Attached files
| file | filename |
|---|---|
| EX-32.1 - EXHIBIT 32.1 - BIOSPECIFICS TECHNOLOGIES CORP | ex32_1.htm |
| EX-31.1 - EXHIBIT 31.1 - BIOSPECIFICS TECHNOLOGIES CORP | ex31_1.htm |
| EX-23.1 - EXHIBIT 23.1 - BIOSPECIFICS TECHNOLOGIES CORP | ex23_1.htm |
| EX-21.1 - EXHIBIT 21.1 - BIOSPECIFICS TECHNOLOGIES CORP | ex21_1.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2016
☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from __________________ to __________________
Commission File Number: 001-34236
BIOSPECIFICS TECHNOLOGIES CORP.
(Exact name of registrant as specified in its charter)
|
Delaware
|
11-3054851
|
|
|
(State or other jurisdiction of incorporation or organization)
|
(I.R.S. Employer Identification No.)
|
|
35 Wilbur Street, Lynbrook, NY
|
11563
|
|
|
(Address of principal executive offices)
|
(Zip Code)
|
Registrant’s telephone number, including area code: 516.593.7000
Securities registered under Section 12(b) of the Exchange Act:
|
Title of each class
|
Name of each exchange on which registered
|
|
Common Stock
|
The Nasdaq Global Market
|
Securities registered under Section 12(g) of the Exchange Act: NONE
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
☐Yes ☑No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act.
☐Yes ☑No
Indicate by check mark whether the registrant (1) filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. ☑Yes ☐No
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the Registrant was required to submit and post such files). ☑Yes ☐No
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☑
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer ☐
|
Accelerated filer ☑
|
|
|
Non-accelerated filer ☐
|
(Do not check if a smaller reporting company)
|
Smaller reporting company ☐
|
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). ☐Yes ☑No
The aggregate market value of voting and non-voting common stock held by non-affiliates of the Registrant as of June 30, 2016, the last business day of the registrant’s most recently completed second fiscal quarter, was approximately $214 million.
The number of shares outstanding of the registrant’s common stock as of March 14, 2017 is 7,162,741.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive proxy statement for its 2017 Annual Meeting of Stockholders, which is expected to be filed with the Securities and Exchange Commission not later than 120 days after the end of the registrant’s fiscal year ended December 31, 2016, are incorporated by reference into Part III of this annual report on Form 10-K. With the exception of the portions of the registrant’s definitive proxy statement for its 2017 Annual Meeting of Stockholders that are expressly incorporated by reference into this Annual Report on Form 10-K, such proxy statement shall not be deemed filed as part of this Annual Report on Form 10-K.
|
Page
|
|||
|
6
|
|||
|
Item1.
|
6
|
||
|
Item1A.
|
29
|
||
|
Item1B.
|
57
|
||
|
Item 2.
|
57
|
||
|
Item 3.
|
57
|
||
|
Item 4.
|
57
|
||
|
|
57
|
||
|
Item 5.
|
57
|
||
|
Item 6.
|
60
|
||
|
Item 7.
|
61
|
||
|
Item 7A.
|
71 | ||
|
Item 8.
|
71 | ||
|
Item 9.
|
72
|
||
| Item 9A. | CONTROLS AND PROCEDURES. |
72
|
|
|
Item 9B.
|
72
|
||
|
73
|
|||
|
Item 10.
|
73
|
||
|
Item 11.
|
73 | ||
|
Item 12.
|
73
|
||
|
Item 13.
|
73
|
||
|
Item 14.
|
73
|
||
|
|
74
|
||
|
Item 15.
|
74
|
||
Overview
We are a biopharmaceutical company involved in the development of an injectable collagenase clostridium histolyticum for multiple indications. We currently have a development and license agreement with Endo Global Ventures, a Bermuda unlimited liability company (“Endo Global Ventures”), an affiliate of Endo International plc (“Endo”), for injectable collagenase for marketed indications and indications in development. Endo assumed this agreement when Endo acquired Auxilium Pharmaceuticals, Inc. (“Auxilium”) on January 29, 2015 (the “Acquisition”). Injectable collagenase clostridium histolyticum is marketed as XIAFLEX® (or Xiapex® in Europe).
On August 31, 2011, we entered into the Second Amended and Restated Development and License Agreement (the “License Agreement”) with Auxilium for XIAFLEX. The License Agreement was filed with the Securities and Exchange Commission (the “SEC”) on September 1, 2011 as Exhibit 10.1 to a Current Report on Form 8-K. Auxilium subsequently assigned the License Agreement to Auxilium Bermuda ULC. As a result of the Acquisition and resulting internal restructuring, the counterparty to the agreement is now Endo Global Ventures.
On February 1, 2016, we entered into with Endo the First Amendment (the “First Amendment”) to the Second Amended and Restated Development and Licensing Agreement (the “Auxilium Agreement”), by and between us and Auxilium, now a wholly-owned subsidiary of Endo, to amend certain provisions of the Auxilium Agreement (as amended by the First Amendment, the “License Agreement”). The First Amendment was filed with the SEC on February 5, 2016 as Exhibit 10.1 to a Current Report on Form 8-K. The effective date of the First Amendment was January 1, 2016. Pursuant to the First Amendment, we and Endo mutually agreed that in exchange for a $8.25 million lump sum payment, we will not receive future additional mark-up on cost of goods sold for sales by non-affiliated sublicensees of Endo outside of the U.S.; provided, however, that Endo will still be required to pay a mark-up on cost of goods sold for sales made in the “Endo Territory,” which includes sales made in the U.S. and sales made in any other country where Endo sells the product directly or through affiliated sublicensees. We received this $8.25 million lump sum payment in February 2016 and began recognizing this income over time based on sales by non-affiliated sublicensees of Endo outside of the U.S. according to our revenue recognition policy in the second quarter of 2016.
Additionally, we agreed that Endo may opt-in early to indications, prior to our submission of a clinical trial report, with our consent, such consent not to be unreasonably withheld. For early opt-ins, Endo will be required to make an opt-in payment of $0.5 million on a per indication basis. For regular opt-ins, following our submission of a clinical trial report, Endo will be required to make an opt-in payment of $0.75 million on a per indication basis.
The two marketed indications involving our injectable collagenase are Dupuytren’s contracture and Peyronie’s disease. Prior to the Acquisition, Auxilium had, and after the Acquisition, Endo has, opted-in to the following indications: frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma. Endo exercised, with our consent, an early opt-in for lateral hip fat and plantar fibromatosis in November 2015. Endo opted-in for human lipoma in July 2016. We manage the development of XIAFLEX for uterine fibroids and initiate the development of XIAFLEX in new potential indications, not licensed by Endo.
Endo is currently selling XIAFLEX in the U.S. for the treatment of Dupuytren’s contracture and Peyronie’s disease and has an agreement with Swedish Orphan Biovitrum AB (“Sobi”), pursuant to which Sobi has marketing rights for Xiapex for Dupuytren’s contracture and Peyronie’s disease in Europe and certain Eurasian countries. Sobi is currently selling Xiapex in Europe and certain Eurasian countries for the treatment of Dupuytren’s contracture and Peyronie’s disease. In addition, Endo has an agreement with Asahi Kasei Pharma Corporation (“Asahi”) pursuant to which Asahi has the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Japan. Asahi is selling XIAFLEX for the treatment of Dupuytren’s contracture in Japan. Endo also had an agreement with Actelion Pharmaceuticals Ltd. (“Actelion”), pursuant to which Actelion had the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Canada and Australia. Actelion received regulatory approval in Canada and Australia for XIAFLEX for the treatment of Dupuytren’s contracture and was selling XIAFLEX in Canada and Australia. Endo terminated its agreement with Actelion as of July 4, 2016 and a transitional services agreement was put in place to cover both Canada and Australia. Endo is currently distributing XIAFLEX in Canada through Paladin Labs Inc. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand.
Operational Highlights
Indications
Endo announced on January 9, 2017 at the J.P. Morgan Healthcare Conference, that, despite the change in Endo’s management, XIAFLEX remains a core asset. In addition, on February 28, 2017, in Endo’s earnings release presentation for the year ended December 31, 2016, Endo described XIAFLEX as its “flagship” product.
Endo-Marketed Indications
Dupuytren’s Contracture. Dupuytren’s contracture is a deforming condition of the hand in which the formation of a collagen cord causes one or more fingers to contract towards the palm. On February 2, 2010, we announced that the FDA had approved XIAFLEX for the treatment of adult Dupuytren’s contracture patients with a palpable cord. Auxilium launched XIAFLEX in March 2010. In May 2015, the U.S. Food and Drug Administration, or the FDA, approved a label expansion for XIAFLEX to include the indication of treatment of recurrent contractures. In October 2014, the FDA approved the sBLA for XIAFLEX for the treatment of up to two Dupuytren’s contracture cords in the same hand. The FDA-approved label expansion permits patients with up to two cords to be treated in a single office visit. In November 2015, the European Medicines Agency, or EMA, approved Sobi’s request for label expansion of Xiapex for the treatment of two Dupuytren’s contracture cords concurrently. In July 2014, Asahi successfully submitted an application to the Japanese Pharmaceutical and Medical Device Agency, or PMDA, for the potential approval of XIAFLEX for the treatment of Dupuytren’s contracture in Japan. On July 20, 2015, we announced that Asahi received approval for its regulatory application to the PMDA for XIAFLEX for the treatment of patients with Dupuytren’s contracture in Japan and on August 31, 2015, we announced that XIAFLEX had been listed on the Japanese National Health Insurance, or NHI, drug price standard for treatment of patients with Dupuytren’s contracture. The first commercial sale of XIAFLEX by Asahi for the treatment of Dupuytren’s in Japan occurred in September 2015. XIAFLEX and Xiapex are currently approved in the U.S., EU, Switzerland, Canada, Australia and Japan, among other jurisdictions, for the treatment of Dupuytren’s contracture.
Peyronie’s Disease. Peyronie’s disease is characterized by the presence of inelastic collagen on the shaft of the penis. In December 2013, the FDA approved Auxilium’s sBLA for XIAFLEX for the treatment of Peyronie’s disease. This is the first and only FDA-approved biologic therapy indicated for the treatment of Peyronie’s disease in men with a palpable plaque and a curvature of 30 degrees or greater at the start of therapy. In February 2015, the EU Commission approved Sobi’s expansion to market Xiapex for the treatment of adult men with Peyronie’s disease with a palpable plaque and curvature deformity of at least 30 degrees at the start of therapy. On May 19, 2015, we announced that on May 18, 2015 at the 2015 Annual Meeting of the American Urological Association, or AUA, the AUA presented the first ever treatment guidelines for Peyronie’s disease, recommending the use of XIAFLEX in combination with modeling in patients with stable Peyronie’s disease, penile curvature greater than 30 degrees and less than 90 degrees and intact erectile function. In addition, at the AUA 2015 Annual meeting, Endo presented positive data evaluating the efficacy of XIAFLEX treatment for Peyronie’s disease as well as the impact of Peyronie’s disease on erectile dysfunction and female partners. In October 2015, Xiapex received approval from Swissmedic, the Swiss Agency for Therapeutic Products, for the treatment of adult men with Peyronie’s disease with a palpable plaque and curvature deformity of at least 30 degrees at the start of therapy. XIAFLEX and Xiapex are currently approved in the U.S., EU, Switzerland, Canada and Australia for the treatment of Peyronie’s disease.
Indications that Endo has Under Development
On November 8, 2016, following the change in Endo management, Endo announced as part of its earnings call that a commercial review is ongoing of the XIAFLEX exercised but non-marketed indications, including frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma, so that Endo can best prioritize its R&D efforts and determine clinical trial timelines moving forward.
Frozen Shoulder (Adhesive Capsulitis). Frozen shoulder is a clinical syndrome of pain and decreased motion in the shoulder joint resulting from inflammation and thickening of the shoulder capsule due to collagen. Auxilium reported positive top-line data in the first quarter of 2013 from its Phase 2a clinical trial of XIAFLEX for the potential treatment of frozen shoulder. In December 2013, Auxilium dosed the first patient in its Phase 2b study of XIAFLEX for the treatment of frozen shoulder. On March 12, 2015, Endo provided an update on the results of the Phase 2b study, which Auxilium had initiated, without releasing all of the data. The data released showed an increased and unexpectedly robust placebo effect in those patients who did not receive XIAFLEX. Endo announced that it plans to initiate another Phase 2b study after a discussion with the FDA scheduled to occur in the first quarter of 2016. No FDA-approved pharmaceutical therapies are currently available for the treatment of frozen shoulder syndrome. We are awaiting an update from Endo’s ongoing commercial review.
Cellulite (Edematous Fibrosclerotic Panniculopathy). Edematous fibrosclerotic panniculopathy, commonly known as cellulite, describes a condition, in which lobules of subcutaneous adipose tissue extend into the dermal layer. No FDA-approved pharmaceutical therapies are currently available for the treatment of cellulite. In August 2014, Auxilium announced positive, statistically significant top-line results from the randomized, double-blind Phase 2a study for the treatment of cellulite. The results showed that all three doses of XIAFLEX used in the study, including a low, medium and high dose, demonstrated an improvement in the appearance of cellulite as measured by the trial endpoints of physician and patient-assessed improvements. Endo announced on January 11, 2016 at the J.P. Morgan Healthcare Conference, that Endo had a productive meeting with the FDA in December 2015 concerning its cellulite development program. On February 17, 2016, Endo announced the initiation of a Phase 2b trial of XIAFLEX in cellulite. On November 17, 2016, we announced positive, highly statistically significant results from Endo’s Phase 2b study of XIAFLEX in cellulite. Trial subjects receiving XIAFLEX showed statistically significant levels of improvement in the appearance of the cellulite with treatement, as measured by the trial’s primary endpoint (p<0.001), compared to those subjects receiving placebo. XIAFLEX was well-tolerated in the actively treated subjects with most adverse events being mild to moderate in severity, and primarily limited to the local injection area. Endo announced on January 9, 2017 at the J.P. Morgan Healthcare Conference that it is currently working with the FDA to efficiently and effectively advance their development of XIAFLEX in cellulite into Phase 3.
Dupuytren’s Disease Nodules. The onset of Dupuytren’s contracture is characterized by the formation of nodules in the palm that are composed primarily of collagen. Thus, the presence of single or multiple nodules in the hand is far more prevalent than the eventual presence of contractures. In December 2014, Auxilium completed a Phase 2a, double-blind, randomized, placebo-controlled, dose-ranging study to evaluate the safety and effectiveness of XIAFLEX to treat Dupuytren’s disease nodules. The study produced statistically significant results which Endo announced in June 2015. We are awaiting an update from Endo’s ongoing commercial review.
Canine Lipoma. In July 2014, we submitted the full study report for Chien-804, a placebo-controlled, double-blind, randomized Phase 2 trial evaluating the efficacy of XIAFLEX in canines with benign subcutaneous lipomas, to Auxilium, which resulted in an opt-in payment and potential future milestone and royalty payments from Auxilium. In November 2014, Auxilium exercised its option to expand its rights to XIAFLEX to include the potential treatment of canine lipomas. Endo is responsible for further development of this indication, but has not yet announced its plans for the indication.
Lateral Hip Fat. Lateral hip fat accumulation is common among women particularly as they age and it is often very difficult to improve its appearance through exercise and diet alone. Patients frequently avoid exercise and are unable to restrict their caloric intake. In some cases, cyrolipolysis and liposuction are performed to remove the unsightly fat deposits in the lateral hip. Currently, there are no pharmaceutical products that are labeled for use on lateral hip fat in the U.S. In November 2015, with our consent, Endo exercised an early opt-in for XIAFLEX for this potential indication. Endo is responsible for further development of this indication. We are awaiting an update on Endo’s ongoing commercial review.
Plantar fibromatosis. Plantar fibromatosis or Ledderhose disease is a medical condition characterized by pain and disability caused by the thickening of the feet’s deep connective tissue resulting in the formation of nodules or cords along the tendons of the foot. Patients with plantar fibromatosis often have Dupuytren’s contracture and adhesive capsulitis. Current treatment options include orthotics and anti-inflammatory drugs in the early stages of the disease, steroid injections and surgery in advanced cases. Currently, there are no pharmaceutical products that are approved for use by the FDA in this indication in the U.S. In November 2015, with our consent, Endo exercised an early opt-in for XIAFLEX for this potential indication. Endo is responsible for further development of this indication. We are awaiting an update on Endo’s ongoing commercial review.
Human Lipoma. Lipomas are encapsulated deposits of benign fatty tumors, often detected as bulges under the skin. In the first quarter of 2014, we announced top-line data from the Phase 2 dose escalation clinical trial of XIAFLEX for the treatment of human lipoma. The primary efficacy outcome of active reduction of the visible surface area of the lipoma as measured by caliper was met, combining all patients (p<0.0001). There were no serious adverse events reported during the trial. In August 2014, we initiated our randomized, double-blind, placebo-controlled Phase 2 clinical trial of XIAFLEX for human lipoma. In June 2016, we announced positive, statistically significant top-line results from our placebo-controlled, double-blind Phase 2 clinical trial. This trial, conducted in 19 patients with two or more benign lipomas, met its primary endpoint of reduction in the visible surface area of the target lipomas relative to placebo, as determined by caliper, at six months post injection (and also met all secondary efficacy endpoints). There were no serious adverse events reported during the trial. Endo opted-in for human lipoma in July 2016. We are awaiting an update on Endo’s ongoing commercial review.
BioSpecifics-Managed Indications
Uterine Fibroids. Uterine fibroids are benign tumors that form on the wall of the uterus that contain large amounts of collagen and are associated with significant co-morbidities. Approximately 200,000 hysterectomies and 30,000 myomectomies are performed annually to treat fibroids. Uterine fibroids have been estimated to result in direct costs of $9.4 billion annually in the U.S., including costs for surgery, hospital admissions, outpatient visits and medications. In October 2014, we announced that a paper titled, “Stiffness of Human Uterine Fibroids is Reduced After Treatment with Purified Clostridial Collagenase due to Collagen Degradation” was presented at the Mechanotransduction in the Reproductive Tract conference hosted by the Campion Fund of the Phyllis and Mark Leppert Foundation for Fertility Research in Durham, North Carolina. The promising preclinical data, resulting from a collaboration with Duke Medicine, showed that highly purified collagenase can reduce the rigidity of human uterine fibroid tissue and potentially shrink uterine fibroid tumors by interrupting the accumulation of poorly aligned and altered collagen. In May 2016, we announced that an article titled, “Loss of Stiffness in Collagen-Rich Uterine Fibroids after Digestion with Purified Collagenase Clostridium Histolyticum” was published in the May 2016 issue of American Journal of Obstetrics & Gynecology. The study, led by Dr. Phyllis Leppert, Professor of Obstetrics and Gynecology at Duke University School of Medicine, showed reduction in stiffness and demonstrated the benefits of XIAFLEX as a potential non-surgical treatment for uterine fibroid patients. We expect to initiate a clinical trial in the first quarter of 2017.
The following sections describe the clinical development and commercialization activities for marketed indications and indications in development.
Background on Collagenase
Collagenase is the only protease that can hydrolyze the triple helical region of collagen under physiological conditions. The specific substrate collagen comprises approximately one-third of the total protein in mammalian organisms, and it is the main constituent of skin, tendon, and cartilage, as well as the organic component of teeth and bone. The body relies on endogenous collagenase production to remove dead tissue, and collagenase production is an essential biological mechanism, which regulates matrix remodeling and the normal turnover of tissue. The Clostridial collagenase produced by us has a broad specificity towards all types of collagen and is acknowledged as much more efficient than mammalian collagenases. Clostridial collagenase cleaves the collagen molecule at multiple sites along the triple helix whereas the mammalian collagenase is only able to cleave the molecule at a single site along the triple helix.
Collagenase is widely used for cell dispersion for tissue disassociation and cell culture because it does not damage the cell membrane. Since the main component of scar tissue is collagen, collagenase has been used in a variety of clinical investigations to remove scar tissue without surgery. Histological and biochemical studies have shown that the tissue responsible for the deformities associated with Dupuytren’s contracture and Peyronie’s disease is primarily composed of collagen.
The two marketed indications involving our injectable collagenase are Dupuytren’s contracture and Peyronie’s disease. Endo has opted-in to develop frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma. Endo exercised its early opt-in for lateral hip fat and plantar fibromatosis in November 2015 and its opt-in for human lipoma in July 2016. We manage the development of XIAFLEX for uterine fibroids and initiate the development of XIAFLEX in new potential indications, not licensed by Endo. ’’
Research and Development of Injectable Collagenase for Multiple Indications
On June 3, 2004, we entered into, and later amended, a development and license agreement with Auxilium pursuant to which we granted to Auxilium an exclusive worldwide license to develop, market and sell products containing our injectable collagenase for the treatment of Dupuytren’s contracture, Peyronie’s disease, frozen shoulder, canine lipoma, cellulite and human lipoma, as well as an exclusive option to develop and license the technology for use in additional indications, such as uterine fibroids, other than dermal formulations labeled for topical administration. We entered into the First Amended and Restated Development and License Agreement on December 11, 2008 in connection with the Development, Commercialization and Supply Agreement, dated December 17, 2008 between an Auxilium subsidiary and Pfizer, Inc. (“Pfizer”). We entered into the License Agreement (the Second Amended and Restated Development and License Agreement) on August 31, 2011. Auxilium then assigned the License Agreement to Auxilium Bermuda ULC. On January 29, 2015 the Acquisition occurred and the License Agreement was assigned to Endo Global Ventures, an affiliate of Endo. We amended the License Agreement once on February 1, 2016.
Endo-Marketed Indications
Collagenase for Treatment of Dupuytren’s Contracture
Dupuytren’s contracture is a deforming condition of the hand in which one or more fingers contract toward the palm, often resulting in physical disability. The onset of Dupuytren’s contracture is characterized by the formation of nodules in the palm that are composed primarily of collagen. As the disease progresses, the collagen nodules begin to form a cord causing the patient’s finger(s) to contract, making it impossible to open the hand fully. Patients often complain about the inability to wash their hands, wear gloves, or grasp some objects. Dupuytren’s contracture is a genetic condition and the incidence of Dupuytren’s contracture is estimated to be between 3% and 9% of the population among adult Caucasians. Dupuytren’s contracture is more common in men than in women, and increases in incidence with age. Well-known individuals with Dupuytren’s contracture include President Ronald Reagan, President George Bush, and Prime Minister Margaret Thatcher.
XIAFLEX is the only drug approved by the FDA, the EMA and the PMDA for the treatment of Dupuytren’s contracture. Prior to FDA approval of XIAFLEX, the only proven treatment for Dupuytren’s contracture was surgery.
Commercialization of XIAFLEX for Dupuytren’s Contracture in the United States
Prior to the Acquisition, Auxilium had been marketing XIAFLEX for the treatment of adult Dupuytren’s contracture patients with a palpable cord since it became available by prescription in March 2010, following Auxilium’s receipt of marketing approval from the FDA. Since the Acquisition, Endo has continued this marketing. The prescribing information for XIAFLEX made available by Auxilium, and now Endo, lists “tendon rupture or other serious injury to the injected extremity,” as well as “pulley rupture, ligament injury, complex regional pain syndrome, sensory abnormality of the hand, and skin laceration (tear),” and one “anaphylactic reaction reported in a post-marketing clinical study in a patient who had previous exposure to XIAFLEX for the treatment of Dupuytren’s contracture” as reported serious adverse reactions to XIAFLEX. The prescribing information for XIAFLEX also states that the most frequently reported adverse drug reactions in XIAFLEX clinical trials included swelling of the injected hand, contusion, injection site reaction, injection site hemorrhage, and pain in the treated extremity. The prescribing information notes that adverse reaction rates observed in clinical trials of a drug may not reflect those observed in practice because such trials “are conducted under widely varying conditions.” As a condition of its approval of XIAFLEX, the FDA and Auxilium had agreed upon a risk evaluation and mitigation strategy, or REMS, program for XIAFLEX, which consists of a communication plan and a medication guide. This REMS program was designed (1) to evaluate and mitigate known and potential risks and serious adverse events; (2) to inform healthcare providers about how to properly inject XIAFLEX and perform finger extension procedures; and (3) to inform patients about the serious risks associated with XIAFLEX. The REMS program is no longer an FDA requirement for Dupuytren’s Contracture only.
In September 2014, Auxilium presented positive safety and efficacy data from the MULTICORD study showing that concurrent injections of XIAFLEX to treat two Dupuytren’s contractures on the same hand reduced fixed flexion contractures and increased range of motion. Delayed manipulation data from the MULTICORD study were also presented which support the ability to vary the time between a XIAFLEX injection and the finger extension procedure from 24, 48 or 72 hours, allowing for greater flexibility for both patients and physicians. Results from the MULTICORD study showed that joints with lower baseline severity showed greater reduction in fixed flexion contractures and higher clinical success rates following concurrent XIAFLEX injections (one injection per treated joint) to two affected joints, compared to those joints with higher baseline severity. Lacerations were more common among patients with more severe pretreatment contractures. A post-hoc analysis of the MULTICORD study examined concurrently treating two affected joints (one injection per treated hand) of the same hand using local anesthesia prior to finger extension, which may result in greater reduction in fixed flexion contractures. Although the risk of skin laceration may be increased with local anesthesia, it was numerically lower when the finger extension was performed at 72 hours as opposed to 24 or 48 hours. All lacerations were treated with wound care or suture placement. Data from an additional study support retreatment of recurrent contractures in joints that were previously treated with XIAFLEX. There were positive outcomes in 85% of retreated joints based on investigator-assessed improvement and patient satisfaction rates. Study results also suggest an improvement in fixed flexion contracture and range of motion in both metacarpophalangeal and proximal interphalangeal joints.
In October 2014, the FDA approved the sBLA for XIAFLEX for the treatment of up to two Dupuytren’s contracture cords in the same hand. The FDA-approved label expansion permits patients with up to two cords to be treated in a single office visit. It is estimated that 35-40% of annual surgical procedures involve two cords.
In May 2015, the FDA approved a label expansion for XIAFLEX to include the indication of treatment of recurrent contractures. The updated U.S. label for XIAFLEX now includes a long-term, observational study demonstrating the rate of recurrence for up to 5 years after successful treatment with XIAFLEX, and the efficacy and safety of retreatment in patients with recurrent Dupuytren’s contracture. The long-term, observational study (referred to as Study 4 in the product label) evaluated the recurrence of contracture and safety at Year 2 to Year 5 in patients who had received up to 8 single injections of XIAFLEX in a previous open-label or double-blind with open-label extension study. A total of 645 patients were enrolled in this study, of whom 30% discontinued the study. Recurrence was assessed in successfully treated joints (i.e., a reduction in contracture to 5 degrees or less 30 days after the last injection of XIAFLEX) and was defined as an increase in joint contracture by at least 20 degrees in the presence of a palpable cord, or the joint underwent medical or surgical intervention primarily to correct a new or worsening Dupuytren’s contracture in that joint. Following successful treatment, the probability of remaining recurrence free was 80% at Year 2 and 50 % at Year 5.
The second study (referred to as Study 5 in the product label) evaluated a subset of patients from Study 4 for a joint that was previously successfully treated but had recurrence. Patients in this study received up to 3 injections of XIAFLEX. Of the 91 patients eligible for the study, 52 enrolled. In the study, 65 % of recurrence in the metacarpophalangeal joints (i.e., the knuckle between the hand and the finger) and 45% of recurrence in the proximal interphalangeal joints (i.e., middle joint of a finger) achieved clinical success after retreatment. No new safety signals were identified among subjects who were retreated with XIAFLEX.
In June 2015, the five-year results from the CORDLESS study were announced. CORDLESS was 5-year noninterventional follow-up study to determine long-term efficacy and safety of XIAFLEX treatment for Dupuytren’s contracture. Patients from previous XIAFLEX clinical studies were eligible. Enrolled patients were evaluated annually for contracture and safety at 2, 3, 4, and 5 years after their first injection (0.58 mg) of XIAFLEX. In successfully treated joints (≤ 5 degrees contracture following XIAFLEX treatment), recurrence was defined as 20 degrees or greater worsening (relative to day 30 after the last injection) with a palpable cord or any medical/surgical intervention to correct new/worsening contracture. A post hoc analysis was also conducted using a less stringent threshold (≥ 30 degrees worsening) for comparison with criteria historically used to assess surgical treatment. Of 950 eligible patients, 644 enrolled (1,081 treated joints). At year 5, 47% (291 of 623) of successfully treated joints had recurrence (≥ 20 degrees worsening)-39% (178 of 451) of metacarpophalangeal and 66% (113 of 172) of proximal interphalangeal joints. At year 5, 32% (198 of 623) of successfully treated joints had 30° or greater worsening (metacarpophalangeal 26% [119 of 451] and proximal interphalangeal 46% [79 of 172] joints). Of 105 secondary interventions performed in the successfully treated joints, 47% (49 of 105) received fasciectomy, 30% (32 of 105) received additional XIAFLEX, and 23% (24 of 105) received other interventions. One mild adverse event was attributed to XIAFLEX treatment (skin atrophy [decreased ring finger circumference from thinning of Dupuytren tissue]). Antibodies to clostridial type I and/or II collagenase were found in 93% of patients, but over the 5 years of follow-up, this did not correspond to any reported clinical adverse events. Five years after successful XIAFLEX treatment, the overall recurrence rate of 47% was comparable with published recurrence rates after surgical treatments, with one reported long-term treatment-related adverse event. Collagenase clostridium histolyticum injection proved to be an effective and safe treatment for Dupuytren contracture. For those receiving treatment during follow-up, both XIAFLEX and fasciectomy were elected options.
Status of Regulatory Approval of XIAFLEX for Dupuytren’s Contracture Outside of the United States
Sobi has exclusive rights to commercialize Xiapex for Dupuytren’s contracture and Peyronie’s disease, subject to applicable regulatory approvals, in 28 EU member countries, Switzerland, Norway, Iceland, 18 Central Eastern Europe/Commonwealth of Independent countries, including Russia and Turkey, and 22 Middle Eastern & North African countries. Sobi Partner Products, a business unit within Sobi, is primarily responsible for the applicable regulatory, clinical and commercialization activities for Xiapex in Dupuytren’s contracture and Peyronie’s disease in these countries. In November 2015, following the October 2014 U.S. approval of the sBLA for XIAFLEX for treatment of up to two Dupuytren’s contracture cords in the same hand during the same office visit, the EU Commission approved Sobi’s label expansion for Xiapex.
In July 2014, Asahi successfully submitted an application to the PMDA for the potential approval of XIAFLEX for the treatment of Dupuytren’s contracture in Japan. In July 2015, Asahi received approval for its regulatory application to the PMDA for XIAFLEX for the treatment of patients with Dupuytren’s contracture in Japan. Asahi has the rights to develop and market XIAFLEX in Japan through an agreement with BioSpecifics’ partner, Endo. In August 2015, XIAFLEX was listed on the Japanese NHI drug price standard for treatment of patients with Dupuytren’s contracture. The first commercial sale of XIAFLEX by Asahi for the treatment of Dupuytren’s contracture in Japan occurred in September 2015.
Endo also had an agreement with Actelion, pursuant to which Actelion has the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture in Canada and Australia. XIAFLEX for the treatment of Dupuytren’s contracture has been approved for sale in Canada and Australia. Endo terminated its agreement with Actelion as of July 4, 2016 and a transitional services agreement was put in place to cover both Canada and Australia. Endo is currently distributing XIAFLEX in Canada through Paladin Labs Inc. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand.
Collagenase for Treatment of Peyronie’s Disease
Peyronie’s disease is characterized by the presence of a collagen plaque on the shaft of the penis, which can distort an erection and make intercourse difficult or impossible in advanced cases. In some mild cases, the plaque can resolve spontaneously without medical intervention. In severe cases, the penis can be bent at a 90-degree angle during erection. Significant psychological distress has been noted in patients with Peyronie’s disease who are sexually active. Frequent patient complaints include increased pain, painful erections, palpable plaque, penile deformity, and erectile dysfunction. Patients with Peyronie’s disease have been reported to have an increased likelihood of having Dupuytren’s contracture, frozen shoulder, plantar fibromatosis, knuckle pads, hypertension and diabetes. Peyronie’s disease is a disease with an initial inflammatory component. This inflammatory phase is poorly understood with a somewhat variable disease course and spontaneous resolution occurring in an estimated 20% of cases. After approximately 12 months of disease, the disease is reported to often develop into a more chronic, stable phase. The incidence of Peyronie’s disease is estimated between 3% and 9% of the population; however, the disease is believe to be underdiagnosed and undertreated. (See L.A. Levine Peyronie’s Disease: A Guide to Clinical Management. Humana Press: 10-17, 2007). The cause of Peyronie’s disease is unknown, although some investigators have proposed that it may be due to trauma or an autoimmune component. A number of researchers have suggested that the incidence of Peyronie’s disease has increased due to the use of erectile dysfunction drugs. Based on U.S. historical medical claims data, it is estimated that around 95,000 patients are diagnosed with Peyronie’s disease every year.
Approval by the FDA and the EMA
In December 2013, the FDA approved the sBLA submitted by Auxilium for XIAFLEX, an in-office, biologic for the treatment of Peyronie’s disease. This is the first and only FDA-approved biologic therapy indicated for the treatment of Peyronie’s disease in men with a palpable plaque and a curvature of 30 degrees or greater at the start of therapy. In June 2014, Sobi filed with the EMA to expand the label for Xiapex to include the indication of Peyronie’s disease. In February 2015, the EU Commission approved Sobi’s expansion to market Xiapex for the treatment of adult men with Peyronie’s disease with a palpable plaque and curvature deformity of at least 30 degrees at the start of therapy. In October 2015, Xiapex received approval from Swissmedic, the Swiss Agency for Therapeutic Products for treatment of Peyronie’s disease.
The approval by the FDA of Auxilium’s sBLA for XIAFLEX for the treatment of Peyronie’s disease is based on safety and efficacy data from Auxilium’s Phase 3 clinical trials and other controlled and open label clinical studies in which over 1,000 patients with Peyronie’s disease were enrolled and received over 7,400 injections of XIAFLEX. In the two identical Phase 3 double-blind placebo-controlled studies, XIAFLEX demonstrated statistically significant improvement in the co-primary endpoints of penile curvature deformity and patient-reported bother versus placebo. The approved dose of XIAFLEX for the treatment of Peyronie’s disease is 0.58 mg per injection administered into a Peyronie’s plaque. Up to eight injections (four treatment cycles) may be administered in the course of treatment. Also, a penile modeling procedure is recommended after every treatment cycle of two injections in an effort to further disrupt the plaque. If more than one plaque is present, it should be injected into the plaque causing the curvature deformity.
The approval by the EU Commission of Sobi’s expansion to market Xiapex for the treatment of adult men with Peyronie’s disease with a palpable plaque and curvature deformity of at least 30 degrees at the start of therapy is based on safety and efficacy data from two Phase 3 double-blind placebo-controlled studies, IMPRESS I and II (The Investigation for Maximal Peyronie’s Reduction Efficacy and Safety Studies), which evaluated XIAFLEX for the treatment of Peyronie’s disease and reported that 75% of men with Peyronie’s disease treated with XIAFLEX in the IMPRESS pivotal studies had a clinically meaningful improvement in their penile curvature deformity by the end of the trials. These subjects reported an improvement of 25% or greater in penile curvature deformity. The mean reduction in penile curvature deformity for XIAFLEX subjects in IMPRESS I trial was 38 degrees. Under the terms of the Endo Agreement, we will receive a certain percentage of milestone payments that Sobi pays to Endo as well as royalties from net sales of Xiapex for Dupuytren’s contracture and Peyronie’s disease.
Auxilium created Auxilium Advantage™ to support access to XIAFLEX and provide a single point of contact for health care providers and patients for help accessing the product. Since the Acquisition, Endo has continued this effort. A REMS for XIAFLEX went into effect after the product first received FDA approval in February 2010 for adults with Dupuytren’s contracture with a palpable cord, and Auxilium further collaborated with the FDA to update the REMS with an Elements to Assure Safe Use, or ETASU, for XIAFLEX for the treatment of Peyronie’s disease in men with a palpable plaque and curvature deformity of 30 degrees or greater at the start of therapy. In November 2016, FDA released the REMS for the Dupuytren’s contracture indication only. Now, because of the risks of corporal rupture or other serious penile injury XIAFLEX is only available for the treatment of Peyronie’s disease through a restricted program called the XIAFLEX REMS. Required components of the XIAFLEX REMS Program include the following: (1) Prescribers must be certified with the program by enrolling and completing training in the administration of XIAFLEX treatment for Peyronie’s disease and (2) Healthcare sites must be certified with the program and ensure that XIAFLEX is only dispensed for use by certified prescribers. The serious risks related to XIAFLEX use for treatment of Peyronie’s disease are highlighted in the Boxed Warning within the Full Prescribing Information (the label).
Indications that Endo has Under Development
On November 8, 2016, following the change in Endo management, Endo announced as part of its earnings call that a commercial review is ongoing of the XIAFLEX exercised but non-marketed indications, including frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma, so that Endo can best prioritize its R&D efforts and determine clinical trial timelines moving forward. We are awaiting an update on Endo’s ongoing commercial review.
Collagenase for Treatment of Frozen Shoulder Syndrome (Adhesive Capsulitis)
Frozen shoulder syndrome is a clinical syndrome of pain and decreased motion in the shoulder joint which results from inflammation and thickening of the shoulder capsule due to collagen. It is estimated to affect 20 to 50 million people worldwide with a slightly higher incidence in women. It is estimated that 300,000 cases of frozen shoulder syndrome are diagnosed annually in the U.S. It typically occurs in adults between the ages of 40-70. It is estimated that 20% of diabetics have frozen shoulder syndrome. No FDA-approved pharmaceutical therapies are currently available for the treatment of frozen shoulder. The most common treatments for frozen shoulder syndrome are longer-term extensive physical therapy, manipulation under anesthesia, corticosteroids and/or arthroscopy, and some drugs are used to manage pain.
Phase 2
In the first quarter of 2013, Auxilium reported the top-line results of its Phase 2a study. The Phase 2a study was an open-label, controlled dose-ranging study designed to assess the safety and efficacy of XIAFLEX for the treatment of Stage 2 unilateral idiopathic frozen shoulder in comparison to an exercise-only control group. The study involved 50 adult men and women at 11 sites throughout the U.S. Four cohorts of 10 patients each received up to three ultrasound-guided extraarticular injections of varying doses of XIAFLEX (ranging from 0.29 mg to 0.58 mg in three different volumes; 0.5, 1.0, or 2.0 ml), separated by a minimum of 21 days. All patients were instructed to perform home shoulder exercises. The fifth cohort of ten patients received no XIAFLEX injections and only performed home shoulder exercises. The study’s primary endpoint was the change (in degrees) from baseline to the day 92 follow-up in active forward flexion in the affected shoulder compared to the exercise-only cohort. Safety assessments were made during all study visits and immunogenicity testing was performed at screening and day 92.
Both the 0.58mg (1ml) and 0.58mg (2ml) dosing arms showed positive, statistically significant improvement from baseline in forward flexion vs. the exercise-only group. The 0.58mg (1ml) dosing arm also showed statistically significant improvement from baseline in shoulder abduction vs. the exercise-only group. Positive trends with improvement in degrees were also seen in other active range of motion, AROM, assessments vs. the exercise-only group. Twenty-nine study patients (72.5%) received three XIAFLEX injections with 5 subjects receiving two injections and 6 subjects receiving one injection only.
Patients were also assessed using the American Shoulder and Elbow Surgeons, or ASES, Scale for function and pain. Both the 0.58 mg(1ml) and 0.58 mg(2ml) cohort demonstrated statistically significant improvement in pain and function over baseline scores vs. the exercise-only group (p<0.05).
Treatment-related adverse events with XIAFLEX were mostly localized bruising, injection site pain and swelling, hematoma, and musculoskeletal pain. All such events resolved without intervention, and are consistent with XIAFLEX use in other approved and potential indications. No subjects discontinued the study due to an adverse event. A shoulder MRI was performed on all patients at screening and day 92. Screening MRIs were performed to exclude the presence of other clinically significant conditions such as concomitant rotator cuff injury. Day 92 MRI evaluations indicated there were no rotator cuff injuries. There were no drug-related serious adverse events reported.
In the fourth quarter of 2013, Auxilium reported that it had initiated a Phase 2b double-blind, placebo-controlled study based on positive, statistically significant results in the Phase 2a study. The Phase 2b study evaluated the safety and efficacy of XIAFLEX for the treatment of Stage 2 unilateral idiopathic frozen shoulder. Following the Acquisition, Endo assumed Auxilium’s responsibilities with respect to the Phase 2b trial. Three hundred twenty one adult men and women were enrolled at approximately 35 sites in the U.S. and Australia. Subjects were randomized 3:1 to receive XIAFLEX or placebo and received up to three ultrasound-guided injections of study drug. Each injection was separated by a minimum of 21 days. All subjects also performed home shoulder exercises after the first injection.
The primary endpoint of the Phase 2b study was change in degrees from baseline to the day 95 follow-up visit in active forward flexion in the affected shoulder compared to placebo. Patients were assessed using the ASES Scale for function and pain as well as additional patient reported outcome measures. Safety assessments will be made during all study visits and immunogenicity testing was performed at screening and at the end of the study.
On March 12, 2015, Endo provided an update on the results of the Phase 2b study without releasing all of the data. Endo noted strong drug effect and similar XIAFLEX patient improvements in flexion, shoulder abduction and external and internal rotation seen across both Phase 2a and 2b trials and similar patient improvement in pain seen across both trials. Endo also noted an increased and unexpectedly robust placebo effect in those patients who did not receive XIAFLEX.
We are awaiting the results of Endo’s ongoing commercial review.
Collagenase for Treatment of Cellulite (Edematous Fibrosclerotic Panniculopathy)
Edematous fibrosclerotic panniculopathy, commonly known as cellulite, describes a condition in which lobules of subcutaneous adipose tissue extend into the dermal layer. Cellulite can involve the loss of elasticity or shrinking of collagen cords, called septae, that attach the skin to lower layers of muscle. When fat in cellulite prone areas swells and expands, the septae tether the skin, which causes surface dimpling characteristic of cellulite. These changes can visibly affect the shape of the epidermis and resemble an orange peel-like dimpling of the skin. (See Avram, Cellulite: a review of its physiology and treatment, Journal of Cosmetic Laser Therapy 2004; 6: 181-185).
Cellulite has been reported to occur in 85-98% (est.) of post-pubertal females and rarely in men, and it is believed to be prevalent in women of all races. (See Avram, Cellulite: a review of its physiology and treatment, Journal of Cosmetic Laser Therapy 2004; 6: 181-185; Khan MH et al. Treatment of cellulite: Part I. Pathophysiology. J Am Acad Dermatol. 2010 Mar;62(3):361-70). Current treatments for cellulite include massage devices, creams, unapproved injectables, laser-based procedures or liposuction. There are no drugs currently approved by the FDA to treat cellulite, and devices cleared by the FDA to treat the condition have varying degrees of success in eliminating cellulite. Cellfina and Cellulaze, the devices of two competitors in the cellulite market, have already received medical device approval. Treatment with XIAFLEX is intended to target and lyse, or break, those collagen tethers with the goal of releasing the skin dimpling and potentially resulting in smoothing of the skin.
In January 2013, Auxilium exercised its exclusive opt-in under the License Agreement to expand the field of its license for injectable collagenase to include the potential treatment of adult patients with cellulite. As a result, we received a one-time license fee payment of $0.5 million, a portion of which we paid to the Research Foundation of the State University of New York at Stony Brook pursuant to the terms of our in-licensing agreement described below in the “In-Licensing and Royalty Agreements” section under the heading “Cellulite”. Auxilium’s license was expanded to include an exclusive, worldwide license, subject to the terms of the License Agreement, which includes all research, development, use, commercialization, marketing, sales and distribution rights for injectable collagenase for the potential treatment of cellulite. Endo assumed this expanded license in the Acquisition.
In October 2013, Auxilium announced the initiation of its Phase 2a study of XIAFLEX for the treatment of cellulite. The Phase 2a study was a randomized, double-blind, multiple-dose study and enrolled approximately 150 women between the ages of 18 and 45 in the U.S. Each subject received up to three treatment sessions of drug or placebo according to randomization (5 high-dose (0.84mg): 5 mid (0.48mg): 5 low (0.06mg): 3 placebo) and each treatment session was approximately 21 days apart. Up to 12 injections were administered into cellulite dimples during each session across an entire treatment quadrant - left or right buttock or left or right posterior thigh. Only the dimples treated on day 1 were able to be retreated on day 22 (Treatment Session 2) and day 43 (Treatment Session 3) if, in the opinion of the investigator, the dimple continued to be evident. A variable number of dimples were able to be treated within one treatment quadrant. The primary trial endpoint was an investigator and a patient score on the Global Aesthetic Improvement Scale, or GAIS, which is an FDA-recognized scale developed as an assessment of degree of improvement and adapted by Auxilium for use in the cellulite study. Investigators and patients used the respective GAIS to compare a day 1 pretreatment digital image of their cellulite to their treatment results. A score of -1 indicated that the results were “Worse.” A score of 0 indicated “No Change.” A score of +1 indicated “Improved.” A score of +2 indicated “Much Improved” and a score of +3 indicated “Very Much Improved.” Additional study endpoints included Physician and Patient-assessed Composite Responder Analyses.
In August 2014, Auxilium announced positive, statistically significant top-line results from the randomized, double-blind Phase 2a study. The results showed that all three doses of XIAFLEX used in the study, including a low, medium and high dose, demonstrated an improvement in the appearance of cellulite as measured by the trial endpoints of physician and patient-assessed improvements. XIAFLEX was well-tolerated by all dose groups with most adverse events being mild to moderate and primarily limited to the local injection area. Specifically, both the mid and high dose groups of XIAFLEX demonstrated a statistically significant improvement in investigators’ assessments of the appearance of cellulite, as measured by GAIS scores, with a p-value of <0.05 versus placebo, as well as in patients’ assessments of the appearance of cellulite, as measured by GAIS scores, with a p-value of <0.02 versus placebo. Sixty-eight percent of both the mid- and high-dose groups reported being “Satisfied” or “Very Satisfied” with their cellulite treatment, compared to only 34% of placebo patients. Both the mid and high dose groups of XIAFLEX demonstrated a statistically significant improvement in the post-hoc composite responder analysis, as measured by combined investigator and patient GAIS scores, with p-values of <0.021 and <0.004, respectively, versus placebo. Eighty-six percent of all related adverse events resolved within 21 days and there was only one serious adverse event in the trial determined to be unrelated to the treatment drug.
On February 17, 2016, Endo announced the initiation of a Phase 2b trial of XIAFLEX in cellulite. The Phase 2b trial enrolled 375 women aged 18 years or older in the U.S. Each subject received three treatment sessions of XIAFLEX (0.84 mg / session) or placebo with each treatment session occurring approximately 21 days apart. Twelve injections were administered into cellulite dimples during each session across an entire treatment quadrant - left or right buttock or left or right posterior thigh. At both the outset and conclusion of treatment, cellulite severity was assessed by each patient and clinician using two photonumeric cellulite severity scales developed by Endo and third-party experts and reviewed by the FDA. The scales - the Photonumeric Cellulite Severity Scale (PCSS) - are 5-point scales ranging from 0 (no cellulite) to 4 (severe cellulite) that measure improvement in the appearance of cellulite. In addition to the patient and physician assessments, an independent, blinded five-member panel of trained aesthetic clinicians evaluated pre-treatment and end-of-study photo images of patients using the PCSS. The Phase 2b trial’s primary endpoint was the proportion of composite responders at Day 71 defined as subjects with a 2-point improvement in severity from baseline in the clinician-rated PCSS (CR-PCSS) and a 2-point improvement in the patient-rated PCSS (PR-PCSS). Additional endpoints include assessment of patient and clinician satisfaction using the Global Aesthetic Improvement Scale (GAIS) and change in the Hexsel cellulite severity scale.
On November 17, 2016, Endo announced positive results from its Phase 2b trial of XIAFLEX in cellulite. Trial subjects receiving XIAFLEX demonstrated a highly statistically significant improvement in the primary endpoint of composite investigators’ and patients’ assessments of the appearance of cellulite, as measured by a two-point improvement in both the CR-PCSS and PR-PCSS scores, with a p-value of <0.001 versus placebo. Subjects receiving XIAFLEX demonstrated a highly statistically significant improvement in the composite investigators’ and patients’ assessments of the appearance of cellulite, as measured by a one-point improvement in both the CR-PCSS and PR-PCSS scores, with a p-value of <0.001 versus placebo. A highly significant proportion of XIAFLEX subjects reported being “Satisfied” or “Very Satisfied” with their cellulite treatment, compared to placebo subjects, with a p-value of <0.001. A highly significant proportion of XIAFLEX subjects were reported as “Improved” or “Very Improved” or “Very Much Improved” in global appearance of their cellulite area as assessed by the subjects and investigators, compared to placebo subjects, with a p-value of <0.001. XIAFLEX was well-tolerated by all dose groups with most adverse events (AEs) being mild to moderate and primarily limited to the local injection area; 92 percent of all related AEs were mild to moderate in the XIAFLEX group compared to 96 percent in the placebo group; the most common AEs were expected and included injection site bruising (approximately 75 percent) and injection site pain (approximately 59 percent). XIAFLEX was well-tolerated in the actively treated subjects with most adverse events AEs being mild to moderate in severity, and primarily limited to the local injection area
On February 28, 2017, in Endo’s earnings release presentation for the year ended December 31, 2016, Endo stated that they plan to initiate Phase 3 in the second half of 2017.
Canine Lipoma
Based on the encouraging results reported in the clinical investigations in human lipoma, we began clinical trials in canine lipoma. As many as 1.7 million canines per year are affected with lipomas in the U.S. Lipomas in older canines are very common, and lipomas that restrict motion in older canines are a serious problem. The only proven therapy for this condition is surgical excision of the lipoma, which necessarily involves the use of general anesthesia. There are approximately 1 million lipomas excised each year from dogs in the U.S.
Chien-804
In December 2013, we announced top-line data from Chien-804, the placebo-controlled, double-blind, randomized Phase 2 trial evaluating the efficacy of XIAFLEX in canines with benign subcutaneous lipomas. The Chien-804 trial enrolled 37 dogs in a single injection study randomized 1:1 XIAFLEX to placebo with lipoma volume being measured by CT scan and lipoma surface area being measured by caliper at baseline, one month and 90 days. The data at 90 days show a post-treatment difference in the mean percent change in lipoma volume by CT scan between the XIAFLEX and placebo-treated groups of -11.58% (p=0.52), which was not statistically significant. The percent change at 90 days in mean visible surface area measured by caliper showed a difference of -44.12% versus 4.0% in the placebo group (p=0.006), which was statistically significant. Among those dogs whose lipomas decreased by 50% or more, the results achieved statistical significance and showed that the visible surface area as measured by caliper decreased by 50% or more in 45.0% of XIAFLEX-treated dogs (9 out of 20) versus 0% of placebo-treated dogs (0 out of 17), with a p-value of 0.0015. A questionnaire administered to pet owners, while blinded to the study, showed 70.0% satisfaction with the results of XIAFLEX treatment versus 23.6% satisfaction with the placebo results (p=0.0027). There were no drug-related serious adverse events reported during the trial. The most frequent treatment-related adverse events were local injection site reactions including bruising, injection site swelling, injection site pain and injection site edema. These adverse events are consistent with those seen previously in clinical experience in humans.
We provided Auxilium with the Chien-804 final study report in July 2014, which triggered the 120 day opt-in period. In November 2014, Auxilium exercised its option to expand its rights to XIAFLEX to include the potential treatment of canine lipomas. Endo is responsible for further development of this indication, but has not yet announced its plans for the indication.
Lateral Hip Fat
Lateral hip fat accumulation is common among women particularly as they age and it is often very difficult to improve its appearance through exercise and diet alone. Patients frequently avoid exercise and are unable to restrict their caloric intake. The prevalence of lateral hip fat is similar to the prevalence of cellulite. In some cases, cyrolipolysis and liposuction are performed to remove the unsightly fat deposits in the lateral hip. There are no pharmaceutical products that are labeled for use on lateral hip fat in the U.S. In November 2015, with our consent, Endo exercised an early opt-in for XIAFLEX for this potential indication. Endo is responsible for further development of this indication. We are awaiting the results of Endo’s ongoing commercial review.
Plantar fibromatosis
Plantar fibromatosis or Ledderhose disease is a medical condition characterized by pain and disability caused by the thickening of the feet’s deep connective tissue resulting in the formation of nodules or cords along the tendons of the foot. Patients with plantar fibromatosis often have Dupuytren’s contracture and adhesive capsulitis. It is estimated that there are approximately 200,000 patients in the U.S. Treatment may include orthotics and anti-inflammatory drugs in the early stages of the disease, steroid injections and surgery in advanced cases. There are no pharmaceutical products that are FDA approved for use in this indication in the U.S. In November 2015, with our consent, Endo exercised an early opt-in for XIAFLEX for this potential indication. Endo is responsible for further development of this indication. We are awaiting the results of Endo’s ongoing commercial review.
Human Lipoma
Lipomas are benign fatty tumors that occur as bulges under the skin and affect humans and canines. It is estimated that lipomas are the primary diagnosis in approximately 600,000 human patients in the U.S. annually. The only proven therapy for lipoma treatment is surgery, which is often not practical for patients with multiple lipomas. Twenty percent of patients have multiple lipomas. Based on observations made during preclinical studies that a collagenase injection decreased the size of fat pads in animals, we initiated, monitored and supplied the requisite study drug for a Phase 1 open label clinical trial for the treatment of human lipomas with a single injection of collagenase. Favorable initial results (10 out of 12 patients had a 50-90% reduction in the size of the lipomas) from this trial for the treatment of human lipomas were presented at a meeting of the American Society of Plastic Surgeons.
In January 2014, we announced the top-line data from the Phase 2 dose escalation clinical trial of XIAFLEX for the treatment of human lipoma. This Phase 2 open-label single-center dose escalation study assessed the safety and efficacy of XIAFLEX in 14 patients with lipoma, divided into four dose cohorts. Each patient received a single injection of XIAFLEX in one of four ascending doses based on the current commercial dose of XIAFLEX in marketed indications, ranging from 0.058mg (10% of commercial dose) to 0.44mg (75% of commercial dose). The primary efficacy outcome was a statistically significant (p<0.0001) reduction in lipoma visible surface area as measured by caliper, combining all patients. Data showed patients in the highest dose group (75% of commercial dose) achieved the best efficacy results with an average of 67% reduction of lipoma visible surface area as measured by caliper at six months post-treatment. Additionally, data demonstrated that 75% of patients in the highest dose group achieved reduction of 50% or more in lipoma visible surface area. There were no drug-related serious adverse events reported during the trial. The most frequent treatment-related adverse events were localized to the injection site and included bruising, injection site swelling and injection site pain. These adverse events are consistent with those seen previously in clinical experience.
In August 2014, we initiated our randomized, double-blind, placebo-controlled Phase 2 clinical trial of XIAFLEX for the treatment of lipoma. We completed patient enrollment during the fourth quarter of 2015. The study was conducted at two centers in the U.S. and enrolled 18 adult men and women presenting with at least two benign lipomas of similar size. Subjects were randomized to have two lipomas treated in immediate succession; one with XIAFLEX and one with placebo. The primary endpoint of the Phase 2 clinical trial is the reduction in the measureable surface area of the target lipomas, as determined by caliper, at six months post injection. The secondary efficacy endpoints include responders at six months post injection who show a ≥50% decrease in lipoma surface area relative to baseline between XIAFLEX and placebo, the change in the length of the target lipoma, the relative change in lipoma surface area as measured by caliper at one month and three months, and the relative change in lipoma volume as measured by MRI. The study also gathered qualitative lipoma characteristics and an assessment of patient satisfaction through a questionnaire administered to each subject prior to injection and at each follow-up visit.
In June 2016, we announced positive, statistically significant top-line results from our placebo-controlled, double-blind Phase 2 clinical trial. This trial, conducted in 19 patients with two or more benign lipomas, met its primary endpoint of reduction in the visible surface area of the target lipomas relative to placebo, as determined by caliper, at six months post injection (and also met all secondary efficacy endpoints). 81.3 percent reduction in the visible surface area for patients who received XIAFLEX compared to a 2.1 percent increase for treatment with placebo in the target lipoma, as measured by caliper at six months post-treatment, resulting in an 83.4 percent difference in favor of XIAFLEX (p˂0.0001). 89.5 percent of XIAFLEX patients (17 of 19 patients) were responders at six months post-injection (showed a ≥50% decrease in lipoma visible surface area relative to baseline) compared to 0 percent for placebo (p˂0.0001). The mean decrease in the length of the target lipoma at 6 months was 64.8 percent from baseline for XIAFLEX treated lipomas and 0.2 percent increase for placebo (p<0.0001). As measured by caliper, the mean decrease in lipoma visible surface area at three months was 62.5 percent for XIAFLEX and 0.4 percent increase for placebo (p<0.0001). As measured by caliper, the mean decrease in lipoma visible surface area at one month was 26.8 percent for XIAFLEX and 0.2 percent increase for placebo (p=0.0042). The mean decrease in lipoma volume as measured by MRI at 6 months was 47.2 percent for XIAFLEX treated lipomas and 4.9 percent for placebo (p=0.0013). Patient satisfaction was assessed through a questionnaire administered to each subject prior to injection and at the one, three and six month follow-up visits. For the lipomas that received XIAFLEX treatment, at six months, 57.9 percent of patients reported being very satisfied; 36.8 were somewhat satisfied and zero were not satisfied verses placebo where 21.1 percent were very satisfied; 15.8 percent were somewhat satisfied and 57.9 percent were not satisfied (p=0.0010 in favor of XIAFLEX). There were no drug-related serious adverse events reported during the trial and XIAFLEX was well-tolerated, with no trial dropouts. The most frequent treatment-related adverse events were localized to the injection site and included bruising, injection site swelling/pain and pruritus. These adverse events are consistent with those seen previously in clinical experience.
In August 2016, we announced that Endo opted in to this indication. We are awaiting the results of Endo’s ongoing commercial review.
BioSpecifics-Managed Indications
Uterine Fibroids
Uterine fibroids are benign tumors that form on the wall of the uterus that contain large amounts of collagen and are associated with significant co-morbidities, which can include pain, decreased fertility, pregnancy complications, miscarriage, heavy menstrual bleeding and frequent urination. Uterine fibroids are the primary indication for hysterectomy in the U.S. Approximately 200,000 hysterectomies and 30,000 myomectomies are performed annually to treat fibroids. Uterine fibroids have been estimated to result in direct costs of $9.4 billion annually in the U.S., including costs for surgery, hospital admissions, outpatient visits and medications.
In October 2014, we announced that a paper titled, “Stiffness of Human Uterine Fibroids is Reduced After Treatment with Purified Clostridial Collagenase due to Collagen Degradation” was presented at the Mechanotransduction in the Reproductive Tract conference hosted by the Campion Fund of the Phyllis and Mark Leppert Foundation for Fertility Research in Durham, North Carolina. The data presented showed that highly purified collagenase can reduce the rigidity of human uterine fibroid tissue and potentially shrink uterine fibroid tumors by interrupting the accumulation of poorly aligned and altered collagen. Accumulation of collagen in uterine fibroid tumors is thought to contribute to the many morbidities associated with uterine fibroids. The preclinical results were presented by Dr. Friederike Jayes, D.V.M., Ph.D. of Duke Medicine. In the ex vivo study, uterine fibroid tissues from eight patients were injected with 50 microliters of highly purified XIAFLEX at four different dose levels (0-1-2-4 mg/ml), and compared to uninjected tissue as a control. Following incubation (37º C for 0-24-48-72-96 hours), tissue samples were confirmed for high collagen content through Masson-Trichrome staining and tested by rheometry to measure stiffness. Collagen content degradation was evident at all dose levels after 96 hours and collagen fibrils were undetectable under electron microscopy in tissue treated with the highest dose. Treatment with 1 mg/ml caused statistically significant softening after 24 hours to 4005±608 Pa compared to vehicle-injected controls (7416±801 Pa; p<0.007). The 2 and 4 mg/ml treatments resulted in statistically significant decreased stiffness after 24 hours (3145±689 Pa; p<0.0005) and 96 hours (1440±115 Pa; p<0.0005). A statistically significant decrease in stiffness was achieved with all doses and at all time points.
This collaborative study was conducted by researchers at Duke Medicine including Dr. Jayes and Dr. Phyllis Leppert, a Professor of Obstetrics and Gynecology and Professor of Pathology at Duke Medicine with our support.
In May 2016, we announced that an article titled, “Loss of Stiffness in Collagen-Rich Uterine Fibroids after Digestion with Purified Collagenase Clostridium Histolyticum” was published in the May 2016 issue of American Journal of Obstetrics & Gynecology. The study, led by Dr. Phyllis Leppert, showed reduction in stiffness and demonstrated the benefits of XIAFLEX as a potential non-surgical treatment for uterine fibroid patients.
We expect to initiate a clinical trial in the first quarter of 2017.
Other Clinical Indications
Other clinical indications for which our collagenase injection has been tested include keloids, hypertrophic scars, scarred tendons, glaucoma, herniated intervertebral discs, and as an adjunct to vitrectomy. We are currently evaluating our options for development of additional indications using collagenase.
LICENSING AND MARKETING AGREEMENTS
Endo Agreement
Under the License Agreement, we granted to Auxilium exclusive worldwide rights to develop, market and sell certain products containing our injectable collagenase. Auxilium subsequently assigned the License Agreement to Auxilium Bermuda ULC. Endo acquired Auxilium on January 29, 2015, and a result of the Acquisition and resulting internal restructuring, the counterparty to the agreement is now Endo Global Ventures. On February 1, 2016, we entered into the First Amendment with Endo Global Ventures.
As noted above, on February 1, 2016 we entered into the First Amendment. The First Amendment has an effective date of January 1, 2016. Pursuant to the First Amendment, the Company and Endo Global Ventures mutually agreed that in exchange for an $8.25 million lump sum payment by Endo Global Ventures to the Company, Endo Global Ventures is no longer required to pay an additional mark-up of cost of goods to the Company for sales by non-affiliated sublicensees of Endo Global Ventures outside of the United States; provided, however, that Endo Global Ventures will still be required to pay a mark-up on cost of goods for sales made in the “Endo Territory”, which will always include sales made in the United States and sales made in any other country where Endo Global Ventures sells the product directly or through affiliated sublicensees. The $8.25 million lump sum payment was received by the Company on February 11, 2016, and will be recognized over time based on sales by non-affiliated sublicensees of Endo Global Ventures outside of the U.S.
In addition, pursuant to the First Amendment, the Company and Endo Global Ventures agreed that Endo Global Ventures may opt-in early to indications, prior to the Company’s submission of a clinical trial report, with the Company’s consent, such consent not to be unreasonably withheld (as Endo Global Ventures did previously with the consent of the Company, in the case of lateral hip fat and plantar fibromatosis as documented by a Current Report on Form 8-K filed with the SEC on November 6, 2015). For early opt-ins, Endo Global Ventures will be required to make an opt-in payment of $0.5 million on a per indication basis. For regular opt-ins, Endo Global Ventures will be required to make an opt-in payment of $0.75 million on a per indication basis, following the submission of a clinical trial report. Endo has opted-in to the following indications: frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma.
Pursuant to the Endo Agreement, we are entitled to receive certain up-front licensing and sublicensing fees, and milestone, mark-up on cost of goods sold and royalty payments. Through December 31, 2016, Auxilium and Endo have collectively paid us up-front licensing and sublicensing fees and milestone, mark-up on cost of goods sold and royalty payments under the Endo Agreement of $107.9 million, including Endo’s agreements with Pfizer, Sobi , Asahi and Actelion. In addition to the payments already received by us and to be received by us with respect to the Dupuytren’s contracture indication and Peyronie’s indication, Endo will be obligated to make contingent milestone payments to us, with respect to each of frozen shoulder, cellulite and canine lipoma, lateral hip fat, plantar fibromatosis indications and human lipoma, upon the acceptance of the regulatory filing and upon receipt by Endo, its affiliate or sublicensee of regulatory approval. The remaining contingent milestone payments that may be received, in the aggregate, from Endo in respect of frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma are $6.0 million.
Endo has partnered with Sobi, Asahi and Actelion to commercialize XIAFLEX and Xiapex outside of the United States. Sobi has exclusive rights to commercialize Xiapex for Dupuytren's contracture and Peyronie's disease, subject to applicable regulatory approvals, in 28 EU member countries, Switzerland, Norway, Iceland, 18 Central Eastern Europe/Commonwealth of Independent countries, including Russia and Turkey, and 22 Middle Eastern & North African countries. Sobi, via its Partner Products business unit, is primarily responsible for the applicable regulatory, and commercialization activities for Xiapex in Dupuytren's contracture and Peyronie's disease in these countries. Endo has granted to Asahi the exclusive right to develop and commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Japan. Endo had granted to Actelion the exclusive right to develop and commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Canada and Australia. Endo terminated its agreement with Actelion as of July 4, 2016 and a transitional services agreement was put in place to cover both Canada and Australia. Endo is currently distributing XIAFLEX in Canada through Paladin Labs Inc. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand.
Pursuant to the Endo Agreement, we will receive a certain percentage of milestone payments that each of Sobi, Asahi and Actelion pays to Endo. We will also receive royalties from net sales in Sobi, Asahi and Actelion territories from Endo, which will be a specified percentage of what Endo receives from Sobi, Asahi and Actelion. To the extent Endo enters into an agreement or agreements related to Dupuytren’s contracture and Peyronie’s disease in other territories, the percentage of sublicense income that Endo would pay us will depend on the territory, the stage of development and approval of XIAFLEX for the particular indication at the time such other agreement or agreements are executed. Pursuant to the First Amendment, BioSpecifics no longer receives a mark-up on COGS for sales made by Endo outside of the U.S. to unaffiliated parties; provided however that if the sale is made outside of the U.S. by Endo directly, Endo is still required to pay us a mark-up on COGS.
Endo must pay us on a country-by-country and product-by-product basis a low double digit royalty as a percentage of net sales for products covered by the Endo Agreement and sold in the United States, Europe, Canada, Australia and certain Eurasian countries and Japan. In the case of products covered by the Endo Agreement and sold in other countries, or the Rest of the World (as defined in the Endo Agreement), Endo must pay us on a country-by-country and product-by-product basis a specified percentage of the royalties it is entitled to receive from a partner or partners with whom it has contracted for such countries. The royalty rate is independent of sales volume and clinical indication in the United States, Europe, Canada, Australia and certain Eurasian countries and Japan, but is subject to set-off in those other countries and the Rest of the World for certain expenses we owe to Endo relating to certain development and patent costs. In addition, the royalty percentage may be reduced if (i) market share of a competing product exceeds a specified threshold; or (ii) Endo is required to obtain a license from a third party in order to practice our patents without infringing such third party’s patent rights. To date, neither Auxilium nor Endo has paid any royalties to third parties. In addition, if Endo out-licenses to a third party, then we will receive a specified percentage of certain payments made to Endo in consideration of such out-licenses.
These royalty obligations extend, on a country-by-country and product-by-product basis, for the longer of the patent life (including pending patents), the expiration of any regulatory exclusivity period based on orphan drug designation or foreign equivalent thereof or June 3, 2016. Endo may terminate the Endo Agreement upon 90 days prior written notice. If Endo terminates the Endo Agreement other than because of an uncured, material breach by us, all rights revert to us. Pursuant to our August 31, 2011 settlement agreement with Endo, we are now co-owners and two of our employees will be co-inventors of U.S. Patent No. 7,811,560 and any continuations and divisionals thereof. We expect that this patent will expire in July 2028.
On top of the payments set forth above, as a result of the First Amendment, Endo must pay to us an amount equal to a specified mark-up of the cost of goods sold for products sold in the Endo Territory, which will always include sales made in the United States and sales made in any other country where Endo Global Ventures sells the product directly or through affiliated sublicensees. Pursuant to the First Amendment, in exchange for the $8.25 million lump sum payment, Endo is no longer required to pay for costs of goods sold for sales within the Partner II Territory or the Japan Territory (as defined in the Endo Agreement).
Endo is generally responsible, at its own cost and expense, for developing the formulation and finished dosage form of products and arranging for the clinical supply of products. Endo is generally responsible for all clinical development and regulatory costs for Peyronie’s disease, Dupuytren’s contracture, frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis, human lipoma and all additional indications for which it exercises its options.
A redacted copy of the License Agreement was filed on Form 8-K with the Securities and Exchange Commission, or the SEC, on September 1, 2011. A redacted copy of the First Amendment was filed on Form 8-K with the SEC, on February 5, 2016. The foregoing descriptions of the License Agreement and the First Amendment do not purport to be complete and are qualified in their entirety by reference to the full text of the License Agreement and the First Amendment.
In-Licensing and Royalty Agreements
We have entered into several in-licensing and royalty agreements with various investigators, universities and other entities throughout the years. It is the policy of the Company not to announce publicly royalty rates for potential future indications under development before commercialization. It is important to emphasize that in-licensing royalty rates vary from indication to indication and it should not be assumed that the in-licensing royalty rates for potential future indications will be the same as those for currently marketed indications.
Dupuytren’s Disease
On November 21, 2006, we entered into a license agreement (the “Dupuytren’s License Agreement”), with the Research Foundation of the State University of New York at Stony Brook, or the Research Foundation, pursuant to which the Research Foundation granted to us and our affiliates an exclusive worldwide license, with the right to sublicense to certain third parties, to know-how owned by the Research Foundation related to the development, manufacture, use or sale of (i) the collagenase enzyme obtained by a fermentation and purification process, the Enzyme, and (ii) all pharmaceutical products containing the Enzyme or injectable collagenase, in each case to the extent it pertains to the treatment and prevention of Dupuytren’s disease.
In consideration of the license granted under the Dupuytren’s License Agreement, we agreed to pay to the Research Foundation certain royalties on net sales (if any) of pharmaceutical products containing the Enzyme or injectable collagenase for the treatment and prevention of Dupuytren’s disease, each a Dupuytren’s Licensed Product.
Our obligation to pay royalties to the Research Foundation with respect to sales by us, our affiliates or any sublicensee of any Dupuytren’s Licensed Product in any country (including the U.S.) arises only upon the first commercial sale of such Dupuytren’s Licensed Product on a country-by-country basis. The royalty rate is 0.5% of net sales. Our obligation to pay royalties to the Research Foundation will continue until the later of (i) the expiration of the last valid claim of a patent pertaining to the Dupuytren’s Licensed Product; (ii) the expiration of the regulatory exclusivity period conveyed by the FDA’s Office of Orphan Products Development, or the OOPD, with respect to the Dupuytren’s Licensed Product; or (iii) June 3, 2016.
Unless terminated earlier in accordance with its termination provisions, the Dupuytren’s License Agreement and the licenses granted under that agreement will continue in effect until the termination of our royalty obligations. After that, all licenses granted to us under the Dupuytren’s License Agreement will become fully paid, irrevocable exclusive licenses.
A redacted copy of the Dupuytren’s License Agreement was filed on Form 8-K with the SEC on November 28, 2006. The foregoing descriptions of the Dupuytren’s License Agreement do not purport to be complete and are qualified in their entirety by reference to the full text of the Dupuytren’s License Agreement.
Peyronie’s Disease
On August 27, 2008, we entered into an agreement with Dr. Martin K. Gelbard to improve the deal terms related to our future royalty obligations for Peyronie’s disease by buying down our future royalty obligations with a one-time cash payment. On March 31, 2012, we entered into an amendment to this agreement, which enables us to buy down a portion of our future royalty obligations in exchange for an initial cash payment and five additional cash payments. We are currently making the payments to buy down the future royalty obligations, which royalty obligations terminate 5 years after first commercial sale.
A redacted copy of the amendment was filed on Form 8-K/A with the SEC on August 8, 2012. The foregoing descriptions of the agreement with Dr. Gelbard and the amendment to that agreement do not comport to be complete and are qualified in their entirety by reference to the full text of that agreement, as amended.
Frozen Shoulder
On November 21, 2006, we entered into a license agreement (the “Frozen Shoulder License Agreement”) with the Research Foundation, pursuant to which the Research Foundation granted to us and our affiliates an exclusive worldwide license, with the right to sublicense to certain third parties, to know-how owned by the Research Foundation related to the development, manufacture, use or sale of (i) the Enzyme and (ii) all pharmaceutical products containing the Enzyme or injectable collagenase, in each case to the extent it pertains to the treatment and prevention of frozen shoulder.
Additionally, the Research Foundation granted to us an exclusive license to the patent applications in respect of frozen shoulder. The license granted to us under the Frozen Shoulder License Agreement is subject to the non-exclusive license (with right to sublicense) granted to the U.S. government by the Research Foundation in connection with the U.S. government’s funding of the initial research.
In consideration of the license granted under the Frozen Shoulder License Agreement, we agreed to pay to the Research Foundation certain royalties on net sales (if any) of pharmaceutical products containing the Enzyme or injectable collagenase for the treatment and prevention of frozen shoulder, each a Frozen Shoulder Licensed Product. In addition, we and the Research Foundation will share in any milestone payments and sublicense income received by us in respect of the rights licensed under the Frozen Shoulder License Agreement.
Our obligation to pay royalties to the Research Foundation with respect to sales by us, our affiliates or any sublicensee of any Frozen Shoulder Licensed Product in any country (including the U.S.) arises only upon the first commercial sale of a Frozen Shoulder Licensed Product. Our obligation to pay royalties to the Research Foundation will continue until, the later of (i) the expiration of the last valid claim of a university patent pertaining to a Frozen Shoulder Licensed Product or (ii) June 3, 2016.
Unless terminated earlier in accordance with its termination provisions, the Frozen Shoulder License Agreement and licenses granted under that agreement will continue in effect until the termination of our royalty obligations. After that, all licenses granted to us under the Frozen Shoulder License Agreement will become fully paid, irrevocable exclusive licenses.
In connection with the execution of the Dupuytren’s License Agreement and the Frozen Shoulder License Agreement, we made certain up-front payments to the Research Foundation for working on the Dupuytren’s disease and frozen shoulder indications for the Enzyme.
A redacted copy of the Frozen Shoulder License Agreement was filed on Form 8-K with the SEC on November 28, 2006. The foregoing descriptions of the Frozen Shoulder License Agreement do not purport to be complete and are qualified in their entirety by reference to the full text of the Frozen Shoulder License Agreement.
Cellulite
We have two in-licensing and royalty agreements related to cellulite. One is a license agreement (“Cellulite License Agreement”), with the Research Foundation that we entered into on August 23, 2007. Pursuant to the Cellulite License Agreement, the Research Foundation granted to us and our affiliates an exclusive worldwide license, with the right to sublicense to certain third parties, to know-how owned by the Research Foundation related to the manufacture, preparation, formulation, use or development of (i) the Enzyme and (ii) all pharmaceutical products containing the Enzyme, which are made, used and sold for the prevention or treatment of cellulite. Additionally, the Research Foundation granted to us an exclusive license to the patent applications in respect of cellulite. The license granted to us under the Cellulite License Agreement is subject to the non-exclusive license (with right to sublicense) granted to the U.S. government by the Research Foundation in connection with the U.S. government’s funding of the initial research.
In consideration of the license granted under the Cellulite License Agreement, we agreed to pay to the Research Foundation certain royalties on net sales (if any) of pharmaceutical products containing the Enzyme, which are made, used and sold for the prevention or treatment of cellulite, each a Cellulite Licensed Product. In addition, we and the Research Foundation will share in any milestone payments and sublicense income received by us in respect of the rights licensed under the Cellulite License Agreement. We paid a portion of the $0.5 million milestone payment we received from Auxilium in respect of its exercise of cellulite as an addition indication under the License Agreement, subject to certain credits for certain up-front payments we made to the Research Foundation.
Our obligation to pay royalties to the Research Foundation with respect to sales by us, our affiliates or any sublicensee of any Cellulite Licensed Product in any country (including the U.S.) arises only upon the first commercial sale of a Cellulite Licensed Product. Our obligation to pay royalties to the Research Foundation will continue until, the later of (i) the expiration of the last valid claim of a patent pertaining to a Cellulite Licensed Product or (ii) June 3, 2016. Valid claim is defined only to include an issued Research Foundation patent.
Unless terminated earlier in accordance with its termination provisions, the Cellulite License Agreement and licenses granted under that agreement will continue in effect until the termination of our royalty obligations. After that, all licenses granted to us under the Cellulite License Agreement will become fully paid, irrevocable exclusive licenses.
The other in-licensing and royalty agreement we have related to cellulite is a license agreement with Dr. Zachary Gerut that we entered into on March 27, 2010 (the “Gerut License Agreement”). Pursuant to the Gerut License Agreement, Dr. Gerut granted to us and our affiliates an exclusive worldwide license, with the right to sublicense to certain third parties to know-how owned by Dr. Gerut related to the manufacture, preparation, formulation, use or development of (i) the Enzyme and (ii) all pharmaceutical products containing the Enzyme or injectable collagenase, in each case to the extent it pertains to the treatment of fat. As the in-license granted in the Gerut License Agreement pertains to the treatment of fat, this in-license also relates to human lipoma and canine lipoma.
In consideration of the license granted under the Gerut License Agreement, we agreed to pay to Dr. Gerut certain royalties on net sales (if any) of pharmaceutical products containing the Enzyme which are made, used and sold for the removal or treatment of fat in humans or animals, each a Gerut Licensed Product. In addition, in the event the FDA approves a Gerut Licensed Product, we agreed to make a one-time stock option grant to Dr. Gerut with a strike price equal to the closing trading price on the day before the date of such grant.
Our obligation to pay royalties to Dr. Gerut with respect to sales by us, our affiliates or any sublicensee of any Gerut Licensed Product in any country (including the U.S.) arises only upon the first commercial sale of a Gerut Licensed Product. Our obligation to pay royalties to Dr. Gerut will continue until June 3, 2016 or such longer period as we continue to receive royalties for such Gerut Licensed Product.
Unless terminated earlier in accordance with its termination provisions, the Gerut License Agreement and licenses granted under that agreement will continue in effect until the termination of our royalty obligations. After that, all licenses granted to us under the Gerut License Agreement will become fully paid, irrevocable exclusive licenses.
Redacted copies of the Cellulite License Agreement and the Gerut License Agreement were filed on our Form 10-K filed with the SEC on March 15, 2013. The foregoing descriptions of the Cellulite License Agreement and the Gerut License Agreement do not purport to be complete and are qualified in their entirety by reference to the full text of these agreements.
Other Indications
We may enter into certain other license and royalty agreements with respect to other indications that we may elect to pursue.
COMPETITION
We and our licensees face worldwide competition from larger pharmaceutical companies, specialty pharmaceutical companies and biotechnology firms, universities and other research institutions and government agencies that are developing and commercializing pharmaceutical products. Many of our competitors have substantially greater financial, technical and human resources than we have and may subsequently develop products that are more effective, safer or less costly than any products that we have developed, are developing, or will develop, or that are generic products. Our success will depend on our ability to acquire, develop and commercialize products and our ability to establish and maintain markets for our products that receive marketing approval. Our marketed indication, Peyronie’s disease, currently enjoys Orphan Drug Protection until December 6, 2020. Orphan drug status for Dupuytren’s contracture expired on February 2, 2017. For more information on orphan drug designations, please see the discussion below. We may face greater competition, including from biosimilars, after the expiration of the orphan drug designations and the expiration of the 12 year marketing exclusivity under certain laws as further described below in “Public Health Service Act and Biologics Price Competition and Innovation Act”.
COST OF RESEARCH AND DEVELOPMENT ACTIVITIES
During fiscal years 2016 and 2015, the company invested $1.3 million dollars and $1.0 million dollars, respectively, in R&D activities.
GOVERNMENT REGULATION
Any product labeled for use in humans requires regulatory approval by government agencies prior to commercialization. In particular, human therapeutic products are subject to rigorous preclinical and clinical trials to demonstrate safety and efficacy and other approval procedures of the FDA and similar regulatory authorities in foreign countries, such as the EMA in Europe and the PMDA in Japan. Clinical and preclinical trials must be conducted in accordance with the applicable regulatory standards, good clinical practices, or GCPs, and good laboratory practices, or GLPs, respectively. Various federal, state, local, and foreign statutes and regulations also govern testing, manufacturing, labeling, distribution, storage, and record-keeping related to such products and their promotion and marketing. The process of obtaining these approvals and the compliance with federal, state, local, and foreign statutes and regulations require the expenditure of substantial time and financial resources. Specifically, in the United States, the FDA regulates our products and product candidates as biologics, which are a drug subset.
Clinical trials involve the administration of the investigational product candidate or approved products to human subjects under the supervision of qualified investigators. Each trial must be conducted under an FDA Investigational New Drug Application, or IND. Prior to commencing the first clinical trial with a product candidate, an IND sponsor must submit the results of the preclinical tests and preclinical literature, together with manufacturing information, analytical data, any available clinical data or literature, and proposed clinical study protocols among other things, to the FDA as part of an IND. An IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day time period, notifies the applicant of safety concerns or questions related to one or more proposed clinical trials and places the trial on a clinical hold. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. Clinical holds also may be imposed by the FDA at any time before or during trials due to safety concerns or non-compliance. As a result, submission of an IND may not result in FDA authorization to commence a clinical trial. A separate submission to an existing IND must also be made for each successive clinical trial conducted during product development.
In addition to FDA review and supervision, each trial must also be reviewed, approved and conducted under the auspices of an independent institutional review board, and each trial must include the patient’s informed consent. Clinical trials are conducted under protocols detailing, among other things, the objectives of the study and the parameters to be used in assessing the safety and the effectiveness of the drug. Typically, clinical evaluation involves a time-consuming and costly three-phase sequential process, but the phases may overlap. There are typically multiple studies conducted within any given phase to collect the data necessary to support a marketing application. The recently passed 21st Century Cures Act, however, provides for FDA acceptance of new kinds of data such as patient experience data and, for appropriate indications sought through supplemental marketing applications, data summaries. ’
Information about certain clinical trials, including a description of the study and study results, must be submitted within specific timeframes to the National Institutes of Health, or NIH, for public dissemination on their clinicaltrials.gov website. Moreover, under the 21st Century Cures Act, manufacturers or distributors of investigational drugs for the diagnosis, monitoring, or treatment of one or more serious diseases or conditions must have a publicly available policy concerning expanded access to investigational drugs.
In addition to requirements concerning the conduct of clinical and preclinical trials, the manufacture of investigational biologics for the conduct of human clinical trials is subject to cGMP requirements. Sponsors of clinical trial must provide FDA annual updates on their development program and more frequent reports in the case of serious adverse events. Investigational biologics and active ingredients imported into the United States are also subject to regulation by the FDA relating to their labeling and distribution. Further, the export of investigational products outside of the United States is subject to regulatory requirements of the receiving country as well as U.S. export requirements.
Clinical testing may not be completed successfully within any specified time period, if at all. The FDA monitors the progress of all clinical trials that are conducted in the U.S. and may, at its discretion, reevaluate, alter, suspend or terminate the testing based upon the data accumulated to that point and the FDA’s assessment of the risk/benefit ratio to the patient. The FDA can also provide specific guidance on the acceptability of protocol design for clinical trials. The FDA, we or our partners may suspend or terminate clinical trials at any time for various reasons, including a finding that the subjects or patients are being exposed to an unacceptable health risk. The FDA can also request that additional clinical trials be conducted as a condition to product approval. During all clinical trials, physicians monitor the patients to determine effectiveness and/or to observe and report any reactions or other safety risks that may result from use of the drug candidate.
Assuming successful completion of the required clinical trials, drug developers submit the results of preclinical studies and clinical trials, together with other detailed information including information on the chemistry, manufacture and control of the product, to the FDA, in the form of a New Drug Application, or NDA, or a Biologics License Application, or BLA, requesting approval to market the product for one or more indications. In most cases, the NDA/BLA must be accompanied by a substantial user fee. The FDA reviews an NDA or BLA to determine, among other things, whether a product is safe and effective for its intended use.
Before approving an NDA or BLA, the FDA will inspect the facility or facilities where the product is manufactured as well as selected clinical trial sites. The FDA will not approve the NDA or BLA unless Current Good Manufacturing Practices, or cGMP, and GCP compliance is satisfactory. The FDA will issue an approval letter if it determines that the NDA or BLA, clinical trial conduct, manufacturing process and manufacturing facilities are acceptable. If the FDA determines that the NDA or BLA, clinical trial conduct, manufacturing process or manufacturing facilities are not acceptable, it will outline the deficiencies in a complete response letter and will often request additional testing or information. Notwithstanding the submission of any requested additional information, the FDA ultimately may decide that the NDA or BLA does not satisfy the regulatory criteria for approval and refuse to approve the NDA or BLA“”.
The testing and approval process requires substantial time, effort and financial resources, which may take several years to complete. The FDA may not grant approval on a timely basis, or at all. We or our partners may encounter difficulties or unanticipated costs in our or their efforts to secure necessary governmental approvals, which could delay or preclude us or them from marketing our products. Furthermore, the FDA may prevent a drug developer from marketing a product under a label for its desired indications or place other conditions, including restrictive labeling, on distribution as a condition of any approvals, which may impair commercialization of the product. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval.
If the FDA approves the NDA or BLA, the drug can be marketed to physicians to prescribe in the U.S. FDA, however, may approve product candidates for fewer or more limited indications or uses than requested, may require significant safety warnings, including black box warnings, contraindications, and precautions, may grant approval contingent on the performance of costly post-marketing clinical trials, surveillance, or other requirements, including REMS, to monitor the safety or efficacy of the product, or may approve a product candidate with a label that does not include the labeling claims necessary or desirable for successful commercialization. After approval, the drug developer must comply with a number of post-approval requirements, including delivering periodic reports to the FDA (i.e., annual reports), submitting descriptions of any adverse reactions reported, biological product deviation reporting, and complying with drug sampling and distribution requirements, including tracking and tracing requirements and suspect and illegitimate product investigation and notification requirements, as well as any other requirements set forth in the FDA’s approval (such as the REMS program, which the FDA has required for XIAFLEX and consists of ETASU, and an implementation system). The holder of an approved NDA or BLA is required to provide updated safety and efficacy information and to comply with requirements concerning advertising and promotional labeling.
Also, quality control and manufacturing procedures must continue to conform to cGMP after approval. Drug manufacturers and their subcontractors are required to register their facilities and are subject to periodic unannounced inspections by the FDA to assess compliance with cGMP which impose procedural and documentation requirements relating to manufacturing, quality assurance and quality control. In some case, after a BLA is approved, the product may also be subject to official lot release as a condition of approval. As part of the manufacturing process, the manufacturer is required to perform certain tests on each lot of the product before it is released for distribution. If the product is subject to official release by the FDA, the manufacturer submits samples of each lot of product to the FDA together with a release protocol showing the results of all of the manufacturer’s tests performed on the lot. The FDA may also perform certain confirmatory tests on lots of some products before releasing the lots for distribution by the manufacturer. Changes to the manufacturing process are further strictly regulated and often require prior FDA approval or notification before being implemented. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain compliance with cGMP and other regulatory requirements. The FDA may require post-market testing and surveillance to monitor the product’s safety or efficacy, including additional studies to evaluate long-term effects. There also are continuing annual user fee requirements for any approved products and the establishments at which such products are manufactured.
In addition to studies requested by the FDA after approval, a drug developer may conduct other trials and studies to explore use of the approved drug for treatment of new indications, which require submission of a supplemental or new NDA or BLA and FDA approval of the new labeling claims. The purpose of these trials and studies is to broaden the application and use of the drug and its acceptance in the medical community.
We use, and will continue to use, third party manufacturers to produce our products in clinical quantities. We additionally use third party contract research organizations, clinical trial sites, and outside laboratories to conduct our clinical and preclinical studies. Future FDA inspections may identify compliance issues at our facilities, at the facilities of our contract manufacturers and other third parties or at those of our partners that may disrupt production or distribution, disrupt clinical or preclinical studies, or require substantial resources to correct. In addition, discovery of problems with a product or the failure to comply with requirements may result in restrictions on a product, studies, manufacturer or holder of an approved NDA/BLA, including withdrawal or recall of the product from the market, clinical holds or suspensions, or other voluntary or FDA-initiated action that could delay, prevent, or restrict further marketing or product approval. Newly discovered or developed safety or effectiveness data may require changes to a product’s approved labeling, including the addition of new warnings and contraindications. Also, new government requirements may be established that could delay or prevent regulatory approval of our products under development.
INTELLECTUAL PROPERTY AND RIGHTS
Our success will depend in part on our ability to protect our existing products and the products we acquire or in-license by obtaining and maintaining a strong proprietary position both in the U.S. and in other countries. To develop and maintain such a position, we intend to continue relying upon patent protection, trade secrets, know-how, continuing technological innovations and licensing opportunities. In addition, we intend to seek patent protection whenever available for any products or product candidates and related technology we develop or acquire in the future.
Patents
We are the assignee or licensee of various U.S. patents, which have received patent protection in various foreign countries. Pursuant to our August 31, 2011 settlement agreement with Auxilium, we are now co-owners and two of our employees will be added as co-inventors of U.S. Patent No. 7,811,560, have been added to a pending continuation, and will be named as co-inventors of any further continuations and divisionals thereof. We expect this patent will expire in July 2028. In addition, we have licenses to other pending patent applications. Although we believe these patent applications, if they issue as patents, will provide a competitive advantage, the scope of the patent positions of pharmaceutical firms involves complex legal, scientific and factual questions and, as such, is generally uncertain. In addition, the coverage claimed in a patent application can be significantly reduced before the patent is issued. Consequently, we do not know whether any of our current patent applications, or the products or product candidates we develop, acquire or license will result in the issuance of patents or, if any patents are issued, whether they will provide significant proprietary protection, will be of any value to us or will be challenged, circumvented or invalidated by our competitors or otherwise.
While we attempt to ensure that our product candidates and the methods we employ to manufacture them do not infringe other parties’ patents and proprietary rights, competitors or other parties may assert that we infringe their proprietary rights. Because patent applications in the U.S. and some other jurisdictions can proceed in secrecy until patents issue, third parties may obtain other patents without our knowledge prior to the issuance of patents relating to our product candidates, which they could attempt to assert against us. Also, since publication of discoveries in the scientific or patent literature often lags behind actual discoveries, we cannot be certain of the priority of inventions covered by pending patent applications.
Although we believe that our product candidates, production methods and other activities do not currently infringe the intellectual property rights of third parties, we cannot be certain that a third party will not challenge our position in the future. If a third party alleges that we are infringing its intellectual property rights, we may need to obtain a license from that third party, but there can be no assurance that any such license will be available on commercially acceptable terms or at all. Any infringement claim that results in litigation could result in substantial cost to us and the diversion of management’s attention from our core business. To enforce patents issued, assigned or licensed to us or to determine the scope and validity of other parties’ proprietary rights, we may also become involved in litigation or in interference proceedings declared by the United States Patent and Trademark Office, or USPTO, which could result in substantial costs to us or an adverse decision as to the priority of our inventions. We may be involved in interference and/or opposition proceedings in the future. We believe there will continue to be litigation in our industry regarding patent and other intellectual property rights.
We have licensed to Endo our injectable collagenase for the treatment of Dupuytren’s contracture, Peyronie’s disease, frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma. We have two use patents in the U.S. covering the enzyme underlying our injectable collagenase, one for the treatment of Dupuytren’s contracture, which issued from a reissue proceeding in December 2007, and one for the treatment of Peyronie’s disease. The Dupuytren’s patent would have expired in 2014 if were it not for an extension based on regulatory delay discussed below. Because of the extension it has not expired yet, and the Peyronie’s patent expires in 2019. Both the Dupuytren’s and Peyronie’s patents are limited to the use of the enzyme for the treatment of Dupuytren’s contracture and Peyronie’s disease within certain dose ranges. An application to extend the term of the Dupuytren’s patent to August 22, 2019 based upon regulatory delay in granting approval to sell XIAFLEX was filed in the USPTO on April 1, 2010. On July 17, 2015, the USPTO granted the application extending the expiration date to August 24, 2019.
Orphan Drug Designations
Two indications, Dupuytren’s contracture and Peyronie’s disease, have received orphan drug designation from the OOPD. These indications did not receive the European equivalent of orphan drug designation.
The orphan drug provisions of the Federal Food, Drug, and Cosmetic Act provide incentives to drug and biologics suppliers to develop and supply drugs for the treatment of rare diseases, currently defined as diseases that affect fewer than 200,000 individuals in the U.S. or, for a disease that affects more than 200,000 individuals in the U.S. and for which there is no reasonable expectation that the cost of developing and making available in the U.S. a drug for such disease or condition will be recovered from its sales in the U.S. Under these provisions the holder of the first FDA approval of a designated orphan product will be granted a seven-year period of marketing exclusivity for that product for the orphan indication. In the case of Dupuytren’s contracture, orphan drug status expired on February 2, 2017; in the case of Peyronie’s Disease, orphan drug status expires on December 6, 2020. It would not prevent other drugs from being approved for the same indication. Companies developing orphan drugs may also be eligible for tax credits for expenses associated with clinical trials including a 20 year tax carry-forward, availability of FDA grants, and advice on design of the clinical development plan.
Public Health Service Act and Biologics Price Competition and Innovation Act
XIAFLEX is regulated and marketed as a biologic product pursuant to BLAs. XIAFLEX was licensed based on a determination by the FDA of safety, purity, and potency as required under the Public Health Service Act, or PHSA. In 2010, Congress enacted the Biologics Price Competition and Innovation Act of 2009, or BPCIA, as part of the Healthcare Reform Law, which amended the PHSA to create an abbreviated licensure pathway for products deemed to be biosimilar to or interchangeable with FDA-licensed reference biological products as well as protections for reference biologics.
Under the BPCIA, a reference biologic is granted 12 years of exclusivity from the time of first licensure. During this 12 year period, no application for a biosimilar product can be submitted for four years from the date of licensure of the reference product and FDA may not make a biosimilar product approval effective until the expiration of the 12 years. Not all reference product biologic applications and supplements, however, will qualify for 12 years of exclusivity. For instance, certain changes and supplements to an approved BLA, and subsequent applications filed by the same sponsor, manufacturer, licensor, predecessor in interest, or other related entity do not qualify for the twelve year exclusivity period. The BPCIA also includes provisions to protect reference products that have patent protection. The biosimilar product sponsor and reference product sponsor may exchange certain patent and product information for the purpose of determining whether there should be a legal patent challenge. Based on the outcome of negotiations surrounding the exchanged information, the reference product sponsor may bring a patent infringement suit and injunction proceedings against the biosimilar product sponsor.
Under the BPCIA, following the expiration of a 12-year reference exclusivity period, the FDA may license under section 351(k) of the PHSA a biologic that it determines is biosimilar to or interchangeable with a reference product licensed under section 351(a) of the PHSA. Biosimilarity is defined to mean that the section 351(k) product is highly similar to the reference product notwithstanding minor differences in clinically inactive components and that there are no clinically meaningful differences between the section 351(k) product and the reference product in terms of the safety, purity, and potency of the product. To be considered interchangeable, a product must be biosimilar to the reference product, be expected to produce the same clinical result as the reference product in any given patient, and, if administered more than once to an individual, the risks in terms of safety or diminished efficacy of alternating or switching between use of the product and its reference product is not greater than the risk of using the reference product without such alternation or switch. Interchangeable products may be substituted for the reference product without the intervention of the prescribing doctor.
Once any reference exclusivity period for our BLA-licensed biologics expires, the FDA may make an approval under section 351(k) of the PHSA ’for a biosimilar or interchangeable version of our product effective. Licensure of a biosimilar or interchangeable under section 351(k) generally requires less than the full complement of product-specific preclinical and clinical data required for innovator products licensed under section 351(a). The FDA has considerable discretion over the kind and amount of scientific evidence required to demonstrate biosimilarity and interchangeability’.
Trade Secrets
We also rely on trade secret protection for our confidential and proprietary information. No assurance can be given that others will not independently develop substantially equivalent proprietary information and techniques or otherwise gain access to our trade secrets or disclose such technology or that we can meaningfully protect our trade secrets.
It is our policy to require certain employees, consultants, outside scientific collaborators, sponsored researchers and other advisors to execute confidentiality agreements upon the commencement of employment or consulting relationships with us. These agreements provide that all confidential information developed or made known to the individual during the course of the individual’s relationship with us is to be kept confidential and not disclosed to third parties except in specific circumstances. In the case of employees, the agreements provide that all inventions conceived by the individual shall be our exclusive property. There can be no assurance, however, that these agreements will provide meaningful protection or adequate remedies for our trade secrets in the event of unauthorized use or disclosure of such information.
EMPLOYEES
The Company currently has five employees, who are all full-time employees.
CORPORATE INFORMATION
BioSpecifics Technologies Corp. was incorporated in Delaware in 1990. ABC-NY was incorporated in New York in 1957. Our telephone number is 516-593-7000. Our corporate headquarters are currently located at 35 Wilbur St., Lynbrook, NY 11563, as further described in this Report under “Item 2 - Properties”.
AVAILABLE INFORMATION
We file annual, quarterly and current reports, proxy statements and other information with the SEC. You may read and copy any document we file with the SEC at the SEC’s public reference room at 100 F. Street, N.E., Washington, DC 20549, at prescribed rates. Please call the SEC at 1-800-SEC-0330 for further information on the public reference room. You may also obtain our SEC filings free of charge from the SEC’s Internet website at www.sec.gov.
Our website address is www.biospecifics.com. We make available free of charge through our website’s “Investors Relations” page most of our filings with the SEC, including our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and other information. These reports and information are available as soon as reasonably practicable after such material is electronically filed with, or furnished to, the SEC.
References to these websites do not constitute incorporation by reference of the information contained therein and should not be considered part of this document.
In addition to the other information included in this Report, the following factors should be considered in evaluating our business and future prospects. Any of the following risks, either alone or taken together, could materially and adversely affect our business, financial position or results of operations. If one or more of these or other risks or uncertainties materialize or if our underlying assumptions prove to be incorrect, our actual results may vary materially from what we projected. There may be additional risks that we do not presently know or that we currently believe are immaterial which could also impair our business or financial position.
Please also see the “Special Note Regarding Forward Looking Statements” on page 2 of this Annual Report.
Risks Related to Our Limited Sources of Revenue
We are dependent on Endo for future opt-in, milestone, mark-up on cost of goods sold and royalty payments and there is uncertainty surrounding Endo’s plans for licensed indications and, therefore, decisions made by Endo may negatively impact our financial position.
Our primary sources of revenues are from opt-in, milestone, mark-up on cost of goods sold and royalty payments from Endo under the Endo Agreement. As described in Item 1 above, under the Endo Agreement, in exchange for the right to receive royalties and other payments, we have granted to Endo the right to develop, manufacture, market and sell worldwide products (other than dermal formulations for topical administration) that contain collagenase for the treatment of Dupuytren’s contracture, Peyronie’s disease, frozen shoulder, cellulite, canine lipoma, plantar fibromatosis, lateral hip fat and human lipoma. However, we have no control over Endo’s ability to successfully market, sell and manufacture products for the treatment of Dupuytren’s contracture and Peyronie’s disease, or, in the case of frozen shoulder, cellulite, canine lipoma, plantar fibromatosis, lateral hip fat and human lipoma, to pursue commercialization, and we may receive limited, if any, royalty payments from Endo. We have no control over Endo’s future plans for any licensed indications. We have received in the past, and are entitled to receive in the future, certain milestone payments from Endo in respect of its efforts to commercialize products, but we have no control over Endo’s ability to achieve the milestones. As also described in Item 1 above, Endo has sublicensed to third parties some of the development and commercialization rights it licenses from us. We have received in the past a percentage of sublicense income that Endo receives from these third parties based on the achievement of certain regulatory and sales related milestones. There is no guarantee that these third parties will continue to pursue development and commercialization of XIAFLEX (or Xiapex in Europe). If any third party stops pursuing such development and commercialization, sublicense income would no longer be payable to Endo or us.
Even if Endo or its sublicensees pursues development and commercialization, there is no guarantee that the FDA or equivalent foreign regulatory body will approve XIAFLEX for a given indication or that commercialization will be successful, if the FDA or equivalent foreign regulatory body does approve XIAFLEX for a given indication. Moreover, under the Endo Agreement, royalty payments are subject to set-off for certain expenses we owe Endo related to development and patent costs. We anticipate that the amount of royalties due to us will exceed the amount of any set-offs on a going forward basis.
In addition, we have granted to Endo an opt-in right to expand its license and development rights to one or more additional indications for injectable collagenase not currently licensed to Endo, including for the treatment of uterine fibroids. Endo may exercise its opt-in prior the Company’s submission of a clinical trial report to Endo, with the Company’s consent. Alternatively, Endo may opt-in following our submission of such a report. If Endo exercises its opt-in with respect to an additional indication, we are entitled to receive a one-time license fee for the rights to, as well as potential milestone, royalty and other payments with respect to, such new indication. If Endo does not exercise its opt-in as to any additional indication, we may offer to any third party such development rights with regard to products in the Endo Territory (as defined in the Endo Agreement), provided that we first offer the same terms to Endo, or develop the product ourselves. Endo has no obligation to exercise its opt-in with respect to any such additional indication, and its decision to do so is in its complete discretion. Clinical trials can be expensive and the results are subject to different interpretations, and therefore, there is no assurance that after conducting Phase 2 clinical trials on any additional indication, and incurring the associated expenses, Endo will exercise its opt-in or we will receive any revenue from it. Under the Endo Agreement, we may only offer to a third party development rights with regard to products in the Endo Territory and not in Europe and certain Eurasian countries. Even if Endo exercises its opt-in as to any additional indication, its obligations to develop the product for such indication are limited to initiating Stage II Development (as defined in the Endo Agreement) for such additional indication within one year of exercising the opt-in as to such indication.
The outcome and effects of Endo’s ongoing commercial review of the XIAFLEX exercised but non-marketed indications is uncertain.
Following the change in Endo management, Endo has announced a commercial review of the XIAFLEX exercised but non-marketed indications, including frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma, so that Endo can best prioritize its R&D efforts and determine clinical trial timelines moving forward. At the present time, it is unclear how long this commercial review will take to complete and the effect that it will have on Endo’s willingness to develop further such exercised but non-marketed indications. It is also unclear what effect, if any, the commercial review will have on the willingness of Endo to exercise its rights to opt in for any additional indications, including uterine fibroid, currently under development by the Company.
Due to our dependence on Endo for future royalty, milestone, cost of goods mark up and sublicense income payments and the commercialization of licensed indications and further development of future indications of XIAFLEX, the restructuring of Endo’s business and Endo’s failure to achieve projected revenues could have a material adverse effect on our business.
Our performance is substantially dependent on Endo’s performance, stability and success. Endo’s operations are substantially dependent on the continued services and performance of its senior management and other key personnel as well as the stability and performance of its various business units. Although the revised guidance on projected revenues and internal restructuring of Endo’s business units are principally related to the generics business, they could have the effect of distracting the attention of management and other resources away from the commercialization and further development of XIAFLEX, thereby materially and adversely our financial condition by slowing down the growth of, or reducing, XIAFLEX sales and development and payments by Endo to us for royalties, cost of goods sold, milestones, and sublicense income.
Endo’s acquisitions, other products and activities, and future resources may divert focus away from XIAFLEX and impact our financial position.
On January 29, 2015, Endo acquired Auxilium and Auxilium became a wholly owned subsidiary of Endo. Our business is now primarily dependent upon our relationship with Endo. It is unclear what long-term effect the acquisition of Auxilium will have on the relationship between the Company and Endo moving forward and the extent to which Endo’s focus on XIAFLEX will be reduced by virtue of other activities that it may undertake.
On September 25, 2015, Endo acquired Par Pharmaceutical Holdings, Inc. (“Par”), a specialty pharmaceutical company that develops, manufactures and markets pharmaceuticals. The Par acquisition expanded Endo’s portfolio, pipeline and manufacturing capabilities. Endo has announced that it expects to launch more than 110 products from 2016 to 2019, including certain first to file opportunities. In the third quarter of 2015, Endo acquired a product portfolio from Aspen. Endo also acquired the rights to commercialize developed technology assets treated as business combinations, which were not individually material. While Endo has noted that mergers and acquisitions were not a priority in 2016 and that in 2016 Endo was focused on advancing their de-risked R&D development pipeline and moving key XIAFLEX programs into clinical trials in 2016, Endo may continue to opportunistically acquire other pharmaceutical companies or engage in other partnerships. It is unclear what effect of the acquisitions or future acquisitions of other companies by Endo will have on the support for the product currently being developed and marketed by Endo that generate milestone payments and royalties for the Company.
Endo has products in its pipeline other than XIAFLEX. Endo may decide to allocate its resources other than to the development of XIAFLEX, and we have no control over that decision. Ultimately, these acquisitions and other products may divert attention away from XIAFLEX, which would materially affect our business, financial condition, and results of operations.
Our dependence upon revenue from Endo makes us subject to the commercialization and other risk factors affecting Endo over which we have limited or no control, including those risk factors identified by Endo in their 10-K for the year ended December 31, 2016, filed on March 1, 2017.
We are dependent upon revenue from Endo and Endo’s operating success or failure has a significant impact on our potential royalty stream and other payment rights. Certain risks effecting Endo and, consequently us, include the following:
Endo is subject to various regulations pertaining to the marketing of their products and services.
Endo is subject to various federal and state laws pertaining to healthcare fraud and abuse, including prohibitions on the offer of payment or acceptance of kickbacks or other remuneration for the purchase of Endo’s products and services, including inducements to potential patients to request Endo’s products and services and inducements to healthcare professionals to prescribe and use Endo’s products. Additionally, product promotion, educational activities, support of continuing medical education programs, and other interactions with healthcare professionals and patients must be conducted in a manner consistent with the FDA regulations and the Anti-Kickback Statute. The Anti-Kickback Statute, with certain exceptions or exemptions published by the Office of the Inspector General of the Department of Health and Human Services, or HHS-OIG, prohibits persons or entities from knowingly and willfully soliciting, receiving, offering or providing remuneration, directly or indirectly, to induce either the referral of an individual, or the furnishing, recommending, or arranging for a good or service, for which payment may be made under federal healthcare programs, such as the Medicare and Medicaid programs. Violations of the Anti-Kickback Statute also carry potential federal False Claims Act liability. Additionally, many states have adopted laws similar to the Anti-Kickback Statute, without identical exceptions or exemptions. Some of these state prohibitions apply to referral of patients for healthcare items or services reimbursed by any third-party payer, not only the Medicare and Medicaid programs. Any such new regulations or requirements may be difficult and expensive for Endo to comply with, may delay Endo’s introduction of new products, may adversely affect Endo’s total revenues and may have a material adverse effect on Endo’s business, results of operations, financial condition and cash flows.
Sanctions for violating these laws include criminal penalties and civil sanctions and possible exclusion from federal funded healthcare programs such as Medicare and Medicaid as well as potential liability under the False Claims Act and applicable state false claims acts. There can be no assurance that Endo’s practices will not be challenged under these laws in the future or that such a challenge would not have a material adverse effect on their business and Endo’s business or results of operations.
In addition, Endo is subject to statutory and regulatory restrictions on the promotion of uses of prescription drugs that are not approved by the FDA. Although the FDA does not regulate a physician’s choice of medications or treatments, the FDCA and FDA regulations and guidance significantly restrict the ability of pharmaceutical companies to communicate with patients, physicians, and other third-parties about unapproved product uses. FDA, FTC, the HHS-OIG, the DOJ and various state Attorneys General actively enforce state and federal prohibitions on the promotion of unapproved uses, as well as prohibitions against promotional practices deemed false or misleading. A company that is found to have improperly promoted its products under these laws may be subject to significant liability, including significant administrative, civil, and criminal sanctions, including but not limited to, significant civil damages, criminal fines, and exclusion from participation in Medicare, Medicaid, and other federal healthcare programs. Applicable laws governing product promotion also provide for administrative, civil, and criminal liability for individuals, including, in some circumstances, potential strict vicarious liability. Conduct giving rise to such liability could also form the basis for private civil litigation by third-party payers or other persons allegedly harmed by such conduct, as well as qui tam actions under the federal False Claims Act in which the government could chose to intervene.
Endo has endeavored to establish and implement a corporate compliance program designed to prevent, detect, and correct violations of state and federal healthcare laws, including laws related to advertising and promotion of Endo’s drugs. Nonetheless, the FDA, FTC, HHS-OIG, the DOJ and/or the state Attorneys General, and qui tam relators may take the position that Endo is not in compliance with such requirements, and, if such non-compliance is proven, Endo and, in some cases, individual employees, may be subject to significant liability, including the aforementioned administrative, civil, and criminal sanctions. This could have a material adverse effect on Endo’s business and financial operations. For instance, while not related to Xiaflex or any of our product candidates, in 2014, Endo entered into a settlement and corporate integrity agreement to resolve criminal and civil liability arising from its marketing of an unrelated drug.
The pharmaceutical industry is heavily regulated, which creates uncertainty about Endo’s ability to bring new products to market and imposes substantial compliance costs on their business.
Governmental authorities such as the FDA impose substantial requirements on the development, manufacture, holding, labeling, marketing, advertising, promotion, distribution and sale of therapeutic pharmaceutical products through lengthy and detailed laboratory and clinical testing and other costly and time-consuming procedures A failure to obtain satisfactory results in required pre-marketing trials may prevent Endo from obtaining required regulatory approvals. The FDA may also require companies to conduct post-approval studies and post-approval surveillance regarding their drug products and does require companies to report adverse events.
Before obtaining regulatory approvals for the sale of any of Endo’s new product candidates, Endo must demonstrate through preclinical studies and clinical trials that the product is safe and effective for each intended use. Preclinical and clinical studies may fail to demonstrate the safety and effectiveness of a product. Likewise, Endo may not be able to demonstrate through clinical trials that a product candidate’s therapeutic benefits outweigh its risks. Even promising results from preclinical and early clinical studies do not always accurately predict results in later, large scale trials. A failure to demonstrate safety and efficacy could or would result in Endo’s failure to obtain regulatory approvals. Clinical trials can be delayed for reasons outside of Endo’s control which can lead to increased development costs and delays in regulatory approval. For example, there is substantial competition to enroll patients in clinical trials and such competition has delayed clinical development of Endo’s products in the past. For example, patients may not enroll in clinical trials at the rate expected or patients may drop out after enrolling in the trials or during the trials. In addition, Endo relies on collaboration partners that may control or make changes in trial protocol and design enhancements, or encounter clinical trial compliance-related issues, which may also delay clinical trials or require that clinical trials be suspended or terminated. Product supplies may be delayed or be insufficient to treat the patients participating in the clinical trials, or manufacturers or suppliers may not meet the requirements of the FDA or foreign regulatory authorities, such as those relating to cGMP or GCPs. Endo also may experience delays in obtaining, or Endo may not obtain, required initial and continuing approval of Endo’s clinical trials from institutional review boards. Endo cannot confirm that it will not experience delays or undesired results their clinical trials.
Endo cannot confirm that the FDA or foreign regulatory agencies will approve, clear for marketing or certify any products developed by Endo or that such approval will not subject the marketing of Endo’s products to certain limits on indicated use. The FDA or foreign regulatory authorities may not agree with Endo’s assessment of the clinical data or they may interpret it differently. Such regulatory authorities may require additional or expanded clinical trials. Any limitation on use imposed by the FDA or delay in or failure to obtain FDA approvals or clearances of products developed by Endo would adversely affect the marketing of these products and Endo’s ability to generate product revenue, which would adversely affect Endo’s financial condition and results of operations.
In addition, with respect specifically to pharmaceutical products, the submission of a marketing application to the FDA with supporting clinical safety and efficacy data, for example, does not guarantee that the FDA will grant approval to market the product. Meeting the FDA’s regulatory requirements to obtain approval to market a drug product, which varies substantially based on the type, complexity and novelty of the pharmaceutical product, typically takes years and is subject to uncertainty. The approval process for a new product varies in time. Approvals, if granted, may not include all uses (known as indications) for which a company may seek to market a product.
Further, once a product is approved for marketing, failure to comply with applicable regulatory requirements can result in, among other things, suspensions or withdrawals of approvals or clearances, seizures or recalls of products, injunctions against the manufacture, holding, distribution, marketing and sale of a product, and civil and criminal sanctions. Furthermore, changes in existing regulations or the adoption of new regulations could prevent Endo from obtaining, or affect the timing of, future regulatory approvals or clearances. Meeting regulatory requirements and evolving government standards may delay marketing of Endo’s new products for a considerable period of time, impose costly procedures upon Endo’s activities and result in a competitive advantage to larger companies that compete against Endo.
Based on scientific developments, post-market experience, or other legislative or regulatory changes, the current FDA standards of review for approving new pharmaceutical products, or new indications or uses for approved products, are sometimes more stringent than those that were applied in the past.
The FDA has the authority to require companies to undertake additional post-approval studies to assess known or signaled safety risks and to make any labeling changes to address those risks. The FDA also can require companies to formulate approved REMS to ensure a drug’s benefits outweigh its risks either for approval or following approval. The FDA’s exercise of its authority under the FFDCA could result in delays or increased costs during product development, clinical trials and regulatory review, increased costs to comply with additional post-approval regulatory requirements and potential restrictions on sales of approved products. Foreign regulatory agencies often have similar authority and may impose comparable requirements and costs. Post-marketing studies and other emerging data about marketed products, such as adverse event reports, may also adversely affect sales of Endo’s products or prompt regulatory authorities to take regulatory actions with regard to the product. Furthermore, the discovery of significant safety or efficacy concerns or problems with a product in the same therapeutic class as one of Endo’s products that implicate or appear to implicate the entire class of products could have an adverse effect on sales of Endo’s product or, in some cases, result in product withdrawals or other regulatory action. Furthermore, new data and information, including information about product misuse or abuse at the user level, may lead government agencies, professional societies, practice management groups or patient or trade organizations to recommend or publish guidance or guidelines related to the use of Endo’s products, which may lead to reduced sales of Endo’s products.
The FDA regulates and monitors the quality of drug clinical trials to provide human subject protection and to support marketing applications. The FDA may place a hold on a clinical trial and may cause a suspension or withdrawal of product approvals if regulatory standards are not maintained. The FDA also regulates the facilities, processes, and procedures used to manufacture and market pharmaceutical products in the U.S. both for clinical supply and marketed products. Manufacturing facilities must be registered with the FDA and all commercially distributed products made in such facilities must be manufactured in accordance with the latest cGMP regulations, which are enforced by the FDA. Compliance with clinical trial requirements and cGMP regulations requires the dedication of substantial resources and requires significant expenditures. In the event an approved manufacturing facility for a particular drug is required by the FDA to curtail or cease operations, or otherwise becomes inoperable, or a third party contract manufacturing facility faces manufacturing problems, obtaining the required FDA authorization to manufacture at the same or a different manufacturing site could result in production delays, which could adversely affect Endo’s business, results of operations, financial condition and cash flow.
The FDA is authorized to perform inspections of U.S. and foreign manufacturing facilities and clinical trial sites under the FFDCA. Following such inspections, the FDA may issue an untitled letter as an initial correspondence that cites violations that do not meet the threshold of regulatory significance of a Warning Letter. FDA guidelines also provide for the issuance of Warning Letters for violations of “regulatory significance” for which the failure to adequately and promptly achieve correction may be expected to result in an enforcement action. Finally, the FDA could issue a Form 483 Notice of Inspectional Observations, which could cause Endo to modify certain activities identified during the inspection FDA also may issue Warning Letters and untitled letters in connection with events or circumstances unrelated to an FDA inspection.
Similar to other healthcare companies, during 2016, Endo’s facilities, in multiple countries, across the full range of Endo’s business units, were subject to routine and new-product related inspections by the FDA, MHRA, HPRA and Health Canada. Some of these inspections resulted in non-critical inspection observations (including FDA Form 483 observations). Endo has responded to all inspection observations within the required time frame and have implemented, or are continuing to implement, the corrective action plans as agreed with the relevant regulatory agencies.
Endo cannot determine what effect changes in regulations or legal interpretations or requirements by the FDA or the courts, when and if promulgated or issued, may have on Endo’s business in the future. Changes could, among other things, require different labeling, monitoring of patients, interaction with physicians, education programs for patients or physicians, curtailment of necessary supplies, or limitations on product distribution. These changes, or others required by the FDA or DEA could have an adverse effect on the sales of these products. The evolving and complex nature of regulatory science and regulatory requirements, the broad authority and discretion of the FDA and the generally high level of regulatory oversight results in a continuing possibility that, from time to time, Endo will be adversely affected by regulatory actions despite Endo’s ongoing efforts and commitment to achieve and maintain full compliance with all regulatory requirements.
Any issues that Endo or any other companies to which we grant licensing rights experience concerning regulatory and legal compliance generally, as well as the development, manufacturing, approval, sale, marketing, promotion, and distribution specifically of our products and/or product candidates may limit the opt-in, mark up on COGs, milestone and/or royalty payments that we are due under our agreements.
The availability of third party reimbursement for Endo’s products is uncertain, and thus Endo may find it difficult to maintain current price levels. Additionally, the market may not accept those products for which third party reimbursement is not adequately provided.
Endo’s ability to commercialize Endo’s products depends, in part, on the extent to which reimbursement for the costs of these products is available from government healthcare programs, such as Medicaid and Medicare, private health insurers and others. Endo cannot be certain that, over time, third party reimbursements for Endo’s products will be adequate for Endo to maintain price levels sufficient for realization of an appropriate return on Endo’s investment. Government payers, private insurers and other third party payers are increasingly attempting to contain healthcare costs by (1) limiting both coverage and the level of reimbursement (including adjusting co-pays) for products approved for marketing by the FDA, (2) refusing, in some cases, to provide any coverage for uses of approved products for indications for which the FDA has not granted marketing approval and (3) requiring or encouraging, through more favorable reimbursement levels or otherwise, the substitution of generic alternatives to branded products.
Endo may experience pricing pressure on the price of Endo’s products due to social or political pressure to lower the cost of drugs, which would reduce Endo’s revenue and future profitability.
Endo may experience downward pricing pressure on the price of Endo’s products due to social or political pressure to lower the cost of drugs, which would reduce Endo’s revenue and future profitability. Recent events have resulted in increased public and governmental scrutiny of the cost of drugs, especially in connection with price increases following companies’ acquisitions of the rights to certain drug products. In particular, U.S. federal prosecutors recently issued subpoenas to a pharmaceutical company seeking information about its drug pricing practices, among other issues, and members of the U.S. Congress have sought information from certain pharmaceutical companies relating to post-acquisition drug-price increases. Endo’s revenue and future profitability could be negatively affected if these inquiries were to result in legislative or regulatory proposals that limit Endo’s ability to increase the prices of Endo’s products.
Pressure from social activist groups and future government regulations may also put downward pressure on the price of drugs, which could result in downward pressure on the prices of Endo’s products in the future.
If Endo’s manufacturing facilities are unable to manufacture Endo’s products or the manufacturing process is interrupted due to failure to comply with regulations or for other reasons, it could have a material adverse impact on Endo’s business.
If any of Endo’s manufacturing facilities or contract manufacturers that Endo may use in the future fail to comply with regulatory requirements or encounter other manufacturing difficulties, it could adversely affect Endo’s ability to supply products. All facilities and manufacturing processes used for the manufacture of pharmaceutical products (including many components of such products) are subject to inspection by regulatory agencies at any time and must be operated in conformity with cGMP. Compliance with the FDA’s cGMP requirements applies to both drug products seeking regulatory approval and to approved drug products. In complying with cGMP requirements, pharmaceutical manufacturing facilities must continually expend significant time, money and effort in production, record-keeping and quality assurance and control so that their products meet applicable specifications and other requirements for product safety, efficacy and quality. Failure to comply with applicable legal requirements subjects Endo’s manufacturing facilities to possible legal or regulatory action, including shutdown, which may adversely affect the ability to supply XIAFLEX or any product candidate for clinical and preclinical trials. If Endo or its contract manufacturers are not able to manufacture products at its manufacturing facilities because of regulatory, business or any other reasons, the manufacture and marketing of XIAFLEX would be interrupted. This could have a material adverse impact on Endo’s business, results of operation, financial condition, cash flows and competitive position.
Endo acquired Auxilium on January 29, 2015. Auxilium’s Horsham, Pennsylvania and Rye, New York facilities and the facilities of the manufacturer that Endo is the process of qualifying as an alternate manufacturer for XIAFLEX® (the “Alternate Manufacturer” and such facility, the “Alternate Facility”) are subject to such regulatory requirements and oversight. If Endo or the Alternate Manufacturer fail to comply with cGMP requirements, Endo may not be permitted to sell its products or may be limited in the jurisdictions in which it is permitted to sell them. Such noncompliance could also impact the Company’s ability to supply the necessary product required for clinical and preclinical development. Further, if an inspection by regulatory authorities indicates that there are deficiencies including non-compliance with regulatory requirements, Endo could be required to take remedial actions, stop production or close Endo’s Horsham and/or Rye facilities or the Alternate Facility, which would disrupt the manufacturing processes, limit the supplies of XIAFLEX and delay clinical trials and subsequent licensure, and/or limit the sale of commercial supplies. In addition, future noncompliance with any applicable regulatory requirements may result in refusal by regulatory authorities to allow use of XIAFLEX or any other products or product candidates in clinical trials, refusal of the government to allow distribution of XIAFLEX or any other products or product candidates within the U.S. or other jurisdictions, criminal prosecution and fines, recall or seizure of products, total or partial suspension of production, prohibitions or limitations on the commercial sale of products, refusal to allow the entering into of federal and state supply contracts, and follow-on civil litigation.
Endo has limited experience in manufacturing biologic products and may encounter difficulties in Endo’s manufacturing processes, which could materially adversely affect Endo’s results of operations or delay or disrupt manufacture of those of Endo’s products that are reliant upon Endo’s manufacturing operations.
The manufacture of biologic products requires significant expertise and capital investment. Although Endo’s subsidiary, Auxilium, leased its facilities in Horsham, Pennsylvania in order to have direct control over the manufacturing of the active ingredient of XIAFLEX, Endo has limited experience in manufacturing XIAFLEX or any other biologic product. Biologics such as XIAFLEX require processing steps that are highly complex and generally more difficult than those required for most chemical pharmaceuticals. If Endo’s manufacturing processes at the Rye, New York facility or Horsham facility are disrupted, it may be difficult to find alternate manufacturing sites. Endo may encounter difficulties with the manufacture of the active ingredient of XIAFLEX which could delay, disrupt or halt Endo’s manufacture of XIAFLEX and require write-offs which may affect Endo’s financial results, result in product recalls or product liability claims or otherwise materially affect Endo’s results of operations.
The regulatory approval process outside the U.S. varies depending on foreign regulatory requirements, and failure to obtain regulatory approval in foreign jurisdictions would prevent the marketing of Endo’s products in those jurisdictions.
Endo has worldwide intellectual property rights to market many of Endo’s products and product candidates and intends to seek approval to market certain of Endo’s products outside of the U.S. Approval of a product by the regulatory authorities of foreign countries must be obtained prior to manufacturing or marketing that product in those countries. The approval procedure varies among countries and can involve additional testing and the time required to obtain such approval may differ from that required to obtain FDA approval. The non-U.S. regulatory approval process includes all of the risks associated with obtaining FDA approval set forth herein. Approval by the FDA does not secure approval by the regulatory authorities of any other country, nor does the approval by foreign regulatory authorities in one country secure approval by regulatory authorities in other foreign countries or the FDA. If Endo fails to comply with these regulatory requirements or fails to obtain and maintain required approvals, Endo’s target market will be reduced and Endo’s ability to generate revenue from abroad will be adversely affected.
The expanding nature of Endo’s business in global markets exposes Endo to risks associated with adapting to emerging markets and taking advantage of growth opportunities.
The globalization of Endo’s business may expose Endo to increased risks associated with conducting business in emerging markets. Any difficulties in adapting to emerging markets could impair Endo’s ability to take advantage of growth opportunities in these regions and a decline in the growth of emerging markets could negatively affect Endo’s business, results of operations or financial condition.
The expansion of Endo’s activities in emerging markets may further expose Endo to more volatile economic conditions and political instability. Endo also faces competition from companies that are already well established in these markets. Endo’s inability to adequately respond to the unique characteristics of these markets, particularly with respect to their regulatory frameworks, the difficulties in recruiting qualified personnel, potential exchange controls, weaker intellectual property protection, higher crime levels and corruption and fraud, could have a material adverse effect on Endo’s business.
Endo’s policies and procedures, which are designed to help Endo, Endo’s employees and agents comply with various laws and regulations regarding corrupt practices and anti-bribery, cannot guarantee protection against liability for actions taken by businesses in which Endo invests. Failure to comply with domestic or international laws could result in various adverse consequences, including possible delay in the approval or refusal to approve a product, recalls, seizures, withdrawal of an approved product from the market, or the imposition of criminal or civil sanctions, including substantial monetary penalties.
In addition, differences in banking systems and business cultures could have an adverse effect on the efficiency of internal controls over financial reporting matters. Given the significant learning curve to fully understand the emerging markets’ business, operating environment and the quality of controls in place, Endo may not be able to adequately assess the efficiency of internal controls over financial reporting or the effects of the laws and requirements of the local business jurisdictions.
Many jurisdictions require specific permits or business licenses, particularly if the business is considered foreign. These requirements may affect Endo’s ability to carry out Endo’s business operations in emerging markets.
The risks of selling and shipping products and of purchasing components and products internationally may adversely impact Endo’s revenues, results of operations and financial condition.
The sale and shipping of Endo’s products and services across international borders is subject to extensive U.S. and foreign governmental trade regulations, such as various anti-bribery laws, including the U.S. Foreign Corrupt Practices Act, export control laws, customs and import laws, and anti-boycott laws. Endo’s failure to comply with applicable laws and regulations could result in significant criminal, civil and administrative penalties, including, but not limited to, imprisonment of individuals, fines, denial of export privileges, seizure of shipments, restrictions on certain business activities, and exclusion or debarment from government contracting. Also, the failure to comply with applicable legal and regulatory obligations could result in the disruption of Endo’s shipping and sales activities.
In addition, some countries in which Endo’s subsidiaries sell products are, to some degree, subject to political, economic and/or social instability. Endo’s international sales operations expose Endo and Endo’s representatives, agents and distributors to risks inherent in operating in foreign jurisdictions. These risks include:
| • | the imposition of additional U.S. and foreign governmental controls or regulations; |
| • |
the imposition of costly and lengthy new export licensing requirements;
|
| • |
the imposition of U.S. and/or international sanctions against a country, company, person or entity with whom the company does business that would restrict or prohibit continued business with the sanctioned country, company, person or entity;
|
| • |
economic and political instability or disruptions, including local and regional instability, or disruptions due to natural disasters, such as severe weather and geological events, disruptions due to civil unrest and hostilities, rioting, military activity, terror attacks or armed hostilities;
|
| • |
changes in duties and tariffs, license obligations and other non-tariff barriers to trade;
|
| • |
the imposition of new trade restrictions;
|
| • |
imposition of restrictions on the activities of foreign agents, representatives and distributors;
|
| • |
foreign tax authorities imposing significant fines, penalties and additional taxes;
|
| • |
pricing pressure that Endo may experience internationally;
|
| • |
laws and business practices favoring local companies;
|
| • |
difficulties in enforcing or defending intellectual property rights; and
|
| • |
exposure to different legal and political standards due to Endo’s conducting business in several foreign countries.
|
Endo cannot provide assurance that one or more of these factors will not harm Endo’s business. Additionally, Endo is experiencing fluidity in regulatory and pricing trends as a result of the Patient Protection and Affordable Care Act and the Health Care and Education Reconciliation Act of 2010. Any material decrease in Endo’s international sales would adversely impact Endo’s results of operations and financial condition.
If physicians do not prescribe XIAFLEX or the medical profession or patients do not accept XIAFLEX, our ability to grow or maintain revenues will be limited.
Our revenues are dependent on market acceptance of XIAFLEX. Physician willingness to prescribe, and patients’ willingness to accept, XIAFLEX depend on many factors, including:
| ☐ |
perceived safety and efficacy;
|
| ☐ |
convenience and ease of administration;
|
| ☐ |
incidence and severity of adverse side effects in both clinical trials and commercial use;
|
| ☐ |
availability of alternative treatments or products;
|
| ☐ |
cost effectiveness and pricing;
|
| ☐ |
the adequacy and effectiveness of Endo’s sales force and that of any partner’s sales force;
|
| ☐ |
the adequacy and effectiveness of Endo’s production, distribution and marketing capabilities and those of Endo’s international partners;
|
| ☐ |
publicity concerning Endo’s products or competing products; and
|
| ☐ |
existence and level of third-party or government coverage or reimbursement for XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease.
|
Even though there is regulatory approval for XIAFLEX, physicians may not prescribe, and patients may not accept, XIAFLEX if Endo or its partners do not promote it effectively. If XIAFLEX fails to achieve market acceptance, Endo may not be able to market and sell XIAFLEX successfully, which would limit our ability to receive revenue and could harm our business.
We may not be able to obtain or maintain orphan drug exclusivity for XIAFLEX, which could significantly harm our business.
Some jurisdictions, including Europe and the U.S., may designate drugs intended to treat relatively small patient populations as orphan drugs. The FDA granted orphan drug status to XIAFLEX in the U.S. for the treatment of Dupuytren’s contracture and Peyronie’s disease. The orphan drug designation for Dupuytren’s contracture expired on February 2, 2017. Orphan drug designation must be requested before submitting an application for marketing authorization. Orphan drug designation may not convey any advantage in, or shorten the duration of, the regulatory review and approval process, but does make the product eligible for orphan drug exclusivity and, in the U.S., specific tax credits. Generally, if a product with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to orphan drug exclusivity. Orphan drug exclusivity means that another application to market the same drug for the same indication may not be approved, except in limited circumstances, for a period of up to 10 years in Europe and for a period of seven years in the U.S. Maintaining orphan drug designations and orphan drug exclusivity for XIAFLEX for the treatment Peyronie’s disease may be critical to its success. Peyronie’s disease currently enjoys Orphan Drug Protection until December 6, 2020. Even with orphan drug exclusivity, we may not be able to maintain it. For example, if a competitive product is shown to be different or clinically superior, any orphan drug exclusivity we have obtained will not block the approval of such competitive product.
Endo is dependent upon Endo’s collaborative relationships with third parties to further develop and commercialize XIAFLEX outside of the U.S. There may be circumstances that delay or prevent the ability of any of these third parties’ to develop and commercialize XIAFLEX.
Endo has assumed all agreements that Auxilium entered into with each of Sobi and Asahi under which Auxilium has granted them the right to develop and commercialize XIAFLEX/Xiapex in 71 Eurasian and African countries, in Japan, respectively. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand. In addition, Endo may seek to enter into similar arrangements with other third parties with respect to the development and commercialization of XIAFLEX/Xiapex in the rest of the world. Endo is subject to a number of risks associated with Endo’s dependence on Endo’s collaborative relationship with these third parties, including:
| ☐ |
adverse decisions by a third party regarding the amount and timing of resource expenditures for the development and commercialization of XIAFLEX/Xiapex;
|
| ☐ |
possible disagreements as to the timing, nature and extent of Endo’s development plans, including clinical trials or regulatory approval strategy;
|
| ☐ |
the right of a third party to terminate its collaboration agreement with Endo on limited notice upon the occurrence of certain defined events;
|
| ☐ |
loss of significant rights if Endo fails to meet Endo’s obligations under the collaboration agreement;
|
| ☐ |
withdrawal of support by a third party following change of that third party’s corporate strategy or due to competing priorities;
|
| ☐ |
changes in key management personnel at a third party that are members of the collaboration’s various operating committees; and
|
| ☐ |
possible disagreements with a third party regarding the collaboration agreement or ownership of proprietary rights, including with respect to inventions discovered under the applicable collaborative agreement.
|
Due to these factors and other possible disagreements with a third party, including potential disputes over intellectual property ownership, Endo may be delayed or prevented from further developing, manufacturing or commercializing XIAFLEX outside the U.S., or Endo may become involved in litigation or arbitration, which would be time consuming and expensive.
If a third party were to terminate its collaboration agreement with Endo, Endo would need to undertake development and marketing activities for XIAFLEX in that third party’s territory solely at Endo’s own expense and/or seek another partner for some or all of these activities in that territory. If Endo pursued these activities in that territory on Endo’s own, it would significantly increase Endo’s capital and infrastructure requirements, and might limit the indications Endo is able to pursue and could prevent Endo from effectively developing and commercializing XIAFLEX. If Endo sought to find another pharmaceutical company partner for some or all of these activities, Endo may not be successful in such efforts, or they may result in a collaboration that has Endo expending greater funds and efforts than the relationship with the terminating third party.
In general, Endo cannot control the amount and timing that Endo’s third party partners may devote to Endo’s collaborations. Endo is relying on Endo’s third-party partners to obtain regulatory approvals for and successfully commercialize XIAFLEX in the relevant territories. If a third party fails to adequately market and promote XIAFLEX in its territory, Endo may be unable to obtain any remedy against that third party and sales of XIAFLEX may be harmed, which would negatively impact Endo’s business, results of operations, cash flows and liquidity due to reduced milestone and royalty payments under the applicable third party agreement and, subsequently, our business and results of operations. In addition, third party partners may have difficulty obtaining reimbursement for their products and may withdraw from certain markets outside of the U.S.
As a condition for approval of XIAFLEX for Dupuytren’s contracture and for Peyronie’s disease, Endo is required to comply with post-marketing requirements. Failure to comply with these requirements or any future post-marketing requirements, or the cost of compliance with such requirements, may harm our business.
The FDA or, for products outside the U.S. for which Endo holds the regulatory approvals, international regulatory agencies can establish requirements for XIAFLEX or Xiapex with which Endo must comply. Data from preclinical testing and clinical trials are submitted to the FDA in an NDA or BLA for marketing approval and to foreign government health authorities in a marketing authorization application, consistent with each health authority’s specific regulatory requirements. The process of completing clinical trials for a new drug may take many years and require the expenditures of substantial resources. As a condition of approval, the FDA or foreign regulatory authorities may require further studies, including Phase 4 post-marketing studies and pediatric studies, to provide additional data. In September 2007, Congress passed legislation authorizing the FDA to require companies to undertake such studies to assess the risks of drugs known or signaling potential to have serious safety issues. For some drugs, the FDA may require a Risk Evaluation and Mitigation Strategy (REMS), which could include medication guides, physician communication plans, or restrictions on distribution and use, such as limitations on who may prescribe the drug or where it may be dispensed or administered. Other post-marketing studies could be used to gain approval for the use of a product as a treatment for clinical indications other than those for which the product was initially tested. Also, the FDA or foreign government regulatory authorities require post-marketing reporting to monitor the adverse effects of drugs. Results of post-marketing programs may limit or expand the further marketing of the products. Failure to report or conduct the studies is considered a violation and can result in enforcement action. These studies or clinical trials could be time-consuming and costly and the results could have negative effects on Endo’s ability to market the product.
XIAFLEX is regulated and marketed as biologic products pursuant to BLAs. XIAFLEX is licensed based on a determination by the FDA of safety, purity, and potency as required under the Public Health Service Act (PHSA). In 2010, Congress enacted the Biologics Price Competition and Innovation Act of 2009 (BPCIA), as part of the Healthcare Reform Law, which amended the PHSA to create an abbreviated licensure pathway for products deemed to be biosimilar to or interchangeable with FDA-licensed reference biological products. Under the BPCIA, an approval for a biosimilar product cannot be made effective by the FDA until 12 years after the original branded product was approved under a BLA. Certain changes, however, and supplements to an approved BLA, and subsequent applications filed by the same sponsor, manufacturer, licensor, predecessor in interest, or other related entity do not qualify for the 12-year exclusivity period.
Under the BPCIA, following the expiration of a 12-year reference exclusivity period, FDA may license under section 351(k) of the PHSA effective for a biologic that it determines is biosimilar to or interchangeable with a reference product licensed under section 351(a) of the PHSA. Biosimilarity is defined to mean that the section 351(k) product is highly similar to the reference product notwithstanding minor differences in clinically inactive components and that there are no clinically meaningful differences between the section 351(k) product and the reference product in terms of the safety, purity, and potency of the product. To be considered interchangeable, a product must be biosimilar to the reference product, be expected to produce the same clinical result as the reference product in any given patient, and, if administered more than once to an individual, the risks in terms of safety or diminished efficacy of alternating or switching between use of the product and its reference product is not greater than the risk of using the reference product without such alternation or switch.
Once any reference exclusivity period for a BLA-licensed biologics expires, FDA may make an approval under section 351(k) effective of the PHSA another company’s BLA for a biosimilar or interchangeable version of our product. Although licensure of a biosimilar or interchangeable under section 351(k) is generally expected to require less than the full complement of product-specific preclinical and clinical data required for innovator products licensed under section 351(a), FDA has considerable discretion over the kind and amount of scientific evidence required to demonstrate biosimilarity and interchangeability.’
We believe that Xiaflex, which was initially approved in 2010, would have exclusivity protection through 2022. However, there is a risk that the FDA will not consider our product candidates to be reference products for competing products, potentially creating the opportunity for biosimilar competition sooner than anticipated. Additionally, this period of regulatory exclusivity does not apply to companies pursuing regulatory approval via their own traditional BLA, rather than via the abbreviated pathway. Moreover, the extent to which a biosimilar, once approved, will be substituted for any one of our reference products in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing. It is possible that payers will give reimbursement preference to biosimilars even over reference biologics absent a determination of interchangeability.
For XIAFLEX for Peyronie’s disease, Endo is required to implement a REMS or other programs. Failure to comply, or the cost of compliance with such REMS or other programs, may harm our business.
The FDA is authorized to require Endo as the sponsor of an approved or unapproved marketing application to submit a proposed REMS if the FDA determines that a REMS is necessary to ensure that the benefits of a drug outweigh the risks of the drug. Failure to comply with the requirements of the approved REMS can render the drug misbranded. A violation of a REMS requirement is subject to civil penalties. Complying with the requirements of a REMS can be costly and time-consuming and adversely affect Endo’s operations.
Because of the risks of corporal rupture (penile fracture) or other serious penile injury in the treatment of Peyronie’s disease, XIAFLEX is available only through the XIAFLEX REMS Program. The required components of the XIAFLEX REMS Program include (i) Prescribers must be certified with the program by enrolling and completing training in the administration of XIAFLEX treatment for Peyronie’s disease, and (ii) Healthcare sites must be certified with the program and ensure that XIAFLEX is only dispensed for use by certified prescribers.
If we are unable to obtain opt-in, milestone, mark-up on cost of goods sold and royalty payments from Endo or meet our needs for additional funding from other sources, we may be required to limit, scale back or cease our operations.
Our business strategy contains elements that we will not be able to implement if we do not receive the anticipated opt-in, milestone, royalty or mark-up on cost of goods sold payments from Endo, or secure additional funding from other sources. While we anticipate being profitable on an ongoing, annual basis, our future funding requirements will depend on many factors, including:
| ☐ |
Endo’s ability to manufacture and commercialize XIAFLEX for which we would receive milestone, mark-up on cost of goods sold and royalty payments;
|
| ☐ |
The ability of Endo’s sublicensees to commercialize XIAFLEX/Xiapex in their respective territories;
|
| ☐ |
the amount actually owed by us to Endo for certain patent costs;
|
| ☐ |
the scope, rate of progress, cost and results of our clinical trials on additional indications, including uterine fibroids, for which Endo could exercise its opt-in to acquire its rights;
|
| ☐ |
the terms and timing of any future collaborative, licensing, co-promotion and other arrangements that we may establish;
|
| ☐ |
the cost of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights or defending against any other litigation; and
|
| ☐ |
the extent to which Endo may reallocate priority away from XIAFLEX.
|
These factors could result in variations from our currently projected operating requirements. If our existing resources are insufficient to satisfy our operating requirements, we may need to limit, scale back or cease operations or, in the alternative, borrow money. Given our operations and history, we may not be able to borrow money on commercially reasonable terms, if at all. If we issue any equity or debt securities, the terms of such issuance may not be acceptable to us and would likely result in substantial dilution of our stockholders’ investment. If we do not receive revenues from Endo, and are unable to secure additional financing, we may be required to cease operations.
We depend on Endo for the determination of royalty payments and cost of goods sold. While we have rights to audit Endo, the independent auditors may have difficulty determining the correct royalty and cost of goods sold calculations, we may not be able to detect errors and payment calculations may call for retroactive adjustments. We may have to exercise legal remedies to resolve any disputes resulting from the audit.
The royalty payments we receive are determined by Endo based on reported sales. Endo’s calculation of the royalty payments are subject to and dependent upon the adequacy and accuracy of its sales and accounting functions. Endo’s calculation of cost of goods sold are subject to and dependent upon the adequacy and accuracy of its internal accounting of costs. Errors may occur from time to time in these calculations. The Endo Agreement provides us the right to audit the calculations and sales data for the associated royalty payments. Although we may exercise our audit rights, such audits may occur many months following our recognition of the royalty revenue, may require us to adjust our royalty revenues in later periods and may require expense on the part of the Company. Further, Endo may be uncooperative or have insufficient records, which may complicate and delay the audit process.
Although we may exercise our audit rights, we rely in the first instance on Endo to accurately report sales and calculate and pay applicable royalties. Such audits may occur many months following our recognition of the royalty revenue, may require us to adjust our royalty revenues in later periods and may require expense on the part of the Company. We also rely on Endo’s cooperation and maintenance of sufficient records in performing such audits. If Endo is uncooperative or has insufficient records, it may complicate and delay the audit process. In the absence of such cooperation, we may be forced to exercise legal remedies to enforce our rights.
In order to finance and to secure the rights to conduct clinical trials for products we have licensed to Endo, we have granted to third parties significant rights to share in royalty payments received by us and, in some case, milestone payments to be received by us.
To finance and secure the rights to conduct clinical trials for products we have licensed to Endo, we have granted to third parties certain rights to share in royalty payments and, in some cases milestone payments, received by us from Endo under the Endo Agreement. Consequently, we will be required to share a significant portion of the payments due to us from Endo under the Endo Agreement.
If we breach our agreements with third parties or if there is a dispute concerning any of our agreements with third parties, our business could be materially harmed.
Our agreements with third parties impose on us various obligations, such as those related to intellectual property rights, non-competition, and development of products, as described throughout this Item 1A of this Report. If we fail to comply with such obligations, or a counterparty to our agreements believes that we have failed to comply with such obligations, we may be sued and the costs of the resulting litigation could materially harm our business. Additionally, disputes may arise under these agreements, including with respect to the interpretation of such agreements and fee redeterminations or renegotiations thereof. These disputes may lead to litigation, termination of the agreement, or amendments that change our rights under the agreement, which could materially affect our financial position and materially harm our business. We agreed, for example, to resolve a dispute with Endo, to grant Endo an early opt-in to indications which may, if we consent, limit our ability to conduct clinical trials pursuant to the First Amendment which is described more fully in Item 1 above.
Our results of operations and financial position could be negatively impacted if our tax positions are challenged by tax authorities.
We are a U.S.-based company subject to tax in certain U.S. jurisdictions. U.S. federal, state and local tax laws and regulations are extremely complex and subject to varying interpretations. Although we believe that our tax estimates and tax positions are reasonable, there can be no assurance that our tax positions will not be challenged by relevant tax authorities or that we would be successful in any such challenge. If we are unsuccessful in such a challenge, the relevant tax authorities may assess additional taxes, which could result in adjustments to, or impact the timing or amount of, taxable income, deductions or other tax allocations, which may adversely affect our results of operations and financial position.
Risks Related to Clinical Trials and Development of Drug Candidates
Our ability to conduct future clinical trials and develop products for injectable administration of collagenase may be limited by the Endo Agreement.
Under the Endo Agreement, we have the right to conduct trials, studies or development work for, among other things, uterine fibroids, and, upon approval by the parties’ joint development committee, or the JDC, additional indications. Endo has pre-approved our protocol for uterine fibroids. However, certain material changes to the protocol must be approved by the JDC, and the JDC may decide not to approve such changes if the JDC has reasonable safety concerns. In addition, the JDC has the right to stop our study or trial in uterine fibroids if the rate of serious adverse events exceeds certain thresholds. If the JDC fails to approve changes to our protocol for uterine fibroids or if the JDC stops our studies or trials in uterine fibroids due to safety concerns, our ability to obtain milestones and royalty payments with respect to this indication would be limited. We may only conduct in vivo trials, studies or development work for additional indications beyond the pre-approved indications upon submission to and approval by the JDC of our development plan which includes in vivo studies of uterine fibroids. In the case of indications in keloids, capsular contraction after breast augmentation, arthrofibrosis following total joint replacement in humans and equine suspensory ligament desmitis, the JDC may reject our submission only for reasonable safety concerns. The JDC may reject our submission for any other additional indications for safety or commercial concerns. If the JDC rejects our submissions in any additional indications, our ability to obtain opt-in, milestone and royalty payments with respect to those additional indications would be limited.
Additionally, under the Endo Agreement, we have licensed or granted options to certain of our rights to conduct clinical trials and develop products for injectable administration of collagenase. We agreed, for example, to certain non-competition provisions, which may limit our clinical development activities.
We are dependent on Endo for access to XIAFLEX, which may limit our ability to conduct future clinical trials and to obtain the associated opt-in, milestone, mark-up on cost of goods sold payments and royalty payments under the Endo Agreement.
Under the Endo Agreement, we have agreed to buy at cost plus a mark-up XIAFLEX from Endo for conducting our trials, studies and development work. If Endo does not supply XIAFLEX to us, our ability to conduct clinical trials using XIAFLEX would be limited because we do not have the right to make XIAFLEX or to purchase it from third parties. . Similarly, any interruptions in Endo’s manufacturing as a result of regulatory issues or noncompliance would limit our ability to conduct our trials. We may also be held responsible for any Endo departures from the applicable regulatory manufacturing requirements, to the extent it impacts our clinical supply. Moreover, our ability to use our own clinical material may be limited both by lack of availability and by certain potential regulatory restrictions. Without adequate supply of clinical material our ability to obtain additional opt-in, milestone and royalty payments under the Endo Agreement would be limited.
If clinical trials for our potential new indications are delayed, we may not be able to obtain opt-in, milestone or royalty payments under the Endo Agreement for new indications.
Clinical trials that we, Endo, or our investigators may conduct may not begin on time or may need to be restructured or temporarily suspended after they have begun. Clinical trials can be delayed, may never be completed or may need to be restructured for a variety of reasons, including delays, impediments or restructuring related to:
| ☐ |
changes to the regulatory approval process for product candidates;
|
| ☐ |
obtaining regulatory approval to commence a clinical trial;
|
| ☐ |
timing of responses required from regulatory authorities;
|
| ☐ |
negotiating acceptable clinical trial agreement terms with prospective investigators or trial sites;
|
| ☐ |
obtaining institutional review board, or equivalent, approval to conduct a clinical trial at a prospective site;
|
| ☐ |
recruiting subjects to participate in a clinical trial;
|
| ☐ |
competition in recruiting clinical investigators;
|
| ☐ |
shortage or lack of availability of clinical trial supplies from external and internal sources;
|
| ☐ |
the need to repeat clinical trials as a result of inconclusive results or poorly executed testing, or to conduct additional clinical or preclinical trials or analyses;
|
| ☐ |
failure to validate a patient-reported outcome questionnaire;
|
| ☐ |
the placement of a clinical hold on a study;
|
| ☐ |
the failure of third parties conducting and overseeing the operations of our clinical trials to perform their contractual or regulatory obligations in a timely fashion;
|
| ☐ |
exposure of clinical trial subjects to unexpected and unacceptable health risks or noncompliance with regulatory requirements, which may result in suspension of the trial; and
|
| ☐ |
manufacturing and/or distribution issues associated with clinical supplies.
|
Completion of clinical trials for each product candidate will be required before commercialization. If Endo or we experience delays in, or termination of, clinical trials, or fails to enroll patients in clinical trials in a timely manner, or if the cost or timing of the regulatory approval process increases, our financial results and the commercial prospects for product candidates for new indications will be adversely impacted.
The process of conducting clinical trials and developing product candidates involves a high degree of risk, may take several years, and may ultimately not be successful.
Product candidates that appear promising in the early phases of development may fail to reach the market for several reasons, including:
| ☐ |
clinical trials may show product candidates to be ineffective or not as effective as anticipated or to have harmful side effects or any unforeseen result;
|
| ☐ |
experience with marketed versions of product candidates may reveal harmful side effects or other unforeseen results;
|
| ☐ |
regulatory authorities may disagree with study design and/or data interpretation from preclinical and clinical trials, or may find that a product candidate’s benefits do not outweigh its risks;
|
| ☐ |
regulatory authorities may take longer than anticipated to make a decision on the product candidates;
|
| ☐ |
product candidates may fail to receive regulatory approvals required to bring the products to market;
|
| ☐ |
manufacturing costs, the inability to scale up to produce supplies for clinical trials or other factors may make our product candidates uneconomical;
|
| ☐ |
changes in approval policies, data standards, statutes, and regulations; and
|
| ☐ |
the proprietary rights of others and their competing products and technologies may prevent product candidates from being effectively commercialized or from obtaining exclusivity.
|
Success in preclinical and early clinical trials does not ensure that large-scale clinical trials will be successful. Clinical results are frequently susceptible to varying interpretations that may delay, limit or prevent regulatory approvals. The length of time necessary to complete clinical trials and to submit an application for marketing approval for a final decision by a regulatory authority varies significantly and may be difficult to predict. Any changes to the U.S. regulatory approval process could significantly increase the timing or cost of regulatory approval for product candidates making further development uneconomical or impossible. In addition, once Endo exercises its opt-in with respect to an additional indication, further clinical trials, development, manufacturing, marketing and selling of such product are out of our control. Our interest is limited to receiving opt-in, milestone, mark-up on cost of goods sold payments and royalty payments.
Successful development of drug candidates is inherently difficult and uncertain, and our long-term prospects depend upon our ability and the ability of our partners, particularly with respect to XIAFLEX, to continue to successfully commercialize these drug candidates.
Successful development of drugs is inherently difficult and uncertain. Our business requires investments in R&D over many years, often for drug candidates that may fail during the R&D process. Even if the Company is able to successfully complete the development of our drug candidates, our long-term prospects depend upon our ability and the ability of our partners, particularly with respect to XIAFLEX, to continue to successfully commercialize these drug candidates.
There is significant uncertainty regarding our ability to successfully develop drug candidates in other indications. These risks include the uncertainty of:
| ☐ |
the nature, timing and estimated costs of the efforts necessary to complete the development of our drug candidate projects;
|
| ☐ |
the anticipated completion dates for our drug candidate projects;
|
| ☐ |
the scope, rate of progress and cost of our clinical trials that we are currently running or may commence in the future with respect to our drug candidate projects;
|
| ☐ |
the scope, rate of progress of our preclinical studies and other R&D activities related to our drug candidate projects;
|
| ☐ |
clinical trial results for our drug candidate projects;
|
| ☐ |
the cost of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights relating to our drug candidate projects;
|
| ☐ |
the terms and timing of any strategic alliance, licensing and other arrangements that we have or may establish in the future relating to our drug candidate projects;
|
| ☐ |
the cost and timing of regulatory approvals with respect to our drug candidate projects; and
|
| ☐ |
the cost of establishing clinical supplies for our drug candidate projects.
|
Risks Related to Regulatory Requirements
We are subject to numerous complex regulatory requirements and failure to comply with these regulations, or the cost of compliance with these regulations, may harm our business.
Conducting clinical trials for human drugs and, in certain circumstances, veterinarian trials for animal drugs, and the testing, development and manufacturing and distribution of product candidates are subject to regulation by numerous governmental authorities in the U.S. and other jurisdictions, if we desire to export the resulting products to such other jurisdictions. These regulations govern or affect the testing, manufacture, safety, labeling, storage, record-keeping, approval, distribution, advertising and promotion of product candidates, as well as safe working conditions. Noncompliance with any applicable regulatory requirements can result in suspension or termination of any ongoing clinical trials of a product candidate or refusal of the government to approve a product candidate for commercialization, criminal prosecution and fines, recall or seizure of products, total or partial suspension of production, prohibitions or limitations on the commercial sale of products or refusal to allow the entering into of federal and state supply contracts. The FDA and comparable governmental authorities have the authority to suspend or terminate any ongoing clinical trials of a product candidate or withdraw product approvals that have been previously granted. Even after a product candidate has been approved, the FDA and comparable governmental authorities subject such product to continuing review and regulatory requirements including, for example, requiring the conducting and reporting of the results of certain clinical studies or trials and commitments to voluntarily conduct additional clinical trials. In addition, regulatory approval could impose limitations on the indicated or intended uses for which product candidates may be marketed. With respect to its approval of XIAFLEX for the treatment of adult Dupuytren’s contracture patients with a palpable cord, for example, the FDA and Auxilium agreed upon a REMS program consisting of a communication plan and a medication guide. The REMS program is no longer an FDA requirement for Dupuytren’s Contracture only.. With respect to its approval of XIAFLEX for Peyronie’s disease, Auxilium, and now Endo, has further collaborated with the FDA for a REMS for XIAFLEX for the treatment of Peyronie’s disease in men with a palpable plaque and curvature deformity of 30 degrees or greater at the start of therapy. The required components of the XIAFLEX REMS Program include (i) Prescribers must be certified with the program by enrolling and completing training in the administration of XIAFLEX treatment for Peyronie’s disease, and (ii) Healthcare sites must be certified with the program and ensure that XIAFLEX is only dispensed for use by certified prescribers. Currently, there is a substantial amount of congressional and administrative review of the FDA and the regulatory approval process for drug candidates in the U.S. As a result, there may be significant changes made to the regulatory approval process in the U.S. In addition, the regulatory requirements relating to the development, manufacturing, testing, promotion, marketing and distribution of product candidates may change in the U.S. Such changes may increase our costs and adversely affect our operations.
Additionally, failure to comply with, or changes to applicable regulatory requirements may result in a variety of consequences, including the following:
| ☐ |
restrictions on our products or the manufacturing processes of such products;
|
| ☐ |
warning letters, untitled letters and cyber letters;
|
| ☐ |
withdrawal of a product from the market;
|
| ☐ |
voluntary or mandatory recall of a product;
|
| ☐ |
fines;
|
| ☐ |
suspension or withdrawal of regulatory approvals for a product;
|
| ☐ |
refusal to permit the import or export of our products;
|
| ☐ |
refusal to approve pending applications or supplements to approved applications that we submit;
|
| ☐ |
denial of permission to file an application or supplement in a jurisdiction;
|
| ☐ |
debarment, exclusion from participation in federal healthcare programs, exclusion or debarment from government contracting, consent decrees, or corporate integrity agreements;
|
| ☐ |
product seizure; and
|
| ☐ |
injunctions or the imposition of civil or criminal penalties against us.
|
To the extent that we or our partners do not perform particular regulated functions ourselves but contract out to third parties, including contract manufacturers, contract research organizations, clinical trial sites, and laboratories, we or our partners may be held responsible for such third parties’ failure to follow the applicable regulatory requirements.
Our corporate compliance program cannot guarantee that we are in compliance with all potentially applicable laws and regulations and we have incurred and will continue to incur costs relating to compliance with applicable laws and regulations.
We are a small company and we rely heavily on third parties and outside consultants to conduct many important functions. As a biopharmaceutical company, we are subject to a large body of legal and regulatory requirements. In addition, as a publicly traded company we are subject to significant regulations, including the Sarbanes-Oxley Act of 2002, or SOX, some of which have only recently been revised or adopted. We cannot assure you that we are or will be in compliance with all potentially applicable laws and regulations. Failure to comply with all potentially applicable laws and regulations could lead to the imposition of fines, cause the value of our common stock to decline, and impede our ability to raise capital or list our securities on certain securities exchanges. New rules could make it more difficult or more costly for us to obtain certain types of insurance, including director and officer liability insurance, and we may be forced to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. The impact of these events could also make it more difficult for us to attract and retain qualified persons to serve on our Board, our committees and as executive officers. We cannot predict or estimate the amount of the additional costs we may incur or the timing of such costs to comply with these rules and regulations.
We may fail to maintain effective internal controls over external financial reporting or such controls may fail or be circumvented.
SOX requires us to report annually on our internal controls over financial reporting, and our business and financial results could be adversely effected if we, or our independent registered public accounting firm, determine that these controls are not effective. In addition, any failure or circumvention of our internal controls and procedures or failure to comply with regulations concerning controls and procedures could have a material effect on our business, results of operation and financial condition. The impact of these events could also make it more difficult for us to attract and retain qualified persons to serve on our Board, our committees and as executive officers.
Risks Related to Growth and Employees
Because of the specialized nature of our business, the termination of relationships with key management, consulting and scientific personnel or the inability to recruit and retain additional personnel could prevent us from developing our technologies, conducting clinical trials and/or obtaining financing.
Because of the specialized scientific nature of our business, our ability to develop products and to compete with our current and future competitors largely depends upon our ability to attract, retain and motivate highly qualified managerial, consulting and scientific personnel. If we are unable to retain the services of one or more of the principal members of senior management, consultants or other key employees, our ability to implement our business strategy could be materially harmed. We face intense competition for qualified employees and consultants from biopharmaceutical companies, research organizations and academic institutions. Attracting, retaining or replacing these personnel on acceptable terms may be difficult and time-consuming given the high demand in our industry for similar personnel. There is intense competition for qualified personnel in the areas of our activities, and we cannot assure you that we will be able to continue to attract and retain the qualified personnel necessary for the development of our business.
Adverse events or lack of efficacy in clinical trials may force us and/or our partners upon whom we are wholly dependent to stop development of our product candidates or prevent regulatory approval of our product candidates or significant safety issues could arise after regulatory approval of our products, any of which could materially harm our business.
The prescribing information for XIAFLEX for Dupuytren’s contracture originally made available by Auxilium lists “tendon ruptures or other serious injury to the injected extremity” and one “anaphylactic reaction reported in a post-marketing clinical study in a patient who had previous exposure to XIAFLEX for the treatment of Dupuytren’s contracture” as a reported serious adverse reaction to XIAFLEX and states that the most frequently reported adverse drug reactions in XIAFLEX clinical trials included swelling of the injected hand, contusion, injection site reaction, injection site hemorrhage, and pain in the treated extremity. The prescribing information notes that adverse reaction rates observed in clinical trials of a drug may not reflect those observed in practice because such trials “are conducted under widely varying conditions.”
In the case of Peyronie’s disease, the serious risks include penile fracture (corporal rupture) and other serious injuries to the penis such as hematoma. These serious risks are highlighted in the Boxed Warning within the Full Prescribing Information (the label).
Adverse events or lack of efficacy may force us to stop development of our product candidates or prevent or limit regulatory approval of our product candidates, which could materially harm our business. In addition, any adverse events or lack of efficacy may force Endo to stop development of the products we have licensed to it or prevent or limit regulatory approval of such products, which could materially impair all or a material part of the future revenue we hope to receive from Endo. Even if our product candidates receive regulatory approval, new safety issues may be reported and we or our partners may be required to amend the conditions of use for a product and may make it difficult to obtain product liability insurance for clinical trials.
We and our licensees face competition in our product development and marketing efforts from pharmaceutical and biotechnology companies, universities and other not-for-profit institutions.
We and our licensees face competition in our product development and marketing efforts from entities that have substantially greater research and product development capabilities and greater financial, scientific, marketing and human resources. These entities include pharmaceutical and biotechnology companies, as well as universities and not-for-profit institutions. Our and our licensees’ competitors may succeed in developing products or intellectual property earlier than we or our licensees do, entering into successful collaborations before us or our licensees, obtaining approvals from the FDA or other regulatory agencies for such products before us or our licensees, or developing or marketing products that are more effective than those we or our licensees could develop or market. The success of any one competitor in these or other respects will have a material adverse effect on our business, our ability to receive opt-in payments from Endo or our ability to generate revenues from third party arrangements with respect to additional indications for which Endo does not exercise its opt-in.
We may face financial pressures because of our lack of diversity in our research and product development.
All of our income is derived from products marketed by Endo and Endo has the right under the Endo Agreement to opt-in to all work we do in the Field (as defined in the Endo Agreement). Therefore, with respect to those products for which Endo opts-in, the Company’s upside is limited by the Endo Agreement. For example, Endo may opt-in to an indication and then choose not to vigorously pursue the development of that indication which may result in BioSpecifics negotiating with Endo for repurchase rights to the indication. In order to eliminate this financial pressure and diversify our portfolio, we may choose to acquire or in-license non-collagenase opportunities.
Our strategy of generating growth through acquisitions and in-licensing deals may not be successful.
Because of limits in the Endo Agreement, our business strategy may include growing our business through acquisition and in-licensing transactions. We may not be successful in identifying, effectively evaluating, acquiring or in-licensing, and developing and commercializing additional products on favorable terms, or at all. Competition for attractive product opportunities is intense and may require us to devote substantial resources, both managerial and financial, to an acquisition or in-licensing opportunity.
Acquisition and in-licensing efforts can consume significant management attention and require substantial expenditures, which could detract from our other programs. In addition, we may devote significant resources to potential deals that are never completed. Even if we are successful in acquiring a product or company or obtaining licensing terms favorable to us, it may not result in a successfully developed or commercialized product or, even if an acquired product is commercialized, competing products or technologies could render a product noncompetitive, uneconomical or obsolete. Moreover, the cost of acquiring other companies or in-licensing products could be substantial. If we are unsuccessful in our efforts to acquire other companies or in-license and develop additional products, or if we acquire or in-license unproductive assets, it could have a material adverse effect on the growth of our business.
We may face pressure from activist stockholders to declare dividends which may negatively affect our business.
Campaigns by stockholders to effect changes at publicly-listed companies are sometimes led by investors seeking to increase short-term stockholder value by advocating corporate actions including special dividends. We have built a substantial amount of cash. Given our stockholder composition and other factors, it is possible such stockholder or future activist stockholders may attempt to effect a distribution of this cash. Responding to actions by such activist stockholders or others in the future would be costly and time-consuming, disrupt our operations and divert the attention of our Board and senior management from the pursuit of business strategies, including new collagenase or non-collagenase opportunities, acquisitions or in-licenses of other indications or technologies, which could adversely affect our results of operations and financial condition. Furthermore, if faced with actions by activist stockholders, we may not be able to respond effectively to such actions, which could be disruptive to our business.
If product liability lawsuits are brought against us, we may incur substantial liabilities.
Our business exposes us to potential liability risks that arise from the clinical testing and, if approved, the commercialization of our products. We continue to have product liability exposure for topical products sold by us prior to the sale of our topical business. In addition to direct expenditures for damages, settlement and defense costs, there is a possibility of adverse publicity and loss of revenues as a result of product liability claims. Product liability is a significant commercial risk for us. Some plaintiffs have received substantial damage awards in some jurisdictions against pharmaceutical companies based upon claims for injuries allegedly caused by the use of their products. In addition, in the age of social media, plaintiffs’ counsel now have a wide variety of tools to advertise their services and solicit new clients for litigation. Thus, we could expect that any significant product liability litigation or mass tort in which we are a defendant will have a larger number of plaintiffs than such actions have seen historically because of the increasing use of widespread and media-varied advertising. In addition, under the Endo Agreement, we are obligated to indemnify Endo and its affiliates for any harm or losses they suffer relating to any personal injury and other product liability resulting from our development, manufacture or commercialization of any injectable collagenase product. We have clinical trial and product liability insurance in the aggregate amount of $5.0 million dollars that we believe is adequate in both scope and amount and has been placed with what we believe are reputable insurers. We may not be able to maintain our clinical trial and product liability insurance at an acceptable cost, if at all, and this insurance may not provide adequate coverage against potential claims or losses. If losses from product liability claims exceed our insurance coverage, we may incur substantial liabilities that exceed our financial resources, and our business and results of operations may be harmed. Whether or not we are ultimately successful in product liability litigation, such litigation could consume substantial amounts of our financial and managerial resources, and might result in adverse publicity, all of which could impair our business
In addition, it may be necessary for us to voluntarily or mandatorily recall or withdraw products that do not meet approved specifications or which subsequent data demonstrate may be unsafe or ineffective, which would also result in adverse publicity as well as in costs connected to the recall and loss of revenue.
Risks Related to Intellectual Property Rights
If we are unable to obtain, maintain and enforce intellectual property protection covering our products, others may be able to make, use or sell products substantially the same as ours, which could adversely affect our ability to compete in the market.
Our commercial success depends, in part, on our ability to obtain, maintain and enforce patents, trade secrets, trademarks and other intellectual property rights and to operate without having third parties infringe, misappropriate or circumvent the rights that we own or license. If we are unable to obtain, maintain and enforce intellectual property protection covering our products, others may be able to make, use or sell products that are substantially the same as ours without incurring the sizeable development and licensing costs that we have incurred, which would adversely affect our ability to compete in the market. Our ability to stop third parties from making, using, selling, offering to sell or importing our product candidates is dependent upon the extent to which we have rights under valid and enforceable patents or trade secrets that cover these activities. However, the patent positions of biopharmaceutical companies, including ours, can be highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. Therefore, there is no assurance that our pending patent applications will result in the issuance of patents or that we will develop additional proprietary products which are patentable. Moreover, patents issued or to be issued to us may not provide us with any competitive advantage. Our patent position is subject to numerous additional risks, including the following:
| · |
we may fail to seek patent protection for inventions that are important to our success;
|
| · |
our pending patent applications may not result in issued patents;
|
| · |
we cannot be certain that we were the first to invent the inventions covered by pending pre-America Invents Act patent applications or that we were the first to file such applications and, if we are not, we may be subject to priority disputes;
|
| · |
we may be required to disclaim part or all of the term of certain patents or all of the term of certain patent applications;
|
| · |
we may file patent applications but have claims restricted or we may not be able to supply sufficient data to support our claims and, as a result, may not obtain the original claims desired or we may receive restricted claims. Alternatively, it is possible that we may not receive any patent protection from an application;
|
| · |
we could inadvertently abandon a patent or patent application, resulting in the loss of protection of certain intellectual property rights in a certain country. We, our collaborators or our patent counsel may take action resulting in a patent or patent application becoming abandoned which may not be able to be reinstated or if reinstated, may suffer patent term adjustments;
|
| · |
the claims of our issued patents or patent applications when issued may not cover our products;
|
| · |
no assurance can be given that our patents would be declared by a court to be valid or enforceable or that a competitor’s technology or product would be found by a court to infringe our patents. Our patents or patent applications may be challenged by third parties in patent litigation or in proceedings before the USPTO or its foreign counterparts, and may ultimately be declared invalid or unenforceable, or narrowed in scope;
|
| · |
there may be prior art of which we are not aware that may affect the validity or enforceability of a patent claim. There also may be prior art of which we are aware, but which we do not believe affects the validity or enforceability of a claim, which may, nonetheless, ultimately be found to affect the validity or enforceability of a claim;
|
| · |
third parties may develop products which have the same or similar effect as our products without infringing our patents. Such third parties may also intentionally circumvent our patents by means of alternate designs or processes or file applications or be granted patents that would block or hurt our efforts;
|
| · |
there may be dominating patents relevant to our product candidates of which we are not aware;
|
| · |
our patent counsel, lawyers or advisors may have given us, or may in the future give us incorrect advice or counsel. Opinions from such patent counsel or lawyers may not be correct or may be based on incomplete facts;
|
| · |
obtaining regulatory approval for biopharmaceutical products is a lengthy and complex process, and as a result, any patents covering our product candidates may expire before, or shortly after such product candidates are approved and commercialized;
|
| · |
the patent and patent enforcement laws of some foreign jurisdictions do not protect intellectual property rights to the same extent as laws in the U.S., and many companies have encountered significant difficulties in protecting and defending such rights in foreign jurisdictions. If we encounter such difficulties or we are otherwise precluded from effectively protecting our intellectual property rights in foreign jurisdictions, our business prospects could be substantially harmed; and
|
| · |
we may not develop additional proprietary technologies that are patentable.
|
Any of these factors could hurt our ability to gain full patent protection for our products. Registered trademarks and trademark applications in the U.S. and other countries are subject to similar risks as described above for patents and patent applications.
Moreover, we may be subject to a third-party pre-issuance submission of prior art to the USPTO, or become involved in opposition, nullity, derivation, reexamination, inter partes review, post-grant review or interference proceedings challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our technology or drugs and compete directly with us, without payment to us or result in our inability to manufacture or commercialize drugs without infringing third-party patent rights. In addition, if the breadth or strength of protection provided by our patents and patent applications is threatened, it could dissuade companies from collaborating with us to seek patent protection or to license, develop or commercialize current or future product candidates.
Developments in patent law could have a negative impact on our business.
From time to time, the United States Supreme Court, or the Supreme Court, other federal courts, the United States Congress, or the USPTO, may change the standards of patentability and any such changes could have a negative impact on our business.
Two cases involving diagnostic method claims and “gene patents” have recently been decided by the Supreme Court. On March 20, 2012, the Supreme Court issued a decision in Mayo Collaborative v. Prometheus Laboratories, or Prometheus, a case involving patent claims directed to optimizing the amount of drug administered to a specific patient. According to that decision, Prometheus’ claims failed to incorporate sufficient inventive content above and beyond mere underlying natural correlations to allow the claimed processes to qualify as patent-eligible processes that apply natural laws. On June 13, 2013, the Supreme Court subsequently decided Association for Molecular Pathology v. Myriad Genetics, or Myriad, a case brought by multiple plaintiffs challenging the validity of patent claims held by Myriad Genetics, Inc. relating to the breast cancer susceptibility genes BRCA1 and BRCA2, holding that genomic DNA that exists in nature, even if isolated, such as the DNA constituting the BRCA1 and BRCA2 genes, is not patentable subject matter under 35 U.S.C. §101.
On March 4, 2014, the USPTO issued a memorandum to patent examiners providing guidance for examining claims reciting laws of nature/natural principles, natural phenomena, and/or natural products for patent eligibility in view of the Supreme Court decisions in Prometheus and Myriad. The guidance indicates that claims reciting such natural products, even in combination, that do not significantly differ from such natural products could be rejected as directed to non-statutory subject matter. That guidance was replaced by a memorandum issued December 15, 2014, that modified some of the earlier guidance, but a number of the aspects have not substantially changed, and it is too soon to determine how the revised guidance will be applied. These guidelines, and the Myriad discussion that isolation of natural products may not confer eligibility under 35 U.S.C. §101, is relevant to our patent portfolio and thus enforcement of these patents.
A further case relevant to these issues was decided by the Supreme Court on June 19, 2014, in Alice Corp. v. CLS Bank International, 573 U.S. __, 134 S. Ct. 2347 (2014). While the Alice case related to computer-implemented inventions, the holdings in that case, which also related to natural laws or “abstract ideas” have been used to reject claims in applications directed to other technologies. As a result of the Alice case, the March guidance issued by the USPTO was replaced by a memorandum issued December 15, 2014, that modified some of the earlier guidance. In June of 2015, an additional case was decided by the Federal Circuit, namely, Ariosa Diagnostics, Inc. v. Sequenom, Inc., 788 F.3d 1371 (Fed. Cir. 2015). The Federal Circuit affirmed the district court, finding that methods of detecting paternally inherited nucleic acids were not patent eligible. Sequenom’s petition for rehearing en banc and its petition for certiorari to the Supreme Court were both denied.
On July 30, 2015, the USPTO issued a “July 2015 Update on Subject Matter Eligibility,” which provided further guidance, as well as examples of patent-eligible and patent-ineligible subject matter, which was largely directed to computer-implemented inventions. However, in May of 2016, the Patent Office issued an additional “Subject Matter Eligibility Update,” as well as “Subject Matter Eligibility Examples: Life Sciences,” which included examples of eligible and non-eligible claims relating to vaccines, diagnosis and treatment of disease, dietary sweeteners, screening for gene alterations, a paper-making machine, and a process for hydrolysis of fat. These examples are useful guidance for drafting eligible claims in the chemical and biological arts. In addition, the Patent Office provided an additional memorandum in November of 2016, summarizing more recent decisions by the Federal Circuit in the area of software claim eligibility.
In light of the developing case law and guidance from the USPTO on subject matter eligibility, we cannot assure you that our efforts to seek patent protection for our technology and products will not be negatively impacted by the guidance issued by the USPTO, the decisions described above, rulings in other cases, or changes in guidance or procedures issued by the USPTO, or changes in statutes implemented by Congress.
Furthermore, we cannot fully predict what impact the Supreme Court’s decisions in Prometheus, Myriad and Alice may have on the ability of biopharmaceutical companies or other entities to obtain or enforce patents relating to purified natural products in the future. The Prometheus, Myriad and Alice decisions are new and the contours of when claims to laws of nature, natural phenomena or natural products meet the patent eligibility requirements are not clear and may take many years to develop via interpretation in the courts. Thus, we may not be able to successfully defend the validity of our patents if challenged.
In addition, the Leahy-Smith America Invents Act, or the America Invents Act, which was signed into law in 2011, includes a number of significant changes to U.S. patent law. These changes include a transition from a “first-to-invent” system to a “first-to-file” system, changes to the way issued patents are challenged, and changes to the way patent applications are disputed during the examination process. These changes may favor larger and more established companies that have greater resources to devote to patent application filing and prosecution. The USPTO has developed new and untested regulations and procedures to govern the full implementation of the America Invents Act, and many of the substantive changes to patent law associated with the America Invents Act, and, in particular, the first-to-file provisions, became effective on March 16, 2013. Substantive changes to patent law associated with the America Invents Act may affect our ability to obtain patents, and, if obtained, to enforce or defend them. Accordingly, it is not clear what, if any, impact the America Invents Act will ultimately have on the cost of prosecuting our patent applications, our ability to obtain patents based on our discoveries and our ability to enforce or defend any patents that may issue from our patent applications, all of which could have a material adverse effect on our business.
In addition, the laws of foreign countries may not protect our rights to the same extent as the laws of the U.S. or visa-versa. For example, European patent law restricts the patentability of methods of treatment of the human body more than U.S. law. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and utility, or equivalent, patent applications in the U.S. and other jurisdictions are typically not published until 18 months after the filing date of such patent applications, or in some cases, not at all. Therefore, we cannot know with certainty whether we were the first to make the inventions claimed in our owned or licensed patents or pending patent applications, or that we were the first to file for patent protection of such inventions. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain. Our pending and future patent applications may not result in patents being issued that protect our product candidates, in whole or in part, or which effectively prevent others from commercializing competitive technologies and drugs. Changes in either the patent laws or interpretation of the patent laws in the U.S. and other countries may diminish the value of our patents or narrow the scope of our patent protection.
If we breach any of the agreements under which we license rights to products or technology from others, we could lose license rights that are critical to our business and our business could be harmed.
We are a party to a number of license agreements by which we have acquired rights to use the intellectual property of third parties that are necessary for us to operate our business. If any of the parties terminates its agreement, whether by its terms or due to our breach, our right to use the party’s intellectual property may negatively affect our licenses to Endo, and, in turn, their obligation to make opt-in, milestone, mark-up on cost of goods sold, royalty or other payments to us.
Our ability and the ability of our licensees and collaborators to develop and license products based on our patents may be impaired by the intellectual property of third parties.
Endo’s, and our commercial success in developing and manufacturing collagenase products based on our patents is dependent on these products not infringing the patents or proprietary rights of third parties. While we currently believe that we, our licensees and collaborators have freedom to operate in the collagenase market, others may challenge that position in the future. There has been, and we believe that there will continue to be, significant litigation in the pharmaceutical industry regarding patent and other intellectual property rights.
Third parties could bring legal actions against us, our licensees, licensors or collaborators claiming damages and seeking to enjoin clinical testing, manufacturing and marketing of the affected product or products. A third party might request a court to rule that the patents we in-licensed or licensed to others, or those we may in-license in the future, are invalid or unenforceable. In such a case, even if the validity or enforceability of those patents were upheld, a court might hold that the third party’s actions do not infringe the patent we license to others, which could, in effect, limit the scope of our patent rights and those of our licensees or collaborators. Our agreements with Endo require us to indemnify them against any claims for infringement based on the use of our technology. If we become involved in any litigation, it could consume a substantial portion of our resources, regardless of the outcome of the litigation. If Endo becomes involved in such litigation, it could also consume a substantial portion of their resources, regardless of the outcome of the litigation, thereby jeopardizing their ability to commercialize candidate products and/or their ability to make opt-in, milestone, mark-up on cost of goods sold or royalty payments to us. If any of these actions is successful, in addition to any potential liability for damages, we could be required to obtain a license to permit ourselves, our licensees, licensors or our collaborators to conduct clinical trials, manufacture or market the affected product, in which case we may be required to pay substantial royalties or grant cross-licenses to our patents. However, there can be no assurance that any such license will be available on commercially acceptable terms or at all. Ultimately, we, our licensees or collaborators could be prevented from commercializing a product, or forced to cease some aspect of their or our business, as a result of patent infringement claims, which could harm our business or right to receive opt-in, milestone, mark-up on cost of goods sold and royalty payments.
Our intellectual property may be infringed by a third party.
Third parties may infringe one or more of our issued patents or trademarks. We cannot predict if, when or where a third party may infringe one or more of our issued patents or trademarks. To counter infringement, we may be required to file infringement claims, which can be expensive and time consuming. There is no assurance that we would be successful in a court of law in proving that a third party is infringing one or more of our issued patents or trademarks. Any claims we assert against perceived infringers could also provoke these parties to assert counterclaims against us, alleging that we infringe their intellectual property. In addition, in a patent infringement proceeding, a court may decide that a patent of ours is invalid or unenforceable, in whole or in part, construe the patent’s claims narrowly and/or refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question, any of which may adversely affect our business. Even if we are successful in proving in a court of law that a third party is infringing one or more of our issued patents or trademarks there can be no assurance that we would be successful in halting their infringing activities, for example, through a permanent injunction, or that we would be fully or even partially financially compensated for any harm to our business. We may be forced to enter into a license or other agreement with the infringing third party at terms less profitable or otherwise commercially acceptable to us than if the license or agreement were negotiated under conditions between those of a willing licensee and a willing licensor. We may not become aware of a third-party infringer within legal timeframes for compensation or at all, thereby possibly losing the ability to be compensated for any harm to our business. Such a third party may be operating in a foreign country where the infringer is difficult to locate and/or the intellectual property laws may be more difficult to enforce. Some third-party infringers may be able to sustain the costs of complex infringement litigation more effectively than we can because they have substantially greater resources. Any inability to stop third-party infringement could result in loss in market share of some of our products or even lead to a delay, reduction and/or inhibition of the development, manufacture or sale of certain products by us. There is no assurance that a product produced and sold by a third-party infringer would meet our or other regulatory standards or would be safe for use. Such third‑party infringer products could irreparably harm the reputation of our products thereby resulting in substantial loss in market share and profits.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties.
We employ individuals who were previously employed at other biotechnology or pharmaceutical companies. We may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed confidential information of our employees’ former employers or other third parties. We may also be subject to claims that former employers or other third parties have an ownership interest in our patents. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and if we do not prevail, we could be required to pay substantial damages and could lose rights to important intellectual property. Even if we are successful, litigation could result in substantial cost and be a distraction to our management and other employees.
Risks Related to our Common Stock
We have no current plan to pay dividends on our common stock and investors must rely on an increase in stock price for any return on their investment.
We retain the earnings that we generate and we have no current plans to pay dividends on our common stock. Because we historically have not declared dividends, stockholders must rely on an increase in the stock price for any return on their investment in us. Investors will not receive any funds absent a sale of their shares. We cannot assure investors of a positive return on their investment when they sell their shares.
Our stock price has, in the past, been volatile, and the market price of our common stock may drop below the current price.
Our stock price has, at times, been volatile. Currently, our common stock is traded on The Nasdaq Global Market, or NASDAQ, and is thinly traded.
Market prices for securities of pharmaceutical, biotechnology and specialty pharmaceutical companies have been particularly volatile. Some of the factors that may cause the market price of our common stock to fluctuate include:
| ☐ |
results of our clinical trials;
|
| ☐ |
failure of any product candidates we have licensed to Endo to achieve commercial success;
|
| ☐ |
failure of Endo to exercise any opt in rights to new indications;
|
| ☐ |
regulatory developments in the U.S. and foreign countries;
|
| ☐ |
developments or disputes concerning patents or other proprietary rights;
|
| ☐ |
litigation involving us or our general industry, or both;
|
| ☐ |
future sales of our common stock by the estate of our former Chairman and CEO, directors, officers, or others;
|
| ☐ |
changes in the structure of healthcare payment systems, including developments in price control legislation;
|
| ☐ |
departure of key personnel;
|
| ☐ |
termination of agreements with our licensees or their sublicensees;
|
| ☐ |
announcements of material events by those companies that are our competitors or perceived to be similar to us;
|
| ☐ |
changes in estimates of our financial results;
|
| ☐ |
investors’ general perception of us;
|
| ☐ |
general economic, industry and market conditions; and
|
| ☐ |
the reallocation by Endo of its priorities away from XIAFLEX.
|
If any of these risks occurs, or continues to occur, it could cause our stock price to fall and may expose us to class action lawsuits that, even if unsuccessful, could be costly to defend and a distraction to management.
We cannot guarantee that we will repurchase our common stock pursuant to our stock repurchase program or that our stock repurchase program will enhance long-term stockholder value. Stock repurchases could also increase the volatility of the price of our common stock and could diminish our cash reserves.
In August 2015, our Board authorized an increase in the repurchase amount of our stock repurchase program under which we are authorized to repurchase shares of our common stock for an aggregate purchase price not to exceed $2.5 million in open market transactions in compliance with SEC Rule 10b-18. Although our Board has authorized the stock repurchase program, the stock repurchase program does not obligate us to repurchase any specific dollar amount or to acquire any specific number of shares. Stock will be purchased from time to time, in the open market in compliance with SEC Rule 10b-18, subject to market conditions and applicable state and federal securities laws. The timing and amount of repurchases, if any, will depend upon several factors, including market and business conditions, the trading price of our common stock and the nature of other investment opportunities. In addition, repurchases of our common stock pursuant to our stock repurchase program could affect the market price of our common stock or increase its volatility. For example, the existence of a stock repurchase program could cause our stock price to be higher than it would be in the absence of such a program and could potentially reduce the market liquidity for our stock. Additionally, our stock repurchase program could diminish our cash reserves, which may impact our ability to finance future growth and to pursue possible future strategic opportunities and acquisitions. There can be no assurance that any stock repurchases will enhance stockholder value because the market price of our common stock may decline below the levels at which we determine to repurchase our stock. Although our stock repurchase program is intended to enhance long-term stockholder value, there is no assurance that it will do so and short-term stock price fluctuations could reduce the program’s effectiveness.
Actual or potential sales of our common stock by our directors, employees and consultants, during open trading windows and pursuant to pre-arranged stock trading plans, could cause our stock price to fall or prevent it from increasing for numerous reasons, and actual or potential sales by such persons could be viewed negatively by other investors.
We have a number of insiders that own significant blocks of our Common Stock. If one or more of these stockholders sell large portions of their holdings in a relatively short time, for liquidity, tax, or other reasons, the prevailing market price of our Common Stock could be negatively affected. In addition, it is possible that our executive officer, consultants, or non-employee members of our Board could sell shares of our Common Stock during an open trading window under our Insider Trading Policy. These transactions and the perceived reasons for these transactions could be viewed negatively by other investors and could have a negative effect on the prevailing market price of our Common Stock.
In accordance with the guidelines specified under Rule 10b5-1 of the Exchange Act, and our policies regarding stock transactions, certain of our directors and consultants have adopted and may continue to adopt stock trading plans pursuant to which they have arranged to sell shares of our common stock from time to time in the future. Generally, sales under such plans by our directors require public filings. Actual or potential sales of our common stock by such persons could cause the price of our common stock to fall or prevent it from increasing for numerous reasons. For example, a substantial number of shares of our common stock becoming available (or being perceived to become available) for sale in the public market could cause the market price of our common stock to fall or prevent it from increasing.
Our outstanding options to purchase shares of common stock could have a possible dilutive effect.
As of December 31, 2016, options to purchase 297,000 shares of common stock were outstanding. In addition, as of December 31, 2016, a total of 209,098 options were available for grant under our stock option plans. The issuance of common stock upon the exercise of these options could adversely affect the market price of the common stock or result in substantial dilution to our existing stockholders.
If securities analysts do not publish research reports about our or Endo’s business or if they downgrade us, Endo or our sector, the price of our common stock could decline.
The trading market for our common stock will depend in part on research reports that industry or financial analysts publish about us or our business or about Endo. If analysts downgrade us or any of our licensees, including Endo, or other research analysts downgrade the industry in which we operate or the stock of any of our competitors or licensees, the price of our common stock may decline. We currently have one analyst covering our stock. We lack the potential benefit that coverage by other analysts may provide.
Provisions in our certificate of incorporation and bylaws may prevent or frustrate a change in control.
Provisions of our certificate of incorporation and bylaws may discourage, delay or prevent a merger, acquisition or other change in control that stockholders may consider favorable, including transactions in which you might otherwise receive a premium for your shares. These provisions:
| ☐ |
provide for a classified Board;
|
| ☐ |
give our Board the ability to designate the terms of and issue new series of preferred stock without stockholder approval, commonly referred to as “blank check” preferred stock, with rights senior to those of our common stock;
|
| ☐ |
limit the ability of the stockholders to call special meetings; and
|
| ☐ |
impose advance notice requirements on stockholders concerning the election of directors and other proposals to be presented at stockholder meetings.
|
In addition, during May 2002, the Board implemented a rights agreement, commonly known as a Poison Pill, which effectively discourages or prevents acquisitions of more than 15% of our common stock in transactions (mergers, consolidations, tender offer, etc.) that have not been approved by our Board. The Board amended the Poison Pill in February 2011 to increase the threshold from 15% to 18% and extended the expiration date of the Poison Pill for an additional two years, to May 31, 2014. In February 2014, the Board amended the Poison Pill again to extend the term for an additional two years, to May 31, 2016. In May 2016, the Board again amended the Poison Pill to extend the term for an additional two years, to May 31, 2018. These provisions could make it more difficult for common stockholders to replace members of the Board. Because our Board is responsible for appointing the members of our management team, these provisions could in turn affect any attempt to replace the current management team.
If our principal stockholders, executive officer and directors choose to act together, they may be able to control our operations, acting in their own best interests and not necessarily those of other stockholders.
As of March 14, 2017 our executive officer, directors and their affiliates, in the aggregate, beneficially owned shares representing approximately 21% of our common stock. Beneficial ownership includes shares over which an individual or entity has investment or voting power and includes shares that could be issued upon the exercise of options within 60 days. As a result, if these stockholders were to choose to act together, they may be able to control all matters submitted to our stockholders for approval, as well as our management and affairs. For example, these individuals, if they chose to act together, could control the election of directors and approval of any merger, consolidation or sale of all or substantially all of our assets. This concentration of ownership could have the effect of delaying, deferring or preventing a change in control or impeding a merger or consolidation, takeover or other business combination that could be favorable to other stockholders.
This significant concentration of share ownership may adversely affect the trading price for our common stock because investors often perceive disadvantages in owning stock in companies with controlling stockholders.
None.
Our corporate headquarters are currently located at 35 Wilbur St., Lynbrook, NY 11563 (the “Headquarters”). As previously reported, the Company formerly leased the Headquarters from Wilbur St. Corp. (“WSC”), which was owned by Edward H. Wegman, the former CEO and Chairman of BioSpecifics. On November 21, 2013, WSC sold the Headquarters to 35 Wilbur Street Associates, LLC (the “Landlord”), and the Company entered into an Agreement of Lease (the “Lease”) with the Landlord for the Company’s Headquarters and simultaneously terminated the existing lease. Neither the Company nor its affiliates have a material relationship or affiliation with the Landlord. The term of the Lease was for twenty-four months and the base rent was $12,000 per month, provided, however, that the Company had the option to cancel the Lease after the first year by giving three months’ notice to the Landlord. The Lease was filed with the SEC as Exhibit 10.1 to the Company’s Annual Report on Form 10-K filed with the SEC on March 7, 2014. In 2014 the Company leased approximately 2,300 square feet back to the Landlord and the Company’s base rent was adjusted to approximately $10,200 per month.
On August 14, 2015, the Company entered into an agreement with the Landlord to extend the term of the lease to the Headquarters for an additional one year period (the “Extended Lease Agreement”). The one year extension ended on November 30, 2016. Pursuant to the Extended Lease Agreement, the Landlord will take occupancy of 1,000 square feet in the front of the building, the base rent will be $10,213 per month and the Company may cancel the lease with three months’ prior written notice to the Landlord at any time during the term. The Agreement is incorporated by reference to Exhibit 10.1 to the Quarterly Report on Form 10-Q filed with the SEC on November 9, 2015.
On November 1, 2016, the Company entered into an agreement with the Landlord to extend the term of the lease to the Headquarters for an additional one year period (the “2016 Extended Lease Agreement”). The one year extension will end on November 30, 2017. Pursuant to the 2016 Extended Lease Agreement, the base rent is $10,757 per month and the Company may cancel the lease with three months’ prior written notice to the Landlord at any time during the term. The 2016 Extended Lease Agreement was filed with the SEC as Exhibit 10.1 to the Company’s Quarterly Report on Form 10Q on November 9, 2016.
None.
Not Applicable.
| Item 5. |
MARKET FOR COMMON EQUITY, RELATED STOCKHOLDER MATTERS, AND ISSUER PURCHASES OF EQUITY SECURITIES.
|
Market Information
Our common stock currently trades under the symbol BSTC on NASDAQ. On March 14, 2017, the last reported sale price of our common stock was $53.95 per share.
The table below sets forth the high and low closing sale prices for our common stock as reported by and as quoted by NASDAQ for each of the quarterly periods in 2016 and 2015:
|
2016
|
HIGH
|
LOW
|
||||||
|
Fourth Quarter
|
$
|
55.70
|
$
|
41.01
|
||||
|
Third Quarter
|
$
|
46.87
|
$
|
36.10
|
||||
|
Second Quarter
|
$
|
39.94
|
$
|
33.79
|
||||
|
First Quarter
|
$
|
40.10
|
$
|
31.32
|
||||
|
2015
|
HIGH
|
LOW
|
||||||
|
Fourth Quarter
|
$
|
62.48
|
$
|
40.41
|
||||
|
Third Quarter
|
$
|
68.72
|
$
|
42.07
|
||||
|
Second Quarter
|
$
|
55.19
|
$
|
36.96
|
||||
|
First Quarter
|
$
|
41.32
|
$
|
37.51
|
||||
These quotations reflect inter-dealer prices, without retail mark-up, mark-down or commission and may not represent actual transactions.
Holders of Record
As of March 14, 2017, there were approximately 57 holders of record of our common stock. Because many of such shares are held by brokers and other institutions on behalf of stockholders, we are unable to estimate the total number of stockholders represented by these nominees and we believe that the total number of beneficial owners is considerably higher.
Dividends
It has been our policy to retain potential earnings to finance the growth and development of our business and not pay dividends, and we have no current plans to pay dividends. Any payment of cash dividends in the future will depend upon our financial condition, capital requirements and earnings as well as such other factors as our Board of Directors (the “Board”) may deem relevant.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of December 31, 2016 with respect to the shares of our common stock that may be issued under our existing equity compensation plans:
|
Plan Category
|
Number of securities to be
issued upon exercise of
outstanding options,
warrants and rights
(a)
|
Weighted-average
exercise price of
outstanding options,
warrants and rights
(b)
|
Number of securities
remaining available
for future issuance
under equity
compensation plans
(excluding securities
reflected in column (a))
(c)
|
|
Equity compensation plans
approved by security holders(1)
|
297,000
|
$20.14
|
209,098
|
|
Equity compensation plans not
approved by security holders
|
-
|
-
|
-
|
|
Total
|
297,000
|
$20.14
|
209,098
|
(1) Please see Note 9, “Stockholders’ Equity,” of the notes to the consolidated financial statements for a description of the material features of each of our plans.
Recent Sales of Unregistered Securities
For the year ended December 31, 2016, we did not issue any unregistered shares of securities.
Issuer Purchases of Equity Securities(1)
|
Month
|
Total Number
of Shares
Purchased(2)
|
Average
Price Paid
Per Share (3)
|
Total
Cumulative
Number of
Shares
Purchased as
Part of Publicly
Announced Plan
|
Maximum
Dollar Value
of Shares
that may yet
be Purchased
under the
Plan
|
|||
|
October 1, 2016 to October 31, 2016
|
1,700
|
$45.06
|
261,388
|
$645,379
|
|||
|
November 1, 2016 to November 30, 2016
|
1,295
|
$45.80
|
262,683
|
$586,073
|
|||
|
December 1, 2016 to December 31, 2016
|
283
|
$51.78
|
262,966
|
$571,419
|
|||
|
Total
|
3,278
|
The following table presents a summary of share repurchases made by us during the quarter ended December 31, 2016.
| (1) |
On August 17, 2015, we announced that our Board had authorized the repurchase of up to $2.5 million of our common stock under the stock repurchase program.
|
| (2) |
The purchases were made in open-market transactions in compliance with rule 10b-18 or under the Company’s 10b-18 plan.
|
| (3) |
Includes commissions paid, if any, related to the stock repurchase transactions.
|
Performance Graph
The graph below compares the cumulative total stockholder return on our common stock with the cumulative total stockholder return of (i) the NASDAQ Biotechnology Index, and (ii) the NASDAQ Composite Index, assuming an investment of $100 on December 31, 2011, in our common stock; the stocks comprising the NASDAQ Composite Index; and the stocks comprising the NASDAQ Biotechnology Index.
Comparison of Cumulative Total Return* Among BioSpecifics Technologies Corp, the NASDAQ Biotechnology Index and the NASDAQ Composite Index
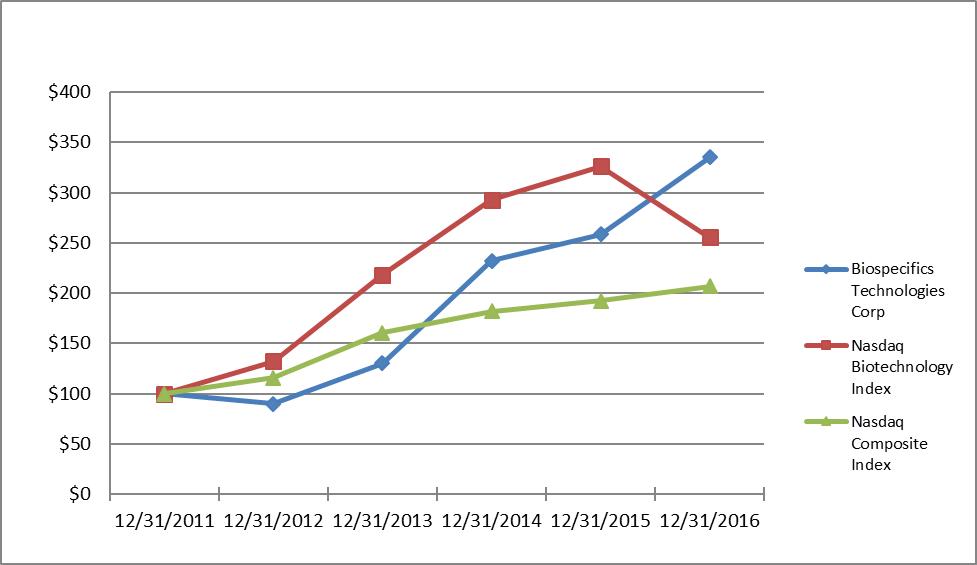
|
12/31/2011
|
12/31/2012
|
12/31/2013
|
12/31/2014
|
12/31/2015
|
12/31/2016
|
|||||||||||||||||||
|
BioSpecifics
Technologies Corp.
|
$
|
100.00
|
$
|
89.95
|
$
|
130.39
|
$
|
232.37
|
$
|
258.54
|
$
|
335.14
|
||||||||||||
|
NASDAQ
Biotechnology Index
|
$
|
100.00
|
$
|
131.91
|
$
|
218.45
|
$
|
292.93
|
$
|
326.39
|
$
|
255.62
|
||||||||||||
|
NASDAQ Composite
Index
|
$
|
100.00
|
$
|
115.91
|
$
|
160.32
|
$
|
181.80
|
$
|
192.21
|
$
|
206.63
|
||||||||||||
*Total return assumes $100 invested on December 31, 2011 in our common stock, the NASDAQ Composite Index, and the NASDAQ Biotechnology Index and reinvestment of dividends through fiscal year ended December 31, 2016.
The following selected consolidated financial data should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our consolidated financial statements and the related notes appearing elsewhere in this Report. The consolidated statements of income data for the years ended December 31, 2016, 2015 and 2014 and the consolidated balance sheet data as of December 31, 2016 and 2015 have been derived from our audited consolidated financial statements and related notes, which are included elsewhere in this Report. The consolidated statement of income data for the years ended December 31, 2013 and 2012 and the consolidated balance sheet data as of December 31, 2014, 2013 and 2012 have been derived from audited financial statements which do not appear in this Report. The historical results presented are not necessarily indicative of results to be expected in any future period.
|
Consolidated Statement of Income Data
|
Years Ended December 31,
|
|||||||||||||||||||
|
2016
|
2015
|
2014
|
2013
|
2012
|
||||||||||||||||
|
Total revenues
|
$
|
26,250,955
|
$
|
22,750,135
|
$
|
14,044,624
|
$
|
14,429,782
|
$
|
11,126,859
|
||||||||||
|
Operating expenses:
|
||||||||||||||||||||
|
Research and development
|
1,327,923
|
1,034,288
|
1,263,512
|
1,484,416
|
1,249,755
|
|||||||||||||||
|
General and administrative
|
7,896,616
|
7,272,532
|
5,814,185
|
5,038,363
|
4,774,828
|
|||||||||||||||
|
Total costs and expenses
|
9,224,539
|
8,306,820
|
7,077,697
|
6,522,779
|
6,024,583
|
|||||||||||||||
|
Operating income
|
17,026,416
|
14,443,315
|
6,966,927
|
7,907,003
|
5,102,276
|
|||||||||||||||
|
Other income:
|
||||||||||||||||||||
|
Interest income
|
295,783
|
92,926
|
32,158
|
26,202
|
34,634
|
|||||||||||||||
|
Other
|
52,805
|
14,719
|
33,582
|
37,458
|
18,219
|
|||||||||||||||
|
348,588
|
107,645
|
65,740
|
63,660
|
52,853
|
||||||||||||||||
|
Income before income tax
|
17,375,004
|
14,550,960
|
7,032,667
|
7,970,663
|
5,155,129
|
|||||||||||||||
|
Provision for income tax expense
|
(6,002,765
|
)
|
(4,933,328
|
)
|
(2,386,707
|
)
|
(2,684,816
|
)
|
(2,174,054
|
)
|
||||||||||
|
Net income
|
$
|
11,372,239
|
$
|
9,617,632
|
$
|
4,645,960
|
$
|
5,285,847
|
$
|
2,981,075
|
||||||||||
|
Earnings per common share:
|
||||||||||||||||||||
|
Basic
|
$
|
1.61
|
$
|
1.41
|
$
|
0.72
|
$
|
0.83
|
$
|
0.47
|
||||||||||
|
Diluted
|
$
|
1.56
|
$
|
1.32
|
$
|
0.66
|
$
|
0.76
|
$
|
0.43
|
||||||||||
|
Shares used in calculation of net income per common share:
|
||||||||||||||||||||
|
Basic
|
7,061,404
|
6,827,355
|
6,477,457
|
6,345,615
|
6,351,245
|
|||||||||||||||
|
Diluted
|
7,283,262
|
7,272,989
|
7,079,570
|
6,922,274
|
6,981,527
|
|||||||||||||||
|
Years Ended December 31,
|
||||||||||||||||||||
|
Consolidated Balance
Sheet Data:
|
2016
|
2015
|
2014
|
2013
|
2012
|
|||||||||||||||
|
Cash and cash equivalents
|
$
|
4,763,364
|
$
|
5,137,875
|
$
|
9,810,816
|
$
|
5,624,860
|
$
|
3,383,737
|
||||||||||
|
Investments
|
48,026,242
|
31,944,083
|
12,150,436
|
6,966,964
|
5,120,000
|
|||||||||||||||
|
Total assets
|
64,696,280
|
45,698,113
|
31,026,824
|
23,252,244
|
18,390,264
|
|||||||||||||||
|
Total stockholders’ equity
|
56,281,943
|
44,810,209
|
30,256,855
|
22,332,439
|
17,458,346
|
|||||||||||||||
|
MANAGEMENT’S DISCUSSION AND ANALYSIS OR PLAN OF OPERATION OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS.
|
You should read the following discussion and analysis of our financial condition and results of operations together with our consolidated financial statements and the related notes appearing at the end of this Report. Some of the information contained in this discussion and analysis or set forth elsewhere in this Report, including information with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks and uncertainties. You should review the “Risk Factors” section of this Report for a discussion of important factors that could cause actual results to differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
We are a biopharmaceutical company involved in the development of an injectable collagenase clostridium histolyticum for multiple indications. We currently have a development and license agreement with Endo Global Ventures, a Bermuda unlimited liability company (“Endo Global Ventures”), an affiliate of Endo International plc (“Endo”), for injectable collagenase for marketed indications and indications in development. Endo assumed this agreement when Endo acquired Auxilium Pharmaceuticals, Inc. (“Auxilium”) on January 29, 2015 (the “Acquisition”). Injectable collagenase clostridium histolyticum is marketed as XIAFLEX® (or Xiapex® in Europe).
On August 31, 2011, we entered into the Second Amended and Restated Development and License Agreement (the “License Agreement”) with Auxilium for XIAFLEX. The License Agreement was filed with the Securities and Exchange Commission (the “SEC”) on September 1, 2011 as Exhibit 10.1 to a Current Report on Form 8-K. Auxilium subsequently assigned the License Agreement to Auxilium Bermuda ULC. As a result of the Acquisition and resulting internal restructuring, the counterparty to the agreement is now Endo Global Ventures.
On February 1, 2016, we entered into with Endo the First Amendment (the “First Amendment”) to the Second Amended and Restated Development and Licensing Agreement (the “Auxilium Agreement”), by and between us and Auxilium, now a wholly-owned subsidiary of Endo, to amend certain provisions of the Auxilium Agreement (as amended by the First Amendment, the “License Agreement”). The First Amendment was filed with the SEC on February 5, 2016 as Exhibit 10.1 to a Current Report on Form 8-K. The effective date of the First Amendment was January 1, 2016. Pursuant to the First Amendment, we and Endo mutually agreed that in exchange for a $8.25 million lump sum payment, we will not receive future additional mark-up on cost of goods sold for sales by non-affiliated sublicensees of Endo outside of the U.S.; provided, however, that Endo will still be required to pay a mark-up on cost of goods sold for sales made in the “Endo Territory,” which includes sales made in the U.S. and sales made in any other country where Endo sells the product directly or through affiliated sublicensees. We received this $8.25 million lump sum payment in February 2016 and began recognizing this income over time based on sales by non-affiliated sublicensees of Endo outside of the U.S. according to our revenue recognition policy in the second quarter of 2016.
Additionally, we agreed that Endo may opt-in early to indications, prior to our submission of a clinical trial report, with our consent, such consent not to be unreasonably withheld. For early opt-ins, Endo will be required to make an opt-in payment of $0.5 million on a per indication basis. For regular opt-ins, following our submission of a clinical trial report, Endo will be required to make an opt-in payment of $0.75 million on a per indication basis.
The two marketed indications involving our injectable collagenase are Dupuytren’s contracture and Peyronie’s disease. Prior to the Acquisition, Auxilium had, and after the Acquisition, Endo has, opted-in to the following indications: frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma. Endo exercised, with our consent, an early opt-in for lateral hip fat and plantar fibromatosis in November 2015. Endo opted-in for human lipoma in July 2016. We manage the development of XIAFLEX for uterine fibroids and initiate the development of XIAFLEX in new potential indications, not licensed by Endo.
Endo is currently selling XIAFLEX in the U.S. for the treatment of Dupuytren’s contracture and Peyronie’s disease and has an agreement with Swedish Orphan Biovitrum AB (“Sobi”), pursuant to which Sobi has marketing rights for Xiapex for Dupuytren’s contracture and Peyronie’s disease in Europe and certain Eurasian countries. Sobi is currently selling Xiapex in Europe and certain Eurasian countries for the treatment of Dupuytren’s contracture and Peyronie’s disease. In addition, Endo has an agreement with Asahi Kasei Pharma Corporation (“Asahi”) pursuant to which Asahi has the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Japan. Asahi is selling XIAFLEX for the treatment of Dupuytren’s contracture in Japan. Endo also had an agreement with Actelion Pharmaceuticals Ltd. (“Actelion”), pursuant to which Actelion had the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Canada and Australia. Actelion received regulatory approval in Canada and Australia for XIAFLEX for the treatment of Dupuytren’s contracture and was selling XIAFLEX in Canada and Australia. Endo terminated its agreement with Actelion as of July 4, 2016 and a transitional services agreement was put in place to cover both Canada and Australia. Endo is currently distributing XIAFLEX in Canada through Paladin Labs Inc. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand.
Outlook
We generated revenue from primarily one source, the License Agreement. Under the License Agreement, we receive license, sublicense income, royalties, milestones and mark-up on cost of goods sold payments related to the sale, regulatory submissions and approval of XIAFLEX as described above.
Significant Risks
We are dependent to a significant extent on third parties, and our principal licensee, Endo, may not be able to continue successfully commercializing XIAFLEX for Dupuytren’s contracture and Peyronie’s disease, successfully develop XIAFLEX for additional indications, obtain required regulatory approvals, manufacture XIAFLEX at an acceptable cost, in a timely manner and with appropriate quality, or successfully market products or maintain desired margins for products sold, and, as a result, we may not achieve sustained profitable operations.
The Company maintains bank account balances, which, at times, may exceed insured limits. The Company has not experienced any losses with these accounts and believes that it is not exposed to any significant credit risk on cash. The Company maintains its investment in FDIC insured certificates of deposits with several banks, municipal bonds and corporate bonds.
For more information regarding the risks facing the Company, please see the risk factors discussed under the heading “Risk Factors” under Item. 1A of Part 1 within this Report for the year ended December 31, 2016.
Critical Accounting Policies, Estimates and Assumptions
The preparation of consolidated financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. These estimates are based on historical experience and on various other assumptions that we believe are reasonable under the circumstances. Actual results could differ from those estimates. While our significant accounting policies are described in more detail in the notes to our consolidated financial statements, we believe the following accounting policies to be critical to the judgments and estimates used in the preparation of our consolidated financial statements.
Revenue Recognition. We recognize revenues from product sales when there is persuasive evidence that an arrangement exists, title passes, the price is fixed and determinable, and payment is reasonably assured. We currently recognize revenues resulting from the licensing, sublicensing and use of our technology and from services we sometimes perform in connection with the licensed technology.
We enter into product development licenses and collaboration agreements that may contain multiple elements, such as upfront license and sublicense fees, milestones related to the achievement of particular stages in product development and royalties. As a result, significant contract interpretation is sometimes required to determine the appropriate accounting, including whether the deliverables specified in a multiple-element arrangement should be treated as separate units of accounting for revenue recognition purposes, and if so, how the aggregate contract value should be allocated among the deliverable elements and when to recognize revenue for each element.
We recognize revenue for delivered elements only when the fair values of undelivered elements are known, when the associated earnings process is complete and, to the extent the milestone amount relates to our performance obligation, when our licensee confirms that we have met the requirements under the terms of the agreement, and when payment is reasonably assured. Changes in the allocation of the contract value between various deliverable elements might impact the timing of revenue recognition, but in any event, would not change the total revenue recognized on the contract. For example, nonrefundable upfront product license fees, for product candidates for which we are providing continuing services related to product development, are deferred and recognized as revenue over the development period.
Milestones, in the form of additional license fees, typically represent nonrefundable payments to be received in conjunction with the achievement of a specific event identified in a contract, such as completion of specified clinical development activities and/or regulatory submissions and/or approvals. We believe that a milestone represents the culmination of a distinct earnings process when it is not associated with ongoing research, development or other performance on our part. We recognize such milestones as revenue when they become due and payment is reasonably assured. When a milestone does not represent the culmination of a distinct earnings process, we recognize revenue in a manner similar to that of an upfront product license fee.
Royalty / Mark-up on Cost of Goods Sold / Earn-Out Revenue. For those arrangements for which royalty, mark-up on cost of goods sold or earn-out payment information becomes available and collectability is reasonably assured, we recognize revenue during the applicable period earned. For interim quarterly reporting purposes and year end, when collectability is reasonably assured but a reasonable estimate of royalty, mark-up on cost of goods sold or earn-out payment revenues cannot be made, the royalty, mark-up on cost of goods sold or earn-out payment revenues are generally recognized in the quarter that the applicable licensee provides the written report and related information to us.
Under the License Agreement, we do not participate in the selling, marketing or manufacturing of products for which we receive royalties and a mark-up of the cost of goods sold revenues. The royalty and mark-up on cost of goods sold revenues will generally be recognized in the quarter that Endo provides the written reports and related information to us, that is, royalty and mark-up on cost of goods sold revenues are generally recognized one quarter following the quarter in which the underlying sales by Endo occurred. The royalties payable by Endo to us are subject to set-off for certain patent costs.
Under the DFB Agreement, pursuant to which we sold our topical collagenase business to DFB Biotech, Inc. (“DFB”), we had the right to receive earn-out payments based on sales of certain products. This right to receive payments on Santyl sales expired in August 2013. Generally, under the DFB Agreement we received payments and a report within ninety (90) days from the end of each calendar year after DFB sold the royalty-bearing product. DFB provided us earn-out reports on a quarterly basis. BioSpecifics has now recognized all income from the Santyl sales under the DFB Agreement. We received the final earn-out payment for revenue recognized during 2013 in March 2014.
Reimbursable Third Party Development Costs. We accrue patent expenses for research and development (“R&D”) that are reimbursable by us under the License Agreement. We capitalize certain patent costs related to estimated third party development costs that are reimbursable under the License Agreement.
Receivables. Trade accounts receivable are stated at the amount the Company expects to collect. We consider the following factors when determining the collectability of specific customer accounts: customer credit-worthiness; past transaction history with the customer; current economic industry trends; and changes in customer payment terms. Our accounts receivable balance is typically due from Endo, our one large specialty pharmaceutical customer. Endo has historically paid timely and has been a financially stable organization. Due to the nature of the accounts receivable balance, we believe the risk of doubtful accounts is minimal. If the financial condition of our customer were to deteriorate, adversely affecting its ability to make payments, allowances would be required. Balances that remain outstanding after we have used reasonable collection efforts are written off through a charge to the valuation allowance and a credit to accounts receivable.
Deferred Revenue. Nonrefundable upfront product license fees, for product candidates for which we are providing continuing services related to product development, are deferred and recognized as revenue over the development period.
Deferred revenue consists of the remaining $7.4 million related to the First Amendment with Endo of mark-up on cost of goods sold revenue for sales by non-affiliated sublicensees, approximately $53,000 related to nonrefundable upfront product license fees for product candidates for which we are providing continuing services related to product development and $100,000 related to a milestone payment withheld by Endo due to a foreign tax withholding which remains uncollected. Currently, the Company expects to recover the full amount. As of December 31, 2016 and 2015, deferred revenue was $7.6 million and $0.2 million, respectively.
Third Party Royalties. We have entered into licensing and royalty agreements with third parties and agreed to pay certain royalties on net sales of products for specific indications. The royalty rates differ from agreement to agreement and, in certain cases, have been redacted with the permission of the SEC. No assumptions should be made that any disclosed royalty rate payable to a particular third party is the same or similar with respect to any royalty rate payable to any other third parties. We accrue third-party royalty expenses on net sales reported to us by Endo. Third-party royalty costs are generally expensed in the quarter that Endo provides the written reports and related information to us; that is, generally one quarter following the quarter in which the underlying sales by Endo occurred. Our third-party royalty expense under general and administrative expenses may increase if net sales by Endo and its partners for XIAFLEX and XIAPEX increase and potential new indications for XIAFLEX are approved.
Royalty Buy-Down. On March 31, 2012, we entered into an amendment to our existing agreement with Dr. Martin K. Gelbard, dated August 27, 2008, related to our future royalty obligations in connection with Peyronie’s disease. The amendment enables us to buy down a portion of our future royalty obligations in exchange for an initial cash payment of $1.5 million and five additional cash payments of $600,000, four of which have been paid as of December 31, 2016. We are currently making the payments to buy down the future royalty obligations, which royalty obligations terminate five years after first commercial sale. The Company amortizes long-term contracts with finite lives in a manner that reflects the pattern in which the economic benefits of the assets are consumed or otherwise used up. Dr. Gelbard’s agreement is amortized based on an income forecast method by estimating sales of XIAFLEX for Peyronie’s disease on an annual basis as measured by the proportion of the total estimated sales over the five year period. We perform an evaluation of the recoverability of the carrying value to determine if facts and circumstances indicate that the carrying value of the assets may be impaired and if any adjustment is warranted. Based on our evaluation as of December 31, 2016, no impairment existed and no adjustment was warranted.
Stock-Based Compensation. Under Accounting Standards Codification 718, Compensation - Stock Compensation, or ASC 718, we estimate the fair value of our employee stock awards at the date of grant using the Black-Scholes option-pricing model, which requires the use of certain subjective assumptions. The most significant assumptions are our estimates of the expected volatility of the market price of our common stock and the expected term of an award. Expected volatility is based on the historical volatility of our common stock. When establishing an estimate of the expected term of an award, we consider the vesting period for the award, our historical experience of employee stock option exercises (including forfeitures) and the expected volatility. As required under the accounting rules, we review our valuation assumptions at each grant date and, as a result, we are likely to change our valuation assumptions used to value future employee stock-based awards granted, to the extent any such awards are granted.
Further, ASC 718 requires that employee stock-based compensation costs to be recognized over the requisite service period, or the vesting period, in a manner similar to all other forms of compensation paid to employees. The allocation of employee stock-based compensation costs to each operating expense line are estimated based on specific employee headcount information at each grant date and estimated stock option forfeiture rates and revised, if necessary, in future periods if actual employee headcount information or forfeitures differ materially from those estimates. As a result, the amount of employee stock-based compensation costs we recognize in each operating expense category in future periods may differ significantly from what we have recorded in the current period.
R&D Expenses. R&D expenses include, but are not limited to, internal costs, such as salaries and benefits, costs of materials, lab expenses, facility costs and overhead. R&D expenses also consist of third party costs, such as medical professional fees, product costs used in clinical trials, consulting fees and costs associated with clinical study arrangements. We may fund R&D at medical research institutions under agreements that are generally cancelable. All of these costs are charged to R&D as incurred, which may be measured by percentage of completion, contract milestones, patient enrollment, or the passage of time.
Clinical Trial Expenses. Our cost accruals for clinical trials are based on estimates of the services received and efforts expended pursuant to contracts with various clinical trial centers and clinical research organizations. In the normal course of business we contract with third parties to perform various clinical trial activities in the ongoing development of potential drugs. The financial terms of these agreements are subject to negotiation and vary from contract to contract and may result in uneven payment flows. Payments under the contracts depend on factors such as the achievement of certain events, the successful enrollment of patients, the completion of portions of the clinical trial, and other similar conditions. The objective of our accrual policy is to match the recording of expenses in our financial statements to the actual cost of services received and efforts expended. As such, expenses related to each patient enrolled in a clinical trial are recognized ratably beginning upon entry into the trial and over the course of the patient’s continued participation in the trial. In the event of early termination of a clinical trial, we accrue an amount based on our estimate of the remaining non-cancelable obligations associated with the winding down of the clinical trial. Our estimates and assumptions could differ significantly from the amounts that may actually be incurred.
Income Taxes. Our deferred tax liabilities and deferred tax assets are impacted by events and transactions arising in the ordinary course of business, R&D activities, vesting of nonqualified options, deferred revenues and other items. We account for income taxes using an asset and liability approach to financial accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on the difference between the financial statement carrying amounts and tax bases of assets and liabilities using enacted tax rates. We periodically assess the likelihood of the realization of deferred tax assets, and reduce the carrying amount of these deferred tax assets to an amount that is considered to be more-likely-than-not realizable. Our assessment considers recent cumulative earnings experience, estimated future taxable income and ongoing prudent and feasible tax planning strategies. Significant judgment is required in making this assessment.
New Accounting Pronouncements. The Financial Accounting Standards Board, or FASB, issued in May 2014, in August 2015, March 2016 and April 2016, respectively, Accounting Standards Updates No. 2014-09, No. 2015-14, No. 2016-08, and No. 2016-10 (the “ASUs”). These ASUs were issued in connection with revenue from contracts with customers. The new standard provides a five-step approach to be applied to all contracts with customers and also requires expanded disclosures about revenue recognition. In August 2015, the FASB deferred the effective date of the guidance to reporting periods, including interim periods, beginning after December 15, 2017, and will be applied retrospectively. Early adoption is not permitted. We are currently evaluating the timing, method of adoption and the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In January 2016, the FASB issued new guidance on recognition and measurement of financial assets and financial liabilities. The new guidance will impact the accounting for equity investments, financial liabilities under the fair value option, and the presentation and disclosure requirements for financial instruments. All equity investments in unconsolidated entities (other than those accounted for under the equity method of accounting) will generally be measured at fair value with changes in fair value recognized through earnings. There will no longer be an available-for-sale classification (changes in fair value reported in other comprehensive income (loss) for equity securities with readily determinable fair values. In addition, the FASB clarified the need for a valuation allowance on deferred tax assets resulting from unrealized losses on available-for-sale debt securities. In general, the new guidance will require modified retrospective application to all outstanding instruments, with a cumulative effect adjustment recorded to opening retained earnings. This guidance will be effective for us on January 1, 2018. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In February 2016, FASB issued Accounting Standards Update (ASU) No. 2016-02, Leases (Topic 842). Under the new guidance, lessees will be required to recognize the following for all leases (with the exception of short-term leases) at the lease commencement date: a lease liability, which is a lessee’s obligation to make lease payments arising from a lease, measured on a discounted basis; and a right-of-use asset, which is an asset that represents the lessee’s right to use, or control the use of, a specified asset for the lease term. Under the new guidance, lessor accounting is largely unchanged. Certain targeted improvements were made to align, where necessary, lessor accounting with the lessee accounting model and Topic 606, Revenue from Contracts with Customers. The new lease guidance simplified the accounting for sale and leaseback transactions primarily because lessees must recognize lease assets and lease liabilities. Lessees will no longer be provided with a source of off-balance sheet financing. Public business entities should apply the amendments in ASU 2016-02 for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years (i.e., January 1, 2019, for a calendar year entity). Early application is permitted. Lessees (for capital and operating leases) and lessors (for sales-type, direct financing, and operating leases) must apply a modified retrospective transition approach for leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements. The modified retrospective approach would not require any transition accounting for leases that expired before the earliest comparative period presented. Lessees and lessors may not apply a full retrospective transition approach. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In March 2016, FASB issued ASU No. 2016-09 related to stock-based compensation. The new guidance simplifies the accounting for stock-based compensation transactions, including income tax consequences, classification of awards as either equity or liabilities, and classification on the statement of cash flows. This update is effective in fiscal years, including interim periods, beginning after December 15, 2016, and early adoption is permitted. We are currently evaluating this guidance and the impact it will have on the consolidated financial statements and related disclosures.
In May 2016, FASB issued ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients, which is intended to not change the core principle of the guidance in Topic 606, but rather affect only the narrow aspects of Topic 606 by reducing the potential for diversity in practice at initial application and by reducing the cost and complexity of applying Topic 606 both at transition and on an ongoing basis. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In June 2016, FASB issued ASU 2016-13, Financial Instruments - Credit Losses. The amendment revises the impairment model to utilize an expected loss methodology in place of the currently used incurred loss methodology, which will result in more timely recognition of losses on financial instruments, including, but not limited to, available for sale debt securities and accounts receivable. The Company is required to adopt this standard starting in the first quarter of fiscal year 2021. Early adoption is permitted. We are currently evaluating the impact of the adoption of this standard on our consolidated financial statements and related disclosures.
In January 2017, FASB issued ASU 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business. The amended definition of a business is an integrated set of activities and assets that is capable of being conducted and managed for the purpose of providing a return in the form of dividends, lower costs, or other economic benefits directly to investors or other owners, members or participants. In order to be considered a business, the three elements of inputs, processes and outputs must be present. In a business acquisition, if substantially all of the fair value of the gross assets acquired is concentrated in a single identifiable asset or group of similar identifiable assets, the integrated set of assets and activities acquired is not considered a business. The amendments are effective for fiscal years beginning after December 15, 2017, and interim periods within those fiscal years. Early adoption is permitted. This amendment may impact the allocation of purchase price in future acquisitions depending on the structure of future acquisitions.
Results of Operations for Years Ended December 31, 2016, 2015 and 2014
Revenues
The following table summarizes our primary sources of revenue during the periods presented:
|
Year Ended December 31
|
||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Royalties
|
$
|
25,431,012
|
$
|
20,800,757
|
$
|
12,985,370
|
||||||
|
Licensing revenue
|
819,943
|
1,949,378
|
1,059,254
|
|||||||||
|
Total revenues
|
$
|
26,250,955
|
$
|
22,750,135
|
$
|
14,044,624
|
||||||
Royalties
Royalties consist of royalties and the mark-up on cost of goods sold under the License Agreement.
Royalty and the mark-up on cost of goods sold revenues recognized under the License Agreement for years ended December 31, 2016 and 2015 were $25.4 million and $20.8 million, respectively. The increase in 2016 as compared to the same period in 2015 of $4.6 million, or 22%, was primarily due to the increased sales of XIAFLEX for the treatment of Peyronie’s disease and a moderate increase in sales of XIAFLEX for the treatment of Dupuytren’s contracture reported to us by Endo.
Royalty and the mark-up on cost of goods sold revenues recognized under the License Agreement for years ended December 31, 2015 and 2014 were $20.8 million and $13.0 million, respectively. The increase in 2015 as compared to the same period in 2014 of $7.8 million, or 60%, was primarily due to the increased sales of XIAFLEX for the treatment of Peyronie’s disease and a moderate increase in sales of XIAFLEX for the treatment of Dupuytren’s contracture reported to us by Endo.
Licensing Revenue
Licensing revenue consists of licensing fees, sublicensing fees and milestones.
The following table summarizes our licensing revenues under our agreement with Endo during the periods presented:
|
Year Ended December 31
|
||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Licensing fees
|
$
|
750,000
|
$
|
1,000,000
|
$
|
500,000
|
||||||
|
Development licensing fees
|
41,443
|
49,378
|
59,254
|
|||||||||
|
Milestones
|
28,500
|
900,000
|
500,000
|
|||||||||
|
Total Licensing revenues
|
$
|
819,943
|
$
|
1,949,378
|
$
|
1,059,254
|
||||||
Licensing fees recognized for the years ended December 31, 2016 were $0.8 million, $1.0 million in 2015 and $0.5 million in the 2014 period. In the 2016 period, licensing fees recognized of $0.8 million were related to the exercise of an opt-in right by Endo for the human lipoma indication. In 2015 period, licensing fees recognized of $1.0 million were related to the early opt-in exercise by Endo for XIAFLEX to two new potential indications, lateral hip fat and plantar fibromatosis. The Company received a $0.5 million opt-in fee for each indication. In the 2014 period, licensing fees recognized of $0.5 million were related to the exercise by Auxilium of its exclusive option to expand the field of its license for injectable collagenase to include the potential treatment of canine lipomas.
Development licensing fees recognized for XIAFLEX are related to the cash payments received under the License Agreement in prior years and amortized over the expected development period. For the year ended December 31, 2016, we recognized development licensing fees of $41,433 as compared to $49,378 in the 2015 period. This decrease was directly related to the stage of development for certain indications. For the year ended December 31, 2015, we recognized development licensing fees of $49,378 as compared to $59,254 in the 2014 period. This decrease was directly related to the completion of certain clinical trials for certain indications.
Milestone revenue recognized for the years ended December 31, 2016 and 2015 were $28,500 and $0.9 million, respectively. The $28,500 milestone revenue recognized in the 2016 period related to the approval of XIAFLEX in Australia for the treatment of Peyronie’s Disease by Actelion. The $0.9 million (net of foreign tax withholding) milestone revenue recognized in the 2015 period related to the first commercial sale of XIAFLEX by Asahi for the treatment of Dupuytren's contracture in Japan.
Milestone revenue recognized for the years ended December 31, 2015 and 2014 were $0.9 million and $0.5 million, respectively. The $0.5 million milestone revenue recognized in the 2014 period related to a regulatory milestone for the successful submission in July 2014 of a regulatory application to the Japanese Pharmaceutical and Medical Device Agency, or PMDA, for the potential approval of XIAFLEX for the treatment of Dupuytren's contracture in Japan by Asahi Kasei Pharma Corporation.
Under current accounting guidance, nonrefundable upfront license fees for product candidates for which we are providing continuing services related to product development are deferred and recognized as revenue over the development period. The remaining balance will be recognized over the respective development periods or when we determine that we have no ongoing performance obligations.
Research and Development Activities
R&D expenses include, but are not limited to, internal costs, such as salaries and benefits, costs of materials, lab expense, facility costs and overhead. R&D expenses also consist of third party costs, such as medical professional fees, product costs used in clinical trials, consulting fees and costs associated with clinical study arrangements.
R&D expenses were $1.3 million and $1.0 million, respectively, for the years ended December 31, 2016 and 2015, representing an increase in 2016 of $0.3 million, or 30%. This increase in R&D expenses was primarily due to the completion of the phase 2 clinical trial of XIAFLEX for the treatment of human lipoma and the development of our uterine fibroid program.
R&D expenses were $1.0 million and $1.3 million, respectively, for the years ended December 31, 2015 and 2014, representing a decrease in 2015 of $0.3 million, or 23%. This decrease in R&D expenses was primarily due to the completion of the canine lipoma trials, the completion of the human lipoma phase 1 clinical trial and a decrease in pre-clinical costs associated with the uterine fibroid program, which was partially offset by the initiation of the phase 2 clinical trial of XIAFLEX for the treatment of human lipoma.
We manage the development of XIAFLEX for uterine fibroids and initiate the development of XIAFLEX in new potential indications, not licensed by Endo. We have finished the development work on human lipomas. On July 29, 2016, Endo exercised its opt-in right under the license agreement with respect to the human lipoma indication.
The following table summarizes our R&D expenses related to our pre-clinical and clinical development programs:
|
Year Ended
December 31, 2016
|
Year Ended
December 31, 2015
|
Year Ended
December 31, 2014
|
||||||||||
|
Program
|
||||||||||||
|
Canine Lipoma
|
$
|
-
|
$
|
-
|
$
|
307,962
|
||||||
|
Human Lipoma
|
412,933
|
252,029
|
240,304
|
|||||||||
|
Uterine Fibroids
|
214,221
|
65,152
|
83,368
|
|||||||||
|
Pre-clinical/other research projects
|
700,769
|
717,108
|
631,878
|
|||||||||
The successful development of drugs is inherently difficult and uncertain. Our business requires investments in R&D over many years, often for drug candidates that may fail during the R&D process. Even if the Company is able to successfully complete the development of our drug candidates, our long-term prospects depend upon our ability and the ability of our partners, particularly with respect to XIAFLEX and XIAFLEX, to continue to successfully commercialize these drug candidates.
There is significant uncertainty regarding our ability to successfully develop drug candidates in other indications. These risks include the uncertainty of:
| · |
the nature, timing and estimated costs of the efforts necessary to complete the development of our drug candidate projects;
|
| · |
the anticipated completion dates for our drug candidate projects;
|
| · |
the scope, rate of progress and cost of our clinical trials that we are currently running or may commence in the future with respect to our drug candidate projects;
|
| · |
the scope, rate of progress of our preclinical studies and other R&D activities related to our drug candidate projects;
|
| · |
clinical trial results for our drug candidate projects;
|
| · |
the cost of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights relating to our drug candidate projects;
|
| · |
the terms and timing of any strategic alliance, licensing and other arrangements that we have or may establish in the future relating to our drug candidate projects;
|
| · |
the cost and timing of regulatory approvals with respect to our drug candidate projects; and
|
| · |
the cost of establishing clinical supplies for our drug candidate projects.
|
Our current resources and liquidity are sufficient to advance our significant current R&D projects and Endo will have the option to exclusively license the human lipoma indication upon completion of the current opt-in study.
General and Administrative Expenses
General and administrative expenses consist primarily of salaries and other related costs for personnel, third party royalty fees, amortization of deferred royalty buy-down, consultant costs, legal fees, investor relations, professional fees and overhead costs.
General and administrative expenses were $7.9 million and $7.3 million for the years ended December 31, 2016 and 2015, respectively. The increase in general and administrative expenses of $0.6 million, or 8%, in the 2016 period as compared to 2015 was mainly due to the increased amortization of the deferred royalty buy-down, third party royalties, patent fees partially offset by lower legal and consulting fees.
General and administrative expenses were $7.3 million and $5.8 million for the years ended December 31, 2015 and 2014, respectively. The increase in general and administrative expenses of $1.5 million, or 26%, in the 2015 period as compared to 2014 was mainly due to increased third party royalty fees, consulting fees, amortization of the royalty buy down and stock-based compensation expense partially offset by lower legal fees.
Other Income
Other income consists of interest earned on our investments and product sales of collagenase for laboratory use. Other income for the years ended December 31, 2016, 2105 and 2014 was $348,588, $107,645 and $65,740, respectively.
Provision for Income Taxes
Our deferred tax liabilities and deferred tax assets are impacted by events and transactions arising in the ordinary course of business, R&D activities, vesting of nonqualified options, deferred revenues and other items. The provision for income taxes is based on an estimated effective tax rate derived from the consolidated earnings before taxes, adjusted for nondeductible expenses and other permanent differences for the fiscal year.
The provision for income taxes in 2016 was $6.0 million as compared to $4.9 million in 2015. In 2016, our deferred tax assets increased by $2.7 million due to the deferred revenue associated with the receipt of $8.25 million under the First Amendment with Endo on sales by non-affiliated sublicensees of Endo outside of the U.S. During 2016, the Company has recorded $0.3 million of excess tax benefits resulting from the exercise of stock options which was recorded in additional paid in capital.
The provision for income taxes in 2015 was $4.9 million as compared to $2.4 million in 2014. In 2015, we utilized tax assets of $0.5 million related to deferred licensing revenue, stock based compensation and a R&D credit to reduce our taxes payable which was partially offset by an increase to our deferred taxes for employee based compensation. During 2015, the Company has recorded $3.8 million of excess tax benefits resulting from the exercise of stock options which was recorded in additional paid in capital. The amount of refundable federal income taxes as of December 31, 2015 was approximately $0.9 million.
Financial Condition, Liquidity and Capital Resources
To date, we have financed our operations primarily through product sales, licensing revenues and royalties under agreements with third parties and sales of our common stock. At December 31, 2016, 2015 and 2014, we had cash and cash equivalents and investments in the aggregate of approximately $52.8 million, $37.1 million and $22.0 million, respectively.
Sources and Uses of Cash
Operating Activities
Net cash provided by operating activities was $16.4 million, $10.6 million and $6.1 million for the 2016, 2015 and 2014 periods.
Net cash provided by operating activities for 2016 was primarily attributable to our net income of $11.4 million, an increase in operating assets and liabilities of $5.8 million of which $7.4 million was related to the First Amendment with Endo for mark-up on cost of goods sold for sales by non-affiliated sublicensees of Endo outside of the U.S. partially offset by an increase in accounts receivable of $1.3 million related to royalties due from Endo. Non-cash items included amortization, stock-based compensation expense, and deferred taxes which was reduced by adjustments to reconcile net income to net cash provided by operating activities of $0.8 million.
Net cash provided by operating activities for 2015 was primarily attributable to our net income of $9.6 million, adjustments to reconcile net income to net cash provided by operating activities of $1.5 million and offset by changes in operating assets and liabilities of $0.5 million. Non-cash items included amortization, stock-based compensation expense, deferred taxes and deferred revenue.
Net cash provided by operating activities for 2014 was primarily attributable our net income of $4.6 million, adjustments to reconcile net income to net cash provided by operating activities of $0.7 million and changes in operating assets and liabilities of $0.8 million. Non-cash items included amortization, stock-based compensation expense, deferred taxes and deferred revenue.
The majority of our cash expenditures in 2016, 2015, and 2014 were to fund R&D, our general and administrative business activities and our stock repurchase program.
Investing Activities
Net cash used in investing activities was $16.7 million, $20.1 million and $5.2 million in 2016, 2015 and 2014, respectively.
The net cash used in investing activities in the 2016 period reflects the maturing of investments of $43.2 million and reinvestment of $59.9 million in marketable securities.
The net cash used in investing activities in the 2015 period reflects the maturing of investments of $14.1 million and reinvestment of $34.2 million in marketable securities.
The net cash used in investing activities in the 2014 period reflects the maturing of investments of $7.6 million and reinvestment of $12.8 million in marketable securities.
Financing Activities
Net cash used in financing activities for 2016 was approximately $34,000 as compared to net cash provided by financing activities of $4.8 million and $3.3 million in 2015 and 2014, respectively.
In 2016, net cash used in financing activities was mainly related to the repurchase of our common stock under our stock repurchase program of $1.0 million offset by excess tax benefits related to share-based payments and stock option exercise proceeds of $1.0 million.
In 2015, net cash provided by financing activities was mainly related to stock option exercise proceeds of $2.8 million and excess tax benefits related to share-based payments of $3.8 million partially offset by the repurchase of our common stock under our stock repurchase program of $1.8 million.
In 2014, net cash provided by financing activities was mainly related to stock option exercise proceeds of $2.1 million and excess tax benefits related to share-based payments of $1.9 million partially offset by the repurchase of our common stock under our stock repurchase program of $0.8 million.
Contractual Commitments
We are involved with licensing of products which are generally associated with payments to third parties from whom we have licensed the product. Such payments may take the form of an up-front payment; milestone payments which are paid when certain parts of the overall development program are accomplished; payments upon certain regulatory events, such as the filing of an IND, an NDA or BLA or approval of an NDA or BLA, or the equivalents in other countries; and payments based on a percentage of sales.
We may also out-license products, for which we hold the rights, to other companies for commercialization in other territories, or at times, for other uses. When this happens, the payments to us would also take the same form as described above.
Operating Leases
Our operating leases are principally for facilities and equipment. We currently lease approximately 10,000 square feet of space at our headquarters in Lynbrook, New York which expires in November 2017. Additionally, we lease certain vehicle and certain office equipment which generally expire in 2020 and 2017, respectively.
Operating lease expenses amounted to approximately $127,000, $130,000 and $140,000 for the years ended December 31, 2016, 2015 and 2014, respectively.
Future minimum annual payments required under non-cancelable operating leases are approximated as follows:
|
Year ending December 31,
|
||||
|
2017
|
$
|
125,000
|
||
|
2018
|
4,200
|
|||
|
2019
|
4,200
|
|||
|
2020
|
1,000
|
|||
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements as defined in Item 303(a)(4) of Regulation S-K.
We are exposed to market risk related to changes in interest rates. As of December 31, 2016, we invested our cash in a variety of financial instruments, principally money market funds, pre-refunded municipal bonds, and certificates of deposit. Most of our interest-bearing securities are subject to interest rate risk and could decline in value if interest rates fluctuate. Our investment portfolio is comprised of marketable securities of highly rated financial institutions and investment-grade debt instruments, and we have guidelines to limit the term-to-maturity of our investments. Based on the type of securities we hold, we do not believe a change in interest rates would have a material impact on our financial statements. If interest rates were to increase or decrease by 100 basis points the fair value of our investment portfolio would (decrease) increase by approximately ($76,000) and $463,000, respectively. All investments are classified as held to maturity.
For the discussion of Item 8, “Financial Statements” please see the Consolidated Financial Statements, beginning on page F-1 of this Report.
None
Evaluation of Disclosure Controls and Procedures
The Company, under the supervision and with the participation of Thomas L. Wegman, the Company’s President, Principal Executive Officer, Principal Financial Officer and Principal Accounting Officer, evaluated the effectiveness of its disclosure controls and procedures as of the end of the period covered by this Report. Based on that evaluation, management has concluded that the Company’s disclosure controls and procedures are effective to ensure that information required to be disclosed in reports filed under the Securities Exchange Act of 1934, as amended, or the Exchange Act, is recorded, processed, summarized and reported within the time periods specified in the rules and forms of the SEC, and that such information is accumulated and communicated to the Company’s management, to allow timely decisions regarding required disclosure. Because of the inherent limitations in all control systems, any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives, and management necessarily is required to apply its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Furthermore, our controls and procedures can be circumvented by the individual acts of some persons, by collusion of two or more people or by management override of the control and misstatements due to error or fraud may occur and not be detected on a timely basis.
Management’s Annual Report on Internal Control Over Financial Reporting
Management of the Company is responsible for establishing and maintaining adequate internal control over financial reporting for the Company as defined in Rule 13a-15(f) under the Exchange Act. The Company’s internal control over financial reporting is designed to provide reasonable assurance to the Company’s management and Board regarding the preparation and fair presentation of published financial statements and the reliability of financial reporting.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation.
Management assessed the effectiveness of the Company’s internal control over financial reporting as of December 31, 2016. In making this assessment, management used the 2013 criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission in Internal Control – Integrated Framework. We believe that, as of December 31, 2016, the Company’s internal control over financial reporting was effective based on this criteria.
EisnerAmper LLP, the independent registered public accounting firm that audited our Consolidated Financial Statements included in this Report, audited the effectiveness of our internal control over financial reporting as of December 31, 2016, as stated in their report which is included in Part IV, Item 15 of this Report.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting during our most recent fiscal quarter identified in connection with the evaluation of our controls and procedures that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Not applicable.
The information required by this Item is set forth in our Proxy Statement for the 2017 Annual Meeting of Stockholders to be filed with the SEC within 120 days of December 31, 2016, and is incorporated into this Annual Report on Form 10-K by reference.
The information required by this Item is set forth in our Proxy Statement for the 2017 Annual Meeting of Stockholders to be filed with the SEC within 120 days of December 31, 2016, and is incorporated into this Annual Report on Form 10-K by reference.
|
SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS.
|
The information required by this Item is set forth in our Proxy Statement for the 2017 Annual Meeting of Stockholders to be filed with the SEC within 120 days of December 31, 2016, and is incorporated into this Annual Report on Form 10-K by reference and is also included in under the heading “Securities Authorized for Issuance under Equity Compensation Plans”, in Item 5 of Part II of this Annual Report on Form 10-K.
The information required by this Item is set forth in our Proxy Statement for the 2017 Annual Meeting of Stockholders to be filed with the SEC within 120 days of December 31, 2016, and is incorporated into this Annual Report on Form 10-K by reference.
The information required by this Item is set forth in our Proxy Statement for the 2017 Annual Meeting of Stockholders to be filed with the SEC within 120 days of December 31, 2016, and is incorporated into this Annual Report on Form 10-K by reference.
|
a)
|
The following documents are filed as part of this Annual Report:
|
| (1) |
Consolidated Financial Statements (See Index to Consolidated Financial Statements on page F-1)
|
| (2) |
Financial Statement Schedules
|
All schedules to the consolidated financial statements are omitted as the required information is either inapplicable or presented in the consolidated financial statements.
| (3) |
Exhibits
|
The information required by this Item is set forth in the Exhibit Index hereto which is incorporated herein by reference.
|
b)
|
Exhibits
|
The information required by this Item is set forth in the Exhibit Index hereto which is incorporated herein by reference.
BIOSPECIFICS TECHNOLOGIES CORP.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS FOR THE YEAR
ENDED DECEMBER 31, 2016, 2015 and 2014
|
Page
|
|
|
Reports of Independent Registered Public Accounting Firm
|
F-2
|
|
Consolidated Balance Sheets
|
F-4
|
|
Consolidated Statements of Income
|
F-5
|
|
Consolidated Statements of Stockholders’ Equity
|
F-6
|
|
Consolidated Statements of Cash Flows
|
F-7
|
|
Notes to Consolidated Financial Statements
|
F-8
|
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of
BioSpecifics Technologies Corp.
We have audited the accompanying consolidated balance sheets of BioSpecifics Technologies Corp. and its subsidiary (the “Company”) as of December 31, 2016 and 2015, and the related consolidated statements of income, stockholders’ equity, and cash flows for each of the years in the three-year period ended December 31, 2016. The financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of BioSpecifics Technologies Corp. and its subsidiary as of December 31, 2016 and 2015, and the consolidated results of their operations and their cash flows for each of the years in the three-year period ended December 31, 2016, in conformity with accounting principles generally accepted in the United States of America.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), BioSpecifics Technologies Corp. and its subsidiary’s internal control over financial reporting as of December 31, 2016, based on criteria established in the Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”), and our report dated March 16, 2017 expressed an unqualified opinion thereon.
/s/ EisnerAmper LLP
New York, New York
March 16, 2017
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of BioSpecifics Technologies Corp.
We have audited BioSpecifics Technologies Corp. and its subsidiary’s (the “Company”) internal control over financial reporting as of December 31, 2016, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”). The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Annual Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
An entity’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. An entity’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the entity; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the entity are being made only in accordance with authorizations of management and directors of the entity; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the entity’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2016, based on criteria established in the Internal Control - Integrated Framework (2013) issued by COSO.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of BioSpecifics Technologies Corp. and its subsidiary as of December 31, 2016 and 2015, and the related consolidated statements of income, stockholders’ equity, and cash flows for each of the years in the three-year period ended December 31, 2016, and our report dated March 16, 2017 expressed an unqualified opinion thereon.
/s/ EisnerAmper LLP
New York, New York
March 16, 2017
BioSpecifics Technologies Corp.
Consolidated Balance Sheets
|
December 31,
|
||||||||
|
2016
|
2015
|
|||||||
|
Assets
|
||||||||
|
Current assets:
|
||||||||
|
Cash and cash equivalents
|
$
|
4,763,364
|
$
|
5,137,875
|
||||
|
Short term investments
|
44,254,862
|
28,347,542
|
||||||
|
Accounts receivable
|
3,810,792
|
2,547,920
|
||||||
|
Income tax receivable
|
494,711
|
916,843
|
||||||
|
Deferred royalty buy-down
|
1,451,893
|
1,017,981
|
||||||
|
Prepaid expenses and other current assets
|
624,345
|
383,810
|
||||||
|
Total current assets
|
55,399,967
|
38,351,971
|
||||||
|
Long-term investments
|
3,771,380
|
3,596,541
|
||||||
|
Deferred royalty buy-down – long term, net
|
1,976,456
|
2,851,423
|
||||||
|
Deferred tax assets, net
|
3,290,122
|
622,972
|
||||||
|
Patent costs, net
|
258,355
|
275,206
|
||||||
|
Total assets
|
$
|
64,696,280
|
$
|
45,698,113
|
||||
|
Liabilities and Stockholders' Equity
|
||||||||
|
Current liabilities:
|
||||||||
|
Accounts payable and accrued expenses
|
$
|
738,649
|
$
|
611,009
|
||||
|
Deferred revenue
|
1,179,848
|
149,378
|
||||||
|
Accrued liabilities of discontinued operations
|
78,138
|
78,138
|
||||||
|
Total current liabilities
|
1,996,635
|
838,525
|
||||||
|
Long-term deferred revenue
|
6,417,702
|
49,379
|
||||||
|
Commitments and contingencies (Note 10)
|
||||||||
|
Stockholders' equity:
|
||||||||
|
Series A Preferred stock, $.50 par value, 700,000 shares authorized; none outstanding
|
-
|
-
|
||||||
|
Common stock, $.001 par value; 10,000,000 shares authorized; 7,555,167 and 7,290,167 shares issued, 7,156,281 and 6,918,579 outstanding at December 31, 2016 and 2015, respectively
|
7,555
|
7,290
|
||||||
|
Additional paid-in capital
|
32,945,240
|
31,797,418
|
||||||
|
Retained earnings
|
30,610,849
|
19,238,610
|
||||||
|
Treasury stock, 398,886 and 371,588 shares at cost as of December 31, 2016 and 2015
|
(7,281,701
|
)
|
(6,233,109
|
)
|
||||
|
Total stockholders' equity
|
56,281,943
|
44,810,209
|
||||||
|
Total liabilities and stockholders’ equity
|
$
|
64,696,280
|
$
|
45,698,113
|
||||
See accompanying notes to consolidated financial statements
BioSpecifics Technologies Corp.
Consolidated Statements of Income
|
Years Ended December 31,
|
||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Revenues:
|
||||||||||||
|
Royalties
|
$
|
25,431,012
|
$
|
20,800,757
|
$
|
12,985,370
|
||||||
|
Licensing revenue
|
819,943
|
1,949,378
|
1,059,254
|
|||||||||
|
Total revenues
|
26,250,955
|
22,750,135
|
14,044,624
|
|||||||||
|
Costs and expenses:
|
||||||||||||
|
Research and development
|
1,327,923
|
1,034,288
|
1,263,512
|
|||||||||
|
General and administrative
|
7,896,616
|
7,272,532
|
5,814,185
|
|||||||||
|
Total costs and expenses
|
9,224,539
|
8,306,820
|
7,077,697
|
|||||||||
|
Operating income
|
17,026,416
|
14,443,315
|
6,966,927
|
|||||||||
|
Other income:
|
||||||||||||
|
Interest income
|
295,783
|
92,926
|
32,158
|
|||||||||
|
Other
|
52,805
|
14,719
|
33,582
|
|||||||||
|
348,588
|
107,645
|
65,740
|
||||||||||
|
Income before income tax
|
17,375,004
|
14,550,960
|
7,032,667
|
|||||||||
|
Income tax provision
|
(6,002,765
|
)
|
(4,933,328
|
)
|
(2,386,707
|
)
|
||||||
|
Net income
|
$
|
11,372,239
|
$
|
9,617,632
|
$
|
4,645,960
|
||||||
|
Earnings per common share:
|
||||||||||||
|
Basic
|
$
|
1.61
|
$
|
1.41
|
$
|
0.72
|
||||||
|
Diluted
|
$
|
1.56
|
$
|
1.32
|
$
|
0.66
|
||||||
|
Shares used in calculation of net income per common share:
|
||||||||||||
|
Basic
|
7,061,404
|
6,827,355
|
6,477,457
|
|||||||||
|
Diluted
|
7,283,262
|
7,272,989
|
7,079,570
|
|||||||||
See accompanying notes to consolidated financial statements
BioSpecifics Technologies Corp.
Consolidated Statements of Stockholders' Equity
|
Common Stock
|
||||||||||||||||||||||||
|
Shares
|
Amount |
Additional
Paid in
Capital
|
Retained
Earnings
|
Treasury
Stock
|
Stockholder
Equity
Total
|
|||||||||||||||||||
|
Balances - December 31, 2013
|
6,655,168
|
$
|
6,655
|
$
|
20,951,796
|
$
|
4,975,018
|
$
|
(3,601,030
|
)
|
$
|
22,332,439
|
||||||||||||
|
Issuance of common stock upon stock option exercise
|
407,041
|
407
|
2,146,414
|
-
|
-
|
2,146,821
|
||||||||||||||||||
|
Stock compensation expense
|
-
|
-
|
21,416
|
-
|
-
|
21,416
|
||||||||||||||||||
|
Repurchases of common stock
|
-
|
-
|
-
|
-
|
(829,613
|
)
|
(829,613
|
)
|
||||||||||||||||
|
Excess tax benefits from share-based payment arrangements
|
-
|
-
|
1,939,832
|
-
|
-
|
1,939,832
|
||||||||||||||||||
|
Net income
|
-
|
-
|
-
|
4,645,960
|
-
|
4,645,960
|
||||||||||||||||||
|
Balances - December 31, 2014
|
7,062,209
|
7,062
|
25,059,458
|
9,620,978
|
(4,430,643
|
)
|
30,256,855
|
|||||||||||||||||
|
Issuance of common stock upon stock option exercise
|
227,958
|
228
|
2,823,755
|
-
|
-
|
2,823,983
|
||||||||||||||||||
|
Stock compensation expense
|
-
|
-
|
105,782
|
-
|
-
|
105,782
|
||||||||||||||||||
|
Repurchases of common stock
|
-
|
-
|
-
|
-
|
(1,802,466
|
)
|
(1,802,466
|
)
|
||||||||||||||||
|
Excess tax benefits from share-based payment arrangements
|
-
|
-
|
3,808,423
|
-
|
-
|
3,808,423
|
||||||||||||||||||
|
Net income
|
-
|
-
|
-
|
9,617,632
|
-
|
9,617,632
|
||||||||||||||||||
|
Balances - December 31, 2015
|
7,290,167
|
7,290
|
31,797,418
|
19,238,610
|
(6,233,109
|
)
|
44,810,209
|
|||||||||||||||||
|
Issuance of common stock upon stock option exercise
|
265,000
|
265
|
711,135
|
-
|
-
|
711,400
|
||||||||||||||||||
|
Stock compensation expense
|
-
|
-
|
133,904
|
-
|
-
|
133,904
|
||||||||||||||||||
|
Repurchases of common stock
|
-
|
-
|
-
|
-
|
(1,048,592
|
)
|
(1,048,592
|
)
|
||||||||||||||||
|
Excess tax benefits from share-based payment arrangements
|
-
|
-
|
302,783
|
-
|
-
|
302,783
|
||||||||||||||||||
|
Net income
|
-
|
-
|
-
|
11,372,239
|
-
|
11,372,239
|
||||||||||||||||||
|
Balances - December 31, 2016
|
7,555,167
|
$
|
7,555
|
$
|
32,945,240
|
$
|
30,610,849
|
$
|
(7,281,701
|
)
|
$
|
56,281,943
|
||||||||||||
See accompanying notes to consolidated financial statements
BioSpecifics Technologies Corp.
Consolidated Statements of Cash Flows
|
Cash flows from operating activities:
|
Years Ended December 31,
|
|||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Net income
|
$
|
11,372,239
|
$
|
9,617,632
|
$
|
4,645,960
|
||||||
|
Adjustments to reconcile net income to net cash provided in operating activities:
|
||||||||||||
|
Amortization
|
1,691,539
|
933,009
|
247,097
|
|||||||||
|
Stock-based compensation expense
|
133,904
|
105,782
|
21,416
|
|||||||||
|
Deferred tax expense
|
(2,667,150
|
)
|
455,799
|
429,005
|
||||||||
|
Gain on the sale of fixed assets
|
-
|
-
|
(1,150
|
)
|
||||||||
|
Changes in operating assets and liabilities:
|
||||||||||||
|
Accounts receivable
|
(1,262,872
|
)
|
390,811
|
2,051,335
|
||||||||
|
Income tax receivable
|
422,132
|
(263,727
|
)
|
(397,408
|
)
|
|||||||
|
Prepaid expenses and other current assets
|
(240,535
|
)
|
(124,647
|
)
|
81,708
|
|||||||
|
Patent costs
|
(23,341
|
)
|
(25,934
|
)
|
(198,952
|
)
|
||||||
|
Accounts payable and accrued expenses
|
127,640
|
67,313
|
(90,580
|
)
|
||||||||
|
Deferred royalty buy-down
|
(600,000
|
)
|
(600,000
|
)
|
(600,000
|
)
|
||||||
|
Deferred revenue
|
7,398,793
|
50,622
|
(59,255
|
)
|
||||||||
|
Net cash provided by operating activities from operations
|
16,352,349
|
10,606,660
|
6,129,176
|
|||||||||
|
Cash flows from investing activities:
|
||||||||||||
|
Maturities of marketable securities
|
43,242,679
|
14,070,544
|
7,646,964
|
|||||||||
|
Purchases of marketable securities
|
(59,935,130
|
)
|
(34,180,085
|
)
|
(12,848,374
|
)
|
||||||
|
Proceeds from sale of fixed assets
|
-
|
-
|
1,150
|
|||||||||
|
Net cash used in investing activities from operations
|
(16,692,451
|
)
|
(20,109,541
|
)
|
(5,200,260
|
)
|
||||||
|
Cash flows from financing activities:
|
||||||||||||
|
Proceeds from stock option exercises
|
711,400
|
2,823,983
|
2,146,821
|
|||||||||
|
Repurchases of common stock
|
(1,048,592
|
)
|
(1,802,466
|
)
|
(829,613
|
)
|
||||||
|
Excess tax benefits from share-based payment arrangements
|
302,783
|
3,808,423
|
1,939,832
|
|||||||||
|
Net cash (used in) provided by financing activities from operations
|
(34,409
|
)
|
4,829,940
|
3,257,040
|
||||||||
|
(Decrease) increase in cash and cash equivalents
|
(374,511
|
)
|
(4,672,941
|
)
|
4,185,956
|
|||||||
|
Cash and cash equivalents at beginning of year
|
5,137,875
|
9,810,816
|
5,624,860
|
|||||||||
|
Cash and cash equivalents at end of year
|
$
|
4,763,364
|
$
|
5,137,875
|
$
|
9,810,816
|
||||||
|
Supplemental disclosures of cash flow information:
|
||||||||||||
|
Cash paid during the year for:
|
||||||||||||
|
Interest
|
$
|
-
|
$
|
-
|
$
|
-
|
||||||
|
Taxes
|
$
|
7,945,000
|
$
|
1,906,000
|
$
|
415,279
|
||||||
See accompanying notes to consolidated financial statements
BIOSPECIFICS TECHNOLOGIES CORP.
Notes to Consolidated Financial Statements
December 31, 2016, 2015 and 2014
1. ORGANIZATION AND DESCRIPTION OF BUSINESS
We are a biopharmaceutical company involved in the development of an injectable collagenase clostridium histolyticum for multiple indications. We currently have a development and license agreement with Endo Global Ventures, a Bermuda unlimited liability company (“Endo Global Ventures”), an affiliate of Endo International plc (“Endo”), for injectable collagenase for marketed indications and indications in development. Endo assumed this agreement when Endo acquired Auxilium Pharmaceuticals, Inc. (“Auxilium”) on January 29, 2015 (the “Acquisition”). Injectable collagenase clostridium histolyticum is marketed as XIAFLEX® (or Xiapex® in Europe).
On August 31, 2011, we entered into the Second Amended and Restated Development and License Agreement (the “License Agreement”) with Auxilium for XIAFLEX. The License Agreement was filed with the Securities and Exchange Commission (the “SEC”) on September 1, 2011 as Exhibit 10.1 to a Current Report on Form 8-K. Auxilium subsequently assigned the License Agreement to Auxilium Bermuda ULC. As a result of the Acquisition and resulting internal restructuring, the counterparty to the agreement is now Endo Global Ventures.
On February 1, 2016, we entered into with Endo the First Amendment (the “First Amendment”) to the Second Amended and Restated Development and Licensing Agreement (the “Auxilium Agreement”), by and between us and Auxilium, now a wholly-owned subsidiary of Endo, to amend certain provisions of the Auxilium Agreement (as amended by the First Amendment, the “License Agreement”). The First Amendment was filed with the SEC on February 5, 2016 as Exhibit 10.1 to a Current Report on Form 8-K. The effective date of the First Amendment was January 1, 2016. Pursuant to the First Amendment, we and Endo mutually agreed that in exchange for a $8.25 million lump sum payment, we will not receive future additional mark-up on cost of goods sold for sales by non-affiliated sublicensees of Endo outside of the U.S.; provided, however, that Endo will still be required to pay a mark-up on cost of goods sold for sales made in the “Endo Territory,” which includes sales made in the U.S. and sales made in any other country where Endo sells the product directly or through affiliated sublicensees. We received this $8.25 million lump sum payment in February 2016 and began recognizing this income over time based on sales by non-affiliated sublicensees of Endo outside of the U.S. according to our revenue recognition policy in the second quarter of 2016.
Additionally, we agreed that Endo may opt-in early to indications, prior to our submission of a clinical trial report, with our consent, such consent not to be unreasonably withheld. For early opt-ins, Endo will be required to make an opt-in payment of $0.5 million on a per indication basis. For regular opt-ins, following our submission of a clinical trial report, Endo will be required to make an opt-in payment of $0.75 million on a per indication basis.
The two marketed indications involving our injectable collagenase are Dupuytren’s contracture and Peyronie’s disease. Prior to the Acquisition, Auxilium had, and after the Acquisition, Endo has, opted-in to the following indications: frozen shoulder, cellulite, canine lipoma, lateral hip fat, plantar fibromatosis and human lipoma. Endo exercised, with our consent, an early opt-in for lateral hip fat and plantar fibromatosis in November 2015. Endo opted-in for human lipoma in July 2016. We manage the development of XIAFLEX for uterine fibroids and initiate the development of XIAFLEX in new potential indications, not licensed by Endo.
Endo is currently selling XIAFLEX in the U.S. for the treatment of Dupuytren’s contracture and Peyronie’s disease and has an agreement with Swedish Orphan Biovitrum AB (“Sobi”), pursuant to which Sobi has marketing rights for Xiapex for Dupuytren’s contracture and Peyronie’s disease in Europe and certain Eurasian countries. Sobi is currently selling Xiapex in Europe and certain Eurasian countries for the treatment of Dupuytren’s contracture and Peyronie’s disease. In addition, Endo has an agreement with Asahi Kasei Pharma Corporation (“Asahi”) pursuant to which Asahi has the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Japan. Asahi is selling XIAFLEX for the treatment of Dupuytren’s contracture in Japan. Endo also had an agreement with Actelion Pharmaceuticals Ltd. (“Actelion”), pursuant to which Actelion had the right to commercialize XIAFLEX for the treatment of Dupuytren’s contracture and Peyronie’s disease in Canada and Australia. Actelion received regulatory approval in Canada and Australia for XIAFLEX for the treatment of Dupuytren’s contracture and was selling XIAFLEX in Canada and Australia. Endo terminated its agreement with Actelion as of July 4, 2016 and a transitional services agreement was put in place to cover both Canada and Australia. Endo is currently distributing XIAFLEX in Canada through Paladin Labs Inc. In December 2016, Endo entered into a new out-licensing agreement with Actelion, pursuant to which Actelion obtained marketing and commercial rights for XIAFLEX in Australia and New Zealand.
2. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Principles of Consolidation
The consolidated financial statements include the accounts of the Company and its subsidiary, Advance Biofactures Corp., a New York corporation (“ABC-NY”). All intercompany balances and transactions have been eliminated.
Reclassification
Certain reclassifications have been made to prior year balances to conform to the current year’s presentation.
Critical Accounting Policies, Estimates and Assumptions
The preparation of consolidated financial statements in conformity with U.S. Generally Accepted Accounting Principles (“GAAP”) requires the use of management’s estimates and assumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. The Company makes certain assumptions and estimates for its deferred tax assets and deferred royalty buy-down. For further details see footnote “Provision for Income Taxes, Third Party Royalties and Royalty Buy-Down”. Actual results could differ from those estimates.
Cash, Cash Equivalents and Investments
Cash equivalents include only securities having a maturity of three months or less at the time of purchase. Investments are stated on an amortized cost basis. The Company limits its credit risk associated with cash, cash equivalents and investments by placing its investments with banks it believes are highly creditworthy and with highly rated money market funds, certificates of deposit, pre-refunded municipal bonds, municipal bonds and corporate bonds. All investments are classified as held to maturity. As of December 31, 2016 and 2015, the aggregate fair value of these investments was $48.0 million and $31.9 million, respectively. No unrealized gains or losses were recorded in the balance sheet in either period.
Fair Value Measurements
Management believes that the carrying amounts of the Company’s financial instruments, including cash, cash equivalents, held to maturity investments, accounts receivable, accounts payable and accrued expenses approximate fair value due to the short-term nature of those instruments. As of December 31, 2016 and 2015, there were no recorded unrealized gains or losses on our investments as they are held to maturity. As of December 31, 2016, amortized cost basis of the investments approximate their fair value. In 2016 and 2015, the amortized premium included in interest income was $610,000 and $316,000, respectively.
The schedule of maturities at December 31, 2016 and 2015 are as follows:
|
Maturities as of
December 31, 2016
|
Maturities as of
December 31, 2015
|
|||||||||||||||
|
1 Year or
Less
|
Greater than 1
Year
|
1 Year or
Less
|
Greater than 1
Year
|
|||||||||||||
|
Municipal bonds
|
$
|
6,967,954
|
$
|
586,074
|
$
|
6,461,216
|
$
|
155,826
|
||||||||
|
Corporate Bonds
|
30,418,120
|
2,936,287
|
9,882,285
|
1,597,715
|
||||||||||||
|
Certificates of deposit
|
6,868,788
|
249,019
|
12,004,041
|
1,843,000
|
||||||||||||
|
Total
|
$
|
44,254,862
|
$
|
3,771,380
|
$
|
28,347,542
|
$
|
3,596,541
|
||||||||
Concentration of Credit Risk and Major Customers
The Company maintains bank account balances, which, at times, may exceed insured limits. The Company has not experienced any losses with these accounts and believes that it is not exposed to any significant credit risk on cash.
The Company maintains its investment in FDIC insured certificates of deposits with several banks, pre-refunded municipal bonds, municipal bonds and corporate bonds.
At December 31, 2016 our accounts receivable balance was $3.8 million and was from one customer, Endo.
At December 31, 2015 our accounts receivable balance was $2.5 million and was from one customer, Endo.
The Company is currently dependent on one customer, Endo, who generates almost all its revenues. For the years ended December 31, 2016, 2015 and 2014, the licensing, sublicensing, milestones and royalty revenues under the License Agreement with Endo were approximately $26.3 million, $22.8 million and $14.0 million, respectively.
Revenue Recognition
We currently recognize revenues resulting from the licensing and sublicensing of the use of our technology and from services we sometimes perform in connection with the licensed technology under the guidance of Accounting Standards Codification 605, Revenue Recognition (“ASC 605”).
If we determine that separate elements exist in a revenue arrangement under ASC 605, we recognize revenue for delivered elements only when the fair values of undelivered elements are known, when the associated earnings process is complete, when payment is reasonably assured and, to the extent the milestone amount relates to our performance obligation, when our customer confirms that we have met the requirements under the terms of the agreement.
Revenues, and their respective treatment for financial reporting purposes, are as follows:
Royalty / Mark-Up on Cost of Goods Sold
For those arrangements for which royalty and mark-up on cost of goods sold information becomes available and collectability is reasonably assured, we recognize revenue during the applicable period in which it is earned. For interim quarterly and year-end reporting purposes, when collectability is reasonably assured, but a reasonable estimate of royalty and mark-up on cost of goods sold cannot be made, the royalty and mark-up on cost of goods sold are generally recognized in the quarter that the applicable licensee provides the written report and related information to us.
Under the License Agreement, we do not participate in the selling, marketing or manufacturing of products for which we receive royalties and a mark-up on the cost of goods sold. The royalty and mark-up on cost of goods sold will generally be recognized in the quarter that Endo provides the written reports and related information to us; that is, royalty and mark-up on cost of goods sold are generally recognized one quarter following the quarter in which the underlying sales by Endo occurred. The royalties payable by Endo to us are subject to set-off for certain patent costs.
Pursuant to the First Amendment with Endo, in exchange for a $8.25 million lump sum payment, we will not receive future additional mark-up on cost of goods sold for sales by non-affiliated sublicensees of Endo outside of the U.S.; provided, however, that Endo will still be required to pay a mark-up on cost of goods sold for sales made in the “Endo Territory,” which includes sales made in the U.S. and sales made in any other country where Endo sells the product directly or through affiliated sublicensees. We received this $8.25 million lump sum payment in February 2016. We classified this payment as deferred revenue in our balance sheet and began recognizing this income over time in the second quarter of 2016 based on sales by non-affiliated sublicensees of Endo outside of the U.S. according to our revenue recognition policy. We recognized approximately $0.8 million for the year ended December 31, 2016, and zero in the 2015 and 2014 corresponding periods.
Licensing Revenue
We include revenue recognized from upfront licensing, sublicensing and milestone payments in “License Revenues” in our consolidated statements of income in this Report.
Upfront License and Sublicensing Fees
We generally recognize revenue from upfront licensing and sublicensing fees when the agreement is signed, we have completed the earnings process and we have no ongoing performance obligation with respect to the arrangement. Nonrefundable upfront technology license for product candidates for which we are providing continuing services related to product development are deferred and recognized as revenue over the development period.
Milestones
Milestones, in the form of additional license fees, typically represent nonrefundable payments to be received in conjunction with the achievement of a specific event identified in the contract, such as completion of specified development activities and/or regulatory submissions and/or approvals. We believe that a milestone represents the culmination of a distinct earnings process when it is not associated with ongoing research, development or other performance on our part. We recognize such milestones as revenue when they become due and collection is reasonably assured. When a milestone does not represent the culmination of a distinct earnings process, we recognize revenue in a manner similar to that of an upfront license fee.
The timing and amount of revenue that we recognize from licenses of technology, either from upfront fees or milestones where we are providing continuing services related to product development, is primarily dependent upon our estimates of the development period. We define the development period as the point from which research activities commence up to regulatory approval of either our, or our partners’, submission assuming no further research is necessary. As product candidates move through the development process, it is necessary to revise these estimates to consider changes to the product development cycle, such as changes in the clinical development plan, regulatory requirements, or various other factors, many of which may be outside of our control. Should the FDA or other regulatory agencies require additional data or information, we would adjust our development period estimates accordingly. The impact on revenue of changes in our estimates and the timing thereof is recognized prospectively over the remaining estimated product development period.
Treasury Stock
The Company accounts for treasury stock under the cost method and includes treasury stock as a component of stockholders’ equity. For the year ended December 31, 2016, we repurchased 27,298 shares at an average price of $38.41 as compared to 40,001 shares at an average price of $45.06 in the 2015 period. In the 2014 period, we purchased 30,848 shares at an average price of $26.89.
Receivables
Trade accounts receivable are stated at the amount the Company expects to collect. We may maintain allowances for doubtful accounts for estimated losses resulting from the inability of our customers to make required payments. We consider the following factors when determining the collectability of specific customer accounts: customer credit-worthiness, past transaction history with the customer, current economic industry trends, and changes in customer payment terms. Our accounts receivable balance is typically due from Endo, our one large specialty pharmaceutical customer. Endo has historically paid timely and has been a financially stable organization. Due to the nature of the accounts receivable balance, we believe the risk of doubtful accounts is minimal. If the financial condition of our customer were to deteriorate, adversely affecting its ability to make payments, additional allowances would be required. We may provide for estimated uncollectible amounts through a charge to earnings and a credit to a valuation allowance. Balances that remain outstanding after we have used reasonable collection efforts are written off through a charge to the valuation allowance and a credit to accounts receivable.
At December 31, 2016 and 2015, our accounts receivable balance was $3.8 million and $2.5 million, respectively and was from one customer, Endo.
Deferred Revenue
Deferred revenue consists of the remaining $7.4 million related to the First Amendment with Endo of mark-up on cost of goods sold revenue for sales by non-affiliated sublicensees, approximately $53,000 related to nonrefundable upfront product license fees for product candidates for which we are providing continuing services related to product development and $100,000 related to a milestone payment withheld by Endo due to a foreign tax withholding which remains uncollected. Currently, the Company expects to recover the full amount. As of December 31, 2016 and 2015, deferred revenue was $7.6 million and $0.2 million, respectively.
Reimbursable Third Party Development Costs
We accrued patent expenses that are reimbursable by us under the License Agreement. We capitalize certain patent costs related to estimated third-party development costs that are reimbursable under the License Agreement. As of December 31, 2016 and 2015, our net reimbursable third party patent expense accrual was approximately $25,000 and $20,000, respectively.
Third Party Royalties
We have entered into licensing and royalty agreements with third parties and agreed to pay certain royalties on net sales of products for specific indications. The royalty rates differ from agreement to agreement and, in certain cases, have been redacted with the permission of the SEC. No assumptions should be made that any disclosed royalty rate payable to a particular third party is the same or similar with respect to any royalty rate payable to any other third parties. We accrue third-party royalty expenses on net sales reported to us by Endo. Third-party royalty costs are generally expensed under general and administrative in the quarter that Endo provides the written reports and related information to us; that is, generally one quarter following the quarter in which the underlying sales by Endo occurred. For the years ended December 31, 2016, 2015 and 2014, third party royalty expenses was $1.6 million, $1.4 million and $0.8 million, respectively. Our third-party royalty expense under general and administrative expenses may increase if net sales by Endo and its partners for XIAFLEX and XIAPEX increase and potential new indications for XIAFLEX are approved.
Royalty Buy-Down
On March 31, 2012, we entered into an amendment to our existing agreement with Dr. Martin K. Gelbard, dated August 27, 2008, related to our future royalty obligations in connection with Peyronie’s disease. The amendment enables us to buy down a portion of our future royalty obligations in exchange for an initial cash payment of $1.5 million and five additional cash payments of $600,000, four of which have been paid as of December 31, 2016. We are currently making the payments to buy down the future royalty obligations, which royalty obligations terminate five years after first commercial sale. The Company amortizes long-term contracts with finite lives in a manner that reflects the pattern in which the economic benefits of the assets are consumed or otherwise used up. Dr. Gelbard’s agreement is amortized based on an income forecast method by estimating sales of XIAFLEX for Peyronie’s disease on an annual basis as measured by the proportion of the total estimated sales over the five year period. For the years ended December 31, 2016, 2015, and 2014, we amortized approximately $1.0 million, $0.6 million and $0.1 million related to this agreement, respectively. As of December 31, 2016 and 2015, the remaining capitalized balances were approximately $3.4 million and $3.9 million, respectively. We perform an evaluation of the recoverability of the carrying value to determine if facts and circumstances indicate that the carrying value of the assets may be impaired and if any adjustment is warranted. As of December 31, 2016, there was no indicator that an impairment existed.
Research and Development Expenses
R&D expenses include, but are not limited to, internal costs, such as salaries and benefits, costs of materials, lab expense, facility costs and overhead. R&D expenses also consist of third party costs, such as medical professional fees, product costs used in clinical trials, consulting fees and costs associated with clinical study arrangements. We may fund R&D at medical research institutions under agreements that are generally cancelable. All of these costs are charged to R&D as incurred, which may be measured by percentage of completion, contract milestones, patient enrollment, or the passage of time.
Clinical Trial Expenses
Our cost accruals for clinical trials are based on estimates of the services received and efforts expended pursuant to contracts with various clinical trial centers and clinical research organizations. In the normal course of business we contract with third parties to perform various clinical trial activities in the ongoing development of potential drugs. The financial terms of these agreements are subject to negotiation and vary from contract to contract and may result in uneven payment flows. Payments under the contracts depend on factors such as the achievement of certain events, the successful enrollment of patients, the completion of portions of the clinical trial, or similar conditions. The objective of our accrual policy is to match the recording of expenses in our financial statements to the actual cost of services received and efforts expended. As such, expenses related to each patient enrolled in a clinical trial are recognized ratably beginning upon entry into the trial and over the course of the patient’s continued participation in the trial. In the event of early termination of a clinical trial, we accrue an amount based on our estimate of the remaining non-cancelable obligations associated with the winding down of the clinical trial. Our estimates and assumptions could differ significantly from the amounts that may actually be incurred.
Income Taxes
Deferred tax assets and liabilities are recognized based on the expected future tax consequences, using current tax rates, of temporary differences between the financial statement carrying amounts and the income tax basis of assets and liabilities. A valuation allowance is applied against any net deferred tax asset if, based on the weighted available evidence, it is more likely than not that some or all of the deferred tax assets will not be realized.
We use the asset and liability method of accounting for income taxes, as set forth in Accounting Standards Codification 740-10-25-2. Under this method, deferred income taxes, when required, are provided on the basis of the difference between the financial reporting and income tax basis of assets and liabilities at the statutory rates enacted for future periods. In accordance with Accounting Standards Codification 740-10-45-25, Income Statement Classification of Interest and Penalties, we classify interest associated with income taxes under interest expense and tax penalties under other.
The Company recognizes a tax benefit from an uncertain tax position only if it is more likely than not that the tax position will be sustained on examination by taxing authorities, based on the technical merits of the position. The tax benefit recognized in the consolidated financial statements from such position are measured based on the largest benefit that has a greater than 50% likelihood of being realized upon the ultimate settlement. As of December 31, 2016 and 2015, the Company has not recorded any unrecognized tax benefits.
Stock-Based Compensation
The Company has one stock-based compensation plan in effect which is described more fully in Note 10. Accounting Standards Codification 718, Compensation - Stock Compensation (“ASC 718”) requires the recognition of compensation expense, using a fair-value based method, for costs related to all share-based awards including stock options and common stock issued to our employees and directors under our stock plan. It requires companies to estimate the fair value of share-based awards on the date of grant using an option-pricing model. The value of the portion of the award that is ultimately expected to vest is recognized as expense on a straight-line basis over the requisite service periods in our consolidated statements of income.
Under ASC 718, we estimate the fair value of our employee stock awards at the date of grant using the Black-Scholes option-pricing model, which requires the use of certain subjective assumptions. The most significant of these assumptions are our estimates of the expected volatility of the market price of our stock and the expected term of an award. When establishing an estimate of the expected term of an award, we consider the vesting period for the award, our recent historical experience of employee stock option exercises (including forfeitures) and the expected volatility. When there is uncertainty in the factors used to determine the expected term of an award, we use the simplified method. As required under the accounting rules, we review our valuation assumptions at each grant date and, as a result, our valuation assumptions used to value employee stock-based awards granted in future periods may change.
We account for stock options granted to persons other than employees or directors at fair value using the Black-Scholes option-pricing model in accordance with Accounting Standards Codification 505-50, Equity Based Payments to Non-Employees (“ASC 505-50”). Stock options granted to such persons and stock options that are modified and continue to vest when an employee has a change in employment status are subject to periodic revaluation over their vesting terms. We recognize the resulting stock-based compensation expense during the service period over which the non-employee provides services to us.
Patent Costs
We amortize intangible assets with definite lives on a straight-line basis over their remaining estimated useful lives, ranging from 3 to 10 years, and review for impairment on an annual basis and when events or changes in circumstances indicate that the carrying amount of such assets may not be recoverable. As of December 31, 2016, there was no indicator that an impairment existed.
For the year ended December 31, 2016, we capitalized patent costs related to patent prosecution and maintenance of approximately $23,000 based on the most current information reported to us by Endo. As of December 31, 2016, the Company’s estimated costs related to certain patent costs are approximately $25,000 which are reimbursable to Endo under the License Agreement. These patent costs are creditable against future royalty revenues. For each period presented below net patent costs consisted of:
|
December 31,
|
||||||||
|
2016
|
2015
|
|||||||
|
Patents
|
$
|
720,601
|
$
|
697,260
|
||||
|
Accumulated Amortization
|
(462,246
|
)
|
(422,054
|
)
|
||||
|
Net Patent Costs
|
$
|
258,355
|
$
|
275,206
|
||||
The amortization expense for patents for the years ended December 31, 2016, 2015 and 2014 were $40,192, $45,758 and $119,920, respectively. The estimated aggregate amortization expense for each of the next five years is approximately as follows:
|
2017
|
$
|
39,000
|
||
|
2018
|
39,000
|
|||
|
2019
|
39,000
|
|||
|
2020
|
27,000
|
|||
|
2021
|
16,000
|
New Accounting Pronouncements
The Financial Accounting Standards Board, or FASB, issued in May 2014, in August 2015, March 2016 and April 2016, respectively, Accounting Standards Updates No. 2014-09, No. 2015-14, No. 2016-08, and No. 2016-10 (the “ASUs”). These ASUs were issued in connection with revenue from contracts with customers. The new standard provides a five-step approach to be applied to all contracts with customers and also requires expanded disclosures about revenue recognition. In August 2015, the FASB deferred the effective date of the guidance to reporting periods, including interim periods, beginning after December 15, 2017, and will be applied retrospectively. Early adoption is not permitted. We are currently evaluating the timing, method of adoption and the expected impact that the standard could have on our consolidated financial statements and related disclosures. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In January 2016, the FASB issued new guidance on recognition and measurement of financial assets and financial liabilities. The new guidance will impact the accounting for equity investments, financial liabilities under the fair value option, and the presentation and disclosure requirements for financial instruments. All equity investments in unconsolidated entities (other than those accounted for under the equity method of accounting) will generally be measured at fair value with changes in fair value recognized through earnings. There will no longer be an available-for-sale classification (changes in fair value reported in other comprehensive income (loss) for equity securities with readily determinable fair values. In addition, the FASB clarified the need for a valuation allowance on deferred tax assets resulting from unrealized losses on available-for-sale debt securities. In general, the new guidance will require modified retrospective application to all outstanding instruments, with a cumulative effect adjustment recorded to opening retained earnings. This guidance will be effective for us on January 1, 2018. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures however the Company does not classify any securities as available for sale.
In February 2016, FASB issued Accounting Standards Update (ASU) No. 2016-02, Leases (Topic 842). Under the new guidance, lessees will be required to recognize the following for all leases (with the exception of short-term leases) at the lease commencement date: a lease liability, which is a lessee’s obligation to make lease payments arising from a lease, measured on a discounted basis; and a right-of-use asset, which is an asset that represents the lessee’s right to use, or control the use of, a specified asset for the lease term. Under the new guidance, lessor accounting is largely unchanged. Certain targeted improvements were made to align, where necessary, lessor accounting with the lessee accounting model and Topic 606, Revenue from Contracts with Customers. The new lease guidance simplified the accounting for sale and leaseback transactions primarily because lessees must recognize lease assets and lease liabilities. Lessees will no longer be provided with a source of off-balance sheet financing. Public business entities should apply the amendments in ASU 2016-02 for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years (i.e., January 1, 2019, for a calendar year entity). Early application is permitted. Lessees (for capital and operating leases) and lessors (for sales-type, direct financing, and operating leases) must apply a modified retrospective transition approach for leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements. The modified retrospective approach would not require any transition accounting for leases that expired before the earliest comparative period presented. Lessees and lessors may not apply a full retrospective transition approach. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In March 2016, FASB issued ASU No. 2016-09 related to stock-based compensation. The new guidance simplifies the accounting for stock-based compensation transactions, including income tax consequences, classification of awards as either equity or liabilities, and classification on the statement of cash flows. This update is effective in fiscal years, including interim periods, beginning after December 15, 2016, and early adoption is permitted. We are currently evaluating this guidance and the impact it will have on the consolidated financial statements and related disclosures.
In May 2016, FASB issued ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients, which is intended to not change the core principle of the guidance in Topic 606, but rather affect only the narrow aspects of Topic 606 by reducing the potential for diversity in practice at initial application and by reducing the cost and complexity of applying Topic 606 both at transition and on an ongoing basis. We are currently evaluating the expected impact that the standard could have on our consolidated financial statements and related disclosures.
In June 2016, FASB issued ASU 2016-13, Financial Instruments - Credit Losses. The amendment revises the impairment model to utilize an expected loss methodology in place of the currently used incurred loss methodology, which will result in more timely recognition of losses on financial instruments, including, but not limited to, available for sale debt securities and accounts receivable. The Company is required to adopt this standard starting in the first quarter of fiscal year 2021. Early adoption is permitted. We are currently evaluating the impact of the adoption of this standard on our consolidated financial statements and related disclosures.
In January 2017, FASB issued ASU 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business. The amended definition of a business is an integrated set of activities and assets that is capable of being conducted and managed for the purpose of providing a return in the form of dividends, lower costs, or other economic benefits directly to investors or other owners, members or participants. In order to be considered a business, the three elements of inputs, processes and outputs must be present. In a business acquisition, if substantially all of the fair value of the gross assets acquired is concentrated in a single identifiable asset or group of similar identifiable assets, the integrated set of assets and activities acquired is not considered a business. The amendments are effective for fiscal years beginning after December 15, 2017, and interim periods within those fiscal years. Early adoption is permitted. This amendment may impact the allocation of purchase price in future acquisitions depending on the structure of future acquisitions.
3. FAIR VALUE MEASUREMENTS
The authoritative literature for fair value measurements established a three-tier fair value hierarchy, which prioritizes the inputs in measuring fair value. These tiers are as follows: Level 1, defined as observable inputs such as quoted market prices in active markets; Level 2, defined as inputs other than the quoted prices in active markets that are either directly or indirectly observable; and Level 3, defined as significant unobservable inputs (entity developed assumptions) in which little or no market data exists.
As of December 31, 2016, the Company held certain investments that are required to be measured at fair value on a recurring basis. The following tables present the Company’s fair value hierarchy for these financial assets as of December 31, 2016 and 2015:
|
December 31, 2016
|
Type of Instrument
|
Fair Value
|
Level 1
|
Level 2
|
Level 3
|
||||||||||||
|
Cash equivalents
|
Institutional Money Market
|
$
|
2,290,331
|
$
|
2,290,331
|
-
|
-
|
||||||||||
|
Investments
|
Municipal Bonds
|
7,554,028
|
-
|
7,554,028
|
-
|
||||||||||||
|
Investments
|
Corporate Bonds
|
33,354,407
|
-
|
33,354,407
|
-
|
||||||||||||
|
Investments
|
Certificates of Deposit
|
7,117,807
|
7,117,807
|
-
|
-
|
||||||||||||
|
December 31, 2015
|
Type of Instrument
|
Fair Value
|
Level 1
|
Level 2
|
Level 3
|
||||||||||||
|
Cash equivalents
|
Institutional Money Market
|
$
|
715,784
|
$
|
715,784
|
-
|
-
|
||||||||||
|
Investments
|
Municipal Bonds
|
6,617,042
|
-
|
6,617,042
|
-
|
||||||||||||
|
Investments
|
Corporate Bonds
|
11,480,000
|
-
|
11,480,000
|
-
|
||||||||||||
|
Investments
|
Certificates of Deposit
|
13,847,041
|
13,847,041
|
-
|
-
|
||||||||||||
4. EARNINGS PER SHARE
Basic earnings per share is computed by dividing net income by the weighted-average number of common shares outstanding during the period. Diluted earnings per share is computed by dividing net income by the weighted-average number of common shares outstanding during the period increased to include all additional common shares that would have been outstanding assuming potentially dilutive common shares, resulting from option exercises, had been issued and any proceeds thereof used to repurchase common stock at the average market price during the period.
|
2016
|
2015
|
2014
|
||||||||||
|
Net income for diluted computation
|
$
|
11,372,239
|
$
|
9,617,632
|
$
|
4,645,960
|
||||||
|
Weighted average shares:
|
||||||||||||
|
Basic
|
7,061,404
|
6,827,355
|
6,477,457
|
|||||||||
|
Effect of dilutive securities:
|
||||||||||||
|
Stock options
|
221,858
|
445,634
|
602,113
|
|||||||||
|
Diluted
|
7,283,262
|
7,272,989
|
7,079,570
|
|||||||||
|
Net income per share:
|
||||||||||||
|
Basic
|
$
|
1.61
|
$
|
1.41
|
$
|
0.72
|
||||||
|
Diluted
|
$
|
1.56
|
$
|
1.32
|
$
|
0.66
|
||||||
We exclude from earnings per share the weighted-average number of securities whose effect is anti-dilutive. Excluded from the calculation of earnings per share for each of the years ended December 31, 2016, 2015 and 2014 were 20,000 options to purchase shares of common stock, because their effect is anti-dilutive.
5. PROPERTY, PLANT AND EQUIPMENT
Property and equipment are stated at cost, less accumulated depreciation. Machinery and equipment, furniture and fixtures, and autos are depreciated on the straight-line basis over their estimated useful lives of 5 to 10 years. Leasehold improvements are amortized over the lesser of their estimated useful lives or the remaining life of the lease. As of December 31, 2016, 2015 and 2014, property and equipment were fully depreciated.
6. COMPREHENSIVE INCOME
For the years ended 2016, 2015, 2014, we had no components of other comprehensive income other than net income itself.
7. ACCOUNTS PAYABLE AND ACCRUED LIABILITIES
Accounts payable and accrued expenses consist of the following:
|
December 31,
|
||||||||
|
2016
|
2015
|
|||||||
|
Trade accounts payable and accrued expenses
|
$
|
505,098
|
$
|
372,367
|
||||
|
Accrued legal and other professional fees
|
51,000
|
74,138
|
||||||
|
Accrued payroll and related costs
|
182,551
|
164,504
|
||||||
|
$
|
738,649
|
$
|
611,009
|
|||||
8. INCOME TAXES
The provision for income taxes consists of the following:
|
Year ended December 31,
|
||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Current taxes:
|
||||||||||||
|
Federal
|
$
|
8,571,034
|
4,428,344
|
$
|
1,939,830
|
|||||||
|
State
|
98,881
|
49,185
|
17,872
|
|||||||||
|
Total current taxes
|
8,669,915
|
4,477,529
|
1,957,702
|
|||||||||
|
Deferred taxes:
|
||||||||||||
|
Federal
|
(2,647,363
|
)
|
452,761
|
425,127
|
||||||||
|
State
|
(19,787
|
)
|
3,038
|
3,878
|
||||||||
|
Total deferred taxes
|
(2,667,150
|
)
|
455,799
|
429,005
|
||||||||
|
Total provision for income taxes
|
$
|
6,002,765
|
4,933,328
|
$
|
2,386,707
|
|||||||
The effective income tax rate of the Company differs from the federal statutory tax rate due to the following items:
| Year ended December 31, | ||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Statutory rate
|
35.00
|
%
|
34.00
|
%
|
34.00
|
%
|
||||||
|
State income taxes, net of federal income tax benefit
|
0.26
|
%
|
0.25
|
%
|
0.17
|
%
|
||||||
|
Stock-based compensation
|
(0.50
|
)%
|
(0.46
|
)%
|
(0.40
|
)%
|
||||||
|
Miscellaneous other, net
|
(0.21
|
)%
|
0.11
|
%
|
0.17
|
%
|
||||||
|
Effective tax rate
|
34.55
|
%
|
33.90
|
%
|
33.94
|
%
|
||||||
The effective rate reconciliation includes the permanent differences and changes for windfalls and stock-based compensation, and net operating loss.
Deferred income taxes reflect the tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. The components of deferred income tax assets and liabilities are as follows:
|
December 31,
|
||||||||
|
2016
|
2015
|
|||||||
|
Deferred revenue
|
$
|
2,643,678
|
$
|
33,823
|
||||
|
Stock option based compensation
|
536,065
|
490,405
|
||||||
|
Other
|
110,379
|
98,744
|
||||||
|
Net deferred tax asset
|
$
|
3,290,122
|
$
|
622,972
|
||||
Stock option based compensation, recorded in the Company's consolidated financial statements, is non-deductible for tax purposes and increases the Company's effective tax rate. Deferred tax assets, including those associated with stock option based compensation, are reviewed and adjusted for apportionment and potential tax rates changes in various jurisdictions.
During 2016, the Company has recorded $0.3 million of excess tax benefits resulting from the exercise of stock options which was recorded in additional paid in capital.
As of December 31, 2016, the Company believes that there are no significant uncertain tax positions, and no amounts have been recorded for interest and penalties. The tax periods open to examination by the major taxing jurisdictions to which the Company is subject include fiscal years 2013 through 2016.
9. STOCKHOLDERS’ EQUITY
Stock Option Plan
At December 31, 2016, we have one stock option plan, the Amended and Restated 2001 Stock Option Plan (“2001 Plan”). Under the 2001 Plan, qualified incentive stock options and non-qualified stock options may be granted to purchase up to an aggregate of 2,050,000 shares of the Company's common stock, subject to certain anti-dilution provisions. The exercise price per share of common stock may not be less than 100% (110% for qualified incentive stock options granted to stockholders owning at least 10% of common shares) of the fair market value of the Company's common stock on the date of grant. In general, the options vest and become exercisable in four equal annual installments following the date of grant, although the Company’s Board, at its discretion, may provide for different vesting schedules. The options expire 10 years (five years for qualified incentive stock options granted to stockholders owning at least 10% of common shares) after such date. As of December 31, 2016, options to purchase 297,000 shares of common stock were outstanding under the 2001 Plan, and a total of 209,098 shares remain available for grant under the 2001 Plan.
Stock-Based Compensation
ASC 718 requires that employee stock-based compensation costs to be recognized over the requisite service period, or the vesting period, in a manner similar to all other forms of compensation paid to employees. The allocation of employee stock-based compensation costs to each operating expense line are estimated based on specific employee headcount information at each grant date and estimated stock option forfeiture rates and revised, if necessary, in future periods if actual employee headcount information or forfeitures differ materially from those estimates. As a result, the amount of employee stock-based compensation costs we recognize in each operating expense category in future periods may differ significantly from what we have recorded in the current period.
Stock-based compensation expense recognized under ASC 718 was as follows:
|
December 31,
|
||||||||||||
|
2016
|
2015
|
2014
|
||||||||||
|
Research and development
|
$
|
-
|
$
|
-
|
$
|
-
|
||||||
|
General and administrative
|
133,904
|
105,782
|
21,416
|
|||||||||
|
Total stock-based compensation expense
|
$
|
133,904
|
$
|
105,782
|
$
|
21,416
|
||||||
Stock Options
No stock options were granted during the year ended December 31, 2016. During the year ended December 31, 2015, 30,000 stock options valued at approximately $450,000 were granted to two new members of the Board (Jennifer Chao and Jyrki Mattila, M.D., Ph.D.). 15,000 stock options valued at approximately $123,000 were granted to a new member of the Board (Max Link, Ph.D.) during the year ended December 31, 2014. At the time of Dr. Link’s sudden death on October 6, 2014, none of these options had vested and, in accordance with the applicable terms, they expired upon his death. The following table presents the assumptions used to estimate the fair values of the stock options granted in the periods presented:
|
2016
|
2015
|
2014
|
||||||||||
|
Risk-free interest rate
|
-
|
1.41
|
%
|
1.66
|
%
|
|||||||
|
Expected volatility
|
-
|
39
|
%
|
32
|
%
|
|||||||
|
Expected life (in years)
|
-
|
6.25
|
5.00
|
|||||||||
|
Dividend yield
|
-
|
-
|
-
|
|||||||||
The summary of the stock options activity is as follows for year ended:
|
Shares
|
Weighted-
Average
Exercise
Price
|
Weighted-
Average
Remaining
Contractual
Term
|
Aggregate
Intrinsic
Value
|
|||||||||||||
|
Outstanding at January 1, 2015
|
759,958
|
$
|
11.04
|
3.12
|
$
|
23,483,235
|
||||||||||
|
Grants
|
30,000
|
37.64
|
10.00
|
-
|
||||||||||||
|
Exercised
|
(227,958
|
)
|
12.39
|
-
|
9,251,027
|
|||||||||||
|
Forfeitures or expirations
|
-
|
-
|
-
|
-
|
||||||||||||
|
Outstanding at December 31, 2015
|
562,000
|
11.91
|
2.51
|
17,456,220
|
||||||||||||
|
Grants
|
-
|
-
|
-
|
-
|
||||||||||||
|
Exercised
|
(265,000
|
)
|
2.68
|
-
|
9,392,150
|
|||||||||||
|
Forfeitures or expirations
|
-
|
-
|
-
|
-
|
||||||||||||
|
Outstanding at December 31, 2016
|
297,000
|
20.14
|
3.10
|
10,561,380
|
||||||||||||
|
Vested and expected to vest at December 31, 2016
|
297,000
|
20.14
|
3.10
|
10,561,380
|
||||||||||||
|
Exercisable at December 31, 2016
|
250,750
|
$
|
17.88
|
2.60
|
$
|
9,483,518
|
||||||||||
The following table summarizes information relating to stock options by exercise price at December 31, 2016:
|
Outstanding Shares
|
Exercisable Shares
|
||||||||||||||||||||||||
|
Option
Exercise Price
|
Number of
Shares
|
Weighted
Average
Life
(years)
|
Weighted
Average
Exercise Price
|
Number
of
Shares
|
Weighted
Average
Option
Price
|
Weighted
Average
Life
(years)
|
|||||||||||||||||||
|
4.00 - 5.50
|
35,000
|
0.71
|
$
|
5.24
|
35,000
|
$
|
5.24
|
0.71
|
|||||||||||||||||
|
13.24 - 15.85
|
60,000
|
3.58
|
14.61
|
60,000
|
14.61
|
3.58
|
|||||||||||||||||||
|
17.00 - 21.00
|
125,000
|
2.39
|
19.69
|
121,250
|
19.74
|
2.26
|
|||||||||||||||||||
|
26.43 - 37.64
|
77,000
|
4.97
|
31.95
|
34,500
|
29.83
|
3.99
|
|||||||||||||||||||
|
297,000
|
3.10
|
$
|
20.14
|
250,750
|
$
|
17.88
|
2.60
|
||||||||||||||||||
During the years 2016, 2015 and 2014, $0.7 million, $2.8 million and $2.1 million proceeds were received from stock options exercised, respectively. Aggregate intrinsic value represents the total pre-tax intrinsic value, based on the closing price of our common stock of $55.70 on December 31, 2016, which would have been received by the option holders had all option holders exercised their options as of that date. Total unrecognized compensation cost related to non-vested stock options outstanding as of December 31, 2016 was approximately $0.3 million which we expect to recognize over a weighted-average period of 2.42 years.
10. COMMITMENTS AND CONTINGENCIES
Lease Agreements
The Company’s corporate headquarters are currently located at 35 Wilbur St., Lynbrook, NY 11563 (the “Headquarters”). As previously reported, the Company formerly leased the Headquarters from Wilbur St. Corp. (“WSC”), which was owned by Edward H. Wegman, the former CEO and Chairman of BioSpecifics. On November 21, 2013, WSC sold the Headquarters to 35 Wilbur Street Associates, LLC (the “Landlord”), and the Company entered into an Agreement of Lease (the “Lease”) with the Landlord for the Company’s Headquarters and simultaneously terminated the existing lease. Neither the Company nor its affiliates have a material relationship or affiliation with the Landlord. The term of the Lease was for twenty-four months and the base rent was $12,000 per month, provided, however, that the Company had the option to cancel the Lease after the first year by giving three months’ notice to the Landlord. The Lease was filed with the SEC as Exhibit 10.1 to the Company’s Annual Report on Form 10-K filed with the SEC on March 7, 2014. In 2014 the Company leased approximately 2,300 square feet back to the Landlord and the Company’s base rent was adjusted to approximately $10,200 per month.
On August 14, 2015, the Company entered into an agreement with the Landlord to extend the term of the lease to the Headquarters for an additional one year period (the “Extended Lease Agreement”). The one year extension ended on November 30, 2016. Pursuant to the Extended Lease Agreement, the Landlord will take occupancy of 1,000 square feet in the front of the building, the base rent will be $10,213 per month and the Company may cancel the lease with three months’ prior written notice to the Landlord at any time during the term. In addition, the Company leases a vehicle and certain office equipment which expire in mid-2017.
On November 1, 2016, the Company entered into an agreement with the Landlord to extend the term of the lease to the Headquarters for an additional one year period (the “Extended Lease Agreement”). The one year extension will end on November 30, 2017. Pursuant to the Extended Lease Agreement, the base rent is $10,757 per month and the Company may cancel the lease with three months’ prior written notice to the Landlord at any time during the term. The Extended Lease Agreement was filed with the SEC as Exhibit 10.1 to the Company’s Quarterly Report on Form 10Q on November 9, 2016.
Future minimum annual rental payments required under non-cancelable operating leases are $134,450 at year end December 31, 2016.
Expense under all operating leases amounted to approximately $127,000, $130,000 and $140,000 for 2016, 2015 and 2014, respectively.
Future minimum annual payments required under non-cancelable operating leases are approximated as follows:
Year ending December 31,
|
2017
|
$
|
125,000
|
||
| 2018 |
4,200
|
|||
|
2019
|
4,200
|
|||
| 2020 |
1,050
|
11. RELATED PARTY TRANSACTIONS
During the fiscal years ended December 31, 2016, 2015 and 2014 there were no related party transactions.
12. EMPLOYEE BENEFIT PLANS
ABC-NY has a 401(k) Profit Sharing Plan for employees who meet minimum age and service requirements. Contributions to the plan by ABC-NY are discretionary and subject to certain vesting provisions. The Company made no contributions to this plan for fiscal years 2016, 2015 or 2014.
14. SELECTED QUARTERLY DATA (Unaudited)
The following table sets forth certain unaudited quarterly data for each of the four quarters in the years ended December 31, 2016 and 2015. The data has been derived from the Company's unaudited Consolidated Financial Statements that, in management's opinion, include all adjustments (consisting of normal recurring adjustments) necessary for a fair presentation of such information when read in conjunction with the Consolidated Financial Statements and Notes thereto. The results of operations for any quarter are not necessarily indicative of the results of operations for any future period.
|
First
Quarter
|
Second
Quarter
|
Third
Quarter
|
Fourth
Quarter
|
|||||||||||||
|
Year ended December 31, 2016
|
||||||||||||||||
|
Net revenues
|
$
|
6,567,991
|
$
|
6,180,156
|
$
|
6,882,160
|
$
|
6,620,648
|
||||||||
|
Operating profit
|
4,155,158
|
3,833,596
|
4,725,885
|
4,311,777
|
||||||||||||
|
Net income
|
2,829,124
|
2,572,715
|
3,053,593
|
2,916,807
|
||||||||||||
|
Basic earnings per share
|
$
|
0.40
|
$
|
0.37
|
$
|
0.43
|
$
|
0.41
|
||||||||
|
Diluted earnings per share
|
$
|
0.39
|
$
|
0.35
|
$
|
0.42
|
$
|
0.40
|
||||||||
|
|
||||||||||||||||
|
First
Quarter |
Second
Quarter |
Third
Quarter |
Fourth
Quarter |
|||||||||||||
|
Year ended December 31, 2015
|
||||||||||||||||
|
Net revenues
|
$
|
5,606,454
|
$
|
4,714,975
|
$
|
6,289,839
|
$
|
6,138,867
|
||||||||
|
Operating profit
|
3,563,867
|
2,662,974
|
4,321,958
|
3,894,516
|
||||||||||||
|
Net income
|
2,330,900
|
1,757,204
|
2,870,979
|
2,658,549
|
||||||||||||
|
Basic earnings per share
|
$
|
0.35
|
$
|
0.26
|
$
|
0.42
|
$
|
0.38
|
||||||||
|
Diluted earnings per share
|
$
|
0.32
|
$
|
0.24
|
$
|
0.39
|
$
|
0.36
|
||||||||
EXHIBIT INDEX
|
Exhibit
Number
|
Description
|
|
3.1
|
Registrant’s Certificate of Incorporation, as amended (incorporated by reference to Exhibit 3.1 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on March 2, 2007)
|
|
3.2
|
Registrant’s Amended and Restated By-laws, as amended February 25, 2014 (incorporated by reference to Exhibit 3.2 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 7, 2014)
|
|
3.3
|
Amendment to Amended and Restated By-laws (incorporated by reference to Exhibit 3.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on February 26, 2014)
|
|
4.1
|
Rights Agreement dated as of May 14, 2002 (incorporated by reference to Exhibit 1 to the Registrant’s Form 8-A filed with the Commission on May 30, 2002)
|
|
4.2
|
Amendment No. 1 to Rights Agreement, dated June 19, 2003 (incorporated by reference to Exhibit 10.19 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on March 2, 2007)
|
|
4.3
|
Amendment No. 2 to Rights Agreement, dated as of February 3, 2011 (incorporated by reference to Exhibit 4.1 to the Registrant’s Current Report on Form 8-K filed with the Commission on February 4, 2011)
|
|
4.4
|
Amendment No. 3 Rights Agreement, dated as of March 5, 2014 (incorporated by reference to Exhibit 4.4 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 7, 2014)
|
|
10.1
|
Agreement of Lease, dated as of November 21, 2013, among the Company, ABC-NY and 35 Wilbur Street Associates, LLC (incorporated by reference to Exhibit 10.1 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 7, 2014)
|
|
10.2
|
Consulting Agreement, dated as of August 4, 2014, by and between BioSpecifics Technologies Corp. and Mr. Henry Morgan (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on August 5, 2014)
|
|
10.3
|
Asset Purchase Agreement among the Company, ABC-NY and DFB dated March 3, 2006 (incorporated by reference to Exhibit 2.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on March 9, 2006)
|
|
10.4
|
Amendment to Asset Purchase Agreement between the Company, ABC-NY and DFB dated January 8, 2007 (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on January 12, 2007)
|
|
10.5
|
Dupuytren’s License Agreement dated November 21, 2006 between the Company and the Research Foundation (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on November 28, 2006)
|
|
10.6
|
Frozen Shoulder License Agreement dated November 21, 2006 between the Company and the Research Foundation (incorporated by reference to Exhibit 10.2 of the Registrant’s Current Report on Form 8-K filed with the Commission on November 28, 2006)
|
|
10.7
|
Cellulite License Agreement dated August 23, 2007 between the Company and the Research Foundation (incorporated by reference to Exhibit 10.7 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 15, 2013)
|
|
10.8
|
License Agreement dated March 27, 2010 between the Company and Zachary Gerut, M.D. (incorporated by reference as Exhibit 10.8 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 15, 2013)
|
|
10.9
|
Form of 1997 Stock Option Plan of Registrant (incorporated by reference to Exhibit 4.1 of the Registrant’s Form S-8 filed with the Commission on September 26, 1997)
|
|
10.10
|
Amended and Restated 2001 Stock Option Plan of Registrant (incorporated by reference to Appendix D of the Registrant’s Schedule 14A filed with the Commission on April 30, 2009)
|
|
10.11
|
Change of Control Agreement, dated June 18, 2007 between the Company and Henry Morgan (incorporated by reference to Exhibit 10.21 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on September 26, 2007)
|
|
10.12
|
Change of Control Agreement, dated June 18, 2007 between the Company and Michael Schamroth (incorporated by reference to Exhibit 10.22 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on September 26, 2007)
|
|
10.13
|
Change of Control Agreement, dated June 18, 2007 between the Company and Dr. Paul Gitman (incorporated by reference to Exhibit 10.23 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on September 26, 2007)
|
|
10.14
|
Amendment to Amended and Restated Agreement between the Company and Dr. Marty Gelbard dated March 31, 2012 between the Company and Marty Gelbard (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-KA filed with the Commission on August 13, 2012)
|
|
10.15
|
Amended and Restated Development and License Agreement, dated December 11, 2008, between the Company and Auxilium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on December 19, 2008)
|
|
10.16
|
Executive Employment Agreement, dated August 5, 2008 between the Company and Thomas L. Wegman (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the Commission on August 8, 2008)
|
|
10.17
|
Change of Control Agreement, dated October 1, 2008 between the Company and Dr. Matthew Geller (incorporated by reference to Exhibit 10.23 of the Registrant’s Form 10-K filed with the Commission on March 31, 2009)
|
|
10.18
|
Change of Control Agreement, dated as of September 17, 2013, between the Company and George Gould (incorporated by reference to Exhibit 10.18 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 7, 2014)
|
|
10.19
|
Change of Control Agreement, dated as of April 22, 2015, between the Company and Jyrki Mattila (incorporated by reference to Exhibit 10.19 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 14, 2016)
|
|
10.20
|
Change of Control Agreement, dated as of April 22, 2015, between the Company and Jennifer Chao (incorporated by reference to Exhibit 10.20 of the Registrant’s Annual Report on Form 10-K filed with the Commission on March 14, 2016)
|
|
10.21
|
Second Amended and Restated Development and License Agreement, dated as of August 31, 2011, by and between BioSpecifics Technologies Corp. and Auxilium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 10.1 of the Registrant's Current Report on Form 8-K filed with the SEC on September 1, 2011)
|
|
10.22
|
Settlement Agreement, dated as of August 31, 2011, by and between BioSpecifics Technologies Corp. and Auxilium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 10.2 of the Registrant's Current Report on Form 8-K filed with the SEC on September 1, 2011)
|
|
10.23
|
Amended Agreement of Lease, dated as of August 14, 2015, among the company, ABC NY and 35 Wilbur Street Associates (incorporated by reference to Exhibit 10.1 of the Registrant’s Quarterly Report on Form 10-Q filed with the SEC on November 9, 2015)
|
|
10.24
|
First Amendment to Second Amended and Restated Development and License Agreement, dated as of February 1, 2016, by and between BioSpecifics Technologies Corp. and Endo Global Ventures. (incorporated by reference to Exhibit 10.1 of the Registrant’s Current Report on Form 8-K filed with the SEC on February 5, 2016)
|
|
14.1
|
Amended and Restated Code of Business Conduct and Ethics (incorporated by reference to Exhibit 14.1 of the Registrant’s Annual Report on Form 10-KSB filed with the Commission on March 2, 2007)
|
|
Subsidiaries of the Registrant
|
|
|
Consent of EisnerAmper LLP
|
|
|
Certification of Principal Executive Officer and Principal Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002
|
|
|
Certification of Principal Executive Officer and Principal Financial Officer pursuant to Section 906 of the Sarbanes-Oxley Act of 2002
|
101* The following materials from BioSpecifics Technologies Corp. Annual Report on Form 10-K for the year ended December 31, 2016, formatted in XBRL (Extensible Business Reporting Language): (i) the Consolidated Balance Sheets, (ii) the Consolidated Statements of Income, (iii) Consolidated Statements of Stockholders’ Equity, (iv) the Consolidated Statements of Cash Flows, and (v) Notes to Consolidated Financial Statements
| * |
filed herewith
|
| ** |
furnished herewith.
|
SIGNATURES
In accordance with section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant caused this Report on Form 10-K to be signed on its behalf by the undersigned, thereto duly authorized individual.
Date: March 16, 2017
|
BIOSPECIFICS TECHNOLOGIES CORP.
|
|||
|
By:
|
/s/ Thomas L. Wegman
|
||
|
Name:
|
Thomas L. Wegman
|
||
|
Title:
|
President
|
||
In accordance with the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the Registrant and in the capacities and on the dates indicated.
|
SIGNATURE
|
TITLE
|
|
|
/s/ Thomas L. Wegman
|
President, Director, and Principal Executive, Financial
|
|
|
Name: Thomas L. Wegman
|
and Accounting Officer
|
|
|
Date: March 16, 2017
|
||
|
|
Director
|
|
|
Name: Dr. Paul Gitman
|
||
|
Date: March 16, 2017
|
||
|
/s/ George Gould
|
Director
|
|
|
Name: George Gould
|
||
|
Date: March 16, 2017
|
||
|
/s/ Michael Schamroth
|
Director
|
|
|
Name: Michael Schamroth
|
||
|
Date: March 16, 2017
|
||
|
/s/ Dr. Mark Wegman
|
Director
|
|
|
Name: Dr. Mark Wegman
|
||
|
Date: March 16, 2017
|
||
|
/s/ Toby Wegman
|
Director
|
|
|
Name: Toby Wegman
|
||
|
Date: March 16, 2017
|
||
|
/s/ Dr. Jyrki Mattila
|
Director
|
|
|
Name: Dr. Jyrki Mattila
|
||
|
Date: March 16, 2017
|
||
|
/s/ Jennifer Chao
|
Director
|
|
|
Name: Jennifer Chao
|
||
|
Date: March 16, 2017
|
||