Attached files
| file | filename |
|---|---|
| EX-99.1 - EX-99.1 - Minerva Neurosciences, Inc. | d831554dex991.htm |
| 8-K - 8-K - Minerva Neurosciences, Inc. | d831554d8k.htm |
 Exhibit 99.2
Minerva Neurosciences, Inc.
1601 Trapelo Road, Suite 284, Waltham, MA
02451 |
 2
Forward-Looking Statement Safe-Harbor
All trademarks, trade names and service marks appearing in this presentation are
the property of their respective owners. This presentation contains certain forward-looking
statements about Minerva Neurosciences that are intended to be covered by the safe harbor for
“forward-looking statements” provided by the Private Securities Litigation Reform Act of 1995, as amended.
Forward-looking statements are statements that are not historical facts. Words such as
“expect(s),” “feel(s),” “believe(s),” “will,”
“may,” “anticipate(s)” and similar expressions are intended to identify
forward-looking statements. These statements include, but are not limited to: the benefits,
efficacy and safety of the new once-a-day formulation of MIN-101; the timing and results of
future clinical milestones; the timing of future clinical trials and results of such clinical trials;
statements regarding our ability to successfully develop and commercialize our therapeutic
products; our ability to expand our long-term business opportunities; our expectations
regarding approval for our products by the U.S. Food and Drug Administration or equivalent foreign regulatory
agencies; estimates regarding the market potential for our products; financial projections and
estimates and their underlying assumptions; and future performance. All of such statements are
subject to certain risks and uncertainties, many of which are difficult to predict and
generally beyond the control of the Company, that could cause actual results to differ materially from
those expressed in, or implied or projected by, the forward-looking statements. These risks and
uncertainties include, but are not limited to: the benefits, efficacy and safety of the new
once-a-day formulation of MIN-101; the timing and results of future clinical
milestones; the timing of future clinical trials and results of such clinical trials; whether any of our therapeutic candidates
will advance further in the clinical trials process and whether and when, if at all, they will receive
final approval from the U.S. Food and Drug Administration or equivalent foreign regulatory
agencies and for which indications; whether any of our therapeutic candidates will be
successfully marketed if approved; whether our therapeutic product discovery and development
efforts will be successful; our ability to achieve the results contemplated by our collaboration
agreements; the strength and enforceability of our intellectual property rights; competition
from pharmaceutical and biotechnology companies; the development of and our ability to take
advantage of the market for our therapeutic products; our ability to raise additional capital to
fund our operations on terms acceptable to us; general economic conditions; and the other risk factors contained in our
periodic and interim reports filed with the Securities and Exchange Commission which are available on
the SEC website at www.sec.gov. Our audience is cautioned not to place undue reliance on these
forward-looking statements that speak only as of the date hereof, and we do not undertake
any obligation to revise and disseminate forward-looking statements to reflect events or
circumstances after the date hereof, or to reflect the occurrence of or non-occurrence of any events. |
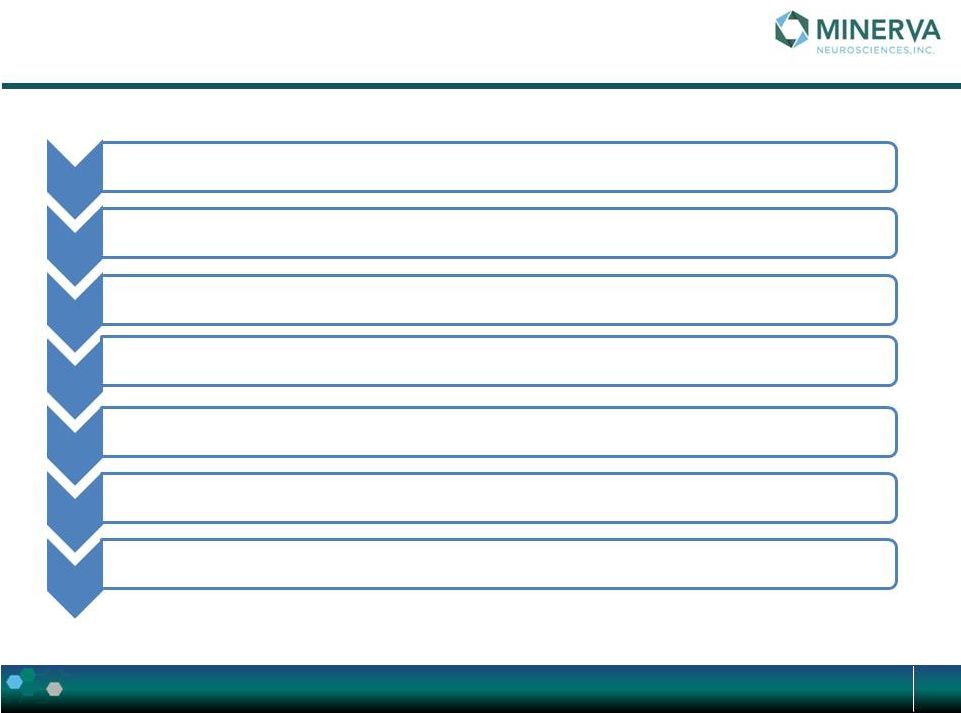
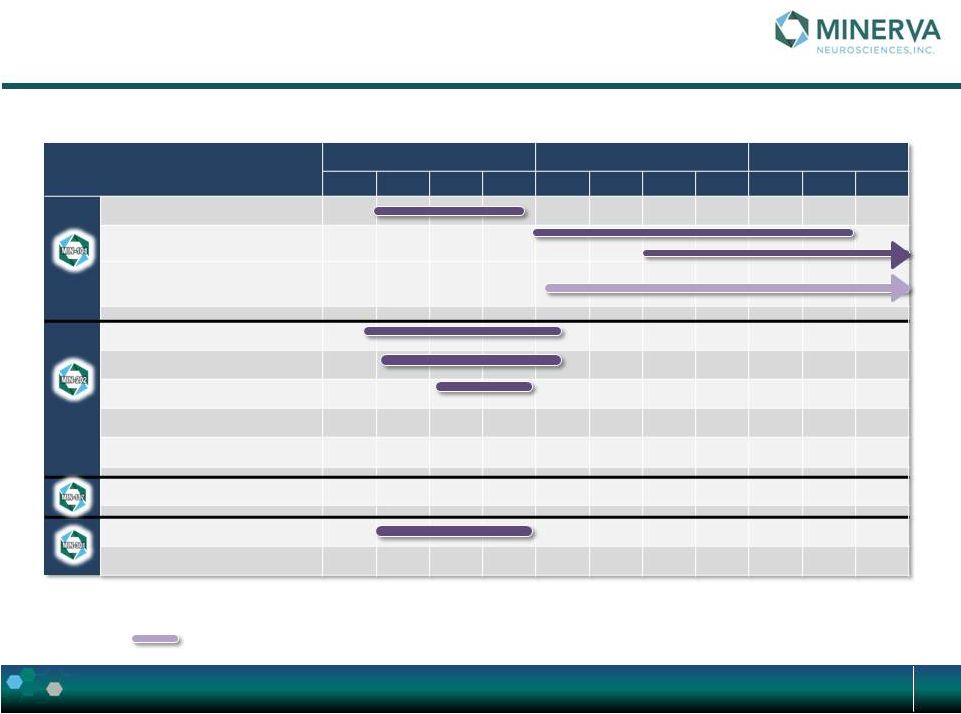 Minerva:
Overview R&D Current Status 3
Subject to additional financing
*
TBC –
subject to Ph1 results
‡
Planning in progress; subject to additional financing
End of bar = expected availability of topline results
Phase / Event
Q1
Q1
Q1
Q2
Q2
Q2
Q3
Q3
Q3
Q4
Q4
2014
2015
2016
Once A Day Formulation
Ph IIB in Schizophrenia
Ph IIB Extension
Parallel clinical development & phase III
preparation
Phase IB in MDD (single dose)
PK/Safety Study in HV (MAD)
BA Study in HV (solid)
Ph IIA in Primary Insomnia
*
Ph IIA in Sec. Insomnia (MDD)
*
Ph II in MDD
‡
MPTP Primate Study
Ph I in Healthy Volunteers
‡ |
 MIN-101
4 |
 R&D update
Once a day formulation results
Phase IIB study design
5 |
 MIN-101C02: Once a day formulation
6
MIN-101C02
Study Title:
A Two-Part Study Designed to Evaluate the Pharmacokinetic Profile of MIN-101
and its Main Metabolites Following Single and Multiple Dose Modified Release
Prototype Formulation Administration in Healthy CYP2D6 Extensive Metaboliser
Male and Female Subjects, and to Evaluate the Relationship Between the
Pharmacokinetic Profile of MIN-101 and its Main Metabolites and
Cardiovascular Parameters |
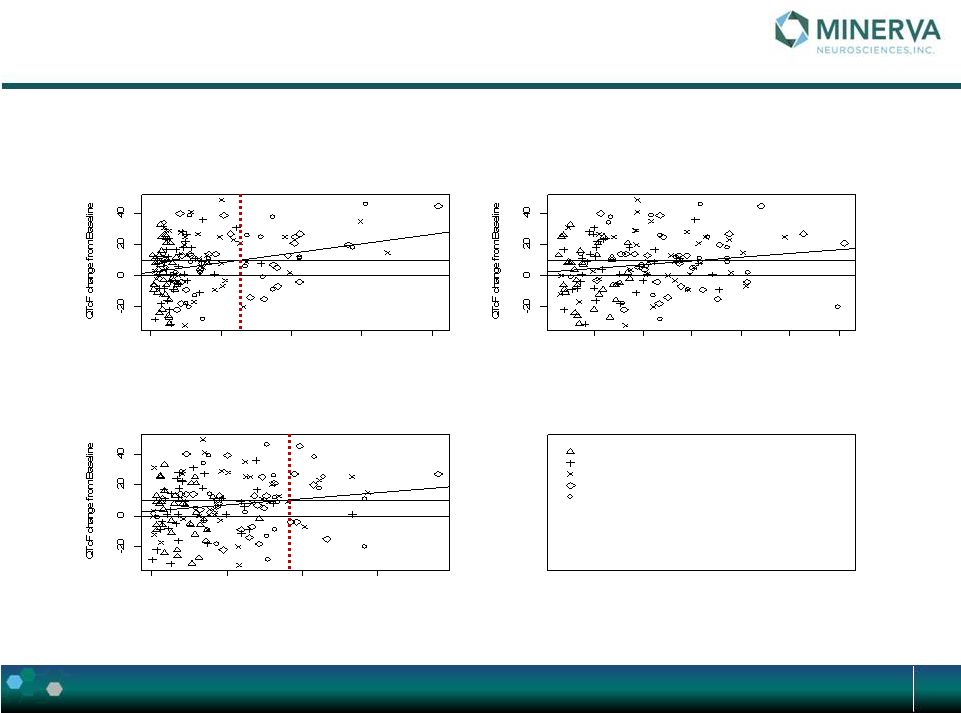 7
0
10
20
30
40
Change in QTcF by BFB-520 concentration
Plasma concentration
1
2
3
4
5
6
Change in QTcF by BFB-999 concentration
Plasma concentration
0
50
100
150
Change in QTcF by CYR-101 concentration
Plasma concentration
2 subjects with outlying values removed
Dose adjustment period D2
Dose adjustment period D4
Dose adjustment period D6
Fixed dose period D14
Ambulatory and fixed dose period D28
Exposure levels not to exceed…. |
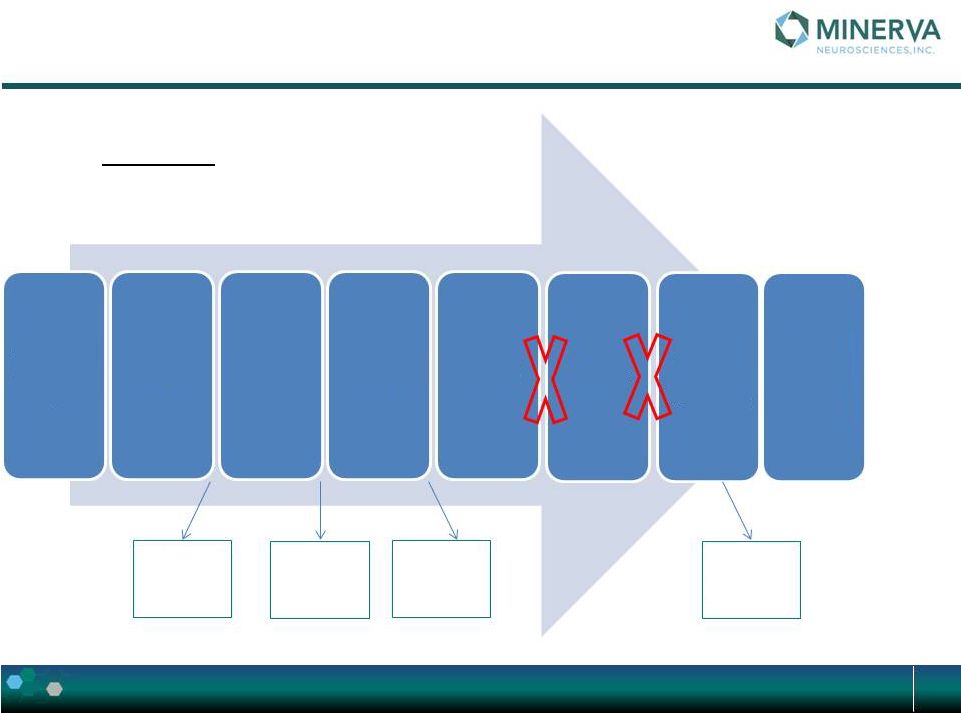 Part 1
Study Design 8
PART 1
32 mg
slow
release
32 mg
medium
release
40 mg
slow
release
32 mg
slow
release
Screening
Day -28 to
Day -2
Period
1
Period
2
Period
3
Period
4
Period
5
Period
6
Food
interaction
Follow
up
call 3 to 5
days
after
last |
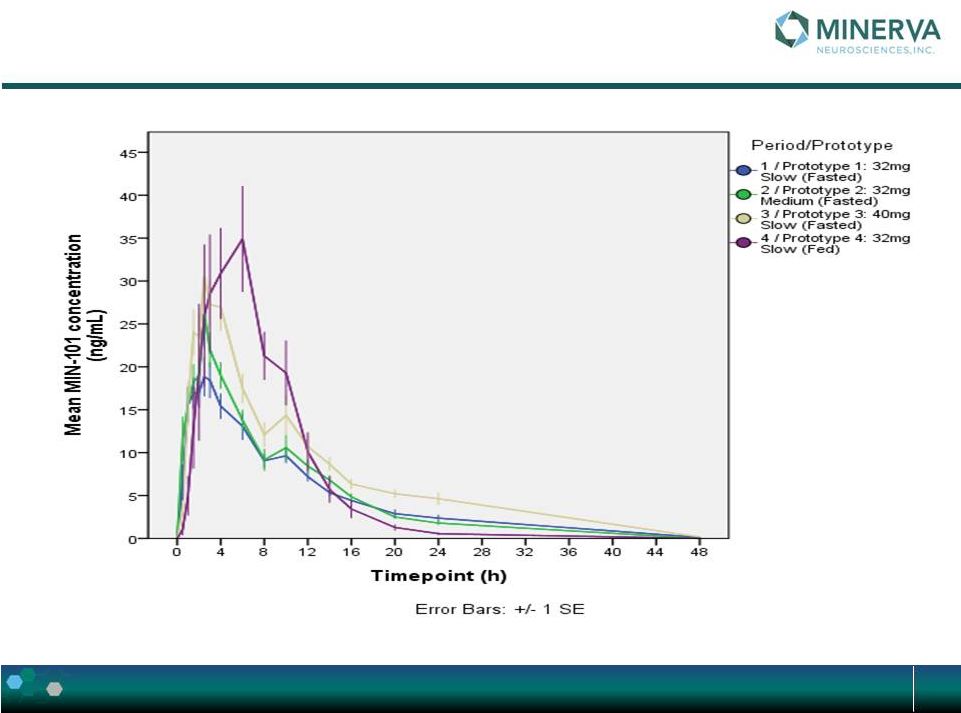 Plasma
Concentration-Time Profiles: MIN-101 Linear Scale 9
|
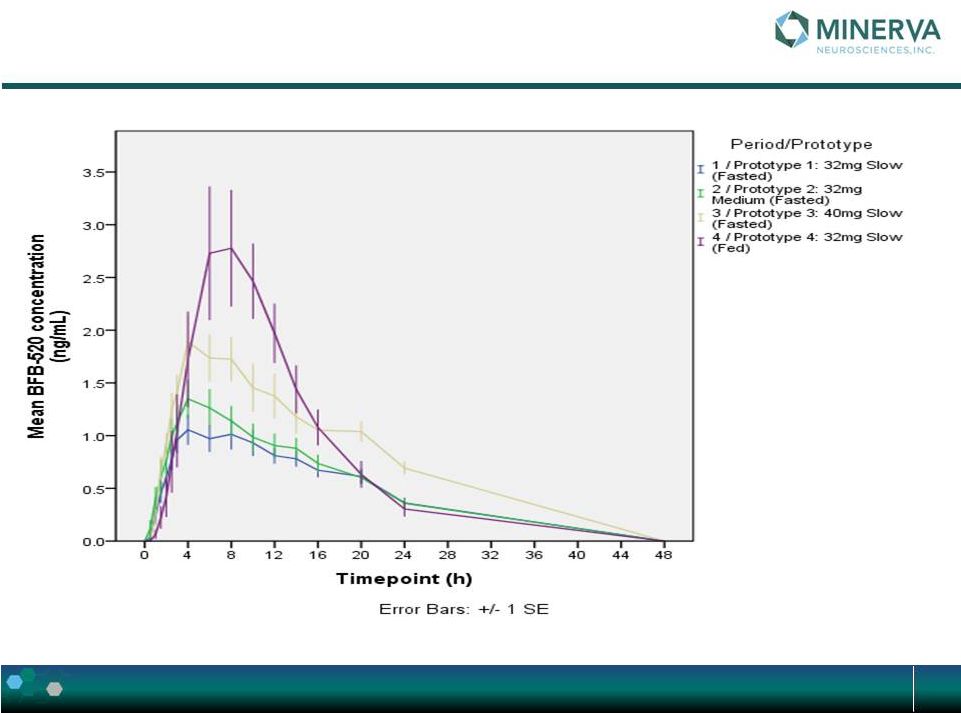 Plasma
Concentration-Time Profiles: BFB-520 Linear Scale 10
|
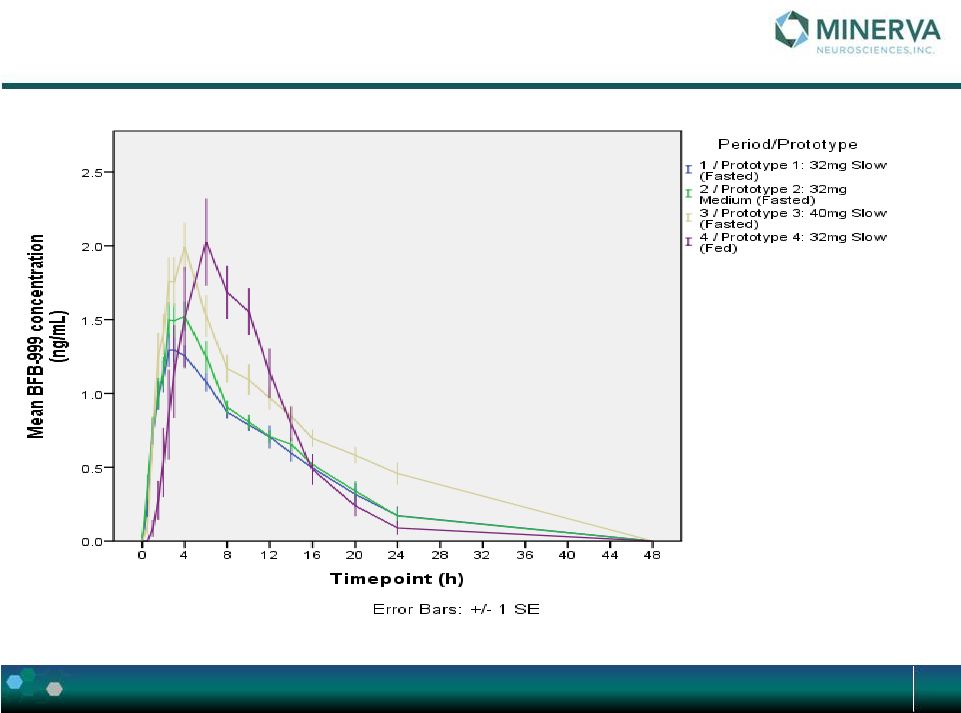 Plasma
Concentration-Time Profiles: BFB-999 Linear Scale 11
|
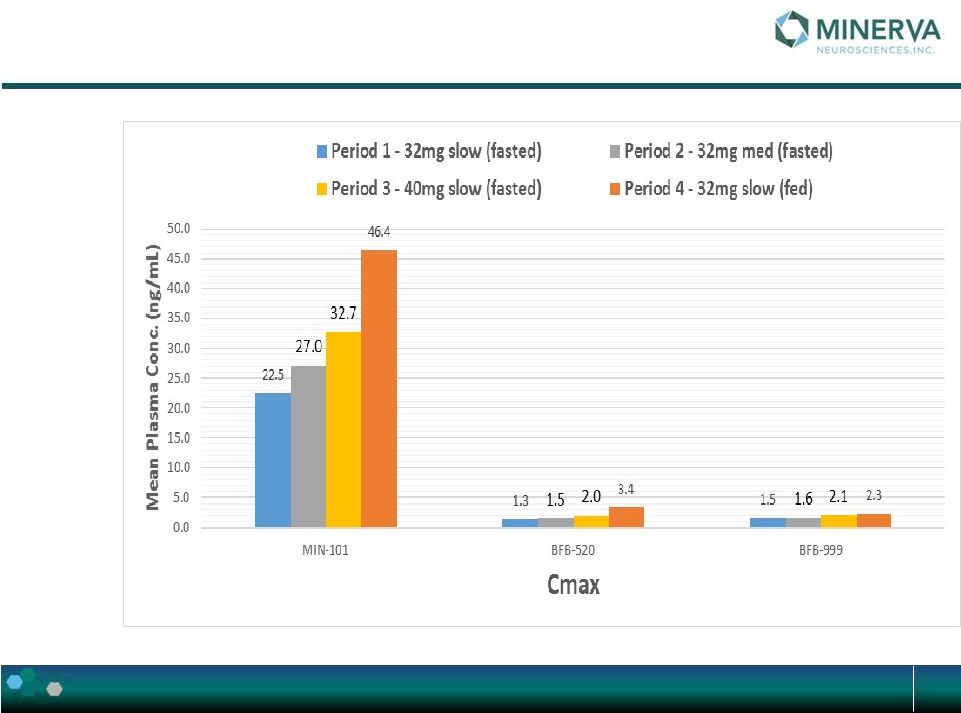 C
max
by Period
12 |
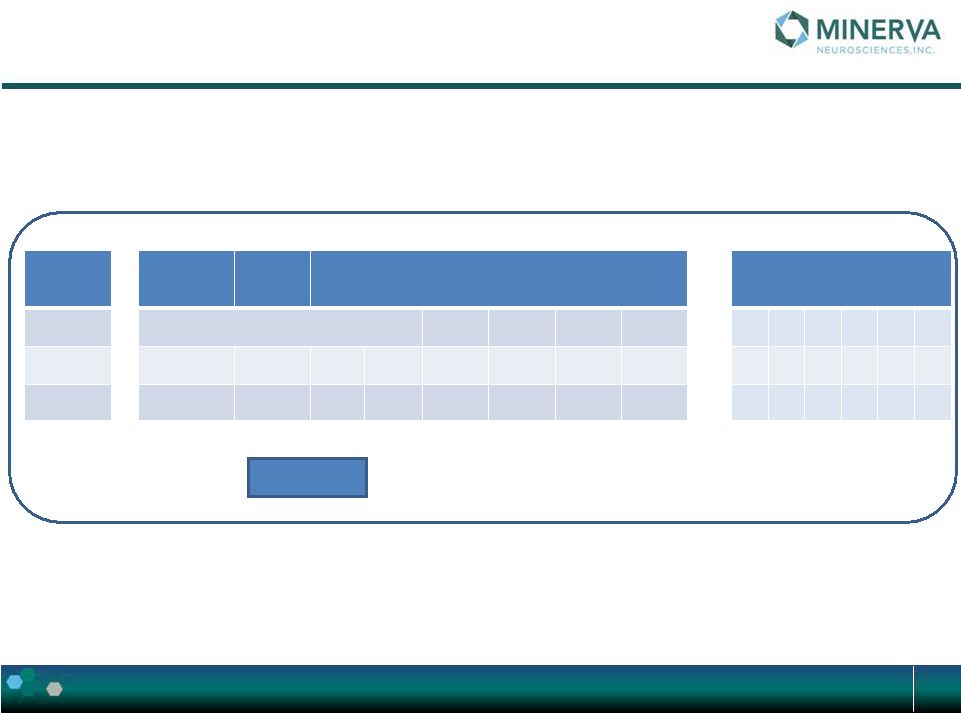
 Summary
of Select PK Parameters – Period 1 (32 mg Slow Release, Fasted)
13
MIN-101
Tmax
(h)
Cmax
(ng/mL)
Tlag
(h)
t1/2
(h)
AUClast
(h*ng/mL)
N
10
10
10
9
10
Mean
NA
22.52
NA
6.257
211.9
Median
2.25
23.74
0
5.353
220.4
CV%
NA
28.3
NA
38.1
18.6
BFB-520
Tmax
(h)
Cmax
(ng/mL)
Tlag
(h)
t1/2
(h)
AUClast
(h*ng/mL)
N
10
10
10
4
10
Mean
NA
1.321
NA
6.540
18.60
Median
4
1.294
0.5
6.458
18.04
CV%
NA
27.7
NA
21.1
24.7
BFB-999
Tmax
(h)
Cmax
(ng/mL)
Tlag
(h)
t1/2
(h)
AUClast
(h*ng/mL)
N
10
10
10
5
10
Mean
NA
1.510
NA
6.202
16.02
Median
3
1.436
0.25
5.486
15.22
CV%
NA
19.5
NA
27.3
22.3 |
 Conclusions –
MR Formulation Under Fasted Conditions
14
Short lag time suggestive of fast bioavailability
Exposure variability is generally low
Low to non-quantifiable values for most by Hour 24
PK is generally dose proportional for MIN-101 & BFB-999, and less so for
BFB-520 Inversion of BFB-520 & BFB-999 occurred with generally
suppressed levels of BFB- 520, and a higher BFB-999 to BFB-520
ratio MR formulation findings suggest shorter time in small intestine is helpful
in suppressing BFB-520 levels
Halflife for MIN-101 and 2 metabolite in 3-8 hour range, longer for 40 mg slow
release most likely due to flip-flop (absorption & elimination balanced
during terminal phase) Simulation results indicate steady state within 10-14
days, and no accumulation for all 3 analytes |
 Conclusions –
Food Effect
15
Positive food effect evident –
Higher exposure
MR formulation behaved similar to IR formulation with rapid release and absorption,
mostly prior to reaching colon
•
This explains further increase in BFB-520 levels
Due to rapid absorption MIN-101 Cmax increase was ~ 2x, BFB-520 Cmax increase
was ~ 3x, and BFB-999 Cmax increase was ~ 0.5x
Halflife was shortened substantially: Fed to Fasted ratios were
•
0.5 for MIN-101
•
0.8 for BFB-520
•
0.6 for BFB-999
Consequently, accumulation is not expected
AUC increase was minimal (compared to Cmax): 1.3 to 1.8 multiples with highest
increase to BFB-520 |
 16
32 mg slow release in fasted condition
will be the formulation used in the C03 upcoming patient
study in patients suffering from schizophrenia
Conclusion |
 QBR117055_ MIN-101C02
17
Study Part 2:
16 and 32 mg will be explored
Screening
Day -28 to
Day -2
Period 1
Period 2
Period 3
Follow
up
visit
5
days
after
last dose
of IMP |
 18
Period Scheme
•
Admission
•
Dosing, PK profile and ECG/vital sign
s
•
Dosing
•
Dosing; sleep
at 22:00
•
Dosing; PK profile, Triplicate
ECGs
•
Discharge
24h post dose
•
Optional
visit
(PK 48 h post dose)
Day -1
Day 1
Day 2-5
Day 6
Day 7
Day 8
Day 9 |
 MIN-101C03:
Phase
IIB
in
patients
suffering
from
schizophrenia
19
MIN-101C03
Study Title:
A Phase IIb, Multi-centre, Randomized, Double-blind, Parallel-group,
Placebo-controlled Study to Evaluate the Efficacy, Tolerability and Safety
of MIN-101 in Patients with Negative Symptoms of Schizophrenia
Followed by a 24-week, Open-label extension. |
 MIN-101C03: Phase IIB in patients with schizophrenia
20
Screening
Wash out
Period
Baseline
Core Study
Treatment period (12 weeks): MIN-101 (64 or 32 mg) or
PLACEBO
Extension
6-month: MIN-101 64 or 32 mg
Obligatory In patient Day -3 to day +2 afterwards
up to the end of study at the discretion of the PI
A
A
IN
A
IN
A
D-21
D-3 to D-1
Day-1
D1
D2
W2
W4
W8
W12
W
14
W
18
W
24
W
30
W
36
W
37
V1
V2
V3
V4
V5
V6
V7
V8
V9
V
10
V
11
V
12
V
13
V
14
V
15
Global Study Design
RANDOMIZATION |
 MIN-101C03: Phase IIB in patients with schizophrenia
Study Objectives
21
Primary
To evaluate the efficacy of MIN-101 compared to placebo in
improving the negative symptoms of schizophrenia as
measured
by
the
change
from
Baseline
in
the
Positive
and Negative Syndrome Scale (PANSS) negative
subscale score of the pentagonal model over 12 weeks
of treatment. |
 MIN-101C03: Phase IIB in patients with schizophrenia
Study Objectives
22
Main Secondary
•
To evaluate the efficacy of MIN-101 compared to placebo in improving other
symptoms of schizophrenia as measured by the change from baseline in the
PANSS
total
score,
and
sub-scores
of
the
pentagonal
model
AND
3
factors
analysis
over
12
weeks
of
double
blind
treatment.
•
To evaluate the efficacy of MIN-101 compared to placebo in improving
negative symptoms of schizophrenia as measured by the change from
Baseline
in
the
Brief
Negative
Symptoms
Scale
(BNSS)
total
score
over
12
weeks of double blind treatment.
•
To assess the effects versus placebo of MIN-101 on cognitive function as
measured
by
the
Brief
Assessment
of
Cognition
in
Schizophrenia
(BACS)
battery over 12 weeks of double blind treatment.
•
To assess the persistence of efficacy, and the safety and tolerability of
MIN- 101 during the 24-week, of open-label extension phase.
|
 MIN-101C03: Phase IIB in patients with schizophrenia
Study Objectives
23
Exploratory objectives
•
To
evaluate
the
effects
versus
placebo
of
MIN-101
on
depressive
symptoms
as
measured
by
the
Calgary
Depression
Scale
for
Schizophrenia (CDSS) over 12 weeks of double blind treatment.
•
To
evaluate
the
effects
versus
placebo
of
MIN-101
on
social
functioning
by
means
of
the
Personal
and
Social
Performance
(PSP) over 12 weeks of double blind treatment.
•
To
assess
the
effects
versus
placebo
of
MIN-101
on
sleep
architecture
and
continuity
as
measured
with
the
help
of
the
V-Watch
methodology
over
12
weeks
of
double
blind
treatment. |
 MIN-101C03: Phase IIB in patients with schizophrenia
Inclusion/ Exclusion Criteria
24
Main Inclusion Criteria
•
Male or female patient, 18 to 60 years of age, inclusive.
•
Patient meets the diagnostic criteria for schizophrenia as defined in the
Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition
(DSM-V) •
Patient being stable in terms of positive symptoms over the last three
months according to his treating psychiatrist
•
Patient presenting with negative symptoms over the last three months
according to his treating psychiatrist
•
Patient with PANSS negative sub-score of at least 20.
•
Patient with PANSS item score of <4
on: P4 Excitement, hyperactivity P7
Hostility P6 Suspiciousness G8 Uncooperativeness G14 Poor impulse control
•
No change in psychotropic medication during the last month
•
Patient must be extensive metabolizers for P450 CYP2D6, as determined by
genotyping test before the first drug dose is administered.
|
 MIN-101C03: Phase IIB in patients with schizophrenia
Inclusion/ Exclusion Criteria
25
Main Exclusion Criteria
•
Current bipolar disorder, panic disorder, obsessive compulsive disorder, or
evidence of mental retardation.
•
Patient’s
condition
is
due
to
direct
physiological
effects
of
a
substance
(e.g.,
a
drug
of
abuse, or medication) or a general medical condition.
•
Significant risk of suicide or attempted suicide, or of danger to self or
others. •
Patient
who
cannot
be
discontinued
from
psychotropics
other
than
those
allowed.
•
Patient who received clozapine within 6
months of the Screening visit.
•
Patient receiving treatment with depot antipsychotic medication can be enrolled in
the study 4 weeks after the last injection.
•
Patient with a history of significant other major or unstable neurological,
neurosurgical (e.g., head trauma), metabolic, hepatic, renal, hematological,
pulmonary, cardiovascular, metabolic, gastrointestinal, or urological
disorder. •
Patient with a clinically significant electrocardiogram (ECG) abnormality that
could be a safety issue in the study, including QT interval value corrected
for heart rate using the
Fridericia’s
formula
(QTcF)
>
430
msec
for
males
and
>
450
msec
for
females. |
 MIN-101C03: Phase IIB in patients with schizophrenia
Assessments
26
Main Efficacy Assessments
–
Positive and Negative Symptoms Scale (PANSS)
–
Brief Negative Symptoms Scale (BNSS): semi structured interview, designed to
measure the current level of severity of negative symptoms in schizophrenia and
schizoaffective disorder (Kirkpatrick et al.)
•
Anhedonia
•
Distress
•
Asociality
•
Avolition
•
Blunted affect
•
Alogia
–
Brief Assessment of Cognition in Schizophrenia (BACS)
–
Personal and Social Performance (PSP): assess social functioning;
clinician rated –
socially useful activities,
–
personal and social relationships,
–
self-care
–
disturbing and aggressive behavior
–
Sleep architecture and continuity |
 MIN-101C03: Phase IIB in patients with schizophrenia
-
Sleep assessment
27
WHY?
–
Sleep and circadian rhythm disruptions are reported in 30% to 80% of patients with
schizophrenia.
–
Patients with insomnia report •
lower quality of life
•
greater symptom severity
•
worse adherence/compliance to treatment –
Sleep disturbances have also been associated with enhanced psychosis –
Sleep is important for memory consolidation, thus disturbances in sleep architecture,
or circadian de-synchronization could also contribute to the cognitive
impairment observed in schizophrenia. –
MIN-101 showed effects on sleep architecture in the previous Phase 2a study that
could possibly be linked to the improvements observed on negative symptoms and
cognition, thus they will be further investigated in the present study. •
In a subgroup of patients (20) who underwent sleep recordings (PSG), sleep was
evaluated at Baseline and Day 14. MIN-101 had an effect on –
Slow Wave Sleep (SWS) distribution: it shifted SWS from the end to the
beginning of the night: MIN-101 significantly increased SWS in the first
third of the night and decreased it in the last third of the night.
–
Sleep initiation parameters (sleep onset latency, latency to persistent sleep).
•
Subjective sleep quality as measured by PSQI improved and this improvement was greater
with MIN-101 than with placebo although not statistically significant. |
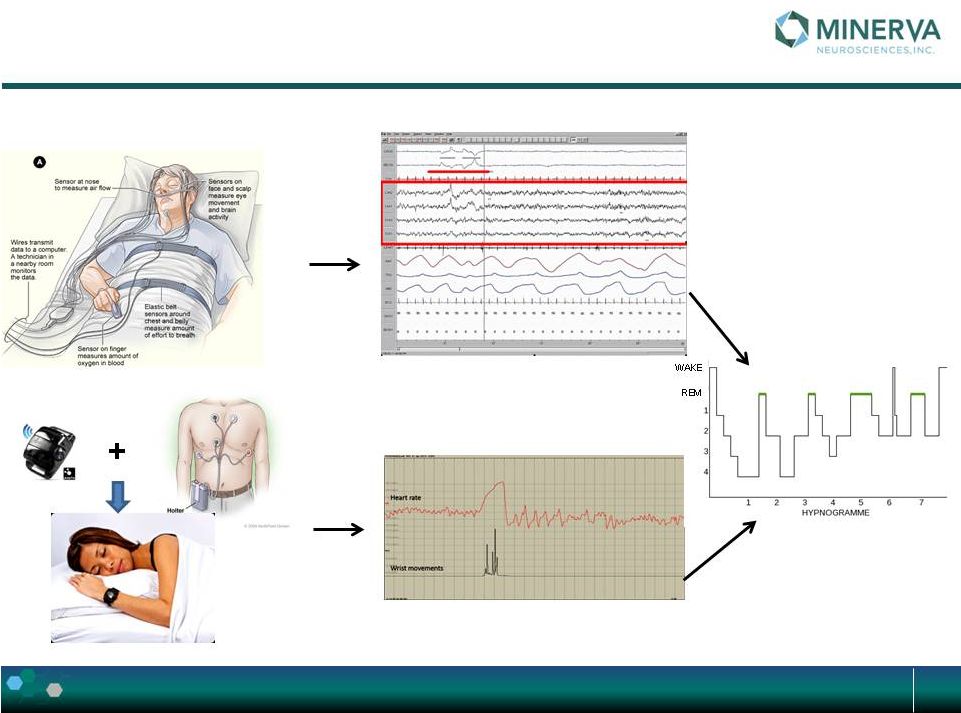 Monitoring sleep in MIN-101C03 using
V-Watch, a
sleep biomarker & companion diagnostic tool
28
PSG
VWATCH
VWatch methodology overview-2 |
 The
Submissions Status is: (1) 29
Romania (22 sites):
End November / Beginning December
Russia (11 sites):
December
Latvia (4 sites):
December
Estonia (3 sites):
End December/ Beginning January
Bulgaria (3 sites):
January
Ukraine (12 sites):
January |
 30
Thank you |