Attached files
| file | filename |
|---|---|
| 8-K - 8-K - PIERIS PHARMACEUTICALS, INC. | d266594d8k.htm |
Exhibit 99.1
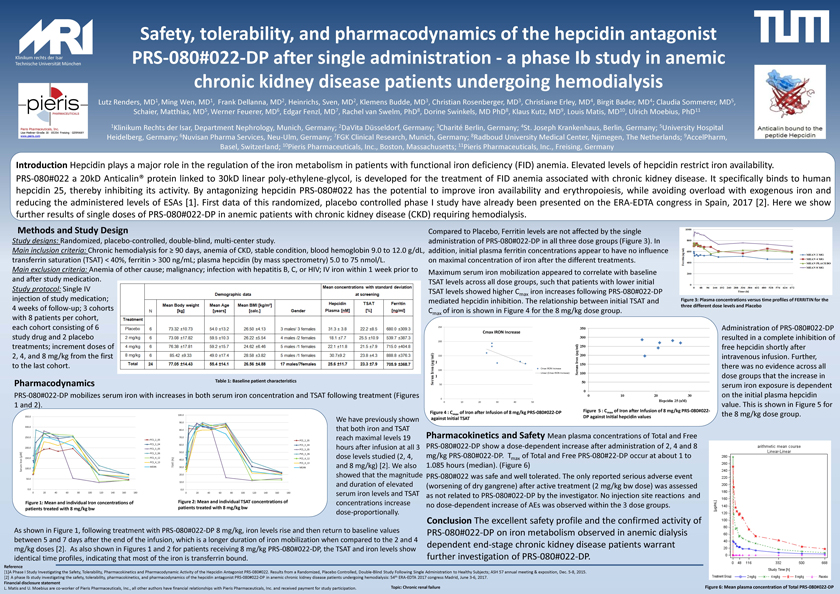
Klinikum rechts der Isar Technische Universität München Safety, tolerability, and pharmacodynamics of the hepcidin antagonist PRS-080#022-DP after single administration -a phase Ib study in anemic chronic kidney disease patients undergoing hemodialysisPieris Pharmaceuticals, Inc. Lise-Meitner-Straße 30 l 85354 Freising l GERMANY www.pieris.com There is also evidence that the serum iron exposure is independent from the initial ferritin and initial TSAT values in all dosegroups (Figure 3). Reference[1]APhaseIStudyInvestigatingtheSafety,Tolerability,PharmacokineticsandPharmacodynamicActivityofthe HepcidinAntagonistPRS-080#022.ResultsfromaRandomized,PlaceboControlled,Double-BlindStudyFollowingSingleAdministrationtoHealthySubjects;ASH57annualmeeting&exposition,Dec.5-8,2015. [2]AphaseIbstudyinvestigatingthesafety,tolerability,pharmacokinetics,and pharmacodynamicsofthehepcidinantagonistPRS-080#022-DPinanemicchronickidneydiseasepatients undergoinghemodialysis:54thERA-EDTA2017congressMadrid,June3-6,2017. Financial disclosure statement L.MatisandU.MoebiusarecoworkerofPierisPharmaceuticals,Inc.,allotherauthorshavefinancialrelationshipswithPierisPharmaceuticals, Inc.andreceivedpaymentforstudyparticipation. Topic: Chronic renal failure Lutz Renders, MD1,Ming Wen, MD1,Frank Dellanna, MD2, Heinrichs, Sven, MD2, Klemens Budde, MD3, Christian Rosenberger, MD3, Christiane Erley, MD4, Birgit Bader, MD4; Claudia Sommerer, MD5, Schaier, Matthias, MD5,Werner Feuerer, MD6, Edgar Fenzl, MD7, Rachel van Swelm, PhD8, Dorine Swinkels, MD PhD8, Klaus Kutz, MD9, Louis Matis, MD10, Ulrich Moebius, PhD11 1Klinikum Rechts der Isar, Department Nephrology, Munich, Germany; 2DaVita Düsseldorf, Germany; 3Charité Berlin, Germany; 4St. Joseph Krankenhaus, Berlin, Germany; 5University Hospital Heidelberg, Germany; 6Nuvisan Pharma Services, Neu-Ulm, Germany; 7FGK Clinical Research, Munich, Germany; 8Radboud University Medical Center, Njimegen, The Netherlands; 9AccelPharm, Basel, Switzerland; 10Pieris Pharmaceuticals, Inc., Boston, Massachusetts; 11Pieris Pharmaceuticals, Inc., Freising, Germany IntroductionHepcidinplaysamajorroleintheregulationoftheironmetabolisminpatients withfunctionalirondeficiency(FID)anemia.Elevatedlevelsofhepcidinrestrictironavailability. PRS-080#022a20kDAnticalin®proteinlinkedto30kDlinearpoly-ethylene-glycol,isdevelopedforthetreatmentofFIDanemiaassociatedwithchronickidneydisease. Itspecificallybindstohumanhepcidin25,therebyinhibitingitsactivity.ByantagonizinghepcidinPRS-080#022 hasthepotentialtoimproveironavailabilityanderythropoiesis,whileavoidingoverloadwithexogenousironandreducing theadministeredlevelsofESAs[1].Firstdataofthisrandomized,placebocontrolledphaseIstudyhavealreadybenpresentedonthe ERA-EDTAcongressinSpain,2017[2].HereweshowfurtherresultsofsingledosesofPRS-080#022-DPinanemicpatients withchronickidneydisease(CKD)requiringhemodialysis. Methods and Study Design Studydesigns:Randomized,placebo-controlled,double-blind,multi-centerstudy. Main inclusion criteria: Chronic hemodialysis for ³ 90 days, anemia of CKD, stable condition, blood hemoglobin 9.0 to 12.0 g/dL, transferrin saturation (TSAT) < 40%, ferritin > 300 ng/mL; plasma hepcidin (by mass spectrometry) 5.0 to 75 nmol/L. Main exclusion criteria: Anemia of other cause; malignancy; infection with hepatitis B, C, or HIV; IV iron within 1 week prior to and after study medication. Study protocol:Single IV injection of study medication; 4 weeks of follow-up; 3 cohorts with 8 patients per cohort, each cohort consisting of 6 study drug and 2 placebo treatments; increment doses of 2, 4, and 8 mg/kg from the first to the last cohort. Table 1: Baseline patient characteristics Pharmacodynamics PRS-080#022-DP mobilizes serum iron with increases in both serum iron concentration and TSAT following treatment (Figures 1 and 2). As shown in Figure 1, following treatment with PRS-080#022-DP 8 mg/kg, iron levels rise and then return to baseline values between 5 and 7 days after the end of the infusion, which is a longer duration of iron mobilization when compared to the 2 and 4mg/kg doses [2]. As also shown in Figures 1 and 2 for patients receiving 8 mg/kg PRS-080#022-DP, the TSAT and iron levels show identical time profiles, indicating that most of the iron is transferrin bound. 0.0 50.0 100.0 150.0 200.0 250.0 300.0 350.0 0 20 40 60 80 100 120 140 160 180 PCS_2_05 PCS_3_04 PCS_3_05 PCS_3_06 PCS_4_12 PCS_4_13 MEAN 0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0 100.0 0 20 40 60 80 100 120 140 160 180 PCS_2_05 PCS_3_04 PCS_3_05 PVS_3_06 PCS_4_12 PCS_4_13 MEAN Figure 1: Mean and individual Iron concentrations of patients treated with 8 mg/kg bw Figure 2: Mean and individual TSAT concentrations of patients treated with 8 mg/kg bw We have previously shown that both iron and TSAT reach maximal levels 19 hours after infusion at all 3 dose levels studied (2, 4, and 8 mg/kg) [2]. We also showed that the magnitude and duration of elevated serum iron levels and TSAT concentrations increase dose-proportionally. Compared to Placebo, Ferritin levels are not affected by the single administration of PRS-080#022-DP in all three dose groups (Figure 3). In addition, initial plasma ferritin concentrations appear to have no influence on maximal concentration of iron after the different treatments. Figure 3: Plasma concentrations versus time profiles of FERRITIN for the three different dose levels and Placebo Serum Iron [µM] TSAT (%) There is also evidence that the serum iron exposure is independent from the initial ferritin and initial TSAT values in all dosegroups (Figure 3). 0 50 100 150 200 250 0 10 20 30 40 50 Cmax IRON Increase Cmax IRON Increase Linear (Cmax IRON Increase) Figure 4 : Cmaxof Iron after Infusion of 8 mg/kg PRS-080#022-DP against Initial TSAT Figure 5 : Cmaxof Iron after Infusion of 8 mg/kg PRS-080#022-DP against Initial hepcidin values Maximum serum iron mobilization appeared to correlate with baseline TSAT levels across all dose groups, such that patients with lower initial TSAT levels showed higher Cmaxiron increases following PRS-080#022-DP mediated hepcidin inhibition. The relationship between initial TSAT and Cmax of iron is shown in Figure 4 for the 8 mg/kg dose group. Administration of PRS-080#022-DP resulted in a complete inhibition of free hepcidin shortly after intravenous infusion.Further, there was no evidence across all dose groups that the increase in serum iron exposure is dependent on the initial plasma hepcidin value. This is shown in Figure 5 for the 8 mg/kg dose group. Pharmacokinetics and Safety Mean plasma concentrations of Total and Free PRS-080#022-DP show a dose-dependent increase after administration of 2, 4 and 8 mg/kg PRS-080#022-DP. Tmaxof Total and Free PRS-080#22-DP occur at about 1 to 1.085 hours (median). (Figure 6) PRS-080#022 was safe and well tolerated. The only reported serious adverse event (worsening of dry gangrene) after active treatment (2 mg/kg bw dose) was assessed as not related to PRS-080#022-DP by the investigator. No injection site reactions and no dose-dependent increase of AEs was observed within the 3 dose groups. Figure 6: Mean plasma concentration of Total PRS-080#022-DP Conclusion The excellent safety profile and the confirmed activity of PRS-080#022-DP on iron metabolism observed in anemic dialysis dependent end-stage chronic kidney disease patients warrant further investigation of PRS-080#022-DP.