Attached files
| file | filename |
|---|---|
| EX-99.01 - EXHIBIT 99.01 - Inspyr Therapeutics, Inc. | v428794_ex99-01.htm |
| 8-K - FORM 8-K - Inspyr Therapeutics, Inc. | v428794_8k.htm |
Exhibit 99.02

1 Corporate Presentation January 2016 OTC QB : GNSZ www.GenSpera.com Craig A. Dionne, PhD President & CEO
2 Safe Harbor Statement Safe Harbor Statement Under the Private Securities Litigation Reform Act of 1995: Any statements that are not historical facts are forward - looking statements that involve risks and uncertainties that could cause actual results to differ materially from those in the forward - looking statements, which may include, but are not limited to, factors related to GenSpera's anticipated growth strategies, the outcome of its clinical trials, future business development, ability to develop new products, expand to other related industries or markets in other geographical locations, and other information detailed from time to time in the Company's filings and future filings made with the United States Securities and Exchange Commission. Readers are advised that this information is intended for the use of investment professionals. Anyone interested in obtaining information on GenSpera should contact GenSpera directly. This presentation was developed by GenSpera and is intended solely for informational purposes and is not to be construed as an offer to sell or the solicitation of an offer to buy the Company's stock. This presentation is based upon information available to the public, as well as other information from sources which management believes to be reliable, but is not guaranteed by the Company as being accurate nor does it purport to be complete. Opinions expressed herein are those of management as of the date of the presentation and are subject to change without notice.

3 • Publicly listed in 2009 ( OTC QB: GNSZ) with IP exclusively licensed from inventors out of John Hopkins • Deep experience in oncology drug discovery and development • A leader in prodrug therapeutics for the treatment of cancer • Robust, global Intellectual Property platform • Highly - differentiated drugs utilizing natural, plant - derived toxin • World - class manufacturing and supply partners • Global barrier to generic entry via exclusive manufacturing and farming controls of raw goods • Multiple value creation catalysts in 2016 Corporate Overview
4 • Developing a naturally occurring toxin in a peptide delivery system to target solid tumors without the side - effect profile of chemotherapeutic agents • Large market opportunities in multiple cancers including liver, brain and prostate with potential for combination with immunotherapy • Efficacy being demonstrated in mid - stage clinical trials in 2 orphan indications • Positive proof - of - concept Phase 2 liver cancer trial • Highly encouraging data from ongoing Phase 2 brain cancer trial • Mechanism of action protected by robust , global patent estate including exclusive license to technology developed at Johns Hopkins University • Exclusive rights with world - class partners for commercial - scale production and raw material supply • Management has a history of success in oncology drug discovery and development Investment Highlights

5 Experienced Leadership and Scientific Development Team Management and Board (Prior Experience / Affiliations) Craig A. Dionne, PhD Chairman and Chief Executive Officer Russell Richerson, PhD COO and Corporate Secretary Peter E. Grebow, PhD Director Bo Jesper Hansen, MD, PhD Director Scott V. Ogilvie Director Scientific Advisory Board John T. Isaacs, PhD Chief Scientific Advisor, Co - Founder Professor at Johns Hopkins School of Medicine, Co - Inventor of GenSpera’s technologies Samuel R. Denmeade, MD Chief Clinical Advisor and Co - Founder Professor at Johns Hopkins and Board Certified Medical Oncologist, Co - Inventor of GenSpera’s technologies Søren Brøgger Christensen, PhD Scientific Advisory Board Member Professor at University of Copenhagen; expert in chemistry of thapsigargin, exploring further derivatives and manufacturing efficiencies for thapsigargin Santosh Kesari , MD, PhD Science Advisory Board Member Chair, Department of Translational Neuro - Oncology and Neurotherapeutics , John Wayne Cancer Institute, Board Certified Neurologist and Neuro - Oncologist AFIN International, Inc. Gulf Enterprises International, Ltd.

6 Evaluating Multiple Oncology Indications RESEARCH PRE - CLINICAL PHASE 1 PHASE 2 HCC TARGET SITE DRUG INDICATION GBM PCa Mipsagargin Blood vessels of most solid tumors DEVELOPMENT STAGE HUMAN CLINICAL TRIALS PHASE 3 25 pts treated in Ph2 study at 5 sites – Study Complete – Results presented 19 patients treated in Ph2 study at UCSD* - Trial expanded to 34 patients Ph2 to begin Q2 2016 at UTHSC Houston* * Ph2 costs primarily supported by investigator funds 2016 Partner Outreach • Glioblastoma Phase 2 trial ongoing in 2016 • Data with IP = increased corporate valuation • Provides expanded options for partnering • Global market = partnership opportunities driven by disease type T hapsigargin prodrug development candidate
7 Scientific Background & IP

8 • GenSpera’s platform is based on exclusively licensed technology developed at Johns Hopkins University and the University of Copenhagen • Platform combines a cytotoxin with a protective peptide, creating a blood soluble prodrug that remains inactive until in the presence of a specific enzyme ▪ Selected enzyme is chosen due to its high level of expression in tumors ▪ The peptide helps solubilize the prodrug and prevents its internalization into cells until the peptide is removed ▪ The enzyme cleaves the peptide from the prodrug and releases the active ingredient only within the tumor, resulting in tumor death • Unique mechanism of action with enhanced anti - tumor activity • Targeted and localized cytotoxic presence minimizes side effects • Target cells unable to acquire resistance Platform Overview

9 Prostate - Specific Membrane Antigen (PSMA): Pan - Tumor Target • Type II transmembrane glycoprotein • Unique proteolytic activity • Highly expressed in normal and malignant prostate epithelial cells • Selective expression in the vascular endothelium of solid tumors – both established and new growth PSMA PSMA is expressed by tumor vasculature

10 Mechanism of Action 1. Blood vessels feed living tumor 2. Drug circulates in bloodstream in benign fashion 3. PSMA enzyme within tumor blood vessels activates drug 4. Activated drug kills blood vessels and tumor cells 5. Death of t umor Precision Targeting by Design → Potential for Complete Tumor Kill → Fewer Side Effects

11 • Exclusive license to use technology developed at Johns Hopkins University and the University of Copenhagen • Current i nfusion composition • Patent coverage in U.S. to 2023 – additional years via patent restoration and ODD • Data exclusivity outside of U.S. − up to 10 years after drug approval in EU • New composition - of - matter Patent Application • Worldwide exclusivity expected through 2033 • Other applications filed for methods of use, formulations, process improvements • Exclusive partnership with Phyton Biotech for commercial - scale thapsigargin production • The name mipsagargin has novel stem – new drug class differentiation value Intellectual Property

12 Mipsagargin: First - in - class Oncologic A gent

13 • A prodrug that becomes active only at tumor site • Plant - based toxin (thapsigargin derivative, 12ADT) is combined with a protective peptide • Peptide targets the PSMA enzyme, which is highly expressed on the surface of tumor vasculature • PSMA removes the peptide, releasing toxin that kills blood vessels feeding tumor and also cancer cells • Targeted drug delivery significantly reduces side effects • No apparent effect on bone marrow – combination with immunotherapy is viable • Manageable side effect profile • Orphan drug designation for liver cancer; pending for brain cancer • Prolonged disease stabilization (via RECIST) in a significant percentage of liver cancer patients Mipsagargin – Lead Drug Candidate 12ADT Extraction and chemical modification Masking and targeting peptide attached PSMA removes peptide, releasing toxin at tumor site
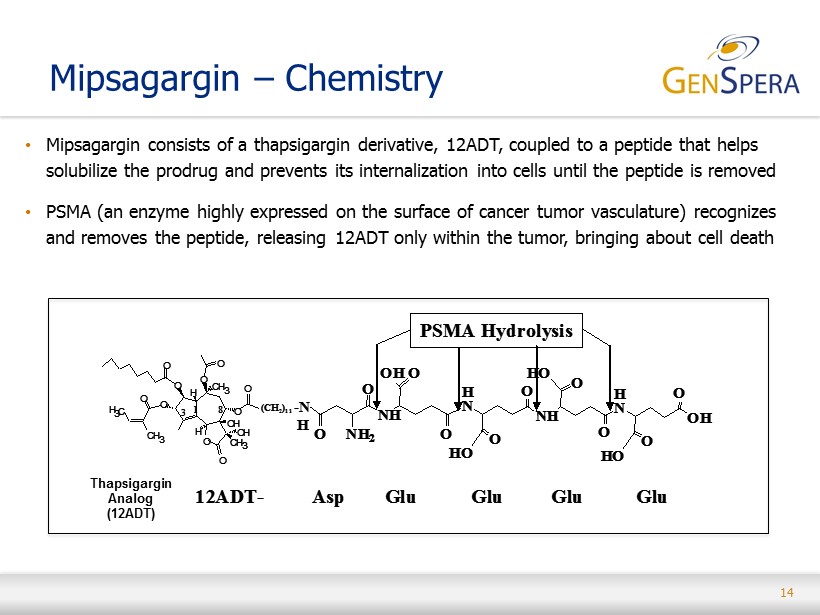
14 • Mipsagargin consists of a thapsigargin derivative, 12ADT, coupled to a peptide that helps solubilize the prodrug and prevents its internalization into cells until the peptide is removed • PSMA (an enzyme highly expressed on the surface of cancer tumor vasculature) recognizes and removes the peptide , releasing 12ADT only within the tumor, bringing about cell death Mipsagargin – Chemistry O O H OH CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 H N N H H N N H H N N H H N N H O O NH 2 O O O H 2 N O HO O OH O HN N N O O H N O (CH 2 ) 11 His (H) Ser- (S) Ser- (S) Lys- (K) Leu- (L) Gln- (Q) Leu- (L)12ADT - PSA Hydrolysis O O H OH CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 H N N H H N N H H N N H H N N H O O NH 2 O O O H 2 N O HO O OH O HN N N O O H N O (CH 2 ) 11 His (H) Ser- (S) Ser- (S) Lys- (K) Leu- (L) Gln- (Q) Leu- (L)12ADT - O O H OH CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 O O H OH CH 3 CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 H N N H H N N H H N N H H N N H O O NH 2 O O O H 2 N O HO O OH O HN N N O O H N O H N N H H N N H H N N H H N N H O O NH 2 O O O H 2 N O HO O OH O HN N N O O H N O (CH 2 ) 11 His (H) Ser- (S) Ser- (S) Lys- (K) Leu- (L) Gln- (Q) Leu- (L)12ADT - PSA Hydrolysis O O H OH CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 (CH 2 ) 11 12ADT- NH O O O ONH 2 OH H N N H O HO O H N OH O HO O O HO O NH O O O ONH 2 OH H N N H O HO O H N OH O HO O O HO O -N H Asp Glu Glu Glu Glu PSMA Hydrolysis O O H OH CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 O O H OH CH 3 CH 3 OH O CH 3 O O O O O CH 3 O H 3 C O H 3 8 1 (CH 2 ) 11 12ADT- NH O O O ONH 2 OH H N N H O HO O H N OH O HO O O HO O NH O O O ONH 2 OH H N N H O HO O H N OH O HO O O HO O -N H Asp Glu Glu Glu Glu PSMA Hydrolysis Thapsigargin Analog (12ADT)

15 Mipsagargin – Compelling Preclinical Data Efficacy Pharmacology • Complete tumor regression with monotherapy in mouse tumor models – No need to combine with other drugs – Fewer side effects • Safety margin of 7 - to 10 - fold in mouse • No acquired resistance to mipsagargin Bioanalytical • In blood, can only find intact mipsagargin and no released active 12ADT • 12ADT is found at very high levels in tumors, less found in liver and kidneys, not found elsewhere - Targeted Delivery! Toxicology • No effect on liver or cardiovascular system • No effect on bone marrow – no immunosuppression or anemia • Kidney is the affected organ at high doses – dose - dependent, non - cumulative, easily monitored and 100% rapidly reversible
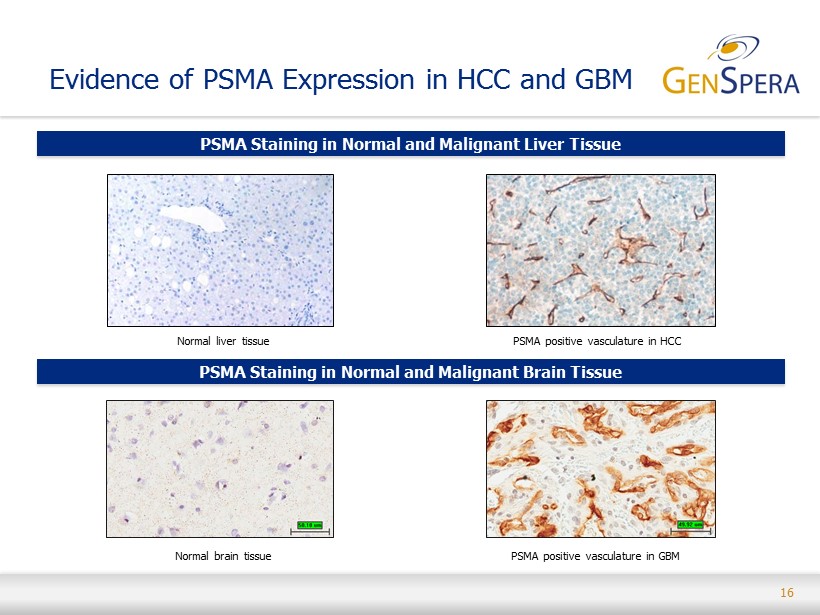
16 Evidence of PSMA Expression in HCC and GBM Normal liver tissue PSMA positive vasculature in HCC Normal brain tissue PSMA Staining in Normal and Malignant Liver Tissue PSMA Staining in Normal and Malignant Brain Tissue PSMA positive vasculature in GBM
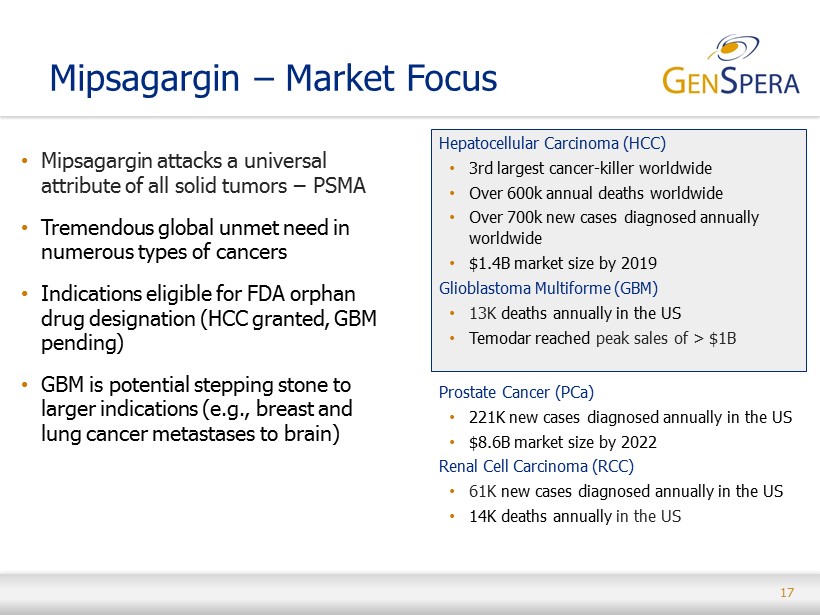
17 Mipsagargin – Market Focus • Mipsagargin attacks a universal attribute of all solid tumors − PSMA • Tremendous global unmet need in numerous types of cancers • Indications eligible for FDA orphan drug designation (HCC granted, GBM pending) • GBM is potential stepping stone to larger indications (e.g., breast and lung cancer metastases to brain) Hepatocellular Carcinoma (HCC) • 3rd largest cancer - killer worldwide • Over 600k annual deaths worldwide • Over 700k new cases diagnosed annually worldwide • $1.4B ma rket size by 2019 Glioblastoma Multiforme (GBM) • 13K deaths annually in the US • Temodar reached peak sales of > $1B Prostate Cancer ( PCa ) • 221K new cases diagnosed annually in the US • $8.6B market size by 2022 Renal Cell Carcinoma (RCC) • 61K new cases diagnosed annually in the US • 14K deaths annually in the US
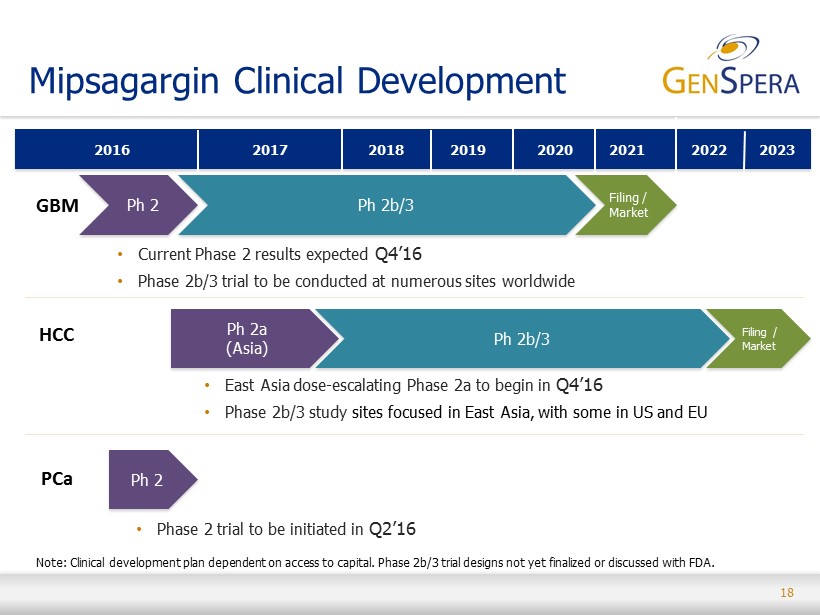
18 Mipsagargin Clinical Development • Phase 2 trial to be initiated in Q2’16 2021 2016 2018 2020 2017 2019 Ph 2 Ph 2b/3 Filing / Market • East Asia dose - escalating Phase 2a to begin in Q4’16 • Phase 2b/3 study sites focused in East Asia, with some in US and EU • Current Phase 2 results expected Q4’16 • Phase 2b/3 trial to be conducted at numerous sites worldwide HCC Ph 2a (Asia) Ph 2 Note: Clinical development plan dependent on access to capital . Phase 2b/3 trial designs not yet finalized or discussed with FDA. GBM PCa 2022 Ph 2b/3 2023 Filing / Market

19 Mipsagargin for Glioblastoma

20 GBM Phase 2 Trial Interim Data • Recurrent GBM patients (prior surgery, radiation, temozolomide) • Simon two - stage design • Data in first 12 patients exceeded criteria required for expansion • Variable expression of PSMA – only 60% have 2+ or 3+ staining • Biomarker development funded by FDA grant • 3 of 11 evaluable patients experience clinical benefit • SD for at least 2 months, reduction in tumor volume • All 3 pts have > 2+ staining • 1 patient with partial response at 11 months • Dramatic reduction in edema, off steroids • Side - effect profile similar to HCC trial
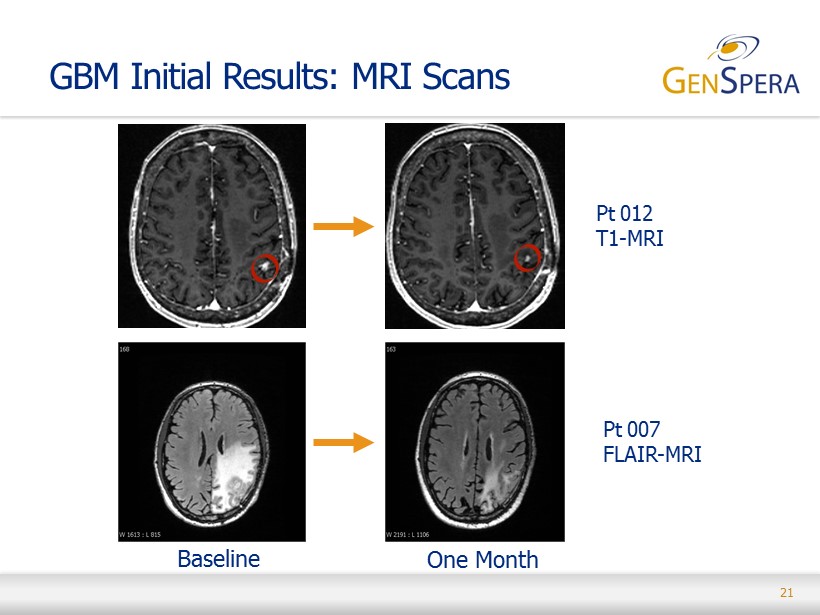
21 Pt 012 T1 - MRI Pt 007 FLAIR - MRI GBM Initial Results: MRI Scans Baseline One Month

22 Proposed (Phase 2/3) Trial Design • Indication: GBM • Geography(s) : Worldwide • Partners: TBD • KOLs: Santosh Kesari, MD, PhD • Possible Trial Design : Two stage adaptive trial design ▪ Stage 1: 75 patients in a Phase 2 trial (20 sites ) ▪ Stage 2: 400 patients in a Phase 3 (100 sites ) • Primary Study Endpoints : Overall Survival • Expected Timing : ▪ Initiation: Stage 1 to begin in Q4’16 ▪ Completion: Stage 2 component expected to conclude by 2H’20

23 Mipsagargin for HCC

24 Clinical Trials of Mipsagargin Phase 1 First - in Human Study • Multi - center, dose escalation, 3+3 design • Advanced solid tumors • One - hour intravenous infusion in saline on Days 1, 2 and 3 of 28 - day cycle • Protocol - defined MTD not reached; 66.8 mg/m 2 established as MTD with 40 mg/m 2 on Day 1 to avoid infusion - related reactions • 44 patients treated, including 5 with HCC at 40/66.8/66.8 mg/m 2 • Prolonged disease stabilization in HCC (12 and 25 months) observed in 2 of 5 patients Phase 2 Study in HCC after Progression on Sorafenib • 25 patients treated • 40 mg/m 2 on Days 1, 2 and 3 accepted for this patient population ▪ 40 mg/m 2 on Days 1, 2 and 3 for patients 1 - 3 and 10 - 25 ▪ 40/66.8/66.8 mg/m 2 on Days 1, 2 and 3 for patients 4 - 9; dose reduction due to SAEs • Study complete

25 Patient Demographics – Phase 2 Indication Hepatocellular carcinoma, progressed on sorafenib (25, 100%) Dose and Schedule 40 mg/m 2 on Days 1, 2 and 3 of 28-day cycle (19 pts) 40 mg/m 2 on Day 1, 66.8 mg/m 2 on Days 2 and 3 of 28-day cycle (6 pts) Performance Status ECOG 0 (8 pts, 32%) ECOG 1 (17 pts, 68%) Child-Pugh Score A5 or A6 (18, 72%) B7 or B8 (7, 28%) Extra-Hepatic Disease No (6 pts, 24%) Yes (19 pts, 76%) Age Mean 64.5 years (range 51 - 73) Gender Male (18 pts, 72%) Female (7 pts, 28%)

26 Safety Observations – Phase 2 Most Frequently - Occurring Mipsagargin - Related AEs Grade ≥ 2 * Number (%) of Patients Creatinine increased 8 (32%) Fatigue 7 (28%) ALT increased 6 (24%) AST increased 6 (24%) Bilirubin increased 6 (24%) LDH increased 5 (20%) Blood urea increased 5 (20%) Thrombocytopenia 4 (16%) Hyperkalemia 3 (12%) * Observed in at least 3 patients
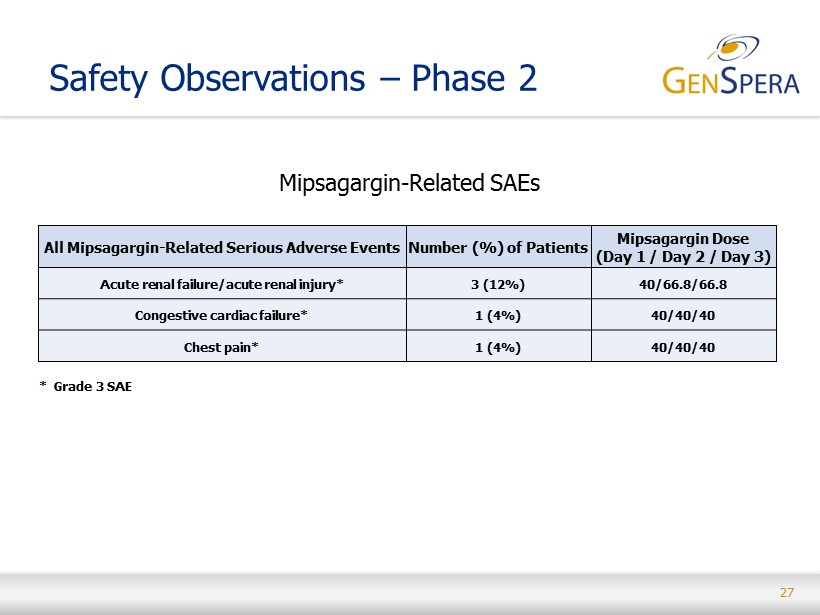
27 Safety Observations – Phase 2 Mipsagargin - Related SAEs All Mipsagargin - Related Serious Adverse Events Number (%) of Patients Mipsagargin Dose (Day 1 / Day 2 / Day 3) Acute renal failure/acute renal injury* 3 (12%) 40/66.8/66.8 Congestive cardiac failure* 1 (4%) 40/40/40 Chest pain* 1 (4%) 40/40/40 * Grade 3 SAE

28 Clinical Observations – Phase 2 Number of Cycles (n=25 patients) 75 total (average 3 per pt; range 1 - 9) 63 cycles at 40/40/40 12 cycles at 40/66.8/66.8 Evaluable for Response (EE Population) 19 patients (76%) Best Response (EE Population) CR + PR 0 pts SD 12 pts (63%) SD ≥ 5 cycles 6 pts (24%) TTP (EE Population) 134 days* (4.5 months; 95% Cl: 58.0, NE)** OS (EE Population) 205 days (6.8 months; 95% Cl: 138, NE)*** PFS (EE Population) 129 days (4.3 months; 95% Cl: 58.0, 205.0)**** * p < 0.001 vs. historic control of 2.1 months ** 7 patients censored *** 8 patients censored **** 2 patients censored

29 Best Change in Tumor Size – Phase 2 C h a ng e f r o m B ase lin e ( % ) 100 80 60 40 20 0 -20 -30% -40 -60 -80 -100 03 20 16 12 05 19 14 01 09 22 07 15 18 08 02 21 11 23 *10 Patient Number Note: *Patient 010 exhibited new metastatic disease and was removed from study; post-treatment target lesion measurement not performed.
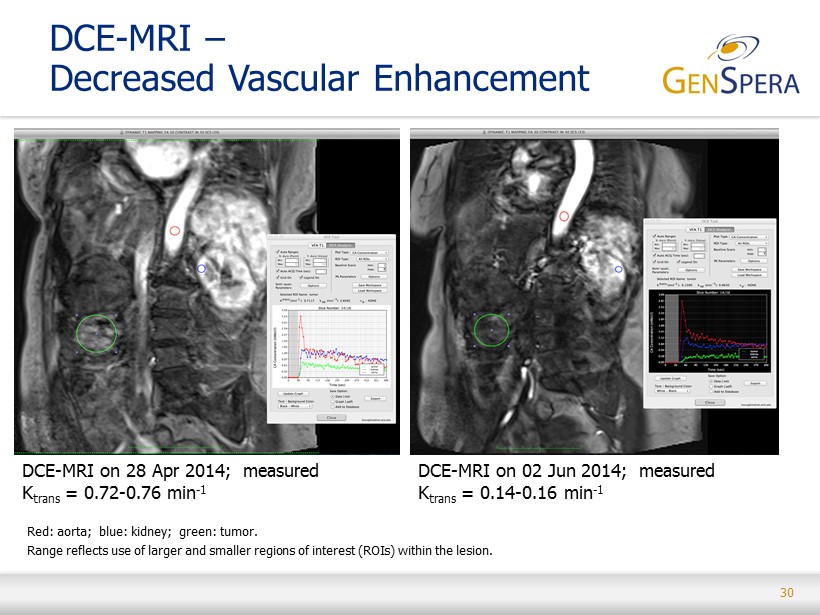
30 DCE - MRI – Decreased Vascular Enhancement DCE - MRI on 28 Apr 2014; measured K trans = 0.72 - 0.76 min - 1 DCE - MRI on 02 Jun 2014; measured K trans = 0.14 - 0.16 min - 1 Red: aorta; blue: kidney; green: tumor. Range reflects use of larger and smaller regions of interest (ROIs) within the lesion.

31 • RECIST criteria is limited by lack of tumor viability information • HCC patient with gastrohepatic metastatic lymph node involvement (gold arrows) • Increased hypoenhancement after mipsagargin treatment (right panel) suggests response HCC – Pharmacodynamic Proof of Principle via DCE - MRI Baseline Five weeks
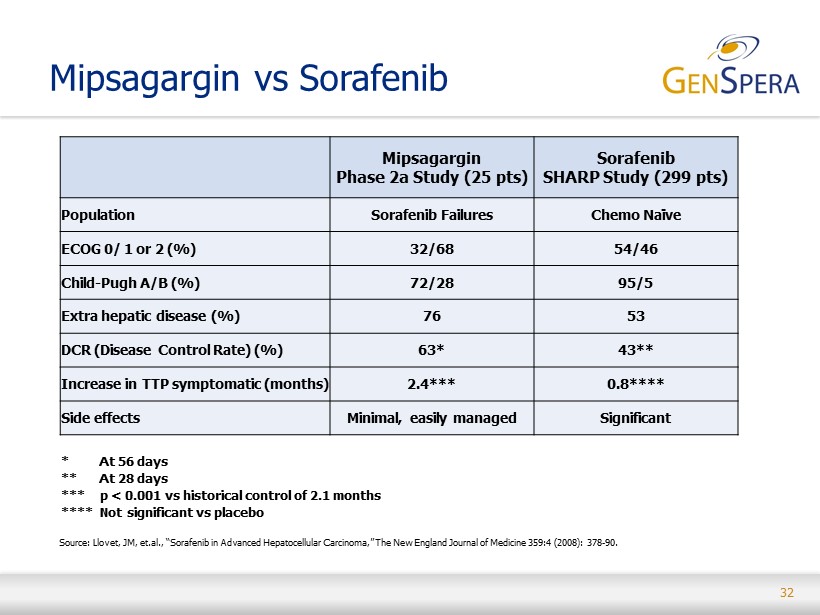
32 Mipsagargin vs Sorafenib Mipsagargin Phase 2a Study (25 pts) Sorafenib SHARP Study (299 pts) Population Sorafenib Failures Chemo Naïve ECOG 0/ 1 or 2 (%) 32/68 54/46 Child - Pugh A/B (%) 72/28 95/5 Extra hepatic disease (%) 76 53 DCR (Disease Control Rate) (%) 63* 43** Increase in TTP symptomatic (months) 2.4*** 0.8**** Side effects Minimal, easily managed Significant * At 56 days ** At 28 days *** p < 0.001 vs historical control of 2.1 months **** Not significant vs placebo Source: Llovet, JM, et.al., “Sorafenib in Advanced Hepatocellular Carcinoma,” The New England Journal of Medicine 359:4 (2008 ): 378 - 90.

33 Impressive clinical activity • Highly differentiated from other anti - cancer approaches • Outstanding clinical safety profile • Minimal and manageable side effects ▪ Fatigue, nausea, rash, reversible creatinine increase ▪ No apparent effect on bone marrow • Data strongly suggestive of clinical activity in second - line HCC ▪ Study participants experienced a median time to progression of 4.5 months (p<0.001), more than twice the time demonstrated in prior studies with placebo or ineffective agents ▪ 6 3 % of patients experienced disease stabilization (via RECIST) at 2 months ▪ Prolonged disease stabilization in a significant percentage of patients – 24% with stable disease > 5 months • Additionally, mipsagargin demonstrated decreased blood flow in liver tumors as measured by DCE - MRI Phase 2 HCC Trial Results Overview

34 Next HCC Clinical Development Steps

35 • Liver cancer is the most common type of cancer in Southeast Asia • Three fourths of worldwide liver cancer cases in males, and two thirds in females, occur in 15 Asian countries ▪ Compared to the US and EU, high rates of Hepatitis B virus (HBV) prevalence, and to a lesser extent HCV, are leading factors for higher liver cancer rates • Regular screening of high - risk HBV carriers in Eastern Asia allows for early detection of liver cancer when potentially curative treatment can still be offered ▪ Clinical development program for mipsagargin will initially be focused in East Asia ▪ Rapid trial initiation in Singapore, Taiwan and/or Hong Kong because of potential to access US INDs Next Steps: Asia Represents Advantageous Environment for Clinical Development Source: Pfizer Facts: The Burden of Cancer in Asia, 2008.

36 3.4 3.8 4.4 4.6 5.0 5.3 6.3 6.8 7.2 7.2 7.3 7.5 9.5 9.8 12.9 13.9 16.6 18.9 21.4 35.5 1.6 1.6 2.3 1.9 2.0 3.9 4.4 2.2 3.6 2.1 7.0 2.5 3.4 3.2 5.0 5.1 8.0 9.6 9.0 12.7 -50 -40 -30 -20 -10 0 10 20 30 40 50 South-Central Asia Northern Europe Western Asia Central and Eastern Europe Australia/New Zealand South America Caribbean Northern America Eastern Africa Western Europe Central America Northern Africa Micronesia/Polynesia Southern Europe Melanesia Southern Africa Western Africa Middle Africa South-Eastern Asia Eastern Asia Males Females Market Focus: Liver Cancer in Asia Age - Standardized Liver Cancer Incidence Rates by Sex and Geography (per 100,000) Source : GLOBOCAN 2008 . China 56.8 Japan 6.2 Korea 2.5 US 2.3 RoW 20.9 China 51.6 Japan 6.8 Korea 1.8 US 2.6 RoW 26.9 Annual WW New Liver Cancer Cases by Country (‘000s) Males Females

37 Phase 2a Dose Escalation Trial • Indication: HCC • Geography(s) : Taiwan , Singapore and potentially Hong Kong • Partners: TBD • KOLs: TBD • Trial Design : Dose escalation study in East Asian population; typical 3+3 design • Trial Size : 9 - 18 patients • Study Endpoints : Safety, Tolerability, Response Rate • Expected Timing : ▪ Initiation: Phase 2a trial to be initiated in Q4’16 ▪ Results: 2H’17 ▪ Trial to be followed by Phase 2b/3, scheduled to begin in Q4’17

38 Mipsagargin for Prostate

39 Mipsagargin in PCa Phase 2 Neoadjuvant PCa Study • Site: University of Texas Health Science Center in Houston ; investigator - sponsored • Initiate in Q2’16 • Expected completion Q4’16 Prostate Cancer (PCa) • 221K new cases diagnosed annually in the U.S. • Est. $8.6B market by 2022* * Source: Decision Resources Prodrug Candidate Activating Enzyme Target Location of Active Enzyme Status G - 115 Prostate - Specific Antigen (PSA) Prostate Cancer Pilot toxicology completed; limited preclinical development G - 114 Prostate - Specific Antigen (PSA) Prostate Cancer Validated efficacy in preclinical animal models (Johns Hopkins) G - 301 Human Glandular Kallikrein 2 (hK2) Prostate Cancer Validated efficacy in preclinical animal models (Johns Hopkins) Other Drug Candidates

40 GenSpera : Going Forward
41 Business Strategy • O ptimize value across multiple indications, territories, and technologies • Continue developing drug candidates independently • Expand management and staffing • Continue business development discussions and partnership opportunities • Develop pipeline through internal efforts, licensing, or acquisition
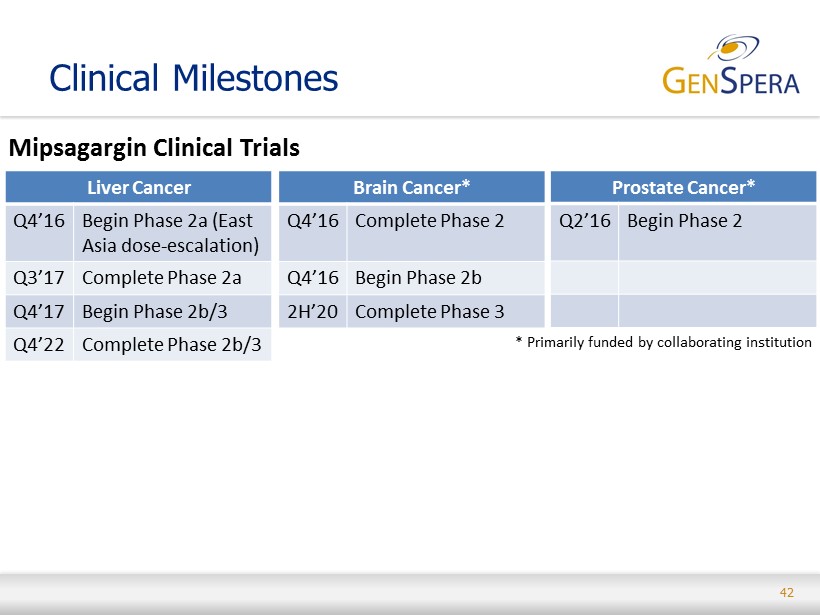
42 Clinical Milestones Mipsagargin Clinical Trials Liver Cancer Q4’16 Begin Phase 2a (East Asia dose - escalation) Q3’17 Complete Phase 2a Q4’17 Begin Phase 2b/3 Q4’22 Complete Phase 2b/3 Brain Cancer* Q4’16 Complete Phase 2 Q4’16 Begin Phase 2b 2H’20 Complete Phase 3 Prostate Cancer* Q2’16 Begin Phase 2 * Primarily funded by collaborating institution
43 • Developing a naturally occurring toxin in a peptide delivery system to target solid tumors without the side - effect profile of chemotherapeutic agents • Large market opportunities in multiple cancers including liver, brain and prostate with potential for combination with immunotherapy • Efficacy being demonstrated in mid - stage clinical trials in 2 orphan indications • Positive proof - of - concept Phase 2 liver cancer trial • Highly encouraging data from ongoing Phase 2 brain cancer trial • Mechanism of action protected by robust , global patent estate including exclusive license to technology developed at Johns Hopkins University • Exclusive rights with world - class partners for commercial - scale production and raw material supply • Management has a history of success in oncology drug discovery and development Investment Highlights