Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - INSMED Inc | d418353d8k.htm |
| EX-5.1 - OPINION OF PEPPER HAMILTON LLP - INSMED Inc | d418353dex51.htm |
| EX-10.1 - FORM SUBSCRIPTION AGREEMENT - INSMED Inc | d418353dex101.htm |
| EX-99.1 - PRESS RELEASE - INSMED Inc | d418353dex991.htm |
 Developing
Innovative Inhaled Treatments for Serious Lung Infections
August 2012
Free Writing Prospectus
Registration Statement No. 333-182124
Exhibit 99.2 |
 This presentation
contains forward-looking statements which are made pursuant to provisions of Section 21E
of the Securities Exchange Act of 1934. Investors are cautioned that such statements in this
presentation, including statements relating to our financial position, projected year
end cash and cash runway, the status and the results of preclinical studies and
clinical trials and preclinical and clinical data described herein, the timing of
responses to information and data requests from FDA, the development of our products, our
estimates of the size of the potential markets for our product candidates, and the business
strategies, evaluations, plans and objectives of management, constitute
forward-looking statements which involve risks and uncertainties that could cause
actual results to differ materially from those anticipated by the forward-
looking
statements.
Our
results
may
be
affected
by
such
factors
as
the
receipt
and
timing
of
FDA
and
other
regulatory reviews and approvals, if at all, competitive developments affecting our product
development, delays in product development or clinical trials, and patent disputes
involving currently developing products. The risks and uncertainties include,
without limitation, we may experience unexpected regulatory actions, delays or
requests, our future clinical trials may not be successful, we may be unsuccessful in developing our
product candidates or receiving necessary regulatory approvals, we may experience delays in
our product development or clinical trials, our product candidates may not prove to be
commercially successful, our expenses may be higher than anticipated and other risks
and challenges detailed in our filings with the U.S. Securities and Exchange
Commission, including our Annual Report on Form 10-K for the year ended
December
31,
2011
and
our
Quarterly
Report
on
Form
10-Q
for
the
quarter
ended
June
30,
2012.
Investors
are cautioned not to place undue reliance on any forward-looking statements which speak
only as of the date of this presentation. We undertake no obligation to publicly
release the results of any revisions to these forward-looking statements that may
be made to reflect events or circumstances that occur after the date of this release or
to reflect the occurrence of unanticipated events. Safe Harbor Statement
|
 2
Insmed: Value Proposition
Attractive
Late-Stage
Opportunity
ARIKACE has strong Phase 2 efficacy and safety data in CF
Amikacin is an FDA-approved antibiotic, long recognized as one of the most
effective treatments for gram-negative infections
Compelling
Business Model
Two orphan indications with high unmet need and combined global market
potential of over $1 billion
Limited commercial infrastructure required
Strong IP and potential for extended exclusivity
Strong Balance
Sheet &
Experienced
Management
As of 6/30/12, company reported ~$75 million in cash, investments & CD
We believe cash is sufficient to take Company through the availability of
top-line data for both CF CLEAR-108 trial and TARGET-NTM trial
Management has extensive anti-infective development, regulatory, and
commercial experience
ARIKACE
®
* is a highly differentiated product that offers a compelling
business opportunity in two orphan diseases
* ARIKACE
®
is a registered trademark of Insmed Incorporated
ARIKACE (liposomal amikacin for inhalation), is in Phase 3 (CLEAR-108)
for cystic fibrosis (CF) Pseudomonas (Pa) lung infections and Phase 2
(TARGET-NTM) for non-TB mycobacteria (NTM) lung infections |
 3
ARIKACE: Amikacin Summary
Amikacin is an FDA-approved antibiotic with proven efficacy in the
treatment of gram-negative infections, including Pseudomonas and NTM
Aminoglycoside antibiotic
Value of the IV use has been limited
by nephro-toxicity and ototoxicity
ARIKACE (liposomal amikacin for inhalation) delivers high, sustained levels of drug to
the lung while reducing systemic exposure to well below established toxicity
levels |
 4
ARIKACE: Proprietary Liposomal Formulation Provides Basis
for Important Potential Benefits
Potential Benefit
Lipid Polar Head Groups
(at Both Surfaces)
Lipid Hydrophobic Chains
(Bi-Layer Interior)
Water Core (where Amikacin resides)
ARIKACE delivers the potency of Amikacin at the site of the lung
infection;
engineered specifically for improved PK-PD* profile in the lung providing for
potential enhanced efficacy, safety and convenience benefits
Greater efficacy by reaching infection site
Greater efficacy by reaching infection site
Greater efficacy and once-a-day dosing
Reduces potential for systemic toxicity
Engineered Specifically for Lung Delivery
Prolonged lung residence time
Biofilm penetration
Preferential uptake into macrophages
Minimal systemic exposure
* Pharmacokinetic-Pharmacodynamic (PK-PD) |
 5
ARIKACE: Delivery Using Proprietary eFlow
®
Technology
ARIKACE is delivered once daily via the state-of-the-art PARI Optimized,
Investigational eFlow Nebulizer System with Advanced Mesh Technology
Fast
drug delivery with efficient
lung deposition
Small, portable, silent and
cordless
device weighs less than
10 ounces.
eFlow Technology Device
exclusivity
from PARI Pharma for
15 years after first commercial
sale of ARIKACE
* eFlow
®
is a registered trademark of PARI Pharma GmbH |
 6
ARIKACE: Development Plan
Target-NTM
Study in U.S.
ARIKACE vs. placebo in recalcitrant patients who are on a stable ATS/IDSA
guidelines-based
multi-drug
treatment
regimen;
N
100
No
inhaled
antibiotics
approved
for
treating
NTM
lung
infections
and
little
known competitive activity in clinic
Study
initiated
in
May-2012
top-line
results
from
randomized
portion
of
trial projected in 4Q13
CLEAR-109
CF Pseudomonas
Study for U.S.
FDA
removed
the
clinical
hold
for
CF
Pa
Phase
3
study
in
May
Insmed
will
defer
plans
to
initiate
a
Phase
3
study
of
ARIKACE
in
the
U.S.
for
CF patients until the Company reviews top-line results from CLEAR-108
Insmed is focusing on CLEAR-108 (CF Pa Phase 3 Study) and TARGET-NTM
(NTM Phase 2 Study)
CLEAR-108
CF Pseudomonas
Study for
EU/Canada
ARIKACE
vs.
Tobi
®
(inhaled
tobramycin
solution);
N
300
Builds off of strong Phase 2 efficacy and safety data
Broad population with preferred trial design
Trial
initiated
in
April
2012
top-line
results
projected
in
mid-2013
Eligible
patients
roll-over
into
open-label
ARIKACE®
long
term
safety
and
tolerability study, CLEAR-110
* Tobi
®
is a Registered Trademark of Novartis Pharmaceuticals Corporation
|
 7
Arikace—Cystic Fibrosis
Epidemiology and Disease Description
Cystic fibrosis is a life-threatening disease with significant unmet needs
Affects about 70,000 children
and adults worldwide (30,000 in
U.S. and Europe, each)
Inherited disease that causes
thick, sticky mucus to build up
in the lungs
Despite expanded use of current
products, lung function often
continues to decline
High treatment burden
major compliance issue
Source: Adapted from Cystic Fibrosis Foundation, Patient Registry
Annual Data Reports 2010
Mean = 51.2%
Pseudomonas Lung Infections Increase with Patient Age
Age (Years)
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
<2
2 to 5
6 to 10
11 to 17
18 to 24
25 to 34
35 to 44
45+ |
 8
ARIKACE: Cystic Fibrosis
Need for New Inhaled Antibiotics
Current inhaled antibiotics produce modest efficacy in a limited
patient
population providing an opportunity for ARIKACE to become first-line
treatment
Current inhaled antibiotics are not indicated for a significant segment of the
CF population --
patients with FEV-1 % predicted of greater than 75%
Improvement in lung function with current inhaled antibiotics is
not sustained
in the off-treatment period, and appears to decline over multiple cycles
Lung function continues to decline at an average rate of 1% to 3% per year
with some patients experiencing much greater declines |
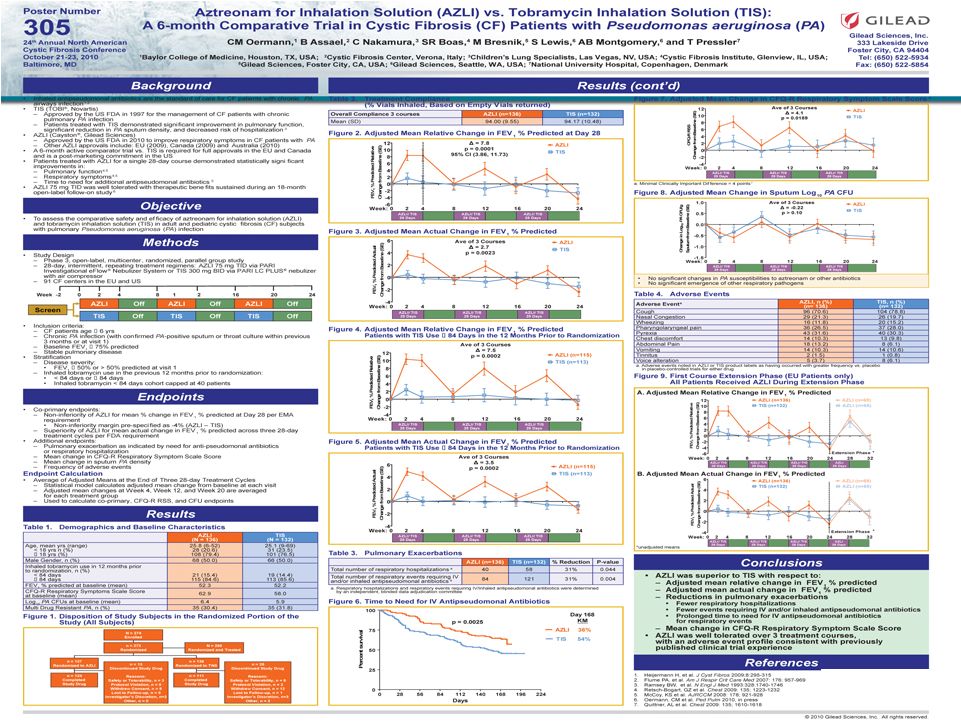
 9
Cayston
®
vs. Tobi
®
CF Phase 3 Trial Results: Pulmonary Function
Lung Function
Adjusted
Mean
Relative
Change
in
FEV
1
%
Predicted
Source: 2010 North American CF Conference Poster 305 and Slide Presentation,
10/10. * Cayston
®
(aztreonam
for
inhalation
solution)
is
a
registered
trademark
of
Gilead
Sciences.
** Tobi
®
(Tobramycin Inhalation Solution) is a registered trademark of Novartis.
*** AZLI = Cayston; TIS = Tobi
Lung function returned to baseline or lower during each off treatment
period and at the end of 24 weeks, both treatment groups showed a
decline in lung function from baseline
Week:
2
AZLI
TIS
+ 7.8
P
= 0.0001
95% CI (3.86, 11.73)
-6
-4
-2
0
2
4
6
8
10
12
0
4
8
12
16
20
24
AZLI/
TIS
28 Days
AZLI/
TIS
28 Days
AZLI/
TIS
28 Days |
 10
Off-Treatment
Period
P = 0.033
P = 0.003
(36/36)
(36/35)
(33/36)
(32/35)
(34/35)
(34/34)
(N=ARIKACE/Placebo)
ARIKACE: Cystic Fibrosis
Phase 2 Pooled Results (560mg QD): Pulmonary Function
(N)
Mean (SE)
ARIKACE demonstrated statistically significant and clinically meaningful
improvement in pulmonary function throughout the 28-day treatment
period that was sustained through the off-treatment period
-6%
-3%
0%
3%
6%
9%
12%
15%
18%
0
7
14
21
28
56
Visit Day
% Change in FEV
1
(ml) vs. Baseline
Arikace
560mg
Placebo |
 11
Visit Days
ARIKACE: Cystic Fibrosis
Open Label Extension (TR02-105): Durability of Response
Treatment
Period
* Significance at end of treatment over 6 cycles
** Significance 56 days off-treatment over 6 cycles
An open label extension study demonstrated the sustained efficacy
of ARIKACE during and between multiple cycles of therapy
Patients Receiving 560 mg ARIKACE Once Daily for 28 Days and Off-Treatment for 56
Days p=0.0001**
p<0.0001*
Cycle
1
Cycle
2
Cycle
3
Cycle
4
Cycle
5
Cycle
6
0
5
10
15
20
14
28
56
70
85
98
112
140
154
169
182
196
224
238
253
266
280
308
322
337
350
364
392
406
421
434
448
476
490
504 |
 12
ARIKACE: Cystic Fibrosis
Phase 3 Program Has Been Initiated in Europe and Canada
Insmed has reached agreement with EMA and Health Canada on pivotal study
requirements for CF patients with Pseudomonas lung infections
* Patients who complete CLEAR-108 are eligible to participate in CLEAR-110,
which is a long term open-label extension study in which patients receive
ARIKACE every other month for up to 2 years CLEAR-108: Phase 3 Primary
Efficacy Study (vs. Tobi ®
, N
300)*
Primary End-Point: Relative Change in FEV-1 at week 24
Key Secondary End-Point: Time to First Pulmonary
Exacerbation Patient
Population:
Patients
ages
6
and
above
with
FEV-1
%
Predicted
25%
Approximately 260 patients required to demonstrate non-inferiority at agreed
upon Top-Line results projected in mid-2013
margin with 80% power |
 13
ARIKACE: Non-TB Mycobacteria
Disease Description and High Unmet Need
NTM
are
intracellular
organisms
that
invade
and
multiply
chiefly
within
macrophages
in
the lung and are characteristically resistant to most antibiotics
NTM lung infections occurs commonly in patients with structural lung disease (e.g.
COPD, bronchiectasis and CF), patients taking immunosuppressive medications, and
in postmenopausal women without clear risk factors
NTM lung infections are often debilitating and progressive
Virtually all patients experience chronic or recurring cough
Other frequent symptoms including sputum production, fatigue, malaise, dyspnea,
fever, hemoptysis, chest pain and weight loss
Non-TB mycobacteria (NTM) are intracellular pathogens that can cause
severe, chronic pulmonary disease with limited effective treatment options
ATS -
American Thoracic Society;
IDSA -
Infectious Disease Society of America
Current
treatment
for
NTM
lung
disease
requires
lengthy
multi-drug
regimens
that
can
be
poorly
tolerated
and
have
limited
efficacy,
especially
in
patients
with
severe
disease
or
in
those
who
have
failed
prior
treatment
attempts”
David
E.
Griffith,
M.D.,
Lead
author
of
the
ATS/IDSA's
diagnosis
and
treatment
guidelines
for
NTM,
and
Professor
of
Medicine
at
the
University
of
Texas
Health
Science
Center
at
Tyler;(Insmed
Press
Release,
6/27/12)
“ |
 14
ARIKACE: Non-TB Mycobacteria
Market Opportunity
“The prevalence of this debilitating chronic disease continues to
grow, and
the current NTM treatment paradigm lacks acceptable treatment options”*
Sources: 1. Clarity Pharma Research, Patient Chart Study, 2012.
2.
Adjemian et al. Prevalence of Pulmonary Nontuberculous Mycobacterial Disease among
Medicare Beneficiaries, USA, 1997-2007, American Journal of Respiratory
and Critical Care Medicine. Apr 2012. 3. SDI Healthcare Database, July
2009. Mycobacterium avium Complex; M. abscessus –
Mycobacterium abscessus
U.S. Patients Diagnosed with NTM Lung Infections in 2011
50K
40K
21K
Diagnosis
growing
at~
8%
annually
2
MAC and M. abscessus* account for
75%-85% of NTM lung disease in U.S.
Mean age is ~ 57 years with
53% treated
with
antibiotics
1
Treated patients use an average of 7.6
antibiotic
courses
per
year
3
Average length of inpatient hospital
stay
is
10.2
days
3
Patients over the age of 65 years were
40% more likely to die than those
without
NTM
from
1997
to
2007
2
* Mark Rolfe, M.D. FCCP, President of New Lung Associates P.A., Medical Director of the
Lung Transplant and Adult Cystic F Fibrosis Programs at Tampa General
Hospital; Insmed press release, June 27, 2012 0
10,000
20,000
30,000
40,000
50,000
60,000
NTM Patients
Diagnosed
NTM Patients
Diagnosed with
MAC or M.
Abscessus
MAC & M.
abscessus
Patients Treated
with Anitbiotics
1 |
 15
ARIKACE: Non-TB Mycobacteria
Rationale for ARIKACE
NTM lung infections are difficult to treat since NTM are taken
up and multiply inside lung macrophages and most antibiotics
have poor macrophage penetration
Amikacin IV is a recommended treatment for MAC and
M. abscessus in the ATS/IDSA's NTM diagnosis and treatment
guidelines
1
but
use
is
limited
due
to
nephro-
and
oto-toxicity
The proprietary liposomal formulation enables ARIKACE to be
preferentially
taken
up
and
concentrated
in
the
lung
macrophages
while
potentially
decreasing systemic exposure and related toxicities
ARIKACE
was
shown
to
have
superior
in
vitro
activity
against
MAC
and
M.
abscessus
vs.
“free”
amikacin
2
ARIKACE
is
well
positioned
to
become
the
first
drug
approved
for
NTM
lung
infections
ARIKACE opportunity: achieve superior efficacy in NTM treatment by
better penetrating lung macrophages where NTM bacteria reside while
limiting systemic drug exposure
Sources: 1. Griffith et al. ATS/IDSA Statement: Diagnosis, Treatment, and Prevention of
NTM Diseases, American Journal of Respiratory and Critical Care Medicine,
2007. 2.
Study conducted by L. E. Bermudez at Oregon State University. (Data on
File) |
 16
ARIKACE: Non-TB Mycobacteria
TARGET-NTM Clinical Study Initiated in Mid-2012
Trial Design and Patient Population (N
100):
–
Randomized, double-blind, placebo controlled Phase 2 study in patients with
recalcitrant/persistent NTM lung infections who are on a stable ATS/IDSA
guidelines-based multi-drug treatment regimen
–
Patients receive ARIKACE or placebo daily for 84 days; then all patients can
receive ARIKACE 560 mg in an open-label manner for an additional 84 days
–
Study population: patients ages 18 to 75
Key Inclusion Criteria: History of chronic infection with either Mycobacterium
avium complex
(MAC)
or
Mycobacterium
abscessus
or
mixed
infection
with
both
species
Primary endpoint: Change in mycobacterial culture results from baseline to end of
treatment [Time
Frame:
84 days]
Insmed appears to be the only company with an NTM clinical program;
top-line Phase 2 data projected in 4Q 2013
There have been very few clinical trials to support current NTM treatment
recommendations, and no new drugs have been assessed in randomized trials
for NTM lung disease in many years. (Insmed Press Release, June 27,
2012) according to Kenneth N. Olivier, M.D., M.P.H., Principal
Investigator of the study and staff pulmonologist at the NIAID, part of
NIH |
 17
Projected
Cash at year
end 2012
(including cash,
investments & CD
)
Approximately $60 to $64 million currently forecast
We believe cash is sufficient to take Company through the
availability of top-line data for both CLEAR-108 and TARGET-NTM
top-line results
Current Overview: Capital Structure and Key Financials
Balance Sheet
Cash of ~$75 million as of June 30, 2012 consisting of cash,
investments & CD
Present Capital
Structure
(INSM)
26.5 million fully diluted shares:
24.9 million Common Shares
1.6 million options, restricted stock units, and warrants
Insmed has a strong cash position |
 18
Appendix
Addressing the Potential for Cross-Resistance of ARIKACE
|
 19
Summary: Addressing Potential for Cross-Resistance in
ARIKACE
While resistance to TOBI (tobramycin) has been documented,
we believe there is no cross-resistance in ARIKACE (amikacin) for the
following reasons. Well-characterized clinical isolates of Pseudomonas
aeruginosa (Pa) from Dr. Burns’ collection have been tested against
amikacin and
ARIKACE.
ARIKACE
has
shown
activity
against
aminoglycoside-resistant
and
multi-drug
resistant
isolates.
Dr.
Burns
felt
ARIKACE performed a bit better than free amikacin. (Report on file.)
Overall, amikacin has lower potential for inducing resistance as
compared to tobramycin (literature).
Additionally,
aminoglycoside-inactivating enzymes elaborated by Pa are different for these two
aminoglycosides. Thus, we there is no complete cross resistance. The issue of
emerging tobramycin resistance secondary to TOBI (inhaled antibiotic) use is not
completely
quantified.
However,
it
is
primarily
due
to
poor
compliance
with
the
prescribed
regimen
of
TOBI.
Patients
do
not take
the drug twice a day consistently. This leads to drug levels much below the MICs of
most phenotypes of Pa for prolonged periods, and thus increased potential for
emergence of resistance. Additionally, there is non-specific binding of
cationic tobramycin to sputum and further low levels available to microbes.
Typically, levels >10x of the MICs are needed for entire dosing interval.
Thus, compliance with dosing regimen is critical as is penetration of antibiotics into
biofilms. Features of ARIKACE that overcome some of the issues responsible
for resistance include: charge neutral liposomes shield
amikacin, providing penetration into biofilm, and high Cmax and AUC, enabling once a
day dosing and improved compliance. The unique features of ARIKACE will reduce
potential for emergence of amikacin resistance vs. free aminoglycoside for inhalation.
Most importantly, the sustained clinical benefit of Arikace in the “off
month” and convenience of once a day will shape the use of
inhalation antibiotics in CF patients.
Use of ciprofloxacin is known to contribute to emergence of Pa isolates with
antimicrobial resistance. Tobramycin is also used as IV
for
treatment
of
exacerbations
and
for
tune-ups.
This
may
also
be
contributing
to
emergence
of
resistance
as
low
levels
of
drug reach the lung after IV use.
Our phase 2 data have shown that 65% of isolates were resistant to aminoglycosides and
~90% were mucoid variant. However, we were able to demonstrate reduction in
bacterial density and improvement in lung function and pros. Thus, we expect to have
significant treatment effect in phase 3 studies even if isolates
are resistant. We have also done in vitro work against mdr isolates
and shown ARIKACE to be effective. |
 20 |
 21
Percent Change in FEV
1
—ITT
Visit Day
Arikace 560 *
15.4% (16.5)
18.4% (21.3)
13.2% (15.3)
13.2% (16.2)
11.5% (16.4)
13.2% (24.3)
Arikace 280 *
10.9% (10.6)
9.4% (12.6)
9.6% (12.5)
10.1% (12.8)
1.7% (9.0)
2.0% (8.6)
Placebo *
0.6% (11.7)
-3.2% (12.2)
1.8% (10.9)
2.2% (11.9)
-0.3% (12.0)
-4.4% (13.0)
* Mean (SD)
Arikace 280
Placebo
Arikace 560
p=0.016
p=0.005
p=0.07
p=0.04 |
 22
Change in FEV
1
(% predicted)—ITT
Visit Day
Arikace 560 *
12.9% (17.2)
15.8% (22.5)
10.5% (15.6)
11.0% (16.4)
8.6% (17.7)
13.8% (26.2)
Arikace 280 *
10.8% (10.8)
9.2% (13.1)
9.4% (12.9)
9.6% (13.7)
1.6% (9.6)
1.8% (8.8)
Placebo *
-0.9% (10.7)
-4.4% (11.3)
0.3% (9.9)
0.5% (10.5)
0.7% (9.6)
-3.8% (13.5)
Arikace 280
Placebo
Arikace 560
P=0.009
P=0.019
P=0.124
P=0.021
* Mean (SD) |
 23
ARIKACE—TR02-05
PFT: Prior Use of Inhalation Antibiotic
Arikace ™
( N = 8 )
Placebo
( N = 4 )
Day 28
10 %
-5 %
Day 56
5 %
-1 %
Relative Change FEV
1
(ml) |
 24
Tobramycin
FEV
1
(L) Absolute |
 25
ARIKACE—TR02-05
By Prior Tobramycin Use
Patients With Prior
Tobramycin Use
Patients Without Prior
Tobramycin Use
Arikace ™
N=5
Placebo
N=3
Arikace ™
N=16
Placebo
N=8
Day 28
0.326 (0.290)
5
-0.083 (0.123)
3
0.126 (0.203)
16
-0.016 (0.144)
8
Day 56
0.152 (0.186)
5
-0.040 (0.284)
3
0.001 (0.161)
15
-0.120 (0.168)
8
*
Absolute
Change
from
Baseline
-
FEV
1
(L)
Cohort I –
280 mg |
 ARIKACE—TR02-05
By Prior Tobramycin Use
26
* Mean (SD)
280mg Cohort
Patients without Tobramycin
280mg Cohort
Patients with Tobramycin
Arikace
Placebo
Arikace
Placebo
Visit Day
Visit Day
Arikace *
326 (290)
152 (186)
Placebo *
-83 (123)
-40 (284)
Arikace *
126 (203)
1 (161)
Placebo *
-16 (144)
-120 (168)
RUN12AUG2008
26 |
 27
Tobramycin
FEV
1
(L) Relative |
 28
ARIKACE—TR02-05
By Prior Tobramycin Use
Patients With Prior
Tobramycin Use
Patients Without Prior
Tobramycin Use
Arikace ™
N=5
Placebo
N=3
Arikace ™
N=16
Placebo
N=8
Day 28
0.136 (0.088)
5
-0.052 (0.075)
3
0.091 (0.138)
16
-0.002 (0.067)
8
Day 56
0.051 (0.093)
5
-0.010 (0.148)
3
0.009 (0.084)
15
-0.053 (0.083)
8
* Mean (SD)
*
Relative
Change
from
Baseline
-
FEV
1
(L)
RUN12AUG2008
Cohort I –
280 mg |
 29
ARIKACE—TR02-05
By Prior Tobramycin Use
* Mean (SD)
RUN12AUG2008
280mg Cohort
Patients without Tobramycin
280mg Cohort
Patients with Tobramycin
Arikace
Placebo
Arikace
Placebo
Visit Day
Visit Day
Arikace *
13.6% (8.8)
5.1% (9.3)
Placebo *
-5.2% (7.5)
-1.0% (14.8)
Arikace *
9.1% (13.8)
0.9% (8.4)
Placebo *
-0.2% (6.7)
-5.3% (8.3) |
 30
Arikace™
-
Efficacy in Patients with Prior Tobramycin Use:
TR02-106
Mean
Change in Log
10
CFU
Subjects with 5-6 Cycles of TOBI in
prior 12 months
Change in FEV1
(ml)
Subjects with 5-6 Cycles of TOBI in
prior 12 months
Placebo
Visit Day
Visit Day
Arikace 560
90 (220)
90 (30)
230 (60)
90 (90)
Placebo
-140 (210)
-110 (350)
-200 (20)
-290 (10)
Arikace 560
Arikace 560
-1.99
(0.70)
-1.26
(0.86)
-0.93
(1.19)
-1.43
(0.89)
-0.27
(0.44)
Placebo
0.15
0.03
-0.55
-0.29
0.08
Placebo
Arikace 560
Mean
-3
-2
-1
0
1
2
3
0
7
14
21
28
35
-300
-250
-200
-150
-100
-50
0
50
100
150
200
250
0
28
56
70
84 |
 31
Insmed has filed a registration statement (including a prospectus) with the Securities
and Exchange Commission (the “SEC”) for the offering to which this
communication relates. Before you invest, you should read the prospectus in that
registration statement and other documents Insmed has filed with the SEC for more
complete information about Insmed and this offering. You may get these documents
for free by visiting EDGAR on the SEC web site at
www.sec.gov.
Alternatively,
Insmed
will
arrange
to
send
you
a
copy
of
the
prospectus
if
you request it by calling Insmed’s corporate secretary at: (732) 997-4600.
|