Attached files
| file | filename |
|---|---|
| 8-K - 8-K - BROWN FORMAN CORP | d726131d8k.htm |
Exhibit 10.1
May 12, 2014
Donald Berg
14212 Reserve Cove
Prospect, KY 40059
Dear Don:
Congratulations on your retirement from Brown-Forman (the “Company”), and thank you again for your many years of service. As we have discussed, you handed off your duties as Chief Financial Officer effective January 31, 2014, and you will retire from employment with the Company effective April 30, 2014. In the interim period between January 31, 2014, and April 30, 2014, you will continue to be employed by the Company and will help transition your duties. This letter outlines the ways the Company is offering to support you during and after this transition.
Don, you are entitled to receive the first category of benefits contained in Section 1 of this letter whether or not you sign the Release and Agreement (Section 3). The benefits contained in Section 2 however, require your agreement and signature. If you decide to sign the Release and Agreement, note that you are also agreeing to everything contained in Sections 1 and 2 as explained below.
We would like to call your attention to one specific item that is discussed below – understanding how to continue your health care and other insurance coverages after you move from employment status to retirement. To avoid any interruption in your medical coverage, we encourage you to act quickly on the information you will be sent shortly after your last date of employment.
Section 1 – General Information
This section describes your status and rights in various matters, and explains steps you may need to take. To confirm, you do not have to sign the Release and Agreement to receive any of the benefits listed in this Section 1.
Vacation
You will be paid for the number of unused vacation days remaining as of your last date of employment, in the payroll cycle following your last date of employment. Either you or Sue Smith can provide this information to us; please let us know how you would like to handle. To the extent your last date of employment is before April 30, 2014, however, you will be paid for the number of unused vacation days remaining as of your last date of employment, in the payroll cycle following your last date of employment, and those unused days will be counted as days of employment for purposes of your short-term cash incentive.
Holiday Bonus
You will receive a pro-rated holiday bonus based on your last date of employment with the Company. (The holiday bonus is accrued on a December-November cycle.) This amount will be paid in the payroll cycle following your last date of employment.
Page 2
American Express and Other Amounts Owed to the Company
You are responsible for completing any outstanding expense reports and making arrangements to reimburse any amounts owed the Company. You must take these actions whether or not you sign the Release and Agreement. Let’s discuss the easiest way to manage these matters, with help from Sue Smith.
Employee Benefits
Following is a brief explanation of what happens to your Company benefits upon the end of your employment. You will receive additional personalized information directly from the Brown-Forman Benefits Service Center. Please contact the Brown-Forman Benefits Service Center by calling 1-877-775-1477 with questions regarding any of these items, or to change an address on file. Don, you are also welcome to contact Cheryl Beckman (502-774-6747) or Donna Wimbec (502-774-7306) directly if you prefer.
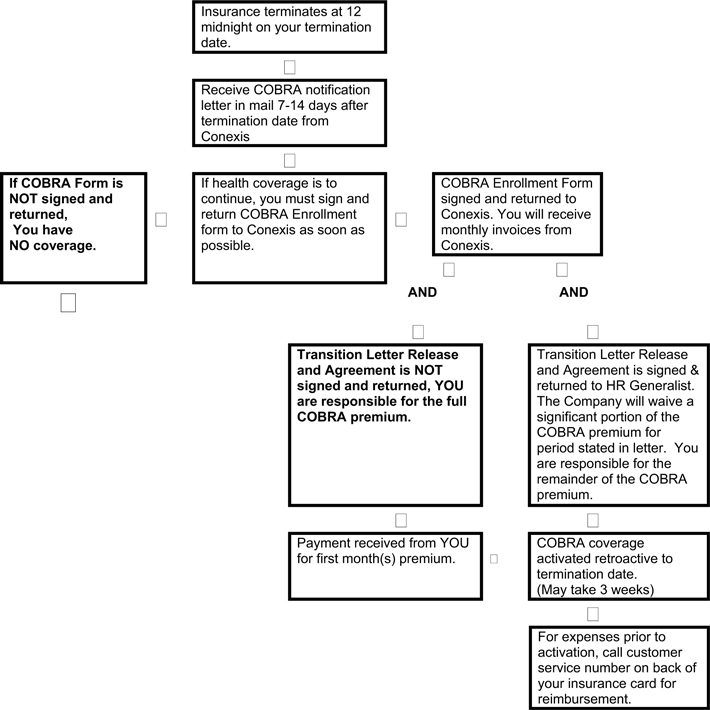
Medical, Vision and Dental Coverage Continuation. Your medical, vision, and dental coverages end on the last date of your employment. If you so elect, those coverages can be continued for up to 18 months under a law known as COBRA. Shortly after your last date of employment, you will receive, at your home address as prescribed by the COBRA law, an “Election and Enrollment” form which you must complete, sign and return as directed in that letter. Please note: COBRA information will come from Conexis, our partner for administering COBRA. If you do not receive a COBRA packet within two weeks following your last date of employment, please notify the B-F Benefits Service Center at 1-877-775-1477. Note the attached flow chart describing the COBRA administration process.
Reinstatement of your medical, vision, and dental coverages under COBRA require completion of the COBRA enrollment form and forwarding the document, along with any required premium, to the address specified on the form. You will have 60 days from the date of your COBRA package to enroll in COBRA benefits. The premium notice will follow soon after your enrollment form is received by Conexis. Failure to pay the premium will result in your coverage not being continued. Reinstatement can take up to three weeks from the mailing of the required information. Once coverages are reinstated, they will be retroactive to the last date of your employment, so no lapse in coverage will occur. If you have claims denied during this period, please request that your provider re-file once reinstatement has occurred.
Retiree Medical. You and your spouse are eligible for retiree medical coverage under the B-F Retiree Medical plan. If you choose to elect that benefit, you may do so within 31 days of your last date of employment. Alternatively, you can elect COBRA through the subsidy period (ending January 31, 2015) to take advantage of the subsidized premiums. You will then have 31 days from the subsidy end date to elect retiree medical. If however, you are eligible for other employer sponsored coverage (i.e., coverage from a new employer), you may elect to waive enrollment in the B-F Retiree Medical plan until such time your other employer coverage ends by contacting the B-F Benefits Service Center at 1-877-775-1477. The B-F Retiree Medical waiver due to other employer coverage must be made within 31 days of your last date of employment, or within 31 days of the end of the subsidy period (if applicable), in order to be eligible to enroll at a later date. Once waived, the coverage can be later be elected within 31 days of your other employer sponsored coverage ending by contacting the B-F Benefits Service Center.
Page 3
Flexible Spending Accounts (FSAs)
Health Care FSA – You may elect COBRA for your Health Care FSA following your last date of employment (after deducting submitted expenses from contributions thus far from payroll). If you elect to continue the Health Care FSA benefit under COBRA, please note that the Your Spending Account (YSA) Debit card will no longer be active after your last date of employment. Reimbursement is requested for eligible FSA expenses by completing claim forms (“Health Care Claim Forms”) which can be requested through YSA at 1-877-775-1477. If you elect not to continue the Health Care FSA under COBRA, you have until March 1 following the end of the year to submit claims for reimbursement for eligible services incurred through your last date of employment.
If you elect COBRA for your Health Care FSA and continue that coverage through the end of the plan year, you have until March 1 following the end of the year to file claims for reimbursement for eligible services and items received or purchased up to December 31 of the plan year. Should you drop your COBRA coverage at any point prior to the end of the plan year, you have until March 1 following the end of the year to file for reimbursement for eligible services and items received or purchased prior to the date of the COBRA termination.
IMPORTANT REMINDER FOR FSA REIMBURSEMENTS: Keep copies of all receipts for services and/or items for which you receive reimbursement from either a Health Care or Dependent Care FSA with your tax records for as long as you retain those tax records (recommended seven years). YSA, as required by the IRS, may request verification of expenses well after the end of the plan year.
For questions about your FSA account(s), contact YSA at 1-877-775-1477.
B-F Live Well Health Incentive Account (LWIA)
You may elect COBRA for your LWIA if you have a positive balance in your account as of your last date of employment (after deducting submitted expenses from incentives earned). If you elect to continue the LWIA benefit under COBRA, please note that the Your Spending Account (YSA) Debit card will no longer be active after your last date of employment. Reimbursement is requested for eligible expenses by completing claim forms (“Health Care Claim Forms”) which can be requested by contacting YSA at 1-877-775-1477. If you elect not to continue the LWIA under COBRA, you have until March 1 following the end of the year to submit claims for reimbursement for eligible services incurred through December 31st.
If you elect COBRA for your LWIA and continue that coverage through the end of the calendar year, you have until March 1 following the end of the year to file claims for reimbursement for eligible expenses incurred through December 31st. Should you drop your COBRA coverage at any point prior to the end of the year, you have until March 1 following the end of the year to file for reimbursement for eligible expenses incurred prior to the date of the COBRA termination.
IMPORTANT REMINDER FOR LWIA REIMBURSEMENTS: Keep copies of all receipts for services and/or items for which you receive reimbursement from Health Care providers with your tax records for as long as you retain those tax records (recommended seven years). YSA, as required by the IRS, may request verification of expenses well after the end of the plan year.
Page 4
For questions about your LWIA account, contact YSA at 1-877-775-1477.
| • | Group Life Insurance. All life insurance benefits end on your last date of employment. These include Company paid life insurance plus any additional life insurance coverage for yourself, your spouse, or your dependent child(ren) that you have elected on a contributory basis. The plan allows you in most cases to continue life coverage under an individual conversion policy, which is a whole life policy with The Hartford. The plan also allows you in most cases to “port” your coverage, that is, to continue coverage under a group term life policy with The Hartford. To apply for conversion or portability coverage, you must apply within 31 days of your last date of employment by calling The Hartford at 1-877-320-0484. |
| • | Short-Term and Long-Term Disability coverage for any future disability ends upon your last date of employment and cannot be converted to a private policy. If you are on a long-term disability leave as of your last date of employment, information about your current disability benefits will be provided separately. |
| • | 401(k) Savings Plan. As a 401(k) savings plan participant, you will be entitled to a distribution, either through a cash payout or through a rollover into a personal Individual Retirement Account (IRA) or another employer’s plan. This is an important tax decision that should be discussed with your financial advisor. You should contact Fidelity Investments directly at 1-800-835-5093 to better understand your alternatives. You are also welcome to contact Cheryl Beckman (502-774-6747) or Donna Wimbec (502-774-7306) directly with questions. Please note that it will take approximately four weeks from your last date of employment for your final contributions and dividends to be credited to your account. Your account continues to participate in market performance (both up and down) during this period. Further, you may continue to direct your investments and make changes regarding your asset allocation until your account is distributed. |
| • | Executive Savings Plan (Nonqualified Deferred Compensation Plan). As a participant in this executive benefit plan, you will be contacted within four weeks of your last date of employment with specific information concerning the payment of this benefit. If you do not receive information within four weeks of this date, please contact Mullin TBG at 1-800-824-0040. Please note, if you enrolled in the Plan for the current calendar year and made an election for a portion of your STIP or LTIP to be deferred, by law, this deferral must still be made into the plan even if your employment ended prior to the actual payment of these bonuses. |
| • | Pension. Because you are a vested participant in the pension plan, the Brown-Forman Pension Center will send you detailed pension information approximately six weeks after your last date of employment. That detailed information will also provide you with the lump sum benefit available to you from the Plan. You have a 120 day window from your last date of employment to elect the lump sum benefit. If you do not request a lump sum within that window, your only option for form of payment will be monthly installment payments. If you have questions regarding your pension information, please contact the Brown-Forman Pension Center at 1-877-775-1477. You are also welcome to contact Cheryl Beckman (502-774-6747) or Donna Wimbec (502-774-7306) directly with questions. |
Page 5
| • | SERP (Supplemental Executive Retirement Plan). As a participant in this executive benefit plan, you will be contacted approximately six weeks after your last date of employment with specific information concerning the payment of this benefit. If you do not receive information six weeks after this date, please contact the Brown-Forman Pension Center at 1-877-775-1477. You are also welcome to contact Cheryl Beckman (502-774-6747) or Donna Wimbec (502-774-7306) directly with questions. |
| • | B-F Live Well Work Life Services. Should you or your dependents want professional counseling, the Company encourages you to contact the Work Life Services Program. These completely confidential services are provided by the Company through United Behavioral Health for 30 days after your last date of employment. Continuation of this benefit is also available under COBRA for 18 months at no cost to you. Even though this benefit is provided at no cost to you, you still must elect it on the COBRA continuation form to be entitled to the benefit. United Behavioral Health may be reached at 1-866-374-6061. |
Short-Term Cash Incentive
You will receive a short-term cash incentive for F’14 prorated by the number of calendar days you were employed during the F’14 fiscal year. It will be paid in the same manner as to other participants after the end of the fiscal year. Your plan has been designed so that 80% of your short-term incentive is based on Brown-Forman’s actual performance and 20% is based on your Individual Performance Objectives (IPO’s). Company performance will be used as a proxy for your IPO score; thus, 100% of your short-term incentive payout will be based on Brown-Forman’s actual performance.
Long-Term Cash, Stock Options, SSARs, and Performance-Based Restricted Stock
You will receive a long-term cash incentive for the performance period F’14-F’16 prorated by the number of whole months you were employed during F’14. Long-term cash incentives for the performance periods F’12-F’14, F’13-F’15, and F’14-F’16, respectively, will be adjusted for actual Company performance and be paid at the same time and in the same manner as to employee participants, unless otherwise provided herein.
You will be treated as a retiree for purposes of your stock options and stock-settled stock appreciation rights (“SSARs”). You will have 7 years from your last date of employment to exercise stock options and SSARs that are vested and exercisable as of your last date of employment (however, you may not exercise stock options or SSARs beyond the expiration date indicated on the award agreement). SSARs granted in F’12, F’13, and F’14, respectively, will vest on the date indicated on the award agreements. Upon vesting, you will have 7 years to exercise these awards. Your SSAR award issued in F’14 will be prorated based on the number of whole months worked during F’14.
Performance-based restricted stock awards for the period F’11-F’14 are no longer subject to performance conditions and restrictions will lapse on April 30, 2014. Performance-based restricted stock awards for the periods F’12-F’15, F’13-F’16, and F’14-F’17, respectively, will be adjusted for actual Company performance and paid at the same time and in the same manner as to employee participants. Your performance-based restricted stock award issued in F’14 will be prorated based on the number of whole months worked during F’14.
Please note that your short-term and long-term cash incentives, stock options, SSARs and performance-based restricted stock awards remain subject to the terms and conditions of their respective award agreements and the Brown-Forman Omnibus Compensation Plan under which they were issued.
Page 6
Section 2 – Additional Benefits
This section describes the additional compensation that the Company will pay you in return for your signing and fully complying with the Release and Agreement in Section 3 of this letter (“Additional Benefits”).
Transition Payment
The Company will pay you a one-time transition payment of Five Hundred Ninety-Eight Thousand Nine Hundred Fifty-Eight Dollars ($598,958) (“Transition Payment”) payable in the payroll cycle following your last date of employment. This payment, less required withholdings, will be automatically deposited to your bank account through the normal semi-monthly payroll process.
Fiscal 2014 Make-Whole Benefit
Should your last date of employment be April 30, 2014, the Company shall provide you with the Transition Payment, to be paid in the payroll cycle following April 30, 2014.
Should you determine that your last date of employment be before April 30, 2014, the Company shall pay you the Transition Payment, to be paid in the payroll cycle following your last date of employment and the following additional payments:
Salary and Holiday Bonus. The Company will pay you for any additional base salary or holiday bonus to which you otherwise would have been entitled had your last day of employment with the Company been April 30, 2014. This additional base salary and holiday bonus amount will be paid in the payroll cycle following your last date of employment based on your current annualized rate of Five Hundred Ninety Eight Thousand Nine Hundred Fifty Eight Dollars ($598,958).
Short-Term Cash Incentive. The Company will pay you your target short-term cash incentive for F’14 prorated by the number of calendar days that you were not employed during the F’14 fiscal year. This amount will be paid in the payroll cycle following your last date of employment based on your current annualized rate of Four Hundred Fifteen Thousand Dollars ($415,000).
Long-Term Incentive. The Company will pay you your target long-term incentive for F’14 prorated by the number of whole months that you were not employed during the F’14 fiscal year. The long-term incentive will be paid in cash in the payroll cycle following your last date of employment based on your current annualized rate of Seven Hundred Sixty Thousand Dollars ($760,000).
Should the Company determine that your last day of employment be before April 30, 2014, the Company shall pay you the Transition Payment and a payment equal in value to your Salary and Holiday Bonus, your Short-Term Cash Incentive, and your Long-Term Incentive as if you had been employed through April 30, 2014. The lump sum Transition Payment of Five Hundred Ninety Eight Thousand Nine Hundred Fifty Eight Dollars ($598,958) and the payment for Salary and Holiday Bonus will be paid in the payroll cycle following your last date of employment. The Short-Term Cash Incentive and the Long-Term incentive will be paid at the same time and in the same manner as is normal for such bonusable employees.
Health Insurance and COBRA
The Company will pay for its portion of your health and dental coverage under COBRA for nine (9) months following April 30, 2014. In the event that you continue to receive health and dental coverage under COBRA past January 31, 2015, you will be responsible for full payment of the cost of such coverage in order to ensure that the coverage is uninterrupted.
Page 7
Summary
If you have any questions about this letter or the Release and Agreement, or if there is any other transition matter you wish to discuss, please contact me at 502-774-7747. I encourage you to take your time in reviewing these materials. If you decide to sign the Release and Agreement, please return one complete copy of this entire document (the letter as well as the signed Release and Agreement) to me, in the self-addressed envelope provided.
Don, again, congratulations on your retirement from Brown-Forman, and on behalf of Paul Varga and the Brown-Forman Board of Directors, thank you for your dedicated service and important contributions to the Company over the years. I wish you all the best in the future.
| Yours truly, |
| /s/ Lisa Steiner |
| Lisa Steiner, |
| SVP, Chief HR Officer |
Page 8
Section 3 – Release and Agreement
1. GENERAL
(a) PURPOSE. I understand that I am entitled to the compensation and benefits described in Section 1 above (General Information), even if I do not sign this Section 3 Release and Agreement. I further understand that the Additional Benefits described in Section 2 above are being offered by the Company to me conditioned upon and as consideration for my signing and fully complying with all aspects of this Section 3 Release and Agreement, and that I am not otherwise eligible for these Additional Benefits.
(b) ENCOURAGEMENT TO CONSULT WITH ATTORNEY. I acknowledge that this Release and Agreement is a binding legal document and that the Company advises me to consult with an attorney before signing this Release and Agreement.
(c) REVIEW AND CONSIDERATION PERIOD. I acknowledge that I have been given at least 21 days to review and consider this Release and Agreement and have had the opportunity to use as much of that time as I wish before signing it.
I wish to accept the Additional Benefits described in Section 2 of this letter and in exchange agree as follows:
2. RELEASE AND COVENANT NOT TO SUE. I hereby release, to the extent permitted by law, the Company and all of its divisions, subsidiaries, affiliates, employees, officers, directors, successors and assigns (hereinafter “the Company’) from all claims, actions, causes of action, direct or derivative suits, demands, grievances, promises, rights, warranties, debts, judgments, obligations, liabilities, damages, losses, costs and expenses of every kind and nature, known or unknown, suspected or unsuspected, foreseen or unforeseen, which I may have or claim to have against the Company except as noted in Paragraph 2(d) below.
(a) This release includes but is not limited to all claims that I may have for discrimination on the basis of religion, national origin, race, sex, disability, age (including all claims under the Age Discrimination in Employment Act of 1967 as amended (ADEA)), and all other protected classifications under any other federal, state or local laws or regulations, except as noted in Paragraph 2(d) below. I also release, to the extent permitted by law, and except as noted in Paragraph 2(d) below, any and all common law and statutory claims, including but not limited to, contract, tort, or wrongful discharge claims.
(b) Except as provided in Paragraph 2(d) below and to the extent permitted by law, I agree never to file any lawsuit, complaint, proceeding, grievance or action of any sort arising from my employment or the termination of my employment with the Company prior to the Effective Date of this Agreement as set forth in Paragraph 4(a) below. If I violate this promise by suing the Company, then I agree that I will forfeit any outstanding payments or benefits due under Section 2 of this letter and will repay to the Company any amounts and benefits already paid or provided pursuant to Section 2 of this letter.
(c) This Release and Covenant Not to Sue covers both known and unknown claims that may exist prior to the Effective Date of this Agreement, as set forth in Paragraph 4(a) below.
(d) This Release and Covenant Not to Sue does NOT cover:
| (i) | any rights or claims arising after the Effective Date of this Release and Agreement; or |
| (ii) | my right to communicate with, file a charge with, or participate in an investigation conducted by any federal, state, or local government |
Page 9
| agency or law enforcement entity, or to bring an action under Equal Employment Opportunity Commission (“EEOC”)-enforced statutes with respect to rights that I cannot be required to waive; or |
| (iii) | my rights to commence an action or proceeding to enforce this Release and Agreement or to file a suit challenging its validity under the ADEA; or |
| (iv) | any rights or claims I may have for benefits under the provisions of any pension benefit plan maintained by the Company and which is applicable to me; or |
| (v) | any rights which I may have under the existing or then-current indemnification provision in the Company’s Articles, Bylaws, or any employee benefit plan with which I worked at the Company’s request, or any such provisions applying to employees generally, for any actions or claims against me arising out of my tenure as an officer and employee of the Company; or |
| (vi) | any rights preserved by or created under this Agreement and/or the law. |
(e) I agree that I will not file any claim or suit against the Company for any reason without first engaging in discussions with a designated Company representative in a good faith effort to resolve the dispute. Any such claim or suit shall be filed in the state or federal courts located in Jefferson County, Kentucky. In any claim or suit that I file, the prevailing party shall be entitled to its reasonable attorneys’ fees and costs.
3. AGREEMENTS.
(a) MUTUAL NON-DISPARAGEMENT. I will not make any statements (whether orally or in writing) which are intended to be derogatory or damaging to the Company, its business, the business reputation, practices, or conduct of its Board of Directors, or any of the Company’s assets, businesses, or relations with customers, suppliers, or consumers. The Company’s Directors and the Executive Leadership Team in office as of the Effective Date shall also not make any statements (whether orally or in writing) which are intended to be derogatory or damaging to me. This paragraph shall not restrict my ability or the ability of the Company to (i) respond to any inquiry from applicable regulatory or other authorities or to provide information pursuant to legal process, court order, subpoena, or other effective directive by a court, administrative agency, arbitration panel, or legislative body, or pursuant to law, rule, regulation, or other requirement; (ii) enforce this Agreement; (iii) discuss any person or the Company generally with legal counsel in a context in which it reasonably is expected that the attorney will maintain as confidential under the attorney-client privilege; or (iv) communicate with, or participate in an investigation conducted by, the EEOC or any other federal, state, or local government agency or law enforcement entity. Further, this paragraph shall not require me to affirmatively take actions to enhance or support the Company or other stakeholders.
(b) CONFIDENTIALITY. I acknowledge and reaffirm my ongoing legal and professional obligations to maintain confidential and not use or disclose to any other person or entity other than as permitted or required by law any trade secrets or other non-public, confidential information belonging to the Company. Confidential information includes all non-public: manufacturing, marketing and strategic information and data; costs and pricing structures; financial and accounting data; information regarding customers and suppliers; trade secrets and trademarks; information regarding the Board of Directors’ Committees and their activities; information regarding the shareholders’ shareholdings and relationships with the Company; and legal and/or regulatory information. Nothing in this Agreement shall prohibit or restrict me (or my attorney) from
Page 10
responding to any inquiry, or providing testimony, about the Company’s confidential or proprietary information by or before any federal or state administrative or regulatory agency or authority, including pursuant to legal process, court order, subpoena, or other effective directive by a court, administrative agency, arbitration panel, or legislative body, or pursuant to law, rule, regulation, or other requirement, or in connection with any communication with, or participation in an investigation conducted by, the EEOC or any other federal, state, or local government agency or law enforcement entity.
(c) NON-COMPETITION. I agree, for a period of twelve (12) months following April 30, 2014, not to accept employment with or serve as a Board member of, or consultant to, or have any other advisory or ownership relationship with (other than as an owner of less than one percent of its stock or as a consumer of its products) any spirits Supplier (“Supplier” being defined as any U.S. or non-U.S. spirits producer, manufacturer, brand owner, primary brand marketer, or importer). Notwithstanding the foregoing, the Company agrees and acknowledges that this non-competition provision does not prohibit my employment with, consultancy to, or ownership of (i) any company whose primary business is as a beverage alcohol distributor in the U.S., even if such distributor owns brands and/or is also licensed as a spirits supplier or importer; or (ii) any Supplier whose annual volume is less than 100,000 cases, except Suppliers (x) of bourbon whiskey or Tennessee whiskey, or (y) whose principal place of business is in the Commonwealth of Kentucky or the State of Tennessee.
(d) STANDSTILL. I agree that I will not directly or indirectly, enter into any discussions, negotiations, arrangements or understandings with, or assist, advise, encourage, or otherwise participate in any attempt to take over the Company, the term “take over” being defined in the broadest possible manner to include without limitation the acquisition of greater than one percent (1%) of the Company’s Class A Common Stock, any proxy solicitation involving the Company, the acquisition of a material portion of the Company’s assets, any attempt to elect Directors to the Company’s Board of Directors who have not been nominated by the Board, advocating for the Company’s restructuring, merger or involvement in another business combination, or gaining any material voting interest in the Company, provided, however, that nothing in this Agreement shall prohibit or restrict me (or my family or heirs) from acquiring or selling Class A Common Stock or other securities of the Company in amounts not to exceed 1% of any class thereof. Nothing in this paragraph shall be construed to prohibit or restrict me from voting any shares that I own so long as those shares do not constitute more than 1% in the aggregate of any class of shares.
(e) PROSPECTIVE EMPLOYMENT. I and the Company agree that all third party inquiries regarding my employment at Brown Forman, including, but not limited to, all inquiries from prospective employers, shall be referred to the Company’s Human Resources Department and shall be handled pursuant to (i) what is the current Company policy, which policy provides that such inquiries shall be responded to with only the following information: my dates of employment; the positions held during my employment with the Company; and if requested by the party making the inquiry, confirmation of my final compensation package; as well as (ii) the attached December 4, 2013 commentary. In addition, the Company will fund executive outplacement services at a total cost not to exceed Fifty Thousand Dollars ($50,000.00), which Fifty Thousand Dollars ($50,000) will be paid directly to the outplacement agency I select upon presentation to the Company of an invoice. Such invoice must be submitted to the Company for payment within six months of the date of this Release and Agreement
(f) UNEMPLOYMENT CLAIM. The Company agrees not to contest any claim that I may make for unemployment compensation benefits.
Page 11
(g) INDEMNIFICATION. As of the execution date of this Release and Agreement, the Company confirms that it has no intent to assert any legal cause of action against me. Moreover, the Company agrees to indemnify and hold me harmless to the fullest extent permitted by applicable law and/or, at a minimum, the organizational documents and policies of the Company, including all policies allowing the advancement of reasonable and documented attorneys’ fees and expenses and all policies concerning amounts paid in settlement, for my actions or inactions in accordance with my performance of duties as an officer, employee, or agent of the Company or as a fiduciary of any benefit plan of the Company. The Company also agrees to provide me with directors’ and officers’ liability insurance coverage after my employment with regard to matters occurring during my employment with the Company, which coverage will be at a level at least equal to the greatest level afforded other current officers of the Company.
(h) COOPERATION. I agree to (i) cooperate with reasonable requests made to me by the Company to provide information and to respond to questions related to matters that occurred while I was employed by the Company and of which I have knowledge; and (ii) at the Company’s request, participate in any proceeding or litigation before any arbitral, administrative, judicial, legislative, or other body or agency related to such matters. My agreement to cooperate or participate in this regard, however, is premised upon being compensated for reasonable attorneys’ fees and expenses, including but not limited to, reasonable fees and expenses of any lawyer I choose to retain in connection with, as well as reasonable travel, lodging, and meal expenses incurred by me in, performing all acts and executing and delivering any documents that may be reasonably necessary to carry out the provisions of this paragraph.
4. OTHER MATTERS
(a) RIGHT TO REVOKE. I understand that I may revoke this Release and Agreement within seven (7) days after I sign it by delivering or sending a written notice of revocation to Lisa Steiner, SVP Chief HR Officer (with a copy to the General Counsel) at 850 Dixie Highway, Louisville, KY 40210, by no later than the close of business on the seventh day after I sign this Release and Agreement. I understand that if I revoke this Release and Agreement, it shall not be effective or enforceable, and I will not receive the Additional Benefits described in Section 2 of this letter. I also understand that if I sign this Release and Agreement, Additional Benefits will not be paid until this revocation period expires. This Release and Agreement becomes effective on the eighth day after it is signed by me and not revoked (“the Effective Date”). To the extent that the end of the revocation period or the Effective Date fall on a Saturday, Sunday or holiday, the date will be considered the next business day.
(b) ENTIRE AGREEMENT. I agree that this is the entire agreement between me and the Company, that the Company has not made any promises to me other than in this letter, and that no changes may be made to this agreement unless in writing and signed by me and the Company.
(c) SEVERABILITY; GOVERNING LAW; VENUE. I agree that if any part of this Release and Agreement is found to be illegal or unenforceable, the rest of the Release and Agreement will nevertheless be enforceable. This Release and Agreement shall be governed by and construed in accordance with the laws of the Commonwealth of Kentucky, without giving effect to the principles of conflict of laws; all disputes arising under or relating to this Agreement, or its breach, shall be decided in the state or federal courts located in Jefferson County, Kentucky, except that the Company may seek enforcement of any of the covenants or commitments contained herein in any jurisdiction where it is necessary in its judgment to do so. In the event I fail to comply with any of the commitments set forth in this Release and Agreement, the Company may seek to terminate this agreement and recover the Additional Benefits provided to me.
Page 12
I ACKNOWLEDGE AND AFFIRM THAT I HAVE CAREFULLY READ THIS RELEASE AND AGREEMENT. I UNDERSTAND IT AND HAVE NO QUESTIONS ABOUT WHAT IT MEANS. I HAVE NOT BEEN FORCED OR INTIMIDATED IN ANY WAY TO SIGN IT, AND I AM KNOWINGLY AND VOLUNTARILY ENTERING INTO IT.
| /s/ Donald C. Berg |
| Donald C. Berg |
| May 14, 2014 |
| Dated |
| BROWN-FORMAN: | ||
| By: | /s/ Lisa Steiner | |
| Printed Name: | Lisa Steiner | |
| Date: | May 15, 2014 | |
Page 13
IMPORTANT!
Your health care stops at termination and must be activated
under COBRA before any claims can be considered.
In order for the Company to pay your COBRA premiums under the terms of your Release and Agreement you must sign and return the COBRA forms for coverage to be activated.