Attached files
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d)
OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended September 30, 2010
Commission File Number: 0-13265
UCI MEDICAL AFFILIATES, INC.
(Name of Registrant as Specified in its Charter)
| Delaware | 59-2225346 | |
| (State or Other Jurisdiction of Incorporation or Organization) |
(IRS Employer Identification Number) |
1818 Henderson Street,
Columbia, South Carolina 29201
(Address of Principal Executive Offices, Including Zip Code)
(803) 782-4278
(Registrant’s Telephone Number, Including Area Code)
| Securities registered pursuant to Section 12(b) of the Act: |
None | |
| Securities registered pursuant to Section 12(g) of the Act: |
Common Stock, $.05 par value |
Indicate by check mark whether the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months, and (2) has been subject to the filing requirements for the past 90 days. Yes ¨ No x
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ¨ No ¨
Indicate by check mark if the disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definition of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act
| Large Accelerated Filer |
¨ |
Accelerated Filer |
¨ | |||
| Non-Accelerated Filer |
x |
Smaller Reporting Company |
¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the common equity held by non-affiliates of the registrant on September 30, 2010 was approximately $6,955,843, based on the number of shares held by non-affiliates of the registrant and the reported last sale price of common stock on September 30, 2010 ($2.41), which was the last business day of the registrant’s most recently completed quarter. This calculation does not reflect a determination that persons are affiliates for any other purposes. The registrant has no non-voting common stock outstanding.
APPLICABLE ONLY TO REGISTRANTS INVOLVED IN BANKRUPTCY
PROCEEDINGS DURING THE PRECEDING FIVE YEARS
Indicate by check mark whether the registrant has filed all documents and reports required to be filed by Section 12, 13, or 15(d) of the Securities Exchange Act of 1934 subsequent to the distribution of securities under a plan confirmed by a court. Yes x No ¨
The number of shares outstanding of the registrant’s common stock, $.05 par value, was 9,934,072 at September 30, 2010.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive proxy statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrants fiscal year ended September 30, 2010, are incorporated by reference in Part III hereof.
Table of Contents
UCI MEDICAL AFFILIATES, INC.
| PAGE | ||||||
| PART I |
||||||
| Item 1. |
3 | |||||
| Item 1A. |
10 | |||||
| Item 1B. |
16 | |||||
| Item 2. |
16 | |||||
| Item 3. |
17 | |||||
| Item 4. |
17 | |||||
| PART II |
||||||
| Item 5. |
18 | |||||
| Item 6. |
21 | |||||
| Item 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
22 | ||||
| Item 7A. |
28 | |||||
| Item 8. |
29 | |||||
| Item 9. |
Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
49 | ||||
| Item 9A. |
49 | |||||
| Item 9B. |
49 | |||||
| PART III |
||||||
| Item 10. |
50 | |||||
| Item 11. |
50 | |||||
| Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
50 | ||||
| Item 13. |
Certain Relationships and Related Transactions and Director Independence |
50 | ||||
| Item 14. |
50 | |||||
| PART IV |
||||||
| Item 15. |
51 | |||||
| 52 | ||||||
2
Table of Contents
Advisory Note Regarding Forward-Looking Statements
Certain of the statements contained in this Report on Form 10-K that are not historical facts are forward-looking statements subject to the safe harbor created by the Private Securities Litigation Reform Act of 1995. We caution readers of this Form 10-K that such forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from those expressed or implied by such forward-looking statements. Although our management believes that their expectations of future performance are based on reasonable assumptions within the bounds of their knowledge of their business and operations, we can give no assurance that actual results will not differ materially from their expectations. Factors that could cause actual results to differ from expectations include, among other things, (1) the difficulty in controlling our costs of providing healthcare and administering our network of centers; (2) the possible negative effects from changes in reimbursement and capitation payment levels and payment practices by insurance companies, healthcare plans, government payers and other payment sources; (3) the difficulty of attracting primary care physicians; (4) the increasing competition for patients among healthcare providers; (5) possible government regulations negatively impacting our existing organizational structure; (6) the possible negative effects of healthcare reform; (7) the challenges and uncertainties in the implementation of our expansion and development strategy; (8) the dependence on key personnel; (9) adverse conditions in the stock market, the public debt market, and other capital markets (including changes in interest rate conditions); (10) the strength of the United States economy in general and the strength of the local economies in which we conduct operations may be different than expected resulting in, among other things, a reduced demand for practice management services; (11) the demand for our products and services; (12) technological changes; (13) the ability to increase market share; (14) the adequacy of expense projections and estimates of impairment loss; (15) the impact of changes in accounting policies by the Securities and Exchange Commission; (16) unanticipated regulatory or judicial proceedings; (17) the impact on our business, as well as on the risks set forth above, of various domestic or international military or terrorist activities or conflicts; (18) other factors described in this Form 10-K, including, but not limited to, those matters described under the caption “PART I – ITEM 1A. – RISK FACTORS,” and in our other reports filed with the Securities and Exchange Commission; and (19) our success at managing the risks involved in the foregoing.
PART I
| ITEM 1. | BUSINESS |
General
UCI Medical Affiliates, Inc. (“UCI”) is a Delaware corporation incorporated on August 25, 1982. Operating through its wholly-owned subsidiary, UCI Medical Affiliates of South Carolina, Inc. (“UCI-SC”), UCI provides nonmedical management and administrative services for a network of freestanding medical centers. As of September 30, 2010, UCI provided services to 67 medical centers, 66 of which are located throughout South Carolina and one is located in Knoxville, Tennessee (43 operating as Doctors Care in South Carolina, one as Doctors Care in Knoxville, Tennessee, 20 as Progressive Physical Therapy Services in South Carolina, one as Luberoff Pediatrics in South Carolina, one as Carolina Orthopedic & Sports Medicine in South Carolina and one as Doctors Wellness Center in South Carolina). We refer to these 67 medical centers as the “centers” throughout this Report. As such terms are defined below in PART I – ITEM 1. – BUSINESS – Organizational Structure,” we sometimes refer to the P.A., UCI, UCI-SC, and UCI-LLC collectively as the “Company” or as “we,” “us” and “our” throughout this Report.
Organizational Structure
Federal law and the laws of many states, including South Carolina and Tennessee, generally specify who may practice medicine and limit the scope of relationships between medical practitioners and other parties. Under such laws, UCI and UCI-SC are prohibited from practicing medicine or exercising control over the provision of medical services. In order to comply with such laws, all medical services at the centers are provided by or under the supervision of Doctors Care, P.A., Progressive Physical Therapy, P.A. (“PPT”), Carolina Orthopedic & Sports Medicine, P.A. (“COSM”) or Doctors Care of Tennessee, P.C. (the four together as the “P.A.”), each of which has contracted with UCI-SC to be the sole provider of all non-medical direction and supervision of the centers operating in its respective state of organization. We sometimes refer to the P.A., UCI, UCI-SC, and UCI Properties, LLC (“UCI-LLC”) collectively as the “Company” or as “we,” “us” and “our” throughout this Report. The P.A. is organized so that all physician services are offered by the physicians who are employed by the P.A. Neither UCI, UCI-LLC nor UCI-SC employ practicing physicians as practitioners, exert control over their decisions regarding medical care, or represent to the public that it offers medical services.
3
Table of Contents
UCI-SC has entered into an Administrative Services Agreement with each P.A. pursuant to which UCI-SC performs all non-medical management of the P.A. and has exclusive authority over all aspects of the business of the P.A. (other than those directly related to the provision of patient medical services or as otherwise prohibited by state law). The non-medical management provided by UCI-SC includes, among other functions, treasury and capital planning, financial reporting and accounting, pricing decisions, patient acceptance policies, setting office hours, contracting with third-party payers, and all administrative services. UCI-SC provides all of the resources (systems, procedures, and staffing) to bill third-party payers or patients and provides all of the resources for cash collection and management of accounts receivable, including custody of the lockbox where cash receipts are deposited. From the cash receipts, UCI-SC pays all physician salaries and operating expenses of the centers and of UCI-SC. Compensation guidelines for the licensed medical professionals at the P.A. are set by UCI-SC, and UCI-SC establishes guidelines for selecting, hiring, and terminating the licensed medical professionals. UCI-SC also negotiates and executes substantially all of the provider contracts with third-party payers. UCI-SC does not loan or otherwise advance funds to the P.A. for any purpose.
The P.A. and UCI-SC share a common management team. In each case, the same individuals serve in the same executive offices of each entity.
UCI-SC believes that the services it provides to the P.A. do not constitute the practice of medicine under applicable laws. Because of the unique structure of the relationships described above, many aspects of our business operations have not been the subject of state or federal regulatory interpretation. We can give no assurance that a review of our business by the courts or regulatory authorities will not result in a determination that could adversely affect our operations or that the healthcare regulatory environment will not change so as to restrict our existing operations or future expansion.
The Centers
The centers are staffed by licensed physicians, physical therapists, other healthcare providers (including physician assistants and nurse practitioners), medical support staff, and administrative support staff. The medical support staff includes licensed nurses, certified medical assistants, laboratory technicians, and registered radiographic technologists.
The centers typically are open for extended hours (weekends and evenings) and provide out-patient care only. When hospitalization or specialty care is needed, referrals to appropriate specialists are made. Carolina Orthopedic & Sports Medicine is an exception since it does provide in-patient care.
Over the past five fiscal years we have increased the number of our centers by 56%. The number of centers in operation increased from 43 to 47 during fiscal year 2005. We added three Doctors Care offices (two in the Columbia, South Carolina region and one in the Myrtle Beach, South Carolina region) and one physical therapy office (in the Charleston, South Carolina region). The number of centers in operation increased from 47 to 52 during fiscal year 2006. We added two Doctors Care offices (one in the Columbia, South Carolina region and one in the Charleston, South Carolina region), three physical therapy offices (two in the Columbia, South Carolina region and one in the Charleston, South Carolina region), and one Wellness center (in the Columbia, South Carolina region), and we closed one physical therapy office (in the Columbia, South Carolina region). The number of centers increased from 52 to 58 during fiscal year 2007. We added five Doctors Care offices (three in the Charleston, South Carolina region and two in the Greenville-Spartanburg, South Carolina region) and one physical therapy office (in the Myrtle Beach, South Carolina region). The number of centers increased from 58 to 62 during fiscal year 2008. We added three Doctors Care offices (two in the Pee Dee, South Carolina region and one in the Myrtle Beach, South Carolina region) and one physical therapy office (in the Pee Dee, South Carolina region). The number of centers increased from 62 to 67 during fiscal year 2009. We added five Doctors Care offices (three in the Columbia, South Carolina region, one in the Myrtle Beach, South Carolina region and one in the Charleston, South Carolina region) and one physical therapy office (in the Columbia, South Carolina region). During 2009, we closed one Doctors Care office in the Columbia, South Carolina region). During 2010, we relocated one Doctors Care office in the Columbia, South Carolina region.
Our centers are broadly distributed throughout the State of South Carolina, and one is in Knoxville, Tennessee. Twenty-eight centers are in the Columbia, South Carolina region (including nine physical therapy centers, one pediatric center, one orthopedic center, and one wellness center), seventeen in the Charleston, South Carolina region (including six physical therapy offices), eight in the Myrtle Beach, South Carolina region (including one physical therapy office), three in the Pee Dee, South Carolina region (including one physical therapy office), ten in the Greenville-Spartanburg, South Carolina region (including three physical therapy offices), and one in Knoxville, Tennessee.
4
Table of Contents
Medical Services Provided at the Centers
Our centers offer out-patient medical care for treatment of acute, episodic, and some minor chronic medical problems. The centers provide a broad range of medical services that would generally be classified as within the scope of urgent care, family practice, primary care, and occupational medicine. We also offer pediatric and orthopedic medical services at two of our centers, and physical therapy at our 20 physical therapy centers. Licensed medical providers, nurses, and auxiliary support personnel provide the medical services. The services provided at the centers include, but are not limited to, the following:
| • | Routine care of general medical problems, including colds, flu, ear infections, hypertension, asthma, pneumonia, and other conditions typically treated by primary care providers; |
| • | Treatment of injuries, such as simple fractures, dislocations, sprains, bruises, and cuts; |
| • | Minor surgery, including suturing of lacerations and removal of cysts and foreign bodies; |
| • | Diagnostic tests, such as x-rays, electrocardiograms, complete blood counts, and urinalyses; and, |
| • | Occupational and industrial medical services, including drug testing, workers’ compensation cases, and physical examinations. |
Patient Charges and Payments
The fees charged to a patient are determined by the nature of medical services rendered. Our management believes that the charges at our centers are significantly lower than the charges of hospital emergency departments and are generally competitive with the charges of local physicians and other providers in the area. For the majority of our patients the charges are established by third-party payers.
Our centers accept payment from a wide range of sources. These include patient payments at time of service (by cash, check, or credit card), patient billing, and assignment of insurance benefits (including Blue Cross Blue Shield, Workers’ Compensation, and other private insurance). We also provide services for members of the three largest health maintenance organizations (“HMOs”) operating in South Carolina – BlueChoice HealthPlan (“BCHP”), Cigna/HealthSource South Carolina, Inc., and SuperMed.
Revenues generated from billings to Blue Cross Blue Shield of South Carolina (“BCBS”) and its subsidiaries, BCHP and Companion Property and Casualty Insurance Company (“CP&C”), totaled approximately 38%, 40% and 40% of the Company’s total revenues for fiscal years 2010, 2009 and 2008, respectively. BCBS and its subsidiaries own approximately 68% of our outstanding common stock. (See Footnote 12 to audited Consolidated Financial Statements for information on related parties.)
During the past three fiscal years, we have continued our services provided to members of HMOs. In these arrangements, we, through the P.A., act as the designated primary caregiver for members of HMOs who have selected one of our centers or providers as their primary care provider. In fiscal year 1994, we began participating in an HMO operated by BCHP and CP&C, wholly owned subsidiaries of BCBS. (See Footnote 11 to audited Consolidated Financial Statements for information on related parties.) As of September 30, 2010, all of these HMOs use a discounted fee-for-service basis for payment. HMOs do not, at this time, have a significant penetration into the South Carolina market. We are not certain if the market share of HMOs will grow in the areas in which we operate centers.
Revenues in fiscal years 2010, 2009 and 2008, also reflect our occupational medicine and industrial healthcare services (these revenues are referred to as “employer paid” and “workers’ compensation” on the table depicted below). Approximately 13% of our total revenue was derived from these occupational medicine services in fiscal year 2010, while 13% and 15% were derived in fiscal years 2009 and 2008, respectively.
5
Table of Contents
The following table sets forth our revenue and patient visits by revenue source for fiscal years 2010, 2009 and 2008:
| Percent of Patient Visits | Percent of Revenue | |||||||||||||||||||||||
| 2010 | 2009 | 2008 | 2010 | 2009 | 2008 | |||||||||||||||||||
| Patient Pay |
12 | 15 | 16 | 9 | 8 | 8 | ||||||||||||||||||
| Employer Paid |
7 | 6 | 8 | 2 | 2 | 3 | ||||||||||||||||||
| HMO |
4 | 5 | 6 | 4 | 6 | 7 | ||||||||||||||||||
| Workers’ Compensation |
8 | 9 | 10 | 11 | 11 | 12 | ||||||||||||||||||
| Medicare/Medicaid |
19 | 16 | 14 | 17 | 15 | 13 | ||||||||||||||||||
| Insured Patients |
46 | 45 | 43 | 53 | 54 | 55 | ||||||||||||||||||
| Other (Commercial Indemnity, Champus, etc.) |
4 | 4 | 3 | 4 | 4 | 2 | ||||||||||||||||||
| 100 | 100 | 100 | 100 | 100 | 100 | |||||||||||||||||||
As insurers attempt to cut costs, they typically increase the administrative burden placed on providers by requiring referral approvals and by requesting hard copies of medical records before they will pay claims. The number of patients at our centers that are covered by managed care plans is significant and accounted for 53%, 54%, and 55% of our revenues in 2010, 2009 and 2008, respectively.
In accordance with the Administrative Services Agreements described previously, UCI-SC, as the agent for each P.A., processes all payments for the P.A. When payments for the P.A. are received, they are deposited in accounts owned by each P.A. and are automatically transferred to a lockbox account owned by UCI-SC. In no event are the physicians entitled to receive such payments. The patient mix in no way affects our management service fees per the Administrative Services Agreement.
Fee Arrangements
Medical services traditionally have been provided on a fee-for-service basis with insurance companies assuming responsibility for paying all or a portion of such fees. The increase in medical costs under traditional indemnity healthcare plans has been caused by a number of factors. These factors include: (i) the lack of incentives on the part of healthcare providers to deliver cost-effective medical care; (ii) the absence of controls over the utilization of costly specialty care physicians and hospitals; (iii) a growing and aging population that requires increased healthcare expenditures; and (iv) the expense involved with the introduction and use of advanced pharmaceuticals and medical technology.
As a result of escalating healthcare costs, employers, insurers, and governmental entities all have sought cost-effective approaches to the delivery of and payment for quality healthcare services. HMOs and other managed healthcare organizations have emerged as integral components in this effort. HMOs and managed care organizations enroll members by entering into contracts with employer groups or directly with individuals to provide a broad range of healthcare services for a capitation payment (we have no capitation arrangements at the present time) or a discounted fee-for-service schedule, with minimal or no deductibles or co-payments required of the members. HMOs and other managed care groups, in turn, contract with healthcare providers like us to administer medical care to their members. These contracts provide for payment to us on a discounted fee-for-service basis.
Certain third-party payers constantly seek various alternatives for reducing medical costs, some of which, if implemented, could affect our payment levels. Our management cannot predict whether changes in present payment methods will affect payments for services provided by the centers and, if so, whether they will have an adverse impact upon our business.
Competition and Marketing
All of our centers face competition, in varying degrees, from hospital emergency rooms, private doctor’s offices, other competing freestanding medical centers, hospital-supported urgent care offices and physical therapy offices. Some of these providers have financial resources that are greater than our resources. Our centers compete on the basis of accessibility, including evening and weekend hours, walk-in care, as well as limited appointment opportunities, and the attractiveness of our state-wide network to large employers and third-party payers. We have implemented substantial marketing efforts, which currently include radio, television and billboard advertisements. We employ a marketing director and also employ regional marketing representatives who develop and focus on promotional material. In addition, our regional marketing representatives use direct sales methods to support our occupational medical initiatives.
6
Table of Contents
Government Regulation
As participants in the healthcare industry, our operations and relationships are subject to extensive and increasing regulation by a number of governmental entities at the federal, state, and local levels.
Limitations on the Corporate Practice of Medicine
Federal law and the laws of many states, including South Carolina and Tennessee, generally specify who may practice medicine and limit the scope of relationships between medical practitioners and other parties. Under such laws, business corporations such as UCI and UCI-SC are prohibited from practicing medicine or exercising control over the provision of medical services. In order to comply with such laws, all medical services at our centers are provided by or are under the supervision of the P.A. pursuant to contracts with UCI-SC. The P.A. is organized so that the physicians who are employed by the P.A. offer all physician services. Neither UCI nor UCI-SC employs practicing physicians as practitioners, exerts control over any physician’s decisions regarding medical care, or represents to the public that it offers medical services.
As described previously, UCI-SC has entered into an Administrative Services Agreement with each P.A. to perform all non-medical management of the applicable P.A. and has exclusive authority over all aspects of the business of the P.A., other than those directly related to the provision of patient medical services or as otherwise prohibited by state law. (See “PART I – ITEM 1. – BUSINESS – Organizational Structure” above).
Because of the unique structure of the relationships existing between UCI-SC and each P.A., many aspects of our business operations have not been the subject of state or federal regulatory interpretation. We can give no assurance that a review by the courts or regulatory authorities of the business formerly or currently conducted by us will not result in a determination that could adversely affect our operations or that the healthcare regulatory environment will not change so as to restrict the existing operations or any potential expansion of our business.
Third Party Payments
Approximately 17%, 15%, and 13% of our revenue in 2010, 2009 and 2008, respectively, was derived from payments made by government-sponsored healthcare programs (principally, Medicare and Medicaid). As a result, any change in the laws, regulations, or policies governing reimbursements could adversely affect our operations. See “PART I – ITEM 1. – BUSINESS – Healthcare Reform Initiatives” and “PART I – ITEM 1A. – RISK FACTORS – Changes to the laws, regulations, and policies governing government-sponsored healthcare programs could materially adversely affect our programs,” below. State and federal civil and criminal statutes also impose substantial penalties, including civil and criminal fines and imprisonment, on healthcare providers that fraudulently or erroneously bill governmental or other third-party payers for healthcare services. We believe we are in compliance with such laws, but we can give no assurance that our activities will not be challenged or scrutinized by governmental authorities.
Federal Anti-Kickback and Self-Referral Laws
Certain provisions of the Social Security Act, commonly referred to as the “Anti-kickback Statute,” prohibit the offer, payment, solicitation, or receipt of any form of remuneration in return for the referral of Medicare or state healthcare program patients or patient care opportunities, or in return for the recommendation, arrangement, purchase, lease, or order of items or services that are covered by Medicare or state healthcare programs. We believe that we are not in violation of the Anti-kickback Statute or similar state statutes.
On April 14, 1998, the Office of the Inspector General (the “OIG”), the government office that is charged with the enforcement of the federal Anti-kickback Statute, issued an advisory opinion regarding a proposed management services contract unrelated to us that involved a cost plus a percentage of net revenue payment arrangement (“Advisory Opinion 98-4”). Based on its analysis of the intent and scope of the Anti-kickback Statute, the OIG determined that it could not approve the arrangement because the structure of the management agreement raised the following concerns under the Anti-kickback Statute: (i) the agreement might include financial incentives to increase patient referrals; (ii) the agreement did not include any controls to prevent over utilization; and (iii) the percentage billing arrangement may include financial incentives that increase the risk of abusive billing practices. The OIG opinion did not find that the management arrangement violated the Anti-kickback Statute, rather that the arrangement may involve prohibited remuneration absent sufficient controls to minimize potential fraud and abuse. An OIG advisory opinion is only legally binding on the Department of Health and Human Services (including the OIG) and the requesting party and is limited to the specific conduct of the requesting party because additional facts and circumstances could be involved in each particular case. Accordingly, we believe that Advisory Opinion 98-4 does
7
Table of Contents
not have broad application to the provision by UCI and UCI-SC of nonmedical management and administrative services for the centers. We also believe that we have implemented appropriate controls to ensure that the arrangements between UCI and UCI-SC and the centers do not result in abusive billing practices or the over utilization of items and services paid for by federal healthcare programs.
The applicability of the Anti-kickback Statute to many business transactions in the healthcare industry, including the service agreements with the centers and the development of ancillary services by UCI and UCI-SC, has not been subject to any significant judicial and regulatory interpretation. We believe that although remuneration for the management services is provided for under our service agreements with the centers, UCI and UCI-SC are not in a position to make or influence referrals of patients or services reimbursed under Medicare or state healthcare programs to the centers. In addition, UCI and UCI-SC is not a separate provider of Medicare or state healthcare program reimbursed services. Consequently, we do not believe that the service and management fees payable to UCI and UCI-SC should be viewed as remuneration for referring or influencing referrals of patients or services covered by such programs as prohibited by the Anti-kickback Statute.
The U.S. Congress in the Omnibus Budget Reconciliation Act of 1993 enacted significant prohibitions against physician referrals. Subject to certain exemptions, a physician or a member of his or her immediate family is prohibited from referring Medicare or Medicaid patients to an entity providing “designated health services” in which the physician has an ownership or investment interest or with which the physician has entered into a compensation arrangement. While we believe we are currently in compliance with such legislation, future regulations could require us to modify the form of our relationships with physician groups.
State Anti-Kickback and Self-Referral Laws
Some states have also enacted similar self-referral laws, and we believe that more states will likely follow. We believe that our practices fit within exemptions contained in such laws. Nevertheless, in the event we expand our operations to certain additional jurisdictions, structural and organizational modifications of our relationships with physician groups might be required to comply with new or revised state statutes. Such modifications could adversely affect our operations.
Through UCI’s wholly owned subsidiary, UCI-SC, we provide non-medical management and administrative services to the centers in South Carolina and Tennessee. South Carolina and Tennessee have adopted anti-kickback and self-referral laws that regulate financial relationships between healthcare providers and entities that provide healthcare services. The following is a summary of the applicable state anti-kickback and self-referral laws.
South Carolina
South Carolina’s Provider Self-Referral Act of 1993 generally provides that a healthcare provider may not refer a patient for the provision of any designated healthcare service to an entity in which the healthcare provider is an investor or has an investment interest. Under our current operations, we do not believe UCI or UCI-SC is an entity providing designated healthcare services for purposes of the South Carolina Provider Self-Referral Act. The centers provide all healthcare services to patients through employees of the P.A. No provider investors in the P.A. refer patients to the centers for designated healthcare services. Accordingly, under South Carolina law, we believe that the provider self-referral prohibition would not apply to our centers or operations in South Carolina.
In addition to self-referral prohibitions, South Carolina’s Provider Self-Referral Act of 1993 also prohibits the offer, payment, solicitation, or receipt of a kickback, directly or indirectly, overtly or covertly, in cash or in kind, for referring or soliciting patients. We believe that payment arrangements are reasonable compensation for services rendered and do not constitute payments for referrals.
Tennessee
The Tennessee physician conflict of interest/disclosure law provides that physicians are free to enter into lawful contractual relationships, including the acquisition of ownership interests in healthcare facilities. The law further recognizes that these relationships can create potential conflicts of interests, which shall be addressed by the following: (a) the physician has a duty to disclose to the patient or referring colleagues such physician’s ownership interest in the facility or therapy at the time of referral and prior to utilization; (b) the physician shall not exploit the patient in any way, as by inappropriate or unnecessary utilization; (c) the physician’s activities shall be in strict conformity with the law; (d) the patient shall have free choice either to use the physician’s proprietary facility or therapy or to seek the needed medical services elsewhere; and (e) when a physician’s commercial interest conflicts so greatly with the patient’s interest as to be incompatible, the physician shall make alternative arrangements for the care of the patient.
8
Table of Contents
We believe that Tennessee’s conflict of interest/disclosure law does not apply to our current operations because UCI and UCI-SC are not providers of healthcare services. The centers provide all healthcare services to patients through employees of the P.A. Even if the Tennessee conflict of interest/disclosure law were to apply, our internal quality assurance/utilization review programs will help identify any inappropriate utilization by a center.
Tennessee also has a law regulating healthcare referrals. The general rule is that a physician who has an investment interest in a healthcare entity shall not refer patients to the entity unless a statutory exception exists. A healthcare entity is defined as an entity that provides healthcare services. We believe that UCI and UCI-SC do not fit within the definition of a “healthcare entity” because UCI and UCI-SC are not providers of healthcare services. The centers provide all healthcare services to patients through employees of the P.A. No provider investors in the P.A. refer patients for designated healthcare services except the sole physician shareholder of the P.A. We believe that referrals by the sole shareholder of the P.A. come within a statutory exception. Accordingly, under Tennessee law, we believe that the provider self-referral prohibition would not apply to our center or operations in Tennessee.
Tennessee’s anti-kickback provision prohibits a physician from making payments in exchange for the referral of a patient. In addition, under Tennessee law a physician may not split or divide fees with any person for referring a patient. The Tennessee Attorney General has issued opinions that determined that the fee-splitting prohibition applied to management services arrangements. The Tennessee fee-splitting prohibition contains an exception for reasonable compensation for goods or services. We believe that the payment arrangements between UCI and UCI-SC, as applicable, and the centers are reasonable compensation for services rendered and do not constitute payments for referrals or a fee-splitting arrangement.
Antitrust Laws
Because each P.A. is a separate legal entity, each may be deemed a competitor subject to a range of antitrust laws that prohibit anti-competitive conduct, including price fixing, concerted refusals to deal, and division of market. We believe we are in compliance with such state and federal laws that may affect our development of integrated healthcare delivery networks, but we can give no assurance that a review of our business by courts or regulatory authorities will not result in a determination that could adversely affect our operations.
Healthcare Reform Initiatives
Congress recently enacted the Patient Protection and Affordable Care Act (the “2010 Act”) which is a significant reform to the U.S. healthcare system, including limits to Medicare payments and increased taxes. Various healthcare reform proposals have also emerged at the state level. We cannot predict the effect the 2010 Act and any future legislation or regulation will have on us.
Regulation of Provider Networks
Many states regulate the establishment and operation of networks of healthcare providers. Generally, these laws do not apply to the hiring and contracting of physicians by other healthcare providers. South Carolina and Tennessee do not currently regulate the establishment or operation of networks of healthcare providers except where such entities provide utilization review services through private review agents. We believe that we are in compliance with these laws in the states in which we currently do business, but we can give no assurance that future interpretations of these laws by the regulatory authorities in South Carolina, Tennessee, or the states in which we may expand in the future will not require licensure of our operations as an insurer or provider network or a restructuring of some or all of our operations. In the event we are required to become licensed under these laws, the licensure process can be lengthy, costly and time consuming and, unless the regulatory authority permits us to continue to operate while the licensure process is progressing, we could experience a material adverse change in our business while the licensure process is pending. In addition, many of the licensing requirements mandate strict financial and other requirements that we may not immediately be able to meet. Further, once licensed, we would be subject to continuing oversight by and reporting to the respective regulatory agency.
9
Table of Contents
HIPAA
Under the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), the Secretary of Health and Human Services (“HHS”) has adopted national data interchange standards for some types of electronic transactions and the data elements used in those transactions; adopted security standards to protect the confidentiality, integrity and availability of patient healthcare information; and adopted privacy standards to prevent inappropriate access, use and disclosure of patient healthcare information. In December 2000, HHS published the final privacy regulations that took effect in April 2003. These regulations restrict the use and disclosure of individually identifiable healthcare information without the prior informed consent of the patient. In February 2003, HHS published the final security regulations, which took effect in April 2005. These regulations mandate that healthcare facilities implement operational, physical and technical security measures to reasonably prevent accidental, negligent, or intentional inappropriate access or disclosure of patient healthcare information. A violation of HIPAA’s standard transactions, privacy and security provisions may result in criminal and civil penalties, which could adversely affect our financial condition and results of operations. See “PART I – ITEM 1A. – RISK FACTORS – We are required to comply with laws governing the transmission, security and privacy of healthcare information that require significant compliance costs, and any failure to comply with these laws could result in material criminal and civil penalties,” below. We conduct our operations in an attempt to comply with all applicable HIPAA requirements, but we can give no assurance that our activities or interpretations of applicable law will not be challenged or scrutinized by governmental authorities.
Employees
As of September 30, 2010, we had 1,070 employees (767 on a full-time equivalent basis). This amount includes 193 medical providers employed by the P.A.
| ITEM 1A. | RISK FACTORS. |
Investing in our common stock involves various risks which are particular to our Company, our industry and our market area. Several risk factors regarding investing in our common stock are discussed below. This listing should not be considered as all-inclusive. Any of the following risks, as well as other risks, uncertainties, and possibly inaccurate assumptions underlying our plans and expectations, could result in material harm to our business, results of operations and financial condition and cause the value of our securities to decline, which in turn could cause investors to lose all or part of their investment in our Company. These factors, among others, could also cause actual results to differ from those we have experienced in the past or those we may express or imply from time to time in any forward-looking statements we make. See “Advisory Note Regarding Forward-Looking Statements” above in this Report. Investors are advised that it is impossible to identify or predict all risks, and that risks not currently known to us or that we currently deem immaterial also could affect us in the future.
We can provide no assurance that our medical centers will be able to compete effectively with other existing healthcare providers.
The business of providing healthcare-related services is highly competitive. Many companies, including professionally managed physician practice management companies like ours, manage medical clinics, and employ clinic physicians at the clinics. Large hospitals, other physician practice centers, retail healthcare providers, private doctor’s offices and healthcare companies, HMOs, and insurance companies are also involved in activities similar to ours. Because our main business is the provision of medical services to the general public, our primary competitors are the local physician practices and hospital emergency rooms in the markets where we operate medical centers. Increased competition is expected in our markets from retail healthcare providers, often located in retail businesses such as drug stores and discount store operations, which offer treatment without an appointment for certain permitted routine diagnoses. Some of these competitors have longer operating histories or significantly greater resources than we do. In addition, traditional sources of medical services, such as hospital emergency rooms and private physicians, have had in the past a higher degree of recognition and acceptance than the medical centers that we operate. We cannot assure you that we will be able to compete effectively or that additional competitors will not enter the market in the future.
If a regulatory authority finds that our organization and relationships do not comply with existing or future laws and regulations, our operations could be materially adversely affected.
As a participant in the healthcare industry, our operations and relationships are subject to extensive and increasing regulation by a number of governmental bodies at the federal, state and local levels. Although we have tried to structure our business to comply with these existing laws and regulations, we have had little guidance as to whether we comply or not because of the unique structure of our business operations. We cannot assure you that a review by the courts or regulatory authorities of our former or current business will not result in a determination that could adversely affect our operations. In particular, we can provide you with no assurance that a court or regulatory body would find that our structure and business operations comply with the following:
| • | State and federal laws limiting the provision of medical services by business corporations; |
10
Table of Contents
| • | State and federal anti-kickback and self-referral laws; |
| • | Antitrust laws; and, |
| • | Federal and state laws and regulations governing insurance companies, HMOs, and other managed care organizations. |
We have provided you with a discussion of each of these areas in the section titled “Government Regulation” under PART 1 – ITEM 1, above.
Furthermore, the laws and regulations governing the healthcare industry change rapidly and constantly. Political, economic and regulatory influences are currently subjecting the healthcare industry to fundamental changes. We anticipate that the current presidential administration, Congress and certain state legislatures will continue to review and assess alternative healthcare delivery systems and payment methods with an objective of ultimately reducing healthcare costs and expanding access. Public debate of these issues will likely continue in the future. At this time, we cannot predict which, if any, healthcare reform proposals will be adopted, but any initiatives that force us to modify or restrict our existing operations and any proposed expansion of our business could materially affect our business.
Changes to the laws, regulations, and policies governing government-sponsored healthcare programs could materially adversely affect our operations.
We have derived approximately 17%, 15% and 13% of our revenues in 2010, 2009 and 2008, respectively, from payments made by government-funded healthcare programs (principally, Medicare and Medicaid). Congress recently adopted the Patient Protection and Affordable Care Act (the “2010 Act”) which reforms the structure and funding for the U.S. healthcare system, including the Medicare and Medicaid programs. Various items of the 2010 Act could have a material adverse impact on government-sponsored healthcare programs, such as Medicare payments and increased taxes. Also, many states have enacted or are considering enacting measures designed to reduce Medicaid expenditures. States have also adopted, or are considering, legislation designed to reduce coverage and program eligibility and/or impose additional taxes on hospitals to help finance or expand states’ Medicaid systems. We are unable to predict the future course of federal or state healthcare legislation. The 2010 Act and further changes in the law or regulatory framework that reduce our revenues or increase our costs could have a material adverse effect on our business, financial condition or results of operation.
We are subject to healthcare fraud and abuse regulations that could result in significant liability, require us to change our business practices and restrict our operations in the future.
We are subject to various U.S. federal and state laws targeting fraud and abuse in the healthcare industry, including anti-kickback and false claims laws. Violations of these laws are punishable by criminal or civil sanctions, including substantial fines, imprisonment and exclusion from participation in healthcare programs such as Medicare and Medicaid. Additionally, state and federal civil and criminal statutes impose substantial penalties, including civil and criminal fines and imprisonment, on healthcare providers that fraudulently or wrongfully bill governmental or other third-party payers for healthcare services. We believe we are in material compliance with these laws, but we cannot assure you that our activities will not be challenged or scrutinized by governmental authorities.
We are required to comply with laws governing the transmission, security and privacy of healthcare information that require significant compliance costs, and any failure to comply with these laws could result in material criminal and civil penalties.
Numerous state and federal laws and regulations govern the collection, dissemination, use and confidentiality of patient-identifiable healthcare information, including HIPAA and its related rules and regulations. The HIPAA privacy rules restrict the use and disclosure of patient information and requires entities to safeguard that information and to provide certain rights to individuals with respect to that information. The HIPAA security rules establish elaborate requirements for safeguarding patient information transmitted or stored electronically. We conduct our operations in an attempt to comply with all applicable HIPAA requirements. Given the complexity of the HIPAA regulations, the possibility that the regulations may change and the fact that the regulations are subject to changing and sometimes conflicting interpretation, our ongoing ability to comply with the HIPAA requirements is uncertain. Additionally, the costs of complying with any changes to the HIPAA regulations may have a negative impact on our operations. Sanctions for failing to comply with the HIPAA healthcare information provisions include criminal penalties and civil sanctions, including significant monetary penalties. A failure by us to comply with state healthcare laws that may be more restrictive than the HIPAA regulations could result in additional penalties.
11
Table of Contents
In 2008, we determined that our previously issued consolidated financial statements should no longer be relied upon and we restated our consolidated financial statements for the six year period ended September 30, 2007. The restatements subjected us to significant cost and a number of additional risks and uncertainties, including increased costs for accounting and legal fees and the increased possibility of legal proceedings.
As previously disclosed in our 2008 Annual Report on Form 10-K which was filed on February 2, 2010, we determined that our previously issued consolidated financial statements for all prior years and interim periods dating back to our fiscal year ended September 30, 2002 should no longer be relied upon because of errors in such financial statements. The restatement subjected us to significant cost and a number of additional risks and uncertainties, including the following:
| • | Substantial unanticipated costs in the form of accounting, legal fees and similar professional fees, in addition to the substantial diversion of time and attention of our Chief Financial Officer and members of our finance department in preparing the restatement. Although the restatement is complete, we can give no assurance that we will not incur additional costs associated with the restatement. |
| • | As a result of the determination that our previously issued financial statements could no longer be relied upon and the restatement of certain prior financial statements, we may be susceptible to legal claims by current or former stockholders, regulators or others. If such events occur, we may incur substantial defense costs regardless of the outcome of these actions and insurance and indemnification may not be sufficient to cover the losses we may incur. Likewise, such events might cause a further diversion of our management’s time and attention. If we do not prevail in one or more of these potential actions, we could be required to pay substantial damages or settlement costs, which could adversely affect our business, financial condition, results of operations and liquidity. |
Departures of our key personnel or directors may impair our business operations.
We have two executive officers. D. Michael Stout, M.D., serves as our President and Chief Executive Officer. Joseph A. Boyle, CPA, serves as our Executive Vice President and Chief Financial Officer. They are instrumental in our organization and are the key executives in charge of our medical and business operations. We cannot be assured of the continued service of either of them and each of them would be difficult to replace. Additionally, our directors’ community involvement, diverse backgrounds, and extensive business relationships are important to our success.
Because of the nature of our business, we run the risk that we will be unable to collect the fees that we have earned.
Virtually all of our consolidated net revenue was earned in the past, and we believe will be earned in the future, from our medical centers’ charges for services on a fee-for-service basis. Accordingly, we assume the financial risk related to collection, including the potential uncollectability of accounts, long collection cycles for accounts receivable, and delays associated with reimbursement by third-party payers, such as governmental programs, private insurance plans and managed care organizations. Increases in write-offs of doubtful accounts, delays in receiving payments or potential retroactive adjustments, and penalties resulting from audits by payers may require us to borrow funds to meet our current obligations or may otherwise have a material adverse effect on our financial condition, results of operations and liquidity.
We are subject to certain special risks in connection with goodwill reported on our balance sheet.
As a result of our various acquisition transactions, goodwill (net of accumulated amortization) of approximately $3.4 million has been recorded on our balance sheet as of September 30, 2010. Because of a change in accounting principles adopted by the accounting profession, we ceased amortizing our goodwill in the fiscal year ending September 30, 2002. Instead, after an initial review of our goodwill for impairment in connection with our adoption of this new accounting principle, we analyze our goodwill on an annual basis for impairment of value. During 2009, we deemed $41,000 of goodwill to be impaired due to the closure of the center with which it was related. Otherwise, under these current accounting principles, our net unamortized balance of goodwill was not considered to be impaired as of September 30, 2010.
We cannot assure you that we will ever realize the value of our remaining goodwill in the future. We may be required to recognize that the value of our goodwill has been impaired in our subsequent annual reviews upon analyzing our operating results. Any future determination that a significant impairment has occurred would require us to write-off the impaired portion of our remaining goodwill, which could have a material adverse effect on our results of operations and financial condition.
12
Table of Contents
Changes in accounting standards could impact reported earnings.
The accounting standard setters, including the FASB, the SEC and other regulatory bodies, periodically change the financial accounting and reporting standards that govern the preparation of our consolidated financial statements. These changes can be hard to predict and can materially impact how we record and report our financial condition and results of operations. Among other possible impacts, we could be required to apply a new or revised standard retroactively, which could result in material changes to, and restatements of, prior period financial statements.
You may have difficulty in selling your shares because of the absence of an active public market.
On February 13, 2009, our common stock was delisted from the Over-the-Counter Bulletin Board (“OTCBB”) as a result of our failure to timely file with the SEC our Annual Report on Form 10-K. Such failure was due to an investigation of the fraudulent activities of our former Chief Financial Officer. Since February 13, 2009, our common stock has traded on the Pink Sheets Electronic Over-the-Counter Market (“Pink Sheets”). Consequently, our stockholders may find disposing of shares of our common stock and obtaining accurate quotations of its market value more difficult. In addition, the delisting may make our common stock substantially less attractive as:
| • | collateral for loans; |
| • | an investment by financial institutions because of their internal policies or state legal investment laws; |
| • | consideration to finance any future acquisitions of medical practices; and, |
| • | an investment opportunity by investors should we desire to raise additional capital in the future. |
We have been informed that the NASD may be considering higher standards for permitting quotations of securities on the OTCBB. If the NASD does raise its standards, relisting on the OTCBB may no longer be available as a trading market for our stockholders. Consequently, potential investors should only invest in our common stock if they have a long-term investment intent. If an active market does not develop and a stockholder desires to sell its shares of our common stock, the stockholder will be required to locate a buyer on its own and may not be able to do so.
The absence of a public market makes the price of our common stock particularly volatile and susceptible to market fluctuations.
Trading in our common stock has historically been very limited, and we cannot assure stockholders that an active trading market for our common stock will ever develop or be sustained. Because of the limited trading activity in our common stock, the market price of our common stock has been vulnerable to significant fluctuations in response to very limited market trading in our shares. Sales of substantial amounts of our common stock in the public market, or the perception that these sales could occur, could adversely affect prevailing market prices of our common stock and could impair our future ability to raise capital through the sale of our equity securities. The market price of our common stock will remain subject to significant fluctuations in response to these factors as well as in response to operating results and other factors affecting stock prices generally. The stock market in recent years has experienced price and volume fluctuations that often have been unrelated or disproportionate to the operating performance of companies. These fluctuations, as well as general economic and market conditions, may adversely affect the market price of our common stock in the future. We are unable to predict the effect, if any, that future sales of our common stock or the availability of our common stock for sale may have on the market price of our common stock from time to time.
Stockholders may have difficulty selling their shares because our common stock is a “penny stock” and is subject to special SEC rules that make transactions in our common stock burdensome for broker-dealers.
Our stock is a “penny stock.” The Commission has adopted regulations which generally define “penny stock” as any equity security that has a market price (as defined) less than $5.00 per share or an exercise price of less than $5.00 per share, subject to certain exceptions. Our common stock is covered by the Commission’s penny stock rules, which impose additional sales practice requirements on broker-dealers who sell to persons other than established customers and “accredited investors.” The term “accredited investor” refers generally to institutions with assets in excess of $5,000,000 or individuals with a net worth in excess of $1,000,000 or annual income exceeding $200,000 or $300,000 jointly with their spouse. If a penny stock is traded in the secondary market, the Commission rules require the broker-dealer to provide to the purchaser a standardized risk disclosure schedule prepared by the Commission explaining the nature of the penny stock market and the risks associated with it. The broker-dealer also must provide to the purchaser the current bid and offer quotations for the penny stock, the compensation payable to both the broker-dealer and its registered representative, and the rights and remedies available to an investor in cases of fraud in penny stock transactions. If the
13
Table of Contents
broker-dealer is the sole market maker, the broker-dealer must disclose to the purchaser this fact and the broker-dealer’s presumed control over the market. The foregoing information must be given to the purchaser orally or in writing prior to effecting the transaction and must be given to the purchaser in writing before or with the purchaser’s confirmation. In addition, the penny stock rules require that prior to a transaction in a penny stock not otherwise exempt from the rules, the broker-dealer must make a special written determination that the penny stock is a suitable investment for the purchaser and that the purchaser has sufficient knowledge and experience in financial matters to be capable of evaluating the risks of transactions in penny stocks and must receive the purchaser’s written agreement to the transaction. Finally, after the sale, the broker-dealer must provide to the purchaser monthly account statements showing the market value of each penny stock held in the purchaser’s account and containing information on the limited market in penny stocks. The additional burdens that these Commission rules impose upon broker-dealers may discourage broker-dealers from effecting transactions in our common stock and could severely limit a stockholder’s ability to sell its shares in the secondary market.
The market price of our common stock may fluctuate widely in the future.
The trading price of our common stock could be subject to wide fluctuations in response to quarter-to-quarter variations in our operating results, material announcements made by us from time to time, governmental regulatory action, general conditions in the healthcare industry, or other events, or factors, many of which are beyond our control. In addition, the stock market has experienced extreme price and volume fluctuations, which have particularly affected the market prices of many healthcare services companies and which have often been unrelated to the operating performance of these companies. Our operating results in future quarters may be below the expectations of securities analysts and investors. In this event, the price of our common stock would likely decline, perhaps substantially.
Anti-takeover provisions in our certificate of incorporation and state corporate laws could deter or prevent take-over attempts by a potential purchaser of our common stock and deprive you of the opportunity to obtain a takeover premium for your shares.
In many cases, stockholders receive a premium for their shares when a company is purchased by another. Various provisions in our certificate of incorporation and bylaws and state corporate laws could deter and make it more difficult for a third party to bring about a merger, sale of control, or similar transaction without approval of our board of directors. These provisions tend to perpetuate existing management. As a result, our stockholders may be deprived of opportunities to sell some or all of their shares at prices that represent a premium over market prices.
These provisions, which could make it less likely that a change in control will occur, include:
| • | provisions in our certificate of incorporation establishing three classes of directors with staggered terms, which means that only one-third of the members of the board of directors is elected each year and each director serves for a term of three years. |
| • | provisions in our certificate of incorporation authorizing the board of directors to issue a series of preferred stock without stockholder action, which issuance could discourage a third party from attempting to acquire, or make it more difficult for a third party to acquire, a controlling interest in us. |
Currently, we have no plans to pay dividends on our common stock in the foreseeable future.
It is our current intention to retain future earnings, if any, for use in the operation and expansion of our business. Consequently, we do not currently plan to pay dividends until we recover any losses that we have incurred. Additionally, our future dividend policy will depend on our earnings, financial condition, liquidity and other factors that our Board of Directors considers relevant.
Stockholders may suffer dilution in their interests in our common stock if we offer additional shares of common stock in the future or if certain third parties exercise their option rights to acquire additional shares of our common stock.
Although we have no present intent to offer for sale additional shares of common stock, we cannot ensure that, in the future, we will not have to seek additional capital by offering and selling additional shares of common stock in order to continue to operate, acquire additional medical practices in our current or other markets, or achieve successful operations. If it becomes necessary to raise additional capital to support our operations, there is no assurance that additional capital will be available to us, that additional capital
14
Table of Contents
can be obtained on terms favorable to us, or that the price of any additional shares that may be offered by us in the future will not be less than the subscription price paid by our stockholders. Although the precise effect on existing stockholders of sales of additional shares of common stock cannot presently be determined, either or both the ownership and voting percentage and the relative value of shares of common stock held by our existing stockholders could be diluted by our issuance of additional stock.
As of September 30, 2010, BCBS owned in the aggregate 6,726,019 shares, or approximately 68 percent, of our outstanding common stock. Under various agreements among BCHP and us, we have given these companies the right at any time to purchase from us the number of shares of our voting stock as is necessary for BCBS and its affiliated entity, as a group, to obtain and then maintain an aggregate ownership of not less than 48 percent of our outstanding voting stock. To the extent the BCBS subsidiary exercises its right in conjunction with a sale of voting stock by us to other parties, the price to be paid by the BCBS subsidiary is the average price to be paid by the other purchasers in that sale. Otherwise, the price is the average closing bid price of our voting stock on the ten trading days immediately preceding the election by the BCBS subsidiary to exercise its purchase rights. Consequently, to the extent the BCBS subsidiary elects to exercise any or a portion of its rights under these anti-dilution agreements, the sale of shares of common stock to the BCBS subsidiary will have the effect of further reducing the percentage voting interest in us represented by a share of the common stock.
Certain affiliates have the ability to exercise substantial influence.
The substantial ownership of our common stock by the BCBS subsidiary and other of our affiliates may provide them with the ability to exercise substantial influence over, or based on the present ownership of the BCBS subsidiary, determine the outcome of, the election of directors and other matters submitted for approval by our stockholders. As a result, other stockholders may be unable to successfully oppose matters that are presented by these entities for action by stockholders, or to take actions that are opposed by these entities. The ownership by these entities may also have the effect of delaying, deterring, or preventing a change in our control without the consent of these entities. These effects could reduce the value of our stock. In addition, sales of common stock by these entities could result in another stockholder obtaining control over us.
We are dependent upon the good reputation of our physicians.
The success of our business is dependent upon quality medical services being rendered by our physicians. As the patient-physician relationship involves inherent trust and confidence, any negative publicity, whether from civil litigation, allegations of criminal misconduct, or forfeiture of medical licenses, with respect to any of our physicians and/or our facilities could adversely affect our results of operations.
Our revenues and profits could be diminished if we lose the services of key physicians.
Substantially all of our revenues are derived from medical services performed by physicians. Some of our physicians produce more revenue than other physicians in our Company. Certain of these higher producing physicians could retire, become disabled, terminate their employment agreements or provider contracts, or otherwise become unable or unwilling to continue generating revenues at the current level, or discontinue practicing medicine within our organization. Patients who have been served by those physicians could choose to request medical services from our competitors, reducing our revenues and profits. Moreover, we may not be able to attract or retain other qualified physicians into our Company to replace the services of such physicians.
We may become subject to claims of medical malpractice for which our insurance coverage may not be adequate. Such claims could materially increase our costs and reduce our profitability.
Since we are involved in the delivery of healthcare services to the public, we are exposed to the risk of professional liability claims. Claims of this nature, if successful, could result in substantial damage awards to the claimants, which may exceed the limits of any applicable insurance coverage. We are currently insured under policies in amounts management deems appropriate, based upon historical claims and the nature and risk of our business. Nevertheless, there are exclusions and exceptions to coverage under each insurance policy that may make coverage for any claim unavailable, future claims could exceed the limits of available insurance coverage, existing insurers could become insolvent and fail to meet their obligations to provide coverage for such claims, and such coverage may not always be available with sufficient limits and at reasonable cost to adequately and economically insure us in the future. A judgment against us could materially increase our costs and reduce our profitability.
15
Table of Contents
Our business is concentrated in specific geographic locations and could be affected by a depressed economy in these areas.
We provide our services primarily in South Carolina and have one center in Tennessee. A stagnant or depressed economy in South Carolina could affect all of our markets and adversely affect our business and results of operations.
Terrorist attacks, acts of war, natural disasters or other catastrophic events may adversely affect our operating results and financial condition.
Our centers are vulnerable to damage from hurricanes, tornados, fires, floods, power losses, telecommunications failures, computer viruses, acts of terrorism, acts of war and similar events that may cause an interruption in our business. Any such catastrophic event or other unexpected disruption of one or more of our centers could have a material adverse effect on our business, results of operations and financial condition. Furthermore, future terrorist attacks, acts of war, natural disasters or other catastrophic events may adversely affect prevailing economic conditions generally. These events, depending on their magnitude, could have a material effect on our operating results and financial condition.
| ITEM 1B. | UNRESOLVED STAFF COMMENTS |
There are no comments from the staff of the SEC regarding our periodic or current reports under the Exchange Act that remain unresolved.
| ITEM 2. | PROPERTIES |
In September 2007, the Company formed a South Carolina limited liability company, UCI Properties, LLC (“UCI-LLC”), for the purpose of holding certain real estate. The sole member of UCI-LLC is UCI-SC.
During fiscal year 2008, UCI-LLC entered into a loan agreement with a financial institution to finance the purchase of, and renovations to, a new corporate headquarters located in Columbia, South Carolina. At September 30, 2010, the outstanding balance on the loan was approximately $2,036,000. The note has a variable interest rate based on the Adjusted Libor Rate and the balance is payable in equal monthly installments of principal and interest in the amount of $11,407 with the balance due on March 5, 2015. The promissory note is collateralized by a lien on the property.
During fiscal year 2008, a center located in Surfside Beach, South Carolina was purchased by UCI-LLC for a total purchase price of $815,000. This property was previously rented by UCI-SC and occupied as a medical center. A portion of the purchase price was funded by a promissory note in the original principal amount of $695,000, and is collateralized by a lien on the property. At September 30, 2010, the outstanding balance on the mortgage loan was approximately $628,000. The promissory note accrues interest at a rate of 5.95 percent per annum. Monthly principal and interest payments are $5,890. The entire unpaid balance of principal and interest will be due on July 16, 2013.
Our centers are broadly distributed throughout the State of South Carolina, and one is in Knoxville, Tennessee. The locations of our centers are more fully described under the caption, “PART 1. – ITEM 1. BUSINESS – The Centers.” Our corporate offices are located in a newly renovated free-standing building in Columbia, South Carolina which is owned by UCI-LLC.
All of our centers are leased by UCI-SC, except for the two centers which are owned by UCI-LLC. The centers are generally located on well-traveled streets or highways, with easy access. Each property offers free, off-street parking immediately adjacent to the center. Our lease terms range from five to twenty years. Most of our leases are classified as operating leases; however, we have seventeen leases that are classified as capital leases as of September 30, 2010. All of our capital leases have lease terms of twenty years and all have been executed since 2004. At September 30, 2010, we reported assets and liabilities of $12,396,711 and $13,723,418, respectively, associated with our capital leases related to real estate leases. Two centers are leased from physician employees of the P.A.
In November 2010, we completed the renovation of and opened a new Doctors Care center located in Columbia, South Carolina. In addition, in November 2010, we acquired a property in Newberry, South Carolina for $285,000 and have commenced the construction of a new facility which will house a Doctors Care and Progressive Physical Therapy center. We expect the new centers will be opened late in our second quarter or early in our third quarter of 2011.
16
Table of Contents
| ITEM 3. | LEGAL PROCEEDINGS |
We are a party to various claims, legal activities, and complaints arising in the normal course of business. In the opinion of management and legal counsel, aggregate liabilities, if any, arising from currently known or pending legal actions would not have a material adverse effect on our financial position.
On December 10, 2008, our Audit Committee of the Board of Directors (the “Audit Committee”) commenced an internal investigation (the “Investigation”) of certain accounting irregularities with respect to our internal controls and improper expense reimbursements to Jerry F. Wells, Jr., the Company’s former Executive Vice-President of Finance, Chief Financial Officer, and Secretary. As a result of the Investigation, on February 27, 2009, Mr. Wells executed a Confession of Judgment (the “Judgment”) in our favor in the amount of $2,967,382.
In conjunction with our collection efforts pursuant to the Judgment, we filed claims with two insurance carriers under fidelity bond and employee dishonesty insurance policies. In conjunction with such claims, we received an insurance settlement in the amount of $2,732,840 which was recognized in 2010. The recovery reflects a reduction from the amount of the Judgment for the policy deductible and other adjustments related to amounts we have collected from Mr. Wells and expenses we incurred in conjunction with our collection efforts. In conjunction with the recovery, we assigned our claims against certain third parties to the insurance carrier that paid the recovery. We, however, retained our right to pursue certain claims against our former independent registered public accounting firm which are unrelated to the fraud losses recovered from the insurance carrier. Our initial claim against our former registered independent public accounting firm is approximately $2.1 million; however, we may claim additional damages as they are ascertained. Efforts to collect such losses from our former independent registered public accounting firm have commenced. Even though we intend to vigorously pursue such claim, we can give no assurances that our claim will result in any recovery from our former independent registered public accounting firm.
| ITEM 4. | REMOVED AND RESERVED |
17
Table of Contents
PART II
| ITEM 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Until October 19, 1998, UCI’s common stock was traded on the NASDAQ SmallCap Market under the symbol UCIA. On October 20, 1998, UCI’s common stock was delisted from trading on the NASDAQ SmallCap Market as a consequence of UCI’s failure to meet certain quantitative requirements under the NASD’s expanded listing criteria. Subsequent to October 20, 1998, trading in UCI’s common stock was conducted through the OTCBB. On February 13, 2009 UCI’s common stock was delisted from the OTCBB as a result of UCI’s failure to file its Annual Report on Form 10-K with the SEC. Since February 13, 2009 UCI’s common stock has traded on the “Pink Sheets.”
The prices set forth below indicate the high and low bid prices reported on the Pink Sheets. The quotations reflect inter-dealer prices without retail markup, markdown, or commission and may not necessarily reflect actual transactions.
| Bid Price | ||||||||
| High | Low | |||||||
| Fiscal Year Ended September 30, 2010 |
||||||||
|
1st quarter (10/01/09 - 12/31/09) |
$ | 2.60 | $ | 1.56 | ||||
|
2nd quarter (01/01/10 - 03/31/10) |
2.75 | 1.91 | ||||||
|
3rd quarter (04/01/10 - 06/30/10) |
2.69 | 1.15 | ||||||
|
4th quarter (07/01/10 - 09/30/10) |
2.45 | 1.45 | ||||||
| Fiscal Year Ended September 30, 2009 |
||||||||
|
1st quarter (10/01/08 - 12/31/08) |
$ | 2.49 | $ | 1.80 | ||||
|
2nd quarter (01/01/09 - 03/31/09) |
2.13 | 0.35 | ||||||
|
3rd quarter (04/01/09 - 06/30/09) |
3.00 | 0.75 | ||||||
|
4th quarter (07/01/09 - 09/30/09) |
2.75 | 1.01 | ||||||
As of September 30, 2010, there were 233 stockholders of record of UCI’s common stock, excluding shareholders whose shares are held by a broker in street name.
UCI has not paid cash dividends on its common stock since its inception and has no current plans to declare cash dividends in the foreseeable future.
During the fiscal year ended September 30, 2010, there were no shares of common stock issued by UCI upon the exercise of options which were registered under the Securities Act.
As of September 30, 2010, the high and low bid prices for our common stock on the Pink Sheets were $2.41 and $2.41, respectively.
No equity securities of UCI were repurchased by UCI during the fiscal year ended September 30, 2010.
Equity Compensation Plan Information
During the fiscal year ended September 30, 2010, there were no securities issued upon exercise of outstanding options, warrants and rights, and no securities remaining available for future issuance, under equity compensation plans approved or not approved by security holders.
18
Table of Contents
PERFORMANCE GRAPH
This Section is not soliciting material, is not deemed filed with the SEC or subject to Regulation 14A or 14C, or to the liabilities of Section 18 of the Securities Exchange Act of 1934, as amended, and is not to be incorporated by reference in any filing of the Company under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, whether made before or after the date hereof and irrespective of any general incorporation language in any such filing.
The following graph compares cumulative total shareholder return of UCI’s common stock over a five-year period with The NASDAQ Composite Index, Morningstar Medical Care Index, and the 2009 Peer Group of companies for the same period. Total shareholder return represents stock price changes and assumes the reinvestment of dividends. The graph assumes the investment of $100 on October 1, 2005.
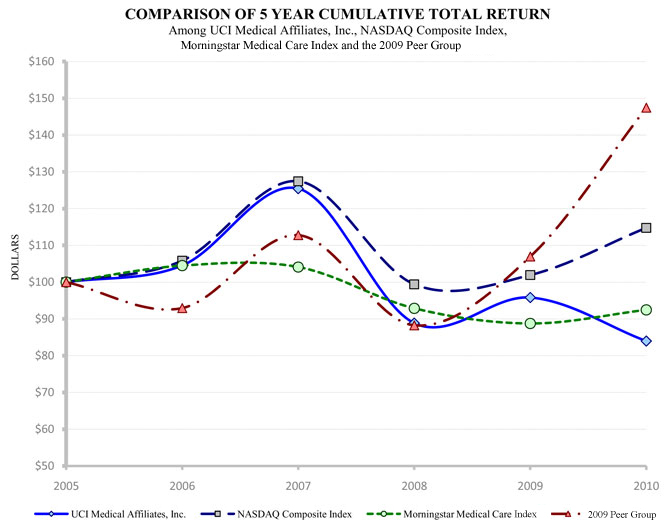
19
Table of Contents
| Fiscal Year Ended | ||||||||||||||||||||||||
| 9/30/2005 | 9/30/2006 | 9/30/2007 | 9/30/2008 | 9/30/2009 | 9/30/2010 | |||||||||||||||||||
| UCI Medical Affiliates, Inc. |
$ | 100.00 | $ | 104.53 | $ | 125.44 | $ | 88.85 | $ | 95.82 | $ | 83.97 | ||||||||||||
| NASDAQ Composite Index |
$ | 100.00 | $ | 105.83 | $ | 127.44 | $ | 99.42 | $ | 101.93 | $ | 114.78 | ||||||||||||
| Morningstar Medical Care Index |
$ | 100.00 | $ | 104.49 | $ | 104.11 | $ | 92.87 | $ | 88.75 | $ | 92.45 | ||||||||||||
| 2009 Peer Group |
$ | 100.00 | $ | 92.94 | $ | 112.77 | $ | 88.24 | $ | 106.96 | $ | 147.43 | ||||||||||||
The members of the 2009 Peer Group are Continucare Corporation, IntegraMed America, Inc., and Metropolitan Health Networks. Pediatrix Medical Group, Inc. was removed from the 2009 Peer Group following their acquisition by MEDNAX, Inc. The returns of each company in the 2009 Peer Group and the Morningstar Medical Care Index have been weighted according to their respective stock market capitalization for purposes of arriving at a Peer Group average. The Morningstar Medical Care Index contains approximately 110 companies in our industry. We will discontinue comparing our total shareholder return to the 2009 Peer Group which contains only three companies. The prices of UCI’s common stock used in computing the returns reflected above are the average of the high and low bid prices reported for UCI’s common stock during the fiscal year ended on such dates.
20
Table of Contents
| ITEM 6. | SELECTED FINANCIAL DATA |
STATEMENTS OF INCOME DATA
| Years ended September 30, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| Revenues |
$ | 86,905,329 | $ | 80,350,452 | $ | 77,045,256 | $ | 71,645,715 | $ | 62,287,914 | ||||||||||
| Operating expenses |
71,574,779 | 63,613,355 | 61,244,515 | 56,804,833 | 49,319,085 | |||||||||||||||
| Operating margin |
15,330,550 | 16,737,097 | 15,800,741 | 14,840,882 | 12,968,829 | |||||||||||||||
| General and administrative expenses |
13,021,060 | 12,472,412 | 14,056,608 | 12,588,646 | 11,085,785 | |||||||||||||||
| Income from operations |
2,309,490 | 4,264,685 | 1,744,133 | 2,252,236 | 1,883,044 | |||||||||||||||
| Recovery of misappropriation loss |
2,732,840 | 776,672 | — | — | — | |||||||||||||||
| Income before income taxes |
5,042,330 | 5,041,357 | 1,744,133 | 2,252,236 | 1,883,044 | |||||||||||||||
| Income tax expense |
1,906,370 | 1,946,468 | 666,714 | 910,195 | 771,320 | |||||||||||||||
| Net income |
$ | 3,135,960 | $ | 3,094,889 | $ | 1,077,419 | $ | 1,342,041 | $ | 1,111,724 | ||||||||||
| Basic earnings per share |
$ | 0.32 | $ | 0.31 | $ | 0.11 | $ | 0.14 | $ | 0.11 | ||||||||||
| Basic weighted average common shares outstanding |
9,934,072 | 9,941,544 | 9,914,122 | 9,881,613 | 9,783,502 | |||||||||||||||
| Diluted earnings per share |
$ | 0.32 | $ | 0.31 | $ | 0.11 | $ | 0.14 | $ | 0.11 | ||||||||||
| Diluted weighted average common shares outstanding |
9,934,072 | 9,941,544 | 9,914,122 | 9,915,524 | 9,858,959 | |||||||||||||||
BALANCE SHEET DATA
| As of September 30, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| unaudited (1) | ||||||||||||||||||||
| Working capital |
$ | 5,347,998 | $ | 3,220,224 | $ | 2,893,448 | $ | 3,131,840 | $ | 3,327,514 | ||||||||||
| Property and equipment, net |
14,747,283 | 14,203,029 | 10,935,156 | 8,533,327 | 7,495,676 | |||||||||||||||
| Capital leases, net |
12,488,271 | 13,279,797 | 9,334,040 | 6,667,718 | 3,335,790 | |||||||||||||||
| Total assets |
47,052,485 | 45,917,358 | 37,539,241 | 34,015,661 | 27,347,424 | |||||||||||||||
| Long-term debt, including current portion |
3,580,618 | 4,545,278 | 3,754,139 | 2,587,164 | 3,519,410 | |||||||||||||||
| Capital lease obligations, including current portion |
13,723,418 | 14,050,450 | 9,784,416 | 6,830,339 | 3,320,163 | |||||||||||||||
| Stockholders’ equity |
20,647,483 | 17,511,523 | 14,377,447 | 13,300,028 | 11,778,516 | |||||||||||||||
| Book value per share |
$ | 2.08 | $ | 1.76 | $ | 1.45 | $ | 1.34 | $ | 1.20 | ||||||||||
| (1) | The “BALANCE SHEET DATA” as of September 30, 2006 was restated in our 2008 Annual Report on Form 10-K. Such restatement and an explanation of the restatement adjustments are described in our 2008 Annual Report on Form 10-K under the caption, “PART II – ITEM 6. – MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS, Restatements and Related Matters. The restatement adjustments as of September 30, 2006 were not audited and, accordingly, such information is deemed to be unaudited data. |
21
Table of Contents
| ITEM 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
The following discussion and analysis provides information that we believe is relevant to an assessment and understanding of our consolidated results of operations and financial condition. This discussion should be read in conjunction with the Consolidated Financial Statements and notes thereto.
Overview
UCI Medical Affiliates, Inc. (“UCI”) is a Delaware corporation incorporated on August 25, 1982. Through our wholly-owned subsidiary, UCI Medical Affiliates of South Carolina, Inc. (“UCI-SC”), we provide nonmedical management and administrative services for a network of 67 freestanding medical centers. With the exception of one center which is located in Knoxville, Tennessee, all of the centers are located in South Carolina. The centers operate under the names of Doctors Care (44 centers), Progressive Physical Therapy (20 centers), Carolina Orthopedic & Sports Medicine (1 center), Luberoff Pediatrics (1 center) and Doctors Wellness Center (1 center).
The centers offer out-patient medical care for treatment of acute, episodic, and some minor chronic medical problems. The centers provide a broad range of medical services that would generally be classified as within the scope of family practice, primary care, and occupational medicine. We also offer pediatric and orthopedic medical services at two of our centers, and physical therapy at our 20 physical therapy centers. Licensed medical providers, nurses, and auxiliary support personnel provide the medical services. The services provided at the centers include, but are not limited to, the following:
| • | Routine care of general medical problems, including colds, flu, ear infections, hypertension, asthma, pneumonia, and other conditions typically treated by primary care providers; |
| • | Treatment of injuries, such as simple fractures, dislocations, sprains, bruises, and cuts; |
| • | Minor surgery, including suturing of lacerations and removal of cysts and foreign bodies; |
| • | Diagnostic tests, such as x-rays, electrocardiograms, complete blood counts, and urinalyses; and, |
| • | Occupational and industrial medical services, including drug testing, workers’ compensation cases, and physical examinations. |
Critical Accounting Policies
Our discussion and analysis of our financial condition and results of operations is based upon our Consolidated Financial Statements included in this Report, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, revenues and expenses, and related disclosure of contingent assets and liabilities. We consider critical accounting policies to be those that require more significant judgments and estimates in the preparation of our financial statements and include the following: (1) revenue recognition; (2) accounts receivable; (3) allowance for doubtful accounts; (4) consideration of impairment of intangible assets; and (5) valuation reserve on net deferred tax assets.
Revenue recognition -
We record revenues at the estimated net amount that we expect to receive from patients, employers, third-party payers, and others at the time we perform the services. The amount of revenue we recognize pursuant to the services we provide is subject to significant judgments and estimates. We have stated billing rates which are billed as gross revenues when services are performed. The amounts we bill are then reduced by our estimate of amounts we do not expect to collect due to discounts (“Contractual Adjustments”) that are taken by third-party payers or otherwise given to patients who pay us directly. We estimate Contractual Adjustments based on the ratio of cash collected in the preceding periods to gross revenues we billed.
22
Table of Contents
Accounts receivable -
Accounts receivable represent the net receivables we expect to collect related to the services we provide. The amount we record as net accounts receivable is subject to significant judgments and estimates. As explained in the above caption, “Revenue recognition,” the amounts we bill and record as accounts receivable are reduced by our estimate of amounts we will not collect due to Contractual Adjustments that are taken by third-party payers or otherwise given to patients who pay us directly. Additionally, as explained below in the caption, “Allowance for doubtful accounts,” our accounts receivable are also reduced by our estimate of losses which may result from the inability of some of our patients or other third-party payers to make required payments.
Allowance for doubtful accounts -
We maintain our allowance for doubtful accounts for estimated losses, which may result from the inability of our patients to make required payments. Most of our allowance for doubtful accounts relate to amounts owed to us by patients who are or become responsible for the payments associated with the services we provided. We base our allowance on the likelihood of recoverability of accounts receivable considering such factors as past experience and current collection trends. Factors taken into consideration in estimating the allowance include: amounts past due, in dispute, or a client that we believe might be having financial difficulties. If economic, industry, or business trends worsen beyond earlier estimates, we increase the allowance for doubtful accounts by recording additional bad debt expense.
Consideration of impairment of intangible assets -
We evaluate the recovery of the carrying amount of excess of cost over fair value of assets acquired, primarily goodwill, by determining if a permanent impairment has occurred. This evaluation is done annually as of September 30th of each year or more frequently if indicators of permanent impairment arise. Indicators of a permanent impairment include, among other things, a significant adverse change in legal factors or the business climate, an adverse action by a regulator, unanticipated competition, loss of key personnel or allocation of goodwill to a portion of the business that is to be sold or otherwise disposed. At such time as impairment is determined, the intangible assets are written off during that period.
Valuation reserve on net deferred tax assets -
We record a valuation allowance to reduce our deferred tax assets to the amount that management considers is more likely than not to be realized. Based upon our current financial position, results from operations, and our forecast of future earnings, we do not believe we currently need a valuation allowance.
Comparison of Fiscal Year Ended September 30, 2010 to Fiscal Year Ended September 30, 2009 and Comparison of Fiscal Year Ended September 30, 2009 to Fiscal Year Ended September 30, 2008
Revenues and Operating Expenses
Our revenues are derived from the medical services we provide to our patients. Amounts we earn as revenues are paid by our patients or collected from third-party payers, including insurance carriers, employers or other third-parties. Our revenues are affected by a number of different factors, including increases or decreases in reimbursement rates from third-party payers, the mix of our patients between the nature of the payment source, competitive factors, the severity of seasonal illnesses, the general economic environment and most importantly, the new centers we open in the current and preceding year.
Operating expenses are those costs that we incur in the direct delivery of our services to patients and include the costs to operate and maintain our medical centers. Such costs include the salaries and benefits associated with our medical providers and other center employees, rent, depreciation, interest expense on our capital leases, medical supplies and other expenses incurred by our medical centers.
23
Table of Contents
The following table sets forth our revenues, operating expenses and operating margin for the three fiscal years ended September 30, 2010.
| For the years ended September 30, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Revenues |
$ | 86,905,329 | $ | 80,350,452 | $ | 77,045,256 | ||||||
| Operating Expenses |
71,574,779 | 63,613,355 | 61,244,515 | |||||||||
| Operating Margin |
$ | 15,330,550 | $ | 16,737,097 | $ | 15,800,741 | ||||||
Comparison of Revenues and Operating Expenses in 2010 to 2009
We recognized revenues of $86,905,329 in fiscal year 2010 compared to revenues of $80,350,452 in fiscal year 2009. The increase in our revenues between our 2010 and 2009 fiscal years of $6,554,877, or 8.16% was the result of two primary factors. First, we opened four new Doctors Care centers during the third and fourth quarters of 2009 which contributed significantly to the increase in revenues for the year ended September 30, 2010. The centers we opened during the third and fourth quarters of 2009 contributed revenues of approximately $4,671,000 in the year ended September 30, 2010 in excess of the revenues those centers contributed in 2009. Revenues related to centers that were opened prior to the third quarter of 2009 increased by approximately $1,743,000 in the year ended September 30, 2010 compared to the revenues of those centers in 2009. Most of the revenue increase associated with those centers was realized in the first quarter of 2010. We believe the revenue increase was primarily due to the severity of the H1N1 flu virus during the first quarter of 2010.
Our operating expenses were $71,574,779 in fiscal year 2010 compared to operating expenses of $63,613,355 in fiscal year 2009, an increase of $7,961,424, or 12.52%. Of the total increase, operating expenses associated with the four new Doctors Care centers we opened in the third and fourth quarter of 2009 increased by approximately $4,585,000 in 2010 compared to the operating expenses of those centers in 2009. In addition, operating expenses associated with centers opened prior to the third quarter of 2009 increased by approximately $3,377,000, of which $3,305,000 related to increased compensation-related cost.
Comparison of Revenues and Operating Expenses in 2009 to 2008
We recognized revenues of $80,350,452 in fiscal year 2009 compared to revenues of $77,045,256 in fiscal year 2008. The increase in our revenues between our 2009 and 2008 fiscal years of approximately $3,305,196, or 4.29% was primarily the result of the revenues contributed by the six centers we opened in 2009 and the revenues of the four centers we opened at various times in 2008. In 2009, centers that were opened in 2009 contributed revenues of approximately $3,327,000 to total revenues. Centers that were opened in 2008 contributed approximately $1,167,000 of revenues in 2009 in excess of the amount of revenues the same centers contributed in 2008. A decrease of approximately $1,189,000 in revenues associated with our other centers was due to two principal factors. First, we closed one Doctors Care center in January of 2009. That center contributed revenues of approximately $600,000 in 2008 in excess of the revenues it contributed in 2009. In addition, the number of patient encounters at centers, including the center that we closed, which were open prior to 2008 decreased by approximately 3.0% during 2009. The decrease in patient encounters was partially offset by slight increases in other variables such as increases in our charges and reimbursement rates. We believe the decrease in patient encounters primarily resulted from the generally poor economic conditions in 2008 which carried over into 2009 and increased competition.
Our operating expenses were $63,613,355 in fiscal year 2009 compared to $61,244,515 in fiscal year 2008. The increase of $2,368,840, or 3.87%, was due primarily to the costs associated with the opening of the new centers in 2009 and the full year effect of the costs associated with the centers opened in 2008. In 2009, operating expenses related to centers that were opened in 2009 were approximately $2,478,000. Operating expenses related to centers that were opened in 2008 were approximately $1,080,000 higher in 2009 than the operating expenses related to the centers in 2008. Operating expenses related to the center we closed in 2009 were approximately $429,000 lower in 2009 than the operating expenses related to the same center in 2008. In addition, depreciation expense which was classified as an operating expense was impacted in 2008 by approximately $600,000 due to a change in estimate. Operating expenses in 2009 were also favorably impacted by reduced bad debt expense in 2009 compared to 2008 of $337,412. This decrease was a result of more aggressive collection efforts and the continued improvements in account management related to the migration to a new billing and receivables management system.
24
Table of Contents
General and Administrative Expenses (G&A)
G&A expenses consist of the costs and expenses to administer and support our medical centers. Such costs include salaries and benefits of corporate employees (administrative, maintenance and billing departments), postage and shipping, professional fees, advertising, banking fees and other costs incidental to operating our corporate office.
The following table sets forth our G&A expenses for the three fiscal years ended September 30, 2010.
| For the years ended September 30, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| General and administrative expenses |
$ | 13,021,060 | $ | 12,472,412 | $ | 14,056,608 | ||||||
Comparison of G&A Expenses in 2010 to 2009
Our G&A expenses were $13,021,060 in fiscal year 2010 compared to $12,472,412 in fiscal year 2009. The increase of $548,648, or 4.40%, was due to several factors. First, compensation related cost increased approximately $566,000. The increase was due to the increase in the payment of nonexecutive bonuses in 2010 compared to 2009 and the addition of several management employees. In addition, depreciation and maintenance and utilities increased by approximately $212,000 and $127,000, respectively, primarily as a result of a full year of occupancy in our new corporate headquarters building. The overall increase in G&A expenses was offset by a reduction in professional fees and misappropriation losses of approximately $334,000 and $102,000, respectively. Such reductions were due to the commencement and conclusion of an investigation of our previous Chief Financial Officer in 2009 as more fully discussed below under the caption, “Recovery of Misappropriation Loss.”
Comparison of G&A Expenses in 2009 to 2008
Our G&A expenses were $12,472,412 in fiscal year 2009 compared to $14,056,608 in fiscal year 2008. The decrease of $1,584,196, or 11.27%, was due to several factors, a significant factor of which was a decrease in advertising expenses of $807,207, in 2009 compared to 2008. In addition, salaries and benefits expenses decreased by $737,617 in 2009 compared to 2008. Most of the decrease related to the effect in 2009 of the termination of approximately twenty employees in the third quarter of 2008. Interest expense decreased by $223,981 and misappropriation losses decreased by $381,118 in 2009 compared to 2008. The decrease in interest expense was due to the reduction in our debt on which we recognized interest expense during 2009. The overall decrease was offset by increases in professional fees of $726,760 in 2009 compared to 2008. The increase in professional fees was related to the investigation of our former CFO, Jerry F. Wells, Jr.
Recovery of Misappropriation Loss
On December 10, 2008, our Audit Committee of the Board of Directors (the “Audit Committee”) commenced an internal investigation (the “Investigation”) of certain accounting irregularities with respect to our internal controls and improper expense reimbursements to Jerry F. Wells, Jr., the Company’s former Executive Vice-President of Finance, Chief Financial Officer, and Secretary. As a result of the Investigation, on February 27, 2009, Mr. Wells executed a Confession of Judgment (the “Judgment”) in our favor in the amount of $2,967,382.
In conjunction with our collection efforts pursuant to the Judgment, we filed claims with two insurance carriers under fidelity bond and employee dishonesty insurance policies. In conjunction with such claims, we received an insurance settlement in the amount of $2,732,840 which was recognized in 2010. The recovery reflects a reduction from the amount of the Judgment for the policy deductible and other adjustments related to amounts we have collected from Mr. Wells and expenses we incurred in conjunction with our collection efforts. In conjunction with the recovery, we assigned our claims against certain third parties to the insurance carrier that paid the recovery. We, however, retained our right to pursue certain claims against our former independent registered public accounting firm which are unrelated to the fraud losses recovered from the insurance carrier. Our initial claim against our former registered independent public accounting firm is approximately $2.1 million; however, we may claim additional damages as they are ascertained. Efforts to collect such losses from our former independent registered public accounting firm have commenced. Even though we intend to vigorously pursue such claim, we can give no assurances that our claim will result in any recovery from our former independent registered public accounting firm.
25
Table of Contents
Further, on February 20, 2009, our Board of Directors passed a resolution declaring a forfeiture of Mr. Wells’ interest in our deferred compensation plan. On February 23, 2009, Mr. Wells signed a voluntary relinquishment of his interest in the deferred compensation plan. We do not deem the forfeiture of Mr. Wells’ interest in the deferred compensation plan as a partial settlement of amounts he owes us under the Judgment. Rather, we deem such amount as a nullity as of the date of the resolution of our Board of Directors because any such interest in the deferred compensation plan had been conditionally credited to Mr. Wells under false pretenses. The amount of the conditional liability associated with the deferred compensation plan at the time of forfeiture was $585,422. In addition, in 2009 we recovered 11,400 shares of our common stock which had been previously issued to Mr. Wells as compensation, the aggregate value of which was $31,350 on the date of recovery. During 2009, we also recovered other miscellaneous items of personal property from Mr. Wells which was valued at $49,900 and collected $110,000 from the sales of other assets in which Mr. Wells had an interest.
Comparison of Income Tax Expenses in 2010 to 2009 and 2009 to 2008
Our income tax expense was $1,906,370 in fiscal year 2010 compared to $1,946,468 in fiscal year 2009 and our effective tax rates were 37.8% and 38.6%, respectively. Our income tax expense was $666,714 in fiscal year 2008 and our effective tax rate was 38.2%. Our effective tax rates vary from the combined enacted federal and state tax rates due to the net effect of nondeductible expenses, offset by certain tax credits we recognized for tax purposes.
Liquidity and Capital Resources
Our primary liquidity and capital requirements are to fund working capital for current operations, including the expansion of our business through opening new centers, and servicing our long-term debt. Typically, the cash requirements associated with the opening of new centers involve the funding of real estate, the purchase of furniture and medical equipment necessary to provide medical services and funding the operations of the new centers until such time as they generate positive cash flows. The primary sources to meet our liquidity and capital requirements are funds generated from operations, a $1,000,000 line of credit with a commercial bank and other term and mortgage loans.
The line of credit bears interest at the commercial bank’s prime interest rate which was 3.25% at September 30, 2010 and is secured by our accounts receivable. At September 30, 2010 and 2009, we had no outstanding borrowings under the line of credit. During 2010, the maximum amount outstanding under the line of credit was $1,000,000, the average amount outstanding was approximately $305,000 and we recognized interest expense of $2,800 related to the line of credit. During 2009, the maximum amount outstanding under the line of credit was $1,000,000, the average amount outstanding was approximately $295,000 and we recognized interest expense of $9,602 related to the line of credit.
In 2008 we secured a mortgage loan commitment and agreement from a commercial bank in the amount of $3,200,000 for the purpose of acquiring and renovating our new corporate headquarters property. Under the terms of the mortgage loan agreement we paid interest only at one-month LIBOR plus 2.5% until the modification date, at which time $2,100,000 of the amount outstanding converted to a permanent mortgage loan. The mortgage loan was modified on November 23, 2009. As explained below, approximately $1,050,000 of the $3,150,000 amount then outstanding was transferred to a term loan. At September 30, 2010, $2,035,635 was outstanding under the mortgage loan agreement. Interest on the permanent mortgage loan will continue to be paid based on one-month LIBOR (0.257% at September 30, 2010) plus 2.5%, and we will pay total monthly payments of $11,407. Any amount outstanding on March 5, 2015 will be due and payable on that date.
At September 30, 2010, we had a term loan outstanding with a commercial bank in the amount of $916,378. The term loan is payable in monthly installments of $76,033 and was originally scheduled for maturity on June 16, 2009. The interest rate on the term loan is the commercial bank’s prime interest rate (3.25% at September 30, 2010) plus 1/2%. Prior to June 2009, the term loan was extended, and it was modified on November 23, 2009. Under the modified terms, $1,050,000 of the amount outstanding under the mortgage loan was added to the outstanding balance of the term loan. After modification, the aggregate balance of the term loan was $1,785,000. The term loan agreement was further modified to extend the maturity date until October 2013.
Additionally, in the fiscal year ending September 30, 2008 we acquired a center in Surfside Beach, SC for $815,000. We financed the acquisition of the center with a mortgage loan in the amount of $695,000, of which $628,605 was outstanding at September 30, 2010. Monthly principal and interest payments are $5,890. Remaining unpaid principal and interest will be due on July 16, 2013.
26
Table of Contents
Long-term debt decreased from $4,545,278 at September 30, 2009 to $3,580,618 at September 30, 2010, due to regular principal pay-downs. Our management believes that for the next 12 months and the foreseeable future thereafter it will be able to continue to fund debt service requirements out of cash generated through operations.
Cash provided by operating activities for the fiscal year ended September 30, 2010 was $7,394,233 compared to $7,654,538 for the fiscal year ended September 30, 2009. Cash provided by operating activities for the fiscal year ended September 30, 2008 was $5,270,143. In each of the three years ended September 30, 2010, cash provided by operations resulted primarily from net income, and was increased by non-cash charges to net income, the primary components of which were the provision for losses on accounts receivable, depreciation and amortization and the provision for deferred income taxes. In aggregate, such non-cash charges increased cash provided by operating activities by $6,505,062, $7,399,971 and $5,944,600 for the years ended September 30, 2010, 2009 and 2008, respectively. Such increase was partially offset by continued growth in our accounts receivable of $1,783,131, $2,811,304, and $2,037,045 for the years ended September 30, 2010, 2009 and 2008, respectively. In the year ended September 30, 2010, activities related to other operating assets and liabilities decreased cash provided by operating activities by $437,882. In the year ended September 30, 2009 and 2008, activities related to other operating assets and liabilities decreased cash provided by operating activities by $262,516 and $258,342, respectively.
Cash used in investing activities for the fiscal year ended September 30, 2010 was $4,271,083 compared to $6,069,188 for the fiscal year ended September 30, 2009. Cash used by investing activities for the fiscal year ended September 30, 2008 was $5,335,089. In each of the three years ended September 30, 2010, a major use of cash in investing activities related to the purchases of property and equipment, a significant amount of which related to the purchase of furniture and medical equipment to outfit the new centers we opened in each of the three years ended September 30, 2010. In 2010, cash used by investing activities included approximately $956,000 related to the acquisition of two properties in which we have opened or will open new Doctors Care centers. Further, in 2010, we invested cash of approximately $801,000 in renovation of those centers and another leased property in which we relocated an existing Doctors Care and Progressive Physical Therapy center. Additionally, as discussed above, in fiscal year 2008, we purchased a medical office and acquired and began renovations of a new corporate office which was completed in 2009. In 2009 and 2008, we expended approximately $2,300,000 and $1,800,000, respectively, of cash resources to acquire and renovate the new corporate office.
Cash used in financing activities for the fiscal year ended September 30, 2010 was $1,291,692 and related to regular principal paydowns on loans and capital lease obligations. Cash provided by financing activities for the fiscal years ended September 30, 2009 and 2008 was $400,157 and $347,172, respectively. In 2009 and 2008, the increase in our financing activities resulted primarily from the financing activities related to the acquisition and renovation of the property for a new corporate office. In addition, in the year ended September 30, 2009, we financed the acquisition of one medical office. Such financing activities were offset by the liquidation in 2008 of amounts outstanding under our line of credit as of September 30, 2007.
At September 30, 2010, we had cash and cash equivalents of $4,586,614 compared to $2,755,156 at September 30, 2009, an increase of $1,831,458. Our working capital was $5,347,998 at September 30, 2010 compared to $3,220,224 at September 30, 2009.
Contractual Obligations
The following table summarizes our contractual obligations, including interest as applicable, as of September 30, 2010:
| Payment Due By Period | ||||||||||||||||||||
| Contractual Obligations |
Total | < 1 Year | 1-3 Years | 3-5 Years | >5 Years | |||||||||||||||
| Long-term Debt |
$ | 3,947,503 | $ | 1,119,960 | $ | 948,963 | $ | 1,878,580 | $ | — | ||||||||||
| Capital Leases |
28,664,465 | 1,682,252 | 3,364,504 | 3,364,504 | 20,253,205 | |||||||||||||||
| Operating Leases |
28,295,387 | 3,607,183 | 6,170,733 | 4,679,431 | 13,838,040 | |||||||||||||||
Please refer to Footnotes 4 and 6 to our Consolidated Financial Statements included in this report.
We are also subject to purchase obligations related to the construction of a new center in Newberry, SC. Under the terms of the contracts we expect to incur approximately $1,100,000 of costs within the next twelve months.
27
Table of Contents
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
We are exposed to changes in interest rates primarily as a result of our borrowing activities, which includes credit facilities with financial institutions used to maintain liquidity and fund our business operations, as well as notes payable to various third parties in connection with certain acquisitions of property and equipment. The nature and amount of our debt may vary as a result of future business requirements, market conditions and other factors. The definitive extent of our interest rate risk is not quantifiable or predictable because of the variability of future interest rates and business financing requirements. We do not currently use derivative instruments to adjust our interest rate risk profile.
Approximately $628,000 of our debt at September 30, 2010 was subject to fixed interest rates. Approximately $2,953,000 of our debt at September 30, 2010 was subject to variable interest rates. Based on the outstanding amounts of variable rate debt at September 30, 2010, our interest expense on an annualized basis would increase approximately $30,000 for each increase of one percent in the prime rate.
We also have exposure to increases in the consumer price index associated with certain operating and capital leases we have entered, all of which relate to our leased real estate. At September 30, 2010, we had $3,833,738 in aggregate annual lease payments that are subject to increases based on future changes in the consumer price index. Typically, the lease agreements stipulate that the lease payments will increase every three years based on the aggregate increase in the consumer price index over the preceding three years. Of the aggregate annual lease payments subject to change based on the consumer price index, annual payments subject to change in 2011, 2012 and 2013 are $2,240,901, $946,769 and $646,068, respectively.
We do not utilize financial instruments for trading or other speculative purposes, nor do we utilize leveraged financial instruments.
28
Table of Contents
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Schedule II, Valuation and Qualifying Accounts, is omitted because the information is included in the consolidated financial statements and notes.
29
Table of Contents
Report of Independent Registered Accounting Firm
To the Board of Directors and Stockholders
UCI Medical Affiliates, Inc.
Columbia, South Carolina
We have audited the accompanying consolidated balance sheets of UCI Medical Affiliates, Inc. as of September 30, 2010 and 2009, and the related consolidated statements of income, changes in stockholders' equity, and cash flows for each of the three years in the period ended September 30, 2010. These consolidated financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform an audit of its internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall consolidated financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of UCI Medical Affiliates, Inc. as of September 30, 2010 and 2009, and the results of their operations and their cash flows for each of the three years in the period ended September 30, 2010, in conformity with U.S. generally accepted accounting principles.
| /s/ ELLIOTT DAVIS, LLC |
| Columbia, South Carolina |
| December 28, 2010 |
SIGNED ORIGINAL ON ELLIOTT DAVIS, LLC LETTERHEAD
IS ON FILE IN THE CORPORATE OFFICE OF
UCI MEDICAL AFFILIATES, INC.
30
Table of Contents
Consolidated Balance Sheets
September 30, 2010 and 2009
| 2010 | 2009 | |||||||
| Assets |
||||||||
| Current Assets |
||||||||
| Cash |
$ | 4,586,614 | $ | 2,755,156 | ||||
| Certificates of deposit |
755,990 | — | ||||||
| Accounts receivable, net of allowance for doubtful accounts of $1,375,856 and $1,547,367 |
5,810,442 | 6,648,194 | ||||||
| Inventory |
1,066,555 | 1,196,903 | ||||||
| Income taxes receivable |
187,346 | 411,948 | ||||||
| Deferred taxes |
910,568 | 1,374,385 | ||||||
| Prepaid expenses and other current assets |
331,356 | 434,613 | ||||||
| Total current assets |
13,648,871 | 12,821,199 | ||||||
| Property and equipment, less accumulated depreciation of $16,424,672 and $15,959,380 |
14,747,283 | 14,203,029 | ||||||
| Leased property under capital leases, less accumulated amortization of $2,736,632 and $1,911,931 |
12,448,271 | 13,279,797 | ||||||
| Deferred taxes |
94,634 | 114,805 | ||||||
| Restricted investments |
2,172,840 | 1,765,294 | ||||||
| Goodwill, less accumulated amortization of $2,493,255 |
3,350,501 | 3,350,501 | ||||||
| Other assets |
590,085 | 382,733 | ||||||
| Total Assets |
$ | 47,052,485 | $ | 45,917,358 | ||||
| Liabilities and Stockholders’ Equity |
||||||||
| Current liabilities |
||||||||
| Current portion of long-term debt |
$ | 995,042 | $ | 924,839 | ||||
| Obligations under capital leases |
329,841 | 327,031 | ||||||
| Accounts payable |
566,667 | 865,119 | ||||||
| Payable to patients and insurance carriers |
1,586,050 | 1,927,039 | ||||||
| Accrued salaries and payroll taxes |
3,019,380 | 3,736,387 | ||||||
| Accrued compensated absences |
638,026 | 618,025 | ||||||
| Other accrued liabilities |
1,165,867 | 1,202,535 | ||||||
| Total current liabilities |
8,300,873 | 9,600,975 | ||||||
| Long-term liabilities |
||||||||
| Deferred compensation liability |
2,124,976 | 1,461,002 | ||||||
| Long-term debt, net of current portion |
2,585,576 | 3,620,439 | ||||||
| Obligations under capital leases |
13,393,577 | 13,723,419 | ||||||
| Total long-term liabilities |
18,104,129 | 18,804,860 | ||||||
| Total Liabilities |
26,405,002 | 28,405,835 | ||||||
| Commitments and contingencies (Note 10) |
— | — | ||||||
| Stockholders’ Equity |
||||||||
| Preferred stock, par value $.01 per share: Authorized shares - 10,000,000; none issued |
— | — | ||||||
| Common stock, par value $.05 per share: Authorized shares - 50,000,000; issued - 9,945,472 shares; outstanding - 9,934,072 shares |
497,274 | 497,274 | ||||||
| Treasury stock - 11,400 shares |
(31,350 | ) | (31,350 | ) | ||||
| Paid-in capital |
22,173,993 | 22,173,993 | ||||||
| Accumulated deficit |
(1,992,434 | ) | (5,128,394 | ) | ||||
| Total Stockholders’ Equity |
20,647,483 | 17,511,523 | ||||||
| Total Liabilities and Stockholders’ Equity |
$ | 47,052,485 | $ | 45,917,358 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
31
Table of Contents
Consolidated Statements of Income
Years ended September 30, 2010, 2009 and 2008
| 2010 | 2009 | 2008 | ||||||||||
| Revenues |
$ | 86,905,329 | $ | 80,350,452 | $ | 77,045,256 | ||||||
| Operating expenses |
71,574,779 | 63,613,355 | 61,244,515 | |||||||||
| Operating margin |
15,330,550 | 16,737,097 | 15,800,741 | |||||||||
| General and administrative expenses |
13,021,060 | 12,472,412 | 14,056,608 | |||||||||
| Income from operations |
2,309,490 | 4,264,685 | 1,744,133 | |||||||||
| Recovery of misappropriation loss |
2,732,840 | 776,672 | — | |||||||||
| Income before income taxes |
5,042,330 | 5,041,357 | 1,744,133 | |||||||||
| Income tax expense |
1,906,370 | 1,946,468 | 666,714 | |||||||||
| Net income |
$ | 3,135,960 | $ | 3,094,889 | $ | 1,077,419 | ||||||
| Basic earnings per share |
$ | 0.32 | $ | 0.31 | $ | 0.11 | ||||||
| Basic weighted average common shares outstanding |
9,934,072 | 9,941,544 | 9,914,122 | |||||||||
| Diluted earnings per share |
$ | 0.32 | $ | 0.31 | $ | 0.11 | ||||||
| Diluted weighted average common shares outstanding |
9,934,072 | 9,941,544 | 9,914,122 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
32
Table of Contents
Consolidated Statements of Changes in Stockholders’ Equity
Years ended September 30, 2010, 2009 and 2008
| Common Stock | Paid-in | Treasury | Accumulated | Total Stockholders’ |
||||||||||||||||||||
| Shares | Amount | Capital | Stock | Deficit | Equity | |||||||||||||||||||
| Balance at September 30, 2007 |
9,914,122 | $ | 495,706 | $ | 22,105,024 | $ | — | $ | (9,300,702 | ) | $ | 13,300,028 | ||||||||||||
| Net income |
— | — | — | — | 1,077,419 | 1,077,419 | ||||||||||||||||||
| Balance at September 30, 2008 |
9,914,122 | 495,706 | 22,105,024 | — | (8,223,283 | ) | 14,377,447 | |||||||||||||||||
| Net income |
— | — | — | — | 3,094,889 | 3,094,889 | ||||||||||||||||||
| Common stock issued for compensation |
31,350 | 1,568 | 68,969 | — | — | 70,537 | ||||||||||||||||||
| Recovery of common stock issued for compensation |
— | — | — | (31,350 | ) | — | (31,350 | ) | ||||||||||||||||
| Balance at September 30, 2009 |
9,945,472 | 497,274 | 22,173,993 | (31,350 | ) | (5,128,394 | ) | 17,511,523 | ||||||||||||||||
| Net income |
— | — | — | — | 3,135,960 | 3,135,960 | ||||||||||||||||||
| Balance at September 30, 2010 |
9,945,472 | $ | 497,274 | $ | 22,173,993 | $ | (31,350 | ) | $ | (1,992,434 | ) | $ | 20,647,483 | |||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
33
Table of Contents
Consolidated Statements of Cash Flows
Years ended September 30, 2010, 2009 and 2008
| 2010 | 2009 | 2008 | ||||||||||
| Operating activities: |
||||||||||||
| Net income |
$ | 3,135,960 | $ | 3,094,889 | $ | 1,077,419 | ||||||
| Adjustments to reconcile net income to net cash provided by operating activities: |
||||||||||||
| Provision for losses on accounts receivable |
2,620,883 | 2,349,485 | 2,686,897 | |||||||||
| Depreciation and amortization |
3,213,243 | 3,104,017 | 3,024,853 | |||||||||
| Loss (gain) on disposal of property and equipment |
74,605 | (400 | ) | 59,756 | ||||||||
| Deferred taxes |
483,988 | 1,946,469 | 232,850 | |||||||||
| Unrealized (gain) loss on restricted and other investments |
(100,381 | ) | 265,248 | 483,755 | ||||||||
| Recovery of common stock issued for compensation |
— | (31,350 | ) | — | ||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Accounts receivable |
(1,783,131 | ) | (2,811,304 | ) | (2,037,045 | ) | ||||||
| Inventory |
130,348 | (241,011 | ) | 1,677 | ||||||||
| Income taxes receivable |
224,602 | (225,000 | ) | 771,152 | ||||||||
| Prepaid expenses and other current assets |
103,257 | (53,910 | ) | 123,756 | ||||||||
| Accounts payable and accrued expenses |
(1,373,115 | ) | 816,887 | (1,106,975 | ) | |||||||
| Deferred compensation |
663,974 | (559,482 | ) | (47,952 | ) | |||||||
| Cash provided by operating activities |
7,394,233 | 7,654,538 | 5,270,143 | |||||||||
| Investing activities: |
||||||||||||
| Purchases of property and equipment |
(3,000,576 | ) | (5,619,190 | ) | (4,891,279 | ) | ||||||
| Proceeds from sale of property |
— | 400 | — | |||||||||
| Increase in other assets |
(168,786 | ) | (59,049 | ) | (9,999 | ) | ||||||
| Purchase of certificates of deposit |
(755,990 | ) | — | — | ||||||||
| Purchase of restricted investments |
(345,731 | ) | (391,349 | ) | (433,811 | ) | ||||||
| Cash used in investing activities |
(4,271,083 | ) | (6,069,188 | ) | (5,335,089 | ) | ||||||
| Financing activities: |
||||||||||||
| Net payments on line of credit |
— | — | (415,888 | ) | ||||||||
| Proceeds from borrowings on loans |
— | 1,750,070 | 2,095,487 | |||||||||
| Principal payments on loans |
(964,660 | ) | (958,931 | ) | (928,512 | ) | ||||||
| Principal payments on capital lease obligations |
(327,032 | ) | (390,982 | ) | (307,404 | ) | ||||||
| Payments on other long-term obligations |
— | — | (96,511 | ) | ||||||||
| Cash provided by (used in) financing activities |
(1,291,692 | ) | 400,157 | 347,172 | ||||||||
| Increase in cash and cash equivalents |
1,831,458 | 1,985,507 | 282,226 | |||||||||
| Cash and cash equivalents at beginning of year |
2,755,156 | 769,649 | 487,423 | |||||||||
| Cash and cash equivalents at end of year |
$ | 4,586,614 | $ | 2,755,156 | $ | 769,649 | ||||||
| Supplemental cash flow information: |
||||||||||||
| Cash paid during the year for: |
||||||||||||
| Interest |
$ | 1,534,411 | $ | 1,319,279 | $ | 1,241,691 | ||||||
| Income taxes |
$ | 1,422,778 | $ | 225,000 | $ | 412,000 | ||||||
| Supplemental disclosure of non-cash investing and financing activities: |
||||||||||||
| Capital lease obligations incurred |
$ | — | $ | 4,657,016 | $ | 3,261,481 | ||||||
| Issuance of common stock for compensation |
$ | — | $ | 70,537 | $ | — | ||||||
| Transfer of restricted investments to other assets |
$ | — | $ | 266,950 | $ | — | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
34
Table of Contents
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
NOTE 1. DESCRIPTION OF COMPANY AND SIGNIFICANT ACCOUNTING POLICIES
Description of Company
UCI Medical Affiliates, Inc. (“UCI”) is a Delaware corporation incorporated on August 25, 1982. Operating through its wholly-owned subsidiary, UCI Medical Affiliates of South Carolina, Inc. (“UCI-SC”), UCI provides nonmedical management and administrative services for a network of 67 freestanding medical centers, 66 of which are located throughout South Carolina and one is located in Knoxville, Tennessee (43 operating as Doctors Care in South Carolina, one as Doctors Care in Knoxville, Tennessee, 20 as Progressive Physical Therapy Services in South Carolina, one as Luberoff Pediatrics in South Carolina, one as Carolina Orthopedic & Sports Medicine in South Carolina and one as Doctors Wellness Center in South Carolina).
Basis of Preparation
The Company’s consolidated financial statements have been prepared in conformity with accounting principles generally accepted in the United States of America.
Principles of Consolidation
The consolidated financial statements include the accounts of UCI, UCI-SC, UCI Properties, LLC (“UCI-LLC”), Doctors Care, P.A., Progressive Physical Therapy, P.A. (“PPT”), Carolina Orthopedic & Sports Medicine, P.A. (“COSM”), and Doctors Care of Tennessee, P.C. (the four together as the “P.A.” and together with UCI, UCI-SC and UCI-LLC, the “Company”). Because of the corporate practice of medicine laws in the states in which the Company operates, the Company does not own medical practices but instead enters into exclusive long-term management and administrative services agreements with the P.A.s that operate the medical practices. UCI-SC, in its sole discretion, can effect a change in the nominee shareholder of each of the P.A.s at any time for a payment of $100 from the new nominee shareholder to the old nominee shareholder, with no limits placed on the identity of any new nominee shareholder and no adverse impact resulting to UCI-SC or the P.A. from such change. Because of the agreements between UCI-SC and the P.A.s, and the rights held by UCI-SC under those agreements, the financial statements of the P.A.s are consolidated with UCI, UCI-SC and UCI-LLC, in accordance with accounting principles generally accepted in the United States of America. All significant intercompany accounts and transactions are eliminated in consolidation, including management fees.
Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make certain estimates and assumptions that affect the reported amounts of assets and liabilities and disclosures of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. The most significant estimates are related to the allowance for doubtful accounts, goodwill and intangible assets, income taxes, depreciation and amortization, contingencies, and revenue recognition. The Company bases its estimates on historical experience and on various other assumptions that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates in the near term.
Cash and Cash Equivalents
The Company considers all short-term deposits with a maturity of three months or less at their acquisition date to be cash equivalents. At September 30, 2010, the Company had cash deposits in excess of federally insured limits in the approximate amount of $5,192,754.
35
Table of Contents
Accounts Receivable
Accounts receivable, which are recognized at estimated net contracted amounts, are primarily amounts due from patients and amounts due under fee-for-service contracts from third-party payers, such as insurance companies, self-insured employers and government-sponsored healthcare programs. Concentration of credit risk related to accounts receivable is limited by number, diversity and the state-wide geographic dispersion of the business units managed by the Company, as well as by the large number of patients and payers, including the various governmental agencies in the state. The accounts receivable balances serve as collateral for certain of the Company’s financing arrangements.
Allowance for Doubtful Accounts
The Company maintains an allowance for doubtful accounts for estimated losses, which may result from the inability of patients or third-party payers to make required payments. The allowance is based on the likelihood of recoverability of accounts receivable considering such factors as past experience and current collection trends. Factors taken into consideration in estimating the allowance include: amounts past due, charge-off trends and amounts in dispute. If economic, industry, or specific customer business trends worsen beyond estimates, the allowance for doubtful accounts is increased by recording additional bad debt expense.
Inventory
The Company’s inventory consists of medical supplies and drugs and both are carried at the lower of average cost or market. The volume of supplies carried at a center varies very little from month to month; therefore, management performs only an annual physical inventory count and does not maintain a perpetual inventory system.
Property and Equipment
Property and equipment is recorded at cost. Depreciation is provided principally by the straight-line method over the estimated useful lives of the assets, ranging from five to forty years.
Maintenance, repairs and minor renewals are charged to expense. Major renewals or betterments, which prolong the life of the assets, are capitalized.
Upon disposal of depreciable property, the asset accounts are reduced by the related cost and accumulated depreciation. The resulting gains and losses are reflected in the consolidated statements of income.
Long-Lived Asset Impairment
The Company periodically evaluates its long-lived assets for impairment. An impairment of a long-lived asset exists when the carrying value of an asset exceeds its fair value and when the carrying value is not recoverable through future operations. The carrying values of long-lived assets are reviewed for impairment when events or changes in circumstances indicate that the carrying amount of assets may not be recoverable. For the three years ended September 30, 2010, the Company recognized no material impairment losses related to long-lived assets.
Goodwill
Goodwill represents the excess of cost over the fair value of assets acquired. Goodwill and intangible assets with indefinite lives are assessed for impairment at least annually using a fair-value-based approach. For the three years ended September 30, 2010, the Company recognized no material impairment losses related to goodwill.
Fair Value of Financial Instruments
The estimated fair value of financial instruments has been determined by the Company using available market information and appropriate valuation methodologies. Available market information includes current market rates and instruments with the same or similar risk and maturities. Judgment is required in interpreting data to develop the estimates of fair value. Accordingly, management’s estimates are not necessarily indicative of the amounts that the Company could realize in a current market exchange. Management’s fair value estimates are based on pertinent information available to management as of September 30, 2010 and 2009. The Company’s financial instruments consist mainly of cash, certificates of deposit, accounts receivable, restricted and other investments, notes payable, lines of credit, all accounts payable, the deferred compensation liability and capital lease obligations. The Company’s capital lease obligations are reported at the net present
36
Table of Contents
value of future minimum lease payments based on rates of interest implicit in the lease at the lease inception and are not reported at fair value in the accompanying financial statements. The Company’s restricted and other investments consist of Company owned life insurance policies that are reported at the cash surrender value of the policies as of the reporting date. The Company’s deferred compensation liability is reported at the balances accrued to participants, based on their participation and elections under the plan, as of the reporting date. The carrying amounts of the Company’s cash, certificates of deposit, accounts receivable, and all accounts payable approximate fair value due to the short-term nature of these instruments. At September 30, 2010 and 2009, the carrying value of the Company’s loans payable approximate fair value based on the terms of the obligations.
Restricted Investments
Restricted investments represent Company-owned life insurance policies used to fund the Company’s deferred compensation liability. Changes in cash surrender value are recorded in the Company’s statement of income.
Revenue Recognition
Revenue is recognized at estimated net contracted amounts to be received from patients, employers, third-party payers, and others at the time the related services are rendered. The Company records an estimate for contractual adjustments at the time bills are generated for services rendered.
Concentration of Credit Risk
In the normal course of providing healthcare services, the Company extends credit to patients without requiring collateral. The Company assesses its ability to collect balances due and allowances are established to provide for management’s estimate of uncollectible balances. Approximately 18% of the Company’s year end accounts receivable balance is due from Blue Cross and Blue Shield of South Carolina and its subsidiaries (“BCBS”). No other single payer represents more than 5% of the year end balance. Future revenues of the Company are largely dependent on third-party payers and private insurance companies.
Revenues generated from billings to a major third-party payer, BCBS, totaled approximately 38%, 40% and 40% of the Company’s total revenues for fiscal years 2010, 2009 and 2008, respectively. BCBS owns approximately 68% of the Company’s common stock. Revenues generated from billings to state worker’s compensation plans totaled approximately 11%, 11% and 12% of the Company’s total revenues for the fiscal years 2010, 2009 and 2008, respectively.
Stock Based Compensation
The Company recognizes compensation costs related to share-based payment transactions ratably in its financial statements over the period that an employee provides service in exchange for the award. The Company applies the modified prospective method to account for its share-based payments. Under the modified prospective method, companies are allowed to record compensation cost for new and modified awards over the related vesting period of such awards prospectively and record compensation cost prospectively on the nonvested portion, at the date of adoption, of previously issued and outstanding awards over the remaining vesting period of such awards. No change to prior periods presented is permitted under the modified prospective method. At September 30, 2010 and 2009, the Company had no nonvested stock options outstanding in any of its plans.
The fair value at the date of grant of the stock option is estimated using the Black-Scholes option-pricing model. The dividend yield is based on estimated future dividend yields. The risk-free rate for periods within the contractual term of the share option is based on the U.S. Treasury yield curve in effect at the time of grant. Expected volatilities are generally based on the historical volatility of the Company’s stock. The expected term of share options granted is generally derived from historical experience. Compensation expense is recognized on a straight-line basis over the stock option vesting period.
Income Taxes
Deferred tax assets and liabilities are recorded based on the difference between the financial statement and tax bases of assets and liabilities as measured by the enacted tax rates which are anticipated to be in effect when these differences reverse. The deferred tax provision is the result of the net change in the deferred tax assets to amounts expected to be realized. Valuation allowances are provided against deferred tax assets when the Company determines it is more likely than not that the deferred tax asset will not be realized. The tax returns for the eight fiscal years ending September 30, 2010 are open for examination.
37
Table of Contents
When tax returns are filed, it is highly certain that some positions taken would be sustained upon examination by the taxing authorities, while others are subject to uncertainty about the merits of the position taken or the amount of the position that would be ultimately sustained. The benefit of a tax position is recognized in the financial statements in the period during which, based on all available evidence, management believes it is more likely than not that the position will be sustained upon examination, including the resolution of appeals or litigation processes, if any. Tax positions taken are not offset or aggregated with other positions. Tax positions that meet the more-likely-than-not recognition threshold are measured as the largest amount of tax benefit that is more than 50% likely of being realized upon settlement with the applicable taxing authority. The portion of the benefits associated with tax positions taken that exceeds the amount measured as described above is reflected as a liability for unrecognized tax benefits in the accompanying balance sheet along with any associated interest and penalties that would be payable to the taxing authorities upon examination. Management is not aware of any material uncertain tax positions and no liability has been recognized at September 30, 2010. Interest and penalties associated with unrecognized tax benefits are classified as additional income taxes in the statement of income as they occur.
Leases
The Company leases office locations and various equipment under non-cancellable operating and capital leases. The Company performs an evaluation of each lease agreement at the lease inception date and at any lease modification date to determine if the leases, based on their terms, are operating leases or capital leases as defined under accounting principles generally accepted in the United States of America. Capital leases are recognized as an obligation in the Company’s financial statements at the net present value of future minimum lease payments. A corresponding asset is also recognized and depreciated over the lease term.
Advertising Costs
Advertising and marketing costs are expensed as incurred.
Earnings Per Share
Basic earnings per share are calculated by dividing income available to common shareholders by the weighted-average number of shares outstanding for each period. Diluted earnings per common share are calculated by adjusting the weighted-average shares outstanding assuming conversion of all potentially dilutive stock options.
Segment Information
The Company has a number of operating segments as defined in accounting principles generally accepted in the United States of America. All the Company’s operating segments are aggregated into one reportable segment. In its determination of aggregating its operating segments into one reportable segment management considered the following factors: the consistency of the services (direct to patient medical services) provided to its patients; the consistent manner in which its services are delivered to its patients; the similarity in which the Company is reimbursed for its services; the relative close geographic proximity of the operating segments; and, the comparable regulatory environment in which its operating segments operate.
New Accounting Pronouncements
In February 2010, the FASB issued ASU No. 2010-09, Subsequent Events (ASC Topic 855) Amendments to Certain Recognition and Disclosure Requirements. The amendments in this ASU requires an entity that is an SEC filer to evaluate subsequent events through the date that the financial statements are issued and removes the requirement for an SEC filer to disclose a date, in both issued and revised financial statements, through which the filer had evaluated subsequent events. The adoption did not have a material effect on the Company’s financial statements.
Other accounting standards that have been issued or proposed by the FASB or other standards-setting bodies are not expected to have a material impact on the Company’s financial position, results of operations or cash flows.
Reclassifications
Certain amounts in the prior period financial statements have been reclassified to conform to the current period presentation.
38
Table of Contents
NOTE 2. ALLOWANCE FOR DOUBTFUL ACCOUNTS
The changes in the allowance for doubtful accounts for the fiscal years ending September 30, 2010, 2009 and 2008 are as follows:
| Fiscal Year | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Balance at beginning of year |
$ | 1,547,367 | $ | 2,872,120 | $ | 2,267,794 | ||||||
| Additions |
2,620,883 | 2,349,485 | 4,549,479 | |||||||||
| Write-offs, net of recoveries |
(2,792,394 | ) | (3,674,238 | ) | (3,945,153 | ) | ||||||
| Balance at end of year |
$ | 1,375,856 | $ | 1,547,367 | $ | 2,872,120 | ||||||
NOTE 3. PROPERTY AND EQUIPMENT
Property and equipment consists of the following at September 30:
| Useful Life | 2010 | 2009 | ||||||||||||||||
| Range |
Cost | Accumulated Depreciation |
Cost | Accumulated Depreciation |
||||||||||||||
| Land |
N/A | $ | 461,098 | $ | — | $ | 461,098 | $ | — | |||||||||
| Building |
5 - 40 | 3,812,533 | 172,530 | 3,801,065 | 58,745 | |||||||||||||
| Leasehold Improvements |
5 - 15 | 7,189,734 | 3,984,202 | 7,007,873 | 3,904,282 | |||||||||||||
| Construction In Progress |
N/A | 1,254,294 | — | — | — | |||||||||||||
| Furniture & Fixtures |
5 - 10 | 3,856,360 | 2,916,724 | 4,246,250 | 2,930,983 | |||||||||||||
| EDP – Companion |
5 | 1,294,958 | 1,294,958 | 1,175,676 | 1,175,676 | |||||||||||||
| EDP – Other |
5 - 10 | 4,279,398 | 2,539,496 | 3,789,837 | 1,992,152 | |||||||||||||
| Medical Equipment |
5 - 10 | 6,610,907 | 3,638,756 | 7,021,126 | 3,982,499 | |||||||||||||
| Other Equipment |
5 - 10 | 2,299,834 | 1,794,623 | 2,545,700 | 1,842,360 | |||||||||||||
| Autos |
5 - 10 | 112,839 | 83,383 | 113,784 | 72,683 | |||||||||||||
| Totals |
$ | 31,171,955 | $ | 16,424,672 | $ | 30,162,409 | $ | 15,959,380 | ||||||||||
At September 30, 2010, property and equipment included $1,254,294 of construction in progress assets that had not yet been placed in service, and therefore had no related depreciation. These assets include the land, building and related costs for the new Doctors Care offices that are undergoing renovations. Management plans to place these assets into service during fiscal year 2011.
Depreciation expense totaled $2,381,717, $2,351,305, and $2,429,705 for the years ended September 30, 2010, 2009 and 2008, respectively. Based on historical data, the Company re-evaluated the salvage values of the property and equipment during fiscal year 2008. As a result of this review, the Company reduced the salvage values to zero and recognized additional depreciation expense of $941,236 for fiscal year 2008.
39
Table of Contents
NOTE 4. CAPITAL AND OPERATING LEASES
Capital Leases
The following is an analysis of the leased property under capital leases by major classes at September 30:
| Classes of property: |
2010 | 2009 | ||||||
| Buildings |
$ | 14,557,363 | $ | 14,557,363 | ||||
| Medical Equipment |
111,943 | 118,768 | ||||||
| EDP - Other |
515,597 | 515,597 | ||||||
| 15,184,903 | 15,191,728 | |||||||
| Less: Accumulated Amortization |
(2,736,632 | ) | (1,911,931 | ) | ||||
| $ | 12,448,271 | $ | 13,279,797 | |||||
Amortization expense on capital leases totaled $831,526, $711,271 and $595,148 for the years ended September 30, 2010, 2009 and 2008, respectively. Contingent lease payment increases under capital leases totaled $60,575, $27,215 and $8,995 for the years ended September 30, 2010, 2009 and 2008 respectively.
The following is a schedule by years of future minimum lease payments under capital leases together with the present value of the net minimum lease payments as of September 30, 2010:
| Year ending September 30: |
||||
| 2011 |
$ | 1,682,252 | ||
| 2012 |
1,682,252 | |||
| 2013 |
1,682,252 | |||
| 2014 |
1,682,252 | |||
| 2015 |
1,682,252 | |||
| Thereafter |
20,253,205 | |||
| Total minimum lease payments |
28,664,465 | |||
| Less: Amount representing interest |
(14,941,047 | ) | ||
| Present value of net minimum lease payments |
$ | 13,723,418 | ||
Operating Leases
UCI-SC leases office and medical center space under various operating lease agreements. Certain operating leases provide for escalation payments, exclusive of renewal options.
Future minimum lease payments under noncancellable operating leases with a remaining term in excess of one year as of September 30, 2010 are as follows:
| Year ending September 30: |
||||
| 2011 |
3,607,183 | |||
| 2012 |
3,262,197 | |||
| 2013 |
2,908,536 | |||
| 2014 |
2,435,146 | |||
| 2015 |
2,244,285 | |||
| Thereafter |
13,838,040 | |||
| Total minimum lease payments |
$ | 28,295,387 | ||
Total rental expense under operating leases for fiscal years 2010, 2009 and 2008 was $3,700,420, $3,587,318, and $3,585,090, respectively.
40
Table of Contents
NOTE 5. INCOME TAXES
The components of the provision for income taxes for the years ended September 30 are as follows:
| 2010 | 2009 | 2008 | ||||||||||
| Current: |
||||||||||||
| Federal |
$ | 1,231,689 | $ | — | $ | 359,766 | ||||||
| State |
190,693 | — | 74,098 | |||||||||
| 1,422,382 | — | 433,864 | ||||||||||
| Deferred: |
||||||||||||
| Federal |
496,548 | 1,692,031 | 213,065 | |||||||||
| State |
(12,560 | ) | 254,437 | 19,785 | ||||||||
| 483,988 | 1,946,468 | 232,850 | ||||||||||
| Total income tax provision |
$ | 1,906,370 | $ | 1,946,468 | $ | 666,714 | ||||||
Deferred taxes result from temporary differences in the recognition of certain items of income and expense, and the changes in the valuation allowance attributable to deferred tax assets.
At September 30, 2010, 2009 and 2008, the Company’s deferred tax assets (liabilities) are as follows:
| 2010 | 2009 | 2008 | ||||||||||
| Accounts receivable |
$ | 526,235 | $ | 591,870 | $ | 2,860,145 | ||||||
| Operating loss carryforwards |
— | 256,012 | — | |||||||||
| Property and equipment |
17,732 | 454,727 | 207,833 | |||||||||
| Goodwill |
(576,796 | ) | (552,197 | ) | (483,700 | ) | ||||||
| Accruals |
971,154 | 568,453 | 719,189 | |||||||||
| Other |
66,877 | 170,325 | 132,192 | |||||||||
| $ | 1,005,202 | $ | 1,489,190 | $ | 3,435,659 | |||||||
The principal reasons for the differences between the consolidated income tax (benefit) expense and the amount computed by applying the statutory federal income tax rate of 35% to pre-tax income were as follows for the years ended September 30:
| 2010 | 2009 | 2008 | ||||||||||
| Tax at federal statutory rate |
$ | 1,764,816 | $ | 1,764,475 | $ | 610,447 | ||||||
| Effect on rate of: |
||||||||||||
| Nondeductible expenses |
15,531 | 11,626 | 25,218 | |||||||||
| State income tax |
117,568 | 167,928 | 56,330 | |||||||||
| Other |
8,455 | 2,439 | (25,281 | ) | ||||||||
| $ | 1,906,370 | $ | 1,946,468 | $ | 666,714 | |||||||
The Company has analyzed the tax positions taken or expected to be taken in its federal, state and local tax filings and has concluded that it has no material liability related to uncertain tax positions.
NOTE 6. FINANCING ARRANGEMENTS
The Company maintains a line of credit of $1,000,000 with a commercial bank. At September 30, 2010 and 2009, there were no outstanding borrowings under the line of credit. During 2010 and 2009, the average amounts outstanding under the line of credit were $305,000 and $295,000, respectively, and the maximum amount outstanding for each year was $1,000,000. Interest expense was $2,800 and $9,602 in 2010 and 2009, respectively. The line of credit bears interest at the commercial bank’s prime rate, which was 3.25% at September 30, 2010. Borrowings are collateralized by the Company’s accounts receivable and the maturity date of the line of credit is May 5, 2012.
In 2008 the Company secured a mortgage loan commitment and agreement from a commercial bank in the amount of $3,200,000 for the purpose of acquiring and renovating a new corporate headquarters property. Under the terms of the mortgage loan agreement the
41
Table of Contents
Company paid interest only at one-month LIBOR plus 2.5% until the modification date, at which time $2,100,000 of the amount outstanding converted to a permanent mortgage loan. The mortgage loan was modified on November 23, 2009. As explained below, approximately $1,050,000 of the $3,150,000 amount then outstanding was transferred to a term loan. At September 30, 2010, $2,035,635 was outstanding under the mortgage loan agreement. Interest on the permanent mortgage loan will continue to be paid based on one-month LIBOR (0.257% at September 30, 2010) plus 2.5%, and the Company will pay total monthly payments of $11,407. Any amount outstanding on March 5, 2015 will be due and payable on that date.
At September 30, 2010, the Company had a term loan outstanding with a commercial bank in the amount of $916,378. The term loan is payable in monthly installments of $76,033 and was originally scheduled for maturity on June 16, 2009. The interest rate on the term loan is the commercial bank’s prime interest rate (3.25% at September 30, 2010) plus 1/2%. Prior to June 2009, the term loan was extended, and it was modified on November 23, 2009. Under the modified terms, $1,050,000 of the amount outstanding under the mortgage loan was added to the outstanding balance of the term loan. After modification, the aggregate balance of the term loan was $1,785,000. The term loan agreement was further modified to extend the maturity date until October 2013.
On July 17, 2008, the Company purchased a Doctors Care building for a total purchase price of $815,000. This property was previously rented by the Company and occupied as a medical center. A portion of the purchase price was funded by a promissory note in the original principal amount of $695,000, and is collateralized by a lien on the property. At September 30, 2010, the outstanding balance on the mortgage loan was $628,605. The promissory note accrues interest at a rate of 5.95 percent per annum. Monthly principal and interest payments are $5,890. Remaining unpaid principal and interest will be due on July 16, 2013.
The Company’s loans include various covenant restrictions which include ratios on maximum debt to net worth, debt service coverage, maximum funded debt to earnings before interest, taxes, depreciation and amortization, and minimum tangible net worth requirements. The Company was in compliance with all loan covenants as of the period ending September 30, 2010.
Long-term debt consists of the following at September 30:
| 2010 | 2009 | |||||||
| Term note in the amount of $3,200,000 dated June 16, 2005, payable in monthly installments including interest at a rate of prime plus 1/2 % (prime rate is 3.25% as of September 30, 2010) of $76,033, maturing October, 2013, collateralized by substantially all assets of the Company. |
$ | 916,378 | $ | 735,061 | ||||
| Term note with a commitment level up to $3,200,000 payable to a financial institution, with a variable interest rate based on the one month Libor Rate (0.257% at September 30, 2010), plus 2.5% interest only payments due through September 2009. In November 2009, $1,050,000 was transferred to the term loan described above and the remaining balance of $2,100,000 was converted to a mortgage loan and is payable in monthly installments of $11,407 including interest. The loan matures on March 5, 2015, and is collateralized by a lien on the property. |
2,035,635 | 3,150,557 | ||||||
| Mortgage loan payable to a financial institution in the amount of $695,000 with monthly installments of $5,890 including interest at 5.95% from August 16, 2008 through July 16, 2013, with a final payment of all remaining prinicipal and accrued interest due in July 2013, collateralized by a lien on the property and substantially all the assets of the Company. |
628,605 | 659,660 | ||||||
| Subtotal |
3,580,618 | 4,545,278 | ||||||
| Less, current portion |
(995,042 | ) | (924,839 | ) | ||||
| Total Long-term Debt |
$ | 2,585,576 | $ | 3,620,439 | ||||
42
Table of Contents
Aggregate maturities of long-term debt are as follows:
| Year ending September 30, |
||||
| 2011 |
$ | 995,042 | ||
| 2012 |
136,357 | |||
| 2013 |
638,253 | |||
| 2014 |
84,026 | |||
| 2015 |
1,726,940 | |||
| Thereafter |
— | |||
| $ | 3,580,618 | |||
NOTE 7. EMPLOYEE BENEFIT AND STOCK OPTION PLANS
Employee Benefit Plans
The Company has an employee savings plan (the “Savings Plan”) that qualifies as a deferred salary arrangement under Section 401(k) of the Internal Revenue Code. Under the Savings Plan participating employees may defer a portion of their pretax earnings, up to the Internal Revenue Service annual contribution limit. The Company matches 150% of each employee’s contribution up to a maximum of 4% of the employee’s earnings. The Company’s matching contributions were approximately $1,105,000, $935,000, and $920,000, in fiscal years 2010, 2009 and 2008, respectively.
During June 1997, the Company’s Board of Directors approved the UCI/Doctors Care Deferred Compensation Plan (the “Plan”) for key employees of the Company with an effective date of June 1998. Under the Plan, as amended and restated effective January 1, 2005, key employees may defer up to 30% of their pre-tax earnings. The Company may match up to three times the employee's contribution percentage up to a limit of 10% of the employee’s pre-tax earnings. The Company’s matching contribution vests immediately. Distributions from the Plan to the employee or their beneficiaries may occur if the employee resigns or is terminated, becomes disabled or deceased, reaches the normal retirement age of 65, or if there is a change of control of the Company. Participating employees may elect a lump-sum payment or be paid in annual installments; however, in no event may the employee receive the first payment until six months after the event which precipitated the distribution. The Company’s matching contributions were approximately $317,000, $232,000, and $261,000, in fiscal years 2010, 2009 and 2008, respectively. The Company establishes and maintains insurance contracts, classified as “Restricted investments” in the Company’s balance sheets, to fund the Deferred Compensation Plan. The “Deferred compensation liability” increases or decreases based on employee and Company contributions plus or minus earnings or losses on the deemed investment selections of the participants less any payments to participants.
The Company established the 2007 Equity Incentive Plan (the “Plan”), effective as of March 7, 2007, to use Common Stock of UCI (“Common Stock”) as a tool to encourage employees of UCI and its subsidiaries, its affiliates and its joint ventures to work together to increase the overall value of UCI Common Stock. The Company believes the Plan will serve the interests of UCI and its stockholders because it allows employees to have a greater personal financial interest in UCI through ownership of its Common Stock, the right to acquire its Common Stock, or other plan awards and rights that are measured and paid based on UCI’s performance. The types of equity incentives under this Plan include:
| (a) | Incentive Stock Options; |
| (b) | Nonqualified Stock Options; |
| (c) | Stock Appreciation Rights; |
| (d) | Restricted Stock Grants; |
| (e) | Performance Shares; |
| (f) | Share Awards; and |
| (g) | Phantom Stock Awards. |
43
Table of Contents
In 2008, two executives and two physician employees were awarded 31,350 shares of common stock under the Plan. The shares were issued in 2009. The shares were valued at $2.25 per share and vested immediately. The Company recognized compensation expense of $70,537 in 2008 related to the stock award. Subsequently, in 2009, 11,400 shares of stock were recovered from the Company’s former Chief Financial Officer, as further discussed in Note 10. The stock was valued at $2.75 per share and the aggregate value of $31,350 was recorded as treasury stock.
NOTE 8. OPERATING EXPENSES
The components of operating expenses for each of the three years ended September 30 are as follows:
| 2010 | 2009 | 2008 | ||||||||||
| Salaries and benefits |
$ | 49,046,005 | $ | 42,438,788 | $ | 41,125,450 | ||||||
| Rent |
3,612,997 | 3,509,244 | 3,430,919 | |||||||||
| Maintenance and utilities |
2,099,134 | 1,907,733 | 1,674,017 | |||||||||
| Taxes and insurance |
2,176,901 | 2,120,782 | 1,949,824 | |||||||||
| Communications expense |
750,039 | 719,098 | 828,657 | |||||||||
| Medical and other supplies |
6,446,687 | 6,082,973 | 5,682,964 | |||||||||
| Provision for doubtful accounts |
2,620,883 | 2,349,485 | 2,686,897 | |||||||||
| Depreciation and amortization |
2,350,424 | 2,453,024 | 2,290,479 | |||||||||
| Interest expense |
1,421,800 | 1,214,498 | 900,046 | |||||||||
| Other expenses |
1,049,909 | 817,730 | 675,262 | |||||||||
| $ | 71,574,779 | $ | 63,613,355 | $ | 61,244,515 | |||||||
NOTE 9. GENERAL AND ADMINISTRATIVE EXPENSES
The components of general and administrative expenses for each of the three years ended September 30 are as follows:
| 2010 | 2009 | 2008 | ||||||||||
| Salaries and benefits |
$ | 7,138,915 | $ | 6,572,878 | $ | 7,310,495 | ||||||
| Maintenance and utilities |
418,382 | 291,699 | 374,259 | |||||||||
| Postage and shipping |
736,789 | 698,209 | 721,625 | |||||||||
| Office supplies |
151,139 | 152,544 | 162,901 | |||||||||
| Advertising |
657,683 | 693,092 | 1,500,300 | |||||||||
| Professional fees |
782,444 | 1,116,291 | 389,531 | |||||||||
| Depreciation and amortization |
862,819 | 650,993 | 734,374 | |||||||||
| Interest expense |
107,613 | 117,664 | 341,645 | |||||||||
| Banking fees |
615,392 | 573,680 | 543,904 | |||||||||
| Misappropriation loss |
— | 102,030 | 483,148 | |||||||||
| Other expenses |
1,549,884 | 1,503,332 | 1,494,426 | |||||||||
| $ | 13,021,060 | $ | 12,472,412 | $ | 14,056,608 | |||||||
NOTE 10. RECOVERY OF MISAPPROPRIATION LOSSES
On December 10, 2008, the Company’s Audit Committee of the Board of Directors (the “Audit Committee”) commenced an internal investigation (the “Investigation”) of certain accounting irregularities with respect to its internal controls and improper expense reimbursements to Jerry F. Wells, Jr., the Company’s former Executive Vice-President of Finance, Chief Financial Officer, and Secretary. On December 17, 2008, the Board of Directors terminated the employment of Mr. Wells based upon the preliminary results of the Investigation. On February 27, 2009, Mr. Wells executed a Confession of Judgment (the “Judgment”) in favor of the Company in the amount of Two Million Nine Hundred Sixty-Seven Thousand Three Hundred and Eighty-Two ($2,967,382) Dollars.
In conjunction with the Company’s collection efforts pursuant to the Judgment, it filed claims with two insurance carriers under fidelity bond and employee dishonesty insurance policies. In conjunction with such claims, the Company received an insurance
44
Table of Contents
settlement in the amount of $2,732,840 which was recognized in 2010. The recovery reflects a reduction from the amount of the Judgment for the policy deductible and other adjustments related to amounts the Company has collected from Mr. Wells and expenses it incurred in conjunction with its collection efforts. In conjunction with the recovery, the Company assigned its claims against certain third parties to the insurance carrier that paid the recovery. The Company, however, retained its right to pursue certain claims against its former independent registered public accounting firm which are unrelated to the fraud losses recovered from the insurance carrier. Efforts to collect such losses from its former independent registered public accounting firm have commenced. The Company’s initial claim against its former registered independent public accounting firm is approximately $2,100,000; however, the Company may claim additional damages as they are ascertained.
On February 20, 2009, the Company’s Board of Directors passed a resolution declaring a forfeiture of Mr. Wells’ interest in the Company’s deferred compensation plan. On February 23, 2009, Mr. Wells signed a voluntary relinquishment of his interest in the deferred compensation plan. The Company does not deem the relinquishment of Mr. Wells’ interest in the deferred compensation plan as a partial settlement of amounts he owes the Company under the Judgment. Rather, the Company deems such amount as being a nullity as of the date of the resolution of its Board of Directors because such interest in the deferred compensation plan had been conditionally credited to Mr. Wells under false pretenses. The amount of the liability associated with the deferred compensation plan at the time of relinquishment was $585,422.
Furthermore, during 2009, the Company recovered 11,400 shares of its common stock previously issued to Mr. Wells as compensation. At the date of recovery the common stock was valued at $31,350. In addition, during 2009, the Company recovered other miscellaneous items of personal property from Mr. Wells which it valued at $49,900 and collected $110,000 from the sales of other assets in which Mr. Wells had an interest.
NOTE 11. COMMITMENTS AND CONTINGENCIES
The Company is insured for professional liability on a claims-made basis and general liability on an occurrence basis, with additional tail coverage being obtained when necessary.
In the ordinary course of conducting its business, the Company becomes involved in litigation, claims, and administrative proceedings. Certain litigation, claims, and proceedings were pending at September 30, 2010, and management intends to vigorously defend the Company in such matters.
The healthcare industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government healthcare program participation requirements, reimbursement for patient services and Medicare and Medicaid fraud and abuse. Recently, government activity has increased with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by healthcare providers.
Violations of these laws and regulations could result in expulsion from government healthcare programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed. Management believes that the Company is in compliance with fraud and abuse laws and regulations as well as other applicable government laws and regulations; however, the possibility for future governmental review and interpretation exists.
The Company is exposed to changes in interest rates primarily as a result of its borrowing activities, which includes credit facilities with financial institutions used to maintain liquidity and fund its business operations, as well as notes payable to various third parties in connection with certain acquisitions of property and equipment. The nature and amount of the Company’s debt may vary as a result of future business requirements, market conditions and other factors. The definitive extent of the Company’s interest rate risk is not quantifiable or predictable because of the variability of future interest rates and business financing requirements. The Company does not currently use derivative instruments to adjust its interest rate risk profile.
Approximately $628,000 of the Company’s debt at September 30, 2010 was subject to fixed interest rates. Approximately $2,953,000 of its debt at September 30, 2010 was subject to variable interest rates. Based on the outstanding amounts of variable rate debt at September 30, 2010, the Company’s interest expense on an annualized basis would increase approximately $30,000 for each increase of one percent in the prime rate.
45
Table of Contents
The Company also has exposure to increases in the consumer price index associated with certain operating and capital leases it has entered, all of which relate to its leased real estate. At September 30, 2010, the Company had $3,833,738 in aggregate annual lease payments that are subject to increases based on future changes in the consumer price index. Typically, the lease agreements stipulate that the lease payments will increase every three years based on the aggregate increase in the consumer price index over the preceding three years. Of the aggregate annual lease payments subject to change based on the consumer price index, annual payments subject to change in 2011, 2012 and 2013 are $2,240,901, $946,769 and $646,068, respectively.
The Company does not utilize financial instruments for trading or other speculative purposes, nor does it utilize leveraged financial instruments.
NOTE 12. RELATED PARTY TRANSACTIONS
Relationship between UCI-SC and the P.A.
Pursuant to agreements between UCI-SC and the P.A., UCI-SC provides non-medical management services and personnel, facilities, equipment and other assets to the medical centers. UCI-SC guarantees the compensation of the physicians employed by the P.A. The agreements also allow UCI-SC to negotiate contracts with HMOs and other organizations for the provision of medical services by the P.A. physicians. Under the terms of the agreement, the P.A. assigns all revenue generated from providing medical services to UCI-SC. UCI-SC pays on the P.A.’s behalf the cost of medical services, including physician salaries. The P.A. is owned by D. Michael Stout, M.D., who is also the Chief Executive Officer for UCI and UCI-SC.
Relationship between the Company and Blue Cross Blue Shield of South Carolina
Blue Cross Blue Shield of South Carolina (“BCBS”) owns 100% of BlueChoice HealthPlan (“BCHP”) and Companion Property & Casualty Insurance Company (“CP&C”). At September 30, 2010, BCHP owned 6,107,838 shares of the Company’s outstanding common stock and CP&C owned 618,181 shares of the Company’s outstanding common stock, which combine to approximately 68% of the Company’s outstanding common stock.
Facility Leases
Two medical facilities operated by UCI-SC are leased from physician employees of the P.A. Total lease payments made by UCI-SC under these leases during the Company’s fiscal years ended September 30, 2010, 2009 and 2008, were approximately $117,000, $140,000 and, $126,000, respectively.
Other Transactions with Related Parties
At September 30, 2010, BCBS and its subsidiaries control 6,726,019 shares, or approximately 68% of the Company’s outstanding common stock. The shares acquired by BlueChoice HealthPlan (“BCHP”) and Companion Property & Casualty Insurance Company (“CP&C”) from the Company were purchased pursuant to stock purchase agreements and were not registered. BCHP and CP&C have the right to require registration of the stock under certain circumstances as described in the agreement. BCBS and its subsidiaries have the option to purchase as many shares as may be necessary for BCBS to obtain ownership of not less than 48% of the outstanding common stock of the Company in the event that the Company issues additional stock to other parties (excluding shares issued to employees or directors of the Company).
During the three year period ended September 30, 2010 the Company maintained an agreement with CP&C pursuant to which UCI-SC, through the P.A., acts as the primary care provider for injured workers of firms carrying workers’ compensation insurance through CP&C.
UCI-SC, through the P.A., provides services to members of a health maintenance organization (“HMO”) operated by BlueChoice HealthPlan (“BCHP”) who has selected the P.A. as their primary care provider.
In January 2009, the Company terminated its self-insured healthcare plan and entered into an insurance contract with BCBS to cover the Company’s employees. The total annual premiums paid to BCBS (including Company and employee contributions) were approximately $3,362,000 and $1,992,000 for the fiscal years ended September 30, 2010 and 2009, respectively.
46
Table of Contents
Revenues generated from billings to BCBS and its subsidiaries totaled approximately 38%, 40%, and 40% of the Company’s total revenues for fiscal years 2010, 2009 and 2008, respectively. Amounts receivable from BCBS and its subsidiaries approximated $1,903,000 and $2,469,000 at September 30, 2010 and 2009, respectively.
NOTE 13. SUBSEQUENT EVENTS
In November 2010, the Company completed the renovation of and opened a new Doctors Care center located in Columbia, South Carolina. In addition, in November 2010, the Company acquired a property in Newberry, South Carolina for $285,000 and has commenced the construction of a new facility which will house a Doctors Care and Progressive Physical Therapy center.
Subsequent events are events or transactions that occur after the balance sheet date but before financial statements are issued. Recognized subsequent events are events or transactions that provide additional evidence about conditions that existed at the date of the balance sheet, including the estimates inherent in the process of preparing financial statements. Nonrecognized subsequent events are events that provide evidence about conditions that did not exist at the date of the balance sheet but arose after that date. Management has reviewed events occurring through the date the financial statements were issued and no subsequent events occurred requiring additional accrual or disclosure.
47
Table of Contents
NOTE 14. QUARTERLY FINANCIAL DATA (unaudited)
The following table sets forth unaudited selected financial information for the quarters indicated. The quarterly financial information has been derived from unaudited consolidated financial statements, which, in the opinion of management, include all adjustments (consisting of normal recurring adjustments) necessary for a fair presentation of such information. The results of any quarter are not necessarily indicative of the results to be expected for any future period. The sum of certain amounts listed below differs from the annual reported total due to rounding.
| Year ended September 30, 2010 - Quarters ended | ||||||||||||||||
| December 31, 2009 | March 31, 2010 | June 30, 2010 | September 30, 2010 | |||||||||||||
| Revenues |
$ | 21,868,730 | $ | 22,114,808 | $ | 21,041,896 | $ | 21,879,895 | ||||||||
| Operating expenses |
18,172,658 | 17,499,878 | 17,631,114 | 18,271,129 | ||||||||||||
| Operating margin |
3,696,072 | 4,614,930 | 3,410,782 | 3,608,766 | ||||||||||||
| General and administrative expenses |
3,314,419 | 3,423,641 | 3,181,937 | 3,101,063 | ||||||||||||
| Income from operations |
381,653 | 1,191,289 | 228,845 | 507,703 | ||||||||||||
| Recovery of misappropriation loss |
— | — | 2,732,840 | — | ||||||||||||
| Income before income taxes |
381,653 | 1,191,289 | 2,961,685 | 507,703 | ||||||||||||
| Income tax expense |
147,356 | 459,957 | 1,107,324 | 191,733 | ||||||||||||
| Net income (loss) after provision for income taxes |
$ | 234,297 | $ | 731,332 | $ | 1,854,361 | $ | 315,970 | ||||||||
| Basic earnings (loss) per common share |
$ | 0.02 | $ | 0.07 | $ | 0.19 | $ | 0.04 | ||||||||
| Diluted earnings (loss) per common share |
$ | 0.02 | $ | 0.07 | $ | 0.19 | $ | 0.04 | ||||||||
| Year ended September 30, 2009 - Quarters ended | ||||||||||||||||
| December 31, 2008 | March 31, 2009 | June 30, 2009 | September 30, 2009 | |||||||||||||
| Revenues |
$ | 18,307,786 | $ | 20,544,839 | $ | 19,264,467 | $ | 22,233,360 | ||||||||
| Operating expenses |
15,418,449 | 15,539,153 | 15,589,446 | 17,066,307 | ||||||||||||
| Operating margin |
2,889,337 | 5,005,686 | 3,675,021 | 5,167,053 | ||||||||||||
| General and administrative expenses |
3,160,454 | 3,079,675 | 2,954,050 | 3,278,233 | ||||||||||||
| Income (loss) from operations |
(271,117 | ) | 1,926,011 | 720,971 | 1,888,820 | |||||||||||
| Recovery of misappropriation loss |
— | 585,422 | 78,884 | 112,366 | ||||||||||||
| Income (loss) before income taxes |
(271,117 | ) | 2,511,433 | 799,855 | 2,001,186 | |||||||||||
| Income tax (benefit) expense |
(104,689 | ) | 969,662 | 308,824 | 772,671 | |||||||||||
| Net income (loss) after provision for income taxes |
$ | (166,428 | ) | $ | 1,541,771 | $ | 491,031 | $ | 1,228,515 | |||||||
| Basic earnings (loss) per common share |
$ | (0.02 | ) | $ | 0.16 | $ | 0.05 | $ | 0.12 | |||||||
| Diluted earnings (loss) per common share |
$ | (0.02 | ) | $ | 0.16 | $ | 0.05 | $ | 0.12 | |||||||
48
Table of Contents
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
We maintain “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”), that are designed to ensure that information required to be disclosed by us in reports we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate, to allow timely decisions regarding required disclosure. In designing and evaluating our disclosure controls and procedures, our management recognized that disclosure controls and procedures, no matter how well conceived and operated, can provide only reasonable assurance of achieving the desired control objectives, and we necessarily are required to apply our judgment in evaluating the cost-benefit relationship of possible disclosure controls and procedures.
Our management, including our principal executive officer and principal financial officer, evaluated the effectiveness of the design and operation of our disclosure controls and procedures as of September 30, 2010 and concluded that the disclosure controls and procedures were effective.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) of the Exchange Act. Our system of internal control over financial reporting was designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes, in conformity with accounting principles generally accepted in the United States of America. Because of inherent limitations, a system of internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate due to a change in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management, including our principal executive officer and principal financial officer, conducted an evaluation of the effectiveness of our internal control over financial reporting using the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control—Integrated Framework. Based on the evaluation, our management concluded that our internal control over financial reporting was effective as of September 30, 2010.
Changes in Internal Control over Financial Reporting
There were no changes in our internal control over financial reporting during the fourth quarter of 2010 that materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
None.
49
Table of Contents
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by Item 10 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrant’s fiscal year ended September 30, 2010.
ITEM 11. EXECUTIVE COMPENSATION
The information required by Item 11 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrant’s fiscal year ended September 30, 2010.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
The information required by Item 12 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrant’s fiscal year ended September 30, 2010.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS AND DIRECTOR INDEPENDENCE
The information required by Item 13 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrant’s fiscal year ended September 30, 2010.
ITEM 14. PRINCIPAL ACCOUNTING FEES AND SERVICES
The information required by Item 14 of Form 10-K is incorporated by reference from the information contained in the Definitive Proxy Statement for the Annual Meeting of Stockholders, which is expected to be filed within 120 days after the registrant’s fiscal year ended September 30, 2010.
50
Table of Contents
PART IV
ITEM 15. EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
| (a) | Financial Statements |
The Consolidated Financial Statements listed on the Index to the Consolidated Financial Statements on page 29 are filed as part of this Form 10-K.
| (b) | Exhibits, Required by Item 601 of Regulation S-K |
A listing of the exhibits to the Form 10-K is set forth on the Exhibit Index that immediately precedes such exhibits in this Form 10-K.
| (c) | Financial Statement Schedules. Financial Statement Schedules Required by Item 8. |
51
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant, UCI Medical Affiliates, Inc., has duly caused this Report to be signed on its behalf by the undersigned, thereunto duly authorized.
| UCI MEDICAL AFFILIATES, INC. | Date | |||
| /s/ D. Michael Stout, M.D. D. Michael Stout, M.D. |
December 28, 2010 | |||
| Its: President and Chief Executive Officer |
||||
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
| /s/ D. Michael Stout, M.D. D. Michael Stout, M.D. |
President and Chief Executive Officer (principal executive officer) |
December 28, 2010 | ||
| /s/ Joseph A. Boyle, CPA Joseph A. Boyle, CPA |
Executive Vice President and Chief Financial Officer, and Director (principal financial and accounting officer) |
December 28, 2010 | ||
| /s/ Harold H. Adams, Jr., CPCU Harold H. Adams, Jr., CPCU |
Director |
December 28, 2010 | ||
| /s/ Charles M. Potok Charles M. Potok |
Director |
December 28, 2010 | ||
| /s/ Thomas G. Faulds Thomas G. Faulds |
Director |
December 28, 2010 | ||
| /s/ John M. Little, Jr., M.D., MBA John M. Little, Jr., M.D., MBA |
Director |
December 28, 2010 | ||
| /s/ Timothy L. Vaughn, CPA Timothy L. Vaughn, CPA |
Director |
December 28, 2010 | ||
| /s/ Jean E. Duke, CPA Jean E. Duke, CPA |
Director |
December 28, 2010 | ||
| /s/ Ann Thomas Burnett Ann Thomas Burnett |
Director |
December 28, 2010 | ||
52
Table of Contents
UCI MEDICAL AFFILIATES, INC.
EXHIBIT INDEX
| Exhibit |
Description | |
| 2.1 | Order of Confirmation of UCI Medical Affiliates, Inc. (“UCI”) Dated August 7, 2002 (Incorporated by reference to Exhibit 2.1 on the Form 8-K filed August 16, 2002) | |
| 2.2 | Order of Confirmation of UCI Medical Affiliates of South Carolina Dated August 5, 2002 (Incorporated by reference to Exhibit 2.2 on the Form 8-K filed August 16, 2002) | |
| 2.3 | Order of Confirmation of UCI Medical Affiliates of Georgia, Inc. Dated August 7, 2002 (Incorporated by reference to Exhibit 2.3 on the Form 8-K filed August 16, 2002) | |
| 2.4 | Order of Confirmation of Doctors Care, P.A. Dated August 8, 2002 (Incorporated by reference to Exhibit 2.4 on the Form 8-K filed August 16, 2002) | |
| 2.5 | Order of Confirmation of Doctors Care of Tennessee, P.C. Dated August 6, 2002 (Incorporated by reference to Exhibit 2.5 on the Form 8-K filed August 16, 2002) | |
| 2.6 | Order of Confirmation of Doctors Care of Georgia, P.C. Dated August 7, 2002 (Incorporated by reference to Exhibit 2.6 on the Form 8-K filed August 16, 2002) | |
| 2.7 | Plan of Reorganization for UCI (Incorporated by reference to Exhibit 2.7 on the Form 8-K filed August 16, 2002) | |
| 2.8 | Plan of Reorganization for UCI Medical Affiliates of South Carolina, Inc. (Incorporated by reference to Exhibit 2.8 on the Form 8-K filed August 16, 2002) | |
| 2.9 | Plan of Reorganization of UCI Medical Affiliates of Georgia, Inc. (Incorporated by reference to Exhibit 2.9 on the Form 8-K filed August 16, 2002) | |
| 2.10 | Plan of Reorganization of Doctors Care, P.A. (Incorporated by reference to Exhibit 2.10 on the Form 8-K filed August 16, 2002) | |
| 2.11 | Plan of Reorganization of Doctors Care of Tennessee, P.C. (Incorporated by reference to Exhibit 2.11 on the Form 8-K filed August 16, 2002) | |
| 2.12 | Plan of Reorganization for Doctors Care of Georgia, P.C. (Incorporated by reference to Exhibit 2.12 on the Form 8-K filed August 16, 2002) | |
| 2.13 | Joint Disclosure Statement Filed as of May 3, 2002 (Incorporated by reference to Exhibit 2.13 on the Form 8-K filed August 16, 2002) | |
| 2.14 | Addendum to Joint Disclosure Statement and Plans of Reorganization Filed as of June 14, 2002 (Incorporated by reference to Exhibit 2.14 on the Form 8-K filed August 16, 2002) | |
| 2.15 | Second Addendum to Plans of Reorganization Filed as of July 29, 2002 (Incorporated by reference to Exhibit 2.15 on the Form 8-K filed August 16, 2002) | |
| 3.1 | Amended and Restated Certificate of Incorporation of UCI filed with the Delaware Secretary of State as of July 27, 1994 (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 3.2 | Amended and Restated Bylaws of UCI dated as of November 23, 1993 (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
53
Table of Contents
| 3.3 | Amendment to Amended and Restated Bylaws of UCI dated as of August 21, 1996 (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 3.4 | Amendment to Amended and Restated Bylaws of UCI dated as of August 15, 2002 (Incorporated by reference to Exhibit 3.4 on the Form 8-K filed as of October 28, 2002) | |
| 3.5 | Certificate of Amendment of Certificate of Incorporation filed with the Delaware Secretary of State as of February 24, 1999 (Exhibit 3.5 on the Form 10-K filed for fiscal year 2002) | |
| 4.1 | The rights of security holders of the registrant are set forth in the registrant’s Certificate of Incorporation and Bylaws, as amended, included as Exhibits 3. 1 through 3. 5 | |
| 10.17 | Administrative Services Agreement dated April 24, 1998 by and between Doctors Care of Georgia, P.C. and UCI Medical Affiliates of Georgia, Inc. (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 10.18 | Administrative Services Agreement dated April 24, 1998 by and between Doctors Care of Tennessee, P.C. and UCI Medical Affiliates of Georgia, Inc. (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 10.19 | Administrative Services Agreement dated August 11, 1998 between UCI Medical Affiliates of South Carolina, Inc. and Doctors Care, P.A. (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 10.21 | Stock Purchase Option and Restriction Agreement dated September 1, 1998 by and among D. Michael Stout, M.D.; UCI Medical Affiliates of Georgia, Inc. and Doctors Care of Georgia, P.C. (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 10.22 | Stock Purchase Option and Restriction Agreement dated July 15, 1998 by and among D. Michael Stout, M.D.; UCI Medical Affiliates of Georgia, Inc.; and Doctors Care of Georgia, P.C. (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 10.31 | Stock Purchase Option and Restriction Agreement dated as of October 31, 2002 by and among D. Michael Stout, M.D.; UCI Medical Affiliates of South Carolina, Inc.; and Doctors Care, P.A. (Incorporated by reference to Exhibit 10.31 filed on Form 10-K for fiscal year 2002) | |
| 10.32* | UCI Medical Affiliates, Inc. 2007 Equity Incentive Plan (Incorporated by reference to Exhibit 10.32 filed on Form 10-K for fiscal year 2007) | |
| 10.33* | The Executive Nonqualified Excess Plan (Incorporated by reference to Exhibit 10.33 filed on Form 10-K for fiscal year 2007) | |
| 10.34* | The Executive Nonqualified Excess Plan Adoption Agreement (Incorporated by reference to Exhibit 10.34 filed on Form 10-K for fiscal year 2007) | |
| 10.35 | BB&T Promissory Note (Incorporated by reference to Exhibit 10.35 filed on Form 10-Q for quarter ended June 30, 2008) | |
| 10.36 | Carolina First Promissory Note (Incorporated by reference to Exhibit 10.36 filed on Form 10-Q for quarter ended June 30, 2008) | |
| 10.37* | Employment Agreement of Joseph A. Boyle dated March 16, 2009 (Incorporated by reference to Exhibit 10.37 filed on Form 8-K on March 18, 2009) | |
54
Table of Contents
| 10.38 | First Amended and Restated Loan Agreement dated November 23, 2009, by and among UCI Medical Affiliates, Inc.; UCI Medical Affiliates of South Carolina, Inc.; Doctors Care, P.A.; Doctor’s Care of Tennessee, P.C.; Progressive Physical Therapy, P.A.; Carolina Orthopedic & Sports Medicine, P.A.; and Branch Banking and Trust Company (Incorporated by reference to Exhibit 10.38 filed on Form 8-K on December 2, 2009). | |
| 10.39 | Second Amendment and Modification to Loan Agreement dated November 23, 2009, by and between UCI Properties, LLC and Branch Banking and Trust Company (Incorporated by reference to Exhibit 10.39 filed on Form 8-K on December 2, 2009). | |
| 14 | Code of Ethics dated as of November 25, 2003 (Incorporated by reference to the exhibit of same number on the Form 10-K filed for fiscal year 2003) | |
| 21 | Subsidiaries of the Registrant (Incorporated by reference to Exhibit 21 filed on Form 10-K for fiscal year 2007) | |
| 23# | Consent of Independent Auditors | |
| 31.1# | Rule 13a-14(a)/15d-14(a) Certification of D. Michael Stout, M.D. | |
| 31.2# | Rule 13a-14(a)/15d-14(a) Certification of Joseph A. Boyle, CPA | |
| 32# | Section 1350 Certification | |
| 99# | Press Release dated December 28, 2010 | |
| # | Filed herewith |
| * | Denotes a management contract or compensatory plan or arrangement. |
55