|
| Exhibit 99.1 |
|
Prevention of Chemotherapy-induced Myelosuppression in SCLC Patients Treated with the Dual MDMX/MDM2 Inhibitor ALRN-6924 Zoran Andric1,
Timur Ceric2, Mirko Stanetic3, Milan Rancic4, Marko Jakopovic5, Santiago Ponce Aix6, Rodryg Ramlau7, Egbert Smit8, Malgorzata Ulanska9, Christopher Caldwell10, Dora Ferrari10, Allen Annis10, Vojislav Vukovic10, Bojan Zaric11 1CHC Bezanijska Kosa,
Belgrade, Serbia, 2Clinical Center University of Sarajevo, Sarajevo, Bosnia and Herzegovina, 3University Clinical Center Lung Clinic, Banja Luka, Bosnia and Herzegovina, 4Clinic for Pulmonary Diseases, Clinical Center Nis, Serbia, 5Clinic for Lung
Disease Jordanovac, Zagreb, Croatia, 6Hospital Universitario 12 de Octubre, Madrid, Spain, 7Poznan University of Medical Sciences, Poland, 8Stichting Het Nederlands Kanker Instituut – Antoni van Leeuwenhoek Ziekenhuis, Amsterdam, Netherlands,
9Centrum Terapii Współczesnej, Lodz, Poland, 10Aileron Therapeutics Inc., Watertown, MA, 11Institute for Pulmonary Diseases of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia Abstract Table 3: TEAEs Occurring in
10% of All Patients ALL AEs ALL AEs GRADE 3 Figure 2: ALRN-6924 Plasma Pharmacokinetics Figure 3: Dose-response Between ALRN-6924 and Serum MIC-1, a Biomarker of p53 Activation Background: ALRN-6924 is a cell-permeating, stabilized alpha-helical
peptide that binds with high affinity to endogenous p53 inhibitors MDM2 and MDMX. Treatment with ALRN-6924 increases intracellular p53 levels and initiates its transcriptional activity, leading to cell cycle arrest. This effect is limited to cells
with wild-type, functional p53; therefore, for patients with tumors 0.3 mg/kg (N=14) N (%) 0.6 mg/kg (N=5) N (%) 1.2 mg/kg (N=6) N (%) Total (N=25) N (%) 0.3 mg/kg (N=14) N (%) 0.6 mg/kg (N=5) N (%) 1.2 mg/kg (N=6) N (%) Total (N=25) N (%) PARAMETER
(AVERAGE) 0.3 mg/kg 0.6 mg/kg 1.2 mg/kg A 60 55 50 >ZE Ğ ŵ Ŭ harboring mutated P53, pre-treatment with ALRN-6924 may selectively induce cell cycle arrest in normal cells allowing chemotherapy to selectively target cancer cells that
are actively cycling. Materials and Methods: A Phase 1b study in extensive disease small-cell lung cancer (ED SCLC) patients with ECOG PS 0-2 receiving topotecan was conducted to evaluate the ability of ALRN-6924 to reduce bone marrow toxicity
without impacting the efficacy of topotecan. Inclusion criteria included the presence of p53 mutations in tumor tissue as measured by next-generation sequencing. Prophylactic use of growth factors was not permitted in the first treatment cycle.
ALRN-6924 was given at three dose levels: 0.3, 0.6 and 1.2 mg/kg on days 0-4 of each treatment cycle. Topotecan was administered 24 hrs after ALRN-6924 on days 1-5 at 1.5 ALL AEs 14 (100) 5 (100) 6 (100) 25 (100) 13 (93) 5 (100) 6 (100) 24 (96)
NEUTROPENIA 11 (79) 5 (100) 6 (100) 22 (88) 11 (79) 5 (100) 6 (100) 22 (88) THROMBOCYTOPENIA 9 (64) 4 (80) 5 (83) 18 (72) 5 (36) 2 (40) 2 (33) 9 (36) LEUKOPENIA 6 (43) 4 (80) 4 (67) 14 (56) 2 (14) 4 (80) 4 (66) 10 (40) ANEMIA 5 (36) 4 (80) 3 (50) 12
(48) 3 (21) 2 (40) 1 (17) 6 (24) FATIGUE 3 (21) 2 (40) 2 (33) 7 (28) 0 1 (20) 0 1 (4) FEVER 2 (14) 1 (20) 0 3 (12) 0 0 0 0 45 > 40 ŵ Cmax µg/mL 5.0 9.9 21.9 Ő 35 Ŷ 30 25 / 20 D AUC0-24hr ng·hr/mL 35,862 83,030 250,519
15 ŵ 10 Ğ ^ 5 0 t½ hr 3.4 4.5 7.1 0 5 10 15 20 25 30 35 40 45 50 55 60 mg/m2 of each treatment cycle. Hematological laboratory values were coded as AEs based on NCI CTC v5.0. Plasma and serum samples were analyzed for ALRN-6924
pharmacokinetics and pharmacodynamic biomarkers of p53 activation. Table 4: Historical Controls Trial Phase N* Cycles 100000 Hematological Toxicity Grade 3 (%) B Note: Data points <5 ng/mL at 24 hrs not shown Ž Ğ 70 65 60 55
dŝŵ ŌĞ >ZE Ž Ğ Ś >ZE Ž Ğ ŵ Ŭ Results: As of 31-August-2020, 26 patients were enrolled (6 per dose level and 8 additional patients in the expansion cohort); Median Comments > > 50
ŵ 10000 ŵ 45 Ő Ő 25/26 patients were evaluable. Baseline characteristics were typical for this patient population (median age 67 years, 80% males, ECOG PS 0 60%, baseline LDH ULN 40%, chemosensitive population 48%). Median number
of completed topotecan treatment cycles was 3. 12% of patients required topotecan dose reduction. Disease control rate was 64%. No patients reported Grade 3 Neutropenia Febrile Neutropenia Hematological Toxicity Reported by Laboratory Values Thrombo
cytopeniaAnemia Ŷ Ŷ Ž Ă Ŷ 1000 Ŷ / D 40 35 30 25 events of nausea, vomiting, diarrhea, and 1 patient had fatigue Grade 3. Grade 3/4 anemia, thrombocytopenia and neutropenia were reported in 24%, 36% and 88% of patients
and compare favorably to recent historical results of Grade 3/4 anemia, thrombocytopenia and neutropenia of 63%, 70% and 86%.1 JCO, 20191 2 28 3 86 17 70 63 Chemosensitive population not reported; GCSF not Hart, et al. Ğ 100 D prophylactic in
C; Transfusions: Plt 31%, RBC 41% Ŷ Ž Hematological Toxicity Reported as AEs 10 JCO, 20142 3 213 5 54 3 54 31 Chemosensitive population 55%; RBC transfusions 53%; Pawel, et al. 20 ŵ 15 Ğ 10 ^ 5 0 0 10 20 30 0 10 20 30 40 50
60 70 80 90 100 110 120 130 140 150 The 0.3 mgkg ALRN-6924 dose level showed the most consistent chemoprotection results, with NCI CTC Grade 3/4 anemia, Mandatory prophylactic growth factors Time (hr) Dose Ž Ğ JCO, 20073 3 151 4 88 5 43 31
Chemosensitive population 100%; RBC transfusions43%; dŝŵ ŌĞ >ZE Ž Ğ Ś Eckardt, et al. thrombocytopenia and neutropenia limited to 21%, 37% and 79% of patients, respectively, and a 43% rate of neutropenia Grade 4
GCSF 16% • Monophasic clearance, low patient-to-patient variability • Slightly less than dose-proportional exposure A) Serum MIC-1 following a single ALRN-6924 dose. B) Serum MIC-1 following fivedaily in the 1st treatment cycle (historical
result: 76%); none of the patients treated at this dose level had hematological SAEs nor did they require RBC/platelet transfusions (historical result: 41% and 36%, respectively). Figure 1: ALRN-6924 Phase 1b StudySchema JCO, 20114 2 26 2 78 9 61 30
Chemosensitive population 100%; Growth factors as Jotte, et al. necessary; Worst toxicities in cycle #1 Inoue, et al. JCO, 20085 2 30 2 87 3 40 30 Chemosensitive population 63%;GCSF not prophylactic Table 5: Key Toxicities Relative to Recent
Hisorical Control with AE’s Graded by Objective Laboratory Values • 3.4 to 7.1 hr half-life yields no accumulation on repeated dosing Figure 4: Radiological Evaluation of Tumor Response 40 ALRN-6924 doses. Data modelled from this trial and
other ALRN-6924 clinical studies.6 Dose Optimization 24h ALRN-6924 Before Topotecan 3 Dose Levels Tested 0.3 mg/kg Expansion Enrollment Completed Dose Optimization Part of Phase 1b/2 Clinical Trial of ALRN-6924 as a ChemoprotectionAgent Topotecan
± Trilaciclib in SCLC Patients‡ s n o is e L te 35 30 25 AEs* NCI CTC GRADE 3 AEs* NCICTC GRADE 3 g 20 r Schedule Optimization 6h ALRN-6924 Before Topotecan Test up to 2 Dose Levels Ongoing ALRN-6924 0.3 mg/kg+ Topotecan N (%) N=14
ALRN-6924 + Topotecan, All Patients N (%) N=25 Placebo + Topotecan N (%) N=28 Trilaciclib + Topotecan N (%) N=32 a T r o f e n il e s a B 15 10 5 0 Color by Best Overall Response Stable Disease WĂ ZĞ ŽŶ Ğ Anemia
Thrombocytopenia Neutropenia Endpoints ALL AEs 13 (93) 24 (96) 27 (96) 28 (88) m -5 NEUTROPENIA 11 (79) 22 (88) 24 (86) 22 (69) o r f THROMBOCYTOPENIA 5 (37) 9 (36) 20 (70) 22 (68) -10 e g ANEMIA 3 (21) 6 (24) 18 (63) 10 (39) n -15 a FEBRILE
NEUTROPENIA 0 0 5 (17) 2 (6) h Progression % NCI CTC Gr 3 Table 1: Demographics and Key Baseline Characteristics % NCI CTC Gr 3 % NCI CTC Gr 3 Table 2: Study Drug Exposure C -20 FATIGUE 0 0 2 (7) 3 (9) e g NAUSEA 0 0 1 (4) 0 a -25 t n e -30 c r
NEUTROPENIA e NCI CTC GRADE 4** 6 (43) 12 (48) 21 (76) 13 (41) P -35 t s *AEs based on laboratory values, as applicable e 0.3 mg/kg N (%) N=14 0.6 mg/kg N (%) N=5 1.2 mg/kg N (%) N=6 Total N (%) N=25 0.3 mg/kg N=14 0.6 mg/kg N=5 1.2 mg/kg N=6 -40 **
in the first treatment cycle Hart et al. ASCO, 2019 – G1 Therapeutics; Phase 2 Clinical Trial B Total -45 N=25 AGE Median 68.5 67 58 67 GENDER Male 14 (100) 2 (40) 4 (67) 20 (80) ECOG PS 0 10 (71) 2 (40) 3 (50) 15 (60) 1 4 (29) 3 (60) 3 (50) 10
(40) BASELINE LDH ULN 5 (36) 3 (60) 2 (33) 10 (40) TIME SINCE DURATION OF EXPOSURE (DAYS) Mean 62 41 61 57 Median (Min, Max) 59 (6, 204) 27 (6, 90) 42 (27, 157) 55 (6, 204) NUMBER OF CYCLES COMPLETED Mean 3.2 2 3.3 3 Median (Min, Max) 3 (1, 6) 1 (1,
4) 2.5 (1, 8) 3 (1, 8) Table 6: Other Results Support Chemoprotection Signal with ALRN-6924 Treatment SAEs 0.3 mg/kg, N (%), N=14 Total, N (%), N=25 NEUTROPENIA 0 3 (12) LEUKOPENIA 0 1 (4) THROMBOCYTOPENIA 0 2 (8) ANEMIA 0 1 (4) ANGINA PECTORIS 1
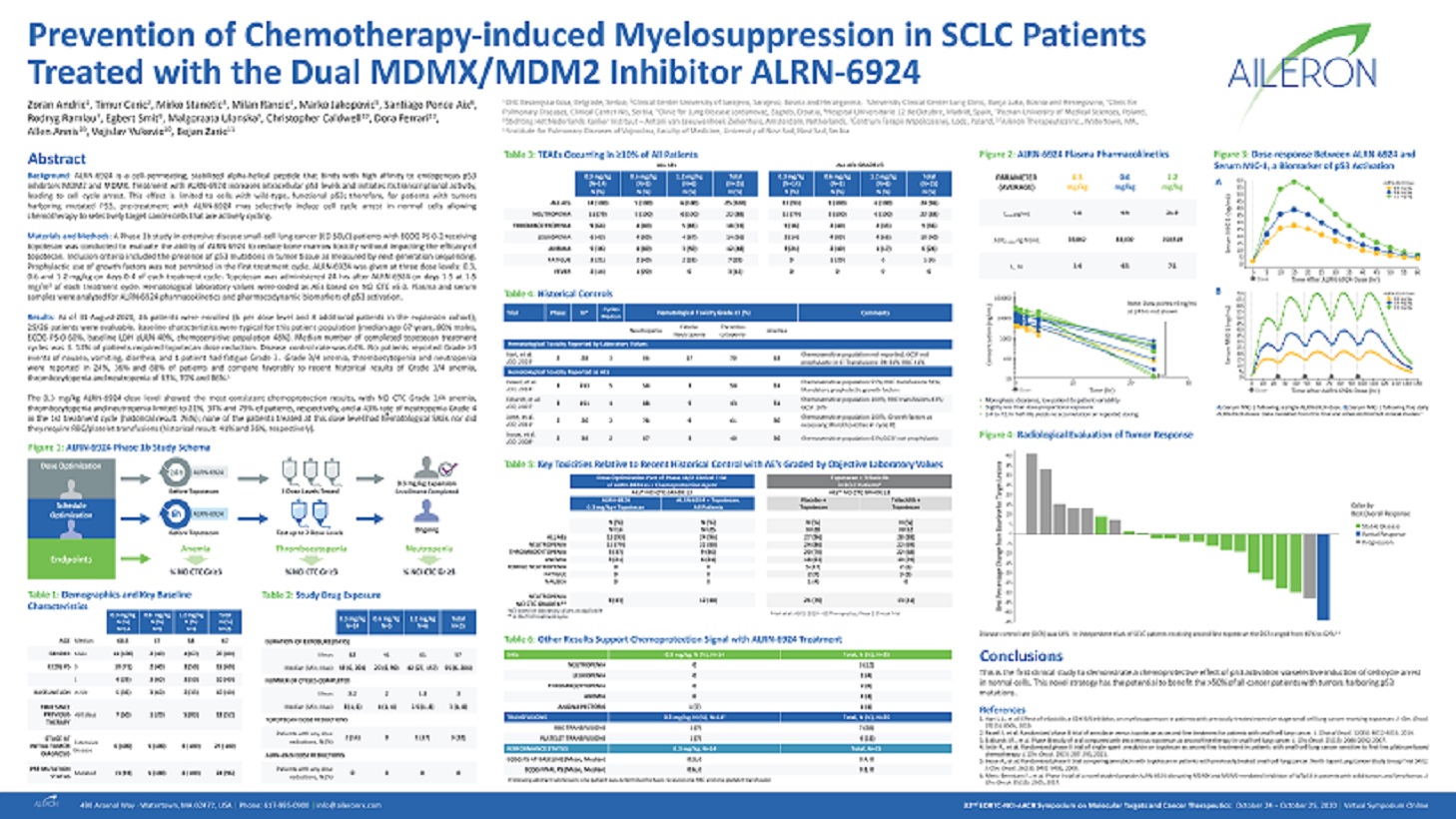
(7) 1 (4) Disease control rate (DCR) was 64%. In independent trials of SCLC patients receiving second-line topotecan the DCR ranged from 4% to 62%.2-5 Conclusions This is the first clinical study to demonstrate a chemoprotective effect of p53
activation via selective induction of cell cycle arrest in normal cells. This novel strategy has the potential to benefit the >50% of all cancer patients with tumors harboring p53 mutations. References PREVIOUS THERAPY STAGE AT INITIAL TUMOR
DIAGNOSIS P53 MUTATION <60 days 7 (50) 1 (20) 5 (83) 13 (52) Extensive Disease 6 (100) 5 (100) 6 (100) 25 (100) TOPOTECAN DOSE REDUCTIONS Patients with any dose reductions, N (%) 2 (14) 0 1 (17) 3 (12) ALRN-6924 DOSE REDUCTIONS Patients with any
dose TRANSFUSIONS 0.3 mg/kg, N (%), N=14 Total, N (%), N=25 RBC TRANSFUSIONS 1 (7) 7 (28) PLATELET TRANSUSIONS 1 (7) 4 (16) PERFORMANCE STATUS 0.3 mg/kg, N=14 Total, N=25 ECOG PS AT BASELINE (Mean, Median) 0.3, 0 0.4, 0 ECOG FINAL PS (Mean, Median)
0.6, 0 0.8, 0 1.Hart L.L., et al. Effect of trilaciclib, a CDK 4/6 inhibitor, on myelosuppression in patients with previously treated extensive-stage small cell lung cancer receiving topotecan. J. Clin. Oncol. 37(15): 8505, 2019. 2.Pawel J., et al.
Randomized phase III trial of amrubicin versus topotecan as second-line treatment for patients with small-cell lung cancer. J. Clinical Oncol. 32(35): 4012-4019, 2014. 3. Eckhardt J.R., et al. Phase III study of oral compared with intravenous
topotecan as second-line therapy in small-cell lung cancer. J. Clin. Oncol. 25(15): 2086-2092, 2007. 4.Jotte R., et al. Randomized phase II trial of single-agent amrubicin or topotecan as second-line treatment in patients with small-cell lung cancer
sensitive to first-line platinum-based chemotherapy. J. Clin. Oncol. 29(3): 287-293, 2011. 5.Inoue A., et al. Randomized phase II trial comparing amrubicin with topotecan in patients with previously treated small-cell lung cancer: North Japan Lung
Cancer Study Group Trial 0402. J. Clin. Oncol. 26(33): 5401-5406, 2008. STATUS Mutated 13 (93) 5 (100) 6 (100) 24 (96) reductions, N (%) 0 0 0 0 Following abstract submission, one patient was determined to have received one RBC and one platelet
transfusion 6.Meric-Bernstam F., et al. Phase I trial of a novel stapled peptide ALRN-6924 disrupting MDMX and MDM2-mediated inhibition of WTp53 in patients with solid tumors and lymphomas. J. Clin. Oncol. 35(15): 2505, 2017. 32nd 490 Arsenal Way -
Watertown, MA 02472, USA | Phone: 617-995-0900 | info@aileronrx.com EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics: October 24 – October 25, 2020 | Virtual Symposium Online