Attached files
| file | filename |
|---|---|
| EX-99.1 - EX-99.1 - Forte Biosciences, Inc. | d88635dex991.htm |
| 8-K - 8-K - Forte Biosciences, Inc. | d88635d8k.htm |

Exhibit 99.2 FORTE BIOSCIENCES TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE CORPORATE PRESENTATION SEPTEMBER 2020Exhibit 99.2 FORTE BIOSCIENCES TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE CORPORATE PRESENTATION SEPTEMBER 2020

CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS ¡ Certain statements contained in this presentation regarding matters that are not historical facts, are forward-looking statements within the meaning of Section 21E of the Securities and Exchange Act of 1934, as amended, and the Private Securities Litigation Act of 1995, known as the PSLRA. These include statements regarding management’s intention, plans, beliefs, expectations or forecasts for the future, and, therefore, you are cautioned not to place undue reliance on them. No forward-looking statement can be guaranteed, and actual results may differ materially from those projected. Forte Biosciences, Inc. (“we”, the “Company” or “Forte”) undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future events or otherwise, except to the extent required by law. We use words such as “anticipates,” “believes,” “plans,” “expects,” “projects,” “intends,” “may,” “will,” “should,” “could,” “estimates,” “predicts,” “potential,” “continue,” “guidance,” and similar expressions to identify these forward-looking statements that are intended to be covered by the safe-harbor provisions of the PSLRA. ¡ Such forward-looking statements are based on our expectations and involve risks and uncertainties; consequently, actual results may differ materially from those expressed or implied in the statements due to a number of factors, including, but not limited to, risks relating to the sufficiency of the Company’s cash balance to fund the Company’s activities, and the expectation with respect thereto; the business and prospects of the Company; Forte’s plans to develop and potentially commercialize its product candidates, including FB-401; the timing of initiation of Forte’s planned clinical trials; the timing of the availability of data from Forte’s clinical trials; the timing of any planned investigational new drug application or new drug application; Forte’s plans to research, develop and commercialize its current and future product candidates; Forte’s ability to successfully enter into collaborations, and to fulfill its obligations under any such collaboration agreements; the clinical utility, potential benefits and market acceptance of Forte’s product candidates; Forte’s commercialization, marketing and manufacturing capabilities and strategy; Forte’s ability to identify additional products or product candidates with significant commercial potential; developments and projections relating to Forte’s competitors and its industry; the impact of government laws and regulations; Forte’s ability to protect its intellectual property position; Forte’s estimates regarding future revenue, expenses, capital requirements and need for additional financing following the proposed transaction; and the impact of COVID-19 on the Company, the Company’s industry or the economy generally. ¡ The known risks and uncertainties are described in detail under the caption “Risk Factors” and elsewhere in the Company’s Annual Report on Form 10-K for the year ending December 31, 2019, Quarterly Report on Form 10-Q for the quarter ended June 30, 2020, and the Registration Statement/Proxy Statement/Prospectus filed on Form S-4 (Registration No. 333-237371), initially filed on March 25, 2020, as amended, and declared effective by the Securities and Exchange Commission, or SEC, on May 13, 2020, and our subsequent reports filed with the SEC and other documents filed from time to time with the SEC. Forward-looking statements included in this presentation are based on information available to Forte as of the date of this presentation. Accordingly, our actual results may materially differ from our current expectations, estimates and projections. Forte undertakes no obligation to update such forward-looking statements to reflect events or circumstances after the date of this presentation. 2CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS ¡ Certain statements contained in this presentation regarding matters that are not historical facts, are forward-looking statements within the meaning of Section 21E of the Securities and Exchange Act of 1934, as amended, and the Private Securities Litigation Act of 1995, known as the PSLRA. These include statements regarding management’s intention, plans, beliefs, expectations or forecasts for the future, and, therefore, you are cautioned not to place undue reliance on them. No forward-looking statement can be guaranteed, and actual results may differ materially from those projected. Forte Biosciences, Inc. (“we”, the “Company” or “Forte”) undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future events or otherwise, except to the extent required by law. We use words such as “anticipates,” “believes,” “plans,” “expects,” “projects,” “intends,” “may,” “will,” “should,” “could,” “estimates,” “predicts,” “potential,” “continue,” “guidance,” and similar expressions to identify these forward-looking statements that are intended to be covered by the safe-harbor provisions of the PSLRA. ¡ Such forward-looking statements are based on our expectations and involve risks and uncertainties; consequently, actual results may differ materially from those expressed or implied in the statements due to a number of factors, including, but not limited to, risks relating to the sufficiency of the Company’s cash balance to fund the Company’s activities, and the expectation with respect thereto; the business and prospects of the Company; Forte’s plans to develop and potentially commercialize its product candidates, including FB-401; the timing of initiation of Forte’s planned clinical trials; the timing of the availability of data from Forte’s clinical trials; the timing of any planned investigational new drug application or new drug application; Forte’s plans to research, develop and commercialize its current and future product candidates; Forte’s ability to successfully enter into collaborations, and to fulfill its obligations under any such collaboration agreements; the clinical utility, potential benefits and market acceptance of Forte’s product candidates; Forte’s commercialization, marketing and manufacturing capabilities and strategy; Forte’s ability to identify additional products or product candidates with significant commercial potential; developments and projections relating to Forte’s competitors and its industry; the impact of government laws and regulations; Forte’s ability to protect its intellectual property position; Forte’s estimates regarding future revenue, expenses, capital requirements and need for additional financing following the proposed transaction; and the impact of COVID-19 on the Company, the Company’s industry or the economy generally. ¡ The known risks and uncertainties are described in detail under the caption “Risk Factors” and elsewhere in the Company’s Annual Report on Form 10-K for the year ending December 31, 2019, Quarterly Report on Form 10-Q for the quarter ended June 30, 2020, and the Registration Statement/Proxy Statement/Prospectus filed on Form S-4 (Registration No. 333-237371), initially filed on March 25, 2020, as amended, and declared effective by the Securities and Exchange Commission, or SEC, on May 13, 2020, and our subsequent reports filed with the SEC and other documents filed from time to time with the SEC. Forward-looking statements included in this presentation are based on information available to Forte as of the date of this presentation. Accordingly, our actual results may materially differ from our current expectations, estimates and projections. Forte undertakes no obligation to update such forward-looking statements to reflect events or circumstances after the date of this presentation. 2
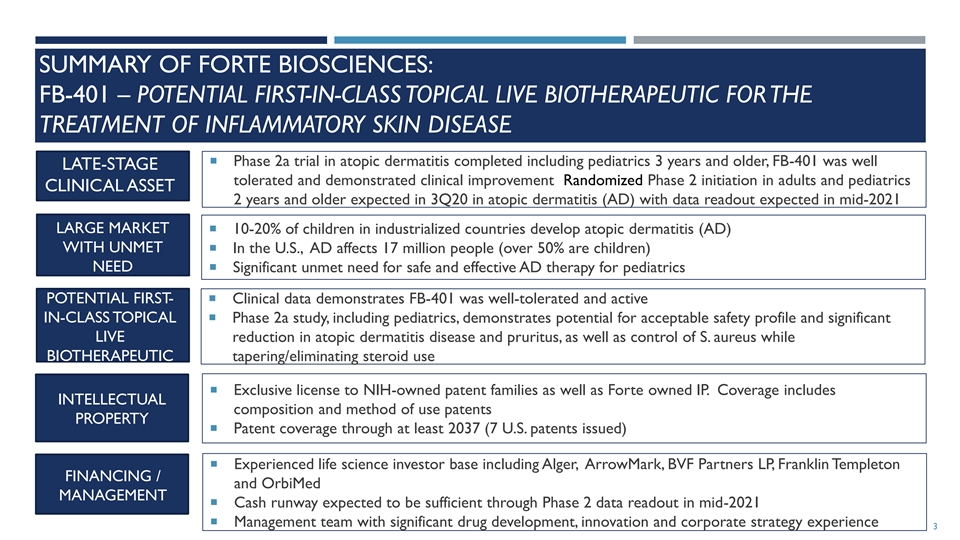
SUMMARY OF FORTE BIOSCIENCES: FB-401 – POTENTIAL FIRST-IN-CLASS TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE ¡ Phase 2a trial in atopic dermatitis completed including pediatrics 3 years and older, FB-401 was well LATE-STAGE tolerated and demonstrated clinical improvement Randomized Phase 2 initiation in adults and pediatrics CLINICAL ASSET 2 years and older expected in 3Q20 in atopic dermatitis (AD) with data readout expected in mid-2021 LARGE MARKET ¡ 10-20% of children in industrialized countries develop atopic dermatitis (AD) WITH UNMET ¡ In the U.S., AD affects 17 million people (over 50% are children) NEED¡ Significant unmet need for safe and effective AD therapy for pediatrics POTENTIAL FIRST- ¡ Clinical data demonstrates FB-401 was well-tolerated and active IN-CLASS TOPICAL ¡ Phase 2a study, including pediatrics, demonstrates potential for acceptable safety profile and significant LIVE reduction in atopic dermatitis disease and pruritus, as well as control of S. aureus while BIOTHERAPEUTIC tapering/eliminating steroid use ¡ Exclusive license to NIH-owned patent families as well as Forte owned IP. Coverage includes INTELLECTUAL composition and method of use patents PROPERTY ¡ Patent coverage through at least 2037 (7 U.S. patents issued) ¡ Experienced life science investor base including Alger, ArrowMark, BVF Partners LP, Franklin Templeton FINANCING / and OrbiMed MANAGEMENT ¡ Cash runway expected to be sufficient through Phase 2 data readout in mid-2021 ¡ Management team with significant drug development, innovation and corporate strategy experience 3SUMMARY OF FORTE BIOSCIENCES: FB-401 – POTENTIAL FIRST-IN-CLASS TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE ¡ Phase 2a trial in atopic dermatitis completed including pediatrics 3 years and older, FB-401 was well LATE-STAGE tolerated and demonstrated clinical improvement Randomized Phase 2 initiation in adults and pediatrics CLINICAL ASSET 2 years and older expected in 3Q20 in atopic dermatitis (AD) with data readout expected in mid-2021 LARGE MARKET ¡ 10-20% of children in industrialized countries develop atopic dermatitis (AD) WITH UNMET ¡ In the U.S., AD affects 17 million people (over 50% are children) NEED¡ Significant unmet need for safe and effective AD therapy for pediatrics POTENTIAL FIRST- ¡ Clinical data demonstrates FB-401 was well-tolerated and active IN-CLASS TOPICAL ¡ Phase 2a study, including pediatrics, demonstrates potential for acceptable safety profile and significant LIVE reduction in atopic dermatitis disease and pruritus, as well as control of S. aureus while BIOTHERAPEUTIC tapering/eliminating steroid use ¡ Exclusive license to NIH-owned patent families as well as Forte owned IP. Coverage includes INTELLECTUAL composition and method of use patents PROPERTY ¡ Patent coverage through at least 2037 (7 U.S. patents issued) ¡ Experienced life science investor base including Alger, ArrowMark, BVF Partners LP, Franklin Templeton FINANCING / and OrbiMed MANAGEMENT ¡ Cash runway expected to be sufficient through Phase 2 data readout in mid-2021 ¡ Management team with significant drug development, innovation and corporate strategy experience 3

FORTE BIOSCIENCES: OVERVIEW OF FB-401 ¡ FB-401 drug product consists of 3 therapeutic bacterial strains of commensal gram negative R. mucosa specifically selected based on screening for impact on inflammatory skin disease parameters ¡ Topical application of the specifically selected therapeutic bacterial strains of R. mucosa drug product: ¡ Drives immune pathways that are defective ¡ Suppresses Staphylococcus aureus growth ¡ Improves skin barrier function ¡ Clinical data demonstrates FB-401 live biotherapeutic therapy was well-tolerated and active in both adults and pediatric ¡ Phase 2a study, including pediatrics, well tolerated and demonstrated clinical improvement in atopic dermatitis disease and pruritus, as well as control of S. aureus while tapering/eliminating steroid use ¡ Randomized Phase 2 trial initiation expected in 3Q20 4FORTE BIOSCIENCES: OVERVIEW OF FB-401 ¡ FB-401 drug product consists of 3 therapeutic bacterial strains of commensal gram negative R. mucosa specifically selected based on screening for impact on inflammatory skin disease parameters ¡ Topical application of the specifically selected therapeutic bacterial strains of R. mucosa drug product: ¡ Drives immune pathways that are defective ¡ Suppresses Staphylococcus aureus growth ¡ Improves skin barrier function ¡ Clinical data demonstrates FB-401 live biotherapeutic therapy was well-tolerated and active in both adults and pediatric ¡ Phase 2a study, including pediatrics, well tolerated and demonstrated clinical improvement in atopic dermatitis disease and pruritus, as well as control of S. aureus while tapering/eliminating steroid use ¡ Randomized Phase 2 trial initiation expected in 3Q20 4

EXPERIENCED MANAGEMENT AND ADVISORY TEAMS ¡ Forte BioSciences team has extensive experience in microbial manufacturing, quality, regulatory and clinical development in dermatology Paul Wagner, Ph.D. – CEO Dan Burge, MD – Head of Clinical Development Eric Emery – Head of Downstream Manufacturing Tony Riley – Chief Financial Officer Hank Talbot, Ph.D. – Head of Process Development and Quality Scientific Advisory Board (SAB) ¡ Prof. Amy Paller, MD – Chair, Department of Dermatology Northwestern University Feinberg School of Medicine ¡ Prof. Lawrence Eichenfield, MD – Chief of Pediatric and Adolescent Dermatology at Rady Children's Hospital-San Diego, Editor in Chief of Pediatric Dermatology ¡ Prof. Eric Simpson, MD –Professor of Dermatology, Oregon Health & Science University, Portland ¡ Dr. Patricia Walker, MD, Ph.D. – Former CMO of Allergan Medical and Dermatology TA Head 5EXPERIENCED MANAGEMENT AND ADVISORY TEAMS ¡ Forte BioSciences team has extensive experience in microbial manufacturing, quality, regulatory and clinical development in dermatology Paul Wagner, Ph.D. – CEO Dan Burge, MD – Head of Clinical Development Eric Emery – Head of Downstream Manufacturing Tony Riley – Chief Financial Officer Hank Talbot, Ph.D. – Head of Process Development and Quality Scientific Advisory Board (SAB) ¡ Prof. Amy Paller, MD – Chair, Department of Dermatology Northwestern University Feinberg School of Medicine ¡ Prof. Lawrence Eichenfield, MD – Chief of Pediatric and Adolescent Dermatology at Rady Children's Hospital-San Diego, Editor in Chief of Pediatric Dermatology ¡ Prof. Eric Simpson, MD –Professor of Dermatology, Oregon Health & Science University, Portland ¡ Dr. Patricia Walker, MD, Ph.D. – Former CMO of Allergan Medical and Dermatology TA Head 5

ATOPIC DERMATITIS ¡ Atopic dermatitis (AD) is characterized by itching, a scaly rash, dry skin, and cutaneous sensitization to allergens. The underlying pathology of AD consists of a triad of defective skin barrier function, susceptibility to Staphylococcus aureus skin infection, and immune imbalance (overactive adaptive immunity in lieu of innate immunity) ¡ 10-20% of children in industrialized countries develop atopic dermatitis with increasing incidence. 80% of children with severe disease continue to have lifelong exacerbations ¡ There is currently no cure for AD ¡ In the US, the prevalence of atopic dermatitis is approximately 17 million ¡ More than half of that prevalence is pediatric (<17 years old) ¡ Treatment options for pediatrics are very limited Lichenified, Erythematous ill- erythematous plaques defined patches Affects flexural behind the knees with overlying areas of neck, scale and erosions Erythematous, elbows, knees, on her cheeks excoriated papules with wrists, and overlying crust in the ankles antecubital fossa FDA Pediatric Subcommittee October 29-30, 2003 American Academy of Dermatology 6ATOPIC DERMATITIS ¡ Atopic dermatitis (AD) is characterized by itching, a scaly rash, dry skin, and cutaneous sensitization to allergens. The underlying pathology of AD consists of a triad of defective skin barrier function, susceptibility to Staphylococcus aureus skin infection, and immune imbalance (overactive adaptive immunity in lieu of innate immunity) ¡ 10-20% of children in industrialized countries develop atopic dermatitis with increasing incidence. 80% of children with severe disease continue to have lifelong exacerbations ¡ There is currently no cure for AD ¡ In the US, the prevalence of atopic dermatitis is approximately 17 million ¡ More than half of that prevalence is pediatric (<17 years old) ¡ Treatment options for pediatrics are very limited Lichenified, Erythematous ill- erythematous plaques defined patches Affects flexural behind the knees with overlying areas of neck, scale and erosions Erythematous, elbows, knees, on her cheeks excoriated papules with wrists, and overlying crust in the ankles antecubital fossa FDA Pediatric Subcommittee October 29-30, 2003 American Academy of Dermatology 6
SKIN MICROBIOME The skin is a complex barrier organ characterized by symbiotic relationship between microbial communities and host tissue via complex signals provided by the innate and the adaptive immune systems Exposure to various endogenous and exogenous factors impact the system balance potentially leading to inflammatory skin conditions comprising infections, allergies or autoimmune diseases Researchers in microbiology and dermatology identified and characterized the microorganisms present on the skin, to evaluate the bacterial diversity and their relative abundance and to understand how microbial diversity may contribute to skin health and dermatological conditions Recent work has revealed that the skin microbiome is significantly different between healthy controls and patients with AD and that symptoms are associated with a loss of commensal diversity Dreno et al, European Academy of Dermatology and Venerology 2016, 30, 2038-2047 7 Kong HH et al. Genome research. 2012;22(5):850-859SKIN MICROBIOME The skin is a complex barrier organ characterized by symbiotic relationship between microbial communities and host tissue via complex signals provided by the innate and the adaptive immune systems Exposure to various endogenous and exogenous factors impact the system balance potentially leading to inflammatory skin conditions comprising infections, allergies or autoimmune diseases Researchers in microbiology and dermatology identified and characterized the microorganisms present on the skin, to evaluate the bacterial diversity and their relative abundance and to understand how microbial diversity may contribute to skin health and dermatological conditions Recent work has revealed that the skin microbiome is significantly different between healthy controls and patients with AD and that symptoms are associated with a loss of commensal diversity Dreno et al, European Academy of Dermatology and Venerology 2016, 30, 2038-2047 7 Kong HH et al. Genome research. 2012;22(5):850-859

SKIN MICROBIOME DIFFERENCES IN ATOPIC DERMATITIS Genetic-based microbiome identification revealed significant differences in the Gram-negative skin biome between atopic dermatitis (AD) patients and healthy controls (HV) NIH (Myles et. al.) identified substantial differences in the gram-negative microbiome present on the skin of AD patients and healthy volunteers The predominant species of skin commensal Gram-negative bacteria (CGN) in HV found to be Roseomonas mucosa Over 50% of AD patients did not have any culturable Gram- negative flora, consistent with DNA-based analysis Myles IA, Williams KW, Reckhow JD, et al. JCI Insight. 2016;1(10) Kong HH et al. Genome research. 2012;22(5):850-859 8SKIN MICROBIOME DIFFERENCES IN ATOPIC DERMATITIS Genetic-based microbiome identification revealed significant differences in the Gram-negative skin biome between atopic dermatitis (AD) patients and healthy controls (HV) NIH (Myles et. al.) identified substantial differences in the gram-negative microbiome present on the skin of AD patients and healthy volunteers The predominant species of skin commensal Gram-negative bacteria (CGN) in HV found to be Roseomonas mucosa Over 50% of AD patients did not have any culturable Gram- negative flora, consistent with DNA-based analysis Myles IA, Williams KW, Reckhow JD, et al. JCI Insight. 2016;1(10) Kong HH et al. Genome research. 2012;22(5):850-859 8
MECHANISM OF FB-401 Extensive preclinical work by Forte in collaboration with NIH, investigating the activity of FB-401 has demonstrated: 1) FB-401 activates tissue repair and anti-inflammation pathways in keratinocytes, dendritic cells and fibroblasts 1) Gene sequencing of the FB-401 strains and mRNAseq highlights the activation of TLR5, TNFR and CXCR2 (IL-8 signaling) 2) FB-401 inhibits S. aureus through metabolites produced by the 3 strains of R. mucosa 1) The 3 strains of R mucosa were specifically selected based on their ability to suppress different strains of S aureus including methicillin resistant S. aureus (MRSA) 2) Phosphatidylcholine and phosphatidylethanolamine metabolites produced by FB-401 suppress S. aureus CONFIDENTIAL 9MECHANISM OF FB-401 Extensive preclinical work by Forte in collaboration with NIH, investigating the activity of FB-401 has demonstrated: 1) FB-401 activates tissue repair and anti-inflammation pathways in keratinocytes, dendritic cells and fibroblasts 1) Gene sequencing of the FB-401 strains and mRNAseq highlights the activation of TLR5, TNFR and CXCR2 (IL-8 signaling) 2) FB-401 inhibits S. aureus through metabolites produced by the 3 strains of R. mucosa 1) The 3 strains of R mucosa were specifically selected based on their ability to suppress different strains of S aureus including methicillin resistant S. aureus (MRSA) 2) Phosphatidylcholine and phosphatidylethanolamine metabolites produced by FB-401 suppress S. aureus CONFIDENTIAL 9

MULTIPLEX GENE PATHWAY ANALYSIS (RNASEQ): FB-401 ACTIVATES TISSUE REPAIR/ANTI-INFLAMMATION PATHWAYS Gene FB ESC KC DC GPRIN3 2.76 Fibroblast, keratinocyte, embryonic stem cell and dendritic cell demonstrate TLR5 2.30 LY6D 1.99 tissue repair pathway activation following exposure to FB-401 including TLR5, SOX9 0.46 IL6R -0.33 CYP27b1 -0.78 3.22 TNFR and CXCR2 driving epithelial to mesenchymal transition (EMT) tissue CXCL8 -1.39 3.25 6.74 GSTM1 -3.29 repair/anti-inflammation SF3B5 1.39 MKNK1 1.38 -0.47 SOX4 1.24 0.61 UAP1 -0.91 RAP1GDS1 -1.40 WDR26 -1.41 AC013271.3 2.88 FIRRE 2.43 OPCML 2.29 RP11-261C10.5 2.23 GRAMD1B 1.97 AC009336.24 1.66 RP4-621F18.2 1.58 BIRC3 0.83 4.04 DACT2 -1.56 RTL1 -2.76 CMB9-75A1.1 -2.99 CCL15 8.45 CCL20 7.76 TNFAIP6 7.34 CXCL5 7.31 WNT5A 5.41 GJC2 2.30 PNPLA1 2.27 JAM2 2.23 NEURL2 2.01 CD200R1 -2.01 PRUNE2 -2.62 GCOM1 -3.09 ICAM4 -3.43 CONFIDENTIAL 10 Skin Fibroblast (FB), keratinocyte (KC), Embryonic Stem cell (ESC) and Dendritic cell (DC) Myles IA et al. Science Translational Medicine. 2020; 12MULTIPLEX GENE PATHWAY ANALYSIS (RNASEQ): FB-401 ACTIVATES TISSUE REPAIR/ANTI-INFLAMMATION PATHWAYS Gene FB ESC KC DC GPRIN3 2.76 Fibroblast, keratinocyte, embryonic stem cell and dendritic cell demonstrate TLR5 2.30 LY6D 1.99 tissue repair pathway activation following exposure to FB-401 including TLR5, SOX9 0.46 IL6R -0.33 CYP27b1 -0.78 3.22 TNFR and CXCR2 driving epithelial to mesenchymal transition (EMT) tissue CXCL8 -1.39 3.25 6.74 GSTM1 -3.29 repair/anti-inflammation SF3B5 1.39 MKNK1 1.38 -0.47 SOX4 1.24 0.61 UAP1 -0.91 RAP1GDS1 -1.40 WDR26 -1.41 AC013271.3 2.88 FIRRE 2.43 OPCML 2.29 RP11-261C10.5 2.23 GRAMD1B 1.97 AC009336.24 1.66 RP4-621F18.2 1.58 BIRC3 0.83 4.04 DACT2 -1.56 RTL1 -2.76 CMB9-75A1.1 -2.99 CCL15 8.45 CCL20 7.76 TNFAIP6 7.34 CXCL5 7.31 WNT5A 5.41 GJC2 2.30 PNPLA1 2.27 JAM2 2.23 NEURL2 2.01 CD200R1 -2.01 PRUNE2 -2.62 GCOM1 -3.09 ICAM4 -3.43 CONFIDENTIAL 10 Skin Fibroblast (FB), keratinocyte (KC), Embryonic Stem cell (ESC) and Dendritic cell (DC) Myles IA et al. Science Translational Medicine. 2020; 12

FIBROBLAST AND KERATINOCYTE SCRATCH MODELS CONFIRM TISSUE REPAIR THROUGH TLR5 PATHWAY ACTIVATION BY FB-401 Scratch model for Blocking TLR5 both keratinocytes (anti-TLR5 and fibroblasts antibody) demonstrates prevents tissue tissue repair by repair by FB-401 CONFIDENTIAL 11 PBS RmHV FB-401 FB Coverage KC Coverage Myles IA et al. Science Translational Medicine. 2020; 12FIBROBLAST AND KERATINOCYTE SCRATCH MODELS CONFIRM TISSUE REPAIR THROUGH TLR5 PATHWAY ACTIVATION BY FB-401 Scratch model for Blocking TLR5 both keratinocytes (anti-TLR5 and fibroblasts antibody) demonstrates prevents tissue tissue repair by repair by FB-401 CONFIDENTIAL 11 PBS RmHV FB-401 FB Coverage KC Coverage Myles IA et al. Science Translational Medicine. 2020; 12
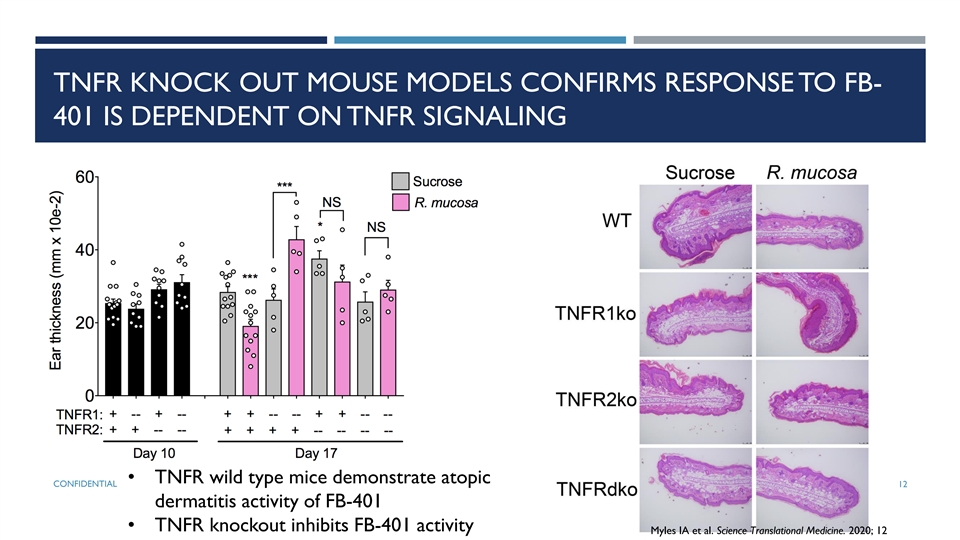
TNFR KNOCK OUT MOUSE MODELS CONFIRMS RESPONSE TO FB- 401 IS DEPENDENT ON TNFR SIGNALING • TNFR wild type mice demonstrate atopic CONFIDENTIAL 12 dermatitis activity of FB-401 • TNFR knockout inhibits FB-401 activity Myles IA et al. Science Translational Medicine. 2020; 12TNFR KNOCK OUT MOUSE MODELS CONFIRMS RESPONSE TO FB- 401 IS DEPENDENT ON TNFR SIGNALING • TNFR wild type mice demonstrate atopic CONFIDENTIAL 12 dermatitis activity of FB-401 • TNFR knockout inhibits FB-401 activity Myles IA et al. Science Translational Medicine. 2020; 12
PHASE 2A FIRST HUMAN STUDY OF FB-401 - CUTANEOUS LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF ATOPIC DERMATITIS Drug product: FB-401 (3 specifically selected therapeutic R. mucosa strains) lyophilized and reconstituted with sterile water in single-use, self-administered spray Design: Phase 1/2a enrolled 2 cohorts: ¡ Initial cohort enrolled 10 adult atopic dermatitis patients 18 years and older ¡ Following positive safety assessment from cohort I, the second cohort of 20 pediatric patients was enrolled Primary Objective: To evaluate the safety and activity of R mucosa as a live biotherapeutic for treatment of AD Secondary Objective: To evaluate the effect of R mucosa live biotherapy on quality of life of participants with AD Exploratory Objectives ¡ Measure trans epidermal water loss (TEWL) ¡ Characterize changes to total and specific IgE ¡ Evaluate potential changes to pre-diagnosed asthma and/or food allergies ¡ Evaluate incidence of S aureus infections that require treatment 13 ¡ Persistence of R mucosa colonization after treatmentPHASE 2A FIRST HUMAN STUDY OF FB-401 - CUTANEOUS LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF ATOPIC DERMATITIS Drug product: FB-401 (3 specifically selected therapeutic R. mucosa strains) lyophilized and reconstituted with sterile water in single-use, self-administered spray Design: Phase 1/2a enrolled 2 cohorts: ¡ Initial cohort enrolled 10 adult atopic dermatitis patients 18 years and older ¡ Following positive safety assessment from cohort I, the second cohort of 20 pediatric patients was enrolled Primary Objective: To evaluate the safety and activity of R mucosa as a live biotherapeutic for treatment of AD Secondary Objective: To evaluate the effect of R mucosa live biotherapy on quality of life of participants with AD Exploratory Objectives ¡ Measure trans epidermal water loss (TEWL) ¡ Characterize changes to total and specific IgE ¡ Evaluate potential changes to pre-diagnosed asthma and/or food allergies ¡ Evaluate incidence of S aureus infections that require treatment 13 ¡ Persistence of R mucosa colonization after treatment
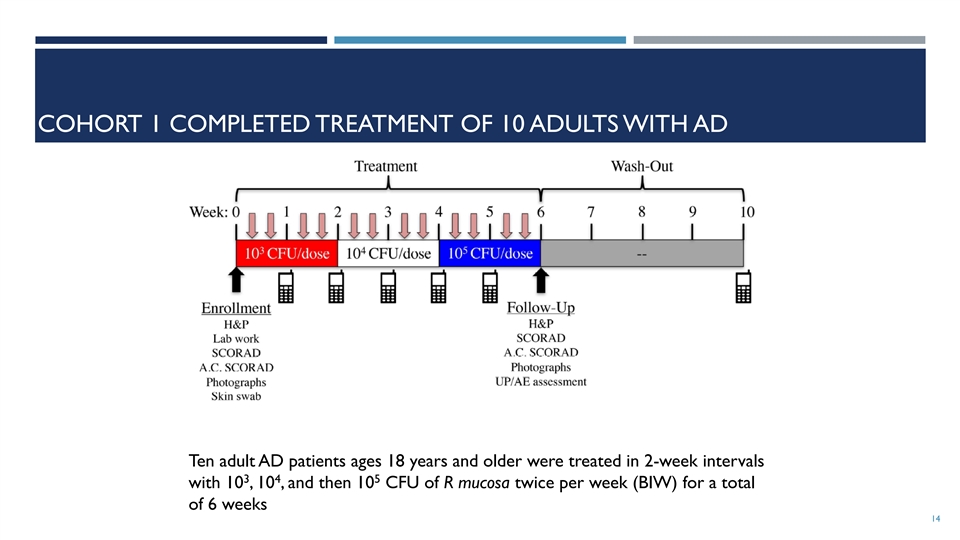
COHORT 1 COMPLETED TREATMENT OF 10 ADULTS WITH AD Ten adult AD patients ages 18 years and older were treated in 2-week intervals 3 4 5 with 10 , 10 , and then 10 CFU of R mucosa twice per week (BIW) for a total of 6 weeks 14COHORT 1 COMPLETED TREATMENT OF 10 ADULTS WITH AD Ten adult AD patients ages 18 years and older were treated in 2-week intervals 3 4 5 with 10 , 10 , and then 10 CFU of R mucosa twice per week (BIW) for a total of 6 weeks 14

STATISTICALLY SIGNIFICANT, DOSE-DEPENDENT IMPROVEMENTS OBSERVED IN ADULT COHORT OF PHASE 1/2a STUDY Only treated areas responded. No AD lesions that were untreated resolved over the course of the study Results from Cohort 1 indicate that six patients responded (60%) with mean improvement of 85%, one patient reported partial response with 44% improvement and three were non (A) Intensity of AD disease (B) Subjective pruritus (C) Antecubital-specific was measured in a blinded reported by the SCORAD (blinded) responders with 9% mean improvement manner using SCORAD patient on 0-10 scale assessed antecubital measures of dryness, region by summing local redness, lichenification, intensity and pruritic excoriation, crusting and scores edema (0-3 scale for each * p<0.05 ** p<0.01 15 measure) Myles et al, JCI Insight, 2018;3(9):e120608STATISTICALLY SIGNIFICANT, DOSE-DEPENDENT IMPROVEMENTS OBSERVED IN ADULT COHORT OF PHASE 1/2a STUDY Only treated areas responded. No AD lesions that were untreated resolved over the course of the study Results from Cohort 1 indicate that six patients responded (60%) with mean improvement of 85%, one patient reported partial response with 44% improvement and three were non (A) Intensity of AD disease (B) Subjective pruritus (C) Antecubital-specific was measured in a blinded reported by the SCORAD (blinded) responders with 9% mean improvement manner using SCORAD patient on 0-10 scale assessed antecubital measures of dryness, region by summing local redness, lichenification, intensity and pruritic excoriation, crusting and scores edema (0-3 scale for each * p<0.05 ** p<0.01 15 measure) Myles et al, JCI Insight, 2018;3(9):e120608

COHORT 2: FB-401 TREATMENT OF 20 CHILDREN WITH AD 20 pediatric/adolescent patients with active AD: ¡ First 5, ages 7-17 ¡ Remainder, ages 3-17 ¡ Baseline SCORAD >10 Pediatric Cohort Treatment Period Design: ¡ Treat AD-involved skin with FB-401 3 ¡ 10 CFU BIW for 4 weeks 4 ¡ 10 CFU BIW for 4 weeks 5 ¡ 10 CFU BIW for 4 weeks 5 Baseline Week 4 ¡ 10 CFU QOD for 4 weeks Week 8 Week 16 Week 12 ¡ Efficacy assessments at baseline and Q4W ¡ SCORAD, pruritus, EASI (%, -50,-75,-90) TEWL, FDLQI, CDLQI ¡ Microbiome assessment ¡ Adverse events throughout and at F/U 16COHORT 2: FB-401 TREATMENT OF 20 CHILDREN WITH AD 20 pediatric/adolescent patients with active AD: ¡ First 5, ages 7-17 ¡ Remainder, ages 3-17 ¡ Baseline SCORAD >10 Pediatric Cohort Treatment Period Design: ¡ Treat AD-involved skin with FB-401 3 ¡ 10 CFU BIW for 4 weeks 4 ¡ 10 CFU BIW for 4 weeks 5 ¡ 10 CFU BIW for 4 weeks 5 Baseline Week 4 ¡ 10 CFU QOD for 4 weeks Week 8 Week 16 Week 12 ¡ Efficacy assessments at baseline and Q4W ¡ SCORAD, pruritus, EASI (%, -50,-75,-90) TEWL, FDLQI, CDLQI ¡ Microbiome assessment ¡ Adverse events throughout and at F/U 16

PATIENT DEMOGRAPHICS Part 1 (Adult Cohort) Part 2 (Pediatric Cohort) N=10 N=21 Age (years) Mean (min, max) 41.5 (19–70) 9.0 (3–16) Gender, n (%) Male 1 (10.0%) 11 (52.4%) Female 9 (90.0%) 10 (47.6%) Race, n (%) Asian 3 (30.0%) 5 (23.8%) Black 0 3 (14.3%) White 7 (70.0%) 13 (61.9%) 17 CONFIDENTIALPATIENT DEMOGRAPHICS Part 1 (Adult Cohort) Part 2 (Pediatric Cohort) N=10 N=21 Age (years) Mean (min, max) 41.5 (19–70) 9.0 (3–16) Gender, n (%) Male 1 (10.0%) 11 (52.4%) Female 9 (90.0%) 10 (47.6%) Race, n (%) Asian 3 (30.0%) 5 (23.8%) Black 0 3 (14.3%) White 7 (70.0%) 13 (61.9%) 17 CONFIDENTIAL

PEDIATRIC PATIENT DATA SHOWS SIGNIFICANT ACTIVITY – TREATMENT THROUGH W16, FOLLOW UP 6 M AFTER TREATMENT COMPLETION Dotted lines are data from patients that went direct to 10^5 Solid lines are dose escalation patients * p<0.05 ** P<0.01 Average Response *** p<0.001 Ave **** p<0.0001 baseline N SCORAD Responder % All Responders 18 SCORAD (50% improvement) 20 36.1 17 85.0% 65.6% 73.2% CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12PEDIATRIC PATIENT DATA SHOWS SIGNIFICANT ACTIVITY – TREATMENT THROUGH W16, FOLLOW UP 6 M AFTER TREATMENT COMPLETION Dotted lines are data from patients that went direct to 10^5 Solid lines are dose escalation patients * p<0.05 ** P<0.01 Average Response *** p<0.001 Ave **** p<0.0001 baseline N SCORAD Responder % All Responders 18 SCORAD (50% improvement) 20 36.1 17 85.0% 65.6% 73.2% CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12
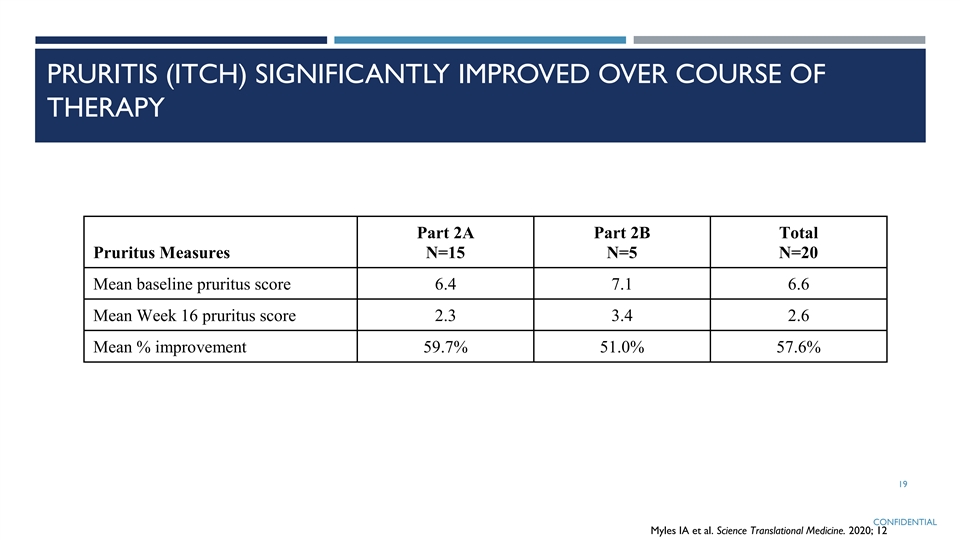
PRURITIS (ITCH) SIGNIFICANTLY IMPROVED OVER COURSE OF THERAPY Part 2A Part 2B Total Pruritus Measures N=15 N=5 N=20 Mean baseline pruritus score 6.4 7.1 6.6 Mean Week 16 pruritus score 2.3 3.4 2.6 Mean % improvement 59.7% 51.0% 57.6% 19 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12PRURITIS (ITCH) SIGNIFICANTLY IMPROVED OVER COURSE OF THERAPY Part 2A Part 2B Total Pruritus Measures N=15 N=5 N=20 Mean baseline pruritus score 6.4 7.1 6.6 Mean Week 16 pruritus score 2.3 3.4 2.6 Mean % improvement 59.7% 51.0% 57.6% 19 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12

PEDIATRIC PATIENT EASI EFFICACY DATA SHOWS SIGNIFICANT ACTIVITY Average Response Ave baseline N EASI Responders % All Responders EASI-50 20 7.8 18 90.0% 76.8% 83.6% Ave baseline N EASI Responders % EASI-75 20 7.8 14 70.0% • Dotted lines are data from patients that went Ave baseline direct to 10^5 N EASI Responders % • Solid lines are dose escalation patients EASI-90 20 7.8 6 30.0% EASI Severity * p<0.05 Mild<7 20 ** P<0.01 Moderate 7-21 *** p<0.001 Severe>21 CONFIDENTIAL **** p<0.0001 Myles IA et al. Science Translational Medicine. 2020; 12PEDIATRIC PATIENT EASI EFFICACY DATA SHOWS SIGNIFICANT ACTIVITY Average Response Ave baseline N EASI Responders % All Responders EASI-50 20 7.8 18 90.0% 76.8% 83.6% Ave baseline N EASI Responders % EASI-75 20 7.8 14 70.0% • Dotted lines are data from patients that went Ave baseline direct to 10^5 N EASI Responders % • Solid lines are dose escalation patients EASI-90 20 7.8 6 30.0% EASI Severity * p<0.05 Mild<7 20 ** P<0.01 Moderate 7-21 *** p<0.001 Severe>21 CONFIDENTIAL **** p<0.0001 Myles IA et al. Science Translational Medicine. 2020; 12

PEDIATRIC PATIENT EFFICACY DATA SHOWS SIGNIFICANT ACTIVITY ACROSS DISEASE SEVERITY Mild Disease Moderate/Severe Disease Trial Protocol Total EASI=<7 at baseline EASI>=7 at baseline EASI =>5 at baseline N=11 N=9 N=14 N=20 EASI 50 81.8% (9/11) 100% (9/9) 100% (14/14) 90% (18/20) EASI 75 54.5% (6/11) 88.9% (8/9) 78.6% (11/14) 70% (14/20) EASI 90 27.2% (3/11) 33.3% (3/9) 35.7% (5/14) 30.0% (6/20) 21 CONFIDENTIALPEDIATRIC PATIENT EFFICACY DATA SHOWS SIGNIFICANT ACTIVITY ACROSS DISEASE SEVERITY Mild Disease Moderate/Severe Disease Trial Protocol Total EASI=<7 at baseline EASI>=7 at baseline EASI =>5 at baseline N=11 N=9 N=14 N=20 EASI 50 81.8% (9/11) 100% (9/9) 100% (14/14) 90% (18/20) EASI 75 54.5% (6/11) 88.9% (8/9) 78.6% (11/14) 70% (14/20) EASI 90 27.2% (3/11) 33.3% (3/9) 35.7% (5/14) 30.0% (6/20) 21 CONFIDENTIAL

TREATMENT WITH FB-401 DEMONSTRATES SIGNIFICANT IMPROVEMENT Myles et al, JCI Insight, 2018;3(9):e120608 22TREATMENT WITH FB-401 DEMONSTRATES SIGNIFICANT IMPROVEMENT Myles et al, JCI Insight, 2018;3(9):e120608 22

REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 23 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 23 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12

REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 16 Week 0 24 CONFIDENTIALREPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 16 Week 0 24 CONFIDENTIAL

REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 25 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 25 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12

REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 26 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY Week 0 Week 16 26 CONFIDENTIAL Myles IA et al. Science Translational Medicine. 2020; 12

REPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY 27 CONFIDENTIALREPRESENTATIVE IMAGE OF IMPROVEMENT FOLLOWING THERAPY 27 CONFIDENTIAL

PLANNED FB-401 RANDOMIZED PHASE 2 STUDY • Randomized, placebo-controlled, multi-center study • Includes children (2 years and older), adolescents and adults with mild to moderate atopic dermatitis • Approximately 124 subjects randomized 1:1 to receive FB-401 or placebo for 16 weeks • Endpoints include Eczema Area and Severity Index (EASI), Investigator Global Assessment (IGA), pruritus CONFIDENTIAL 28PLANNED FB-401 RANDOMIZED PHASE 2 STUDY • Randomized, placebo-controlled, multi-center study • Includes children (2 years and older), adolescents and adults with mild to moderate atopic dermatitis • Approximately 124 subjects randomized 1:1 to receive FB-401 or placebo for 16 weeks • Endpoints include Eczema Area and Severity Index (EASI), Investigator Global Assessment (IGA), pruritus CONFIDENTIAL 28

INTELLECTUAL PROPERTY OVERVIEW ¡ Exclusive license to NIH-owned patent family focused on treatment of AD with a consortia of gram negative bacteria from healthy donors ¡ Patent coverage through at least 2037 ¡ 7 US patents issued ¡ Entered in 10 Ex-US jurisdictions ¡ Europe, China, Canada, Japan, South Korea, Australia, Singapore, Mexico, Israel, and Hong Kong ¡ Company-owned IP directed to compositions for treatment of skin conditions associated with dysbiosis ¡ Broadly covers use of gram negative bacteria for treatment of atopic disorders 29INTELLECTUAL PROPERTY OVERVIEW ¡ Exclusive license to NIH-owned patent family focused on treatment of AD with a consortia of gram negative bacteria from healthy donors ¡ Patent coverage through at least 2037 ¡ 7 US patents issued ¡ Entered in 10 Ex-US jurisdictions ¡ Europe, China, Canada, Japan, South Korea, Australia, Singapore, Mexico, Israel, and Hong Kong ¡ Company-owned IP directed to compositions for treatment of skin conditions associated with dysbiosis ¡ Broadly covers use of gram negative bacteria for treatment of atopic disorders 29

SUMMARY OF FORTE BIOSCIENCES: FB-401 – POTENTIAL FIRST-IN-CLASS TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE ¡ Phase 2a trial in atopic dermatitis completed including pediatrics 3 years and older, FB-401 was well LATE-STAGE tolerated and demonstrated clinical improvement Randomized Phase 2 initiation in adults and pediatrics CLINICAL ASSET 2 years and older expected in 3Q20 in atopic dermatitis (AD) with data readout expected in mid-2021 LARGE MARKET ¡ 10-20% of children in industrialized countries develop atopic dermatitis (AD) WITH UNMET ¡ In the U.S., AD affects 17 million people (over 50% are children) NEED¡ Significant unmet need for safe and effective AD therapy for pediatrics POTENTIAL FIRST- ¡ Clinical data demonstrates FB-401 was well-tolerated and active IN-CLASS TOPICAL ¡ Phase 2a study, including pediatrics, demonstrates potential for acceptable safety profile and significant LIVE reduction in atopic dermatitis disease and pruritus, as well as control of S. aureus while BIOTHERAPEUTIC tapering/eliminating steroid use ¡ Exclusive license to NIH-owned patent families as well as Forte owned IP. Coverage includes INTELLECTUAL composition and method of use patents PROPERTY ¡ Patent coverage through at least 2037 (7 U.S. patents issued) ¡ Experienced life science investor base including Alger, ArrowMark, BVF Partners LP, Franklin Templeton FINANCING / and OrbiMed MANAGEMENT ¡ Cash runway expected to be sufficient through Phase 2 data readout in mid-2021 ¡ Management team with significant drug development, innovation and corporate strategy experience 30SUMMARY OF FORTE BIOSCIENCES: FB-401 – POTENTIAL FIRST-IN-CLASS TOPICAL LIVE BIOTHERAPEUTIC FOR THE TREATMENT OF INFLAMMATORY SKIN DISEASE ¡ Phase 2a trial in atopic dermatitis completed including pediatrics 3 years and older, FB-401 was well LATE-STAGE tolerated and demonstrated clinical improvement Randomized Phase 2 initiation in adults and pediatrics CLINICAL ASSET 2 years and older expected in 3Q20 in atopic dermatitis (AD) with data readout expected in mid-2021 LARGE MARKET ¡ 10-20% of children in industrialized countries develop atopic dermatitis (AD) WITH UNMET ¡ In the U.S., AD affects 17 million people (over 50% are children) NEED¡ Significant unmet need for safe and effective AD therapy for pediatrics POTENTIAL FIRST- ¡ Clinical data demonstrates FB-401 was well-tolerated and active IN-CLASS TOPICAL ¡ Phase 2a study, including pediatrics, demonstrates potential for acceptable safety profile and significant LIVE reduction in atopic dermatitis disease and pruritus, as well as control of S. aureus while BIOTHERAPEUTIC tapering/eliminating steroid use ¡ Exclusive license to NIH-owned patent families as well as Forte owned IP. Coverage includes INTELLECTUAL composition and method of use patents PROPERTY ¡ Patent coverage through at least 2037 (7 U.S. patents issued) ¡ Experienced life science investor base including Alger, ArrowMark, BVF Partners LP, Franklin Templeton FINANCING / and OrbiMed MANAGEMENT ¡ Cash runway expected to be sufficient through Phase 2 data readout in mid-2021 ¡ Management team with significant drug development, innovation and corporate strategy experience 30