Attached files
Exhibit 99.1

April 2016 NASDAQ: WINT
Forward Looking Statement 2 To the extent that statements in this presentation are not strictly historical, including statements about the Company’s business strategy, outlook, objectives, plans, intentions, goals, future financial conditions, future collaboration agreements, the success of the Company’s product development, or otherwise as to future events, such statements are forward-looking, and are made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. The forward-looking statements contained in this presentation are subject to certain risks and uncertainties that could cause actual results to differ materially from the statements made. These risks are further described in the Company's periodic filings with the Securities and Exchange Commission (SEC), including the most recent reports on Forms 10-K, 8-K and 10-Q, and any amendments thereto (“Company Filings”). This presentation under no circumstances shall be construed as an offer to sell or as a solicitation of an offer to buy any of the Company’s securities. In addition, the information presented in this deck is qualified in its entirety by the Company Filings. The reader is encouraged to refer to the Company Filings for a fuller discussion of the matters presented here.
3 Public biotherapeutic / medical device company; Nasdaq: WINT Based in Warrington, PA with 55 employees Lead program focused in the acute respiratory area

4 Experienced Management Team Very experienced management team averaging over 20 years of experience developing drugs and devices and building and leading businesses

Well characterized asset and target applicationPotential to develop a transformative therapy for an established market that has a clear unmet needBuilding a data base of potential safety, clinical effect and benefit informationOpportunity to build a positive health economic positionStrong IP with the potential to build a pipeline of aerosolized KL4 surfactant therapies to address a variety of respiratory diseasesExperienced management team focused on rigorous clinical execution and effective cash management High Value-Creating Potential Innovative synthetic KL4 surfactant and breakthrough aerosolized delivery systemInitially focused on respiratory distress syndrome (RDS) in premature infants – 5

AEROSURF®Aerosolized Surfactant for RDS Potential to transform the treatment of premature infants with RDS by making surfactant therapy available through non-invasive delivery technology Proprietary Synthetic KL4 Surfactant Designed to be structurally similar to human lung surfactantLiquid KL4 surfactant (intratracheal instillate) for RDS approved by the FDA Lyophilized (freeze-dried) KL4 surfactant – developed initially for AEROSURF® Innovative Aerosol Delivery Technology Designed specifically to aerosolize and deliver surfactant 6
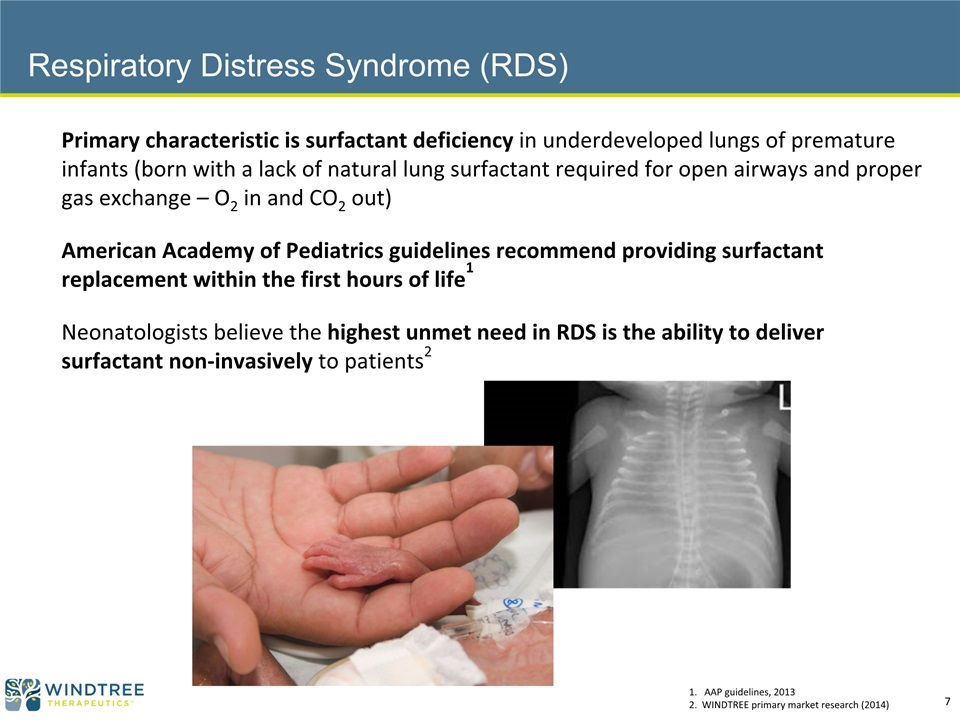
Primary characteristic is surfactant deficiency in underdeveloped lungs of premature infants (born with a lack of natural lung surfactant required for open airways and proper gas exchange – O2 in and CO2 out)American Academy of Pediatrics guidelines recommend providing surfactant replacement within the first hours of life1Neonatologists believe the highest unmet need in RDS is the ability to deliver surfactant non-invasively to patients2 1. AAP guidelines, 20132. WINDTREE primary market research (2014) Respiratory Distress Syndrome (RDS) 7

Current Treatment of RDS: Intubate or Not? Current surfactant replacement therapy (SRT) requires intubation and mechanical ventilation (MV); available surfactants are animal-derivedInvasive intubation and MV can result in serious respiratory conditions and other complications, such as higher risk of infection and bronchopulmonary dysplasia (BPD) Considered less invasive but does not address underlying condition – surfactant deficiencyMany infants respond poorly and require delayed rescue SRT via intubation and MV (“nCPAP failure”) Earlier SRT produces better outcomes compared to late SRT1 Invasive Intubation Nasal continuous positive airway pressure (nCPAP) 1. AAP guidelines, 2013 8

nCPAP Used Across All Gestational Ages (GA) and Severity of RDS Frequency and Severity of RDS & Incidence of CPAP Failure Rate HIGHER LOWER GA 26-28 wks(85-95% have RDS) GA 29-32 wks(65-75% have RDS) GA 33-34 wks(40-50% have RDS) 30% ETT/SRT CPAP 70% 55% ETT/SRT CPAP 45% 70% ETT/SRT CPAP 30% Source: WINDTREE primary market research (2014); IMS MIDAS data (2012); CDC National Vital Statistics, 2014, Healthcare Costs and Utilization Project (HCUP), 2013; Agency for Healthcare Research and Quality (AHRQ), 2012; Births by birth weight (CDC Website). Note: ETT/SRT – administration of surfactant replacement therapy via intubation with an endotracheal tube 9 HIGHER LOWER Size of Sub-Population

Trends in Non-Invasive Care of Neonates – Increasing Use of nCPAP to Avoid Intubation However, still experience high nCPAP failure rates First-line nCPAP use has been trending up across all gestational ages up to 32 weeks GA Est. GA: < 24 wks ~24-27 wks ~28-29 wks ~30-32 wks Source: Soll, Obstetric and Neonatal Care Practices for Infants 501 to 1500 g From 2000 to 2009; Pediatrics; July 2013 Source: Soll, Obstetric and Neonatal Care Practices for Infants 501 to 1500 g From 2000 to 2009; Pediatrics; July 2013 10
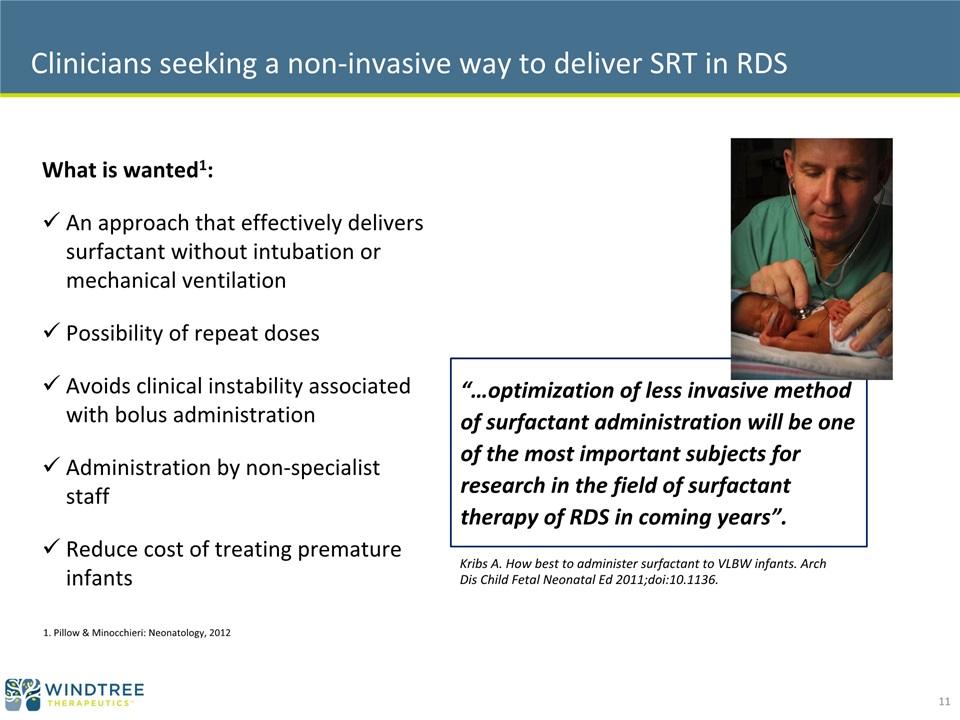
Clinicians seeking a non-invasive way to deliver SRT in RDS What is wanted1:An approach that effectively delivers surfactant without intubation or mechanical ventilationPossibility of repeat dosesAvoids clinical instability associated with bolus administrationAdministration by non-specialist staffReduce cost of treating premature infants 1. Pillow & Minocchieri: Neonatology, 2012 “…optimization of less invasive method of surfactant administration will be one of the most important subjects for research in the field of surfactant therapy of RDS in coming years”. Kribs A. How best to administer surfactant to VLBW infants. Arch Dis Child Fetal Neonatal Ed 2011;doi:10.1136. 11

12 Innovative, Proprietary Device Provides the Breakthrough Capillary Drug pumped through capillary Energy Input Aerosolized KL4 Surfactant via nCPAP Transformative administration of KL4 surfactant without invasive intubation and early in the management of RDS in premature infants AEROSURF®
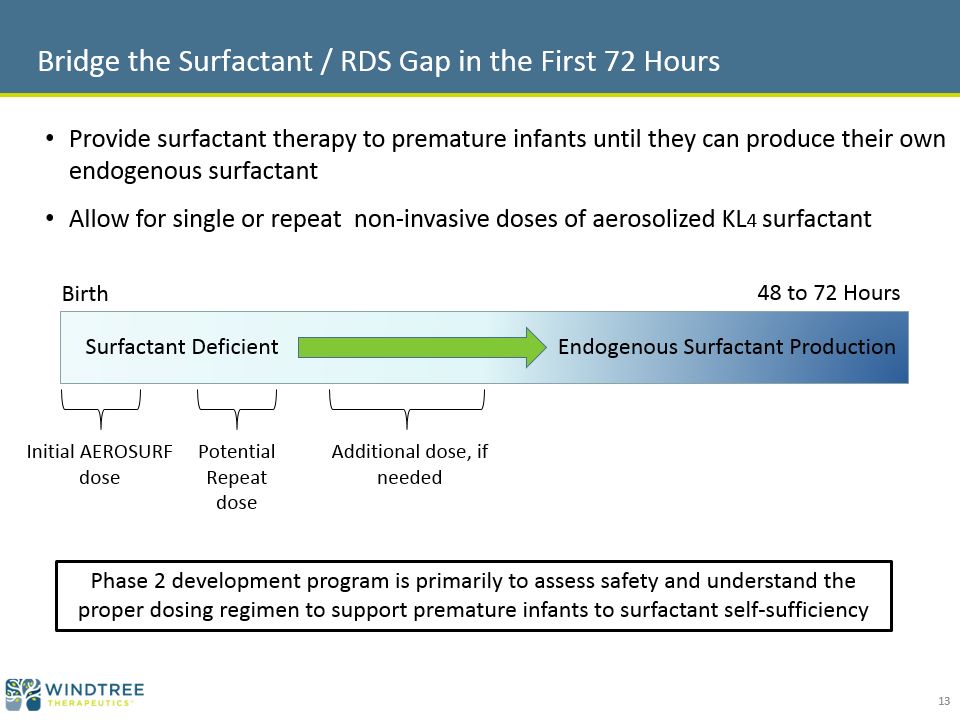
Bridge the Surfactant / RDS Gap in the First 72 Hours 48 to 72 Hours Surfactant Deficient Endogenous Surfactant Production Birth Provide surfactant therapy to premature infants until they can produce their own endogenous surfactantAllow for single or repeat non-invasive doses of aerosolized KL4 surfactant Initial AEROSURF dose Potential Repeat dose Additional dose, if needed Phase 2 development program is primarily to assess safety and understand the proper dosing regimen to support premature infants to surfactant self-sufficiency 13

Phase 2a Phase 2a Expansion Gestational Age (wks) 29 – 34 Dose Groups 15 min; 30 min; 45 min( 25, 50, 75 TPL mg/kg)(8 active, 8 control per group)Single dose 60 min; 90 min (100 and 150 TPL mg/kg)(8 active, 8 control per group)Primarily single dose # of patients 48 32 Objective(s) Safety and tolerabilityPhysiological data suggesting delivery of KL4 surfactant to the lungsPerformance of Aerosol Delivery System Safety and tolerability of higher doses and determine therapeutic index (safety window)Continue physiological assessment # of sites Initiated with 3; increased to 8 (US) 12 (US) Timeline / Milestones Completed May 2015; key objectives achieved Completed Oct 2015 Comprehensive Phase 2 Program – Completed Trials 14
Phase 2a Study (29 to 34 wks GA)Study Objectives Primary ObjectiveSafety and tolerability of AEROSURF® compared to nCPAP aloneOther Key ObjectivesAssess physiological data indicating that aerosolized KL4 surfactant is being delivered into the lungs of premature infantsGas exchange: FiO2 requirements and changes in CO2Need for rescue therapy and requirement for invasive respiratory supportAcceptable performance of the Aerosol Delivery System (ADS) in the NICU 15

Phase 2a Study (29 to 34 wks GA)Safety and Tolerability - Summary The safety and tolerability profile of AEROSURF® was generally comparable to the control groupThe Independent Safety Review Committee supports proceeding to the next studies in our programThe Aerosol Delivery System delivered KL4 surfactant to the infants in a way that was well toleratedThe adverse events and serious adverse events (SAE) seen were expected for this patient population and generally comparable between AEROSURF® and control groupsMost common adverse events were jaundice, constipation, apnea and anemiaMost common SAE’s were air leaks (including pneumothorax, pneumomediastinum and pulmonary interstitial emphysema) There was no pattern of increased adverse events or serious adverse events with increasing AEROSURF dose 16
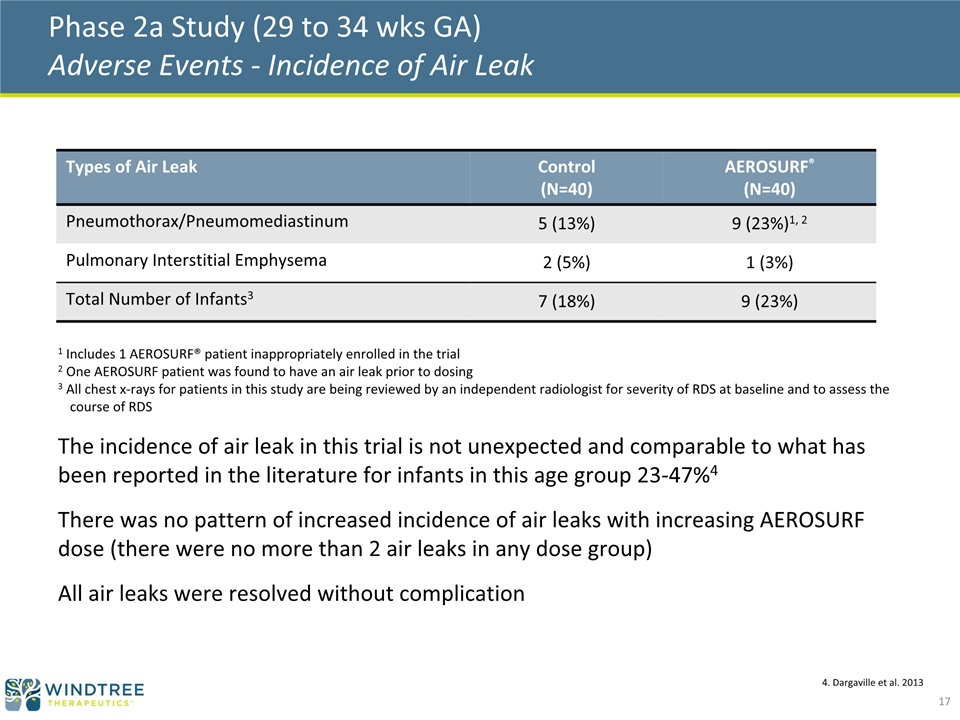
Phase 2a Study (29 to 34 wks GA) Adverse Events - Incidence of Air Leak Types of Air Leak Control(N=40) AEROSURF®(N=40) Pneumothorax/Pneumomediastinum 5 (13%) 9 (23%)1, 2 Pulmonary Interstitial Emphysema 2 (5%) 1 (3%) Total Number of Infants3 7 (18%) 9 (23%) 1 Includes 1 AEROSURF® patient inappropriately enrolled in the trial2 One AEROSURF patient was found to have an air leak prior to dosing3 All chest x-rays for patients in this study are being reviewed by an independent radiologist for severity of RDS at baseline and to assess the course of RDSThe incidence of air leak in this trial is not unexpected and comparable to what has been reported in the literature for infants in this age group 23-47%4There was no pattern of increased incidence of air leaks with increasing AEROSURF dose (there were no more than 2 air leaks in any dose group)All air leaks were resolved without complication 4. Dargaville et al. 2013 17

Phase 2a Study (29 to 34 wks GA)Physiological Data ObjectiveEstablish proof of concept that aerosolized KL4 surfactant is being delivered into the lungs of premature infants by assessing: Need for rescue therapy and requirement for invasive respiratory support, andGas exchangeSummaryAerosolized KL4 surfactant produces physiological changes that are expected with surfactant replacement therapyThe goal of decreasing nCPAP failure and intubations appears achievable - data to date suggest that AEROSURF® may be decreasing nCPAP failure and the need for intubationRepeat dosing may be important to extend this effect to surfactant self-sufficiency 18

Phase 2a Study (29 to 34 wks GA) Time to Intubation for nCPAP Failure by Treatment Group AEROSURF® may prolong the time to intubation; repeat dosing may be important to extend this effect to surfactant self-sufficiency Control Dose Groups 3,4 & 5 Dose Groups 1 & 2 (15 & 30 min) (45, 60 & 90 min) 19

* One intubated patient excluded due to being inappropriately enrolled 1/7* 3/8 3/8 21/40 5/8 6/8 (15 min) (30 min) (45 min) (60 min) (90 min) Phase 2a Study (29 to 34 wks GA)nCPAP Failure by Treatment Group through 72 hours AEROSURF® treatment, primarily in single doses of 45 minutes and greater, appears to be associated with lower rates of nCPAP failure. Focus for dose selection going forward 20

Phase 2a Study (29 to 34 wks GA) 45 and 60 Minute Dose Groups - nCPAP Failure through 72 hours Time to nCPAP Failure * One intubated patient excluded due to being inappropriately enrolled At 72 hours post-dosing, 27% of AEROSURF® patients in the combined 45 and 60 minute dose groups required intubation compared to 53% in the control group; a relative reduction in nCPAP failure of 49% (45 & 60 min) 21/40 (45 & 60 min) 4/15* 21

Phase 2a Study (29 to 34 wks GA)45 and 60 Minute Dose Groups - nCPAP Failure through 72 hours No AEROSURF patients in the 45 and 60 minute dose groups required intubation at 3 or 6 hours post-dosing compared to 18% (7/40) of control patientsAEROSURF 45 and 60 minute doses may be reducing the rates of intubation and also prolonging the time to intubation – repeat dosing may be important to extend this effect to surfactant self-sufficiency 45 and 60 minute Dose Groups AEROSURF® treated patients experienced a 26% absolute reduction or a 49% relative reduction in nCPAP failure compared to control 22 * One intubated patient excluded due to being inappropriately enrolled

Phase 2a Study (29 to 34 wks GA)Moving Forward – Window for Repeat Dosing Potential repeat dose Additional dose if needed 45 and 60 minute Dose Groups 23 * One intubated patient excluded due to being inappropriately enrolled

Phase 2a in 29-34 week GA radiographic changes post-AEROSURF® in a treated patient* * These radiographs are illustrative of one particular patient only. They are not intended to imply that the same result can be achieved in another individual infant or group of infants or that the FDA will find AEROSURF® to be safe and effective. Day 2 Baseline ~9 Hrs Post-Treatment 24
Summary - Encouraging Phase 2a Results in 29 to 34 wks Gestational Age Premature Infants The goal of decreasing nCPAP failure and intubations appears achievable Aerosolized KL4 surfactant produces physiological changes that are expected with surfactant replacement therapyData to date suggest that AEROSURF® may be decreasing nCPAP failure and the need for intubationAdvancing AEROSURF to a phase 2b clinical trial; repeat dosing may be important to enhancing the reduction in nCPAP failures and extend this effect to surfactant self-sufficiencyOverall, the safety and tolerability profile of the AEROSURF group in the trial was generally comparable to the control group There was acceptable performance by the novel Aerosol Delivery System technology in the NICU 25

Phase 2a Phase 2a Expansion Phase 2a Phase 2b Gestational Age (wks) 29 – 34 26 - 28 26 – 32(Begin with 29 – 32) Dose Groups 15 min; 30 min; 45 min( 25, 50, 75 TPL mg/kg)(8 active, 8 control per group)Single dose 60 min; 90 min (100 and 150 TPL mg/kg)(8 active, 8 control per group)Primarily single dose 30 min; 45 min (50 and 75 TPL mg/kg)(8 active, 8 control per group)Up to two doses 25 min; 50 min; Control(40 and 80 TPL mg/kg)Up to 3 doses # of patients 48 32 32 Up to 240 Objective(s) Safety and tolerabilityPhysiological data suggesting delivery of KL4 surfactant to the lungsPerformance of Aerosol Delivery System Safety and tolerability of higher doses and determine therapeutic index (safety window)Continue physiological assessment Safety and tolerabilityPhysiological assessment Provide evidence of efficacy on an acceptable endpointIdentify dose regimens for phase 3 studyProvide estimate of effect size # of sites Initiated with 3; increased to 8 (US) 12 (US) Up to 20 (US) 50+ (US, EU, Canada, LATAM) Timeline / Milestones Completed May 2015; key objectives achieved Completed Oct 2015 Target enrollment completion – Q2’16; top line data – Q3’16 Target enrollment completion – end of 2016; top line data – Q1’17 Comprehensive Phase 2 Program – Ongoing Trials 26

Large Global Revenue Opportunity Regions Current Annual RevenueInvasive SRT only† Revenue Potential of AEROSURF‡ US $70 - $75 million EU $60 - $70 million LATAM $50 - $100 million ROW $50 - $100 million GLOBAL $230 - $345 million $600 million to $1.0b+ Developed World – 250k to 350k RDS PatientsOnly 50% to 60% of RDS patients currently treated with SRTCurrent market: invasive, undifferentiated, animal-derived productsOpportunity to expand treatment population and increase the pharmacoeconomic value of SRT Developing World – 1.0 million+ RDS PatientsCurrent SRT market as large as the developed world – fewer than 50% treated with SRTOpportunity for growth as access to neonatal care continues to increase world-wide 8 to 10 Million LBW Children Born Every Year Globally † Current global revenue based on ~$900 to $1000 per treatment‡ Windtree primary market research (2014)In addition to expanding the number of patients treated, value of AEROSURF® therapy potentially significantly higher than current treatments – potentially reduces the largest cost-drivers for treating premature infants with RDS: in the U.S. the average cost to treat low birth weight (LBW) infants with RDS on MV is over $50,000; cost to treat patient with chronic lung disease is over $100,000 CDC National Vital Statistics; UNICEF data; Windtree market research; IMS MIDAS data; private companies with access to government purchasing records for Latin America, China and Middle East 27

Technology Platform Exclusivities Broad Multi-Faceted Exclusivity Portfolio PatentsLyophilized KL4 Surfactant Portfolio - to 2033Aerosol Delivery System Portfolio - through 2031+Trade Secrets/Know-HowMethods of ManufactureNon-USP Analytical ProcessesPotential Regulatory ExclusivitiesMultiple Orphan Drug Designations in Respiratory DiseasesPotential Challenges to Generic EntryBioequivalence Complexities – Surfactants are Non-Receptor Based 28

29 Development Pipeline The preclinical development activities listed above have been or are being funded by grants issued by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health (NIH) to study influenza (contract HHSN272201500027C) and radiation (award number R44AI102308) induced lung injury, and by the NIH Office of the Director and the Countermeasures Against Chemical Threats (CounterACT) program to study chemical-induced lung injury. The foregoing content concerning these initiatives is solely the responsibility of Windtree Therapeutics and does not necessarily represent the official views of the NIH. Windtree is focused on developing novel treatments for respiratory critical care patients using its proprietary synthetic KL4 surfactant and aerosol delivery technologies, beginning with the treatment of RDS in premature infants. Windtree believes that its aerosolized KL4 surfactant , alone or in combination with other pharmaceutical compounds, has the potential to be developed to address a range of serious respiratory conditions.

Q4’15 Financial Update Cash of $38.7M as of December 31, 2015Operating cash outflows of $7.6 million in Q4’15The Company anticipates that it has sufficient cash to fund operations through Q1’17 including the completion of the AEROSURF® phase 2b trialCurrent Liabilities and Long-term debt as of December 31, 2015Accounts payable and accrued expenses of $10.8 million$25 million of long-term debt with Deerfield: $12.5 million due in February 2018 (subject to potential deferral) and in February 2019Q4’15 Operating Results 30

Well characterized asset and target application in RDSPotentially transformative therapy for an established market that has a clear unmet needBuilding data base of potential safety, clinical effect and benefit informationSignificant opportunity to build a positive health economic positionStrong IP with the potential to build a pipeline of aerosolized surfactant therapies to address a variety of respiratory diseasesExperienced management team focused on rigorous clinical execution and effective cash management 31 High Value-Creating Potential