Attached files
| file | filename |
|---|---|
| 8-K - 8-K - Aravive, Inc. | d743904d8k.htm |
| EX-99.2 - EX-99.2 - Aravive, Inc. | d743904dex992.htm |
| Exhibit 99.1
|
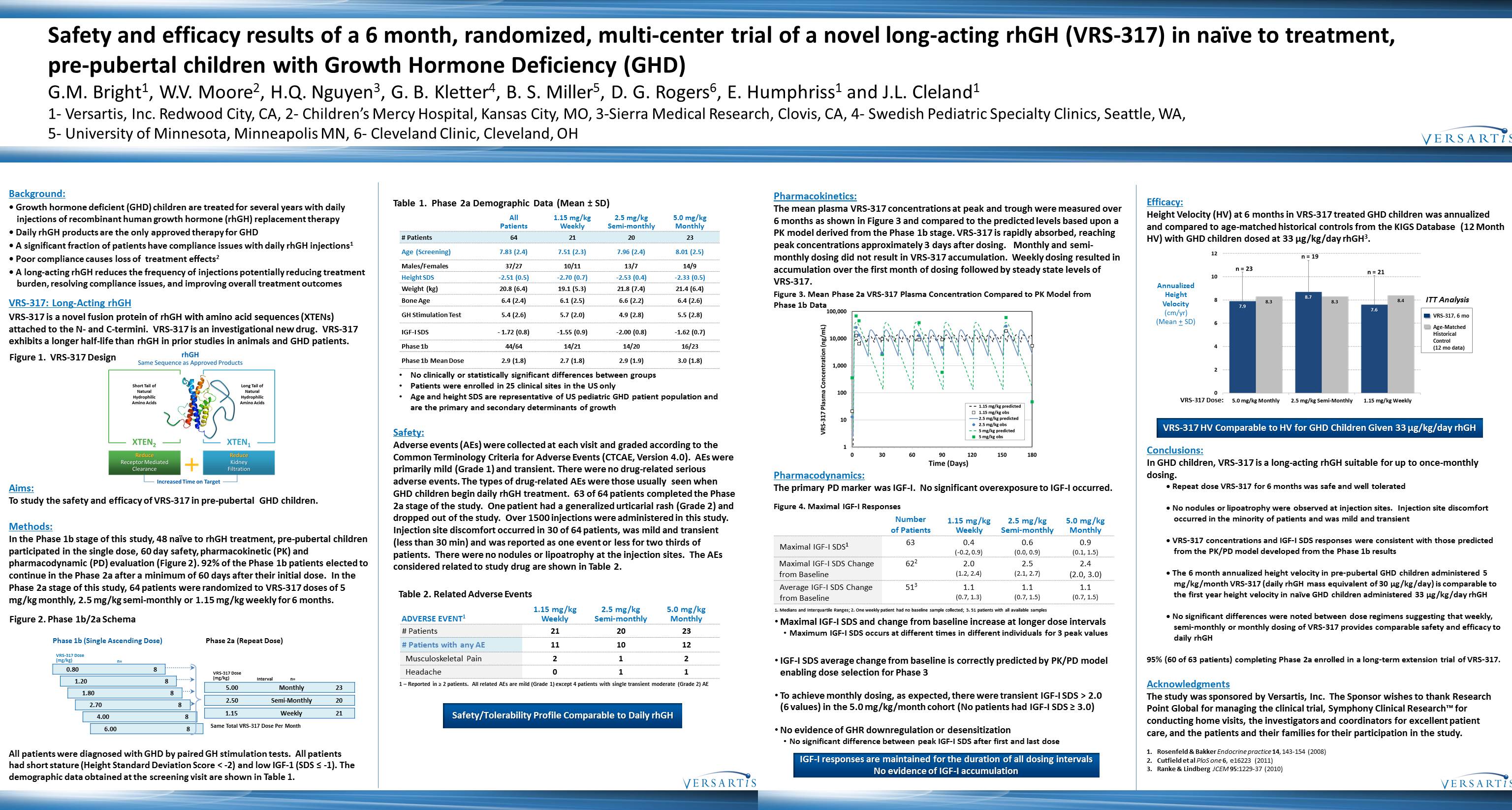
Safety and efficacy results of a 6 month, randomized, multi-center trial of a novel long-acting rhGH (VRS-317) in naïve to treatment, pre-pubertal children with Growth Hormone Deficiency (GHD)
G.M. Bright1, W.V. Moore2, H.Q. Nguyen3, G. B. Kletter4, B. S. Miller5, D. G. Rogers6, E. Humphriss1 and J.L. Cleland1
1-Versartis, Inc. Redwood City, CA, 2-Children’s Mercy Hospital, Kansas City, MO, 3-Sierra Medical Research, Clovis, CA, 4-Swedish Pediatric Specialty Clinics, Seattle, WA, 5-University of Minnesota, Minneapolis MN, 6-Cleveland Clinic, Cleveland, OH
Background:
Growth hormone deficient (GHD) children are treated for several years with daily injections of recombinant human growth hormone (rhGH) replacement therapy
Daily rhGH products are the only approved therapy for GHD
A significant fraction of patients have compliance issues with daily rhGH injections1
Poor compliance causes loss of treatment effects2
A long-acting rhGH reduces the frequency of injections potentially reducing treatment burden, resolving compliance issues, and improving overall treatment outcomes
VRS-317: Long-Acting rhGH
VRS-317 is a novel fusion protein of rhGH with amino acid sequences (XTENs) attached to the N-and C-termini. VRS-317 is an investigational new drug. VRS 317 exhibits a longer half-life than rhGH in prior studies in animals and GHD patients.
Figure 1. VRS-317 Design
rhGH
Same Sequence as Approved Products
Short Tail of Natural Hydrophilic Amino Acids
Long Tail of Natural Hydrophilic Amino Acids
Reduce
Receptor Mediated Clearance
+
Reduce Kidney Filtration
Increased Time on Target
Aims:
To study the safety and efficacy of VRS-317 in pre pubertal GHD children.
Methods:
In the Phase 1b stage of this study, 48 naïve to rhGH treatment, pre-pubertal children participated in the single dose, 60 day safety, pharmacokinetic (PK) and pharmacodynamic (PD) evaluation (Figure 2). 92% of the Phase 1b patients elected to continue in the Phase 2a after a minimum of 60 days after their initial dose. In the Phase 2a stage of this study, 64 patients were randomized to VRS 317 doses of 5 mg/kg monthly, 2.5 mg/kg semi-monthly or 1.15 mg/kg weekly for 6 months.
Figure 2. Phase 1b/2a Schema
Phase 1b (Single Ascending Dose) Phase 2a (Repeat Dose)
VRS-317 Dose
(mg/kg) n=
0.80 8
VRS-317 Dose
1.20 8(mg/kg) Interval n=
5.00 Monthly 23
1.80 8
2.50 Semi Monthly 20
2.70 8
1.15 Weekly 21
4.00 8
6.00 8 Same Total VRS 317 Dose Per Month
All patients were diagnosed with GHD by paired GH stimulation tests. All patients had short stature (Height Standard Deviation Score £ 2) and low IGF 1 (SDS 1). The demographic data obtained at the screening visit are shown in Table 1.
Table 1. Phase 2a Demographic Data (Mean ± SD)
All 1.15 mg/kg 2.5 mg/kg 5.0 mg/kg
Patients Weekly Semi-monthly Monthly
# Patients 64 21 20 23
Age (Screening) 7.83 (2.4) 7.51 (2.3) 7.96 (2.4) 8.01 (2.5)
Males/Females 37/27 10/11 13/7 14/9
Height SDS-2.51 (0.5)-2.70 (0.7)-2.53 (0.4)-2.33 (0.5)
Weight (kg) 20.8 (6.4) 19.1 (5.3) 21.8 (7.4) 21.4 (6.4)
Bone Age 6.4 (2.4) 6.1 (2.5) 6.6 (2.2) 6.4 (2.6)
GH Stimulation Test 5.4 (2.6) 5.7 (2.0) 4.9 (2.8) 5.5 (2.8)
IGF-I SDS-1.72 (0.8)-1.55 (0.9)-2.00 (0.8)-1.62 (0.7)
Phase 1b 44/64 14/21 14/20 16/23
Phase 1b Mean Dose 2.9 (1.8) 2.7 (1.8) 2.9 (1.9) 3.0 (1.8)
No clinically or statistically significant differences between groups
Patients were enrolled in 25 clinical sites in the US only
Age and height SDS are representative of US pediatric GHD patient population and are the primary and secondary determinants of growth
Safety:
Adverse events (AEs) were collected at each visit and graded according to the Common Terminology Criteria for Adverse Events (CTCAE, Version 4.0). AEs were primarily mild (Grade 1) and transient. There were no drug related serious adverse events. The types of drug related AEs were those usually seen when GHD children begin daily rhGH treatment. 63 of 64 patients completed the Phase 2a stage of the study. One patient had a generalized urticarial rash (Grade 2) and dropped out of the study. Over 1500 injections were administered in this study. Injection site discomfort occurred in 30 of 64 patients, was mild and transient (less than 30 min) and was reported as one event or less for two thirds of patients. There were no nodules or lipoatrophy at the injection sites. The AEs considered related to study drug are shown in Table 2.
Table 2. Related Adverse Events
1.15 mg/kg 2.5 mg/kg 5.0 mg/kg
ADVERSE EVENT1 Weekly Semi-monthly Monthly
# Patients 21 20 23
# Patients with any AE 11 10 12
Musculoskeletal Pain 2 1 2
Headache 0 1 1
1 – Reported in 2³patients. All related AEs are mild (Grade 1) except 4 patients with single transient moderate (Grade 2) AE
Safety/Tolerability Profile Comparable to Daily rhGH
Pharmacokinetics:
The mean plasma VRS-317 concentrations at peak and trough were measured
over 6 months as shown in Figure 3 and compared to the predicted levels based upon a PK model derived from the Phase 1b stage. VRS-317 is rapidly absorbed, reaching peak concentrations approximately 3 days after dosing. Monthly and semi monthly dosing did not result in VRS-317 accumulation. Weekly dosing resulted in accumulation over the first month of dosing followed by steady state levels of VRS317.
Figure 3. Mean Phase 2a VRS-317 Plasma Concentration Compared to PK Model from Phase 1b Data
100,000 10,000 1,000 100 10 1
0 30 60 90 120 150 180
Time (Days)
VRS-317 Plasma Concentration (ng/mL)
Pharmacodynamics:
The primary PD marker was IGF-I. No significant overexposure to IGF-I occurred.
Figure 4. Maximal IGF-I Responses
Number 1.15 mg/kg 2.5 mg/kg 5.0 mg/kg
of Patients Weekly Semi-monthly Monthly
Maximal IGF-I SDS1 63 0.4 0.6 0.9
(- minus 0.2, 0.9)(0.0, 0.9)(0.1, 1.5)
Maximal IGF-I SDS Change 622 2.0 2.5 2.4
from Baseline(1.2, 2.4)(2.1, 2.7)(2.0, 3.0)
Average IGF-I SDS Change 513 1.1 1.1 1.1
from Baseline(0.7, 1.3)(0.7, 1.5)(0.7, 1.5)
1. Medians and Interquartile Ranges; 2. One weekly patient had no baseline sample collected; 3. 51 patients with all available samples
Maximal IGF-I SDS and change from baseline increase at longer dose intervals Maximum IGF I SDS occurs at different times in different individuals for 3 peak values
IGF-I SDS average change from baseline is correctly predicted by PK/PD model enabling dose selection for Phase 3
To achieve monthly dosing, as expected, there were transient IGF-I SDS > 2.0 (6 values) in the 5.0 mg/kg/month cohort (No patients had IGF-I SDS-3.0)
No evidence of GHR downregulation or desensitization
No significant difference between peak IGF-I SDS after first and last dose
IGF-I responses are maintained for the duration of all dosing intervals No evidence of IGF I accumulation
Efficacy:
Height Velocity (HV) at 6 months in VRS-317 treated GHD children was annualized and compared to age- matched historical controls from the KIGS Database (12 Month HV) with GHD children dosed at 33 µg/kg/day rhGH3.
Annualized Height Velocity (cm/yr) (Mean+-SD)
12 10 8 6 4 2 0
n=23 n=19 n=21
7.9 8.3 8.7 8.3 7.6 8.4
ITT Analysis VRS-317, 6 mo
Age-Matched Historical Control (12 mo data)
VRS-317 Dose: 5.0mg/kg Monthly
2.5mg/kg Semi-Monthly
1.15mg/kg Weekly
VRS-317 HV Comparable to HV for GHD Children Given 33 µg/kg/day rhGH
Conclusions:
In GHD children, VRS-317 is a long-acting rhGH suitable for up to once-monthly
dosing.
Repeat dose VRS-317 for 6 months was safe and well tolerated
No nodules or lipoatrophy were observed at injection sites. Injection site discomfort
occurred in the minority of patients and was mild and transient
VRS-317 concentrations and IGF-I SDS responses were consistent with those predicted
from the PK/PD model developed from the Phase 1b results
The 6 month annualized height velocity in pre-pubertal GHD children administered 5
mg/kg/month VRS-317 (daily rhGH mass equivalent of 30 µg/kg/day) is comparable to
the first year height velocity in naïve GHD children administered 33 µg/kg/day rhGH
No significant differences were noted between dose regimens suggesting that weekly,
semi-monthly or monthly dosing of VRS-317 provides comparable safety and efficacy to
daily rhGH
95% (60 of 63 patients) completing Phase 2a enrolled in a long-term extension trial of VRS-317.
Acknowledgments
The study was sponsored by Versartis, Inc. The Sponsor wishes to thank Research Point Global for managing the clinical trial,
Symphony Clinical Research™ for conducting home visits, the investigators and coordinators for excellent patient care, and the patients and their families for their participation in the study.
1. Rosenfeld & Bakker Endocrine practice 14, 143-154 (2008)
2. Cutfield et al PloS one 6, e16223 (2011)
3. Ranke & Lindberg JCEM 95:1229 37 (2010)