Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - REPROS THERAPEUTICS INC. | v421109_8k.htm |
Exhibit 99.1

Enclomiphene ( EnCyzix ™) A Mechanistically Consistent Approach to the Treatment of Secondary Hypogonadism

Repros Disclaimer Any statements made by the Company that are not historical facts contained in these slides (or in any oral accompanying discussion) are forward - looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 and are subject to various risks, uncertainties and other factors that could cause the Company’s actual results, performance or achievements to differ materially from those expressed or implied by such forward - looking statements . These statements often include words such as “may,” “will,” “expect,” “anticipate,” “continue,” “estimate,” “project,” “potential,” “intend,” “believe,” “plan,” “seek,” “could,” “can,” “should” or similar expressions . These statements are based on assumptions that the Company has made in light of the Company’s experience in the industry, as well as the Company’s perceptions of historical trends, current conditions, expected future developments and other factors the Company believes are appropriate in these circumstances . Forward - looking statements include, but are not limited to, those relating to anticipated milestones for Enclomiphene and Proellex®, the conduct of planned clinical studies and the timing and nature of the results thereof, the markets for the Company’s products and the potential success of the Company in penetrating those markets and that the Company’s need for and use of financial resources . Such statements are based on current expectations that involve a number of known and unknown risks, uncertainties and other factors that may cause actual events to be materially different from those expressed or implied by such forward - looking statements, including the ability to raise additional needed capital on a timely basis in order for it to continue to fund development of its Enclomiphene and Proellex® programs, the ability to have success in the clinical development of its technologies, the reliability of interim results to predict final study outcomes, and such other risks as are identified in the Company's most recent Annual Report on Form 10 - K and the subsequent quarterly report on Form 10 - Q and in the prospectus supplement and the accompanying prospectus included in the registration statement mentioned below . These documents are available on request from Repros or at www . sec . gov . Repros disclaims any intention or obligation to update or revise any forward - looking statements, whether as a result of new information, future events or otherwise . In this presentation, we rely on and refer to information and statistics regarding the pharmaceutical industry . We obtained this information and these statistics from third - party sources, which we have supplemented where necessary with information from publicly available sources and our own internal estimates . Industry publications and surveys generally state that they have obtained information from sources believed to be reliable, but do not guarantee the accuracy and completeness of such information . While we believe that each of these studies and publications is reliable, we have not independently verified such data, and we make no any representation as to the accuracy of such information . Similarly, we believe our internal research is reliable, but it has not been verified by any independent sources . 2
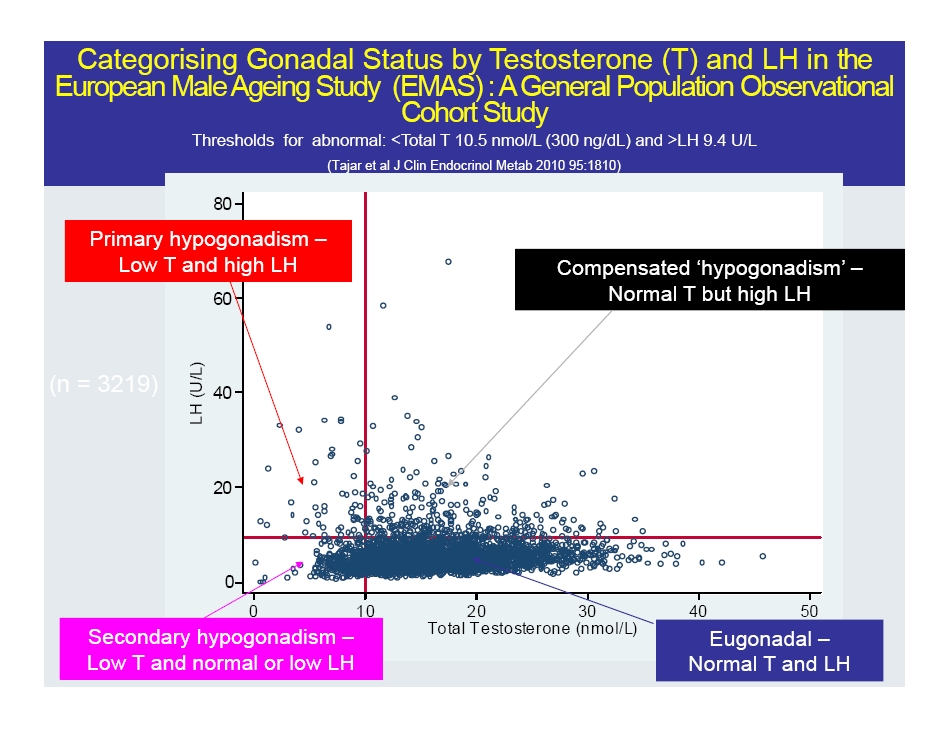
Categorising Gonadal Status by Testosterone (T) and LH in the European Male Ageing Study (EMAS) : A General Population Observational Cohort Study Thresholds for abnormal: <Total T 10.5 nmol /L (300 ng/ dL ) and >LH 9.4 U/L (Tajar et al J Clin Endocrinol Metab 2010 95:1810) 0 20 40 60 80 LH (U/L) 0 10 20 30 40 50 Total Testosterone (nmol/L) Secondary hypogonadism – Low T and normal or low LH Eugonadal – Normal T and LH Primary hypogonadism – Low T and high LH Compensated ‘ hypogonadism ’ – Normal T but high LH (n = 3219)

CM - 4 Risk Factors Age ( yrs ) BMI ≥ 25 - <30 kg/m 2 BMI ≥ 30 kg/m 2 Smoking ( current) Alcohol ( frequent) Co - morbidity ( ≥ 1) 0 5 10 15 *** *** * Adjusted Relative Risk Ratio Secondary Obesity Related Hypogonadism EMAS Tajar, JCEM 2010 0 5 10 15 *** Hypogonadism of Aging * p<0.05 *** p<0.001 Primary
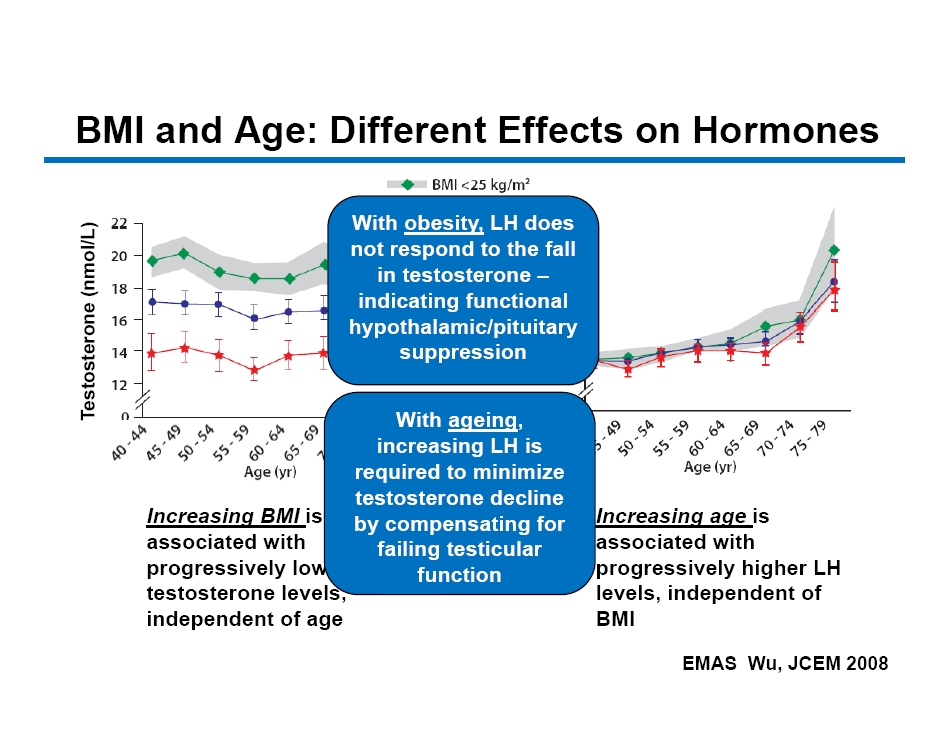
CM - 5 EMAS Wu, JCEM 2008 BMI and Age: Different Effects on Hormones Increasing BMI is associated with progressively lower testosterone levels, independent of age Increasing age is associated with progressively higher LH levels, independent of BMI Testosterone ( nmol /L) LH (U/L) With obesity, LH does not respond to the fall in testosterone – indicating functional hypothalamic/pituitary suppression With ageing , increasing LH is required to minimize testosterone decline by compensating for failing testicular function
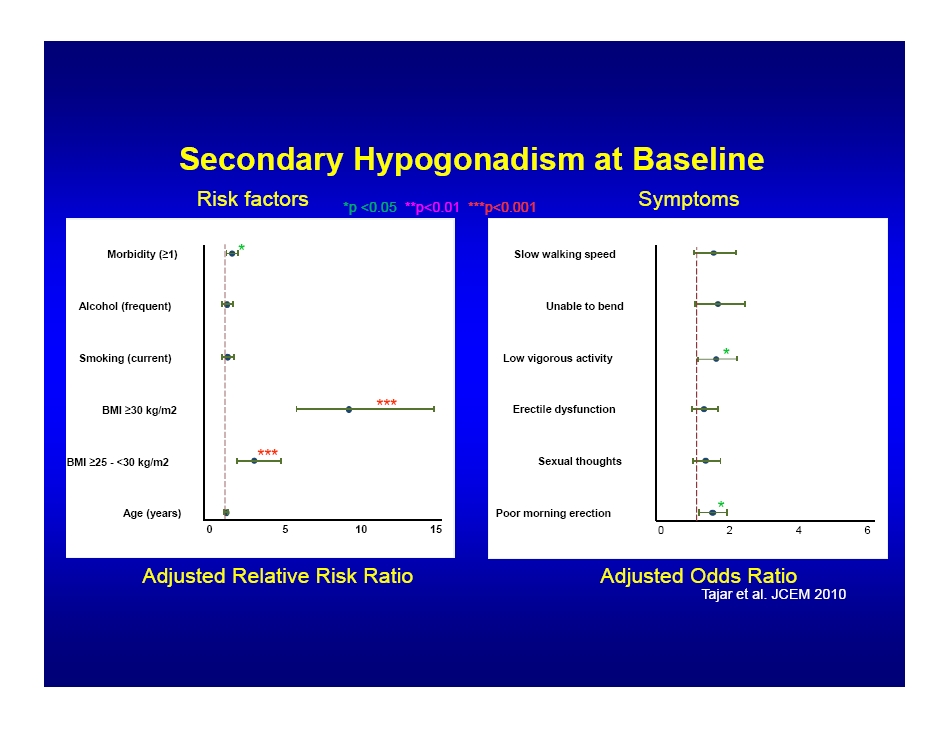
Secondary Hypogonadism at Baseline Age (years) BMI ≥ 25 - <30 kg/m2 BMI ≥ 30 kg/m2 Smoking (current) Alcohol (frequent) Morbidity ( ≥ 1) 0 5 10 15 *** *** * Poor morning erection Sexual thoughts Erectile dysfunction Low vigorous activity Unable to bend Slow walking speed 0 2 4 6 * * Adjusted Relative Risk Ratio *p <0.05 **p<0.01 ***p<0.001 Adjusted Odds Ratio Risk factors Symptoms Tajar et al. JCEM 2010
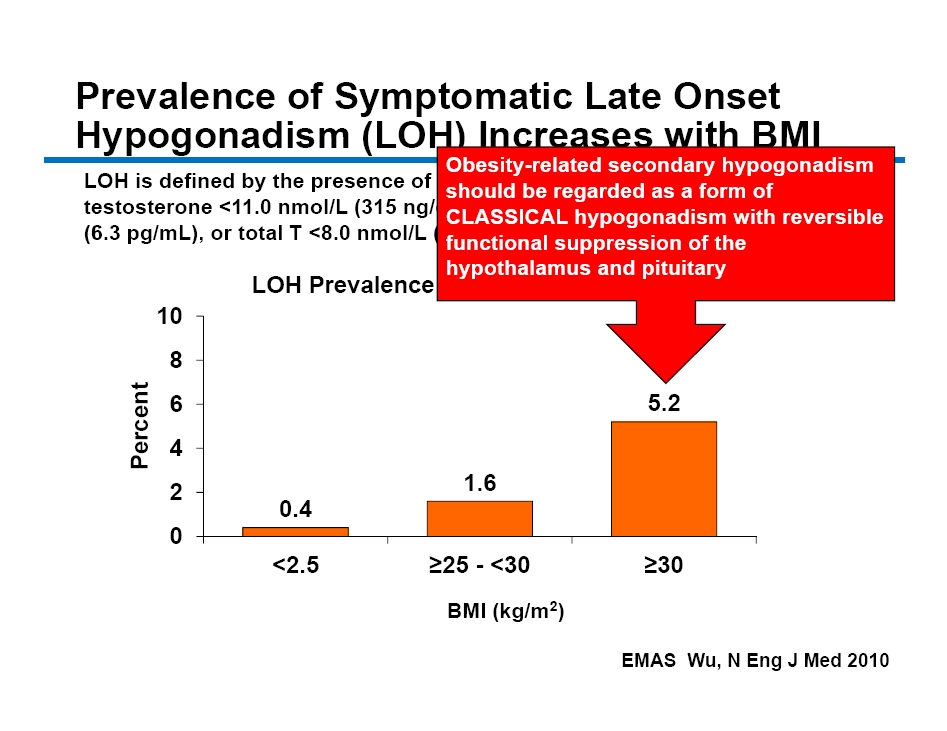
CM - 7 Prevalence of Symptomatic Late Onset Hypogonadism (LOH) Increases with BMI Wu et al New Eng J Med 2010 EMAS Wu, N Eng J Med 2010 LOH is defined by the presence of 3 sexual symptoms associated with total testosterone <11.0 nmol /L (315 ng/ dL ) and free testosterone of <220 pmol /L (6.3 pg /mL), or total T <8.0 nmol /L (230 ng/ dL ) 0.4 1.6 5.2 0 2 4 6 8 10 <2.5 ≥25 - <30 ≥30 Percent BMI (kg/m 2 ) LOH Prevalence by BMI Categories Obesity - related secondary hypogonadism should be regarded as a form of CLASSICAL hypogonadism with reversible functional suppression of the hypothalamus and pituitary
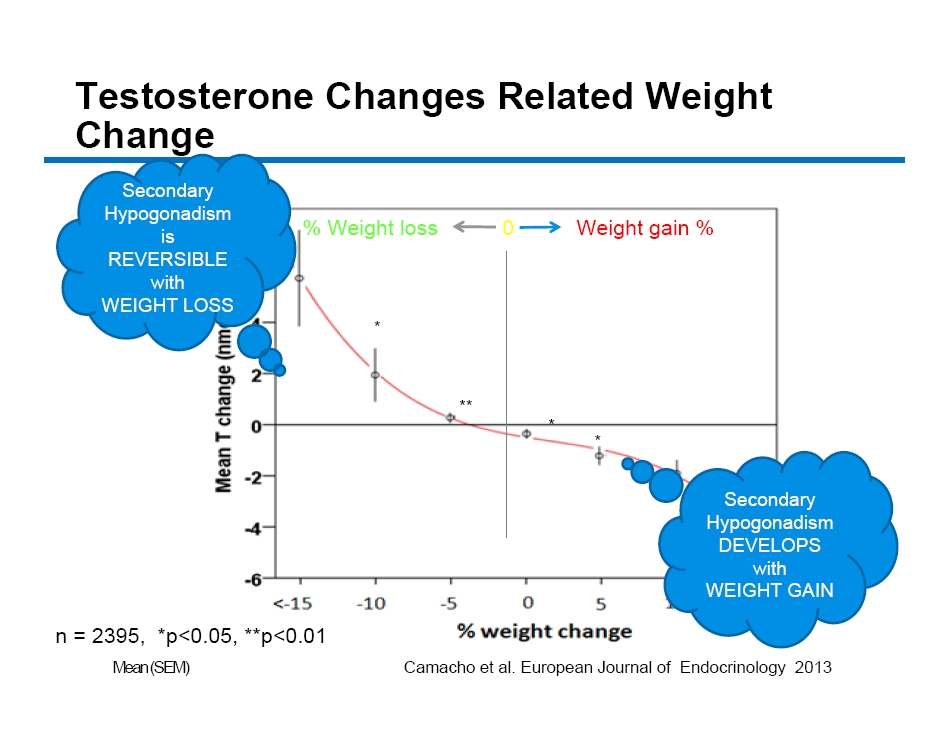
CM - 8 n = 2395, *p<0.05, **p<0.01 % Weight loss Weight gain % 0 * ** * * * Camacho et al. European Journal of Endocrinology 2013 Mean (SEM) Secondary Hypogonadism is REVERSIBLE with WEIGHT LOSS Secondary Hypogonadism DEVELOPS with WEIGHT GAIN Testosterone Changes Related Weight Change

CM - 9 Age - Related Hypogonadism In recent years, use of testosterone therapies has increased markedly among middle - aged and elderly men for a controversial condition that the FDA calls “ age - related hypogonadism , ” also referred to as “ late onset hypogonadism , ” a condition which is typically diagnosed in men who, for no discernable reason other than older age , have serum testosterone concentrations below the normal range for healthy young men, as well as signs and symptoms that may or may not be caused by low testosterone concentrations . (Nguyen NEJM 2015)

CM - 10 Increasing Number of Prescription Claims for Testosterone Products from U.S. Outpatient Retail Pharmacies, Stratified According to Age, 2010 – 2013 Nguyen et al N Eng J Med 2015 9% 3%
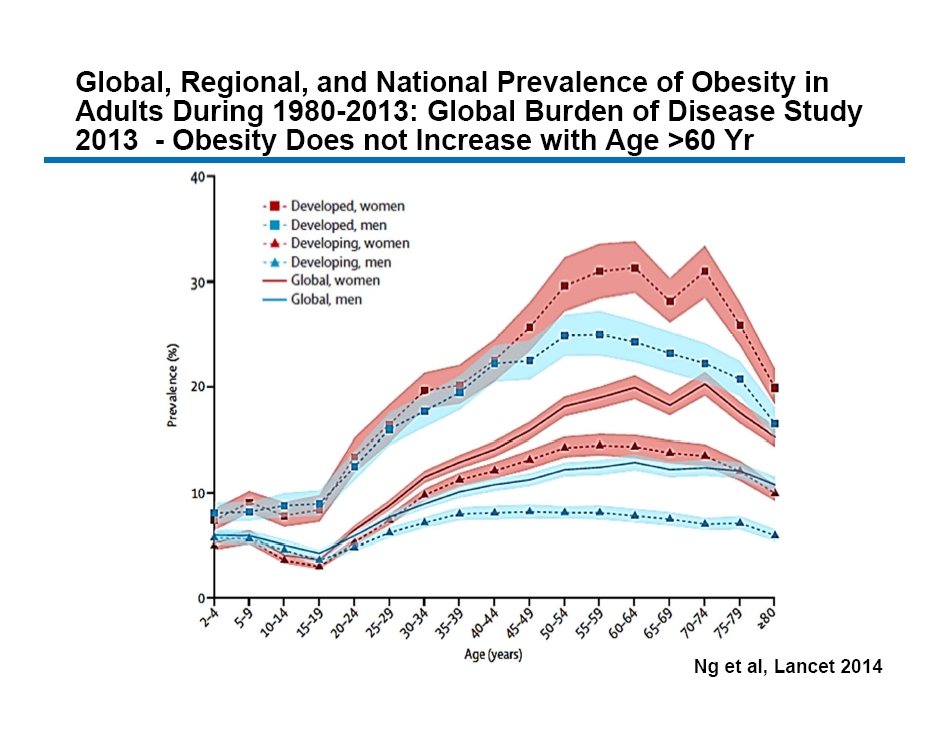
CM - 11 Global, Regional, and National Prevalence of Obesity in Adults During 1980 - 2013: Global Burden of Disease Study 2013 - Obesity Does not Increase with Age >60 Yr Ng et al, Lancet 2014

CM - 12 So What Do We Know About the Current Group of Men Seeking Treatment for Hypogonadism? The majority are secondary hypogonadal and are fertile Confirmatory diagnosis not practiced in the US No studies conducted by hormone replacement sponsors to assess impact on spermatogenesis “But these men don’t care about fertility” – True for some – Not true for all Modest increase in “off label” scripts for Clomid being written by physicians

Units of Testosterone and Clomiphene Sold 0 200 400 600 800 1000 1200 0 5000 10000 15000 20000 25000 30000 35000 40000 45000 Mar Apr May June July Aug Sep Oct Nov Dec Jan Feb Mar Apr May June July Aug Sep Oct Nov Dec Jan Feb Units of Clomiphene Sold (000) Units of Testosterone Sold (000) Monthly Units Sold Testosterone Clomiphene IMS Data through 11/14

CM - 14 “So is there anything else to worry about if I take T?” “I don’t want to have any more kids” You have a reversible disorder if you are willing to make a lifestyle change If you start taking testosterone you may need to take it for the rest of your life Conclusions : Interruption of TRT resulted in worsening of symptoms. Hypogonadism may require lifelong TRT .* *HOW LONG SHOULD HYPOGONADAL SUBJECTS BE TREATED? INTERMISSION AND RESUMPTION OF LONG−TERM TESTOSTERONE REPLACEMENT THERAPY (TRT) AND EFFECTS ON HORMONAL AND ANTHROPOMETRIC PARAMETERS IN HYPOGONADAL ELDERLY MEN Farid Saad, DVM, PhD1, Aksam Yassin, MD, PhD2, Yousef Al Mehmadi , MD, PhD2, Gheorghe Doros , PhD3 and Abdulmaged Traish , PhD4 1Global Medical Affairs Andrology, Bayer Pharma AG, Berlin, Germany; 2Institute of Urology and Andrology; 3Boston University Sch ool of Public Health; 4Boston University School of Medicine (Presented By: Farid Saad, DVM, PhD )
CM - 15 Conclusions: Clinical Implications Diagnostic differentiation of secondary from primary hypogonadism is essential – measure T and LH – The commonest form of T deficiency in ‘aging’ men is Secondary Hypogonadism associated with obesity (independent of ageing) due to reversible functional suppression of hypothalamic/ pituitary function – Primary hypogonadism is age - related , rare and irreversible First line standard of care for obese men with low T should be weight loss, but results are variable and not always practical Other strategies to reverse gonadotrophin suppression, and encourage recovery of endogenous T safely, and preserving fertility, are preferable to exogenous T in the treatment of men with secondary hypogonadism

Why Not Just Use Clomid ? Enclomiphene (Patented) Trans Isomer (Pure Estrogen Antagonist) of Clomiphene Commercial Clomid (60% Trans, 40% Cis) 0 20 40 60 80 100 0.01 1 100 10000 % Concentration ( nM ) Estrogen Receptor Binding Affinity zu en Trough Concentration of Enclomiphene In Serum at Steady State Achieved within 10 Days Of Administration Cis Isomer Exhibits Agonist/Antagonist Activity Mikkelson et al, Fertility & Sterility, Vol. 46, No. 3, Sept. 1986 In animal studies the zu isomer achieves > 10 fold concentrations in serum and prolonged residence in all tissues including the eye and male reproductive tissues

Clomiphene Isomers Exhibit Different Impact on Animal Urogenital Tract Tissues 0 5 10 15 20 25 Blood Testis Epididymis Seminal vesicles Kidneys ng Equivalent [ 14 C] clomiphene isomers /Kg Zuc 4 Hr Zuc 24 Hr Enc 4 Hr Enc 24 Hr Single 20 mg/kg radiolabeled dose 90 Day Exposure @ 40 and 4 mg/kg Control 40 mg Enclomiphen 4 mg Enclomiphene 40 mg Zuclomiphene 4 mg Zuclomiphene
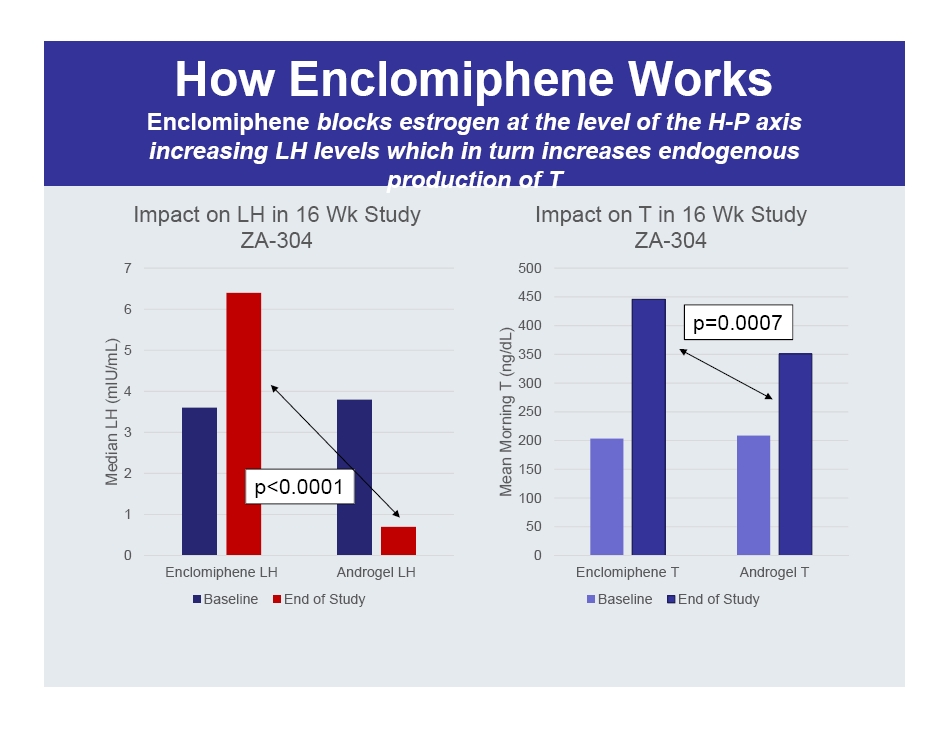
How Enclomiphene Works Enclomiphene blocks estrogen at the level of the H - P axis increasing LH levels which in turn increases endogenous production of T 0 1 2 3 4 5 6 7 Enclomiphene LH Androgel LH Median LH ( mIU /mL) Impact on LH in 16 Wk Study ZA - 304 Baseline End of Study 0 50 100 150 200 250 300 350 400 450 500 Enclomiphene T Androgel T Mean Morning T (ng/ dL ) Impact on T in 16 Wk Study ZA - 304 Baseline End of Study p<0.0001 p=0.0007

ZA - 304 & ZA - 305 Results Enclomiphene Yields Meaningful Reproducible Outcomes Study ZA - 304 (p - values Treatment vs Enclomiphene) ZA - 305 (p - values Treatment vs Enclomiphene) Treatment Enclomiphene Androgel Placebo Enclomiphene Androgel Placebo N 41 43 45 44 42 41 Age (SD) 49.1 (7.4) 47.4 (7.2) 47.2 (9.0) 47.3 (8.8) 45.0 (8.2) 47.5 (8.9) BMI 33.1 (4.4) 34.0 (4.4) 32.6 (4.3) 33.8 (4.6) 33.1 (4.6) 33.5 (4.4) Baseline T (ng/dL) 203.3 (52.4) 208.6 (54.0) 200.3 (43.1) 212.9 (48.0) 229.8 (44.0) 206.0 (48.2) Baseline Sperm (10 6 /ml) 98.3 (87.2) 78.9 (68.5) 95.3 (90.8) 79.0 (55.2) 75.1 (45.8) 80.5 (62.3) 16 Wk T 445.8 (186.4) 350.6 (338.1)) p = 0.0007 236.4 (144.7) p < 0.0001 412.9 (130.3) 387.4 (244.8) p = 0.0368 214.4 (58.7) p < 0.0001 % Change Sperm @ 16 Wk 11.7 (80.3) - 56.6 (48.2) p < 0.0001 4.1 (57.2) p = 0.5482 15.2 (55.8) - 32.8 (63.2) p = 0.0003 + 7.6 (89.6) p = 0.2007 % Sperm < 15 MM/mL 4.9 48.8 p < 0.0001 4.4 p = 1.0000 2.3 23.8 p = 0.0031 2.4 p = 1.000
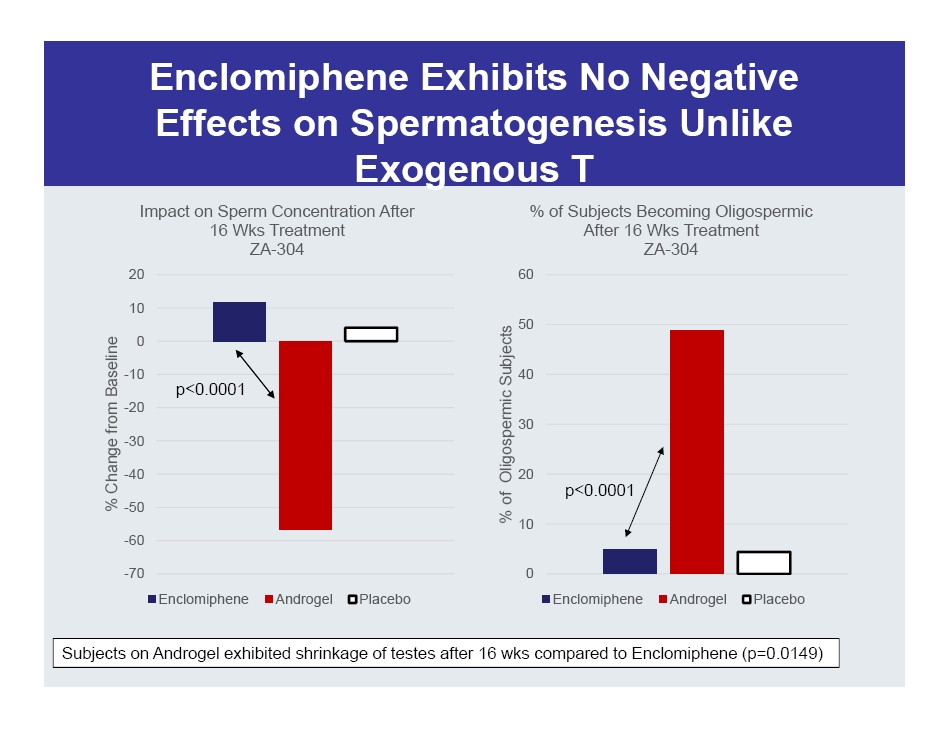
Enclomiphene Exhibits No Negative Effects on Spermatogenesis Unlike Exogenous T -70 -60 -50 -40 -30 -20 -10 0 10 20 % Change from Baseline Impact on Sperm Concentration After 16 Wks Treatment ZA - 304 Enclomiphene Androgel Placebo 0 10 20 30 40 50 60 % of Oligospermic Subjects % of Subjects Becoming Oligospermic After 16 Wks Treatment ZA - 304 Enclomiphene Androgel Placebo Subjects on Androgel exhibited shrinkage of testes after 16 wks compared to Enclomiphene (p=0.0149) p<0.0001 p<0.0001
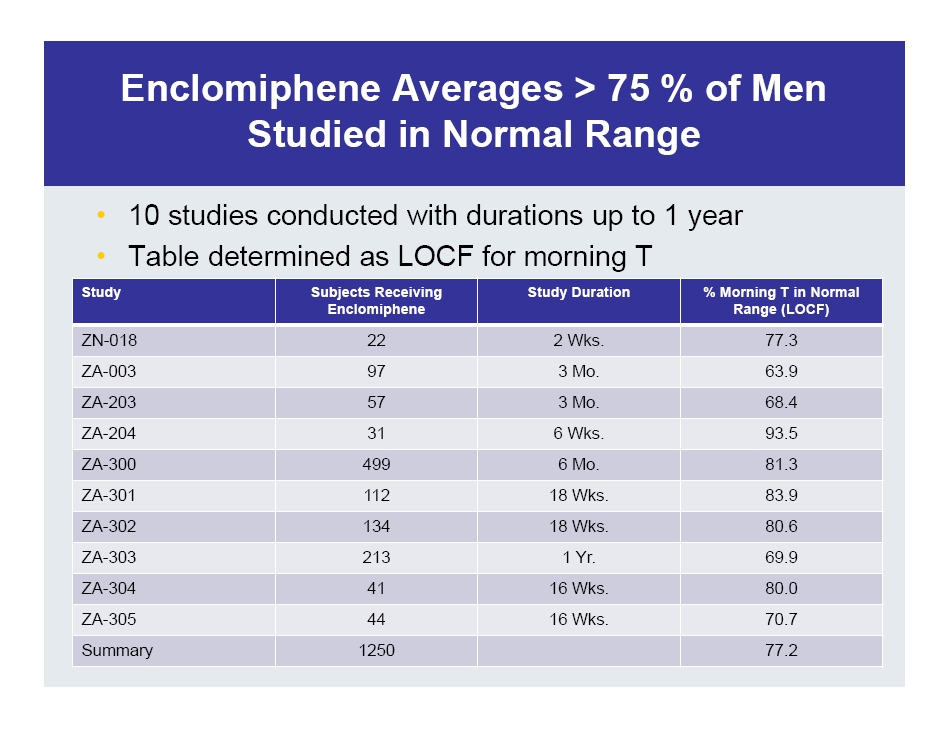
Enclomiphene Averages > 75 % of Men Studied in Normal Range • 10 studies conducted with durations up to 1 year • Table determined as LOCF for morning T Study Subjects Receiving Enclomiphene Study Duration % Morning T in Normal Range (LOCF) ZN - 018 22 2 Wks. 77.3 ZA - 003 97 3 Mo. 63.9 ZA - 203 57 3 Mo. 68.4 ZA - 204 31 6 Wks. 93.5 ZA - 300 499 6 Mo. 81.3 ZA - 301 112 18 Wks. 83.9 ZA - 302 134 18 Wks. 80.6 ZA - 303 213 1 Yr. 69.9 ZA - 304 41 16 Wks. 80.0 ZA - 305 44 16 Wks. 70.7 Summary 1250 77.2

Enclomiphene Exhibits Unique Profile with Numerous Advantages vs Approved Hormone Replacement • The Enclomiphene Advantages – Oral – Not controlled substance, cannot be abused – No supernormal levels of T achieved – No transference risk – Restores normal function (no loss of testicular function) – Does not develop dependency – Avoids withdrawal symptoms – With lifestyle change can reverse disorder and result in no need for therapy

Enclomiphene Regulatory Status • NDA accepted by FDA – Treatment of secondary hypogonadism in overweight men – NDA filing requests NCE (New Chemical Entity) status • EMA (European Medicines Agency) notes enclomiphene is eligible for submission for a centralized marketing authorisation application (MAA) as a New Active Substance – MAA anticipated filing in 2016 – If approved potential for extended patent life
Enclomiphene US Commercial Plan/Schedule • Completed Activities Year - to - Date – NDA filed – Initiated EU filing activities (anticipate central filing 2/16) – Adcom consultancy ( Pharmapprove ) hired and active • Two Mock Panels conducted • Q4 - 15 – Build launch inventory – Award sales contract – Nov. 30 PDUFA date • Q2 - 16 – Launch into Endo & Uro Spec space (~ 25% of all prescriptions) NOTE: Commercial plan/schedule contingent on FDA approval of Enclomiphene

Proellex Status and Plans Going Forward • Ongoing Phase 2b Proellex studies – Uterine fibroids (vaginal and oral administration studies) • Rapid and maintained reduction in bleeding • Reduction of fibroid bulk • Reduction of bulk associated symptoms – Endometriosis • Rapid reduction in menstrual and non - menstrual pain • Significant reduction in narcotic and non - narcotic analgesic use • Proellex safety profile very encouraging at lower doses – General adverse events are mild to moderate and transient
Financial Summary • Cash and equivalents: (unaudited end of Q2 2015) $32.2 M • Cash used in 2015 (through June 30, 2015) : $14.5 M • Cash runway: H2 2016 • Current shares outstanding: 24.3 M shares – Warrants Outstanding – Series A – 2,502 (purchased in unit deal @ $2.45); Series B – 429,704 @ $2.49 exercise price.