Attached files
| file | filename |
|---|---|
| EX-32.2 - MEDICAL INNOVATION HOLDINGS, INC. | ex32-2.htm |
| EX-32.1 - MEDICAL INNOVATION HOLDINGS, INC. | ex32-1.htm |
| EX-31.2 - MEDICAL INNOVATION HOLDINGS, INC. | ex31-2.htm |
| EX-31.1 - MEDICAL INNOVATION HOLDINGS, INC. | ex31-1.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D. C. 20549
FORM 10-Q
[X] QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the quarterly period ended July 31, 2017
OR
[ ] TRANSITION REPORT UNDER SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from ____________________ to ____________________.
Commission file number: 000-27211
MEDICAL INNOVATION HOLDINGS, INC.
(Exact name of registrant as specified in its charter)
| Colorado | 84-1469319 | |
(State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
5805 State Bridge Rd, Suite G-328, Duluth, GA 30097
(Address of principal executive offices)
(909) 522-4414
(Registrant’s telephone number, including area code)
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the past 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to the filing requirements for the past 90 days.
| Yes | [X] | No | [ ] |
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files).
| Yes | [X] | No | [ ] |
Indicate by check mark whether the registrant is a large accelerated file, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | [ ] | Accelerated filer | [ ] | ||
| Non-accelerated filer | [ ] | Smaller reporting company | [X] | ||
| (Do not check if a smaller reporting company) |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act).
| Yes | [ ] | No | [X] |
Indicate the number of shares outstanding of each of the issuer’s classes of common stock, as of the latest practicable date.
As of July 31, 2017, there were 39,235,022 shares of the registrant’s common stock issued and outstanding.
Table of Contents
| 2 |
PART I. - FINANCIAL INFORMATION
ITEM 1. Financial Statements (Unaudited)
MEDICAL INNOVATION HOLDINGS, INC. AND SUBSIDIARY
| July 31, 2017 | April 30, 2017 | |||||||
| Unaudited | Audited | |||||||
| ASSETS | ||||||||
| Current assets: | ||||||||
| Cash | $ | 30,692 | $ | 8,895 | ||||
| Total Current Assets | 30,692 | 8,895 | ||||||
| Total assets | $ | 30,692 | $ | 8,895 | ||||
| LIABILITIES AND STOCKHOLDERS’ DEFICIT | ||||||||
| Current liabilities: | ||||||||
| Accounts Payable and Accrued Liabilities | $ | 900,852 | $ | 804,852 | ||||
| Notes Payable | 341,573 | 322,209 | ||||||
| Derivative Liability | 108,205 | - | ||||||
| Total liabilities | 1,350,630 | 1,127,061 | ||||||
| Stockholders’ deficit: | ||||||||
| Common stock; authorized 500,000,000; 39,235,022 shares at $0.0001 par value as of July 31, 2017 and 39,175,022 shares at $0.0001 par value as of April 30, 2017 | 3,924 | 3,918 | ||||||
| Additional Paid in Capital | 589,059 | 440,855 | ||||||
| Deficit accumulated | (1,912,921 | ) | (1,562,939 | ) | ||||
| Total stockholders’ deficit | (1,319,938 | ) | (1,118,166 | ) | ||||
| Total liabilities and stockholders’ deficit | $ | 30,692 | $ | 8,895 | ||||
The accompanying notes are an integral part of these financial statements
| 3 |
MEDICAL INNOVATION HOLDINGS, INC. AND SUBSIDIARY
Consolidated Statements of Operations
(Unaudited)
| For
the Three Month Period Ended July 31, 2017 | For
the Three Month Period Ended July 31, 2016 | |||||||
| Operating Expenses: | ||||||||
| General and administrative | $ | 179,203 | $ | 246,678 | ||||
| Non-Operating expense | ||||||||
| Changes in fair value of derivative liability | 5,824 | - | ||||||
| Other Expenses | ||||||||
| Interest Expense, net | 46,755 | - | ||||||
| Loss on settlement of debt | 118,200 | - | ||||||
| Total non-operating expense | 170,779 | - | ||||||
| Net loss for the period | $ | (349,982 | ) | $ | (246,678 | ) | ||
| Net loss per share: | ||||||||
| Basic and diluted | $ | (0.01 | ) | $ | (0.01 | ) | ||
| Weighted average number of shares outstanding: | ||||||||
| Basic and diluted | 39,235,022 | 37,639,012 | ||||||
The accompanying notes are an integral part of these financial statements
| 4 |
MEDICAL INNOVATION HOLDINGS, INC. AND SUBSIDIARY
Consolidated Statements of Cash Flows
(Unaudited)
| For
the Three Month Period Ended July 31, 2017 | For
the Three Month Period Ended July 31, 2016 | |||||||
| Cash flow from operating activities: | ||||||||
| Net loss | $ | (349,982 | ) | $ | (246,678 | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
| Loss on settlement of debt | 118,200 | - | ||||||
| Change in value of derivative liability | 5,824 | - | ||||||
| Amortization of debt discount | 5,137 | - | ||||||
| Financing costs | 27,382 | - | ||||||
| Changes in operating assets and liabilities: | ||||||||
| Accrued interest | 14,236 | - | ||||||
| Accounts Payable | 126,000 | - | ||||||
| 141,000 | ||||||||
| Net Cash Used in Operating activities | (53,203 | ) | $ | (105,678 | ) | |||
| Cash flows from financing activities: | ||||||||
| Issuance of Common Stock | - | 172,000 | ||||||
| Change due to Shareholders | - | 1,900 | ||||||
| Proceeds from Note Payable- Unrelated Party | 75,000 | - | ||||||
| Net cash provided by financing activities | 75,000 | 173,900 | ||||||
| Increase in cash during the period | 21,797 | 68,222 | ||||||
| Cash, beginning of period | 8,895 | 1,600 | ||||||
| Cash, end of period | $ | 30,692 | $ | 69,822 | ||||
| Supplemental disclosure of cash flow information: | ||||||||
| Cash paid during the period | ||||||||
| Taxes | $ | - | $ | - | ||||
| Interest | $ | - | $ | - | ||||
The accompanying notes are an integral part of these financial statements
| 5 |
MEDICAL INNOVATION HOLDINGS, INC. AND SUBSIDIARY
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
JULY 31, 2017
(Unaudited)
NOTE 1 - INTRODUCTION
On April 29, 2016, Medina International Holdings, Inc. (the “Company”) entered into an Acquisition and Purchase Agreement with Medical Innovation Holdings, a Joint Venture (“MedHold”) effective April 29, 2016, whereby all the assets of MedHold were acquired by the Company. In conjunction therewith, 35,100,000 shares (post-reverse split 1-for-10) were issued. Since the owners of MedHold now own approximately 94% of Medina, this transaction was accounted for as a reverse acquisition of Medina by MedHold resulting in a recapitalization of Medhold. Accordingly, the financial statements presented herein contain comparisons to the prior fiscal year, as operations began April 29, 2016.
Prior to the acquisition, Medina went through a restructuring and divesture. For details, please see the 8-K/A filed by Medina on June 6, 2016.
On or about June 24, 2016, the Company proposed a reverse split of the common stock issued and outstanding on a one new share for 10 old shares basis, with fractional shares being rounded up to the next whole share, and sought authorization to change the Company’s name to Medical Innovation Holdings, Inc. (note these actions required an amendment to the Articles of Incorporation and required the approval of the Financial Industry Regulatory Authority (“FINRA”), which was granted). The majority shareholders approved both proposals and a Schedule 14C Information Statement was filed on August 8, 2016. The stock split and name change were effective September 15, 2016, and as such, the numbers reflected in the financial statements are post-split figures; all per share data was retroactively restated.
The Company is establishing a nationwide, state-by-state, multi-disciplinary medical specialist provider/practice network, staffed by 16 types of Physician Specialists. These Physician Specialists will provide virtual medical consultations to rural patients who are chronically underserved. The Company intends to accomplish this via a comprehensive and sophisticated end-to-end virtual medicine program.
On June 28, 2016, the Company formed a wholly-owned subsidiary, BKare Diagnostics, Inc., in the state of Georgia. BKare Diagnostics is a full-scale provider of high quality laboratory and pharmaceutical services providing personalized services for small and mid-size medical practices and Virtual Health Medical Providers. All BKare Referral Laboratories are certified to provide services to Medicare, Medicaid, HMO and all private and commercial insurance companies. Their personalized services include custom testing protocols, tailored to meet client’s needs and includes services as an online private portal to order tests, supplies, online results 24 hours per day with board certified pathologists.
On August 9, 2016 the Company announced it set up a subsidiary, 3PointCare, Inc. (“3P”), a Georgia corporation, to provide services critical to the Company for the administration, scheduling, claims processing, technical support as well as delivering medical and health related services. The subsidiary is in the development stage.
On September 8, 2016 the Company announced that 3P entered into a Management Services Agreement to exclusively provide management services to TeleLife MD, Inc. with this agreement, the Company acquired the services of TeleLife MD, a multi-disciplinary specialty care practice formed for the purpose of providing telemedicine services to patients in rural underserved areas in various States. The Company also licensed its cloud-based tele-health technology platform to TeleLife. Additionally, the Company will provide core MSO services such as claims processing, billing and collection, physician services that include support and recruiting.
Going Concern
The accompanying financial statements were prepared in conformity with GAAP in the United States (“GAAP”), which contemplates continuation of the Company as a going concern. In addition, the Company’s notes are currently in default. The Company is a development stage enterprise and has limited operations as of July 31, 2017. As of July 31, 2017, the Company had an accumulated deficit of $1,912,921.
| 6 |
Management is devoting considerable effort to establish a business as discussed above. Management has taken various steps in that direction and it believes that its actions will allow the Company to continue its operations through the next fiscal year.
The future success of the Company is likely dependent on its ability to attain additional capital to develop its proposed products and ultimately, upon its ability to attain future profitable operations. There can be no assurance that the Company will be successful in obtaining such financing, or that it will obtain positive cash flow.
NOTE 2 - SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES:
The accompanying consolidated financial statements (“CFS”) of Medical Innovation Holdings, Inc. and its subsidiaries were prepared in accordance with GAAP and include the assets, liabilities, revenues, and expenses of subsidiaries. All intercompany balances and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of our CFS in conformity with GAAP requires the use of estimates and assumptions that affect the reported amounts of assets and liabilities, the disclosure of contingent assets and liabilities at the date of the consolidated financial statements, and the reported amounts of revenues and expenses during the reporting periods. Significant estimates and assumptions are used for, but are not limited to;
| 1) | Revenue recognition; |
| 2) | Allowance for doubtful accounts; |
| 3) | Inventory costs; |
| 4) | Asset impairments; |
| 5) | Depreciable lives of assets; |
| 6) | Income tax reserves and valuation allowances; |
| 7) | Fair value of stock options; |
| 8) | Allocation of direct and indirect cost of sales; and |
| 9) | Contingent liabilities. |
Future events and their effects cannot be predicted with certainty; accordingly, our accounting estimates require judgment. We base our estimates on historical experience, available market information, appropriate valuation methodologies, and on various other assumptions that we believe to be reasonable. We evaluate and update our assumptions and estimates on an ongoing basis and may employ outside experts to assist in our evaluation, when necessary. Actual results could differ materially from these estimates.
Revenue Recognition
Revenue is recognized when earned. The Company’s revenue recognition policies comply with SEC Staff Accounting Bulletin (SAB) 104. Sales revenue is recognized at the date services are rendered and no other significant obligations of the Company exist and collectability is reasonably assured. Payments received before all of the relevant criteria for revenue recognition are satisfied, are recorded as unearned revenue.
Cash and Cash Equivalents
The Company considers all liquid investments with a maturity of three months or less from the date of purchase that are readily convertible into cash to be cash equivalents. The Company maintains its cash in bank deposit accounts that does not exceed federally insured limits. The Company has not experienced any losses in such accounts.
| 7 |
Accounts Receivable
The Company reviews its accounts receivables accounts periodically for collectability and establishes an allowance for doubtful accounts and records bad debt expense when deemed necessary.
Advertising costs
Advertising costs are expensed as incurred. The Company recorded no advertising costs in the three months ended July 31, 2017 and 2016.
Inventory
We carry our inventories at the lower of cost or market value. Cost is determined using first-in, first-out (“FIFO”) method. Market is determined based on net realizable value. We also provide due consideration to obsolescence, excess quantities, and other factors in evaluating net realizable value.
Fixed Assets
Capital assets are stated at cost. Equipment consists of medical equipment and related assets. Depreciation of fixed assets is provided using the straight-line method over the estimated useful lives (3-7 years) of the assets. Expenditures for maintenance and repairs are charged to expense as incurred.
| Property and Equipment | No. of Years | |
| Medical Equipment | 7 years | |
| Telemedicine Equipment | 3 years | |
| Computers | 3 years | |
| Furniture | 5 years | |
| Office Equipment | 5 years | |
| Office Phone | 3 years |
Long Lived Assets
The Company follows Statement of Financial Accounting Standard No. 144, “Accounting for the Impairment or Disposal of Long-Lived Assets” (“SFAS 144”), now codified in ASC 350,which addresses financial accounting and reporting for the impairment or disposal of long-lived assets and supersedes SFAS No. 121, “Accounting for the Impairment of Long-Lived Assets and for Long-Lived Assets to be Disposed Of,” and the accounting and reporting provisions of APB Opinion No. 30, “Reporting the Results of Operations for a Disposal of a Segment of a Business.” The Company periodically evaluates the carrying value of long-lived assets to be held and used in accordance with ASC 350. ASC 350 requires impairment losses to be recorded on long-lived assets used in operations when indicators of impairment are present and the undiscounted cash flows estimated to be generated by those assets are less than the assets’ carrying amounts. In that event, a loss is recognized based on the amount by which the carrying amount exceeds the fair market value of the long-lived assets. Loss on long-lived assets to be disposed of is determined in a similar manner, except that fair market values are reduced.
Income Taxes
The Company uses the liability method of accounting for income taxes under which deferred tax assets and liabilities are recognized for the future tax consequences of temporary differences between the accounting bases and the tax bases of the Company’s assets and liabilities. Any deferred tax assets and liabilities are computed using enacted tax rates in effect for the year in which the temporary differences are expected to reverse.
GAAP generally requires that recognized revenue, expenses, gains and losses be included in net income. Certain statements, however, require entities to report specific changes in assets and liabilities, such as unrealized gains and losses on available-for-sale securities, as a separate component of the equity section of the balance sheet. Such items, along with net income, are components of comprehensive income.
| 8 |
Issuance of Shares for Service
The Company accounts for employee and non-employee stock awards under ASC 718, whereby equity instruments issued to employees for services are recorded based on the fair value of the instrument issued and those issued to non-employees are recorded based on the fair value of the consideration received or the fair value of the equity instrument, whichever is more reliably measurable.
Foreign Currency Translations and Hedging
The Company will be exposed to foreign currency fluctuations due to international trade. Management does not intend to enter into forward exchange contracts or any derivative financial investments for trading purposes. There is no present international trade and as such management does not currently hedge foreign currency exposure.
Basic and Diluted Net Loss per Share
Net loss per share is calculated in accordance with FASB ASC 105. Basic net loss per share is based upon the weighted average number of common shares outstanding. Diluted net loss per share is based on the assumption that all dilutive convertible shares and stock options were converted or exercised. Dilution is computed by applying the treasury stock method. Under this method, options and warrants are assumed to be exercised at the beginning of the period (or at the time of issuance, if later), and as if funds obtained thereby were used to purchase common stock at the average market price during the period.
Products and Services, Geographic Areas and Major Customers
The Company intends to establish a nationwide, state-by-state, multi-disciplinary medical specialist provider/practice network, staffed by sixteen types of physician specialists. These specialist physicians will provide virtual medical consultations to the potential millions of rural patients who are chronically underserved. This will be accomplished via a seamless, comprehensive, sophisticated end-to-end virtual medicine program.
Recently issued accounting pronouncements
In May 2014, the Financial Accounting Standards Board (“FASB”) issued an Accounting Standards Update (“ASU”) amending revenue recognition guidance and requiring more detailed disclosures to enable users of financial statements to understand the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers. In August 2015, the FASB deferred the effective date of the revenue recognition guidance to reporting periods beginning after December 15, 2017. Early adoption is permitted for reporting periods beginning after December 15, 2016. This standard has no material effect on our CFS.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842). The guidance in ASU 2016-02 supersedes the lease recognition requirements in ASC Topic 840, Leases (FAS 13). ASU 2016-02 requires an entity to recognize assets and liabilities arising from a lease for both financing and operating leases, along with additional qualitative and quantitative disclosures. ASU 2016-02 is effective for fiscal years beginning after December 15, 2018, with early adoption permitted. The Company is in the process of evaluating the impact of this ASU on its CFS.
In March 2016, the FASB issued an ASU amending the accounting for stock-based compensation and requiring excess tax benefits and deficiencies to be recognized as a component of income tax expense rather than equity. This guidance also requires excess tax benefits to be presented as an operating activity on the statement of cash flows and allows an entity to make an accounting policy election to either estimate expected forfeitures or to account for them as they occur. The ASU is effective for reporting periods beginning after December 15, 2016, with early adoption permitted. This standard has no material effect on our CFS.
In August 2016, the FASB issued ASU 2016-15, Statement of Cash Flows (Topic 230), Classification of Certain Cash Receipts and Cash Payments. ASU 2016-15 provides guidance for targeted changes with respect to how cash receipts and cash payments are classified in the statements of cash flows, with the objective of reducing diversity in practice. ASU 2016- 15 is effective for interim and annual periods beginning after December 15, 2017, with early adoption permitted. The Company is in the process of evaluating the impact of this ASU on its CFS.
| 9 |
In October 2016, the FASB issued ASU 2016-16, Income Taxes (Topic 740): Intra-Entity Transfer of Assets Other than Inventory, which requires the recognition of the income tax consequences of an intra-entity transfer of an asset, other than inventory, when the transfer occurs. ASU 2016-16 is effective for interim and annual periods beginning after December 15, 2018, with early adoption permitted. The Company is in the process of evaluating the impact of this ASU on its CFS.
In November 2016, the FASB issued ASU 2016-18, Statement of Cash Flows (Topic 230): Restricted Cash, which requires restricted cash to be presented with cash and cash equivalents on the statement of cash flows and disclosure of how the statement of cash flows reconciles to the balance sheet if restricted cash is shown separately from cash and cash equivalents on the balance sheet. ASU 2016-18 is effective for interim and annual periods beginning after December 15, 2017, with early adoption permitted. The Company is in the process of evaluating the impact of this ASU on its CFS.
In January 2017, the FASB issued an ASU 2017-01, Business Combinations (Topic 805) Clarifying the Definition of a Business. The amendments in this update clarify the definition of a business with the objective of adding guidance to assist entities with evaluating whether transactions should be accounted for as acquisitions or disposals of assets or businesses. The definition of a business affects many areas of accounting including acquisitions, disposals, goodwill, and consolidation. The guidance is effective for interim and annual periods beginning after December 15, 2017 and should be applied prospectively on or after the effective date. The Company is in the process of evaluating the impact of this ASU on its CFS.
In July 2017, FASB issued ASU 2017-11, Earnings Per Share (Topic 260) Distinguishing Liabilities from Equity (Topic 480) Derivatives and Hedging (Topic 815): I. Accounting for Certain Financial Instruments with Down Round Features, II. Replacement of the Indefinite Deferral for Mandatorily Redeemable Financial Instruments of Certain Nonpublic Entities and Certain Mandatorily Redeemable Noncontrolling Interests with a Scope Exception. Part I of this ASU changes the classification analysis of certain equity-linked financial instruments (or embedded features) with down round features and clarifies existing disclosure requirements. Part II does not have an accounting effect. The ASU is effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2018 with early adoption permitted. Management is currently evaluating the potential impact of these changes on the CFS of the Company.
As of July 31, 2017, there are no recently issued accounting standards not yet adopted that would have a material effect on the Company’s financial statements to have a material impact on the Company’s CFS.
NOTE 3 - ACCOUNTS PAYABLE AND ACCRUED EXPENSES
Accounts payable and accrued expenses consisted of the following as of July 31 and April 30, 2017.
| July 31, 2017 | April 30, 2017 | |||||||
| Attorney fees | $ | 272,748 | $ | 272,748 | ||||
| Related party-Accrued Salaries | 218,400 | 182,400 | ||||||
| Other | 5,204 | 5,204 | ||||||
| Amount due for consultant BBVI, LLC | 404,500 | 344,500 | ||||||
| Total | $ | 900,852 | $ | 804,852 | ||||
NOTE 4 - NOTES PAYABLE
Notes payable consisted of the following as of July 31 and April 30, 2017
| July 31, 2017 | April 30, 2017 | |||||||
| Syndicated Equity, Inc. | $ | 316,020 | $ | 302,209 | ||||
| C. S. Seshadri | 20,000 | 20,000 | ||||||
| Eagle Equities LLC, net of discount of $69,863 | 5,553 | |||||||
| Total | $ | 341,573 | $ | 322,209 | ||||
| 10 |
The Company retained a Note payable of $256,025. The Note was issued on June 18, 2015 and was due in one month at 1%. The Note carries a default interest rate of 18% and is convertible at 60% of the Volume Weighted Average Price for 5 days prior to conversion. This note is currently in default. The Company evaluated and recorded beneficial conversion on this note in prior years’ financial statements. The Company has recorded $13,820 in accrued interest for the three month period ending July 31, 2017 as compared to accrued interest of $11,695 for the comparable period in 2016.
The Seshadri note was agreed to be settled with a payment of $20,000. Prior to the settlement the note carried interest and was convertible into the Company’s common stock.
On July 6, 2017, Medical Innovation Holdings, Inc., a Colorado corporation (the “Company”) issued an 8% Convertible Promissory Note, convertible 180 days after the execution (the “Note”) to Eagle Equities LLC. (“Eagle”) of $75,000 to evidence funds lent by Eagle to the Company on July 6, 2017. The Note has a maturity date of July 6, 2018. The Company has recorded $416 in accrued interest for the three month period ending July 31, 2017.
The aforementioned Note is classified as a hybrid instrument with an embedded feature. The embedded feature has exhibited all of the following characteristics to qualify as a derivative:
1. The Note has an underlying and notional amount which is defined as the number of shares into which the may be converted into.
2. The Note requires little or no initial net investment. The initial net investment, which equals the fair value of the conversion feature, is generally less than the fair value of the underlying shares and therefore complies with the second criterion.
3. The Note provides for net settlement. The Company’s shares are publicly traded, then the conversion feature is considered to provide for net settlement, because the holder can readily sell the shares received upon conversion for cash.
The Company uses a weighted average Black-Scholes-Merton option pricing model to value the derivative instruments at inception and on subsequent valuation dates.
NOTE 5 – DERIVATIVE LIABILITY
Derivative instruments
The fair value of derivative instruments is recorded and shown separately under current liabilities. Changes in the fair value of derivatives liability are recorded in the statement of operations under non-operating income (expense).
Our Company evaluates all of its financial instruments to determine if such instruments are derivatives or contain features that qualify as embedded derivatives. For derivative financial instruments that are accounted for as liabilities, the derivative instrument is initially recorded at its fair value and is then re-valued at each reporting date, with changes in the fair value reported in the consolidated statements of operations. For stock-based derivative financial instruments, the Company uses a weighted average Black-Scholes-Merton option pricing model to value the derivative instruments at inception and on subsequent valuation dates. The classification of derivative instruments, including whether such instruments should be recorded as liabilities or as equity, is evaluated at the end of each reporting period. Derivative instrument liabilities are classified in the balance sheet as current or non-current based on whether or not net-cash settlement of the derivative instrument could be required within 12 months of the balance sheet date.
6. Derivative liabilities
The derivative liability is derived from the conversion features in the promissory note issued on July 6, 2017. As of July 31, 2017, the derivative liability was $108,205. The Company recorded $27,382 of financing costs, which is the difference between the derivative liability and the face value of the note, and $5,824 expense from changes in derivative liability during the period ended July 31, 2017 respectively.
| 11 |
| July 31, 2017 | ||||
| Annual dividend yield | — | |||
| Expected life (years) | 1 | |||
| Risk-free interest rate | 1.14 | % | ||
| Expected volatility | 270 | % | ||
NOTE 6 - EMPLOYMENT AGREEMENT
As of July 31, 2017 there are no employment agreements with any management personal. However, on April 1, 2016 the Company entered into a memorandum of understanding with its CEO that includes a tentative salary of $144,000 per annum based upon certain conditions and other provisions. However, as of the date of this report, no definitive agreement has been signed.
NOTE 7 - PREFERRED STOCK
As of July 31, 2017 the Company had 30 shares of convertible preferred stock outstanding. Each share of preferred share is convertible in to 1% of the outstanding common shares at the date of conversion. At July 31, 2017 the preferred shares were convertible into approximately 11,770.500 shares of common stock.
NOTE 8- PENDING LITIGATION
Under a contract, the Company had liabilities due to a former law firm of $200,000 (see note 3 above). The law firm filed suit against multiple defendants, including the Company, and was awarded a judgment against the parties to collect its fees, including costs. The Company intends to settle this matter.
NOTE 9 - CONTRACTUAL OBLIGATIONS
As part of the acquisition on April 29, 2016, the Company assumed a consulting agreement entered into on February 20, 2016 by MedHold JV, which obligates MedHold JV to pay BBV International Consulting, LLC (“BBVI”) $30,000 per month through February 19, 2019 for strategic and corporate planning. The agreement was ratified by the Company’s Board of Directors effective May 1, 2016. A major shareholder of the Company is a consultant for BBVI. During the year ended April 30, 2017 the Company expensed $360,000 of consulting fees. The outstanding balance as of December 31, 2016 was converted into restricted shares of common stock at $0.50 per share, the value of the shares as of the date of issue was $149,310. Upon board approval, the remaining balance through July 31, 2017 will be converted to restricted shares of common stock.
During the three month period ending July 31, 2017 the Company issued 60,000 shares to settle $30,000 of previous debt owed to BBVI, a related party, the fair value of the 60,000 common shares was $148,200 which resulted in a loss on settlement of debt of $118,200. The Company also recorded $90,000 in accrued fees to BBVI during the three month period ending July 31, 2017.
On June 27, 2017, the Registrant entered into an Asset Acquisition Agreement with Renaissance Health Publishing LLC. a Florida Limited Liability Company.
The consideration to be paid to Seller for the Purchased Assets (the “Purchase Price”) shall consist of:
a) a cash payment at Closing of $1,000,000 (the “Closing Date Payment”), payable via certified check or wire transfer of immediately available funds to an account that shall have been designated by Seller to Buyer prior to Closing; and
b) payment of: (x) four (4) times Seller’s earnings before interest, taxes, depreciation and amortization (“EBITDA”) for the 12 month period ending on the last day of the calendar month immediately preceding the month in which the audit is completed (the “Audit Date”), as determined by an audit of Seller’s financial statements conducted by Assurance Dimensions, Inc. (the “Auditor”), plus (y) the value of Seller’s fully-paid inventory (calculated at Seller’s actual cost) of supplements and pre-printed direct mail pieces as of the Closing, minus (z) the Closing Date Payment (the “Formula Payment”). The Formula Payment shall be payable pursuant to the Convertible Promissory Note attached as Exhibit “A” hereto (the “Convertible Note”) and the obligations of Buyer under the Convertible Note shall be secured by the Security Agreement in the form attached as Exhibit “B” hereto. Seller shall be required to execute an inter-creditor agreement with the Senior Lender in form and substance reasonably satisfactory to the Senior Lender pursuant to which the Seller shall subordinate the priority of its lien on the collateral described in the Security Agreement to the lien on such collateral arising under the Senior Loan documents. To date the Transaction has not closed.
| 12 |
NOTE 10 - STOCKHOLDERS’ EQUITY
1,866,000 common shares (post-reverse split 1-for-10) were issued during the year ended April 30, 2017 for $295,463 through a private placement to unrelated parties under Rule 506 of Regulation D. During the 12 months ended April 30, 2017 100,000 shares were issued to a consultant for worked performed. The valuation of those shares was $149,310.
On April 25, 2017 the Company issued 60,000 shares of common stock to BBVI Consulting, a related party, to settle a portion of previous debt owed to BBVI. The fair value of the 60,000 common shares was $148,200, which resulted in a loss on settlement of debt of $118,200.
NOTE 11-SUBSEQUENT EVENTS
On August 7, 2017 the Company entered into a Letter of Intent (LOI) with Orange Care Group of Miami lakes Florida. Medical Innovation Holdings, Inc. is to provide Information Technology management services to practices enrolled in Orange Care Group’s Accountable Care Organizations, including Total Care ACO, LLC d/b/a Orange Accountable Care of New York, Orange Accountable Care of New Jersey, LLC, Orange Accountable Care of Texas, LLC, Orange Accountable Care of South Florida, LLC or Orange Accountable Care Organization of South Florida, LLC (collectively known as “ACO”).
It is the understanding of the parties to this Letter that the products and services which Manager will provide to providers, practices and physicians that are members of the ACO (“ACO Participants”) will support the ACO’s mission of Advancing Care Information in connection with the provision of healthcare services by such ACO Participants to their patients who are Medicare beneficiaries
The term of this Letter of intent shall not be less than five months and at the end of such five-month period, an option to renew for a term of not less than one year.
Compensation for the Services provided by Medical Innovation Holdings, Inc. (“MIHI”) pursuant to this Agreement is according to the following schedule:
| ● | A $50,000 set up fee will be paid to MIHI by Orange Care Group upon signing of this Agreement by Orange Care Group. Such fee shall be used by MIHI to initiate performance of the services listed in Exhibit A. | |
| ● | MIHI shall charge ACO providers, practices and physicians who elect to purchase any of the products and services being provided by MIHI a 20% service fee on a cost plus basis of Fair Market Value for any fee for service. This fee will be subject to negotiation by MIHI with Orange Care Group, its providers, practices and physicians. |
| 13 |
ITEM 2. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion should be read in conjunction with our unaudited financial statements and notes thereto included herein. In connection with, and because we desire to take advantage of, the “safe harbor” provisions of the Private Securities Litigation Reform Act of 1995, we caution readers regarding certain forward looking statements in the following discussion and elsewhere in this report and in any other statement made by, or on our behalf, whether or not in future filings with the Securities and Exchange Commission. Forward-looking statements are statements not based on historical information and which relate to future operations, strategies, financial results or other developments. Forward looking statements are necessarily based upon estimates and assumptions that are inherently subject to significant business, economic and competitive uncertainties and contingencies, many of which are beyond our control and many of which, with respect to future business decisions, are subject to change. These uncertainties and contingencies can affect actual results and could cause actual results to differ materially from those expressed in any forward looking statements made by, or on our behalf. We disclaim any obligation to update forward-looking statements.,
The independent registered public accounting firm’s report on the Company’s financial statements as of April 30, 2017, and for each of the years in the two-year period then ended, includes a “going concern” explanatory paragraph, that describes substantial doubt about the Company’s ability to continue as a going concern.
History
Medical Innovation Holdings, Inc. (“MedHold,” “we,” “us,” “Company”) was incorporated on June 23, 1998 in the state of Colorado as Colorado Community Broadcasting, Inc. In 2005, the Company changed its name to Medina International Holdings, Inc. We changed our name to Medical Innovation Holdings, Inc. effective September 15, 2016, and our name change with FINRA was approved. The Company’s Stock trades on the OTC Market under the symbol “MIHI”.
On April 29, 2016, we completed a Definitive Agreement by which we acquired the business concepts, plan, and intellectual property of Medical Innovations Holdings, and thereafter, divested Harbor Guard Boats, Inc. business to the former management, thereby releasing $3,112,599 in debt associated with the Harbor Guard assets and business. The Harbor Guard assets had not generated any significant revenue for several years, and required major capital to relaunch and manufacture boats, in a very competitive market. The Board deemed it was in the best interest of the shareholders to move in a new business direction with the elimination of a large amount of debt that had been carried. The Company issued 351 million common shares (post-reverse split 1 for 10) for the new Medical Innovations assets and business plan, and 30 Series “A” Convertible Preferred shares were transferred to Medhold, and the Company received 35 million shares of common stock from prior management to retire to treasury in conjunction with the simultaneous divestiture of the old Harbor Guard Boats, Inc. subsidiary and the relief of $3,112,599 in debt from the Company liabilities.
Our majority shareholders as of June 24, 2016 also approved a reverse split (1 for 10 old common shares) effective September 15, 2016 for which a Definitive Form 14C was filed and mailed to shareholders. We have changed control, divested the Company of its prior operations including old assets and liabilities and restructured to continue in the business described in this filing. Our corporate offices are located at 5805 State Bridge Road, Suite G-328, Duluth, Georgia 30097 and our telephone number is (866) 883-3793.
On June 28, 2016, the Company formed a wholly-owned subsidiary, BKare Diagnostics, Inc., in the state of Georgia. BKare Diagnostics is a full-scale provider of high quality laboratory and pharmaceutical services providing personalized services for small and mid-size medical practices and Virtual Health Medical Providers. All BKare Referral Laboratories are certified to provide services to Medicare, Medicaid, HMO and all private and commercial insurance companies. Their personalized services include custom testing protocols, tailored to meet client’s needs and includes services as an online private portal to order tests, supplies, online results 24 hours per day with board certified pathologists.
| 14 |
On August 9, 2016, the Company formed a wholly-owned subsidiary, 3PointCare, Inc. (“3P”), in the state of Georgia to provide services critical to the Company for the administration, scheduling, claims processing, technical support, as well as delivering medical and health related services. The subsidiary is in the development stage.
On September 8, 2016, MedHold’s wholly owned subsidiary, 3P, entered into a Management Services Agreement to exclusively provide management services to TeleLife MD, Inc. The Company will be the exclusive provider to TeleLife. The agreement has an initial term of 10 years together with certain renewal rights. TeleLife MD is a multi-disciplinary specialty care practice formed to provide telemedicine services to patients in rural underserved areas in various states.
On November 14, 2016, the Company announced that its wholly owned subsidiary, BKare, entered into a Marketing & Services Agreement with Vantari Genetics. Under the agreement BKare will provide certain marketing and other services to the Company’s network of clients and Vantari will provide genetic based testing and conduct the molecular laboratory and toxicology testing services. Vantari is a nationally known molecular diagnostic services and toxicology company, and has experience with the development and delivery of molecular laboratory and toxicology testing. It offers full array of genetic testing across the health spectrum, from pharmacogenetics to non-invasive prenatal testing and testing for inherited cancers.
On January 24, 2017, the Company entered into an exclusive agreement for Moody Capital Solutions, Inc., to be the Company’s investment banker in connection with the Company’s efforts to secure financing and to make strategic acquisitions.
On January 13, 2017, the Company entered into a Letter of Intent (LOI) with a Florida-based nutraceutical company, Renaissance Health Publishing, LLC (“RHP”). Under the agreement, the Company will acquire 100% of the assets of RHP in a cash and stock transaction valued between $2.5-$3.5 million. RHP will provide a proprietary product line with specialized formulations along with Trademark product names. Also with the acquisition, the Company will receive a more robust customer base, existing staff and management, and certain marketing material designed to promote RHP product line. RHP is a nationally known research and development company recognized for its portfolio of physician-developed, natural health supplements designed to provide their customers with a better quality of life.
On June 27, 2017, the Company entered into an Asset Purchase Agreement with RHP, details of which are included in the Form 8-K filed on July 3, 2017.
On April 26, 2017, the Company entered into a LOI with a Florida-based international consulting company (“BBVI”). Under the agreement MIHI will acquire 100% of the assets of BBVI in a stock transaction. BBVI will provide immediate access to its strategic client/customer base, share in the sale, ordering, and delivery of products and services to its customers. The acquisition would potentially provide revenue and profits for MIHI once the transaction is complete along with the beginning of building out a global footprint for the Company. The transaction is contingent on the delivery of audited financials. BBVI has been providing strategic consulting services to MIHI for the last year and a half. Through this relationship, the Company has been working with MIHI to expand its presence into international markets. BBVI has been successful in introducing MIHI to these markets and has taken the lead in penetrating certain foreign markets with high-level business professionals and government entities/individuals. This has resulted in securing government bids that may allow MIHI to fulfill the orders and book the resulting revenue.
Our business plan is to establish a nationwide, state by state, multi-disciplinary medical specialist provider/practice network, staffed by 16 types of Physician Specialists who will serve the rural patient population within the States it practices, via a seamless, comprehensive, sophisticated telemedicine program. Our platform is designed to bring unparalleled access to quality healthcare in real time, as needed, and create huge cost savings and efficiencies. Our fully integrated practice management system provides EMR/EHR, patient scheduling, real time insurance verification, billing, video conferencing and all systems in an end to end technology platform coupled with all the components of a dynamic telehealth delivery system. Our telemedicine platform brings together many different modalities of telemedicine to create a virtual multi-specialty practice within our referring partner’s primary clinic practice. Our business model is designed to increase the access to specialty providers, including, neurology, dermatology, ENT, tele-stroke, management of high risk pregnancy, mental health, dermatology, endocrinology, pediatrics, cardiology, nephrology, pulmonology, OBGYN, maternal and fetal and others.
| 15 |
Corporate Structure:
MEDICAL INNOVATION HOLDINGS, INC. (A Colorado Corporation) | ||
3PointCare, Inc. (A Georgia Corporation) |
BKare Diagnostics, Inc. (A Georgia Corporation) | |
The Problem We Solve
Our Management believes it is recognized by government officials, healthcare executives, healthcare practitioners including physicians, and noted academics that the current medical system is dysfunctional and not in line with the intended goals of effective, affordable and accessible healthcare.
Our Management believes the current medical system and its technological advances as well as the current regulatory trajectory are trapped in outdated, high cost, and ineffective business models. Our mission is to implement cost-effective technological management and develop business models around them to make health care and wellness more affordable and accessible.
Our plan is to have state licensed medical practice locations managed by our Management Services Organization (“MSO”). Our MSO staff and Medical Director will have the necessary backgrounds in their service area and be responsible for business development, clinic and service delivery, and profit and loss.
Sales and Marketing
Our sales and marketing strategy is to present our specialty practice medical services to underserved rural patients in the setting of their primary practice provider. We intend to offer a business-oriented approach to practice management systems, differing from the current medical model. Our model is to enhance medicine for patients, and offer the most efficient administrative system solution for medical practices. We believe we can do that because our business model and profit motive is aligned properly with patient goals and successful outcomes.
We intend to work to leverage success with client practices by implementing for each practice a strategy to use our telehealth platform and our focused management system demonstrating measurable patient and medical professional satisfaction results.
We believe sales and marketing also includes recruiting and developing relationships with candidate health practitioners, unaffiliated care facilities, and medical specialists who will provide efficient service without excessive overhead. Therefore, marketing our service involves enlisting primary care physicians who are interested in expanding their patient base and care services, and increasing their profits through elimination of the excessive administrative staffs. We intend to transmit images electronically through our HIPPA compliant PACS System (acronym for Picture Archiving Communication and Storage). We utilize the eclinicalworks integrated platform to manage all functions of our medical practices. Our Services Agreement grants the Company access to the technology platform and systems, which are licensed.
Key Success Drivers
Our Management believes there is a relatively low cost in opening an MSO to operate across the United States. Our business model is scalable and efficient. However, there is a relatively high barrier to entry in developing a fully integrated platform of trained telehealth practitioners with primary care referring partners.
We believe executing solid operations and market strategy is key. Here are our perceived drivers to success:
| ● | Operational Excellence | |
| ● | Marketing to Physicians and Deploying Locations |
| 16 |
| ● | Marketing and Servicing to Clinics | |
| ● | Building Relationships and Enlisting Specialists to Perform Diagnosis | |
| ● | Staff Training and Service Excellence | |
| ● | Integrity in honoring the value-chain, the patient, and the payers by minimizing the administrative costs with conservative treatments and effective documented outcomes |
Competition
Our current competition is mostly based on the current “dysfunctional” large hospital / holding company medical model. Our primary competition is various hospitals conglomerates, and local health groups.
The local groups are typically either hospital-based health services or independent primary care physicians who may not be focused on availability of add-on expertise through our model.
Neither the large conglomerate hospital chain nor the local hospital-based groups may soon adopt our model because of the burden of their overhead and capital costs. Moreover, their revenue model is based on treatment delivery to specific geographic areas within driving distance not broader efficient health solutions. Their expertise, overhead structure, revenue model and mindset simply preclude them from breaking out of their current business models.
OUR TELEHEALTH BUSINESS PLAN
GENERAL
Our premise is the current healthcare delivery system, which serves the 87 million rural US patients, is inadequate. Because specialists are primarily based in urban areas, rural patients do not have direct access to these specialists and are forced to travel great distances, wasting time and money to get the care they need. Because of this, the care continuum is beginning to embrace the new models of communication; information transfer and collaboration in order to fulfill the required healthcare needs of those patients. A transformation of the traditional health system is underway in the US, which incentivizes providers, payers and patients toward improved quality and lower costs.
We believe telemedicine has the ability to greatly improve the accessibility and quality of medical services by extending the reach and increasing the efficiency of the existing system. Succinctly stated, we intend to establish a nationwide multi-disciplinary specialist provider/practice network, staffed by 16 types of specialists who serve the rural patient population via a telemedicine program. This platform will bring unparalleled access to quality healthcare in real time, as needed, and create huge cost savings and efficiencies. Our fully integrated practice management system provides electronic medical records/electronic health records (“EMR/EHR”), patient scheduling, real time insurance verification, billing, video conferencing and all systems in an end to end technology platform coupled with all the components of a seamless telehealth delivery system.
Our proprietary telemedicine platform brings together many different modalities of telemedicine to create a virtual multi-specialty practice within our referring partner’s primary clinic practice. Our business model is designed to greatly increase the access to specialty providers, including, neurology, dermatology, ear nose and throat (“ENT”), tele-stroke, management of high-risk pregnancy, psychiatry, dermatology, endocrinology, pediatrics, cardiology, nephrology, pulmonology, OBGYN, maternal and fetal, and others.
Our plan is to develop an extensive and robust specialty telemedicine program in the US with the capability to implement telemedicine programs and develop networks throughout the 50 states and eventually around the world.
| 17 |
OUR COMPANY
3P is the newly formed operating MSO subsidiary of our Company and is being developed to:
| ● | Manage, improve and promote the availability and provision of specialized healthcare services in rural and underserved areas. | |
| ● | Empower our rural primary clinic referring partners with new revenue streams, improved profitability and better care for their patients. | |
| ● | Reduce the service barriers that exist for patients in remote areas or otherwise living at a significant distance from needed medical resources. |
One hallmark of our business model is the recruitment of top specialists in each state making that collective expertise available and accessible to the largest amount of participating healthcare facilities and primary healthcare providers and their patients. This network model maximizes the ability of people in isolated areas to transcend distance and obtain specialty care close to home. The model and our management team intends to provide expertise and services to primary care organizations and providers seeking a reliable, high quality and cost effective means to access specialty healthcare for its patients.
Our Core Business: Our Management Service Organization (MSO) and Friendly PC (Medical Practice) structure
We are an applied telehealth platform with three integrated components.
1. Our MSO, 3P, Inc., is powered by an integrated end-to-end software system that enables our team to manage all aspects of our Specialty Medical Practices. We handle all aspects of managing the delivery of our physician services in the delivery of telemedicine/telehealth in consultation encounters.
2. The multi-state Specialty Medical Practice, TeleLifeMD, Inc.
3. Loaning and installing of the telemedicine platform and peripherals to our referring partner clinics/ primary care doctor offices. These become the pipeline for patients into our specialty medical practice.
THE MARKET
We Believe the Time is Right:
The US is the world’s largest national economy with over $17.4 trillion of annual economic activity. This is more than one fifth of the world’s total economic output. Healthcare, a key economic driver, comprises approximately 18% of the nation’s gross domestic product, with Americans spending more than any other country on their care at $8,608 per person. Yet despite devoting many resources to this industry, the U.S. has consistently ranked lower in many measures of health and wellness including: life expectancy, infant mortality, and diabetes care. The government has made numerous attempts throughout the nation’s history in reforming healthcare with few successes. A big stride in healthcare reform came in 2010 with the signing of the Patient Protection and Affordable Care Act (ACA). Although the ACA intends to reduce costs and improve quality within the U.S. healthcare system, many agree that the key to achieving that goal will not be legislation, but technology.
The two major sweeping changes from the ACA that will have tremendous impact on the U.S. healthcare system, should they stay in place through regulatory changes, are Accountable Care Organizations (ACOs) and nearly universal coverage. According to the ACA, ACOs are networks of physicians, hospitals, and other providers that take both clinical and financial responsibility for the care of patients. By breaking individual silos among hospitals, pharmacies, home health care agencies, hospices, primary care physicians, and other providers, ACOs attempt to make it easier for all of these providers to coordinate a patient’s care. We face the risk that the ACA is modified or replaced with new healthcare laws, and that many of our base assumptions will change as a result. The Company believes that our business will adapt to any future healthcare reforms.
| 18 |
The implications of ACOs are that technology will be more important in the delivery of healthcare to improve patient outcomes and keep costs down. As patients leave the hospital or a primary care doctor’s office to return home, care will need to be maintained and coordinated. For this to take place, technologies that collect health data, promote communication among providers and patients, and that facilitate treatment will need to be implemented. Many of these technologies fall under the telemedicine umbrella, which will be discussed later in this plan. A key facet to remember is that technology is the bridge that fills the gap between all these providers (pharmacies, hospitals, primary care doctors, nurses, etc.) and since coordination is needed to comply with the ACO mandate, more companies will seek out the services of telemedicine and health technology companies. The Company is uncertain about what changes to healthcare laws may affect these premises, however, the Company believes that its services will be beneficial to the market, regardless of the healthcare laws.
Telemedicine is the provision of healthcare services by physicians from one location to patients at another. Telemedicine has gained momentum in the last 50 years thanks to improvements in technology, changes in healthcare policy, and increased consumer demand for such services. Telemedicine not only encompasses technologies related to patient-doctor communication, but also tools used in the delivery and management of diseases, wellness, critical care, and post-acute care.
The deployment of telemedicine services is increasing in tandem with the development of telecommunications technology. The shortage of physicians in rural and remote areas is providing the opportunity for telemedicine to increase its services to millions of patients. This widespread deployment of services will continue at a rapid pace for the foreseeable future.
Telemedicine applications are increasing due to the high prevalence of chronic diseases, consistent need for improved quality services and rising elderly population across countries which demand telemedicine to deliver improved products with higher patient satisfaction. Rapid pace of innovation among hardware and software vendors, along with the speed and coverage of broadband and mobile technologies is enabling the availability and optimized delivery of healthcare.
The continuing rise in healthcare costs, the change from fee-based payment models to value-based payment models and the current and projected shortage of physicians are driving healthcare providers and technology companies to collaborate and innovate to address these challenges. In addition, there is tremendous patient demand for access to affordable care. Consumers are playing a more direct role in their care. Physicians are demanding better ways to provide that care.
We believe consumer demand will cause telehealth to become “mainstream” health care.
| ● | Consumers want telemedicine. | |
| ● | The greatest impact of telemedicine is on the patient, their family and their community. | |
| ● | Using telemedicine technologies reduces travel time and stress for the patient. | |
| ● | Over the past 15 years several studies have documented patient satisfaction and support for telehealth services. Such services offer patients the access to providers that might not be available otherwise, as well as medical services without the need to travel long distances. |
THE POTENTIAL MARKET FOR 3P
Based on our telehealth strategy, 3P and TeleLifeMD will focus on penetrating into markets where there are favorable telemedicine reimbursement regulations. The acceptance of telemedicine throughout the states is expanding the potential market for us. Taking into consideration physician practices, hospitals, nursing homes and skilled nursing facilities and urgent care centers, we estimate the immediate market includes over 500,000 potential referrer partners in the U.S. Currently there are 60-80 million patients in Medically Underserved Areas (MUAs) as defined by the federal government. This represents a large market segment in the rural areas we wish to serve.
| 19 |
| Primary Target Customers | Approximate Addressable Market | |||
| Hospitals | 5,724 of which 1,984 are rural | |||
| Nursing Homes | 15,465 | |||
| Urgent Care Clinics | 9,300 | |||
| Physicians | 468,819 | |||
| Emerging: Employers (Fortune 500) | 500 (each with multiple locations | ) | ||
The initial and primary focus for 3P will be to build an MSO capable of servicing each state where we intend to operate, create a professional medical corporation, managed by a Medical Director and recruit the necessary part time medical specialist employees required to serve our patients. This model will be expanded and scaled with solid leadership in developing, delivering and managing comprehensive telehealth solutions. The expansion of the model and market penetration will be achieved with a direct to referring primary practice sales and marketing strategy. We intend to follow or chart best practices for the specialty medicine telemedicine delivery model.
Hospitals:
Hospitals and health systems in the U.S. are undergoing a dramatic shift in their business models due to a number of forces that may be expected to eventually turn the industry on its head — from providers concerned with the volume of services they provide, to providers who focus on offering high-value services that emphasize keeping populations healthy
| ● | There are 5,724 hospitals in the U.S., according to the American Hospital Association. (2015) | |
| ● | Of all hospitals in the U.S. 1,984, or 35 percent, serve rural communities and are considered rural hospitals. | |
| ● | Of rural hospitals, 1,328 have been designated as Critical Access Hospitals by CMS.2 CAHs are rural hospitals with no more than 25 beds and are at least 35 miles (15 miles in areas with mountainous terrain or only secondary roads) away from another hospital. |
Our target for Nursing Homes:
There are estimated to be 15,000 nursing homes in the United States. Results of several studies conducted by leading institutions (such as Dartmouth, Commonwealth Fund), showed that based on the reduced hospitalization rates of the more telemedicine engaged facilities, Medicare might see up to $150,000 in savings per nursing home per year. We believe the annual cost of the telemedicine service is estimated at $36,000 per nursing home per year, suggesting that there could be $114,000 in net savings per year.
Top Telemedicine Encounters:
| ● | Mental Health (medication management, screening/assessment) | |
| ● | Wound Care (wound images, diagnosis/treatment) | |
| ● | Episodic Care (non-emergent issues – sore throat, flu, etc.) |
Benefits for the Resident:
| ● | Decrease transports to the emergency department | |
| ● | Decrease stress on the resident and family | |
| ● | Decrease the chances of a fall | |
| ● | Decrease hospital acquired illness |
Our Target for K-12 Schools:
The estimated number of K-12 Schools: 130,000. According to the Center for Education Reform, of the total number of schools, about 2,000 have School Based Health Centers (SCHCs), and, few of these are using telehealth. This market segment can experience significant growth with an access solution, which we intend to offer.
| 20 |
Health has a direct impact on student learning (improves education, absenteeism and the learning experience.
For Schools our business intends to offer solutions resolving an unfulfilled need:
| ● | Increased access to primary and episodic care (many would not have otherwise). | |
| ● | Mental Healthcare | |
| ● | Specialists | |
| ● | Oral Healthcare | |
| ● | Pharmacy |
Our Program Benefits:
| ● | Students like the technology | |
| ● | School-based health centers are five minutes or 50 feet from the student’s world | |
| ● | Increase in yearly medical visits | |
| ● | 3.4 hours saved from parents missing work (avg. of $43 in lost wages) per year | |
| ● | Reduced emergency department visits (avg. savings per family $224) per year | |
| ● | Creates a true system of care for the student |
Our Target for Urgent Care Facilities (Estimated at over 9,000 Facilities):
Based upon a statement on their website from the American Academy of Urgent Care Medicine, the growth and development of Urgent Care Medicine should be no surprise to anyone. Fueled by frustration over long waits in the emergency room (for non-emergency care), and a reduction in available primary care appointments (often resulting in patients waiting for weeks to see their primary care physician), a new growth spurt for the Urgent Care industry began in the mid-1990s and continues today. The public’s desire for immediate access to quality and affordable medical care has been the driving force behind this monumental growth.
We intend to develop this market.
THE TELEHEALTH TOOLS AND SERVICES
The following is a detailed description of the products and services that our operating subsidiary, 3P, intends to provide.
Our Proposed Process:
Our in-house dedicated business development team identifies referring primary clinic locations where their patient base will benefit from our solution and we:
| ● | Provide detailed site assessment for equipment needs based on medical specialty and available connectivity. | |
| ● | Order equipment, install equipment, and train all staff and providers. | |
| ● | Carry out ongoing education and support for the program. | |
| ● | Implement telehealth program, monitor use, and track use and outcomes associated with goals and objectives. |
| 21 |
Our Proposed Telehealth Services Include:
| ● | Training and implementation of telehealth for specialist practitioners and presenting sites by our field based Liaisons’ | |
| ● | Network Infrastructure/mobility/flexibility | |
| ● | Centralized Scheduling | |
| ● | Image grid and cloud-based PACS system to enable access to CT scans and MRIs remotely by physicians. | |
| ● | Credentialing Assistance | |
| ● | 24/7 IT and Program Support |
Our Proposed Network Technology and Architecture:
Our proposed specialty practice network is designed to be a highly secure environment and a working IP network that allows access to the Internet. Videoconference, either point-to-point or multipoint, is readily available to all users for consultations, education and business applications.
The network is expandable in both scope and size. The network platform has an integrated electronic health record system practice management, insurance eligibility for claims, billing and all other functions of a practice and supports an image grid and PACS system to enable access to CT scans and MRIs, and to then store and forward images. In addition, the network has enough capacity to take on considerably more applications as desired or needed.
Dedicated Support
3P provides 24 hour per day help desk support. The maintenance program and help desk support gives us a single point of contact for quick problem resolution.
Scheduling System
Our licensed software scheduling system is manned by our staff and is integrated into our platform. This advanced, user-friendly scheduling system coordinates all patient / facility / physician / distant learning appointments.
Back office practice Management
We are using the Eclinical works EMR and practice management system to manage all aspects of our medical practices. Our front office, mid office and back office team does real time eligibility, claims and secondary claims, claims management, billing etc.
Credentialing Support/ Management
To meet the physician credentialing requirements of partnering hospitals and institutions, 3P assists with the process to credential and privilege clinicians / practitioners who provide telemedicine consultations via the network. All providers must meet the minimum standards of criminal background and certification specific (varies with license, education, training, experience, and competence) screening, as well as additional quality controls.
3P’s Telehealth practice offers our partners technology services, patient services, comprehensive program services and educational services.
| 22 |
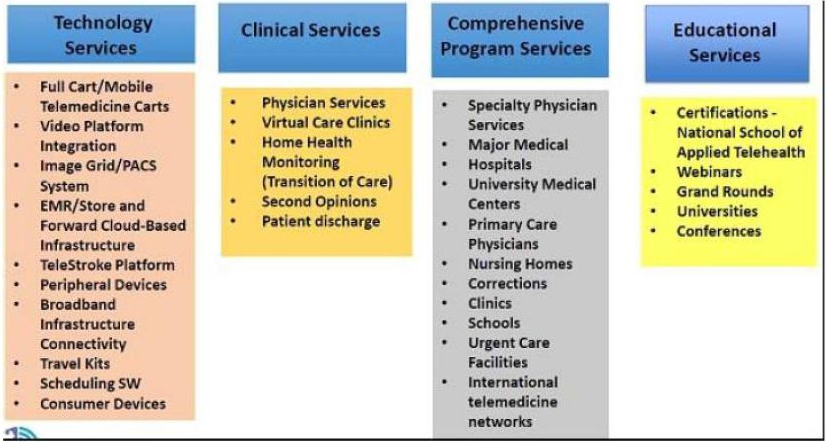
The Benefits of 3P’s service offering:
| ● | Our network supports the ability to read images, CT scan, MRI, and other diagnostic resources. | |
| ● | We provide a comprehensive telehealth program including centralized scheduling, credentialing support, 24/7 IT support, dedicated telehealth liaison, as well as training and on-going education for site staff. |
3P offers a value proposition to its referring partners:
| ● | Increased and enhanced access to our specialty services | |
| ● | Increased revenues to physicians by increasing their patient volumes | |
| ● | Increased revenues to hospitals through patient retention | |
| ● | Alignment with value-based payment models | |
| ● | Improved patient outcomes | |
| ● | Overall healthcare delivery optimization and cost reduction |
MARKETING AND SALES STRATEGY
We intend our business and growth will come through direct presentations to primary care facilities and may also grow by word of mouth and referrals, which we hope will develop a brand and positive reputation. We intend to operate with a dedicated field sales and marketing team. Generally, each state where we operate will be staffed by one business development team member per 20 county territories. The business development and revenue growth may also come from the visibility and efforts of the leadership team, along with the support of business developers in the field. In order to sustain our success, maintain the integrity of our brand, keep pace with rising demand, ride the rapid expansion of the market and capture more market share, we must obtain the required funding, estimated at $5,000,000 which is not committed at this time.
| 23 |
Our sales and marketing strategy is outlined below.
Market Development Strategies
a. Our initial focus is to grow the core business: Align solutions, go-to-market strategy and tactics for each of our existing customer market segments where believe there are proven need, benefit, and return on investment.
b. Target Prospects: We will solicit the following:
| i) | Nursing Homes | |
| ii) | Hospitals | |
| iii) | Urgent Care Facilities | |
| iv) | Schools | |
| v) | Correctional Facilities | |
| vi) | Physicians |
c. We intend to prioritize and drive sales growth where State Laws support telehealth.
| i. | States: There are currently 35 States where we would target expansion |
d. We intend to launch to “policy friendly” telemedicine States
| i. | 7 States with American Telemedicine Association top composite score (GA, CO, VA, TN, MS, NM, CA) | |
| ii. | 30 States plus DC ranked second highest for telemedicine “friendly” |
Sales and Distribution Strategy
We plan that sales will be driven through a combination of a 3P direct sales force and strategic partner/indirect channels (in a “sell with” and “sell through” model). Our strategy will also be to develop and monetize partnerships to promote business and revenue opportunities throughout the ecosystem.
Partnering and “marketing cooperative” relationships with hardware, software, service providers, healthcare systems, insurance companies and others may help provide the synergy for growth in our traditional telehealth consulting and managed services lines. Lead generation and referral may come from partners and strategic alignment with several industry leaders with the applied application being the genesis for sales and services.
Sales Velocity
Our sales strategy will incorporate a process to facilitate sales to enable scale, operational marketing success and sustainability (with continuous improvements to increase sales velocity) to include:
| ● | Implement a sales funnel methodology and ongoing sales process (qualification, prioritization, revenue forecasting, performance tracking). | |
| ● | Invest and implement a customer relationship management (CRM) platform for visibility, opportunity development and management. | |
| ● | Create sales enablement tools: training, baseline proposals, and value propositions by market segment, pricing, etc. to enable, replicate success and empower sales executives and partner distribution channels. | |
| ● | Procure business intelligence and lead generation tools (for target lists, sales leads). |
| 24 |
Plans to Expand Brand Awareness
We plan to hire/invest in marketing/messaging expertise to drive brand awareness
i. We plan to market the 3P brand to be known for:
| ● | Renowned telehealth experts | |
| ● | Passion, commitment and partnership collaboration | |
| ● | Advocates and champions for the integrity of telemedicine |
ii. We plan to pro-actively increase visibility of our projects and thought leadership through active participation in social media outlets
iii. We plan to continue to participate in healthcare technology/telehealth conferences, panels
iv. We plan to host conferences, webinars with strategic partners
v. We plan to create marketing communications (newsletters to network partners, prospects, distribution partners, employees)
vi. We plan to engage with key technology hardware and software technology partners.
vii. We plan to maintain active participation and sponsorship in professional industry and technology associations.
viii. We plan to create a world-class “experience” center – to showcase and demo the virtual care center and patient centered medical home.
ix. We plan to forge strategic alliances for differentiation and market visibility.
REVENUE MODEL
The 3P Telehealth revenue model and projections are based upon performance, expansion of core telehealth services, and implementation of new and telehealth service lines. Opportunities for revenue from additional telehealth services lines will be realized over the next five years in the areas of consumer telehealth, consulting, and home healthcare. The national projections include revenue associated with these areas with the most robust being home healthcare. It is believed that the migration of telehealth into the home and to the consumer may account for a larger portion of health services revenue in the future.
Management believes that given the growing market and changes in healthcare i.e., Affordable Care Act, penalties for readmissions, and financial rewards for high quality care and lower cost care, the potential market and pricing options for our core business and additional telehealth services lines is robust.
Competition and Defensibility:
There are a broad range of telehealth products and services available to today’s health care industry. The healthcare industry, in its current state, is uncoordinated and fragmented across the care continuum. There is no shortage of technology companies rapidly innovating to address these challenges. However, like the healthcare industry, the myriad of hardware, software and platform solution offerings are also uncoordinated and fragmented. Each, typically addresses one particular aspect of the continuum of care or its product represents only one piece of the entire “telemedicine network” ecosystem. This leaves healthcare providers and systems confused and overwhelmed with how best to implement a telehealth program.
We intend to be a specialty telehealth medical practice management provider utilizing a proprietary technology and hardware platform to deliver those services to patients via our referring physicians. 3P intends to orchestrate, deliver, train and manage an end-to-end customized telehealth program for its primary care referring partners. We believe 3P is unique in its approach and the assets that it brings to the marketplace. 3P brings the healthcare and technology providers together to create a full and comprehensive healthcare delivery system.
| 25 |
We intend to break down the silos and coordinate an entire program to create a cohesive, holistic solution for healthcare delivery. Our key differentiator we believe is our ability to optimize, deliver and manage across the entire patient-centered medical home (“PCMH”) spectrum.
Renaissance Health Publishing-Asset Acquisition
On June 27, 2017, the Registrant entered into an Asset Acquisition Agreement with Renaissance Health Publishing LLC. a Florida Limited Liability Company.
The consideration of the Asset Acquisition shall be due and payable as follows:
Purchase and Sale of Assets.
Subject to the terms and conditions set forth in this Agreement, Seller does hereby sell, convey, transfer, assign and deliver to Buyer, and Buyer does hereby purchase from Seller, all of the goodwill and all of the assets used by or in connection with the Business, tangible or intangible, wherever located (the assets being transferred hereunder are collectively referred to as the “Purchased Assets”), including without limitation, all inventory of products and supplies and work in progress owned by Seller, all of Seller’s contracts (including, without limitation, all of Seller’s real property, computer, telephone and equipment leases) (collectively, the “Assigned Contracts”), prepaid expenses, machinery and equipment, manufacturer’s warranties, licenses, consents and permits, customer lists, training materials, trademarks, trade names, servicemarks, copyrights, techniques, know-how, show-how and other intangibles, except for the assets specifically set forth on Schedule 2.1 hereto (the “Excluded Assets”).
Purchase Price.
The consideration to be paid to Seller for the Purchased Assets (the “Purchase Price”) shall consist of:
a) a cash payment at Closing of $1,000,000 (the “Closing Date Payment”), payable via certified check or wire transfer of immediately available funds to an account that shall have been designated by Seller to Buyer prior to Closing; and
b) payment of: (x) four (4) times Seller’s earnings before interest, taxes, depreciation and amortization (“EBITDA”) for the 12 month period ending on the last day of the calendar month immediately preceding the month in which the audit is completed (the “Audit Date”), as determined by an audit of Seller’s financial statements conducted by Assurance Dimensions, Inc. (the “Auditor”), plus (y) the value of Seller’s fully-paid inventory (calculated at Seller’s actual cost) of supplements and pre-printed direct mail pieces as of the Closing, minus (z) the Closing Date Payment (the “Formula Payment”). The Formula Payment shall be payable pursuant to the Convertible Promissory Note attached as Exhibit “A” hereto (the “Convertible Note”) and the obligations of Buyer under the Convertible Note shall be secured by the Security Agreement in the form attached as Exhibit “B” hereto. Seller shall be required to execute an inter-creditor agreement with the Senior Lender in form and substance reasonably satisfactory to the Senior Lender pursuant to which the Seller shall subordinate the priority of its lien on the collateral described in the Security Agreement to the lien on such collateral arising under the Senior Loan documents.
Allocation of Purchase Price.
Within five days after the Closing Date, Seller shall deliver a schedule allocating the Purchase Price (the “Allocation Schedule”). The Allocation Schedule shall be prepared in accordance with Section 1060 of the Code. The Allocation Schedule shall be deemed final unless Buyer notifies Seller in writing that Buyer objects to one or more items reflected in the Allocation Schedule within five (5) days after delivery of the Allocation Schedule to Buyer. In the event of any such objection, Seller and Buyer shall negotiate in good faith to resolve such dispute; provided, however, that if Seller and Buyer are unable to resolve any dispute with respect to the Allocation Schedule within thirty (30) days after the delivery of the Allocation Schedule to Buyer, such dispute shall be resolved by the Auditor or, if the Auditor is unable to serve, another impartial nationally recognized firm of independent certified public accountants mutually appointed by Buyer and Seller. The fees and expenses of such accounting firm shall be borne equally by Seller and Buyer. Seller and Buyer agree to file their respective IRS Forms 8594 and all federal, state and local tax returns in accordance with the Allocation Schedule.
| 26 |
No Assumption of Liabilities.
Buyer does not and shall not assume any debts, obligations or liabilities of any nature whatsoever of the Seller arising before or after the date hereof or in connection with any of the Purchased Assets or the Business of Seller (the “Excluded Liabilities”) other than the liabilities of the Seller disclosed on Schedule 2.4 hereto (the “Assumed Liabilities”). Seller agrees to satisfy and discharge the Excluded Liabilities as the same shall become due. Buyer agrees to satisfy and discharge the Assumed Liabilities as the same shall become due.
Non-assignable Assets.
Notwithstanding anything to the contrary in this Agreement, and subject to the provisions of this Section 2.5, to the extent that the sale, assignment, transfer, conveyance or delivery, or attempted sale, assignment, transfer, conveyance or delivery, to Buyer of any Purchased Asset would result in a violation of applicable Law, or would require the consent, authorization, approval or waiver of a Person who is not a party to this Agreement or an Affiliate of a party to this Agreement (including any Governmental Entity), and such consent, authorization, approval or waiver shall not have been obtained prior to the Closing, this Agreement shall not constitute a sale, assignment, transfer, conveyance or delivery, or an attempted sale, assignment, transfer, conveyance or delivery, thereof; provided, however, that, subject to the satisfaction or waiver of the conditions contained in Section 8.1 hereof, the Closing shall occur notwithstanding the foregoing without any adjustment to the Purchase Price on account thereof. Following the Closing, Seller and Buyer shall use commercially reasonable efforts, and shall cooperate with each other, to obtain any such required consent, authorization, approval or waiver. Once such consent, authorization, approval or waiver is obtained, Seller shall sell, assign, transfer, convey and deliver to Buyer the relevant Purchased Asset to which such consent, authorization, approval or waiver relates for no additional consideration.
To the extent that any Purchased Asset cannot be transferred to Buyer following the Closing pursuant to this Section 2.5, Buyer and Seller shall use commercially reasonable efforts to enter into such arrangements (such as subleasing, sublicensing or subcontracting) to provide to the Parties the economic and, to the extent permitted under applicable Law, operational equivalent of the transfer of such Purchased Asset to Buyer as of the Closing and the performance by Buyer of its obligations with respect thereto. Buyer shall, as agent or subcontractor for Seller pay, perform and discharge fully the liabilities and obligations of Seller thereunder from and after the Closing Date. To the extent permitted under applicable Law, Seller shall, at Buyer’s expense, hold in trust for and pay to Buyer promptly upon receipt thereof, such Purchased Asset and all income, proceeds and other monies received by Seller to the extent related to such Purchased Asset in connection with the arrangements under this Section 2.5. Seller shall be permitted to set off against such amounts all direct costs associated with the retention and maintenance of such Purchased Assets.
The Asset Acquisition Agreement contains customary representations and warranties and pre and post-closing covenants of each party and customary closing conditions. Breaches of the representations and warranties will be subject to customary indemnification provisions, subject to specified aggregate limits of liability. The registrant has not completed the funding of this acquisition, and with the execution of this agreement it allows the Registrant to source funding for this acquisition. The foregoing summary description of the terms of the Asset Acquisition Agreement may not contain all information that is of interest to the reader. For further information regarding the terms and conditions of the Asset Acquisition Agreement, this reference is made to such agreement, which is filed as Exhibit 10.1 hereto and is incorporated herein by this reference as filed on Form 8-K with the Securities and Exchange Commission
Events Subsequent to July 31, 2017
On August 7, 2017 Medical Innovation Holdings, Inc. (“MIHI”), a Colorado corporation (the “Company”) entered into a Letter of Intent (LOI) with Orange Care Group of Miami lakes Florida. Medical Innovation Holdings, Inc. is to provide Information Technology management services to practices enrolled in Orange Care Group’s Accountable Care Organizations, including Total Care ACO, LLC d/b/a Orange Accountable Care of New York, Orange Accountable Care of New Jersey, LLC, Orange Accountable Care of Texas, LLC, Orange Accountable Care of South Florida, LLC or Orange Accountable Care Organization of South Florida, LLC (collectively known as “ACO”).
| 27 |
It is the understanding of the parties to this Letter that the products and services which Manager will provide to providers, practices and physicians that are members of the ACO (“ACO Participants”) will support the ACO’s mission of Advancing Care Information in connection with the provision of healthcare services by such ACO Participants to their patients who are Medicare beneficiaries
The term of this Letter of intent shall not be less than five months and at the end of such five-month period, an option to renew for a term of not less than one year.
Compensation for the Services provided by Medical Innovation Holdings, Inc. (“MIHI”) pursuant to this Agreement is according to the following schedule:
| ● | A $50,000 set up fee will be paid to MIHI by Orange Care Group upon signing of this Agreement by Orange Care Group. Such fee shall be used by MIHI to initiate performance of the services listed in Exhibit A. | |
| ● | Medical Innovation Holdings, Inc. (“MIHI”) shall charge ACO providers, practices and physicians who elect to purchase any of the products and services being provided by MIHI a 20% service fee on a cost plus basis of Fair Market Value for any fee for service. This fee will be subject to negotiation by MIHI with Orange Care Group, its providers, practices and physicians. |
The above description of the Letter of Intent is intended as a summary only and is qualified in its entirety by the terms and conditions set forth therein, and may not contain all information that is of interest to the reader. For further information regarding the terms and conditions of the Letter of Intent, this reference is made to the Letter of Intent, which is filed hereto as Exhibit 10.1 and is incorporated herein by this reference.
RESULTS OF OPERATIONS
The Company recognized no revenues during the three months ended July 31, 2017.
During the three months ended July 31, 2017, we incurred general and administrative expenses of $179,203, which were mainly due to the ongoing costs of operations of a fully reporting company
During the three months ended July 31, 2017, the Company recognized a net loss of $349,982 due to the general and administrative expenses.
The Company recognized no revenues during the three months ended July 31, 2017.
LIQUIDITY AND CAPITAL RESOURCES
As of July 31, 2017, the Company had $30,692 cash on hand. The Company’s total current liabilities were $1,350,630 as of July 31, 2017, which was mainly accounts payable and accrued expenses of $900,852, and notes payable of $341,573. At July 31, 2017, the Company’s current liabilities exceeded current assets by $1,319,938.
The Company received $75,000 in financing activities, but used $53,203 of cash in operating activities for the three-month period ended July 31, 2017.
The Company did not have any investment activities during the three months ended July 31, 2017.
The Company has an accumulated deficit, as of July 31, 2017, of $1,912,921 compared to $1,562,939 as of April 30, 2017, an increase in the deficit of $349,982 in the three-month period.
Going Concern
The Company’s auditors issued a “going concern” statement as part of their opinion in the Audit Report for the year ended April 30, 2017 and for each of the years in the two-year period then ended, including a “going concern” explanatory paragraph, that describes substantial doubt about the Company’s ability of the Company to continue as a “going concern.”
| 28 |
Short Term
On a short-term basis, we do not generate revenues sufficient to cover operations. Based on prior history, we will continue to have insufficient revenue to satisfy current and recurring liabilities as we continue to develop our operations. For short term needs we will be dependent on receipt, if any, of offering proceeds.
Need for Additional Financing
We do not have capital sufficient to meet our cash needs. We will have to seek loans or equity placements to cover such cash needs. No commitments to provide additional funds have been made by our management or other stockholders. Accordingly, there can be no assurance that any additional funds will be available to us to allow it to cover our expenses as they may be incurred.
There is no assurance the Company will be profitable, the Company may not be able to successfully develop, manage or market its products and services, the Company may not be able to attract or retain qualified executives and personnel, the Company’s products and services may become obsolete, government regulation may hinder the Company’s business, additional dilution in outstanding stock ownership may be incurred due to the issuance of more shares, warrants and stock options, or the exercise of warrants and stock options, and other risks inherent in the Company’s businesses.
The Company undertakes no obligation to publicly revise these forward-looking statements to reflect events or circumstances that arise after the date hereof. Readers should carefully review the factors described in other documents the Company files from time to time with the Securities and Exchange Commission, including the Annual Report on Form 10-K and Quarterly Reports on Form 10-Q filed by the Company and any Current Reports on Form 8-K filed by the Company.
Contractual Obligations and Other Commercial Commitments
The Company does not have sufficient capital to meet its cash needs, including the costs of compliance with the continuing reporting requirements of the Securities Exchange Act of 1934. Management will have to seek loans or equity placements to cover such cash needs and cover outstanding payables. Lack of existing capital may be a sufficient impediment to prevent the Company from accomplishing its goal of expanding operations. There is no assurance that the Company will be able to carry out our business. No commitments to provide additional funds have been made by the Company’s management or other shareholders. Accordingly, there can be no assurance that any additional funds will be available to the Company to cover its expenses as they are incurred.
Irrespective of whether the Company’s cash assets prove to be inadequate to meet its operational needs, the management might seek to compensate providers of services by issuances of stock in lieu of cash.
Off-Balance Sheet Arrangements
In accordance with the definition under SEC rules, the following qualify as off-balance sheet arrangements:
| a) | Any obligation under certain guarantees or contracts; | |
| b) | A retained or contingent interest in assets transferred to an unconsolidated entity or similar entity or similar arrangement that serves as credit, liquidity, or market risk support to that entity for such assets; | |
| c) | Any obligation under certain derivative instruments; and | |
| d) | Any obligation under a material variable interest held by the registrant in an unconsolidated entity that provides financing, liquidity, market risk, or credit risk support to the registrant, or engages in leasing, hedging, or research and development services with the registrant. |
The following will address each of the above items pertaining to the Company.
As of July 31, 2017, we do not have any obligation under certain guarantees or contracts as defined above.
| 29 |
As of July 31, 2017, we do not have any retained or contingent interest in assets as defined above.
As of July 31, 2017, we hold one derivative financial instrument.
Accounting for Derivative Instrument and Hedging Activities, as amended.
As of July 31, 2017, we did not participate in transactions that generate relationships with unconsolidated entities or financial partnerships, such as entities often referred to as structured finance or special purpose entities (“SPEs”), which would have been established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purposes. As of July 31, 2017 and April 30, 2017, we were not involved in any unconsolidated SPE transactions.
Dividends
The Company has not declared or paid any cash dividend on its common stock and does not anticipate paying dividends for the foreseeable future.
ITEM 3. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK.
Not Applicable.
ITEM 4. CONTROLS AND PROCEDURES
Disclosures Controls and Procedures
We have adopted and maintained disclosure controls and procedures (as such term is defined in Rules 13a 15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”) that are designed to ensure that information required to be disclosed in our reports under the Exchange Act, is recorded, processed, summarized and reported within the time periods required under the SEC’s rules and forms and that the information is gathered and communicated to our management, including our Chief Executive Officer (Principal Executive Officer) and Chief Financial Officer (Principal Financial Officer), as appropriate, to allow for timely decisions regarding required disclosure.
As required by SEC Rule 15d-15(b), our Chief Executive Officer carried out an evaluation under the supervision and with the participation of our management, of the effectiveness of the design and operation of our disclosure controls and procedures pursuant to Exchange Act Rule 15d-14 as of the end of the period covered by this report. Based on the foregoing evaluation, our Chief Executive Officer and our Chief Financial Officer have concluded that our disclosure controls and procedures are not effective in timely alerting them to material information required to be included in our periodic SEC filings and to ensure that information required to be disclosed in our periodic SEC filings is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, to allow timely decisions regarding required disclosure as a result of the deficiency in our internal control over financial reporting discussed below.
Management’s assessment of the effectiveness of the small business issuer’s internal control over financial reporting is as of the quarter ended July 31, 2017. We believe that internal control over financial reporting is not effective because of the small size of the business. We have not identified any current, material weaknesses considering the nature and extent of our current operations and any risks or errors in financial reporting under current operations.
There was no change in our internal control over financial reporting that occurred during the quarter ended July 31, 2017, that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
| 30 |
The Company assumed liabilities due to a former law firm of $140,000. The law firm has filed suit against the Company and other guarantors to collect its fees, including costs. The Company is presently attempting to settle this matter.
None.
ITEM 2. UNREGISTERED SALES OF EQUITY SECURITIES AND USE OF PROCEEDS.
None.
ITEM 3. DEFAULTS UPON SENIOR SECURITIES.
None.
ITEM 4. MINE SAFETY DISCLOSURES.
None.
None.
Exhibits.
The following is a complete list of exhibits filed as part of this Form 10-Q. Exhibit numbers correspond to the numbers in the Exhibit Table of Item 601 of Regulation S-K.
| 101.INS | XBRL Instance Document (1) | ||
| 101.SCH | XBRL Taxonomy Extension Schema Document (1) | ||
| 101.CAL | XBRL Taxonomy Extension Calculation Linkbase Document (1) | ||
| 101.DEF | XBRL Taxonomy Extension Definition Linkbase Document (1) | ||
| 101.LAB | XBRL Taxonomy Extension Label Linkbase Document (1) | ||
| 101.PRE | XBRL Taxonomy Extension Presentation Linkbase Document (1) |
| (1) Pursuant to Rule 406T of Regulation S-T, this interactive data file is deemed not filed or part of a registration statement or prospectus for purposes of Sections 11 or 12 of the Securities Act of 1933, is deemed not filed for purposes of Section 18 of the Securities Exchange Act of 1934, and otherwise is not subject to liability under these sections. |
| 31 |
Pursuant to the requirements of Section 12 of the Securities and Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| MEDICAL INNOVATION HOLDINGS, INC. | ||
| (Registrant) | ||
| Dated: October 4, 2017 | By: | /s/ Arturo Sanchez |
| Arturo “Jake” Sanchez, | ||
| Chief Executive Officer | ||
| (Principal Executive Officer) | ||
| 32 |