Attached files
| file | filename |
|---|---|
| EX-32.1 - EX-32.1 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex3210c2734.htm |
| EX-31.2 - EX-31.2 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex312bc6e82.htm |
| EX-31.1 - EX-31.1 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex311da44ef.htm |
| EX-23.1 - EX-23.1 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex23136b88e.htm |
| EX-10.18 - EX-10.18 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex1018cd3ce.htm |
| EX-10.17(B) - EX-10.17(B) - Corvus Pharmaceuticals, Inc. | crvs-20191231ex1017b16cd.htm |
| EX-10.16(C) - EX-10.16(C) - Corvus Pharmaceuticals, Inc. | crvs-20191231ex1016cdf22.htm |
| EX-10.16(B) - EX-10.16(B) - Corvus Pharmaceuticals, Inc. | crvs-20191231ex1016b82ec.htm |
| EX-4.5 - EX-4.5 - Corvus Pharmaceuticals, Inc. | crvs-20191231ex45adb3c49.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
(Mark One)
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the Fiscal Year Ended December 31, 2019
OR
☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
Corvus Pharmaceuticals, Inc.
(Exact name of registrant as specified in its charter)
|
Delaware |
001-37719 |
46-4670809 |
|
(State or other jurisdiction |
(Commission |
(IRS Employer |
863 Mitten Road, Suite 102, Burlingame, CA 94010
(Address of principal executive offices, including Zip Code)
Registrant’s telephone number, including area code: (650) 900-4520
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class |
Trading symbol(s) |
Name of each exchange on which registered |
|
Common Stock, Par Value $0.0001 per share |
CRVS |
Nasdaq Global Market |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the issuer (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer ☐ |
|
|
Accelerated filer ☒ |
|
Non‑accelerated filer ☐ |
|
|
Smaller reporting company ☒ |
|
|
|
|
Emerging growth company ☒ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☒
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
As of June 30, 2019, the aggregate market value of Common Stock held by non-affiliates of the registrant was approximately $65.7 million, computed by reference to the closing price as reported on The Nasdaq Stock Market. As of March 9, 2020, 29,326,900 shares of the registrant’s common stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
None.
CORVUS PHARMACEUTICALS, INC.
ANNUAL REPORT ON FORM 10‑K
i
Forward‑Looking Statements
This Annual Report on Form 10‑K contains forward‑looking statements that involve risks and uncertainties. All statements other than statements of historical facts contained in this report are forward‑looking statements. In some cases, you can identify forward‑looking statements by terminology such as “may,” “could,” “will,” “would,” “should,” “expect,” “plan,” “anticipate,” “believe,” “estimate,” “intend,” “predict,” “seek,” “contemplate,” “potential” or “continue” or the negative of these terms or other comparable terminology. These forward‑looking statements include, but are not limited to, statements about:
|
· |
our expectations and beliefs regarding the potential benefits of our product candidates; |
|
· |
our expectations regarding the clinical effectiveness of our product candidates and utility of our biomarker data; |
|
· |
the anticipated timing, costs and conduct of our ongoing and planned clinical trials for ciforadenant (formerly CPI‑444), CPI‑006 and CPI-818, and planned preclinical studies and clinical trials for other product candidates in our development programs; |
|
· |
our ability to develop, acquire and advance product candidates into, and successfully complete, clinical trials; |
|
· |
the timing of the completion of our ongoing clinical trials of ciforadenant, CPI-006 and CPI-818 and the timing and availability of clinical data from such clinical trials; |
|
· |
clinical and regulatory development plans with respect to ciforadenant, CPI‑006, CPI-818 and our other product candidates; |
|
· |
our expectations regarding the potential market size and the size of the patient populations for ciforadenant, CPI‑006, CPI-818 and our other product candidates, if approved for commercial use; |
|
· |
our ability to commercialize ciforadenant and our other product candidates, if approved; |
|
· |
our commercialization, marketing and manufacturing capabilities and strategy; |
|
· |
the pricing and reimbursement of our product candidates, if approved; |
|
· |
the scope of protection we are able to establish and maintain for intellectual property rights covering our product candidates, including the projected terms of patent protection; |
|
· |
our or any existing or future collaborator’s ability to obtain and maintain intellectual property protection for our technologies and product candidates and our ability to operate our business without infringing the intellectual property rights of others; |
|
· |
our ability to establish and maintain collaborations and retain commercial rights for our product candidates in such collaborations; |
|
· |
the potential benefits of strategic collaborations and our ability to enter into strategic arrangements; |
|
· |
developments and projections relating to our competitors and our industry, including competing therapies; |
|
· |
our estimates regarding the effect of changes in the tax code as a result of recent federal tax legislation and uncertainty as to how some of those changes may be applied; |
ii
|
· |
our estimates regarding expenses, future revenue, capital requirements and needs for additional financing; and |
|
· |
our financial performance. |
Any forward‑looking statements in this Annual Report on Form 10‑K reflect our current views with respect to future events or to our future financial performance and involve known and unknown risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by these forward‑looking statements. Factors that may cause actual results to differ materially from current expectations include, among other things, those listed under Part I, Item 1A. Risk Factors and discussed elsewhere in this Annual Report on Form 10‑K. Given these uncertainties, you should not place undue reliance on these forward‑looking statements. Except as required by law, we assume no obligation to update or revise these forward‑looking statements for any reason, even if new information becomes available in the future.
This Annual Report on Form 10‑K also contains estimates, projections and other information concerning our industry, our business and the markets for certain drugs, including data regarding the estimated size of those markets, their projected growth rates and the incidence of certain medical conditions. Information that is based on estimates, forecasts, projections or similar methodologies is inherently subject to uncertainties, and actual events or circumstances may differ materially from events and circumstances reflected in this information. Unless otherwise expressly stated, we obtained this industry, business, market and other data from reports, research surveys, studies and similar data prepared by third parties, industry, medical and general publications, government data and similar sources. In some cases, we do not expressly refer to the sources from which this data is derived. In that regard, when we refer to one or more sources of this type of data in any paragraph, you should assume that other data of this type appearing in the same paragraph is derived from the same sources, unless otherwise expressly stated or the context otherwise requires.
Except where the context otherwise requires, in this Annual Report on Form 10‑K, “we,” “us,” “our” and the “Company” refer to Corvus Pharmaceuticals, Inc.
Trademarks
This Annual Report on Form 10‑K includes trademarks, service marks and trade names owned by us or other companies. All trademarks, service marks and trade names included in this Annual Report on Form 10‑K are the property of their respective owners.
iii
Overview
We are a clinical stage biopharmaceutical company focused on the development and commercialization of precisely targeted oncology therapies. Our strategy is to identify and utilize novel biomarkers to enhance selection of patients we believe will be most likely to benefit from treatment with our product candidates. We have utilized adaptive clinical protocol designs that enable us to evaluate our agents in multiple dosing regimens and for a range of cancer types. Since we began operations in November 2014, we have built a pipeline of five oncology programs. Three of these product candidates are now in international multicenter trials directed against a broad number of cancer indications. To date, we have evaluated our product candidates in over 350 patients. We are developing small molecules that are designed to selectively inhibit the binding of immunosuppressive adenosine to either A2A receptors or to A2B receptors. Another small molecule inhibitor is designed to block the function of ITK, a kinase protein inside T cells that is crucial to T-cell activation and differentiation. We also are developing injectable monoclonal antibodies. One of these antibodies is designed to block the production of adenosine by tumors by inhibiting the cell surface enzyme CD73. This antibody is designed to have dual properties; in addition to blocking production of immunosuppressive adenosine, the antibody is designed to stimulate various immune cells. Another antibody that is designed to bind to the chemokine receptor CXCR2 on myeloid cells to block the activity of immunosuppressive myeloid cells that infiltrate tumors is in preclinical development. Our product candidates’ designed specificity has the potential to provide greater safety and facilitate their development either as monotherapies or in combination with other cancer therapies such as immune checkpoint inhibitors or chemotherapy.
Ciforadenant (formerly CPI-444), is an oral, small molecule antagonist of the A2A receptor for adenosine and is currently being studied under a Phase 2 expansion protocol in combination with Genentech, Inc.’s cancer immunotherapy, Tecentriq® (atezolizumab) for patients with either advanced, refractory renal cell cancer (“RCC”) or patients with refractory metastatic castration resistant prostate cancer (“mCRPC”). Our second clinical product candidate, CPI-006, is an anti‑CD73 monoclonal antibody that is designed to both inhibit the production of adenosine and stimulate various immune cells. CPI-006 is currently being studied in a Phase 1/1b clinical trial as a monotherapy and in combination with ciforadenant, in combination with pembrolizumab and in triplet combination with both ciforadenant and pembrolizumab. Our third clinical product candidate, CPI-818, is a selective, covalent inhibitor of ITK and is in a multi-center Phase 1/1b clinical trial in patients with various malignant T-cell lymphomas. CPI-818 is designed to be directly cytotoxic to certain malignant T-cells and we believe has the potential to regulate immune responses to tumors. We believe the breadth and status of our pipeline demonstrates our management team’s expertise in understanding and developing oncology assets as well as in identifying product candidates that can be in‑licensed and further developed internally to treat many types of cancer. We hold worldwide rights to all of our product candidates.
Oncology therapies that stimulate or enhance immune responses to tumors have become a commonly used approach with several potential benefits over existing therapies. First, the immune system exhibits immunologic diversity and selectivity, which enables it to respond selectively to a large number of potential targets. Second, once triggered, the immune response can be amplified, offering the potential to enhance the efficacy of treatment. Third, once activated, the immune system possesses immunologic memory, potentially providing for a durable and long‑lasting response. Some of the most successful types of immuno‑oncology therapies are immune checkpoint inhibitors. Immune checkpoints are signaling molecules produced by or expressed on immune cells that act to shut down or block an immune response. In a healthy person, these checkpoints function to limit an immune response to ensure that the immune system does not overreact, which could lead to excessive inflammation and tissue damage, as occurs in patients with autoimmune diseases or allergies. Tumor cells have evolved to activate these checkpoints to shield the tumor from immune response attacks, but studies have shown that immune checkpoint inhibitors can counter these tumor‑protective measures and unleash the immune system’s cancer‑destroying properties.
The FDA has approved agents that target specific immune checkpoints, including antibodies against the cytotoxic T‑lymphocyte‑associated antigen‑4 (“CTLA‑4”), programmed death 1 (“PD‑1”) receptors, and programmed death receptor‑ligand 1 (“PD‑L1”). These antibodies represent the first immune checkpoint inhibitors to demonstrate effectiveness in the clinic, and preclinical data suggest that there are many other immune checkpoints or targets that may
1
be modulated to promote the activation of a patient’s anti‑tumor immune system. To date, antibodies targeting immune checkpoints have been approved to treat melanoma, lung, renal cell, breast, bladder, head and neck and other cancers.
Product Pipeline
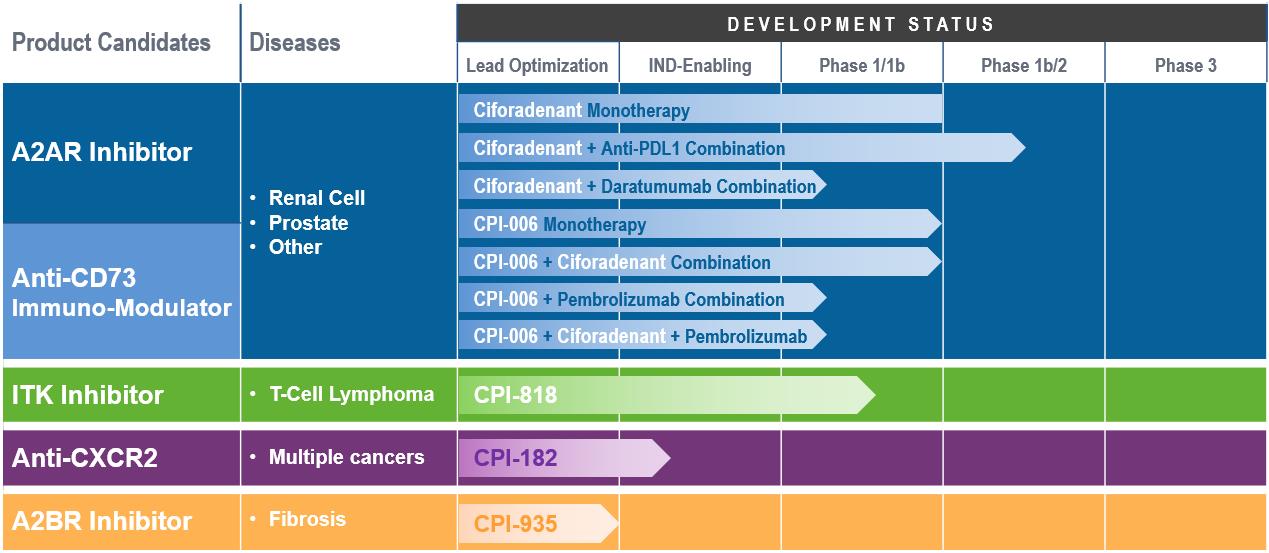
Our oncology product candidate pipeline includes the following:
Ciforadenant Adenosine A2A Receptor Antagonist. Our initial product candidate, ciforadenant, is an oral, small molecule antagonist of the A2A receptor for adenosine that we in-licensed from Vernalis (R&D) Limited (“Vernalis”) in February 2015. In January 2016, we began enrolling patients in a large expansion cohort trial for ciforadenant. This Phase 1/1b clinical trial is designed to examine safety, tolerability, biomarkers and preliminary efficacy of ciforadenant in several solid tumor types, both as a single agent and in combination with Genentech, Inc.’s cancer immunotherapy, Tecentriq, a fully humanized monoclonal antibody targeting PD‑L1. In November 2016, we completed enrollment of 48 patients in the first step of the Phase 1/1b clinical trial, which was designed to determine the optimal dose of ciforadenant as both a single agent therapy and in combination with Tecentriq for use in the cohort expansion stage of the trial. The expansion cohort portion of the trial enrolled patients with non‑small cell lung cancer (“NSCLC”), RCC, melanoma (“MEL”), triple negative breast cancer (“TNBC”) and other cancers including colorectal cancer, prostate cancer, head and neck cancer and bladder cancer at leading medical centers in the U.S., Australia and Canada. We have enrolled over 300 patients in this clinical trial to date. In 2017, both the single agent and combination arms of the NSCLC and RCC cohorts met the protocol‑defined criteria for expansion from 14 to 26 patients, and both arms of the RCC cohort further met the protocol‑defined criteria for expansion to 48 patients. In December 2017, Genentech began enrolling patients in a Phase 1b/2 clinical trial that is evaluating ciforadenant in combination with Tecentriq in patients with NSCLC under an umbrella protocol known as Morpheus. In 2018, we amended our Phase 1/1b protocol to enroll patients in a Phase 1b/2 clinical trial with RCC who have failed therapies with both anti-PD-(L)1 antibodies and tyrosine kinase inhibitors (“TKI”). Based on data observed in the Phase 1b/2 trial in 2019, we began enrolling patients with metastatic castration-resistant prostate cancer (“mCRPC”) in a Phase 2 expansion arm of our ongoing Phase 1/1b clinical trial with mCRPC who will receive the combination of ciforadenant with Tecentriq based on data from the Phase 1b/2 trial that showed activity in this disease.
As of November 2019, the key findings from these clinical trials include:
|
· |
Ciforadenant has been well-tolerated at doses that achieved substantial receptor blockade; |
|
· |
Ciforadenant has shown evidence of anti-tumor activity as a monotherapy and in combination with atezolizumab; |
2
|
· |
Of cancers studied, RCC, mCRPC and NSCLC have appeared most responsive to therapy; and |
|
· |
Identification of a gene expression signature, known as the adenosine gene signature, that enhances selection of patients we believe are most likely to benefit from therapy and may be a useful biomarker for selection of patients in future clinical trials. |
The issued U.S. patents that we in‑licensed from Vernalis for ciforadenant are directed to the composition of matter of ciforadenant and its method of use for treating disorders treatable by purine receptor blocking. The composition of matter patent covering ciforadenant is expected to expire in the United States in July 2029, excluding any patent term extension that may be available. We hold an exclusive, worldwide license under these patent rights and related know‑how, including a limited right to grant sublicenses, for all fields of use, to develop, manufacture and commercialize products containing certain adenosine receptor antagonists, including ciforadenant. We have also filed patent applications covering the use of ciforadenant in combination with other checkpoint inhibitors, and the use of various biomarkers to select and monitor patients receiving therapy.
CPI-006, Immunomodulatory Anti‑CD73 Antibody. Our second clinical product candidate, CPI-006, is an anti‑CD73 monoclonal antibody that is designed to inhibit the production of adenosine, which we in‑licensed from The Scripps Research Institute (“Scripps”) in December 2014. CPI-006 was developed into a humanized anti‑CD73 monoclonal antibody from a mouse hybridoma clone expressing an anti‑human CD73 antibody. We have further modified CPI‑006 to improve binding to CD73 and maximize its inhibition of catalytic activity. CD73 is an ectonucleotidase often found on lymphocytes, tumors and other tissues and is believed to play an important role in tumor immune suppression by catalyzing the production of extracellular adenosine. In preclinical in vitro studies, our humanized monoclonal anti‑CD73 antibody has been shown to inhibit the catalytic activity of CD73, resulting in the blocking of extracellular adenosine production by tumor cells, which we believe could stimulate or enhance immune response to tumors. In addition to its role in the production of adenosine, CD73 also functions as an immunomodulatory receptor present on B-cells, T-cells and certain myeloid cells. In February 2018, we initiated a Phase 1/1b clinical trial with CPI-006 administered alone and in combination with ciforadenant and in combination with pembrolizumab. In addition, we recently added a treatment arm to the study to evaluate the triplet combination of CPI-006, ciforadenant and pembrolizumab. As of February 2020, the key findings from this clinical trial include the observation that CPI-006 has been well-tolerated and has resulted in changes in lymphocyte migration and activation in peripheral blood.
We hold a non‑exclusive, world‑wide license for all fields of use under Scripps’ rights in a hybridoma clone expressing an anti‑CD73 antibody, and to progeny, mutants or unmodified derivatives of such hybridoma and any antibodies expressed by such hybridoma. In 2016, we filed a patent application covering the composition of matter of CPI‑006. In 2019, we filed patent applications covering the use of this CPI-006 for immunomodulation and enhancement of anti-tumor immunity.
CPI-818, ITK Inhibitor. Our third clinical product candidate, CPI-818, is a selective, covalent inhibitor of ITK. ITK, an enzyme that functions in T‑cell signaling and differentiation, is expressed predominantly in T‑cells, which are lymphocytes that play a vital role in immune responses. One of the key survival mechanisms of tumors is believed to be the reprogramming of T‑cells to create an inflammatory environment that inhibits anti‑tumor immune response and favors tumor growth. We believe highly selective inhibitors of this enzyme will facilitate induction of T‑cell anti‑tumor immunity and also may be useful in the treatment of T‑cell lymphomas. CPI-818 is orally bioavailable and has been shown to achieve cellular occupancy of the target in vivo in various animal models. Pre-clinical studies have demonstrated that CPI-818 was well-tolerated in vivo and resulted in inhibition of T-cell activation. In March of 2019, we initiated a phase 1/1b study of CPI-818 in patients with advanced refractory T-cell lymphomas. Early interim results from the dose-escalation portion of the study were presented in December 2019 at the American Society of Hematology (ASH) meeting and in February 2020 at the 12th Annual T-cell Lymphoma Forum, showing that, CPI-818 was well tolerated and achieved substantial ITK target occupancy, one of the goals of the study.
We have filed patent applications covering composition of matter and uses of our ITK inhibitors and hold exclusive worldwide rights for all indications.
CPI-182, Anti-CXCR2 Antibody designed to block Myeloid Suppression. In 2017, we in-licensed this monoclonal antibody designed to block CXCR2, a novel target expressed on myeloid derived suppressor cells
3
(“MDSC”). Preclinical studies have demonstrated that this antibody blocked MDSCs and also may have reacted with CXCR2 present on certain cancers such as acute myeloid leukemia cells and other cancers. This product candidate is now in Investigational New Drug (“IND”)-enabling studies and scale-up manufacturing.
CPI-935, Adenosine A2B Receptor Antagonist. Adenosine A2B receptors have been found to play an important role in the immune response to tumors as well as in inflammation and fibrosis. Similar to adenosine A2A receptors, adenosine binds to adenosine A2B receptors, which leads to immunosuppression. Preclinical models have shown that inhibition of A2B receptors prevents fibrosis. In 2018, we selected a development candidate for this program, a small molecule antagonist of the A2B receptor.
Our Company Origins and Team
Since we began operations in November 2014, our focus has been on improving and expanding upon the recent success achieved with immune checkpoint inhibitors and on developing agents to new targets in the evolving immuno‑oncology field. Our founders and management team consist of industry veterans who have played significant roles in the discovery and development of successful oncology and immunology antibodies and drugs, including rituximab and ibrutinib. Our co‑founders include our Chief Executive Officer, Richard A. Miller, M.D., our Chief Financial Officer, Leiv Lea, and our Executive Vice President, Discovery Research, Joseph Buggy, Ph.D. Dr. Miller previously co‑founded IDEC (which merged to form Biogen IDEC, now Biogen), where he led research efforts on lymphoma, culminating in the development of rituximab. Dr. Miller, an oncologist, also co‑founded and was the initial CEO of Pharmacyclics, Inc. where he and colleagues in‑licensed ibrutinib and, together with Dr. Buggy and other members of our executive team, led its development. Our Chief Financial Officer, Leiv Lea, has previously led finance teams for emerging biotechnology companies, including Pharmacyclics. Mr. Lea has extensive commercial and operating experience in addition to having completed a number of financial and strategic transactions. We have recruited industry veterans and experts to join our management team, and established collaborations with leading biotechnology companies, including Genentech, and collaborative relationships with many leading academic research institutions. With our management team’s expertise in developing both small molecule and antibody‑based oncology treatments, we believe we are well positioned to identify and develop novel therapeutic agents that have diverse but complementary mechanisms of action, allowing for their potential integration into oncology treatment regimens for a broad variety of cancers.
Our Strategy
Our goal is to become a leader in the discovery and development of precisely targeted treatments for multiple cancer indications. Specific elements of our strategy are:
•Leverage our expertise in immunology and oncology to identify, develop and commercialize new product candidates. We have established development expertise and capabilities in synthetic chemistry, molecular biology, immunology and clinical oncology, which we believe will help us advance product candidates in the oncology field. We plan to become a leader in the development and commercialization of product candidates targeting adenosine and other components involved in cancer immunity. Our ITK inhibitor, CPI-818, leverages our expertise in development of covalent kinase inhibitors. We have also in‑licensed CPI-182, a monoclonal antibody to a novel immuno‑oncology target. In addition to our internal research programs, we intend to seek opportunities to in‑license other product candidates with a focus on the potential to address unmet needs within our areas of expertise.
•Utilize efficient clinical trial designs to enable us to identify the most promising clinical indications. Our adaptive clinical trials are efficiently designed to evaluate multiple variables, such as single agent and combination therapy, impact of prior therapy with immuno‑oncology agents and the role of various biomarkers, which may allow us to determine tumor types that are most responsive to our product candidates. This approach has the potential to shorten development time by quickly identifying the most promising clinical indications, which would then be evaluated in subsequent definitive pivotal trials. To date, over 350 patients have been treated in our clinical studies, with results presented at several major medical meetings.
4
•Advance product candidates for use alone or in combination with other oncology treatments. We intend to focus on product candidates with single agent activity, which are also designed to be combined synergistically with other cancer therapies. We believe focusing on single agent activity allows us to better understand safety, mechanism of action, potential efficacy and use of biomarkers before testing our product candidates in combination with other therapies, where interpretation of results becomes more difficult. This approach may enable us to more strategically combine our agents with other therapies.
•Identify and utilize biomarker-driven patient selection strategies. Predicting optimal drug responses in patients requires the identification and validation of predictive biomarkers. We believe that developing the ability to identify patient subsets most likely to respond to our product candidates will increase the clinical benefit to patients and improve the probability of success of our clinical trials. Our Phase 1/1b clinical trials of ciforadenant, CPI-006 and CPI-818 include the examination of numerous biomarkers to identify those that may correlate with clinical efficacy and increase our likelihood of success. For instance, from our clinical data we believe we have discovered a novel adenosine gene expression signature, which could identify patients most likely to respond to treatment with adenosine blockade with ciforadenant. In patients with RCC, expression of the adenosine signature has correlated with tumor response and progression free survival.
•Pursue collaborative relationships, partnerships and in‑licensing opportunities to help advance and expand our product candidate portfolio. In addition to developing product candidates through preclinical and clinical stages of development, we plan to identify and pursue strategic collaborative relationships, partnerships and in‑licensing opportunities, which could enhance the development of our programs and product candidates. As evidenced by our collaboration with Genentech for ciforadenant, we intend to build upon our relationships with leading biotechnology companies and research institutions to identify and expand new opportunities in cancer treatment.
Cancer Treatment and Immuno‑oncology
Cancer is the second leading cause of mortality in the United States, accounting for nearly one in every four deaths. Approximately 40% of Americans will develop some form of cancer, and, according to the American Cancer Society, there were an estimated 1.8 million new cases of cancer and 600,000 deaths due to cancer in the United States in 2019. Cancer treatment has traditionally included chemotherapy, biologic therapy, radiation, surgery or a combination of these approaches. Treatment with targeted agents that block cell signaling pathways or inhibit driver mutations in cancer cells is becoming more widely used. These agents often react with specifically mutated proteins in cancer or signaling molecules involved in cellular activation and proliferation. Many different mutations are now known to occur in cancer and, in many cases, are responsible for driving tumor progression.
Immuno‑oncology is an approach to treating cancer that is based on stimulating or enhancing an immune response to the tumor and is founded on the findings that the mutations occurring in cancer cells may be immunogenic and capable of eliciting an immune response against the tumor. Immuno‑oncology therapies offer several potential advantages over existing cancer therapies due to the intrinsic features of the immune system. For instance, the immune system exhibits immunologic diversity and selectivity, which enables it to respond to a large number of potential targets. In addition, once triggered, the immune response can be amplified, offering the potential to enhance the efficacy of treatment. Furthermore, once activated, the immune system possesses immunologic memory, potentially providing for a durable and long‑lasting response. Finally, because immunotherapy mechanisms are indifferent to tissue origin and are instead focused on immunogenic mutations, which are often expressed across tumor types, immunotherapy may be widely applicable to many types of cancer and not limited to a particular tumor type. This allows for these agents to be potentially active in a multitude of cancer histologies.
Recently, the reasons for the historical failures of immunologic approaches to cancer treatment have become better understood. Tumors evolve sophisticated survival mechanisms, allowing them to avoid immune‑mediated destruction as occurs with pathogens, such as bacteria or viruses. These mechanisms include the activation of immune checkpoints on cells of the immune system, which act to block immune responses, and the reprogramming of T‑cells to create an inflammatory environment that inhibits immune response and favors tumor growth. Immune checkpoints are signaling molecules produced by or expressed on immune cells that shut down or block an immune response. In a
5
healthy person, these checkpoints function to limit an immune response to ensure that the immune system does not overreact, which could lead to excessive inflammation and tissue damage, as occurs in patients with autoimmune diseases or allergies. Tumors have evolved to activate these checkpoints to shield them from immune response attacks. However, studies have shown that these mechanisms can be countered using immune checkpoint inhibitors, which can unleash the immune system’s cancer‑destroying properties. The new found understanding of immune checkpoints has led to a revolution in cancer treatment and the growing field of immuno‑oncology. Specific immune checkpoint inhibitors, including antibodies against CTLA‑4, PD‑1 receptor or its ligand PD‑L1 have produced impressive results in the clinic in a range of cancers, leading to FDA approvals for ipilimumab (anti‑CTLA‑4), nivolumab (anti‑PD‑1), pembrolizumab (anti‑PD‑1), Tecentriq (anti‑PD‑L1), durvalumab (anti‑PD‑L1) and avelumab (anti‑PD‑L1).
Despite their recent success, current checkpoint inhibitors suffer from several limitations. Only a subset of patients treated with checkpoint inhibitors exhibit robust anti‑tumor responses, and responses are often partial and temporary. Many patients initially respond, but then relapse due to the emergence of resistant pathways, which may occur due to tumor cell expression of other checkpoints. Some patients experience unusual toxicities related to an over‑exuberant immune response against normal tissues leading to pneumonitis, hepatitis, colitis and other autoimmune related disorders. These limitations have motivated a search for other immune checkpoint targets and the use of combinations of various checkpoint inhibitors in an attempt to improve efficacy, reduce resistance and limit or reduce toxicity.
The recent success of checkpoint inhibitors has stimulated increased interest in utilizing various immunotherapy approaches to treating cancer, including vaccines, cellular therapies and other immunomodulatory agents. These approaches include modulating the function of various immune cells.
In addition to the search for more precisely targeted therapeutic agents, much attention has focused on the use of biomarkers to identify and enrich clinical trial enrollment with patients who are more likely to benefit from a treatment. We believe this approach has the potential to result in more efficient clinical design and to reduce the cost of clinical trials. The ultimate goal of this personalized approach is to select the optimum treatment for a patient based on the biologic characteristics of the patient and tumor. The use of protein, genetic or other biomarkers to select the right patient for the right treatment is growing in importance in oncology.
Product Pipeline
We are developing novel, precisely targeted agents that we believe may overcome some of the limitations of current therapies. Two of our clinical programs are aimed at disabling cancer’s ability to subvert immune attack by inhibiting adenosine in the tumor microenvironment or by both blocking its production by tumors and concomitantly stimulating host tumor immunity. Our third clinical program is aimed at developing product candidates that regulate T‑cell activation and differentiation by inhibiting ITK, an enzyme important in T-cell differentiation and function. Our two preclinical product candidates are designed to enhance anti-tumor immunity by blocking immunosuppressive cells present in the tumor microenvironment. We intend to commercialize any approved product candidates primarily in the United States, Asia and Europe for any oncology indications our product candidates are approved for. We expect cancer patients or their healthcare providers to be our primary customers for any approved product candidates and expect that our commercial sales of such product candidates will depend on the availability of adequate coverage and reimbursement from government health administration authorities, private health insurers and other third‑party payors.
6
The following chart summarizes key information regarding our current product candidate pipeline:
Adenosine Inhibitors
Adenosine activates an immune checkpoint, the adenosine A2A receptor, that is used by the body to limit inflammation and immune responses. It is produced during acute, inflammatory processes in two steps. The first step is the catalytic conversion of adenosine triphosphate (“ATP”) to adenosine monophosphate (“AMP”) by the enzyme CD39. The second and rate‑limiting step is the conversion of AMP to adenosine by CD73, an enzyme expressed on the surface of several types of immune cells, tumor cells and cells of certain other tissues. Under normal circumstances, the level of adenosine is increased to protect a person from over‑injury in response to such stimuli as inflammation, infection or ischemia. However, as a self‑protective maneuver, many tumor types actively sustain increased levels of extracellular adenosine by production through CD73 or by direct secretion of adenosine. These increased levels of adenosine interact with the A2A and A2B receptors expressed on several cells of the immune system, including T‑cells, NK cells, macrophages, dendritic cells and myeloid derived suppressor cells, as well as other cells, which has the effect of dampening the immune response to the tumor, a system known as the adenosine‑cancer axis.
7
The following figure provides an overview of adenosine production by tumors and its effects on the immune system:
Adenosine‑Cancer Axis
Immunosuppressive Effects of Adenosine Mediated through Multiple Pathways
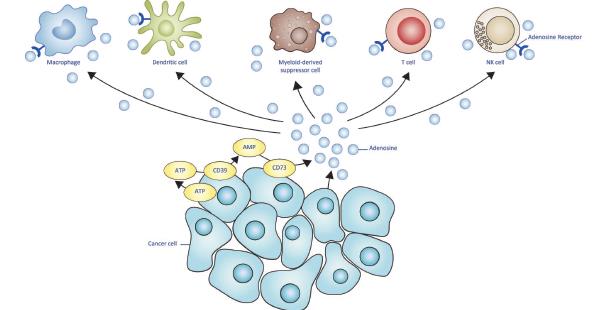
The immune system is composed of several cellular components that mediate a variety of functions in response to tumor cells and foreign pathogens. For instance, macrophages and dendritic cells function primarily to process foreign antigens and tumor antigens. These cells then present such antigens to other cells, such as T‑cells. The presentation of these antigens to T‑cells stimulates cytotoxic T‑cells (also known as killer T‑cells) to destroy the tumor cells or foreign pathogens. Other cells, such as NK cells, are capable of destroying tumor cells without the need for antigen presentation from macrophages or dendritic cells. In addition, certain immune cells, such as myeloid derived suppressor cells and T-regulatory cells, function to suppress or dampen immune responses. The various cellular components of the immune system work in a coordinated manner to recognize and destroy pathogens and tumor cells, and then return the tissue to its normal state.
Adenosine hinders the immune response to tumors by both blocking the activation and effectiveness of immune cells capable of destroying tumor cells, and by increasing the number of immune cells that act to suppress immune cells from responding to the tumor. For instance, adenosine reduces T‑cell and NK cell production of cytokines, such as interleukin‑2 (“IL‑2”) and gamma interferon (“IFNg”), which results in the blockade or reduction in the ability of such cells to destroy tumor cells. Adenosine also leads to activation and proliferation of T-regulatory cells, which function to suppress or dampen immune responses. In addition, adenosine causes dendritic cells to both decrease the rate at which they present antigens to T‑cells, thereby inhibiting the ability of T‑cells to destroy tumor cells, and decrease their production of co‑stimulatory cytokines, which also has the effect of suppressing or dampening the immune response. Macrophages exposed to adenosine will similarly decrease their function, which results in the suppression of immune activity. Finally, adenosine stimulates and increases the number of myeloid derived suppressor cells in the tumor microenvironment, which suppresses immune responses to the tumor. As tumor cells evolve and form cancerous growths, they utilize these processes to evade immune attack and promote their survival. Many of the effects of adenosine on the immune system are mediated through binding to A2A receptors present on several immune cells. Much less is known about A2B receptors, but they have recently been found on certain immune cells, such as macrophages and myeloid derived suppressor cells, and adenosine binding to A2B receptors also appears to play a role in tumor induced immune suppression.
8
Cancer cells also appear to directly utilize adenosine to promote their own growth. Many solid tumors upregulate CD73 for increased adenosine production. In some cases, it appears adenosine can stimulate growth in tumors by increasing a tumor’s blood supply.
A significant body of data indicates that targeting the adenosine‑cancer axis through the A2A receptor can promote anti‑tumor immune responses leading to tumor regression. Consistent with studies of the inhibition of the A2A receptor, A2A receptor gene knockout mice, which completely lack expression of the A2A receptor, exhibit improved anti‑tumor immunity. In addition, several preclinical tumor model studies have shown that treatment with A2A receptor inhibitors leads to tumor regression that is enhanced when administered in combination with various other checkpoint inhibitors, such as anti‑PD‑1 therapies and anti‑CTLA‑4 therapies. Treatment with anti‑CD73 antibodies has been shown to inhibit tumor growth in several pre‑clinical animal tumor models.
Lead Product Candidate: Ciforadenant, an A2A selective, orally administered antagonist of the adenosine A2A receptor
Overview
Our lead product candidate, ciforadenant, is a selective oral adenosine A2A receptor antagonist that we licensed from Vernalis in February 2015. Since licensing ciforadenant, we have conducted extensive laboratory studies in vitro and in vivo in animal models to evaluate ciforadenant’s immune‑enhancing and anti‑tumor properties. In these studies, orally administered ciforadenant inhibited tumor growth in multiple mouse models of cancer as a single agent, in combination with anti‑PD‑1, in combination with anti‑PD‑L1, in combination with other immuno‑oncology agents and in combination with certain chemotherapy drugs. We also have shown in vitro that ciforadenant bound potently and selectively to human activated T‑cells and blocked adenosine mediated immunosuppression by restoring T‑cell function. In addition, we have shown anti‑tumor activity in mice for a significant time following oral administration, which appeared to be mediated through a long‑lasting memory immune response. Furthermore, we have shown in animal models that the treatment was well tolerated. Our IND in oncology was filed in October 2015, and we began enrolling patients in a Phase 1/1b clinical trial in January 2016. Preclinical data with ciforadenant was published in the journal Cancer Immunology Research in October 2018 demonstrating that ciforadenant was active as a monotherapy and in combination with other agents in several tumor models.
Ciforadenant Clinical Development Plan
In January 2016, we began enrolling patients in a Phase 1/1b, open‑label, expansion cohort design clinical trial for patients with selected advanced, incurable cancers. The trial was designed to examine oral ciforadenant administered as both a single agent and in combination with Tecentriq. Under our clinical trial collaboration agreement with Genentech, we are responsible for the design, conduct and cost of the relevant studies, which are under the review of a joint development committee made up of our representatives and representatives of Genentech. Genentech supplies Tecentriq. Pre‑treatment and on‑treatment tissue, blood and serum samples are collected and tested for a wide range of biomarkers including the characteristics of immune cell infiltrates and expression of numerous genes in tumor tissue samples.
We are currently conducting the trial at leading medical centers in the United States, Australia and Canada. We have enrolled over 300 patients to date. Initially, patients with NSCLC, MEL, RCC, TNBC, bladder cancer, prostate cancer or colorectal cancer with high mutation rates were eligible for participation. The objectives of this portion of the trial were to identify the optimum and safe dose of ciforadenant when used as a monotherapy or in combination with Tecentriq, and to evaluate anti-tumor activity in various cancers. Extensive biomarker analysis was performed to search for biomarkers that may be associated with disease response.
Key interim findings of our clinical trial for ciforadenant, as a single agent and in combination with Tecentriq, include:
|
· |
Ciforadenant has been well-tolerated at doses that achieved substantial receptor blockade; |
9
|
· |
Ciforadenant demonstrated evidence of anti-tumor activity as both a monotherapy and in combination with atezolizumab; |
|
· |
Of cancers studied, RCC, mCRPC and NSCLC have appeared most responsive to therapy; and |
|
· |
Expression of adenosine induced genes was observed in tumor biopsies, and we believe may provide useful biomarkers for selection of patients in future clinical trials. |
Ciforadenant Interim Clinical Trial Results
Results Presented at the Society for Immunotherapy of Cancer Annual Meeting—November 2018
|
· |
Clinical and biomarker data in 68 patients with treatment-refractory RCC from our Phase 1/1b clinical trial were presented in November 2018 at the Society for Immunotherapy of Cancer Annual Meeting. Data from 33 patients receiving ciforadenant as a monotherapy and 35 receiving ciforadenant in combination with atezolizumab who were evaluable for response were reported. |
Interim Results Published in the Journal Cancer Discovery
Updated results in 68 patients with treatment-refractory RCC demonstrated an overall survival (“OS”) of 90% at more than 25 months follow-up with ciforadenant administered in combination with atezolizumab. The OS for patients receiving ciforadenant alone was over 69% at 16 months. At the time of enrollment, study participants had advanced refractory disease and a poor prognosis. They had been treated with a median of three prior therapies (range: 1 to 5), and approximately 72% had failed prior anti-PD-(L)1 therapy. The results from this study were published in January 2020 in the journal Cancer Discovery.
Key findings from the published results include:
|
· |
Disease control for more than 6 months was observed in 39% and 17% of patients receiving combination therapy and monotherapy, respectively. |
|
· |
For patients receiving combination therapy, 11% experienced a confirmed partial response (“PR”) (as determined by RECIST criteria). Several additional patients experienced tumor regression not meeting the criteria for a PR. For patients receiving monotherapy, one patient experienced a confirmed PR, one experienced an unconfirmed PR, and several patients experienced tumor regression not meeting the PR criteria. |
|
· |
Responses were seen in both the combination therapy and monotherapy arms, and in patients who failed prior anti-PD-(L)1 therapy. |
|
· |
Progression-free survival (as assessed by RECIST criteria) was 5.8 months with combination therapy and 4.1 months with monotherapy. |
|
· |
OS was 90% at 25 months follow-up with combination therapy and 69% at 16 months follow-up with monotherapy. |
|
· |
Combination therapy was superior to monotherapy with respect to OS, response rate, disease control rate and progression-free survival. |
|
· |
Evaluation of pre- and on-treatment tumor biopsies showed a statistically significant correlation between treatment-induced CD8+ T-cell infiltration in tumors and response (p<0.016). |
|
· |
The recently described adenosine gene signature showed a statistically significant correlation with tumor response and disease control rates (p<0.008). We evaluated adenosine gene signatures in pretreatment |
10
biopsies from 30 patients. Of the patients showing a low adenosine gene signature, none exhibited signs of tumor regression. In contrast, patients with a high adenosine gene signature had a 17% (N=18) overall response rate by RECIST criteria. |
|
· |
Ciforadenant was well tolerated with grade 3 adverse events that were infrequent (less than 5%) and reversible. |
This study supports the tumor immune enhancing potential of adenosine pathway blockade. The unique mechanism of action and safety results suggest that this treatment, if successfully developed and approved, may be valuable, particularly in patients who have failed anti-PD-(L)1 therapy or as a combination to prevent the development of resistance. The studies also demonstrate that RCC exhibited high levels of adenosine pathway related genes. We expect to be able to utilize this biomarker in future studies to target patients most likely to benefit from therapy with ciforadenant.
Current Ciforadenant Clinical Trials
The preliminary data from our ongoing clinical trial indicate that ciforadenant has shown activity as a single agent and when used in combination with Tecentriq in multiple tumor histologies and in patients refractory to prior therapies with anti‑PD‑(L)1 antibodies. Based on these preliminary results, we amended our Phase 1b/2 trial to focus on ciforadenant in combination with Tecentriq in patients with either advanced refractory RCC or mCRPC. This trial is currently evaluating safety and efficacy of the combination as well as providing additional evidence regarding the potential role of the adenosine gene signature biomarker in predicting outcome.
The mCRPC arm of the study began enrolling patients in October 2019 and in February 2020 we presented data at ASCO GU from 35 patients with advanced mCRPC, including 11 that received ciforadenant as a monotherapy (100 mg twice daily) and 24 that received ciforadenant (100 mg twice daily) in combination with Tecentriq (840 mg delivered intravenously every two weeks). These patients had failed a median of three prior therapies and 43% had visceral metastases, which is a negative prognostic factor for patients with mCRPC. Key updates from the clinical trial include:
|
· |
With median follow up of 3.2+ months, there was one partial response (PR, RECIST), wich such patient exhibiting a prostate-specific antigen (PSA) level drop from 98 to less than 1. Ten additional patients had tumor regression not meeting the criteria for PR. Seven patients had confirmed stable disease exceeding 6 months; one of these patients remained on therapy. Five patients have unconfirmed stable disease and were continuing on therapy. A total of nine patients were continuing on therapy. |
|
· |
Gene expression profiling of tumor biopsies demonstrated a significant correlation of tumor CD73 expression with the adenosine signature (p=0.02). We believes this correlation supports the relevance of adenosine in prostate cancer, its production by CD73 and the expression of adenosine induced immunosuppressive genes. |
|
· |
Treatment was well tolerated with one Grade 3 adverse event of fatigue in monotherapy and one Grade 3 adverse event of anemia in the combination arm. |
Ciforadenant is also being evaluated in combination with the anti-CD38 antibody, daratumumab (Darzalex) in patients with advanced refractory multiple myeloma. The objective of this Phase 1 clinical trial is to evaluate whether ciforadenant can overcome resistance in patients who have failed daratumumab treatment.
In May 2017, we entered into a second collaboration agreement with Genentech, pursuant to which Genentech will evaluate ciforadenant in combination with atezolizumab in patients with NSCLC that have previously failed a platinum containing chemotherapy regimen and an anti‑PD‑(L)1. Enrollment in this Phase 1b/2 clinical trial, which was being conducted under an umbrella protocol known as Morpheus, has been completed and patients are in follow-up.
11
Product Candidate: CPI-006, A monoclonal anti‑CD73 immunomodulatory antibody for cancer
Overview
In December 2014, we in‑licensed from Scripps a mouse anti‑human CD73 antibody, CPI‑006. We have genetically engineered CPI‑006 to be humanized by replacing the immunoglobulin (“Ig”) heavy and light chain constant regions, and by replacing the murine variable framework regions with human heavy and light chain Ig frameworks. In addition, we have further engineered CPI‑006 to enhance binding to CD73 in order to both block its catalytic activity and to activate its immunomodulatory properties.
The Role of CD73 in Cancer
CD73 is a multifunctional enzyme expressed on immune cells, tumor cells and certain other tissues. CD73 converts AMP to adenosine in the extracellular space. The catalytic production of adenosine by CD73 may play an important role in tumor immune suppression by increasing the concentration of adenosine in the tumor microenvironment. CD73 is overexpressed in many cancers, and high levels of CD73 have been shown to be associated with poor disease prognosis. CD73 expression on tumor cells as well as on the host immune cells has been shown to promote tumor immune suppression and metastasis in mice. Other studies in mice have shown that the targeted blockade of CD73 with antibodies can enhance the therapeutic activity of anti‑PD‑1 and anti‑CTLA‑4 checkpoint blockade. CD73 also exhibits additional immunomodulatory functions including cellular adhesion, lymphocyte migration and T and B-cell activation. While most investigators have focused on its role in adenosine production, we have concentrated efforts on understanding both its role in adenosine production as well as its immunomodulatory properties. We believe, that together, these properties will be complementary and potentially lead to synergistic anti-tumor activity.
Preclinical Proof of Concept
In preclinical studies using tumor cells that express the CD73 enzyme, the addition of various concentrations of CPI‑006 to such cells in culture substantially inhibited the catalytic activity of the enzyme to background levels of the assay. This was studied by measuring the conversion of AMP to adenosine. These studies demonstrated that at concentrations of 10 µg/ml, CPI‑006 was capable of substantially inhibiting the production of adenosine, which indicates that CPI‑006 binds to a critical site in the CD73 enzyme necessary for its function. By blocking the cellular production of adenosine, we believe CPI‑006 could lead to enhancement of the anti‑tumor immune response by lowering the amount of adenosine in the tumor environment. As compared to other reported anti‑CD73 antibodies, CPI‑006 has been shown in these preclinical studies to react with the active site of the CD73 enzyme and has not caused internalization of CD73. We believe this means it will act as a more potent blockade of the enzyme. In in vitro studies with human lymphocytes, CPI‑006 restored T-cell activation in the presence of AMP, indicating blockade of CD73 activity. CPI-006 has been found to bind to CD73, resulting in activation of some lymphocytes and redistribution from blood to other lymphoid tissues. In other preclinical studies we conducted, CPI‑006 bound to a variety of different types of cancer cell lines in vitro, including those derived from human breast cancer, lung cancer, lymphoma, leukemias and sarcomas.
In in vitro studies using human immune cells, CPI-006 led to activation of B-cells and differentiation into antibody producing plasmablasts. Changes on monocytes were also observed and included increased expression of cell surface markers involved in enhanced antigen presentation. Together, we believe these results suggest that CPI-006 has the potential to function as an immunostimulant. We are not aware of any other anti-CD73 antibody that has been reported to possess these properties.
CPI-006 Anti-CD73 Development Plan
In March 2018, we began enrollment in a multicenter Phase 1/1b expansion design trial with four arms that will evaluate CPI‑006 as a single agent, in combination with our adenosine antagonist, ciforadenant, in combination with pembrolizumab (anti‑PD‑1), and in a triplet combination arm of CPI-006, ciforadenant and pembrolizumab. In each arm, CPI‑006 will be administered in increasing doses to cohorts of patients until a maximally tolerated dose is determined for each arm. This will be followed by an expansion stage that will evaluate various tumor types, including RCC, mCRPC and NSCLC.
12
Interim results from this trial have been reported in oral presentations at both the June 2019 American Society of Clinical Oncology (ASCO) and the November 2019 Society for Immunotherapy of Cancer (SITC) meetings. As of February 2020, we have dosed patients in the single agent arm of the trial, in the CPI-006 combination arm with ciforadenant and in the combination arm of CPI-006 with pembrolizumab. No dose limiting toxicity up to doses of 18 mg/kg have been observed as of February 2020. Interim data from the single-agent arm of the trial has suggested that CPI-006 blocked production of adenosine by inhibiting the enzymatic active site of CD73, activated peripheral blood B-cells, and affected B-lymphocyte trafficking in the blood. The interim results as of February 2020 are summarized below:
|
· |
CPI-006 has shown novel immunomodulatory activities: |
|
· |
Induced differentiation of B-cells, class switching, secretion of immunoglobulin (in vitro), and generation of memory B-cells; and |
|
· |
Increased expression of CD69 and other markers consistent with increased antigen presentation by APCs. |
|
· |
The recommended dose of CPI-006 for further study was 18 mg/kg or a fixed dose of 1200 mg and led to sustained target occupancy. This dose was well tolerated. |
|
· |
Treatment with CPI-006 induced redistribution of T-cells and B-cells with an observed increase in returning memory B-cells and expansion of new B-cell clones. |
|
· |
Changes in lymphocytes were consistent with induction of adaptive humoral immunity. |
|
· |
Tumor regression was observed in protocol predefined cohorts of patients with RCC and mCRPC. |
Enrollment in this trial continues and has entered the disease specific expansion cohorts for monotherapy with CPI-006 and for CPI-006 in combination with ciforadenant. Dose escalation continues in the CPI-006 with pembrolizumab arm of the trial.
ITK Inhibitor
ITK and Anti‑tumor Immune Response
ITK is an enzyme expressed predominantly in T‑cells where it plays a key role in T‑cell signaling. T‑cell signaling involving ITK is required in the development of T‑cells within the thymus, where ITK regulates the production of various T‑cell subsets and functions. The ITK cell signaling pathway is similar to the signaling that occurs in B‑cells, which is mediated by a homologous enzyme known as BTK, the target of ibrutinib, an approved treatment for patients with B‑cell lymphomas and leukemias. We believe that inhibiting ITK in malignant T‑cells may be of therapeutic benefit in patients with T‑cell leukemias and lymphomas, analogous to the effects of ibrutinib on B‑cell lymphomas and leukemias. In malignant T‑cells, ITK was found to be over‑expressed specifically in certain T‑cell lymphomas, including peripheral T‑cell lymphoma (“PTCL”), angioimmunoblastic T‑cell lymphoma (“AITL”) and in a subgroup of T‑lymphoblastic leukemia and lymphoma (“T‑ALL”).
In ITK genetic knockout mice, which completely lack expression of ITK, T‑cells exhibit defects in T‑helper cell differentiation and cytokine secretion but retain the ability to differentiate into cytotoxic T‑cells that secrete IL‑2 and IFNg, which are the cells responsible for tumor rejection. We believe that skewing T‑helper cell differentiation to favor cytotoxic T‑cells may be beneficial in treating many types of cancer.
13
Product Candidate: CPI-818, An ITK kinase inhibitor
CPI-818 is a selective, small molecule designed as a covalent inhibitor of ITK that we have selected as our lead development candidate for our ITK program. We identified ITK as a product candidate target because it plays a key role in T‑cell receptor signaling and in the differentiation of T‑cells responsible for tumor immunity.
We have developed CPI-818 by targeting the cysteine amino acid residue at position 442 in the ITK protein. Covalent targeting of ITK is expected to provide a selective and prolonged duration of activity without the need for high systemic exposures and thereby improve the therapeutic window. This approach was previously used by our co‑founders to generate ibrutinib. We anticipate that the selectivity of CPI-818 will mimic the immune properties seen in ITK knockout mice and skew the immune response toward a more favorable anti‑tumor immune response. In addition, ITK plays a role in the proliferation of some T-cell lymphomas and its inhibition may lead to growth arrest and/or tumor cell cytotoxicity. In our preclinical studies of CPI-818, objective tumor response has been seen in a preclinical study in dogs with spontaneous T-cell lymphomas.
Our Phase 1/1b clinical trial of CPI-818 is currently enrolling patients with several types of advanced, refractory T-cell lymphomas, including peripheral T-cell lymphoma-not otherwise specified (PTCL-NOS), angioimmunoblastic T-cell lymphoma (AITL), cutaneous T-cell lymphoma (CTCL) and other T-cell lymphomas. The study employs an adaptive, expansion cohort design to select the dose and evaluate the safety, pharmacokinetics (PK), target occupancy, biomarkers and efficacy of CPI-818. The initial phase of the trial is evaluating escalating doses in successive cohorts of patients in order to determine the optimum dose. A second phase will evaluate safety and tumor response to this optimum dose of CPI-818 in disease-specific patient cohorts that may be expanded based on early signs of efficacy. The study is enrolling patients at major medical centers in the United States, Australia and South Korea.
In December 2019, we presented preliminary preclinical and Phase 1/1b clinical data with CPI-818 at the American Society of Hematology meeting. In vitro studies with human malignant Sezary cells indicated that CPI-818 inhibited proliferation of the malignant cells but not normal T-cells.
In February 2020, we presented additional preliminary preclinical and Phase 1/1b clinical data with CPI-818. The key updates at such time included that:
|
· |
16 patients have been enrolled in the first four dose cohorts in the initial phase of the trial, receiving a 100 mg, 200 mg, 400 mg or 600 mg oral dose of CPI-818 two times per day, with no dose limiting toxicities and no grade 3 or 4 treatment related adverse events observed. |
|
· |
The median patient follow-up period is now three months, with 11 patients remaining on therapy. One patient with CTCL treated with the 200 mg dose of CPI-818 achieved a reduction in lymphadenopathy and improvement of PET scan imaging; another patient with CTCL receiving the 400 mg dose has exhibited improvement in cutaneous disease. These patients continue on therapy. |
|
· |
The results from the pharmacokinetic and occupancy studies for the first 12 patients have been in-line with expectations, with increasing target occupancy with higher doses based on available data from the 100 mg, 200 mg, and 400 mg doses. |
We plan to continue to advance CPI-818 in our Phase 1/1b clinical trial in patients with several types of T‑cell lymphomas including peripheral T-cell lymphoma (“PTCL”), cutaneous T-cell lymphoma, angioimmunoblastic T-cell lymphoma and others.
CPI-182 Anti-CXCR2 Antibody for Myeloid Suppression
In 2017, we in-licensed a monoclonal antibody to the chemokine receptor CXCR2, a novel target in immuno‑oncology. CXCR2 is a receptor expressed on myeloid cells, particularly myeloid cells known as MDSC that infiltrate tumors and play a role in tumor induced immunosuppression. This antibody is now undergoing IND‑enabling studies and scale-up manufacturing.
14
Product Candidate: An antagonist of the adenosine A2B receptor
We have identified a selective A2B receptor antagonist from our internal research program. Adenosine A2B receptors have recently been found to play an important role in the immune response to tumors. Similar to adenosine A2A receptors, adenosine binds to adenosine A2B receptors, which leads to immunosuppression. However, adenosine A2B receptor expression is found on different immune cells, and its function in tumor induced immune suppression is not yet well understood. We have selected a development candidate and expect to begin IND-enabling studies in 2020 for potential use in cancer and fibrotic diseases.
Manufacturing
We do not own or operate, and currently have no plans to establish, any manufacturing facilities. We currently rely, and expect to continue to rely, on third parties for the manufacture of our product candidates for clinical testing, as well as for manufacture of any products that we may commercialize. We are able to internally produce small quantities of our product candidates required for relatively short preclinical animal studies. We believe that this allows us to accelerate the drug development process by not having to rely on third parties for all of our research and development needs. However, we currently rely, and expect to continue to rely, on a number of contract manufacturers to produce sufficient quantities of our product candidates for use in more lengthy preclinical development and clinical trials and in relation to any future commercialization of our product candidates. Additional contract manufacturers are used to fill, label, package and distribute investigational drug products. This strategy allows us to maintain a more efficient infrastructure, avoid depending on our own manufacturing facility and equipment while simultaneously enabling us to focus our expertise on developing our products. Although we believe we have multiple potential sources for the manufacturing of our product candidates, we currently rely on several different manufacturers who supply different components of the ciforadenant and CPI-818 molecules, on one manufacturer for CPI-006 drug substance and other third-party manufacturers to produce our other product candidates.
Competition
The pharmaceutical and biotechnology industries are characterized by intense competition and rely heavily on the ability to move quickly, adapt to changing medical and market needs, and to develop and maintain strong intellectual property positions. We believe that the development experience of our scientific and management team, as well as the strength and promise of our product candidates, provide us with a competitive advantage; nevertheless, we face potential competition from myriad sources, including pharmaceutical and biotechnology companies, academic institutions, governmental agencies and public and private research institutions.
Kyowa Hakko Kirin has approval in Japan and the United States for istradefylline, an A2A antagonist, in Parkinson’s disease. Within oncology, Novartis has announced an exclusive licensing agreement with Palobiofarma SL and is conducting a Phase 1 trial with an A2A antagonist. AstraZeneca plc is conducting clinical trials with an A2A antagonist for use in cancer therapy. Merck KgaA has entered into a pre-clinical collaboration with Domain Therapeutics Inc. to develop programs targeting the adenosine pathway. In addition, Redoxtherapies, Inc., which was acquired by Juno Therapeutics and subsequently by Celgene, and Arcus Biosciences, Inc. are developing A2A receptor antagonists for cancer. Astra Zeneca, Bristol-Myers Squib, and Novartis in partnership with Surface Oncology, Inc. have initiated clinical trials with anti-CD73 antibodies in cancer patients. More generally, in the field of immuno-oncology, there are large pharmaceutical companies with approved products or products in late-stage development that target other immune checkpoints, including PD-1, PD-L1 or CTLA-4. These companies include Bristol-Myers Squibb (nivolumab, ipilimumab), Merck (pembrolizumab), Genentech (atezolizumab) and AstraZeneca (durvalumab, tremelimumab). Janssen Pharmaceuticals, Inc. and AbbVie Inc. are co-marketing Imbruvica (ibrutinib), which is a small molecule inhibitor of the kinase BTK that has also been reported to inhibit ITK.
Intellectual Property
We strive to protect and enhance the proprietary technology, inventions, and improvements that are commercially important to our business, including seeking, maintaining and defending patent rights, whether developed internally or licensed from our collaborators or other third parties. We do not yet own any issued patents relating to our
15
product candidates. Our policy is to seek to protect our proprietary position by, among other methods, filing patent applications in the United States and in jurisdictions outside of the United States covering our proprietary technology, inventions, improvements and product candidates that are important to the development and implementation of our business. We also rely on trade secrets and know‑how relating to our proprietary technology and product candidates, continuing innovation, and in‑licensing opportunities to develop, strengthen and maintain our proprietary position in the field of immuno‑oncology. We also plan to rely on data exclusivity, market exclusivity, and patent term extensions when available. Our commercial success will depend in part on our ability to obtain and maintain patent and other proprietary protection for our technology, inventions, and improvements; to preserve the confidentiality of our trade secrets; to obtain and maintain licenses to use intellectual property owned by third parties; to defend and enforce our proprietary rights, including any patents that we may own in the future; and to operate without infringing on the valid and enforceable patents and other proprietary rights of third parties.
We have in‑licensed patents and patent applications directed to certain of our product candidates and related uses thereof. We also possess and in‑license substantial know‑how and trade secrets relating to the development and commercialization of our product candidates, including related manufacturing processes and technology. As of March 2, 2020, our owned and licensed patent portfolio consisted of fourteen licensed U.S. issued patents, four licensed U.S. pending patent applications, twelve owned U.S. pending patent applications, four owned U.S. provisional patent applications, and seven owned PCT International patent applications directed to ciforadenant, CPI‑006, and CPI-818, and certain of our other proprietary technology, inventions, improvements or other potential product candidates. In addition, our owned and licensed patent portfolio included forty‑four licensed patents, nine licensed patent applications, and sixty-three owned patent applications pending in jurisdictions outside of the United States that are foreign counterparts to one or more of the foregoing U.S. patents and patent applications. The patents and patent applications outside of the United States in our portfolio are held primarily in Europe, Canada, Japan, Australia and China.
With respect to the immuno‑oncology product candidates and processes we intend to develop and commercialize in the normal course of business, we intend to pursue patent protection covering, when possible, compositions, methods of use, dosing and formulations. We may also pursue patent protection with respect to manufacturing and drug development processes and technologies.
Issued patents can provide protection for varying periods of time, depending upon the date of filing of the patent application, the date of patent issuance, and the legal term of patents in the countries in which they are obtained. In general, patents issued for applications filed in the United States can provide exclusionary rights for 20 years from the earliest effective filing date. In addition, in certain instances, the term of an issued United States patent that covers or claims an FDA approved product can be extended to recapture a portion of the term effectively lost as a result of the FDA regulatory review period, which is called patent term extension. The restoration period cannot be longer than five years and the total patent term, including the restoration period, must not exceed 14 years following FDA approval. The term of patents outside of the United States varies in accordance with the laws of the foreign jurisdiction, but typically is also 20 years from the earliest effective filing date. The issued United States patents we license from Vernalis directed to the composition of matter of ciforadenant and its method of use for treating disorders treatable by purine receptor blocking are expected to expire between January 2022 and July 2029, excluding any patent term extension that may be available. The pending U.S. patent application and PCT International patent applications, if granted as patents, that we own directed to the composition of matter and methods of treatment for CPI‑006 are expected to expire between December 2036 and June 2037, excluding any patent term extension that may be available. The pending U.S. and foreign patent applications, if granted as patents, that we own directed to the composition of matter and methods of treatment for CPI 818 are expected to expire November 2037, excluding any patent term extension that may be available. However, the actual protection afforded by a patent varies on a product‑by‑product basis, from country‑to‑country, and depends upon many factors, including the type of patent, the scope of its coverage, the availability of regulatory‑related extensions, the availability of legal remedies in a particular country, and the validity and enforceability of the patent.
The patent positions of companies like ours are generally uncertain and involve complex legal and factual questions. No consistent policy regarding the scope of claims allowable in patents in the field of immuno‑oncology has emerged in the United States. The relevant patent laws and their interpretation outside of the United States is also uncertain. Changes in either the patent laws or their interpretation in the United States and other countries may diminish
16
our ability to protect our technology or product candidates and enforce the patent rights that we license, and could affect the value of such intellectual property. In particular, our ability to stop third parties from making, using, selling, offering to sell, or importing products that infringe our intellectual property will depend in part on our success in obtaining and enforcing patent claims that cover our technology, inventions, and improvements. With respect to both licensed and company‑owned intellectual property, we cannot guarantee that patents will be granted with respect to any of our pending patent applications or with respect to any patent applications we may file in the future, nor can we be sure that any patents that may be granted to us in the future will be commercially useful in protecting our products, the methods of use or manufacture of those products. Moreover, even the issued patents that we license do not guarantee us the right to practice our technology in relation to the commercialization of our products. Patent and other intellectual property rights in the pharmaceutical and biotechnology space are evolving and involve many risks and uncertainties. For example, third parties may have blocking patents that could be used to prevent us from commercializing our product candidates and practicing our proprietary technology, and the issued patents that we in‑license and those that may issue in the future may be challenged, invalidated, or circumvented, which could limit our ability to stop competitors from marketing related products or could limit the term of patent protection that otherwise may exist for our product candidates. In addition, the scope of the rights granted under any issued patents may not provide us with protection or competitive advantages against competitors with similar technology. Furthermore, our competitors may independently develop similar technologies that are outside the scope of the rights granted under any issued patents that we own or exclusively in‑license. For these reasons, we may face competition with respect to our product candidates. Moreover, because of the extensive time required for development, testing and regulatory review of a potential product, it is possible that, before any particular product candidate can be commercialized, any patent protection for such product may expire or remain in force for only a short period following commercialization, thereby reducing the commercial advantage the patent provides.
Licenses and Collaborations
Vernalis Licensing Agreement
In February 2015, we entered into a license agreement with Vernalis, pursuant to which we were granted an exclusive, worldwide license under certain patent rights and know‑how, including a limited right to grant sublicenses, for all fields of use to develop, manufacture and commercialize products containing certain adenosine receptor antagonists, including ciforadenant. The issued U.S. patents that we in‑licensed from Vernalis pursuant to this agreement are directed to the composition of matter of ciforadenant and its method of use for treating disorders treatable by purine receptor blocking. These patents are expected to expire in the United States between January 2022 and July 2029, excluding any patent term extension that may be available. Vernalis has the first right to prosecute and maintain the licensed patent rights worldwide, subject to our right with respect to certain of the licensed patents to continue prosecution and maintenance if Vernalis elects not to do so. We also have the right to prosecute and maintain any patent rights that we may own that cover the licensed compounds that do not fall within the licensed patent rights. Pursuant to this agreement, we are required to use commercially reasonable efforts to conduct certain activities to obtain marketing authorizations for licensed products and to conduct certain preclinical and clinical studies for ciforadenant. We also must use commercially reasonable efforts to conduct certain preclinical and clinical studies to support the use of ciforadenant as an immunotherapeutic agent for cancer studies, and to meet certain specified development, regulatory and commercial milestones within specified time periods.
Pursuant to this agreement, we made a one‑time cash payment to Vernalis in the amount of $1.0 million upon entering into the agreement. We are also required to make cash milestone payments to Vernalis upon the successful completion of clinical and regulatory milestones for licensed products depending on the indications for which such licensed products are developed and upon achievement of certain sales milestones. In February 2017, we made a milestone payment of $3 million to Vernalis following the expansion of a cohort of patients with renal cell cancer treated with single‑agent ciforadenant in our Phase 1/1b clinical trial. The aggregate potential milestone payments are approximately $220 million for all indications.
We have also agreed to pay Vernalis tiered incremental royalties based on the annual net sales of licensed products containing ciforadenant on a product‑by‑product and country‑by‑country basis, subject to certain offsets and reductions. The tiered royalty rates for products containing ciforadenant range from the mid‑single digits up to the
17
low‑double digits on a country‑by‑country net sales basis. The royalties on other licensed products that do not include ciforadenant also increase with the amount of net sales on a product‑by‑product and country‑by‑country basis and range from the low‑single digits up to the mid‑single digits on a country‑by‑country net sales basis.
The agreement will expire on a product‑by‑product and country‑by‑country basis upon the expiration of our payment obligations to Vernalis in respect of a particular product and country. Both parties have the right to terminate the agreement in the event of an uncured material breach by the other party. We may also terminate the agreement at our convenience by providing 90 days written notice, provided that we have not received notice of our own default under the agreement at the time we exercise such termination right. Vernalis may also terminate the agreement if we challenge a licensed patent or undergo a bankruptcy event.
Scripps Licensing Agreement
In December 2014, we entered into a license agreement with Scripps, pursuant to which we were granted a non‑exclusive, world‑wide license for all fields of use under Scripps’ rights in certain know‑how and technology related to a mouse hybridoma clone expressing an anti‑human CD73 antibody, and to progeny, mutants or unmodified derivatives of such hybridoma and any antibodies expressed by such hybridoma, from which we developed CPI-006. Scripps also granted us the right to grant sublicenses in conjunction with other proprietary rights we hold, or to others collaborating with or performing services for us. Under this license agreement, Scripps has agreed not to grant any additional commercial licenses with respect to such materials, other than march‑in rights granted to the U.S. government.
Upon execution of the agreement, we made a one‑time cash payment to Scripps of $10,000 and are also obligated to pay a minimum annual fee to Scripps of $25,000. The first minimum annual fee payment is due on the first anniversary of effective date of the agreement and will be due on each subsequent anniversary of the effective date for the term of the agreement. We are also required to make performance‑based cash payments upon successful completion of clinical and sales milestones. The aggregate potential milestone payments are $2.6 million. We are also required to pay royalties on net sales of licensed products (including CPI-006) sold by us, our affiliates and our sublicensees at a rate in the low‑single digits. In addition, should we sublicense the rights licensed under the agreement, we have agreed to pay a percentage of sublicense revenue received at single digit percentages based on the achievement of development milestones.
Our license agreement with Scripps will terminate upon expiration of our obligation to pay royalties to Scripps under the license agreement. The license agreement is terminable by the consent of the parties, at will by us or upon providing 90 days written notice to Scripps, or by Scripps for certain material breaches by us, or if we undergo a bankruptcy event. In addition, Scripps may terminate our license on a product‑by‑product basis, or the entire agreement, if we fail to meet specified diligence obligations related to the development and commercialization of licensed products. Scripps may also terminate the agreement after the third anniversary of the effective date of the agreement if it reasonably believes, based on reports we provide to Scripps, that we have not used commercially reasonable efforts as required under the agreement, subject to a specified notice and cure period.
Genentech Collaboration Agreements
In October 2015, we entered into a clinical trial collaboration agreement with Genentech to evaluate the safety, tolerability and preliminary efficacy of ciforadenant combined with Genentech’s investigational cancer immunotherapy, Tecentriq, a fully humanized monoclonal antibody targeting PD‑L1, in a variety of solid tumors in our Phase 1/1b clinical trial. Pursuant to this agreement, we will be responsible for the conduct and cost of the relevant studies, under the supervision of a joint development committee made up of our representatives and representatives of Genentech. Genentech will supply Tecentriq. As part of the agreement, we granted Genentech certain rights of first negotiation to participate in future clinical trials that we may conduct evaluating the administration of ciforadenant in combination with an anti‑PD‑1 or anti‑PD‑L1 antibody. If we do not reach agreement on the terms of any such participation by Genentech within a specified time period, we retain the right to collaborate with third parties in such activities. We also granted Genentech certain rights of first negotiation should we decide to license development and commercialization rights to ciforadenant. Should we not reach agreement on the terms of such a license within a specified time period, we retain the right to enter into a license with another third party.
18
We and Genentech each have the right to terminate the agreement for material breach by the other party. In addition, the agreement may be terminated by either party due to safety considerations, if directed by a regulatory authority or if development of ciforadenant or Tecentriq is discontinued. Further, the agreement will expire after a set period of time following the provision by us of the final clinical study report to Genentech.
In May 2017, we entered into a second clinical trial collaboration agreement with Genentech. Under the new agreement, ciforadenant administered in combination with Tecentriq will be evaluated in a Phase 1b/2 randomized, controlled clinical study as second‑line therapy in patients with NSCLC who are resistant and/or refractory to prior therapy with an anti‑PD‑(L)1 antibody. It is anticipated that the study will enroll up to 65 patients in the treatment arm. Genentech will be responsible for the conduct of the study and we will share the cost of the Phase 1b/2 trial, which began enrolling patients in the fourth quarter of 2017. We are responsible for supplying ciforadenant and retain global development and commercialization rights to ciforadenant. We and Genentech each have the right to terminate the agreement for material breach by the other party. In addition, the agreement may be terminated by either party due to safety considerations, if directed by a regulatory authority or if development of ciforadenant or Tecentriq is discontinued. Further, the agreement will expire after a set period of time following the provision by us of the final clinical study report to Genentech.
Monash License Agreement
In April 2017, we entered into a license agreement with Monash University (Monash), pursuant to which we were granted an exclusive, sublicensable worldwide license under certain know‑how, patent rights and other intellectual property rights controlled by Monash to research, develop, and commercialize certain antibodies directed to CXCR2 for the treatment of human diseases.
Upon execution of the agreement, we made a one‑time cash payment to Monash of $275,000 and reimbursed Monash for certain patent prosecution costs incurred prior to execution of the agreement. We are also obligated to pay an annual license maintenance fee to Monash of $25,000 until a certain development milestone is met with respect to the licensed product, after which no further maintenance fee will be due. We are also required to make development and sales milestone payments to Monash with respect to the licensed products in the aggregate of up to $45.1 million. We are also required to pay to Monash tiered royalties on net sales of licensed products sold by us, our affiliates and our sublicensees at a rate ranging in the low‑single digits. In addition, should we sublicense our rights under the agreement, we have agreed to pay a percentage of sublicense revenue received at specified rates that are currently at low double digit percentages and decrease to single digit percentages based on the achievement of development milestones.
The term of our agreement with Monash continues until the expiration of our obligation to pay royalties to Monash thereunder. The license agreement is terminable at will by us upon providing 30 days written notice to Monash, or by either party for material breaches by the other party. In addition, Monash may terminate the entire agreement or convert the license to a non-exclusive license if we have materially breached our obligation to use commercially reasonable efforts to develop and commercialize a licensed product, subject to a specified notice and cure mechanism.
Regulation
Government authorities in the United States, at the federal, state and local level, and other countries extensively regulate, among other things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record‑keeping, promotion, advertising, distribution, marketing and export and import of products such as those we are developing. A new drug must be approved by the FDA through the New Drug Application (“NDA”) process and a new biologic must be approved by the FDA through the Biologics License Application (“BLA”) process before it may be legally marketed in the United States.
United States Drug Development Process
In the United States, the FDA regulates drugs under the federal Food, Drug, and Cosmetic Act (“FDCA”), and in the case of biologics, also under the Public Health Service Act (“PHSA”), and their implementing regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and
19
foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or after approval may subject an applicant to administrative or judicial sanctions. These sanctions could include the FDA’s refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us.
The process required by the FDA before a drug or biologic may be marketed in the United States generally involves the following:
|
· |
completion of preclinical laboratory tests, animal studies and formulation studies in accordance with Good Laboratory Practice (“GLP”) regulations and other applicable regulations; |
|
· |
submission to the FDA of an Investigational New Drug application (“IND”), which must become effective before human clinical trials may begin; |
|
· |
performance of adequate and well‑controlled human clinical trials in accordance with Good Clinical Practice (“GCP”) regulations to establish the safety and efficacy of the proposed drug, or safety, purity and potency of the proposed biologic for its intended use; |
|
· |
submission to the FDA of an NDA or BLA; |
|
· |
satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the drug is produced to assess compliance with current Good Manufacturing Practice (“cGMP”) requirements to assure that the facilities, methods and controls are adequate to preserve the drug’s identity, strength, quality and purity; and |
|
· |
FDA review and approval of the NDA or BLA. |
Once a pharmaceutical candidate is identified for development, it enters the preclinical testing stage. Preclinical tests include laboratory evaluations of product chemistry, toxicity and formulation, as well as animal studies. An IND sponsor must submit the results of the preclinical tests, together with manufacturing information and analytical data, to the FDA as part of the IND. The sponsor will also include a protocol detailing, among other things, the objectives of the first phase of the clinical trial, the parameters to be used in monitoring safety, and the effectiveness criteria to be evaluated, if the first phase lends itself to an efficacy evaluation. Some preclinical testing may continue even after the IND is submitted. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30‑day time period, places the clinical trial on a clinical hold. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. Clinical holds also may be imposed by the FDA at any time before or during clinical trials due to safety concerns about on‑going or proposed clinical trials or non‑compliance with specific FDA requirements, and the trials may not begin or continue until the FDA notifies the sponsor that the hold has been lifted. All clinical trials must be conducted under the supervision of one or more qualified investigators in accordance with GCP regulations. They must be conducted under protocols detailing the objectives of the trial, dosing procedures, subject selection and exclusion criteria and the safety and effectiveness criteria to be evaluated. Each protocol must be submitted to the FDA as part of the IND, and timely safety reports must be submitted to the FDA and the investigators for serious and unexpected adverse events. An institutional review board (“IRB”) at each institution participating in the clinical trial must review and approve each protocol before a clinical trial commences at that institution and must also approve the information regarding the trial and the consent form that must be provided to each trial subject or his or her legal representative, monitor the study until completed and otherwise comply with IRB regulations.
20
Human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
|
· |
Phase 1: The product candidate is initially introduced into healthy human subjects and tested for safety, dosage tolerance, absorption, metabolism, distribution and excretion. In the case of some products for severe or life‑threatening diseases, such as cancer, especially when the product may be too inherently toxic to ethically administer to healthy volunteers, the initial human testing is often conducted in patients. Sponsors sometimes designate their Phase 1 trials as Phase 1a or Phase 1b. Phase 1b trials are typically aimed at confirming dosing, pharmacokinetics and safety in larger number of patients. Some Phase 1b studies evaluate biomarkers or surrogate markers that may be associated with efficacy in patients with specific types of diseases. |
|
· |
Phase 2: This phase involves clinical trials in a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance and appropriate dosage. |
|
· |
Phase 3: Clinical trials are undertaken to further evaluate dosage, clinical efficacy and safety in an expanded patient population at geographically dispersed clinical study sites. These clinical trials are intended to establish the overall risk‑benefit ratio of the product candidate and provide, if appropriate, an adequate basis for product labeling. |
Post‑approval trials, sometimes referred to as Phase 4 studies, may be conducted after initial marketing approval. These trials are used to gain additional experience from the treatment of patients in the intended therapeutic indication. In certain instances, the FDA may mandate the performance of Phase 4 clinical trials as a condition of approval of an NDA or BLA.
The FDA or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the research subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients. In addition, some clinical trials are overseen by an independent group of qualified experts organized by the sponsor, known as a data safety monitoring board or committee. Depending on its charter, this group may determine whether a trial may move forward at designated check points based on access to certain data from the trial.
During the development of a new drug or biologic, sponsors are given opportunities to meet with the FDA at certain points. These points may be prior to submission of an IND, at the end of Phase 2, and before an NDA or BLA is submitted. Meetings at other times may be requested. These meetings can provide an opportunity for the sponsor to share information about the data gathered to date, for the FDA to provide advice, and for the sponsor and the FDA to reach agreement on the next phase of development. Sponsors typically use the meetings at the end of the Phase 2 trial to discuss Phase 2 clinical results and present plans for the pivotal Phase 3 clinical trial that they believe will support approval of the new drug or biologic.
Concurrent with clinical trials, companies usually complete additional animal studies and must also develop additional information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, the manufacturer must develop methods for testing the identity, strength, quality and purity of the final drug. In addition, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the product candidate does not undergo unacceptable deterioration over its shelf life. While the IND is active and before approval, progress reports summarizing the results of the clinical trials and nonclinical studies performed since the last progress report must be submitted at least annually to the FDA, and written IND safety reports must be submitted to the FDA and investigators for serious and unexpected suspected adverse events, findings from other studies suggesting a significant risk to humans exposed to the same or similar drugs, findings from animal or in vitro testing suggesting a significant risk to humans, and any clinically important increased incidence of a serious suspected adverse reaction compared to that listed in the protocol or investigator brochure.
21
There are also requirements governing the reporting of ongoing clinical trials and completed trial results to public registries. Sponsors of certain clinical trials of FDA‑regulated products are required to register and disclose specified clinical trial information, which is publicly available at www.clinicaltrials.gov. Information related to the product, patient population, phase of investigation, trial sites and investigators and other aspects of the clinical trial is then made public as part of the registration. Sponsors are also obligated to discuss the results of their clinical trials after completion.
Disclosure of the results of these trials can be delayed until the new product or new indication being studied has been approved.
United States Review and Approval Process
The results of product development, preclinical and other non‑clinical studies and clinical trials, along with descriptions of the manufacturing process, analytical tests conducted on the chemistry of the drug, proposed labeling and other relevant information are submitted to the FDA as part of an NDA or BLA requesting approval to market the product. The submission of an NDA or BLA is subject to the payment of user fees; a waiver of such fees may be obtained under certain limited circumstances.
The FDA reviews all NDAs and BLAs submitted to ensure that they are sufficiently complete for substantive review before it accepts them for filing. The FDA may request additional information rather than accept an NDA or BLA for filing. In this event, the NDA or BLA must be resubmitted with the additional information. The resubmitted application also is subject to review before the FDA accepts it for filing.
Once the submission is accepted for filing, the FDA begins an in‑depth substantive review. The FDA may refer the NDA or BLA to an advisory committee for review, evaluation and recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendation of an advisory committee, but it generally follows such recommendations. The approval process is lengthy and often difficult, and the FDA may refuse to approve an NDA or BLA if the applicable regulatory criteria are not satisfied or may require additional clinical or other data and information. Even if such data and information are submitted, the FDA may ultimately decide that the NDA or BLA does not satisfy the criteria for approval. The FDA reviews an NDA to determine, among other things, whether a product is safe and effective for its intended use and whether its manufacturing is cGMP‑compliant to assure and preserve the product’s identity, strength, quality and purity. The FDA reviews a BLA to determine, among other things whether the product is safe, pure and potent and the facility in which it is manufactured, processed, packed or held meets standards designed to assure the product’s continued safety, purity and potency. Before approving an NDA or BLA, the FDA will inspect the facility or facilities where the product is manufactured.
After the FDA evaluates an NDA or BLA, it will issue an approval letter or a Complete Response Letter. An approval letter authorizes commercial marketing of the drug with prescribing information for specific indications. A Complete Response Letter indicates that the review cycle of the application is complete and the application will not be approved in its present form. A Complete Response Letter usually describes the specific deficiencies in the NDA or BLA identified by the FDA and may require additional clinical data, such as an additional pivotal Phase 3 trial or other significant and time‑consuming requirements related to clinical trials, nonclinical studies or manufacturing. If a Complete Response Letter is issued, the sponsor must resubmit the NDA or BLA, addressing all of the deficiencies identified in the letter, or withdraw the application. Even if such data and information are submitted, the FDA may decide that the NDA or BLA does not satisfy the criteria for approval. If a product receives regulatory approval, the approval may be significantly limited to specific diseases and dosages or the indications for use may otherwise be limited, which could restrict the commercial value of the product. In addition, the FDA may require a sponsor to conduct Phase 4 testing, which involves clinical trials designed to further assess a drug’s safety and effectiveness after NDA or BLA approval, and may require testing and surveillance programs to monitor the safety of approved products which have been commercialized. The FDA may also place other conditions on approval including the requirement for a risk evaluation and mitigation strategy (“REMS”) to assure the safe use of the drug. If the FDA concludes a REMS is needed, the sponsor of the NDA must submit a proposed REMS. The FDA will not approve the NDA without an approved REMS, if required. A REMS could include medication guides, physician communication plans or elements to
22
assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. Any of these limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of products. Marketing approval may be withdrawn for non‑compliance with regulatory requirements or if problems occur following initial marketing.
The Food and Drug Administration Safety and Innovation Act (“FDASIA”) made permanent the Pediatric Research Equity Act (“PREA”), which requires a sponsor to conduct pediatric clinical trials for most drugs and biologics, for a new active ingredient, new indication, new dosage form, new dosing regimen or new route of administration. Under PREA, original NDAs, BLAs and supplements thereto must contain a pediatric assessment unless the sponsor has received a deferral or waiver. The required assessment must evaluate the safety and effectiveness of the product for the claimed indications in all relevant pediatric subpopulations and support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The sponsor or FDA may request a deferral of pediatric clinical trials for some or all of the pediatric subpopulations. A deferral may be granted for several reasons, including a finding that the drug or biologic is ready for approval for use in adults before pediatric clinical trials are complete or that additional safety or effectiveness data needs to be collected before the pediatric clinical trials begin. The FDA must send a non‑compliance letter to any sponsor that fails to submit the required assessment, keep a deferral current or fails to submit a request for approval of a pediatric formulation.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan designation to a drug or biologic intended to treat a rare disease or condition, which is a disease or condition that affects fewer than 200,000 individuals in the United States or, if it affects more than 200,000 individuals in the United States, there is no reasonable expectation that the cost of developing and making a drug or biologic product available in the United States for this type of disease or condition will be recovered from sales of the product. Orphan designation must be requested before submitting an NDA or BLA. After the FDA grants orphan designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan designation does not convey any advantage in or shorten the duration of the regulatory review and approval process.
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan product exclusivity, which means that the FDA may not approve any other applications to market the same drug or biological product for the same indication for seven years, except in limited circumstances, such as a showing of clinical superiority to the product with orphan exclusivity or inability to manufacture the product in sufficient quantities. The designation of such drug or biologic also entitles a party to financial incentives such as opportunities for grant funding towards clinical trial costs, tax advantages and user‑fee waivers. However, competitors, may receive approval of different products for the indication for which the orphan product has exclusivity or obtain approval for the same product but for a different indication for which the orphan product has exclusivity. Orphan exclusivity also could block the approval of a product candidate for seven years if a competitor obtains approval of the same drug or biologic as defined by the FDA or if such product candidate is determined to be contained within the competitor’s product for the same indication or disease. If an orphan designated product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan exclusivity. Orphan drug status in the European Union has similar but not identical benefits in that jurisdiction.
Although we have not sought or obtained orphan designation for any of our product candidates, we may pursue such designation in the future if we determine that our proposed indications meet the qualifying criteria for such designation.
Expedited Development and Review Programs
The FDA has a Fast Track program that is intended to expedite or facilitate the process for reviewing new drug products that meet certain criteria. Specifically, new drugs are eligible for Fast Track designation if they are intended to treat a serious or life‑threatening disease or condition and nonclinical or clinical data demonstrate the potential to address unmet medical needs for the disease or condition. Fast Track designation applies to the combination of the product and the specific indication for which it is being studied. The FDA may consider for review sections of the NDA or BLA for a
23
Fast Track review designation on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the NDA or BLA, the FDA agrees to accept sections of the NDA or BLA and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the NDA or BLA.
Any product submitted to the FDA for approval, including a product with a Fast Track designation, may also be eligible for other types of FDA programs intended to expedite development and review, such as priority review and accelerated approval. A product is eligible for priority review if it is designed to treat a serious condition, and if approved, would provide a significant improvement in safety or effectiveness compared to marketed products. The FDA will attempt to direct additional resources to the evaluation of an application for a new drug designated for priority review in an effort to facilitate the review. The FDA endeavors to review applications with priority review designations within six months of the filing date as compared to ten months for review of original BLAs and new molecular entity NDAs under its standard review goals.
In addition, a product may be eligible for accelerated approval. Drug and biologic products intended to treat serious or life‑threatening diseases or conditions may be eligible for accelerated approval upon a determination that the product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. As a condition of approval, the FDA may require that a sponsor of a drug receiving accelerated approval perform adequate and well‑controlled post‑marketing clinical trials. In addition, the FDA currently requires as a condition for accelerated approval pre‑approval of promotional materials, which could adversely impact the timing of the commercial launch of the product.
FDASIA established a category of drugs and biologics referred to as “breakthrough therapies” that may be eligible to receive Breakthrough Therapy Designation. A sponsor may seek FDA designation of a drug or biologic candidate as a “breakthrough therapy” if the product is intended, alone or in combination with one or more other products, to treat a serious or life‑threatening disease or condition and preliminary clinical evidence indicates that the product may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. The designation includes all of the Fast Track program features, as well as more intensive FDA interaction and guidance. The Breakthrough Therapy Designation is a distinct status from both accelerated approval and priority review, which can also be granted to the same drug if relevant criteria are met. If a product is designated as breakthrough therapy, the FDA will expedite the development and review of such drug. All requests for breakthrough therapy designation will be reviewed within 60 days of receipt, and the FDA will either grant or deny the request.
Fast Track designation, Breakthrough Therapy designation, priority review and accelerated approval do not change the standards for approval but may expedite the development or approval process.
Post‑approval requirements
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market. After approval, some types of changes to the approved product, such as adding new indications, certain manufacturing changes and additional labeling claims, are subject to further FDA review and approval. Drug and biologics manufacturers and other entities involved in the manufacture and distribution of approved drugs and biologics are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMP regulations and other laws and regulations.
Any drug products manufactured or distributed by us or our partners pursuant to FDA approvals will be subject to continuing regulation by the FDA, including, among other things, record‑keeping requirements, reporting of adverse experiences with the drug, providing the FDA with updated safety and efficacy information, drug sampling and
24
distribution requirements, complying with certain electronic records and signature requirements, and complying with FDA promotion and advertising requirements. The FDA strictly regulates labeling, advertising, promotion and other types of information on products that are placed on the market and imposes requirements and restrictions on drug and biologics manufacturers, such as those related to direct‑to‑consumer advertising, the prohibition on promoting products for uses or in patient populations that are not described in the product’s approved labeling (known as “off‑label use”), industry‑sponsored scientific and educational activities, and promotional activities involving the internet. Discovery of previously unknown problems or the failure to comply with the applicable regulatory requirements may result in restrictions on the marketing of a product or withdrawal of the product from the market as well as possible civil or criminal sanctions. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or after approval, may subject an applicant or manufacturer to administrative or judicial civil or criminal sanctions and adverse publicity. FDA sanctions could include refusal to approve pending applications, withdrawal of an approval, clinical hold, warning or untitled letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, mandated corrective advertising or communications with doctors, debarment, restitution, disgorgement of profits, or civil or criminal penalties.
Patent Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of FDA approval of our product candidates, some of the U.S. patents that we may be granted in the future may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, referred to as the Hatch‑Waxman Amendments. The Hatch‑Waxman Amendments permit a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The patent term restoration period is generally one‑half the time between the effective date of an IND and the submission date of an NDA or BLA, plus the time between the submission date of an NDA or BLA and the approval of that application, less any time the applicant did not act with due diligence. Only one patent applicable to an approved drug is eligible for the extension, and the extension must be applied for prior to expiration of the patent. The United States Patent and Trademark Office, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, we intend to apply for restorations of patent term for patents that may be issued to us, depending on the expected length of clinical trials and other factors involved in the filing of the relevant marketing application.
Market exclusivity provisions under the FDCA can also delay the submission or the approval of certain marketing applications. The FDCA provides a five‑year period of non‑patent marketing exclusivity within the United States to the first applicant to obtain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety, which is the molecule or ion responsible for the action of the drug substance. During the exclusivity period, the FDA may not approve or even accept for review an abbreviated new drug application (“ANDA”) or a NDA submitted under Section 505(b)(2), or 505(b)(2) NDA, submitted by another company for another drug based on the same active moiety, regardless of whether the drug is intended for the same indication as the original innovative drug or for another indication, where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non‑infringement to one of the patents listed with the FDA by the innovator NDA holder. The FDCA alternatively provides three years of marketing exclusivity for an NDA, or supplement to an existing NDA if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by the FDA to be essential to the approval of the application, for example new indications, dosages or strengths of an existing drug. This three‑year exclusivity covers only the modification for which the drug received approval on the basis of the new clinical investigations and does not prohibit the FDA from approving ANDAs or 505(b)(2) NDAs for drugs containing the active agent for the original indication or condition of use. Five‑year and three‑year exclusivity will not delay the submission or approval of a full NDA. However, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well‑controlled clinical trials necessary to demonstrate safety and effectiveness.
Pediatric exclusivity is a type of marketing exclusivity available in the United States. Pediatric exclusivity under the Best Pharmaceuticals for Children Act provides for an additional six months of marketing exclusivity if a
25
sponsor conducts clinical trials in children in response to a written request from the FDA. If such written request does not include clinical trials in neonates, the FDA is required to include its rationale for not requesting those clinical trials. The FDA may request studies on approved or unapproved indications in separate written requests. The issuance of a written request does not require the sponsor to undertake the described clinical trials. In addition, orphan drug exclusivity, as described above, may offer a seven‑year period of marketing exclusivity, except in certain circumstances.
Biosimilars and Exclusivity
The Affordable Care Act includes a subtitle called the Biologics Price Competition and Innovation Act of 2009 (“BPCIA”), which created an abbreviated approval pathway for biological products that are biosimilar to or interchangeable with an FDA‑licensed reference biological product. The FDA has issued several guidance documents outlining an approach to review and approval of biosimilars.
Biosimilarity, which requires that there be no clinically meaningful differences between the biological product and the reference product in terms of safety, purity, and potency, can be shown through analytical studies, animal studies, and a clinical study or studies. Interchangeability requires that a product is biosimilar to the reference product and the product must demonstrate that it can be expected to produce the same clinical results as the reference product in any given patient and, for products that are administered multiple times to an individual, the biologic and the reference biologic may be alternated or switched after one has been previously administered without increasing safety risks or risks of diminished efficacy relative to exclusive use of the reference biologic. However, complexities associated with the larger, and often more complex, structures of biological products, as well as the processes by which such products are manufactured, pose significant hurdles to implementation of the abbreviated approval pathway that are still being addressed by the FDA.
Under the BPCIA, an application for a biosimilar product may not be submitted to the FDA until four years following the date that the reference product was first licensed by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until twelve years from the date on which the reference product was first licensed. During this twelve‑year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing the sponsor’s own preclinical data and data from adequate and well‑controlled clinical trials to demonstrate the safety, purity and potency of their product. The BPCIA also created certain exclusivity periods for biosimilars approved as interchangeable products. At this juncture, it is unclear whether products deemed “interchangeable” by the FDA will, in fact, be readily substituted by pharmacies, which are governed by state pharmacy law.
The BPCIA is complex and continues to be interpreted and implemented by the FDA. In addition, recent government proposals have sought to reduce the twelve‑year reference product exclusivity period. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. As a result, the ultimate impact, implementation and meaning of the BPCIA is subject to significant uncertainty.
FDA Regulation of Companion Diagnostics
We expect that certain of our product candidates may require an in vitro diagnostic to identify appropriate patient populations for our product candidates. These diagnostics, often referred to as companion diagnostics, are regulated as medical devices. In the United States, the FDCA and its implementing regulations, and other federal and state statutes and regulations govern, among other things, medical device design and development, preclinical and clinical testing, premarket clearance or approval, registration and listing, manufacturing, labeling, storage, advertising and promotion, sales and distribution, export and import, and post-market surveillance. Unless an exemption applies, diagnostic tests require marketing clearance or approval from the FDA prior to commercial distribution. The two primary types of FDA marketing authorization applicable to a medical device are premarket notification, also called 510(k) clearance, and premarket approval (“PMA”). We expect that any companion diagnostic developed for our product candidates will utilize the PMA pathway.
If use of companion diagnostic is essential to safe and effective use of a drug or biologic product, then the FDA generally will require approval or clearance of the diagnostic contemporaneously with the approval of the therapeutic
26
product. On August 6, 2014, the FDA issued a final guidance document addressing the development and approval process for “In Vitro Companion Diagnostic Devices.” According to the guidance, for novel product candidates, a companion diagnostic device and its corresponding drug candidate should be approved or cleared contemporaneously by FDA for the use indicated in the therapeutic product labeling. The guidance also explains that a companion diagnostic device used to make treatment decisions in clinical trials of a drug generally will be considered an investigational device, unless it is employed for an intended use for which the device is already approved or cleared. If used to make critical treatment decisions, such as patient selection, the diagnostic device generally will be considered a significant risk device under the FDA’s Investigational Device Exemption (“IDE”) regulations. Thus, the sponsor of the diagnostic device will be required to comply with the IDE regulations. According to the guidance, if a diagnostic device and a drug are to be studied together to support their respective approvals, both products can be studied in the same investigational study, if the study meets both the requirements of the IDE regulations and the IND regulations. The guidance provides that depending on the details of the study plan and subjects, a sponsor may seek to submit an IND alone, or both an IND and an IDE.
The FDA has generally required companion diagnostics intended to select the patients who will respond to cancer treatment to obtain approval of a PMA for that diagnostic simultaneously with approval of the therapeutic. The PMA process, including the gathering of clinical and preclinical data and the submission to and review by the FDA, can take several years or longer. It involves a rigorous premarket review during which the applicant must prepare and provide the FDA with reasonable assurance of the device’s safety and effectiveness and information about the device and its components regarding, among other things, device design, manufacturing and labeling. In addition, PMAs for certain devices must generally include the results from extensive preclinical and adequate and well-controlled clinical trials to establish the safety and effectiveness of the device for each indication for which FDA approval is sought. In particular, for a diagnostic, the applicant must demonstrate that the diagnostic produces reproducible results when the same sample is tested multiple times by multiple users at multiple laboratories. As part of the PMA review, the FDA will typically inspect the manufacturer’s facilities for compliance with the Quality System Regulation (“QSR”),which imposes elaborate testing, control, documentation and other quality assurance requirements.
If the FDA evaluations of both the PMA application and the manufacturing facilities are favorable, the FDA will either issue an approval letter or an approvable letter, which usually contains a number of conditions that must be met in order to secure the final approval of the PMA, such as changes in labeling, or specific additional information, such as submission of final labeling, in order to secure final approval of the PMA. If the FDA concludes that the applicable criteria have been met, the FDA will issue a PMA for the approved indications, which can be more limited than those originally sought by the applicant. The PMA can include post-approval conditions that the FDA believes necessary to ensure the safety and effectiveness of the device, including, among other things, restrictions on labeling, promotion, sale and distribution.
If the FDA’s evaluation of the PMA or manufacturing facilities is not favorable, the FDA will deny approval of the PMA or issue a not approvable letter. A not approvable letter will outline the deficiencies in the application and, where practical, will identify what is necessary to make the PMA approvable. The FDA may also determine that additional clinical trials are necessary, in which case the PMA approval may be delayed for several months or years while the trials are conducted and then the data submitted in an amendment to the PMA. Once granted, PMA approval may be withdrawn by the FDA if compliance with post approval requirements, conditions of approval or other regulatory standards is not maintained or problems are identified following initial marketing. PMA approval is not guaranteed, and the FDA may ultimately respond to a PMA submission with a not approvable determination based on deficiencies in the application and require additional clinical trial or other data that may be expensive and time-consuming to generate and that can substantially delay approval.
27
After a device is placed on the market, it remains subject to significant regulatory requirements. Medical devices may be marketed only for the uses and indications for which they are cleared or approved. Device manufacturers must also establish registration and device listings with the FDA. A medical device manufacturer’s manufacturing processes and those of its suppliers are required to comply with the applicable portions of the QSR, which cover the methods and documentation of the design, testing, production, processes, controls, quality assurance, labeling, packaging and shipping of medical devices. Domestic facility records and manufacturing processes are subject to periodic unscheduled inspections by the FDA. The FDA also may inspect foreign facilities that export products to the United States.
Government Regulation Outside of the United States
In addition to regulations in the United States, we will be subject to a variety of regulations in other jurisdictions governing, among other things, clinical studies and any commercial sales and distribution of our product candidates.
Whether or not we obtain FDA approval for a product candidates, we must obtain the requisite approvals from regulatory authorities in foreign countries prior to the commencement of clinical studies or marketing of the product candidates in those countries. Certain countries outside of the United States have a similar process that requires the submission of a clinical study application much like the IND prior to the commencement of human clinical studies. In the European Union, for example, a clinical trial authorization (“CTA”) must be submitted to each country’s national health authority and an independent ethics committee, much like the FDA and the IRB, respectively. Once the CTA is approved in accordance with a country’s requirements, clinical study development may proceed.
The requirements and process governing the conduct of clinical studies, product licensing, pricing and reimbursement vary from country to country. In all cases, the clinical studies are conducted in accordance with GCP and the applicable regulatory requirements and the ethical principles that have their origin in the Declaration of Helsinki.
To obtain regulatory approval of an investigational biological product under European Union regulatory systems, we must submit a marketing authorization application. The application used to file the BLA in the United States is similar to that required in the European Union, with the exception of, among other things, country‑specific document requirements. The European Union also provides opportunities for market exclusivity. For example, in the European Union, upon receiving marketing authorization, new chemical entities generally receive eight years of data exclusivity and an additional two years of market exclusivity. If granted, data exclusivity prevents regulatory authorities in the European Union from referencing the innovator’s data to assess a generic application. During the additional two‑year period of market exclusivity, a generic marketing authorization can be submitted, and the innovator’s data may be referenced, but no generic product can be marketed until the expiration of the market exclusivity. However, there is no guarantee that a product will be considered by the European Union’s regulatory authorities to be a new chemical entity, and products may not qualify for data exclusivity. Products receiving orphan designation in the European Union can receive ten years of market exclusivity, during which time no similar medicinal product for the same indication may be placed on the market. An orphan product can also obtain an additional two years of market exclusivity in the European Union for pediatric studies. No extension to any supplementary protection certificate can be granted on the basis of pediatric studies for orphan indications.
The criteria for designating an “orphan medicinal product” in the European Union are similar in principle to those in the United States. Under Article 3 of Regulation (EC) 141/2000, a medicinal product may be designated as orphan if (1) it is intended for the diagnosis, prevention or treatment of a life‑threatening or chronically debilitating condition; (2) either (a) such condition affects no more than five in 10,000 persons in the European Union when the application is made, or (b) the product, without the benefits derived from orphan status, would not generate sufficient return in the European Union to justify investment; and (3) there exists no satisfactory method of diagnosis, prevention or treatment of such condition authorized for marketing in the European Union, or if such a method exists, the product will be of significant benefit to those affected by the condition, as defined in Regulation (EC) 847/2000. Orphan medicinal products are eligible for financial incentives such as reduction of fees or fee waivers and are, upon grant of a marketing authorization, entitled to ten years of market exclusivity for the approved therapeutic indication. The application for orphan drug designation must be submitted before the application for marketing authorization. The
28
applicant will receive a fee reduction for the marketing authorization application if the orphan drug designation has been granted, but not if the designation is still pending at the time the marketing authorization is submitted. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process.
The 10‑year market exclusivity may be reduced to six years if, at the end of the fifth year, it is established that the product no longer meets the criteria for orphan designation, for example, if the product is sufficiently profitable not to justify maintenance of market exclusivity. In addition, marketing authorization may be granted to a similar product for the same indication at any time if:
|
· |
the second applicant can establish that its product, although similar, is safer, more effective or otherwise clinically superior; |
|
· |
the applicant consents to a second orphan medicinal product application; or |
|
· |
the applicant cannot supply enough orphan medicinal product. |
When conducting clinical trials in the EU, we must adhere to the provisions of the European Union Clinical Trials Directive (Directive 2001/20/EC) and the laws and regulations of the EU Member States implementing them. These provisions require, among other things, that the prior authorization of an Ethics Committee and the competent Member State authority is obtained before commencing the clinical trial. In April 2014, the EU passed the Clinical Trials Regulation (Regulation 536/2014), which will replace the current Clinical Trials Directive. To ensure that the rules for clinical trials are identical throughout the European Union, the EU Clinical Trials Regulation was passed as a regulation that is directly applicable in all EU member states. All clinical trials performed in the European Union are required to be conducted in accordance with the Clinical Trials Directive until the Clinical Trials Regulation becomes applicable. According to the current plans of the EMA, the Clinical Trials Regulation is expected to become applicable in 2020.
For other countries outside of the European Union, such as countries in Eastern Europe, Latin America or Asia, the requirements governing the conduct of clinical studies, product licensing, pricing and reimbursement vary from country to country. In all cases, again, the clinical studies are conducted in accordance with GCP and the applicable regulatory requirements and the ethical principles that have their origin in the Declaration of Helsinki.
If we fail to comply with applicable foreign regulatory requirements, we may be subject to, among other things, fines, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions and criminal prosecution.
Other Healthcare Laws
In addition to FDA restrictions on marketing of pharmaceutical and biological products, other U.S. federal and state healthcare regulatory laws restrict business practices in the pharmaceutical industry, which include, but are not limited to, state and federal anti‑kickback, fraud & abuse, false claims, price reporting, consumer fraud, data privacy and security and physician payment transparency laws. These laws may affect our sales, marketing and other promotional activities by limiting the kinds of financial arrangements we may have with physicians, customers and third‑party payors including discount practices, customer support, education and training programs, physician consulting and other service arrangements. In addition, manufacturers can be held liable under the False Claims Act even when they do not submit claims directly to government payors if they are deemed to “cause” the submission of false or fraudulent claims by, for example, providing inaccurate billing or coding information to customers or promoting a product off‑label. These laws are broadly written, and it is often difficult to determine precisely how these laws will be applied to specific circumstances. Such laws include:
|
· |
The federal Anti‑Kickback Statute, which prohibits, among other things, any person or entity from knowingly and willfully offering, paying, soliciting, receiving or providing any remuneration, directly or indirectly, overtly or covertly, to induce or in return for purchasing, leasing, ordering or arranging for or recommending the purchase, lease or order of any item or service reimbursable, in whole or in part, under Medicare, Medicaid or other federal healthcare programs. A person or entity does not need to have actual |
29
knowledge of the federal Anti‑Kickback Statute or specific intent to violate it to have committed a violation. In addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti‑Kickback Statute constitutes a false or fraudulent claim for purposes of the False Claims Act; |
|
· |
The federal false claims and civil monetary penalties laws, including the False Claims Act, which prohibit any person or entity from, among other things, knowingly presenting, or causing to be presented, a false, fictitious or fraudulent claim for payment to, or approval by, the federal government or knowingly making, using or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government; |
|
· |
The federal Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), which prohibits, among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third‑party payors, knowingly and willfully embezzling or stealing from a healthcare benefit program, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services; |
|
· |
The Physician Payments Sunshine Act, which imposed, among other things, new annual reporting requirements for covered manufacturers for certain payments and “transfers of value” provided to physicians and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members and will be expanded to include certain other healthcare professionals in 2022 for payments made in 2021; |
|
· |
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act (“HITECH”), and their respective implementing regulations, impose specified requirements relating to the privacy, security and transmission of individually identifiable health information held by covered entities and their business associates; and |
|
· |
Analogous state laws and regulations, such as state anti‑kickback and false claims laws, may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non‑governmental third‑party payors, including private insurers. |
If our operations are found to be in violation of any of such laws or any other governmental regulations that apply to us, we may be subject to penalties, including, without limitation, administrative, civil and criminal penalties, damages, fines, disgorgement, contractual damages, reputational harm, diminished profits and future earnings, the curtailment or restructuring of our operations, exclusion from participation in federal and state healthcare programs and individual imprisonment, any of which could adversely affect our ability to operate our business and our financial results.
To the extent that any of our product candidates, once approved, are sold in a foreign country, we may be subject to similar foreign laws and regulations, which may include, for instance, applicable post‑marketing requirements, including safety surveillance, anti‑fraud and abuse laws, and implementation of corporate compliance programs and reporting of payments or other transfers of value to healthcare professionals.
Coverage and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any pharmaceutical or biological product for which we obtain regulatory approval. In the United States and markets in other countries, patients who are prescribed treatments for their conditions and providers performing the prescribed services generally rely on third‑party payors to reimburse all or part of the associated healthcare costs. Patients are unlikely to use our products unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost of our products. Sales of any product candidates for which we receive regulatory approval for commercial sale will therefore depend, in part, on
30
the availability of coverage and adequate reimbursement from third‑party payors. Third‑ party payors include government authorities, managed care plans, private health insurers and other organizations.
The process for determining whether a third‑party payor will provide coverage for a pharmaceutical or biological product typically is separate from the process for setting the price of such product or for establishing the reimbursement rate that the payor will pay for the product once coverage is approved. Third‑party payors may limit coverage to specific products on an approved list, also known as a formulary, which might not include all of the FDA‑approved products for a particular indication. A decision by a third‑party payor not to cover our product candidates could reduce physician utilization of our products once approved and have a material adverse effect on our sales, results of operations and financial condition. Moreover, a third‑party payor’s decision to provide coverage for a pharmaceutical or biological product does not imply that an adequate reimbursement rate will be approved. Adequate third‑party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment in product development. In addition, coverage and reimbursement for new products can differ significantly from payor to payor. One third‑party payor’s decision to cover a particular medical product or service does not ensure that other payors will also provide coverage for the medical product or service, or will provide coverage at an adequate reimbursement rate. As a result, the coverage determination process will require us to provide scientific and clinical support for the use of our products to each payor separately and will be a time consuming process.
The containment of healthcare costs has become a priority of federal, state and foreign governments, and the prices of pharmaceutical or biological products have been a focus in this effort. Third‑party payors are increasingly challenging the prices charged for medical products and services, examining the medical necessity and reviewing the cost‑effectiveness of pharmaceutical products, biological products, medical devices and medical services, in addition to questioning safety and efficacy. If these third‑party payors do not consider our product candidates to be cost‑effective compared to other available therapies, they may not cover our products after FDA approval or, if they do, the level of payment may not be sufficient to allow us to sell our products at a profit.
Healthcare Reform
A primary trend in the U.S. healthcare industry and elsewhere is cost containment. Government authorities and other third‑party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medical products. For example, in March 2010, the Affordable Care Act was enacted, which, among other things, increased the minimum Medicaid rebates owed by most manufacturers under the Medicaid Drug Rebate Program; introduced a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected; extended the Medicaid Drug Rebate Program to utilization of prescriptions of individuals enrolled in Medicaid managed care plans; imposed mandatory discounts for certain Medicare Part D beneficiaries as a condition for manufacturers’ outpatient drugs coverage under Medicare Part D; subjected drug manufacturers to new annual fees based on pharmaceutical companies’ share of sales to federal healthcare programs, and created a new Patient Centered Outcomes Research Institute to oversee, identify priorities in and conduct comparative clinical effectiveness research, along with funding for such research.
We expect that the current presidential administration and U.S. Congress will likely continue to seek to challenge, replace, modify, repeal, or otherwise invalidate all, or certain provisions of, the Affordable Care Act.
For example, the Tax Cuts and Jobs Act was enacted, which, among other things, removes penalties for not complying with the Affordable Care Act’s individual mandate to carry health insurance. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas, ruled that the individual mandate is a critical and inseverable feature of the ACA, and therefore, because it was repealed as part of the Tax Act, the remaining provisions of the ACA are invalid as well. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit upheld the District Court's decision that the individual mandate was unconstitutional but remanded the case back to the District Court to determine whether the remaining provisions of the Affordable Care Act are invalid as well. It is unclear how these decisions, subsequent appeals, and other efforts to challenge, replace, modify, repeal or otherwise invalidate the Affordable Care Act will impact the Act or our business. We expect that the Affordable Care Act, as well as other healthcare reform measures that may be adopted in the future, may result in more rigorous coverage criteria and lower reimbursement, and
31
additional downward pressure on the price that we receive for any approved product. Any reduction in reimbursement from Medicare or other government‑funded programs may result in a similar reduction in payments from private payors. Recently there has been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, reform government program reimbursement methodologies. Additionally, individual states in the United States have also become increasingly active in passing legislation and implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability or commercialize our product candidates.
In addition, the Budget Control Act of 2011 and the Bipartisan Budget Act of 2015 led to aggregate reductions of Medicare payments to providers of up to 2% per fiscal year that will remain in effect through 2029 unless additional Congressional action is taken. On January 2, 2013, the American Taxpayer Relief Act was signed into law, which, among other things, further reduced Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
Moreover, there has recently been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed and enacted legislation designed, among other things, to bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs and reform government program reimbursement methodologies for pharmaceutical products. In addition, individual states in the United States have also become increasingly active in implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures and, in some cases, mechanisms to encourage importation from other countries and bulk purchasing. Furthermore, there has been increased interest by third party payors and governmental authorities in reference pricing systems and publication of discounts and list prices.
Similar political, economic and regulatory developments are occurring in the EU and may affect the ability of pharmaceutical companies to profitably commercialize their products. In addition to continuing pressure on prices and cost containment measures, legislative developments at the EU or member state level may result in significant additional requirements or obstacles. The delivery of healthcare in the EU, including the establishment and operation of health services and the pricing and reimbursement of medicines, is almost exclusively a matter for national, rather than EU, law and policy. National governments and health service providers have different priorities and approaches to the delivery of health care and the pricing and reimbursement of products in that context. In general, however, the healthcare budgetary constraints in most EU member states have resulted in restrictions on the pricing and reimbursement of medicines by relevant health service providers. Coupled with ever-increasing EU and national regulatory burdens on those wishing to develop and market products, this could restrict or regulate post-approval activities and affect the ability of pharmaceutical companies to commercialize their products. In international markets, reimbursement and healthcare payment systems vary significantly by country, and many countries have instituted price ceilings on specific products and therapies
In the future, there may continue to be additional proposals relating to the reform of the U.S. healthcare system and international healthcare systems. We expect that additional state and federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in limited coverage and reimbursement and reduced demand for our products, once approved, or additional pricing pressures.
Research and Development Expenses
Our research and development expenses were $38.0 million, $38.6 million and $46.3 million for the years ended December 31, 2019, 2018, and 2017, respectively. Please see “Management’s Discussion and Analysis of
32
Financial Condition and Results of Operations‑Research and Development Expenses” for additional detail regarding our research and development activities.
Environment
Our third‑party manufacturers are subject to inspections by the FDA for compliance with cGMP and other U.S. regulatory requirements, including U.S. federal, state and local regulations regarding environmental protection and hazardous and controlled substance controls, among others. Environmental laws and regulations are complex, change frequently and have tended to become more stringent over time. We have incurred, and may continue to incur, significant expenditures to ensure we are in compliance with these laws and regulations. We would be subject to significant penalties for failure to comply with these laws and regulations.
Employees
As of December 31, 2019, we had 53 total employees, one of whom was part-time and 42 of whom were primarily engaged in research and development activities.
Facilities
We currently lease a total of approximately 27,280 square feet of office and research and development facilities in Burlingame, California. Our lease expires in 2023. We regularly explore alternatives which would provide us with additional space to accommodate our anticipated growth.
Legal Proceedings
We are not currently a party to any material legal proceedings.
Corporate Information
We were incorporated in Delaware on January 27, 2014 and began operations in November 2014. Our principal executive offices are located at 863 Mitten Road, Suite 102, Burlingame, California 94010, and our telephone number is (650) 900‑4520. Our website address is http://www.corvuspharma.com. The information on our website is not incorporated by reference in this Annual Report on Form 10‑K or in any other filings we make with the SEC.
We are an emerging growth company as defined in the Jumpstart Our Business Startups Act of 2012 (JOBS Act). We will remain an emerging growth company until the earlier of (1) December 31, 2021, (2) the last day of the fiscal year in which we have total annual gross revenue of at least $1.07 billion, (3) the last day of the fiscal year in which we are deemed to be a “large accelerated filer” as defined in Rule 12b‑2 under the Exchange Act, which would occur if the market value of our common stock held by non‑affiliates exceeded $700.0 million as of the last business day of the second fiscal quarter of such fiscal year, or (4) the date on which we have issued more than $1.0 billion in non‑convertible debt securities during the prior three‑year period. An emerging growth company may take advantage of specified reduced reporting requirements and is relieved of certain other significant requirements that are otherwise generally applicable to public companies. As an emerging growth company,
|
· |
We may present only two years of audited financial statements, plus unaudited condensed financial statements for any interim period, and related management’s discussion and analysis of financial condition and results of operations; |
|
· |
We may avail ourselves of the exemption from the requirement to obtain an attestation and report from our auditors on the assessment of our internal control over financial reporting pursuant to the Sarbanes‑Oxley Act of 2002 (Sarbanes‑Oxley); |
|
· |
We may provide less extensive disclosure about our executive compensation arrangements; and |
33
|
· |
We may not require stockholder non‑binding advisory votes on executive compensation or golden parachute arrangements. |
We have chosen to opt out of the extended transition periods available to emerging growth companies under the JOBS Act for complying with new or revised accounting standards. Section 107 of the JOBS Act provides that our decision to opt out of the extended transition periods for complying with new or revised accounting standards is irrevocable.
Financial Information about Segments
We view our operations and manage our business as one reportable segment. See Note 2 to our audited financial statements included in this Annual Report on Form 10‑K. Additional information required by this item is incorporated herein by reference to Part II, Item 6, “Selected Financial Data.”
Available Information
We file electronically with the SEC our annual reports on Form 10‑K, quarterly reports on Form 10‑Q and current reports on Form 8‑K pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended. We make available on our website at http://www.corvuspharma.com, free of charge, copies of these reports, as soon as reasonably practicable after we electronically file such material with, or furnish it to, the SEC. The public may read or copy any materials we file with the SEC. The SEC maintains a website that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC. The address of that website is www.sec.gov. The information on or accessible through the SEC and our website is not incorporated into, and is not considered part of, this filing. Further, our references to the URLs for these websites are intended to be inactive textual references only.
Our business involves significant risks, some of which are described below. You should consider carefully the risks and uncertainties described below, together with all of the other information in this Annual Report on Form 10‑K, including our audited financial statements and related notes included elsewhere in this Annual Report on Form 10‑K and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” If any of the following risks are realized, our business, financial condition, results of operations and prospects could be materially and adversely affected. Additional risks and uncertainties not presently known to us or that we currently deem immaterial may also impair our business operations.
Risks Related to Our Limited Operating History, Financial Condition and Capital Requirements
We have a limited operating history, have incurred significant operating losses since our inception and expect to incur significant losses for the foreseeable future. We may never generate any revenue or become profitable or, if we achieve profitability, we may not be able to sustain it.
We are a clinical-stage biopharmaceutical company with a limited operating history. Biopharmaceutical product development is a highly speculative undertaking and involves a substantial degree of risk. To date, we have focused primarily on developing our lead product candidates, ciforadenant, CPI-006 and CPI-818, and researching additional product candidates. We have incurred significant operating losses since we were founded in January 2014 and have not yet generated any revenue from sales. If our product candidates are not approved, we may never generate any revenue. We incurred a net loss of $46.7 million, $46.9 million and $55.7 million for the years ended December 31, 2019, 2018 and 2017, respectively. We had an accumulated deficit of $217.1 million as of December 31, 2019. We expect to continue to incur losses for the foreseeable future, and we anticipate these losses will increase as we continue our development of, seek regulatory approval for and, if approved, begin to commercialize ciforadenant, CPI-006 and CPI-818, and as we develop other product candidates. Even if we achieve profitability in the future, we may not be able to
34
sustain it in subsequent periods. Our prior losses, combined with expected future losses, have had and will continue to have an adverse effect on our stockholders’ equity and results of operations.
We will require substantial additional financing to achieve our goals, and a failure to obtain this necessary capital when needed on acceptable terms, or at all, could force us to delay, limit, reduce or terminate our product development, other operations or commercialization efforts.
Since commencing our operations in 2014, the majority of our efforts have been focused on the research and development of ciforadenant, CPI-006 and CPI-818. We believe that we will continue to expend substantial resources for the foreseeable future as we continue clinical development of, seek regulatory approval for and, if approved, prepare for the commercialization of ciforadenant, CPI-006, and CPI-818, as well as product candidates under our other development programs. These expenditures will include costs associated with research and development, conducting preclinical studies and clinical trials, obtaining regulatory approvals, manufacturing and supply, sales and marketing and general operations. In addition, other unanticipated costs may arise. Because the outcome of any clinical trial and/or regulatory approval process is highly uncertain, we may not be able to accurately estimate the actual amounts necessary to successfully complete the development, regulatory approval process and commercialization of ciforadenant, CPI-006, CPI-818 or any other product candidates.
In March and April 2016, we completed our initial public offering (“IPO”) of our common stock pursuant to which we received proceeds of approximately $70.6 million, net of underwriting discounts and commission, and offering expenses, which included shares issued pursuant to the underwriters’ exercise of their option in full to purchase additional shares of common stock. In March 2018, in a follow-on offering, we sold 8,117,647 shares of our common stock at a price of $8.50 per share, which included 1,058,823 shares issued pursuant to the underwriters’ exercise of their option to purchase additional shares of common stock. We received aggregate net proceeds of approximately $64.9 million, after underwriting discounts, commissions and offering expenses.
As of December 31, 2019, we had capital resources consisting of cash, cash equivalents and marketable securities of $78.0 million. We do not expect our existing capital resources to be sufficient to enable us to fund the completion of our clinical trials and remaining development program of any of ciforadenant, CPI-006 or CPI-818 through commercialization. In addition, our operating plan may change as a result of many factors, including those described below as well as others currently unknown to us, and we may need to seek additional funds sooner than planned, through public or private equity, including pursuant to the Sales Agreement we entered into with Cowen and Company, LLC in September 2017 in connection with our at-the-market offering (the “Sales Agreement”), debt financings or other sources, such as strategic collaborations. Such financing would result in dilution to stockholders, imposition of debt covenants and repayment obligations or other restrictions that may affect our business. If we raise additional capital through strategic collaboration agreements, we may have to relinquish valuable rights to our product candidates, including possible future revenue streams. In addition, additional funding may not be available to us on acceptable terms, or at all, and any additional fundraising efforts may divert our management from their day-to-day activities, which may adversely affect our ability to develop and commercialize our product candidates. Furthermore, even if we believe we have sufficient funds for our current or future operating plans, we may seek additional capital due to favorable market conditions or strategic considerations.
The amount and timing of any expenditures needed to implement our development and commercialization programs will depend on numerous factors, including, but not limited to:
|
· |
the type, number, scope, progress, expansions, results of and timing of our ongoing and planned clinical trials of ciforadenant, CPI-006 and CPI-818 and any of our planned preclinical studies and clinical trials of other product candidates which we are pursuing or may choose to pursue in the future; |
|
· |
the need for, and the progress, costs and results of, any additional clinical trials of ciforadenant, CPI-006, CPI-818 or any of our other product candidates we may initiate based on the results of our planned clinical |
35
trials or discussions with the FDA, including any additional trials the FDA or other regulatory agencies may require; |
|
· |
the costs of obtaining, maintaining and enforcing our patents and other intellectual property rights; |
|
· |
the costs and timing of obtaining or maintaining manufacturing for ciforadenant, CPI-006, CPI-818 and our other product candidates, including commercial manufacturing if any product candidate is approved; |
|
· |
the costs and timing of establishing sales and marketing capabilities; |
|
· |
our ability to achieve sufficient market acceptance, coverage and reimbursement from third-party payors and adequate market share for our product candidates; |
|
· |
the terms and timing of establishing collaborations, license agreements and other partnerships; |
|
· |
costs associated with any new product candidates that we may develop, in-license or acquire; |
|
· |
the effect of competing technological and market developments; |
|
· |
our ability to attract, hire and retain qualified personnel; |
|
· |
our ability to establish and maintain partnering arrangements for development; and |
|
· |
the costs associated with being a public company. |
Several of these factors are outside of our control and if we are unable to obtain funding on a timely basis, we will be unable to complete the clinical trials for ciforadenant, CPI-006, CPI-818 and our other product candidates, and we may be required to significantly curtail some or all of our activities.
Risks Related to the Discovery and Development of Our Product Candidates
Our product candidates are in early stages of development and may fail or suffer delays that materially and adversely affect their commercial viability. If we are unable to advance our product candidates through clinical development, obtain regulatory approval and ultimately commercialize such product candidates, or experience significant delays in doing so, our business will be materially harmed.
We are very early in our development efforts, with three product candidates, ciforadenant, CPI-006 and CPI-818, currently in early stage clinical development. We have no products on the market and our ability to achieve and sustain profitability depends on obtaining regulatory approvals for and successfully commercializing our product candidates, either alone or with third parties. Before obtaining regulatory approval for the commercial distribution of our product candidates, we or our collaborator must conduct extensive preclinical tests and clinical trials to demonstrate sufficient safety and efficacy of our product candidates in patients.
As a result, we may not have the financial resources to continue development of, or to modify existing or enter into new collaborations for, a product candidate if we experience any issues that delay or prevent regulatory approval of, or our ability to commercialize, product candidates, including:
|
· |
negative or inconclusive results from our clinical trials, the clinical trials of our collaborators or the clinical trials of others for product candidates similar to ours, leading to a decision or requirement to conduct additional preclinical testing or clinical trials or abandon a program; |
|
· |
product-related side effects experienced by participants in our clinical trials, the clinical trials of our collaborators or by individuals using drugs or therapeutic biologics similar to our product candidates; |
36
|
· |
delays in submitting INDs or comparable foreign applications or delays or failure in obtaining the necessary approvals from regulators to commence a clinical trial, or a suspension or termination of a clinical trial once commenced; |
|
· |
conditions imposed by the United States Food and Drug Administration (“FDA”) or comparable foreign authorities regarding the scope or design of our clinical trials; |
|
· |
delays in enrolling research subjects in clinical trials; |
|
· |
high drop-out rates of research subjects; |
|
· |
inadequate supply or quality of product candidate components or materials or other supplies necessary for the conduct of our clinical trials or the clinical trials of our collaborators; |
|
· |
greater than anticipated clinical trial costs; |
|
· |
delay in the development or approval of companion diagnostic tests for our product candidates; |
|
· |
unfavorable FDA or other regulatory agency inspection and review of a clinical trial site; |
|
· |
failure of our third-party contractors or investigators to comply with regulatory requirements or otherwise meet their contractual obligations in a timely manner, or at all; |
|
· |
delays and changes in regulatory requirements, policy and guidelines, including the imposition of additional regulatory oversight around clinical testing generally or with respect to our technology in particular; or |
|
· |
varying interpretations of data by the FDA and similar foreign regulatory agencies. |
In addition, disruptions at the FDA and other regulatory agencies that are unrelated to our company or our products could also cause delays to the regulatory approval process for our products. For example, over the last several years, including from December 2018 into January 2019, the U.S. government has shut down several times and certain regulatory agencies, including the FDA, have had to furlough critical employees and stop critical activities. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions.
We could find that the product candidates we or our collaborators pursue are not safe or efficacious. Furthermore, if one or more of our product candidates, particularly in relation to the adenosine pathway, generally prove to be ineffective, unsafe or commercially unviable, the development of our entire platform and pipeline could be delayed, potentially permanently. Any of these occurrences may materially and adversely affect our business, financial condition, results of operations and prospects.
Of the large number of drugs in development in the pharmaceutical industry, only a small percentage result in the submission of a New Drug Application (“NDA”) or Biologics License Application (“BLA”) to the FDA or comparable marketing applications to foreign regulatory authorities, and even fewer are approved for commercialization. Furthermore, even if we do receive regulatory approval to market ciforadenant, CPI-006 or CPI-818, any such approval may be subject to limitations on the indicated uses for which we may market the product. Accordingly, even if we are able to obtain the requisite financing to continue to fund our development programs, we cannot assure our stockholders that ciforadenant, CPI-006 or CPI-818 will be successfully developed or commercialized. If we or any of our potential future collaborators are unable to develop, or obtain regulatory approval for, or, if approved, successfully commercialize ciforadenant, CPI-006 or CPI-818, we may not be able to generate sufficient revenue to continue our business.
37
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and the results of preclinical studies and early clinical trials are not necessarily predictive of future results. Any product candidate we or any of our potential future collaborators advance into clinical trials, including ciforadenant, CPI-006 and CPI-818, may not have favorable results in later clinical trials, if any, or receive regulatory approval.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of preclinical studies and early clinical trials of our product candidates may not be predictive of the results of later-stage clinical trials. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through preclinical studies and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials.
Furthermore, our ongoing and planned clinical trials will need to demonstrate sufficient safety and efficacy for approval by regulatory authorities in larger patient populations. Since the initiation of our Phase 1/1b clinical trial in January 2016, ciforadenant has been administered to more than 300 cancer patients and, while it has generally been well tolerated, there have been possibly drug-related or drug-related serious adverse events observed during the trial, and limited information is available concerning long-term safety and efficacy. It remains possible that patients enrolled in our Phase 1/1b clinical trial or our amended Phase 1b/2 clinical trial for ciforadenant could respond in unexpected ways. Our Phase 1/1b and our amended Phase 1b/2 clinical trial are conducted in patients with advanced cancers who have failed other approved therapies for their disease, and as such, it may be difficult to establish safety and efficacy in this type of patient population. Furthermore, a portion of our Phase 1/1b clinical trial, our amended Phase 1b/2 clinical trial and Genentech’s Phase 1b/2 clinical trial under our collaboration agreement, includes the administration of ciforadenant in combination with Genentech’s cancer immunotherapy, Tecentriq, which could exacerbate immune system related adverse events, cause increased toxicity or otherwise lead to unexpected adverse events. As a result, there can be no assurance that the results of historical clinical studies of ciforadenant conducted by third parties or the results of our clinical studies to-date will be indicative of the ongoing results of our Phase 1/1b clinical trial or amended Phase 1b/2 clinical trial, Genentech’s Phase 1b/2 clinical trial or any future clinical trial of ciforadenant.
In March 2018, we began enrolling patients in our Phase 1/1b trial evaluating CPI-006. The protocol is designed to enroll successive cohorts of patients with advanced cancers who will receive increasing doses of CPI-006 both alone, or in combination with ciforadenant or an anti-PD-1. CPI-006 has been well tolerated in the clinical trial at doses up to 18mg/kg, although a limited number of patients have been enrolled and the follow-up period has necessarily been short, and we have observed one patient with Grade 3 anemia. We have seen 1 patient develop Grade 3 hyponatremia at a dose of 24mg/kg. However, CD73 is involved in several physiological systems and the administration of anti-CD73 antibodies such as CPI-006 could result in unforeseen safety issues. Similar to our Phase 1/1b clinical trial of ciforadenant, it is possible that patients enrolled in our Phase 1/1b clinical trial for CPI-006 could respond in unexpected ways and that the administration of CPI-006 in combination with ciforadenant and pembrolizumab could exacerbate immune system related adverse events. As a result, there can be no assurance that we will be able to establish the safety and efficacy of CPI-006 or that we will be able to successfully complete our Phase 1/1b clinical trial.
In March 2019, we initiated a multi-center Phase 1/1b clinical trial evaluating CPI-818 in patients with various malignant T-cell lymphomas. Similar to our clinical trials of ciforadenant and CPI-006, it is possible that patients enrolled in our Phase 1/1b clinical trial for CPI-818 could respond in unexpected ways
For the foregoing reasons, we cannot be certain that our ongoing or planned clinical trials or any other future clinical trials will be successful. Any safety concerns observed in any one of our clinical trials in our targeted indications could limit the prospects for regulatory approval of our product candidates in those and other indications, which could have a material adverse effect on our business, financial condition and results of operations.
38
Any termination or suspension of, or delays in the commencement or completion of, our planned clinical trials could result in increased costs to us, delay or limit our ability to generate revenue and adversely affect our commercial prospects.
Before we can initiate clinical trials in the United States for any of our product and development candidates, we must submit the results of preclinical testing to the FDA along with other information, including information about product candidate chemistry, manufacturing and controls and our proposed clinical trial protocol, as part of an investigational new drug (“IND”) application. In addition, we may rely in part on preclinical, clinical and quality data generated by clinical research organizations (“CROs”) and other third parties for regulatory submissions for our product candidates. If these third parties do not make timely regulatory submissions for our product candidates, it will delay our plans for our clinical trials. If those third parties do not make this data available to us, we will likely have to develop all necessary preclinical and clinical data on our own, which will lead to significant delays and increase development costs of the product candidate. In addition, the FDA may require us to conduct additional preclinical testing for any product candidate before it allows us to initiate clinical testing under any IND, which may lead to additional delays and increase the costs of our preclinical development. Delays in the completion of our planned clinical trials for product candidates could significantly affect our product development costs.
While we initiated our Phase 1/1b trial for ciforadenant in January 2016, our Phase 1/1b trial for CPI-006 in March 2018, and our Phase 1/1b trial for CPI-818 in March 2019, we do not know whether any of our other planned trials will begin on time in the future or whether any of our trials will be completed on schedule, if at all. The commencement and completion of clinical trials can be delayed for a number of reasons, including delays related to:
|
· |
the FDA failing to grant permission to proceed or placing the clinical trial on hold; |
|
· |
subjects failing to enroll or remain in our trial at the rate we expect; |
|
· |
subjects choosing an alternative treatment for the indication for which we are developing ciforadenant, CPI-006, CPI-818 or other product candidates, or participating in competing clinical trials; |
|
· |
lack of adequate funding to continue the clinical trial; |
|
· |
subjects experiencing severe or unexpected drug-related adverse effects; |
|
· |
a facility manufacturing ciforadenant, CPI-006, CPI-818, any of our other product candidates or any of their components being ordered by the FDA or other regulatory authorities to temporarily or permanently shut down due to violations of good manufacturing practice (“cGMP”) regulations or other applicable requirements, or infections or cross-contaminations of product candidates in the manufacturing process; |
|
· |
any changes to our manufacturing process that may be necessary or desired; |
|
· |
any failure or delay in reaching an agreement with CROs and clinical trial sites; |
|
· |
third-party clinical investigators losing the licenses or permits necessary to perform our clinical trials, not performing our clinical trials on our anticipated schedule or consistent with the clinical trial protocol, good clinical practices (“GCP”) or regulatory requirements or other third parties not performing data collection or analysis in a timely or accurate manner; |
|
· |
third-party contractors becoming debarred or suspended or otherwise penalized by the FDA or other government or regulatory authorities for violations of regulatory requirements, in which case we may need to find a substitute contractor, and we may not be able to use some or all of the data produced by such contractors in support of our marketing applications; |
39
|
· |
one or more Institutional Review Boards (“IRBs”) refusing to approve, suspending or terminating the trial at an investigational site, precluding enrollment of additional subjects, or withdrawing its approval of the trial; or |
|
· |
patients failing to complete a trial or return for post-treatment follow-up. |
We could also encounter delays if a clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such trials are being conducted, by the Data Safety Monitoring Board for such trial or by the FDA or other regulatory authorities. Such authorities may impose such a suspension or termination due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. In addition, changes in regulatory requirements and policies may occur, and we may need to amend clinical trial protocols to comply with these changes. Amendments may require us to resubmit our clinical trial protocols to IRBs for reexamination, which may impact the costs, timing or successful completion of a clinical trial.
If we experience delays in the completion of, or termination of, any clinical trial of our product candidates, the commercial prospects of our product candidates will be harmed, and our ability to generate product revenues from any of these product candidates will be delayed. In addition, any delays in completing our clinical trials will increase our costs, slow down our product candidate development and approval process and jeopardize our ability to commence product sales and generate revenues. See also the risk factor below titled “If we encounter difficulties enrolling subjects in our clinical trials, our clinical development activities could be delayed or otherwise adversely affected.”
In addition, many of the factors that cause, or lead to, termination or suspension of, or a delay in the commencement or completion of, clinical trials may also ultimately lead to the denial of regulatory approval of a product candidate. For example, if we make manufacturing or formulation changes to our product candidates, we may need to conduct additional studies to bridge our modified product candidates to earlier versions. Further, if one or more clinical trials are delayed, our competitors may be able to bring products to market before we do, and the commercial viability of ciforadenant, CPI-006, CPI-818 or other product candidates could be significantly reduced. Any of these occurrences may harm our business, financial condition and prospects significantly.
|
1 Interim “top-line” and preliminary data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final data. |
From time to time, we may publicly disclose interim, top-line or preliminary data from our clinical trials, which is based on a preliminary analysis of then-available data, and the results and related findings and conclusions are subject to change following a more comprehensive review of the data related to the particular study or trial. We also make assumptions, estimations, calculations and conclusions as part of our analyses of data, and we may not have received or had the opportunity to fully and carefully evaluate all data. As a result, the top-line or preliminary results that we report may differ from future results of the same studies, or different conclusions or considerations may qualify such results, once additional data have been received and fully evaluated. Top-line or preliminary data also remain subject to audit and verification procedures that may result in the final data being materially different from the top-line or preliminary data we previously published. As a result, top-line and preliminary data should be viewed with caution until the final data are available.
From time to time, we may also disclose interim data from our preclinical studies and clinical trials. Interim data from clinical trials that we may complete are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data become available. Adverse differences between interim data and final data could significantly harm our business prospects. Further, disclosure of interim data by us or by our competitors could result in volatility in the price of our common stock after this offering.
40
Further, others, including regulatory agencies, may not accept or agree with our assumptions, estimates, calculations, conclusions or analyses or may interpret or weigh the importance of data differently, which could impact the value of the particular program, the approvability or commercialization of the particular product candidate or product and our company in general. In addition, the information we choose to publicly disclose regarding a particular study or clinical trial is based on what is typically extensive information, and you or others may not agree with what we determine is material or otherwise appropriate information to include in our disclosure.
If the interim, top-line or preliminary data that we report differ from actual results, or if others, including regulatory authorities, disagree with the conclusions reached, our ability to obtain approval for, and commercialize, our product candidates may be harmed, which could harm our business, operating results, prospects or financial condition.
Our product candidates are subject to extensive regulation, compliance with which is costly and time consuming, and such regulation may cause unanticipated delays or prevent the receipt of the required approvals to commercialize our product candidates.
The clinical development, manufacturing, labeling, storage, record-keeping, advertising, promotion, import, export, marketing and distribution of our product candidates are subject to extensive regulation by the FDA in the United States and by comparable authorities in foreign markets. In the United States, we are not permitted to market our product candidates until we receive regulatory approval from the FDA. The process of obtaining regulatory approval is expensive, often takes many years and can vary substantially based upon the type, complexity and novelty of the product candidates involved, as well as the target indications and patient population. Approval policies or regulations may change, and the FDA has substantial discretion in the drug approval process, including the ability to delay, limit or deny approval of a product candidate for many reasons. Despite the time and expense invested in clinical development of product candidates, regulatory approval is never guaranteed.
The FDA or comparable foreign regulatory authorities can delay, limit or deny approval of a product candidate for many reasons, including:
|
· |
such authorities may disagree with the design or implementation of our or any of our potential future collaborators’ clinical trials; |
|
· |
we or any of our potential future collaborators may be unable to demonstrate to the satisfaction of the FDA or other regulatory authorities that a product candidate is safe and effective for any indication; |
|
· |
such authorities may not accept clinical data from trials which are conducted at clinical facilities or in countries where the standard of care is potentially different from that of the United States; |
|
· |
we or any of our potential future collaborators may be unable to demonstrate that a product candidate’s clinical and other benefits outweigh its safety risks; |
|
· |
such authorities may disagree with our interpretation of data from preclinical studies or clinical trials; |
|
· |
approval may be granted only for indications that are significantly more limited than what we apply for and/or with other significant restrictions on distribution and use; |
|
· |
such authorities may find deficiencies in the manufacturing processes or facilities of third-party manufacturers with which we or any of our potential future collaborators contract for clinical and commercial supplies; or |
|
· |
the approval policies or regulations of such authorities may significantly change in a manner rendering our or any of our potential future collaborators’ clinical data insufficient for approval. |
41
With respect to foreign markets, approval procedures vary among countries and, in addition to the foregoing risks, may involve additional product testing, administrative review periods and agreements with pricing authorities. In addition, events raising questions about the safety of certain marketed pharmaceuticals may result in increased cautiousness by the FDA and comparable foreign regulatory authorities in reviewing new drugs based on safety, efficacy or other regulatory considerations and may result in significant delays in obtaining regulatory approvals. Any delay in obtaining, or inability to obtain, applicable regulatory approvals would prevent us or any of our potential future collaborators from commercializing our product candidates.
If we are required by the FDA to obtain approval of a companion diagnostic device in connection with approval of one of our product candidates, and we do not obtain or face delays in obtaining FDA approval of a companion diagnostic device, we will not be able to commercialize the product candidate and our ability to generate revenue will be materially impaired.
According to FDA guidance, if the FDA determines that a companion diagnostic device is essential to the safe and effective use of a novel therapeutic product or indication, the FDA generally will not approve the therapeutic product or new therapeutic product indication if the companion diagnostic is not also approved or cleared for that indication. We plan to collaborate with patient diagnostic companies during our clinical trial enrollment process to help identify patients with tumor gene alterations that we believe are most likely to respond to our product candidates. If a satisfactory companion diagnostic is not commercially available, we may be required to create or obtain one that would be subject to regulatory approval requirements. The process of obtaining or creating such diagnostic is time consuming and costly.
Companion diagnostics are developed in conjunction with clinical programs for the associated product and are subject to regulation as medical devices by the FDA and comparable foreign regulatory authorities, and, to date, the FDA has required premarket approval of all companion diagnostics for cancer therapies. Generally, when a companion diagnostic is essential to the safe and effective use of a therapeutic product, the FDA requires that the companion diagnostic be approved before or concurrent with approval of the therapeutic product and before a product can be commercialized. The approval of a companion diagnostic as part of the therapeutic product’s labeling limits the use of the therapeutic product to only those patients who express the specific genetic alteration that the companion diagnostic was developed to detect.
If the FDA or a comparable foreign regulatory authority requires approval of a companion diagnostic for any of our product candidates, whether before or after the product candidate obtains marketing approval, we and/ or third-party collaborators may encounter difficulties in developing and obtaining approval for these companion diagnostics. Any delay or failure by us or third-party collaborators to develop or obtain regulatory approval of a companion diagnostic could delay or prevent approval or continued marketing of our related product candidates. We may also experience delays in developing a sustainable, reproducible and scalable manufacturing process for the companion diagnostic or in transferring that process to commercial partners or negotiating insurance reimbursement plans, all of which may prevent us from completing our clinical trials or commercializing our product candidates, if approved, on a timely or profitable basis, if at all.
If we encounter difficulties enrolling subjects in our clinical trials, our clinical development activities could be delayed or otherwise adversely affected.
Subject enrollment, a significant factor in the timing of clinical trials, is affected by many factors including the size and nature of the patient population, the proximity of patients to clinical sites, the eligibility criteria for the trial, the design of the clinical trial, the risk that enrolled patients will not complete a clinical trial, our ability to recruit clinical trial investigators with the appropriate competencies and experience, competing clinical trials and clinicians’ and patients’ perceptions as to the potential advantages of the product candidate being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. We will be required to identify and enroll a sufficient number of subjects for each of our clinical trials. Potential subjects for any planned clinical trials may not be adequately diagnosed or identified with the diseases which we are targeting or may not meet the entry criteria for our studies. We also may encounter difficulties in identifying and enrolling subjects with a stage of disease appropriate for our planned clinical trials. We may not be able to initiate or continue clinical trials if we are
42
unable to locate a sufficient number of eligible subjects to participate in the clinical trials required by the FDA or other foreign regulatory agencies. In addition, the process of finding and diagnosing subjects may prove costly.
In our ongoing trial of ciforadenant, we have enrolled over 300 patients with many different types of cancer and the disease-specific cohorts for renal cell cancer and prostate cancer are continuing to enroll. We have also added patients with various cancers to investigate higher doses of our drug as part of a protocol amendment. Lung cancer patients are also in the follow-up phase in a Phase 1b/2 trial being conducted by Genentech under our collaboration agreement. We are also enrolling patients with many different types of cancer in our Phase 1/1b trial of CPI-006 and patients with many different types of T-cell lymphomas in our Phase 1/1b trial of CPI-818. If patients are unwilling to participate in our studies for any reason, including the existence of competitive clinical trials for similar patient populations, the availability of approved therapies or negative perceptions of the safety or efficacy of our product candidates, the timeline for recruiting subjects, conducting studies and obtaining regulatory approval of our product candidates may be delayed. Our inability to enroll a sufficient number of subjects for any of our future clinical trials would result in significant delays or may require us to abandon one or more clinical trials altogether.
We believe we have appropriately accounted for the above factors in our trials when determining expected clinical trial timelines, but we cannot assure our stockholders that our assumptions are correct or that we will not experience delays in enrollment, which would result in the delay of completion of such trials beyond our expected timelines.
The occurrence of serious complications or side effects in connection with use of our product candidates, either in clinical trials or post-approval, could lead to discontinuation of our clinical development programs, refusal of regulatory authorities to approve our product candidates or, post-approval, revocation of marketing authorizations or refusal to approve new indications, which could severely harm our business, prospects, operating results and financial condition.
During the conduct of clinical trials, patients report changes in their health, including illnesses, injuries and discomforts, to their study doctor. Often, it is not possible to determine whether or not the product candidate being studied caused these conditions. It is possible that as we test our product candidates in larger, longer and more extensive clinical programs with different dosing regimens and in combination with other immunotherapies, or as use of these product candidates becomes more widespread if they receive regulatory approval, illnesses, injuries, discomforts and other adverse events that were observed in earlier trials, as well as conditions that did not occur or went undetected in previous trials, will be reported by subjects. For example, possibly drug-related or drug-related serious adverse events have been observed during our Phase 1/1b clinical trial and our amended Phase 1b/2 clinical trial in patients receiving combination therapy with ciforadenant and Tecentriq include hemolytic anemia, encephalitis, hepatitis, pneumonitis, mucositis, myocarditis and dermatitis. Other toxicities observed during our Phase 1/1b clinical trial and our amended Phase 1b/2 clinical trial were mild and are commonly seen in patients with advanced cancers, such as nausea, vomiting, fatigue, rash, diarrhea, fever, abdominal pain, cough, constipation and decreased appetite. Other immune-oncology drugs also have been found occasionally to induce immune related toxicities such as colitis, hepatitis, pneumonitis, meningitis, myocarditis and various endocrine diseases. Such side effects could also be exacerbated when ciforadenant is administered in combination with Tecentriq which is provided for in a portion of our Phase 1/1b clinical trial and amended Phase 1b/2 clinical trial as well as in Genentech’s Phase 1b/2 clinical trial under our collaboration agreement, or when ciforadenant is administered in higher doses, which we added as part of a protocol amendment.
In March 2018, we began enrolling patients in our Phase 1/1b trial evaluating CPI-006. We have completed the dose escalation stage where patients receive CPI-006 alone and in combination with ciforadenant and we recently selected the recommended dose of 18 mg/kg and initiated the disease expansion phase in both the monotherapy and the combination arm with ciforadenant of our CPI-006 clinical trial. We are also enrolling patients in the dose escalation phase in the pembrolizumab combination arm of the trial. We expect that successive cohorts of enrolled patients will receive increasing doses of CPI-006 in combination with pembrolizumab or in combination with ciforadenant and pembrolizumab. To date, although only a limited number of patients have been enrolled and the follow-up period has been necessarily short, we have observed one patient with Grade 3 anemia. We have seen one patient develop Grade 3 hyponatremia at a dose of 24 mg/kg.
43
In March 2019, we initiated a multi-center Phase 1/1b clinical trial evaluating CPI-818 in patients with various malignant T-cell lymphomas. To date, a limited number of patients have been enrolled and, although no serious adverse events have been observed, the follow-up period has necessarily been short.
Many times side effects are only detectable after investigational products are tested in large-scale, Phase 3 clinical trials or, in some cases, after they are made available to patients on a commercial scale after approval. Results of our current clinical trials and any future clinical trials we undertake could reveal a high and unacceptable severity and prevalence of these or other side effects. In such an event, our trials could be suspended or terminated, and the FDA or comparable foreign regulatory authorities could order us to cease further development of or deny approval of our product candidates for any or all targeted indications. Drug-related side effects could affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition and prospects significantly.
In addition, if one or more of our product candidates receives marketing approval, and we or others later identify undesirable side effects caused by such products, a number of potentially significant negative consequences could result, including:
|
· |
regulatory authorities may withdraw approvals of such product; |
|
· |
regulatory authorities may require additional warnings on the label; |
|
· |
we may be required to create a medication guide outlining the risks of such side effects for distribution to patients; |
|
· |
we could be sued and held liable for harm caused to patients; and |
|
· |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate, if approved, and could significantly harm our business, results of operations and prospects.
We may not be successful in our efforts to identify or discover additional product candidates.
The success of our business depends primarily upon our ability to develop and commercialize ciforadenant, CPI-006 and CPI-818. Although ciforadenant, CPI-006 and CPI-818 are currently in clinical development, our research programs may fail to identify other potential product candidates, or advance them into and through clinical development for a number of reasons. Our research methodology may be unsuccessful in identifying other potential product candidates or our other potential product candidates may be shown to have harmful side effects or may have other characteristics that may make the products unmarketable or unlikely to receive marketing approval. It may also take greater human and financial resources to identify additional therapeutic opportunities for our product candidates or to develop suitable potential product candidates through our research programs than we will possess, thereby limiting our ability to diversify and expand our product candidate portfolio.
We are conducting clinical trials for ciforadenant, CPI-006 and CPI-818, and may in the future, conduct clinical trials of other product candidates, at sites outside the United States, and the FDA may not accept data from trials conducted in foreign locations.
We are currently conducting our clinical trial for ciforadenant at leading medical centers in the U.S., Australia and Canada. We are also conducting our clinical trials for CPI-006 in the U.S. and Australia and CPI-818 in the U.S., Australia and South Korea. In the future, we may add additional clinical sites outside of the United States in our clinical trials for ciforadenant, CPI-006 and CPI-818. Although the FDA may accept data from clinical trials conducted outside the United States, acceptance of this data is subject to certain conditions imposed by the FDA. For example, the clinical trial must be well designed and conducted in accordance with GCP requirements, and the FDA must be able to validate
44
the clinical trial data through an on-site inspection, if necessary. If a marketing application is based solely on foreign clinical data, the FDA also requires such data to be applicable to the U.S. population and U.S. medical practice, and for the clinical trials to have been performed by clinical investigators of recognized competence. There can be no assurance the FDA will accept data from trials conducted outside of the United States. If the FDA does not accept the data from our clinical trials for ciforadenant, CPI-006 and CPI-818, or any other product candidates, it would likely result in the need for additional trials, which would be costly and time-consuming and delay or permanently halt our development of ciforadenant, CPI-006, CPI-818 or any other product candidates.
Risks Related to Our Reliance on Third Parties
We rely, and expect to continue to rely, on third parties to conduct our clinical trials. If these third parties do not meet our deadlines or otherwise conduct the trials as required, our clinical development programs could be delayed or unsuccessful and we may not be able to obtain regulatory approval for or commercialize our product candidates when expected, or at all.
We do not have the ability to conduct all aspects of our preclinical testing or clinical trials ourselves. As a result, we are dependent on third parties to conduct our Phase 1/1b clinical trial and our amended Phase 1b/2 clinical trial for ciforadenant, our Phase 1/1b clinical trial for CPI-006, and our Phase 1/1b trial for CPI-818, and expect to continue to be dependent on third parties to conduct any future clinical studies of ciforadenant, CPI-006, CPI-818 and preclinical and clinical trials for our other product candidates. The timing of the initiation and completion of these trials will therefore be controlled by such third parties and may occur at times substantially different from our estimates. Specifically, we use and rely on medical institutions, clinical investigators, CROs and consultants to conduct our trials in accordance with our clinical protocols and regulatory requirements. Such CROs, investigators and other third parties play a significant role in the conduct of these trials and subsequent collection and analysis of data, and we will control only certain aspects of their activities. Nevertheless, we are responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol and legal, regulatory and scientific standards, and our reliance on the CROs and other third parties does not relieve us of our regulatory responsibilities. We and our CROs are required to comply with GCP requirements, which are regulations and guidelines enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area (“EEA”) and comparable foreign regulatory authorities for all of our product candidates in clinical development.
Regulatory authorities enforce these GCPs through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of our CROs or trial sites fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable, and the FDA, EMA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. In addition, our clinical trials must be conducted with product produced under cGMP regulations. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process.
There is no guarantee that any such CROs, investigators or other third parties will devote adequate time and resources to such trials or perform as contractually required. If any of these third parties fail to meet expected deadlines, adhere to our clinical protocols or meet regulatory requirements, or otherwise performs in a substandard manner, our clinical trials may be extended, delayed or terminated.
If any of our clinical trial sites terminates for any reason, we may experience the loss of follow-up information on subjects enrolled in such clinical trials unless we are able to transfer those subjects to another qualified clinical trial site, which may be difficult or impossible.
In addition, principal investigators for our clinical trials may serve as scientific advisors or consultants to us from time to time and may receive cash or equity compensation in connection with such services. If these relationships and any related compensation result in perceived or actual conflicts of interest, or the FDA concludes that the financial relationship may have affected the interpretation of the study, the integrity of the data generated at the applicable clinical trial site may be questioned and the utility of the clinical trial itself may be jeopardized, which could result in the delay or rejection of any NDA or BLA we submit by the FDA. Any such delay or rejection could prevent us from commercializing ciforadenant, CPI-006, CPI-818 or our other product candidates.
45
We rely on third parties to conduct some or all aspects of our manufacturing, research and preclinical and clinical testing, and these third parties may not perform satisfactorily.
We do not expect to independently conduct all aspects of our manufacturing, research and preclinical and clinical testing. We currently rely, and expect to continue to rely, on third parties with respect to these items. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our studies in accordance with regulatory requirements or our stated study plans and protocols, we may not be able to complete, or may be delayed in completing, the preclinical and clinical studies required to support future IND submissions and approval of our product candidates. Furthermore, any of these third parties may terminate its engagement with us at any time. If we need to enter into alternative arrangements, it could delay our product development activities, and we may not be able to negotiate alternative arrangements on commercially reasonable terms, or at all.
We and our contract manufacturers are subject to significant regulation with respect to manufacturing our products and the contract manufacturers on which we rely may not continue to meet regulatory requirements.
We do not currently have nor do we plan to acquire the infrastructure or internal capability to manufacture our clinical drug supplies for use in the conduct of our trials, and we lack the resources and the capability to manufacture any of our product candidates on a clinical or commercial scale. We currently rely on several different manufacturers who supply different parts of the ciforadenant and CPI-818 molecules, on one manufacturer for CPI-006 drug substance and on other third-party manufacturers to produce our other product candidates.
All entities involved in the preparation of therapeutics for clinical studies or commercial sale, including our existing contract manufacturers for our product candidates, are subject to extensive regulation. Components of a finished therapeutic product approved for commercial sale or used in late-stage clinical studies must be manufactured in accordance with cGMP requirements. These regulations govern manufacturing processes and procedures, including record keeping, and the implementation and operation of quality systems to control and assure the quality of investigational products and products approved for sale. Poor control of production processes can lead to the introduction of adventitious agents or other contaminants, or to inadvertent changes in the properties or stability of our product candidates that may not be detectable in final product testing. We or our contract manufacturers must supply all necessary documentation in support of an NDA or BLA on a timely basis and must adhere to the FDA’s Good Laboratory Practice regulations and cGMP regulations enforced by the FDA through its facilities inspection program. Our facilities and quality systems and the facilities and quality systems of some or all of our third-party contractors must pass a pre-approval inspection for compliance with the applicable regulations as a condition of regulatory approval of our product candidates or any of our other potential products. In addition, the regulatory authorities may, at any time, audit or inspect our manufacturing facilities or those of our third-party contractors involved with the preparation of our product candidates or the associated quality systems for compliance with the regulations applicable to the activities being conducted. We do not control the manufacturing process of, and are completely dependent on, our contract manufacturing partners for compliance with cGMPs.
The regulatory authorities also may, at any time following approval of a product for sale, audit the manufacturing facilities of our third-party contractors. If any such inspection or audit identifies a failure to comply with applicable regulations or if a violation of our product specifications or applicable regulations occurs independent of such an inspection or audit, we or the relevant regulatory authority may require remedial measures that may be costly and/or time-consuming for us or a third party to implement and that may include the temporary or permanent suspension of a clinical study or commercial sales or the temporary or permanent closure of a facility. Such violations could also result in civil and/or criminal penalties, and the FDA may impose regulatory sanctions including, among other things, refusal to approve a pending application for a new drug product or biologic product, revocation of a pre-existing approval or closing one or more manufacturing facilities.
In addition, if supply from an approved manufacturer is interrupted, there could be a significant disruption in commercial supply. An alternative manufacturer would need to be qualified through an NDA or BLA supplement which could result in further delay. The regulatory agencies may also require additional studies if a new manufacturer is relied upon for commercial production. Changing manufacturers may involve substantial costs and is likely to result in a delay in our desired clinical and commercial timelines.
46
We, or our third-party manufacturers, may be unable to successfully scale-up manufacturing of our product candidates in sufficient quality and quantity, which would delay or prevent us from developing our product candidates and commercializing approved products, if any.
In order to conduct clinical trials of our product candidates, we will need to manufacture them in large quantities. We, or any manufacturing partners, may be unable to successfully increase the manufacturing capacity for any of our product candidates in a timely or cost-effective manner, or at all. In addition, quality issues may arise during scale-up activities. If we or any manufacturing partners are unable to successfully scale up the manufacture of our product candidates in sufficient quality and quantity, the development, testing and clinical trials of that product candidate may be delayed or become infeasible, and regulatory approval or commercial launch of any resulting product may be delayed or not obtained, which could significantly harm our business.
In addition, the supply chain for the manufacturing of our product candidates is complicated and can involve several parties. If we were to experience any supply chain issues, our product supply could be seriously disrupted. We expect that the logistical challenges associated with our supply chain will grow more complex as we expand enrollment in our clinical trials for CPI-006 and CPI-818 and as we commence any clinical trials for additional product candidates.
Our reliance on third parties requires us to share our trade secrets, which increases the possibility that a competitor will discover them or that our trade secrets will be misappropriated or disclosed.
Because we rely on third parties to research and develop and to manufacture our product candidates, we must share trade secrets with them. We seek to protect our proprietary technology in part by entering into confidentiality agreements and, if applicable, material transfer agreements, consulting agreements or other similar agreements with our advisors, employees, third-party contractors and consultants prior to beginning research or disclosing proprietary information. These agreements typically limit the rights of the third parties to use or disclose our confidential information, including our trade secrets. Despite the contractual provisions employed when working with third parties, the need to share trade secrets and other confidential information increases the risk that such trade secrets become known by our competitors, are inadvertently incorporated into the technology of others, or are disclosed or used in violation of these agreements. Given that our proprietary position is based, in part, on our know-how and trade secrets, a competitor’s independent discovery of our trade secrets or other unauthorized use or disclosure would impair our competitive position and may have a material adverse effect on our business.
In addition, these agreements typically restrict the ability of our advisors, employees, third-party contractors and consultants to publish data potentially relating to our trade secrets, although our agreements may contain certain limited publication rights. For example, any academic institution that we may collaborate with in the future will likely expect to be granted rights to publish data arising out of such collaboration. In the future we may also conduct joint research and development programs that may require us to share trade secrets under the terms of our research and development or similar agreements. Despite our efforts to protect our trade secrets, our competitors may discover our trade secrets, either through breach of our agreements with third parties, independent development or publication of information by any of our third-party collaborators. A competitor’s discovery of our trade secrets would impair our competitive position and have an adverse impact on our business.
Risks Related to Commercialization of Our Product Candidates
If we are unable to commercialize our product candidates or if we experience significant delays in obtaining regulatory approval for, or commercializing, any or all of our product candidates, our business will be materially and adversely affected.
Our ability to generate product revenue will depend heavily on our ability to successfully develop and commercialize our product candidates. We do not expect that such commercialization of any of our product candidates
47
will occur for at least the next several years, if ever. Our ability to commercialize our product candidates effectively will depend on several factors, including the following:
|
· |
successful completion of preclinical studies and clinical trials, including the ability to demonstrate safety and efficacy of our product candidates; |
|
· |
managing the complexity of our clinical trial designs; |
|
· |
receipt of marketing approvals from the FDA and similar foreign regulatory authorities; |
|
· |
establishing commercial manufacturing capabilities by making arrangements with third-party manufacturers; |
|
· |
successfully launching commercial sales of any approved products, whether alone or in collaboration with others; |
|
· |
acceptance of any approved products by patients, the medical community and third-party payors; |
|
· |
establishing market share while competing with other therapies; |
|
· |
a continued acceptable safety profile of any approved products; |
|
· |
maintaining compliance with post-approval regulation and other requirements; and |
|
· |
qualifying for, identifying, registering, maintaining, enforcing and defending intellectual property rights and claims covering our product candidates. |
If we experience significant delays or an inability to commercialize our product candidates, our business, financial condition and results of operations will be materially adversely affected.
If we do not achieve our projected development goals in the time frames we announce and expect, the commercialization of our products may be delayed and, as a result, our stock price may decline.
We estimate the timing of the accomplishment of various scientific, clinical, regulatory and other product development goals, which we sometimes refer to as milestones. These milestones may include the commencement or completion of scientific studies and clinical trials and the submission of regulatory filings. From time to time, we may publicly announce the expected timing of some of these milestones. All of these milestones will be based on a variety of assumptions, and the actual timing of these milestones can vary dramatically compared to our estimates, in some cases for reasons beyond our control. If we do not meet these milestones as publicly announced, the commercialization of our products may be delayed and, as a result, our stock price may decline.
Any approved products could be subject to restrictions or withdrawal from the market, and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with our product candidates, when and if any of them are approved.
Following potential approval of any of our product candidates, the FDA may impose significant restrictions on a product’s indicated uses or marketing or impose ongoing requirements for potentially costly and time consuming post-approval studies, post-market surveillance or clinical trials. Following approval, if any, of ciforadenant, CPI-006, CPI-818 or any other product candidate, such candidate will also be subject to ongoing FDA requirements governing the labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, recordkeeping and reporting of safety and other post-market information. If we or a regulatory agency discovers previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is
48
manufactured, a regulatory agency may impose restrictions on that product, the manufacturing facility or us, including requesting recall or withdrawal of the product from the market or suspension of manufacturing.
If we or the manufacturing facilities for ciforadenant, CPI-006, CPI-818 or any other product candidate that may receive regulatory approval, if any, fail to comply with applicable regulatory requirements, a regulatory agency may:
|
· |
issue warning letters or untitled letters; |
|
· |
seek an injunction or impose civil or criminal penalties or monetary fines; |
|
· |
suspend or withdraw regulatory approval; |
|
· |
suspend any ongoing clinical trials; |
|
· |
refuse to approve pending applications or supplements or applications filed by us; |
|
· |
suspend or impose restrictions on operations, including costly new manufacturing requirements; or |
|
· |
seize or detain products, refuse to permit the import or export of product or request that we initiate a product recall. |
The occurrence of any event or penalty described above may inhibit our ability to commercialize our product candidates and generate revenue.
The FDA has the authority to require a risk evaluation and mitigation strategy (“REMS”) as part of an NDA or BLA or after approval, which may impose further requirements or restrictions on the distribution or use of an approved drug, such as limiting prescribing to certain physicians or medical centers that have undergone specialized training, limiting treatment to patients who meet certain safe-use criteria and requiring treated patients to enroll in a registry.
In addition, if ciforadenant, CPI-006, CPI-818 or any of our other product candidates is approved, our product labeling, advertising and promotion will be subject to regulatory requirements and continuing regulatory review. The FDA strictly regulates the promotional claims that may be made about prescription products. In particular, a product may not be promoted for uses that are not approved by the FDA as reflected in the product’s approved labeling. If we receive marketing approval for a product candidate, physicians may nevertheless prescribe it to their patients in a manner that is inconsistent with the approved label. If we are found to have promoted such off-label uses, we may become subject to significant liability. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant sanctions. The federal government has levied large civil and criminal fines against companies for alleged improper promotion and has enjoined several companies from engaging in off-label promotion. The FDA has also requested that companies enter into consent decrees or permanent injunctions under which specified promotional conduct is changed or curtailed.
Any government investigation of alleged violations of law could require us to expend significant time and resources in response, and could generate negative publicity. Any failure to comply with ongoing regulatory requirements may significantly and adversely affect our ability to commercialize our product candidates.
Further, the FDA’s policies may change and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our product candidates. If we are slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose any marketing approval that we may have obtained, which would adversely affect our business, prospects and ability to achieve or sustain profitability.
49
We also cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative or executive action, either in the United States or abroad. For example, certain policies of the Trump administration may impact our business and industry. Namely, the Trump administration has taken several executive actions, including the issuance of a number of Executive Orders, that could impose significant burdens on, or otherwise materially delay, FDA’s ability to engage in routine regulatory and oversight activities such as implementing statutes through rulemaking, issuance of guidance, and review and approval of marketing applications. It is difficult to predict how these Executive Orders will be implemented, and the extent to which they will impact the FDA’s ability to exercise its regulatory authority. If these executive actions impose constraints on FDA’s ability to engage in oversight and implementation activities in the normal course, our business may be negatively impacted.
Changes in funding for the FDA and other government agencies could hinder their ability to hire and retain key leadership and other personnel, or otherwise prevent new products and services from being developed or commercialized in a timely manner, which could negatively impact our business.
The ability of the FDA to review and approve new products can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, and statutory, regulatory, and policy changes. Average review times at the agency have fluctuated in recent years as a result. In addition, government funding of other government agencies that fund research and development activities is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other agencies may also slow the time necessary for new drugs to be reviewed and/or approved by necessary government agencies, which would adversely affect our business. For example, over the last several years, including from December 2018 into January 2019, the U.S. government has shut down several times and certain regulatory agencies, such as the FDA, have had to furlough critical FDA employees and stop critical activities. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business.
Even if we receive regulatory approval we still may not be able to successfully commercialize ciforadenant, CPI-006, CPI-818 or any other product candidate, and the revenue that we generate from sales, if any, could be limited.
Even if ciforadenant, CPI-006, CPI-818 or any of our other product candidates receive regulatory approval, they may not gain market acceptance among physicians, patients, healthcare payors or the medical community. The degree of market acceptance of our product candidates will depend on a number of factors, including:
|
· |
demonstration of clinical efficacy and safety compared to other more-established products; |
|
· |
the indications for which our product candidates are approved; |
|
· |
the limitation of our targeted patient population and other limitations or warnings contained in any FDA-approved labeling; |
|
· |
acceptance of a new formulation by healthcare providers and their patients; |
|
· |
our ability to obtain and maintain sufficient third-party coverage and reimbursement from government healthcare programs, including Medicare and Medicaid, private health insurers and other third-party payors; |
|
· |
the willingness of patients to pay out-of-pocket in the absence of third-party coverage and reimbursement; |
|
· |
the prevalence and severity of any adverse effects; |
50
|
· |
pricing and cost-effectiveness; |
|
· |
the timing of market introduction of our product candidates as well as competitive drugs; |
|
· |
the effectiveness of our or any of our potential future collaborators’ sales and marketing strategies; and |
|
· |
unfavorable publicity relating to the product candidate |
If any product candidate is approved but does not achieve an adequate level of acceptance by physicians, hospitals, healthcare payors or patients, we may not generate sufficient revenue from that product candidate and may not become or remain profitable. Our efforts to educate the medical community and third-party payors regarding the benefits of ciforadenant, CPI-006, CPI-818 or any of our other product candidates may require significant resources and may never be successful.
Failure to obtain or maintain adequate coverage and reimbursement for our product candidates, if approved, could limit our ability to market those products and decrease our ability to generate revenue.
Successful commercial sales of any approved products will depend on the availability of adequate coverage and reimbursement from government health administration authorities, private health insurers and other third-party payors. Each third-party payor separately decides which products it will cover and establishes the reimbursement level, and there is no guarantee that any of our product candidates that may be approved for marketing by regulatory authorities will receive adequate coverage or reimbursement levels. Obtaining and maintaining coverage approval for a product candidate is time-consuming, costly and may be difficult. We may be required to conduct expensive pharmacoeconomic studies to justify coverage and reimbursement or the level of coverage and reimbursement relative to other therapies. If coverage and adequate reimbursement are not available or limited, we may not be able to successfully commercialize any product candidate for which we obtain marketing approval. Government authorities and third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for drugs and biologics. Even if we obtain coverage for a given product, the resulting reimbursement rates may be inadequate and may affect the demand for, or the price of, any product candidate for which we obtain marketing approval.
Recently enacted legislation, future legislation and healthcare reform measures may increase the difficulty and cost for us to obtain marketing approval for and commercialize our product candidates and affect the prices we may obtain.
In the United States and some foreign jurisdictions, there have been, and we expect there will continue to be, a number of legislative and regulatory changes to the healthcare system, including cost-containment measures that may reduce or limit coverage and reimbursement for newly approved drugs and biologics and affect our ability to profitably sell any product candidates for which we obtain marketing approval.
For example, in March 2010, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively referred to as the Affordable Care Act, was enacted with a goal of reducing the cost of healthcare and substantially changing the way healthcare is financed by both governmental and private insurers. The Affordable Care Act, among other things, subjected biological products to potential competition by lower-cost biosimilars; addressed a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected; increased the minimum Medicaid rebates owed by manufacturers under the Medicaid Drug Rebate Program; extended the rebate program to individuals enrolled in Medicaid managed care organizations; established annual fees and taxes on manufacturers of certain prescription drugs; created a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D; and established a new Patient-Centered Outcomes Research Institute to oversee, identify priorities and conduct comparative clinical effectiveness research, along with funding for such research.
51
Since its enactment, there have been judicial and Congressional challenges to certain aspects of the Affordable Care Act, and we expect there will be additional challenges and amendments to the Affordable Care Act in the future. The current Presidential Administration and U.S. Congress has sought and will likely continue to seek to modify, repeal, or otherwise invalidate all, or certain provisions of, the Affordable Care Act. For example, the Tax Cuts and Jobs Act was enacted, which, among other things, removes penalties for not complying with the Affordable Care Act’s individual mandate to carry health insurance. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas, ruled that the individual mandate is a critical and inseverable feature of the ACA, and therefore, because it was repealed as part of the Tax Act, the remaining provisions of the ACA are invalid as well. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit upheld the District Court's decision that the individual mandate was unconstitutional but remanded the case back to the District Court to determine whether the remaining provisions of the Affordable Care Act are invalid as well. It is unclear how these decisions, subsequent appeals, and other efforts to challenge, replace, modify, repeal, or otherwise invalidate the Affordable Care Act will impact the Act or our business. There may be additional challenges and amendments to the ACA in the future, and it is uncertain the extent to which any such changes may impact our business or financial condition.
In addition, other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. These new laws, among other things, included aggregate reductions of Medicare payments to providers of 2% per fiscal year that will remain in effect through 2029 unless additional Congressional action is taken and additional specific reductions in Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers. Recently there has been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, reform government program reimbursement methodologies. Additionally, individual states in the United States have also become increasingly active in passing legislation and implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
We expect that the Affordable Care Act, these new laws and other healthcare reform measures that may be adopted in the future may result in additional reductions in Medicare and other healthcare funding, more rigorous coverage criteria, new payment methodologies and additional downward pressure on the price that we receive for any approved product. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability or commercialize our product candidates, if approved.
In the European Union, similar political, economic and regulatory developments may affect our ability to profitably commercialize our product candidates, if approved. In addition to continuing pressure on prices and cost containment measures, legislative developments at the European Union or member state level may result in significant additional requirements or obstacles that may increase our operating costs. The delivery of healthcare in the European Union, including the establishment and operation of health services and the pricing and reimbursement of medicines, is almost exclusively a matter for national, rather than European Union, law and policy. National governments and health service providers have different priorities and approaches to the delivery of health care and the pricing and reimbursement of products in that context. In general, however, the healthcare budgetary constraints in most European Union member states have resulted in restrictions on the pricing and reimbursement of medicines by relevant health service providers. Coupled with ever-increasing European Union and national regulatory burdens on those wishing to develop and market products, this could prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities and affect our ability to commercialize our product candidates, if approved. In markets outside of the United States and European Union, reimbursement and healthcare payment systems vary significantly by country, and many countries have instituted price ceilings on specific products and therapies.
We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action in the United States, the European Union or any other jurisdiction. If we or any third parties we may engage are slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we or such third parties are not able to maintain regulatory compliance, our product
52
candidates may lose any regulatory approval that may have been obtained and we may not achieve or sustain profitability.
Any product candidates for which we intend to seek approval as biologic products may face competition sooner than anticipated.
The Affordable Care Act includes a subtitle called the Biologics Price Competition and Innovation Act of 2009 (“BPCIA”), which created an abbreviated approval pathway for biological products that are biosimilar to or interchangeable with an FDA-licensed reference biological product. Under the BPCIA, an application for a biosimilar product may not be submitted to the FDA until four years following the date that the reference product was first licensed by the FDA. In addition, the approval of a biosimilar product may not be made effective by the FDA until twelve years from the date on which the reference product was first licensed. During this twelve-year period of exclusivity, another company may still market a competing version of the reference product if the FDA approves a full BLA for the competing product containing the sponsor’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of its product. The law is complex and is still being interpreted and implemented by the FDA. Any processes adopted by the FDA to implement the BPCIA could have a material adverse effect on the future commercial prospects for our biological products.
Though ciforadenant and CPI-818 are small molecules and will not be regulated as biological products, CPI-006, which we have begun evaluating in a Phase 1/1b clinical trial, is a biological product. We believe that any of our future product candidates approved as a biological product under a BLA should qualify for the twelve-year period of exclusivity. However, there is a risk that this exclusivity could be shortened due to Congressional action or otherwise, or that the FDA will not consider our product candidates to be reference products for competing products, potentially creating the opportunity for generic competition sooner than anticipated. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. Moreover, the extent to which a biosimilar, once approved, could be substituted for any one of our reference products in a way that is similar to traditional generic substitution for non-biological products will depend on a number of marketplace and regulatory factors that are still developing.
We may fail to obtain orphan drug designations from the FDA for our product candidates, and even if we obtain such designations, we may be unable to maintain the benefits associated with orphan drug designation, including the potential for market exclusivity.
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug or biologic intended to treat a rare disease or condition, which is defined as one occurring in a patient population of fewer than 200,000 in the United States, or a patient population greater than 200,000 in the United States where there is no reasonable expectation that the cost of developing the drug or biologic will be recovered from sales in the United States. In the United States, orphan drug designation entitles a party to financial incentives such as opportunities for grant funding towards clinical trial costs, tax advantages and user-fee waivers. In addition, if a product that has orphan drug designation subsequently receives the first FDA approval for the disease for which it has such designation, the product is entitled to orphan drug exclusivity, which means that the FDA may not approve any other applications, including a full NDA or BLA, to market the same drug or biologic for the same indication for seven years, except in limited circumstances, such as a showing of clinical superiority to the product with orphan drug exclusivity or where the manufacturer is unable to assure sufficient product quantity.
While we have not obtained nor have we sought to obtain orphan designation for any product candidate, we believe many of the potential indications of our product candidates, if approved, could qualify for orphan drug designation. For instance, if ciforadenant, CPI-006 or CPI-818 is approved for the treatment of certain solid tumors with small patient populations, such as melanoma, renal or triple-negative breast cancer, it is possible that it could qualify for orphan drug designation with respect to such indications. As a result, we may seek to obtain orphan drug designation for our product candidates for any qualifying indications they may be approved for in the future. Even if we obtain such designations, we may not be the first to obtain marketing approval of our product candidate for the orphan-designated indication due to the uncertainties associated with developing pharmaceutical products. In addition, exclusive marketing rights in the United States may be limited if we seek approval for an indication broader than the orphan-designated
53
indication or may be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantities of the product to meet the needs of patients with the rare disease or condition. Further, even if we obtain orphan drug exclusivity for a product, that exclusivity may not effectively protect the product from competition because different drugs with different active moieties can be approved for the same condition. Even after an orphan product is approved, the FDA can subsequently approve the same drug with the same active moiety for the same condition if the FDA concludes that the later drug is safer, more effective or makes a major contribution to patient care. Orphan drug designation neither shortens the development time or regulatory review time of a drug, nor gives the drug any advantage in the regulatory review or approval process. In addition, while we may seek orphan drug designation for our product candidates, we may never receive such designations.
We may expend our limited resources to pursue a particular product candidate and fail to capitalize on product candidates that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and managerial resources, we focus on specific product candidates, including ciforadenant, CPI-006 and CPI-818. As a result, we may forgo or delay pursuit of opportunities with other product candidates that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on current and future research and development programs and product candidates for specific indications may not yield any commercially viable product candidates. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such product candidate.
We may not be successful in establishing and maintaining development or other strategic collaborations, which could adversely affect our ability to develop and commercialize product candidates.
In connection with our Phase 1/1b clinical trial for ciforadenant, we entered into a clinical trial collaboration agreement with Genentech in October 2015. Pursuant to the agreement, Genentech provides access to, and supplies of, its cancer immunotherapy, Tecentriq, to be used in combination with ciforadenant during the clinical trial. The collaboration operates under a joint development committee with equal representation from both companies. In May 2017, we signed a second clinical trial collaboration agreement with Genentech. Under this second agreement, ciforadenant administered in combination with Tecentriq is being evaluated in a Phase 1b/2 randomized, controlled clinical study as second-line therapy in patients with non-small cell lung cancer who are resistant and/or refractory to prior therapy with an anti-PD-(L)1 antibody. However, we and Genentech each have the right to terminate the respective collaboration agreements due to material breach by either party, for safety considerations, if directed by a regulatory authority or if development of ciforadenant or Tecentriq is discontinued. If we fail to maintain these strategic collaborations with Genentech (1) the development of ciforadenant in combination with Tecentriq may be terminated or delayed; (2) our cash expenditures related to development of ciforadenant could increase significantly, and we may need to seek additional financing; (3) we may be required to hire additional employees or otherwise develop expertise for which we have not budgeted; (4) we will bear all of the risk related to the development of ciforadenant as a combination therapy; and (5) we will need to seek collaborations with other companies that have anti-PD-1 or anti-PD-L1 antibodies, which will significantly delay our development program and could have a material adverse effect on our business, financial condition and results of operations.
We may form strategic alliances and collaborative partnerships in the future, and we may not realize the benefits of such alliances.
In addition to our collaboration agreements with Genentech, we may form additional strategic alliances, create joint ventures or collaborations or enter into licensing arrangements with third parties that we believe will complement or augment our existing business, including for the continued development or commercialization of our product candidates. These relationships may result in or include non-recurring and other charges, increased near- and long-term expenditures, the issuance of securities that dilute our existing stockholders or disruptions to our management and business. In addition, we face significant competition in seeking appropriate strategic partners, and the negotiation process is time-consuming and complex. Moreover, we may not be successful in our efforts to establish a strategic
54
partnership or other alternative arrangements for our product candidates because third parties may view the risk of failure in future clinical trials as too significant or the commercial opportunity for our product candidates as too limited. We cannot be certain that, following a strategic transaction or license, we will achieve the revenue or specific net income that justifies such transaction.
Even if we are successful in our efforts to establish strategic alliances or collaborative partnerships, the terms that we agree upon may not be favorable to us, and we may not be able to maintain such strategic alliances or collaborative partnerships if, for example, development or approval of a product candidate is delayed, the safety of a product candidate is questioned or sales of an approved product candidate are unsatisfactory. In addition, any potential future strategic alliances or collaborative partnerships may be terminable by our strategic partners, and we may not be able to adequately protect our rights under these agreements. Furthermore, strategic partners may negotiate for certain rights to control decisions regarding the development and commercialization of our product candidates, if approved, and may not conduct those activities in the same manner as we do. Any termination of strategic alliances or collaborative partnerships we enter into in the future, or any delay in entering into collaborative partnership agreements related to our product candidates, could delay the development and commercialization of our product candidates and reduce their competitiveness if they reach the market, which could have a material adverse effect on our business, financial condition and results of operations.
We face competition from entities that have developed or may develop product candidates for cancer, including companies developing novel treatments and technology platforms. If these companies develop technologies or product candidates more rapidly than we do or their technologies are more effective, our ability to develop and successfully commercialize product candidates may be adversely affected.
Our competitors have developed, are developing or will develop product candidates and processes competitive with our product candidates. Competitive therapeutic treatments include those that have already been approved and accepted by the medical community and any new treatments that enter the market. We believe that a significant number of products are currently under development, and may become commercially available in the future, for the treatment of conditions for which we may attempt to develop product candidates. In particular, there is intense and rapidly evolving competition in the immunoregulatory therapeutics field. Our competitors include larger and better funded pharmaceutical, biopharmaceutical, biotechnological and therapeutics companies. Moreover, we also compete with universities and other research institutions that may be active in oncology research and could be in direct competition with us. We also compete with these organizations to recruit management, scientists and clinical development personnel, which could negatively affect our level of expertise and our ability to execute our business plan. We will also face competition in establishing clinical trial sites, registering subjects for clinical trials and in identifying and in-licensing new product candidates. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
Kyowa Hakko Kirin has approval in Japan and the US for istradefylline, an A2A antagonist, in Parkinson’s disease. Within oncology, Novartis has announced an exclusive licensing agreement with Palobiofarma SL and is conducting a Phase 1 trial with an A2A antagonist. AstraZeneca plc is conducting clinical trials with an A2A antagonist for use in cancer therapy. Merck KgaA has entered into a pre-clinical collaboration with Domain Therapeutics Inc. to develop programs targeting the adenosine pathway. In addition, Redoxtherapies, Inc., which was acquired by Juno Therapeutics and subsequently by Celgene, and Arcus Biosciences, Inc. are developing A2A receptor antagonists for cancer. Astra Zeneca, Bristol-Myers Squib, and Novartis in partnership with Surface Oncology, Inc. have initiated clinical trials with anti-CD73 antibodies in cancer patients. More generally, in the field of immuno-oncology, there are large pharmaceutical companies with approved products or products in late-stage development that target other immune checkpoints, including PD-1, PD-L1 or CTLA-4. These companies include Bristol-Myers Squibb (nivolumab, ipilimumab), Merck (pembrolizumab), Genentech (atezolizumab) and AstraZeneca (durvalumab, tremelimumab). Janssen Pharmaceuticals, Inc. and AbbVie Inc. are co-marketing Imbruvica (ibrutinib), which is a small molecule inhibitor of the kinase BTK that has also been reported to inhibit ITK.
Many of our competitors have significantly greater financial, technical, manufacturing, marketing, sales and supply resources or experience than we do. If we successfully obtain approval for any product candidate, we will face competition based on many different factors, including the safety and effectiveness of our products, the ease with which
55
our products can be administered and the extent to which patients accept relatively new routes of administration, the timing and scope of regulatory approvals for these products, the availability and cost of manufacturing, marketing and sales capabilities, price, reimbursement coverage and patent position. Competing products could present superior treatment alternatives, including by being more effective, safer, less expensive or marketed and sold more effectively than any products we may develop. Competitive products may make any products we develop obsolete or noncompetitive before we recover the expense of developing and commercializing our product candidates.
The market opportunities for our product candidates may be limited to those patients who are ineligible for or have failed prior treatments and may be small.
Cancer therapies are sometimes characterized as first-line, second-line or third-line, and the FDA often approves new therapies initially only for third-line use. When cancer is detected early enough, first line therapy is sometimes adequate to cure the cancer or prolong life without a cure. Whenever first-line therapy, usually chemotherapy, hormone therapy, surgery or a combination of these, proves unsuccessful, second-line therapy may be administered. Second-line therapies often consist of more chemotherapy, radiation, antibody drugs, tumor targeted small molecules or a combination of these. Third-line therapies can include bone marrow transplantation, antibody and small molecule targeted therapies, more invasive forms of surgery and new technologies. In markets with approved therapies, we expect to initially seek approval of our product candidates as a later stage therapy for patients who have failed other approved treatments. Subsequently, for those drugs that prove to be sufficiently beneficial, if any, we would expect to seek approval as a second-line therapy and potentially as a first-line therapy, but there is no guarantee that our product candidates, even if approved, would be approved for second-line or first-line therapy. In addition, we may have to conduct additional clinical trials prior to gaining approval for second-line or first-line therapy.
Our projections of both the number of people who have the cancers we are targeting, as well as the subset of people with these cancers in a position to receive later stage therapy and who have the potential to benefit from treatment with our product candidates, are based on our beliefs and estimates. These estimates have been derived from a variety of sources, including scientific literature, surveys of clinics, patient foundations or market research and may prove to be incorrect. Further, new studies may change the estimated incidence or prevalence of these cancers. The number of patients may turn out to be lower than expected. In addition, the potentially addressable patient population for our product candidates may be limited or may not be amenable to treatment with our product candidates. Even if we obtain significant market share for our product candidates, we may never achieve profitability without obtaining regulatory approval for additional indications, including use as a first or second-line therapy.
We have no sales, marketing or distribution capabilities, and we may have to invest significant resources to develop these capabilities.
We have no internal sales, marketing or distribution capabilities. If ciforadenant, CPI-006, CPI-818 or any of our other product candidates ultimately receives regulatory approval, we may not be able to effectively market and distribute the product candidate. We may have to seek collaborators or invest significant amounts of financial and management resources to develop internal sales, distribution and marketing capabilities, some of which will be committed prior to any confirmation that ciforadenant, CPI-006, CPI-818 or any of our other product candidates will be approved, if at all. We may not be able to enter into collaborations or hire consultants or external service providers to assist us in sales, marketing and distribution functions on acceptable financial terms or at all. Even if we determine to perform sales, marketing and distribution functions ourselves, we could face a number of additional related risks, including:
|
· |
we may not be able to attract and build an effective marketing department or sales force; |
|
· |
the cost of establishing a marketing department or sales force may exceed our available financial resources and the revenue generated by ciforadenant, CPI-006, CPI-818 or any other product candidates that we may develop, in-license or acquire; and |
|
· |
our direct sales and marketing efforts may not be successful. |
56
Our future growth may depend, in part, on our ability to operate in foreign markets, where we would be subject to additional regulatory burdens and other risks and uncertainties.
Our future growth may depend, in part, on our ability to develop and commercialize our product candidates in foreign markets. We are not permitted to market or promote any of our product candidates before we receive regulatory approval from applicable regulatory authorities in foreign markets, and we may never receive such regulatory approvals for any of our product candidates. To obtain separate regulatory approval in many other countries we must comply with numerous and varying regulatory requirements regarding safety and efficacy and governing, among other things, clinical trials, commercial sales, pricing and distribution of our product candidates. If we obtain regulatory approval of our product candidates and ultimately commercialize our product candidates in foreign markets, we would be subject to additional risks and uncertainties, including the burden of complying with complex and changing foreign regulatory, tax, accounting and legal requirements and the reduced protection of intellectual property rights in some foreign countries.
Governments may impose price controls, which may adversely affect our future profitability.
We intend to seek approval to market our product candidates in both the United States and in foreign jurisdictions. In some foreign countries, particularly in the European Union, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a product candidate. To obtain reimbursement or pricing approval in some countries, we may be required to conduct clinical trials to compare the cost-effectiveness of our product candidates to other available therapies, which is time-consuming and costly. If reimbursement of our future products is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, we may be unable to achieve or sustain profitability.
Recent U.S. tax legislation and future changes to applicable U.S. or foreign tax laws and regulations may have a material adverse effect on our business, financial condition and results of operations.
We are subject to income and other taxes in the U.S. and foreign jurisdictions. Changes in laws and policy relating to taxes or trade may have an adverse effect on our business, financial condition and results of operations. For example, the U.S. government recently enacted significant tax reform, and certain provisions of the new law may adversely affect us. Changes include, but are not limited to, a federal corporate tax rate decrease from 34% to 21% for tax years beginning after December 31, 2017, the transition of U.S. international taxation from a worldwide tax system to a more generally territorial system, and a one-time transition tax on the mandatory deemed repatriation of foreign earnings. The legislation is unclear in many respects and could be subject to potential amendments and technical corrections, and will be subject to interpretations and implementing regulations by the Treasury and Internal Revenue Service, any of which could mitigate or increase certain adverse effects of the legislation. In addition, it is unclear how these U.S. federal income tax changes will affect state and local taxation. Generally, future changes in applicable U.S. or foreign tax laws and regulations, or their interpretation and application could have an adverse effect on our business, financial conditions and results of operations.
Risks Related to Our Business Operations
Our operating results may fluctuate significantly, which makes our future operating results difficult to predict and could cause our operating results to fall below expectations or any guidance we may provide.
Our quarterly and annual operating results may fluctuate significantly, which makes it difficult for us to predict our future operating results. These fluctuations may occur due to a variety of factors, many of which are outside of our control, including, but not limited to:
|
· |
the timing and cost of, and level of investment in, research, development and commercialization activities relating to our product candidates, which may change from time to time; |
|
· |
coverage and reimbursement policies with respect to our product candidates, if approved, and potential future drugs that compete with our product candidates; |
57
|
· |
the cost of manufacturing our product candidates, which may vary depending on the quantity of production and the terms of our agreements with manufacturers; |
|
· |
expenditures that we may incur to acquire, develop or commercialize additional product candidates and technologies; |
|
· |
the level of demand for any approved products, which may vary significantly; |
|
· |
future accounting pronouncements or changes in our accounting policies; and |
|
· |
the timing and success or failure of clinical trials for our product candidates or competing product candidates, or any other change in the competitive landscape of our industry, including consolidation among our competitors or partners. |
The cumulative effects of these factors could result in large fluctuations and unpredictability in our quarterly and annual operating results. As a result, comparing our operating results on a period-to-period basis may not be meaningful. Investors should not rely on our past results as an indication of our future performance.
This variability and unpredictability could also result in our failing to meet the expectations of industry or financial analysts or investors for any period. If our revenue or operating results fall below the expectations of analysts or investors or below any forecasts we may provide to the market, or if the forecasts we provide to the market are below the expectations of analysts or investors, the price of our common stock could decline substantially. Such a stock price decline could occur even when we have met any previously publicly stated revenue or earnings guidance we may provide.
We are dependent on the services of our President and Chief Executive Officer, Richard A. Miller, M.D., and other key executives, and if we are not able to retain these members of our management or recruit additional management, clinical and scientific personnel, our business will suffer.
We are dependent on the principal members of our management and scientific staff. The loss of service of any of our management could harm our business. In addition, we are dependent on our continued ability to attract, retain and motivate highly qualified management, clinical and scientific personnel. If we are not able to retain our management, particularly our President and Chief Executive Officer, Dr. Miller, and to attract, on acceptable terms, additional qualified personnel necessary for the continued development of our business, we may not be able to sustain our operations or grow. Although we have executed employment agreements with each member of our current executive management team, including Dr. Miller, these agreements are terminable at will with or without notice and, therefore, we may not be able to retain their services as expected.
We will need to expand and effectively manage our managerial, operational, financial and other resources in order to successfully pursue our clinical development and commercialization efforts. We may not be able to attract or retain qualified management and scientific and clinical personnel in the future due to the intense competition for qualified personnel among pharmaceutical, biotechnology and other businesses, particularly in the San Francisco Bay Area. Our industry has experienced a high rate of turnover of management personnel in recent years. If we are not able to attract, integrate, retain and motivate necessary personnel to accomplish our business objectives, we may experience constraints that will significantly impede the achievement of our development objectives, our ability to raise additional capital and our ability to implement our business strategy.
In addition, we do not currently maintain “key person” life insurance on the lives of our executives or any of our employees. This lack of insurance means that we may not have adequate compensation for the loss of the services of these individuals.
58
We may encounter difficulties in managing our growth and expanding our operations successfully.
We will need to grow our organization substantially to continue development and pursue the potential commercialization of ciforadenant, CPI-006, CPI-818 and our other product candidates. As we seek to advance ciforadenant, CPI-006, CPI-818 and other product candidates, we will need to expand our financial, development, regulatory, manufacturing, marketing and sales capabilities or contract with third parties to provide these capabilities for us. As our operations expand, we expect that we will need to manage additional relationships with various strategic partners, suppliers and other third parties. Our future financial performance and our ability to commercialize our product candidates and to compete effectively will depend, in part, on our ability to manage any future growth effectively.
We are subject to various federal and state healthcare laws and regulations, and our failure to comply with these laws and regulations could harm our results of operations and financial condition.
Although we do not currently have any products on the market, if we obtain FDA approval for any of our product candidates and begin commercializing those products in the United States, our operations may be directly, or indirectly through our customers and third-party payors, subject to various U.S. federal and state healthcare laws and regulations. These laws will affect our operations, sales and marketing practices, and our relationships with physicians and other customers and third-party payors. Such laws include:
|
· |
the federal Anti-Kickback Statute, which prohibits, among other things, persons or entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the federal Anti-Kickback Statute or specific intent to violate it to have committed a violation; in addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act; |
|
· |
the federal False Claims Act, which imposes criminal and civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
|
· |
the federal Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), which imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation; |
|
· |
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act and its implementing regulations, which also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
|
· |
the federal Physician Payment Sunshine Act, which requires manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to report annually to the government information related to payments or other “transfers of value” made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and requires applicable manufacturers and group purchasing organizations to report annually to the government ownership and investment interests held by the physicians described above and their immediate family members and payments or other “transfers of value” to such physician owners (manufacturers are required to submit reports to the government by the 90th day of each calendar year). Additional reporting and transparency requirements for |
59
payments to physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse midwives go into effect in 2022 for payments made in 2021; and |
|
· |
analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, which may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payors, including private insurers; state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government; state laws that require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures and pricing information; and state and foreign laws governing the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts. |
Ensuring that our internal operations and business arrangements with third-parties comply with applicable healthcare laws and regulations could involve substantial costs. If our operations are found to be in violation of such laws or any other governmental laws and regulations that may apply to us, we may be subject to significant penalties, including civil, criminal and administrative penalties, damages, fines, exclusion from U.S. government funded healthcare programs, such as Medicare and Medicaid, disgorgement, individual imprisonment, contractual damages, reputational harm, diminished profits and the curtailment or restructuring of our operations.
We and our current and any future collaborators, third-party manufacturers and suppliers will or may use biological materials and may use hazardous materials, and any claims relating to improper handling, storage or disposal of these materials could be time consuming or costly.
We and our current and any future collaborators, third-party manufacturers or suppliers will or may use biological materials and may use hazardous materials, including chemicals and biological agents and compounds that could be dangerous to human health and safety of the environment. Our operations and the operations of our third-party manufacturers and suppliers also produce hazardous waste products. Federal, state and local laws and regulations govern the use, generation, manufacture, storage, handling and disposal of these materials and wastes. Compliance with applicable environmental laws and regulations may be expensive, and current or future environmental laws and regulations may impair our product development efforts. In addition, we cannot eliminate the risk of accidental injury or contamination from these materials or wastes. We do not carry specific biological or hazardous waste insurance coverage, and our property, casualty and general liability insurance policies specifically exclude coverage for damages and fines arising from biological or hazardous waste exposure or contamination. In the event of contamination or injury, we could be held liable for damages or be penalized with fines in an amount exceeding our resources, and our clinical trials or regulatory approvals could be suspended.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of ciforadenant, CPI-006, CPI-818 or our other product candidates.
We face an inherent risk of product liability as a result of the clinical testing of ciforadenant, CPI-006, CPI-818, and the planned clinical testing of our other product candidates and will face an even greater risk if we commercialize our product candidates. For example, we may be sued if ciforadenant, CPI-006, CPI-818 or our other product candidates allegedly cause injury or are found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product candidate, negligence, strict liability and a breach of warranties. Claims could also be asserted under state consumer protection acts.
If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit or cease the commercialization of our product candidates. Even a successful defense would
60
require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in:
|
· |
decreased demand for ciforadenant, CPI-006, CPI-818 or our other product candidates; |
|
· |
injury to our reputation; |
|
· |
withdrawal of clinical trial participants; |
|
· |
costs to defend the related litigation; |
|
· |
a diversion of management’s time and our resources; |
|
· |
substantial monetary awards to trial participants or patients; |
|
· |
product recalls, withdrawals or labeling, marketing or promotional restrictions; |
|
· |
loss of revenue; |
|
· |
the inability to commercialize ciforadenant, CPI-006, CPI-818 or our other product candidates; and |
|
· |
a decline in our stock price. |
We have product liability insurance coverage in an amount and on terms and conditions that are customary for similarly situated companies and that are satisfactory to our board of directors. Our inability to retain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of ciforadenant, CPI-006, CPI-818 or our other product candidates. Although we plan to maintain such insurance, any claim that may be brought against us could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by our insurance or that is in excess of the limits of our insurance coverage. Our insurance policies will also have various exclusions, and we may be subject to a product liability claim for which we have no coverage. We may have to pay any amounts awarded by a court or negotiated in a settlement that exceed our coverage limitations or that are not covered by our insurance, and we may not have, or be able to obtain, sufficient capital to pay such amounts.
We and any of our potential future collaborators will be required to report to regulatory authorities if any of our approved products cause or contribute to adverse medical events, and any failure to do so would result in sanctions that would materially harm our business.
If we and any of our potential future collaborators are successful in commercializing our products, the FDA and foreign regulatory authorities would require that we and any of our potential future collaborators report certain information about adverse medical events if those products may have caused or contributed to those adverse events. The timing of our obligation to report would be triggered by the date we become aware of the adverse event as well as the nature of the event. We and any of our potential future collaborators or CROs may fail to report adverse events within the prescribed timeframe. If we or any of our potential future collaborators or CROs fail to comply with such reporting obligations, the FDA or a foreign regulatory authority could take action, including criminal prosecution, the imposition of civil monetary penalties, seizure of our products or delay in approval or clearance of future products.
Our internal computer systems, or those of any of our potential future collaborators, CROs or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our product development programs.
Despite the implementation of security measures, our internal computer systems and those of our current and any future CROs and other contractors, consultants and collaborators are vulnerable to damage from computer viruses,
61
unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our development programs and our business operations, whether due to a loss of our trade secrets or other similar disruptions. For example, the loss of clinical trial data from completed or future clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. In addition, such a breach may require notification to governmental agencies, the media or individuals pursuant to various federal and state privacy and security laws, if applicable, including the Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Clinical Health Act of 2009, or HITECH, and its implementing rules and regulations, as well as regulations promulgated by the Federal Trade Commission and state breach notification laws. We would also be exposed to a risk of loss, including financial assets or litigation and potential liability, which could materially adversely affect our business, financial condition, results of operations and prospects. We also rely on third parties to manufacture our product candidates, and similar events relating to their computer systems could also have a material adverse effect on our business. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development and commercialization of our product candidates could be delayed.
Changes in and failures to comply with U.S. and foreign privacy and data protection laws, regulations and standards may adversely affect our business, operations and financial performance.
We are subject to or affected by numerous federal, state and foreign laws and regulations, as well as regulatory guidance, governing the collection, use, disclosure, retention, and security of personal data, such as information that we collect about patients and healthcare providers in connection with clinical trials in the United States and abroad. The global data protection landscape is rapidly evolving, and implementation standards and enforcement practices are likely to remain uncertain for the foreseeable future. This evolution may create uncertainty in our business, affect our or our collaborators’, service providers’ and contractors’ ability to operate in certain jurisdictions or to collect, store, transfer use and share personal information, necessitate the acceptance of more onerous obligations in our contracts, result in liability or impose additional costs on us. The cost of compliance with these laws, regulations and standards is high and is likely to increase in the future. Any failure or perceived failure by us or our collaborators, service providers and contractors to comply with federal, state or foreign laws or regulation, our internal policies and procedures or our contracts governing processing of personal information could result in negative publicity, diversion of management time and effort and proceedings against us by governmental entities or others. In many jurisdictions, enforcement actions and consequences for noncompliance are rising.
In the United States, California enacted the California Consumer Privacy Act, or the CCPA, on June 28, 2018, which went into effect on January 1, 2020. The CCPA gives California residents expanded rights to access and delete their personal information, opt out of certain personal information sharing, and receive detailed information about how their personal information is used. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches that is expected to increase data breach litigation. The CCPA may increase our compliance costs and potential liability. Some observers have noted that the CCPA could mark the beginning of a trend toward more stringent privacy legislation in the United States, which could increase our potential liability and adversely affect our business.
Our operations abroad may also be subject to increased scrutiny or attention from data protection authorities. Many countries in these regions have established or are in the process of establishing privacy and data security legal frameworks with which we, our collaborators, service providers, including our CRO, and contractors must comply. For example, the EU has adopted the EU General Data Protection Regulation (EU) 2016/679, or GDPR, which went into effect in May 2018 and introduces strict requirements for processing the personal information of EU subjects, including clinical trial data. The GDPR has and will continue to increase compliance burdens on us, including by mandating potentially burdensome documentation requirements and granting certain rights to individuals to control how we collect, use, disclose, retain and process information about them. The processing of sensitive personal data, such as physical health condition, may impose heightened compliance burdens under the GDPR and is a topic of active interest among foreign regulators. In addition, the GDPR provides for more robust regulatory enforcement and fines of up to €20 million or 4% of the annual global revenue of the noncompliant company, whichever is greater. As we expand into other
62
foreign countries and jurisdictions, we may be subject to additional laws and regulations that may affect how we conduct business.
Our information technology systems could face serious disruptions that could adversely affect our business.
Our information technology and other internal infrastructure systems, including corporate firewalls, servers, leased lines and connection to the Internet, face the risk of systemic failure that could disrupt our operations. A significant disruption in the availability of our information technology and other internal infrastructure systems could cause interruptions and delays in our research and development work.
Cybersecurity breaches could expose us to liability, damage our reputation, compromise our confidential information or otherwise adversely affect our business.
We maintain sensitive company data on our computer networks, including our intellectual property and proprietary business information. We face a number of threats to our networks from unauthorized access, security breaches and other system disruptions. Despite our security measures, our infrastructure may be vulnerable to attacks by hackers or other disruptive problems. Any such security breach may compromise information stored on our networks, or those of our vendors, and may result in significant data losses or theft of our intellectual property or proprietary business information. A cybersecurity breach could adversely affect our reputation and could result in other negative consequences, including disruption of our internal operations, increased cyber security protection costs, lost revenues or litigation.
Business disruptions could seriously harm our future revenue and financial condition and increase our costs and expenses.
Our operations could be subject to earthquakes, power shortages, telecommunications failures, water shortages, floods, hurricanes, typhoons, fires, extreme weather conditions, medical epidemics and other natural or manmade disasters or business interruptions, for which we are predominantly self-insured. We currently rely on several different manufacturers who supply different parts of the ciforadenant molecule and CPI-818 molecule, on one manufacturer for CPI-006 drug substance and on other third-party manufacturers to produce our other product candidates. Our ability to obtain clinical supplies of ciforadenant, CPI-006, CPI-818 or our other product candidates could be disrupted if the operations of these suppliers were affected by a man-made or natural disaster or other business interruption. The occurrence of any of these business disruptions could seriously harm our operations and financial condition and increase our costs and expenses.
Our employees, independent contractors, principal investigators, CROs, consultants and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements.
We are exposed to the risk that our employees, independent contractors, principal investigators, CROs, consultants and vendors may engage in misconduct or other illegal activity. Misconduct by these parties could include intentional, reckless and/or negligent conduct involving the improper use or misrepresentation of information obtained in the course of clinical trials, the creation of fraudulent data in our preclinical studies or clinical trials or illegal misappropriation of drug product, which could result in regulatory sanctions and cause serious harm to our reputation. It is not always possible to identify and deter misconduct by employees and other third parties, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. In addition, we are subject to the risk that a person or government could allege such fraud or other misconduct, even if none occurred. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of fines and other sanctions.
63
Risks Related to Our Intellectual Property
Our rights to develop and commercialize our product candidates are subject in part to the terms and conditions of licenses granted to us by other companies. The patent protection, prosecution and enforcement for some of our product candidates may be dependent on third parties.
We currently are heavily reliant upon licenses of certain patent rights and proprietary technology from third parties that is important or necessary to the development of our technology and products, including technology related to our product candidates. For example, we rely on our license agreement with Vernalis for rights with respect to the intellectual property covering ciforadenant and certain development candidates under our A2B receptor antagonist program. Further, we rely on our license agreement with The Scripps Research Institute for rights related to our lead development candidate for our anti-CD73 program, CPI-006. These and other licenses we may enter into in the future may not provide adequate rights to use such intellectual property and technology in all relevant fields of use or in all territories in which we may wish to develop or commercialize our technology and products in the future. As a result, we may not be able to develop and commercialize our technology and products in fields of use and territories for which we are not granted rights pursuant to such licenses.
Licenses to additional third-party technology that may be required for our development programs may not be available in the future or may not be available on commercially reasonable terms, which could have a material adverse effect on our business and financial condition.
In some circumstances, we may not have the right to control the preparation, filing, prosecution and enforcement of patent applications, or to maintain the patents, covering technology that we license from third parties. In addition, some of our agreements with our licensors require us to obtain consent from the licensor before we can enforce patent rights, and our licensor may withhold such consent or may not provide it on a timely basis. Therefore, we cannot be certain that our licensors or collaborators will prosecute, maintain, enforce and defend such intellectual property rights in a manner consistent with the best interests of our business, including by taking reasonable measures to protect the confidentiality of know-how and trade secrets, or by paying all applicable prosecution and maintenance fees related to intellectual property registrations for any of our product candidates. We also cannot be certain that our licensors have drafted or prosecuted the patents and patent applications licensed to us in compliance with applicable laws and regulations, which may affect the validity and enforceability of such patents or any patents that may issue from such applications. If they fail to do so, this could cause us to lose rights in any applicable intellectual property that we in-license, and as a result our ability to develop and commercialize products or product candidates may be adversely affected and we may be unable to prevent competitors from making, using and selling competing products.
Our success depends on our ability to protect our intellectual property and our proprietary technologies.
Our commercial success depends in part on our ability to obtain and maintain patent protection and trade secret protection for our product candidates, proprietary technologies and their uses as well as our ability to operate without infringing upon the proprietary rights of others. We generally seek to protect our proprietary position by filing patent applications in the United States and abroad related to our product candidates, proprietary technologies and their uses that are important to our business. There can be no assurance that our patent applications or those of our licensors will result in additional patents being issued or that issued patents will afford sufficient protection against competitors with similar technology, nor can there be any assurance that the patents issued will not be infringed, designed around or invalidated by third parties. Even issued patents may later be found invalid or unenforceable or may be modified or revoked in proceedings instituted by third parties before various patent offices or in courts. The degree of future protection for our proprietary rights is uncertain. Only limited protection may be available and may not adequately protect our rights or permit us to gain or keep any competitive advantage. This failure to properly protect the intellectual property rights relating to our product candidates could have a material adverse effect on our financial condition and results of operations.
While we have rights to an issued composition-of-matter patent in the United States and corresponding issued patents in certain foreign territories covering ciforadenant, we cannot be certain that the claims in any of our patent applications covering composition-of-matter of our other product candidates will be considered patentable by the United
64
States Patent and Trademark Office (“USPTO”), courts in the United States or by the patent offices and courts in foreign countries, nor can we be certain that the claims in our issued composition-of-matter patents will not be found invalid or unenforceable if challenged.
The patent application process is subject to numerous risks and uncertainties, and there can be no assurance that we or any of our potential future collaborators will be successful in protecting our product candidates by obtaining and defending patents. These risks and uncertainties include the following:
|
· |
the USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other provisions during the patent process, the noncompliance with which can result in abandonment or lapse of a patent or patent application, and partial or complete loss of patent rights in the relevant jurisdiction; |
|
· |
patent applications may not result in any patents being issued; |
|
· |
patents that may be issued or in-licensed may be challenged, invalidated, modified, revoked, circumvented, found to be unenforceable or otherwise may not provide any competitive advantage; |
|
· |
our competitors, many of whom have substantially greater resources than we do and many of whom have made significant investments in competing technologies, may seek or may have already obtained patents that will limit, interfere with or eliminate our ability to make, use and sell our potential product candidates; |
|
· |
there may be significant pressure on the U.S. government and international governmental bodies to limit the scope of patent protection both inside and outside the United States for disease treatments that prove successful, as a matter of public policy regarding worldwide health concerns; and |
|
· |
countries other than the United States may have patent laws less favorable to patentees than those upheld by U.S. courts, allowing foreign competitors a better opportunity to create, develop and market competing product candidates. |
The patent prosecution process is also expensive and time-consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. Although we enter into non-disclosure and confidentiality agreements with parties who have access to patentable aspects of our research and development output, such as our employees, corporate collaborators, outside scientific collaborators, CROs, contract manufacturers, consultants, advisors and other third parties, any of these parties may breach such agreements and disclose such output before a patent application is filed, thereby jeopardizing our ability to seek patent protection.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our patents, if issued, or the patent rights that we license from others, may be challenged in the courts or patent offices in the United States and abroad. Such challenges may result in loss of exclusivity or in patent claims being narrowed, invalidated or held unenforceable, which could limit our ability to stop others from using or commercializing similar or identical products, or limit the duration of the patent protection of our products and product candidates. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our intellectual property may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
65
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition, we rely on the protection of our trade secrets, including unpatented know-how, technology and other proprietary information to maintain our competitive position. Although we have taken steps to protect our trade secrets and unpatented know-how, including entering into confidentiality agreements with third parties, and confidential information and inventions agreements with employees, consultants and advisors. Despite these efforts, we cannot provide any assurances that all such agreements have been duly executed, and any of these parties may breach the agreements and disclose our proprietary information, including our trade secrets, and we may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the United States are less willing or unwilling to protect trade secrets. Moreover, third parties may still obtain this information or may come upon this or similar information independently, and we would have no right to prevent them from using that technology or information to compete with us. If any of these events occurs or if we otherwise lose protection for our trade secrets, the value of this information may be greatly reduced and our competitive position would be harmed. If we do not apply for patent protection prior to such publication or if we cannot otherwise maintain the confidentiality of our proprietary technology and other confidential information, then our ability to obtain patent protection or to protect our trade secret information may be jeopardized.
Our commercial success depends significantly on our ability to operate without infringing the patents and other proprietary rights of third parties. Claims by third parties that we infringe their proprietary rights may result in liability for damages or prevent or delay our developmental and commercialization efforts.
Our commercial success depends in part on our avoiding infringement of the patents and proprietary rights of third parties. Other entities may have or obtain patents or proprietary rights that could limit our ability to make, use, sell, offer for sale or import our product candidates and future approved products or impair our competitive position. There is a substantial amount of litigation, both within and outside the United States, involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries, including patent infringement lawsuits, interferences, oppositions, reexaminations, inter partes review (“IPR”) proceedings and post-grant review (“PGR”) proceedings before the USPTO and/or corresponding foreign patent offices. Numerous third-party U.S. and foreign issued patents and pending patent applications exist in the fields in which we are developing product candidates. There may be third-party patents or patent applications with claims to materials, formulations, methods of manufacture or methods for treatment related to the use or manufacture of our product candidates. For example, we are aware of an issued patent in Australia that may be relevant to commercialization of ciforadenant in that country. That Australian patent is expected to expire in 2022. Our ability to commercialize ciforadenant in Australia prior to 2022 could be adversely affected if we do not obtain a license under such patent. We are also aware of a corresponding patent application that has been issued in the United States and which is expected to expire in 2023. However, to the extent that any claims of this patent may be interpreted to cover our potential uses of ciforadenant, we do not believe that such claims would be valid and enforceable if asserted. We have filed a PGR petition challenging the patentability of certain claims of the patent and the patentee subsequently disclaimed every challenged claim. As the biotechnology industry expands and more patents are issued, the risk increases that our product candidates may be subject to claims of infringement of the patent rights of third parties. Because patent applications are maintained as confidential for a certain period of time, until the relevant application is published we may be unaware of third-party patent applications that, if issued as patents, may be infringed by commercialization of ciforadenant, CPI-006, CPI-818 or our other product candidates, and cannot be certain that we were the first to file a patent application related to a product candidate or technology. Moreover, because patent applications can take many years to issue, there may be currently-pending patent applications that may later result in issued patents that our product candidates may infringe. In addition, identification of third-party patent rights that may be relevant to our technology is difficult because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. Any claims of patent infringement asserted by third parties would be time consuming and could:
|
· |
result in costly litigation; |
|
· |
divert the time and attention of our technical personnel and management; |
66
|
· |
cause development delays; |
|
· |
prevent us from commercializing ciforadenant, CPI-006, CPI-818 or our other product candidates until the asserted patent expires or is held finally invalid or not infringed in a court of law; |
|
· |
require us to develop non-infringing technology, which may not be possible on a cost-effective basis; or |
|
· |
require us to enter into royalty or licensing agreements, which may not be available on commercially reasonable terms, or at all. |
Although no third party has asserted a claim of patent infringement against us as of the date of this report, others may hold proprietary rights that could prevent ciforadenant, CPI-006, CPI-818 or our other product candidates from being marketed. Any patent-related legal action against us claiming damages and seeking to enjoin commercial activities relating to our product candidates or processes could subject us to potential liability for damages, including treble damages if we were determined to willfully infringe, and require us to obtain a license to manufacture or market ciforadenant, CPI-006, CPI-818 or our other product candidates.
Defense of these claims, regardless of their merit, would involve substantial litigation expense and would be a substantial diversion of employee resources from our business. We cannot predict whether we would prevail in any such actions or that any license required under any of these patents would be made available on commercially acceptable terms, if at all. Moreover, even if we or our future strategic partners were able to obtain a license, the rights may be nonexclusive, which could result in our competitors gaining access to the same intellectual property. In addition, we cannot be certain that we could redesign our product candidates or processes to avoid infringement, if necessary. Accordingly, an adverse determination in a judicial or administrative proceeding, or the failure to obtain necessary licenses, could prevent us from developing and commercializing ciforadenant, CPI-006, CPI-818 or our other product candidates, which could harm our business, financial condition and operating results. In addition, intellectual property litigation, regardless of its outcome, may cause negative publicity and could prohibit us from marketing or otherwise commercializing our product candidates and technology.
We may be involved in lawsuits to protect or enforce our patents or the patents of our licensors, which could be expensive, time consuming, and unsuccessful. Further, our issued patents could be found invalid or unenforceable if challenged in court.
Competitors may infringe our intellectual property rights or those of our licensors. To prevent infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming. In addition, in a patent infringement proceeding, a court may decide that a patent we own or in-license is not valid, is unenforceable and/or is not infringed. If we or any of our potential future collaborators were to initiate legal proceedings against a third party to enforce a patent directed at one of our product candidates, the defendant could counterclaim that our patent is invalid and/or unenforceable in whole or in part. In patent litigation in the United States, defendant counterclaims alleging invalidity and/or unenforceability are commonplace. Grounds for a validity challenge include an alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness or non-enablement. Grounds for an unenforceability assertion could include an allegation that someone connected with prosecution of the patent withheld relevant information from the USPTO or made a misleading statement during prosecution. Third parties may also raise similar claims before the USPTO, even outside the context of litigation. The outcome following legal assertions of invalidity and unenforceability is unpredictable, and prior art could render our patents or those of our licensors invalid. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability, we would lose at least part, and perhaps all, of the patent protection on such product candidate. Such a loss of patent protection would have a material adverse impact on our business.
Interference proceedings provoked by third parties or brought by us or declared by the USPTO may be necessary to determine the priority of inventions with respect to our patents or patent applications or those of our licensors. An unfavorable outcome could require us to cease using the related technology or to attempt to license rights to it from the prevailing party. Our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms. Our defense of litigation or interference proceedings may fail and, even if successful,
67
may result in substantial costs and distract our management and other employees. In addition, the uncertainties associated with litigation could have a material adverse effect on our ability to raise the funds necessary to continue our clinical trials, continue our research programs, license necessary technology from third parties or enter into development or manufacturing partnerships that would help us bring our product candidates to market.
Even if resolved in our favor, litigation or other legal proceedings relating to our intellectual property rights may cause us to incur significant expenses, and could distract our technical and management personnel from their normal responsibilities. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments and if securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our common stock. Such litigation or proceedings could substantially increase our operating losses and reduce the resources available for development activities or any future sales, marketing or distribution activities. We may not have sufficient financial or other resources to conduct such litigation or proceedings adequately. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could compromise our ability to compete in the marketplace.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock.
Recent patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents.
On September 16, 2011, the Leahy-Smith America Invents Act (“Leahy-Smith Act”) was signed into law. The Leahy-Smith Act includes a number of significant changes to U.S. patent law. These include provisions that affect the way patent applications will be prosecuted and may also affect patent litigation. In particular, under the Leahy-Smith Act, the United States transitioned in March 2013 to a “first to file” system in which the first inventor to file a patent application will be entitled to the patent. Third parties are allowed to submit prior art before the issuance of a patent by the USPTO, and may become involved in post-grant proceedings including opposition, derivation, reexamination, inter-partes review or interference proceedings challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope or enforceability of, or invalidate, our patent rights, which could adversely affect our competitive position.
We may not be successful in obtaining or maintaining necessary rights to our product candidates through acquisitions and in-licenses.
We currently have rights to the intellectual property, through licenses from third parties and under patents that we own, to develop our product candidates. Because our programs may require the use of proprietary rights held by third parties, the growth of our business will depend in part on our ability to acquire, in-license or use these proprietary rights. For example, our product candidates may require specific formulations to work effectively and efficiently and the rights to these formulations may be held by others. We may be unable to acquire or in-license any compositions, methods of use, processes or other third-party intellectual property rights from third parties that we identify as necessary for our product candidates. The licensing and acquisition of third-party intellectual property rights is a competitive area, and a number of more established companies are also pursuing strategies to license or acquire third-party intellectual property rights that we may consider attractive. These established companies may have a competitive advantage over us due to their size, cash resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment.
We have collaborated with U.S. academic institutions and may in the future collaborate with U.S. and foreign academic institutions to accelerate our preclinical research or development under written agreements with these
68
institutions. These institutions may provide us with an option to negotiate a license to any of the institution’s rights in technology resulting from the collaboration. Regardless of such option, we may be unable to negotiate a license within the specified timeframe or under terms that are acceptable to us. If we are unable to do so, the institution may offer the intellectual property rights to other parties, potentially blocking our ability to pursue our program.
If we are unable to successfully obtain rights to required third-party intellectual property rights or maintain the existing intellectual property rights we have, we may have to abandon development of that program and our business and financial condition could suffer.
We may fail to comply with any of our obligations under existing agreements pursuant to which we license or have otherwise acquired intellectual property rights or technology, which could result in the loss of rights or technology that are material to our business.
Licensing of intellectual property is of critical importance to our business and involves complex legal, business and scientific issues. We are party to various agreements that we depend on for rights to use various technologies that are material to our business, including intellectual property rights covering ciforadenant and methods relating to its use and manufacture. In each of these cases, our rights to use the licensed intellectual property are subject to the continuation of and our compliance with the terms of these agreements. Disputes may arise regarding our rights to intellectual property licensed to us from a third party, including but not limited to:
|
· |
the scope of rights granted under the license agreement and other interpretation-related issues; |
|
· |
the extent to which our technology and processes infringe on intellectual property of the licensor that is not subject to the licensing agreement; |
|
· |
the sublicensing of patent and other rights; |
|
· |
our diligence obligations under the license agreement and what activities satisfy those diligence obligations; |
|
· |
the ownership of inventions and know-how resulting from the creation or use of intellectual property by us, alone or with our licensors and collaborators; |
|
· |
the scope and duration of our payment obligations; |
|
· |
our rights upon termination of such agreement; and |
|
· |
the scope and duration of exclusivity obligations of each party to the agreement. |
If disputes over intellectual property and other rights that we have licensed or acquired from third parties prevent or impair our ability to maintain our current licensing arrangements on acceptable terms, we may be unable to successfully develop and commercialize the affected product candidates. If we fail to comply with our obligations under current or future licensing agreements, these agreements may be terminated or the scope of our rights under them may be reduced and we might be unable to develop, manufacture or market any product that is licensed under these agreements.
We may be subject to claims that we have wrongfully hired an employee from a competitor or that we or our employees have wrongfully used or disclosed alleged confidential information or trade secrets of their former employers.
As is common in the pharmaceutical industry, in addition to our employees, we engage the services of consultants to assist us in the development of our product candidates. Many of these consultants, and many of our employees, were previously employed at, or may have previously provided or may be currently providing consulting services to, other pharmaceutical companies including our competitors or potential competitors. We may become subject
69
to claims that we, our employees or a consultant inadvertently or otherwise used or disclosed trade secrets or other information proprietary to their former employers or their former or current clients. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, which could adversely affect our business. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to our management team.
We may be subject to claims challenging the inventorship or ownership of our patents and other intellectual property.
We may also be subject to claims that former employees, collaborators or other third parties have an ownership interest in our patents or other intellectual property. Litigation may be necessary to defend against these and other claims challenging inventorship or ownership. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and distraction to management and other employees.
If we do not obtain patent term extension for our product candidates, our business may be materially harmed.
Depending upon the timing, duration and specifics of potential FDA marketing approval of ciforadenant, CPI-006 , CPI-818 or other product candidates, one or more of our U.S. patents may be eligible for limited patent term restoration under the Drug Price Competition and Patent Term Restoration Act of 1984 (“Hatch-Waxman Amendments”). The Hatch-Waxman Amendments permit a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, we may not be granted an extension because of, for example, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents or otherwise failing to satisfy applicable requirements. Moreover, the applicable time period or the scope of patent protection afforded could be less than we request. If we are unable to obtain patent term extension or restoration or the term of any such extension is less than we request, our competitors may obtain approval of competing products following our patent expiration, and our revenue could be reduced, possibly materially.
If our trademarks and trade names are not adequately protected, then we may not be able to build name recognition in our markets of interest and our business may be adversely affected.
Our registered or unregistered trademarks or trade names may be challenged, infringed, circumvented or declared generic or determined to be infringing on other marks. We may not be able to protect our rights to these trademarks and trade names, which we need to build name recognition among potential partners or customers in our markets of interest. At times, competitors may adopt trade names or trademarks similar to ours, thereby impeding our ability to build brand identity and possibly leading to market confusion. In addition, there could be potential trade name or trademark infringement claims brought by owners of other registered trademarks or trademarks that incorporate variations of our registered or unregistered trademarks or trade names. Over the long term, if we are unable to establish name recognition based on our trademarks and trade names, then we may not be able to compete effectively and our business may be adversely affected. Our efforts to enforce or protect our proprietary rights related to trademarks, trade secrets, domain names, copyrights or other intellectual property may be ineffective and could result in substantial costs and diversion of resources and could adversely affect our financial condition or results of operations.
Changes in U.S. patent law could diminish the value of patents in general, thereby impairing our ability to protect our product candidates.
As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involve a high degree of technological and legal complexity. Therefore, obtaining and enforcing biopharmaceutical patents is costly, time consuming and inherently uncertain. In addition, Congress may pass patent reform legislation that is unfavorable to us. The Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on decisions by Congress, the federal courts and the
70
USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents we might obtain in the future.
We may not be able to protect our intellectual property rights throughout the world.
While we have issued patents directed at ciforadenant in the United States and certain foreign territories, and pending patent applications directed at ciforadenant, CPI-006, CPI-818 and other product candidates in the United States and other countries, filing, prosecuting and defending patents on ciforadenant, CPI-006, CPI-818 and our other product candidates in all countries throughout the world would be prohibitively expensive, and our intellectual property rights in some countries outside the United States can be less extensive than those in the United States. In addition, the laws of some foreign countries do not protect intellectual property rights to the same extent as federal and state laws in the United States. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the United States, or from selling or importing products made using our inventions in and into the United States or other jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we have patent protection but enforcement is not as strong as that in the United States. These products may compete with our product candidates, and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
The legal systems of many foreign countries do not favor the enforcement of patents and other intellectual property protection, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
Intellectual property rights do not necessarily address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations, and may not adequately protect our business or permit us to maintain our competitive advantage. For example:
|
· |
others may be able to make adenosine antagonists that are similar to our product candidates but that are not covered by the claims of the patents that we own or have exclusively licensed; |
|
· |
we or our licensors or future collaborators might not have been the first to make the inventions covered by the issued patent or pending patent application that we own or have exclusively licensed; |
|
· |
we or our licensors or future collaborators might not have been the first to file patent applications covering certain of our inventions; |
|
· |
others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; |
|
· |
it is possible that our pending patent applications will not lead to issued patents; |
|
· |
issued patents that we own or have exclusively licensed may be held invalid or unenforceable, as a result of legal challenges by our competitors; |
71
|
· |
our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; |
|
· |
we may not develop additional proprietary technologies that are patentable; and |
|
· |
the patents of others may have an adverse effect on our business. |
Should any of these events occur, they could significantly harm our business, results of operations and prospects.
Risks Related to Our Common Stock
An active, liquid and orderly market for our common stock may not be maintained.
Prior to our IPO in March 2016, there had been no public market for our common stock. Although our common stock is listed on The Nasdaq Global Market (“Nasdaq”), an active trading market for our common stock may not be sustained on Nasdaq or any other exchange in the future. The lack of an active market may impair our stockholders’ ability to sell their shares at the time they wish to sell them or at a price that they consider reasonable. If an active market for our common stock is not maintained, it may also be difficult for our stockholders to sell shares without depressing the market price for the shares or at all. An inactive market may also impair our ability to raise capital by selling shares and may impair our ability to acquire other businesses, applications or technologies using our shares as consideration, which, in turn, could materially adversely affect our business.
The trading price of the shares of our common stock could be highly volatile, and investors in our common stock could incur substantial losses.
Our stock price has been volatile. The stock market in general and the market for stock of pharmaceutical companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. The market price for our common stock may be influenced by those factors discussed in this “Risk Factors” section and many others, including:
|
· |
our ability to enroll subjects in our planned clinical trials; |
|
· |
results of the clinical trials, and the results of trials of our competitors or those of other companies in our market sector; |
|
· |
regulatory approval of ciforadenant, CPI-006, CPI-818 and our other product candidates, or limitations to specific label indications or patient populations for its use, or changes or delays in the regulatory review process; |
|
· |
regulatory developments in the United States and foreign countries; |
|
· |
changes in the structure of healthcare payment systems, especially in light of current reforms to the U.S. healthcare system; |
|
· |
the success or failure of our efforts to acquire, license or develop additional product candidates; |
|
· |
innovations or new products developed by us or our competitors; |
|
· |
announcements by us or our competitors of significant acquisitions, strategic partnerships, joint ventures or capital commitments; |
72
|
· |
manufacturing, supply or distribution delays or shortages; |
|
· |
any changes to our relationship with any manufacturers, suppliers, collaborators or other strategic partners; |
|
· |
achievement of expected product sales and profitability; |
|
· |
variations in our financial results or those of companies that are perceived to be similar to us; |
|
· |
market conditions in the pharmaceutical sector and issuance of securities analysts’ reports or recommendations; |
|
· |
trading volume of our common stock; |
|
· |
an inability to obtain additional funding; |
|
· |
sales of our stock by insiders and stockholders; |
|
· |
general economic, industry and market conditions other events or factors, many of which are beyond our control; |
|
· |
additions or departures of key personnel; and |
|
· |
intellectual property, product liability or other litigation against us. |
As a result of this volatility, investors may experience losses on their investment in our common stock.
In addition, in the past, stockholders have initiated class action lawsuits against pharmaceutical companies following periods of volatility in the market prices of these companies’ stock. Such litigation, if instituted against us, could cause us to incur substantial costs and divert management’s attention and resources, which could have a material adverse effect on our business, financial condition and results of operations.
Our failure to meet the continued listing requirements of Nasdaq could result in a delisting of our common stock.
If we fail to satisfy the continued listing requirements of Nasdaq, such as the corporate governance requirements or the minimum closing bid price requirement, Nasdaq may take steps to delist our common stock. Such a delisting would likely have a negative effect on the price of our common stock and would impair our stockholders’ ability to sell or purchase our common stock when they wish to do so. In the event of a delisting, we can provide no assurance that any action taken by us to restore compliance with listing requirements would allow our common stock to become listed again, stabilize the market price or improve the liquidity of our common stock, prevent our common stock from dropping below the Nasdaq minimum bid price requirement or prevent future non-compliance with Nasdaq’s listing requirements.
Because a small number of our existing stockholders own a majority of our voting stock, a stockholder’s ability to influence corporate matters will be limited.
As of December 31, 2019, our executive officers, directors and greater than 5% stockholders, in the aggregate, owned approximately 43% of our outstanding common stock, excluding 1,458,000 shares of our common stock subject to prefunded warrants as described in Note 1 in Item 8, Financial Statements and Supplementary Data. As a result, such persons, acting together, have the ability to control our management and affairs and substantially all matters submitted to our stockholders for approval, including the election and removal of directors and approval of any significant transaction. This concentration of ownership may have the effect of delaying, deferring or preventing a change in control, impeding a merger, consolidation, takeover or other business combination involving us, or discouraging a
73
potential acquiror from making a tender offer or otherwise attempting to obtain control of our business, even if such a transaction would benefit other stockholders.
We do not currently intend to pay dividends on our common stock, and, consequently, our stockholders’ ability to achieve a return on their investment will depend on appreciation, if any, in the price of our common stock.
We have never declared or paid any cash dividend on our common stock. We currently anticipate that we will retain future earnings for the development, operation and expansion of our business and do not anticipate declaring or paying any cash dividends for the foreseeable future. Any return to stockholders will therefore be limited to the appreciation of their stock. There is no guarantee that shares of our common stock will appreciate in value or even maintain the price at which stockholders have purchased their shares.
Raising additional funds by issuing securities may cause dilution to our existing stockholders.
To the extent that we raise additional capital by issuing equity securities, the share ownership of existing stockholders will be diluted. For example, on April 3, 2017, we filed a Registration Statement on Form S-3 (File No. 333-217102), covering the offering of up to $250 million of shares of common stock, preferred stock, warrants and units. On September 20, 2017, we filed a prospectus supplement and entered into the Sales Agreement with Cowen and Company, LLC (“Cowen”) to sell shares of our common stock, from time to time, with aggregate gross sales proceeds of up to $125,000,000, through an at-the-market equity offering program under which Cowen will act as our sales agent. As of December 31, 2019, we have sold 52,569 shares of common stock for gross proceeds of approximately $894,000 pursuant to the Sales Agreement. In March 2018, we sold 8,117,647 shares of our common stock for net proceeds of $64.9 million in an underwritten public offering pursuant to our Registration Statement on Form S-3 (File No. 333-217102).
Sales of a substantial number of shares of our common stock by our existing stockholders in the public market could cause our stock price to fall.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock. Moreover, certain holders of shares of our common stock have rights, subject to certain conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders. We have registered and intend to continue to register all shares of common stock that we may issue under our equity compensation plans. Once we register these shares, they can be freely sold in the public market upon issuance, subject to volume limitations applicable to affiliates.
We are an emerging growth company, and the reduced reporting requirements applicable to emerging growth companies may make our common stock less attractive to investors.
We are an “emerging growth company,” as defined in the JOBS Act. For as long as we continue to be an emerging growth company, we may take advantage of exemptions from various reporting requirements that are applicable to other public companies that are not emerging growth companies, including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of Sarbanes-Oxley, reduced disclosure obligations regarding executive compensation in our Annual Report on Form 10-K and our periodic reports and proxy statements and exemptions from the requirements of holding nonbinding advisory votes on executive compensation and stockholder approval of any golden parachute payments not previously approved. We will remain an emerging growth company until the earlier of (1) December 31, 2021, (2) the last day of the fiscal year in which we have total annual gross revenue of at least $1.07 billion, (3) the last day of the fiscal year in which we are deemed to be a “large accelerated filer” as defined in Rule 12b-2 under the Exchange Act, which would occur if the market value of our common stock held by non-affiliates exceeded $700.0 million as of the last business day of the second fiscal quarter of such fiscal year, or (4) the date on which we have issued more than $1.0 billion in non-convertible debt securities during the prior three-year period. If investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile.
74
If securities or industry analysts do not publish research or reports or publish unfavorable research or reports about our business, our stock price and trading volume could decline.
The trading market for our common stock is influenced by the research and reports that industry or securities analysts publish about us or our business. If any of the analysts who cover us issue an adverse or misleading opinion regarding us, our business model, our intellectual property or our stock performance, or if our target studies and operating results fail to meet the expectations of analysts, our stock price would likely decline. If one or more of these analysts cease coverage of us or fail to publish reports on us regularly, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline.
If we fail to maintain proper and effective internal control over financial reporting, our ability to produce accurate and timely financial statements could be impaired, investors may lose confidence in our financial reporting and the trading price of our common stock may decline.
Pursuant to Section 404 of Sarbanes-Oxley, when we lose our status as an “emerging growth company” and are an accelerated filer, our independent registered public accounting firm will be required to attest to the effectiveness of our internal control over financial reporting. The rules governing the standards that must be met for management to assess our internal control over financial reporting are complex and require significant documentation, testing and possible remediation. To continue to comply with the requirements of being a reporting company under the Exchange Act, as we continue to grow, we will need to upgrade our systems including information technology; implement additional financial and management controls, reporting systems and procedures; and hire additional accounting and finance staff. If we or, if required, our auditors are unable to conclude that our internal control over financial reporting is effective, investors may lose confidence in our financial reporting and the trading price of our common stock may decline.
We cannot assure our stockholders that there will not be material weaknesses or significant deficiencies in our internal control over financial reporting in the future. Any failure to maintain internal control over financial reporting could severely inhibit our ability to accurately report our financial condition, results of operations or cash flows. If we are unable to conclude that our internal control over financial reporting is effective, or if our independent registered public accounting firm determines we have a material weakness or significant deficiency in our internal control over financial reporting once that firm begin its Section 404 reviews, investors may lose confidence in the accuracy and completeness of our financial reports, the market price of our common stock could decline, and we could be subject to sanctions or investigations by Nasdaq, the SEC or other regulatory authorities. Failure to remedy any material weakness in our internal control over financial reporting, or to implement or maintain other effective control systems required of public companies, could also restrict our future access to the capital markets.
Provisions in our charter documents and under Delaware law could discourage a takeover that stockholders may consider favorable and may lead to entrenchment of management.
Our amended and restated certificate of incorporation and amended and restated bylaws contain provisions that could significantly reduce the value of our shares to a potential acquiror or delay or prevent changes in control or changes in our management without the consent of our board of directors. The provisions in our charter documents include the following:
|
· |
a classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors; |
|
· |
no cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates; |
|
· |
the exclusive right of our board of directors, unless the board of directors grants such right to the stockholders, to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors; |
75
|
· |
the required approval of at least 66 2/3% of the shares entitled to vote to remove a director for cause, and the prohibition on removal of directors without cause; |
|
· |
the ability of our board of directors to authorize the issuance of shares of preferred stock and to determine the price and other terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquiror; |
|
· |
the ability of our board of directors to alter our amended and restated bylaws without obtaining stockholder approval; |
|
· |
the required approval of at least 66 2/3% of the shares entitled to vote to adopt, amend or repeal our amended and restated bylaws or repeal the provisions of our amended and restated certificate of incorporation regarding the election and removal of directors; |
|
· |
a prohibition on stockholder action by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders; |
|
· |
an exclusive forum provision providing that the Court of Chancery of the State of Delaware will be the exclusive forum for certain actions and proceedings; |
|
· |
the requirement that a special meeting of stockholders may be called only by the board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors; and |
|
· |
advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquiror from conducting a solicitation of proxies to elect the acquiror’s own slate of directors or otherwise attempting to obtain control of us. |
We are also subject to the anti-takeover provisions contained in Section 203 of the Delaware General Corporation Law. Under Section 203, a corporation may not, in general, engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other exceptions, the board of directors has approved the transaction.
Our amended and restated certificate of incorporation and amended and restated bylaws provide that the Court of Chancery of the State of Delaware is the exclusive forum for substantially all disputes between us and our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us or our directors, officers or employees.
Our amended and restated certificate of incorporation and amended and restated bylaws provide that the Court of Chancery of the State of Delaware is the exclusive forum for any derivative action or proceeding brought on our behalf, any action asserting a breach of fiduciary duty, any action asserting a claim against us arising pursuant to the Delaware General Corporation Law, our amended and restated certificate of incorporation or our amended and restated bylaws, or any action asserting a claim against us that is governed by the internal affairs doctrine. This provision may limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes with us or our directors, officers or other employees, which may discourage such lawsuits against us and our directors, officers and other employees. Alternatively, if a court were to find this provision in our amended and restated certificate of incorporation and amended and restated bylaws to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving such action in other jurisdictions, which could adversely affect our business and financial condition.
76
Our ability to use net operating loss carryforwards and other tax attributes may be limited.
We have incurred substantial losses during our history and do not expect to become profitable in the near future, and we may never achieve profitability. To the extent that we continue to generate taxable losses, unused losses will carry forward to offset future taxable income, if any, until such unused losses expire. As of December 31, 2019, we had federal net operating loss (“NOL”) carryforwards of approximately $144.5 million and state NOL carryforwards of approximately $173.9 million available to offset future taxable income. If not utilized, the federal and state NOL carryforwards will begin to expire in various years beginning in 2034. As of December 31, 2019, we also had $6.1 million of federal and $3.3 million of state research and development tax credit carryforwards available to reduce future income taxes. The federal research and development tax credits will begin to expire in 2035, if not utilized. The state research and development tax credits have no expiration date. Utilization of NOL carryforwards and credits may be subject to an annual limitation due to the “ownership change” provisions under Sections 382 and 383 of the Internal Revenue Code of 1986, as amended. An “ownership change” is generally defined as a cumulative change in the ownership interest of significant stockholders over a three‑year period in excess of 50 percentage points. Similar provisions under state tax law may also apply. We may experience an ownership change in the future as a result of subsequent shifts in our stock ownership, some of which changes are outside our control. Such ownership changes could result in the expiration of our NOL carryforwards and other tax attributes before they can be utilized and, if we are profitable, our future cash flows could be adversely affected due to our increased tax liability.
Item 1B. Unresolved Staff Comments
None
We currently lease approximately 27,280 square feet of office and research and development facilities in Burlingame, California. Our lease expires in 2023. We frequently explore alternatives that would provide us with additional space to accommodate our anticipated growth.
We are not currently a party to any material litigation or legal proceedings; however, we may from time to time be involved in various legal proceedings incident to the ordinary course of our business.
Item 4. Mine Safety Disclosures
Not applicable.
77
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters, and Issuer Purchases of Equity Securities
Market Information for Common Stock
Our common stock has been listed on The Nasdaq Global Market under the symbol “CRVS” since March 23, 2016. Prior to that there was no public trading market for our common stock. The following table sets forth for the indicated periods the high and low sales prices per share for our common stock on the Nasdaq stock market.
|
|
|
Price Range |
||||
|
|
|
High |
|
Low |
||
|
2019 |
|
|
|
|
|
|
|
First Quarter |
|
$ |
5.44 |
|
$ |
3.55 |
|
Second Quarter |
|
$ |
4.75 |
|
$ |
3.23 |
|
Third Quarter |
|
$ |
8.10 |
|
$ |
2.91 |
|
Fourth Quarter |
|
$ |
5.10 |
|
$ |
2.53 |
|
2018 |
|
|
|
|
|
|
|
First Quarter |
|
$ |
11.64 |
|
$ |
7.42 |
|
Second Quarter |
|
$ |
13.91 |
|
$ |
9.05 |
|
Third Quarter |
|
$ |
11.53 |
|
$ |
8.50 |
|
Fourth Quarter |
|
$ |
9.19 |
|
$ |
3.22 |
Holders of Record
As of March 9, 2020, there were approximately 25 stockholders of record of our common stock. The actual number of stockholders is greater than this number of record holders, and includes stockholders who are beneficial owners, but whose shares are held in street name by brokers and other nominees. This number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
Dividend Policy
We currently intend to retain future earnings, if any, for use in operation of our business and to fund future growth. We have never declared or paid any cash dividends on our capital stock and do not anticipate paying any cash dividends in the foreseeable future. Payment of cash dividends, if any, in the future will be at the discretion of our board of directors and will depend on then‑existing conditions, including our financial condition, operating results, contractual restrictions, capital requirements, business prospects and other factors our board of directors may deem relevant.
Stock Performance Graph
The following graph shows the total stockholder’s return on an investment of $100 in cash at market close on March 23, 2016 (the first day of trading of our common stock), through December 31, 2019 for (i) our common stock, (ii) the Nasdaq Composite Index and (iii) the Nasdaq Biotechnology Index.
Pursuant to applicable Securities and Exchange Commission rules, all values assume reinvestment of the full amount of all dividends, however, no dividends have been declared on our common stock to date. The stockholder return shown on the graph below is not necessarily indicative of future performance, and we do not make or endorse any predictions as to future stockholder return. This graph and the table below it shall not be deemed “soliciting material” or be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934 as amended (the “Exchange Act”), or otherwise subject to the liabilities under that Section, and shall not be deemed to be incorporated by reference into any
78
of our filings under the Securities Act of 1933, as amended (the “Securities Act”), whether made before or after the date hereof and irrespective of any general incorporation language in any such filing.
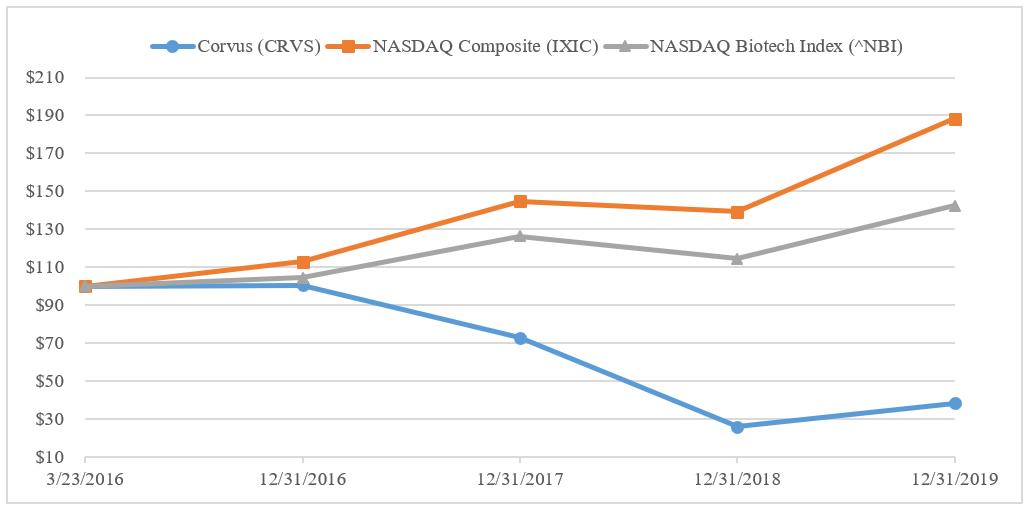
|
|
|
March 23, |
|
December 31, |
|
December 31, |
|
December 31, |
|
December 31, |
|||||
|
$100 investment in stock or index |
|
2016 |
|
2016 |
|
2017 |
|
2018 |
|
2019 |
|||||
|
Corvus (CRVS) |
|
$ |
100.00 |
|
$ |
100.35 |
|
$ |
72.70 |
|
$ |
25.75 |
|
$ |
38.18 |
|
NASDAQ Composite Index (IXIC) |
|
$ |
100.00 |
|
$ |
112.88 |
|
$ |
144.76 |
|
$ |
139.14 |
|
$ |
188.15 |
|
NASDAQ Biotech Index (^NBI) |
|
$ |
100.00 |
|
$ |
104.36 |
|
$ |
126.33 |
|
$ |
114.55 |
|
$ |
142.51 |
Securities Authorized for Issuance Under Equity Compensation Plans
The information required by this Item regarding equity compensation plans is incorporated by reference to the information set forth in PART III Item 12 of this Annual Report on Form 10‑K.
Use of Proceeds from Registered Securities
None.
Recent Sales of Unregistered Equity Securities
In November 2019, we entered into an exchange agreement (the “Exchange Agreement”) with entities affiliated with Biotechnology Value Fund, L.P. (the “Exchanging Stockholders”), pursuant to which we exchanged an aggregate of 1,458,000 shares of our common stock owned by the Exchanging Stockholders for warrants (the “Exchange Warrants”) to purchase an aggregate of 1,458,000 shares of common stock (subject to adjustment in the event of stock splits, recapitalizations and other similar events affecting common stock), with an exercise price of $0.0001 per share. The Exchange Warrants were issued without registration under the Securities Act of 1933, as amended (the “Securities Act”), in reliance on the exemption from registration contained in Section 3(a)(9) of the Securities Act.
Issuer Purchases of Equity Securities by the Issuer and Affiliated Purchasers
None.
79
Item 6. Selected Financial Data
You should read the following selected financial data together with the information under “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and related notes included in Part II, Item 8 of this Annual Report on Form 10 K. The selected statement of operations data for each of the years ended December 31, 2019, 2018 and 2017 and the balance sheet data as of December 31, 2019 and 2018 are derived from our audited financial statements included elsewhere in this Annual Report on Form 10 K. The statement of operations data for the years ended December 31, 2016 and 2015 and the balance sheet data as of December 31, 2017, 2016 and 2015 are derived from our audited financial statements which are not included in this Annual Report on Form 10 K. Our historical results of any prior periods are not necessary indicative of results to be expected in any future period.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|
|||||||||||||
|
Statements of Operations and Comprehensive Loss Data: |
|
2019 |
|
2018 |
|
2017 |
|
2016 |
|
2015 |
|
|||||
|
|
|
(In thousands, except share and per share amounts) |
|
|||||||||||||
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
37,975 |
|
$ |
38,586 |
|
$ |
46,305 |
|
$ |
29,356 |
|
$ |
11,352 |
|
|
General and administrative |
|
|
10,879 |
|
|
10,636 |
|
|
10,219 |
|
|
7,620 |
|
|
2,418 |
|
|
Total operating expenses |
|
|
48,854 |
|
|
49,222 |
|
|
56,524 |
|
|
36,976 |
|
|
13,770 |
|
|
Loss from operations |
|
|
(48,854) |
|
|
(49,222) |
|
|
(56,524) |
|
|
(36,976) |
|
|
(13,770) |
|
|
Change in fair value of convertible preferred stock liability |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(17,600) |
|
|
Interest income and other expense, net. |
|
|
2,182 |
|
|
2,283 |
|
|
861 |
|
|
601 |
|
|
35 |
|
|
Net loss |
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
|
$ |
(36,375) |
|
$ |
(31,335) |
|
|
Net loss per share, basic and diluted |
|
$ |
(1.59) |
|
$ |
(1.71) |
|
$ |
(2.72) |
|
$ |
(2.36) |
|
$ |
(83.86) |
|
|
Shares used to compute net loss per share, basic and diluted |
|
|
29,349,810 |
|
|
27,509,960 |
|
|
20,488,506 |
|
|
15,422,041 |
|
|
373,643 |
|
|
Other comprehensive income (loss): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unrealized gain (loss) on marketable securities |
|
|
63 |
|
|
7 |
|
|
(2) |
|
|
6 |
|
|
(45) |
|
|
Comprehensive loss |
|
$ |
(46,609) |
|
$ |
(46,932) |
|
$ |
(55,665) |
|
$ |
(36,369) |
|
$ |
(31,380) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||||||||
|
Balance Sheet Data: |
|
2019 |
|
2018 |
|
2017 |
|
2016 |
|
2015 |
|||||
|
|
|
(In thousands) |
|
|
|
||||||||||
|
Cash, cash equivalents and marketable securities |
|
$ |
77,982 |
|
$ |
114,597 |
|
$ |
90,055 |
|
$ |
134,896 |
|
$ |
94,386 |
|
Working capital |
|
|
69,119 |
|
|
108,562 |
|
|
82,265 |
|
|
130,089 |
|
|
92,593 |
|
Total assets |
|
|
83,646 |
|
|
118,232 |
|
|
94,775 |
|
|
140,150 |
|
|
98,459 |
|
Convertible preferred stock |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
125,780 |
|
Total stockholders’ equity (deficit) |
|
$ |
71,111 |
|
$ |
110,336 |
|
$ |
84,835 |
|
$ |
132,801 |
|
$ |
(31,101) |
80
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion should be read in conjunction with the consolidated financial statements and notes thereto included elsewhere in this Annual report on Form 10‑K. This Annual Report on Form 10‑K, including the following sections, contains forward‑looking statements within the meaning of the federal securities laws. These statements are subject to risks and uncertainties that could cause actual results and events to differ materially from those expressed or implied by such forward‑looking statements. For a detailed discussion of these risks and uncertainties, see the “Risk Factors” section in Item 1A of this Annual Report on Form 10‑K. We caution the reader not to place undue reliance on these forward‑looking statements, which reflect management’s analysis only as of the date of this Form 10‑K. We undertake no obligation to update forward‑looking statements, which reflect events or circumstances occurring after the date of this Form 10‑K.
Overview
We are a clinical stage biopharmaceutical company focused on the development and commercialization of precisely targeted oncology therapies. Our strategy is to identify and utilize novel biomarkers to enhance selection of patients we believe will be most likely to benefit from treatment with our product candidates. We have utilized adaptive clinical protocol designs that enable us to evaluate our agents in multiple dosing regimens and for a range of cancer types. Since we began operations in November 2014, we have built a pipeline of five oncology programs. Three of these product candidates are now in international multicenter trials directed against a broad number of cancer indications. To date, we have evaluated our product candidates in over 350 patients. We are developing small molecules that are designed to selectively inhibit the binding of immunosuppressive adenosine to either A2A receptors or to A2B receptors. Another small molecule inhibitor is designed to block the function of ITK, a kinase protein inside T cells that is crucial to T-cell activation and differentiation. We also are developing injectable monoclonal antibodies. One of these antibodies is designed to block the production of adenosine by tumors by inhibiting the cell surface enzyme CD73. This antibody is designed to have dual properties; in addition to blocking production of immunosuppressive adenosine, the antibody is designed to stimulate various immune cells. Another antibody that is designed to bind to the chemokine receptor CXCR2 on myeloid cells to block the activity of immunosuppressive myeloid cells that infiltrate tumors is in preclinical development. Our product candidates’ designed specificity has the potential to provide greater safety and facilitate their development either as monotherapies or in combination with other cancer therapies such as immune checkpoint inhibitors or chemotherapy.
Ciforadenant (formerly CPI-444), is an oral, small molecule antagonist of the A2A receptor for adenosine and is currently being studied under a Phase 2 expansion protocol in combination with Genentech, Inc.’s cancer immunotherapy, Tecentriq® (atezolizumab), for patients with either advanced, refractory renal cell cancer (“RCC”) or patients with refractory metastatic castration resistant prostate cancer (“mCRPC”). Our second clinical product candidate, CPI-006, is an anti‑CD73 monoclonal antibody that is designed to both inhibit the production of adenosine and stimulate various immune cells. CPI-006 is currently being studied in a Phase 1/1b clinical trial as a monotherapy and in combination with ciforadenant, in combination with pembrolizumab and in triplet combination with both ciforadenant and pembrolizumab. Our third clinical product candidate, CPI-818, is a selective, covalent inhibitor of ITK and is in a multi-center Phase 1/1b clinical trial in patients with various malignant T-cell lymphomas. CPI-818 is designed to be directly cytotoxic to certain malignant T-cells and we believe has the potential to regulate immune responses to tumors. We believe the breadth and status of our pipeline demonstrates our management team’s expertise in understanding and developing oncology assets as well as in identifying product candidates that can be in‑licensed and further developed internally to treat many types of cancer. We hold worldwide rights to all of our product candidates.
To date, the majority of our efforts have been focused on the research, development and advancement of ciforadenant, CPI-006 and CPI-818, and we have not generated any revenue from product sales and, as a result, we have incurred significant losses. We expect to continue to incur significant research and development and general and administrative expenses related to our operations. Our net loss for the years ended December 31, 2019 and 2018 was $46.7 million and $46.9 million, respectively. As of December 31, 2019, we had an accumulated deficit of $217.1 million. We expect to continue to incur losses for the foreseeable future, and we anticipate these losses will increase as we continue our development of, seek regulatory approval for and begin to commercialize ciforadenant, CPI-006 and CPI-818, and as we develop other product candidates. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods.
81
Since our inception and through December 31, 2019, we have funded our operations primarily through the sale and issuance of stock. On March 22, 2016, our registration statement on Form S‑1 (File No. 333‑208850) relating to our initial public offering (“IPO”) of our common stock was declared effective by the SEC. Shares of our common stock began trading on the Nasdaq Global Market on March 23, 2016. The IPO closed on March 29, 2016, pursuant to which we sold 4,700,000 shares of our common stock at a public offering price of $15.00 per share. In April 2016, we sold an additional 502,618 shares of our common stock to the underwriters upon partial exercise of their over‑allotment option, at the initial offering price of $15.00 per share. We received aggregate net proceeds of approximately $70.6 million, after underwriting discounts, commissions and offering expenses. Immediately prior to the consummation of the IPO, all of our outstanding shares of convertible preferred stock were converted into 14.3 million shares of our common stock. In March 2018, in a follow-on offering, we sold 8,117,647 shares of our common stock at a price of $8.50 per share, which included 1,058,823 shares issued pursuant to the underwriters’ exercise of their option to purchase additional shares of common stock. We received aggregate net proceeds of approximately $64.9 million, after underwriting discounts, commissions and offering expenses
In September 2017, we entered into a sales agreement (the “Sales Agreement”) with Cowen and Company, LLC (“Cowen”) to sell shares of the Company’s common stock, from time to time, with aggregate gross sales proceeds of up to $125,000,000, through an at‑the‑market equity offering program under which Cowen acted as our sales agent. Cowen was entitled to compensation for its services equal to up to 3.0% of the gross proceeds of any shares of common stock sold through Cowen under the Sales Agreement. As of December 31, 2019, we had sold 52,569 shares of our common stock for gross proceed of approximately $894,000 pursuant to the Sales Agreement. We terminated the Sales Agreement in February 2020.
As of December 31, 2019, we had capital resources consisting of cash, cash equivalents and marketable securities of approximately $78.0 million. We do not expect our existing capital resources to be sufficient to enable us to fund the completion of our clinical trials and remaining development program of any of ciforadenant, CPI-006 or CPI-818 through commercialization. In addition, our operating plan may change as a result of many factors, including those described in the section of this report entitled “Risk Factors” and others currently unknown to us, and we may need to seek additional funds sooner than planned, through public or private equity, debt financings or other sources, such as strategic collaborations. Such financing would result in dilution to stockholders, imposition of debt covenants and repayment obligations or other restrictions that may affect our business. If we raise additional capital through strategic collaboration agreements, we may have to relinquish valuable rights to our product candidates, including possible future revenue streams. In addition, additional funding may not be available to us on acceptable terms or at all and any additional fundraising efforts may divert our management from its day-to-day activities, which may adversely affect our ability to develop and commercialize our product candidates. Furthermore, even if we believe we have sufficient funds for our current or future operating plans, we may seek additional capital due to favorable market conditions or strategic considerations.
We currently have no manufacturing capabilities and do not intend to establish any such capabilities. We have no commercial manufacturing facilities for our product candidates. As such, we are dependent on third parties to supply our product candidates according to our specifications, in sufficient quantities, on time, in compliance with appropriate regulatory standards and at competitive prices.
Components of Results of Operations
Revenue
To date, we have not generated any revenues. We do not expect to receive any revenues from any product candidates that we develop unless and until we obtain regulatory approval and commercialize our products or enter into revenue‑generating collaboration agreements with third parties.
82
Research and Development Expenses
Our research and development expenses consist primarily of costs incurred to conduct research and development of our product candidates. We record research and development expenses as incurred. Research and development expenses include:
|
· |
employee-related expenses, including salaries, benefits, travel and non-cash stock-based compensation expense; |
|
· |
external research and development expenses incurred under arrangements with third parties, such as contract research organizations, preclinical testing organizations, contract manufacturing organizations, academic and non-profit institutions and consultants; |
|
· |
costs to acquire technologies to be used in research and development that have not reached technological feasibility and have no alternative future use; |
|
· |
license fees; and |
|
· |
other expenses, which include direct and allocated expenses for laboratory, facilities and other costs. |
We plan to increase our research and development expenses substantially as we continue the development and potential commercialization of our product candidates. Our current planned research and development activities include the following:
|
· |
enrollment and completion of our Phase 1/1b clinical trial and amended Phase 1b/2 clinical trial of ciforadenant; |
|
· |
enrollment of our ongoing Phase 1/1b clinical trial of CPI-006; |
|
· |
enrollment of our ongoing Phase 1/1b clinical trial of CPI-818; |
|
· |
process development and manufacturing of drug supply of ciforadenant, CPI-006 and CPI-818; and |
|
· |
preclinical studies under our other programs in order to select development product candidates. |
In addition to our product candidates that are in clinical development, we believe it is important to continue substantial investment in potential new product candidates to build the value of our product candidate pipeline and our business.
Our expenditures on current and future preclinical and clinical development programs are subject to numerous uncertainties related to timing and cost to completion. The duration, costs and timing of clinical trials and development of product candidates will depend on a variety of factors, including many of which are beyond our control. The process of conducting the necessary clinical research to obtain regulatory approval is costly and time consuming, and the successful development of our product candidates is uncertain. The risks and uncertainties associated with our research and development projects are discussed more fully in “Part 1, Item 1A—Risk Factors.” As a result of these risks and uncertainties, we are unable to determine with any degree of certainty the duration and completion costs of our research and development projects or if, when or to what extent we will generate revenues from the commercialization and sale of any of our product candidates that obtain regulatory approval. We may never succeed in achieving regulatory approval for any of our product candidates.
83
General and Administrative Expenses
General and administrative expenses include personnel costs, expenses for outside professional services and allocated expenses. Personnel costs consist of salaries, benefits and stock‑based compensation. Outside professional services consist of legal, accounting and audit services and other consulting fees. Allocated expenses consist of rent expense related to our office and research and development facility.
We expect that our general and administrative expenses will increase in the future as we increase our headcount to support our continued research and development and potential commercialization of one or more of our product candidates.
Results of Operations
Comparison of the periods below as indicated (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended December 31, |
|
Change |
|
Change |
|||||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
2018 to 2019 |
|
2017 to 2018 |
|||||
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
37,975 |
|
$ |
38,586 |
|
$ |
46,305 |
|
$ |
(611) |
|
$ |
(7,719) |
|
General and administrative |
|
|
10,879 |
|
|
10,636 |
|
|
10,219 |
|
|
243 |
|
|
417 |
|
Total operating expenses |
|
|
48,854 |
|
|
49,222 |
|
|
56,524 |
|
|
(368) |
|
|
(7,302) |
|
Loss from operations |
|
|
(48,854) |
|
|
(49,222) |
|
|
(56,524) |
|
|
368 |
|
|
7,302 |
|
Interest income and other expense, net |
|
|
2,182 |
|
|
2,283 |
|
|
861 |
|
|
(101) |
|
|
1,422 |
|
Net loss |
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
|
$ |
267 |
|
$ |
8,724 |
Research and Development Expenses
Research and development expense for the years ended December 31, 2019 and 2018, consisted of the following costs by program (specific program costs consist solely of external costs):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended December 31, |
|
Change |
|
Change |
|
|||||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
2018 to 2019 |
|
2017 to 2018 |
|
|||||
|
Ciforadenant (formerly CPI-444) |
|
$ |
5,750 |
|
$ |
10,378 |
|
$ |
23,156 |
|
$ |
(4,628) |
|
$ |
(12,778) |
|
|
CPI‑006 |
|
|
6,774 |
|
|
6,108 |
|
|
6,008 |
|
|
666 |
|
|
100 |
|
|
CPI-818 |
|
|
6,577 |
|
|
4,707 |
|
|
1,791 |
|
|
1,870 |
|
|
2,916 |
|
|
Other programs |
|
|
981 |
|
|
877 |
|
|
581 |
|
|
104 |
|
|
296 |
|
|
Unallocated employee and overhead costs |
|
|
17,893 |
|
|
16,516 |
|
|
14,769 |
|
|
1,377 |
|
|
1,747 |
|
|
|
|
$ |
37,975 |
|
$ |
38,586 |
|
$ |
46,305 |
|
$ |
(611) |
|
$ |
(7,719) |
|
For the year ended December 31, 2019, the decrease in ciforadenant costs of $4.6 million as compared to the year ended December 31, 2018, primarily consisted of a decrease of $2.8 million in drug manufacturing costs, a decrease of $1.3 million in clinical trial expenses associated with lower enrollment in accordance with our protocol amendment focusing on RCC and mCRPC patients and a decrease of $0.5 million in other outside services.
For the year ended December 31, 2019, the increase in CPI-006 costs of $0.7 million as compared to the year ended December 31, 2018, primarily consisted of an increase of $1.2 million in clinical trial expenses, partially offset by a decrease of $0.3 million in drug manufacturing costs and a decrease of $0.2 million in other outside services.
For the year ended December 31, 2019, the increase in CPI-818 costs of $1.9 million as compared to the year ended December 31, 2018, primarily consisted of an increase of $2.2 million in clinical trial expenses, an increase of $0.6 million in drug manufacturing costs, and an increase of $0.2 million in other outside services, partially offset by a decrease of $1.1 million in IND-enabling study costs.
84
For the year ended December 31, 2019, the increase in costs related to other programs of $0.1 million as compared to the year ended December 31, 2018, primarily consisted of outside chemical synthesis and testing of research compounds.
For the year ended December 31, 2019, the increase in unallocated costs of $1.4 million as compared to the year ended December 31, 2018, primarily consisted of an increase in personnel and related costs.
For the year ended December 31, 2018, the decrease in ciforadenant costs of $12.8 million as compared to the year ended December 31, 2017, primarily consisted of a $3.0 million milestone payment to Vernalis in 2017, a decrease of $7.4 million in clinical trial expenses associated with lower enrollment in accordance with our protocol amendment focusing on RCC patients, a decrease of $1.8 million in contracted research costs, and a decrease of $0.6 million in drug manufacturing costs.
For the year ended December 31, 2018, the increase in CPI-006 costs of $0.1 million as compared to the year ended December 31, 2017, primarily consisted of a $2.5 million increase in clinical trial expenses, partially offset by a $1.6 million decrease in drug manufacturing costs and a $0.8 million decrease in IND-enabling study costs.
For the year ended December 31, 2018, the increase in CPI-818 costs of $2.9 million as compared to the year ended December 31, 2017, primarily consisted of a $1.9 million increase in drug manufacturing costs and a $1.0 million increase in IND-enabling study costs.
For the year ended December 31, 2018, the increase in costs related to other programs of $0.3 million as compared to the year ended December 31, 2017, primarily consisted of outside chemical synthesis and testing of research compounds.
For the year ended December 31, 2018, the increase in unallocated costs of $1.7 million as compared to the year ended December 31, 2017, primarily consisted of an increase of $1.2 million in personnel and related costs (including an increase in stock compensation expense of $0.2 million) and an increase of $0.5 million in contracted research costs.
General and Administrative Expenses
For the year ended December 31, 2019, the increase in general and administrative expenses of $0.2 million as compared to the year ended December 31, 2018, primarily consisted of an increase in personnel and related costs.
For the year ended December 31, 2018, the increase in general and administrative expenses of $0.4 million as compared to the year ended December 31, 2017, primarily consisted of an increase of $0.7 million in stock compensation expense, partially offset by a decrease of $0.3 million in professional services costs.
Interest Income and Other Expense, net
For the year ended December 31, 2019, the decrease in interest income and other expense, net of $0.1 million as compared to the year ended December 31, 2018, primarily consisted of a decrease in interest income earned due to a decrease in cash equivalents and marketable securities.
For the year ended December 31, 2018, the increase in interest income and other expense, net of $1.4 million as compared to the year ended December 31, 2017, primarily consisted of additional interest income earned due to a higher rate of return on investments.
85
Liquidity and Capital Resources
Sources of Liquidity
As of December 31, 2019, we had cash, cash equivalents and marketable securities of $78.0 million and an accumulated deficit of $217.1 million, compared to cash, cash equivalents and marketable securities of $114.6 million and an accumulated deficit of $170.5 million as of December 31, 2018. We have financed our operations primarily through sales of our common stock and convertible preferred stock.
In March 2016, we consummated our IPO and sold 4,700,000 shares of our common stock at a price of $15.00 per share, and in April 2016, sold 502,618 shares at a price of $15.00 per share pursuant to the partial exercise of the underwriters’ option to purchase additional shares of common stock. We received net proceeds of approximately $70.6 million, after deducting underwriting discounts, commissions and offering expenses. Immediately prior to the consummation of our IPO, all outstanding shares of the convertible preferred stock were converted into common stock on a one‑for‑one basis.
In March 2018, in a follow-on offering, we sold 8,117,647 shares of our common stock at a price of $8.50 per share, which included 1,058,823 shares issued pursuant to the underwriters’ exercise of their option to purchase additional shares of common stock. We received aggregate net proceeds of approximately $64.9 million, after underwriting discounts, commissions and offering expenses.
We believe our current cash, cash equivalents and marketable securities will be sufficient to fund our planned expenditures and meet our obligations through at least the next twelve months from the issuance of our financial statements as of and for year ended December 31, 2019. The amounts and timing of our actual expenditures depend on numerous factors, including:
|
· |
the progress, timing, costs and results of clinical trials for ciforadenant, CPI-006 and CPI-818; |
|
· |
the timing, progress, costs and results of preclinical and clinical development activities for our other product candidates; |
|
· |
the number and scope of preclinical and clinical programs we decide to pursue; |
|
· |
the costs involved in prosecuting, maintaining and enforcing patent and other intellectual property rights; |
|
· |
the cost and timing of regulatory approvals; |
|
· |
our efforts to enhance operational systems and hire additional personnel, including personnel to support development of our product candidates and satisfy our obligations as a public company; and |
|
· |
other factors described in the section of this report entitled “Risk Factors.” |
We expect to increase our spending in connection with the development and commercialization of our product candidates. Until such time, if ever, as we can generate substantial revenue from product sales, we expect to fund our operations and capital funding needs through equity and/or debt financings. We may also enter into additional collaboration arrangements or selectively partner for clinical development and commercialization. The sale of additional equity would result in dilution to our stockholders. The incurrence of debt financing would result in debt service obligations and the governing documents would likely include operating and financing covenants that would restrict our operations. In addition, sufficient additional funding may not be available on acceptable terms, or at all. If we are not able to secure adequate additional funding, we may be forced to make reductions in spending, extend payment terms with suppliers, liquidate assets where possible and/or suspend or curtail planned programs. Any of these actions could have a material effect on our business, financial condition and results of operations.
86
Summary of Statement of Cash Flows
The following table summarizes our cash flows for the periods indicated (in thousands):
|
|
|
Year ended December 31, |
|
Change |
|
Change |
|||||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
2018 to 2019 |
|
2017 to 2018 |
|||||
|
Net cash provided by (used in): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Operating activities |
|
$ |
(37,321) |
|
$ |
(40,988) |
|
$ |
(46,212) |
|
$ |
3,667 |
|
$ |
5,224 |
|
Investing activities |
|
|
3,255 |
|
|
(30,192) |
|
|
84,826 |
|
|
33,447 |
|
|
(115,018) |
|
Financing activities |
|
|
24 |
|
|
65,270 |
|
|
1,442 |
|
|
(65,246) |
|
|
63,828 |
|
Net increase (decrease) in cash and cash equivalents |
|
$ |
(34,042) |
|
$ |
(5,910) |
|
$ |
40,056 |
|
$ |
(28,132) |
|
$ |
(45,966) |
Cash Flows from Operating Activities
Cash used in operating activities during the year ended December 31, 2019 was $37.3 million, which primarily consisted of a net loss of $46.7 million, adjusted by non‑cash charges of $7.4 million, primarily consisting of $7.3 million of stock compensation expense, an increase of $2.5 million in accounts payable and accrued and other liabilities and an increase of $0.4 million in prepaid and other current assets, primarily associated with the timing of payments to vendors.
Cash used in operating activities during the year ended December 31, 2018 was $41.0 million, which primarily consisted of a net loss of $46.9 million, adjusted by non‑cash charges of $7.4 million, primarily consisting of $7.1 million of stock compensation expense, a decrease of $2.0 million in accounts payable and accrued and other liabilities and a decrease of $0.6 million in current and other assets, primarily associated with the timing of payments to vendors.
Cash used in operating activities during the year ended December 31, 2017 was $46.2 million, which primarily consisted of a net loss of $55.7 million, adjusted by non‑cash charges of $6.9 million, primarily consisting of $6.2 million of stock compensation expense and $0.8 million of depreciation expense, an increase of $3.1 million in accounts payable and accrued and other liabilities, primarily associated with our increased research and development activities.
Cash Flows from Investing Activities
Cash provided by investing activities during the year ended December 31, 2019 was $3.3 million, which consisted of proceeds from maturities of marketable securities of $141.9 million, which were partially offset by purchases of marketable securities of $138.6 million.
Cash used in investing activities during the year ended December 31, 2018 was $30.2 million, which consisted of purchases of marketable securities of $161.9 million and purchases of property and equipment of $0.4 million, which were partially offset by proceeds from maturities of marketable securities of $132.0 million.
Cash provided by investing activities during the year ended December 31, 2017 was $84.8 million, which consisted of proceeds from maturities of marketable securities of $173.4 million, which was partially offset by purchases of marketable securities of $88.3 million and purchases of property and equipment of $0.3 million.
Cash Flows from Financing Activities
Cash provided by financing activities during the year ended December 31, 2019 was negligible.
Cash provided by financing activities during the year ended December 31, 2018 was $65.3 million, consisting of $64.9 million of net proceeds from our follow-on offering and $0.4 million of proceeds from the exercise of stock options.
87
Cash provided by financing activities during the year ended December 31, 2017 was $1.4 million, consisting of $0.7 million of stock sales and $0.7 million of proceeds from the exercise of stock options.
Off‑Balance Sheet Arrangements
We have not entered into any off‑balance sheet arrangements and do not have any holdings in variable interest entities.
Contractual Obligations
We lease our facilities under a non‑cancelable operating lease that expires in 2023. As of December 31, 2019, contractual obligations were as follows (in thousands):
|
|
|
Payment Due by Period |
|||||||||||||
|
|
|
|
|
|
Less than |
|
|
|
|
|
|
|
More than |
||
|
|
|
Total |
|
1 year |
|
2 - 3 years |
|
4 - 5 years |
|
5 years |
|||||
|
Contractual obligations: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Operating lease obligations |
|
$ |
3,718 |
|
$ |
1,159 |
|
$ |
2,559 |
|
$ |
— |
|
$ |
— |
|
Total contractual obligations |
|
$ |
3,718 |
|
$ |
1,159 |
|
$ |
2,559 |
|
$ |
— |
|
$ |
— |
In August 2015 we entered into an agreement for a line of credit of $0.1 million for the purpose of issuing our landlord a letter of credit of $0.1 million as a security deposit under our facility lease. We pledged money market funds and marketable securities as collateral for the line of credit. Pursuant to our license agreements with each of Vernalis and Scripps, we have obligations to make future milestone and royalty payments to these parties. However, because these amounts are contingent, they have not been included on our balance sheet.
Critical Accounting Policies
Our management’s discussion and analysis of our financial condition and results of operations is based on our financial statements, which have been prepared in accordance with United States generally accepted accounting principles (“U.S. GAAP”). The preparation of these financial statements requires our management to make judgments and estimates that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements, as well as the reported revenue generated and expenses incurred during the reporting periods. Our estimates are based on our historical experience and on various other factors that we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these judgments and estimates under different assumptions or conditions and any such differences may be material. We believe that the accounting policies discussed below are critical to understanding our historical and future performance, as these policies relate to the more significant areas involving management’s judgments and estimates. Our significant accounting policies are more fully described in Note 2 of Notes to Financial Statements in Part II, Item 8 of this Annual Report on Form 10‑K.
Cash, Cash Equivalents and Marketable Securities
We consider all highly liquid investment securities with remaining maturities at the date of purchase of three months or less to be cash equivalents.
Investments with remaining maturities, at the date of purchase, greater than three months, but less than one year are considered short‑term. We determined the appropriate classification of marketable securities at the time of purchase and evaluates such designation as of each balance sheet date. To date, all marketable securities have been classified as available‑for‑sale and are carried at fair value with unrealized gains and losses, if any, included as a component of accumulated other comprehensive income (loss) in stockholders’ equity (deficit). Interest and realized gains and losses are included in interest income. Realized gains and losses are recognized based on the specific identification method.
88
Research and Development Expenses
We record research and development expenses as incurred. We account for nonrefundable advance payments for goods and services that will be used in future research and development activities as expenses when the goods have been received or when the service has been performed rather than when the payment is made. Research and development expenses consist of costs incurred by us for the discovery and development of our product candidates and include:
|
· |
employee‑related expenses, including salaries, benefits, travel and non‑cash stock‑based compensation expense; |
|
· |
external research and development expenses incurred under arrangements with third parties, such as contract research organizations, contract manufacturing organizations, academic and non‑profit institutions and consultants; |
|
· |
costs to acquire technologies to be used in research and development that have not reached technological feasibility and have no alternative future use; |
|
· |
license fees; and |
|
· |
other expenses, which include direct and allocated expenses for laboratory, facilities and other costs. |
Clinical Trial Accruals
Costs for preclinical studies and clinical trial activities are recognized based on an evaluation of the vendors’ progress towards completion of specific tasks, using data such as clinical site activations, patient enrollment or information provided to us by our vendors regarding their actual costs incurred. Payments for these activities are based on the terms of individual contracts and payment timing may differ significantly from the period in which the services are performed. We determine accrual estimates through reports from and discussions with applicable personnel and outside service providers as to the progress or state of completion, or the services completed. Our estimates of accrued expenses as of each balance sheet date are based on the facts and circumstances known at the time
Recent Accounting Pronouncements
See Note 2 in Item 8 “Financial Statements and Supplementary Data.”
Segment Information
We have one primary business activity and operate as one reportable segment.
JOBS Act Accounting Election
We are an emerging growth company, as defined in the JOBS Act. Under the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards issued subsequent to the enactment of the JOBS Act until such time as those standards apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, will be subject to the same new or revised accounting standards as other public companies that are not emerging growth companies. We also intend to rely on other exemptions provided by the JOBS Act, including, without limitation, providing an auditor’s attestation report on our system of internal controls over financial reporting pursuant to Section 404(b) of the Sarbanes‑Oxley Act. We will remain an emerging growth company until the earlier of (1) December 31, 2021, (2) the last day of the fiscal year in which we have total annual gross revenue of at least $1.07 billion, (3) the last day of the fiscal year in which we are deemed to be a “large accelerated filer” as defined in Rule 12b‑2 under the Exchange Act, which would occur if the market value of our common stock held by non‑affiliates exceeded $700.0 million as of the last business day of the
89
second fiscal quarter of such fiscal year, or (4) the date on which we have issued more than $1.0 billion in non‑convertible debt securities during the prior three‑year period.
Item 7A. Quantitative and Qualitative Disclosures about Market Risk
We are exposed to market risk related to changes in interest rates. We had cash, cash equivalents and marketable securities of $78.0 million as of December 31, 2019, which consisted of U.S. Treasury securities, U.S. government agency securities and corporate debt obligations. Such interest‑earning instruments carry a degree of interest rate risk; however, historical fluctuations of interest income have not been significant. Due to the short‑term duration of our investment portfolio and the low risk profile of our investments, an immediate 10% increase in interest rates would not have a material effect on the fair market value of our portfolio.
We do not have any foreign currency or other derivative financial instruments.
90
Item 8. Financial Statements and Supplementary Data
CORVUS PHARMACEUTICALS, INC.
ANNUAL REPORT ON FORM 10‑K
INDEX TO FINANCIAL STATEMENTS
|
|
Page |
| 92 | |
|
Financial Statements |
|
| 93 | |
| 94 | |
| 95 | |
| 96 | |
| 97 |
91
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of Corvus Pharmaceuticals, Inc.
Opinion on the Financial Statements
We have audited the accompanying balance sheet of Corvus Pharmaceuticals, Inc. (the “Company”) as of December 31, 2019 and 2018, and the related statements of operations and comprehensive loss, changes in stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2019, including the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2019 , and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2019 in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audit. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit of these financial statements in accordance with the standards of the PCAOB and in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audit we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audit included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audit also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audit provides a reasonable basis for our opinion.
/s/ PricewaterhouseCoopers LLP
San Jose, California
March 9, 2020
We have served as the Company’s auditor since 2015
92
CORVUS PHARMACEUTICALS, INC.
(in thousands, except share data)
|
|
|
December 31, |
|
December 31, |
||
|
|
|
2019 |
|
2018 |
||
|
Assets |
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
5,154 |
|
$ |
39,196 |
|
Marketable securities |
|
|
72,828 |
|
|
75,401 |
|
Prepaid and other current assets |
|
|
1,362 |
|
|
992 |
|
Total current assets |
|
|
79,344 |
|
|
115,589 |
|
Property and equipment, net |
|
|
1,462 |
|
|
2,180 |
|
Operating lease right-of-use asset |
|
|
2,327 |
|
|
— |
|
Other assets |
|
|
513 |
|
|
463 |
|
Total assets |
|
$ |
83,646 |
|
$ |
118,232 |
|
|
|
|
|
|
|
|
|
Liabilities and Stockholders’ Equity |
|
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
|
Accounts payable |
|
$ |
2,448 |
|
$ |
1,998 |
|
Operating lease liability |
|
|
878 |
|
|
— |
|
Accrued and other liabilities |
|
|
6,899 |
|
|
5,029 |
|
Total current liabilities |
|
|
10,225 |
|
|
7,027 |
|
Operating lease liability |
|
|
2,310 |
|
|
— |
|
Other liabilities |
|
|
— |
|
|
869 |
|
Total liabilities |
|
|
12,535 |
|
|
7,896 |
|
Commitments and contingencies (Note 12) |
|
|
|
|
|
|
|
Stockholders’ equity: |
|
|
|
|
|
|
|
Preferred stock: $0.0001 par value; 10,000,000 shares authorized at December 31, 2019 and December 31, 2018; 0 shares issued and outstanding at December 31, 2019 and December 31, 2018 |
|
|
— |
|
|
— |
|
Common stock: $0.0001 par value; 290,000,000 shares authorized at December 31, 2019 and December 31, 2018; 27,953,233 and 29,323,930 shares issued and outstanding at December 31, 2019 and December 31, 2018, respectively |
|
|
3 |
|
|
3 |
|
Additional paid-in capital |
|
|
288,224 |
|
|
280,840 |
|
Accumulated other comprehensive income (loss) |
|
|
29 |
|
|
(34) |
|
Accumulated deficit |
|
|
(217,145) |
|
|
(170,473) |
|
Total stockholders’ equity |
|
|
71,111 |
|
|
110,336 |
|
Total liabilities and stockholders’ equity |
|
$ |
83,646 |
|
$ |
118,232 |
The accompanying notes are an integral part of these financial statements.
93
CORVUS PHARMACEUTICALS, INC.
STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
(in thousands, except share and per share data)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
37,975 |
|
$ |
38,586 |
|
$ |
46,305 |
|
General and administrative |
|
|
10,879 |
|
|
10,636 |
|
|
10,219 |
|
Total operating expenses |
|
|
48,854 |
|
|
49,222 |
|
|
56,524 |
|
Loss from operations |
|
|
(48,854) |
|
|
(49,222) |
|
|
(56,524) |
|
Interest income and other expense, net |
|
|
2,182 |
|
|
2,283 |
|
|
861 |
|
Net loss |
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
|
Net loss per share, basic and diluted |
|
$ |
(1.59) |
|
$ |
(1.71) |
|
$ |
(2.72) |
|
Shares used to compute net loss per share, basic and diluted |
|
|
29,349,810 |
|
|
27,509,960 |
|
|
20,488,506 |
|
Other comprehensive loss: |
|
|
|
|
|
|
|
|
|
|
Unrealized gain (loss) on marketable securities |
|
|
63 |
|
|
7 |
|
|
(2) |
|
Comprehensive loss |
|
$ |
(46,609) |
|
$ |
(46,932) |
|
$ |
(55,665) |
The accompanying notes are an integral part of these financial statements.
94
CORVUS PHARMACEUTICALS, INC.
STATEMENTS OF CHANGES IN STOCKHOLDERS’ EQUITY
(in thousands, except share and per share data)
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
Other |
|
|
|
|
Total |
|||
|
|
|
Common Stock |
|
Paid-in |
|
Comprehensive |
|
Accumulated |
|
Stockholders’ |
|||||||
|
|
|
Shares |
|
Amount |
|
Capital |
|
Income (Loss) |
|
Deficit |
|
Equity |
|||||
|
Balance at December 31, 2016 |
|
20,922,428 |
|
$ |
2 |
|
$ |
200,709 |
|
$ |
(39) |
|
$ |
(67,871) |
|
$ |
132,801 |
|
Issuance of common stock in conjunction with the Sales Agreement, net |
|
52,569 |
|
|
— |
|
|
711 |
|
|
— |
|
|
— |
|
|
711 |
|
Common stock issued on exercise of stock options |
|
66,253 |
|
|
— |
|
|
731 |
|
|
— |
|
|
— |
|
|
731 |
|
Vesting of restricted stock issued upon early exercise of stock options |
|
— |
|
|
— |
|
|
28 |
|
|
— |
|
|
— |
|
|
28 |
|
Stock-based compensation expense |
|
— |
|
|
— |
|
|
6,229 |
|
|
— |
|
|
— |
|
|
6,229 |
|
Unrealized loss on marketable securities |
|
— |
|
|
— |
|
|
— |
|
|
(2) |
|
|
— |
|
|
(2) |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(55,663) |
|
|
(55,663) |
|
Balance at December 31, 2017 |
|
21,041,250 |
|
$ |
2 |
|
$ |
208,408 |
|
$ |
(41) |
|
$ |
(123,534) |
|
$ |
84,835 |
|
Issuance of common stock upon follow-on public offering, net |
|
8,117,647 |
|
|
1 |
|
|
64,876 |
|
|
— |
|
|
— |
|
|
64,877 |
|
Common stock issued on exercise of stock options |
|
165,033 |
|
|
— |
|
|
393 |
|
|
— |
|
|
— |
|
|
393 |
|
Vesting of restricted stock issued upon early exercise of stock options |
|
— |
|
|
— |
|
|
28 |
|
|
— |
|
|
— |
|
|
28 |
|
Stock-based compensation expense |
|
— |
|
|
— |
|
|
7,135 |
|
|
— |
|
|
— |
|
|
7,135 |
|
Unrealized gain on marketable securities |
|
— |
|
|
— |
|
|
— |
|
|
7 |
|
|
— |
|
|
7 |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(46,939) |
|
|
(46,939) |
|
Balance at December 31, 2018 |
|
29,323,930 |
|
$ |
3 |
|
$ |
280,840 |
|
$ |
(34) |
|
$ |
(170,473) |
|
$ |
110,336 |
|
Retirement of common stock in exchange for common stock warrant |
|
(1,458,000) |
|
|
— |
|
|
(5,030) |
|
|
— |
|
|
— |
|
|
(5,030) |
|
Issuance of common stock warrant in exchange for retirement of common stock |
|
— |
|
|
— |
|
|
5,030 |
|
|
— |
|
|
— |
|
|
5,030 |
|
Common stock issued on exercise of stock options |
|
87,303 |
|
|
— |
|
|
24 |
|
|
— |
|
|
— |
|
|
24 |
|
Vesting of restricted stock issued upon early exercise of stock options |
|
— |
|
|
— |
|
|
12 |
|
|
— |
|
|
— |
|
|
12 |
|
Stock-based compensation expense |
|
— |
|
|
— |
|
|
7,348 |
|
|
— |
|
|
— |
|
|
7,348 |
|
Unrealized gain on marketable securities |
|
— |
|
|
— |
|
|
— |
|
|
63 |
|
|
— |
|
|
63 |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(46,672) |
|
|
(46,672) |
|
Balance at December 31, 2019 |
|
27,953,233 |
|
$ |
3 |
|
$ |
288,224 |
|
$ |
29 |
|
$ |
(217,145) |
|
$ |
71,111 |
The accompanying notes are an integral part of these financial statements.
95
CORVUS PHARMACEUTICALS, INC.
(in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Cash flows from operating activities |
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
|
Depreciation and amortization |
|
|
743 |
|
|
847 |
|
|
842 |
|
Accretion related to marketable securities |
|
|
(644) |
|
|
(608) |
|
|
(195) |
|
Stock-based compensation |
|
|
7,348 |
|
|
7,135 |
|
|
6,229 |
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
Prepaid and other current assets |
|
|
(370) |
|
|
187 |
|
|
(44) |
|
Operating lease right-of-use asset |
|
|
599 |
|
|
— |
|
|
— |
|
Other assets |
|
|
(50) |
|
|
406 |
|
|
— |
|
Accounts payable |
|
|
450 |
|
|
(1,456) |
|
|
1,554 |
|
Accrued and other liabilities |
|
|
2,030 |
|
|
(458) |
|
|
1,499 |
|
Operating lease liability |
|
|
(767) |
|
|
— |
|
|
— |
|
Other long-term liabilities |
|
|
12 |
|
|
(102) |
|
|
(434) |
|
Net cash used in operating activities |
|
|
(37,321) |
|
|
(40,988) |
|
|
(46,212) |
|
Cash flows from investing activities |
|
|
|
|
|
|
|
|
|
|
Purchases of marketable securities |
|
|
(138,586) |
|
|
(161,861) |
|
|
(88,309) |
|
Maturities of marketable securities |
|
|
141,866 |
|
|
132,024 |
|
|
173,401 |
|
Purchases of property and equipment |
|
|
(25) |
|
|
(355) |
|
|
(266) |
|
Net cash provided by (used in) investing activities |
|
|
3,255 |
|
|
(30,192) |
|
|
84,826 |
|
Cash flows from financing activities |
|
|
|
|
|
|
|
|
|
|
Proceeds from issuance of common stock, net (includes $30,850 in aggregate gross proceeds from related parties for the year ended December 31, 2018) |
|
|
— |
|
|
64,877 |
|
|
711 |
|
Proceeds from exercise of common stock options |
|
|
24 |
|
|
393 |
|
|
731 |
|
Net cash provided by financing activities |
|
|
24 |
|
|
65,270 |
|
|
1,442 |
|
Net decrease in cash and cash equivalents |
|
|
(34,042) |
|
|
(5,910) |
|
|
40,056 |
|
Cash and cash equivalents at beginning of the period |
|
|
39,196 |
|
|
45,106 |
|
|
5,050 |
|
Cash and cash equivalents at end of the period |
|
$ |
5,154 |
|
$ |
39,196 |
|
$ |
45,106 |
|
Supplemental disclosures of cash flow information |
|
|
|
|
|
|
|
|
|
|
Purchases of property and equipment incurred but not paid |
|
$ |
— |
|
$ |
84 |
|
$ |
— |
The accompanying notes are an integral part of these financial statements.
96
CORVUS PHARMACEUTICALS, INC.
1. Organization
Corvus Pharmaceuticals, Inc. (“Corvus” or the “Company”) was incorporated in Delaware on January 27, 2014 and commenced operations in November 2014. Corvus is a clinical stage biopharmaceutical company focused on the development and commercialization of precisely targeted oncology therapies. The Company’s operations are located in Burlingame, California.
Initial Public Offering
On March 22, 2016, the Company’s registration statement on Form S-1 (File No. 333-208850) relating to its initial public offering (“IPO”) of its common stock was declared effective by the Securities and Exchange Commission (“SEC”) and the shares of its common stock began trading on the Nasdaq Global Market on March 23, 2016. The public offering price of the shares sold in the IPO was $15.00 per share. The IPO closed on March 29, 2016, pursuant to which the Company sold 4,700,000 shares of its common stock. On April 26, 2016, the Company sold an additional 502,618 shares of its common stock to the underwriters upon partial exercise of their over-allotment option, at the initial offering price of $15.00 per share. The Company received aggregate net proceeds of approximately $70.6 million, after underwriting discounts, commissions and offering expenses. Immediately prior to the consummation of the IPO, all outstanding shares of convertible preferred stock were converted into common stock.
Follow-on Public Offering
In March 2018, the Company completed a follow-on public offering in which the Company sold 8,117,647 shares of common stock at a price of $8.50 per share, which included 1,058,823 shares issued pursuant to the underwriters’ exercise of their option to purchase additional shares of common stock. The aggregate net proceeds received by the Company from the offering were approximately $64.9 million, net of underwriting discounts and commissions and offering expenses payable by the Company.
Liquidity
The Company is subject to risks and uncertainties common to early-stage companies in the biotechnology industry, including, but not limited to, development by competitors of new technological innovations, protection of proprietary technology, dependence on key personnel, contract manufacturer and contract research organizations, compliance with government regulations and the need to obtain additional financing to fund operations. Since commencing operations in 2014, the majority of the Company’s efforts have been focused on the research and development of ciforadenant, CPI-006 and CPI-818. The Company believes that it will continue to expend substantial resources for the foreseeable future as it continues clinical development of, seek regulatory approval for and, if approved, prepare for the commercialization of ciforadenant, CPI-006, and CPI-818, as well as product candidates under the Company’s other development programs. These expenditures will include costs associated with research and development, conducting preclinical studies and clinical trials, obtaining regulatory approvals, manufacturing and supply, sales and marketing and general operations. In addition, other unanticipated costs may arise. Because the outcome of any clinical trial and/or regulatory approval process is highly uncertain, the Company may not be able to accurately estimate the actual amounts necessary to successfully complete the development, regulatory approval process and commercialization of ciforadenant, CPI-006, CPI-818 or any other product candidates. The Company does not expect its existing capital resources to be sufficient to enable it to fund the completion of its clinical trials and remaining development program of ciforadenant, CPI-006 or CPI-818 through commercialization. In addition, its operating plan may change as a result of many factors, including those described in this Annual Report on Form 10-K for the year ended December 31, 2019.
The Company has incurred significant losses and negative cash flows from operations in all periods since inception and had an accumulated deficit of $217.1 million as of December 31, 2019. The Company has historically
97
financed its operations primarily through the sale of redeemable convertible preferred stock and common stock. While the Company has been able to raise multiple rounds of financing, there can be no assurance that in the event the Company requires additional financing, such financing will be available on terms which are favorable or at all. Failure to generate sufficient cash flows from operations, raise additional capital or reduce certain discretionary spending would have a material adverse effect on the Company’s ability to achieve its intended business objectives.
As of December 31, 2019, the Company had cash, cash equivalents and short-term marketable securities of $78.0 million. Management believes that the Company’s current cash, cash equivalents and short-term marketable securities will be sufficient to fund its planned operations for at least 12 months from the date of the issuance of these financial statements
Exchange Warrants
On November 8, 2019, the Company entered into an exchange agreement (the “Exchange Agreement”) with an Investor and its affiliates (the “Exchanging Stockholders”), pursuant to which the Company exchanged an aggregate of 1,458,000 shares of the Company’s common stock, par value $0.0001 per share, owned by the Exchanging Stockholders for pre-funded warrants (the “Exchange Warrants”) to purchase an aggregate of 1,458,000 shares of common stock (subject to adjustment in the event of any stock dividends and splits, reverse stock split, recapitalization, reorganization or similar transaction, as described in the Exchange Warrants), with an exercise price of $0.0001 per share. The Exchange Warrants will expire ten years from the date of issuance. The Exchange Warrants are exercisable at any time prior to expiration except that the Exchange Warrants cannot be exercised by the Exchanging Stockholders if, after giving effect thereto, the Exchanging Stockholders would beneficially own more than 9.99% of the Company’s common stock, subject to certain exceptions. In accordance with Accounting Standards Codification Topic 505, Equity, and Accounting Research Bulletin 43, the Company recorded the retirement of the common stock exchanged as a reduction of common shares outstanding and elected to record the excess over par value as a debit to additional paid-in-capital at the fair value of the Exchange Warrants on the issuance date. The Exchange Warrants are classified as equity in accordance with Accounting Standards Codification Topic 480, Distinguishing Liabilities from Equity, and Accounting Standards Codification Topic 815, Derivatives and Hedging, and the fair value of the Exchange Warrants was recorded as a credit to additional paid-in capital and is not subject to remeasurement. The Company determined that the fair value of the Exchange Warrants is substantially similar to the fair value of the retired shares on the issuance date due to the negligible exercise price for the Exchange Warrants. As of December 31, 2019, none of the Exchange Warrants have been exercised.
2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America (“U.S. GAAP”). The Company’s functional and reporting currency is the U.S. dollar. The accompanying financial statements have been prepared on a going-concern basis, which contemplates the realization of assets and discharge of liabilities in the normal course of business. Since its inception, the Company has incurred significant losses and negative cash flows from operations. As of December 31, 2019, the Company had an accumulated deficit of $217.1 million and cash, cash equivalents and marketable securities of $78.0 million. The Company has financed its operations primarily with the proceeds from the sale of stock. The Company will need to raise additional capital to meet its business objectives. The Company believes that its current cash, cash equivalents and marketable securities will be sufficient to fund its planned expenditures and meet its obligations through at least the next twelve months from the issuance of these financial statements.
Use of Estimates
The preparation of the Company’s financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Actual results could differ from such estimates.
98
Concentrations of Credit Risk and Other Risks and Uncertainties
Substantially all of the Company’s cash and cash equivalents are deposited in accounts with two financial institutions that management believes are of high credit quality. Such deposits may, at times, exceed federally insured limits. The Company maintains its cash with an accredited financial institution and accordingly, such funds are subject to minimal credit risk. The Company’s marketable securities consist of investments in U.S. Treasury securities, U.S. government agency securities and corporate debt obligations, which can be subject to certain credit risks. However, the Company mitigates the risks by investing in high-grade instruments, limiting its exposure to any one issuer, and monitoring the ongoing creditworthiness of the financial institutions and issuers. The Company has not experienced any losses on its deposits of cash, cash equivalents or marketable securities.
The Company is subject to a number of risks similar to other early stage biopharmaceutical companies, including, but not limited to, the need to obtain adequate additional funding, possible failure of preclinical testing or clinical trials, its reliance on third parties to conduct its clinical trials, the need to obtain marketing approval for its product candidates, competitors developing new technological innovations, the need to successfully commercialize and gain market acceptance of the Company’s product candidates, its right to develop and commercialize its product candidates pursuant to the terms and conditions of the licenses granted to the Company, and protection of proprietary technology. If the Company does not successfully commercialize or partner any of its product candidates, it will be unable to generate product revenue or achieve profitability.
Segments
Operating segments are identified as components of an enterprise about which separate discrete financial information is available for evaluation by the chief operating decision‑maker in making decisions regarding resource allocation and assessing performance. The Company views its operations and manages its business in one operating segment, that of the development of and commercialization of precisely targeted oncology therapies.
Cash, Cash Equivalents and Marketable Securities
The Company considers all highly liquid investment securities with remaining maturities at the date of purchase of three months or less to be cash equivalents.
Investments with remaining maturities, at the date of purchase, greater than three months are classified as “available-for-sale” and are carried at fair value with unrealized gains and losses, if any, included as a component of accumulated other comprehensive income (loss) in stockholders’ equity. Interest and realized gains and losses are included in interest income. Realized gains and losses are recognized based on the specific identification model.
Fair Value Measurements
Fair value accounting is applied for all financial assets and liabilities and non-financial assets and liabilities that are recognized or disclosed at fair value in the financial statements on a recurring basis (at least annually). The carrying amount of the Company’s financial instruments, including cash equivalents, accounts payable and accrued liabilities, approximate fair value due to their short-term maturities.
Property and Equipment, Net
Property and equipment are stated at cost and depreciated using the straight‑line method over the estimated useful lives of the respective assets:
|
Laboratory equipment |
|
5 |
years |
|
Computer equipment and purchased software |
|
3 |
years |
|
Leasehold improvements |
|
Shorter of asset's useful life or remaining term of lease |
|
99
Maintenance and repairs that do not extend the life or improve the asset are expensed when incurred. When assets are retired or otherwise disposed of, the cost and accumulated depreciation or amortization are removed from the balance sheet and any resulting gain or loss is reflected in operations.
Impairment of Long‑Lived Assets
The Company regularly reviews the carrying value and estimated lives of all of its long-lived assets, including property and equipment, to determine whether indicators of impairment may exist which warrant adjustments to carrying values or estimated useful lives. The determinants used for this evaluation include management’s estimate of the asset’s ability to generate positive income from operations and positive cash flow in future periods as well as the strategic significance of the assets to the Company’s business objectives. Should impairment exist, the impairment loss to be recognized is measured by the amount by which the carrying amount of the asset exceeds the projected discounted future net cash flows arising from the asset. All long-lived assets are maintained in the United States of America.
Research and Development Expenses
The Company records research and development expenses as incurred. The Company accounts for nonrefundable advance payments for goods and services that will be used in future research and development activities as expenses when the goods have been received or when the service has been performed rather than when the payment is made. Research and development expenses consist of costs incurred by the Company for the discovery and development of the Company’s product candidates and include:
|
· |
employee‑related expenses, including salaries, benefits, travel and non‑cash stock‑based compensation expense; |
|
· |
external research and development expenses incurred under arrangements with third parties, such as contract research organizations, contract manufacturing organizations, academic and non‑profit institutions and consultants; |
|
· |
costs to acquire technologies to be used in research and development that have not reached technological feasibility and have no alternative future use; |
|
· |
license fees; and |
|
· |
other expenses, which include direct and allocated expenses for laboratory, facilities and other costs. |
Clinical Trial Accruals
Costs for preclinical studies and clinical trial activities are recognized based on an evaluation of the vendors’ progress towards completion of specific tasks, using data such as clinical site activations, patient enrollment or information provided to the Company by its vendors regarding their actual costs incurred. Payments for these activities are based on the terms of individual contracts and payment timing may differ significantly from the period in which the services are performed. The Company determines accrual estimates through reports from and discussions with applicable personnel and outside service providers as to the progress or state of completion, or the services completed. The Company’s estimates of accrued expenses as of each balance sheet date are based on the facts and circumstances known at the time.
Stock‑Based Compensation
The Company maintains incentive plans under which incentive stock options and nonqualified stock options may be granted to employees and non‑employee service providers.
100
The Company accounts for stock-based employee compensation arrangements in accordance with the provisions of ASC 718, “Compensation—Stock Compensation.” For stock options granted to employees, the Company recognizes compensation expense for all stock-based awards based on the grant-date estimated fair values. The value of the award is recognized as an expense ratably over the requisite service period. The fair value of stock options is determined using the Black-Scholes option pricing model. Forfeitures are accounted for when they occur.
Stock-based compensation expense related to stock options granted to non-employees is recognized based on the fair value of the stock options, determined using the Black-Scholes option pricing model. The awards generally vest over the time period the Company expects to receive service from the non-employee.
Income Taxes
The Company accounts for income taxes under the asset and liability method. The Company estimates actual current tax exposure together with assessing temporary differences resulting from differences in accounting for reporting purposes and tax purposes for certain items, such as accruals and allowances not currently deductible for tax purposes. These temporary differences result in deferred tax assets and liabilities, which are included in the Company’s balance sheets. In general, deferred tax assets represent future tax benefits to be received when certain expenses previously recognized in the Company’s statements of operations and comprehensive loss become deductible expenses, under applicable income tax laws or when net operating loss or credit carryforwards are utilized. Accordingly, realization of the Company’s deferred tax assets is dependent on future taxable income against which these deductions, losses and credits can be utilized.
The Company must assess the likelihood that the Company’s deferred tax assets will be recovered from future taxable income and a valuation allowance is recorded when it is more likely than not that the deferred tax asset will not be recovered. The Company applies judgment in the determination of the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. Based on the available evidence, the Company is unable, at this time, to support the determination that it is more likely than not that its deferred tax assets will be utilized in the future. Accordingly, the Company recorded a full valuation allowance for all periods presented. The Company intends to maintain a valuation allowance until sufficient evidence exists to support its reversal.
The Company recognizes benefits of uncertain tax positions if it is more likely than not such positions will be sustained upon examination based solely on their technical merits as the largest amount of benefit that is more likely than not to be realized upon the ultimate settlement. The Company recognizes any material interest and penalties related to unrecognized tax benefits in income tax expense. The Company is required to file income tax returns in the U.S. federal jurisdiction. The Company currently is not under examination by the Internal Revenue Service or other jurisdictions for any tax years.
Comprehensive Loss
Comprehensive loss includes net loss as well as other changes in stockholders’ equity that result from transactions and economic events other than those with stockholders. The Company’s only element of other comprehensive loss in any period presented was unrealized gains and losses on available-for-sale marketable securities.
Net Loss per Share
Basic net loss per share is calculated by dividing the net loss by the weighted average number of common shares outstanding and Exchange Warrants outstanding during the period, without consideration of potentially dilutive securities. In accordance with Accounting Standards Codification Topic 260, Earnings Per Share, the Exchange Warrants are included in the computation of basic net loss per share because the exercise price is negligible and they are fully vested and exercisable at any time after the original issuance date. Diluted net loss per share is computed by dividing the net loss by the weighted average number of common shares, Exchange Warrants, and potentially dilutive securities outstanding for the period. Diluted net loss per share is the same as basic net loss per share for all periods presented since the effect of potentially dilutive securities is anti-dilutive given the net loss of the Company.
101
Recent Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) No. 2014-09, Revenue from Contracts with Customers, which required an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. ASU No. 2014-09 will replace most existing revenue recognition guidance in U.S. GAAP when it becomes effective. The new standard is effective January 1, 2018 for public companies. Early application is permitted as of January 1, 2017. The standard permits the use of either the retrospective or cumulative effect transition method. In March 2016, the FASB issued ASU No. 2016-08, Revenue from Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net), which clarifies the implementation guidance on principal versus agent considerations in ASU No. 2014-09. In April 2016, the FASB issued ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing, which clarifies certain aspects of identifying performance obligations and licensing implementation guidance. In May 2016, the FASB issued ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients, which relates to disclosures of remaining performance obligations, as well as other amendments to guidance on collectability, non-cash consideration and the presentation of sales and other similar taxes collected from customers. These standards have the same effective date and transition date of January 1, 2018. The Company adopted this guidance on January 1, 2018. The adoption of this guidance did not have a material impact on its condensed financial statements as the Company is not yet generating revenues.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842), which requires lessees to recognize leases on-balance sheet and disclose key information about leasing arrangements. Topic 842 was subsequently amended by ASU No. 2018-01, Land Easement Practical Expedient for Transition to Topic 842; ASU No. 2018-10, Codification Improvements to Topic 842, Leases; and ASU No. 2018-11, Targeted Improvements. The new standard establishes a right-of-use (ROU) model that requires a lessee to recognize an ROU asset and lease liability on the balance sheet. Leases will be classified as finance or operating, with classification affecting the pattern and classification of expense recognition in the statement of operations. The Company adopted the new standard on January 1, 2019 and chose to apply the provisions of ASC 842 as of the effective date with no restatement of prior periods. Additionally, the Company has elected the ‘package of practical expedients’, which permit it not to reassess under the new standard its prior conclusions about lease identification, lease classification and initial direct costs. The Company did not elect the use-of-hindsight or the practical expedient pertaining to land easements; the latter is not applicable to the Company. The Company determines if an arrangement is a lease at inception and accounts for lease and non-lease components separately. The Company has elected not to apply the recognition requirements of Topic 842 for leases with a term of 12 months or less. Upon adoption of ASU 2016-02, the Company recognized an operating lease, right-of-use asset of $2.8 million and a corresponding liability of $3.8 million and eliminated $1.0 million of deferred rent in the Company’s condensed balance sheet. The adoption of ASU 2016-02 did not have any impact on the Company’s condensed statements of operations and comprehensive loss. See also Note 11.
In May 2017, the FASB issued ASU No 2017-09, Compensation—Stock Compensation (Topic 718) — Scope of Modification Accounting, to clarify when to account for a change to the terms or conditions of a share-based payment award as a modification. Under the new standard, modification is required only if the fair value, the vesting conditions, or the classification of an award as equity or liability changes as a result of the change in terms or conditions. ASU 2017-09 was effective for the Company beginning January 1, 2018 and is applied prospectively. Early adoption is permitted. The Company adopted this guidance on January 1, 2018. The adoption of this guidance did not have a material impact on its financial statements as the Company has not made any changes to the terms or conditions of its share-based payment awards.
102
3. Net Loss per Share
The following table shows the calculation of net loss per share (in thousands, except share and per share data):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Numerator: |
|
|
|
|
|
|
|
|
|
|
Net loss - basic and diluted |
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
|
Denominator: |
|
|
|
|
|
|
|
|
|
|
Weighted average common shares outstanding |
|
|
29,364,535 |
|
|
27,686,909 |
|
|
20,958,557 |
|
Less: weighted average common shares subject to repurchase |
|
|
(14,725) |
|
|
(176,949) |
|
|
(470,051) |
|
Weighted average common shares outstanding used to compute basic and diluted net loss per share |
|
|
29,349,810 |
|
|
27,509,960 |
|
|
20,488,506 |
|
Net loss per share, basic and diluted |
|
$ |
(1.59) |
|
$ |
(1.71) |
|
$ |
(2.72) |
The amounts in the table below were excluded from the calculation of diluted net loss per share, due to their anti-dilutive effect:
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
Common stock subject to repurchase |
|
— |
|
43,076 |
|
319,203 |
|
Outstanding options |
|
5,643,410 |
|
3,778,259 |
|
3,013,394 |
|
Total shares of common stock equivalents |
|
5,643,410 |
|
3,821,335 |
|
3,332,597 |
4. Fair Value Measurements
Financial assets and liabilities are measured and recorded at fair value. The Company is required to disclose information on all assets and liabilities reported at fair value that enables an assessment of the inputs used in determining the reported fair values. The fair value hierarchy prioritizes valuation inputs based on the observable nature of those inputs. The fair value hierarchy applies only to the valuation inputs used in determining the reported fair value of the investments and is not a measure of the investment credit quality. The hierarchy defines three levels of valuation inputs:
|
· |
Level 1—Quoted prices in active markets for identical assets or liabilities |
|
· |
Level 2—Inputs other than quoted prices included within Level 1 that are observable for the asset or liability, either directly or indirectly |
|
· |
Level 3—Unobservable inputs that reflect the Company’s own assumptions about the assumptions market participants would use in pricing the asset or liability |
There have been no transfers of assets and liabilities between levels of hierarchy.
The Company’s Level 2 investments are valued using third-party pricing sources. The pricing services utilize industry standard valuation models, including both income and market-based approaches, for which all significant inputs are observable, either directly or indirectly, to estimate fair value. These inputs include reported trades of and broker/dealer quotes on the same or similar investments, issuer credit spreads, benchmark investments, prepayment/default projections based on historical data and other observable inputs.
103
The following tables present information as of December 31, 2019 and 2018 about the Company’s assets that are measured at fair value on a recurring basis and indicate the level of the fair value hierarchy the Company utilized to determine such fair values (in thousands):
|
|
|
December 31, 2019 |
||||||||||
|
|
|
Fair Value Measured Using |
|
Total |
||||||||
|
|
|
(Level 1) |
|
(Level 2) |
|
(Level 3) |
|
Balance |
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash equivalents |
|
$ |
4,252 |
|
$ |
— |
|
$ |
— |
|
$ |
4,252 |
|
Marketable securities |
|
|
7,023 |
|
|
65,805 |
|
|
— |
|
|
72,828 |
|
|
|
$ |
11,275 |
|
$ |
65,805 |
|
$ |
— |
|
$ |
77,080 |
|
|
|
December 31, 2018 |
||||||||||
|
|
|
Fair Value Measured Using |
|
Total |
||||||||
|
|
|
(Level 1) |
|
(Level 2) |
|
(Level 3) |
|
Balance |
||||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash equivalents |
|
$ |
38,698 |
|
$ |
— |
|
$ |
— |
|
$ |
38,698 |
|
Marketable securities |
|
|
— |
|
|
75,401 |
|
|
— |
|
|
75,401 |
|
|
|
$ |
38,698 |
|
$ |
75,401 |
|
$ |
— |
|
$ |
114,099 |
As of December 31, 2019, marketable securities had a maximum remaining maturity of ten months.
As of December 31, 2019 and 2018, the fair value of available for sale marketable securities by type of security were as follows (in thousands):
|
|
|
December 31, 2019 |
||||||||||
|
|
|
|
|
|
Gross |
|
Gross |
|
|
|
||
|
|
|
Amortized |
|
Unrealized |
|
Unrealized |
|
Fair |
||||
|
|
|
Cost |
|
Gains |
|
Losses |
|
Value |
||||
|
U.S. Treasury securities |
|
$ |
7,019 |
|
$ |
4 |
|
$ |
— |
|
$ |
7,023 |
|
U.S. Government agency securities |
|
|
17,701 |
|
|
16 |
|
|
— |
|
|
17,717 |
|
Corporate debt obligations |
|
|
48,079 |
|
|
17 |
|
|
(8) |
|
|
48,088 |
|
|
|
$ |
72,799 |
|
$ |
37 |
|
$ |
(8) |
|
$ |
72,828 |
|
|
|
December 31, 2018 |
||||||||||
|
|
|
|
|
|
Gross |
|
Gross |
|
|
|
||
|
|
|
Amortized |
|
Unrealized |
|
Unrealized |
|
Fair |
||||
|
|
|
Cost |
|
Gains |
|
Losses |
|
Value |
||||
|
U.S. Government agency securities |
|
$ |
49,124 |
|
$ |
— |
|
$ |
(27) |
|
$ |
49,097 |
|
Corporate debt obligations |
|
|
26,311 |
|
|
— |
|
|
(7) |
|
|
26,304 |
|
|
|
$ |
75,435 |
|
$ |
— |
|
$ |
(34) |
|
$ |
75,401 |
5. License and Collaboration Agreements
Scripps Licensing Agreement
In December 2014, the Company entered into a license agreement with The Scripps Research Institute (“Scripps”), pursuant to which it was granted a non-exclusive, world-wide license for all fields of use under Scripps’ rights in certain know-how and technology related to a mouse hybridoma clone expressing an anti-human CD73 antibody, and to progeny, mutants or unmodified derivatives of such hybridoma and any antibodies expressed by such hybridoma, from which we developed CPI-006. Scripps also granted the Company the right to grant sublicenses in conjunction with other proprietary rights the Company holds, or to others collaborating with or performing services for the Company. Under this license agreement, Scripps has agreed not to grant any additional commercial licenses with respect to such materials, other than march-in rights granted to the U.S. government.
104
Upon execution of the agreement, the Company made a one‑time cash payment to Scripps of $10,000 in 2015 and is also obligated to pay a minimum annual fee to Scripps of $25,000. The one‑time cash payment was recorded as research and development expense as technological feasibility of the asset had not been established and there was no alternative future use. A minimum annual fee payment is due on each anniversary of the effective date of the agreement for the term of the agreement. The Company is also required to make performance‑based cash payments upon successful completion of clinical and sales milestones. The aggregate potential milestone payments are $2.6 million. The Company is also required to pay royalties on net sales of licensed products (including CPI-006) sold by it, its affiliates and its sublicensees at a rate in the low‑single digits. In addition, should the Company sublicense the rights licensed under the agreement, it has agreed to pay a percentage of sublicense revenue received at specified rates that start at double digit percentages and decrease to single digit percentages based on the elapsed time from the effective date of the agreement and the time of entry into such sublicense. To date, no milestone payments have been made.
The Company’s license agreement with Scripps will terminate upon expiration of its obligation to pay royalties to Scripps under the license agreement. The Company’s license agreement with Scripps is terminable by the consent of the parties, at will by the Company upon providing 90 days written notice to Scripps, or by Scripps for certain material breaches, or if the Company undergoes a bankruptcy event. In addition, Scripps may terminate the license on a product‑by‑product basis, or the entire agreement, if the Company fails to meet specified diligence obligations related to the development and commercialization of licensed products. Scripps may also terminate the agreement after the third anniversary of the effective date of the agreement if it reasonably believes, based on reports the Company provides to Scripps, that the Company has not used commercially reasonable efforts as required under the agreement, subject to a specified notice and cure period.
Vernalis Licensing Agreement
In February 2015, the Company entered into a license agreement with Vernalis (R&D) Limited (“Vernalis”), which was subsequently amended as of November 5, 2015, and, pursuant to which the Company was granted an exclusive, worldwide license under certain patent rights and know-how, including a limited right to grant sublicenses, for all fields of use to develop, manufacture and commercialize products containing certain adenosine receptor antagonists, including ciforadenant. Pursuant to this agreement, the Company made a one-time cash payment to Vernalis in the amount of $1.0 million, which was recorded as research and development expense as technological feasibility of the asset had not been established and there was no alternative future use. The Company is also required to make cash milestone payments to Vernalis upon the successful completion of clinical and regulatory milestones for licensed products depending on the indications for which such licensed products are developed and upon achievement of certain sales milestones. In February 2017, the Company made a milestone payment of $3.0 million to Vernalis following the expansion of a cohort of patients with renal cell cancer treated with single agent ciforadenant in the Company’s Phase 1/1b clinical trial. The aggregate potential milestone payments are approximately $220 million for all The Company has also agreed to pay Vernalis tiered incremental royalties based on the annual net sales of licensed products containing ciforadenant on a product‑by‑product and country‑by‑country basis, subject to certain offsets and reductions. The tiered royalty rates for products containing ciforadenant range from the mid‑single digits up to the low‑double digits on a country‑by‑country net sales basis. The royalties on other licensed products that do not include ciforadenant also increase with the amount of net sales on a product-by-product and country‑by‑country basis and range from the low‑single digits up to the mid‑single digits on a country‑by‑country net sales basis. The Company is also obligated to pay to Vernalis certain sales milestones as indicated above when worldwide net sales reach specified levels over an agreed upon time period.
The agreement will expire on a product‑by‑product and country‑by‑country basis upon the expiration of the Company’s payment obligations to Vernalis in respect of a particular product and country. Both parties have the right to terminate the agreement for an uncured material breach by the other party. The Company may also terminate the agreement at its convenience by providing 90 days written notice, provided that the Company has not received notice of its own default under the agreement at the time the Company exercises such termination right. Vernalis may also terminate the agreement if the Company challenges a licensed patent or undergoes a bankruptcy event.
105
Genentech Collaboration Agreement
In October 2015, the Company entered into a clinical trial collaboration agreement with Genentech to evaluate the safety, tolerability and preliminary efficacy of ciforadenant combined with Genentech’s investigational cancer immunotherapy, Tecentriq (atezolizumab), a fully humanized monoclonal antibody targeting protein programmed cell death ligand 1(“PD-L1”), in a variety of solid tumors in a Phase 1/1b clinical trial. Pursuant to this agreement, the Company will be responsible for the conduct and cost of the relevant studies, under the supervision of a joint development committee made up of representatives of the Company and representatives of Genentech. Genentech will supply Tecentriq. As part of the agreement, the Company granted Genentech certain rights of first negotiation to participate in future clinical trials that the Company may conduct evaluating the administration of ciforadenant in combination with an anti-PD-1 or anti-PD-L1 antibody. If the Company and Genentech do not reach agreement on the terms of any such participation by Genentech within a specified time period, the Company retains the right to collaborate with third parties in such activities. The Company also granted Genentech certain rights of first negotiation should it decide to license development and commercialization rights to ciforadenant. Should the Company and Genentech not reach agreement on the terms of such a license within a specified time period, it retains the right to enter into a license with another third party.
The Company and Genentech each have the right to terminate the agreement for material breach by the other party. In addition, the agreement may be terminated by either party due to safety considerations, if directed by a regulatory authority or if development of ciforadenant or Tecentriq is discontinued. Further, the agreement will expire after a set period of time following the provision by the Company of the final clinical study report to Genentech.
In May, 2017, the Company signed a second clinical trial collaboration agreement with Genentech. Under the second agreement, ciforadenant administered in combination with Tecentriq is being evaluated in a Phase 1b/2 randomized, controlled clinical study, known as Morpheus, as second-line therapy in patients with non-small cell lung cancer who are resistant and/or refractory to prior therapy with an anti-PD-(L)1 antibody. The patients in the Morpheus trial are currently in the follow-up phase of the trial. Genentech is responsible for the conduct of the study and the parties share the cost of the Morpheus trial, which began enrolling patients in the fourth quarter of 2017. The Company is responsible for supplying ciforadenant and retains global development and commercialization rights to ciforadenant. The Company and Genentech each have the right to terminate the agreement for material breach by the other party. In addition, the agreement may be terminated by either party due to safety considerations, if directed by a regulatory authority or if development of ciforadenant or Tecentriq is discontinued.
Monash License Agreement
In April 2017, the Company entered into a license agreement with Monash University (Monash), pursuant to which the Company was granted an exclusive, sublicensable worldwide license under certain know‑how, patent rights and other intellectual property rights controlled by Monash to research, develop, and commercialize certain antibodies directed to CXCR2 for the treatment of human diseases.
Upon execution of the agreement, the Company made a one‑time cash payment to Monash of $275,000 and reimbursed Monash for certain patent prosecution costs incurred prior to execution of the agreement. The Company us also obligated to pay an annual license maintenance fee to Monash of $25,000 until a certain development milestone is met with respect to the licensed product, after which no further maintenance fee will be due. The Company is also required to make development and sales milestone payments to Monash with respect to the licensed products in the aggregate of up to $45.1 million. The Company is also required to pay to Monash tiered royalties on net sales of licensed products sold by it, its affiliates and its sublicensees at a rate ranging in the low‑single digits. In addition, should the Company sublicense its rights under the agreement, the Company has agreed to pay a percentage of sublicense revenue received at specified rates that are currently at low double digit percentages and decrease to single digit percentages based on the achievement of development milestones.
The term of the Company’s agreement with Monash continues until the expiration of its obligation to pay royalties to Monash thereunder. The license agreement is terminable at will by the Company upon providing 30 days written notice to Monash, or by either party for material breaches by the other party. In addition, Monash may terminate
106
the entire agreement or convert the license to a non-exclusive license if the Company has materially breached our obligation to use commercially reasonable efforts to develop and commercialize a licensed product, subject to a specified notice and cure mechanism.
6. Balance Sheet Components (in thousands):
|
|
|
December 31, |
||||
|
|
|
2019 |
|
2018 |
||
|
Prepaid and Other Current Assets |
|
|
|
|
|
|
|
Interest receivable |
|
$ |
329 |
|
$ |
337 |
|
Prepaid research and development manufacturing expenses |
|
|
240 |
|
|
75 |
|
Prepaid facility expenses |
|
|
157 |
|
|
149 |
|
Prepaid insurance |
|
|
150 |
|
|
166 |
|
Other |
|
|
486 |
|
|
265 |
|
|
|
$ |
1,362 |
|
$ |
992 |
|
Property and Equipment |
|
|
|
|
|
|
|
Laboratory equipment |
|
$ |
2,396 |
|
$ |
2,371 |
|
Computer equipment and purchased software |
|
|
142 |
|
|
142 |
|
Leasehold improvements |
|
|
2,084 |
|
|
2,084 |
|
|
|
|
4,622 |
|
|
4,597 |
|
Less: accumulated depreciation and amortization |
|
|
(3,160) |
|
|
(2,417) |
|
|
|
$ |
1,462 |
|
$ |
2,180 |
|
Accrued and Other Liabilities |
|
|
|
|
|
|
|
Accrued clinical trial related |
|
$ |
4,300 |
|
$ |
2,718 |
|
Accrued manufacturing expense |
|
|
696 |
|
|
1,077 |
|
Personnel related |
|
|
1,624 |
|
|
649 |
|
Other |
|
|
279 |
|
|
585 |
|
|
|
$ |
6,899 |
|
$ |
5,029 |
|
Other Liabilities |
|
|
|
|
|
|
|
Deferred rent |
|
$ |
— |
|
$ |
869 |
|
|
|
$ |
— |
|
$ |
869 |
7. Common Stock
As of December 31, 2019, the amended and restated certificate of incorporation authorizes the Company to issue 290 million shares of common stock and 10 million shares of preferred stock.
Each share of common stock is entitled to one vote. Common stockholders are entitled to dividends if and when declared by the board of directors. As of December 31, 2019, no dividends on common stock had been declared.
107
The Company has reserved shares of common stock, for issuance as follows:
|
|
|
December 31, |
||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
Exchange warrants |
|
1,458,000 |
|
— |
|
— |
|
Shares available for future option grants |
|
1,704,183 |
|
2,486,637 |
|
2,576,535 |
|
Outstanding options |
|
5,643,410 |
|
3,778,259 |
|
3,013,394 |
|
Unvested restricted common stock (founders and early exercise of stock options) |
|
— |
|
43,076 |
|
319,203 |
|
Shares reserved for employee stock purchase plan |
|
400,000 |
|
400,000 |
|
400,000 |
|
Total |
|
9,205,593 |
|
6,707,972 |
|
6,309,132 |
8. Stock Option Plans
In February 2014, the Company adopted the 2014 Equity Incentive Plan (the “2014 Plan”), which was subsequently amended in November 2014, July 2015 and September 2015, under which it granted incentive stock options (“ISOs”) or non-qualified stock options (“NSOs”). Terms of stock agreements, including vesting requirements, are determined by the board of directors or a committee authorized by the board of directors, subject to the provisions of the 2014 Plan. In general, awards granted by the Company vest over four years and have maximum exercise term of 10 years. The 2014 Plan provides that grants must be at an exercise price of 100% of fair market value of the Company’s common stock as determined by the board of directors on the date of the grant.
In connection with the consummation of the IPO in March 2016, the 2016 Equity Incentive Award Plan (the “2016 Plan”), became effective. Under the 2016 Plan, incentive stock options, non-statutory stock options, stock purchase rights and other stock-based awards may be granted. Terms of stock agreements, including vesting requirements, are determined by the board of directors or a committee authorized by the board of directors, subject to the provisions of the 2016 Plan. In general, awards granted by the Company vest over four years and have maximum exercise term of 10 years. The 2016 Plan provides that grants must be at an exercise price of 100% of fair market value of the Company’s common stock as determined by the board of directors on the date of the grant. In conjunction with adopting the 2016 Plan, the 2014 Plan was terminated and no further awards will be granted under the 2014 Plan. Options outstanding under the 2014 Plan as of the effective date of the 2016 Plan that are forfeited or lapse unexercised may be re-issued under the 2016 Plan, up to a maximum of 1,136,229 shares.
Activity under the Company’s stock option plans is set forth below:
|
|
|
|
|
Options Outstanding |
|||
|
|
|
|
|
|
|
Weighted ‑ |
|
|
|
|
Shares |
|
|
|
Average |
|
|
|
|
Available |
|
Number of |
|
Exercise |
|
|
|
|
for Grant |
|
Options |
|
Price |
|
|
Balance at December 31, 2018 |
|
2,486,637 |
|
3,778,259 |
|
$ |
10.32 |
|
Additional shares authorized |
|
1,170,000 |
|
— |
|
|
— |
|
Options granted |
|
(2,029,000) |
|
2,029,000 |
|
|
3.61 |
|
Options exercised |
|
— |
|
(87,303) |
|
|
0.28 |
|
Options forfeited |
|
76,546 |
|
(76,546) |
|
|
11.67 |
|
Balance at December 31, 2019 |
|
1,704,183 |
|
5,643,410 |
|
$ |
8.05 |
108
The following table summarizes information about stock options outstanding at December 31, 2019 and 2018:
|
|
|
|
|
Options Outstanding |
|
Options Vested |
||||||||||
|
|
|
|
|
at December 31, 2019 |
|
at December 31, 2019 |
||||||||||
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
Average |
|
Weighted |
|
|
|
|
|
|
|
|
Remaining |
|
Weighted |
|
|
|
Remaining |
|
Average |
||
|
|
|
|
|
|
|
Contractual |
|
Average |
|
|
|
Contractual |
|
Exercise |
||
|
Exercise Price |
|
Number |
|
Life (in Years) |
|
Exercise Price |
|
Number |
|
Life (in Years) |
|
Price |
||||
|
$0.28 |
- |
$2.56 |
|
191,000 |
|
5.66 |
|
$ |
0.36 |
|
184,730 |
|
5.52 |
|
$ |
0.29 |
|
$3.01 |
- |
$4.65 |
|
2,027,500 |
|
9.75 |
|
$ |
3.61 |
|
32,375 |
|
6.01 |
|
$ |
4.64 |
|
$4.84 |
|
$7.59 |
|
1,061,522 |
|
8.94 |
|
$ |
5.95 |
|
261,504 |
|
8.90 |
|
$ |
5.98 |
|
$9.52 |
- |
$14.43 |
|
1,051,738 |
|
7.98 |
|
$ |
10.83 |
|
593,596 |
|
7.93 |
|
$ |
10.90 |
|
$15.00 |
- |
$16.70 |
|
1,311,650 |
|
6.51 |
|
$ |
15.49 |
|
1,138,764 |
|
6.44 |
|
$ |
15.40 |
|
|
|
|
|
5,643,410 |
|
8.38 |
|
$ |
8.05 |
|
2,210,969 |
|
7.05 |
|
$ |
11.66 |
|
|
|
|
|
Options Outstanding |
|
Options Vested |
||||||||||
|
|
|
|
|
at December 31, 2018 |
|
at December 31, 2018 |
||||||||||
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
|
Average |
|
|
|
|
|
|
Average |
|
Weighted |
|
|
|
|
|
|
|
|
Remaining |
|
Weighted |
|
|
|
Remaining |
|
Average |
||
|
|
|
|
|
|
|
Contractual |
|
Average |
|
|
|
Contractual |
|
Exercise |
||
|
Exercise Price |
|
Number |
|
Life (in Years) |
|
Exercise Price |
|
Number |
|
Life (in Years) |
|
Price |
||||
|
$0.28 |
- |
$4.65 |
|
301,803 |
|
6.44 |
|
$ |
0.72 |
|
261,373 |
|
6.42 |
|
$ |
0.68 |
|
$5.94 |
- |
$9.52 |
|
1,101,750 |
|
9.92 |
|
$ |
6.10 |
|
3,585 |
|
8.69 |
|
$ |
8.92 |
|
$9.60 |
- |
$14.43 |
|
1,026,180 |
|
8.97 |
|
$ |
10.89 |
|
269,731 |
|
8.70 |
|
$ |
10.56 |
|
$15.00 |
- |
$16.70 |
|
1,348,526 |
|
7.50 |
|
$ |
15.49 |
|
834,456 |
|
7.38 |
|
$ |
15.37 |
|
|
|
|
|
3,778,259 |
|
8.52 |
|
$ |
10.32 |
|
1,369,145 |
|
7.46 |
|
$ |
11.60 |
The weighted average grant date fair value of options granted for the years ended December 31, 2019, 2018 and 2017, was $2.53, $5.23 and $8.93, respectively.
Options outstanding and exercisable that had vested or were expected to vest at December 31, 2019 were as follows:
|
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
|
|
Average |
|
Aggregate |
|
|
|
|
|
|
Weighted |
|
Remaining |
|
Intrinsic |
||
|
|
|
Number |
|
Average |
|
Contractual |
|
Value |
||
|
|
|
of shares |
|
Exercise Price |
|
Life (years) |
|
(in thousands) |
||
|
Vested |
|
2,210,969 |
|
$ |
11.66 |
|
7.05 |
|
$ |
977,587 |
|
Expected to vest |
|
3,432,441 |
|
$ |
5.72 |
|
9.24 |
|
$ |
3,713,778 |
In the table above, aggregate intrinsic value represents the difference between the exercise price of the options to purchase common stock and the estimated fair value of the Company’s common stock of $5.44.
The aggregate intrinsic value of stock options exercised in the years ended December 31, 2019, 2018 and 2017, was $0.4 million, $1.1 million and $0.3 million, respectively.
The total fair value of options that vested in the year ended December 31, 2019, 2018 and 2017, was $7.8 million, $7.1 million, and $5.8 million, respectively.
109
9. Stock‑Based Compensation
The Company’s results of operations include expenses relating to stock‑based awards as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Research and development |
|
$ |
3,103 |
|
$ |
2,919 |
|
$ |
2,692 |
|
General and administrative |
|
|
4,245 |
|
|
4,216 |
|
|
3,537 |
|
Total |
|
$ |
7,348 |
|
$ |
7,135 |
|
$ |
6,229 |
Valuation Assumptions
The Company estimated the fair value of employee stock options using the Black-Scholes valuation model. The fair value of employee stock options is being amortized on a straight-line basis over the requisite service period of the awards. The fair value of employee stock options were estimated using the following assumptions for the years ended December 31, 2019, 2018 and 2017:
|
|
|
Year Ended December 31, |
|
||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
|
Risk-free interest rate |
|
1.9 |
% |
2.8 |
% |
2.1 |
% |
|
Expected volatility |
|
82.1 |
% |
82.7 |
% |
91.4 |
% |
|
Expected term (in years) |
|
6.0 |
|
6.0 |
|
6.0 |
|
|
Expected dividend yield |
|
0 |
% |
0 |
% |
0 |
% |
Risk-free Interest Rate: The Company based the risk-free interest rate over the expected term of the options based on the constant maturity rate of U.S. Treasury securities with similar maturities as of the date of the grant.
Volatility: The Company used an average historical stock price volatility of comparable public companies within the biotechnology and pharmaceutical industry that have been identified as the Company’s industry peers.
Expected Term: The Company uses the simplified method prescribed in the ASC 718, Compensation—Stock Compensation, to calculate the expected term of options granted to employees and directors.
Expected Dividends: The Company has not paid and does not anticipate paying any dividends in the near future.
At December 31, 2019, 2018 and 2017, the unrecognized compensation expense associated with respect to options granted to employees was $13.4 million, $15.8 million and $18.6 million, respectively, and is expected to be recognized on a straight‑line basis over 2.71, 2.72, and 2.85 years, respectively.
10. Income Taxes
The components of loss before income tax is as follows (in thousands):
|
|
|
December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Domestic |
|
$ |
(46,672) |
|
$ |
(47,096) |
|
$ |
(28,253) |
|
Foreign |
|
|
— |
|
|
157 |
|
|
(27,410) |
|
|
|
$ |
(46,672) |
|
$ |
(46,939) |
|
$ |
(55,663) |
During the years ended December 31, 2019, 2018 and 2017, the Company recorded no income tax benefits for the net operating losses (NOLs) incurred due to the uncertainty of realizing a benefit from those items.
110
A reconciliation of the Company’s effective tax rate to the U.S. Federal statutory rate is as follows:
|
|
|
December 31, |
|
||||
|
|
|
2019 |
|
2018 |
|
2017 |
|
|
Federal tax benefit at statutory rate |
|
21 |
% |
21 |
% |
34 |
% |
|
State tax, net of Federal benefit |
|
6 |
% |
9 |
% |
7 |
% |
|
Foreign rate differential |
|
— |
|
— |
% |
(17) |
% |
|
Federal rate change impact |
|
— |
|
— |
% |
(9) |
|
|
Change in valuation allowance |
|
(28) |
% |
(41) |
% |
(16) |
% |
|
Research and development tax credits |
|
3 |
% |
2 |
% |
2 |
% |
|
Prior year federal true-up |
|
— |
% |
10 |
% |
(3) |
% |
|
Other |
|
(2) |
% |
(1) |
% |
2 |
|
|
Effective income tax rate |
|
0 |
% |
0 |
% |
0 |
% |
The effective tax rate is different from the federal statutory tax rate primarily due to a foreign rate differential and a valuation allowance against deferred tax assets as a result of the Company’s history of losses.
The principal components of the Company’s net deferred tax assets are as follows (in thousands)
|
|
|
December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Deferred tax assets |
|
|
|
|
|
|
|
|
|
|
Net operating loss carryforwards |
|
$ |
42,486 |
|
$ |
31,533 |
|
$ |
15,438 |
|
Tax credit carryforwards |
|
|
6,990 |
|
|
6,441 |
|
|
4,351 |
|
Capitalized tax assets |
|
|
(3) |
|
|
138 |
|
|
131 |
|
Accruals |
|
|
152 |
|
|
188 |
|
|
183 |
|
Stock compensation |
|
|
4,317 |
|
|
2,879 |
|
|
1,730 |
|
Operating lease liability |
|
|
892 |
|
|
— |
|
|
— |
|
Other |
|
|
40 |
|
|
58 |
|
|
52 |
|
Total deferred tax assets |
|
$ |
54,874 |
|
$ |
41,237 |
|
$ |
21,885 |
|
Deferred tax liabilities |
|
|
|
|
|
|
|
|
|
|
Operating lease right-of-use asset |
|
$ |
(651) |
|
$ |
— |
|
$ |
— |
|
Valuation allowance |
|
|
(54,223) |
|
|
(41,237) |
|
|
(21,885) |
|
Net deferred tax assets |
|
$ |
— |
|
$ |
— |
|
$ |
— |
The Company recorded a valuation allowance against its deferred tax assets at December 31, 2019 and 2018 because Company management believed that it was more likely than not that these assets would not be fully realized in the future. The valuation allowance increased by approximately $13.0 million and $19.4 million for the years ended December 31, 2019 and 2018, respectively. Changes in the valuation allowance for deferred tax assets relate primarily to the increase in the Company’s net operating loss carryforward.
As of December 31, 2019, the Company had federal NOL carryforwards of approximately $144.5 million and state NOL carryforwards of approximately $173.9 million which are available to reduce future taxable income. The NOLs will begin to expire in 2034, if not utilized. Utilization of the net operating loss carryforwards are subject to various limitations due to the ownership change limitations provided by Internal Revenue Code (IRC) Section 382 and similar state provisions.
As of December 31, 2019, the Company also had $6.1 million of federal and $3.3 million of state research and development tax credit carryforwards available to reduce future income taxes. The federal research and development tax credits will begin to expire 2035, if not utilized. The state research and development tax credits have no expiration date.
111
As of December 31, 2019, the Company had unrecognized tax benefits (“UTBs”) of approximately $1.9 million. All of the deferred tax assets associated with these UTBs are fully offset by a valuation allowance. The following table summarizes the activity related to UTBs:
|
|
|
December 31, |
|||||||
|
|
|
2019 |
|
2018 |
|
2017 |
|||
|
Unrecognized tax benefits beginning of the period |
|
$ |
1,804 |
|
$ |
1,219 |
|
$ |
604 |
|
Decrease related to the prior year |
|
|
(365) |
|
|
— |
|
|
(51) |
|
Increased related to the current year |
|
|
446 |
|
|
585 |
|
|
666 |
|
Unrecognized tax benefits, end of the period |
|
$ |
1,885 |
|
$ |
1,804 |
|
$ |
1,219 |
The Company follows the provisions of ASC 740, Accounting for Income Taxes, and the accounting guidance related to accounting for uncertainty in income taxes. The Company determines its uncertain tax positions based on a determination of whether and how much of a tax benefit taken by the Company in its tax filings or positions is more likely than not to be sustained upon examination by the relevant income tax authorities. None of the Company’s unrecognized tax benefits that, if recognized, would affect its effective tax rate. The Company does not anticipate the total amounts of unrecognized tax benefits will significantly increase or decrease in the next 12 months. The Company will recognize both accrued interest and penalties related to unrecognized benefits in income tax expense. Management determined that no accrual for interest or penalties was required as of December 31, 2019, 2018 and 2017. The Company currently has no federal or state tax examinations in progress nor has it had any federal or state examinations since inception. As a result of the Company’s net operating loss carryforwards, all of its tax years are subject to federal and state tax examinations.
11. Facility Lease
In January 2015, the Company signed an initial operating lease, effective February 1, 2015 for 8,138 square feet of office and laboratory space with a one year term. Between January 2015 and October 2018, the Company entered into a series of lease amendments to increase the amount of leased space to 27,280 square feet and extend the expiration of the lease to February 2023. The lease agreement includes annual rent escalations. Under the lease and subsequent amendments, the landlord provided approximately $1.9 million in free rent and lease incentives. The Company records rent expense on a straight-line basis over the effective term of the lease, including any free rent periods and incentives. As the interest rate implicit in lease arrangements is typically not readily available, in calculating the present value of the lease payments, the Company has utilized its incremental borrowing rate, which is determined based on the prevailing market rates for collateralized debt with maturity dates commensurate with the term of its lease. The Company’s facility lease is a net lease, as the non-lease components (i.e. common area maintenance) are paid separately from rent based on actual costs incurred. Therefore, the non-lease components were not included in the right-of-use asset and liability and are reflected as an expense in the period incurred.
As of December 31, 2019 and 2018, the right-of-use asset under operating lease was $2.3 million and $0, respectively. The elements of lease expense were as follows (in thousands):
|
|
|
|
|
|
|
|||||||
|
|
|
Statements of operations and |
|
Year Ended December 31, |
|
|||||||
|
|
|
comprehensive loss location |
|
2019 |
|
2018 |
|
2017 |
|
|||
|
Costs of operating lease |
|
|
|
|
|
|
|
|
|
|
|
|
|
Operating lease costs |
|
Research and development, |
|
$ |
960 |
|
$ |
748 |
|
$ |
734 |
|
|
Costs of non-lease components (previously common area maintenance) |
|
Research and development, |
|
|
324 |
|
|
296 |
|
|
281 |
|
|
Total operating lease cost |
|
|
|
$ |
1,284 |
|
$ |
1,044 |
|
$ |
1,015 |
|
|
Other Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
Operating cash flows used for operating lease |
|
|
|
$ |
1,449 |
|
$ |
1,389 |
|
$ |
1,398 |
|
|
Remaining lease term |
|
|
|
|
3.1 years |
|
|
4.1 years |
|
|
3.1 years |
|
|
Discount rate |
|
|
|
|
10.0% |
|
|
— |
|
|
— |
|
112
As of December 31, 2019, minimum rental commitments under this lease were as follows (in thousands)
|
Year Ended December 31 (in thousands) |
|
|
|
|
2020 |
|
$ |
1,159 |
|
2021 |
|
|
1,260 |
|
2022 |
|
|
1,299 |
|
Total lease payments |
|
|
3,718 |
|
Less: imputed interest |
|
|
(530) |
|
Total |
|
$ |
3,188 |
As of December 31, 2018, minimum rental commitments under this lease were as follows (in thousands)
|
Year Ended December 31 (in thousands) |
|
|
|
|
2019 |
|
$ |
1,110 |
|
2020 |
|
|
1,142 |
|
2021 |
|
|
1,251 |
|
2022 |
|
|
1,296 |
|
2023 |
|
|
109 |
|
Total |
|
$ |
4,908 |
12. Commitments and Contingencies
In August 2015 the Company entered into an agreement for a line of credit of $0.1 million for the purpose of issuing its landlord a letter of credit of $0.1 million as a security deposit under its facility lease. The Company pledged money market funds and marketable securities as collateral for the line of credit. For further discussion of the Company’s facility lease agreement, see Note 11.
Pursuant to the Company’s license agreements with each of Vernalis and Scripps, it has obligations to make future milestone and royalty payments to these parties, respectively. However, because these amounts are contingent, they have not been included on the Company’s balance sheet. For further discussion of the Vernalis and Scripps licensing agreements, see Note 5.
Indemnifications
In the ordinary course of business, the Company enters into agreements that may include indemnification provisions. Pursuant to such agreements, the Company may indemnify, hold harmless and defend an indemnified party for losses suffered or incurred by the indemnified party. Some of the provisions will limit losses to those arising from third‑party actions. In some cases, the indemnification will continue after the termination of the agreement. The maximum potential amount of future payments the Company could be required to make under these provisions is not determinable. The Company has never incurred material costs to defend lawsuits or settle claims related to these indemnification provisions. The Company has also entered into indemnification agreements with its directors and officers that may require the Company to indemnify its directors and officers against liabilities that may arise by reason of their status or service as directors or officers to the fullest extent permitted by Delaware corporate law. There have been no claims to date and the Company has a directors and officers insurance policy that may enable it to recover a portion of any amounts paid for future claims.
113
Legal Proceedings
The Company is not a party to any material legal proceedings.
13. Related Party Transactions
In 2017, the Company purchased $461,000 of research services from a vendor during the normal course of business, where a Corvus director is also a member of the vendor's board of directors.
In March 2018, the Company completed a follow-on public offering in which the Company sold 8,117,647 shares of common stock at a price of $8.50 per share, which included 1,058,823 shares issued pursuant to the underwriters’ exercise of their option to purchase additional shares of common stock. The aggregate net proceeds received by the Company from the offering were approximately $64.9 million, net of underwriting discounts and commissions and offering expenses payable by the Company.
The following aggregate number of shares of common stock were sold to our owners of more than 5% of our common stock, directors, or executive officers during the March 2018 underwritten public offering:
|
|
|
March 2018 Public Offering |
||||
|
|
|
Number of |
|
Aggregate |
||
|
|
|
|
Shares of |
|
Purchase |
|
|
|
|
Common Stock |
|
Price |
||
|
Owners of More Than 5% of Our Common Stock |
|
|
|
|
|
|
|
FMR LLC |
|
|
1,176,470 |
|
$ |
9,999,995 |
|
OrbiMed Advisors LLC (1) |
|
|
588,235 |
|
|
4,999,998 |
|
Novo Holdings A/S (2) |
|
|
1,176,470 |
|
|
9,999,995 |
|
Adams Street Partners (3) |
|
|
588,235 |
|
|
4,999,998 |
|
Board of Directors |
|
|
|
|
|
|
|
Richard A. Miller, M.D. |
|
|
100,000 |
|
|
850,000 |
|
(1) |
Peter Thompson, M.D., a member of our Board of Directors since November 2014, is a Private Equity Partner at OrbiMed Advisors, LLC. |
|
(2) |
Peter Moldt, Ph.D., a Partner at Novo Ventures (US) Inc., which provide certain consultancy services to Novo Holdings A/S, served as a member of our Board of Directors from January 2015 to January 2019. |
|
(3) |
Elisha P. (Terry) Gould III, a member of our Board of Directors since November 2014, is a Partner at Adams Street Partners, LLC. |
14. Quarterly Selected Financial Data (unaudited)
|
|
|
Quarter Ended |
||||||||||
|
|
|
December 31, |
|
September 30, |
|
June 30, |
|
March 31, |
||||
|
(in thousands, except per share amounts) |
|
2019 |
|
2019 |
|
2019 |
|
2019 |
||||
|
Operating expenses |
|
$ |
11,440 |
|
$ |
11,513 |
|
$ |
13,596 |
|
$ |
12,305 |
|
Net loss |
|
|
(11,047) |
|
|
(11,004) |
|
|
(12,978) |
|
|
(11,643) |
|
Net loss per share, basic and diluted |
|
$ |
(0.38) |
|
$ |
(0.37) |
|
$ |
(0.44) |
|
$ |
(0.40) |
|
|
|
Quarter Ended |
||||||||||
|
|
|
December 31, |
|
September 30, |
|
June 30, |
|
March 31, |
||||
|
(in thousands, except per share amounts) |
|
2018 |
|
2018 |
|
2018 |
|
2018 |
||||
|
Operating expenses |
|
$ |
11,171 |
|
$ |
11,149 |
|
$ |
12,258 |
|
$ |
14,644 |
|
Net loss |
|
|
(10,509) |
|
|
(10,498) |
|
|
(11,631) |
|
|
(14,301) |
|
Net loss per share, basic and diluted |
|
$ |
(0.36) |
|
$ |
(0.36) |
|
$ |
(0.40) |
|
$ |
(0.63) |
114
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures.
The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”) refers to controls and procedures that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure. Our management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and our management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Due to the inherent limitations of control systems, not all misstatements may be detected. These inherent limitations include the realities that judgments in decision-making can be faulty and that breakdowns can occur because of a simple error or mistake. Our disclosure controls and procedures are designed to provide reasonable assurance of achieving their control objectives.
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2019, the end of the period covered by this Annual Report on Form 10-K. Based upon such evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that our disclosure controls and procedures were effective at the reasonable assurance level as of such date.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rule 13a-15(f) and 15d-15(f) of the Exchange Act). Internal control over financial reporting is a process designed by, or under the supervision of, our Chief Executive Officer and Chief Financial Officer, and effected by our Board of Directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
|
· |
Pertain to the maintenance of records that accurately and fairly reflect in reasonable detail the transactions and dispositions of the assets of our company; |
|
· |
Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
|
· |
Provide reasonable assurances regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material adverse effect on our financial statements. |
Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2019 based on the criteria established in Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission, or COSO 2013. Based on our evaluation under the criteria set forth in Internal Control - Integrated Framework issued by the COSO, our management concluded our internal control over financial reporting was effective as of December 31, 2019.
115
Internal control over financial reporting has inherent limitations. Internal control over financial reporting is a process that involves human diligence and compliance and is subject to lapses in judgment and breakdowns resulting from human failures. Internal control over financial reporting also can be circumvented by collusion or improper management override. Because of such limitations, there is a risk that material misstatements will not be prevented or detected on a timely basis by internal control over financial reporting. However, these inherent limitations are known features of the financial reporting process. Therefore, it is possible to design into the process safeguards to reduce, though not eliminate, this risk.
Attestation Report of the Registered Public Accounting Firm
This Annual Report on Form 10‑K does not include an attestation report of our registered public accounting firm on our internal controls due to an exemption established by the JOBS Act for “emerging growth companies.”
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during the fiscal year ended December 31, 2019 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Not applicable.
116
Item 10. Directors, Executive Officers and Corporate Governance
Information about our Board of Directors
The following sets forth information about our directors as of January 31, 2020.
|
Name |
|
Age |
|
Position/Office Held With the Company |
|
Director Since |
|
Class I Directors whose terms expire at the 2020 Annual Meeting of Stockholders |
||||||
|
Richard A. Miller, M.D. |
68 |
President, Chief Executive Officer and Chairman of the Board |
2014 |
|||
|
Linda S. Grais, M.D. J.D.(1)(3) |
63 |
Director |
2019 |
|||
|
Class II Directors whose terms expire at the 2021 Annual Meeting of Stockholders |
||||||
|
Steve E. Krognes(1)(2) |
51 |
Director |
2016 |
|||
|
Scott W. Morrison(1)(2) |
62 |
Director |
2015 |
|||
|
Class III Directors whose terms expire at the 2022 Annual Meeting of Stockholders |
||||||
|
Ian T. Clark(2)(3) |
59 |
Director |
2017 |
|||
|
Elisha P. (Terry) Gould III(3) |
63 |
Director |
2014 |
|||
|
Peter Thompson, M.D.(2) |
60 |
Director |
2014 |
|||
|
(1) |
Member of the Audit Committee. |
|
(2) |
Member of the Compensation Committee. |
|
(3) |
Member of the Nominating and Corporate Governance Committee. |
Board Experience and Directorships
Richard A. Miller, M.D. Dr. Miller has served as our President and Chief Executive Officer since February 2014 and chairman of our board of directors since January 2014. From April 2012 to October 2014, Dr. Miller was Chairman and Chief Executive Officer of Graphea, Inc., a privately‑held chemical company, which he founded. Dr. Miller served as Chief Commercialization Officer, Associate Dean and Research Professor in Chemistry at The University of Texas at Austin from September 2010 to December 2011. Dr. Miller founded Principia Biopharma Inc., a privately‑held biopharmaceutical company, and served as its President and Chief Executive Officer and a member of its board of directors from January 2009 to February 2011. He served as President, Chief Executive Officer and Director of Pharmacyclics, Inc., a public biopharmaceutical company, from 1991, when he co‑founded the company, to 2008. At Pharmacyclics, Dr. Miller led the initial discovery and development efforts for ibrutinib. Dr. Miller was a co‑founder, Vice President and Director of IDEC Pharmaceuticals Corporation, a biotechnology company that merged with Biogen, Inc. in June 2003, where he led research efforts on lymphoma leading to the development of rituximab. Dr. Miller has been Adjunct Clinical Professor of Medicine (Oncology) at Stanford University Medical Center since 1991. Dr. Miller currently serves on the board of directors of a private biopharmaceutical company. Dr. Miller received a B.A. in Chemistry from Franklin & Marshall College and an M.D. from the State University of New York Medical School. He is board certified in both Internal Medicine and Medical Oncology. We believe Dr. Miller’s experience as an officer and director of pharmaceutical and biopharmaceutical companies provides him with the qualifications and skills to serve as a member of our board of directors.
Linda S. Grais, M.D. J.D. Dr. Grais has served as a member of our board of directors since January 2019. Dr. Grais previously served as President and Chief Executive Officer of Ocera Therapeutics, Inc. from June 2012 to December 2017 and as a member of its board of directors from January 2008 through December 2017. Prior to her employment by Ocera, Dr. Grais served as a managing member at InterWest Partners, a venture capital firm, from May
117
2005 until February 2011. From July 1998 to July 2003, Dr. Grais was a founder and executive vice president of SGX Pharmaceuticals Inc., a drug discovery company focusing on new treatments for cancer. Prior to that, she was a corporate attorney at Wilson Sonsini Goodrich & Rosati, where she practiced in such areas as venture financings, public offerings and strategic partnerships. Before practicing law, Dr. Grais worked as an assistant clinical professor of Internal Medicine and Critical Care at the University of California, San Francisco. She currently serves on the board of directors of Arca Biopharma, Inc., a public biotechnology company, Zosano Pharma Corporation, a public pharmaceutical company, and PRA Health Sciences, Inc., a public contract research organization. Dr. Grais received a B.A. from Yale University, an M.D. from Yale Medical School and a J.D. from Stanford Law School. We believe Dr. Grais’ experience as an officer and director of pharmaceutical and biopharmaceutical companies provides her with the qualifications and skills to serve as a member of our board of directors.
Steve E. Krognes. Mr. Krognes has served as a member of our board of directors since January 2016. Mr. Krognes has served as Chief Financial Officer of Denali Therapeutics Inc., a public biotechnology company, since October 2015. From 2009 to September 2015, Mr. Krognes served as Senior Vice President and Chief Financial Officer at Genentech, Inc., a biotechnology company. From 2004 to 2009, he was Head of Mergers & Acquisitions at Roche Holding AG, a biotechnology company. Mr. Krognes served as Director of Mergers & Acquisitions at Danske Bank A/S, a Danish bank, from 2002 to 2003. He was a Venture Capitalist with Pylonia Ventures, a Norwegian venture investments company, from 2000 to 2002. From 1996 to 2000, he was a Management Consultant for McKinsey & Company, a consulting firm. Mr. Krognes currently serves as a member of the boards of directors of Gritstone Oncology, a public biopharmaceutical company, and RLS Global, a Swedish life sciences company. He was a member of the board of directors and board executive committee of the California Life Sciences Association, an industry organization, from September 2010 to September 2015. Mr. Krognes received a B.S. in Economics from the Wharton School of the University of Pennsylvania and an M.B.A. from Harvard Business School. We believe Mr. Krognes’ experience in finance and the biotechnology industry provides him with the qualifications and skills to serve as a member of our board of directors.
Scott W. Morrison. Mr. Morrison has served as a member of our board of directors since December 2015. From 1996 to December 2015, Mr. Morrison was a Partner with Ernst & Young LLP, a public accounting firm, where he also served as U.S. Life Sciences Leader from 2002 to December 2015. He also serves on the board of directors of Global Blood Therapeutics, Inc., a public biopharmaceutical company, since January 2016 and on the board of directors of Ideaya Biosciences, Inc., a public biopharmaceutical company, since July 2018. Mr. Morrison has held roles on the boards of directors of numerous life sciences industry organizations. Since 1999, he has served on the board of directors of the Biotechnology Institute, a non-profit organization, where has also served on the audit committee since 2002. Mr. Morrison has previously served on the boards of directors of the Life Sciences Foundation, a biotechnology non-profit organization, the Bay Area Biosciences Association, a 501(c)(3) organization, and the Emerging Companies Section of the Biotechnology Innovation Organization, a trade organization. He received a B.S. in Business Administration from the University of California-Berkeley and is a certified public accountant (inactive). We believe Mr. Morrison’s experience in public accounting and the life sciences industry provides him with the qualifications and skills to serve as a member of our board of directors.
Ian T. Clark. Mr. Clark has served as a member of our board of directors since January 2017. Mr. Clark has more than 34 years of experience in the biotechnology and pharmaceutical industry, most recently serving as CEO and member of the board of directors for Genentech, until his retirement in December 2016. During his seven-year tenure as CEO, Mr. Clark and his team brought eleven new medicines to market for patients fighting rheumatoid arthritis, idiopathic pulmonary fibrosis and various types of cancer. Ian was among the highest rated CEOs by Glassdoor, recognized as the Bay Area’s most admired CEO by the San Francisco Business Times and awarded the Honorable Mentor of the Year by the Heath Business Woman's Association. Prior to joining Genentech, Mr. Clark held various positions of increasing responsibility at Novartis, Sanofi, Ivax and Searle, working in the USA, UK, Canada, Eastern Europe and France. Currently, Mr. Clark is on the board of directors for Takeda Pharmaceutical Company Limited, Agios Pharmaceuticals, Inc., Guardant Health, Inc., Forty Seven, Inc., and Avrobio, Inc. He is an Operating Partner of Blackstone Life Sciences. He is also on the BioFulcrum Board of the Gladstone Institute. Mr. Clark previously served on the Boards of Shire, Kite Pharma, Dendreon, Solazyme and Vernalis. He was also on the Board of Biotechnology Industry Association and on the Economic Advisory Council of the 12th District of the Federal Reserve. Mr. Clark received his Bachelor of Science in Biological Sciences and an Honorary Doctorate of Science from
118
Southampton University in the United Kingdom. We believe Mr. Clark’s executive experience in the biopharmaceutical industry provides him with the qualifications and skills to serve as a member of our board of directors.
Elisha P. (Terry) Gould III. Mr. Gould has served as a member of our board of directors since November 2014. Mr. Gould is currently a Partner and Head of Venture/Growth Equity Investments at Adams Street Partners, LLC, a global private equity firm, and has been employed by Adams Street Partners or its predecessor organizations since 1994. Mr. Gould has served on the board of Aptinyx Inc., a biopharmaceutical company, since July 2015 and currently serves on the boards of directors of several private biopharmaceutical and/or healthcare companies. Mr. Gould received an A.B. in Engineering Science from Dartmouth College and an M.B.A. from the Stanford University Graduate School of Business. We believe Mr. Gould’s experience in the venture capital industry and as a director of several biopharmaceutical and/or healthcare companies provides him with the qualifications and skills to serve as a member of our board of directors.
Peter Thompson, M.D. Dr. Thompson has served as a member of our board of directors since November 2014. Dr. Thompson currently serves as a Private Equity Partner at OrbiMed Advisors LLC, an investment firm focused on the healthcare sector, where he previously served as a Venture Partner. Dr. Thompson also serves as the chief executive officer of Silverback Therapeutics, Inc. In addition, Dr. Thompson currently serves on the board of directors of several public biopharmaceutical companies: Alpine Immune Sciences, Inc. since June 2016, Synthorx, Inc., since April 2018 and Prevail Therapeutics Inc. since August 2017. Dr. Thompson also currently serves on the board of directors of several private companies. Dr. Thompson is a board-certified internist and oncologist and has served as Affiliate Professor of Neurosurgery at the University of Washington since January 2010. Dr. Thompson co-founded and served as the chief executive officer of Trubion Pharmaceuticals, Inc., a biopharmaceutical company, from 2002 to 2009. Previously, Dr. Thompson served as a medical staff fellow at the National Cancer Institute from 1985 to 1992. Dr. Thompson holds a Sc. B. in Molecular Biology and Mathematics from Brown University and an M.D. from Brown University Medical School. We believe Dr. Thompson’s experience in management and venture capital in the biopharmaceutical industry provides him with the qualifications and skills to serve as a member of our board of directors.
Meetings of the Board of Directors, Board and Committee Member Attendance and Annual Meeting Attendance
The board of directors met four times and acted once by unanimous written consent during the fiscal year ended December 31, 2019. The audit committee met five times, the compensation committee met two times and the nominating and corporate governance committee met one time. Each member of the board of directors attended at least 75% of the aggregate number of meetings of our board of directors, and of the committees on which he or she served, held during the last fiscal year.
Corporate Governance Guidelines
The board of directors has documented our governance practices in our corporate governance guidelines to assure that the board will have the necessary authority and practices in place to review and evaluate our business operations as needed and to make decisions that are independent of our management. The guidelines are also intended to align the interests of directors and management with those of our stockholders. The corporate governance guidelines set forth certain practices the board will follow with respect to board composition, board committees, board nomination, director qualifications and evaluation of the board and committees. The corporate governance guidelines and the charter for each committee of the board of directors may be viewed at www.corvuspharma.com.
Leadership Structure of the Board
Our Bylaws and corporate governance guidelines provide our board of directors with flexibility to combine or separate the positions of chairperson of the board of directors and Chief Executive Officer and/or the implementation of a lead director in accordance with its determination that utilizing one or the other structure would be in our best interests. Dr. Miller currently serves as the chairperson of our board of directors. In that role, Dr. Miller presides over the meetings of our board of directors.
119
Our board of directors has concluded that our current leadership structure is appropriate at this time. However, our board of directors will continue to periodically review our leadership structure and may make such changes in the future as it deems appropriate.
Role of Board in Risk Oversight Process
Risk assessment and oversight are an integral part of our governance and management processes. Our board of directors encourages management to promote a culture that incorporates risk management into our corporate strategy and day‑to‑day business operations. Management discusses strategic and operational risks with the board of directors at regular board meetings as part of management presentations that focus on particular business functions, operations or strategies, and presents the steps taken by management to mitigate or eliminate such risks.
Our board of directors does not have a standing risk management committee, but rather administers this oversight function directly through our board of directors as a whole, as well as through various standing committees of our board of directors that address risks inherent in their respective areas of oversight. In particular, our board of directors is responsible for monitoring and assessing strategic risk exposure. Our audit committee is responsible for overseeing our major financial risk exposures and the steps our management has taken to monitor and control these exposures. The audit committee also monitors compliance with legal and regulatory requirements and considers and approves or disapproves any related person transactions. Our nominating and governance committee monitors the effectiveness of our corporate governance guidelines. Our compensation committee assesses and monitors whether any of our compensation policies and programs has the potential to encourage excessive risk‑taking.
Committees of the Board of Directors
Our board of directors has the following standing committees: an audit committee, a compensation committee and a nominating and corporate governance committee. Our board of directors may establish other committees to facilitate the management of our business. The composition and functions of each committee are described below.
|
|
|
|
|
|
|
Nominating and Corporate |
|
|
Name |
|
Audit |
|
Compensation |
|
Governance |
|
|
Richard A. Miller, M.D. |
|
— |
|
— |
|
— |
|
|
Linda S. Grais, M.D. J.D. |
|
X |
|
— |
|
X |
|
|
Scott W. Morrison |
|
X |
(1) |
X |
|
— |
|
|
Steve E. Krognes |
|
X |
|
X |
|
— |
|
|
Peter Thompson, M.D. |
|
— |
|
X |
(1) |
— |
|
|
Elisha P. (Terry) Gould III |
|
— |
|
— |
|
X |
(1) |
|
Ian T. Clark |
|
— |
|
X |
|
X |
|
|
Total meetings in 2019 |
|
5 |
|
2 |
|
1 |
|
|
(1) Committee Chairman. |
Below is a description of each committee of the board of directors.
Audit Committee
Our audit committee oversees our corporate accounting and financial reporting process. Among other matters, the audit committee:
|
· |
appoints our independent registered public accounting firm; |
|
· |
evaluates the independent registered public accounting firm’s qualifications, independence and performance; |
120
|
· |
determines the engagement of the independent registered public accounting firm; |
|
· |
reviews and approves the scope of the annual audit and the audit fee; |
|
· |
discusses with management and the independent registered public accounting firm the results of the annual audit and the review of our quarterly financial statements; |
|
· |
approves the retention of the independent registered public accounting firm to perform any proposed permissible audit and non‑audit services; |
|
· |
monitors the rotation of partners of the independent registered public accounting firm on our engagement team in accordance with requirements established by the SEC; |
|
· |
is responsible for reviewing our financial statements and our management’s discussion and analysis of financial condition and results of operations to be included in our annual and quarterly reports to be filed with the SEC; |
|
· |
reviews our critical accounting policies and estimates; and |
|
· |
annually reviews the audit committee charter and the audit committee’s performance. |
The current members of our audit committee are Mr. Krognes, Dr. Grais and Mr. Morrison. Mr. Morrison serves as the chairperson of the committee. All members of our audit committee meet the requirements for financial literacy under the applicable rules and regulations of the SEC and Nasdaq. Our board of directors has determined that Mr. Morrison and Mr. Krognes are audit committee financial experts as defined under the applicable rules of the SEC and has the requisite financial sophistication as defined under the applicable rules and regulations of Nasdaq. Under the rules of the SEC, members of the audit committee must also meet heightened independence standards. Our board of directors has determined that each of the members of our audit committee is independent under the applicable rules of Nasdaq. The audit committee operates under a written charter that satisfies the applicable standards of the SEC and Nasdaq which is available on our corporate website at www.corvuspharma.com.
Compensation Committee
Our compensation committee reviews and recommends policies relating to compensation and benefits of our officers and employees. The compensation committee reviews and sets or makes recommendations to our board of directors regarding the compensation of our Chief Executive Officer and other executive officers. The compensation committee also reviews and makes recommendations to our board of directors regarding director compensation. In addition, the compensation committee reviews and approves or makes recommendations to our board of directors regarding our incentive compensation and equity‑based plans. The compensation committee periodically reviews and evaluates the performance of the compensation committee and its members and must annually review and reassess the compensation committee charter and recommend any changes to our board of directors.
The current members of our compensation committee are Mr. Clark, Mr. Krognes, Mr. Morrison, and Dr. Thompson. Dr. Thompson serves as the chairperson of the committee. Each of the members of our compensation committee is independent under the applicable rules and regulations of Nasdaq. Each of Mr. Clark, Mr. Krognes, and Mr. Morrison is also a “non‑employee director” as defined in Rule 16b‑3 under the Exchange Act. Dr. Thompson will not be a “non‑employee director” if OrbiMed Private Investments V, LP continues to own more than ten percent (10%) of our capital stock. In such event and until such time as the compensation committee is comprised solely of “non‑employee directors,” equity compensation awards to directors and executive officers will be approved by our board of directors. The compensation committee operates under a written charter which is available on our corporate website at www.corvuspharma.com.
121
Our executive officers submit proposals to the board and the compensation committee regarding our executive and director compensation. Our Chief Executive Officer also annually reviews the performance of each executive officer and makes recommendations regarding their compensation. The compensation committee considers those recommendations in determining base salaries, adjustments to base salaries, annual cash bonus program targets and awards and equity awards, if any, for the executive officers and other members of senior management.
Nominating and Corporate Governance Committee
The nominating and corporate governance committee is responsible for making recommendations to our board of directors regarding candidates for directorships and the size and composition of our board of directors. In addition, the nominating and corporate governance committee is responsible for overseeing our corporate governance policies and reporting and making recommendations to our board of directors concerning governance matters.
The current members of our nominating and corporate governance committee are Mr. Clark, Mr. Gould and Dr. Grais. Mr. Gould serves as the chairperson of the committee. Each of the members of our nominating and corporate governance committee is an independent director under the applicable rules and regulations of Nasdaq relating to nominating and corporate governance committee independence. The nominating and corporate governance committee operates under a written charter which is available on our corporate website at www.corvuspharma.com.
The nominating and corporate governance committee will consider director candidates recommended by stockholders. For a stockholder to make any recommendation or nomination for election to the board of directors at an annual meeting, the stockholder must provide notice to the Company, which notice must be delivered to, or mailed and received at, the Company’s principal executive offices not less than 90 days and not more than 120 days prior to the one‑year anniversary of the preceding year’s annual meeting, or, if later, the 10th day following the date on which public disclosure of the date of such annual meeting is made. Further updates and supplements to such notice may be required at the times, and in the forms, required under our bylaws. As set forth in our bylaws, submissions must include the name and address of the proposed nominee, information regarding the proposed nominee that is required to be disclosed in a proxy statement or other filings in a contested election pursuant to Section 14(a) under the Exchange Act, information regarding the proposed nominee’s indirect and direct interests in shares of the Company’s common stock, and a completed and signed questionnaire, representation and agreement of the proposed nominee. Our Bylaws also specify further requirements as to the form and content of a stockholder’s notice. We recommend that any stockholder wishing to make a nomination for director review a copy of our Bylaws, as amended and restated to date, which is available, without charge, from our Secretary, Corvus Pharmaceuticals, Inc., 863 Mitten Road, Suite 102, Burlingame, CA 94010.
Board Diversity
Our nominating and corporate governance committee is responsible for reviewing with the board of directors, on an annual basis, the appropriate characteristics, skills and experience required for the board of directors as a whole and its individual members. In evaluating the suitability of individual candidates (both new candidates and current members), the nominating and corporate governance committee, in recommending candidates for election, and the board of directors, in approving (and, in the case of vacancies, appointing) such candidates, may take into account many factors, including, but not limited to, the following:
|
· |
diversity of personal and professional background, perspective and experience; |
|
· |
personal and professional integrity, ethics and values; |
|
· |
experience in corporate management, operations or finance, such as serving as an officer or former officer of a publicly held company, and a general understanding of marketing, finance and other elements relevant to the success of a publicly‑traded company in today’s business environment; |
|
· |
experience relevant to our industry and relevant social policy concerns; |
|
· |
experience as a board member or executive officer of another publicly held company; |
122
|
· |
relevant academic expertise or other proficiency in an area of the our operations; |
|
· |
practical and mature business judgment, including ability to make independent analytical inquiries; |
|
· |
promotion of a diversity of business or career experience relevant to our success; and |
|
· |
any other relevant qualifications, attributes or skills. |
Our board of directors evaluates each individual in the context of the board of directors as a whole, with the objective of assembling a group that can best maximize the success of the business and represent stockholder interests through the exercise of sound judgment using its diversity of experience in these various areas.
Stockholder Communications with the Board of Directors
The board of directors will consider any written or electronic communication from our stockholders to the board, a committee of the board or any individual director. Any stockholder who wishes to communicate to the board of directors, a committee of the board or any individual director should submit written or electronic communications to our Secretary at our principal executive offices, which shall include contact information for such stockholder. All communications from stockholders received shall be forwarded by our Secretary to the board of directors, a committee of the board or an individual director, as appropriate, on a periodic basis, but in any event no later than the board of director’s next scheduled meeting. The board of directors, a committee of the board, or individual directors, as appropriate, will consider and review carefully any communications from stockholders forwarded by our Secretary.
Material Changes to Nominee Recommendation Procedures
There have been no material changes to the procedures by which stockholders may recommend nominees to our board in 2019.
Information about our Executive Officers
The following sets forth information about our executive officers as of January 31, 2020.
|
Name |
|
Position |
|
Age |
|
Richard A. Miller, M.D. |
President, Chief Executive Officer and Chairman of the Board |
68 |
||
|
Joseph J. Buggy, Ph.D. |
Executive Vice President, Discovery Research |
53 |
||
|
Daniel W. Hunt, J.D. |
Senior Vice President and Chief Business Officer |
58 |
||
|
William B. Jones, Ph.D. |
Senior Vice President, Pharmaceutical Development |
55 |
||
|
Leiv Lea |
Chief Financial Officer |
66 |
||
|
Mehrdad Mobasher, M.D. M.P.H. |
Vice President and Chief Medical Officer |
47 |
||
|
Erik J. Verner, Ph.D. |
Vice President, Chemistry Research |
55 |
The following is biographical information as of January 31, 2020 for our executive officers other than Richard A. Miller, M.D., whose biographical information is included in the section above titled “Information about our Board of Directors.”
Joseph J. Buggy, Ph.D., Executive Vice President, Discovery Research. Mr. Buggy has served as our Executive Vice President, Discovery Research since November 2014 and previously served as a member of our board of directors from January 2014, when he co-founded the Company, to November 2014. From 2006 to August 2013, Dr. Buggy held several positions with Pharmacyclics, Inc., a biopharmaceutical company, including, most recently, Vice President, Research. From 2001 to 2006, Dr. Buggy held several positions with Celera Genomics Corporation, a biotechnology company, where he was most recently Director and, prior to that, Principal Scientist. Dr. Buggy served as Senior Scientist and, later, Group Leader, at Axys Pharmaceuticals, Inc., a biotechnology company, from 1996 to 2001.
123
From 1993 to 1996, Dr. Buggy was Scientist for Bayer Pharmaceuticals Corporation, a subsidiary of Bayer HealthCare AG, a health care company. Dr. Buggy received a B.S. in Microbiology from the University of Pittsburgh and a Ph.D. in Molecular, Cellular, and Development Biology from Indiana University.
Daniel W. Hunt, J.D., Senior Vice President and Chief Business Officer. Mr. Hunt has served as our Senior Vice President and Chief Business Officer since December 2017. Prior to joining the Company, Mr. Hunt served as General Counsel and Vice President of Corporate Development at CoMentis, Inc., a biotechnology company, from July 2009 to September 2016. Mr. Hunt was an Associate General Counsel at Genentech, Inc. from 2003 to 2009 and prior to that held senior legal and transactional positions at Abgenix, Inc., Roche Molecular Systems, Inc. and Chiron Corporation. Mr. Hunt received a B.S in Biology from the University of Colorado at Boulder and his J.D. from the Boalt Hall School of Law at the University of California, Berkeley.
William B. Jones, Ph.D., Senior Vice President, Pharmaceutical Development. Dr. Jones has served as our Vice President, Pharmaceutical Development since December 2014. Dr. Jones was Director of Global Regulatory Affairs in the oncology business unit of Sanofi US, LLC, a pharmaceutical company, from December 2012 to December 2014. From 2008 to March 2012, Dr. Jones was Director of Project Management & Regulatory at Pharmacyclics, Inc., a biopharmaceutical company. Dr. Jones served as Associate Director of Development for Plexxikon, Inc., a pharmaceutical company, from 2005 to 2007. From 2002 to 2005, he was Senior Project Manager at Vertex Pharmaceuticals, Inc., a biotechnology company. Dr. Jones received a B.S. and a Ph.D. in Chemistry from the University of Cincinnati and an M.B.A. from Babson College. He completed a post‑doctoral fellowship at the University of Oxford.
Leiv Lea, Chief Financial Officer. Mr. Lea has served as our Chief Financial Officer since November 2014. Mr. Lea was a financial consultant from 2009 to November 2014. From 1998 to 2008, Mr. Lea served as Chief Financial Officer of Pharmacyclics, Inc., a biopharmaceutical company. From 1996 to 1997, he was a financial consultant. From 1986 to 1996, Mr. Lea served as Chief Financial Officer of Margaux, Inc., a refrigeration equipment manufacturer. He received a B.S. in Agricultural Economics from the University of California, Davis and an M.B.A. from the Anderson School at the University of California, Los Angeles.
Mehrdad Mobasher, M.D., M.P.H., Vice President, Chief Medical Officer. Dr. Mobasher has served as our Vice President and Chief Medical Officer since January 2019. Prior to joining the Company, Dr. Mobasher was employed by Genentech/Roche from August 2010 to January 2019, most recently as a Group Medical Director and Development Lead for venetoclax. He has also served as an adjunct clinical faculty member in the Division of Medical Oncology at Stanford University from September 2011 to September 2012. Dr. Mobasher received an M.D. from Tehran University of Medical Sciences, and an M.P.H. in general epidemiology from the School of Public Health at the University of Michigan. He completed an internship and residency in internal medicine at the University of California, Irvine, and post-doctoral fellowships in hematology and medical oncology at Stanford University.
Erik J. Verner, Ph.D., Vice President, Chemistry Research. Dr. Verner has served as our Vice President, Chemistry Research since January 2015. From March 2011 to December 2014, Dr. Verner was Director of Chemistry for Principia Biopharma Inc., a biopharmaceutical company. Dr. Verner served as Director of Chemistry of Pharmacyclics, Inc., a biopharmaceutical company, from 2008 to February 2011, where he served as a principal scientist from 2006 to 2008. From 1996 to 2006, Dr. Verner was a principal scientist at Axys Pharmaceuticals, Inc. (formerly Arris Pharmaceuticals, Incorporated), a biotechnology company, and Celera Corporation, a subsidiary of Axys Pharmaceuticals, Inc. He was a senior scientist at Immunopharmaceutics, Inc., a biotechnology company, from 1993 to 1996. Dr. Verner received a B.S. in Chemistry from the University of Idaho and a Ph.D. in Organic Chemistry from the University of Pittsburgh.
Family Relationships
There are no family relationships among any of our directors or executive officers.
124
Code of Business Conduct and Ethics
We have adopted a code of business conduct and ethics that applies to all of our employees, officers and directors, including those officers responsible for financial reporting. The code of business conduct and ethics is available on our corporate website at www.corvuspharma.com. Any amendments to the code, or any waivers of its requirements, will be disclosed on our website.
Section 16(A) Beneficial Ownership Reporting Compliance
Section 16(a) of the Exchange Act requires our directors and executive officers, and persons who beneficially own more than ten percent of a registered class of our equity securities, to file with the SEC initial reports of ownership and reports of changes in ownership of our common stock and other equity securities. Officers, directors and greater than ten percent beneficial owners are required by SEC regulations to furnish us with copies of all Section 16(a) forms they file.
To our knowledge, based solely on our review of Forms 3, 4 and 5, and any amendments thereto, furnished to us or written representations that no Form 5 was required, we believe that during the fiscal year ended December 31, 2019, all filing requirements applicable to our executive officers and directors under the Exchange Act were met in a timely manner.
Item 11. Executive Compensation
Director Compensation
Director Compensation Table—Year Ended December 31, 2019
The following table presents information regarding the compensation paid for the fiscal year ended December 31, 2019 to members of our board of directors who are not also employed by us or any of our subsidiaries (our non-employee directors). The compensation paid to Richard A. Miller, who is also our president and chief executive officer, is set forth in the section titled “Executive Compensation” below. Dr. Miller was not entitled to receive additional compensation for his service as a director:
|
|
|
FEES |
|
|
|
|
|
|
|
EARNED OR |
|
OPTION |
|
|
|
|
|
PAID IN CASH |
|
AWARDS(1) |
|
TOTAL |
|
NAME |
|
($) |
|
($) |
|
($) |
|
Ian T. Clark |
|
45,000 |
|
38,552 |
|
83,552 |
|
Elisha P. (Terry) Gould III |
|
43,000 |
|
38,552 |
|
81,552 |
|
Linda S. Grais, M.D. J.D. (2) |
|
32,667 |
|
123,622 |
|
156,289 |
|
Steve E. Krognes |
|
51,000 |
|
38,552 |
|
89,552 |
|
Peter Moldt, Ph.D. (3) |
|
— |
|
— |
|
— |
|
Scott W. Morrison |
|
61,000 |
|
38,552 |
|
99,552 |
|
Peter Thompson, M.D. |
|
47,000 |
|
38,552 |
|
85,552 |
|
(1) |
Amounts reported in the Option Awards column represent the grant date fair values of stock options calculated in accordance with Financial Account Standards Board (FASB) ASC Topic 718, Compensation—Stock Compensation. For a discussion of the assumptions used to calculate the value of our stock options, see Note 8, Stock Option Plans, to our audited financial statements included in this report on Form 10-K for the year ended December 31, 2019. Other than in the case of Dr. Grais, during fiscal year 2019, each non-employee director was granted one option grant of 15,000 shares on June 20, 2019 with the aggregate grant date fair value set forth in the table above. As of December 31, 2019, our non-employee directors held outstanding options to purchase shares of our common stock as follows: Mr. Clark, 75,000; Mr. Gould, 75,000; Ms. Grais, 45,000; Mr. Krognes, 75,000; Mr. Morrison, 75,000; and Dr. Thompson, 75,000. Other than these options, none of our non-employee directors held any other equity awards in the Company on that date. |
|
(2) |
Dr. Grais was appointed as a director in January 2019 and received two option grants during fiscal year 2019, an option for 30,000 shares granted on January 28,2019 with an aggregate grant date fair value of $85,069 and an option for 15,000 shares granted on June 20, 2019 with an aggregate grant date fair value of $38,553. |
125
|
(3) |
Dr. Moldt resigned from our board of directors on January 28, 2019. |
Director Compensation
In December 2015, our board of directors approved a compensation policy for our non‑employee directors (the “Director Compensation Program”). Pursuant to our Director Compensation Program, our non‑employee directors are entitled to cash compensation, paid quarterly in arrears, as follows:
|
· |
Each non‑employee director is entitled to receive an annual cash retainer in the amount of $35,000. |
|
· |
The chairperson of the board is entitled to receive additional annual cash compensation of $30,000 for such chairperson’s service on the board of directors. |
|
· |
The chairperson of the audit committee is entitled to receive additional annual cash compensation in the amount of $20,000 for such chairperson’s service on the audit committee. Each non‑chairperson member of the audit committee is entitled to receive additional annual cash compensation in the amount of $10,000 for such member’s service on the audit committee. |
|
· |
The chairperson of the compensation committee is entitled to receive additional annual cash compensation in the amount of $12,000 for such chairperson’s service on the compensation committee. Each non‑chairperson member of the compensation committee is entitled to receive additional annual cash compensation in the amount of $6,000 for such member’s service on the compensation committee. |
|
· |
The chairperson of the nominating and corporate governance committee is entitled to receive additional annual cash compensation in the amount of $8,000 for such chairperson’s service on the nominating and corporate governance committee. Each non‑chairperson member of the nominating and corporate governance committee is entitled to receive additional annual cash compensation in the amount of $4,000 for such member’s service on the nominating and corporate governance committee. |
In addition, unless waived in advance, under the Director Compensation Program, each non‑employee director who is elected or appointed to our board of directors will automatically be granted an option to purchase 30,000 shares of our common stock upon the director’s initial appointment or election to our board of directors, referred to as the Initial Grant. In addition, unless waived in advance, each non‑employee director who is serving on our board of directors immediately following an annual stockholder’s meeting will automatically be granted an annual option to purchase 15,000 shares of our common stock on the date of such annual stockholder’s meeting, referred to as the Annual Grant. The Initial Grant will vest as to 1/3rd of the shares subject to the Initial Grant on each anniversary of the applicable grant date, subject to continued service through the applicable vesting date. The Annual Grant will vest as to all of the shares subject to the Annual Grant on the earlier of the first anniversary of the applicable grant date or the next annual stockholders’ meeting, subject to continued service through the vesting date. All equity awards, including any Initial Grants and Annual Grants, held by our non‑employee directors will vest in full immediately prior to the occurrence of a change in control.
Executive Compensation
This section discusses the material components of our executive compensation program and compensation for our named executive officers (“NEOs”) for the year ended December 31, 2019. As an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, we are not required to include a Compensation Discussion and Analysis section and have elected to comply with the scaled disclosure requirements applicable to emerging growth companies. In addition, as an emerging growth company, we are not required to hold an advisory vote to approve the compensation of our named executive officers, or “say‑on‑pay” vote.
Our NEOs for the year ended December 31, 2019 are:
|
· |
Richard A. Miller, M.D., President and Chief Executive Officer; |
126
|
· |
Leiv Lea, Chief Financial Officer; and |
|
· |
Mehrdad Mobasher, Vice President and Chief Medical Officer. |
Summary Compensation Table
The following table sets forth information for each of the last two completed fiscal years regarding compensation awarded to our NEOs.
|
|
|
|
|
|
|
|
|
|
|
|
|
Non‑equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Incentive |
|
|
|
|
|
|
|
|
|
Base |
|
|
|
Stock |
|
Option |
|
plan |
|
All other |
|
|
|
|
|
Fiscal |
|
salary |
|
|
|
awards |
|
awards |
|
compensation |
|
compensation |
|
Total |
|
Name and principal position |
|
year |
|
($) |
|
Bonus($)(3) |
|
($) |
|
($)(1) |
|
($) |
|
($) (2) |
|
($) |
|
Richard A. Miller, M.D. |
|
2019 |
|
300,000 |
|
— |
|
— |
|
795,039 |
|
— |
|
3,000 |
|
1,098,039 |
|
President and Chief Executive Officer |
|
2018 |
|
300,000 |
|
— |
|
— |
|
1,056,352 |
|
— |
|
3,000 |
|
1,359,352 |
|
Leiv Lea |
|
2019 |
|
349,308 |
|
— |
|
— |
|
397,520 |
|
— |
|
3,000 |
|
749,828 |
|
Chief Financial Officer |
|
2018 |
|
319,342 |
|
— |
|
— |
|
422,540 |
|
— |
|
3,000 |
|
744,882 |
|
Mehrdad Mobasaher, M.D. |
|
2019 |
|
406,731 |
|
245,000 |
|
— |
|
702,425 |
|
— |
|
3,000 |
|
1,357,156 |
|
Vice President and Chief Medical Officer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) |
The amounts reported in this column reflect the grant date fair values of stock options granted to the named executive officers calculated in accordance with Financial Accounting Standards Board (FASB) ASC Topic 718, Compensation-Stock Compensation. For a discussion of the assumptions used to calculate the value of our stock options, see Note 8, Stock Option Plans, to our audited financial statements included in this report on Form 10-K for the year ended December 31, 2019. |
|
(2) |
For 2019, each named executive officer’s other compensation includes a $3,000 401(k) matching contribution. |
|
(3) |
Reflects a $200,000 sign-on bonus and a discretionary bonus in the amount of $45,000 to be paid in 2020 for 2019 performance. |
127
Outstanding Equity Awards at December 31, 2019
The following table presents information regarding the outstanding stock options and stock awards held by each of the named executive officers as of December 31, 2019.
|
|
|
|
|
Option Awards |
||||||
|
|
|
|
|
Number of |
|
Option |
|
|
||
|
|
|
Vesting |
|
Securities Underlying |
|
Exercise |
|
Option |
||
|
|
|
Commencement |
|
Unexercised Options (#) |
|
Price |
|
Expiration |
||
|
Name |
|
Date |
|
Exercisable |
|
Unexercisable |
|
($) |
|
Date |
|
Richard A. Miller, M.D. |
|
3/22/2016 |
(1)(2) |
500,000 |
|
— |
|
15.00 |
|
3/21/2026 |
|
|
|
12/7/2016 |
(1) |
120,000 |
|
40,000 |
|
16.37 |
|
12/6/2026 |
|
|
|
12/13/2017 |
(1) |
62,501 |
|
62,499 |
|
10.60 |
|
12/12/2027 |
|
|
|
12/12/2018 |
(1) |
62,500 |
|
187,500 |
|
5.94 |
|
12/11/2028 |
|
|
|
12/12/2019 |
(1) |
— |
|
320,000 |
|
3.54 |
|
12/11/2029 |
|
Leiv Lea |
|
3/22/2016 |
(1) |
56,250 |
|
3,750 |
|
15.00 |
|
3/21/2026 |
|
|
|
12/7/2016 |
(1) |
18,750 |
|
6,250 |
|
16.37 |
|
12/6/2026 |
|
|
|
12/13/2017 |
(1) |
20,000 |
|
20,000 |
|
10.60 |
|
12/12/2027 |
|
|
|
12/12/2018 |
(1) |
25,000 |
|
75,000 |
|
5.94 |
|
12/11/2028 |
|
|
|
12/12/2019 |
(1) |
— |
|
160,000 |
|
3.54 |
|
12/11/2029 |
|
Mehrdad Mobasher, M.D. |
|
1/28/2019 |
(3) |
— |
|
210,000 |
|
3.88 |
|
1/27/2029 |
|
|
|
12/12/2019 |
(1) |
— |
|
50,000 |
|
3.54 |
|
12/12/2029 |
|
(1) |
This option vests monthly over 48 months from the vesting commencement date, subject to the named executive officer’s continued service to us through the vesting date. |
|
(2) |
This option is immediately exercisable, provided that any shares acquired prior to vesting are subject to a right of repurchase in favor of the Company in the event the named executive officer terminates employment with us prior to vesting. |
|
(3) |
This option vests as to 25% of the total number of shares subject to the option on the first anniversary of the vesting commencement date and the remaining 75% of the total number of shares subject to the option will vest in 36 substantially equal installments on the last day of each of the 36 months following the first anniversary of the vesting commencement date, subject to the named executive officer’s continuous employment through each vesting date. |
Base Salaries and Annual Bonuses
Our NEOs receive a base salary to compensate them for services rendered to our company. The base salary payable to each NEO is intended to provide a fixed component of compensation reflecting the executive’s skill set, experience, role and responsibilities. In December 2018, our board of directors set each of Dr. Miller’s and Mr. Lea’s annual base salary for 2019 at $300,000 and $350,000, respectively . Dr. Mobasher’s joined the Company in February 2019. Pursuant to Dr. Mobasher’s offer letter, he received a base salary of $450,000 per year. In addition to his salary, he received a sign-on bonus of $200,000 that was paid on a periodic basis through November 2019. In December 2019, our board of directors approved increasing Mr. Lea’s annual base salary to $360,500 and Dr. Mobasher’s annual base salary to $463,500 effective as of January 1, 2020. Dr. Miller’s annual base salary remains at $300,000. Our named executive officers are eligible to receive annual performance-based bonuses in the discretion of the board of directors. In December 2019, the board of directors granted Dr. Mobasher a bonus of $45,000 to be paid in 2020.
Equity Awards
In December 2019, the board of directors granted to Dr. Miller, Mr. Lea, and Dr. Mobasher options to purchase 320,000, 160,000 and 50,000 shares of our common stock, respectively, with an exercise price of $3.54 per share, which vest as to 1/48th of the shares underlying the option on each monthly anniversary of December 12, 2019, subject to the executive’s continued service to us.
128
Employment, Severance and Change in Control Arrangements
We are party to an employment agreement or offer letter with each of Dr. Miller, Mr. Lea and Dr. Mobasher, which sets forth the terms of their employment as our President and Chief Executive Officer, Chief Financial Officer and Vice President and Chief Medical Officer, respectively. These agreements provided for initial base salaries, eligibility for annual discretionary bonuses and the grants of discretionary equity awards, and standard benefit plan participation.
Change in Control and Severance Benefits.
Pursuant to Dr. Miller’s and Mr. Lea’s employment agreements and Dr. Mobasher’s change in control severance agreement, in the event that the executive’s employment is terminated by us other than for “cause,” or by the executive for “good reason” (each as defined below) at any time other than during the three month period prior to and twelve month period immediately following a change in control of the Company, the executive is entitled to receive (i) severance payments in an amount equal to nine, or, in the case of Dr. Miller, twelve, months of his then‑existing base salary; and (ii) continued healthcare coverage for the earlier of nine, or, in the case of Dr. Miller, twelve, months, or the date the executive and his dependents, if any, become eligible for healthcare coverage under another employer’s plan(s). In addition, each outstanding equity award that vests subject to the executive’s continued employment will automatically become vested, and, if applicable, all restrictions thereon will lapse, in each case, with respect to (i) in the case of Mr. Lea and Dr. Mobasher, the number of shares that would have vested in the nine month period following such termination had the executive remained employed or (ii) in the case of Dr. Miller, 100% of the number of shares that would have vested following such termination.
Furthermore, pursuant to Dr. Miller’s and Mr. Lea’s employment agreements, as amended and restated, and Dr. Mobasher’s employment agreement, in the event that the executive’s employment is terminated by us other than for “cause”, or by the executive for “good reason” (each as defined below) during the twelve month period immediately following a change in control of the Company, the executive is entitled to receive (i) severance payments in an amount equal to the sum of twelve, or in the case of Dr. Miller, eighteen, months of his then‑existing base salary plus 100%, or, in the case of Dr. Miller, 150%, of his target bonus opportunity, payable in a cash lump sum, less applicable withholdings; and (ii) continued healthcare coverage until the earlier of twelve, or in the case of Dr. Miller, eighteen, months following termination, or the date the executive and his dependents, if any, become eligible for healthcare coverage under another employer’s plan(s). In addition, for Mr. Lea and Dr. Mobasher, each outstanding equity award that vests subject to executive’s continued employment will automatically become vested, and, if applicable, all restrictions thereon will lapse, in each case, with respect to 100% of the shares subject thereto. For Dr. Miller, immediately following a change in control of the Company, each outstanding unvested equity award will automatically become vested and, if applicable, all restrictions thereon will lapse, in each case, with respect to 100% of the shares subject thereto.
Any such severance payments and accelerated vesting are subject to the executive’s timely execution and non‑revocation of a general release of claims against us and our affiliates.
With respect to each of Dr. Miller’s, Mr. Lea’s and Dr. Mobasher’s employment agreements:
|
· |
“Cause” generally means, subject to certain notice requirements and cure rights, the occurrence of any of the following events, as determined by our board of directors or a committee designated by our board, in its sole discretion: the executive’s (i) commission of any felony or any crime involving fraud, dishonesty, or moral turpitude under the laws of the United States or any state thereof; (ii) attempted commission of, or participation in, a fraud or act of dishonesty against us; (iii)intentional, material violation of any contract or agreement with us or of any statutory duty owed to us; (iv) unauthorized use or disclosure of our confidential information or trade secrets; (v) gross misconduct; or, with respect to Dr. Miller’s employment agreement, (vi) willful failure to perform his duties and responsibilities to us. |
|
· |
“Good Reason” means, subject to certain notice requirements and cure rights, the executive’s resignation from all positions he then holds with us if (i) there is a material diminution in his duties and responsibilities with us; provided, however, that a change in title or reporting relationship will not constitute good reason; |
129
(ii) there is a material reduction of his base salary; provided, however, that a material reduction in base salary pursuant to a salary reduction program affecting all or substantially all of our employees and that does not adversely affect the executive to a greater extent than other similarly situated employees shall not constitute good reason; or (iii) the executive is required to relocate his primary work location to a facility or location that would increase his one‑way commute distance by more than twenty‑five (25) miles from his primary work location as of immediately prior to such change. |
Pursuant to their respective agreements, our named executive officers are bound by certain restrictive covenants, including covenants relating to confidentiality and/or assignment of intellectual property rights. In addition, Dr. Miller and Mr. Lea are bound by covenants not to solicit our officers or employees during employment and for a specified period following termination of employment. Each named executive officer is also bound by a covenant not to disparage us or our employees, clients, directors or agents or divert or attempt to divert any of our actual or potential business.
Defined Contribution Plan
We maintain a 401(k) retirement savings plan for the benefit of our employees, including our named executive officers, who satisfy certain eligibility requirements. Under the 401(k) plan, eligible employees may elect to defer a portion of their compensation, within the limits prescribed by the Internal Revenue Code, on a pre‑tax or after‑tax (Roth) basis through contributions to the 401(k) plan. In 2019, we matched 100% of each participant’s contribution to our 401(k) plan up to a maximum match of $3,000 per participant. We believe that providing a vehicle for tax‑deferred retirement savings though our 401(k) plan adds to the overall desirability of our executive compensation package and further incentivizes our employees, including our named executive officers, in accordance with our compensation policies.
Perquisites
We provide limited perquisites and other personal benefits to our named executive officers, including the payment of life insurance premiums to the same extent provided to our other employees. We do not view these benefits as a significant component of our executive compensation program.
The Compensation Committee monitors our compensation programs on an annual basis and expects to make modifications as necessary to address any changes in our business or risk profile.
Compensation Committee Interlocks and Insider Participation
None of the members of our compensation committee has at any time been one of our officers or employees. None of our executive officers currently serves, or in the past fiscal year has served, as a member of our board of directors or compensation committee of any entity that has one or more executive officers on our board of directors or compensation committee.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
Security Ownership of Certain Beneficial Owners and Management
The following table sets forth certain information regarding the ownership of our common stock as of January 31, 2020, by: (i) each of our directors; (ii) each of our named executive officers as set forth in the summary compensation table above; (iii) all of our executive officers and directors as a group; and (iv) all those known by us to be beneficial owners of more than five percent (5%) of our common stock.
Beneficial ownership is determined in accordance with the rules of the SEC and generally includes voting or investment power with respect to securities. This table is based upon information supplied by officers, directors and principal stockholders and Forms 3, Forms 4, Forms 5 and Schedules 13D and 13G filed with the SEC. Unless otherwise indicated in the footnotes to this table, we believe that each of the stockholders named in the table has sole voting and
130
dispositive power with respect to the shares indicated as beneficially owned, subject to community property laws where applicable. Shares of our common stock subject to options that are currently exercisable or exercisable within 60 days of January 31, 2020 are deemed to be outstanding and to be beneficially owned by the person holding the options for the purpose of computing the percentage ownership of that person, but are not treated as outstanding for the purpose of computing the percentage ownership of any other person.
Applicable percentages are based on 27,953,233 shares outstanding on January 31, 2020, adjusted as required by rules promulgated by the SEC. Unless otherwise indicated, the address of each of the individuals and entities named below is c/o Corvus Pharmaceuticals, Inc., 863 Mitten Road, Suite 102, Burlingame, CA 94010.
|
|
|
Shares of Common Stock Beneficial Ownership |
|
||||||
|
|
|
|
|
Securities |
|
Number of |
|
|
|
|
|
|
|
|
Exercisable |
|
Shares |
|
|
|
|
|
|
|
|
Within |
|
Beneficially |
|
|
|
|
Name of Beneficial Owner |
|
Common Stock |
|
60 Days |
|
Owned |
|
Percent of Total |
|
|
5% and Greater Stockholders |
|
|
|
|
|
|
|
|
|
|
OrbiMed Private Investments V, L.P.(1) |
|
6,767,584 |
|
— |
|
6,767,584 |
|
24.21 |
% |
|
Entities affiliated with Adams Street Partners(2) |
|
3,275,616 |
|
— |
|
3,275,616 |
|
11.72 |
% |
|
BVF, Inc.(3) |
|
1,627,568 |
|
1,293,609 |
|
2,921,177 |
|
9.99 |
% |
|
Novo Holdings A/S(4) |
|
2,927,560 |
|
— |
|
2,927,560 |
|
10.47 |
% |
|
Named Executive Officers and Directors |
|
|
|
|
|
|
|
|
|
|
Richard A. Miller, M.D.(5) |
|
1,178,515 |
|
798,439 |
|
1,976,954 |
|
6.88 |
% |
|
Ian T. Clark(6) |
|
— |
|
60,000 |
|
60,000 |
|
* |
|
|
Elisha P. (Terry) Gould III(7) |
|
3,275,616 |
|
60,000 |
|
3,335,616 |
|
11.91 |
% |
|
Linda S. Grais, M.D. J.D.(8) |
|
— |
|
10,000 |
|
10,000 |
|
— |
|
|
Steve E. Krognes(9) |
|
— |
|
60,000 |
|
60,000 |
|
* |
|
|
Scott W. Morrison(10) |
|
— |
|
60,000 |
|
60,000 |
|
* |
|
|
Peter Thompson, M.D.(11) |
|
6,767,584 |
|
60,000 |
|
6,827,584 |
|
24.37 |
% |
|
Leiv Lea(12) |
|
199,406 |
|
144,064 |
|
343,470 |
|
1.22 |
|
|
Mehrdad Mobasher, M.D.(13) |
|
— |
|
64,375 |
|
64,375 |
|
* |
|
|
All executive officers and directors as a group (13 persons)(14) |
|
11,949,853 |
|
1,844,799 |
|
13,794,652 |
|
46.29 |
% |
* Denotes ownership percentage less than one percent.
|
(1) |
As reported on a Form 4 filed with the SEC on August 8, 2019 by Peter A. Thompson, M.D., these securities are held of record by OrbiMed Private Investments V, LP ("OPI V"). OrbiMed Capital GP V LLC ("GP V") is the sole general partner of OPI V, and OrbiMed Advisors LLC ("Advisors"), a registered adviser under the Investment Advisors Act of 1940, as amended, is the sole managing member of GP V. By virtue of such relationships, GP V and Advisors may be deemed to have voting and investment power with respect to the securities held by OPI V noted above and as a result may be deemed to beneficially own such securities for purposes of Rule 13d-3 under the Securities Exchange Act of 1934, as amended (the "Exchange Act"). Advisors exercised this investment and voting power through a management committee comprised of Carl L. Gordon, Sven H. Borho and Jonathan T. Silverstein, each of whom disclaims beneficial ownership of the Shares held by OPI V. Peter Thompson, M.D., a member of our board of directors, is an employee of Advisors. Each of GP V, Advisors and Dr. Thompson, disclaims beneficial ownership of the shares held by OPI V, except to the extent of its or his pecuniary interest therein, if any. Dr. Thompson is obligated to transfer all stock options or other awards of equity-based compensation arrangements for non-employee directors received to OPI V. The address of OrbiMed Advisors is 601 Lexington Avenue (at 53rd Street), 54th Floor, New York, NY 10022 4629. |
|
(2) |
As reported on a Form 4 filed with the SEC on June 24, 2019 by Adams Street Partners, LLC. Consists of (a) 69,864 shares held by Adams Street 2015 Direct Venture/Growth Fund LP ("AS 2015"), 236,128 shares held by Adams Street Venture/Growth Fund VI LP ("ASVG VI"), 67,769 shares held by Adams Street 2016 Direct Venture/Growth Fund LP ("AS 2016"), 87,668 shares held by Adams Street 2017 Direct Venture/Growth Fund LP ("AS 2017"), 126,806 shares held by Adams Street 2018 Direct Venture/Growth Fund LP ("AS 2018"), 694,854 shares held by Adams Street 2011 Direct Fund LP ("AS 2011"), 715,361 shares held by Adams Street 2012 Direct Fund LP ("AS 2012"), 541,133 shares held by Adams Street 2013 Direct Fund LP ("AS 2013") and 736,033 shares held by Adams Street 2014 Direct Fund LP ("AS 2014"). Elisha P. Gould, a member of our board of directors, is a partner of Adams Street Partners, LLC. Adams Street Partners, LLC, as the managing member of the general partner of the general partner of AS 2015, ASVG VI, AS 2016, AS 2017, AS2018, AS2011, AS2012, AS2013 and AS2014, may be deemed to beneficially own the shares held by AS 2015, ASVG VI, AS 2016, AS 2017, AS2018, AS2011, AS2012, AS2013 and AS2014. Thomas S. Bremner, Jeffrey T. Diehl, Elisha P. Gould, Robin Murray, Fred Wang and Michael R. Zappert, each of whom is a partner of Adams Street Partners, LLC (or a subsidiary thereof), may be deemed to have shared voting and investment power over the shares held by AS 2015, ASVG VI, AS 2016, AS 2017, AS2018AS 2011, AS 2012, AS 2013 and AS 2014. Adams Street Partners, LLC and Thomas S. Bremner, Jeffrey T. Diehl, Elisha P. Gould, Robin Murray, Fred Wang and Michael R. Zappert disclaim beneficial ownership of the |
131
shares held by each of AS 2015, ASVG VI, AS 2016, AS 2017, AS2018AS 2011, AS 2012, AS 2013 and AS 2014 except to the extent of their pecuniary interest therein. The address of Adams Street Partners, LLC is One North Wacker Drive, Suite 2700, Chicago, IL 60606 2823. |
|
(3) |
As reported on a Form 13 G/A filed with the SEC on February 18, 2020 by Biotechnology Value Fund, L.P. (BVF). As of the close of business on December 31, 2019, BVF held 1,458,000 Warrants exercisable for an aggregate of 1,458,000 Shares (the “Warrants”). The Warrants may not be exercised if, after such exercise, BVF would beneficially own, as determined in accordance with Section 13(d) of the Securities Exchange Act of 1934, more than 9.99% of the number of Shares then issued and outstanding (the “Beneficial Ownership Limitation”). Such Warrants have an initial exercise price of $0.0001 per share, subject to adjustment pursuant to the terms of the Warrants. As of December 31, 2019, the Beneficial Ownership Limitation limits the aggregate exercise of the Warrants by the Reporting Persons to 1,293,609 out of the 1,458,000 Shares underlying the Warrants owned by the Reporting Persons in the aggregate. In providing beneficial ownership described herein, the Reporting Persons have assumed 746,000 out of 746,000 Warrants owned by BVF would be exercised, 547,609 out of 606,000 Warrants owned by BVF2 would be exercised, and zero out of 106,000 Warrants owned by Trading Fund OS would be exercised. As of the close of business on December 31, 2019, (i) BVF beneficially owned 1,559,939 Shares, including 746,000 Shares issuable upon the exercise of certain Warrants, (ii) BVF2 beneficially owned 1,155,971 Shares, including 547,609 Shares issuable upon the exercise of certain Warrants and (iii) Trading Fund OS beneficially owned 107,396 Shares. BVF GP, as the general partner of BVF, may be deemed to beneficially own the 1,559,939 Shares beneficially owned by BVF. BVF2 GP, as the general partner of BVF2, may be deemed to beneficially own the 1,155,971 Shares beneficially owned by BVF2. Partners OS, as the general partner of Trading Fund OS, may be deemed to beneficially own the 107,396 Shares beneficially owned by Trading Fund OS. BVF GPH, as the sole member of each of BVF GP and BVF2 GP, may be deemed to beneficially own the 2,715,910 Shares beneficially owned in the aggregate by BVF and BVF2. Partners, as the investment manager of BVF, BVF2 and Trading Fund OS, and the sole member of Partners OS, may be deemed to beneficially own the 2,921,177 Shares beneficially owned in the aggregate by BVF, BVF2, Trading Fund OS, and a certain Partners managed account (the “Partners Managed Account”), including 97,871 Shares held in the Partners Managed Account. BVF Inc., as the general partner of Partners, may be deemed to beneficially own the 2,921,177 Shares beneficially owned by Partners. The address of Biotechnology Value Fund, L.P. is 44 Montgomery Street, 40th Floor, San Francisco, California 94104. |
|
(4) |
As reported on a Form 13F-HR filed with the SEC on February 14, 2020 by Novo Holdings A/S. The address of Novo A/S is Tuborg Havnevej 19, 2900 Hellerup, Denmark. |
|
(5) |
Consists of 1,178,515 shares of common stock held by Richard A. Miller and Sandra J. Horning, Trustees of the Miller Horning Family Trust u/a/d January 25, 1985 (Miller Horning Trust), and 798,439 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. Dr. Miller has shared voting, investment and dispositive power over the shares held by the Miller Horning Trust. |
|
(6) |
Consists of 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(7) |
Consists of 69,864 shares held directly by Adams Street 2015 Direct Venture/Growth Fund LP, 236,128 shares held by Adams Street Venture/Growth Fund VI LP, 67,769 shares held by Adams Street 2016 Direct Venture/Growth Fund LP, 87,668 shares held by Adams Street 2017 Direct Venture/Growth Fund LP, 126,806 shares held by Adams Street 2018 Direct Venture/Growth Fund LP, 694,854 shares held by Adams Street 2011 Direct Fund LP, 715,361 shares held by Adams Street 2012 Direct Fund LP, 541,133 shares held by Adams Street 2013 Direct Fund LP and 736,033 shares held by Adams Street 2014 Direct Fund LP and 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. Mr. Gould disclaims beneficial ownership of the shares listed in footnote (2), except to the extent of his pecuniary interest therein. |
|
(8) |
Consists of 10,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(9) |
Consists of 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(10) |
Consists of 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(11) |
Consists of 6,767,584 shares of our common stock held by OrbiMed Private Investments V, L.P. (“OrbiMed”). Dr. Thompson disclaims beneficial ownership of the shares held by OrbiMed except to the extent of his pecuniary interest therein. Also consists of 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(12) |
Consists of 149,206 shares of our common stock held by Mr. Lea and Deborah Karlson, Trustees of the Karlson Lea Family Trust UTA dated February 11, 1998 (Karlson Lea Trust), 50,200 shares of our common stock held by the Leiv Lea IRA Contributory and 144,064 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. Mr. Lea has shared voting, investment and dispositive power over the shares held by the Karlson Lea Trust. |
|
(13) |
Consists of 64,375 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(14) |
Includes 11,949,853 shares of our common stock and 1,844,799 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
132
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information about the securities authorized for issuance under our equity compensation plans as of December 31, 2019.
|
|
|
|
|
|
|
|
Number of |
|
|
|
|
|
|
|
|
|
shares |
|
|
|
|
|
|
|
|
|
remaining |
|
|
|
|
Number of |
|
|
|
|
available for |
|
|
|
|
shares to be |
|
Weighted‑ |
|
future issuance |
|
|
|
|
|
issued upon |
|
average exercise |
|
under equity |
|
|
|
|
|
exercise of |
|
price of |
|
compensation |
|
|
|
|
|
outstanding |
|
outstanding |
|
plans (excluding |
|
|
|
|
|
options, |
|
options, |
|
securities |
|
|
|
|
|
warrants and |
|
warrants and |
|
reflected in |
|
|
|
Plan category |
|
rights |
|
rights |
|
column (a)) |
|
|
|
|
|
(a) |
|
(b) |
|
(c) |
|
|
|
Equity compensation plans approved by stockholders(1)(2)(3) |
|
5,643,410 |
|
$ |
8.05 |
|
2,104,183 |
(4) |
|
Equity compensation plans not approved by stockholders |
|
— |
|
|
— |
|
— |
|
|
Total |
|
5,643,410 |
|
$ |
8.05 |
|
2,104,183 |
|
|
(1) |
Consists of 6,767,584 shares of our common stock held by OrbiMed Private Investments V, L.P. (“OrbiMed”). Dr. Thompson disclaims beneficial ownership of the shares held by OrbiMed except to the extent of his pecuniary interest therein. Also consists of 60,000 shares of our common stock issuable upon exercise of stock options exercisable within 60 days of January 31, 2020. |
|
(2) |
The 2016 Equity Incentive Award Plan contains an “evergreen” provision, pursuant to which the number of shares of common stock reserved for issuance or transfer pursuant to awards under the 2016 Equity Incentive Award Plan shall be increased on the first day of each year beginning in 2017 and ending in 2026, equal to the lesser of (A) four percent (4.0%) of the shares of common stock outstanding (on an as converted basis) on the last day of the immediately preceding fiscal year and (B) such smaller number of shares of stock as determined by our board of directors; provided, however, that no more than 15,000,000 shares of stock (subject to stock splits, dividends, recapitalizations and the like) may be issued upon the exercise of incentive stock options. |
|
(3) |
The 2016 Employee Stock Purchase Plan contains an “evergreen” provision, pursuant to which the maximum number of shares of our common stock authorized for sale under the 2016 Employee Stock Purchase Plan shall be increased on the first day of each year beginning in 2017 and ending in 2026, equal to the lesser of (A) one percent (1.0%) of the shares of common stock outstanding (on an as converted basis) on the last day of the immediately preceding fiscal year and (B) such number of shares of common stock as determined by our Board; provided, however, no more than 3,000,000 shares of our common stock may be issued thereunder. |
|
(4) |
Includes 400,000 shares available for issuance under the 2016 Employee Stock Purchase Plan. |
Item 13. Certain Relationships and Related Transactions and Director Independence
Certain Relationships and Related Party Transactions
Policies and Procedures for Related Party Transactions
Our board of directors has adopted a written related party transaction policy to set forth the policies and procedures for the review and approval or ratification of related person transactions. This policy will cover, with certain exceptions set forth in Item 404 of Regulation S‑K, any transaction, arrangement or relationship, or any series of similar transactions, arrangements or relationships in which we were or are to be a participant, where the amount involved exceeds $120,000 and a related party had, has or will have a direct or indirect material interest, including, without limitation, purchases of goods or services by or from the related party or entities in which the related party has a material interest, indebtedness, guarantees of indebtedness and employment by us of a related party. As provided by our related party transaction policy, our audit committee will be responsible for reviewing and approving in advance the related party transactions covered by our related party transaction policies and procedures.
133
Certain Related Party Transactions
We describe below transactions and series of similar transactions since January 1, 2019, to which we were a party or will be a party, in which (i) the amounts involved exceeded or will exceed $120,000 and (ii) any of our directors, executive officers, holders of more than five percent of our capital stock or any member of their immediate family had or will have a direct or indirect material interest.
Director and Executive Officer Agreements and Compensation
See the sections titled “Director Compensation” and “Executive Compensation” for more information regarding compensation of our directors and executive officers.
Employment Agreements
We have entered into employment agreements with our executive officers. For more information regarding these agreements, see the section titled “Executive Compensation.”
Indemnification Agreements and Directors’ and Officers’ Liability Insurance
We have entered into indemnification agreements with each of our directors and executive officers. These agreements require us to, among other things, indemnify each director and executive officer to the fullest extent permitted by Delaware law, including indemnification of expenses such as attorneys’ fees, judgments, penalties, fines and settlement amounts incurred by the director or executive officer in any action or proceeding, including any action or proceeding by or in right of us, arising out of the person’s services as a director or executive officer. We have obtained an insurance policy that insures our directors and officers against certain liabilities, including liabilities arising under applicable securities laws.
Investors’ Rights Agreement
We are party to an amended and restated investors’ rights agreement, dated as of September 16, 2015, pursuant to which certain of our stockholders, including certain holders of five percent (5%) or more of our capital stock and entities affiliated with certain of our directors, have the right to demand that we file a registration statement for their shares of our common stock or request that their shares of our common stock be covered by a registration statement that we are otherwise filing. As of December 31, 2019, the holders of approximately 10 million shares of our common stock are entitled to rights with respect to the registration of such shares under the Securities Act.
Independence of the Board of Directors
Our board of directors currently consists of seven (7) members. Our board of directors has determined that all of our directors, other than Dr. Miller, qualify as independent directors in accordance with the Nasdaq Global Market (“Nasdaq”) listing requirements. Dr. Miller is not considered independent because he is an employee of the Company. Nasdaq’s independence definition includes a series of objective tests, such as that the director is not, and has not been for at least three (3) years, one of our employees and that neither the director nor any of his or her family members has engaged in various types of business dealings with us. In addition, as required by Nasdaq rules, our board of directors has made a subjective determination as to each independent director that no relationships exist that, in the opinion of our board of directors, would interfere with the exercise of independent judgment in carrying out the responsibilities of a director. In making these determinations, our board of directors reviewed and discussed information provided by the directors and us with regard to each director’s business and personal activities and relationships as they may relate to us and our management. There are no family relationships among any of our directors or executive officers.
As required under Nasdaq rules and regulations, our independent directors meet in regularly scheduled executive sessions at which only independent directors are present.
134
Item 14. Principal Accountant Fees and Services
Independent Registered Public Accounting Firm Fees And Services
The following table represents aggregate fees billed or to be billed to us for fiscal years ended December 31, 2019 and 2018, respectively, by PricewaterhouseCoopers LLP, our independent registered public accounting firm.
|
|
|
Fiscal Year Ended |
||||
|
|
|
December 31, |
||||
|
|
|
2019 |
|
2018 |
||
|
Audit Fees(1) |
|
$ |
551,000 |
|
$ |
625,226 |
|
Audit‑Related Fees(2) |
|
|
— |
|
|
— |
|
Tax Fees(3) |
|
|
— |
|
|
— |
|
All Other Fees(4) |
|
|
900 |
|
|
900 |
|
Total |
|
$ |
551,900 |
|
$ |
626,126 |
|
(1) |
Audit Fees. This category consists of fees for professional services rendered in connection with the audit of our annual financial statements, review of our quarterly financial statements, assistance with registration statements filed with the SEC and services that are normally provided by the independent registered public accounting firm in connection with statutory and regulatory filings or engagements. Audit fees for 2018 included fees associated with our follow-on offering in March 2018. |
|
(2) |
Audit-Related Fees. This category consists of fees for professional services rendered that are reasonably related to the performance of the audit or review of our financial statements. |
|
(3) |
Tax Fees. This category consists of fees for services provided for tax consultation services. |
|
(4) |
All Other Fees. This category consists of fees for all other services that are not reported above. |
All fees described above were approved by our board of directors or the audit committee of the board of directors.
Pre-Approval Policies and Procedures
The audit committee has adopted policies and procedures for the pre‑approval of audit and non‑audit services provided by our independent registered public accounting firm, PricewaterhouseCoopers LLP. The policy generally requires pre‑approval for specified services in the defined categories of audit services, audit‑related services and tax services. The pre‑approval of services may be delegated to one or more of the audit committee’s members, but the decision must be reported to the full audit committee at its next scheduled meeting.
The audit committee reviews both audit and non‑audit services performed by PricewaterhouseCoopers LLP and the fees charged for such services. Among other things, the audit committee reviews non‑audit services proposed to be provided by PricewaterhouseCoopers LLP and pre‑approve such services only if they are compatible with maintaining PricewaterhouseCoopers LLP’s status as an independent registered public accounting firm. All services provided by PricewaterhouseCoopers LLP in 2019 and 2018 were pre‑approved by our board of directors or the audit committee after review of each of the services proposed for approval.
135
Item 15. Exhibits and Financial Statement Schedules
|
(1) |
Financial Statements: |
The financial statements required by Item 15(a) are filed as part of this Annual Report on Form 10‑K under Item 8 “Financial Statements and Supplementary Data.”
|
(2) |
Financial Statement Schedules: |
All schedules are omitted because they are not applicable or the required information is shown in the financial statements or notes thereto.
|
(3) |
Exhibits. |
136
EXHIBIT INDEX
|
|
Exhibit |
|
|
|
Incorporated by Reference |
|
Filed |
||||
|
|
Number |
|
Exhibit Description |
|
Form |
|
Date |
|
Number |
|
Herewith |
|
|
3.1 |
|
|
8‑K |
|
3/29/2016 |
|
3.1 |
|
|
|
|
|
3.2 |
|
|
8‑K |
|
3/29/2016 |
|
3.2 |
|
|
|
|
|
4.1 |
|
Reference is made to Exhibits 3.1 through 3.2. |
|
|
|
|
|
|
|
|
|
|
4.2 |
|
|
S‑1 |
|
1/4/2016 |
|
4.2 |
|
|
|
|
|
4.3 |
|
|
S‑1/A |
|
2/8/2016 |
|
4.3 |
|
|
|
|
|
4.4 |
|
|
8-K |
|
11/12/2019 |
|
4.1 |
|
|
|
|
|
4.5 |
|
|
|
|
|
|
|
|
X |
|
|
|
10.1(a) |
|
|
S‑1 |
|
1/4/2016 |
|
10.2(a) |
|
|
|
|
|
10.1(b) |
|
|
S‑1 |
|
1/4/2016 |
|
10.2(b) |
|
|
|
|
|
10.1(c) |
|
|
S‑1 |
|
1/4/2016 |
|
10.2(c) |
|
|
|
|
|
10.1(d) |
|
|
10‑Q |
|
8/4/2016 |
|
10.1(d) |
|
|
|
|
|
10.1(e) |
|
|
10‑Q |
|
11/3/2016 |
|
10.1(e) |
|
|
|
|
|
10.1(f) |
|
|
10‑Q |
|
5/3/2018 |
|
10.3 |
|
|
|
|
|
10.1(g) |
|
|
10‑Q |
|
8/2/2018 |
|
10.2 |
|
|
|
|
|
10.1(h) |
|
|
10-K |
|
3/7/2019 |
|
10.1(h) |
|
|
|
|
|
10.2(a)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.4(a) |
|
|
|
|
|
10.2(b)# |
|
Amendment to the 2014 Equity Incentive Plan, dated November 26, 2014. |
|
S‑1 |
|
1/4/2016 |
|
10.4(b) |
|
|
|
|
10.2(c)# |
|
Amendment to the 2014 Equity Incentive Plan, dated July 24, 2015. |
|
S‑1 |
|
1/4/2016 |
|
10.4(c) |
|
|
|
|
10.2(d)# |
|
Amendment to the 2014 Equity Incentive Plan, dated September 14, 2015. |
|
S‑1 |
|
1/4/2016 |
|
10.4(d) |
|
|
|
|
10.2(e)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.4(e) |
|
|
|
|
|
10.2(f)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.4(f) |
|
|
|
|
|
10.3(a)# |
|
|
S‑8 |
|
3/29/2016 |
|
99.2(a) |
|
|
|
|
|
10.3(b)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.5(b) |
|
|
|
137
|
|
Exhibit |
|
|
|
Incorporated by Reference |
|
Filed |
||||
|
|
Number |
|
Exhibit Description |
|
Form |
|
Date |
|
Number |
|
Herewith |
|
|
10.3(c)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.5(c) |
|
|
|
|
|
10.3(d)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.5(d) |
|
|
|
|
|
10.4# |
|
Form of Indemnification Agreement for directors and officers. |
|
S‑1 |
|
1/4/2016 |
|
10.6 |
|
|
|
|
10.5# |
|
|
S‑1 |
|
1/4/2016 |
|
10.7 |
|
|
|
|
|
10.6# |
|
|
S‑1 |
|
1/4/2016 |
|
10.8 |
|
|
|
|
|
10.7(a)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.9(a) |
|
|
|
|
|
10.7(b)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.9(b) |
|
|
|
|
|
10.8(a)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.10(a) |
|
|
|
|
|
10.8(b)# |
|
|
S‑1 |
|
1/4/2016 |
|
10.10(b) |
|
|
|
|
|
10.9(a)# |
|
|
10-K |
|
3/1/2018 |
|
10.9(a) |
|
|
|
|
|
10.9(b)# |
|
|
10-K |
|
3/1/2018 |
|
10.9(b) |
|
|
|
|
|
10.10# |
|
|
10-Q |
|
5/3/2018 |
|
10.2 |
|
|
|
|
|
10.11(a)# |
|
|
10-K |
|
3/7/2019 |
|
10.11(a) |
|
|
|
|
|
10.11(b)# |
|
|
10-K |
|
3/7/2019 |
|
10.11(b) |
|
|
|
|
|
10.12# |
|
Corvus Pharmaceuticals, Inc. 2016 Employee Stock Purchase Plan. |
|
S‑8 |
|
3/29/2016 |
|
99.3 |
|
|
|
|
10.13# |
|
|
S‑1 |
|
1/4/2016 |
|
10.12 |
|
|
|
|
|
10.14(a)† |
|
|
S‑1/A |
|
3/10/2016 |
|
10.13(a) |
|
|
|
|
|
10.14(b)† |
|
|
S‑1 |
|
1/4/2016 |
|
10.13(b) |
|
|
|
|
|
10.15† |
|
|
S‑1 |
|
1/4/2016 |
|
10.14 |
|
|
|
|
|
10.16(a)† |
|
|
S‑1/A |
|
2/8/2016 |
|
10.15 |
|
|
|
138
|
|
Exhibit |
|
|
|
Incorporated by Reference |
|
Filed |
||||
|
|
Number |
|
Exhibit Description |
|
Form |
|
Date |
|
Number |
|
Herewith |
|
|
10.16(b) |
|
|
|
|
|
|
|
|
X |
|
|
|
10.16(c) †† |
|
|
|
|
|
|
|
|
X |
|
|
|
10.17(a) |
|
|
10‑Q |
|
8/3/2017 |
|
10.1 |
|
|
|
|
|
10.17(b) |
|
|
|
|
|
|
|
|
X |
|
|
|
10.18†† |
|
|
|
|
|
|
|
|
X |
|
|
|
10.19 |
|
|
8-K |
|
11/12/2019 |
|
10.1 |
|
|
|
|
|
23.1 |
|
|
|
|
|
|
|
|
X |
|
|
|
24.1 |
|
Power of Attorney (included on signature page) |
|
|
|
|
|
|
|
X |
|
|
31.1 |
|
Certification by Chief Executive Officer pursuant to Section 302 of the Sarbanes‑Oxley Act of 2002. |
|
|
|
|
|
|
|
X |
|
|
31.2 |
|
Certification by Chief Financial Officer pursuant to Section 302 of the Sarbanes‑Oxley Act of 2002. |
|
|
|
|
|
|
|
X |
|
|
32.1** |
|
|
|
|
|
|
|
|
X |
|
|
|
101.INS |
|
XBRL Instance Document. |
|
|
|
|
|
|
|
X |
|
|
101.SCH |
|
XBRL Taxonomy Extension Schema Document. |
|
|
|
|
|
|
|
X |
|
|
101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase Document. |
|
|
|
|
|
|
|
X |
|
|
101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase Document. |
|
|
|
|
|
|
|
X |
|
|
101.LAB |
|
XBRL Taxonomy Extension Label Linkbase Document. |
|
|
|
|
|
|
|
X |
|
|
101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase Document. |
|
|
|
|
|
|
|
X |
† Confidential treatment has been granted for a portion of this exhibit.
††Portions of this exhibit have been omitted in accordance with Item 601(b)(10) of Regulation S-K.
# Indicates management contract or compensatory plan.
** The certification attached as Exhibit 32.1 that accompanies this Annual Report on Form 10‑K is not deemed filed with the Securities and Exchange Commission and is not to be incorporated by reference into any filing of Corvus Pharmaceuticals, Inc. under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, whether made before or after the date of this Annual Report on Form 10‑K, irrespective of any general incorporation language contained in such filing.
Registrants may voluntarily include a summary of information required by Form 10‑K under this Item 16. We have elected not to include such summary.
139
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
|
|
CORVUS PHARMACEUTICALS, INC. |
|
|
|
|
|
|
Date: March 9, 2020 |
By: |
/s/ RICHARD. A. MILLER |
|
|
|
Richard A. Miller, M.D. |
|
|
|
President, Chief Executive Officer and Director |
|
|
|
(Principal Executive Officer) |
|
|
|
|
|
Date: March 9, 2020 |
By: |
/s/ LEIV LEA |
|
|
|
Leiv Lea |
|
|
|
Chief Financial Officer |
|
|
|
(Principal Financial and Accounting Officer) |
POWER OF ATTORNEY
Each person whose individual signature appears below hereby authorizes and appoints Richard A. Miller, M.D. and Leiv Lea and each of them, with full power of substitution and resubstitution, as his or her true and lawful attorney‑in‑fact and agent to act in his or her name, place and stead and to execute in the name and on behalf of each person, individually and in each capacity stated below, and to file any and all amendments to this Annual Report on Form 10‑K and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorney‑in‑fact and agents full power and authority to do and perform each and every act and thing, ratifying and confirming all that said attorney‑in‑fact and agents or his substitute or substitutes may lawfully do or cause to be done by virtue thereof. Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
/s/ RICHARD A. MILLER, M.D. |
|
President, Chief Executive Officer and Director |
|
|
|
Richard A. Miller, M.D. |
|
(Principal Executive Officer) |
|
March 9, 2020 |
|
|
|
|
|
|
|
/s/ LEIV LEA |
|
Chief Financial Officer |
|
|
|
Leiv Lea |
|
(Principal Financial and Accounting Officer) |
|
March 9, 2020 |
|
|
|
|
|
|
|
/s/ IAN T. CLARK |
|
Director |
|
March 9, 2020 |
|
Ian T. Clark |
|
|
||
|
|
|
|
|
|
|
/s/ TERRY GOULD |
|
Director |
|
March 9, 2020 |
|
Elisha P. (Terry) Gould III |
|
|
||
|
|
|
|
|
|
|
/s/ LINDA S. GRAIS, M.D., J.D. |
|
Director |
|
March 9, 2020 |
|
Linda S. Grais, M.D., J.D. |
|
|
||
|
|
|
|
|
|
|
/s/ STEVE E. KROGNES |
|
Director |
|
March 9, 2020 |
|
Steve E. Krognes |
|
|
||
|
|
|
|
|
|
|
/s/ SCOTT W. MORRISON |
|
Director |
|
March 9, 2020 |
|
Scott W. Morrison |
|
|
||
|
|
|
|
|
|
|
/s/ PETER THOMPSON, M.D. |
|
Director |
|
March 9, 2020 |
|
Peter Thompson, M.D. |
|
|
140