Attached files
| file | filename |
|---|---|
| 8-K - 8-K - Minerva Neurosciences, Inc. | d509395d8k.htm |
 Confidential & Proprietary
San Francisco January 2018 CORPORATE PRESENTATION Exhibit 99.1 |
 All
trademarks, trade names and service marks appearing in this presentation are the property of their respective owners. Forward-Looking Statement Safe-Harbor 2 This presentation contains forward-looking statements about Minerva Neurosciences which are subject to the safe harbor provisions
of the Private Securities Litigation Reform Act of 1995, as amended.
Forward-looking statements are statements that are not historical
facts, reflect management’s expectations as of the date of this presentation, and involve certain risks and uncertainties. Forward-looking statements include, but are not limited to: the benefits, efficacy and safety of our new formulations; whether studies
performed on analogs or backups of our compounds are a good predictor of
the clinical efficacy of our compounds; statements with respect to the
timing and results of future clinical milestones with MIN-101, seltorexant (MIN-202), MIN-117 and MIN-301, including the Phase 3 trial of MIN-101; the potential for a single Phase 3 trial with supportive Phase 2b results to support the basis for an NDA
for MIN-101; the Phase 2b trials of seltorexant; the planned Phase 2b
trial of MIN-117; statements regarding our ability to successfully
develop and commercialize our therapeutic products; our ability to expand our long-term business opportunities; our expectations regarding approval for our products by the U.S. Food and Drug Administration or equivalent foreign regulatory
agencies; estimates regarding the market potential for our products; financial
projections and estimates and their underlying assumptions; and future
performance. All of such statements are subject to certain risks and uncertainties, many of which are difficult to predict and generally beyond the control of the Company, that could cause actual results to differ materially from those
expressed in, or implied or projected by, the forward-looking
statements. These forward-looking statements are based on our current
expectations and may differ materially from actual results due to a variety of factors including, without limitation, whether any of our therapeutic products will advance further in the clinical trials process and whether and when, if at all, they will receive final approval
from the U.S. Food and Drug Administration or equivalent foreign
regulatory agencies and for which indications; whether the results of
future clinical trials of MIN-101, seltorexant, MIN-117 and MIN-301, if any, will be consistent with the results of past clinical trials; whether MIN-101, seltorexant, MIN-117 and MIN-301 will be successfully marketed if approved; whether our therapeutic product
discovery and development efforts will be successful; our ability to
achieve the results contemplated by our co-development agreements;
the strength and enforceability of our intellectual property rights; competition from pharmaceutical and biotechnology companies; the development of and our ability to take advantage of the market for our therapeutic products; our ability to raise
additional capital to fund our operations on terms acceptable to us; and general
economic conditions. These and other potential risks and
uncertainties that could cause actual results to differ from the results predicted are more fully detailed under the caption “Risk Factors” in our filings with the Securities and Exchange Commission, including our Quarterly Report on Form 10-Q for the
quarter ended September 30, 2017, filed with the Securities and Exchange
Commission on November 6, 2017. Copies of reports filed with the SEC are
posted on our website at www.minervaneurosciences.com. Our audience is cautioned not to place undue reliance on these forward-looking statements that speak only as of the date hereof, and we disclaim any obligation to update any
forward-looking statements, except as required by law.
|
 Focus: to
address the debilitating unmet needs of millions of patients afflicted by
neuropsychiatric illnesses 3
Differentiated assets • Targeting clearly recognized unmet needs • Innovative mechanisms of action Advanced clinical development • Lead product in pivotal Phase 3 trial • Three Phase 2b studies ongoing, one planned to begin in 2018 Commercially attractive CNS markets • Negative symptoms in schizophrenia & beyond • Major depressive and anxiety disorders • Insomnia with and without comorbid psychiatric symptoms • Parkinson’s disease & other neurodegenerative disorders Funded beyond multiple significant data read-outs in 2019 • $143.3 million cash balance at 9/30/17 |
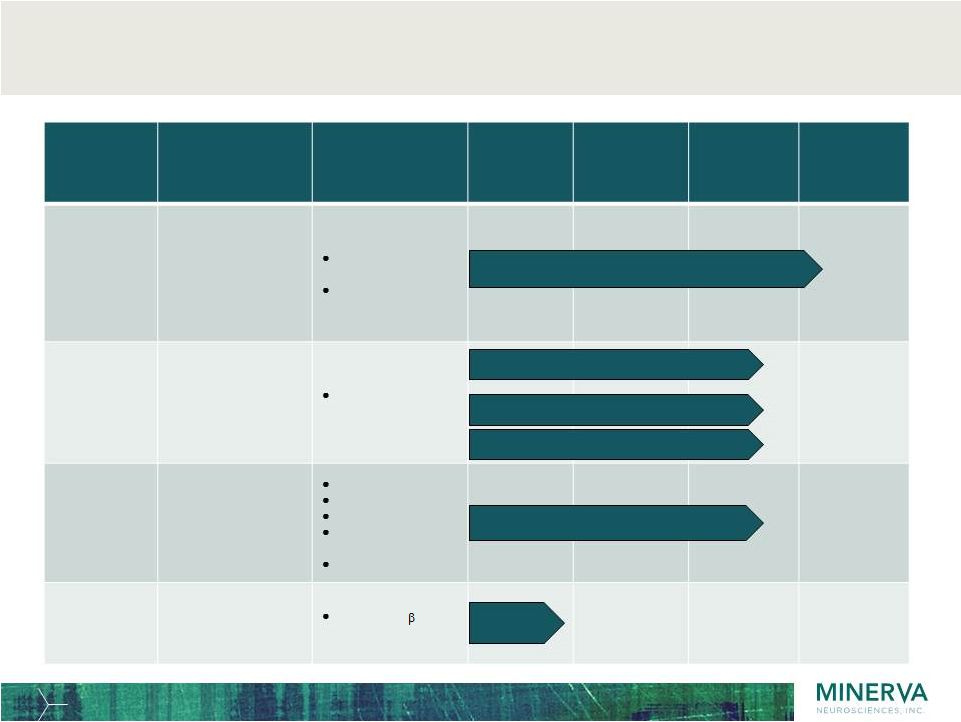 4 Innovative pipeline of four compounds and multiple indications in the CNS space Program Primary Indications MoA Pre- clinical Phase 1 Phase 2 Phase 3 MIN-101 Negative symptoms in Schizophrenia Seltorexant MIN-202 Primary Insomnia Major Depressive Disorder as adjunctive therapy MIN-117 Major Depressive Disorder in monotherapy MIN-301 Parkinson’s Disease Phase 3 initiated Dec 2017 (MIN-101-C07) Phase 2b initiated Dec 2017 (ISM2005) Pre-clinical Phase 2b planned H1 2018 (MIN-117-C03) Phase 2b initiated Sep 2017 (MDD2001) Phase 2b initiated Dec 2017 (MDD2002) 5-HT 2A antagonist Sigma 2 antagonist Selective Orexin2 antagonist 5-HT 1A 5HT transporter Alpha-1a, b Dopamine transporter 5-HT 2A antagonist Neuregulin 1 1 activating ErbB4 |
 5 Five clinical trials anticipated to read out in 2019 Lead program MIN-101: Negative symptoms in schizophrenia, monotherapy – MIN-101C07 Phase 3 ongoing (~500 patients worldwide) Seltorexant (MIN-202): Primary
insomnia and major depressive disorder (MDD) –
MDD2001 Phase 2b ongoing in adjunctive MDD & placebo (~280 patients
worldwide) –
MDD2002 Phase 2b ongoing in adjunctive MDD & comparator (~100 patients
U.S.) –
ISM2005 Phase 2b ongoing in insomnia monotherapy (~360 patients
worldwide) MIN-117:
MDD with prominent anxiety in monotherapy
– MIN-117C03 Phase 2b expected to begin in early 2018 (~325 patients worldwide) |
 Confidential & Proprietary
MIN-101 6 A new paradigm for the treatment of schizophrenia |
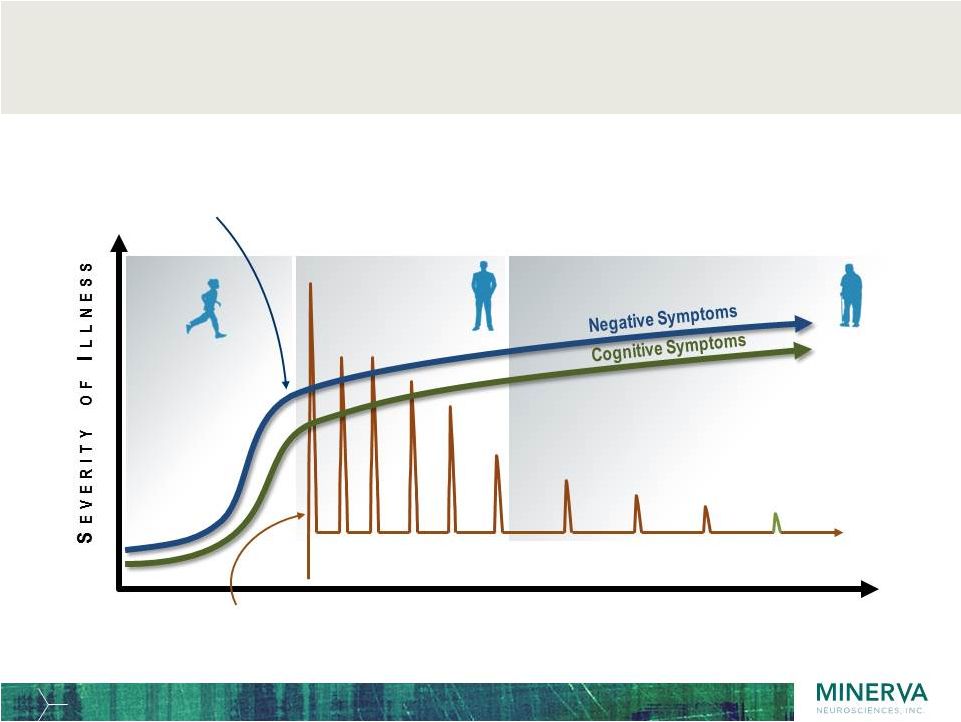 7 Youth 0-18 Adult 18-40 Positive Symptoms Schizophrenia has three symptom domains: positive symptoms fluctuate over time while negative & cognitive symptoms persist and cause lifelong disability Intermittent acute episodes of positive symptoms decline in frequency and severity Negative symptoms and cognitive impairment are evident at onset of illness and are lifelong debilitating symptoms All antipsychotics directly target dopamine (DA) receptors and have only shown efficacy against positive symptoms; none are indicated for negative symptoms or cognitive impairment Mature >40 |
 8 MIN-101 has a unique MoA with the potential to be the first to address negative symptoms and shift the treatment paradigm of schizophrenia • A unique MOA: 5-HT 2A antagonist + Sigma 2 antagonist • No direct dopamine blocking, unlike most available antipsychotics • Avoids antipsychotic side-effects • Exclusive worldwide rights outside of Asia • Granted formulation patent and method of use exclusivity until at least 2035 • Major commercial opportunity as potential first therapy in indication |
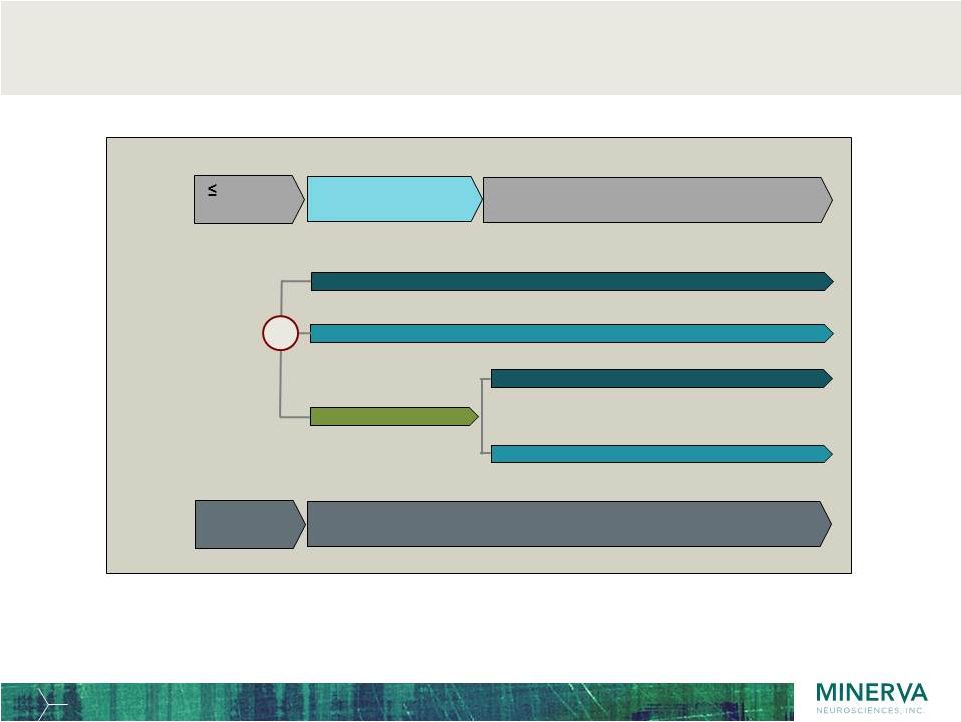
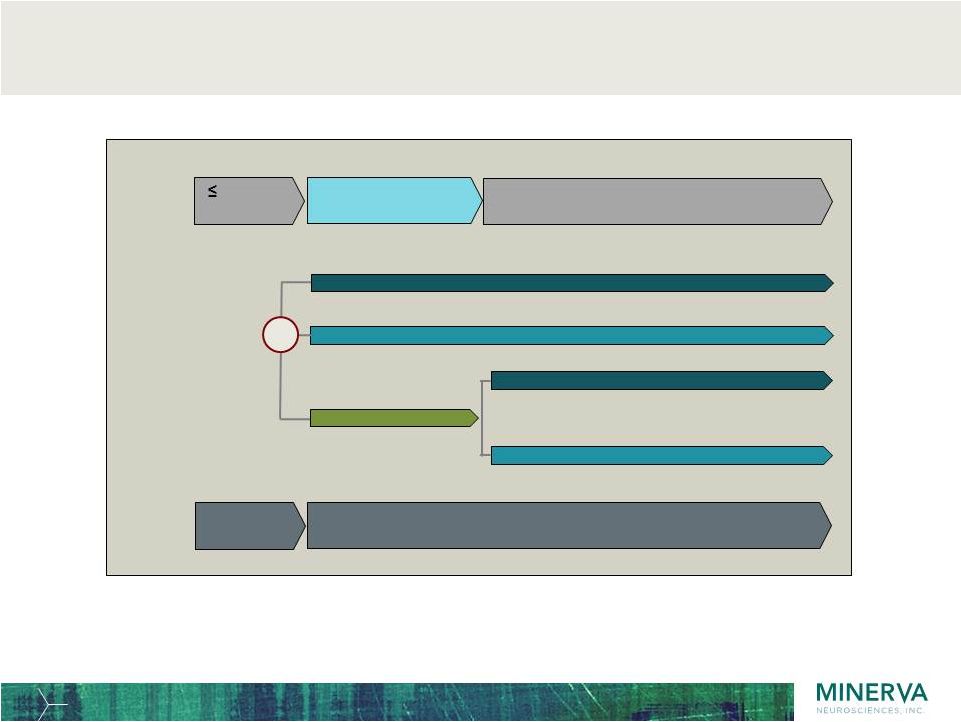 MIN-101: Phase 2b study design: monotherapy, double-blind,
placebo- controlled in schizophrenic patients with confirmed negative
symptoms 9
MIN-101 64mg (n = 83)
Screening Treatment & Assessments 4 weeks Screening 12 week double-blind phase ‘core study’ 24 week open-label ‘extension’ phase
Placebo (n = 83) MIN-101 32mg (n = 78) R MIN-101 64mg MIN-101 32mg Crossover Randomization Specific effects on negative symptoms can only be determined in a placebo-controlled study |
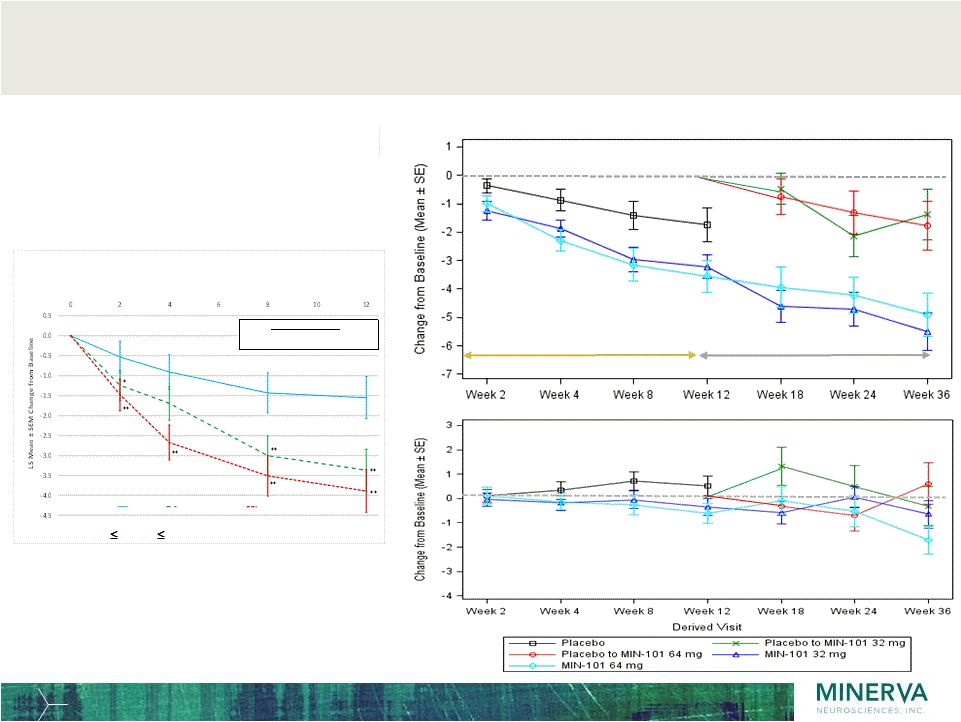 Phase 2b
study showed specific improvements in negative symptoms over 12 weeks and 36
weeks in both doses and stable positive symptoms 10
PANSS Positive Symptoms Subscale Change from Baseline
PANSS Negative Symptoms Subscale Change from Baseline
Statistically significant
improvements in the primary endpoint Extension Core Phase Extension Phase p-value: * 0.05; ** 0.01 versus placebo WEEK PANSS Negative Symptoms Factor Score (Marder) Change from Baseline (MMRM) (ITT Population) Baseline Mean (SD) Placebo 25.1 (4.0) MIN-101 32 mg 25.3 (4.2) MIN-101 64 mg 25.2 (4.0) Placebo MIN-101 32 mg MIN-101 64 mg |
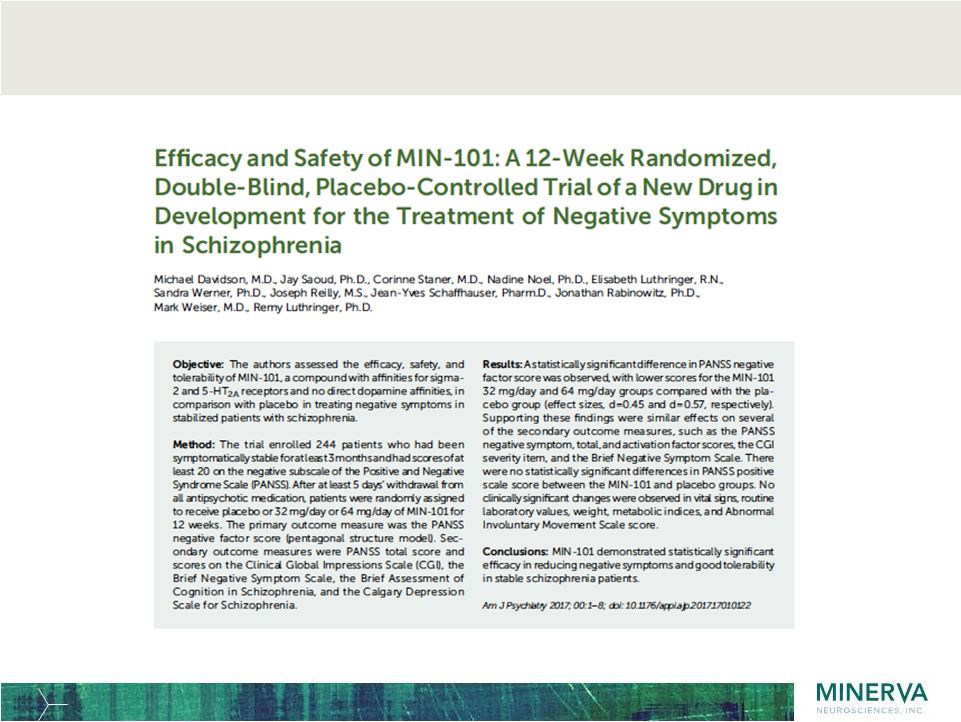 11 MIN-101 Phase 2b: American Journal of Psychiatry 2017; 00:1- 8 |
 12 MIN-101: Phase 3 initiated December 2017 |
 Phase 3
efficacy study: confirmatory study design guided by insights from Phase 2b
and dialogue with FDA 13
• Primary endpoint: PANSS Negative Symptoms Factor Score
(NSFS) according to Marder
after 12 weeks administration
• Secondary endpoints: Clinical Global Impression of Severity
(CGI-S) and Personal and Social Performance scale (PSP)
• 40 weeks (9 months) open-label extension • 501 patients randomized 1:1:1 to 32mg & 64mg doses of MIN-101 vs placebo • Symptomatically stable patients for several months with moderate to severe negative symptoms (>20 PANSS NSFS) and stable positive symptoms • If patients are on antipsychotic medication, switch to MIN-101 without long wash-out periods so as to mimic clinical practice • Study carried out in US (approx 30% of patients) and Europe |
 MIN-101 Phase 3 study design: monotherapy, double-blind, placebo- controlled in schizophrenic patients with negative symptoms 14 MIN-101 64mg (n = 167) Screening Treatment & Assessments 4 weeks Screening 12 week double-blind phase ‘core study’ 40 week open-label ‘extension’ phase
Placebo (n = 167) MIN-101 32mg (n = 167) R MIN-101 64mg MIN-101 32mg Crossover Randomization Phase 3 compared to Phase 2b: same patient population; same double-blind duration; same doses; PANSS negative
score primary endpoint; CGI & PSP secondary endpoints; 40 weeks extension allows 1
year safety coverage |
 15 MIN-101: Route to the schizophrenia market |
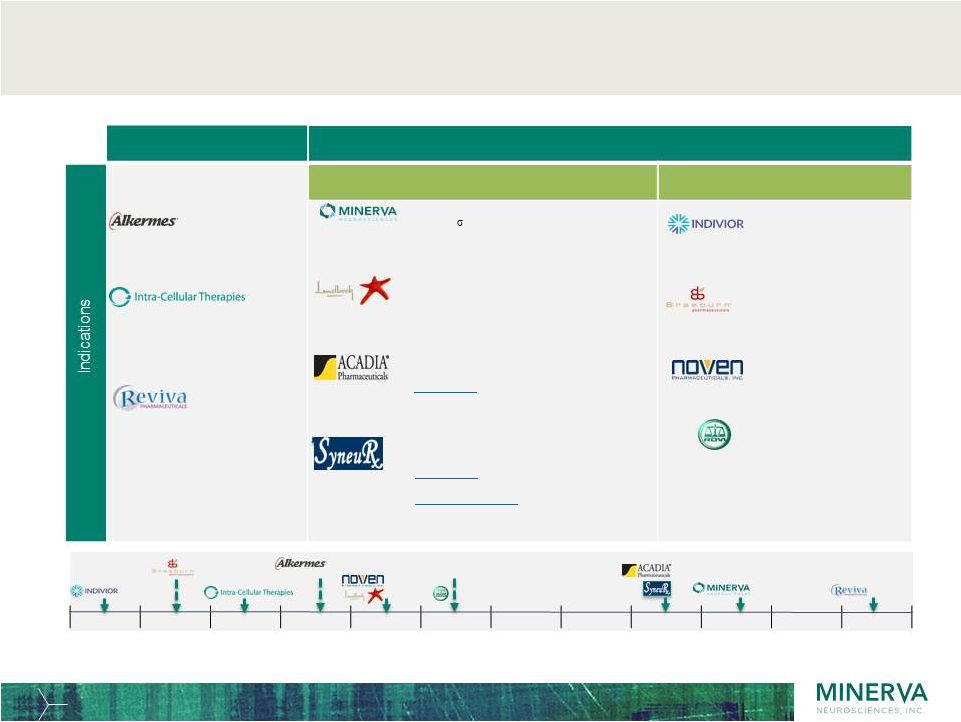 16 MIN-101 is unique in the late-stage schizophrenia pipeline: a monotherapy targeting negative symptoms in maintenance phase Q1-19 Q2-19 Q3-19 Q4-19 Q1-20 Q2-20 Q3-20 Q4-20 Q1-21 Q2-21 Q3-21 Q4-21 CHR assumed earliest launch timeline Source: Dec 2017; Cambridge Healthcare Research (CHR) Limited. UK ITI-007 (lumateperone) (5-HT 2A antagonist, D2 /D1
modulator, SSRI)
ALKS 3831 (Mu-opioid antagonist + olanzapine) Risperidone implant (6 monthly, nonbiodegradable risperidone drug-eluting stent) RBP-7000 (once-monthly, SR
risperidone) HP 3070
(transdermal patch of
asenapine) MIN-101 (5-HT 2A & 2 R antagonist) RP 5063 (D 2,3,4 & 5-HT 1A +2A partial agonist
+ 5-HT
2B,6,7 antagonist) Risperidone ISM (once-monthly IM risperidone) Lu AF35700 (D1, 5-HT 2A & 5-HT 6 antagonist) ACP-103 (pimavanserin) (5-HT 2A inverse agonist) NaBen sodium benzoate) (D-amino acid oxidase inhibitor) 3 indications: -Residual positive symptoms as add-on Orphan designations: -Adolescent monotherapy -Clozapine refractory add-on 2 indications; -Residual positive symptoms as add-on -Negative symptoms as add-on Tx-resistant monotherapy with switch study vs. RIS and OLA (2ry EP negative symptoms) Negative symptoms
monotherapy in stable patients with switch study Maintenance & Sub-population studies Negative Symptoms, Residual positive symptoms,
and Niche populations Long-Acting Injectables or Patch Acute studies Doria |
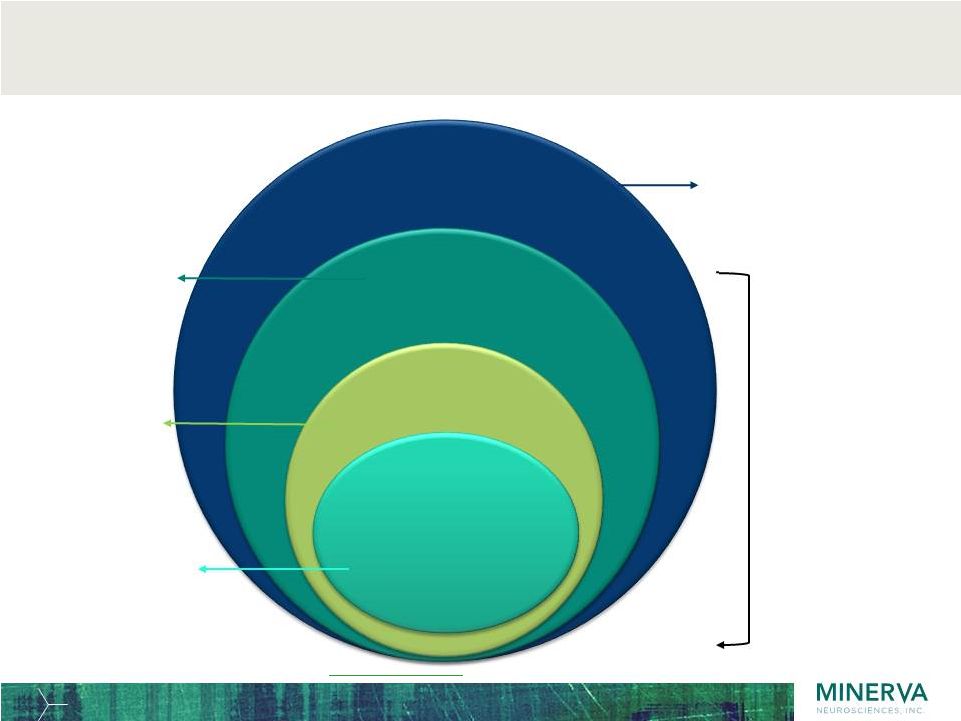 Studies
show 69% of adult patients with schizophrenia have negative symptoms and 85%
are clinically stable, U.S. 2016 patient estimates below
17 Estimated prevalence Of SZ (0.88%) (2.2 million US adults) Treatment prevalence of SZ (0.53%) (1.3 million US adults 5 ) Negative Sx (69%) (919,553 US adults) Stable patients (85%): (781,620 US adults) 59% of all adult patients have negative symptoms and are clinically stable based on these numbers => MIN-101 eligible 15% 2,3 weighted-average 6-month relapse rate among patients with varying severity of negative symptoms 69% of patients have negative symptoms: ~42% 2,3 predominant/ prominent symptoms; ~27% 4 mild symptoms 1. Wu 2006; 2. Toumi 2017; 3. Haro 2015; 4. Nordstroem 2017; 5. www.census.gov/quickfacts (July 1, 2016 adult population) Prevalence of US adults with schizophrenia in treatment/yr: 0.53% 1 Schizophrenia.com: 2.2 million patients in U.S. WHO website: 26 million with schizophrenia worldwide (0.34% prevalence) and 0.1-0.75% 1-yr prevalence. |
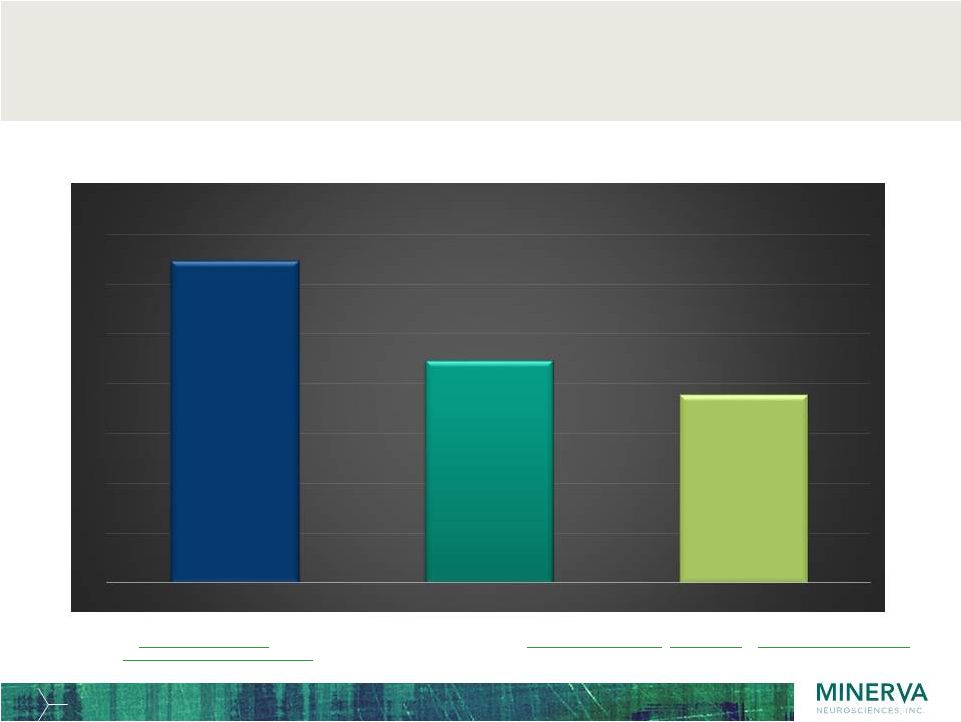 Approximately 2.2 million patients with schizophrenia in major
markets (US, EU5, Japan) have negative symptoms and nearly 2
million are stable and may be eligible for MIN-101 monotherapy
18 Population estimates: www.census.gov/quickfacts/, www.ons.gov.uk/peoplepopulationandcommunity/, www.insee.fr/en/statistiques/, www.istat.it/en/, www.ine.es/dyngs/INEbase/en/,
www.destatis.de/EN/www.stat.go.jp/english/data/jinsui/tsuki/
, en.wikipedia.org
(populations of IT, DE, ES), populationpymamid.net (for % adults in IT, DE, ES) Schizophrenia treatment prevalence estimate, proportion of patients with negative symptoms and % clinically stable(same as prior slide, same references). 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 Adults with schizophrenia Negative Symptoms Clinically stable Number of patients in major markets (millions) Treated patients 3.2 M Patient with negative symptoms 2.2 M Clinically stable patients 1.9 M |
 Confidential & Proprietary
19 A drug to treat insomnia & major depressive disorder by restoring physiological sleep A co-development/co-commercialization program with: Seltorexant MIN-202 / JNJ42847922 |
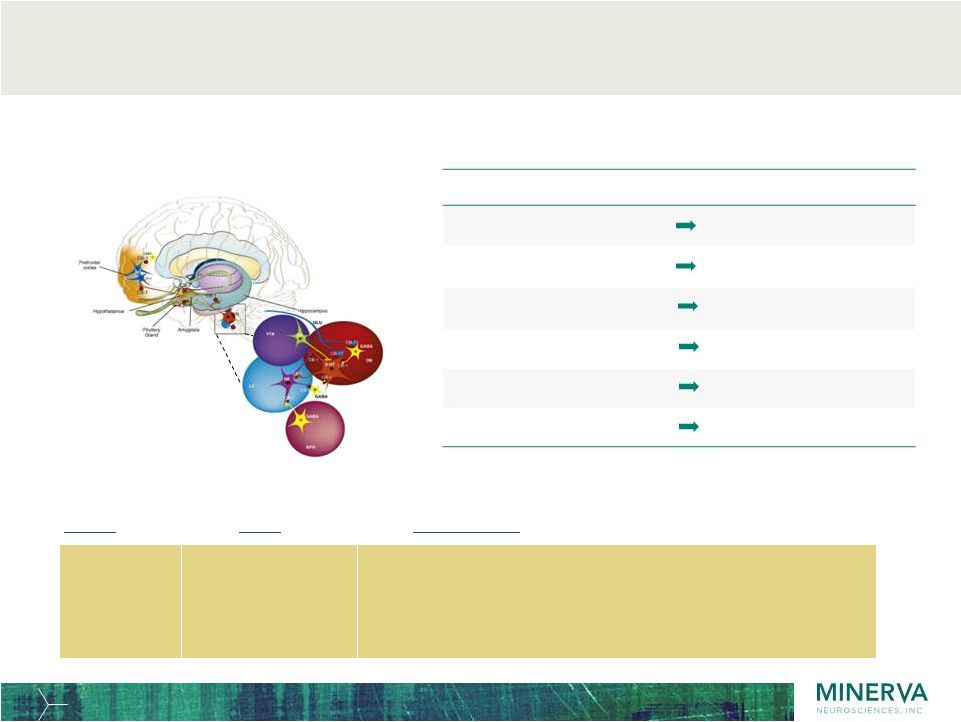 Name MoA PK/PD profile Depressive Symptom Orexinergic Domain Depression/Irritability Emotion/Arousal Low Self View/Guilt Emotion Loss of Interest & Pleasure Reward/Motivation Suicide/Death Ideation Reward/Motivation Sleep Disturbance Sleep-Wake Agitation, Restlessness Arousal/Energy Balance Orexin system: neurobiology targets circuits that mediate sleep and mood symptoms 20 Seltorexant Selective Orexin-2 Antagonist • Highly selective for Orexin-2 (relative to Orexin-1) • Short Tmax (30 minutes) - produces rapid onset of effect • Short half-life (2 hours) - minimizes daytime “hangover” |
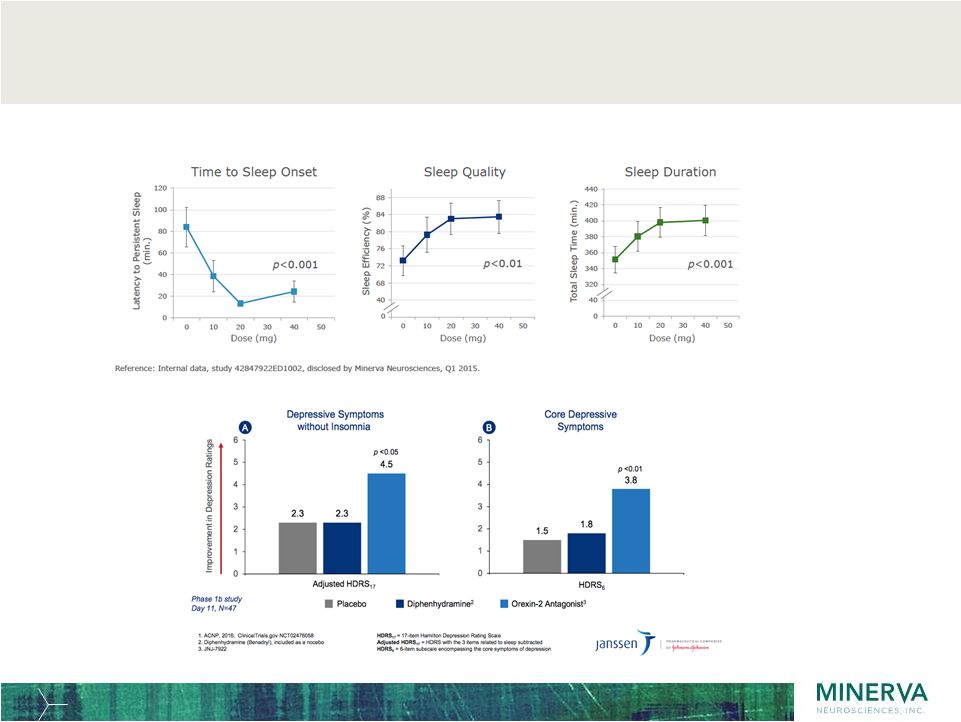 Seltorexant studies in MDD with comorbid insomnia shows improvements of insomnia and depressive symptoms 21 |
 Seltorexant Phase 2b program: two trials in MDD and one in Insomnia ongoing
22 First MDD trial initiated Sep 2017 (clinicaltrials.gov: NCT03227224) • Double-blind, randomized, parallel-group, placebo-controlled adaptive-dose finding study
• 4-week screening, 6-week double-blind treatment and 2-week follow-up
• ~ 280 patients planned to be enrolled at >85 clinical sites in the U.S., Europe, Russia and Japan
- safety & tolerability and dose response and efficacy in up to 3 doses of seltorexant
Second MDD trial initiated Dec 2017 (clinicaltrials.gov: NCT03321526) • Double-blind, randomized, flexible-dose parallel-group study • 4-week screening, 6-month double-blind treatment and 2-week follow-up
• ~ 100 patients planned to be enrolled at ~34 clinical sites in the U.S. - assess the efficacy of flexibly dosed seltorexant compared to flexibly dosed quetiapine as adjunctive therapy to baseline antidepressant therapy (either an SSRI or SNRI) in delaying
time to all-cause discontinuation of study drug over a 6-month treatment
period Insomnia
trial initiated Dec 2017 (clinicaltrials.gov: NCT03375203) • Double-blind, randomized, parallel-group, active- and placebo-controlled dose finding study • Up to 61-day duration, including screening and follow-up • ~ 360 patients planned to be enrolled at clinical sites in the U.S., Europe and Japan
- assess the dose-response of three doses of seltorexant compared to placebo on sleep onset as measured by latency to persistent sleep (LPS) using polysomnography (PSG)
- assess the dose-response of these doses compared to placebo on wake after sleep onset
(WASO) over the first six hours using PSG)
- compare the effects of seltorexant on sleep and cognition to those effects of zolpidem |
 Confidential & Proprietary
MIN-117 23 Addressing the unmet medical needs of patients with Major Depressive Disorder and anxiety symptoms |
 Phase 2a
study designed to explore unmet needs in patients with MDD 24
MIN-117 2.5mg (n = 21)
Screening Treatment & Assessments 4 weeks Screening Day -28 to -1* 6 week double blind treatment phase 2 wk post treatment follow-up phase MIN-117 0.5mg (n = 21) R Paroxetine 20mg (n = 21) Placebo (n = 21) *Includes overlapping washout period of up to 4 weeks Study drug is double-blind and double- dummy |
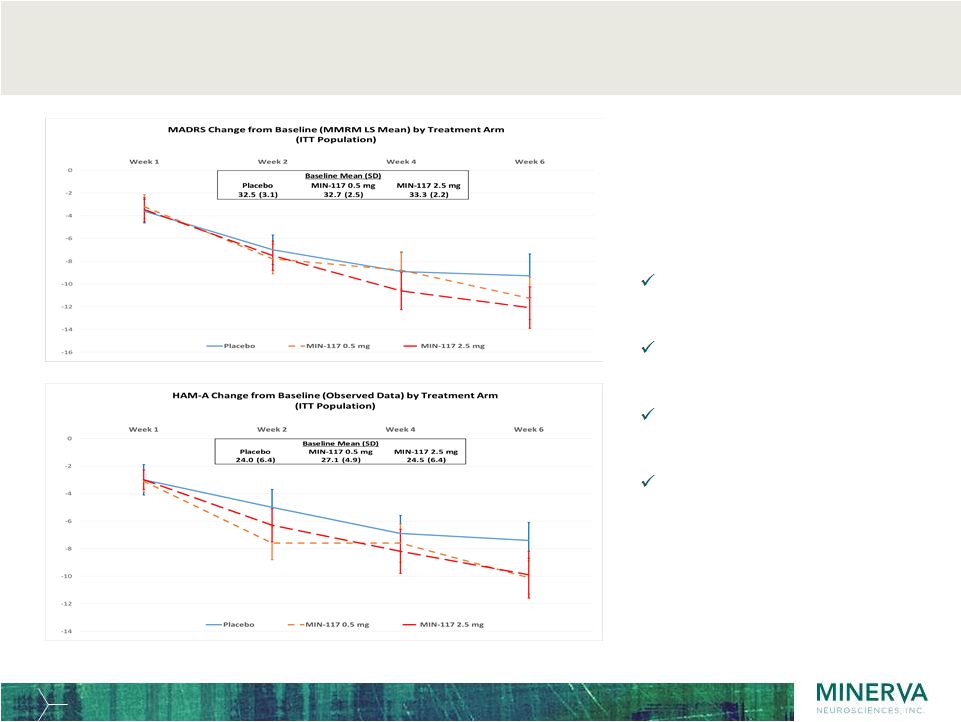 The Phase
2a results show effect on primary endpoint in depression as well as noted
effect on anxiety 25
Exploratory study for dose
finding, safety and efficacy
– not statistically powered: Results: Efficacy on depressive symptoms Onset evident as early as 2 weeks Efficacy on anxiety symptoms Both doses of MIN-117 are well tolerated, no sexual s/e, cognitive benefits Assay sensitivity confirmed by positive separation of Paroxetine from placebo |
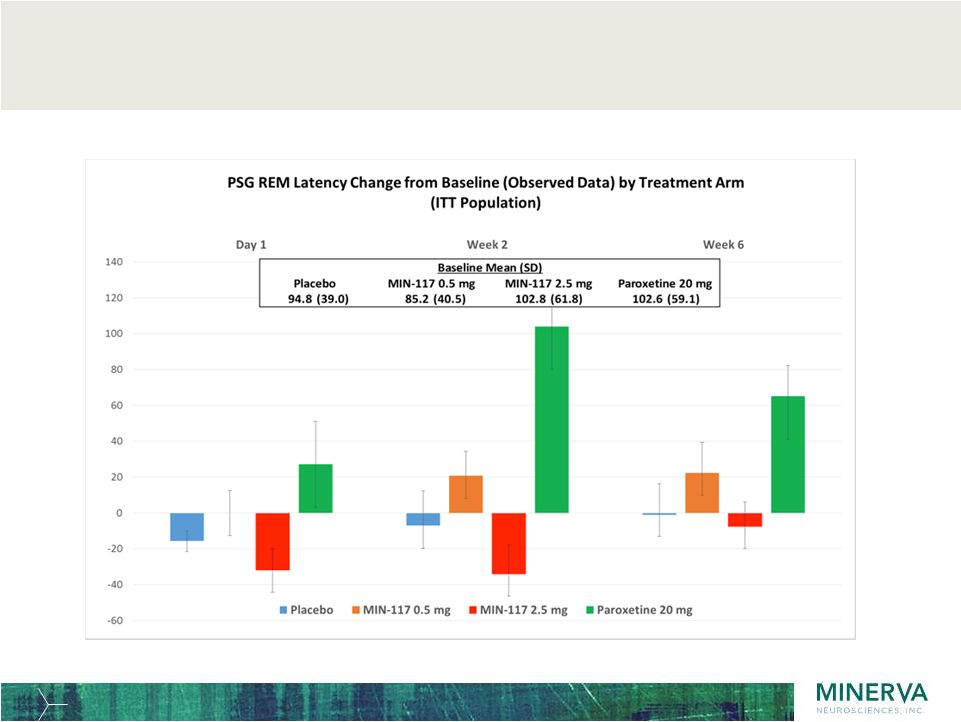 Sleep
polysomnography shows intact REM latency resulting in preservation of sleep
architecture and continuity of sleep, an important product
differentiator 26 |
 Confidential & Proprietary
MIN-301 27 A protein drug with disease modifying potential for the treatment of unmet medical needs in Parkinson’s Disease and other major CNS indications |
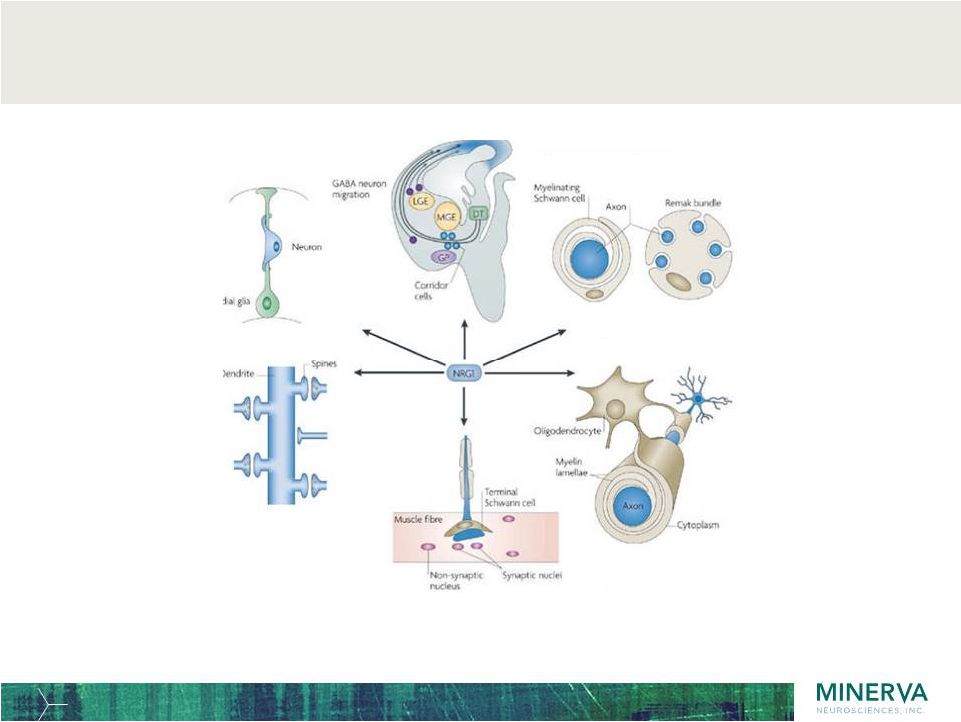 Neuregulin-1 (NGR1) has multiple roles in neuronal development
offering potential for neuronal repair in several CNS indications 28 Axon guidance Radial neuron migration Myelination and ensheathment Synapse formation Oligodendrocyte development Neuromuscular junction formation Mei and Xiong, 2008 NRG1 controls key neuronal development pathways Initial clinical focus will be on treatment of Parkinson’s Disease based on preclinical models. |
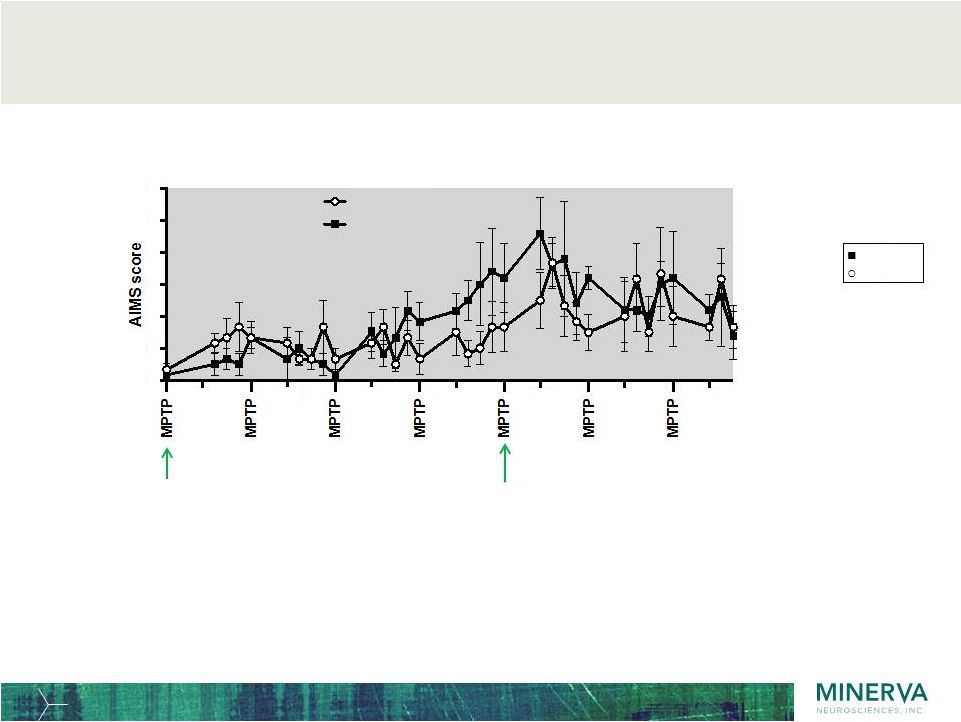 Animal
models (non-human primates): Effect of treatment on abnormal
involuntary movements scale (AIMS) 29
• Clear MPTP-induced increase in AIMS scores • Scores in MIN-301-treated animals lower during low MPTP (< 1 mg/kg) induction as compared to placebo Saline MIN-301 Start MPTP 1 mg / kg Increase MPTP 1.5 mg / kg Day number AIMS score MPTP effect NRG -101 Saline 14 21 28 35 42 49 56 0 1 2 3 4 5 6 |
 Financial
position ~$143.3 million cash balance (cash, cash equivalents and
marketable securities) at September 30, 2017
Q3 2017 cash inflow – Public offering July 5, 2017 net proceeds ~ $41.6 M – $30 M received from J&J in connection with renegotiation of collaboration in
August 29, 2017 Shares outstanding October 31, 2017: ~38.7 M (~42.9 M fully diluted) 30 |
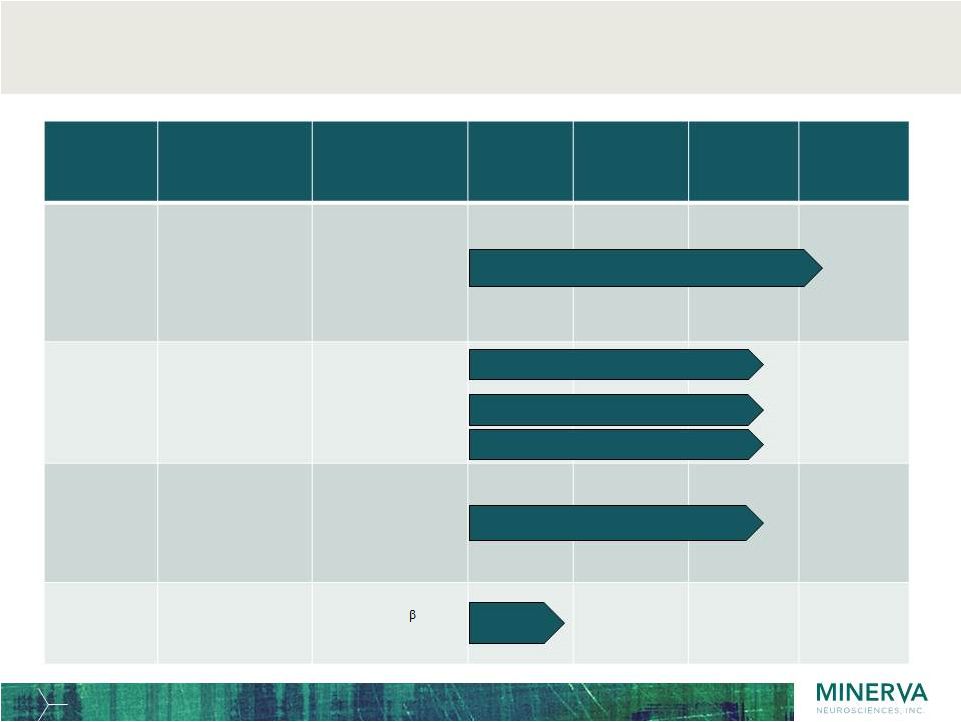 31 Innovative pipeline of four compounds and multiple indications in the CNS space Program Primary Indications MoA Pre- clinical Phase 1 Phase 2 Phase 3 MIN-101 Negative symptoms in Schizophrenia • 5-HT 2A antagonist • Sigma 2 antagonist Seltorexant MIN-202 Primary Insomnia Major Depressive Disorder as adjunctive therapy • Selective Orexin2 antagonist MIN-117 Major Depressive Disorder in monotherapy • 5-HT 1A • 5HT transporter • Alpha-1a, b • Dopamine • 5-HT 2A antagonist MIN-301 Parkinson’s Disease • Neuregulin 1 1 activating ErbB4 Phase 3 initiated Dec 2017 (MIN-101-C07) Phase 2b initiated Dec 2017 (ISM2005) Pre-clinical Phase 2b planned H1 2018 (MIN-117-C03) Phase 2b initiated Sep 2017 (MDD2001) Phase 2b initiated Dec 2017 (MDD2002) transporter |