., F.F.P.M., age 50, has served as our Chief Medical Officer and Head of Research and Development since June 2020. Dr. Prasad has served as principal of Suyash Prasad Consulting LLC, a consulting firm, since October 2019. He previously served as Senior Vice President and Chief Medical Officer of Audentes Therapeutics, Inc., a gene therapy company, from 2014 to June 2019. Dr. Prasad earned a medical degree from the University of Newcastle-upon-Tyne, United Kingdom, a master’s degree (with distinction) in translational science from Kings College, London, United Kingdom, and a diploma in pharmaceutical medicine from the Faculty of Pharmaceutical Medicine of the Royal Colleges of Physicians of the United Kingdom. Dr. Prasad is a United Kingdom board-certified physician and is a member of the Royal College of Physicians and the Royal College of Pediatrics and Child Health and is a Fellow of the Faculty of Pharmaceutical Medicine of the Royal College of Physicians of the United Kingdom.
Non-Employee Directors
Sean P. Nolan, age 53, has served as the Chairman of our board of directors since March 2020. He has served as the President of Nolan Capital, LLC, an investment fund, since October 2019. Mr. Nolan most recently served as President, Chief Executive Officer and a member of the board of directors of AveXis, Inc., a gene therapy company, from June 2015 to May 2018 until its acquisition by Novartis International AG. Mr. Nolan has served on the board of directors of Ventas, Inc., a healthcare real estate investment trust company, since July 2019 and previously served on the board of directors of Neoleukin Therapeutics, Inc., a biopharmaceutical company, from February 2015 to June 2020. Mr. Nolan serves on the boards of several privately held companies including Chairman of Encoded Therapeutics and Affinia Therapeutics, and Executive Chairman of Jaguar Gene Therapy, LLC and Istari Oncology. Mr. Nolan earned a B.S. in biology from John Carroll University. Our board of directors believes that Mr. Nolan is qualified to serve as a director based upon his more than 29 years of broad leadership and management experience in the biopharmaceutical industry.
Phillip B. Donenberg, age 60, has served as a member of our board of directors since August 2020. Mr. Donenberg currently serves as Senior Vice President and Chief Financial Officer of Jaguar Gene Therapy, LLC, a privately held early-stage gene therapy company, and has served in such role since February 2020. Mr. Donenberg has served on the board of directors and as chairman of the
104
audit committee of AVROBIO, Inc., a gene therapy company, since June 2018. Previously, Mr. Donenberg served as Chief Financial Officer and Senior Vice President of Assertio Therapeutics, Inc., a pharmaceutical company, from July 2018 to November 2018. He served as Senior Vice President and Chief Financial Officer of AveXis, Inc., a gene therapy company, from October 2017 to June 2018 and as Vice President, Corporate Controller from September 2016 to October 2017. Mr. Donenberg served as Chief Financial Officer of RestorGenex Corporation from 2014 until its merger with Diffusion Pharmaceuticals LLC, a pharmaceutical company, in January 2016, and served as the merged company’s consultant Chief Financial Officer until September 2016. Mr. Donenberg earned a B.S. in accountancy from the University of Illinois Champaign-Urbana College of Business and is a Certified Public Accountant. Our board of directors believes that Mr. Donenberg is qualified to serve as a director based on his financial expertise and his experience as a director and executive of companies in the biotechnology and pharmaceutical industries.
Paul B. Manning, age 65, has served as a member of our board of directors since March 2020. Mr. Manning currently serves as the Chief Executive Officer of PBM Capital Group, LLC, a private equity investment firm in the business of investing in healthcare and life-science related companies, which he founded in 2010. Mr. Manning currently serves as Chairman of the board of directors of Verrica Pharmaceuticals Inc., a biopharmaceutical company, and on the board of directors of Liquidia Corporation, a biopharmaceutical company. Additionally, he previously served on the boards of directors of Dova Pharmaceuticals, Inc., a biopharmaceutical company, from September 2016 to November 2019 and AveXis, Inc., a gene therapy company, from April 2014 to May 2018. Mr. Manning earned a B.S. in microbiology from the University of Massachusetts. Our board of directors believes that Mr. Manning is qualified to serve as a director based upon his more than 30 years of managerial and operational experience in the healthcare industry and as an investor in healthcare-related companies.
Sukumar Nagendran, M.D., age 55, has served as a member of our board of directors since July 2020. Dr. Nagendran currently serves as President, Research and Development at Jaguar Gene Therapy, LLC, a position he has held since February 2020. Dr. Nagendran has served on the board of directors of Solid Biosciences Inc., a life sciences company, since September 2018 and currently serves as an advisor to Encoded Therapeutics, Inc., a biotechnology company. He previously served on the board of directors of Health Sciences Acquisition Corp., a special purpose acquisition company, from March 2019 to December 2019 prior to its merger with Immunovant, Inc. Dr. Nagendran most recently served as Senior Vice President and Chief Medical Officer of AveXis, Inc., a gene therapy company, from September 2015 to May 2018, and previously served as Vice President, Head of Medical Affairs of U.S. and International Business for Quest Diagnostics Inc., a clinical laboratory, from March 2013 to September 2015. Dr. Nagendran earned a B.A. from Rutgers University and an M.D. from the University of Medicine and Dentistry of New Jersey and trained in Internal Medicine at Mayo Clinic in Rochester, Minnesota. Our board of directors believes that Dr. Nagendran is qualified to serve as a director based upon his more than 30 years of experience with gene therapy development and clinical development strategy.
Kathleen Reape, M.D., age 55, served as Chief Medical Officer of Spark Therapeutics, Inc. from September 2018 to March 2020 and as the Head of Clinical Research and Development of Spark from January 2016 to September 2018. Prior to joining Spark, Dr. Reape served as President of Ark Medical Consulting from August 2015 to January 2016. She served as Senior Vice President, Clinical Development, Global Brands R&D of Allergan plc from March 2015 to July 2015 following its merger with Actavis plc where Dr. Reape served as Vice President, Clinical Development, Global Brands R&D from August 2014 to March 2015. Dr. Reape earned a B.A. in biology and an M.D. from the University of Pennsylvania. Our board of directors believes that Dr. Reape is qualified to serve as a director based upon her extensive experience in gene therapy and clinical research and development as well as her involvement with the regulatory approval of products, including small molecules, biologics, biosimilars and therapeutic devices.
Laura Sepp-Lorenzino, Ph.D., age 60, has served as Executive Vice President, Chief Scientific Officer of Intellia Therapeutics, Inc. since May 2019. From September 2017 to May 2019, Dr. Sepp-Lorenzino served as Vice President, Head of Nucleic Acid Therapies at Vertex Pharmaceuticals, Inc. She served as Vice President, Entrepreneur-in-Residence at Alnylam Pharmaceuticals, Inc. from 2014 to September 2017. She also served in roles of increasing responsibility at Merck & Co. from December 1999 to March 2014, including most recently as Executive Director and Department Head of the RNA Therapeutics Discovery Biology Unit. Dr. Sepp-Lorenzino earned a professional degree in biochemistry from the Universidad de Buenos Aires in Argentina and an M.S. and Ph.D. in biochemistry from New York University. Our board of directors believes that Dr. Sepp-Lorenzino is qualified to serve as a director based upon her extensive experience in research and development of nucleic acid therapies.
Section 16(a) Beneficial Ownership Reporting Compliance
Section 16(a) of the Securities Exchange Act of 1934, as amended, or the Exchange Act, requires our directors and executive officers, and persons who own more than ten percent of a registered class of our equity securities, to file with the SEC initial reports of ownership and reports of changes in ownership of common stock and other equity securities of the Company. Officers, directors and
105
greater than ten percent stockholders are required by SEC regulation to furnish the Company with copies of all Section 16(a) forms they file.
To our knowledge, based solely on a review of the copies of such reports furnished to us and written representations that no other reports were required, during the fiscal year ended December 31, 2020, all Section 16(a) filing requirements applicable to its officers, directors and greater than ten percent beneficial owners were complied with.
Audit Committee and Audit Committee Financial Expert
The Audit Committee of the board of directors was established by the board in accordance with Section 3(a)(58)(A) of the Exchange Act to oversee the Company’s corporate accounting and financial reporting processes and audits of its financial statements. The Audit Committee is comprised of three directors: Mr. Donenberg and Drs. Nagendran and Sepp-Lorenzino, with Mr. Donenberg serving as chair.
The board of directors reviews the Nasdaq Stock Market, or Nasdaq, listing standards definition of independence for Audit Committee members on an annual basis and has determined that all members of the Company’s Audit Committee are independent (as independence is currently defined in Rule 5605(c)(2)(A)(i) and (ii) of the Nasdaq listing standards and Rule 10A-3 of the Exchange Act).
The board of directors has also determined that Mr. Donenberg qualifies as an “audit committee financial expert,” as defined in applicable SEC rules. The board made a qualitative assessment of Mr. Donenberg’s level of knowledge and experience based on a number of factors, including his formal education, that he is a Certified Public Accountant and his experience as a chief financial officer for several public reporting companies.
Stockholder Recommendations for Director Candidates
Historically, we have not provided a formal process related to stockholder communications with the board of directors. Nevertheless, every effort has been made to ensure that the views of stockholders are heard by the board or individual directors, as applicable, and that appropriate responses are provided to stockholders in a timely manner. The Company believes its responsiveness to stockholder communications to the board has been excellent.
Code of Business Conduct and Ethics
We have adopted a Code of Business Conduct and Ethics, which is applicable to all of our employees, executive officers and directors. This includes our principal executive officer, principal financial officer and principal accounting officer or controller, or persons performing similar functions. The full text of the Code of Business Conduct and Ethics is available on our website at www.tayshagtx.com. We intend to post on our website all disclosures that are required by law or the listing standards of the Nasdaq Stock Market concerning any amendments to, or waivers from, any provision of the Code of Business Conduct and Ethics.
Item 11. Executive Compensation.
This section provides a summary of the compensation of our “named executive officers,” who are the three executive officers listed in the “Summary Compensation Table” below. In addition to presenting quantitative compensation information in the tables below, this section also provides a qualitative description of the material factors helpful to an understanding of such data.
106
The following table sets forth information regarding compensation awarded to, earned by and paid to our named executive officers with respect to the year ended December 31, 2020.
|
Name and Principal Position |
|
Salary ($) |
|
|
Stock Awards ($) |
|
|
Non-Equity Incentive Plan Compensation(2) ($) |
|
|
All Other Compensation ($) |
|
Total ($) |
|
||||
|
President, Chief Executive Officer and Director(3) |
|
|
362,594 |
|
|
|
4,060,626 |
|
|
|
271,878 |
|
|
154(4) |
|
|
4,695,252 |
|
|
Kamran Alam Chief Financial Officer |
|
142,088(5) |
|
|
|
4,933,703 |
|
|
|
85,217 |
|
|
330,153(6) |
|
|
5,491,161 |
|
|
|
Suyash Prasad, M.B.B.S, F.F.P.M. Chief Medical Officer |
|
216,833(7) |
|
|
|
3,668,409 |
|
|
|
129,975 |
|
|
152(4) |
|
|
4,015,369 |
|
|
|
(2) |
See “—Narrative to Summary Compensation Table—Non-Equity Incentive Plan Compensation” below for a description of the material terms of the program pursuant to which this compensation was awarded. |
|
(3) |
Mr. Session is also a member of our board of directors, but did not receive any additional compensation in his capacity as a director. Mr. Session’s employment commenced with us in April 2020. The 2020 salary reported reflects the pro rata portion of Mr. Session’s annual salary earned during 2020 from commencement of his employment through December 31, 2020. |
|
(4) |
Represents a holiday meal stipend. |
|
(5) |
Mr. Alam’s employment with us commenced in August 2020. The 2020 salary reported reflects the pro rata portion of Mr. Alam’s annual salary earned during 2020 from commencement of his employment through December 31, 2020. |
|
(6) |
Represents (a) a reimbursement of $107,021 for out-of-pocket expenses associated with Mr. Alam repaying his sign-on bonus to his former employer and related gross-up payment in the amount of $106,560 to cover Mr. Alam’s tax liability with respect to such reimbursement, (b) a reimbursement of $63,714 for certain out-of-pocket indemnification expenses associated with Mr. Alam’s resignation from his former employer and related gross-up payment in the amount of $52,704 to cover Mr. Alam’s tax liability with respect to such reimbursement and (c) a holiday meal stipend of $154. |
|
(7) |
Dr. Prasad’s employment with us commenced in June 2020. The 2020 salary reported reflects the pro rata portion of Dr. Prasad’s annual salary earned during 2020 from commencement of his employment through December 31, 2020. |
Narrative to Summary Compensation Table
The Compensation Committee of our board of directors has historically determined our executives’ compensation, including the compensation of our named executive officers. Our Compensation Committee typically reviews and discusses management’s proposed compensation with the Chief Executive Officer for all executives other than the Chief Executive Officer. Based on those discussions and its discretion, the Compensation Committee then approves the compensation of each executive officer without members of management present.
Annual Base Salary
We have entered into employment agreements with each of our named executive officers that establish annual base salaries, which are generally determined, approved and reviewed periodically by our Compensation Committee in order to compensate our named executive officers for the satisfactory performance of duties to the Company. Annual base salaries are intended to provide a fixed component of compensation to our named executive officers, reflecting their expertise, experience, knowledge, roles and responsibilities. Base salaries for our named executive officers have generally been set at levels deemed necessary to attract and retain individuals with superior talent. Merit-based increases to salaries are based on management’s
107
assessment of the individual executive’s performance, the recommendations made by the Chief Executive Officer to the Compensation Committee and the competitive market in which we operate for talent.
Prior to our initial public offering, Mr. Session’s executive employment agreement provided for an annual base salary of $450,000, Mr. Alam’s offer letter provided for an annual base salary of $350,000 and Dr. Prasad’s offer letter provided for an annual base salary of $420,000. In connection with our initial public offering in September 2020, the Compensation Committee approved base salaries of $542,800, $390,000 and $432,600 for each of Messrs. Session and Alam and Dr. Prasad.
Non-Equity Incentive Plan Compensation
Our named executive officers are eligible to receive annual incentive compensation based on the satisfaction of individual and corporate performance objectives established by the board. Each named executive officer has a target annual incentive opportunity, calculated as a percentage of annual base salary, and may earn more or less than the target amount based on our company’s and his or her individual performance. For 2020, the target annual incentive opportunities as a percentage of base salary for our named executive officers were 50% for Mr. Session and 40% for each of Mr. Alam and Dr. Prasad. The amounts of any annual incentives earned are determined after the end of the year, based on the achievement of the designated corporate and individual performance objectives, and may be paid in cash or equity. The Compensation Committee determined that the percentage attainment of our corporate goals for 2020 was 150% and approved individual performance achievement payouts for each named executive officer in the amounts reflected in the column of the Summary Compensation Table above entitled “Non-Equity Incentive Plan Compensation.”
Equity-Based Awards
Our equity-based incentive awards granted to our named executive officers are designed to align the interests of our named executive officers with those of our stockholders. Vesting of equity awards is generally tied to each officer’s continuous service with us and serves as an additional retention measure. Our executives generally are awarded an initial new hire grant upon commencement of employment and thereafter on an annual basis. Additional grants may occur periodically in order to specifically incentivize executives with respect to achieving certain corporate goals or to reward executives for exceptional performance. Following the completion of our initial public offering, we grant all equity awards pursuant to our 2020 Stock Incentive Plan.
Outstanding Equity Awards at December 31, 2020
The following table sets forth certain information about outstanding equity awards granted to our named executive officers that were outstanding as of December 31, 2020.
|
|
|
Stock Awards |
|
|||||
|
Name |
|
Number of Shares or Units of Stock That Have Not Vested (#) |
|
|
Market Value of Shares or Units of Stock That Have Not Vested ($)(1) |
|
||
|
RA Session II |
|
|
769,058 |
|
|
|
20,410,799 |
|
|
Kamran Alam |
|
|
331,121 |
|
|
|
8,787,951 |
|
|
Suyash Prasad, M.B.B.S, F.F.P.M. |
|
|
668,745 |
|
|
|
17,748,492 |
|
|
(1) |
The market value of our common stock is based on the closing price of our common stock on the Nasdaq Global Select Market on December 31, 2020. |
Employment Agreements with our Named Executive Officers and Potential Payments and Benefits Upon Termination or Change in Control
Amended and Restated Employment Agreement with Mr. Session
We have entered into an amended and restated executive employment agreement with Mr. Session, which reflects an initial annual base salary of $542,800, which is subject to adjustment at the discretion of our board of directors, and an annual bonus target equal to 50% of Mr. Session’s annual base salary based upon the achievement of individual and company performance goals as determined by our board of directors.
108
Pursuant to the amended and restated executive employment agreement, if we terminate Mr. Session’s employment without “cause,” or if Mr. Session terminates his employment for “good reason” (each, as defined in the executive employment agreement), he will be entitled to continued payment of his base salary for 12 months and his then-outstanding equity awards will vest in full. Such severance and acceleration benefits are conditioned upon Mr. Session’s execution of and compliance with an effective and irrevocable general release, compliance with certain non-competition and non-solicitation obligations, resignation from all positions with us and return of all our property. The amended and restated executive employment agreement further provides that Mr. Session are entitled to the severance benefits described in “—Change in Control Severance Plan.”
Amended and Restated Offer Letters with Mr. Alam and Dr. Prasad
We have entered into amended and restated offer letters with Mr. Alam and Dr. Prasad. For Dr. Prasad, the amended and restated offer letter reflects an initial annual base salary of $432,600, which is subject to adjustment at the discretion of our board of directors, and an annual bonus target equal to 40% of Dr. Prasad’s annual base salary based upon the achievement of individual and company performance goals as determined by our board of directors. For Mr. Alam, the amended and restated offer letter reflects an initial annual base salary of $390,000, which is subject to adjustment at the discretion of our board of directors, and an annual bonus target equal to 40% of Mr. Alam’s annual base salary based upon the achievement of individual and company performance goals as determined by our board of directors.
Pursuant to the amended and restated offer letters, if we terminate Dr. Prasad or Mr. Alam’s employment without “cause,” or if Dr. Prasad or Mr. Alam terminates his employment for “good reason” (each, as to be defined in such executive’s amended and restated offer letter), he will be entitled to continued payment of his base salary for 12 months. Such severance benefits are conditioned upon the executive’s execution of and compliance with an effective and irrevocable general release, compliance with certain non-competition and non-solicitation obligations, resignation from all positions with us and return of all our property. The amended and restated offer letters further provide that Dr. Prasad and Mr. Alam are entitled to the severance benefits described in “—Change in Control Severance Plan.”
Change in Control Severance Plan
Each of our named executive officers is eligible to receive severance benefits under the terms of our Change in Control Severance Plan adopted by the board of directors in September 2020.
The Change in Control Severance Plan provides for severance benefits upon a “covered termination” that occurs during a “change in control period” (each as described below). Upon a covered termination that occurs during a change in control period, participants will be entitled to a lump sum payment equal to the participant’s base salary for a period of months (18 months for Mr. Session, 12 months for each of Mr. Alam and Dr. Prasad), a lump sum payment equal to a multiple of the participant’s target annual bonus (150% for Mr. Session, 100% for each of Mr. Alam and Dr. Prasad), payment of continued group health benefits for a period of months (18 months for Mr. Session, 12 months for each of Mr. Alam and Dr. Prasad) and full accelerated vesting of all outstanding equity awards (including performance-based awards, which shall vest at 100% of target).
All severance benefits under the Change in Control Severance Plan are subject to the participant’s execution of an effective release of claims against the company and compliance with the terms of any confidential information agreement, proprietary information and inventions agreement and any other agreement between the participant and the company. For purposes of the Change in Control Severance Plan, a “covered termination” is a termination of employment by the company without “cause,” as defined in the Change in Control Severance Plan, or as a result of the participant’s resignation for “good reason,” as defined in the Change in Control Severance Plan, in either case, not as a result of death or disability. For purposes of the Change in Control Severance Plan, a “change in control period” is the period of time beginning on the date on which a “change in control,” as defined in the 2020 Stock Incentive Plan, becomes effective (or, in the case of Mr. Session, the period beginning three months prior to the date on which a change in control becomes effective) and ending on the first anniversary of the effective date of such change in control.
Non-Employee Director Compensation
Non-Employee Director Compensation Policy
Our board of directors has adopted a non-employee director compensation policy, pursuant to which each of our directors who is not an employee or consultant of our company is eligible to receive compensation for service on our board of directors and committees of our board of directors.
109
Each eligible director will receive an annual cash retainer of $35,000 for serving on our board of directors, and the independent chairperson of the board of directors will receive an additional annual cash retainer of $30,000 for his or her service. The chairperson of the audit committee of our board of directors will be entitled to additional annual cash retainer of $15,000, the chairperson of the compensation committee of our board of directors will be entitled to additional annual cash retainer of $10,000 and the chairperson of the nominating and corporate governance committee of our board of directors will be entitled to additional annual cash retainer of $8,000. The members of the audit committee will be entitled to an additional annual cash retainer of $7,500, the members of the compensation committee of our board of directors will be entitled to additional annual cash retainer of $5,000 and the members of the nominating and corporate governance committee of our board of directors will be entitled to an additional annual cash retainer of $4,000; however, in each case such cash retainer is payable only to members who are not the chairperson of such committee.
In addition, upon the pricing of our initial public offering, each eligible director was granted a non-statutory stock option to purchase 31,000 shares of our common stock at the initial public offering price under our 2020 Stock Incentive Plan, with the shares vesting in 36 equal monthly installments, subject to continued service as a director through the vesting date. Each new eligible director who joins our board of directors will be granted a non-statutory stock option to purchase 31,000 shares of our common stock under our 2020 Stock Incentive Plan, with the shares vesting in 36 equal monthly installments, subject to continued service as a director through the vesting date.
On the date of each annual meeting of our stockholders, each eligible director who continues to serve as a director of our company following the meeting will be granted a non-statutory stock option to purchase 15,500 shares of our common stock under our 2020 Stock Incentive Plan, with the shares vesting on the earlier of the first anniversary of the date of grant or the next annual stockholders meeting, subject to continued service as a director though the applicable vesting date.
Each option awarded to eligible directors under the non-employee director compensation policy will be subject to accelerated vesting upon a Change in Control (as defined in the 2020 Stock Incentive Plan).
The exercise price per share of each stock option granted under the non-employee director compensation policy will be equal to the closing price of our common stock on the Nasdaq Global Select Market on the date of grant. Each stock option will have a term of ten years from the date of grant, subject to earlier termination in connection with a termination of the eligible directors continuous service with us (provided that upon a termination of service other than for death, disability or cause, the post-termination exercise period will be 12 months from the date of termination).
Director Compensation Table
The following table sets forth information regarding the compensation earned for service on our board of directors in 2020 by our non-employee directors. RA Session II, our President and Chief Executive Officer, is also a member of our board of directors but did not receive any additional compensation for service as a director.
|
Name |
|
Fees Earned or Paid in Cash ($) |
|
|
Option Awards ($) (1)(2) |
|
|
Total ($) |
|
|||
|
Claire Aldridge, Ph.D.(3) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Phillip B. Donenberg |
|
|
14,808 |
|
|
|
519,079 |
|
|
|
533,887 |
|
|
Paul B. Manning |
|
|
11,577 |
|
|
|
432,140 |
|
|
|
443,717 |
|
|
Sukumar Nagendran, M.D. |
|
|
14,135 |
|
|
|
518,916 |
|
|
|
533,051 |
|
|
Sean P. Nolan |
|
|
24,435 |
|
|
|
432,140 |
|
|
|
456,575 |
|
|
Kathleen Reape, M.D. |
|
|
4,071 |
|
|
|
430,484 |
|
|
|
434,555 |
|
|
Laura Sepp-Lorenzino, Ph.D. |
|
|
4,437 |
|
|
|
430,484 |
|
|
|
434,921 |
|
110
|
(2) |
The table below shows the aggregate number of option awards outstanding for each of our directors who is not a named executive officer, as of December 31, 2020: |
|
Name |
|
Number of Outstanding Options |
|
|
|
Claire Aldridge, Ph.D. |
|
-- |
|
|
|
Phillip B. Donenberg |
|
|
39,171 |
|
|
Paul B. Manning |
|
|
31,000 |
|
|
Sukumar Nagendran, M.D. |
|
|
39,171 |
|
|
Sean P. Nolan |
|
|
31,000 |
|
|
Kathleen Reape, M.D. |
|
|
31,000 |
|
|
Laura Sepp-Lorenzino, Ph.D. |
|
|
31,000 |
|
(3)Dr. Aldridge resigned from our board of directors in July 2020.
Compensation Committee Interlocks and Insider Participation
None of our directors who serve as a member of our compensation committee is, or has at any time during the past year been, one of our officers or employees. None of our executive officers currently serves, or in the past year has served, as a member of the board of directors or compensation committee of any other entity that has one or more executive officers serving on our board of directors or compensation committee.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The following table sets forth information regarding beneficial ownership of our capital stock by:
|
|
• |
each person, or group of affiliated persons, known by us to beneficially own more than 5% of our common stock; |
|
|
• |
each of our directors; |
|
|
• |
our named executive officer; and |
|
|
• |
all of our current executive officers and directors as a group. |
We have determined beneficial ownership in accordance with the rules of the SEC. Under these rules, beneficial ownership includes any shares of common stock as to which the individual or entity has sole or shared voting power or investment power. Applicable percentage ownership is based on 37,761,435 shares of common stock outstanding as of February 15, 2021. In computing the number of shares beneficially owned by an individual or entity and the percentage ownership of that person, shares of common stock subject to options held by such person that are currently exercisable or will become exercisable within 60 days of February 15, 2021 are considered outstanding, although these shares are not considered outstanding for purposes of computing the percentage ownership of any other person.
Unless noted otherwise, the address of all listed stockholders is c/o Taysha Gene Therapies, Inc., 2280 Inwood Road, Dallas, Texas 75235.
111
Except as indicated by the footnotes below, we believe, based on information furnished to us, that each of the stockholders listed has sole voting and investment power with respect to the shares beneficially owned by the stockholder unless noted otherwise, subject to community property laws where applicable.
|
Name of Beneficial Owner |
|
Number of Shares Beneficially Owned |
|
|
Percentage of Shares Beneficially Owned |
|
||
|
Greater than 5% stockholders |
|
|
|
|
|
|
|
|
|
RA Session II(1) |
|
|
9,430,582 |
|
|
|
25.0 |
% |
|
FMR LLC(2) |
|
|
5,664,215 |
|
|
|
15.0 |
|
|
BlackRock, Inc.(3) |
|
|
2,229,816 |
|
|
|
5.9 |
|
|
UT Southwestern(4) |
|
|
2,179,000 |
|
|
|
5.8 |
|
|
Named Executive Officers and Directors |
|
|
|
|
|
|
|
|
|
RA Session II(1) |
|
|
9,430,582 |
|
|
|
25.0 |
|
|
Kamran Alam |
|
-- |
|
|
-- |
|
||
|
Suyash Prasad, M.B.B.S, F.F.P.M.(5) |
|
|
3,844 |
|
|
* |
|
|
|
Phillip B. Donenberg(6) |
|
|
5,166 |
|
|
* |
|
|
|
Paul B. Manning(7) |
|
|
5,220,473 |
|
|
|
13.8 |
|
|
Sean P. Nolan(8) |
|
|
1,096,267 |
|
|
|
2.9 |
|
|
Sukumar Nagendran, M.D.(9) |
|
|
24,392 |
|
|
* |
|
|
|
Kathleen Reape, M.D.(10) |
|
|
3,444 |
|
|
* |
|
|
|
Laura Sepp-Lorenzino, Ph.D.(11) |
|
|
3,444 |
|
|
* |
|
|
|
All current executive officers and directors as a group (9 persons) |
|
|
15,787,612 |
|
|
|
41.8 |
|
|
(1) |
Consists of (a) 9,148,402 shares of common stock (including 769,058 shares of unvested restricted common stock), (b) 141,090 shares of common stock held by the Session 2020 Annuity Trust I, of which Mr. Session is the trustee and has sole voting and investment power with respect to the shares held by such trust and (c) 141,090 shares of common stock held by the Session 2020 Annuity Trust II, of which Mr. Session is the trustee and has sole voting and investment power with respect to the shares held by such trust. |
|
(2) |
This information has been obtained from a Schedule 13G/A filed on February 16, 2021 by FMR LLC. Abigail P. Johnson is a director, the chairman, the chief executive officer and the president of FMR LLC. Members of the Johnson family, including Abigail P. Johnson, are the predominant owners, directly or through trusts, of Series B voting common shares of FMR LLC, representing 49% of the voting power of FMR LLC. The Johnson family group and all other Series B shareholders of FMR LLC have entered into a shareholders’ voting agreement under which all Series B voting common shares will be voted in accordance with the majority vote of Series B voting common shares. Accordingly, through their ownership of voting common shares and the execution of the shareholders’ voting agreement, members of the Johnson family may be deemed, under the Investment Company Act of 1940, to form a controlling group with respect to FMR LLC. Neither FMR LLC nor Abigail P. Johnson has the sole power to vote or direct the voting of the shares owned directly by the various investment companies registered under the Investment Company Act of 1940, or the Fidelity Funds, advised by Fidelity Management & Research Company, a wholly owned subsidiary of FMR LLC, which power resides with the Fidelity Funds’ Boards of Trustees. Fidelity Management & Research Company carries out the voting of the shares under written guidelines established by the Fidelity Funds’ Boards of Trustees. The business address for FMR LLC is 245 Summer Street, Boston, Massachusetts 02110. |
|
(3) |
This information has been obtained from a Schedule 13G filed on February 2, 2021 by BlackRock, Inc., pursuant to which BlackRock, Inc. reported having sole voting power over 2,221,008 shares, shared voting power over no shares, sole dispositive power over 2,229,816 shares and shared dispositive power over no shares. The address of BlackRock, Inc. is 55 East 52nd Street, New York, NY 10055. |
|
(4) |
This information has been obtained from a Schedule 13G filed on February 16, 2021 by entities and individuals associated with The University of Texas/Texas A&M Investment Management Company. Consists of 2,179,000 shares of common stock held by The Board of Regents of the University of Texas System on behalf of UT Southwestern. The business address for The Board of Regents of the University of Texas System is 5323 Harry Hines Boulevard, Dallas, Texas 75390-9094. |
|
(5) |
Consists of 3,844 shares of common stock. |
|
(6) |
Consists of 5,166 shares of common stock issuable upon the exercise of options within 60 days of February 15, 2021. |
112
|
Investments, LLC. The business address for each person and entity named in this footnote is 200 Garrett Street, Suite S, Charlottesville, Virginia 22902. |
|
(8) |
Consists of (a) 1,091,101 shares of common stock held by Nolan Capital, LLC and (b) 5,166 shares of common stock issuable upon the exercise of options within 60 days of February 15, 2021. Mr. Nolan is the President of Nolan Capital, LLC and has shared voting and investment power with respect to the shares held by Nolan Capital, LLC. The business address for each person and entity named in this footnote is 8 The Green, Ste. R, Dover, Delaware 19901. |
|
(9) |
Consists of (a) 19,226 shares of common stock and (b) 5,166 shares of common stock issuable upon the exercise of options within 60 days of February 15, 2021. |
|
(10) |
Consists of 3,444 shares of common stock issuable upon the exercise of options within 60 days of February 15, 2021. |
|
(11) |
Consists of 3,444 shares of common stock issuable upon the exercise of options within 60 days of February 15, 2021. |
Item 13. Certain Relationships and Related Transactions, and Director Independence.
Related-Person Transactions Policy and Procedures
In September 2020, we adopted a related person transaction policy that sets forth our procedures for the identification, review, consideration and approval or ratification of related person transactions. For purposes of our policy only, a related person transaction is a transaction, arrangement or relationship, or any series of similar transactions, arrangements or relationships, in which we and any related person are, were or will be participants in which the amount involved exceeds $120,000. Transactions involving compensation for services provided to us as an employee or director are not covered by this policy. A related person is any executive officer, director or beneficial owner of more than 5% of any class of our voting securities, including any of their immediate family members and any entity owned or controlled by such persons.
Under the policy, if a transaction has been identified as a related person transaction, including any transaction that was not a related person transaction when originally consummated or any transaction that was not initially identified as a related person transaction prior to consummation, our management must present information regarding the related person transaction to our audit committee, or, if audit committee approval would be inappropriate, to another independent body of our board of directors, for review, consideration and approval or ratification. The presentation must include a description of, among other things, the material facts, the interests, direct and indirect, of the related persons, the benefits to us of the transaction and whether the transaction is on terms that are comparable to the terms available to or from, as the case may be, an unrelated third party or to or from employees generally. Under the policy, we will collect information that we deem reasonably necessary from each director, executive officer and, to the extent feasible, significant stockholder to enable us to identify any existing or potential related-person transactions and to effectuate the terms of the policy. In addition, under our Code of Business Conduct and Ethics, our employees and directors have an affirmative responsibility to disclose any transaction or relationship that reasonably could be expected to give rise to a conflict of interest. In considering related person transactions, our audit committee, or other independent body of our board of directors, will take into account the relevant available facts and circumstances including:
|
|
• |
the risks, costs and benefits to us; |
|
|
• |
the impact on a director’s independence in the event that the related person is a director, immediate family member of a director or an entity with which a director is affiliated; |
|
|
• |
the availability of other sources for comparable services or products; and |
|
|
• |
the terms available to or from, as the case may be, unrelated third parties or to or from employees generally. |
The policy requires that, in determining whether to approve, ratify or reject a related person transaction, our audit committee, or other independent body of our board of directors, must consider, in light of known circumstances, whether the transaction is in, or is not inconsistent with, our best interests and those of our stockholders, as our audit committee, or other independent body of our board of directors, determines in the good faith exercise of its discretion.
Certain Related Person Transactions
Our Relationship with UT Southwestern
In November 2019, we entered into the UT Southwestern Agreement with UT Southwestern, a beneficial owner of more than 5% of our capital stock. Claire Aldridge, Ph.D., a former member of our board of directors, was the Associate Vice President of Commercialization and Business Development at UT Southwestern. In accordance with the terms of, and as consideration for, the UT Southwestern Agreement, we issued 2,179,000 shares of our common stock to UT Southwestern in November 2019. We do not have
113
any future milestone or royalty obligations to UT Southwestern under the UT Southwestern Agreement. See “Business—Research, Collaboration and License Agreement with the University of Texas Southwestern Medical Center” for additional information.
We are also obligated to provide research and development funding pursuant to certain sponsored research agreements entered into beginning in April 2020 in connection with the UT Southwestern Agreement. We paid an aggregate of $3.6 million to UT Southwestern under the sponsored research agreements during the year ended December 31, 2020.
In January 2021, we launched an innovation fund with UT Southwestern, pursuant to which we support UT Southwestern’s gene therapy discovery activities. We will have an exclusive option on new programs and intellectual property associated with, and arising from, the research conducted under this arrangement.
Agreements with RA Session II
Guarantee and Security Agreement
In December 2019, Mr. Session, our President and Chief Executive Officer and a member of our board of directors, entered into a guarantee and security agreement by and among Queen’s University, our company and himself, pursuant to which Mr. Session has personally guaranteed payments due by us to Queen’s University in the event that we fail to fund our obligations under a research grant agreement by and between Queen’s University and us.
Loan Agreement
In January 2020, Mr. Session loaned us the principal amount of approximately $1.7 million with interest accruing at a rate of 10% per annum, and we granted Mr. Session a first priority security interest in certain of our assets as collateral for the loan. We repaid Mr. Session an aggregate of approximately $1.7 million, including interest, in payments made in March 2020 and July 2020, and Mr. Session released his security interest in the collateral.
Private Placements of Our Securities
Series A Convertible Preferred Stock Financing
In March 2020, we entered into a preferred stock purchase agreement with certain investors, including beneficial owners of greater than 5% of our capital stock and affiliates of members of our board of directors, pursuant to which we issued and sold to such investors an aggregate of 6,000,000 shares of our Series A convertible preferred stock at a purchase price of $3.00 per share for aggregate gross proceeds of $18.0 million.
Under the agreement, such investors were required to purchase up to an aggregate of 4,000,000 additional shares of our Series A convertible preferred stock upon our achievement of certain milestones. Moreover, such investors had the right, in their sole discretion, to purchase any or all of such additional shares whether or not we achieved the specified milestones. In June and July 2020, such investors exercised in full their option to purchase these additional shares prior to our achievement of such milestones, and we issued and sold to such investors an aggregate of 4,000,000 shares of Series A convertible preferred stock at a purchase price of $3.00 per share for aggregate gross proceeds of $12.0 million.
The table below sets forth the aggregate number of shares of Series A convertible preferred stock issued to our related parties in this financing:
|
Name |
|
Series A Convertible Preferred Stock (#) |
|
|
Aggregate Purchase Price ($) |
|
||
|
PBM TGT Holdings, LLC(1) |
|
|
8,166,667 |
|
|
|
24,500,001.00 |
|
|
Nolan Capital, LLC(2) |
|
|
1,000,000 |
|
|
|
3,000,000.00 |
|
|
(1) |
Paul B. Manning, a member of our board of directors and a holder of more than 5% of our capital stock, is the Chief Executive Officer of PBM Capital Group, LLC and has sole voting and investment power with respect to the shares held by PBM TGT Holdings, LLC. In September 2020, PBM TGT Holdings, LLC distributed all of the shares of Series A convertible preferred stock it previously held to its beneficial owners, including Mr. Manning and entities controlled by Mr. Manning, for no additional consideration in accordance with the terms of its operating agreement. |
|
(2) |
Sean Nolan, the Chairman of our board of directors, is the President of Nolan Capital, LLC. |
114
Series B Convertible Preferred Stock Financing
In July 2020, we entered into a preferred stock purchase agreement with certain investors, including beneficial owners of greater than 5% of our capital stock, members of our board of directors and affiliates of members of our board of directors, pursuant to which we issued and sold to such investors an aggregate of 5,647,048 shares of our Series B convertible preferred stock at a purchase price of $17.00 per share for aggregate gross proceeds of $96.0 million. The financing closed in July and August 2020.
The table below sets forth the aggregate number of shares of Series B convertible preferred stock issued to our related parties in this financing:
|
Name |
|
Series B Convertible Preferred Stock (#) |
|
|
Aggregate Purchase Price ($) |
|
||
|
Entities affiliated with FMR, LLC(1) |
|
|
1,705,882 |
|
|
|
28,999,994.00 |
|
|
PBM Capital Group, LLC(2) |
|
|
117,647 |
|
|
|
1,999,999.00 |
|
|
Sukumar Nagendran, M.D. |
|
|
17,647 |
|
|
|
299,999.00 |
|
|
Suyash Prasad, M.B.B.S., F.F.P.M |
|
|
3,529 |
|
|
|
59,993.00 |
|
|
Nolan Capital, LLC(3) |
|
|
1,470 |
|
|
|
24,990.00 |
|
|
(1) |
Entities affiliated with FMR, LLC collectively hold more than 5% of our capital stock. |
|
(2) |
Paul B. Manning, a member of our board of directors, and a holder of more than 5% of our capital stock, is the Chief Executive Officer of PBM Capital Group, LLC. |
|
(3) |
Sean Nolan, the Chairman of our board of directors, is the President of Nolan Capital, LLC. |
Our Relationship with PBM Capital Group, LLC
In March 2020, we entered into a services agreement with PBM Capital Group, LLC, or the PBM Services Agreement. Under the PBM Services Agreement, PBM Capital Group, LLC provides accounting and other administrative and management services related to payroll administration, human resources, bookkeeping, preparation of financial statements and tax returns, accounts payable and receivable, and other similar functions for a fee of $2,500 per month. We paid PBM Capital Group, LLC an aggregate of $127,000, which includes certain passthrough costs under the PBM Services Agreement during the year ended December 31, 2020.
Employment Arrangements
We have entered into employment agreements or offer letter agreements with certain of our executive officers. For more information regarding our employment agreements with our named executive officers, see “Executive Compensation—Employment Agreements.”
We also employ Patrick Nolan as our Business Development Manager. Patrick Nolan is the son of Sean P. Nolan, the Chairman of our board of directors. We expect that total compensation for Patrick Nolan will exceed $120,000 in 2021.
Indemnification Agreements
We provide indemnification for our directors and executive officers so that they will be free from undue concern about personal liability in connection with their service to our company. Under our amended and restated bylaws, we are required to indemnify our directors and executive officers to the extent not prohibited under Delaware law. We have also entered into indemnity agreements with our executive officers and directors. These agreements provide, among other things, that we will indemnify the officer or director, under the circumstances and to the extent provided for in the agreement, for expenses, damages, judgments, fines and settlements he or she may be required to pay in actions or proceedings which he or she is or may be made a party by reason of his or her position as a director, officer or other agent of our company, and otherwise to the fullest extent permitted under Delaware law and our amended and restated bylaws.
Director Independence
Applicable Nasdaq rules, or the Nasdaq Listing Rules, require a majority of a listed company’s board of directors to be comprised of independent directors. In addition, the Nasdaq Listing Rules require that, subject to specified exceptions, each member of a listed company’s audit, compensation and nominating and corporate governance committees be independent and that audit committee members also satisfy independence criteria set forth in Rule 10A-3 under the Exchange Act of 1934, as amended, or the
115
Exchange Act. The Nasdaq independence definition includes a series of objective tests, such as that the director is not, and has not been for at least three years, one of our employees, that neither the director nor any of his family members has engaged in various types of business dealings with us and that the director is not associated with the holders of more than 5% of our common stock. In addition, under applicable Nasdaq rules, a director will only qualify as an “independent director” if, in the opinion of the listed company’s board of directors, that person does not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of a director.
Our board of directors has determined that all of our directors other than Mr. Session, representing six of our seven directors, are “independent directors” as defined under applicable Nasdaq rules. In making such determination, our board of directors considered the current and prior relationships that each such director has with our company and all other facts and circumstances that our board of directors deemed relevant in determining his independence, including the beneficial ownership of our capital stock by each director and the transactions described in this section.
Item 14. Principal Accounting Fees and Services.
The following table represents aggregate fees billed to us for the fiscal year ended December 31, 2020 by Deloitte & Touche LLP, our principal accountant. No fees were billed to us by Deloitte & Touche LLP during the period from September 2, 2019 (date of our inception) through December 31, 2019.
|
|
|
Year Ended December 31, 2020 |
|
|
|
Audit Fees(1) |
|
$ |
1,311,459 |
|
|
Total Fees |
|
$ |
1,311,459 |
|
|
(1) |
Audit fees consist of fees billed for professional services provided in connection with the audit of our annual financial statements, the review of our quarterly financial statements and audit services that are normally provided by the independent registered public accounting firm in connection with regulatory filings. The audit fees also include fees for professional services provided in connection with our initial public offering in 2020. |
Pre-Approval Policies and Procedures
The Audit Committee has adopted a policy and procedures for the pre-approval of audit and non-audit services rendered by our independent registered public accounting firm, Deloitte & Touche LLP. The policy generally pre-approves specified services in the defined categories of audit services, audit-related services and tax services up to specified amounts. Pre-approval may also be given as part of the Audit Committee’s approval of the scope of the engagement of the independent auditor or on an individual, explicit, case-by-case basis before the independent auditor is engaged to provide each service. The pre-approval of services may be delegated to one or more of the Audit Committee’s members, but the decision must be reported to the full Audit Committee at its next scheduled meeting.
The Audit Committee has determined that the rendering of services other than audit services by Deloitte & Touche LLP is compatible with maintaining the principal accountant’s independence.
116
Item 15. Exhibits and Financial Statement Schedules.
Financial Statements
The following report and financial statements of the Company are included in this Annual Report on Form 10-K:
|
|
• |
Report of Independent Registered Public Accounting Firm |
|
|
• |
Consolidated Balance Sheets |
|
|
• |
Consolidated Statements of Operations |
|
|
• |
Consolidated Statements of Convertible Preferred Stock and Stockholders’ Equity (Deficit) |
|
|
• |
Consolidated Statement of Cash Flows |
|
|
• |
Notes to Consolidated Financial Statements |
Financial Statements Schedules
All financial statement schedules have been omitted as they are not required, they are not applicable, or the required information is included in the financial statements or notes to the financial statements.
Exhibits
|
Exhibit Number |
|
Description |
|
3.1 |
|
|
|
3.2 |
|
|
|
4.1 |
|
|
|
4.2* |
|
|
|
10.1† |
|
|
|
10.2† |
|
|
|
10.3† |
|
|
|
10.4†# |
|
|
|
10.5†#* |
|
|
|
10.6+ |
|
|
|
10.7+ |
|
117
|
|
||
|
10.9+ |
|
|
|
10.10+ |
|
|
|
10.11+ |
|
|
|
10.12+ |
|
|
|
10.13+* |
|
|
|
10.14+* |
|
|
|
10.15* |
|
Lease, dated December 17, 2020, by and between Patriot Park Partners II, LLC and the Company. |
|
|
|
|
|
23.1* |
|
|
|
31.1* |
|
|
|
31.2* |
|
|
|
32.1*## |
|
|
|
32.2*## |
|
|
|
101.INS |
|
XBRL Instance Document |
|
101.SCH |
|
XBRL Taxonomy Extension Schema Document |
|
101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
101.LAB |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
* |
Filed herewith. |
|
† |
Portions of this agreement (indicated by asterisks) have been omitted because the registrant has determined they are not material and would likely cause competitive harm to the registrant if publicly disclosed. |
|
# |
Certain schedules to this agreement have been omitted in accordance with Item 601(b)(2) of Regulation S-K. A copy of any omitted schedules will be furnished supplementally to the SEC upon request. |
|
+ |
Indicates management contract or compensatory plan. |
|
## |
These certifications are being furnished solely to accompany this annual report pursuant to 18 U.S.C. Section 1350, and are not being filed for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, and are not to be incorporated by reference into any filing of the registrant, whether made before or after the date hereof, regardless of any general incorporation language in such filing. |
Not applicable.
118
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
TAYSHA GENE THERAPIES, INC. |
||
|
|
|
|
|
|
Date: March 3, 2021 |
By: |
|
/s/ RA Session II |
|
|
|
|
RA Session II President and Chief Executive Officer |
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints RA Session II and Kamran Alam, jointly and severally, as his or her true and lawful attorneys-in-fact and agents, with full power of substitution and resubstitution, for him or her and in his or her name, place and stead, in any and all capacities, to sign this Annual Report on Form 10-K of Taysha Gene Therapies, Inc., and any or all amendments thereto, and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents full power and authority to do and perform each and every act and thing requisite or necessary to be done in and about the premises hereby ratifying and confirming all that said attorneys-in-fact and agents, or his, her or their substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
Signature |
|
Title |
|
Date |
|
|
|
|
|
|
|
/s/ RA Session II |
|
President, Chief Executive Officer and Director (Principal Executive Officer) |
|
March 3, 2021 |
|
RA Session II |
|
|
|
|
|
|
|
|
|
|
|
/s/ Kamran Alam |
|
Chief Financial Officer (Principal Financial Officer and Principal Accounting Officer) |
|
March 3, 2021 |
|
Kamran Alam |
|
|
|
|
|
|
|
|
|
|
|
/s/ Phillip B. Donenberg |
|
Director |
|
March 3, 2021 |
|
Phillip B. Donenberg |
|
|
|
|
|
|
|
|
|
|
|
/s/ Sean P. Nolan |
|
Director |
|
March 3, 2021 |
|
Sean P. Nolan |
|
|
|
|
|
|
|
|
|
|
|
/s/ Paul B. Manning |
|
Director |
|
March 3, 2021 |
|
Paul B. Manning |
|
|
|
|
|
|
|
|
|
|
|
/s/ Sukumar Nagendran, M.D. |
|
Director |
|
March 3, 2021 |
|
Sukumar Nagendran, M.D. |
|
|
|
|
|
|
|
|
|
|
|
/s/ Kathleen Reape, M.D. |
|
Director |
|
March 3, 2021 |
|
Kathleen Reape, M.D. |
|
|
|
|
|
|
|
|
|
|
|
/s/ Laura Sepp-Lorenzino, Ph.D. |
|
Director |
|
March 3, 2021 |
|
Laura Sepp-Lorenzino, Ph.D. |
|
|
|
|
119