Attached files
| file | filename |
|---|---|
| 8-K - 8-K - REPROS THERAPEUTICS INC. | v328279_8k.htm |
Developing clinical stage small molecule therapeutics to treat hormonal and reproductive system disorders
Repros Disclaimer Any statements that are not historical facts contained in this release are forward - looking statements that involve risks and uncertainties, including Repros ' ability to have the partial hold on Proellex ® lifted and to determine a safe and effective dose for Proellex ®, raise needed additional capital on a timely basis in order for it to continue to fund its operations and pursue its development activities, and such other risks which are identified in the Company's most recent Annual Report on Form 10 - K and in any subsequent quarterly reports on Form 10 - Q. These documents are available on request from Repros Therapeutics or at www.sec.gov . Repros disclaims any intention or obligation to update or revise any forward - looking statements, whether as a result of new information, future events or otherwise.
Investment Highlights • Focused strategy: small molecule therapeutics for reproductive disorders • Two late stage clinical programs each with +$1B sales potential • Androxal ® : PHASE 3 (SPA) oral treatment for Low Testosterone with pending patent/ patent life to the mid 2020’s(growing +$1B market) – Restoration of testicular function and testosterone levels in treatment of 2 º hypogonadism (most common cause of low T) • Proellex : PHASE 2 treatment for uterine fibroids and endometriosis with pending patent/ patent life to the mid 2020’s (+$5B market) – Chronic relief of uterine fibroid symptoms – Fibroid de - bulking – Chronic relief of the symptoms associated with endometriosis • Key late stage clinical & regulatory events driven news flow in 2012
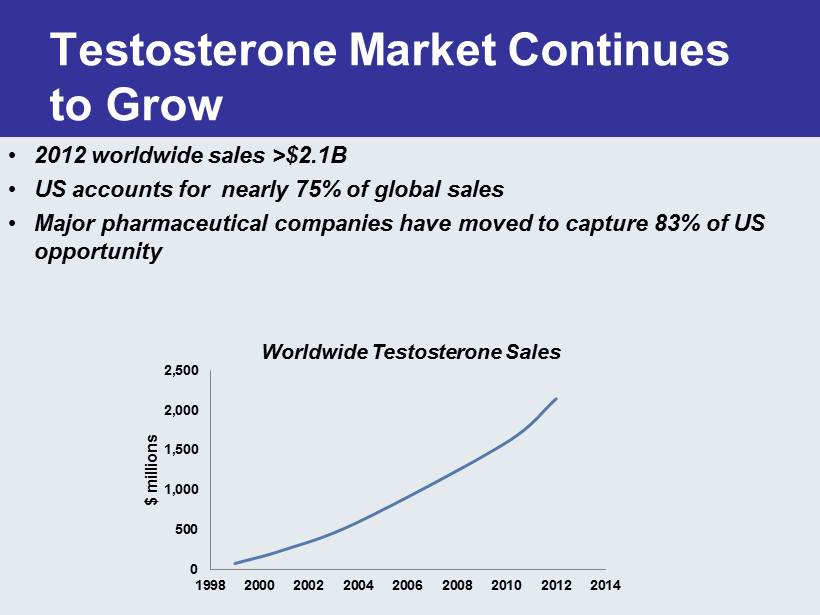
Testosterone Market Continues to Grow 0 500 1,000 1,500 2,000 2,500 1998 2000 2002 2004 2006 2008 2010 2012 2014 $ millions • 2012 worldwide sales >$2.1B • US accounts for nearly 75% of global sales • Major pharmaceutical companies have moved to capture 83% of US opportunity Worldwide Testosterone Sales
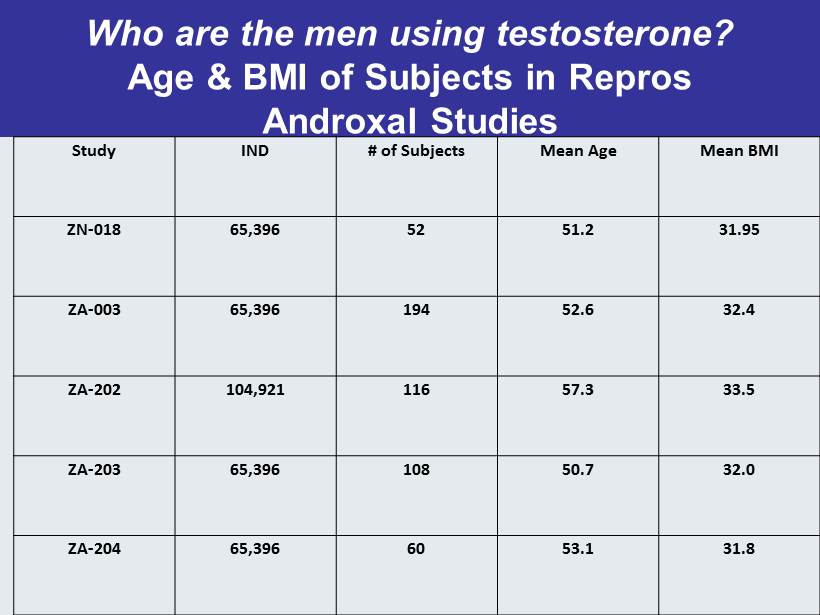
Who are the men using testosterone? Age & BMI of Subjects in Repros Androxal Studies Study IND # of Subjects Mean Age Mean BMI ZN - 018 65,396 52 51.2 31.95 ZA - 003 65,396 194 52.6 32.4 ZA - 202 104,921 116 57.3 33.5 ZA - 203 65,396 108 50.7 32.0 ZA - 204 65,396 60 53.1 31.8
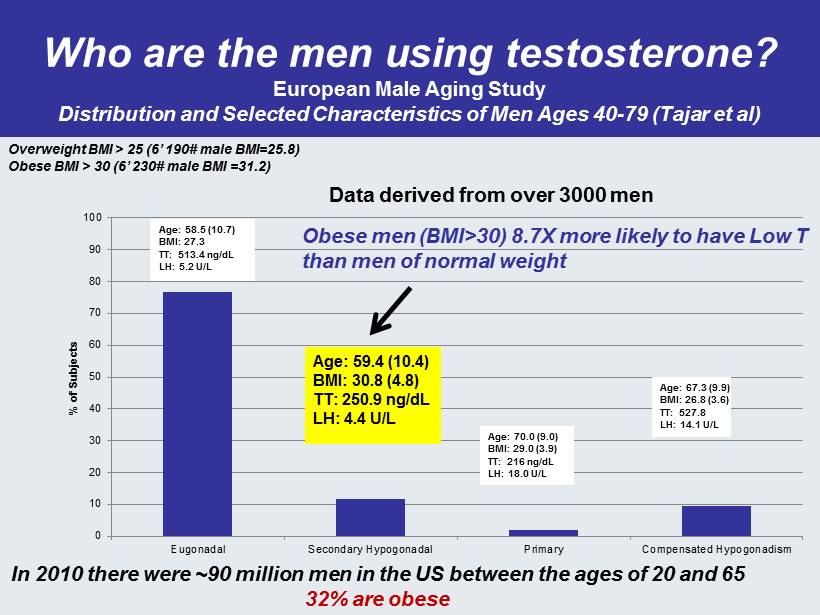
Who are the men using testosterone? European Male Aging Study Distribution and Selected Characteristics of Men Ages 40 - 79 ( Tajar et al) 0 10 20 30 40 50 60 70 80 90 100 Eugonadal Secondary Hypogonadal Primary Compensated Hypogonadism % of Subjects Age: 58.5 (10.7) BMI: 27.3 TT: 513.4 ng / dL LH: 5.2 U/L Age: 59.4 (10.4) BMI: 30.8 (4.8) TT: 250.9 ng / dL LH: 4.4 U/L Age: 70.0 (9.0) BMI: 29.0 (3.9) TT: 216 ng / dL LH: 18.0 U/L Age: 67.3 (9.9) BMI: 26.8 (3.6) TT: 527.8 LH: 14.1 U/L Data derived from over 3000 men Obese men (BMI>30) 8.7X more likely to have Low T than men of normal weight In 2010 there were ~90 million men in the US between the ages of 20 and 65 32% are obese Overweight BMI > 25 (6’ 190# male BMI=25.8) Obese BMI > 30 (6’ 230# male BMI =31.2)
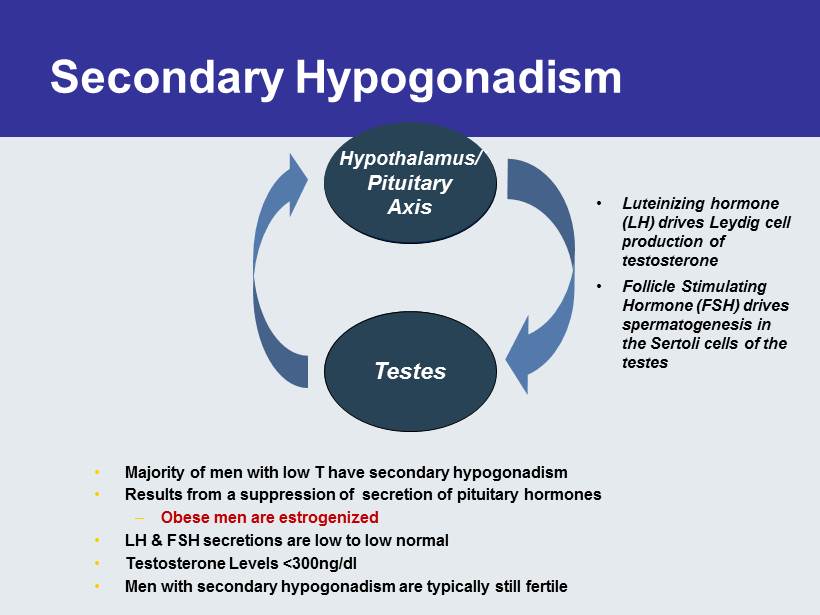
Secondary Hypogonadism • Majority of men with low T have secondary hypogonadism • Results from a suppression of secretion of pituitary hormones – Obese men are estrogenized • LH & FSH secretions are low to low normal • Testosterone Levels <300ng/dl • Men with secondary h ypogonadism are typically s till f ertile Testes Hypothalamus/ Pituitary Axis • Luteinizing hormone (LH) drives Leydig cell production of testosterone • Follicle Stimulating Hormone (FSH) drives spermatogenesis in the Sertoli cells of the testes Testes Hypothalamus / Pituitary Axis
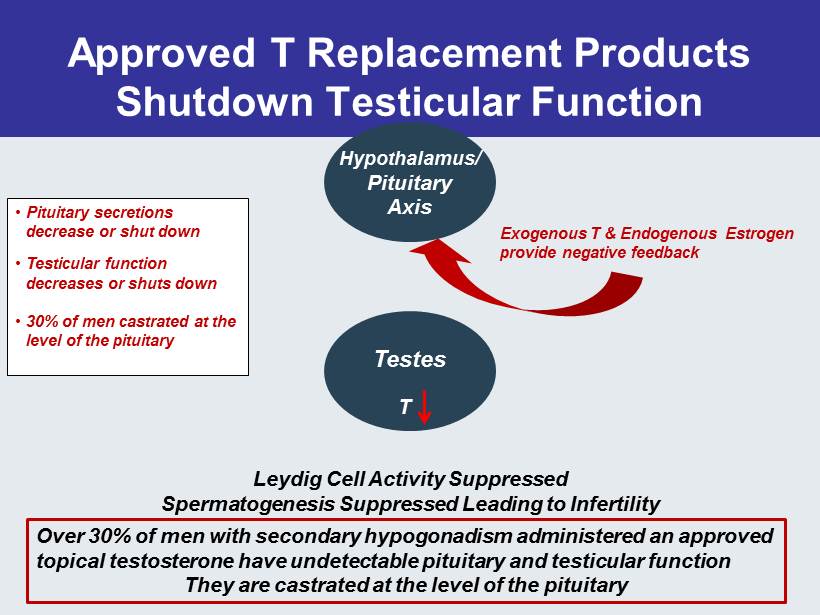
Approved T Replacement Products Shutdown Testicular Function Testes Hypothalamus / Pituitary Axis • Pituitary secretions decrease or shut down • Testicular function decreases or shuts down • 30% of men castrated at the level of the pituitary Leydig Cell Activity Suppressed Spermatogenesis Suppressed Leading to Infertility T Over 30% of men with secondary hypogonadism administered an approved topical testosterone have undetectable pituitary and testicular function They are castrated at the level of the pituitary Exogenous T & Endogenous Estrogen provide negative feedback
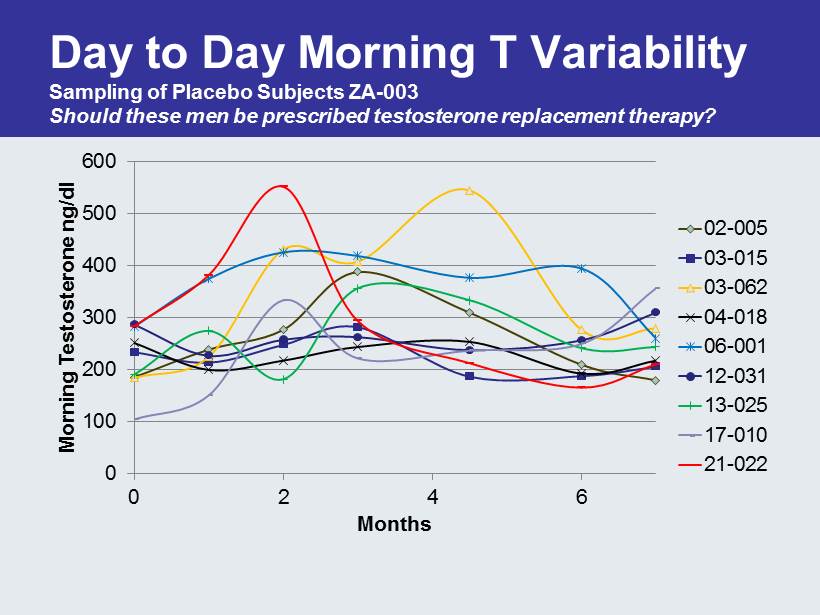
Day to Day Morning T Variability Sampling of Placebo Subjects ZA - 003 Should these men be prescribed testosterone replacement therapy? 0 100 200 300 400 500 600 0 2 4 6 Morning Testosterone ng /dl Months 02-005 03-015 03-062 04-018 06-001 12-031 13-025 17-010 21-022
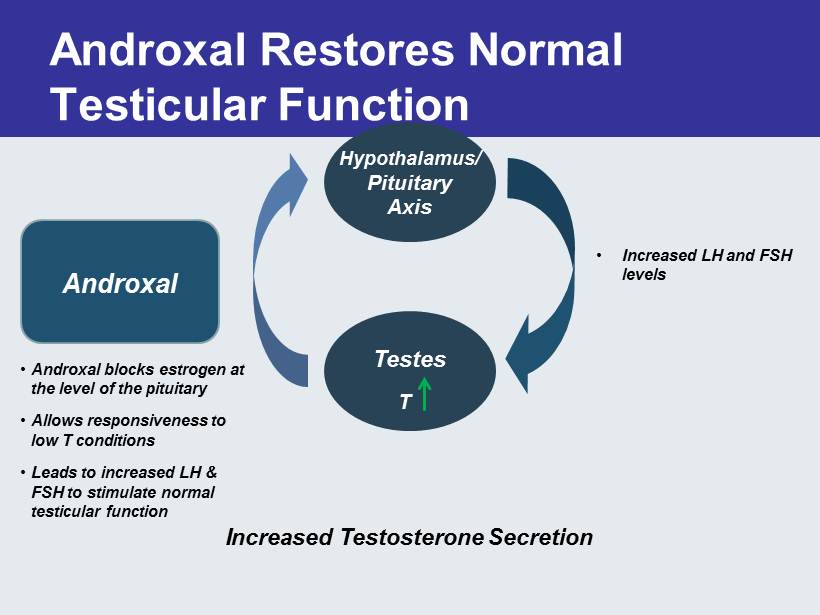
Androxal Restores Normal Testicular Function Testes Increased T estosterone Secretion Androxal • Androxal blocks estrogen at the level of the pituitary • Allows responsiveness to low T conditions • Leads to increased LH & FSH to stimulate normal testicular function • Increased LH and FSH levels T Hypothalamus / Pituitary Axis
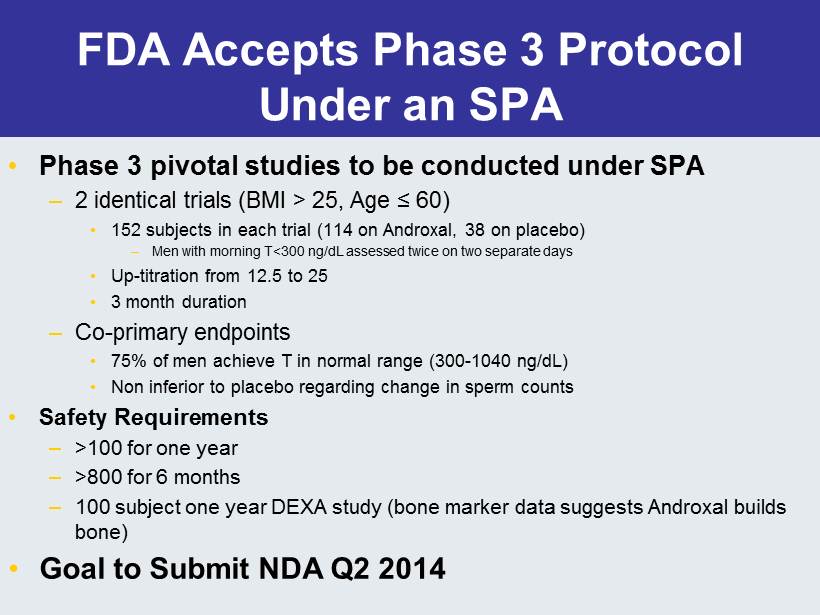
FDA Accepts Phase 3 Protocol Under an SPA • Phase 3 pivotal studies to be conducted under SPA – 2 identical trials (BMI > 25, Age ≤ 60) • 152 subjects in each trial (114 on Androxal , 38 on placebo) – Men with morning T<300 ng / dL assessed twice on two separate days • Up - titration from 12.5 to 25 • 3 month duration – Co - primary endpoints • 75% of men achieve T in normal range (300 - 1040 ng / dL ) • Non inferior to placebo regarding change in sperm counts • Safety Requirements – >100 for one year – >800 for 6 months – 100 subject one year DEXA study (bone marker data suggests Androxal builds bone) • Goal to Submit NDA Q2 2014
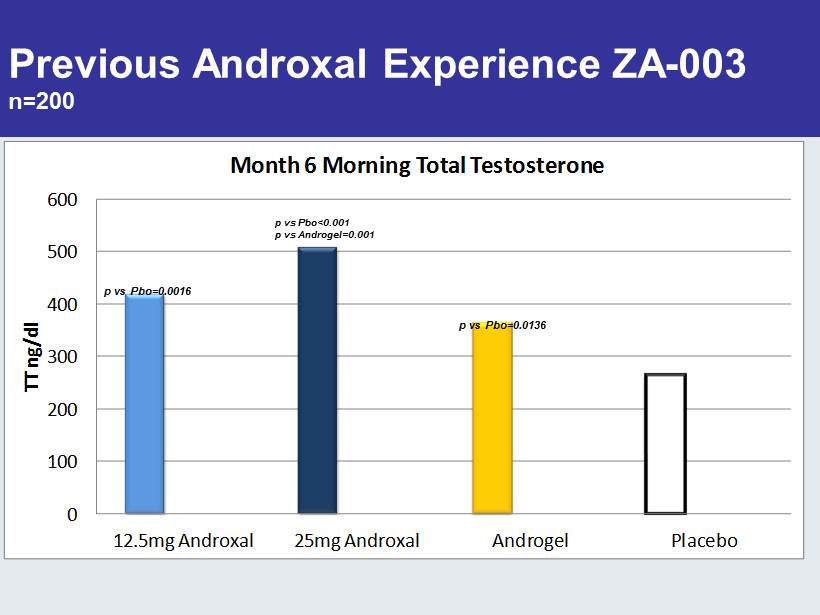
Previous Androxal Experience ZA - 003 n=200 0 100 200 300 400 500 600 12.5mg Androxal 25mg Androxal Androgel Placebo TT ng/dl Month 6 Morning Total Testosterone p vs Pbo=0.0016 p vs Pbo<0.001 p vs Androgel=0.001 p vs Pbo=0.0136
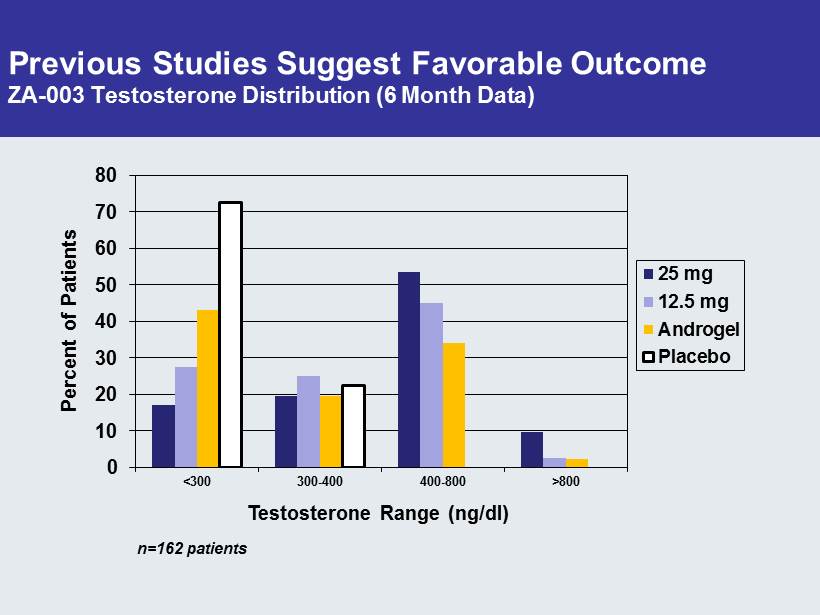
Previous Studies Suggest Favorable Outcome ZA - 003 Testosterone Distribution (6 Month Data) 0 10 20 30 40 50 60 70 80 <300 300-400 400-800 >800 Percent of Patients Testosterone Range (ng/dl) 25 mg 12.5 mg Androgel Placebo n=162 patients
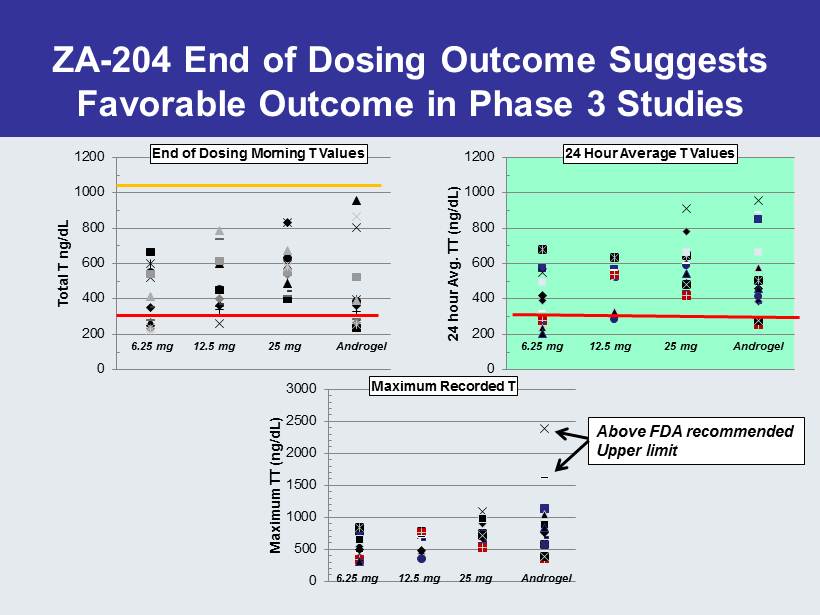
0 200 400 600 800 1000 1200 Total T ng / dL End of Dosing Morning T Values 0 200 400 600 800 1000 1200 24 hour Avg. TT ( ng / dL ) 24 Hour Average T Values 0 500 1000 1500 2000 2500 3000 Maximum TT ( ng / dL ) Maximum Recorded T 6.25 mg 12.5 mg 25 mg Androgel Androgel Androgel Above FDA recommended Upper limit ZA - 204 End of Dosing Outcome Suggests Favorable Outcome in Phase 3 Studies 25 mg 12.5 mg 6.25 mg 6.25 mg 12.5 mg 25 mg
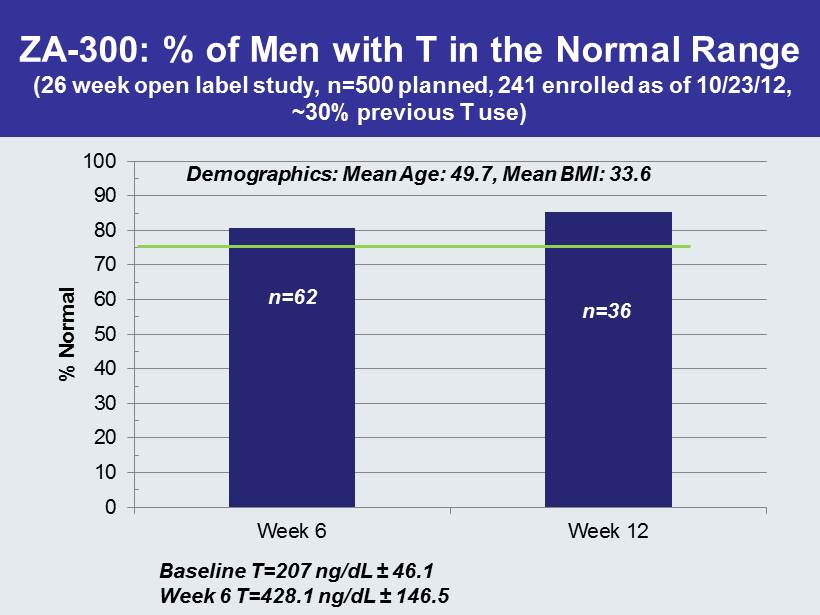
ZA - 300: % of Men with T in the Normal Range (26 week open label study, n=500 planned, 241 enrolled as of 10/23/12, ~30% previous T use) 0 10 20 30 40 50 60 70 80 90 100 Week 6 Week 12 % Normal n=62 n=36 Baseline T=207 ng / dL ± 46.1 Week 6 T=428.1 ng / dL ± 146.5 Demographics: Mean Age: 49.7, Mean BMI: 33.6
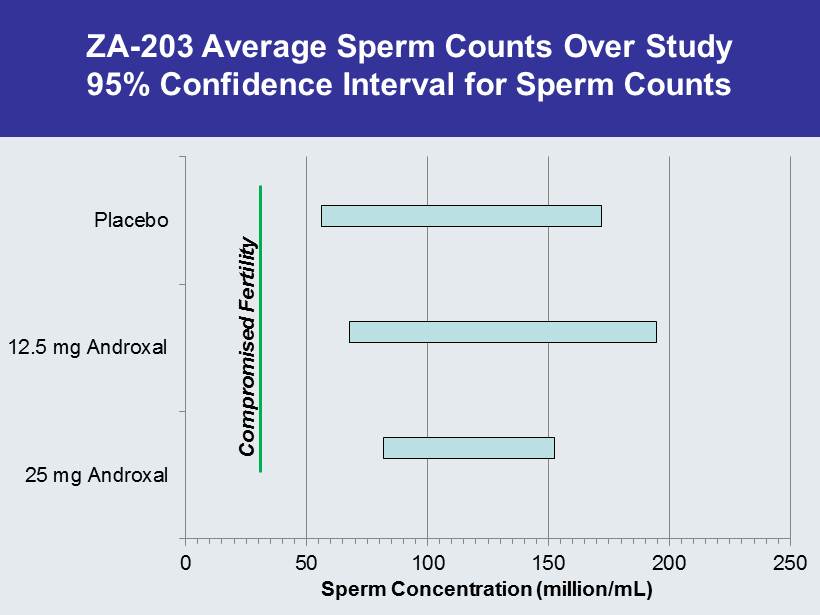
ZA - 203 Average Sperm Counts Over Study 95% Confidence Interval for Sperm Counts 0 50 100 150 200 250 25 mg Androxal 12.5 mg Androxal Placebo Sperm Concentration (million/ mL ) Compromised Fertility
Androxal Preserves Testicular Function Approved Topical Products Suppress the Hypothalamic - Pituitary - Testes Axis
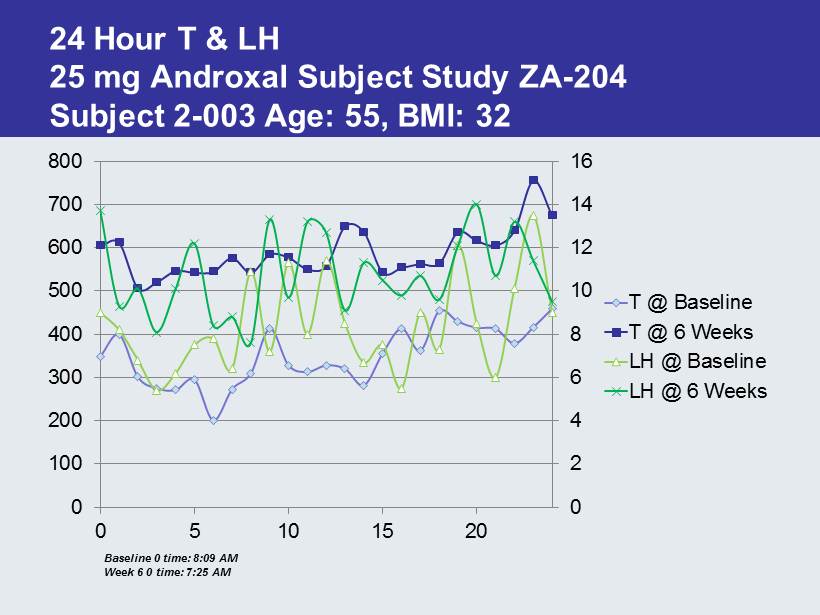
24 Hour T & LH 25 mg Androxal Subject Study ZA - 204 Subject 2 - 003 Age: 55, BMI: 32 0 2 4 6 8 10 12 14 16 0 100 200 300 400 500 600 700 800 0 5 10 15 20 T @ Baseline T @ 6 Weeks LH @ Baseline LH @ 6 Weeks Baseline 0 time: 8:09 AM Week 6 0 time: 7:25 AM
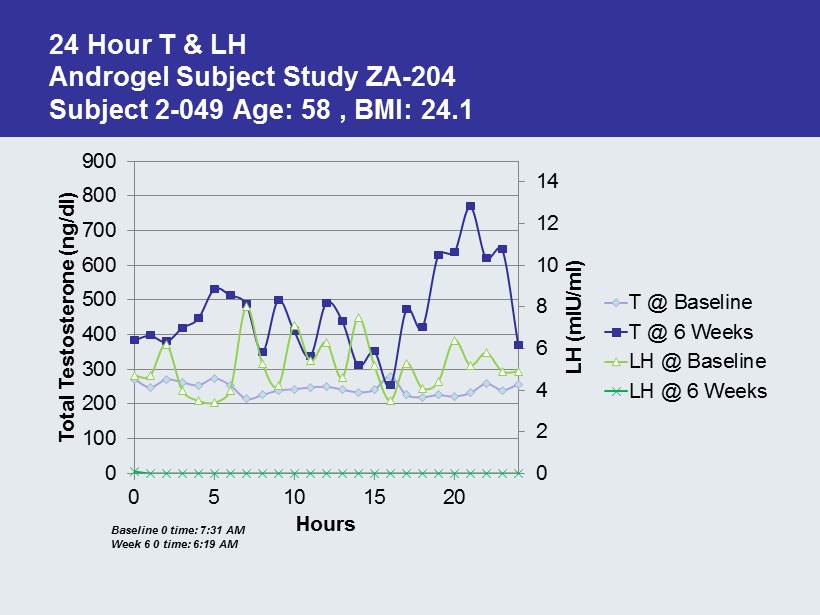
24 Hour T & LH Androgel Subject Study ZA - 204 Subject 2 - 049 Age: 58 , BMI: 24.1 0 2 4 6 8 10 12 14 0 100 200 300 400 500 600 700 800 900 0 5 10 15 20 LH ( mIU /ml) Total Testosterone ( ng /dl) Hours T @ Baseline T @ 6 Weeks LH @ Baseline LH @ 6 Weeks Baseline 0 time: 7:31 AM Week 6 0 time: 6:19 AM
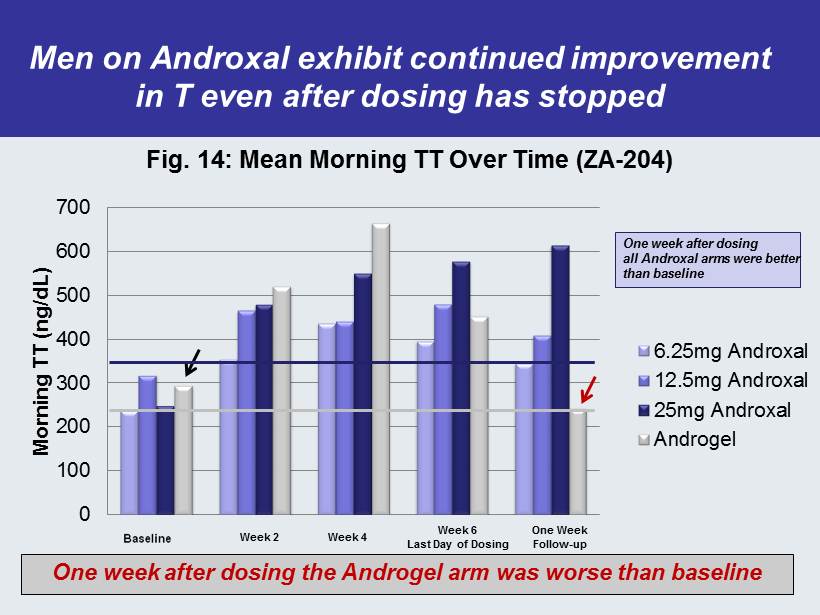
0 100 200 300 400 500 600 700 Morning TT (ng/dL) Fig. 14: Mean Morning TT Over Time (ZA - 204) 6.25mg Androxal 12.5mg Androxal 25mg Androxal Androgel Week 2 Week 4 Week 6 Last Day of Dosing One Week Follow - up One week after dosing all Androxal arms were better than baseline One week after dosing the Androgel arm was worse than baseline Men on Androxal exhibit continued improvement in T even after dosing has stopped
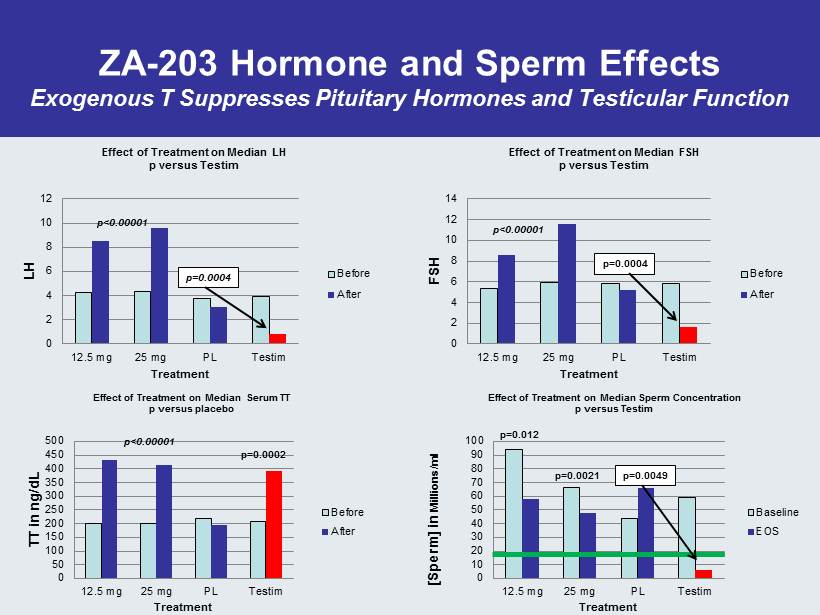
ZA - 203 Hormone and Sperm Effects Exogenous T Suppresses Pituitary Hormones and Testicular Function 0 2 4 6 8 10 12 14 12.5 mg 25 mg PL Testim FSH Treatment Effect of Treatment on Median FSH p versus Testim Before After p<0.00001 p=0.0004 0 10 20 30 40 50 60 70 80 90 100 12.5 mg 25 mg PL Testim [Sperm] in Millions/ml Treatment Effect of Treatment on Median Sperm Concentration p versus Testim Baseline EOS p=0.012 p=0.0021 p=0.0049 0 2 4 6 8 10 12 12.5 mg 25 mg PL Testim LH Treatment Effect of Treatment on Median LH p versus Testim Before After p=0.0004 0 50 100 150 200 250 300 350 400 450 500 12.5 mg 25 mg PL Testim TT in ng/dL Treatment Effect of Treatment on Median Serum TT p versus placebo Before After p<0.00001 p=0.0002 p<0.00001
Recent Findings from ZA - 300 (11/10/12) 37.8% were previous T replacement users Is Hormone Replacement the Right Therapy? • 151 men have completed 6 weeks of treatment – At baseline after washout only 3 subjects exhibited T < 100 ng / dL • All three subjects had been on T therapy for multiple years • 0 of 3 responded to Androxal • 2 of 3 recorded no pituitary stimulation or change in T – Of the 11 patients that remained < 225 ng / dL at 12.5 mg, 7 were previous T users • Of the 42 men that achieved T levels greater than 500 ng / dL , 27 were naïve to any T treatment – In the previous T users, after washout , average LH remained in the normal range and T was above 200 ng / dL
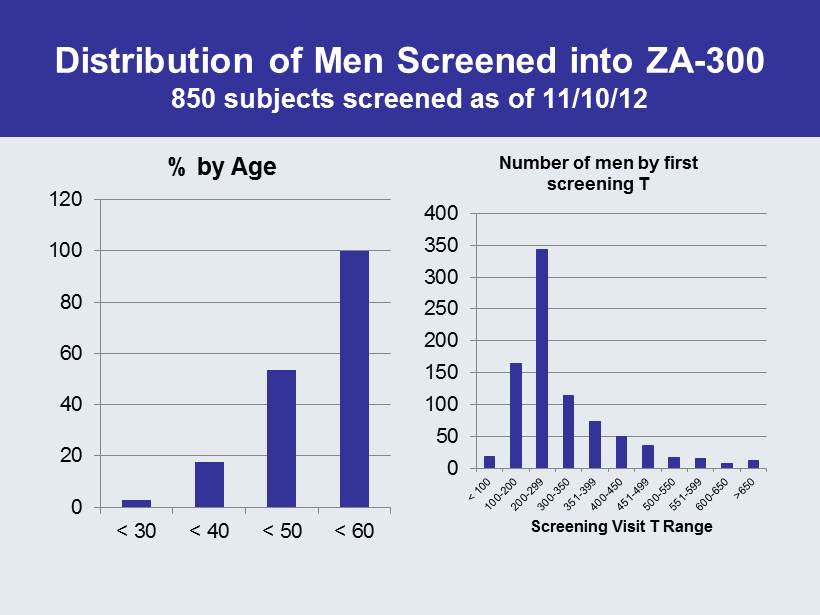
Distribution of Men Screened into ZA - 300 850 subjects screened as of 11/10/12 0 20 40 60 80 100 120 < 30 < 40 < 50 < 60 % by Age 0 50 100 150 200 250 300 350 400 Screening Visit T Range Number of men by first screening T
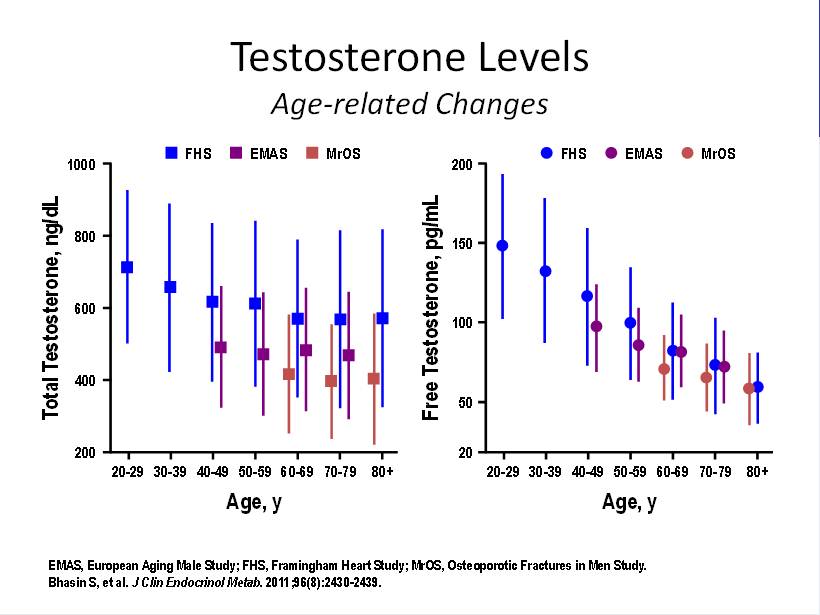
Testosterone Levels Age - related Changes EMAS, European Aging Male Study; FHS, Framingham Heart Study; MrOS, Osteoporotic Fractures in Men Study. Bhasin S, et al. J Clin Endocrinol Metab . 2011;96(8):2430 - 2439. Total Testosterone, ng/dL 20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 1000 800 200 600 400 80+ Age, y FHS EMAS MrOS Free Testosterone, pg/mL 20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 200 150 20 100 50 80+ Age, y FHS EMAS MrOS
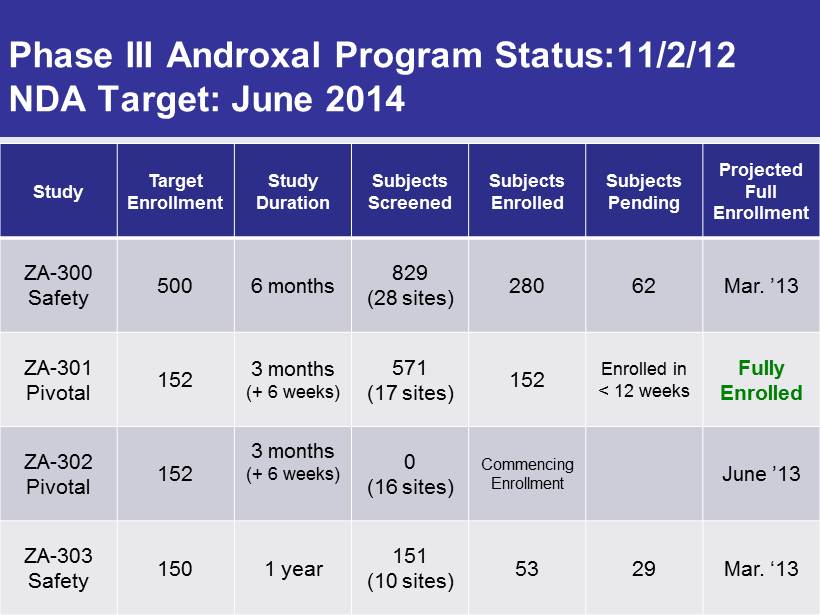
Phase III Androxal Program Status:11/2/12 NDA Target: June 2014 Study Target Enrollment Study Duration Subjects Screened Subjects Enrolled Subjects Pending Projected Full Enrollment ZA - 300 Safety 500 6 months 829 (28 sites) 280 62 Mar. ’13 ZA - 301 Pivotal 152 3 months (+ 6 weeks) 571 (17 sites) 152 Enrolled in < 12 weeks Fully Enrolled ZA - 302 Pivotal 152 3 months (+ 6 weeks) 0 (16 sites) Commencing Enrollment June ’13 ZA - 303 Safety 150 1 year 151 (10 sites) 53 29 Mar. ‘13
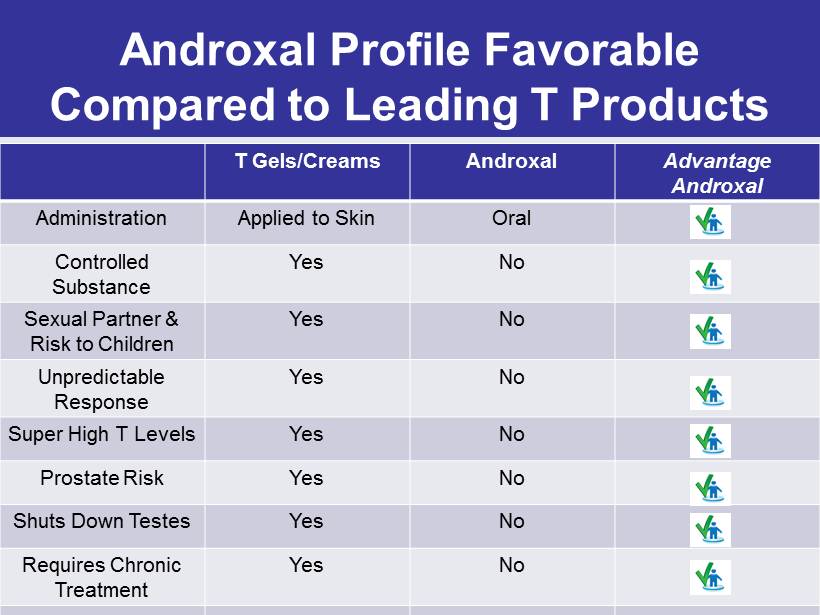
Androxal Profile Favorable Compared to Leading T Products T Gels/Creams Androxal Advantage Androxal Administration Applied to Skin Oral Controlled Substance Yes No Sexual Partner & Risk to Children Yes No Unpredictable Response Yes No Super High T Levels Yes No Prostate Risk Yes No Shuts Down Testes Yes No Requires Chronic Treatment Yes No
Third Party Study Indicates Favorable Reimbursement Potential for Androxal Majority of payers believe Androxal’s oral administration and non - chronic use may offer overall cost savings – Third party assessment of payers indicates vast majority (>90%) would add Androxal to formularies • Cost will be key for tier placement • 50% of plans indicated they would require a PA(Prior Authorization) to show proper diagnosis • 62 % of respondents expect Androxal to be priced at parity to Androgel • Anticipated Androxal pricing of $170 - 350/month would be competitive with Androgel
Androxal Take Home Message • Because of Obesity, 30% of American Males are at Risk of Secondary Hypogonadism – Co - morbidities include diabetes and cardiovascular disease • Approved T Products Worsen the Underlying Condition • We believe only Androxal + Diet + Exercise can reverse this disorder
Proellex for the Treatment of Uterine Fibroids and Endometriosis Over 30 million women of reproductive age in the US afflicted with symptomatic uterine fibroids or endometriosis Over 300,000 hysterectomies performed every year in the US to treat these two disorders No acceptable chronic therapeutic options available today
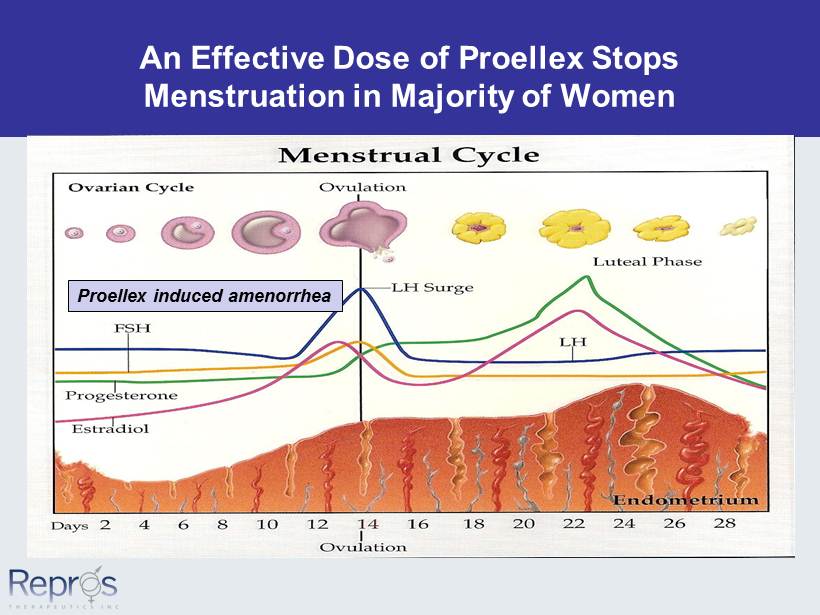
An Effective Dose of Proellex Stops Menstruation in Majority of Women Proellex induced amenorrhea
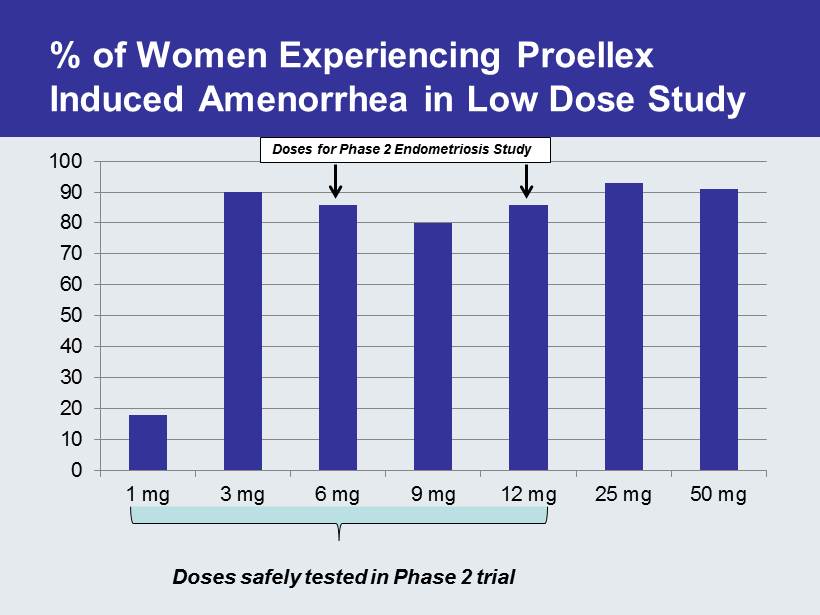
% of Women Experiencing Proellex Induced Amenorrhea in Low Dose Study 0 10 20 30 40 50 60 70 80 90 100 1 mg 3 mg 6 mg 9 mg 12 mg 25 mg 50 mg Doses for Phase 2 Endometriosis Study Doses safely tested in Phase 2 trial
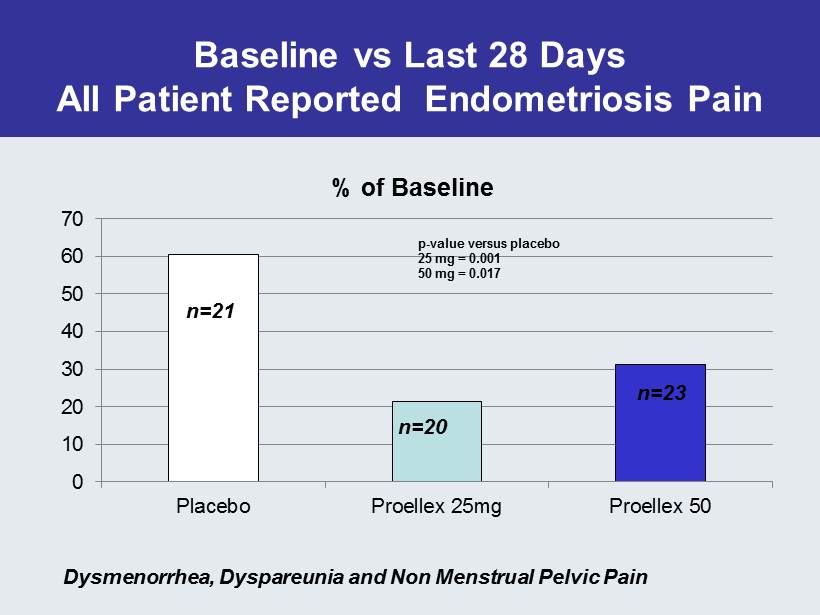
Baseline vs Last 28 Days All Patient Reported Endometriosis Pain 0 10 20 30 40 50 60 70 Placebo Proellex 25mg Proellex 50 % of Baseline n=23 p - value versus placebo 25 mg = 0.001 50 mg = 0.017 n=20 n=21 Dysmenorrhea , Dyspareunia and Non Menstrual Pelvic Pain
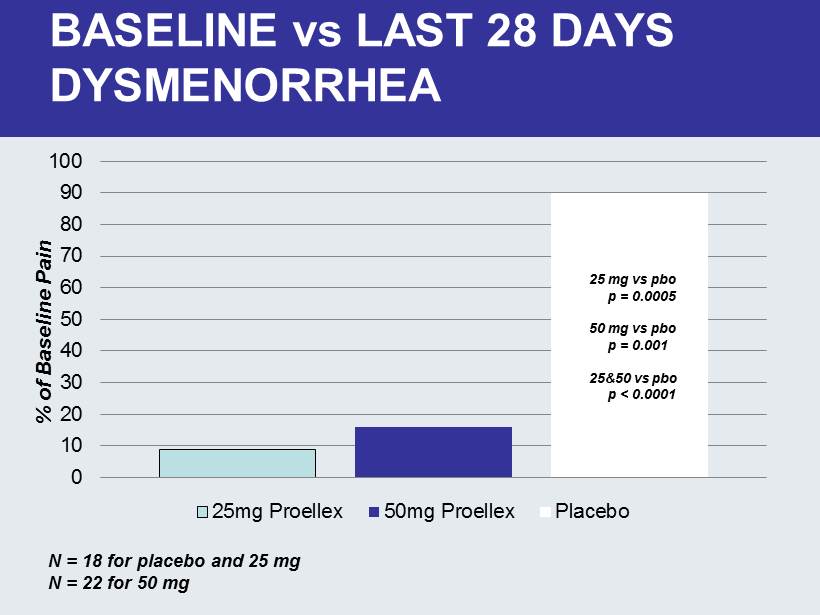
0 10 20 30 40 50 60 70 80 90 100 25mg Proellex 50mg Proellex Placebo BASELINE vs LAST 28 DAYS DYSMENORRHEA N = 18 for placebo and 25 mg N = 22 for 50 mg 25 mg vs pbo p = 0.0005 50 mg vs pbo p = 0.001 25&50 vs pbo p < 0.0001 % of Baseline Pain
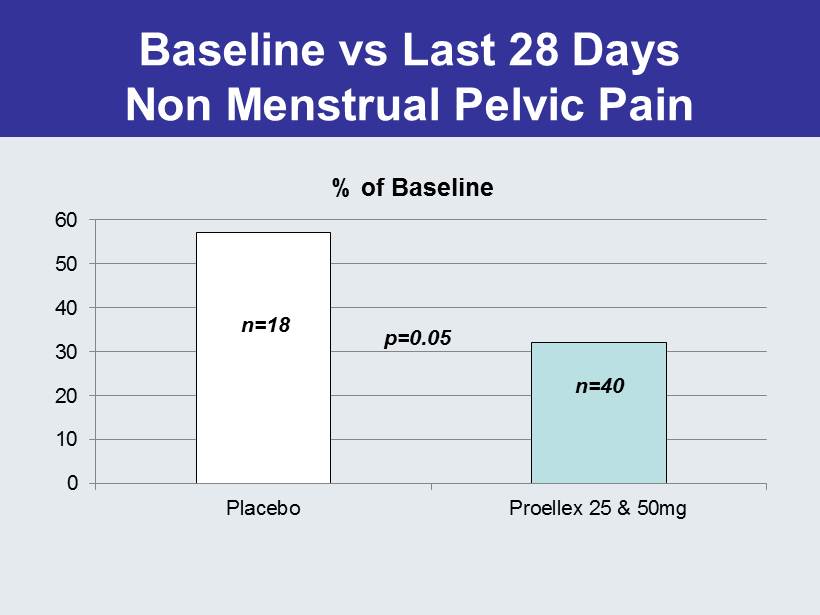
Baseline vs Last 28 Days Non Menstrual Pelvic Pain 0 10 20 30 40 50 60 Placebo Proellex 25 & 50mg % of Baseline n=40 p=0.05 n=18
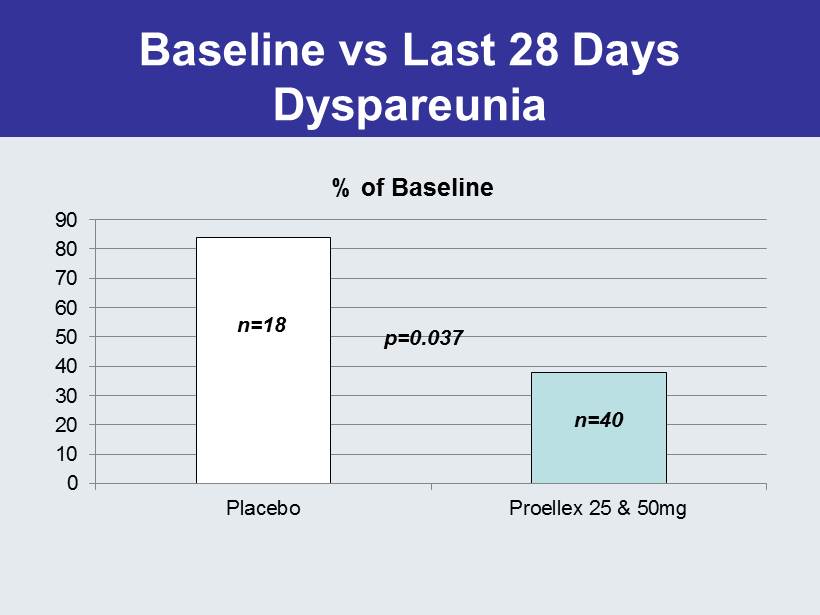
Baseline vs Last 28 Days Dyspareunia 0 10 20 30 40 50 60 70 80 90 Placebo Proellex 25 & 50mg % of Baseline p=0.037 n=18 n=40
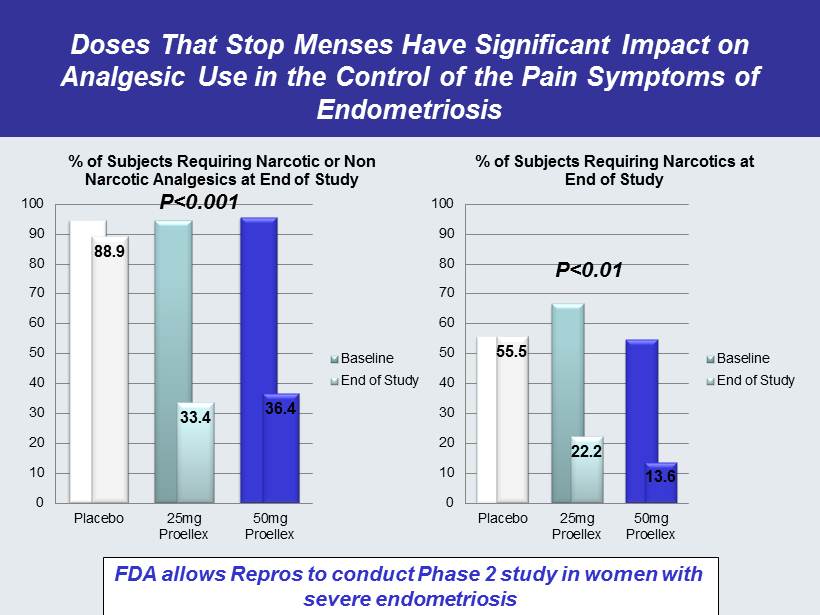
Doses That Stop Menses Have Significant Impact on Analgesic Use in the Control of the Pain Symptoms of Endometriosis 88.9 33.4 36.4 0 10 20 30 40 50 60 70 80 90 100 Placebo 25mg Proellex 50mg Proellex % of Subjects Requiring Narcotic or Non Narcotic Analgesics at End of Study Baseline End of Study 55.5 22.2 13.6 0 10 20 30 40 50 60 70 80 90 100 Placebo 25mg Proellex 50mg Proellex % of Subjects Requiring Narcotics at End of Study Baseline End of Study FDA allows Repros to conduct Phase 2 study in women with severe endometriosis P<0.01 P<0.001
Vaginal Proellex to Eliminate the Need for Hysterectomy in Most Situations – New IND effective • Unaffected by oral outcomes – Initial Phase 2 study to test four doses of vaginal administration in the treatment of uterine fibroids • Assess reduction of fibroid size and elimination of symptoms • Company anticipates efficacy effects greater than highest dose tested in humans (50mg) with systemic exposure less than 3 mg oral.
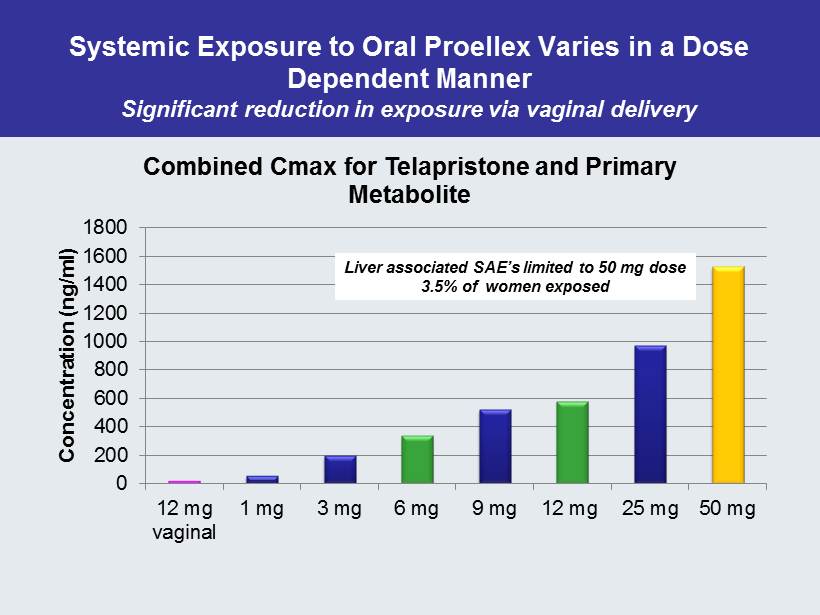
Systemic Exposure to Oral Proellex Varies in a Dose Dependent Manner Significant reduction in exposure via vaginal delivery 0 200 400 600 800 1000 1200 1400 1600 1800 12 mg vaginal 1 mg 3 mg 6 mg 9 mg 12 mg 25 mg 50 mg Concentration ( ng /ml) Combined Cmax for Telapristone and Primary Metabolite Liver associated SAE’s limited to 50 mg dose 3.5% of women exposed
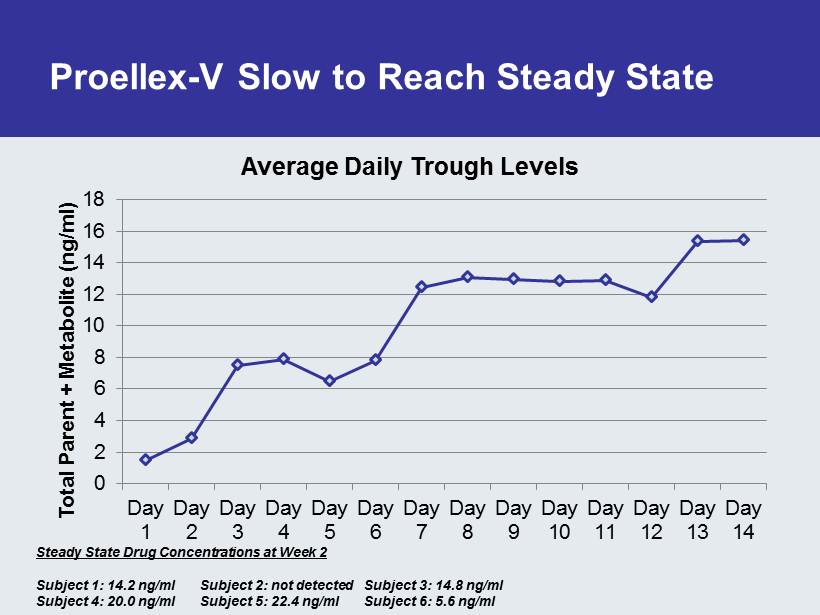
Proellex - V Slow to Reach Steady State 0 2 4 6 8 10 12 14 16 18 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Total Parent + Metabolite ( ng /ml) Average Daily Trough Levels Steady State Drug Concentrations at Week 2 Subject 1: 14.2 ng /ml Subject 2: not detected Subject 3: 14.8 ng /ml Subject 4: 20.0 ng /ml Subject 5: 22.4 ng /ml Subject 6: 5.6 ng /ml
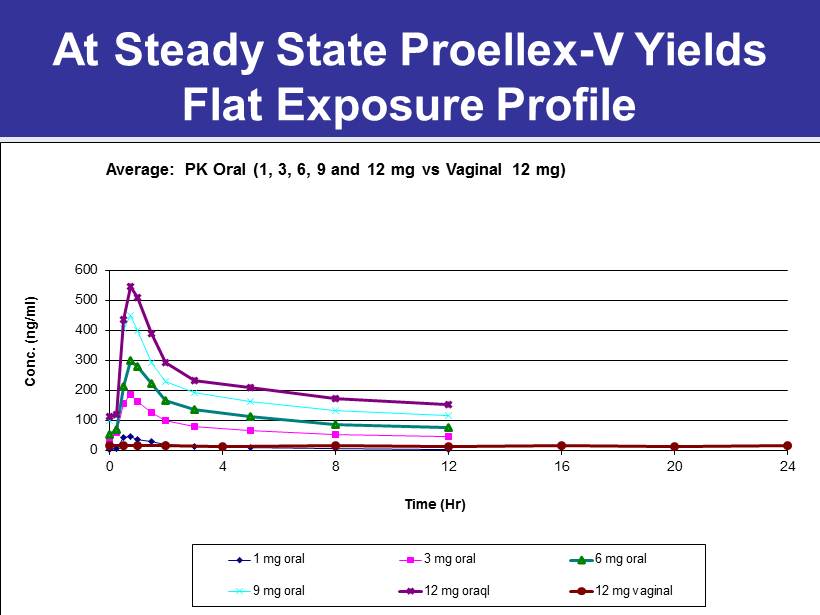
At Steady State Proellex - V Yields Flat Exposure Profile 0 100 200 300 400 500 600 0 4 8 12 16 20 24 Conc. (ng/ml) Time (Hr) Average: PK Oral (1, 3, 6, 9 and 12 mg vs Vaginal 12 mg) 1 mg oral 3 mg oral 6 mg oral 9 mg oral 12 mg oraql 12 mg vaginal
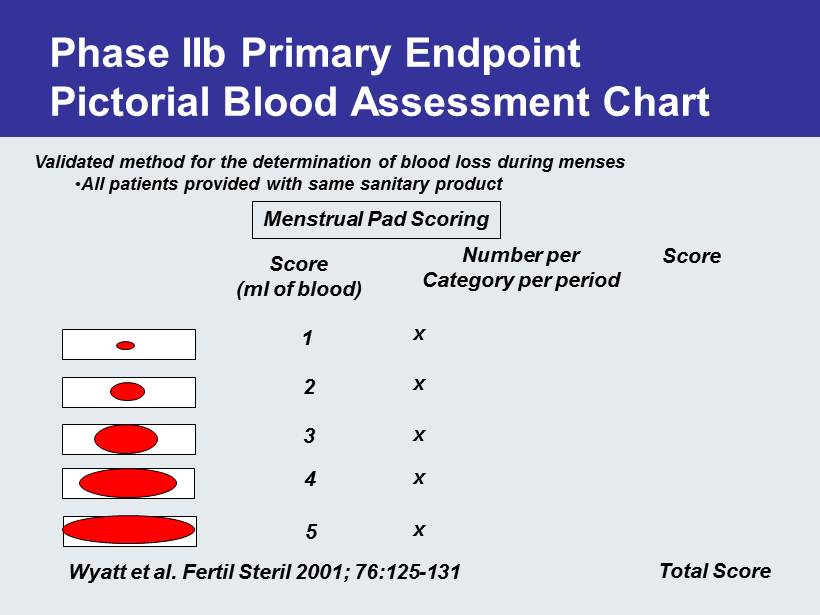
Phase IIb Primary Endpoint Pictorial Blood Assessment Chart Validated method for the determination of blood loss during menses • All patients provided with same sanitary product Menstrual Pad Scoring Score (ml of blood) 1 2 3 4 5 Number per Category per period Score Total Score x x x x x Wyatt et al. Fertil Steril 2001; 76:125 - 131
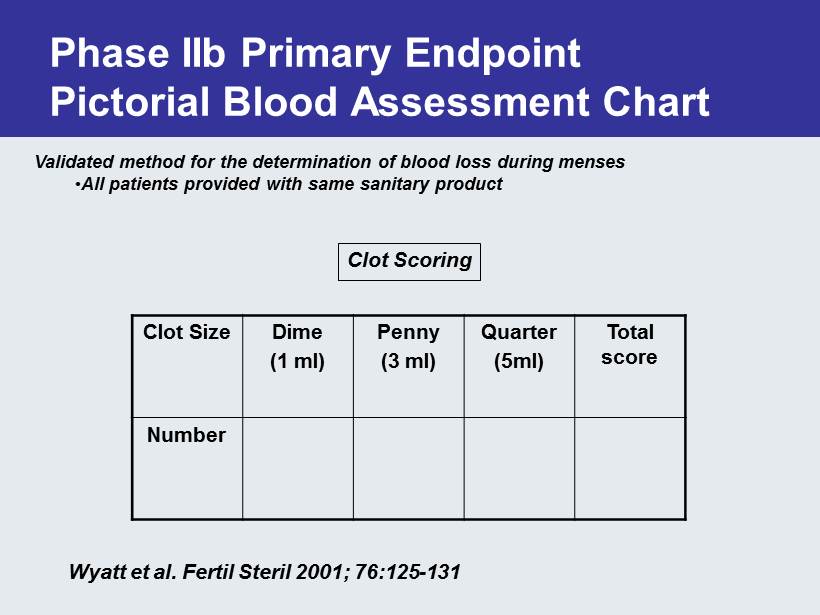
Phase IIb Primary Endpoint Pictorial Blood Assessment Chart Validated method for the determination of blood loss during menses • All patients provided with same sanitary product Clot Scoring Wyatt et al. Fertil Steril 2001; 76:125 - 131 Clot Size Dime (1 ml) Penny (3 ml) Quarter (5ml) Total score Number
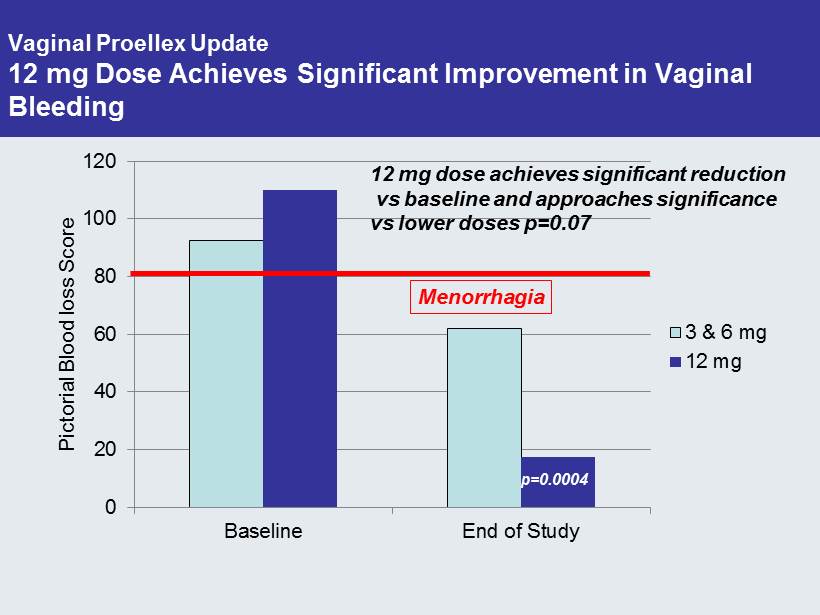
Vaginal Proellex Update 12 mg Dose Achieves Significant Improvement in Vaginal Bleeding 0 20 40 60 80 100 120 Baseline End of Study Pictorial Blood loss Score 3 & 6 mg 12 mg p=0.0004 12 mg dose achieves significant reduction vs baseline and approaches significance vs lower doses p=0.07 Menorrhagia
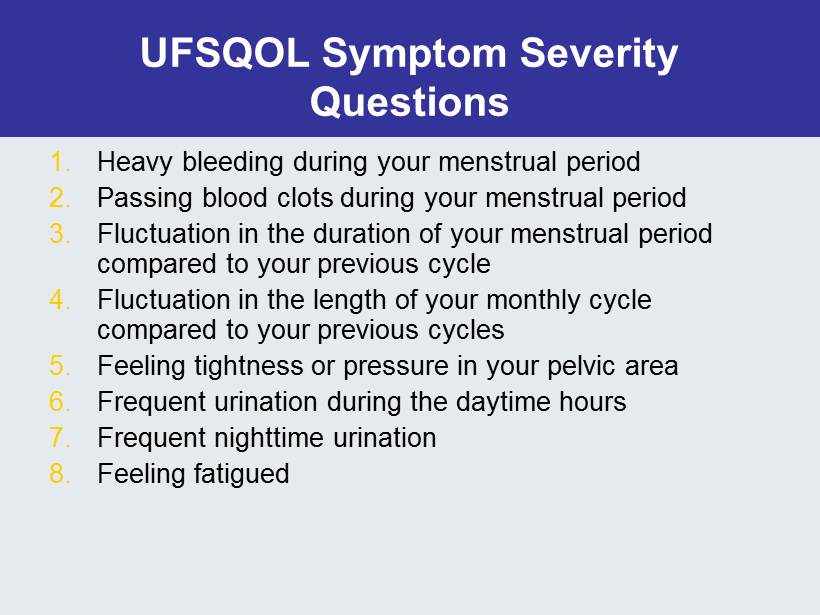
UFSQOL Symptom Severity Questions 1. Heavy bleeding during your menstrual period 2. Passing blood clots during your menstrual period 3. Fluctuation in the duration of your menstrual period compared to your previous cycle 4. Fluctuation in the length of your monthly cycle compared to your previous cycles 5. Feeling tightness or pressure in your pelvic area 6. Frequent urination during the daytime hours 7. Frequent nighttime urination 8. Feeling fatigued
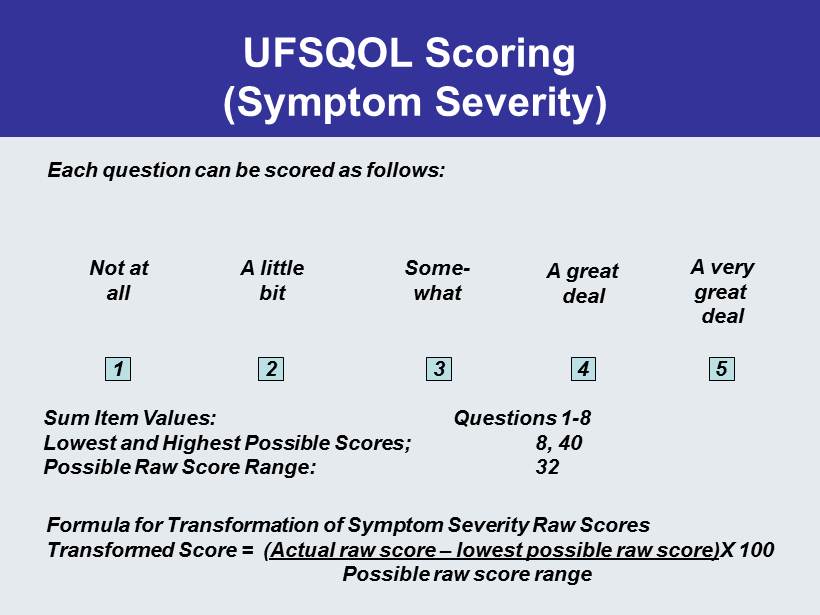
UFSQOL Scoring (Symptom Severity) Each question can be scored as follows: Not at all A little bit Some - what A great deal A very great deal 1 2 3 4 5 Sum Item Values: Questions 1 - 8 Lowest and Highest Possible Scores; 8, 40 Possible Raw Score Range: 32 Formula for Transformation of Symptom Severity Raw Scores Transformed Score = ( Actual raw score – lowest possible raw score) X 100 Possible raw score range
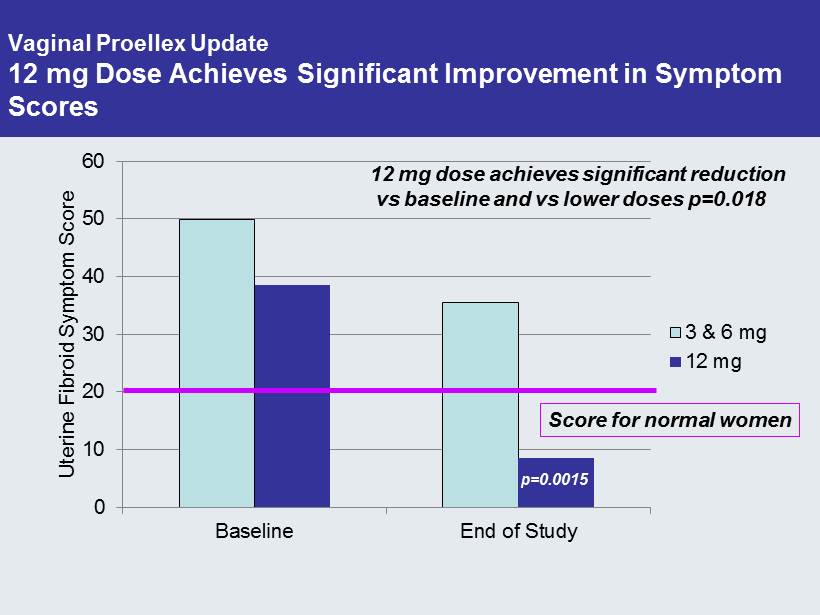
Vaginal Proellex Update 12 mg Dose Achieves Significant Improvement in Symptom Scores 0 10 20 30 40 50 60 Baseline End of Study Uterine Fibroid Symptom Score 3 & 6 mg 12 mg p=0.0015 12 mg dose achieves significant reduction vs baseline and vs lower doses p=0.018 Score for normal women
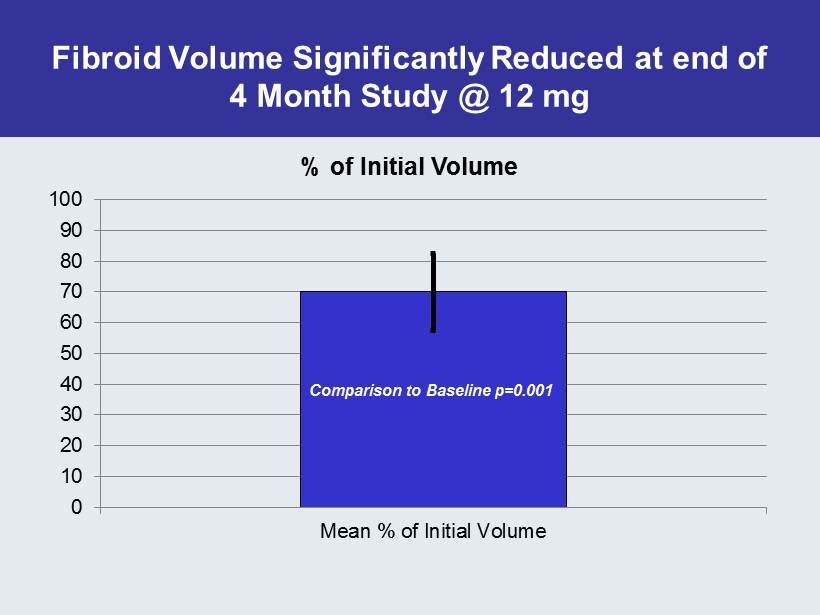
Fibroid Volume Significantly Reduced at end of 4 Month Study @ 12 mg 0 10 20 30 40 50 60 70 80 90 100 Mean % of Initial Volume % of Initial Volume Comparison to Baseline p=0.001
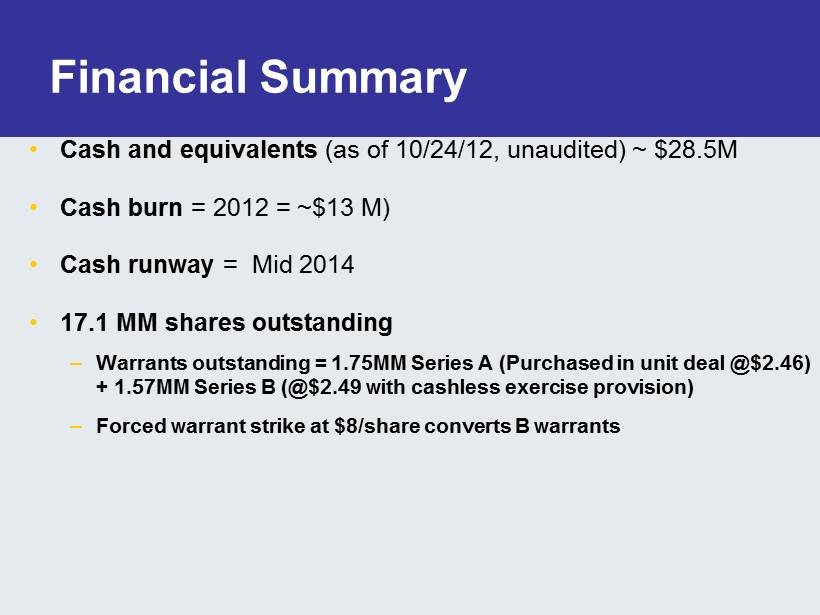
Financial Summary • Cash and equivalents (as of 10/24/12, unaudited) ~ $28.5M • Cash burn = 2012 = ~$13 M) • Cash runway = Mid 2014 • 17.1 MM shares outstanding – Warrants outstanding = 1.75MM Series A (Purchased in unit deal @$2.46) + 1.57MM Series B (@$2.49 with cashless exercise provision) – Forced warrant strike at $8/share converts B warrants

Recently Completed & Upcoming Milestones • Reported results for two Phase 2 Androxal Studies Q4 - 11 • Reported results for low dose Phase 2 Proellex Study Q4 - 11 • Reported effective IND for Vaginal Proellex Phase 2 Q1 - 12 • Commence Dosing Phase 2 UF Vaginal Proellex Q1 - 12 • Held Meeting with FDA for Phase 3 Androxal May ’12 • SPA accepted Androxal Phase 3 July’12 • Commence Phase 3 Pivotal Androxal Studies Aug - 12 • Commence Phase 2 low dose Oral Proellex Study Q4 - 12 • Report Phase 2 UF Vaginal Proellex Study Q4 - 12 • Report top - line results for 1 st Androxal Pivotal Study Q2 - 13