Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - TETRAPHASE PHARMACEUTICALS INC | d847135dex322.htm |
| EX-31.2 - EX-31.2 - TETRAPHASE PHARMACEUTICALS INC | d847135dex312.htm |
| EX-31.1 - EX-31.1 - TETRAPHASE PHARMACEUTICALS INC | d847135dex311.htm |
| EX-21.1 - EX-21.1 - TETRAPHASE PHARMACEUTICALS INC | d847135dex211.htm |
| EX-23.1 - EX-23.1 - TETRAPHASE PHARMACEUTICALS INC | d847135dex231.htm |
| EX-32.1 - EX-32.1 - TETRAPHASE PHARMACEUTICALS INC | d847135dex321.htm |
| EX-10.27 - EX-10.27 - TETRAPHASE PHARMACEUTICALS INC | d847135dex1027.htm |
| EX-10.26 - EX-10.26 - TETRAPHASE PHARMACEUTICALS INC | d847135dex1026.htm |
| EXCEL - IDEA: XBRL DOCUMENT - TETRAPHASE PHARMACEUTICALS INC | Financial_Report.xls |
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended: December 31, 2014
Or
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number: 001-35837
TETRAPHASE PHARMACEUTICALS, INC.
(Exact Name of Registrant as Specified in Its Charter)
| Delaware | 04-3581650 | |
| (State or Other Jurisdiction of Incorporation or Organization) |
(I.R.S. Employer Identification No.) |
480 Arsenal Street, Suite 110
Watertown, Massachusetts 02472
(Address of Principal Executive Offices) (zip code)
Registrant’s telephone number, including area code: (617) 715-3600
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class |
Name of each exchange on which registered | |
| Common Stock, $.001 par value | NASDAQ Global Select Market |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer | ¨ | Accelerated filer | x | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | ¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the registrant’s common stock, $0.001 par value per share (“Common Stock”), held by non-affiliates of the registrant, based on the last reported sale price of the Common Stock on the NASDAQ Global Select Market at the close of business on June 30, 2014, was $294,692,854. For purposes hereof, shares of Common Stock held by each executive officer and director of the registrant and entities affiliated with such executive officers and directors have been excluded from the foregoing calculation because such persons and entities may be deemed to be affiliates of the registrant. This determination of affiliate status is not necessarily a conclusive determination for other purposes.
The number of shares outstanding of the registrant’s Common Stock as of February 28, 2015: 30,976,618
Documents incorporated by reference:
Portions of our definitive proxy statement for our 2015 annual meeting of stockholders are incorporated by reference into Part III of this annual report on Form 10-K.
Table of Contents
TETRAPHASE PHARMACEUTICALS, INC.
Table of Contents
References to Tetraphase
Throughout this annual report on Form 10-K, the “Company,” “Tetraphase,” “we,” “us,” and “our,” except where the context requires otherwise, refer to Tetraphase Pharmaceuticals, Inc. and its consolidated subsidiaries, and “our board of directors” refers to the board of directors of Tetraphase Pharmaceuticals, Inc.
The trademarks, trade names and service marks appearing in this Annual Report on Form 10-K are the property of their respective owners.
Forward-Looking Information
This annual report on Form 10-K contains forward-looking statements regarding, among other things, our future discovery and development efforts, our future operating results and financial position, our business strategy, and other objectives for our operations. The words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “plan,” “predict,” “project,” “would” and similar expressions are intended to identify forward-looking statements, although not all forward-looking statements contain these identifying words. You also can identify them by the fact that they do not relate strictly to historical or current facts. There are a number of important risks and uncertainties that could cause our actual results to differ materially from those indicated by forward-looking statements. These risks and uncertainties include those inherent in pharmaceutical research and development, such as adverse results in our drug discovery and clinical development activities, decisions made by the U.S. Food and Drug Administration and other regulatory authorities with respect to the development and commercialization of our drug candidates, our ability to obtain, maintain and enforce intellectual property rights for our drug candidates, our ability to obtain any necessary financing to conduct our planned activities, and other risk factors. We may not actually achieve the plans, intentions or expectations disclosed in our forward-looking statements, and you should not place undue reliance on our forward-looking statements. Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward-looking statements we make. We have included important factors in the cautionary statements included in this annual report on Form 10-K, particularly in the section entitled “Risk Factors” in Part I that could cause actual results or events to differ materially from the forward-looking statements that we make. Our forward-looking statements do not reflect the potential impact of any future acquisitions, mergers, dispositions, joint ventures or investments that we may make. Unless required by law, we do not undertake any obligation to publicly update any forward-looking statements.
1
Table of Contents
| ITEM 1. | Business |
Overview
We are a clinical-stage biopharmaceutical company using our proprietary chemistry technology to create novel antibiotics for serious and life-threatening multidrug-resistant infections. We are developing our lead product candidate, eravacycline, a fully synthetic tetracycline derivative, as a broad-spectrum intravenous, or IV, and oral antibiotic for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections, including multidrug-resistant Gram-negative infections. We are conducting a global Phase 3 clinical program for eravacycline called IGNITE (Investigating Gram-Negative Infections Treated with Eravacycline), consisting of two Phase 3 clinical trials. IGNITE 1 is a Phase 3 clinical trial evaluating the safety and efficacy of eravacycline with IV administration for the treatment of complicated intra-abdominal infections, or cIAI, for which we announced top-line data in December 2014. IGNITE 2, a second Phase 3 clinical trial of eravacycline for the treatment of complicated urinary tract infections, or cUTI, with IV-to-oral transition therapy, is ongoing.
Consistent with guidance issued by the United States Food and Drug Administration, or FDA, with respect to the development of antibiotics for cIAI and our discussions with the FDA, we expect that positive results from these two Phase 3 clinical trials will be sufficient to support submission of a new drug application, or NDA, for eravacycline in the treatment of cIAI and cUTI. In December 2014, we announced positive top-line data from IGNITE 1. In September 2014, we announced positive data from the lead-in portion of IGNITE 2, and in October 2014, we announced the selection of the oral dose for the IV-to-oral transition therapy (1.5 mg/kg IV followed by 200 mg oral dose) to be evaluated in the pivotal portion of IGNITE 2 and the initiation of patient enrollment. We expect to have top-line data from the pivotal portion of IGNITE 2 in mid-2015. If we complete the pivotal portion of IGNITE 2 when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and a marketing authorization application, or MAA, to the European Medicines Agency, or EMA, in the first half of 2016.
IGNITE 1 is a global, multi-center, randomized, double-blind, double-dummy Phase 3 clinical trial that we conducted to assess the efficacy, safety and pharmacokinetics of eravacycline compared to ertapenem in patients with cIAI. In the trial, we enrolled 541 patients at 66 clinical sites worldwide. These patients were randomized into two arms of the trial on a 1:1 basis. Patients in the eravacycline arm received 1.0 mg/kg IV administered twice per day. Patients in the ertapenem arm received 1.0 g IV administered once per day. Eravacycline met the primary endpoint of statistical non-inferiority of clinical response at the test-of-cure, or TOC, visit, under the guidance set by the FDA and the EMA. The secondary analyses were consistent with and supportive of the primary outcome. There were no drug-related serious adverse events in the trial. The most commonly reported drug-related adverse events for eravacycline were gastrointestinal, including nausea (3.3%) and emesis (2.2%). This adverse event profile for eravacycline was consistent with that seen in the Phase 2 clinical trial of eravacycline in cIAI. The spectrum of pathogens in this trial was similar to that seen in other pivotal trials of antibiotics in this patient population. The most common Gram-negative pathogens in the trial included Escherichia coli, Klebsiella pneumonia, Pseudomonas and Bacteroides.
IGNITE 2 is a global, multi-center, randomized, double-blind clinical trial that we are conducting to assess the efficacy and safety of eravacycline compared with levofloxacin in the treatment of cUTI. We enrolled 143 patients in the lead-in portion of the trial, which we designed to inform the selection of an oral dose to be evaluated in the pivotal portion of the trial. These patients were randomized into three arms on a 1:1:1 basis receiving 1.5 mg/kg IV eravacycline every 24 hours followed by 200 mg of eravacycline orally every 12 hours, 1.5 mg/kg IV eravacycline every 24 hours followed by 250 mg of eravacycline orally every 12 hours or 750 mg IV levofloxacin every 24 hours followed by 750 mg of levofloxacin orally every 24 hours. After treatment completed in the lead-in portion of the trial, we evaluated primary efficacy, safety and tolerability endpoints to determine the dose regimen for eravacycline to be studied in the pivotal portion of the trial. In both IV-to-oral dosing regimens of eravacycline, eravacycline compared favorably to levofloxicin. In addition, treatment was generally well tolerated in all three groups with the most common adverse events reported being nausea and
2
Table of Contents
emesis. Based on these results, we selected the IV-to-oral transition therapy (1.5 mg/kg IV followed by 200 mg oral dose) to be evaluated in the pivotal portion of the trial. We are currently enrolling approximately 720 patients in the pivotal portion of the IGNITE 2 trial who will be randomized on a 1:1 basis to receive 1.5 mg/kg IV eravacycline every 24 hours followed by 200 mg of eravacycline orally every 12 hours or 750 mg IV levofloxacin every 24 hours followed by 750 mg of levofloxacin orally every 24 hours. Under FDA guidance, the primary endpoint of the pivotal portion of the trial is non-inferiority of clinical and microbiological response compared to levofloxacin at the post-treatment, or PT, visit, which takes place approximately seven days after completion of treatment. Under EMA guidance, the primary endpoint is non-inferiority of microbiological response compared to levofloxacin at the PT visit. A key secondary endpoint in IGNITE 2 is to test for superiority of eravacycline over levofloxacin in the treatment of cUTI for those subjects with infections caused by quinolone-resistant pathogens by evaluation of clinical and microbiological response at the PT visit.
Eravacycline has been designated by the FDA as a Qualified Infectious Disease Product, or QIDP, for both the cIAI and cUTI indications. The QIDP designation makes eravacycline eligible for priority review and an additional five years of U.S. market exclusivity, if approved. In April 2014, the FDA granted Fast Track designations for both the cIAI and cUTI indications and the IV and oral formulations of eravacycline. Fast Track designation is awarded to expedite the study and regulatory review of drugs intended to treat serious or life-threatening conditions that demonstrate the potential to address unmet medical needs.
In clinical trials to date, eravacycline monotherapy, either administered intravenously once or twice per day for the treatment of cIAI or administered as an IV-to-oral step-down therapy for the treatment of cUTI, has demonstrated a favorable safety and tolerability profile and a high cure rate, including against multidrug-resistant Gram-negative bacteria. In in vitro experiments, eravacycline has demonstrated the ability to cover a wide variety of multidrug-resistant Gram-negative, Gram-positive, anaerobic and atypical bacteria, including multidrug-resistant Klebsiella pneumoniae. Multidrug-resistant Klebsiella pneumoniae is one of the carbapenem-resistant Enterobacteriaceae listed as an urgent threat by the Centers for Disease Control and Prevention, or CDC, in a September 2013 report, and confirmed as an area of great concern by the World Health Organization in an April 2014 global surveillance report. Gram-negative bacteria that are resistant to all available antibiotics are increasingly common and a growing threat to public health. We believe that the ability of eravacycline to cover multidrug-resistant Gram-negative bacteria, as well as multidrug-resistant Gram-positive, anaerobic and atypical bacteria, and its potential for IV-to-oral transition therapy, will enable eravacycline to become the drug of choice for first-line empiric treatment of a wide variety of serious and life-threatening infections.
We believe that our proprietary chemistry technology, licensed from Harvard University on an exclusive worldwide basis and enhanced by us, represents a significant innovation in the creation of tetracycline drugs that has the potential to reinvigorate the clinical and market potential of the class. Our proprietary chemistry technology makes it possible to create novel tetracycline antibiotics using a practical, fully synthetic process for what we believe is the first time. This fully synthetic process avoids the limitations of bacterially-derived tetracyclines and allows us to chemically modify many positions in the tetracycline scaffold, including most of the positions that we believe could not practically be modified by any previous conventional method, which only allowed for limited chemical diversity. Using our proprietary chemistry technology, we can create a wider variety of tetracycline-based compounds than was previously possible, enabling us to pursue novel tetracycline derivatives for the treatment of multidrug-resistant bacteria that are resistant to existing tetracyclines and other classes of antibiotic products. To date, we have used our proprietary chemistry technology to create more than 3,000 new tetracycline derivatives that we believe could not be practically created with conventional methods. We own exclusive worldwide rights to these compounds and our technology.
In 2011 and 2012, the U.S. government awarded contracts for potential funding of over $100 million for the development of our antibiotic compounds. These awards include a contract for up to $67 million from the Biomedical Advanced Research and Development Authority, or BARDA, an agency of the U.S. Department of Health and Human Services, for the development of eravacycline for the treatment of disease caused by bacterial
3
Table of Contents
biothreat pathogens, which we refer to as the BARDA Contract. The funding under the BARDA Contract is also being used for certain activities in the development of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria. These awards also include a contract for up to $36 million from the National Institute of Allergy and Infectious Diseases, or NIAID, a division of the National Institutes of Health, for the development of TP-271, a broad-spectrum preclinical compound that we are developing for respiratory diseases caused by bacterial biothreat pathogens, which we refer to as the NIAID Contract. These awards were made to CUBRC, Inc., or CUBRC, an independent, not-for-profit, research corporation that specializes in U.S. government-based contracts, with which we are collaborating. CUBRC serves as the prime contractor under these awards, primarily carrying out a program management and administrative role with additional responsibility for the management of preclinical studies. We serve as lead technical expert on all aspects of these awards and also serve as a subcontractor of CUBRC responsible for management of chemistry, manufacturing and control activities and clinical studies. Under our subcontracts with CUBRC, we may receive funding of up to approximately $39.8 million reflecting the portion of the BARDA Contract funding that may be paid to us for our activities, and up to approximately $13.3 million reflecting the portion of the NIAID Contract funding that may be paid to us for our activities. The BARDA Contract includes funding for some of the activities that we would otherwise be required to fund on our own in connection with an NDA filing for eravacycline.
In addition to eravacycline and TP-271, we are pursuing the discovery and development of additional antibiotics to target unmet medical needs, including multidrug-resistant Gram-negative bacteria. We have selected TP-6076 as a lead candidate under this program which we have advanced into IND-enabling studies.
Strategy
Our goal is to become a fully integrated biopharmaceutical company that discovers, develops and commercializes novel antibiotics for use in areas of unmet medical need. Key elements of our strategy include:
| • | Complete clinical development of eravacycline in its lead indications and seek regulatory approval. We have completed a Phase 3 clinical trial of the IV formulation of eravacycline in patients with cIAI. We are also conducting a global Phase 3 clinical trial of eravacycline for the treatment of cUTI, which we initiated in the first quarter of 2014. We announced top-line data from the Phase 3 cIAI clinical trial in December 2014, data from the lead-in portion of the Phase 3 cUTI clinical trial in September 2014 and expect to announce top-line data from the pivotal portion of the Phase 3 cUTI clinical trial in mid-2015. If we complete the pivotal portion of IGNITE 2 when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and an MAA to the EMA in the first half of 2016. |
| • | Maximize the commercial potential of eravacycline. If eravacycline is approved, we intend to directly commercialize eravacycline in the United States with a targeted hospital sales force and to commercialize eravacycline outside the United States through collaboration arrangements. We believe that eravacycline’s broad-spectrum coverage of multidrug-resistant Gram-negative bacteria and other multidrug-resistant bacteria, with the potential for IV-to-oral transition therapy, will allow it to be used to treat patients successfully in hospitals, emergency rooms and out-patient clinic settings. |
| • | Pursue development of eravacycline in additional indications. We are initially developing eravacycline for the treatment of cIAI and cUTI, and, subject to obtaining additional financing, intend to pursue development of eravacycline for the treatment of additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections. We may pursue these development activities either by ourselves or with collaborators. |
| • | Opportunistically advance development of other product candidates created using our proprietary chemistry technology. We have used our proprietary chemistry technology to create more than 3,000 new tetracycline derivatives that we believe could not be practically created with conventional methods. We intend to advance our antibiotic product pipeline with differentiated product candidates created using our proprietary chemistry technology and targeting hospital and acute care markets. We may pursue these activities either by ourselves or with collaborators. |
4
Table of Contents
Drug-Resistant Antibiotic Market
Physicians commonly prescribe antibiotics to treat patients with acute and chronic infectious diseases that are either known, or presumed, to be caused by bacteria. According to IMS Health, in 2011, approximately $41 billion was spent on antibiotic drugs worldwide, of which almost $9 billion was spent in the United States. The widespread use of antibiotics has resulted in a rapid increase in bacterial infections that are resistant to multiple antibacterial agents. For example, the bacterial pathogen Klebsiella pneumoniae is responsible for roughly 14% of Gram-negative infections in hospital intensive care units. Multidrug-resistant Klebsiella pneumoniae are typically treated with the carbapenem class of antibiotics. However, in recent years, strains resistant to carbapenem antibiotics have emerged and markedly increased the threat posed by Klebsiella pneumoniae, as infections caused by carbapenem-resistant strains have few treatment options.
As a result of the increasing prevalence of such multidrug-resistant bacteria, some antibiotics targeting these bacteria have been highly successful commercially. These include:
| • | linezolid, an intravenously and orally administered antibiotic marketed by Pfizer, Inc., or Pfizer, as Zyvox, which had worldwide sales in 2014 of $1.35 billion; |
| • | levofloxacin, an intravenously and orally administered antibiotic marketed by Ortho-McNeil Pharmaceutical, or Ortho McNeil, and Johnson & Johnson as Levaquin, which had worldwide sales in 2012 of $75 million, down from worldwide sales of $1.4 billion in 2010 after losing U.S. market exclusivity in June 2011; |
| • | meropenem, an intravenously administered antibiotic marketed by AstraZeneca plc, or AstraZeneca, as Merrem, which had worldwide sales in 2014 of $253 million, down from worldwide sales of $817 million in 2010 after losing U.S. market exclusivity in June 2010; and |
| • | daptomycin, an intravenously administered antibiotic marketed by Cubist Pharmaceuticals, Inc., or Cubist, as Cubicin, which had worldwide sales of more than $1 billion in 2013. |
Bacterial infections are caused by a variety of different types of bacteria and the infections they cause can range from mild to serious, life-threatening infections requiring immediate treatment. Bacteria are broadly categorized as Gram-positive, Gram-negative, atypical or anaerobic. Gram-positive bacteria possess a single membrane and a thick cell wall and turn dark-blue or violet when subjected to a laboratory staining method known as Gram’s method. Common causes of Gram-positive bacterial infections include species of Staphylococcus, such as methicillin-resistant Staph aureus, or MRSA, Streptococcus and Enterococcus. Gram-negative bacteria have two membranes with a thin cell wall and, when subjected to Gram’s method of staining, lose the stain or are decolorized. According to The New England Journal of Medicine, the most common cause of Gram-negative infection is Escherichia coli, or E. coli. Less prevalent Gram-negative bacteria strains include species of Acinetobacter, Klebsiella and Pseudomonas. Atypical bacteria, such as Mycoplasma species, have modified cell walls and are neither Gram-positive nor Gram-negative. Anaerobic bacteria, such as Bacteroides species, either cannot grow in the presence of oxygen or do not require oxygen to grow and are classified as either Gram-positive or Gram-negative.
Antibiotics that treat bacterial infections can be classified as broad-spectrum or narrow-spectrum. Antibiotics that are active against a mixture of Gram-positive, Gram-negative and anaerobic bacteria are referred to as broad-spectrum. Antibiotics that are active only against a select subset of bacteria are referred to as narrow-spectrum. Because it usually takes from 24 to 72 hours from the time a specimen is received in the laboratory to definitively diagnose a particular bacterial infection, physicians may be required to prescribe antibiotics for serious infections without having identified the bacteria. As such, effective first-line treatment of serious infections requires the use of broad-spectrum antibiotics with activity against a broad range of bacteria at least until the bacterial infection can be diagnosed.
Many strains of bacteria have mutated over time and have developed resistance to existing drugs, resulting in infections that are increasingly serious or more difficult to treat. These drug-resistant pathogens have become a
5
Table of Contents
growing menace to all people, regardless of age, gender or socioeconomic background. They endanger people in affluent, industrial societies like the United States, as well as in less-developed nations. Gram-positive bacteria that have developed resistance to existing drugs include:
| • | Streptococcus pneumoniae that cause pneumonia, ear infections, bloodstream infections and meningitis; |
| • | Staphylococcus aureus that cause skin, bone, lung and bloodstream infections; and |
| • | Enterococci that are responsible for infections transmitted in healthcare settings. |
Gram-negative bacteria that have developed resistance to existing drugs include:
| • | Escherichia coli that cause urinary tract, skin and bloodstream infections; |
| • | Salmonella and Escherichia coli that cause foodborne infections; and |
| • | Acinetobacter baumannii, Pseudomonas aeruginosa and Klebsiella spp. that are responsible for infections transmitted in healthcare settings. |
Broad-spectrum antibiotics are used to treat major hospital infections such as cIAI, cUTI, hospital-acquired pneumonia, or HAP, and ventilator-associated pneumonia, or VAP. Based on an analysis from a variety of industry sources, we estimate that the number of patients treated with antibiotics in hospitals in the United States annually include approximately 1.9 million cIAI patients with each patient being treated for an average of 8.6 average days for a combined estimated 16.3 million annual average days of treatment; approximately 4.0 million cUTI patients with each patient being treated for an average of 6.9 days for a combined estimated 27.9 million annual average days of treatment; and 1.1 million HAP/VAP patients with each patient being treated for an average of 9.6 days for a combined estimated 10.6 million annual average days of treatment. Of these patients, we believe that approximately 45% of cIAI patients and 25% of cUTI patients have infections caused at least in part by multidrug-resistant Gram-negative bacteria. Gram-negative bacteria account for 55-85% of HAP/VAP infections. In hospitalized patients, rates of HAP/VAP due to MDR pathogens are increasing. Late-onset HAP/VAP are more likely to be caused by MDR pathogens, and are associated with increased patient mortality and morbidity.
According to a September 2013 report of the CDC, each year in the United States, at least two million people acquire serious infections with bacteria that are resistant to one or more of the antibiotics designed to treat those infections. At least 23,000 people die each year as a direct result of these antibiotic-resistant infections, with many more dying from other conditions that are complicated by the occurrence of an antibiotic-resistant infection. These antibiotic-resistant infections add considerable and avoidable costs to the already overburdened U.S. healthcare system. In the same September 2013 report, the CDC noted that the total economic cost of antibiotic infections to the U.S. economy has been estimated to be as high as $20 billion in excess of direct healthcare costs. In addition, the CDC reported that, among all of the bacterial resistance problems, Gram-negative pathogens are particularly worrisome because they are becoming resistant to nearly all drugs that would be considered for treatment, with the most serious Gram-negative infections being healthcare associated and the most common pathogens being Enterobacteriaceae, Pseudomonas aeruginosa and Acinetobacter.
As such, at present, there is an acute need for new drugs to treat multidrug-resistant Gram-negative bacteria. Currently approved products, such as Merrem and Levaquin, are becoming increasingly ineffective against Gram-negative bacteria due to increasing resistance, limiting patients’ treatment options, particularly for patients with multidrug-resistant infections, and few new therapeutic agents are in clinical development.
The need for new drugs to treat multidrug-resistant Gram-negative bacteria can be seen in both cIAI and cUTI. Specifically, patients with cIAI need early, rapid treatment as nearly 38% of these patients have mixed infections, meaning that there is more than one pathogen causing the infection, and only 64% of patients are treated with first-line empiric therapy while 36% require treatment with second-line therapies. We estimate that of the cIAI patients treated with current antibiotic treatments, approximately 23% are prescribed piperacillin/
6
Table of Contents
tazobactam and of those patients, nearly 10% fail therapy; approximately 22% are prescribed an antibiotic from the quinolone class and nearly 19% fail therapy; approximately 21% are prescribed an antibiotic from the carbapenem class and nearly 7% fail therapy; and approximately 3% are prescribed ceftriaxone and nearly 14% fail therapy.
The resistance rates for cUTI to current antibiotics are between 20-60% and appear to be increasing. Seventy percent (70%) of cUTI patients are treated with first-line empiric therapy while 30% require treatment with second-line therapies. We estimate that of the cUTI patients treated with current antibiotic treatments, approximately 38% are prescribed an antibiotic from the quinolone class (with IV to oral transition) and of those patients, nearly 22% fail therapy; approximately 15% are prescribed ceftriaxone (a once a day antibiotic) and nearly 18% fail therapy; approximately 9% are prescribed an antibiotic from the carbapenem class and nearly 7% fail therapy; and approximately 7% are prescribed piperacillin/tazobactam and nearly 10% fail therapy.
A survey of infectious disease specialists published in the June 2012 edition of Clinical Infectious Disease rated multidrug-resistant Gram-negative infections as the most important unmet clinical need in current practice. In the survey, 63% of physicians reported treating a patient in the past year whose bacterial infection was resistant to all available antibacterial agents. This resistance was confirmed by the SENTRY Antimicrobial Surveillance Program which evaluated Enterobacteriaceae and Acinetobacter spp., two Gram-negative species of bacteria, from 31 U.S. medical centers from 2005 to 2009. Specifically, the SENTRY Program found that, with respect to the Enterobacteriaceae family of bacteria, 6.8% of the Escherichia coli strains studied and 15.4% of the Klebsiella spp. strains studied exhibited an extended-spectrum beta lactamase, or ESBL, phenotype, and that 22.2% of Enterobacter spp. strains studies were ceftazidime-resistant. ESBLs are enzymes present in certain multidrug-resistant bacteria that destroy classes of beta lactam antibiotics, such as penicillins, cephalosporins and carbapenems. In addition, Klebsiella pneumoniae carbapenemase-, or KPC-, producing bacteria have emerged as a highly drug resistant Gram-negative bacteria associated with mortality rates ranging from 32% to 48%, as compared to 9% to 17% for strains of Klebsiella pneumoniae that are not carbapenem-resistant.
As a further example of the seriousness of the threat of Gram-negative bacteria resistant to all available antibacterial agents, in 2014, the national media including The Wall Street Journal, CBS and Fox News reported on an outbreak, primarily in one suburban Chicago, Illinois hospital, of carbapenem-resistant enterobacteriaceae, or CRE, with more than 40 cases reported in 2013. Additionally, in February 2015, an outbreak of CRE occurred at the Ronald Reagan UCLA Medical Center in which a total of seven people became infected and the infection was a contributing factor in the death of two patients. A similar report came from the Carolinas HealthCare System in February 2015, in which 18 people contracted CRE at a hospital in Charlotte, North Carolina and one person died. According to the CDC, CRE are a nightmare bacteria, are resistant to nearly all known antibiotics and kill up to 50% of people infected.
The growing issue of antibiotic-resistant bacterial infections has been widely recognized as an increasingly urgent public health threat, including by the World Health Organization, or WHO, the CDC and the Infectious Disease Society of America, or IDSA. In April 2014, the WHO issued an antimicrobial resistance global surveillance report stating that resistance to common bacteria has reached alarming levels worldwide indicating that many available treatment options are becoming ineffective, and leading to a negative impact in patient outcomes and health-care spending. The WHO warns that unless significant measures are taken, people will start to die from common, formerly treatable infections, and medical interventions such as surgery, chemotherapy, organ transplantation and care of premature infants will become increasingly risky. The important need for new treatment options for serious bacterial infections was further highlighted by the passage in the United States in July 2012 of the Generating Antibiotic Incentives Now, or GAIN, Act, which provides regulatory incentives for the development of new antibacterial or antifungal drugs intended to treat serious or life-threatening infections that are resistant to existing treatment. In September 2014, the United States’ President’s Council of Advisors on Science and Technology issued a report providing recommendations to combat the rise in antibiotic resistant bacteria and advising that without rapid action, the United States risks losing the tremendous progress made in
7
Table of Contents
antibiotic development over the last century. Their recommendations focused on three areas: improving surveillance, increasing longevity of current antibiotics and increasing the rate at which new antibiotics are discovered and developed.
Additionally, legislative initiatives have recently been introduced as part of the 21st Century Cures discussion document, including the Antibiotic Development to Advance Patient Treatment, or ADAPT, Act which would provide a pathway for approval of antibiotics in limited populations of patients with few or no suitable treatment options, the Developing an Innovating Strategy for Antimicrobial Resistant Microorganisms, or DISARM, Act which would designate certain novel antibiotics used to treat serious bacterial infections to receive higher Medicare reimbursement, and an amendment to the GAIN Act which would allow successful QIDP sponsors to transfer up to one year of exclusivity to another product, including products marketed by other companies.
Limitations of Available Treatment Options
When confronted with a new patient suffering from a serious infection caused by an unknown pathogen, a physician may be required to quickly initiate first-line empiric antibiotic treatment to stabilize the patient prior to definitively diagnosing the particular bacterial infection. However, current antibiotics for first-line empiric treatment of serious bacterial infections suffer from significant limitations, including one or more of the following:
Insufficient Coverage of Multidrug-resistant Bacteria. A physician cannot afford to be too limited in the spectrum of bacteria covered by antibiotics when initially treating a patient for a serious infection that has not yet been definitively identified. Frequently used products, such as Zyvox and Cubicin, are limited to Gram-positive bacteria and thus are rarely used as a first-line empiric monotherapy if broad bacterial coverage is required. In addition, other popular antibiotics that have been used as first-line empiric monotherapies, such as Levaquin, piperacillin/tazobactam, which is marketed by Pfizer as Zosyn, carbapenems, such as Merrem, and imipenem/cilastatin, which is marketed by Merck as Primaxin, have seen their utility as first-line empiric monotherapies diminished as the number of bacterial strains resistant to these therapies has increased.
Complicated and Expensive Multi-Drug Cocktails and Multi-Dose Regimens. Due to gaps in the spectrum of coverage of antibiotics, physicians are often confronted with the need to design complicated multi-drug cocktails for the first-line empiric treatment of patients with serious infections. The clinical situation is further complicated when each drug in the multi-drug cocktail has a different dosing regimen, such as two, three or four times a day, resulting in an added burden on the pharmacy and nursing staff, higher costs due to multiple drug administrations and an increased potential for medical errors or drug-drug interactions. We believe that, with the exception of eravacycline, most of the antibiotics that are in development or have recently been approved by the FDA that are intended to cover a broad spectrum of bacteria, including Gram-negative bacteria, or solely to address Gram-negative bacteria, are being developed or are approved for use in combination with one or more other antibiotics, and require the addition of a third drug such as metronidazole to address the presence of anaerobic bacteria.
Safety and Tolerability Concerns. Concerns about antibiotic safety and tolerability are among the leading reasons why patients stop treatment and fail therapy. Antibiotics on the market have been associated with adverse effects such as myelosuppression, seizures, nephrotoxicity and gastrointestinal disorders.
Lack of Oral Dosage Forms to Permit Transition Therapy. When a patient comes to the emergency room or hospital for treatment of a serious infection, the patient initially receives IV treatment, which allows the drug to be delivered more rapidly and in a larger dose than oral treatment. Once the infection begins to respond to treatment and the patient is stabilized, depending on the infection, hospitals and physicians generally seek to minimize in-hospital treatment and, if possible, discharge patients from the hospital in order to reduce costs, avoid hospital-acquired infections, and improve the patients’ quality of life. Upon discharge, physicians typically prefer to prescribe transition therapy treatment with an oral formulation of the same antibiotic. A transition
8
Table of Contents
therapy to oral treatment allows for more convenient and cost-effective out-patient treatment, with the oral antibiotic providing enhanced patient comfort and mobility and avoiding the risk of infection from the IV catheter. In addition, the use of the same antibiotic allows the physician to avoid switching the patient from the antibiotic that has proven effective during IV administration to a different antibiotic that may be less effective and carries the risk of new or different side effects. Many of the antibiotics that are most commonly used as first-line empiric monotherapies are only available in an IV formulation. Very few of the antibiotics that cover or are focused on the treatment of Gram-negative bacteria have oral dosage forms.
Given these limitations, there is an unmet medical need for a first-line empiric antibiotic treatment that has the following characteristics:
| • | Potency and effectiveness against a broad spectrum of bacteria, including multidrug-resistant Gram-negative, Gram-positive, atypical and anaerobic bacteria; |
| • | Capability of being used as a monotherapy in the majority of patients in the hospital with cIAI, cUTI and other multidrug-resistant infections; |
| • | A convenient dosing regimen, such as once or twice-daily; |
| • | A favorable safety and tolerability profile; and |
| • | Availability in both IV dosage and oral dosage form. |
Based on our belief that eravacycline has, or potentially has, each of these characteristics, our goal is to develop eravacycline to be the drug of choice for first-line empiric treatment of a wide variety of serious and life-threatening infections.
Eravacycline
Overview
We are developing our lead product candidate, eravacycline, as a broad-spectrum IV and oral antibiotic for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections, including multidrug-resistant Gram-negative bacteria. We developed eravacycline using our proprietary chemistry technology. We believe our fully synthetic process will enable us to have a cost of manufacturing that is sufficiently low to enable us to sell eravacycline, when and if approved, for a cost that is similar to other hospital-based antibiotics. Our patent strategy to broadly protect eravacycline includes the filing of patent applications directed towards the composition of matter of eravacycline as well as our proprietary chemistry technology, which we used to create eravacycline. We own exclusive worldwide rights for the development and commercialization of eravacycline.
In 2012, we completed a successful Phase 2 clinical trial of eravacycline with IV administration for the treatment of patients with cIAI. We initiated IGNITE 1, a Phase 3 clinical trial of eravacycline with IV administration for the treatment of cIAI, in the third quarter of 2013, and subsequently initiated the lead-in portion of IGNITE 2, a two-part Phase 3 clinical trial of eravacycline for the treatment of cUTI with IV-to-oral transition therapy, during the first quarter of 2014. In December 2014, we announced positive top-line data from IGNITE 1. In September 2014, we announced positive data from the lead-in portion of IGNITE 2, and in October 2014, we announced the selection of the oral dose to be evaluated in the pivotal portion of the trial and the initiation of patient enrollment. We expect to have top-line data from the Phase 3 cUTI clinical trial in mid-2015. If we complete the pivotal portion of IGNITE 2 when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and an MAA to the EMA in the first half of 2016.
Tetracycline antibiotics have been in clinical use for over 50 years and have a demonstrated record of safety and effectiveness. However, as with most classes of antibiotics, a high incidence of resistance among many bacteria has limited their effectiveness and resulted in tetracyclines being relegated to second- or third-line
9
Table of Contents
therapy several decades after their introduction. Chemists have generally been unable to synthesize new tetracyclines that could overcome bacterial resistance mechanisms. We have used our proprietary chemistry technology to create more than 3,000 new tetracycline derivatives that we believe could not be practically created with conventional methods. Many of these new derivatives, including eravacycline, have been able to overcome bacterial resistance in in vitro studies.
Eravacycline is a novel, fully synthetic tetracycline antibiotic. We selected eravacycline for development from tetracycline derivatives that we generated using our proprietary chemistry technology on the basis of the following characteristics of the compound that we observed in in vitro studies of the compound:
| • | potent antibacterial activity against a broad spectrum of susceptible and multidrug-resistant bacteria, including Gram-negative, Gram-positive, atypical and anaerobic bacteria; |
| • | potential to treat the majority of patients as a first-line empiric monotherapy with convenient dosing; and |
| • | potential for IV-to-oral transition therapy. |
In designing eravacycline, we inserted a fluorine atom into the tetracycline scaffold, which we call a fluorocycline, and modified the scaffold at another position. We believe that these modifications enable eravacycline to not be subject to tetracycline-specific mechanisms of drug resistance. As a result, we believe that eravacycline is active against multidrug-resistant bacteria in ways that tetracyclines currently on the market or in development are not.
In in vitro studies, including a surveillance study published in December 2014 using over 4,000 patient bacterial isolates collected in New York City, eravacycline has been highly active against emerging multidrug-resistant pathogens like Acinetobacter baumannii as well as clinically important species of Enterobacteriaceae, including those isolates that produce ESBLs or are resistant to the carbapenem class of antibiotics, and anaerobes, in comparison to commonly used antibiotics.
Based on in vitro studies we have completed, we believe that eravacycline shares a similar potency profile with carbapenems except that it more broadly covers Gram-positive pathogens like MRSA and enterococci, is active against carbapenem-resistant Gram-negative bacteria and, unlike carbapenems like Primaxin and Merrem, has reduced activity against Pseudomanas aeruginosa. Eravacycline has demonstrated strong activity in vitro against Gram-positive pathogens, including both nosocomial and community-acquired methicillin susceptible or resistant Staphylococcus aureus strains, vancomycin susceptible or resistant Enterococcus faecium and Enterococcus faecalis, and penicillin-susceptible or resistant strains of Streptococcus pneumoniae. In in vitro studies of pathogens most prevalent in cIAI infections, eravacycline consistently exhibited strong activity against enterococci and streptococci. One of the most frequently isolated anaerobic pathogens in cIAI, either as the sole pathogen or often in conjunction with another Gram-negative bacterium, is Bacteroides fragilis. In these studies eravacycline demonstrated activity against Bacteroides fragilis and a wide range of Gram-positive and Gram-negative anaerobes.
Key Differentiating Attributes of Eravacycline
We believe that the following key attributes of eravacycline, observed in clinical trials and preclinical studies, differentiate eravacycline from other antibiotics targeting multidrug-resistant infections, including multidrug-resistant Gram-negative infections. We believe these attributes will make eravacycline a safe and effective treatment for cIAI, cUTI and other serious and life-threatening infections for which we may develop eravacycline, such as hospital-acquired bacterial pneumonias.
| • | Broad-spectrum activity against a wide variety of multidrug-resistant Gram-negative, Gram-positive and anaerobic bacteria. In our Phase 2 clinical trial of the IV formulation of eravacycline, eravacycline demonstrated a high cure rate against a wide variety of multidrug-resistant |
10
Table of Contents
| Gram-negative, Gram-positive and anaerobic bacteria. In addition, in in vitro studies, eravacycline demonstrated potent antibacterial activity against Gram-negative bacteria, including E. coli; ESBL-producing Klebsiella pneumoniae; Acinetobacter baumannii; Gram-positive bacteria, including MRSA and vancomycin-resistant enterococcus, or VRE; and anaerobic pathogens. As a result of this broad-spectrum coverage, we believe that eravacycline has the potential to be used as a first-line empiric monotherapy for the treatment of cIAI, cUTI, hospital-acquired bacterial pneumonias and other serious and life-threatening infections. |
| • | Lower probability of drug resistance. To date, in the clinical trials and preclinical studies of eravacycline that we have conducted we have seen little decrease in susceptibility that would suggest increased resistance to eravacycline. We believe that, as a fluorocycline, eravacycline will not be subject to tetracycline-specific mechanisms of drug resistance. |
| • | Favorable safety and tolerability profile. Eravacycline has been evaluated in more than 800 subjects in the Phase 1, Phase 2 and Phase 3 clinical trials that we have conducted. In these trials, eravacycline has demonstrated a favorable safety and tolerability profile. In our Phase 2 and Phase 3 clinical trials of eravacycline in patients with cIAI, no patients suffered any drug-related serious adverse events, and safety and tolerability were comparable to ertapenem, the control therapy in the trials. In addition, in these Phase 2 and Phase 3 clinical trials, the rate at which gastrointestinal adverse events such as nausea and emesis that occurred in the eravacycline arms was low. |
| • | Convenient dosing regimen. In our clinical trials to date, we have dosed eravacycline once or twice a day as a monotherapy. We believe that eravacycline will be able to be administered as a first-line empiric monotherapy with once- or twice-daily dosing, avoiding the need for complicated dosing regimens typical of multi-drug cocktails and the increased risk of negative drug-drug interactions inherent to multi-drug cocktails. |
| • | Potential for convenient IV-to-oral transition therapy. In addition to the IV formulation of eravacycline, we have developed an oral formulation of eravacycline that we are evaluating in IGNITE 2. If successful, this oral formulation would enable patients who begin IV treatment with eravacycline in the hospital setting to transition to oral dosing of eravacycline either in hospital or upon patient discharge for convenient home-based care. We believe that the availability of both IV and oral transition therapy may reduce the length of a patient’s hospital stay and the overall cost of care. |
Clinical Experience
We have studied IV and oral formulations of eravacycline in 818 subjects in sixteen clinical trials conducted from October 2009 to December 2014, which includes those subjects treated in the lead-in portion of our ongoing Phase 3 clinical trial of eravacycline for cUTI.
Phase 3 Clinical Program
We designed our Phase 3 program for eravacycline to enable us to position eravacycline as a first-line empiric monotherapy for the treatment of cIAI and cUTI due to eravacycline’s broad-spectrum coverage of multidrug-resistant infections, including multidrug-resistant Gram-negative infections. Our program is consistent with the guidance issued by the FDA for drug development for cIAI and cUTI. The cIAI guidance indicates that, for companies developing a drug for cIAI and an additional indication caused by similar bacterial pathogens, such as cUTI, a single trial in cIAI and a single trial in that additional indication could be sufficient to provide evidence of effectiveness in both indications. We believe that prior to the issuance of this guidance, a company that was developing a drug for cIAI and an additional indication would have been required to conduct two Phase 3 clinical trials of the drug for the treatment of cIAI, enrolling 500 to 600 patients in each trial, and additional Phase 3 clinical trials of the drug for the treatment of the additional indication, even where cIAI and the additional indication were caused by similar bacterial pathogens. We believe that the opportunity provided by the guidance to submit an NDA package for two indications on the basis of only two Phase 3 clinical trials makes the process of developing and seeking approval of drugs for cIAI and a second indication more cost-effective. The trials can be conducted at the same time, and because the patient populations are different for the two trials, patient enrollment can be faster.
11
Table of Contents
Phase 3 cIAI Clinical Trial
Eravacycline Phase 3 IGNITE 1 Study Design
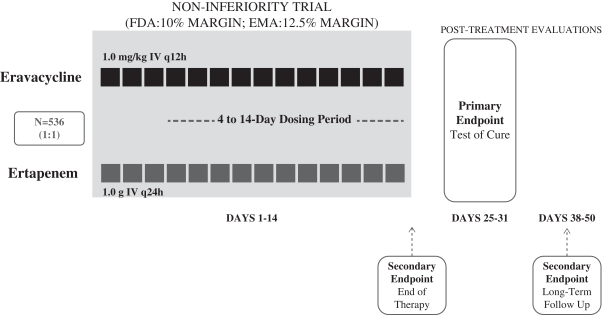
In the third quarter of 2013, we initiated a global, multi-center, randomized, double-blind, double-dummy Phase 3 clinical trial, our IGNITE 1 trial, to assess the efficacy, safety and pharmacokinetics of eravacycline compared to ertapenem in patients with cIAI. We enrolled 541 patients in the trial at 66 clinical sites worldwide. These patients were randomized into two arms on a 1:1 basis. Patients in the eravacycline arm received 1.0 mg/kg IV eravacycline administered twice per day. Patients in the ertapenem arm received 1.0 g IV ertapenem administered once per day.
Investigators obtained baseline intra-abdominal cultures at the time of operation and treated patients for a minimum of four days and a maximum of 14 days following the time of operation and until symptoms of cIAI were resolved. A TOC visit took place 25 to 31 days after the initial dose of treatment and a final or follow-up visit occurred 38 to 50 days after the initial dose of treatment.
We designed the trial as a non-inferiority study, and to be responsive to both FDA and EMA guidance. Under FDA guidance, the primary endpoint of the trial was clinical response at the TOC visit in the microbiological intent-to-treat, or micro-ITT, population which consisted of all randomized patients in the trial who had baseline bacterial pathogens that cause cIAI and against which eravacycline has antibacterial activity. Under EMA guidance, the primary endpoint of the trial was clinical response at the TOC visit in the modified intent-to-treat, or MITT, population which consisted of all patients who received at least one dose of study drug, and in the clinically evaluable, or CE, patient population, which consisted of all randomized patients in the trial who meet key inclusion/exclusion criteria and follow other important components of the trial. Secondary endpoints included clinical response at the end-of-treatment, TOC and follow-up visits in the intent-to-treat population, the CE population, the micro-ITT population and the microbiologically evaluable, or ME, population. The ME population consists of all micro-ITT patients who meet key inclusion/exclusion criteria and follow other important components of the trial. In the trial, we also studied microbiologic response at the end-of-treatment and TOC visits in the micro-ITT and ME populations, the safety and tolerability of eravacycline in the safety population and pharmacokinetic parameters after eravacycline administration. We designed the trial to be
12
Table of Contents
consistent with the FDA’s cIAI guidance, in which the FDA suggested that the primary efficacy endpoint for a trial of cIAI should be complete resolution of baseline signs and symptoms attributable to cIAI in the micro-ITT patient population 28 days after randomization and the absence of clinical failure including death and unplanned surgical procedures through the period ending 28 days following randomization.
In December 2014, we announced top-line data from IGNITE 1. In the trial, eravacycline met the primary endpoint of statistical non-inferiority of clinical response at the TOC visit, under the guidance set by the FDA and the EMA. The primary analysis under the FDA guidance was conducted using a 10% non-inferiority margin in the micro-ITT population. In the micro-ITT population, the lower and upper bounds of the 95% confidence interval were -7.1% and 5.5%, respectively. Under the EMA guidance, the primary analysis was conducted using a 12.5% non-inferiority margin in the CE and MITT patient populations. In the CE population, the lower and upper bounds of the 95% confidence interval were -6.3% and 2.8%, respectively, and the lower and upper bounds of the 99% confidence interval were -7.9% and 4.4%, respectively. In the MITT population, the lower and upper bounds of the 95% confidence interval were -7.4% and 3.8%, respectively, and the lower and upper bounds of the 99% confidence interval were -9.2% and 5.6%, respectively. The secondary analyses were consistent with and supportive of the primary outcome. There were no drug-related serious adverse events in the trial. The most commonly reported drug-related adverse events for eravacycline were gastrointestinal, including nausea (3.3%) and emesis (2.2%). This adverse event profile for eravacycline was consistent with that seen in the Phase 2 clinical trial of eravacycline in cIAI. The spectrum of pathogens in this trial was similar to that seen in other pivotal trials of antibiotics in this patient population. The most common Gram-negative pathogens in the trial included Escherichia coli, Klebsiella pneumonia, Pseudomonas and Bacteroides.
Phase 3 cUTI Clinical Trial
Eravacycline Phase 3 IGNITE 2 Study Design
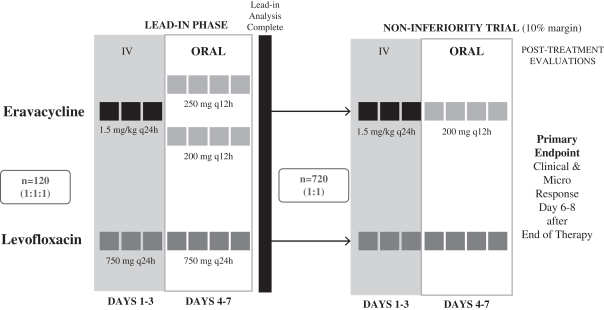
In the first quarter of 2014, we initiated a two-part, multi-center, randomized, double-blind Phase 3 clinical trial, our IGNITE 2 trial, to assess the efficacy and safety of eravacycline compared with levofloxacin in the treatment of cUTI. We enrolled 143 patients in the lead-in portion of the trial. These patients were randomized into three arms on a 1:1:1 basis: an arm in which patients received 1.5 mg/kg IV eravacycline every 24 hours followed by 200 mg of eravacycline orally every 12 hours; an arm in which patients received 1.5 mg/kg IV
13
Table of Contents
eravacycline every 24 hours followed by 250 mg of eravacycline orally every 12 hours; and an arm in which patients received 750 mg IV levofloxacin every 24 hours followed by 750 mg of levofloxacin orally every 24 hours.
After treatment was completed in the lead-in portion of the trial, we evaluated efficacy, safety and tolerability endpoints to determine the dose regimen for eravacycline to be studied in the pivotal portion of the trial. In the lead-in portion of IGNITE 2 both IV-to-oral dosing regimens of eravacycline compared favorably to levofloxacin. The responder outcome, the primary endpoint for the FDA, is determined as the number of micro-ITT patients at the PT visit with both clinical response and microbiological response. Clinical response is measured by a complete or significant improvement in signs or symptoms and microbiological response is demonstrated if the baseline pathogen is cleared or reduced below a specified level in a urine sample. The responder rates in the micro-ITT population for the IV-to-oral 200 mg, IV-to-oral 250 mg and levofloxacin groups were 70.8% (n=24), 64.3% (n=28) and 52.2% (n=23), respectively. The microbiological response rates in the micro-ITT population were 75.0% (n=24), 64.3% (n=28) and 56.5% (n=23), respectively. The pharmacokinetics of both oral doses of eravacycline were comparable to the IV formulation in the trial. Overall, treatment was generally well tolerated in all three groups with the most common adverse events reported being nausea and emesis. Only two patients discontinued treatment as a result of drug related adverse events. In October 2014, we selected the 1.5 mg/kg IV followed by 200 mg oral dose as the IV-to-oral transition therapy to be evaluated in the pivotal portion of the trial and initiated patient enrollment.
We are currently enrolling in the pivotal portion of the trial approximately 720 patients who will be randomized on a 1:1 basis to receive 1.5 mg/kg IV eravacycline every 24 hours followed by 200 mg of eravacycline orally every 12 hours or 750 mg IV levofloxacin every 24 hours followed by 750 mg of levofloxacin orally every 24 hours. We have designed the pivotal portion of the trial as a non-inferiority study and to be responsive to both FDA and EMA guidance. Under FDA guidance, the primary endpoint of the pivotal portion of the trial is clinical and microbiological response in the micro-ITT population at the PT visit. Under EMA guidance, the primary endpoint of the pivotal portion of the trial is microbiological response in the micro-MITT and ME populations. The micro-MITT population consists of any patient who received study drug who had baseline bacterial pathogens that cause cUTI and against which eravacycline has antibacterial activity. The ME population consists of all micro-ITT patients who meet key inclusion/exclusion criteria and follow other important components of the trial. In order to achieve the primary endpoint, eravacycline would need to demonstrate non-inferiority as compared to levofloxacin within a margin of no more than 10%. A key secondary endpoint in IGNITE 2 is to test for superiority of eravacycline over levofloxacin in the treatment of cUTI for those subjects with infections caused by quinolone-resistant pathogens by evaluation of clinical and microbiological response in the micro-ITT population at the PT visit.
Regulatory Filing Timeline
We expect to have top-line data from the Phase 3 cUTI clinical trial in mid-2015. If we successfully complete the trial when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and an MAA to the EMA in the first half of 2016. Our goal is to develop eravacycline to be the drug of choice for first-line empiric treatment of a wide variety of serious and life-threatening infections.
Phase 2 clinical trial of IV formulation in cIAI
In June 2012, we completed a global, multi-center, randomized, double-blind Phase 2 clinical trial to evaluate the efficacy, safety and pharmacokinetics of the IV formulation of eravacycline compared to ertapenem in patients with cIAI. We selected cIAI as the indication for the trial because we wanted to ensure that there would be a significant population of patients in the study with multidrug-resistant Gram-negative bacteria and because Gram-negative bacteria are prevalent in cIAI. We selected ertapenem as the comparison therapy because ertapenem is one of the antibiotics recommended by IDSA guidelines for the treatment of cIAI. We also established clinical sites in countries such as India, where multidrug-resistant Gram-negative pathogens have higher prevalence.
14
Table of Contents
Trial Design. We enrolled 143 hospitalized patients with cIAI in the trial. These patients were randomized into three arms on a 2:2:1 basis: an arm in which patients received 1.5 mg/kg IV eravacycline administered once per day; an arm in which patients received 1.0 mg/kg IV eravacycline administered twice per day; and a control arm in which patients received 1.0 g IV ertapenem administered once per day, which is the standard dosing regimen for ertapenem.
Investigators obtained baseline intra-abdominal cultures at the time of operation and treated patients for a minimum of four days and a maximum of 14 days. The length of treatment for each patient was determined by the physician based on pre-set parameters. A TOC visit took place ten to 14 days after the last dose of drug was administered and a final or follow-up visit occurred within four to six weeks after the last dose of drug was administered.
Patient Disposition. Of the 143 patients in the trial, four did not receive drug. Two were excluded because of incorrect randomization, one withdrew consent for inclusion in the trial after randomization, and one was excluded for having received non-study antibiotics prior to the first dose. At least one pathogen or bacterium responsible for the cIAI was identified following enrollment in 119 of the 139 patients who received drug in the trial. We refer to this subset of patients as the microbiologically-modified intent-to-treat, or micro-MITT, patients. Of the 119 micro-MITT patients, 109 were deemed clinically evaluable based on key inclusion and exclusion criteria being validated and key visits and assessments having been performed. We refer to this subset of the micro-MITT patients as the microbiologically evaluable, or ME, patients. The 10 micro-MITT patients that were not considered clinically evaluable were not classified as ME patients as a result of their withdrawing consent, failing to complete the trial, failing to attend a TOC visit or having indeterminate results at the TOC visit. The primary endpoint of the trial was clinical response at the TOC visit in the ME patients. Clinical response was defined as complete resolution or significant improvement of signs or symptoms of infection with no further systemic antibiotic treatment required. Clinical response was also included as one of the secondary endpoints in the trial at the follow-up visit in the micro-MITT population.
Patient Demographics. Patient demographics were similar across all three trial arms except for APACHE scores as, at baseline, the patients in the 1.5 mg/kg dose group exhibited slightly higher APACHE scores than the other treatment groups. APACHE scores are a commonly used severity of disease scoring system, where a higher number means that the patient had more severe disease and higher risk of death. In the majority of the MITT patient population, complicated appendicitis was the diagnosed disease underlying the infections, which were being treated with the antibiotics in the trial. Other diseases including perforation of intestine, complicated diverticulitis, gastric/duodenal perforation and complicated cholecystitis, comprised the other diagnoses.
Efficacy. In the trial, ME patients in the eravacycline arms experienced similar infection cure rates to the ME patients in the ertapenem arm, as summarized in the table below. The table also shows the 95% confidence interval, a statistical determination that demonstrates the range of possible differences in the point estimates of success that will arise 95% of the time the endpoint is measured.
Eravacycline Phase 2 Trial Primary Endpoint Analysis
| Population |
Eravacycline (1.5 mg/kg every 24 hours) |
Eravacycline (1.0 mg/kg every 12 hours) |
Ertapenem (1.0 g Every 24 hours) |
|||||||||
| Microbiologically Evaluable (ME) |
N=42 | N=41 | N=26 | |||||||||
| % Cure in ME (95% Confidence Interval) |
92.9 (80.5-98.5) | 100 (91.4-100) | 92.3 (74.9-99.1) | |||||||||
|
|
|
|
|
|
|
|||||||
Investigators in the trial had the discretion to determine the period that patients remained on the applicable treatment. The mean duration of treatment in the trial was 6.1 days for the patients receiving 1.5 mg/kg IV eravacycline administered once per day; 5.6 days for the patients receiving 1.0 mg/kg IV eravacycline administered twice per day; and 6.0 days for the patients receiving 1.0 g IV ertapenem administered once per day.
15
Table of Contents
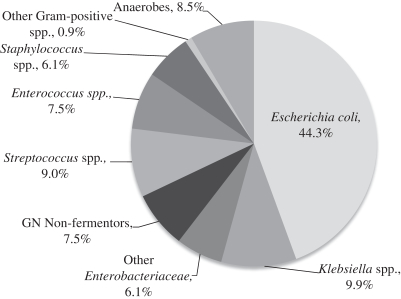
The figure below shows the overall pathogen mix identified in the Phase 2 cIAI clinical trial. Of the pathogens isolated from the micro-MITT patients enrolled in the Phase 2 clinical trial, approximately 60% were members of the Enterobacteriaceae family. Micro-MITT patients in the trial were infected with an average of 1.8 pathogens. The Gram-negative aerobic pathogens occurring most frequently were Escherichia coli, Klebsiella pneumonia, Klebsiella oxytoca, Pseudomonas aeruginosa, Acinetobacter baumannii complex and Morganella morganii. The Gram-positive aerobic pathogens occurring most frequently were Streptococcus spp., Enterococcus faecalis and Staphylococcus aureus. The anaerobic pathogens occurring most frequently were Bacteroides fragilis and Clostridium spp.
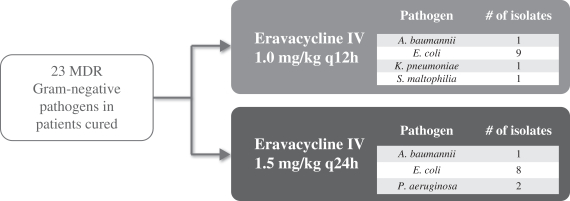
Of particular importance in the trial results was the performance of eravacycline against confirmed drug-resistant Gram-negative pathogens as well as other challenging Gram-negative pathogens. Due to the global, multi-center nature of the trial and our emphasis on sites in known geographic “hot spots” for multidrug-resistant Gram-negative bacteria, 25% of the Gram-negative pathogens identified in micro-MITT patients were confirmed to be multidrug-resistant as a result of being ESBL-positive and/or carbapenem-resistant. The figure below shows that the patients cured with eravacycline in the Phase 2 cIAI clinical trial had 23 confirmed multidrug-resistant Gram-negative pathogens.
16
Table of Contents
Safety and Tolerability. In the Phase 2 clinical trial, eravacycline demonstrated a comparable safety and tolerability profile to ertapenem. No patients in the trial suffered any serious adverse events that were found to be related to eravacycline, and the percentage of patients in the trial arms that experienced treatment emergent adverse events, or TEAEs, were similar. In addition, gastrointestinal adverse events known to be associated with tetracyclines such as nausea and emesis, occurred at low rates in the eravacycline arms that were similar to the rates for the ertapenem arm. Adverse events associated with infusion sites were limited and similar in all treatment groups.
Pharmacokinetics. Patients in the Phase 2 clinical trial were subjected to pharmacokinetic sampling during the period of treatment to enable us to assess plasma exposure levels of eravacycline in the trial. The mean area under the curve, or AUC, was 4,349.9 ng*h/mL (50% CV) for the 1.5 mg/kg dose of eravacycline administered every 24 hours (n=48) and 3,240.7 ng*h/mL (53.5% CV) for the 1.0 mg/kg dose of eravacycline administered every 12 hours (n=51). The Cmax, which refers to the maximum observed peak plasma concentration, was 1,445.6 ng/mL (80.8% CV) for the 1.5 mg/kg dose of eravacycline administered every 24 hours and 952.6 ng/mL (79.8% CV) for the 1.0 mg/kg dose of eravacycline administered every 12 hours.
Efficacy for tetracycline-class molecules is driven by the ratio of AUC to MIC. MIC refers to minimum inhibitory concentration, which is the minimum concentration of an antibiotic needed to inhibit the growth of an organism. In the Phase 2 clinical trial, we measured AUC for the 12 hours following dosing. As a result, in order to understand the AUC of the dose groups we studied in the trial over the 24 hours following dosing, we relied on modeling to predict the AUC of eravacycline in differing dose sizes and schedules over the 24 hours following dosing. We believe that these estimated AUCs for eravacycline are supportive of eravacycline’s potential to treat multidrug-resistant Gram-negative and other bacteria.
Phase 1 clinical trials of IV formulation
We studied the IV formulation of eravacycline in several Phase 1 clinical trials in a total of 140 healthy volunteers and at doses ranging from 0.1 mg/kg to 3.0 mg/kg. No serious adverse events were reported during the Phase 1 clinical trials and no clinically significant dose-related safety signals were reported. As expected in this class of antibiotics, transient gastrointestinal adverse events such as nausea and emesis were observed at the higher dose levels in the Phase 1 clinical trials. Additionally, pharmacokinetic data demonstrates that eravacycline achieves high concentration levels in the blood and urine.
Phase 1 clinical trials of oral formulation
In order to assess the potential for eravacycline to be developed as an orally administered drug, we conducted a Phase 1 single ascending dose clinical trial in 2010, a Phase 1 multiple ascending dose clinical trial in 2011 and a second Phase 1 multiple ascending dose clinical trial in 2013. In each of these trials, we evaluated the compound for safety, tolerability and pharmacokinetics. In these trials the oral formulation of eravacycline achieved drug levels equivalent to those in the patients that received IV infusions of 1.5 mg/kg of eravacycline once per day in our Phase 2 cIAI clinical trial. As part of the Phase 1 clinical trials, we evaluated the impact of food and fasting on the absorption of orally administered eravacycline and observed a significant food effect. As a result, we focused our development efforts on patients in a fasted state.
Across the Phase 1 studies of the oral formulation, the most common adverse events reported were nausea and emesis. Doses up to 300 mg once daily were well tolerated with all adverse events mild to moderate in intensity. A single daily dose of 400 mg was not tolerated due to gastrointestinal-related adverse events.
In the second Phase 1 multiple ascending dose clinical trial, oral doses of 200 mg and 250 mg provided twice-daily were well tolerated. The Day 7 mean AUC was 4520 ng*h/mL (43% CV) for the 200 mg twice-daily dose of eravacycline and 6200 ng*h/mL (17% CV) for the 250 mg twice-daily dose of eravacycline. The Cmax was 261 ng/mL (47% CV) for the 200 mg twice-daily dose of eravacycline and 398 ng/mL (14% CV) for the 250 mg twice-daily dose of eravacycline.
17
Table of Contents
We carried out extensive modeling of the IV and oral pharmacokinetic data from our clinical trials of eravacycline in order to establish an oral transition therapy dose following IV administration. Based on our modeling results of eravacycline, we believe that a twice-daily dose of either 200 mg or 250 mg of oral eravacycline will achieve plasma exposure levels equivalent to those resulting from daily administration of the IV formulation of eravacycline at 1.5 mg/kg and that a twice per day oral dosage form of eravacycline can be developed to permit oral transition therapy treatment of serious infections. As these twice-daily oral doses of 200 mg and 250 mg were safe and well tolerated in the second Phase 1 MAD clinical trial, we evaluated these doses in the lead-in portion of the Phase 3 clinical trial of eravacycline with IV-to-oral transition therapy for the treatment of cUTI.
Preclinical Studies
In preclinical studies, we have evaluated the in vitro activity of eravacycline against a broad range of bacterial pathogens including Gram-negative, Gram-positive, atypical and anaerobic pathogens. In these studies, we also compared the potency of eravacycline to the potency of other antibiotic compounds against the same pathogens. In many cases, the isolates measured were resistant to one or more of the antibiotic compounds against which eravacycline was compared. In each case, we measured potency by determining the concentration of drug required to inhibit the growth of 90% of a panel of bacterial strains isolated from patients. We refer to this measurement as a MIC90 measurement. A lower MIC90 indicates greater potency against a particular bacterium in vitro. Historically, with tetracyclines, MIC90 values of up to 2 µg/mL have indicated that Gram-positive bacteria were susceptible to tetracyclines and for most Gram-negative bacteria up to 4 µg/mL. Traditionally, bacteria considered resistant to an antibiotic have MIC90 values for Gram-positive bacteria of 8 µg/mL and for Gram-negative bacteria of 16 µg/mL and higher.
18
Table of Contents
In Vitro Activity Against Gram-negative Bacteria
The figure below summarizes the in vitro activity of eravacycline and various antibiotics commonly used in hospitals today for the treatment of Gram-negative bacteria in panels that included 1,059 Gram-negative isolates. In each panel, isolates of a single species of bacteria were separately treated with each of the antibiotics in the study. The number specified in the table below for each species of bacteria indicates the number of isolates of that species that were included in the studies. The bacteria selected for evaluation were chosen because they are commonly found in serious hospital infections.
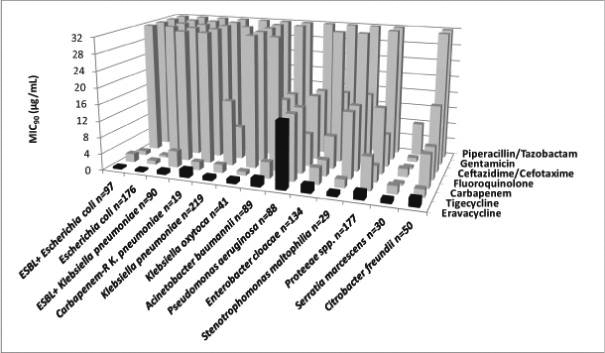
As shown in the figure, eravacycline demonstrated potent, broad-spectrum Gram-negative antibacterial activity. In the majority of instances, the MIC90 of eravacycline was equivalent to or lower than the MIC90 values of the other antibiotics studied for each bacterium. Key observations from these in vitro studies include:
| • | Eravacycline had MIC90 values of under 2 µg/mL against clinical isolates of E. cloacae, A. baumannii, K. pneumoniae, including ESBL-producing and carbapenem-resistant isolates, C. freundii, S. maltophilia, M. morganii, P. vulgaris, P. stuartii, and K. oxytoca. |
| • | Eravacycline was twice as potent as the next most active comparator, tigecycline, against A. baumannii in a panel that was 44% resistant to carbapenems, 53% resistant to tetracyclines and 64% resistant to fluoroquinolones. |
| • | Eravacycline was four times more potent than tigecycline against ESBL-producing K. pneumoniae isolates. |
| • | 83%, 29%, and 43% of the isolates were fully resistant to fluoroquinolones, carbapenems and gentamicin, respectively. |
| • | Isolates of Proteus mirabilis, one of the proteeae species included in the figure above, were two times more susceptible to eravacycline (MIC90 of 4 µg/mL) than to tigecycline. |
| • | P. aeruginosa isolates were largely not susceptible to eravacycline (MIC90 of 16 µg/mL) or tigecycline (MIC90 in excess of 16 µg/mL). |
19
Table of Contents
The figure below further demonstrates the potent activity of eravacycline against Gram-negative bacteria, including multidrug-resistant Gram-negative pathogens, in comparison to commonly used antibiotic treatments. This surveillance study was conducted using over 4,000 patient bacterial isolates collected in New York City from November 2013 through January 2014, and was published in the Antimicrobial Agents and Chemotherapy Journal in December 2014.
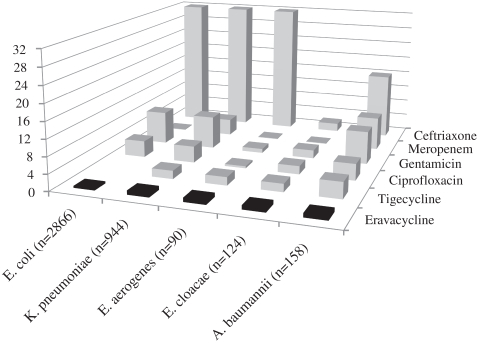
20
Table of Contents
In Vitro Activity Against Gram-positive Bacteria
The figure below summarizes the in vitro activity of eravacycline and various antibiotics commonly used in hospitals today for the treatment of Gram-positive bacteria in panels that included 762 Gram-positive isolates. The bacteria selected for evaluation were chosen because they are commonly found in serious hospital infections.
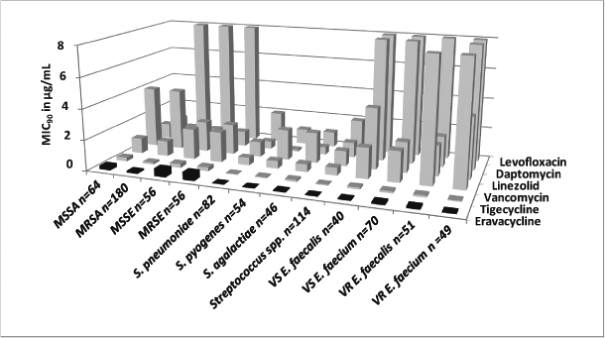
Eravacycline demonstrated excellent in vitro potency against methicillin-susceptible and resistant Staphylococcus aureus and Staphylococcus epidermidis, vancomycin-susceptible and resistant Enterococcus faecium and Enterococcus faecalis, penicillin-susceptible and -resistant Streptococcus pneumoniae, Streptococcus anginosus, Streptococcus intermedius, Streptococcus mitis, Streptococcus sanguis, Streptococcus pyogenes, and Streptococcus agalactiae. The MIC90 values for eravacycline against all of the streptococci and enterococci in the panels were less than 0.12 µg/mL. For staphylococci, including MRSA confirmed to contain Panton-Valentine leukocidin virulence factor, the MIC90 values were less than 0.5 µg/mL in 180 MRSA isolates tested.
21
Table of Contents
In Vitro Activity Against Anaerobic Bacteria
The figure below summarizes the in vitro activity of eravacycline and various antibiotics commonly used in hospitals today for the treatment of anaerobic bacteria in panels that included 190 anaerobic isolates. The bacteria selected for evaluation were chosen because they are commonly found in serious hospital infections.
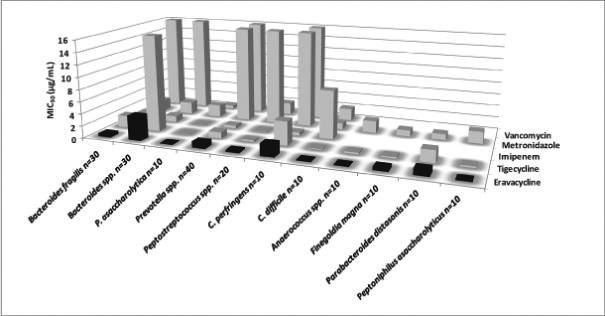
Key observations from these in vitro studies include that eravacycline:
| • | had a MIC90 against B. fragilis, the most prevalent anaerobe in human infections, of 1 µg/mL, which was four times lower than tigecycline; |
| • | had excellent activity against a wide range of Gram-positive and Gram-negative anaerobes; and |
| • | provided broader coverage than the other antibiotics tested in the panel. |
In addition, in the studies, many of the isolates from the Bacteroides, Prevotella and Clostridium perfringens species were vancomycin-resistant, and many of the isolates of the Peptostreptococcus spp. and C. perfringens species were metronidazole-resistant. Eravacycline showed strong activity against these isolates.
Other Indications
Subject to obtaining additional financing, we intend to pursue development of eravacycline for the treatment of additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections following our development of eravacycline for the treatment of cIAI and cUTI.
The Company has received funding for its lead product candidate, eravacycline, under an award from BARDA. In January 2012, BARDA awarded to CUBRC a five-year contract that provides a total of up to $67 million in funding for the development, manufacturing and clinical evaluation of eravacycline as a potential empiric countermeasure for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, including Francisella tularensis, which causes tularemia, Yersinia pestis, which causes plague, and Bacillus anthracis, which causes anthrax disease, as well as bacterial pathogens associated with moderate-to-severe community-acquired bacterial pneumonia and other serious hospital infections. The funding under the
22
Table of Contents
BARDA Contract is also being used for certain activities in the development of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria. Under this program, we have conducted a number of in vitro, toxicology and animal studies to evaluate the efficacy of eravacycline against biothreat pathogens. Eravacycline has performed as well as, or better than, standard-of-care comparators in studies in murine respiratory infection models challenged with public health pathogens. In addition we have also completed a Phase 1 clinical trial assessing the bronchial pulmonary disposition, safety and tolerability of eravacycline, the first clinical assessment of its potential use for treating pneumonia. In connection with the BARDA Contract, in February 2012, we entered into with CUBRC a five-year cost-plus-fixed-fee subcontract under which we may receive funding of up to approximately $39.8 million, reflecting the portion of the BARDA funding that may be paid to us for our activities.
Although the BARDA Contract, and our subcontract with CUBRC under the BARDA Contract, have five-year terms, BARDA is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond current-year amounts from Congressionally approved annual appropriations. To the extent that BARDA ceases to provide funding of the program to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our BARDA subcontract is $31.0 million from the initial contract date through September 9, 2016, of which $16.4 million had been received through December 31, 2014. If BARDA continues to support the program under the contract for the full five-year term, we believe BARDA funding for this program will be sufficient to provide the funds to advance eravacycline through enabling studies for an NDA, and to potentially support the development of eravacycline for other indications.
Technology Platform
We believe that our proprietary chemistry technology, licensed from Harvard on an exclusive worldwide basis and enhanced at our company, represents a significant innovation in the creation of tetracycline drugs and has the potential to reinvigorate the clinical and market potential of the class.
The tetracycline class of antibiotics has been used successfully for more than 50 years. Unlike our tetracycline compounds, all tetracyclines on the market and under development of which we are aware are produced semi-synthetically, first in bacteria and then modified in a limited number of ways by available chemistry. These conventional methods have only been able to produce tetracycline antibiotics with limited chemical diversity, making it difficult for conventional technology to create tetracycline antibiotics that address a wide variety of multidrug-resistant bacteria. In part, because of the challenges in creating novel tetracycline molecules, only one tetracycline antibiotic has been developed and approved by the FDA for sale in the United States in the past 30 years.
By contrast, our proprietary technology makes it possible to create novel tetracycline antibiotics using a practical, fully synthetic process for what we believe is the first time. This fully synthetic process avoids the limitations of bacterially derived tetracyclines and allows us to chemically modify many positions in the tetracycline scaffold, including most of the positions that we believe could not practically be modified by any previous method. Using our proprietary chemistry technology, we can create a wider variety of tetracycline-based compounds than was previously possible, enabling us to pursue novel tetracycline derivatives for the treatment of multidrug-resistant bacteria that are resistant to existing tetracyclines and other classes of antibiotic products.
23
Table of Contents
The diagram below illustrates the tetracycline core scaffold. Scaffold positions marked with dots have been modified to date using conventional chemistry to create either tetracycline drugs that have been marketed or drug candidates of which we are aware that are currently in development. Our fully synthetic process also allows for modification of the positions marked with dots, but with greater opportunity for substitution than is possible using conventional chemistry. The scaffold positions marked with stars in the diagram below indicate useful positions that we have modified through our fully synthetic process that could not practically be modified by conventional chemistry.
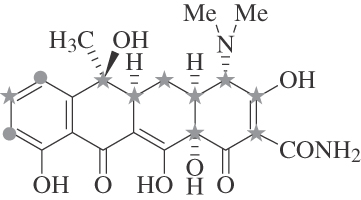
While the four positions on the bottom of the scaffold in the diagram above that are not marked with dots or stars can also be modified using our proprietary chemistry technology, these positions are involved in the binding of tetracyclines to the bacterial ribosome and, consequently, changes to these positions greatly reduce antibacterial activity of compounds. As a result, we are not pursuing compounds based on modifications of these positions.
We believe that our approach to tetracycline drug development provides us with strong intellectual property protection. We hold or have licensed rights under patents and patent applications that protect both our synthetic processes for developing tetracyclines and the compositions of matter of the individual compounds themselves. These include patents and patent applications directed towards the composition of matter for key intermediates like the enone used in the synthesis of eravacycline and our other product candidates. Unless a new synthetic method is created, we believe that, for the life of our intellectual property, our proprietary chemistry technology will be the only practical way of modifying the positions on the tetracycline core scaffold that have not been previously modified using conventional chemistry.
Our proprietary chemistry technology has allowed us to develop compounds that have been highly active in in vitro studies against tetracycline-resistant bacterial strains, including multidrug-resistant Gram-negative bacteria, and that have novel pharmacokinetic properties. To date, we have used our proprietary chemistry technology to create more than 3,000 new tetracycline derivatives that we believe could not be practically created with conventional methods. Our discovery program is focused on identifying novel compounds that will be effective against the toughest multidrug-resistant Gram-negative bacteria.
24
Table of Contents
Drug Development Programs
The following table sets forth our clinical and earlier-stage antibiotic compounds that we are developing for the treatment of serious and life-threatening infections and their status.
| Candidate |
Indication |
Status | ||
| Eravacycline |
cIAI (IV) | Top-line Phase 3 results reported | ||
| cUTI (IV/oral) | Phase 3 started first quarter of 2014 | |||
| Pneumonia (IV) | Phase 1 completed | |||
| TP-271 |
Bacterial biothreats | IND submission planned in 2015 | ||
| TP-6076 |
Multidrug-resistant Gram- negative infections |
IND-enabling studies ongoing |
TP-271
TP-271 is a fully synthetic broad-spectrum preclinical compound that we are developing for respiratory diseases caused by bacterial biothreat pathogens under funding provided by NIAID. We are collaborating with CUBRC on the TP-271 program funded by NIAID.
We created TP-271 using our proprietary chemistry technology. In doing so, we made modifications to the tetracycline scaffold that were designed to improve potency and effectiveness against a broader spectrum of bacteria as compared to tetracycline and doxycycline, which are currently used for the treatment of pneumonia and other respiratory ailments.
In our development program for TP-271, we have conducted a number of in vitro, toxicology and animal studies to evaluate the efficacy of TP-271 against biothreat pathogens. TP-271 has performed as well as, or better than, standard-of-care comparators in studies in murine respiratory infection models challenged with public health pathogens. In susceptibility studies, TP-271 also demonstrated broad-spectrum activity against NIAID Category A and B public health bacterial pathogens including Francisella tularensis, Yersinia pestis, Burkholderia mallei, Burkholderia pseudomallei, Bacillus anthracis, and NIAID Category C public health bacterial pathogens (in vitro and in vivo) that are associated with CABP, including Streptococcus pneumoniae, including multidrug-resistant pneumococci, Staphylococcus aureus (methicillin-susceptible and methicillin-resistant), Haemophilus influenzae, Moraxella catarrhalis and Legionella pneumophila, including strains that are tetracycline-resistant. Given our progress on TP-271, we expect to submit an investigational new drug, or IND, application with the FDA for TP-271 in 2015.
Funding for TP-271 is covered by two awards from NIAID. The first award is a grant awarded to CUBRC in July 2011 that provides up to approximately $2.8 million in funding over five years, which we refer to as the NIAID Grant. The second award is a contract awarded to CUBRC in September 2011 that provides up to approximately $35.8 million in funding over five years. The NIAID Grant and the NIAID Contract each support the development, manufacturing and clinical evaluation of TP-271 for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, including Francisella tularensis, Yersinia pestis and Bacillus anthracis, as well as bacterial pathogens associated with community-acquired bacterial pneumonia.
In connection with the NIAID Contract, in October 2011, we entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which we may receive funding of up to approximately $13.3 million, reflecting the portion of the NIAID Contract funding that may be paid to us for our activities. In connection with the NIAID Grant, in November 2011, CUBRC awarded us a 55-month, no-fee subaward of approximately $980,000 reflecting the portion of the NIAID Grant funding that may be paid to us for our activities.
Although the NIAID Contract and our subcontract with CUBRC under the NIAID Contract have five-year terms, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond September 30, 2016. To the extent NIAID ceases to provide funding of the programs
25
Table of Contents
to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subcontract with respect to the NIAID Contract is $8.3 million, of which $7.1 million had been received through December 31, 2014. In addition, although the NIAID Grant has a term of five years and our subaward from CUBRC has a term of 55 months, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond May 31, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subaward with respect to the NIAID Grant is $0.8 million from the initial grant date through May 31, 2016, of which $0.7 million had been received through December 31, 2014. If NIAID continues to support the program for the full term, we believe NIAID funding for our TP-271 program will provide funding sufficient to advance TP-271 into Phase 1 clinical trials.
Second-generation Gram-negative Program
We are using our proprietary chemistry technology to pursue the discovery and development of tetracycline-derived compounds effective against the most urgent multidrug-resistant Gram-negative bacterial health threats identified by the CDC, in a September 2013 report. Pathogens targeted include carbapenem-resistant variants of Klebsiella pneumoniae, Acinetobacter baumanni, Escherichia coli and Pseudomonas aeruginosa. We have generated compounds that have demonstrated potent activity against a broad range of these multidrug-resistant Gram-negative pathogens. We have identified TP-6076 as a lead preclinical candidate from these compounds and began IND-enabling studies during the fourth quarter of 2014.
Commercialization Strategy
Our commercialization strategy is to develop our product candidates into leading therapies that will be available worldwide for the treatment of serious multidrug-resistant infections. We have retained worldwide commercial rights to all of our product candidates. We intend to retain control over the commercial execution of each of our product candidates in the United States.
We are currently developing our lead product candidate, eravacycline, as a broad-spectrum IV and oral antibiotic for use as a first-line empiric monotherapy for the treatment of serious and life-threatening infections, including a wide variety of multidrug-resistant infections. Assuming the successful completion of clinical trials and receipt of regulatory approvals, we intend to directly commercialize eravacycline in the United States. We currently have limited marketing capabilities and no sales or distribution capabilities. We intend to build a commercial organization in the United States and recruit experienced marketing, sales and medical education professionals and to develop a commercial strategy to target institutions with the greatest use of drugs for multidrug-resistant serious and life-threatening infections. We expect that our sales force will focus on educating hospital and institution-based physicians, nurses, pharmacy directors and payers about the benefits of eravacycline for the product’s approved indications.
If we complete the pivotal portion of IGNITE 2 when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and an MAA to the EMA in the first half of 2016. Our current plan is to develop and commercialize eravacycline outside the United States with collaborators.
Manufacturing and Supply
We do not own or operate manufacturing facilities for the production of any of our product candidates, nor do we have plans to develop our own manufacturing operations in the foreseeable future. All of our product candidates are organic compounds of low molecular weight, commonly referred to as small molecules. They are manufactured in a fully synthetic process from readily available starting materials. As a result, we believe that our use of synthetic process will enable us to have a cost of manufacturing for our product candidates that is sufficiently low to enable us to sell our product candidates, when and if approved, for a cost that is similar to other hospital-based antibiotics.
26
Table of Contents
We currently rely on a limited number of third-party contract manufacturers for all of our required raw materials, drug substance and finished product for our preclinical research and clinical trials. We do not have long-term agreements with any of these third parties. We also do not have any current contractual relationships for the manufacture of commercial supplies of any of our product candidates after they are approved. If any of our products are approved by any regulatory agency, we intend to enter into agreements with third-party contract manufacturers for the commercial production of those products. We currently employ internal resources to manage our manufacturing.
Intellectual Property
We strive to protect the proprietary technology that we believe is important to our business, including seeking and maintaining patents intended to cover our product candidates and compositions, their methods of use and processes for their manufacture and any other inventions that are commercially important to the development of our business. We also rely on trade secrets to protect aspects of our business that are not amenable to, or that we do not consider appropriate for, patent protection.
Our success will significantly depend on our ability to obtain and maintain patent and other proprietary protection for commercially important technology and inventions and know-how related to our business, defend and enforce our patents, preserve the confidentiality of our trade secrets and operate without infringing the valid and enforceable patents and proprietary rights of third parties. We also rely on know-how and continuing technological innovation to develop and maintain our proprietary position.
As of March 2, 2015, we owned five U.S. patents, thirteen foreign patents, six pending U.S. patent applications and 55 pending foreign patent applications in Europe and 17 other jurisdictions. In addition we have exclusively licensed from Harvard University rights under eight U.S. patents, 18 foreign patents, two pending U.S. patent applications and 18 pending foreign patent applications in Europe and ten other jurisdictions. Certain of our patents and patent applications are directed to the composition of matter and/or use of eravacycline and applications are pending in the United States, Europe, Japan and other countries.
Tetraphase-Owned Intellectual Property Relating to Eravacycline and Other Compounds Under Development
We have patent applications directed to the composition of matter and/or use of eravacycline and other fluorocyclines, such as TP-271, pending in the United States, Europe, Japan and other countries. Patents specific to the composition and/or use of eravacycline have been granted in the United States, Europe, Australia, China, Colombia, Japan, Mexico, New Zealand, Hong Kong, Taiwan and Singapore. The granted patents have an expiration date of August 7, 2029, and any patents that may issue from the pending applications will also have an expiration date of August 7, 2029, absent any term extensions or adjustments that may be available. The term of one of the U.S. patents has received 508 days of patent term adjustment under the America Invents Act.
We have also filed patent applications directed to the composition of matter and use of various derivatives of tetracycline and pentacycline (a tetracycline scaffold extended to five rings) in the United States, Europe and other foreign countries. Any patents that might issue from these pending applications will have an expiration date no earlier than 2030, with some expiration dates as late as 2033.
Exclusively Licensed Intellectual Property Relating to Our Proprietary Chemistry Technology
The patents and patent applications that we exclusively license from Harvard provide patent protection for the proprietary chemistry technology used in our fully synthetic process to make eravacycline and other tetracycline derivatives. The key intermediates that enable our fully synthetic process are commonly referred to as enone intermediates. The licensed patents and patent applications are directed towards the composition of matter of enone intermediates and compounds used to make the enone intermediates, referred to as key precursors, as well as synthetic routes to those enone intermediates, precursors and our tetracycline derivatives under development.
27
Table of Contents
Composition of matter for the enone intermediates and precursors used in preparing the enone intermediates, as well as methods of making the precursors and enone intermediates are covered by the U.S. patents we license from Harvard, which will expire no earlier than 2027, taking into consideration patent term adjustment. Corresponding patent applications have been filed in foreign jurisdictions and any patents that have issued and might issue from these applications expire or will expire no earlier than 2025.
Exclusively Licensed Intellectual Property Relating to Pentacycline and Tetracycline Derivatives
Our license from Harvard also includes patent applications directed to the composition of matter and use of other novel tetracycline or pentacycline derivatives. These applications are pending in the United States, Europe and other countries. Any patents that might issue from these pending applications will have an expiration date no earlier than 2027.
Trademark Applications Relating to the Company Name and Logo
In December 2014 we filed four intent-to-use trademark applications at the United States Patent and Trademark Office relating to the Company Name, the Company Logo and combinations of the Company Name and Logo.
The term of individual patents depends upon the legal term for patents in the countries in which they are obtained. In most countries, including the United States, the patent term is 20 years from the earliest filing date of a non-provisional patent application. In the United States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the U.S. Patent and Trademark Office in examining and granting a patent, or may be shortened if a patent is terminally disclaimed over an earlier filed patent. The term of a patent that covers a drug, biological product or medical device approved pursuant to a pre-market approval, or PMA, may also be eligible for patent term extension when FDA approval is granted, provided statutory and regulatory requirements are met. The length of the patent term extension is related to the length of time the drug is under regulatory review while the patent is in force. The Drug Price Competition and Patent Term Restoration Act of 1984, or the Hatch-Waxman Act, permits a patent term extension of up to five years beyond the expiration date set for the patent. Patent extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, only one patent applicable to each regulatory review period may be granted an extension and only those claims reading on the approved drug are extended. Similar provisions are available in Europe and other foreign jurisdictions to extend the term of a patent that covers an approved drug.
We rely, in some circumstances, on trade secrets to protect our unpatented technology. However, trade secrets can be difficult to protect. We seek to protect our trade secrets and proprietary technology and processes, in part, by confidentiality agreements with our employees, consultants, scientific advisors and contractors. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, agreements or security measures may be breached. We may not have adequate remedies for any breach and could lose our trade secrets through such a breach. In addition, our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our consultants, contractors or collaborators use intellectual property owned by others in their work for us, disputes may arise as to the rights in related or resulting trade secrets, know-how and inventions.
License Agreement
On August 3, 2006, we entered into a license agreement with The President and Fellows of Harvard College, under which Harvard granted us an exclusive worldwide license under specified Harvard patent rights to develop and commercialize tetracycline-based products such as eravacycline. Under the license agreement, we also have
28
Table of Contents
the right to expand the patent rights subject to the license to include improvement patents that may be owned by Harvard in the future and that meet specified criteria by paying to Harvard an additional license issuance fee in an amount to be agreed between Harvard and us. We also have a right of negotiation to expand the license to include additional patents relating to tetracycline chemistry within a specified category that may be owned by Harvard in the future, including patents covering inventions made by Andrew Myers, Ph.D., our scientific founder, under his consulting agreement with us. Since entering into the license agreement, we have entered into amendments to the license agreement pursuant to which we expanded the patent rights subject to the license in accordance with these rights. Under the license agreement, we are obligated to satisfy diligence requirements, including using commercially reasonable efforts to develop and commercialize licensed compounds and to implement a specified development plan, meeting specified development milestones and providing an update on progress on an annual basis. Our license grant from Harvard is subject to academic rights retained by Harvard and United States government rights and obligations that are customary in patent license agreements with universities in the United States.
In consideration for the rights granted to us by Harvard under the license agreement, as of December 31, 2014, we have paid Harvard an aggregate of $3.8 million in upfront license fees and development milestone payments, and issued 31,379 shares of our common stock to Harvard. In addition, we have agreed to make payments to Harvard upon the achievement of specified future development and regulatory milestones totaling up to $15.1 million for each licensed product candidate ($3.1 million of which has already been paid with respect to eravacycline), and to pay tiered royalties in the single digits based on annual worldwide net sales, if any, of licensed products by us, our affiliates and sublicensees. We are also obligated to pay Harvard a specified share of non-royalty sublicensing revenues that we receive from sublicensees for the grant of sublicenses under the license and to reimburse Harvard for specified patent prosecution and maintenance costs.
The license agreement expires on a licensed product-by-licensed product and country-by-country basis upon the expiration of the last-to-expire patent covering the applicable product in the applicable country that is included in the license. Harvard may terminate the license agreement based on our uncured material breach or insolvency or bankruptcy. We have the right to terminate the license agreement for any or no reason at any time on sixty (60) days prior written notice to Harvard.
Government Contracts
Eravacycline
We received funding for eravacycline under an award from BARDA. In January 2012, BARDA awarded a five-year contract that provides a total of up to $67 million in funding that BARDA awarded to CUBRC in January 2012. The contract contemplates that CUBRC will collaborate with us on the development, manufacturing and clinical evaluation of a novel broad-spectrum tetracycline antibiotic with potential as an empiric countermeasure for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, including Francisella tularensis, which causes tularemia, Yersinia pestis, which causes plague, and Bacillus anthracis, which causes anthrax disease, as well as bacterial pathogens associated with moderate-to-severe CABP and other serious hospital infections. The funding under the BARDA Contract is also being used for certain activities in the development of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria. In connection with the BARDA Contract, in February 2012, we entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which we may receive funding of up to approximately $39.8 million, reflecting the portion of the BARDA funding that may be paid to us for our activities.
We collaborated with CUBRC in seeking government funding of this development program because we did not have any expertise in bidding for, or the administration and management of, government-funded contracts. Because CUBRC had the expertise to manage and administer awards issued by government funding agencies, we agreed with CUBRC that CUBRC would serve as the prime contractor under the BARDA Contract, primarily carrying out a program management and administrative role with additional responsibility for the management of
29
Table of Contents
certain preclinical studies. We serve as lead technical experts on all aspects of the BARDA Contract and serve as a subcontractor of CUBRC responsible for management of chemistry, manufacturing and control activities and clinical studies. The flow of funds under this arrangement follows the respective activities being conducted by us and by CUBRC, with funds being paid to us under our subcontract with CUBRC reflecting payment for our activities.
We have agreed upon a research plan with CUBRC detailing the activities to be conducted by CUBRC and by us. In addition to our obligations to conduct the activities provided for by the research plan, we are also obligated under the CUBRC subcontract to satisfy various federal reporting requirements, extending to technical reporting with respect to our activities, reporting with respect to intellectual property and financial reporting.
Payments under our subcontract with CUBRC are made in installments as activities are conducted in accordance with the research plan. Payments are based on direct and indirect costs incurred plus fixed fees, where applicable.
Under the subcontract, CUBRC’s use of our eravacycline data is expressly limited to purposes of performing CUBRC’s obligations under the BARDA Contract, and CUBRC and its other subcontractors must assign to us, subject to government rights, all intellectual property rights relating to our compounds and related data that arise from the project. Under standard government contracting terms, the government receives only limited rights for government use of certain of our pre-existing data and certain data produced with non-federal funding, to the extent such data are required for delivery to BARDA under the project. The government receives unlimited rights to use and disclose new data first produced under the project with BARDA funding, and the government is entitled to at least a nonexclusive, worldwide, royalty-free license to practice or have practiced any patent on an invention that is conceived or first reduced to practice under the project.
BARDA is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond current-year amounts from Congressionally approved annual appropriations, and CUBRC has a right to terminate its subcontract with us only to the extent that BARDA first cancels the corresponding portions of CUBRC’s prime contract.
We retain a right to terminate CUBRC’s rights to use eravacycline. Permissible grounds for such termination of CUBRC’s rights include but are not limited to the sale of our assets relating to the project, an acquisition of us or our granting an exclusive or partially exclusive license to use eravacycline to a licensee that declines to continue CUBRC’s license rights. In such an event, the subcontract may be terminated upon CUBRC’s negotiation of a corresponding termination of CUBRC’s obligations to BARDA.
TP-271
Our program to develop TP-271 is funded by NIAID through the NIAID Grant, a grant awarded in July 2011 that provides up to approximately $2.8 million in funding over five years, and the NIAID Contract, a separate a five-year contract that provides up to $35.8 million in funding that NIAID awarded to CUBRC in October 2011. The NIAID Contract contemplates that CUBRC will collaborate with us on the development, manufacturing and clinical evaluation of a novel broad-spectrum tetracycline antibiotic for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, including Francisella tularensis, Yersinia pestis and Bacillus anthracis, as well as bacterial pathogens associated with CABP.
In connection with the NIAID Contract, in October 2011, we entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which we may receive funding of up to approximately $13.3 million, reflecting the portion of the NIAID Contract funding that may be paid to us for our activities. In connection with the NIAID Grant, in November 2011, CUBRC awarded us a 55-month, no-fee subaward of approximately $980,000 reflecting the portion of the NIAID Grant funding that may be paid to us for our activities.
30
Table of Contents
We collaborated with CUBRC in seeking government funding of this development program because we did not have any expertise in bidding for, or the administration and management of, government-funded contracts. Because CUBRC had the expertise to manage and administer awards issued by government funding agencies, we agreed with CUBRC that CUBRC would serve as the prime contractor under the NIAID Contract, primarily carrying out a program management and administrative role with additional responsibility for the management of certain preclinical studies. We serve as lead technical experts on all aspects of the NIAID Contract and serve as a subcontractor of CUBRC responsible for management of chemistry, manufacturing and control activities and clinical studies. The flow of funds under this arrangement follows the respective activities being conducted by us and by CUBRC, with funds being paid to us under our subcontract with, and subaward from, CUBRC reflecting payment for our activities.
We have agreed upon a research plan with CUBRC detailing the activities to be conducted by CUBRC and by us. In addition to our obligations to conduct the activities provided for by the research plan, we are also obligated under the CUBRC subcontract to satisfy various federal reporting requirements, extending to technical reporting with respect to our activities, reporting with respect to intellectual property and financial reporting.
Payments under our subcontract with CUBRC are made in installments as activities are conducted in accordance with the research plan. Payments are based on direct and indirect costs incurred plus fixed fees, where applicable.
Under the subcontract, CUBRC’s use and disclosure of our proprietary data pertaining to the project are expressly subject to a separate confidentiality agreement between CUBRC and us. CUBRC and its other subcontractors or subawardees must assign to us, subject to government rights, all intellectual property rights relating to our compounds and related data that arise from the project. Under standard government contracting terms and grant conditions, the government is entitled to at least a nonexclusive, worldwide, royalty-free license to practice or have practiced any patent on an invention that is conceived or first reduced to practice under the project.
NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond May 31, 2016 in the case of the NIAID Grant, and September 30, 2016 in the case of the NIAID Contract, and CUBRC has a right to terminate its subcontract with, or subaward to, us only to the extent that NIAID first cancels the corresponding portions of CUBRC’s prime contract or award.
We retain rights to terminate the subcontract if CUBRC breaches the subcontract, subject in certain cases to CUBRC’s failure to cure such breach, or by written notice to CUBRC, effective upon CUBRC’s negotiation of a corresponding termination of CUBRC’s obligations to NIAID.
Research and Development Expenses
For the years ended December 31, 2014, 2013 and 2012, we incurred $61.9 million, $31.5 million, and $17.3 million in expenses on research and development activities.
Competition
The biopharmaceutical industry is characterized by intense competition and rapid innovation. Our potential competitors include large pharmaceutical and biotechnology companies, specialty pharmaceutical companies and generic drug companies. Many of our potential competitors have substantially greater financial, technical and human resources than we do, as well as greater experience in the discovery and development of product candidates, obtaining FDA and other regulatory approvals of products and the commercialization of those products. Accordingly, our potential competitors may be more successful than us in obtaining FDA approval for drugs and achieving widespread market acceptance. Our potential competitors’ drugs may be more effective, or more effectively marketed and sold, than any product candidate we may commercialize and may render our
31
Table of Contents
product candidates obsolete or non-competitive before we can recover the expenses of their development and commercialization. We anticipate that we will face intense and increasing competition as new drugs enter the market and advanced technologies become available. Finally, the development of new treatment methods for the diseases we are targeting could render our product candidates non-competitive or obsolete.
We believe the key competitive factors that will affect the development and commercial success of our most advanced product candidate, eravacycline, if approved, will be efficacy, coverage of drug-resistant strains of bacteria, safety and tolerability profile, reliability, convenience of dosing, including capability for IV-to-oral transition therapy, price, availability of reimbursement from governmental and other third-party payers and susceptibility to drug resistance.
We are developing eravacycline as a broad-spectrum IV and oral antibiotic for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections, including multidrug-resistant Gram-negative infections. If approved, eravacycline would compete with a number of currently marketed antibiotics, including meropenem, which is marketed by AstraZeneca as Merrem, imipenem/cilastatin, which is marketed by Merck & Co., or Merck, as Primaxin, tigecycline, which is marketed by Pfizer as Tygacil, levofloxacin, which is marketed by Ortho-McNeil and Johnson & Johnson as Levaquin, piperacillin/tazobactam, which is marketed by Pfizer as Zosyn, ceftolozane/tazobactam, which is marketed by Merck/Cubist as Zerbaxa, and ceftazidime/avibactam, which is marketed by Allergan, Inc. and AstraZeneca as Avycaz, as well as antibiotics currently under FDA review or in Phase 3 development, including meropenem/RPX7009, which is being developed by The Medicines Company as Carbavance, and plazomicin, which is being developed by Achaogen, Inc. We also expect that eravacycline, if approved, would compete with future generic versions of currently marketed antibiotics.
If approved, we believe that eravacycline would compete effectively against these compounds on the basis of:
| • | broad-spectrum activity against a wide variety of multidrug-resistant Gram-negative, Gram-positive and anaerobic bacteria; |
| • | lower probability of drug resistance; |
| • | a favorable safety and tolerability profile; |
| • | a convenient dosing regimen; and |
| • | potentially, convenient IV-to-oral transition therapy. |
Recent Changes in the Regulatory Landscape
The FDA’s Anti-Infective Drugs Division has undergone evolution in recent years, primarily driven by concerns that increasingly less effective antibiotics may have been approved in the last 10 to 15 years and a desire to bring what they perceive to be greater statistical rigor to their analyses. The impact of this was a rethinking of how antibiotic efficacy is measured in clinical trials, and a review of the statistical tools used to analyze the data. In February 2015, the FDA published guidance entitled “Guidance for Industry Complicated Urinary Tract Infections: Developing Drugs for Treatment” and guidance entitled “Guidance for Industry Complicated Intra-Abdominal Infections: Developing Drugs for Treatment.” The purpose of these guidelines was to address any uncertainties regarding what the FDA expected from sponsors and clinical trials for the indications of cUTI and cIAI.
There are several additional legislative initiatives under consideration in the U.S. Congress, such as the ADAPT Act which would provide a pathway for approval of antibiotics in limited populations of patients with few or no suitable treatment options, the DISARM Act which would designate certain novel antibiotics used to treat serious bacterial infections to receive higher Medicare reimbursement, and an amendment to the GAIN Act
32
Table of Contents
which would allow successful QIDP sponsors to transfer up to one year of exclusivity to another product, including products marketed by other companies. These three initiatives have been recently re-introduced as part of the 21st Century Cures discussion document and have not been approved.
Government Regulation and Product Approval
Government authorities in the United States, at the federal, state and local level, and in other countries extensively regulate, among other things, the research, development, testing, manufacture, including any manufacturing changes, packaging, storage, recordkeeping, labeling, advertising, promotion, distribution, marketing, import and export of pharmaceutical products such as those we are developing. The processes for obtaining regulatory approvals in the United States and in foreign countries, along with subsequent compliance with applicable statutes and regulations, require the expenditure of substantial time and financial resources.
U.S. Government Regulation
In the United States, the FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act, or FDCA, and implementing regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations requires the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or after approval, may subject an applicant to a variety of administrative or judicial sanctions, such as the FDA’s refusal to approve pending NDAs, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement or civil or criminal penalties.
The process required by the FDA before a drug may be marketed in the United States generally involves the following:
| • | completion of preclinical laboratory tests, animal studies and formulation studies in compliance with the FDA’s good laboratory practice, or GLP, regulations; |
| • | submission to the FDA of an IND which must become effective before human clinical trials may begin; |
| • | approval by an independent institutional review board, or IRB, at each clinical site before each trial may be initiated; |
| • | performance of adequate and well-controlled human clinical trials in accordance with good clinical practices, or GCP, to establish the safety and efficacy of the proposed drug product for each indication; |
| • | submission to the FDA of an NDA; |
| • | satisfactory completion of an FDA advisory committee review, if applicable; |
| • | satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the product is produced to assess compliance with current good manufacturing practices, or cGMP, and to assure that the facilities, methods and controls are adequate to preserve the drug’s identity, strength, quality and purity; and |
| • | FDA review and approval of the NDA. |
Preclinical Studies
Preclinical studies include laboratory evaluation of product chemistry, toxicity and formulation, as well as animal studies to assess potential safety and efficacy. An IND sponsor must submit the results of the preclinical tests, together with manufacturing information, analytical data and any available clinical data or literature, among other things, to the FDA as part of an IND. Some preclinical testing may continue even after the IND is
33
Table of Contents
submitted. An IND automatically becomes effective 30 days after receipt by the FDA, unless before that time the FDA raises concerns or questions related to one or more proposed clinical trials and places the clinical trial on a clinical hold. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. As a result, submission of an IND may not result in the FDA allowing clinical trials to commence.
Clinical Trials
Clinical trials involve the administration of the investigational new drug to human subjects under the supervision of qualified investigators in accordance with GCP requirements, which include the requirement that all research subjects provide their informed consent in writing for their participation in any clinical trial. Clinical trials are conducted under protocols detailing, among other things, the objectives of the trial, the parameters to be used in monitoring safety, and the effectiveness criteria to be evaluated. A protocol for each clinical trial and any subsequent protocol amendments must be submitted to the FDA as part of the IND. In addition, an IRB at each institution participating in the clinical trial must review and approve the plan for any clinical trial before it commences at that institution. Information about certain clinical trials must be submitted within specific timeframes to the National Institutes of Health, or NIH, for public dissemination on their www.clinicaltrials.gov website.
Human clinical trials are typically conducted in three sequential phases, which may overlap or be combined:
Phase 1: The drug is initially introduced into healthy human subjects or patients with the target disease or condition and tested for safety, dosage tolerance, absorption, metabolism, distribution, excretion and, if possible, to gain an early indication of its effectiveness. During Phase 1 clinical trials, sufficient information about the investigational drug’s or biological product’s pharmacokinetics and pharmacological effects may be obtained to permit the design of well-controlled and scientifically valid Phase 2 clinical trials.
Phase 2: The drug is administered to a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance and optimal dosage. Phase 2 clinical trials are typically well-controlled, closely monitored, and conducted in a limited patient population.
Phase 3: The drug is administered to an expanded patient population, generally at geographically dispersed clinical trial sites, in well-controlled clinical trials to generate enough data to statistically evaluate the efficacy and safety of the product for approval, to establish the overall risk-benefit profile of the product, and to provide adequate information for the labeling of the product. Phase 3 clinical trials usually involve a larger number of participants than a Phase 2 clinical trial.
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA and more frequently if serious adverse events occur. Phase 1, Phase 2 and Phase 3 clinical trials may not be completed successfully within any specified period, or at all. Furthermore, the FDA or the sponsor may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients.
Special Protocol Assessment
The special protocol assessment, or SPA, process is designed to facilitate the FDA’s review and approval of drugs by allowing the FDA to evaluate the proposed design and size of Phase 3 clinical trials that are intended to form the primary basis for determining a drug product’s efficacy. Upon specific request by a clinical trial sponsor, the FDA will evaluate the protocol and respond to a sponsor’s questions regarding, among other things, primary efficacy endpoints, trial conduct and data analysis, within 45 days of receipt of the request.
34
Table of Contents
The FDA ultimately assesses whether the protocol design and planned analysis of the trial are acceptable to support regulatory approval of the product candidate with respect to effectiveness of the indication studied. All agreements and disagreements between the FDA and the sponsor regarding an SPA must be clearly documented in an SPA letter or the minutes of a meeting between the sponsor and the FDA.
Even if the FDA agrees to the design, execution and analyses proposed in protocols reviewed under the SPA process, the FDA may revoke or alter its agreement under the following circumstances:
| • | public health concerns emerge that were unrecognized at the time of the protocol assessment, or the director of the review division determines that a substantial scientific issue essential to determining safety or efficacy has been identified after testing has begun; |
| • | a sponsor fails to follow a protocol that was agreed upon with the FDA; or |
| • | the relevant data, assumptions, or information provided by the sponsor in a request for SPA change, are found to be false statements or misstatements, or are found to omit relevant facts. |
A documented SPA may be modified, and such modification will be deemed binding on the FDA review division, except under the circumstances described above, if FDA and the sponsor agree in writing to modify the protocol and such modification is intended to improve the study.
Marketing Approval
Assuming successful completion of the required clinical testing, the results of the preclinical and clinical studies, together with detailed information relating to the product’s chemistry, manufacture, controls and proposed labeling, among other things, are submitted to the FDA as part of an NDA requesting approval to market the product for one or more indications. In most cases, the submission of an NDA is subject to a substantial application user fee. Under the Prescription Drug User Fee Act, or PDUFA, guidelines that are currently in effect, the FDA has a goal of ten months from the date of “filing” of a standard NDA for a new molecular entity to review and act on the submission. This review typically takes twelve months from the date the NDA is submitted to FDA because the FDA has approximately two months to make a “filing” decision.
In addition, under the Pediatric Research Equity Act of 2003, or PREA, as amended and reauthorized, certain NDAs or supplements to an NDA must contain data that are adequate to assess the safety and effectiveness of the drug for the claimed indications in all relevant pediatric subpopulations, and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may, on its own initiative or at the request of the applicant, grant deferrals for submission of some or all pediatric data until after approval of the product for use in adults, or full or partial waivers from the pediatric data requirements.
Unless otherwise required by regulation, the pediatric data requirements do not apply to products with orphan designation. Our product candidates are not designated as orphan drugs.
The FDA also may require submission of a risk evaluation and mitigation strategy, or REMS, plan to mitigate any identified or suspected serious risks. The REMS plan could include medication guides, physician communication plans, assessment plans, and elements to assure safe use, such as restricted distribution methods, patient registries, or other risk minimization tools.
The FDA conducts a preliminary review of all NDAs within the first 60 days after submission, before accepting them for filing, to determine whether they are sufficiently complete to permit substantive review. The FDA may request additional information rather than accept an NDA for filing. In this event, the application must be resubmitted with the additional information. The resubmitted application is also subject to review before the FDA accepts it for filing. Once the submission is accepted for filing, the FDA begins an in-depth substantive
35
Table of Contents
review. The FDA reviews an NDA to determine, among other things, whether the drug is safe and effective and whether the facility in which it is manufactured, processed, packaged or held meets standards designed to assure the product’s continued safety, quality and purity.
The FDA is required to refer an application for a novel drug to an advisory committee or explain why such referral was not made. An advisory committee is a panel of independent experts, including clinicians and other scientific experts, that reviews, evaluates and provides a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions.
Before approving an NDA, the FDA typically will inspect the facility or facilities where the product is manufactured. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA will typically inspect one or more clinical trial sites to assure compliance with GCP.
The FDA generally accepts data from foreign clinical trials in support of an NDA if the trials were conducted under an IND. If a foreign clinical trial is not conducted under an IND, the FDA nevertheless may accept the data in support of an NDA if the study was conducted in accordance with GCPs and the FDA is able to validate the data through an on-site inspection, if deemed necessary. Although the FDA generally requests that marketing applications be supported by some data from domestic clinical studies, the FDA may accept foreign data as the sole basis for marketing approval if (1) the foreign data are applicable to the U.S. population and U.S. medical practice, (2) the studies were performed by clinical investigators with recognized competence, and (3) the data may be considered valid without the need for an on-site inspection or, if the FDA considers the inspection to be necessary, the FDA is able to validate the data through an on-site inspection or other appropriate means.
The testing and approval process for an NDA requires substantial time, effort and financial resources, and each may take several years to complete. Data obtained from preclinical and clinical testing are not always conclusive and may be susceptible to varying interpretations, which could delay, limit or prevent regulatory approval. The FDA may not grant approval on a timely basis, or at all.
After evaluating the NDA and all related information, including the advisory committee recommendation, if any, and inspection reports regarding the manufacturing facilities and clinical trial sites, the FDA may issue an approval letter, or, in some cases, a complete response letter. A complete response letter generally contains a statement of specific conditions that must be met in order to secure final approval of the NDA and may require additional clinical or preclinical testing in order for FDA to reconsider the application. Even with submission of this additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval. If and when those conditions have been met to the FDA’s satisfaction, the FDA will typically issue an approval letter. An approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications.
Even if the FDA approves a product, it may limit the approved indications for use of the product, require that contraindications, warnings or precautions be included in the product labeling, require that post-approval studies, including Phase 4 clinical trials, be conducted to further assess a drug’s safety after approval, require testing and surveillance programs to monitor the product after commercialization, or impose other conditions, including distribution and use restrictions or other risk management mechanisms under a REMS which can materially affect the potential market and profitability of the product. The FDA may prevent or limit further marketing of a product based on the results of post-marketing studies or surveillance programs. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes, and additional labeling claims, are subject to further testing requirements and FDA review and approval.
36
Table of Contents
Special FDA Expedited Review and Approval Programs
The FDA has various programs, including fast track designation, accelerated approval and priority review, that are intended to expedite or simplify the process for the development and FDA review of drugs that are intended for the treatment of serious or life threatening diseases or conditions and demonstrate the potential to address unmet medical needs. The purpose of these programs is to provide important new drugs to patients earlier than under standard FDA review procedures.
To be eligible for a fast track designation, the FDA must determine, based on the request of a sponsor, that a product is intended to treat a serious or life threatening disease or condition and demonstrates the potential to address an unmet medical need, or if the drug qualifies as a qualified infectious disease product under the recently enacted Generating Antibiotic Incentives Now, or GAIN Act. The FDA will determine that a product will fill an unmet medical need if it will provide a therapy where none exists or provide a therapy that may be potentially superior to existing therapy based on efficacy or safety factors. We have requested fast track designation for eravacycline and are awaiting a response from the FDA.
The FDA may give a priority review designation to drugs that offer major advances in treatment, or provide a treatment where no adequate therapy exists. A priority review means that the goal for the FDA to review an application is six months, rather than the standard review of ten months under current PDUFA guidelines. Under the new PDUFA agreement, these six and ten month review periods are measured from the “filing” date rather than the receipt date for NDAs for new molecular entities, which typically adds approximately two months to the timeline for review and decision from the date of submission. Most products that are eligible for fast track designation are also likely to be considered appropriate to receive a priority review.
In addition, products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may receive accelerated approval and may be approved on the basis of adequate and well-controlled clinical trials establishing that the drug product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity or prevalence of the condition and the availability or lack of alternative treatments. As a condition of approval, the FDA may require a sponsor of a drug receiving accelerated approval to perform post-marketing studies to verify and describe the predicted effect on irreversible morbidity or mortality or other clinical endpoint, and the drug may be subject to accelerated withdrawal procedures.
Moreover, under the provisions of the new Food and Drug Administration Safety and Innovation Act, or FDASIA, enacted in 2012, a sponsor can request designation of a product candidate as a “breakthrough therapy.” A breakthrough therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. Drugs designated as breakthrough therapies are also eligible for accelerated approval. The FDA must take certain actions, such as holding timely meetings and providing advice, intended to expedite the development and review of an application for approval of a breakthrough therapy.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened.
Post-Approval Requirements
Drugs manufactured or distributed pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to recordkeeping, periodic reporting,
37
Table of Contents
product sampling and distribution, advertising and promotion and reporting of adverse experiences with the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims are subject to prior FDA review and approval. There also are continuing, annual user fee requirements for any marketed products and the establishments at which such products are manufactured, as well as new application fees for supplemental applications with clinical data.
The FDA may impose a number of post-approval requirements as a condition of approval of an NDA. For example, the FDA may require post-marketing testing, including Phase 4 clinical trials, and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization.
In addition, drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and state agencies, and are subject to periodic unannounced inspections by the FDA and these state agencies for compliance with cGMP requirements. Changes to the manufacturing process are strictly regulated and often require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMP and impose reporting and documentation requirements upon the sponsor and any third-party manufacturers that the sponsor may decide to use. Accordingly, manufacturers must continue to expend time, money, and effort in the area of production and quality control to maintain cGMP compliance.
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market.
Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in mandatory revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical trials to assess new safety risks; or imposition of distribution or other restrictions under a REMS program. Other potential consequences include, among other things:
| • | restrictions on the marketing or manufacturing of the product, complete withdrawal of the product from the market or product recalls; |
| • | fines, warning letters or holds on post-approval clinical trials; |
| • | refusal of the FDA to approve pending NDAs or supplements to approved NDAs, or suspension or revocation of product license approvals; |
| • | product seizure or detention, or refusal to permit the import or export of products; or |
| • | injunctions or the imposition of civil or criminal penalties. |
The FDA strictly regulates marketing, labeling, advertising and promotion of products that are placed on the market. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability.
In addition, the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act, or PDMA, which regulates the distribution of drugs and drug samples at the federal level, and sets minimum standards for the registration and regulation of drug distributors by the states. Both the PDMA and state laws limit the distribution of prescription pharmaceutical product samples and impose requirements to ensure accountability in distribution.
38
Table of Contents
Exclusivity and Approval of Competing Products
Hatch-Waxman Exclusivity
Market and data exclusivity provisions under the FDCA can delay the submission or the approval of certain applications for competing products. The FDCA provides a five-year period of non-patent data exclusivity within the United States to the first applicant to gain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety, which is the molecule or ion responsible for the activity of the drug substance. We believe that eravacycline and our other product candidates are new chemical entities. During the exclusivity period, the FDA may not accept for review an abbreviated new drug application, or ANDA, or a 505(b)(2) NDA submitted by another company that references the previously approved drug. However, an ANDA or 505(b)(2) NDA may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The FDCA also provides three years of marketing exclusivity for an NDA, 505(b)(2) NDA, or supplement to an existing NDA or 505(b)(2) NDA if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant, are deemed by the FDA to be essential to the approval of the application or supplement. Three year exclusivity may be awarded for changes to a previously approved drug product, such as new indications, dosages, strengths or dosage forms of an existing drug. This three-year exclusivity covers only the conditions of use associated with the new clinical investigations and, as a general matter, does not prohibit the FDA from approving ANDAs or 505(b)(2) NDAs for generic versions of the original, unmodified drug product. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA; however, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness. For drug products that contain an “antibiotic” ingredient approved prior to 1997, such as tetracycline, the statute imposes certain limitations on the award of non-patent exclusivity. However, we do not believe these limitations would apply to eravacycline or any of our other investigational antibiotics.
Qualified Infectious Disease Product Exclusivity
Under the GAIN provisions of FDASIA, which was signed into law in July 2012, the FDA may designate a product as a “qualified infectious disease product,” or QIDP. In order to receive this designation, a drug must qualify as an antibacterial or antifungal drug for human use intended to treat serious or life-threatening infections, including those caused by either (1) an antibacterial or antifungal resistant pathogen, including novel or emerging infectious pathogens, or (2) a so-called “qualifying pathogen” found on a list of potentially dangerous, drug-resistant organisms to be established and maintained by the FDA under the new law. A sponsor must request such designation before submitting a marketing application. We obtained a QIDP designation for the IV formulation of eravacycline for cUTI and cIAI in July 2013 and expect to request QIDP designations for our other product candidates prior to submitting a marketing application for such product candidates, as appropriate.
Upon approving an application for a qualified infectious disease product, the FDA will extend by an additional five years any non-patent marketing exclusivity period awarded, such as a five-year exclusivity period awarded for a new molecular entity. This extension is in addition to any pediatric exclusivity extension awarded, and the extension will be awarded only to a drug first approved on or after the date of enactment.
The GAIN provisions prohibit the grant of an exclusivity extension where the application is a supplement to an application for which an extension is in effect or has expired, is a subsequent application for a specified change to an approved product, or is an application for a product that does not meet the definition of qualified infectious disease product based on the uses for which it is ultimately approved.
Foreign Regulation
In addition to regulations in the United States, we will be subject to a variety of foreign regulations governing clinical trials and commercial sales and distribution of our products. Whether or not we obtain FDA
39
Table of Contents
approval for a product, we must obtain approval by the comparable regulatory authorities of foreign countries or economic areas, such as the European Union, before we may commence clinical trials or market products in those countries or areas. The approval process and requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from place to place, and the time may be longer or shorter than that required for FDA approval.
Under European Union regulatory systems, a company may submit marketing authorization applications either under a centralized or decentralized procedure. The centralized procedure, which is compulsory for medicinal products produced by biotechnology or those medicinal products containing new active substances for specific indications such as the treatment of AIDS, cancer, neurodegenerative disorders, diabetes, viral diseases and designated orphan medicines, and optional for other medicines which are highly innovative. Under the centralized procedure, a marketing application is submitted to the European Medicines Agency where it will be evaluated by the Committee for Medicinal Products for Human Use and a favorable opinion typically results in the grant by the European Commission of a single marketing authorization that is valid for all European Union member states within 67 days of receipt of the opinion. The initial marketing authorization is valid for five years, but once renewed is usually valid for an unlimited period. The decentralized procedure provides for approval by one or more “concerned” member states based on an assessment of an application performed by one member state, known as the “reference” member state. Under the decentralized approval procedure, an applicant submits an application, or dossier, and related materials to the reference member state and concerned member states. The reference member state prepares a draft assessment and drafts of the related materials within 120 days after receipt of a valid application. Within 90 days of receiving the reference member state’s assessment report, each concerned member state must decide whether to approve the assessment report and related materials. If a member state does not recognize the marketing authorization, the disputed points are eventually referred to the European Commission, whose decision is binding on all member states.
Coverage and Reimbursement
Sales of our products will depend, in part, on the extent to which our products will be covered and reimbursed by third-party payors, such as government health programs, including Medicare and Medicaid, commercial insurance and managed healthcare organizations. These third-party payors are increasingly reducing coverage and reimbursement amounts for medical products and services. Additionally, the containment of healthcare costs has become a priority of federal and state governments, and the prices of drugs have been a focus in this effort. The U.S. government, state legislatures and foreign governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on coverage and reimbursement and requirements for substitution of generic products. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit our net revenue and results. Decreases in third-party reimbursement for our product candidates or a decision by a third-party payor to not cover our product candidates could reduce physician usage of the product candidate and have a material adverse effect on our sales, results of operations and financial condition.
In the United States, a number of recent legislative reform measures have been passed to contain healthcare reimbursement for pharmaceuticals, including drugs such as our product candidates. For example, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010, known collectively as ACA, among other things, establishes annual fees to be paid by manufacturers for certain branded prescription drugs, requires manufacturers to participate in a discount program for certain outpatient drugs under Medicare Part D, increases manufacturer rebate responsibilities under the Medicaid Drug Rebate Program for outpatient drugs dispensed to Medicaid recipients, addresses a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected and expands oversight and support for the federal government’s comparative effectiveness research of services and products. In addition, other legislative changes have been proposed and adopted since the ACA was enacted. We cannot predict the full impact of ACA or future reform measures on our operations.
40
Table of Contents
In addition, in some foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the European Union provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products. Historically, products launched in the European Union do not follow price structures of the United States and generally tend to be significantly lower.
Other Healthcare Laws
Although we currently do not have any products on the market, if our drug candidates are approved and we begin commercialization, we may be subject to additional healthcare regulation and enforcement by the federal government and by authorities in the states and foreign jurisdictions in which we conduct our business. Such laws include, without limitation, state and federal anti-kickback, fraud and abuse, false claims, privacy and security and physician sunshine laws and regulations. If our operations are found to be in violation of any of such laws or any other governmental regulations that apply to us, we may be subject to penalties, including, without limitation, civil and criminal penalties, damages, fines, the curtailment or restructuring of our operations, exclusion from participation in federal and state healthcare programs and imprisonment, any of which could adversely affect our ability to operate our business and our financial results.
Legal Proceedings
We are not currently a party to any material legal proceedings.
Employees
As of February 28, 2015, we had 55 full-time employees, 38 of whom were primarily engaged in research and development activities. A total of 23 employees have an M.D. or Ph.D. degree. None of our employees is represented by a labor union and we consider our employee relations to be good.
Executive Officers
The following table lists the positions, names and ages of our executive officers as of February 28, 2015:
Executive Officers
| Guy Macdonald | 56 President and Chief Executive Officer, Director | |
| David C. Lubner | 50 Senior Vice President and Chief Financial Officer | |
| Patrick T. Horn, M.D., Ph.D. | 60 Chief Medical Officer | |
| J. Craig Thompson | 48 Chief Operating Officer | |
| Maria Stahl* | 44 Senior Vice President and General Counsel |
| * | Ms. Stahl commenced employment with us on March 4, 2015. |
Guy Macdonald has served as our President and Chief Executive Officer and a member of our board of directors since January 2008. From August 2003 until January 2008, Mr. Macdonald served as Executive Vice President, Operations, of Idenix Pharmaceuticals, Inc., a biopharmaceutical company. Prior to joining Idenix, he served in various positions at Merck & Co., Inc., a pharmaceutical company, from 1981 to 2003, most recently serving as the Vice President for Anti-Infective and Hospital Products. Mr. Macdonald currently serves as
41
Table of Contents
Chairman of the board of directors of Spring Bank Pharmaceuticals, Inc., a privately held company, and as a member of the Board of Directors for Synexis, Inc., a publicly-traded company. Mr. Macdonald received an Honours Degree in biochemistry from Dundee University in Dundee, Scotland.
David C. Lubner has served as our Senior Vice President and Chief Financial Officer since October 2010 and from our inception in 2006 until October 2010 he served on a part-time basis as our Senior Vice President and Chief Operating Officer. Mr. Lubner also served as Chief Financial Officer of Mediphase Venture Partners, a venture capital firm, from 2006 until October 2010. From 1999 to 2005, he served as Vice President and Chief Financial Officer at PharMetrics, Inc., a pharmacy and medical claims data informatics company, until its acquisition by IMS Health in 2005. Prior to joining PharMetrics, Mr. Lubner served as Vice President and Chief Financial Officer of ProScript, Inc., a biotechnology company, from 1996 to 1999. Mr. Lubner is a member of the American Institute of CPAs and is a certified public accountant in the Commonwealth of Massachusetts. Mr. Lubner received a B.S. in business administration from Northeastern University and an M.S. in Taxation from Bentley University.
Patrick T. Horn, M.D., Ph.D. has served as our Chief Medical Officer since January 2011. From September 2007 until December 2010, he served as Vice President, Clinical & Medical Affairs at Dyax Corporation, a biopharmaceutical company. Prior to joining Dyax, Dr. Horn served in various positions at Abbott Laboratories, a pharmaceutical company, from 2001 to 2006, most recently serving as Medical Director, Head of Clinical Pharmacology. Dr. Horn received a B.S. in Chemistry from the University of Illinois, doctorate in the Pharmacological and Physiological Sciences from the University of Chicago and an M.D. from the University of Chicago, Pritzker School of Medicine.
J. Craig Thompson has served as our Chief Operating Officer since February 2014. From January 2011 to December 2013, Mr. Thompson served as Chief Commercial Officer with Trius Therapeutics, Inc., a biopharmaceutical company. From 2003 to December 2010, Mr. Thompson served in various global and U.S. commercial roles with Pfizer Inc., a pharmaceutical and consumer healthcare company, most recently as Vice President of Marketing for Pfizer’s Specialty Care Business Unit. From 1992 to 2003, Mr. Thompson served in positions of increasing responsibility at Merck & Co., Inc., where he most notably worked on the commercial planning and marketing activities for the company’s anti-infectives as well as on major cardiovascular brands. Mr. Thompson received a Bachelor’s degree in Commerce from McMaster University and an MBA from the University of Notre Dame.
Maria Stahl has served as our Senior Vice President and General Counsel since March 2015. From October 2010 to August 2014, Ms. Stahl served in several capacities at Idenix Pharmaceuticals, Inc., a biotechnology company, most recently as Senior Vice President, General Counsel. Prior to rejoining Idenix in October 2010, Ms. Stahl served as General Counsel of Zipcar, Inc., a car sharing company, from November 2009 to October 2010. From February 2005 to February 2007, Ms. Stahl served as Vice President, Corporate Counsel of Capital Crossing Bank. Prior to that, Ms. Stahl was at Wilmer Cutler Pickering Hale and Dorr LLP. Ms. Stahl received a B.A. from Providence College and a J.D. from Yale Law School.
Available Information
We file reports and other information with the Securities and Exchange Commission as required by the Securities Exchange Act of 1934, as amended, which we refer to as the Exchange Act. You can find, copy and inspect information we file at the SEC’s Public Reference Room, which is located at 100 F Street, N.E., Room 1580, Washington, DC 20549, on official business days during the hours of 10:00 a.m. to 3:00 p.m. Please call the SEC at 1-800-SEC-0330 for more information about the operation of the SEC’s Public Reference Room. You can review our electronically filed reports and other information that we file with the SEC on the SEC’s web site at http://www.sec.gov.
42
Table of Contents
We were incorporated under the laws of the State of Delaware on July 7, 2006 as Tetraphase Pharmaceuticals, Inc. Our principal executive offices are located at 480 Arsenal Street, Suite 110, Watertown, Massachusetts, 02472, and our telephone number is (617) 715-3600. Our Internet website is http://www.tphase.com. We make available free of charge through our website our Annual Report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Sections 13(a) and 15(d) of the Exchange Act. We make these reports available through our website as soon as reasonably practicable after we electronically file such reports with, or furnish such reports to, the SEC. In addition, we regularly use our website to post information regarding our business, product development programs and governance, and we encourage investors to use our website, particularly the information in the section entitled “Investor Relations,” as a source of information about us.
The foregoing references to our website are not intended to, nor shall they be deemed to, incorporate information on our website into this annual report on Form 10-K by reference.
43
Table of Contents
| Item 1A. | Risk Factors |
Our business is subject to numerous risks. We caution you that the following important factors, among others, could cause our actual results to differ materially from those expressed in forward-looking statements made by us or on our behalf in this annual report on Form 10-K and other filings with the SEC, press releases, communications with investors and oral statements. Actual future results may differ materially from those anticipated in our forward-looking statements. We undertake no obligation to update any forward-looking statements, whether as a result of new information, future events or otherwise.
Risks Relating to Our Financial Position and Need for Additional Capital
We have incurred significant losses since inception, expect to incur losses for at least the next several years and may never achieve or sustain profitability.
We have incurred annual net operating losses in every year since our inception. Our net loss was $66.7 million for the year ended December 31, 2014, $29.6 million for the year ended December 31, 2013 and $15.1 million for the year ended December 31, 2012. As of December 31, 2014, we had an accumulated deficit of $186.5 million. We have not generated any product revenues and have financed our operations primarily through the public offering and private placements of our equity securities, debt financings and revenue from U.S. government awards. We have not completed development of any product candidate and have devoted substantially all of our financial resources and efforts to research and development, including preclinical and clinical development. We expect to continue to incur significant expenses and increasing operating losses for at least the next several years. The net losses we incur may fluctuate significantly from quarter to quarter. Net losses and negative cash flows have had, and will continue to have, an adverse effect on our stockholders’ equity and working capital.
We expect that our expenses will increase substantially as we continue our ongoing Phase 3 clinical trial of our lead product candidate, eravacycline, for the treatment of patients with complicated urinary tract infections, or cUTI, seek marketing approval for eravacycline, pursue development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections, conduct pre-commercialization and launch-related activities for eravacycline, advance our other product candidates and satisfy our obligations under our license agreement with Harvard University. If we obtain marketing approval of eravacycline, we also expect to incur significant sales, marketing, distribution and outsourced manufacturing expenses, as well as ongoing research and development expenses. Our expenses also will increase if and as we:
| • | maintain, expand and protect our intellectual property portfolio; |
| • | in-license or acquire other products and technologies; |
| • | hire additional clinical, quality control and scientific personnel; and |
| • | add operational, financial and management information systems and personnel, including personnel to support our product development and planned future commercialization efforts. |
Our ability to become and remain profitable depends on our ability to generate revenue. We do not expect to generate significant revenue unless and until we obtain marketing approval for, and commercialize, eravacycline, which will require us to be successful in a range of challenging activities, including:
| • | conducting and successfully completing our Phase 3 clinical trial of eravacycline for the treatment of cUTI; |
| • | applying for and obtaining marketing approval for eravacycline; |
| • | protecting and maintaining our rights to our intellectual property portfolio related to eravacycline; |
| • | contracting for the manufacture of commercial quantities of eravacycline; and |
| • | establishing sales, marketing and distribution capabilities to effectively market and sell eravacycline. |
44
Table of Contents
Because of the numerous risks and uncertainties associated with pharmaceutical product development, we are unable to accurately predict the timing or amount of increased expenses or when, or if, we will be able to achieve profitability. Our expenses could increase if we are required by the United States Food and Drug Administration, or FDA, or the European Medicines Agency, or EMA, to perform studies in addition to those currently expected, or if there are any delays in completing our clinical trials or the development of any of our product candidates.
We may be unable to develop and commercialize eravacycline or any other product candidate and, even if we do, may never achieve profitability. Even if we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would decrease the value of our company and could impair our ability to raise capital, expand our business or continue our operations. A decline in the value of our company could cause our stockholders to lose all or part of their investment in us.
We expect that we will need substantial additional funding. If we are unable to raise capital when needed, we could be forced to delay, reduce or eliminate our product development programs or commercialization efforts.
Developing pharmaceutical products, including conducting preclinical studies and clinical trials, is a time-consuming, expensive and uncertain process that takes years to complete. We expect that our expenses will increase substantially as we continue our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, seek marketing approval for eravacycline, pursue development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections, conduct pre-commercialization and launch-related activities for eravacycline, advance our other product candidates and satisfy our obligations under our license agreement with Harvard University. We expect that the total external costs of our Phase 3 clinical trials of eravacycline for the treatment of cIAI and cUTI will be approximately $65.0 million to $75.0 million. If we obtain marketing approval for eravacycline or any other product candidate that we develop, we expect to incur significant commercialization expenses related to product sales, marketing, distribution and manufacturing.
We believe that our available funds will enable us to fund our current operating plan and capital expenditure requirements into at least the third quarter of 2016. We believe that our available funds will be sufficient to enable us to obtain top-line data from our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, submit a new drug application, or NDA, to the FDA for eravacycline and to perform pre-commercialization activities for eravacycline. We expect that these funds will not, however, be sufficient to enable us to commercially launch eravacycline. As a result, we will be required to obtain further funding through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources.
These estimates are based on assumptions that may prove to be wrong, and we could use our available capital resources sooner than we currently expect. Changing circumstances could cause us to consume capital significantly faster than we currently anticipate, and we may need to spend more money than currently expected because of circumstances beyond our control. It is also possible that we will not achieve the progress that we expect with respect to eravacycline because the actual costs and timing of clinical development activities are difficult to predict and are subject to substantial risks and delays.
Adequate additional financing may not be available to us on acceptable terms, or at all. Our failure to raise capital as and when needed would have a negative impact on our financial condition and our ability to pursue our business strategy.
Our future funding requirements, both short-term and long-term, will depend on many factors, including:
| • | the timing and costs of our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI; |
| • | manufacturing costs related to regulatory filings and anticipated commercial launch; |
45
Table of Contents
| • | the initiation, progress, timing, costs and results of preclinical studies and clinical trials for our other product candidates and potential product candidates; |
| • | the amount of funding that we receive under our subcontracts awarded to us by our collaborator CUBRC, Inc., or CUBRC, under its government contracts with the Biomedical Advanced Research and Development Authority, or BARDA, and with the National Institutes of Health’s, or NIH’s, National Institute of Allergy and Infectious Diseases, or NIAID, and under our subaward from CUBRC under its grant from NIAID, and the activities funded under these contracts; |
| • | the number and characteristics of product candidates that we pursue; |
| • | the timing and costs of developing eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections; |
| • | the outcome, timing and costs of seeking regulatory approvals; |
| • | the costs of commercialization activities for eravacycline and other product candidates if we receive marketing approval, including the timing and costs of establishing product sales, marketing, distribution and manufacturing capabilities; |
| • | revenue received from commercial sales of eravacycline, subject to receipt of marketing approval; |
| • | the terms and timing of any future collaborations, licensing, consulting or other arrangements that we may establish; |
| • | the amount and timing of any payments we may be required to make, or that we may receive, in connection with the licensing, filing, prosecution, defense and enforcement of any patents or other intellectual property rights, including milestone and royalty payments and patent prosecution fees that we are obligated to pay to Harvard pursuant to our license agreement; |
| • | the costs of preparing, filing and prosecuting patent applications, maintaining and protecting our intellectual property rights and defending against intellectual property related claims; and |
| • | the extent to which we in-license or acquire other products and technologies. |
Raising additional capital may cause dilution to our stockholders, restrict our operations or require us to relinquish rights to our technologies or product candidates.
Currently, our only external source of funds is funding under subcontracts and a subaward awarded to us by CUBRC pursuant to government contracts from BARDA and NIAID and a grant from NIAID. Although the BARDA contract, and our subcontract with CUBRC under the BARDA contract, have five-year terms, BARDA is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond current-year amounts from Congressionally approved annual appropriations. To the extent that BARDA ceases to provide funding of the program to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our BARDA subcontract is $31.0 million from the initial contract date through September 9, 2016, of which $16.4 million had been received through December 31, 2014.
Similarly, although the NIAID contract and our subcontract with CUBRC under the NIAID contract have five-year terms, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond September 30, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subcontract with respect to the NIAID contract is $8.3 million, of which $7.1 million had been received through December 31, 2014. In addition, although the NIAID grant has a term of five years and our subaward from CUBRC has a term of 55 months, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond May 30, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subaward with respect to the NIAID grant is $0.8 million from the initial grant date through May 30, 2016, of which $0.7 million had been received through December 31, 2014.
46
Table of Contents
As a result, unless and until we can generate a substantial amount of revenue from our product candidates, we expect to finance our future cash needs through public or private equity offerings, debt financings or collaborations and licensing arrangements. In addition, we may seek additional capital due to favorable market conditions or strategic considerations, even if we believe that we have sufficient funds for our current or future operating plans.
To the extent that we raise additional capital through the sale of common stock, convertible securities or other equity securities, the ownership interest of our stockholders may be materially diluted, and the terms of these securities could include liquidation or other preferences and anti-dilution protections that could adversely affect their rights. In addition, debt financing, if available, would result in increased fixed payment obligations and may involve agreements that include restrictive covenants that limit our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends, that could adversely impact our ability to conduct our business. For example, our debt facility with Silicon Valley Bank and Oxford Finance contains restrictive covenants that, subject to certain exceptions, prohibit us from transferring all or any part of our business or property, changing our business, liquidating or dissolving, merging with or acquiring another entity, entering into a transaction that will result in a change of control, incurring additional indebtedness, creating any lien on our property, paying dividends, entering into material transactions with affiliates, changing key management or adding new offices or business locations. Future debt securities or other financing arrangements could contain similar or more restrictive negative covenants. In addition, securing additional financing would require a substantial amount of time and attention from our management and may divert a disproportionate amount of their attention away from day-to-day activities, which may adversely affect our management’s ability to oversee the development of our product candidates.
If we raise additional funds through collaborations, strategic alliances or marketing, distribution or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams or product candidates or to grant licenses on terms that may not be favorable to us.
We have a limited operating history and no history of commercializing pharmaceutical products, which may make it difficult to evaluate the prospects for our future viability.
We began operations in the third quarter of 2006. Our operations to date have been limited to financing and staffing our company, developing our technology and developing eravacycline and other product candidates. We have not yet demonstrated an ability to obtain marketing approval, manufacture a commercial scale product, or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful product commercialization. Consequently, predictions about our future success or viability may not be as accurate as they could be if we had a longer operating history or a history of successfully developing and commercializing pharmaceutical products.
Risks Related to Product Development and Commercialization
We are dependent on the success of our lead product candidate, eravacycline, and our ability to develop, obtain marketing approval for and successfully commercialize eravacycline. If we are unable to develop, obtain marketing approval for and successfully commercialize eravacycline or experience significant delays in doing so, our business could be materially harmed.
We currently have no products approved for sale and have invested a significant portion of our efforts and financial resources in the development of eravacycline for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections. Our prospects are substantially dependent on our ability to develop, obtain marketing approval for and successfully commercialize eravacycline. The success of eravacycline will depend on several factors, including the following:
| • | successful completion of clinical trials; |
| • | successful manufacturing of registration batches for regulatory filings for eravacycline; |
47
Table of Contents
| • | timely filing for and receipt of marketing approvals from applicable regulatory authorities; |
| • | establishment of arrangements with third-party manufacturers to obtain manufacturing supply; |
| • | obtainment and maintenance of patent and trade secret protection and regulatory exclusivity; |
| • | protection of our rights in our intellectual property portfolio; |
| • | commercial launch of eravacycline, if and when approved, whether alone or in collaboration with others; |
| • | acceptance of eravacycline, if and when approved, by patients, the medical community and third-party payors; |
| • | competition with other therapies; and |
| • | a continued acceptable safety profile of eravacycline following approval. |
Successful development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections, will be subject to these same risks.
If we are unable to develop, receive marketing approval for, or successfully commercialize eravacycline, or experience delays as a result of any of these matters or otherwise, our business could be materially harmed.
If clinical trials of eravacycline or of any other product candidate that we advance to clinical trials fail to demonstrate safety and efficacy to the satisfaction of the FDA or comparable foreign regulatory authorities or do not otherwise produce favorable results, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of eravacycline or any other product candidate.
We are not permitted to commercialize, market, promote, or sell any product candidate in the United States without obtaining marketing approval from the FDA or in other countries without obtaining approvals from comparable foreign regulatory authorities, such as the EMA, and we may never receive such approvals. We must complete extensive preclinical development and clinical trials to demonstrate the safety and efficacy of our product candidates in humans before we will be able to obtain these approvals. Clinical testing is expensive, difficult to design and implement, can take many years to complete and is inherently uncertain as to outcome. We have not previously submitted an NDA to the FDA or similar drug approval filings to comparable foreign regulatory authorities for any of our product candidates.
The clinical development of eravacycline and other product candidates is susceptible to the risk of failure inherent at any stage of drug development, including failure to achieve efficacy in a trial or across a broad population of patients, the occurrence of severe adverse events, failure to comply with protocols or applicable regulatory requirements, and determination by the FDA or any comparable foreign regulatory authority that a drug product is not approvable. The outcome of preclinical studies and early clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. For example, although eravacycline achieved favorable results in the lead-in part of our Phase 3 clinical trial in cUTI, we may nonetheless fail to achieve success in our Phase 3 clinical trial for eravacycline for the treatment of cUTI.
In addition, preclinical and clinical data are often susceptible to varying interpretations and analyses. Many companies that believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval for the product candidates. Even if we believe that the results of our clinical trials warrant marketing approval, the FDA or comparable foreign regulatory authorities may disagree and may not grant marketing approval of our product candidates.
In some instances, there can be significant variability in safety and/or efficacy results between different trials of the same product candidate due to numerous factors, including changes in trial procedures set forth in
48
Table of Contents
protocols, differences in the size and type of the patient populations, adherence to the dosing regimen and other trial protocols and the rate of dropout among clinical trial participants. In the case of our clinical trials, results may differ on the basis of the type of bacteria with which patients are infected. We cannot be certain that any Phase 2, Phase 3 or other clinical trials that we may conduct will demonstrate consistent or adequate efficacy and safety to obtain regulatory approval to market our product candidates.
We may experience numerous unforeseen events during, or as a result of, clinical trials that could delay or prevent us from obtaining regulatory approval for eravacycline or any of our other product candidates, including:
| • | clinical trials of our product candidates may produce unfavorable or inconclusive results; |
| • | we may decide, or regulators may require us, to conduct additional clinical trials or abandon product development programs; |
| • | the number of patients required for clinical trials of our product candidates may be larger than we anticipate, enrollment in these clinical trials may be slower than we anticipate or participants may drop out of these clinical trials at a higher rate than we anticipate; |
| • | our third-party contractors, including those manufacturing our product candidates or conducting clinical trials on our behalf, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
| • | regulators or institutional review boards may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| • | we may have delays in reaching or fail to reach agreement on acceptable clinical trial contracts or clinical trial protocols with prospective trial sites; |
| • | we may have to suspend or terminate clinical trials of our product candidates for various reasons, including a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate; |
| • | regulators or institutional review boards may require that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate; |
| • | the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes or facilities of third-party manufacturers with which we enter into agreement for clinical and commercial supplies; |
| • | the supply or quality of our product candidates or other materials necessary to conduct clinical trials of our product candidates may be insufficient or inadequate; and |
| • | the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval. |
If we are required to conduct additional clinical trials or other testing of eravacycline, either in an intravenous or oral dosage form, or any other product candidate that we develop beyond the trials and testing that we contemplate, if we are unable to successfully complete clinical trials of our product candidates or other testing, if the results of these trials or tests are unfavorable or are only modestly favorable or if there are safety concerns associated with eravacycline or our other product candidates, we may:
| • | be delayed in obtaining marketing approval for our product candidates; |
| • | not obtain marketing approval at all; |
| • | obtain approval for indications or patient populations that are not as broad as intended or desired; |
49
Table of Contents
| • | obtain approval with labeling that includes significant use or distribution restrictions or significant safety warnings, including boxed warnings; |
| • | be subject to additional post-marketing testing or other requirements; or |
| • | remove the product from the market after obtaining marketing approval. |
Our product development costs will also increase if we experience delays in testing or marketing approvals and we may be required to obtain additional funds to complete clinical trials. We cannot be certain that our clinical trials will begin as planned or be completed on schedule, if at all, or that we will not need to restructure our trials after they have begun. Significant clinical trial delays also could shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before we do and impair our ability to successfully commercialize our product candidates, which may harm our business and results of operations. In addition, many of the factors that cause, or lead to, clinical trial delays may ultimately lead to the denial of regulatory approval of eravacycline or any other product candidate.
If we experience delays or difficulties in the enrollment of patients in clinical trials, our receipt of necessary regulatory approvals could be delayed or prevented.
We may not be able to initiate or continue clinical trials for eravacycline or any other product candidate that we develop if we are unable to locate and enroll a sufficient number of eligible patients to participate in clinical trials for eravacycline or such other product candidate as required by the FDA or comparable foreign regulatory authorities, such as the EMA. Patient enrollment is a significant factor in the timing of clinical trials, and is affected by many factors, including:
| • | the size and nature of the patient population; |
| • | the severity of the disease under investigation; |
| • | the proximity of patients to clinical sites; |
| • | the eligibility criteria for the trial; |
| • | the design of the clinical trial; and |
| • | competing clinical trials and clinicians’ and patients’ perceptions as to the potential advantages and risks of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. |
The inclusion and exclusion criteria for our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI may adversely affect our enrollment rates for patients in this trial. Additionally, if we enroll an insufficient number of micro-ITT patients in the trial, we will need to enroll more patients than planned. In addition, many of our competitors also have ongoing clinical trials for product candidates that treat the same indications as eravacycline, and patients who would otherwise be eligible for our clinical trials may instead enroll in clinical trials of our competitors’ product candidates.
Our inability to enroll a sufficient number of patients for our clinical trials would result in significant delays or may require us to abandon one or more clinical trials altogether. Enrollment delays in our clinical trials may result in increased development costs for our product candidates, slow down or halt our product development and approval process and jeopardize our ability to commence product sales and generate revenues, which would cause the value of our company to decline and limit our ability to obtain additional financing if needed.
50
Table of Contents
Serious adverse events or undesirable side effects or other unexpected properties of eravacycline or any other product candidate may be identified during development or after approval, if obtained, that could delay, prevent or cause the withdrawal of the product candidates’ regulatory approval, limit the commercial profile of an approved label, or result in significant negative consequences following marketing approval, if obtained.
Serious adverse events or undesirable side effects caused by, or other unexpected properties of, our product candidates could cause us, an institutional review board, or regulatory authorities to interrupt, delay or halt our clinical trials and could result in a more restrictive label, the imposition of distribution or use restrictions or the delay or denial of regulatory approval by the FDA or comparable foreign regulatory authorities. If eravacycline or any of our other product candidates are associated with serious adverse events or undesirable side effects or have properties that are unexpected, we may need to abandon their development or limit development to certain uses or subpopulations in which the undesirable side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective. Many compounds that initially showed promise in clinical or earlier stage testing have later been found to cause undesirable or unexpected side effects that prevented further development of the compound.
In our clinical trials of eravacycline, some treatment-related adverse events have been reported. The most common treatment-related adverse events observed in clinical trials of eravacycline have been nausea and emesis. Additional adverse events, undesirable side effects or other unexpected properties of eravacycline or any of our other product candidates could arise or become known either during clinical development or, if approved, after the approved product has been marketed. If such an event occurs during development, our trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to cease further development of, or deny approval of, eravacycline or our other product candidates. If such an event occurs after eravacycline or such other product candidates are approved, a number of potentially significant negative consequences may result, including:
| • | regulatory authorities may withdraw the approval of such product; |
| • | regulatory authorities may require additional warnings on the label or impose distribution or use restrictions; |
| • | regulatory authorities may require one or more postmarket studies; |
| • | we may be required to create a medication guide outlining the risks of such side effects for distribution to patients; |
| • | we could be sued and held liable for harm caused to patients; and |
| • | our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product candidate, if approved, or could substantially increase commercialization costs and expenses, which could delay or prevent us from generating revenues from the sale of our products and harm our business and results of operations.
Even if eravacycline or any other product candidate that we develop receives marketing approval, it may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success and the market opportunity for eravacycline or other product candidates may be smaller than we estimate.
We have never commercialized a product candidate for any indication. Even if eravacycline or any other product candidates that we develop are approved by the appropriate regulatory authorities for marketing and sale, they may nonetheless fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. Efforts to educate the medical community and third-party payors on the benefits of our product candidates may require significant resources and may not be successful. If physicians, rightly or wrongly, associate our product candidates with antibiotic resistance issues of other products of the
51
Table of Contents
same class, physicians might not prescribe our product candidates for treating a broad range of infections. If eravacycline or any other product candidate that we develop does not achieve an adequate level of market acceptance, we may not generate significant product revenues and, therefore, we may not become profitable. The degree of market acceptance of eravacycline, if approved, or any other product candidate that is approved for commercial sale, will depend on a number of factors, including:
| • | the efficacy and safety of the product; |
| • | the potential advantages of the product compared to alternative treatments; |
| • | the prevalence and severity of any side effects; |
| • | the clinical indications for which the product is approved; |
| • | limitations or warnings, including distribution or use restrictions, contained in the product’s approved labeling or an approved risk evaluation and mitigation strategy; |
| • | our ability to offer the product for sale at competitive prices; |
| • | the product’s convenience and ease of administration compared to alternative treatments, including, in the case of eravacycline, the availability of the oral formulation that we are developing for use in intravenous-to-oral transition therapy; |
| • | the willingness of the target patient population to try, and of physicians to prescribe, the product; |
| • | whether the product is designated under physician treatment guidelines as a first-line therapy or as a second- or third-line therapy for particular infections; |
| • | the strength of marketing and distribution support; |
| • | the approval of other new products for the same indications; |
| • | the timing of market introduction of our approved products as well as competitive products; |
| • | the cost of treatment in relation to alternative treatments; |
| • | availability and level of coverage and amount of reimbursement from government payors, managed care plans and other third party payors; |
| • | the effectiveness of our sales and marketing efforts; |
| • | adverse publicity about the product or favorable publicity about competitive products; and |
| • | the development of resistance by bacterial strains to the product. |
In addition, the potential market opportunity for eravacycline is difficult to estimate. Our estimates of the potential market opportunity are predicated on several key assumptions such as industry knowledge, third-party research reports and other surveys. While we believe that our internal assumptions are reasonable, these assumptions involve the exercise of significant judgment on the part of our management, are inherently uncertain and the reasonableness of these assumptions has not been assessed by an independent source. If any of the assumptions proves to be inaccurate, then the actual market for eravacycline could be smaller than our estimates of the potential market opportunity. If the actual market for eravacycline is smaller than we expect, or if the product fails to achieve an adequate level of acceptance by physicians, health care payors and patients, our product revenue may be limited and it may be more difficult for us to achieve or maintain profitability.
If we are unable to establish sales, marketing and distribution capabilities or enter into sales, marketing and distribution agreements with third parties, we may not be successful in commercializing eravacycline or such other product candidates that we develop if and when eravacycline or any other product candidates are approved.
We do not have a sales, marketing or distribution infrastructure and have no experience in the sale, marketing or distribution of pharmaceutical products. To achieve commercial success for any approved product,
52
Table of Contents
we must either develop a sales and marketing organization or outsource these functions to third parties. We intend to develop and build a commercial organization in the United States and recruit experienced sales, marketing and distribution professionals, which will require substantial resources, will be time-consuming and could delay any product launch. If the commercial launch of a product candidate for which we recruit a sales force and establish marketing and distribution capabilities is delayed or does not occur for any reason, we would have prematurely or unnecessarily incurred these commercialization costs. This may be costly, and our investment would be lost if we cannot retain or reposition our sales and marketing personnel. In addition, we may not be able to hire a sales force in the United States that is sufficient in size or has adequate expertise in the medical markets that we intend to target. If we are unable to establish a sales force and marketing and distribution capabilities, our operating results may be adversely affected.
Factors that may inhibit our efforts to commercialize our products on our own include:
| • | our inability to recruit and retain adequate numbers of effective sales and marketing personnel; |
| • | the ability of sales personnel to obtain access to or persuade adequate numbers of physicians to prescribe any future products; |
| • | the lack of complementary products to be offered by sales personnel, which may put us at a competitive disadvantage relative to companies with more extensive product lines; and |
| • | unforeseen costs and expenses associated with creating an independent sales and marketing organization. |
We plan to commercialize eravacycline outside the United States with the assistance of collaborators. As a result of entering into arrangements with third parties to perform sales, marketing and distribution services, our product revenues or the profitability of these product revenues to us may be lower than if we were to directly market and sell products in those markets. Furthermore, we may be unsuccessful in entering into the necessary arrangements with third parties or may be unable to do so on terms that are favorable to us. In addition, we likely will have little control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our products effectively.
If we do not establish sales and marketing capabilities successfully, either on our own or in collaboration with third parties, we will not be successful in commercializing our product candidates.
We face substantial competition from other pharmaceutical and biotechnology companies and our operating results may suffer if we fail to compete effectively.
The development and commercialization of new drug products is highly competitive. We face competition from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide with respect to eravacycline and our other product candidates that we may seek to develop or commercialize in the future. There are a number of large pharmaceutical and biotechnology companies that currently market and sell products or are pursuing the development of product candidates for the treatment of multidrug-resistant infections. Potential competitors also include academic institutions, government agencies and other public and private research organizations. Our competitors may succeed in developing, acquiring or licensing technologies and drug products that are more effective or less costly than eravacycline or any other product candidates that we are currently developing or that we may develop, which could render our product candidates obsolete or noncompetitive.
There are a variety of available therapies marketed for the treatment of multidrug-resistant infections that we would expect would compete with eravacycline, including meropenem, which is marketed by AstraZeneca as Merrem, imipenem/cilastatin, which is marketed by Merck as Primaxin, tigecycline, which is marketed by Pfizer as Tygacil, levofloxacin, which is marketed by Ortho-McNeil and Johnson & Johnson as Levaquin, piperacillin/tazobactam, which is marketed by Pfizer as Zosyn and ceftolozane/tazobactam, which is marketed by Merck/
53
Table of Contents
Cubist as Zerbaxa. Many of the available therapies are well established and widely accepted by physicians, patients and third-party payors. Insurers and other third-party payors may also encourage the use of generic products. If eravacycline is approved, it may be priced at a significant premium over other competitive products. This may make it difficult for eravacycline to compete with these products.
There are also a number of products either currently under FDA review or in Phase 3 development by third parties to treat multidrug-resistant infections, including ceftazidime/avibactam, which is being developed by Allergan Inc. and AstraZeneca plc, meropenem/RPX7009, which is being developed by The Medicines Company as Carbavance, and plazomicin, which is being developed by Achaogen, Inc. If our competitors obtain marketing approval from the FDA or comparable foreign regulatory authorities for their product candidates more rapidly than we do, it could result in our competitors establishing a strong market position before we are able to enter the market.
Many of our competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller and other early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
In July 2012, the Food and Drug Administration Safety and Innovation Act was passed, which included the Generating Antibiotics Incentives Now Act, or the GAIN Act. The GAIN Act is intended to provide incentives for the development of new, qualified infectious disease products. These incentives may result in more competition in the market for new antibiotics, and may cause pharmaceutical and biotechnology companies with more resources than we have to shift their efforts towards the development of products that could be competitive with eravacycline and our other product candidates.
Even if we are able to commercialize eravacycline or any other product candidate that we develop, the product may become subject to unfavorable pricing regulations, third-party payor coverage and reimbursement policies or healthcare reform initiatives that could harm our business.
Marketing approvals, pricing, coverage and reimbursement for new drug products vary widely from country to country. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing or product licensing approval is granted. In some foreign markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain marketing approval for a product in a particular country, but then be subject to price regulations that delay our commercial launch of the product, possibly for lengthy time periods, which may negatively impact the revenues we are able to generate from the sale of the product in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more product candidates, even if our product candidates obtain marketing approval.
Our ability to commercialize eravacycline or any other product candidate will depend in part on the extent to which coverage and reimbursement for these products and related treatments will be available from government authorities, private health insurers, health maintenance organizations and other third-party payors. The healthcare industry is acutely focused on cost containment, both in the United States and elsewhere. As a result, government authorities and third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications, which could affect our ability to sell our product candidates profitably.
There may also be delays in obtaining coverage and reimbursement for newly approved drugs, and coverage may be more limited than the indications for which the drug is approved by the FDA or comparable foreign
54
Table of Contents
regulatory authorities. Increasingly, third-party payors are requiring higher levels of evidence of the benefits and clinical outcomes of new technologies and are challenging the prices charged. Moreover, obtaining coverage does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Reimbursement rates may vary, by way of example, according to the use of the drug and the clinical setting in which it is used. Reimbursement rates may also be based in part on existing reimbursement amounts for lower cost drugs or may be bundled into the payments for other services.
We cannot be sure that coverage will be available for eravacycline or any other product candidate that we commercialize and, if available, that the reimbursement rates will be adequate. Further, the net reimbursement for drug products may be subject to additional reductions if there are changes to laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the United States. An inability to promptly obtain coverage and adequate payment rates from both government-funded and private payors for any approved products that we develop could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Product liability lawsuits against us could divert our resources, cause us to incur substantial liabilities and limit commercialization of any products that we may develop.
We face an inherent risk of product liability claims as a result of the clinical testing of our product candidates despite obtaining appropriate informed consents from our clinical trial participants. We will face an even greater risk if we commercially sell eravacycline or any other product candidate that we develop. For example, we may be sued if any product we develop allegedly causes injury or is found to be otherwise unsuitable during clinical testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability or a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our product candidates. Regardless of the merits or eventual outcome, liability claims may result in:
| • | reduced resources of our management to pursue our business strategy; |
| • | decreased demand for our product candidates or products that we may develop; |
| • | injury to our reputation and significant negative media attention; |
| • | withdrawal of clinical trial participants; |
| • | initiation of investigations by regulators; |
| • | product recalls, withdrawals or labeling, marketing or promotional restrictions; |
| • | significant costs to defend resulting litigation; |
| • | substantial monetary awards to trial participants or patients; |
| • | loss of revenue; and |
| • | the inability to commercialize any products that we may develop. |
Although we maintain general liability insurance of $6 million in the aggregate and clinical trial liability insurance of $6 million in the aggregate for eravacycline, this insurance may not fully cover potential liabilities that we may incur. The cost of any product liability litigation or other proceeding, even if resolved in our favor, could be substantial. We will need to increase our insurance coverage if and when we begin selling eravacycline or any other product candidate that receives marketing approval. In addition, insurance coverage is becoming increasingly expensive. If we are unable to obtain or maintain sufficient insurance coverage at an acceptable cost or to otherwise protect against potential product liability claims, it could prevent or inhibit the development and commercial production and sale of our product candidates, which could adversely affect our business, financial condition, results of operations and prospects.
55
Table of Contents
If we fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could have a material adverse effect on our business.
We are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment and disposal of hazardous materials and wastes. From time to time and in the future, our operations may involve the use of hazardous and flammable materials, including chemicals and biological materials, and may also produce hazardous waste products. Even if we contract with third parties for the disposal of these materials and wastes, we cannot completely eliminate the risk of contamination or injury resulting from these materials. In the event of contamination or injury resulting from our use of hazardous materials, we could be held liable for any resulting damages, and any liability could exceed our resources. We also could incur significant costs associated with civil or criminal fines and penalties for failure to comply with such laws and regulations.
We maintain workers’ compensation insurance to cover us for costs and expenses we may incur due to injuries to our employees resulting from the use of hazardous materials, but this insurance may not provide adequate coverage against potential liabilities. However, we do not maintain insurance for environmental liability or toxic tort claims that may be asserted against us.
In addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and regulations. Current or future environmental laws and regulations may impair our research, development or production efforts, which could adversely affect our business, financial condition, results of operations or prospects. In addition, failure to comply with these laws and regulations may result in substantial fines, penalties or other sanctions.
Risks Related to Our Dependence on Third Parties
We expect to depend on collaborations with third parties for the development and commercialization of some of our product candidates. Our prospects with respect to those product candidates will depend in part on the success of those collaborations.
Although we expect to commercialize eravacycline ourselves in the United States, we intend to seek to commercialize eravacycline outside the United States through collaboration arrangements. In addition, we may seek third-party collaborators for development and commercialization of other product candidates. Our likely collaborators for any marketing, distribution, development, licensing or broader collaboration arrangements include large and mid-size pharmaceutical companies, regional and national pharmaceutical companies and biotechnology companies. We are not currently party to any such arrangements.
We may derive revenue from research and development fees, license fees, milestone payments and royalties under any collaborative arrangement into which we enter. Our ability to generate revenues from these arrangements will depend on our collaborators’ abilities to successfully perform the functions assigned to them in these arrangements. In addition, our collaborators may have the right to abandon research or development projects and terminate applicable agreements, including funding obligations, prior to or upon the expiration of the agreed upon terms. As a result, we can expect to relinquish some or all of the control over the future success of a product candidate that we license to a third party.
Collaborations involving our product candidates may pose a number of risks, including the following:
| • | collaborators have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
| • | collaborators may not perform their obligations as expected or in compliance with applicable regulatory requirements; |
| • | collaborators may not pursue development and commercialization of our product candidates or may elect not to continue or renew development or commercialization programs based on clinical trial |
56
Table of Contents
| results, changes in the collaborators’ strategic focus or available funding, or external factors, such as an acquisition, that divert resources or create competing priorities; |
| • | collaborators may delay clinical trials, provide insufficient funding for a clinical trial program, stop a clinical trial or abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
| • | product candidates discovered in collaboration with us may be viewed by our collaborators as competitive with their own product candidates or products, which may cause collaborators to cease to devote resources to the commercialization of our product candidates; |
| • | a collaborator with marketing and distribution rights to one or more products may not commit sufficient resources to the marketing and distribution of such product or products; |
| • | disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the preferred course of development, might cause delays or termination of the research, development or commercialization of product candidates, might lead to additional responsibilities for us with respect to product candidates, or might result in litigation or arbitration, any of which would be time-consuming and expensive; |
| • | collaborators may not properly maintain or defend our intellectual property rights or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential litigation; |
| • | collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; and |
| • | collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development or commercialization of the applicable product candidates. |
Collaboration agreements may not lead to development or commercialization of product candidates in the most efficient manner or at all. If a collaborator of ours is involved in a business combination, it could decide to delay, diminish or terminate the development or commercialization of any product candidate licensed to it by us.
We may have to alter our development and commercialization plans if we are not able to establish collaborations.
We will require additional funds to complete the development and potential commercialization of eravacycline and our other product candidates. For some of our product candidates, we may decide to collaborate with pharmaceutical and biotechnology companies for the development and potential commercialization of those product candidates. For example, we intend to utilize a variety of types of collaboration arrangements for commercialization outside the United States.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include:
| • | the design or results of clinical trials; |
| • | the likelihood of approval by the FDA or comparable foreign regulatory authorities; |
| • | the potential market for the subject product candidate; |
| • | the costs and complexities of manufacturing and delivering such product candidate to patients; |
| • | the potential for competing products; |
57
Table of Contents
| • | our patent position protecting the product candidate, including any uncertainty with respect to our ownership of our technology or our licensor’s ownership of technology we license from them, which can exist if there is a challenge to such ownership without regard to the merits of the challenge; |
| • | the need to seek licenses or sub-licenses to third-party intellectual property; and |
| • | industry and market conditions generally. |
The collaborator may also consider alternative product candidates or technologies for similar indications that may be available for collaboration and whether such collaboration could be more attractive than the one with us for our product candidate. We may also be restricted under future license agreements from entering into agreements on certain terms with potential collaborators. In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators.
If we are unable to reach agreements with suitable collaborators on a timely basis, on acceptable terms, or at all, we may have to curtail the development of a product candidate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to fund and undertake development or commercialization activities on our own, we may need to obtain additional expertise and additional capital, which may not be available to us on acceptable terms or at all. If we fail to enter into collaborations and do not have sufficient funds or expertise to undertake the necessary development and commercialization activities, we may not be able to further develop our product candidates or bring them to market and our business may be materially and adversely affected.
We rely on third parties to conduct our clinical trials. If they do not perform satisfactorily, our business may be materially harmed.
We do not independently conduct clinical trials of eravacycline. We rely on third parties, such as contract research organizations, clinical data management organizations, medical institutions and clinical investigators, to conduct our clinical trials for eravacycline and expect to rely on these third parties to conduct clinical trials of any other product candidate that we develop. Any of these third parties may terminate their engagements with us at any time. If we need to enter into alternative arrangements, it would delay our product development activities.
Our reliance on these third parties for clinical development activities limits our control over these activities but we remain responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards. For example, notwithstanding the obligations of a contract research organization for a trial of one of our product candidates, we remain responsible for ensuring that each of our clinical trials is conducted in accordance with the general investigational plan and protocols for the trial. Moreover, the FDA requires us to comply with standards, commonly referred to as current Good Clinical Practices, or cGCPs, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. The FDA enforces these cGCPs through periodic inspections of trial sponsors, principal investigators, clinical trial sites and institutional review boards. If we or our third party contractors fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA may require us to perform additional clinical trials before approving our product candidates, which would delay the regulatory approval process. We cannot be certain that, upon inspection, the FDA will determine that any of our clinical trials comply with cGCPs. We are also required to register clinical trials and post the results of completed clinical trials on a government-sponsored database, ClinicalTrials.gov, within certain timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
Furthermore, the third parties conducting clinical trials on our behalf are not our employees, and except for remedies available to us under our agreements with such contractors, we cannot control whether or not they devote sufficient time and resources to our ongoing development programs. These contractors may also have
58
Table of Contents
relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical trials or other drug development activities, which could impede their ability to devote appropriate time to our clinical programs. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with regulatory requirements or our stated protocols, we may not be able to obtain, or may be delayed in obtaining, marketing approvals for our product candidates. If that occurs, we will not be able to, or may be delayed in our efforts to, successfully commercialize our product candidates. In such an event, our financial results and the commercial prospects for eravacycline or any other product candidates that we seek to develop could be harmed, our costs could increase and our ability to generate revenues could be delayed, impaired or foreclosed.
We also rely on other third parties to store and distribute drug supplies for our clinical trials. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidates or commercialization of any resulting products, producing additional losses and depriving us of potential product revenue.
We contract with third parties for the manufacture of eravacycline for clinical trials and expect to continue to do so in connection with the commercialization of eravacycline and for clinical trials and commercialization of any other product candidates that we develop. This reliance on third parties increases the risk that we will not have sufficient quantities of our product candidates or such quantities at an acceptable cost, which could delay, prevent or impair our development or commercialization efforts.
We do not currently have nor do we plan to build the internal infrastructure or capability to manufacture eravacycline or our other product candidates for use in the conduct of our clinical trials or for commercial supply. We currently rely on and expect to continue to rely on third-party contract manufacturers to manufacture clinical supplies of eravacycline and our other product candidates, and we expect to rely on third party contract manufacturers to manufacture registration batches and commercial quantities of any product candidate that we commercialize following approval for marketing by applicable regulatory authorities. Reliance on third-party manufacturers entails risks, including:
| • | delays in the manufacture of our registration batches and commercial supply if our third-party manufacturers give greater priority to the supply of other products over our product candidates or otherwise do not satisfactorily perform according to the terms of the agreement between us; |
| • | the possible termination or nonrenewal of the agreement by the third party at a time that is costly or inconvenient for us; |
| • | the possible breach of the manufacturing agreement by the third party; |
| • | the failure of the third-party manufacturer to comply with applicable regulatory requirements; and |
| • | the possible misappropriation of our proprietary information, including our trade secrets and know-how. |
We currently rely on a small number of third-party contract manufacturers for all of our required raw materials, drug substance and finished product for our preclinical research and clinical trials. We do not have long-term agreements with any of these third parties. We also do not have any current contractual relationships for the manufacture of commercial supplies of any of our other product candidates. If any of our existing manufacturers should become unavailable to us for any reason, we may incur some delay in identifying or qualifying replacements.
If any of our product candidates are approved by any regulatory agency, we intend to enter into agreements with third-party contract manufacturers for the commercial production of those products. This process is difficult and time consuming and we may face competition for access to manufacturing facilities as there are a limited number of contract manufacturers operating under cGMPs that are capable of manufacturing our product candidates. Consequently, we may not be able to reach agreement with third-party manufacturers on satisfactory terms, which could delay our commercialization.
59
Table of Contents
Third-party manufacturers are required to comply with cGMPs and similar regulatory requirements outside the United States. Facilities used by our third-party manufacturers must be inspected by the FDA after we submit an NDA and before potential approval of the product candidate. Similar regulations apply to manufacturers of our product candidates for use or sale in foreign countries. We do not control the manufacturing process and are completely dependent on our third-party manufacturers for compliance with the applicable regulatory requirements for the manufacture of our product candidates. If our manufacturers cannot successfully manufacture material that conforms to the strict regulatory requirements of the FDA and any applicable foreign regulatory authority, they will not be able to secure the applicable approval for their manufacturing facilities. If these facilities are not approved for commercial manufacture, we may need to find alternative manufacturing facilities, which could result in delays in obtaining approval for the applicable product candidate. In addition, our manufacturers are subject to ongoing periodic unannounced inspections by the FDA and corresponding state and foreign agencies for compliance with cGMPs and similar regulatory requirements. Failure by any of our manufacturers to comply with applicable cGMPs or other regulatory requirements could result in sanctions being imposed on us or the contract manufacturer, including fines, injunctions, civil penalties, delays, suspensions or withdrawals of approvals, operating restrictions, interruptions in supply and criminal prosecutions, any of which could significantly and adversely affect supplies of our product candidates and have a material adverse impact on our business, financial condition and results of operations.
Our current and anticipated future dependence upon others for the manufacture of eravacycline and any other product candidate that we develop may adversely affect our future profit margins and our ability to commercialize any products that receive marketing approval on a timely and competitive basis.
If we fail to comply with our obligations in the agreements under which we in-license or acquire development or commercialization rights to products or technology from third parties, we could lose commercial rights that are important to our business.
We are a party to a license agreement with Harvard that imposes, and we may enter into additional agreements, including license agreements, with other parties in the future that impose, diligence, development and commercialization timelines, milestone payment, royalty, insurance and other obligations on us. For instance, under our license agreement with Harvard, we are obligated to satisfy diligence requirements, including using commercially reasonable efforts to develop and commercialize licensed compounds and to implement a specified development plan, meeting specified development milestones and providing an update on progress on an annual basis. If we fail to comply with these obligations, our counterparties may have the right to terminate these agreements, in which event we might not be able to develop, manufacture or market any product that is covered by these agreements, which could materially adversely affect the value of the product candidate being developed under any such agreement. Termination of these agreements or reduction or elimination of our rights under these agreements may result in our having to negotiate new or reinstated agreements with less favorable terms, or cause us to lose our rights under these agreements, including our rights to important intellectual property or technology.
Our reliance on government funding for certain of our programs adds uncertainty to our research and commercialization efforts with respect to those programs and may impose requirements that increase the costs of commercialization and production of product candidates developed under those government-funded programs.
Our development of eravacycline for the treatment of disease caused by bacterial biothreat pathogens and certain life-threatening multidrug-resistant bacteria is currently being funded through a subcontract with funding from BARDA. In addition, our development of TP-271 is being funded through a subcontract and grant subaward with funding from the NIH’s NIAID division. Contracts and grants funded by the U.S. government and its agencies, including our agreements funded by BARDA and NIAID, include provisions that reflect the government’s substantial rights and remedies, many of which are not typically found in commercial contracts, including powers of the government to:
| • | terminate agreements, in whole or in part, for any reason or no reason; |
60
Table of Contents
| • | reduce or modify the government’s obligations under such agreements without the consent of the other party; |
| • | claim rights, including intellectual property rights, in products and data developed under such agreements; |
| • | audit contract-related costs and fees, including allocated indirect costs; |
| • | suspend the contractor or grantee from receiving new contracts pending resolution of alleged violations of procurement laws or regulations; |
| • | impose U.S. manufacturing requirements for products that embody inventions conceived or first reduced to practice under such agreements; |
| • | suspend or debar the contractor or grantee from doing future business with the government; |
| • | control and potentially prohibit the export of products; |
| • | pursue criminal or civil remedies under the False Claims Act, False Statements Act and similar remedy provisions specific to government agreements; and |
| • | limit the government’s financial liability to amounts appropriated by the U.S. Congress on a fiscal-year basis, thereby leaving some uncertainty about the future availability of funding for a program even after it has been funded for an initial period. |
We may not have the right to prohibit the U.S. government from using certain technologies developed by us, and we may not be able to prohibit third party companies, including our competitors, from using those technologies in providing products and services to the U.S. government. The U.S. government generally takes the position that it has the right to royalty-free use of technologies that are developed under U.S. government contracts.
In addition, government contracts and grants, and subcontracts and subawards awarded in the performance of those contracts and grants, normally contain additional requirements that may increase our costs of doing business, reduce our profits, and expose us to liability for failure to comply with these terms and conditions. These requirements include, for example:
| • | specialized accounting systems unique to government contracts and grants; |
| • | mandatory financial audits and potential liability for price adjustments or recoupment of government funds after such funds have been spent; |
| • | public disclosures of certain contract and grant information, which may enable competitors to gain insights into our research program; and |
| • | mandatory socioeconomic compliance requirements, including labor standards, non-discrimination and affirmative action programs and environmental compliance requirements. |
As an organization, we are relatively new to government contracting and new to the regulatory compliance obligations that such contracting entails. If we fail to maintain compliance with those obligations, we may be subject to potential liability and to termination of our contracts.
As a U.S. government contractor, we are subject to financial audits and other reviews by the U.S. government of our costs and performance on their contracts, as well as our accounting and general business practices related to these contracts. Based on the results of its audits, the government may adjust our contract-related costs and fees, including allocated indirect costs. Although adjustments arising from government audits and reviews have not had a material adverse effect on our financial condition or results of operations in the past, we cannot be certain that future audits and reviews will not have those effects.
61
Table of Contents
Risks Related to Our Intellectual Property
If we are unable to obtain and maintain sufficient patent protection for our technology or our product candidates, or if the scope of the patent protection is not sufficiently broad, our competitors could develop and commercialize technology and products similar or identical to ours, and our ability to successfully commercialize our technology and product candidates may be adversely affected.
Our success depends in large part on our ability to obtain and maintain patent protection in the United States and other countries with respect to our proprietary chemistry technology and product candidates. If we do not adequately protect our intellectual property, competitors may be able to use our technologies and erode or negate any competitive advantage we may have, which could harm our business and ability to achieve profitability. To protect our proprietary position, we file patent applications in the United States and abroad related to our novel technologies and product candidates that are important to our business. The patent application and approval process is expensive and time consuming. We may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. We may also fail to identify patentable aspects of our research and development before it is too late to obtain patent protection.
Under our license agreement with Harvard, Harvard retains the right to prosecute and maintain specified Harvard patents and patent applications in the field of tetracycline chemistry, which are exclusively licensed to us under the agreement. Moreover, if we license technology or product candidates from third parties in the future, those licensors may retain the right to prosecute, maintain and enforce the patent rights that they license to us with or without our involvement. Because control of prosecution and maintenance rests with Harvard, and prosecution, maintenance and enforcement could rest with future licensors, we cannot be certain that these in-licensed patents and applications will be prosecuted, maintained and enforced in a manner consistent with the best interests of our business. If Harvard fails to prosecute or maintain, or future licensors fail to prosecute, maintain or enforce, those patents necessary for any of our product candidates, our ability to develop and commercialize those product candidates may be adversely affected and we may not be able to prevent competitors from making and selling competing products.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain. No consistent policy regarding the breadth of claims allowed in biotechnology and pharmaceutical patents has emerged to date in the United States or in many foreign jurisdictions. In addition, the determination of patent rights with respect to pharmaceutical compounds and technologies commonly involves complex legal and factual questions, which has in recent years been the subject of much litigation. As a result, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain. Furthermore, recent changes in patent laws in the United States, including the America Invents Act of 2011, may affect the scope, strength and enforceability of our patent rights or the nature of proceedings which may be brought by us related to our patent rights.
Our pending and future patent applications may not result in patents being issued that protect our technology or product candidates, in whole or in part, or that effectively prevent others from commercializing competitive technologies and products. Changes in either the patent laws or interpretation of the patent laws in the United States and other countries may diminish the value of our patents or narrow the scope of our patent protection.
As a result of the America Invents Act of 2011, the United States transitioned to a first-inventor-to-file system in March 2013, under which, assuming the other requirements for patentability are met, the first inventor to file a patent application is entitled to the patent. However, as a result of the lag in the publication of patent applications following filing in the United States, we are not be able to be certain upon filing that we are the first to file for patent protection for any invention. Moreover, we may be subject to a third party preissuance submission of prior art to the U.S. Patent and Trademark Office, or become involved in opposition, derivation, reexamination, inter partes review or interference proceedings, in the United States or elsewhere, challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of or invalidate our patent rights, allow third parties to commercialize our
62
Table of Contents
technology or product candidates and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights.
Even if our patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our owned or licensed patents by developing similar or alternative technologies or products in a non-infringing manner. Our competitors may seek to market generic versions of any approved products by submitting Abbreviated New Drug Applications to the FDA in which they claim that patents owned or licensed by us are invalid, unenforceable and/or not infringed. Alternatively, our competitors may seek approval to market their own products similar to or otherwise competitive with our products. In these circumstances, we may need to defend and/or assert our patents, including by filing lawsuits alleging patent infringement. In any of these types of proceedings, a court or other agency with jurisdiction may find our patents invalid and/or unenforceable. Even if we have valid and enforceable patents, these patents still may not provide protection against competing products or processes sufficient to achieve our business objectives.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our owned and licensed patents may be challenged in the courts or patent offices in the United States and abroad. Such challenges may result in loss of exclusivity or freedom to operate or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. In addition, given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized.
We may become involved in lawsuits to protect or enforce our patents or other intellectual property, which could be expensive, time consuming and unsuccessful.
Competitors may infringe our patents, trademarks, copyrights or other intellectual property, or those of our licensors. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time consuming and divert the time and attention of our management and scientific personnel. Any claims we assert against perceived infringers could provoke these parties to assert counterclaims against us alleging that we infringe their patents. In addition, in a patent infringement proceeding, there is a risk that a court will decide that a patent of ours is invalid or unenforceable, in whole or in part, and that we do not have the right to stop the other party from using the invention at issue. There is also a risk that, even if the validity of such patents is upheld, the court will construe the patent’s claims narrowly or decide that we do not have the right to stop the other party from using the invention at issue on the grounds that our patents do not cover the invention. An adverse outcome in a litigation or proceeding involving our patents could limit our ability to assert our patents against those parties or other competitors, and may curtail or preclude our ability to exclude third parties from making and selling similar or competitive products. Any of these occurrences could adversely affect our competitive business position, business prospects and financial condition. Similarly, if we assert trademark infringement claims, a court may determine that the marks we have asserted are invalid or unenforceable, or that the party against whom we have asserted trademark infringement has superior rights to the marks in question. In this case, we could ultimately be forced to cease use of such trademarks.
In any infringement litigation, any award of monetary damages we receive may not be commercially valuable. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during litigation. Moreover, there can be no assurance that we will have sufficient financial or other resources to file and pursue such infringement claims, which typically last for years before they are concluded. Even if we ultimately prevail in such claims, the monetary cost of such litigation and the diversion of the attention of our management and scientific personnel could outweigh any benefit we receive as a result of the proceedings.
63
Table of Contents
If we are sued for infringing intellectual property rights of third parties, such litigation could be costly and time consuming and could prevent or delay us from developing or commercializing our product candidates.
Our commercial success depends, in part, on our ability to develop, manufacture, market and sell our product candidates and use our proprietary chemistry technology without infringing the intellectual property and other proprietary rights of third parties. Numerous third-party U.S. and non-U.S. issued patents and pending applications exist in the area of antibacterial treatment, including compounds, formulations, treatment methods and synthetic processes that may be applied towards the synthesis of antibiotics. If any of their patents or patent applications cover our product candidates or technologies, we may not be free to manufacture or market our product candidates as planned.
There is a substantial amount of intellectual property litigation in the biotechnology and pharmaceutical industries, and we may become party to, or threatened with, litigation or other adversarial proceedings regarding intellectual property rights with respect to our technology or products candidates, including interference proceedings before the U.S. Patent and Trademark Office. Third parties may assert infringement claims against us based on existing or future intellectual property rights. The outcome of intellectual property litigation is subject to uncertainties that cannot be adequately quantified in advance. The pharmaceutical and biotechnology industries have produced a significant number of patents, and it may not always be clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform. If we are sued for patent infringement, we would need to demonstrate that our product candidates, products or methods either do not infringe the patent claims of the relevant patent or that the patent claims are invalid, and we may not be able to do this. Proving invalidity is difficult. For example, in the United States, proving invalidity requires a showing of clear and convincing evidence to overcome the presumption of validity enjoyed by issued patents. Even if we are successful in these proceedings, we may incur substantial costs and the time and attention of our management and scientific personnel could be diverted in pursuing these proceedings, which could have a material adverse effect on us. In addition, we may not have sufficient resources to bring these actions to a successful conclusion.
If we are found to infringe a third party’s intellectual property rights, we could be forced, including by court order, to cease developing, manufacturing or commercializing the infringing product candidate or product. Alternatively, we may be required to obtain a license from such third party in order to use the infringing technology and continue developing, manufacturing or marketing the infringing product candidate. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if we were able to obtain a license, it could be non-exclusive, thereby giving our competitors access to the same technologies licensed to us. In addition, we could be found liable for monetary damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent. A finding of infringement could prevent us from commercializing our product candidates or force us to cease some of our business operations, which could materially harm our business. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative impact on our business.
We may be subject to claims that we or our employees have misappropriated the intellectual property of a third party, or claiming ownership of what we regard as our own intellectual property.
Many of our employees were previously employed at universities or other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although we try to ensure that our employees do not use the intellectual property and other proprietary information or know-how of others in their work for us, we may be subject to claims that we or these employees have used or disclosed such intellectual property or other proprietary information. Litigation may be necessary to defend against these claims.
In addition, while we typically require our employees, consultants and contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact develops intellectual property that
64
Table of Contents
we regard as our own. Moreover, because we have licensed intellectual property from Harvard, we must rely on Harvard’s practices with regard to the assignment of intellectual property to it. To the extent we or Harvard have failed to obtain such assignments or such assignments are breached, we may be forced to bring claims against third parties, or defend claims they may bring against us, to determine the ownership of what we regard as our intellectual property. If we fail in prosecuting or defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in prosecuting or defending against such claims, litigation could result in substantial costs and be a distraction to our management and scientific personnel.
If we are unable to protect the confidentiality of our trade secrets, the value of our technology could be materially adversely affected and our business would be harmed.
In addition to seeking patents for some of our technology and products, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, in seeking to develop and maintain a competitive position. We seek to protect these trade secrets, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our consultants, independent contractors, advisors, corporate collaborators, outside scientific collaborators, contract manufacturers, suppliers and other third parties. We, as well as our licensors, also enter into confidentiality and invention or patent assignment agreements with employees and certain consultants. Any party with whom we or Harvard have executed such an agreement may breach that agreement and disclose our proprietary information, including our trade secrets, and we may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, if any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent such third party, or those to whom they communicate such technology or information, from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our business and competitive position could be harmed.
We have not yet registered our trademarks. Failure to secure those registrations could adversely affect our business.
We have not yet registered our trademarks in the United States or other countries. If we do not secure registrations for our trademarks, we may encounter more difficulty in enforcing them against third parties than we otherwise would, which could adversely affect our business. We have also not yet registered trademarks for any of our product candidates in any jurisdiction. When we file trademark applications for our product candidates those applications may not be allowed for registration, and registered trademarks may not be obtained, maintained or enforced. During trademark registration proceedings in the United States and foreign jurisdictions, we may receive rejections. We are given an opportunity to respond to those rejections, but we may not be able to overcome such rejections. In addition, in the United States Patent and Trademark Office and in comparable agencies in many foreign jurisdictions, third parties are given an opportunity to oppose pending trademark applications and to seek to cancel registered trademarks. Opposition or cancellation proceedings may be filed against our trademarks, and our trademarks may not survive such proceedings.
In addition, any proprietary name we propose to use with eravacycline or any other product candidate in the United States must be approved by the FDA, regardless of whether we have registered it, or applied to register it, as a trademark. The FDA typically conducts a review of proposed product names, including an evaluation of potential for confusion with other product names. If the FDA objects to any of our proposed proprietary product names, we may be required to expend significant additional resources in an effort to identify a suitable proprietary product name that would qualify under applicable trademark laws, not infringe the existing rights of third parties and be acceptable to the FDA.
65
Table of Contents
Risks Related to Regulatory Approval and Other Legal Compliance Matters
If we are not able to obtain, or if there are delays in obtaining, required regulatory approvals, we will not be able to commercialize eravacycline or any other product candidate that we develop, and our ability to generate revenue will be materially impaired.
Our product candidates, including eravacycline, and the activities associated with their development and commercialization, including their design, testing, manufacture, safety, efficacy, recordkeeping, labeling, storage, approval, advertising, promotion, sale and distribution, are subject to comprehensive regulation by the FDA and other regulatory agencies in the United States and by comparable foreign regulatory authorities, with regulations differing from country to country. Failure to obtain marketing approval for a product candidate will prevent us from commercializing the product candidate. We currently do not have any products approved for sale in any jurisdiction. We have only limited experience in filing and supporting the applications necessary to gain marketing approvals and expect to rely on third-party contract research organizations to assist us in this process.
We are not permitted to market our product candidates in the United States until we receive approval of an NDA from the FDA. We have not submitted an NDA for any of our product candidates. An NDA must include extensive preclinical and clinical data and supporting information to establish the product candidate’s safety and efficacy for each desired indication. The NDA must also include significant information regarding the chemistry, manufacturing and controls for the product candidate. Obtaining approval of an NDA is a lengthy, expensive and uncertain process. The FDA review process typically takes years to complete. The FDA has substantial discretion in the approval process and may refuse to accept for filing any application or may decide that our data are insufficient for approval and require additional preclinical, clinical or other studies. Foreign regulatory authorities have differing requirements for approval of drug candidates with which we must comply prior to marketing. Obtaining marketing approval for marketing of a product candidate in one country does not ensure that we will be able to obtain marketing approval in other countries, but the failure to obtain marketing approval in one jurisdiction could negatively impact our ability to obtain marketing approval in other jurisdictions. Delays in approvals or rejections of marketing applications in the United States or foreign countries may be based upon many factors, including regulatory requests for additional analyses, reports, data and studies, regulatory questions regarding, or different interpretations of, data and results, changes in regulatory policy during the period of product development and the emergence of new information regarding product candidates or related products. The FDA or other regulatory authorities may determine that eravacycline or any other product candidate that we develop is not effective, or is only moderately effective, or has undesirable or unintended side effects, toxicities, safety profile or other characteristics that preclude marketing approval or prevent or limit commercial use. In addition, any marketing approval we ultimately obtain may be limited or subject to restrictions or post-approval commitments that render the approved product not commercially viable. If we experience delays in obtaining approval or if we fail to obtain approval of eravacycline or any other product candidate that we develop, the commercial prospects for eravacycline or such other product candidate may be harmed and our ability to generate revenues will be materially impaired.
A fast track designation by the FDA does not guarantee approval and may not actually lead to a faster development, regulatory review or approval process.
If a product is intended for the treatment of a serious or life-threatening condition and the product demonstrates the potential to address unmet medical needs for that condition, the treatment sponsor may apply for FDA fast track designation. In April 2014, the FDA notified us that we received fast track designation for both the cIAI and cUTI indications and the intravenous and oral formulations of eravacycline. Fast track designation does not ensure approval or a faster development, regulatory review or approval process compared to conventional FDA procedures. Additionally, the FDA may withdraw fast track designation if it believes that the designation is no longer supported by data from our clinical development program.
66
Table of Contents
If we are unable to obtain marketing approval in international jurisdictions, we will not be able to market our product candidates abroad.
In order to market and sell eravacycline and any other product candidate that we develop in the European Union and many other jurisdictions, we must obtain separate marketing approvals and comply with numerous and varying regulatory requirements. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA. The approval procedure varies among countries and can involve additional testing. In addition, clinical trials conducted in one country may not be accepted by regulatory authorities in other countries. The time required to obtain approval may differ substantially from that required to obtain FDA approval. The regulatory approval process outside the United States generally includes all of the risks associated with obtaining FDA approval. In addition, in many countries outside the United States, it is required that the product be approved for reimbursement before the product can be approved for sale in that country. We may not obtain approvals from regulatory authorities outside the United States on a timely basis or at all.
If we receive regulatory approval for any product candidates, including eravacycline, we will be subject to ongoing obligations and continuing regulatory review, which may result in significant additional expense. Our product candidates, including eravacycline, if approved, could be subject to restrictions or withdrawal from the market, and we may be subject to penalties, if we fail to comply with regulatory requirements or if we experience unanticipated problems with our product candidates, when and if approved.
Any product candidate, including eravacycline, for which we obtain marketing approval, will also be subject to ongoing regulatory requirements for labeling, packaging, storage, distribution, advertising, promotion, record-keeping and submission of safety and other post-market information. For example, approved products, manufacturers and manufacturers’ facilities are required to comply with extensive FDA requirements, including ensuring that quality control and manufacturing procedures conform to cGMPs. As such, we and our contract manufacturers will be subject to continual review and periodic inspections to assess compliance with cGMPs. Accordingly, we and others with whom we work must continue to expend time, money and effort in all areas of regulatory compliance, including manufacturing, production and quality control. We will also be required to report certain adverse reactions and production problems, if any, to the FDA and to comply with requirements concerning advertising and promotion for our products.
In addition, even if marketing approval of a product candidate is granted, the approval may be subject to limitations on the indicated uses for which the product may be marketed, may be subject to significant conditions of approval or may impose requirements for costly post-marketing testing and surveillance to monitor the safety or efficacy of the product. The FDA closely regulates the post-approval marketing and promotion of drugs to ensure drugs are marketed only for the approved indications and in accordance with the provisions of the approved labeling and regulatory requirements. The FDA also imposes stringent restrictions on manufacturers’ communications regarding off-label use and if we do not restrict the marketing of our products only to their approved indications, we may be subject to enforcement action for off-label marketing.
If a regulatory agency discovers previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is manufactured, or disagrees with the promotion, marketing or labeling of a product, it may impose restrictions on that product or us. In addition, if any product fails to comply with applicable regulatory requirements, a regulatory agency may:
| • | issue warning or untitled letters; |
| • | mandate modifications to promotional materials or require provision of corrective information to healthcare practitioners; |
| • | impose restrictions on the product or its manufacturers or manufacturing processes; |
| • | impose restrictions on the labeling or marketing of the product; |
67
Table of Contents
| • | impose restrictions on product distribution or use; |
| • | require post-marketing clinical trials; |
| • | require withdrawal of the product from the market; |
| • | refuse to approve pending applications or supplements to approved applications that we submit; |
| • | require recall of the product; |
| • | require entry into a consent decree, which can include imposition of various fines (including restitution or disgorgement of profits or revenue), reimbursements for inspection costs, required due dates for specific actions and penalties for noncompliance; |
| • | suspend or withdraw marketing approvals; |
| • | refuse to permit the import or export of the product; |
| • | seize or detain supplies of the product; or |
| • | issue injunctions or impose civil or criminal penalties. |
Our relationships with customers and third-party payors will be subject to applicable anti-kickback, fraud and abuse and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Our future arrangements with third-party payors, healthcare professionals and customers who purchase, recommend or prescribe our product candidates will be subject to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute any products for which we obtain marketing approval. These laws and regulations include, for example, the false claims and anti-kickback statutes and regulations. At such time as we market, sell and distribute any products for which we obtain marketing approval, it is possible that our business activities could be subject to challenge under one or more of these laws and regulations. Restrictions under applicable federal and state healthcare laws and regulations include the following:
| • | the federal Anti-Kickback Statute, among other things, prohibits persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federally funded healthcare programs such as Medicare and Medicaid; |
| • | the federal False Claims Act imposes criminal and civil penalties, which can be enforced by private citizens through civil whistleblower and qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| • | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program and creates federal criminal laws that prohibit knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| • | the federal false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| • | the federal transparency requirements under the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively, the ACA, requires |
68
Table of Contents
| manufacturers of covered drugs, devices, biologics and medical supplies to report to the Department of Health and Human Services information related to payments and other transfers of value to physicians and teaching hospitals and physician ownership and investment interests; and |
| • | analogous state laws and regulations, such as state anti-kickback and false claims laws that may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payors, including private insurers; state laws that require pharmaceutical companies to implement compliance programs, comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government or track and report gifts, compensation and other remuneration provided to physicians and other health care providers; and state and foreign laws that govern the privacy and security of health information in specified circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, which complicates compliance efforts. |
We will be required to spend substantial time and money to ensure that our business arrangements with third parties comply with applicable healthcare laws and regulations. Even then, governmental authorities may conclude that our business practices do not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. Recent healthcare reform legislation has strengthened these federal and state healthcare laws. For example, the ACA amends the intent requirement of the federal anti-kickback and criminal healthcare fraud statutes. A person or entity no longer needs to have actual knowledge of these statutes or a specific intent to violate them. In addition, the ACA provides that the government may assert that a claim that includes items or services resulting from a violation of the federal anti-kickback statute constitutes a false or fraudulent claim for purposes of the False Claims Act. If governmental authorities find that our operations violate any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, exclusion from government funded healthcare programs, such as Medicare and Medicaid, and we may be required to curtail or restructure our operations. Moreover, we expect that there will continue to be federal and state laws and regulations, proposed and implemented, that could impact our operations and business. The extent to which future legislation or regulations, if any, relating to healthcare fraud and abuse laws or enforcement, may be enacted or what effect such legislation or regulation would have on our business remains uncertain.
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain.
Among policy makers and payors in the United States and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality and expanding access to healthcare. In the United States, the pharmaceutical industry has been a particular focus of these efforts and has been significantly affected by major legislative initiatives. We expect to experience pricing pressures in connection with the sale of any products that we develop, due to the trend toward managed healthcare, the increasing influence of health maintenance organizations and additional legislative proposals.
In March 2010, the ACA became law in the United States with the goals of broadening access to health insurance, reducing or constraining the growth of healthcare spending, enhancing remedies against fraud and abuse, adding new transparency requirements for health care and health insurance industries and imposing additional health policy reforms. Further, the new law includes annual fees to be paid by manufacturers for certain branded prescription drugs, requires manufacturers to participate in a discount program for certain outpatient drugs under Medicare Part D, increases manufacturer rebate responsibilities under the Medicaid Drug Rebate Program for outpatient drugs dispensed to Medicaid recipients, addresses a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for line extensions and for drugs that are inhaled, infused, instilled, implanted or injected and expands oversight and support for the federal government’s comparative effectiveness research of services and products.
69
Table of Contents
In addition, other legislative changes have been proposed and adopted in the United States since the ACA was enacted. On August 2, 2011, the Budget Control Act of 2011 created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs. This includes aggregate reductions of Medicare payments to providers of up to 2% per fiscal year, which went into effect on April 1, 2013. On January 2, 2013, President Obama signed into law the American Taxpayer Relief Act of 2012 which reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. We expect that additional state and federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our product candidates or additional pricing pressures.
Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be. In addition, increased scrutiny by the United States Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
Risks Related to Employee Matters and Managing Growth
Our future success depends on our ability to retain our chief executive officer and other key executives and to attract, retain and motivate qualified personnel.
Our industry has experienced a high rate of turnover of management personnel in recent years. We are highly dependent on the development, regulatory, commercialization and business development expertise of Guy Macdonald, our President and Chief Executive Officer, Patrick T. Horn, our Chief Medical Officer, David C. Lubner, our Senior Vice President and Chief Financial Officer, and J. Craig Thompson, our Chief Operating Officer, as well as the other principal members of our management, scientific and clinical team. Although we have formal employment agreements with our executive officers, these agreements do not prevent them from terminating their employment with us at any time.
We do not have formal employment agreements with any of our other employees. If we lose one or more of our executive officers or key employees, our ability to implement our business strategy successfully could be seriously harmed. Furthermore, replacing executive officers and key employees may be difficult and may take an extended period of time because of the limited number of individuals in our industry with the breadth of skills and experience required to develop, gain regulatory approval of and commercialize products successfully. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these additional key personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. We also experience competition for the hiring of scientific and clinical personnel from universities and research institutions. In addition, we rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our research and development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us. If we are unable to continue to attract and retain high quality personnel, our ability to develop and commercialize drug candidates will be limited.
We expect to grow our organization, and as a result, we may encounter difficulties in managing our growth, which could disrupt our operations.
We expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of drug development, regulatory affairs and sales, marketing and distribution. Our
70
Table of Contents
management may need to divert a disproportionate amount of its attention away from our day-to-day activities to devote time to managing these growth activities. To manage these growth activities, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel. Our inability to effectively manage the expansion of our operations may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. Our expected growth could require significant capital expenditures and may divert financial resources from other projects, such as the development of additional product candidates. If our management is unable to effectively manage our expected growth, our expenses may increase more than expected, our ability to generate revenues could be reduced and we may not be able to implement our business strategy.
The business that we conduct outside the United States may be adversely affected by international risk and uncertainties.
Although our operations are based in the United States, we conduct business outside the United States and expect to continue to do so in the future. For instance, many of the sites at which our clinical trial is being conducted are outside the United States. In addition, we plan to seek approvals to sell our products in foreign countries. Any business that we conduct outside the United States will be subject to additional risks that may materially adversely affect our ability to conduct business in international markets, including:
| • | potentially reduced protection for intellectual property rights; |
| • | the potential for so-called parallel importing, which is what happens when a local seller, faced with high or higher local prices, opts to import goods from a foreign market (with low or lower prices) rather than buying them locally; |
| • | unexpected changes in tariffs, trade barriers and regulatory requirements; |
| • | economic weakness, including inflation, or political instability in particular foreign economies and markets; |
| • | workforce uncertainty in countries where labor unrest is more common than in the United States; |
| • | production shortages resulting from any events affecting a product candidate and/or finished drug product supply or manufacturing capabilities abroad; |
| • | business interruptions resulting from geo-political actions, including war and terrorism, or natural disasters, including earthquakes, hurricanes, typhoons, floods and fires; and |
| • | failure to comply with Office of Foreign Asset Control rules and regulations and the Foreign Corrupt Practices Act. |
As an example, some of the sites in our ongoing Phase 3 clinical trial of eravacycline are located in Ukraine and Russia and we expect a considerable portion of the patients enrolled in the clinical trial to be from Ukraine and Russia. If the dispute between Ukraine and Russia were to further destabilize the region, our ability to conduct and complete our Phase 3 clinical trial on a timely basis could be impacted, and our business, financial condition and results of operations could be materially adversely affected.
71
Table of Contents
Risks Related to Our Common Stock
The price of our common stock may be volatile and fluctuate substantially, which could result in substantial losses for purchasers of our common stock.
Our stock price may be volatile. The stock market in general and the market for smaller pharmaceutical and biotechnology companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. For example, our stock traded within a range of a high price of $44.55 per share and a low price of $6.62 per share for the period beginning March 20, 2013, our first day of trading on the NASDAQ Global Select Market, through February 28, 2015. As a result of this volatility, investors may not be able to sell their common stock at or above the prices they paid for it. The market price for our common stock may be influenced by many factors, including:
| • | the success of existing or new competitive products or technologies; |
| • | the timing of clinical trials of eravacycline and any other product candidate; |
| • | results of clinical trials of eravacycline and any other product candidate; |
| • | regulatory actions by the FDA or equivalent authorities in foreign jurisdictions with respect to eravacycline and any other product candidate; |
| • | failure or discontinuation of any of our development programs; |
| • | results of clinical trials of product candidates of our competitors; |
| • | regulatory or legal developments in the United States and other countries; |
| • | developments or disputes concerning patent applications, issued patents or other proprietary rights; |
| • | the recruitment or departure of key personnel; |
| • | the level of expenses related to any of our product candidates or clinical development programs; |
| • | the results of our efforts to develop, in-license or acquire additional product candidates or products; |
| • | actual or anticipated changes in estimates as to financial results, development timelines or recommendations by securities analysts; |
| • | announcement or expectation of additional financing efforts; |
| • | sales of our common stock by us, our insiders or other stockholders |
| • | variations in our financial results or those of companies that are perceived to be similar to us; |
| • | changes in estimates or recommendations by securities analysts, if any, that cover our stock; |
| • | changes in the structure of healthcare payment systems; |
| • | market conditions in the pharmaceutical and biotechnology sectors; |
| • | general economic, industry and market conditions; and |
| • | the other factors described in this “Risk Factors” section. |
An active trading market for our common stock may not be sustained.
Although we have listed our common stock on The NASDAQ Global Select Market, an active trading market for our common stock may not be sustained. In the absence of an active trading market for our common stock, investors may not be able to sell their common stock at or above the price at which they acquired the common stock or at the times that they would like to sell. An inactive trading market may also impair our ability to raise capital to continue to fund operations by selling shares and may impair our ability to acquire other companies or technologies by using our shares as consideration.
72
Table of Contents
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our share price and trading volume could decline.
The trading market for our common stock will depend on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. There can be no assurance that analysts will cover us, or provide favorable coverage. If one or more analysts downgrade our stock or change their opinion of our stock, our share price would likely decline. In addition, if one or more analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause our share price or trading volume to decline.
We have broad discretion in the use of our cash reserves and may not use them effectively.
Our management has broad discretion to use our cash reserves and could spend these reserves in ways that do not improve our results of operations or enhance the value of our common stock. The failure by our management to apply these funds effectively could result in financial losses that could have a material adverse effect on our business, cause the price of our common stock to decline and delay the development of our product candidates. Pending their use, we may invest our cash reserves in a manner that does not produce income or that loses value.
We are an “emerging growth company,” and the reduced disclosure requirements applicable to emerging growth companies may make our common stock less attractive to investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, and may remain an emerging growth company for up to five years following our initial public offering in March 2013. For so long as we remain an emerging growth company, we are permitted and intend to rely on exemptions from certain disclosure requirements that are applicable to other public companies that are not emerging growth companies. These exemptions include not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, not being required to comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements, reduced disclosure obligations regarding executive compensation and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and shareholder approval of any golden parachute payments not previously approved. We cannot predict whether investors will find our common stock less attractive if we rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards and, therefore, are subject to the same new or revised accounting standards as other public companies that are not emerging growth companies.
Failure to maintain effective internal controls in accordance with Section 404 of the Sarbanes-Oxley Act could have a material adverse effect on our ability to produce accurate financial statements and on our stock price.
Section 404 of the Sarbanes-Oxley Act of 2002 requires us, on an annual basis beginning in 2014, to review and evaluate our internal controls. However, while we remain an emerging growth company, we will not be required to include an attestation report on internal control over financial reporting issued by our independent registered public accounting firm. To achieve compliance with Section 404 within the prescribed period, we have been engaged in a process to document and evaluate our internal control over financial reporting, which has been
73
Table of Contents
both costly and challenging. In this regard, we will need to continue to dedicate internal resources, continue to engage outside consultants and adopt a detailed work plan to continue to assess and document the adequacy of internal control over financial reporting, continue to improve control processes as appropriate, validate through testing that controls are functioning as documented and implement a continuous reporting and improvement process for internal control over financial reporting. There is a risk that neither we nor our independent registered public accounting firm will be able to conclude within the prescribed timeframe that our internal control over financial reporting is effective as required by Section 404. If we identify one or more material weaknesses, it could result in an adverse reaction in the financial markets due to a loss of confidence in the reliability of our financial statements.
We do not anticipate paying any cash dividends on our capital stock in the foreseeable future, accordingly, stockholders must rely on capital appreciation, if any, for any return on their investment.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the operation, development and growth of our business. The terms of our debt facility with Silicon Valley Bank and Oxford Finance preclude us from paying dividends, and any future debt agreements may also preclude us from paying dividends. As a result, capital appreciation, if any, of our common stock will be the sole source of gain for our stockholders for the foreseeable future.
Provisions in our corporate charter documents and under Delaware law could make an acquisition of us, which may be beneficial to our stockholders, more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our corporate charter and our by-laws may discourage, delay or prevent a merger, acquisition or other change in control of us that stockholders may consider favorable, including transactions in which our stockholders might otherwise receive a premium for their shares. These provisions could also limit the price that investors might be willing to pay in the future for shares of our common stock, thereby depressing the market price of our common stock. In addition, because our board of directors is responsible for appointing the members of our management team, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors. Among other things, these provisions:
| • | establish a classified board of directors such that all members of the board are not elected at one time; |
| • | allow the authorized number of our directors to be changed only by resolution of our board of directors; |
| • | limit the manner in which stockholders can remove directors from the board; |
| • | establish advance notice requirements for nominations for election to the board of directors or for proposing matters that can be acted on at stockholder meetings; |
| • | require that stockholder actions must be effected at a duly called stockholder meeting and prohibit actions by our stockholders by written consent; |
| • | limit who may call a special meeting of stockholder meetings; |
| • | authorize our board of directors to issue preferred stock without stockholder approval, which could be used to institute a “poison pill” that would work to dilute the stock ownership of a potential hostile acquirer, effectively preventing acquisitions that have not been approved by our board of directors; and |
| • | require the approval of the holders of at least 75% of the votes that all our stockholders would be entitled to cast to amend or repeal certain provisions of our charter or by-laws. |
Moreover, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which prohibits a person who owns in excess of 15% of our outstanding voting stock from merging or combining with us for a period of three years after the date of the transaction in
74
Table of Contents
which the person acquired in excess of 15% of our outstanding voting stock, unless the merger or combination is approved in a prescribed manner. This could discourage, delay or prevent someone from acquiring us or merging with us, whether or not it is desired by, or beneficial to, our stockholders.
| ITEM 1B. | Unresolved Staff Comments |
None
| ITEM 2. | Properties |
We lease our principal facilities, which consist of approximately 38,902 square feet of office, research and laboratory space located at 480 Arsenal Street, Watertown, Massachusetts. The leases covering this space expire on November 30, 2016. We believe that our existing facilities are sufficient for our current needs for the foreseeable future.
| ITEM 3. | Legal Proceedings |
We are not currently a party to any material legal proceedings.
| ITEM 4. | Mine Safety Disclosures |
Not applicable.
75
Table of Contents
| ITEM 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Market Price Information
Our common stock began trading on the NASDAQ Global Select Market on March 20, 2013 under the symbol “TTPH”. Prior to that date, there was no established public trading market for our common stock. The following table sets forth, for the periods indicated, the high and low intraday sales prices of our common stock as reported by the NASDAQ Global Select Market:
| High | Low | |||||||
| 2014 |
||||||||
| First Quarter |
$ | 17.74 | $ | 9.85 | ||||
| Second Quarter |
$ | 14.05 | $ | 8.01 | ||||
| Third Quarter |
$ | 20.62 | $ | 10.03 | ||||
| Fourth Quarter |
$ | 41.83 | $ | 19.55 | ||||
| High | Low | |||||||
| 2013 |
||||||||
| First Quarter from and after March 20, 2013 |
$ | 7.50 | $ | 6.62 | ||||
| Second Quarter |
$ | 9.66 | $ | 7.00 | ||||
| Third Quarter |
$ | 11.77 | $ | 7.04 | ||||
| Fourth Quarter |
$ | 13.89 | $ | 9.85 | ||||
Holders
At February 28, 2015, there were approximately 10 holders of record of our common stock. We believe that the number of beneficial owners of our common stock at that date was substantially greater.
Dividends
We have never declared or paid any cash dividends on our common stock and our ability to pay cash dividends is currently prohibited by the terms of our debt financing arrangements. We currently intend to retain earnings, if any, for use in our business and do not anticipate paying cash dividends on our common stock in the foreseeable future. Payment of future dividends, if any, on our common stock will be at the discretion of our board of directors after taking into account various factors, including our financial condition, operating results, anticipated cash needs, and plans for expansion.
Unregistered Sales of Equity Securities
On December 19, 2014, we issued to an affiliate of Oxford Finance (“Oxford Finance”) 20,488 shares of our common stock pursuant to the cashless exercise feature of warrants we had granted to Oxford Finance on May 16, 2011. Warrants to purchase 6,336 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants. We received no cash proceeds from the issuance of these shares upon exercise of the warrants.
On December 19, 2014, we issued to Oxford Finance 12,703 shares of our common stock pursuant to the cashless exercise feature of warrants we had granted to Oxford Finance on December 20, 2012. Warrants to purchase 3,928 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants. We received no cash proceeds from the issuance of these shares upon exercise of the warrants.
76
Table of Contents
On December 19, 2014, we issued to Oxford Finance 6,146 shares of our common stock pursuant to the cashless exercise feature of warrants we had granted to Oxford Finance on February 28, 2013. Warrants to purchase 1,901 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants. We received no cash proceeds from the issuance of these shares upon exercise of the warrants.
These warrants were granted, and the shares of common stock were issued upon exercise of these warrants, in reliance upon the exemption from the registration requirements of the Securities Act provided by Sections 3(a)(9) and 4(a)(2) of the Securities Act. No underwriters were involved in such issuances, and no commissions were paid in connection with such issuances.
Use Of Proceeds
We effected the initial public offering, or IPO, of our common stock through a Registration Statement on Form S-1 (File No. 333-186574) that was declared effective by the Securities and Exchange Commission on March 19, 2013. As of December 31, 2014, we had used all of the net proceeds from the IPO to fund the clinical development of eravacycline and for working capital, capital expenditures and other general corporate purposes. There was no material change in our planned use of proceeds from the IPO from that described in the final prospectus filed with the Securities and Exchange Commission pursuant to Rule 424(b) on March 20, 2013.
Comparative Stock Performance Graph
The information included under the heading “Comparative Stock Performance Graph” in this Item 5 of Part II of this annual report on Form 10-K shall not be deemed to be “soliciting material” or subject to Regulation 14A or 14C, shall not be deemed “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities of that section, nor shall it be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act.
77
Table of Contents
Set forth below is a graph comparing the total cumulative returns of Tetraphase, the NASDAQ Composite Index and the NASDAQ Biotechnology Index. The graph assumes $100 was invested on March 20, 2013 in our common stock and each of the indices and that all dividends, if any, are reinvested.
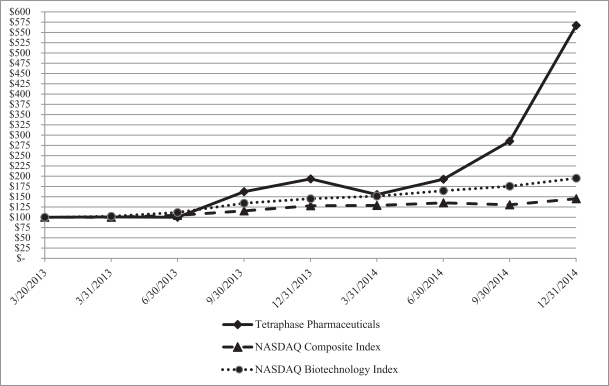
| 3/20/13 | 3/31/13 | 6/30/13 | 9/30/13 | 12/31/13 | 3/31/14 | 6/30/14 | 9/30/14 | 12/31/14 | ||||||||||||||||||||||||||||
| Tetraphase Pharmaceuticals |
$ | 100.00 | $ | 101.00 | $ | 100.43 | $ | 162.57 | $ | 193.14 | $ | 155.57 | $ | 192.71 | $ | 285.00 | $ | 567.29 | ||||||||||||||||||
| NASDAQ Composite Index |
$ | 100.00 | $ | 100.41 | $ | 104.58 | $ | 115.90 | $ | 128.34 | $ | 129.03 | $ | 135.46 | $ | 130.08 | $ | 145.54 | ||||||||||||||||||
| NASDAQ Biotechnology Index |
$ | 100.00 | $ | 102.51 | $ | 111.35 | $ | 134.43 | $ | 145.52 | $ | 151.62 | $ | 164.98 | $ | 175.58 | $ | 195.14 | ||||||||||||||||||
78
Table of Contents
| ITEM 6. | Selected Financial Data |
The following selected consolidated financial data should be read in conjunction with our Consolidated Financial Statements and the Notes thereto and Management’s Discussion and Analysis of Financial Condition and Results of Operations included elsewhere in this annual report on Form 10-K. The selected consolidated financial data in this section are not intended to replace our financial statements and the related notes. Our historical results are not necessarily indicative of the results that may be expected in the future.
The consolidated statement of operations data for each of the three years in the period ended December 31, 2014 and the consolidated balance sheet data at December 31, 2014 and 2013 have been derived from our audited consolidated financial statements for such years, included elsewhere in this annual report on Form 10-K. The statement of operations data for the year ended December 31, 2011 and the consolidated balance sheet data at December 31, 2012 and December 31, 2011 have been derived from the audited consolidated financial statements for such years not included in this annual report on Form 10-K.
Our historical results for any prior period are not necessarily indicative of results to be expected in any future period.
| Year Ended December 31, | ||||||||||||||||
| 2014 | 2013 | 2012 | 2011 | |||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| Statement of Operations data: |
||||||||||||||||
| Contract and grant revenue |
$ | 9,098 | $ | 10,486 | $ | 7,600 | $ | 185 | ||||||||
| Operating expenses: |
||||||||||||||||
| Research and development |
61,932 | 31,508 | 17,294 | 17,737 | ||||||||||||
| General and administrative |
12,932 | 7,168 | 4,309 | 3,874 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Total operating expenses |
74,864 | 38,676 | 21,603 | 21,611 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Loss from operations |
(65,766 | ) | (28,190 | ) | (14,003 | ) | (21,426 | ) | ||||||||
| Other income (expense): |
||||||||||||||||
| Interest income |
17 | 10 | — | 1 | ||||||||||||
| Interest expense |
(1,017 | ) | (1,719 | ) | (1,021 | ) | (161 | ) | ||||||||
| Other income (expense) |
24 | 263 | (63 | ) | 22 | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Total other income (expense) |
(976 | ) | (1,446 | ) | (1,084 | ) | (138 | ) | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Net loss |
$ | (66,742 | ) | $ | (29,636 | ) | $ | (15,087 | ) | $ | (21,564 | ) | ||||
|
|
|
|
|
|
|
|
|
|||||||||
| Net loss per share-basic and diluted |
$ | (2.49 | ) | $ | (1.78 | ) | $ | (47.54 | ) | $ | (73.34 | ) | ||||
|
|
|
|
|
|
|
|
|
|||||||||
| Weighted-average number of common shares used in net loss per share-basic and diluted |
26,807 | 16,665 | 317 | 294 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| As of December 31, | ||||||||||||||||
| 2014 | 2013 | 2012 | 2011 | |||||||||||||
| (in thousands) | ||||||||||||||||
| Balance Sheet Data: |
||||||||||||||||
| Cash and cash equivalents |
$ | 121,042 | $ | 102,712 | $ | 9,079 | $ | 22,454 | ||||||||
| Working capital |
109,321 | 92,229 | 3,720 | 16,400 | ||||||||||||
| Total assets |
127,204 | 105,886 | 14,072 | 24,069 | ||||||||||||
| Current liabilities |
17,276 | 13,191 | 8,661 | 6,974 | ||||||||||||
| Long-term obligations |
1,362 | 4,887 | 8,619 | 5,857 | ||||||||||||
| Convertible preferred stock |
— | — | 79,841 | 79,841 | ||||||||||||
| Accumulated deficit |
(186,463 | ) | (119,721 | ) | (90,085 | ) | (74,998 | ) | ||||||||
| Total stockholders’ equity (deficit) |
$ | 108,566 | $ | 87,808 | $ | (83,049 | ) | (68,603 | ) | |||||||
79
Table of Contents
| ITEM 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
You should read the following discussion and analysis of our financial condition and results of operations together with our consolidated financial statements and related notes appearing in this annual report on Form 10-K. Some of the information contained in this discussion and analysis or set forth elsewhere in this annual report on Form 10-K, including information with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks and uncertainties. As a result of many factors, including those factors set forth in the “Risk Factors” section of this annual report on Form 10-K, our actual results could differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
We are a clinical-stage biopharmaceutical company using our proprietary chemistry technology to create novel antibiotics for serious and life-threatening multidrug-resistant infections. We are developing our lead product candidate, eravacycline, a fully synthetic tetracycline derivative, as a broad-spectrum intravenous, or IV, and oral antibiotic for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections, including multidrug-resistant Gram-negative infections. We are conducting a global Phase 3 clinical program for eravacycline called IGNITE (Investigating Gram-Negative Infections Treated with Eravacycline), consisting of two Phase 3 clinical trials. IGNITE 1 is a Phase 3 clinical trial evaluating the safety and efficacy of eravacycline with IV administration for the treatment of complicated intra-abdominal infections, or cIAI, for which we announced top-line data in December 2014. IGNITE 2, a second Phase 3 clinical trial of eravacycline for the treatment of complicated urinary tract infections, or cUTI, with IV-to-oral transition therapy, is ongoing.
Consistent with guidance issued by the United States Food and Drug Administration, or FDA, with respect to the development of antibiotics for cIAI and our discussions with the FDA, we expect that positive results from these two Phase 3 clinical trials will be sufficient to support submission of a new drug application, or NDA, for eravacycline in the treatment of cIAI and cUTI. In December 2014, we announced positive top-line data from IGNITE 1. In September 2014, we announced positive data from the lead-in portion of IGNITE 2, and in October 2014 announced the selection of the oral dose for the IV-to-oral transition therapy (1.5 mg/kg IV followed by 200 mg oral dose) to be evaluated in the pivotal portion of IGNITE 2 and the initiation of patient enrollment. We expect to have top-line data from the pivotal portion of IGNITE 2 in mid-2015. If we complete the pivotal portion of IGNITE 2 when we anticipate, and it is successful, we expect to submit an NDA to the FDA by the end of 2015 and a marketing authorization application, or MAA, to the European Medicines Agency, or EMA, in the first half of 2016.
Subject to obtaining additional financing, we intend to pursue development of eravacycline for the treatment of additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections following our development of eravacycline for the treatment of cIAI and cUTI. We are also pursuing the discovery and development of TP-271, a broad-spectrum preclinical compound that we are developing for respiratory diseases caused by bacterial biothreat pathogens, and additional antibiotics, including TP-6076, our lead candidate from our second-generation Gram-negative program.
We commenced business operations in July 2006. Our operations to date have been limited to organizing and staffing our company, business planning, raising capital, acquiring and developing our proprietary chemistry technology, identifying potential product candidates and undertaking preclinical studies and clinical trials of our product candidates. To date, we have not generated any product revenue and have primarily financed our operations through public offerings and private placements of our equity securities, debt financings and funding from the United States government. As of December 31, 2014, we had received an aggregate of $298.2 million in net proceeds from the issuance of equity securities and borrowings under debt facilities and an aggregate of $24.2 million from government grants and contracts. As of December 31, 2014, our principal source of liquidity was cash and cash equivalents, which totaled $121.0 million.
80
Table of Contents
As of December 31, 2014, we had an accumulated deficit of $186.5 million. Our net losses were $66.7 million, $29.6 million and $15.1 million for the years ended December 31, 2014, 2013 and 2012, respectively. We expect that our expenses will increase substantially as we continue our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, seek marketing approval for eravacycline, conduct pre-commercialization and launch-related activities for eravacycline, pursue development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections, advance our other product candidates and satisfy our obligations under our license agreement with Harvard University. If we obtain marketing approval of eravacycline, we also expect to incur significant sales, marketing, distribution and manufacturing expenses. Furthermore, we expect to incur ongoing research and development expenses relating to our product candidates other than eravacycline and that our general and administrative costs will increase as we grow and continue to operate as a public company. We will need to generate significant revenue to achieve profitability, and we may never do so.
We believe that our available funds will be sufficient to enable us to obtain top-line data from our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, to submit an NDA to the FDA for eravacycline and to perform pre-commercialization activities for eravacycline. We expect that these funds will not, however, be sufficient to enable us to commercially launch eravacycline. It is also possible that we will not achieve the progress that we expect with respect to eravacycline because the actual costs and timing of clinical development activities are difficult to predict and are subject to substantial risks and delays. We will be required to obtain further funding through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources. Adequate additional financing may not be available to us on acceptable terms, or at all. Our failure to raise capital as and when needed would have a negative impact on our financial condition and our ability to pursue our business strategy.
Financial overview
Contract and Grant Revenue
We have derived all of our revenue to date from funding provided under three U.S. government awards for the development of our compounds as potential counter measures for the treatment of disease caused by bacterial biothreat pathogens through our collaborator CUBRC Inc., or CUBRC, an independent, not-for-profit, research corporation that specializes in U.S. government-based contracts:
| • | We have received funding for our lead product candidate, eravacycline, under an award from the Biomedical Advanced Research and Development Authority, or BARDA, an agency of the U.S. Department of Health and Human Services. In January 2012, BARDA awarded CUBRC a five-year contract that provides for up to a total of $67.0 million in funding for the development, manufacturing and clinical evaluation of eravacycline for the treatment of disease caused by bacterial biothreat pathogens. The funding under the BARDA Contract is also being used for the development, manufacturing and clinical evaluation of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria. We refer to this contract as the BARDA Contract. |
| • | We have received funding for our preclinical compound TP-271 under two awards from the National Institute of Allergy and Infectious Diseases, or NIAID, a division of National Institutes of Health, for the development, manufacturing and clinical evaluation of TP-271 for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, as well as bacterial pathogens associated with community-acquired bacterial pneumonia: |
| • | a grant awarded to CUBRC in July 2011 that provides up to a total of approximately $2.8 million over five years, which we refer to as the NIAID Grant; and |
| • | a contract awarded to CUBRC in September 2011 that provides up to a total of approximately $35.8 million in funding over five years, which we refer to as the NIAID Contract. |
81
Table of Contents
We are collaborating with CUBRC, because when we initially decided to seek government funding, we recognized that we did not have any expertise in bidding for, administrating or managing government-funded contracts. CUBRC serves as the prime contractor under the BARDA Contract, the NIAID Grant and the NIAID Contract, primarily carrying out a program management and administrative role with additional responsibility for the management of preclinical studies. We serve as lead technical expert on all aspects of these awards and also serve as a subcontractor responsible for management of chemistry, manufacturing and control activities and clinical studies. We derive all of our revenue under these collaborations through subcontracts with, and a subaward from, CUBRC, with the flow of funds following the respective activities being conducted by us and by CUBRC.
| • | In connection with the BARDA Contract, in February 2012, we entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which we may receive funding of up to approximately $39.8 million, reflecting the portion of the BARDA Contract funding that may be paid to us for our activities. |
| • | In connection with the NIAID Contract, in October 2011, we entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which we may receive funding of up to approximately $13.3 million, reflecting the portion of the NIAID Contract funding that may be paid to us for our activities. |
| • | In connection with the NIAID Grant, in November 2011, CUBRC awarded us a 55-month, no-fee subaward of approximately $980,000, reflecting the portion of the NIAID Grant funding that may be paid to us for our activities. |
Although the BARDA Contract, and our subcontract with CUBRC under the BARDA Contract, have five-year terms, BARDA is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond current-year amounts from Congressionally approved annual appropriations. To the extent that BARDA ceases to provide funding of the program to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our BARDA subcontract is $31.0 million from the initial contract date through September 9, 2016, of which $16.4 million had been received through December 31, 2014.
Similarly, although the NIAID Contract and our subcontract with CUBRC under the NIAID Contract have five-year terms, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond September 30, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subcontract with respect to the NIAID Contract is $8.3 million, from the initial contract date through September 30, 2016, of which $7.1 million had been received through December 31, 2014. In addition, although the NIAID Grant has a term of five years and our subaward from CUBRC has a term of 55 months, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond May 30, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to us. Committed funding from CUBRC under our subaward with respect to the NIAID Grant is $0.8 million from the initial grant date through May 30, 2016, of which $0.7 million had been received through December 31, 2014.
We have no products approved for sale. Other than the government funding described above, we do not expect to receive any revenue from any product candidates that we develop, including eravacycline, until we obtain regulatory approval and commercialize such products, which we do not expect will occur before 2016, or until we potentially enter into collaborative agreements with third parties for the development and commercialization of such product candidates. We continue to pursue government funding for other preclinical and clinical programs. If our development efforts for any of our product candidates result in clinical success and regulatory approval, or collaboration agreements with third parties, we may generate revenue from those product candidates.
82
Table of Contents
We expect that our revenue will be less than our expenses for the foreseeable future and that we will experience increasing losses as we continue our development of, and seek regulatory approvals for, our product candidates, and begin to commercialize any approved products. Even if we are able to generate revenue from the sale of one or more products, we may not become profitable.
Research and Development Expenses
Research and development expenses consist primarily of costs incurred for the research and development of our preclinical and clinical candidates, and include:
| • | personnel-related expenses, including salaries, benefits and stock-based compensation expense; |
| • | expenses incurred under agreements with contract research organizations, or CROs, contract manufacturing organizations, or CMOs, and consultants that provide preclinical, clinical, regulatory and manufacturing services; |
| • | payments made under our license agreement with Harvard University; |
| • | the cost of acquiring, developing and manufacturing clinical trial materials and lab supplies; |
| • | facility, depreciation and other expenses, which include direct and allocated expenses for rent, maintenance of our facility, insurance and other supplies; and |
| • | costs associated with preclinical and regulatory activities. |
We expense research and development costs to operations as incurred. We recognize costs for certain development activities, such as clinical trials, based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations or information provided to us by our vendors.
We track external development expenses and personnel expense on a program-by-program basis and allocate common expenses, such as scientific consultants and laboratory supplies, to each program based on the personnel resources allocated to such program. Expenses related to facilities, consulting, travel, conferences, stock-based compensation and depreciation are not allocated to a program and are separately classified as other research and development expenses. The following table identifies research and development expenses on a program-specific basis for our product candidates for the years ended December 31, 2014, 2013 and 2012:
| Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| (in thousands) | ||||||||||||
| Eravacycline |
$ | 46,595 | $ | 17,671 | $ | 6,932 | ||||||
| BARDA Contract |
6,782 | 7,341 | 4,279 | |||||||||
| NIAID Contract and NIAID Grant |
2,149 | 2,625 | 2,537 | |||||||||
| Other development programs |
1,219 | 1,041 | 1,071 | |||||||||
| Other research and development |
5,187 | 2,830 | 2,475 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total research and development |
$ | 61,932 | $ | 31,508 | $ | 17,294 | ||||||
|
|
|
|
|
|
|
|||||||
Research and development activities are central to our business model. Product candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical development, primarily due to the increased size and duration of later-stage clinical trials.
As of December 31, 2014, we had incurred an aggregate of $95.0 million in research and development expenses related to the development of eravacycline, excluding $18.4 million of expenses that were funded under the BARDA Contract. We expect that our research and development expenses will increase substantially as we continue our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, pursue development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and
83
Table of Contents
life-threatening infections, advance our other product candidates and satisfy our obligations under our license agreement with Harvard University. We expect that the total external costs of the Phase 3 clinical trials of eravacycline for the treatment of cIAI and cUTI will be approximately $65.0 million to $75.0 million, of which $44.3 million had been incurred through December 31, 2014.
Because of the numerous risks and uncertainties associated with product development, however, we cannot determine with certainty the duration and completion costs of these or other current or future clinical trials of eravacycline or our other product candidates. We may never succeed in achieving regulatory approval for eravacycline or any of our other product candidates. The duration, costs and timing of clinical trials and development of our product candidates will depend on a variety of factors, including the uncertainties of future clinical and preclinical studies, uncertainties in clinical trial enrollment rate and significant and changing government regulation. In addition, the probability of success for each product candidate will depend on numerous factors, including competition, manufacturing capability and commercial viability.
We have licensed our proprietary chemistry technology from Harvard University on an exclusive worldwide basis under a license agreement that we entered into in August 2006. Under our license agreement, we have paid Harvard an aggregate of $3.8 million in upfront license fees and development milestone payments, including a $2.0 million milestone fee that we paid in October 2013 in connection with the dosing of the first patient in our Phase 3 clinical trial of eravacycline for the treatment of cIAI. We have also issued 31,379 shares of our common stock to Harvard under the license agreement. In addition, we have agreed to make payments to Harvard upon the achievement of specified future development and regulatory milestones totaling up to $15.1 million for each licensed product candidate ($3.1 million of which has already been paid with respect to eravacycline), and to pay tiered royalties in the single digits based on annual worldwide net sales, if any, of licensed products, our affiliates and our sublicensees. We are also obligated to pay Harvard a specified share of non-royalty sublicensing revenues that we receive from sublicensees for the grant of sublicenses under the license and to reimburse Harvard for specified patent prosecution and maintenance costs. The next milestone payment due under the license agreement with respect to eravacycline would be a $3.0 million payment upon acceptance of an NDA filing to the FDA.
General and Administrative Expenses
General and administrative expenses consist principally of personnel-related costs, including salaries and related costs such as benefits and stock-based compensation for personnel in executive, finance, operational, business development, corporate communications and human resource functions. Other significant general and administrative expenses include professional fees for legal, patent, auditing and tax services, consulting, and facility costs not otherwise included in research and development expenses.
We anticipate that our general and administrative expenses will increase for a number of reasons, including:
| • | support of the anticipated expansion of our research and development activities as we continue the development of our product candidates; |
| • | increases in personnel-related costs, expansion of infrastructure and higher consulting, legal, accounting and investor relations costs, and directors and officers insurance premiums; and |
| • | if and when we believe a regulatory approval of our first product candidate appears likely, anticipated increases in our personnel-related and consulting costs as a result of our preparation for commercial operations, especially as it relates to the sales and marketing of our product candidates. |
Interest Income
Interest income consists of interest earned on our cash and cash equivalents. The primary objective of our investment policy is capital preservation.
84
Table of Contents
Interest Expense
Interest expense consists primarily of interest accrued on our outstanding indebtedness and non-cash interest related to the amortization of debt discount costs associated with our term loan facility with Silicon Valley Bank and Oxford Finance. We expect that our interest expense will decrease in future periods as we pay down principal on our indebtedness to Silicon Valley Bank and Oxford Finance over the term of the loan facility.
Other Income
Other income consists primarily of fair value adjustments on warrants for the purchase of our preferred stock. We do not anticipate that we will recognize any further amounts with respect to these fair value adjustments as a result of the conversion of all outstanding warrants to purchase our preferred stock into warrants to purchase our common stock in connection with the completion of our initial public offering, or IPO.
Critical Accounting Policies and Significant Judgments and Estimates
Our management’s discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, revenues and expenses and the disclosure of contingent assets and liabilities in our financial statements. On an ongoing basis, we evaluate our estimates and judgments, including those related to revenue recognition, accrued clinical expenses, and stock-based compensation. We base our estimates on historical experience, known trends and events and various other factors that we and our management believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
While our significant accounting policies are described in more detail in the notes to our consolidated financial statements appearing elsewhere in this annual report on Form 10-K, we believe the following accounting policies to be most critical to the judgments and estimates used in the preparation of our financial statements.
Revenue Recognition
We have derived all of our revenue to date from our subcontracts with CUBRC under the BARDA Contract and the NIAID Contract and our subaward under the NIAID Grant. We recognize revenue under these best-efforts, cost-reimbursable and cost-plus-fixed-fee subcontracts and subaward as we perform services under the subcontracts and subaward so long as a subcontract and subaward has been executed and the fees for these services are fixed or determinable, legally billable and reasonably assured of collection. Recognized amounts reflect our partial performance under the subcontracts and subaward and equal direct and indirect costs incurred plus fixed fees, where applicable. We do not recognize revenue under these arrangements for amounts related to contract periods where funding is not yet committed as amounts above committed funding thresholds would not be considered fixed or determinable or reasonably assured of collection. Revenues and expenses under these arrangements are presented gross on our statements of operations and comprehensive loss as we have determined we are the primary obligor under these arrangements relative to the research and development services we perform as lead technical expert.
Revenue under our subcontracts under both the NIAID Contract and the BARDA Contract are earned under a cost-plus-fixed-fee arrangement in which we are reimbursed for direct costs incurred plus allowable indirect costs and a fixed-fee earned. Billings under these contracts are based on approved provisional indirect billing rates, which permit recovery of fringe benefits, allowable overhead and general and administrative expenses and a fixed fee.
85
Table of Contents
Revenue under our subaward under the NIAID Grant is earned under a cost-reimbursable arrangement in which we are reimbursed for direct costs incurred plus allowable indirect costs. Billings under the NIAID Grant are based on approved provisional indirect billing rates, which permit recovery of fringe benefits and allowable general and administrative expenses.
Accrued Research and Development Expenses
As part of the process of preparing our financial statements, we are required to estimate our accrued expenses. This process involves reviewing open contracts and purchase orders, communicating with our personnel to identify services that have been performed for us and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed or when contractual milestones are met. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include fees paid to:
| • | CROs in connection with the conduct of our clinical trials; |
| • | CMOs with respect to the manufacture of drug supply for clinical trials and manufacture of drug substance and finished product; and |
| • | vendors and consultants in connection with preclinical development activities. |
We base our expenses related to clinical studies on our estimates of the services completed and efforts expended pursuant to contracts with multiple CROs that conduct and manage clinical studies on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the clinical expense. Payments under some of these contracts depend on factors such as the successful enrollment of subjects and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which services will be performed, enrollment of subjects, number of sites activated and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual or prepaid accordingly. Although we do not expect our estimates to be materially different from amounts actually incurred, if our estimates of the status and timing of services performed differ from the actual status and timing of services performed we may report amounts that are too high or too low in any particular period. To date, there have been no material differences from our estimates to the amount actually incurred.
Stock-Based Compensation
We apply the fair value recognition provisions of Financial Accounting Standards Board Accounting Standards Codification Topic 718, Compensation-Stock Compensation, or ASC 718, to account for all stock-based compensation. We recognize compensation costs related to stock options granted to employees based on the estimated fair value of the awards on the date of grant. Stock compensation related to non-employee awards is remeasured at each reporting period until the awards are vested.
Determining the amount of stock-based compensation to be recorded requires us to develop estimates of the fair value of stock-based awards as of their grant date for awards granted to employees and as of their measurement date for awards granted to non-employees. For awards granted to employees, we recognize stock-based compensation expense ratably over the requisite service period, which in most cases is the vesting period of the award. For awards granted to non-employees, we recognize stock-based compensation expense over the requisite service period using the accelerated attribution method. Calculating the fair value of stock-based awards requires that we make highly subjective assumptions. We use the Black-Scholes option pricing model to value our stock option awards. Use of this valuation methodology requires that we make assumptions as to the
86
Table of Contents
volatility of our common stock, the fair value of our common stock on the grant date for the period prior to our IPO, the expected term of our stock options, the risk free interest rate for a period that approximates the expected term of our stock options and our expected dividend yield. Because there had been no public market for our common stock prior to our IPO, we believe that we have insufficient data from our limited public trading history to appropriately utilize company-specific historical and implied volatility information. Accordingly, we utilize data from a representative group of publicly traded companies to estimate expected stock price volatility. We selected representative companies from the biopharmaceutical industry with similar characteristics as us, including stage of product development and therapeutic focus. We use the simplified method as prescribed by the Securities and Exchange Commission Staff Accounting Bulletin No. 107, Share-Based Payment as we do not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term of stock options granted to employees. For non-employee grants, we use an expected term equal to the remaining contractual term of the award. We utilize a dividend yield of zero based on the fact that we have never paid cash dividends and have no current intention of paying cash dividends. The risk-free interest rate used for each grant is based on the U.S. Treasury yield curve in effect at the time of measurement for instruments with a similar expected term.
Under ASC 718, we are also required to estimate the level of forfeitures expected to occur and record compensation expense only for those awards that we ultimately expect will vest. We have performed an historical analysis of option awards that were forfeited prior to vesting and recorded total stock option expense that reflected this estimated forfeiture rate. ASC 718 requires forfeitures to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. During the years ended December 31, 2014, 2013 and 2012 our estimated annual forfeiture rate was 5.9%, 3% and 3%, respectively.
Stock-based compensation expense includes options granted to employees and non-employees and has been reported in our statements of operations and comprehensive loss as follows (in thousands):
| Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Research and development |
$ | 1,845 | $ | 690 | $ | 463 | ||||||
| General and administrative |
3,385 | 611 | 149 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
$ | 5,230 | $ | 1,301 | $ | 612 | ||||||
|
|
|
|
|
|
|
|||||||
We estimated the fair value of each employee and director stock option award on the grant date using the Black-Scholes option-pricing model based on the following assumptions:
| Year Ended December 31, | ||||||
| 2014 | 2013 | 2012 | ||||
| Volatility factor |
53.41-58.13% | 54.50-60.54% | 56.89-68.12% | |||
| Expected life (in years) |
5.31-6.11 | 5.8-7.1 | 6.0-6.1 | |||
| Risk-free interest rate |
1.71%-2.13% | 0.91%-2.01% | 0.85%-1.21% | |||
| Dividend yield |
0% | 0% | 0% | |||
87
Table of Contents
Prior to our IPO, due to the absence of an active market for our common stock, the fair value of our common stock was determined in good faith by our board of directors, with the assistance and upon the recommendations of management, based on objective and subjective factors consistent with the methodologies outlined in the American Institute of Certified Public Accountants Practice Aid, Valuation of Privately-Held-Company Equity Securities Issued as Compensation.
Since our IPO, the exercise price per share of all option grants has been set at the closing price of our common stock on the NASDAQ Global Select Market on the applicable date of grant, which our board of directors believes represents the fair value of our common stock.
Stock-based compensation expense related to awards granted to employees was $4.0 million, $1.3 million and $0.3 million for the years ended December 31, 2014, 2013 and 2012, respectively. As of December 31, 2014, we had approximately $11.7 million of total unrecognized stock-based compensation expense related to unvested stock options, expected to be recognized over a weighted-average period of 2.6 years. We expect that our stock-based compensation expense related to stock options granted will grow in future periods due to the potential increases in the value of our common stock and headcount.
During April 2014, we granted an option to a non-employee to purchase 100,000 shares of common stock. This option vests with respect to 25% of the underlying shares eighteen months after the date of grant, an additional 25% of the underlying shares two years after the date of grant, and the remaining 50% of the underlying shares in eight equal quarterly installments starting on the date three months after the two year anniversary of the original date of grant. This option has a contractual term of ten years. During October 2014, we granted an option to a non-employee to purchase 10,000 shares of common stock. This option vests with respect to 50% of the underlying shares one year after the date of grant, with the remaining 50% of the underlying shares vesting two years after the date of grant. This option has a contractual term of ten years. We did not grant stock options to non-employees during 2013 or 2012.
The total expense related to non-employee stock options was $1.2 million, $39,000 and $0.3 million for the years ended December 31, 2014, 2013 and 2012, respectively.
Results of Operations
Comparison of Years Ended December 31, 2014 and 2013
The following tables summarize the results of our operations for each of the years ended December 31, 2014 and 2013, together with the changes in those items in dollars and as a percentage:
| Years Ended December 31, |
Increase/ (decrease) |
% | ||||||||||||||
| 2014 | 2013 | |||||||||||||||
| (in thousands) | ||||||||||||||||
| Revenues |
$ | 9,098 | $ | 10,486 | $ | (1,388 | ) | (13 | )% | |||||||
| Operating expenses: |
||||||||||||||||
| Research and development |
61,932 | 31,508 | 30,424 | 97 | % | |||||||||||
| General and administrative |
12,932 | 7,168 | 5,764 | 80 | % | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Total operating expenses |
74,864 | 38,676 | 36,188 | 94 | % | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Loss from operations |
(65,766 | ) | (28,190 | ) | (37,576 | ) | 133 | % | ||||||||
| Interest income |
17 | 10 | 7 | 70 | % | |||||||||||
| Interest expense |
(1,017 | ) | (1,719 | ) | 702 | (41 | )% | |||||||||
| Other income |
24 | 263 | (239 | ) | (91 | )% | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Net loss |
$ | (66,742 | ) | $ | (29,636 | ) | $ | (37,106 | ) | 125 | % | |||||
|
|
|
|
|
|
|
|
|
|||||||||
88
Table of Contents
Revenue from U.S. Government Contracts and Grants
The following table sets forth our contract and grant revenue for the years ended December 31, 2014 and 2013:
| Years Ended December 31, |
Increase/ (decrease) |
% | ||||||||||||||
| Revenue |
2014 | 2013 | ||||||||||||||
| (in thousands) | ||||||||||||||||
| BARDA |
$ | 6,886 | $ | 7,707 | $ | (821 | ) | (11 | )% | |||||||
| NIAID Contract |
2,077 | 2,512 | (435 | ) | (17 | )% | ||||||||||
| NIAID Grant |
135 | 267 | (132 | ) | (49 | )% | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 9,098 | $ | 10,486 | $ | (1,388 | ) | (13 | )% | ||||||||
|
|
|
|
|
|
|
|
|
|||||||||
Contract and grant revenue was $9.1 million for the year ended December 31, 2014 compared to $10.5 million for the year ended December 31, 2013, a decrease of $1.4 million, or 13%. This decrease was primarily due to the scope and timing of activities under our subcontracts with respect to the BARDA and NIAID Contracts conducted during the year ended December 31, 2014 as compared to the year ended December 31, 2013.
Research and Development Expenses
Research and development expenses were $61.9 million for the year ended December 31, 2014 compared to $31.5 million for the year ended December 31, 2013, an increase of $30.4 million or 97%. This increase was due to higher clinical costs of $18.4 million primarily associated with our two Phase 3 clinical trials of eravacycline for the treatment of cIAI and cUTI; an increase of $8.5 million in non-clinical and drug manufacturing costs principally in support of NDA-related activities; an increase in personnel-related costs of $1.9 million in connection with additional headcount to support our eravacycline Phase 3 clinical trials; an increase of $1.8 million in drug manufacturing costs related to our activities under our BARDA subcontract; and an increase in stock-based compensation expense of $1.2 million resulting from additional headcount and our annual stock option awards to employees granted during the quarter ended March 31, 2014. These increases were offset in part by a $2.0 million milestone fee under our license agreement with Harvard University that we incurred during the year ended December 31, 2013 in connection with the dosing of the first patient in our Phase 3 cIAI clinical trial. No milestone fees were incurred during the year ended December 31, 2014.
General and Administrative Expenses
General and administrative expenses for the year ended December 31, 2014 were $12.9 million compared to $7.2 million for the year ended December 31, 2013, an increase of approximately $5.8 million or 80%. This increase was primarily due to an increase in stock-based compensation expense of $2.8 million resulting from additional headcount, our annual stock option awards to employees granted during the quarter ended March 31, 2014, as well as a stock option granted to a non-employee during 2014; an increase in personnel-related costs of $1.0 million in connection with additional headcount to support our increased level of research and development and pre-commercialization activities; an increase of $0.9 million in consulting costs primarily related to planning and pre-commercialization activities; and an increase in legal costs of $0.3 million primarily related to patent costs.
Interest Income
Interest income for the years ended December 31, 2014 and December 31, 2013 was de minimis.
89
Table of Contents
Interest Expense
Interest expense for the year ended December 31, 2014 was $1.0 million compared to $1.7 million for the year ended December 31, 2013, a decrease of $0.7 million or 41%. The decrease in interest expense was primarily attributable to a decrease in the principal balance under our term loan facility with Silicon Valley Bank and Oxford Finance associated with our principal payments made. We expect that our interest expense will continue to decrease in future periods as we continue to pay down principal on our indebtedness to Silicon Valley Bank and Oxford Finance over the term of the loan facility.
Other Income
Other income for the year ended December 31, 2014 was de minimis compared to $0.3 million for the year ended December 31, 2013. Other income during the year ended December 31, 2013 was primarily due to a decrease in the fair value of the underlying preferred stock, which impacted the fair value of our preferred stock warrants issued in connection with various debt financings. We do not anticipate that we will recognize any further amounts with respect to these fair value adjustments as a result of the conversion of all outstanding warrants to purchase our preferred stock into warrants to purchase our common stock in connection with the completion of our IPO.
Comparison of Years Ended December 31, 2013 and 2012
The following tables summarize the results of our operations for each of the years ended December 31, 2013 and 2012, together with the changes in those items in dollars and as a percentage:
| Years Ended December 31, |
Increase/ (decrease) |
% | ||||||||||||||
| 2013 | 2012 | |||||||||||||||
| (in thousands) | ||||||||||||||||
| Revenues |
$ | 10,486 | $ | 7,600 | $ | 2,886 | 38 | % | ||||||||
| Operating expenses: |
||||||||||||||||
| Research and development |
31,508 | 17,294 | 14,214 | 82 | % | |||||||||||
| General and administrative |
7,168 | 4,309 | 2,859 | 66 | % | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Total operating expenses |
38,676 | 21,603 | 17,073 | 79 | % | |||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Loss from operations |
(28,190 | ) | (14,003 | ) | (14,187 | ) | 101 | % | ||||||||
| Interest income |
10 | — | 10 | 100 | % | |||||||||||
| Interest expense |
(1,719 | ) | (1,021 | ) | (698 | ) | 68 | % | ||||||||
| Other income (expense) |
263 | (63 | ) | 326 | (517 | )% | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Net loss |
$ | (29,636 | ) | $ | (15,087 | ) | $ | (14,549 | ) | 96 | % | |||||
|
|
|
|
|
|
|
|
|
|||||||||
Revenue from U.S. Government Contracts and Grants
The following table sets forth our contract and grant revenue for the years ended December 31, 2013 and 2012:
| Years Ended December 31, |
Increase/ (decrease) |
% | ||||||||||||||
| Revenue |
2013 | 2012 | ||||||||||||||
| (in thousands) | ||||||||||||||||
| BARDA |
$ | 7,707 | $ | 4,876 | $ | 2,831 | 58 | % | ||||||||
| NIAID Contract |
2,512 | 2,451 | 61 | 2 | % | |||||||||||
| NIAID Grant |
267 | 273 | (6 | ) | (2 | )% | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| $ | 10,486 | $ | 7,600 | $ | 2,886 | 38 | % | |||||||||
|
|
|
|
|
|
|
|
|
|||||||||
90
Table of Contents
Contract and grant revenue was $10.5 million for the year ended December 31, 2013 compared to $7.6 million for the year ended December 31, 2012, an increase of $2.9 million, or 38%. This increase was primarily due to revenue associated with an increase in the activities under our subcontract with respect to the BARDA Contract.
Research and Development Expenses
Research and development expenses were $31.5 million for the year ended December 31, 2013 compared to $17.3 million for the year ended December 31, 2012, an increase of $14.2 million or 82%. This increase was primarily due to an increase of $8.5 million in clinical costs related to our Phase 3 clinical program for eravacycline for the treatment of cIAI and cUTI; an increase of $3.1 million in expenses related to activities under our subcontract with CUBRC with respect to the BARDA Contract; a $2.0 million milestone fee due under our license agreement with Harvard University that became payable during the year ended December 31, 2013 in connection with the dosing of the first patient in our Phase 3 cIAI clinical trial; an increase of $1.9 million in drug manufacturing costs associated with our Phase 3 clinical program for eravacycline for the treatment of cIAI and cUTI; an increase in personnel-related costs of $0.9 million to support our increased activities related to the Phase 3 clinical program for eravacycline, the BARDA Contract, the NIAID Contract, and the NIAID Grant; and an increase of $0.6 million in development costs associated with the oral formulation of eravacycline. These increases were offset in part by a decrease in clinical and drug manufacturing costs of $3.3 million attributable to the completion of our Phase 2 clinical trial of eravacycline in the first half of 2012.
General and Administrative Expenses
General and administrative expenses for the year ended December 31, 2013 were $7.2 million compared to $4.3 million for the year ended December 31, 2012, an increase of $2.9 million or 66%. This increase was primarily due to an increase of $1.3 million in audit, legal, insurance and consulting costs primarily due to operating as a public company; an increase in personnel-related costs of $0.8 million; and an increase in stock-based compensation expense of $0.5 million.
Interest Income
Interest income for the years ended December 31, 2013 and December 31, 2012 was de minimis.
Interest Expense
Interest expense for the year ended December 31, 2013 was $1.7 million compared to $1.0 million for the year ended December 31, 2012, an increase of approximately $0.7 million or 68%. The increase in interest expense was primarily attributable to an increase in debt under the term loan facility with Silicon Valley Bank and Oxford Finance associated with our borrowings in December 2012 and February 2013.
Other Income (Expense)
Other income (expense) for the year ended December 31, 2013 was $0.3 million compared to $(0.1) million for the year ended December 31, 2012. The increase in other income was primarily due to a decrease in the fair value of the underlying preferred stock, which impacted the fair value of our preferred stock warrants issued in connection with our December 2012 and February 2013 debt facility with Silicon Valley Bank and Oxford Finance.
91
Table of Contents
Liquidity and Capital Resources
We have incurred losses since our inception and anticipate that we will continue to incur losses for at least the next several years. We expect that our research and development and general and administrative expenses will continue to increase and, as a result, we will need additional capital to fund our operations, which we may obtain from additional financings, research funding, collaborations, contract and grant revenue or other sources.
Since our inception, we have funded our operations principally through the receipt of funds from public offerings and private placements of equity securities, debt financings and contract research funding and research grants from the United States government. As of December 31, 2014, we had cash and cash equivalents of approximately $121.0 million. We invest cash in excess of immediate requirements in accordance with our investment policy, primarily with a view to liquidity and capital preservation. As of December 31, 2014, our funds were held in cash and money market funds.
On March 25, 2013, we completed the sale of 10,714,286 shares of common stock in our IPO at a price to the public of $7.00 per share, resulting in net proceeds to us of $68.0 million after deducting underwriting discounts and commissions of $4.4 million and offering costs of $2.5 million. On April 12, 2013, we completed the sale of an additional 797,792 shares of common stock to the underwriters under the underwriters’ option in the IPO to purchase additional shares of common stock at a price to the public of $7.00 per share, resulting in net proceeds to us of $5.2 million after deducting underwriting discounts and commissions.
On November 13, 2013, we completed the sale of 4,500,000 shares of common stock in a follow-on public offering at a price to the public of $10.00 per share, resulting in net proceeds to us of $41.8 million after deducting underwriting discounts and commissions of $2.7 million and offering costs of $0.5 million. On November 19, 2013, we completed the sale of an additional 407,403 shares of common stock to the underwriters under the underwriters’ option in the follow-on public offering to purchase additional shares of common stock at a price to the public of $10.00 per share, resulting in net proceeds to us of $3.8 million after deducting underwriting discounts and commissions.
On October 22, 2014, we completed the sale of 4,542,500 shares of common stock in a follow-on public offering at a price to the public of $19.00 per share, which number of shares includes the underwriters’ exercise in full of their option to purchase additional shares. This offering resulted in net proceeds to us of $80.8 million after deducting underwriting discounts and commissions of $5.2 million and offering costs of $0.4 million.
The following table summarizes our sources and uses of cash for each of the periods set forth below:
| Years Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| (in thousands) | ||||||||||||
| Net cash used in operating activities |
$ | (57,623 | ) | $ | (24,506 | ) | $ | (16,657 | ) | |||
| Net cash used in investing activities |
(191 | ) | (129 | ) | (54 | ) | ||||||
| Net cash provided by financing activities |
76,144 | 118,268 | 3,336 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net increase (decrease) in cash and cash equivalents |
$ | 18,330 | $ | 93,633 | $ | (13,375 | ) | |||||
|
|
|
|
|
|
|
|||||||
During the years ended December 31, 2014, 2013 and 2012, our operating activities used net cash of $57.6 million, $24.5 million and $16.7 million, respectively. The net cash used in operating activities in these periods primarily resulted from our net losses and changes in our working capital accounts. The increase in net cash used in operations for the year ended December 31, 2014 as compared to the year ended December 31, 2013 was due primarily to higher operating expenses during the year ended December 31, 2014 of $74.9 million as compared to $38.7 million for the year ended December 31, 2013. The increase in net cash used in operations for the year ended December 31, 2013 as compared to the year ended December 31, 2012 was due primarily to higher operating expenses during the year ended December 31, 2013 of $38.7 million as compared to $21.6 million for the year ended December 31, 2012.
92
Table of Contents
During the years ended December 31, 2014, 2013 and 2012, our investing activities used net cash of $191,000, $129,000 and $54,000, respectively. The net cash used by investing activities during these periods resulted from purchases of property, plant and equipment to facilitate our increased research and development activities and increased headcount.
During the years ended December 31, 2014, 2013 and 2012 our net cash provided by financing activities was $76.1 million, $118.3 million and $3.3 million, respectively. The net cash provided by financing activities during the year ended December 31, 2014 was primarily related to proceeds from our follow-on public offering of $80.8 million, as well as proceeds from the exercise of stock options of $1.5 million, offset in part by principal payments on our loans payable of $6.1 million. The net cash provided by financing activities during the year ended December 31, 2013 primarily included proceeds from our IPO of $73.8 million, proceeds from our follow-on public offering of $45.6 million, and $3.0 million in borrowings that we made under our debt facility with Silicon Valley Bank and Oxford Finance, offset in part by repayments on our debt facility of $4.2 million. The net cash provided by financing activities during the year ended December 31, 2012 was primarily related to $6.2 million in borrowings made under our debt facility with Silicon Valley Bank and Oxford Finance, offset in part by $2.2 million in principal payments on our loans payable.
Credit Facilities
In May 2011, we executed a Loan and Security Agreement with two financial institutions, Silicon Valley Bank and Oxford Finance, which provided for up to $8.0 million in funding, to be made available in two tranches. We borrowed the first $1.5 million in May 2011 and the second tranche for the remaining $6.5 million in December 2011. As of December 31, 2014, these amounts have been paid in full and there is no outstanding principal or interest balance related to these two tranches. On December 20, 2012, we amended the Loan and Security Agreement to provide for up to an additional $9.2 million in funding, to be made available in two tranches. We borrowed the first $6.2 million on December 20, 2012, of which $3.0 million of principal and accrued interest remained outstanding at December 31, 2014. The second tranche of $3.0 million was borrowed by us on February 28, 2013, of which $1.6 million of principal and accrued interest remained outstanding at December 31, 2014. As of December 31, 2014, the aggregate principal balance outstanding was $4.6 million.
The $4.6 million of principal outstanding under the debt facility as of December 31, 2014 bears interest at 9% per annum with an additional payment of 2.9% of the original $6.2 million of principal due at the maturity date of March 1, 2016. We were required to pay interest only on the 2012 borrowing through June 1, 2013. We are now repaying this indebtedness in 33 equal monthly payments of $0.2 million through March 1, 2016. The additional payment of 2.9% of the original $6.2 million of principal will be due at the same time as the last loan payment. The remaining $1.6 million of outstanding principal, which we borrowed under the debt facility in February 2013, bears interest at 9% per annum with an additional payment of 2.9% of the original $3.0 million of principal due at the maturity date of May 1, 2016. We were required to pay interest only on the 2013 borrowing through August 1, 2013. We are now repaying this indebtedness in 33 equal monthly payments of $0.1 million through May 1, 2016. The additional payment of 2.9% of the original $3.0 million will be due at the same time as the last loan payment.
The outstanding loans under the debt facility are collateralized by a blanket lien on all of our corporate assets, excluding intellectual property, and by a negative pledge on our intellectual property. The loan and security agreement contains customary default provisions that include material adverse events, as defined therein, that would entitle the lenders to declare all principal, interest and other amounts owed by us under the loan and security agreement immediately due and payable.
93
Table of Contents
In connection with the December 2012 borrowing under the debt facility, we issued to the lenders 10-year warrants to purchase an aggregate of 964,605 shares of Series C preferred stock with an exercise price of $0.2571 per share. In connection with the February 2013 borrowing under the debt facility, the warrant we issued to Silicon Valley Bank automatically became exercisable for an additional 233,372 shares of Series C preferred stock. In addition, we issued to Oxford Finance a 10-year warrant to purchase an additional 233,372 shares of Series C preferred stock with an exercise price of $0.2571 per share. Upon completion of the IPO, the warrants issued in connection with the December 2012 borrowing and the February 2013 borrowing became exercisable for an aggregate of 49,356 shares of our common stock at an exercise price of $7.46 per share and the related warrant liability was reclassified to additional paid-in capital.
All warrants issued in connection with the loans from Silicon Valley Bank and Oxford Finance have been exercised and no warrants remain outstanding as of December 31, 2014. The only warrants that remain outstanding are warrants to purchase 1,103 shares of common stock issued to Silicon Valley Bank in September 2007 in relation to an equipment loan at an exercise price of $29.00.
Operating Capital Requirements
We expect to incur increasing operating losses for at least the next several years as we continue our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, seek marketing approval for eravacycline, pursue development of eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections, conduct pre-commercialization and launch-related activities for eravacycline, advance our other product candidates and satisfy our obligations under our license agreement with Harvard University. We may not be able to complete the development and initiate commercialization of eravacycline or our other product candidates if, among other things, our preclinical research and clinical trials are not successful, the FDA or the EMA does not approve eravacycline or our other product candidates when we expect, or at all, or funding under the NIAID Contract, the NIAID Grant or the BARDA Contract is discontinued.
We believe that our available funds will be sufficient to fund our current operating plan into at least the third quarter of 2016, enable us to obtain top-line data from our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI, to submit an NDA to the FDA for eravacycline, and to perform pre-commercialization activities for eravacycline. We expect that these funds will not, however, be sufficient to enable us to commercially launch eravacycline. As a result, we will be required to obtain further funding through public or private equity offerings, debt financings, collaborations and licensing arrangements or other sources.
We have based our projections of operating capital requirements on assumptions that may prove to be incorrect and we may use all of our available capital resources sooner than we expect. Because of the numerous risks and uncertainties associated with research, development and commercialization of pharmaceutical products, we are unable to estimate the exact amount of our operating capital requirements. Our future funding requirements will depend on many factors, including, but not limited to:
| • | the timing and costs of our ongoing Phase 3 clinical trial of eravacycline for the treatment of cUTI; |
| • | manufacturing costs related to regulatory filings and anticipated commercial launch; |
| • | the initiation, progress, timing, costs and results of preclinical studies and clinical trials for our other product candidates and potential product candidates; |
| • | the amount of funding that we receive under our subcontracts under the BARDA Contract and the NIAID Contract and under our subaward under the NIAID Grant, and the activities funded under the BARDA Contract, the NIAID Contract and the NIAID Grant; |
| • | the number and characteristics of product candidates that we pursue; |
| • | the timing and costs of developing eravacycline for additional indications, including hospital-acquired bacterial pneumonias and other serious and life-threatening infections; |
94
Table of Contents
| • | the outcome, timing and costs of seeking regulatory approvals; |
| • | the costs of commercialization activities for eravacycline and other product candidates if we receive marketing approval, including the timing and costs of establishing product sales, marketing, distribution and manufacturing capabilities; |
| • | revenue received from commercial sales of eravacycline, subject to receipt of marketing approval; |
| • | the terms and timing of any future collaborations, licensing, consulting or other arrangements that we may establish; |
| • | the amount and timing of any payments we may be required to make, or that we may receive, in connection with the licensing, filing, prosecution, defense and enforcement of any patents or other intellectual property rights, including milestone and royalty payments and patent prosecution fees that we are obligated to pay to Harvard pursuant to our license agreement; |
| • | the costs of preparing, filing and prosecuting patent applications, maintaining and protecting our intellectual property rights and defending against intellectual property related claims; and |
| • | the extent to which we in-license or acquire other products and technologies. |
We expect that we will need to obtain substantial additional funding in order to commercialize eravacycline. To the extent that we raise additional capital through the sale of common stock, convertible securities or other equity securities, the ownership interests of our existing stockholders may be materially diluted and the terms of these securities could include liquidation or other preferences that could adversely affect the rights of our existing stockholders. In addition, debt financing, if available, would result in increased fixed payment obligations and may involve agreements that include restrictive covenants that limit our ability to take specific actions, such as incurring additional debt, making capital expenditures or declaring dividends, that could adversely impact our ability to conduct our business. If we are unable to raise capital when needed or on attractive terms, we could be forced to significantly delay, scale back or discontinue the development or commercialization of eravacycline or other product candidates, seek collaborators at an earlier stage than otherwise would be desirable or on terms that are less favorable than might otherwise be available, and relinquish or license, potentially on unfavorable terms, our rights to eravacycline or other product candidates that we otherwise would seek to develop or commercialize ourselves.
Contractual Obligations and Commitments
The following table summarizes our outstanding contractual obligations as of payment due date by period at December 31, 2014:
| Contractual Obligations |
Payment due by period | |||||||||||||||||||
| Total | Less than 1 Year |
1 -3 Years | 3-5 Years | More than 5Years |
||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Term loan (1) |
$ | 5,209 | $ | 3,789 | $ | 1,420 | — | — | ||||||||||||
| Operating leases (2) |
2,669 | 1,431 | 1,238 | — | — | |||||||||||||||
| Harvard milestone payment (3) |
3,325 | 25 | 3,300 | — | — | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| Total contractual cash obligations |
$ | 11,203 | $ | 5,245 | $ | 5,958 | — | — | ||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
| (1) | Consists of repayment obligations relating to principal and interest outstanding under our debt facility with Silicon Valley Bank and Oxford Finance as of December 31, 2014. |
| (2) | On September 4, 2014, we amended our existing operating lease which extended our lease term through November 30, 2016, and entered into a new operating sublease for additional space with a lease term through November 30, 2016. |
95
Table of Contents
| (3) | Consists of milestone payments that would become due to Harvard of (i) $3.0 million upon acceptance from the FDA of an NDA filing for eravacycline, and (ii) an aggregate amount of $325,000 related to various development milestones for certain preclinical compounds. |
We are contractually obligated under our license agreement with Harvard University to make payments to Harvard upon the achievement of specified future development and regulatory milestones totaling up to $15.1 million for each licensed product candidate ($3.1 million of which has already been paid with respect to eravacycline), and to pay tiered royalties in the single digits based on annual worldwide net sales, if any, of licensed products by us, our affiliates and sublicensees. We are also obligated to pay Harvard a specified share of non-royalty sublicensing revenue that we receive from sublicensees for the grant of sublicenses under the license and to reimburse Harvard for specified patent prosecution and maintenance costs. Many of these potential payments are contingent upon the occurrence of certain future events and, given the nature of those events, it is unclear when, if ever, we may be required to pay such amounts or what the total amount of such payments will be. Except for the milestone payments referenced in the contractual obligations table and described in the footnote above, the table does not include any other potential milestone or royalty payments to Harvard.
We have employment agreements with certain employees which require the funding of a specific level of payments, if certain events, such as a change in control or termination without cause, occur.
In the course of normal business operations, we also have agreements with contract service providers to assist in the performance of our research and development and manufacturing activities. We can elect to discontinue the work under these agreements at any time. We could also enter into additional collaborative research, contract research, manufacturing, and supplier agreements in the future, which may require up-front payments and even long-term commitments of cash.
Off-Balance Sheet Arrangements
We did not have, during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined under applicable SEC rules.
| ITEM 7A. | Quantitative and Qualitative Disclosures About Market Risk |
We are exposed to market risk related to changes in interest rates. Our cash equivalents are classified as available-for-sale and consisted of money market funds at December 31, 2014 and 2013. The investments in these financial instruments are made in accordance with an investment policy approved by our board of directors which specifies the categories, allocations and ratings of securities we may consider for investment. The primary objective of our investment activities is to preserve principal while at the same time maximizing the income we receive without significantly increasing risk. Some of the financial instruments that we invest in could be subject to market risk. This means that a change in prevailing interest rates may cause the value of the instruments to fluctuate. For example, if we purchase a security that was issued with a fixed interest rate and the prevailing interest rate later rises, the value of that security will probably decline. To minimize this risk, we intend to maintain a portfolio which may include cash, cash equivalents and investment securities available-for-sale in a variety of securities which may include money market funds, government and non-government debt securities and commercial paper, all with various maturity dates. Based on our current investment portfolio, we do not believe that our results of operations or our financial condition would be materially impacted by an immediate change of 10% in interest rates.
We do not hold or issue derivatives, derivative commodity instruments or other financial instruments for speculative trading purposes. Further, we do not believe our cash equivalents and investment securities have significant risk of default or illiquidity. We made this determination based on discussions with our investment advisors and a review of our holdings. While we believe our cash equivalents and investment securities do not contain excessive risk, we cannot provide absolute assurance that in the future our investments will not be subject to adverse changes in market value. All of our investments are recorded at fair value.
96
Table of Contents
| ITEM 8. | Financial Statements and Supplementary Data |
TETRAPHASE PHARMACEUTICALS, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
| 98 | ||||
| Consolidated Balance Sheets as of December 31, 2014 and 2013 |
99 | |||
| 100 | ||||
| 101 | ||||
| Consolidated Statements of Cash Flows for the Years Ended December 31, 2014, 2013 and 2012 |
102 | |||
| 103 |
97
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders of
Tetraphase Pharmaceuticals, Inc.
We have audited the accompanying consolidated balance sheets of Tetraphase Pharmaceuticals, Inc. (the Company) as of December 31, 2014 and 2013, and the related consolidated statements of operations and comprehensive loss, convertible preferred stock and stockholders’ equity (deficit) and cash flows for each of the three years in the period ended December 31, 2014 These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. We were not engaged to perform an audit of the Company’s internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Tetraphase Pharmaceuticals, Inc. as of December 31, 2014 and 2013 and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2014, in conformity with U.S. generally accepted accounting principles.
/s/ Ernst & Young LLP
Boston, Massachusetts
March 6, 2015
98
Table of Contents
Tetraphase Pharmaceuticals, Inc.
(In thousands, except par value amounts)
| December 31, 2014 |
December 31, 2013 |
|||||||
| Assets |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 121,042 | $ | 102,712 | ||||
| Accounts receivable |
3,458 | 1,706 | ||||||
| Prepaid expenses and other current assets |
2,097 | 1,002 | ||||||
|
|
|
|
|
|||||
| Total current assets |
126,597 | 105,420 | ||||||
| Property and equipment, net |
300 | 235 | ||||||
| Restricted cash |
199 | 199 | ||||||
| Other assets |
108 | 32 | ||||||
|
|
|
|
|
|||||
| Total assets |
$ | 127,204 | $ | 105,886 | ||||
|
|
|
|
|
|||||
| Liabilities and stockholders’ equity |
||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 4,105 | $ | 1,881 | ||||
| Accrued expenses |
9,477 | 5,290 | ||||||
| Deferred revenue |
258 | 92 | ||||||
| Current portion of term loan payable |
3,436 | 5,928 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
17,276 | 13,191 | ||||||
| Accrued final interest payment on term loan |
222 | 327 | ||||||
| Deferred rent, net of current portion |
16 | — | ||||||
| Term loan payable |
1,124 | 4,560 | ||||||
| Commitments and contingencies |
||||||||
| Preferred stock, par value $0.001 per share; 5,000 shares authorized; no shares issued and outstanding |
— | — | ||||||
| Common stock, par value $0.001 per share; 125,000 shares authorized; 30,806 and 25,629 shares issued and outstanding at December 31, 2014 and 2013, respectively |
31 | 26 | ||||||
| Additional paid-in capital |
294,998 | 207,503 | ||||||
| Accumulated deficit |
(186,463 | ) | (119,721 | ) | ||||
|
|
|
|
|
|||||
| Total stockholders’ equity |
108,566 | 87,808 | ||||||
|
|
|
|
|
|||||
| Total liabilities and stockholders’ equity |
$ | 127,204 | $ | 105,886 | ||||
|
|
|
|
|
|||||
See accompanying notes to consolidated financial statements.
99
Table of Contents
Tetraphase Pharmaceuticals, Inc.
Consolidated Statements of Operations and Comprehensive Loss
(In thousands, except per share data)
| Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Revenues |
$ | 9,098 | $ | 10,486 | $ | 7,600 | ||||||
|
|
|
|
|
|
|
|||||||
| Operating expenses: |
||||||||||||
| Research and development |
61,932 | 31,508 | 17,294 | |||||||||
| General and administrative |
12,932 | 7,168 | 4,309 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total operating expenses |
74,864 | 38,676 | 21,603 | |||||||||
|
|
|
|
|
|
|
|||||||
| Loss from operations |
(65,766 | ) | (28,190 | ) | (14,003 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Other income (expense): |
||||||||||||
| Interest income |
17 | 10 | — | |||||||||
| Interest expense |
(1,017 | ) | (1,719 | ) | (1,021 | ) | ||||||
| Other income (expense) |
24 | 263 | (63 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| Other expense, net |
(976 | ) | (1,446 | ) | (1,084 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net loss |
$ | (66,742 | ) | $ | (29,636 | ) | $ | (15,087 | ) | |||
|
|
|
|
|
|
|
|||||||
| Net loss per share-basic and diluted |
$ | (2.49 | ) | $ | (1.78 | ) | $ | (47.54 | ) | |||
|
|
|
|
|
|
|
|||||||
| Weighted-average number of common shares used in net loss per share-basic and diluted |
26,807 | 16,665 | 317 | |||||||||
|
|
|
|
|
|
|
|||||||
| Comprehensive loss |
$ | (66,742 | ) | $ | (29,636 | ) | $ | (15,087 | ) | |||
|
|
|
|
|
|
|
|||||||
See accompanying notes to consolidated financial statements.
100
Table of Contents
Tetraphase Pharmaceuticals, Inc.
Consolidated Statements of Convertible Preferred Stock and Stockholders’ Equity (Deficit)
(In thousands)
| Series A-1 Convertible Preferred Shares |
Series A-2 Convertible Preferred Shares |
Series B Convertible Preferred Shares |
Series C Convertible Preferred Shares |
Common Shares | Additional Paid-In Capital |
Accumulated Deficit |
Total Stockholders’ Equity (Deficit) |
|||||||||||||||||||||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||||||||||||||||
| Balance at December 31, 2011 |
10,040 | $ | 9,925 | 13,096 | $ | 15,055 | 57,471 | $ | 9,946 | 175,418 | $ | 44,915 | 306 | $ | — | $ | 6,395 | $ | (74,998 | ) | $ | (68,603 | ) | |||||||||||||||||||||||||||||
| Exercise of stock options |
— | — | — | — | — | — | — | — | 19 | — | 29 | — | 29 | |||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | 612 | — | 612 | |||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | (15,087 | ) | (15,087 | ) | |||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
| Balance at December 31, 2012 |
10,040 | $ | 9,925 | 13,096 | $ | 15,055 | 57,471 | $ | 9,946 | 175,418 | $ | 44,915 | 325 | $ | — | $ | 7,036 | $ | (90,085 | ) | $ | (83,049 | ) | |||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
| Exercise of stock options |
— | — | — | — | — | — | — | — | 56 | — | 96 | — | 96 | |||||||||||||||||||||||||||||||||||||||
| Issuance of common stock from initial public offering (net of underwriters discounts and issuance costs of $7,391) |
— | — | — | — | — | — | — | — | 11,512 | 12 | 73,182 | — | 73,194 | |||||||||||||||||||||||||||||||||||||||
| Conversion of convertible preferred stock into common stock |
(10,040 | ) | (9,925 | ) | (13,096 | ) | (15,055 | ) | (57,471 | ) | (9,946 | ) | (175,418 | ) | (44,915 | ) | 8,829 | 9 | 79,832 | — | 79,841 | |||||||||||||||||||||||||||||||
| Reclassification of warrants for common stock |
— | — | — | — | — | — | — | — | — | — | 462 | — | 462 | |||||||||||||||||||||||||||||||||||||||
| Issuance of common stock from follow-on public offering (net of underwriters discounts and issuance costs of $3,475) |
— | — | — | — | — | — | — | — | 4,907 | 5 | 45,594 | — | 45,599 | |||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | 1,301 | — | 1,301 | |||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | (29,636 | ) | (29,636 | ) | |||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
| Balance at December 31, 2013 |
— | $ | — | — | $ | — | — | $ | — | — | $ | — | 25,629 | $ | 26 | $ | 207,503 | $ | (119,721 | ) | $ | 87,808 | ||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
| Exercise of stock options |
— | — | — | — | — | — | — | — | 563 | — | 1,421 | — | 1,421 | |||||||||||||||||||||||||||||||||||||||
| Issuance of common stock from follow-on public offering (net of underwriters discounts and issuance costs of $5,542) |
— | — | — | — | — | — | — | — | 4,543 | 5 | 80,761 | — | 80,766 | |||||||||||||||||||||||||||||||||||||||
| Issuance of common stock under employee stock purchase plan |
— | — | — | — | — | — | — | — | 8 | — | 83 | — | 83 | |||||||||||||||||||||||||||||||||||||||
| Issuance of common stock from warrant exercise |
— | — | — | — | — | — | — | — | 63 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Stock-based compensation expense |
— | — | — | — | — | — | — | — | — | — | 5,230 | — | 5,230 | |||||||||||||||||||||||||||||||||||||||
| Net loss |
— | — | — | — | — | — | — | — | — | — | — | (66,742 | ) | (66,742 | ) | |||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
| Balance at December 31, 2014 |
— | $ | — | — | $ | — | — | $ | — | — | $ | — | 30,806 | $ | 31 | $ | 294,998 | $ | (186,463 | ) | $ | 108,566 | ||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
See accompanying notes to consolidated financial statements.
101
Table of Contents
Tetraphase Pharmaceuticals, Inc.
Consolidated Statements of Cash Flows
(In thousands)
| Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Operating activities |
||||||||||||
| Net loss |
$ | (66,742 | ) | $ | (29,636 | ) | $ | (15,087 | ) | |||
| Adjustments to reconcile net loss to net cash used in operating activities |
||||||||||||
| Depreciation and amortization |
124 | 129 | 353 | |||||||||
| Amortization of deferred financing costs and debt discount |
226 | 342 | 175 | |||||||||
| Accretion of final interest payment on term loans |
115 | 199 | 128 | |||||||||
| Fair value adjustment of warrants and investor right obligation |
— | (263 | ) | 63 | ||||||||
| Stock-based compensation expense |
5,230 | 1,301 | 612 | |||||||||
| Loss from disposal of property and equipment |
2 | — | — | |||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Restricted cash |
— | (63 | ) | — | ||||||||
| Accounts receivable |
(1,752 | ) | 746 | (2,267 | ) | |||||||
| Prepaid expenses and other current assets |
(1,199 | ) | (154 | ) | (227 | ) | ||||||
| Accounts payable |
2,224 | 310 | 772 | |||||||||
| Accrued expenses and accrued final interest payment on term loan |
3,983 | 3,190 | (1,878 | ) | ||||||||
| Deferred revenue |
166 | (607 | ) | 699 | ||||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in operating activities |
(57,623 | ) | (24,506 | ) | (16,657 | ) | ||||||
| Investing activities |
||||||||||||
| Purchases of property and equipment |
(191 | ) | (129 | ) | (54 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in investing activities |
(191 | ) | (129 | ) | (54 | ) | ||||||
| Financing activities |
||||||||||||
| Proceeds from sale of common stock, net of underwriter discounts and issuance costs |
80,766 | 119,404 | (611 | ) | ||||||||
| Deferred financing fees |
— | — | (85 | ) | ||||||||
| Proceeds from issuance of term loan payable |
— | 3,000 | 6,200 | |||||||||
| Repayment of term loan payable |
(6,126 | ) | (4,232 | ) | (2,197 | ) | ||||||
| Proceeds from issuance of stock under stock plans |
1,504 | 96 | 29 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by financing activities |
76,144 | 118,268 | 3,336 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net increase (decrease) in cash and cash equivalents |
$ | 18,330 | $ | 93,633 | $ | (13,375 | ) | |||||
| Cash and cash equivalents at beginning of period |
102,712 | 9,079 | 22,454 | |||||||||
|
|
|
|
|
|
|
|||||||
| Cash and cash equivalents at end of period |
$ | 121,042 | $ | 102,712 | $ | 9,079 | ||||||
|
|
|
|
|
|
|
|||||||
| Supplemental cash flow information |
||||||||||||
| Cash paid for interest |
$ | 945 | $ | 1,142 | $ | 702 | ||||||
|
|
|
|
|
|
|
|||||||
| Fair value of warrants issued in connection with issuance of term loan |
$ | — | $ | 115 | $ | 241 | ||||||
|
|
|
|
|
|
|
|||||||
| Conversion of convertible preferred stock into common stock |
$ | — | $ | 79,841 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
| Reclassification of warrant liability to additional paid-in-capital |
$ | — | $ | 462 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
| Reclassification of deferred financing costs to additional paid-in-capital |
$ | — | $ | 1,261 | $ | — | ||||||
|
|
|
|
|
|
|
|||||||
See accompanying notes to consolidated financial statements.
102
Table of Contents
Tetraphase Pharmaceuticals, Inc.
Notes to Consolidated Financial Statements
(1) Organization and Operations
The Company
Tetraphase Pharmaceuticals, Inc. (the “Company”), is a clinical-stage biopharmaceutical company that was incorporated in Delaware on July 7, 2006 and has a principal place of business in Watertown, Massachusetts. The Company is using its proprietary chemistry technology to create novel antibiotics for serious and life-threatening multidrug-resistant infections. The Company is developing its lead product candidate eravacycline, a fully synthetic tetracycline derivative, as a broad-spectrum intravenous (“IV”) and oral antibiotic for use as a first-line empiric monotherapy for the treatment of multidrug-resistant infections, including multidrug-resistant Gram-negative infections. The Company is conducting a global Phase 3 clinical program for eravacycline called IGNITE (Investigating Gram-Negative Infections Treated with Eravacycline) consisting of two Phase 3 clinical trials. IGNITE 1 is a Phase 3 clinical trial evaluating the safety and efficacy of eravacycline with IV administration for the treatment of complicated intra-abdominal infections (“cIAI”), for which the Company announced top-line data in December 2014. IGNITE 2, a second Phase 3 clinical trial of eravacycline for the treatment of complicated urinary tract infections (“cUTI”), with IV-to-oral transition therapy, is ongoing.
Consistent with guidance issued by the United States Food and Drug Administration (“FDA”), with respect to the development of antibiotics for cIAI and the Company’s discussions with the FDA, the Company expects that positive results from these two Phase 3 clinical trials will be sufficient to support submission of a new drug application (“NDA”) for eravacycline in the treatment of cIAI and cUTI. In December 2014, the Company announced positive top-line data from IGNITE 1. In September 2014, the Company announced positive data from the lead-in portion of IGNITE 2, and in October 2014, the Company announced the selection of the oral dose for the IV-to-oral transition therapy (1.5 mg/kg IV followed by 200 mg oral dose) to be evaluated by the pivotal portion of IGNITE 2 and the initiation of patient enrollment. The Company expects to have top-line data from the pivotal portion of IGNITE 2 in mid-2015. If the Company completes the pivotal portion of IGNITE 2 when anticipated, and it is successful, the Company expects to submit an NDA to the FDA by the end of 2015 and a marketing authorization application (“MAA”), to the European Medicines Agency (“EMA”), in the first half of 2016. The Company is also pursuing the discovery and development of additional antibiotics that target unmet medical needs, including multidrug-resistant Gram-negative bacteria.
The Company is devoting substantially all of its efforts to product research and development, market development, and raising capital. The Company is subject to a number of risks similar to those of other life science companies in a similar stage of development, including rapid technological change, dependence on key individuals, competition from other companies, compliance with government regulations, protection of proprietary technology, dependence on third parties, product liability, the need for development of commercially viable products, regulatory approval of products, uncertainty of market acceptance of products, and the need to obtain additional financing to fund the development of its product candidates. The Company has not completed development of any product candidate and has devoted substantially all of its financial resources and efforts to research and development, including preclinical and clinical development. The Company expects to continue to incur significant expenses and increasing operating losses for at least the next several years, and expects to require additional financial resources to advance its product candidates to either commercial stage or liquidity events.
The Company has incurred annual net operating losses in every year since its inception. As of December 31, 2014, the Company had incurred losses since inception of $186.5 million. The Company has not generated any product revenues related to its primary business purpose and has financed its operations primarily through public offerings and private placements of its equity securities, debt financings and funding from the United States government. In March 2013, the Company completed the sale of 10,714,286 shares of common stock in the Company’s initial public offering (“IPO”) at a price to the public of $7.00 per share. In April 2013, the Company
103
Table of Contents
completed the sale of an additional 797,792 shares of common stock to the underwriters for the IPO upon the exercise of the underwriters’ option in the IPO to purchase additional shares of common stock at a price to the public of $7.00. In November 2013, the Company completed the sale of 4,907,403 shares of common stock in a follow-on public offering at a price to the public of $10.00 per share. In October 2014, the Company completed the sale of 4,542,500 shares of common stock in a follow-on public offering at a price to the public of $19.00 per share.
There can be no assurance that the Company will be able to obtain additional debt or equity financing or generate revenues from collaborative partners, on terms acceptable to the Company, on a timely basis or at all. The failure of the Company to obtain sufficient funds on acceptable terms when needed could have a material adverse effect on the Company’s business, results of operations and financial condition.
(2) Summary of Significant Accounting Policies
Segment Information
Operating segments are defined as components of an enterprise about which separate discrete information is available for evaluation by the chief operating decision maker, or decision-making group, in deciding how to allocate resources and in assessing performance. The Company views its operations and manages its business in one operating segment, which is the business of developing and commercializing its proprietary chemistry technology to create novel antibiotics for serious and life-threatening infections, including multidrug-resistant infections.
Use of Estimates
The preparation of financial statements in conformity with generally accepted accounting principles requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenue and expenses and related disclosures. On an ongoing basis, the Company’s management evaluates its estimates, including estimates related to clinical trial accruals, stock-based compensation expense, contract and grant revenues, and expenses. The Company bases its estimates on historical experience and other market-specific or other relevant assumptions that it believes to be reasonable under the circumstances. Actual results may differ from those estimates or assumptions.
Concentrations of Credit Risk and Off-Balance Sheet Risk
Financial instruments that potentially subject the Company to concentrations of credit risk are primarily cash, cash equivalents and restricted cash. The Company maintains its cash and cash equivalent balances in the form of cash and money market accounts with financial institutions that management believes are creditworthy. The Company’s investment policy includes guidelines on the quality of the institutions and financial instruments and defines allowable investments that the Company believes minimize its exposure to concentration of credit risk. The Company has no financial instruments with off-balance-sheet risk of loss.
Principles of Consolidation
The consolidated financial statements include the accounts of the Company and its wholly owned subsidiaries, Tetraphase Securities Corporation and Tetraphase Pharma Securities Inc., Massachusetts Securities Corporations, and Tetraphase Pharmaceuticals (Bermuda) Ltd. All significant intercompany balances and transactions have been eliminated in consolidation.
Cash and Cash Equivalents
The Company considers all highly liquid investments with maturities of three months or less from the date of purchase to be cash equivalents. Cash and cash equivalents at December 31, 2014 and 2013 consisted of cash and money market funds.
104
Table of Contents
Fair Value Measurements
The Company’s financial instruments consist principally of cash and cash equivalents, accounts receivable, accounts payable, accrued liabilities, and term loan payable. Fair value measurements are classified and disclosed in one of the following three categories:
| Level 1 | — | Quoted prices in active markets for identical assets or liabilities. | ||
| Level 2 | — | Inputs other than Level 1 that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities. | ||
| Level 3 | — | Unobservable inputs that are supported by little or no market activity and that are significant to the fair value of the assets or liabilities. | ||
Financial instruments measured at fair value as of December 31, 2014 and 2013 are classified below based on the three fair value hierarchy tiers described above (in thousands):
| Fair Value Measurements at Reporting Date Using |
||||||||||||||||
| Balance | Level 1 | Level 2 | Level 3 | |||||||||||||
| December 31, 2014 |
||||||||||||||||
| Cash |
$ | 2,919 | $ | 2,919 | $ | — | $ | — | ||||||||
| Money market funds, included in cash equivalents |
$ | 118,123 | $ | 118,123 | $ | — | $ | — | ||||||||
| December 31, 2013 |
||||||||||||||||
| Cash |
$ | 2,704 | $ | 2,704 | $ | — | $ | — | ||||||||
| Money market funds, included in cash equivalents |
$ | 100,008 | $ | 100,008 | $ | — | $ | — | ||||||||
The Company measures cash equivalents at fair value on a recurring basis. The fair value of cash equivalents is determined based on “Level 1” inputs, which consist of quoted prices in active markets for identical assets.
The fair value of the Company’s term loan payable is determined using current applicable rates for similar instruments as of the balance sheet date. The Company’s term loan payable is a Level 3 liability within the fair value hierarchy. The fair value of the Company’s term loan payable at December 31, 2014, computed pursuant to a discounted cash flow technique using the effective interest rate based on the Company’s estimated borrowing rate at December 31, 2014, was $4.9 million.
The fair value of the preferred stock warrant liability as of March 25, 2013 was determined based on “Level 3” inputs utilizing the Black-Scholes option pricing model (Note 7). On March 25, 2013, upon completion of the Company’s IPO, the warrants to purchase preferred stock converted into warrants to purchase common stock and the Company reclassified the fair value of the warrants as of March 25, 2013 to additional paid-in capital. The following table presents activity in the preferred stock warrant liability during the year ended December 31, 2013 (in thousands):
| Balance | ||||
| Fair value at December 31, 2012 |
$ | 610 | ||
| Value of warrants issued in 2013 |
115 | |||
| Decrease in fair value recognized in net loss |
(263 | ) | ||
| Reclassification of fair value to additional paid-in capital |
(462 | ) | ||
|
|
|
|||
| Fair value at December 31, 2013 |
$ | — | ||
|
|
|
|||
105
Table of Contents
Accounts Receivable
In September 2011, the National Institutes of Health’s (“NIH”) National Institute of Allergy and Infectious Diseases (“NIAID”) division awarded a contract of up to $35.8 million over a five-year term for the development of TP-271, a preclinical compound, for respiratory disease caused by bacterial biothreat pathogens (“NIAID Contract”) (Note 3). The Company is collaborating with CUBRC Inc. (“CUBRC”), an independent, not for profit, research corporation that specializes in U.S. government-based contracts, on this NIAID Contract and has entered into a subcontract with CUBRC that could potentially provide funding to the Company of up to approximately $13.3 million over the five-year term, including committed funding of $8.3 million from the initial contract date through September 30, 2016, of which $7.1 million had been received by the Company through December 31, 2014. In addition during 2011, the Company was a subawardee under a separate grant from the NIAID (“NIAID Grant”) (Note 3).
In January 2012, the Biomedical Advanced Research and Development Authority (“BARDA”), an agency of the U.S. Department of Health and Human Services, awarded a contract of up to $67.0 million for the development of eravacycline as a potential countermeasure for the treatment of disease caused by bacterial biothreat pathogens (“BARDA Contract”). The funding under the BARDA Contract is also being used for certain activities in the development of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria. The Company is also collaborating with CUBRC on the BARDA Contract and has entered into a subcontract with CUBRC that could potentially provide funding to the Company of up to approximately $39.8 million, including committed funding of $31.0 million from the initial contract date through September 9, 2016, of which $16.4 million had been received by the Company through December 31, 2014 (Note 3).
Accounts receivable at December 31, 2014 and 2013 represent amounts due from CUBRC under the Company’s subcontracts under the NIAID Contract and the BARDA Contract and under the Company’s subaward under the NIAID Grant. The Company’s practice is to bill the prime contractor, CUBRC, amounts for which the Company has been invoiced by third parties in the case of contract research or subcontractor costs or for internal costs incurred. Expenses directly associated with the Company’s NIAID and BARDA Contracts and NIAID Grant that have been accrued at the end of the reporting period are not billed to the prime contractor until third party invoices have been received or until internal costs have been paid. Unbilled accounts receivable was $2.9 million and $0.8 million at December 31, 2014 and 2013, respectively.
Property and Equipment, Net
Property and equipment are stated at cost, less accumulated depreciation and amortization. Depreciation and amortization are recognized using the straight-line method over the estimated useful lives of the respective assets, which is generally three to five years. Leasehold improvements are amortized over the shorter of the lease term or the estimated useful economic lives of the related assets.
Restricted Cash
At December 31, 2014 and 2013 the Company had $199,000 in restricted cash deposits with a bank, of which $159,000 is collateral for a letter of credit issued to the landlord of the Company’s leased facility. If the Company defaults on its rental obligations, $159,000 will be payable to the lessor of the leased facility. In addition, the Company has $40,000 in restricted cash to secure the Company’s corporate credit card issued through the same bank.
Revenue Recognition
The Company’s revenue is derived from its subcontracts with CUBRC under the BARDA Contract and the NIAID Contract and its subaward under the NIAID Grant (Note 3). The Company recognizes revenue under these best-efforts, cost-reimbursable and cost-plus-fixed-fee subcontracts and subaward as the Company performs services under the subcontracts and subaward so long as a subcontract and subaward has been executed
106
Table of Contents
and the fees for these services are fixed or determinable, legally billable and reasonably assured of collection. Recognized amounts reflect the Company’s partial performance under the subcontracts and subaward and equal direct and indirect costs incurred plus fixed fees, where applicable. The Company does not recognize revenue under these arrangements for amounts related to contract periods where funding is not yet committed as amounts above committed funding thresholds would not be considered fixed or determinable or reasonably assured of collection. Revenues and expenses under these arrangements are presented gross on the consolidated statements of operations and comprehensive loss as the Company has determined it is the primary obligor under these arrangements relative to the research and development services it performs as lead technical expert.
Revenue under the Company’s subcontracts with respect to the BARDA Contract and NIAID Contract is earned under a cost-plus-fixed-fee contract through which the Company is reimbursed for direct costs incurred plus allowable indirect costs and a fixed fee earned. Billings under the Company’s subcontracts under the BARDA Contract and NIAID Contract are based on approved provisional indirect billing rates that permit recovery of allowable fringe benefits, overhead and general and administrative expenses and a fixed fee.
Revenue under the Company’s subaward with respect to the NIAID Grant is earned under a cost-reimbursable contract through which the Company is reimbursed for direct costs incurred plus allowable indirect costs. Billings under the Company’s subaward under the NIAID Grant are based on approved provisional indirect billing rates that permit recovery of allowable fringe benefits and general and administrative expenses.
Research and Development Expenses
Research and development costs are charged to expense as incurred and include, but are not limited to:
| • | personnel-related expenses, including salaries, benefits, and stock-based compensation expense; |
| • | expenses incurred under agreements with contract research organizations, contract manufacturing organizations and consultants that provide preclinical, clinical, regulatory and manufacturing services; |
| • | payments made under the Company’s license agreement with Harvard University; |
| • | the cost of acquiring, developing and manufacturing clinical trial materials and lab supplies; |
| • | facility, depreciation and other expenses, which include direct and allocated expenses for rent, maintenance of the Company’s facilities, insurance and other supplies; and |
| • | costs associated with preclinical and regulatory activities. |
Costs for certain development activities, such as clinical trials, are recognized based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations, or information provided to the Company by its vendors on their actual costs incurred. Payments for these activities are based on the terms of the individual arrangements, which may differ from the pattern of costs incurred, and are reflected in the financial statements as prepaid or accrued research and development. In certain circumstances, the Company is required to make nonrefundable advance payments to vendors for goods or services that will be received in the future for use in research and development activities. In such circumstances, the nonrefundable advance payments are deferred and capitalized, even when there is no alternative future use for the research and development, until related goods or services are provided.
Comprehensive Loss
Comprehensive loss consists of net income or loss and changes in equity during a period from transactions and other events and circumstances generated from non-owner sources. The Company’s net loss equals comprehensive loss for all periods presented.
107
Table of Contents
Income Taxes
The Company uses the liability method of accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on the difference between the financial reporting and the tax reporting basis of assets and liabilities and are measured using the enacted tax rates and laws that are expected to be in effect when the differences are expected to reverse. The Company provides a valuation allowance against net deferred tax assets unless, based upon the available evidence, it is more likely than not that the deferred tax assets will be realized. The Company has evaluated available evidence and concluded that the Company may not realize the benefit of its deferred tax assets; therefore a valuation allowance has been established for the full amount of the deferred tax assets. The Company’s practice is to recognize interest and/or penalties related to income tax matters in income tax expense.
Stock-Based Compensation
The Company applies the provisions of Accounting Standards Codification (“ASC”) 718, Compensation-Stock Compensation to stock-based awards. Under ASC 718, the Company determines equity-based compensation at the grant date using the Black-Scholes option pricing model to estimate fair value for employee equity awards. The Company recognizes the value of the award that is ultimately expected to vest as an expense on a straight-line basis over the requisite service period using the estimated fair market value of the stock. Any changes to the estimated forfeiture rates are accounted for prospectively. The Company records stock-based compensation expense for share-based payments issued to non-employees based on the fair value of the awards using the Black-Scholes option pricing model. Share-based payments issued to non-employees are revalued at each reporting period and as the equity instruments vest and are recognized as expense using the accelerated attribution method over the related service period.
Recent Accounting Pronouncements Issued and Adopted
In May 2014, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) No. 2014-09, Revenue from Contracts with Customers (Topic 606), which supersedes all existing revenue recognition requirements, including most industry-specific guidance. The new standard requires a company to recognize revenue when it transfers goods or services to customers in an amount that reflects the consideration that the company expects to receive for those goods or services. The new standard will be effective for the Company on January 1, 2017. The Company is currently evaluating the potential impact that this update may have on the Company’s financial position and results of operations.
In June 2014, the FASB issued ASU 2014-10, which simplifies financial reporting for development stage entities by eliminating requirements specific to development stage entities. As a result, entities in a development stage will no longer need to present inception-to-date information about income statement line items, cash flows, and equity transactions. Instead, the new guidance clarifies how these entities should tailor existing disclosures to explain the risks and uncertainties related to their activities. This update is effective for annual periods beginning after December 15, 2014, and early application is permitted for any annual or interim period for which the entity’s financial statements have not yet been issued. The Company adopted this guidance prior to issuing the financial statements in the Company’s quarterly report on Form 10-Q for the period ended June 30, 2014. The adoption of ASU 2014-10 impacted disclosure only and did not have any impact on the Company’s financial position or results of operations.
In 2014, the FASB issued new guidance on management’s responsibility in evaluating whether or not there is substantial doubt about a company’s ability to continue as a going concern within one year from the date the financial statements are issued each reporting period. This new accounting guidance is effective for annual periods ending after December 15, 2016. Early adoption is permitted. The Company is in process of evaluating the new guidance and determining the expected effect on its financial statements.
108
Table of Contents
Net Loss per Common Share
Basic net loss per share is calculated by dividing the net loss by the weighted average number of shares of Common Stock outstanding for the period, without consideration for common stock equivalents. Diluted net loss per share is computed by dividing the net loss by the weighted average number of common share equivalents outstanding for the period determined using the treasury-stock method. For purposes of this calculation, preferred stock, stock options and warrants are considered to be common stock equivalents and are only included in the calculation of diluted net loss per share when their effect is dilutive.
On February 28, 2013, the Company’s board of directors approved an amendment to the Company’s certificate of incorporation to effect a 1-for-29 reverse split of its common stock. The Company effected this amendment to its certificate of incorporation on March 5, 2013. Following the Company’s reverse split, and effective as of the completion of the Company’s IPO on March 25, 2013, all of the Company’s preferred stock was converted to common stock at a 1-for-29 ratio. For purposes of calculating net loss per common share for the year ended December 31, 2013, the preferred stock that converted to common stock was included in the net loss per common share calculation on a post-conversion basis as of March 25, 2013, the effective date of conversion, and the corresponding converted shares were included on a pro-rata basis for each applicable reporting period. As a result, the weighted-average common shares outstanding during the year ended December 31, 2013 was 16.7 million, as compared to 25.6 million shares outstanding as of December 31, 2013.
The amounts in the table below were excluded from the calculation of diluted weighted-average shares outstanding, prior to the use of the treasury stock method, due to their anti-dilutive effect:
| Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Preferred stock |
— | — | 8,828,438 | |||||||||
| Warrants |
1,103 | 104,107 | 88,013 | |||||||||
| Outstanding stock options |
3,409,497 | 2,844,343 | 1,442,810 | |||||||||
(3) Significant Agreements and Contracts
License Agreement
In August 2006, the Company entered into a license agreement for certain intellectual property with Harvard University (the “University”). Under the license agreement, as of December 31, 2014, the Company has paid the University an aggregate of $3.8 million in upfront license fees and development milestone payments, and has issued 31,379 shares of common stock to the University.
The Company is obligated to make certain payments totaling up to approximately $15.1 million upon achievement of certain development and regulatory milestones and royalties on net sales of products covered by the agreement. In January 2007 and April 2010, the Company and the University amended the license agreement to include certain additional intellectual property. The Company paid an additional $25,000 to the University with each amendment. In February 2011, the license agreement was further amended to include additional intellectual property in the license granted by the University without the payment of any additional consideration. The Company also paid a $2.0 million milestone fee in October 2013 in connection with the dosing of the first patient in the Company’s Phase 3 clinical trial of eravacycline for the treatment of cIAI. This amount was recorded as research and development expense during the year ended December 31, 2013.
Government Grant and Contracts
BARDA Contract for Eravacycline
The Company has received funding for its lead product candidate, eravacycline, under an award from BARDA. In January 2012, BARDA awarded a five-year contract that provides for up to a total of $67.0 million
109
Table of Contents
in funding for the development, manufacturing and clinical evaluation of eravacycline for the treatment of disease caused by bacterial biothreat pathogens. The funding under the BARDA Contract is also being used for the development, manufacturing and clinical evaluation of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria.
In connection with the BARDA Contract, in February 2012, the Company entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which it may receive funding of up to approximately $39.8 million, reflecting the portion of the BARDA funding that may be paid to the Company for its activities.
Although the BARDA Contract and the Company’s subcontract with CUBRC under the BARDA Contract, have five-year terms, BARDA is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond current-year amounts from Congressionally approved annual appropriations. To the extent that BARDA ceases to provide funding of the program to CUBRC, CUBRC has the right to cease providing funding to the Company. Committed funding from CUBRC under the Company’s BARDA subcontract is $31.0 million through September 9, 2016, the current contract end date, as a result of the exercise of several options by BARDA under the BARDA Contract. Total funds of $16.4 million had been received by the Company through December 31, 2014 under this contract. During the years ended December 31, 2014, 2013 and 2012, the Company recognized revenue of $6.9 million, $7.7 million and $4.9 million, respectively, from the Company’s subcontract under the BARDA Contract.
NIAID Grant and Contract for TP-271
The Company has received funding for its preclinical compound TP-271 under two awards from NIAID for the development, manufacturing and clinical evaluation of TP-271 for respiratory diseases caused by biothreat and antibiotic-resistant public health pathogens, as well as bacterial pathogens associated with community-acquired bacterial pneumonia:
| • | the NIAID Grant awarded in July 2011 that provides up to a total of approximately $2.8 million over five years; and |
| • | the NIAID Contract awarded in September 2011 that provides up to a total of approximately $35.8 million in funding over five years. |
In connection with the NIAID Grant, in November 2011, CUBRC awarded the Company a 55-month, no-fee subaward of approximately $980,000, reflecting the portion of the NIAID Grant funding that may be paid to the Company for its activities.
In connection with the NIAID Contract, in October 2011, the Company entered into a five-year cost-plus-fixed-fee subcontract with CUBRC under which the Company may receive funding of up to approximately $13.3 million, reflecting the portion of the NIAID Contract funding that may be paid to the Company for its activities.
Although the NIAID Contract, the NIAID Grant and the Company’s subcontract with CUBRC under the NIAID Contract have terms of five years, and the Company’s subaward under the NIAID Grant has a term of 55 months, NIAID is entitled to terminate the project for convenience at any time, and is not obligated to provide continued funding beyond September 30, 2016. To the extent NIAID ceases to provide funding of the programs to CUBRC, CUBRC has the right to cease providing funding to the Company. As of December 31, 2014, committed funding from CUBRC under the Company’s subcontract with respect to the NIAID Contract is $8.3 million through the current contract end date which has been extended to September 30, 2016, of which $7.1 million had been received through December 31, 2014. Committed funding from CUBRC under the Company’s subaward with respect to the NIAID Grant is $0.8 million through the current contract end date which has been extended to May 30, 2016, of which $0.7 million had been received through December 31, 2014.
110
Table of Contents
During the years ended December 31, 2014, 2013 and 2012, the Company recognized revenue of $2.1 million, $2.5 million, and $2.5 million, respectively, from the Company’s subcontract under the NIAID Contract. During the years ended December 31, 2014, 2013 and 2012, the Company recognized revenue of $135,000, $267,000 and $273,000, respectively, from the Company’s subaward under the NIAID Grant.
(4) Property and Equipment
Property and equipment at December 31, 2014 and 2013 consisted of the following (in thousands):
| Estimated Useful Life In Years |
December 31, | |||||||||||
| 2014 | 2013 | |||||||||||
| Laboratory equipment |
5 | $ | 1,932 | $ | 1,806 | |||||||
| Furniture and fixtures |
5 | 178 | 170 | |||||||||
| Office and computer equipment |
3 | 163 | 176 | |||||||||
| Leasehold improvements |
527 | 527 | ||||||||||
|
|
|
|
|
|||||||||
| 2,800 | 2,679 | |||||||||||
| Less accumulated depreciation and amortization |
(2,500 | ) | (2,444 | ) | ||||||||
|
|
|
|
|
|||||||||
| Property and equipment, net |
$ | 300 | $ | 235 | ||||||||
|
|
|
|
|
|||||||||
Depreciation and amortization expense for the years ended December 31, 2014, 2013 and 2012 was $124,000, $129,000 and $353,000, respectively.
(5) Accrued Expenses
Accrued expenses at December 31, 2014 and 2013 consisted of the following (in thousands):
| December 31, 2014 |
December 31, 2013 |
|||||||
| Drug supply and development |
$ | 5,440 | $ | 970 | ||||
| Salaries and benefits |
2,358 | 1,554 | ||||||
| Clinical trial related |
724 | 1,849 | ||||||
| Preclinical |
328 | 78 | ||||||
| Professional fees |
346 | 246 | ||||||
| Other |
281 | 593 | ||||||
|
|
|
|
|
|||||
| Total |
$ | 9,477 | $ | 5,290 | ||||
|
|
|
|
|
|||||
(6) Long-Term Debt
In May 2011, the Company executed a Loan and Security Agreement with Silicon Valley Bank and Oxford Finance (the “Term Loan”), which provided for up to $8.0 million of funding, to be made available in two tranches. The Company borrowed the first $1.5 million in May 2011 and the second tranche for the remaining $6.5 million in December 2011. The Term Loan bore interest at 10% per annum and provided for a final payment of 2.75% of the original principal due at the maturity date of November 1, 2014. Under the terms of the Term Loan, the Company was only required to pay interest (and not principal) through February 28, 2012. Each tranche was being repaid in 33 monthly payments of equal principal, plus accrued interest, after the interest only period that ended on February 28, 2012. The final payment of 2.75% was due at the same time as the last loan payment. The Term Loan matured on November 1, 2014, and has been paid in full.
In December 2012, the Company amended the Term Loan (the “2012 Term Loan”) to provide for up to an additional $9.2 million in funding, to be made available in two tranches. The Company borrowed the first tranche
111
Table of Contents
totaling $6.2 million under the 2012 Term Loan in December 2012 (“2012 Term A Loan”) and borrowed the remaining $3.0 million in February 2013 (“2012 Term B Loan”). Both the 2012 Term A Loan and the 2012 Term B Loan bear interest at 9% per annum.
The Company was only required to pay interest (and not principal) for the first six months of each tranche of the 2012 Term Loan. Each tranche of the 2012 Term Loan is being repaid in 33 equal monthly payments of principal, plus accrued interest, after the interest only period. An additional payment of 2.90% of the original principal amount of each tranche will be due at the same time as the last loan payment for the tranche. The 2012 Term A Loan matures on March 1, 2016.
The 2012 Term Loan is collateralized by a blanket lien on all corporate assets, excluding intellectual property, and by a negative pledge of the Company’s intellectual property. The 2012 Term Loan contains customary default provisions that include material adverse events, as defined therein. The Company has determined that the risk of subjective acceleration under the material adverse events clause is remote and therefore has classified the outstanding principal in current and long-term liabilities based on scheduled principal payments.
Future principal payments on the 2012 Term Loan are as follows (in thousands):
| December 31, 2014 |
||||
| 2015 |
3,513 | |||
| 2016 |
1,132 | |||
|
|
|
|||
| Total term loan payments |
4,645 | |||
| Current term loan payable |
3,513 | |||
| Less debt discount and issuance costs |
(77 | ) | ||
|
|
|
|||
| Current term loan payable, net |
3,436 | |||
| Term loan payable, less current portion |
1,132 | |||
| Less debt discount and issuance costs |
(8 | ) | ||
|
|
|
|||
| Term loan payable, less current portion, net |
$ | 1,124 | ||
|
|
|
|||
(7) Warrants
In May 2011, the Company issued warrants to purchase an aggregate of 1,555,815 shares of Series C Preferred Stock at an exercise price of $0.2571 per share in connection with the Term Loan (Note 6). The warrants are exercisable immediately and have a ten year life. The warrants were initially valued at $302,000 using the Black-Scholes pricing model with the following assumptions; risk free interest rate of 3.2%; dividend yield of zero; expected volatility of 67%; with an expected life of ten years, and were being expensed as additional interest over the term of the loan. In accordance with ASC 480, the characteristics of these warrants and the rights and privileges of the underlying Series C Preferred Stock resulted in the classification of these warrants as a liability and changes to the fair value of the warrants were recognized as a component of other income (expense) in the statement of operations and comprehensive loss.
In December 2012, the Company issued warrants to purchase an aggregate of 964,605 shares of Series C Preferred Stock at an exercise price of $0.2571 per share in connection with the 2012 Term Loan (Note 6). The warrants are exercisable immediately and have a ten year life. The warrants were initially valued at $241,000 using the Black-Scholes pricing model with the following assumptions; risk free interest rate of 1.8%; dividend yield of zero; expected volatility of 61%; with an expected life of ten years, and are being expensed as additional interest over the term of the loan. In accordance with ASC 480, the characteristics of these warrants and the
112
Table of Contents
rights and privileges of the underlying Series C Preferred Stock resulted in the classification of these warrants as a liability and changes to the fair value of the warrants were recognized as a component of other income (expense) in the statement of operations and comprehensive loss.
In connection with the February 2013 borrowing under the Term Loan, the warrant that the Company issued to Silicon Valley Bank in December 2012 automatically became exercisable for an additional 233,372 shares of Series C preferred stock. In addition, the Company issued to Oxford Finance a 10-year warrant to purchase an additional 233,372 shares of Series C preferred stock with an exercise price of $0.2571 per share. The warrants were initially valued at $115,000 using the Black-Scholes option pricing model with the following assumptions: risk-free interest rate of 1.89%, dividend yield of zero, expected volatility rate of 59% and an expected life of ten years, and are being expensed as additional interest over the term of the loan. The warrant was classified as a liability in accordance with ASC 480 and was subject to remeasurement at each balance sheet date and changes to the fair value were recognized as a component of other income (expense) in the statement of operations and comprehensive loss.
The Company estimated the fair value of the preferred stock warrants using the Black-Scholes option pricing model based on the following assumptions:
| December 31, 2012 | ||
| Expected volatility |
60% | |
| Expected term (in years) |
5.0-10.0 | |
| Risk-free interest rate |
0.72%-1.78% | |
| Expected dividend yield |
0% | |
| Estimated fair value of Series A-1 Preferred Stock |
$0.45 | |
| Estimated fair value of Series C Preferred Stock |
$0.34 |
Upon completion of the IPO, the warrants related to the Term Loan became exercisable for 53,648 shares of the Company’s common stock at an exercise price of $7.46 per share, the warrants related to the 2012 Term A Loan became exercisable for 33,262 shares of the Company’s common stock at an exercise price of $7.46 per share and the warrants related to the 2012 Term B Loan became exercisable for 16,094 shares of the Company’s common stock at an exercise price of $7.46 per share. On the date of the conversion of the warrants, the Company revalued the outstanding warrants using the Black-Scholes option pricing model with the following assumptions: risk-free interest rate of 0.67% to 1.84%, dividend yield of zero, expected volatility rate of 59%, expected term of 5 to 10 years and stock price of $7.00. The fair value of the warrants at March 25, 2013 was $462,000. The Company recorded other income of $263,000 in the statement of operations and comprehensive loss during the year ended December 31, 2013 equal to the change in fair value of the warrants from December 31, 2012 to March 25, 2013. The Company reclassified the fair value of the warrants at March 25, 2013, of $462,000, to additional paid-in capital.
On June 23, 2014, Silicon Valley Bank exercised its warrants under the Term Loan and 2012 Term Loan described above pursuant to the cashless exercise feature of the warrants. In connection with the exercise of the warrants under the Term Loan, the Company issued 12,354 shares of the Company’s common stock. Warrants to purchase 14,470 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants. In connection with the exercise of the warrants under the 2012 Term Loan, the Company issued 11,366 shares of the Company’s common stock. Warrants to purchase 13,312 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants.
On December 13, 2014, Oxford Finance exercised its warrants under the Term Loan and 2012 Term Loan described above pursuant to the cashless exercise feature of the warrants. In connection with the exercise of the warrants under the Term Loan, the Company issued 20,488 shares of the Company’s common stock. Warrants to purchase 6,336 shares of common stock were cancelled as payment for the aggregate exercise price of the
113
Table of Contents
warrants. In connection with the exercise of the warrants under the 2012 Term Loan, the Company issued 18,849 shares of the Company’s common stock. Warrants to purchase 5,829 shares of common stock were cancelled as payment for the aggregate exercise price of the warrants.
(8) Stockholders’ Equity
Initial Public Offering
In March, 2013, the Company completed its IPO, issuing 10,714,286 shares of common stock at a price to the public of $7.00 per share, resulting in net proceeds to the Company of $68.0 million after deducting underwriting discounts of $4.4 million and offering costs of $2.5 million.
In connection with the IPO, all of the Company’s outstanding preferred stock automatically converted into a total of 8,828,438 shares of its common stock.
In April 2013, the Company completed the sale of an additional 797,792 shares to the underwriters upon the exercise of the underwriters’ option in the IPO to purchase additional shares of common stock at a price to the public of $7.00, resulting in net proceeds to the Company of $5.2 million after deducting underwriting discounts and commissions.
2013 Follow-on Public Offering
In November 2013, the Company completed a follow-on public offering, issuing 4,907,403 shares of common stock at a price to the public of $10.00 per share, resulting in net proceeds to the Company of $45.6 million after deducting underwriting discounts and commissions of $2.9 million and offering costs of $0.5 million.
2014 Follow-on Public Offering
In October 2014, the Company sold 4,542,500 shares of common stock in a follow-on public offering at a price to the public of $19.00 per share, resulting in net proceeds to the Company of $80.8 million after deducting underwriting discounts and commissions of $5.2 million and offering costs of $0.4 million.
(9) Stock-based Compensation
In August 2006, the Company adopted the Tetraphase Pharmaceuticals, Inc. Stock Incentive Plan (the “2006 Plan”) under which it was able to grant incentive stock options, nonqualified stock options, restricted stock, and stock grants to purchase up to 1,128,183 shares of Common Stock. In May 2010, the Company amended the plan to increase the number of shares of Common Stock issuable under the 2006 Plan to 1,853,288. The options expire ten years after the grant date. As of December 31, 2014, no shares were available for future issuance under the 2006 Plan.
In February 2013, the Company’s board of directors and stockholders approved, effective upon the closing of the IPO, the 2013 Stock Incentive Plan (the “2013 Plan”). Under the 2013 Plan, the Company may grant incentive stock options, nonstatutory stock options, stock appreciation rights, restricted stock, restricted stock units and other stock-based awards for the purchase of that number of shares of Common Stock equal to the sum of (i) 1,688,777 shares of Common Stock, (ii) 258,265 shares of Common Stock that were reserved for issuance under the 2006 Plan that remained available for issuance under the 2006 Plan upon the closing of the IPO, (iii) any shares of Common Stock subject to awards under the 2006 Plan which awards expire, terminate or are otherwise surrendered, canceled, forfeited or repurchased by the Company without having been fully exercised or resulting in any Common Stock being issued. In addition, the number of shares of Common Stock that may be issued under the 2013 Plan is subject to automatic annual increases, to be added on January 1 of each year from January 1, 2014 through and including January 1, 2023, equal to the number of shares that is the lesser of
114
Table of Contents
(a) 3,000,000, (b) 4% of the then outstanding shares of Common Stock or (c) an amount determined by the Company’s board of directors. In January 2014, the number of shares authorized for issuance under the 2013 Plan increased by 1,025,171 shares. As of December 31, 2014, 386,147 shares were available for future issuance under the 2013 Plan. In January 2015, the number of shares authorized for issuance under the 2013 Plan increased by 1,232,232 shares.
Terms of stock award agreements, including vesting requirements, are determined by the board of directors, subject to the provisions of the 2013 Plan. Options granted by the Company typically vest over a four year period. Certain of the options are subject to acceleration of vesting in the event of certain change of control transactions. The options are exercisable from the date of grant for a period of ten years. For options granted prior to the Company’s IPO, the exercise price equaled the estimated fair value of the Common Stock as determined by the board of directors on the date of grant. For options granted subsequent to the Company’s IPO, the exercise price equaled the closing price of the Company’s stock on the NASDAQ Global Select Market on the date of grant.
Stock option activity at December 31, 2014 and changes during the year then ended are presented in the table and narrative below (in thousands, except share and per share data):
| Shares | Weighted- Average Exercise Price |
Weighted- Average Remaining Contractual Term (years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at December 31, 2013 |
2,844,343 | $ | 5.10 | 7.97 | $ | 23,960 | ||||||||||
| Granted |
1,292,650 | 14.33 | ||||||||||||||
| Exercised |
(562,569 | ) | 2.53 | |||||||||||||
| Canceled |
(164,927 | ) | 10.63 | |||||||||||||
|
|
|
|||||||||||||||
| Options outstanding at December 31, 2014 |
3,409,497 | $ | 8.75 | 7.92 | $ | 105,550 | ||||||||||
|
|
|
|||||||||||||||
| Options vested or expected to vest at December 31, 2014 (1) |
3,256,816 | $ | 8.61 | 7.88 | $ | 101,276 | ||||||||||
|
|
|
|||||||||||||||
| Options exercisable at December 31, 2014 |
1,415,555 | $ | 5.30 | 6.76 | $ | 48,716 | ||||||||||
|
|
|
|||||||||||||||
| (1) | This represents the number of vested options as of December 31, 2014, plus the number of unvested options that the Company estimated as of December 31, 2014 would vest, based on the unvested options at December 31, 2014, as adjusted for the estimated forfeiture rate of 5.9%. |
The aggregate intrinsic value in the table above represents the difference between the Company’s closing common stock price on the last trading day during the year ended December 31, 2014 and the exercise price of the options, multiplied by the number of in-the-money options. The total intrinsic value of options exercised in the years ended December 31, 2014, 2013, and 2012 was $8.1 million, $0.5 million and $25,000, respectively. As of December 31, 2014, there was $11.7 million of total unrecognized stock-based compensation cost related to employee and non-employee unvested stock options granted under the 2006 Plan and the 2013 Plan. Total unrecognized compensation cost will be adjusted for future forfeitures. The Company expects to recognize that cost over a remaining weighted-average period of 2.6 years.
Since the Company completed its IPO on March 25, 2013, it has not had sufficient historical data to support a calculation of volatility and expected life. As such, the Company has used a weighted-average volatility considering the Company’s own volatility and the volatilities of a representative group of publicly traded companies. For purposes of identifying similar entities, the Company selected a group of publicly traded life science/biotechnology companies based on their disease focus, stage of development, number of compounds in clinical trials and number of years as a publicly-traded company. The risk-free interest rate is based on the
115
Table of Contents
U.S. Treasury yield curve in effect at the time of grant, commensurate with the expected life assumption. The expected life of stock options granted represents the weighted-average period of time that stock options granted are expected to be outstanding determined using the simplified method for employee grants. For non-employee grants, the expected life is equal to the remaining contractual term. The expected life is applied to the stock option grant group as a whole, as the Company does not expect substantially different exercise or post-vesting termination behavior among its employee population.
The Company estimates the fair value of each employee and director stock option award on the grant date using the Black-Scholes option-pricing model based on the following assumptions:
| Year Ended December 31, | ||||||
| 2014 | 2013 | 2012 | ||||
| Volatility factor |
53.41-58.13% | 54.50-60.54% | 56.89-68.12% | |||
| Expected life (in years) |
5.31-6.11 | 5.8-7.1 | 6.0-6.1 | |||
| Risk-free interest rate |
1.71%-2.13% | 0.91%-2.01% | 0.85% -1.21% | |||
| Dividend yield |
0% | 0% | 0% | |||
Compensation cost for stock options granted to employees is based on the estimated grant-date fair value and is recognized over the vesting period of the applicable option on a straight-line basis. Stock-based compensation expense related to stock options granted to employees was $4.0 million, $1.3 million, and $0.3 million during the years ended December 31, 2014, 2013, and 2012, respectively. The amount of stock-based compensation expense recognized during a period is based on the value of the portion of the awards that the Company determines are expected to vest. Forfeitures are required to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. The term “forfeitures” is distinct from “cancellations” and represents only the unvested portion of the surrendered option. The Company re-evaluates this analysis quarterly, and adjusts the forfeiture rate as necessary. Ultimately, the actual expense recognized over the vesting period will only be for those options that vest.
Using the Black-Scholes option-pricing model, the weighted-average grant date fair values of options granted to employees for the years ended December 31, 2014, 2013 and 2012 was $7.54, $4.52 and $2.32, respectively.
Stock-based compensation expense recognized in the Company’s consolidated statements of operations for stock options granted during the periods presented was as follows (in thousands):
| Year Ended December 31, |
||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Research and development |
$ | 1,845 | $ | 690 | $ | 463 | ||||||
| General and administrative |
3,385 | 611 | 149 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
$ | 5,230 | $ | 1,301 | $ | 612 | ||||||
|
|
|
|
|
|
|
|||||||
Stock Option Grants to Non-employees
During the year ended December 31, 2014, the Company granted nonqualified options to purchase 110,000 shares of common stock to non-employee consultants, with an average exercise price of $12.56 per share. There were no stock options granted to non-employee consultants during the years ended December 31, 2013 or 2012. The Company valued these options using the Black-Scholes option-pricing model and the options are revalued at each reporting period and as the equity instruments vest and are recognized as expense using the accelerated attribution method over the related service period. Stock-based compensation expense related to stock options granted to non-employees was $1.2 million, $39,000, and $0.3 million for the years ended December 31, 2014,
116
Table of Contents
2013, and 2012, respectively. Stock-based compensation expense for the year ended December 31, 2014 was estimated using the Black-Scholes option pricing model with the following assumptions: risk-free interest rate of 2.11%; dividend rate of 0%; expected volatility of 56.69%; and an expected term of 9.3 years.
(10) Employee Stock Purchase Plan
On February 27, 2014, upon the recommendation of the Company’s compensation committee, the Company’s board of directors adopted, subject to stockholder approval, the 2014 Employee Stock Purchase Plan (the “ESPP”) pursuant to which the Company may sell up to an aggregate of 300,000 shares of Common Stock. The ESPP was approved by the Company’s stockholders on June 12, 2014. The ESPP allows eligible employees to purchase common stock at a price per share equal to 85% of the lower of the fair market value of the common stock at the beginning or end of each period during the term of the ESPP. The first offering period began on August 15, 2014, and concluded on November 14, 2014. The next offering period began on November 15, 2014, and will conclude on May 14, 2015. Pursuant to the ESPP, the Company sold a total of 8,394 shares of common stock during the year ended December 31, 2014 at a purchase price of $9.88, which represented 85% of the closing price of the Company’s common stock on August 15, 2014. The Company records stock-based compensation expense under the ESPP based on the fair value of the purchase rights using the Black-Scholes option pricing model. The total stock-based compensation expense recorded as a result of the ESPP was approximately $46,000 during the year ended December 31, 2014.
(11) Income Taxes
The Company accounts for income taxes under ASC 740. Deferred income tax assets and liabilities are determined based upon differences between financial reporting and tax bases of assets and liabilities and are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse.
For the years ended December 31, 2014, 2013 and 2012, the Company did not have a current or deferred income tax expense or benefit.
As of December 31, 2014 the Company had federal net operating loss carryforwards of approximately $170.4 million and state net operating loss carryforwards of $140.5 million, which are available to reduce future taxable income. The federal net operating loss carryforwards exclude approximately $5.5 million of deductions related to the exercise of stock options. This amount represents an excess tax benefit and has not been included in the gross deferred tax asset reflected for net operating losses. The Company also had federal tax credits of $4.1 million and state tax credits of $1.7 million, which may be used to offset future tax liabilities. The net operating loss (NOL) and tax credit carryforwards will expire at various dates through 2034. The NOL and tax credit carryforwards are subject to review and possible adjustment by the Internal Revenue Service and state tax authorities. Net operating loss and tax credit carryforwards may become subject to an annual limitation in the event of certain cumulative changes in the ownership interest of significant shareholders over a three-year period in excess of 50%, as defined under Sections 382 and 383 of the Internal Revenue Code, respectively, as well as similar state provisions. This could limit the amount of tax attributes that can be utilized annually to offset future taxable income or tax liabilities. The amount of the annual limitation is determined based on the value of the Company immediately prior to the ownership change. Subsequent ownership changes may further affect the limitation in future years. The Company has not, as yet, conducted a study of research and development (“R&D”) credit carryforwards. This study may result in an adjustment to the Company’s R&D credit carryforwards; however, until a study is completed and any adjustment is known, no amounts are being presented as an uncertain tax position.
The Company has recorded no reserves or unrecognized tax benefits for tax positions taken. Since a full valuation allowance has been provided against the Company’s deferred tax assets, the effect of any unrecognized tax benefits would simply be to reduce the gross amount of the deferred tax asset and the corresponding valuation allowance. As of December 31, 2014 and 2013, the Company had no accrued interest or penalties related to uncertain tax positions.
117
Table of Contents
The principal components of the Company’s deferred tax assets are as follows (in thousands):
| Year ended December 31, |
||||||||
| 2014 | 2013 | |||||||
| Deferred tax assets: |
||||||||
| Net operating loss carry forwards |
$ | 65,370 | $ | 41,574 | ||||
| Temporary differences |
3,224 | 1,976 | ||||||
| Research and development credit and carry forwards |
5,170 | 3,609 | ||||||
|
|
|
|
|
|||||
| Deferred tax assets |
73,764 | 47,159 | ||||||
| Less valuation allowance |
(73,764 | ) | (47,159 | ) | ||||
|
|
|
|
|
|||||
| Net deferred tax assets |
$ | — | $ | — | ||||
|
|
|
|
|
|||||
ASC 740 requires a valuation allowance to reduce the deferred tax assets reported, if based on the weight of available evidence, it is more likely than not that some portion or all of the deferred tax assets will not be realized. After consideration of all the evidence, both positive and negative, the Company has recorded a valuation allowance against its deferred tax assets at December 31, 2014 and 2013, respectively, because the Company’s management has determined that is it more likely than not that these assets will not be realized. The $26.6 million increase in the valuation allowance in 2014 primarily relates to the net loss incurred by the Company.
The Company is currently open to examination under the statute of limitations by the Internal Revenue Service and state jurisdictions for the tax years ended 2010 through 2013. Carryforward tax attributes generated in years past may still be adjusted upon future examination if they have or will be used in a future period. The Company is currently not under examination by the Internal Revenue Service or any other jurisdictions for any tax years.
A reconciliation of the Federal statutory tax rate of 34% to the Company’s effective income tax rate follows:
| Year ended December 31, |
||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Statutory tax rate |
(34.00 | )% | (34.00 | )% | (34.00 | )% | ||||||
| State taxes, net of Federal benefits |
(5.28 | )% | (5.28 | )% | (5.28 | )% | ||||||
| Permanent differences |
0.61 | % | 0.93 | % | 1.01 | % | ||||||
| Credits |
(2.34 | )% | (4.33 | )% | (0.09 | )% | ||||||
| Change in valuation allowance |
39.87 | % | 39.92 | % | 38.92 | % | ||||||
| Other |
1.14 | % | 2.76 | % | (0.56 | )% | ||||||
|
|
|
|
|
|
|
|||||||
| Effective tax rate |
— | % | — | % | — | % | ||||||
|
|
|
|
|
|
|
|||||||
(12) Commitments and Contingencies
Lease Commitments
The Company leases its facilities under an operating lease for 15,899 square feet of office and laboratory space that was set to expire on July 31, 2015. In September 2014, the Company amended its operating lease to extend the lease term from July 31, 2015 through November 30, 2016 and also entered into a new sublease covering an additional 15,174 square feet of office and laboratory space, located next to the Company’s current headquarters, with a lease term from February 1, 2015 through November 30, 2016. The Company recognizes rent expense on a straight-line basis over the non-cancelable lease term.
118
Table of Contents
As of December 31, 2014, the aggregate minimum future rent payments under the lease and sublease agreements are as follows (in thousands):
| December 31, 2014 |
||||
| 2015 |
1,431 | |||
| 2016 |
1,238 | |||
|
|
|
|||
| Total minimum lease payments |
$ | 2,669 | ||
|
|
|
|||
The Company recorded $1.0 million, $0.6 million and $0.6 million in rent expense for the years ended December 31, 2014, 2013 and 2012, respectively.
Litigation
The Company is not a party to any litigation and does not have contingency reserves established for any litigation liabilities.
(13) Quarterly Results (Unaudited)
| Three Months Ended | ||||||||||||||||
| March 31, 2014 |
June 30, 2014 |
September 30, 2014 |
December 31, 2014 |
|||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| (unaudited) | ||||||||||||||||
| Revenue |
$ | 2,457 | $ | 1,275 | $ | 2,294 | $ | 3,072 | ||||||||
| Operating expenses |
15,675 | 19,460 | 16,274 | 23,455 | ||||||||||||
| Loss from operations |
(13,218 | ) | (18,185 | ) | (13,980 | ) | (20,383 | ) | ||||||||
| Other expense, net |
(305 | ) | (278 | ) | (226 | ) | (167 | ) | ||||||||
| Net loss |
$ | (13,523 | ) | $ | (18,463 | ) | $ | (14,206 | ) | $ | (20,550 | ) | ||||
| Net loss per share—basic and diluted |
$ | (0.53 | ) | $ | (0.71 | ) | $ | (0.55 | ) | $ | (0.69 | ) | ||||
| Three Months Ended | ||||||||||||||||
| March 31, 2013 |
June 30, 2013 |
September 30, 2013 |
December 31, 2013 |
|||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| (unaudited) | ||||||||||||||||
| Revenue |
$ | 2,700 | $ | 3,722 | $ | 2,166 | $ | 1,898 | ||||||||
| Operating expenses |
5,323 | 8,680 | 11,852 | 12,821 | ||||||||||||
| Loss from operations |
(2,623 | ) | (4,958 | ) | (9,686 | ) | (10,923 | ) | ||||||||
| Other expense, net |
(168 | ) | (468 | ) | (430 | ) | (380 | ) | ||||||||
| Net loss |
$ | (2,791 | ) | $ | (5,426 | ) | $ | (10,116 | ) | $ | (11,303 | ) | ||||
| Net loss per share—basic and diluted |
$ | (1.51 | ) | $ | (0.26 | ) | $ | (0.49 | ) | $ | (0.49 | ) | ||||
119
Table of Contents
| ITEM 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
None.
| ITEM 9A. | Controls and Procedures |
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2014. In designing and evaluating our disclosure controls and procedures, management recognized that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and our management necessarily applied its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on this evaluation, our Chief Executive Officer and Chief Financial Officer concluded that as of December 31, 2014, our disclosure controls and procedures were (1) designed to ensure that material information relating to us is made known to our management including our principal executive officer and principal financial officer by others, particularly during the period in which this annual report on Form 10-K was prepared and (2) effective, in that they provide reasonable assurance that information required to be disclosed by us in the reports we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms.
Management’s report on the Company’s internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) appears below.
Internal Control Over Financial Reporting
Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is defined in Rules 13a-15(f) and 15d-15(f) promulgated under the Exchange Act as a process designed by, or under the supervision of, the company’s principal executive and principal financial officers and effected by the company’s board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
| • | Pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of the assets of the company; |
| • | Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and |
| • | Provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation. Projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2014. In making this assessment, management used the criteria set forth by the Committee of
120
Table of Contents
Sponsoring Organizations of the Treadway Commission in Internal Control—Integrated Framework (2013 framework) (COSO). Based on its assessment, management believes that, as of December 31, 2014, our internal control over financial reporting is effective based on those criteria.
Our independent registered public accounting firm has not issued an attestation report of our internal control over financial reporting due to a transition period established by rules of the SEC for newly public companies.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during the quarter ended December 31, 2014 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
| ITEM 9B. | Other Information |
None.
121
Table of Contents
| ITEM 10. | Directors, Executive Officers and Corporate Governance |
The information required by this Item 10 will be contained in the sections entitled “Election of Directors” and “Section 16(a) Beneficial Ownership Reporting Compliance” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein. The information required by this item concerning our code of ethics is set forth in the section entitled “Code of Business Conduct and Ethics” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein. The information required by this item relating to executive officers may be found in Part I, Item 1 of this annual report on Form 10-K under the heading “Business—Executive Officers” and is incorporated herein by reference.
| ITEM 11. | Executive Compensation |
The information required by this Item 11 will be contained in the sections entitled “Executive and Director Compensation,” “Compensation Committee Interlocks and Insider Participation” and “Compensation Committee Report” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein.
| ITEM 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
The information required by this Item 12 will be contained in the sections entitled “Ownership of Our Common Stock” and “Executive and Director Compensation—Equity Compensation Plan Information” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein.
| ITEM 13. | Certain Relationships and Related Person Transactions, and Director Independence |
The information required by this Item 13 will be contained in the sections entitled “Certain Relationships and Related Person Transactions” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein.
| ITEM 14. | Principal Accounting Fees and Services |
The information required by this Item 14 will be contained in the section entitled “Corporate Governance—Principal Accountant Fees and Services” appearing in the definitive proxy statement we will file in connection with our 2015 Annual Meeting of Stockholders and is incorporated by reference herein.
122
Table of Contents
| ITEM 15. | Exhibits and Financial Statement Schedules |
| (a) | Documents filed as part of Form 10-K. |
| (1) | Financial Statements |
Report of Independent Registered Public Accounting Firm
Consolidated Balance Sheets
Consolidated Statements of Operations and Comprehensive Loss
Consolidated Statements of Stockholders’ Equity (Deficit)
Consolidated Statements of Cash Flows
Notes to Consolidated Financial Statements
| (2) | Schedules |
Schedules have been omitted as all required information has been disclosed in the financial statements and related footnotes.
| (3) | Exhibits |
The Exhibits listed in the Exhibit Index are filed as a part of this Form 10-K.
123
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| TETRAPHASE PHARMACEUTICALS, INC. | ||||
| Date: March 6, 2015 | By: | /s/ Guy Macdonald | ||
| Guy Macdonald President & Chief Executive Officer (Principal Executive Officer) | ||||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
| /s/ Guy Macdonald Guy Macdonald |
Director, President and Chief Executive Officer (Principal Executive Officer) |
March 6, 2015 | ||
| /s/ David C. Lubner David C. Lubner |
Senior Vice President and Chief Financial Officer (Principal Financial and Accounting Officer) |
March 6, 2015 | ||
| /s/ L. Patrick Gage L. Patrick Gage, Ph.D. |
Chairman | March 6, 2015 | ||
| /s/ Garen Bohlin Garen Bohlin |
Director | March 6, 2015 | ||
| /s/ Jeffrey A. Chodakewitz Jeffrey A. Chodakewitz |
Director | March 6, 2015 | ||
| /s/ John G. Freund John G. Freund |
Director | March 6, 2015 | ||
| /s/ Steven R. Gullans Steven R. Gullans |
Director | March 6, 2015 | ||
| /s/ Nancy Wysenski Nancy Wysenki |
Director | March 6, 2015 | ||
124
Table of Contents
EXHIBIT INDEX
| Incorporated by Reference from | ||||||||
| Exhibit Number |
Description |
Registrant’s Form |
Date Filed with the SEC |
Exhibit Number | ||||
| 3.1 | Restated Certificate of Incorporation of the Registrant | 10-Q | 5/13/13 | 3.1 | ||||
| 3.2 | Amended and Restated Bylaws of the Registrant | 10-Q | 5/13/13 | 3.2 | ||||
| 4.1 | Specimen certificate evidencing shares of common stock | S-1/A | 3/5/13 | 4.1 | ||||
| 10.1# | 2006 Stock Incentive Plan, as amended | S-1 | 2/11/13 | 10.5 | ||||
| 10.2# | Form of Incentive Stock Option Agreement under 2006 Stock Incentive Plan | S-1 | 2/11/13 | 10.6 | ||||
| 10.3# | Form of Nonstatutory Stock Option Agreement under 2006 Stock Incentive Plan | S-1 | 2/11/13 | 10.7 | ||||
| 10.4# | 2013 Stock Incentive Plan | S-1/A | 3/5/13 | 10.8 | ||||
| 10.5# | Form of Incentive Stock Option Agreement under 2013 Stock Incentive Plan | S-1/A | 3/5/13 | 10.9 | ||||
| 10.6# | Form of Nonstatutory Stock Option Agreement under 2013 Stock Incentive Plan | S-1/A | 3/5/13 | 10.10 | ||||
| 10.7# | 2014 Employee Stock Purchase Plan | 10-Q | 8/12/14 | 10.1 | ||||
| 10.8# | Offer letter, dated as of December 4, 2007, by and between the Registrant and Guy Macdonald, as amended | S-1 | 2/11/13 | 10.11 | ||||
| 10.9# | Second Amendment to Offer Letter, dated as of March 5, 2014, by and between the Registrant and Guy Macdonald | 10-Q | 5/12/14 | 10.2 | ||||
| 10.10# | Offer letter, dated as of August 10, 2006, by and between the Registrant and David Lubner, as amended | S-1 | 2/11/13 | 10.12 | ||||
| 10.11# | Third Amendment to Offer Letter, dated March 5, 2014, by and between the Registrant and David Lubner | 10-Q | 5/12/14 | 10.3 | ||||
| 10.12# | Offer letter, dated as of December 22, 2010, by and between the Registrant and Patrick T. Horn | S-1 | 2/11/13 | 10.13 | ||||
| 10.13# | Amendment to Offer Letter, dated March 5, 2014, by and between the Registrant and Patrick Horn | 10-Q | 5/12/14 | 10.4 | ||||
| 10.14# | Offer letter, dated as of March 20, 2009, by and between the Registrant and Joyce Sutcliffe | S-1 | 2/11/13 | 10.14 | ||||
| 10.15# | Offer letter, dated as of March 20, 2009, by and between the Registrant and Craig Thompson dated January 30, 2014 | 8-K | 2/5/14 | 99.1 | ||||
| 10.16# | Form of Indemnification Agreement entered into between the Registrant and each of its directors and executive officers | S-1/A | 3/5/13 | 10.27 | ||||
| 10.17 | Lease Agreement, dated as of November 16, 2006, by and between the Registrant and ARE-480 Arsenal Street, LLC, as amended on September 9, 2011, March 15, 2012, September 18, 2012 and November 20, 2013 | 10-K | 3/6/14 | 10.17 | ||||
| 10.18 | Amendment, dated September 4, 2014, to Lease Agreement, dated as of November 16, 2006, by and between the Registrant and ARE-480 Arsenal Street, LLC, as amended | 10-Q | 11/10/14 | 10.1 | ||||
Table of Contents
| 10.19† | License Agreement, dated as of August 3, 2006, by and between the Registrant and the President and Fellows of Harvard College, as amended | S-1 | 2/11/13 | 10.20 | ||||
| 10.20† | Subcontract Agreement, dated as of February 1, 2012, by and between the Registrant and CUBRC, Inc. | S-1 | 2/11/13 | 10.21 | ||||
| 10.21† | Subcontract Agreement, dated as of September 30, 2011, by and between the Registrant and CUBRC, Inc. | S-1 | 2/11/13 | 10.22 | ||||
| 10.22 | Second Amended and Restated Registration Rights Agreement, dated as of May 14, 2010, as amended | S-1 | 2/11/13 | 10.1 | ||||
| 10.23 | Warrant to purchase shares of Series A Convertible Preferred Stock issued by the Registrant to Silicon Valley Bank expiring on September 27, 2017 | S-1 | 2/11/13 | 10.2 | ||||
| 10.24 | Loan and Security Agreement, dated as of May 16, 2011, among the Registrant, Tetraphase Securities Corporation, Silicon Valley Bank and Oxford Finance LLC | S-1 | 2/11/13 | 10.18 | ||||
| 10.25 | First Amendment to Loan and Security Agreement, dated December 20, 2012, by and among the Registrant, Tetraphase Securities Corporation, Silicon Valley Bank and Oxford Finance LLC | S-1 | 2/11/13 | 10.23 | ||||
| 10.26* | Consent and Second Amendment to Loan and Security Agreement, dated December 1, 2014, by and among the Registrant, Tetraphase Securities Corporation, Silicon Valley Bank, Oxford Finance LLC, the other Lenders named therein, and Silicon Valley Bank, as agent for the Lenders | |||||||
| 10.27* | Consent and Third Amendment to Loan and Security Agreement, dated December 18, 2014, by and among the Registrant, Tetraphase Securities Corporation, Silicon Valley Bank, Oxford Finance LLC, the other Lenders named therein, and Silicon Valley Bank, as agent for the Lenders | |||||||
| 21.1* | Subsidiaries of the Registrant | |||||||
| 23.1* | Consent of Ernst & Young LLP | |||||||
| 31.1* | Chief Executive Officer—Certification pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |||||||
| 31.2* | Chief Financial Officer—Certification pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |||||||
| 32.1* | Chief Executive Officer—Certification pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |||||||
| 32.2* | Chief Financial Officer—Certification pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |||||||
| 101.INS* | XBRL Instance Document | |||||||
Table of Contents
| 101.SCH* | XBRL Taxonomy Extension Schema Document | |||||||
| 101.CAL* | XBRL Taxonomy Extension Calculation Linkbase Document | |||||||
| 101.DEF* | XBRL Taxonomy Extension Definition Linkbase Document | |||||||
| 101.LAB* | XBRL Taxonomy Extension Label Linkbase Document | |||||||
| 101.PRE* | XBRL Taxonomy Extension Presentation Linkbase Document | |||||||
| * | Filed herewith. |
| # | Indicates management contract or compensatory plan or arrangement. |
| † | Confidential treatment requested as to certain portions, which portions have been omitted and filed separately with the Securities and Exchange Commission. |