Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - Akero Therapeutics, Inc. | tm2033079-1_8k.htm |
Exhibit 99.1

A Global Disease, A Pioneering Treatment Akero Therapeutics, Inc. Corporate Presentation October 2020

- CONFIDENTIAL - SAFE HARBOR This presentation may contain “forward - looking statements” of Akero Therapeutics, Inc. (“we,” “us,” “our,” “Akero” or the “Compa ny”) within the meaning of the Private Securities Litigation Reform Act of 1995 relating to our business, operations, and financial condition s, including but not limited to current beliefs, expectations and assumptions regarding: the future of our business; future plans and strategies, including o ur expectations around the therapeutic potential and clinical benefits of Efruxifermin ; our development plans for Efruxifermin , including our belief in the unique potential of Efruxifermin as a foundational NASH therapy; our preclinical and clinical results, including our top - line safety/tolerability, laboratory me asures and paired biopsy data from our Phase 2a BALANCED study; risks related to the competitive landscape; and the potential impact of COVID - 19 o n strategy, our employees, supply chain, future operations and clinical trials. Words such as, but not limited to, “look forward to,” “believ e,” “expect,” “anticipate,” “estimate,” “intend,” “plan,” “would,” “should” and “could,” and similar expressions or words, identify forward - looking statemen ts. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Except as required by law, we assume no obligation to update these forward looking statements publicly, or to update the reasons actual results could differ material ly from those anticipated in the forward - looking statements, even if new information becomes available in the future. For a discussion of these and other ris ks and uncertainties, and other important factors, any of which could cause our actual results to differ from those contained in the forward - looking state ments, see the section entitled “Risk Factors” in our most recent annual report on Form 10 - K filed with the Securities and Exchange Commission, as well as discussions of potential risks, uncertainties, and other important factors in our other filings with the Securities and Exchange Commission. Al l information in this presentation is as of the date hereof, and we undertake no duty to update this information unless required by law. Certain in for mation Certain information contained in this presentation relates to or is based on studies, publications, surveys and other data ob tai ned from third - party sources and the Company’s own internal estimates and research. While the Company believes these third - party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or comple ten ess of, any information obtained from third - party sources. In addition, all of the market data included in this presentation involves a number of assump tions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our own internal r ese arch is reliable, such research has not been verified by any independent source. 2
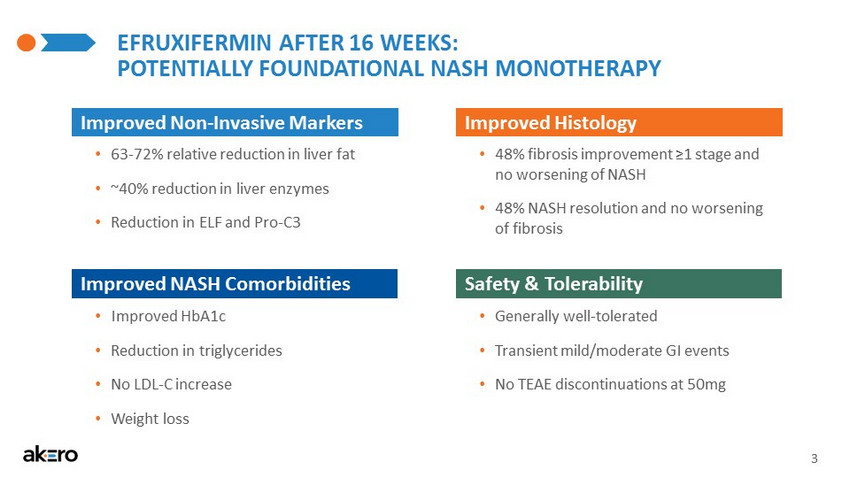
- CONFIDENTIAL - Safety & Tolerability 3 EFRUXIFERMIN AFTER 16 WEEKS: POTENTIALLY FOUNDATIONAL NASH MONOTHERAPY Improved Non - Invasive Markers Improved NASH Comorbidities Improved Histology • 63 - 72% relative reduction in liver fat • ~40% reduction in liver enzymes • Reduction in ELF and Pro - C3 • 48% fibrosis improvement ≥1 stage and no worsening of NASH • 48% NASH resolution and no worsening of fibrosis • Improved HbA1c • Reduction in triglycerides • No LDL - C increase • Weight loss • Generally well - tolerated • Transient mild/moderate GI events • No TEAE discontinuations at 50mg

- CONFIDENTIAL - 4 EXTENSIVE DEVELOPMENT AND COMMERCIALIZATION EXPERIENCE INVOLVED IN 20+ MEDICINE APPROVALS Andrew Cheng, MD, PhD | President & CEO • 19 years at Gilead • Chief Medical Officer & HIV Division Head • Major role in 11 NDA/MAA approvals Kitty Yale | EVP & Chief Development Officer • Over 25 years at Gilead, Roche, Pfizer • VP, Gilead Worldwide Clinical Operations • Major role in 8 global approvals NDA, MAA, JNDA and CFDA William White | EVP, CFO & Head of Corporate Development • 18 years in life sciences investment banking at Goldman Sachs, Citigroup and Deutsche Bank • Most recently, Head of US Life Sciences Investment Banking at Deutsche Bank • Advised on more than $70bn in M&A and $25bn in financing transactions Jonathan Young, PhD, JD | Founder, EVP & COO • Over 15 years in biotechnology product development, law and regulatory policy • General Counsel and VP Policy, Braeburn • Partner and General Counsel, FoxKiser Tim Rolph , D.Phil | Founder & CSO • Over 30 years at Pfizer & Glaxo • CSO of Pfizer’s cardiovascular and metabolic disease unit • Head of Groton & UK Discovery Research, Pfizer • Major role in discovery and early clinical evaluation of two medicines: Selzentry (HIV) and Steglatro (Diabetes)
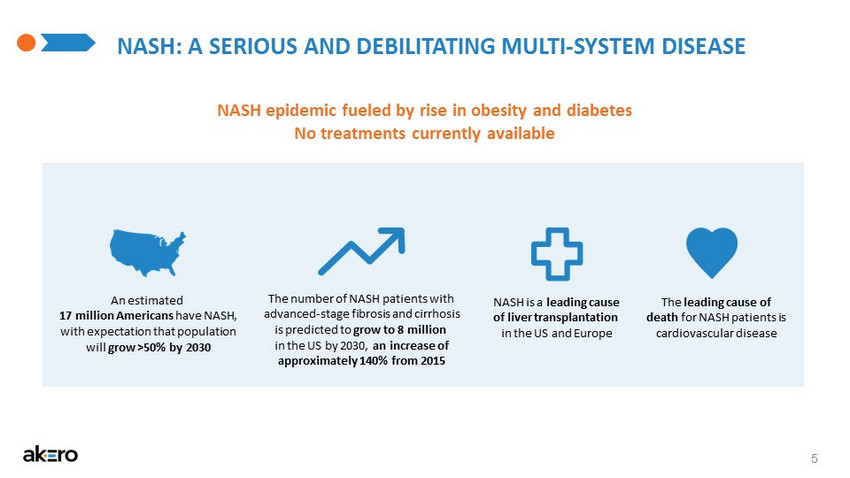
- CONFIDENTIAL - NASH: A SERIOUS AND DEBILITATING MULTI - SYSTEM DISEASE 5 An estimated 17 million Americans have NASH, with expectation that population will grow >50% by 2030 The number of NASH patients with advanced - stage fibrosis and cirrhosis is predicted to grow to 8 million in the US by 2030, an increase of approximately 140% from 2015 NASH is a leading cause of liver transplantation in the US and Europe NASH epidemic fueled by rise in obesity and diabetes No treatments currently available The leading cause of death for NASH patients is cardiovascular disease
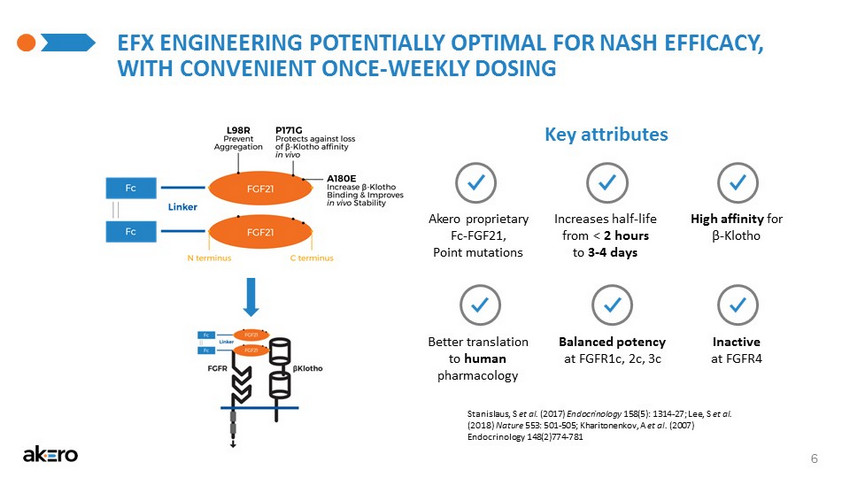
- CONFIDENTIAL - EFX ENGINEERING POTENTIALLY OPTIMAL FOR NASH EFFICACY, WITH CONVENIENT ONCE - WEEKLY DOSING 6 Key attributes Stanislaus, S et al. (2017) Endocrinology 158(5): 1314 - 27; Lee, S et al. (2018) Nature 553: 501 - 505; Kharitonenkov, A et al. (2007) Endocrinology 148(2)774 - 781 Akero proprietary Fc - FGF21, Point mutations Increases half - life from < 2 hours to 3 - 4 days High affinity for β - Klotho Balanced potency at FGFR1c, 2c, 3c Better translation to human pharmacology Inactive at FGFR4
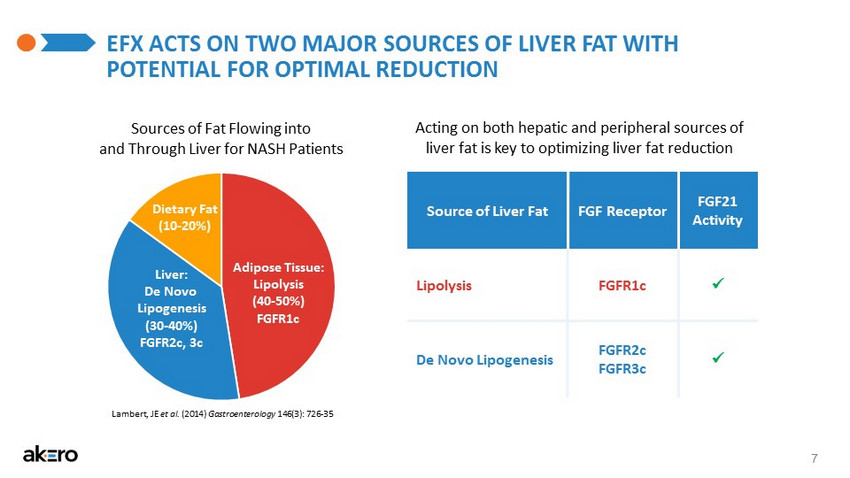
- CONFIDENTIAL - EFX ACTS ON TWO MAJOR SOURCES OF LIVER FAT WITH POTENTIAL FOR OPTIMAL REDUCTION 7 Source of Liver Fat FGF Receptor FGF21 Activity Lipolysis FGFR1c x De Novo Lipogenesis FGFR2c FGFR3c x Sources of Fat Flowing into and Through Liver for NASH Patients Adipose Tissue: Lipolysis (40 - 50%) FGFR1c Liver: De Novo Lipogenesis (30 - 40%) FGFR2c, 3c Dietary Fat (10 - 20%) Lambert, JE et al. (2014) Gastroenterology 146(3): 726 - 35 Acting on both hepatic and peripheral sources of liver fat is key to optimizing liver fat reduction

- CONFIDENTIAL - EFX DIRECT AND INDIRECT ANTI - FIBROTIC EFFECTS 8 Myofibrobl asts *Cited literature available on company website Direct Effect Indirect Effect Bao, L et al. (2018) Br J Pharmacol 175:3379 - 3393; Fisher, FM et al. (2014) Gastroenterology 147:1073 - 1083.e6; Jimenez, V et al. (2018) EMBO Mol Med 10:e8791; Lee, JH et al. (2016) Am J Transl Res 8:4750 - 4763; Sanyal, A et al. (2018) Lancet 392:2705 - 2717; Le, CT et al. (2018) PLOS one 13:e0192146; Xu, P et al. (2016) Toxicol Appl Pharmacol 290:43 - 53; Yu, Y et al. (2016) Int Immunopharmacol 38:144 - 152 EFX Hepatocyte Stress & Death Myofibroblast Differentiation Kupffer Cell Activation Fibrosis

- CONFIDENTIAL - 9 BALANCED STUDY TRIAL DESIGN MRI - PDFF Liver Biopsy Screening Randomization EFX 70mg (n=20) QW SC Injection EFX 50mg (n=20) QW SC Injection EFX 28mg (n=20) QW SC Injection Placebo (n=20) QW SC Injection Safety Follow - Up Liver Biopsies for Responders Week 6 Week 12 Screening Post - Treatment PRIMARY ENDPOINT Absolute change from baseline in hepatic fat fraction (MRI - PDFF) at Week 12 PAIRED BIOPSIES Subjects achieving ≥30% relative reduction of hepatic fat at week 12 are eligible for post - treatment biopsy KEY INCLUSION CRITERIA • F1 - F3 NASH • NAS ≥4 • Liver fat ≥10% KEY SECONDARY EFFICACY ENDPOINTS • Relative Liver Fat • Response Rate • ALT KEY EXPLORATORY EFFICACY ENDPOINTS • 2 - Point NAS Improvement • Fibrosis Improvement • NASH Resolution • Serum Pro - C3 16 WEEKS

BASELINE DEMOGRAPHICS Parameter Mean Placebo (N=21) EFX 28mg (N=19) EFX 50mg (N=20) EFX 70mg (N=20) Age (Years) 52 50 53 53 Sex (Male/Female) 6/15 9/10 10/10 9/11 Weight (kg) 99.6 108.2 103.6 103.1 BMI (kg/m2) 37.6 38.8 36.7 37.2 Liver Fat Content (% by MRI-PDFF) 19.3 21.4 18.3 19.4 NAFLD Activity Score (NAS) 5.1 5.6 5.1 5.6 Fibrosis Stage (% F2-F3) 62 63 65 65 Alanine Aminotransferase (ALT) (U/L) 50.7 62.5 53.4 56.8 Aspartate Aminotransferase (AST) (U/L) 38.6 41.1 35.4 44.6 % Type 2 Diabetes 67 37 50 50 10

- CONFIDENTIAL - 11 PATIENT DISPOSITION Full Analysis Set All subjects who were randomized into the study Safety Set All subjects who received at least one dose of study drug MRI - PDFF Evaluable Analysis Set All FAS subjects who have Baseline and Week 12 MRI - PDFF Liver Biopsy Evaluable Analysis Set All responders who have Baseline and End - of - Treatment liver biopsy results Randomized (80) MRI - PDFF Responders (50) (≥ 30% Relative Reduction) Week 12 MRI - PDFF (68) End - of - Treatment Biopsies Collected (42) Randomized Not Dosed EFX (1) Discontinued (11) Non - Responders Placebo (18) Dosed (79) Due to AEs EFX (6) - Pbo (1) Administrative EFX (4) Biopsies Not Collected Due to COVID - 19 EFX (8) 28mg (13) 50mg (13) 70mg (14) Placebo (2)

SUBSTANTIAL REDUCTIONS IN LIVER FAT AT WEEK 12 ACROSS ALL DOSE GROUPS 12 1Source Data: Full Analysis Set; 2Source Data: MRI-PDFF Evaluable Analysis Set -15 -12 -9 -6 -3 0 Placebo 28mg 50mg 70mg Placebo 28mg 50mg 70mg -72% -0% -12.3*** -13.4*** -14.1*** Absolute Reduction (%) ***p<0.001, versus placebo (ANCOVA) LS Mean Reduction in Liver Fat1 -63% -71% Placebo (N=20) EFX 28mg (N=16) EFX 50mg (N=17) EFX 70mg (N=15) 10% 100% 100% 100%

SUBSTANTIAL NORMALIZATION OF LIVER FAT AT WEEK 12 13 1Source Data: MRI-PDFF Evaluable Analysis Set Baseline 22.2% Liver Fat Week 12 2.0% Liver Fat (↓90%) Analyzed with LiverMultiScan MRI-PDFF Images for Patient 207-012 (50mg EFX) Proton Density Fat Fraction (PDFF) 0% 10% 20% 30% 40% 50% 60% 70% Overall Placebo N=20 5% 1 28mg N=16 25% 4 50mg N=17 53% 9 70mg N=15 67% 10 Proportion of Patients Achieving Normalized Liver Fat (≤5% absolute liver fat content at Week 12)1
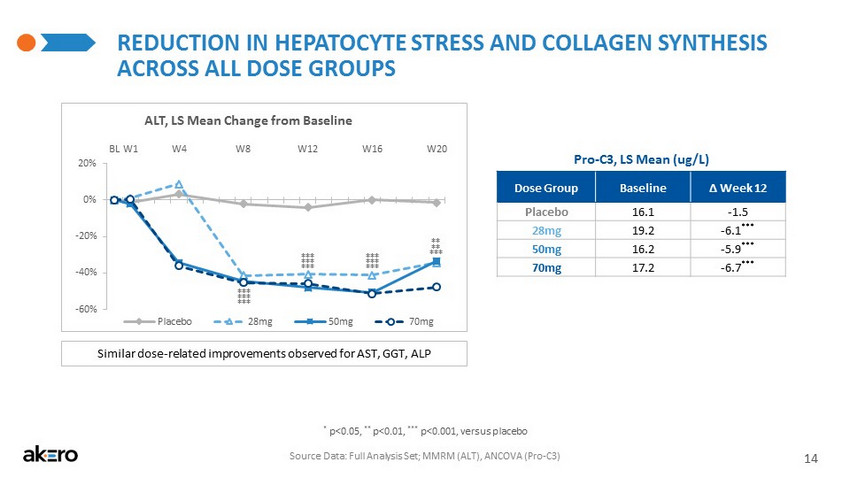
- CONFIDENTIAL - REDUCTION IN HEPATOCYTE STRESS AND COLLAGEN SYNTHESIS ACROSS ALL DOSE GROUPS 14 * p<0.05, ** p<0.01, *** p<0.001, versus placebo (MMRM) Source Data: FAS; ANCOVA LS Mean Serum Pro - C3 (ug/L) Mean Change from Baseline to Week 16 Placebo - 1.5 28mg - 6.1 *** 50mg - 5.9 *** 70mg - 6.7 *** Similar dose - related improvements observed for AST, GGT, ALP -60% -40% -20% 0% 20% BL W1 W4 W8 W12 W16 W20 Placebo 28mg 50mg 70mg *** *** *** *** ** ** *** *** *** ALT, LS Mean Change from Baseline *** *** *** *** p<0.001 versus placebo (ANCOVA)

HIGH RESPONSE RATES ON NASH RESOLUTION AFTER 16 WEEKS ACROSS ALL DOSE GROUPS 15 Source Data: LiverBiopsyEvaluable Analysis Set 1 NAS score of 0 or 1 for lobular inflammation and a score of 0 for ballooning 2 Secondary and exploratory histological endpoints were not powered for statistical significance * A single placebo responder lost 25 pounds over 16 weeks (11% weight reduction) 0% 10% 20% 30% 40% 50% 60% 70% Overall 0% 10% 20% 30% 40% 50% 60% 70% Overall NASH Resolution1,2and No Worsening of Fibrosis Placebo N=2 50% 1* All EFX N=40 48% 19 28mg N=13 46% 6 50mg N=13 54% 7 70mg N=14 43% 6 Biopsy Reading •All baseline and end-of-treatment biopsies were centrally read by a single NASH-CRN pathologist •Baseline biopsies were not re-read with end-of-treatment biopsies •All biopsies were read blinded to both treatment assignment and patient

HIGH RATES OF FIBROSIS IMPROVEMENT AFTER 16 WEEKS ACROSS ALL TREATED PATIENTS 16 Source Data: LiverBiopsyEvaluableAnalysisSet 0% 10% 20% 30% 40% 50% 60% 70% Overall 0% 10% 20% 30% 40% 50% 60% 70% Overall Fibrosis Improvement ≥1 Stage and No Worsening of NAS1,2 1 Improvement in liver fibrosis greater than or equal to one stage and no worsening of NASH (defined as no increase in NAS for ballooning, inflammation, or steatosis) 2 Secondary and exploratory histological endpoints were not powered for statistical significance Placebo N=2 0% All EFX N=40 48% 19 28mg N=13 46% 6 50mg N=13 62% 8 70mg N=14 36% 5 ≥2-Stage Improvement in Fibrosis 11 of 40 EFX patients (28%) had a ≥2-stage improvement

- CONFIDENTIAL - DRUG - RELATED TREATMENT - EMERGENT ADVERSE EVENTS (TEAE) Most Common (>10%) Drug - Related AEs * Placebo (N=21) All EFX (N=58) EFX 28mg (N=19) EFX 50mg (N=19) EFX 70mg (N=20) Diarrhea 2 (10%) 21 (36%) 5 (26%) 10 (53%) 6 (30%) Nausea 0 (0%) 20 (34%) 6 (32%) 4 (21%) 10 (50%) Increased appetite 1 (5%) 13 (22%) 4 (21%) 4 (21%) 5 (25%) Vomiting 0 (0%) 9 (16%) 5 (26%) 2 (11%) 2 (10%) Frequent bowel movements 0 (0%) 8 (14%) 3 (16%) 2 (11%) 3 (15%) Abdominal pain 0 (0%) 7 (12%) 1 (5%) 3 (16%) 3 (15%) Injection site erythema 0 (0%) 7 (12%) 2 (11%) 0 (0%) 5 (25%) Injection site reaction 0 (0%) 6 (10%) 2 (11%) 1 (5%) 3 (15%) Fatigue 2 (10%) 6 (10%) 0 (0%) 1 (5%) 5 (25%) TEAE/SAE Disposition Placebo All EFX 28mg 50mg 70mg TEAE Leading to Death 0 0 0 0 0 TEAE Leading to Discontinuation 1 a 6 2 b 0 4 c Serious Adverse Event (SAE) 0 2 1 d 0 1 17 *Across EFX dose groups Source Data: Safety Set a Muscular Weakness & Myalgia; b Nausea, Vomiting & Dysgeusia; Panic Attack and Anxiety - Linked Tremor; c Dysphagia (Not Drug Related); Acute Pancreatitis (also an SAE); Vomiting; Fatigue & Nausea; d Related to pre - dosing liver biopsy

- CONFIDENTIAL - -0.5 -0.4 -0.3 -0.2 -0.1 0.0 0.1 W16 CLINICALLY MEANINGFUL IMPROVEMENTS IN GLYCEMIC CONTROL AFTER 16 WEEKS Source Data: FAS; ANCOVA LS Mean 18 * p<0.05, ** p<0.01, *** p<0.001, versus placebo (ANCOVA) LS Mean Change From Baseline to Week 16 (%) 1 1 HbA1c is presented in absolute percent change from baseline, whereas HOMA - IR, C - Peptide, and Adiponectin are presented in relative percent change from baseline HbA1c Placebo 28mg 50mg 70mg * ** - 0.1 - 0.4 - 0.5 +0.1 -30% -20% -10% 0% 10% 20% W16 * Placebo 28mg 50mg 70mg C - Peptide - 24% - 22% - 29% + 21% * * -20% 0% 20% 40% 60% 80% 100% 120% W16 Adiponectin + 65% + 88% + 122% - 8% Placebo 28mg 50mg 70mg ** *** *** -50% -20% 10% 40% 70% 100% 130% W16 HOMA - IR - 9% - 46% + 138% Placebo 28mg 50mg 70mg - 23%

- CONFIDENTIAL - -4 -3 -2 -1 0 W16 70mg -4.0 -3.0 -2.0 -1.0 0.0 BL W1 W4 W8 W12 W16 Placebo 28mg 50mg 70mg Mean Change in Body Weight (kg) 19 WEIGHT LOSSES OBSERVED FOR ALL DOSE GROUPS Mean Change in Body Weight at Week 16 (kg) Source Data: Full Analysis Set; ANCOVA LS Mean Placebo 28mg 50mg -0.3 -2.3 -3.7 +0.1

- CONFIDENTIAL - -20% -15% -10% -5% 0% W16 - 16% - 2% - 6% 0% * Placebo 28mg 50mg 70mg -25% -20% -15% -10% -5% 0% W16 - 22% - 15% - 17% - 1% *** * ** Placebo 28mg 50mg 70mg 0% 10% 20% 30% 40% 50% W16 + 34% + 39% + 41% + 4% *** *** *** Placebo 28mg 50mg 70mg IMPROVED LIPOPROTEIN PROFILE FOR CARDIOVASCULAR HEALTH 20 LDL Cholesterol HDL Cholesterol Non - HDL Cholesterol LS Mean Change From Baseline to Week 16 (%) * p<0.05, ** p<0.01, *** p<0.001 versus placebo (ANCOVA) -50% -40% -30% -20% -10% 0% 10% W16 - 39% - 48% - 46% + 6% *** *** *** Placebo 28mg 50mg 70mg Triglycerides Source Data: Full Analysis Set

- CONFIDENTIAL - FGF21 DEVELOPMENT LANDSCAPE Noninvasive Measures: Percent Change From Baseline to End of Study Akero (EFX) 16 weeks BMS ( Pegbelfermin ) 16 weeks 89Bio (BIO89 - 100) 12 weeks Dose pbo 28 QW 50 QW pbo 20 QW 10 QD pbo 18 QW 27 QW 36 Q2W Patient Population Biopsy - confirmed NASH Biopsy - confirmed NASH 80% NAFLD; 20% biopsy - confirmed NASH ≥1 Stage Fibrosis Improvement and No Worsening of NASH, % of Subjects 0% 46% 62% No end - of - study biopsy No end - of - study biopsy MRI - PDFF, % relative reduction 0 - 63 - 71 - 6 - 26 - 38 +10 - 36 - 60 - 50 ALT 0 - 41 - 51 - 5 - 22 - 33 - 4 - 27 - 44 - 40 Triglycerides +6 - 39 - 48 0 - 5 - 5 - 2 - 18 - 28 - 21 HDL - C +4 +34 +39 - 2 +12 +13 +2 +9 +3 +10 LDL - C 0 - 16 - 2 +1 +1 - 11 +1 +3 - 16 - 4 Adiponectin - 8 +65 +80 - 4 +16 +15 - 4 +29 +61 +24 % HbA1c, absolute change +0.1 - 0.1 - 0.4 NR 0 +0.1 - 0.3 +0.5 NR, not reported Note: These data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. No head - to - head clinical trials have been conducted. Sanyal et al (2019) Lancet; 89Bio October 5 Corporate Presentation

- CONFIDENTIAL - -10% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 110% 120% -50% -40% -30% -20% -10% 0% 10% 22 MARKERS OF PERIPHERAL FGFR1c ACTIVATION Note: These data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. No head - to - head clinical trials have been conducted. Sanyal et al (2019) Lancet; 89Bio October 5 Corporate Presentation Adiponectin EFX (Akero) 89Bio Triglycerides BMS Change from Baseline to End of Study Change from Baseline to End of Study pbo 28 QW 50 QW pbo 18 QW 27 QW 36 Q2W pbo 20 QW 10 QD pbo 28 QW 50 QW pbo 18 QW 27 QW 36 Q2W pbo 20 QW 10 QD EFX (Akero) 89Bio BMS

- CONFIDENTIAL - 23 FGF21 DEVELOPMENT LANDSCAPE: SUMMARY Consideration Fc - FGF21 Fusion Protein (Akero) Pegylated FGF21 (BMS or 89Bio) Patient Population: NASH diagnosed only by biopsy; NASH patients have more advanced disease and worse comorbidities Biopsy - confirmed NASH BMS: biopsy - confirmed NASH; 89Bio: ~20% biopsy - confirmed NASH Histology: Fibrosis only histological endpoint correlated with liver outcomes Demonstrated fibrosis improvement by histology BMS: histology data pending 89Bio: no histology data Liver Fat Reduction: Max reduction requires inhibition of both hepatic fat synthesis and adipose tissue lipolysis 71% (50mg QW) BMS: 38% (10mg QD) 89Bio: 60% (27mg QW) Liver Enzymes (LFTs): Reductions indicate improved liver health Large reductions in LFTs; Consistent dose response BMS/89Bio: Smaller effects on LFTs Lipids: Cardiovascular risk #1 cause of mortality for NASH patients. Reflects liver and adipose effects Robust and consistent TG and HDL - C effects BMS/89Bio: Smaller effects on TG and HDL - C Glycemic Control: Improvement in HbA1c mediated by peripheral insulin sensitization; 50% NASH patients diabetic Significant decrease in HbA1c BMS: HbA1c not reported 89Bio: no significant change in HbA1c Safety & Tolerability: Baseline patient population influences profile; Mild GI events common for FGF21 in NASH patients In line with FGF21 class BMS: In line with FGF21 class 89Bio: ~80% NAFLD EFX delivered numerically largest effects, a clear dose response, with maximal or near - maximal effect at 50mg QW

- CONFIDENTIAL - Pbo 0.8g 1.2g Increasing dosing duration NASH DEVELOPMENT LANDSCAPE: NASH RESOLUTION 24 Proportion of Subjects with Resolution of NASH and No Worsening of Fibrosis 1 1 FDA Guidance for Industry: Noncirrhotic Nonalcoholic Steatohepatitis With Liver Fibrosis: Developing Drugs for Treatment (201 8) Pbo 20mg 50mg Pbo 10mg 25mg Pbo 0.2mg 0.4mg Pbo All Pbo 1mg Intercept Ocaliva 78 Wks (Ph3) Daily Oral NGM Bio Aldafermin 24 Wks (Ph2a) Daily Injection (N=22) (N=50) Madrigal Resmetirom 36 Wks (Ph2a) Daily Oral (N=34) (N=79) (N=311) (N=308) Novo Nordisk Semaglutide 72 Wks (Ph2b) Daily Injection Cymabay Seladelpar 52 Wks (Ph2a) Daily Oral (N=25) (N=46) Inventiva Lanifibranor 24 Wks (Ph2b) Daily Oral (N=62) (N=69) Akero Efruxifermin 16 Wks (Ph2a) Weekly Injection (N=80) (N=82) 9 % 24 % 25 % 15 % 8 % 26 % 23 % 23 % 67 % 8 % 12 % (N=312) (N=78) (N=42) 19% 11% (N=63) 40 % 47% 78 Wks * A single placebo responder lost 25 pounds over 16 weeks (11% weight reduction) Note: These data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. No head - to - head clinical trials have been conducted. Inventiva (2020) June 16 Corporate Presentation; NGM Bio (2020) June 3 Corporate Presentation; Harrison, S et al. (2019) Lancet 394(10213):2012 - 24; CymaBay (2020) March 12 Press Release; Novo Nordisk (2020) June 19 R&D Investor Presentation; Younossi Z et al. (2019) Lancet 394(10215):2184 - 96. All trademarks are the property of their respective owners. Pbo All EFX 50mg (N=2) (N=13) 48% 54 % (N=40) * 50 % * 49 % 24 Wks
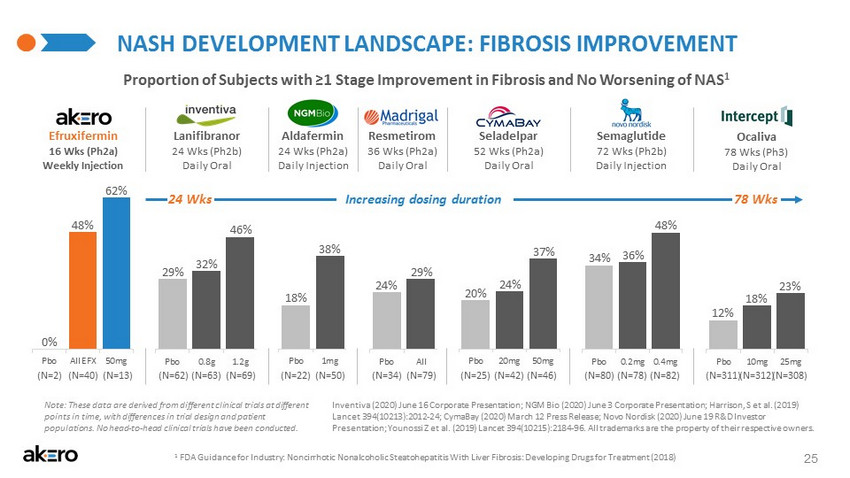
- CONFIDENTIAL - NASH DEVELOPMENT LANDSCAPE: FIBROSIS IMPROVEMENT 25 Proportion of Subjects with ≥1 Stage Improvement in Fibrosis and No Worsening of NAS 1 1 FDA Guidance for Industry: Noncirrhotic Nonalcoholic Steatohepatitis With Liver Fibrosis: Developing Drugs for Treatment (201 8) Pbo All Pbo 1mg Pbo 0.8g 1.2g Pbo 10mg 25mg Pbo 0.2mg 0.4mg Pbo 20mg 50mg Intercept Ocaliva 78 Wks (Ph3) Daily Oral NGM Bio Aldafermin 24 Wks (Ph2a) Daily Injection (N=22) (N=50) Madrigal Resmetirom 36 Wks (Ph2a) Daily Oral (N=34) (N=79) (N=311) (N=308) Novo Nordisk Semaglutide 72 Wks (Ph2b) Daily Injection Cymabay Seladelpar 52 Wks (Ph2a) Daily Oral (N=25) (N=46) Inventiva Lanifibranor 24 Wks (Ph2b) Daily Oral (N=62) (N=69) Akero Efruxifermin 16 Wks (Ph2a) Weekly Injection (N=80) (N=82) (N=312) (N=78) (N=42) (N=63) 18 % 38 % 29 % 24 % 12 % 18 % 23 % 34 % 36% 48 % 20 % 24% 37 % 32% 46 % 29% Note: These data are derived from different clinical trials at different points in time, with differences in trial design and patient populations. No head - to - head clinical trials have been conducted. Inventiva (2020) June 16 Corporate Presentation; NGM Bio (2020) June 3 Corporate Presentation; Harrison, S et al. (2019) Lancet 394(10213):2012 - 24; CymaBay (2020) March 12 Press Release; Novo Nordisk (2020) June 19 R&D Investor Presentation; Younossi Z et al. (2019) Lancet 394(10215):2184 - 96. All trademarks are the property of their respective owners. Increasing dosing duration 78 Wks Pbo All EFX 50mg (N=2) (N=13) (N=40) 0 % 62% 48% 24 Wks
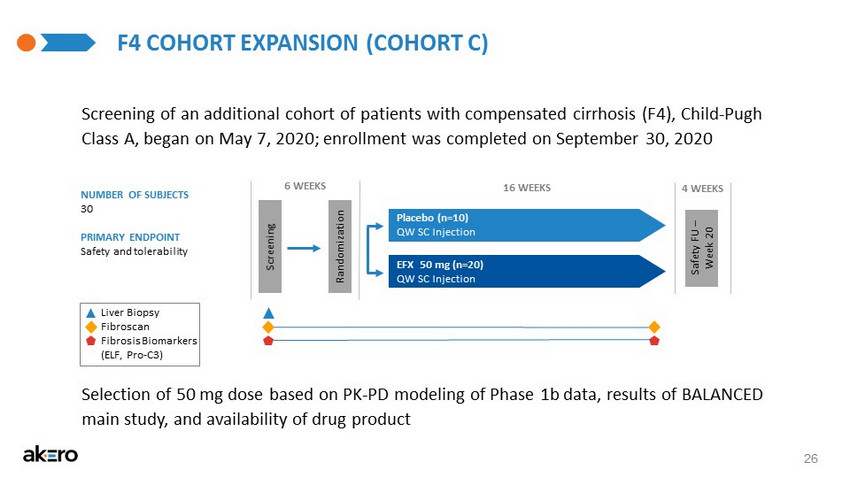
- CONFIDENTIAL - F4 COHORT EXPANSION (COHORT C) 26 NUMBER OF SUBJECTS 30 PRIMARY ENDPOINT Safety and tolerability Screening of an additional cohort of patients with compensated cirrhosis (F4), Child - Pugh Class A, began on May 7, 2020; enrollment was completed on September 30, 2020 6 WEEKS 16 WEEKS 4 WEEKS Screening Randomization EFX 50 mg (n=20) QW SC Injection Placebo (n=10) QW SC Injection Safety FU – Week 20 Selection of 50 mg dose based on PK - PD modeling of Phase 1b data, results of BALANCED main study, and availability of drug product Fibroscan Liver Biopsy Fibrosis Biomarkers (ELF, Pro - C3)

- CONFIDENTIAL - JUN 8 MAR 31 JUN 30 $45.5M Series B MRI-PDFF Read-out JUN20 MAR 13 JUL 2 DEC 16 Last Patient 1st Dose ~$106M Upsized IPO 1stPatient Dosed Amgen License $45M Series A DEC 5 Liver Biopsy Read-out 2018 2019 2020 MILESTONES PROJECTEDMILESTONES DELIVERED 27 SEP 24 FDA Alignment on Ph2b/3 Path JUL 10 ~$216M Upsized Offering

- CONFIDENTIAL - 28 STRONG FINANCIAL POSITION * As of July 10, 2020, we had approximately $305.6 million of cash, cash equivalents and short - term marketable securities. These a mounts have not been audited, reviewed, or compiled by our independent registered public accounting firm. Our actual cash, cash equivalents and short - term marketable se curities as of July 10, 2020 may differ from these amounts after we complete our comprehensive accounting procedures for the three months ended September 30, 2020. ~$ 106M Raised in aggregate gross proceeds ~$ 306M* cash, cash equivalents and short - term marketable securities COMPLETED UPSIZED FOLLOW - ON OFFERING July 10, 2020 ~$ 216M Raised in aggregate gross proceeds

- CONFIDENTIAL - EFRUXIFERMIN: POTENTIALLY FOUNDATIONAL NASH MONOTHERAPY 29 x Substantial fibrosis improvement x Substantial reductions in liver fat • Confirmed by NASH resolution x Ameliorated dyslipidemia • No LDL cholesterol increase x Improved glycemic control x Weight loss across all dose groups x Large, sustained reductions in ALT x Few discontinuations due to AEs

A Global Disease, A Pioneering Treatment NASDAQ: AKRO