Attached files
| file | filename |
|---|---|
| EX-99.1 - EXHIBIT 99.1 - Scholar Rock Holding Corp | a52314353ex99_1.htm |
| 8-K - SCHOLAR ROCK HOLDING CORPORATION 8-K - Scholar Rock Holding Corp | a52314353.htm |
|
|
Exhibit 99.2
|

TOPAZ Interim Analysis: SRK-015 Demonstrates Clinical Proof-of-Concept in Spinal Muscular
Atrophy October 27, 2020

Disclaimers Various statements in this presentation concerning the future expectations, plans and
prospects of Scholar Rock, Inc. (“Scholar Rock”), including without limitation, Scholar Rock’s expectations regarding its strategy, its product candidate selection and development timing, including timing for the initiation of and reporting
results from its clinical trials for its product candidates, its disease indication selection and timing for such selection, the ability of SRK-015 to affect the treatment of patients suffering from Spinal Muscular Atrophy (SMA) either as a
monotherapy or in conjunction with the current standard of care, and the ability of SRK-181 to affect the treatment of cancer patients in a manner consistent with preclinical data constitute forward-looking statements for the purposes of the
safe harbor provisions under The Private Securities Litigation Reform Act of 1995. The use of words such as “may,” “might,” “will,” “should,” “expect,” “plan,” “anticipate,” “believe,” “estimate,” “target,” “project,” “intend,” “future,”
“potential,” or “continue,” and other similar expressions are intended to identify such forward-looking statements. Actual results may differ materially from those indicated by these forward-looking statements as a result of various important
factors, including, without limitation, Scholar Rock’s ability to provide the financial support and resources necessary to identify and develop multiple product candidates on the expected timeline, competition from others developing products
for similar uses, the preliminary nature of interim clinical data, Scholar Rock’s ability to obtain, maintain and protect its intellectual property, Scholar Rock’s dependence on third parties for development and manufacture of product
candidates including to supply any clinical trials, and Scholar Rock’s ability to manage expenses and to obtain additional funding when needed to support its business activities and establish and maintain strategic business alliances and new
business initiatives as well as those risks more fully discussed in the section entitled "Risk Factors" in the Quarterly Report on Form 10-Q for the quarter ended June 30, 2020, which is on file with the Securities and Exchange Commission, as
well as discussions of potential risks, uncertainties, and other important factors in Scholar Rock’s subsequent filings with the Securities and Exchange Commission. Any forward-looking statements represent Scholar Rock’s views only as of
today and should not be relied upon as representing its views as of any subsequent date. Scholar Rock explicitly disclaims any obligation to update any forward-looking statements unless required by law. © Scholar Rock, Inc. All rights
reserved. October 2020.

Agenda 3 Opening Remarks Trial Design and Baseline Characteristics 6-month Interim Efficacy and
Safety Results Summary and Next Steps Tony Kingsley, President & CEO Yung Chyung M.D., Chief Medical Officer Yung Chyung M.D., Chief Medical Officer Tony Kingsley, President & CEO Questions and Answers Tony Kingsley,
President & CEOYung Chyung M.D., Chief Medical OfficerTed Myles, Chief Financial Officer

SRK-015 Has Potential to Pioneer a New Treatment Era to Improve Motor Function in Patients with
SMA 4 SMN = survival motor neuron. *Also referred to as SMN correctors. **SRK-015 is an investigational therapyunder development. SMN Upregulator Therapies* + Muscle-Directed Therapy (SRK-015) Could Potentially Enhance Outcomes for
Patients SRK-015** SMN Upregulator TherapiesAddress SMN deficiency to prevent further motor neuron deterioration Muscle-Directed TherapiesAct directly on muscle with aim to improve motor function

Fully human monoclonal antibody (mAb)Half-life of ~23-33 daysAvoids related growth factors (e.g. GDF11,
BMP9, Activin A)Rare Pediatric Disease Designation for SMA granted by FDA Orphan Drug Designation for SMA granted by the FDAOrphan Medicinal Product Designation for SMA granted by the European Commission SRK-015: Highly Selective Inhibitor
of the Activation of Pro and Latent Myostatin 5 Highlights of strong patent portfolio protecting SRK-015:US Patent 10,751,413 (expiry in 2037): Covers composition of matter and methods of use for SRK-015US Patent 9,758,576 (expiry in 2034):
Covers mAbs that inhibit the activation of myostatin precursorUS 10,287,345 (expiry in 2037): Treatment methods for various myostatin-related conditions

6 Bringing a Revolutionary Approach to Highly Sought-After Growth Factors Implicated in Devastating
Diseases Scholar Rock’s Target Growth Factor Precursor (Latent Form) Scholar Rock’s R&D PlatformTransform Medical Practice Pursue important targets with well-validated biology but are difficult to drugApply revolutionary approach to
tough targetsLeverage deep insights into structure and function Engineer antibodies for exquisite selectivity First demonstration of the therapeutic potential of inhibiting the latent forms of growth factors

7 Mean improvements from baseline in HFMSE/RHS observed in each of the 3 cohorts67% of total patients
achieved ≥1-point improvement in Hammersmith scoresSubstantial proportion of patients in each cohort attained ≥3-point improvement in HFMSE/RHSHigh bar and uncommon to observe in any given patient35% of total patients achieved ≥3-point
improvement in Hammersmith scoresDose response demonstrated in Cohort 3 (randomized, double-blind, parallel arm design)Greater improvements in HFMSE scores for high-dose arm across evaluated timepointsSupportive PK/PD results; high dose led
to higher drug exposure and target engagement TOPAZ Interim Analysis Results Demonstrate Proof-of-ConceptMultiple lines of evidence supporting the potential clinical effect of SRK-015 Ambulatory Patients(Revised Hammersmith
Scale) Non-Ambulatory Patients(Hammersmith Functional Motor Scale Expanded) Cohort 1 Cohort 2* Cohort 3* 20 mg/kg pooled (n=23) 20 mg/kgmonotherapy (n=11) 20 mg/kg +nusinersen (n=12) 20 mg/kg +nusinersen (n=14) 2
mg/kg +nusinersen(n=9) 20 mg/kg +nusinersen(n=9) Mean change from baseline (95% CI) 0.5 (-1.1, 2.2) 0.7 (-2.5, 4.0) 0.3 (-1.4, 2.0) 1.4 (0.1, 2.7) 2.4 (-0.9, 5.8) 5.6 (2.5, 8.7) # (%) patients achieving ≥1-pt increase 12/23
(52%) 7/11 (64%) 5/12 (42%) 10/14 (71%) 6/9 (67%) 9/9 (100%) # (%) patients achieving ≥3-pt increase 6/23 (26%) 4/11 (36%) 2/12 (17%) 3/14 (21%) 4/9 (44%) 6/9 (67%) *3 patients (1 in Cohort 2 and 2 in Cohort 3) each missed 3
doses of SRK-015 and the 6-month interim analysis timepoint due to COVID-19-related site access restrictions; the six-month timepoint from these patients was not included in the interim analysis. Data on file. Scholar Rock, Inc. Cambridge,
MA

Phase 2 Trial Design and Baseline Characteristics Yung Chyung, M.D.Chief Medical Officer
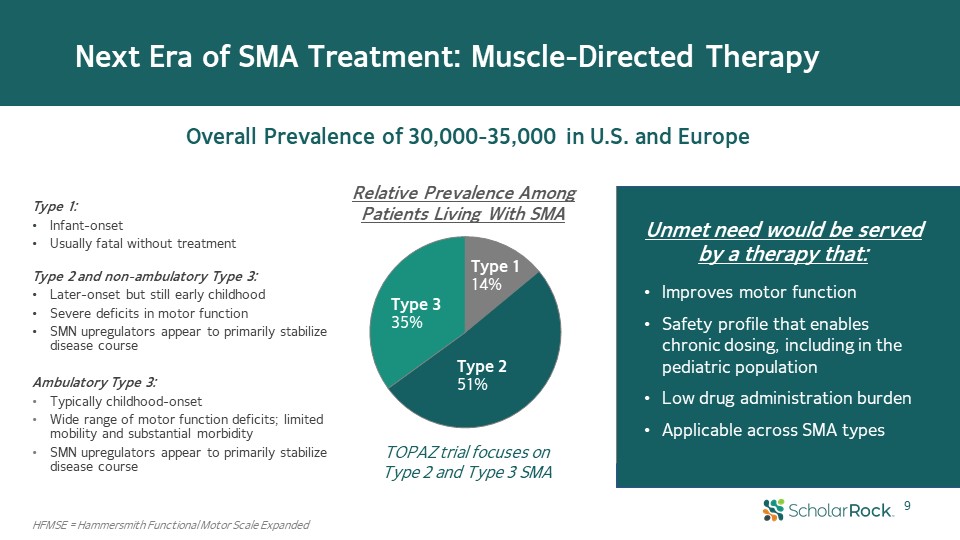
9 Next Era of SMA Treatment: Muscle-Directed Therapy Overall Prevalence of 30,000-35,000 in U.S.
and Europe Type 114% Type 251% Type 335% HFMSE = Hammersmith Functional Motor Scale Expanded Relative Prevalence Among Patients Living With SMA Unmet need would be served by a therapy that:Improves motor functionSafety profile that
enables chronic dosing, including in the pediatric populationLow drug administration burdenApplicable across SMA types TOPAZ trial focuses on Type 2 and Type 3 SMA Type 1: Infant-onsetUsually fatal without treatment Type 2 and
non-ambulatory Type 3: Later-onset but still early childhoodSevere deficits in motor functionSMN upregulators appear to primarily stabilize disease courseAmbulatory Type 3: Typically childhood-onsetWide range of motor function deficits;
limited mobility and substantial morbiditySMN upregulators appear to primarily stabilize disease course
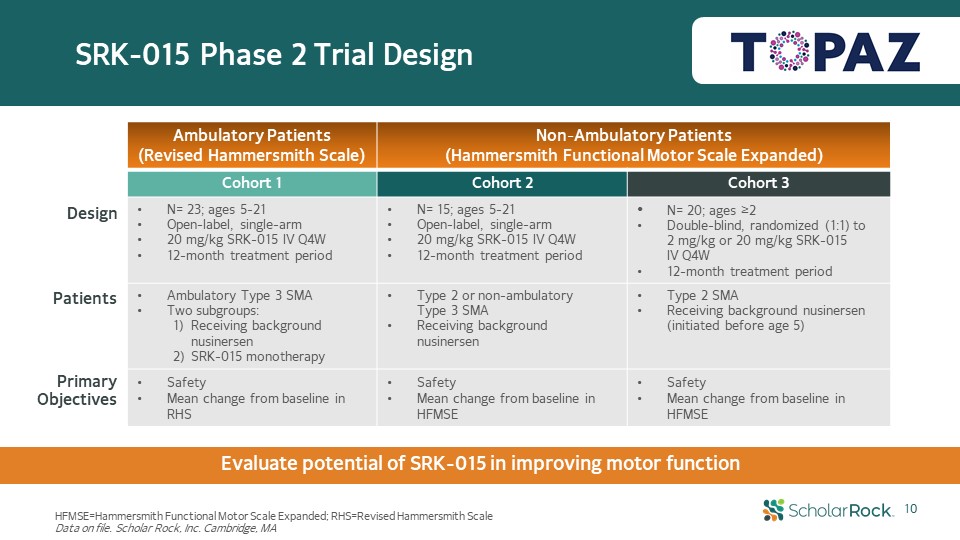
SRK-015 Phase 2 Trial Design Design Patients Primary Objectives HFMSE=Hammersmith Functional Motor
Scale Expanded; RHS=Revised Hammersmith ScaleData on file. Scholar Rock, Inc. Cambridge, MA Evaluate potential of SRK-015 in improving motor function 10 Ambulatory Patients(Revised Hammersmith Scale) Non-Ambulatory Patients(Hammersmith
Functional Motor Scale Expanded) Cohort 1 Cohort 2 Cohort 3 N= 23; ages 5-21Open-label, single-arm20 mg/kg SRK-015 IV Q4W12-month treatment period N= 15; ages 5-21 Open-label, single-arm20 mg/kg SRK-015 IV Q4W12-month treatment
period N= 20; ages ≥2Double-blind, randomized (1:1) to 2 mg/kg or 20 mg/kg SRK-015 IV Q4W12-month treatment period Ambulatory Type 3 SMATwo subgroups: Receiving background nusinersen SRK-015 monotherapy Type 2 or non-ambulatory Type 3
SMAReceiving background nusinersen Type 2 SMA Receiving background nusinersen (initiated before age 5) SafetyMean change from baseline in RHS SafetyMean change from baseline in HFMSE SafetyMean change from baseline in HFMSE

Baseline Characteristics 11 Ambulatory Patients Non-Ambulatory Patients Cohort
1 Cohort 2 Cohort 3 20 mg/kgpooled 20 mg/kgmonotherapy 20 mg/kg +nusinersen 20 mg/kg +nusinersen 2 mg/kg +nusinersen 20 mg/kg +nusinersen N 23 11 12 15 10 10 Mean age (min, max) 12.6 (7, 21) 12.1 (7, 19) 13.1 (7,
21) 11.7 (8, 19) 4.1 (2, 6) 3.8 (2, 6) Female (%) 65% 73% 58% 53% 30% 50% SMN2 Gene Copy* (#, %) 2 1 (4%) 1 (9%) 0 (0%) 1 (10%) 1 (10%) 3 13 (57%) 4 (36%) 9 (75%) 11 (73%) 8 (80%) 8 (80%) 4 5 (22%) 4
(36%) 1 (8%) 2 (13%) 1 (10%) 0 (0%) Mean # of nusinersen maintenance doses N/A N/A 5.6 5.1 5.5 5.4 Discontinuation(s) 1** 0 1** 0 0 0 Mean RHS score (min, max) 49.6 (26, 63) 47.6 (26, 63) 51.3 (43, 62) Mean HFMSE
score (min, max) 22.7 (13, 39) 26.1 (12, 44) 23.5 (14, 42) *data not available for all patients**patient who discontinued study for reasons unrelated to study drug HFMSE=Hammersmith Functional Motor Scale Expanded; RHS=Revised
Hammersmith ScaleData on file. Scholar Rock, Inc. Cambridge, MA

12 Key Strengths of TOPAZ Trial Design and Conduct Large and diverse group of study sites for a rare
disease trialPatients enrolled across 16 study sites in the U.S. and EuropePatient enrollment was not skewed to any one site for any cohort or across the studyPrimary efficacy endpoints are well-validated outcome measuresHammersmith
Functional Motor Scale Expanded (HFMSE) was specifically designed for SMA and served as primary efficacy endpoint in Phase 3 CHERISH trial of nusinersenRevised Hammersmith Scale (RHS) is very similar to the HFMSE, with some modification to
reduce ceiling effects in assessing patients who are ambulatory Efficacy assessments are being conducted in a rigorous fashion:Standardized conduct of Hammersmith scale assessments; extensive training of all trial sitesAssessors of the
Hammersmith scale measures are blinded to baseline and prior visit scoresEmbedded randomized, double-blind portion of trial (Cohort 3) to evaluate dose response between high and low dose arms of SRK-015

13 Six-Month Interim Analysis Results Yung Chyung, M.D.Chief Medical Officer

14 Mean improvements from baseline in HFMSE/RHS observed in each of the 3 cohorts67% of total patients
achieved ≥1-point improvement in Hammersmith scoresSubstantial proportion of patients in each cohort attained ≥3-point improvement in HFMSE/RHSHigh bar and uncommon to observe in any given patient35% of total patients achieved ≥3-point
improvement in Hammersmith scoresDose response demonstrated in Cohort 3 (randomized, double-blind, parallel arm design)Greater improvements in HFMSE scores for high-dose arm across evaluated timepointsSupportive PK/PD results; high dose led
to higher drug exposure and target engagement TOPAZ Interim Analysis Results Demonstrate Proof-of-ConceptMultiple lines of evidence supporting the potential clinical effect of SRK-015 Ambulatory Patients(Revised Hammersmith
Scale) Non-Ambulatory Patients(Hammersmith Functional Motor Scale Expanded) Cohort 1 Cohort 2* Cohort 3* 20 mg/kg pooled (n=23) 20 mg/kgmonotherapy (n=11) 20 mg/kg +nusinersen (n=12) 20 mg/kg +nusinersen (n=14) 2
mg/kg +nusinersen(n=9) 20 mg/kg +nusinersen(n=9) Mean change from baseline (95% CI) 0.5 (-1.1, 2.2) 0.7 (-2.5, 4.0) 0.3 (-1.4, 2.0) 1.4 (0.1, 2.7) 2.4 (-0.9, 5.8) 5.6 (2.5, 8.7) # (%) patients achieving ≥1-pt increase 12/23
(52%) 7/11 (64%) 5/12 (42%) 10/14 (71%) 6/9 (67%) 9/9 (100%) # (%) patients achieving ≥3-pt increase 6/23 (26%) 4/11 (36%) 2/12 (17%) 3/14 (21%) 4/9 (44%) 6/9 (67%) *3 patients (1 in Cohort 2 and 2 in Cohort 3) each missed 3
doses of SRK-015 and the 6-month interim analysis timepoint due to COVID-19-related site access restrictions; the six-month timepoint from these patients was not included in the interim analysis. Data on file. Scholar Rock, Inc. Cambridge,
MA

Cohort 1: Improvement in RHS Observed with Both SRK-015 Monotherapy and as Add-on to Background
Nusinersen 15 Individual RHS responses Ambulatory Type 3 SMA SRK-015 (20 mg/kg)pooled (n=23) SRK-015 (20 mg/kg)monotherapy (n=11) SRK-015 (20 mg/kg) +nusinersen (n=12) Mean change from baseline in RHS (95% CI) 0.5 (-1.1, 2.2) 0.7
(-2.5, 4.0) 0.3 (-1.4, 2.0) # (%) patients achieving ≥1-pt increase in RHS 12/23 (52%) 7/11 (64%) 5/12 (42%) # (%) patients achieving ≥3-pt increase in RHS 6/23 (26%) 4/11 (36%) 2/12 (17%) # (%) patients achieving ≥5-pt increase in
RHS 2/23 (9%) 1/11 (9%) 1/12 (8%) Mean (±SEM) change from baseline in RHS scores N= Data on file. Scholar Rock, Inc. Cambridge, MA

Cohort 2: Meaningful and Consistent Improvements in HFMSE Observed in Type 2 and Non-Ambulatory Type
3 SMA Individual HFMSE responses Type 2 and Non-Ambulatory Type 3 SMA SRK-015 (20 mg/kg) + nusinersen (n=14) Mean change from baseline in HFMSE (95% CI) 1.4 (0.1, 2.7) # (%) patients achieving ≥1-pt increase in HFMSE 10/14 (71%) # (%)
patients achieving ≥3-pt increase in HFMSE 3/14 (21%) # (%) patients achieving ≥5-pt increase in HFMSE 2/14 (14%) 16 Mean (±SEM) change from baseline in HFMSE scores N= Data on file. Scholar Rock, Inc. Cambridge, MA

Cohort 3: SRK-015 High Dose Showed Substantially Greater Improvements in HFMSE scores Than Low Dose
17 Individual HFMSE responses Type 2 SMA SRK-015 low dose (2 mg/kg) +nusinersen (n=9) SRK-015 high dose (20 mg/kg) +nusinersen (n=9) Mean change from baseline in HFMSE (95% CI) 2.4 (-0.9, 5.8) 5.6 (2.5, 8.7) # (%) patients achieving
≥1-pt increase in HFMSE 6/9 (67%) 9/9 (100%) # (%) patients achieving ≥3-pt increase in HFMSE 4/9 (44%) 6/9 (67%) # (%) patients achieving ≥5-pt increase in HFMSE 3/9 (33%) 5/9 (56%) Cohort 3 has a randomized, double-blind, parallel
arm design embedded within TOPAZ Mean (±SEM) change from baseline in HFMSE scores N= Data on file. Scholar Rock, Inc. Cambridge, MA
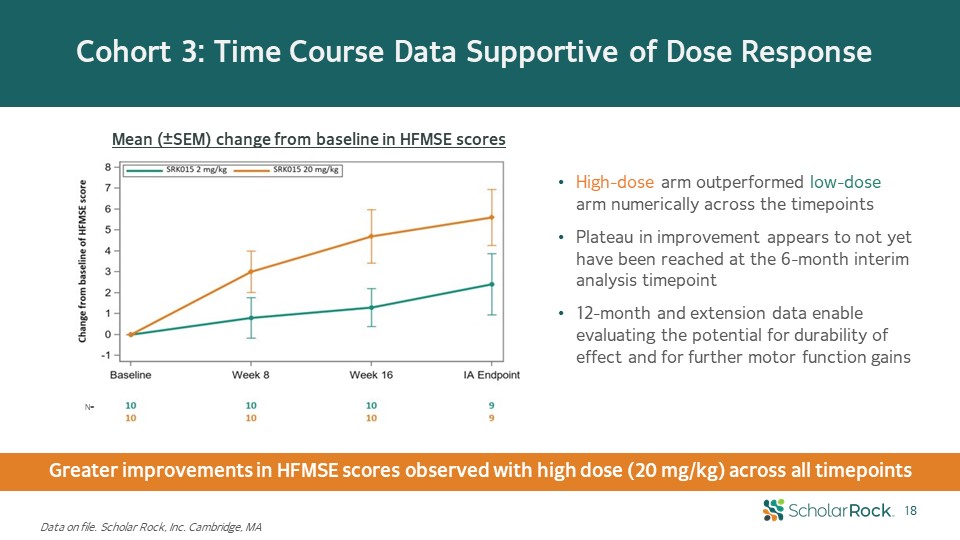
Cohort 3: Time Course Data Supportive of Dose Response 18 Mean (±SEM) change from baseline in HFMSE
scores Greater improvements in HFMSE scores observed with high dose (20 mg/kg) across all timepoints High-dose arm outperformed low-dose arm numerically across the timepointsPlateau in improvement appears to not yet have been reached at
the 6-month interim analysis timepoint12-month and extension data enable evaluating the potential for durability of effect and for further motor function gains N= Data on file. Scholar Rock, Inc. Cambridge, MA

Well-behaved PK profile consistent with that commonly observed with monoclonal antibodiesDrug exposure
was dose proportional Pharmacokinetic and Pharmacodynamic Data are Supportive of Clinically Observed Dose Response Pharmacokinetics* (PK) Pharmacodynamics (PD) Target engagement by SRK-015 was confirmedLow dose (2 mg/kg) yielded lower
level of target engagement and did not achieve full target saturation High dose (20 mg/kg) yielded higher levels of drug exposure and target engagement than low dose (2 mg/kg) 19 *Starting at day 28, measures are pre-dose trough
levels Data on file. Scholar Rock, Inc. Cambridge, MA

No Safety Signals Identified from Interim Analysis 20 Treatment-emergent adverse events
(TEAEs) SRK-015 2 mg/kg dose (n=10) SRK-015 20 mg/kg dose (n=48) Total(n=58) Any TEAE 9 (90%) 40 (83.3%) 49 (84.5%) Any Serious TEAE 0 (0.0%) 1 (2.1%) 1 (1.7%) Any TEAE leading to study drug discontinuation 0 (0.0%) 1 (2.1%) 1
(1.7%) Any Grade 3 (severe) or higher TEAE 0 (0.0%) 0 (0.0%) 0 (0.0%) Treatment-emergent adverse events (TEAEs) are defined as AEs that start after the first dose of study drug or start prior to the administration of study drug and
worsen in severity/grade or relationship to investigational medication after the administration of study drug.Data on file. Scholar Rock, Inc. Cambridge, MA Five most frequently reported TEAEs: Headache, upper respiratory tract infection,
pyrexia, nasopharyngitis, and cough.1 serious TEAE (Cohort 1): Assessed by trial investigator as unrelated to SRK-015. Grade 2 viral upper respiratory infection (prior history) and was hospitalized. Event resolved without sequelae.1 study
drug discontinuation (Cohort 1): Assessed by trial investigator as unrelated to SRK-015. Grade 2 leg muscle fatigue (developed prior to enrollment). Withdrew consent after ~2 months on trial. Incidence and severity of AEs are consistent
with underlying patient population and background therapy

21 TOPAZ Interim Analysis Results Demonstrate Proof-of-Concept Mean improvements in Hammersmith
scores observed across all 3 cohortsMost patients experienced an improvement (≥1-pt increase in Hammersmith scores)Cohort 1: 52% (pooled)Cohort 2: 71% Cohort 3: 100% high dose, 67% low dosePotential for durability and further
improvementsEffects observed through 6 months of treatmentPlateau in improvement has not yet been observed in Cohorts 2 or 312-month and extension data enable evaluation for potential durability of effect and further improvements Dose
response demonstrated in randomized, double-blind, parallel arm Cohort 3High-dose arm showed greater improvements in HFMSE scoresSupportive PK/PD resultsCohort 2 observed improvements from baselineIn population for which SMN upregulator
therapy alone offers motor function stabilization rather than improvementSubstantial % of patients in each cohort attained ≥3-pt increase in Hammersmith scoreHigh bar and uncommon to observe in any given patient 2. SRK-015’s broad and
meaningful therapeutic potential in SMA 1. Multiple lines of evidence supporting the potential clinical effect of SRK-015 Data on file. Scholar Rock, Inc. Cambridge, MA

22 Summary and Next StepsTony KingsleyPresident & CEO

23 Top-line data for 12-month treatment period expected 2Q21Longer-term evaluation of efficacy for
potential durability of clinical effect and continued motor function gainsLonger-term safety, PK, PD, and anti-drug antibody39 of 39 patients who have completed 12-month study have opted into the extension period (as of October 23,
2020)Registrational trial preparations ongoingLook forward to meeting with regulatory authorities to discuss regulatory path Beyond the TOPAZ Interim Analysis Interim results highlight SRK-015’s potential as an important treatment for
patients with SMA

24 Unlocking the Potential of the Scholar Rock R&D Engine Scholar Rock seeks to unlock the
therapeutic potential of modulating growth factor biology Targeting the latent forms of growth factors Opportunities to Further Investigate Therapeutic Potential Broader exploration of SMA types, age range, and background SMN
therapiesPotential for motor function improvement in other neuromuscular disordersExploration of additional indications related to broader myostatin and fast-twitch fiber biologyAntibodies against the latent forms of additional well-validated
targets in oncology (e.g. SRK-181 program) and fibrosisDiscovery platform to generate mAbs against other latent growth factors Emerging Insights Demonstration of proof-of-concept for SRK-015 in SMA Validation of therapeutic potential for
blocking the activation of latent myostatin with SRK-015 Validation of therapeutic potential in targeting latent forms of growth factors Emerging Insights Opportunities Beyond TOPAZ TGFβ Superfamily: More than 30 Related Growth
Factors that Mediate Diverse Biological Processes

DRAGON Part B Initiation Gilead Fibrosis-focused TGFβ Collaboration DRAGON Clinical Response
and Safety Data Across Multiple Tumor TypesPart A2 Combo Efficacy and Safety DataPart B – MelanomaPart B – NSCLCPart B – Urothelial CarcinomaPart B – Other Solid Tumor Types SRK-015SMA SRK-181 Immuno-Oncology and Oncology Preclinical /
Platform TOPAZ Topline12M Data(3 Cohorts) Potential SRK-015 Phase 3 in SMA TOPAZ Interim Analysis(3 Cohorts) Differentiated Pipeline with a Series of Anticipated Milestones TOPAZ 2 Year Extension Continue to Discover and Advance
Preclinical Programs Update on Dose Escalation Multiple Opportunities for Additional Indications Beyond SMA Multiple Additional Opportunities: 1) SRK-181 in Oncology; 2) Latent TGFβ1 Immune Cell in IO; 3) Latent TGFβ1 Immune Cell in
Oncology SRK-015Other Indications Gilead Fibrosis collaboration 2022 and Beyond 2021 Q4 2020 Q3 Q4 Q1 Q2 Latent TGFβ1 Immune Cell Immuno-Oncology and Oncology 25
