Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - CTI BIOPHARMA CORP | d253882d8k.htm |
 Cell
Therapeutics, Inc. James A. Bianco, M.D.
CEO
Exhibit 99.1 |
 2
Forward Looking Statement
The following factors, among others, could cause actual results to differ materially from those
described in the forward-looking statements: risks associated with preclinical,
clinical and sales and marketing developments in the biopharmaceutical industry in general and in particular, including, without limitation:
the potential failure of Opaxio™ (“Opaxio”) to prove safe and effective for treatment
of non-small cell lung and ovarian cancers; that the interim survival
results for the phase III clinical trial for Opaxio may not be ready in 2012; the potential failure of
PixuvriTM (pixantrone dimaleate) (“pixantrone”) to prove
safe and effective (including complete and overall response rates) for treatment of relapsed or
refractory, aggressive non-Hodgkin’s lymphoma (“NHL”) as determined by
the U.S. Food and Drug Administration (the “FDA”) and/or the European Medicines Agency (the “EMA”); that accelerated approval by the
FDA of pixantrone may not be possible or occur; that CTI may not be able to address satisfactorily the
two key matters raised by the FDA’s Office of New Drugs (the “OND”) or
other matters raised by the OND and/or the FDA; that CTI’s interpretation of the guidance provided by the OND may be different than
the intent of the OND; that the OND may change its guidance; that the PIX301 study may not be deemed
successful; that a re-review of the pixantrone NDA may not be warranted and, if warranted,
that the FDA may find pixantrone to not be safe and/or effective; that the PIX301 study may still be deemed to be a
failed study; that the FDA may require an additional clinical trial of pixantrone; that if CTI
conducts an additional clinical trial, it may not demonstrate the
safety and effectiveness of pixantrone; that CTI may not be able to provide satisfactory information
in response to the FDA’s Complete Response Letter;
that the FDA may not approve the NDA in the first half of 2012 or at all; that CTI may not obtain a
PDUFA date of April 2012; that CTI cannot predict or guarantee the pace or geography of
enrollment of its clinical trials, including whether or not the majority of the patients will be enrolled in the U.S.; that the
commercial launch of pixantrone may not commence in the first half of 2012; that the EMA may not
approve the MAA; that CTI cannot guarantee the timing of the approval
and launch of its products; that CTI cannot predict the results of the EMA’s Committee for Medicinal Products for Human Use (“CHMP”)
opinion or guarantee that the CHMP will provide its recommendation regarding the MAA during the first
half of 2012; that CTI cannot guarantee exclusivity in the
market for its products; that CTI cannot predict or guarantee that Novartis will exercise its option to negotiate a license for pixantrone or what the actual
milestone amounts will be; that CTI cannot guarantee that the Gynecologic Oncology Group will conduct
an interim survival analysis in 2012 or what the market size or outcome of such analysis
will be; the potential failure of tosedostat to prove safe and effective for the treatment of Acute Myeloid Leukemia
(“AML”); that the FDA may not accept the proposed clinical trial design of tosedostat and/or
may request additional clinical trials; that clinical trials may not demonstrate the safety and
effectiveness of tosedostat; that the phase III pivotal trial for tosedostat for AML and/or myelodysplastic syndromes may not start
during the second quarter of 2012; that CTI may not be able to retire its outstanding convertible
senior notes due in December 2011; that CTI may not consummate additional financings; that CTI
may not be able to maintain its expected burn rate; that CTI’s ability to continue to raise capital as needed to
fund its operations; that CTI may not be able to maintain its burn rate as expected; that CTI may be
unable to comply with NASDAQ listing standards; determinations by regulatory, patent and
administrative governmental authorities; competitive factors; technological developments; costs of developing,
producing and selling CTI’s products under development; and other economic, business,
competitive, and/or regulatory factors affecting CTI’s business generally, including those
set forth in CTI’s filings with the U.S. Securities and Exchange Commission, including its Annual Report on Form 10-K for its most
recent fiscal year and its Quarterly Reports on Form 10-Q since its most recent Annual
Report on Form 10-K, especially in the “Factors Affecting Our Operating
Results” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” sections, and its Current Reports on
Form 8-K. Except as may be required by law, CTI does not intend to update or alter its
forward-looking statements whether as a result of new information, future events, or
otherwise. |
 3
Important Advances in Treating Cancer
3 novel
“late
stage”
cancer
drug candidates
•
Pixantrone
–
marketing
authorizations
filed;
potential
approval
2012
•
Opaxio
–
completing
final
stage
(III)
clinical
testing
2013
•
Tosedostat
–
entering
final
stage
(III)
clinical
testing
2012
Large market opportunities addressing unmet medical
needs
Concentrated cancer market makes go to market strategy
manageable with attractive ROI
Potential for Novartis to exercise option to co-develop and
co-commercialize pixantrone |
 4
Innovative & Established Cancer Drug Pipeline
*Tosedostat
phase III study expected to initiate Q2-2012
Bisplatinates
Brostallicin
Tosedostat
Preclinical
Phase I
Phase II
Phase III
MAA/NDA
Under Review
>
Third-line r/r aggressive NHL (PIX301)
>
Second-line r/r aggressive NHL (PIX306)
First-line aggressive NHL (PIX203)
Second-line
metastatic
breast
cancer
(NCCTG)
First-line Ovarian cancer
First-line GBM cancer + XRT
Elderly high-risk r/r AML (OPAL)
Myelodysplastic Syndrome (MDS)*
ER-, PR-, HER2-
Metastatic Breast cancer |
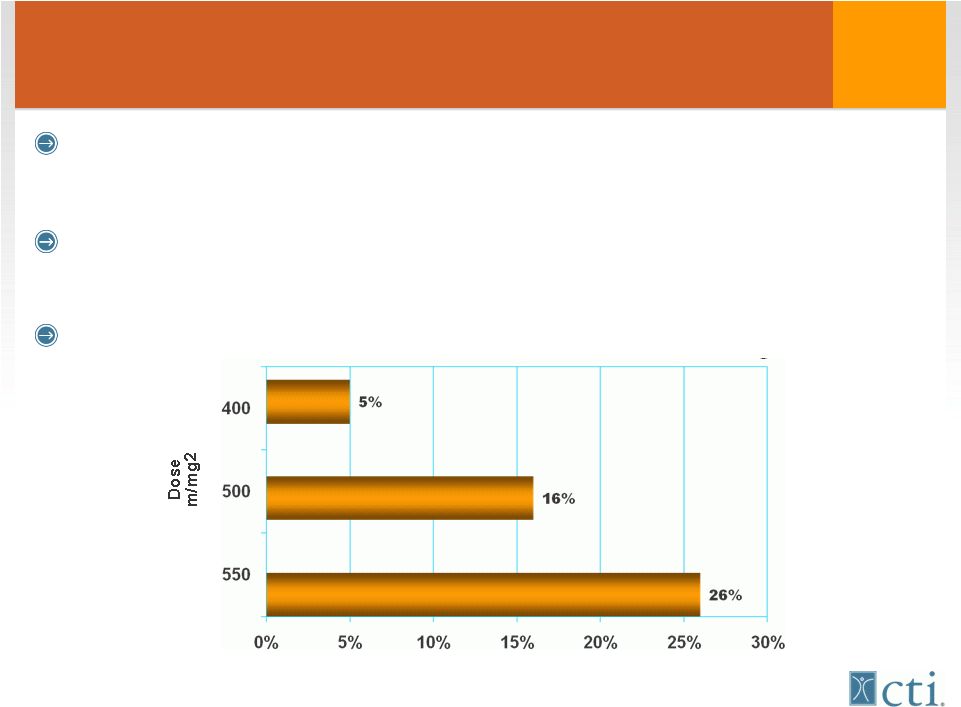 5
Anthracyclines
“Cornerstone”
potentially
curative
therapy 1
st
line
therapy
•
Breast cancer / acute leukemia / NHL
However all anthracyclines cause cumulative, irreversible
damage to heart muscle
Patients
limited
to
life
time
maximum
dose
450mg/m
2*
* Swain et al, chest XRT or cyclophosmaide
Incidence of Congestive Heart Failure |
 6
Pixuvri™
(pixantrone) Product Advantages
More potent DNA alkylator than doxorubicin
Lacks structural motifs that lead to cardiac toxicity
Significant reductions in biochemical, echo-cardiographic
and severe clinical symptoms (CHF) Vs doxorubicin
O
O
O
O
H
O
H
O
H
O
O
H
O
O
O
H
N
H
2
H
N
O
O
N
H
N
H
N
H
2
N
H
2
C
O
O
H
C
O
O
H
O
O
N
H
N
H
N
H
N
H
O
H
O
H
O
H
O
H
Mitoxantrone
Doxorubicin
2 HCl
Pixantrone
Pixantrone
2 |
 7
Pixuvri™
(pixantrone): Overview
Pivotal (PIX301)Trial
•
Significant increase in Complete and Overall Response rates
compared to standard chemotherapy
•
Significant (40%) decrease in risk of dying or progression of
disease over 2 years
•
Well
tolerated,
most
common
side
effect
–
low
white
cell
counts
Marketing Applications filed
•
EU (MAA) –
day 180 responses pending
•
US (NDA) –
re-submitted based on FDA (OND) recommendations
–
expected action date April 2012
Initial indication: r/r aggressive NHL
•
No approved drugs in EU or US for this patient population
Initial market size–
53,000 patients/year (US/EU) |
 8
Novartis Pixantrone Option
NVS has option to negotiate a license to pixantrone
Potentially up to $104 million in registration/sales milestones
•
$17.5mm on approval for r/r aNHL
•
28% to 32% royalty on US net sales
•
NVS assumes certain costs and pays CTI to field 35 sales people
CTI not obligated to license pixantrone to NVS if terms are not
favorable |
 US
Patients/year Treated with Anthracyclines Pixuvri™
Phase II NDA/MAA
o
Development program to enhance
commercial potential post approval
o
Competitive advantages
o
Potential to become standard of care
Source: Tandem Cancer Audit 2004
9 |
 10
Tosedostat: Overview
New drug class: tumor selective targeted agent
•
Works by depriving cancer cells building blocks needed to make
proteins essential for their survival
•
Oral, once daily dosing, well tolerated
Encouraging data in elderly r/r AML (Acute Myeloid
Leukemia) and r/r MDS (Myelodysplasia or pre-leukemia) Pivotal
Phase
III
study
targeted
to
start
Q2
-
2012
Leverages CTI’s access to and expertise in blood-related
cancer market
•
Potential development cost and sales synergies with pixantrone
Exclusive development and marketing rights in the
Americas |
 11
Tosedostat Phase I/II Study |
 12
Unmet Medical Need in MDS and AML
AML and MDS are common diseases
•
MDS often progresses to AML
Is a disease of elderly
•
70% of patients are over age 60
The majority of elderly patients with MDS and AML do
not tolerate standard intensive chemotherapy
•
35% will die from side effects of standard intensive therapy
•
Most are currently treated with low dose chemotherapy or hypo-
methylating agents
There are no approved agents for patients who relapse
Significant unmet medical need for better tolerated
agents in elderly patients with MDS or AML |
 13
Tosedostat: OPAL Interim Study Results
Phase II-
r/r elderly AML (n=75 patients)
•
Oral once-a-day dosing for 6 months
Encouraging interim data presented at ASCO
•
15 of 50 (30%) evaluable patients had bone marrow response;
-
6 (12%) of which were complete bone marrow responses
•
9 of 23 (39%) patients who previously failed therapy with HMA
had a bone marrow response
•
Well tolerated without chemotherapy like side effects
Patients who responded to therapy demonstrated
encouraging survival
Data to be updated at ASH |
 14
Tosedostat
Summary Deal Terms & Structure
Exclusive co-development and marketing rights
in the Americas from Chroma Therapeutics, Ltd
Cost-sharing
•
CTI bears 75% of all development costs
•
Registration trials aimed at US/EU regulatory approval
Initial Payments
•
$5mm upon execution
•
$5mm upon initiation of first pivotal trial
Success based milestones
Royalty rate based on net sales volume |
 15
Relapsed
or
refractory
MDS
(IPSS>2)
•
Currently no approved drugs
•
Existing therapies come off patent in 2011, and 2013
•
18,000 patients/year
Relapsed or refractory elderly AML
•
Currently no approved drugs
•
18,300 patients/year
Other potential indications (patients/year)
•
r/r Myeloma –
19,000
•
1
st
line MDS: 20,100
•
1
st
line Myeloma: 36,000
US Market Size:
Selective Blood Related Cancers |
 16
Indication
WW 2010
sales*
Patent
expiration
MDS
$200MM
2013
MDS
$534MM
2011
Multiple Myeloma/
Mantle Cell
$1.5B
2017
Multiple Myeloma
MDS Deletion 5q
$2.5B
2019
Tosedostat Market Opportunity:
Current targeted agents
VELCADE
*Information from SEC filings. |
 17
A bioengineered
version
of
Taxol®
(paclitaxel)
Singer et al. In: Adv Exp Med Biol. 2003; 519:81-99
|
 18
A
bioengineered
version
of
Taxol®
(paclitaxel)
Taxol®
(paclitaxel)
3hr to 24 hr infusion,
pre-medications required
Opaxio™
15-20 minute infusion,
NO pre-medications required |
 19
Opaxio™
95% of women with advanced Ovarian Cancer achieve CR
with standard (taxol/platinum) chemotherapy
•
Half (median) will relapse within 8 months, and die in 44 months
Ovarian Cancer Pivotal trial (GOG212)
•
Can monthly OPAXIO for 12 months prolong time to
progression and improve survival in women with advanced
Ovarian cancer when compared to no treatment (observation)
•
NIH supported cooperative group study
•
817 of 1100 patients enrolled
•
Interim survival analysis anticipated in 2012
-
Early stopping criteria for success |
 20
Opaxio™
Potential registration route as radiation sensitizer
•
Tumor selective, 8-12X increase in radiation sensitization vs Taxol
(0.8x increase)
Malignant Brain Tumor Study (n=25 patients )
•
Opaxio added to standard therapy (TMZ+XRT)
•
Compared to landmark trial*
-
Median PFS 13.5 months vs. 6.9 months
-
>50% patients alive at 22 months Vs. historically <25% survive 24
months
Randomized multi-center Phase II study underway in
high-risk malignant brain tumors
•
If survival advantage confirmed could serve as basis for approval
*Historical landmark study-
Stupp R, et al, N. Engl. J. Med. 352:987-09, 2005
|
 21
US Patients/year Treated with Taxanes
Source: Tandem Cancer Audit 2004
NSC Lung
Breast
Ovarian
H&N
Prostate
92,400
81,600
27,200
13,600
13,600 |
 22
Capital Structure/Financials
Dual Listed NASDAQ:CTIC, MTA:CTIC.MI
•
Shares outstanding ~193 million
Only $11mm convertible senior notes outstanding
•
Due December 2011
Only common shares outstanding
Manageable burn rate
Cash end of Q3-2011 ~$45.2 million
•
Excludes :~$8.2 million from settlement agreement |
 23
2012 Potential News Flow & Key Milestones
Pixantrone
•
CHMP opinion on MAA and potential approval
•
FDA review of NDA and potential approval
•
Novartis decision on pixantrone option
Tosedostat
•
Final OPAL data to be highlighted at ASH
•
Start of Tosedostat phase III r/r MDS trial
Opaxio
•
OPAXIO phase III ovarian cancer trial interim results
|