Attached files
| file | filename |
|---|---|
| EX-32.1 - EXHIBIT 32.1 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex321.htm |
| EX-31.2 - EXHIBIT 31.2 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex312.htm |
| EX-31.1 - EXHIBIT 31.1 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex311.htm |
| EX-23 - EXHIBIT 23 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex23.htm |
| EX-21.1 - EXHIBIT 21.1 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex211.htm |
| EX-12 - EXHIBIT 12 - SELECT MEDICAL HOLDINGS CORP | sem-12311710kex12.htm |
Use these links to rapidly review the document
1
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
ý | ANNUAL REPORT PURSUANT TO SECTION 13 or 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 | |
For fiscal year ended December 31, 2017 | ||
OR | ||
o | TRANSITION REPORT PURSUANT TO SECTION 13 or 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 | |
For the transition period from to | ||
Commission file numbers: 001-34465 and 001-31441
SELECT MEDICAL HOLDINGS CORPORATION
SELECT MEDICAL CORPORATION
(Exact name of Registrants as specified in their Charter)
Delaware Delaware (State or Other Jurisdiction of Incorporation or Organization) | 20-1764048 23-2872718 (I.R.S. Employer Identification Number) | |
4714 Gettysburg Road, P.O. Box 2034 Mechanicsburg, PA (Address of Principal Executive Offices) | 17055 (Zip Code) | |
(717) 972-1100
(Registrants’ telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
Title of Each Class | Name of Each Exchange on Which Registered | |
Select Medical Holdings Corporation, Common Stock, $0.001 par value | New York Stock Exchange | |
Securities registered pursuant to Section 12(g) of the Act: NONE
Indicate by check mark if the registrants are well-known seasoned issuers, as defined in Rule 405 of the Securities Act.
Select Medical Holdings Corporation Yes ý No o
Select Medical Corporation Yes o No ý
Indicate by check mark if the registrants are not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No ý
Indicate by check mark whether the registrants (1) have filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding twelve months (or for such shorter period that the registrants were required to file such reports), and (2) have been subject to such filing requirements for the past 90 days. Yes ý No o
Indicate by check mark whether the registrants have submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding twelve months (or for such shorter period that the registrants were required to submit and post such files). Yes ý No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrants’ knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by check mark whether the registrant, Select Medical Holdings Corporation, is a large accelerated filer, an accelerated filer, a non- accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer ý | Accelerated filer o | Non-accelerated filer o (Do not check if a smaller reporting company) | Smaller reporting company o | Emerging growth company o | ||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. o
Indicate by check mark whether the registrant, Select Medical Corporation, is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” or “emerging growth company” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer o | Accelerated filer o | Non-accelerated filer ý (Do not check if a smaller reporting company) | Smaller reporting company o | Emerging growth company o | ||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. o
Indicate by check mark whether the registrants are shell companies (as defined in Rule 12b-2 of the Act). Yes o No ý
The aggregate market value of Holdings’ voting stock held by non-affiliates at June 30, 2017 (the last business day of Holdings’ most recently completed second fiscal quarter) was approximately $1,636,498,421, based on the closing price per share of common stock on that date of $15.35 as reported on the New York Stock Exchange. Shares of common stock known by the registrants to be beneficially owned by directors and officers of Holdings subject to the reporting and other requirements of Section 16 of the Securities Exchange Act of 1934 are not included in the computation. The registrants, however, have made no determination that such persons are “affiliates” within the meaning of Rule 12b-2 under the Securities Exchange Act of 1934.
The number of shares of Holdings’ Common Stock, $0.001 par value, outstanding as of February 1, 2018 was 134,103,978.
This Form 10-K is a combined annual report being filed separately by two registrants: Select Medical Holdings Corporation and Select Medical Corporation. Unless the context indicates otherwise, any reference in this report to “Holdings” refers to Select Medical Holdings Corporation and any reference to “Select” refers to Select Medical Corporation, the wholly owned operating subsidiary of Holdings, and any of Select’s subsidiaries. Any reference to “Concentra” refers to Concentra Inc., the indirect operating subsidiary of Concentra Group Holdings Parent, LLC (“Concentra Group Holdings Parent”), and its subsidiaries. References to the “Company,” “we,” “us,” and “our” refer collectively to Holdings, Select, and Concentra Group Holdings Parent and its subsidiaries.
Documents Incorporated by Reference
Listed hereunder are the documents, any portions of which are incorporated by reference and the Parts of this Form 10-K into which such portions are incorporated:
1. The registrant's definitive proxy statement for use in connection with the 2018 Annual Meeting of Stockholders to be held on or about May 1, 2018 to be filed within 120 days after the registrant’s fiscal year ended December 31, 2017, portions of which are incorporated by reference into Part III of this Form 10-K. Such definitive proxy statement, except for the parts therein which have been specifically incorporated by reference, should not be deemed “filed” for the purposes of this form 10-K.
SELECT MEDICAL HOLDINGS CORPORATION
SELECT MEDICAL CORPORATION
ANNUAL REPORT ON FORM 10-K
FOR THE YEAR ENDED DECEMBER 31, 2017
Item | Page | |||
PART I
Forward-Looking Statements
This annual report on Form 10-K contains forward-looking statements within the meaning of the federal securities laws. Statements that are not historical facts, including statements about our beliefs and expectations, are forward-looking statements. Forward-looking statements include statements preceded by, followed by or that include the words “may,” “could,” “would,” “should,” “believe,” “expect,” “anticipate,” “plan,” “target,” “estimate,” “project,” “intend,” and similar expressions. These statements include, among others, statements regarding our expected business outlook, anticipated financial and operating results, our business strategy and means to implement our strategy, our objectives, the amount and timing of capital expenditures, the likelihood of our success in expanding our business, financing plans, budgets, working capital needs, and sources of liquidity.
Forward-looking statements are only predictions and are not guarantees of performance. These statements are based on our management’s beliefs and assumptions, which in turn are based on currently available information. Important assumptions relating to the forward-looking statements include, among others, assumptions regarding our services, the expansion of our services, competitive conditions, and general economic conditions. These assumptions could prove inaccurate. Forward-looking statements also involve known and unknown risks and uncertainties, which could cause actual results to differ materially from those contained in any forward-looking statement. Many of these factors are beyond our ability to control or predict. Such factors include, but are not limited to, the following:
• | changes in government reimbursement for our services and/or new payment policies (including, for example, the expiration of the moratorium limiting the full application of the 25 Percent Rule that would reduce our Medicare payments for those patients admitted to a long term acute care hospital from a referring hospital in excess of an applicable percentage admissions threshold) may result in a reduction in net operating revenues, an increase in costs, and a reduction in profitability; |
• | the failure of our long term acute care hospitals or inpatient rehabilitation facilities to maintain their Medicare certifications may cause our net operating revenues and profitability to decline; |
• | the failure of our long term acute care hospitals and inpatient rehabilitation facilities operated as “hospitals within hospitals” to qualify as hospitals separate from their host hospitals may cause our net operating revenues and profitability to decline; |
• | a government investigation or assertion that we have violated applicable regulations may result in sanctions or reputational harm and increased costs; |
• | acquisitions or joint ventures may prove difficult or unsuccessful, use significant resources, or expose us to unforeseen liabilities; |
• | our plans and expectations related to the acquisition of U.S. HealthWorks by Concentra and our ability to realize anticipated synergies; |
• | private third-party payors for our services may adopt payment policies that could limit our future net operating revenues and profitability; |
• | the failure to maintain established relationships with the physicians in the areas we serve could reduce our net operating revenues and profitability; |
• | shortages in qualified nurses, therapists, physicians, or other licensed providers could increase our operating costs significantly or limit our ability to staff our facilities; |
• | competition may limit our ability to grow and result in a decrease in our net operating revenues and profitability; |
• | the loss of key members of our management team could significantly disrupt our operations; |
• | the effect of claims asserted against us could subject us to substantial uninsured liabilities; |
• | a security breach of our or our third-party vendors’ information technology systems may subject us to potential legal and reputational harm and may result in a violation of the Health Insurance Portability and Accountability Act of 1996 or the Health Information Technology for Economic and Clinical Health Act; and |
• | other factors discussed from time to time in our filings with the Securities and Exchange Commission (the “SEC”), including factors discussed under the heading “Risk Factors” of this annual report on Form 10-K. |
1
Except as required by applicable law, including the securities laws of the United States and the rules and regulations of the SEC, we are under no obligation to publicly update or revise any forward-looking statements, whether as a result of any new information, future events, or otherwise. You should not place undue reliance on our forward-looking statements. Although we believe that the expectations reflected in forward-looking statements are reasonable, we cannot guarantee future results or performance.
Investors should also be aware that while we do, from time to time, communicate with securities analysts, it is against our policy to disclose to securities analysts any material non-public information or other confidential commercial information. Accordingly, stockholders should not assume that we agree with any statement or report issued by any securities analyst irrespective of the content of the statement or report. Thus, to the extent that reports issued by securities analysts contain any projections, forecasts or opinions, such reports are not the responsibility of the Company.
2
Item 1. Business.
Overview
We began operations in 1997 and, based on number of facilities, are one of the largest operators of long term acute care hospitals, or “LTCHs,” inpatient rehabilitation facilities, or “IRFs,” outpatient rehabilitation clinics, and occupational medicine centers in the United States. As of December 31, 2017, we had operations in 47 states and the District of Columbia. As of December 31, 2017, we operated 100 LTCHs, 24 IRFs, and 1,616 outpatient rehabilitation clinics in 39 states and the District of Columbia. Concentra, which is operated through a joint venture subsidiary, operated 312 medical centers in 38 states as of December 31, 2017. Concentra also provides contract services at employer worksites and Department of Veterans Affairs community-based outpatient clinics, or “CBOCs.”
In 2017, we changed our internal segment reporting structure to reflect how we now manage the operations of our business, review operating performance, and allocate resources for our LTCHs and IRFs. All prior period information has been recast to conform to our new reportable segments. We now manage our Company through four business segments: long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. We had net operating revenues of $4,443.6 million for the year ended December 31, 2017. Of this total, we earned approximately 40% of our net operating revenues from our long term acute care segment, approximately 14% of our net operating revenues from our inpatient rehabilitation segment, approximately 23% from our outpatient rehabilitation segment, and approximately 23% from our Concentra segment. Our long term acute care segment consists of hospitals designed to serve the needs of long term acute patients, and our inpatient rehabilitation segment consists of hospitals designed to serve patients that require intensive rehabilitation care. Patients are typically admitted to our LTCHs and IRFs from general acute care hospitals. Patients in each of these segments have specialized needs, with serious and often complex medical conditions. Our outpatient rehabilitation segment consists of clinics that provide physical, occupational, and speech rehabilitation services. Our Concentra segment consists of medical centers and contract services provided at employer worksites and Department of Veterans Affairs CBOCs that deliver occupational medicine, physical therapy, veteran’s healthcare, and consumer health services. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Results of Operations” and “Notes to Consolidated Financial Statements—Note 10. Segment Information” beginning on F-33 for financial information for each of our segments for the past three fiscal years, which have been recast to reflect the current reportable segment structure of our Company. The financial and statistical information related to the operation of our Concentra segment, and used for calculations in the “Management’s Discussion and Analysis of Financial Condition and Results of Operations” section, which is contained elsewhere herein, began as of June 1, 2015, which is the date the Concentra acquisition was consummated.
Long Term Acute Care
We are a leading operator of LTCHs in the United States. As of December 31, 2017, we operated 100 LTCHs in 27 states. For the years ended December 31, 2015, 2016, and 2017, approximately 58%, 53% and 52%, respectively, of the net operating revenues of our long term acute care segment came from Medicare reimbursement. This percentage declined in 2017 as compared to the prior year because of the changes we implemented at LTCHs operating under new Medicare patient criteria, which have resulted in lower Medicare patient volume. As of December 31, 2017, we operated a total of 4,159 available licensed beds and employed approximately 14,100 people in our long term acute care segment, consisting primarily of registered nurses, respiratory therapists, physical therapists, occupational therapists, and speech therapists.
We operate the majority of our LTCHs as a hospital within a hospital, or an “HIH.” An LTCH that operates as an HIH leases space from a general acute care hospital, or “host hospital,” and operates as a separately licensed hospital within the host hospital, or on the same campus as the host hospital. In contrast, a free-standing LTCH does not operate on a host hospital campus. We operated 100 LTCHs at December 31, 2017, of which 99 were owned and one was managed. Of the 99 LTCHs we owned, 73 were operated as HIHs and 26 were operated as free-standing hospitals.
Patients are typically admitted to our LTCHs from general acute care hospitals, likely following an intensive care unit stay, suffering from chronic illness. These patients have highly specialized needs, with serious and complex medical conditions involving multiple organ systems. These conditions are often a result of complications related to heart failure, complex infectious disease, respiratory failure and pulmonary disease, complex surgery requiring prolonged recovery, renal disease, neurological events, and trauma. Given their complex medical needs, these patients require a longer length of stay than patients in a general acute care hospital and benefit from being treated in an LTCH that is designed to meet their unique medical needs. For the year ended December 31, 2017, the average length of stay for patients in our LTCHs was 28 days.
3
Additionally, we continually seek to increase our admissions by demonstrating our quality of care and, by doing so, expanding and improving our relationships with the physicians and general acute care hospitals in the markets where we operate. We maintain a strong focus on the provision of high-quality medical care within our facilities. The Joint Commission (“TJC”) and DNV GL Healthcare USA, Inc. (“DNV”) are independent, not-for-profit organizations that establish standards related to the operation and management of healthcare facilities. As of December 31, 2017, we operated 100 LTCHs, 99 of which were accredited by TJC. One of our LTCHs was accredited by DNV. Also as of December 31, 2017, all of our LTCHs were certified as Medicare providers. Each of our LTCHs must regularly demonstrate to a survey team conformance to the applicable standards established by TJC, DNV or the Medicare program, as applicable.
When a patient is referred to one of our LTCHs by a physician, case manager, discharge planner, health maintenance organization, or payor, a clinical assessment is performed to determine patient eligibility for admission. Based on the determinations reached in this clinical assessment, an admission decision is made.
Upon admission, an interdisciplinary team meets to perform a comprehensive review of the patient’s condition. The interdisciplinary team is composed of a number of clinicians and may include any or all of the following: an attending physician; a registered nurse; a physical, occupational, and speech therapist; a respiratory therapist; a dietitian; a pharmacist; and a case manager. Upon completion of an initial evaluation by each member of the treatment team, an individualized treatment plan is established and immediately initiated. Case management coordinates all aspects of the patient’s hospital stay and serves as a liaison to the insurance carrier’s case management staff as appropriate. The case manager specifically communicates clinical progress, resource utilization, and treatment goals to the patient, the treatment team, and the payor.
Each of our LTCHs has a distinct medical staff that is composed of physicians from multiple specialties that have successfully completed the required privileging and credentialing process; In general, physicians on the medical staff are not directly employed but are more commonly independent, practicing at multiple hospitals in the community. Attending physicians conduct daily rounds on their patients while consulting physicians provide consulting services based on the specific medical needs of our patients. Each LTCH develops on-call arrangements with individual physicians to ensure that a physician is available to care for our patients. When determining the appropriate composition of the medical staff of an LTCH, we consider the size of the LTCH, services provided by the LTCH, if applicable, the size and capabilities of the medical staff of the general acute care hospital that hosts that HIH and, if applicable, the proximity of an acute care hospital to the free-standing LTCH. The medical staff of each of our LTCHs meets the applicable requirements set forth by Medicare, the hospital’s applicable accrediting organizations, and the state in which that LTCH is located.
Our long term acute care segment is led by a President, Chief Operating Officer, Chief Medical Officer, and Chief Quality Officer. Each of our LTCHs has an onsite management team consisting of a chief executive officer, a chief nursing officer, and a director of business development. These teams manage local strategy and day-to-day operations, including oversight of clinical care and treatment. They also assume primary responsibility for developing relationships with the general acute care providers and clinicians in the local areas we serve that refer patients to our LTCHs. We provide our LTCHs with centralized accounting, treasury, payroll, legal, operational support, human resources, compliance, management information systems, and billing and collection services. The centralization of these services improves efficiency and permits staff at our LTCHs to focus their time on patient care.
For a description of government regulations and Medicare payments made to our LTCHs, see “—Government Regulations” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Regulatory Changes.”
Long Term Acute Care Strategy
The key elements of our long term acute care strategy are to:
Focus on Specialized Inpatient Services. We serve highly acute patients and patients with debilitating injuries and rehabilitation needs that cannot be adequately cared for in a less medically intensive environment, such as a skilled nursing facility. Chronically critically ill patients admitted to our LTCHs require long stays, benefitting from a more specialized and targeted clinical approach. Our care model is distinct from what patients experience in general acute care hospitals.
Provide High-Quality Care and Service. Our LTCHs serve a critical role in comprehensive healthcare delivery. Through our specialized treatment programs and staffing models, we treat patients with acute, highly complex, and specialized medical needs. Our treatment programs focus on specific patient needs and medical conditions, such as ventilator weaning protocols, comprehensive wound care assessments and treatment protocols, medication review and antibiotic stewardship, infection control prevention, and customized mobility, speech, and swallow programs. Our staffing models ensure that patients have the appropriate clinical resources over the course of their stay. We maintain quality assurance programs to support and monitor quality of care standards and to meet regulatory requirements and maintain Medicare certifications. We believe that we are recognized for providing quality care and service, which helps develop brand loyalty in the local areas we serve.
4
Our treatment programs are continuously reassessed and updated based on peer-reviewed literature. This approach provides our clinicians access to the best practices and protocols that we have found to be effective in treating various conditions in this population such as respiratory failure, non-healing wounds, brain injury, renal dysfunction, and complex infectious diseases. In addition, we customize these programs to provide a treatment plan tailored to meet our patients’ unique needs. The collaborative team-based approach coupled with the intense focus on patient safety and quality affords these highly complex patients the best opportunity to recover from catastrophic illness. This comprehensive care model is ultimately measured by the functional recovery of each of our patients.
The quality of the patient care we provide is continually monitored using several measures, including clinical outcomes data and analyses and patient satisfaction surveys. Quality metrics from our LTCHs are submitted to our corporate offices and used to create monthly, quarterly, and annual reports. In order to benchmark ourselves against other hospitals, we collect our clinical and patient satisfaction information and compare it to national standards and the results of other healthcare organizations. We are required to report quality measures to individual states based on unique requirements and laws. We also submit required LTCH quality data elements to CMS. See “—Government Regulations—Other Medicare Regulations—Medicare Quality Reporting.”
Control Operating Costs. We continually seek to improve operating efficiency and control costs at our LTCHs by standardizing operations and centralizing key administrative functions. These initiatives include:
• | centralizing administrative functions such as accounting, finance, treasury, payroll, legal, operational support, human resources, compliance, and billing and collection; |
• | standardizing management information systems to assist in capturing the medical record, accounting, billing, collections, and data capture and analysis; and |
• | centralizing sourcing and contracting to receive discounted prices for pharmaceuticals, medical supplies, and other commodities used in our operations. |
Increase Commercial Volume. We have focused on continued expansion of our relationships with commercial insurers to increase our volume of patients with commercial insurance in our LTCHs. We believe that commercial payors seek to contract with our hospitals because we offer our patients high-quality, cost-effective care at more attractive rates than general acute care hospitals. We also offer commercial enrollees customized treatment programs not typically offered in general acute care hospitals.
Inpatient Rehabilitation
Our IRFs provide comprehensive physical medicine, as well as rehabilitation programs and services, which serve to optimize patient health, function, and quality of life in the United States. As of December 31, 2017, we operated 24 IRFs in 10 states. For the years ended December 31, 2015, 2016, and 2017, approximately 39%, 38% and 42%, respectively, of the net operating revenues of our inpatient rehabilitation segment came from Medicare reimbursement. As of December 31, 2017, we operated a total of 1,133 available licensed beds and employed approximately 8,800 people in our inpatient rehabilitation segment, consisting primarily of registered nurses, respiratory therapists, physical therapists, occupational therapists, speech therapists, neuropsychologists, and other psychologists.
Patients at our IRFs have specialized needs, with serious and often complex medical conditions requiring rehabilitative healthcare services in an inpatient setting. These conditions require targeted therapy and rehabilitation treatment, including comprehensive rehabilitative services for brain and spinal cord injuries, strokes, amputations, neurological disorders, orthopedic conditions, pediatric congenital or acquired disabilities, and cancer. Given their complex medical needs and gradual and prolonged recovery, these patients generally require a longer length of stay than patients in a general acute care hospital. For the year ended December 31, 2017, the average length of stay for patients in our IRFs was 14 days.
Additionally, we continually seek to increase our admissions by demonstrating our quality of care and, by doing so, expanding and improving our relationships with the physicians and general acute care hospitals in the markets where we operate. We maintain a strong focus on the provision of high-quality medical care within our facilities. As of December 31, 2017, we operated 24 IRFs, 23 of which were accredited by TJC. One of our IRFs was accredited by DNV. Also as of December 31, 2017, 23 of our IRFs were certified as Medicare providers. Medicare certification of one IRF is pending. Ten of our IRFs also received accreditation from the Commission on Accreditation of Rehabilitation Facilities (“CARF”), an independent, not-for-profit organization that establishes standards related to the operation of medical rehabilitation facilities. Each of our IRFs must regularly demonstrate to a survey team conformance to the applicable standards established by TJC, DNV, the Medicare program or CARF, as applicable.
5
When a patient is referred to one of our IRFs by a physician, case manager, discharge planner, health maintenance organization, or insurance company, we perform a clinical assessment of the patient to determine if the patient meets criteria for admission. Based on the determinations reached in this clinical assessment, an admission decision is made.
Upon admission, an interdisciplinary team reviews a new patient’s condition. The interdisciplinary team is composed of a number of clinicians and may include any or all of the following: an attending physician; a registered nurse; a physical, occupational, and speech therapist; a respiratory therapist; a dietician; a pharmacist; and a case manager. Upon completion of an initial evaluation by each member of the treatment team, an individualized treatment plan is established and implemented. The case manager coordinates all aspects of the patient’s hospital stay and serves as a liaison with the insurance carrier’s case management staff when appropriate. The case manager communicates progress, resource utilization, and treatment goals between the patient, the treatment team, and the payor.
Each of our IRFs has a multispecialty medical staff that is composed of physicians that have completed the privileging and credentialing process required by that IRF, and have been approved by the governing board of that IRF. Physicians on the medical staff of our IRFs are generally not directly employed by our IRFs, but instead have staff privileges at one or more hospitals. At each of our IRFs, attending physicians conduct rounds on their patients on a regular basis and consulting physicians provide consulting services based on the medical needs of our patients. Our IRFs also have on-call arrangements with physicians to ensure that a physician is available to care for our patients. We staff our IRFs with the number of physicians, therapists, and other medical practitioners that we believe is appropriate to address the varying needs of our patients. When determining the appropriate composition of the medical staff of an IRF, we consider the size of the IRF, services provided by the IRF, if applicable, the proximity of an acute care hospital to the free-standing IRF. The medical staff of each of our IRFs meets the applicable requirements set forth by Medicare, the facility’s applicable accrediting organizations, and the state in which that IRF is located.
Our inpatient rehabilitation segment is led by a President, Medical Director, Chief Academic Officer, and Chief Quality Officer and each of our IRFs has an onsite management team consisting of a chief executive officer, a chief nursing officer, and a director of business development. These teams manage local strategy and day-to-day operations, including oversight of clinical care and treatment. They also assume primary responsibility for developing relationships with the general acute care providers and clinicians in the local areas we serve that refer patients to our IRFs. We provide our facilities within our inpatient rehabilitation segment with centralized accounting, treasury, payroll, legal, operational support, human resources, compliance, management information systems, and billing and collection services. The centralization of these services improves efficiency and permits the staff at our IRFs to focus their time on patient care.
For a description of government regulations and Medicare payments made to our IRFs, see “—Government Regulations” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Regulatory Changes.”
Inpatient Rehabilitation Strategy
The key elements of our inpatient rehabilitation strategy are to:
Focus on Specialized Inpatient Services. We serve patients with debilitating injuries and rehabilitation needs that cannot be adequately cared for in a less medically intensive environment, such as a skilled nursing facility. Generally, patients in our IRFs require longer stays and can benefit from more specialized and intensive clinical care than patients treated in general acute care hospitals and require more intensive therapy than that provided in outpatient rehabilitation clinics.
Provide High-Quality Care and Service. Our IRFs serve a critical role in comprehensive healthcare delivery. Through our specialized treatment programs and staffing models, we treat patients with complex and specialized medical needs. Our specialized treatment programs focus on specific patient needs and medical conditions, such as rehabilitation programs for brain trauma and spinal cord injuries. We also focus on specific programs of care designed to restore strength, improve physical and cognitive function, and promote independence in activities of daily living for patients who have suffered complications from strokes, amputations, cancer, and neurological and orthopedic conditions. Our staffing models ensure that patients have the appropriate clinical resources over the course of their stay. We maintain quality assurance programs to support and monitor quality of care standards and to meet regulatory requirements and maintain Medicare certifications. We believe that we are recognized for providing quality care and service, which helps develop brand loyalty in the local areas we serve.
Our treatment programs, which are continuously reassessed and updated, benefit patients because they give our clinicians access to the best practices and protocols that we have found to be most effective in treating various conditions such as brain and spinal cord injuries, strokes, and neuromuscular disorders. In addition, we combine or modify these programs to provide a treatment plan tailored to meet our patients’ unique needs. We measure the outcomes and successes of our patients’ recovery in order to provide the best possible patient care and service.
6
The quality of the patient care we provide is continually monitored using several measures, including clinical outcomes data and analyses and patient satisfaction surveys. Quality metrics from our IRFs are submitted to our corporate offices and used to create monthly, quarterly, and annual reports. In order to benchmark ourselves against other hospitals, we collect our clinical and patient satisfaction information and compare it to national standards and the results of other healthcare organizations. We are required to report quality measures to individual states based on unique requirements and laws. We also submit required IRF quality data elements to CMS. See “—Government Regulations—Other Medicare Regulations—Medicare Quality Reporting.”
Control Operating Costs. We continually seek to improve operating efficiency and control costs at our IRFs by standardizing operations and centralizing key administrative functions. These initiatives include:
• | centralizing administrative functions such as accounting, finance, treasury, payroll, legal, operational support, human resources, compliance, and billing and collection; |
• | standardizing management information systems to assist in capturing the medical record, accounting, billing, collections, and data capture and analysis; and |
• | centralizing sourcing and contracting to receive discounted prices for pharmaceuticals, medical supplies, and other commodities used in our operations. |
Increase Commercial Volume. We have focused on continued expansion of our relationships with commercial insurers to increase our volume of patients with commercial insurance in our IRFs. We believe that commercial payors seek to contract with our IRFs because we offer our patients high-quality, cost-effective care at more attractive rates than general acute care hospitals. We also offer commercial enrollees customized and comprehensive rehabilitation treatment programs not typically offered in general acute care hospitals.
Develop IRFs through Pursuing Joint Ventures with Large Healthcare Systems. By leveraging the experience of our senior management and development team, we believe that we are well positioned to expand our portfolio of joint ventured operations. When we identify joint venture opportunities, our development team conducts an extensive review of the area’s referral patterns and commercial insurance rates to determine the general reimbursement trends and payor mix. Once discussions commence with a healthcare system, we refine the specific needs of a joint venture, which could include working capital, the construction of new space, or the leasing and renovation of existing space. A joint venture typically consists of us and the healthcare system contributing certain post-acute care businesses into a newly formed entity. We typically function as the manager and hold either a majority or minority ownership interest. We bring clinical expertise and clinical programs that attract commercial payors and implement our standardized resource management programs, which may improve the clinical outcome and enhance the financial performance of the joint venture.
Pursue Opportunistic Acquisitions. We may grow our network of IRFs through opportunistic acquisitions. When we acquire an IRF or a group of related facilities, a team of our professionals is responsible for formulating and executing an integration plan. We seek to improve financial performance at such facilities by adding clinical programs that attract commercial payors, centralizing administrative functions, and implementing our standardized resource management programs.
Outpatient Rehabilitation
We believe that we are the largest operator of outpatient rehabilitation clinics in the United States based on number of facilities, with 1,616 facilities throughout 37 states and the District of Columbia as of December 31, 2017. Our outpatient rehabilitation clinics are typically located in a medical complex or retail location. On March 4, 2016, we acquired Physiotherapy, a national provider of outpatient physical rehabilitation care offering a wide range of services. On March 31, 2016, we sold our contract therapy businesses. Our outpatient rehabilitation segment employed approximately 9,900 people as of December 31, 2017.
In our rehabilitation clinics, we provide physical, occupational, and speech rehabilitation programs and services. We also provide certain specialized programs such as functional programs for work related injuries, hand therapy, post-concussion rehabilitation, and athletic training services. The typical patient in one of our rehabilitation clinics suffers from musculoskeletal impairments that restrict his or her ability to perform normal activities of daily living. These impairments are often associated with accidents, sports injuries, work related injuries, or post-operative orthopedic and other medical conditions. Our rehabilitation programs and services are designed to help these patients minimize physical and cognitive impairments and maximize functional ability. We also provide services designed to prevent short term disabilities from becoming chronic conditions. Our rehabilitation services are provided by our professionals including licensed physical therapists, occupational therapists, and speech-language pathologists.
7
Outpatient rehabilitation patients are generally referred or directed to our clinics by a physician, employer, or health insurer who believes that a patient, employee, or member can benefit from the level of therapy we provide in an outpatient setting. In recent years a number of states have enacted laws that allow individuals to seek outpatient physical rehabilitation services without a physician order. Currently, this population of patients is not significant. In our outpatient rehabilitation segment, for the year ended December 31, 2017, approximately 85% of our net operating revenues come from commercial payors, including healthcare insurers, managed care organizations and workers’ compensation programs, contract management services, and private pay sources. We believe that our services are attractive to healthcare payors who are seeking to provide high-quality and cost-effective care to their enrollees. The balance of our reimbursement is derived from Medicare and other government sponsored programs.
For a description of government regulations and Medicare payments made to our outpatient rehabilitation services see “—Government Regulations” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Regulatory Changes.”
Outpatient Rehabilitation Strategy
The key elements of our outpatient rehabilitation strategy are to:
Provide High-Quality Care and Service. We are focused on providing a high level of service to our patients throughout their entire course of treatment. To measure satisfaction with our service we have developed surveys for both patients and physicians. Our clinics utilize the feedback from these surveys to continuously refine and improve service levels. We believe that by focusing on quality care and offering a high level of customer service we develop brand loyalty which allows us to strengthen our relationships with referring physicians, employers, and health insurers to drive additional patient volume.
Increase Market Share. We strive to establish a leading presence within the local areas we serve. To increase our presence, we seek to open new clinics in our existing markets. This allows us to realize economies of scale, heightened brand loyalty, and workforce continuity. We also focus on increasing our workers’ compensation and commercial/managed care payor mix.
Expand Rehabilitation Programs and Services. Through our local clinical directors of operations and clinic managers within their service areas, we assess the healthcare needs of the areas we serve. Based on these assessments, we implement additional programs and services specifically targeted to meet demand in the local community. In designing these programs we benefit from the knowledge we gain through our national network of clinics. This knowledge is used to design programs that optimize treatment methods and measure changes in health status, clinical outcomes, and patient satisfaction.
Optimize Payor Contract Reimbursements. We review payor contracts scheduled for renewal and potential new payor contracts to assure reasonable reimbursements for the services we provide. Before we enter into a new contract with a commercial payor, we evaluate it with the aid of our contract management system. We assess the reasonableness of the reimbursements by evaluating past and projected patient volume and clinic capacity. We create a retention strategy for the top performing contracts and a renegotiation strategy for contracts that do not meet our defined criteria. We believe that our national footprint and our strong reputation enable us to negotiate favorable reimbursement rates with commercial insurers.
Maintain Strong Community and Employee Relations. We believe that the relationships between our employees and the referral sources in their communities are critical to our success. Our referral sources, such as physicians and healthcare case managers, send their patients to our clinics based on three factors: the quality of our care, the customer service we provide, and their familiarity with our therapists. We seek to retain and motivate our therapists by implementing a performance-based bonus program, a defined career path with the ability to be promoted from within, timely communication on company developments, and internal training programs. We also focus on empowering our employees by giving them a high degree of autonomy in determining local area strategy. We seek to identify therapists who are potential business leaders. This management approach reflects the unique nature of each local area in which we operate and the importance of encouraging our employees to assume responsibility for their clinic’s financial and operational performance.
Pursue Opportunistic Acquisitions. We may grow our network of outpatient rehabilitation facilities through opportunistic acquisitions such as Physiotherapy. We believe our size and centralized infrastructure allow us to take advantage of operational efficiencies and improve financial performance at acquired facilities.
8
Concentra
We believe that we are the largest provider of occupational health services in the United States based on the number of facilities. As of December 31, 2017, we operated 312 medical centers, 105 onsite clinics at employer worksites, and 32 CBOCs throughout 43 states. We deliver occupational medicine, consumer health, physical therapy, and veteran’s healthcare services in our medical centers, onsite clinics located at the workplaces of our employer customers, and our CBOCs. Our Concentra segment employed approximately 7,700 people as of December 31, 2017.
We offer a range of occupational and consumer health services through our medical centers and onsite clinics. Occupational health services include workers’ compensation injury care as well as employer services, clinical testing, wellness programs, and preventative care. Our services at the CBOCs include primary care, specialty care, subspecialty care, mental health, and pharmacy benefits. Consumer health consists of non-employer, patient-directed treatment of injuries, and illnesses. Our consumer service offerings include urgent care, wellness programs, and preventative care.
Occupational medicine refers to the diagnosis and treatment of work-related injuries (workers’ compensation), compliance services, such as preventive services, including pre-employment, fitness-for-duty, and post-accident physical examinations and substance abuse screening. Utilization is driven by the needs of labor-intensive industries such as transportation, distribution/warehousing, manufacturing, construction, healthcare, police/fire, and other occupations that have historically posed a higher than average risk of workplace injury or that require a workplace physical. Workers’ compensation is the form of insurance that provides medical coverage to employees with work-related illnesses or injuries.
Workers’ compensation is administered on a state-by-state basis and each state is responsible for implementing and regulating its own workers’ compensation program. Because workers’ compensation benefits are mandated by law and subject to extensive regulation, insurers, third-party administrators, and employers do not have the same flexibility to alter benefits as they have with other health benefit programs. In addition, because programs vary by state, it is difficult for insurance companies and multi-state employers to adopt uniform policies to administer, manage and control the costs of benefits across states. As a result, managing the cost of workers’ compensation requires approaches that are tailored to the specific regulatory environments in which the employer operates. For the year ended December 31, 2017, approximately 53% of our Concentra segment operating revenues came from workers’ compensation.
Acquisition of U.S. HealthWorks
On October 23, 2017, we announced that Concentra Group Holdings, LLC, or Concentra Group Holdings, entered into an Equity Purchase and Contribution Agreement, or “Purchase Agreement,” dated October 22, 2017 with Concentra, Concentra Group Holdings Parent, U.S. HealthWorks, Inc., or “U.S. HealthWorks,” and Dignity Health Holding Corporation, or “DHHC.” On February 1, 2018, pursuant to the terms of the Purchase Agreement, Concentra acquired all of the issued and outstanding shares of stock of U.S. HealthWorks, an occupational medicine and urgent care service provider.
In connection with the closing of the transaction, Concentra Group Holdings redeemed certain of its outstanding equity interests from existing minority equity holders and subsequently, Concentra Group Holdings and a wholly owned subsidiary of Concentra Group Holdings Parent merged, with Concentra Group Holdings surviving the merger and becoming a wholly owned subsidiary of Concentra Group Holdings Parent. As a result of the merger, the equity interests of Concentra Group Holdings outstanding after the redemption described above were exchanged for membership interests in Concentra Group Holdings Parent.
The transaction valued U.S. HealthWorks at $753.0 million. DHHC, a subsidiary of Dignity Health, was issued a 20% equity interest in Concentra Group Holdings Parent, which was valued at $238.0 million. The remainder of the purchase price was paid in cash. Select currently retains a majority voting interest in Concentra Group Holdings Parent.
Concentra financed the transaction and related expenses using a $555.0 million senior secured incremental term facility under its existing credit facility and a $240.0 million second lien term facility.
Concentra Strategy
The key elements of our Concentra strategy are to:
Provide High-Quality Care and Service. We strive to provide a high level of service to our patients and our employer customers. We measure and monitor patient and employer satisfaction and focus on treatment programs to provide the best clinical outcomes in a consistent manner. Our programs and services have proven that aggressive treatment and management of workers injuries can more rapidly restore employees to better health which reduces workers’ compensation indemnity claim costs for our employer customers.
9
Focus on Occupational Medicine. Our history as an industry leader in the provision of occupational medicine services provides the platform for Concentra to grow this service offering. Complementary service offerings help drive additional growth in this business line.
Pursue Direct Employer Relationships. We believe we provide occupational health services in a cost-effective manner to our employer customers. By establishing direct relationships with these customers we seek to reduce overall costs of their workers’ compensation claims, while improving employee health, and getting their employees back to work faster.
Increase Presence in the Areas We Serve. We strive to establish a strong presence within the local areas we serve. To increase our presence, we seek to expand our services and programs, and to open new medical centers and employer onsite locations. This allows us to realize economies of scale, heightened brand loyalty, and workforce continuity.
Pursue Opportunistic Acquisitions. We may grow our network and expand our geographic reach through opportunistic acquisitions, such as the acquisition of U.S. HealthWorks. We believe our size and centralized infrastructure allow us to take advantage of operational efficiencies and improve financial performance at acquired facilities.
Other
Other activities include our corporate services and certain other minority investments in other healthcare related businesses. These include investments in companies that provide specialized technology, services to healthcare entities and providers of complementary services.
Our Competitive Strengths
We believe that the success of our business model is based on a number of competitive strengths, including our position as a leading operator in each of our business segments, proven financial performance and strong cash flow, significant scale, experience in completing and integrating acquisitions and partnering with large healthcare systems, ability to capitalize on consolidation opportunities, and an experienced management team.
Leading Operator in Distinct but Complementary Lines of Business. We believe that we are a leading operator in our business segments, based on number of facilities in the United States. Our leadership position and reputation as a high-quality, cost-effective healthcare provider in each of our business segments allows us to attract patients and employees, aids us in our marketing efforts to referral sources, and helps us negotiate payor contracts. In our long term acute care segment, we operated 100 LTCHs in 27 states as of December 31, 2017. In our inpatient rehabilitation segment, we operated 24 IRFs in 10 states as of December 31, 2017. In our outpatient rehabilitation segment, we operated 1,616 outpatient rehabilitation clinics in 37 states and the District of Columbia as of December 31, 2017. In our Concentra segment, we operated 312 medical centers in 38 states as of December 31, 2017. With these leading positions in the areas we serve, we believe that we are well-positioned to benefit from the rising demand for medical services due to an aging population in the United States, which will drive growth across our business segments.
Proven Financial Performance and Strong Cash Flow. We have established a track record of improving the financial performance of our facilities due to our disciplined approach to revenue growth, expense management, and focus on free cash flow generation. This includes regular review of specific financial metrics of our business to determine trends in our revenue generation, expenses, billing, and cash collection. Based on the ongoing analysis of such trends, we make adjustments to our operations to optimize our financial performance and cash flow.
Significant Scale. By building significant scale in each of our business segments, we have been able to leverage our operating costs by centralizing administrative functions at our corporate office.
Experience in Successfully Completing and Integrating Acquisitions. Since our inception in 1997 through 2017, we completed nine significant acquisitions for approximately $2.57 billion, which includes $418.6 million paid to acquire Physiotherapy and $1.05 billion paid to acquire Concentra. On February 1, 2018, we paid $753.0 million to acquire U.S. HealthWorks. We believe that we have improved the operating performance of these businesses over time by applying our standard operating practices and by realizing efficiencies from our centralized operations and management.
Experience in Partnering with Large Healthcare Systems. Over the past several years we have partnered with large healthcare systems to provide post-acute care services. We believe that we provide operating expertise through our experience in operating LTCHs, IRFs, and outpatient rehabilitation services to these ventures and have improved and expanded the level of post-acute care services provided in these communities, as well as the financial performance of these operations.
10
Well-Positioned to Capitalize on Consolidation Opportunities. We believe that we are well-positioned to capitalize on consolidation opportunities within each of our business segments and selectively augment our internal growth. We believe that each of our business segments is largely fragmented, with many of the nation’s LTCHs, IRFs, outpatient rehabilitation facilities, and occupational medical centers operated by independent operators lacking national or broad regional scope. With our geographically diversified portfolio of facilities in the United States, we believe that our footprint provides us with a wide-ranging perspective on multiple potential acquisition opportunities.
Experienced and Proven Management Team. Prior to co-founding our company with our current Executive Chairman and Co-Founder, our Vice Chairman and Co-Founder founded and operated three other healthcare companies focused on inpatient and outpatient rehabilitation services. In addition, our senior management team has extensive experience in the healthcare industry. Our President and Chief Executive Officer has more than two decades of management experience in the healthcare industry. Many of our other executives, such as our Chief Financial Officer, our General Counsel, our Chief Human Resources Officer, and our Chief Accounting Officer, have each served at our company for more than 18 years. In recent years, we have reorganized our operations to expand executive talent and ensure management continuity.
Sources of Net Operating Revenues
The following table presents the approximate percentages by source of net operating revenue received for healthcare services we provided for the periods indicated:
Year Ended December 31, | ||||||||||
Net Operating Revenues by Payor Source | 2015 | 2016 | 2017 | |||||||
Medicare | 36.5 | % | 30.0 | % | 30.0 | % | ||||
Commercial insurance(1) | 34.1 | % | 33.0 | % | 33.1 | % | ||||
Workers’ Compensation | 12.6 | % | 17.2 | % | 17.2 | % | ||||
Private and other(2) | 12.8 | % | 15.8 | % | 15.4 | % | ||||
Medicaid | 4.0 | % | 4.0 | % | 4.3 | % | ||||
Total | 100.0 | % | 100.0 | % | 100.0 | % | ||||
_______________________________________________________________________________
(1) | Includes commercial healthcare insurance carriers, health maintenance organizations, preferred provider organizations and managed care programs. |
(2) | Includes self-payors, management services and non-patient related payments. Self-pay revenues represent less than 1% of total net operating revenues for all periods. |
Government Sources
Medicare is a federal program that provides medical insurance benefits to persons age 65 and over, some disabled persons, and persons with end-stage renal disease. Medicaid is a federal-state funded program, administered by the states, which provides medical benefits to individuals who are unable to afford healthcare. As of December 31, 2017, we operated 100 LTCHs, all of which were certified as Medicare providers. Also as of December 31, 2017, we operated 24 IRFs, 23 of which were certified as Medicare providers and one of which was in the process of obtaining its certification. Our outpatient rehabilitation clinics regularly receive Medicare payments for their services. Our Concentra segment receives payments from the Department of Veterans Affairs and other governmental programs. Additionally, many of our LTCHs and IRFs participate in state Medicaid programs. Amounts received under the Medicare and Medicaid programs are generally less than the customary charges for the services provided. In recent years, there have been significant changes made to the Medicare and Medicaid programs. Since a significant portion of our revenues come from patients under the Medicare program, our ability to operate our business successfully in the future will depend in large measure on our ability to adapt to changes in the Medicare program. See “—Government Regulations—Overview of U.S. and State Government Reimbursements.”
11
Non-Government Sources
Our non-government sources of net operating revenue include insurance companies, workers’ compensation programs, health maintenance organizations, preferred provider organizations, other managed care companies and employers, as well as patients directly. Patients are generally not responsible for any difference between customary charges for our services and amounts paid by Medicare and Medicaid programs, insurance companies, workers’ compensation programs, health maintenance organizations, preferred provider organizations, and other managed care companies, but are responsible for services not covered by these programs or plans, as well as for deductibles and co-insurance obligations of their coverage. The amount of these deductibles and co-insurance obligations has increased in recent years. Collection of amounts due from individuals is typically more difficult than collection of amounts due from government or commercial payors.
Employees
As of December 31, 2017, we employed approximately 42,200 people throughout the United States. Approximately 29,900 of our employees are full-time and the remaining approximately 12,300 are part-time employees. Our long term acute care segment employees totaled approximately 14,100, inpatient rehabilitation segment employees totaled approximately 8,800, outpatient rehabilitation segment employees totaled approximately 9,900, and Concentra segment employees totaled approximately 7,700. The remaining approximately 1,700 employees performed corporate management, administration, and other support services primarily at our Mechanicsburg, Pennsylvania headquarters.
Competition
Long Term Acute Care Hospitals and Inpatient Rehabilitation Facilities
Our long term acute care hospitals and inpatient rehabilitation facilities both compete on the basis of the quality of the patient services we provide, the outcomes we achieve for our patients, and the prices we charge for our services. The primary competitive factors in both of our long term acute care and inpatient rehabilitation segments include quality of services, charges for services, and responsiveness to the needs of patients, families, payors, and physicians. Other companies operate LTCHs and IRFs that compete with our own LTCHs and IRFs, including large operators of similar facilities, such as Kindred Healthcare Inc. and Encompass Health Corporation, and rehabilitation units and stepdown units operated by acute care hospitals in the markets we serve. The competitive position of an LTCH or IRF is also affected by the ability of its management to negotiate contracts with purchasers of group healthcare services, including private employers, managed care companies, preferred provider organizations, and health maintenance organizations. Such organizations attempt to obtain discounts from established LTCH or IRF charges. The importance of obtaining contracts with preferred provider organizations, health maintenance organizations, and other organizations which finance healthcare, and its effect on an LTCH or IRF’s competitive position, vary from area to area depending on the number and strength of such organizations.
Outpatient Rehabilitation Clinics
Our outpatient rehabilitation clinics face a highly fragmented and competitive environment. The primary competitors that provide outpatient rehabilitation services include physician-owned physical therapy clinics, dedicated locally owned and managed outpatient rehabilitation clinics, and hospital or university owned or affiliated ventures, as well as national and regional providers in select areas, including Athletico Physical Therapy, ATI Physical Therapy, Drayer Physical Therapy Institute, U.S. Physical Therapy, and Upstream Physical Therapy. Some of these competing clinics have longer operating histories and greater name recognition in these communities than our clinics, and they may have stronger relations with physicians in these communities on whom we rely for patient referrals. Because the barriers to entry are not substantial and current customers have the flexibility to move easily to new healthcare service providers, we believe that new outpatient physical therapy competitors can emerge relatively quickly.
Concentra
Our Concentra segment’s occupational health services, consumer health, and veteran’s healthcare business face a highly fragmented and competitive environment. The primary competitors that provide occupational health services have typically been independent physicians, hospital emergency departments, and hospital-owned or hospital-affiliated medical facilities. Because the barriers to entry are not substantial and its current customers have the flexibility to move easily to new healthcare service providers, we believe that new competitors to Concentra can emerge relatively quickly. Furthermore, urgent care clinics in the local communities Concentra serves provide services similar to those Concentra offers, and, in some cases, competing facilities are more established or newer than Concentra’s, may offer a broader array of services to patients than Concentra’s, and may have larger or more specialized medical staffs to treat and serve patients.
12
Government Regulations
General
The healthcare industry is required to comply with many complex laws and regulations at the federal, state and local government levels. These laws and regulations require that hospitals and facilities furnishing outpatient services (including outpatient rehabilitation clinics, Concentra medical centers, onsite clinics and CBOCs) comply with various requirements and standards. These laws and regulations include those relating to the adequacy of medical care, facilities and equipment, personnel, operating policies and procedures and recordkeeping as well as standards for reimbursement, fraud and abuse prevention and health information privacy and security. These laws and regulations are extremely complex, often overlap and, in many instances, the industry does not have the benefit of significant regulatory or judicial interpretation. If we fail to comply with applicable laws and regulations, we could suffer civil or criminal penalties, including the loss of our licenses to operate and our ability to participate in the Medicare, Medicaid and other federal and state healthcare programs.
Facility Licensure
Our healthcare facilities are subject to state and local licensing statutes and regulations ranging from the adequacy of medical care to compliance with building codes and environmental protection laws. In order to assure continued compliance with these various regulations, governmental and other authorities periodically inspect our facilities, both at scheduled intervals and in response to complaints from patients and others. While our facilities intend to comply with existing licensing standards, there can be no assurance that regulatory authorities will determine that all applicable requirements are fully met at any given time. In addition, the state and local licensing laws are subject to changes or new interpretations that could impose additional burdens on our facilities. A determination by an applicable regulatory authority that a facility is not in compliance with these requirements could lead to the imposition of corrective action, assessment of fines and penalties, or loss of licensure, Medicare enrollment or certification or accreditation. These consequences could have an adverse effect on our company.
Some states still require us to get approval under certificate of need regulations when we create, acquire or expand our facilities or services, or alter the ownership of such facilities, whether directly or indirectly. The certificate of need regulations vary from state to state, and are subject to change and new interpretation. If we fail to show public need and obtain approval in these states for our new facilities or changes to the ownership structure of existing facilities, we may be subject to civil or even criminal penalties, lose our facility license or become ineligible for reimbursement.
Professional Licensure, Corporate Practice and Fee-Splitting Laws
Healthcare professionals at our LTCHs, IRFs, and facilities furnishing outpatient services are required to be individually licensed or certified under applicable state law. We take steps to ensure that our employees and agents possess all necessary licenses and certifications.
Some states prohibit the “corporate practice of medicine,” which restricts business corporations from practicing medicine through the direct employment of physicians or from exercising control over medical decisions by physicians. Some states similarly prohibit the “corporate practice of therapy.” The laws relating to corporate practice vary from state to state and are not fully developed in each state in which we have facilities. Typically, however, professional corporations owned and controlled by licensed professionals are exempt from corporate practice restrictions and may employ physicians or therapists to furnish professional services. Also, in some states hospitals are permitted to employ physicians.
Some states also prohibit entities from engaging in certain financial arrangements, such as fee-splitting, with physicians or therapists. The laws relating to fee-splitting also vary from state to state and are not fully developed. Generally, these laws restrict business arrangements that involve a physician or therapist sharing medical fees with a referral source, but in some states these laws have been interpreted to extend to management agreements between physicians or therapists and business entities under some circumstances.
We believe that each of our facilities, licensed physicians, and therapists comply with any current corporate practice and fee-splitting laws of the state in which they are located. In states where we are prohibited by the corporate practice of medicine from directly employing licensed physicians, we typically enter into management agreements with professional corporations that are owned by licensed physicians, which, in turn, employ or contract with physicians who provide professional medical services in our facilities. Under those management agreements, we perform only non-medical administrative services, do not exercise control over the practice of medicine by the physicians and structure compensation to avoid fee-splitting. In those states that apply the corporate practice of therapy prohibition, we either contract to obtain therapy services from an entity permitted to employ therapists or we manage the physical therapy practice owned by licensed therapists through which the therapy services are provided.
13
Although we believe that our facilities comply with corporate practice and fee-splitting laws, if new regulations or judicial or administrative interpretations establish that our facilities do not comply with these laws, we could be subject to civil and perhaps criminal penalties. In addition, if any of our facilities is determined not to comply with corporate practice and fee-splitting laws, certain of our agreements relating to the facility may be determined to be unenforceable, including our management agreements with the professional corporations furnishing physician services or our payment arrangements with insurers or employers. Future interpretations of corporate practice and fee-splitting laws, the enactment of new legislation or the adoption of new regulations relating to these laws could cause us to have to restructure our business operations or close our facilities in a particular state. Any such penalties, determinations of unenforceability or interpretations could have a material adverse effect on our business.
Medicare Enrollment and Certification
In order to participate in the Medicare program and receive Medicare reimbursement, each facility must comply with the applicable regulations of the United States Department of Health and Human Services relating to, among other things, the type of facility, its equipment, its personnel and its standards of medical care, as well as compliance with all applicable state and local laws and regulations. As of December 31, 2017, all of the LTCHs we operated were certified as Medicare providers. As of December 31, 2017, we operated 24 IRFs, 23 of which were certified as Medicare providers and one of which was in the process of obtaining its certification. In addition, we provide the majority of our outpatient rehabilitation services through outpatient rehabilitation clinics certified by Medicare as rehabilitation agencies or “rehab agencies.” Our Concentra medical centers furnishing outpatient services are generally enrolled in Medicare as suppliers.
Accreditation
Our LTCHs and IRFs receive accreditation from TJC, DNV and/or CARF. As of December 31, 2017, all of the 100 LTCHS and all of the 24 IRFs we operated were accredited by TJC or DNV. In addition, ten of our IRFs have also received accreditation from CARF. Where required under our contracts with the Department of Veterans Affairs, our facilities furnishing outpatient services that operate as CBOCs are accredited by TJC or another healthcare accrediting organization. See “—Government Regulations—Veterans Affairs.”
Workers’ Compensation
Workers’ compensation is a state mandated, comprehensive insurance program that requires employers to fund or insure medical expenses, lost wages and other costs resulting from work related injuries and illnesses. Workers’ compensation benefits and arrangements vary from state to state, and are often highly complex. In some states, payment for services covered by workers’ compensation programs are subject to cost containment features, such as requirements that all workers’ compensation injuries be treated through a managed care program, or the imposition of fee schedules or payment caps for services furnished to injured employees. Some state workers’ compensation laws limit the ability of an employer to select the providers furnishing care to injured employees. Several states require that physicians furnishing non-emergency services to workers’ compensation patients must register with the applicable state agency and undergo special continuing education and training. Workers’ compensation programs may also impose other requirements that affect the operations of our facilities furnishing outpatient services. Net operating revenues generated directly from workers’ compensation programs represented approximately 18% of our net operating revenue from outpatient rehabilitation services, 1% of our net operating revenue from our LTCHs, 2% of our net operating revenue from our IRFs, and 53% of our net operating revenue from our Concentra segment for the year ended December 31, 2017.
Our facilities furnishing outpatient services are reimbursed for services furnished to injured workers by payors pursuant to the applicable state workers’ compensation statutes. Most of the states in which we maintain operations reimburse providers for services payable under workers’ compensation laws pursuant to a treatment-specific fee schedule with established maximum reimbursement levels. In states without such fee schedules, healthcare providers are often reimbursed based on “usual and customary” fees benchmarked by market data and negotiated by providers with payors and networks.
Inadequate increases to the applicable fee schedule amounts for our services, and changes in state workers’ compensation laws, including cost containment initiatives, could have a negative impact on the operations and financial performance of those facilities.
Veterans Affairs
As of December 31, 2017, we had 32 CBOCs, which were established to provide services to veterans residing in catchment areas under agreements with the Department of Veterans Affairs. The awarding of such agreements is regulated by laws related to federal government procurements generally, including the Federal Acquisition Regulations. Our contracts with the Department of Veterans Affairs include administrative and clinical services, performance standards, qualifications and other contractor requirements and information and security requirements. In general, our facilities furnishing outpatient services that are CBOCs provide outpatient primary care in exchange for a capitated monthly fee based on the number of eligible patients then enrolled in that CBOC.
14
Overview of U.S. and State Government Reimbursements
Medicare Program in General
The Medicare program reimburses healthcare providers for services furnished to Medicare beneficiaries, which are generally persons age 65 and older, those who are chronically disabled, and those suffering from end stage renal disease. The program is governed by the Social Security Act of 1965 and is administered primarily by the Department of Health and Human Services and CMS. Net operating revenues generated directly from the Medicare program represented approximately 37% for the year ended December 31, 2015, 30% for the year ended December 31, 2016, and 30% for the year ended December 31, 2017.
The Medicare program reimburses various types of providers, including LTCHs, IRFs, and outpatient rehabilitation providers, using different payment methodologies. The Medicare reimbursement systems specific to LTCHs, IRFs, and outpatient rehabilitation providers, as described below, are different than the system applicable to general acute care hospitals. If any of our hospitals fail to comply with requirements for payment under Medicare reimbursement systems for LTCHs or IRFs, as applicable, that hospital will be paid under the system applicable to general acute care hospitals. For general acute care hospitals, Medicare payments for inpatient care are made under the inpatient prospective payment system, or “IPPS,” under which a hospital receives a fixed payment amount per discharge (adjusted for area wage differences) using Medicare severity diagnosis-related groups, or “MS-DRGs.” The general acute care hospital MS-DRG payment rate is based upon the national average cost of treating a Medicare patient’s condition, based on severity levels of illness, in that type of facility. Although the average length of stay varies for each MS-DRG, the average stay of all Medicare patients in a general acute care hospital is substantially less than the average length of stay in LTCHs and IRFs. Thus, the prospective payment system for general acute care hospitals creates an economic incentive for those hospitals to discharge medically complex Medicare patients to a post-acute care setting as soon as clinically possible. Effective October 1, 2005, CMS expanded its post-acute care transfer policy under which general acute care hospitals are paid on a per diem basis rather than the full MS-DRG rate if a patient is discharged early to certain post-acute care settings, including LTCHs and IRFs. When a patient is discharged from selected MS-DRGs to, among other providers, an LTCH or IRF, the general acute care hospital may be reimbursed below the full MS-DRG payment if the patient’s length of stay is less than the geometric mean length of stay for the MS-DRG.
Medicare Reimbursement of Long Term Acute Care Hospital Services
The Medicare payment system for long term acute care hospitals is based on a prospective payment system specifically applicable to LTCHs, or “LTCH-PPS.” The policies and payment rates under LTCH-PPS are subject to annual updates and revisions. Under LTCH-PPS, each patient discharged from an LTCH is assigned to a distinct “MS-LTC-DRG,” which is a Medicare severity long-term care diagnosis-related group for LTCHs, and an LTCH is generally paid a pre-determined fixed amount applicable to the assigned MS-LTC-DRG (adjusted for area wage differences), subject to exceptions for short stay and high cost outlier patients (described below). CMS assigns relative weights to each MS-LTC-DRG to reflect their relative use of medical care resources. The payment amount for each MS-LTC-DRG is intended to reflect the average cost of treating a Medicare patient assigned to that MS-LTC-DRG in an LTCH.
Standard Federal Rate
Payment under the LTCH-PPS is dependent on determining the patient classification, that is, the assignment of the case to a particular MS-LTC-DRG, the weight of the MS-LTC-DRG, and the standard federal payment rate. There is a single standard federal rate that encompasses both the inpatient operating costs, which includes a labor and non-labor component, and capital-related costs that CMS updates on an annual basis. LTCH-PPS also includes special payment policies that adjust the payments for some patients based on the patient’s length of stay, the facility’s costs, whether the patient was discharged and readmitted, and other factors.
Patient Criteria
The BBA of 2013, enacted December 26, 2013, establishes a dual-rate LTCH-PPS for Medicare patients discharged from an LTCH. Specifically, for Medicare patients discharged in cost reporting periods beginning on or after October 1, 2015, LTCHs will be reimbursed at the LTCH-PPS standard federal payment rate only if, immediately preceding the patient’s LTCH admission, the patient was discharged from a “subsection (d) hospital” (generally, a short-term acute care hospital paid under IPPS) and either the patient’s stay included at least three days in an intensive care unit (ICU) or coronary care unit (CCU) at the subsection (d) hospital, or the patient was assigned to an MS-LTC-DRG for cases receiving at least 96 hours of ventilator services in the LTCH. In addition, to be paid at the LTCH-PPS standard federal payment rate, the patient’s discharge from the LTCH may not include a principal diagnosis relating to psychiatric or rehabilitation services. For any Medicare patient who does not meet these criteria, the LTCH will be paid a lower “site-neutral” payment rate, which will be the lower of: (i) the IPPS comparable per-diem payment rate capped at the MS-DRG payment rate plus any outlier payments; or (ii) 100 percent of the estimated costs for services.
15
The site neutral payment rate for those patients not paid at the LTCH-PPS standard federal payment rate is subject to a transition period. During the transition period (applicable to hospital cost reporting periods beginning on or after October 1, 2015 through September 30, 2019), a blended rate will be paid for Medicare patients not meeting the new criteria that is equal to 50% of the site neutral payment rate amount and 50% of the standard federal payment rate amount. For discharges in cost reporting periods beginning on or after October 1, 2019, only the site neutral payment rate will apply for Medicare patients not meeting the new criteria. For hospital cost reporting periods beginning on or after October 1, 2017 through September 30, 2026, the IPPS comparable per diem payment amount (including any applicable outlier payment) used to determine the site neutral payment rate will be reduced by 4.6% after any annual payment rate update.
In addition, for cost reporting periods beginning on or after October 1, 2019, qualifying discharges from an LTCH will continue to be paid at the LTCH-PPS standard federal payment rate, unless the number of discharges for which payment is made under the site-neutral payment rate is greater than 50% of the total number of discharges from the LTCH for that period. If the number of discharges for which payment is made under the site-neutral payment rate is greater than 50%, then beginning in the next cost reporting period all discharges from the LTCH will be reimbursed at the site-neutral payment rate. The BBA of 2013 requires CMS to establish a process for an LTCH subject to only the site-neutral payment rate to be reinstated for payment under the dual-rate LTCH-PPS.
Payment adjustments, including the interrupted stay policy and the 25 Percent Rule (discussed below), apply to LTCH discharges regardless of whether the case is paid at the standard federal payment rate or the site-neutral payment rate. However, short stay outlier payment adjustments do not apply to cases paid at the site-neutral payment rate. CMS calculates the annual recalibration of the MS-LTC-DRG relative payment weighting factors using only data from LTCH discharges that meet the criteria for exclusion from the site-neutral payment rate. In addition, CMS applies the IPPS fixed-loss amount for high cost outliers to site-neutral cases, rather than the LTCH-PPS fixed-loss amount. CMS calculates the LTCH-PPS fixed-loss amount using only data from cases paid at the LTCH-PPS payment rate, excluding cases paid at the site-neutral rate. For fiscal year 2018, the IPPS fixed-loss amount is set at $26,537 and the LTCH-PPS fixed-loss amount is $27,381.
Short Stay Outlier Policy
CMS established a different payment methodology for Medicare patients with a length of stay less than or equal to five-sixths of the geometric average length of stay for that particular MS-LTC-DRG, referred to as a short stay outlier, or “SSO.” For discharges before October 1, 2017, SSO cases were paid based on the lesser of: (i) 100% of the average cost of the case; (ii) 120% of the MS-LTC-DRG specific per diem amount multiplied by the patient’s length of stay; (iii) the full MS-LTC-DRG payment; or (iv) a per diem rate derived from blending 120% of the MS-LTC-DRG specific per diem amount with a per diem rate based on the general acute care hospital IPPS.
The SSO rule also had a category referred to as a “very short stay outlier,” which applied to cases with a length of stay that is less than the average length of stay plus one standard deviation for the same MS-DRG under IPPS, referred to as the so-called “IPPS comparable threshold.” The LTCH payment for very short stay outlier cases was equivalent to the general acute care hospital IPPS per diem rate.
For fiscal year 2018, CMS adopted changes to the SSO policy such that all SSO cases discharged on or after October 1, 2017 are paid based on a per diem rate derived from blending 120% of the MS‑LTC‑DRG specific per diem amount with a per diem rate based on the general acute care hospital IPPS (i.e., the fourth option under the prior policy). Under this policy, as the length of stay of a SSO case increases, the percentage of the per diem payment amounts based on the full MS-LTCH-DRG standard federal payment rate increases and the percentage of the payment based on the IPPS comparable amount decreases. In addition, the very short stay outlier category was eliminated.
High Cost Outliers
Some cases are extraordinarily costly, producing losses that may be too large for hospitals to offset. Cases with unusually high costs, referred to as “high cost outliers,” receive a payment adjustment to reflect the additional resources utilized. CMS provides an additional payment if the estimated costs for the patient exceed the adjusted MS-LTC-DRG payment plus a fixed-loss amount that is established in the annual payment rate update.
Interrupted Stays
An interrupted stay is defined as a case in which an LTCH patient, upon discharge, is admitted to a general acute care hospital, IRF or skilled nursing facility/swing-bed and then returns to the same LTCH within a specified period of time. If the length of stay at the receiving provider is equal to or less than the applicable fixed period of time, it is considered to be an interrupted stay case and the case is treated as a single discharge for the purposes of payment to the LTCH.
16
Freestanding, HIH, and Satellite LTCHs
LTCHs may be organized and operated as freestanding facilities or as HIHs. As its name suggests, a freestanding LTCH is not located on the campus of another hospital. For such purpose, “campus” means the physical area immediately adjacent to a hospital’s main buildings, other areas and structures that are not strictly contiguous to a hospital’s main buildings but are located within 250 yards of its main buildings, and any other areas determined, on an individual case basis by the applicable CMS regional office, to be part of a hospital’s campus. Conversely, an HIH is an LTCH that is located on the campus of another hospital. An LTCH, whether freestanding or an HIH, that uses the same Medicare provider number of an affiliated “primary site” LTCH is known as a “satellite.” Under Medicare policy, a satellite LTCH must be located within 35 miles of its primary site LTCH and be administered by such primary site LTCH. A primary site LTCH may have more than one satellite LTCH. CMS sometimes refers to a satellite LTCH that is freestanding as a “remote location.”
Facility Certification Criteria
The LTCH-PPS regulations define the criteria that must be met in order for a hospital to be certified as an LTCH. To be eligible for payment under the LTCH-PPS, a hospital must be primarily engaged in providing inpatient services to Medicare beneficiaries with medically complex conditions that require a long hospital stay. In addition, by definition, LTCHs must meet certain facility criteria, including: (i) instituting a review process that screens patients for appropriateness of an admission and validates the patient criteria within 48 hours of each patient’s admission, evaluates regularly their patients for continuation of care and assesses the available discharge options; (ii) having active physician involvement with patient care that includes a physician available on-site daily and additional consulting physicians on call; and (iii) having an interdisciplinary team of healthcare professionals to prepare and carry out an individualized treatment plan for each patient.
An LTCH must have an average inpatient length of stay for Medicare patients (including both Medicare covered and non-covered days) of greater than 25 days. LTCH cases paid at the site-neutral rate and Medicare Advantage cases are excluded from the LTCH average length of stay calculation. LTCHs that fail to exceed an average length of stay of 25 days during any cost reporting period may be paid under the general acute care hospital IPPS if not corrected within established timeframes. CMS, through its contractors, determines whether an LTCH has maintained an average length of stay of greater than 25 days during each annual cost reporting period.
Prior to qualifying under the payment system applicable to LTCHs, a new LTCH initially receives payments under the general acute care hospital IPPS. The LTCH must continue to be paid under this system for a minimum of six months while meeting certain Medicare LTCH requirements, the most significant requirement being an average length of stay for Medicare patients (including both Medicare covered and non-covered days) greater than 25 days.
25 Percent Rule
The “25 Percent Rule” is a downward payment adjustment that applies if the percentage of Medicare patients discharged from LTCHs who were admitted from a referring hospital (regardless of whether the LTCH or LTCH satellite is co-located with the referring hospital) exceeds the applicable percentage admissions threshold during a particular cost reporting period. Specifically, the payment rate for only Medicare patients above the percentage admissions threshold are subject to a downward payment adjustment. For Medicare patients above the applicable percentage admissions threshold, the LTCH is reimbursed at a rate equivalent to that under general acute care hospital IPPS, which is generally lower than LTCH-PPS rates. Cases that reach outlier status in the referring hospital do not count toward the admissions threshold and are paid under LTCH-PPS.
Current law, as amended by the 21st Century Cures Act, precludes CMS from applying the 25 Percent Rule for freestanding LTCHs to cost reporting years beginning before July 1, 2016 and for discharges occurring on or after October 1, 2016 and before October 1, 2017. In addition, current law applies higher percentage admissions thresholds under the 25 Percent Rule for most HIHs and satellites for cost reporting years beginning before July 1, 2016 and effective for discharges occurring on or after October 1, 2016 and before October 1, 2017. For freestanding LTCHs the percentage admissions threshold is suspended during the relief periods. For most HIHs and satellites, the percentage admissions threshold is raised from 25% to 50% during the relief periods. In the special case of rural LTCHs, LTCHs co-located with an urban single hospital, or LTCHs co-located with an MSA-dominant hospital the referral percentage was raised from 50% to 75%. Grandfathered HIHs are exempt from the 25 Percent Rule regulations.
For fiscal year 2018, CMS adopted a regulatory moratorium on the implementation of the 25 Percent Rule. As a result, the 25 Percent Rule does not apply until discharges occurring on or after October 1, 2018.
17
After the expiration of the regulatory moratorium, as described above, our LTCHs (whether freestanding, HIH or satellite) will be subject to a downward payment adjustment for any Medicare patients who were admitted from a co-located or a non-co-located hospital and that exceed the applicable percentage admissions threshold of all Medicare patients discharged from the LTCH during the cost reporting period. These regulatory changes have the potential to cause an adverse financial impact on the net operating revenues and profitability of many of these hospitals for discharges on or after October 1, 2018.
Expiration of Moratorium on New LTCHs, LTCH Satellite Facilities, and LTCH Beds
Federal law imposed a temporary moratorium on the establishment and classification of new LTCHs or LTCH satellite facilities, and on the increase of LTCH beds in existing LTCHs or satellite facilities through September 30, 2017, subject to certain exceptions. As a result of the expiration of the moratorium, qualifying hospitals may now be classified as new LTCHs or LTCH satellite facilities, and existing LTCHs may increase their bed count.
Annual Payment Rate Update
Fiscal Year 2016. On August 17, 2015, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2016 (affecting discharges and cost reporting periods beginning on or after October 1, 2015 through September 30, 2016). The standard federal rate was set at $41,763, an increase from the standard federal rate applicable during fiscal year 2015 of $41,044. The update to the standard federal rate for fiscal year 2016 included a market basket increase of 2.4%, less a productivity adjustment of 0.5%, and less a reduction of 0.2% mandated by the Affordable Care Act, or the “ACA.” The fixed loss amount for high cost outlier cases paid under LTCH-PPS was set at $16,423, an increase from the fixed loss amount in the 2015 fiscal year of $14,972. The fixed loss amount for high cost outlier cases paid under the site neutral payment rate described above was set at $22,538.
Fiscal Year 2017. On August 22, 2016, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2017 (affecting discharges and cost reporting periods beginning on or after October 1, 2016 through September 30, 2017). The standard federal rate was set at $42,476, an increase from the standard federal rate applicable during fiscal year 2016 of $41,763. The update to the standard federal rate for fiscal year 2017 included a market basket increase of 2.8%, less a productivity adjustment of 0.3%, and less a reduction of 0.75% mandated by the ACA. The fixed-loss amount for high cost outlier cases paid under LTCH-PPS was set at $21,943, an increase from the fixed-loss amount in the 2016 fiscal year of $16,423. The fixed-loss amount for high cost outlier cases paid under the site-neutral payment rate was set at $23,573, an increase from the fixed-loss amount in the 2016 fiscal year of $22,538.
Fiscal Year 2018. On August 14, 2017, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2018 (affecting discharges and cost reporting periods beginning on or after October 1, 2017 through September 30, 2018). Certain errors in the final rule were corrected in a final rule published October 4, 2017. The standard federal rate was set at $41,415, a decrease from the standard federal rate applicable during fiscal year 2017 of $42,476. The update to the standard federal rate for fiscal year 2018 included a market basket increase of 2.7%, less a productivity adjustment of 0.6%, and less a reduction of 0.75% mandated by the ACA. The update to the standard federal rate for fiscal year 2018 is impacted further by the Medicare Access and CHIP Reauthorization Act of 2015, which limits the update for fiscal year 2018 to 1.0%. The fixed-loss amount for high cost outlier cases paid under LTCH-PPS was set at $27,381, an increase from the fixed-loss amount in the 2017 fiscal year of $21,943. The fixed-loss amount for high cost outlier cases paid under the site-neutral payment rate was set at $26,537, an increase from the fixed-loss amount in the 2017 fiscal year of $23,573.
Medicare Market Basket Adjustments
The ACA instituted a market basket payment adjustment to LTCHs. In fiscal year 2019, the market basket update will be reduced by 0.75%. The ACA specifically allows these market basket reductions to result in less than a 0% payment update and payment rates that are less than the prior year.
Medicare Reimbursement of Inpatient Rehabilitation Facility Services
IRFs are paid under a prospective payment system specifically applicable to this provider type, which is referred to as “IRF-PPS.” Under the IRF-PPS, each patient discharged from an IRF is assigned to a case mix group, or “IRF-CMG,” containing patients with similar clinical conditions that are expected to require similar amounts of resources. An IRF is generally paid a pre-determined fixed amount applicable to the assigned IRF-CMG (subject to applicable case adjustments related to length of stay and facility level adjustments for location and low income patients). The payment amount for each IRF-CMG is intended to reflect the average cost of treating a Medicare patient’s condition in an IRF relative to patients with conditions described by other IRF-CMGs. The IRF-PPS also includes special payment policies that adjust the payments for some patients based on the patient’s length of stay, the facility’s costs, whether the patient was discharged and readmitted and other factors.
18
Facility Certification Criteria
Our rehabilitation hospitals must meet certain facility criteria to be classified as an IRF by the Medicare program, including: (i) a provider agreement to participate as a hospital in Medicare; (ii) a preadmission screening procedure; (iii) ensuring that patients receive close medical supervision and furnish, through the use of qualified personnel, rehabilitation nursing, physical therapy, and occupational therapy, plus, as needed, speech therapy, social or psychological services, and orthotic and prosthetic services; (iv) a full-time, qualified director of rehabilitation; (v) a plan of treatment for each inpatient that is established, reviewed, and revised as needed by a physician in consultation with other professional personnel who provide services to the patient; and (vi) a coordinated multidisciplinary team approach in the rehabilitation of each inpatient, as documented by periodic clinical entries made in the patient’s medical record to note the patient’s status in relationship to goal attainment, and that team conferences are held at least every two weeks to determine the appropriateness of treatment. Failure to comply with any of the classification criteria may result in the denial of claims for payment or cause a hospital to lose its status as an IRF and be paid under the prospective payment system that applies to general acute care hospitals.
Patient Classification Criteria
In order to qualify as an IRF, a hospital must demonstrate that during its most recent 12-month cost reporting period, it served an inpatient population of whom at least 60% required intensive rehabilitation services for one or more of 13 conditions specified by regulation. Compliance with the 60% Rule is demonstrated through either medical review or the “presumptive” method, in which a patient’s diagnosis codes are compared to a “presumptive compliance” list. For fiscal year 2018, CMS revised the 60% Rule’s presumptive methodology (i) including certain International Classification of Diseases, Tenth Revision, Clinical Modification, or “ICD-10-CM,” diagnosis codes for patients with traumatic brain injury and hip fracture conditions and (ii) revising the presumptive methodology list for major multiple trauma by counting IRF cases that contain two or more of the ICD-10-CM codes from three major multiple trauma lists in the specified combinations.
Annual Payment Rate Update
Fiscal Year 2016. On August 6, 2015, CMS published the final rule updating policies and payment rates for the IRF-PPS for fiscal year 2016 (affecting discharges and cost reporting periods beginning on or after October 1, 2015 through September 30, 2016). The standard payment conversion factor for discharges for fiscal year 2016 was set at $15,478, an increase from the standard payment conversion factor applicable during fiscal year 2015 of $15,198. The update to the standard payment conversion factor for fiscal year 2016 included a market basket increase of 2.4%, less a productivity adjustment of 0.5%, and less a reduction of 0.2% mandated by the ACA. CMS decreased the outlier threshold amount for fiscal year 2016 to $8,658 from $8,848 established in the final rule for fiscal year 2015.
Fiscal Year 2017. On August 5, 2016, CMS published the final rule updating policies and payment rates for the IRF-PPS for fiscal year 2017 (affecting discharges and cost reporting periods beginning on or after October 1, 2016 through September 30, 2017). The standard payment conversion factor for discharges for fiscal year 2017 was set at $15,708, an increase from the standard payment conversion factor applicable during fiscal year 2016 of $15,478. The update to the standard payment conversion factor for fiscal year 2017 included a market basket increase of 2.7%, less a productivity adjustment of 0.3%, and less a reduction of 0.75% mandated by the ACA. CMS decreased the outlier threshold amount for fiscal year 2017 to $7,984 from $8,658 established in the final rule for fiscal year 2016.
Fiscal Year 2018. On August 3, 2017, CMS published the final rule updating policies and payment rates for the IRF-PPS for fiscal year 2018 (affecting discharges and cost reporting periods beginning on or after October 1, 2017 through September 30, 2018). The standard payment conversion factor for discharges for fiscal year 2018 was set at $15,838, an increase from the standard payment conversion factor applicable during fiscal year 2017 of $15,708. The update to the standard payment conversion factor for fiscal year 2018 included a market basket increase of 2.6%, less a productivity adjustment of 0.6%, and less a reduction of 0.75% mandated by the ACA. The standard payment conversion factor for fiscal year 2018 is impacted further by the Medicare Access and CHIP Reauthorization Act of 2015, which limits the update for fiscal year 2018 to 1.0%. CMS increased the outlier threshold amount for fiscal year 2018 to $8,679 from $7,984 established in the final rule for fiscal year 2017.
Medicare Market Basket Adjustments
The ACA instituted a market basket payment adjustment for IRFs. In fiscal year 2019, the market basket update will be reduced by 0.75%. The ACA specifically allows these market basket reductions to result in less than a 0% payment update and payment rates that are less than the prior year.
19
Medicare Reimbursement of Outpatient Rehabilitation Clinic Services
The Medicare program reimburses outpatient rehabilitation providers based on the Medicare physician fee schedule. For services provided in 2017 through 2019, a 0.5% update will be applied each year to the fee schedule payment rates, subject to an adjustment beginning in 2019 under the Merit-Based Incentive Payment System (“MIPS”). For services provided in 2020 through 2025, a 0.0% percent update will be applied each year to the fee schedule payment rates, subject to adjustments under MIPS and the alternative payment models (“APMs”). In 2026 and subsequent years eligible professionals participating in APMs that meet certain criteria would receive annual updates of 0.75%, while all other professionals would receive annual updates of 0.25%.
Beginning in 2019, payments under the fee schedule are subject to adjustment based on performance in MIPS, which measures performance based on certain quality metrics, resource use, and meaningful use of electronic health records. Under the MIPS requirements a provider’s performance is assessed according to established performance standards and used to determine an adjustment factor that is then applied to the professional’s payment for a year. Each year from 2019 through 2024, professionals who receive a significant share of their revenues through an APM (such as accountable care organizations or bundled payment arrangements) that involves risk of financial losses and a quality measurement component will receive a 5% bonus. The bonus payment for APM participation is intended to encourage participation and testing of new APMs and to promote the alignment of incentives across payors. The specifics of the MIPS and APM adjustments beginning in 2019 and 2020, respectively, will be subject to future notice and comment rule-making. For the year ended December 31, 2017, we received approximately 15% of our outpatient rehabilitation net operating revenues from Medicare.
Therapy Caps
Outpatient therapy providers reimbursed under the Medicare physician fee schedule have been subject to annual limits for therapy expenses. For example, for the calendar year beginning January 1, 2017, the annual limit on outpatient therapy services was $1,980 for combined physical and speech language pathology services and $1,980 for occupational therapy services. The Bipartisan Budget Act of 2018 repealed the annual limits on outpatient therapy.
The annual limits for therapy expenses historically did not apply to services furnished and billed by outpatient hospital departments. However, the Medicare Access and CHIP Reauthorization Act of 2015, and prior legislation, extended the annual limits on therapy expenses in hospital outpatient department settings through December 31, 2017. The application of annual limits to hospital outpatient department settings sunset on December 31, 2017.
Prior to calendar year 2028, all therapy claims exceeding $3,000 are subject to a manual medical review process. The $3,000 threshold is applied to physical therapy and speech therapy services combined and separately applied to occupational therapy. CMS will continue to require that an appropriate modifier be included on claims over the current exception threshold indicating that the therapy services are medically necessary. Beginning in 2028 and in each calendar year thereafter, the threshold amount for claims requiring manual medical review will increase by the percentage increase in the Medicare Economic Index.
Other Requirements for Payment
Historically, outpatient rehabilitation services have been subject to scrutiny by the Medicare program for, among other things, medical necessity for services, appropriate documentation for services, supervision of therapy aides and students, and billing for single rather than group therapy when services are furnished to more than one patient. CMS has issued guidance to clarify that services performed by a student are not reimbursed even if provided under “line of sight” supervision of the therapist. Likewise, CMS has reiterated that Medicare does not pay for services provided by aides regardless of the level of supervision. CMS also has issued instructions that outpatient physical and occupational therapy services provided simultaneously to two or more individuals by a practitioner should be billed as group therapy services.
Medicare claims for outpatient therapy services furnished by therapy assistants on or after January 1, 2022 must include a modifier indicating the service was furnished by a therapy assistant. CMS is required to develop a modifier to mark services provided by a therapy assistant by January 1, 2019, and then submitted claims have to report the modifier mark starting January 1, 2020. Outpatient therapy services furnished on or after January 1, 2022 in whole or part by a therapy assistant will be paid at an amount equal to 85% of the payment amount otherwise applicable for the service.
20
Medicaid Reimbursement of Long Term Acute Care Hospital and Inpatient Rehabilitation Facility Services
The Medicaid program is designed to provide medical assistance to individuals unable to afford care. The program is governed by the Social Security Act of 1965, funded jointly by each individual state and the federal government, and administered by state agencies. Medicaid payments are made under a number of different systems, which include cost based reimbursement, prospective payment systems, or programs that negotiate payment levels with individual hospitals. In addition, Medicaid programs are subject to statutory and regulatory changes, administrative rulings, interpretations of policy by the state agencies, and certain government funding limitations, all of which may increase or decrease the level of program payments to our hospitals. Net operating revenues generated directly from the Medicaid program represented approximately 9% of our LTCH net operating revenues and 4% of our IRF net operating revenues for the year ended December 31, 2017.
Other Healthcare Regulations
Medicare Quality Reporting
Our LTCHs and IRFs are subject to mandatory quality reporting requirements. LTCHs and IRFs that do not submit the required quality data will be subject to a 2% reduction in their annual payment update. The reduction can result in payment rates less than the prior year. However, the reduction will not carry over into the subsequent fiscal years.
Our LTCHs and IRFs are required to collect and report patient assessment data and clinical measures on each Medicare beneficiary who receives inpatient services in our facilities. Our LTCHs and IRFs began reporting this data on October 1, 2012. CMS began making this data available to the public on the CMS website in December 2016. CMS is now adding cross-setting quality measures to compare quality and resource data across post-acute settings pursuant to the Improving Medicare Post-Acute Care Transformation Act of 2014 (IMPACT) (Pub. L. 113-185).
Medicare Hospital Wage Index Adjustment
As part of the methodology for determining prospective payments to LTCHs and IRFs, CMS adjusts the standard payment amounts for area differences in hospital wage levels by a factor reflecting the relative hospital wage level in the geographic area of the hospital compared to the national average hospital wage level. This adjustment factor is the hospital wage index. CMS currently defines hospital geographic areas (labor market areas) based on the definitions of Core-Based Statistical Areas established by the Office of Management and Budget. The ACA calls for CMS to develop and present to Congress a comprehensive reform plan using Bureau of Labor Statistics data, or other data or methodologies, to calculate relative wages for each geographic area involved. In the preamble to the proposed rule for LTCH-PPS for fiscal year 2012, CMS solicited public comments on ways to redefine the geographic reclassification requirements to more accurately define labor markets. To date, CMS has not presented a comprehensive reform plan to Congress.
Physician-Owned Hospital Limitations
CMS regulations include a number of hospital ownership and physician referral provisions, including certain obligations requiring physician-owned hospitals to disclose ownership or investment interests held by the referring physician or his or her immediate family members. In particular, physician-owned hospitals must furnish to patients, on request, a list of physicians or immediate family members who own or invest in the hospital. Moreover, a physician-owned hospital must require all physician owners or investors who are also active members of the hospital’s medical staff to disclose in writing their ownership or investment interests in the hospital to all patients they refer to the hospital. CMS can terminate the Medicare provider agreement of a physician-owned hospital if it fails to comply with these disclosure provisions or with the requirement that a hospital disclose in writing to all patients whether there is a physician on-site at the hospital, 24 hours per day, seven days per week.
Under the transparency and program integrity provisions of the ACA, the exception to the federal self-referral law, or “Stark Law,” that permits physicians to refer patients to hospitals in which they have an ownership or investment interest has been dramatically curtailed. Only hospitals with physician ownership and a provider agreement in place on December 31, 2010 are exempt from the general ban on self-referral. Existing physician-owned hospitals are prohibited from increasing the percentage of physician ownership or investment interests held in the hospital after March 23, 2010. In addition, physician-owned hospitals are prohibited from increasing the number of licensed beds after March 23, 2010, unless meeting specific exceptions related to the hospital’s location and patient population. In order to retain their exemption from the general ban on self-referrals, our physician-owned hospitals are required to adopt specific measures relating to conflicts of interest, bona fide investments and patient safety. As of December 31, 2017, we operated six hospitals that are owned in-part by physicians.
21
Medicare Recovery Audit Contractors
CMS contracts with third-party organizations, known as Recovery Audit Contractors, or “RACs,” to identify Medicare underpayments and overpayments, and to authorize RACs to recoup any overpayments. The compensation paid to each RAC is based on a percentage of overpayment recoveries identified by the RAC. CMS has selected and entered into contracts with four RACs, each of which has begun their audit activities in specific jurisdictions. RAC audits of our Medicare reimbursement may lead to assertions that we have been overpaid, require us to incur additional costs to respond to requests for records and pursue the reversal of payment denials, and ultimately require us to refund any amounts determined to have been overpaid. We cannot predict the impact of future RAC reviews on our results of operations or cash flows.
Fraud and Abuse Enforcement
Various federal and state laws prohibit the submission of false or fraudulent claims, including claims to obtain payment under Medicare, Medicaid, and other government healthcare programs. Penalties for violation of these laws include civil and criminal fines, imprisonment, and exclusion from participation in federal and state healthcare programs. In recent years, federal and state government agencies have increased the level of enforcement resources and activities targeted at the healthcare industry. In addition, the federal False Claims Act and similar state statutes allow individuals to bring lawsuits on behalf of the government, in what are known as qui tam or “whistleblower” actions, alleging false or fraudulent Medicare or Medicaid claims or other violations of the statute. The use of these private enforcement actions against healthcare providers has increased dramatically in recent years, in part because the individual filing the initial complaint is entitled to share in a portion of any settlement or judgment. Revisions to the False Claims Act enacted in 2009 expanded significantly the scope of liability, provided for new investigative tools, and made it easier for whistleblowers to bring and maintain False Claims Act suits on behalf of the government. See “—Legal Proceedings.”
From time to time, various federal and state agencies, such as the Office of Inspector General of the Department of Health and Human Services, or “OIG,” issue a variety of pronouncements, including fraud alerts, the OIG’s Annual Work Plan, and other reports, identifying practices that may be subject to heightened scrutiny. These pronouncements can identify issues relating to LTCHs, IRFs, or outpatient rehabilitation services or providers. For example, the OIG stated in its 2017 Work Plan that it would identify the factors contributing to adverse and temporary harm events for Medicare beneficiaries receiving care in LTCHs for the purpose of determining the extent to which the events were preventable. In the 2017 Work Plan, the OIG also indicated it would review IRF claims for compliance with Medicare documentation and coverage requirements. Additionally, the 2017 Work Plan described the OIG’s plan to review IRF admissions to determine whether patients who participated in intensive therapy caps were suitable candidates. Our IRFs and LTCHs may be required to provide information related to these reviews. We monitor government publications applicable to us to supplement and enhance our compliance efforts.
We endeavor to conduct our operations in compliance with applicable laws, including healthcare fraud and abuse laws. If we identify any practices as being potentially contrary to applicable law, we will take appropriate action to address the matter, including, where appropriate, disclosure to the proper authorities, which may result in a voluntary refund of monies to Medicare, Medicaid, or other governmental healthcare programs.
Remuneration and Fraud Measures
The federal anti-kickback statute prohibits some business practices and relationships under Medicare, Medicaid, and other federal healthcare programs. These practices include the payment, receipt, offer, or solicitation of remuneration in connection with, to induce, or to arrange for, the referral of patients covered by a federal or state healthcare program. Violations of the anti-kickback law may be punished by a criminal fine of up to $50,000 or imprisonment for each violation, or both, civil monetary penalties of $50,000 and damages of up to three times the total amount of remuneration, and exclusion from participation in federal or state healthcare programs.
The Stark Law prohibits referrals for designated health services by physicians under the Medicare and Medicaid programs to other healthcare providers in which the physicians have an ownership or compensation arrangement unless an exception applies. Sanctions for violating the Stark Law include civil monetary penalties of up to $15,000 per prohibited service provided, assessments equal to three times the dollar value of each such service provided, and exclusion from the Medicare and Medicaid programs and other federal and state healthcare programs. The statute also provides a penalty of up to $100,000 for a circumvention scheme. In addition, many states have adopted or may adopt similar anti-kickback or anti-self-referral statutes. Some of these statutes prohibit the payment or receipt of remuneration for the referral of patients, regardless of the source of the payment for the care. While we do not believe our arrangements are in violation of these prohibitions, we cannot assure you that governmental officials charged with the responsibility for enforcing the provisions of these prohibitions will not assert that one or more of our arrangements are in violation of the provisions of such laws and regulations.
22
Provider-Based Status
The designation “provider-based” refers to circumstances in which a subordinate facility (e.g., a separately certified Medicare provider, a department of a provider, or a satellite facility) is treated as part of a provider for Medicare payment purposes. In these cases, the services of the subordinate facility are included on the “main” provider’s cost report and overhead costs of the main provider can be allocated to the subordinate facility, to the extent that they are shared. As of December 31, 2017, we operated 16 LTCHs and six IRFs that were treated as provider-based satellites of certain of our other facilities, 205 of the outpatient rehabilitation clinics we operated were provider-based and are operated as departments of the IRFs we operated, and we provide rehabilitation management and staffing services to hospital rehabilitation departments that may be treated as provider-based. These facilities are required to satisfy certain operational standards in order to retain their provider-based status.
Health Information Practices
The Health Insurance Portability and Accountability Act of 1996, or “HIPAA,” mandates the adoption of standards for the exchange of electronic health information in an effort to encourage overall administrative simplification and enhance the effectiveness and efficiency of the healthcare industry, while maintaining the privacy and security of health information. Among the standards that the Department of Health and Human Services has adopted or will adopt pursuant to HIPAA are standards for electronic transactions and code sets, unique identifiers for providers (referred to as National Provider Identifier), employers, health plans and individuals, security and electronic signatures, privacy, and enforcement. If we fail to comply with the HIPAA requirements, we could be subject to criminal penalties and civil sanctions. The privacy, security and enforcement provisions of HIPAA were enhanced by the Health Information Technology for Economic and Clinical Health Act, or “HITECH,” which was included in the ARRA. Among other things, HITECH establishes security breach notification requirements, allows enforcement of HIPAA by state attorneys general, and increases penalties for HIPAA violations.
The Department of Health and Human Services has adopted standards in three areas in which we are required to comply that affect our operations.
Standards relating to the privacy of individually identifiable health information govern our use and disclosure of protected health information and require us to impose those rules, by contract, on any business associate to whom such information is disclosed.
Standards relating to electronic transactions and code sets require the use of uniform standards for common healthcare transactions, including healthcare claims information, plan eligibility, referral certification and authorization, claims status, plan enrollment and disenrollment, payment and remittance advice, plan premium payments, and coordination of benefits.
Standards for the security of electronic health information require us to implement various administrative, physical, and technical safeguards to ensure the integrity and confidentiality of electronic protected health information.
We maintain a HIPAA committee that is charged with evaluating and monitoring our compliance with HIPAA. The HIPAA committee monitors regulations promulgated under HIPAA as they have been adopted to date and as additional standards and modifications are adopted. Although health information standards have had a significant effect on the manner in which we handle health data and communicate with payors, the cost of our compliance has not had a material adverse effect on our business, financial condition, or results of operations. We cannot estimate the cost of compliance with standards that have not been issued or finalized by the Department of Health and Human Services.
In addition to HIPAA, there are numerous federal and state laws and regulations addressing patient and consumer privacy concerns, including unauthorized access or theft of personal information. State statutes and regulations vary from state to state. Lawsuits, including class actions and action by state attorneys general, directed at companies that have experienced a privacy or security breach also can occur. Although our policies and procedures are aimed at complying with privacy and security requirements and minimizing the risks of any breach of privacy or security, there can be no assurance that a breach of privacy or security will not occur. If there is a breach, we may be subject to various penalties and damages and may be required to incur costs to mitigate the impact of the breach on affected individuals.
Compliance Program
Our Compliance Program
We maintain a written code of conduct that provides guidelines for principles and regulatory rules that are applicable to our patient care and business activities. The code is reviewed and amended as necessary and is the basis for our company-wide compliance program. These guidelines are implemented by a compliance officer, a compliance and audit committee, and employee education and training. We also have established a reporting system, auditing and monitoring programs, and a disciplinary system as a means for enforcing the code’s policies.
23
Compliance and Audit Committee
Our compliance and audit committee is made up of members of our senior management and in-house counsel. The compliance and audit committee meets on a quarterly basis and reviews the activities, reports, and operation of our compliance program. In addition, the HIPAA committee provides reports to the compliance and audit committee. The vice president of compliance and audit services meets with the compliance and audit committee on a quarterly basis to provide an overview of the activities and operation of our compliance program.
Operating Our Compliance Program
We focus on integrating compliance responsibilities with operational functions. We recognize that our compliance with applicable laws and regulations depends upon individual employee actions as well as company operations. As a result, we have adopted an operations team approach to compliance. Our corporate executives, with the assistance of corporate experts, designed the programs of the compliance and audit committee. We utilize facility leaders for employee-level implementation of our code of conduct. This approach is intended to reinforce our company-wide commitment to operate in accordance with the laws and regulations that govern our business.
Compliance Issue Reporting
In order to facilitate our employees’ ability to report known, suspected, or potential violations of our code of conduct, we have developed a system of reporting. This reporting, anonymous or attributable, may be accomplished through our toll-free compliance hotline, compliance e-mail address, or our compliance post office box. The compliance officer and the compliance and audit committee are responsible for reviewing and investigating each compliance incident in accordance with the compliance and audit services department’s investigation policy.
Compliance Monitoring and Auditing / Comprehensive Training and Education
Monitoring reports and the results of compliance for each of our business segments are reported to the compliance and audit committee on a quarterly basis. We train and educate our employees regarding the code of conduct, as well as the legal and regulatory requirements relevant to each employee’s work environment. New and current employees are required to acknowledge and certify that the employee has read, understood and has agreed to abide by the code of conduct. Additionally, all employees are required to re-certify compliance with the code on an annual basis.
Policies and Procedures Reflecting Compliance Focus Areas
We review our policies and procedures for our compliance program from time to time in order to improve operations and to ensure compliance with requirements of standards, laws, and regulations and to reflect the ongoing compliance focus areas which have been identified by the compliance and audit committee.
Internal Audit
We have a compliance and audit department, which has an internal audit function. The vice president of compliance and audit services manages the combined compliance and audit department and meets with the audit and compliance committee of the board of directors on a quarterly basis to discuss audit results and provide an overview of the activities and operation of our compliance program.
Available Information
We are subject to the information and periodic reporting requirements of the Securities Exchange Act of 1934, as amended, and, in accordance therewith, file periodic reports, proxy statements, and other information with the SEC. Such periodic reports, proxy statements, and other information are available for inspection and copying at the SEC’s Public Reference Room at 100 F Street, NE., Washington, DC 20549, or may be obtained by calling the SEC at 1-800-SEC-0330. In addition, the SEC maintains a website at www.sec.gov that contains reports, proxy statements, and other information regarding issuers that file electronically with the SEC.
Our website address is www.selectmedicalholdings.com and can be used to access free of charge, through the investor relations section, our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and any amendments to those reports, as soon as reasonably practicable after we electronically file such material with or furnish it to the SEC. The information on our website is not incorporated as a part of this annual report.
24
Executive Officers of the Registrant
The following table sets forth the names, ages and titles, as well as a brief account of the business experience, of each person who was an executive officer of the Company as of January 1, 2017:
Name | Age | Position | |||
Robert A. Ortenzio | 60 | Executive Chairman and Co-Founder | |||
Rocco A. Ortenzio | 85 | Vice Chairman and Co-Founder | |||
David S. Chernow | 60 | President and Chief Executive Officer | |||
Martin F. Jackson | 63 | Executive Vice President and Chief Financial Officer | |||
John A. Saich | 49 | Executive Vice President and Chief Human Resources Officer | |||
Michael E. Tarvin | 57 | Executive Vice President, General Counsel and Secretary | |||
Scott A. Romberger | 57 | Senior Vice President, Controller and Chief Accounting Officer | |||
Robert G. Breighner, Jr. | 49 | Vice President, Compliance and Audit Services and Corporate Compliance Officer | |||
Robert A. Ortenzio has served as our Executive Chairman and Co-Founder since January 1, 2014. Mr. Ortenzio served as our Chief Executive Officer from January 1, 2005 until December 31, 2013, and. Mr. Ortenzio served as our President and Chief Executive Officer from September 2001 to January 1, 2005. Mr. Ortenzio also served as our President and Chief Operating Officer from February 1997 to September 2001. Mr. Ortenzio co-founded the Company and has served as a director since February 1997. Mr. Ortenzio also serves on the board of directors of Concentra Group Holdings Parent. He was an Executive Vice President and a director of Horizon/CMS Healthcare Corporation from July 1995 until July 1996. In 1986, Mr. Ortenzio co-founded Continental Medical Systems, Inc., and served in a number of different capacities, including as a Senior Vice President from February 1986 until April 1988, as Chief Operating Officer from April 1988 until July 1995, as President from May 1989 until August 1996 and as Chief Executive Officer from July 1995 until August 1996. Before co-founding Continental Medical Systems, Inc., he was a Vice President of Rehab Hospital Services Corporation. Mr. Ortenzio is the son of Rocco A. Ortenzio, our Vice Chairman and Co-Founder.
Rocco A. Ortenzio has served as our Vice Chairman and Co-Founder since January 1, 2014. Mr. Ortenzio served as our Executive Chairman from September 2001 until December 2013. From February 1997 to September 2001, Mr. Ortenzio served as our Chief Executive Officer. Mr. Ortenzio co-founded the Company and has served as a director since February 1997. In 1986, he co-founded Continental Medical Systems, Inc., and served as its Chairman and Chief Executive Officer until July 1995. In 1979, Mr. Ortenzio founded Rehab Hospital Services Corporation, and served as its Chairman and Chief Executive Officer until June 1986. In 1969, Mr. Ortenzio founded Rehab Corporation and served as its Chairman and Chief Executive Officer until 1974. Mr. Ortenzio is the father of Robert A. Ortenzio, our Executive Chairman and Co-Founder.
David S. Chernow has served as our President and Chief Executive Officer since January 1, 2014. Mr. Chernow has served as our President and previously held various additional executive officer titles since September 2010. Mr. Chernow served as a director of the Company from January 2002 until February 2005 and from August 2005 until September 2010. Mr. Chernow also serves on the board of directors of Concentra Group Holdings Parent. From May 2007 to February 2010, Mr. Chernow served as the President and Chief Executive Officer of Oncure Medical Corp., one of the largest providers of free-standing radiation oncology care in the United States. From July 2001 to June 2007, Mr. Chernow served as the President and Chief Executive Officer of JA Worldwide, a nonprofit organization dedicated to the education of young people about business (formerly, Junior Achievement, Inc.). From 1999 to 2001, he was the President of the Physician Services Group at US Oncology, Inc. Mr. Chernow co-founded American Oncology Resources in 1992 and served as its Chief Development Officer until the time of the merger with Physician Reliance Network, Inc., which created US Oncology, Inc. in 1999.
Martin F. Jackson has served as our Executive Vice President and Chief Financial Officer since February 2007. He served as our Senior Vice President and Chief Financial Officer from May 1999 to February 2007. Mr. Jackson also serves on the board of directors of Concentra Group Holdings Parent. Mr. Jackson previously served as a Managing Director in the Health Care Investment Banking Group for CIBC Oppenheimer from January 1997 to May 1999. Prior to that time, he served as Senior Vice President, Health Care Finance with McDonald & Company Securities, Inc. from January 1994 to January 1997. Prior to 1994, Mr. Jackson held senior financial positions with Van Kampen Merritt, Touche Ross, Honeywell and L’Nard Associates.
John A. Saich has served as our Executive Vice President and Chief Human Resources Officer since December 15, 2010. He served as our Senior Vice President, Human Resources from February 2007 to December 2010. He served as our Vice President, Human Resources from November 1999 to January 2007. He joined the Company as Director, Human Resources and HRIS in February 1998. Previously, Mr. Saich served as Director of Benefits and Human Resources for Integrated Health Services in 1997 and as Director of Human Resources for Continental Medical Systems, Inc. from August 1993 to January 1997.
25
Michael E. Tarvin has served as our Executive Vice President, General Counsel and Secretary since February 2007. He served as our Senior Vice President, General Counsel and Secretary from November 1999 to February 2007. He served as our Vice President, General Counsel and Secretary from February 1997 to November 1999. He was Vice President—Senior Counsel of Continental Medical Systems from February 1993 until February 1997. Prior to that time, he was Associate Counsel of Continental Medical Systems from March 1992. Mr. Tarvin was an associate at the Philadelphia law firm of Drinker Biddle & Reath, LLP from September 1985 until March 1992.
Scott A. Romberger has served as our Senior Vice President and Controller since February 2007. He served as our Vice President and Controller from February 1997 to February 2007. In addition, he has served as our Chief Accounting Officer since December 2000. Prior to February 1997, he was Vice President—Controller of Continental Medical Systems from January 1991 until January 1997. Prior to that time, he served as Acting Corporate Controller and Assistant Controller of Continental Medical Systems from June 1990 and December 1988, respectively. Mr. Romberger is a certified public accountant and was employed by a national accounting firm from April 1985 until December 1988.
Robert G. Breighner, Jr. has served as our Vice President, Compliance and Audit Services since August 2003. He served as our Director of Internal Audit from November 2001 to August 2003. Previously, Mr. Breighner was Director of Internal Audit for Susquehanna Pfaltzgraff Co. from June 1997 until November 2001. Mr. Breighner held other positions with Susquehanna Pfaltzgraff Co. from May 1991 until June 1997.
26
Item 1A. Risk Factors.
In addition to the factors discussed elsewhere in this Form 10-K, the following are important factors which could cause actual results or events to differ materially from those contained in any forward-looking statements made by or on behalf of us.
Risks Related to Our Business
If there are changes in the rates or methods of government reimbursements for our services, our net operating revenues and profitability could decline.
Approximately 37% of our net operating revenues for the year ended December 31, 2015, 30% of our net operating revenues for the year ended December 31, 2016, and 30% of our net operating revenues for the year ended December 31, 2017, came from the highly regulated federal Medicare program.
In recent years, through legislative and regulatory actions, the federal government has made substantial changes to various payment systems under the Medicare program. President Obama signed into law comprehensive reforms to the healthcare system, including changes to the methods for, and amounts of, Medicare reimbursement. Additional reforms or other changes to these payment systems, including modifications to the conditions on qualification for payment, bundling payments to cover both acute and post-acute care or the imposition of enrollment limitations on new providers, may be proposed or could be adopted, either by Congress or CMS. If revised regulations are adopted, the availability, methods, and rates of Medicare reimbursements for services of the type furnished at our facilities could change. Some of these changes and proposed changes could adversely affect our business strategy, operations, and financial results. In addition, there can be no assurance that any increases in Medicare reimbursement rates established by CMS will fully reflect increases in our operating costs.
We conduct business in a heavily regulated industry, and changes in regulations, new interpretations of existing regulations or violations of regulations may result in increased costs or sanctions that reduce our net operating revenues and profitability.
The healthcare industry is subject to extensive federal, state and local laws and regulations relating to: (i) facility and professional licensure, including certificates of need; (ii) conduct of operations, including financial relationships among healthcare providers, Medicare fraud and abuse, and physician self-referral; (iii) addition of facilities and services and enrollment of newly developed facilities in the Medicare program; (iv) payment for services; and (v) safeguarding protected health information.
Both federal and state regulatory agencies inspect, survey and audit our facilities to review our compliance with these laws and regulations. While our facilities intend to comply with existing licensing, Medicare certification requirements, and accreditation standards, there can be no assurance that these regulatory authorities will determine that all applicable requirements are fully met at any given time. A determination by any of these regulatory authorities that a facility is not in compliance with these requirements could lead to the imposition of requirements that the facility takes corrective action, assessment of fines and penalties, or loss of licensure, Medicare certification, or accreditation. These consequences could have an adverse effect on our company.
In addition, there have been heightened coordinated civil and criminal enforcement efforts by both federal and state government agencies relating to the healthcare industry. The ongoing investigations relate to, among other things, various referral practices, billing practices, and physician ownership. In the future, different interpretations or enforcement of these laws and regulations could subject us to allegations of impropriety or illegality or could require us to make changes in our facilities, equipment, personnel, services, and capital expenditure programs. These changes may increase our operating expenses and reduce our operating revenues. If we fail to comply with these extensive laws and government regulations, we could become ineligible to receive government program reimbursement, suffer civil or criminal penalties, or be required to make significant changes to our operations. In addition, we could be forced to expend considerable resources responding to any related investigation or other enforcement action.
Full implementation of the Medicare 25 Percent Rule applicable to LTCHs will have an adverse effect on our future net operating revenues and profitability.
Under the 25 Percent Rule, the Medicare payment rate for LTCHs is subject to a downward payment adjustment if the percentage of Medicare patients discharged from an LTCH who were admitted from a referring hospital (regardless of whether the LTCH or LTCH satellite is co-located with the referring hospital) exceeds an applicable percentage admissions threshold during a particular cost reporting period. Cases admitted to an LTCH in excess of the applicable percentage admissions threshold are reimbursed at a rate equivalent to that under IPPS. IPPS rates are generally lower than LTCH-PPS rates. Cases that reach outlier status in the discharging hospital do not count toward the admission threshold and are paid under LTCH-PPS.
27
For fiscal year 2018, CMS adopted a regulatory moratorium on the implementation of the 25 Percent Rule. As a result, the 25 Percent Rule does not apply until discharges occurring on or after October 1, 2018. Unless Congress or CMS take further action, beginning on or after October 1, 2018, our LTCHs (whether freestanding, HIH, or satellite) will be subject to a downward payment adjustment for any Medicare patients who were admitted from a co-located or a non-co-located hospital and that exceed the applicable percentage admissions threshold of all Medicare patients discharged from the LTCH during the cost reporting period. See “Business—Government Regulations—Overview of U.S. and State Government Reimbursements—Long Term Acute Care Hospital Medicare Reimbursement—25 Percent Rule.”
Because these rules are complex and are based on the volume of Medicare admissions from other referring hospitals as a percent of our overall Medicare admissions, we cannot predict with any certainty the impact on our future net operating revenues and profitability of compliance with these regulations. We expect many of our LTCHs will experience an adverse financial impact when implementation of the Medicare percentage admissions thresholds goes back into effect. Our LTCHs have cost reporting periods that commence on various dates throughout the calendar year. Therefore, the application of the lower percentage admissions thresholds could be staggered, depending on how CMS implements the new statutory relief. In any event, the regular percentage admissions thresholds would not be in effect for all of our affected LTCHs until October 1, 2018 at the earliest, and we would not experience potential payment adjustments at the regular percentage thresholds until after Medicare cost reports are filed for cost reporting periods that include October 1, 2018.
If our LTCHs fail to maintain their certifications as LTCHs or if our facilities operated as HIHs fail to qualify as hospitals separate from their host hospitals, our net operating revenues and profitability may decline.
As of December 31, 2017, we operated 100 LTCHs, all of which are currently certified by Medicare as LTCHs. LTCHs must meet certain conditions of participation to enroll in, and seek payment from, the Medicare program as an LTCH, including, among other things, maintaining an average length of stay for Medicare patients in excess of 25 days. An LTCH that fails to maintain this average length of stay for Medicare patients in excess of 25 days during a single cost reporting period is generally allowed an opportunity to show that it meets the length of stay criteria during a subsequent cure period. If the LTCH can show that it meets the length of stay criteria during this cure period, it will continue to be paid under the LTCH-PPS. If the LTCH again fails to meet the average length of stay criteria during the cure period, it will be paid under the general acute care IPPS at rates generally lower than the rates under the LTCH-PPS.
Similarly, our HIHs must meet conditions of participation in the Medicare program, which include additional criteria establishing separateness from the hospital with which the HIH shares space. If our LTCHs or HIHs fail to meet or maintain the standards for certification as LTCHs, they will receive payment under the general acute care hospitals IPPS which is generally lower than payment under the system applicable to LTCHs. Payments at rates applicable to general acute care hospitals would result in our LTCHs receiving significantly less Medicare reimbursement than they currently receive for their patient services.
Decreases in Medicare reimbursement rates received by our outpatient rehabilitation clinics may reduce our future net operating revenues and profitability.
Our outpatient rehabilitation clinics receive payments from the Medicare program under a fee schedule. The Medicare Access and CHIP Reauthorization Act of 2015 requires that payments under the fee schedule be adjusted starting in 2019 based on performance in a new Merit-Based Incentive Payment System and, beginning in 2020, incentives for participation in alternative payment models. The specifics of the Merit-Based Incentive Payment System and incentives for participation in alternative payment models will be subject to future notice and comment rule-making. It is unclear what impact, if any, the Merit-Based Incentive Payment System and incentives for participation in alternative payment models will have on our business and operating results, but any resulting decrease in payment may reduce our future net operating revenues and profitability.
The nature of the markets that Concentra serves may constrain its ability to raise prices at rates sufficient to keep pace with the inflation of its costs.
Rates of reimbursement for work-related injury or illness visits in Concentra’s occupational health services business are established through a legislative or regulatory process within each state that Concentra serves. Currently, 32 states have fee schedules pursuant to which all healthcare providers are uniformly reimbursed. The fee schedules are determined by each state and generally prescribe the maximum amounts that may be reimbursed for a designated procedure. In the states without fee schedules, healthcare providers are generally reimbursed based on usual, customary and reasonable rates charged in the particular state in which the services are provided. Given that Concentra does not control these processes, it may be subject to financial risks if individual jurisdictions reduce rates or do not routinely raise rates of reimbursement in a manner that keeps pace with the inflation of Concentra’s costs of service.
28
In Concentra’s veteran’s healthcare business, reimbursement rates are generally set according to the capitated monthly rate based on the number of then enrolled patients at that CBOC. Evolving legislative and regulatory changes aimed at improving veteran’s access to care in the wake of Department of Veterans Affairs scandals (none of which involved Concentra’s CBOCs) could result in fewer patients enrolling in CBOCs. Federal legislation that permits certain veterans to receive their healthcare outside of the Department of Veterans Affairs facilities, for example, may reduce demand for services at some of Concentra’s CBOCs. Moreover, changes in the methods, manner or amounts of compensation payable for Concentra’s services, including, amounts reimbursable to the CBOCs under its agreements with the Department of Veterans Affairs, due to legislative or other changes or shifting budget priorities could result in lower reimbursement for services provided at Concentra’s CBOCs. Concentra may receive lower payments from the Veterans Health Administration if fewer eligible veterans are considered to live within the catchments of its CBOCs. These trends could have an adverse effect on our financial condition and results of operations.
If our IRFs fail to comply with the 60% Rule or admissions to our IRFs are limited due to changes to the diagnosis codes on the presumptive compliance list, our net operating revenues and profitability may decline.
As of December 31, 2017, we operated 24 IRFs, 23 of which were certified as Medicare providers and one of which is in the process of obtaining its certification. IRFs must meet certain conditions of participation to enroll in, and seek payment from, the Medicare program as an IRF. Among other things, at least 60% of the IRF’s total inpatient population must require treatment for one or more of 13 conditions specified by regulation. This requirement is now commonly referred to as the “60% Rule.” Compliance with the 60% Rule is demonstrated through a two step process. The first step is the “presumptive” method, in which patient diagnosis codes are compared to a “presumptive compliance” list. IRFs that fail to demonstrate compliance with the 60% Rule using this presumptive test may demonstrate compliance through a second step involving an audit of the facility’s medical records to assess compliance.
If an IRF does not demonstrate compliance with the 60% Rule by either the presumptive method or through a review of medical records, then the facility’s classification as an IRF may be terminated at the start of its next cost reporting period causing the facility to be paid as a general acute care hospital under IPPS. If our IRFs fail to demonstrate compliance with the 60% Rule through either method and are classified as general acute care hospitals, our net operating revenue and profitability may be adversely affected.
As a result of post-payment reviews of claims we submit to Medicare for our services, we may incur additional costs and may be required to repay amounts already paid to us.
We are subject to regular post-payment inquiries, investigations, and audits of the claims we submit to Medicare for payment for our services. These post-payment reviews include medical necessity reviews for Medicare patients admitted to our LTCHs and IRFs, and audits of Medicare claims under the Recovery Audit Contractor program. These post-payment reviews may require us to incur additional costs to respond to requests for records and to pursue the reversal of payment denials, and ultimately may require us to refund amounts paid to us by Medicare that are determined to have been overpaid.
Our facilities are subject to extensive federal and state laws and regulations relating to the privacy of individually identifiable information.
HIPAA required the United States Department of Health and Human Services to adopt standards to protect the privacy and security of individually identifiable health information. The department released final regulations containing privacy standards in December 2000 and published revisions to the final regulations in August 2002. The privacy regulations extensively regulate the use and disclosure of individually identifiable health information. The regulations also provide patients with significant new rights related to understanding and controlling how their health information is used or disclosed. The security regulations require healthcare providers to implement administrative, physical and technical practices to protect the security of individually identifiable health information that is maintained or transmitted electronically. HITECH, which was signed into law in February 2009, enhanced the privacy, security, and enforcement provisions of HIPAA by, among other things, establishing security breach notification requirements, allowing enforcement of HIPAA by state attorneys general, and increasing penalties for HIPAA violations. Violations of HIPAA or HITECH could result in civil or criminal penalties.
In addition to HIPAA, there are numerous federal and state laws and regulations addressing patient and consumer privacy concerns, including unauthorized access, or theft of patient’s identifiable health information. State statutes and regulations vary from state to state. Lawsuits, including class actions and action by state attorneys general, directed at companies that have experienced a privacy or security breach also can occur.
29
In the conduct of our business, we process, maintain, and transmit sensitive data, including our patient’s individually identifiable health information. We have developed a comprehensive set of policies and procedures in our efforts to comply with HIPAA and other privacy laws. Our compliance officer, privacy officer, and information security officer are responsible for implementing and monitoring compliance with our privacy and security policies and procedures at our facilities. We believe that the cost of our compliance with HIPAA and other federal and state privacy laws will not have a material adverse effect on our business, financial condition, results of operations, or cash flows. However, there can be no assurance that a breach of privacy or security will not occur. If there is a breach, we may be subject to various lawsuits, penalties and damages and may be required to incur costs to mitigate the impact of the breach on affected individuals.
We may be adversely affected by a security breach of our, or our third-party vendors’, information technology systems, such as a cyber attack, which may cause a violation of HIPAA or HITECH and subject us to potential legal and reputational harm.
In the normal course of business, our information technology systems hold sensitive patient information including patient demographic data, eligibility for various medical plans including Medicare and Medicaid, and protected health information, which is subject to HIPAA and HITECH. Additionally, we utilize those same systems to perform our day-to-day activities, such as receiving referrals, assigning medical teams to patients, documenting medical information, maintaining an accurate record of all transactions, processing payments, and maintaining our employee’s personal information. We also contract with third-party vendors to maintain and store our patient’s individually identifiable health information. Numerous state and federal laws and regulations address privacy and information security concerns resulting from our access to our patient’s and employee’s personal information.
Our information technology systems and those of our vendors that process, maintain, and transmit such data are subject to computer viruses, cyber attacks, or breaches. We adhere to policies and procedures designed to ensure compliance with HIPAA and other privacy and information security laws and require our third-party vendors to do so as well. If, however, we or our third-party vendors experience a breach, loss, or other compromise of unsecured protected health information or other personal information, such an event could result in significant civil and criminal penalties, lawsuits, reputational harm, and increased costs to us, any of which could have a material adverse effect on our financial condition and results of operations.
Furthermore, while our information technology systems, and those of our third-party vendors, are maintained with safeguards protecting against cyber attacks, including passive intrusion protection, firewalls, and virus detection software, these safeguards do not ensure that a significant cyber attack could not occur. A cyber attack that bypasses our information technology security systems, or those of our third-party vendors, could cause the loss of protected health information, or other data subject to privacy laws, the loss of proprietary business information, or a material disruption to our or a third-party vendor’s information technology business systems resulting in a material adverse effect on our business, financial condition, results of operations, or cash flows. In addition, our future results could be adversely affected due to the theft, destruction, loss, misappropriation, or release of protected health information, other confidential data or proprietary business information, operational or business delays resulting from the disruption of information technology systems and subsequent clean-up and mitigation activities, negative publicity resulting in reputation or brand damage with clients, members, or industry peers, or regulatory action taken as a result of such incident. We provide our employees training and regular reminders on important measures they can take to prevent breaches. We routinely identify attempts to gain unauthorized access to our systems. However, given the rapidly evolving nature and proliferation of cyber threats, there can be no assurance our training and network security measures or other controls will detect, prevent, or remediate security or data breaches in a timely manner or otherwise prevent unauthorized access to, damage to, or interruption of our systems and operations. For example, it has been widely reported that many well-organized international interests, in certain cases with the backing of sovereign governments, are targeting the theft of patient information through the use of advance persistent threats. Similarly, in recent years, several hospitals have reported being the victim of ransomware attacks in which they lost access to their systems, including clinical systems, during the course of the attacks. We are likely to face attempted attacks in the future. Accordingly, we may be vulnerable to losses associated with the improper functioning, security breach, or unavailability of our information systems as well as any systems used in acquired operations.
Our acquisitions require transitions and integration of various information technology systems, and we regularly upgrade and expand our information technology systems’ capabilities. If we experience difficulties with the transition and integration of these systems or are unable to implement, maintain, or expand our systems properly, we could suffer from, among other things, operational disruptions, regulatory problems, working capital disruptions and increases in administrative expenses. While we make significant efforts to address any information security issues and vulnerabilities with respect to the companies we acquire, we may still inherit risks of security breaches or other compromises when we integrate these companies within our business.
30
We may be adversely affected by negative publicity which can result in increased governmental and regulatory scrutiny and possibly adverse regulatory changes.
Negative press coverage can result in increased governmental and regulatory scrutiny and possibly adverse regulatory changes. Adverse publicity and increased governmental scrutiny can have a negative impact on our reputation with referral sources and patients and on the morale and performance of our employees, both of which could adversely affect our businesses and results of operations.
The acquisition of U.S. HealthWorks by Concentra and future acquisitions may use significant resources, may be unsuccessful, and could expose us to unforeseen liabilities.
As part of our growth strategy, we may pursue acquisitions of LTCHs, IRFs, outpatient rehabilitation clinics, and other related healthcare facilities and services. These acquisitions, including the acquisition of U.S. HealthWorks by Concentra, may involve significant cash expenditures, debt incurrence, additional operating losses and expenses and compliance risks that could have a material adverse effect on our financial condition and results of operations.
We may not be able to successfully integrate U.S. HealthWorks or other acquired businesses into ours, and therefore, we may not be able to realize the intended benefits from an acquisition. If we fail to successfully integrate U.S. HealthWorks or other acquisitions, our financial condition and results of operations may be materially adversely affected. The acquisition of U.S. HealthWorks by Concentra and other acquisitions could result in difficulties integrating acquired operations, technologies, and personnel into our business. Such difficulties may divert significant financial, operational, and managerial resources from our existing operations and make it more difficult to achieve our operating and strategic objectives. We may fail to retain employees or patients acquired through the acquisition of U.S. HealthWorks by Concentra or other acquisitions, which may negatively impact the integration efforts. These acquisitions, including the acquisition of U.S. HealthWorks by Concentra, could also have a negative impact on our results of operations if it is subsequently determined that goodwill or other acquired intangible assets are impaired, thus resulting in an impairment charge in a future period. See “Business—Concentra—Acquisition of U.S. HealthWorks.”
In addition, the acquisition of U.S. HealthWorks by Concentra and other acquisitions involve risks that the acquired businesses will not perform in accordance with expectations; that we may become liable for unforeseen financial or business liabilities of the acquired businesses, including liabilities for failure to comply with healthcare regulations; that the expected synergies associated with acquisitions will not be achieved; and that business judgments concerning the value, strengths and weaknesses of businesses acquired will prove incorrect, which could have a material adverse effect on our financial condition and results of operations.
Risks associated with our potential international operations.
We intend to expand our operations into other countries. International operations are subject to risks that may materially adversely affect our business, results of operations, and financial condition. The risks that our potential international operations would be subject to include, among other things: difficulties and costs relating to staffing and managing foreign operations; fluctuations in the value of foreign currencies; repatriation of cash from our foreign operations to the United States; foreign countries may impose additional withholding taxes or otherwise tax our foreign income; separate operating and financial systems; disaster recovery; and unexpected regulatory, economic, and political changes in foreign markets. In addition to the foregoing, our potential international operations will face risks associated with complying with laws governing our foreign business operations, including the United States Foreign Corrupt Practices Act and applicable regulatory requirements.
Future joint ventures may use significant resources, may be unsuccessful and could expose us to unforeseen liabilities.
As part of our growth strategy, we may partner with large healthcare systems to provide post-acute care services. These joint ventures may involve significant cash expenditures, debt incurrence, additional operating losses and expenses, and compliance risks that could have a material adverse effect on our financial condition and results of operations.
A joint venture involves the combining of corporate cultures and mission. As a result, we may not be able to successfully operate a joint venture, and therefore, we may not be able to realize the intended benefits. If we fail to successfully execute a joint venture relationship, our financial condition and results of operations may be materially adversely affected. A new joint venture could result in difficulties in combining operations, technologies, and personnel. Such difficulties may divert significant financial, operational, and managerial resources from our existing operations and make it more difficult to achieve our operating and strategic objectives. We may fail to retain employees or patients as a result of the integration efforts.
A joint venture is operated through a board of directors that contains representatives of Select and other parties to the joint venture. We may not control the board or some actions of the board may require supermajority votes. As a result, the joint venture may elect certain actions that could have adverse effects on our financial condition and results of operations.
31
If we fail to compete effectively with other hospitals, clinics, medical centers and healthcare providers in the local areas we serve, our net operating revenues and profitability may decline.
The healthcare business is highly competitive, and we compete with other hospitals, rehabilitation clinics, medical centers, and other healthcare providers for patients. If we are unable to compete effectively in the long term acute care, inpatient rehabilitation, outpatient rehabilitation, and occupational health services businesses, our ability to retain customers and physicians, or maintain or increase our revenue growth, price flexibility, control over medical cost trends, and marketing expenses may be compromised and our net operating revenues and profitability may decline.
Many of our LTCHs and IRFs operate in geographic areas where we compete with at least one other facility that provides similar services.
Our outpatient rehabilitation clinics face competition from a variety of local and national outpatient rehabilitation providers, including physician-owned physical therapy clinics, dedicated locally owned and managed outpatient rehabilitation clinics, and hospital or university owned or affiliated ventures, as well as national and regional providers in select areas. Other competing outpatient rehabilitation clinics in local areas we serve may have greater name recognition and longer operating histories than our clinics. The managers of these competing clinics may also have stronger relationships with physicians in their communities, which could give them a competitive advantage for patient referrals. Because the barriers to entry are not substantial and current customers have the flexibility to move easily to new healthcare service providers, we believe that new outpatient physical therapy competitors can emerge relatively quickly.
Concentra’s primary competitors have typically been independent physicians, hospital emergency departments, and hospital-owned or hospital-affiliated medical facilities. Because the barriers to entry in Concentra’s geographic markets are not substantial and its current customers have the flexibility to move easily to new healthcare service providers, new competitors to Concentra can emerge relatively quickly. The markets for Concentra’s consumer health and veteran’s healthcare businesses are also fragmented and competitive. If Concentra’s competitors are better able to attract patients or expand services at their facilities than Concentra is, Concentra may experience an overall decline in revenue. Similarly, competitive pricing pressures from our competitors could cause Concentra to lose existing or future CBOC contracts with the Department of Veterans Affairs, which may also cause Concentra to experience an overall decline in revenue.
Future cost containment initiatives undertaken by private third-party payors may limit our future net operating revenues and profitability.
Initiatives undertaken by major insurers and managed care companies to contain healthcare costs affect our profitability. These payors attempt to control healthcare costs by contracting with hospitals and other healthcare providers to obtain services on a discounted basis. We believe that this trend may continue and may limit reimbursements for healthcare services. If insurers or managed care companies from whom we receive substantial payments reduce the amounts they pay for services, our profit margins may decline, or we may lose patients if we choose not to renew our contracts with these insurers at lower rates.
If we fail to maintain established relationships with the physicians in the areas we serve, our net operating revenues may decrease.
Our success is partially dependent upon the admissions and referral practices of the physicians in the communities our LTCHs, IRFs, and outpatient rehabilitation clinics serve, and our ability to maintain good relations with these physicians. Physicians referring patients to our hospitals and clinics are generally not our employees and, in many of the local areas that we serve, most physicians have admitting privileges at other hospitals and are free to refer their patients to other providers. If we are unable to successfully cultivate and maintain strong relationships with these physicians, our hospitals’ admissions and our facilities’ and clinics’ businesses may decrease, and our net operating revenues may decline.
We could experience significant increases to our operating costs due to shortages of healthcare professionals or union activity.
Our LTCHs and IRFs are highly dependent on nurses, our outpatient rehabilitation division is highly dependent on therapists for patient care, and Concentra is highly dependent upon the ability of its affiliated professional groups to recruit and retain qualified physicians and other licensed providers. The market for qualified healthcare professionals is highly competitive. We have sometimes experienced difficulties in attracting and retaining qualified healthcare personnel. We cannot assure you we will be able to attract and retain qualified healthcare professionals in the future. Additionally, the cost of attracting and retaining qualified healthcare personnel may be higher than we anticipate, and as a result, our profitability could decline.
In addition, United States healthcare providers are continuing to see an increase in the amount of union activity. Though we cannot predict the degree to which we will be affected by future union activity, there may be continuing legislative proposals that could result in increased union activity. We could experience an increase in labor and other costs from such union activity.
32
Our business operations could be significantly disrupted if we lose key members of our management team.
Our success depends to a significant degree upon the continued contributions of our senior officers and other key employees, and our ability to retain and motivate these individuals. We currently have employment agreements in place with three executive officers and change in control agreements and/or non-competition agreements with several other officers. Many of these individuals also have significant equity ownership in our company. We do not maintain any key life insurance policies for any of our employees. The loss of the services of certain of these individuals could disrupt significant aspects of our business, could prevent us from successfully executing our business strategy, and could have a material adverse effect on our results of operations.
In conducting our business, we are required to comply with applicable laws regarding fee-splitting and the corporate practice of medicine.
Some states prohibit the “corporate practice of medicine” that restricts business corporations from practicing medicine through the direct employment of physicians or from exercising control over medical decisions by physicians. Some states similarly prohibit the “corporate practice of therapy.” The laws relating to corporate practice vary from state to state and are not fully developed in each state in which we have facilities. Typically, however, professional corporations owned and controlled by licensed professionals are exempt from corporate practice restrictions and may employ physicians or therapists to furnish professional services. Also, in some states hospitals are permitted to employ physicians.
Some states also prohibit entities from engaging in certain financial arrangements, such as fee-splitting, with physicians or therapists. The laws relating to fee-splitting also vary from state to state and are not fully developed. Generally, these laws restrict business arrangements that involve a physician or therapist sharing medical fees with a referral source, but in some states, these laws have been interpreted to extend to management agreements between physicians or therapists and business entities under some circumstances.
We believe that the Company’s current and planned activities do not constitute fee-splitting or the unlawful corporate practice of medicine as contemplated by these state laws. However, there can be no assurance that future interpretations of such laws will not require structural and organizational modification of our existing relationships with the practices. If a court or regulatory body determines that we have violated these laws or if new laws are introduced that would render our arrangements illegal, we could be subject to civil or criminal penalties, our contracts could be found legally invalid and unenforceable (in whole or in part), or we could be required to restructure our contractual arrangements with our affiliated physicians and other licensed providers.
If the frequency of workplace injuries and illnesses continues to decline, Concentra’s results may be negatively affected.
Approximately 53% of Concentra’s revenue in 2017 was generated from the treatment or review of workers’ compensation claims. In the past decade, the number of workers’ compensation claims has decreased, which Concentra primarily attributes to improvements in workplace safety, improved risk management by employers, and changes in the type and composition of jobs. During the economic downturn, the number of employees with workers’ compensation insurance substantially decreased. Although the number of covered employees has increased more in recent years as the employment rate has increased, adverse economic conditions can cause the number of covered employees to decline which can cause further declines in workers’ compensation claims. In addition, because of the greater access to health insurance and the fact that the United States economy has continued to shift from a manufacturing-based to a service-based economy along with general improvements in workplace safety, workers are generally healthier and less prone to work injuries. Increases in employer-sponsored wellness and health promotion programs, spurred in part by the ACA, have led to fitter and healthier employees who may be less likely to injure themselves on the job. Concentra’s business model is based, in part, on its ability to expand its relative share of the market for the treatment and review of claims for workplace injuries and illnesses. If workplace injuries and illnesses decline at a greater rate than the increase in total employment, or if total employment declines at a greater rate than the increase in incident rates, the number of claims in the workers’ compensation market will decrease and may adversely affect Concentra’s business.
If Concentra loses several significant employer customers, its results may be adversely affected.
Concentra’s results may decline if it loses several significant employer customers. One or more of Concentra’s significant employer customers could be acquired. Additionally, Concentra could lose significant employer customers due to competitive pricing pressures or other reasons. The loss of several significant employer customers could cause a material decline in Concentra’s profitability and operating performance.
33
Significant legal actions could subject us to substantial uninsured liabilities.
Physicians, hospitals, and other healthcare providers have become subject to an increasing number of legal actions alleging malpractice, product liability, or related legal theories. Many of these actions involve large claims and significant defense costs. We are also subject to lawsuits under federal and state whistleblower statutes designed to combat fraud and abuse in the healthcare industry. These whistleblower lawsuits are not covered by insurance and can involve significant monetary damages and award bounties to private plaintiffs who successfully bring the suits. See “Legal Proceedings” and Note 15 in our audited consolidated financial statements.
We currently maintain professional malpractice liability insurance and general liability insurance coverages through a number of different programs that are dependent upon such factors as the state where we are operating and whether the operations are wholly owned or are operated through a joint venture. For our wholly owned operations, we maintain insurance coverages under a combination of policies with a total annual aggregate limit of $35.0 million. Our insurance for the professional liability coverage is written on a “claims-made” basis, and our commercial general liability coverage is maintained on an “occurrence” basis. These coverages apply after a self-insured retention limit is exceeded. For our joint venture operations, we have numerous programs that are designed to respond to the risks of the specific joint venture. The annual aggregate limit under these programs ranges from $5.0 million to $20.0 million. The policies are generally written on a “claims-made” basis. Each of these programs has either a deductible or self-insured retention limit. We review our insurance program annually and may make adjustments to the amount of insurance coverage and self-insured retentions in future years. In addition, our insurance coverage does not generally cover punitive damages and may not cover all claims against us. See “Business—Government Regulations—Other Healthcare Regulations.”
Concentration of ownership among our existing executives and directors may prevent new investors from influencing significant corporate decisions.
Our executives and directors, beneficially own, in the aggregate, approximately 19.9% of Holdings’ outstanding common stock as of February 1, 2018. As a result, these stockholders have significant control over our management and policies and are able to exercise influence over all matters requiring stockholder approval, including the election of directors, amendment of our certificate of incorporation, and approval of significant corporate transactions. The directors elected by these stockholders are able to make decisions affecting our capital structure, including decisions to issue additional capital stock, implement stock repurchase programs, and incur indebtedness. This influence may have the effect of deterring hostile takeovers, delaying or preventing changes in control or changes in management, or limiting the ability of our other stockholders to approve transactions that they may deem to be in their best interest.
Risks Related to Our Capital Structure
If WCAS and the other members of Concentra Group Holdings Parent or Dignity Health exercise their Put Right, it may have an adverse effect on our liquidity. Additionally, we may not have adequate funds to pay amounts due in connection with the Put Right, if exercised, in which case we would be required to issue Holdings’ common stock to purchase interests of Concentra Group Holdings Parent and our stockholders’ ownership interest will be diluted.
Pursuant to the Amended and Restated Limited Liability Company Agreement of Concentra Group Holdings Parent, WCAS and the other members of Concentra Group Holdings Parent and Dignity Health have separate put rights, each, a “Put Right,” with respect to their equity interests in Concentra Group Holdings Parent. If a Put Right is exercised by WCAS or Dignity Health, Select will be obligated to purchase up to 331/3% of the equity interests of Concentra Group Holdings Parent that WCAS or Dignity Health, respectively, owned as of February 1, 2018, at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA (as defined in the Amended and Restated Limited Liability Company Agreement of Concentra Group Holdings Parent) and capped at an agreed upon multiple of EBITDA. Select has the right to elect to pay the purchase price in cash or in shares of Holdings’ common stock. WCAS and Dignity Health may first exercise their respective Put Right during a sixty-day period following the second anniversary of the date of the Amended and Restated LLC Agreement in 2020, and then may exercise their respective Put Right again annually during a sixty-day period in each calendar year thereafter. If WCAS exercises its Put Right, the other members of Concentra Group Holdings Parent, other than Dignity Health, may elect to sell to Select, on the same terms as WCAS, a percentage of their equity interests of Concentra Group Holdings Parent that such member owned as of the date of the Amended and Restated LLC Agreement, up to but not exceeding the percentage of equity interests owned by WCAS as of the date of the Amended and Restated LLC Agreement that WCAS has determined to sell to Select in the exercise of its Put Right.
34
Furthermore, WCAS, Dignity Health, and the other members of Concentra Group Holdings Parent have a put right with respect to their equity interest in Concentra Group Holdings Parent that may only be exercised in the event Holdings or Select experiences a change of control that has not been previously approved by WCAS and Dignity Health, and which results in change in the senior management of Select (an “SEM COC Put Right”). If an SEM COC Put Right is exercised by WCAS, Select will be obligated to purchase all (but not less than all) of the equity interests of WCAS and the other members of Concentra Group Holdings Parent (other than Dignity Health) at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA and capped at an agreed upon multiple of EBITDA. Similarly, if an SEM COC Put Right is exercised by Dignity Health, Select will be obligated to purchase all (but not less than all) of the equity interests of Dignity Health at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA and capped at an agreed upon multiple of EBITDA.
We may not have sufficient funds, borrowing capacity, or other capital resources available to pay for the interests of Concentra Group Holdings Parent in cash if WCAS, Dignity Health, and the other members of Concentra Group Holdings Parent exercise the Put Right or the SEM COC Put Right or may be prohibited from doing so under the terms of our debt agreements. Such lack of available funds upon the exercising of the Put Right or the SEM COC Put Right would force us to issue stock at a time we might not otherwise desire to do so in order to purchase the interests of Concentra Group Holdings Parent. To the extent that the interests of Concentra Group Holdings Parent are purchased by issuing shares of our common stock, the increase in the number of shares of our common stock issued and outstanding may depress the price of our common stock and our stockholders will experience dilution in their respective percentage ownership in us. In addition, shares issued to purchase the interests in Concentra Group Holdings Parent will be valued at the twenty-one trading day volume-weighted average sales price of such shares for the period beginning ten trading days immediately preceding the first public announcement of the Put Right or the SEM COC Put Right being exercised and ending ten trading days immediately following such announcement. Because the value of the common stock issued to purchase the interests in Concentra Group Holdings Parent is, in part, determined by the sales price of our common stock following the announcement that the Put Right or the SEM COC Put Right is being exercised, which may cause the sales price of our common stock to decline, the amount of common stock we may have to issue to purchase the interests in Concentra Group Holdings Parent may increase, resulting in further dilution to our existing stockholders.
Our substantial indebtedness may limit the amount of cash flow available to invest in the ongoing needs of our business.
We have a substantial amount of indebtedness. As of December 31, 2017, Select had approximately $2,087.0 million of total indebtedness, and Concentra had approximately $612.9 million of total indebtedness, which is nonrecourse to Select. As of December 31, 2017, our total indebtedness was $2,699.9 million. On February 1, 2018, Concentra acquired all of the issued and outstanding shares of stock of U.S. HealthWorks. In connection with the acquisition of U.S. HealthWorks, Concentra added a $555.0 million senior secured incremental term facility under its existing credit facilities and entered into a $240.0 million second lien term facility, which matures on June 1, 2023. Our indebtedness could have important consequences to you. For example, it:
• | requires us to dedicate a substantial portion of our cash flow from operations to payments on our indebtedness, reducing the availability of our cash flow to fund working capital, capital expenditures, development activity, acquisitions, and other general corporate purposes; |
• | increases our vulnerability to adverse general economic or industry conditions; |
• | limits our flexibility in planning for, or reacting to, changes in our business or the industries in which we operate; |
• | makes us more vulnerable to increases in interest rates, as borrowings under our senior secured credit facilities are at variable rates; |
• | limits our ability to obtain additional financing in the future for working capital or other purposes; and |
• | places us at a competitive disadvantage compared to our competitors that have less indebtedness. |
Any of these consequences could have a material adverse effect on our business, financial condition, results of operations, prospects, and ability to satisfy our obligations under our indebtedness. In addition, there would be a material adverse effect on our business, financial condition, results of operations and cash flows if we were unable to service our indebtedness or obtain additional financing, as needed.
See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources.”
35
The Select credit facilities and the indenture governing Select’s 6.375% senior notes require Select to comply with certain financial covenants and obligations, the default of which may result in the acceleration of certain of Select’s indebtedness.
In the case of an event of default under the agreements governing the Select credit facilities (as defined below), the lenders under such agreements could elect to declare all amounts borrowed, together with accrued and unpaid interest and other fees, to be due and payable. If Select is unable to obtain a waiver from the requisite lenders under such circumstances, these lenders could exercise their rights, then Select’s financial condition and results of operations could be adversely affected, and Select could become bankrupt or insolvent.
The Select credit facilities require Select to maintain a leverage ratio (based upon the ratio of indebtedness to consolidated EBITDA as defined in the agreements governing the Select credit facilities), which is tested quarterly. Failure to comply with these covenants would result in an event of default under the Select credit facilities and, absent a waiver or an amendment from the lenders, preclude Select from making further borrowings under its revolving facility and permit the lenders to accelerate all outstanding borrowings under the Select credit facilities.
As of December 31, 2017, Select was required to maintain its leverage ratio (its ratio of total indebtedness to consolidated EBITDA for the prior four consecutive fiscal quarters) at less than 6.25 to 1.00. For the four consecutive fiscal quarters ended December 31, 2017, Select’s leverage ratio was 5.27 to 1.00.
While Select has never defaulted on compliance with any of its financial covenants, Select’s ability to comply with these ratios in the future may be affected by events beyond its control. Inability to comply with the required financial covenants could result in a default under the Select credit facilities. In the event of any default under Select’s credit facilities, the lenders could elect to terminate borrowing commitments and declare all borrowings outstanding, together with accrued and unpaid interest and other fees, to be immediately due and payable. In the event of any default under Select’s indenture, the trustee or holders of 25% of the notes could declare all outstanding 6.375% senior notes immediately due and payable.
The Concentra credit facilities require Concentra to comply with certain financial covenants and obligations, the default of which may result in the acceleration of certain of Concentra’s indebtedness.
In the case of an event of default under the agreements governing the Concentra credit facilities (as defined below), which is nonrecourse to Select, the lenders under such agreements could elect to declare all amounts borrowed, together with accrued and unpaid interest and other fees, to be due and payable. If Concentra is unable to obtain a waiver from these lenders under such circumstances, the lenders could exercise their rights, then Concentra’s financial condition and results of operations could be adversely affected, and Concentra could become bankrupt or insolvent.
The Concentra first lien credit agreement (as defined below) requires Concentra to maintain a leverage ratio (based upon the ratio of indebtedness for money borrowed to consolidated EBITDA) of 5.75 to 1.00, which is tested quarterly, but only if Revolving Exposure (as defined in the Concentra credit facilities) exceeds 30% of Revolving Commitments (as defined in the Concentra credit facilities) on such day. Failure to comply with this covenant would result in an event of default under the Concentra revolving facility (as defined below) only and, absent a waiver or an amendment from the lenders, preclude Concentra from making further borrowings under the Concentra revolving facility and permit the lenders to accelerate all outstanding borrowings under the Concentra revolving facility. Upon such acceleration, Concentra’s failure to comply with the financial covenant would result in an Event of Default (as defined in the Concentra credit facilities) with respect to the Concentra first lien term loan (as defined below).
The Concentra credit facilities also contain a number of affirmative and restrictive covenants, including limitations on mergers, consolidations, and dissolutions; sales of assets; investments and acquisitions; indebtedness; liens; affiliate transactions; and dividends and restricted payments. The Concentra credit facilities contain events of default for non-payment of principal and interest when due (subject to a grace period for interest), cross-default and cross-acceleration provisions and an event of default that would be triggered by a change of control.
While Concentra has never defaulted on compliance with any of its financial covenants, Concentra’s ability to comply with these ratios in the future may be affected by events beyond our control. Inability to comply with the required financial covenants could result in a default under the Concentra credit facilities. In the event of any default under the Concentra credit facilities, the lenders could elect to terminate borrowing commitments and declare all borrowings outstanding, together with accrued and unpaid interest and other fees, to be immediately due and payable.
36
Payment of interest on, and repayment of principal of, our indebtedness is dependent in part on cash flow generated by our subsidiaries.
Payment of interest on, and repayment of, principal of our indebtedness will be dependent in part upon cash flow generated by our subsidiaries and their ability to make such cash available to us, by dividend, debt repayment, or otherwise. Our subsidiaries may not be able to, or be permitted to, make distributions to enable us to make payments in respect of our indebtedness. For example, as a general matter, Concentra is restricted from paying dividends under the Concentra credit facilities and therefore we cannot rely on Concentra’s cash flow to repay Select’s indebtedness. Each of our subsidiaries is a distinct legal entity and, under certain circumstances, legal and contractual restrictions may limit our ability to obtain cash from our subsidiaries. In the event that we do not receive distributions from our subsidiaries, we may be unable to make required principal and interest payments on our indebtedness. In addition, any payment of interest, dividends, distributions, loans, or advances by our subsidiaries to us could be subject to restrictions on dividends or repatriation of distributions under applicable local law, monetary transfer restrictions, and foreign currency exchange regulations in the jurisdictions in which the subsidiaries operate or under arrangements with local partners. Furthermore, the ability of our subsidiaries to make such payments of interest, dividends, distributions, loans, or advances may be contested by taxing authorities in the relevant jurisdictions.
Despite our substantial level of indebtedness, we and our subsidiaries may be able to incur additional indebtedness. This could further exacerbate the risks described above.
We and our subsidiaries may be able to incur additional indebtedness in the future. Although the Select credit facilities and the Concentra credit facilities contain restrictions on the incurrence of additional indebtedness, these restrictions are subject to a number of qualifications and exceptions, and the indebtedness incurred in compliance with these restrictions could be substantial. Also, these restrictions do not prevent us or our subsidiaries from incurring obligations that do not constitute indebtedness. As of December 31, 2017, Select had $181.4 million of availability under the Select revolving facility (as defined below) (after giving effect to $38.6 million of outstanding letters of credit) and Concentra had $43.4 million of availability under the Concentra revolving facility (after giving effect to $6.6 million of outstanding letters of credit). In addition, to the extent new debt is added to us and our subsidiaries’ current debt levels, the substantial leverage risks described above would increase.
Concentra’s inability to meet the conditions and payments under the Concentra credit facilities, although nonrecourse to Select, could jeopardize Select’s equity contribution to Concentra Group Holdings Parent.
Select is not a party to the Concentra credit facilities and is not an obligor with respect to Concentra’s debt under such agreements; however, if Concentra fails to meet its obligations and defaults on the Concentra credit facilities, a portion of or all of Select’s equity investment in Concentra Group Holdings Parent, the indirect parent company of Concentra, could be at risk of loss.
We may be unable to refinance our debt on terms favorable to us or at all, which would negatively impact our business and financial condition.
We are subject to risks normally associated with debt financing, including the risk that our cash flow will be insufficient to meet required payments of principal and interest. While we intend to refinance all of our indebtedness before it matures, there can be no assurance that we will be able to refinance any maturing indebtedness, that such refinancing will be on terms as favorable to us as the terms of the maturing indebtedness or, if the indebtedness cannot be refinanced, that we will be able to otherwise obtain funds by selling assets or raising equity to make required payments on our maturing indebtedness. Furthermore, if prevailing interest rates or other factors at the time of refinancing result in higher interest rates upon refinancing, then the interest expense relating to that refinanced indebtedness would increase. If we are unable to refinance our indebtedness at or before maturity or otherwise meet our payment obligations, our business and financial condition will be negatively impacted, and we may be in default under our indebtedness. Any default under the Select senior secured credit facilities would permit lenders to foreclose on our assets and would also be deemed a default under the indenture governing Select’s 6.375% senior notes, which may also result in the acceleration of that indebtedness, and, although Select is not a party to the Concentra credit facilities and is not an obligor with respect to Concentra’s debt under such agreements, if Concentra fails to meet its obligations and defaults on the Concentra credit facilities, a portion of or all of Select’s equity investment in Concentra Group Holdings Parent, the indirect parent company of Concentra, could be at risk of loss.
See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources.”
Item 1B. Unresolved Staff Comments.
None.
37
Item 2. Properties.
We currently lease most of our facilities, including LTCHs, IRFs, outpatient rehabilitation clinics, medical centers, CBOCs, and our corporate headquarters. We own 20 of our LTCHs, seven of our IRFs, one of our outpatient rehabilitation clinics, and six of our Concentra medical centers throughout the United States. As of December 31, 2017, we leased 79 of our LTCHs, 9 of our IRFs, 1,446 of our outpatient rehabilitation clinics, 306 of our Concentra medical centers, and 32 CBOCs throughout the United States.
We lease our corporate headquarters from companies owned by a related party affiliated with us through common ownership or management. Our corporate headquarters is approximately 221,453 square feet and is located in Mechanicsburg, Pennsylvania.
The following is a list by state of the number of facilities we operated as of December 31, 2017.
Long Term Acute Care Hospitals(1) | Inpatient Rehabilitation Facilities(1) | Outpatient Clinics(1) | Concentra Medical Centers(2) | Total Facilities | |||||||||||
Alabama | 1 | 27 | 28 | ||||||||||||
Alaska | 7 | 7 | |||||||||||||
Arizona | 2 | 1 | 26 | 12 | 41 | ||||||||||
Arkansas | 2 | 1 | 2 | 5 | |||||||||||
California | 1 | 69 | 19 | 89 | |||||||||||
Colorado | 46 | 19 | 65 | ||||||||||||
Connecticut | 52 | 10 | 62 | ||||||||||||
Delaware | 1 | 11 | 1 | 13 | |||||||||||
District of Columbia | 5 | 5 | |||||||||||||
Florida | 10 | 1 | 117 | 9 | 137 | ||||||||||
Georgia | 5 | 1 | 68 | 13 | 87 | ||||||||||
Hawaii | 1 | 1 | |||||||||||||
Illinois | 63 | 13 | 76 | ||||||||||||
Indiana | 3 | 29 | 4 | 36 | |||||||||||
Iowa | 2 | 19 | 3 | 24 | |||||||||||
Kansas | 2 | 14 | 2 | 18 | |||||||||||
Kentucky | 2 | 52 | 6 | 60 | |||||||||||
Louisiana | 3 | 3 | 6 | ||||||||||||
Maine | 13 | 5 | 18 | ||||||||||||
Maryland | 63 | 12 | 75 | ||||||||||||
Massachusetts | 12 | 2 | 14 | ||||||||||||
Michigan | 11 | 37 | 18 | 66 | |||||||||||
Minnesota | 1 | 27 | 28 | ||||||||||||
Mississippi | 5 | 1 | 6 | ||||||||||||
Missouri | 3 | 3 | 89 | 11 | 106 | ||||||||||
Nebraska | 2 | 2 | 3 | 7 | |||||||||||
Nevada | 11 | 7 | 18 | ||||||||||||
New Hampshire | 3 | 3 | |||||||||||||
New Jersey | 1 | 4 | 160 | 13 | 178 | ||||||||||
New Mexico | 2 | 4 | 6 | ||||||||||||
North Carolina | 2 | 36 | 6 | 44 | |||||||||||
Ohio | 17 | 5 | 84 | 10 | 116 | ||||||||||
Oklahoma | 2 | 22 | 7 | 31 | |||||||||||
Oregon | 4 | 4 | |||||||||||||
Pennsylvania | 9 | 2 | 220 | 14 | 245 | ||||||||||
Rhode Island | 2 | 2 | |||||||||||||
South Carolina | 2 | 26 | 2 | 30 | |||||||||||
38
South Dakota | 1 | 1 | |||||||||||||
Tennessee | 5 | 23 | 7 | 35 | |||||||||||
Texas | 4 | 5 | 115 | 43 | 167 | ||||||||||
Utah | 6 | 6 | |||||||||||||
Vermont | 2 | 2 | |||||||||||||
Virginia | 1 | 1 | 45 | 6 | 53 | ||||||||||
Washington | 5 | 5 | |||||||||||||
West Virginia | 1 | 1 | |||||||||||||
Wisconsin | 3 | 14 | 8 | 25 | |||||||||||
Total Company | 100 | 24 | 1,616 | 312 | 2,052 | ||||||||||
_______________________________________________________________________________
(1) | Includes managed LTCHs, IRFs, and outpatient clinics, respectively. |
(2) | Our Concentra segment also had operations in New York and Wyoming. |
Item 3. Legal Proceedings.
We are a party to various legal actions, proceedings, and claims (some of which are not insured), and regulatory and other governmental audits and investigations in the ordinary course of its business. We cannot predict the ultimate outcome of pending litigation, proceedings, and regulatory and other governmental audits and investigations. These matters could potentially subject us to sanctions, damages, recoupments, fines, and other penalties. The Department of Justice, CMS, or other federal and state enforcement and regulatory agencies may conduct additional investigations related to our businesses in the future that may, either individually or in the aggregate, have a material adverse effect on our business, financial position, results of operations, and liquidity.
To address claims arising out of the our operations, we maintain professional malpractice liability insurance and general liability insurance coverages through a number of different programs that are dependent upon such factors as the state where we are operating and whether the operations are wholly owned or are operated through a joint venture. For our wholly owned operations, we maintain insurance coverages under a combination of policies with a total annual aggregate limit of $ 35.0 million. Our insurance for the professional liability coverage is written on a “claims-made” basis, and our commercial general liability coverage is maintained on an “occurrence” basis. These coverages apply after a self-insured retention limit is exceeded. For our joint venture operations, we have numerous programs that are designed to respond to the risks of the specific joint venture. The annual aggregate limit under these programs ranges from $5.0 million to $20.0 million. The policies are generally written on a “claims-made” basis. Each of these programs has either a deductible or self-insured retention limit. We review our insurance program annually and may make adjustments to the amount of insurance coverage and self-insured retentions in future years. We also maintain umbrella liability insurance covering claims which, due to their nature or amount, are not covered by or not fully covered by our other insurance policies. These insurance policies also do not generally cover punitive damages and are subject to various deductibles and policy limits. Significant legal actions, as well as the cost and possible lack of available insurance, could subject us to substantial uninsured liabilities. In our opinion, the outcome of these actions, individually or in the aggregate, will not have a material adverse effect on its financial position, results of operations, or cash flows.
Healthcare providers are subject to lawsuits under the qui tam provisions of the federal False Claims Act. Qui tam lawsuits typically remain under seal (hence, usually unknown to the defendant) for some time while the government decides whether or not to intervene on behalf of a private qui tam plaintiff (known as a relator) and take the lead in the litigation. These lawsuits can involve significant monetary damages and penalties and award bounties to private plaintiffs who successfully bring the suits. We are and have been a defendant in these cases in the past, and may be named as a defendant in similar cases from time to time in the future.
39
Evansville Litigation
On October 19, 2015, the plaintiff-relators filed a Second Amended Complaint in United States of America, ex rel. Tracy Conroy, Pamela Schenk and Lisa Wilson v. Select Medical Corporation, Select Specialty Hospital—Evansville, LLC (“SSH-Evansville”), Select Employment Services, Inc., and Dr. Richard Sloan. The case is a civil action filed in the United States District Court for the Southern District of Indiana by private plaintiff-relators on behalf of the United States under the federal False Claims Act. The plaintiff-relators are the former CEO and two former case managers at SSH-Evansville, and the defendants currently include us, SSH-Evansville, one of our subsidiaries serving as common paymaster for its employees, and a physician who practices at SSH-Evansville. The plaintiff-relators allege that SSH-Evansville discharged patients too early or held patients too long, improperly discharged patients to and readmitted them from short stay hospitals, up-coded diagnoses at admission, and admitted patients for whom long term acute care was not medically necessary. They also allege that the defendants engaged in retaliation in violation of federal and state law. The Second Amended Complaint replaced a prior complaint that was filed under seal on September 28, 2012 and served on us on February 15, 2013, after a federal magistrate judge unsealed it on January 8, 2013. All deadlines in the case had been stayed after the seal was lifted in order to allow the government time to complete its investigation and to decide whether or not to intervene. On June 19, 2015, the United States Department of Justice notified the District Court of its decision not to intervene in the case.
In December 2015, the defendants filed a Motion to Dismiss the Second Amended Complaint on multiple grounds, including that the action is disallowed by the False Claims Act’s public disclosure bar, which disqualifies qui tam actions that are based on fraud already publicly disclosed through enumerated sources, unless the relator is an original source, and that the plaintiff-relators did not plead their claims with sufficient particularity, as required by the Federal Rules of Civil Procedure.
Thereafter, the United States filed a notice asserting a veto of the defendants’ use of the public disclosure bar for claims arising from conduct from and after March 23, 2010, which was based on certain statutory changes to the public disclosure bar language included in the ACA. On September 30, 2016, the District Court partially granted and partially denied the defendants’ Motion to Dismiss. It ruled that the plaintiff-relators alleged substantially the same conduct as had been publicly disclosed and that the plaintiff-relators are not original sources, so that the public disclosure bar requires dismissal of all non-retaliation claims arising from conduct before March 23, 2010. The District Court also ruled that the statutory changes to the public disclosure bar gave the United States the power to veto its applicability to claims arising from conduct on and after March 23, 2010, and therefore did not dismiss those claims based on the public disclosure bar. However, the District Court ruled that the plaintiff-relators did not plead certain of their claims relating to interrupted stay manipulation and premature discharging of patients with the requisite particularity, and dismissed those claims. The District Court declined to dismiss the plaintiff-relators’ claims arising from conduct from and after March 23, 2010 relating to delayed discharging of patients and up-coding and the plaintiff-relators’ retaliation claims. The plaintiff-relators then proposed a case management plan seeking nationwide discovery involving all of the Company’s LTCHs for the period from March 23, 2010 through the present, which the defendants have opposed.
We intend to vigorously defend this action, but at this time we are unable to predict the timing and outcome of this matter.
Knoxville Litigation
On July 13, 2015, the United States District Court for the Eastern District of Tennessee unsealed a qui tam Complaint in Armes v. Garman, et al, No. 3:14-cv-00172-TAV-CCS, which named as defendants Select, Select Specialty Hospital—Knoxville, Inc. (“SSH-Knoxville”), Select Specialty Hospital—North Knoxville, Inc. and ten current or former employees of these facilities. The Complaint was unsealed after the United States and the State of Tennessee notified the court on July 13, 2015 that each had decided not to intervene in the case. The Complaint is a civil action that was filed under seal on April 29, 2014 by a respiratory therapist formerly employed at SSH-Knoxville. The Complaint alleges violations of the federal False Claims Act and the Tennessee Medicaid False Claims Act based on extending patient stays to increase reimbursement and to increase average length of stay; artificially prolonging the lives of patients to increase Medicare reimbursements and decrease inspections; admitting patients who do not require medically necessary care; performing unnecessary procedures and services; and delaying performance of procedures to increase billing. The Complaint was served on some of the defendants during October 2015.
In November 2015, the defendants filed a Motion to Dismiss the Complaint on multiple grounds. The defendants first argued that False Claims Act’s first-to-file bar required dismissal of plaintiff-relator’s claims. Under the first-to-file bar, if a qui tam case is pending, no person may bring a related action based on the facts underlying the first action. The defendants asserted that the plaintiff-relator’s claims were based on the same underlying facts as were asserted in the Evansville litigation, discussed above. The defendants also argued that the plaintiff-relator’s claims must be dismissed under the public disclosure bar, and because the plaintiff-relator did not plead his claims with sufficient particularity.
40
In June 2016, the District Court granted the defendants’ Motion to Dismiss and dismissed with prejudice the plaintiff-relator’s lawsuit in its entirety. The District Court ruled that the first-to-file bar precludes all but one of the plaintiff-relator’s claims, and that the remaining claim must also be dismissed because the plaintiff-relator failed to plead it with sufficient particularity. In July 2016, the plaintiff-relator filed a Notice of Appeal to the United States Court of Appeals for the Sixth Circuit. Then, on October 11, 2016, the plaintiff-relator filed a Motion to Remand the case to the District Court for further proceedings, arguing that the September 30, 2016 decision in the Evansville litigation, discussed above, undermines the basis for the District Court’s dismissal. After the Court of Appeals denied the Motion to Remand, the plaintiff-relator then sought an indicative ruling from the District Court that it would vacate its prior dismissal ruling and allow plaintiff-relator to supplement his Complaint, but the District Court denied such request. In December 2017, the Court of Appeals, relying on the public disclosure bar, denied the appeal of the plaintiff-relator and affirmed the judgment of the District Court. In February 2018, the Court of Appeals denied a petition for rehearing that the plaintiff-relator filed in January 2018.
We intend to vigorously defend this action, but at this time we are unable to predict the timing and outcome of this matter.
Wilmington Litigation
On January 19, 2017, the United States District Court for the District of Delaware unsealed a qui tam Complaint in United States of America and State of Delaware ex rel. Theresa Kelly v. Select Specialty Hospital—Wilmington, Inc. (“SSH-Wilmington”), Select Specialty Hospitals, Inc., Select Employment Services, Inc., Select Medical Corporation, and Crystal Cheek, No. 16-347-LPS. The Complaint was initially filed under seal in May 2016 by a former chief nursing officer at SSH-Wilmington and was unsealed after the United States filed a Notice of Election to Decline Intervention in January 2017. The corporate defendants were served in March 2017. In the complaint, the plaintiff-relator alleges that the Select defendants and an individual defendant, who is a former health information manager at SSH-Wilmington, violated the False Claims Act and the Delaware False Claims and Reporting Act based on allegedly falsifying medical practitioner signatures on medical records and failing to properly examine the credentials of medical practitioners at SSH-Wilmington. In response to the Select defendants’ motion to dismiss the Complaint, in May 2017, the plaintiff-relator filed an Amended Complaint asserting the same causes of action. The Select defendants filed a Motion to Dismiss the Amended Complaint, which is now pending, based on numerous grounds, including that the Amended Complaint did not plead any alleged fraud with sufficient particularity, failed to plead that the alleged fraud was material to the government’s payment decision, failed to plead sufficient facts to establish that the Select defendants knowingly submitted false claims or records, and failed to allege any reverse false claim.
In March 2017, the plaintiff-relator initiated a second action by filing a Complaint in the Superior Court of the State of Delaware in Theresa Kelly v. Select Medical Corporation, Select Employment Services, Inc. and SSH-Wilmington, C.A. No. N17C-03-293 CLS. The Delaware Complaint alleges that the defendants retaliated against her in violation of the Delaware Whistleblowers’ Protection Act for reporting the same alleged violations that are the subject of the federal Amended Complaint. The defendants filed a motion to dismiss, or alternatively to stay, the Delaware Complaint based on the pending federal Amended Complaint and the failure to allege facts to support a violation of the Delaware Whistleblowers’ Protection Act. In January 2018, the Court stayed the Delaware Complaint pending the outcome of the federal case.
We intend to vigorously defend these actions, but at this time we are unable to predict the timing and outcome of this matter.
Contract Therapy Subpoena
On May 18, 2017, we received a subpoena from the U.S. Attorney’s Office for the District of New Jersey seeking various documents principally relating to our contract therapy division, which contracted to furnish rehabilitation therapy services to residents of skilled nursing facilities (“SNFs”) and other providers. We operated our contract therapy division through a subsidiary until March 31, 2016, when we sold the stock of the subsidiary. The subpoena seeks documents that appear to be aimed at assessing whether therapy services were furnished and billed in compliance with Medicare SNF billing requirements, including whether therapy services were coded at inappropriate levels and whether excessive or unnecessary therapy was furnished to justify coding at higher paying levels. We do not know whether the subpoena has been issued in connection with a qui tam lawsuit or in connection with possible civil, criminal, or administrative proceedings by the government. We are producing documents in response to the subpoena and intends to fully cooperate with this investigation. At this time, we are unable to predict the timing and outcome of this matter.
Northern District of Alabama Investigation
On October 30, 2017, we were contacted by the U.S. Attorney’s Office for the Northern District of Alabama to request cooperation in connection with an investigation that may involve Medicare billing compliance at certain of our Physiotherapy outpatient rehabilitation clinics. We intend to cooperate with this investigation. At this time, we are unable to predict the timing and outcome of this matter.
41
Item 4. Mine Safety Disclosures.
None.
42
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Information
Select Medical Holdings Corporation common stock is quoted on the New York Stock Exchange under the symbol “SEM.” The following table sets forth, for the periods indicated, the high and low sales prices of our common stock, reported by the New York Stock Exchange.
Market Prices | ||||||||
Fiscal Year Ended December 31, 2016 | High | Low | ||||||
First Quarter | $ | 12.10 | $ | 7.33 | ||||
Second Quarter | $ | 14.30 | $ | 10.31 | ||||
Third Quarter | $ | 13.61 | $ | 10.08 | ||||
Fourth Quarter | $ | 14.25 | $ | 10.20 | ||||
Market Prices | ||||||||
Fiscal Year Ended December 31, 2017 | High | Low | ||||||
First Quarter | $ | 15.15 | $ | 12.00 | ||||
Second Quarter | $ | 15.60 | $ | 12.90 | ||||
Third Quarter | $ | 19.60 | $ | 14.80 | ||||
Fourth Quarter | $ | 19.77 | $ | 16.10 | ||||
Holders
At the close of business on February 1, 2018, Holdings had 134,103,978 shares of common stock issued and outstanding. As of that date, there were 124 registered holders of record. This does not reflect beneficial stockholders who hold their stock in nominee or “street” name through brokerage firms.
Dividend Policy
Holdings has not paid or declared any dividends on its common stock at any point during the last two fiscal years. We do not anticipate paying any further dividends on Holdings’ common stock in the foreseeable future. We intend to retain future earnings to finance the ongoing operations and growth of our business. Any future determination relating to our dividend policy will be made at the discretion of our board of directors and will depend on conditions at that time, including our financial condition, results of operations, contractual restrictions, capital requirements, business prospects, and other factors our board of directors may deem relevant. Additionally, certain contractual agreements we are party to, including the Select credit facilities and the Indenture governing Select’s 6.375% senior notes, restrict our capacity to pay dividends.
Securities Authorized For Issuance Under Equity Compensation Plans
For information regarding securities authorized for issuance under equity compensation plans, see Part III “Item 12—Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.”
43
Stock Performance Graph
The graph below compares the cumulative total stockholder return on $100 invested at the close of the market on December 31, 2012, with dividends being reinvested on the date paid through and including the market close on December 31, 2017 with the cumulative total return of the same time period on the same amount invested in the Standard & Poor’s 500 Index (S&P 500) and the S&P Health Care Services Select Industry Index (SPSIHP). The chart below the graph sets forth the actual numbers depicted on the graph.
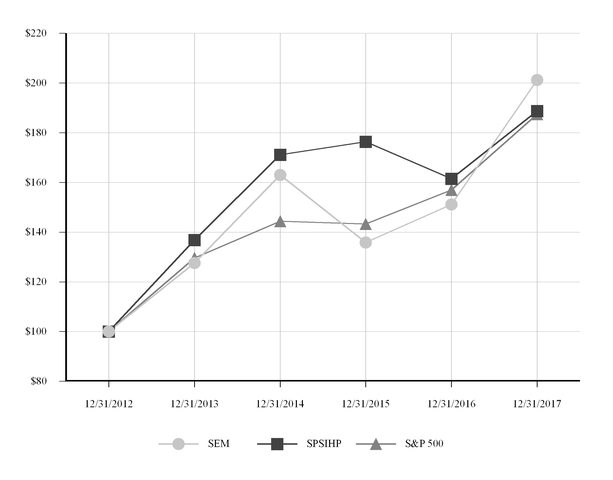
12/31/2012 | 12/31/2013 | 12/31/2014 | 12/31/2015 | 12/31/2016 | 12/31/2017 | |||||||||||||||||||
Select Medical Holdings Corporation (SEM) | $ | 100.00 | $ | 127.61 | $ | 162.98 | $ | 135.82 | $ | 151.10 | $ | 201.27 | ||||||||||||
S&P Health Care Services Select Industry Index (SPSIHP) | $ | 100.00 | $ | 136.89 | $ | 171.13 | $ | 176.41 | $ | 161.51 | $ | 188.78 | ||||||||||||
S&P 500 | $ | 100.00 | $ | 129.64 | $ | 144.36 | $ | 143.28 | $ | 156.98 | $ | 187.47 | ||||||||||||
44
Purchases of Equity Securities by the Issuer
Holdings’ board of directors has authorized a common stock repurchase program to repurchase up to $500.0 million worth of shares of its common stock. The program has been extended until December 31, 2018 and will remain in effect until then, unless further extended or earlier terminated by the board of directors. Stock repurchases under this program may be made in the open market or through privately negotiated transactions, and at times and in such amounts as Holdings deems appropriate. Holdings did not repurchase shares during the three months ended December 31, 2017 under the authorized common stock repurchase program.
The following table provides information regarding repurchases of our common stock during the three months ended December 31, 2017. As set forth below, the shares repurchased during the three months ended December 31, 2017 relate entirely to shares of common stock surrendered to us to satisfy tax withholding obligations associated with the vesting of restricted shares issued to employees, pursuant to the provisions of our equity incentive plans.
Total Number of Shares Purchased(1) | Average Price Paid Per Share | Total Number of Shares Purchased as Part of Publically Announced Plans or Programs | Approximate Dollar Value of Shares that May Yet Be Purchased Under Plans or Programs | ||||||||||||
October 1 - October 31, 2017 | 60,404 | $ | 19.05 | — | $ | 185,249,048 | |||||||||
November 1 - November 30, 2017 | — | — | — | 185,249,048 | |||||||||||
December 1 - December 31, 2017 | — | — | — | 185,249,048 | |||||||||||
Total | 60,404 | $ | 19.05 | — | $ | 185,249,048 | |||||||||
45
Item 6. Selected Financial Data.
You should read the following selected historical consolidated financial data in conjunction with our consolidated financial statements and the accompanying notes. Upon the consummation of the Concentra and Physiotherapy acquisitions, their financial results are consolidated with Select’s effective June 1, 2015 and March 4, 2016, respectively. You should also read “Management’s Discussion and Analysis of Financial Condition and Results of Operations” which is contained elsewhere herein. The selected historical financial data as of December 31, 2013, 2014, 2015, 2016, and 2017 and for the years ended December 31, 2013, 2014, 2015, 2016, and 2017 have been derived from consolidated financial statements audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm. The selected historical consolidated financial data as of December 31, 2016 and 2017, and for the years ended December 31, 2015, 2016, and 2017 have been derived from our consolidated financial information included elsewhere herein. The selected historical consolidated financial data as of December 31, 2013, 2014, and 2015 and for the years ended December 31, 2013 and 2014 have been derived from our audited consolidated financial information not included elsewhere herein.
Select Medical Holdings Corporation(1) | ||||||||||||||||||||
For the Year Ended December 31, | ||||||||||||||||||||
2013 | 2014 | 2015 | 2016 | 2017 | ||||||||||||||||
(In thousands, except per share data) | ||||||||||||||||||||
Statement of Operations Data: | ||||||||||||||||||||
Net operating revenues | $ | 2,975,648 | $ | 3,065,017 | $ | 3,742,736 | $ | 4,286,021 | $ | 4,443,603 | ||||||||||
Operating expenses(2) | 2,609,820 | 2,712,187 | 3,362,965 | 3,840,863 | 3,927,714 | |||||||||||||||
Depreciation and amortization | 64,392 | 68,354 | 104,981 | 145,311 | 160,011 | |||||||||||||||
Income from operations | 301,436 | 284,476 | 274,790 | 299,847 | 355,878 | |||||||||||||||
Loss on early retirement of debt(3) | (18,747 | ) | (2,277 | ) | — | (11,626 | ) | (19,719 | ) | |||||||||||
Equity in earnings of unconsolidated subsidiaries | 2,476 | 7,044 | 16,811 | 19,943 | 21,054 | |||||||||||||||
Non-operating gain (loss) | — | — | 29,647 | 42,651 | (49 | ) | ||||||||||||||
Interest expense, net(4) | (87,364 | ) | (85,446 | ) | (112,816 | ) | (170,081 | ) | (154,703 | ) | ||||||||||
Income before income taxes | 197,801 | 203,797 | 208,432 | 180,734 | 202,461 | |||||||||||||||
Income tax expense (benefit) | 74,792 | 75,622 | 72,436 | 55,464 | (18,184 | ) | ||||||||||||||
Net income | 123,009 | 128,175 | 135,996 | 125,270 | 220,645 | |||||||||||||||
Less: Net income attributable to non-controlling interests(5) | 8,619 | 7,548 | 5,260 | 9,859 | 43,461 | |||||||||||||||
Net income attributable to Select Medical Holdings Corporation | $ | 114,390 | $ | 120,627 | $ | 130,736 | $ | 115,411 | $ | 177,184 | ||||||||||
Income per common share: | ||||||||||||||||||||
Basic | $ | 0.82 | $ | 0.91 | $ | 1.00 | $ | 0.88 | $ | 1.33 | ||||||||||
Diluted | $ | 0.82 | $ | 0.91 | $ | 0.99 | $ | 0.87 | $ | 1.33 | ||||||||||
Weighted average common shares outstanding: | ||||||||||||||||||||
Basic | 136,879 | 129,026 | 127,478 | 127,813 | 128,955 | |||||||||||||||
Diluted | 137,047 | 129,465 | 127,752 | 127,968 | 129,126 | |||||||||||||||
Dividends per share | $ | 0.30 | $ | 0.40 | $ | 0.10 | $ | — | $ | — | ||||||||||
Balance Sheet Data (at end of period): | ||||||||||||||||||||
Cash and cash equivalents | $ | 4,319 | $ | 3,354 | $ | 14,435 | $ | 99,029 | $ | 122,549 | ||||||||||
Working capital(6)(7) | 82,878 | 133,220 | 19,869 | 191,268 | 315,423 | |||||||||||||||
Total assets(6)(7) | 2,817,622 | 2,924,809 | 4,388,678 | 4,920,626 | 5,127,166 | |||||||||||||||
Total debt(6) | 1,445,275 | 1,552,976 | 2,385,896 | 2,698,989 | 2,699,902 | |||||||||||||||
Total Select Medical Holdings Corporation stockholders’ equity | 786,234 | 739,515 | 859,253 | 815,725 | 823,368 | |||||||||||||||
46
Select Medical Corporation(1) | |||||||||||||||||||||
For the Year Ended December 31, | |||||||||||||||||||||
2013 | 2014 | 2015 | 2016 | 2017 | |||||||||||||||||
(In thousands) | |||||||||||||||||||||
Statement of Operations Data: | |||||||||||||||||||||
Net operating revenues | $ | 2,975,648 | $ | 3,065,017 | $ | 3,742,736 | $ | 4,286,021 | $ | 4,443,603 | |||||||||||
Operating expenses(2) | 2,609,820 | 2,712,187 | 3,362,965 | 3,840,863 | 3,927,714 | ||||||||||||||||
Depreciation and amortization | 64,392 | 68,354 | 104,981 | 145,311 | 160,011 | ||||||||||||||||
Income from operations | 301,436 | 284,476 | 274,790 | 299,847 | 355,878 | ||||||||||||||||
Loss on early retirement of debt(3) | (17,788 | ) | (2,277 | ) | — | (11,626 | ) | (19,719 | ) | ||||||||||||
Equity in earnings of unconsolidated subsidiaries | 2,476 | 7,044 | 16,811 | 19,943 | 21,054 | ||||||||||||||||
Non-operating gain (loss) | — | — | 29,647 | 42,651 | (49 | ) | |||||||||||||||
Interest expense, net(4) | (84,954 | ) | (85,446 | ) | (112,816 | ) | (170,081 | ) | (154,703 | ) | |||||||||||
Income before income taxes | 201,170 | 203,797 | 208,432 | 180,734 | 202,461 | ||||||||||||||||
Income tax expense (benefit) | 75,971 | 75,622 | 72,436 | 55,464 | (18,184 | ) | |||||||||||||||
Net income | 125,199 | 128,175 | 135,996 | 125,270 | 220,645 | ||||||||||||||||
Less: Net income attributable to non-controlling interests(5) | 8,619 | 7,548 | 5,260 | 9,859 | 43,461 | ||||||||||||||||
Net income attributable to Select Medical Corporation | $ | 116,580 | $ | 120,627 | $ | 130,736 | $ | 115,411 | $ | 177,184 | |||||||||||
Balance Sheet Data (at end of period): | |||||||||||||||||||||
Cash and cash equivalents | $ | 4,319 | $ | 3,354 | $ | 14,435 | $ | 99,029 | $ | 122,549 | |||||||||||
Working capital(6)(7) | 82,878 | 133,220 | 19,869 | 191,268 | 315,423 | ||||||||||||||||
Total assets(6)(7) | 2,817,622 | 2,924,809 | 4,388,678 | 4,920,626 | 5,127,166 | ||||||||||||||||
Total debt(6) | 1,445,275 | 1,552,976 | 2,385,896 | 2,698,989 | 2,699,902 | ||||||||||||||||
Total Select Medical Corporation stockholders’ equity | 786,234 | 739,515 | 859,253 | 815,725 | 823,368 | ||||||||||||||||
_______________________________________________________________________________
(1) | The results of Holdings are identical to those of Select for the years ended December 2014, 2015, 2016, and 2017. The amounts recognized as loss on early retirement of debt, interest expense, net and income tax expense by Holdings and Select differ for the year ended December 31, 2013. |
(2) | Operating expenses include cost of services, general and administrative expenses, bad debt expenses, and stock compensation expense. |
(3) | During the year ended December 31, 2013, Select entered into a credit extension amendment on February 20, 2013, the proceeds of which were used to redeem all of its outstanding 75/8% senior subordinated notes, to finance Holdings’ redemption of all of its 10% senior floating rate, and to repay a portion of the balance outstanding under Select’s 2011 senior secured credit facility. Additionally, on May 28, 2013, Select issued and sold $600.0 million aggregate principal amount of its 6.375% senior notes due 2021, the proceeds of which were used to pay a portion of the Select term loans then outstanding and to pay related fees and expenses. A loss on early retirement of debt of $18.7 million and $17.8 million for Holdings and Select, respectively, was recognized for the year ended December 31, 2013, which included the write-off of unamortized debt issuance costs. |
During the year ended December 31, 2014, Select amended its term loans under Select’s 2011 senior secured credit facility. A loss on early retirement of debt of $2.3 million was recognized for unamortized debt issuance costs, unamortized original issue discount and certain fees incurred related to term loan modifications.
During the year ended December 31, 2016, the Company recognized a loss on early retirement debt of $0.8 million relating to the repayment of series D tranche B term loans under Select’s 2011 senior secured credit facility. Additionally, on September 26, 2016, Concentra prepaid the second lien term loan under the Concentra credit facilities. The premium plus the expensing of unamortized deferred financing costs and original issuance discount resulted in a loss on early retirement of debt of $10.9 million.
47
During the year ended December 31, 2017, Select refinanced its 2011 senior secured credit facility. A loss on early retirement of debt of $19.7 million was recognized for unamortized debt issuance costs, unamortized original issue discount and certain fees incurred in connection with the refinancing.
(4) | Interest expense, net equals interest expense minus interest income. |
(5) | Reflects interests held by other parties in subsidiaries, limited liability companies and limited partnerships owned and controlled by us. |
(6) | The balance sheet data as of December 31, 2015, 2016, and 2017 reflects the adoption of ASU 2015-03 and ASU 2015-15, which requires unamortized debt issuance costs to be reflected as a direct reduction of debt, rather than a component of other assets. The balance sheet data as of December 31, 2013 and 2014 was not retrospectively conformed. |
(7) The balance sheet data as of December 31, 2016 and 2017 reflects the adoption of ASU 2015-17, which requires all deferred tax liabilities and assets be classified as non-current. The balance sheet data as of December 31, 2013, 2014, and 2015 was not retrospectively conformed.
Non-GAAP Measure Reconciliation
The following table reconciles Holdings’ net income and income from operations to Adjusted EBITDA and should be referenced when we discuss Adjusted EBITDA. Refer to “Management’s Discussion and Analysis of Financial Condition and Results of Operations” for further information on Adjusted EBITDA as a non-GAAP measure.
Select Medical Holdings Corporation | |||||||||||||||||||||
For the Year Ended December 31, | |||||||||||||||||||||
2013 | 2014 | 2015 | 2016 | 2017 | |||||||||||||||||
(In thousands) | |||||||||||||||||||||
Net income | $ | 123,009 | $ | 128,175 | $ | 135,996 | $ | 125,270 | $ | 220,645 | |||||||||||
Income tax expense (benefit) | 74,792 | 75,622 | 72,436 | 55,464 | (18,184 | ) | |||||||||||||||
Interest expense | 87,364 | 85,446 | 112,816 | 170,081 | 154,703 | ||||||||||||||||
Non-operating loss (gain) | — | — | (29,647 | ) | (42,651 | ) | 49 | ||||||||||||||
Equity in earnings of unconsolidated subsidiaries | (2,476 | ) | (7,044 | ) | (16,811 | ) | (19,943 | ) | (21,054 | ) | |||||||||||
Loss on early retirement of debt | 18,747 | 2,277 | — | 11,626 | 19,719 | ||||||||||||||||
Income from operations | 301,436 | 284,476 | 274,790 | 299,847 | 355,878 | ||||||||||||||||
Stock compensation expense: | |||||||||||||||||||||
Included in general and administrative | 5,276 | 9,027 | 11,633 | 14,607 | 15,706 | ||||||||||||||||
Included in cost of services | 1,757 | 2,015 | 3,046 | 2,806 | 3,578 | ||||||||||||||||
Depreciation and amortization | 64,392 | 68,354 | 104,981 | 145,311 | 160,011 | ||||||||||||||||
Concentra acquisition costs | — | — | 4,715 | — | — | ||||||||||||||||
Physiotherapy acquisition costs | — | — | — | 3,236 | — | ||||||||||||||||
U.S. HealthWorks acquisition costs | — | — | — | — | 2,819 | ||||||||||||||||
Adjusted EBITDA | $ | 372,861 | $ | 363,872 | $ | 399,165 | $ | 465,807 | $ | 537,992 | |||||||||||
48
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
You should read this discussion together with the “Selected Financial Data” and consolidated financial statements and accompanying notes included elsewhere herein.
Overview
We began operations in 1997 and have grown to be one of the largest operators of long term acute care hospitals (“LTCHs”), inpatient rehabilitation facilities (“IRFs”), outpatient rehabilitation clinics and occupational health centers in the United States based on the number of facilities. As of December 31, 2017, we operated 100 LTCHs in 27 states, 24 IRFs in 10 states, and 1,616 outpatient rehabilitation clinics in 37 states and the District of Columbia. Concentra, which is operated through a joint venture subsidiary, operated 312 occupational health centers in 38 states as of December 31, 2017. Concentra also provides contract services at employer worksites and Department of Veterans Affairs community-based outpatient clinics, or “CBOCs.” As of December 31, 2017, we had operations in 47 states and the District of Columbia.
In 2017, we changed our internal segment reporting structure to reflect how we now manage our business operations, review operating performance, and allocate resources. For the year ended December 31, 2017, our reportable segments include long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. Prior year results for the year ended December 31, 2016 presented herein have been recast to conform to the current presentation. Prior to 2017, we disclosed our financial information in three reportable segments: specialty hospitals, outpatient rehabilitation, and Concentra.
We had net operating revenues of $4,443.6 million for the year ended December 31, 2017. Of this total, we earned approximately 40% of our net operating revenues from our long term acute care segment, approximately 14% from our inpatient rehabilitation segment, approximately 23% from our outpatient rehabilitation segment, and approximately 23% from our Concentra segment. Patients are typically admitted to the Company’s LTCHs and IRFs from general acute care hospitals. These patients have specialized needs, with serious and often complex medical conditions. Our outpatient rehabilitation segment consists of clinics that provide physical, occupational, and speech rehabilitation services. Our Concentra segment consists of occupational health centers and contract services provided at employer worksites and Department of Veterans Affairs CBOCs that deliver occupational medicine, physical therapy, veteran’s healthcare, and consumer health services.
Non-GAAP Measure
We believe that the presentation of Adjusted EBITDA, as defined below, is important to investors because Adjusted EBITDA is commonly used as an analytical indicator of performance by investors within the healthcare industry. Adjusted EBITDA is used by management to evaluate financial performance and determine resource allocation for each of our operating segments. Adjusted EBITDA is not a measure of financial performance under accounting principles generally accepted in the United States of America (“GAAP”). Items excluded from Adjusted EBITDA are significant components in understanding and assessing financial performance. Adjusted EBITDA should not be considered in isolation or as an alternative to, or substitute for, net income, income from operations, cash flows generated by operations, investing or financing activities, or other financial statement data presented in the consolidated financial statements as indicators of financial performance or liquidity. Because Adjusted EBITDA is not a measurement determined in accordance with GAAP and is thus susceptible to varying calculations, Adjusted EBITDA as presented may not be comparable to other similarly titled measures of other companies.
We define Adjusted EBITDA as earnings excluding interest, income taxes, depreciation and amortization, gain (loss) on early retirement of debt, stock compensation expense, acquisition costs associated with Concentra, Physiotherapy, and U.S. HealthWorks, non-operating gain (loss), and equity in earnings (losses) of unconsolidated subsidiaries. We will refer to Adjusted EBITDA throughout the remainder of Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The table in “Selected Financial Data” reconciles net income and income from operations to Adjusted EBITDA and should be referenced when we discuss Adjusted EBITDA.
49
Summary Financial Results
Year Ended December 31, 2017
For the year ended December 31, 2017, our net operating revenues increased 3.7% to $4,443.6 million, compared to $4,286.0 million for the year ended December 31, 2016. Income from operations increased 18.7% to $355.9 million for the year ended December 31, 2017, compared to $299.8 million for the year ended December 31, 2016.
Our Adjusted EBITDA increased $72.2 million, or 15.5%, to $538.0 million for the year ended December 31, 2017, compared to $465.8 million for the year ended December 31, 2016. Our Adjusted EBITDA margin improved to 12.1% for the year ended December 31, 2017, compared to 10.9% for the year ended December 31, 2016.
The following table provides a reconciliation of our segment performance measures to our consolidated operating results for the year ended December 31, 2017.
Year Ended December 31, 2017 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net operating revenues | $ | 1,756,243 | $ | 631,777 | $ | 1,020,848 | $ | 1,034,035 | $ | 700 | $ | 4,443,603 | |||||||||||
Operating expenses | 1,503,564 | 541,736 | 888,315 | 880,286 | 113,813 | 3,927,714 | |||||||||||||||||
Depreciation and amortization | 45,743 | 20,176 | 24,607 | 61,945 | 7,540 | 160,011 | |||||||||||||||||
Income from operations | 206,936 | 69,865 | 107,926 | 91,804 | (120,653 | ) | 355,878 | ||||||||||||||||
Depreciation and amortization | 45,743 | 20,176 | 24,607 | 61,945 | 7,540 | 160,011 | |||||||||||||||||
Stock compensation expense | — | — | — | 993 | 18,291 | 19,284 | |||||||||||||||||
U.S. HealthWorks acquisition costs | — | — | — | 2,819 | — | 2,819 | |||||||||||||||||
Adjusted EBITDA | $ | 252,679 | $ | 90,041 | $ | 132,533 | $ | 157,561 | $ | (94,822 | ) | $ | 537,992 | ||||||||||
Adjusted EBITDA margin | 14.4 | % | 14.3 | % | 13.0 | % | 15.2 | % | N/M | 12.1 | % | ||||||||||||
N/M — Not Meaningful.
The following table provides the change in segment performance measures for the year ended December 31, 2017, compared to the year ended December 31, 2016.
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||
Change in net operating revenues | (1.6 | )% | 25.3 | % | 2.6 | % | 3.3 | % | N/M | 3.7 | % | ||||||
Change in income from operations | 14.5 | % | 58.1 | % | 0.7 | % | 12.6 | % | (6.0 | )% | 18.7 | % | |||||
Change in Adjusted EBITDA | 12.5 | % | 58.2 | % | 2.1 | % | 10.2 | % | (7.1 | )% | 15.5 | % | |||||
N/M—Not Meaningful.
Long Term Acute Care Segment. We operated 100 LTCHs at December 31, 2017, compared to 103 LTCHs at December 31, 2016. While our bed counts, admissions, and patient days decreased during the year ended December 31, 2017 due to a decline in the number of hospitals we operated, our revenue per patient day and occupancy rate improved. Since fully transitioning to operating under the new Medicare patient criteria regulations, our LTCHs have experienced improvements in income from operations and Adjusted EBITDA as a result of increases in net revenue per patient day and lower relative operating expenses. Our long term acute care segment contributed to increases in consolidated income from operations of $26.2 million and Adjusted EBITDA of $28.1 million for the year ended December 31, 2017, compared to the year ended December 31, 2016. Our Adjusted EBITDA margin improved to 14.4% for the year ended December 31, 2017, compared to 12.6% for the year ended December 31, 2016.
50
Inpatient Rehabilitation Segment. We operated 24 IRFs at December 31, 2017, compared to 20 IRFs at December 31, 2016. Our admissions, patient days, net revenue per patient day, and occupancy rate increased during the year ended December 31, 2017. These increases are principally due to several of our new inpatient rehabilitation facilities which commenced operations during 2016 and 2017. Our inpatient rehabilitation segment contributed to increases in our consolidated net operating revenues of $127.5 million, income from operations of $25.7 million, and Adjusted EBITDA of $33.1 million for the year ended December 31, 2017, compared to the year ended December 31, 2016. Our Adjusted EBITDA margin improved to 14.3% for the year ended December 31, 2017, compared to 11.3% for the year ended December 31, 2016.
Outpatient Rehabilitation Segment. We operated 1,616 clinics at December 31, 2017, compared to 1,611 clinics at December 31, 2016. We acquired Physiotherapy on March 4, 2016, and sold our contract therapy business on March 31, 2016, which affects our year-to-year comparisons as of the date for each of these events. Our visits and net revenue per visit increased during the year ended December 31, 2017, resulting in increases of $25.5 million in our consolidated net operating revenues compared to the year ended December 31, 2016. Our relative operating expenses also increased for the year ended December 31, 2017 compared to the year ended December 31, 2016, resulting in nominal increases in income from operations and Adjusted EBITDA during the year ended December 31, 2017. Our Adjusted EBITDA margin was 13.0% for both the years ended December 31, 2017 and December 31, 2016.
Concentra Segment. We operated 312 centers at December 31, 2017, compared to 300 centers at December 31, 2016. Visits in our centers increased during the year ended December 31, 2017, which contributed to increases in our consolidated net operating revenues of $33.4 million, and our relative operating expenses also improved. This resulted in increases to our consolidated income from operations of $10.3 million and Adjusted EBITDA of $14.6 million for the year ended December 31, 2017, compared to the year ended December 31, 2016. Our Adjusted EBITDA margin improved to 15.2% for the year ended December 31, 2017, compared to 14.3% for the year ended December 31, 2016.
Our consolidated net income increased $95.4 million, or 76.1%, to $220.6 million for the year ended December 31, 2017, compared to $125.3 million for the year ended December 31, 2016. The increase in our net income is principally due to an increase in income from operations for the year ended December 31, 2017, compared to the year ended December 31, 2016 and the recognition of an income tax benefit for the year ended December 31, 2017. The tax benefit principally related to the effects resulting from the federal tax reform legislation enacted during the year ended December 31, 2017.
51
Year Ended December 31, 2016
For the year ended December 31, 2016, our net operating revenues increased 14.5% to $4,286.0 million, compared to $3,742.7 million for the year ended December 31, 2015. Income from operations increased 9.1% to $299.8 million for the year ended December 31, 2016, compared to $274.8 million for the year ended December 31, 2015.
Our Adjusted EBITDA increased $66.6 million, or 16.7%, to $465.8 million for the year ended December 31, 2016, compared to $399.2 million for the year ended December 31, 2015. Our Adjusted EBITDA margin improved to 10.9% for the year ended December 31, 2016, compared to 10.7% for the year ended December 31, 2015.
The following table provides a reconciliation of our segment performance measures to our consolidated operating results for the year ended December 31, 2016.
Year Ended December 31, 2016 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net operating revenues | $ | 1,785,164 | $ | 504,318 | $ | 995,374 | $ | 1,000,624 | $ | 541 | $ | 4,286,021 | |||||||||||
Operating expenses | 1,560,555 | 447,416 | 865,544 | 858,385 | 108,963 | 3,840,863 | |||||||||||||||||
Depreciation and amortization | 43,862 | 12,723 | 22,661 | 60,717 | 5,348 | 145,311 | |||||||||||||||||
Income from operations | 180,747 | 44,179 | 107,169 | 81,522 | (113,770 | ) | 299,847 | ||||||||||||||||
Depreciation and amortization | 43,862 | 12,723 | 22,661 | 60,717 | 5,348 | 145,311 | |||||||||||||||||
Stock compensation expense | — | — | — | 770 | 16,643 | 17,413 | |||||||||||||||||
Physiotherapy acquisition costs | — | — | — | — | 3,236 | 3,236 | |||||||||||||||||
Adjusted EBITDA | $ | 224,609 | $ | 56,902 | $ | 129,830 | $ | 143,009 | $ | (88,543 | ) | $ | 465,807 | ||||||||||
Adjusted EBITDA margin | 12.6 | % | 11.3 | % | 13.0 | % | 14.3 | % | N/M | 10.9 | % | ||||||||||||
N/M — Not Meaningful.
The following table provides the change in segment performance measures for the year ended December 31, 2016, compared to the year ended December 31, 2015.
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||
Change in net operating revenues | (6.2 | )% | 13.6 | % | 22.9 | % | 71.0 | % | N/M | 14.5 | % | ||||||
Change in income from operations | (15.1 | )% | (27.1 | )% | 25.8 | % | 813.3 | % | (22.4 | )% | 9.1 | % | |||||
Change in Adjusted EBITDA | (13.0 | )% | (18.0 | )% | 32.2 | % | 196.1 | % | (18.1 | )% | 16.7 | % | |||||
N/M—Not Meaningful.
Long Term Acute Care Segment. We operated 103 LTCHs at December 31, 2016, compared to 109 LTCHs at December 31, 2015. Our bed counts, admissions, patient days, and occupancy rate decreased during the year ended December 31, 2016 due to a decline in the number of hospitals we operated and as a result of transitioning to operating under the new Medicare patient criteria regulations. The decline in patient days, which was offset in part by an increase in net revenue per day, resulted in a decrease in net operating revenues of $117.6 million, income from operations of $32.2 million, and Adjusted EBITDA of $33.6 million for the year ended December 31, 2016, compared to the year ended December 31, 2015. Our Adjusted EBITDA margin declined to 12.6% for the year ended December 31, 2016, compared to 13.6% for the year ended December 31, 2015.
52
Inpatient Rehabilitation Segment. We operated 20 IRFs at December 31, 2016, compared to 18 IRFs at December 31, 2015. Our admissions, patient days, and net revenue per patient day increased during the year ended December 31, 2016, principally as a result of two new facilities which commenced operations during the year ended December 31, 2016. Our occupancy rate declined during the year ended December 31, 2016, which is principally attributable to our start-up facilities. Our inpatient rehabilitation segment contributed to an increase in our consolidated net operating revenues of $60.3 million; however, we experienced declines in our consolidated income from operations of $16.5 million and Adjusted EBITDA of $12.5 million for the year ended December 31, 2016 compared to the year ended December 31, 2015. The decline was principally due to several start-up facilities which recently commenced operations. These facilities incurred $21.8 million of Adjusted EBITDA losses for the year ended December 31, 2016, compared to $6.4 million for the year ended December 31, 2015. The higher relative operating expenses of our inpatient rehabilitation segment resulting, in part, from our start-up facilities caused our Adjusted EBITDA margin to decline to 11.3% for the year ended December 31, 2016, compared to 15.6% for the year ended December 31, 2015.
Outpatient Rehabilitation Segment. We acquired Physiotherapy on March 4, 2016, which caused a significant increase in the number of clinics we operated during the year ended December 31, 2016. We operated 1,611 clinics at December 31, 2016, compared to 1,038 clinics at December 31, 2015. Our visits increased by 2.6 million during the year ended December 31, 2016, which was the principal cause of the increase in our consolidated net operating revenues of $185.4 million, income from operations of $22.0 million, and Adjusted EBITDA of $31.6 million during the year ended December 31, 2016, compared to the year ended December 31, 2015. The increase in our net operating revenues due to the increase in visits was offset in part by a decline in net revenue per visit for the year ended December 31, 2016. Our Adjusted EBITDA margin increased during the year ended December 31, 2016, principally due to the sale of our contract therapy businesses on March 31, 2016, which operated at lower Adjusted EBITDA margins than our outpatient rehabilitation clinics. The Adjusted EBITDA margin for the outpatient rehabilitation segment was 13.0% for the year ended December 31, 2016, compared to 12.1% for the year ended December 31, 2015.
Concentra Segment. We operated 300 centers at both December 31, 2016 and December 31, 2015. We acquired Concentra on June 1, 2015; accordingly, our operating results for the year ended December 31, 2015 include Concentra for the period June 1, 2015 through December 31, 2015. Our visits and net revenue per visit increased significantly during the year ended December 31, 2016. Our Concentra segment contributed to increases in our consolidated net operating revenues of $415.4 million, income from operations of $72.6 million, and Adjusted EBITDA of $94.7 million during the year ended December 31, 2016, compared to the year ended December 31, 2015. Our Adjusted EBITDA margin improved to 14.3% for the year ended December 31, 2016, compared to 8.3% for the year ended December 31, 2015.
Our consolidated net income declined $10.7 million to $125.3 million for the year ended December 31, 2016, compared to $136.0 million for the year ended December 31, 2015, despite increases in income from operations, equity in earnings of unconsolidated subsidiaries, non-operating gains, and a lower effective income tax rate. The decrease in net income was principally due to increased interest expense and losses on early retirement of debt of $11.6 million. Interest expense increased $57.3 million to $170.1 million for the year ended December 31, 2016, compared to $112.8 million for the year ended December 31, 2015. The increase was the result of increases in our indebtedness used to finance the acquisitions of Concentra and Physiotherapy and increases in our interest rates associated with amendments of Select’s 2011 senior secured credit facility.
53
Implementation of Patient Criteria
As discussed below under “Regulatory Changes - Medicare Reimbursement of LTCH Services - Patient Criteria,” our LTCHs transitioned to operating under new Medicare regulations, which established payment limits for Medicare patients discharged from an LTCH who do not meet specified patient criteria, beginning October 1, 2015. Since completing our transition to operating under the new LTCH Medicare patient criteria regulations during the third quarter of 2016, we have experienced an increase in admissions of patients eligible for the full LTCH-PPS standard reimbursement rate.
The table below illustrates the trends of our case mix index and occupancy percentages prior to and during the periods in which our LTCHs became subject to the new patient criteria requirements.
2015 | 2016 | 2017 | ||||||||||||
Occupancy Percentage | Case Mix Index(1) | Occupancy Percentage | Case Mix Index(1) | Occupancy Percentage | Case Mix Index(1) | |||||||||
Three months ended: | ||||||||||||||
March 31 | 71 | % | 1.22 | 71 | % | 1.24 | 68 | % | 1.28 | |||||
June 30 | 70 | % | 1.21 | 67 | % | 1.27 | 66 | % | 1.28 | |||||
September 30 | 70 | % | 1.18 | 61 | % | 1.26 | 65 | % | 1.27 | |||||
December 31 | 70 | % | 1.21 | 63 | % | 1.26 | 65 | % | 1.26 | |||||
(1) | Case mix index, which is calculated as the sum of all diagnostic-related group weights for the period divided by the sum of discharges for the same period, is reflective of the level of patient-acuity in our LTCHs. |
From 2015 to 2017, our case mix index has increased, which is reflective of the higher-acuity patients we are now admitting under patient criteria. This has resulted in increases in our net revenue per patient day due to higher reimbursement rates for these cases. Our LTCH occupancy percentage reached its lowest level during the third quarter of 2016, which is the first quarter in which all of our LTCHs operated under the new Medicare payment rules.
Significant Events
Refinancing
On March 6, 2017, Select entered into a new senior secured credit agreement (the “Select credit agreement”) that provides for $1.6 billion in senior secured credit facilities comprising a $1.15 billion, seven-year term loan (the “Select term loan”) and a $450.0 million, five-year revolving credit facility (the “Select revolving facility” and together with the Select term loan, the “Select credit facilities”), including a $75.0 million sublimit for the issuance of standby letters of credit. Select used borrowings under the new Select credit facilities to: (i) repay the series E tranche B term loans due June 1, 2018, the series F tranche B term loans due March 31, 2021, and the revolving facility maturing March 1, 2018 under Select’s 2011 senior secured credit facility; and (ii) pay fees and expenses in connection with the refinancing.
Acquisition of U.S. HealthWorks and Financing
On October 23, 2017, Select announced that Concentra Group Holdings, LLC (“Concentra Group Holdings”) entered into an Equity Purchase and Contribution Agreement (the “Purchase Agreement”) dated October 22, 2017 with Concentra, Concentra Group Holdings Parent, U.S. HealthWorks, Inc. (“U.S. HealthWorks”), and Dignity Health Holding Company (“DHHC”). On February 1, 2018, pursuant to the terms of the Purchase Agreement, Concentra acquired all of the issued and outstanding shares of stock of U.S. HealthWorks, an occupational medicine and urgent care service provider.
In connection with the closing of the transaction, Concentra Group Holdings redeemed certain of its outstanding equity interests from existing minority equity holders and subsequently, Concentra Group Holdings and a wholly owned subsidiary of Concentra Group Holdings Parent merged, with Concentra Group Holdings surviving the merger and becoming a wholly owned subsidiary of Concentra Group Holdings Parent. As a result of the merger, the equity interests of Concentra Group Holdings outstanding after the redemption described above were exchanged for membership interests in Concentra Group Holdings Parent.
Concentra acquired U.S. HealthWorks for $753.0 million. DHHC, a subsidiary of Dignity Health, was issued a 20% equity interest in Concentra Group Holdings Parent, which was valued at $238.0 million. Select retained a majority voting interest in Concentra Group Holdings Parent following the closing of the transaction.
54
On February 1, 2018, in connection with the transactions contemplated under the Purchase Agreement, Concentra amended its first lien credit agreement (the “Concentra first lien credit agreement”) to, among other things, provide for (i) an additional $555.0 million in tranche B term loans that, along with the existing tranche B term loans under the Concentra first lien credit agreement, have a maturity date of June 1, 2022 and (ii) an additional $25.0 million to the $50.0 million, five-year revolving credit facility under the terms of the existing Concentra first lien credit agreement. The tranche B term loans bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra first lien credit agreement) plus 2.75% (subject to an Adjusted LIBO Rate floor of 1.00%) for Eurodollar Borrowings (as defined in the Concentra first lien credit agreement), or Alternate Base Rate (as defined in the Concentra first lien credit agreement) plus 1.75% (subject to an Alternate Base Rate floor of 2.00%) for ABR Borrowings (as defined in the Concentra first lien credit agreement). All other material terms and conditions applicable to the original tranche B term loan commitments are applicable to the additional tranche B term loans created under this amendment.
In addition, Concentra entered into a second lien credit agreement (the “Concentra 2018 second lien credit agreement”) that provides for $240.0 million in term loans with an initial maturity date of June 1, 2023. Borrowings under the Concentra 2018 second lien credit agreement will bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra 2018 second lien credit agreement) plus 6.50% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Concentra 2018 second lien credit agreement) plus 5.50% (subject to an Alternate Base Rate floor of 2.00%).
Concentra used borrowings under the Concentra first lien credit agreement and the Concentra 2018 second lien credit agreement, together with cash on hand, to pay the purchase price for all of the issued and outstanding stock of U.S. HealthWorks to DHHC and to finance the redemption and reorganization transactions contemplated by the Purchase Agreement (as described above).
55
Regulatory Changes
The Medicare program reimburses us for services furnished to Medicare beneficiaries, which are generally persons age 65 and older, those who are chronically disabled, and those suffering from end stage renal disease. Net operating revenues generated directly from the Medicare program represented approximately 37%, 30%, and 30% of the Company’s net operating revenues for the years ended December 31, 2015, 2016, and 2017, respectively. The principal causes of the decrease in Medicare net operating revenues as a percentage of our total net operating revenues are the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016, which both have a significantly lower relative percentage of Medicare net operating revenues as compared to our historical business prior to the acquisitions. Since the percentage of net operating revenues generated directly from the Medicare program has been historically higher in our long term acute care and inpatient rehabilitation segments as compared to our outpatient rehabilitation and Concentra segments, we anticipate that the percentage of net operating revenues generated directly from the Medicare program will continue to decrease to the extent growth in our outpatient rehabilitation and Concentra segments outpaces growth in our long term acute care and inpatient rehabilitation segments.
The Medicare program reimburses various types of providers, including LTCHs, IRFs, and outpatient rehabilitation providers, using different payment methodologies. Those payment methodologies are complex and are described elsewhere in this report under “Business—Government Regulations.” The following is a summary of some of the more significant healthcare regulatory changes that have affected our financial performance in the periods covered by this report or are likely to affect our financial performance and financial condition in the future.
Medicare Reimbursement of Long Term Acute Care Hospital Services
There have been significant regulatory changes affecting LTCHs that have affected our net operating revenues and, in some cases, caused us to change our operating models and strategies. We have been subject to regulatory changes that occur through the rulemaking procedures of CMS. All Medicare payments to our LTCHs are made in accordance with LTCH-PPS. Proposed rules specifically related to LTCHs are generally published in May, finalized in August and effective on October 1 of each year.
The following is a summary of significant changes to the Medicare prospective payment system for LTCHs which have affected our results of operations, as well as the policies and payment rates for fiscal year 2018 that may affect our future results of operations.
Fiscal Year 2016. On August 17, 2015, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2016 (affecting discharges and cost reporting periods beginning on or after October 1, 2015 through September 30, 2016). The standard federal rate was set at $41,763, an increase from the standard federal rate applicable during fiscal year 2015 of $41,044. The update to the standard federal rate for fiscal year 2016 included a market basket increase of 2.4%, less a productivity adjustment of 0.5%, and less a reduction of 0.2% mandated by the Affordable Care Act, or the ACA. The fixed loss amount for high cost outlier cases paid under LTCH-PPS was set at $16,423, an increase from the fixed loss amount in the 2015 fiscal year of $14,972. The fixed loss amount for high cost outlier cases paid under the site neutral payment rate described below was set at $22,538.
Fiscal Year 2017. On August 22, 2016, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2017 (affecting discharges and cost reporting periods beginning on or after October 1, 2016 through September 30, 2017). The standard federal rate was set at $42,476, an increase from the standard federal rate applicable during fiscal year 2016 of $41,763. The update to the standard federal rate for fiscal year 2017 included a market basket increase of 2.8%, less a productivity adjustment of 0.3%, and less a reduction of 0.75% mandated by the ACA. The fixed‑loss amount for high cost outlier cases paid under LTCH‑PPS was set at $21,943, an increase from the fixed‑loss amount in the 2016 fiscal year of $16,423. The fixed‑loss amount for high cost outlier cases paid under the site‑neutral payment rate was set at $23,573, an increase from the fixed‑loss amount in the 2016 fiscal year of $22,538.
Fiscal Year 2018. On August 14, 2017, CMS published the final rule updating policies and payment rates for the LTCH-PPS for fiscal year 2018 (affecting discharges and cost reporting periods beginning on or after October 1, 2017 through September 30, 2018). Certain errors in the final rule were corrected in a final rule published October 4, 2017. The standard federal rate was set at $41,415, a decrease from the standard federal rate applicable during fiscal year 2017 of $42,476. The update to the standard federal rate for fiscal year 2018 included a market basket increase of 2.7%, less a productivity adjustment of 0.6%, and less a reduction of 0.75% mandated by the ACA. The update to the standard federal rate for fiscal year 2018 is impacted further by the Medicare Access and CHIP Reauthorization Act of 2015, which limits the update for fiscal year 2018 to 1.0%. The fixed-loss amount for high cost outlier cases paid under LTCH-PPS was set at $27,381, an increase from the fixed-loss amount in the 2017 fiscal year of $21,943. The fixed-loss amount for high cost outlier cases paid under the site-neutral payment rate was set at $26,537, an increase from the fixed-loss amount in the 2017 fiscal year of $23,573.
56
Patient Criteria
The BBA of 2013, enacted December 26, 2013, establishes a dual‑rate LTCH-PPS for Medicare patients discharged from an LTCH. Specifically, for Medicare patients discharged in cost reporting periods beginning on or after October 1, 2015, LTCHs will be reimbursed at the LTCH-PPS standard federal payment rate only if, immediately preceding the patient’s LTCH admission, the patient was discharged from a “subsection (d) hospital” (generally, a short‑term acute care hospital paid under IPPS) and either the patient’s stay included at least three days in an intensive care unit (ICU) or coronary care unit (CCU) at the subsection (d) hospital, or the patient was assigned to an MS-LTC-DRG for cases receiving at least 96 hours of ventilator services in the LTCH. In addition, to be paid at the LTCH-PPS standard federal payment rate, the patient’s discharge from the LTCH may not include a principal diagnosis relating to psychiatric or rehabilitation services. For any Medicare patient who does not meet these criteria, the LTCH will be paid a lower “site neutral” payment rate, which will be the lower of: (i) the IPPS comparable per diem payment rate capped at the MS-DRG payment rate plus any outlier payments; or (ii) 100 percent of the estimated costs for services.
The site neutral payment rate for those patients not paid at the LTCH-PPS standard federal payment rate is subject to a transition period. During the transition period (applicable to hospital cost reporting periods beginning on or after October 1, 2015 through September 30, 2019), a blended rate will be paid for Medicare patients not meeting the new criteria that is equal to 50% of the site neutral payment rate amount and 50% of the standard federal payment rate amount. For discharges in cost reporting periods beginning on or after October 1, 2019, only the site neutral payment rate will apply for Medicare patients not meeting the new criteria. For hospital cost reporting periods beginning on or after October 1, 2017 through September 30, 2026, the IPPS comparable per diem payment amount (including any applicable outlier payment) used to determine the site neutral payment rate will be reduced by 4.6% after any annual payment rate update.
In addition, for cost reporting periods beginning on or after October 1, 2019, qualifying discharges from an LTCH will continue to be paid at the LTCH-PPS standard federal payment rate, unless the number of discharges for which payment is made under the site‑neutral payment rate is greater than 50% of the total number of discharges from the LTCH for that period. If the number of discharges for which payment is made under the site‑neutral payment rate is greater than 50%, then beginning in the next cost reporting period all discharges from the LTCH will be reimbursed at the site‑neutral payment rate. The BBA of 2013 requires CMS to establish a process for an LTCH subject to only the site‑neutral payment rate to be reinstated for payment under the dual-rate LTCH‑PPS.
Payment adjustments, including the interrupted stay policy and the 25 Percent Rule (discussed below), apply to LTCH discharges regardless of whether the case is paid at the standard federal payment rate or the site‑neutral payment rate. However, short stay outlier payment adjustments do not apply to cases paid at the site‑neutral payment rate. CMS calculates the annual recalibration of the MS-LTC-DRG relative payment weighting factors using only data from LTCH discharges that meet the criteria for exclusion from the site‑neutral payment rate. In addition, CMS applies the IPPS fixed‑loss amount for high cost outliers to site‑neutral cases, rather than the LTCH-PPS fixed‑loss amount. CMS calculates the LTCH‑PPS fixed‑loss amount using only data from cases paid at the LTCH-PPS payment rate, excluding cases paid at the site‑neutral rate. For fiscal year 2018, the IPPS fixed-loss amount is set at $26,537 and the LTCH-PPS fixed-loss amount is $27,381.
Medicare Market Basket Adjustments
The ACA instituted a market basket payment adjustment to LTCHs. In fiscal year 2019, the market basket update will be reduced by 0.75%. The ACA specifically allows these market basket reductions to result in less than a 0% payment update and payment rates that are less than the prior year.
25 Percent Rule
The “25 Percent Rule” is a downward payment adjustment that applies if the percentage of Medicare patients discharged from LTCHs who were admitted from a referring hospital (regardless of whether the LTCH or LTCH satellite is co‑located with the referring hospital) exceeds the applicable percentage admissions threshold during a particular cost reporting period. Specifically, the payment rate for only Medicare patients above the percentage admissions threshold are subject to a downward payment adjustment. For Medicare patients above the applicable percentage admissions threshold, the LTCH is reimbursed at a rate equivalent to that under general acute care hospital IPPS, which is generally lower than LTCH-PPS rates. Cases that reach outlier status in the referring hospital do not count toward the admissions threshold and are paid under LTCH-PPS.
57
Current law, as amended by the 21st Century Cures Act, precludes CMS from applying the 25 Percent Rule for freestanding LTCHs to cost reporting years beginning before July 1, 2016 and for discharges occurring on or after October 1, 2016 and before October 1, 2017. In addition, current law applies higher percentage admissions thresholds under the 25 Percent Rule for most HIHs and satellites for cost reporting years beginning before July 1, 2016 and effective for discharges occurring on or after October 1, 2016 and before October 1, 2017. For freestanding LTCHs the percentage admissions threshold is suspended during the relief periods. For most HIHs and satellites the percentage admissions threshold is raised from 25% to 50% during the relief periods. In the special case of rural LTCHs, LTCHs co‑located with an urban single hospital, or LTCHs co‑located with an MSA dominant hospital the referral percentage was raised from 50% to 75%. Grandfathered HIHs are exempt from the 25 Percent Rule regulations.
For fiscal year 2018, CMS adopted a regulatory moratorium on the implementation of the 25 Percent Rule. As a result, the 25 Percent Rule does not apply until discharges occurring on or after October 1, 2018. After the expiration of the regulatory moratorium, as described above, our LTCHs (whether freestanding, HIH or satellite) will be subject to a downward payment adjustment for any Medicare patients who were admitted from a co‑located or a non-co-located hospital and that exceed the applicable percentage admissions threshold of all Medicare patients discharged from the LTCH during the cost reporting period. These regulatory changes have the potential to cause an adverse financial impact on the net operating revenues and profitability of many of these hospitals for discharges on or after October 1, 2018.
Short Stay Outlier Policy
CMS established a different payment methodology for Medicare patients with a length of stay less than or equal to five‑sixths of the geometric average length of stay for that particular MS-LTC-DRG, referred to as a short stay outlier, or “SSO.” For discharges before October 1, 2017, SSO cases were paid based on the lesser of (i) 100% of the average cost of the case, (ii) 120% of the MS-LTC-DRG specific per diem amount multiplied by the patient’s length of stay, (iii) the full MS-LTC-DRG payment, or (iv) a per diem rate derived from blending 120% of the MS-LTC-DRG specific per diem amount with a per diem rate based on the general acute care hospital IPPS.
The SSO rule also had a category referred to as a “very short stay outlier,” which applied to cases with a length of stay that is less than the average length of stay plus one standard deviation for the same MS-DRG under IPPS, referred to as the so-called “IPPS comparable threshold.” The LTCH payment for very short stay outlier cases was equivalent to the general acute care hospital IPPS per diem rate.
For fiscal year 2018, CMS adopted changes to the SSO policy such that all SSO cases discharged on or after October 1, 2017 are paid based on a per diem rate derived from blending 120% of the MS-LTC-DRG specific per diem amount with a per diem rate based on the general acute care hospital IPPS (i.e., the fourth option under the prior policy). Under this policy, as the length of stay of a SSO case increases, the percentage of the per diem payment amounts based on the full MS-LTCH-DRG standard federal payment rate increases and the percentage of the payment based on the IPPS comparable amount decreases. In addition, the very short stay outlier category was eliminated.
Expiration of Moratorium on New LTCHs, LTCH Satellite Facilities and LTCH Beds
Federal law imposed a temporary moratorium on the establishment and classification of new LTCHs or LTCH satellite facilities, and on the increase of LTCH beds in existing LTCHs or satellite facilities through September 30, 2017, subject to certain exceptions. As a result of the expiration of the moratorium, qualifying hospitals may now be classified as new LTCHs or LTCH satellite facilities, and existing LTCHs may increase their bed count.
Medicare Reimbursement of Inpatient Rehabilitation Facility Services
The following is a summary of significant changes to the Medicare prospective payment system for IRFs which have affected our results of operations, as well as the policies and payment rates for fiscal year 2017 that may affect our future results of operations.
Fiscal Year 2016. On August 6, 2015, CMS published the final rule updating policies and payment rates for the IRF-PPS for fiscal year 2016 (affecting discharges and cost reporting periods beginning on or after October 1, 2015 through September 30, 2016). The standard payment conversion factor for discharges for fiscal year 2016 was set at $15,478, an increase from the standard payment conversion factor applicable during fiscal year 2015 of $15,198. The update to the standard payment conversion factor for fiscal year 2016 included a market basket increase of 2.4%, less a productivity adjustment of 0.5%, and less a reduction of 0.2% mandated by the ACA. CMS decreased the outlier threshold amount for fiscal year 2016 to $8,658 from $8,848 established in the final rule for fiscal year 2015.
58
Fiscal Year 2017. On August 5, 2016, CMS published the final rule updating policies and payment rates for the IRF‑PPS for fiscal year 2017 (affecting discharges and cost reporting periods beginning on or after October 1, 2016 through September 30, 2017). The standard payment conversion factor for discharges for fiscal year 2017 was set at $15,708, an increase from the standard payment conversion factor applicable during fiscal year 2016 of $15,478. The update to the standard payment conversion factor for fiscal year 2017 included a market basket increase of 2.7%, less a productivity adjustment of 0.3%, and less a reduction of 0.75% mandated by the ACA. CMS decreased the outlier threshold amount for fiscal year 2017 to $7,984 from $8,658 established in the final rule for fiscal year 2016.
Fiscal Year 2018. On August 3, 2017, CMS published the final rule updating policies and payment rates for the IRF‑PPS for fiscal year 2018 (affecting discharges and cost reporting periods beginning on or after October 1, 2017 through September 30, 2018). The standard payment conversion factor for discharges for fiscal year 2018 was set at $15,838, an increase from the standard payment conversion factor applicable during fiscal year 2017 of $15,708. The update to the standard payment conversion factor for fiscal year 2018 included a market basket increase of 2.6%, less a productivity adjustment of 0.6%, and less a reduction of 0.75% mandated by the ACA. The standard payment conversion factor for fiscal year 2018 is impacted further by the Medicare Access and CHIP Reauthorization Act of 2015, which limits the update for fiscal year 2018 to 1.0%. CMS increased the outlier threshold amount for fiscal year 2018 to $8,679 from $7,984 established in the final rule for fiscal year 2017.
Medicare Market Basket Adjustments
The ACA instituted a market basket payment adjustment for IRFs. In fiscal year 2019, the market basket update will be reduced by 0.75%. The ACA specifically allows these market basket reductions to result in less than a 0% payment update and payment rates that are less than the prior year.
Patient Classification Criteria
In order to qualify as an IRF, a hospital must demonstrate that during its most recent 12-month cost reporting period it served an inpatient population of whom at least 60% required intensive rehabilitation services for one or more of 13 conditions specified by regulation. Compliance with the 60% Rule is demonstrated through either medical review or the “presumptive” method, in which a patient’s diagnosis codes are compared to a “presumptive compliance” list. For fiscal year 2018, CMS revised the 60% Rule’s presumptive methodology (i) including certain International Classification of Diseases, Tenth Revision, Clinical Modification, or ICD-10-CM, diagnosis codes for patients with traumatic brain injury and hip fracture conditions and (ii) revising the presumptive methodology list for major multiple trauma by counting IRF cases that contain two or more of the ICD-10-CM codes from three major multiple trauma lists in the specified combinations.
Medicare Reimbursement of Outpatient Rehabilitation Clinic Services
The Medicare program reimburses outpatient rehabilitation providers based on the Medicare physician fee schedule. For services provided in 2017 through 2019, a 0.5% update will be applied each year to the fee schedule payment rates, subject to an adjustment beginning in 2019 under the Merit‑Based Incentive Payment System (“MIPS”). For services provided in 2020 through 2025, a 0.0% percent update will be applied each year to the fee schedule payment rates, subject to adjustments under MIPS and the alternative payment models (“APMs”). In 2026 and subsequent years eligible professionals participating in APMs that meet certain criteria would receive annual updates of 0.75%, while all other professionals would receive annual updates of 0.25%.
Beginning in 2019, payments under the fee schedule are subject to adjustment based on performance in MIPS, which measures performance based on certain quality metrics, resource use, and meaningful use of electronic health records. Under the MIPS requirements a provider’s performance is assessed according to established performance standards and used to determine an adjustment factor that is then applied to the professional’s payment for a year. Each year from 2019 through 2024 professionals who receive a significant share of their revenues through an APM (such as accountable care organizations or bundled payment arrangements) that involves risk of financial losses and a quality measurement component will receive a 5% bonus. The bonus payment for APM participation is intended to encourage participation and testing of new APMs and to promote the alignment of incentives across payors. The specifics of the MIPS and APM adjustments beginning in 2019 and 2020, respectively, will be subject to future notice and comment rule‑making. For the year ended December 31, 2017, we received approximately 15% of our outpatient rehabilitation net operating revenues from Medicare.
Therapy Caps
Outpatient therapy providers reimbursed under the Medicare physician fee schedule have been subject to annual limits for therapy expenses. For example, for the calendar year beginning January 1, 2017, the annual limit on outpatient therapy services was $1,980 for combined physical and speech language pathology services and $1,980 for occupational therapy services. The Bipartisan Budget Act of 2018 repealed the annual limits on outpatient therapy.
59
The annual limits for therapy expenses historically did not apply to services furnished and billed by outpatient hospital departments. However, the Medicare Access and CHIP Reauthorization Act of 2015, and prior legislation, extended the annual limits on therapy expenses in hospital outpatient department settings through December 31, 2017. The application of annual limits to hospital outpatient department settings sunset on December 31, 2017.
Prior to calendar year 2028, all therapy claims exceeding $3,000 are subject to a manual medical review process. The $3,000 threshold is applied to physical therapy and speech therapy services combined and separately applied to occupational therapy. CMS will continue to require that an appropriate modifier be included on claims over the current exception threshold indicating that the therapy services are medically necessary. Beginning in 2028 and in each calendar year thereafter, the threshold amount for claims requiring manual medical review will increase by the percentage increase in the Medicare Economic Index.
60
Critical Accounting Matters
Contractual Adjustments
Net operating revenues include amounts estimated by us to be reimbursable by Medicare and Medicaid under prospective payment systems and provisions of cost-reimbursement and other payment methods. In addition, we are reimbursed by non-governmental payors using a variety of payment methodologies. Amounts we receive for treatment of patients covered by these programs are generally less than the standard billing rates. Contractual allowances are calculated and recorded through our internally developed systems. In our long term acute care and inpatient rehabilitation segments, our billing system automatically calculates estimated Medicare reimbursement and associated contractual allowances. For non-governmental payors in our long term acute care segment, we manually calculate the contractual allowance for each patient based upon the contractual provisions associated with the specific payor. For non-governmental payors in our inpatient rehabilitation segment, we monitor payors’ historical closed paid claims data and apply those payment rates to the existing patient population. The net payments are converted into per diem rates. The per diem rates are applied to unpaid patient days to determine the expected payment and a contractual adjustment is recorded to adjust the recorded amount to agree with the expected payment. Quarterly, we update our analysis of historical closed paid claims. In our outpatient rehabilitation and Concentra segments, we perform provision testing using internally developed systems. We monitor our payors’ historical paid claims data and compare it against the associated gross charges. The difference is determined as a percentage of gross charges and is applied against gross billing revenue to determine the contractual allowances for the period. Additionally, these contractual percentages are applied against our gross receivables to determine that adequate contractual reserves are maintained for the gross accounts receivables reported on the balance sheet. We account for any difference as additional contractual adjustments to gross revenues to arrive at net operating revenues in the period that the difference is determined. We believe the processes used in recording our contractual adjustments, as described above, have resulted in reasonable estimates determined on a consistent basis.
Allowance for Doubtful Accounts
Substantially all of our accounts receivable are related to providing healthcare services to patients. Collection of these accounts receivable is our primary source of cash and is critical to our financial performance. Our primary collection risks relate to non-governmental payors who insure these patients and deductibles, co-payments, and self-insured amounts owed by the patient. Deductibles, co-payments, and self-insured amounts are an immaterial portion of our net accounts receivable balance. At December 31, 2017, deductibles, co-payments, and self-insured amounts owed by patients accounted for approximately 0.6% of our net accounts receivable balance before doubtful accounts. Our general policy is to verify insurance coverage prior to the date of admission for patients admitted to our LTCHs and IRFs. Within our outpatient rehabilitation clinics, we verify insurance coverage prior to the patient’s visit. Within our Concentra centers, we verify insurance coverage or receive authorization from the patient’s employer prior to the patient’s visit. Our estimate for the allowance for doubtful accounts is calculated by applying a reserve allowance based upon the age of an account balance. This method is monitored based on historical cash collections experience and write-off experience. Collections are impacted by the effectiveness of our collection efforts with non-governmental payors and regulatory or administrative disruptions with the fiscal intermediaries that pay our governmental receivables.
We estimate bad debts for total accounts receivable within each of our operating units. We believe our policies have resulted in reasonable estimates determined on a consistent basis. We have historically collected substantially all of our third-party insured receivables (net of contractual allowances) which include receivables from governmental agencies. Historically, there has not been a material difference between our bad debt allowances and the ultimate historical collection rates on accounts receivable. We review our overall reserve adequacy by monitoring historical cash collections as a percentage of net revenue less the provision for bad debts. Uncollected accounts are charged against the reserve when they are turned over to an outside collection agency, or when management determines that the balance is uncollectible, whichever occurs first.
The following table is an aging of our accounts receivable (after allowances for contractual adjustments but before doubtful accounts) as of the dates indicated (in thousands):
December 31, | |||||||||||||||||
2016 | 2017 | ||||||||||||||||
0 - 180 Days | Over 180 Days | 0 - 180 Days | Over 180 Days | ||||||||||||||
Commercial insurance and other | $ | 415,858 | $ | 59,218 | $ | 436,098 | $ | 76,493 | |||||||||
Medicare and Medicaid | 148,395 | 14,068 | 241,927 | 12,758 | |||||||||||||
Total accounts receivable | $ | 564,253 | $ | 73,286 | $ | 678,025 | $ | 89,251 | |||||||||
61
The approximate percentage of total accounts receivable (after allowance for contractual adjustments but before doubtful accounts) summarized by aging categories as of the dates indicated is as follows:
December 31, | |||||||
2016 | 2017 | ||||||
0 to 90 days | 77.8 | % | 80.0 | % | |||
91 to 180 days | 10.7 | % | 8.4 | % | |||
181 to 365 days | 6.9 | % | 6.5 | % | |||
Over 365 days | 4.6 | % | 5.1 | % | |||
Total | 100.0 | % | 100.0 | % | |||
The approximate percentage of total accounts receivable (after allowance for contractual adjustments but before doubtful accounts) summarized by insured status as of the dates indicated is as follows:
December 31, | |||||||
2016 | 2017 | ||||||
Commercial insurance and other | 73.3 | % | 66.2 | % | |||
Medicare and Medicaid | 25.5 | % | 33.2 | % | |||
Self-pay receivables (including deductibles and co-payments) | 1.2 | % | 0.6 | % | |||
Total | 100.0 | % | 100.0 | % | |||
Insurance
Under a number of our insurance programs, which include our employee health insurance, workers’ compensation, and professional malpractice liability insurance programs, we are liable for a portion of our losses before we can attempt to recover from the applicable insurance carrier. We accrue for losses for which we will be ultimately responsible under an occurrence-based approach, whereby we estimate the losses that will be incurred in a respective accounting period and accrue that estimated liability using actuarial methods. We monitor these programs quarterly and revise our estimates as necessary to take into account additional information. We recorded a liability of $147.4 million and $157.1 million for our estimated losses under these insurance programs at December 31, 2016 and 2017, respectively.
Related Party Transactions
We are party to various rental and other agreements with related parties. Our payments to these related parties amounted to $4.7 million, $5.0 million, and $6.2 million for the years ended December 31, 2015, 2016, and 2017, respectively. Our future commitments are related to commercial office space we lease for our corporate headquarters in Mechanicsburg, Pennsylvania. These future commitments as of December 31, 2017 amount to $34.1 million payable through 2027. These transactions and commitments are described more fully in the notes to our consolidated financial statements included herein. Our practice is that any such transaction must receive the prior approval of both the audit and compliance committee of the board of directors and a majority of non-interested members of the board of directors. It is our practice that an independent third-party appraisal supporting the amount of rent for such leased space is obtained prior to approving the related party lease of office space.
We also provide contracted services, principally employee leasing services, and charge management fees to related parties affiliated through our equity investments. Net operating revenues generated from contracted services and management fees charged to related parties affiliated through our equity investments were $146.0 million, $164.2 million, and $178.1 million for the years ended December 31, 2015, 2016 and 2017, respectively.
62
Intangible Assets
Goodwill and other indefinite‑lived intangible assets are not amortized, but instead are subject to periodic impairment evaluations. Impairment tests are required to be conducted at least annually or when events or conditions occur that might suggest a possible impairment. These events or conditions include, but are not limited to: a significant adverse change in the business environment, regulatory environment or legal factors; a current period operating or cash flow loss combined with a history of such losses or a projection of continuing losses; or a sale or disposition of a significant portion of a reporting unit. The occurrence of one of these events or conditions could significantly impact an impairment assessment, necessitating an impairment charge.
In performing the quantitative periodic impairment tests for goodwill, the fair value of the reporting unit is compared to its carrying value, including goodwill and other intangible assets. If the carrying value exceeds the fair value and an impairment condition exists, an impairment loss would be recognized. When we determine the fair value of its reporting units, we consider both the income and market approach. Included in the income approach, specific for each reporting unit, are assumptions regarding revenue growth rate, future Adjusted EBITDA margin estimates, future general and administrative expense rates, and the industry’s weighted average cost of capital and industry specific, market comparable implied Adjusted EBITDA multiples. We also must estimate residual values at the end of the forecast period and future capital expenditure requirements. Each of these assumptions requires us to use our knowledge of the industry, our recent transactions, and reasonable performance expectations for our operations. If any one of the above assumptions changes or fails to materialize, the resulting decline in our estimated fair value could result in an impairment charge to the goodwill associated with any one of the reporting units. Additionally, regulatory changes governing the provision of our services and development activities can have both positive and negative effects on our results of operations and future cash flows which impact the fair value of our reporting units.
At December 31, 2017, our indefinite-lived intangible assets consist of trademarks, certificates of need, and accreditations. In performing the quantitative periodic impairment tests for our trademarks, the fair value of the trademark is compared to its carrying value. If the carrying value exceeds the fair value and an impairment condition exists, an impairment loss would be recognized. To determine the fair value of the trademark, we use a relief from royalty income approach. For our certificates of need and accreditations, we perform a qualitative assessment. As part of this assessment, we evaluate the current business environment, regulatory environment, legal and other company-specific factors. If it is more likely than not that the fair value is less than the carrying value, we perform a quantitative impairment test.
Our most recent impairment assessment was completed during the fourth quarter of 2017 utilizing financial information as of October 1, 2017. We did not identify any instances of impairment with respect to goodwill or other indefinite-lived intangible assets as of October 1, 2017. The percentages by which the fair values exceed the carrying values for our specialty hospitals, outpatient rehabilitation, and Concentra reporting units were approximately 151%, 186%, and 168%, respectively, at October 1, 2017. Our impairment assessments completed during the fourth quarters of 2015 and 2016 indicated that there was no impairment with respect to goodwill or other identifiable intangible assets.
During the fourth quarter of 2017, we determined that we were operating through four operating segments, which resulted in a change to our reporting units. As of December 31, 2017, our reporting units include long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. Goodwill was allocated to the long term acute care and inpatient rehabilitation reporting units based upon the relative fair values of these reporting units. The Company completed an assessment of potential goodwill impairment for each of these reporting units immediately after the allocation of goodwill and determined that no impairment existed. The percentages by which the fair values exceed the carrying values for our long term acute care and inpatient rehabilitation reporting units were approximately 158% and 135%.
We have recorded total goodwill and other identifiable intangible assets of $3.1 billion at December 31, 2017, of which $1.1 billion relates to our long term acute care reporting unit, $439.9 million relates to our inpatient rehabilitation reporting unit, $709.0 million relates to our outpatient rehabilitation reporting unit, and $891.9 million relates to the Concentra reporting unit.
63
Realization of Deferred Tax Assets
Deferred tax assets and liabilities are required to be recognized using enacted tax rates for the effect of temporary differences between the book and tax bases of recorded assets and liabilities. Deferred tax assets are also required to be reduced by a valuation allowance if it is more likely than not that some portion or all of the deferred tax asset will not be realized. As part of the process of preparing our consolidated financial statements, we estimate our income taxes based on our actual current tax exposure together with assessing temporary differences resulting from differing treatment of items for tax and accounting purposes. We also recognize as deferred tax assets the future tax benefits from net operating loss carry forwards. We evaluate the realizability of these deferred tax assets by assessing their valuation allowances and by adjusting the amount of such allowances, if necessary. Among the factors used to assess the likelihood of realization are our projections of future taxable income streams, the expected timing of the reversals of existing temporary differences, and the impact of tax planning strategies that could be implemented to avoid the potential loss of future tax benefits. However, changes in tax codes, statutory tax rates or future taxable income levels could materially impact our valuation of tax accruals and assets and could cause our provision for income taxes to vary significantly from period to period.
At December 31, 2017, we had deferred tax liabilities in excess of deferred tax assets of approximately $105.5 million million principally due to depreciation deductions that have been accelerated for tax purposes and amortization of intangibles and goodwill. This amount includes approximately $13.0 million of valuation reserves related primarily to state net operating losses.
64
Operating Statistics
The following table sets forth operating statistics for each of our operating segments for each of the periods presented. The operating statistics reflect data for the period of time we managed these operations:
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Long term acute care data: | |||||||||||||
Number of hospitals owned—start of period | 112 | 108 | 102 | ||||||||||
Number of hospitals acquired | — | 4 | 1 | ||||||||||
Number of hospital start-ups | 1 | — | 1 | ||||||||||
Number of hospitals closed/sold | (5 | ) | (10 | ) | (5 | ) | |||||||
Number of hospitals owned—end of period | 108 | 102 | 99 | ||||||||||
Number of hospitals managed—end of period | 1 | 1 | 1 | ||||||||||
Total number of hospitals (all)—end of period | 109 | 103 | 100 | ||||||||||
Available licensed beds(1) | 4,448 | 4,254 | 4,159 | ||||||||||
Admissions(1) | 41,993 | 36,859 | 35,793 | ||||||||||
Patient days(1) | 1,179,020 | 1,041,074 | 1,003,161 | ||||||||||
Average length of stay (days)(1) | 28 | 28 | 28 | ||||||||||
Net revenue per patient day(1)(2) | $ | 1,596 | $ | 1,690 | $ | 1,735 | |||||||
Occupancy rate(1) | 70 | % | 65 | % | 66 | % | |||||||
Percent patient days—Medicare(1) | 61 | % | 55 | % | 54 | % | |||||||
Inpatient rehabilitation data: | |||||||||||||
Number of facilities owned—start of period | 8 | 10 | 13 | ||||||||||
Number of facilities acquired | 1 | 1 | — | ||||||||||
Number of facilities start-ups | 1 | 2 | 3 | ||||||||||
Number of facilities closed/sold | — | — | — | ||||||||||
Number of facilities owned—end of period | 10 | 13 | 16 | ||||||||||
Number of facilities managed—end of period | 8 | 7 | 8 | ||||||||||
Total number of facilities (all)—end of period | 18 | 20 | 24 | ||||||||||
Available licensed beds(1) | 724 | 983 | 1,133 | ||||||||||
Admissions(1) | 13,598 | 14,670 | 18,841 | ||||||||||
Patient days(1) | 194,760 | 216,994 | 269,905 | ||||||||||
Average length of stay (days)(1) | 14 | 15 | 14 | ||||||||||
Net revenue per patient day(1)(2) | $ | 1,406 | $ | 1,465 | $ | 1,609 | |||||||
Occupancy rate(1) | 80 | % | 71 | % | 72 | % | |||||||
Percent patient days—Medicare(1) | 53 | % | 53 | % | 54 | % | |||||||
Outpatient rehabilitation data: | |||||||||||||
Number of clinics owned—start of period | 880 | 896 | 1,445 | ||||||||||
Number of clinics acquired | 7 | 559 | 13 | ||||||||||
Number of clinic start-ups | 34 | 28 | 28 | ||||||||||
Number of clinics closed/sold | (25 | ) | (38 | ) | (39 | ) | |||||||
Number of clinics owned—end of period | 896 | 1,445 | 1,447 | ||||||||||
Number of clinics managed—end of period | 142 | 166 | 169 | ||||||||||
Total number of clinics (all)—end of period | 1,038 | 1,611 | 1,616 | ||||||||||
Number of visits(1) | 5,218,532 | 7,799,208 | 8,232,536 | ||||||||||
Net revenue per visit(1)(3) | $ | 103 | $ | 102 | $ | 103 | |||||||
65
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Concentra data:(4) | |||||||||||||
Number of centers owned—start of period | — | 300 | 300 | ||||||||||
Number of centers acquired | 300 | 4 | 11 | ||||||||||
Number of clinic start-ups | — | — | 4 | ||||||||||
Number of centers closed/sold | — | (4 | ) | (3 | ) | ||||||||
Number of centers owned—end of period | 300 | 300 | 312 | ||||||||||
Number of visits(1) | 4,436,977 | 7,373,751 | 7,709,508 | ||||||||||
Net revenue per visit(1)(3) | $ | 114 | $ | 118 | $ | 117 | |||||||
_______________________________________________________________________________
(1) | Data excludes locations managed by the Company. For purposes of our Concentra segment, onsite clinics and community-based outpatient clinics are excluded. |
(2) | Net revenue per patient day is calculated by dividing direct patient service revenues by the total number of patient days. |
(3) | Net revenue per visit is calculated by dividing direct patient service revenue by the total number of visits. For purposes of this computation for our outpatient rehabilitation segment, direct patient service clinic revenue does not include contract therapy revenue. For purposes of this computation for our Concentra segment, direct patient service revenue does not include onsite clinics and community-based outpatient clinics. |
(4) | The selected financial data for the Company’s Concentra segment for the periods presented begins as of June 1, 2015, which is the date the Concentra acquisition was consummated. |
Results of Operations
The following table outlines selected operating data as a percentage of net operating revenues for the periods indicated:
For the Year Ended December 31, | ||||||||||
2015 | 2016 | 2017 | ||||||||
Net operating revenues | 100.0 | % | 100.0 | % | 100.0 | % | ||||
Cost of services(1) | 85.8 | 85.5 | 84.0 | |||||||
General and administrative | 2.5 | 2.5 | 2.6 | |||||||
Bad debt expense | 1.6 | 1.6 | 1.8 | |||||||
Depreciation and amortization | 2.8 | 3.4 | 3.6 | |||||||
Income from operations | 7.3 | 7.0 | 8.0 | |||||||
Loss on early retirement of debt | — | (0.3 | ) | (0.4 | ) | |||||
Equity in earnings of unconsolidated subsidiaries | 0.4 | 0.5 | 0.5 | |||||||
Non-operating gain (loss) | 0.8 | 1.0 | — | |||||||
Interest expense, net | (2.9 | ) | (4.0 | ) | (3.5 | ) | ||||
Income before income taxes | 5.6 | 4.2 | 4.6 | |||||||
Income tax expense (benefit) | 2.0 | 1.3 | (0.4 | ) | ||||||
Net income | 3.6 | 2.9 | 5.0 | |||||||
Net income attributable to non-controlling interests | 0.1 | 0.2 | 1.0 | |||||||
Net income attributable to Holdings and Select | 3.5 | % | 2.7 | % | 4.0 | % | ||||
_______________________________________________________________________________
(1) | Cost of services includes salaries, wages and benefits, operating supplies, lease and rent expense and other operating costs. |
66
The following table summarizes selected financial data by business segment for the periods indicated:
Year Ended December 31, | |||||||||||||||||||
2015 | 2016 | 2017 | % Change 2015 - 2016 | % Change 2016 - 2017 | |||||||||||||||
Net operating revenues: | |||||||||||||||||||
Long term acute care | $ | 1,902,776 | $ | 1,785,164 | $ | 1,756,243 | (6.2 | )% | (1.6 | )% | |||||||||
Inpatient rehabilitation | 444,005 | 504,318 | 631,777 | 13.6 | 25.3 | ||||||||||||||
Outpatient rehabilitation(1) | 810,009 | 995,374 | 1,020,848 | 22.9 | 2.6 | ||||||||||||||
Concentra(2) | 585,222 | 1,000,624 | 1,034,035 | N/M | 3.3 | ||||||||||||||
Other(3) | 724 | 541 | 700 | N/M | N/M | ||||||||||||||
Total company | $ | 3,742,736 | $ | 4,286,021 | $ | 4,443,603 | 14.5 | % | 3.7 | % | |||||||||
Income (loss) from operations: | |||||||||||||||||||
Long term acute care | $ | 212,989 | $ | 180,747 | $ | 206,936 | (15.1 | )% | 14.5 | % | |||||||||
Inpatient rehabilitation | 60,642 | 44,179 | 69,865 | (27.1 | ) | 58.1 | |||||||||||||
Outpatient rehabilitation(1) | 85,167 | 107,169 | 107,926 | 25.8 | 0.7 | ||||||||||||||
Concentra(2) | 8,926 | 81,522 | 91,804 | N/M | 12.6 | ||||||||||||||
Other(3) | (92,934 | ) | (113,770 | ) | (120,653 | ) | (22.4 | ) | (6.0 | ) | |||||||||
Total company | $ | 274,790 | $ | 299,847 | $ | 355,878 | 9.1 | % | 18.7 | % | |||||||||
Adjusted EBITDA: | |||||||||||||||||||
Long term acute care | $ | 258,223 | $ | 224,609 | $ | 252,679 | (13.0 | )% | 12.5 | % | |||||||||
Inpatient rehabilitation | 69,400 | 56,902 | 90,041 | (18.0 | ) | 58.2 | |||||||||||||
Outpatient rehabilitation(1) | 98,220 | 129,830 | 132,533 | 32.2 | 2.1 | ||||||||||||||
Concentra(2) | 48,301 | 143,009 | 157,561 | N/M | 10.2 | ||||||||||||||
Other(3) | (74,979 | ) | (88,543 | ) | (94,822 | ) | (18.1 | ) | (7.1 | ) | |||||||||
Total company | $ | 399,165 | $ | 465,807 | $ | 537,992 | 16.7 | % | 15.5 | % | |||||||||
Adjusted EBITDA margins: | |||||||||||||||||||
Long term acute care | 13.6 | % | 12.6 | % | 14.4 | % | |||||||||||||
Inpatient rehabilitation | 15.6 | 11.3 | 14.3 | ||||||||||||||||
Outpatient rehabilitation(1) | 12.1 | 13.0 | 13.0 | ||||||||||||||||
Concentra(2) | 8.3 | 14.3 | 15.2 | ||||||||||||||||
Other(3) | N/M | N/M | N/M | ||||||||||||||||
Total company | 10.7 | % | 10.9 | % | 12.1 | % | |||||||||||||
Total assets:(4) | |||||||||||||||||||
Long term acute care | $ | 1,954,823 | $ | 1,910,013 | $ | 1,848,783 | |||||||||||||
Inpatient rehabilitation | 470,290 | 621,105 | 868,517 | ||||||||||||||||
Outpatient rehabilitation | 548,242 | 969,014 | 954,661 | ||||||||||||||||
Concentra | 1,311,631 | 1,313,176 | 1,340,919 | ||||||||||||||||
Other(3) | 103,692 | 107,318 | 114,286 | ||||||||||||||||
Total company | $ | 4,388,678 | $ | 4,920,626 | $ | 5,127,166 | |||||||||||||
Purchases of property and equipment, net: | |||||||||||||||||||
Long term acute care | $ | 39,784 | $ | 48,626 | $ | 49,720 | |||||||||||||
Inpatient rehabilitation | 86,230 | 60,513 | 96,477 | ||||||||||||||||
Outpatient rehabilitation(1) | 17,768 | 21,286 | 27,721 | ||||||||||||||||
Concentra(2) | 26,771 | 15,946 | 28,912 | ||||||||||||||||
Other(3) | 12,089 | 15,262 | 30,413 | ||||||||||||||||
Total company | $ | 182,642 | $ | 161,633 | $ | 233,243 | |||||||||||||
67
_______________________________________________________________________________
N/M—Not Meaningful.
(1) | The outpatient rehabilitation segment includes the operating results of our contract therapy businesses through March 31, 2016 and Physiotherapy beginning March 4, 2016. |
(2) | Concentra’s financial results are consolidated with Select’s effective June 1, 2015. |
(3) | Other includes our corporate services and certain other non-consolidating joint ventures and minority investments in other healthcare related businesses. |
(4) | As of December 31, 2016, total assets were retrospectively conformed to reflect the adoption ASU 2015-17, Balance Sheet Classification of Deferred Taxes, which resulted in a reduction to total assets of $23.8 million. |
Year Ended December 31, 2017 Compared to Year Ended December 31, 2016
In the following, we discuss our results of operations related to net operating revenues, operating expenses, Adjusted EBITDA, depreciation and amortization, income from operations, loss on early retirement of debt, equity in earnings of unconsolidated subsidiaries, non-operating gain (loss), interest expense, income taxes, and non-controlling interest, which, in each case, are the same for Holdings and Select.
Net Operating Revenues
Our net operating revenues increased 3.7% to $4,443.6 million for the year ended December 31, 2017, compared to $4,286.0 million for the year ended December 31, 2016.
Long Term Acute Care Segment. Net operating revenues were $1,756.2 million for the year ended December 31, 2017, compared to $1,785.2 million for the year ended December 31, 2016. The decline in net operating revenues was principally due to a decrease in patient days as a result of hospital closures. We had 1,003,161 patient days for the year ended December 31, 2017, compared to 1,041,074 days for the year ended December 31, 2016. The decline in net operating revenues attributable to a decrease in patient days was offset in part by an increase in our net revenue per patient day. Our net revenue per patient day increased 2.7% to $1,735 for the year ended December 31, 2017, compared to $1,690 for the year ended December 31, 2016. The increase in net revenue per patient day was principally due to higher-acuity patient populations in our LTCHs, which was caused by the changes in operations we made in response to Medicare patient criteria regulations.
Inpatient Rehabilitation Segment. Net operating revenues increased 25.3% to $631.8 million for the year ended December 31, 2017, compared to $504.3 million for the year ended December 31, 2016. The increase in net operating revenues is principally due to several new inpatient rehabilitation facilities which commenced operations during 2016 and 2017. Our patient days increased 24.4% to 269,905 days for the year ended December 31, 2017, compared to 216,994 days for the year ended December 31, 2016. Our net revenue per patient day increased 9.8% to $1,609 for the year ended December 31, 2017, compared to $1,465 for the year ended December 31, 2016.
Outpatient Rehabilitation Segment. Net operating revenues increased 2.6% to $1,020.8 million for the year ended December 31, 2017, compared to $995.4 million for the year ended December 31, 2016. The increase in net operating revenues was principally due to the acquisition of Physiotherapy on March 4, 2016, offset in part by the sale of our contract therapy businesses on March 31, 2016. Visits increased 5.6% to 8,232,536 for the year ended December 31, 2017, compared to 7,799,208 visits for the year ended December 31, 2016. The increase in visits was principally due to Physiotherapy. Net revenue per visit increased 1.0% to $103 for the year ended December 31, 2017, compared to $102 for the year ended December 31, 2016.
Concentra Segment. Net operating revenues increased 3.3% to $1,034.0 million for the year ended December 31, 2017, compared to $1,000.6 million for the year ended December 31, 2016. The increase in net operating revenues was principally due to newly acquired and developed centers. Visits in our centers increased 4.6% to 7,709,508 for the year ended December 31, 2017, compared to 7,373,751 visits for the year ended December 31, 2016. The growth in visits principally related to an increase in employer services visits. Net revenue per visit was $117 for the year ended December 31, 2017, compared to $118 for the year ended December 31, 2016. The decrease in net revenue per visit is principally due to an increased proportion of employer service visits, which yield lower per visit rates.
68
Operating Expenses
Our operating expenses include our cost of services, general and administrative expense, and bad debt expense. Our operating expenses were $3,927.7 million, or 88.4% of net operating revenues, for the year ended December 31, 2017, compared to $3,840.9 million, or 89.6% of net operating revenues, for the year ended December 31, 2016. Our cost of services, a major component of which is labor expense, was $3,734.2 million, or 84.0% of net operating revenues, for the year ended December 31, 2017, compared to $3,664.8 million, or 85.5% of net operating revenues, for the year ended December 31, 2016. The decrease in our operating expenses relative to our net operating revenues is principally due to the improved operating performance of our start-up inpatient rehabilitation facilities and cost reductions achieved within our long term acute care and Concentra segments. Facility rent expense, a component of cost of services, was $230.1 million for the year ended December 31, 2017, compared to $225.6 million for the year ended December 31, 2016. General and administrative expenses were $114.0 million, or 2.6% of net operating revenues, for the year ended December 31, 2017, compared to $106.9 million, or 2.5% of net operating revenues, for the year ended December 31, 2016. General and administrative expenses included $2.8 million of U.S. HealthWorks acquisition costs and $3.2 million of Physiotherapy acquisition costs for the years ended December 31, 2017 and 2016, respectively. Our bad debt expense was $79.5 million, or 1.8% of net operating revenues, for the year ended December 31, 2017, compared to $69.1 million, or 1.6% of net operating revenues, for the year ended December 31, 2016. The increase was principally the result of increases in bad debt expense in our long term acute care, inpatient rehabilitation, and Concentra segments.
Adjusted EBITDA
Long Term Acute Care Segment. Adjusted EBITDA increased 12.5% to $252.7 million for the year ended December 31, 2017, compared to $224.6 million for the year ended December 31, 2016. Our Adjusted EBITDA margin for the long term acute care segment was 14.4% for the year ended December 31, 2017, compared to 12.6% for the year ended December 31, 2016. The increases in Adjusted EBITDA and Adjusted EBITDA margin for the year ended December 31, 2017, compared to the year ended December 31, 2016 are principally due to an increase in our net revenue per patient day, as described above under “Net Operating Revenues,” while maintaining a consistent cost structure.
Inpatient Rehabilitation Segment. Adjusted EBITDA increased 58.2% to $90.0 million for the year ended December 31, 2017, compared to $56.9 million for the year ended December 31, 2016. Our Adjusted EBITDA margin for the inpatient rehabilitation segment was 14.3% for the year ended December 31, 2017, compared to 11.3% for the year ended December 31, 2016. The increases in Adjusted EBITDA and Adjusted EBITDA margin for our inpatient rehabilitation segment were primarily driven by increased patient volumes at our start-up inpatient rehabilitation facilities, as discussed above under “Net Operating Revenues.” Adjusted EBITDA losses in our start-up facilities were $7.5 million for the year ended December 31, 2017, compared to $21.8 million for the year ended December 31, 2016.
Outpatient Rehabilitation Segment. Adjusted EBITDA increased 2.1% to $132.5 million for the year ended December 31, 2017, compared to $129.8 million for the year ended December 31, 2016. The increase in Adjusted EBITDA was principally due to growth in visits and an increase in net revenue per visit, as discussed above under “Net Operating Revenues.” Our Adjusted EBITDA margins for the outpatient rehabilitation segment were 13.0% for both the years ended December 31, 2017 and 2016. Our Adjusted EBITDA margin for our outpatient rehabilitation segment for the year ended December 31, 2017 was impacted by higher relative labor expenses within markets which have experienced a decline in patient volumes. We also experienced higher relative operating costs in some of our start-up and recently acquired outpatient rehabilitation clinics.
Concentra Segment. Adjusted EBITDA increased 10.2% to $157.6 million for the year ended December 31, 2017, compared to $143.0 million for the year ended December 31, 2016. Our Adjusted EBITDA margin for the Concentra segment was 15.2% for the year ended December 31, 2017, compared to 14.3% for the year ended December 31, 2016. The increases in Adjusted EBITDA and Adjusted EBITDA margin for our Concentra segment for the year ended December 31, 2017, compared to the year ended December 31, 2016 are principally due to an increase in net operating revenues from newly acquired and developed centers, as described above under “Net Operating Revenues,” while leveraging our existing cost structure.
Other. The Adjusted EBITDA loss was $94.8 million for the year ended December 31, 2017, compared to an Adjusted EBITDA loss of $88.5 million for the year ended December 31, 2016. The increase in our Adjusted EBITDA loss was due to an increase in general and administrative costs, which resulted from the expansion of our corporate shared services activities.
Depreciation and Amortization
Depreciation and amortization expense was $160.0 million for the year ended December 31, 2017, compared to $145.3 million for the year ended December 31, 2016. The increase principally occurred in our inpatient rehabilitation segment due to new facilities operating within the segment.
69
Income from Operations
For the year ended December 31, 2017, we had income from operations of $355.9 million, compared to $299.8 million for the year ended December 31, 2016. The increase in income from operations resulted principally from the increases in Adjusted EBITDA, as described above.
Loss on Early Retirement of Debt
On March 6, 2017, we refinanced Select’s 2011 senior secured credit facility which resulted in losses on early retirement of debt of $19.7 million during the year ended December 31, 2017.
On March 4, 2016, we refinanced a portion of our term loans under Select’s 2011 senior secured credit facility which resulted in a loss on early retirement of debt of $0.8 million. On September 26, 2016, Concentra prepaid the second lien term loan under the Concentra credit facilities, resulting in a loss on early retirement of debt of approximately $10.9 million.
Equity in Earnings of Unconsolidated Subsidiaries
For the year ended December 31, 2017, we had equity in earnings of unconsolidated subsidiaries of $21.1 million, compared to $19.9 million for the year ended December 31, 2016. The increase in our equity in earnings of unconsolidated subsidiaries resulted principally from the improved performance of rehabilitation businesses in which we own a minority interest.
Non-Operating Gain
We recognized a non-operating gain of $42.7 million for the year ended December 31, 2016, principally due to the sale of our contract therapy businesses for $65.0 million, which resulted in a non-operating gain of $33.9 million.
Interest Expense
Interest expense was $154.7 million for the year ended December 31, 2017, compared to $170.1 million for the year ended December 31, 2016. The decrease in interest expense was principally the result of decreases in our interest rates associated with the refinancing of Select’s 2011 senior secured credit facility during the quarter ended March 31, 2017 and the Concentra credit facilities during the quarter ended September 30, 2016.
Income Taxes
We recorded an income tax benefit of $18.2 million for the year ended December 31, 2017. We recorded income tax expense of $55.5 million for the year ended December 31, 2016, which represented an effective tax rate of 30.7%. Our income tax benefit for the year ended December 31, 2017 was principally related to the effects resulting from the federal tax reform legislation enacted during the year ended December 31, 2017 on our net deferred tax liability that resulted in an income tax benefit of $71.5 million. Additionally we were able to realize the benefit of a prior net operating loss deduction of $14.1 million.
On December 22, 2017 the Tax Cuts and Jobs Act (the “Act") was signed into law. The Act reduces the federal statutory tax rate to 21% from 35%. Accounting Standards Codification 740, Income Taxes, requires the effects of changes in tax rates and laws on deferred tax balances to be recognized in the period in which the legislation is enacted. While the effective date of the new corporate tax rate is January 1, 2018, we recorded the effect on our December 31, 2017 deferred tax balances.
Net Income Attributable to Non-Controlling Interests
Net income attributable to non-controlling interests was $43.5 million for the year ended December 31, 2017, compared to $9.9 million for the year ended December 31, 2016. The increase is principally due to increases in net income of our joint venture subsidiary, Concentra, and the improved operating performance of joint venture inpatient rehabilitation facilities.
70
Year Ended December 31, 2016 Compared to Year Ended December 31, 2015
In the following, we discuss our results of operations related to net operating revenues, operating expenses, Adjusted EBITDA, depreciation and amortization, income from operations, loss on early retirement of debt, equity in earnings of unconsolidated subsidiaries, non-operating gain (loss), interest expense, income taxes, and non-controlling interest, which, in each case, are the same for Holdings and Select.
Net Operating Revenues
Our net operating revenues increased by 14.5% to $4,286.0 million for the year ended December 31, 2016, compared to $3,742.7 million for the year ended December 31, 2015, principally due to the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016.
Long Term Acute Care Segment. Net operating revenues were $1,785.2 million for the year ended December 31, 2016, compared to $1,902.8 million for the year ended December 31, 2015. The decline in net operating revenues was principally due to a decrease in patient days as a result of the changes in operations we made in response to new Medicare patient criteria regulations. Our hospitals began transitioning to operating under the new patient criteria regulations during the fourth quarter of 2015 and, by the end of the third quarter of 2016, all of our hospitals were operating under the new regulations. We also experienced fewer patient days in 2016 as compared to 2015 as a result of hospital closures. We had 1,041,074 patient days for the year ended December 31, 2016, compared to 1,179,020 days for the year ended December 31, 2015. The decline in net operating revenues attributable to the decrease in patient days was offset in part by an increase in our net revenue per patient day. Our net revenue per patient day increased 5.9% to $1,690 for the year ended December 31, 2016, compared to $1,596 for the year ended December 31, 2015. The increase in net revenue per patient day was principally due to higher-acuity patient populations in our LTCHs, which was caused by the changes in operations we made in response to Medicare patient criteria regulations.
Inpatient Rehabilitation Segment. Net operating revenues increased 13.6% to $504.3 million for the year ended December 31, 2016, compared to $444.0 million for the year ended December 31, 2015. The increase in net operating revenues was caused by increases in patient days and net revenue per day, which was principally driven by several inpatient rehabilitation facilities which commenced operations in 2016. Our patient days increased 11.4% to 216,994 days for the year ended December 31, 2016, compared to 194,760 days for the year ended December 31, 2015. Our net revenue per patient day increased 4.2% to $1,465 for the year ended December 31, 2016, compared to $1,406 for the year ended December 31, 2015.
Outpatient Rehabilitation Segment. Net operating revenues increased 22.9% to $995.4 million for the year ended December 31, 2016, compared to $810.0 million for the year ended December 31, 2015. This increase was due to an increase in visits resulting principally from our newly acquired outpatient rehabilitation clinics and growth in our existing outpatient rehabilitation clinics. Net revenue per visit in our owned outpatient rehabilitation clinics was $102 for the year ended December 31, 2016, compared to $103 for the year ended December 31, 2015.
Concentra Segment. Net operating revenues were $1,000.6 million for the year ended December 31, 2016, compared to $585.2 million for the year ended December 31, 2015, which includes results beginning June 1, 2015. Net revenue per visit was $118 and visits were 7,373,751 in the centers for the year ended December 31, 2016, compared to net revenue per visit of $114 and 4,436,977 visits in the centers for the year ended December 31, 2015, which includes results beginning June 1, 2015.
71
Operating Expenses
Our operating expenses include our cost of services, general and administrative expense, and bad debt expense. Our operating expenses increased to $3,840.9 million, or 89.6% of net operating revenues, for the year ended December 31, 2016, compared to $3,363.0 million, or 89.9% of net operating revenues, for the year ended December 31, 2015. The increase in operating expenses is principally due to the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016. Our cost of services, a major component of which is labor expense, was $3,664.8 million, or 85.5% of net operating revenues, for the year ended December 31, 2016, compared to $3,211.5 million, or 85.8% of net operating revenues, for the year ended December 31, 2015. The decrease in cost of services, as a percentage of net operating revenues, resulted principally from cost reductions achieved by Concentra, partially offset by an increase in expenses relative to revenues within our long term acute care and inpatient rehabilitation segments. Facility rent expense, a component of cost of services, was $225.6 million for the year ended December 31, 2016, compared to $169.8 million for the year ended December 31, 2015. General and administrative expenses were $106.9 million for the year ended December 31, 2016, which included $3.2 million of Physiotherapy acquisition costs, compared to $92.1 million for the year ended December 31, 2015, which included $4.7 million of Concentra acquisition costs. General and administrative expenses as a percentage of net operating revenues were 2.5% for both the years ended December 31, 2016 and 2015. Our general and administrative function includes our shared services activities which have grown and expanded as a result of our significant business acquisitions. Our bad debt expense was $69.1 million for the year ended December 31, 2016, compared to $59.4 million for the year ended December 31, 2015. Bad debt expense as a percentage of net operating revenues was 1.6% for both the years ended December 31, 2016 and 2015.
Adjusted EBITDA
Long Term Acute Care Segment. Adjusted EBITDA was $224.6 million for the year ended December 31, 2016, compared to $258.2 million for the year ended December 31, 2015. Our Adjusted EBITDA margin for the long term acute care segment was 12.6% for the year ended December 31, 2016, compared to 13.6% for the year ended December 31, 2015. The decreases in Adjusted EBITDA and Adjusted EBITDA margin for our long term acute care segment were primarily driven by a decrease in patient days as a result of the changes in operations we made in response to new Medicare patient criteria regulations and hospital closures, as discussed above under “Net Operating Revenues,” and an increase in expenses, as discussed above under ‘‘Operating Expenses.” Additionally, we incurred Adjusted EBITDA losses in some of our newly acquired hospitals.
Inpatient Rehabilitation Segment. Adjusted EBITDA was $56.9 million for the year ended December 31, 2016, compared to $69.4 million for the year ended December 31, 2015. Our Adjusted EBITDA margin for the inpatient rehabilitation segment was 11.3% for the year ended December 31, 2016, compared to 15.6% for the year ended December 31, 2015. The decreases in Adjusted EBITDA and Adjusted EBITDA margin for our inpatient rehabilitation segment were primarily driven by an increase in Adjusted EBITDA losses in our start-up facilities. Start‑up facilities incurred $21.8 million of Adjusted EBITDA losses for the year ended December 31, 2016, compared to $6.4 million for the year ended December 31, 2015.
Outpatient Rehabilitation Segment. Our Adjusted EBITDA for our outpatient rehabilitation segment increased 32.2% to $129.8 million for the year ended December 31, 2016, compared to $98.2 million for the year ended December 31, 2015. This increase was principally due to the acquisition of Physiotherapy on March 4, 2016. Our Adjusted EBITDA margin for the outpatient rehabilitation segment was 13.0% for the year ended December 31, 2016, compared to 12.1% for the year ended December 31, 2015. The increase was principally due to the sale of our contract therapy businesses, which operated at lower Adjusted EBITDA margins than our outpatient rehabilitation clinics.
Concentra Segment. Adjusted EBITDA for our Concentra segment was $143.0 million for the year ended December 31, 2016, compared to $48.3 million for the year ended December 31, 2015, which includes results beginning June 1, 2015. Our Adjusted EBITDA margin for the Concentra segment was 14.3% for the year ended December 31, 2016, compared to 8.3% for the year ended December 31, 2015. The increase in Adjusted EBITDA was principally due to our ownership of Concentra for the entirety of fiscal year 2016, compared to our ownership of Concentra beginning June 1, 2015 for fiscal year 2015. The increase in Concentra’s Adjusted EBITDA margin was principally due to cost reductions in 2016 compared to the prior year.
Other. The Adjusted EBITDA loss was $88.5 million for the year ended December 31, 2016, compared to an Adjusted EBITDA loss of $75.0 million for the year ended December 31, 2015.
Depreciation and Amortization
Depreciation and amortization expense was $145.3 million for the year ended December 31, 2016, compared to $105.0 million for the year ended December 31, 2015. The increase was principally due to the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016.
72
Income from Operations
For the year ended December 31, 2016, we had income from operations of $299.8 million, compared to $274.8 million for the year ended December 31, 2015. The increase was principally due to the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016.
Loss on Early Retirement of Debt
On March 4, 2016, we refinanced a portion of our term loans under Select’s 2011 senior secured credit facility which resulted in a loss on early retirement of debt of $0.8 million. On September 26, 2016, Concentra prepaid the second lien term loan under the Concentra credit facilities, resulting in a loss on early retirement of debt of approximately $10.9 million.
Equity in Earnings of Unconsolidated Subsidiaries
For the year ended December 31, 2016, we had equity in earnings of unconsolidated subsidiaries of $19.9 million, compared to $16.8 million for the year ended December 31, 2015. The increase in our equity in earnings of unconsolidated subsidiaries resulted principally from the improved performance of rehabilitation businesses in which we own a minority interest.
Non-Operating Gain
We recognized a non-operating gain of $42.7 million for the year ended December 31, 2016, principally due to the sale of our contract therapy businesses for $65.0 million, which resulted in a non-operating gain of $33.9 million.
During the year ended December 31, 2015, we recognized a non-operating gain of $29.6 million related to the sale of an equity method investment.
Interest Expense
Interest expense was $170.1 million for the year ended December 31, 2016, compared to $112.8 million for the year ended December 31, 2015. The increase in interest expense was principally the result of increases in our indebtedness used to finance the acquisitions of Concentra on June 1, 2015 and Physiotherapy on March 4, 2016 in addition to increases in our interest rates resulting from amendments to the Select’s 2011 senior secured credit facility in the fourth quarter of 2015 and the first quarter of 2016.
Income Taxes
We recorded income tax expense of $55.5 million for the year ended December 31, 2016, which represented an effective tax rate of 30.7%. We recorded income tax expense of $72.4 million for the year ended December 31, 2015, which represented an effective tax rate of 34.8%.
Our effective tax rate for the year ended December 31, 2016 benefited from the sale of our contract therapy businesses. Our tax basis in our contract therapy businesses exceeded our selling price. As a result, we had no tax expense from the sale. Our effective tax rate for the year ended December 31, 2015 benefited from the resolution of uncertain tax positions.
Net Income Attributable to Non-Controlling Interests
Net income attributable to non-controlling interests was $9.9 million for the year ended December 31, 2016, compared to $5.3 million for the year ended December 31, 2015. The increase is principally due to the acquisition of Concentra, offset in part by the minority interest owners’ share of losses from new joint venture inpatient rehabilitation facilities.
73
Liquidity and Capital Resources
Years Ended December 31, 2015, 2016, and 2017
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Cash flows provided by operating activities | $ | 208,415 | $ | 346,603 | $ | 238,131 | |||||||
Cash flows used in investing activities | (1,211,754 | ) | (554,320 | ) | (192,965 | ) | |||||||
Cash flows provided by (used in) financing activities | 1,014,420 | 292,311 | (21,646 | ) | |||||||||
Net increase in cash and cash equivalents | 11,081 | 84,594 | 23,520 | ||||||||||
Cash and cash equivalents at beginning of period | 3,354 | 14,435 | 99,029 | ||||||||||
Cash and cash equivalents at end of period | $ | 14,435 | $ | 99,029 | $ | 122,549 | |||||||
Operating activities provided $238.1 million of cash flows for the year ended December 31, 2017. The decrease in operating cash flows for the year ended December 31, 2017 compared to the year ended December 31, 2016 is principally due to increases in our accounts receivable. Our days sales outstanding was 57 days at December 31, 2017, 51 days at December 31, 2016, and 53 days at December 31, 2015. The timing of our periodic interim payments received from Medicare in our LTCHs has had an impact on our days sales outstanding for the years ended December 31, 2017 and 2016.
Operating activities provided $346.6 million of cash flows for the year ended December 31, 2016. The increase in operating cash flows for the year ended December 31, 2016 compared to the year ended December 31, 2015 is principally due to cash flows provided from Concentra which was acquired on June 1, 2015.
Investing activities used $193.0 million, $554.3 million and $1,211.8 million of cash flows for the years ended December 31, 2017, 2016 and 2015, respectively. For the year ended December 31, 2017, the principal uses of cash were $233.2 million for purchases of property and equipment and $27.4 million for the acquisition of businesses, offset in part by $80.4 million of proceeds received from the sale of assets. For the year ended December 31, 2016, the principal uses of cash were $406.3 million for the Physiotherapy acquisition and $161.6 million for purchases of property and equipment, offset in part by $80.5 million of proceeds received from the sale of assets and businesses. For the year ended December 31, 2015, the principal uses of cash were $1,047.2 million for the Concentra acquisition and $182.6 million for purchases of property and equipment, offset in part by the proceeds from the sale of an equity investment.
Financing activities used $21.6 million of cash flows for the year ended December 31, 2017. The principal uses of cash were $23.1 million for a principal prepayment associated with the Concentra credit facilities, $8.6 million for term loan payments associated with the Select credit facilities, and cash used for the payment of financing costs related to the refinancing of the Select credit facilities, offset in part by $10.0 million of net borrowings under the Select revolving facility.
Financing activities provided $292.3 million of cash flows for the year ended December 31, 2016. The principal source of cash was the issuance of $625.0 million series F tranche B term loans under Select’s 2011 senior secured credit facility, resulting in net proceeds of $600.1 million. This was offset by $215.7 million of cash used to repay the series D tranche B term loans under Select’s 2011 senior secured credit facility and $80.0 million of net repayments under the Select and Concentra revolving facilities.
Financing activities provided $1,014.4 million of cash flows for the year ended December 31, 2015. The principal sources of cash were $235.0 million of net borrowings under the Select revolving facility, $5.0 million of net borrowings under the Concentra revolving facility, $646.9 million borrowed under the Concentra credit facilities, and $217.1 million attributable to the issuance of non-controlling interests in Concentra Group Holdings. The principal uses of cash for financing activities were $26.9 million for the mandatory prepayment of term loans under Select’s 2011 senior secured credit facility, $23.3 million for Concentra’s debt issuance costs, $13.6 million for common stock repurchases, and $13.1 million for dividend payments to common stockholders.
74
Capital Resources
Working capital. We had net working capital of $315.4 million at December 31, 2017 compared to net working capital of $191.3 million at December 31, 2016. The increase in net working capital is primarily due to an increase in our accounts receivable.
Select credit facilities. On March 6, 2017, Select entered into the Select credit agreement that provides for $1.6 billion in senior secured credit facilities comprising a $1.15 billion, seven-year term loan and a $450.0 million, five-year revolving credit facility, including a $75.0 million sublimit for the issuance of standby letters of credit. Select used borrowings under the Select credit facilities to: (i) repay the series E tranche B term loans due June 1, 2018, the series F tranche B term loans due March 3, 2021, and the revolving facility maturing March 1, 2018 under Select’s 2011 senior secured credit facility; and (ii) pay fees and expenses in connection with the refinancing.
Borrowings under the Select credit facilities bear interest at a rate equal to: (i) in the case of the Select term loan, the Adjusted LIBO Rate (as defined in the Select credit agreement) plus 3.50% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Select credit agreement) plus 2.50% (subject to an Alternate Base Rate floor of 2.00%); and (ii) in the case of the Select revolving facility, the Adjusted LIBO Rate plus a percentage ranging from 3.00% to 3.25% or Alternate Base Rate plus a percentage ranging from 2.00% to 2.25%, in each case based on Select’s leverage ratio, as defined in the Select credit facilities.
The Select term loan amortizes in equal quarterly installments in amounts equal to 0.25% of the aggregate original principal amount of the Select term loan commencing on June 30, 2017. The balance of the Select term loan will be payable on March 6, 2024; however, if the Select 6.375% senior notes, which are due June 1, 2021, are outstanding on March 1, 2021, the maturity date for the Select term loan will become March 1, 2021. The Select revolving facility will be payable on March 6, 2022; however, if the Select 6.375% senior notes are outstanding on February 1, 2021, the maturity date for the Select revolving facility will become February 1, 2021.
Select will be required to prepay borrowings under the Select credit facilities with (i) 100% of the net cash proceeds received from non-ordinary course asset sales or other dispositions, or as a result of a casualty or condemnation, subject to reinvestment provisions and other customary carveouts and, to the extent required, the payment of certain indebtedness secured by liens having priority over the debt under the Select credit facilities or subject to a first lien intercreditor agreement, (ii) 100% of the net cash proceeds received from the issuance of debt obligations other than certain permitted debt obligations, and (iii) 50% of excess cash flow (as defined in the Select credit agreement) if Select’s leverage ratio is greater than 4.50 to 1.00 and 25% of excess cash flow if Select’s leverage ratio is less than or equal to 4.50 to 1.00 and greater than 4.00 to 1.00, in each case, reduced by the aggregate amount of term loans, revolving loans and certain other debt optionally prepaid during the applicable fiscal year. Select will not be required to prepay borrowings with excess cash flow if Select’s leverage ratio is less than or equal to 4.00 to 1.00.
The Select revolving facility requires Select to maintain a leverage ratio (as defined in the Select credit agreement), which is tested quarterly, not to exceed 6.25 to 1.00. After March 31, 2019, the leverage ratio must not exceed 6.00 to 1.00. The leverage ratio is tested quarterly. Failure to comply with this covenant would result in an event of default under the Select revolving facility and, absent a waiver or an amendment from the revolving lenders, preclude Select from making further borrowings under the Select revolving facility and permit the revolving lenders to accelerate all outstanding borrowings under the Select revolving facility. The termination of the Select revolving facility commitments and the acceleration of amounts outstanding thereunder would constitute an event of default with respect to the Select term loan. For each of the four fiscal quarters during the year ended December 31, 2017, Select was required to maintain its leverage ratio at less than 6.25 to 1.00. As of December 31, 2017, Select’s leverage ratio was 5.27 to 1.00.
The Select credit facilities also contain a number of other affirmative and restrictive covenants, including limitations on mergers, consolidations and dissolutions; sales of assets; investments and acquisitions; indebtedness; liens; affiliate transactions; and dividends and restricted payments. The Select credit facilities contain events of default for non-payment of principal and interest when due (subject, as to interest, to a grace period), cross-default and cross-acceleration provisions and an event of default that would be triggered by a change of control.
Borrowings under the Select credit facilities are guaranteed by Holdings and substantially all of Select’s current domestic subsidiaries and will be guaranteed by substantially all of Select’s future domestic subsidiaries. Borrowings under the Select credit facilities are secured by substantially all of Select’s existing and future property and assets and by a pledge of Select’s capital stock, the capital stock of Select’s domestic subsidiaries and up to 65% of the capital stock of Select’s foreign subsidiaries held directly by Select or a domestic subsidiary.
At December 31, 2017, Select had outstanding borrowings under the Select credit facilities consisting of a $1,141.4 million Select term loan (excluding unamortized original issue discounts and debt issuance costs of $24.9 million) and borrowings of $230.0 million (excluding letters of credit) under the Select revolving facility. At December 31, 2017, Select had $181.4 million of availability under the Select revolving facility after giving effect to $38.6 million of outstanding letters of credit.
75
Concentra credit facilities. Select and Holdings are not parties to the Concentra credit facilities and are not obligors with respect to Concentra’s debt under such agreements. While this debt is non-recourse to Select, it is included in Select’s consolidated financial statements.
On March 1, 2017, Concentra made a principal prepayment of $23.1 million associated with its first lien term loan in accordance with the provision in the Concentra credit facilities that requires mandatory prepayments of term loans as a result of annual excess cash flow, as defined in the Concentra credit facilities.
At December 31, 2017, Concentra had outstanding borrowings under the Concentra credit facilities of $619.2 million of term loans (excluding unamortized discounts and debt issuance costs of $12.9 million). Concentra did not have any borrowings under the Concentra revolving facility. At December 31, 2017, Concentra had $43.4 million of availability under its revolving facility after giving effect to $6.6 million of outstanding letters of credit.
On February 1, 2018, in connection with the transactions contemplated under the Purchase Agreement, as described above under “Significant Events,” Concentra amended the Concentra first lien credit agreement to, among other things, provide for (i) an additional $555.0 million in tranche B term loans that, along with the existing tranche B term loans under the Concentra first lien credit agreement, have a maturity date of June 1, 2022 and (ii) an additional $25.0 million to the $50.0 million, five-year revolving credit facility under the terms of the existing Concentra first lien credit agreement. The tranche B term loans bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra first lien credit agreement) plus 2.75% (subject to an Adjusted LIBO Rate floor of 1.00%) for Eurodollar Borrowings (as defined in the Concentra first lien credit agreement), or Alternate Base Rate (as defined in the Concentra first lien credit agreement) plus 1.75% (subject to an Alternate Base Rate floor of 2.00%) for ABR Borrowings (as defined in the Concentra first lien credit agreement). All other material terms and conditions applicable to the original tranche B term loan commitments are applicable to the additional tranche B term loans created under this amendment.
In addition, Concentra entered into the Concentra 2018 second lien credit agreement that provides for $240.0 million in term loans with an initial maturity date of June 1, 2023. Borrowings under the Concentra 2018 second lien credit agreement will bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra 2018 second lien credit agreement) plus 6.50% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Concentra 2018 second lien credit agreement) plus 5.50% (subject to an Alternate Base Rate floor of 2.00%).
In the event that, on or prior to February 1, 2019, Concentra prepays any of the 2018 second lien term loans to refinance such term loans, Concentra shall pay a premium of 2.00% of the aggregate principal amount of the 2018 second lien term loans prepaid. If Concentra prepays any of the 2018 second lien term loans to refinance such term loans on or prior to February 1, 2020, Concentra shall pay a premium of 1.00% of the aggregate principal amount of the 2018 second lien term loans prepaid. The 2018 second lien term loans will be payable on June 1, 2023.
Concentra used borrowings under the Concentra first lien credit agreement and the Concentra 2018 second lien credit agreement, together with cash on hand, to pay the purchase price for all of the issued and outstanding stock of U.S. HealthWorks to DHHC and to finance the redemption and reorganization transactions contemplated by the Purchase Agreement.
Stock Repurchase Program. Holdings’ board of directors has authorized a common stock repurchase program to repurchase up to $500.0 million worth of shares of its common stock. The program has been extended until December 31, 2018, and will remain in effect until then, unless further extended or earlier terminated by the board of directors. Stock repurchases under this program may be made in the open market or through privately negotiated transactions, and at times and in such amounts as Holdings deems appropriate. Holdings funds this program with cash on hand and borrowings under the Select revolving facility. Holdings did not repurchase shares during the year ended December 31, 2017. Since the inception of the program through December 31, 2017, Holdings has repurchased 35,924,128 shares at a cost of approximately $314.7 million, or $8.76 per share, which includes transaction costs.
Liquidity. We believe our internally generated cash flows and borrowing capacity under the Select and Concentra credit facilities will be sufficient to finance operations over the next twelve months. We may from time to time seek to retire or purchase our outstanding debt through cash purchases and/or exchanges for equity securities, in open market purchases, privately negotiated transactions, tender offers or otherwise. Such repurchases or exchanges, if any, may be funded from operating cash flows or other sources and will depend on prevailing market conditions, our liquidity requirements, contractual restrictions and other factors. The amounts involved may be material.
Use of Capital Resources. We may from time to time pursue opportunities to develop new joint venture relationships with significant health systems and other healthcare providers and from time to time we may also develop new inpatient rehabilitation hospitals and occupational health centers. We also intend to open new outpatient rehabilitation clinics in local areas that we currently serve where we can benefit from existing referral relationships and brand awareness to produce incremental growth. In addition to our development activities, we may grow through opportunistic acquisitions, such as the acquisition of U.S. HealthWorks.
76
Commitments and Contingencies
The following contractual obligation table summarizes the contractual obligations for Select and Concentra at December 31, 2017, and the effect such obligations are expected to have on liquidity and cash flow in future periods.
Total | 2018 | 2019 - 2021 | 2022 - 2023 | After 2023 | |||||||||||||||||
(in thousands) | |||||||||||||||||||||
Debt(1) | $ | 2,744,080 | $ | 22,186 | $ | 781,288 | $ | 863,042 | $ | 1,077,564 | |||||||||||
Interest(2)(3) | 645,111 | 137,223 | 380,155 | 116,920 | 10,813 | ||||||||||||||||
Letters of credit outstanding(1) | 45,202 | — | 6,579 | 38,623 | — | ||||||||||||||||
Purchase obligations(4) | 154,525 | 56,984 | 61,142 | 21,888 | 14,511 | ||||||||||||||||
Construction contracts(5) | 38,595 | 38,595 | — | — | — | ||||||||||||||||
Operating leases(5) | 1,209,845 | 224,359 | 469,495 | 157,751 | 358,240 | ||||||||||||||||
Related party operating leases(5) | 34,062 | 5,667 | 17,855 | 7,241 | 3,299 | ||||||||||||||||
Total contractual cash obligations(6) | $ | 4,871,420 | $ | 485,014 | $ | 1,716,514 | $ | 1,205,465 | $ | 1,464,427 | |||||||||||
_______________________________________________________________________________
(1) | See Note 8 – Long-Term Debt and Notes Payable of the Notes to Consolidated Financial Statements (Part II, Item 8 of this Form 10-K). This table does not include the incremental $555.0 million in tranche B term loans provided for under the Concentra first lien credit agreement, the $240.0 million of term loans provided for under the Concentra 2018 second lien credit agreement, or the additional $25.0 million five-year revolving credit facility made available under the Concentra first lien credit agreement on February 1, 2018 in connection with the acquisition of U.S. HealthWorks. |
(2) | The interest obligation for the Select credit facilities was calculated using the average interest rate at December 31, 2017 of 4.7% for the Select term loan and 4.7% for the Select revolving facility. The interest obligation for the 6.375% senior notes was calculated using the stated interest rate and a weighted average interest rate of 2.5% was used for the other debt obligations. |
(3) | The interest obligation for the Concentra credit facilities was calculated using the average interest rate at December 31, 2017 of 4.2% for the Concentra first lien term loan. The weighted average interest rate for Concentra’s other debt obligations was 7.8%. |
(4) | Amounts represent purchase commitments that are not presented as construction contract commitments above. Our purchase obligations primarily relate to software licensing and support. |
(5) | See Note 15 – Commitments and Contingencies of the Notes to Consolidated Financial Statements (Part II, Item 8 of this Form 10-K). |
(6) | Reserves for uncertain tax positions of $3.1 million and workers’ compensation and professional malpractice liability insurance liabilities of $101.8 million, which are included as components of other non-current liabilities on the consolidated balance sheets, have been excluded from the table above as we cannot reasonably estimate the amounts or periods in which these liabilities will be paid. |
Concentra Put Right
Pursuant to the Amended and Restated Limited Liability Company Agreement of Concentra Group Holdings Parent, WCAS and the other members of Concentra Group Holdings Parent and Dignity Health have separate put rights, each, a “Put Right,” with respect to their equity interests in Concentra Group Holdings Parent. If a Put Right is exercised by WCAS or Dignity Health, Select will be obligated to purchase up to 331/3% of the equity interests of Concentra Group Holdings Parent that WCAS or Dignity Health, respectively, owned as of February 1, 2018, at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA (as defined in the Amended and Restated Limited Liability Company Agreement of Concentra Group Holdings Parent) and capped at an agreed upon multiple of EBITDA. Select has the right to elect to pay the purchase price in cash or in shares of Holdings’ common stock. WCAS and Dignity Health may first exercise their respective Put Right during a sixty-day period following the second anniversary of the date of the Amended and Restated LLC Agreement in 2020, and then may exercise their respective Put Right again annually during a sixty-day period in each calendar year thereafter. If WCAS exercises its Put Right, the other members of Concentra Group Holdings Parent, other than Dignity Health, may elect to sell to Select, on the same terms as WCAS, a percentage of their equity interests of Concentra Group Holdings Parent that such member owned as of the date of the Amended and Restated LLC Agreement, up to but not exceeding the percentage of equity interests owned by WCAS as of the date of the Amended and Restated LLC Agreement that WCAS has determined to sell to Select in the exercise of its Put Right.
77
Furthermore, WCAS, Dignity Health, and the other members of Concentra Group Holdings Parent have a put right with respect to their equity interest in Concentra Group Holdings Parent that may only be exercised in the event Holdings or Select experiences a change of control that has not been previously approved by WCAS and Dignity Health, and which results in change in the senior management of Select (an “SEM COC Put Right”). If an SEM COC Put Right is exercised by WCAS, Select will be obligated to purchase all (but not less than all) of the equity interests of WCAS and the other members of Concentra Group Holdings Parent (other than Dignity Health) at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA and capped at an agreed upon multiple of EBITDA. Similarly, if an SEM COC Put Right is exercised by Dignity Health, Select will be obligated to purchase all (but not less than all) of the equity interests of Dignity Health at a purchase price based on a valuation of Concentra Group Holdings Parent performed by an investment bank to be agreed between Select and one of WCAS or Dignity Health, which valuation will be based on certain precedent transactions using multiples of EBITDA and capped at an agreed upon multiple of EBITDA.
Furthermore, Select has a call right (the “Call Right”), whereby each other member of Concentra Group Holdings Parent will be obligated to sell all or a portion of their equity interests in Concentra Group Holdings Parent to Select at a purchase price based on a valuation of Concentra Group Holdings performed by an investment bank to be mutually agreed upon by Select and either WCAS or Dignity Health. The valuation will be based on certain precedent transactions using multiples of EBITDA and capped at an agreed upon multiple of EBITDA. Select may first exercise the Call Right after February 1, 2022.
We exclude the approximate amount that we may be required to pay to purchase these equity interests in Concentra Group Holdings Parent from the contractual obligations table above because of the uncertainty as to: (i) whether or not the Put Right, if exercisable, or the Call Right, will actually be exercised; (ii) the dollar amounts that would be paid if the Put Right or Call Right is exercised; and (iii) the timing and form of consideration of any such payments.
Effects of Inflation and Changing Prices
We derive a substantial portion of our revenues from the Medicare program. We have been, and could be in the future, affected by the continuing efforts of governmental and private third-party payors to contain healthcare costs by limiting or reducing reimbursement payments.
Additionally, reimbursement payments under governmental and private third-party payor programs may not increase to sufficiently cover increasing costs. Medicare reimbursement in our LTCHs and IRFs is subject to fixed payments under the Medicare prospective payment systems. In accordance with Medicare laws, CMS makes annual adjustments to Medicare payments under what is commonly known as a “market basket update.” Generally, these rates are adjusted for inflation. However, these adjustments may not reflect the actual increase in the costs of providing healthcare services and may be reduced by CMS for other adjustments.
The healthcare industry is labor intensive and the Company’s largest expenses are labor related costs. Wage and other expenses increase during periods of inflation and when labor shortages occur in the marketplace. There can be no guarantee we will not experience increases in the cost of labor, as the need for clinical healthcare professionals is expected to grow. In addition, suppliers pass along rising costs to us in the form of higher prices. We have little or no ability to pass on these increased costs associated with providing services due to federal laws that establish fixed reimbursement rates.
78
Recent Accounting Pronouncements
Revenue from Contracts with Customers
Beginning in May 2014, the Financial Accounting Standards Board (“FASB”) issued several Accounting Standards Updates which established Topic 606, Revenue from Contracts with Customers (the “standard”). This standard supersedes existing revenue recognition requirements and seeks to eliminate most industry-specific guidance under current GAAP. The core principle of the new guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. New disclosures about the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers are also required. The standard requires the selection of a full retrospective or cumulative effect transition method.
The Company has completed its implementation efforts and will adopt the new standard beginning January 1, 2018 using the full retrospective transition method. The presentation of the amount of income from operations and net income will be unchanged upon adoption of the new standard; however, adoption of the new standard will result in significant changes to the presentation of net operating revenues and bad debt expense in the consolidated statements of operations and comprehensive income. The principal change affecting the Company results from the presentation of variable consideration that under the accounting standard is included in the transaction price up to an amount which is probable that a significant reversal will not occur. The most common form of variable consideration the Company experiences are amounts for services provided that are ultimately not realizable from a patient. Under the current standard, the Company’s estimate for unrealizable amounts was recorded to bad debt expense. Under the new standard, the Company’s estimate for unrealizable amounts will be recognized as an additional allowance to revenue and will be reflected as a reduction to accounts receivable.
Adoption of the revenue recognition standard will impact our reported results for December 31, 2016 and December 31, 2017 as follows:
December 31, 2016 | December 31, 2017 | ||||||||||||||
As Reported | As Adjusted | As Reported | As Adjusted | ||||||||||||
(in thousands) | |||||||||||||||
Net operating revenues | $ | 4,286,021 | $ | 4,217,460 | $ | 4,443,603 | $ | 4,365,245 | |||||||
Bad debt expense | 69,093 | 532 | 79,491 | 1,133 | |||||||||||
Leases
In February 2016, the FASB issued Accounting Standards Update (“ASU”) 2016‑02, Leases. This ASU includes a lessee accounting model that recognizes two types of leases: finance and operating. This ASU requires that a lessee recognize on the balance sheet assets and liabilities for all leases with lease terms of more than twelve months. Lessees will need to recognize almost all leases on the balance sheet as a right-of-use asset and a lease liability. For income statement purposes, the FASB retained the dual model, requiring leases to be classified as either operating or finance. The recognition, measurement, and presentation of expenses and cash flows arising from a lease by a lessee will depend on its classification as finance or operating lease. For short-term leases of twelve months or less, lessees are permitted to make an accounting election by class of underlying asset not to recognize right-of-use assets or lease liabilities. If the alternative is elected, lease expense would be recognized generally on the straight-line basis over the respective lease term.
The amendments in ASU 2016‑02 will take effect for public companies for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Earlier application is permitted as of the beginning of an interim or annual reporting period. A modified retrospective approach is required for leases that exist or are entered into after the beginning of the earliest comparative period in the financial statements.
Upon adoption, the Company will recognize significant assets and liabilities on the consolidated balance sheets as a result of the operating lease obligations of the Company. Operating lease expense will still be recognized as rent expense on a straight-line basis over the respective lease terms in the consolidated statements of operations and comprehensive income.
The Company will implement the new standard beginning January 1, 2019. The Company’s implementation efforts are focused on designing accounting processes, disclosure processes, and internal controls in order to account for its leases under the new standard.
79
Income Taxes
In October 2016, the FASB issued ASU 2016-16, Income Taxes (Topic 740), Intra-Entity Transfers of Assets Other Than Inventory. Current GAAP prohibits the recognition of current and deferred income taxes for an intra-entity asset transfer until the asset has been sold to an outside party. The ASU requires an entity to recognize the income tax consequences of an intra‑entity transfer of an asset other than inventory when the transfer occurs. The standard will be effective for fiscal years beginning after December 15, 2017. The Company plans to adopt the guidance effective January 1, 2018. Adoption of the guidance will be applied on a modified retrospective approach through a cumulative effect adjustment to retained earnings as of the effective date.
Business Combinations
In January 2017, the FASB issued ASU 2017-01, Business Combinations (Topic 805), Clarifying the Definition of a Business, which clarifies the definition of a business with the objective of adding guidance to assist entities with evaluating whether transactions should be accounted for as acquisitions or disposals of assets or businesses. ASU 2017-01 states that if substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the transaction should be accounted for as an asset acquisition. In addition, the ASU clarifies the requirements for a set of activities to be considered a business and narrows the definition of an output. The definition of a business affects many areas of accounting including acquisitions, disposals, goodwill and consolidation. ASU 2017-01 is effective for annual periods beginning after December 15, 2017. Early adoption is permitted.
Financial Instruments
In June 2016, the FASB issued ASU 2016-13, Financial Instruments - Credit Losses: Measurement of Credit Losses on Financial Instruments. The current standard delays the recognition of a credit loss on a financial asset until the loss is probable of occurring. The new standard removes the requirement that a credit loss be probable of occurring for it to be recognized and requires entities to use historical experience, current conditions, and reasonable and supportable forecasts to estimate their future expected credit losses. The Company’s accounts receivable derived from contracts with customers will be subject to ASU 2016-13.
The standard will be effective for fiscal years beginning after December 15, 2019, including interim periods within those fiscal years. The guidance must be applied using a modified retrospective approach through a cumulative-effect adjustment to retained earnings as of the beginning of the earliest comparative period in the financial statements. Given the very high rate of collectability of the Company’s accounts receivable derived from contracts with customers, the impact of ASU 2016-13 is unlikely to be material.
Recently Adopted Accounting Pronouncements
Income Taxes
In November 2015, the FASB issued ASU 2015-17, Balance Sheet Classification of Deferred Taxes, which changed the presentation of deferred income taxes. The standard changed the presentation of deferred income taxes through the requirement that all deferred tax liabilities and assets be classified as non-current in a classified statement of financial position. The Company adopted the standard on January 1, 2017. The consolidated balance sheet at December 31, 2016 has been retrospectively adjusted. Adoption of the new standard impacted the Company’s previously reported results as follows:
December 31, 2016 | |||||||
As Reported | As Adjusted | ||||||
(in thousands) | |||||||
Current deferred tax asset | $ | 45,165 | $ | — | |||
Total current assets | 808,068 | 762,903 | |||||
Other assets | 152,548 | 173,944 | |||||
Total assets | 4,944,395 | 4,920,626 | |||||
Non-current deferred tax liability | 222,847 | 199,078 | |||||
Total liabilities | 3,616,335 | 3,592,566 | |||||
Total liabilities and equity | 4,944,395 | 4,920,626 | |||||
80
Stock Compensation
In March 2016, the FASB issued ASU 2016-09, Compensation‑Stock Compensation, which simplifies various aspects of accounting for share-based payments. The areas for simplification involve several aspects of the accounting for share-based payment transactions, including the income tax consequences and classification on the statements of cash flows. During the fourth quarter of 2016, the Company adopted and applied the standard on a prospective basis beginning January 1, 2016. The Company has elected to recognize the effect of forfeitures in compensation cost when they occur. There was no retrospective impact to the consolidated financial statements, including the consolidated statements of cash flows, as a result of the adoption of this standard.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
We are subject to interest rate risk in connection with our variable rate long-term indebtedness. Our principal interest rate exposure relates to the loans outstanding under the Select credit facilities and Concentra credit facilities.
As of December 31, 2017, Select had outstanding borrowings under the Select credit facilities consisting of a $1,141.4 million Select term loan (excluding unamortized original issue discounts and debt issuance costs totaling $24.9 million) and borrowings of $230.0 million under the Select revolving facility, which bear interest at variable rates.
As of December 31, 2017, Concentra had outstanding borrowings under the Concentra credit facilities of $619.2 million of term loans (excluding unamortized discounts and debt issuance costs of $12.9 million), which bear interest at variable rates. Concentra did not have any borrowings under the Concentra revolving facility.
As of December 31, 2017, the three-month LIBOR rate was 1.69%. Consequently, each 0.25% increase in market interest rates will impact the interest expense on Select’s and Concentra’s variable rate debt by $5.0 million per annum.
Concentra’s long-term indebtedness, as described above, does not include the incremental $555.0 million in tranche B term loans provided for under the Concentra first lien credit agreement, the $240.0 million of term loans provided for under the Concentra 2018 second lien credit agreement, or the additional $25.0 million five-year revolving credit facility made available under the Concentra first lien credit agreement on February 1, 2018 in connection with the acquisition of U.S. HealthWorks. The acquisition of U.S. HealthWorks is described further under “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Significant Events.”
Item 8. Financial Statements and Supplementary Data.
See Consolidated Financial Statements and Notes thereto commencing at Page F-1.
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
We carried out an evaluation, under the supervision and with the participation of our principal executive officer and principal financial officer, of the effectiveness of the design and operation of our disclosure controls and procedures (as defined in Rule 13a-15(e) of the Securities Exchange Act of 1934) as of the end of the period covered in this report. Based on this evaluation, our principal executive officer and principal financial officer concluded that our disclosure controls and procedures, including the accumulation and communication of disclosure to our principal executive officer and principal financial officer as appropriate to allow timely decisions regarding disclosure, are effective as of December 31, 2017 to provide reasonable assurance that material information required to be included in our periodic SEC reports is recorded, processed, summarized, and reported within the time periods specified in the relevant SEC rules and forms.
Changes in Internal Control over Financial Reporting
There was no change in our internal control over financial reporting (as defined in Rule 13a-15(f) of the Securities Exchange Act of 1934) identified in connection with the evaluation required by Rule 13a-15(d) of the Securities Exchange Act of 1934 that occurred during the fourth quarter of the year ended December 31, 2017 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
81
Inherent Limitations on Effectiveness of Controls
It should be noted that any system of controls, however well designed and operated, can provide only reasonable, and not absolute, assurance that the objectives of the system will be met. In addition, the design of any control system is based in part upon certain assumptions about the likelihood of future events. Because of these and other inherent limitations of control systems, there is only reasonable assurance that our controls will succeed in achieving their goals under all potential future conditions.
Management’s Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining an adequate system of internal control over our financial reporting. In order to evaluate the effectiveness of internal control over financial reporting, as required by Section 404 of the Sarbanes-Oxley Act, management has conducted an assessment, including testing, using the criteria of “Internal Control—Integrated Framework (2013)” issued by the Committee of Sponsoring Organizations of the Treadway Commission, or “COSO,” as of December 31, 2017. Our system of internal control over financial reporting is designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation and fair presentation of financial statements for external purposes in accordance with U.S. generally accepted accounting principles.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness of internal control over financial reporting to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Management assessed the effectiveness of the Company’s internal control over financial reporting as of December 31, 2017. This assessment was based on criteria for effective internal control over financial reporting described in “Internal Control—Integrated Framework (2013)” issued by COSO. Based on this assessment, management concludes that, as of December 31, 2017, internal control over financial reporting was effective to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements in accordance with U.S. generally accepted accounting principles. The effectiveness of the Company’s internal control over financial reporting as of December 31, 2017 has been audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm as stated in their report which appears herein.
Item 9B. Other Information.
None.
82
PART III
Item 10. Directors, Executive Officers and Corporate Governance.
The information regarding directors and nominees for directors of the Company, including identification of the audit committee and audit committee financial expert, and Compliance with Section 16(a) of the Exchange Act is presented under the headings “Corporate Governance—Committees of the Board of Directors,” “Election of Directors—Directors and Nominees” and “Section 16(a) Beneficial Ownership Reporting Compliance” in the Company’s definitive proxy statement for use in connection with the 2018 Annual Meeting of Stockholders (the “Proxy Statement”) to be filed within 120 days after the end of the Company’s fiscal year ended December 31, 2017. The information contained under these headings is incorporated herein by reference. Information regarding the executive officers of the Company is included in this Annual Report on Form 10-K under Item 1 of Part I as permitted by Instruction 3 to Item 401(b) of Regulation S-K.
We have adopted a written code of business conduct and ethics, known as our code of conduct, which applies to all of our directors, officers, and employees, as well as a code of ethics applicable to our senior financial officers, including our chief executive officer, our chief financial officer and our chief accounting officer. Our code of conduct and code of ethics for senior financial officers are available on our Internet website, www.selectmedicalholdings.com. Our code of conduct and code of ethics for senior financial officers may also be obtained by contacting investor relations at (717) 972-1100. Any amendments to our code of conduct or code of ethics for senior financial officers or waivers from the provisions of the codes for our chief executive officer, our chief financial officer and our chief accounting officer will be disclosed on our Internet website promptly following the date of such amendment or waiver.
Item 11. Executive Compensation.
Information concerning executive compensation is presented under the headings “Executive Compensation” and “Compensation Committee Report” in the Proxy Statement. The information contained under these headings is incorporated herein by reference.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
Information with respect to security ownership of certain beneficial owners and management is set forth under the heading “Security Ownership of Certain Beneficial Owners and Directors and Officers” in the Proxy Statement. The information contained under this heading is incorporated herein by reference.
Equity Compensation Plan Information
Set forth in the table below is a list of all of our equity compensation plans and the number of securities to be issued on exercise of equity rights, average exercise price, and number of securities that would remain available under each plan if outstanding equity rights were exercised as of December 31, 2017.
Plan Category | Number of securities to be issued upon exercise of outstanding options, warrants and rights (a) | Weighted-average exercise price of outstanding options, warrants and rights (b) | Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a))(c) | ||||||||
Equity compensation plans approved by security holders: | |||||||||||
Select Medical Holdings Corporation 2005 Equity Incentive Plan | 282,775 | $ | 9.24 | — | (1) | ||||||
Select Medical Holdings Corporation 2011 Equity Incentive Plan | — | — | — | (2) | |||||||
Director Equity Incentive Plan | 9,000 | 10.00 | — | (2) | |||||||
Select Medical Holdings Corporation 2016 Equity Incentive Plan | — | — | 4,505,801 | ||||||||
Equity compensation plans not approved by security holders | — | — | — | ||||||||
_____________________________________________________________________________
(1) | In connection with the approval of the Select Medical Holdings Corporation 2011 Equity Incentive Plan, we no longer issue awards under the Select Medical Holdings Corporation 2005 Equity Incentive Plan. |
(2) | In connection with the approval of the Select Medical Holdings Corporation 2016 Equity Incentive Plan, we no longer issue awards under the Select Medical Holdings 2011 Equity Incentive Plan and the Director Equity Incentive Plan. |
83
Item 13. Certain Relationships, Related Transactions and Director Independence.
Information concerning related transactions is presented under the heading “Certain Relationships, Related Transactions and Director Independence” in the Proxy Statement. The information contained under this heading is incorporated herein by reference.
Item 14. Principal Accountant Fees and Services.
Information concerning principal accountant fees and services is presented under the heading “Ratification of Appointment of Independent Registered Public Accounting Firm” in the Proxy Statement. The information contained under this heading is incorporated herein by reference.
84
PART IV
Item 15. Exhibits and Financial Statement Schedules.
a. | The following documents are filed as part of this report: |
i. | Financial Statements: See Index to Financial Statements appearing on page F-1 of this report. |
ii. | Financial Statement Schedule: See Schedule II—Valuation and Qualifying Accounts appearing on page F-56 of this report. |
iii. | The following exhibits are filed as part of, or incorporated by reference into, this report: |
Number | Description | ||
2.1 | |||
2.2 | |||
2.3 | |||
2.4 | |||
2.5 | |||
2.6 | |||
3.1 | |||
3.2 | |||
3.3 | |||
3.4 | |||
4.1 | |||
4.2 | |||
4.3 | |||
85
Number | Description | ||
10.1 | |||
10.2 | |||
10.3 | |||
10.4 | |||
10.5 | |||
10.6 | |||
10.7 | |||
10.8 | |||
10.9 | |||
10.10 | |||
10.11 | |||
10.12 | |||
10.13 | |||
10.14 | |||
10.15 | |||
10.16 | |||
10.17 | |||
10.18 | |||
10.19 | |||
86
Number | Description | ||
10.20 | |||
10.21 | |||
10.22 | |||
10.23 | |||
10.24 | |||
10.25 | |||
10.26 | |||
10.27 | |||
10.28 | |||
10.29 | |||
10.30 | |||
10.31 | |||
10.32 | |||
10.33 | |||
10.34 | |||
10.35 | |||
10.36 | |||
10.37 | |||
87
Number | Description | ||
10.38 | |||
10.39 | |||
10.40 | |||
10.41 | |||
10.42 | |||
10.43 | |||
10.44 | |||
10.45 | |||
10.46 | |||
10.47 | |||
10.48 | |||
10.49 | |||
10.50 | |||
10.51 | |||
10.52 | |||
10.53 | |||
10.54 | |||
88
Number | Description | ||
10.55 | |||
10.56 | |||
10.57 | |||
10.58 | |||
10.59 | |||
10.60 | |||
10.61 | |||
10.62 | |||
10.63 | |||
10.64 | |||
10.65 | |||
10.66 | |||
10.67 | |||
10.68 | |||
89
Number | Description | ||
12 | |||
21.1 | |||
23 | |||
31.1 | |||
31.2 | |||
32.1 | |||
101 | The following financial information from the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2017 formatted in XBRL (eXtensible Business Reporting Language): (i) Consolidated Statements of Operations and Comprehensive Income for the years ended December 31, 2017, 2016 and 2015 (ii) Consolidated Balance Sheets as of December 31, 2017 and 2016, (iii) Consolidated Statements of Cash Flows for the years ended December 31, 2017, 2016 and 2015, (iv) Consolidated Statements of Changes in Equity and Income for the years ended December 31, 2017, 2016 and 2015 and (v) Notes to Consolidated Financial Statements. | ||
The representations, warranties, and covenants contained in the agreements set forth in this Exhibit Index were made only as of specified dates for the purposes of the applicable agreement, were made solely for the benefit of the parties to such agreement, and may be subject to qualifications and limitations agreed upon by the parties. In particular, the representations, warranties, and covenants contained in such agreement were negotiated with the principal purpose of allocating risk between the parties, rather than establishing matters as facts, and may have been qualified by confidential disclosures. Such representations, warranties, and covenants may also be subject to a contractual standard of materiality different from those generally applicable to stockholders and to reports and documents filed with the SEC. Accordingly, investors should not rely on such representations, warranties, and covenants as characterizations of the actual state of facts or circumstances described therein. Information concerning the subject matter of such representations, warranties, and covenants may change after the date of such agreement, which subsequent information may or may not be fully reflected in the parties’ public disclosures.
Item 16. Form 10-K Summary.
None.
90
Signatures
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
SELECT MEDICAL HOLDINGS CORPORATION SELECT MEDICAL CORPORATION | ||||
By: | /s/ MICHAEL E. TARVIN Michael E. Tarvin (Executive Vice President, General Counsel and Secretary) | |||
Date: February 22, 2018
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities indicated as of February 22, 2018.
/s/ ROCCO A. ORTENZIO Rocco A. Ortenzio Director, Vice Chairman and Co-Founder | /s/ ROBERT A. ORTENZIO Robert A. Ortenzio Director, Executive Chairman and Co-Founder | |
/s/ DAVID S. CHERNOW David S. Chernow President and Chief Executive Officer (principal executive officer) | /s/ MARTIN F. JACKSON Martin F. Jackson Executive Vice President and Chief Financial Officer (principal financial officer) | |
/s/ SCOTT A. ROMBERGER Scott A. Romberger Senior Vice President, Controller and Chief Accounting Officer (principal accounting officer) | /s/ RUSSELL L. CARSON Russell L. Carson Director | |
/s/ BRYAN C. CRESSEY Bryan C. Cressey Director | /s/ WILLIAM H. FRIST, M.D. William H. Frist, M.D. Director | |
/s/ JAMES S. ELY III James S. Ely III Director | /s/ LEOPOLD SWERGOLD Leopold Swergold Director | |
/s/ THOMAS A. SCULLY Thomas A. Scully Director | /s/ HAROLD L. PAZ Harold L. Paz Director | |
91
SELECT MEDICAL HOLDINGS CORPORATION AND SELECT MEDICAL CORPORATION
INDEX TO FINANCIAL STATEMENTS
F-2 | ||
F-4 | ||
F-5 | ||
F-7 | ||
F-9 | ||
F-11 | ||
F-56 | ||
F-1
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders
of Select Medical Holdings Corporation
Opinions on the Financial Statements and Internal Control over Financial Reporting
We have audited the accompanying consolidated balance sheets of Select Medical Holdings Corporation and its subsidiaries as of December 31, 2017 and 2016, and the related consolidated statements of operations and comprehensive income, of changes in equity and income, and of cash flows for each of the three years in the period ended December 31, 2017, including the related notes and schedule of valuation and qualifying accounts for each of the three years in the period ended December 31, 2017 appearing under Item 15(a) (collectively referred to as the “consolidated financial statements”). We also have audited the Company's internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2017 and 2016, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2017 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the COSO.
Basis for Opinions
The Company's management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Report on Internal Control over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on the Company’s consolidated financial statements and on the Company's internal control over financial reporting based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud, and whether effective internal control over financial reporting was maintained in all material respects.
Our audits of the consolidated financial statements included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
Definition and Limitations of Internal Control over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
Harrisburg, Pennsylvania
February 22, 2018
We have served as the Company’s auditor since 2005.
F-2
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholder
of Select Medical Corporation
Opinions on the Financial Statements and Internal Control over Financial Reporting
We have audited the accompanying consolidated balance sheets of Select Medical Corporation and its subsidiaries as of December 31, 2017 and 2016, and the related consolidated statements of operations and comprehensive income, of changes in equity and income, and of cash flows for each of the three years in the period ended December 31, 2017, including the related notes and schedule of valuation and qualifying accounts for each of the three years in the period ended December 31, 2017 appearing under Item 15(a) (collectively referred to as the “consolidated financial statements”). We also have audited the Company's internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2017 and 2016, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2017 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the COSO.
Basis for Opinions
The Company's management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Report on Internal Control over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on the Company’s consolidated financial statements and on the Company's internal control over financial reporting based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud, and whether effective internal control over financial reporting was maintained in all material respects.
Our audits of the consolidated financial statements included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
Definition and Limitations of Internal Control over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
Harrisburg, Pennsylvania
February 22, 2018
We have served as the Company’s auditor since 1999, which includes periods before the Company became subject to SEC reporting requirements.
F-3
PART I FINANCIAL INFORMATION
ITEM 1. CONSOLIDATED FINANCIAL STATEMENTS
Consolidated Balance Sheets
(in thousands, except share and per share amounts)
Select Medical Holdings Corporation | Select Medical Corporation | ||||||||||||||||
December 31, 2016 | December 31, 2017 | December 31, 2016 | December 31, 2017 | ||||||||||||||
ASSETS | |||||||||||||||||
Current Assets: | |||||||||||||||||
Cash and cash equivalents | $ | 99,029 | $ | 122,549 | $ | 99,029 | $ | 122,549 | |||||||||
Accounts receivable, net of allowance for doubtful accounts of $63,787 and $75,544 at 2016 and 2017, respectively | 573,752 | 691,732 | 573,752 | 691,732 | |||||||||||||
Prepaid income taxes | 12,423 | 31,387 | 12,423 | 31,387 | |||||||||||||
Other current assets | 77,699 | 75,158 | 77,699 | 75,158 | |||||||||||||
Total Current Assets | 762,903 | 920,826 | 762,903 | 920,826 | |||||||||||||
Property and equipment, net | 892,217 | 912,591 | 892,217 | 912,591 | |||||||||||||
Goodwill | 2,751,000 | 2,782,812 | 2,751,000 | 2,782,812 | |||||||||||||
Identifiable intangible assets, net | 340,562 | 326,519 | 340,562 | 326,519 | |||||||||||||
Other assets | 173,944 | 184,418 | 173,944 | 184,418 | |||||||||||||
Total Assets | $ | 4,920,626 | $ | 5,127,166 | $ | 4,920,626 | $ | 5,127,166 | |||||||||
LIABILITIES AND EQUITY | |||||||||||||||||
Current Liabilities: | |||||||||||||||||
Overdrafts | $ | 39,362 | $ | 29,463 | $ | 39,362 | $ | 29,463 | |||||||||
Current portion of long-term debt and notes payable | 13,656 | 22,187 | 13,656 | 22,187 | |||||||||||||
Accounts payable | 126,558 | 128,194 | 126,558 | 128,194 | |||||||||||||
Accrued payroll | 146,397 | 160,562 | 146,397 | 160,562 | |||||||||||||
Accrued vacation | 83,261 | 92,875 | 83,261 | 92,875 | |||||||||||||
Accrued interest | 22,325 | 19,885 | 22,325 | 19,885 | |||||||||||||
Accrued other | 140,076 | 143,166 | 140,076 | 143,166 | |||||||||||||
Income taxes payable | — | 9,071 | — | 9,071 | |||||||||||||
Total Current Liabilities | 571,635 | 605,403 | 571,635 | 605,403 | |||||||||||||
Long-term debt, net of current portion | 2,685,333 | 2,677,715 | 2,685,333 | 2,677,715 | |||||||||||||
Non-current deferred tax liability | 199,078 | 124,917 | 199,078 | 124,917 | |||||||||||||
Other non-current liabilities | 136,520 | 145,709 | 136,520 | 145,709 | |||||||||||||
Total Liabilities | 3,592,566 | 3,553,744 | 3,592,566 | 3,553,744 | |||||||||||||
Commitments and contingencies (Note 15) | |||||||||||||||||
Redeemable non-controlling interests | 422,159 | 640,818 | 422,159 | 640,818 | |||||||||||||
Stockholders’ Equity: | |||||||||||||||||
Common stock of Holdings, $0.001 par value, 700,000,000 shares authorized, 132,596,758 and 134,114,715 shares issued and outstanding at 2016 and 2017, respectively | 132 | 134 | — | — | |||||||||||||
Common stock of Select, $0.01 par value, 100 shares issued and outstanding | — | — | 0 | 0 | |||||||||||||
Capital in excess of par | 443,908 | 463,499 | 925,111 | 947,370 | |||||||||||||
Retained earnings (accumulated deficit) | 371,685 | 359,735 | (109,386 | ) | (124,002 | ) | |||||||||||
Total Select Medical Holdings Corporation and Select Medical Corporation Stockholders’ Equity | 815,725 | 823,368 | 815,725 | 823,368 | |||||||||||||
Non-controlling interests | 90,176 | 109,236 | 90,176 | 109,236 | |||||||||||||
Total Equity | 905,901 | 932,604 | 905,901 | 932,604 | |||||||||||||
Total Liabilities and Equity | $ | 4,920,626 | $ | 5,127,166 | $ | 4,920,626 | $ | 5,127,166 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Select Medical Holdings Corporation
Consolidated Statements of Operations and Comprehensive Income
(in thousands, except per share amounts)
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Net operating revenues | $ | 3,742,736 | $ | 4,286,021 | $ | 4,443,603 | |||||||
Costs and expenses: | |||||||||||||
Cost of services | 3,211,541 | 3,664,843 | 3,734,176 | ||||||||||
General and administrative | 92,052 | 106,927 | 114,047 | ||||||||||
Bad debt expense | 59,372 | 69,093 | 79,491 | ||||||||||
Depreciation and amortization | 104,981 | 145,311 | 160,011 | ||||||||||
Total costs and expenses | 3,467,946 | 3,986,174 | 4,087,725 | ||||||||||
Income from operations | 274,790 | 299,847 | 355,878 | ||||||||||
Other income and expense: | |||||||||||||
Loss on early retirement of debt | — | (11,626 | ) | (19,719 | ) | ||||||||
Equity in earnings of unconsolidated subsidiaries | 16,811 | 19,943 | 21,054 | ||||||||||
Non-operating gain (loss) | 29,647 | 42,651 | (49 | ) | |||||||||
Interest expense | (112,816 | ) | (170,081 | ) | (154,703 | ) | |||||||
Income before income taxes | 208,432 | 180,734 | 202,461 | ||||||||||
Income tax expense (benefit) | 72,436 | 55,464 | (18,184 | ) | |||||||||
Net income | 135,996 | 125,270 | 220,645 | ||||||||||
Less: Net income attributable to non-controlling interests | 5,260 | 9,859 | 43,461 | ||||||||||
Net income attributable to Select Medical Holdings Corporation | $ | 130,736 | $ | 115,411 | $ | 177,184 | |||||||
Income per common share: | |||||||||||||
Basic | $ | 1.00 | $ | 0.88 | $ | 1.33 | |||||||
Diluted | $ | 0.99 | $ | 0.87 | $ | 1.33 | |||||||
Dividends paid per share | $ | 0.10 | $ | — | $ | — | |||||||
Weighted average shares outstanding: | |||||||||||||
Basic | 127,478 | 127,813 | 128,955 | ||||||||||
Diluted | 127,752 | 127,968 | 129,126 | ||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Select Medical Corporation
Consolidated Statements of Operations and Comprehensive Income
(in thousands)
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Net operating revenues | $ | 3,742,736 | $ | 4,286,021 | $ | 4,443,603 | |||||||
Costs and expenses: | |||||||||||||
Cost of services | 3,211,541 | 3,664,843 | 3,734,176 | ||||||||||
General and administrative | 92,052 | 106,927 | 114,047 | ||||||||||
Bad debt expense | 59,372 | 69,093 | 79,491 | ||||||||||
Depreciation and amortization | 104,981 | 145,311 | 160,011 | ||||||||||
Total costs and expenses | 3,467,946 | 3,986,174 | 4,087,725 | ||||||||||
Income from operations | 274,790 | 299,847 | 355,878 | ||||||||||
Other income and expense: | |||||||||||||
Loss on early retirement of debt | — | (11,626 | ) | (19,719 | ) | ||||||||
Equity in earnings of unconsolidated subsidiaries | 16,811 | 19,943 | 21,054 | ||||||||||
Non-operating gain (loss) | 29,647 | 42,651 | (49 | ) | |||||||||
Interest expense | (112,816 | ) | (170,081 | ) | (154,703 | ) | |||||||
Income before income taxes | 208,432 | 180,734 | 202,461 | ||||||||||
Income tax expense (benefit) | 72,436 | 55,464 | (18,184 | ) | |||||||||
Net income | 135,996 | 125,270 | 220,645 | ||||||||||
Less: Net income attributable to non-controlling interests | 5,260 | 9,859 | 43,461 | ||||||||||
Net income attributable to Select Medical Corporation | $ | 130,736 | $ | 115,411 | $ | 177,184 | |||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-6
Select Medical Holdings Corporation
Consolidated Statements of Changes in Equity and Income
(in thousands)
Select Medical Holdings Corporation Stockholders | |||||||||||||||||||||||||||||||||
Redeemable Non-controlling interests | Common Stock Issued | Common Stock Par Value | Capital in Excess of Par | Retained Earnings | Total Stockholders’ Equity | Non-controlling Interests | Total Equity | ||||||||||||||||||||||||||
Balance at December 31, 2014 | $ | 10,985 | 131,233 | $ | 131 | $ | 413,706 | $ | 325,678 | $ | 739,515 | $ | 35,725 | $ | 775,240 | ||||||||||||||||||
Net income attributable to Select Medical Holdings Corporation | 130,736 | 130,736 | 130,736 | ||||||||||||||||||||||||||||||
Net income (loss) attributable to non-controlling interests | (2,190 | ) | — | 7,450 | 7,450 | ||||||||||||||||||||||||||||
Dividends paid to common stockholders | (13,129 | ) | (13,129 | ) | (13,129 | ) | |||||||||||||||||||||||||||
Issuance and vesting of restricted stock | 1,385 | 0 | 13,916 | 13,916 | 13,916 | ||||||||||||||||||||||||||||
Tax benefit from stock based awards | 1,846 | 1,846 | 1,846 | ||||||||||||||||||||||||||||||
Repurchase of common shares | (1,518 | ) | 0 | (8,168 | ) | (7,659 | ) | (15,827 | ) | (15,827 | ) | ||||||||||||||||||||||
Stock option expense | 53 | 53 | 53 | ||||||||||||||||||||||||||||||
Exercise of stock options | 183 | 0 | 1,649 | 1,649 | 1,649 | ||||||||||||||||||||||||||||
Issuance of non-controlling interests | 218,005 | 1,689 | 1,689 | 12,880 | 14,569 | ||||||||||||||||||||||||||||
Acquired non-controlling interests | 14,196 | — | 2,888 | 2,888 | |||||||||||||||||||||||||||||
Purchase of non-controlling interests | (876 | ) | (194 | ) | (194 | ) | (25 | ) | (219 | ) | |||||||||||||||||||||||
Distributions to non-controlling interests | (2,909 | ) | — | (9,732 | ) | (9,732 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 1,010 | (1,010 | ) | (1,010 | ) | (1,010 | ) | ||||||||||||||||||||||||||
Other | 9 | 9 | 78 | 87 | |||||||||||||||||||||||||||||
Balance at December 31, 2015 | $ | 238,221 | 131,283 | $ | 131 | $ | 424,506 | $ | 434,616 | $ | 859,253 | $ | 49,264 | $ | 908,517 | ||||||||||||||||||
Net income attributable to Select Medical Holdings Corporation | 115,411 | 115,411 | 115,411 | ||||||||||||||||||||||||||||||
Net income (loss) attributable to non-controlling interests | 12,479 | — | (2,620 | ) | (2,620 | ) | |||||||||||||||||||||||||||
Issuance and vesting of restricted stock | 1,344 | 1 | 16,639 | 16,640 | 16,640 | ||||||||||||||||||||||||||||
Repurchase of common shares | (232 | ) | 0 | (1,333 | ) | (1,596 | ) | (2,929 | ) | (2,929 | ) | ||||||||||||||||||||||
Stock option expense | 4 | 4 | 4 | ||||||||||||||||||||||||||||||
Exercise of stock options | 202 | 0 | 1,672 | 1,672 | 1,672 | ||||||||||||||||||||||||||||
Issuance of non-controlling interests | 2,377 | 2,377 | 47,801 | 50,178 | |||||||||||||||||||||||||||||
Acquired non-controlling interests | — | 2,514 | 2,514 | ||||||||||||||||||||||||||||||
Purchase of non-controlling interests | (2,753 | ) | 75 | 579 | 654 | 654 | |||||||||||||||||||||||||||
Distributions to non-controlling interests | (3,231 | ) | — | (7,324 | ) | (7,324 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 177,216 | (177,216 | ) | (177,216 | ) | (177,216 | ) | ||||||||||||||||||||||||||
Other | 227 | (32 | ) | (109 | ) | (141 | ) | 541 | 400 | ||||||||||||||||||||||||
Balance at December 31, 2016 | $ | 422,159 | 132,597 | $ | 132 | $ | 443,908 | $ | 371,685 | $ | 815,725 | $ | 90,176 | $ | 905,901 | ||||||||||||||||||
Net income attributable to Select Medical Holdings Corporation | 177,184 | 177,184 | 177,184 | ||||||||||||||||||||||||||||||
Net income attributable to non-controlling interests | 35,639 | — | 7,822 | 7,822 | |||||||||||||||||||||||||||||
Issuance and vesting of restricted stock | 1,571 | 2 | 18,289 | 18,291 | 18,291 | ||||||||||||||||||||||||||||
Repurchase of common shares | (280 | ) | 0 | (2,666 | ) | (2,087 | ) | (4,753 | ) | (4,753 | ) | ||||||||||||||||||||||
Exercise of stock options | 227 | 0 | 2,017 | 2,017 | 2,017 | ||||||||||||||||||||||||||||
Issuance of non-controlling interests | 1,951 | 1,951 | 16,329 | 18,280 | |||||||||||||||||||||||||||||
Purchase of non-controlling interests | (127 | ) | 7 | 7 | 7 | ||||||||||||||||||||||||||||
Distributions to non-controlling interests | (5,207 | ) | — | (5,293 | ) | (5,293 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 187,506 | (187,506 | ) | (187,506 | ) | (187,506 | ) | ||||||||||||||||||||||||||
Other | 848 | 452 | 452 | 202 | 654 | ||||||||||||||||||||||||||||
Balance at December 31, 2017 | $ | 640,818 | 134,115 | $ | 134 | $ | 463,499 | $ | 359,735 | $ | 823,368 | $ | 109,236 | $ | 932,604 | ||||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-7
Select Medical Corporation
Consolidated Statements of Changes in Equity and Income
(in thousands)
Select Medical Stockholders | |||||||||||||||||||||||||||||||||
Redeemable Non-controlling interests | Common Stock Issued | Common Stock Par Value | Capital in Excess of Par | Retained Earnings | Total Stockholders’ Equity | Non-controlling Interests | Total Equity | ||||||||||||||||||||||||||
Balance at December 31, 2014 | $ | 10,985 | 0 | $ | 0 | $ | 885,407 | $ | (145,892 | ) | $ | 739,515 | $ | 35,725 | $ | 775,240 | |||||||||||||||||
Net income attributable to Select Medical Corporation | 130,736 | 130,736 | 130,736 | ||||||||||||||||||||||||||||||
Net income (loss) attributable to non-controlling interests | (2,190 | ) | — | 7,450 | 7,450 | ||||||||||||||||||||||||||||
Additional investment by Holdings | 1,649 | 1,649 | 1,649 | ||||||||||||||||||||||||||||||
Dividends declared and paid to Holdings | (28,956 | ) | (28,956 | ) | (28,956 | ) | |||||||||||||||||||||||||||
Contribution related to restricted stock awards and stock option issuances by Holdings | 13,969 | 13,969 | 13,969 | ||||||||||||||||||||||||||||||
Tax benefit from stock based awards | 1,846 | 1,846 | 1,846 | ||||||||||||||||||||||||||||||
Issuance of non-controlling interests | 218,005 | 1,689 | 1,689 | 12,880 | 14,569 | ||||||||||||||||||||||||||||
Acquired non-controlling interests | 14,196 | — | 2,888 | 2,888 | |||||||||||||||||||||||||||||
Purchase of non-controlling interests | (876 | ) | (194 | ) | (194 | ) | (25 | ) | (219 | ) | |||||||||||||||||||||||
Distributions to non-controlling interests | (2,909 | ) | — | (9,732 | ) | (9,732 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 1,010 | (1,010 | ) | (1,010 | ) | (1,010 | ) | ||||||||||||||||||||||||||
Other | 9 | 9 | 78 | 87 | |||||||||||||||||||||||||||||
Balance at December 31, 2015 | $ | 238,221 | 0 | $ | 0 | $ | 904,375 | $ | (45,122 | ) | $ | 859,253 | $ | 49,264 | $ | 908,517 | |||||||||||||||||
Net income attributable to Select Medical Corporation | 115,411 | 115,411 | 115,411 | ||||||||||||||||||||||||||||||
Net income (loss) attributable to non-controlling interests | 12,479 | — | (2,620 | ) | (2,620 | ) | |||||||||||||||||||||||||||
Additional investment by Holdings | 1,672 | 1,672 | 1,672 | ||||||||||||||||||||||||||||||
Dividends declared and paid to Holdings | (2,929 | ) | (2,929 | ) | (2,929 | ) | |||||||||||||||||||||||||||
Contribution related to restricted stock awards and stock option issuances by Holdings | 16,644 | 16,644 | 16,644 | ||||||||||||||||||||||||||||||
Issuance of non-controlling interests | 2,377 | 2,377 | 47,801 | 50,178 | |||||||||||||||||||||||||||||
Acquired non-controlling interests | — | 2,514 | 2,514 | ||||||||||||||||||||||||||||||
Purchase of non-controlling interests | (2,753 | ) | 75 | 579 | 654 | 654 | |||||||||||||||||||||||||||
Distributions to non-controlling interests | (3,231 | ) | — | (7,324 | ) | (7,324 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 177,216 | (177,216 | ) | (177,216 | ) | (177,216 | ) | ||||||||||||||||||||||||||
Other | 227 | (32 | ) | (109 | ) | (141 | ) | 541 | 400 | ||||||||||||||||||||||||
Balance at December 31, 2016 | $ | 422,159 | 0 | $ | 0 | $ | 925,111 | $ | (109,386 | ) | $ | 815,725 | $ | 90,176 | $ | 905,901 | |||||||||||||||||
Net income attributable to Select Medical Corporation | 177,184 | 177,184 | 177,184 | ||||||||||||||||||||||||||||||
Net income attributable to non-controlling interests | 35,639 | — | 7,822 | 7,822 | |||||||||||||||||||||||||||||
Additional investment by Holdings | 2,017 | 2,017 | 2,017 | ||||||||||||||||||||||||||||||
Dividends declared and paid to Holdings | (4,753 | ) | (4,753 | ) | (4,753 | ) | |||||||||||||||||||||||||||
Contribution related to restricted stock award issuances by Holdings | 18,291 | 18,291 | 18,291 | ||||||||||||||||||||||||||||||
Issuance of non-controlling interests | 1,951 | 1,951 | 16,329 | 18,280 | |||||||||||||||||||||||||||||
Purchase of non-controlling interests | (127 | ) | 7 | 7 | 7 | ||||||||||||||||||||||||||||
Distributions to non-controlling interests | (5,207 | ) | — | (5,293 | ) | (5,293 | ) | ||||||||||||||||||||||||||
Redemption adjustment on non-controlling interests | 187,506 | (187,506 | ) | (187,506 | ) | (187,506 | ) | ||||||||||||||||||||||||||
Other | 848 | 452 | 452 | 202 | 654 | ||||||||||||||||||||||||||||
Balance at December 31, 2017 | $ | 640,818 | 0 | $ | 0 | $ | 947,370 | $ | (124,002 | ) | $ | 823,368 | $ | 109,236 | $ | 932,604 | |||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-8
Select Medical Holdings Corporation
Consolidated Statements of Cash Flows
(in thousands)
For the Year Ended December 31, | ||||||||||||||
2015 | 2016 | 2017 | ||||||||||||
Operating activities | ||||||||||||||
Net income | $ | 135,996 | $ | 125,270 | $ | 220,645 | ||||||||
Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||||||
Distributions from unconsolidated subsidiaries | 13,969 | 20,476 | 20,006 | |||||||||||
Depreciation and amortization | 104,981 | 145,311 | 160,011 | |||||||||||
Provision for bad debts | 59,372 | 69,093 | 79,491 | |||||||||||
Equity in earnings of unconsolidated subsidiaries | (16,811 | ) | (19,943 | ) | (21,054 | ) | ||||||||
Loss on extinguishment of debt | — | 11,626 | 6,527 | |||||||||||
Gain on sale of assets and businesses | (1,098 | ) | (46,488 | ) | (10,349 | ) | ||||||||
Gain on sale of equity investment | (29,647 | ) | (2,779 | ) | — | |||||||||
Impairment of equity investment | — | 5,339 | — | |||||||||||
Stock compensation expense | 14,985 | 17,413 | 19,284 | |||||||||||
Amortization of debt discount, premium and issuance costs | 9,543 | 15,656 | 11,130 | |||||||||||
Deferred income taxes | (2,058 | ) | (12,591 | ) | (72,324 | ) | ||||||||
Changes in operating assets and liabilities, net of effects of business combinations: | ||||||||||||||
Accounts receivable | (92,572 | ) | (39,320 | ) | (197,191 | ) | ||||||||
Other current assets | (2,503 | ) | 17,450 | 1,597 | ||||||||||
Other assets | 4,713 | 9,290 | (886 | ) | ||||||||||
Accounts payable | 2,345 | (15,492 | ) | 3,903 | ||||||||||
Accrued expenses | 7,200 | 46,292 | 17,341 | |||||||||||
Net cash provided by operating activities | 208,415 | 346,603 | 238,131 | |||||||||||
Investing activities | ||||||||||||||
Business combinations, net of cash acquired | (1,061,628 | ) | (472,206 | ) | (27,390 | ) | ||||||||
Purchases of property and equipment | (182,642 | ) | (161,633 | ) | (233,243 | ) | ||||||||
Investment in businesses | (2,347 | ) | (4,723 | ) | (12,682 | ) | ||||||||
Proceeds from sale of assets and businesses | 1,767 | 80,463 | 80,350 | |||||||||||
Proceeds from sale of equity investment | 33,096 | 3,779 | — | |||||||||||
Net cash used in investing activities | (1,211,754 | ) | (554,320 | ) | (192,965 | ) | ||||||||
Financing activities | ||||||||||||||
Borrowings on revolving facilities | 1,135,000 | 575,000 | 970,000 | |||||||||||
Payments on revolving facilities | (895,000 | ) | (655,000 | ) | (960,000 | ) | ||||||||
Proceeds from term loans | 623,575 | 795,344 | 1,139,487 | |||||||||||
Payments on term loans | (29,134 | ) | (438,034 | ) | (1,179,442 | ) | ||||||||
Revolving facility debt issuance costs | — | — | (4,392 | ) | ||||||||||
Borrowings of other debt | 13,374 | 27,721 | 46,621 | |||||||||||
Principal payments on other debt | (18,136 | ) | (21,401 | ) | (20,647 | ) | ||||||||
Dividends paid to common stockholders | (13,129 | ) | — | — | ||||||||||
Repurchase of common stock | (15,827 | ) | (2,929 | ) | (4,753 | ) | ||||||||
Proceeds from exercise of stock options | 1,649 | 1,672 | 2,017 | |||||||||||
Tax benefit from stock based awards | 1,846 | — | — | |||||||||||
Increase (decrease) in overdrafts | 6,869 | 10,746 | (9,899 | ) | ||||||||||
Proceeds from issuance of non-controlling interests | 217,065 | 11,846 | 9,982 | |||||||||||
Purchase of non-controlling interests | (1,095 | ) | (2,099 | ) | (120 | ) | ||||||||
Distributions to non-controlling interests | (12,637 | ) | (10,555 | ) | (10,500 | ) | ||||||||
Net cash provided by (used in) financing activities | 1,014,420 | 292,311 | (21,646 | ) | ||||||||||
Net increase in cash and cash equivalents | 11,081 | 84,594 | 23,520 | |||||||||||
Cash and cash equivalents at beginning of period | 3,354 | 14,435 | 99,029 | |||||||||||
Cash and cash equivalents at end of period | $ | 14,435 | $ | 99,029 | $ | 122,549 | ||||||||
Supplemental Information | ||||||||||||||
Cash paid for interest | $ | 103,166 | $ | 142,640 | $ | 149,156 | ||||||||
Cash paid for taxes | $ | 79,420 | $ | 70,756 | $ | 64,991 | ||||||||
Liabilities for purchases of property and equipment | $ | 36,744 | $ | 32,861 | $ | 30,043 | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-9
Select Medical Corporation
Consolidated Statements of Cash Flows
(in thousands)
For the Year Ended December 31, | |||||||||||||
2015 | 2016 | 2017 | |||||||||||
Operating activities | |||||||||||||
Net income | $ | 135,996 | $ | 125,270 | $ | 220,645 | |||||||
Adjustments to reconcile net income to net cash provided by operating activities: | |||||||||||||
Distributions from unconsolidated subsidiaries | 13,969 | 20,476 | 20,006 | ||||||||||
Depreciation and amortization | 104,981 | 145,311 | 160,011 | ||||||||||
Provision for bad debts | 59,372 | 69,093 | 79,491 | ||||||||||
Equity in earnings of unconsolidated subsidiaries | (16,811 | ) | (19,943 | ) | (21,054 | ) | |||||||
Loss on extinguishment of debt | — | 11,626 | 6,527 | ||||||||||
Gain on sale of assets and businesses | (1,098 | ) | (46,488 | ) | (10,349 | ) | |||||||
Gain on sale of equity investment | (29,647 | ) | (2,779 | ) | — | ||||||||
Impairment of equity investment | — | 5,339 | — | ||||||||||
Stock compensation expense | 14,985 | 17,413 | 19,284 | ||||||||||
Amortization of debt discount, premium and issuance costs | 9,543 | 15,656 | 11,130 | ||||||||||
Deferred income taxes | (2,058 | ) | (12,591 | ) | (72,324 | ) | |||||||
Changes in operating assets and liabilities, net of effects of business combinations: | |||||||||||||
Accounts receivable | (92,572 | ) | (39,320 | ) | (197,191 | ) | |||||||
Other current assets | (2,503 | ) | 17,450 | 1,597 | |||||||||
Other assets | 4,713 | 9,290 | (886 | ) | |||||||||
Accounts payable | 2,345 | (15,492 | ) | 3,903 | |||||||||
Accrued expenses | 7,200 | 46,292 | 17,341 | ||||||||||
Net cash provided by operating activities | 208,415 | 346,603 | 238,131 | ||||||||||
Investing activities | |||||||||||||
Business combinations, net of cash acquired | (1,061,628 | ) | (472,206 | ) | (27,390 | ) | |||||||
Purchases of property and equipment | (182,642 | ) | (161,633 | ) | (233,243 | ) | |||||||
Investment in businesses | (2,347 | ) | (4,723 | ) | (12,682 | ) | |||||||
Proceeds from sale of assets and businesses | 1,767 | 80,463 | 80,350 | ||||||||||
Proceeds from sale of equity investment | 33,096 | 3,779 | — | ||||||||||
Net cash used in investing activities | (1,211,754 | ) | (554,320 | ) | (192,965 | ) | |||||||
Financing activities | |||||||||||||
Borrowings on revolving facilities | 1,135,000 | 575,000 | 970,000 | ||||||||||
Payments on revolving facilities | (895,000 | ) | (655,000 | ) | (960,000 | ) | |||||||
Proceeds from term loans | 623,575 | 795,344 | 1,139,487 | ||||||||||
Payments on term loans | (29,134 | ) | (438,034 | ) | (1,179,442 | ) | |||||||
Revolving facility debt issuance costs | — | — | (4,392 | ) | |||||||||
Borrowings of other debt | 13,374 | 27,721 | 46,621 | ||||||||||
Principal payments on other debt | (18,136 | ) | (21,401 | ) | (20,647 | ) | |||||||
Dividends paid to Holdings | (28,956 | ) | (2,929 | ) | (4,753 | ) | |||||||
Equity investment by Holdings | 1,649 | 1,672 | 2,017 | ||||||||||
Tax benefit from stock based awards | 1,846 | — | — | ||||||||||
Increase (decrease) in overdrafts | 6,869 | 10,746 | (9,899 | ) | |||||||||
Proceeds from issuance of non-controlling interests | 217,065 | 11,846 | 9,982 | ||||||||||
Purchase of non-controlling interests | (1,095 | ) | (2,099 | ) | (120 | ) | |||||||
Distributions to non-controlling interests | (12,637 | ) | (10,555 | ) | (10,500 | ) | |||||||
Net cash provided by (used in) financing activities | 1,014,420 | 292,311 | (21,646 | ) | |||||||||
Net increase in cash and cash equivalents | 11,081 | 84,594 | 23,520 | ||||||||||
Cash and cash equivalents at beginning of period | 3,354 | 14,435 | 99,029 | ||||||||||
Cash and cash equivalents at end of period | $ | 14,435 | $ | 99,029 | $ | 122,549 | |||||||
Supplemental Information | |||||||||||||
Cash paid for interest | $ | 103,166 | $ | 142,640 | $ | 149,156 | |||||||
Cash paid for taxes | $ | 79,420 | $ | 70,756 | $ | 64,991 | |||||||
Liabilities for purchases of property and equipment | $ | 36,744 | $ | 32,861 | $ | 30,043 | |||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-10
SELECT MEDICAL HOLDINGS CORPORATION AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Organization and Significant Accounting Policies
Business Description
Select Medical Corporation (“Select”) was formed in December 1996 and commenced operations during February 1997 upon the completion of its first acquisition. Select Medical Holdings Corporation (“Holdings”) was formed in October 2004 for the purpose of effecting a leveraged buyout of Select, which was a publicly traded entity. On February 24, 2005, Select merged with a subsidiary of Holdings, which resulted in Select becoming a wholly owned subsidiary of Holdings (the “Merger”). On September 30, 2009, Holdings completed its initial public offering of common stock. At the time of the transaction, generally accepted accounting principles (“GAAP”) required that any amounts recorded or incurred (such as goodwill and compensation expense) by the parent as a result of the Merger or for the benefit of the subsidiary be “pushed down” and recorded in Select’s consolidated financial statements. Holdings and Select and their subsidiaries are collectively referred to as the “Company.” The consolidated financial statements of Holdings include the accounts of its wholly owned subsidiary Select. Holdings conducts substantially all of its business through Select and its subsidiaries.
The Company is managed through four business segments: long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. The Company’s long term acute care segment consists of hospitals designed to serve the needs of long term acute patients and the inpatient rehabilitation segment consists of hospitals designed to serve patients that require intensive rehabilitation care. Patients are typically admitted to the Company’s long term acute care hospitals (“LTCHs”) and inpatient rehabilitation facilities (“IRFs”) from general acute care hospitals. These patients have specialized needs, with serious and often complex medical conditions. The Company operated 100 LTCHs and 24 IRFs at December 31, 2017. The Company’s outpatient rehabilitation segment consists of clinics that provide physical, occupational, and speech rehabilitation services. At December 31, 2017, the Company operated 1,616 outpatient clinics. The Company’s Concentra segment consists of occupational health centers and contract services provided at employer worksites and Department of Veterans Affairs community-based outpatient clinics (“CBOCs”) that deliver occupational medicine, physical therapy, veteran’s healthcare, and consumer health services. At December 31, 2017, the Company operated 312 occupational health centers, 105 medical facilities located at the workplaces of Concentra’s employer customers, and 32 Department of Veterans Affairs CBOCs. At December 31, 2017, the Company had operations in 47 states and the District of Columbia.
Principles of Consolidation
The consolidated financial statements include the accounts of the Company; the subsidiaries, limited liability companies, and limited partnerships in which the Company has a controlling financial interest; and its subsidiaries’ controlling financial interests in limited partnerships and limited liability companies. All intercompany balances and transactions are eliminated in consolidation.
Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities, including disclosure of contingencies, at the date of the financial statements and reported amounts of revenues and expenses during the reporting period. Significant estimates and assumptions are used for, but not limited to: accounts receivable and allowance for doubtful accounts, depreciable lives of assets, intangible assets, insurance, and income taxes. Future events and their effects cannot be predicted with certainty; accordingly, the Company’s accounting estimates require the exercise of judgment. The accounting estimates used in the preparation of the financial statements will change as new events occur, as more experience is acquired, as additional information is obtained, and as the Company’s operating environment changes. The Company’s management evaluates and updates assumptions and estimates on an ongoing basis. Actual results could differ from those estimates.
F-11
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Segment Reporting
The Company identifies its operating segments according to how the chief operating decision maker evaluates financial performance and allocates resources. During 2017, the Company changed its internal segment reporting structure which is reflective of how the Company now manages its business operations, reviews operating performance, and allocates resources. For the year ended December 31, 2017, the Company’s reportable segments include long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. Prior year results for the years ended December 31, 2015 and 2016 presented herein have been recast to conform to the current presentation. Prior to 2017, the Company disclosed financial information for the following reportable segments: specialty hospitals, outpatient rehabilitation, and Concentra.
Cash and Cash Equivalents
The Company considers all highly liquid investments with a maturity of three months or less when purchased to be cash equivalents. Cash equivalents are stated at cost which approximates fair value.
Accounts Receivable and Allowance for Doubtful Accounts
The Company reports accounts receivable at estimated net realizable values. Substantially all of the Company’s accounts receivable are related to providing healthcare services to patients whose costs are primarily paid by federal and state governmental authorities, managed care health plans, commercial insurance companies, and workers’ compensation and employer programs. Collection of these accounts receivable is the Company’s primary source of cash and is critical to its operating performance. The Company’s primary collection risks relate to non-governmental payors who insure these patients and deductibles, co-payments, and amounts owed by the patient. Deductibles, co-payments, and self-insured amounts owed by the patient are an immaterial portion of the Company’s net accounts receivable balance and accounted for approximately 1.2% and 0.6% of the net accounts receivable balance before doubtful accounts at December 31, 2016 and 2017, respectively. The Company’s general policy is to verify insurance coverage prior to the date of admission for patients admitted to the Company’s LTCHs and IRFs. Within the Company’s outpatient rehabilitation clinics, the Company verifies insurance coverage prior to the patient’s visit. Within the Company’s Concentra centers, the Company verifies insurance coverage or receives authorization from the patient’s employer prior to the patient’s visit. The Company’s estimate for the allowance for doubtful accounts is calculated by applying a reserve allowance based upon the age of an account balance. This method is monitored based on historical cash collections experience and write-off experience. Collections are impacted by the effectiveness of the Company’s collection efforts with non-governmental payors and regulatory or administrative disruptions with the fiscal intermediaries that pay the Company’s governmental receivables. Uncollected accounts are written off the balance sheet when they are turned over to an outside collection agency, or when management determines that the balance is uncollectible, whichever occurs first.
Concentration of Credit Risk
Financial instruments that potentially subject the Company to concentration of credit risk consist primarily of cash balances and trade receivables. The Company invests its excess cash with large financial institutions. The Company grants unsecured credit to its patients, most of who reside in the service area of the Company’s facilities and are insured under third-party payor agreements. Because of the geographic diversity of the Company’s facilities and non-governmental third-party payors, Medicare represents the Company’s only significant concentration of credit risk.
Financial Instruments
The Company accounts for its financial instruments in accordance with Accounting Standards Codification (“ASC”) Topic 820, Fair Value Measurements and Disclosure. The Company’s financial instruments include cash and cash equivalents, accounts receivable, accounts payable, and indebtedness. The carrying amount of cash and cash equivalents, accounts receivable, and accounts payable approximate fair value because of the short-term maturity of these instruments. The face values, carrying values, and fair values of the Company’s indebtedness are presented in Note 8.
F-12
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Property and Equipment
Property and equipment are stated at cost, net of accumulated depreciation. Maintenance and repairs of property and equipment are expensed as incurred. Improvements that increase the estimated useful life of an asset are capitalized. Direct internal and external costs of developing software for internal use, including programming and enhancements, are capitalized and depreciated over the estimated useful lives once the software is placed in service. Capitalized software costs are included within furniture and equipment. Software training costs, maintenance, and repairs are expensed as incurred. Depreciation and amortization are computed using the straight-line method over the estimated useful lives of the assets or the term of the lease, as appropriate. The general range of useful lives is as follows:
Land improvements | 2 - 25 years |
Leasehold improvements | 1 - 15 years |
Buildings | 40 years |
Building improvements | 5 - 20 years |
Furniture and equipment | 1 - 20 years |
The Company reviews the realizability of long-lived assets whenever events or circumstances occur which indicate recorded costs may not be recoverable. Gains or losses related to the retirement or disposal of property and equipment are reported as a component of income from operations.
Intangible Assets
Goodwill and other indefinite-lived intangible assets
Goodwill and other indefinite-lived intangible assets are recognized primarily as the result of business combinations. Goodwill is assigned to reporting units based upon the specific nature of the business acquired. When a business combination contains business components related to more than one reporting unit, goodwill is assigned to each reporting unit based upon an allocation determined by the relative fair values of the business acquired.
Goodwill and other indefinite‑lived intangible assets are not amortized, but instead are subject to periodic impairment evaluations. Impairment tests are required to be conducted at least annually or when events or conditions occur that might suggest a possible impairment. These events or conditions include, but are not limited to: a significant adverse change in the business environment, regulatory environment or legal factors; a current period operating or cash flow loss combined with a history of such losses or a projection of continuing losses; or a sale or disposition of a significant portion of a reporting unit. The occurrence of one of these events or conditions could significantly impact an impairment assessment, necessitating an impairment charge.
In performing the quantitative periodic impairment tests for goodwill, the fair value of the reporting unit is compared to its carrying value, including goodwill and other intangible assets. If the carrying value exceeds the fair value and an impairment condition exists, an impairment loss would be recognized. When the Company determines the fair value of its reporting units, the Company considers both the income and market approach. Included in the income approach, specific for each reporting unit, are assumptions regarding revenue growth rate, future Adjusted EBITDA margin estimates, future general and administrative expense rates, and the industry’s weighted average cost of capital and industry specific, market comparable implied Adjusted EBITDA multiples. The Company also must estimate residual values at the end of the forecast period and future capital expenditure requirements. Each of these assumptions requires the Company to use its knowledge of its industry, its recent transactions, and reasonable performance expectations for its operations. If any one of the above assumptions changes or fails to materialize, the resulting decline in the Company’s estimated fair value could result in an impairment charge to the goodwill associated with any one of the reporting units.
F-13
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
At December 31, 2017, the Company’s indefinite-lived intangible assets consist of trademarks, certificates of need, and accreditations. In performing the quantitative periodic impairment tests for the Company’s trademarks, the fair value of the trademark is compared to its carrying value. If the carrying value exceeds the fair value and an impairment condition exists, an impairment loss would be recognized. To determine the fair value of the trademark, the Company uses a relief from royalty income approach. For the Company’s certificates of need and accreditations, the Company performs a qualitative assessment. As part of this assessment, the Company evaluates the current business environment, regulatory environment, legal and other company-specific factors. If it is more likely than not that the fair value is less than the carrying value, the Company performs a quantitative impairment test.
The Company’s most recent impairment assessment was completed during the fourth quarter of 2017 utilizing financial information as of October 1, 2017. The Company did not identify any instances of impairment with respect to goodwill or other indefinite-lived intangible assets as of October 1, 2017.
During the fourth quarter of 2017, the Company determined that it was operating through four operating segments, which resulted in a change to the Company’s reporting units. As of December 31, 2017 , our reporting units include long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. Previously, the Company had three reporting units: specialty hospitals, outpatient rehabilitation, and Concentra. Goodwill was allocated to the long term acute care and inpatient rehabilitation reporting units based upon the relative fair values of these reporting units. The Company completed an assessment of potential goodwill impairment for each of these reporting units immediately after the allocation of goodwill and determined that no impairment existed.
Other finite-lived intangible assets
At December 31, 2017, the Company’s finite-lived intangible assets consist of customer relationships, non-compete agreements, and leasehold interests. Finite-lived intangible assets are amortized based on the pattern in which the economic benefits are consumed or otherwise depleted. If such a pattern cannot be reliably determined, finite-lived intangible assets are amortized on a straight-line basis over their estimated lives. Management believes that the below estimated useful lives are reasonable based on the economic factors applicable to each class of finite-lived intangible asset.
Customer relationships | 6 - 17 years |
Leasehold interests | 1 - 15 years |
Non-compete agreements | 1 - 15 years |
The Company reviews the realizability of finite-lived intangible assets whenever events or circumstances occur which indicate recorded amounts may not be recoverable. If the expected undiscounted future cash flows are less than the carrying amount of such assets, the Company recognizes an impairment loss to the extent the carrying amount of the assets exceeds their estimated fair value.
Equity Method Investments
Investments in equity method investees are accounted for using the equity method based upon the level of ownership and/or the Company’s ability to exercise significant influence over the operating and financial policies of the investee. Investments of this nature are recorded at original cost and adjusted periodically to recognize the Company’s proportionate share of the investees’ net income or losses after the date of investment. When net losses from an investment accounted for under the equity method exceed its carrying amount, the investment balance is reduced to zero. The Company resumes accounting for the investment under the equity method if the entity subsequently reports net income and the Company’s share of that net income exceeds the share of the net losses not recognized during the period the equity method was suspended. Investments are written down only when there is clear evidence that a decline in value that is other than temporary has occurred. The Company evaluates its investments in companies accounted for using the equity method for impairment when there is evidence or indicators that a decrease in value may be other than temporary.
F-14
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Debt Issuance Costs
Debt issuance costs related to notes and loans are recognized as a direct deduction from the carrying value of the debt liability on the consolidated balance sheets. Debt issuance costs related to line-of-credit arrangements are presented as part of other assets on the consolidated balance sheets. Debt issuance costs are subsequently amortized and recognized as interest expense using the effective interest method over the term of the related indebtedness. Whenever indebtedness is modified from its original terms or exchanged, an evaluation is made whether an accounting modification or accounting extinguishment has occurred.
Due to Third-Party Payors
Due to third-party payors represents the difference between amounts received under interim payment plans from Medicare for services rendered and amounts estimated to be reimbursed upon settlement of cost reports.
Income Taxes
Deferred tax assets and liabilities are recognized using enacted tax rates for the effect of temporary differences between the book and tax basis of recorded assets and liabilities. Deferred tax assets are reduced by a valuation allowance if it is more likely than not that some portion or all of the deferred tax asset will not be realized. As part of the process of preparing its consolidated financial statements, the Company estimates income taxes based on its actual current tax exposure together with assessing temporary differences resulting from differing treatment of items for book and tax purposes. The Company also recognizes as deferred tax assets the future tax benefits from net operating loss carryforwards. The Company evaluates the realizability of these deferred tax assets by assessing their valuation allowances and by adjusting the amount of such allowances, if necessary. Among the factors used to assess the likelihood of realization are projections of future taxable income streams, the expected timing of the reversals of existing temporary differences, and the impact of tax planning strategies that could be implemented to avoid the potential loss of future tax benefits.
Reserves for uncertain tax positions are established for exposure items related to various federal and state tax matters. Income tax reserves are recorded when an exposure is identified and when, in the opinion of management, it is more likely than not that a tax position will not be sustained and the amount of the liability can be estimated.
Tax Cuts and Jobs Act
On December 22, 2017 the Tax Cuts and Jobs Act (the “Act") was signed into law. The Act reduces the federal statutory tax rate to 21% from 35%. ASC 740, Income Taxes, requires the effects of changes in tax rates and laws on deferred tax balances to be recognized in the period in which the legislation is enacted. While the effective date of the new corporate tax rate is January 1, 2018, the Company recorded the effect on its December 31, 2017 deferred tax balances.
Applying the effects of a lower corporate tax rate to deferred tax assets and liabilities and considering provisions of the Act in a relatively short period of time requires significant estimation and judgment. The Company has been able to make reasonable estimates of the Act's provisions and has recorded an income tax benefit of $71.5 million to reflect these effects.
Insurance Risk Programs
Under a number of the Company’s insurance programs, which include the Company’s employee health insurance, workers’ compensation, and professional malpractice liability insurance programs, the Company is liable for a portion of its losses before it can attempt to recover from the applicable insurance carrier. The Company accrues for losses for which it will be ultimately responsible under an occurrence-based approach whereby the Company estimates the losses that will be incurred in a respective accounting period and accrues that estimated liability using actuarial methods. These programs are monitored quarterly and estimates are revised as necessary to take into account additional information.
F-15
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Non-Controlling Interests
The ownership interests held by outside parties in subsidiaries, limited liability companies and limited partnerships controlled by the Company are classified as non-controlling interests.
Some of our non-controlling ownership interests consist of outside parties that have certain redemption rights that, if exercised, require the Company to purchase the parties’ ownership interest. These interests are classified and reported as redeemable non-controlling interests and have been adjusted to their approximate redemption values. As of December 31, 2016 and 2017, the Company believes the redemption amounts of these ownership interests approximate fair value.
Net income or loss is attributed to each non-controlling ownership interest and to the Company in the consolidated statements of operations and comprehensive income. The following table summarizes the net income or loss attributable to non-controlling interests and redeemable non-controlling interests. The results of Holdings are identical to those of Select.
For the Year Ended December 31, | |||||||||||
2015 | 2016 | 2017 | |||||||||
(in thousands) | |||||||||||
Attributable to non-controlling interests | $ | 7,450 | $ | (2,620 | ) | $ | 7,822 | ||||
Attributable to redeemable non-controlling interests | (2,190 | ) | 12,479 | 35,639 | |||||||
Net income attributable to non-controlling interests | $ | 5,260 | $ | 9,859 | $ | 43,461 | |||||
Revenue Recognition
Net operating revenues consists primarily of patient service revenues and revenues generated from services provided to healthcare institutions under contractual arrangements and are recognized as services are rendered.
Patient service revenue is reported net of provisions for contractual allowances from third-party payors and patients. The Company has agreements with third-party payors that provide for payments to the Company at amounts which differ from its established billing rates. The differences between the estimated program reimbursement rates and the standard billing rates are accounted for as contractual adjustments, which are deducted from gross revenues to arrive at net operating revenues. Payment arrangements include prospectively determined rates per discharge, reimbursed costs, discounted charges, per diem, and per visit payments. Retroactive adjustments are accrued on an estimated basis in the period the related services are rendered and adjusted in future periods as final settlements are determined. Accounts receivable resulting from such payment arrangements are recorded net of contractual allowances.
A significant portion of the Company’s net operating revenues are generated directly from the Medicare program. Net operating revenues generated directly from the Medicare program represented approximately 37%, 30%, and 30% of the Company’s net operating revenues for the years ended December 31, 2015, 2016, and 2017, respectively. Approximately 18% and 27% of the Company’s accounts receivable (after allowances for contractual adjustments but before doubtful accounts) are from Medicare at December 31, 2016 and 2017, respectively. As a provider of services to the Medicare program, the Company is subject to extensive regulations. The inability of any of the Company’s long term acute care hospitals, inpatient rehabilitation facilities, or outpatient rehabilitation clinics to comply with Medicare regulations can result in significant changes in the net operating revenues generated from the Medicare program.
F-16
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Recent Accounting Pronouncements
Revenue from Contracts with Customers
Beginning in May 2014, the Financial Accounting Standards Board (“FASB”) issued several Accounting Standards Updates which established Topic 606, Revenue from Contracts with Customers (the “standard”). This standard supersedes existing revenue recognition requirements and seeks to eliminate most industry-specific guidance under current GAAP. The core principle of the new guidance is that an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. New disclosures about the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers are also required. The standard requires the selection of a full retrospective or cumulative effect transition method.
The Company has completed its implementation efforts and will adopt the new standard beginning January 1, 2018 using the full retrospective transition method. The presentation of the amount of income from operations and net income will be unchanged upon adoption of the new standard; however, adoption of the new standard will result in significant changes to the presentation of net operating revenues and bad debt expense in the consolidated statements of operations and comprehensive income. The principal change affecting the Company results from the presentation of variable consideration that under the accounting standard is included in the transaction price up to an amount which is probable that a significant reversal will not occur. The most common form of variable consideration the Company experiences are amounts for services provided that are ultimately not realizable from a patient. Under the current standard, the Company’s estimate for unrealizable amounts was recorded to bad debt expense. Under the new standard, the Company’s estimate for unrealizable amounts will be recognized as an additional allowance to revenue and will be reflected as a reduction to accounts receivable.
Adoption of the revenue recognition standard will impact our reported results for December 31, 2016 and December 31, 2017 as follows:
December 31, 2016 | December 31, 2017 | ||||||||||||||
As Reported | As Adjusted | As Reported | As Adjusted | ||||||||||||
(in thousands) | |||||||||||||||
Net operating revenues | $ | 4,286,021 | $ | 4,217,460 | $ | 4,443,603 | $ | 4,365,245 | |||||||
Bad debt expense | 69,093 | 532 | 79,491 | 1,133 | |||||||||||
Leases
In February 2016, the FASB issued Accounting Standards Update (“ASU”) 2016-02, Leases. This ASU includes a lessee accounting model that recognizes two types of leases: finance and operating. This ASU requires that a lessee recognize on the balance sheet assets and liabilities for all leases with lease terms of more than twelve months. Lessees will need to recognize almost all leases on the balance sheet as a right-of-use asset and a lease liability. For income statement purposes, the FASB retained the dual model, requiring leases to be classified as either operating or finance. The recognition, measurement, and presentation of expenses and cash flows arising from a lease by a lessee will depend on its classification as finance or operating lease. For short-term leases of twelve months or less, lessees are permitted to make an accounting election by class of underlying asset not to recognize right-of-use assets or lease liabilities. If the alternative is elected, lease expense would be recognized generally on the straight-line basis over the respective lease term.
The amendments in ASU 2016-02 will take effect for public companies for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Earlier application is permitted as of the beginning of an interim or annual reporting period. A modified retrospective approach is required for leases that exist or are entered into after the beginning of the earliest comparative period in the financial statements.
Upon adoption, the Company will recognize significant assets and liabilities on the consolidated balance sheets as a result of the operating lease obligations of the Company. Operating lease expense will still be recognized as rent expense on a straight-line basis over the respective lease terms in the consolidated statements of operations and comprehensive income.
F-17
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
The Company will implement the new standard beginning January 1, 2019. The Company’s implementation efforts are focused on designing accounting processes, disclosure processes, and internal controls in order to account for its leases under the new standard.
Income Taxes
In October 2016, the FASB issued ASU 2016-16, Income Taxes (Topic 740), Intra-Entity Transfers of Assets Other Than Inventory. Current GAAP prohibits the recognition of current and deferred income taxes for an intra-entity asset transfer until the asset has been sold to an outside party. The ASU requires an entity to recognize the income tax consequences of an intra‑entity transfer of an asset other than inventory when the transfer occurs. The standard will be effective for fiscal years beginning after December 15, 2017. The Company plans to adopt the guidance effective January 1, 2018. Adoption of the guidance will be applied on a modified retrospective approach through a cumulative effect adjustment to retained earnings as of the effective date.
Business Combinations
In January 2017, the FASB issued ASU 2017-01, Business Combinations (Topic 805), Clarifying the Definition of a Business, which clarifies the definition of a business with the objective of adding guidance to assist entities with evaluating whether transactions should be accounted for as acquisitions or disposals of assets or businesses. ASU 2017-01 states that if substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the transaction should be accounted for as an asset acquisition. In addition, the ASU clarifies the requirements for a set of activities to be considered a business and narrows the definition of an output. The definition of a business affects many areas of accounting including acquisitions, disposals, goodwill and consolidation. ASU 2017-01 is effective for annual periods beginning after December 15, 2017. Early adoption is permitted.
Financial Instruments
In June 2016, the FASB issued ASU 2016-13, Financial Instruments - Credit Losses: Measurement of Credit Losses on Financial Instruments. The current standard delays the recognition of a credit loss on a financial asset until the loss is probable of occurring. The new standard removes the requirement that a credit loss be probable of occurring for it to be recognized and requires entities to use historical experience, current conditions, and reasonable and supportable forecasts to estimate their future expected credit losses. The Company’s accounts receivable derived from contracts with customers will be subject to ASU 2016-13.
The standard will be effective for fiscal years beginning after December 15, 2019, including interim periods within those fiscal years. The guidance must be applied using a modified retrospective approach through a cumulative-effect adjustment to retained earnings as of the beginning of the earliest comparative period in the financial statements. Given the very high rate of collectability of the Company’s accounts receivable derived from contracts with customers, the impact of ASU 2016-13 is unlikely to be material.
F-18
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Organization and Significant Accounting Policies (Continued)
Recently Adopted Accounting Pronouncements
Income Taxes
In November 2015, the FASB issued ASU 2015-17, Balance Sheet Classification of Deferred Taxes, which changed the presentation of deferred income taxes. The standard changed the presentation of deferred income taxes through the requirement that all deferred tax liabilities and assets be classified as non-current in a classified statement of financial position. The Company adopted the standard on January 1, 2017. The consolidated balance sheet at December 31, 2016 has been retrospectively adjusted. Adoption of the new standard impacted the Company’s previously reported results as follows:
December 31, 2016 | |||||||
As Reported | As Adjusted | ||||||
(in thousands) | |||||||
Current deferred tax asset | $ | 45,165 | $ | — | |||
Total current assets | 808,068 | 762,903 | |||||
Other assets | 152,548 | 173,944 | |||||
Total assets | 4,944,395 | 4,920,626 | |||||
Non-current deferred tax liability | 222,847 | 199,078 | |||||
Total liabilities | 3,616,335 | 3,592,566 | |||||
Total liabilities and equity | 4,944,395 | 4,920,626 | |||||
Stock Compensation
In March 2016, the FASB issued ASU 2016-09, Compensation‑Stock Compensation, which simplifies various aspects of accounting for share-based payments. The areas for simplification involve several aspects of the accounting for share-based payment transactions, including the income tax consequences and classification on the statements of cash flows. During the fourth quarter of 2016, the Company adopted and applied the standard on a prospective basis beginning January 1, 2016. The Company has elected to recognize the effect of forfeitures in compensation cost when they occur. There was no retrospective impact to the consolidated financial statements, including the consolidated statements of cash flows, as a result of the adoption of this standard.
Reclassifications
Certain reclassifications have been made to prior year amounts in order to conform to current year presentation. As discussed above, the condensed consolidated balance sheet at December 31, 2016 has been changed in order to conform to the current year balance sheet presentation for the adoption of ASU 2015-17, Balance Sheet Classification of Deferred Taxes.
F-19
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Acquisitions
Physiotherapy Acquisition
On March 4, 2016, Select acquired 100% of the issued and outstanding equity securities of Physiotherapy Associates Holdings, Inc. (“Physiotherapy”) for $406.3 million, net of $12.3 million of cash acquired. For the year ended December 31, 2016, $3.2 million of Physiotherapy acquisition costs were recognized in general and administrative expense.
Physiotherapy is a national provider of outpatient physical rehabilitation care offering a wide range of services, including general orthopedics, spinal care and neurological rehabilitation, as well as orthotics and prosthetics services.
For the Physiotherapy acquisition, the Company allocated the purchase price to tangible and identifiable intangible assets acquired and liabilities assumed based on their estimated fair value in accordance with the provisions of ASC 805, Business Combinations. During the year ended December 31, 2016, the Company finalized the accounting for identifiable intangible assets and liabilities, fixed assets, non-controlling interests, and certain pre-acquisition contingencies. During the quarter ended March 31, 2017, the Company completed the accounting for certain deferred tax matters.
The following table reconciles the allocation of the consideration given for identifiable net assets and goodwill acquired to the net cash paid for the acquired business (in thousands):
Cash and cash equivalents | $ | 12,340 | |
Identifiable tangible assets, excluding cash and cash equivalents | 87,832 | ||
Identifiable intangible assets | 32,484 | ||
Goodwill | 343,187 | ||
Total assets | 475,843 | ||
Total liabilities | 54,685 | ||
Acquired non-controlling interests | 2,514 | ||
Net assets acquired | 418,644 | ||
Less: Cash and cash equivalents acquired | (12,340 | ) | |
Net cash paid | $ | 406,304 | |
Goodwill of $343.2 million has been recognized in the business combination, representing the excess of the consideration given over the fair value of identifiable net assets acquired. The value of goodwill is derived from Physiotherapy’s future earnings potential and its assembled workforce. Goodwill has been assigned to the outpatient rehabilitation reporting unit and is not deductible for tax purposes. However, prior to its acquisition by the Company, Physiotherapy completed certain acquisitions that resulted in tax deductible goodwill with an estimated value of $8.8 million, which the Company will deduct through 2030.
Due to the integration of Physiotherapy into our outpatient rehabilitation operations, it is not practicable to separately identify net revenue and earnings of Physiotherapy on a stand-alone basis.
Concentra Acquisition
On June 1, 2015, MJ Acquisition Corporation, a joint venture that Select created with Welsh, Carson, Anderson & Stowe XII, L.P., consummated the acquisition of Concentra, the indirect operating subsidiary of Concentra Group Holdings, LLC (“Concentra Group Holdings”) and its subsidiaries. Pursuant to the terms of the stock purchase agreement, dated as of March 22, 2015, by and among MJ Acquisition Corporation, Concentra and Humana, Inc., MJ Acquisition Corporation acquired 100% of the issued and outstanding equity securities of Concentra from Humana, Inc. for $1,047.2 million, net of $3.8 million of cash acquired. For the year ended December 31, 2015, $4.7 million of Concentra acquisition costs were recognized in general and administrative expense.
During the year ended December 31, 2015, the Company finalized the accounting for identifiable intangible assets and liabilities, fixed assets, non-controlling interests, and certain pre-acquisition contingencies. During the quarter ended June 30, 2016, the Company completed the accounting for certain deferred tax matters.
F-20
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Acquisitions (Continued)
The following table reconciles the allocation of the consideration given for identifiable net assets and goodwill acquired to the net cash paid for the acquired business (in thousands):
Cash and cash equivalents | $ | 3,772 | |
Identifiable tangible assets, excluding cash and cash equivalents | 406,926 | ||
Identifiable intangible assets | 254,990 | ||
Goodwill | 651,152 | ||
Total assets | 1,316,840 | ||
Total liabilities | 248,797 | ||
Acquired non-controlling interests | 17,084 | ||
Net assets acquired | 1,050,959 | ||
Less: Cash and cash equivalents acquired | (3,772 | ) | |
Net cash paid | $ | 1,047,187 | |
Goodwill of $651.2 million was recognized in the business combination, representing the excess of the consideration given over the fair value of the identifiable net assets acquired. The value of goodwill is derived from Concentra’s future earnings potential and its assembled workforce. The goodwill is assigned to the Concentra reporting unit and is not deductible for tax purposes. However, prior to its acquisition by MJ Acquisition Corporation, Concentra completed certain acquisitions that resulted in tax deductible goodwill with an estimated value of $23.9 million, which the Company will deduct through 2025.
For the years ended December 31, 2015, 2016, and 2017, Concentra had net revenue of $585.2 million, $1.0 billion, and $1.0 billion, respectively, which is reflected in the Company’s consolidated statements of operations and comprehensive income.
For the year ended December 31, 2015, Concentra had a net loss of $10.0 million, which is reflected in the Company’s consolidated statements of operations and comprehensive income. For the years ended December 31, 2016, and 2017, Concentra had net income of $19.7 million and $68.7 million, respectively, which is reflected in the Company’s consolidated statements of operations and comprehensive income.
Pro Forma Results
The following pro forma unaudited results of operations have been prepared assuming the acquisitions of Concentra and Physiotherapy occurred January 1, 2014 and 2015, respectively. These results are not necessarily indicative of results of future operations nor of the results that would have actually occurred had the acquisitions been consummated on the aforementioned dates. The Company’s results of operations for year ended December 31, 2017 include Concentra and Physiotherapy for the entire period and there were no pro forma adjustments during these periods. Accordingly, no pro forma information is presented.
For the Year Ended December 31, | |||||||
2015 | 2016 | ||||||
(in thousands, except per share amounts) | |||||||
Net revenue | $ | 4,477,088 | $ | 4,339,551 | |||
Net income | 119,763 | 113,590 | |||||
Income per common share: | |||||||
Basic | $ | 0.91 | $ | 0.86 | |||
Diluted | $ | 0.91 | $ | 0.86 | |||
The pro forma financial information is based on the allocation of the purchase price of both the Concentra and Physiotherapy acquisitions. The net income tax impact was calculated at a statutory rate, as if Concentra and Physiotherapy had been subsidiaries of the Company as of January 1, 2014 and 2015, respectively.
F-21
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Acquisitions (Continued)
Pro forma results for the year ended December 31, 2015 were adjusted to include $3.2 million of Physiotherapy acquisition costs and exclude $4.7 million of Concentra acquisition costs. Pro forma results for the year ended December 31, 2016 were adjusted to exclude approximately $3.2 million of Physiotherapy acquisition costs.
Other Acquisitions
In addition to the acquisition of Concentra, the Company completed acquisitions consisting principally of inpatient rehabilitation businesses and other Concentra businesses during the year ended December 31, 2015. Consideration given for these acquisitions consisted of $14.4 million of cash, net of cash received, and the issuance of $14.7 million of non-controlling interests. The assets received in these acquisitions consisted principally of accounts receivable, property and equipment, and goodwill, of which $21.9 million and $4.2 million was recognized in our specialty hospitals and Concentra reporting units, respectively.
In addition to the acquisition of Physiotherapy, the Company completed acquisitions consisting of long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra businesses during the year ended December 31, 2016. Consideration given for these acquisitions consisted of $65.6 million of cash, net of cash received, the issuance of $38.3 million of non-controlling interests, and $17.7 million of business net assets. The Company’s acquisition of certain hospitals resulted in a non-operating gain totaling $9.5 million due, in part, to a bargain purchase because the fair values of the identifiable assets acquired exceeded the fair value of the consideration given in an exchange transaction. The assets received in these acquisitions consisted principally of cash, real property, and goodwill, of which $96.8 million, $2.3 million, and $4.6 million of goodwill was recognized in our specialty hospitals, outpatient rehabilitation, and Concentra reporting units, respectively.
The Company completed acquisitions consisting of long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra businesses during the year ended December 31, 2017. The Company provided total consideration of $36.1 million, consisting principally of $27.4 million of cash and the issuance of non-controlling interests. The assets received in these acquisitions consisted principally of accounts receivable, property and equipment, identifiable intangible assets, and goodwill, of which $12.9 million, $3.8 million, and $14.5 million of goodwill was recognized in our inpatient rehabilitation, outpatient rehabilitation, and Concentra reporting units, respectively. Prior to the change in the Company’s reporting units, goodwill of $0.8 million was recognized in our specialty hospitals reporting unit.
3. Sale of Businesses
The Company recognized a non-operating gain of $35.6 million resulting from the sale of businesses during the year ended December 31, 2016. The non-operating gain was the result of the sale of the Company’s contract therapy businesses for $65.0 million, resulting in a non-operating gain of $33.9 million, and the sale of nine outpatient rehabilitation clinics to an entity the Company holds as an equity method investment, resulting in a non-operating gain of $1.7 million.
F-22
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
4. Property and Equipment
The Company’s property and equipment consists of the following:
December 31, | |||||||
2016 | 2017 | ||||||
(in thousands) | |||||||
Land | $ | 76,987 | $ | 77,077 | |||
Leasehold improvements | 309,504 | 420,632 | |||||
Buildings | 421,017 | 414,704 | |||||
Furniture and equipment | 432,944 | 517,912 | |||||
Construction-in-progress | 164,516 | 112,930 | |||||
Total property and equipment | 1,404,968 | 1,543,255 | |||||
Accumulated depreciation | (512,751 | ) | (630,664 | ) | |||
Property and equipment, net | $ | 892,217 | $ | 912,591 | |||
Depreciation expense was $96.1 million, $129.0 million, and $142.6 million for the years ended December 31, 2015, 2016 and 2017, respectively.
5. Intangible Assets
Goodwill
The following table shows changes in the carrying amounts of goodwill by reporting unit for the years ended December 31, 2016 and 2017:
Long Term Acute Care | Inpatient Rehabilitation | Specialty Hospitals | Outpatient Rehabilitation | Concentra | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Balance as of January 1, 2016 | $ | — | $ | — | $ | 1,357,379 | $ | 306,595 | $ | 650,650 | $ | 2,314,624 | |||||||||||
Acquired | — | — | 96,785 | 345,355 | 4,562 | 446,702 | |||||||||||||||||
Measurement period adjustment | — | — | — | — | 4,825 | 4,825 | |||||||||||||||||
Sold | — | — | (6,758 | ) | (8,393 | ) | — | (15,151 | ) | ||||||||||||||
Balance as of December 31, 2016 | $ | — | $ | — | $ | 1,447,406 | $ | 643,557 | $ | 660,037 | $ | 2,751,000 | |||||||||||
Acquired | — | 12,887 | 797 | 3,797 | 14,505 | 31,986 | |||||||||||||||||
Measurement period adjustment | — | — | (342 | ) | 168 | — | (174 | ) | |||||||||||||||
Reorganization of reporting units | 1,045,220 | 402,641 | (1,447,861 | ) | — | — | — | ||||||||||||||||
Balance as of December 31, 2017 | $ | 1,045,220 | $ | 415,528 | $ | — | $ | 647,522 | $ | 674,542 | $ | 2,782,812 | |||||||||||
See Note 2 for details of the goodwill acquired during the period.
F-23
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
5. Intangible Assets (Continued)
Identifiable Intangible Assets
The following table provides the gross carrying amounts, accumulated amortization, and net carrying amounts for the Company’s identifiable intangible assets:
December 31, | |||||||||||||||||||||||
2016 | 2017 | ||||||||||||||||||||||
Gross Carrying Amount | Accumulated Amortization | Net Carrying Amount | Gross Carrying Amount | Accumulated Amortization | Net Carrying Amount | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Identifiable intangibles—Indefinite lived assets: | |||||||||||||||||||||||
Trademarks | $ | 166,698 | $ | — | $ | 166,698 | $ | 166,698 | $ | — | $ | 166,698 | |||||||||||
Certificates of need | 17,026 | — | 17,026 | 19,155 | — | 19,155 | |||||||||||||||||
Accreditations | 2,235 | — | 2,235 | 1,895 | — | 1,895 | |||||||||||||||||
Identifiable intangibles—Finite lived assets: | |||||||||||||||||||||||
Customer relationships | 142,198 | (23,185 | ) | 119,013 | 143,953 | (38,281 | ) | 105,672 | |||||||||||||||
Favorable leasehold interests | 13,089 | (2,317 | ) | 10,772 | 13,295 | (4,319 | ) | 8,976 | |||||||||||||||
Non-compete agreements | 26,655 | (1,837 | ) | 24,818 | 28,023 | (3,900 | ) | 24,123 | |||||||||||||||
Total identifiable intangible assets | $ | 367,901 | $ | (27,339 | ) | $ | 340,562 | $ | 373,019 | $ | (46,500 | ) | $ | 326,519 | |||||||||
The Company’s accreditations and trademarks have renewal terms. The costs to renew these intangibles are expensed as incurred. At December 31, 2017, the accreditations and trademarks have a weighted average time until next renewal of 1.5 years and 1.9 years, respectively.
The Company’s customer relationships and non-compete agreements amortize over their estimated useful lives. Amortization expense was $8.9 million, $16.3 million, and $17.4 million for the years ended December 31, 2015, 2016, and 2017, respectively.
Estimated amortization expense of the Company’s customer relationships and non-compete agreements for each of the five succeeding years is as follows:
2018 | 2019 | 2020 | 2021 | 2022 | |||||||||||||||
(in thousands | |||||||||||||||||||
Amortization expense | $ | 16,831 | $ | 16,802 | $ | 16,647 | $ | 16,483 | $ | 16,332 | |||||||||
The Company’s leasehold interests have finite lives and are amortized to rent expense over the remaining term of their respective leases to reflect a market rent per period based upon the market conditions present at the acquisition date.
F-24
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
6. Equity Method Investments
The Company’s equity method investments consist principally of minority ownership interests in rehabilitation businesses. Equity method investments of $100.0 million and $114.2 million are presented as part of other assets on the consolidated balance sheets as of December 31, 2016 and 2017, respectively. As of December 31, 2016 and 2017, these businesses consist primarily of the following ownership interests:
BIR JV, LLP | 49.0 | % |
OHRH, LLC | 49.0 | % |
GlobalRehab—Scottsdale, LLC | 49.0 | % |
Rehabilitation Institute of Denton, LLC | 50.0 | % |
ES Rehabilitation, LLC | 49.0 | % |
Coastal Virginia Rehabilitation, LLC | 49.0 | % |
Summarized combined financial information of the rehabilitation entities in which the Company has a minority ownership interest is as follows:
December 31, | ||||||||
2016 | 2017 | |||||||
(in thousands) | ||||||||
Current assets | $ | 90,656 | $ | 102,908 | ||||
Non-current assets | 78,913 | 79,364 | ||||||
Total assets | $ | 169,569 | $ | 182,272 | ||||
Current liabilities | $ | 32,520 | $ | 37,113 | ||||
Non-current liabilities | 14,384 | 13,751 | ||||||
Equity | 122,665 | 131,408 | ||||||
Total liabilities and equity | $ | 169,569 | $ | 182,272 | ||||
December 31, | ||||||||||||
2015 | 2016 | 2017 | ||||||||||
(in thousands) | ||||||||||||
Revenues | $ | 289,994 | $ | 320,078 | $ | 336,349 | ||||||
Operating expenses | 250,170 | 274,952 | 289,224 | |||||||||
Net income | 37,951 | 43,410 | 45,648 | |||||||||
The Company provides contracted services, principally employee leasing services, and charges management fees to related parties affiliated through its equity investments. Net operating revenues generated from contracted services and management fees charged to related parties affiliated through the Company’s equity investments were $146.0 million, $164.2 million, and $178.1 million for the years ended December 31, 2015, 2016 and 2017, respectively.
During the year ended December 31, 2016, the Company recognized a non-operating loss of $5.1 million related to the sale of an equity method investment. Additionally, the Company received contingent proceeds related to the final settlement of its 2015 sale of an equity method investment, resulting in a non-operating gain of $2.5 million recognized during the year ended December 31, 2016.
During the year ended December 31, 2015, the Company recognized a non-operating gain of $29.6 million related to the sale of an equity method investment.
F-25
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
7. Insurance Risk Programs
Under a number of the Company’s insurance programs, which include the Company’s employee health insurance, workers’ compensation, and professional malpractice liability insurance programs, the Company is liable for a portion of its losses before it can attempt to recover from the applicable insurance carrier. The Company accrues for losses for which it will be ultimately responsible under an occurrence-based approach whereby the Company estimates the losses that will be incurred in a respective accounting period and accrues that estimated liability using actuarial methods. Provisions for losses for professional liability risks retained by the Company at December 31, 2016 and 2017 have been discounted at 3%. The Company recorded a liability of $147.4 million and $157.1 million related to these programs at December 31, 2016 and 2017, respectively. If the Company did not discount the provisions for losses for professional liability risks, the aggregate liability for all of the insurance risk programs would be approximately $152.7 million and $162.1 million at December 31, 2016 and 2017, respectively.
8. Long-Term Debt and Notes Payable
For purposes of this indebtedness footnote, references to Select exclude Concentra because the Concentra credit facilities are non-recourse to Holdings and Select.
The Company’s long‑term debt and notes payable as of December 31, 2017 are as follows (in thousands):
Principal Outstanding | Unamortized Premium (Discount) | Unamortized Issuance Costs | Carrying Value | Fair Value | ||||||||||||||||
Select: | ||||||||||||||||||||
6.375% senior notes | $ | 710,000 | $ | 778 | $ | (6,553 | ) | $ | 704,225 | $ | 727,750 | |||||||||
Credit facilities: | ||||||||||||||||||||
Revolving facility | 230,000 | — | — | 230,000 | 211,600 | |||||||||||||||
Term loan | 1,141,375 | (12,445 | ) | (12,500 | ) | 1,116,430 | 1,154,215 | |||||||||||||
Other | 36,877 | — | (533 | ) | 36,344 | 36,344 | ||||||||||||||
Total Select debt | 2,118,252 | (11,667 | ) | (19,586 | ) | 2,086,999 | 2,129,909 | |||||||||||||
Concentra: | ||||||||||||||||||||
Credit facilities: | ||||||||||||||||||||
Term loan | 619,175 | (2,257 | ) | (10,668 | ) | 606,250 | 625,173 | |||||||||||||
Other | 6,653 | — | — | 6,653 | 6,653 | |||||||||||||||
Total Concentra debt | 625,828 | (2,257 | ) | (10,668 | ) | 612,903 | 631,826 | |||||||||||||
Total debt | $ | 2,744,080 | $ | (13,924 | ) | $ | (30,254 | ) | $ | 2,699,902 | $ | 2,761,735 | ||||||||
F-26
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
Principal maturities of the Company’s long‑term debt and notes payable are approximately as follows (in thousands):
2018 | 2019 | 2020 | 2021 | 2022 | Thereafter | Total | |||||||||||||||||||||
Select: | |||||||||||||||||||||||||||
6.375% senior notes | $ | — | $ | — | $ | — | $ | 710,000 | $ | — | $ | — | $ | 710,000 | |||||||||||||
Credit facilities: | |||||||||||||||||||||||||||
Revolving facility | — | — | — | — | 230,000 | — | 230,000 | ||||||||||||||||||||
Term loan | 11,500 | 11,500 | 11,500 | 11,500 | 11,500 | 1,083,875 | 1,141,375 | ||||||||||||||||||||
Other | 8,086 | 3,221 | 23,299 | 236 | 10 | 2,025 | 36,877 | ||||||||||||||||||||
Total Select debt | 19,586 | 14,721 | 34,799 | 721,736 | 241,510 | 1,085,900 | 2,118,252 | ||||||||||||||||||||
Concentra: | |||||||||||||||||||||||||||
Credit facilities: | |||||||||||||||||||||||||||
Term loan | — | — | 3,016 | 6,520 | 609,639 | — | 619,175 | ||||||||||||||||||||
Other | 2,600 | 154 | 172 | 170 | 183 | 3,374 | 6,653 | ||||||||||||||||||||
Total Concentra debt | 2,600 | 154 | 3,188 | 6,690 | 609,822 | 3,374 | 625,828 | ||||||||||||||||||||
Total debt | $ | 22,186 | $ | 14,875 | $ | 37,987 | $ | 728,426 | $ | 851,332 | $ | 1,089,274 | $ | 2,744,080 | |||||||||||||
The Company’s long‑term debt and notes payable as of December 31, 2016 were as follows (in thousands):
Principal Outstanding | Unamortized Premium (Discount) | Unamortized Issuance Costs | Carrying Value | Fair Value | ||||||||||||||||
Select: | ||||||||||||||||||||
6.375% senior notes | $ | 710,000 | $ | 1,006 | $ | (8,461 | ) | $ | 702,545 | $ | 710,000 | |||||||||
Credit facilities: | ||||||||||||||||||||
Revolving facility | 220,000 | — | — | 220,000 | 204,600 | |||||||||||||||
Term loan | 1,147,751 | (11,967 | ) | (13,581 | ) | 1,122,203 | 1,165,860 | |||||||||||||
Other | 22,688 | — | — | 22,688 | 22,688 | |||||||||||||||
Total Select debt | 2,100,439 | (10,961 | ) | (22,042 | ) | 2,067,436 | 2,103,148 | |||||||||||||
Concentra: | ||||||||||||||||||||
Credit facilities: | ||||||||||||||||||||
Term loan | 642,239 | (2,773 | ) | (13,091 | ) | 626,375 | 644,648 | |||||||||||||
Other | 5,178 | — | — | 5,178 | 5,178 | |||||||||||||||
Total Concentra debt | 647,417 | (2,773 | ) | (13,091 | ) | 631,553 | 649,826 | |||||||||||||
Total debt | $ | 2,747,856 | $ | (13,734 | ) | $ | (35,133 | ) | $ | 2,698,989 | $ | 2,752,974 | ||||||||
2011 Select Credit Facilities
The following discussion summarizes the amendments and significant transactions affecting Select’s 2011 senior secured credit facility which occurred during the years ended December 31, 2015 and 2016. The series E tranche B term loans, the series F tranche B term loans, and the revolving facility under Select’s 2011 senior secured credit facility (the “2011 Select credit facilities”) were repaid in full on March 6, 2017, as described below.
On May 20, 2015 Select entered into an additional credit extension amendment of the revolving facility to obtain $100.0 million of incremental revolving commitments. The revolving commitments had a maturity date of March 1, 2018.
F-27
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
On December 11, 2015, Select amended the 2011 Select credit facilities in order to, among other things: (i) convert $56.2 million of its series D tranche B term loans into series E tranche B term loans, which would have a maturity date of June 1, 2018; (ii) increase the interest rate payable on the series E tranche B term loans from Adjusted LIBO plus 2.75% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate plus 1.75%, to Adjusted LIBO plus 4.00% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate plus 3.00%; (iii) beginning with the quarter ending December 31, 2015, increase the quarterly compliance threshold set forth in the leverage ratio financial maintenance covenant to a level of 5.75 to 1.00 from 5.00 to 1.00; (iv) increase the capacity for incremental extensions of credit to $450.0 million; and (v) amend the definition of “consolidated EBITDA” to add back certain start-up losses.
On March 4, 2016, Select amended the 2011 Select credit facilities in order to, among other things: (i) have the lenders named therein make available an aggregate of $625.0 million series F tranche B term loans, (ii) extend the financial covenants through March 3, 2021, (iii) add a 1.00% prepayment premium for prepayments made with new term loans on or prior to March 4, 2017 if such new term loans have a lower yield than the series F tranche B term loans, (iv) increase the interest rate payable on the series E tranche B term loans from Adjusted LIBO plus 4.00% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate plus 3.00%, to Adjusted LIBO plus 5.00% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate plus 4.00%; and (v) made certain other technical amendments to the 2011 Select credit facilities. The series F tranche B term loans bore interest at a rate per annum equal to the Adjusted LIBO Rate (as defined in the 2011 Select credit facilities, subject to an Adjusted LIBO Rate floor of 1.00%) plus 5.00% for Eurodollar Loans or the Alternate Base Rate (as defined in the 2011 Select credit facilities) plus 4.00% for Alternate Base Rate Loans (as defined in the 2011 Select credit facilities). Select was required to make principal payments on the series F tranche B term loans in quarterly installments on the last day of each of March, June, September and December, beginning June 30, 2016, in amounts equal to 0.25% of the aggregate principal amount of the series F tranche B term loans outstanding as of the date of the credit extension amendment. The balance of the series F tranche B term loans was payable on March 3, 2021. Except as specifically set forth in the credit extension amendment, the terms and conditions of the series F tranche B term loans were identical to the terms of the outstanding series E tranche B term loans under the 2011 Select credit facilities and the other loan documents to which Select was party.
Select used the proceeds of the series F tranche B term loans to: (i) refinance in full the series D tranche B term loans due December 20, 2016, (ii) consummate the acquisition of Physiotherapy, and (iii) pay fees and expenses incurred in connection with the acquisition of Physiotherapy, the refinancing, and the Select credit extension amendment.
Excess Cash Flow Payments
On March 4, 2015 and March 2, 2016, Select made principal prepayments of $26.9 million and $10.2 million, respectively, in accordance with the provision in the 2011 Select credit facilities that required mandatory repayments of term loans as a result of annual excess cash flow.
2017 Select Credit Facilities
On March 6, 2017, Select entered into a new senior secured credit agreement (the “Select credit agreement”) that provides for $1.6 billion in senior secured credit facilities comprising a $1.15 billion, seven-year term loan (the “Select term loan”) and a $450.0 million, five-year revolving credit facility (the “Select revolving facility” and together with the Select term loan, the “Select credit facilities”), including a $75.0 million sublimit for the issuance of standby letters of credit.
Select used borrowings under the Select credit facilities to: (i) repay the series E tranche B term loans due June 1, 2018, the series F tranche B term loans due March 3, 2021, and the revolving facility maturing March 1, 2018 under Select’s 2011 credit facilities; and (ii) pay fees and expenses in connection with the refinancing.
Borrowings under the Select credit facilities bear interest at a rate equal to: (i) in the case of the Select term loan, the Adjusted LIBO Rate (as defined in the Select credit agreement) plus 3.50% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Select credit agreement) plus 2.50% (subject to an Alternate Base Rate floor of 2.00%); and (ii) in the case of the Select revolving facility, the Adjusted LIBO Rate plus a percentage ranging from 3.00% to 3.25% or Alternate Base Rate plus a percentage ranging from 2.00% to 2.25%, in each case based on Select’s leverage ratio, as defined in the Select credit facilities. The applicable interest rate for revolving loans as of December 31, 2017 was the Adjusted LIBO Rate plus 3.25% for Eurodollar Loans and Alternate Base Rate plus 2.25% for Alternate Base Rate Loans.
F-28
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
The Select term loan amortizes in equal quarterly installments in amounts equal to 0.25% of the aggregate original principal amount of the Select term loan commencing on June 30, 2017. The balance of the Select term loan will be payable on March 6, 2024; however, if the Select 6.375% senior notes, which are due June 1, 2021, are outstanding on March 1, 2021, the maturity date for the Select term loan will become March 1, 2021. The Select revolving facility will be payable on March 6, 2022; however, if the Select 6.375% senior notes are outstanding on February 1, 2021, the maturity date for the Select revolving facility will become February 1, 2021.
Select will be required to prepay borrowings under the Select credit facilities with (i) 100% of the net cash proceeds received from non-ordinary course asset sales or other dispositions, or as a result of a casualty or condemnation, subject to reinvestment provisions and other customary carveouts and, to the extent required, the payment of certain indebtedness secured by liens having priority over the debt under the Select credit facilities or subject to a first lien intercreditor agreement, (ii) 100% of the net cash proceeds received from the issuance of debt obligations other than certain permitted debt obligations, and (iii) 50% of excess cash flow (as defined in the Select credit agreement) if Select’s leverage ratio is greater than 4.50 to 1.00 and 25% of excess cash flow if Select’s leverage ratio is less than or equal to 4.50 to 1.00 and greater than 4.00 to 1.00, in each case, reduced by the aggregate amount of term loans, revolving loans and certain other debt optionally prepaid during the applicable fiscal year. Select will not be required to prepay borrowings with excess cash flow if Select’s leverage ratio is less than or equal to 4.00 to 1.00.
The Select revolving facility requires Select to maintain a leverage ratio (as defined in the Select credit agreement), which is tested quarterly, not to exceed 6.25 to 1.00. The leverage ratio is tested quarterly. After March 31, 2019, the leverage ratio must not exceed 6.00 to 1.00. Failure to comply with this covenant would result in an event of default under the Select revolving facility and, absent a waiver or an amendment from the revolving lenders, preclude Select from making further borrowings under the Select revolving facility and permit the revolving lenders to accelerate all outstanding borrowings under the Select revolving facility. The termination of the Select revolving facility commitments and the acceleration of amounts outstanding thereunder would constitute an event of default with respect to the Select term loan. For each of the four fiscal quarters during the year ended December 31, 2017, Select was required to maintain its leverage ratio at less than 6.25 to 1.00. As of December 31, 2017, Select’s leverage ratio was 5.27 to 1.00.
The Select credit facilities also contain a number of other affirmative and restrictive covenants, including limitations on mergers, consolidations and dissolutions; sales of assets; investments and acquisitions; indebtedness; liens; affiliate transactions; and dividends and restricted payments. The Select credit facilities contain events of default for non-payment of principal and interest when due (subject, as to interest, to a grace period), cross-default and cross-acceleration provisions and an event of default that would be triggered by a change of control.
Borrowings under the Select credit facilities are guaranteed by Holdings and substantially all of Select’s current domestic subsidiaries and will be guaranteed by substantially all of Select’s future domestic subsidiaries. Borrowings under the Select credit facilities are secured by substantially all of Select’s existing and future property and assets and by a pledge of Select’s capital stock, the capital stock of Select’s domestic subsidiaries and up to 65% of the capital stock of Select’s foreign subsidiaries held directly by Select or a domestic subsidiary.
On the last day of each calendar quarter, Select is required to pay each lender a commitment fee in respect of any unused commitments under the revolving facility, which is currently 0.50% per annum subject to adjustment based Select’s leverage ratio (as defined in the Select credit facilities).
At December 31, 2017, Select had outstanding borrowings under the Select credit facilities consisting of a $1,141.4 million Select term loan (excluding unamortized original issue discounts and debt issuance costs totaling $24.9 million) which matures on March 6, 2024, and borrowings of $230.0 million (excluding letters of credit) under the Select revolving facility which matures on March 6, 2022. At December 31, 2017, Select had $181.4 million of availability under the Select revolving facility after giving effect to $38.6 million of outstanding letters of credit.
F-29
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
Senior Notes
On May 28, 2013, Select issued and sold $600.0 million aggregate principal amount of 6.375% senior notes due June 1, 2021. On March 11, 2014, Select issued and sold $110.0 million aggregate principal amount of additional 6.375% senior notes due June 1, 2021 (the “Additional Notes”) at 101.50% of the aggregate principal amount resulting in gross proceeds of $111.7 million. The notes were issued as additional notes under the indenture pursuant to which it previously issued $600.0 million of 6.375% senior notes due June 1, 2021 (the “Existing Notes” and, together with the Additional Notes, the “Notes”). The Additional Notes are treated as a single series with the Existing Notes and have the same terms as those of the Existing Notes.
Interest on the Notes accrues at the rate of 6.375% per annum and is payable semi-annually in cash in arrears on June 1 and December 1 of each year. The Notes are Select’s senior unsecured obligations and rank equally in right of payment with all of its other existing and future senior unsecured indebtedness and senior in right of payment to all of its existing and future subordinated indebtedness. The Notes are fully and unconditionally guaranteed by all of Select’s wholly owned subsidiaries. The Notes are guaranteed, jointly and severally, by Select’s direct or indirect existing and future domestic restricted subsidiaries other than certain non-guarantor subsidiaries.
Select may redeem some or all of the Notes at the following redemption prices (expressed in percentages of principal amount on the redemption date), plus accrued interest, if any, if redeemed during the twelve-month period beginning on June 1 of the years indicated below:
Year | Redemption Price | |
2017 | 103.188 | % |
2018 | 101.594 | % |
2019 | 100.000 | % |
Select is obligated to offer to repurchase the Notes at a price of 101% of their principal amount plus accrued and unpaid interest, if any, as a result of certain change of control events. These restrictions and prohibitions are subject to certain qualifications and exceptions.
The indenture relating to the Notes contains covenants that, among other things, limit Select’s ability and the ability of certain of its subsidiaries to grant liens on its assets; make dividend payments, other distributions or other restricted payments; incur restrictions on the ability of Select’s restricted subsidiaries to pay dividends or make other payments; enter into sale and leaseback transactions; merge, consolidate, transfer or dispose of substantially all of their assets; incur additional indebtedness; make investments; sell assets, including capital stock of subsidiaries; use the proceeds from sales of assets, including capital stock of restricted subsidiaries; and enter into transactions with affiliates. In addition, the indenture requires, among other things, Select to provide financial and current reports to holders of the Notes or file such reports electronically with the SEC. These covenants are subject to a number of exceptions, limitations and qualifications set forth in the indenture.
F-30
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
Concentra credit facilities
The following discussion summarizes the amendments and significant transactions affecting the Concentra first lien credit agreement, which occurred during the years ended December 31, 2015, 2016, and 2017.
On June 1, 2015, MJ Acquisition Corporation, as the initial borrower, entered into a first lien credit agreement (the “Concentra first lien credit agreement”) and a second lien credit agreement (the “Concentra second lien credit agreement”). Concentra, as the surviving entity of the merger between MJ Acquisition Corporation and Concentra, became the borrower.
The Concentra first lien credit agreement provided for $500.0 million in first lien loans comprised of a $450.0 million, seven-year term loan (“Concentra first lien term loan”) and a $50.0 million, five-year revolving credit facility (the “Concentra revolving facility” and, together with the Concentra first lien term loan, the “Concentra credit facilities”). The borrowings under the Concentra first lien credit agreement are guaranteed, on a first lien basis, by Concentra Holdings, Inc., the direct parent of Concentra. Select and Holdings are not parties to the Concentra first lien credit agreement and are not obligors with respect to Concentra’s debt under such agreement. Borrowings under the Concentra first lien credit agreement bear interest at a rate equal to:
• | in the case of the Concentra first lien term loan, the Adjusted LIBO Rate (as defined in the Concentra first lien credit agreement) plus 3.00% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Concentra first lien credit agreement) plus 2.00% (subject to an Alternate Base Rate floor of 2.00%); and |
• | in the case of the Concentra revolving facility, the Adjusted LIBO Rate plus a percentage ranging from 2.75% to 3.00%, or Alternate Base Rate plus a percentage ranging from 1.75% to 2.00%, in each case based on Concentra’s leverage ratio. |
The Concentra second lien credit agreement provided for a $200.0 million eight-year second lien term loan (“Concentra second lien term loan”). The borrowings under the Concentra second lien credit agreement were guaranteed, on a second lien basis, by Concentra Holdings, Inc., the direct parent of Concentra. Select and Holdings are not parties to the Concentra second lien credit agreement and are not obligors with respect to Concentra’s debt under such agreement. Borrowings under the Concentra second lien term loan bore interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra second lien credit agreement) plus 8.00% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Concentra second lien credit agreement) plus 7.00% (subject to an Alternate Base Rate floor of 2.00%).
On September 26, 2016, Concentra entered into a credit agreement amendment to the Concentra first lien credit agreement dated June 1, 2015. The credit agreement amendment provided an additional $200.0 million of first lien term loans due June 1, 2022, the proceeds of which were used to prepay in full the Concentra second lien term loan due June 1, 2023; and also amended certain restrictive covenants to give Concentra greater operational flexibility.
The Concentra first lien term loan amortizes in equal quarterly installments of $1.6 million. As a result of the principal prepayment made on March 1, 2017, the next quarterly installment will be due in 2020, with the remaining unamortized aggregate principal due at maturity on June 1, 2022. The Concentra revolving facility matures on June 1, 2020.
Concentra will be required to prepay borrowings under the Concentra first lien credit agreement with (i) 100% of the net cash proceeds received from non-ordinary course asset sales or other dispositions, or as a result of a casualty or condemnation, subject to reinvestment provisions and other customary carveouts and the payment of certain indebtedness secured by liens, (ii) 100% of the net cash proceeds received from the issuance of debt obligations other than certain permitted debt obligations, and (iii) 50% of excess cash flow (as defined in the Concentra first lien credit agreement) if Concentra’s leverage ratio is greater than 4.25 to 1.00 and 25% of excess cash flow if Concentra’s leverage ratio is less than or equal to 4.25 to 1.00 and greater than 3.75 to 1.00, in each case, reduced by the aggregate amount of term loans and certain debt secured on a pari passu basis optionally prepaid during the applicable fiscal year and the aggregate amount of revolving commitments hereunder reduced permanently during the applicable fiscal year (other than in connection with a refinancing). Concentra will not be required to prepay borrowings with excess cash flow if Concentra’s leverage ratio is less than or equal to 3.75 to 1.00.
F-31
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Long-Term Debt and Notes Payable (Continued)
The Concentra first lien credit agreement requires Concentra to maintain a leverage ratio (based upon the ratio of indebtedness for money borrowed to consolidated EBITDA, as defined in the Concentra first lien credit agreement) of 5.75 to 1.00 which is tested quarterly, but only if Revolving Exposure (as defined in the Concentra first lien credit agreement) exceeds 30% of Revolving Commitments (as defined in the Concentra first lien credit agreement) on such day. Failure to comply with this covenant would result in an event of default under the Concentra revolving facility only and, absent a waiver or an amendment from the lenders, preclude Concentra from making further borrowings under the Concentra revolving facility and permit the lenders to accelerate all outstanding borrowings under the Concentra revolving facility. Upon such acceleration, Concentra’s failure to comply with the financial covenant would result in an event of default with respect to the Concentra first lien term loan.
The Concentra credit facilities also contain a number of affirmative and restrictive covenants, including limitations on mergers, consolidations and dissolutions; sales of assets; investments and acquisitions; indebtedness; liens; affiliate transactions; and dividends and restricted payments. The Concentra credit facilities contain events of default for non-payment of principal and interest when due (subject to a grace period for interest), cross-default and cross-acceleration provisions and an event of default that would be triggered by a change of control.
At December 31, 2017, Concentra had outstanding borrowings under the Concentra credit facilities of $619.2 million of term loans (excluding unamortized discounts and debt issuance costs totaling $12.9 million). Concentra did not have any borrowings under the Concentra revolving facility. At December 31, 2017, Concentra had $43.4 million of availability under its revolving facility after giving effect to $6.6 million of outstanding letters of credit.
Excess Cash Flow Payment
On March 1, 2017, Concentra made a principal prepayment of $23.1 million associated with the Concentra first lien term loan in accordance with the provision in the Concentra credit facilities that requires mandatory prepayments of term loans as a result of annual excess cash flow.
Fair Value
The Company considers the inputs in the valuation process to be Level 2 in the fair value hierarchy for Select’s 6.375% senior notes and for its credit facilities. Level 2 in the fair value hierarchy is defined as inputs that are observable for the asset or liability, either directly or indirectly, which includes quoted prices for identical assets or liabilities in markets that are not active.
The fair values of the Select credit facilities and the Concentra credit facilities were based on quoted market prices for this debt in the syndicated loan market. The fair value of Select’s 6.375% senior notes was based on quoted market prices. The carrying amount of other debt, principally short-term notes payable, approximates fair value.
Loss on Early Retirement of Debt
During the year ended December 31, 2016, the Company refinanced a portion of the term loans outstanding under the 2011 Select credit facilities, which resulted in a loss on early retirement of debt of $0.8 million. Additionally, Concentra prepaid the second lien term loan under the Concentra credit facilities, which resulted in a loss on early retirement of debt of $10.9 million.
During the year ended December 31, 2017, the Company refinanced the 2011 Select credit facilities which resulted in $6.5 million of debt extinguishment losses and $13.2 million of debt modification losses.
F-32
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Stockholders’ Equity
The following table summarizes the share activity for Holdings:
For the Year Ended December 31, | ||||||||
2015 | 2016 | 2017 | ||||||
(in thousands) | ||||||||
Restricted stock granted | 1,385 | 1,426 | 1,598 | |||||
Common stock issued through stock option exercise | 183 | 202 | 227 | |||||
Unvested restricted stock forfeitures | 304 | 82 | 27 | |||||
Stock repurchases for satisfaction of tax obligations | 183 | 232 | 280 | |||||
Holdings’ board of directors has authorized a common stock repurchase program to repurchase up to $500.0 million worth of shares of its common stock. The program has been extended until December 31, 2018, and will remain in effect until then, unless further extended or earlier terminated by the board of directors. Stock repurchases under this program may be made in the open market or through privately negotiated transactions, and at times and in such amounts as Holdings deems appropriate. Holdings is funding this program with cash on hand and borrowings under the Select revolving facility.
For the year ended December 31, 2015, Holdings repurchased 1,032,334 shares at a cost of $13.6 million, which includes transaction costs. Holdings did not repurchase shares during the years ended December 31, 2016 and 2017. The common stock repurchase program has available capacity of $185.2 million as of December 31, 2017.
10. Segment Information
The Company’s reportable segments consist of: long term acute care, inpatient rehabilitation, outpatient rehabilitation, and Concentra. Other activities include the Company’s corporate shared services and certain other non-consolidating joint ventures and minority investments in other healthcare related businesses. The accounting policies of the segments are the same as those described in the summary of significant accounting policies. The Company evaluates performance of the segments based on Adjusted EBITDA. Adjusted EBITDA is defined as earnings excluding interest, income taxes, depreciation and amortization, gain (loss) on early retirement of debt, stock compensation expense, acquisition costs associated with Concentra, Physiotherapy, and U.S. HealthWorks, non-operating gain (loss), and equity in earnings (losses) of unconsolidated subsidiaries. The Company has provided additional information regarding its reportable segments, such as total assets, which contributes to the understanding of the Company and provides useful information to the users of the consolidated financial statements.
The following tables summarize selected financial data for the Company’s reportable segments. The segment results of Holdings are identical to those of Select.
Year Ended December 31, 2015 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra(3) | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net revenue | $ | 1,902,776 | $ | 444,005 | $ | 810,009 | $ | 585,222 | $ | 724 | $ | 3,742,736 | |||||||||||
Adjusted EBITDA | 258,223 | 69,400 | 98,220 | 48,301 | (74,979 | ) | 399,165 | ||||||||||||||||
Total assets(1) | 1,954,823 | 470,290 | 548,242 | 1,311,631 | 103,692 | 4,388,678 | |||||||||||||||||
Capital expenditures | 39,784 | 86,230 | 17,768 | 26,771 | 12,089 | 182,642 | |||||||||||||||||
F-33
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Segment Information (Continued)
Year Ended December 31, 2016 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation(4) | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net revenue | $ | 1,785,164 | $ | 504,318 | $ | 995,374 | $ | 1,000,624 | $ | 541 | $ | 4,286,021 | |||||||||||
Adjusted EBITDA | 224,609 | 56,902 | 129,830 | 143,009 | (88,543 | ) | 465,807 | ||||||||||||||||
Total assets(1)(2) | 1,910,013 | 621,105 | 969,014 | 1,313,176 | 107,318 | 4,920,626 | |||||||||||||||||
Capital expenditures | 48,626 | 60,513 | 21,286 | 15,946 | 15,262 | 161,633 | |||||||||||||||||
Year Ended December 31, 2017 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net revenue | $ | 1,756,243 | $ | 631,777 | $ | 1,020,848 | $ | 1,034,035 | $ | 700 | $ | 4,443,603 | |||||||||||
Adjusted EBITDA | 252,679 | 90,041 | 132,533 | 157,561 | (94,822 | ) | 537,992 | ||||||||||||||||
Total assets(1) | 1,848,783 | 868,517 | 954,661 | 1,340,919 | 114,286 | 5,127,166 | |||||||||||||||||
Capital expenditures | 49,720 | 96,477 | 27,721 | 28,912 | 30,413 | 233,243 | |||||||||||||||||
A reconciliation of Adjusted EBITDA to income before income taxes is as follows:
Year Ended December 31, 2015 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra(3) | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Adjusted EBITDA | $ | 258,223 | $ | 69,400 | $ | 98,220 | $ | 48,301 | $ | (74,979 | ) | ||||||||||||
Depreciation and amortization | (45,234 | ) | (8,758 | ) | (13,053 | ) | (33,644 | ) | (4,292 | ) | |||||||||||||
Stock compensation expense | — | — | — | (1,016 | ) | (13,663 | ) | ||||||||||||||||
Concentra acquisition costs | — | — | — | (4,715 | ) | — | |||||||||||||||||
Income (loss) from operations | $ | 212,989 | $ | 60,642 | $ | 85,167 | $ | 8,926 | $ | (92,934 | ) | $ | 274,790 | ||||||||||
Equity in earnings of unconsolidated subsidiaries | 16,811 | ||||||||||||||||||||||
Non-operating gain | 29,647 | ||||||||||||||||||||||
Interest expense | (112,816 | ) | |||||||||||||||||||||
Income before income taxes | $ | 208,432 | |||||||||||||||||||||
F-34
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Segment Information (Continued)
Year Ended December 31, 2016 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation(4) | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Adjusted EBITDA | $ | 224,609 | $ | 56,902 | $ | 129,830 | $ | 143,009 | $ | (88,543 | ) | ||||||||||||
Depreciation and amortization | (43,862 | ) | (12,723 | ) | (22,661 | ) | (60,717 | ) | (5,348 | ) | |||||||||||||
Stock compensation expense | — | — | — | (770 | ) | (16,643 | ) | ||||||||||||||||
Physiotherapy acquisition costs | — | — | — | — | (3,236 | ) | |||||||||||||||||
Income (loss) from operations | $ | 180,747 | $ | 44,179 | $ | 107,169 | $ | 81,522 | $ | (113,770 | ) | $ | 299,847 | ||||||||||
Loss on early retirement of debt | (11,626 | ) | |||||||||||||||||||||
Equity in earnings of unconsolidated subsidiaries | 19,943 | ||||||||||||||||||||||
Non-operating gain | 42,651 | ||||||||||||||||||||||
Interest expense | (170,081 | ) | |||||||||||||||||||||
Income before income taxes | $ | 180,734 | |||||||||||||||||||||
Year Ended December 31, 2017 | |||||||||||||||||||||||
Long Term Acute Care | Inpatient Rehabilitation | Outpatient Rehabilitation | Concentra | Other | Total | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Adjusted EBITDA | $ | 252,679 | $ | 90,041 | $ | 132,533 | $ | 157,561 | $ | (94,822 | ) | ||||||||||||
Depreciation and amortization | (45,743 | ) | (20,176 | ) | (24,607 | ) | (61,945 | ) | (7,540 | ) | |||||||||||||
Stock compensation expense | — | — | — | (993 | ) | (18,291 | ) | ||||||||||||||||
U.S. HealthWorks acquisition costs | — | — | — | (2,819 | ) | — | |||||||||||||||||
Income (loss) from operations | $ | 206,936 | $ | 69,865 | $ | 107,926 | $ | 91,804 | $ | (120,653 | ) | $ | 355,878 | ||||||||||
Loss on early retirement of debt | (19,719 | ) | |||||||||||||||||||||
Equity in earnings of unconsolidated subsidiaries | 21,054 | ||||||||||||||||||||||
Non-operating loss | (49 | ) | |||||||||||||||||||||
Interest expense | (154,703 | ) | |||||||||||||||||||||
Income before income taxes | $ | 202,461 | |||||||||||||||||||||
_______________________________________________________________________________
(1) | The long term acute care segment includes $2.7 million, $24.4 million, and $9.8 million in real estate assets held for sale on December 31, 2015, 2016, and 2017, respectively. |
(2) | Total assets were retrospectively conformed to reflect the adoption ASU 2015-17, Balance Sheet Classification of Deferred Taxes, which resulted in a reduction to total assets of $23.8 million. |
(3) | The selected financial data for the Company’s Concentra segment begins as of June 1, 2015, which is the date the Concentra acquisition was consummated. |
(4) | The outpatient rehabilitation segment includes the operating results of the Company’s contract therapy businesses through March 31, 2016 and Physiotherapy beginning March 4, 2016. |
F-35
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
11. Stock-based Compensation
Holdings awards stock-based compensation in the form of stock options and restricted stock awards under its equity incentive plans. On June 2, 2016, Holdings adopted the Select Medical Holdings Corporation 2016 Equity Incentive Plan (the “Plan”) and its existing plans were frozen. The total capacity for restricted stock and stock option awards under the Plan is 7,529,200 awards, as adjusted for forfeited restricted stock and stock options awards through December 31, 2017. As of December 31, 2017, Holdings has capacity to issue 4,505,801 restricted stock and stock option awards under the Plan. Holdings’ equity plan allows for authorized but previously unissued shares or shares previously issued and outstanding and reacquired by Holdings to satisfy these awards.
On November 8, 2005, the board of directors of Holdings adopted a director equity incentive plan (“Director Plan”) and on August 12, 2009, the board of directors and stockholders of Holdings approved an amendment and restatement of the Director Plan. This amendment authorized Holdings to issue under the Director Plan options to purchase up to 75,000 shares of its common stock and restricted stock awards covering up to 150,000 shares of its common stock. On June 2, 2016, upon the adoption of the Select Medical Holdings Corporation 2016 Equity Incentive Plan, the Director Plan was frozen.
The Company measures the compensation costs of stock-based compensation arrangements based on the grant-date fair value and recognizes the costs over the period during which employees are required to provide services. The Company values restricted stock awards by using the closing market price of its stock on the date of grant. The Company values stock options using the Black-Scholes option-pricing model. There were no options granted during the year ended December 31, 2017.
Transactions related to restricted stock awards are as follows:
Shares | Weighted Average Grant Date Fair Value | |||||
(share amounts in thousands) | ||||||
Unvested balance, January 1, 2017 | 4,201 | $ | 12.86 | |||
Granted | 1,598 | 15.84 | ||||
Vested | (1,304 | ) | 13.09 | |||
Forfeited | (27 | ) | 14.44 | |||
Unvested balance, December 31, 2017 | 4,468 | $ | 13.85 | |||
The weighted average grant date fair value of restricted stock awards granted for the years ended December 31, 2015, 2016, and 2017 was $13.94, $11.57, and $15.84, respectively. The total weighted average grant date fair value of restricted stock awards vested for the years ended December 31, 2015, 2016, and 2017 was $9.0 million, $8.4 million, and $17.1 million, respectively.
As of December 31, 2017, there were 291,775 stock options outstanding and exercisable. The outstanding and exercisable shares have a weighted average exercise price of $9.26 and a weighted average remaining contractual life of 1.8 years. As of December 31, 2016, there were 529,720 stock options outstanding and exercisable which had a weighted average exercise price of $9.09.
During the year ended December 31, 2017, 226,845 options were exercised, which had a weighted average exercise price of $8.89, and 11,100 options were canceled, which had a weighted average exercise price of $8.51. The total intrinsic value of options exercised for the years ended December 31, 2015, 2016, and 2017 was $1.0 million, $0.8 million, and $1.6 million, respectively. The aggregate intrinsic value of options outstanding and options exercisable at December 31, 2017 was $2.4 million.
F-36
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
11. Stock-based Compensation (Continued)
Stock compensation expense recognized by the Company was as follows:
For the Year Ended December 31, | |||||||||||
2015 | 2016 | 2017 | |||||||||
(in thousands) | |||||||||||
Stock compensation expense: | |||||||||||
Included in general and administrative | $ | 11,633 | $ | 14,607 | $ | 15,706 | |||||
Included in cost of services | 3,046 | 2,806 | 3,578 | ||||||||
Total | $ | 14,679 | $ | 17,413 | $ | 19,284 | |||||
Stock compensation expense based on current stock-based awards for each of the next five years is estimated to be as follows:
2018 | 2019 | 2020 | 2021 | 2022 | |||||||||||||||
(in thousands) | |||||||||||||||||||
Stock compensation expense | $ | 17,547 | $ | 11,946 | $ | 6,315 | $ | 1,472 | $ | 6 | |||||||||
12. Income Taxes
The components of the Company’s income tax expense for the years ended December 31, 2015, 2016, and 2017 were as follows:
For the Year Ended December 31, | |||||||||||
2015 | 2016 | 2017 | |||||||||
(in thousands) | |||||||||||
Current income tax expense: | |||||||||||
Federal | $ | 63,626 | $ | 54,726 | $ | 45,809 | |||||
State and local | 10,868 | 13,329 | 8,331 | ||||||||
Total current income tax expense | 74,494 | 68,055 | 54,140 | ||||||||
Deferred income tax expense (benefit) | (2,058 | ) | (12,591 | ) | (72,324 | ) | |||||
Total income tax expense (benefit) | $ | 72,436 | $ | 55,464 | $ | (18,184 | ) | ||||
Reconciliations of the statutory federal income tax rate to the effective income tax rate are as follows:
For the Year Ended December 31, | ||||||||
2015 | 2016 | 2017 | ||||||
Federal income tax at statutory rate | 35.0 | % | 35.0 | % | 35.0 | % | ||
State and local income taxes, less federal income tax benefit | 4.0 | 3.6 | 3.7 | |||||
Permanent differences | 1.4 | 1.4 | 1.7 | |||||
Tax benefit from the sale of businesses | — | (6.7 | ) | — | ||||
Valuation allowance | (0.9 | ) | 0.2 | (7.3 | ) | |||
Uncertain tax positions | (2.3 | ) | (1.3 | ) | (0.6 | ) | ||
Non-controlling interest | (2.0 | ) | (0.5 | ) | 0.5 | |||
Stock-based compensation | — | (0.7 | ) | (1.3 | ) | |||
Deferred income taxes - state income tax rate adjustment | — | — | (2.8 | ) | ||||
Deferred income taxes - tax legislation rate adjustment | — | — | (37.5 | ) | ||||
Other | (0.4 | ) | (0.3 | ) | (0.4 | ) | ||
Total effective income tax rate | 34.8 | % | 30.7 | % | (9.0 | )% | ||
F-37
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
12. Income Taxes (Continued)
The Company’s deferred tax assets and liabilities are as follows:
December 31, | |||||||
2016 | 2017 | ||||||
(in thousands) | |||||||
Deferred tax assets | |||||||
Allowance for doubtful accounts | $ | 10,735 | $ | 8,792 | |||
Compensation and benefit-related accruals | 70,199 | 50,936 | |||||
Professional malpractice liability insurance | 19,763 | 11,036 | |||||
Deferred revenue | 746 | 319 | |||||
Net operating loss carryforwards | 39,481 | 36,112 | |||||
Stock options | 9,533 | 6,591 | |||||
Equity investments | 1,567 | 1,452 | |||||
Uncertain tax positions | 499 | 503 | |||||
Other | 3,496 | 3,040 | |||||
Deferred tax assets | $ | 156,019 | $ | 118,781 | |||
Valuation allowance | (26,421 | ) | (12,986 | ) | |||
Deferred tax assets, net of valuation allowance | $ | 129,598 | $ | 105,795 | |||
Deferred tax liabilities | |||||||
Deferred income | $ | (26,068 | ) | $ | (19,608 | ) | |
Investment in unconsolidated affiliates | (3,885 | ) | (4,457 | ) | |||
Depreciation and amortization | (271,914 | ) | (179,055 | ) | |||
Deferred financing costs | — | (4,528 | ) | ||||
Other | (5,413 | ) | (3,673 | ) | |||
Deferred tax liabilities | $ | (307,280 | ) | $ | (211,321 | ) | |
Deferred tax liabilities, net of deferred tax assets | $ | (177,682 | ) | $ | (105,526 | ) | |
The Company’s deferred tax assets and liabilities are included in the consolidated balance sheet captions as follows:
December 31, | |||||||
2016 | 2017 | ||||||
(in thousands) | |||||||
Other assets | $ | 21,396 | $ | 19,391 | |||
Non-current deferred tax liability | (199,078 | ) | (124,917 | ) | |||
$ | (177,682 | ) | $ | (105,526 | ) | ||
The valuation allowance as of December 31, 2017 is primarily attributable to the uncertainty regarding the realization of state net operating losses and other net deferred tax assets of loss entities. The state net deferred tax assets have a full valuation allowance recorded for entities that have a cumulative history of pre-tax losses (current year in addition to the two prior years). For the year ended December 31, 2017, the Company recorded a net valuation allowance release of $13.4 million (comprised of a valuation release of $14.1 million related to federal net operating losses acquired as part of the Physiotherapy acquisition and $0.2 million of expired state net operating losses, partially offset by a $0.9 million increase in the valuation allowance for newly generated state net operating losses) on the basis of management’s reassessment of the amount of its deferred tax assets that are more likely than not to be realized.
F-38
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
12. Income Taxes (Continued)
The net deferred tax liabilities at December 31, 2016 and 2017 of approximately $177.7 million and $105.5 million, respectively, consist of items which have been recognized for tax reporting purposes, but which will increase tax on returns to be filed in the future, and include the use of net operating loss carryforwards. The Company has performed an assessment of positive and negative evidence regarding the realization of the net deferred tax assets. This assessment included a review of legal entities with three years of cumulative losses, estimates of projected future taxable income, generation of income from the turning of existing deferred tax liabilities and the impact of tax planning strategies that management would and could implement in order to keep deferred tax assets from expiring unused. Although realization is not assured, based on the Company’s assessment, it has concluded that it is more likely than not that such assets, net of the determined valuation allowance, will be realized.
The total state net operating losses are approximately $596.7 million. State net operating loss carryforwards expire and are subject to valuation allowances as follows:
State Net Operating Losses | Gross Valuation Allowance | ||||||
(in thousands) | |||||||
2018 | $ | 1,812 | $ | 1,081 | |||
2019 | 9,770 | 8,788 | |||||
2020 | 10,483 | 8,333 | |||||
2021 | 12,269 | 6,817 | |||||
Thereafter through 2036 | 562,326 | 426,138 | |||||
Reserves for Uncertain Tax Positions:
The Company and its subsidiaries are subject to U.S. federal income tax as well as income tax of multiple state jurisdictions. Significant judgment is required in evaluating the Company’s tax positions and determining its provision for income taxes. During the ordinary course of business, there are many transactions and calculations for which the ultimate tax determination is uncertain. The Company establishes reserves for tax related uncertainties based on estimates of whether, and the extent to which, additional taxes will be due. These reserves are established when it is believed that certain positions might be challenged despite the Company’s belief that its tax return positions are fully supportable. The Company adjusts these reserves in light of changing facts and circumstances. The provision for income taxes includes the impact of reserve provisions and changes to reserves that have resulted from resolution of the tax position or expirations of statutes of limitations. As of December 31, 2016 and 2017, the Company had $3.8 million and $2.8 million of unrecognized tax benefits, respectively, all of which, if fully recognized, would affect the Company’s effective income tax rate.
The federal statute of limitations remains open for tax years 2014 through 2017.
State jurisdictions generally have statutes of limitations for tax returns ranging from three to five years. The state impact of any federal income tax changes remains subject to examination for a period of up to one year after formal notification to the states. Currently, the Company has one state income tax return under examination.
F-39
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
13. Retirement Savings Plan
Select sponsors a defined contribution retirement savings plan for substantially all of its employees. Employees who are not classified as highly compensated employees (“HCE’s”) may contribute up to 30% of their salary; HCE’s may contribute up to 7% of their salary. The plan provides a discretionary company match which is determined annually. Currently, Select matches 25% of the first 6% of compensation employees contribute to the plan. The employees vest in the employer contributions over a three-year period beginning on the employee’s hire date. The expense incurred by Select related to this plan was $10.0 million, $14.7 million, and $15.2 million during the years ended December 31, 2015, 2016, and 2017, respectively.
For the period June 1, 2015 through December 31, 2015, Concentra sponsored a separate defined contribution retirement savings plan and incurred expenses related to this plan of $8.8 million. For the years ended December 31, 2016 and 2017, Concentra employees participated in the defined contribution retirement savings plan sponsored by Select.
14. Income per Share
The Company applies the two-class method for calculating and presenting income per common share. The two-class method is an earnings allocation formula that determines earnings per share for each class of stock participation rights in undistributed earnings. Under the two class method:
(i) | Net income attributable to Select Medical Holdings Corporation is reduced by any contractual amount of dividends in the current period for each class of stock. There were no contractual dividends for the years ended December 31, 2015, 2016, and 2017. |
(ii) | The remaining income is allocated to common stock and unvested restricted stock, to the extent that each security may participate in income, as if all of the earnings for the period had been distributed. The total income allocated to each security is determined by adding together the amount allocated for dividends in (i) above and the amount allocated for participation features. |
(iii) | The income allocated to common stock is then divided by the weighted average number of outstanding shares for the period to which the earnings are allocated to determine the income per share for common stock. |
In applying the two-class method, the Company determined that undistributed earnings should be allocated equally on a per share basis between common stock and unvested restricted stock due to the equal participation rights of common stock and unvested restricted stock (i.e., the voting conversion rights).
The following table sets forth the calculation of income per share in the Company’s consolidated statements of operations and comprehensive income and the differences between basic weighted average shares outstanding and diluted weighted average shares outstanding used to compute basic and diluted earnings per share, respectively:
For the Year Ended December 31, | |||||||||||
2015 | 2016 | 2017 | |||||||||
(in thousands, except per share amounts) | |||||||||||
Numerator: | |||||||||||
Net income attributable to Select Medical Holdings Corporation | $ | 130,736 | $ | 115,411 | $ | 177,184 | |||||
Less: Earnings allocated to unvested restricted stockholders | 3,830 | 3,521 | 5,758 | ||||||||
Net income available to common stockholders | $ | 126,906 | $ | 111,890 | $ | 171,426 | |||||
Denominator: | |||||||||||
Weighted average shares—basic | 127,478 | 127,813 | 128,955 | ||||||||
Effect of dilutive securities: | |||||||||||
Stock options | 274 | 155 | 171 | ||||||||
Weighted average shares—diluted | 127,752 | 127,968 | 129,126 | ||||||||
Basic income per common share: | $ | 1.00 | $ | 0.88 | $ | 1.33 | |||||
Diluted income per common share: | $ | 0.99 | $ | 0.87 | $ | 1.33 | |||||
F-40
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
15. Commitments and Contingencies
Leases
The Company leases facilities and equipment from unrelated parties under operating leases. Minimum future non-cancelable lease obligations on long-term operating leases in effect at December 31, 2017 are approximately as follows (in thousands):
2018 | $ | 224,359 | |
2019 | 191,120 | ||
2020 | 156,494 | ||
2021 | 121,881 | ||
2022 | 91,351 | ||
Thereafter | 424,640 | ||
$ | 1,209,845 | ||
Total rent expense for facility and equipment operating leases, including cancelable leases, for the years ended December 31, 2015, 2016, and 2017 was $214.9 million, $265.1 million, and $267.4 million, respectively. Facility rent expense to unrelated parties, a component of total rent expense, for the years ended December 31, 2015, 2016, and 2017 was $165.3 million, $220.8 million, and $224.2 million, respectively.
The Company rents its corporate office space from related parties. The Company made payments for office rent, leasehold improvements, and miscellaneous expenses aggregating $4.7 million, $5.0 million, and $6.2 million for the years ended December 31, 2015, 2016, and 2017, respectively, to related parties.
As of December 31, 2017, future rental commitments under outstanding agreements with related parties are approximately as follows (in thousands):
2018 | $ | 5,667 | |
2019 | 5,811 | ||
2020 | 5,958 | ||
2021 | 6,086 | ||
2022 | 5,981 | ||
Thereafter | 4,559 | ||
$ | 34,062 | ||
Construction Commitments
At December 31, 2017, the Company had outstanding commitments under construction contracts related to new construction, improvements, and renovations totaling approximately $38.6 million.
F-41
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
15. Commitments and Contingencies (Continued)
Litigation
The Company is a party to various legal actions, proceedings, and claims (some of which are not insured), and regulatory and other governmental audits and investigations in the ordinary course of its business. The Company cannot predict the ultimate outcome of pending litigation, proceedings, and regulatory and other governmental audits and investigations. These matters could potentially subject the Company to sanctions, damages, recoupments, fines, and other penalties. The Department of Justice, Centers for Medicare & Medicaid Services (“CMS”), or other federal and state enforcement and regulatory agencies may conduct additional investigations related to the Company’s businesses in the future that may, either individually or in the aggregate, have a material adverse effect on the Company’s business, financial position, results of operations, and liquidity.
To address claims arising out of the the Company’s operations, the Company maintains professional malpractice liability insurance and general liability insurance coverages through a number of different programs that are dependent upon such factors as the state where the Company is operating and whether the operations are wholly owned or are operated through a joint venture. For the Company’s wholly owned operations, the Company maintains insurance coverages under a combination of policies with a total annual aggregate limit of $35.0 million. The Company’s insurance for the professional liability coverage is written on a “claims-made” basis, and its commercial general liability coverage is maintained on an “occurrence” basis. These coverages apply after a self-insured retention limit is exceeded. For the Company’s joint venture operations, the Company has numerous programs that are designed to respond to the risks of the specific joint venture. The annual aggregate limit under these programs ranges from $5.0 million to $20.0 million. The policies are generally written on a “claims-made” basis. Each of these programs has either a deductible or self-insured retention limit. The Company reviews its insurance program annually and may make adjustments to the amount of insurance coverage and self-insured retentions in future years. The Company also maintains umbrella liability insurance covering claims which, due to their nature or amount, are not covered by or not fully covered by the Company’s other insurance policies. These insurance policies also do not generally cover punitive damages and are subject to various deductibles and policy limits. Significant legal actions, as well as the cost and possible lack of available insurance, could subject the Company to substantial uninsured liabilities. In the Company’s opinion, the outcome of these actions, individually or in the aggregate, will not have a material adverse effect on its financial position, results of operations, or cash flows.
Healthcare providers are subject to lawsuits under the qui tam provisions of the federal False Claims Act. Qui tam lawsuits typically remain under seal (hence, usually unknown to the defendant) for some time while the government decides whether or not to intervene on behalf of a private qui tam plaintiff (known as a relator) and take the lead in the litigation. These lawsuits can involve significant monetary damages and penalties and award bounties to private plaintiffs who successfully bring the suits. The Company is and has been a defendant in these cases in the past, and may be named as a defendant in similar cases from time to time in the future.
Evansville Litigation. On October 19, 2015, the plaintiff‑relators filed a Second Amended Complaint in United States of America, ex rel. Tracy Conroy, Pamela Schenk and Lisa Wilson v. Select Medical Corporation, Select Specialty Hospital-Evansville, LLC (“SSH‑Evansville”), Select Employment Services, Inc., and Dr. Richard Sloan. The case is a civil action filed in the United States District Court for the Southern District of Indiana by private plaintiff‑relators on behalf of the United States under the federal False Claims Act. The plaintiff‑relators are the former CEO and two former case managers at SSH‑Evansville, and the defendants currently include the Company, SSH‑Evansville, a subsidiary of the Company serving as common paymaster for its employees, and a physician who practices at SSH‑Evansville. The plaintiff‑relators allege that SSH‑Evansville discharged patients too early or held patients too long, improperly discharged patients to and readmitted them from short stay hospitals, up‑coded diagnoses at admission, and admitted patients for whom long‑term acute care was not medically necessary. They also allege that the defendants engaged in retaliation in violation of federal and state law. The Second Amended Complaint replaced a prior complaint that was filed under seal on September 28, 2012 and served on the Company on February 15, 2013, after a federal magistrate judge unsealed it on January 8, 2013. All deadlines in the case had been stayed after the seal was lifted in order to allow the government time to complete its investigation and to decide whether or not to intervene. On June 19, 2015, the United States Department of Justice notified the District Court of its decision not to intervene in the case.
In December 2015, the defendants filed a Motion to Dismiss the Second Amended Complaint on multiple grounds, including that the action is disallowed by the False Claims Act’s public disclosure bar, which disqualifies qui tam actions that are based on fraud already publicly disclosed through enumerated sources, unless the relator is an original source, and that the plaintiff‑relators did not plead their claims with sufficient particularity, as required by the Federal Rules of Civil Procedure.
F-42
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
15. Commitments and Contingencies (Continued)
Thereafter, the United States filed a notice asserting a veto of the defendants’ use of the public disclosure bar for claims arising from conduct from and after March 23, 2010, which was based on certain statutory changes to the public disclosure bar language included in the Affordable Care Act. On September 30, 2016, the District Court partially granted and partially denied the defendants’ Motion to Dismiss. It ruled that the plaintiff‑relators alleged substantially the same conduct as had been publicly disclosed and that the plaintiff relators are not original sources, so that the public disclosure bar requires dismissal of all non‑retaliation claims arising from conduct before March 23, 2010. The District Court also ruled that the statutory changes to the public disclosure bar gave the United States the power to veto its applicability to claims arising from conduct on and after March 23, 2010, and therefore did not dismiss those claims based on the public disclosure bar. However, the District Court ruled that the plaintiff‑relators did not plead certain of their claims relating to interrupted stay manipulation and premature discharging of patients with the requisite particularity, and dismissed those claims. The District Court declined to dismiss the plaintiff relators’ claims arising from conduct from and after March 23, 2010 relating to delayed discharging of patients and up-coding and the plaintiff relators’ retaliation claims. The plaintiff-relators then proposed a case management plan seeking nationwide discovery involving all of the Company’s LTCHs for the period from March 23, 2010 through the present, which the defendants have opposed. The Company intends to vigorously defend this action, but at this time the Company is unable to predict the timing and outcome of this matter.
Knoxville Litigation. On July 13, 2015, the United States District Court for the Eastern District of Tennessee unsealed a qui tam Complaint in Armes v. Garman, et al, No. 3:14‑cv‑00172‑TAV‑CCS, which named as defendants Select, Select Specialty Hospital-Knoxville, Inc. (“SSH‑Knoxville”), Select Specialty Hospital-North Knoxville, Inc. and ten current or former employees of these facilities. The Complaint was unsealed after the United States and the State of Tennessee notified the court on July 13, 2015 that each had decided not to intervene in the case. The Complaint is a civil action that was filed under seal on April 29, 2014 by a respiratory therapist formerly employed at SSH‑Knoxville. The Complaint alleges violations of the federal False Claims Act and the Tennessee Medicaid False Claims Act based on extending patient stays to increase reimbursement and to increase average length of stay; artificially prolonging the lives of patients to increase Medicare reimbursements and decrease inspections; admitting patients who do not require medically necessary care; performing unnecessary procedures and services; and delaying performance of procedures to increase billing. The Complaint was served on some of the defendants during October 2015.
In November 2015, the defendants filed a Motion to Dismiss the Complaint on multiple grounds. The defendants first argued that False Claims Act’s first‑to‑file bar required dismissal of plaintiff‑relator’s claims. Under the first‑to‑file bar, if a qui tam case is pending, no person may bring a related action based on the facts underlying the first action. The defendants asserted that the plaintiff‑relator’s claims were based on the same underlying facts as were asserted in the Evansville litigation, discussed above. The defendants also argued that the plaintiff‑relator’s claims must be dismissed under the public disclosure bar, and because the plaintiff‑relator did not plead his claims with sufficient particularity.
In June 2016, the District Court granted the defendants’ Motion to Dismiss and dismissed with prejudice the plaintiff‑relator’s lawsuit in its entirety. The District Court ruled that the first‑to‑file bar precludes all but one of the plaintiff‑relator’s claims, and that the remaining claim must also be dismissed because the plaintiff‑relator failed to plead it with sufficient particularity. In July 2016, the plaintiff‑relator filed a Notice of Appeal to the United States Court of Appeals for the Sixth Circuit. Then, on October 11, 2016, the plaintiff‑relator filed a Motion to Remand the case to the District Court for further proceedings, arguing that the September 30, 2016 decision in the Evansville litigation, discussed above, undermines the basis for the District Court’s dismissal. After the Court of Appeals denied the Motion to Remand, the plaintiff‑relator then sought an indicative ruling from the District Court that it would vacate its prior dismissal ruling and allow plaintiff‑relator to supplement his Complaint, but the District Court denied such request. In December 2017, the Court of Appeals, relying on the public disclosure bar, denied the appeal of the plaintiff‑relator and affirmed the judgment of the District Court. In February 2018, the Court of Appeals denied a petition for rehearing that the plaintiff-relator filed in January 2018. The Company intends to vigorously defend this action, but at this time the Company is unable to predict the timing and outcome of this matter.
F-43
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
15. Commitments and Contingencies (Continued)
Wilmington Litigation. On January 19, 2017, the United States District Court for the District of Delaware unsealed a qui tam Complaint in United States of America and State of Delaware ex rel. Theresa Kelly v. Select Specialty Hospital-Wilmington, Inc. (“SSH‑Wilmington”), Select Specialty Hospitals, Inc., Select Employment Services, Inc., Select Medical Corporation, and Crystal Cheek, No. 16‑347‑LPS. The Complaint was initially filed under seal in May 2016 by a former chief nursing officer at SSH‑Wilmington and was unsealed after the United States filed a Notice of Election to Decline Intervention in January 2017. The corporate defendants were served in March 2017. In the complaint, the plaintiff‑relator alleges that the Select defendants and an individual defendant, who is a former health information manager at SSH‑Wilmington, violated the False Claims Act and the Delaware False Claims and Reporting Act based on allegedly falsifying medical practitioner signatures on medical records and failing to properly examine the credentials of medical practitioners at SSH‑Wilmington. In response to the Select defendants’ motion to dismiss the Complaint, in May 2017 the plaintiff-relator filed an Amended Complaint asserting the same causes of action. The Select defendants filed a Motion to Dismiss the Amended Complaint, which is now pending, based on numerous grounds, including that the Amended Complaint did not plead any alleged fraud with sufficient particularity, failed to plead that the alleged fraud was material to the government’s payment decision, failed to plead sufficient facts to establish that the Select defendants knowingly submitted false claims or records, and failed to allege any reverse false claim.
In March 2017, the plaintiff-relator initiated a second action by filing a Complaint in the Superior Court of the State of Delaware in Theresa Kelly v. Select Medical Corporation, Select Employment Services, Inc., and SSH‑Wilmington, C.A. No. N17C-03-293 CLS. The Delaware Complaint alleges that the defendants retaliated against her in violation of the Delaware Whistleblowers’ Protection Act for reporting the same alleged violations that are the subject of the federal Amended Complaint. The defendants filed a motion to dismiss, or alternatively to stay, the Delaware Complaint based on the pending federal Amended Complaint and the failure to allege facts to support a violation of the Delaware Whistleblowers’ Protection Act. In January 2018, the Court stayed the Delaware Complaint pending the outcome of the federal case.
The Company intends to vigorously defend these actions, but at this time the Company is unable to predict the timing and outcome of this matter.
Contract Therapy Subpoena
On May 18, 2017, the Company received a subpoena from the U.S. Attorney’s Office for the District of New Jersey seeking various documents principally relating to the Company’s contract therapy division, which contracted to furnish rehabilitation therapy services to residents of skilled nursing facilities (“SNFs”) and other providers. The Company operated its contract therapy division through a subsidiary until March 31, 2016, when the Company sold the stock of the subsidiary. The subpoena seeks documents that appear to be aimed at assessing whether therapy services were furnished and billed in compliance with Medicare SNF billing requirements, including whether therapy services were coded at inappropriate levels and whether excessive or unnecessary therapy was furnished to justify coding at higher paying levels. The Company does not know whether the subpoena has been issued in connection with a qui tam lawsuit or in connection with possible civil, criminal or administrative proceedings by the government. The Company is producing documents in response to the subpoena and intends to fully cooperate with this investigation. At this time, the Company is unable to predict the timing and outcome of this matter.
Northern District of Alabama Investigation
On October 30, 2017, the Company was contacted by the U.S. Attorney’s Office for the Northern District of Alabama to request cooperation in connection with an investigation that may involve Medicare billing compliance at certain of the Company’s Physiotherapy outpatient rehabilitation clinics. The Company intends to cooperate with this investigation. At this time, the Company is unable to predict the timing and outcome of this matter.
F-44
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes
Select’s 6.375% senior notes are fully and unconditionally and jointly and severally guaranteed, except for customary limitations, on a senior basis by all of Select’s wholly owned subsidiaries (the “Subsidiary Guarantors”). The Subsidiary Guarantors are defined as subsidiaries where Select, or a subsidiary of Select, holds all of the outstanding ownership interests. Certain of Select’s subsidiaries did not guarantee the 6.375% senior notes (the “Non-Guarantor Subsidiaries” and Concentra Group Holdings and its subsidiaries, or “Non-Guarantor Concentra”).
Select conducts a significant portion of its business through its subsidiaries. Presented below is condensed consolidating financial information for Select, the Subsidiary Guarantors, the Non-Guarantor Subsidiaries, and Non-Guarantor Concentra at December 31, 2016 and 2017 and for the years ended December 31, 2015, 2016, and 2017.
The equity method has been used by Select with respect to investments in subsidiaries. The equity method has been used by Subsidiary Guarantors with respect to investments in Non-Guarantor Subsidiaries. Separate financial statements for Subsidiary Guarantors are not presented.
Certain reclassifications have been made to prior reported amounts in order to conform to the current year guarantor structure.
F-45
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Balance Sheet
December 31, 2017
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
ASSETS | |||||||||||||||||||||||
Current Assets: | |||||||||||||||||||||||
Cash and cash equivalents | $ | 73 | $ | 4,856 | $ | 4,561 | $ | 113,059 | $ | — | $ | 122,549 | |||||||||||
Accounts receivable, net | — | 445,942 | 126,279 | 119,511 | — | 691,732 | |||||||||||||||||
Intercompany receivables | — | 1,595,692 | 62,990 | — | (1,658,682 | ) | (a) | — | |||||||||||||||
Prepaid income taxes | 22,704 | 5,703 | 31 | 2,949 | — | 31,387 | |||||||||||||||||
Other current assets | 13,021 | 29,547 | 13,693 | 18,897 | — | 75,158 | |||||||||||||||||
Total Current Assets | 35,798 | 2,081,740 | 207,554 | 254,416 | (1,658,682 | ) | 920,826 | ||||||||||||||||
Property and equipment, net | 39,836 | 622,445 | 79,653 | 170,657 | — | 912,591 | |||||||||||||||||
Investment in affiliates | 4,521,865 | 128,319 | — | — | (4,650,184 | ) | (b)(c) | — | |||||||||||||||
Goodwill | — | 2,108,270 | — | 674,542 | — | 2,782,812 | |||||||||||||||||
Identifiable intangible assets, net | — | 103,913 | 5,200 | 217,406 | — | 326,519 | |||||||||||||||||
Other assets | 36,494 | 98,492 | 35,523 | 23,898 | (9,989 | ) | (e) | 184,418 | |||||||||||||||
Total Assets | $ | 4,633,993 | $ | 5,143,179 | $ | 327,930 | $ | 1,340,919 | $ | (6,318,855 | ) | $ | 5,127,166 | ||||||||||
LIABILITIES AND EQUITY | |||||||||||||||||||||||
Current Liabilities: | |||||||||||||||||||||||
Overdrafts | $ | 29,463 | $ | — | $ | — | $ | — | $ | — | $ | 29,463 | |||||||||||
Current portion of long-term debt and notes payable | 16,635 | 740 | 2,212 | 2,600 | — | 22,187 | |||||||||||||||||
Accounts payable | 12,504 | 85,096 | 17,868 | 12,726 | — | 128,194 | |||||||||||||||||
Intercompany payables | 1,595,692 | 62,990 | — | — | (1,658,682 | ) | (a) | — | |||||||||||||||
Accrued payroll | 16,736 | 98,834 | 4,872 | 40,120 | — | 160,562 | |||||||||||||||||
Accrued vacation | 4,083 | 58,043 | 12,607 | 18,142 | — | 92,875 | |||||||||||||||||
Accrued interest | 17,479 | 7 | 6 | 2,393 | — | 19,885 | |||||||||||||||||
Accrued other | 39,219 | 57,121 | 12,856 | 33,970 | — | 143,166 | |||||||||||||||||
Income taxes payable | — | 1,190 | 142 | 7,739 | — | 9,071 | |||||||||||||||||
Total Current Liabilities | 1,731,811 | 364,021 | 50,563 | 117,690 | (1,658,682 | ) | 605,403 | ||||||||||||||||
Long-term debt, net of current portion | 2,042,555 | 127 | 24,730 | 610,303 | — | 2,677,715 | |||||||||||||||||
Non-current deferred tax liability | — | 88,376 | 780 | 45,750 | (9,989 | ) | (e) | 124,917 | |||||||||||||||
Other non-current liabilities | 36,259 | 56,718 | 8,141 | 44,591 | — | 145,709 | |||||||||||||||||
Total Liabilities | 3,810,625 | 509,242 | 84,214 | 818,334 | (1,668,671 | ) | 3,553,744 | ||||||||||||||||
Redeemable non-controlling interests | — | — | — | 16,270 | 624,548 | (d) | 640,818 | ||||||||||||||||
Stockholder’s Equity: | |||||||||||||||||||||||
Common stock | 0 | — | — | — | — | 0 | |||||||||||||||||
Capital in excess of par | 947,370 | — | — | — | — | 947,370 | |||||||||||||||||
Retained earnings (accumulated deficit) | (124,002 | ) | 1,415,978 | (33,368 | ) | 64,626 | (1,447,236 | ) | (c)(d) | (124,002 | ) | ||||||||||||
Subsidiary investment | — | 3,217,959 | 277,084 | 437,779 | (3,932,822 | ) | (b)(d) | — | |||||||||||||||
Total Select Medical Corporation Stockholder’s Equity | 823,368 | 4,633,937 | 243,716 | 502,405 | (5,380,058 | ) | 823,368 | ||||||||||||||||
Non-controlling interests | — | — | — | 3,910 | 105,326 | (d) | 109,236 | ||||||||||||||||
Total Equity | 823,368 | 4,633,937 | 243,716 | 506,315 | (5,274,732 | ) | 932,604 | ||||||||||||||||
Total Liabilities and Equity | $ | 4,633,993 | $ | 5,143,179 | $ | 327,930 | $ | 1,340,919 | $ | (6,318,855 | ) | $ | 5,127,166 | ||||||||||
_______________________________________________________________________________
(a) | Elimination of intercompany. |
(b) | Elimination of investments in consolidated subsidiaries. |
(c) | Elimination of investments in consolidated subsidiaries’ earnings. |
(d) | Reclassification of equity attributable to non-controlling interests. |
(e) | Reclassification of non-current deferred tax asset to report net non-current deferred tax liability in consolidation. |
F-46
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Operations
For the Year Ended December 31, 2017
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net operating revenues | $ | 700 | $ | 2,711,321 | $ | 697,547 | $ | 1,034,035 | $ | — | $ | 4,443,603 | |||||||||||
Costs and expenses: | |||||||||||||||||||||||
Cost of services | 2,585 | 2,283,360 | 591,641 | 856,590 | — | 3,734,176 | |||||||||||||||||
General and administrative | 111,069 | 159 | — | 2,819 | — | 114,047 | |||||||||||||||||
Bad debt expense | — | 44,080 | 14,534 | 20,877 | — | 79,491 | |||||||||||||||||
Depreciation and amortization | 7,540 | 76,268 | 14,258 | 61,945 | — | 160,011 | |||||||||||||||||
Total costs and expenses | 121,194 | 2,403,867 | 620,433 | 942,231 | — | 4,087,725 | |||||||||||||||||
Income (loss) from operations | (120,494 | ) | 307,454 | 77,114 | 91,804 | — | 355,878 | ||||||||||||||||
Other income and expense: | |||||||||||||||||||||||
Intercompany interest and royalty fees | 32,828 | (17,864 | ) | (14,964 | ) | — | — | — | |||||||||||||||
Intercompany management fees | 220,601 | (180,697 | ) | (39,904 | ) | — | — | — | |||||||||||||||
Loss on early retirement of debt | (19,719 | ) | — | — | — | — | (19,719 | ) | |||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | 20,973 | 81 | — | — | 21,054 | |||||||||||||||||
Non-operating loss | — | (49 | ) | — | — | — | (49 | ) | |||||||||||||||
Interest income (expense) | (124,406 | ) | 381 | (170 | ) | (30,508 | ) | — | (154,703 | ) | |||||||||||||
Income (loss) from operations before income taxes | (11,190 | ) | 130,198 | 22,157 | 61,296 | — | 202,461 | ||||||||||||||||
Income tax expense (benefit) | (8,753 | ) | (3,178 | ) | 1,186 | (7,439 | ) | — | (18,184 | ) | |||||||||||||
Equity in earnings of consolidated subsidiaries | 179,621 | 13,588 | — | — | (193,209 | ) | (a) | — | |||||||||||||||
Net income | 177,184 | 146,964 | 20,971 | 68,735 | (193,209 | ) | 220,645 | ||||||||||||||||
Less: Net income attributable to non-controlling interests | — | — | 6,736 | 36,725 | — | 43,461 | |||||||||||||||||
Net income attributable to Select Medical Corporation | $ | 177,184 | $ | 146,964 | $ | 14,235 | $ | 32,010 | $ | (193,209 | ) | $ | 177,184 | ||||||||||
_______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-47
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Cash Flows
For the Year Ended December 31, 2017
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Operating activities | |||||||||||||||||||||||
Net income | $ | 177,184 | $ | 146,964 | $ | 20,971 | $ | 68,735 | $ | (193,209 | ) | (a) | $ | 220,645 | |||||||||
Adjustments to reconcile net income to net cash provided by operating activities: | |||||||||||||||||||||||
Distributions from unconsolidated subsidiaries | — | 19,940 | 66 | — | — | 20,006 | |||||||||||||||||
Depreciation and amortization | 7,540 | 76,268 | 14,258 | 61,945 | — | 160,011 | |||||||||||||||||
Provision for bad debts | — | 44,080 | 14,534 | 20,877 | — | 79,491 | |||||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | (20,973 | ) | (81 | ) | — | — | (21,054 | ) | ||||||||||||||
Equity in earnings of consolidated subsidiaries | (179,621 | ) | (13,588 | ) | — | — | 193,209 | (a) | — | ||||||||||||||
Loss on extinguishment of debt | 6,527 | — | — | — | — | 6,527 | |||||||||||||||||
Loss (gain) on sale of assets and businesses | (939 | ) | (4,828 | ) | (4,602 | ) | 20 | — | (10,349 | ) | |||||||||||||
Stock compensation expense | 18,291 | — | — | 993 | — | 19,284 | |||||||||||||||||
Amortization of debt discount, premium and issuance costs | 7,895 | — | — | 3,235 | — | 11,130 | |||||||||||||||||
Deferred income taxes | 14,041 | (40,788 | ) | 156 | (45,733 | ) | — | (72,324 | ) | ||||||||||||||
Changes in operating assets and liabilities, net of effects of business combinations: | |||||||||||||||||||||||
Accounts receivable | — | (126,451 | ) | (43,043 | ) | (27,697 | ) | — | (197,191 | ) | |||||||||||||
Other current assets | (1,068 | ) | 4,411 | (3,697 | ) | 1,951 | — | 1,597 | |||||||||||||||
Other assets | 168 | (4,235 | ) | 3,413 | (232 | ) | — | (886 | ) | ||||||||||||||
Accounts payable | 1,450 | 2,534 | 828 | (909 | ) | — | 3,903 | ||||||||||||||||
Accrued expenses | (25,396 | ) | 2,168 | 13,244 | 27,325 | — | 17,341 | ||||||||||||||||
Net cash provided by operating activities | 26,072 | 85,502 | 16,047 | 110,510 | — | 238,131 | |||||||||||||||||
Investing activities | |||||||||||||||||||||||
Business combinations, net of cash acquired | — | (10,006 | ) | (1,664 | ) | (15,720 | ) | — | (27,390 | ) | |||||||||||||
Purchases of property and equipment | (30,413 | ) | (136,075 | ) | (37,843 | ) | (28,912 | ) | — | (233,243 | ) | ||||||||||||
Investment in businesses | — | (12,682 | ) | — | — | — | (12,682 | ) | |||||||||||||||
Proceeds from sale of assets and businesses | 45,788 | 15,022 | 19,537 | 3 | — | 80,350 | |||||||||||||||||
Net cash provided by (used in) investing activities | 15,375 | (143,741 | ) | (19,970 | ) | (44,629 | ) | — | (192,965 | ) | |||||||||||||
Financing activities | |||||||||||||||||||||||
Borrowings on revolving facilities | 970,000 | — | — | — | — | 970,000 | |||||||||||||||||
Payments on revolving facilities | (960,000 | ) | — | — | — | — | (960,000 | ) | |||||||||||||||
Proceeds from term loans | 1,139,487 | — | — | — | — | 1,139,487 | |||||||||||||||||
Payments on term loans | (1,156,377 | ) | — | — | (23,065 | ) | — | (1,179,442 | ) | ||||||||||||||
Revolving facility debt issuance costs | (4,392 | ) | — | — | — | — | (4,392 | ) | |||||||||||||||
Borrowings of other debt | 25,630 | — | 18,224 | 2,767 | — | 46,621 | |||||||||||||||||
Principal payments on other debt | (13,748 | ) | (456 | ) | (3,036 | ) | (3,407 | ) | — | (20,647 | ) | ||||||||||||
Dividends paid to Holdings | (4,753 | ) | — | — | — | — | (4,753 | ) | |||||||||||||||
Equity investment by Holdings | 2,017 | — | — | — | — | 2,017 | |||||||||||||||||
Intercompany | (40,410 | ) | 57,204 | (16,794 | ) | — | — | — | |||||||||||||||
Decrease in overdrafts | (9,899 | ) | — | — | — | — | (9,899 | ) | |||||||||||||||
Proceeds from issuance of non-controlling interests | — | — | 9,982 | — | — | 9,982 | |||||||||||||||||
Purchase of non-controlling interests | — | (120 | ) | — | — | — | (120 | ) | |||||||||||||||
Distributions to non-controlling interests | — | — | (4,948 | ) | (5,552 | ) | — | (10,500 | ) | ||||||||||||||
Net cash provided by (used in) financing activities | (52,445 | ) | 56,628 | 3,428 | (29,257 | ) | — | (21,646 | ) | ||||||||||||||
Net increase (decrease) in cash and cash equivalents | (10,998 | ) | (1,611 | ) | (495 | ) | 36,624 | — | 23,520 | ||||||||||||||
Cash and cash equivalents at beginning of period | 11,071 | 6,467 | 5,056 | 76,435 | — | 99,029 | |||||||||||||||||
Cash and cash equivalents at end of period | $ | 73 | $ | 4,856 | $ | 4,561 | $ | 113,059 | $ | — | $ | 122,549 | |||||||||||
_______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-48
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Balance Sheet
December 31, 2016
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
ASSETS | |||||||||||||||||||||||
Current Assets: | |||||||||||||||||||||||
Cash and cash equivalents | $ | 11,071 | $ | 6,467 | $ | 5,056 | $ | 76,435 | $ | — | $ | 99,029 | |||||||||||
Accounts receivable, net | — | 363,470 | 97,770 | 112,512 | — | 573,752 | |||||||||||||||||
Intercompany receivables | — | 1,573,960 | 25,578 | — | (1,599,538 | ) | (a) | — | |||||||||||||||
Prepaid income taxes | 6,658 | — | — | 5,765 | — | 12,423 | |||||||||||||||||
Other current assets | 11,953 | 33,958 | 10,269 | 21,519 | — | 77,699 | |||||||||||||||||
Total Current Assets | 29,682 | 1,977,855 | 138,673 | 216,231 | (1,599,538 | ) | 762,903 | ||||||||||||||||
Property and equipment, net | 48,697 | 603,408 | 50,869 | 189,243 | — | 892,217 | |||||||||||||||||
Investment in affiliates | 4,493,684 | 89,288 | — | — | (4,582,972 | ) | (b) (c) | — | |||||||||||||||
Goodwill | — | 2,090,963 | — | 660,037 | — | 2,751,000 | |||||||||||||||||
Identifiable intangible assets, net | — | 106,439 | 2,693 | 231,430 | — | 340,562 | |||||||||||||||||
Other assets | 45,636 | 84,803 | 53,954 | 16,235 | (26,684 | ) | (e) | 173,944 | |||||||||||||||
Total Assets | $ | 4,617,699 | $ | 4,952,756 | $ | 246,189 | $ | 1,313,176 | $ | (6,209,194 | ) | $ | 4,920,626 | ||||||||||
LIABILITIES AND EQUITY | |||||||||||||||||||||||
Current Liabilities: | |||||||||||||||||||||||
Overdrafts | $ | 39,362 | $ | — | $ | — | $ | — | $ | — | $ | 39,362 | |||||||||||
Current portion of long-term debt and notes payable | 7,227 | 445 | 1,324 | 4,660 | — | 13,656 | |||||||||||||||||
Accounts payable | 10,775 | 78,608 | 22,397 | 14,778 | — | 126,558 | |||||||||||||||||
Intercompany payables | 1,573,960 | 25,578 | — | — | (1,599,538 | ) | (a) | — | |||||||||||||||
Accrued payroll | 16,963 | 92,216 | 4,246 | 32,972 | — | 146,397 | |||||||||||||||||
Accrued vacation | 3,440 | 55,486 | 10,668 | 13,667 | — | 83,261 | |||||||||||||||||
Accrued interest | 20,114 | — | — | 2,211 | — | 22,325 | |||||||||||||||||
Accrued other | 39,155 | 62,384 | 4,639 | 33,898 | — | 140,076 | |||||||||||||||||
Total Current Liabilities | 1,710,996 | 314,717 | 43,274 | 102,186 | (1,599,538 | ) | 571,635 | ||||||||||||||||
Long-term debt, net of current portion | 2,048,154 | 601 | 9,685 | 626,893 | — | 2,685,333 | |||||||||||||||||
Non-current deferred tax liability | — | 133,852 | 596 | 91,314 | (26,684 | ) | (e) | 199,078 | |||||||||||||||
Other non-current liabilities | 42,824 | 53,537 | 5,727 | 34,432 | — | 136,520 | |||||||||||||||||
Total Liabilities | 3,801,974 | 502,707 | 59,282 | 854,825 | (1,626,222 | ) | 3,592,566 | ||||||||||||||||
Redeemable non-controlling interests | — | — | — | 15,493 | 406,666 | (d) | 422,159 | ||||||||||||||||
Stockholder’s Equity: | |||||||||||||||||||||||
Common stock | 0 | — | — | — | — | 0 | |||||||||||||||||
Capital in excess of par | 925,111 | — | — | — | — | 925,111 | |||||||||||||||||
Retained earnings (accumulated deficit) | (109,386 | ) | 1,269,009 | (32,826 | ) | 2,723 | (1,238,906 | ) | (c) (d) | (109,386 | ) | ||||||||||||
Subsidiary investment | — | 3,181,040 | 219,733 | 436,786 | (3,837,559 | ) | (b) (d) | — | |||||||||||||||
Total Select Medical Corporation Stockholder’s Equity | 815,725 | 4,450,049 | 186,907 | 439,509 | (5,076,465 | ) | 815,725 | ||||||||||||||||
Non-controlling interests | — | — | — | 3,349 | 86,827 | (d) | 90,176 | ||||||||||||||||
Total Equity | 815,725 | 4,450,049 | 186,907 | 442,858 | (4,989,638 | ) | 905,901 | ||||||||||||||||
Total Liabilities and Equity | $ | 4,617,699 | $ | 4,952,756 | $ | 246,189 | $ | 1,313,176 | $ | (6,209,194 | ) | $ | 4,920,626 | ||||||||||
_______________________________________________________________________________
(a) | Elimination of intercompany. |
(b) | Elimination of investments in consolidated subsidiaries. |
(c) | Elimination of investments in consolidated subsidiaries’ earnings. |
(d) | Reclassification of equity attributable to non-controlling interests. |
(e) | Reclassification of non-current deferred tax asset to report net non-current deferred tax liability in consolidation. |
F-49
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Operations
For the Year Ended December 31, 2016
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net operating revenues | $ | 541 | $ | 2,752,676 | $ | 532,180 | $ | 1,000,624 | $ | — | $ | 4,286,021 | |||||||||||
Costs and expenses: | |||||||||||||||||||||||
Cost of services | 2,037 | 2,346,487 | 476,084 | 840,235 | — | 3,664,843 | |||||||||||||||||
General and administrative | 106,864 | 63 | — | — | — | 106,927 | |||||||||||||||||
Bad debt expense | — | 41,737 | 9,206 | 18,150 | — | 69,093 | |||||||||||||||||
Depreciation and amortization | 5,348 | 67,932 | 11,314 | 60,717 | — | 145,311 | |||||||||||||||||
Total costs and expenses | 114,249 | 2,456,219 | 496,604 | 919,102 | — | 3,986,174 | |||||||||||||||||
Income (loss) from operations | (113,708 | ) | 296,457 | 35,576 | 81,522 | — | 299,847 | ||||||||||||||||
Other income and expense: | |||||||||||||||||||||||
Intercompany interest and royalty fees | 31,083 | (16,998 | ) | (14,085 | ) | — | — | — | |||||||||||||||
Intercompany management fees | 168,915 | (140,347 | ) | (28,568 | ) | — | — | — | |||||||||||||||
Loss on early retirement of debt | (773 | ) | — | — | (10,853 | ) | — | (11,626 | ) | ||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | 19,838 | 105 | — | — | 19,943 | |||||||||||||||||
Non-operating gain | 33,932 | 8,719 | — | — | — | 42,651 | |||||||||||||||||
Interest income (expense) | (132,066 | ) | 382 | (101 | ) | (38,296 | ) | — | (170,081 | ) | |||||||||||||
Income (loss) from operations before income taxes | (12,617 | ) | 168,051 | (7,073 | ) | 32,373 | — | 180,734 | |||||||||||||||
Income tax expense (benefit) | (14,461 | ) | 54,047 | 3,166 | 12,712 | — | 55,464 | ||||||||||||||||
Equity in earnings (losses) of consolidated subsidiaries | 113,567 | (8,061 | ) | — | — | (105,506 | ) | (a) | — | ||||||||||||||
Net income (loss) | 115,411 | 105,943 | (10,239 | ) | 19,661 | (105,506 | ) | 125,270 | |||||||||||||||
Less: Net income (loss) attributable to non-controlling interests | — | 28 | (2,346 | ) | 12,177 | — | 9,859 | ||||||||||||||||
Net income (loss) attributable to Select Medical Corporation | $ | 115,411 | $ | 105,915 | $ | (7,893 | ) | $ | 7,484 | $ | (105,506 | ) | $ | 115,411 | |||||||||
______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-50
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Cash Flows
For the Year Ended December 31, 2016
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Operating activities | |||||||||||||||||||||||
Net income (loss) | $ | 115,411 | $ | 105,943 | $ | (10,239 | ) | $ | 19,661 | $ | (105,506 | ) | (a) | $ | 125,270 | ||||||||
Adjustments to reconcile net income (loss) to net cash provided by (used in) operating activities: | |||||||||||||||||||||||
Distributions from unconsolidated subsidiaries | — | 20,380 | 96 | — | — | 20,476 | |||||||||||||||||
Depreciation and amortization | 5,348 | 67,932 | 11,314 | 60,717 | — | 145,311 | |||||||||||||||||
Provision for bad debts | — | 41,737 | 9,206 | 18,150 | — | 69,093 | |||||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | (19,838 | ) | (105 | ) | — | — | (19,943 | ) | ||||||||||||||
Equity in earnings of consolidated subsidiaries | (113,567 | ) | 8,061 | — | — | 105,506 | (a) | — | |||||||||||||||
Loss on extinguishment of debt | 773 | — | — | 10,853 | — | 11,626 | |||||||||||||||||
Loss (gain) on sale of assets and businesses | (33,738 | ) | (12,975 | ) | 246 | (21 | ) | — | (46,488 | ) | |||||||||||||
Gain on sale of equity investment | — | (2,779 | ) | — | — | — | (2,779 | ) | |||||||||||||||
Impairment of equity investment | — | 5,339 | — | — | — | 5,339 | |||||||||||||||||
Stock compensation expense | 16,643 | — | — | 770 | — | 17,413 | |||||||||||||||||
Amortization of debt discount, premium and issuance costs | 12,358 | — | — | 3,298 | — | 15,656 | |||||||||||||||||
Deferred income taxes | (709 | ) | — | — | (11,882 | ) | — | (12,591 | ) | ||||||||||||||
Changes in operating assets and liabilities, net of effects of business combinations: | |||||||||||||||||||||||
Accounts receivable | — | 15,768 | (40,080 | ) | (15,008 | ) | — | (39,320 | ) | ||||||||||||||
Other current assets | (1,432 | ) | 10,310 | (4,619 | ) | 13,191 | — | 17,450 | |||||||||||||||
Other assets | (2,978 | ) | 51,586 | (53,295 | ) | 13,977 | — | 9,290 | |||||||||||||||
Accounts payable | 330 | (24,877 | ) | 5,979 | 3,076 | — | (15,492 | ) | |||||||||||||||
Accrued expenses | (1,287 | ) | 53,764 | (2,091 | ) | (4,094 | ) | — | 46,292 | ||||||||||||||
Net cash provided by (used in) operating activities | (2,848 | ) | 320,351 | (83,588 | ) | 112,688 | — | 346,603 | |||||||||||||||
Investing activities | |||||||||||||||||||||||
Business combinations, net of cash acquired | (406,305 | ) | (59,520 | ) | (953 | ) | (5,428 | ) | — | (472,206 | ) | ||||||||||||
Purchases of property and equipment | (15,262 | ) | (101,564 | ) | (28,861 | ) | (15,946 | ) | — | (161,633 | ) | ||||||||||||
Investment in businesses | — | (4,723 | ) | — | — | — | (4,723 | ) | |||||||||||||||
Proceeds from sale of assets and businesses | 63,418 | 16,978 | 67 | — | — | 80,463 | |||||||||||||||||
Proceeds from sale of equity investment | — | 3,779 | — | — | — | 3,779 | |||||||||||||||||
Net cash used in investing activities | (358,149 | ) | (145,050 | ) | (29,747 | ) | (21,374 | ) | — | (554,320 | ) | ||||||||||||
Financing activities | |||||||||||||||||||||||
Borrowings on revolving facilities | 575,000 | — | — | — | — | 575,000 | |||||||||||||||||
Payments on revolving facilities | (650,000 | ) | — | — | (5,000 | ) | — | (655,000 | ) | ||||||||||||||
Proceeds from term loans | 600,127 | — | — | 195,217 | — | 795,344 | |||||||||||||||||
Payments on term loans | (230,524 | ) | — | — | (207,510 | ) | — | (438,034 | ) | ||||||||||||||
Borrowings of other debt | 11,935 | — | 12,970 | 2,816 | — | 27,721 | |||||||||||||||||
Principal payments on other debt | (15,144 | ) | (751 | ) | (2,554 | ) | (2,952 | ) | — | (21,401 | ) | ||||||||||||
Dividends paid to Holdings | (2,929 | ) | — | — | — | — | (2,929 | ) | |||||||||||||||
Equity investment by Holdings | 1,672 | — | — | — | — | 1,672 | |||||||||||||||||
Intercompany | 67,115 | (169,473 | ) | 102,358 | — | — | — | ||||||||||||||||
Increase in overdrafts | 10,746 | — | — | — | — | 10,746 | |||||||||||||||||
Proceeds from issuance of non-controlling interests | — | — | 11,846 | — | — | 11,846 | |||||||||||||||||
Purchase of non-controlling interests | — | (2,099 | ) | — | — | — | (2,099 | ) | |||||||||||||||
Distributions to non-controlling interests | — | (217 | ) | (6,854 | ) | (3,484 | ) | — | (10,555 | ) | |||||||||||||
Net cash provided by (used in) financing activities | 367,998 | (172,540 | ) | 117,766 | (20,913 | ) | — | 292,311 | |||||||||||||||
Net increase in cash and cash equivalents | 7,001 | 2,761 | 4,431 | 70,401 | — | 84,594 | |||||||||||||||||
Cash and cash equivalents at beginning of period | 4,070 | 3,706 | 625 | 6,034 | — | 14,435 | |||||||||||||||||
Cash and cash equivalents at end of period | $ | 11,071 | $ | 6,467 | $ | 5,056 | $ | 76,435 | $ | — | $ | 99,029 | |||||||||||
_______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-51
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Operations
For the Year Ended December 31, 2015
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Net operating revenues | $ | 724 | $ | 2,691,851 | $ | 464,939 | $ | 585,222 | $ | — | $ | 3,742,736 | |||||||||||
Costs and expenses: | |||||||||||||||||||||||
Cost of services | 2,029 | 2,280,986 | 400,179 | 528,347 | — | 3,211,541 | |||||||||||||||||
General and administrative | 88,227 | (890 | ) | — | 4,715 | — | 92,052 | ||||||||||||||||
Bad debt expense | — | 40,708 | 9,073 | 9,591 | — | 59,372 | |||||||||||||||||
Depreciation and amortization | 4,292 | 56,957 | 10,088 | 33,644 | — | 104,981 | |||||||||||||||||
Total costs and expenses | 94,548 | 2,377,761 | 419,340 | 576,297 | — | 3,467,946 | |||||||||||||||||
Income (loss) from operations | (93,824 | ) | 314,090 | 45,599 | 8,925 | — | 274,790 | ||||||||||||||||
Other income and expense: | |||||||||||||||||||||||
Intercompany interest and royalty fees | 29,393 | (23,274 | ) | (6,119 | ) | — | — | — | |||||||||||||||
Intercompany management fees | 143,939 | (120,356 | ) | (23,583 | ) | — | — | — | |||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | 16,719 | 92 | — | — | 16,811 | |||||||||||||||||
Non-operating gain | — | 29,647 | — | — | — | 29,647 | |||||||||||||||||
Interest income (expense) | (89,160 | ) | 408 | (2 | ) | (24,062 | ) | — | (112,816 | ) | |||||||||||||
Income (loss) from operations before income taxes | (9,652 | ) | 217,234 | 15,987 | (15,137 | ) | — | 208,432 | |||||||||||||||
Income tax expense (benefit) | (7,869 | ) | 85,949 | (512 | ) | (5,132 | ) | — | 72,436 | ||||||||||||||
Equity in earnings of consolidated subsidiaries | 132,519 | 7,527 | — | — | (140,046 | ) | (a) | — | |||||||||||||||
Net income (loss) | 130,736 | 138,812 | 16,499 | (10,005 | ) | (140,046 | ) | 135,996 | |||||||||||||||
Less: Net income (loss) attributable to non-controlling interests | — | 245 | 8,899 | (3,884 | ) | — | 5,260 | ||||||||||||||||
Net income (loss) attributable to Select Medical Corporation | $ | 130,736 | $ | 138,567 | $ | 7,600 | $ | (6,121 | ) | $ | (140,046 | ) | $ | 130,736 | |||||||||
_______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-52
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
16. Financial Information for Subsidiary Guarantors and Non-Guarantor Subsidiaries under Select’s 6.375% Senior Notes (Continued)
Select Medical Corporation
Condensed Consolidating Statement of Cash Flows
For the Year Ended December 31, 2015
Select (Parent Company Only) | Subsidiary Guarantors | Non-Guarantor Subsidiaries | Non-Guarantor Concentra | Eliminations | Consolidated Select Medical Corporation | ||||||||||||||||||
(in thousands) | |||||||||||||||||||||||
Operating activities | |||||||||||||||||||||||
Net income (loss) | $ | 130,736 | $ | 138,812 | $ | 16,499 | $ | (10,005 | ) | $ | (140,046 | ) | (a) | $ | 135,996 | ||||||||
Adjustments to reconcile net income (loss) to net cash provided by operating activities: | |||||||||||||||||||||||
Distributions from unconsolidated subsidiaries | — | 13,870 | 99 | — | — | 13,969 | |||||||||||||||||
Depreciation and amortization | 4,292 | 56,957 | 10,088 | 33,644 | — | 104,981 | |||||||||||||||||
Provision for bad debts | — | 40,708 | 9,073 | 9,591 | — | 59,372 | |||||||||||||||||
Equity in earnings of unconsolidated subsidiaries | — | (16,719 | ) | (92 | ) | — | — | (16,811 | ) | ||||||||||||||
Equity in earnings of consolidated subsidiaries | (132,519 | ) | (7,527 | ) | — | — | 140,046 | (a) | — | ||||||||||||||
Loss (gain) on sale of assets and businesses | — | (1,128 | ) | 16 | 14 | — | (1,098 | ) | |||||||||||||||
Gain on sale of equity investment | — | (29,647 | ) | — | — | — | (29,647 | ) | |||||||||||||||
Stock compensation expense | 13,969 | — | — | 1,016 | — | 14,985 | |||||||||||||||||
Amortization of debt discount, premium and issuance costs | 7,404 | — | — | 2,139 | — | 9,543 | |||||||||||||||||
Deferred income taxes | (3,484 | ) | — | — | 1,426 | — | (2,058 | ) | |||||||||||||||
Changes in operating assets and liabilities, net of effects of business combinations: | |||||||||||||||||||||||
Accounts receivable | — | (83,142 | ) | (10,255 | ) | 825 | — | (92,572 | ) | ||||||||||||||
Other current assets | (2,661 | ) | (2,236 | ) | (396 | ) | 2,790 | — | (2,503 | ) | |||||||||||||
Other assets | 10,840 | (6,415 | ) | 288 | — | — | 4,713 | ||||||||||||||||
Accounts payable | 560 | 8,569 | 2,654 | (9,438 | ) | — | 2,345 | ||||||||||||||||
Accrued expenses | (1,508 | ) | 9,569 | 5,696 | (6,557 | ) | — | 7,200 | |||||||||||||||
Net cash provided by operating activities | 27,629 | 121,671 | 33,670 | 25,445 | — | 208,415 | |||||||||||||||||
Investing activities | |||||||||||||||||||||||
Business combinations, net of cash acquired | — | — | (8,832 | ) | (1,052,796 | ) | — | (1,061,628 | ) | ||||||||||||||
Purchases of property and equipment | (10,890 | ) | (134,002 | ) | (10,979 | ) | (26,771 | ) | — | (182,642 | ) | ||||||||||||
Investment in businesses | — | (2,347 | ) | — | — | — | (2,347 | ) | |||||||||||||||
Proceeds from sale of assets and businesses | — | 1,742 | 24 | 1 | — | 1,767 | |||||||||||||||||
Proceeds from sale of equity investment | — | 33,096 | — | — | — | 33,096 | |||||||||||||||||
Net cash used in investing activities | (10,890 | ) | (101,511 | ) | (19,787 | ) | (1,079,566 | ) | — | (1,211,754 | ) | ||||||||||||
Financing activities | |||||||||||||||||||||||
Borrowings on revolving facilities | 1,115,000 | — | — | 20,000 | — | 1,135,000 | |||||||||||||||||
Payments on revolving facilities | (880,000 | ) | — | — | (15,000 | ) | — | (895,000 | ) | ||||||||||||||
Proceeds from term loans | — | — | — | 623,575 | — | 623,575 | |||||||||||||||||
Payments on term loans | (26,884 | ) | — | — | (2,250 | ) | — | (29,134 | ) | ||||||||||||||
Borrowings of other debt | 8,684 | — | 1,681 | 3,009 | — | 13,374 | |||||||||||||||||
Principal payments on other debt | (11,923 | ) | (2,736 | ) | (1,513 | ) | (1,964 | ) | — | (18,136 | ) | ||||||||||||
Dividends paid to Holdings | (28,956 | ) | — | — | — | — | (28,956 | ) | |||||||||||||||
Equity investment by Holdings | 1,649 | — | — | — | — | 1,649 | |||||||||||||||||
Intercompany | (199,024 | ) | (15,930 | ) | (2,981 | ) | 217,935 | — | — | ||||||||||||||
Tax benefit from stock based awards | 1,846 | — | — | — | — | 1,846 | |||||||||||||||||
Increase in overdrafts | 6,869 | — | — | — | — | 6,869 | |||||||||||||||||
Proceeds from issuance of non-controlling interests | — | — | — | 217,065 | — | 217,065 | |||||||||||||||||
Purchase of non-controlling interests | — | — | (1,095 | ) | — | — | (1,095 | ) | |||||||||||||||
Distributions to non-controlling interests | — | (242 | ) | (10,180 | ) | (2,215 | ) | — | (12,637 | ) | |||||||||||||
Net cash provided by (used in) financing activities | (12,739 | ) | (18,908 | ) | (14,088 | ) | 1,060,155 | — | 1,014,420 | ||||||||||||||
Net increase (decrease) in cash and cash equivalents | 4,000 | 1,252 | (205 | ) | 6,034 | — | 11,081 | ||||||||||||||||
Cash and cash equivalents at beginning of period | 70 | 2,454 | 830 | — | — | 3,354 | |||||||||||||||||
Cash and cash equivalents at end of period | $ | 4,070 | $ | 3,706 | $ | 625 | $ | 6,034 | $ | — | $ | 14,435 | |||||||||||
_______________________________________________________________________________
(a) | Elimination of equity in earnings of consolidated subsidiaries. |
F-53
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
17. Subsequent Events
Acquisition of U.S. HealthWorks and Financing
On October 23, 2017, Select announced that Concentra Group Holdings entered into an Equity Purchase and Contribution Agreement (the “Purchase Agreement”) dated October 22, 2017 with Concentra, Concentra Group Holdings Parent, LLC (“Concentra Group Holdings Parent”), U.S. HealthWorks, and Dignity Health Holding Company (“DHHC”). On February 1, 2018, pursuant to the terms of the Purchase Agreement, Concentra acquired all of the issued and outstanding shares of stock of U.S. HealthWorks, an occupational medicine and urgent care service provider. For the year ended December 31, 2017, $2.8 million of U.S. HealthWorks acquisition costs were recognized in general and administrative expense.
In connection with the closing of the transaction, Concentra Group Holdings redeemed certain of its outstanding equity interests from existing minority equity holders and subsequently, Concentra Group Holdings and a wholly owned subsidiary of Concentra Group Holdings Parent merged, with Concentra Group Holdings surviving the merger and becoming a wholly owned subsidiary of Concentra Group Holdings Parent. As a result of the merger, the equity interests of Concentra Group Holdings outstanding after the redemption described above were exchanged for membership interests in Concentra Group Holdings Parent.
Concentra acquired U.S. HealthWorks for $753.0 million. DHHC, a subsidiary of Dignity Health, was issued a 20% equity interest in Concentra Group Holdings Parent, which was valued at $238.0 million. Select retained a majority voting interest in Concentra Group Holdings Parent following the closing of the transaction.
The U.S. HealthWorks acquisition is being accounted for under the provisions of ASC 805, Business Combinations. The Company will allocate the purchase price to tangible and identifiable intangible assets acquired and liabilities assumed based on their estimated fair values. The assessment of the acquisition-date fair values of the assets acquired and the liabilities assumed and the determination of estimated useful lives of long-lived assets and finite-lived intangibles are pending the completion of appraisals; therefore, the Company is unable to disclose the purchase price allocation or pro forma results of operations for the year ended December 31, 2017.
On February 1, 2018, in connection with the transactions contemplated under the Purchase Agreement, Concentra amended the Concentra first lien credit agreement to, among other things, provide for (i) an additional $555.0 million in tranche B term loans that, along with the existing tranche B term loans under the Concentra first lien credit agreement, have a maturity date of June 1, 2022 and (ii) an additional $25.0 million to the $50.0 million, five-year revolving credit facility under the terms of the existing Concentra first lien credit agreement. The tranche B term loans bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra first lien credit agreement) plus 2.75% (subject to an Adjusted LIBO Rate floor of 1.00%) for Eurodollar Borrowings (as defined in the Concentra first lien credit agreement), or Alternate Base Rate (as defined in the Concentra first lien credit agreement) plus 1.75% (subject to an Alternate Base Rate floor of 2.00%) for ABR Borrowings (as defined in the Concentra first lien credit agreement). All other material terms and conditions applicable to the original tranche B term loan commitments are applicable to the additional tranche B term loans created under this amendment.
In addition, Concentra entered into a second lien credit agreement (the “Concentra 2018 second lien credit agreement”) that provides for $240.0 million in term loans with an initial maturity date of June 1, 2023. Borrowings under the Concentra 2018 second lien credit agreement will bear interest at a rate equal to the Adjusted LIBO Rate (as defined in the Concentra 2018 second lien credit agreement) plus 6.50% (subject to an Adjusted LIBO Rate floor of 1.00%), or Alternate Base Rate (as defined in the Concentra 2018 second lien credit agreement) plus 5.50% (subject to an Alternate Base Rate floor of 2.00%).
Concentra used borrowings under the Concentra first lien credit agreement and the Concentra 2018 second lien credit agreement, together with cash on hand, to pay the purchase price for all of the issued and outstanding stock of U.S. HealthWorks to DHHC and to finance the redemption and reorganization transactions contemplated by the Purchase Agreement (as described above).
F-54
SELECT MEDICAL HOLDINGS CORPORATION
AND SELECT MEDICAL CORPORATION
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
18. Selected Quarterly Financial Data (Unaudited)
The tables below sets forth selected unaudited financial data for each quarter of the last two years. The financial data presented below is the same for both Select Medical Holdings Corporation and Select Medical Corporation, except for income per common share which is limited to Select Medical Holdings Corporation.
First Quarter | Second Quarter | Third Quarter | Fourth Quarter | ||||||||||||
(in thousands, except per share amounts) | |||||||||||||||
Year ended December 31, 2016 | |||||||||||||||
Net operating revenues | $ | 1,088,330 | $ | 1,097,631 | $ | 1,053,795 | $ | 1,046,265 | |||||||
Income from operations | 86,886 | 101,054 | 56,162 | 55,745 | |||||||||||
Net income attributable to Select Medical Holdings Corporation | 54,833 | 33,935 | 6,471 | 20,172 | |||||||||||
Income per common share(1): | |||||||||||||||
Basic | $ | 0.42 | $ | 0.26 | $ | 0.05 | $ | 0.15 | |||||||
Diluted | $ | 0.42 | $ | 0.26 | $ | 0.05 | $ | 0.15 | |||||||
First Quarter | Second Quarter | Third Quarter | Fourth Quarter | ||||||||||||
(in thousands, except per share amounts) | |||||||||||||||
Year ended December 31, 2017 | |||||||||||||||
Net operating revenues | $ | 1,111,361 | $ | 1,120,675 | $ | 1,097,166 | $ | 1,114,401 | |||||||
Income from operations | 91,765 | 115,663 | 72,098 | 76,352 | |||||||||||
Net income attributable to Select Medical Holdings Corporation | 15,870 | 42,055 | 18,462 | 100,797 | |||||||||||
Income per common share(1): | |||||||||||||||
Basic | $ | 0.12 | $ | 0.32 | $ | 0.14 | $ | 0.75 | |||||||
Diluted | $ | 0.12 | $ | 0.32 | $ | 0.14 | $ | 0.75 | |||||||
_______________________________________________________________________________
(1) | Due to rounding, the summation of quarterly income per share balances may not equal year to date equivalents. |
F-55
The following Financial Statement Schedule along with the report thereon of PricewaterhouseCoopers LLP dated February 22, 2018, should be read in conjunction with the consolidated financial statements. Financial Statement Schedules not included in this filing have been omitted because they are not applicable or the required information is shown in the consolidated financial statements or notes thereto.
Select Medical Holdings Corporation
Select Medical Corporation
Schedule II—Valuation and Qualifying Accounts
Balance at Beginning of Year | Charged to Cost and Expenses | Deductions(1) | Balance at End of Year | |||||||||||||
(in thousands) | ||||||||||||||||
Allowance for Doubtful Accounts | ||||||||||||||||
Year ended December 31, 2017 | $ | 63,787 | $ | 79,491 | $ | (67,734 | ) | $ | 75,544 | |||||||
Year ended December 31, 2016 | $ | 61,133 | $ | 69,093 | $ | (66,439 | ) | $ | 63,787 | |||||||
Year ended December 31, 2015 | $ | 46,425 | $ | 59,372 | $ | (44,664 | ) | $ | 61,133 | |||||||
Income Tax Valuation Allowance | ||||||||||||||||
Year ended December 31, 2017 | $ | 26,421 | $ | (13,435 | ) | $ | — | $ | 12,986 | |||||||
Year ended December 31, 2016 | $ | 7,586 | $ | 18,835 | $ | — | $ | 26,421 | ||||||||
Year ended December 31, 2015 | $ | 9,641 | $ | (2,055 | ) | $ | — | $ | 7,586 | |||||||
_______________________________________________________________________________
(1) | Allowance for doubtful accounts deductions represent write-offs against the reserve for 2015, 2016, and 2017. |
F-56