Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - TACTILE SYSTEMS TECHNOLOGY INC | tcmd-20161231ex32250f412.htm |
| EX-32.1 - EX-32.1 - TACTILE SYSTEMS TECHNOLOGY INC | tcmd-20161231ex321228d61.htm |
| EX-31.2 - EX-31.2 - TACTILE SYSTEMS TECHNOLOGY INC | tcmd-20161231ex312b95414.htm |
| EX-31.1 - EX-31.1 - TACTILE SYSTEMS TECHNOLOGY INC | tcmd-20161231ex311de9de3.htm |
| EX-23.1 - EX-23.1 - TACTILE SYSTEMS TECHNOLOGY INC | tcmd-20161231ex2310128a7.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
☒ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2016
OR
☐TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from to
Commission file number: 001-37799
Tactile Systems Technology, Inc.
(Exact Name of Registrant as Specified in Its Charter)
|
Delaware |
41-1801204 |
|
(State or Other Jurisdiction of Incorporation or Organization) |
(I.R.S. Employer Identification Number) |
|
|
|
|
1331 Tyler Street NE, Suite 200 Minneapolis, Minnesota |
55413 |
|
(Address of Principal Executive Offices) |
(Zip Code) |
(612) 355-5100
(Registrant’s Telephone Number, Including Area Code)
Securities registered pursuant to Section 12(b) of the Act:
|
Common Stock, Par Value $0.001 Per Share |
The NASDAQ Stock Market |
|
(Title of each class) |
(Name of each exchange on which registered) |
Securities registered pursuant to Section 12(g) of the Act:
None
(Title of class)
Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the Registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the Registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the Registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the Registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405) is not contained herein, and will not be contained, to the best of Registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☐
Indicate by check mark whether the Registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definition of “large accelerated filer”, “accelerated filer”, and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
|
Large accelerated filer |
☐ |
|
|
|
Accelerated filer |
☐ |
|
|
|
|
|
|
|
|
|
Non-accelerated filer |
☒ |
|
(Do not check if a smaller reporting company) |
|
Smaller reporting company |
☐ |
Indicate by check mark whether the Registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
The aggregate market value of the voting and non-voting common equity held by non-affiliates of the Registrant, based on $13.16, the closing price of the shares of common stock on August 2, 2016 as reported by the Nasdaq Global Market on such date, was approximately $117,891,360. The Registrant has elected to use August 2, 2016, which was the closing date of the Registrant’s initial public offering, as the calculation date because on June 30, 2016 (the last business day of the Registrant’s most recently completed second fiscal quarter), the Registrant was a privately held company. August 2, 2016 was also the date that the Registrant’s previously outstanding preferred stock was converted to common stock.
The number of shares of Registrant’s Common Stock outstanding as of February 22, 2017 was 16,896,099.
Portions of the Registrant’s Definitive Proxy Statement relating to the Annual Meeting of Stockholders, scheduled to be held on May 9, 2017, are incorporated by reference into Part III of this Report.
i
SPECIAL NOTE REGARDING FORWARD-LOOKING INFORMATION
This Annual Report on Form 10-K contains forward-looking statements regarding us, our business prospects and our results of operations that are subject to certain risks and uncertainties posed by many factors and events that could cause our actual business, prospects and results of operations to differ materially from those that may be anticipated by such forward-looking statements. Factors that could cause or contribute to such differences include, but are not limited to, those described in Part I, Item 1A. “Risk Factors” and elsewhere in this report. Readers are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this report. We expressly disclaim any intent or obligation to update or revise any forward-looking statements, whether as a result of new information, future events or otherwise. Readers are urged to carefully review and consider the various disclosures made by us in this report and in our other reports filed with the Securities and Exchange Commission that advise interested parties of the risks and factors that may affect our business.
All statements, other than statements of historical facts, contained in this Annual Report on Form 10-K, including statements regarding our business, operations and financial performance and condition, as well as our plans, objectives and expectations for our business, operations and financial performance and condition, are forward-looking statements. In some cases, you can identify forward-looking statements by the following words: "anticipate," "believe," "continue," "could," "estimate," "expect," "intend," "may," "might," "target," "ongoing," "plan," "potential," "predict," "project," "should," "will," "would," or the negative of these terms or other comparable terminology, although not all forward-looking statements contain these words. Forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause our results, levels of activity, performance or achievements to be materially different from the information expressed or implied by the forward-looking statements in this Annual Report on Form 10-K. Forward-looking statements may include, among other things, statements relating to:
|
· |
our expectations regarding the potential market size and widespread adoption of our products; |
|
· |
our ability to increase awareness of lymphedema and chronic venous insufficiency and to demonstrate the clinical and economic benefits of our solutions to clinicians and patients; |
|
· |
developments and projections relating to our competitors or our industry; |
|
· |
the expected growth in our business and our organization, including outside of the United States; |
|
· |
our ability to achieve and maintain adequate levels of coverage or reimbursement for our products and the effect of changes to the level of Medicare coverage; |
|
· |
our financial performance, our estimates of our expenses, future revenues, capital requirements and our needs for, or ability to obtain, additional financing; |
|
· |
our ability to retain and recruit key personnel, including the continued development and expansion of our sales and marketing organization; |
|
· |
our ability to obtain an adequate supply of components for our products from our third party suppliers; |
|
· |
our ability to obtain and maintain intellectual property protection for our products or avoid claims of infringement; |
|
· |
our ability to identify and develop new products; |
|
· |
our compliance with extensive government regulation; |
|
· |
the volatility of our stock price; and |
|
· |
our expectations regarding the time during which we will be an emerging growth company under the JOBS Act. |
1
You should read the matters described in Part I, Item 1A. "Risk Factors" and the other cautionary statements made in this Annual Report on Form 10-K. We cannot assure you that the forward-looking statements in this report will prove to be accurate and therefore you are encouraged not to place undue reliance on forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements we make. You are urged to carefully review and consider the various disclosures made by us in this report and in other filings with the SEC that advise of the risks and factors that may affect our business. Other than as required by law, we undertake no obligation to update or revise these forward-looking statements, even though our situation may change in the future. Our forward-looking statements do not reflect the potential impact of any future acquisitions, mergers, dispositions, joint ventures or investments that we may make.
2
Overview
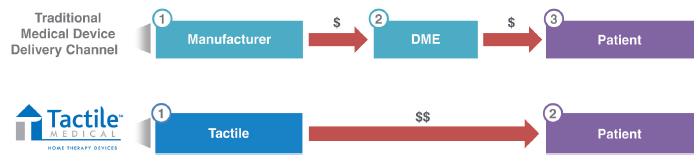
Tactile Systems Technology, Inc. (“we,” “us,” and “our”) is a medical technology company that develops and provides innovative medical devices for the treatment of chronic diseases at home. We focus on advancing the standard of care in treating chronic diseases in the home setting to improve patient outcomes and quality of life and help control rising healthcare expenditures. We possess a unique, scalable platform to deliver at-home healthcare solutions throughout the United States. This evolving care delivery model is recognized by policy-makers and payers as a key for controlling rising healthcare expenditures. Our initial area of therapeutic focus is vascular disease, with a goal of advancing the standard of care in treating lymphedema and chronic venous insufficiency. Our proprietary Flexitouch System is an at-home solution for lymphedema patients. Our proprietary ACTitouch System is a home-based solution for chronic venous insufficiency patients that may be worn throughout the day. Our products deliver cost-effective, clinically proven, long-term treatment of chronic diseases. We employ a direct-to-patient and -provider model, through which we obtain patient referrals from clinicians, manage insurance claims on behalf of our patients and their clinicians, deliver our solutions to patients and train them on the proper use of our solutions in their homes. This model allows us to directly approach patients and clinicians, whereby we disintermediate the traditional durable medical equipment channel and capture both the manufacturer and distributor margins. For the year ended December 31, 2016, we generated revenues of $84.5 million and had net income of $2.9 million. Our revenues increased 34% during the year ended December 31, 2016 compared to the year ended December 31, 2015.
Lymphedema is a type of chronic swelling, or edema, which occurs in the arms, legs, neck, trunk or other body parts when the lymphatic vessels are unable to adequately drain protein-rich lymph fluid from these regions. Lymphedema is progressive in nature, worsens over time, and has no known cure. Chronic venous insufficiency is a condition that occurs when the venous wall and/or valves in the veins are not working effectively, making it difficult for blood to return to the heart from the affected region. This pooling or collecting of blood in the veins can result in painful, slow-healing wounds on the lower leg, called venous leg ulcers. Patients with lymphedema or chronic venous insufficiency are typically treated by vascular surgeons, vascular medicine physicians, wound physicians, wound nurses and lymphedema therapists.
Our advanced at-home Flexitouch System mimics the clinic-based manual lymphatic drainage therapy through an easy-to-use, one-hour daily, self-applied system. The predecessor version to our Flexitouch System received 510(k) clearance from the FDA in July 2002 and our current Flexitouch System received 510(k) clearance from the FDA in October 2006. In September 2016, we received 510(k) clearance from the FDA for the Flexitouch System in treating lymphedema in the head and neck. Our Flexitouch System generated $73.4 million, or 87%, of our revenues in 2016, and $54.8 million, or 87%, of our revenues in 2015.
Our ACTitouch System provides precise, consistent and wearable compression that a patient may apply, remove and reapply at home. This system was developed to provide maximum convenience for patients by providing them with the freedom to remain active while simultaneously receiving the benefits of sustained and intermittent pneumatic compression, which we refer to as dual-compression. Our ACTitouch System received 510(k) clearance from the FDA in June 2013 and we began selling the product in September 2013. We also introduced the Entré System in the United States in February 2013. The Entré System is sold to patients for whom a basic pump is suitable or who do not yet qualify for insurance reimbursement for an advanced compression device such as our Flexitouch System. Our ACTitouch System and Entré System combined generated $11.1 million, or 13%, of our revenues in 2016, and $8.1 million, or 13%, of our revenues in 2015.
To support the growth of our business, we invest heavily in our commercial infrastructure, consisting of our direct sales force, reimbursement capabilities and clinical expertise. We are a national, accredited provider of home medical equipment services approved for coverage by private payers, Medicare, the Veterans Administration and certain Medicaid programs in the United States. We market our products using a direct-to-patient and -provider model. Our direct sales force is focused on increasing clinician awareness of our solutions, and has grown from three representatives in March 2005 to a team of over 125 people as of December 31, 2016. We also utilize over 400 licensed, independent healthcare practitioners as home trainers who educate patients on the proper use of our solutions. Our experienced reimbursement operations group of over 70 people focuses on verifying case-by-case benefits, obtaining prior
3
authorization, billing and collecting payments from payers and providing customer support services. Our payer relationships group of 30 people is responsible for developing relationships with payer decision-makers to educate them on our product efficacy, develop overall payer coverage policies and reimbursement criteria, manage Medicare patient claims and contracts with payers and serve as an advocacy liaison between patients, clinicians and payers throughout the appeals process. Our clinical team, consisting of a scientific advisory board, in-house therapists and nurses, and a medical director (part-time), serves as a resource to clinicians and patients and guides our development of clinical evidence in support of our products. We believe these investments are critical to driving patient adoption of our technologies, and together with our commercial infrastructure represents a significant competitive advantage. Health insurance coverage for our Flexitouch System and our ACTitouch System is in place with private payers, Medicare, the Veterans Administration and certain Medicaid programs. Based on our estimates, we have contracts as an in-network provider covering over 270 million lives in the United States. Over 65,000 patients have been treated with our Flexitouch System since its launch in 2004, and over 16,000 Flexitouch Systems were shipped in 2016. More than 17,000 patients were treated with our ACTitouch and Entré Systems since their launch in 2013, and over 7,500 ACTitouch and Entré Systems were shipped in 2016. We do not currently have any international operations or sales outside the United States.
We were originally incorporated in Minnesota under the name Tactile Systems Technology, Inc. on January 30, 1995. During 2006, we established a merger corporation and subsequently, on July 21, 2006, merged with and into this merger corporation. The resulting corporation assumed the name Tactile Systems Technology, Inc. In September 2013, we began doing business as “Tactile Medical.”
Overview of the Lymphedema and Chronic Venous Insufficiency Markets
Lymphedema
The lymphatic system performs a fundamental role in maintaining health through balancing fluids and regulating immunity by removing harmful bacteria, viruses and waste products. Lymphatic structures are situated throughout the body and are comprised of a series of vessels, lymph nodes and lymphoid organs that act as a drainage system by collecting protein rich lymph fluid and sending it to the venous system. Lymph nodes are located in several areas of the body with superficial and deep lymph nodes under each arm, at the hip, in the groin, above the collar bones in the neck, in the abdomen, tonsils and spleen, and in bone marrow.
Lymphedema refers to a type of chronic swelling, or edema, which may occur in the arms, legs, neck, trunk or other body parts and causes severe and debilitating symptoms, including decreased mobility, skin breakdown, pain, increased risk of serious infection and marked psychosocial impairment, resulting in significantly negative implications for a patient's health and quality of life. The disease occurs when the lymphatic vessels are unable to adequately drain protein-rich lymph fluid from the arms, legs or other regions of the body. Any condition or procedure that damages the lymph nodes or lymphatic vessels, such as surgery or treatment for breast and other cancers, obesity, infection, scar tissue formation, trauma or chronic venous insufficiency can cause lymphedema. The disease may also be caused from congenital malformation of the lymphatic system. Lymphedema is progressive in nature, worsens over time, and has no known cure.
Misdiagnosis of lymphedema is fairly common, as many conditions that cause swelling are not related to lymphedema. Correct diagnosis of lymphedema may require evaluation by a physician or other healthcare provider with knowledge of lymphedema who may choose to perform diagnostic testing. Diagnostic tests for lymphedema include history and physical examination, soft tissue and vascular imaging, lymph node imaging, volume measurements, changes in electrical conductance, changes in biomechanical properties, genetic testing, and blood tests for other conditions that have similar symptoms to lymphedema. The International Society of Lymphology categorizes the progression of lymphedema from Stage 0, the least severe stage, to Stage 3, the most severe stage.
Chronic Venous Insufficiency
Chronic venous insufficiency occurs when the venous wall and/or valves in the veins are not working effectively, making it difficult for blood to return to the heart. The disease is prevalent among patients who are obese or pregnant and may also be caused by high blood pressure, trauma, lack of exercise, smoking, deep vein thrombosis and inflammation of the vein walls. As the valves deteriorate, blood leaks or flows backward, leading to increased pressure in veins, stretched and dilated vessels and pooling of blood in the veins. As blood accumulates, swelling occurs, leading
4
to progressive tissue breakdown and venous leg ulcers. Ulcers develop in areas where blood collects as swelling interferes with the movement of oxygen and nutrients through tissues, and if left untreated, these ulcers can quickly become infected or even gangrenous. Prolonged or untreated chronic venous insufficiency may damage the lymphatic system. Physicians diagnose chronic venous insufficiency based on appearance, symptoms and imaging techniques and classify it based upon a scale endorsed by the Society for Vascular Surgery.
Market Opportunity
Lymphedema and chronic venous insufficiency are costly and lifelong conditions with debilitating physical and psychological impacts on patients. We estimate the addressable market opportunity for our solutions treating lymphedema and chronic venous insufficiency in the United States is in excess of $4 billion. We believe that between three to five million people in the United States are living with lymphedema. Based on an analysis of claims data commissioned by us, we estimate approximately 700,000 patients were diagnosed with lymphedema during the 12 months ended June 30, 2014. Based on a separate analysis of claims data commissioned by us, we estimate approximately 820,000 patients were diagnosed with lymphedema during the 12 months ended December 31, 2015. This represents a 17% increase in the number of patients diagnosed with lymphedema over the 18-month period from June 30, 2014 to December 31, 2015. We estimate that the addressable market opportunity for our Flexitouch System is approximately $4 billion in the United States, which is based on the number of patients diagnosed with lymphedema and our average selling price per device.
In the fourth quarter of 2016 we expanded the indications for the Flexitouch System. We received U.S. FDA clearance to market a first-of-kind system to treat patients suffering from lymphedema of the head and neck, a frequent consequence of head and neck cancer and its treatment. Patient symptoms often include significant skin changes, pain and discomfort, as well as difficulty breathing and swallowing. The American Cancer Society estimates that 450,000 people in the United States suffer from cancers of the head and neck, and more than 60,000 new patients are diagnosed each year. In a recent clinical publication, researchers at Vanderbilt University School of Medicine estimated that more than 75% of patients with head and neck cancer will develop lymphedema requiring treatment. Our Flexitouch Head and Neck System is the only pneumatic compression device with an indication to treat patients suffering from this debilitating condition.
We believe that chronic venous insufficiency afflicts approximately 8% of the U.S. population, and this percentage may rise due to the growing prevalence of obesity, as well as an aging population. Based on an analysis of claims data commissioned by us, we estimate there were over 1.5 million patients diagnosed with venous leg ulcers in the United States during the 12 months ended June 30, 2014. We estimate that our immediately addressable patient population consists of the 30% to 40% of these patients, or approximately 525,000 patients, for whom we believe device reimbursement is available because their venous leg ulcers have not resolved after six months of treatment. We estimate the addressable market opportunity for our ACTitouch System is in excess of $500 million in the United States, which is based on the number of patients diagnosed with unresolved leg venous ulcers and our average selling price per device.
Current Treatment and Limitations
A traditional treatment for lymphedema is complete decongestive therapy consisting of manual lymphatic drainage, which is a specialized application of gentle pressure to the skin applied by a therapist that encourages drainage of lymph fluid, as well as decongestive exercises, skin care and compression with multilayered bandages, compression garments or pumps. Typically, this therapy begins with clinic visits three to five times per week for four to eight weeks, which is costly, inconvenient for the patient and time consuming. At that point, clinical improvement plateaus or reimbursement for the therapy ends and patients transition to self-administered home-based care. Manual lymphatic drainage is difficult for patients to self-administer due to limited range of motion and treatment techniques that are difficult to replicate, and basic pump-based compression is uncomfortable and has not demonstrated the benefits of our advanced pneumatic pump. To address these limitations, our at-home Flexitouch System mimics the clinic-based manual lymphatic drainage therapy through an advanced, easy-to-use, self-applied system. Peer-reviewed, published studies have shown that our Flexitouch System provides improved quality of life and clinical outcomes and delivers significant cost-savings to payers and patients.
The standard of care treatment for chronic venous insufficiency is compression therapy. As the disease progresses, patients may develop a venous leg ulcer, which is commonly treated using multilayered bandages to minimize swelling and enhance blood flow. A clinician applies these non-removable bandages to patients at a precise pressure and patients
5
wear the bandages between weekly visits to the wound clinic during which they are then removed and reapplied. Treatment typically occurs for several months and impairs patient quality of life by limiting bathing, range of motion and other activities. Treatment efficacy is inconsistent because bandages can lose their precise pressure between treatments. Patients also use our ACTitouch System to administer intermittent pneumatic compression therapy to assist with the circulation of blood through affected veins. Our ACTitouch System provides precise, sustained and wearable compression that a patient may apply, remove and reapply at home, allowing patients to bathe, sleep comfortably and increase mobility. In a clinical study, our ACTitouch System was shown to have comparable efficacy in healing venous leg ulcers and achieved higher patient quality of life scores as compared to multilayered bandages.
Our Strategy
Our goal is to become a leader in the at-home treatment of chronic diseases. We intend to leverage our established platform to be a global provider of clinically proven, easy-to-use and cost-effective solutions. The key elements of our strategy include:
|
· |
Increase awareness of our solutions and establish them as the standards of care. We believe that many patients with lymphedema and chronic venous insufficiency are undiagnosed or undertreated, and we intend to further educate physicians, wound nurses and lymphedema therapists, patients and payers to raise awareness of these diseases, the associated health burdens of such diseases on patients and society and the clinical and economic benefits of using our products. We intend to continue promoting this awareness through advertising campaigns, exhibiting at tradeshows and physician meetings, training and educating clinicians and publishing additional clinical and economic outcome data demonstrating the benefits of our solutions. Our ongoing marketing initiatives focus on increasing referrals to physicians trained in venous and lymphatic diseases. In addition, we plan to launch more extensive direct-to-patient and -provider marketing programs that we believe will further increase awareness of our solutions. |
|
· |
Expand our direct sales and customer support teams. We plan to expand our direct sales and marketing organization to drive greater product adoption by patients and their clinicians. We intend to strengthen our distribution network by continuing to recruit, train and retain talented sales representatives and increasing the number of licensed home trainers. With an expanded sales force, we believe we could target additional clinical call points. |
|
· |
Introduce new features and products to grow our technology platform. We intend to pursue new features for our products, and introduce new solutions to expand the number of patients using our products and allow us to enter new clinical adjacencies. We pursue internal research, design and development, and work with external collaborators to expand our product offerings. For example, we are developing new garment offerings and controller improvements for our Flexitouch System which we intend to launch in the second half of 2017. In addition, we evaluate opportunities to license or acquire additional technologies and products to expand our total addressable market opportunity. |
|
· |
Continue the development of clinical and economic outcome data. A key part of our success is our ability to demonstrate the effectiveness of our products through clinical and economic outcome data. We intend to invest in additional studies to support peer-reviewed, published studies that evidence the clinical and economic benefits of our solutions as compared to traditional treatments. We intend to use these data to continue to educate clinicians, payers and patients on the proven advantages of our products compared to other therapies and expand our network of key opinion leader advocates. |
|
· |
Expand third-party reimbursement. Our products are covered under existing reimbursement codes, and we have secured coverage for our solutions with private payers, Medicare, the Veterans Administration and certain Medicaid programs. Our team has experienced significant success in obtaining positive coverage policies from payers by developing direct relationships with payer decision-makers, leveraging our relationships with physician societies and key opinion leaders, providing clinical data, demonstrating the efficacy of our products and educating payers on the limitations of traditional treatments. We intend to continue this strategic approach to further expand coverage for our solutions, as well as to meet payer-specific requirements on behalf of patients. |
6
|
· |
Introduce our solutions outside the United States. We currently sell our products only within the United States. While our plan is to continue to focus our direct sales efforts on penetrating the U.S. market, we plan to pursue future international expansion. We have European CE Mark approval for our current Flexitouch System and are seeking CE Mark approval for our ACTitouch System. We also have a Medical Device License in Canada for our Flexitouch System. |
Our Products
We market our Flexitouch, ACTitouch and Entré systems, as at-home therapies for the treatment of lymphedema and chronic venous insufficiency. These products have received 510(k) clearance from the FDA to be marketed in the United States. We believe our products have unique features and benefits that address the shortcomings of traditional treatments, are more cost-effective and enable more consistent and effective therapy, leading to improved patient quality of life.
Flexitouch System
We introduced a predecessor to our Flexitouch System in the United States in 2003 and our Flexitouch System in 2006. Our Flexitouch System is a fully-automated, programmable, advanced pneumatic compression device designed for treatment of lymphedema in the home setting. Our Flexitouch System has received 510(k) clearance for the treatment of lymphedema, certain types of edema, venous insufficiencies and certain types of leg ulcers. In September 2016, we received 510(k) clearance from the FDA for the Flexitouch System for treating lymphedema of the head and neck. The mechanism of action of our patented Flexitouch System is designed to mimic manual lymphatic drainage therapy, the current standard of care in patient treatment. By automating this technique, we believe our system offers an effective, cost-efficient, convenient and accessible treatment for patients.
Our Flexitouch System consists of an electronic controller unit that offers 15 treatment settings and multiple contoured garment configurations for the trunk and the arm or leg. Our Flexitouch System offers flexibility for treating upper and lower extremities and the head and neck, as well as the trunk and chest. The electronic controller is a pneumatic compressor with four connector outlets. Each connector has eight outflow ports into which the garment hoses are connected. Our unique garments contain up to 32 air chambers, are made of a soft, pliable fabric and are designed with hook-and-loop fasteners to fit snugly around affected areas for maximum comfort and optimum pressure delivery. The garments come in a variety of sizes that can be easily adjusted to patients of all sizes. When our system is activated, air passes through the hoses delivering sequential inflation and deflation to the garments, applying gentle pressure to the skin. The inflation sequence is designed to stimulate the lymphatic system moving lymph fluid from the impaired areas towards healthy regions of the body to be processed.
The electronic controller unit adjusts the amount of pressure and the timing of the pressure and release cycles. This unit is lightweight and easily portable, providing maximum convenience for at-home treatment. A typical therapy session using our Flexitouch System lasts one hour, with additional treatment options available if prescribed by a clinician.
ACTitouch System
We introduced our ACTitouch System in the United States in September 2013. Our wearable ACTitouch System combines intermittent pneumatic compression with sustained gradient compression to the lower leg, ankle and foot to improve and accelerate healing, as compared to the current standard of care, which involves sustained compression applied with compression wraps.
Our ACTitouch System consists of a compression sleeve, a control unit, an undersock and a power adapter/charger. The compression sleeve has four chambers that inflate to apply pressure to the leg, is designed with hook and loop fasteners to accommodate a wide range of leg shapes and sizes and may be worn under clothing and with most shoes. The control unit is concealed within the compression sleeve and monitors and adjusts the air pressure to ensure the correct level of compression is applied to the leg. It offers a therapy tracker that monitors and displays average daily use to reinforce therapy goals. The undersock is designed to draw perspiration and moisture away from the skin and has padding in key areas to provide additional comfort. The system comes with a power adapter/charger that is used to power the device directly during intermittent pneumatic compression mode or to charge the battery for ambulatory use. The battery life allows the patient to wear the system all day without recharging.
7
Our ACTitouch System operates in sustained compression mode or intermittent pneumatic compression mode. In sustained compression mode, the system provides sustained, graduated compression to the leg at preset pressures, and the compact, lightweight design gives patients the freedom to stay active while experiencing the benefits of a more comfortable compression therapy. The system ensures consistent compression regardless of variations in sleeve application, and throughout the day monitors and adjusts pressure automatically every 30 minutes in response to changes in leg circumference. In intermittent pneumatic compression mode, the system performs cyclic inflation/deflation sequences to preset gradient pressures. Standard daily treatment involves two hours of intermittent compression while seated or reclining and 10 hours of sustained compression while active. The system is worn throughout the day and has the advantage of being removable for bathing or showering and when driving or operating machinery. The patient removes the system for sleep, allowing the battery to be recharged overnight.
Entré System
We introduced our Entré System in the United States in February 2013 to offer a lightweight, portable pneumatic compression solution for patients who need a basic pump or who do not yet qualify for insurance coverage of an advanced compression device such as our Flexitouch System. Our Entré System is a basic pneumatic compression device used for the at-home treatment of venous disorders including lymphedema and chronic venous insufficiency, including venous leg ulcers. Our Entré System is a pump with garments covering the arm or leg with eight chambers that inflate in sequence and remain inflated for a preset time period. All chambers deflate at once. Our Entré System moves fluid from fingers or toes toward areas closer to the trunk. The system can be programmed to a variety of pressures delivering a prescribed treatment customized to meet the patient's needs.
Clinical Results and Studies
Overview
A key part of our success is our ability to demonstrate the effectiveness of our products by funding studies that generate clinical and economic outcome data supporting our products. We have developed a significant body of clinical data supporting the safety and effectiveness of our products. We intend to continue to invest in additional studies to support peer-reviewed, published articles that evidence the clinical and economic benefits of our solutions as compared to traditional treatments. To date, 14 studies regarding the safety and efficacy of our products have been completed, in which over 1,400 subjects have been included.
Impact on Clinical Outcomes and Healthcare Costs with Use of our Flexitouch System
A retrospective study published by the American Medical Association in JAMA Dermatology demonstrated significant improvement in key clinical endpoints and immediate cost reductions for individuals with lymphedema following receipt of our Flexitouch System. The study was conducted in the United States and included 718 patients with a lymphedema diagnosis who had continuous insurance coverage during the 12 months prior to and the 12 months after receiving our Flexitouch System.
The study evaluated a broad, clinically relevant set of healthcare use outcomes for each patient for the 12 months before and the 12 months after receipt of our Flexitouch System, including cellulitis infections, inpatient hospitalizations, manual therapy and outpatient hospital visits. Receipt of our Flexitouch System was associated with a significant decline in the rate of cellulitis diagnosis in the cancer-related lymphedema patients of 79% (from 21.1% to 4.5%; p<.001) and in the non-cancer-related lymphedema patients of 75% (from 28.8% to 7.3%; p<.001). The inpatient hospitalization rate declined 22% in the cancer-related group (from 2.7% to 2.1%; p=.63) and declined 54% in the non-cancer-related group (from 7.0% to 3.2%; p=.02). The manual therapy rate decreased 30% in the cancer-related lymphedema patients (from 35.6% to 24.9%; p=.001) and decreased 34% in the non-cancer-related lymphedema patients (from 32.3% to 21.2%; p=.001). In addition, outpatient hospital visits declined 29% in the cancer-related patients (from 58.6% to 41.4%; p<.001) and 40% in the non-cancer-related patients (from 52.6% to 31.4%; p<.001).
The study also reviewed lymphedema-related healthcare costs for each patient in the study for the 12 months before and the 12 months after receipt of our Flexitouch System. Among the cancer-related lymphedema patients, total costs per patient, excluding durable medical equipment costs, were reduced by 37%, from $2,597 to $1,642 (p=.002) following receipt of our Flexitouch System. The greatest contributor to this change was a 54% reduction in outpatient hospital costs from $1,517 to $694 (p<.001). Total costs per non-cancer-related lymphedema patients, excluding durable
8
medical equipment costs, were reduced by 36% from $2,937 to $1,883 (p=.007). Outpatient hospital costs for the non-cancer patients declined by 65% from $1,726 to $606 (p<.001).
Flexitouch System Impact on Limb Volume and Patient-Reported Outcomes
A prospective study published in the European Journal of Vascular and Endovascular Surgery demonstrated that use of our Flexitouch System is associated with consistent lower extremity limb volume and pain reduction while achieving improvement in patient health outcomes. The study was conducted in the United States and collected data from a patient registry required by a third-party payer for 196 patients with lower extremity lymphedema who were prescribed our Flexitouch System from January 2009 to May 2012. The primary objective of the study was to examine the effectiveness of our Flexitouch System in reducing lower extremity limb volume, with a secondary objective of evaluating clinician-assessed and patient-reported outcomes.
Use of our Flexitouch System was associated with a reduction in limb volume, with 88% of patients experiencing a reduction in limb volume and with 35% enjoying a reduction in limb volume of greater than 10%. Twelve percent of patients experienced an increase in limb volume. Clinician assessment indicated that the majority of patients experienced improvement in the condition of their skin. In 168, or 86%, of the patients, a reduction in skin hardening or fibrosis was reported based on manual assessment of the skin. Based on clinical observation of function, all but three of these patients demonstrated an increased ability to perform activities of daily living. Additionally, 149, or 77%, of the patients demonstrated improved range of motion.
Patients reported a significant increase in their ability to control lymphedema through treatment with our Flexitouch System, with an increase in function and a reduction in pain. Of the 98 patients who responded, 66% reported being "very satisfied" with the treatment by our Flexitouch System and 29, or 30%, of patients reported being "satisfied" with the treatment by our Flexitouch System.
Comparison of our Flexitouch System with Pneumatic Compression Devices
A prospective, randomized controlled study published in Supportive Care in Cancer demonstrated that our Flexitouch System provides better clinical outcomes as compared to those achieved with a basic pneumatic compression device for home-based treatment of breast cancer-related lymphedema. The study was conducted in the United States and involved 36 patients. This number of participants in the study is considered to be a small sample size and a limitation of the study. The patients were randomized to our Flexitouch System or a basic pneumatic compression device used for home treatment of one-hour per day for 12 weeks. The basic pneumatic compression device used in the study was a Bio Compression 2004 Sequential Circulator pneumatic compression device. The primary objective of the study was to determine whether our Flexitouch System provides better outcomes, as measured by arm edema and tissue water reductions, compared to a basic pneumatic compression device in patients with arm lymphedema. The study does not reflect a comparison of our Flexitouch System to a product that is billed under the same HCPCS Code as our Flexitouch System.
Thirty-six patients with unilateral upper extremity lymphedema with at least 5% arm edema volume at the time of enrollment completed treatments over the 12-week period, with 26 patients being evaluated for edema volume change and 28 patients being evaluated for changes in arm tissue water content. Arm edema volumes were determined from arm girth measurements and suitable model calculations, and tissue water was determined based on measurements of the arm tissue. The patients were randomized into two groups of 18 patients each, with one group receiving treatment with our Flexitouch System and the other group receiving treatment using a basic pneumatic compression device. The group using our Flexitouch System experienced an average reduction in edema of 29% compared to a 16% increase in the group using a basic pneumatic compression device.
Study of Patient-Reported Satisfaction with Use of our Flexitouch System
A retrospective study published in the Oncology Nursing Forum demonstrated that patients using our Flexitouch System were satisfied with the device and perceived it to be beneficial in managing their lymphedema. The study was conducted in the United States and involved 155 patients with lymphedema. The primary objective of the study was to compare treatment protocol adherence, satisfaction and perceived changes in emotional and functional status between patients with cancer-related lymphedema and non-cancer-related lymphedema using our Flexitouch System.
9
Ninety percent of the 155 study patients reported being "satisfied" with our Flexitouch System. Of these patients, more than 65% reported being "extremely satisfied." Further, 95% of patients reported a positive limb volume outcome, which was defined as a patient perceiving that limb volume had been maintained or reduced with device use. Of these patients, 42% reported limb volume decreases as much as 20%, and an additional 20% reported decreases of less than 20%. In addition, clinically and statistically significant improvements occurred in all areas of physical and emotional health (p < 0.006).
Flexitouch System Impact on Patient-Reported Improved Quality-of-Life
A prospective observational study published in Annals of Vascular Surgery demonstrated that use of our Flexitouch System is associated with patient-reported overall improvement in quality-of-life and lower extremity-related symptoms. The study was conducted in the United States and collected data from patients presenting for treatment of lower-extremity lymphedema from March 2011 to September 2014. A total of 100 consecutive patients with lower-extremity lymphedema met inclusion criteria and were included in the study. The primary objective of the study was to demonstrate improved quality-of-life in patients with lower-extremity lymphedema with Flexitouch System treatment. The secondary objective was to demonstrate reduced infectious complications of lymphedema with Flexitouch System treatment, and to determine the incidence of concomitant venous insufficiency in patients with lymphedema.
Use of our Flexitouch System was associated with overall improvement in lower extremity-related symptoms, with 54% of patients reporting greatly improved symptom control after use of our Flexitouch System, 35% moderately improved and 11% mildly improved. In the year before use of our Flexitouch System, 15% of the patients reported 26 episodes of cellulitis, which decreased to five episodes after initiation of the Flexitouch System (P = 0.002) in subsequent median follow-up of 12.7 months. Eight percent of patients reported skin ulceration of the affected extremity in the year before presentation for treatment. The number of lower-extremity ulcers pre- and post-Flexitouch System use decreased from seven to two (P = 0.007). Overall, 46% of the patients had complete limb girth measurements at the ankle and calf, and there was a statistically significant decreased overall limb girth after Flexitouch System treatment in pre- and post-ankle (28.3 cm vs. 27.5 cm, P = 0.01), and calf mean girths (44.7 cm vs. 43.8 cm, P = 0.018). In addition, venous reflux was present in 18% of patients, 14% and 4% within the superficial and deep venous system respectively. In patients with venous reflux, moderate to great improvement in symptoms was reported in 7% and 11%, respectively compared with 28% and 43% in patients without venous reflux (P = 0.257).
Comparison of Conventional Treatment for Venous Leg Ulcers with our ACTitouch System
A prospective, randomized study published in the International Wound Journal demonstrated that our ACTitouch System provides a comparable degree of effectiveness in venous leg ulcer healing to conventional treatment and an improved quality of life for patients. The study was conducted in the United States and Europe, involving a total of 90 patients over a 12-week period. The primary objective of the study was to evaluate the efficacy, functionality, safety, patient perceptions and impact on patient quality of life of two compression methods for venous leg ulcers, including our ACTitouch System and a traditional four-layer bandage system. Of the 90 patients, 38 patients used our ACTitouch System and 52 patients used a traditional four-layer bandage system.
The study demonstrated a comparable degree of effectiveness in venous leg ulcer healing, with healing rate differences not reaching statistical significance. The type and frequency of adverse events reported were similar between the treatment groups and there were no serious adverse events related to treatment in either group. In addition to demonstrating a comparable degree of effectiveness in venous leg ulcer healing, this study also demonstrated that using our ACTitouch System yielded greater improvements in quality of life as compared to those using the bandage system. The only area that our ACTitouch System did not rate higher than the bandage system was discreteness under clothing.
10
Sales and Marketing
Unlike many of our competitors, we utilize a direct-to-patient and -provider model to market our solutions directly to patients and clinics, whereby we disintermediate the traditional durable medical equipment channel and capture both the manufacturer and distributor margins. The below chart shows this disintermediation:
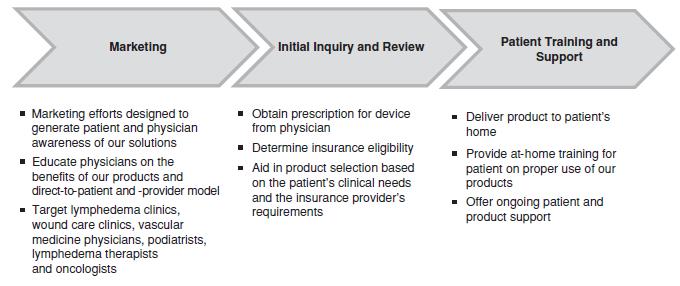
Our direct-to-patient and -provider model is comprised of a direct sales force, contract at-home trainers, reimbursement capabilities and medical expertise to expand awareness, garner referrals and obtain payment for our products. As of December 31, 2016, we employed over 125 full-time sales representatives, including 11 sales managers, who provide coverage throughout the United States. The below chart describes our U.S. direct-to-patient and -provider model.
Our marketing team leads our efforts in brand development, tradeshow attendance, educational forums, product messaging, website development, social media and advertising.
Reimbursement, Payer Relations and Customer Support Process
Private insurance payers represented approximately 74% of our revenues in both 2016 and 2015, while Medicare represented approximately 12% of our revenues in 2016 and 13% of our revenues in 2015. Other payers, including the Veterans Administration, represented the remainder of our revenues. When we sell our solutions directly to patients, we bill third-party payers, such as private insurance or Medicare, on behalf of our patients and bill the patient for their co-payment obligations and deductibles. Any regulatory or legislative developments that eliminate or reduce reimbursement rates for our products could harm our ability to sell our products or cause increasing downward pressure on the prices of our products, either of which would negatively affect our ability to generate the revenues necessary to support our business. For example, changes to the level of Medicare coverage for our products, including a 2015 revision to the criteria that administrative contractors use for Medicare coverage, could reduce the number of Medicare patients who have access to our products. Changes to, or repeal of, the Patient Protection and Affordable Care Act could also potentially impact the number of patients who have access to our products.
11
As a nationwide provider, we have developed a broad expertise in obtaining billing codes, developing coverage policies, overcoming payer barriers, and obtaining authorization and payment from payers across all regions of the United States. Our model utilizes our strategic and operational reimbursement proficiency to meet the varying requirements of hundreds of payers across the country.
To achieve ongoing success in both the strategic and operational reimbursement arenas, we have developed two teams with specialized focus on these respective competencies. Our payer relations group is comprised of 30 employees and is responsible for developing relationships with payer decision-makers. Specifically, this group educates payers on our product efficacy, develops overall payer coverage policies and reimbursement criteria, and manages our Medicare strategy, patient claims, reimbursement codes, and contracts with payers. Our payer relations team is also the advocacy liaison between patients, clinicians and payers through the appeals process. Our reimbursement operations group is comprised of over 70 employees and is responsible for verifying case-by-case benefits, obtaining prior authorization, billing and collecting payments from payers, analyzing payer data to help understand trends, developing processes and patient programs and providing customer support services.
We have strong and established payer relationships, including some of the largest private payers in the United States. Based on our estimates, we are contracted or enrolled as an in-network provider with payers covering over 270 million lives. These contracts allow us to be an in-network provider for patients, enabling them to access our systems at a competitive rate and copay comparable to other suppliers and easing our administrative burden in processing authorizations and claims. We have enjoyed a consistent commercial payer approval rate of greater than 80% for the last eight years, and a greater than 90% Medicare claims submitted approval rate (post-arbitration and based on the number of claims, not dollar amount of claims, submitted across all our products) since we began doing business with Medicare in 2007. We have an in-depth understanding of specific payer coverage criteria, and our submission materials are tailored to address individual payer's distinct requirements. Our dedicated customer service team is available to answer patient questions regarding reimbursement, account status, device operation and troubleshooting during normal business hours. We receive no additional reimbursement for patient support, but provide high-quality customer service and continuity of care to enhance patient comfort, satisfaction, compliance and safety with our products.
Our Flexitouch System is reimbursed under HCPCS code E0652, and our ACTitouch System and Entré System are reimbursed under HCPCS code E0651. Garments that cover various parts of the body are used with these systems and billed using HCPCS codes E0667, E0668 and E0669. As of December 31, 2016, over 900 payers have paid for our products.
Research and Clinical Operations
We are committed to ongoing research and development as part of our efforts to be at the forefront of patient preference in the area of chronic disease, especially lymphedema and chronic venous insufficiency. As of December 31, 2016, our research and development and clinical operations staff included more than 10 engineers, scientists, clinical monitors and project managers with expertise in trial management, pneumatics, electronics, garment design, embedded software, mechanical design, sensors and manufacturing technologies. Our research and development expenses, including spending on our clinical evidence development efforts, totaled $4.5 million and $4.3 million for the years ended December 31, 2016 and 2015, respectively. Our current research and development efforts are focused primarily on increasing efficacy, improving design for ease-of-use, enhancing clinical functionality and reducing production costs of our solutions. Our clinical development efforts are focused on further differentiating our products from our competitors. We coordinate our development efforts with our intellectual property strategies in order to enhance our ability to obtain patent and other intellectual property protection.
Manufacturing and Quality Assurance
Our manufacturing and quality assurance model combines our internal manufacturing resources and expertise, including assembly, quality assurance, material procurement and inventory control, with approved third-party manufacturers and suppliers of system components. Our internal manufacturing activities, located in Minneapolis, Minnesota, include quality inspection, assembly, packaging, warehousing and shipping of our products. We outsource the manufacture of components, which are produced to our specifications and shipped to our facilities for inspection and final assembly. We use third-party manufacturers and suppliers worldwide to source our components, maintaining dual-source vendors of critical components whenever possible, and leveraging competitive bids among third-party
12
manufacturers and suppliers to control costs. We have elected to source certain key components from single sources of supply, including our ACTitouch controller. While we believe alternate sources exist for the ACTitouch controller, we have not yet qualified an alternate supplier. Quality control, risk management, efficiency and the ability to respond quickly to changing requirements are the primary goals of our manufacturing operations. We believe our manufacturing model permits us to operate with low capital expenditure requirements. We carefully manage our supply chain in an effort to take costs out of the manufacturing process, as demonstrated by a 58% reduction in controller costs for our Flexitouch System since 2008.
We manage our arrangements with our third-party manufacturers and suppliers to adjust delivery schedules and quantities of components to match our changing manufacturing requirements. We forecast our component needs based on historical trends, current utilization patterns and sales forecasts of future demand. We establish our relationships with our third-party manufacturers and suppliers through supplier contracts and purchase orders. In most cases, these supplier relationships may be terminated by either party upon short notice.
In order to mitigate against the risks related to a single-source of supply, we qualify alternative suppliers, when possible, and develop contingency plans for responding to disruptions, including maintaining adequate inventory of any single source components, along with requiring each supplier to maintain specified quantities of inventory. To date, we have not experienced material delays in obtaining any of our components, nor has the ready supply of finished products to our patients or clinicians been adversely affected by component supply issues.
We have implemented a quality management system designed to comply with FDA regulations and International Standards Organization, or ISO, standards governing medical device products. In the United States, we and certain of our manufacturers are required to manufacture our products in compliance with the FDA's Quality System Regulation, which covers the methods and documentation of the design, testing, control, manufacturing, labeling, quality assurance, packaging, storage, and shipping for our products. We maintain a quality management system to control compliance with such requirements and have procedures in place designed to ensure that all products and materials purchased by us conform to our requirements and FDA regulations. As of December 31, 2016, we had over 25 employees in operations, manufacturing and quality assurance. Our quality management system has been certified to ISO in 2012 and 2014, including ISO 13485:2003. Many of our manufacturers' quality management systems also have been certified to ISO.
Order Fulfillment and Patient Training
Once we have a complete order and prior authorization from the payer, we package and ship a system, configured to their physician's prescription, directly to the patient. Our primary logistics partner is United Parcel Service, which we use for delivery and pick up of our devices. After delivery, we coordinate a visit from one of our over 400 licensed, independent contract trainers that go to our patients' homes to provide individualized training to our patients, when requested. These trainers are healthcare professionals, licensed in their state of residence, who we have identified through our sales and marketing interest and instructed on proper use of our products. Training visits are coordinated from our offices in Minneapolis and training sessions assigned by our staff. Upon completion of training, the independent contractor submits an invoice to us for payment for the patient's training and their travel.
Competition
The pneumatic compression pump market is a competitive industry, and we compete with a number of manufacturers and distributors of pneumatic compression pumps. Our most significant competitors are Bio Compression Systems, Inc. and Lympha Press USA. Other competitors are Wright Therapy Products (which was acquired by BSN Medical GmbH in 2015), Devon Medical Products, Inc. and NormaTec Industries. If we expand internationally, we expect that ArjoHuntleigh, an affiliate of Getinge Group, would become a competitor, in addition to other potential international competitors.
Given the growth of the pneumatic compression pump market, we expect that the industry will become increasingly competitive in the future. Manufacturing companies compete for sales to patients primarily based on product features and service.
We believe we are the only pneumatic compression home-therapy device company with a meaningful U.S. market position supported by a direct sales force. We believe our manufacturing competitors' complete reliance on home medical equipment distribution intermediaries compresses their margins and limits their ability to invest in product
13
features that address consumer preferences. To pursue a direct-to-patient and -provider sales model, our manufacturing competitors would need to meet national accreditation and state-by-state licensing requirements and secure Medicare billing privileges, as well as compete directly with the home medical equipment providers that many rely on across their entire home care businesses.
Some of our competitors and potential competitors are large, well-capitalized companies with greater resources than we have. As a consequence, they are able to spend more aggressively on product development, marketing, sales and other product initiatives than we can. Some of these competitors have:
|
· |
significantly greater name recognition; |
|
· |
established relations with healthcare professionals, customers, and third-party payers; |
|
· |
established distribution networks; |
|
· |
additional lines of products, and the ability to offer rebates or bundle products to offer higher discounts or other incentives to gain a competitive advantage; |
|
· |
greater history in conducting research and development, manufacturing, marketing, and obtaining regulatory approval for homecare devices; and |
|
· |
greater financial and human resources for product development, sales and marketing, patent litigation and customer financing. |
As a result, our competitors may be able to respond more quickly and effectively than we can to new or changing opportunities, technologies, standards or customer requirements. In light of our competitors' advantages, even if our technology and direct-to-patient and -provider marketing strategy is more effective than the technology and marketing strategy of our competitors, current or potential customers might accept competitor products and services in lieu of purchasing our products. We anticipate that we will face increased competition in the future as existing companies and competitors develop new or improved products and distribution strategies and as new companies enter the market with new technologies and distribution strategies. We may not be able to compete effectively against these organizations. Our ability to compete successfully and to increase our market share is dependent upon our reputation for providing responsive, professional and high-quality products and services and achieving strong customer satisfaction. Increased competition in the future could adversely affect our revenues, revenues growth rate, if any, margins and market share.
Government Regulation
Our systems are medical devices subject to extensive and ongoing regulation by numerous governmental authorities, principally the FDA, and corresponding state and foreign regulatory agencies.
FDA Regulation
In the United States, the FDA regulates medical devices, including the following activities that we perform, or that are performed on our behalf with respect to our devices: product design and development, pre-clinical and clinical testing, manufacturing, labeling, storage, premarket clearance or approval, record keeping, product marketing, advertising and promotion, sales and distribution, and post-marketing surveillance. Failure to comply with applicable U.S. requirements may subject us to a variety of administrative or judicial sanctions, such as warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, civil penalties, and criminal prosecution. The FDA can also refuse to clear or approve pending applications.
Unless an exemption applies, each medical device we seek to distribute commercially in the United States requires marketing authorization from the FDA prior to distribution. The two primary types of FDA marketing authorization applicable to a device are premarket notification, also called 510(k) clearance, and premarket approval. The type of marketing authorization is generally linked to the classification of the device. The FDA classifies medical devices into one of three classes — Class I, Class II or Class III — based on the degree of risk the FDA determines to be associated with a device and the level of regulatory control deemed necessary to ensure the device's safety and effectiveness.
14
Devices requiring fewer controls because they are deemed to pose lower risk are placed in Class I or II. Class I devices are deemed to pose the least risk and are subject only to general controls applicable to all devices, such as requirements for device labeling, premarket notification, and adherence to the FDA's Good Manufacturing Practices. Class II devices are intermediate risk devices that are subject to general controls and may also be subject to special controls such as performance standards, product-specific guidance documents, special labeling requirements, patient registries, or post-market surveillance. Class III devices are those for which insufficient information exists to assure safety and effectiveness solely through general controls or if the device is a life-sustaining, life-supporting or a device of substantial importance in preventing impairment of human health, or which presents a potential, unreasonable risk of illness or injury and special controls are not adequate to assure safety and effectiveness.
Most Class I devices and some Class II devices are exempted by regulation from the 510(k) clearance requirement and can be marketed without prior authorization from the FDA. Most Class II devices (and certain Class I devices that are not exempt) are eligible for marketing through the 510(k) clearance pathway. By contrast, devices placed in Class III generally require premarket approval or 510(k) de novo clearance prior to commercial marketing. The premarket approval process is more stringent, time-consuming, and expensive than the 510(k) clearance process. However, the 510(k) clearance process has also become increasingly stringent and expensive.
510(k) Clearance Pathway. When a 510(k) clearance is required, we must submit a premarket notification to the FDA demonstrating that our proposed device is "substantially equivalent" to a previously cleared and legally marketed 510(k) device or a device that was in commercial distribution before May 28, 1976 for which the FDA has not yet called for the submission of a premarket approval application, which is commonly known as the "predicate device." A device is substantially equivalent if, with respect to the predicate device, it has the same intended use and has either (i) the same technological characteristics or (ii) different technological characteristics and the information submitted demonstrates that the device is as safe and effective as a legally marked device and does not raise different questions of safety or effectiveness. By law, the FDA is required to clear or deny a 510(k) premarket notification within 90 days of submission of the application. As a practical matter, clearance often takes significantly longer. The FDA may require further information, including clinical data, to make a determination regarding substantial equivalence. If the FDA determines that the device, or its intended use, is not substantially equivalent to a previously-cleared device or use, the FDA will issue a not substantially equivalent decision. This means the device cannot be cleared through the 510k process and will require marketing authorization through the premarket approval pathway. We obtained 510(k) clearance for our Flexitouch System in October 2006 and for a discontinued predecessor system in July 2002. In September 2016, we received 510(k) clearance from the FDA for the Flexitouch System for treating lymphedema of the head and neck. We obtained 510(k) clearance for our ACTitouch System in June 2013 and our Entré System in May 2015.
Premarket Approval Pathway. A premarket approval application must be submitted to the FDA if the device cannot be cleared through the 510(k) process. The premarket approval application process is much more demanding than the 510(k) premarket notification process and requires the payment of significant user fees. A premarket approval application must be supported by valid scientific evidence, which typically requires extensive data, including but not limited to technical, preclinical, clinical trials, manufacturing and labeling to demonstrate to the FDA's satisfaction reasonable evidence of safety and effectiveness of the device.
The FDA has 45 days from its receipt of a premarket approval application to determine whether the application will be accepted for filing based on the FDA's threshold determination that it is sufficiently complete to permit substantive review. After the FDA determines that the application is sufficiently complete to permit a substantive review, the FDA will accept the application and begin its in-depth review. The FDA has 180 days to review an "accepted" premarket approval application, although this process typically takes significantly longer and may require several years to complete. During this review period, the FDA may request additional information or clarification of the information already provided. Also, an advisory panel of experts from outside the FDA may be convened to review and evaluate the application and provide recommendations to the FDA as to the approvability of the device. In addition, the FDA will conduct a preapproval inspection of the manufacturing facility to ensure compliance with quality system regulations. The FDA may delay, limit or deny approval of a premarket approval application for many reasons, including:
|
· |
failure of the applicant to demonstrate that there is reasonable assurance that the medical device is safe or effective under the conditions of use prescribed, recommended or suggested in the proposed labeling; |
|
· |
insufficient data from the preclinical studies and clinical trials; or |
15
|
· |
the manufacturing processes, methods, controls or facilities used for the manufacture, processing, packing or installation of the device do not meet applicable requirements. |
If the FDA evaluations of both the premarket approval application and the manufacturing facilities are favorable, the FDA will either issue an approval order or an approvable letter, which usually contains a number of conditions that must be met in order to secure final approval of the premarket approval application. If the FDA's evaluation of the premarket approval application or manufacturing facilities is not favorable, the FDA will deny approval of the premarket approval application or issue a not approvable letter. A not approvable letter will outline the deficiencies in the application and, where practical, will identify what is necessary to make the premarket approval application. The FDA may also determine that additional clinical trials are necessary, in which case the premarket approval application may be delayed for several months or years while the trials are conducted and then the data submitted in an amendment to the premarket approval application. Once granted, premarket approval application may be withdrawn by the FDA if compliance with post approval requirements, conditions of approval or other regulatory standards is not maintained or problems are identified following initial marketing.
Clinical Trials. Clinical trials are almost always required to support premarket approval and are sometimes required for 510(k) clearance. In the United States, these trials generally require submission of an application for an Investigational Device Exemption, or IDE, to the FDA. The IDE application must be supported by appropriate data, such as animal and laboratory testing results, showing it is safe to test the device in humans and that the testing protocol is scientifically sound. The FDA must approve the IDE in advance of trials for a specific number of patients unless the product is deemed a non-significant risk device eligible for more abbreviated IDE requirements or the clinical investigation is exempt from the IDE regulations. Clinical trials for significant risk devices may not begin until the IDE application is approved by the FDA and the appropriate institutional review boards, or IRBs, at the clinical trial sites. We, the FDA or the IRB at each site at which a clinical trial is being performed may suspend a clinical trial at any time for various reasons, including a belief that the risks to study subjects outweigh the benefits. Even if a trial is completed, the results of clinical testing may not demonstrate the safety and efficacy of the device, may be equivocal or may otherwise not be sufficient to obtain approval or clearance of the product.
FDA Ongoing Regulation. Even after a device receives clearance or approval by the FDA and is placed on the market, numerous regulatory requirements apply. These include:
|
· |
establishment registration and device listing; |
|
· |
quality system regulation, which requires manufacturers, including third-party manufacturers, to follow stringent design, testing, control, documentation and other quality assurance procedures during all aspects of the manufacturing process; |
|
· |
labeling regulations and the FDA prohibitions against the promotion of products for un-cleared, unapproved or "off-label" uses, and other requirements related to promotional activities; |
|
· |
medical device reporting regulations, which require that manufacturers report to the FDA if their device may have caused or contributed to a death or serious injury or malfunctioned in a way that would likely cause or contribute to a death or serious injury if the malfunction were to recur; |
|
· |
corrections and removals reporting regulations, which require that manufacturers report to the FDA field corrections and product recalls or removals if undertaken to reduce a risk to health posed by the device or to remedy a violation that may present a risk to health; and |
|
· |
post-market surveillance regulations, which apply when necessary to protect the public health or to provide additional safety and effectiveness data for the device. |
After a device receives 510(k) clearance or a premarket approval, in general any modification that could significantly affect its safety or effectiveness, or that would constitute a major change in its intended use, will require a new clearance or approval. The FDA requires each manufacturer to make this determination, but the FDA can review any such decision and can disagree with a manufacturer's determination. We have modified various aspects of our systems since receiving regulatory clearance, but we believe that new 510(k) clearances are not required for these
16
modifications. If the FDA disagrees with our determination not to seek a new 510(k) clearance, the FDA may retroactively require us to seek 510(k) clearance or premarket approval. The FDA could also require us to cease marketing and distribution and/or recall the modified device until 510(k) clearance or premarket approval is obtained. Also, in these circumstances, we may be subject to significant regulatory fines and penalties.
Failure to comply with applicable regulatory requirements can result in enforcement action by the FDA, which may include any of the following sanctions: Warning Letters, fines, injunctions, civil or criminal penalties, recall or seizure of our products, operating restrictions, partial suspension or total shutdown of production, refusing our request for 510(k) clearance or premarket approval of new products, rescinding previously granted 510(k) clearances or withdrawing previously granted premarket approvals.
We are also subject to announced and unannounced inspections by the FDA, and these inspections may include the manufacturing facilities of our subcontractors. We were audited two times since January 2010 by the FDA and found to be in compliance with the Quality System Regulation. We cannot assure you that we can maintain a comparable level of regulatory compliance in the future at our facility.
FTC Regulation
Device advertising and promotional activity in certain circumstances is also subject to scrutiny by the Federal Trade Commission, as well as similar state consumer protection agencies, which enforce laws related to false and deceptive trade practices. A company that is found to have advertised its product in violation of these laws may be subject to liability, including monetary penalties.
Centers for Medicare and Medicaid Services
Centers for Medicare and Medicaid Services, or CMS, requires providers of product or services to attain and maintain accreditation. To attain and maintain accreditation, companies are required to institute policies and procedures that, among other things, formalize the interaction of the company with patients. Accrediting bodies that are approved by CMS will perform audits of these policies and procedures every three years. Should a company fall out of compliance with the requirements of the Accrediting body, expulsion from the Medicare program could follow. In May 2008, we became a Durable, Medical Equipment, Prosthetics, Orthotics, and Supplies accredited Medicare supplier by the Accreditation Commission for Health Care for our solutions. Our Medicare accreditation must be renewed every three years through passage of an on-site inspection. Our current accreditation with Medicare is due to expire in May 2017. We are in the process of renewing our accreditation. Maintaining our accreditation and Medicare enrollment requires that we comply with numerous business and customer support standards. If we are found to be out of compliance with accreditation standards, our enrollment status in the Medicare program could be jeopardized, up to and including termination.
Licensure
Several states require that durable medical equipment providers be licensed in order to sell products to patients in that state. Certain of these states require that durable medical equipment providers maintain an in-state location. Most of our state licenses are renewed on an annual or bi-annual basis. Although we believe we are in compliance with all applicable state regulations regarding licensure requirements, if we were found to be noncompliant, we could lose our licensure in that state, which could prohibit us from selling our current or future products to patients in that state. In addition, we are subject to certain state laws regarding professional licensure. We believe that our certified clinicians are in compliance with all such state laws. If our clinicians were to be found non-compliant in a given state, we would need to modify our approach to providing education, clinical support and customer service in such state.
Fraud and Abuse Regulations
Federal Anti-Kickback and Self-Referral Laws. The Federal Anti-Kickback Statute, among other things, prohibits the knowing and willful offer, payment, solicitation or receipt of any form of remuneration, whether directly or indirectly and overtly or covertly, in return for, or to induce the referral of an individual for the:
|
· |
furnishing or arranging for the furnishing of items or services reimbursable in whole or in part under Medicare, Medicaid or other federal healthcare programs; or |
17
|
· |
purchase, lease, or order of, or the arrangement or recommendation of the purchasing, leasing, or ordering of any item or service reimbursable in whole or in part under Medicare, Medicaid or other federal healthcare programs. |
There are a number of safe harbors to the Federal Anti-Kickback Statute. Such safe harbors permit certain payments and business practices that, although they would otherwise potentially implicate the Federal Anti-Kickback Statute, are not treated as an offense under the same if the requirements of the specific applicable safe harbor are met.
The Federal Anti-Kickback Statute applies to certain arrangements with healthcare providers, product end users, and other parties, including marketing arrangements and discounts and other financial incentives offered to our clinicians in connection with the sales of our products. Although we believe that we have structured such arrangements to be in compliance with the Anti-Kickback Statute and other applicable laws, regulatory authorities may determine that our marketing, pricing, or other activities violate the Federal Anti-Kickback Statute or other applicable laws. Noncompliance with the Federal Anti-Kickback Statute can result in civil, administrative, and criminal penalties, restrictions on our ability to operate in certain jurisdictions, and exclusion from participation in Medicare, Medicaid or other federal healthcare programs. In addition, to the extent we are found to not be in compliance, we may be required to curtail or restructure our operations. Any penalties, damages, fines, exclusions, curtailment or restructuring of our operations could adversely affect our ability to operate our business, our financial condition, and our results of operations.
The Ethics in Patient Referrals Act, commonly known as the "Stark Law," prohibits a physician from making referrals for certain "designated health services" payable by Medicare to an entity, including a company that furnishes durable medical equipment, in which the physician or an immediate family member of such physician has an ownership or investment interest or with which the physician has entered into a compensation arrangement unless an exception applies. Violation of the Stark Law could result in denial of payment, disgorgement of reimbursements received under a noncompliant arrangement, civil penalties, and exclusion from Medicare or other governmental programs. Although we believe that we have structured our provider arrangements to comply with current Stark Law requirements, these requirements are highly technical and there can be no guarantee that regulatory authorities will not determine or assert that our arrangements do not meet applicable Stark Law exceptions.
Additionally, because some of these laws continue to evolve, we lack definitive guidance as to the application of certain key aspects of these laws as they relate to our arrangements with providers with respect to patient training. We cannot predict the final form that these regulations will take or the effect that the final regulations will have on us. As a result, our provider arrangements may ultimately be found to be non-compliant with applicable federal law.
False statements. The federal false statements statute prohibits knowingly and willfully falsifying, concealing, or omitting a material fact or making any materially false statement in connection with the delivery of healthcare benefits, items, or services. In addition to criminal penalties, violation of this statute may result in collateral administrative sanctions, including exclusion from participation in Medicare, Medicaid, and other federal health care programs.
Federal False Claims Act and Civil Monetary Penalties Law. The Federal False Claims Act provides, in part, that the federal government may bring a lawsuit against any person whom it believes has knowingly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim paid or to avoid, decrease or conceal an obligation to pay money to the federal government or who has knowingly retained an overpayment. In addition, amendments in 1986 to the Federal False Claims Act have made it easier for private parties to bring "qui tam" whistleblower lawsuits against companies.
The Civil Monetary Penalties Law provides, in part, that the federal government may seek civil monetary penalties against any person that, like under the False Claims Act, presents or causes to be presented claims to a Federal health care program that the person knows or should know is for an item or services that was not provided as claimed or is false or fraudulent or that has made a false statement or used a false record to get a claim paid. The federal government may also seek civil monetary penalties for a wide variety of other conduct, including offering remuneration to influence a Medicare or Medicaid beneficiary's selection of providers and violations of the Federal Anti-Kickback Statute.
Although we believe that we are in compliance with the Federal False Claims Act as well as the Civil Monetary Penalties laws, if we are found in violation of the same, penalties include fines ranging from $5,500 to $11,000 for each false claim violation of the Federal False Claims Act and varying amounts based on the type of violation of the Civil Monetary Penalties Law), plus up to three times the amount of damages that the federal government sustained because of
18
the act of that person. In addition, the federal government may also seek exclusion from participation in all federal health care programs.
In addition, we bill Medicare Part B and other insurers directly for each sale to patients. As a result, we must comply with all laws, rules and regulations associated with filing claims with the Medicare program, including the Social Security Act, Medicare regulations, the Federal False Claims Act and the Civil Monetary Penalties Law, as well as a variety of additional federal and state laws. During an audit, insurers typically expect to find explicit documentation in the medical record to support a claim. Physicians and other clinicians, who are responsible for prescribing our products for patients, are expected to create and maintain the medical records that form the basis for the claims we submit to Medicare and other insurers. Any failure by physicians and other clinicians to properly document the medical records for patients using our products could invalidate claims, impair our ability to collect submitted claims and subject us to overpayment liabilities, Federal False Claims Act liabilities and other penalties including exclusion from the Medicare, Medicaid or private insurance programs.
To the extent we are found to not be in compliance, we may be required to curtail or restructure our operations. Any penalties, damages, fines, exclusions, curtailment or restructuring of our operations could adversely affect our ability to operate our business, our financial condition, and our results of operations.
The U.S. Foreign Corrupt Practices Act and Other Anti-Corruption Laws. We may be subject to a variety of domestic and foreign anti-corruption laws with respect to our regulatory compliance efforts and operations. The U.S. Foreign Corrupt Practices Act, commonly known as the FCPA, is a criminal statute that prohibits an individual or business from paying, offering, promising or authorizing the provision of money (such as a bribe or kickback) or anything else of value (such as an improper gift, hospitality, or favor), directly or indirectly, to any foreign official, political party or candidate for the purpose of influencing any act or decision in order to assist the individual or business in obtaining, retaining, or directing business or other advantages (such as favorable regulatory rulings). The FCPA also obligates companies with securities listed in the United States to comply with certain accounting provisions. Those provisions require a company such as ours to (i) maintain books and records that accurately and fairly reflect all transactions, expenses, and asset dispositions, and (ii) devise and maintain an adequate system of internal accounting controls sufficient to provide reasonable assurances that transactions are properly authorized, executed and recorded. The FCPA is subject to broad interpretation by the U.S. government. The past decade has seen a significant increase in enforcement activity. In addition to the FCPA, there are a number of other federal and state anti-corruption laws to which we may be subject, including, the U.S. domestic bribery statute contained in 18 USC § 201 (which prohibits bribing U.S. government officials) and the U.S. Travel Act (which in some instances addresses private-sector or commercial bribery both within and outside the United States). Also, a number of the countries in which we conduct activities have their own domestic and international anti-corruption laws, such as the UK Bribery Act 2010. There have been cases where companies have faced multi-jurisdictional liability under the FCPA and the anti-corruption laws of other countries for the same illegal act.
We could be held liable under the FCPA and other anti-corruption laws for the illegal activities of our employees, representatives, contractors, collaborators, agents, subsidiaries, or affiliates, even if we did not explicitly authorize such activity. Although we will seek to comply with anti-corruption laws, there can be no assurance that all of our employees, representatives, contractors, collaborators, agents, subsidiaries or affiliates will comply with these laws at all times. Violation of these laws could subject us to whistleblower complaints, investigations, sanctions, settlements, prosecution, other enforcement actions, disgorgement of profits, significant fines, damages, other civil and criminal penalties or injunctions, suspension and/or debarment from contracting with certain governments or other persons, the loss of export privileges, reputational harm, adverse media coverage, and other collateral consequences. In addition, our directors, officers, employees, and other representatives who engage in violations of the FCPA and certain other anti-corruption statutes may face imprisonment, fines, and penalties. If any subpoenas or investigations are launched, or governmental or other sanctions are imposed, or if we do not prevail in any possible civil or criminal litigation, our business, financial condition, and results of operations could be materially harmed. In addition, responding to any action will likely result in a materially significant diversion of management's attention and resources and significant defense costs and other professional fees. Enforcement actions and sanctions could further harm our business, financial condition, and results of operations.
State fraud and abuse provisions. Many states have also adopted some form of anti-kickback and anti-referral laws and false claims acts that apply regardless of payer, in addition to items and services reimbursed under Medicaid and other state programs. In some states, these laws apply and we believe that we are in compliance with such laws.
19
Nevertheless, a determination of liability under such laws could result in fines and penalties and restrictions on our ability to operate in these jurisdictions.
State and federal transparency/reporting requirements. As part of the Patient Protection and Affordable Care Act, the Federal government has created a transparency program known as Open Payments (the Physician Payments Sunshine Act) which requires manufacturers of drugs, devices, biologicals and medical supplies to report annually to the Centers for Medicare & Medicaid Services, or CMS, an agency within the U.S. Department of Health and Human Services, or HHS, information related to payments and other transfers of value provided to physicians and teaching hospitals and certain ownership and investment interests held by physicians and their immediate family members. Failure to submit timely, accurate and complete information may result in civil monetary penalties of up to an aggregate of $150,000 per year and up to an aggregate of $1.0 million per year for "knowing failures to report." Certain states require implementation of commercial compliance programs and compliance with the device industry's voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government, impose restrictions on marketing practices, and/or prohibition and tracking and reporting of gifts, compensation and other remuneration or items of value provided to physicians and other healthcare professionals and entities.
The laws described above impact the kinds of financial arrangements we may have with hospitals, healthcare professionals or other potential purchasers of our products. If our operations are found to be in violation of any of the laws or regulations described above or others that apply to us, we may be subject to penalties, including potentially significant criminal, civil and/or administrative penalties, damages, fines, disgorgement, exclusion from participation in government healthcare programs, contractual damages, reputational harm, administrative burdens, diminished profits and future earnings, and the curtailment or restructuring of our operations.
HIPAA. The Health Insurance Portability and Accountability Act of 1996, or HIPAA, established uniform standards governing the conduct of certain electronic healthcare transactions and protecting the security and privacy of individually identifiable health information maintained or transmitted by healthcare providers, health plans and healthcare clearinghouses, which are referred to as covered entities. The following standards have been promulgated under HIPAA's regulations:
|
· |
the Standards for Privacy of Individually Identifiable Health Information, which restrict the use and disclosure of individually identifiable health information, or "protected health information"; |
|
· |
the Standards for Electronic Transactions, which establish standards for common healthcare transactions, such as claims information, plan eligibility, payment information and the use of electronic signatures; |
|
· |
the Security Standards, which require covered entities to implement and maintain certain security measures to safeguard certain electronic health information, including the adoption of administrative, physical and technical safeguards to protect such information; and |
|
· |
the breach notification rules, which require covered entitles to provide notification to affected individuals, the Department of Health and Human Services, and the media in the event of a breach of unsecured protected health information. |
In 2009, Congress passed the American Recovery and Reinvestment Act of 2009, or ARRA, which included sweeping changes to HIPAA, including an expansion of HIPAA's privacy and security standards. ARRA includes the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, which, among other things, made HIPAA's privacy and security standards directly applicable to business associates of covered entities. A business associate is a person or entity that performs certain functions or activities on behalf of a covered entity that involve the use or disclosure of protected health information. As a result, business associates are now subject to significant civil and criminal penalties for failure to comply with applicable standards. Moreover, HITECH creates a new requirement to report certain breaches of unsecured, individually identifiable health information and imposes penalties on entities that fail to do so. HITECH also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney fees and costs associated with pursuing federal civil actions. The 2013 final HITECH omnibus rule modifies the breach reporting standard in a manner that will likely make more data security incidents qualify as reportable breaches.
20
In addition to federal regulations issued under HIPAA, some states have enacted privacy and security statutes or regulations that, in certain cases, are more stringent than those issued under HIPAA. In those cases, it may be necessary to modify our planned operations and procedures to comply with the more stringent state laws. Most states have also adopted breach notification laws that require notification to affected individuals and certain state agencies if there is a security breach of certain individually-identifiable information. If we suffer a privacy or security breach, we could be required to expend significant resources to provide notification to the affected individuals and address the breach, as well as reputational harm associated with the breach. If we fail to comply with applicable state laws and regulations, we could be subject to additional sanctions. Any liability from failure to comply with the requirements of HIPAA, HITECH or state privacy and security statutes or regulations could adversely affect our financial condition. The costs of complying with privacy and security related legal and regulatory requirements are burdensome and could have a material adverse effect on our business, financial condition and results of operations.
Environmental Regulation
Our research and development and manufacturing processes and operations involve the controlled use of hazardous materials, including flammables, toxics, and corrosives and produce hazardous chemical waste products. We are subject to numerous foreign, federal, state, and local environmental, health and safety laws and regulations relating to, among other matters, safe working conditions, product stewardship and end-of-life handling or disposition of products, and environmental protection, including those governing the generation, storage, handling, use, transportation and disposal of hazardous or potentially hazardous materials. Some of these laws and regulations require us to obtain licenses or permits to conduct our operations. Environmental laws and regulations are complex, change frequently and have tended to become more stringent over time. Although the costs to comply with applicable laws and regulations, including requirements in the European Union relating to the restriction of use of hazardous substances in products, have not been material, we cannot predict the impact on our business of new or amended laws or regulations or any changes in the way existing and future laws and regulations are interpreted or enforced, nor can we ensure we will be able to obtain or maintain any required licenses or permits. Also, we cannot eliminate the risk of accidental contamination or discharge and any resultant injury from these materials. We do not currently maintain separate environmental liability coverage and any such contamination or discharge could result in significant cost to us in penalties, damages, and suspension of our operations.
Foreign Government Regulation
International sales of medical devices are subject to foreign governmental regulations, which vary substantially from country to country. The time required to obtain clearance or approval by a foreign country may be longer or shorter than that required for FDA clearance or approval, and the requirements may be different. Many countries also impose product standards, packaging requirements, environmental requirements, labeling requirements, and import restrictions on medical devices. Each country has its own tariff regulations, duties, and tax requirements. Failure to comply with applicable foreign regulatory requirements may subject a company to fines, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions, criminal prosecution or other consequences.
The European Union is the primary regulator in Europe, which has adopted numerous directives and has promulgated voluntary standards regulating the design, manufacture, clinical trials, labeling and adverse event reporting for medical devices. Medical devices that comply with the requirements of applicable directives will be entitled to bear the CE conformity marking, indicating that the device conforms with the essential requirements of the applicable directives and, accordingly, can be commercially distributed throughout the member states of the European Union, and other countries that comply with or mirror these directives. The method of assessing conformity varies depending on the type and class of the product, but typically involves a combination of self-assessment by the manufacturer and a third-party assessment by a notified body, an independent and neutral institution appointed by a country to conduct the conformity assessment. This third-party assessment may consist of an audit of the manufacturer's quality system, technical or design file and specific testing of the manufacturer's device. Such an assessment may be required in order for a manufacturer to commercially distribute the product throughout these countries. Compliance establishes the presumption of conformity with the essential requirements for a CE Marking. We have the authorization to affix the CE Mark to our Flexitouch System and our Entré System and to commercialize these devices in the European Union. The notified body who inspected us issued our ISO 13485 certification in October 2014 and our EC-Certificate in December 2014.
21
In March 2012, we received our Medical Device License in Canada for our Flexitouch System. Before we are permitted to sell our devices in Canada, we must submit and obtain clearance of a license application, implement and comply with ISO Standard 13485, the Canadian Medical Device Regulations, and undergo an audit by a registrar accredited by Health Canada.
General Regulatory Compliance and Health Care Reform
The evolving regulatory and compliance environment and the need to build and maintain robust systems to comply with different compliance or reporting requirements in multiple jurisdictions increase the possibility that a healthcare company may fail to comply fully with one or more of these requirements. If our operations are found to be in violation of any of the health regulatory laws described above or any other laws that apply to us, we may be subject to penalties, including potentially significant criminal and civil and administrative penalties, damages, fines, disgorgement, imprisonment, exclusion from participation in government healthcare programs, contractual damages, reputational harm, administrative burdens, diminished profits and future earnings, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business, financial condition, and our results of operations.
In March 2010, the Patient Protection and Affordable Care Act and Health Care and Education Reconciliation Act, which we refer to as the Patient Protection and Affordable Care Act was enacted into law in the United States. This healthcare reform, which included a number of provisions aimed at improving the quality and decreasing the cost of healthcare, has resulted in significant reimbursement cuts in Medicare payments to hospitals and other healthcare providers and in the healthcare reimbursement system evolving toward value- and outcomes-based reimbursement methodologies. It is uncertain what long-term consequences these provisions will have on patient access to new technologies and what impacts these provisions will have on Medicare reimbursement rates. Other elements of the Patient Protection and Affordable Care Act, including comparative effectiveness research, an independent payment advisory board, and payment systems reform, including shared savings pilots and other reforms, may result in fundamental changes to federal healthcare reimbursement programs. Changes to the Patient Protection and Affordable Care Act could impact the number of patients who have access to our products. Existing and additional legislative or administrative reforms, or any repeal of provisions, of the U.S. healthcare reimbursement systems may significantly reduce reimbursement or otherwise impact coverage for our medical devices, or adverse decisions relating to our products by administrators of such systems in coverage or reimbursement issues could have an adverse impact on our financial condition and results of operations.
Third-Party Reimbursement
In the United States and elsewhere, sales of medical devices depend in significant part on the availability of coverage and reimbursement to providers and patients from third party payers. Third party payers include private insurance plans and governmental programs. As with other medical devices, reimbursement for our products can differ significantly from payer to payer and our products are not universally covered by third party commercial payers. Further, third party payers continually review existing technologies for continued coverage and can, with limited notice, deny or reverse coverage for existing products.
Two principal governmental third party payers in the United States are Medicaid and Medicare. Medicare is a federal program that provides certain medical insurance benefits to persons age 65 and over, certain disabled persons and others. In contrast, Medicaid is a medical assistance program jointly funded by federal and state governments to serve certain individuals and families with low incomes and who meet other eligibility requirements. Each state administers its own Medicaid program which determines the benefits made available to the Medicaid recipients in that state. The Medicare and Medicaid statutory framework is subject to administrative rulings, interpretations and discretion that affect the amount and timing of reimbursement made under Medicare and Medicaid.
The Center for Medicare and Medicaid Services (CMS), which is the agency within the Department of Health and Human Services that administers both Medicare and Medicaid, has the authority to decline to cover particular products or services if it determines that they are not "reasonable and necessary" for the treatment of Medicare beneficiaries. A coverage determination for a product, which establishes the indications that will be covered, and any restrictions or limitations, can be developed at the national level by CMS through a National Coverage Determination, or NCD, or at the local level through a Local Coverage Determination, or LCD, by a regional Medicare administrative contractor, which is a private contractor that processes and pays claims on behalf of CMS for the geographic area where the services were rendered. Obtaining a coverage determination, whether an NCD or LCD, is a time consuming, expensive and
22
highly uncertain proposition, especially for a new device. Under an NCD that has been effective since January 14, 2002, pneumatic devices, including our products, are covered for the treatment of lymphedema or for the treatment of chronic venous insufficiency with venous stasis ulcers.
In December 2015, the four Medicare Administrative Contractors responsible for processing Medicare claims for durable medical equipment released an LCD that included additional restrictive criteria that limits Medicare coverage of our Flexitouch System and our Entré System for certain patients. Compared to the previous LCD, this LCD increased the severity of lymphedema symptoms that a patient must exhibit before such patient is eligible for Medicare reimbursement for a pneumatic compression device. The 2015 LCD also inserted more restrictive criteria that require a patient to potentially endure a longer period of conservative therapy to prove that it fails to control their lymphedema, instead of requiring completion of just one four-week round of conservative therapy as stated in the NCD. The LCD states that to qualify for any PCD, the patient must complete four consecutive weeks of conservative therapy with no significant improvement in symptoms during those four weeks. Further, the LCD does not cover use of an advanced pneumatic compression device, such as our Flexitouch System, unless the patient's lymphedema is present in the chest, trunk or abdomen. Although many patients with lymphedema likely do have some level of chest, trunk or abdominal involvement, this criteria in the LCD means that patients with lymphedema that is confined to the limb will not have access to advanced pneumatic compression devices until the lymphedema progresses to impact the trunk, chest or abdomen. The LCD pneumatic compression device coverage criteria for chronic venous insufficiency with venous stasis ulcers largely track existing NCD criteria, while defining the elements of a required conservative therapy trial. Under the 2015 LCD, advanced pneumatic compression devices like our Flexitouch System are no longer covered at all for the treatment of venous stasis ulcers.
Since the LCD was released, we continue to work with physicians, advocacy groups, patients and legislators regarding the potentially negative consequences to patients that the LCD could cause. Many stakeholders met with CMS leadership to discuss these concerns and share clinical data on lymphedema treatment and PCDs. While the LCD is still in place, CMS was receptive to the information shared. Further, we provided significant educational data to prescribers to help them understand the new criteria and explicit documentation requirements in the LCD. As a result of these communication strategies, we have not experienced any significant negative impact on our Medicare fee-for-service business. We continue to maintain open communication with physician stakeholders and with Medicare contractors to provide data as it becomes available that could potentially influence coverage decisions. We also continue to closely monitor our Medicare business to identify trends that could have a negative impact on certain Medicare patients' access to our products, which in turn could have an adverse effect on our business and results of operations.
Private payers that reimburse for our products do so in a variety of ways, depending on the insurance plan's policies, employer and benefit manager input and contracts with their physician network. Moreover, Medicaid programs and private insurance plans are frequently influenced by Medicare coverage determinations. In the year since the release of the LCD referenced above, we have seen, and continue to see, certain Medicare Advantage plans (commercial insurers that are administering Medicare benefits to certain beneficiaries) and a few other private insurers change their policies to reflect the LCD criteria, which has resulted in some patients being denied coverage due to lack of explicit documentation. To mitigate these developments, we have initiated communications with insurers to ensure mutual understanding of criteria interpretation, which differs significantly among the plans from very restrictive to quite lenient, and have educated prescribers accordingly. While this approach has had positive impact, we do not know if or when additional payers may adopt the LCD criteria nor do we know how they will choose to interpret it.
We believe a reduction or elimination of coverage or reimbursement of our products by Medicare, such as the LCD discussed above or another unfavorable NCD or LCD that may go into effect in the future, would likely cause some commercial third party payers to implement similar reductions in their coverage or reimbursement of our products. If we are unable to expand coverage of our products by additional commercial payers, or if third party payers that currently cover or reimburse for our products reverse or limit their coverage in the future, our business and results of operations could be adversely affected.
Intellectual Property
Our intellectual property consists of patented designs and methods and proprietary know-how. In addition to the patented designs and methods discussed below, we have made significant investments in proprietary know-how, including the manufacture of fabrics and garments used in our systems and the algorithms used to manage the inflation and deflation of our systems and other functions of the controllers. To maintain and protect our proprietary technologies
23
and products, we rely on a combination of patent, copyright, trademark, trade secret and other intellectual property laws, and confidentiality provisions in our contracts. We have a policy to enter into confidentiality agreements with employees, consultants, third parties and our advisors to protect our intellectual property and maintain our competitive position. We also require our employees and consultants to sign agreements requiring that they assign to us their interest in intellectual property such as patents and copyrights arising from their work for us. We also require all employees to sign an agreement not to compete unfairly with us during their employment and upon termination of their employment through the misuse of confidential information, soliciting employees, and soliciting customers. Despite any measures taken to protect our intellectual property, unauthorized parties may attempt to copy aspects of our systems or to obtain and use information that we regard as proprietary.
On September 14, 2012, we completed an acquisition of certain assets, including inventory, equipment and tooling and patents for the ACTitouch System and a technology known as SMM from ConvaTec, Inc. and ConvaTec Technologies, Inc., or the Sellers. In addition to $5.0 million of earlier payments, we are required to pay quarterly royalty payments to the Sellers through September 1, 2017 equal to 9% of sales for the ACTitouch System and 7% of sales of SMM. For each quarterly calculation period beginning thereafter and ending on September 1, 2023, we will make quarterly payments to the Sellers equal to 6% of the sales of the ACTitouch System and 5% of the sales of SMM. If ACTitouch System and SMM sales in any calendar year beginning in 2018 exceed $40.0 million, the sales percentage amount relating to ACTitouch System sales shall equal 6% of the sales of the ACTitouch System up to $40.0 million and 7% on the sales of the ACTitouch System over $40.0 million.
Patents
Our patent portfolio consists of three sets of patents, including patents relating to our Flexitouch System, our ACTitouch System and other compression-related technologies, each of which is described in further detail below. As of December 31, 2016, we owned more than 75 issued patents globally, of which 20 were issued U.S. patents. As of December 31, 2016, we owned 25 patent applications pending globally, of which 16 were patent applications pending in the United States. Our U.S. issued patents have varying patent terms expiring between 2017 and through at least 2029, subject to payment of required maintenance fees, annuities and other charges.
Flexitouch System Patent Family. The following is a summary of patents relating to our Flexitouch System:
|
· |
On January 30, 2001, our first patent, directed to our unique wrap structure, was issued (U.S. Pat. No. 6,179,796). This patent is specifically directed to an arcuate design and other features of a garment for wrapping about a patient. This arcuate design is one of the keys to the success of our Flexitouch System, as it facilitates the movement of the lymph fluid from the damaged lymph node area to other functioning lymph node areas. Similar patents have been issued in Europe and Canada. |
|
· |
On November 11, 2003, a patent directed to our preparation and drainage methodology was issued (U.S. Pat. No. 6,645,165). This second patent is directed to body preparation for receipt of lymph fluid via pressurization and depressurization of chambers, and the subsequent lymph drainage from a body extremity via select pressurization and depressurization of chambers. This preparation and subsequent drainage of the lymph fluid is another key to our Flexitouch System, as it allows stimulation of the lymphatic system to promote reabsorption of the lymph fluid. |
|
· |
On March 1, 2005, a patent directed to our wrap structure and fabrication was issued (U.S. Pat. No. 6,860,862). This third patent is directed to the unique aspects of the fabrication of our wrap. In particular, a "four way stretch" and "axial stretch" of our garment allow us to stretch the patient's skin in the same manner as manual lymphatic drainage therapy. |
|
· |
On November 22, 2005, a patent directed to our preparation and drainage methodology was issued (U.S. Pat. No. 6,966,884). This fourth patent is directed to a lymphedema treatment methodology, entailing optimum sequencing of air chamber inflation/deflation. |
24
ACTitouch System Patents. The following is a summary of our patent families relating to our ACTitouch System:
|
· |
On October 14, 2008, a "Medical Compress" patent directed to the ornamental aspects of the compression sleeve was issued (U.S. Design Pat. No. D578,652). Similar patents have been issued in Europe, Japan, Canada, Mexico, Australia, China and Taiwan. |
|
· |
On June 22, 2010, a "Proximity Detection Apparatus" patent directed to control unit proximity detection allowing a different mode of operation was issued (U.S. Pat. No. 7,741,966). Similar patents have been issued in Japan, Canada, Mexico, China and Taiwan, and an application is pending in Europe. |
|
· |
On March 22, 2011, a "Compression Device for the Limb" patent directed to the storage of data related to duration of use was issued (U.S. Pat. No. 7,909,786). Similar patents have been issued in Japan, Canada, Mexico, China, the United Kingdom, Germany, France, Ireland, Italy, Sweden and Taiwan. |
|
· |
On May 24, 2011, a "Pressurized Medical Device" patent directed to the detection of malfunctioning pressure sensors was issued (U.S. Pat. No. 7,947,003). Similar patents have been issued in Japan, Canada, Mexico, China and Taiwan and an application is pending in Europe. |
|
· |
On December 13, 2011, a "Relating to Socks" patent directed to a sock and compression device kit was issued (U.S. Pat. No. 8,075,507). Similar patents have been issued in Japan, Canada, Mexico, China, the United Kingdom, Germany, France, Ireland, Italy and Sweden. |
|
· |
On July 23, 2013, a "Medical Compress" patent directed to the ornamental aspects of the compression sleeve and control unit was issued (U.S. Design Pat. No. D686,738). Similar patents have been issued in Europe, Canada, Mexico, Australia, China and Taiwan. |
|
· |
On November 5, 2013, a "Compression Device for the Foot" patent directed to a Y-shaped foot wrap was issued (U.S. Pat. No. 8,574,180). Similar patents have been issued in Japan, Canada, China, the United Kingdom, Germany, France, Ireland, Sweden and Taiwan. A continuation application (U.S. Pub. No. 2014/0058302) directed to the subject matter of this patent family issued in the United States as U.S. Patent No. 9,463,135. Another continuation application directed to the subject matter of this patent family is pending in the United States. |
|
· |
On January 28, 2014, a "Compression Device for the Limb" patent directed to the compression sleeve configuration was issued (U.S. Pat. No. 8,636,679). Similar patents have been issued in Japan, Canada, Mexico and Taiwan, an application for similar subject matter is pending in Europe, and a continuation application (U.S. Pub. No. 2014/0128787) is pending in the United States. |
|
· |
On March 8, 2016, a "Cuff for Providing Compression to a Limb" patent directed to a compression cuff including an abutting spacer configuration was issued (U.S. Patent No. 9,278,043). Similar patents have been issued in Japan, Canada, China, the United Kingdom, Germany, France, Ireland, Sweden and Taiwan. |
|
· |
On January 10, 2017, a “Compression Device for the Limb” patent directed to a compression device including silent mode was issued (U.S. Pat. No. 9,539,166). Similar patents have been issued in France, Germany, Ireland, Sweden, and the United Kingdom. A continuation application directed to the subject matter of this patent family is pending in the United States. |
Trademarks
We have registered the trademarks Flexitouch, the Flexitouch logo design, and ACTitouch with the United States Patent and Trademark Office on the Principal Register. We rely in the United States on common law rights to the Entré, Tactile Medical and Tactile Medical design trademarks and have applied to register the Tactile Medical trademark in the United States, Australia, China, the European Union, and Japan.
25
Employees
As of December 31, 2016, we had 335 employees, including 173 in sales and marketing; 102 in reimbursement and payer relations; 32 in manufacturing, quality assurance, and research and development; 20 in general administration, finance, information technology and human resources; and 8 in clinical research and operations. None of our employees are represented by a collective bargaining agreement. We believe that our employee relations are positive, as evidenced by our being selected as a Top Workplace in Minnesota by our employees for the last seven years.
Risk factors which could cause actual results to differ from our expectations and which could negatively impact our financial condition and results of operations are discussed below and elsewhere in this report. Additional risks and uncertainties not presently known to us or that are currently not believed to be significant to our business may also affect our actual results and could harm our business, financial condition and results of operations. If any of the risks or uncertainties described below or any additional risks and uncertainties actually occur, our business, results of operations and financial condition could be materially and adversely affected.
Risks Related to Our Business
Our revenues are primarily generated from our Flexitouch System and we are therefore highly dependent on only one product.
Our Flexitouch System accounted for 87% of our revenues for each of the years ended December 31, 2016 and 2015. We expect that sales of this product will continue to account for the substantial majority of our revenues going forward. Therefore, our ability to execute our growth strategy will depend not only upon increasing awareness of lymphedema, but also on the adoption of our Flexitouch System to treat this condition. Many physicians and clinicians may have experience with, and/or invested substantial resources in, developing expertise in traditional treatments for lymphedema, which may make them less willing to adopt our Flexitouch System. If our Flexitouch System fails to achieve wide market acceptance for any reason, our business, financial condition and results of operations could be adversely affected.
Our long-term growth depends on awareness and adoption of our products.
A primary growth strategy is to establish our products as the standard of care for the treatment of lymphedema and chronic venous insufficiency. In order to achieve this growth strategy, we must:
|
· |
increase clinician and consumer awareness of these diseases, which are often undertreated; |
|
· |
introduce the clinical and economic benefits of our solutions to physicians, therapists and other clinicians across several specialties and in various clinical settings; and |
|
· |
demonstrate consistent coverage and reimbursement for our solutions by private payers, Medicare, the Veterans Administration and certain Medicaid programs. |
Clinicians may not adopt our solutions as the standard of care for lymphedema and chronic venous insufficiency or may not prescribe our products for a number of reasons, including:
|
· |
our inability to educate a sufficient number of clinicians on these diseases or our products; |
|
· |
the unavailability or inadequacy of insurance coverage or reimbursement for our products; |
|
· |
failure of evidence supporting clinical benefits or cost-effectiveness of our products over existing alternatives to convince clinicians to change their treatment methods; and |
|
· |
resistance from clinicians to replace traditional treatments with our solutions. |
26
We believe recommendations and support of our products by key opinion leaders can influence market acceptance and adoption. If these key opinion leaders choose to not support our products, our ability to achieve broad market acceptance for our products may be impaired.
If we are unable to achieve and maintain adequate levels of coverage or reimbursement for our products, our business and results of operations will be adversely affected.
Any decline in the amount payers are willing to reimburse patients for our products could cause difficulty for patients to purchase our products and could create pricing pressure for us. If we are forced to lower the price we charge for our products, our gross margins will decrease, which will adversely affect our business, financial condition and results of operations.
Third-party payers, whether foreign or domestic, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In the United States, no uniform policy of coverage and reimbursement for our products exists among third-party payers. Therefore, reimbursement for our products can differ significantly from payer to payer and our products are not universally covered by third-party commercial payers. In addition, payers, including Medicare, continually review existing technologies for continued coverage and can, without notice, deny or reverse coverage for existing products. We believe a reduction or elimination of coverage or reimbursement of our products by Medicare would likely cause commercial third-party payers to implement similar reductions in their coverage or reimbursement of our products. If we are unable to expand coverage of our products by additional commercial payers, or if third-party payers that currently cover or reimburse for our products reverse or limit their coverage in the future, our business and results of operations could be adversely affected.
Further, we believe that future coverage and reimbursement may be subject to increased restrictions, such as additional preauthorization requirements, both in the United States and in international markets. If we are unable to satisfy any new preauthorization requirements or adjust to any future new restrictions on our products, third-party coverage and reimbursement may be limited in the future, which could have an adverse impact on our business.
A change to the criteria for Medicare coverage for our products could have an adverse effect on our business and results of operations.
The Medicare Administrative Contractors, or MACs, responsible for processing Medicare claims for durable medical equipment released a Local Coverage Determination, or LCD, document that included additional restrictive criteria that limit Medicare coverage of our products for certain patients. This LCD, released by the MACs on December 17, 2015, was retroactively effective, beginning December 1, 2015. The LCD increased the severity of lymphedema symptoms that a patient must exhibit before such patient is eligible for Medicare reimbursement for a pneumatic compression device, or PCD. The LCD also inserted more restrictive criteria that require a patient to potentially endure a longer period of conservative therapy to prove that it fails to control their lymphedema, instead of requiring completion of just one four-week round of conservative therapy as stated in the National Coverage Determination, or NCD. The LCD states that to qualify for any PCD, the patient must complete four consecutive weeks of conservative therapy with no significant improvement in symptoms during those four weeks. Further, the LCD does not cover use of an advanced pneumatic compression device, such as our Flexitouch System, unless the patient's lymphedema is present in the chest, trunk or abdomen. Although many patients with lymphedema likely do have some level of chest, trunk or abdominal involvement, this criteria in the LCD means that patients with lymphedema that is confined to the limb do not have access to advanced pneumatic compression devices until the lymphedema progresses to impact the trunk, chest or abdomen. The LCD pneumatic compression device coverage criteria for chronic venous insufficiency with venous stasis ulcers largely track existing NCD criteria, while defining the elements of a required conservative therapy trial. Under this LCD, advanced pneumatic compression devices like our Flexitouch System are no longer covered at all for the treatment of venous stasis ulcers. Since the LCD was released, we continue to work with physicians, advocacy groups, patients and legislators regarding the potentially negative consequences to patients that the LCD could cause. Although we have not experienced a significant negative impact on our Medicare fee-for-service business, the LCD could yet have an adverse effect on our business and results of operations. In addition, private payers often follow Medicare's lead in setting reimbursement criteria, and private payers may adopt the same or similar coverage standards as set forth in the LCD.
27
The U.S. patent protection for our Flexitouch System will expire in 2017, which may subject us to increased competition and reduce or eliminate our opportunity to generate product revenues.
The four U.S. patents for our Flexitouch System will expire in 2017. Upon expiration of such patents, our Flexitouch System could be subject to increased competition from products attempting to replicate our technology and our opportunity to increase or maintain revenues from our Flexitouch System could be substantially reduced.
If we are unable to expand, manage and maintain our direct sales and marketing organizations, we may not be able to generate anticipated revenues.
Our operating results are directly dependent upon the sales and marketing efforts of our employees. If our direct sales force fails to adequately promote, market and sell our products, our sales may suffer. Our direct sales force has grown from three representatives in March 2005 to a team of over 125 people as of December 31, 2016.
In order to generate future sales growth, we will need to expand the size and geographic scope of our direct sales organization. Accordingly, our future success will depend largely on our ability to continue to hire, train, retain and motivate skilled sales personnel with significant technical knowledge of lymphedema and chronic venous insufficiency. Because the competition for their services is high, we cannot assure you we will be able to hire and retain additional personnel on favorable or commercially reasonable terms, if at all. Failure to hire or retain qualified sales personnel would prevent us from building awareness of our solutions, expanding our business and generating additional sales. If we are unable to expand our sales and marketing capabilities, we may not be able to effectively commercialize our products, which could have an adverse impact on our business.
Increases in our operating costs could have an adverse effect on our financial condition and results of operations.
Reimbursement rates are established by fee schedules mandated by private payers, Medicare, the Veterans Administration and certain Medicaid programs and are likely to remain constant or decrease due, in part, to federal and state government budgetary constraints. As a result, with respect to Medicare and Medicaid related revenues, we may not be able to offset the effects of general inflation on our operating costs through increases in prices for our products. In particular, labor and related costs account for a significant portion of our operating costs and we compete with other healthcare providers to attract and retain qualified or skilled personnel and with various industries for administrative and service employees. This competitive environment could result in increased labor costs. As such, we must control our operating costs, particularly labor and related costs, and failing to do so could adversely affect our financial conditions and results of operations.
Our operating costs may fluctuate significantly in the future as a result of a variety of factors, many of which are outside of our control. These factors include:
|
· |
increased sales and marketing costs to increase awareness of our products; |
|
· |
costs to develop new and enhanced features for current products and research and development costs for new products; |
|
· |
the time, resources, and expense required to develop and conduct clinical trials and seek additional regulatory clearances and approvals for additional treatment indications for our products and for any additional products we develop; |
|
· |
the costs of preparing, filing, prosecuting, defending, and enforcing patent claims and other patent related costs, including litigation costs and the results of such litigation; |
|
· |
any product liability or other lawsuits related to our products and the costs associated with defending them or the costs related to the results of such lawsuits; |
|
· |
the costs to attract and retain personnel with the skills required for effective operations; |
|
· |
the costs associated with being a public company; and |
28
|
· |
costs associated with entering international markets. |
Our failure to anticipate and minimize the impact of these costs could adversely affect our business and results of operations.
We compete and may compete in the future against other companies, some of which have longer operating histories, more established products or greater resources than we do, which may harm our business.
The medical device industry is highly competitive. Our success depends, in part, upon our ability to maintain a competitive position in the development of technologies and solutions for the at-home treatment of lymphedema and chronic venous insufficiency or for market adjacencies. Any product we develop will have to compete for market acceptance and market share. We face significant competition in the United States, and we expect the intensity of competition will increase over time. Our primary competitors are Bio Compression Systems, Inc. and Lympha Press USA. Other competitors include Wright Therapy Products (which was acquired by BSN Medical GmbH in 2015), Devon Medical Products and NormaTec Industries. If we expand internationally, we expect that ArjoHuntleigh, an affiliate of the Getinge Group, would become a competitor, in addition to other potential international competitors. Many of the companies developing or marketing competing products enjoy several competitive advantages, including:
|
· |
significantly greater name recognition; |
|
· |
established relations with healthcare professionals, customers, and third-party payers; |
|
· |
established distribution networks; |
|
· |
additional lines of products, and the ability to offer rebates or bundle products to offer higher discounts or other incentives to gain a competitive advantage; |
|
· |
greater history in conducting research and development, manufacturing, marketing, and obtaining regulatory approval for homecare devices; and |
|
· |
greater financial and human resources for product development, sales and marketing, patent litigation and customer financing. |
Our competitors may develop and patent processes or products earlier than us, obtain regulatory clearance or approvals for competing devices more rapidly than us or develop more effective or less expensive products or technologies that render our technology or products obsolete or less competitive. We also face fierce competition in recruiting and retaining qualified sales, scientific, reimbursement and management personnel, particularly those with direct-to-patient and -provider experience. If our competitors are more successful than us in these matters, our business may be harmed.
Physicians and payers may require additional clinical studies prior to prescribing our products or to providing or maintaining coverage and reimbursement for our products. Any subsequent clinical studies that are conducted and published may not be positive or consistent with our existing data, which would adversely affect the rate of adoption of our products.
Our success depends in large part on the medical and third-party payer community's acceptance of our products as being useful in treating patients with lymphedema or chronic venous insufficiency. While the results of our studies collectively indicate a favorable safety and efficacy profile, the study designs and results may not be viewed as compelling to physicians and insurers. In particular, payers and physicians may see limitations in the design and results of the studies because certain studies were not specifically based on our products, involved a limited number of total subjects or subjects outside the control group and made "quality of life" conclusions based upon criteria contained in patient questionnaires that required subjective conclusions. Certain physicians and insurers may also prefer to see longer-term efficacy data than we have produced or are able to produce. If physicians or insurers do not find our data compelling or wish to wait for additional or independently-performed studies, they may choose not to prescribe or to provide coverage and reimbursement for our products.
29
We cannot assure you that any data that we or others generate will be consistent with that observed in the existing studies or that results will be maintained beyond the time points studied. We also cannot assure you that any data that may be collected will be compelling to the medical community because the data may not be scientifically meaningful or may not demonstrate that our products are attractive alternatives to traditional treatments. If subsequent studies are not positive or consistent with our existing data, adoption of our products may suffer and, accordingly, our business could be adversely impacted.
Our long-term growth depends on our ability to develop and commercialize additional products.
The medical device industry is highly competitive and subject to rapid change and technological advancements. Therefore, it is important to our business that we continue to enhance our product offerings and introduce new products. Developing products is expensive and time-consuming and could divert management's attention away from our business. We may not be successful in developing new products or enhancements to existing products. Our ability to develop and commercialize additional products or enhancements to existing products will depend on several factors, including our ability to:
|
· |
properly identify and anticipate physician and patient needs; |
|
· |
develop and introduce new products or product enhancements in a timely manner; |
|
· |
avoid infringing upon the intellectual property rights of third-parties; |
|
· |
demonstrate the safety and efficacy of new products with data from clinical studies; |
|
· |
obtain the necessary regulatory clearances or approvals for new products or product enhancements; |
|
· |
be fully FDA-compliant with the development, manufacturing and marketing of new devices or modified products; |
|
· |
provide adequate training to potential users of our products; |
|
· |
secure adequate coverage and reimbursement for our products; and |
|
· |
develop an effective and dedicated sales and marketing team. |
If we are unsuccessful in developing and commercializing new products, our ability to increase our revenues may be impaired.
It is difficult to forecast future performance and our financial results may vary from forecasts and may fluctuate from quarter to quarter.
Our limited operating history and commercial experience make it difficult for us to predict future performance. A number of factors over which we have limited control, such as seasonal variations in revenues, may contribute to fluctuations in our financial results. In the first and second quarters, our results of operations have been negatively impacted by resetting of annual patient healthcare insurance plan deductibles, which may cause patients to delay purchase of elective products. In the third and fourth quarters, our revenues have been higher because patients often spend the remaining balances in their flexible-spending accounts or because of lower out-of-pocket costs to patients who have met their annual deductibles under their health insurance plans. To the extent that the prevalence of high deductible insurance plans and higher copay and coinsurance plans continue to grow in the private payer market, the seasonal variations in our revenues could become even more pronounced.
Other factors that may cause fluctuation in our quarterly results or variations from our forecasts include:
|
· |
physician adoption of our products; |
|
· |
timing of new product offerings, acquisitions, licenses or other significant events by us or our competitors; |
30
|
· |
unanticipated pricing pressure; |
|
· |
the hiring, retention and continued productivity of our sales representatives; |
|
· |
our ability to expand the geographic reach of our sales and marketing efforts; |
|
· |
our ability to obtain regulatory clearance or approval for our products in development or for our current products outside the United States; |
|
· |
the impact of results from clinical research and trials on our existing products and products in development; |
|
· |
delays in receipt of anticipated purchase orders; |
|
· |
delays in, or failure of, component deliveries from our suppliers; and |
|
· |
positive or negative coverage in the media or clinical publications of our products or products of our competitors or our industry. |
In the event our actual revenues and operating results do not meet our forecasts or the forecasts or estimates of the research analysts that cover us for a particular period, the market price of our common stock may decline substantially.
We utilize third-party, single-source suppliers for some components and materials used in our products, and the loss of any of these suppliers could have an adverse impact on our business.
We rely on third-party manufacturers and suppliers to supply all components and materials used in our Flexitouch, ACTitouch and Entré Systems. We rely on a single-source supplier for the controller in our ACTitouch System. Our ability to supply our products commercially depends, in part, on our ability to obtain components and materials in accordance with our specifications and with regulatory requirements and in sufficient quantities to meet demand for our products. Our ability to obtain components and materials may be affected by matters outside our control, including that our suppliers may cancel our arrangements on short notice, we may be relatively less important as a customer to certain suppliers and our suppliers may have disruptions to their operations.
If we are required to establish additional or replacement suppliers for any of our components or materials, it may not be accomplished quickly and our operations could be disrupted. Even if we are able to find replacement suppliers, the replacement suppliers would need to be qualified and may require additional regulatory authority approval, which could result in further delay. In the event of a supply disruption, our product inventories may be insufficient to supply our patients.
If our third-party suppliers fail to deliver the required commercial quantities of materials on a timely basis and at commercially reasonable prices, and we are unable to find one or more replacement suppliers capable of production at a substantially equivalent cost in substantially equivalent volumes and quality on a timely basis, the continued commercialization of our products, the supply of our products to customers and the development of any future products would be delayed, limited or prevented, which could have an adverse impact on our business.
Consolidation in the healthcare industry could lead to demands for price concessions, which may impact our ability to sell our products at prices necessary to support our current business strategies.
Healthcare costs have risen significantly over the past decade, which has resulted in or led to numerous cost reform initiatives by legislators, regulators and third-party payers. Cost reform has triggered a consolidation trend in the healthcare industry to aggregate purchasing power, which may create more requests for pricing concessions in the future. We expect that market demand, government regulation, third-party coverage and reimbursement policies and societal pressures will continue to change the healthcare industry worldwide, resulting in further business consolidations and alliances among our payers, which may exert increasing downward pressure on the prices of our products in the future.
31
We may be unable to collect all of our Medicare accounts receivable.
At December 31, 2016, we had approximately $3.8 million of accounts receivable for sales of our Flexitouch System to patients covered by Medicare. A portion of the related claims to Medicare are initially denied and enter the appeals process, where many are ultimately reviewed by an Administrative Law Judge. The appeal process can be lengthy, lasting more than a year in most cases. At December 31, 2016, we classified $2.8 million of our Medicare accounts receivable related to Flexitouch System sales as long-term assets on our balance sheet due to the estimated amount of receivables that will be paid more than one year from December 31, 2016, as a result of delays with the Administrative Law Judge appeal process. A significant increase in Medicare denial of submitted claims or an increase in the proportion of Medicare denials that are upheld by an Administrative Law Judge could adversely affect our results of operations or cause us to reduce the carrying value of our Medicare accounts receivable related to Flexitouch System sales.
As an alternative to individual appeals, Medicare may seek to settle a number of outstanding appeals at one time through a settlement conference. On September 3, 2015, we entered into a settlement agreement with the Centers for Medicare and Medicaid Services, or CMS, for 247 claims, representing approximately $1.5 million of original claims based on the Medicare allowable rates, in which we had submitted a request for an Administrative Law Judge hearing in 2013. The settlement entitled us to receive a payment of approximately $0.9 million. We received this full amount during the fourth quarter of 2015. The settlement resulted in a reduction in the fourth quarter of 2015 of $0.8 million in our accounts receivable for shipment of products to patients covered by Medicare. The settlement was part of a pilot program, facilitated by the Office of Medicare Hearings and Appeals, to address a backlog of overdue claims awaiting Administrative Law Judge adjudication. Because the settlement was part of a pilot program, we cannot predict whether we will be able to conclude future settlements with Medicare or achieve settlements on similar terms. Any future settlement of claims for amounts less than the corresponding amounts receivable could result in a write off.
If physicians fail to properly document medical records for patients using our products, our business could be adversely impacted.
We bill Medicare Part B and other insurers directly for each sale to patients. As a result, we must comply with all laws, rules and regulations associated with filing claims with the Medicare program, including the Social Security Act, Medicare regulations, the Federal False Claims Act and the Civil Monetary Penalties Law, as well as a variety of additional federal and state laws. During an audit, insurers typically expect to find explicit documentation in the medical record to support a claim. Physicians and other clinicians, who are responsible for prescribing our products for patients, are expected to create and maintain the medical records that form the basis for the claims we submit to Medicare and other insurers. Any failure by physicians and other clinicians to properly document the medical records for patients using our products could invalidate claims, impair our ability to collect submitted claims and subject us to overpayment liabilities, False Claims Act liabilities and other penalties including exclusion from the Medicare, Medicaid or private insurance programs. Our payer relations group is responsible for verifying and managing patient claims. This group works with physicians and other clinicians to educate physicians and other clinicians on their record keeping responsibilities. From time to time our payer relations group identifies situations where the physician documentation could be questioned by Medicare or other insurers, and revises its procedures to strengthen our compliance systems based on our experience with Medicare contractors, Medicaid, insurers, physicians and other clinicians. If our procedures are not sufficient to detect deficiencies in the medical records of patients or such procedures are not updated in a timely manner before claims are submitted to Medicare or other insurers, or if the Medicare program or other insurer disagrees with the way physicians and other clinicians document the medical necessity support for prescribing our products, we could face potential liabilities for submitting claims based on inadequate records, even though those records are prepared and maintained by physicians and other clinicians.
Changes to the level of Medicare coverage for our products could have an adverse effect on our business and results of operations.
Determinations of which products or services will be reimbursed under Medicare can be developed at the national level through an NCD, by CMS, or at the local level through an LCD, by one or all of the four regional Medicare Administrative Contractors, which are private contractors that process and pay claims on behalf of CMS for different regions. These NCDs and LCDs may be subject to review and revision from time to time, which revisions may not be favorable for coverage of our products, and the NCDs and LCDs may not always be consistent. We have in the past been required to respond to potential changes in LCDs for our products, which, if enacted, would have had adverse effects on
32
our business. Further, we believe that a reduction in coverage by Medicare would likely cause some commercial third-party payers to implement similar reductions in their coverage or reimbursement of our products. Given the evolving nature of the healthcare industry and on-going healthcare cost reforms, we are and will continue to be subject to changes in the level of Medicare coverage for our products, and unfavorable coverage determinations at the national or local level could adversely affect our business and results of operations. See also "A change to the criteria for Medicare coverage for our products could have an adverse effect on our business and results of operations."
The size of the market for our products is an estimate, and may be smaller than we believe.
Our estimate of the annual total addressable market for our products is based on a number of internal and third-party estimates. In addition, our internal estimates are based in large part on current trends in diagnosing lymphedema and chronic venous insufficiency. While we believe these factors have historically provided and may continue to provide us with effective tools in estimating the total market for lymphedema, chronic venous insufficiency and our products, these estimates may not be correct and the conditions supporting our estimates may change at any time, thereby reducing the predictive accuracy of these underlying factors. As a result, our estimates of the annual total addressable market for our products may prove to be incorrect. If the actual number of patients who would benefit from our products and the annual total addressable market for our products is smaller than we have estimated, our future growth could be adversely impacted.
We may be unable to manage our growth effectively.
Our past growth has provided, and our future growth may create, challenges to our organization. For instance, from March 2005 to December 31, 2016, the number of our employees increased from 10 to 335. We intend to continue to grow and may experience periods of rapid growth and expansion. Future growth will impose significant added responsibilities on management, including the need to identify, recruit, train, integrate, retain and motivate additional employees. In addition, rapid and significant growth will place a strain on our administrative personnel, information technology systems and other operational infrastructure. Any failure by us to manage our growth effectively could have an adverse effect on our ability to achieve our development and commercialization goals.
Successful growth is also dependent upon our ability to implement appropriate financial and management controls, systems and procedures. In order to manage our operations and growth, we will need to continue to improve our operational and management controls, reporting and information technology systems and financial internal control procedures. If we are unable to manage our growth effectively, it may be difficult for us to execute our business strategy and there could be an adverse impact on our business.
Our ability to maintain our competitive position depends on our ability to attract, integrate and retain key executives and highly qualified personnel.
We believe that our continued success depends to a significant extent upon the efforts and abilities of our executive officers and other key personnel. Our executive officers and other key personnel are critical to the strategic direction and overall management of our company as well as our research and development process. Some key personnel have only joined us in the last year as part of our investment in the expansion of our business, including a new Vice President of Business Development who joined us in January 2016, a new Chief Financial Officer who joined us in April 2016, and a new Vice President of Supply Chain and Manufacturing who joined us in September 2016.
Our future success also depends on our ability to continue to attract and retain additional executive officers and other key employees. We invest significant time and expense in training our employees, which increases their value to competitors who may seek to recruit them. Many of our competitors have greater resources than we have that allows them to offer more competitive remuneration, which could adversely impact our ability to attract and retain experienced executives and other key employees. We carry a "key person" insurance policy on only our Chief Executive Officer. The replacement of any of our key personnel likely would involve significant time and costs and may significantly delay or prevent the achievement of our business objectives and would harm our business. Our productivity may be adversely affected if we do not integrate and train our new employees quickly and effectively
Many of our employees have become or will soon become vested in a substantial amount of our common stock or a number of common stock options. Our employees may be more likely to leave us if the shares they own have significantly appreciated in value relative to the original purchase prices of the shares, or if the exercise prices of the
33
options that they hold are significantly below the market price of our common stock, particularly after the expiration of the lock-up agreements described herein.
We face the risk of product liability claims that could be expensive, divert management's attention and harm our reputation and business. We may not be able to maintain adequate product liability insurance.
Our business exposes us to the risk of product liability claims that are inherent in the testing, manufacturing and marketing of medical devices. This risk exists even if a device is cleared or approved for commercial sale by the FDA and manufactured in facilities licensed and regulated by the FDA or an applicable foreign regulatory authority. Our products are designed to affect, and any future products will be designed to affect, important bodily functions and processes. Any side effects, manufacturing defects, misuse or abuse associated with our products or our products in development could result in patient injury or death. The medical device industry has historically been subject to extensive litigation over product liability claims, and we cannot offer any assurance that we will not face product liability suits. We may be subject to product liability claims if our products cause, or merely appear to have caused, patient injury or death. In addition, an injury that is caused by the activities of our suppliers, such as those who provide us with components and materials, may be the basis for a claim against us. Product liability claims may be brought against us by patients, clinicians or others selling or otherwise coming into contact with our products, among others. If we cannot successfully defend ourselves against product liability claims, we will incur substantial liabilities and reputational harm. In addition, regardless of merit or eventual outcome, product liability claims may result in:
|
· |
costs of litigation; |
|
· |
distraction of management's attention from our primary business; |
|
· |
the inability to commercialize our existing or new products; |
|
· |
decreased demand for our products or, if cleared or approved, products in development; |
|
· |
damage to our business reputation; |
|
· |
product recalls or withdrawals from the market; |
|
· |
withdrawal of clinical trial participants; |
|
· |
substantial monetary awards to patients or other claimants; or |
|
· |
loss of revenues. |
While we may attempt to manage our product liability exposure by proactively recalling or withdrawing from the market any defective products, any recall or market withdrawal of our products would delay the supply of those products to our clinicians and patients and may impact our reputation. We can provide no assurance that we will be successful in initiating appropriate market recall or market withdrawal efforts that may be required in the future or that these efforts will have the intended effect of preventing product malfunctions and the accompanying product liability that may result. Such recalls and withdrawals may also be used by our competitors to harm our reputation for safety or be perceived by patients as a safety risk when considering the use of our products, either of which could have an adverse impact on our business.
In addition, our product liability insurance is subject to deductibles and coverage limitations. Our current product liability insurance may not continue to be available to us on acceptable terms, if at all, and, if available, coverage may not be adequate to protect us against any future product liability claims. If we are unable to obtain insurance at an acceptable cost or on acceptable terms or otherwise protect against potential product liability claims, we could be exposed to significant liabilities. A product liability claim, recall or other claim with respect to uninsured liabilities or for amounts in excess of insured liabilities could have an adverse impact on our business.
34
Changes in reimbursement coding could impair our ability to receive reimbursement for our products.
Our Flexitouch System is reimbursed under Healthcare Common Procedure Coding System (HCPCS) code E0652, and our ACTitouch System and Entré System are reimbursed under HCPCS code E0651. Garments that cover various parts of the body are used with these systems and billed using HCPCS codes E0667, E0668 and E0669. These are tied to specific existing International Statistical Classification of Diseases and Related Health Problems Revision 10 (ICD-10) diagnoses. Many private payers have paid for our products using these codes as well. These contracts allow us to be an in-network provider for these payers, which eases our administrative burden in processing at both prior authorization and billing levels. With the ICD-10 requirements, it is possible the we or our patients may have difficulty properly submitting claims for reimbursement and, even if the claims are properly submitted, private payers, Medicare and Medicaid may have problems processing the claims. This could have an adverse impact on our reimbursement rates, results of operations and cash flows.
If the quality of our products does not meet the expectations of physicians or patients, then our brand and reputation could suffer and our business could be adversely impacted.
In the course of conducting our business, we must adequately address quality issues that may arise with our products, as well as defects in third-party components included in our products. There can be no assurance that our internal procedures to minimize risks that may arise from quality issues will be able to eliminate or mitigate occurrences of these issues and associated liabilities. If the quality of our products does not meet the expectations of physicians or patients, then our brand and reputation could suffer with those physicians or patients and our business could be adversely impacted.
If our facilities are damaged or become inoperable, we will be unable to continue to research, develop, manufacture and commercialize our products and, as a result, there will be an adverse impact on our business until we are able to secure a new facility.
We do not have redundant facilities. We perform substantially all of our research and development, assembly and back office activity and maintain all our finished goods inventory at two locations in Minneapolis, Minnesota. Our facilities and equipment would be costly to replace and could require substantial lead time to repair or replace. The facilities may be harmed or rendered inoperable by natural or man-made disasters, including, but not limited to, tornadoes, flooding, fire and power outages, which may render it difficult or impossible for us to perform our research, development, manufacturing and commercialization activities for some period of time. The inability to perform those activities, combined with our limited inventory of reserve raw materials and finished product, may result in the inability to continue manufacturing our products during such periods and the loss of customers or harm to our reputation. Our insurance for damage to our property and the disruption of our business may not be sufficient to cover all of our potential losses, and this insurance may not continue to be available to us on acceptable terms, or at all.
If we choose to acquire new and complementary businesses, products or technologies, we may be unable to complete these acquisitions or to successfully integrate them in a cost-effective and non-disruptive manner.
Our success depends on our ability to continually enhance and broaden our product offerings in response to changing customer demands, competitive pressures and advances in technologies. Accordingly, although we have no current commitments with respect to any acquisition or investment, we may in the future pursue the acquisition of, or joint ventures relating to, complementary businesses, products or technologies instead of developing them ourselves. We do not know if we will be able to successfully complete any future acquisitions or joint ventures, or whether we will be able to successfully integrate any acquired business, product or technology or retain any key employees related thereto. Integrating any business, product or technology we acquire could be expensive and time-consuming, disrupt our ongoing business and distract our management. If we are unable to integrate any acquired businesses, products or technologies effectively, our business will suffer. In addition, any amortization or charges resulting from the costs of acquisitions could increase our expenses.
35
Failure to protect our information technology infrastructure against cyber-based attacks, network security breaches, service interruptions or data corruption could significantly disrupt our operations and adversely affect our business and operating results.
We rely extensively on information technology systems and telephone networks and systems, including the Internet, to process and transmit sensitive electronic information and to manage or support a variety of business processes and activities, including sales, billing, customer service, procurement and supply chain, manufacturing, and distribution. We use enterprise information technology systems to record, process, and summarize financial information and results of operations for internal reporting purposes and to comply with regulatory financial reporting, legal, and tax requirements. Our information technology systems, some of which are managed by third-parties, may be susceptible to damage, disruptions or shutdowns due to computer viruses, attacks by computer hackers, failures during the process of upgrading or replacing software, databases or components thereof, power outages, hardware failures, telecommunication failures, user errors or catastrophic events. Despite the precautionary measures we have taken to prevent breakdowns in our information technology and telephone systems, if our systems suffer severe damage or disruption or shutdown and we are unable to effectively resolve the issues in a timely manner, our business and operating results may suffer.
In addition, we accept payments for many of our sales through credit and debit card transactions, which are handled through a third-party payment processor. As a result, we are subject to a number of risks related to credit and debit card payments, including that we pay interchange and other fees, which may increase over time and could require us to either increase the prices we charge for our products or experience an increase in our costs and expenses. In addition, as part of the payment processing process, we transmit our patients' and clinicians' credit and debit card information to our third-party payment processor. We may in the future become subject to lawsuits or other proceedings for purportedly fraudulent transactions arising out of the actual or alleged theft of our patients' credit or debit card information if the security of our third-party credit card payment processor is breached. We and our third-party credit card payment processor are also subject to payment card association operating rules, certification requirements and rules governing electronic funds transfers, which could change or be reinterpreted to make it difficult or impossible for us to comply. If we or our third-party credit card payment processor fail to comply with these rules or requirements, we may be subject to fines and higher transaction fees and lose our ability to accept credit and debit card payments from our patients, and there may be an adverse impact on our business.
We have no experience selling our products outside of the United States and cannot predict if we will be successful in achieving adoption of our products and revenue growth outside of the United States in a timely manner or at all. If we commercialize any products outside of the United States, a variety of risks associated with international operations could impact our strategy and adversely affect our future growth.
We expect that we would be subject to additional risks related to entering into international markets, including:
|
· |
difficulty successfully training patients and physicians on using our products; |
|
· |
difficulty hiring a qualified direct-sales force or finding and entering into commercially-acceptable agreements with suitable third-parties to market our products; |
|
· |
reduced protection for intellectual property rights; |
|
· |
unexpected changes in tariffs, trade barriers and regulatory requirements; |
|
· |
economic weakness, including inflation, or political instability in particular foreign economies and markets; |
|
· |
compliance with tax, employment, immigration and labor laws for employees living or traveling abroad; |
|
· |
foreign taxes, including withholding of payroll taxes; |
|
· |
foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country; |
|
· |
workforce uncertainty in countries where labor unrest is more common than in the United States; |
36
|
· |
international regulators and third-party payers may require additional clinical studies prior to approving or allowing reimbursement for our products; |
|
· |
disadvantages of competing against companies from countries that are not subject to U.S. laws and regulations, including the U.S. Foreign Corrupt Practices Act, regulations of the U.S. Office of Foreign Assets Controls, and U.S. anti-money laundering regulations, as well as exposure of our foreign operations to liability under these regulatory regimes; and |
|
· |
business interruptions resulting from geopolitical actions, including war and terrorism, or natural disasters including earthquakes, typhoons, floods and fires. |
If we experience any of these risks, our strategy to expand internationally could be impacted and our future growth could be adversely affected.
Our employees, independent contractors, consultants, collaborators and suppliers may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements and insider trading.
We are exposed to the risk that our employees and other third parties may engage in fraudulent conduct or other illegal activity. Misconduct by employees and other third parties could include intentional, reckless and/or negligent conduct or disclosure of unauthorized activities to us that violate FDA regulations, including those laws requiring the reporting of true, complete and accurate information to the FDA, manufacturing standards, federal and state healthcare fraud and abuse laws and regulations, or laws that require the reporting of financial information or data accurately. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Activities subject to these laws also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter employee and other third-party misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant civil, criminal and administrative penalties, damages, monetary fines, disgorgement, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings and curtailment or restructuring of our operations, any of which could adversely affect our ability to operate.
A reclassification of our independent contractor home trainers by tax authorities could require us to pay retroactive taxes and penalties, which could have a material adverse effect on our business, financial condition and operating results.
We contract with over 400 licensed healthcare practitioners as home trainers, who educate our patients on the proper use of our solutions. Because we consider these licensed practitioners to be independent contractors, as opposed to employees, we do not withhold federal or state income or other employment related taxes or make federal or state unemployment tax or Federal Insurance Contributions Act payments. Our contracts with these independent contractors obligate them to pay these taxes. The classification of healthcare practitioners as independent contractors depends on the facts and circumstances of the relationship. In the event federal or state taxing authorities determine that the healthcare practitioners are employees, our business may be adversely affected and subject to retroactive taxes and penalties. Under current federal tax law, a safe harbor from reclassification, and consequently retroactive taxes and penalties, is available if our current treatment is consistent with a long-standing practice of a significant segment of our industry and if we meet certain other requirements. If challenged, we may not prevail in demonstrating the applicability of the safe harbor to our operations. Further, interested persons have recently proposed to eliminate the safe harbor and may do so again in the future. If such proposals are reintroduced and passed by Congress, they could impact our classification of healthcare practitioners as independent contractors, which could have a material adverse effect on our business, financial condition and results of operations.
37
Risks Relating to Government Regulation
We are subject to extensive federal and state regulation, and if we fail to comply with applicable regulations, we could suffer severe criminal or civil sanctions or be required to make significant changes to our operations that could adversely affect our business, financial condition and operating results.
The federal government and all states in which we currently operate regulate various aspects of our business. Our operations also are subject to state laws governing, among other things, distribution of medical equipment and certain types of home health activities, and we are required to obtain and maintain licenses in each state to act as a durable medical equipment supplier.
As a healthcare provider participating in governmental healthcare programs, we are subject to laws directed at preventing fraud and abuse, which subject our marketing, billing, documentation and other practices to government scrutiny. To ensure compliance with Medicare, Medicaid and other regulations, government agencies or their contractors often conduct routine audits and request customer records and other documents to support our claims submitted for payment of services rendered. Government agencies or their contractors also periodically open investigations and obtain information from healthcare providers. Violations of federal and state regulations can result in severe criminal, civil and administrative penalties and sanctions, including debarment, suspension or exclusion from Medicare, Medicaid and other government reimbursement programs, any of which would have a material adverse effect on our business.
Changes in healthcare laws and regulations and new interpretations of existing laws and regulations may affect permissible activities, the relative costs associated with doing business, and reimbursement amounts paid by federal, state and other third-party payers. There have been and will continue to be regulatory initiatives affecting our business and we cannot predict the extent to which future legislation and regulatory changes could have a material adverse effect on our business, financial condition and results of operations.
We are subject to significant regulation by numerous government agencies, including the FDA. We cannot market or commercially distribute our products without obtaining and maintaining necessary regulatory clearances or approvals.
Our products are medical devices subject to extensive regulation in the United States. The FDA and other U.S. and foreign governmental agencies regulate, among other things, with respect to medical devices:
|
· |
design, development and manufacturing; |
|
· |
establishment registration and product listing; |
|
· |
testing, labeling, content and language of instructions for use and storage; |
|
· |
clinical trials; |
|
· |
product safety; |
|
· |
marketing, sales and distribution; |
|
· |
unique device identifiers; |
|
· |
premarket clearance and approval; |
|
· |
record keeping procedures; |
|
· |
advertising and promotion; |
|
· |
recalls and field safety corrective actions; |
38
|
· |
post-market surveillance, including reporting of deaths or serious injuries and malfunctions that, if they were to recur, could lead to death or serious injury; |
|
· |
post-market approval studies; and |
|
· |
product import and export. |
Unless an exemption applies, each medical device we seek to distribute commercially in the United States requires marketing authorization from the FDA prior to distribution. The two primary types of FDA marketing authorization applicable to a device are premarket notification, also called 510(k) clearance, and premarket approval. The type of marketing authorization is generally linked to the classification of the device. When a 510(k) clearance is required, we must submit a premarket notification to the FDA demonstrating that our proposed device is "substantially equivalent" to a legally marketed device previously found substantially equivalent through a 510(k) premarket notification, a legally marketed device which has been reclassified from high to low or moderate risk or a legally marketed device in commercial distribution before May 28, 1976 for which the FDA does not require the submission of a premarket approval application. Such a device is commonly known as a ‘‘predicate device.’’ The FDA may require further information, including clinical data, to make a determination regarding substantial equivalence. A medical device may be found not to be equivalent if it has different intended uses from the predicate device or possesses different technological characteristics from the predicate device which raise new questions of safety and effectiveness. A premarket approval application must be submitted to the FDA if the device cannot be cleared through the 510(k) process. The premarket approval application process is much more demanding than the 510(k) premarket notification process and requires the payment of significant user fees. A premarket approval application must be supported by valid scientific evidence, which typically requires extensive data to demonstrate the reasonable assurance of safety and effectiveness of the device. The approval process involves FDA review of information, including but not limited to, technical, preclinical (bench and/or animal), clinical trials, manufacturing and labeling. The FDA clearance and approval processes frequently take longer than anticipated due to increasing FDA demands for clarification of data or new data requirements.
If there is no predicate device that would permit the device to be cleared through the 510(k) path, then the FDA will automatically classify the device as a Class III high risk premarket approval device. In the event of this possibility, the sponsor can request a risk-based classification determination for the device in accordance with the de novo process, which is a route to market for novel medical devices that are low to moderate risk and are not substantially equivalent to a predicate device. A company files a de novo request when it does not have a predicate to which it can claim substantial equivalence. The FDA reviews the request for a de novo decision and grants or denies the request. If the request is granted, the FDA issues an order indicating that the device may legally be marketed and the device is classified as a Class I or II device, depending on risk. Once a device is classified through the de novo process, future devices from the company or a competitor may use that device as a 510(k) predicate. The advantage of the de novo process is that it generally requires less data than a premarket approval. The disadvantage is that it may require more data than a 510(k) and most often will include human clinical data. The FDA is increasingly moving devices with slightly different proposed indication statements or different technological features off the 510(k) path and on to the de novo path resulting in more time and expense for the company.
Both the 510(k) and premarket approval processes can be expensive and lengthy and require the payment of significant fees, unless an exemption applies. The FDA's 510(k) clearance process usually takes from approximately three to 12 months, but may take longer. The process of obtaining a premarket approval is much more costly and uncertain than the 510(k) clearance process and generally takes from approximately one to five years, or longer, from the time the application is submitted to the FDA until an approval is obtained. The process of obtaining regulatory clearances or approvals to market a medical device can be costly and time consuming, and we may not be able to obtain these clearances or approvals on a timely basis, if at all.
In the United States, our currently commercialized products are marketed pursuant to premarket clearance under Section 510(k) of the Federal Food, Drug and Cosmetic Act, or FDCA. If the FDA requires us to go through a lengthier, more rigorous examination for future products or modifications to existing products than we had expected, our product introductions or modifications could be delayed or canceled, which could cause our sales to decline. In addition, the FDA may determine that future products will require the more costly, lengthy and uncertain premarket approval process. Although we do not currently market any devices under a premarket approval, the FDA may demand that we obtain a premarket approval prior to marketing certain of our future products. In addition, if the FDA disagrees with our determination that a product we currently market is subject to an exemption from premarket review, the FDA may
39
require us to submit a 510(k) or premarket approval application in order to continue marketing the product. Further, even with respect to those future products where a premarket approval is not required, we cannot assure you that we will be able to obtain the 510(k) clearances required with respect to those products.
The FDA can delay, limit or deny clearance or approval of a device for many reasons, including:
|
· |
for non-premarket approval devices, failure of the applicant to demonstrate to the FDA's satisfaction that its products meet the definition of "substantial equivalence" or meet the standard for the FDA to grant a petition for de novo classification; |
|
· |
failure of the applicant to demonstrate that there is reasonable assurance that the medical device is safe or effective under the conditions of use prescribed, recommended or suggested in the proposed labeling; |
|
· |
insufficient data from the preclinical studies and clinical trials; or |
|
· |
the manufacturing processes, methods, controls or facilities used for the manufacture, processing, packing or installation of the device do not meet applicable requirements. |
Any delay in, or failure to receive or maintain, clearances or approvals for our products could prevent us from generating revenue from these products or achieving profitability. Additionally, the FDA and other governmental authorities have broad enforcement powers. Our failure to comply with applicable regulatory requirements could lead governmental authorities or a court to take action against us, including, but not limited to:
|
· |
issuing untitled (notice of violation) letters or public warning letters to us; |
|
· |
imposing fines and penalties on us; |
|
· |
obtaining an injunction or administrative detention preventing us from manufacturing or selling our products; |
|
· |
seizing products to prevent sale or transport or export; |
|
· |
bringing civil or criminal charges against us; |
|
· |
recalling our products or mandating a product correction; |
|
· |
detaining our products at U.S. Customs; |
|
· |
delaying the introduction of our products into the market; |
|
· |
delaying pending requests for clearance or approval of new uses or modifications to our existing products; and |
|
· |
withdrawing or denying approvals or clearances for our products. |
If we fail to obtain and maintain regulatory clearances or approvals, our ability to sell our products and generate revenue will be materially harmed.
In addition, the FDA may change its clearance and approval policies, adopt additional regulations or revise existing regulations, or take other actions which may prevent or delay approval or clearance of our products under development or impact our ability to modify our currently approved or cleared products on a timely basis. For example, in response to industry and healthcare provider concerns regarding the predictability, consistency and rigor of the 510(k) regulatory pathway, the FDA published new guidance on the 510(k) regulatory pathway in 2014, which alters the manner in which the 510(k) regulatory pathway is administered and interpreted. The FDA intends these reform actions to improve the efficiency and transparency of the clearance process, as well as bolster patient safety. This new guidance could impose additional regulatory requirements upon us which could delay our ability to obtain new 510(k) clearances, increase the costs of compliance or restrict our ability to maintain our current clearances. In addition, as part of the Food and Drug Administration Safety and Innovation Act, Congress reauthorized the Medical Device User Fee Amendments with
40
various FDA performance goal commitments and enacted several "Medical Device Regulatory Improvements" and miscellaneous reforms which are further intended to clarify and improve medical device regulation both pre- and post-market.
Medical devices may only be promoted and sold for the indications for which they are approved or cleared. In addition, even if the FDA has approved or cleared a product, it can take action affecting such product approvals or clearances if serious safety or other problems develop in the marketplace. Delays in obtaining clearances or approvals could adversely affect our ability to introduce new products or modifications to our existing products in a timely manner, which would delay or prevent commercial sales of our products. Additionally, the FDA and other regulatory authorities have broad enforcement powers. Regulatory enforcement or inquiries, or other increased scrutiny on us, could affect the perceived safety and efficacy of our products and dissuade patients and clinicians from using our products.
If we modify our FDA cleared devices, we may need to seek additional clearances or approvals, which, if not granted, would prevent us from selling our modified products.
The FDA regulations require the submission and clearance of a new 510(k) premarket notification, or possibly, premarket approval, for significant changes or modifications made in the design, components, method of manufacture or intended use of a device including changes or modifications to a 510(k)-cleared device that could significantly affect the device's safety or effectiveness, or would constitute a major change or modification in the device's intended use. The FDA requires each manufacturer to make this determination, but the FDA may review any manufacturer's decision. The FDA may not agree with our decisions regarding whether new clearances or approvals are necessary. We have modified some of our 510(k) cleared products, and have determined based on our review of the applicable FDA guidance that in certain instances new 510(k) clearances or premarket approval are not required. If the FDA disagrees with our determination and requires us to submit new 510(k) notifications or premarket approval for modifications to our previously cleared products for which we have concluded that new clearances or approvals are unnecessary, we may be required to cease marketing or to recall the modified product until we obtain clearance or approval, and we may be subject to significant regulatory fines or penalties.
Furthermore, the FDA's ongoing review of the 510(k) program may make it more difficult for us to make modifications to our previously cleared products, either by imposing more strict requirements on when a manufacturer must submit a new 510(k) for a modification to a previously cleared product, or by applying more onerous review criteria to such submissions. If the FDA requires us to cease marketing a modified device until we obtain a new 510(k) clearance or premarket approval, our business, financial condition, operating results and future growth prospects could be materially adversely affected. Further in this situation, our products could be subject to recall. Any recall or FDA requirement that we seek additional approvals or clearances could result in significant delays, fines, increased costs associated with modification of a product, loss of revenue and potential operating restrictions imposed by the FDA.
The misuse or off-label use of our products may harm our image in the marketplace, result in injuries that lead to product liability suits or result in costly investigations, fines or sanctions by regulatory bodies if we are deemed to have engaged in the promotion of these uses, any of which could be costly to our business.
The products we currently market have been cleared by the FDA for specific treatments. We train our marketing and direct sales force to not promote our products for uses outside of the FDA-cleared indications for use, known as "off-label uses." We cannot, however, prevent a physician from using our products off-label, when in the physician's independent professional medical judgment he or she deems it appropriate. The FDA does not restrict or regulate a physician's choice of treatment. There may be increased risk of injury to patients if physicians use our products off-label. Furthermore, the use of our products for indications other than those cleared by the governing regulatory body may not effectively treat such conditions, which could harm our reputation in the marketplace among physicians and patients.
If the FDA determines that our promotional materials, communications or training constitute promotion of or encourage off-label uses, it could request that we modify our training or promotional materials or subject us to regulatory or enforcement actions, including the issuance of untitled letters, warning letters, injunctions, seizures, civil fines or criminal penalties. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our business activities to constitute promotion of an off-label use, which could result in significant penalties, including, but not limited to, criminal, civil and administrative penalties, damages, fines, disgorgement, exclusion from participation in government healthcare programs, and the curtailment of our operations.
41
In addition, physicians or patients may misuse our products or use improper techniques, potentially leading to injury and an increased risk of product liability. If our products are misused or used with improper technique, we may become subject to costly litigation by our clinicians or their patients. As noted above, we can be subject to lawsuits, whether or not our product is proven to be defective and whether or not our employees have adequately trained the physicians. Similarly, in an effort to decrease costs, physicians may also reuse those of our products that are intended for a single use or may purchase reprocessed products from third-party reprocessors in lieu of purchasing new products from us, which could result in product failure and liability. As described immediately above, product liability claims could divert management's attention from our core business, be expensive to defend and result in sizeable damage awards against us that may not be covered by insurance.
Our products may cause or contribute to adverse medical events that we are required to report to the FDA, and if we fail to do so, we would be subject to sanctions that would materially harm our business.
Our marketed products are subject to Medical Device Reporting, or MDR, obligations, which require that we report to the FDA any incident in which our products may have caused or contributed to a death or serious injury, or in which our products malfunctioned and, if the malfunction were to recur, it could likely cause or contribute to a death or serious injury. The timing of our obligation to report under the MDR regulations is triggered by the date we become aware of the adverse event as well as the nature of the event. We may fail to report adverse events of which we become aware within the prescribed timeframe. We may also fail to recognize that we have become aware of a reportable adverse event, especially if it is not reported to us as an adverse event or if it is an adverse event that is unexpected or removed in time from the use of our products. If we fail to comply with our reporting obligations, the FDA could take action including warning letters, untitled letters, administrative actions, criminal prosecution, imposition of civil monetary penalties, revocation of our device clearances, seizure of our products, or delay in clearance of future products.
Our products may in the future be subject to product recalls. A recall of our products, either voluntarily or at the direction of the FDA or another governmental authority, or the discovery of serious safety issues with our products, could have a significant adverse impact on us.
The FDA and similar foreign governmental authorities have the authority to require the recall of commercialized products in the event of material deficiencies or defects in their design or manufacture. The FDA's authority to require a recall must be based on a finding that there is reasonable probability that the device would cause serious, adverse health consequences or death. We may also choose to voluntarily recall a product if any material deficiency is found. A government-mandated or voluntary recall could occur as a result of an unacceptable risk to health, component failures, malfunctions, manufacturing errors, design or labeling defects or other deficiencies and issues. Recalls of any of our products would divert managerial and financial resources and have an adverse effect on our reputation and business, which could impair our ability to produce our products in a cost-effective and timely manner in order to meet our patients' demands. We may also be subject to liability claims, be required to bear other costs, or take other actions that may have a negative impact on our future sales and our ability to generate profits.
Companies are required to maintain certain records of recalls and corrections, even if they are not reportable to the FDA. We may initiate voluntary recalls or corrections for our products in the future that we determine do not require notification of the FDA. If the FDA disagrees with our determinations, they could require us to report those actions as recalls and we may be subject to enforcement action.
If we or our component manufacturers fail to comply with the FDA's Quality System Regulation, our manufacturing operations could be interrupted, and our product sales and operating results could suffer.
We and many of our component manufacturers are required to comply with the FDA's Quality System Regulation, or QSR, which covers the procedures and documentation of the design, testing, production, control, quality assurance, labeling, packaging, sterilization, storage and shipping of our devices. The FDA audits compliance with the QSR through periodic announced and unannounced inspections of manufacturing and other facilities. We and our component manufacturers have been, and anticipate in the future being, subject to such inspections. We cannot provide assurance that any future inspection will not result in adverse findings with respect to our QSR compliance. If our manufacturing facilities or those of any of our component manufacturers or suppliers are found to be in violation of applicable laws and
42
regulations, or we or our manufacturers or suppliers fail to take satisfactory corrective action in response to an adverse inspection, the FDA could take enforcement action, including one or more of the following non-exclusive sanctions:
|
· |
untitled letters, warning letters, fines, injunctions, consent decrees and civil penalties; |
|
· |
customer notifications or repair, replacement, refunds, recall, detention or seizure of our products; |
|
· |
operating restrictions or partial suspension or total shutdown of production; |
|
· |
refusing or delaying our requests for 510(k) clearance or premarket approval of new products or modified products; |
|
· |
withdrawing 510(k) clearances or premarket approvals that have already been granted; |
|
· |
refusal to grant export approval for our products; or |
|
· |
criminal prosecution. |
Any of these sanctions could adversely affect our business, financial condition and results of operations.
If we begin selling our products outside the United States, our products and operations would also be required to comply with standards set by industrial standards bodies, such as the International Organization for Standardization, or ISO. Foreign regulatory bodies may evaluate our products or the testing that our products undergo against these or other standards. The specific standards, types of evaluation and scope of review differ among foreign regulatory bodies. If we fail to adequately comply with any of these standards, a foreign regulatory body may take adverse actions similar to those within the power of the FDA.
Any of these actions could prevent us from marketing, distributing or selling our products and would likely harm our business.
If clinical studies of our future products do not produce results necessary to support regulatory clearance or approval in the United States or, with respect to our current or future products, elsewhere, we will be unable to expand the indications for or commercialize these products.
We will likely need to conduct additional clinical studies in the future to support new indications for our products or for clearances of new product lines, or for the approval of the use of our products in some foreign countries. Clinical testing can take many years, can be expensive and carries uncertain outcomes. The initiation and completion of any of these studies may be prevented, delayed, or halted for numerous reasons.
Clinical failure can occur at any stage of testing. Our clinical studies may produce negative, unanticipated or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical and non-clinical testing in addition to those we have planned. Our failure to adequately demonstrate the safety and efficacy of any of our devices would prevent receipt of regulatory clearance or approval and, ultimately, the commercialization of that device or indication for use. Even if our future products are cleared in the United States, commercialization of our products in foreign countries would require approval by regulatory authorities in those countries. Approval procedures vary among jurisdictions and can involve requirements and administrative review periods different from, and greater than, those in the United States, including additional preclinical studies or clinical trials. Any of these occurrences could have an adverse impact on our business.
If the third parties on which we rely to conduct our clinical trials and to assist us with pre-clinical development do not perform as contractually required or expected, we may not be able to obtain regulatory clearance or approval for or commercialize our products.
We often must rely on third parties, such as contract research organizations, medical institutions, clinical investigators and contract laboratories to conduct our clinical trials. If these third parties do not successfully carry out their contractual duties or regulatory obligations, have difficulty recruiting sufficient subjects for clinical studies or fail
43
to meet expected deadlines, if these third parties need to be replaced, or if the quality or accuracy of the data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for other reasons, our pre-clinical development activities or clinical trials may be extended, delayed, suspended or terminated, and we may not be able to obtain regulatory approval for, or successfully commercialize, our products on a timely basis, if at all, and our business, operating results and prospects may be adversely affected. Furthermore, our third-party clinical trial investigators may be delayed in conducting our clinical trials for reasons outside of their control.
Future regulatory actions may adversely affect our ability to sell our products profitably.
From time to time, legislation is drafted and introduced that could significantly change the statutory provisions governing the clearance or approval, manufacture and marketing of a medical device. In addition, FDA and other regulations and guidance are often revised or reinterpreted in ways that may significantly affect our business and our products, and new regulations or guidance documents may be promulgated. It is impossible to predict whether legislative changes will be enacted or regulations, guidance or interpretations changed or added, and what the impact of such changes or additions, if any, may be.
Healthcare regulatory reform may affect our ability to sell our products profitably.
In the United States, the legislative landscape, particularly as it relates to healthcare regulation and reimbursement coverage, continues to evolve. In March 2010, the Patient Protection and Affordable Care Act and Health Care and Education Reconciliation Act, which we refer to as the Patient Protection and Affordable Care Act, was passed, which has the potential to substantially change healthcare financing by both governmental and private insurers, and significantly impact the U.S. medical device industry. The Patient Protection and Affordable Care Act, among other things, imposes a new excise tax, which began in 2013, on entities that manufacture, produce or import medical devices in an amount equal to 2.3% of the price for which such devices are sold in the United States. While we believe that our current products are exempt from this tax under an exemption for retail products, if our belief is determined to be incorrect, we could be subject to significant tax liabilities and penalties, which could have a material adverse effect on our results of operations and cash position. Moreover, products that we introduce in the future could be subject to this tax.
In addition, the Patient Protection and Affordable Care Act also expands the round two of competitive bidding to a total of 91 competitive bidding areas, and by 2016, the process must be nationalized or prices in non-competitive bidding areas must be adjusted to match competitive bidding prices. Other legislative changes have been proposed and adopted in the United States since the Patient Protection and Affordable Care Act was enacted. On August 2, 2011, the Budget Control Act of 2011 among other things, created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation's automatic reduction to several government programs. This includes aggregate reductions of Medicare payments to providers up to 2% per fiscal year, which went into effect on April 1, 2013. On January 2, 2013, President Obama signed into law the American Taxpayer Relief Act of 2012 which, among other things, further reduced Medicare payments to certain providers, including physicians, hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. We expect that additional state and federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our products or additional pricing pressures.
There have been judicial and Congressional challenges to certain aspects of the Patient Protection and Affordable Care Act. Additional state and federal health care reform measures that may be adopted in the future could have a material adverse effect on our industry generally and on our customers. Any changes in, or uncertainty with respect to future reimbursement rates, or changes in hospital admission rates could impact our customers' demand for our products and services, which in turn could impact our ability to successfully commercialize our products, or could limit or eliminate our spending on certain development projects. These changes could adversely affect our business and results of operations.
44
While our products are not currently subject to the competitive bidding process under Medicare, if our products were to become subject to such process in the future, it could negatively affect our business and financial condition.
The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 required the Secretary of Health and Human Services to establish and implement programs under which competitive acquisition areas are established throughout the United States for purposes of awarding contracts for the furnishing of competitively priced items of durable medical equipment.
CMS, the agency responsible for administering the Medicare program, conducts a competition for each competitive acquisition area under which providers submit bids to supply certain covered items of durable medical equipment. Successful bidders must meet certain program quality standards in order to be awarded a contract and only successful bidders can supply the covered items to Medicare beneficiaries in the acquisition area. There are, however, regulations in place that allow non-contracted providers to continue to provide products and services to their existing customers at the new competitive bidding payment amounts. The contracts are expected to be re-bid every three years. CMS is required to award contracts to multiple entities submitting bids in each area for an item or service, but has the authority to limit the number of contractors in a competitive acquisition area to the number it determines to be necessary to meet projected demand.
Although CMS concluded the bidding process for the first round of Metropolitan Statistical Areas in September 2007, in July 2008, Congress enacted Medicare Improvements for Patients and Providers Act of 2008, which retroactively delayed the implementation of competitive bidding. Medicare Improvements for Patients and Providers Act of 2008 also reduced Medicare prices nationwide by 9.5% beginning in 2009 for the product categories that were initially included in competitive bidding.
The Patient Protection and Affordable Care Act legislation requires CMS to expand competitive bidding further to additional geographic markets or to use competitive bid pricing information to adjust the payment amounts otherwise in effect for areas that are not competitive acquisition areas by January 1, 2016.
Although we continue to monitor developments regarding the implementation of the competitive bidding program, we cannot predict the outcome of the competitive bidding program on our business when fully implemented, nor the Medicare payment rates that will be in effect in future years for the items subjected to competitive bidding, including our products. We expect that payment rates will continue to fluctuate, and a large negative payment adjustment could adversely affect our business, financial conditions and results of operations.
We are subject to additional federal, state and foreign laws and regulations relating to our healthcare business; our failure to comply with those laws could have an adverse impact on our business.
We are subject to healthcare fraud and abuse regulation and enforcement by federal and state governments, which could adversely impact our business. Healthcare fraud and abuse and health information privacy and security laws potentially applicable to our operations include:
|
· |
the federal Anti-Kickback Statute, which applies to our marketing practices, educational programs, pricing policies and relationships with healthcare providers, by prohibiting, among other things, soliciting, receiving, offering or providing remuneration, whether directly or indirectly and overtly or covertly, intended to induce the referral of an individual for (i) the furnishing or the arranging for the furnishing of items or services reimbursable under a federal healthcare program, such as Medicare or Medicaid; or (ii) the purchase, lease or order of, or the arrangement or recommendation of the purchasing, leasing or ordering of, of an item or service reimbursable under a federal healthcare program. A person or entity does not need to have actual knowledge of this statute or specific intent to violate it to have committed a violation; |
|
· |
federal civil and criminal false claims laws and civil monetary penalty laws, including civil whistleblower or qui tam actions that prohibit, among other things, knowingly presenting, or causing to be presented, claims for payment or approval to the federal government that are false or fraudulent, knowingly making a false statement material to an obligation to pay or transmit money or property to the federal government, knowingly concealing or knowingly and improperly avoiding or decreasing an obligation to pay or transmit money or property to the federal government or knowingly offering remuneration to influence a Medicare or Medicaid beneficiary's selection of health care providers. The government may assert that a claim, including items or |
45
services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the false claims statutes; |
|
· |
HIPAA and its implementing regulations, which created federal criminal laws that prohibit, among other things, executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; |
|
· |
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, also imposes certain regulatory and contractual requirements regarding the privacy, security and transmission of individually identifiable health information; |
|
· |
federal Open Payments (the Physician Payments Sunshine Act) requirements imposed by the Patient Protection and Affordable Care Act on device manufacturers regarding certain "transfers of value" made or distributed to physicians and teaching hospitals. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $150,000 per year (or up to an aggregate of $1.0 million per year for "knowing failures"), for all payments, transfers of value or ownership or investment interests that are not timely, accurately, and completely reported in an annual submission. The period between August 1, 2013 and December 31, 2013 was the first reporting period, and manufacturers were required to report aggregate payment data by March 31, 2014, and to report detailed payment data and submit legal attestation to the accuracy of such data by June 30, 2014. Thereafter, manufacturers must submit reports by the 90th day of each subsequent calendar year; |
|
· |
federal consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm consumers; and |
|
· |
state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws that may apply to items or services reimbursed by any third-party payer, including commercial insurers; state laws that require device companies to comply with the industry's voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government or otherwise restrict payments that may be made to healthcare providers; state laws that require device manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; and state laws governing the privacy and security of certain health information, many of which differ from each other in significant ways and often are not preempted by HIPAA. |
The risk of our being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. We are unable to predict what additional federal or state legislation or regulatory initiatives may be enacted in the future regarding our business or the healthcare industry in general, or what effect such legislation or regulations may have on us. Federal or state governments may impose additional restrictions or adopt interpretations of existing laws that could have a material adverse effect on us.
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available under such laws, it is possible that some of our business activities, including certain sales and marketing practices and financial arrangements, including the provision of stock options as partial compensation for consulting services, with physicians, some of whom use or purchase our products, and other customers, could be subject to challenge under one or more of such laws. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management's attention from the operation of our business. If our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, exclusion from governmental healthcare programs, disgorgement, contractual damages, reputational harm, diminished profits and future earnings, and the curtailment or restructuring of our operations, any of which could adversely impact our business.
Failure to comply with regulations affecting the transmission, security and privacy of health information could result in significant penalties.
Numerous federal and state laws and regulations, including HIPAA and the Health Information Technology for Economic and Clinical Health Act, or the HITECH Act, govern the collection, dissemination, security, use and
46
confidentiality of patient-identifiable health information. HIPAA and the HITECH Act require us to comply with standards for the use and disclosure of health information within our company and with third parties. The Privacy Standards and Security Standards under HIPAA establish a set of basic national privacy and security standards for the protection of individually identifiable health information by health plans, healthcare clearinghouses and certain healthcare providers, referred to as covered entities, and the business associates with whom such covered entities contract for services. Notably, whereas HIPAA previously directly regulated only these covered entities, the HITECH Act, which was signed into law as part of the stimulus package in February 2009, makes certain of HIPAA's privacy and security standards also directly applicable to covered entities' business associates. As a result, both covered entities and business associates are now subject to significant civil and criminal penalties for failure to comply with Privacy Standards and Security Standards.
HIPAA and the HITECH Act also include standards for common healthcare electronic transactions and code sets, such as claims information, plan eligibility, payment information and the use of electronic signatures, and privacy and electronic security of individually identifiable health information. Covered entities, such as healthcare providers, are required to conform to such transaction set standards pursuant to HIPAA.
HIPAA requires healthcare providers like us to develop and maintain policies and procedures with respect to protected health information that is used or disclosed, including the adoption of administrative, physical and technical safeguards to protect such information. The HITECH Act expands the notification requirement for breaches of patient-identifiable health information, restricts certain disclosures and sales of patient-identifiable health information and provides a tiered system for civil monetary penalties for HIPAA violations. The HITECH Act also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney fees and costs associated with pursuing federal civil actions. Additionally, certain states have adopted comparable privacy and security laws and regulations, some of which may be more stringent than HIPAA.
If we do not comply with existing or new laws and regulations related to patient health information, we could be subject to criminal or civil sanctions. New health information standards, whether implemented pursuant to HIPAA, the HITECH Act, congressional action or otherwise, could have a significant effect on the manner in which we handle healthcare related data and communicate with payors, and the cost of complying with these standards could be significant.
The 2013 final HITECH omnibus rule modifies the breach reporting standard in a manner that will likely make more data security incidents qualify as reportable breaches. Any liability from a failure to comply with the requirements of HIPAA or the HITECH Act could adversely affect our financial condition. The costs of complying with privacy and security related legal and regulatory requirements are burdensome and could have a material adverse effect on our results of operations. These new provisions, as modified, will be subject to interpretation by various courts and other governmental authorities, thus creating potentially complex compliance issues for us, as well as our clients and strategic partners. In addition, we are unable to predict what changes to the HIPAA Privacy Standards and Security Standards might be made in the future or how those changes could affect our business. Any new legislation or regulation in the area of privacy and security of personal information, including personal health information, could also adversely affect our business operations.
Additionally, the Federal Trade Commission has issued and several states have issued or are considering new regulations to require holders of certain types of personally identifiable information to implement formal policies and programs to prevent, detect and mitigate the risk of identity theft and other unauthorized access to or use of such information. Further, the U.S. Congress and a number of states have considered or are considering prohibitions or limitations on the disclosure of medical or other information to individuals or entities located outside of the United States. If we begin selling our products outside the United States, we will need to comply with applicable laws in those jurisdictions that regulate the use and disclosure of individually identifiable information.
47
If we fail to comply with state and federal fraud and abuse laws, including anti-kickback, false claims and anti-inducement laws, we could face substantial penalties and our business, operations, and financial condition could be adversely affected.
The federal anti-kickback statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration, whether directly or indirectly and overtly or covertly, to induce or in return for purchasing, leasing, ordering, or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid, or other federal financed healthcare programs. The statutory exceptions and regulatory safe harbors protecting certain common activities from prosecution are drawn narrowly, and any remuneration to or from a prescriber or purchaser of healthcare products or services may be subject to scrutiny if they do not qualify for an exception or safe harbor. Our practices may not in all cases meet all of the criteria for safe harbor protection from anti-kickback liability.
Federal false claims laws prohibit, in part, any person from knowingly presenting or causing to be presented a false claim for payment to the federal government, or knowingly making or causing to be made a false statement to get a false claim paid. The majority of states also have statutes or regulations similar to the federal anti-kickback law and false claims laws, which apply to items or services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of payer. These false claims statutes allow any person to bring suit in the name of the government alleging false and fraudulent claims presented to or paid by the government (or other violations of the statutes) and to share in any amounts paid by the entity to the government in fines or settlement. Such suits, known as qui tam actions, have increased significantly in the healthcare industry in recent years. Sanctions under these federal and state laws may include civil monetary penalties, exclusion of a manufacturer's products from reimbursement under government programs, criminal fines and imprisonment. In addition, the Patient Protection and Affordable Care Act, among other things, amends the intent requirement of the federal anti-kickback and criminal healthcare fraud statutes. A person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, the Patient Protection and Affordable Care Act provides that the government may assert that a claim, including items or services resulting from a violation of the federal anti-kickback statute constitutes a false or fraudulent claim for purposes of the false claims statutes. Because of the breadth of these laws and the narrowness of the safe harbors and exceptions, it is possible that some of our business activities could be subject to challenge under one or more of such laws. Such a challenge, regardless of the outcome, could have a material adverse effect on our business, business relationships, reputation, financial condition and results of operations.
In addition, there has been a recent trend of increased federal and state regulation of payments made to physicians. The Patient Protection and Affordable Care Act imposed new reporting and disclosure requirements on device and drug manufacturers for any "transfer of value" made or distributed to prescribers and other healthcare providers. Device and drug manufacturers will also be required to report and disclose any investment interests held by physicians and their immediate family members during the preceding calendar year. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $150,000 per year (and up to an aggregate of $1.0 million per year for "knowing failures to report"), for all payments, transfers of value or ownership or investment interests not reported in an annual submission. As of August 1, 2013, manufacturers are required to collect data and are required to submit their data reports to CMS by the 90th day of each calendar year.
Certain states mandate implementation of compliance programs and/or the tracking and reporting of gifts, compensation and other remuneration to physicians. The shifting compliance environment and the need to build and maintain robust and expandable systems to comply with different compliance and/or reporting requirements in multiple jurisdictions increase the possibility that a healthcare company many violate one or more of the requirements.
The Federal Civil Monetary Penalties Law prohibits, in part, the offering or giving of remuneration to a Medicare or Medicaid beneficiary that the person knows or should know is likely to influence the beneficiary's selection of a particular supplier of items or services reimbursable by a Federal or state governmental program. We sometimes offer customers various discounts and other financial incentives in connection with the sales of our products. While it is our intent to comply with all applicable laws, the government may find that our marketing activities violate the Civil Monetary Penalties Law. If we are found to be in noncompliance, we could be subject to civil money penalties of up to $10,000 for each wrongful act, assessment of three times the amount claimed for each item or service and exclusion from the Federal healthcare programs.
48
The scope and enforcement of each of these laws is uncertain and subject to rapid change in the current environment of healthcare reform, especially in light of the lack of applicable precedent and regulations. If our operations are found to be in violation of any of the laws described above or any other government regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines and the curtailment, restructuring, or restricting of our operations. Any penalties, damages, fines, curtailment or restructuring or our operations could harm our ability to operate our business and our financial results. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management's attention from operation of our business. Moreover, achieving and sustaining compliance with applicable federal and state fraud laws may prove costly.
Failure to maintain the licenses and accreditations necessary to operate under our direct-to-patient and -provider model would adversely affect our business.
To continue operating our business under our direct-to-patient and -provider model, we must maintain our Durable Medical Equipment license and certification from the Accreditation Commission for Health Care. In May 2008, we became a Durable, Medical Equipment, Prosthetics, Orthotics, and Supplies accredited Medicare supplier by the Accreditation Commission for Health Care for our solutions and our Medicare accreditation must be renewed every three years through passage of an on-site inspection. Our current accreditation with Medicare is due to expire in May 2017. In addition to maintaining our Durable Medical Equipment license and certification from the Accreditation Commission for Health Care, we also must maintain certain state-required licenses. If we were found to be noncompliant, we could lose our licensure in that state. Losing our licensure could prohibit us from selling our current or future products to patients in such state and our business, financial condition and results of operations could be adversely affected as a result of any such prohibition.
Our products are currently made available to authorized users of the Department of Veterans Affairs Federal Supply Schedule and if we were no longer eligible to sell our products through such channel, our business may be adversely affected.
For our products to be eligible for reimbursement by the Veterans Administration, we must participate in the Department of Veterans Affairs Federal Supply Schedule pricing program, established by Section 603 of the Veterans Health Care Act of 1992. To be eligible for this program, we must comply with additional laws and requirements applicable to our operations and manufacturing processes. If we were to lose eligibility for reimbursement by the Veterans Administration, our business, financial condition and results of operations could be adversely affected.
We may be unable to obtain or maintain international regulatory registrations or approvals for our current or future products and indications, which could adversely impact our business.
Any future sales of our devices outside the United States are subject to foreign regulatory requirements that vary widely from country to country. In addition, the FDA regulates exports of medical devices from the United States. Complying with international regulatory requirements can be an expensive and time-consuming process and approval is not certain. The time required to obtain registration or approvals, if required by other countries, may be longer than that required for FDA clearance, and requirements for such registrations or approvals may significantly differ from FDA requirements. In certain countries we intend to rely upon third-party distributors to obtain all required regulatory registrations and approvals, and these distributors may be unable to obtain or maintain such registrations or approvals. Our distributors in these countries may also incur significant costs in attempting to obtain and in maintaining foreign regulatory approvals or registrations, which could increase the difficulty of attracting and retaining qualified distributors. If these distributors experience delays in receiving necessary registrations or approvals to market our products outside the United States, or if they fail to receive those registrations or approvals, we may be unable to market our products or enhancements in certain international markets effectively, or at all.
Our operations involve the use of hazardous and toxic materials, and we must comply with environmental, health and safety laws and regulations, which can be expensive, and could have an adverse impact on our business.
Our operations use or generate small volumes of hazardous or toxic materials. We are therefore subject to a variety of federal, state and local regulations relating to the use, handling, storage, disposal and human exposure to hazardous and toxic materials. Liability under environmental laws can be joint and several and without regard to comparative fault, and environmental laws could become more stringent over time, imposing greater compliance costs and increasing risks
49
and penalties associated with violations, which could have an adverse impact on our business. There can be no assurance that violations of environmental, health and safety laws will not occur in the future as a result of human error, accident, equipment failure or other causes. The failure to comply with past, present or future laws could result in the imposition of fines, third-party property damage and personal injury claims, investigation and remediation costs, the suspension of production or a cessation of operations. We also expect that our operations will be affected by other new environmental and health and safety laws and regulations on an ongoing basis. Although we cannot predict the ultimate impact of any such new laws and regulations, they will likely result in additional costs, and may require us to change how we manufacture our products, which could have an adverse impact on our business.
Risks Related to Our Financial Condition
We may need substantial additional funding and may be unable to raise capital when needed, which could force us to delay or reduce our commercialization efforts or product development programs.
We believe the net proceeds from our initial public offering, together with our existing cash and cash equivalents and revenues, will be sufficient to meet our capital requirements and fund our operations indefinitely. However, we have based these estimates on assumptions that may prove to be incorrect, and we could spend our available financial resources much faster than we currently expect. Any future funding requirements will depend on many factors, including:
|
· |
market acceptance of our products; |
|
· |
the scope, rate of progress and cost of our clinical studies; |
|
· |
the cost of our research and development activities; |
|
· |
the cost of filing and prosecuting patent applications and defending and enforcing our patent or other intellectual property rights; |
|
· |
the cost of defending, in litigation or otherwise, any claims that we infringe third-party patents or other intellectual property rights; |
|
· |
the cost and timing of additional regulatory clearances or approvals; |
|
· |
the cost and timing of establishing additional sales, marketing and distribution capabilities; |
|
· |
costs associated with any product recall that may occur; |
|
· |
the effect of competing technological and market developments; |
|
· |
the extent to which we acquire or invest in products, technologies and businesses, although we currently have no commitments or agreements relating to any of these types of transactions; and |
|
· |
the costs of operating as a public company. |
If we raise additional funds by issuing equity securities, our stockholders may experience dilution. Any future debt financing into which we enter may impose upon us covenants that restrict our operations, including limitations on our ability to incur liens or additional debt, pay dividends, repurchase our common stock, make certain investments and engage in certain merger, consolidation or asset sale transactions. Any debt financing or additional equity that we raise may contain terms that are not favorable to us or our stockholders. If we raise additional funds through collaboration and licensing arrangements with third parties, it may be necessary to relinquish some rights to our technologies or our products, or grant licenses on terms that are not favorable to us.
Furthermore, we cannot be certain that additional funding will be available on acceptable terms, if at all. If we do not have, or are not able to obtain, sufficient funds, we may have to delay development or commercialization of our products or license to third parties the rights to commercialize products or technologies that we would otherwise seek to
50
commercialize. We also may have to reduce marketing, customer support or other resources devoted to our products or cease operations. Any of these factors could harm our operating results.
Risks Related to Our Intellectual Property
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on products in all countries throughout the world would be prohibitively expensive, and our intellectual property rights in some countries outside the United States may be less extensive than those in the United States. In addition, the laws of some foreign countries do not protect intellectual property rights to the same extent as federal and state laws in the United States. For example, many foreign countries have compulsory licensing laws, under which a patent owner must grant licenses to third parties. Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the United States, or from selling or importing products made using our inventions in and into the United States or other jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products, and further, competitors may export otherwise infringing products to territories where we have patent protection but enforcement rights are not as strong as those in the United States. These products may compete with our products in jurisdictions where we do not have any issued patents, and our patent claims or other intellectual rights may not be effective or sufficient to prevent them from so competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries do not favor the enforcement of patents and other intellectual property protection, which could make it difficult for us to stop the infringement of our patents generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing, and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
The patent protection for our products may expire before we are able to maximize their commercial value, which may subject us to increased competition and reduce or eliminate our opportunity to generate product revenues.
The patents for our products have varying expiration dates and, if these patents expire, we may be subject to increased competition and we may not be able to recover our development costs or market any of our approved products profitably. For instance, our patents for our Flexitouch System will expire in 2017. Upon expiration of our patents, we may be subject to increased competition and our opportunity to establish or maintain product revenues could be substantially reduced or eliminated. Further, we may not have sufficient time to recover our development costs prior to the expiration of our U.S. and foreign patents.
We may not identify relevant patents or may incorrectly interpret the relevance, scope or expiration of a patent, which may adversely affect our ability to develop and market our products.
We cannot guarantee that any of our patent searches or analyses, including but not limited to the identification of relevant patents, the scope of patent claims or the expiration of relevant patents, are complete or thorough, nor can we be certain that we have identified each and every patent and pending application in the United States and abroad that is relevant to or necessary for the commercialization of our products in any jurisdiction.
The scope of a patent claim is determined by an interpretation of the law, the written disclosure in a patent and the patent family's prosecution history. Our interpretation of the relevance or the scope of a patent or a pending application may be incorrect, which may negatively impact our ability to market our products. We may incorrectly determine that our products are not covered by a third-party patent.
Many patents may cover a marketed product, including but not limited to patents covering the product or portions thereof, methods of use or methods relating to the product, and production processes of or for the product. The identification of all patents and their expiration dates relevant to the production and sale of a therapeutic product is extraordinarily complex and requires sophisticated legal knowledge in the relevant jurisdiction. It may be impossible to
51
identify all patents in all jurisdictions relevant to a marketed product. Our determination of the expiration date of any patent in the United States or abroad that we consider relevant may be incorrect, which may negatively impact our ability to develop and market our products.
Obtaining and maintaining our patent protection depends on compliance with various procedural, documentary, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The United States Patent and Trademark Office, or USPTO, and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent prosecution process. Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on any issued patent and/or pending patent applications are due to be paid to the USPTO and foreign patent agencies in several stages over the lifetime of a patent or patent application. We have systems in place to remind us to pay these fees, and we employ an outside firm and rely on our outside counsel to pay these fees. While an inadvertent lapse may sometimes be cured by payment of a late fee or by other means in accordance with the applicable rules, there are many situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. If we fail to maintain the patents and patent applications directed to our products, our competitors might be able to enter the market earlier than should otherwise have been the case, which would have a material adverse effect on our business.
We may become involved in lawsuits to protect our patents or other intellectual property rights, which could be expensive, time-consuming and ultimately unsuccessful.
Competitors may infringe our patents or other intellectual property rights. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours is not valid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation or defense proceedings could put one or more of our patents at risk of being invalidated or interpreted narrowly and could put our patent applications at risk of not issuing.
Various proceedings brought before the USPTO may be necessary to determine the priority of inventions with respect to our patents and patent applications or those of our current or future collaborators. An unfavorable outcome could require us to cease using the technology or to attempt to license rights to it from the prevailing party. Our business could be harmed if a prevailing party does not offer us a license on terms that are acceptable to us. Litigation or other proceedings may fail and, even if successful, may result in substantial costs and distraction of our management and other employees. We may not be able to prevent misappropriation of our proprietary rights, particularly in countries where the laws may not protect those rights as fully as in the United States.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential and proprietary information could be compromised by disclosure during this type of litigation. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our common stock.
Third-party claims of intellectual property infringement or misappropriation may adversely affect our business and could prevent us from developing or commercializing our products.
Our commercial success depends in part on us not infringing the patents and proprietary rights of third parties. There is a substantial amount of litigation, both within and outside the United States, involving patent and other intellectual property rights in the medical device industry, including patent infringement lawsuits, interferences, oppositions, ex-parte review and inter partes reexamination and post-grant review proceedings before the USPTO and corresponding foreign patent offices. Numerous U.S. and foreign issued patents and pending patent applications owned by third parties exist in the fields in which we are developing and may develop our products. As the medical device industry expands and more patents are issued, the risk increases that our products may be subject to claims of
52
infringement of the patent rights of third parties. If a third party claims that we infringe on their products or technology, we could face a number of issues, including:
|
· |
infringement and other intellectual property claims which, with or without merit, can be expensive and time-consuming to litigate and can divert management's attention from our core business; |
|
· |
substantial damages for past infringement, which we may have to pay if a court decides that our product infringes on a competitor's patent; |
|
· |
a court prohibiting us from selling or licensing our product, unless the patent holder licenses the patent to us; |
|
· |
if a license is available from a patent holder, we may have to pay substantial royalties or grant cross licenses to our patents; and |
|
· |
redesigning our processes so they do not infringe, which may not be possible or could require substantial funds and time. |
Third parties may assert that we are employing their proprietary technology without authorization. There may be third-party patents or patent applications with claims to products, materials, formulations, methods of manufacture or methods for treatment related to the use or manufacture of our products, that we failed to identify. For example, applications filed before November 29, 2000 and certain applications filed after that date that will not be filed outside the United States remain confidential until issued as patents. Except for the preceding exceptions, patent applications in the United States and elsewhere are generally published only after a waiting period of approximately 18 months after the earliest filing. Therefore, patent applications covering our technology or our products could have been filed by others without our knowledge. Additionally, pending patent applications that have been published can, subject to certain limitations, be later amended in a manner that could cover our technologies, our products or the use or manufacture of our products. We may also face a claim of misappropriation, if a third party believes that we inappropriately obtained and used trade secrets of such third parties. If we are found to have misappropriated a third party's trade secrets, we may be prevented from further using such trade secrets, limiting our ability to develop our products, and we may be required to pay damages.
If any third-party patents were held by a court of competent jurisdiction to cover aspects of our products, materials, formulations, methods of manufacture or methods for treatment, the holders of any such patents would be able to block our ability to develop and commercialize the applicable product candidate until such patent expired or unless we obtain a license. These licenses may not be available on acceptable terms, if at all. Even if we were able to obtain a license, the rights may be nonexclusive, which could result in our competitors gaining access to the same intellectual property. Ultimately, we could be prevented from commercializing a product, or be forced to cease some aspect of our business operations, if, as a result of actual or threatened patent infringement claims, we are unable to enter into licenses on acceptable terms. In addition, during the course of any patent or other intellectual property litigation, there could be public announcements of the results of hearings, rulings on motions, and other interim proceedings in the litigation. If securities analysts or investors regard these announcements as negative, the perceived value of our products, programs, or intellectual property could be diminished. Accordingly, the market price of our common stock may decline.
Parties making claims against us may obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our products. Defending against claims of patent infringement or misappropriation of trade secrets could be costly and time-consuming, regardless of the outcome. Thus, even if we were to ultimately prevail, or to settle at an early stage, such litigation could burden us with substantial unanticipated costs. In addition, litigation or threatened litigation could result in significant demands on the time and attention of our management team, distracting them from the pursuit of other company business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys' fees for willful infringement, pay royalties, redesign our infringing products or obtain one or more licenses from third parties, which may be impossible or require substantial time and monetary expenditure. In addition, the uncertainties associated with litigation could have a material adverse effect on our ability to raise the funds necessary to continue our clinical trials, continue our research programs, license necessary technology from third parties, or enter into development collaborations that would help us bring our products to market.
53
Changes in U.S. patent law could diminish the value of patents in general, thereby impairing our ability to protect our products.
As is the case with other medical device companies, our success is heavily dependent on intellectual property, particularly on obtaining and enforcing patents. Obtaining and enforcing patents in the medical device industry involves both technological and legal complexity, and therefore is costly, time-consuming and inherently uncertain. In addition, the United States has recently enacted and is currently implementing wide-ranging patent reform legislation. Further, several recent judicial rulings have either narrowed the scope of patent protection available in certain circumstances or weakened the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained.
For our U.S. patent applications containing a claim not entitled to priority before March 16, 2013, there is a greater level of uncertainty in the patent law. In September 2011, the Leahy-Smith America Invents Act, or the American Invents Act, or AIA, was signed into law. The AIA includes a number of significant changes to U.S. patent law, including provisions that affect the way patent applications will be prosecuted, reviewed after issuance, and may also affect patent litigation. The USPTO is currently developing regulations and procedures to govern administration of the AIA and many of the substantive changes to patent law associated with the AIA. It is not clear what other, if any, impact the AIA will have on the operation of our business. Moreover, the AIA and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents, all of which could have a material adverse effect on our business and financial condition.
An important change introduced by the AIA is that, as of March 16, 2013, the United States transitioned to a "first-inventor-to-file" system for deciding which party should be granted a patent when two or more patent applications are filed by different parties claiming the same invention. A third party that files a patent application in the USPTO after that date but before us could therefore be awarded a patent covering an invention of ours, even if we had made the invention before it was made by the third party. This will require us to be cognizant, going forward, of the time from invention to filing of a patent application, but early filing of patent applications may not always be possible. Furthermore, our ability to obtain and maintain valid and enforceable patents depends on whether the differences between our technology and the prior art allow our technology to be patentable over the prior art. Since patent applications in the United States and most other countries are confidential for a period of time after filing, we cannot be certain that we were the first to either (a) file any patent application related to our products or (b) invent any of the inventions claimed in our patents or patent applications.
Among some of the other changes introduced by the AIA are changes that limit where a patentee may file a patent infringement suit and provide opportunities for third parties to challenge any issued patent in the USPTO. This applies to all of our U.S. patents, even those issued before March 16, 2013. Because of a lower evidentiary standard in USPTO proceedings compared to the evidentiary standard in United States federal court necessary to invalidate a patent claim, a third party could potentially provide evidence in a USPTO proceeding sufficient for the USPTO to hold a claim invalid as unpatentable, even though the same evidence may be insufficient to invalidate the claim if first presented in a district court action. Accordingly, a third party may attempt to use the USPTO procedures to invalidate our patent claims that would not have been invalidated if first challenged by the third party as a defendant in a district court action.
Depending on decisions by the U.S. Congress, the federal courts, and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future.
Because of the expense and uncertainty of litigation, we may not be in a position to enforce our intellectual property rights against third parties.
We have become aware from time to time that third parties may be infringing on our patents or other intellectual property rights. Because of the expense and uncertainty of litigation, we have concluded in the past and may conclude in the future that even if a third party is infringing our patents or other intellectual property rights, the risk-adjusted cost of bringing and enforcing such a claim or action may be too high or not in the best interest of our company or our stockholders. In such cases, we may decide that the more prudent course of action is to simply monitor the situation or initiate or seek some other non-litigious action or solution.
54
Intellectual property rights do not address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain, because intellectual property rights have limitations and may not adequately protect our business or permit us to maintain our competitive advantage. The following examples are illustrative:
|
· |
Others may be able to make products that are similar to our products but that are not covered by the claims of the patents that we own or license from others. |
|
· |
Others may independently develop similar or alternative technologies or otherwise circumvent any of our technologies without infringing our intellectual property rights. |
|
· |
We might not have been the first to conceive and reduce to practice the inventions covered by the patents or patent applications that we own, license or will own or license. |
|
· |
We might not have been the first to file patent applications covering certain subject matter of the patents or patent applications that we own or for which we have obtained a license, or will own or for which we will obtain a license. |
|
· |
It is possible that our pending patent applications will not lead to issued patents. |
|
· |
Issued patents that we own may not provide us with any competitive advantage, or may be held invalid or unenforceable, as a result of legal challenges by our competitors. |
|
· |
Our competitors might conduct research and development activities in countries where we do not have patent rights, or in countries where research and development safe harbor laws exist, and then use the information learned from such activities to develop competitive products for sale in our major commercial markets. |
|
· |
Ownership of our patents or patent applications may be challenged by third parties. |
|
· |
The patents of third parties or pending or future applications of third parties, if issued, may have an adverse effect on our business. |
Confidentiality agreements with employees and others may not adequately prevent disclosure of trade secrets and protect other proprietary information.
We consider proprietary trade secrets and/or confidential know-how and unpatented know-how to be important to our business. We may rely on trade secrets and/or confidential know-how to protect our technology, especially where patent protection is believed by us to be of limited value. However, trade secrets and/or confidential know-how can be difficult to maintain as confidential.
To protect this type of information against disclosure or appropriation by competitors, our policy is to require our employees, consultants, contractors and advisors to enter into confidentiality agreements with us. However, current or former employees, consultants, contractors and advisers may unintentionally or willfully disclose our confidential information to competitors, and confidentiality agreements may not provide an adequate remedy in the event of unauthorized disclosure of confidential information. Enforcing a claim that a third party obtained illegally and is using trade secrets and/or confidential know-how is expensive, time consuming and unpredictable. The enforceability of confidentiality agreements may vary from jurisdiction to jurisdiction.
Failure to obtain or maintain trade secrets and/or confidential know-how trade protection could adversely affect our competitive position. Moreover, our competitors may independently develop substantially equivalent proprietary information and may even apply for patent protection in respect of the same. If successful in obtaining such patent protection, our competitors could limit our use of our trade secrets and/or confidential know-how.
55
We may need to license certain intellectual property from third parties, and such licenses may not be available or may not be available on commercially reasonable terms.
A third party may hold intellectual property, including patent rights that are important or necessary to the development or commercialization of any future products. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our products, in which case we would be required to obtain a license from these third parties. Such a license may not be available on commercially reasonable terms or at all, which could materially harm our business.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of third parties.
We have received confidential and proprietary information from third parties. In addition, we employ individuals who were previously employed at other medical device companies. We may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise improperly used or disclosed confidential information of these third parties or our employees' former employers. Further, we may be subject to ownership disputes in the future, arising, for example, from conflicting obligations of consultants or others who are involved in developing our products. We may also be subject to claims that former employees, consultants, independent contractors, collaborators or other third parties have an ownership interest in our patents or other intellectual property. Litigation may be necessary to defend against these and other claims challenging our right to and use of confidential and proprietary information. If we fail in defending any such claims, in addition to paying monetary damages, we may lose our rights therein. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against these claims, litigation could result in substantial cost and be a distraction to our management and employees.
We may be subject to claims challenging the inventorship or ownership of our patents and other intellectual property.
We may also be subject to claims that former employees, collaborators or other third parties have an ownership interest in our patents or other intellectual property. We may be subject to ownership disputes in the future, arising, for example, from conflicting obligations of consultants or others who are involved in developing our products. Litigation may be necessary to defend against these and other claims challenging inventorship or ownership. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Our reliance on third parties requires us to share our trade secrets, which increases the possibility that a competitor will discover them or that our trade secrets will be misappropriated or disclosed.
Because we rely on third parties to assist with research and development and to manufacture our products, we must, at times, share trade secrets with them. We seek to protect our proprietary technology in part by entering into confidentiality agreements and, if applicable, material transfer agreements, consulting agreements or other similar agreements with our advisors, employees, third-party contractors and consultants, prior to beginning research or disclosing proprietary information. These agreements typically limit the rights of the third parties to use or disclose our confidential information, including our trade secrets. Despite the contractual provisions employed when working with third parties, the need to share trade secrets and other confidential information increases the risk that such trade secrets become known by our competitors, are inadvertently incorporated into the technology of others, or are disclosed or used in violation of these agreements. Given that our proprietary position is based, in part, on our know-how and trade secrets, a competitor's discovery of our trade secrets or other unauthorized use or disclosure would impair our competitive position and may have a material adverse effect on our business.
In addition, these agreements typically restrict the ability of our advisors, employees, third-party contractors and consultants to publish data potentially relating to our trade secrets, although our agreements may contain certain limited publication rights. For example, any academic institution that we may collaborate with in the future will usually expect to be granted rights to publish data arising out of such collaboration, provided that we are notified in advance and given the opportunity to delay publication for a limited time period in order for us to secure patent protection of intellectual property rights arising from the collaboration, in addition to the opportunity to remove confidential or trade secret
56
information from any such publication. In the future, we may also conduct joint research and development programs that may require us to share trade secrets under the terms of our research and development or similar agreements. Despite our efforts to protect our trade secrets, our competitors may discover our trade secrets, either through breach of our agreements with third parties, independent development or publication of information by any of our third-party collaborators. A competitor's discovery of our trade secrets would impair our competitive position and have an adverse impact on our business.
If our trademarks and trade names are not adequately protected, then we may not be able to build name recognition in our markets of interest and our business may be adversely affected.
If our trademarks and trade names are not adequately protected, then we may not be able to build name recognition in our markets of interest, and our business may be adversely affected. We currently have registered and unregistered trademarks in the United States. Our trademarks or trade names may be challenged, infringed, circumvented or declared generic or determined to be infringing on other marks. We may not be able to protect our rights to these trademarks and trade names, which we need to build name recognition among potential collaborators or customers in our markets of interest. At times, competitors may adopt trade names or trademarks similar to ours, thereby impeding our ability to build brand identity and possibly leading to market confusion. Further, there could be potential trade name or trademark infringement claims brought by owners of other trademarks or trade names that incorporate variations of our trademarks or trade names. In addition, we have not registered our trademarks internationally, and the laws of certain foreign countries may not protect proprietary rights to the same extent as do the laws of the United States. Over the long term, if we are unable to successfully register our trademarks and trade names and/or establish name recognition based on our trademarks and trade names, then we may not be able to compete effectively and our business may be adversely affected. Our efforts to enforce or protect our proprietary rights related to trademarks, trade secrets, domain names, copyrights or other intellectual property may be ineffective and could result in substantial costs and diversion of resources and could adversely impact our financial condition or results of operations.
Risks Related to Ownership of Our Common Stock
The trading price of the shares of our common stock has been and could continue to be highly volatile, and purchasers of our common stock may not be able to resell the shares of our common stock at or above the price at which they purchased their shares and could incur substantial losses.
Our stock price has been and is likely to continue to be volatile. The stock market in general has experienced extreme volatility that has often been unrelated to the operating performance of particular companies. As a result of this volatility, investors may not be able to sell their shares of our common stock at or above the price at which they purchased their shares. The market price for our common stock may be influenced by many factors, including:
|
· |
the passage of legislation or other regulatory developments in the United States and foreign countries; |
|
· |
actual or anticipated variations in our financial results or those of companies that are perceived to be similar to us; |
|
· |
changes in the structure of healthcare payment systems, especially in light of current reforms to the U.S. healthcare system; |
|
· |
our ability to develop and commercialize additional products; |
|
· |
announcements by us or our competitors of significant acquisitions, strategic collaborations, joint ventures or capital commitments; |
|
· |
market conditions in medical device sectors and issuance of securities analysts' research reports or recommendations; |
|
· |
sales of our stock by us, our insiders and our other stockholders; |
|
· |
the trading volume of our common stock; |
57
|
· |
speculation in the press or investment community; |
|
· |
general economic, industry and market conditions, or other events or factors, many of which are beyond our control; |
|
· |
additions or departures of key personnel; and |
|
· |
intellectual property, product liability or other litigation against us. |
In addition, the stock market has recently experienced significant volatility with respect to medical device and other life sciences company stocks. The volatility of medical device and other medical technology company stocks often does not relate to the operating performance of the companies represented by the stock. As we operate in a single industry, we are especially vulnerable to these factors to the extent that they affect our industry or our products, or to a lesser extent our markets.
We are an "emerging growth company," and the reduced disclosure requirements applicable to emerging growth companies may make our common stock less attractive to investors.
We are an "emerging growth company," as defined in the JOBS Act and may remain an emerging growth company for up to five years following our initial public offering. For so long as we remain an emerging growth company, we are permitted and intend to rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth companies. These exemptions include:
|
· |
not being required to comply with the auditor attestation requirements in the assessment of our internal control over financial reporting; |
|
· |
not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor's report providing additional information about the audit and the financial statements; |
|
· |
reduced disclosure obligations regarding executive compensation; and |
|
· |
exemptions from the requirements of holding a non-binding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. |
We have taken advantage of reduced reporting burdens in this report. We cannot predict whether investors will find our common stock less attractive if we rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be reduced or more volatile. In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of these accounting standards until they would otherwise apply to private companies. We have elected to avail ourselves of this exemption and, as a result, our financial statements may not be comparable to the financial statements of issuers that are required to comply with the effective dates for new or revised accounting standards that are applicable to public companies. We cannot predict whether investors will find our common stock less attractive if we rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be reduced or more volatile.
Sales of a substantial number of shares of our common stock by our existing stockholders in the public market could cause our stock price to fall.
Sales of a substantial number of shares of our common stock in the public market, or the perception that these sales might occur, could significantly reduce the market price of our common stock and impair our ability to raise adequate capital through the sale of additional equity securities.
As of February 16, 2017, approximately 47% of our outstanding shares are held by directors, executive officers and other affiliates. Although these shares are subject to volume limitations under Rule 144 under the Securities Act of
58
1933, as amended, or the Securities Act, if these shares of common stock are sold, or if it is perceived that they will be sold, in the public market, the trading price of our common stock could decline
As of February 16, 2017, the holders of 7,242,903 shares of our outstanding common stock, or approximately 43% of our total outstanding common stock, are entitled to rights with respect to the registration of their shares under the Securities Act. Registration of these shares under the Securities Act would result in the shares becoming freely tradable without restriction under the Securities Act, except for shares held by affiliates, as defined in Rule 144 under the Securities Act. Any sales of securities by these stockholders could have a material adverse effect on the trading price of our common stock.
We do not intend to pay dividends on our common stock, and, consequently, your ability to achieve a return on your investment will depend on appreciation, if any, in the price of our common stock.
We have never declared or paid any cash dividend on our common stock and do not currently intend to do so for the foreseeable future. We currently anticipate that we will retain future earnings for the development, operation and expansion of our business. In addition, any future debt financing arrangement may contain terms prohibiting or limiting the amount of dividends that may be declared or paid on our common stock. Any return to stockholders will therefore be limited to any appreciation of their stock. Therefore, the success of an investment in shares of our common stock will depend upon any future appreciation in their value. There is no guarantee that shares of our common stock will appreciate in value or even maintain the price at which our stockholders purchased their shares.
We are incurring increased costs and are subject to additional regulations and requirements as a result of being a public company, which could lower our profits or make it more difficult to run our business.
As a public company, we are incurring significant legal, accounting and other expenses that we did not incur as a private company, including costs associated with public company reporting requirements. We also have incurred and will continue to incur costs associated with the Sarbanes-Oxley Act and related rules implemented by the SEC and Nasdaq. The expenses incurred by public companies generally for reporting and corporate governance purposes have been increasing. We expect these rules and regulations to increase our legal and financial compliance costs and to make some activities more time-consuming and costly, although we are currently unable to estimate these costs with any degree of certainty. These laws and regulations also could make it more difficult or costly for us to obtain certain types of insurance, including director and officer liability insurance, and we may be forced to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. These laws and regulations could also make it more difficult for us to attract and retain qualified persons to serve on our board of directors, our board committees or as our executive officers. Furthermore, if we are unable to satisfy our obligations as a public company, we could be subject to delisting of our common stock, fines, sanctions and other regulatory action and potentially civil litigation.
If we fail to maintain proper and effective internal control over financial reporting in the future, our ability to produce accurate and timely financial statements could be impaired, which could harm our operating results, investors' views of us and, as a result, the value of our common stock.
Pursuant to Section 404 of the Sarbanes-Oxley Act, our management is required to report upon the effectiveness of our internal control over financial reporting beginning with the Annual Report on Form 10-K for our fiscal year ending December 31, 2017. When and if we are a "large accelerated filer" or an "accelerated filer" and are no longer an "emerging growth company," each as defined in the Exchange Act, our independent registered public accounting firm will be required to attest to the effectiveness of our internal control over financial reporting. However, for so long as we remain an emerging growth company, we intend to take advantage of an exemption available to emerging growth companies from these auditor attestation requirements. We could be an "emerging growth company" for up to five years following our initial public offering. The rules governing the standards that must be met for management to assess our internal control over financial reporting are complex and require significant documentation, testing, and possible remediation. To comply with the requirements of being a reporting company under the Exchange Act, we will need to upgrade our systems, including information technology; implement additional financial and management controls, reporting systems, and procedures; and hire additional accounting and finance staff.
Any failure to implement required new or improved controls, or difficulties encountered in their implementation, could cause us to fail to meet our reporting obligations. In addition, any testing by us conducted in connection with
59
Section 404 of the Sarbanes-Oxley Act, or any subsequent testing by our independent registered public accounting firm, may reveal deficiencies in our internal control over financial reporting that are deemed to be material weaknesses or that may require prospective or retroactive changes to our financial statements or identify other areas for further attention or improvement. Inferior internal controls could also cause investors to lose confidence in our reported financial information, which could have a negative effect on the trading price of our common stock.
In addition, we may encounter problems or delays in implementing any changes necessary to make a favorable assessment of our internal control over financial reporting. Further, once we are no longer an emerging growth company, we may encounter problems or delays in completing the implementation of any requested improvements and receiving a favorable attestation in connection with the attestation provided by our independent registered public accounting firm. If we cannot favorably assess the effectiveness of our internal control over financial reporting, or if our independent registered public accounting firm is unable to provide an unqualified attestation report on our internal controls, investors could lose confidence in our financial information and the trading price of our common stock could decline.
In connection with our future evaluation of our internal control over financial reporting, we may need to upgrade our systems or create new systems, implement additional financial and management controls, update our reporting systems and procedures, create or outsource an internal audit function or hire additional accounting and finance staff. If we are unable to accomplish these objectives in a timely and effective fashion, our ability to comply with the financial reporting requirements and other rules that apply to reporting companies could be impaired. Any failure to maintain effective internal control over financial reporting could have a material adverse effect on our business, financial condition and results of operations and the trading price of our common stock.
Anti-takeover provisions in our charter documents and under Delaware law could make an acquisition of us, which may be beneficial to our stockholders, more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our amended and restated certificate of incorporation and amended and restated bylaws, as well as provisions of Delaware law, may delay or prevent an acquisition of us or a change in our management. These provisions include:
|
· |
authorizing the issuance of "blank check" preferred stock, the terms of which may be established and shares of which may be issued without stockholder approval; |
|
· |
limiting the removal of directors by the stockholders; |
|
· |
prohibiting cumulative voting in the election of directors, which would otherwise allow for less than a majority of stockholders to elect director candidates; |
|
· |
prohibiting stockholder action by written consent, thereby requiring all stockholder actions to be taken at a meeting of our stockholders; |
|
· |
eliminating the ability of stockholders to call a special meeting of stockholders; and |
|
· |
establishing advance notice requirements for nominations for election to the board of directors or for proposing matters that can be acted upon at stockholder meetings. |
These provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors, who are responsible for appointing the members of our management. In addition, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which limits the ability of stockholders owning in excess of 15% of our outstanding voting stock to merge or combine with us. These provisions would apply even if an offer rejected by our board were considered beneficial by some stockholders. Any provision of our amended and restated certificate of incorporation or our amended and restated bylaws or Delaware law that has the effect of delaying or deterring a change of control could limit the opportunity for our stockholders to receive a premium for their shares of our common stock, and could also affect the price that some investors are willing to pay for our common stock.
60
Our executive officers, directors and principal stockholders, if they choose to act together, have the ability to control all matters submitted to stockholders for approval and may take actions that may not be in the best interests of our other stockholders.
Our executive officers, directors and stockholders who hold more than 5% of our outstanding common stock beneficially own, in the aggregate, shares representing approximately 47% of our outstanding capital stock. As a result, if these stockholders were to act together, they would be able to control all matters submitted to our stockholders for approval, as well as our management and affairs. For example, these persons, if they act together, would control the election of directors and decisions on any merger, consolidation or sale of all or substantially all of our assets. This concentration of voting power could delay or prevent an acquisition of our company on terms that other stockholders may desire or result in management of our company with which our public stockholders disagree.
If securities or industry analysts do not publish research, or publish inaccurate or unfavorable research, about our business, the price of our common stock and our trading volume could decline.
The trading market for our common stock depends in part on the research and reports that securities or industry analysts publish about us or our business. If too few securities or industry analysts commence or maintain coverage of our company, the trading price for our common stock would likely be negatively affected. If one or more of the analysts who cover us downgrade our common stock or publish inaccurate or unfavorable research about our business, the price of our common stock would likely decline. If one or more of these analysts cease coverage of our company or fail to publish reports on us regularly, demand for our common stock could decrease, which might cause the price of our shares and trading volume to decline.
Claims for indemnification by our directors and officers may reduce our available funds to satisfy successful third-party claims against us and may reduce the amount of money available to us.
Our amended and restated certificate of incorporation and amended and restated bylaws provide that we will indemnify our directors and officers, in each case to the fullest extent permitted by Delaware law.
In addition, as permitted by Section 145 of the Delaware General Corporation Law, our amended and restated bylaws and our indemnification agreements with our directors and officers provide that:
|
· |
We will indemnify our directors and officers for serving us in those capacities or for serving other business enterprises at our request, to the fullest extent permitted by Delaware law. Delaware law provides that a corporation may indemnify such person if such person acted in good faith and in a manner such person reasonably believed to be in or not opposed to the best interests of the corporation and, with respect to any criminal proceeding, had no reasonable cause to believe such person's conduct was unlawful. |
|
· |
We may, in our discretion, indemnify employees and agents in those circumstances where indemnification is permitted by applicable law. |
|
· |
We are required to advance expenses, as incurred, to our directors and officers in connection with defending a proceeding, except that such directors or officers shall undertake to repay such advances if it is ultimately determined that such person is not entitled to indemnification. |
|
· |
We will not be obligated pursuant to our amended and restated bylaws to indemnify a person with respect to proceedings initiated by that person against us or our other indemnitees, except with respect to proceedings authorized by our board of directors or brought to enforce a right to indemnification. |
|
· |
The rights conferred in our amended and restated bylaws are not exclusive, and we are authorized to enter into indemnification agreements with our directors, officers, employees and agents and to obtain insurance to indemnify such persons. |
|
· |
We may not retroactively amend our bylaw provisions to reduce our indemnification obligations to directors, officers, employees and agents. |
61
Item 1B. Unresolved Staff Comments.
None
We lease approximately 52,000 square feet of office and assembly space at our corporate headquarters in Minneapolis, Minnesota under a lease that expires in July 2021. We lease an additional 31,200 square feet of office and warehouse space at a second leased facility in Minneapolis, Minnesota under a lease that expires in November 2021. We believe that our existing facilities are adequate to meet our business requirements for the near term and that additional space will be available on commercially reasonable terms, if required.
From time to time, we may be subject to various claims and legal proceedings arising in the ordinary course of business. We are not currently a party to any legal proceedings that, in the opinion of our management, are likely to have a material adverse effect on our business. Regardless of outcome, litigation can have an adverse impact on us because of defense and settlement costs, diversion of management resources, and other factors.
Item 4. Mine Safety Disclosures.
Not applicable.
Item 5. Market For Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Price Information
Our common stock has been listed on the NASDAQ Global Market under the symbol "TCMD" since July 28, 2016. Prior to that date, there was no public trading market for our common stock. Our common stock priced at $10.00 per share in our initial public offering on July 27, 2016. The following table sets forth for the periods indicated the high and low intra-day sale prices per share of our common stock as reported on the NASDAQ Global Market:
|
|
|
High |
|
|
Low |
|
||
|
Year Ended December 31, 2016 |
|
|
|
|
|
|
|
|
|
Third quarter from and after July 28, 2016 |
|
$ |
22.29 |
|
|
$ |
10.00 |
|
|
Fourth quarter |
|
$ |
20.25 |
|
|
$ |
14.70 |
|
Holders
As of February 10, 2017, there were approximately 168 holders of record of our common stock. The actual number of holders of common stock is greater than this number of record holders and includes stockholders who are beneficial owners, but whose shares are held in street name by brokers and nominees. The number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
Dividends
We have never declared or paid any cash dividends on our common stock. We currently intend to retain our future earnings, if any, to finance the operation and expansion of our business. We do not expect to pay cash dividends on our common stock in the foreseeable future. Payment of future cash dividends, if any, will be at the discretion of our board of directors after taking into account various factors, including our financial condition, operating results, current and anticipated cash needs, outstanding indebtedness and plans for expansion and restrictions imposed by lenders, if any.
62
Recent Sales of Unregistered Securities
In August 2016, upon the closing of our initial public offering, (i) all shares of our then-outstanding convertible preferred stock were automatically converted into an aggregate of 5,924,453 shares of common stock, (ii) we issued 2,354,323 additional shares of common stock that our Series A and Series B preferred stockholders were entitled to receive in connection with the initial public offering, and (iii) we issued 956,842 shares of common stock to pay accrued dividends on our Series B convertible preferred stock. These shares of common stock were issued pursuant to an exemption from the registration requirements of the Securities Act provided by Section 3(a)(9) or Section 4(a)(2) of the Securities Act.
Issuer Purchases of Equity Securities
None.
Equity Compensation Plan Information
The information required by this Item concerning equity compensation plans is incorporated herein by reference from Part III, Item 12 of this report.
Use of Proceeds from Registered Securities
On August 2, 2016, we issued and sold 4,120,000 shares of our common stock in the initial public offering at a public offering price of $10.00 per share, for aggregate gross proceeds of $41.2 million. All of the shares issued and sold in the initial public offering were registered under the Securities Act pursuant to a Registration Statement on Form S-1 (File No. 333-209115), which was declared effective by the SEC on July 27, 2016. Piper Jaffray & Co. and William Blair & Company, L.L.C. acted as joint book-running managers for the offering. The offering terminated on August 2, 2016.
The net offering proceeds to us, after deducting underwriting discounts of approximately $2.9 million and offering expenses paid by us totaling approximately $2.9 million, were approximately $35.4 million. No offering expenses were paid directly or indirectly to any of our directors or officers (or their associates) or persons owning 10.0% or more of any class of our equity securities or to any other affiliates. We also paid $8.2 million in cumulative accrued dividends to our Series A preferred stockholders from the issuance proceeds.
At December 31, 2016, the net proceeds from our initial public offering were held in a diversified portfolio of bank deposits, government money market funds, government securities (U.S. Treasury and U.S. government agency securities), and high-grade short-term corporate bonds. All investments were in compliance with our Investment Policy and are highly liquid, with liquidity and capital preservation being the primary investment objectives. There has been no material change in our planned uses of the net proceeds from those described in the Prospectus dated July 27, 2016.
Stock Performance Graph
The graph below compares the cumulative total stockholder return on our common stock with the cumulative total stockholder returns on the NASDAQ Composite Index, Russell 2000 Index and S&P Healthcare Equipment Select Industry Index for the period indicated. The graph assumes that $100 was invested on July 28, 2016 in our common stock and each of the indices and that all dividends, if any, were reinvested. No cash dividends have been declared on
63
our common stock. Stockholder returns over the indicated period should not be considered indicative of future stockholder returns.
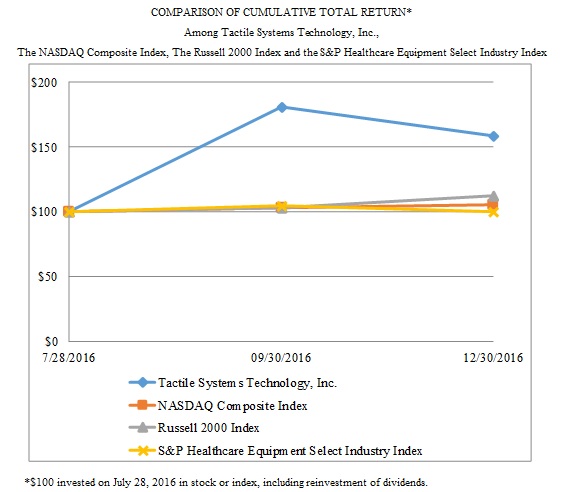
|
|
|
|
Jul. 28, 2016 |
|
|
Sep. 30, 2016 |
|
|
Dec. 31, 2016 |
|
|
Tactile Systems Technology, Inc |
|
$ |
100 |
|
$ |
181 |
|
$ |
159 |
|
|
NASDAQ Composite Index |
|
|
100 |
|
|
103 |
|
|
105 |
|
|
Russell 2000 Index |
|
|
100 |
|
|
103 |
|
|
112 |
|
|
S&P Healthcare Equipment Select Industry Index |
|
|
100 |
|
|
104 |
|
|
100 |
|
Item 6. Selected Financial Data.
The following tables set forth our selected historical consolidated financial data as of and for the periods indicated. The selected consolidated statements of operations data for the years ended December 31, 2016, 2015 and 2014, and the selected consolidated balance sheet data as of December 31, 2016, 2015 and 2014, have been derived from our audited consolidated financial statements included elsewhere in this report. Our historical results are not indicative of the results to be expected in the future. The following financial data should be read in conjunction with, and are qualified in their
64
entirety by reference to, “Management's Discussion and Analysis of Financial Condition and Results of Operations” and our consolidated financial statements and the related notes included elsewhere in this report.
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands, except share and per share data) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Consolidated Statements of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
Revenues, net |
|
$ |
84,542 |
|
$ |
62,872 |
|
$ |
47,736 |
|
|
Cost of goods sold |
|
|
22,940 |
|
|
16,908 |
|
|
12,715 |
|
|
Gross profit |
|
|
61,602 |
|
|
45,964 |
|
|
35,021 |
|
|
Operating expenses |
|
|
|
|
|
|
|
|
|
|
|
Sales and marketing |
|
|
33,794 |
|
|
24,485 |
|
|
18,154 |
|
|
Research and development |
|
|
4,476 |
|
|
4,312 |
|
|
2,843 |
|
|
Reimbursement, general and administrative |
|
|
19,060 |
|
|
13,716 |
|
|
10,225 |
|
|
Total operating expenses |
|
|
57,330 |
|
|
42,513 |
|
|
31,222 |
|
|
Income from operations |
|
|
4,272 |
|
|
3,451 |
|
|
3,799 |
|
|
Other income (expense) |
|
|
38 |
|
|
(194) |
|
|
(4) |
|
|
Income before income taxes |
|
|
4,310 |
|
|
3,257 |
|
|
3,795 |
|
|
Income tax expense |
|
|
1,431 |
|
|
1,864 |
|
|
1,725 |
|
|
Net income |
|
|
2,879 |
|
|
1,393 |
|
|
2,070 |
|
|
Convertible preferred stock dividends |
|
|
1,247 |
|
|
1,845 |
|
|
1,761 |
|
|
Allocation of undistributed earnings to preferred stockholders |
|
|
— |
|
|
— |
|
|
216 |
|
|
Net income (loss) attributable to common stockholders |
|
$ |
1,632 |
|
$ |
(452) |
|
$ |
93 |
|
|
Net income (loss) per common share attributable to common stockholders (1) |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
$ |
0.18 |
|
$ |
(0.15) |
|
$ |
0.04 |
|
|
Diluted |
|
$ |
0.15 |
|
$ |
(0.15) |
|
$ |
0.02 |
|
|
Weighted-average common shares used to compute net income (loss) per common share attributable to common stockholders |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
|
8,913,042 |
|
|
2,929,438 |
|
|
2,491,108 |
|
|
Diluted |
|
|
10,758,684 |
|
|
2,929,438 |
|
|
3,797,688 |
|
|
|
|
As of December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Consolidated Balance Sheet Data: |
|
|
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
30,701 |
|
$ |
7,060 |
|
$ |
5,416 |
|
|
Working capital |
|
|
50,440 |
|
|
19,858 |
|
|
18,927 |
|
|
Total assets |
|
|
73,935 |
|
|
36,973 |
|
|
31,494 |
|
|
Total debt |
|
|
— |
|
|
— |
|
|
13 |
|
|
Convertible preferred stock |
|
|
— |
|
|
32,927 |
|
|
21,082 |
|
|
Accumulated deficit |
|
|
(2,773) |
|
|
(5,652) |
|
|
(6,872) |
|
|
Total stockholders' equity (deficit) |
|
|
59,639 |
|
|
(5,649) |
|
|
(6,427) |
|
|
(1) |
Net income (loss) per common share attributable to common stockholders is calculated under the two-class method, as our convertible preferred stock participated in our undistributed earnings prior to our initial public offering. The two-class method requires earnings for the period to be allocated based upon their respective rights to receive distributed and undistributed earnings. No adjustment is made during periods with a net loss, as the holders of the convertible preferred stock have no obligation to fund losses. |
65
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and the accompanying notes thereto included elsewhere in this report.
Overview
We are a medical technology company that develops and provides innovative medical devices for the treatment of chronic diseases at home. We focus on advancing the standard of care in treating chronic diseases in the home setting to improve patient outcomes and quality of life and help control rising healthcare expenditures. We possess a unique, scalable platform to deliver at-home healthcare solutions throughout the United States. This evolving home care delivery model is recognized by policy-makers and payers as a key for controlling rising healthcare expenditures. Our initial area of therapeutic focus is vascular disease, with a goal of advancing the standard of care in treating lymphedema and chronic venous insufficiency. Our mission is to help people with chronic diseases live better and care for themselves at home. Our solutions deliver cost-effective, clinically proven, long-term treatment for these chronic diseases.
Our proprietary products are the Flexitouch System, the Entré System and the ACTitouch System. A predecessor to our Flexitouch System received 510(k) clearance from the FDA in July 2002, and we introduced the system to address the many limitations of self-administered home-based manual lymphatic drainage therapy. We began selling our more advanced Flexitouch System after receiving 510(k) clearance from the FDA in October 2006. In September 2016, we received 510(k) clearance from the FDA for the Flexitouch System in treating lymphedema in the head and neck. Historically, we derived substantially all of our revenues from our Flexitouch System. For each of 2016 and 2015, sales of our Flexitouch System represented 87% of our revenues.
In September 2012, we acquired our second proprietary product, the ACTitouch System. The system received 510(k) clearance from the FDA in June 2013, and we began selling the product in September 2013 to address the many limitations of non-removable multilayered bandages that are worn by patients suffering from venous leg ulcers. We also introduced our Entré System in the United States in February 2013. The Entré System is sold to patients who need a more basic pump or who do not yet qualify for insurance reimbursement for an advanced compression device such as our Flexitouch System. For each of 2016 and 2015, sales of our ACTitouch and Entré Systems combined represented 13% of our revenues.
To support the growth of our business, we invest heavily in our commercial infrastructure, consisting of our direct sales force, home training resources, reimbursement capabilities and clinical expertise. We market our products in the United States using a direct-to-patient and -provider model. Our direct sales force has grown from three representatives in March 2005 to a team of over 125 people as of December 31, 2016. This model allows us to directly approach patients and clinicians, whereby we disintermediate the traditional durable medical equipment channel, allowing us to capture both the manufacturer and distributor margins. We also utilize over 400 licensed, independent healthcare practitioners as home trainers who educate patients on the proper use of our systems. We invest substantial resources in our reimbursement operations group of over 70 people that focuses on verifying case-by-case benefits, obtaining prior authorization, billing and collecting payments from payers and providing customer support services. Our payer relations group of 30 people is responsible for developing relationships with payer decision-makers to educate them on our product efficacy, develop overall payer coverage policies and reimbursement criteria, manage Medicare patient claims and contracts with payers, and serve as an advocacy liaison between patients, clinicians and payers throughout the appeals process. We also have a clinical team, consisting of a scientific advisory board, in-house therapists and nurses, and a medical director (part-time), that serves as a resource to clinicians and patients and guides our development of clinical evidence in support of our products.
Our patients are reimbursed by government and private payers for the purchase of our products pursuant to established rates with each payer. We rely on third-party contract manufacturers for the sourcing of parts, the assembly of our controllers and the manufacturing of the garments used with our systems. We conduct final assembly of the garments used with our Flexitouch System, perform quality assurance, and ship our products from our facility in Minneapolis, Minnesota.
66
For the year ended December 31, 2016, we generated revenues of $84.5 million and had net income of $2.9 million, compared to revenues of $62.9 million and net income of $1.4 million for the year ended December 31, 2015 and revenues of $47.7 million and net income of $2.1 million for the year ended December 31, 2014.
Our primary sources of capital to date have been from operating income and private placements of our capital stock, as well as our initial public offering, which closed on August 2, 2016. We operate in one segment for financial reporting purposes.
Components of our Results of Operations
Revenues
We derive our revenues from the sale of our Flexitouch, ACTitouch and Entré systems to patients in the United States. Revenue growth has been driven by increased clinician, patient and payer awareness of lymphedema and the clinical efficacy of our Flexitouch System, and the launch of our ACTitouch and Entré systems in 2013. We have expanded our direct sales force that helps us drive and support our revenue growth and intend to continue this expansion. However, any reversal in these recent trends could have a negative impact on our future revenues.
Our revenues have fluctuated, and we expect our revenues to continue to fluctuate, from quarter to quarter due to a variety of factors. For instance, our fourth quarter is consistently our strongest quarter of the year. See Item 7. “Management’s Discussion and Analysis of Financial Condition and Results of Operations – Seasonality” for a further discussion of factors contributing to our seasonality. Further, our revenues are impacted by fluctuations in the mix of products being sold during each period and changes in the mix of our payers and contract pricing.
We sell our products directly to patients, who are referred to us by physicians, therapists or nurses. We bill payers, such as private insurers, Medicare, the Veterans Administration or Medicaid, on behalf of our patients and bill patients directly for their cost-sharing amounts, including any portion of an unsatisfied deductible and any copayments or co-insurance. Approximately 15% of our revenues in 2016 came from the Veterans Administration, comparable to 2015. However, due to pricing changes, our Flexitouch System sales volume with the Veterans Administration increased from 2015 to 2016. Approximately 12% of our revenues in 2016 and 13% of our revenues in 2015 came from Medicare patients. Changes to the level of Medicare coverage for our products, including the 2015 LCD modification to the criteria for Medicare coverage, could reduce the number of Medicare patients who have access to our products. Our products currently are not subject to the competitive bidding process for supplying covered items to Medicare recipients.
We expect our revenues to continue to increase in the future as a result of increased awareness of our solutions, expansion of our direct sales force, enhanced marketing and customer support efforts, continued focus on developing clinical and economic outcome data, expanded third-party reimbursement and introduction of our solutions outside the United States. We also anticipate increasing pricing pressure from commercial insurance payers, which will result in increasing downward pressure on our revenue growth rate.
Cost of Goods Sold and Gross Margin
Cost of goods sold consists primarily of component costs, direct labor, overhead costs, product warranties, provisions for slow-moving and obsolete inventory and delivery costs for items sold. A significant portion of our cost of goods sold consists of manufacturing overhead costs. These overhead costs include the cost of quality assurance, material procurement, inventory control, facilities, equipment and operations supervision and management. We expect overhead costs as a percentage of revenues to decrease as a result of expected increases in production volume and yields. Cost of goods sold also includes depreciation expense for product tooling, production equipment and shipping costs. We expect cost of goods sold to increase in absolute dollars primarily if, and to the extent, our revenues grow.
We provide a warranty on our device controllers ranging from one to two years for commercially insured patients and five years for Medicare patients, as required by CMS. We also provide replacement garments to our patients for up to five years after purchase. We establish a reserve for warranty claims based on historical warranty repair and replacement costs incurred. Provisions for warranty obligations, which are included in cost of goods sold, are recorded at the time of shipment.
67
We calculate gross margin as gross profit divided by revenues. Our gross margin has been and will continue to be affected by a variety of factors, including product and payer mix, production volumes, manufacturing costs and cost-reduction strategies. We expect our gross margin to decrease slightly over the near term as we experience pricing pressure from third-party payers. We continue to work to reduce product manufacturing cost through enhanced product design efforts as well as supply chain initiatives in an effort to offset anticipated price erosion. Our gross margin will likely fluctuate from quarter to quarter.
Sales and Marketing Expenses
Our sales and marketing expenses support our direct-to-patient and -provider model. These expenses consist primarily of personnel-related expenses, including salaries, bonuses, commissions and benefits for employees. They also include expenses for patient home training, social media and advertising, informational kits, public relations and other promotional and marketing activities, field sales travel and entertainment expenses, trade shows and conferences, stock-based compensation, as well as customer service. We expect sales and marketing expenses to continue to increase in absolute dollars as we expand our commercial infrastructure to drive and support our planned revenue growth. To the extent our revenues grow, we expect sales and marketing expenses to decrease as a percentage of revenues over time.
Research and Development Expenses
Research and development, or R&D, expenses consist primarily of personnel-related expenses, third-party product development costs, laboratory supplies, consulting fees and related costs, clinical research expenses, expenses related to clinical and regulatory affairs, patent amortization costs, stock-based compensation and patent legal fees, including defense costs and testing costs for new product launches. Clinical research expenses include clinical trial management and monitoring, payment to clinical investigators, consulting fees, data management, stock-based compensation, travel expenses and the cost of manufacturing products for clinical trials. We have made substantial investments in R&D since our inception. Our R&D efforts have focused primarily on activities designed to enhance our technologies and to support development and commercialization of new and existing products. We expect R&D expenses to increase in absolute dollars for the foreseeable future as we continue to develop, enhance and commercialize new products and expand clinical trial efforts. We expect R&D expenses as a percentage of our revenues to vary over time depending on the level and timing of initiating new product development efforts, as well as our clinical trial activities.
Reimbursement, General and Administrative Expenses
Reimbursement, general and administrative expenses consist primarily of compensation, including salaries, bonuses and benefits for employees in our patient services and advocacy, billing and collections, case management, payer relations and governmental affairs and reimbursement operations departments, as well as finance, human resources and administration, information technology, business development and general management functions, and facilities costs. Our experienced payer relations and reimbursement operations departments of over 100 people focus on verifying case-by-case benefits, obtaining prior authorization, billing and collecting payments from payers and providing customer support services. Payer relations and reimbursement operations department expenses also include consulting, travel to payer case manager seminars, professional development and training and certification expenses. General and administrative expenses also include professional services, such as legal, consulting and accounting services, stock-based compensation, travel expenses and insurance costs. We expect to continue to incur additional legal, accounting, insurance and other professional service fees associated with being a public company, which may increase further when we are no longer able to rely on the "emerging growth company" exemption we are afforded under the JOBS Act.
Other Income (Expense), Net
Other income (expense), net consists primarily of interest expense related to our notes payable and interest income driven by the interest accruing on cash and cash equivalents and past due insurance balances. We do not accrue interest on a majority of past due customer accounts receivable balances.
Income Tax Expense (Benefit)
Our income tax expense (benefit) consists primarily of deferred income taxes resulting from temporary differences between the reporting of amounts for financial statement purposes and income tax purposes.
68
Critical Accounting Policies and Significant Estimates
Our discussion and analysis of our financial condition and results of operations are based upon our financial statements which have been prepared in accordance with generally accepted accounting principles in the United States, or GAAP. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets and liabilities and related disclosure of contingent assets and liabilities, revenues and expenses at the date of the financial statements. Generally, we base our estimates on historical experience and on various other assumptions in accordance with GAAP that we believe to be reasonable under the circumstances. Actual results may differ from these estimates and such differences could be material to our financial position and results of operations.
While our significant accounting policies are more fully described in Note 1 to our consolidated financial statements included elsewhere in this report, we believe the following discussion addresses our most critical accounting policies, which are those that are most important to the portrayal of our financial condition and results of operations and require our most difficult, subjective and complex judgments.
Revenue Recognition
We recognize revenue when persuasive evidence of a sale arrangement exists, delivery of product has occurred through the transfer of title and risks of reward of ownership, the selling price is fixed or determinable and collectability is reasonably assured.
We distribute our products directly to patients. For any of our products sold to patients covered by private payers, such as commercial insurance companies, we recognize revenues from such sales upon shipment of our products. A product is not shipped until we have received a prescription from a physician for our products and, as applicable, receipt of prior authorization from payers. At shipment, we invoice the payer for the total product price and we recognize revenue as a percentage of the invoice based on the policies and payment history of the applicable payer, net of estimated uncollectible patient copayments. The payment history of the applicable payer is drawn from our actual payment experience over the past year. Any differences in payments received as compared to our estimates are recognized in the period in which we actually receive payment for the product. Over time, we adjust the ultimate collection estimates to reflect these differences. After the insurance payer has remitted payment, we separately invoice the patient for their portion of the payment obligation, such as copayments and deductibles.
For our products sold to Medicare patients, we recognize revenues from such sales upon shipment of our products, which can occur only after we have received a prescription from a physician and all applicable Medicare documentation is obtained. For Flexitouch System sales, we estimate the revenue on each shipment to a Medicare patient as a percentage of the total invoice based on collection history. While we have contracted rates with Medicare, to the extent any claims for reimbursement are denied, we will recognize any necessary adjustments in the period for which the adjustment is made or can be estimated.
Accounts Receivable
The majority of our accounts receivable and revenues are from commercial insurance payers and government payers, such as Medicare, the Veterans Administration and Medicaid.
Accounts receivable are carried net of allowances for estimated non-receipt of patient co-payment and deductible obligations and allowances for uncollectible accounts. We believe all accounts receivable in excess of the allowance are fully collectible. We do not accrue interest on a majority of the past due accounts receivable. We determine when accounts become past due on a customer by customer basis. If accounts receivables in excess of the provided allowance are determined uncollectible, the allowance for uncollectible accounts is adjusted as appropriate in the quarter that determination is made, and accounts receivable are written off after all collection efforts have failed. A portion of our claims to Medicare are initially denied, and enter the appeals process, where many are ultimately reviewed by an Administrative Law Judge. After final adjudication of all claims, approximately 90% of the claims submitted are approved (this is on a number of claims, not a dollars claimed, basis across all our products). The appeal process can be lengthy, lasting more than a year in most cases. Accordingly, we classify a portion of our Medicare accounts receivable as non-current based on our experience with Medicare collections.
69
As an alternative to individual appeals, Medicare may seek to settle a number of outstanding appeals at one time through a settlement conference. On September 3, 2015, we entered into a settlement agreement with the Centers for Medicare and Medicaid Services, or CMS, for 247 claims, representing approximately $1.5 million of original claims based on the Medicare allowable rates, in which we had submitted a request for an Administrative Law Judge hearing in 2013. The settlement entitled us to receive a payment of approximately $0.9 million. We received this full amount during the fourth quarter of 2015. The settlement resulted in a reduction in the fourth quarter of 2015 of $0.8 million in our accounts receivable for shipment of products to patients covered by Medicare. The settlement was part of a pilot program, facilitated by the Office of Medicare Hearings and Appeals, to address a backlog of overdue claims awaiting Administrative Law Judge adjudication. Because the settlement was part of a pilot program, we cannot predict whether we will be able to conclude future settlements with Medicare or achieve settlements on similar terms. Any future settlement of claims for amounts less than the corresponding amounts receivable could result in a write off.
Stock-Based Compensation
We account for stock-based compensation awards at the fair value on the date of grant expensed over the applicable vesting period. The fair value of options on the grant date is estimated using the Black-Scholes option-pricing model. We recognize the fair value of each award as an expense on a straight-line basis over the requisite service period, which is generally the vesting period of the equity grant.
The Black-Scholes option-pricing model requires the input of highly subjective assumptions, including the expected term of the option, the expected volatility of the price of our common stock, the risk-free interest rate and the expected dividend yield. These estimates involve inherent uncertainties and the significant application of management's judgment. If factors change and different assumptions are used, our stock-based compensation expense could be materially different in the future. We determined weighted-average valuation assumptions as follows:
|
· |
Expected term. We use the "simplified method" to determine the expected term of the stock option. |
|
· |
Expected volatility. Our expected volatility is derived using the average historical volatility of public companies of similar size and industry because we believe the expected volatility will approximate historical volatility, due to the fact that we had no trading history prior to our initial public offering. |
|
· |
Risk-free interest rate. The risk free interest rate is based on the yields of U.S. Treasury securities with maturities similar to the expected term of the options for each option group. |
|
· |
Expected dividend yield. We have never declared or paid any cash dividends on our common stock and do not presently plan to pay cash dividends on our common stock in the foreseeable future. Consequently, we use an expected dividend yield of zero. |
The following table sets forth the estimated weighted-average fair values of our stock options granted in the years ended December 31, 2016, 2015 and 2014, and the assumptions on which they were based:
|
|
|
|
Year Ended |
|
||||||
|
|
|
|
December 31, |
|
||||||
|
|
|
|
2016 |
|
|
2015 |
|
|
2014 |
|
|
Expected term |
|
|
6 years |
|
|
6 years |
|
|
6 years |
|
|
Expected volatility |
|
|
43% |
|
|
60% |
|
|
60% |
|
|
Risk-free interest rate |
|
|
1% |
|
|
2% |
|
|
2% |
|
|
Expected dividend yield |
|
|
0% |
|
|
0% |
|
|
0% |
|
|
Weighted-average fair value on the date of grant |
|
$ |
4.43 |
|
$ |
1.91 |
|
$ |
0.47 |
|
If in the future we determine that another method is more reasonable, or if another method for calculating these input assumptions is prescribed by authoritative guidance, and, therefore, should be used to estimate volatility or expected life, the fair value calculated for our stock options could change significantly. Higher volatility and longer expected lives result in an increase to stock-based compensation expense determined at the date of grant. Stock-based compensation expense affects our cost of goods sold, sales and marketing expenses, research and development expenses, and reimbursement, general and administrative expenses.
70
We estimate our forfeiture rate based on an analysis of our actual forfeitures and will continue to evaluate the appropriateness of the forfeiture rate based on actual forfeiture experience, analysis of employee turnover behavior and other factors. Quarterly changes in the estimated forfeiture rate can have a significant effect on reported stock-based compensation expense, as the cumulative effect of adjusting the rate for all expense amortization is recognized in the period the forfeiture estimate is changed. If a revised forfeiture rate is higher than the previously estimated forfeiture rate, an adjustment is made that will result in a decrease to the stock-based compensation expense recognized in the consolidated financial statements. If a revised forfeiture rate is lower than the previously estimated forfeiture rate, an adjustment is made that will result in an increase to the stock-based compensation expense recognized in the consolidated financial statements. The effect of forfeiture adjustments was insignificant for the years ended December 31, 2016, 2015 and 2014. We will continue to use significant judgment in evaluating the expected term, volatility and forfeiture rate related to our stock-based compensation.
Prior to our initial public offering, the fair value of the common stock underlying our equity compensation awards was historically determined by our board of directors, with input from management and third-party valuations on an annual basis. We believe that our board of directors has the relevant experience and expertise to determine the fair value of our common stock. However, the fair value of our common stock may vary significantly in the future and from the estimates previously made. Given the absence of a public trading market for our common stock, our board of directors exercised reasonable judgment and considered numerous objective and subjective factors to determine the best estimate of the fair value of our common stock using methodologies, approaches and assumptions consistent with the American Institute of Certified Public Accountants, or AICPA, Audit and Accounting Practice Aid Series: Valuation of Privately Held Company Equity Securities Issued as Compensation, known as the AICPA Accounting and Valuation Guide. The following factors, among others, were considered:
|
· |
our results of operations, history of losses and other financial metrics; |
|
· |
our capital resources and financial condition; |
|
· |
the contemporaneous valuations of our common stock by an unrelated third-party valuation firm; |
|
· |
the prices of our convertible redeemable preferred stock sold to outside investors in arms-length transactions; |
|
· |
the rights, preferences and privileges of our preferred stock relative to those of our common stock; |
|
· |
the rights of freestanding warrants and other similar instruments related to our securities that are redeemable; |
|
· |
the hiring of key personnel; |
|
· |
the introduction of new products; |
|
· |
the fact that the common stock underlying the option grants involves illiquid securities in a private company; |
|
· |
the risks inherent in the development and expansion of our products and services; and |
|
· |
the likelihood of achieving a liquidity event, such as an initial public offering or sale of our company given prevailing market conditions. |
In valuing our common stock, since January 1, 2014, our board of directors determined the equity value of our business using the market approach valuation method and the income approach valuation method to determine the enterprise value. For 2014, our board of directors exclusively used the market approach valuation method. For 2015, these two approaches were initially weighted equally. During 2015, we received a summary valuation from the lead underwriters for our initial public offering. In the second half of 2015 we reviewed our fair value determinations for 2015, effectively modifying our valuation approach for 2015 to include this summary valuation as a third factor in determining fair value, along with the other approaches previously considered. Our board of directors then considered the factors set forth above in reaching its determination of the fair value.
71
Since our initial public offering, our board of directors determines the fair value of our common stock based on the closing market price on The Nasdaq Global Market on the date of grant.
Results of Operations
Comparison of the Years Ended December 31, 2016 and 2015
The following table presents our results of operations for the periods indicated.
|
|
|
Year Ended December 31, |
|
|
|
|
|
|
||||||||
|
(In thousands, except percentages) |
|
2016 |
|
2015 |
|
Change |
|
|||||||||
|
|
|
|
|
% of revenue |
|
|
|
% of revenue |
|
$ |
|
% |
|
|||
|
Condensed Consolidated Statement of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenues |
|
$ |
84,542 |
|
100 |
% |
$ |
62,872 |
|
100 |
% |
$ |
21,670 |
|
34 |
% |
|
Cost of goods sold |
|
|
22,940 |
|
27 |
|
|
16,908 |
|
27 |
|
|
6,032 |
|
36 |
|
|
Gross profit |
|
|
61,602 |
|
73 |
|
|
45,964 |
|
73 |
|
|
15,638 |
|
34 |
|
|
Operating expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sales and marketing |
|
|
33,794 |
|
40 |
|
|
24,485 |
|
39 |
|
|
9,309 |
|
38 |
|
|
Research and development |
|
|
4,476 |
|
5 |
|
|
4,312 |
|
7 |
|
|
164 |
|
4 |
|
|
Reimbursement, general and administrative |
|
|
19,060 |
|
23 |
|
|
13,716 |
|
22 |
|
|
5,344 |
|
39 |
|
|
Total operating expenses |
|
|
57,330 |
|
68 |
|
|
42,513 |
|
68 |
|
|
14,817 |
|
35 |
|
|
Income from operations |
|
|
4,272 |
|
5 |
|
|
3,451 |
|
5 |
|
|
821 |
|
24 |
|
|
Other income (expense) |
|
|
38 |
|
- |
|
|
(194) |
|
- |
|
|
232 |
|
(120) |
|
|
Income before income taxes |
|
|
4,310 |
|
5 |
|
|
3,257 |
|
5 |
|
|
1,053 |
|
32 |
|
|
Income tax expense |
|
|
1,431 |
|
2 |
|
|
1,864 |
|
3 |
|
|
(433) |
|
(23) |
|
|
Net income |
|
$ |
2,879 |
|
3 |
|
$ |
1,393 |
|
2 |
|
$ |
1,486 |
|
107 |
|
Revenues
Revenues increased $21.7 million, or 34%, to $84.5 million in the year ended December 31, 2016, compared to $62.9 million in the year ended December 31, 2015. The growth in revenues was primarily attributable to an increase of approximately $18.7 million, or 34%, in sales of our Flexitouch System in the year ended December 31, 2016. The increase in Flexitouch sales was driven primarily by expansion of our sales force, increased physician and patient awareness of the lymphedema condition, and increased contractual coverage with national and regional insurance payers. The growth in revenues in 2016 was also attributable to an increase of approximately $3.0 million, or 37%, in sales of the ACTitouch and Entré Systems, compared to 2015.
The following table summarizes our revenues by product for the years ended December 31, 2016 and December 31, 2015, both in dollars and percentage of total revenues:
|
|
|
Year Ended December 31, |
|
|
|
||||
|
(In thousands, except percentages) |
|
2016 |
|
2015 |
|
% Change |
|
||
|
Revenues |
|
|
|
|
|
|
|
|
|
|
Flexitouch System |
|
$ |
73,413 |
|
$ |
54,748 |
|
34 |
% |
|
ACTitouch/Entré Systems |
|
|
11,129 |
|
|
8,124 |
|
37 |
% |
|
Total |
|
$ |
84,542 |
|
$ |
62,872 |
|
34 |
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Percentage of total revenues |
|
|
|
|
|
|
|
|
|
|
Flexitouch System |
|
|
87 |
% |
|
87 |
% |
|
|
|
ACTitouch/Entré Systems |
|
|
13 |
% |
|
13 |
% |
|
|
|
Total |
|
|
100 |
% |
|
100 |
% |
|
|
72
Cost of Goods Sold and Gross Margin
Cost of goods sold increased $ 6.0 million, or 36%, to $22.9 million during the year ended December 31, 2016, compared to $16.9 million during the year ended December 31, 2015. The increase in cost of goods sold was primarily attributable to an increase in the number of systems sold. Gross margin for each of the years ended December 31, 2016 and 2015 was 73%.
Sales and Marketing Expenses
Sales and marketing expenses increased $9.3 million, or 38%, to $33.8 million during the year ended December 31, 2016, compared to $24.5 million during the year ended December 31, 2015. The increase was primarily attributable to $6.1 million of increased compensation and related expenses as a result of increased sales and marketing headcount and increased commission and other variable selling expenses associated with favorable sales performance. In addition, other sales and marketing expenses increased $3.3 million primarily due to increased field sales meetings, travel and entertainment, consulting and field sales training expenses.
Research and Development Expenses
R&D expenses increased $0.2 million, or 4%, to $4.5 million during the year ended December 31, 2016, compared to $4.3 million during the year ended December 31, 2015. The increase in R&D expenses was primarily attributable to increased clinical study and product development costs, including those related to the development of our new head and neck Flexitouch System.
Reimbursement, General and Administrative Expenses
Reimbursement, general and administrative expenses increased $5.3 million, or 39%, to $19.1 million during the year ended December 31, 2016, compared to $13.7 million during the year ended December 31, 2015. The increase in reimbursement, general and administrative expenses was primarily attributable to personnel-related expenses as a result of increased headcount in our patient services, contracting, case management, billing and collections, advocacy, reimbursement and administrative teams, as well as increased stock-based compensation expense and incremental expenses associated with public company compliance requirements incurred in the third and fourth quarters of 2016, subsequent to our initial public offering.
Other Income (Expense), Net
Other income, net was $38,000 for the year ended December 31, 2016 compared to other expense of $0.2 million for the year ended December 31, 2015. The other expense in 2015 was primarily due to interest expense recognized on the value of future minimum royalty payments.
Income Tax Expense
Income tax expense was $1.4 million on earnings before tax of $4.3 million for the year ended December 31, 2016, resulting in an effective income tax rate of 33%. This compares to income tax expense of $1.9 million on earnings before tax of $3.3 million for the year ended December 31, 2015, resulting in an effective income tax rate of 57%. The decrease in the effective tax rate in fiscal year 2016 was due to the adoption of Accounting Standards Update (ASU) 2016-09, “Improvements to Employee Share-Based Payment Accounting,” which allows for the recognition of excess tax benefits in earnings.
73
Comparison of the Years Ended December 31, 2015 and 2014
The following table presents our results of operations for the periods indicated.
|
|
|
Year Ended December 31, |
|
|
|
|
|
|
||||||||
|
(In thousands, except percentages) |
|
2015 |
|
2014 |
|
Change |
|
|||||||||
|
|
|
|
|
% of revenue |
|
|
|
% of revenue |
|
$ |
|
% |
|
|||
|
Condensed Consolidated Statement of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenues |
|
$ |
62,872 |
|
100 |
% |
$ |
47,736 |
|
100 |
% |
$ |
15,136 |
|
32 |
% |
|
Cost of goods sold |
|
|
16,908 |
|
27 |
|
|
12,715 |
|
27 |
|
|
4,193 |
|
33 |
|
|
Gross profit |
|
|
45,964 |
|
73 |
|
|
35,021 |
|
73 |
|
|
10,943 |
|
31 |
|
|
Operating expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sales and marketing |
|
|
24,485 |
|
39 |
|
|
18,154 |
|
38 |
|
|
6,331 |
|
35 |
|
|
Research and development |
|
|
4,312 |
|
7 |
|
|
2,843 |
|
6 |
|
|
1,469 |
|
52 |
|
|
Reimbursement, general and administrative |
|
|
13,716 |
|
22 |
|
|
10,225 |
|
21 |
|
|
3,491 |
|
34 |
|
|
Total operating expenses |
|
|
42,513 |
|
68 |
|
|
31,222 |
|
65 |
|
|
11,291 |
|
36 |
|
|
Income from operations |
|
|
3,451 |
|
5 |
|
|
3,799 |
|
8 |
|
|
(348) |
|
(9) |
|
|
Other income (expense) |
|
|
(194) |
|
- |
|
|
(4) |
|
- |
|
|
(190) |
|
N.M. |
|
|
Income before income taxes |
|
|
3,257 |
|
5 |
|
|
3,795 |
|
8 |
|
|
(538) |
|
(14) |
|
|
Income tax expense |
|
|
1,864 |
|
3 |
|
|
1,725 |
|
4 |
|
|
139 |
|
8 |
|
|
Net income |
|
$ |
1,393 |
|
2 |
|
$ |
2,070 |
|
4 |
|
$ |
(677) |
|
(33) |
|
N.M. – Not meaningful
Revenues
Revenues increased $15.1 million, or 32%, to $62.9 million during the year ended December 31, 2015, compared to $47.7 million during the year ended December 31, 2014. The growth in revenues was primarily attributable to an increase of approximately $11.0 million, or 25%, in sales of our Flexitouch System and an increase of approximately $4.1 million, or 103%, in sales of our ACTitouch and Entré Systems. These increases in sales were driven by expansion of our sales force and increased physician and patient awareness.
The following table summarizes our revenues by product for the years ended December 31, 2015 and December 31, 2014, both in dollars and percentage of total revenues:
|
|
|
Year Ended December 31, |
|
|
|
||||
|
(In thousands, except percentages) |
|
2015 |
|
2014 |
|
% Change |
|
||
|
Revenues |
|
|
|
|
|
|
|
|
|
|
Flexitouch System |
|
$ |
54,748 |
|
$ |
43,738 |
|
25 |
% |
|
ACTitouch/Entré Systems |
|
|
8,124 |
|
|
3,998 |
|
103 |
% |
|
Total |
|
$ |
62,872 |
|
$ |
47,736 |
|
32 |
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Percentage of total revenues |
|
|
|
|
|
|
|
|
|
|
Flexitouch System |
|
|
87 |
% |
|
92 |
% |
|
|
|
ACTitouch/Entré Systems |
|
|
13 |
% |
|
8 |
% |
|
|
|
Total |
|
|
100 |
% |
|
100 |
% |
|
|
Cost of Goods Sold and Gross Margin
Cost of goods sold increased $4.2 million, or 33%, to $16.9 million during the year ended December 31, 2015, compared to $12.7 million during the year ended December 31, 2014. The increase in cost of goods sold was primarily attributable to an increase in the number of systems sold, partially offset by reduced material and labor costs for our products associated with better sourcing and increased volumes.
74
Gross margin for the year ended December 31, 2015 of 73.1% was essentially flat compared to gross margin of 73.4% for the year ended December 31, 2014.
Sales and Marketing Expenses
Sales and marketing expenses increased $6.3 million, or 35%, to $24.5 million during the year ended December 31, 2015, compared to $18.2 million during the year ended December 31, 2014. The increase was primarily attributable to a $4.7 million increase in personnel-related compensation expenses as a result of increased sales and marketing headcount. In addition, other sales and marketing expenses increased $1.6 million due to increased field sales travel expenses, trade show and conference expenses and patient training costs.
Research and Development Expenses
R&D expenses increased $1.5 million, or 52%, to $4.3 million during the year ended December 31, 2015, compared to $2.8 million during the year ended December 31, 2014. The increase in R&D expenses was primarily attributable to increases in product development and consulting costs of $1.2 million and clinical study costs of $0.2 million.
Reimbursement, General and Administrative Expenses
Reimbursement, general and administrative expenses increased $3.5 million, or 34%, to $13.7 million during the year ended December 31, 2015, compared to $10.2 million during the year ended December 31, 2014. The increase in reimbursement, general and administrative expenses was primarily attributable to a $1.7 million increase in personnel-related expenses as a result of increased headcount on our patient services, contracting, case management, billing and collections, advocacy, reimbursement and administrative teams, an increase of $1.0 million in professional, legal, accounting and information technology costs, and higher facility costs of $0.2 million for new office space, utilities, property taxes and maintenance.
Other Expense, Net
Other expense increased to $0.2 million during the year ended December 31, 2015 primarily due to interest expense recognized on the value of future minimum royalty payments. Other expense was less than $5,000 during the year ended December 31, 2014.
Seasonality
Our business may be affected by seasonality. In the first quarter of each year, when most patients have started a new insurance year and have not paid their annual insurance deductibles, we experience substantially reduced demand for our products. We typically experience higher sales in the third and fourth quarters as a result of patients having paid their annual insurance deductibles in full, thereby reducing their out-of-pocket costs for our products, or because patients often spend the remaining balances in their flexible-spending accounts.
Liquidity and Capital Resources
Overview
As of December 31, 2016, we had cash and cash equivalents of $30.7 million, marketable securities of $11.0 million and an accumulated deficit of $2.8 million, compared to cash and cash equivalents of $7.1 million and an accumulated deficit of $5.7 million as of December 31, 2015. Our primary sources of capital to date have been from operating income and private placements of our capital stock, as well as our initial public offering, which closed on August 2, 2016.
Cash Flows
At December 31, 2016, our principal sources of liquidity were cash and cash equivalents of $30.7 million, marketable securities of $11.0 million and net accounts receivable of $15.0 million.
75
The following table summarizes our cash flows for the periods indicated:
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Net cash provided by (used in): |
|
|
|
|
|
|
|
|
|
|
|
Operating activities |
|
$ |
7,033 |
|
$ |
2,399 |
|
$ |
(991) |
|
|
Investing activities |
|
|
(11,844) |
|
|
(615) |
|
|
(353) |
|
|
Financing activities |
|
|
28,452 |
|
|
(140) |
|
|
221 |
|
|
Net increase (decrease) in cash and cash equivalents |
|
$ |
23,641 |
|
$ |
1,644 |
|
$ |
(1,123) |
|
Net Cash Provided by (Used in) Operating Activities
Net cash provided by operating activities during the year ended December 31, 2016 was $7.0 million, resulting from net income of $2.9 million, non-cash expenses of $2.6 million and a net decrease in operating assets and liabilities of $1.5 million. The cash provided by operations was primarily due to our increased revenue volume, as well as increased accounts payable, accrued compensation and accrued expenses. The non-cash expense items primarily consisted of $1.9 million of stock-based compensation and $0.8 million of depreciation and amortization of equipment, leasehold improvements and patents of 0.8 million. These non-cash impacts were partially offset by an increase in deferred taxes of $0.6 million.
Net cash provided by operating activities during the year ended December 31, 2015 was $2.4 million, resulting from net income of $1.4 million, non-cash expenses of $1.1 million, a decrease of $0.9 million in deferred income tax assets, and a $0.1 million provision for doubtful accounts. The cash provided by operations was primarily due to the ongoing commercialization of our products, as well as increased accounts payable, accrued compensation and accrued expenses, partially offset by increased accounts receivable, inventory, prepaid expenses and other non-current assets. The non-cash expense items primarily consisted of depreciation and amortization of equipment and leasehold improvements and patents and stock-based compensation. Our net operating assets and liabilities increased $2.1 million. The increase in our net operating assets and liabilities was primarily due to increased accounts receivable, inventory, and other non-current assets.
Net cash used in operating activities during the year ended December 31, 2014 was $1.0 million, consisting primarily of our net income of $2.1 million, a decrease of $1.6 million in deferred income tax assets, a $0.5 million provision for doubtful accounts and non-cash expenses of $0.8 million. The cash used in operations was primarily due to the ongoing commercialization of our products, as well as increased accounts receivable and inventory and decreased accrued compensation, offset by increased accounts payable. The non-cash expense items primarily consisted of depreciation and amortization of equipment, leasehold improvements and patents and stock-based compensation. Our net operating assets and liabilities increased $6.0 million. The increase in our net operating assets and liabilities was primarily due to increased accounts receivable and inventory.
Net Cash Used in Investing Activities
Net cash used in investing activities during the year ended December 31, 2016, was $11.8 million, consisting primarily of purchases of marketable securities of $11.0 million and $0.8 million in purchases of product tooling and computer and manufacturing equipment. Net cash used in investing activities during the year ended December 31, 2015, was $0.6 million, consisting primarily of purchases of product tooling and computer and manufacturing equipment. Net cash used in investing activities during the year ended December 31, 2014 was $0.4 million, consisting of purchases of product tooling and computer and manufacturing equipment.
Net Cash Provided by (Used in) Financing Activities
Until August 2016, when we closed on our initial public offering, we historically funded our operations through the issuance of capital stock. Net cash provided by financing activities during the year ended December 31, 2016, was $28.5 million, which was primarily generated by gross proceeds of $41.2 million from the initial public offering, partially offset by $8.2 million in payments of accrued dividends on preferred stock and $4.8 million of underwriting costs and expenses associated with the initial public offering. We also paid $1.0 million of expenses associated with the initial public offering during the fourth quarter of 2015.
76
Net cash used in financing activities during the year ended December 31, 2015, was $0.1 million, consisting primarily of fees paid in connection with our initial public offering, partially offset by proceeds from exercises of stock options and warrants. Net cash provided by financing activities during the year ended December 31, 2014 was $0.2 million, consisting of proceeds from exercise of stock options, partially offset by minimal repayments of borrowings.
Credit Line
We have a bank credit line with borrowing availability of $2.0 million. As of December 31, 2016, we did not have any outstanding borrowings under our credit line. Our credit line bears interest based on the prime rate, which was 3.75% as of December 31, 2016. On May 11, 2016, we extended our credit agreement until May 11, 2017. Our credit line is secured by substantially all our assets, including property and equipment, accounts receivable and inventory. Our credit line contains customary conditions as to borrowing, events of default and covenants, including covenants that restrict our ability to dispose of assets, merge with or acquire other entities, and incur indebtedness or encumbrances.
Adequacy of Capital Resources
Our future capital requirements may vary significantly from those now planned and will depend on many factors, including:
|
· |
sales and marketing resources needed to further penetrate our market; |
|
· |
expansion of our operations; |
|
· |
response of competitors to our solutions and applications; |
|
· |
costs associated with clinical research activities; |
|
· |
costs to develop and implement new products, if any; and |
|
· |
use of capital for acquisitions, if any. |
Historically, we have experienced increases in our expenditures consistent with the growth in our operations and personnel, and we anticipate that our expenditures will continue to increase as we expand our business.
We believe our cash, cash equivalents, marketable securities, and cash flows from operations will be sufficient to meet our working capital and capital expenditure requirements for at least the next twelve months. We expect increased expenses in connection with meeting our obligations as a public company.
Inflation and changing prices did not have a material effect on our business during the year ended December 31, 2016, and we do not expect that inflation or changing prices will materially affect our business in the foreseeable future.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined under the applicable regulations.
77
Contractual and Commercial Commitments Summary
Our contractual obligations and commercial commitments as of December 31, 2016 are summarized below:
|
|
|
Payments Due By Period |
|
|||||||||||||
|
|
|
|
|
Less Than |
|
|
|
|
|
More Than |
|
|||||
|
(In thousands) |
|
Total |
|
1 Year |
|
1-3 Years |
|
3-5 Years |
|
5 Years |
|
|||||
|
Operating lease obligations (1) |
|
$ |
3,790 |
|
$ |
1,036 |
|
$ |
1,476 |
|
$ |
1,278 |
|
$ |
— |
|
|
Future product royalties (2) |
|
|
67 |
|
|
67 |
|
|
— |
|
|
— |
|
|
— |
|
|
Purchase commitments (3) |
|
|
12,690 |
|
|
10,964 |
|
|
1,726 |
|
|
— |
|
|
— |
|
|
Total |
|
$ |
16,547 |
|
$ |
12,067 |
|
$ |
3,202 |
|
$ |
1,278 |
|
$ |
— |
|
|
(1) |
We currently lease approximately 52,000 square feet of office and assembly space at our corporate headquarters in Minneapolis, Minnesota under a lease that expires in July 2021 and an additional 31,200 square feet of office and warehouse space at a second leased facility in Minneapolis, Minnesota under a lease that expires in November 2021. We also entered into a fleet vehicle program for certain members of our field sales organization in 2016. At December 31, 2016, we had 39 leased vehicles under this program. |
|
(2) |
We are required to make quarterly royalty payments to a third party for our ACTitouch System revenue through August 2023. The payments are equal to 9% of our quarterly revenues attributable to our ACTitouch System through August of 2017, and for the remaining period, equal to 6% of our quarterly revenues attributable to our ACTitouch System. In any year that these revenues exceed $40.0 million, we are required to pay 7% on revenues over $40.0 million and 6% on revenues $40.0 million and under. |
|
(3) |
Represents purchase orders issued in February 2016 and January 2017 to vendors for inventory expected to be received in 2017 and 2018. |
Recent Accounting Pronouncements
Refer to Note 1, “Summary of Significant Accounting Policies,” of our consolidated financial statements contained in this report for a description of recently issued accounting pronouncements that are applicable to our business.
JOBS Act
As an "emerging growth company" under the JOBS Act, we can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption and, as a result, our financial statements may not be comparable to the financial statements of issuers who are required to comply with the effective dates for new or revised accounting standards that are applicable to public companies. Section 107 of the JOBS Act provides that we can elect to opt out of the extended transition period at any time, which election is irrevocable.
We are in the process of evaluating the benefits of relying on other exemptions and reduced reporting requirements under the JOBS Act. Subject to certain conditions, as an emerging growth company, we intend to rely on certain of these exemptions, including without limitation from providing an auditor's attestation report on our system of internal controls over financial reporting pursuant to Section 404(b) of the Sarbanes-Oxley Act of 2002 and from complying with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor's report providing additional information about the audit and the financial statements, known as the auditor discussion and analysis. We will remain an emerging growth company until the earliest of: (a) the last day of the fiscal year in which we have total annual gross revenues of $1 billion or more; (b) the last day of 2021; (c) the date on which we have issued more than $1 billion in nonconvertible debt during the previous three years; and (d) the date on which we are deemed to be a large accelerated filer under the rules of the SEC.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
We are exposed to market risk from changes in interest rates, primarily related to our investment activities. The principal objectives of our investment activities are to preserve principal, provide liquidity and maximize income consistent with minimizing risk of material loss. The recorded carrying amounts of cash and cash equivalents approximate fair value due to their short maturities. Our interest income is sensitive to changes in the general level of interest rates in the United States, particularly since our investments are generally short-term in nature. Due to the nature
78
of our short-term investments, an immediate 100 basis point change in interest rates would not have a material effect on the fair market value of our portfolio.
Additionally, the interest rates for our credit line have both fixed and variable components. If overall interest rates had increased by 100 basis points during the periods presented, our interest expense would not have been materially affected.
Inflation
Inflationary factors, such as increases in our cost of goods sold, sales and marketing expenses and reimbursement expenses, may adversely affect our operating results. Although we do not believe that inflation has had a material impact on our financial condition or results of operations to date, a high rate of inflation in the future may have an adverse effect on our ability to maintain and increase our gross margin, and on our sales and marketing and reimbursement expenses as a percentage of our revenues if the selling prices of our products do not increase as much or more than these increased costs.
Credit Risk
As of December 31, 2016, our cash, cash equivalents and marketable securities were maintained with two financial institutions in the United States. As of December 31, 2015, our cash and cash equivalents were maintained with one financial institution in the United States. We have reviewed the financial statements of these institutions and believe they have sufficient assets and liquidity to conduct their operations in the ordinary course of business with little or no credit risk to us.
Our accounts receivable primarily relate to revenues from the sale of our products to patients in the United States. For the years ended December 31, 2016 and 2015, our accounts receivable were $17.8 million and $16.2 million, respectively. We had accounts receivable from three insurance companies representing approximately 27%, 16% and 8% of accounts receivable as of December 31, 2016, and we had accounts receivable from three insurance companies representing approximately 26%, 18% and 7% of accounts receivable as of December 31, 2015.
Foreign Currency Risk
Our business is conducted in U.S. dollars and foreign transactions have been minimal. As we begin building relationships to commercialize our products internationally, our results of operations and cash flows may become increasingly subject to changes in foreign exchange rates.
79
Item 8. Financial Statements and Supplementary Data.
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Stockholders
Tactile Systems Technology, Inc.
We have audited the accompanying consolidated balance sheets of Tactile Systems Technology, Inc. and its subsidiary (the “Company”) as of December 31, 2016 and 2015, and the related consolidated statements of operations, comprehensive income, stockholders’ equity (deficit), and cash flows for each of the three years in the period ended December 31, 2016. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. We were not engaged to perform an audit of the Company’s internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Tactile Systems Technology, Inc. and subsidiary as of December 31, 2016 and 2015, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2016 in conformity with accounting principles generally accepted in the United States of America.
/s/ Grant Thornton LLP
Minneapolis, Minnesota
February 27, 2017
80
Tactile Systems Technology, Inc.
Consolidated Balance Sheets
|
|
|
As of |
|
||||
|
(In thousands, except share and per share data) |
|
2016 |
|
2015 |
|
||
|
Assets |
|
|
|
|
|
|
|
|
Current assets |
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
30,701 |
|
$ |
7,060 |
|
|
Marketable securities |
|
|
10,994 |
|
|
— |
|
|
Accounts receivable, net |
|
|
15,003 |
|
|
14,151 |
|
|
Inventories |
|
|
6,554 |
|
|
5,781 |
|
|
Deferred income taxes |
|
|
— |
|
|
1,766 |
|
|
Prepaid expenses |
|
|
981 |
|
|
602 |
|
|
Total current assets |
|
|
64,233 |
|
|
29,360 |
|
|
Property and equipment, net |
|
|
1,563 |
|
|
1,346 |
|
|
Other assets |
|
|
|
|
|
|
|
|
Patent costs, net |
|
|
2,394 |
|
|
2,489 |
|
|
Medicare accounts receivable, long-term |
|
|
2,823 |
|
|
2,039 |
|
|
Deferred income taxes |
|
|
2,785 |
|
|
402 |
|
|
Other non-current assets |
|
|
137 |
|
|
1,337 |
|
|
Total other assets |
|
|
8,139 |
|
|
6,267 |
|
|
Total assets |
|
$ |
73,935 |
|
$ |
36,973 |
|
|
|
|
|
|
|
|
|
|
|
Liabilities and Stockholders’ Equity (Deficit) |
|
|
|
|
|
|
|
|
Current liabilities |
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
5,018 |
|
$ |
3,336 |
|
|
Accrued payroll and related taxes |
|
|
6,692 |
|
|
3,355 |
|
|
Accrued expenses |
|
|
1,193 |
|
|
916 |
|
|
Future product royalties |
|
|
67 |
|
|
991 |
|
|
Income taxes payable |
|
|
823 |
|
|
904 |
|
|
Total current liabilities |
|
|
13,793 |
|
|
9,502 |
|
|
Long-term liabilities |
|
|
|
|
|
|
|
|
Deferred compensation |
|
|
— |
|
|
193 |
|
|
Accrued warranty reserve, long-term |
|
|
503 |
|
|
— |
|
|
Total liabilities |
|
|
14,296 |
|
|
9,695 |
|
|
Convertible preferred stock |
|
|
|
|
|
|
|
|
Series B convertible preferred stock; $0.001 par value, no shares authorized, issued or outstanding as of December 31, 2016 and 5,319,066 shares authorized and 2,733,468 shares issued and outstanding as of December 31, 2015 |
|
|
— |
|
|
12,599 |
|
|
Series A convertible preferred stock; $0.001 par value, no shares authorized, issued or outstanding as of December 31, 2016 and 3,112,153 shares authorized and 3,108,589 shares issued and 3,061,488 shares outstanding as of December 31, 2015 |
|
|
— |
|
|
20,328 |
|
|
Stockholders’ equity (deficit) |
|
|
|
|
|
|
|
|
Preferred stock; $0.001 par value, 50,000,000 shares authorized and no shares issued and outstanding as of December 31, 2016 |
|
|
— |
|
|
— |
|
|
Common stock; $0.001 par value, 300,000,000 shares authorized, 16,833,737 shares issued and outstanding as of December 31, 2016, and 14,184,175 shares authorized and 3,222,902 shares issued and outstanding as of December 31, 2015 |
|
|
17 |
|
|
3 |
|
|
Additional paid-in capital |
|
|
62,406 |
|
|
— |
|
|
Accumulated deficit |
|
|
(2,773) |
|
|
(5,652) |
|
|
Accumulated other comprehensive loss |
|
|
(11) |
|
|
— |
|
|
Total stockholders’ equity (deficit) |
|
|
59,639 |
|
|
(5,649) |
|
|
Total liabilities and stockholders’ equity (deficit) |
|
$ |
73,935 |
|
$ |
36,973 |
|
See accompanying notes to the consolidated financial statements.
81
Tactile Systems Technology, Inc.
Consolidated Statements of Operations
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands, except share and per share data) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Revenues, net |
|
$ |
84,542 |
|
$ |
62,872 |
|
$ |
47,736 |
|
|
Cost of goods sold |
|
|
22,940 |
|
|
16,908 |
|
|
12,715 |
|
|
Gross profit |
|
|
61,602 |
|
|
45,964 |
|
|
35,021 |
|
|
Operating expenses |
|
|
|
|
|
|
|
|
|
|
|
Sales and marketing |
|
|
33,794 |
|
|
24,485 |
|
|
18,154 |
|
|
Research and development |
|
|
4,476 |
|
|
4,312 |
|
|
2,843 |
|
|
Reimbursement, general and administrative |
|
|
19,060 |
|
|
13,716 |
|
|
10,225 |
|
|
Total operating expenses |
|
|
57,330 |
|
|
42,513 |
|
|
31,222 |
|
|
Income from operations |
|
|
4,272 |
|
|
3,451 |
|
|
3,799 |
|
|
Other income (expense) |
|
|
38 |
|
|
(194) |
|
|
(4) |
|
|
Income before income taxes |
|
|
4,310 |
|
|
3,257 |
|
|
3,795 |
|
|
Income tax expense |
|
|
1,431 |
|
|
1,864 |
|
|
1,725 |
|
|
Net income |
|
|
2,879 |
|
|
1,393 |
|
|
2,070 |
|
|
Convertible preferred stock dividends |
|
|
1,247 |
|
|
1,845 |
|
|
1,761 |
|
|
Allocation of undistributed earnings to preferred stockholders |
|
|
— |
|
|
— |
|
|
216 |
|
|
Net income (loss) attributable to common stockholders |
|
$ |
1,632 |
|
$ |
(452) |
|
$ |
93 |
|
|
Net income (loss) per common share attributable to common stockholders |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
$ |
0.18 |
|
$ |
(0.15) |
|
$ |
0.04 |
|
|
Diluted |
|
$ |
0.15 |
|
$ |
(0.15) |
|
$ |
0.02 |
|
|
Weighted-average common shares used to compute net income (loss) per common share attributable to common stockholders |
|
|
|
|
|
|
|
|
|
|
|
Basic |
|
|
8,913,042 |
|
|
2,929,438 |
|
|
2,491,108 |
|
|
Diluted |
|
|
10,758,684 |
|
|
2,929,438 |
|
|
3,797,688 |
|
See accompanying notes to the consolidated financial statements.
82
Tactile Systems Technology, Inc.
Consolidated Statements of Comprehensive Income
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Net income |
|
$ |
2,879 |
|
$ |
1,393 |
|
$ |
2,070 |
|
|
Other comprehensive (loss): |
|
|
|
|
|
|
|
|
|
|
|
Unrealized (losses) on available-for-sale securities |
|
|
(17) |
|
|
— |
|
|
— |
|
|
Income tax related to items of other comprehensive (loss) |
|
|
6 |
|
|
— |
|
|
— |
|
|
Total other comprehensive loss |
|
|
(11) |
|
|
— |
|
|
— |
|
|
Comprehensive income |
|
$ |
2,868 |
|
$ |
1,393 |
|
$ |
2,070 |
|
See accompanying notes to the consolidated financial statements.
83
Tactile Systems Technology, Inc.
Consolidated Statements of Stockholders’ Equity (Deficit)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
|
Series B Preferred Stock |
|
Series A Preferred Stock |
|
|
Common Stock |
|
Additional |
|
|
|
Other |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Paid-In |
|
Accumulated |
|
Comprehensive |
|
|
|
|
|||
|
(In thousands, except share data) |
|
Shares |
|
Amount |
|
Shares |
|
Amount |
|
|
Shares |
|
Par Value |
|
Capital |
|
Deficit |
|
Loss |
|
Total |
|
|||||||
|
Balances, December 31, 2013 |
|
2,733,468 |
|
$ |
11,278 |
|
3,061,488 |
|
$ |
18,043 |
|
|
2,226,716 |
|
$ |
2 |
|
$ |
1,826 |
|
$ |
(8,942) |
|
$ |
— |
|
$ |
(7,114) |
|
|
Stock-based compensation |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
148 |
|
|
— |
|
|
— |
|
|
148 |
|
|
Exercise of common stock options and warrants |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
399,903 |
|
|
1 |
|
|
229 |
|
|
— |
|
|
— |
|
|
230 |
|
|
Preferred stock dividends |
|
— |
|
|
616 |
|
— |
|
|
1,145 |
|
|
— |
|
|
— |
|
|
(1,761) |
|
|
— |
|
|
— |
|
|
(1,761) |
|
|
Comprehensive income for the period |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
2,070 |
|
|
— |
|
|
2,070 |
|
|
Balances, December 31, 2014 |
|
2,733,468 |
|
|
11,894 |
|
3,061,488 |
|
|
19,188 |
|
|
2,626,619 |
|
|
3 |
|
|
442 |
|
|
(6,872) |
|
|
— |
|
|
(6,427) |
|
|
Stock-based compensation |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
316 |
|
|
— |
|
|
— |
|
|
316 |
|
|
Exercise of common stock options and warrants |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
596,283 |
|
|
— |
|
|
914 |
|
|
— |
|
|
— |
|
|
914 |
|
|
Preferred stock dividends |
|
— |
|
|
705 |
|
— |
|
|
1,140 |
|
|
— |
|
|
— |
|
|
(1,672) |
|
|
(173) |
|
|
— |
|
|
(1,845) |
|
|
Comprehensive income for the period |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
1,393 |
|
|
— |
|
|
1,393 |
|
|
Balances, December 31, 2015 |
|
2,733,468 |
|
|
12,599 |
|
3,061,488 |
|
|
20,328 |
|
|
3,222,902 |
|
|
3 |
|
|
— |
|
|
(5,652) |
|
|
— |
|
|
(5,649) |
|
|
Stock-based compensation |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
2,082 |
|
|
— |
|
|
— |
|
|
2,082 |
|
|
Exercise of common stock options and warrants |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
255,217 |
|
|
1 |
|
|
235 |
|
|
— |
|
|
— |
|
|
236 |
|
|
Preferred stock dividend |
|
— |
|
|
436 |
|
— |
|
|
811 |
|
|
— |
|
|
— |
|
|
(1,247) |
|
|
— |
|
|
— |
|
|
(1,247) |
|
|
Sale of common stock from initial public offering, net of offering expenses |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
4,120,000 |
|
|
4 |
|
|
35,378 |
|
|
— |
|
|
— |
|
|
35,382 |
|
|
Preferred stock dividends paid in cash |
|
— |
|
|
— |
|
— |
|
|
(8,207) |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Common stock issued in lieu of series B preferred stock dividend |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
956,842 |
|
|
1 |
|
|
(1) |
|
|
— |
|
|
— |
|
|
— |
|
|
Conversion of series B preferred stock to common stock |
|
(2,733,468) |
|
|
(13,035) |
|
— |
|
|
— |
|
|
2,733,468 |
|
|
3 |
|
|
13,032 |
|
|
— |
|
|
— |
|
|
13,035 |
|
|
Conversion of series A preferred stock to common stock |
|
— |
|
|
— |
|
(3,061,488) |
|
|
(12,932) |
|
|
3,190,985 |
|
|
3 |
|
|
12,929 |
|
|
— |
|
|
— |
|
|
12,932 |
|
|
Common stock issued for series A & B preferred stock liquidation preference |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
2,354,323 |
|
|
2 |
|
|
(2) |
|
|
— |
|
|
— |
|
|
— |
|
|
Comprehensive income for the period |
|
— |
|
|
— |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
2,879 |
|
|
(11) |
|
|
2,868 |
|
|
Balances, December 31, 2016 |
|
— |
|
$ |
— |
|
— |
|
$ |
— |
|
|
16,833,737 |
|
$ |
17 |
|
$ |
62,406 |
|
$ |
(2,773) |
|
$ |
(11) |
|
$ |
59,639 |
|
See accompanying notes to the consolidated financial statements.
84
Tactile Systems Technology, Inc.
Consolidated Statements of Cash Flows
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Cash flows from operating activities |
|
|
|
|
|
|
|
|
|
|
|
Net income |
|
$ |
2,879 |
|
$ |
1,393 |
|
$ |
2,070 |
|
|
Adjustments to reconcile net income to net cash provided by (used in) operating activities: |
|
|
|
|
|
|
|
|
|
|
|
Depreciation and amortization |
|
|
799 |
|
|
827 |
|
|
706 |
|
|
Deferred income taxes |
|
|
(611) |
|
|
852 |
|
|
1,558 |
|
|
Stock-based compensation expense |
|
|
1,889 |
|
|
316 |
|
|
148 |
|
|
Deferred compensation |
|
|
— |
|
|
(6) |
|
|
— |
|
|
Change in allowance for doubtful accounts |
|
|
568 |
|
|
100 |
|
|
500 |
|
|
Changes in assets and liabilities |
|
|
|
|
|
|
|
|
|
|
|
Accounts receivable |
|
|
(1,420) |
|
|
(509) |
|
|
(4,671) |
|
|
Inventories |
|
|
(773) |
|
|
(2,260) |
|
|
(608) |
|
|
Prepaid expenses and other non-current assets |
|
|
(407) |
|
|
(452) |
|
|
(142) |
|
|
Medicare accounts receivable – long-term |
|
|
(784) |
|
|
(737) |
|
|
(381) |
|
|
Accounts payable |
|
|
1,737 |
|
|
829 |
|
|
547 |
|
|
Accrued payroll and related taxes |
|
|
3,337 |
|
|
1,352 |
|
|
(601) |
|
|
Accrued expenses and income taxes payable |
|
|
743 |
|
|
1,073 |
|
|
44 |
|
|
Future product royalties |
|
|
(924) |
|
|
(379) |
|
|
(161) |
|
|
Net cash provided by (used in) operating activities |
|
|
7,033 |
|
|
2,399 |
|
|
(991) |
|
|
Cash flows from investing activities |
|
|
|
|
|
|
|
|
|
|
|
Purchases of marketable securities |
|
|
(11,011) |
|
|
— |
|
|
— |
|
|
Purchases of property and equipment |
|
|
(775) |
|
|
(592) |
|
|
(353) |
|
|
Patent costs |
|
|
(58) |
|
|
(23) |
|
|
— |
|
|
Net cash used in investing activities |
|
|
(11,844) |
|
|
(615) |
|
|
(353) |
|
|
Cash flows from financing activities |
|
|
|
|
|
|
|
|
|
|
|
Payments on notes payable |
|
|
— |
|
|
(13) |
|
|
(9) |
|
|
Proceeds from exercise of common stock options and warrants |
|
|
236 |
|
|
914 |
|
|
230 |
|
|
Dividends paid on preferred stock |
|
|
(8,207) |
|
|
— |
|
|
— |
|
|
Fees paid for IPO |
|
|
(4,777) |
|
|
(1,041) |
|
|
— |
|
|
Proceeds from IPO |
|
|
41,200 |
|
|
— |
|
|
— |
|
|
Net cash provided by (used in) financing activities |
|
|
28,452 |
|
|
(140) |
|
|
221 |
|
|
Net change in cash and cash equivalents |
|
|
23,641 |
|
|
1,644 |
|
|
(1,123) |
|
|
Cash and cash equivalents – beginning of period |
|
|
7,060 |
|
|
5,416 |
|
|
6,539 |
|
|
Cash and cash equivalents – end of period |
|
$ |
30,701 |
|
$ |
7,060 |
|
$ |
5,416 |
|
|
Supplemental cash flow disclosure |
|
|
|
|
|
|
|
|
|
|
|
Cash paid for interest |
|
$ |
— |
|
$ |
1 |
|
$ |
1 |
|
|
Cash paid for taxes |
|
$ |
2,158 |
|
$ |
240 |
|
$ |
238 |
|
|
Non-cash investing activities |
|
|
|
|
|
|
|
|
|
|
|
Acquisition of assets included in accounts payable |
|
$ |
174 |
|
$ |
— |
|
$ |
— |
|
See accompanying notes to the consolidated financial statements.
85
Tactile Systems Technology, Inc.
Notes to the Consolidated Financial Statements
Note 1. Summary of Significant Accounting Policies
Nature of Operations
Tactile Systems Technology, Inc. (“we,” “us,” and “our”) is the sole manufacturer and distributor of the Flexitouch and Entré Systems, medical devices that help control symptoms of lymphedema, a chronic and progressive medical condition, and the ACTitouch System, a medical device used to treat venous leg ulcers and chronic venous insufficiency. We provide our products for use in the home and sell them through vascular, wound and lymphedema clinics throughout the United States. We do business as “Tactile Medical.”
Basis of Presentation
Our accompanying consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States (“GAAP”) and pursuant to the rules and regulations of the SEC. The results for the year ended December 31, 2016 are not necessarily indicative of results to be expected for any future year.
Our business is affected by seasonality. In the first quarter of each year, when most patients have started a new insurance year and have not paid their annual deductibles, we experience substantially reduced demand for our products. We typically experience higher sales in the third and fourth quarters as a result of patients having paid their annual insurance deductibles in full, thereby reducing their out-of-pocket costs for our products, or because patients often spend the remaining balances in their flexible spending accounts.
We were originally incorporated in Minnesota under the name Tactile Systems Technology, Inc. on January 30, 1995. During 2006, we established a merger corporation and subsequently, on July 21, 2006, merged with and into this merger corporation. The resulting corporation assumed the name Tactile Systems Technology, Inc. The purpose of this merger was to reincorporate the Company in Delaware, increase the number of authorized common shares to 8.9 million and assign a par value of $0.001 to our common stock. In September 2013, we began doing business as “Tactile Medical.”
In connection with preparing for our initial public offering, our board of directors and stockholders approved a one-for-2.820044 reverse stock split of our capital stock. The reverse stock split became effective in June 2016. All share and per share amounts in these consolidated financial statements and notes thereto have been retroactively adjusted for all periods presented to give effect to this reverse stock split, including reclassifying an amount equal to the reduction in par value of common stock to additional paid-in capital.
On August 2, 2016 we closed the initial public offering of our common stock, which resulted in the sale of 4,120,000 shares of our common stock at a public offering price of $10.00 per share. We received net proceeds from the initial public offering of approximately $35.4 million, after deducting underwriting discounts and approximately $2.9 million of transaction expenses. In connection with the closing of the initial public offering, all of our outstanding redeemable convertible preferred stock automatically converted to common stock on August 2, 2016. At August 2, 2016, we did not have any redeemable convertible preferred stock issued or outstanding. The significant increase in common stock outstanding in connection with the initial public offering impacts the year-over-year comparability of our earnings per share calculations.
Basis of Consolidation
The consolidated financial statements include the accounts of Tactile Systems Technology, Inc. and its wholly owned subsidiary, Swelling Solutions, Inc., after elimination of intercompany accounts and transactions.
JOBS Act Accounting Election
As an emerging growth company under the Jumpstart Our Business Startups (“JOBS”) Act, we are eligible to take advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not emerging growth companies. We have elected to take advantage of the extended transition period for
86
adopting new or revised accounting standards that have different effective dates for public and private companies until such time as those standards apply to private companies.
Estimates
The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
Cash and Cash Equivalents
Cash and cash equivalents consist of all cash on hand, deposits and funds invested in available for sale securities with original maturities of three months or less at the time of purchase. At December 31, 2016, our cash was held primarily in checking and money market accounts. At December 31, 2015, our cash was held primarily in checking accounts.
Accounts Receivable
The majority of our accounts receivable and revenues are from commercial insurance payers and government payers, such as Medicare, the Veterans Administration and Medicaid.
Accounts receivable are carried net of allowances for estimated non-receipt of patient co-payment and deductible obligations and allowances for uncollectible accounts. The allowance for estimated non-receipt of co-payment reimbursements and for uncollectible accounts was $2.6 million and $2.0 million as of December 31, 2016 and 2015, respectively. We believe all accounts receivable in excess of the allowance are fully collectible. We do not accrue interest on a majority of the past due accounts receivable. We determine when accounts become past due on a customer by customer basis. If accounts receivables in excess of the provided allowance are determined uncollectible, the allowance for uncollectible accounts is adjusted as appropriate in the quarter that determination is made, and accounts receivable are written off after all collection efforts have failed. A portion of our claims to Medicare are initially denied, and enter the appeals process, where many are ultimately reviewed by an Administrative Law Judge. After final adjudication of all claims, approximately 90% of the claims submitted are approved (this is on a number of claims, not a dollars claimed, basis across all our products). The appeals process can be lengthy, lasting more than a year in most cases. Accordingly, we classify a portion of our Medicare accounts receivable as non-current based on our experience with Medicare collections.
We had accounts receivable from three insurance companies representing approximately 27%, 16% and 8% of accounts receivable as of December 31, 2016. We had accounts receivable from three insurance companies representing approximately 26%, 18% and 7% of accounts receivable as of December 31, 2015. Revenues from these insurance companies accounted for 28%, 12%, and 12% of our total revenues for the year ended December 31, 2016 and 28%, 13% and 11% for the year ended December 31, 2015.
Accounts receivable include amounts due from Medicare totaling $3.8 million and $4.3 million relating to Flexitouch System sales to patients as of December 31, 2016 and 2015, respectively, that are waiting insurance approval. We estimate the portion of these accounts receivable for which we expect to receive authorization and payment based on our reimbursement history from Medicare.
We classified $2.8 million and $2.0 million of this receivable as of December 31, 2016 and 2015, respectively, as non-current as we do not expect these claims will be paid within the next twelve months due to delays with the Administrative Law Judge appeal process.
On September 3, 2015, we entered into a settlement agreement with the Centers for Medicare and Medicaid Services for 247 claims, representing approximately $1.5 million of original claims based on the Medicare allowable rates, in which we had submitted a request for an Administrative Law Judge hearing in 2013. The settlement entitled us to receive a payment of approximately $0.9 million. We received this full amount during the fourth quarter of 2015. The settlement resulted in a reduction in the fourth quarter of 2015 of $0.8 million in accounts receivable for shipment of products to patients covered by Medicare. The settlement was part of a pilot program, facilitated by the Office of
87
Medicare Hearings and Appeals, to address a backlog of overdue claims awaiting Administrative Law Judge adjudication. Because the settlement was part of a pilot program, we cannot predict whether we will be able to conclude future settlements with Medicare or achieve settlements on similar terms. Any future settlement of claims for amounts less than the corresponding amounts receivable would result in a write off.
The reserves for uncollectible co-payment reimbursements and doubtful accounts were as follows:
|
|
|
Year Ended |
|
||||
|
|
|
December 31, |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Beginning balance |
|
$ |
2,000 |
|
$ |
1,900 |
|
|
Accounts receivable provision |
|
|
7,087 |
|
|
5,973 |
|
|
Write-offs |
|
|
(6,519) |
|
|
(5,873) |
|
|
Ending balance |
|
$ |
2,568 |
|
$ |
2,000 |
|
Advertising
Advertising costs are charged to operations when incurred. Advertising expense was $57,000, $52,000 and $23,000 for the years ended December 31, 2016, 2015 and 2014, respectively.
Research and Development Costs
We expense research and development costs as incurred, including expenses associated with clinical research studies and development.
Shipping and Handling Costs
We do not charge any shipping and handling costs to our customers and the shipping and handling costs incurred are included in cost of goods sold.
Product Warranty
We provide a warranty for our products against defects in material and workmanship for a period of one to five years on garments and one to two years on controllers. We record a liability for future warranty claims at the time of sale for the warranty period offered to a customer. If the assumptions used in calculating the provision were to materially change, resulting in more defects than anticipated, an additional provision may be required.
The warranty reserve was as follows:
|
|
|
Year Ended |
|
||||
|
|
|
December 31, |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Beginning balance |
|
$ |
360 |
|
$ |
250 |
|
|
Warranty provision |
|
|
766 |
|
|
262 |
|
|
Processed warranty claims |
|
|
(333) |
|
|
(152) |
|
|
Ending balance |
|
$ |
793 |
|
$ |
360 |
|
|
|
|
|
|
|
|
|
|
|
Accrued warranty reserve, current |
|
$ |
290 |
|
$ |
360 |
|
|
Accrued warranty reserve, long-term |
|
|
503 |
|
|
— |
|
|
Total accrued warranty reserve |
|
$ |
793 |
|
$ |
360 |
|
88
Inventories
Inventories are valued at the lower of cost (first-in, first-out method) or market, and consisted of the following:
|
|
|
As of |
|
||||
|
|
|
December 31, |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Finished goods |
|
$ |
2,884 |
|
$ |
2,503 |
|
|
Component parts and work-in-process |
|
|
3,670 |
|
|
3,278 |
|
|
Total inventories |
|
$ |
6,554 |
|
$ |
5,781 |
|
Property and Equipment
Property and equipment are stated at cost and are being depreciated using the straight-line method over their estimated useful lives of three to five years and leasehold improvements are depreciated over the remaining life of the building lease agreement. Property and equipment consisted of the following:
|
|
|
As of |
|
||||
|
|
|
December 31, |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Equipment |
|
$ |
2,322 |
|
$ |
1,797 |
|
|
Leasehold improvements |
|
|
501 |
|
|
439 |
|
|
Tooling |
|
|
1,216 |
|
|
960 |
|
|
Furniture and fixtures |
|
|
323 |
|
|
303 |
|
|
Subtotal |
|
|
4,362 |
|
|
3,499 |
|
|
Less: accumulated depreciation |
|
|
(2,799) |
|
|
(2,153) |
|
|
Property and equipment, net |
|
$ |
1,563 |
|
$ |
1,346 |
|
Major expenditures for property and equipment are capitalized. Maintenance, repairs, and minor renewals are expensed as incurred. When assets are retired or otherwise disposed of, their costs and related accumulated depreciation are removed from the accounts and resulting gains or losses are included in income. Depreciation expense was $0.6 million, $0.5 million and $0.4 million for the years ended December 31, 2016, 2015 and 2014, respectively.
Deferred Offering Costs
Deferred offering costs, primarily consisting of legal, accounting and other direct fees and costs relating to the initial public offering were initially capitalized and then reclassified to stockholders’ equity at the conclusion of our initial public offering on August 2, 2016. There was $1.3 million in deferred offering costs capitalized as of December 31, 2015 in other non-current assets on the consolidated balance sheet. There were no deferred offering costs capitalized as of December 31, 2016.
Impairment of Long-Lived Assets
We review long-lived assets, including property and equipment and patents, for impairment whenever events or changes in business circumstances indicate that the carrying amount of an asset may not be fully recoverable. We will assess long-lived assets used in operations for impairment indicators which includes when undiscounted cash flows estimated to be generated by those assets are less than the assets’ carrying amount. To date, we have recorded no such losses other than the write-off of various assets acquired in the ACTitouch transaction.
Revenue Recognition
We recognize revenue when persuasive evidence of a sales arrangement exists, delivery of product has occurred through the transfer of title and risks of reward of ownership, the selling price is fixed or determinable and collectability is reasonably assured.
We distribute our products directly to patients. For any of our products sold to patients covered by private payers, such as commercial insurance companies, we recognize revenues from such sales upon shipment of our products. A
89
product is not shipped until we have received a prescription from a physician for our products and, as applicable, receipt of prior authorization from payers. At shipment, we invoice the payer for the total product price and we recognize revenue as a percentage of the invoice based on the policies and payment history of the applicable payer, net of estimated uncollectible patient copayments. The payment history of the applicable payer is drawn from our actual payment experience over the past year. Any differences in payments received as compared to our estimates are recognized in the period in which we actually receive payment for the product. Over time, we adjust the ultimate collection estimates to reflect these differences. After the insurance payer has remitted payment, we separately invoice the patient for their portion of the payment obligation, such as copayments and deductibles.
For our products sold to Medicare patients, we recognize revenues from such sales upon shipment of our products, which can occur only after we have received a prescription from a physician and all applicable Medicare documentation is obtained. For Flexitouch System sales, we estimate the revenue on each shipment to a Medicare patient as a percentage of the total invoice based on collection history. While we have contracted rates with Medicare, to the extent any claims for reimbursement are denied, we will recognize any necessary adjustments in the period for which the adjustment is made or can be estimated.
Net Income (Loss) per Share Attributable to Common Stockholders
For the reporting periods prior to our initial public offering, we used the two-class method to compute net income (loss) per common share attributable to common stockholders because we had issued securities, other than common stock, that contractually entitled the holders to participate in our dividends and earnings prior to our initial public offering. The two-class method requires earnings for the period to be allocated between common stock and participating securities based upon their respective rights to receive distributed and undistributed earnings. All series of our convertible preferred stock were considered participating securities.
Under the two-class method, for periods with net income, basic net income per share attributable to common stockholders is computed by dividing the net income attributable to common stockholders by the weighted-average number of shares of common stock outstanding during the period. Diluted net income per share attributable to common stockholders is computed by dividing the net income attributable to common stockholders by the weighted-average number of shares of common stock and dilutive potential shares of common stock outstanding during the period. Net income attributable to common stockholders is computed by subtracting from net income the portion of current year earnings that the participating securities would have been entitled to receive pursuant to their dividend rights had all of the year’s earnings been distributed. No such adjustment to earnings is made during periods with a net loss, as the holders of the participating securities have no obligation to fund losses.
Income Taxes
Income taxes are accounted for under the liability method. Deferred income taxes are provided for temporary differences between the financial reporting and the tax bases of assets and liabilities. If we determine in the future that it is more likely than not that we will not realize all or a portion of the deferred tax assets, we will record a valuation allowance in the period the determination is made (see Note 8). Changes in tax rates are reflected in the tax provision as they occur.
Stock-Based Compensation
The valuation of stock options involves the use of the Black-Scholes option-pricing model, which requires the input of highly subjective assumptions. The assumptions include the expected term of the option, the expected volatility of the price of our common stock, expected dividend yield and the risk-free interest rate. These estimates involve inherent uncertainties and the significant application of management’s judgment. If factors change and different assumptions are used, our stock-based compensation expense could be materially different in the future. We recognize compensation expense for these options on a straight-line basis over the requisite service period (see Note 7).
Marketable Securities
We determine the appropriate classification of our marketable securities as available-for-sale or held-to-maturity at the time of purchase and periodically reevaluates such classification. Debt securities are classified as held-to-
90
maturity when we have the positive intent and ability to hold the securities to maturity. Debt securities for which we do not have the intent or ability to hold to maturity are classified as available-for-sale.
Debt securities not classified as held-to-maturity and all equity securities are classified as available-for-sale and are reported at fair value, with unrealized gains and losses included in the determination of comprehensive income, a component of shareholders' equity. We review our available-for-sale securities for impairment to determine if the impairment is temporary or other-than-temporary. A temporary impairment charge results in an unrealized loss being recorded in other comprehensive income. Other-than-temporary impairments are recorded in net income in the period the impairment is determined to be other-than-temporary. Realized gains and losses on the sale of marketable securities are determined using the specific-identification method.
Comprehensive Income
Comprehensive income reflects the change in equity of a business enterprise during a period from transactions and other events and circumstances from non-owner sources. Our comprehensive income represents net income adjusted for unrealized gains and losses on available-for-sale marketable securities.
Recent Accounting Pronouncements
The JOBS Act provides that an "emerging growth company" can take advantage of the extended transition period provided in Section 7(a)(2)(B) of the Securities Act for complying with new or revised accounting standards. In other words, an "emerging growth company" can selectively delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to avail ourselves of this exemption and, as a result, our financial statements may not be comparable to the financial statements of issuers who are required to comply with the effective dates for new or revised accounting standards that are applicable to public companies. Section 107 of the JOBS Act provides that we can elect to opt out of the extended transition period at any time, which election is irrevocable.
In May 2014, the Financial Accounting Standards Board (“FASB”), issued Accounting Standards Update (“ASU”) 2014-09, “Revenue from Contracts with Customers.” The new section will replace Section 605, “Revenue Recognition,” and creates modifications to various other revenue accounting standards for specialized transactions and industries. The section is intended to conform revenue accounting principles with a concurrently issued International Financial Reporting Standards to reconcile previously differing treatment between U.S. practices and those of the rest of the world and to enhance disclosures related to disaggregated revenue information. The updated guidance is effective for interim and annual reporting periods beginning on or after December 15, 2018, for private companies; this effective date is applicable for us due to the JOBS Act exemption described above. Therefore, we plan to further evaluate the timing and anticipated impact of the adoption of this updated guidance on our consolidated financial statements in future periods.
In November 2015, the FASB issued ASU 2015-l7, “Income Taxes: Balance Sheet Classification of Deferred Taxes,” which requires entities to present deferred tax assets and deferred tax liabilities as noncurrent in a classified balance sheet. The ASU is effective for annual periods beginning after December l5, 20l7, and interim periods within annual periods beginning after December 15, 2018. Early adoption is permitted for all entities. We elected to adopt this new standard in the fourth quarter of 2016.
In February 2016, the FASB issued ASU 2016-02, “Leases” (Topic 842), which supersedes the existing guidance for lease accounting, “Leases” (Topic 840). ASU 2016-02 requires lessees to recognize a lease liability and a right-of-use asset for all leases. Lessor accounting remains largely unchanged. The amendments in this ASU are effective for interim and annual periods beginning after December 15, 2019 for private companies; this effective date is applicable to us due to the JOBS Act exemption described above. Early adoption is permitted for all entities. ASU 2016-02 requires a modified retrospective approach for all leases existing at, or entered into after the date of initial adoption, with an option to elect to use certain transition relief. We plan to further evaluate the timing and anticipated impact of the adoption of this ASU on our consolidated financial statements in future periods.
In March 2016, the FASB issued ASU 2016-09, “Improvements to Employee Share-Based Payment Accounting,” which simplifies several aspects of the accounting for employee share-based payment transactions, including the accounting for income taxes and statutory tax withholding requirements and classification within the statement of cash
91
flows. The ASU is effective for fiscal years beginning after December 15, 2016. We elected to adopt this new standard in the fourth quarter of 2016, effective as of January 1, 2016.
In June 2016, the FASB issued ASU No. 2016-13, “Financial Instruments — Credit Losses,” to require the measurement of expected credit losses for financial instruments held at the reporting date based on historical experience, current conditions and reasonable forecasts. The ASU is effective for interim and annual periods beginning after December 15, 2020, for private companies; this effective date is applicable to us due to the JOBS Act exemption described above. Therefore, we plan to further evaluate the timing and anticipated impact of the adoption of this ASU on our consolidated financial statements in future periods.
In August 2016, the FASB issued ASU No. 2016-15, “Statement of Cash Flows (Topic 230) — Classification of Certain Cash Receipts and Cash Payments,” to provide clarity on how certain cash receipt and cash payment transactions are presented and classified within the statement of cash flows. The ASU is effective for interim and annual periods beginning after December 15, 2018, for private companies; this effective date is applicable for us due to the JOBS Act exemption described above. Therefore, we plan to further evaluate the timing and anticipated impact of the adoption of this ASU on our consolidated financial statements in future periods.
Note 2. Marketable Securities
Our investments in marketable securities are classified as available-for-sale and consist of the following:
|
|
|
December 31, 2016 |
|
||||||||||
|
|
|
|
|
|
Unrealized |
|
Unrealized |
|
|
|
|
||
|
(In thousands) |
|
Cost |
|
Gains |
|
Losses |
|
Fair Value |
|
||||
|
U.S. government and agency obligations |
|
$ |
9,011 |
|
$ |
2 |
|
$ |
17 |
|
$ |
8,996 |
|
|
Corporate debt securities and certificates of deposit |
|
|
2,000 |
|
|
— |
|
|
2 |
|
|
1,998 |
|
|
Marketable securities |
|
$ |
11,011 |
|
$ |
2 |
|
$ |
19 |
|
$ |
10,994 |
|
Our investments in marketable debt securities all have contractual maturities of twelve to 24 months from December 31, 2016. At December 31, 2016, marketable debt securities valued at $4.0 million were in an unrealized gain position totaling $2,000 and marketable debt securities valued at $7.0 million were in an unrealized loss position totaling $19,000 (all had been in an unrealized loss position for less than 12 months).
Net pre-tax unrealized losses for marketable securities of $17,000 at December 31, 2016 were recorded as a component of accumulated other comprehensive loss in stockholders' equity. There were no sales of securities during the year ended December 31, 2016.
Note 3. Patent Costs, Net
Our patents, all of which are subject to amortization, are summarized as follows:
|
|
|
As of |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Patents |
|
$ |
3,462 |
|
$ |
3,403 |
|
|
Less: accumulated amortization |
|
|
(1,068) |
|
|
(914) |
|
|
Net patents |
|
$ |
2,394 |
|
$ |
2,489 |
|
92
Amortization expense was $0.3 million, $0.3 million and $0.3 million for the years ended December 31, 2016, 2015 and 2014, respectively. Future amortization expenses are expected as follows:
|
(In thousands) |
|
|
|
|
|
2017 |
|
$ |
249 |
|
|
2018 |
|
|
249 |
|
|
2019 |
|
|
249 |
|
|
2020 |
|
|
249 |
|
|
2021 |
|
|
249 |
|
|
Thereafter |
|
|
1,149 |
|
|
Total |
|
$ |
2,394 |
|
The weighted-average remaining amortization period for these patents was 13.6 years as of December 31, 2016.
Note 4. Accrued Expenses
Accrued expenses consisted of the following:
|
|
|
As of |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
||
|
Accrued warranty |
|
$ |
290 |
|
$ |
360 |
|
|
Accrued clinical |
|
|
45 |
|
|
130 |
|
|
Other |
|
|
858 |
|
|
426 |
|
|
Total |
|
$ |
1,193 |
|
$ |
916 |
|
Note 5. Line of Credit — Bank
We have a $2.0 million line of credit with a bank that bears interest based on the prime rate, which was 3.75% as of December 31, 2016, and expires on May 11, 2017. Our credit line is secured by substantially all of our assets, including property and equipment, accounts receivable and inventory. Our credit line contains customary conditions as to borrowing, events of default and covenants, including covenants that restrict our ability to dispose of assets, merge with or acquire other entities, and incur indebtedness or encumbrances. There was no outstanding balance on the line of credit as of December 31, 2016 and December 31, 2015.
Note 6. Commitments and Contingencies
Lease Obligations
In March 2008, we entered into a non-cancelable operating lease agreement for building space for our corporate headquarters that provides for monthly rent, real estate taxes and operating expenses that was extended to July 31, 2021. Rent expense was $1.0 million, $0.9 million and $0.8 million for the years ended December 31, 2016, 2015 and 2014, respectively.
In July 2016, we entered into a non-cancelable operating lease agreement for building space to accommodate the relocation of our manufacturing, quality, and research and development functions. The lease agreement extends through November 2021 and provides for monthly rent, real estate taxes and operating expenses.
We also have operating lease agreements for certain computer and office equipment that expire in 2020. The leases provide an option to purchase the related equipment at fair market value at the end of the lease.
93
Future base minimum lease payments for all lease obligations are expected to be as follows for the years ending December 31:
|
|
|
|
|
|
Computer/Office |
|
Fleet Car |
|
|
|
|
||
|
(In thousands) |
|
Buildings |
|
Equipment |
|
Program |
|
Total |
|
||||
|
2017 |
|
$ |
696 |
|
$ |
20 |
|
$ |
320 |
|
$ |
1,036 |
|
|
2018 |
|
|
714 |
|
|
18 |
|
|
— |
|
|
732 |
|
|
2019 |
|
|
733 |
|
|
11 |
|
|
— |
|
|
744 |
|
|
2020 |
|
|
752 |
|
|
1 |
|
|
— |
|
|
753 |
|
|
2021 |
|
|
525 |
|
|
— |
|
|
— |
|
|
525 |
|
|
Thereafter |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Total |
|
$ |
3,420 |
|
$ |
50 |
|
$ |
320 |
|
$ |
3,790 |
|
Major Vendors
We had purchases from three vendors that accounted for 37% and 45% of total purchases for the years ended December 31, 2016 and December 31, 2015, respectively.
Purchase Commitment
We issued purchase orders in February 2016 for which $4.9 million remains for inventory that we expect to receive between January and July of 2017. We issued purchase orders in January 2017 totaling $7.8 million that we expect to receive between July of 2017 and February of 2018.
Employment Agreements
We have entered into employment agreements with certain of our officers. The agreements provide for payment of severance ranging from nine to 15 months of then-current annualized base salary in the event of termination by us without cause or by the employee for good reason or, in the case of two of the officers, death, disability, or as a result of a qualifying termination after a change in control. The agreements also provide for payment of an amount equal to nine to 15 months of the then-current annual target bonus in the event of termination by us without cause or by the employee for good reason, or, in the case of two of the officers, death, disability, or as a result of a qualifying termination after a change in control. In addition, the agreements provide for the vesting of certain equity compensation through the date of termination in the event of termination by us without cause or by the employee for good reason.
Retirement Plan
We maintain a 401(k) retirement plan for our employees in which eligible employees can contribute a percentage of their pre-tax compensation. We may also make discretionary contributions to the 401(k) plan. We made contributions of $0.2 million, $0.1 million and $0.1 million for the years ended December 31, 2016, 2015 and 2014, respectively.
Note 7. Stockholders' Equity
In September and October 2012, we received gross proceeds of $10.4 million for issuance of 2,733,468 shares of our Series B preferred stock at $3.80 per share. The Series B preferred stock included a liquidation preference of the original investment plus an accruing dividend at a rate of 6%, compounded annually, whether or not declared. The accruing dividend was payable upon a voluntary or involuntary liquidation or dissolution of our Company, upon conversion of the Series B preferred stock to common stock, upon redemption of the Series B preferred stock or at such time as we paid a dividend on other shares of our capital stock. The accruing dividend could have been paid in cash or, at the option of the stockholder, additional shares of Series B preferred stock determined by dividing the amount of the accruing dividend by the Series B preferred stock purchase price as adjusted. There were $2.6 million of undeclared cumulative preferred dividends as of August 2, 2016, the date we closed our initial public offering, and we paid those dividends in the form of shares of our common stock. Holders of shares of Series B preferred stock were entitled to votes equal to the number of shares of common stock into which such Series B preferred stock could be converted.
94
Each share of Series B preferred stock could be converted into equal shares of common stock at the option of the Series B preferred stock holder at any time. In addition, the Series B preferred stock shares were automatically convertible into common shares upon the sale of shares of common stock to the public at a price per share of at least $11.42 in a firm commitment underwritten public offering pursuant to an effective registration statement under the Securities Act of 1933, as amended, resulting in at least $30 million of proceeds to our company, net of underwriting discounts and commissions and after which the common stock is listed on an United States national securities exchange. Each Series B preferred stockholder was also entitled to receive the number of common shares equal to the Series B preferred stock original issue price divided by the initial public offering price per share. In addition, each Series B Preferred stockholder was entitled to receive the number of common shares equal to (1) the accrued dividends on the shares of Series B preferred stock divided by the original issue price of the Series B preferred stock and (2) the accrued dividends on the shares of Series B preferred stock divided by the initial public offering price per share in the offering.
From 2007 through 2009, we received gross proceeds of $13.0 million for the issuance of 3,061,488 shares of our Series A preferred stock at $4.23 per share. The Series A preferred stock included a liquidation preference of the original investment plus an accruing dividend at a rate of 6%, compounded annually, whether or not declared. The accruing dividend was payable upon a voluntary or involuntary liquidation or dissolution of our company or upon conversion of the Series A preferred stock to common stock, upon redemption of the Series A preferred stock or at such time as we paid a dividend on other shares of our capital stock. The accruing dividend would be paid in cash. There were $8.2 million of undeclared cumulative preferred dividends as of August 2, 2016, the date we closed our initial public offering, and we paid those dividends in cash. Holders of shares of Series A preferred stock were entitled to votes equal to the number of shares of common stock into which such Series A preferred stock could be converted. Purchasers of the Series A preferred stock received anti-dilution rights whereby if we issued or sold additional shares of preferred or common shares at a purchase price below $4.23 per share, we would issue additional shares to these purchasers of Series A preferred stock to effectively reduce their purchase price. The Series B preferred stock was sold at a price less than the Series A preferred stock. As a result, we issued 83,972 shares of common stock for this anti-dilution provision.
Each share of Series A preferred stock could be converted into equal shares of common stock at the option of the Series A preferred stock holder at any time. In addition, the Series A preferred stock shares were automatically convertible into common shares upon the sale of shares of common stock to the public at a minimum price of $11.42 per share in a firm commitment underwritten public offering pursuant to an effective registration statement under the Securities Act of 1933, as amended, resulting in at least $30 million of proceeds to our company, net of underwriting discounts and commissions. Each Series A preferred stockholder was also entitled to receive the number of common shares equal to the Series A preferred stock original issue price divided by the initial public offering price per share.
At the time of its issuance, we determined that the Series B and Series A preferred stock contained two embedded features: (1) optional redemption by the holder and (2) optional conversion by the holder. We determined that each of the embedded features met the definition of a derivative and that the Series B and Series A preferred stock should be considered an equity host for the purposes of assessing the embedded derivatives for potential bifurcation. The following was noted regarding these embedded features:
Optional Redemption by the Holder. We determined that the redemption feature was not clearly and closely related to the equity host instrument but does not meet the definition of a derivative. As such, the redemption feature did not require bifurcation under the guidance for derivatives.
Optional Conversion by the Holder. The optional conversion feature was determined to be clearly and closely related to the Series B and Series A preferred stock host. As such the conversion feature did not require bifurcation under ASC 815, “Derivatives and Hedging.”
The Series B and Series A preferred stock was assessed under ASC 470, "Debt," to determine if there was a beneficial conversion feature. We determined there was no beneficial conversion feature.
We completed the initial public offering of our common stock on August 2, 2016, in which we sold 4,120,000 shares of our common stock at a public offering price of $10.00 per share. Immediately prior to the completion of the initial public offering, all then-outstanding shares of our Series A and Series B preferred stock were converted into 5,924,453 shares of our common stock. Our Series A preferred stock converted to common stock at a ratio of 1-for-1.03 and our Series B preferred stock converted to common stock at a ratio of 1-for-1. In addition, immediately prior to the completion of the initial public offering, we issued 2,354,323 additional shares of our common stock that our Series A
95
and Series B preferred stockholders were entitled to receive in connection with the conversion of the preferred stock, and we issued 956,842 shares of our common stock to pay accrued dividends on our Series B preferred stock. We also paid $8.2 million in cumulative accrued dividends to our Series A convertible preferred stockholders in connection with the initial public offering, including $0.1 million of dividends paid to the holders of the common restricted shares.
Stock-Based Compensation
Our 2016 Equity Incentive Plan (the “2016 Plan”) authorizes us to grant stock options, stock appreciation rights, restricted stock, stock units and other stock-based awards to employees, non-employee directors and certain consultants and advisors. There were up to 4,800,000 shares of our common stock initially reserved for issuance pursuant to the 2016 Plan, of which 4,180,831 shares were available for future issuance as of December 31, 2016. The 2016 Plan provides that the number of shares reserved and available for issuance under the 2016 Plan will automatically increase annually on January 1 of each calendar year, commencing in 2017 and ending on and including January 1, 2026, by an amount equal to the lesser of: (a) 5% of the number of common shares of stock outstanding as of December 31 of the immediately preceding calendar year, or (b) 2,500,000 shares; provided, however, that our Board of Directors may determine that any annual increase be a lesser number. In addition, all awards granted under our 2007 Omnibus Stock Plan and our 2003 Stock Option Plan that were outstanding when the 2016 Plan became effective and that are forfeited, expire, are cancelled, are settled for cash or otherwise not issued, will become available for issuance under the 2016 Plan. Effective January 1, 2017, 841,686 shares were added to the 2016 Plan, as available for issuance thereunder, pursuant to the automatic increase feature of the 2016 Plan.
Upon adoption and approval of the 2016 Equity Incentive Plan, all of our previous equity incentive compensation plans were terminated. However, existing awards under those plans continue to vest in accordance with the original vesting schedules and will expire at the end of their original terms.
We recorded total stock-based compensation expense of $1.9 million, $0.3 million and $0.1 million for the years ended December 31, 2016, 2015 and 2014, respectively. This expense was allocated as follows:
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Cost of goods sold |
|
$ |
112 |
|
$ |
73 |
|
$ |
2 |
|
|
Sales and marketing expenses |
|
|
514 |
|
|
178 |
|
|
48 |
|
|
Research and development expenses |
|
|
36 |
|
|
— |
|
|
— |
|
|
Reimbursement, general and administrative expenses |
|
|
1,227 |
|
|
65 |
|
|
98 |
|
|
Total stock-based compensation expense |
|
$ |
1,889 |
|
$ |
316 |
|
$ |
148 |
|
Stock Options
Stock options issued to participants other than non-employees vest over four years and typically have a contractual term of 10 years. The stock options granted on July 27, 2016 to our non-employee directors vest in full on the earlier of one year after the date of grant or the date of the 2017 annual meeting of stockholders. These options have a contractual term of 7 years.
Stock-based compensation expense included in our Consolidated Statements of Operations for stock options was $1.5 million, $0.1 million and $0.1 million for the years ended December 31, 2016, 2015 and 2014, respectively. The total grant date fair value of options vested during the year was $0.2 million, $0.1 million and $0.1 million for the years ended December 31, 2016, 2015 and 2014 respectively. As of December 31, 2016, there was approximately $1.5 million of total unrecognized pre-tax compensation expense related to non-vested stock option awards that are expected to be recognized over a weighted average period of 2.8 years.
The fair value of each option grant is estimated on the date of grant using the Black-Scholes option pricing model. Annually, we make predictive assumptions regarding future stock price volatility, employee exercise behavior, dividend yield and the forfeiture rate. The dividend yield assumption is based on expected annual dividend yield on the grant date. To date, no dividend on common stock has been paid by us. Expected volatility was estimated using the average historical volatility of public companies of similar size and industry over the similar period as the expected term assumption used for our options. The risk free interest rate is based on the yields of U.S. Treasury securities with
96
maturities similar to the expected term of the options for each option group. We use the “simplified method” to determine the expected term of the stock option.
The following table sets forth the estimated weighted-average fair values of our stock options granted in each of the years indicated, and the assumptions on which the fair values were determined:
|
|
|
|
Year Ended |
|
||||||
|
|
|
|
December 31, |
|
||||||
|
|
|
|
2016 |
|
|
2015 |
|
|
2014 |
|
|
Expected term |
|
|
6 years |
|
|
6 years |
|
|
6 years |
|
|
Expected volatility |
|
|
43% |
|
|
60% |
|
|
60% |
|
|
Risk-free interest rate |
|
|
1% |
|
|
2% |
|
|
2% |
|
|
Expected dividend yield |
|
|
0% |
|
|
0% |
|
|
0% |
|
|
Weighted-average fair value on the date of grant |
|
$ |
4.43 |
|
$ |
1.91 |
|
$ |
0.47 |
|
Stock option activity for the three years ended December 31, 2016 is summarized as follows:
|
|
|
|
|
|
Weighted Average |
|
Weighted Average |
Aggregate |
|
||
|
|
|
Options |
|
|
Exercise Price |
|
Remaining |
Intrinsic |
|
||
|
(In thousands except share, per share and years data) |
|
Outstanding |
|
|
Per Share1 |
|
Contractual Life |
Value2 |
|
||
|
Balance at December 31, 2013 |
|
2,467,834 |
|
$ |
0.79 |
|
6.4 years |
|
$ |
652 |
|
|
Granted |
|
156,558 |
|
|
1.35 |
|
|
|
|
|
|
|
Exercised |
|
(399,903) |
|
|
0.56 |
|
|
|
|
161 |
|
|
Forfeited |
|
(67,191) |
|
|
0.85 |
|
|
|
|
|
|
|
Balance at December 31, 2014 |
|
2,157,298 |
|
|
0.87 |
|
6.2 years |
|
|
5,912 |
|
|
Granted |
|
169,501 |
|
|
4.23 |
|
|
|
|
|
|
|
Exercised |
|
(428,856) |
|
|
0.65 |
|
|
|
|
4,569 |
|
|
Forfeited |
|
(57,495) |
|
|
2.26 |
|
|
|
|
|
|
|
Balance at December 31, 2015 |
|
1,840,448 |
|
|
1.18 |
|
5.8 years |
|
|
18,573 |
|
|
Granted |
|
305,236 |
|
|
10.60 |
|
|
|
|
|
|
|
Exercised |
|
(253,138) |
|
|
0.93 |
|
|
|
|
2,447 |
|
|
Forfeited |
|
(36,247) |
|
|
5.34 |
|
|
|
|
|
|
|
Balance at December 31, 2016 |
|
1,856,299 |
|
|
2.69 |
|
5.5 years |
|
|
25,467 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Options exercisable at December 31, 2016 |
|
1,359,302 |
|
$ |
1.06 |
|
4.5 years |
|
$ |
20,874 |
|
|
(1) |
The exercise price of each option granted during the periods shown was equal to the market price of the underlying stock on the date of grant. |
|
(2) |
The aggregate intrinsic value of options exercised represents the difference between the exercise price of the option and the closing stock price of our common stock on the date of exercise. The aggregate intrinsic value of options outstanding represents the difference between the exercise price of the option and the closing stock price of our common stock on the last day of the year. |
Options exercisable of 1,359,302 at December 31, 2016 and 1,368,047 at December 31, 2015 had weighted average exercise prices of $1.06 and $1.18, respectively.
The following summarizes additional information about the our stock options:
|
|
|
As of |
|
||||
|
|
|
December 31, |
|
||||
|
Number of: |
|
2016 |
|
2015 |
|
||
|
Non-vested options beginning of the year |
|
|
472,401 |
|
|
623,143 |
|
|
Non-vested options end of the year |
|
|
496,997 |
|
|
472,401 |
|
|
Vested options |
|
|
251,968 |
|
|
304,995 |
|
97
|
|
|
As of |
|
||||
|
|
|
December 31, |
|
||||
|
Weighted-average grant date fair value of: |
|
2016 |
|
2015 |
|
||
|
Non-vested options beginning of the year |
$ |
|
2.85 |
$ |
|
0.45 |
|
|
Non-vested options end of the year |
|
|
2.99 |
|
|
2.85 |
|
|
Vested options |
|
|
0.76 |
|
|
0.54 |
|
|
Forfeited options |
|
|
2.71 |
|
|
3.30 |
|
Stock-Settled Restricted Stock Units
Stock-settled restricted stock units granted under the 2016 Equity Incentive Plan vest after one to three years. These awards are stock-settled for common chares. Stock-based compensation expense included in our Consolidated Statement of Operations for stock-settled restricted stock units was $0.7 million for the year ended December 31, 2016. No restricted stock units had been granted prior to fiscal 2016. As of December 31, 2016, there was $2.7 million of total unrecognized pre-tax compensation expense related to outstanding stock-settled restricted stock units that is expected to be recognized over a weighted-average period of 2.0 years.
Stock-settled restricted stock unit activity for the year ended December 31, 2016 is summarized as follows:
|
|
|
|
|
|
Weighted |
|
Aggregate |
|
|
|
|
|
Units |
|
|
Average Grant |
|
Intrinsic |
|
|
|
(In thousands except share and per share data) |
|
Outstanding |
|
|
Date Fair Value |
|
Value2 |
|
|
|
Balance at December 31, 2015 |
|
— |
|
$ |
— |
|
|
|
|
|
Granted |
|
327,454 |
|
|
10.45 |
|
|
|
|
|
Vested1 |
|
(1,726) |
|
|
17.29 |
|
|
|
|
|
Cancelled |
|
(865) |
|
|
17.35 |
|
|
|
|
|
Balance at December 31, 2016 |
|
324,863 |
|
|
10.39 |
|
$ |
1,972 |
|
|
(1) |
The restricted stock units shown as vested during the year represent grants to non-employee directors in lieu of annual retainer installments, which restricted stock units were fully vested upon grant and represent the right to receive one share of common stock upon the earlier of the director’s termination of service as a director of ours or the occurrence of a change in control of us. The shares of common stock underlying these restricted stock units are not issued or outstanding. |
|
(2) |
Intrinsic value of stock-settled restricted stock units vested was based on our closing stock price on the last trading day of the year. |
Restricted Stock Awards
Restricted stock awards were granted in 2009 in lieu of cash bonuses. Stock-based compensation expense included in our Consolidated Statements of Operations for restricted stock was $0.3 million for the year ended December 31, 2016.
Employee Stock Purchase Plan
Our employee stock purchase plan (“ESPP”), which was approved by our Board of Directors on April 27, 2016 and by our stockholders on June 20, 2016, allows participating employees to purchase shares of our common stock at a discount through payroll deductions. The plan is available to all of our employees and employees of participating subsidiaries. Participating employees may purchase common stock, on a voluntary after-tax basis, at a price equal to 85% of the lower of the closing market price per share of our common stock on the first or last trading day of each stock purchase period. The plan ordinarily consists of six-month purchase periods, beginning on May 16 and November 16 of each calendar year, but the initial purchase period began on July 27, 2016 and will end on May 15, 2017. A total of 1.6 million shares of common stock are reserved for issuance under the plan, and this share reserve will automatically be supplemented each January 1, commencing in 2017 and ending on and including January 1, 2026, by an amount equal to the least of (1) 1% of the shares of our common stock outstanding on the immediately preceding December 31, (2) 500,000 shares or (3) such lesser amount as our Board of Directors may determine. Effective January 1, 2017, 168,337 shares will be added to the ESPP, as available for issuance thereunder, pursuant to the automatic increase feature of the plan. No purchases were made under the plan during the year ended December 31, 2016. We recognized $0.4 million in stock-based compensation expense related to the ESPP for the year ended December 31, 2016. We did not recognize any stock-based compensation expense related to the ESPP for the years ended December 31, 2015 and 2014.
98
Stock Warrants
We have also issued warrants to purchase shares of our common stock which are summarized below:
|
|
|
|
|
|
|
|
Weighted-Average |
|
|
|
|
|
|
|
Weighted-Average |
|
Remaining |
|
||
|
|
|
Number |
|
Exercise |
|
Contractual |
|
||
|
|
|
Outstanding |
|
Price |
|
Life |
|
||
|
Warrants outstanding — December 31, 2013 |
|
172,817 |
|
$ |
3.84 |
|
|
|
|
|
Exercised |
|
— |
|
|
— |
|
|
|
|
|
Expired |
|
— |
|
|
— |
|
|
|
|
|
Warrants outstanding — December 31, 2014 |
|
172,817 |
|
|
4.43 |
|
|
|
|
|
Exercised |
|
166,617 |
|
|
3.81 |
|
|
|
|
|
Expired |
|
400 |
|
|
— |
|
|
|
|
|
Warrants outstanding — December 31, 2015 |
|
5,800 |
|
|
4.23 |
|
|
|
|
|
Exercised |
|
2,882 |
|
|
4.23 |
|
|
|
|
|
Expired |
|
— |
|
|
— |
|
|
|
|
|
Warrants outstanding — December 31, 2016 |
|
2,918 |
|
|
4.23 |
|
|
0.56 years |
|
Note 8. Income Taxes
The provision for income tax expense consisted of the following:
|
|
|
Year Ended |
|
|||||||
|
|
|
December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Current income taxes |
|
$ |
2,042 |
|
$ |
1,012 |
|
$ |
167 |
|
|
Deferred income taxes |
|
|
(611) |
|
|
852 |
|
|
1,558 |
|
|
Total provision for income taxes |
|
$ |
1,431 |
|
$ |
1,864 |
|
$ |
1,725 |
|
The components of our deferred tax assets were as follows:
|
|
|
As of December 31, |
|
|||||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Deferred tax assets: |
|
|
|
|
|
|
|
|
|
|
|
Net operating loss carryforwards |
|
$ |
156 |
|
$ |
— |
|
$ |
874 |
|
|
Accounts receivable and inventory reserves |
|
|
1,182 |
|
|
1,253 |
|
|
977 |
|
|
Warranty reserves |
|
|
285 |
|
|
128 |
|
|
100 |
|
|
Intangible assets |
|
|
837 |
|
|
810 |
|
|
886 |
|
|
Accrued liabilities |
|
|
97 |
|
|
181 |
|
|
362 |
|
|
Stock-based compensation |
|
|
410 |
|
|
— |
|
|
— |
|
|
Other |
|
|
157 |
|
|
39 |
|
|
40 |
|
|
Total deferred tax assets |
|
$ |
3,124 |
|
$ |
2,411 |
|
$ |
3,239 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Deferred tax liabilities: |
|
|
|
|
|
|
|
|
|
|
|
Depreciation |
|
|
(339) |
|
|
(243) |
|
|
(219) |
|
|
Total deferred tax liabilities |
|
$ |
(339) |
|
$ |
(243) |
|
$ |
(219) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net deferred tax assets |
|
$ |
2,785 |
|
$ |
2,168 |
|
$ |
3,020 |
|
99
A reconciliation of income tax expense to the statutory federal tax rate of 34% is as follows:
|
|
|
Year Ended |
|
||||
|
|
|
December 31, |
|
||||
|
(In thousands) |
|
2016 |
|
2015 |
|
2014 |
|
|
Tax expense at statutory rate |
|
34.0 |
% |
34.0 |
% |
34.0 |
% |
|
Other Permanent differences |
|
5.6 |
|
3.6 |
|
3.9 |
|
|
Meals & Entertainment |
|
5.4 |
|
4.8 |
|
— |
|
|
State income taxes, net of federal benefit |
|
3.3 |
|
3.6 |
|
3.0 |
|
|
State tax rate adjustment |
|
(0.3) |
|
9.2 |
|
— |
|
|
Deferred true-up adjustment |
|
(7.9) |
|
— |
|
— |
|
|
Excess benefit on non-qualified stock options |
|
(8.0) |
|
— |
|
— |
|
|
Other and uncertain tax positions |
|
1.1 |
|
2.0 |
|
4.5 |
|
|
Net effective rate |
|
33.2 |
% |
57.2 |
% |
45.4 |
% |
Deferred income taxes result from temporary differences between the reporting of amounts for financial statement purposes and income tax purposes. These differences relate primarily to different methods used for income tax purposes including depreciation and amortization, warranty and vacation accruals, and deductions related to allowances for doubtful accounts receivable and inventory reserves.
As of December 31, 2016, we had no U.S. federal net operating loss (“NOL”) carry-forwards and approximately $2.4 million of Minnesota state NOLs. The Minnesota NOL carry-forward amounts expire in tax years 2024 through 2029, if not utilized.
We are subject to income tax examinations in the U.S. federal jurisdiction as well as in various state jurisdictions. U.S. federal and state tax years prior to 2012 were still open to examination at December 31, 2016.
In accounting for uncertainty in income taxes, we recognize the financial statement benefit of a tax position only after determining that the relevant tax authority would more likely than not sustain the position following an audit. For tax positions meeting the more likely than not threshold, the amount recognized in the financial statements is the largest benefit that has a greater than 50 percent likelihood of being realized upon ultimate settlement with the relevant tax authority. As of December 31, 2016 and 2015, we did not have any unrecognized tax benefits. We recognize interest and penalties accrued on any unrecognized tax benefits as a component of income tax expense. We do not expect any material changes in our unrecognized tax benefits over the next 12 months.
In March 2016, the FASB issued ASU 2016-09, “Improvements to Employee Share-Based Payment Accounting.” The standard is required to be adopted by all companies in their first fiscal year beginning after December 15, 2016, but allows companies to elect adoption prior to this date. The standard is intended to simplify various aspects of the accounting and presentation of share-based payments. During the quarter ended December 31, 2016, we elected to early adopt this standard as of January 1, 2016. Adoption of this standard had the following impact on our financial statements:
Statements of Operations – The new accounting standard requires that the tax effects of stock-based compensation be recognized in the income tax provision of our Consolidated Statements of Operations. Previously, all excess tax benefits were recognized in additional paid-in capital, and tax deficiencies were recognized either in the income tax provision or in additional paid-in capital to the extent that there was a sufficient “APIC pool” related to previously recognized excess tax benefits. The new standard requires amounts recognized through additional paid-in capital during 2016 interim periods to be recasted as recognized through our Consolidated Statements of Operations. We did not recognize any excess benefit or deficiency through additional paid-in capital with respect to our 2016 quarterly filings. In our quarterly provisions we made no entries with respect to NQSOs exercised throughout the year as the FMV valuations necessary to compute the excess benefit were not available at the time reports were issued. Accordingly, there is no adjustment as the result of prior entries to APIC. There are, however, favorable adjustments to adjust tax expense for the unrecorded tax benefits for prior quarters in the amounts of $0.3 million, $49,000, and $0.6 million for the first, second, and third quarters of 2016, respectively.
100
Statements of Cash Flows – The standard requires that excess tax benefits from stock-based employee awards be reported as operating activities in our Consolidated Statements of Cash Flows. Previously, these cash flows were included as hypothetical inflows/outflows in both operating and financing activities. We elected to apply this change on a prospective basis, resulting in no change in net cash provided by operating activities and financing activities with respect to our 2016 quarterly filings.
Statements of Shareholders’ Equity (Deficit) – The standard requires that as of the beginning of the annual period of adoption, previously unrecognized excess tax benefits be recognized on a modified retrospective basis and a deferred tax asset be recorded for the balance with an offsetting adjustment to retained earnings. We did not recognize additional deferred tax assets or adjust retained earnings as we did not recognize any excess benefit or deficiency through additional paid-in capital through our third quarter 2016 reporting period.
In recording stock-based compensation expense, the new standard allows companies to make a policy election as to whether they will include an estimate of awards expected to be forfeited or whether they will account for forfeitures as they occur. We have elected to include an estimate of forfeitures in the computation of our stock-based compensation expense. As this treatment is consistent with our previous practice, there is no impact on our consolidated financial statements. The new standard requires that employee taxes paid when an employer withholds shares for tax-withholding purposes be reported as financing activities in the Consolidated Statements of Cash Flows. As this treatment is consistent with our previous practice, this election had no impact on our consolidated financial statements.
Under ASU No. 2016-09, an entity recognizes all excess tax benefits and tax deficiencies relating to stock based compensation as income tax expense or benefit in the Statement of Operations. This change eliminates the notion of the “APIC” pool and related prior year disclosures for excess tax deductions not reflected in our deferred tax asset presentation.
On November 20, 2015, the FASB issued ASU 2015-17, “Balance Sheet Classification of Deferred Taxes.” The ASU is part of the FASB’s simplification initiative aimed at reducing complexity in accounting standards. To simplify presentation, the new guidance requires that all deferred tax assets and liabilities, along with any related valuation allowance, be classified as non-current on the balance sheet. As a result, each jurisdiction will now only have one net non-current deferred tax asset or liability. During the quarter ended December 31, 2016, we early adopted ASU 2015-17 to present balance sheet classification of deferred income taxes as non-current. This adoption was applied prospectively and therefore, prior periods were not retrospectively adjusted.
Note 9. Accumulated Other Comprehensive Loss
At December 31, 2016, 2015 and 2014, the components of accumulated other comprehensive loss were as follows:
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
Available- |
|
Other |
|
||
|
|
|
for-Sale |
|
Comprehensive |
|
||
|
(In thousands) |
|
Securities |
|
Loss |
|
||
|
Balances at December 31, 2013 |
|
$ |
— |
|
$ |
— |
|
|
Other comprehensive income (loss) |
|
|
— |
|
|
— |
|
|
Balances at December 31, 2014 |
|
|
— |
|
|
— |
|
|
Other comprehensive income (loss) |
|
|
— |
|
|
— |
|
|
Balances at December 31, 2015 |
|
|
— |
|
|
— |
|
|
Other comprehensive income (loss) |
|
|
(11) |
|
|
(11) |
|
|
Balances at December 31, 2016 |
|
$ |
(11) |
|
$ |
(11) |
|
101
Note 10. Net Income (Loss) Per Share Attributable to Common Stockholders
The following table sets forth the computation of our basic and diluted net income (loss) per share attributable to common stockholders:
|
|
|
Year Ended December 31, |
|
|||||||
|
(In thousands, except share and per share data) |
|
2016 |
|
2015 |
|
2014 |
|
|||
|
Net income |
|
$ |
2,879 |
|
$ |
1,393 |
|
$ |
2,070 |
|
|
Convertible preferred stock dividends |
|
|
1,247 |
|
|
1,845 |
|
|
1,761 |
|
|
Allocation of undistributed earnings to preferred stockholders |
|
|
— |
|
|
— |
|
|
216 |
|
|
Net income (loss) attributable to common stockholders |
|
$ |
1,632 |
|
$ |
(452) |
|
$ |
93 |
|
|
Weighted average shares outstanding |
|
|
8,913,042 |
|
|
2,929,438 |
|
|
2,491,108 |
|
|
Effect of common stock options, warrants, restricted stock units and employee stock purchase plan shares |
|
|
1,845,642 |
|
|
— |
|
|
1,306,580 |
|
|
Weighted-average shares used to compute diluted net income (loss) per share |
|
|
10,758,684 |
|
|
2,929,438 |
|
|
3,797,688 |
|
|
Net income (loss) per share - Basic |
|
$ |
0.18 |
|
$ |
(0.15) |
|
$ |
0.04 |
|
|
Net income (loss) per share - Diluted |
|
$ |
0.15 |
|
$ |
(0.15) |
|
$ |
0.02 |
|
As of December 31, 2016, total common shares outstanding and the potentially dilutive shares totaled approximately 18.7 million shares.
The following potentially dilutive securities were excluded from the computation of weighted-average shares outstanding for the years ended December 31, 2016, 2015 and 2014 because these securities would have had an anti-dilutive impact:
|
|
|
Year Ended December 31, |
|
||||
|
|
|
2016 |
|
2015 |
|
2014 |
|
|
Convertible preferred stock outstanding |
|
— |
|
5,794,957 |
|
5,794,957 |
|
|
Restricted stock units |
|
— |
|
— |
|
— |
|
|
Common stock options |
|
30,845 |
|
1,840,447 |
|
2,791 |
|
|
Employee stock purchase plan shares |
|
— |
|
— |
|
— |
|
|
Common stock warrants |
|
— |
|
5,800 |
|
172,817 |
|
|
Total |
|
30,845 |
|
7,641,204 |
|
5,970,565 |
|
102
Note 11. Fair Value Measurements
We determine the fair value of our assets and liabilities based on the exchange price that would be received for an asset or paid to transfer a liability (exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value maximize the use of observable inputs and minimize the use of unobservable inputs. We use a fair value hierarchy with three levels of inputs, of which the first two are considered observable and the last unobservable, to measure fair value. The fair value hierarchy gives the highest priority to quoted prices in active markets for identical assets or liabilities (Level 1). The next highest priority is based on quoted prices for similar assets or liabilities in active markets or quoted prices for identical or similar assets or liabilities in non-active markets or other observable inputs (Level 2). The lowest priority is given to unobservable inputs (Level 3). The following provides information regarding fair value measurements for our marketable securities as of December 31, 2016 according to the three-level fair value hierarchy.
|
|
|
Fair Value Measurements at |
||||||||||
|
|
|
December 31, 2016 Using: |
||||||||||
|
|
|
Quoted Prices |
|
|
|
|
|
|
|
|
|
|
|
|
|
in Active |
|
Significant |
|
|
|
|
|
|
||
|
|
|
Markets for |
|
Other |
|
Significant |
|
|
||||
|
|
|
Identical |
|
Observable |
|
Unobservable |
|
|
||||
|
|
|
Assets |
|
Inputs |
|
Inputs |
|
|
||||
|
(In thousands) |
|
(Level 1) |
|
(Level 2) |
|
(Level 3) |
|
Total |
||||
|
Recurring Fair Value Measurements: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Currency |
|
$ |
14 |
|
$ |
— |
|
$ |
— |
|
$ |
14 |
|
Money market mutual funds |
|
|
18,976 |
|
|
|
|
|
|
|
|
18,976 |
|
U.S. government and agency obligations |
|
|
2,017 |
|
|
6,979 |
|
|
— |
|
|
8,996 |
|
Corporate debt securities and certificates of deposit |
|
|
— |
|
|
1,998 |
|
|
— |
|
|
1,998 |
|
Total |
|
$ |
21,007 |
|
$ |
8,977 |
|
$ |
— |
|
$ |
29,984 |
During the year ended December 31, 2016 there were no transfers within the three level hierarchy. A significant transfer is recognized when the inputs used to value a security have been changed which merit a transfer between the disclosed levels of the valuation hierarchy.
The fair value for our currency, money market mutual funds, U.S. government and agency obligations and corporate debt securities are determined based on valuations provided by external investment managers who obtain them from a variety of industry standard data providers.
The carrying amounts of financial instruments such as cash equivalents, accounts receivable, other assets, accounts payable, accrued expenses and other liabilities approximate their related fair values due to the short-term maturities of these instruments. Non-financial assets such as equipment and leasehold improvements, and intangible assets are subject to non-recurring fair value measurements if they are deemed impaired. We had no re-measurements of non-financial assets to fair value in 2016.
103
Note 12. Quarterly Financial Information (Unaudited)
The quarterly financial data presented below should be read in conjunction with the consolidated financial statements and related notes. The adjustment is due to the retrospective application of ASU 2016-09 as further discussed in Note 8 – Income tax above.
|
|
|
Three Months Ended |
|
|||||||||||||||||||
|
|
|
Mar. 31, 2016 |
|
Jun. 30, 2016 |
|
Sep. 30, 2016 |
|
|
|
|
||||||||||||
|
|
|
As |
|
As |
|
As |
|
As |
|
As |
|
As |
|
|
|
|||||||
|
(In thousands, except per share data) |
|
Reported |
|
Adjusted(2) |
|
Reported |
|
Adjusted(2) |
|
Reported |
|
Adjusted(2) |
|
Dec. 31, 2016 |
|
|||||||
|
Revenues |
|
$ |
13,700 |
|
$ |
13,700 |
|
$ |
19,729 |
|
$ |
19,729 |
|
$ |
22,635 |
|
$ |
22,635 |
|
$ |
28,478 |
|
|
Gross margin |
|
|
9,889 |
|
|
9,889 |
|
|
14,405 |
|
|
14,405 |
|
|
16,353 |
|
|
16,353 |
|
|
20,955 |
|
|
Income (loss) from operations |
|
|
(1,786) |
|
|
(1,786) |
|
|
1,792 |
|
|
1,792 |
|
|
974 |
|
|
974 |
|
|
3,292 |
|
|
Net income (loss) attributable to common stockholders |
|
|
(1,494) |
|
|
(1,231) |
|
|
177 |
|
|
204 |
|
|
169 |
|
|
334 |
|
|
2,379 |
|
|
Net income (loss) per share - Basic(1) |
|
|
(0.45) |
|
|
(0.38) |
|
|
0.05 |
|
|
0.06 |
|
|
0.01 |
|
|
0.03 |
|
|
0.14 |
|
|
Net income (loss) per share - Diluted(1) |
|
|
(0.45) |
|
|
(0.38) |
|
|
0.04 |
|
|
0.04 |
|
|
0.01 |
|
|
0.02 |
|
|
0.13 |
|
|
|
|
Three Months Ended |
||||||||||
|
(In thousands, except per share data) |
|
Mar. 31, 2015 |
|
Jun. 30, 2015 |
|
Sep. 30, 2015 |
|
Dec. 31, 2015 |
||||
|
Revenues |
|
$ |
10,121 |
|
$ |
14,771 |
|
$ |
16,820 |
|
$ |
21,160 |
|
Gross margin |
|
|
7,149 |
|
|
10,370 |
|
|
12,354 |
|
|
16,091 |
|
Income (loss) from operations |
|
|
(1,484) |
|
|
228 |
|
|
1,462 |
|
|
3,245 |
|
Net income (loss) attributable to common stockholders |
|
|
(1,340) |
|
|
(328) |
|
|
144 |
|
|
289 |
|
Net income (loss) per share - Basic(1) |
|
|
(0.51) |
|
|
(0.12) |
|
|
0.05 |
|
|
0.09 |
|
Net income (loss) per share - Diluted(1) |
|
|
(0.51) |
|
|
(0.12) |
|
|
0.03 |
|
|
0.06 |
|
(1) |
The summation of quarterly per share amounts may not equal the calculation for the full year, as each quarterly calculation is performed discretely. |
|
(2) |
As adjusted amounts include the impact of adopting ASU 2016-09, “Improvements to Employee Share-Based Payment Accounting,” which simplifies several aspects of the accounting for employee share-based payment transactions, including the accounting for income taxes and statutory tax withholding requirements and classification within the statement of cash flows. The ASU is effective for fiscal years beginning after December 15, 2016. We elected to adopt this new standard in the fourth quarter of 2016, effective as of January 1, 2016. |
104
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure.
None
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2016. The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”), means controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure. Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on the evaluation of our disclosure controls and procedures as of December 31, 2016, our Chief Executive Officer and Chief Financial Officer concluded that, as of such date, our disclosure controls and procedures were effective.
Changes in Internal Control over Financial Reporting
There were no material changes in our internal control over financial reporting during the quarter ended December 31, 2016 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Management Report on Internal Control over Financial Reporting
This annual report does not include a report of management’s assessment regarding internal control over financial reporting or an attestation report of our registered independent public accounting firm due to a transition period established by rules of the SEC for newly public companies.
None.
Item 10. Directors, Executive Officers and Corporate Governance.
Directors
Peter H. Soderberg, age 70, has served as a member of our board of directors since September 2012. Mr. Soderberg currently is the Managing Partner of Worthy Venture Resources, LLC, a company that seeks to add intellectual and financial capital to post start-up companies transitioning to an established national market presence. Beginning in 2006, Mr. Soderberg served as the President and Chief Executive Officer of both Hillenbrand Industries and Hill-Rom. In 2008, Hillenbrand Industries separated its two subsidiaries creating two, separately traded, public companies. Mr. Soderberg continued his role as President and Chief Executive Officer of the medical technology company, Hill-Rom Holdings, Inc. until 2010. Mr. Soderberg served on the board of Hillenbrand Industries/Hill-Rom from 2002 until his semi-retirement in 2011. Previously, he was President and Chief Executive Officer at Welch Allyn, a manufacturer of medical diagnostic equipment, for six years, and served as Group Vice President and Chief Operating Officer from 1993 to 1999. Prior to his role at Welch Allyn Mr. Soderberg's served 23 years at Johnson & Johnson, in a variety of operations, marketing and management positions, including President of Johnson & Johnson Health Management. His career also includes roles as President and Chief Executive Officer of an industrial technology
105
company and the founder and President of a venture capital business. Mr. Soderberg currently serves on the board of directors of Integer Holdings Corp. (NYSE: ITGR, formerly Greatbatch, Inc.), a medical technology company. Mr. Soderberg previously served on the boards of Constellation Brands, Inc. and the Advanced Medical Technology Association.
William W. Burke, age 57, has served as a member of our board of directors since September 2015. Since November 2015, Mr. Burke has served as President of Austin Highlands Advisors, LLC, a provider of corporate advisory services. He served as Executive Vice President and Chief Financial Officer of IDEV Technologies, a peripheral vascular devices company, from November 2009 until the company was acquired by Abbott Laboratories in August 2013. From August 2004 to December 2007, he served as Executive Vice President and Chief Financial Officer of ReAble Therapeutics, a diversified orthopedic device company which was sold to The Blackstone Group in a going private transaction in 2006 and subsequently merged with DJO Incorporated in November 2007. Mr. Burke remained with ReAble until June 2008. From 2001 to 2004, he served as Chief Financial Officer of Cholestech Corporation, a medical diagnostic products company. Mr. Burke has served on the board of directors of numerous public and private companies and currently serves on the board of directors of DeVry Education Group, Invuity, Inc. and Myocardial Solutions, Inc. He previously served on the board of directors of LDR Holding Corporation (acquired by Zimmer Biomet in July 2016) and Medical Action Industries (acquired by Owens & Minor in October 2014). Mr. Burke was selected to serve on our Board of Directors because of his business experience with other medical technology companies and his experience as chief financial officer of other companies, including other publicly traded companies.
Jordan S. Davis, age 55, has served as a member of our board of directors since September 2012. Mr. Davis is a Managing Partner of Radius Ventures, a venture capital firm focused on health and life sciences companies, which he co-founded in 1997. Mr. Davis has served on numerous public and private company boards and currently serves on the board of directors of Athersys, Inc. (Nasdaq: ATHX) and Endogastric Solutions, Inc., which are Radius portfolio companies. In addition, Mr. Davis serves on the board of directors of HealthCorps, a non-profit organization engaged in educating youth on nutrition, fitness and mental resilience. Mr. Davis was a co-founder of Cambridge Heart, Inc., a medical technology company that developed and commercialized a device to non-invasively identify patients at risk of sudden cardiac death, and Voxware, Inc., a speech technology company and early entrant in the VoIP market, both of which completed initial public offerings in 1996.
Gerald R. Mattys, age 58, has served as our Chief Executive Officer and as a member of our board of directors since 2005. From 2002 to 2004, he served as the Chief Executive Officer of Medisyn Technologies, Inc., a development stage biotechnology company. From 2000 to 2002, he was the President and Chief Executive Officer of Timm Medical Technologies, Inc., a medical device company. During the period from 1998 to 2000, he was Vice President and General Manager of Alternate Care for Mallinckrodt, Inc., a pharmaceutical and medical device company. Prior to that, he served 18 years in various roles in product management, sales, marketing and management at several medical device companies.
Richard Nigon, age 69, has served as a member of our board of directors since September 2012. Mr. Nigon is currently Senior Vice President of Cedar Point Capital, Inc., a private company that raises capital for early stage companies, where he has served since 2007. From February 2001 until December 2006, Mr. Nigon was a Director of Equity Corporate Finance for Miller Johnson Steichen Kinnard, a privately held investment firm, which was acquired in December 2006 by Stifel Nicolaus, a brokerage and investment banking firm. After that acquisition, Mr. Nigon became a Managing Director of Private Placements until May 2007. From February 2000 to February 2001, Mr. Nigon served as the Chief Financial Officer of Dantis, Inc., a web hosting company. Prior to joining Dantis, Mr. Nigon was employed by Ernst & Young LLP from 1970 to 2000, where he was a partner from 1981 to 2000. While at Ernst & Young, Mr. Nigon served as the Director of Ernst & Young's Twin Cities Entrepreneurial Services Group and was the coordinating partner on several publicly-traded companies in the consumer retailing and manufacturing sectors. Mr. Nigon is a director of Northern Technologies International Corporation and was previously a director of Vascular Solutions, Inc. before its acquisition by Teleflex, Incorporated, in February 2017. Mr. Nigon also serves as a director of several private companies.
Kevin H. Roche, age 66, has served as a member of our board of directors since October 2004. Mr. Roche was General Counsel of UnitedHealth Group, a health insurance provider, from 1989 to 1996, at which time he founded and operated as the Chief Executive Officer of the Ingenix division of UnitedHealth Group where he served until 2001. Following his retirement from UnitedHealth Group, Mr. Roche has spent several years assisting emerging growth companies as an investor, advisor and board member. He also serves as a Senior Advisor for Triple Tree, LLC. He
106
currently serves as a director for several private healthcare companies. During the past five years, Mr. Roche served on the board of directors of Cogentix Medical, Inc.
Stephen I. Shapiro, age 72, has served as a member of our board of directors since June 2010. From 1983 through 1999, Mr. Shapiro was a Managing Director of The Wilkerson Group, a leading medical products management consulting firm, with a client base including pharmaceutical, diagnostic, device and biotech companies, where he led the medical devices practice. Prior to joining The Wilkerson Group, he was Director of Advanced Research and Development and New Business Development for Becton, Dickinson and Company, and spent eight years at Union Carbide Clinical Diagnostics, becoming engineering group leader. Mr. Shapiro also serves on the board of directors of Pacific Diagnostic Laboratories, LLC, and he previously served on the board of directors of PolyRemedy, Inc., and Cambrooke Therapeutics, Inc. Mr. Shapiro was a Venture Partner with Advanced Technology Ventures (a venture capital firm focused on investments in healthcare companies) from January 2000 through January 2015. Mr. Shapiro served as a consultant to Galen Partners (a venture capital firm focused on investments in healthcare companies) as a Venture Partner from January 2000 through December 2013.
Zubeen Shroff, age 52, has served as a member of our board of directors since September 2007. Mr. Shroff is a Managing Director of Galen Partners, a healthcare growth equity investment firm which he joined in 1996. Prior to joining Galen, Mr. Shroff was a Principal with The Wilkerson Group, where his client base included pharmaceutical, diagnostics, device and biotech companies, plus a select number of venture capital firms. Prior to joining The Wilkerson Group, Mr. Shroff worked at Schering-Plough France, a manufacturer of healthcare products and medicines, where he helped launch their biotech product, alpha-Interferon, in several new indications. Currently, Mr. Shroff is Treasurer and on the Executive Committee of the Board for The Westchester Medical Center Public Benefit Corporation, as well as Chairman of its Foundation. Since 2004, he has served on the Advisory Committees to Boston University Medical School and School of Public Health. Previously, Mr. Shroff was also on the Advisory Board of the Joslin Diabetes Center. In addition to the above positions, Mr. Shroff has served on the board of directors of numerous privately held Galen portfolio companies. Mr. Shroff currently serves on the board of directors of Quotient Biodiagnostics and served on the board of directors of Pet DRx Corporation until July 2010 and Encore Medical until June 2006.
Executive Officers
Information regarding our Chief Executive Officer, Gerald R. Mattys, is included above under the heading “Directors”.
Lynn L. Blake, age 50, has served as our Chief Financial Officer since joining the company in April 2016. Prior to joining our company, Ms. Blake served as Chief Financial Officer and Secretary of Taylor-Wharton International LLC, a global industrial products manufacturer, from September 2014 through December 2015. Prior to joining Taylor-Wharton International LLC, Ms. Blake served as Chief Financial Officer and Treasurer of Analysts International Corporation, a leading national information technology services firm, from July 2012 until its sale in October 2013. Prior to these roles, Ms. Blake held a variety of senior financial leadership positions at companies including Entegris, Inc., MTS Systems Corporation, and Honeywell International Inc.
Robert J. Folkes, age 54, has served as our Chief Operating Officer since February 2015. He served as our Chief Financial Officer from 2005 until April 2016. Prior to joining our company in 2004, Mr. Folkes was the Chief Financial Officer for Advanced Respiratory, a medical device company, from 1997 until its sale in 2003. Prior to joining Advanced Respiratory, Mr. Folkes was an Audit Senior Manager for Ernst & Young LLP.
Mary E. Anderson, age 53, has served as our Vice President, Reimbursement since April 2007, and prior to that was our Director of Reimbursement since she started with our company in 2005. Prior to joining our company, Ms. Anderson served in various roles at Advanced Respiratory, a medical device company, from 1990 until its sale in 2003, including Controller, Chief Financial Officer and Vice President of Internal Operations. Ms. Anderson began her career as an auditor with Ernst & Young LLP.
Bryan F. Rishe, age 61, has served as our Vice President, Sales since 2008. From 2004 to 2008, he served as the Vice President, Sales for BSN Medical, a medical soft goods manufacturer. Mr. Rishe also served as the Vice President, Sales and Marketing for TFX Medical, a surgical equipment manufacturer. Prior to that, Mr. Rishe was the Western Area Manager with Surgical Laser Technologies, a specialty laser company. Mr. Rishe has held other sales leadership and business development roles with Becton Dickinson, Baxter Travenol and American Hospital Supply.
107
Mary M. "Maggie" Thompson, age 59, has served as our Vice President, Payer Relations and Government Affairs since 2006. Prior to joining our company, Ms. Thompson served as Director of Reimbursement for Uroplasty, Inc., a medical device company, from 2005-2006. From 1998 until 2005, Ms. Thompson served as Director of Payer Relations at Advanced Respiratory, a medical device company. A registered nurse, Ms. Thompson first practiced nursing at Gillette Children's Hospital and at a grant-funded community clinic in St. Paul. She then worked for the Minnesota Attorney General's Office as a nurse consultant until she joined a large health plan as the Government Programs Quality Regulatory Manager working closely with the Centers for Medicare and Medicaid Services and Minnesota's Medicaid program. Ms. Thompson is active in the Alliance for Wound Care Stakeholders and is a member of Women's Business Leaders in Healthcare.
Corporate Governance
Our board of directors has adopted a Code of Business Conduct and Ethics that applies to our directors, officers and employees. This code is available on the corporate governance section of our website (which is a subsection of the investor relations section of our website) at the following address: www.tactilemedical.com. We intend to disclose on our website any amendments or waivers to the Code that are required to be disclosed by SEC rules.
Additional information required by this Item 10 will be contained in our definitive proxy statement for our 2017 Annual Meeting of Stockholders (the “Definitive Proxy Statement”) and is incorporated herein by reference.
Item 11. Executive Compensation.
The information required by this Item 11 will be contained in the Definitive Proxy Statement and is incorporated herein by reference.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The information required by this Item 12 will be contained in the Definitive Proxy Statement and is incorporated herein by reference.
Item 13. Certain Relationships and Related Transactions, and Director Independence.
The information required by this Item 13 will be contained in the Definitive Proxy Statement and is incorporated herein by reference.
Item 14. Principal Accountant Fees and Services.
The information required by this Item 14 will be contained in the Definitive Proxy Statement and is incorporated herein by reference.
Item 15. Exhibits, Financial Statement Schedules.
|
1. |
Financial Statements |
The following financial statements of Tactile Systems Technology, Inc. are set forth in Part II, Item 8:
Report of Independent Registered Public Accounting Firm
Consolidated Balance Sheets as of December 31, 2016 and 2015
Consolidated Statements of Operations for the years ended December 31, 2016, 2015 and 2014
Consolidated Statements of Comprehensive Income for the years ended December 31, 2016, 2015 and 2014
Consolidated Statements of Stockholders’ Equity (Deficit) as of December 31, 2016, 2015 and 2014
Consolidated Statements of Cash Flows for the years ended December 31, 2016, 2015 and 2014
Notes to Consolidated Financial Statements
108
|
2. |
Financial Statement Schedules |
Not applicable
|
3. |
Exhibits |
A list of exhibits required to be filed as part of this report is set forth in the Index to Exhibits, which immediately precedes such exhibits and is incorporated herein by reference
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
Tactile Systems Technology, Inc. |
|||
|
Date: February 27, 2017 |
By: |
/s/ Gerald R. Mattys |
|
|
Gerald R. Mattys |
|||
|
Chief Executive Officer |
|||
|
(Principal executive officer) |
|||
Each of the undersigned hereby appoints Gerald R. Mattys and Lynn L. Blake, and each of them (with full power to act alone), as attorneys and agents for the undersigned, with full power of substitution, for and in the name, place and stead of the undersigned, to sign and file with the Securities and Exchange Commission under the Securities Act of 1934, any and all amendments and exhibits to this annual report on Form 10-K and any and all applications, instruments, and other documents to be filed with the Securities and Exchange Commission pertaining to this annual report on Form 10-K or any amendments thereto, with full power and authority to do and perform any and all acts and things whatsoever requisite and necessary or desirable. Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities indicated on February 27, 2017.
|
Name |
|
Title |
|
|
|
|
|
/s/ Gerald R. Mattys |
|
Chief Executive Officer (principal executive officer) and Director |
|
Gerald R. Mattys |
|
|
|
|
|
|
|
/s/ Lynn L. Blake |
|
Chief Financial Officer (principal financial officer and principal accounting officer) |
|
Lynn L. Blake |
|
|
|
|
|
|
|
/s/ Peter H. Soderberg |
|
Chairman of the Board of Directors |
|
Peter H. Soderberg |
|
|
|
|
|
|
|
/s/ William W. Burke |
|
Director |
|
William W. Burke |
|
|
|
|
|
|
|
/s/ Jordan S. Davis |
|
Director |
|
Jordan S. Davis |
|
|
|
|
|
|
|
/s/ Richard Nigon |
Director |
|
|
Richard Nigon |
|
|
109
|
/s/ Kevin H. Roche |
|
Director |
|
Kevin H. Roche |
|
|
|
|
|
|
|
/s/ Stephen I. Shapiro |
|
Director |
|
Stephen I. Shapiro |
|
|
|
|
|
|
|
/s/ Zubeen Shroff |
|
Director |
|
Zubeen Shroff |
|
|
110
EXHIBIT INDEX
|
Exhibit |
|
Description of Exhibit |
|
Incorporated by Reference |
|
Filed |
||||||
|
|
|
|
|
Form |
|
File Number |
|
Date of Filing |
|
Exhibit |
|
|
|
2.1^ |
|
Asset Sale and Purchase Agreement, dated as of September 14, 2012, by and between Tactile Systems Technology, Inc., Swelling Solutions, Inc., ConvaTec Inc. and ConvaTec Technologies, Inc. |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
2.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.1 |
Fourth Amended and Restated Certificate of Incorporation |
S-1 |
333-209115 |
06/09/2016 |
3.1 |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3.2 |
|
Amended and Restated By-laws |
|
S-1 |
|
333-209115 |
|
05/06/2016 |
|
3.2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.1 |
|
Specimen Certificate representing shares of common stock |
|
S-1 |
|
333-209115 |
|
05/06/2016 |
|
4.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4.2 |
|
Amended and Restated Investors' Rights Agreement dated September 14, 2012 |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
4.2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.1* |
|
2003 Stock Option Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.2* |
|
Form of Incentive Stock Option Agreement under 2003 Stock Option Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.3* |
|
Form of Non-Statutory Stock Option Agreement (Employee) under 2003 Stock Option Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.4* |
|
Form of Non-Statutory Stock Option Agreement (Director) under 2003 Stock Option Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.5* |
|
2007 Omnibus Stock Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.6* |
|
Form of Incentive Stock Option Agreement under 2007 Omnibus Stock Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.7* |
|
Form of Non-Statutory Stock Option Agreement (Employee) under 2007 Omnibus Stock Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.8* |
|
Form of Non-Statutory Stock Option Agreement (Directors) under 2007 Omnibus Stock Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.9* |
|
Form of Non-Statutory Stock Option Agreement (Consultants) under 2007 Omnibus Stock Plan |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.10* |
|
Form of Restricted Stock Agreement |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
10.10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.11* |
|
2016 Equity Incentive Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.11 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.12* |
|
Form of Non-Qualified Stock Option Agreement under 2016 Equity Incentive Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.13* |
|
Form of Incentive Stock Option Agreement under 2016 Equity Incentive Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.13 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
111
|
10.14* |
|
Form of Restricted Stock Agreement under 2016 Equity Incentive Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.15* |
|
Form of Restricted Stock Unit Award Agreement under 2016 Equity Incentive Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.16* |
|
Form of Restricted Stock Unit Agreement under 2016 Equity Incentive Plan (Quarterly Awards) |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.17* |
|
Employee Stock Purchase Plan |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.17 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.18* |
|
Non-Employee Director Compensation Policy |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.19* |
|
Form of Director and Officer Indemnification Agreement |
|
S-1 |
|
333-209115 |
|
05/06/2016 |
|
10.19 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.20* |
|
Form of Employment Agreement between Tactile Systems Technology, Inc. and its named executive officers |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.21* |
|
Employment Agreement between Tactile Systems Technology, Inc. and Gerald Mattys |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.22* |
|
Employment Agreement between Tactile Systems Technology, Inc. and Lynn Blake |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.23 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.23* |
|
Employment Agreement between Tactile Systems Technology, Inc. and Bryan Rishe |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.24 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10.24 |
|
Line of credit documents, as amended May 11, 2016 by and between Tactile Systems Technology, Inc. and Venture Bank |
|
S-1 |
|
333-209115 |
|
06/09/2016 |
|
10.21 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21.1 |
|
Subsidiaries |
|
S-1 |
|
333-209115 |
|
01/25/2016 |
|
21.1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23.1 |
|
Consent of Grant Thornton LLP |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24.1 |
|
Power of Attorney (included in signature page) |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.1 |
|
Certification of Principal Executive Officer pursuant to Rule 13a-14(a) / 15d-14(a) of the Securities Exchange Act of 1934, as amended |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31.2 |
|
Certification of Principal Financial Officer pursuant to Rule 13a-14(a) / 15d-14(a) of the Securities Exchange Act of 1934, as amended |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.1 |
|
Certification of Principal Executive Officer pursuant to 18 U.S.C. § 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32.2 |
|
Certification of Principal Financial Officer pursuant to 18 U.S.C. §1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
112
|
101.1 |
|
The following financial statements from the Company’s Annual Report on Form 10-K for the year ended December 31, 2016, formatted in XBRL: (i) Balance Sheets, (ii) Statements of Operations, (iii) Statements of Cash Flows, and (iv) Notes to the Financial Statements |
|
|
|
|
|
|
|
|
|
X |
^Schedules to this exhibit have been omitted pursuant to Item 601(b)(2) of Regulation S-K. A copy of any omitted schedule will be furnished supplementally to the Securities and Exchange Commission upon request.
*Indicates management contract or compensatory plan or arrangement.
113