Attached files
| file | filename |
|---|---|
| EX-99.1 - EXHIBIT 99.1 - Aevi Genomic Medicine, Inc. | v445891_ex99-1.htm |
| 8-K - FORM 8-K - Aevi Genomic Medicine, Inc. | v445891_8k.htm |
Exhibit 99.2
Mid - Year Review and Business Update August 4, 2016
Forward Looking Statement This presentation includes certain estimates and other forward - looking statements within the meaning of Section 21E of the Securities Exchange Act of 1934, as amended, including statements with respect to anticipated operating and financial performance, clinical results, potential partnerships, licensing opportunities and other statements of expectation. Words such as “expects,” “anticipates,” “intends,” “plans,” “believes,” “assumes,” “seeks,” “estimates,” “should” and variations of these words and similar expressions, are intended to identify these forward - looking statements. While we believe these statements are accurate, forward - looking statements are inherently uncertain and we cannot assure you that these expectations will occur and our actual results may be significantly different. These statements by the Company and its management are based on estimates, projections, beliefs and assumptions of management and are not guarantees of future performance. Important factors that could cause actual results to differ from those in the forward - looking statements include the factors described in the Company’s filings with the U.S. Securities and Exchange Commission. The Company disclaims any obligation to update or revise any forward - looking statement based on the occurrence of future events, the receipt of new information, or otherwise. 2
Agenda 3 • Mid - Year Summary • Genomic Medicine Approach • Anti - LIGHT Program Overview • Financials & Milestones
Mid Year - Summary 4 ; NFC – 1 Programs Advancing Rapidly – mGlurR + ADHD • Record response and recruitment to phenotype/genotype study (1,000 Patients) • Confirmation of mGluR + prevalence rate of 25% • Enrolment initiating in June with data expected in 2H2016 • US market opportunity of $2 – 3B – 22q Deletion Syndrome • Orphan program in collaboration with CHOP • Enrolment initiating in August with initial Open - Label data expected 2H2016 ; New Biologics Development Program with KHK in Severe Pediatric IBD – 1st in class P2 ready biologic with minimal investment to POC – Strong genetic thesis and significant unmet medical need – High value commercial opportunity with first US launch anticipated in 2020 ; Strengthened Balance Sheet – Completed registered public offering, raising ~$20M in net proceeds – Extends the cash runway through Q1 2018 ; Genomic Approach – MDGN/CAG translational research continues to prod uce potential development targets
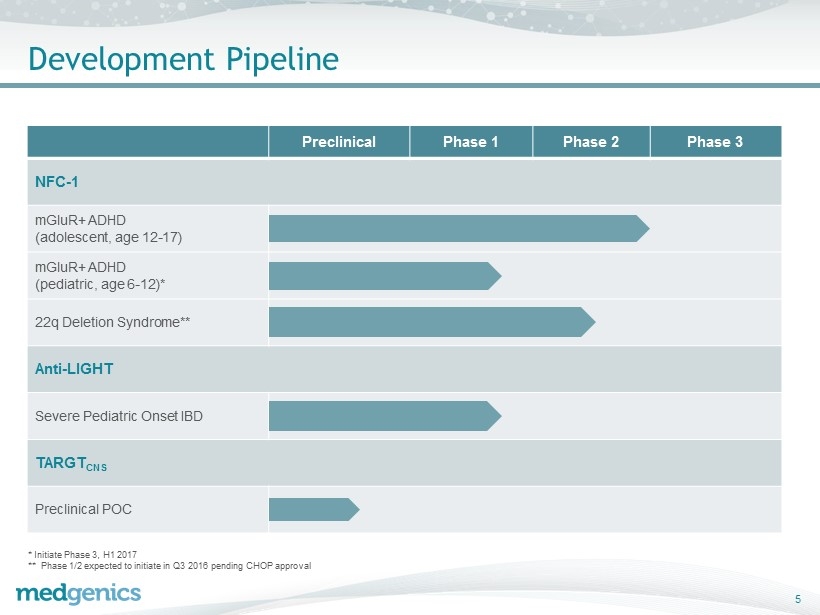
Development Pipeline 5 Preclinical Phase 1 Phase 2 Phase 3 NFC - 1 mGluR+ ADHD (adolescent, age 12 - 17 ) mGluR+ ADHD (pediatric, age 6 - 12 ) * 22q Deletion Syndrome ** Anti - LIGHT Severe Pediatric Onset IBD TARGT CNS Preclinical POC * Initiate Phase 3, H1 2017 ** Phase 1/2 expected to initiate in Q3 2016 pending CHOP approval

Genomic Medicine Approach
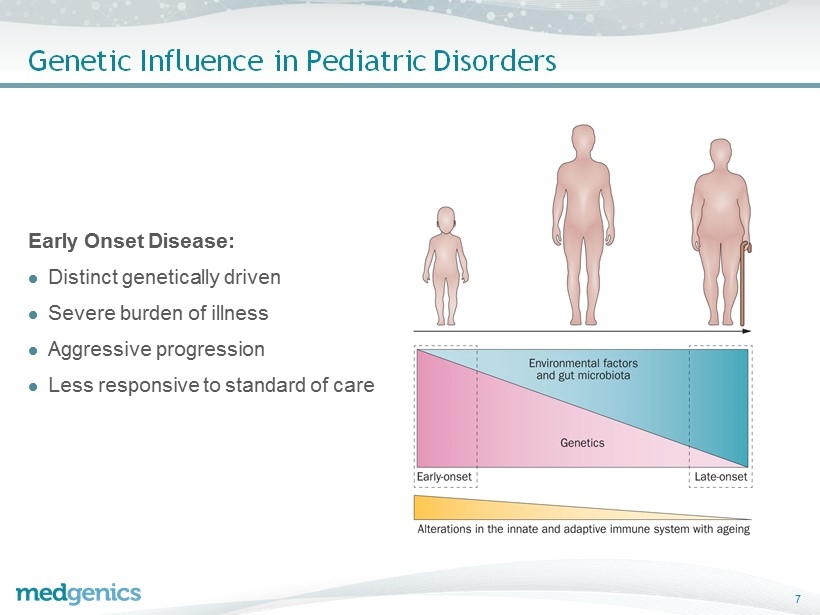
Genetic Influence in Pediatric Disorders E arly Onset Disease: ; Distinct genetically driven ; Severe burden of illness ; Aggressive progression ; Less responsive to standard of care 7
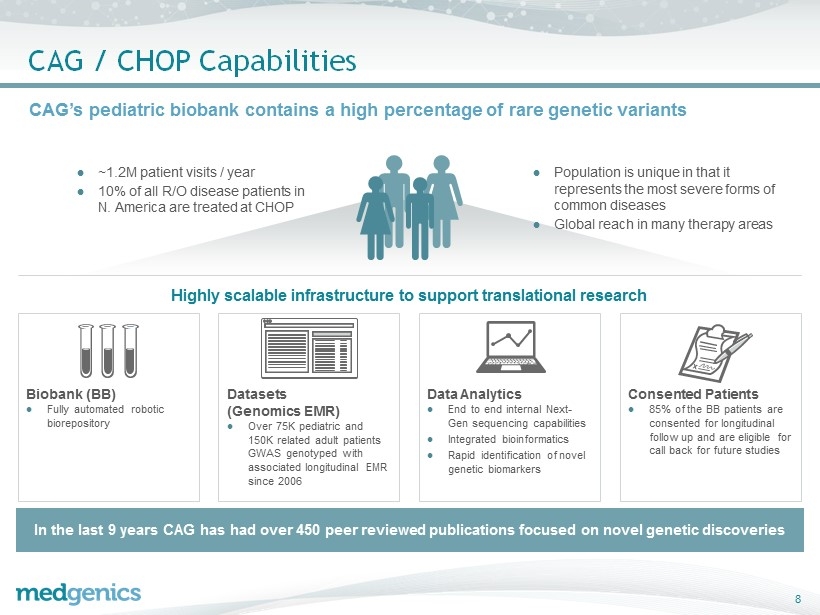
CAG / CHOP Capabilities CAG’s pediatric biobank contains a high percentage of rare genetic variants Datasets (Genomics EMR) ; Over 75K pediatric and 150K related adult patients GWAS genotyped with associated longitudinal EMR since 2006 Data Analytics ; End to end internal Next - Gen sequencing capabilities ; Integrated bioinformatics ; Rapid identification of novel genetic biomarkers Biobank (BB) ; Fully automated robotic biorepository Consented Patients ; 85% of the BB patients are consented for longitudinal follow up and are eligible for call back for future studies ; ~1.2M patient visits / year ; 10% of all R/O disease patients in N. America are treated at CHOP ; Population is unique in that it represents the most severe forms of common diseases ; Global reach in many therapy areas In the last 9 years CAG has had over 450 peer reviewed publications focused on novel genetic discoveries Highly scalable infrastructure to support translational research 8
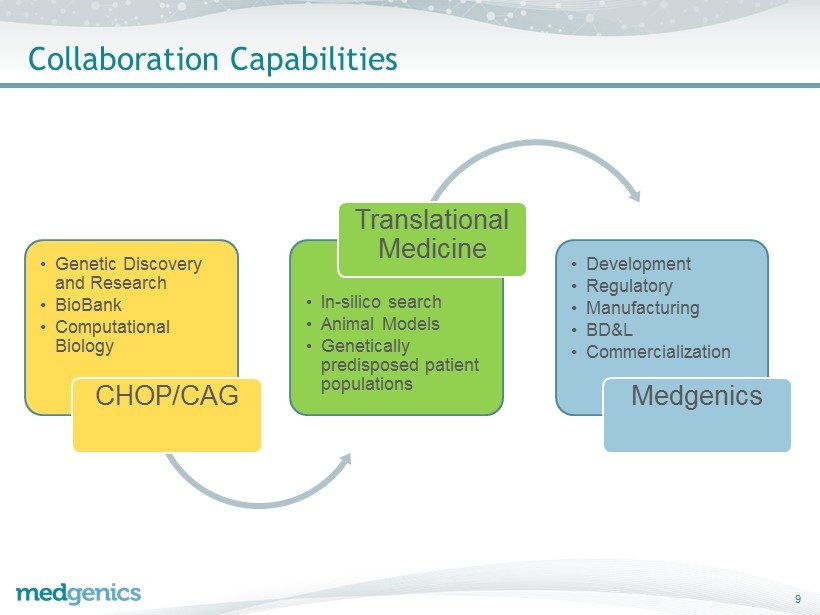
• Genetic Discovery and Research • BioBank • Computational Biology CHOP/CAG • In - silico search • Animal Models • Genetically predisposed patient populations Translational Medicine • Development • Regulatory • Manufacturing • BD&L • Commercialization Medgenics Collaboration Capabilities 9
Benefits of Genomic Guided Drug Development Higher Value Medicines Improved response rates Smaller, faster, clinical trials Increased probability of regulatory success Targeted launch Potential label expansion in adjacent genetic diseases G enomic biomarkers improve overall program outcomes 10

Anti - LIGHT mAb Program
Anti - LIGHT mAb Overview ; First - in - Class Biologic from Kyowa Hakko Kirin – Initial Development in Severe Pediatric Onset IBD – Phase 2 Ready Antibody – Strong Regulatory Exclusivity and Robust Intellectual Property Portfolio – High Value Commercial Opportunity with Potential for Indication Expansion ; World Class Partners – Kyowa Hakko Kirin – The Children’s Hospital of Philadelphia ; Rapid and Capital Efficient Global Development Pathway – Minimal investment to POC – Single Pivotal Trial for registration 12
Deal Terms ; MDGN to: – Requalify KHK clinical supplies – Conduct signal finding study (~$2M) – Exercise option to license on positive data (low single - digit millions USD) ; Following option exercise, KHK elects either: – Partnership • “Co - Development/Co - Commercialization ” – Parties share sales and costs equally in US and Canada; MDGN receives double - digit royalty on ex - North Americ a net sales – License • MDGN funds development and commercializes in North America and EU, and retains approximately 75% of profits, MDGN receives double - digit royalty on ROW sales ; Success - based development milestones payable in both scenarios 13
CAG / CHOP Discovery: Genetic Link to Pediatric Onset IBD 14 Key Points ; Established importance of the DcR3 gene in pediatric IBD ; Loss of function of DcR3 correlates with severity ; Prevalence between 10 - 15% Nature Genetics VOLUME 40 | NUMBER 10 | OCTOBER 2008

Rationale for Anti - LIGHT Approach ; DcR3 is strongly linked to Severe Pediatric Onset IBD 1 ; Initial strategy to augment DcR3 – Very short half life – Toxicity reported with previous DcR3 analog ; “Rational Search” based on biological pathway – LIGHT overexpressed in IBD – DcR3 LOF increases LIGHT 2 15 Decoy Receptor 3 DcR3 LIGHT Immune Cell HVEM LT b R 1 Hakonarson, et al 2008. Loci on 20q13 and 21q22 are associated with pediatric - onset inflammatory bowel disease. Nature Genet ics 40 (10): 1211 - 1215 2 Mauri DN, et al 1998. LIGHT, a new member of the TNF superf amily, and lymphotoxin alpha are ligands for herpesvirus entry med iator.Immunity 8 (1): 21 – 30 Our Approach: Therapeutic antibody which mimics DcR3 regulation by binding LIGHT
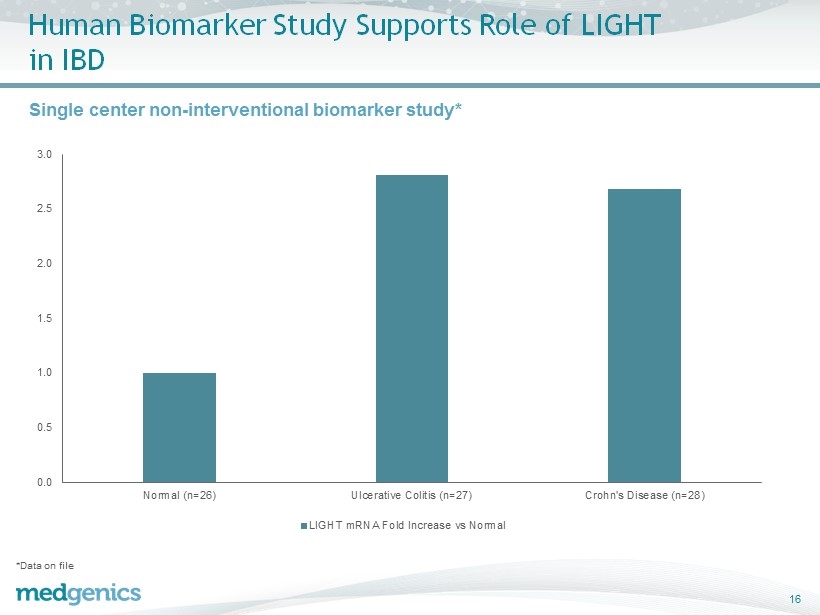
Human Biomarker Study Supports Role of LIGHT in IBD 16 Single center non - interventional biomarker study* 0.0 0.5 1.0 1.5 2.0 2.5 3.0 Normal (n=26) Ulcerative Colitis (n=27) Crohn's Disease (n=28) LIGHT mRNA Fold Increase vs Normal *Data on file
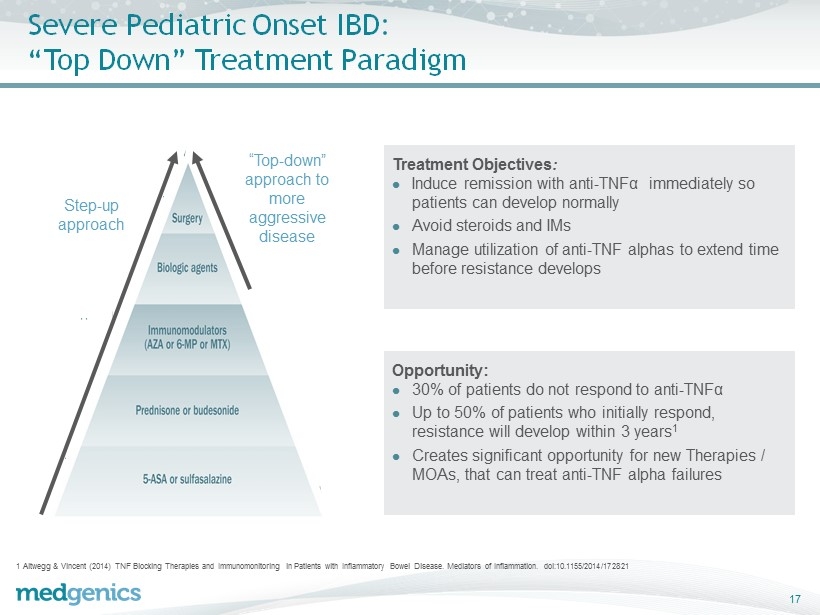
Severe Pediatric Onset IBD: “Top Down” Treatment Paradigm 17 1 Altwegg & Vincent (2014) TNF Blocking Therapies and Immunomonitoring in Patients with Inflammatory Bowel Disease. Mediators of Inflammation. doi:10.1155/2014/172821 Treatment Objectives : ; Induce remission with anti - TNFα immediately so patients can develop normally ; Avoid steroids and IMs ; Manage utilization of anti - TNF alphas to extend time before resistance develops Opportunity: ; 30% of patients do not respond to anti - TNFα ; Up to 50% of patients who initially respond, resistance will develop within 3 years 1 ; Creates significant opportunity for new Therapies / MOAs, that can treat anti - TNF alpha failures Step - up approach “Top - down” approach to more aggressive disease
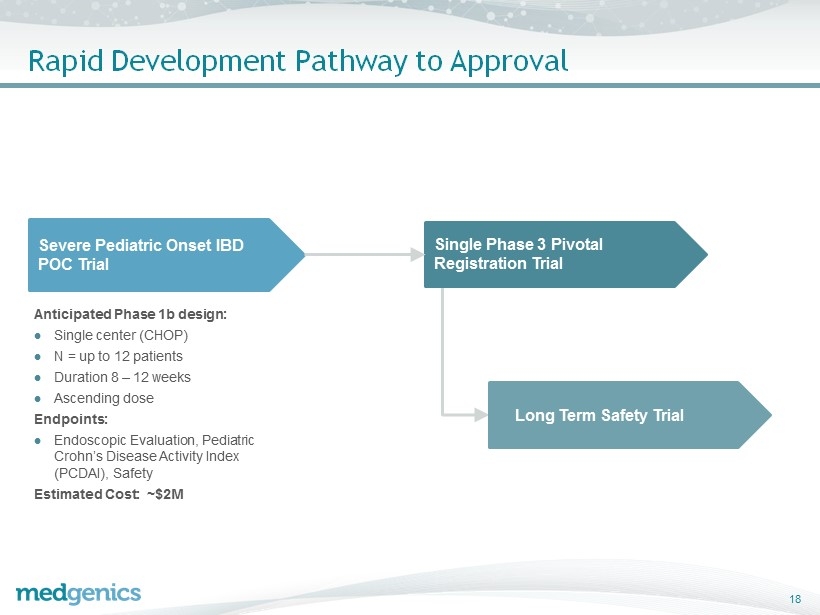
Rapid Development Pathway to Approval 18 Severe Pediatric Onset IBD POC Trial Anticipated Phase 1b design: ; Single center (CHOP) ; N = up to 12 patients ; Duration 8 – 12 weeks ; Ascending dose Endpoints: ; Endoscopic Evaluation, Pediatric Crohn’s Disease Activity Index (PCDAI), Safety Estimated Cost: ~$2M Single Phase 3 Pivotal Registration Trial Long Term Safety Trial
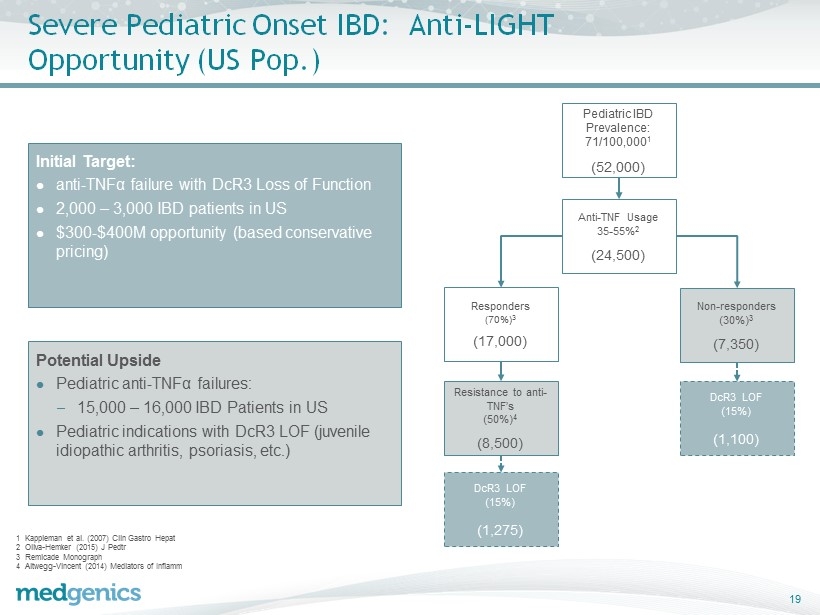
Severe Pediatric Onset IBD: Anti - LIGHT Opportunity (US Pop.) 19 1 Kappleman et al. (2007) Clin Gastro Hepat 2 Oliva - Hemker (2015) J Pedtr 3 Remicade Monograph 4 Altwegg - Vincent (2014) Mediators of Inflamm Initial Target: ; anti - TNFα failure with DcR3 Loss of Function ; 2,000 – 3,000 IBD patients in US ; $300 - $400M opportunity (based conservative pricing) Potential Upside ; Pediatric anti - TNFα failures: – 15,000 – 16,000 IBD Patients in US ; Pediatric indications with DcR3 LOF (juvenile idiopathic arthritis, psoriasis, etc.) Pediatric IBD Prevalence: 71/100,000 1 (52,000) Anti - TNF Usage 35 - 55% 2 (24,500) Responders (70%) 3 (17,000) Resistance to anti - TNF’s (50%) 4 (8,500) DcR3 LOF (15%) (1,275) Non - responders (30%) 3 (7,350) DcR3 LOF (15%) (1,100)

Financials & Milestones
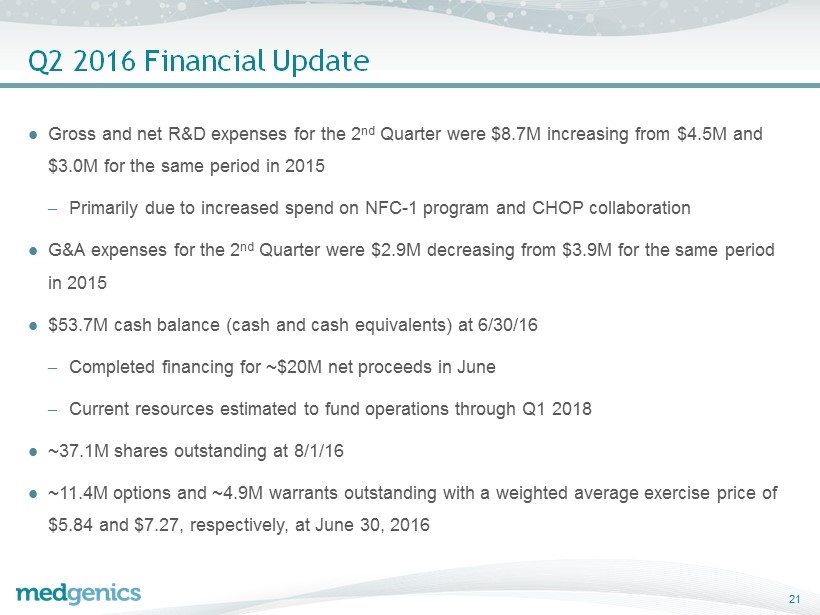
Q2 2016 Financial Update ; Gross and net R&D expenses for the 2 nd Quarter were $8.7M increasing from $4.5M and $3.0M for the same period in 2015 – Primarily due to increased spend on NFC - 1 program and CHOP collaboration ; G&A expenses for the 2 nd Quarter were $2.9M decreasing from $3.9M for the same period in 2015 ; $53.7M cash balance (cash and cash equivalents) at 6/30/16 – Completed financing for ~$20M net proceeds in June – Current resources estimated to fund operations through Q1 2018 ; ~37.1M shares outstanding at 8/1/16 ; ~11.4M options and ~4.9M warrants outstanding with a weighted average exercise price of $5.84 and $7.27, respectively, at June 30, 2016 21
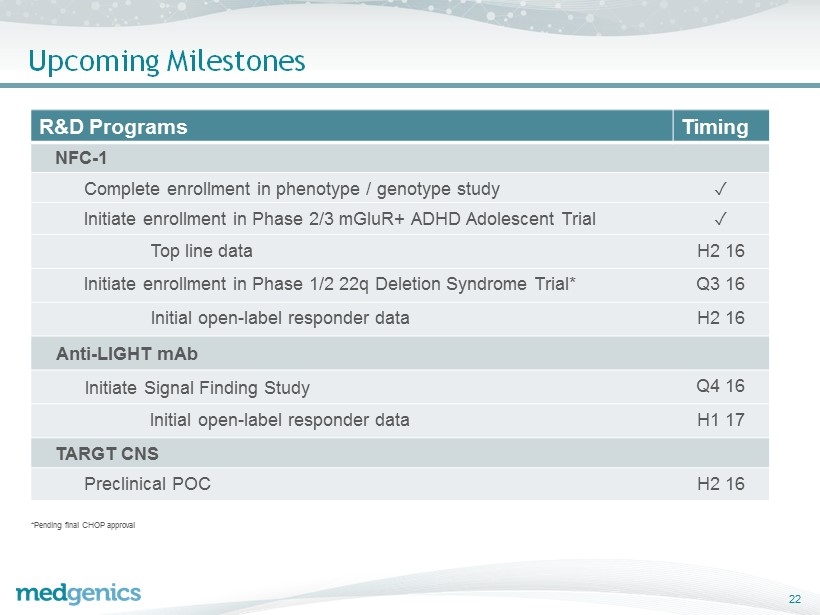
Upcoming Milestones *Pending final CHOP approval 22 R&D Programs Timing NFC - 1 Complete enrollment in phenotype / genotype study ✓ Initiate enrollment in Phase 2/3 mGluR+ ADHD Adolescent Trial ✓ Top line data H2 16 Initiate enrollment in Phase 1/2 22q Deletion Syndrome Trial* Q3 16 Initial open - label responder data H2 16 Anti - LIGHT mAb Initiate Signal Finding Study Q4 16 Initial open - label responder data H1 17 TARGT CNS Preclinical POC H2 16
Thank You