Attached files
| file | filename |
|---|---|
| 8-K - 8-K - AERIE PHARMACEUTICALS INC | d756020d8k.htm |
Exhibit 99.1
Leading Innovation in Glaucoma The Next Generation
Aerie Pharmaceuticals, Inc.
Company Overview July 9, 2014
Important Information
Any discussion of the potential use or expected success of our product candidates is subject to our product candidates being approved by regulatory authorities. In addition, any discussion of clinical data results for our RhopressaTM and RoclatanTM product candidates relate to the results in our Phase 2 clinical trials.
The information in this presentation is current only as of its date and may have changed or may change in the future. We undertake no obligation to update this information in light of new information, future events or otherwise. We are not making any representation or warranty that the information in this presentation is accurate or complete.
Certain statements in this presentation are “forward-looking statements” within the meaning of the federal securities laws, including beliefs, expectations, estimates, projections and statements relating to our business plans, prospects and objectives, and the assumptions upon which those statements are based. Words such as “may,” “will,” “should,” “would,” “could,” “believe,” “expects,” “anticipates,” “plans,” “intends,” “estimates,” “targets,” “projects” or similar expressions are intended to identify these forward-looking statements. These statements are based on the Company’s current plans and expectations. Known and unknown risks, uncertainties and other factors could cause actual results to differ materially from those contemplated by the statements. In evaluating these statements, you should specifically consider various factors that may cause our actual results to differ materially from any forward-looking statements. These risks and uncertainties are described more fully in the quarterly and annual reports that we file with the SEC, particularly in the sections titled “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operation.” Such forward-looking statements only speak as of the date they are made. We undertake no obligation to publicly update or revise any forward-looking statements, whether because of new information, future events or otherwise, except as otherwise required by law.
2
Aerie – Next ext Generation in Glaucoma Therapies
• $4.5B US/EU/JP Market with significant unmet needs
Large Market • Multiple MOAs, once daily, high efficacy and safety
Opportunity
• Late-stage/potential blockbuster revenue opportunity
• Inhibits ROCK and NET, targets diseased tissue
RhopressaTM
Triple Action • Consistent IOP lowering, lowers EVP
• Expect P3 efficacy data mid-2015, NDA filing mid-2016
• Fixed combination of RhopressaTM and latanoprost
RoclatanTM • P2b results achieved all clinical endpoints, P3
Quadruple Action readiness mid-2015
• Potentially most efficacious IOP-lowering therapy
All Products Fully • Full patent protection through at least 2030
Owned by Aerie • Will retain North America rights and plan to
partner in JP/EU
3
Glaucoma Market
Expanding Market
Largest Rx market in ophthalmology: $4.5B US/EU/JP
US Glaucoma patients: 2.7M growing to 4.3M by 20301
Patients on more than one drug to control disease: 50%
Unmet Needs
No commonly prescribed drugs: • target the diseased tissue
relax the main fluid drain and lower EVP
show consistent efficacy across a broad range of pressures
1 National Eye Institute
4
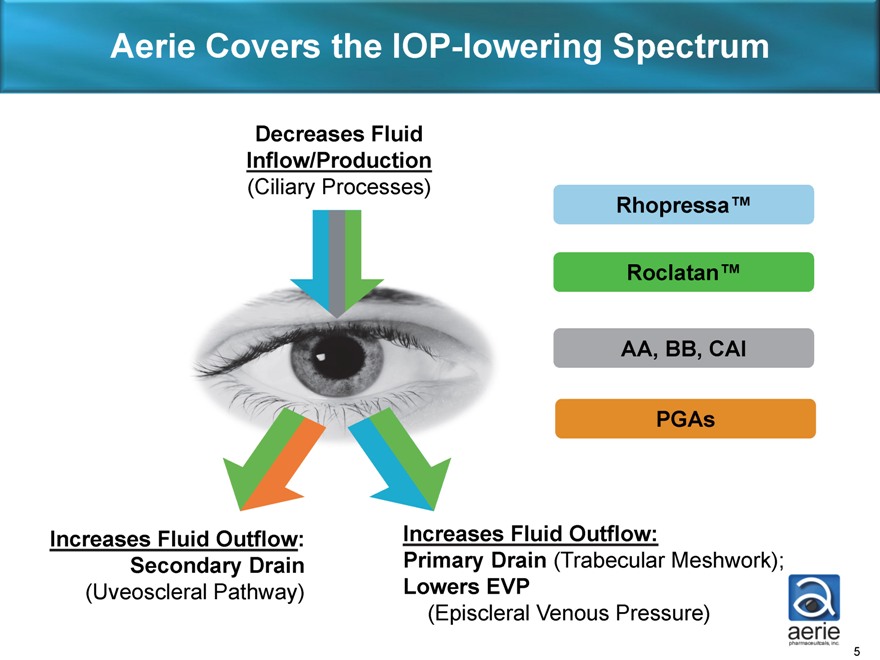
Aerie Covers the IOP-lowering Spectrum
Decreases Fluid
Inflow/Production
(Ciliary Processes)
Rhopressa™
Roclatan™
AA, BB, CAI
PGAs
increase
Increases Fluid Outflow: Increases Fluid Outflow:
Secondary Drain Primary Drain (Trabecular Meshwork);
(Uveoscleral Pathway) Lowers EVP
(Episcleral Venous Pressure)
5
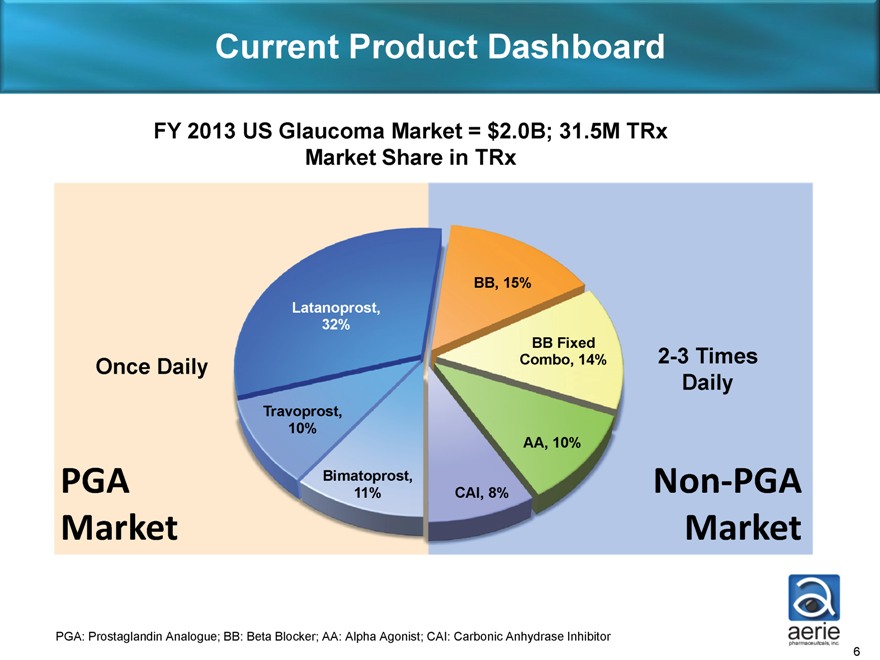
Current Product Dashboard
FY 2013 US Glaucoma Market = $2.0B; 31.5M TRx
Market Share in TRx
BB, 15%
Latanoprost,
32%
BB Fixed
Once Daily Combo, 14% 2-3 Times
Daily
Travoprost,
10%
AA, 10%
PGA Bimatoprost, Non?PGA
11% CAI, 8%
Market Market
PGA: Prostaglandin Analogue; BB: Beta Blocker; AA: Alpha Agonist; CAI: Carbonic Anhydrase Inhibitor
6
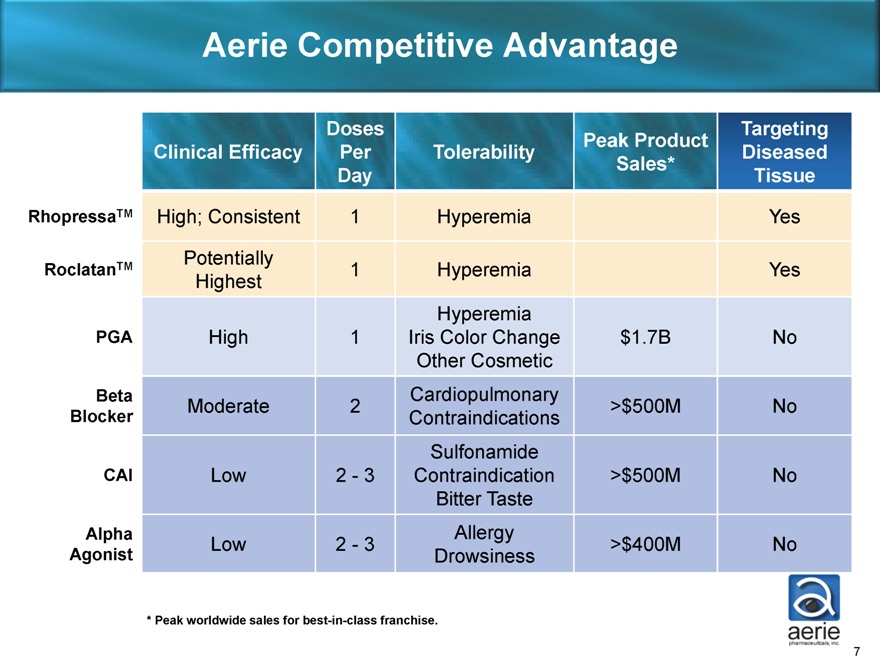
Aerie Competitive Advantage
Doses Peak Product
Clinical Efficacy Per Tolerability Sales*
Day
RhopressaTM High; Consistent 1 Hyperemia Yes
Targeting Diseased Tissue
Potentially
RoclatanTM 1 Hyperemia Yes
Highest
Hyperemia
PGA High 1 Iris Color Change $1.7B No
Other Cosmetic
Beta Cardiopulmonary
Moderate 2 >$500M No
Blocker Contraindications
Sulfonamide
CAI Low 2—3 Contraindication >$500M No
Bitter Taste
Alpha Allergy
Low 2—3 >$400M No
Agonist Drowsiness
* Peak worldwide sales for best-in-class franchise.
7
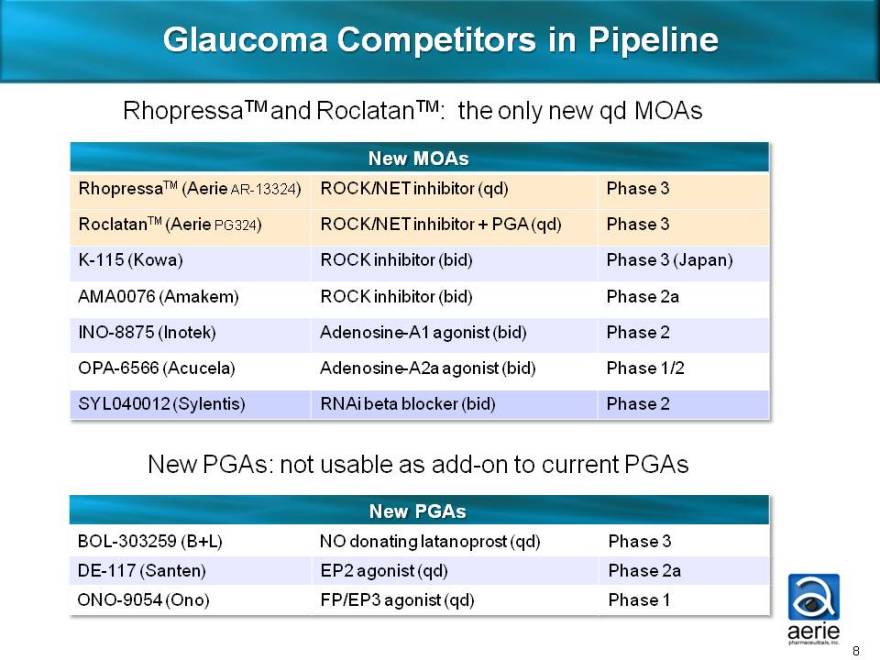
Glaucoma Competitors in Pipeline
RhopressaTM and RoclatanTM: the only new qd MOAs
New MOAs
RhopressaTM (Aerie AR-13324) ROCK/NET inhibitor (qd) Phase 3
RoclatanTM (Aerie PG324) ROCK/NET inhibitor + PGA (qd) Phase 3
K-115 (Kowa) ROCK inhibitor (bid) Phase 3 (Japan)
AMA0076 (Amakem) ROCK inhibitor (bid) Phase 2a
INO-8875 (Inotek) Adenosine-A1 agonist (bid) Phase 2
OPA-6566 (Acucela) Adenosine-A2a agonist (bid) Phase 1/2
SYL040012 (Sylentis) RNAi beta blocker (bid) Phase 2
New PGAs: not usable as add-on to current PGAs
New PGAs
BOL-303259 (B+L) NO donating latanoprost (qd) Phase 3
DE-117 (Santen) EP2 agonist (qd) Phase 2a
ONO-9054 (Ono) FP/EP3 agonist (qd) Phase 1
8
Aerie Market Positioning
Triple-Action RhopressaTM Quadruple-Action RoclatanTM
Future drug of choice for the Future product of choice for
80% of patients with IOP of patients requiring maximal IOP
26 mmHg or less lowering
Also for PGA users as add-on Efficacy potentially greater than all
therapy currently marketed drugs
Also for PGA non-responders and For patients with IOPs above
those with tolerability concerns 26 mmHg
Also for patients with low-tension Also for patients at any IOP with
glaucoma significant disease progression
9
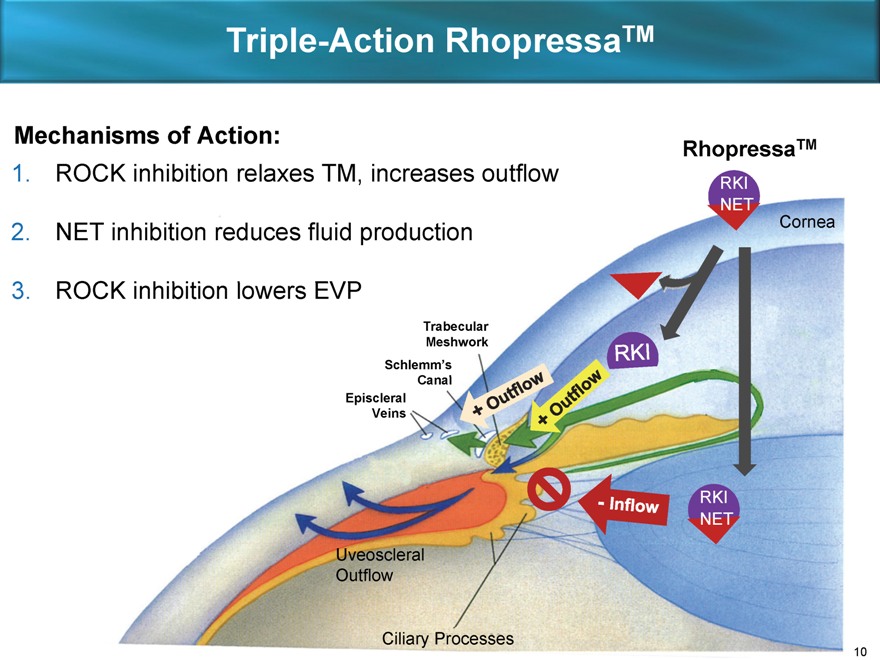
Triple-Action RhopressaTM
Mechanisms of Action: RhopressaTM
1. ROCK inhibition relaxes TM, increases outflow RKI
NET
2. NET inhibition reduces fluid production Cornea
3. ROCK inhibition lowers EVP
Trabecular
Meshwork
Schlemm’s
Canal
Episcleral
Veins
RKI
NET
Uveoscleral
Outflow
Ciliary Processes
10
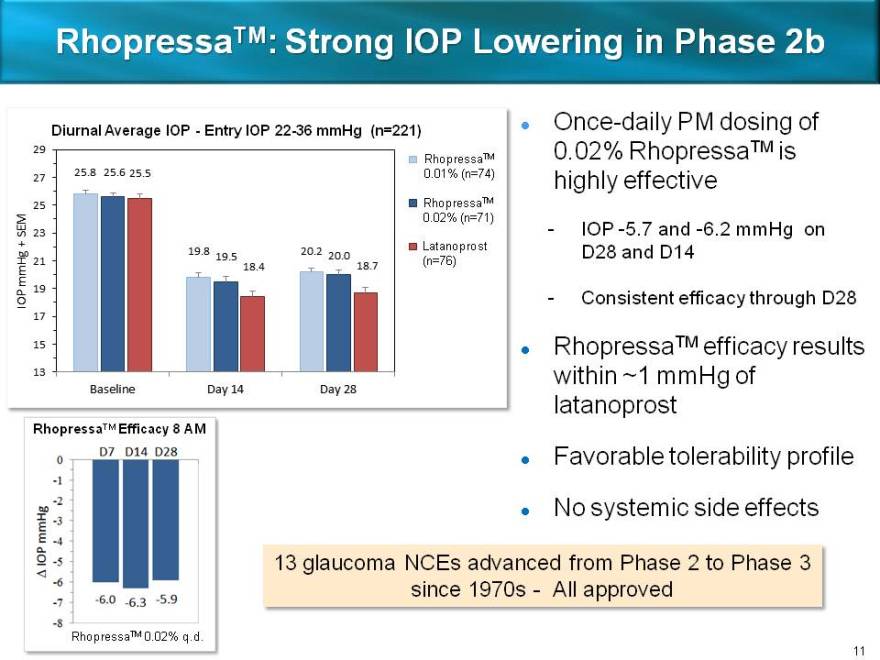
RhopressaTM: Strong IOP Lowering in Phase 2b
Diurnal Average IOP—Entry IOP 22-36 mmHg (n=221) ? Once-daily PM dosing of
RhopressaTM 0.02% RhopressaTM is
0.01% (n=74) highly effective
RhopressaTM
0.02% (n=71)
— IOP -5.7 and -6.2 mmHg on
Latanoprost D28 and D14
(n=76)
— Consistent efficacy through D28
RhopressaTM efficacy results
within ~1 mmHg of
latanoprost
RhopressaTM Efficacy 8 AM
Favorable tolerability profile
No systemic side effects
13 glaucoma NCEs advanced from Phase 2 to Phase 3
since 1970s—All approved
RhopressaTM 0.02% q.d.
11
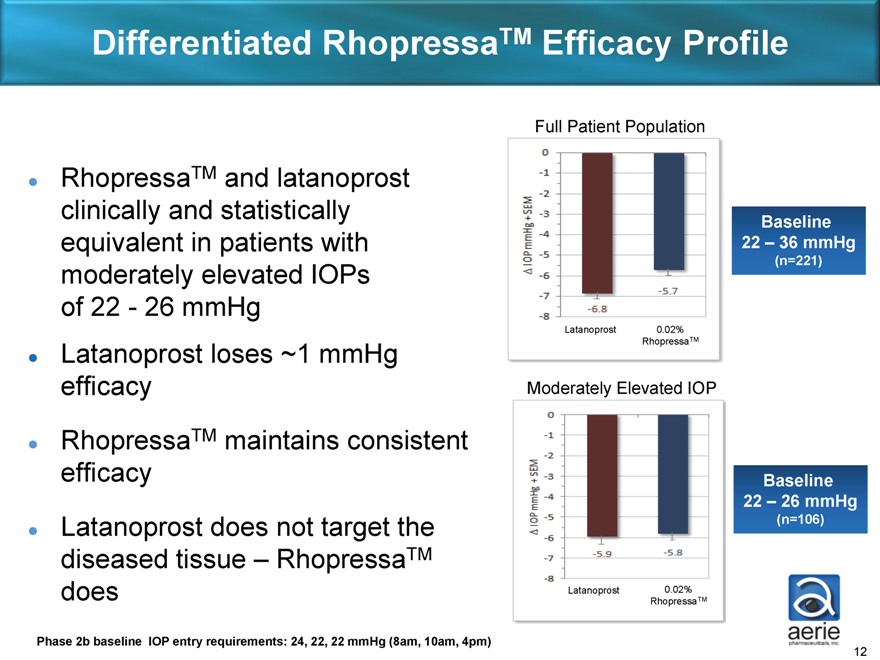
Differentiated RhopressaTM Efficacy Profile
RhopressaTM
and latanoprost clinically and statistically equivalent in patients with moderately elevated IOPs of 22—26 mmHg Latanoprost loses ~1 mmHg efficacy RhopressaTM
maintains consistent efficacy ? Latanoprost does not target the diseased tissue – RhopressaTM does
Full Patient Population
Baseline
22 – 36 mmHg
(n=221)
Latanoprost 0.02%
RhopressaTM
Moderately Elevated IOP
Baseline
22 – 26 mmHg
(n=106)
Latanoprost 0.02%
RhopressaTM
Phase 2b baseline IOP entry requirements: 24, 22, 22 mmHg (8am, 10am, 4pm)
12
RhopressaTM EVP-Lowering Breakthrough
Phase 2b data provided first sign of EVP-lowering:
Consistent efficacy across baseline IOPs
Phase 1 study in low baseline IOP subjects:
Lowered average IOP by over 30% from 16 to 11 mmHg
Preclinical in vivo study:
Lowered EVP by 35%
Note: EVP contributes up to half of IOP in normotensive subjects
13
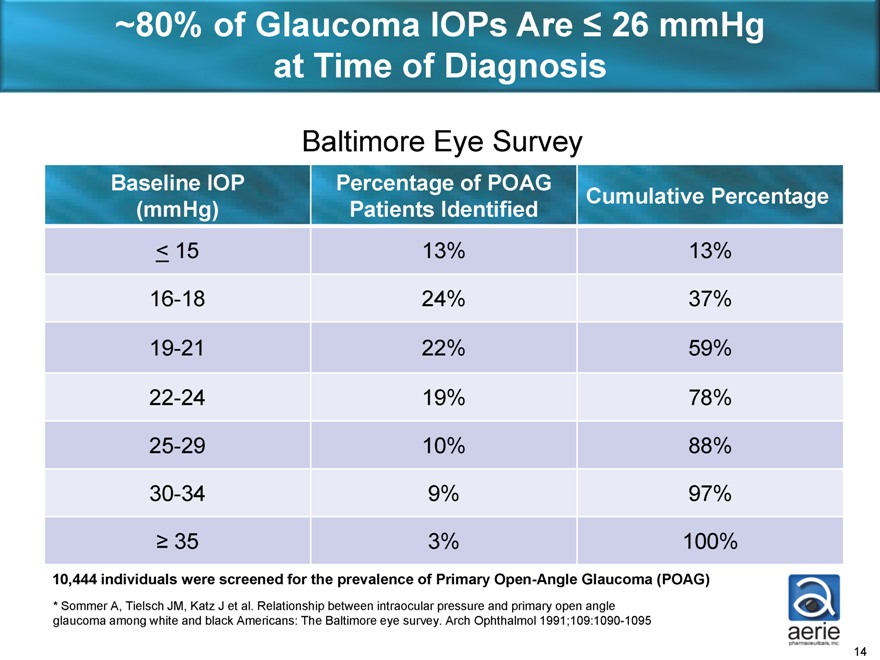
~80% of Glaucoma IOPs Are £ 26 mmHg at Time of Diagnosis
Baltimore Eye Survey
Baseline IOP Percentage of POAG Cumulative Percentage
(mmHg) Patients Identified
£ 15 13% 13%
16-18 24% 37%
19-21 22% 59%
22-24 19% 78%
25-29 10% 88%
30-34 9% 97%
³ 35 3% 100%
10,444 individuals were screened for the prevalence of Primary Open-Angle Glaucoma (POAG)
* Sommer A, Tielsch JM, Katz J et al. Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans: The Baltimore eye survey. Arch Ophthalmol 1991;109:1090-1095
14
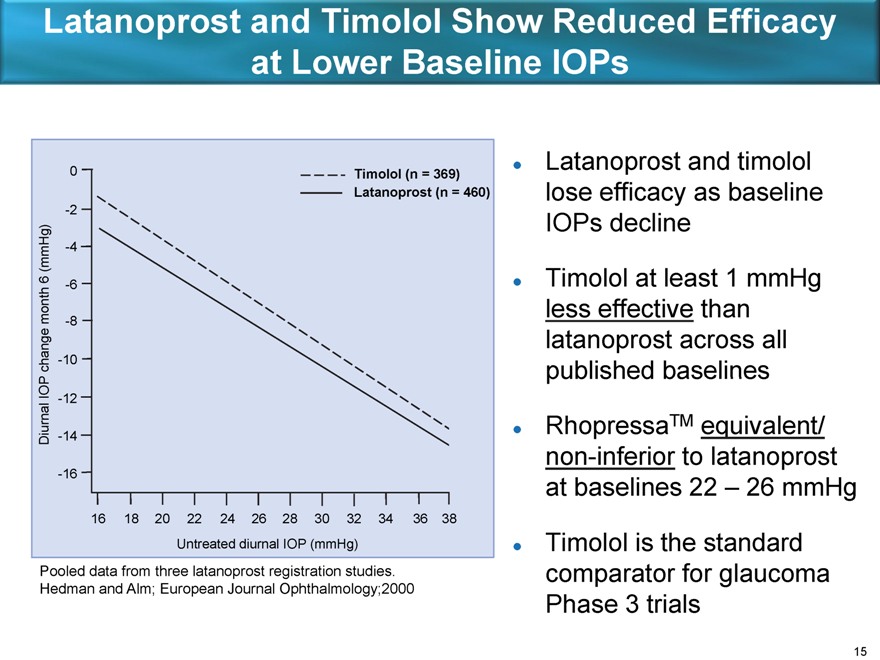
Latanoprost and Timolol Show Reduced Efficacy at Lower Baseline IOPs
0 Timolol (n = 369)
Latanoprost (n = 460)
-2
(mmHg) -4
6 -6
month -8
change -10
IOP -12
Diurnal -14
-16
16 18 20 22 24 26 28 30 32 34 36 38
Untreated diurnal IOP (mmHg)
Pooled data from three latanoprost registration studies.
Hedman and Alm; European Journal Ophthalmology;2000
Latanoprost and timolol lose efficacy as baseline IOPs decline
Timolol at least 1 mmHg less effective than latanoprost across all published baselines
RhopressaTM equivalent/non-inferior to latanoprost at baselines 22 – 26 mmHg
Timolol is the standard comparator for glaucoma Phase 3 trials
15
RhopressaTM Registration Trial Overview
Primary efficacy endpoint: IOP at all time points through Day 90 Non-inferiority design vs. timolol
- 95% CI within 1.5 mmHg at all time points, within 1.0 mmHg at a majority of time points
Entry IOP: Over 20 mmHg and less than 27 mmHg
- FDA has agreed to Aerie proposal for entry IOPs with no expected impact on label
- RhopressaTM non-inferior to latanoprost at entry IOPs of 22-26 mmHg in Phase 2b
FDA discussions on Phase 3 design now complete
- Combined trials to include approximately 1,300 total patients
- 100 patients of 12 month safety data needed for NDA filing
16
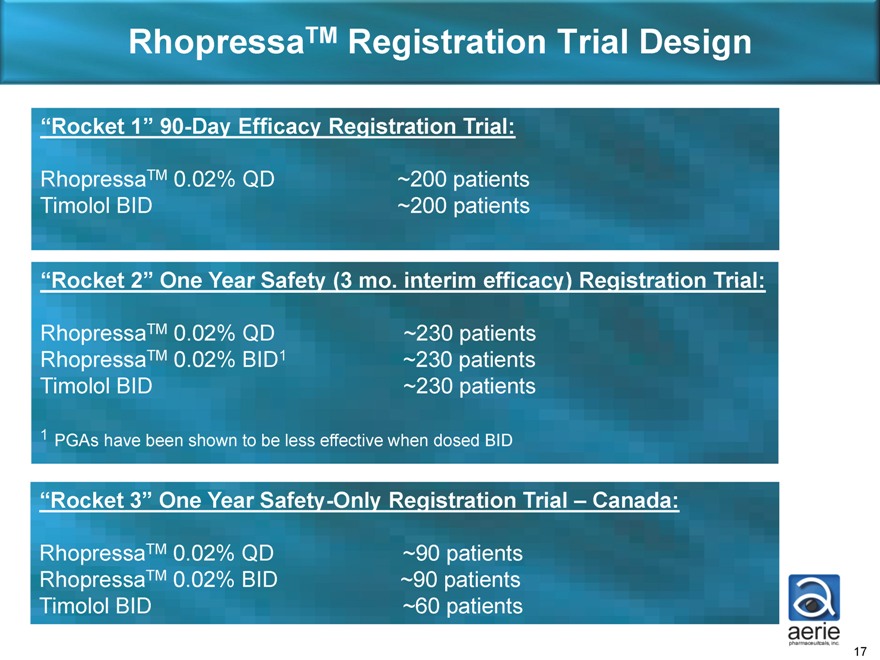
RhopressaTM Registration Trial Design
“Rocket 1” 90-Day Efficacy Registration Trial:
RhopressaTM 0.02% QD ~200 patients Timolol BID ~200 patients
“Rocket 2” One Year Safety (3 mo. interim efficacy) Registration Trial:
RhopressaTM 0.02% QD ~230 patients RhopressaTM 0.02% BID1 ~230 patients Timolol BID ~230 patients
1 PGAs have been shown to be less effective when dosed BID
“Rocket 3” One Year Safety-Only Registration Trial – Canada:
RhopressaTM 0.02% QD ~90 patients RhopressaTM 0.02% BID ~90 patients Timolol BID ~60 patients
17
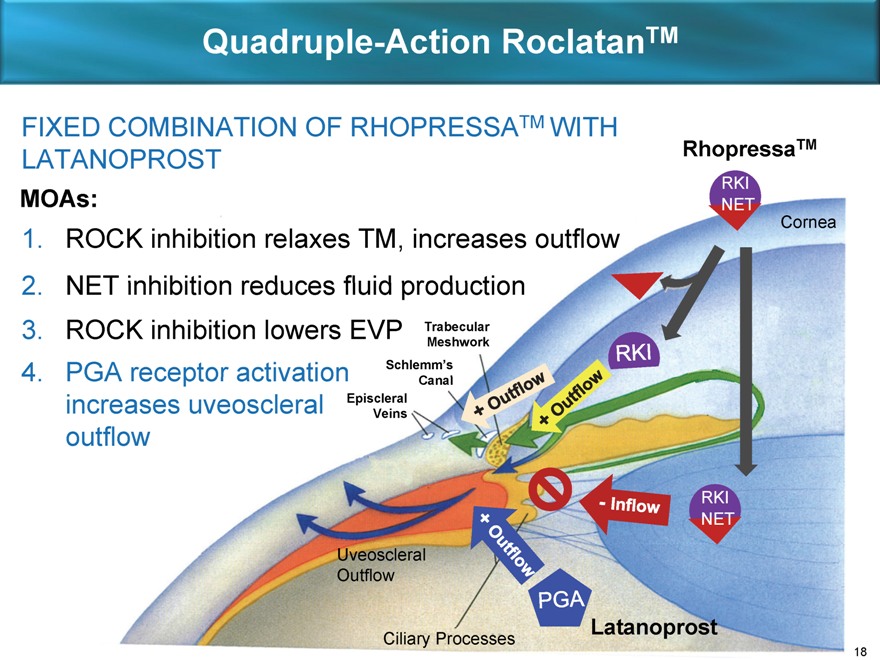
Quadruple-Action RoclatanTM
FIXED COMBINATION OF RHOPRESSATM WITH LATANOPROST
MOAs:
1. ROCK inhibition relaxes TM, increases outflow
2. NET inhibition reduces fluid production
3. ROCK inhibition lowers EVP Trabecular
Meshwork
4. PGA receptor activation Schlemm’s
Canal
increases uveoscleral Episcleral
Veins
outflow
RhopressaTM
RKI
NET
Cornea
Uveoscleral Outflow
Latanoprost
Ciliary Processes
RKI NET
+ Outflow
+ Outflow
RKI
+ Outflow
+ Outflow
- Inflow
PGA
18
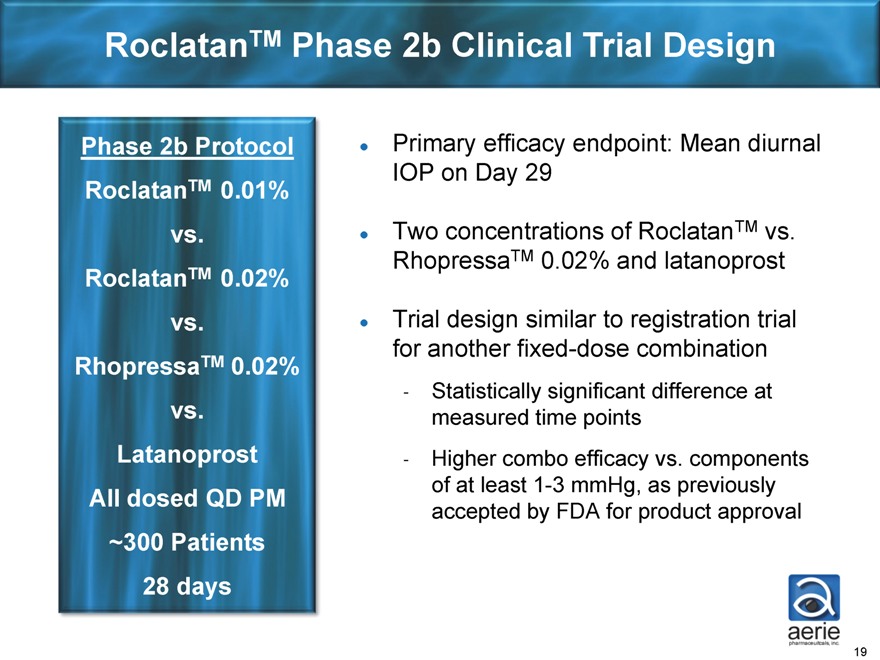
RoclatanTM Phase 2b Clinical Trial Design
Phase 2b Protocol RoclatanTM 0.01% vs. RoclatanTM 0.02% vs. RhopressaTM 0.02% vs.
Latanoprostatanoprost All dosed QD PM
~300 Patients 28 days
Primary efficacy endpoint: Mean diurnal IOP on Day 29
Two concentrations of RoclatanTM vs.
RhopressaTM 0.02% and latanoprost
Trial design similar to registration trial for another fixed-dose combination
- Statistically significant difference at measured time points
- Higher combo efficacy vs. components of at least 1-3 mmHg, as previously accepted by FDA for product approval
19
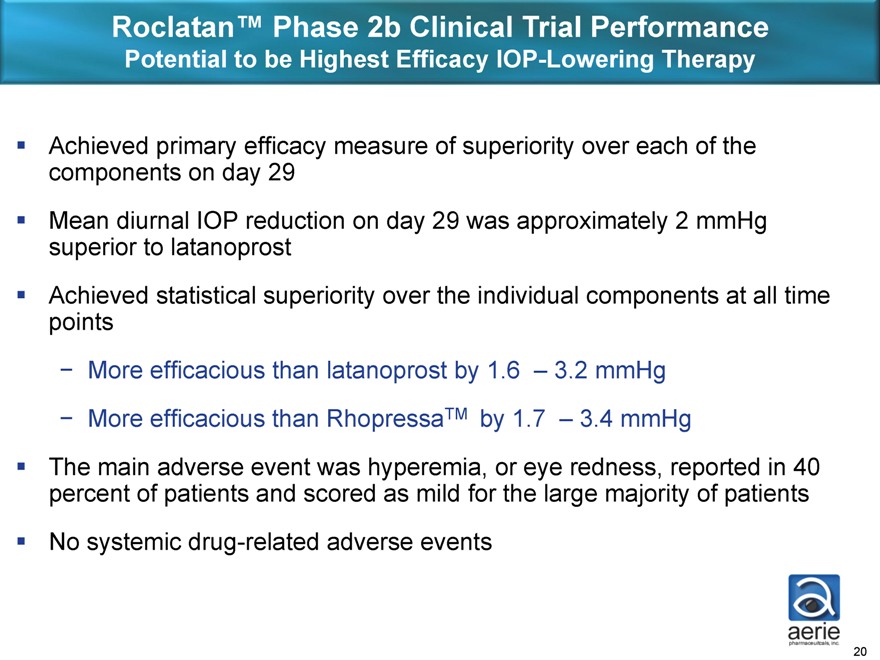
Roclatan™ Phase 2b Clinical Trial Performance
Potential to be Highest Efficacy IOP-Lowering Therapy
Achieved primary efficacy measure of superiority over each of the components on day 29 Mean diurnal IOP reduction on day 29 was approximately 2 mmHg superior to latanoprost Achieved statistical superiority over the individual components at all time points
- More efficacious than latanoprost by 1.6 – 3.2 mmHg
- More efficacious than RhopressaTM by 1.7 – 3.4 mmHg
The main adverse event was hyperemia, or eye redness, reported in 40 percent of patients and scored as mild for the large majority of patients No systemic drug-related adverse events
20
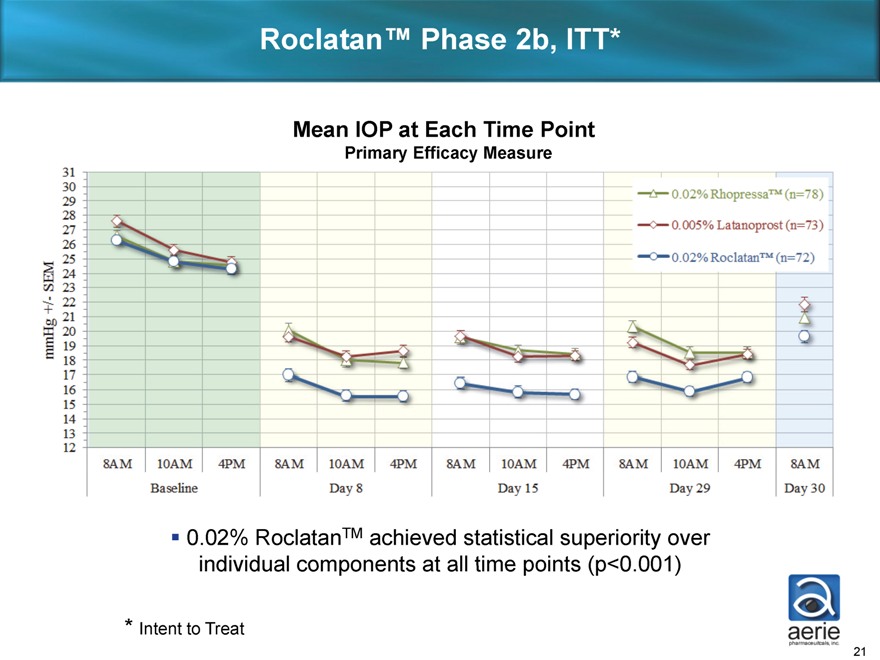
Roclatan™ Phase 2b, ITT*
Mean IOP at Each Time Point
Primary Efficacy Measure
31 30 29 28 27 26 25 24 23 22 21 20 19 18 17 16 15 14 13 12
8AM 10AM 4PM 8AM 10AM 4PM 8AM 10AM 4PM 8AM 10AM 4PM 8AM
Baseline Day 8 Day 15 Day 29 Day 30
0.02% RhopressaTM (n=78)
0.005% Latanoprost (n=73)
0.02% RoclatanTM (n=72)
0.02% RoclatanTM achieved statistical superiority over individual components at all time points (p<0.001)
* Intent to Treat mmHg+/- SEM
21
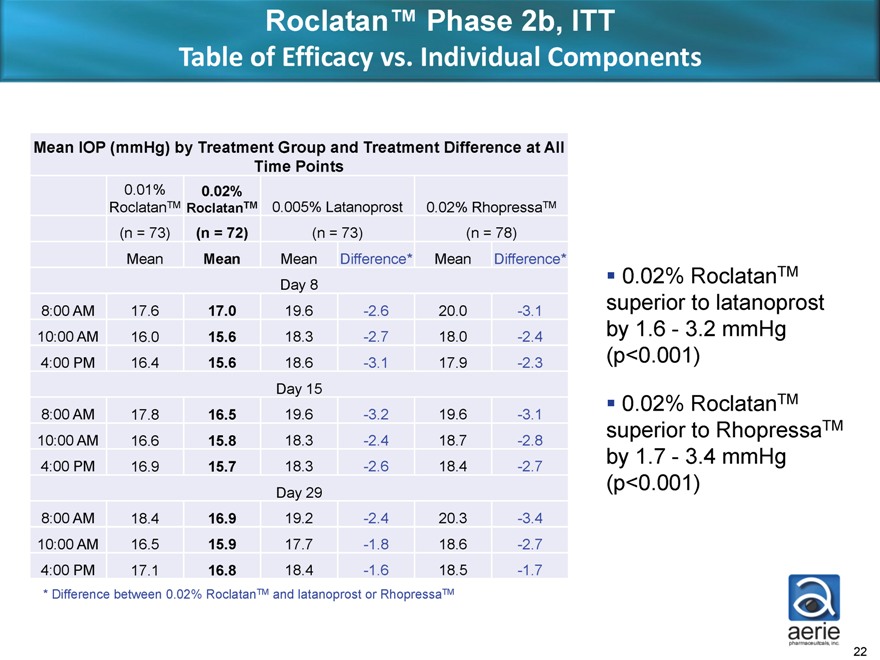
Roclatan™ Phase 2b, ITT
Table of Efficacy vs. Individual Components
Mean IOP (mmHg) by Treatment Group and Treatment Difference at All
Time Points
0.01% 0.02%
RoclatanTM RoclatanTM 0.005% Latanoprost 0.02% RhopressaTM
(n = 73) (n = 72) (n = 73) (n = 78)
Mean Mean Mean Difference* Mean Difference*
Day 8
8:00 AM 17.6 17.0 19.6 -2.6 20.0 -3.1
10:00 AM 16.0 15.6 18.3 -2.7 18.0 -2.4
4:00 PM 16.4 15.6 18.6 -3.1 17.9 -2.3
Day 15
8:00 AM 17.8 16.5 19.6 -3.2 19.6 -3.1
10:00 AM 16.6 15.8 18.3 -2.4 18.7 -2.8
4:00 PM 16.9 15.7 18.3 -2.6 18.4 -2.7
Day 29
8:00 AM 18.4 16.9 19.2 -2.4 20.3 -3.4
10:00 AM 16.5 15.9 17.7 -1.8 18.6 -2.7
4:00 PM 17.1 16.8 18.4 -1.6 18.5 -1.7
* Difference between 0.02% RoclatanTM and latanoprost or RhopressaTM
0.02% RoclatanTM superior to latanoprost by 1.6 - 3.2 mmHg (p<0.001)
0.02% RoclatanTM superior to RhopressaTM by 1.7 - 3.4 mmHg (p<0.001)
22
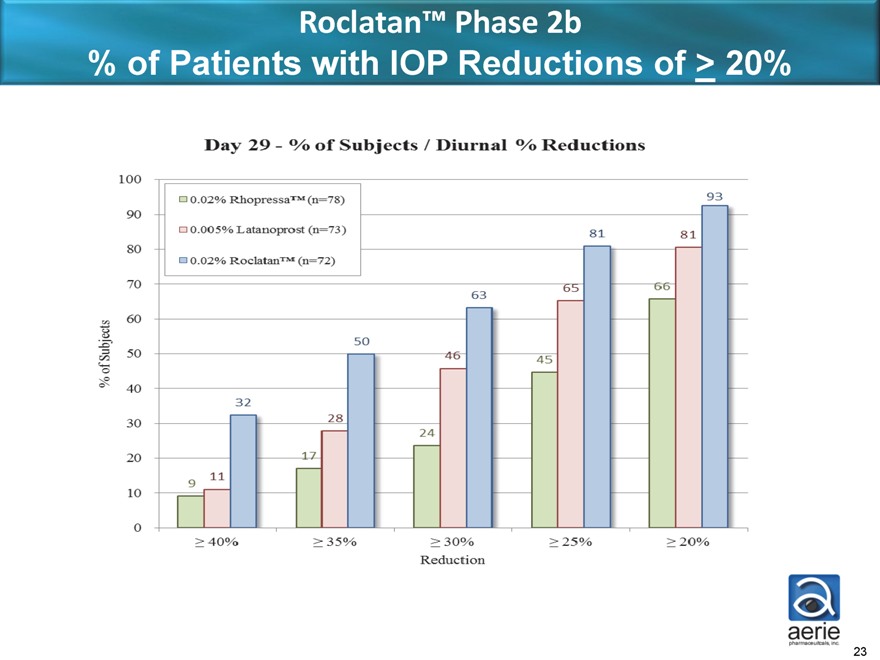
Roclatan™ Phase 2b
% of Patients with IOP Reductions of > 20%%
Day 29—% of Subjects / Diurnal % Reductions
100 90 80 70 60 50 40 30 20 10 0
% of Subjects
9 11 32
17 28 50
24 46 63
45 65 81
66 81 93
40% 35% 30% 25% 20%
Reduction
0.02% Rhopressa TM (n=78)
0.005% Latanoprost (n=73)
0.02% Roclatan TM (n=72)
23
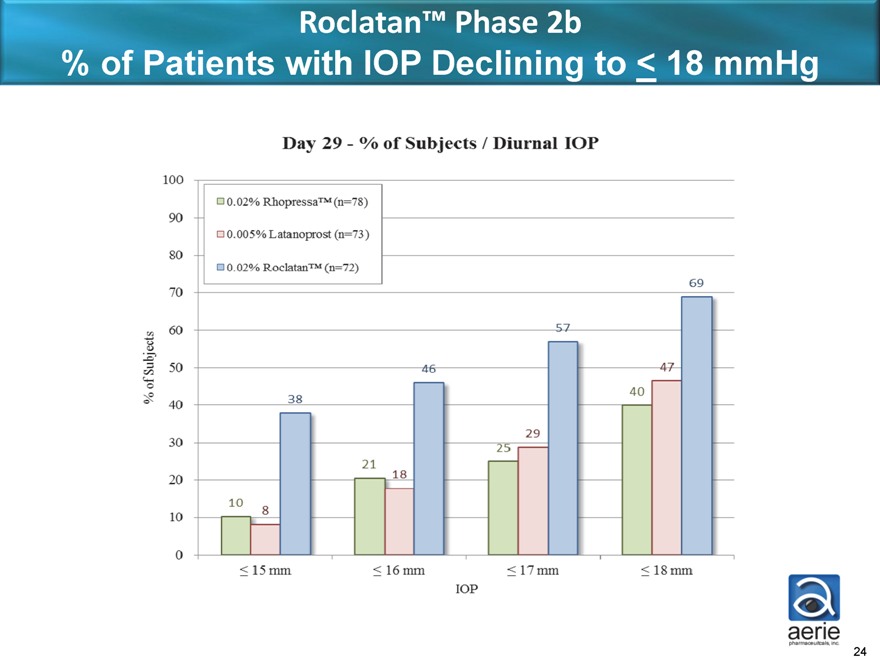
Roclatan™ Phase 2b
% of Patients with IOP Declining to < 18 mmHg
Day 29—% of Subjects / Diurnal IOP
100 90 80 70 60 50 40 30 20 10 0
% of Subjects
15mm 16mm 17mm 18mm
10 8 38
21 18 46
25 29 57
40 47 69
0.02% RhopressaTM (n=78)
0.005% Latanoprost (n=73)
0.02% RoclatanTM (n=72)
IOP
24
Roclatan™
Anticipated Future Milestones
Phase 3 enabling activities (now through 1H2015)
Commencement of Phase 3 registration trials (mid-2015) Phase 3 efficacy and safety results available (mid-2016) NDA filing (mid-2017)
25
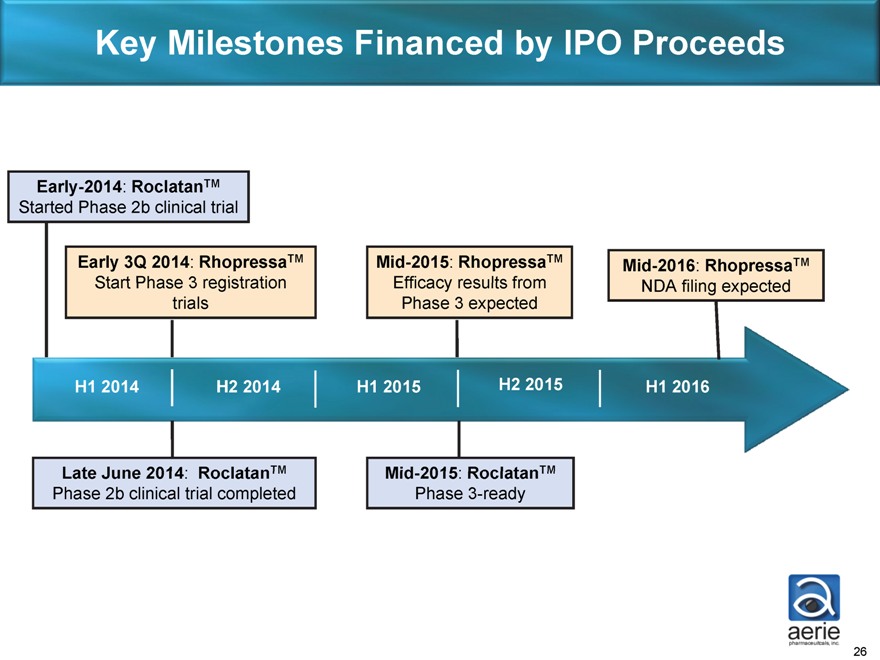
Key Milestones Financed by IPO Proceeds
Early-2014: RoclatanTM
Started Phase 2b clinical trial
Early 3Q 2014: RhopressaTM
Start Phase 3 registration trials
Mid-2015: RhopressaTM
Efficacy results from Phase 3 expected
Mid-2016: RhopressaTM
NDA filing expected
H1 2014 H2 2014 H1 2015 H2 2015 H1 2016
Late June 2014: RoclatanTM
Phase 2b clinical trial completed
Mid-2015: RoclatanTM
Phase 3-ready
26
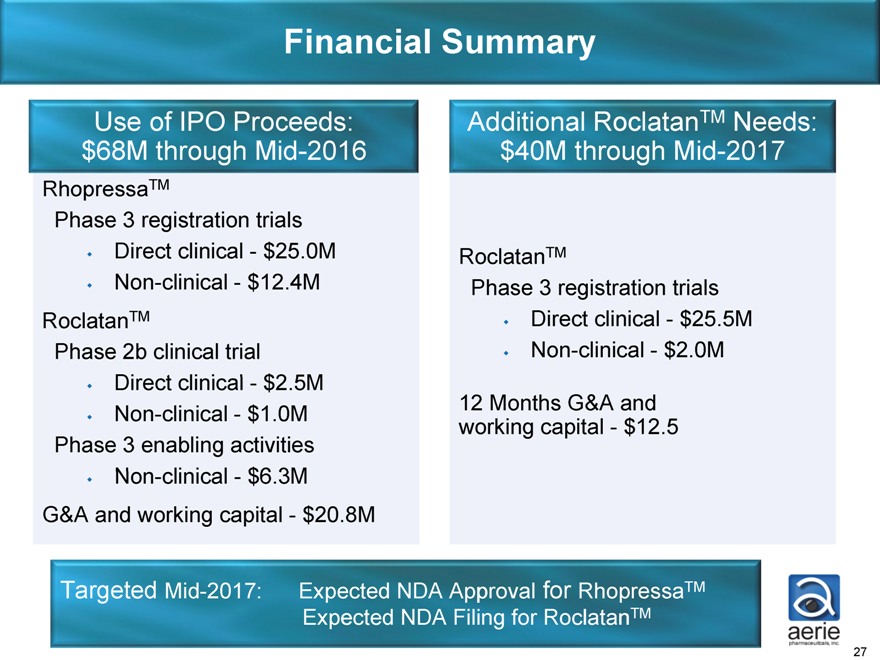
Financial Summary
Use of IPO Proceeds: $68M through Mid-2016
RhopressaTM
Phase 3 registration trials Direct clinical - $25.0M
Non-clinical - $12.4M RoclatanTM
Phase 2b clinical trial Direct clinical - $2.5M
Non-clinical - $1.0M Phase 3 enabling activities Non-clinical - $6.3M G&A and working capital - $20.8M
Additional RoclatanTM Needs: $40M through Mid-2017
RoclatanTM
Phase 3 registration trials Direct clinical - $25.5M
Non-clinical - $2.0M
12 Months G&A and working capital - $12.5
Targeted Mid-2017: Expected NDA Approval for RhopressaTM Expected NDA Filing for RoclatanTM
27

Aerie Stock & Market Cap Performance
Market Cap (dollars in millions)
10/31/13 - $243.7 12/31/13 - $418.2 6/30/14 - $581.5
28 26 24 22 20 18 16 14 12 10
10/31 11/30 12/31 01/31 02/28 03/31 04/30 05/31
4000k
0 10/31 11/30 12/31 01/31 02/28 03/31 04/30 05/31
28
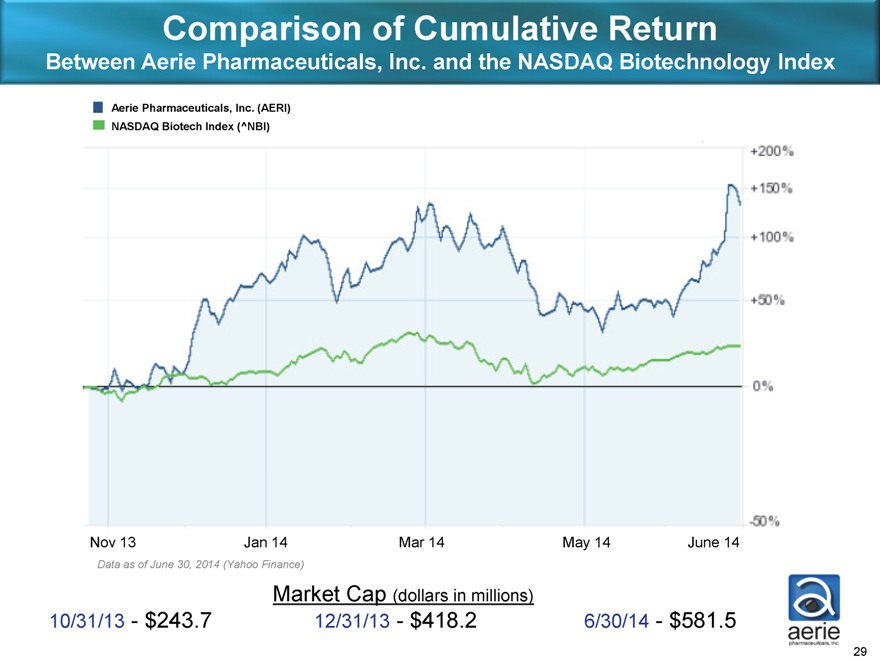
Comparison of Cumulative Return
Between Aerie Pharmaceuticals, Inc. and the NASDAQ Biotechnology Index
Aerie Pharmaceuticals, Inc. (AERI) NASDAQ Biotech Index (^NBI)
+200% +150% +100% +50% 0% -50%
Nov 13 Jan 14 Mar 14 May 14 June 14
Data as of June 30, 2014 (Yahoo Finance)
Market Cap (dollars in millions)
10/31/13—$243.7 12/31/13—$418.2 6/30/14—$581.5
29