Attached files
| file | filename |
|---|---|
| 8-K - 8-K - ACELRX PHARMACEUTICALS INC | d867188d8k.htm |
 February
2015 Exhibit 99.1 |
 Forward
Looking Statements 2
This presentation contains forward-looking statements, including, but not limited to,
statements related to future financial results, potential proceeds under the Grunenthal
agreement, the process and timing of anticipated future development of AcelRx’s product
candidates, including Zalviso, the NDA submission and the CRL, the Type A meeting held with
the FDA to discuss the CRL, AcelRx’s
plans
to
address
the
issues
raised
in
the
CRL,
and
anticipated
resubmission
of
the
Zalviso
NDA
to
the
FDA,
including
the scope
of the resubmission and the timing of the resubmission and FDA review time, the impact, if
any, of the FDA’s review of the amendments to the Zalviso NDA that were not
previously reviewed, planned initiation of the Phase 3 clinical trial for ARX-04,
and the therapeutic and commercial potential of AcelRx Pharmaceuticals' product
candidates, including Zalviso. These forward-looking statements are based on AcelRx
Pharmaceuticals' current expectations and inherently involve significant risks and uncertainties.
AcelRx Pharmaceuticals' actual results and the timing of events could differ materially from
those anticipated in such forward-looking statements as a result of these risks and
uncertainties, which include, without limitation, risks related to: AcelRx Pharmaceuticals'
ability to receive regulatory approval for Zalviso; any delays or inability to obtain and
maintain regulatory approval of its product candidates, including Zalviso, in the
United States and Europe; AcelRx's ability to build an effective commercial organization; its ability
to receive any milestones or royalty payments under the Grunenthal agreement; its ability to
obtain sufficient financing to commercialize Zalviso and proceed with clinical
development of ARX-04; the success, cost and timing of all product development
activities and clinical trials, including the planned Phase 3 ARX-04 trial; the market
potential for its product candidates; the accuracy of AcelRx’s estimates regarding
expenses, capital requirements and needs for financing; and other risks detailed in the "Risk Factors" and
elsewhere
in
AcelRx
Pharmaceuticals'
U.S.
Securities
and
Exchange
Commission
filings
and
reports,
including
its
Quarterly
Report
on
Form 10-Q filed with the SEC on November 10, 2014. AcelRx Pharmaceuticals undertakes no
duty or obligation to update any forward- looking statements contained in this
release as a result of new information, future events or changes in its expectations. |
 3
AcelRx–Working to Improve Acute Pain Management
Zalviso
TM
profile from Phase 3 studies
Efficacy: Demonstrated in two placebo controlled studies, 1 active
comparator study Adverse
events:
Most
common
related
AE’s
were
nausea,
vomiting,
O
2
desaturation,
itching
High patient satisfaction and nurse ease of care reported
Grünenthal partnership to commercialize Zalviso in EU & Australia established
Upcoming regulatory catalysts in US and EU
US:
NDA
resubmission
targeted
Q1
2015
EU:
Day
120
submission
planned
for
Q1
2015
Strong balance sheet with $75 million cash on hand December 31, 2014
(unaudited)
Terms:
$250M
upfront
and
potential
milestones,
mid-teens
to
mid-twenties
%
royalty
Other
Territories:
Continue
to
seek
additional
partnerships
in
Asia
&
South
America
CE
Mark:
Received
December
2014
MAA filed in Switzerland |
 4
AcelRx Update Q1 2015
Zalviso resubmission
•
Received FDA comments on bench testing
•
•
•
–
Healthy volunteers study completed
at risk, testing successful
–
Post-op
patient
study
initiated
Zalviso EU Day 120 Response
•
•
•
Expected submission in Q1
ARX-04
•
Discussion with DoD continues, funding
targeted for H1 2015
•
Pivotal Phase 3 study to be initiated in Q1
without DoD funding
Bench testing initiated, anticipated
completion end of February
Awaiting FDA comments on Human
Factors protocol
Proposed HF study to FDA in two
populations: healthy volunteers, post-op
patients
All questions to be addressed and in
process of preparing a response
CE mark approved and to be included
as part of response |
 Major items in
CRL: System errors were noted in the clinical setting at a single digit rate
Did not appear to impact Phase 3 safety and efficacy results
Improvements have been made to reduce error rate
Formal bench testing in process to confirm error rate reduction
15 misplaced tablets of ~30,000 doses
IFU modified to address this issue
HF studies underway to confirm IFU/GUI changes are adequate
Data to be provided to support 24 month dating
5
Zalviso NDA Status-CRL received July 25, 2014
Demonstration of a reduction in the incidence of system errors
Changes
to
the
Instructions
for
Use
(IFU)
to
address
inadvertent
dosing
Support for shelf life (not approvability issue) |
 Proposed
Indication: Management of Moderate to Severe In-Hospital Acute Pain
Investigational drug and delivery system not FDA approved for commercial use
6
Clinical Data |
 Invasive route
of delivery IV infiltration causes analgesic gaps
IV connection restricts patient mobility
Risk of IV site infection
Programming errors
1/9 harmful hospital errors due to IV PCA
2
IV PCA –
Current Standard of Care
7
In-hospital, post-operative
moderate to severe pain control
Higher Patient satisfaction when
patients control their own pain
IV-PCA
1.
FDA
/
AAMI
Summit
Meeting
held
October
2010;
http://www.aami.org/infusionsummit/AAMI_FDA_Summit_Report.pdf
2.
Calculated from “The rate and costs attributable to intravenous patient-controlled
analgesia errors.” Brian Meissner et al, Hospital Pharmacy April 2009
Infusion pumps large source of morbidity /
mortality
1 |
 Zalviso:
Leveraging Sufentanil High Therapeutic Index Opioid
In animal studies
High Lipophilicity
6 minute brain:plasma equilibration
No active metabolites
OPIOID
THERAPEUTIC
INDEX
Morphine
71
1
Hydromorphone
232
2
Fentanyl
277
1
Sufentanil
26,716
1
8
Sublingual Sufentanil Delivery
May reduce IV peaks & troughs
Small size may minimize swallowed drug
May result in high bioavailability
Helps with goal of consistent dose
delivery
Supplied in cartridge of 40 Tablets
2 days for average patient
1. Mather, Clin Exp Pharmacol Physiol 1995; 22:833.
2. Kumar, Eur J Pharmacol 2008; 597:39 (ED50) and Purdue Pharma MSDS, 2009
(LD50) Enables rapid transmucosal uptake
|
 9
9
Zalviso: Delivery Device Design and Feature Set
Non-invasive (sublingual) delivery
Eliminates IV infection risk
May enhance ambulation
Pre-programmed delivery
Factory set 20-minute lockout period
Addresses end-user programming
error risk
Design safety features
Set-up tablet, RFID cartridge provides full inventory loop tracking of sufentanil
tablets RFID thumb tag co-located to device helps reduce proxy dosing
HCP controlled access, device tether reduces risk of product loss
Battery power ensures 72-hour function even in the event of power outage
Investigational drug and delivery system not FDA
approved for commercial use |
 Zalviso
Phase 3 Program 10
Surgery Type
Study
Type
Sites
N
Data
Primary
Endpoint
Results
Abdominal &
Orthopedic
Surgery (IAP309)
Open-label,
Active-comparator
1
o
EP: Patient Global
Assessment of Method of
Pain Control over 48 hrs
26
359
1:1
Nov
2012
Zalviso
non-inferior to IV PCA
(p<0.001)
Zalviso
also demonstrates
superiority
to IV
PCA
(p=0.007)
Abdominal
Surgery (IAP310)
Double-blind,
Placebo-controlled
1
o
EP:Sum of Pain Intensity
Difference over 48 hrs
13
178
2:1
Mar
2013
Sufentanil treatment
superior to placebo
p=0.001
Orthopedic
Surgery (IAP311)
Double-blind,
Placebo-controlled
1
o
EP:Sum of Pain Intensity
Difference over 48 hrs
34
426
3:1
May
2013
Sufentanil treatment
superior to placebo
p<0.001 |
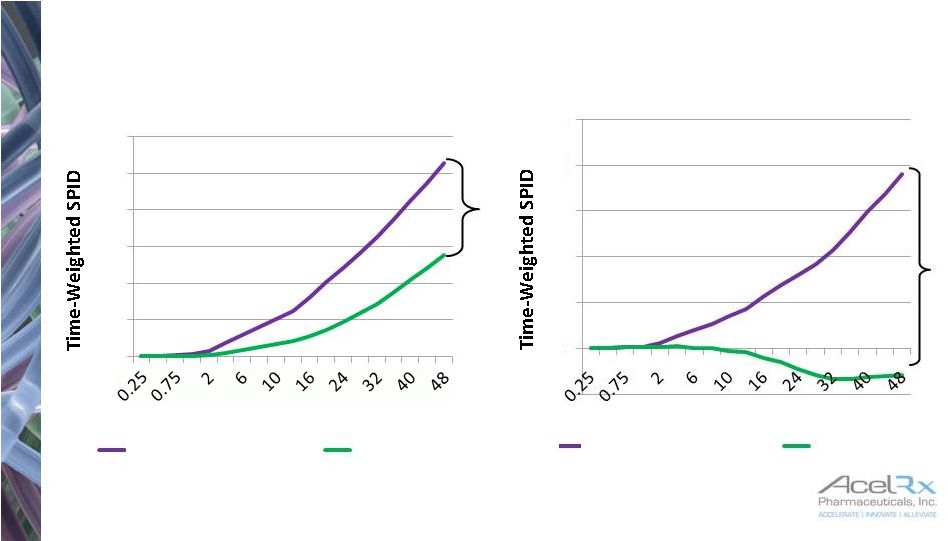 IAP310
& IAP311 Primary Endpoint: SPID-48 –
ITT Population
11
p=0.001
p<0.001
Time (hrs)
Time (hrs)
Zalviso
Zalviso
0
20
40
60
80
100
120
IAP 310 –
Abdominal
Placebo
-20
0
20
40
60
80
100
IAP 311 -
Orthopedic
Placebo |
 12
Time from first dose of study drug (hours)
Zalviso: Studies Indicate Rapid Ability to Control
Moderate to Severe Acute Pain
0
1
2
3
0
0.25
0.5
0.75
1
2
3
4
5
6
Zalviso 309
Zalviso 310
Zalviso 311
IV PCA MS 309 |
 Adverse
Reactions >2% in Placebo Studies 13
* Significantly Different between Zalviso and Placebo (p<0.05)
Possibly or Probably
Related Adverse Reactions
Zalviso
N=429
Placebo
N=162
Nausea
29.4%
22.4%
Vomiting
8.9%
4.9%
Oxygen Saturation Decreased
6.1%
2.5%
Itching*
4.7%
0%
Dizziness
4.4%
1.2%
Constipation
3.7%
0.6%
Headache
3.3%
3.7%
Insomnia
3.3%
1.9%
Hypotension
3.0%
1.2%
Confusional State
2.1%
0.6% |
 Proposed
Indication: Management of Moderate to Severe In-Hospital Acute Pain
Investigational drug and delivery system not FDA approved for commercial use
14
Commercial Opportunity |
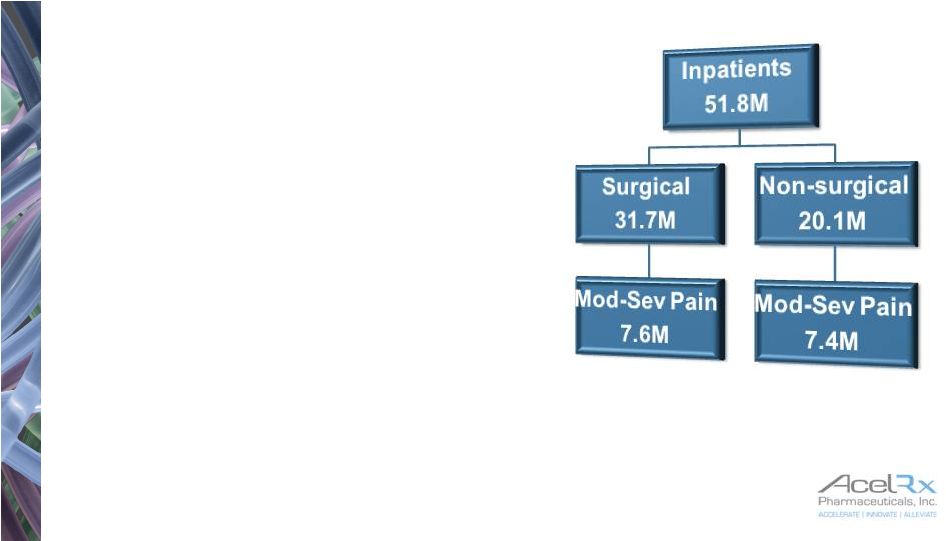 Target
Market Potential 15
1.
Rosetta, 2009 Inpatient sample
2.
Decision Resources, Pain Management Study, Acute Pain, October 2014
•
The potential market for Zalviso is defined as:
•
Acute moderate-to-severe pain population
in the hospital setting
•
Includes post-operative as well as
non-surgical pain
•
The market size for Zalviso is characterized by
hospital in-patient sampling that demonstrates
15M
patients
annually
1
•
7.6M patients post-op
•
7.4M patients non post-op
2013
U.S.
Acute
Pain
Market
$6.7B
2
•
43% of which represents post-op pain
•
20% of which represents other acute pain (non post-op)
1 |
 Anticipated Formulary Adoption after FDA Approval
Earliest –
2 Months; Typical –
8-10 Months
16
42% Very Likely to
Approve
42% Quite Likely to
Approve
16% Early Approval
Unlikely
might be swayed by
additional,
independent clinical
literature
assume product
expensive, might
accept favorable
cost-benefit analysis
looking for relevant
experts to champion
the product
unsure of cost,
looking for favorable
cost-benefit analysis
convinced by the
clinical benefit
demonstrated
assume ability to
demonstrate
economic benefit or
set cost aside
ZS Associates Qualitative Survey Among 45 P&T Committee Members, Fall 2013, sponsored by
AcelRx Pharmaceuticals, Inc. |
 Strong
Positive Reaction to Zalviso Clinical Profile Market
Research
Among
Hospital
Specialists
(n=244)
Predicted Zalviso Share of Procedural Volume
* Size of bubble is
representative of size of Zalviso
opportunity in Specialty
0
10%
20%
30%
40%
50%
60%
17
Orthopedic Surgeons
Cardiothoracic
Surgeons
General Surgeons
Hospitalist
Anesthesiologist
OB / GYN
1. ZS Associates Quantitative Survey Among Hospital Specialists, Winter 2013, sponsored by
AcelRx Pharmaceuticals, Inc.
1 |
 Current
Cost of IV PCA 18
Data from Premier Database, 2010-12
Data for post surgical pain management
involving IV PCA in total knee/hip
replacement and abdominal surgery
Costs for pumps, tubing, carrier saline and
drug range from $200-240 for 2 days
Zalviso may add value:
Addresses programming errors
Elimination of PCA IV site infection risk
Supports early ambulation
Enhanced patient satisfaction
1.
COST OF INTRAVENEOUS PATIENT-CONTROLLED ANALGESIA (IV PCA) EQUIPMENT AND OPIOID MEDICATION
FOR ORTHOPEDIC AND ABDOMINAL SURGERIES IN US HOSPITALS 0
50
100
150
200
250
300
Opioids via PCA/ Other
Tubing / Carrier Saline
IVPCA / Carrier Infusion Pump
Total Knee
Total Hip
Abdominal
Xiang (Jay) Ji, MS, Jennifer Stephens, PharmD, Pamela Palmer, MD, PhD.
Poster presented at ISPOR meeting, June 2014 |
 US
Customer-focused Organization Planned Build 80%
of relevant procedure
volume
identified
in
top
1,400
accounts
65 sales territories planned
Estimated cost/rep $250K
Estimated salesforce cost
around $16.5M per annum
19
Medical
Affairs
8 MSL’s in place
Commercial
7 RBD’s (6 hired)
65 Account
Managers to be
hired |
 20
Zalviso Publication Strategy
Peer Reviewed Manuscripts in Process
A Phase 3 Study of a Sufentanil Sublingual Microtablet System for the Management of
Postoperative Pain Following
Major
Orthopedic
Surgery
(IAP-311
Primary);
Anesthesiology
-
Submitted
Peer-Reviewed Manuscripts Available
Cost of Opioid Intravenous Patient-controlled Analgesia: Results From a Hospital Database
Analysis and Literature Assessment.
(Palmer et al.)
Clinicoeconomics and Outcomes Research
www.dovepress.com/getfile.php?fileID=20509
Pharmacokinetics of Sublingual Sufentanil Tablets and Efficacy and Safety in the Management of
Postoperative
Pain
(Minkowitz
et
al.)
Reg
Anesth
Pain
Med
2013;38:
131-139.
Sufentanil Sublingual Microtablet System versus Intravenous Patient-Controlled Analgesia
with Morphine for Postoperative
Pain
Control:
A
Randomized,
Controlled
Trial
(IAP309
Primary);
Pain
Practice;
http://onlinelibrary.wiley.com/doi/10.1111/papr.12238/full
•
A Phase 3 Study of Sufentanil Sublingual Microtablet System for the Management of Postoperative
Pain Following
Open
Abdominal
Surgery
(IAP-310
Primary);
Reg
Anesth
Pain
Med
–
http://journals.lww.com/rapm/Abstract/onlinefirst/Sufentanil_Sublingual_Tablet_System_for_the.99572.aspx
|
 Investigating
Moderate to Severe acute pain treatment in medically supervised settings
Investigational drug and delivery system not FDA approved for commercial use
21
ARX-04
HCP Administered
Single 30mcg dose
Sufentanil Tablet |
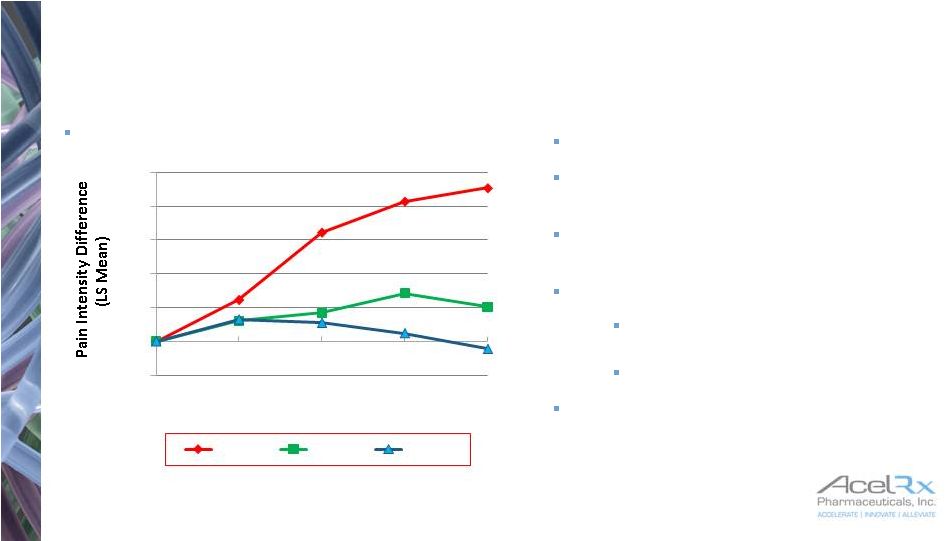 ARX-04 –
Short Term Acute Pain Management
22
End of Phase 2 Meeting held Dec. ‘13
505(b)(2) submission
500 patient safety database ,
100 multiple dose, 400 single dose
Single & repeat dose PK study -
completed
Phase 3 placebo-controlled study
Abdominal surgery, SPID-12
primary, follow for 48 hours
Results expected H2 2015
Small safety study in ER patients
planned -
results expected H2 2015
Will count as pivotal trial
-0.5
0
0.5
1
1.5
2
2.5
0
15
30
45
60
Minutes after Dose
30 mcg
20 mcg
placebo
*
**
**
*p<0.01
**p<0.001
Successful Phase 2 Bunionectomy Study |
 ARX-04 –
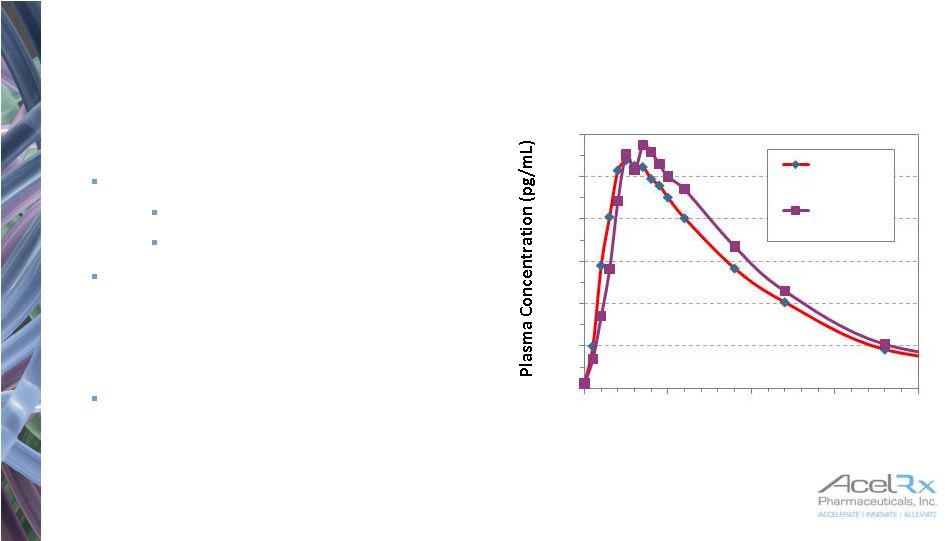
PK Study Results
23
Demonstration of Bioequivalence of
2 x 15 mcg and 1 x 30 mcg sublingual
sufentanil tablets
Bioavailability:
30 mcg 57.6%
2 x 15 mcg 60.9%
Proposed to FDA that demonstration
of bioequivalence for 2 x 15mcg
dosed 20 mins apart and single
30mcg dose would enable use of
Zalviso database to support ARX-04
In Phase 3 Zalviso studies, 323
patients dosed at t=0 and between
t=20-25mins later
0.0
10.0
20.0
30.0
40.0
50.0
60.0
0
100
200
300
400
Time (minutes)
One 30 mcg
tablet
2 x 15 mcg
tablet
BA for 30 mcg 57.6%
BA for 2 x 15 mcg 60.9% |
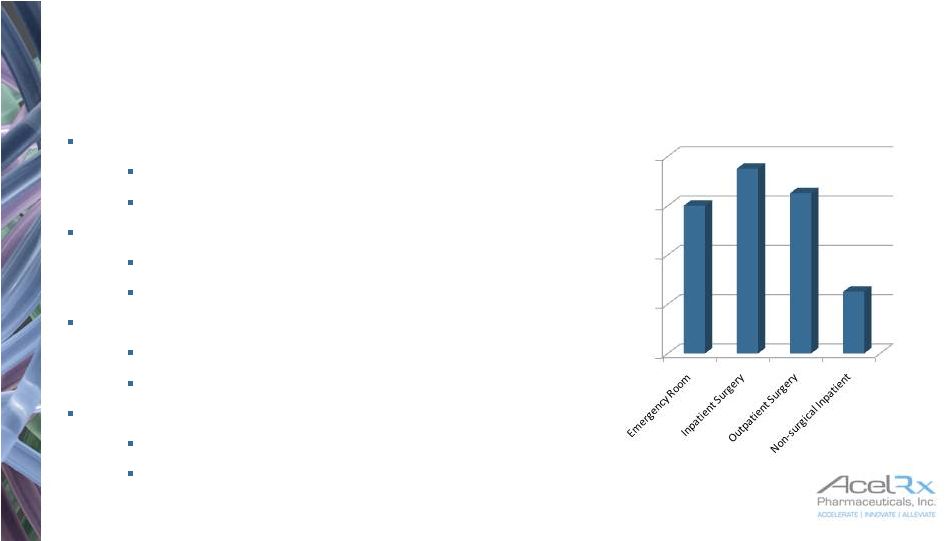 ARX-04 –
Commercial Opportunity
24
Market Research Suggests Broad Opportunity in
Moderate to Severe Acute Pain*
ER Department
51MM patients annually
2 doses per patient on average
Inpatient Surgery
8MM patients annually
2-9 doses per patient
Outpatient Surgery
13MM patients annually
3 doses per patient on average
Non-surgical Acute Pain
4MM patients annually
8 doses per patient on average
ZS Associates US Opportunity Sizing, September 2014; Includes only patients 18+ years of age.
Sponsored by AcelRx Pharmaceuticals, Inc.
0%
20%
40%
60%
80%
Physician Stated Share |
 25
Scientific Conference Schedule -
2015
Minimally Invasive Surgery Symposium (MISS)
February 25-28; Las Vegas, NV –
poster presentation (ARX-
04)
American Academy of Orthopedic Surgeons (AAOS)
March 24-28; Las Vegas, NV –
Booth & Symposium
American Society of Peri-Anesthesia Nurses (ASPAN)
April
26-30;
San
Antonio,
TX
–
Booth
&
Symposium
American Congress of Obstetricians (ACOG)
May
2-6;
San
Francisco
–
Booth
&
Symposium
International Conference on Emergency Medicine (ICEM)
American Society of Pain Management Nursing
(ASPMN)
September
16-19;
Atlanta,
GA
–
Booth
&
Symposium
American College of Surgeons (ACS)
October
4-8;
Chicago,
IL
–
Booth
&
Symposium
American Society of Anesthesiologists (ASA)
October
24-28;
San
Diego,
CA
–
Booth
&
Symposium
American Society of Regional Anesthesia and Pain
Management (ASRA)
November 19-21; Miami, FL –
1 Booth & Symposium
American Society of Health System Pharmacists (ASHP)
December 6-10; New Orleans, LA –
Booth &
Symposium
May
11-12;
Montreal,
Quebec
–
Podium
Presentation
(ARX-04)
February 25-28; Las Vegas, NV –
poster presentation
(ARX-04) |
 Financial Summary
26
Cash position at September 30, 2014: $85 million
$10 million drawn June 2014 under debt facility
$5 million received August 2014 from Grünenthal for MAA submission
Currently available cash resources fund operations through launch
Assumes timely regulatory approval of Zalviso in the US in 2015
Supports execution of all planned US pre-commercial launch efforts
Q3 2014 cash usage of ~$12 million
Headcount at December 31, 2014: 50
Cash balance December 31, 2014 $75 million (unaudited)
44 million shares outstanding at December 31, 2014 |
 Future
Catalysts 27
Event
Timing
120 day question response to Zalviso
MAA review
Q1 2015
Zalviso NDA resubmission (pending protocol approval)
Q1 2015
ARX-04 DOD
contract finalized
H1 2015
Zalviso NDA decision
Q3 2015
Zalviso
MAA decision
Q3 2015
ARX-04 Phase
3 data
H2 2015 |
 28
AcelRx–Working
to
Improve
Acute
Pain
Management
Zalviso
TM
profile from Phase 3 studies
Efficacy: Demonstrated in two placebo controlled studies, 1 active
comparator study Adverse
events:
Most
common
related
AE’s
were
nausea,
vomiting,
O
2
desaturation,
itching
High patient satisfaction and nurse ease of care reported
Grünenthal partnership to commercialize Zalviso in EU & Australia established
Upcoming regulatory catalysts in US and EU
US:
NDA
resubmission
targeted
Q1
2015
EU:
Day
120
submission
planned
for
Q1
2015
Strong balance sheet with $75 million cash on hand December 31, 2014
(unaudited)
MAA
filed
in
Switzerland
CE
Mark:
Received
December
2014
Other
Territories:
Continue
to
seek
additional
partnerships
in
Asia,
South
America
Terms:
$250M
upfront
and
potential
milestones,
mid-teens
to
mid-twenties
%
royalty |