Attached files
| file | filename |
|---|---|
| EX-31.2 - EXHIBIT 31.2 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-31_2.htm |
| EX-23.1 - EXHIBIT 23.1 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-23_1.htm |
| EX-21.1 - EXHIBIT 21.1 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-21_1.htm |
| EX-31.1 - EXHIBIT 31.1 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-31_1.htm |
| EX-32.2 - EXHIBIT 32.2 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-32_2.htm |
| EX-32.1 - EXHIBIT 32.1 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-32_1.htm |
| EX-10.42 - EXHIBIT 10.42 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-10_42.htm |
| EX-10.89 - EXHIBIT 10.89 - PROSPECT MEDICAL HOLDINGS INC | a2195842zex-10_89.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES
EXCHANGE ACT OF 1934
For the fiscal year ended September 30, 2009
Commission File Number 1-32203
PROSPECT MEDICAL HOLDINGS, INC.
| Delaware (State or other jurisdiction of incorporation or organization) |
33-0564370 (IRS Employer Identification No.) |
|
10780 Santa Monica Blvd., Suite 400 Los Angeles, California (Address of principal executive offices) |
90025 (Zip Code) |
(310) 943-4500
(Registrant's telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class: | Name of each exchange on which registered: | |
|---|---|---|
| Common stock, Par value $0.01 per share | The NASDAQ Stock Market LLC |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. o Yes ý No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. o Yes ý No
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. ý Yes o No
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). o Yes o No
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of the registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o Yes ý No
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer," and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer o | Accelerated filer o | Non-accelerated filer o (Do not check if a smaller reporting company) |
Smaller reporting company ý |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). o Yes ý No
The aggregate market value of common stock held by non-affiliates of the registrant as of March 31, 2009 (the last business day of our most recently completed second fiscal quarter) was approximately $12,251,000 based upon the closing price for shares of our common stock as reported by NASDAQ (the exchange upon which our common stock was traded at the time) on such date.
As of December 11, 2009, 20,655,278 shares of the registrant's common stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant's definitive proxy statement for the 2010 annual stockholders meeting, expected to be filed within 120 days of our fiscal year end, are incorporated by reference into Part III of this Form 10-K.
Table of Contents
Form 10-K
2
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
Certain statements in this Annual Report on Form 10-K constitute "forward-looking statements" (rather than historical facts) as defined in the Private Securities Litigation Reform Act of 1995 or by the Securities and Exchange Commission (the"SEC") in its rules, regulations and releases, including Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. All statements in this Annual Report, including under the captions "Business," "Risk Factors," and "Management's Discussion and Analysis of Financial Condition and Results of Operations," other than statements of historical fact, are forward-looking statements for purposes of these provisions, including statements of our current views with respect to our business strategy, business plan, our future financial results, and other future events. In some cases, forward-looking statements can be identified by the use of terminology such as "may," "will," "expects," "plans," "anticipates," "estimates," "potential" or "could" or the negative thereof or other comparable terminology. Although we believe that the expectations reflected in the forward-looking statements contained herein are reasonable, there can be no assurance that such expectations or any of the forward-looking statements will prove to be correct, and actual results could differ materially from those projected or assumed in the forward-looking statements.
All forward-looking statements involve inherent risks and uncertainties, and there are or will be important factors that could cause actual results to differ materially from those indicated in these statements. We believe that these factors include, but are not limited to, those factors set forth in this Annual Report under the captions "Business," "Risk Factors," and "Management's Discussion and Analysis of Financial Condition and Results of Operations," all of which you should review carefully. If one or more of these or other risks or uncertainties materialize, or if our underlying assumptions prove to be incorrect, actual results may vary materially from what we anticipate. Please consider our forward-looking statements in light of those risks as you read this Annual Report. We undertake no obligation to publicly update or review any forward-looking statement, whether as a result of new information, future developments or otherwise.
3
Overview
We provide quality, coordinated healthcare and physician services in Southern California. We own and operate five hospitals, with a total of approximately 759 licensed beds, and currently maintain approximately 829 on-staff physicians, including specialists who cover approximately 35 medical and surgical specialties. Our hospitals are located in high density population areas within Los Angeles County and maintain leading market positions in the areas they serve. We also manage the provision of physician services through ten Medical Groups that consist of physician networks with approximately 7,200 primary care and specialty physicians. Our Medical Groups provide physician services to approximately 177,000 enrollees. Based on our enrollment, our combined Medical Groups represent one of the largest in Southern California and has contracts with nearly all the major (non-Kaiser) HMOs operating in the region. We believe the coordination of our hospitals and Medical Groups will create an efficient healthcare delivery system that positions us to drive growth and profitability.
We operate both our hospitals and Medical Groups by applying highly disciplined, data-driven management to the provision of quality care. Through this in-depth and data-driven approach to analysis and application of various operational and financial metrics, we have been able to achieve a highly-efficient cost structure which enables us to adjust our operations to provide services that generate higher margins and revenue growth. Our management's expertise in executing our operating model has enabled us to increase profitability across a diverse mix of payors and the flexibility to adapt to economic and regulatory changes. Our operating model also allows us to be well-positioned for the future, as we believe that the most cost-efficient providers will be the ones who benefit in this rapidly changing economic and regulatory environment.
We have grown through a series of strategic acquisitions:
- •
- in June 2007, we acquired the ProMed Entities, which, at the time of the acquisition, collectively had approximately
82,000 HMO enrollees;
- •
- in August 2007, we acquired Alta, which owned and operated four community-based hospitals in Los Angeles County with a
combined 339 licensed beds served by approximately 315 on-staff physicians. In connection with the Alta acquisition, Sam Lee, Alta's president, joined our board of directors and the
management team and was later appointed Chief Executive Officer in March 2008. The acquisition of Alta transformed our Company from a business exclusively providing Medical Group management services
to a business capable of providing coordinated hospital and physician management services; and
- •
- in April 2009, we increased our approximately 33% ownership stake in Brotman, a 420-bed hospital located in Culver City, California, to approximately 72%.
We have improved our operating margin and profitability through the following actions:
- •
- managing staffing levels according to patient volumes and acuity levels of care required;
- •
- optimizing resource allocation by utilizing our case management program, which assists in improving clinical care and cost
containment;
- •
- negotiating favorable payor contracts and reductions in uncompensated care and payor claims denial;
- •
- expanding and improving profitable services offered by our hospitals;
- •
- enhancing claims management functions and negotiating more favorable provider contracts for our Medical Groups;
- •
- divesting non-core assets; and
4
- •
- restructuring our senior management team and adding experienced professionals in the areas of finance, operations, claims management, business development and compliance.
We believe that our acquisitions and the successful implementation of our operating model by our management team have both strengthened our infrastructure and positioned us for continued revenue growth and profitability.
Our principal executive offices are located at 10780 Santa Monica Blvd., Suite 400, Los Angeles, CA 90025. Our telephone number is (310) 943-4500. Our web site address is www.prospectmedicalholdings.com. A copy of this filing is posted on our web site. However, our web site and the information contained on our web site or connected to our web site are not incorporated by reference into this Annual Report on Form 10-K.
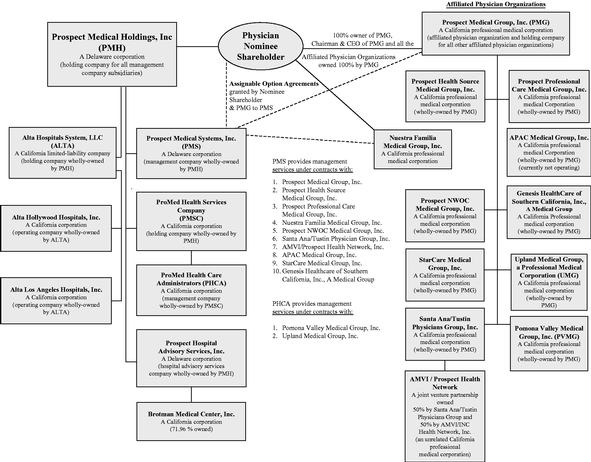
The organizational structure of our business is set forth on the next page.
ORGANIZATIONAL STRUCTURE OF OUR BUSINESS
History and Development of Our Business
Our business effectively commenced in 1996, when we began to implement our growth strategy through a series of acquisitions and affiliations. Between 1996 and 2005, PMG acquired fourteen physician organizations. These acquisitions provided us with a substantial concentration of HMO enrollees in our three Southern California service areas—North and Central Orange County, West Los Angeles and the Antelope Valley region of Los Angeles County. In 2007 we completed two major acquisitions, described below, which resulted in the addition of HMO enrollees in San Bernardino County and in the establishment of our Hospital Services segment.
5
On June 1, 2007, PMG completed the acquisition of the ProMed Entities, for consideration of $48,000,000, consisting of $41,040,000 of cash and 1,543,237 shares of PMH common stock, valued at $6,960,000, or $4.51 per share. As a result of the ProMed Acquisition, PHCA became a wholly-owned subsidiary of PMH and PVMG and UMG became wholly-owned subsidiaries of PMG. At the time of the acquisition, PVMG and UMG had approximately 80,000 HMO enrollees.
On August 8, 2007, we acquired Alta, and we repaid approximately $41,500,000 of Alta's existing debt. Total merger consideration, exclusive of the Alta debt repaid, consisting of approximately $103 million, was paid one-half ($51.3 million) in cash and one-half in stock (valued, for transaction purposes only, at $5.00 per share of our common stock). The equity portion of the merger consideration consisted of 1,887,136 shares of common stock and 1,672,880 shares of Series B Preferred Stock. The Series B Preferred Stock was non-convertible until such time as the stockholders voted to approve its convertibility. Such approval was received at our annual meeting of stockholders held on August 13, 2008. As a result, each share of Series B Preferred Stock automatically became convertible into five shares of common stock at a conversion price of $5.00 per share of common stock. Following such stockholder approval, the holders of all the outstanding shares of Series B Preferred Stock elected to convert their preferred shares into common stock.
Also on August 8, 2007, in connection with the closing of the Alta acquisition, Bank of America, N.A. (the "Lender") agented $155 million of financing for us in the form of term loans totaling $145 million and a $10 million revolving line of credit facility, $3 million of which was drawn at closing. The term loans were used to refinance approximately $41.5 million of existing Alta debt, refinance approximately $48 million of our existing debt that had previously been provided by the Lender in connection with our acquisition of ProMed, and pay the cash portion of the Alta purchase price.
On August 1, 2008, we completed the sale of all of the outstanding stock of the AV Entities for total pre-tax cash consideration of $8,000,000 and entered into a non-competition agreement in the Antelope Valley region of Los Angeles County for the benefit of the buyer.
On August 31, 2005, we initially acquired an approximately 33% ownership interest in Brotman. Although Brotman faced financial and operational challenges, we viewed the investment as having a potential benefit to our Medical Group business. Following our initial investment, Brotman continued to incur substantial losses. In September 2007, following consultation with outside advisors and our new management team, which was experienced in hospital management and turnarounds, Brotman determined that it would be in its best interest to file for bankruptcy protection, which it did in October 2007. Concurrent with the filing, we entered into an amendment to our existing consulting services agreement with Brotman, which provided for an increased level of services and responsibility by our new management team.
On April 14, 2009, Brotman emerged from bankruptcy and we acquired an approximately 39% additional ownership interest, which brought us to our current total ownership of approximately 72% of the outstanding common stock of Brotman. Pursuant to the terms of the bankruptcy plan, we made additional investments in Brotman totaling $2,500,000.
Our Strategy
Our objective is to operate as an entrepreneurial, efficient healthcare delivery system by delivering both hospital and physician services.
Enhance Operating Efficiencies
We seek to use our operating efficiencies to provide an advantage by enabling us to profitably service patients that other providers cannot serve profitably. We monitor our cost trends, operating performance and the regulatory environment in our existing markets to drive operating efficiencies, such as the optimization of staffing and utilization levels. These efficiencies allow us to strengthen our
6
financial performance while improving the services we provide to our patients, physicians and health plan partners, as well as provide us greater flexibility to adapt to regulatory changes.
Cross-Fertilize Revenues among Our Hospitals and Medical Group Networks
We seek to generate organic growth primarily through cross-fertilization between our Medical Group and Hospital Services segments. Specifically, we have undertaken the following initiatives:
- •
- utilizing our existing community hospitals to facilitate referrals to Brotman;
- •
- consolidating the back-office operations and management of our existing Medical Groups to reduce
administrative costs and enhance partnering with HMOs and physicians; and
- •
- integrating Medical Group and Hospital Services operations to:
- •
- utilize our existing hospital-physician relationships to increase enrollment at our Medical Groups;
- •
- use our existing Medical Group enrollment to drive business to our hospital facilities;
- •
- leverage our existing Medical Groups to enhance payor diversification for our hospitals; and
- •
- expand HMO contracts by offering a combined hospital-physician provider solution.
Additionally, we plan to expand our physician networks into areas where we have hospitals and seek hospital acquisition opportunities in areas where we have physician networks. The HMOs with which we contract have increasingly expressed their desires for their medical group partners to provide a combined hospital-physician solution.
Complete the Transformation of Brotman
We believe that our acquisition of a controlling stake in Brotman will allow us to use our proven operating model to drive efficiencies, as well as add new payors, improve reimbursement from existing payors and recruit new physicians to the medical staff. We will continue the implementation of our cost efficiency initiatives, which we expect will improve Brotman's operating results. We will also continue to recruit physicians for our surgical and cardiology groups as well as in primary care, which we believe will create opportunities for both inpatient and outpatient growth. In addition, we are evaluating the expansion of Brotman's emergency room services to better serve its strategic geographic location and facilitate admissions into the hospital.
Grow Through Strategic Acquisitions
We intend to continue growing through select strategic acquisitions of hospitals. We will seek hospital acquisition candidates that we believe are not currently achieving their potential in attractive service areas where our operating model can be applied. Additionally, we expect the number of potential acquisition candidates to increase given the fragmented ownership within the hospital market and the increasing number of underperforming hospitals struggling with inefficient operations and high cost structures.
Our Market
We operate our business in Southern California where we believe market dynamics will favorably impact our growth. There is a shortage of hospital beds in Los Angeles County, with fewer than 100 hospitals to serve approximately ten million people across 4,000 square miles. According to a recent report from the Hospital Association of Southern California ("HASC"), Los Angeles County averages approximately one bed per 1,000 people, well below the national average of over three beds per 1,000 people. High hospital construction costs in Southern California have prevented meaningful increases in bed supply commensurate with demand.
7
Additionally, we expect demographic trends to further increase the supply-demand imbalance for hospital services. California anticipates unprecedented growth in its senior population as the baby boom generation ages and life expectancy continues to increase. California's senior population is projected to more than double between 2000 and 2030, growing to approximately 8.8 million, according to a recent report from the California HealthCare Foundation. Because of these demographic trends and the shortage of hospital beds in our local markets, we believe we are well-positioned to benefit organically from the increased demand for our services.
Closures of competitor hospitals have further added to the hospital bed shortage. Over the past ten years, 14 hospitals in Los Angeles County have closed, mostly because of their inefficient cost structures. HASC reported recently that it expects this trend to continue. Also, the Southern California hospital market is highly fragmented, with approximately 60 different ownership entities. The fragmented and decreasing number of hospitals in our market will facilitate our acquisition strategy, as competitor hospitals become available for acquisition.
Description of Our Business—Hospital Services Segment
Overview
The hospital services sector is comprised of at least three sub-sectors that do not generally compete with each other because they largely serve three distinct patient populations:
- •
- Tertiary Care Hospitals: Tertiary care hospitals are
generally owned by the larger philanthropic organizations and for-profit hospital companies which tend to be well funded and utilize state of the art facilities to treat commercially
insured patients and higher acuity care patients.
- •
- Community Hospitals: Community hospitals are both
for-profit and not-for-profit and operate in generally older properties, use generally less state-of-the-art equipment, and are
equipped to care for patients of lower acuity. Efficient hospitals in this group are able to provide care profitably because of their significantly lower cost structures.
- •
- Public Hospitals: Public hospitals are generally owned by government entities that are set up to treat uninsured, indigent patients with a full range of acuity needs.
Both government and managed care payors are under pressure to reduce the cost of health coverage. One means of doing this is to match patients to the facility best suited to delivering the quality of care required in the most cost-efficient setting. Because of the focused, cost efficient structures of community hospitals, both patients and payors can benefit economically from utilizing community hospitals where feasible. In the managed care context, patient co-pays in many instances increase as the cost structure of the hospital increases, thereby providing an incentive to the patient, as well as the payor, to utilize focused cost efficient community hospitals. Further, government payors generally pay tertiary care hospitals higher per diem amounts for care under Medicare and Medi-Cal than the per diem amounts paid to community hospitals. Companies operating community-based hospitals are positioned to benefit from this market dynamic as focused quality, cost efficient providers.
Our Hospitals
We own and operate five hospitals in Los Angeles County, all accredited by the Joint Commission (formerly the Joint Commission on Accreditation of Healthcare Organizations), with a total of approximately 759 licensed beds served by 829 on-staff physicians at September 30, 2009. We acquired four community hospitals in Hollywood, Los Angeles, Norwalk and Van Nuys in connection with our acquisition of Alta. Our fifth hospital is Brotman Medical Center, located in Culver City. For the 12 months ended September 30, 2009, our hospital services segment generated revenues of approximately $205 million.
8
Our three community hospitals in Hollywood, Los Angeles and Norwalk offer a comprehensive range of medical and surgical services, including general acute care hospital services, pediatrics, obstetrics and gynecology, pediatric sub-acute care, general surgery, medical-surgical services, orthopedic surgery, and diagnostic, outpatient, skilled nursing and urgent care services. Our psychiatric hospital in Van Nuys provides acute inpatient and outpatient psychiatric services on a voluntary basis. Brotman offers a comprehensive range of inpatient and outpatient services, including general surgery, orthopedic, spine and neurosurgery, cardiology, diagnostic outpatient, rehabilitation, psychiatric and detox services. In addition, Brotman has an active emergency room that plays an integral part in providing emergency services to the West Los Angeles area.
The table below gives a brief overview of our hospitals and the locations they serve:
Name/Location
|
Primary Service | Number of Beds | ||
|---|---|---|---|---|
Hollywood Community Hospital |
Medical/Surgical | 100 licensed beds/100 staffed beds | ||
Los Angeles Community Hospital |
Medical/Surgical |
130 licensed beds/130 staffed beds |
||
Norwalk Community Hospital |
Medical/Surgical |
50 licensed beds/50 staffed beds |
||
Brotman Medical Center |
Medical/Surgical |
420 licensed beds/240 staffed beds |
||
Van Nuys Community Hospital |
Psychiatric |
59 licensed beds/59 staffed beds |
Selected Operating Statistics
The table below sets forth selected hospital operating statistics for the years ended September 30, 2009 and 2008.
| |
Year Ended September 30, | ||||||
|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||
Licensed beds as of the end of the period(1) |
759 | 339 | |||||
Admissions(2) |
18,573 | 14,206 | |||||
Adjusted admissions(3) |
20,098 | 15,058 | |||||
Emergency room visits(4) |
25,616 | 13,600 | |||||
Surgeries(5) |
4,146 | 2,935 | |||||
Patient days(6) |
124,004 | 87,463 | |||||
Acute care average length of stay in days(7) |
6.20 | 5.50 | |||||
- (1)
- Licensed beds are beds for which a hospital has obtained approval to operate from the applicable state licensing agency.
9
- (2)
- Admissions
are patients admitted to our hospitals for inpatient treatment. This statistic is used by our management, investors and other readers of our
financial statements as a measure of inpatient volume.
- (3)
- Adjusted
admissions are total admissions adjusted for outpatient volume. Adjusted admissions are computed by multiplying admissions (inpatient volume) by
the sum of gross inpatient charges and gross outpatient charges and then dividing the resulting amount by gross inpatient charges. This statistic is used by our management, investors and other readers
of our financial statements as a measure of inpatient and outpatient volume.
- (4)
- The
number of emergency room visits is an important operational measure that is used by our management, investors and other readers of our financial
statements to gauge our patient volume. Much of our inpatient volume results from a patient's initial encounter with our hospitals through an emergency room visit.
- (5)
- The
number of surgeries includes both inpatient and outpatient surgeries. This statistic is used by our management, investors and other readers of our
financial statements as one component of overall patient volume and business trends.
- (6)
- Patient
days are the total number of days that patients are admitted in our hospitals. This statistic is used by our management, investors and other readers
of our financial statements as a measure of inpatient volume.
- (7)
- Acute
care average length of stay in days represents the average number of days admitted patients stay in our hospitals. This statistic is used by our
management, investors and other readers of our financial statements as a measure of our utilization of hospital resources.
- (8)
- Operating statistics are for the period April 14, 2009 through September 30, 2009.
Our Hospital Operating Model
Our hospital operating model is physician-centric. We have found that a physician friendly environment is key to recruiting physicians. We also strive to provide convenience in scheduling and collaborative patient case management in order to assist in the treatment of the patient and in the physician's time management. We have, for example, developed an admissions process that enables the physician's office to make a hospital admission with a single telephone call to our admissions coordinator. We also provide admissions through our emergency room and urgent care centers to help better evaluate medical necessity.
Our hospital physicians are not employed by us. However, some physicians provide services in our hospitals under contracts which generally describe a term of service, provide and establish the duties and obligations of such physicians, require the maintenance of certain performance criteria and fix compensation for such services. Any licensed physician may apply to be admitted to the medical staff of any of our hospitals in accordance with established credentialing criteria.
We have also developed transfer processes with other area hospitals to receive patients that are more appropriately treated in one of our hospitals. Hospitals with which we have such transfer relationships include community hospitals that do not accept Medi-Cal patients and tertiary care hospitals with high cost structures that consider certain non-tertiary-level care patients to be unprofitable. Correspondingly, our hospitals will transfer patients to another hospital with which we have a transfer relationship when the patient's individual circumstances warrant.
10
Hospital Revenues and Reimbursement
We record gross patient service charges on a patient-by-patient basis in the period in which services are rendered. Patient accounts are billed after the patient is discharged. When a patient's account is billed, our accounting system calculates the reimbursement that we expect to receive based on the type of payor and the contractual terms of such payor. We record the difference between gross patient service charges and expected reimbursement as contractual adjustments.
At the end of each month, we estimate expected reimbursement for unbilled accounts. Estimated reimbursement amounts are calculated on a payor-specific basis and are recorded based on the best information available to us at the time regarding applicable laws, rules, regulations and contract terms. We continually review our contractual adjustment estimation process to consider and incorporate updates to laws, rules and regulations, as well as changes to managed care contract terms that result from negotiations and renewals.
Hospital revenues depend upon inpatient occupancy levels, the ancillary services and therapy programs ordered by physicians and provided to patients, the volume of outpatient procedures and the charges or negotiated payment rates for such services. Charges and reimbursement rates for inpatient services vary significantly depending on the type of service and geographic location of the hospital. Our hospitals receive revenues for patient services from a variety of sources, including the federal Medicare program, California's Medi-Cal program, managed care payors (including PPOs and HMOs), indemnity-based health insurance companies and self-pay patients. The basis for payments involving inpatients is prospectively set Diagnostic Related Group ("DRG") rates for Medicare, negotiated per diem rates for Medi-Cal and percentage of charge or negotiated rates for the other payors. The basis for payments for outpatients is prospectively set rate-per-service based on the Ambulatory Payment Classification ("APC") assigned for Medicare, a fixed rate by procedure for Medi-Cal and percentage of charges or negotiated rates for other payors. Our hospitals are also eligible for State of California Disproportionate Share payments based on a prospective payment system for hospitals that serve large populations of low-income patients.
Our hospitals receive payment for patient services from the federal government, primarily under the Medicare program, the California Medi-Cal program, managed care plans (including PPOs and HMOs), indemnity-based health insurance plans, as well as directly from patients ("self-pay"). All of our hospitals are certified as providers of Medicare and Medi-Cal services. Amounts received under the Medicare and Medi-Cal programs are generally significantly less than a hospital's customary charges for the services provided. Since a substantial portion of our revenue comes from patients under Medicare and Medi-Cal programs, our ability to operate our business successfully in the future will depend in large measure on our ability to adapt to changes in these programs.
The nation's current economic crisis may have a negative impact on reimbursement for our hospitals. A recent American Hospital Association report on the economic crisis indicates that the credit crunch is making it difficult and expensive for hospitals to finance facility and technology needs. The majority of hospitals are experiencing decreased admissions and elective procedures. In addition, rising unemployment is leading to increased uncompensated care. California budget shortfalls may result in decreases in hospital Medi-Cal reimbursement.
Medicare
Medicare is a federal program that provides medical insurance benefits to persons age 65 and over, some disabled persons, and persons with end-stage renal disease. Under the Medicare program, we are paid for inpatient and outpatient services performed by our hospitals. Payments for inpatient acute services are generally made pursuant to a prospective payment system, commonly known as "PPS." Under PPS, our hospitals are paid a predetermined amount for each hospital discharge based on the patient's diagnosis.
11
Specifically, each discharge is assigned to a diagnosis related group, commonly known as a "DRG," based upon the patient's condition and treatment during the relevant inpatient stay. Each DRG is assigned a cost weight based on its severity. The DRG weight is then applied to a national average rate to arrive at the payment. The national average rate is adjusted for labor cost by a predetermined geographic adjustment factor assigned to the geographic area in which the hospital is located. In addition to the DRG payment, hospitals may qualify for an "outlier" payment when the relevant patient's treatment costs are extraordinarily high and exceed a specified regulatory threshold.
The national average rates are adjusted by an update factor on October 1 of each year, the beginning of the federal fiscal year. The index used to adjust the DRG rates, known as the "market basket index," gives consideration to the inflation experienced by hospitals in purchasing goods and services. Under the Medicare Prescription Drug, Improvement and Modernization Act of 2003 ("MMA"), DRG payment rates were increased by the full "market basket index," for the federal fiscal years 2007, 2008 and 2009 or 3.4%, 3.3% and 3.6% respectively. The Deficit Reduction Act of 2005 imposes a 2% reduction to the market basket index beginning in the federal fiscal year 2007, and thereafter, if patient quality data is not submitted. We intend to and have complied with this data submission requirement. Future legislation may decrease the rate of increase for DRG payments, but we are not able to predict the amount of any reduction or the effect that any reduction will have on us.
In an effort to encourage hospitals to improve quality of care, the Medicare program has taken steps to reduce or withhold payments to hospitals for treatment given to patients whose conditions were caused by serious medical error. Under rules that became effective October 1, 2008, Medicare will no longer pay hospitals for the higher costs of care resulting from eight complications, including falls, objects left inside patients during surgery, pressure ulcers and three types of hospital-acquired infections. California hospitals are required to report certain adverse events to a state agency charged with publicizing the events, as well as the results of any ensuing investigation conducted by the agency. We believe that our hospital quality of care programs will address such issues, but we are unable to predict the future impact of these developments on our business.
Medi-Cal
Medi-Cal is a federal/state-funded program, administered by the California Department of Health Services (the "State") which provides medical benefits to individuals that qualify. Our hospitals participate in the Medi-Cal system and are paid a negotiated per diem rate. There can be no assurances that revisions in the Medi-Cal program will not have a material adverse effect on our results of operations.
Pursuant to the terms of the Medi-Cal contracts between the State and each of our hospitals, a significant portion of our hospital business is subject to termination of contracts and subcontracts at the election of the government. The contract between the State and Los Angeles Community Hospital and Norwalk Community Hospital was entered into on September 14, 2000 and most recently amended on September 24, 2009. The agreement may not be terminated without cause prior to December 31, 2010 and after that date it may be terminated without cause, provided that 120 days notice of termination is given. The contract between the State and Hollywood Community Hospital and Van Nuys Community Hospital was entered into on September 14, 2000 and most recently amended on May 10, 2007. The agreement may not be terminated without cause prior to July 10, 2009 and after that date it may be terminated without cause, provided that 120 days notice of termination is given. The contract between the State and Brotman was entered into on September 1, 2005 and most recently amended on June 1, 2009. The agreement may not be terminated without cause prior to July 1, 2010 and after that date it may be terminated without cause, provided that 120 days notice of termination is given. California budgetary shortfalls may result in our inability to renew Medi-Cal contracts at existing rates. Thereafter, the contracts are renewed by negotiation between the parties. We can provide no assurance whether these contracts will be renewed upon their expiration.
12
Disproportionate Share Payments
Hospitals that treat a high percentage of low-income patients may receive additional Disproportionate Share ("DSH") payment adjustment from Medicare and Medi-Cal. We receive both of these adjustments. The Medicare adjustment is based on the hospital's DSH patient percentage, which is the sum of the number of patient days for patients entitled to both Medicare Part A and Supplemental Security Income benefits, divided by the total number of Medicare Part A patient days and a second factor that is a ratio of Medi-Cal eligible days to total DRG days. For fiscal 2009, total Medicare DSH payments received were approximately $27,700,000 compared to approximately $18,000,000 for fiscal 2008. The Medi-Cal adjustment is based either on the Hospital's Medi-Cal utilization or its low income utilization percentage. Our hospitals qualify because their Medi-Cal utilization was greater than one standard deviation above 42% of the hospitals' total patient days. For fiscal 2009, total Medi-Cal DSH payments received by our hospitals were approximately $12,000,000 compared to approximately $11,300,000 for fiscal 2008.
Medicare Bad Debt Reimbursement
Under Medicare, the costs attributable to the deductible and coinsurance amounts which remain unpaid by the Medicare beneficiary can be added to the Medicare share of allowable costs as cost reports are filed. Hospitals generally receive interim pass-through payments during the cost report year which were determined by the fiscal intermediary from the prior cost report filing.
Bad debts must meet the following criteria to be allowable:
- •
- the debt must be related to covered services and derived from deductible and coinsurance amounts;
- •
- the provider must be able to establish that reasonable collection efforts were made;
- •
- the debt was actually uncollectible when claimed as worthless; and
- •
- sound business judgment established that there was no likelihood of recovery at any time in the future.
The amounts uncollectible from specific beneficiaries are to be charged off as bad debts in the accounting period in which the accounts are deemed to be worthless. In some cases, an amount previously written off as a bad debt and allocated to the program may be recovered in a subsequent accounting period. In these cases, the recoveries must be used to reduce the cost of beneficiary services for the period in which the collection is made. In determining reasonable costs for hospitals, the amount of bad debts otherwise treated allowable costs is reduced by 30%. Under this program, our hospitals incurred an aggregate of approximately $4,568,000 and $2,757,000, which are subject to the 30% reduction, for fiscal 2009 and 2008, respectively. Amounts incurred by a hospital as reimbursement for bad debts are subject to audit and recoupment by the fiscal intermediary. Bad debt reimbursement has been a focus of fiscal intermediary audit/recoupment efforts in the past.
Annual Cost Reports
Hospitals participating in the Medicare and some Medi-Cal programs are required to meet specified financial reporting requirements. Federal and state regulations require submission of annual cost reports identifying medical costs and expenses associated with the services provided by each hospital to Medicare beneficiaries and Medi-Cal recipients. Annual cost reports required under the Medicare and Medi-Cal programs are subject to routine governmental audits. These audits may result in adjustments to the amounts ultimately determined to be due to us under these reimbursement programs. Finalization of these audits often takes several years. We can appeal any final determination made in connection with an audit. DRG outlier payments and other cost report abuses have been and
13
continue to be the subject of audit and adjustment by the Centers for Medicare and Medicaid Services ("CMS").
In 2003, Congress passed legislation to enhance and support Medicare's current efforts in identifying and correcting improper payments. In section 306 of the Medicare Modernization Act ("MMA"), Congress directed the Department of Health and Human Services ("DHHS") to conduct a three-year demonstration program using Recovery Audit Contractors ("RAC") to detect and correct improper payments in the Medicare FFS program. In addition, in section 302 to the Tax Relief and Health Care Act of 2006 ("TRHCA"), Congress required DHHS to make the RAC program permanent and nationwide by no later than January 1, 2010. The RAC program does not detect or correct payments for Medicare Advantage or the Medicare prescription drug benefit.
The permanent RAC program is scheduled to begin in California in July 2009. The auditors will be auditing payments made to California healthcare providers to assure correct payment. Payments deemed incorrect will be adjusted at the time of audit. These adjustments can be appealed following the guidelines of the program. As of September 30, 2009, no audits under the RAC program were scheduled for any of our hospitals.
Our hospitals are subject to audit along with other California hospitals during this upcoming year. Our hospitals have taken steps to assure on-going coding and billing accuracy, which will also help ensure successful RAC audits.
Inpatient Psychiatric
As of September 30, 2009, we operated one 70-bed, inpatient psychiatric unit paid under the IPF PPS method at Brotman and one 59 licensed bed, inpatient psychiatric unit paid on the acute PPS method at Van Nuys. Effective for reporting periods after January 1, 2005, CMS replaced the cost-based system with a PPS for inpatient hospital services furnished in freestanding psychiatric hospitals and PPS exempt psychiatric units of general, acute care hospitals and critical access hospitals ("IPF PPS"). IPF PPS is a per diem prospective payment system with adjustments to account for certain patient and facility characteristics. IPF PPS contains an "outlier" policy for extraordinarily costly cases and an adjustment to a facility's base payment if it maintains a full-service emergency department. Under this program, Brotman received an aggregate of approximately $6,392,000 for fiscal 2009. Under the acute MS-DRG, Van Nuys received an aggregate of approximately $8,168,000 and $6,401,000 for fiscal 2009 and 2008 respectively.
Competition
All five of our hospitals are located in Los Angeles County and each hospital serves its own local community.
Within the Los Angeles Community Hospital ("LACH") service area, three urban hospitals are considered competitors of LACH. They are Mission Hospital of Huntington Park, a 127 licensed bed acute care hospital, Monterey Park Hospital, a 101 licensed bed acute care facility, and East Lost Angeles Doctors Hospital, which is licensed for 127 acute care beds and 30 skilled nursing beds.
The Norwalk Community Hospital service area has two main competitors, Coast Plaza Doctors Hospital, located in Norwalk, and Presbyterian Intercommunity Hospital, which is located in Whittier. Coast Plaza Doctors Hospital is licensed for 105 beds, of which 7 are skilled nursing beds. Presbyterian Intercommunity Hospital is licensed for 402 beds, of which 24 are licensed as skilled nursing beds.
In the surrounding service area of Hollywood Community Hospital, there are two main competitors, Olympia Medical Center, an acute care hospital licensed for 204 beds and Valley Presbyterian Hospital, a 350 acute care licensed bed hospital.
14
Brotman, located in Culver City, serves the growing Culver City market as well as parts of West Los Angeles. Its closest competitor, Century City Hospital, closed in the fall of 2008 which provided immediate benefit to Brotman as a number of registered nurses were hired from the hospital. Brotman does not have any significant competitors in its immediate vicinity. Brotman's nearest competitors are UCLA Medical Center, Cedar Sinai Medical Center and Olympia Medical Center, which are located approximately seven miles, five miles and four miles, respectively, from Brotman and all of which have capacity issues for inpatient and emergency care.
Van Nuys Community Hospital is the only psychiatric hospital in the area. There are two competing acute care facilities that offer acute psychiatric services. Mission Community Hospital in Panorama City is licensed for 60 acute psychiatric beds and Pacifica Hospital of the Valley, located in Sun Valley, is licensed for 38 acute psychiatric beds.
We believe that each of our hospitals is able to compete within its respective service areas based upon three primary factors:
- •
- Competitive Cost Structure. We have historically been
successful in increasing operating revenue and developing improved service delivery capabilities. We have been able to achieve a highly-efficient cost structure which allows us to maintain
profitability across all payors. Our cost structure enables us to service patients that many other providers cannot serve profitably. We seek to achieve efficiencies through higher margin revenue
growth and continual process improvements.
- •
- Quality of Service. Our operating model has allowed our
hospitals to develop a reputation for delivering quality care and easy access to the communities in which they serve. We have strengthened the patient care we provide by retaining and recruiting
experienced physicians. Our medical staffs typically practice at several hospitals concurrently, including some major tertiary care facilities located within the same metropolitan areas as our
hospitals.
- •
- Leverageable Platform. Our hospital operations are, over time, expected to provide synergies between our Medical Group business and our Hospital Services segment, allowing us to offer quality, coordinated, healthcare and physician services.
Description of Our Business—Medical Group Segment
Overview
Our affiliated group of Medical Groups is one of the largest providers of physician services for HMO enrollees in Southern California, managing the provision of healthcare services for approximately 135,700 commercial, 19,900 Medi-Cal and 21,800 Medicare lives. Our Medical Group network of approximately 7,200 independent physicians is concentrated in Orange, Los Angeles and San Bernardino Counties. For the fiscal year ended September 30, 2009, our Medical Groups generated revenues of $196.7 million.
Our Medical Groups are networks of independent physicians who collectively contract with HMOs under a capitated payment arrangement. Under the capitated model, an HMO pays our Medical Groups a per-member-per-month ("PMPM") rate, or a "capitation" payment, and then assigns our Medical Groups the responsibility for providing the physician services required by those patients. In certain areas, HMOs find it more efficient to outsource the responsibility of providing physician services through Medical Groups. The relationship between HMOs and Medical Groups is a well-established model in the markets we serve and is designed to motivate physicians to practice preventative medicine and reduce unnecessary procedures. Medical Groups allow independent physicians to participate in contracts with HMOs and obtain patients, while allowing HMOs to more efficiently contract for physician services and outsource certain administrative functions associated with those activities.
15
We provide the following management and administrative support services to our affiliated physician organizations:
- •
- negotiation of contracts with physicians and HMOs;
- •
- physician recruiting and credentialing;
- •
- human resources;
- •
- claims administration;
- •
- provider relations;
- •
- member services;
- •
- medical management, including utilization management and quality assurance; and
- •
- data collection and management information systems.
We employ a variety of methodologies to mitigate the financial risk associated with the capitation model, including passing a portion of our payment through to the physician in a "sub-capitated" payment, pre-negotiating contracts with other providers, requiring prior authorization for services, and other techniques to appropriately manage utilization. All of our primary care physicians and a portion of our specialist physicians receive sub-capitation payments, with capitation representing approximately 53% of our medical costs. The remaining 47% of our medical costs consist of pre-authorized procedures referred to our contracted providers at discounted fee-for-service rates and emergency room services provided by non-contracted providers.
Our Affiliated Physician Organizations
Our two management subsidiaries, PMS and PHCA, currently provide management services to ten affiliated physician organizations. Our affiliated physician organizations include PMG, the nine affiliated physician organizations that PMG owns or controls, and one affiliated physician organization that is a joint venture in which PMG owns a 50% interest.
Physician organizations, by California law, may only be owned by physicians. We have designated Arthur Lipper, M.D., the President of PMG, to be the owner of all of the capital stock of PMG. As such he indirectly controls PMG's ownership interest in each of our other affiliated physician organizations. Dr. Lipper is also the President of all of the affiliated physician organizations that PMG owns (except Nuestra Familia Medical Group, Pomona Valley Medical Group, and Upland Medical Group, where he is a Vice-President) and is one of the two general partners of our joint venture affiliated physician organization.
We control the ownership of each of our affiliated physician organizations through assignable option agreements that we have entered into through our management subsidiary, PMS, with Dr. Lipper and PMG, and with Dr. Lipper and Nuestra. See "Assignable Option Agreement," below. For financial reporting purposes, we are deemed to control PMG under U.S. Generally Accepted Accounting Principles (see "Management's Discussion and Analysis of Financial Condition and Results of Operations—Critical Accounting Policies—Consolidation of Financial Statements") and are therefore required to consolidate the financial statements of PMG with those of our management subsidiaries.
Our affiliated physician organizations consist of affiliated Medical Groups which contract with physicians (primary care and specialist) and other ancillary providers, to provide all of their physician services.
Each of our affiliated physician organizations enters into contracts with HMOs to provide physician services to enrollees of the HMOs. Most of our HMO agreements have an initial term of two years renewing automatically for successive one-year terms. Increased capitation rates under the HMO
16
agreements are usually negotiated at the end of the term of such HMO agreements, typically taking the form of new agreements or amendments for additional two-year terms.
The HMO agreements generally provide for a termination by the HMOs for cause at any time, although we have never experienced a for-cause termination. The HMO agreements generally allow either the HMOs or the affiliated physician organizations to terminate the HMO agreements without cause within a four to six month period immediately preceding the expiration of the term of the agreement.
As of September 30, 2009, our affiliated physician organizations had contracts with approximately 6,200 independent physicians.
The physicians of the affiliated physician organizations are exclusively in control of and responsible for all aspects of the practice of medicine, subject to specialist referral guidelines developed by multi-specialty medical committees composed of our contracted physicians and chaired by one of our medical directors.
Information about our ten affiliated physician organizations is listed in the tables below. Except where noted, each organization is a medical corporation owned either directly or through PMG by a single shareholder, currently, Arthur Lipper, M.D.
| |
As of September 30, 2009 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Affiliated Physician Organizations
|
Primary Care Physicians |
Specialists | Enrollees | Area of Operations | |||||||
Prospect Medical Group, Inc. |
452 | 3,337 | 28,587 | Orange, Los Angeles & Riverside Counties | |||||||
Prospect Health Source Medical Group, Inc. |
72 | 1,845 | 14,055 | West Los Angeles | |||||||
Nuestra Familia Medical Group, Inc.(1) |
75 | 915 | 3,301 | East Los Angeles | |||||||
AMVI/Prospect Health Network(2) |
276 | 1,777 | 13,134 | Orange County | |||||||
Prospect Professional Care Medical Group |
184 | 2,275 | 16,024 | East Los Angeles & North Orange County | |||||||
Prospect NWOC Medical Group, Inc. |
110 | 1,428 | 5,773 | North Orange County | |||||||
StarCare Medical Group, Inc.(3) |
157 | 1,935 | 16,443 | North Orange County | |||||||
Genesis HealthCare of Southern California |
198 | 1,745 | 12,514 | Los Angeles and North Orange County | |||||||
Pomona Valley Medical Group |
126 | 183 | 55,960 | San Bernardino County | |||||||
Upland Medical Group |
85 | 146 | 11,609 | San Bernardino Counties | |||||||
Less: Physicians counted at multiple Medical Group |
(825 | ) | (9,346 | ) | — | ||||||
Total |
910 | 6,240 | 177,400 | ||||||||
- (1)
- 55%
owned by PMG directly with Arthur Lipper, M.D. through a separate assignable option agreement.
- (2)
- 50% owned joint venture partnership with AMVI/IMC Health Network, originally formed to service Medi-Cal, Healthy Families and OneCare members under the CalOPTIMA contract. Included in the total enrollment were approximately 2,900 enrollees that we manage for our own
17
economic benefit, and approximately 10,200 enrollees in the joint venture and in AMVI Care that we manage for the economic benefit of our partner, for which we earn management fee income.
| |
As of September 30, | ||||||
|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||
Commercial |
135,700 | 144,700 | |||||
Medicare |
21,800 | 21,900 | |||||
Medi-Cal |
19,900 | 27,400 | |||||
Totals |
177,400 | 194,000 | |||||
Note: On August 1, 2008, we sold the AV Entities, which had total enrollees of approximately 18,000 as of the date of sale.
The Medi-Cal enrollment statistics above include both enrollees that we manage for our own economic benefit, and enrollees that we manage for the economic benefit of our partner in the AMVI/Prospect Health Network joint venture. The number of enrollees included in the above table for which we provide management services to our joint venture partner, but in which we have no beneficial ownership interest, was 10,200 and 9,100, as of September 30, 2009 and 2008, respectively.
Revenue Concentration Statistics of our Affiliated Physician Organizations
For the Fiscal Years Ended September 30, 2009 and 2008
For the fiscal year ended September 30, 2009, our affiliated physician organizations had contracts with approximately 14 HMOs, from which our revenue was primarily derived. All of the contracts between our affiliated physician organizations and the HMOs provide for the provision of medical services to the HMO enrollees by the affiliated physician organization in consideration for the prepayment of the fixed monthly capitation fee paid by the HMOs.
For the fiscal years ended September 2009 and 2008, our affiliated physician organizations recognized capitation revenue of approximately $193,543,000 and $199,322,000, respectively. During those periods, the five largest HMOs of our affiliated physician organizations, United Healthcare, Health Net of California, Blue Cross of California, Blue Shield of California and Inter Valley Health Plan, accounted for approximately 77% and 79% of total capitation revenue, respectively.
As of June 1, 2009, the latest date for which such date was compiled, our affiliated physician organizations were listed by Cattaneo & Stroud as having a combined market share (based on number of HMO enrollees served) of approximately 6.7% in Orange County (92,000 enrollees compared to 1,378,450 total enrollees in Orange County), approximately 0.4% in Los Angeles County (18,000 enrollees compared to 4,863,050 total enrollees in Los Angeles County), and approximately 8.3% in San Bernardino County (68,000 enrollees compared to 822,900 total enrollees in San Bernardino County).
Assignable Option Agreement
The assignable option agreement is an essential element of our "single shareholder model." The assignable option agreement between our management subsidiary, PMS, and PMG provides PMS the right, at will and on an unlimited basis, to designate a successor physician to purchase the capital stock of PMG for nominal consideration ($1,000) and thereby determine the ownership of PMG. The assignable option agreement terminates or expires coterminous with the management services agreement between PMS and PMG, which has a thirty-year term with successive automatic ten-year
18
renewal terms. There is no limitation on whom we may name as a successor shareholder except that any successor shareholder must be duly licensed as a physician in the State of California or otherwise be permitted by law to be a shareholder of a professional corporation.
As a result of the assignable option agreement and our control of PMS, we have control over the ownership of PMG. Because PMG is the owner of all or a significant amount of the capital stock of all of the other affiliated physician organizations, control over the ownership of PMG ensures that we can control the ownership of each of our affiliated physician organizations.
Arthur Lipper, M.D. is currently the sole shareholder, sole director and President of PMG. He is also the President of each of our other affiliated physician organizations, except for AMVI/Prospect Health Network, Nuestra Familia Medical Group, Pomona Valley Medical Group and Upland Medical Group. As such, Dr. Lipper has a fiduciary duty to protect the interests of each entity and its shareholders.
Management Services Agreements
Upon completion of every Medical Group acquisition, one of our management subsidiaries enters into a long-term management services agreement with the newly-acquired physician organization. Our management subsidiaries provide management services to our affiliated Medical Groups under management services agreements that transfer control of all non-medical components of the business of the affiliated physician organizations to our management subsidiaries to the full extent permissible under federal and state law.
Under the management services agreements, we, through our management subsidiaries, provide management functions only. Under these agreements, each affiliated physician organization delegates to us the non-physician support activities that are required by the affiliated physician organizations in the practice of medicine. The management services agreements require us to provide suitable facilities, fixtures and equipment and non-physician support personnel to each affiliated physician organization. The primary services that we provide under management services agreements include the following:
- •
- utilization management and quality assurance;
- •
- medical management;
- •
- physician contracting;
- •
- physician credentialing;
- •
- HMO contracting;
- •
- claims administration;
- •
- provider relations;
- •
- management information systems;
- •
- patient eligibility and services;
- •
- member services; and
- •
- physician recruiting.
In return for these management and administrative support services we receive a management fee. Our current standard management fee is 15% of each organization's gross revenues, which we receive from each of our affiliated physician organizations, with the exception of AMVI/Prospect Health Network (an amount equal to the sum of $5.25 per CalOPTIMA Medi-Cal enrollee per month, $3.15 per CalOPTIMA Healthy Families enrollee, and 6.5% of the premium per CalOptima OneCare enrollee per month).
19
In addition to these management fees, we receive an incentive bonus based on the net profit or loss of each wholly-owned affiliated physician organization. Generally, we are allocated a 50% residual interest in all profits after the first 8% of the profits or a 50% residual interest in the net losses, after deduction for costs to the management subsidiary and physician compensation.
From time to time, supplemental management fees have been awarded by the physician organizations to the management companies to compensate for, among other things, increased costs associated with specific initiatives for the benefit of the physician organizations.
Because of the ownership of a controlling financial interest by PMG or Dr. Lipper in all of our affiliated physician organizations, other than AMVI/Prospect Health Network, we have the ability to adjust our management fees (other than for AMVI/Prospect Health Network) should we determine that an adjustment is appropriate and warranted, based on increased costs associated with managing the affiliated physicians organizations. In the case of AMVI/Prospect Health Network, because PMG's ownership interest is a 50% interest, in the event we determine that an adjustment of the management fee for AMVI/Prospect Health Network is appropriate, an adjustment would require negotiation with the joint venture partner.
Notwithstanding our ability to control the management fee adjustment process, we are limited by laws affecting management fees of healthcare management service companies. Such laws require that our management fees reflect fair market value for the services being rendered, giving consideration however to the costs of providing the services. Such laws also limit our ability to increase our management fees more frequently than once a year.
The management services agreements with our affiliated physician organizations that are 100% owned by PMG each have a thirty-year term and renew automatically for successive ten-year terms unless either party elects to terminate them 90 days prior to the end of their term. The management services agreements with those affiliated physician organizations in which PMG has less than a 100% interest have different terms. Our contract with Nuestra Familia is for only ten years; however, because Dr. Lipper as the nominee shareholder under an assignable option agreement is a 55% shareholder, any renewal or termination must be approved by Dr. Lipper. Similarly, our joint venture with AMVI is year-to-year, but because PMG is a 50% owner of that joint venture, it cannot be terminated without approval of the board of directors, of which PMG controls the appointment of 50% of the members. The management services agreements are terminable by the unilateral action of the particular physician organization prior to their normal expiration if we materially breach our obligations under the agreements or become subject to bankruptcy-related events, and we are unable to cure a material breach within sixty days of the occurrence. All management fees of consolidated entities are eliminated in our consolidated financial statements.
Risk Management
We control the medical expense or medical risk of our affiliated physician organizations. We use sub-capitation as our primary technique to control this risk. Sub-capitation is where an organization that is paid under capitated contracts with an HMO in turn contracts with other providers on a capitated basis for a portion of the original capitated premium. Historically, approximately half of the medical costs of our affiliated physician organizations are sub-capitated.
The medical costs of our affiliated physician organizations which are not sub-capitated are controlled in various ways. For those specialties for which we cannot, or do not choose to obtain a sub-capitated contract, we negotiate discounted fee-for-service contracts. Further, by contract, our affiliated physician organizations generally do not assume responsibility for the costs of providing medical services ("medical costs") that occur outside of their service area, which has been defined as a 30-mile radius around the office of the HMO enrollee's primary care physician. All non-emergent care requires prior authorization, in order to limit unnecessary procedures and to direct the HMO enrollee
20
requiring care to the physicians contracted with our affiliated physician organizations, and to the most cost effective facility. Our affiliated physician organizations utilize board certified pulmonologists and internists, trained in intensive care to maintain appropriate utilization, reducing unnecessary consultations and facilitating the patient's treatment and discharge. We also review medical costs by Medical Group and by specialty and compare those costs to the trend of patient utilization of medical services by specialty. In those instances where the patient utilization is trending very low, we determine whether it would be less expensive for our affiliated physician organizations to pay their providers on a discounted fee-for-service basis rather than on a capitated basis.
In addition, our affiliated physician organizations' agreements with HMOs and hospitals contain risk-sharing arrangements under which the affiliated physician organizations can earn additional compensation by coordinating the provision of quality, cost-effective healthcare to enrollees, but, in certain very limited cases, they may also be required to assume a portion of any loss sustained from these arrangements. Risk-sharing arrangements are based upon the cost of hospital services or other services for which our physician organizations are not capitated. The terms of the particular risk-sharing arrangement allocate responsibility to the respective parties when the cost of services exceeds a budget, which results in a "deficit," and permit the parties to share in any amounts remaining in the budget, known as a "surplus," which occurs when actual cost is less than the budgeted amount. The amount of non-capitated and hospital costs in any period could be affected by factors beyond our control, such as changes in treatment protocols, new technologies and inflation. To the extent that such non-capitated and hospital costs are higher than anticipated, revenue paid to our affiliated physician organizations may not be sufficient to cover the risk-sharing deficits they are responsible for paying, which could reduce our revenues and profitability. It is our experience that "deficit" amounts for hospital costs are applied to offset any future "surplus" amount we would otherwise be entitled to receive. We have historically not been required to reimburse the HMOs for most hospital cost deficit amounts. Most of our contracts with HMOs specifically provide that we will not have to reimburse the HMO for hospital cost deficit amounts.
HMOs may insist on withholding negotiated amounts from the affiliated physician organizations' professional capitation payments, which the HMOs are permitted to retain, in order to cover the affiliated physician organizations' share of any risk-sharing deficits. Whenever possible, we seek to contractually reduce or eliminate our affiliated physician organizations' liability for risk-sharing deficits.
Provider Agreements
The physicians of our affiliated physician organizations are exclusively in control of, and responsible for all aspects of, the practice of medicine, and are subject to specialist referral guidelines developed by multi-specialty medical committees composed of our contracted physicians and chaired by one of our medical directors. Each affiliated physician organization enters into the following types of contracts for the provision of physician and ancillary health services:
Primary Care Physician Agreement. A primary care physician agreement provides for primary care physicians contracting with independent physician associations to be responsible for both the provision of primary care services to enrollees and for the referral of enrollees to specialists affiliated with the independent physician association, when appropriate. Primary care physicians receive monthly sub-capitation for the provision of primary care services to enrollees assigned to them.
Specialist Agreement. A specialist agreement provides for a specialty care physician contracting with the independent physician association to receive either sub-capitated payments or discounted fee-for-service payments for the provision of specialty services to those enrollees referred to them by the independent physician association's primary care physician.
21
Ancillary Provider Agreement. An ancillary provider agreement provides for ancillary service providers—generally non-physician providers such as physical therapists, laboratories, etc.—to contract with an independent physician association to receive either monthly sub-capitated, discounted fee-for service or case rate payments for the provision of service to enrollees on an as-needed basis.
Competition
The medical group industry is highly competitive and is subject to continuing changes with respect to the manner in which services are provided and how providers are selected and paid. We are subject to significant competition with respect to physicians affiliating with our physician organizations. Generally, both we and our affiliated physician organizations compete with any entity that enters into contracts with HMOs for the provision of prepaid healthcare services, including:
- •
- other companies that provide management services to healthcare providers but do not own the affiliated physician
organization;
- •
- hospitals that affiliate with one or more physician organizations;
- •
- HMOs that contract directly with physicians; and
- •
- other physician organizations.
We believe that we offer competitive services in the Southern California managed care market based upon our historical stability, our competitive compensation relative to other organizations, and our quality of service.
There is competition for patients and primary care physicians in every market in which our affiliated physician organizations operate. The number of significant competitors varies in each region. The following summary of information about our competitors and their estimated enrollment in various markets is based on an industry report updated through June 1, 2009. Enrollment numbers that follow differ from updated enrollment numbers of our affiliated entities provided elsewhere in this filing, due to differing dates of presentation.
Based on these reports, total HMO enrollment in Los Angeles County was approximately 4,863,050, of which we had approximately 18,000 enrollees, or approximately 0.4%. Our five largest competitors in Los Angeles County are Kaiser Foundation, Healthcare Partners Medical Group, Regal Medical Group, La Vida Medical Group, and Facey Medical Foundation. HMO enrollment in Orange County was estimated at approximately 1,378,450, of which Prospect had approximately 92,000 enrollees, or approximately 6.7%. Our five largest competitors in Orange County are Kaiser Foundation, St. Joseph Heritage Healthcare, Monarch Healthcare, Greater Newport Physicians Medical Group, and Bristol Park Medical Group. HMO enrollment in San Bernardino County was estimated at approximately 822,900 of which Prospect had approximately 68,000 enrollees, or approximately 8.3%. Our five largest competitors in San Bernardino County are Kaiser Foundation, Beaver Medical Group, Choice Medical Group, PrimeCare of San Bernardino and Regal Medical Group. As such, we believe that the combined enrollment of our affiliated physician organizations is the eighth largest in California.
Some of our competitors are larger than us, have greater resources and may have longer-established relationships with buyers of their services, giving them greater value in contracting with physicians and HMOs. Such competition may make it difficult to enter into affiliations with physician organizations on acceptable terms and to sustain profitable operations.
22
Health Care Regulation
General Regulatory Overview
Both our hospitals and affiliated physician organizations are subject to numerous federal and state statutes and regulations that are applicable to the management and provision of health care services and to business generally, as summarized below. The healthcare industry is required to comply with extensive government regulation at the federal, state, and local levels. Under these regulations, hospitals must meet requirements to be certified as hospitals and qualified to participate in government programs, including the Medicare and Medi-Cal programs. These requirements relate to the adequacy of medical care, equipment, personnel, operating policies and procedures, maintenance of adequate records, hospital use, rate-setting, compliance with building codes, and environmental protection laws. There are also extensive regulations governing a hospital's participation in these government programs. If we fail to comply with applicable laws and regulations, we can be subject to criminal penalties and civil sanctions, our hospitals can lose their licenses and we could lose our ability to participate in these government programs. In addition, government regulations may change. If that happens, we may have to make changes in our facilities, equipment, personnel, and services so that our hospitals remain certified as hospitals and qualified to participate in these programs. We believe that our hospitals and affiliated physician organizations are in substantial compliance with current federal, state, and local regulations and standards.
In addition to the regulations referenced above, our affiliated physician organization operations may also be affected by changes in ethical guidelines and operating standards of professional and trade associations such as the American Medical Association. Changes in existing ethical guidelines or professional organization standards, adverse judicial or administrative interpretations of such guidelines and standards, or enactment of new legislation could require us to make costly changes to our business that would reduce our profitability. Changes in health care legislation or government regulation may restrict our existing operations, limit the expansion of our business or impose additional compliance requirements and costs, any of which could have a material adverse effect on our business, financial condition, results of operations and the trading price of our stock.
Corporate Practice of Medicine and Professional Licensing
In California, lay entities are generally prohibited from exercising control over the medical or the business aspects of a professional practice, and may be prohibited from sharing the profits of a professional practice. The California Medical Board has taken the position that certain physician practice management agreements that confer too much control over a physician practice violate the prohibition against corporate practice of medicine. The California Medical Board has also taken the position in at least one case that an assignable option agreement, whereby a lay management company can assign to a nominee physician the right to purchase all of the shares of the managed medical group for a nominal price, violates the corporate practice of medicine prohibition. While there is no express provision in the California statutes prohibiting a lay entity from holding an option to purchase stock in a medical corporation, lay entities are prohibited from owning such stock and one court, in an unpublished opinion, has determined that such stock may not be beneficially owned by a lay entity.
State law also imposes licensing requirements on individual physicians and on some facilities operated by physicians. Federal and state laws regulate HMOs and other managed care organizations with which physician organizations may have contracts. Some states also require licensing of third-party administrators and collection agencies. This may affect our operations in states in which we may seek to do business in the future. Our ability to operate profitably will depend, in part, upon our ability and the ability of our affiliated physician organizations to obtain and maintain all necessary licenses and other approvals and operate in compliance with applicable health care laws and regulations, including any new laws and regulations or new interpretations of existing laws and regulations.
23
Anti-Kickback
Medicare and Medi-Cal anti-kickback and anti-fraud and abuse amendments codified under Section 1128B(b) of the Social Security Act (the "Anti-kickback Statute") prohibit certain business practices and relationships that might affect the provision and cost of health care services payable under the Medicare and Medi-Cal programs and other government programs, including the payment or receipt of remuneration for the referral of patients whose care will be paid for by such programs. Sanctions for violating the Anti-kickback Statute include criminal and civil penalties, as well as fines and possible exclusion from government programs, such as Medicare and Medi-Cal. Many states have statutes similar to the federal Anti-kickback Statute, except that the state statutes usually apply to referrals for services reimbursed by all third-party payors, not just federal programs. In addition, it is a violation of the federal Civil Monetary Penalties Law to offer or transfer anything of value to Medicare or Medi-Cal beneficiaries that is likely to influence their decision to obtain covered goods or services from one provider of service over another. The federal government has also issued regulations that describe some of the conduct and business relationships that are permissible under the Anti-kickback Statute. These regulations are often referred to as the "Safe Harbor" regulations. The fact that certain conduct or a given business arrangement does not meet a Safe Harbor does not necessarily render the conduct or business arrangement illegal under the Anti-kickback Statute. Rather, such conduct and business arrangements risk increased scrutiny by government enforcement authorities and should be reviewed on a case-by-case basis.
There are several aspects of our hospitals' relationships with third parties and our relationships with physicians to which the Anti-kickback Statute may be relevant. The government may construe some of the marketing and managed care contracting activities that we historically performed as arranging for the referral of patients to the physicians with whom we had a management agreement. The government may also construe some of the financial arrangements that our hospitals have historically had with physicians, marketers and other referral sources as payment for the referral or arranging for the referral of patients to our hospitals. As a result of our internal compliance review process, we have, from time to time, identified contract relationships we believed posed a risk to the Company, and in such cases, we have changed the payments, modified the terms or terminated these contracts. We believe our business activities are not in violation of the Anti-kickback Statute. Further, we believe that the business operations of our affiliated physician organizations do not involve the offer, payment, solicitation or receipt of remuneration to induce referrals of patients, because compensation arrangements between the physician organizations and the primary care physicians who make referrals are designed to discourage referrals to the extent they are medically unnecessary. These physicians are paid either on a sub-capitation or fee-for-service basis and do not receive any financial benefit from making referrals.
Noncompliance with, or violation of, the Anti-kickback Statute can result in exclusion from the Medicare and Medi-Cal programs and civil and criminal penalties. California also has a similar anti-kickback prohibition with similar penalties. Although we believe our activities to be in compliance, if we were found to be in violation of the anti-kickback legislation, we could suffer civil penalties, criminal fines, imprisonment or possible exclusion from participation in the reimbursement programs, which could reduce our revenues, increase our costs and decrease our profitability.
Self-Referral
Section 1877 of the Social Security Act (commonly referred to as the "Stark law") generally restricts referrals by physicians of Medicare patients to entities with which the physician or an immediate family member has a financial relationship, unless one of several exceptions applies. The referral prohibition applies to a number of statutorily defined "designated health services," such as clinical laboratory, physical therapy, radiology, and inpatient and outpatient hospital services. The exceptions to the referral prohibition cover a broad range of common financial relationships. These
24
statutory, and the subsequent regulatory, exceptions are available to protect certain permitted employment relationships, leases, group practice arrangements, medical directorships, and other common relationships between physicians and providers of designated health services, such as hospitals. A violation of the Stark law may result in a denial of payment, required refunds to patients and the Medicare program, civil monetary penalties of up to $15,000 for each violation, civil monetary penalties of up to $100,000 for "sham" arrangements, civil monetary penalties of up to $10,000 for each day that an entity fails to report required information, and exclusion from participation in the Medicare and Medi-Cal programs and other federal programs. In addition, California has its own self-referral laws which are similar in many ways to the Stark law, but which differ from the federal law in that they apply not just to Medicare patients, but to all categories of patients and they impose disclosure requirements. No payment from any source is permitted for services performed pursuant to referrals which are prohibited by California's self-referral law. Our hospitals' and Medical Groups' participation in and development of financial relationships with physicians could be adversely affected by the Stark law or similar state enactments.
The self-referral prohibition applies to our services, and we believe our relationships comply with the law. We believe our business arrangements do not involve the referral of patients to entities with whom referring physicians have an ownership interest or compensation arrangement within the meaning of federal and state self-referral laws, because referrals are made directly to other providers rather than to entities in which referring physicians have an ownership interest or compensation arrangement. We further believe our financial arrangements with physicians fall within exceptions to state and federal self-referral laws, including exceptions for ownership or compensation arrangements with managed care organizations and for physician incentive plans that limit referrals. In addition, we believe that the methods we use to acquire existing physician organizations and to recruit new physicians do not violate such laws and regulations. Nevertheless, it is possible that the government or a court could construe some of the financial arrangements that our hospitals or Medical Groups have historically had with physicians or may have in the future as non-compliant with state or federal self-referral statutes. If we were found to have violated the self-referral laws, we could be subject to denial of reimbursement, forfeiture of amounts collected in violation of the law, civil monetary penalties, and exclusion from the Medicare and Medi-Cal programs, which could reduce our revenues, increase our costs and decrease our profitability.
False Claims Act
The federal False Claims Act ("FCA") prohibits providers from knowingly submitting false claims for payment to the federal government. This law has been used not only by the federal government, but also by individuals who bring an action on behalf of the government under the law's "qui tam" or "whistleblower" provisions. When a private party brings a qui tam action under the federal FCA, the defendant may not become aware of the lawsuit until the government makes a determination whether it will intervene and take a lead in the litigation.
Civil liability under the federal FCA can be up to three times the actual damages sustained by the government plus civil penalties for each separate false claim. There are many potential bases for liability under the federal FCA, including claims submitted pursuant to a referral found to violate the anti-kickback or self-referral statutes. Although liability under the federal FCA arises when an entity knowingly submits a false claim for reimbursement to the federal government, the federal FCA defines the term "knowingly" broadly. Although simple negligence generally will not give rise to liability under the federal FCA, submitting a claim with reckless disregard for its truth or falsity can constitute "knowingly" submitting a false claim. Recently, the federal FCA was further expanded to cover the improper retention of an overpayment when President Obama signed into law the Fraud Enforcement and Recovery Act of 2009.
25
The State of California has enacted false claims legislation. These California false claims statutes are generally modeled on the federal FCA, with similar damages, penalties, and qui tam enforcement provisions. For example, the California False Claims Act prohibits "knowingly" submitting false claims for payment to California and its agencies, such as the Medi-Cal program. Violations are subject to damages and civil monetary penalties. Similar to the federal statute, the California False Claims Act allows private parties to sue on behalf of the state as qui tam (i.e., whistleblower) plaintiffs, and authorizes qui tam plaintiffs to share in any proceeds recovered as a result of the lawsuit. California's False Claims Act also includes provisions intended to discourage employers from retaliating against employees for initiating, testifying or assisting in qui tam lawsuits, or otherwise furnishing information to government or law enforcement authorities. An increasing number of healthcare false claims cases seek recoveries under both federal and state law. Provisions in the Deficit Reduction Act of 2005 ("DRA") that went into effect on January 1, 2007 give states significant financial incentives to enact false claims laws modeled on the federal FCA. Additionally, the DRA requires every entity that receives annual payments of at least $5 million from a state Medi-Cal plan to establish written policies for its employees that provide detailed information about federal and state false claims statutes and the whistleblower protections that exist under those laws. Both provisions of the DRA are expected to result in increased false claims litigation against health care providers. We believe our Alta hospitals have fully complied with the written policy requirements, and we are in the process of reviewing and, to the extent necessary, updating the written policies of our newly acquired Brotman facility. Since the Brotman facility was not previously controlled or operated by the Company or its subsidiaries, we cannot assure that its prior policies fully complied with the DRA requirements. Compliance with the written policy requirement is a condition of payment by Medi-Cal, and failure to comply could give rise to claims for recoupment of Medi-Cal payments, damages and other sanctions.
Fraud and Abuse
Existing federal laws governing Medi-Cal, Medicare and other federal health care programs, as well as similar state laws, impose on us a variety of fraud and abuse prohibitions. These laws are interpreted broadly and enforced aggressively by multiple government agencies, including the Office of Inspector General of the Department of Health and Human Services, the Department of Justice and various state authorities. In addition, in the DRA, Congress created a new Medicaid Integrity Program to enhance federal and state efforts to detect Medi-Cal fraud, waste and abuse and provide financial incentives for states to enact their own false claims acts as an additional enforcement tool against Medi-Cal fraud and abuse. Violations of these laws are punishable by substantial penalties, including monetary fines, civil penalties, criminal sanctions, exclusion from participation in government-sponsored health care programs, and forfeiture of amounts collected in violation of such laws, any of which could have an adverse effect on our business and results of operations.
Emergency Medical Treatment and Active Labor Act
All of our hospital facilities are subject to the Emergency Medical Treatment and Active Labor Act ("EMTALA"). This federal law requires any hospital that participates in the Medicare program to conduct an appropriate medical screening examination of every person who presents to the hospital's emergency department for treatment and, if the patient is suffering from an emergency medical condition, to either stabilize that condition or make an appropriate transfer of the patient to a facility that can handle the condition. The obligation to screen and stabilize emergency medical conditions exists regardless of a patient's ability to pay for treatment. All hospitals with specialized capabilities are also required to accept appropriate transfers of patients in need of such specialized services if the transferring hospital cannot provide the services required by the patient. There are severe penalties under EMTALA if a hospital fails to screen or appropriately stabilize or transfer a patient or if the hospital delays appropriate treatment in order to first inquire about the patient's ability to pay, or if the hospital fails to accept an appropriate transfer of a patient from another hospital for specialized services. Penalties for violations of EMTALA include civil monetary penalties and exclusion from participation in the Medicare program. In addition, an injured patient, the patient's family or a medical facility that suffers a financial loss as a direct result of another hospital's violation of the law can bring a civil suit against that other hospital.
26
During 2003, CMS published a final rule clarifying a hospital's duties under EMTALA. In the final rule, CMS clarified when a patient is considered to be on a hospital's property for purposes of treating the person pursuant to EMTALA. CMS stated that off-campus facilities such as specialty clinics, surgery centers and other facilities that lack emergency departments should not be subject to EMTALA, but that these locations must have a plan explaining how the location should proceed in an emergency situation such as transferring the patient to the closest hospital with an emergency department. CMS further clarified that hospital-owned ambulances could transport a patient to the closest emergency department instead of to the hospital that owns the ambulance. However, under certain circumstances, when a patient is in a ground or air ambulance owned by one of our hospitals for purposes of examination and treatment for a medical condition at that hospital, EMTALA requires that the patient be screened for, and as needed, treated for an emergency medical condition at least until the patient's condition has been stabilized. CMS's rules did not specify "on-call" physician requirements for an emergency department, but provided a subjective standard stating that "on-call" hospital schedules should meet the hospital's and community's needs. Although we believe that our hospitals comply with EMTALA, we cannot predict whether CMS will implement new requirements in the future and whether our hospitals will comply with any new requirements.
Health Care Facility Licensing, Certification and Accreditation Requirements
All of our hospitals are subject to compliance with various federal, state and local statutes and regulations. Our hospitals must also comply with the conditions of participation and licensing requirements of federal, state and local health agencies, as well as the requirements of municipal building codes, health codes and local fire departments. Various other licenses and permits also are required in order to dispense narcotics, operate pharmacies, handle radioactive materials and operate certain equipment. We believe our health care facilities hold all required governmental approvals, licenses and permits material to the operation of our business.
Hospitals are subject to periodic inspection by federal, state, and local authorities to determine their compliance with applicable regulations and requirements necessary for licensing and certification. All of our hospitals are licensed under appropriate state laws and are qualified to participate in Medicare and Medi-Cal programs. In addition, all of our hospitals are accredited by the Joint Commission. This accreditation indicates that a hospital satisfies the applicable health and administrative standards to participate in Medicare and Medi-Cal programs. If any of our facilities were to lose its Joint Commission accreditation or otherwise lose its certification under the Medicare and Medi-Cal programs, the hospital may be unable to receive reimbursement from the Medicare and Medi-Cal program and other payors. We believe that our hospitals are in substantial compliance with current applicable federal, state, local and independent review body regulations and standards. The requirements for licensure, certification and accreditation are subject to change and, in order to remain qualified, it may become necessary for us to make changes in our facilities, equipment, personnel and services in the future, which could have a material adverse impact on operations.
Recovery Audit Contractors
In 2003, Congress enacted section 306 of the MMA, which directed the Department of Health and Human Services to conduct a three year demonstration program using Recovery Audit Contractors ("RACs") to identify overpayments and underpayments in the Medicare Fee-For-Service program, as a means of fighting fraud, waste and abuse in the Medicare program. The demonstration project operated in New York, Massachusetts, Florida, South Carolina and California and ended on March 27, 2008. In 2006, Congress enacted the Tax Relief and Health Care Act of 2006, which established a permanent and national RAC program to be in place by January 1, 2010. The RACs will review hospitals, physician practices, nursing homes, home health agencies, durable medical suppliers and any other provider or supplier that bills Medicare Parts A and B. The RACs will review claims on a
27
post-payment basis and conduct both automated (no medical record needed) and complex (medical record required) reviews for claims paid after October 1, 2007. CMS and the RAC contractors are currently in the process of phasing in the program. Reviews by the RACs may result in a determination that there have been overpayments by Medicare to facility and recoupment by Medicare of such overpayment amounts, plus interest and potential penalties. As of September 30, 2009 no RAC audit was scheduled for any of our hospitals.
Never Events and Hospital Acquired Conditions
In 2002, the National Quality Form published "Serious Reportable Events in Healthcare: A Consensus Report" that identified 27 adverse events that were "serious, largely preventable and of concern to both the public and healthcare providers." This list (and subsequent revisions) became known as "never events." Historically, Medicare did not distinguish between costs that resulted from patient treatment as opposed to costs that resulted from an adverse event that occurred in the hospital. Section 5001(c) of the Deficit Reduction Act of 2005 required CMS to identify conditions that were high cost or volume or both, resulted in assignment to a DRG that had a higher payment when present as a secondary diagnosis, and that could have reasonably been prevented. As a result, CMS has developed a list of hospital acquired conditions (such as foreign object retained after surgery, Stage III and IV pressure ulcers and catheter-associated urinary tract infections) that are denied higher Medicare payments. In addition, CMS has developed a list of non-covered services that relate to adverse events (e.g., surgery on the wrong body part or correct procedure on the wrong patient) for which the hospital will not be reimbursed. The hospital will be at risk for decreased reimbursement if certain adverse events or hospital acquired conditions occur.
California Reporting of Adverse Events and Immediate Jeopardy Penalties
California is one of many states that have adopted strict reporting requirements for adverse events in general acute-care hospitals (and psychiatric and special hospitals) and initiated penalties for failure to report and for deficiencies identified as situations where the "noncompliance caused or was likely to cause serious harm or death to the patient" (known as "immediate jeopardy" deficiencies). Health and Safety Code section 1279.1 mandates that a health facility report an adverse event (as delineated in the statute) to the Department of Public Health within five days of the date the adverse event is detected or within one day if the issue is an ongoing or emergent threat to a patient, personnel or visitors' welfare, health or safety. Failure to report an adverse event may result in fines of up to $100 per day for each day the event is not reported. If the Department of Public Health issues a deficiency that constitutes immediate jeopardy, the hospital will be responsible for submitting a plan of correction and the Department of Public Health may assess an administrative penalty. Effective January 1, 2009, Health and Safety Code Section 1280.1(d) provides that the amount of the administrative penalty for immediate jeopardy shall be up to $50,000 for the first administrative penalty, up to $75,000 for the second subsequent immediate jeopardy violation and up to $100,000 for the third and every subsequent violation. The statute further provides that an administrative penalty issued after three years from the date of the last immediate jeopardy shall be considered a first administrative penalty as long as the hospital has not received additional immediate jeopardy violations and is determined to be in substantial compliance with all state and federal licensing laws and regulations. The hospital will be at risk for administrative penalties if adverse events occur. The hospital will also be at risk for further oversight from state and federal regulators.
Utilization Review Compliance and Hospital Governance
Federal law contains numerous provisions designed to ensure that services rendered by hospitals to Medicare and Medi-Cal patients meet professionally recognized standards, are medically necessary and that claims for reimbursement are properly filed. These provisions include a requirement that a
28
sampling of admissions of Medicare and Medi-Cal patients must be reviewed by peer review organizations, which review the appropriateness of Medicare and Medi-Cal patient admissions and discharges, the quality of care provided, the validity of DRG classifications and the appropriateness of cases of extraordinary length of stay or cost. Peer review organizations may deny payment for services provided, or assess fines and also have the authority to recommend to the DHHS that a provider which is in substantial noncompliance with the standards of the peer review organization be excluded from participation in the Medicare program. Utilization review is also a requirement of most non-governmental managed care organizations.
Medical and surgical services and practices are extensively supervised by committees of staff doctors at each of our hospitals, are overseen by each facility's local governing board, the members of which primarily are community members and physicians, and are reviewed by our clinical quality personnel. The local hospital governing board also helps maintain standards for quality care, develop long-range plans, establish, review and enforce practices and procedures, and approve the credentials and disciplining of medical staff members.
California Seismic Standards
California's Alfred E. Alquist Hospital Facilities Seismic Safety Act (the "Alquist Act") requires that the California Building Standards Commission adopt earthquake performance categories, seismic evaluation procedures, standards and timeframes for upgrading certain facilities, and seismic retrofit building standards. These regulations require hospitals to meet seismic performance standards to ensure that they are capable of providing medical services to the public after an earthquake or other disaster. The Building Standards Commission completed its adoption of evaluation criteria and retrofit standards in 1998. The Alquist Act requires that within three years after the Building Standards Commission had adopted evaluation criteria and retrofit standards:
- •
- Hospitals in California must conduct seismic evaluations and submit these evaluations to the Office of Statewide Health
Planning and Development ("OSHPD"), Facilities Development Division for its review and approval;
- •
- Hospitals in California must identify the most critical nonstructural systems that represent the greatest risk of failure
during an earthquake and submit timetables for upgrading these systems to the OSHPD, Facilities Development Division for its review and approval; and
- •
- Hospitals in California must prepare a plan and compliance schedule for each regulated building demonstrating the steps a hospital will take to bring the hospital buildings into substantial compliance with the regulations and standards.
We were required to conduct engineering studies at our hospitals to determine whether and to what extent modifications to the hospital facilities will be required. We believe that our hospitals satisfy all current requirements; however, we may be required to make significant capital expenditures in the future to comply with the seismic standards, which could impact our earnings.
OSHPD is currently implementing a new voluntary program to re-evaluate the seismic risk of hospital buildings classified as Structural Performance Category ("SPC-1"). These buildings are considered hazardous and at risk of collapse in the event of an earthquake and must be retrofitted, replaced or removed from providing acute care services by January 1, 2013. OSHPD is using HAZUS, a state-of-the-art methodology, to reassess the seismic risk of SPC-1 buildings and those that are determined to pose a low seismic risk may be reclassified to SPC-2. The SPC-2 buildings would have until January 1, 2030 to comply with the structural seismic safety standards. Any buildings that are denied reclassification will remain in the SPC-1 category, and must meet seismic compliance standards by January 1, 2013, unless further extensions are granted. Participation in the HAZUS program is optional for hospital owners wishing to have their SPC-1 building(s) re-evaluated. We have applied for
29
a HAZUS re-evaluation of the seismic risk for Hollywood Community Hospital, Los Angeles Community Hospital, Norwalk Community Hospital and Brotman. Our Van Nuys Community Hospital is exempt from the seismic retrofitting guidelines because psychiatric hospitals are exempt from seismic retrofitting. The current status of the re-evaluation is as follows:
- •
- Hollywood Community Hospital was denied reclassification, and remains in the SPC-1 category;
- •
- Norwalk Community Hospital was granted the reclassification, and moved into the SPC-2 category;
- •
- Los Angeles Community Hospital and Brotman are awaiting reclassification decisions and currently remain in the
SPC-1 category; and
- •
- Brotman has also qualified for SB 306 extension to 2020 which means it will not have to meet SPC-2 and NPC-3 by 2013. However, if Brotman does not meet SPC-2 and NPC-3 category by 2013, it must retrofit the building to meet SPC-5 and NPC-5 by 2020.
Furthermore, the Alquist Act permits OSHPD to grant an extension to acute care hospitals that lack the financial capacity to meet the January 1, 2013 retrofit deadline, and instead, requires them to replace those buildings by January 1, 2020. Brotman has been approved for this extension.
Pursuant to the Alquist Act, hospital buildings not in compliance by their applicable deadlines may be subject to loss of licensure. Unless the noncompliant hospital places its license in voluntary suspense, the Department of Public Health may suspend or refuse to renew the license of a hospital that has received a notice of violation. However, the license may be reinstated or renewed upon presentation to the Department of Public Health of a written notice of compliance.
Hospital Conversion Legislation
California has adopted legislation regarding the sale or other disposition of hospitals operated by not-for-profit entities. The California attorney general has demonstrated an interest in these transactions under its general obligations to protect charitable assets. These legislative and administrative efforts primarily focus on the appropriate valuation of the assets divested and the use of the proceeds of the sale by the not-for-profit seller. These reviews and, in some instances, approval processes can add additional time to the closing of a not-for-profit hospital acquisition. Future actions by state legislators or attorneys general may seriously delay or even prevent our ability to acquire certain hospitals.
Environmental Regulation
Our hospitals and certain affiliated physician organizations generate medical waste that must be disposed of in compliance with federal, state and local environmental laws, rules and regulations. Our operations, as well as our purchases and sales of hospitals, are also subject to compliance with various other environmental laws, rules and regulations. Such compliance costs are not significant and we do not anticipate that such compliance costs will be significant in the future.
HIPAA Transaction, Privacy and Security Requirements
Federal regulations issued pursuant to the Health Insurance Portability and Accountability Act ("HIPAA") contain, among other measures, provisions that require us to implement very significant and potentially expensive new computer systems, employee training programs and business procedures. The federal regulations are intended to protect the privacy of healthcare information and encourage electronic commerce in the healthcare industry. Our hospitals and affiliated physician organizations are covered entities subject to these regulations. As a business associate of such entities and contracted health plans, we are also subject to many HIPAA requirements pursuant to a business associate
30
contract required between covered entities and their business associates and now, because of Health Information Technology for Economic and Clinical Health Act (the "HITECH Act"), directly under HIPAA. HITECH amended HIPAA, which previously applied only to "covered entities" (i.e., healthcare providers, insurers, and clearinghouses), to now apply directly to business associates, who previously were subject only to contractual liability to covered entities under business associate agreements. As a result, business associates will have to institute the same formalized HIPAA compliance programs that covered entities must, including detailed written policies, training programs, dedicated personnel, and board oversight. We are also subject to California's privacy laws regarding privacy of medical information.
Among other things, HIPAA requires healthcare facilities to use standard data formats and code sets established by DHHS when electronically transmitting information in connection with several transactions, including health claims and equivalent encounter information, healthcare payment and remittance advice and health claim status. We have implemented or upgraded computer system utilizing a third party vendor, as appropriate, at our facilities and at our corporate headquarters to comply with the new transaction and code set regulations and have tested these systems with our payors.
HIPAA also requires DHHS to issue regulations establishing standard unique health identifiers for individuals, employers, health plans and healthcare providers to be used in connection with the standard electronic transactions. All healthcare providers, including our facilities, were required to obtain a new National Provider Identifier to be used in standard transactions instead of other numerical identifiers beginning no later than May 23, 2007. Our facilities have fully implemented use of the Employer Identification Number as the standard unique health identifier for employers without experiencing any payment delays during the transition.
HIPAA regulations also require our facilities to comply with standards to protect the confidentiality, availability and integrity of patient health information, by establishing and maintaining reasonable and appropriate administrative, technical and physical safeguards to ensure the integrity, confidentiality and availability of electronic health and related financial information. The security standards were designed to protect electronic information against reasonably anticipated threats or hazards to the security or integrity of the information and to protect the information against unauthorized use or disclosure. The security standards require our facilities to implement business procedures and training programs, though the regulations do not mandate use of a specific technology. We have performed comprehensive security risk assessments and are currently in the remediation process for the systems/devices that have been identified as having the highest levels of vulnerability. This will be an ongoing process as we update, upgrade, or purchase new systems technology.
DHHS has also established standards for the privacy of individually identifiable health information. These privacy standards apply to all health plans, all healthcare clearinghouses and healthcare providers, such as our facilities, that transmit health information in an electronic form in connection with standard transactions, and apply to individually identifiable information held or disclosed by a covered entity in any form. These standards now also apply to us in our capacity as a business associate of such covered entities. These standards impose extensive administrative requirements on us and our facilities and require compliance with rules governing the use and disclosure of this health information, and they require our facilities to impose these rules, by contract, on any business associate to whom we disclose such information in order for them to perform functions on our facilities' behalf. In addition, our facilities will continue to remain subject to California's privacy laws that are in many instances more restrictive than the privacy regulations issued under HIPAA. California's privacy laws could impose additional penalties.
The restrictions under HIPAA and California's privacy laws have over the years been strengthened and penalties for their breach increased. HITECH greatly enhanced HIPAA's patient privacy and security obligations. HITECH and HIPAA require correspondingly intensive compliance efforts by
31
providers and suppliers, including self-disclosures of breaches to federal officials and a fining system. "Snooping" by covered entity personnel constitutes a breach of HIPAA. These anti-snooping provisions present operational challenges to healthcare providers, including us. HITECH also amends HIPAA to create new enforcement provisions and expanded civil and criminal penalties. The net effect of these amendments is to make HIPAA a more encompassing regulatory scheme for patient privacy. California legislation enacted effective January 1, 2009 mirrors the HIPAA changes enacted by HITECH. The California legislation has more stringent anti-snooping provisions than those enacted by HITECH, contains mandatory breach notice rules applicable to us and enhances penalties for noncompliance. Compliance with these standards requires significant commitment and action by us.
Antitrust
Federal and state antitrust laws prohibit agreements in restraint of trade, price-fixing, division of markets, the exercise of monopoly power and other practices that are considered to be anti-competitive. We must structure and operate our business activities and select and implement our Medical Group and hospital acquisitions in a manner which conforms with antitrust laws. If any of our current or newly acquired Medical Groups were determined to be competitors with one another, it is possible that their common management by us could be claimed to lead to sharing of pricing information or coordinated price negotiations that could be prohibited under antitrust laws. Government authorities have also challenged Medical Groups under the antitrust laws if the Medical Groups negotiate prices on behalf of their physician members with PPOs or insurance companies on a non-capitated (e.g. fee-for-service) basis. If one or more of our Medical Groups were to negotiate PPO prices in such a manner, they could be subject to an antitrust challenge. While we believe that we are in material compliance with federal and state antitrust laws, if we were found to be in violation of these laws, we could be subject to significant financial penalties, possible divestiture of certain assets and a possible injunction that could disrupt our business operations or require a restructuring of our physician relationships.
Health Plan Licensing and Regulation
The California Department of Managed Health Care ("DMHC") is responsible for licensing and regulating health plans in California under the Knox-Keene Health Care Service Plan Act of 1975 (the "Knox-Keene Act").
Our affiliated physician organizations contract with HMOs to provide physician and certain ancillary services to the HMO enrollees. The Knox-Keene Act imposes numerous requirements on health plans regarding the provision of care to health plan enrollees. HMOs, in turn, require their contracted physician organizations to comply with those requirements where applicable. Health plans also require their contracted physician organizations to ensure compliance with applicable Knox-Keene Act requirements on the part of the organizations' sub-contracted physicians. Thus, our physician organizations are indirectly subject to many of the requirements of the Knox-Keene Act. While health plans are bound by the provisions of the Knox-Keene Act directly, our physician organizations are indirectly bound by many of these same provisions as embodied in their contracts with the health plans.
Our affiliated physician organizations typically enter into contracts with HMOs, pursuant to which the affiliated physician organizations are paid on a capitated (per member/per month) basis. Under capitation arrangements, health care providers bear the risk, subject to specified loss limits, that the total costs of providing medical services to members will exceed the premiums received. Because they are compensated on a prepaid basis in exchange for providing or arranging for the provision of health care services to assigned patients, the physician organizations may be deemed, under state law, to be in the business of insurance. If the physician organizations are deemed to be insurers, they will be subject to a variety of regulatory and licensing requirements applicable to insurance companies or HMOs, resulting in increased costs and corresponding reduced profitability.
32
In addition to state regulations, HMOs which contract with the Medicare program under Medicare Advantage, as well as their subcontracting Medical Groups, such as ours, are subject to extensive federal regulations. These regulations govern many aspects of our Medical Groups' operations, including but not limited to, marketing to and enrollment of Medicare beneficiaries into Medicare Advantage plans, reporting requirements, claims payment, disclosure requirements, and physician compensation. Failure to comply with these regulations could result in the imposition of civil monetary penalties or other sanctions.
Financial Solvency Regulations
The DMHC has instituted financial solvency regulations mandated by California Senate Bill 260. The regulations are intended to provide a formal mechanism for monitoring the financial solvency of capitated physician groups. Management believes that our affiliated physician organizations that are subject to these regulations will be able to comply with them. However, these regulations could limit our ability to use our cash resources, including to make future acquisitions.
Under the regulations, our affiliated physician organizations are required to comply with specific criteria, including:
- •
- Maintain, at all times, a minimum "cash-to-claims ratio" (where
"cash-to-claims ratio" means the organization's cash, marketable securities and certain qualified receivables, divided by the organization's total unpaid claims liability). The
regulations require a cash-to-claims ratio of 0.75.
- •
- Submit periodic reports to the DMHC containing various data and attestations regarding performance and financial solvency, including IBNR (incurred but not reported) calculations and documentation, and attestations as to whether or not the organization was in compliance with Knox-Keene Act requirements related to claims payment timeliness, had maintained positive tangible net equity and had maintained positive working capital.
Further, under these regulations, the DMHC will make public some of the information contained in the reports, including, but not limited to, whether or not a particular physician organization met each of the criteria.
In the event we are not able to meet certain of the financial solvency requirements, and fail to meet subsequent corrective action plans, we could be subject to sanction, or limitations on, or removal of, our ability to do business in California.
Our cash-to-claims ratio on September 30, 2009, was 2.3.
Government Investigations
The government increasingly examines arrangements between health care providers and potential referral sources to ensure that they are not designed to exchange remuneration for patient referrals, do not violate self-referral laws and do not involve billing fraud. Investigators are increasingly willing to look behind formalities of business transactions to determine the underlying purpose of payments. Enforcement actions have increased and are highly publicized.
In addition to investigations and enforcement actions initiated by governmental agencies, we could become the subject of an action brought under the False Claims Act by a private individual on behalf of the government. Actions under the False Claims Act, commonly known as "whistleblower" lawsuits, are generally filed under seal to allow the government adequate time to investigate and determine whether it will intervene in the action, and defendant health care providers may have no knowledge of such actions until the government has completed its investigation and the seal is lifted.
33
To our knowledge, we, and our affiliated physician organizations, are not currently the subject of any investigation or action under the False Claims Act. Any such future investigation or action could result in sanctions and unfavorable publicity that could reduce potential revenues and profitability.
Health Care Reform
The U.S. health care industry continues to attract much legislative interest and public attention. In recent years, an increasing number of legislative proposals have been introduced or proposed in Congress and in some state legislatures that would effect major changes in the health care system. Proposals that have been considered include changes in Medicare, Medi-Cal and other programs, cost controls on hospitals and mandatory health insurance coverage for employees. The costs of implementing some of these proposals would be financed, in part, by reduction of payments to health care providers under Medicare, Medi-Cal, and other government programs. We cannot predict the course of future health care legislation or other changes in the administration or interpretation of governmental health care programs. However, future legislation, interpretations, or other changes to the health care system could reduce our revenues and profitability.
Regulatory Compliance Program
It is our policy to conduct our business with integrity and in compliance with the law. We have a Code of Conduct which applies to all directors, officers, employees and consultants, and a confidential disclosure program to enhance the statement of ethical responsibility expected of our employees and business associates who work in the accounting, financial reporting, and asset management areas of our company.
Our Alta hospitals have in place and continue to enhance a company-wide compliance program which focuses on all areas of regulatory compliance including billing, reimbursement and cost reporting practices. We are in the process of modifying the compliance program at Brotman to conform to the program used at our Alta hospitals. This regulatory compliance program is intended to help ensure that high standards of conduct are maintained in the operation of our business and that policies and procedures are implemented so that employees act in full compliance with all applicable laws, regulations and company policies. Specific written policies, procedures, training and educational materials and programs, as well as auditing and monitoring activities have been prepared and implemented to address the functional and operational aspects of our business. Included within these functional areas are materials and activities for business sub-units, including laboratory, radiology, pharmacy, emergency, surgery, observation, home health, skilled nursing, and clinics. Specific areas identified through regulatory interpretation and enforcement activities have also been addressed in our program. Claims preparation and submission, including coding, billing, and cost reports, comprise the bulk of these areas. Financial arrangements with physicians and other referral sources, including compliance with anti-kickback and Stark laws, emergency department treatment and transfer requirements, and other patient disposition issues are also the focus of policy and training, standardized documentation requirements, and review and audit. Another focus of the program is the interpretation and implementation of the HIPAA standards for privacy and security.
Under the regulatory compliance program, every employee, certain contractors involved in patient care, and coding and billing, receive initial and periodic legal compliance and ethics training. In addition, we regularly monitor our ongoing compliance efforts and develop and implement policies and procedures designed to foster compliance with the law. The compliance program also includes a mechanism for employees to report, without fear of retaliation, any suspected legal or ethical violations to their supervisors, designated compliance officers in our hospitals, our compliance hotline or directly to our corporate compliance office. There can be no assurances, however, that our regulatory compliance program will prevent us from being subject to any public or private regulatory actions, claims or investigations.
34
Insurance
We maintain general liability, umbrella liability, property, crime, fiduciary, corporate counsel, automobile and workers' compensation insurance, directors and officers insurance and employment practices liability insurance. Our annual policy limits are $1,000,000 per occurrence and $2,000,000 in the aggregate for general liability coverage, $6,270,000 for property coverage and $8,000,000 for business interruption coverage with total insured value of $13,870,000, $2,000,000 for crime coverage, $2,000,000 for fiduciary coverage, $2,000,000 for corporate counsel coverage, $1,000,000 for automobile coverage, the amounts required by state law for workers' compensation, $5,000,000 for employment practices liability and $8,000,000 in the aggregate for directors and officers liability, and Side A DIC Coverage in the amount of $7,000,000. The umbrella policy limits of $2,000,000 operate as excess limits over the underlying general liability and automobile liability coverage.
Our affiliated physician organizations, Prospect Professional Care Medical Group, Inc., AMVI/Prospect Health Network, Nuestra Familia Medical Group, Inc., Prospect Health Source Medical Group, Inc., Prospect NWOC Medical Group, Inc., StarCare Medical Group, Inc., Genesis HealthCare of Southern California, Prospect Medical Group, Inc., Pomona Valley Medical Group and Upland Medical Group maintain managed care errors and omissions insurance (professional liability) in a minimum coverage amount of $2,000,000 per claim and $5,000,000 in the aggregate. The individual physicians who contract with the Affiliates carry their own medical malpractice insurance. In the Hospital Services segment, Alta purchases professional and general liability insurance to cover medical malpractice claims under a claims-made policy.
Our Alta hospitals maintain professional liability, general liability, property, automobile and workers' compensation insurance. The Alta/Prospect workers' compensation coverage for October 1, 2008 through September 30, 2009 had an aggregate loss limit of $2,019,345. The current workers' compensation policy for the period of October 1, 2009 through September 30, 2010 does not have an aggregate loss limitation. The policy limits are $10,000,000 per occurrence and in the aggregate for the professional and general liability, $38,368,528 for property coverage and $10,346,000 for contents and $20,000,000 for business interruption coverage with total insured value of $70,714,528, $1,000,000 for automobile coverage, and the amount required by law for workers' compensation. The Excess Liability policy for Alta operates as excess coverage over the underlying primary Automobile liability coverage. In 2008 and 2009, Brotman has a commercial occurrence-based insurance policy for workers' compensation claims. In 2005, the policy had a $250,000 deductible per accident. The aggregate loss limitation was $2,500,000. The 2006 policy had a $250,000 loss limitation per accident with an annual aggregate loss limitation of $1,625,000. The 2007 policy had a $250,000 loss limitation per accident with an annual aggregate loss limitation of $1,562,000.
Our insurance, and the insurance of our affiliated physician organizations, contain customary exclusions and exceptions from coverage. Additionally, we are at risk for our self-insured retention ("deductible") on certain policies such as $10,000 for our Prospect property policy, $50,000 for our Alta property policy, and $75,000 for the managed care errors and omissions insurance. Directors & Officers Liability and Employment Practices Liability policies have a $150,000 self-insured retention and the hospital's professional/general liability policy has a $1,000,000 self-insured retention. Brotman has a commercial claims-made insurance policy for malpractice claims in excess of $100,000 per claim with no annual aggregate. The general liability coverage is occurrence coverage with a $100,000 per occurrence retention and an annual aggregate of $12 million. Brotman offers self-insured HMO and PPO plans to employees. Employee health benefits are administered by a local claims processor based on plan coverage and eligibility guidelines determined by Brotman and collective bargaining agreements. A commercial insurance policy covers losses in excess of $200,000 per occurrence.
We believe that the lines and amounts of insurance coverage that we and our affiliated physician organizations maintain, and that we require our contracted physician providers to maintain, are
35
customary in our industry and adequate for the risks insured. We cannot assure, however, that we will not become subject to claims not covered or that exceed our insurance coverage amounts.
Employees
Hospital Services Segment
General. Our hospitals are staffed by licensed physicians who have been admitted to the medical staffs of individual hospitals. Under state laws and other licensing standards, hospital medical staffs are generally self-governing organizations subject to ultimate oversight by the hospital's local governing board. Members of the medical staffs of our hospitals also often serve on the medical staffs of hospitals not owned by us. Members of our medical staffs are free to terminate their affiliation with our hospitals or admit their patients to competing hospitals at any time. Although we operate some physician practices and, where permitted by law, employ some physicians, the overwhelming majority of the physicians who practice at our hospitals are not our employees. Nurses, therapists, lab technicians, facility maintenance workers and the administrative staffs of hospitals, however, normally are our employees. We are subject to federal minimum wage and hour laws and various state labor laws, and maintain a number of different employee benefit plans.
Although we will continue our efforts to successfully attract and retain key employees, qualified physicians and other healthcare professionals, the loss of some or all of our key employees or the inability to attract or retain sufficient numbers of qualified physicians and other healthcare professionals could have a material adverse effect on our business, financial condition, results of operations or cash flows.
Union Activity and Labor Relations. At September 30, 2009, our Hospital Services operation had a total of 1,884 employees, which included 1,004 employees at our four Alta hospitals and 880 employees at Brotman. Of that amount, approximately 5.0% and 80.0% of the total employee headcount at our Alta and Brotman hospitals, respectively, are subject to collective bargaining agreements. On or about May 9, 2008 we entered into a new collective bargaining agreement with the SEIU to replace the expired collective bargaining agreement at Hollywood Community Hospital, which is one of the hospitals under the consolidated group of Alta Hospitals System, LLC. The collective bargaining agreement covers a small number of Hollywood Community Hospital's employees, and expires on May 9, 2011. We do not anticipate that the agreement we reached in 2008 will have a material adverse effect on the results of our Hospital Services operations. Brotman has two collective bargaining agreements with the SEIU and CNA covering approximately 80% of the hospital's employees. Both agreements expire on February 28, 2010.
Corporate and Medical Group Segment
At September 30, 2009, we and our Medical Group subsidiaries had a total of 285 employees. The employees are not subject to any collective bargaining agreements. We believe that employee relations are good.
Executive Officers
The following table summarizes the name, age, title and business experience for the past five years of each of our executive officers. Other than as described below, no family relationships exist between or among any of our officers.
Name
|
Age | Position | |||
|---|---|---|---|---|---|
Samuel S. Lee |
43 | Chairman, Chief Executive Officer and Director | |||
Mike Heather |
51 | Chief Financial Officer | |||
Donna Vigil |
61 | Vice President, Finance | |||
36
Samuel S. Lee. Mr. Lee was appointed our Chief Executive Officer on March 19, 2008 and as Chairman of our Board of Directors on May 14, 2008. Mr. Lee was previously appointed as a member of our Board of Directors and as Chief Executive Officer of our subsidiary, Alta Hospitals System, LLC on August 8, 2007. Mr. Lee is an officer and director of each of our direct and indirect subsidiaries and is sole manager of Alta Hospitals System, LLC. He served previously as the President of Alta from January 2002 until we acquired Alta on August 8, 2007. Effective April 22, 2008, Mr. Lee was also appointed as the Chairman of the Board of Directors of Brotman Medical Center, Inc. Mr. Lee's background involves healthcare and technology related private equity investment management, operational leadership, entrepreneurship, mergers and acquisitions, and leveraged financing for various corporations. Prior to Alta, Mr. Lee was a General Partner with Kline Hawkes & Co., a $500 million private equity firm located in Brentwood, California, that focuses on healthcare, technology, and business services. Mr. Lee has been the lead/principal investor and director of several private and public companies. Additionally, Mr. Lee worked in healthcare reimbursement, business office, and operations for SFS, Inc., and in consulting and systems engineering for Andersen Consulting and Verizon. Mr. Lee received his bachelor's degree in Industrial and Systems Engineering from Georgia Tech and master's degree in business administration from Harvard Business School. Mr. Lee is an active member of the Young President's Organization of Los Angeles, and is also involved with several civic and community organizations.
Mike Heather. Mr. Heather was appointed Chief Financial Officer of the Company in April 2004. Most recently, Mr. Heather served as Co-Chief Executive Officer of WebVision, Inc. from March 2001 to June 2002, and served as the Chief Financial Officer of WebVision beginning in June 2000 and continuing through June 2002. Prior to joining WebVision, Mr. Heather was a partner at Deloitte, which he joined in 1980, and was the founder and Partner-in-Charge of the Healthcare Services Practice of Deloitte in Orange County.
Donna Vigil. Ms. Vigil has served as our Vice President of Finance since April 2004, prior to which she served as our Chief Financial Officer commencing July 1998. Ms. Vigil served as Chief Financial Officer of NetSoft, a privately held, $20 million software development company with five European subsidiaries, from October 1989 to September 1997. Ms. Vigil was Acting Chief Financial Officer/Consultant of Strategic HR Services, the staffing division for a large real estate developer in Southern California, from October 1997 to May 1998.
Terms of Office
Officers are elected by and serve at the discretion of our Board of Directors. They hold office until their successors are chosen and qualified, or until they resign or have been removed from office. The Board of Directors may appoint, or empower the Chief Executive Officer to appoint or terminate, such other officers and agents as the business of the Company may require, each of whom shall hold office for such period, and have such authority, and perform such duties as are provided in our Bylaws, or as the Board of Directors may from time to time determine.
Our business is subject to a number of risks, including those described below.
Medicare, Medi-Cal, other government-sponsored programs and private third-party payor cost containment efforts and reductions in reimbursement rates could reduce our hospital revenue and our cash flow.
For the fiscal year ended September 30, 2009, our hospitals derived approximately 83% of their revenues from the Medicare and Medi-Cal programs. Changes in recent years in the Medicare and Medi-Cal programs, including both fee-for-service and managed care programs, have resulted in
37
limitations on reimbursement and, in some cases, reduced levels of reimbursement for healthcare services. Payments from federal and state government programs are subject to statutory and regulatory changes, administrative rulings, interpretations and determinations, requirements for utilization review, and federal and state funding restrictions, all of which could materially increase or decrease program payments, as well as affect the cost of providing service to patients and the timing of payments to facilities. Future federal and state legislation may further reduce the payments we receive for our services.
The State of California has incurred budget deficits in the past few years. As a result, the state has enacted legislation designed to reduce its Medi-Cal expenditures. Last year, the state reduced Medi-Cal reimbursement for numerous services including hospital outpatient services, hospital sub-acute services, and distinct-part nursing services. In addition, payments to hospitals for inpatient services not furnished under Medi-Cal contracts were reduced. The inpatient reductions do not currently affect our hospitals because our hospitals all have contracts with the state to provide Medi-Cal inpatient services, but these reductions could affect our hospitals if any of our contracts are terminated. All of these reductions are being challenged in court by the state hospital association. The outcome of this litigation is uncertain. A temporary injunction has been issued prohibiting certain of the reductions from being implemented for services on and after April 6, 2009 due to the state's failure to comply with federal Medicaid law. If the courts ultimately find that the rate reductions were lawful, our hospitals may be obligated to return to the state the additional amounts paid under the injunction and future Medi-Cal reimbursement could be reduced. The amount that our hospitals may have to return to the state was estimated to be approximately $180,000.
In addition, in order to balance its projected budget deficit, the State of California is considering various proposals designed to reduce its healthcare-related expenditures. Many of these proposals threaten to reduce our hospital revenue. The State of California has considered numerous proposals reducing Medi-Cal payments directly to private hospitals in the form of Disproportionate Share Hospital ("DSH") payments or distressed hospital supplemental payments. In addition, the State of California has considered other proposals that may impact our hospitals' revenues, including reductions in coverage and reimbursement relating to prescription drugs, AIDS services, family planning services and mental health community-based services, breast and cervical screening, non-emergency services for individuals without documentation status, dialysis and non-digestive nutrition services. The State of California has also considered the reduction of funding for counties to pay local hospitals for uncompensated care, the elimination of funding to Institutions of Mental Disease for ancillary health services not covered under the federal Medicaid program and restricting eligibility for or coverage under the Medi-Cal and Healthy Families programs or eliminating the Healthy Families program altogether. These proposals would increase the number of uninsured individuals or amount of non-covered services, potentially adversely affecting the revenues of our hospitals. In addition to these reductions, due to a state constitutional restriction prohibiting expenditures in a fiscal year absent a budget, the State of California is intending to delay payments for certain mental health treatment and rehabilitation services, which may affect cash flow and profitability at our hospital in Van Nuys. We do not currently anticipate that our other hospitals will be affected by delayed payments because federal law prohibits delays in payment by the State of California for hospital services furnished under Medicaid, but there can be no assurance that there will be funds available to make these payments or that there will be no payment delays for these services in the future. In addition, the State of California may consider other proposals that may reduce Medi-Cal or other state payments to hospitals.
We are unable to predict the effect of future state or federal healthcare funding policy changes on our operations. If the rates paid by governmental payors are reduced, if the scope of services covered by governmental payors is limited, or if we, or one or more of our hospitals, are excluded from participation in the Medicare or Medi-Cal program or any other government healthcare program, there
38
could be a material adverse effect on our business, financial condition, results of operations and cash flows.
Employers have also passed more healthcare benefit costs on to employees to reduce the employers' health insurance expense. This trend has caused the self-pay/deductible component of healthcare services to become more common. This payor shifting increases collection costs and reduces overall collections.
During the past several years, major purchasers of healthcare, such as federal and state governments, insurance companies and employers, have undertaken initiatives to revise payment methodologies and monitor healthcare costs. As part of their efforts to contain healthcare costs, purchasers increasingly are demanding discounted fee structures or the assumption by healthcare providers of all or a portion of the financial risk through prepaid capitation arrangements, often in exchange for exclusive or preferred participation in their benefit plans. We expect efforts to impose greater discounts and more stringent cost controls by government and other payors to continue, thereby reducing the payments we receive for our services. In addition, these payors have instituted policies and procedures to substantially reduce or limit the use of inpatient services. The trends may result in a reduction from historical levels in per patient revenue received by our hospitals and affiliated physician organizations.
In addition, President Obama and Congress have proposed measures intended to expand the number of citizens covered by health insurance and other changes within the healthcare system. The costs of implementing some of these proposals could be financed, in part, by reductions in the payments made to healthcare providers under Medicare, Medi-Cal, and other government programs. See "Future reforms in healthcare legislation and regulation could reduce our revenues and profitability," below.
In our hospital segment, the continued growth of uninsured and underinsured patients or further deterioration in the collectability of the accounts of such patients could harm our results of operations.
Like others in the hospital industry, we have experienced large provisions for bad debts, totaling $17.7 million or 8.6% of total net patient revenue for fiscal 2009, due to a growth in self-pay volume. Although we continue to seek ways of improving collection efforts and implementing appropriate payment plans for our services, if we experience growth in self-pay volume and revenue, our results of operations could be adversely affected. Further, our ability to improve collections for self-pay and other patients may be limited by statutory, regulatory and investigatory initiatives, including private lawsuits directed at hospital charges and collection practices for uninsured and underinsured patients. The principal collection risks for our accounts receivable include uninsured patient accounts and to patient accounts for which the primary insurance carrier has paid the amounts covered by the applicable agreement but patient responsibility amounts (e.g., deductibles, co-payments and other amounts not covered by insurance) remain outstanding. The amount of our provision for doubtful accounts is based upon our assessment of historical cash collections and accounts receivable write-offs, expected net collections, business and economic conditions, trends in federal, state and private employer healthcare coverage and other collection indicators. If we continue to experience significant levels of uninsured and underinsured patients, and bad debt expenses, our results of operations could be negatively impacted.
Because our hospitals are obligated to provide care in certain circumstances regardless of whether we will get paid for providing such care, if the number of uninsured patients treated at our hospitals increases, our results of operations may be harmed.
In accordance with our Code of Business Conduct and Ethics, as well as EMTALA, we provide a medical screening examination to any individual who comes to our hospitals while in active labor
39
and/or seeking medical treatment (whether or not such individual is eligible for insurance benefits and regardless of their ability to pay) to determine if such individual has an emergency medical condition. If it is determined that such person has an emergency medical condition, we provide further medical examination and treatment as is required in order to stabilize the patient's medical condition, within the facility's capability, or arrange for transfer of such individual to another medical facility in accordance with applicable law and the treating hospital's written procedures. If the number of indigent and charity care patients with emergency medical conditions we treat increases significantly, our results of operations may be negatively impacted.
Decreases in the number of HMO enrollees using our Medical Group networks reduce our profitability and inhibit future growth.
During recent periods, the number of HMO enrollees using our physician networks has declined (exclusive of increases resulting from our acquisitions), and management currently anticipates that this trend will continue. The profitability and growth of our business depends largely on the number of HMO members who use our physician networks. We seek to maintain and increase the number of HMO enrollees using our physician networks by partnering with HMOs with which our affiliated physician organizations have contracts. If we are not successful, we may not be able to maintain or achieve profitability. For the years ended September 30, 2009 and 2008, our Medical Group segment saw a decrease in the number of HMO enrollees, using our physician networks of approximately 12,000 and 37,300, respectively, exclusive of the divested AV Entities. Estimated revenue reductions associated with the enrollment decreases for those periods were approximately $4,200,000 and $14,000,000, respectively. These fiscal year estimates assume that enrollment decreased ratably during the indicated periods and, as such, represent approximately 50% of the lost revenue that will be experienced in subsequent periods, when the enrollment decline is in effect for the whole period.
Substantially all of our Medical Group segment revenues are generated from contracts with a limited number of HMOs, and if we were to lose HMO contracts or to renew HMO contracts on less favorable terms, our revenues and profitability could be significantly reduced.
With the consolidation of HMOs, there are a limited number of HMOs doing business in California, which magnifies the risk of loss of any one HMO contract. The potential for risk is also magnified because HMO contracts often have only a one-year term, may be terminated with cause upon short notice, and, upon renewal, are subject to annual negotiation of capitation rates, covered benefits and other terms and conditions.
We are particularly at risk with respect to the potential loss or renewal on less favorable terms of contracts that we have with five of these HMOs due to the concentration of revenue with these HMOs—United Healthcare, Blue Cross of California, Health Net of California, Blue Shield of California and InterValley Health Plan. For the fiscal year ended September 30, 2009, contracts with our five largest HMOs accounted for approximately 63% of our enrollment and accounted approximately $146,862,000, or 75% of our total capitation revenue. The loss of contracts with any one of these HMOs could significantly reduce our revenues and profitability.
We have one-year automatically renewable contracts with most contracted HMOs, including our largest HMO customers discussed above, whereby such contracts are automatically renewed, unless either party provides the other party with four to six months' notice (prior to the expiration of the term) of such party's intent not to renew. Under limited circumstances, the HMOs may immediately terminate the contracts for cause; otherwise, termination for cause requires one to three months' prior written notice with an opportunity to cure. There can be no assurance that we will be able to renew any of these contracts or, if renewed, that they will contain terms favorable to us.
40
In our Medical Group segment, risk-sharing arrangements that our Medical Groups have with HMOs and hospitals could result in their costs exceeding the corresponding revenues, which could reduce or eliminate any shared risk profitability.
Most of our affiliated physician organizations' agreements with HMOs and hospitals contain risk-sharing arrangements under which the affiliated physician organizations can earn additional compensation by coordinating the provision of quality, cost-effective healthcare to enrollees, but they may also be required to assume a portion of any loss sustained from these arrangements, thereby reducing our net income. Risk-sharing arrangements are based upon the cost of hospital services or other services for which our physician organizations are not capitated. The terms of the particular risk-sharing arrangement allocate responsibility to the respective parties when the cost of services exceeds the related revenue, which results in a "deficit," or permit the parties to share in any "surplus" amounts when actual costs are less than the related revenue. The amount of non-capitated and hospital costs in any period could be affected by factors beyond our control, such as changes in treatment protocols, new technologies, longer lengths of stay by the patient and inflation. To the extent that such non-capitated and hospital costs are higher than anticipated, revenue may not be sufficient to cover the risk-sharing deficits they are responsible for, which could reduce our revenues and profitability. It is our experience that "deficit" amounts for hospital costs are applied to offset any future "surplus" amount we would otherwise be entitled to receive. We have historically not been required to reimburse the HMOs for any hospital cost deficit amounts. Most of our contracts with HMOs specifically provide that we will not have to reimburse the HMO for hospital cost deficit amounts.
HMOs often insist on withholding negotiated amounts from professional capitation payments, which the HMOs are permitted to retain, in order to cover our share of any risk-sharing deficits; and hospitals may demand cash settlements of risk-sharing deficits as a "quid pro quo" for joining in these arrangements. Net risk-pool deficits were approximately $6,217,000 and $3,141,000, for the fiscal years ended September 30, 2009 and 2008, respectively.
To date, we have not suffered significant losses due to hospital risk arrangements other than offsets (for deficit amounts) against any future surpluses we otherwise would have received. Whenever possible, we seek to contractually reduce or eliminate our affiliated physician organizations' liability for risk-sharing deficits. Notwithstanding the foregoing, risk-sharing deficits could have a significant impact on our future profitability.
The operating results of our Medical Group segment could be adversely affected if our actual healthcare claims exceed our reserves.
At certain times in our history, we have not had adequate cash resources to retire one hundred percent of our incurred but not reported ("IBNR") medical claims. As of September 30, 2009 and 2008, we had sufficient cash to fully retire our estimated accrued medical claims and other healthcare costs payable of approximately $16,824,000 and $20,480,000, respectively.
Historically, we have been able to satisfy our claims payment obligations each month out of cash flows from operations and existing cash reserves. However, in the event that our revenues are substantially reduced due to a loss of a significant HMO contract or other factors, our cash flow may not be sufficient to pay off claims on a timely basis, or at all. If we are unable to pay claims timely we may be subject to HMO de-delegation wherein the HMO would take away our claims processing functions and perform the functions on our behalf, charging us a fee per enrollee, a requirement by the HMO to comply with a corrective action plan, and/or termination of the HMO contract, which could have a material adverse effect on our operations and results of operations.
We estimate the amount of our reserves for submitted claims and IBNR claims primarily using standard actuarial methodologies based upon historical data. The estimates for submitted claims and IBNR claims liabilities are made on an accrual basis, are continually reviewed and are adjusted in
41
current operations as required. Given the uncertainties inherent in such estimates, the reserves could materially understate or overstate our actual liability for claims payable. Any increases to these prior estimates could adversely affect our results of operations in future periods.
In our Medical Group segment, we may be exposed to liability or fail to estimate IBNR claims accurately if we cannot process any increased volume of claims accurately and timely.
We have regulatory risk for the timely processing and payment of claims. If we are unable to handle increased claims volume, or if we are unable to pay claims timely we may become subject to an HMO corrective action plan or de-delegation until the problem is corrected, and/or termination of the HMO agreement, which could have a material adverse effect on our operations and profitability. In addition, if our claims processing system is unable to process claims accurately, the data we use for our IBNR estimates could be incomplete and our ability to accurately estimate claims liabilities and establish adequate reserves could be adversely affected.
The profitability of our Medical Group segment may be reduced or eliminated if we are not able to manage our healthcare costs effectively.
Our success depends in large part on our effective management of healthcare costs incurred by our affiliated physician organizations and controlling utilization of specialty and ancillary care, and by contracting with our independent physicians at competitive prices.
We attempt to control the healthcare costs of our HMO enrollees through capitated and discounted fee-for-service contracts, by emphasizing preventive care, entering into risk-sharing agreements with HMOs at hospitals that have favorable rate and utilization structures, and requiring prior authorization for specialist physician referrals. If we cannot maintain or improve our management of healthcare costs, our business, results of operations, financial condition, and ability to satisfy our obligations could be adversely affected.
Under all current HMO contracts, our affiliated physician organizations accept the financial risk for the provision of primary care and specialty physician services, and some ancillary healthcare services. If we are unable to negotiate favorable contract rates with providers of these services, or if our affiliated physician organizations are unable to effectively control the utilization of these services, our profitability would be negatively impacted. Our ability to manage healthcare costs is also diminished to the extent that we are unable to sub-capitate the specialists in our service areas at competitive rates. To the extent that our HMO enrollees require more frequent or extensive care, our operating margins may be reduced and the revenues derived from our capitation contracts may be insufficient to cover the costs of the services provided.
The revenue and profitability of our Medical Group segment could be significantly reduced and could also fluctuate significantly from period to period under Medicare's Risk Adjusted payment methodology.
In calendar 2004, CMS began a four-year phase-in of a revised compensation model for Medicare beneficiaries enrolled in Medicare Advantage plans. Previously, monthly capitation revenue was based primarily on age, sex and location.
The CMS revised payment model seeks to compensate Medicare managed care organizations based on the health status of each individual enrollee. Health plans/Medical Groups with enrollees that can be proven to require more care will receive higher compensation, and those with enrollees requiring less care will receive less. This is referred to by CMS as "Risk Adjustment."
42
Increased numbers of office visits by members, and submission of encounter data is required in order to receive incremental revenue, or not lose revenue for any given member. This requires a great deal of continuous effort on our part, and cooperation on the part of our contracted physicians and HMO enrollees. We have not always been able to gain this cooperation from the contracted physicians and enrollees, or devote the resources necessary to obtain incremental Risk Adjustment revenue, or avoid having previously received revenue taken back from us.
Additionally, because of the time required by CMS to process all of the submitted encounter data from all participating entities, we typically do not find out until the latter part of the calendar year what adjustments will be made to our Medicare revenue for the prior year, at which time those adjustments to revenue, which have historically been significant, are recorded.
In fiscal 2009 and 2008, we received approximately $4.3 million and $1.6 million, respectively, in incremental Risk Adjustment revenue, which was recorded in the respective fiscal fourth quarter. This adjustment became known, and was recorded, in the fiscal fourth quarter, even though the majority of the adjustment related to earlier periods.
Given the deadlines for submitting data to CMS, and CMS's processing time in order to calculate these Risk Adjustment revenue changes, we have no way of reliably estimating the impact of Risk Adjustment until such time as those adjustments are made known by CMS. As such, retroactive Risk Adjustments will be recorded each year in the quarter they become known, notwithstanding that a significant portion of those adjustments will relate to earlier periods. These adjustments will continue to be significant and could be materially more or less than our estimates.
An increasing portion of our Medical Group revenue is "at risk" and difficult to project, which increases uncertainty regarding future revenues, cash flow projections, and profitability.
Historically, our Medical Group revenue has primarily consisted of contractually guaranteed capitation revenue from HMOs based on a fixed per-member-per-month rate. In recent years, new revenue sources including pay for performance, risk-sharing and risk adjustment have increased and will represent an increasingly significant portion of our total Medical Group revenue. These revenue sources and reimbursement methods are more difficult to project and have a much longer collection cycle. Pay for performance revenue is paid on an approximate one-year lag basis, and predicated on health plan funding being available as well as on the ability of the organization and its partner physicians to achieve certain criteria. These performance thresholds are typically in the areas of clinical measures, patient satisfaction, IT investment, encounter data submission and generic drug utilization. The ultimate receipt of pay for performance monies can vary with our relative performance in comparison to that of competitor medical groups and our ability to successfully modify physician behavior in these areas. Similarly, risk-sharing and risk adjustment revenues have more variability and volatility than capitated arrangements and can require a lengthy reconciliation and reimbursement process. As mentioned previously, incremental revenue generated by both sources involves not only our ability to control medical costs and influence provider and member behavior (i.e., office visits, encounter data submission, etc.), but also is contingent on certain other factors that are beyond our control.
Our profitability could be adversely affected by any changes that would reduce payments to HMOs under government-sponsored health care programs and recent changes affecting payments to non-contract hospitals under Medi-Cal Managed Care.
Although our affiliated physician organizations do not directly contract with CMS, during the fiscal years ended September 30, 2009 and 2008, our affiliated physician organizations received approximately $89,649,000 and $78,512,000 or 46% and 38%, respectively, of capitation revenues from HMOs related to contracts with Medicare, Medi-Cal and other government-sponsored health care programs.
43
Consequently, any change in the regulations, policies, practices, interpretations or statutes adversely affecting payments made to HMOs under these government-sponsored health care programs could reduce our profitability. The recent California budget included reductions in funding for the Medi-Cal mental health managed care program, which could potentially reduce revenues for our hospital in Van Nuys. California continues to explore further reforms to payments to Medi-Cal managed care plans in light of California's ongoing budget crises. A decline in enrollees in Medicare Advantage could also have a material adverse effect on our profitability.
The State of California enacted legislation in 2008 concerning the amount of payments to providers, including hospitals, for service furnished to Medi-Cal recipients enrolled in managed care plans with which the provider does not have a contract. Our hospitals furnish such services. Under the legislation, payments are limited to the regional average rate under Medi-Cal fee-for-service contracts for emergency services and 95% of this rate for post-stabilization services. Some of these reductions have been enjoined by federal courts. These payment limits could adversely affect our hospitals' revenue.
If any of our hospitals lose their Joint Commission accreditation, such hospitals could become ineligible to receive reimbursement under Medicare or Medi-Cal.
Our hospitals are accredited, meaning that they are properly licensed under appropriate state laws and regulations, certified under the Medicare program and accredited by the Joint Commission (formerly known as the Joint Commission on Accreditation of Healthcare Organizations). The effect of maintaining accredited facilities is to allow such facilities to participate in the Medicare and Medi-Cal programs. We believe that all of our healthcare facilities are in material compliance with applicable federal, state, local and independent review body regulations and standards. However, should any of our healthcare facilities lose their accredited status and thereby lose certification under the Medicare or Medi-Cal programs, such facilities would be unable to receive reimbursement from either of those programs and our business could be harmed. Because the requirements for accreditation are subject to modification, it may be necessary for us to effect changes in our facilities, equipment, personnel and services in order to maintain accreditation. Such changes could be expensive and could harm our results of operations.
Controls designed to reduce inpatient services may reduce our hospital revenue.
Controls imposed by third party payors that are designed to reduce admissions and the average length of hospital stays, commonly referred to as "utilization management," have affected and are expected to continue to affect results for our hospital facilities. Utilization management reviews entail an evaluation of a patient's admission and course of treatment by healthcare payors. Inpatient utilization, average lengths of stay and occupancy rates continue to be negatively impacted by payor-required pre-admission authorization, utilization reviews and payor pressure to maximize outpatient and alternative healthcare delivery services for less acutely ill patients. Efforts to impose more stringent cost controls are expected to continue. Although we cannot predict the effect these changes will have on our operations, limitations on the scope of services for which we are reimbursed and/or downward pressure on reimbursement rates and fees as a result of increasing utilization management efforts by payors could have a material adverse effect on our business, financial position and results of operations.
Relocation of the Brotman emergency room facility in connection with the JHA option will require significant capital and may disrupt operations.
As part of the bankruptcy plan of reorganization for Brotman, replacement financing was secured from JHA West 16, LLC and JHA East 7 LLC, affiliates of the Los Angeles Jewish Home for the Aging (collectively, "JHA"), and exit financing was secured through Gemino Healthcare Finance, LLC ("Gemino"). The JHA transaction was comprised of two term debt components, a $16.0 million
44
tranche secured by assets on the west side of the Brotman campus commonly referred to as "Delmas West" and a $6.25 million tranche on the main hospital pavilion on the east side of the property. The $16.0 tranche contains an option for JHA to acquire the Delmas West parcel, where JHA plans to construct a senior living facility, for a purchase price equal to the outstanding debt within 24 months of the effective date of the bankruptcy. In connection with any JHA exercise of its option to purchase the Delmas West parcel, Brotman will have to relocate its emergency room facilities and other related ancillary services to the main hospital pavilion on the east side of the property. Such relocation could take several years, require a significant amount of capital and disrupt operations during periods of construction.
Hospital operations are capital intensive and could prove to be a drain on cash.
Operating a hospital requires a significant continual investment in capital assets, particularly in hospital machinery and equipment. Due to obsolescence and heavy usage, hospital capital assets may require more frequent replacement, and at a higher cost relative to that in an IPA. With additional acquisitions of hospitals, the capital investment required to maintain hospital operations at an optimal level could be significant.
Additionally, according to the California Hospital Association, 1,022 hospitals statewide would have to be upgraded by the year 2013 to comply with seismic retrofitting guidelines established by legislation enacted in the 1990s. Hollywood Community Hospital is required to meet applicable compliance standards by January 1, 2013 and Norwalk Community Hospital is required to meet applicable compliance standards by January 1, 2030. We have applied for a HAZARDS U.S. ("HAZUS") re-evaluation of the seismic risk for Los Angeles Community Hospital and Brotman. Our Van Nuys Community Hospital is exempt from the seismic retrofitting guidelines because psychiatric hospitals are exempt from seismic retrofitting. (See "Business Description—Health Care Regulation—California Seismic Standards"). Further, Brotman's relocation of the emergency room facility in connection with JHA's exercise of the purchase option may negatively impact the HAZUS evaluation process as well as the related OSHPD approval since Brotman will build new facilities in a building that may have seismic issues prior to HAZUS approval which may complicate the requirements of the approval process. Any upgrading costs we incur in order to comply with seismic retrofitting guidelines for our hospitals may be significant.
If we do not continually enhance our hospitals with the most recent technological advances in diagnostic and surgical equipment, our ability to maintain and expand our markets will be adversely affected.
Technological advances are continually being made regarding computer-assisted tomography scanners, magnetic resonance imaging equipment, positron emission tomography scanners and other similar equipment. In order to effectively compete, we must continually assess our equipment needs and upgrade when technological advances occur. If our hospitals do not invest significantly and stay abreast of technological advances in the healthcare industry, patients may seek treatment from other providers and physicians may refer their patients to alternate sources.
If we are unable to identify suitable acquisition candidates or to negotiate or complete acquisitions on favorable terms, our prospects for growth could be limited. In addition, we may not realize the anticipated benefits of any acquisitions that we are able to complete.
Part of our business strategy is to grow through potential acquisitions in order to achieve economies of scale. Although we are regularly in discussions with potential acquisition candidates, it may be difficult to identify suitable acquisition candidates and to negotiate satisfactory terms with them. If we are unable to identify suitable acquisition candidates at favorable prices, our ability to grow by acquisition could be limited.
45
In addition, to the extent we are successful in identifying suitable acquisition candidates and making acquisitions, these acquisitions involve a number of risks, including:
- •
- we may find that the acquired company or assets do not further our business strategy, or that we overpaid for the company
or assets, or that industry or economic conditions change, all of which may require a future impairment charge;
- •
- we may have difficulty integrating the operations and personnel of the acquired business and may have difficulty retaining
the key personnel of the acquired business;
- •
- we may have difficulty incorporating the acquired services with our existing services;
- •
- there may be customer confusion where our services overlap with those of entities that we acquire;
- •
- our ongoing business and management's attention may be disrupted or diverted by transition or integration issues and the
complexity of managing geographically and culturally diverse locations;
- •
- we may have difficulty maintaining uniform standards, controls, procedures and policies across locations;
- •
- we may acquire companies that have material liabilities, including, among other things, for the failure to comply with
healthcare laws and regulations;
- •
- the acquisition may result in litigation from terminated employees or third parties;
- •
- we may experience significant problems or liabilities associated with service quality, technology and legal contingencies;
- •
- we may spend considerable amounts of money (legal, accounting, diligence, etc.) in seeking an acquisition candidate and
never complete the acquisition; and
- •
- acquisition candidate letters of intent may have large break-up fees that we could be liable for in the event we sign a letter of intent and do not complete the transaction.
In particular, our strategy for growth includes strategic acquisitions of hospitals. However, even if we are successful in completing further acquisitions, it may not be possible to integrate their operations into our operations or it may be difficult and time consuming to integrate the acquired hospitals' management services, information systems, billing and collection systems, finance department, medical records, and other key administrative functions, while at the same time managing a larger entity with a differing history, business model and culture. Management may be required to develop working relationships with providers and vendors with whom they have had no previous business experience. Management also may not be able to obtain the necessary economies of scale. Integration of acquired entities is vital for us to be able to operate effectively and to control variable (staffing) and fixed costs. If we are not successful in integrating acquired operations on a timely basis, or at all, our business could be disrupted and we may not be able to realize the anticipated benefits of our acquisitions, including cost savings. There may be substantial unanticipated costs associated with acquisition and integration activities, any of which could result in significant one-time or on-going charges to earnings or otherwise adversely affect our operating results.
We may not be able to make future acquisitions without obtaining additional financing.
To finance any acquisitions, we may, from time to time, issue additional equity securities or incur additional debt. A greater amount of debt or additional equity financing could be required to the extent that our common stock fails to achieve or to maintain a market value sufficient to warrant its use in future acquisitions, or to the extent that acquisition targets are unwilling to accept common stock in exchange for their businesses. Our ability to incur additional debt will be restricted by our senior
46
secured credit facility and the indenture governing the notes issued under the facility. Even if we were permitted to incur additional debt or determine to sell equity, we may not be able to obtain additional required capital on acceptable terms, if at all, which would limit our plans for growth. In addition, any capital we may be able to raise could result in increased leverage on our balance sheet, additional interest and financing expense, and decreased operating income.
The acquisition of hospitals and subsequent integration with our Medical Group business may prove to be difficult and may outweigh the anticipated benefits of a hospital- Medical Group combination.
Our core business has historically been that of a healthcare management services company that manages independent physician associations providing healthcare services to HMO enrollees. In continuing to diversify acquisition targets beyond our Medical Group business, we will be facing a myriad of unique operational, financial and regulatory issues in a hospital environment that could prove to be a drain on existing resources, and be a significant distraction from other initiatives facing us. For instance, hospital revenue from Medicare, Medi-Cal and other third parties are tentative in nature and subject to audits by third-party fiscal intermediaries. In addition, acquiring, developing and integrating facilities may involve significant cash expenditures, expenses and unforeseen liabilities that could have a material adverse effect on our financial condition and results of operation. Finally, changing legislation on the funding and recognition of hospital revenues could negatively impact financial performance and cause earnings decreases. Moreover, in recent years Congress has enacted legislation DSH payments revisiting the program's intent and methodologies for calculating payments to hospitals. There have recently been other initiatives proposed to reduce the overall funding of Medicare and Medi-Cal programs, coupled with increased regulation on the disbursement methodology for such funds. Unfavorable outcomes on such legislation could cause a reduction in revenues generated as compared to prior years.
Whenever we seek to make an acquisition of an entity that has an HMO contract, the HMO could potentially refuse to consent to the transfer of its contract, and this could effectively stop the acquisition or potentially deprive us of the revenues associated with that HMO contract if we choose to complete the acquisition without the HMO's consent.
Contracts with HMOs typically include provisions requiring the HMO to consent to the transfer of their contract before effecting any change in control of the healthcare provider party thereto. As a result, whenever we seek to make an acquisition, such acquisition may be conditioned upon the acquisition candidate's ability to obtain such consent from the HMOs with which it has contracted. Therefore, an acquisition could be delayed while an HMO seeks to determine whether it will consent to the transfer. While in our experience the HMOs limit their review to satisfying their regulatory responsibility to ensure that, following the acquisition, the post-acquisition entity will meet certain financial and operational thresholds, the language in many of the HMO agreements give the HMO the ability to decline to give their consent if they simply do not want to do business with the acquiring entity. If an HMO is unwilling for any reason to give its consent, this could deter us from completing the acquisition, or, if we complete an acquisition without obtaining an HMO's consent, we could lose the benefits associated with that HMO's contract.
If we were to lose the services of Sam Lee or other key members of management, we might not be able to replace them in a timely manner with qualified personnel, which could disrupt our business and reduce our profitability and revenue growth.
Our success depends, in large part, on the skills, experience and efforts of our senior management team and on the efforts, ability and experience of key members of our local hospital management staffs, including our Chairman and Chief Executive Officer, Sam Lee, who is also Chief Executive Officer of Alta Hospitals System, LLC; our Chief Financial Officer, Mike Heather; our President of
47
Alta Hospitals Subsidiary, David Topper; and Jeereddi Prasad, M.D., President of our ProMed Entities. In addition to these individuals, there are a number of other critical members of management whose loss would very negatively impact our operations. If for any reason we were to lose the services of any key member of management, we would need to find and recruit a qualified replacement quickly to avoid disrupting our business and reducing our profitability and revenue growth. We compete with other companies for executive talent, and it may not be possible for us to recruit a qualified candidate on a timely basis, or at all. The loss of the services of one or more members of our senior management team or of a significant portion of our local hospital management staffs could significantly weaken our management expertise and our ability to efficiently deliver healthcare services, which could harm our business.
Our hospitals face competition for medical support staff, including nurses, pharmacists, medical technicians and other personnel, which may increase our labor costs and harm our results of operations.
We are highly dependent on the efforts, abilities and experience of our medical support personnel, including our nurses, pharmacists and lab technicians. We compete with other healthcare providers in recruiting and retaining qualified hospital management, nurses and other medical personnel. Hospitals are experiencing a severe ongoing shortage of nursing professionals, a trend which we expect to continue for some time. If the supply of qualified nurses declines in the markets in which our hospitals operate, it may require us to enhance wages and benefits to recruit and retain nurses and other medical support personnel or require us to hire expensive temporary personnel, and may result in increased labor expenses and lower operating margins at those hospitals. California has regulatory requirements to maintain specified nurse-staffing levels. To the extent we cannot meet those levels of staffing, the healthcare services that we provide in these markets may be reduced. In addition, to the extent that a significant portion of our employee base unionizes, or attempts to unionize, our labor costs could increase. We cannot predict the degree to which we will be affected by union activity or the future availability or cost of attracting and retaining talented medical support staff. If our general labor and related expenses increase, we may not be able to raise our rates correspondingly. Our failure to either recruit and retain qualified hospital management, nurses and other medical support personnel or control our labor costs could harm the results of our operations.
The performance of our hospital business segment depends on our ability to recruit and retain quality physicians.
Physicians generally direct the majority of hospital admissions, and the success of our hospitals depends, therefore, in part on the number and quality of the physicians on the medical staffs of our hospitals, the admitting practices of those physicians and maintaining good relations with those physicians. Physicians are often not employees of the hospitals at which they practice and, in many of the markets that we serve, most physicians have admitting privileges at other hospitals in addition to our hospitals. Such physicians may terminate their affiliation with our hospitals at any time. If we are unable to provide adequate support, personnel or technologically advanced equipment and hospital facilities that meet the needs of those physicians, they may be discouraged from referring patients to our facilities, admissions may decrease and our operating performance may decline.
Our revenues and profits could be diminished if we lose the services of key primary care physicians.
Substantially all of our Medical Group revenues are derived from our affiliated physician organizations. Key primary care physicians with large patient enrollment could retire, become disabled, terminate their provider contracts, get lured away by a competing IPA, or otherwise become unable or unwilling to continue practicing medicine or contracting with our affiliated physician organizations. Enrollees who have been served by such physicians could choose to enroll with competitors' physician
48
organizations, reducing our revenues and profits. Moreover, we may not be able to attract new physicians into our affiliated physician organizations to replace the services of terminating physicians.
Physicians make hospital admitting decisions and decisions regarding the appropriate course of patient treatment, which, in turn, affect hospital revenue. Therefore, the success of our hospitals depends, in part, on the number and quality of the physicians on the medical staffs of our hospitals, the admitting practices of those physicians and our maintenance of good relations with those physicians. In many instances, physicians are not employees of our hospitals and, in a number of the markets that we serve, physicians have admitting privileges at other hospitals in addition to our hospitals. If we are unable to provide adequate support personnel or technologically advanced equipment and facilities that meet the needs of those physicians, they may be discouraged from referring patients to our facilities and our results of operations could be harmed.
Our ability to control labor and employee benefit costs could be hindered by continued acquisition activity.
As additional acquisitions are completed and our work force continues to grow, maintaining competitive salaries and employee benefits could prove to be cost prohibitive. The impact of inflation and the challenge of blending different benefit programs into our existing structure could lead to either a significant increase in compensation expense and reduced profitability, or a reduction in benefits with the potential outcomes of increased turnover and a reduced ability to attract quality employees.
We operate in a highly competitive market; increased competition could adversely affect our revenues.
A number of factors affect our HMO membership levels and patient census at our hospitals. The healthcare industry, including hospitals and Medical Groups, are highly competitive. In addition to the competition we face for acquisitions and physicians, we must also compete with other hospitals and healthcare providers for patients, which competition has continued to intensify in recent years. Our hospitals face competition from hospitals inside and outside of their primary service areas, including hospitals that operate newer facilities or provide more complex services. Patients in our primary service areas may travel to these other hospitals for a variety of reasons. These reasons include physician referrals or the need for services we do not offer. Patients who seek services from these other hospitals may subsequently shift their preferences to those hospitals for the services that we provide.
Some of the hospitals that compete with our hospitals are owned by government agencies or not-for-profit corporations. Tax-exempt competitors may have certain financial advantages not available to our facilities, such as endowments, charitable contributions, tax-exempt financing, and exemptions from sales, property and income taxes. In California some government hospitals are permitted by law to directly employ physicians while for-profit hospitals are prohibited from doing so. We also face increasing competition from physician-owned specialty hospitals and freestanding surgery, diagnostic and imaging centers for market share in high margin services and for quality physicians and personnel.
If competing healthcare providers are better able to attract patients, recruit and retain physicians, expand services or obtain favorable managed care and other contracts at their facilities, we may experience a decline in inpatient and outpatient volume levels. Our inability to compete effectively with other hospitals and other healthcare providers could cause local residents to use other hospitals. If our hospitals are not able to effectively attract patients, our business could be harmed.
In 2005, CMS began making public performance data relating to ten quality measures that hospitals submit in connection with their Medicare reimbursement. If any of our hospitals should achieve poor results (or results that are lower than our competitors) on these ten quality criteria, patient volumes could decline. In the future, other trends toward clinical transparency may have an unanticipated impact on our competitive position and patient volume.
49
The managed care industry is also highly competitive and is subject to continuing changes in the ways in which services are provided and providers are selected and paid. We are subject to significant competition with respect to physicians affiliating with our affiliated physician organizations. Some of our competitors have substantially greater financial, technical, managerial, marketing and other resources and experience than we do and, as a result, may compete more effectively than we can. Companies in other healthcare industry segments, some of which have financial and other resources greater than we do, may become competitors in providing similar services. We may not be able to continue to compete effectively in this industry. Additional competitors may enter our markets and this increased competition may have an adverse effect on our business, financial condition and results of operations.
Hospitals with union contracts could experience setbacks from unfavorable negotiations with union members.
Our Hollywood Community Hospital has a collective bargaining agreement with the Service Employees International Union ("SEIU") involving a small portion of the hospital staff. This agreement, which expires May 9, 2011, specifies employee benefits for those represented by the collective bargaining agreement, including compensation rates, hours of work, overtime, vacation, holiday, sick, and health and retirement benefits. Unsuccessful negotiations between hospital officials and union representatives could have an unfavorable impact on day-to-day operations of that hospital. In addition, approximately 78% of the employees of Brotman are part of a collective bargaining agreement with the SEIU or the California Nurses Association ("CNA"). Brotman's existing agreements with both unions expire February 28, 2010. Unsuccessful negotiations between hospital officials and union representatives could have an unfavorable impact on day-to-day operations of that hospital and any increased costs that we are required to pay pursuant to a new collective bargaining agreement could materially and adversely affect our results of operations.
We may be required to obtain a Knox-Keene license or otherwise restructure our Medical Group segment if the assignable option agreement or our management services agreements with affiliated physician organizations are deemed invalid under California's prohibition against the corporate practice of medicine.
State laws specify who may practice medicine and limit the scope of relationships, including management agreements and stock purchase agreements, between medical practitioners and other parties. Under these laws, lay companies, like us and our subsidiaries, are prohibited from practicing medicine, exercising control over the medical and business aspects of a medical practice and owning stock in a medical corporation, and may be prohibited from sharing in the profits of a medical practice.
While we exercise control over the ownership of the stock in our affiliated Medical Groups through an assignable option agreement, the option is not exercisable by us or by any non-professional organization, and neither we nor our subsidiaries directly own the stock in our affiliated Medical Groups. Rather, we have the right to designate the physician who will purchase the capital stock of our affiliated physician organizations. We and our subsidiaries do not employ physicians to provide medical services, exert control over medical decision-making or represent to the public that we offer medical services. Our subsidiaries have entered into management services agreements with our affiliated physician organizations pursuant to which the physician organizations reserve exclusive control and responsibility for all aspects of the practice of medicine and the delivery of medical services.
Nevertheless, it is possible that the California Medical Board, a different regulatory agency or a court could determine that the assignable option agreement, either independently or coupled with the management services agreements, confers impermissible control over the business and/or medical operations of the affiliated physician groups or their participating physicians, that the management fee results in profit sharing or that we are the beneficial owner of the Medical Groups' stock in violation of
50
the corporate practice of medicine doctrine. If there were a determination that the assignable option and/or management services agreements constituted a corporate practice of medicine violation, these arrangements could be deemed invalid, potentially resulting in a loss of our Medical Group revenues and we, as well as the shareholder nominee, could be subject to criminal or civil penalties or an injunction for practicing medicine without a license or aiding and abetting the unlicensed practice of medicine. This could also force a restructuring of our Medical Group management arrangements, including possible revisions of the management services agreements, which might include a modification of the management fee or elimination of any portion of the fee tied to Medical Group profits, and/or establishing an alternative structure, such as obtaining a Knox-Keene license which would permit us to operate a physician network without being subject to the corporate practice of medicine prohibition. There can be no assurance that such a restructuring would be feasible, or that it could be accomplished within a reasonable time frame without a material adverse effect on our operations and financial results.
If our assignable option agreements with our physician shareholder nominee of our affiliated physician organizations is deemed invalid under California or federal law, is terminated as a result of changes in California law or application of Financial Accounting Standards Board policies, it would impact our consolidation of our affiliated physician organizations and total revenues.
Our financial statements are consolidated and include the accounts of the Company and all majority owned subsidiaries and controlled entities under Financial Accounting Standards Board ("FASB") ASC 810-10-05, (previously issued as Emerging Issues Task Force ("EITF") No. 97-2, "Application of FASB Statement No. 94 and APB Opinion No. 16 to Physician Practice Management Entities and Certain Other Entities with Contractual Management Arrangements") and FASB ASC 810-10, "Consolidation of Variable Interest Entities, an Interpretation of ARB No. 51" (previously issued as EITF No. 00-06). All adjustments considered necessary for a fair presentation of the results as of the date of, and for the interim periods presented, which consist solely of normal recurring adjustments, have been included. All significant inter-company balances and transactions have been eliminated in consolidation. In the event of a change in FASB interpretations, a determination by a regulatory agency or a court that the assignable option agreement or the Company's management relationships with its affiliated Medical Groups are not valid or if there were a change in California or federal law, we may be forced to no longer consolidate the revenues of our affiliated physician organizations. See "Business Description—Health Care Regulation—Corporate Practice of Medicine and Professional Licenses."
In the event our physician shareholder nominee under the assignable option agreement was to file a personal bankruptcy, we may need court approval to replace such physician nominee under such option agreements.
Under our assignable option agreements with our physician shareholder nominee, we can replace at any time our physician shareholder nominee for consideration of $1,000. In the event our physician shareholder nominee was to file a personal bankruptcy, we may need court approval to replace such physician nominee under such option agreement, which may require a significant amount of time, may require payment of an amount much greater than the normal consideration in such option agreement or may not be given by the bankruptcy court. To the extent we are unable to nominate the physician shareholder, we may lose a certain degree of control over our Medical Groups. In addition, in the event of the bankruptcy of the sole physician shareholder, our stockholders and creditors could experience delays in recovering the value of the IPA-related collateral held by such physician shareholder or could lose the value of these assets entirely.
51
We are subject to extensive government regulation regarding the conduct of our operations. If we fail to comply with any existing or new regulations, we could suffer civil or criminal penalties or be required to make significant changes to our operations.
Failure to comply with federal and state regulations could result in substantial penalties and changes in business operations. Companies that provide healthcare services are required to comply with many highly complex laws and regulations at the federal, state and local levels, including, but not limited to, those relating to the adequacy of medical care, billing for services, patient privacy, equipment, personnel, operating policies and procedures and maintenance of records. We, along with our hospitals and our affiliated physician organizations, are subject to numerous federal and state statutes and regulations that are applicable to healthcare organizations and businesses generally, including the corporate practice of medicine prohibition, federal and state anti-kickback laws and federal and state laws regarding the use and disclosure of patient health information. If our business operations are found to be in violation of any of the laws and regulations to which we are subject, we may be subject to the applicable penalty associated with the violation, including civil and criminal penalties, damages, fines, and increased legal expenses, we may be required to make costly changes to our business operations, and we may be excluded from government reimbursement programs. The laws and regulations that our hospitals and affiliated physician organizations are subject to are complex and subject to varying interpretations. Any action against our hospitals or affiliated physician organizations for violation of these laws or regulations, even if we successfully defended against it, could cause us to incur significant legal expenses and divert management's attention from the operation of our business. All of these consequences could have the effect of reducing our revenues, increasing our costs, decreasing our profitability and curtailing our growth. Although we believe that we are in compliance with all applicable laws and regulations, if we fail to comply with any such laws or regulations, we could suffer civil or criminal penalties, including the loss of licenses to operate our facilities. We could also become unable to participate in Medicare, Medi-Cal, and other federal and state healthcare programs that significantly contribute to our revenue.
Because many of the laws and regulations to which we are subject are relatively new or highly complex, in many cases we do not have the benefit of regulatory or judicial interpretation. In the future, it is possible that different interpretations or enforcement of such laws and regulations could require us to make changes in our facilities, equipment, personnel, services or capital expenditure programs.
Providers in the hospital industry have been the subject of federal and state investigations and we could become subject to such investigations in the future.
Significant media and public attention has been focused on the hospital industry due to ongoing investigations related to referrals, cost reporting and billing practices, laboratory and home healthcare services and physician ownership of joint ventures involving hospitals. Both federal and state government agencies have announced heightened and coordinated civil and criminal enforcement efforts and the Office of the Inspector General of the U.S. Department of Health and Human Services and the U.S. Department of Justice have, from time to time, established enforcement initiatives that focus on specific areas of suspected fraud and abuse. Recent initiatives include a focus on hospital billing practices.
We closely monitor our billing and other hospital practices to maintain compliance with prevailing industry interpretations of applicable laws and regulations and we believe that our practices are consistent with current industry practices. However, government investigations could be initiated that are inconsistent with industry practices and prevailing interpretations of existing laws and regulations. In public statements, governmental authorities have taken positions on issues for which little official interpretation had been previously available. Some of those positions appear to be inconsistent with practices that have been common within the industry and, in some cases, have not yet been challenged.
52
Moreover, some government investigations that were previously conducted under the civil provisions of federal law are now being conducted as criminal investigations under fraud and abuse laws.
We cannot predict whether we will be the subject of future governmental investigations or inquiries. Any determination that we have violated applicable laws or regulations or even a public announcement that we are being investigated for possible violations could harm our business.
The healthcare industry is subject to many laws and regulations designed to deter and prevent practices deemed by the government to be fraudulent or abusive.
Unless an exception applies, the portion of the Social Security Act commonly known as the "Stark law" prohibits physicians from referring Medicare or Medi-Cal patients to providers of enumerated "designated health services" with whom the physician or a member of the physician's immediate family has an ownership interest or compensation arrangement. Such referrals are deemed to be "self referrals" due to the physician's financial relationship with the entity providing the designated health services. Moreover, many states have adopted or are considering similar legislative proposals, some of which extend beyond the scope of the Stark law to prohibit the payment or receipt of remuneration for the prohibited referral of patients for designated healthcare services and physician self-referrals, regardless of the source of the payment for the patient's care.
Companies in the hospital industry are subject to Medicare and Medi-Cal anti-fraud and abuse provisions, known as the "anti-kickback statute." As a company in the hospital industry, we are subject to the anti-kickback statute, which prohibits some business practices and relationships related to items or services reimbursable under Medicare, Medi-Cal and other federal healthcare programs. For example, the anti-kickback statute prohibits hospitals from paying or receiving remuneration to induce or arrange for the referral of patients or purchase of items or services covered by a federal or state healthcare program. If regulatory authorities determine that any of our hospitals' arrangements violate the anti-kickback statute, we could be subject to liabilities under the Social Security Act, including:
- •
- criminal penalties
- •
- civil monetary penalties; and/or
- •
- exclusion from participation in Medicare, Medi-Cal or other federal healthcare programs, any of which could impair our ability to operate one or more of our hospitals profitably.
We systematically review all of our operations on an ongoing basis and believe that we are in compliance with the Stark law and similar state statutes. When evaluating strategic joint ventures or other collaborative relationships with physicians, we consider the scope and effect of these statutes and seek to structure the relationships in full compliance with their provisions. We also maintain a company-wide compliance program in order to monitor and promote our continued compliance with these and other statutory prohibitions and requirements. Nevertheless, if it is determined that certain of our practices or operations violate the Stark law or similar statutes, we could become subject to civil and criminal penalties, including exclusion from the Medicare or Medi-Cal programs and loss of government reimbursement. The imposition of any such penalties could harm our business.
We may be subjected to actions brought by the government under anti-fraud and abuse provisions or by individuals on the government's behalf under the False Claims Act's "qui tam" or whistleblower provisions.
Whistleblower provisions allow private individuals to bring actions on behalf of the government alleging that the defendant has defrauded the federal government. Defendants found to be liable under the False Claims Act may be required to pay three times the actual damages sustained by the government, plus mandatory civil penalties ranging between $5,500 and $11,000 for each separate false claim.
53
There are many potential bases for liability under the False Claims Act. Liability often arises when an entity knowingly submits a false claim for reimbursement to the federal government. The False Claims Act defines the term "knowingly" broadly. Although simple negligence will not give rise to liability under the False Claims Act, submitting a claim with reckless disregard for its truth or falsity constitutes a "knowing" submission under the False Claims Act and, therefore, will give rise to liability. In some cases, whistleblowers or the federal government have taken the position that providers, who allegedly have violated other statutes, such as the anti-kickback statute and the Stark law, have thereby submitted false claims under the False Claims Act. In addition, a number of states, including California, have adopted their own false claims provisions as well as their own whistleblower provisions whereby a private party may file a civil lawsuit in state court. See "Business Description—Health Care Regulations—False Claims Act".
Although we intend and will endeavor to conduct our business in compliance with all applicable federal and state fraud and abuse laws, many of these laws are broadly worded and may be interpreted or applied in ways that cannot be predicted. Therefore, we cannot assure you that our arrangements or business practices will not be subject to government scrutiny or be found to be in compliance with applicable fraud and abuse laws.
We are required to comply with laws governing the transmission, security and privacy of health information that require significant compliance costs, and any failure to comply with these laws could result in material criminal and civil penalties.
HIPAA and California's patient privacy laws require us to comply with standards regarding the exchange of health information and the security and privacy of patient medical information within our company and with third parties, such as healthcare providers, business associates and our members. To the extent that state laws impose stricter privacy standards than HIPAA privacy regulations, HIPAA does not preempt the state standards and laws. The California Medical Information Act, and other California laws contain stringent privacy and security protections, many of which are not preempted by HIPAA, the HITECH Act, Title XIII, Div. A and Title IV, Div. B of the American Recovery and Reinvestment Act of 2009, Pub. L. No. 111-5, greatly enhanced HIPAA's patient privacy and security obligations.
Given the complexity of the HIPAA, HITECH Act and California privacy restrictions, the possibility that the regulations may change, and the fact that the regulations are subject to changing and potentially conflicting interpretation, our ability to comply with the HIPAA, HITECH Act and California privacy requirements is uncertain and the costs of compliance are significant. Furthermore, California's promulgation of stricter laws, and uncertainty regarding many aspects of California's requirements, make compliance more difficult. To the extent that we submit electronic healthcare claims and payment transactions that do not comply with the electronic data transmission standards established under HIPAA, payments to us may be delayed or denied. Additionally, the costs of complying with any changes to the HIPAA and California privacy restrictions may have a negative impact on our operations. We could be subject to criminal penalties and civil sanctions for failing to comply with the HIPAA and California privacy restrictions, which could result in the incurrence of significant monetary penalties. See "Business Description—Health Care Regulation—HIPAA Transaction, Privacy and Security Requirements."
Future reforms in healthcare legislation and regulation could reduce our revenues and profitability.
President Obama and Congress have considered multiple proposals for healthcare reform. These proposals include an expansion of health insurance coverage by (a) expanding the coverage of Medi-Cal and the State Children's Health Insurance Program, (b) requiring that individuals have health insurance and/or (c) requiring that most employers offer health insurance coverage or contribute to the cost of such coverage.
54
Additional changes to the public health care system or the Medi-Cal and/or Medicare programs may impact our profitability. For example, a significant percentage of our revenue is based on payments received from Medicare Advantage plans. As a result, any future changes to the Medicare Advantage program may significantly affect the amounts of payment we receive for services that our providers render and the number of Medicare enrollees that our affiliated Medical Groups serve. Changes to the current system also may increase our administrative costs, particularly during the transition from the current payment model to the new system. Any other changes to the payment system to hospitals, such as tying payment to patient quality of care or bundling payments to hospitals to cover the costs of treating patients during and immediately after their admission, may impact our receipt of payments.
Numerous other legislative initiatives have been introduced or proposed in recent years that would also result in major changes in the healthcare delivery system on a national or a state level. Among the other proposals that have been introduced are California healthcare coverage for the uninsured and price controls on hospitals. Additionally, the State of California is considering a proposal to significantly change the Medi-Cal reimbursement system for hospitals. The proposal includes an exaction on hospitals that would be used to fund increases in Medi-Cal reimbursement to hospitals. While the exact methodology for the exaction and the increases in Medi-Cal reimbursement has not been determined, this proposal could result in lowered revenue at our hospitals. Further, the State of California is considering various other changes to the Medi-Cal program including seeking a federal waiver to implement widespread changes that could have a significant adverse effect on our hospital's Medi-Cal revenue.
We cannot predict whether any of President Obama's proposals, the other proposals listed above or any other proposals will be adopted and, if adopted, no assurances can be given that their implementation will not have a material adverse effect on our business, financial condition or results of operations. The costs of implementing some of these proposals could be financed, in part, by reductions in the payments made to healthcare providers under Medicare, Medi-Cal, and other government programs. Future legislation, regulations, interpretations, or other changes to the healthcare system could reduce our revenues and profitability.
Recently enacted legislation may require us to spend significant capital on an electronic health record system to benefit from Medicare financial incentives and avoid financial and other penalties.
President Obama's desire to encourage the adoption of new health information technology has resulted in the enactment under the HITECH Act, of a system of incentives and disincentives for hospitals and non-hospital based physicians to purchase and use electronic health record technology. Beginning in 2011, the HITECH Act provides a host of financial incentives and penalties to encourage Medicare-participating physicians and hospitals to move quickly toward adopting "certified" electronic health record ("EHR") technology. Early-adopting eligible providers who become "meaningful" EHR users over the next two to three years will maximize their incentive payments under Medicare and Medicaid. Late-adopting providers who wait until after 2015 will have no opportunity to recoup costs associated with the mandated shift toward EHR. The HITECH Act phases down incentive payments significantly starting in 2013, and no incentive payments will be made after 2016. Instead, from 2017-2020, Medicare hospitals and non-hospital based physicians who do not make meaningful use of EHR technology will be penalized a percentage of their Medicare reimbursements. It is possible that any participation in the Medicare and Medicaid programs after 2020 may require meaningful use of certified EHR technology. Therefore, we may have to expend considerable money and administrative effort to implement EHR technology to receive the HITECH Act's Medicare incentive, avoid future penalties and, perhaps, even to continue to participate in the Medicare and Medicaid programs. Implementation of EHR is expensive, and there can be no assurance that the Company will have sufficient financial resources to implement a Medicare compliant EHR system in a timely manner in order to benefit from the financial incentives and avoid financial and other penalties.
55
If our affiliated physician organizations are not able to satisfy California Department of Managed Health Care financial solvency requirements, we could become subject to sanctions and our ability to do business in this segment in California could be limited or terminated.
The California Department of Managed Health Care ("DMHC") has instituted financial solvency regulations. The regulations are intended to provide a formal mechanism for monitoring the financial solvency of capitated physician groups. Management believes that our affiliated physician organizations that are subject to these regulations will be able to comply with them. However, these regulations could limit our ability to use our cash resources to make future hospital acquisitions.
Under the regulations, our affiliated physician organizations are required to comply with specific criteria, including:
- •
- Maintain, at all times, a minimum "cash-to-claims ratio" (where
"cash-to-claims ratio" means the organization's cash, marketable securities and certain qualified receivables, divided by the organization's total unpaid claims liability.) The
regulations currently require a cash-to-claims ratio of 0.75.
- •
- Submit periodic reports to the DMHC containing various data and attestations regarding performance and financial solvency, including IBNR (incurred but not reported) calculations and documentation, and attestations as to whether or not the organization was in compliance with the Knox-Keene Health Care Service Plan Act of 1975 (the "Knox-Keene Act") requirements related to claims payment timeliness, had maintained positive tangible net equity (i.e., at least $1.00), and had maintained positive working capital (i.e., at least $1.00).
In a case where an organization is not in compliance with any of the above criteria, the organization would be required to describe in the report submitted to the DMHC the reasons for non-compliance and actions to be taken to bring the organization into compliance. Further, under these regulations, the DMHC will make public some of the information contained in the reports, including, but not limited to, whether or not a particular physician organization met each of the criteria. In the event our affiliated physician organizations are not able to meet certain of the financial solvency requirements, and fail to meet subsequent corrective action plans, we could be subject to sanction, or limitations on, or removal of, our ability to do business in this segment in California. Our affiliated physician organizations had a cash-to-claims ratio at September 30, 2009 of 2.3 and exceeded the requirement for $1.00 of tangible net equity and $1.00 of positive working capital.
Because our business is currently limited to the Southern California area, any reduction in our revenues and profitability from local economic, regulatory, environmental and other developments would not be offset by operations in other geographic areas.
To date, we have developed our business within only one geographic area to take advantage of economies of scale. Due to this concentration of business in a single geographic area, we are exposed to potential losses resulting from economic, regulatory, environmental and competition changes in Southern California. A natural disaster or other catastrophic event could affect us more significantly than other companies with less geographic concentration. Specifically, mudslides, earthquakes, wildfires and other natural disasters occur frequently in California. Potential damage and disruption in our facilities or employees' homes located in California as a result of mudslides, earthquakes, wildfires or other natural disasters could be substantial. If we experience mudslides, earthquakes, wildfires or other natural disasters at any of our facilities or employees' homes, our reputation and results of operations could be harmed due to financial losses to repair or rebuild our facilities or disruption to our customers or employees that could hurt our ability to effectively provide our services. Should any adverse economic, regulatory, environmental or other developments occur in Southern California, our business, financial condition, results of operation or cash flows could be materially adversely affected.
56
We may be unable to expand into some geographic areas, or may be unable to do so without incurring significant additional costs.
We are likely to incur additional costs if we enter states or other counties in California where we do not currently operate. Our rate of expansion into other geographic areas may also be inhibited by:
- •
- our inability to develop a network of physicians, hospitals and other healthcare providers that meets our requirements,
the requirements of the community and those of government regulators;
- •
- competition for physicians and patients;
- •
- the cost of providing healthcare services in those areas; and
- •
- demographics and population density.
Accordingly, we may be unsuccessful in entering other metropolitan areas, counties or states.
Our overall business results may suffer from the recent economic downturn.
Recently, the U.S. economy has weakened significantly. Tightening credit markets, depressed consumer spending and higher unemployment rates continue to pressure many industries. During economic downturns, governmental entities often experience budgetary constraints as a result of increased costs and lower than expected tax collections. These budgetary constraints may result in decreased spending for health and human service programs, including Medicare, Medicaid and similar programs, which represent significant payor sources for our hospitals and Medical Groups. Other risks we face from general economic weakness include potential declines in the population covered under managed care agreements, patient decisions to postpone or cancel elective and non-emergent healthcare procedures, potential increases in the uninsured and underinsured populations and further difficulties in our collecting patient co-payment and deductible receivables.
We must evaluate the effectiveness of our disclosure controls and internal control over financial reporting on a periodic basis and publicly disclose the results of these evaluations and related matters.
Our management is required to periodically evaluate the effectiveness of our disclosure controls and procedures and our internal control over financial reporting. We are also required to disclose in our periodic reports with the SEC any changes in our internal control over financial reporting that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting. The rules governing the standards that must be met for management to assess the effectiveness of our internal control over financial reporting are complex and require significant documentation, testing and possible remediation. Compliance with these rules has resulted in increased expenses and the devotion of significant management resources.
Our evaluation of our disclosure controls and procedures may reveal material weaknesses in our internal control over financial reporting. If we identify a material weakness, we would be required to conclude that our internal control over financial reporting is ineffective and disclose this conclusion, which could harm our business.
We are required to upgrade and modify our management information systems to accommodate growth in our business and changes in technology and to satisfy new government regulations. As we seek to implement these changes, we may experience complications, delays and increasing costs, which could disrupt our business and reduce our profitability.
We have developed sophisticated management information systems that process and monitor patient case management and utilization of physician, hospital and ancillary services, claims receipt and claims payments, patient eligibility and other operational data required by management. These systems
57
require ongoing modifications, improvements or replacements as we expand and as new technologies become available. We have a centralized business office ("CBO") located in Bellflower, California to meet the management information systems needs of our four Alta hospitals. Although Brotman currently outsources all of its information technology and management information systems needs, we may integrate Brotman into our CBO, which would require improvements or replacements to our existing systems if Brotman requires functionalities that are not available through our current systems. This transition may result in substantial cost and disrupt operations. Full integration of Brotman into our CBO may take up to 24 months, or it may not even be possible.
We may also be required to modify our management information systems in order to comply with new government regulations. For example, regulations adopted under HIPAA have required us to comply with new electronic healthcare transactions and conduct standards, uniform standards for data reporting, formatting and coding, and standards for ensuring the privacy of individually identifiable health information. This required us to make significant changes to our management information systems, at substantial cost. Similar modifications, improvements and replacements may be required in the future at additional substantial cost and could disrupt our operations during periods of implementation. Moreover, implementation of such systems is subject to the availability of information technology and skilled personnel to assist us in creating and implementing the systems. The complications, delays and cost of implementing these changes could disrupt our business and reduce our profitability. In addition, any system failure that causes an interruption in service or availability of our systems could adversely affect operations or delay the collection of revenues.
We and our hospitals and affiliated physician organizations may become subject to claims of medical malpractice or HMO bad-faith liability claims for which our insurance coverage may not be adequate. Such claims could materially increase our costs and reduce our profitability.
In the ordinary course of business, we may be subject to medical malpractice lawsuits and other legal actions arising from our operations. These actions may involve large claims and significant defense costs. In an effort to resolve one or more of these matters, we may choose to negotiate a settlement. Amounts we pay to settle any of these matters may be material. To mitigate a portion of this risk, we maintain professional malpractice liability, general liability insurance coverage and managed care errors and omissions insurance for these potential claims in amounts above our self-insured retention level that we believe to be appropriate for our operations. However, some of these claims could exceed the scope of the coverage in effect, or coverage of particular claims could be denied. It is possible that successful claims against us that are within the self-insured retention level amounts, when considered in the aggregate, could have an adverse effect on our results of operations, cash flows, financial condition or liquidity. Furthermore, insurance coverage in the future may not continue to be available at a cost allowing us to maintain adequate levels of insurance with acceptable self-insured retention level amounts. Also, one or more of our insurance carriers may become insolvent and unable to fulfill its obligation to defend, pay or reimburse us when that obligation becomes due. In addition, physicians using our hospitals may be unable to obtain insurance on acceptable terms. Our subsidiary hospitals are subject to medical malpractice lawsuits, general liability lawsuits and other legal actions. We believe, based on our past experience and actuarial estimates, that our insurance coverage is sufficient to cover claims arising from the operations of our subsidiary hospitals. However, if payments for claims and related expenses exceed our estimates or if payments are required to be made by us that are not covered by insurance, our business could be harmed.
58
If our goodwill and intangible assets become impaired, the impaired portion has to be written off, which will materially reduce the value of our assets and reduce our net income for the year in which the write-off occurs.
As of September 30, 2007, we concluded that the goodwill and other intangible assets related to our pre-2006 acquisitions (i.e., excluding ProMed and Alta) were impaired, and recorded a write-off of approximately $27,512,000 within the continuing legacy Medical Group segment. Following the 2007 acquisitions of ProMed and Alta, our intangible assets represent a substantial portion of our assets. As of September 30, 2009, goodwill totaled approximately $153,250,000 and other intangible assets totaled approximately $46,425,000 for a combined total of $199,675,000, representing approximately 53% of our total assets. Of these amounts, approximately $24,373,000 was attributable to goodwill and approximately $3,000,000 was attributable to identifiable intangible assets recorded in connection with the Brotman Acquisition.
FASB "Accounting Standards Codification" ("ASC") 350 (previously issued as SFAS No. 142 "Goodwill and Other Intangible Assets,") requires, among other things, that the carrying value of goodwill and indefinite life intangible assets will be evaluated for impairment at least on an annual basis, or more frequently if certain indicators are encountered. A two-step impairment test is used to identify potential goodwill impairment and to measure the amount of goodwill impairment loss to be recognized (if any). The first step of the goodwill impairment test, which is used to identify potential impairment, compares the fair value of a reporting unit with its carrying amount, including goodwill. If the fair value of a reporting unit exceeds its carrying amount, goodwill of the reporting unit is considered not impaired, making the second step of the impairment test unnecessary.
A finding that the value of our goodwill and intangible assets has been impaired requires us to write off the impaired portion, which significantly reduces the value of our assets and reduces our net income for the year in which the write-off occurs.
Our hospital revenues and volume trends may be adversely affected by certain factors over which we have no control, including weather conditions, severity of annual flu seasons and other factors.
Our hospital revenues and volume trends are dependent on many factors, including physicians' clinical decisions and availability, payor programs shifting to a more outpatient-based environment, whether or not certain services are offered, seasonal and severe weather conditions, earthquakes, current local economic and demographic changes and the intensity and timing of yearly flu outbreaks. Any of these factors could have a material adverse effect on our revenues and volume trends, and none of these factors will be within the control of our management.
The financial statements of Brotman are being presented on a standalone basis and include a Going Concern emphasis paragraph
The audit opinion for those standalone financial statements reflects the fact that Brotman's auditors have concluded that there is substantial doubt about Brotman's ability to continue as a going concern, resulting from liquidity issues and the potential for the JHA debt to be called within twelve months from the date of issuance of those standalone financial statements. This uncertainty may negatively impact the carrying value of the Company's investment in Brotman and could result in the future impairment of Goodwill. No adjustments have been recorded in the consolidated financial statements from any losses that may result from this uncertainty.
We also face other risks that could adversely affect our business, financial condition or results of operations, which include:
- •
- any requirement to restate financial results in the event of inappropriate application of accounting principles;
59
- •
- a significant failure of our internal control over financial reporting;
- •
- failure of our prevention and control systems related to employee compliance with internal policies, including data
security;
- •
- failure to protect our proprietary information;
- •
- failure of our corporate governance policies or procedures; and
- •
- failing to meet covenants or requirements under our loan agreements which could impact our liquidity and ability to make
future acquisitions.
- •
- Brotman has a history of losses and defaults under indebtedness owed to its creditors. Brotman's ability to return to profitability is subject to its management's ability to revise and implement the turnaround plans and to generate sufficient cash from operations to meet its obligations.
Item 1B. Unresolved Staff Comments.
Not applicable.
60
We own or control through our subsidiaries, Alta Hospitals System, LLC and Prospect Hospital Advisory Services, Inc., the following real property:
Entity
|
Location | Description | ||
|---|---|---|---|---|
Hollywood Community Hospital |
6245 De Longpre Ave. Los Angeles, CA 90028 and 6228 Leland Way Los Angeles, CA 90028 |
Hospital with 100 licensed beds with 49,152 square feet of improvements situated on 1.88 acres of land. | ||
Los Angeles Community Hospital |
4081 East Olympic Blvd. |
Hospital with 130 licensed beds with 64,024 square feet of improvements situated on 2.01 acres of land. |
||
Los Angeles Community Hospital |
4057/4059 East Olympic Blvd. |
Hospital clinic. |
||
Norwalk Community Hospital |
13222 Bloomfield Ave. |
Hospital with 50 licensed beds with 23,530 square feet of improvements situated on 1.88 acres of land. |
||
Van Nuys Community Hospital |
14433 Emelita St. |
Psychiatric hospital with 59 licensed beds with 34,192 square feet of improvements situated on 1.86 acres of land. |
||
Brotman Medical Center |
3828 Delmas Terrace |
Hospital Pavilion with 420 licensed beds with 44,301 square feet of improvements. |
||
Brotman Medical Center |
3847 Delmas Terrace |
Hospital Tower with 14,497 square feet of improvements. |
||
Brotman Medical Center |
3828 Hughes Avenue |
Outpatient and hospital support facilities. |
||
Brotman Medical Center |
3817 Watseka Avenue |
Plan operations building. |
In addition, we, or our affiliated physician organizations, currently lease space for administrative and medical offices, some of which is shared space, as follows:
Medical or Independent Practice Association Offices
Entity
|
Location | Purpose | Lease Term; Renewal | Current Monthly Rent | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Prospect Medical Group(1) |
Santa Ana, CA | Shares space with Prospect Medical Systems | 5 years; 2010 | $ | 47,518 | |||||
61
Entity
|
Location | Purpose | Lease Term; Renewal | Current Monthly Rent | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Prospect Medical Holdings(3) |
Los Angeles, CA | Shares office space with Alta Hospitals System LLC | 7 years; 2015 | $ | 25,039 | ||||||
Prospect Medical Holdings(5) |
Culver City, CA |
Office space |
7 years; 2012 |
$ |
5,656 | ||||||
Prospect Medical Systems(2) |
Santa Ana, CA |
Shares space with Prospect Medical Group |
5 years; 2010 |
$ |
49,031 | ||||||
Prospect Medical Systems(2) |
Santa Ana, CA |
Shares space with Prospect Medical Group |
5 years; 2011 |
$ |
21,600 | ||||||
ProMed Health Care Administrators, Inc. |
Ontario, CA |
Office space shared with Pomona Valley Medical Group and Upland Medical Group |
10 years; 2014 |
$ |
39,305 | ||||||
ProMed Health Care Administrators, Inc. |
Ontario, CA |
Storage Space |
Month-to-month |
$ |
1,210 | ||||||
Alta Hospitals System, LLC(3) |
Los Angeles, CA |
Shares office space with Prospect Medical Holdings |
7 years; 2015 |
$ |
25,039 | ||||||
Alta Hospitals System, LLC(4) |
Los Angeles, CA |
Office space |
5 years; 2010 |
$ |
9,454 | ||||||
Alta Hospitals System, LLC |
Bellflower, CA |
Office space |
6 years; 2011 |
$ |
13,352 | ||||||
Norwalk Community Hospital |
Norwalk, CA |
Medical office space |
5 years; 2014 |
$ |
1,010 | ||||||
Hollywood Community Hospital |
Hollywood, CA |
Administrative office space |
2 years; 2011 |
$ |
3,250 | ||||||
Brotman Medical Center |
Culver City, CA |
Medical office space |
6 years; 2012 |
$ |
6,498 | ||||||
Brotman Medical Center |
Culver City, CA |
Office space |
6 years; 2012 |
$ |
9,370 | ||||||
Brotman Medical Center |
Culver City, CA |
Medical office space |
10 years; 2019 |
$ |
9,037 | ||||||
- (1)
- Prospect
Medical Group includes all affiliated physician organizations that are wholly-owned subsidiaries of Prospect Medical Group.
- (2)
- On
May 10, 2004, Prospect Medical Systems executed a Seventh Addendum to its office lease that provided for an increase in space of 5,298 square feet
effective July 1, 2004, at which date, the base rent increased to $39,951. Since then, the base rent has increased to the current monthly rate of $49,031.
- We
leased additional space in July, 2006 adjacent to the Santa Ana facilities for approximately 12,015 square feet. The lease agreement term is
for 60 months, through 2011, with starting monthly lease payments of approximately $20,400.
- (3)
- On
May 7, 2008, Alta Hospitals System, LLC executed a lease for approximately 7,154 square feet of office space that is shared with Prospect
Medical Holdings. The lease agreement term is for 84 months through 2015 with starting monthly lease payments of approximately $25,039.
- (4)
- Alta Hospitals System, LLC executed a sublease agreement effective August 1, 2008 for the remainder of the original lease. The monthly lease payments are approximately $10,205.
62
- (5)
- Prospect Medical Holdings, Inc. executed a sublease agreement effective November 1, 2008 for the remainder of the original lease. The subtenant left in May 2009. The monthly sublease payments were approximately $6,029, and made through April 2009. We are in the process of locating a replacement tenant.
We believe that this office space is sufficient for our operational needs for the foreseeable future, although we may need to acquire additional space to accommodate our plans for future growth, if successful.
We and our affiliated physician organizations are parties to legal actions arising in the ordinary course of business. We believe that liability, if any, under these claims will not have a material adverse effect on our consolidated financial position or results of operations.
Item 4. Submission of Matters to a Vote of Security Holders.
None.
63
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Common Stock. Beginning on September 30, 2009, our common stock, par value $0.01 per share, commenced listing on the NASDAQ Global Market under the symbol "PZZ" and we voluntarily ceased its trading on the NYSE Amex (formerly the American Stock Exchange) where it had begun trading on May 11, 2005.
The following table sets forth the quarterly high and low sales prices for our common stock for the last two completed fiscal years.
Date Range
|
High Sales Price |
Low Sales Price |
|||||
|---|---|---|---|---|---|---|---|
2008 |
|||||||
First Quarter |
$ | 5.45 | $ | 3.65 | |||
Second Quarter(1)(2) |
$ | 4.35 | $ | 3.83 | |||
Third Quarter(1)(3) |
$ | 4.30 | $ | 2.90 | |||
Fourth Quarter |
$ | 3.50 | $ | 1.78 | |||
2009 |
|||||||
First Quarter |
$ | 3.00 | $ | 1.00 | |||
Second Quarter |
$ | 2.64 | $ | 1.45 | |||
Third Quarter |
$ | 5.00 | $ | 1.23 | |||
Fourth Quarter |
$ | 4.69 | $ | 3.54 | |||
- (1)
- As
a result of non-timely filing of our Form 10-K for the fiscal year ended September 30, 2007, the NYSE Amex
suspended trading in our common stock on January 16, 2008. After we became current in our SEC filings, trading in our common stock resumed on June 17, 2008.
- (2)
- For
the reasons stated in note (1), trading occurred during this quarter only from January 1, 2008 to January 15, 2008.
- (3)
- For the reasons stated in note (1), trading occurred during this quarter only from June 17, 2008 to June 30, 2008.
As of December 11, 2009, we had approximately 354 record owners and approximately 473 beneficial owners of our common stock.
Dividends. We have not paid any cash dividends on our common stock in the past and do not plan to do so in the near future. Under our new credit facilities, we are allowed to make dividend payments, provided that the aggregate amount of such payments do not exceed 50% of our consolidated net income (as defined in the credit agreements) and so long as no default has occurred.
Equity Compensation Plan Information. See Part III, Item 12, Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters, for information regarding securities authorized for issuance under our equity compensation plans.
Item 6. Selected Financial Data.
Not applicable.
64
Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations.
Overview
Prior to the acquisition of Alta and Brotman, we were primarily a physician services organization that provided medical management systems and services to affiliated medical organizations, primarily Independent Physician Associations, also referred to as Medical Groups ("Medical Group"). With the acquisition of Alta and Brotman, we now own and operate five hospitals in Southern California and our operations are now organized into three reporting segments: Hospital Services, Medical Group and Corporate. The Hospital Services segment includes the results of operations and financial position of Brotman since our April 14, 2009 acquisition of a majority stake in Brotman.
Hospital Services Segment
The Hospital Services segment owns and operates five hospitals in Los Angeles County with a total of approximately 759 licensed beds served by 829 on-staff physicians at September 30, 2009. Each of the community hospitals in Hollywood, Los Angeles, Norwalk and Culver City offers a comprehensive range of medical and surgical services, including inpatient, outpatient, skilled nursing and urgent care services. The psychiatric hospital in Van Nuys provides acute inpatient and outpatient psychiatric services to patients admitted on a voluntary basis. Admitting physicians are primarily practitioners in the local area. The hospitals have payment arrangements with Medicare, Medi-Cal and other third-party payers including some commercial insurance carriers, HMOs and Preferred Provider Organizations ("PPOs"). The basis for such payments involving inpatient and outpatient services rendered includes prospectively determined rates per discharge and cost-reimbursed methodologies. The Alta hospitals are eligible to receive additional Disproportionate Share Hospital Program ("DSH") payment adjustments from Medicare and Medi-Cal based on a prospective payment system for hospitals that serve large proportions of low-income patients. The Brotman hospital is also eligible to receive DSH payment adjustments from Medicare and supplemental Distressed Hospital Fund payments from the California Medical Assistance Commission ("CMAC").
Operating revenue of our Hospital Services segment consists primarily of payments for services rendered, including estimated retroactive adjustments under reimbursement arrangements with third-party payers. In some cases, reimbursement is based on formulas and reimbursable amounts are not considered final until cost reports are filed and audited or otherwise settled by the various programs. We accrue for amounts that we believe will ultimately be due to or from Medicare and other third-party payers and report such amounts as net patient revenues in the accompanying financial statements. We closely monitor our historical collection rates, as well as changes in applicable laws, rules and regulations and contract terms, to assure that provisions are made using the most accurate information available. However, due to the complexities involved in these estimations, actual payments from payers may be materially different from the amounts we estimate and record. A summary of the payment arrangements with major third-party payers follows:
Medicare: Medicare is a federal program that provides certain hospital and medical insurance benefits to persons aged 65 and over, some disabled persons with end-stage renal disease and certain other beneficiary categories. Inpatient services rendered to Medicare program beneficiaries are paid at prospectively determined rates per discharge, according to a patient classification system based on clinical, diagnostic, and other factors. Outpatient services are paid based on a blend of prospectively determined rates and cost-reimbursed methodologies. We are also reimbursed for various disproportionate share and Medicare bad debt components at tentative rates, with final settlement determined after submission of annual Medicare cost reports and audit thereof by the Medicare fiscal intermediary. Normal estimation differences between final settlements and amounts accrued in previous years are reflected in net patient service revenue in the year of final settlement.
65
Medi-Cal: Medi-Cal is a joint federal-state funded healthcare benefit program that is administered by the state of California to provide benefits to qualifying individuals who are unable to afford care. As such, Medi-Cal constitutes the version of the federal Medicaid program that is applicable to California residents. Inpatient services rendered to Medi-Cal program beneficiaries are paid at contracted per diem rates. The per diem rates are not subject to retrospective adjustment. Outpatient services are paid based on prospectively determined rates per procedure provided.
Managed Care: We also receive payment from certain commercial insurance carriers, HMOs, and PPOs, though we generally do not enter into contracts with these entities. The basis for payment under these agreements includes our standard charges for services.
Self-Pay: Our hospitals provide services to individuals that do not have any form of healthcare coverage. Such patients are evaluated, at the time of service or shortly thereafter, for their ability to pay based upon federal and state poverty guidelines, qualifications for Medi-Cal, as well as our local hospital's indigent and charity care policy.
Hospital revenues depend upon inpatient occupancy levels, the medical and ancillary services and therapy programs ordered by physicians and provided to patients, the volume of outpatient procedures and the charges or negotiated payment rates for such services. Charges and reimbursement rates for inpatient routine services vary depending on the type of services provided (e.g., medical/surgical, intensive care or behavioral health) and the geographic location of the hospital. Inpatient occupancy levels fluctuate for various reasons, many of which are beyond our control. The percentage of patient service revenue attributable to outpatient services has generally increased in recent years, primarily as a result of advances in medical technology that allow more services to be provided on an outpatient basis, as well as increased pressure from Medicare, Medi-Cal and private insurers to reduce hospital stays and provide services, where possible, on a less expensive outpatient basis. We believe that our experience with respect to our increased outpatient levels mirrors the general trend occurring in the healthcare industry and we are unable to predict the rate of growth and resulting impact on our future revenues.
Patients are generally not responsible for any difference between customary hospital charges and amounts reimbursed for such services under Medicare, Medicaid, some private insurance plans, and managed care plans, but are responsible for services not covered by such plans, exclusions, deductibles or co-insurance features of their coverage. The amount of such exclusions, deductibles and co-insurance has generally been increasing each year. Indications from recent federal and state legislation are that this trend will continue. Collection of amounts due from individuals is typically more difficult than from governmental or business payers and increases in uninsured and self-pay patients unfavorably impact the collectability of our patient accounts, thereby increasing our provision for doubtful accounts and charity care provided.
Operating expenses of our Hospital Services segment generally consist of salaries, benefits and other compensation paid to physicians and healthcare professionals that are employees of our hospitals; medical supplies; consultant and professional services; and provision for doubtful accounts.
General and administrative expenses of our Hospital Services segment generally consists of salaries, benefits and other compensation for our hospital administrative employees, insurance, rent, operating supplies, legal, accounting and marketing.
Hospital Services Results of Operations
The following table sets forth the results of operations for our hospitals and is used in the discussion below for the fiscal years ended September 30, 2009 and 2008 (in thousands).
66
| |
Year Ended September 30, | |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
% Increase (Decrease) |
||||||||||
| |
2009 | 2008 | |||||||||
Net Hospital Services revenues: |
|||||||||||
Medicare |
$ | 96,693 | $ | 66,740 | 44.9 | % | |||||
Medi-Cal |
74,865 | 51,407 | 45.6 | % | |||||||
Managed care |
23,329 | 4,701 | 396.2 | % | |||||||
Self pay |
8,926 | 2,040 | 337.6 | % | |||||||
Other |
1,691 | 1,804 | (6.3 | )% | |||||||
Total Hospital Services revenues |
$ | 205,504 | $ | 126,692 | 62.2 | % | |||||
Hospital operating expenses: |
|||||||||||
Salaries, wages and benefits |
94,547 | 60,213 | 57.0 | % | |||||||
Other operating expenses |
15,754 | 7,919 | 98.9 | % | |||||||
Supplies expense |
16,531 | 9,329 | 77.2 | % | |||||||
Provision for doubtful accounts |
17,715 | 5,782 | 206.4 | % | |||||||
Lease and rental expense |
1,802 | 1,112 | 62.3 | % | |||||||
Total Hospital Services operating expenses |
$ | 146,349 | $ | 84,355 | 73.6 | % | |||||
General and administrative expenses |
18,154 | 12,479 | 45.5 | % | |||||||
Depreciation and amortization expense |
4,301 | 4,286 | 0.4 | % | |||||||
Total non-medical expenses |
$ | 22,455 | $ | 16,765 | 33.9 | % | |||||
Operating income |
$ | 36,700 | $ | 25,572 | 43.5 | % | |||||
The following table sets forth selected operating items, expressed as a percentage of total net hospital services revenue for the fiscal years ended September 30, 2009 and 2008:
| |
Year Ended September 30, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
Net Hospital Services revenues: |
||||||||
Medicare |
47.1 | % | 52.7 | % | ||||
Medi-Cal |
36.4 | % | 40.6 | % | ||||
Medical group |
11.4 | % | 3.7 | % | ||||
Self pay |
4.3 | % | 1.6 | % | ||||
Other |
0.8 | % | 1.4 | % | ||||
Total Hospital Services revenues |
100.0 | % | 100.0 | % | ||||
Hospital operating expenses: |
||||||||
Salaries, wages and benefits |
46.0 | % | 47.5 | % | ||||
Other operating expenses |
7.7 | % | 6.3 | % | ||||
Supplies expense |
8.0 | % | 7.4 | % | ||||
Provision for doubtful accounts |
8.6 | % | 4.6 | % | ||||
Lease and rental expense |
0.9 | % | 0.9 | % | ||||
Total Hospital Services operating expenses |
71.2 | % | 66.6 | % | ||||
General and administrative expenses |
8.8 | % | 9.9 | % | ||||
Depreciation and amortization expense |
2.1 | % | 3.4 | % | ||||
Total non-medical expenses |
10.9 | % | 13.2 | % | ||||
Operating income |
17.9 | % | 20.2 | % | ||||
67
The following table shows certain selected historical operating statistics for our hospitals for the fiscal years ended September 30, 2009 and 2008:
| |
Year Ended September 30, | |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
% Increase (Decrease) |
|||||||||
| |
2009(4) | 2008 | ||||||||
Net inpatient revenues (in thousands)(1) |
$ | 186,253 | $ | 118,219 | 58 | % | ||||
Net outpatient revenues (in thousands)(1) |
$ | 17,560 | $ | 6,668 | 163 | % | ||||
Other hospital services revenues (in thousands) |
$ | 1,691 | $ | 1,806 | (6 | )% | ||||
Number of hospitals at end of period |
5 | 4 | 25 | % | ||||||
Licensed beds at end of period |
759 | 339 | 124 | % | ||||||
Average licensed beds |
759 | 340 | 123 | % | ||||||
Average available beds |
616 | 331 | 86 | % | ||||||
Admissions(2) |
18,573 | 14,206 | 31 | % | ||||||
Adjusted admissions(3) |
20,098 | 15,058 | 33 | % | ||||||
Net inpatient revenue per admission |
$ | 10,028 | $ | 8,322 | 21 | % | ||||
Patient days |
124,004 | 87,463 | 42 | % | ||||||
Adjusted patient days |
135,228 | 92,706 | 46 | % | ||||||
Acute Care average length of stay (days) |
6.20 | 5.50 | 13 | % | ||||||
Net inpatient revenue per patient day |
$ | 1,502 | $ | 1,352 | 11 | % | ||||
Outpatient visits |
34,999 | 17,111 | 105 | % | ||||||
Net outpatient revenue per visit |
$ | 502 | $ | 389 | 29 | % | ||||
- (1)
- Net
inpatient revenues and net outpatient revenues are components of net patient revenues. Net inpatient revenues for the fiscal years ended
September 30, 2009 and 2008 included self-pay revenues of approximately $8,926,000 and $1,931,000, respectively. Net outpatient revenues for the fiscal years ended
September 30, 2009 and 2008 included self-pay revenues of approximately $1,145,000 and $109,000, respectively.
- (2)
- Charity
care admissions represented 0.7% and 0.4% of total admissions for the fiscal years ended September 30, 2009 and 2008, respectively.
- (3)
- Adjusted
admissions are total admissions adjusted for outpatient volume. Adjusted admissions are computed by multiplying admissions (inpatient volume) by
the sum of gross inpatient charges and gross outpatient charges and then dividing the resulting amount by gross inpatient charges.
- (4)
- The above amounts include Brotman operating results since April 14, 2009, when the Company acquired a majority stake in Brotman.
Net Hospital Services Revenues
Net inpatient revenues for fiscal 2009 were approximately $186,253,000, representing an increase of approximately $68,034,000 or 57.6% from net inpatient revenues for fiscal 2008, of approximately $118,219,000. Brotman, which results were included since April 14, 2009, accounted for $49,415,000 or 72.6% of the increase.
Excluding Brotman, same hospital net inpatient revenues increased by approximately $18,619,000 or 15.8% during fiscal 2009 as compared fiscal 2008. The increase was due to higher Medicare reimbursement rates and increases in total admissions.
Same-hospital admissions, excluding the effect of Brotman, for fiscal 2009 increased by 3.5% compared to fiscal 2008, primarily due to net volume increases in many of the service lines emphasized by our targeted growth initiatives and closures of several competing hospital facilities in certain of our hospital operating areas.
68
Net outpatient revenues for fiscal 2009 were approximately $17,560,000, representing an increase of approximately $10,893,000 or 163.3% from net outpatient revenues for fiscal 2008, of approximately $6,668,000. Brotman, which results were included since April 14, 2009, accounted for the majority of the increase.
Excluding Brotman, same hospital net outpatient revenues increased by approximately 11.8% and same hospital net outpatient revenues per outpatient visits decreased by approximately 8%. The increase was due to increases in outpatient surgery cases with higher reimbursement rates.
Salaries, Wages and Benefits
Salaries, wages and benefits for fiscal 2009 were approximately $94,547,000, representing an increase of approximately $34,334,000 or 57.0% over fiscal 2008 of approximately $60,213,000. Brotman, which results were included since April 14, 2009, accounted for $30,271,000 or the majority of the increase.
Excluding Brotman, same hospital salaries, wages and benefits expense as a percentage of Alta's net Hospital Services revenues for fiscal 2009 decreased by approximately 3.3% compared to fiscal 2008. Same hospital salaries, wages and benefits per adjusted patient day for fiscal 2009 were approximately $629, representing a decrease of 3.1% compared to $649 for fiscal 2008. The decrease was primarily due to productivity gained through efficiencies, partially offset by merit increases for our employees.
As of September 30, 2009, approximately 5.0% and 80% of the total employees at our Alta and Brotman hospitals were represented by labor unions, respectively. The collective bargaining agreement entered into between Hollywood Community Hospital, which is one of the hospitals under the consolidated group of Alta Hospitals System, LLC, and Service Employees International Union ("SEIU"), covers a small group of Hollywood Community Hospital's employees and will expire on May 9, 2011. The collective bargaining agreements entered into between Brotman and the California Nurses Association ("CNA"), and Brotman and the SEIU both expire on February 28, 2010. We do not anticipate that any changes in these agreements will have a material adverse effect on results of our Hospital Services operations in fiscal 2009.
Other Operating Expenses
Other operating expenses for fiscal 2009 were approximately $15,754,000, representing an increase of approximately $7,835,000 or 98.9% from other operating expense for fiscal 2008, of approximately $7,919,000. Brotman, which results were included since April 14, 2009, accounted for the majority of the increase.
Excluding Brotman, Alta's same hospital other operating expense as a percentage of Alta's net Hospital Services revenue for fiscal 2009 was approximately decreased by 11.1%, compared to fiscal 2008. Same hospital other operating expenses per adjusted patient day decreased approximately 5.9% to $80 in fiscal 2009 compared to $85 for fiscal 2008, primarily due to the write-off of a certain vendor liability in 2009.
Supplies Expense
Supplies expense for fiscal 2009 was approximately $16,531,000, representing an increase of approximately $7,202,000 or 77.2% from supplies expense for fiscal 2008, of approximately $9,329,000. Brotman, which results were included since April 14, 2009, accounted for substantially all of the increase.
Excluding Brotman, same hospital supplies expense as a percentage of Alta's net Hospital Services revenue for fiscal 2009 decreased by 17.8%, compared to fiscal 2008. Same hospital supplies expense
69
per adjusted patient day for fiscal 2009 was approximately $86, representing a decrease of 14.1%, compared to approximately $101 for fiscal 2008. This decrease in supplies expense per adjusted patient day primarily was due to a decrease in orthopedic cases in one of our hospitals and improved efficiencies gained through continued focus on supply management.
Provision for Doubtful Accounts
The provision for doubtful accounts as a percentage of net Hospital Services revenues was 8.6% for fiscal 2009 compared to 4.6% for fiscal 2008. Brotman, which results were included since April 14, 2009, accounted for substantially all of the increase.
Excluding Brotman, same hospital provision for doubtful accounts as a percentage of Alta's net Hospital Services revenue for fiscal 2009 was approximately 5.5%, as compared to 4.6% for fiscal 2008. The increase was due to lower than usual bad debt experience in the prior year period.
Lease and Rental Expense
Lease and rental expense for fiscal 2009 was approximately $1,802,000, representing an increase of approximately $692,000 or 62.3% from lease and rental expense for fiscal 2008, of approximately $1,111,000. Brotman, which results were included since April 14, 2009, accounted for $263,000 or 38.0% of the increase.
Excluding Brotman, same hospital lease and rental expense as a percentage of Alta's net Hospital Services revenue for fiscal 2009 was 1.1%, representing an increase of 22.2%, compared to 0.9% for fiscal 2008. The increase was due primarily to an increase in rent expense for hospital beds, in line with increased admissions, patient days and length of patients' stay and secondarily to increased rent associated with our new administrative office space, commencing in October 2008.
General and Administrative Expense
General and administrative, or "G&A" expense for fiscal 2009 was approximately $18,154,000, representing an increase of approximately $5,673,000 or 45.5% from G&A for fiscal 2008, of approximately $12,479,000. Brotman, which results were included since April 14, 2009, accounted for the majority of the increase.
Excluding Brotman, same hospital general and administrative expense as a percentage of Alta's net Hospital Services revenue for fiscal 2009 decreased by 3.3%, compared to fiscal 2008. The decrease was due primarily to a decrease in consulting and outside services. Included in G&A expenses were consulting and outside services, supplies, insurance, utilities, taxes and licenses and maintenance, which accounted for approximately 98.4% of the total expenses in fiscal 2009, as compared to 99.9% for fiscal 2008.
Depreciation and Amortization Expense
Depreciation and amortization expense for fiscal 2009 was approximately $4,301,000, representing an increase of approximately $15,000 or 0.3% from depreciation and amortization expense for fiscal 2008, of approximately $4,286,000. Brotman, which results were included since April 14, 2009, accounted for substantially all of the increase.
70
Excluding Brotman, depreciation and amortization expenses as a percentage of Alta's net Hospital Services revenues for fiscal 2009 were approximately 2.7%, representing a decrease of 20.6%, compared to 3.4% for fiscal 2008. Included in depreciation and amortization expense was amortization of identifiable intangibles of approximately $1,267,000 in each of fiscal 2009 and 2008.
Operating Income
Our Hospital Services segment reported an operating income of approximately $36,700,000 and $25,573,000 for fiscal 2009 and 2008, respectively, which increase was the result of the changes discussed above. The pre-tax operating results from the Hospital Services segment include certain corporate expense allocations for insurance, professional fees, and amortization of identifiable intangibles.
Medical Group Segment
The Medical Group segment provides management services to affiliated physician organizations that operate as independent physician associations. The affiliated physician organizations enter into agreements with HMOs to provide HMO enrollees with a full range of medical services in exchange for fixed, prepaid monthly fees known as "capitation" payments. The Medical Groups contract with physicians (primary care and specialist) and other healthcare providers to provide all necessary medical services.
Through our management subsidiaries—Prospect Medical Systems, Inc. ("PMS"), Sierra Medical Management (through August 1, 2008) and ProMed Health Care Administrators—we have entered into long-term agreements to provide management services to each of our affiliated physician organizations in exchange for a management fee. The management services we provide include HMO contracting, physician recruiting, credentialing and contracting, human resources services, claims administration, provider relations, patient eligibility and other services, medical management including utilization management and quality assurance, data collection, and management information systems.
Effective August 1, 2008, we sold the AV Entities. The assets, liabilities and operating results of the AV Entities have been classified as discontinued operations and are excluded from the disclosures below.
Our management subsidiaries currently provide management services to ten affiliated physician organizations, which include PMG, Nuestra Familia Medical Group, Inc. ("Nuestra"), seven other affiliated physician organizations that PMG owns or controls, and one affiliated physician organization (AMVI/Prospect Health Network) that is an unconsolidated joint venture in which PMG owns a 50% interest. PMG, which was our first affiliated physician organization, has acquired the ownership interest in all of our other affiliated physician organizations, except Nuestra. Both PMG and Nuestra are owned by our physician shareholder nominee, Dr. Arthur Lipper, and controlled through assignable option agreements and management services agreements. PMG also serves as a holding company for our other affiliated physician organizations, except Nuestra (see chart at page 5 and Note 7 to the Notes to the Consolidated Financial Statements).
The ten affiliated physician organizations provided medical services to a combined total of approximately 177,000 HMO enrollees at September 30, 2009, including approximately 10,200 AMVI/Prospect Health Network enrollees that we manage for the economic benefit of an independent third party, and for which we earn management fee income.
As of September 30, 2009, our affiliated physician organizations had contracts with approximately 14 HMOs, from which our revenue was primarily derived. HMOs offer a comprehensive healthcare benefits package in exchange for a capitation fee per enrollee that does not vary through the contract period regardless of the quantity or cost of medical services required or used. HMOs enroll members by entering into contracts with employer groups or directly with individuals to provide a broad range of
71
healthcare services for a prepaid charge, with minimal deductibles or co-payments required of the members. All of the contracts between our affiliated physician organizations and the HMOs provide for the provision of medical services by the affiliated physician organization to the HMO enrollees in consideration for the prepayment of the fixed monthly capitation fee per enrollee.
Our Medical Group business has grown through the acquisition of Medical Groups by PMG, and is concentrated in the California counties of Orange, Los Angeles and San Bernardino.
Managed care revenues consist primarily of fees for medical services provided by our affiliated physician organizations under capitated contracts with HMOs. Capitation revenue under HMO contracts is prepaid monthly to the affiliates based on the number of covered HMO enrollees. Capitation revenue may be subsequently adjusted to reflect changes in enrollment as a result of retroactive terminations or additions. These adjustments have not had a material effect on capitation revenue. Capitation revenue is also subject to risk adjustment, whereby capitation with respect to Medicare enrollees is subject to subsequent adjustment for the acuity of the enrollees to whom services were provided. Capitation for the current year is paid based on data submitted for each enrollee for the preceding year. Capitation is paid at interim rates during the year and is adjusted in subsequent periods (generally in our fourth fiscal quarter) after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since we do not currently have the ability to reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated from the health plans, generally in the fourth quarter of the fiscal year to which the adjustments relate. Management fees were primarily comprised of amounts earned from managing the operations of AMVI, Inc., which is our joint venture partner in the AMVI/Prospect Health Network joint venture, related to Medi-Cal members and Medicare members enrolling in CalOPTIMA's OneCare HMO. OneCare is a Medicare Advantage Special Needs Plan serving dually-eligible members in Orange County who are entitled to Medicare benefits and are also Medi-Cal eligible. Management fee revenue is earned in the month the services are delivered.
Managed care revenues also included incentive payments from HMOs under "pay-for-performance" programs for quality medical care based on various criteria. These incentives are generally received in the third and fourth quarters of our fiscal year and are recorded when such amounts are known since we do not have the information to independently and reliably estimate these amounts.
We also potentially earn additional incentive revenue or incur penalties under HMO contracts by sharing in the financial risk for hospitalization based upon inpatient services utilized. These amounts were included in capitation revenue. As of September 30, 2009, except for one minor contract where we were contractually obligated for down-side risk, shared risk deficits were not payable until and unless we generate future risk-sharing surpluses. Risk pools are generally settled in the following year. Due to the lack of access to timely inpatient utilization information and the difficulty in estimating the related costs, shared-risk amounts receivable from the HMOs are recorded when such amounts are known. We also receive incentives under "pay-for-performance" programs for quality medical care based on various criteria. Pay-for-performance payments are generally recorded in the third and fourth quarters of our fiscal year when such amounts are known, since we do not have the ability to reliably estimate these amounts. Risk pool and pay-for-performance incentives are affected by many factors, some of which are beyond our control, and may vary significantly from year to year.
We have increased our membership through acquisitions. These increases through acquisition were offset by HMO enrollment declines at our affiliated physician organizations, not unlike the general
72
HMO enrollment trends in California in recent years. The following table sets forth the approximate number of members, by category (in thousands):
| |
As of September 30, | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
Member Category
|
2009 | 2008 | % Increase (Decrease) |
|||||||
Commercial—owned |
134.1 | 143.4 | (6.5 | )% | ||||||
Commercial—managed(l) |
1.6 | 9.8 | (83.7 | )% | ||||||
Senior—owned |
21.6 | 16.7 | 29.3 | % | ||||||
Senior—managed(1) |
0.2 | 0.1 | 100.0 | % | ||||||
Medi-Cal—owned(2) |
11.6 | 16.3 | (28.8 | )% | ||||||
Medi-Cal—managed(1) |
8.3 | 7.7 | 7.8 | % | ||||||
Total |
177.4 | 194.0 | (8.6 | )% | ||||||
- (1)
- Represent
members of AMVI, Inc., our joint venture partner, which we manage on their behalf in exchange for a fee.
- (2)
- The Company cancelled certain unprofitable Medi-Cal contracts during fiscal 2008.
The following table details total paid member months, by member category, for the years ended September 30, 2009 and 2008 (in thousands):
| |
Years Ended September 30, |
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
% Increase (Decrease) |
|||||||||
| |
2009 | 2008 | ||||||||
Commercial—owned |
1,696.2 | 1,907.5 | (11.1 | )% | ||||||
Commercial—managed(1) |
17.2 | 41.3 | (58.4 | )% | ||||||
Senior—owned |
258.3 | 246.0 | 5.0 | % | ||||||
Senior—managed (1) |
1.6 | 1.7 | (5.9 | )% | ||||||
MediCal—owned (2) |
137.8 | 192.0 | (28.2 | )% | ||||||
MediCal—managed(1) |
96.0 | 86.7 | 10.7 | % | ||||||
Total |
2,207.1 | 2,475.2 | (10.8 | )% | ||||||
- (1)
- Represent
members of AMVI, Inc., our joint venture partner, which we manage on their behalf in exchange for a fee.
- (2)
- The Company cancelled certain unprofitable Medi-Cal contracts during fiscal 2008.
Our operating expenses include expenses related to the provision of medical care services (medical group cost of revenues) and general and administrative costs. Our results of operations depend on our ability to effectively manage expenses related to health-care delivery and accurately predict costs incurred.
Expenses related to medical care services include payments to contracted primary care physicians, payments to contracted specialists and the cost of employed physicians at our medical clinics (through August 1, 2008). In general, primary care physicians are paid on a capitation basis, while specialists are paid on either a capitation or a fee-for-service basis.
Capitation payments are fixed in advance of periods covered and are not subject to significant accounting estimates. These payments are expensed in the period the providers are obligated to provide services. Fee-for-service payments are expensed in the period services are provided to our members. Medical care costs include actual historical claims experience and estimates of incurred but not reported amounts ("IBNR"). We estimate our IBNR monthly, based on a number of factors, including prior claims experience. As part of this review, we also include amounts to cover uncertainties related to fluctuations in provider billing patterns, claims payment patterns, membership and medical cost
73
trends. These estimates are adjusted each month as more information becomes available. In addition to our own IBNR estimation process, we obtain semi-annual assessments of our IBNR liability from independent actuaries. We believe that our process for estimating IBNR is adequate, but there can be no assurance that medical care costs will not exceed such estimates. In addition to contractual reimbursements to providers, we also make discretionary incentive payments to physicians, which are in part based on the pay-for-performance, shared risk revenues and any favorable senior capitation risk adjustment payments we receive. Since we record these revenues generally in the third or fourth quarter of each fiscal year, when the incentives and capitation adjustments due from the health plans are known, we also historically adjust interim accruals of discretionary physician bonuses in the same period. Because incentives and risk-adjustment revenues form a meaningful component in determining these discretionary bonuses, variability in earnings due to fluctuations in revenues are mitigated by reductions in bonuses awarded.
G&A costs are largely comprised of wage and benefit costs related to our employee base and other administrative expenses. G&A functions include claims processing, information systems, provider relations, finance and accounting functions, and legal and regulatory services.
Medical Group Results of Operations
The following tables summarize our net operating revenue, operating expenses and operating income from continuing Medical Group operations and are used in the discussions below for the years ended September 30, 2009 and 2008 (in thousands). Effective August 1, 2008, we sold the AV Entities' operations. The operating results of the AV Entities are reflected as loss from discontinued operations, net of income tax in our 2008 financial statements, and are excluded from the disclosures below for each period presented.
| |
Year Ended September 30, |
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
% Increase (Decrease) |
||||||||||
| |
2009 | 2008 | |||||||||
Medical group revenues: |
|||||||||||
Capitation |
$ | 194,126 | $ | 200,717 | (3.3 | )% | |||||
Management fees |
556 | 553 | 0.5 | % | |||||||
Other revenues |
2,048 | 1,574 | 30.1 | % | |||||||
Total medical group revenues |
196,730 | 202,844 | (3.0 | )% | |||||||
Medical group cost of revenues: |
|||||||||||
PCP capitation |
33,930 | 36,715 | -7.6 | % | |||||||
Specialist capitation |
43,710 | 42,406 | 3.1 | % | |||||||
Claims expense |
71,294 | 77,178 | -7.6 | % | |||||||
Physician salaries |
3,159 | 4,546 | (30.5 | )% | |||||||
Other cost of revenues |
(1,037 | ) | (1,938 | ) | (46.5 | )% | |||||
Total medical group cost of revenues |
151,056 | 158,907 | (4.9 | )% | |||||||
Gross margin |
45,674 | 43,937 | 4.0 | % | |||||||
General and administrative expenses |
28,397 | 29,848 | (4.9 | )% | |||||||
Depreciation and amortization expense |
3,515 | 3,479 | 1.0 | % | |||||||
Total other expenses |
31,912 | 33,327 | (4.2 | )% | |||||||
Income from unconsolidated joint venture |
2,046 | 2,563 | (20.2 | )% | |||||||
Operating income |
$ | 15,808 | $ | 13,173 | 20.0 | % | |||||
Medical cost ratios |
76.8 | % | 78.3 | % | |||||||
74
The following table sets forth selected operating items, expressed as a percentage of total revenue:
| |
Year Ended September 30, |
|||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
Medical group revenues: |
||||||||
Capitation |
98.7 | % | 99.0 | % | ||||
Management fees |
0.3 | % | 0.3 | % | ||||
Other revenues |
1.0 | % | 0.8 | % | ||||
Total medical group revenues |
100.0 | % | 100.0 | % | ||||
Medical group cost of revenues: |
||||||||
PCP capitation |
17.3 | % | 18.1 | % | ||||
Specialist capitation |
22.2 | % | 20.9 | % | ||||
Claims expense |
36.2 | % | 38.0 | % | ||||
Physician salaries |
1.6 | % | 2.2 | % | ||||
Other cost of revenues |
(0.5 | )% | (1.0 | )% | ||||
Total medical group cost of revenues |
76.8 | % | 78.3 | % | ||||
Gross margin |
23.2 | % | 21.7 | % | ||||
General and administrative expenses |
14.4 | % | 14.7 | % | ||||
Depreciation and amortization expense |
1.8 | % | 1.7 | % | ||||
Total other expenses |
16.2 | % | 16.4 | % | ||||
Income from unconsolidated joint venture |
1.0 | % | 1.3 | % | ||||
Operating income |
8.0 | % | 6.5 | % | ||||
Capitation Revenue
Capitation revenue for fiscal 2009 was approximately $194,126,000, representing a decrease of approximately $6,591,000 or 3.3% from capitation revenue for fiscal 2008 of approximately $200,717,000.
The decrease in capitation revenue for fiscal 2009 was due primarily to a decrease in commercial enrollment as a result of increased unemployment and cancellation of certain unprofitable Medi-Cal contracts, offset by rate increases.
Management fee revenue
Management fee revenue for fiscal 2009 was approximately $556,000, representing an increase of approximately $3,000 or 0.5% from management fee revenue for fiscal 2008, of approximately $553,000.
The increase in management fee revenue during fiscal 2009 was primarily due to an increase in management fee, resulting from an increase in the number of members of AMVICare Health Network, Inc.
Other revenue
Other revenue for fiscal 2009 was approximately $2,048,000, representing an increase of $474,000 or 30.1% over other revenue for fiscal 2008, of approximately $1,574,000.
Amounts represent incentive payments from HMOs under "pay-per-performance" programs for quality medical care based on various criteria. The incentives are recorded when such amounts are known.
75
The increase in other revenue during fiscal 2009 was primarily due to the continued efforts to meet and exceed minimum thresholds in measures identified by the various health plans.
PCP Capitation Expense
Primary care physician ("PCP") capitation expense for fiscal 2009 was approximately $33,930,000, representing a decrease of approximately $2,785,000 or 7.6% over PCP capitation expense for fiscal 2008, of approximately $36,715,000.
The decrease in PCP capitation expense during fiscal 2009 was primarily due to decreased enrollment, offset by market rate adjustments made as part of our continued effort to attract new PCPs and their members.
Specialist Capitation Expense
Specialist Capitation expense for fiscal 2009 was approximately $43,710,000, representing an increase of $1,304,000 or 3.1% from specialist capitation expense for fiscal 2008, of approximately $42,406,000.
The increase in specialist capitation expense during fiscal 2009 was primarily due to capitation of a large portion of our radiology services at a number of our Medical Groups, which had previously been provided on a fee-for-service basis.
Claims Expense
Claims expense for fiscal 2009 was approximately $71,294,000, representing a decrease of $5,884,000 or 7.6% over claims expense for fiscal 2008, of approximately $77,178,000.
The decrease in claims expense during fiscal 2009 was primarily due to lower enrollment, capitating radiology and other services and ongoing utilization and cost initiatives.
Physician Salaries Expense
Physician salaries expense for fiscal 2009 was approximately $3,159,000, representing a decrease of $1,387,000 or 30.5%, compared to physician salaries expense for fiscal 2008 of approximately $4,546,000.
The decrease in physician salaries expense was primarily the result of the conversion of certain physicians from employment to capitation basis during fiscal 2009.
Other Cost of Revenues
Other cost of revenues for fiscal 2009 was a negative expense of approximately $1,037,000 compared to a negative expense of approximately $1,938,000 for fiscal 2008. The negative expense represents reinsurance/stop-loss recoveries in excess of premiums paid.
Gross Margin
Medical care costs as a percentage of medical revenues (the medical care ratio) largely determine our gross margin. Our gross margin increased to 23.2% for fiscal 2009, from 21.7% for fiscal 2008.
The increase in our gross margin percentage between fiscal 2009 and 2008 was the result of the factors discussed above, inclusive of improved margins as a result of a more profitable senior/commercial membership mix.
76
General and Administrative Expense
General and administrative expenses were approximately $28,397,000 for fiscal 2009, representing 14.4% of total Medical Group revenues, as compared with $29,848,000, or 14.7% of total revenues, for fiscal 2008.
The decrease in general and administrative expenses during fiscal 2009 was primarily the result of the elimination of certain positions and the consolidation of administrative functions among our Medical Groups.
Depreciation and Amortization Expense
Depreciation and amortization expense for fiscal 2009 increased to approximately $3,515,000 from $3,479,000 for fiscal 2008. This lack of fluctuation in this expense category is consistent with management expectations and the lack of any material change in this segment's depreciable assets.
Income from Unconsolidated Joint Venture
The income from unconsolidated joint venture for fiscal 2009 decreased to approximately $2,046,000 from approximately $2,563,000 for fiscal 2008. The decrease resulted from lower risk pool income due to decreased membership.
Operating Income
Our Medical Group segment reported operating incomes of approximately $15,808,000 and $13,173,000 for fiscal 2009 and 2008, respectively, which increase was the result of the changes discussed above. The pre-tax operating results from the Medical Group segment include certain corporate expense allocations for insurance, professional fees, and amortization of identifiable intangibles.
Corporate Results of Operations
Certain expenses incurred at Prospect Medical Holdings, Inc. (the "Parent Entity") not specifically allocable to the Hospital Services or Medical Group segments are recorded in the Corporate segment. These include salaries, benefits and other compensation for corporate employees, financing, insurance, rent, operating supplies, legal, accounting, SEC compliance, and Sarbanes-Oxley compliance. We do not allocate interest expense, debt extinguishment loss, gain or loss on interest rate swaps and income taxes to the other reporting segments.
77
The following table summarizes our corporate expense for the Parent Entity, and is used in the discussion below for the years ended September 30, 2009 and 2008 (in thousands).
| |
Year Ended September 30, |
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
% Increase (Decrease) |
||||||||||
| |
2009 | 2008 | |||||||||
Operating Expenses: |
|||||||||||
General and administrative expense |
$ | 12,215 | $ | 15,070 | -18.9 | % | |||||
Depreciation and amortization expense |
13 | 24 | (45.8 | )% | |||||||
Total Operating Expense |
12,228 | 15,094 | (19.0 | )% | |||||||
Other (Income) Expense: |
|||||||||||
Investment income |
(62 | ) | (362 | ) | (82.8 | )% | |||||
Interest expense and amortization of deferred financing costs |
26,897 | 22,173 | 21.3 | % | |||||||
(Gain) loss in value of interest rate swaps |
5,299 | (3,096 | ) | 271.2 | % | ||||||
Loss on debt extinguishment |
— | 8,308 | (100.0 | )% | |||||||
Prepayment penalty on debt refinance |
2,588 | — | 100.0 | % | |||||||
Loss on termination of interest rate swap arrangements |
6,861 | — | 100.0 | % | |||||||
Total Other (Income) Expense |
41,583 | 27,023 | 53.9 | % | |||||||
Total Corporate Expenses |
$ | 53,811 | $ | 42,117 | 27.8 | % | |||||
The following table sets forth selected operating items, expressed as a percentage of total consolidated revenues from continuing operations:
| |
Year Ended September 30, |
|||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
Operating Expenses: |
||||||||
General and administrative expense |
3.0 | % | 4.6 | % | ||||
Depreciation and amortization expense |
0.0 | % | 0.0 | % | ||||
Total Operating Expense |
3.0 | % | 4.6 | % | ||||
Other (Income) Expense: |
||||||||
Investment income |
0.0 | % | (0.1 | )% | ||||
Interest expense and amortization of deferred financing costs |
6.7 | % | 6.7 | % | ||||
(Gain) loss in value of interest rate swaps |
1.3 | % | (0.9 | )% | ||||
Loss on debt extinguishment |
0.0 | % | 2.5 | % | ||||
Prepayment penalty on debt refinance |
0.7 | % | 0.0 | % | ||||
Loss on termination of interest rate swap arrangements |
1.7 | % | 0.0 | % | ||||
Total Other (Income) Expense |
10.4 | % | 8.2 | % | ||||
Total Corporate Expenses |
13.4 | % | 12.8 | % | ||||
78
General and Administrative
General and administrative expenses for fiscal 2009 were approximately $12,215,000, representing approximately 3.0% of total revenues from continuing operations, compared to approximately $15,070,000, or approximately 4.6% of total revenues from continuing operations for fiscal 2008, a decrease of approximately 17.0%. The decrease in G&A expenses during fiscal 2009 primarily related to reductions in audit, legal, bank, and outside services costs, including savings related to bringing certain functions in-house, offset by increased compensation expense and lease termination costs of approximately $79,000. In the fourth quarter of fiscal 2009, when the Company lost its tenant for certain office space where a lease obligation still exists.
Depreciation and Amortization Expense
Depreciation and amortization expense for fiscal 2009 was approximately $13,000, compared to approximately $24,000 for fiscal 2008, a decrease of approximately 45.8%. The decrease was primarily due to retirement of certain capital equipment.
Investment Income
Investment income for fiscal 2009 was approximately $62,000, compared to approximately $362,000, for fiscal 2008, a decrease of approximately 82.9%. Following the amendment of our former senior credit facility agreement on May 15, 2008, we were required by Bank of America, N.A. to maintain the majority of our cash in non-interest bearing accounts at that bank.
Interest Expense and Amortization of Deferred Financing Costs
Interest expense and amortization of deferred financing costs for fiscal 2009 was approximately $26,897,000, compared to $22,173,000, for fiscal 2008, an increase of approximately 21.3%. We were in default under our credit facilities and under the resulting April 2008 forbearance agreements, the applicable margins on the first and second lien term loans were permanently increased to 750 and 1,175 basis points, respectively, and the range of applicable margins on the revolving line of credit was increased from 500 to 750 basis points effective April 10, 2008. The agreements also provided for a minimum LIBOR rate of 3.50%. In May 2008, the debt agreements were further modified to add a 1% "payment-in-kind" ("PIK") interest to the outstanding balance of the debt plus an additional 4% PIK interest to the interest rate applicable to the second lien debt. Additionally, effective on the March 19, 2009 notice date for an asserted non-monetary event of default, our lenders began assessing default rates on all borrowings and effective April 14, 2009, following the Brotman transaction we began including interest on all Brotman debt in our consolidated financial statements. As set forth below, following the issuance of the $160 million 12.75% senior secured notes and the repayment of all remaining amounts outstanding under its former $155 million senior secured credit facility, the Company wrote-off approximately $550,000 of deferred financing related to its former credit facilities, which amount was recorded as interest expense in the fourth quarter of fiscal 2009.
Gain (Loss) in Value of Interest Rate Swap Arrangements
We had two interest rate swaps in place for initial notional principal amounts of $48.0 million and $97.8 million, respectively. The interest rate swaps were designated as cash flow hedges of our floating rate term debt, with the effective date of the $48.0 million swap being December 31, 2007 and the effective date of the $97.8 million swap being September 6, 2007. As of April 1, 2008, in anticipation of modifications to the terms of our credit agreements, the swaps were determined to no longer be effective in offsetting the hedged items. As a result, cash flow hedge accounting treatment was discontinued and all further changes in fair value of the swaps were included in earnings. In fiscal 2009, loss on interest rate swaps totaled approximately $5,299,000. In fiscal 2008, gain on interest rate swaps
79
totaled approximately $3,096,000, representing the change in fair value of the $48.0 million swap that was not yet subject to hedge accounting, which amount was charged to earnings.
Concurrent with the Senior Secured Note transaction, the Company terminated the interest rate swap arrangements, paid $11.7 million in final settlement of all amounts owing under the swap arrangements and expensed all previously unamortized swap fluctuation amounts.
Loss on Debt Extinguishments
The $8,308,000 loss on debt extinguishment for fiscal 2008 related to the modification of our first and second-lien term loans and our revolving line of credit in the third quarter of 2008. The charge included amendment fees of $758,000 paid in cash to lenders, $1,514,000 of PIK interest added to the principal of the new debt and the write off of $6,036,000 in unamortized debt issuance costs relating to the early extinguishment of the existing term debt and revolving line of credit.
Prepayment Penalty on Debt Refinance
As discussed in Note 9 to the accompanying consolidated financial statements, following the issuance of the $160 million 12.75% senior secured notes, the Company repaid all remaining amounts outstanding under its former $155 million senior secured credit facility, plus a prepayment premium of approximately $2,588,000.
Loss on Termination of Interest Rate Swap Arrangements
Concurrent with the senior secured note transaction, effective July 23, 2009, the Company terminated the master swap agreement and the swap arrangements thereunder by payment, on July 29, 2009, of $11.7 million to the swap counterparty in final settlement of all amounts owed under the swap arrangements. All related amounts included in accumulated other comprehensive loss, including related deferred income taxes (of approximately $4.2 million) of approximately $6,861,000 was recorded as interest rate swaps termination charge, as of the effective date of the swap terminations.
Consolidated Results of Operations
Provision for Income Taxes
Income tax benefit for fiscal 2009 was approximately $(1,019,000) compared to approximately $(1,327,000) in fiscal 2008. The effective tax rate was lower at 30% in fiscal 2009 compared to 40% in fiscal 2008. The lower effective tax rate in fiscal 2009 was primarily due to change in tax valuation account attributable to the Brotman Acquisition.
Net Income (Loss) from Continuing Operations
Net loss from continuing operations attributable to common stockholders for fiscal 2009 was approximately ($2,420,000), or $0.12 per diluted share, as compared to a net loss of $1,961,000, or $0.68 per diluted share, for fiscal 2008, which decrease in loss was the result of the changes discussed above.
Net Loss from Discontinued Operations
Net income from discontinued operations for fiscal 2008 was approximately $6,169,000 or $0.48 per diluted share, as compared to none for fiscal 2009. We sold the AV Entities effective August 1, 2008.
80
Liquidity and Capital Resources
Our primary sources of cash have been funds provided by borrowings under our credit facilities, by the issuance of equity securities, by cash flow from operations and by proceeds from sales of assets related to discontinued operations. Prior to the August 8, 2007 acquisition of Alta, our primary sources of cash from operations were healthcare capitation revenues, fee-for-service revenues, risk pool payments and pay-for-performance incentives. With the acquisition of Alta and, subsequently Brotman, our sources of cash from operations now include payments for hospital services rendered under reimbursement arrangements with third-party payers, which include the federal government under the Medicare program, the state government under the Medi-Cal program, private insurers, HMOs, PPOs, and self-pay patients.
Our primary uses of cash include healthcare capitation and claims payments by our affiliated physician organizations, administrative expenses, debt service, acquisitions, costs associated with the integration of acquired businesses, information systems development costs and, with the acquisition of Alta and Brotman, operating, capital improvement and administrative expenses related to our hospital operations. Our affiliated physician organizations generally receive capitation revenue in advance of having to make capitation and claims payments to their providers. However, our hospitals receive payments for services rendered, generally 30 to 90 days after the medical care is rendered. For some accounts and payer programs, the time lag between service and reimbursement can exceed one year.
Our investment strategies are designed to provide safety and preservation of capital, sufficient liquidity to meet cash-flow needs, the integration of investment strategy with our business operations and objectives, and attainment of a competitive return. At September 30, 2009, we invested a portion of our cash in interest bearing money market accounts. All of these amounts are classified as current assets and included in cash and cash equivalents in our condensed consolidated balance sheets. We believe that we have sufficient liquidity to fund operations for at least the next twelve months given our expectation of cash flows from operations, cash and cash equivalents on hand and borrowing capacity under our revolving line of credit.
Cash Flow from Continuing Operations
Net cash provided by continuing operations was approximately $23,566,000 for the year ended September 30, 2009 compared to $12,265,000 for the year ended September 30, 2008. The increase in net cash provided by continuing operations for the year ended September 30, 2009 as compared to the year ended September 30, 2008 was due to various factors, including the following:
- •
- earnings, excluding non-cash charges and credits were approximately $35,125,000 in fiscal year 2009 compared
to approximately $16,052,000 in fiscal year 2008;
- •
- changes in patient, government program and other receivables, a use of approximately $12,803,000 in fiscal year 2009
compared to a use of approximately $9,109,000 in fiscal year 2008. The increase in fiscal year 2009 was primarily related to our Hospital Services segment, which saw an increase of approximately 62.0%
in volume, of which approximately 76.4% was contributed by Brotman;
- •
- changes in refundable income tax and taxes payable, a source of approximately $1,096,000 in fiscal year 2009 compared to a
source of $2,388,000 in fiscal year 2008, primarily due to deferred income taxes recorded in connection with Brotman acquisition;
- •
- changes in medical claims and related liabilities, a use of approximately $3,656,000 in fiscal year 2009 compared to a use of approximately $926,000 in fiscal year 2008. The increase in fiscal year 2009 was primarily due to decreased enrollment and payment made during fiscal 2009 to a certain contracted HMO; and
81
- •
- changes in accounts payable and other accrued liabilities, a source of approximately $3,742,000 in fiscal year 2009 compared to a source of approximately $5,040,000 in fiscal year 2008. The decrease in fiscal year 2009 was due primarily to decreased year end bonus accrual at our Medical Group segment.
Net cash used in investing activities totaled approximately $3,543,000 fiscal year 2009, compared to a source of approximately $4,366,000 in fiscal year 2008, the largest component of which was the acquisition costs net paid in connection with the Brotman acquisition totaling approximately $2,310,000, purchases of property, improvements and equipment, a use of approximately $1,558,000 in fiscal year 2009 compared to a use of approximately $1,104,000 in fiscal year 2008.
Net cash used by financing activities totaled approximately $15,838,000 fiscal 2009, compared to a use of approximately $5,143,000 in fiscal 2008. Net cash used in financing activities in fiscal year 2009 was comprised primarily of the repayment of our former first-lien and second-lien term debt of approximately $141,368,000, the repayment of our former line of credit of approximately $7,100,000, and the payment of approximately $7,063,000 in fees in connection with the issuance of the $160 million 12.75% senior secured note (the "Notes"), net of the proceeds from the sale of the Notes totaling approximately $147,736,000. Net cash used by financing activities in fiscal year 2008 included a $17,750,000 borrowing on our former line of credit and $1,200,000 received from the exercise of stock options, net of payments of approximately $13,750,000 on our former line of credit and approximately $9,219,000 on our former long-term debt and payment of approximately $729,000 to our former lenders in connection with loan modifications in May 2008.
Cash Flow from Discontinued Operations
In fiscal year 2008, net cash used in operating activities in our discontinued operations was approximately $546,000, compared to none in fiscal year 2009, and net cash provided from investing activities, was approximately $5,185,000 compared to none in fiscal 2009. As previously discussed, we sold the AV Entities effective August 1, 2008.
At September 30, 2009, we had positive working capital of approximately $9,903,000 as compared to positive working capital of $12,373,000 at September 30, 2008.
At September 30, 2009 and 2008, cash, cash equivalents and investments were approximately $39,828,000 and $34,220,000, respectively.
Prospect's Debt
Former Credit Facility
On August 8, 2007, in connection with the closing of the Alta acquisition, we obtained an aggregate $155 million syndicated senior secured credit facility which was comprised of a first-lien facility and second-lien facility (the "Former Credit Facility"). The term loans were used to refinance approximately $41.5 million of existing Alta debt, to refinance approximately $48 million of our existing debt incurred in connection with our acquisition of the ProMed Entities and to pay the cash portion of the Alta purchase price. The maturity dates of the first-lien revolver, the first-lien term facility and the second-lien term facility were August 8, 2012, August 8, 2014 and February 8, 2015, respectively.
The Former Credit Facility was subject to certain financial and administrative covenants, cross default provisions and other conditions, including a maximum senior debt/EBITDA (earnings before interest, taxes, depreciation and amortization) ratio, a minimum fixed-charge coverage ratio and a minimum EBITDA level. There were also various administrative covenants and other restrictions.
The Company made all scheduled payments of principal and interest since inception of the Former Credit Facility. On March 19, 2009, we received written notices that the Former Credit Facility's lenders
82
deemed us in default of a credit facility requirement regarding the required sale of one of our entities by a specified date. Additionally, on April 17, 2009, we received written notices of an alleged event of default related to our increased ownership interest in Brotman.
Effective with the first asserted event of default, the lenders began assessing default interest; however, they did not exercise any other remedies. We disputed the lenders' characterization of the asserted defaults.
On June 30, 2009, we entered into amendments to our Former Credit Facility pursuant to which, among other things, the lenders waived all asserted events of default and stopped assessing default rates. The amendments further required that we refinance the Former Credit Facility by no later than October 31, 2009.
As discussed in more detail at "Current Credit Facilities" below, on July 29, 2009 we repaid all amounts owing under our Former Credit Facility.
Former Interest Rate Swaps
As required by the Former Credit Facility, on May 16, 2007, we entered into a $48 million interest rate swap, to effectively convert the variable interest rate (the LIBOR component) under the original credit facility to a fixed rate of 5.3%, plus the applicable margin per year throughout the term of the loan. This interest rate swap remained in effect after the related term loan was repaid in August 2007 in contemplation of the $155,000,000 Former Credit Facility entered into in August, 2007. In addition to the pre-existing $48,000,000 interest rate swap described above, on September 5, 2007, we entered into a separate interest rate swap agreement, initially totaling $97,750,000, to effectively convert the variable interest rate (the LIBOR component) under the incremental portion of the Former Credit Facility to a fixed rate of 5.05%, plus the applicable margin, per year, throughout the term of the loan. The notional amounts of these interest rate swaps were structured to decline as the principal balances owing under the term loans declined.
On July 29, 2009, in connection with the issuance of the $160 million Original Notes, the Company terminated its interest rate swap arrangements and paid the swap counterparty approximately $11.7 million in final settlement of all amounts owing under the swap arrangements.
Current Credit Facilities
On July 29, 2009, the Company closed the offering of $160 million in 123/4% Senior Secured Notes, Series A, due 2014 (the "Original Notes"), at an issue price of 92.335%. The sale was executed in accordance with Rule 144A under the Securities Act of 1933 and Regulation S under the Securities Act of 1933. Also, in connection with the issuance of the Original Notes, the Company entered into a three-year $15 million revolving credit facility, which was undrawn at closing, and is still undrawn. The interest rate under the revolving credit facility is at LIBOR plus an applicable margin of 7.00%, with a LIBOR floor of 2.00%. The Company used the net proceeds from the sale of the Original Notes to repay all amounts outstanding under the Former Credit Facility, plus a prepayment premium of approximately $2.6 million.
Pursuant to its definitive Prospectus filed with the SEC on September 26, 2009, the Company commenced an offer to exchange up to $160 million of its newly registered 123/4% Senior Secured Notes, Series B, due 2014 (the "Exchange Notes" and together with the Original Notes, the "Notes") for an equal amount of the Original Notes (the "Exchange Offer"). The Exchange Notes are substantially identical to the Original Notes, except that the offer and sale of the Exchange Notes have been registered under the Securities Act of 1933, as amended, and the Exchange Notes do not bear any legend restricting their transfer. The exchange offer was extended on November 25, 2009 until
83
December 3, 2009, at which time the exchange offer closed with $159 million of the $160 million aggregate principal amount of private notes tendered and accepted for exchange.
Brotman's Debt
As part of Brotman's bankruptcy plan of reorganization, financing was secured from the Los Angeles Jewish Home for the Aging ("JHA") and Gemino.
The JHA financing was comprised of two term debt components, a $16.0 million tranche secured by assets on the west side of the Brotman campus commonly referred to as "Delmas West" and a $6.25 million tranche on the main hospital pavilion on the east side of the property. The $16.0 million tranche contains an option for JHA to acquire the Delmas West parcel for a purchase price equal to the outstanding debt within 24 months of the effective date of the bankruptcy. If JHA does not exercise its option, Brotman will be required to refinance the $16.0 million tranche on or before April 14, 2011. With respect to the $16.0 million tranche of the JHA facility, JHA also has the right to declare the unpaid loan amount, including remaining interest and any other amounts due and payable, immediately due and payable at any time after April 14, 2010 and prior to April 14, 2011, provided that JHA gives 180 days' written notice of exercise. JHA may not however provide notification of its exercise of this option prior to the first anniversary of the April 14, 2009 closing date. As such, the loan is presented within long term debt in the consolidated balance sheet. In addition, the $6.25 million tranche of the JHA transaction will mature on April 14, 2012 and Brotman will need to secure financing to retire this portion of the debt.
The Gemino financing was comprised of a $6.0 million, senior credit facility secured by accounts receivable. The facility expires on the earlier of April 14, 2012 and the JHA loan (see above) maturity date and bears interest at LIBOR plus 7% per annum, with a LIBOR floor of 4%. Interest is incurred based on the greater of $2 million or the outstanding principal balance. The agreement also includes an unused line fee at 0.5% per annum and a collateral line fee, based on the average outstanding principal balance, of 0.5% per annum. The senior credit facility agreement contains customary covenants for facilities of this type including restrictions on the payment of dividends, change in ownership/management, asset sales, incurrence of additional indebtedness, sale-leaseback transactions, and related party transactions. In addition, Brotman must also comply with financial covenants, originally including a fixed charge coverage ratio of not less than (i) 1.10:1.00 for the fiscal quarter ended June 30, 2009, (ii) 1.15:1.00 for the fiscal quarter ended September 30, 2009; and (iii) 1.20:1.00 for each fiscal quarter ending thereafter. As of September 30, 2009, Brotman was not in compliance with the required financial covenants under the Gemino credit agreement. Pursuant to an amendment entered into effective December 11, 2009, the Gemino credit agreement was amended to provide, among other things, a waiver of the specified events of default and the amendment to the definition of fixed charge ratio. Under the amended credit agreement, fixed charge coverage ratio was amended to require not less than (i) 1.00:1.00 for the fiscal quarters ending December 31, 2009 and March 31, 2010; (ii) 1.05:1.00 for the fiscal quarters ending June 30, 2010 and September 30, 2010, (iii) 1.10:1.00 for the fiscal quarters ending December 31, 2010 and March 31, 2011, and (iv) 1.20:1.00 for the fiscal quarter ending June 30, 2011 and each fiscal quarter ending thereafter. The first calculation of the Fixed Charge Coverage Ratio shall be for the quarter ending December 31, 2009.
We anticipate attempting to finance future acquisitions and potential business expansion with a combination of debt, issuances of equity, and cash flow from operations.
In order to meet our long-term liquidity needs, we may incur, from time to time, additional bank indebtedness. Banks and traditional commercial lenders do not generally make loans to companies without substantial tangible net worth. Since, by the nature of our business, we accumulate substantial goodwill and intangibles on our balance sheet, it may be difficult for us to obtain this type of financing in the future. We may issue additional equity and debt securities, the availability and terms of which
84
will depend upon market and other conditions. The corporate lending and equity markets have been disrupted by the current credit market conditions, resulting in both a reduction in the number of transactions as well as the amount of funds raised. Transactions that have been consummated are completed at lower valuations in the case of equity offerings and at higher interest costs in the case of debt offerings. Our ability to issue any debt or equity instruments in a public or private sale is also restricted under certain circumstances, pursuant to contractual restrictions in agreements with our lenders and the indenture governing the Notes (see above). There can be no assurance that additional financing will be available upon terms acceptable to us, if at all. The failure to raise the funds necessary to finance our future cash requirements could adversely affect our ability to pursue our strategy and could adversely affect our future results of operations.
Off-Balance Sheet Arrangements
None.
Critical Accounting Policies
The accounting policies described below are considered critical in preparing our financial statements. Critical accounting policies require difficult, subjective or complex judgments, often as a result of the need to make estimates about the effect of matters that are inherently uncertain. The judgments and uncertainties affecting the application of these policies include significant estimates and assumptions made by us using information available at the time the estimates are made. Actual results could differ materially from those estimates.
Consolidation of Financial Statements
Under applicable financial reporting requirements, the financial statements of the affiliated physician organizations with which we have management services agreements are consolidated with our own financial statements. This consolidation is required under FASB ASC 810-10 (previously issued as EITF Issue No. 97-2, "Application of FASB Statement No. 94 and APB Opinion No. 16 to Physician Practice Management Entities and Certain Other Entities with Contractual Management Arrangements") because we are deemed to hold a controlling financial interest in such organizations through a nominee shareholder. We can, through two assignable option agreements, change the nominee shareholder at will on an unlimited basis and for nominal cost. There is no limitation on our designation of a nominee shareholder except that any nominee shareholder must be a licensed physician or otherwise permitted by law to hold shares in a professional medical corporation. We have also concluded that we are required to consolidate our affiliated physician organizations. The operations of our affiliated physician organizations have a significant impact on our financial statements. The financial statements of Brotman have been included in our consolidated financial statements since April 14, 2009, when we acquired a majority stake in Brotman. All inter-company accounts and balances have been eliminated in consolidation.
Revenue Recognition
Hospital Services Segment
Operating revenue of the Hospital Services segment consists primarily of net patient service revenue. We report net patient service revenue at the estimated net realizable amounts from patients, third-party payers and others in the period in which services are rendered. A summary of the payment arrangements with major third-party payers follows:
Medicare: Medicare is a federal program that provides certain hospital and medical insurance benefits to persons aged 65 and over, some disabled persons and persons with end-stage renal disease. Inpatient services rendered to Medicare program beneficiaries are paid at prospectively determined
85
rates per discharge, according to a patient classification system based on clinical, diagnostic, and other factors. Outpatient services are paid based on a blend of prospectively determined rates and cost-reimbursed methodologies. We are also reimbursed for various disproportionate share and Medicare bad debt components at tentative rates, with final settlement determined after submission of annual Medicare cost reports and audits thereof by the Medicare fiscal intermediary. Normal estimation differences between final settlements and amounts accrued in previous years are reflected in net patient service revenue in the year of final settlement.
Medi-Cal: Medi-Cal is a joint federal-state funded healthcare benefit program that is administered by the state of California to provide benefits to qualifying individuals who are unable to afford care. Inpatient services rendered to Medi-Cal program beneficiaries are paid at contracted per diem rates. The per diem rates are not subject to retrospective adjustment. Outpatient services are paid based on prospectively determined rates per procedure provided.
Managed care: We also receive payment from certain commercial insurance carriers, HMOs and PPOs. The basis for payment is in accordance with contracted rates or at our standard charges for services provided where no prior contract is in place.
Self-Pay: Our hospitals also provide services to certain individuals that do not have any form of healthcare coverage. Such patients are evaluated, at the time of service or shortly thereafter, for their ability to pay based upon federal and state poverty guidelines, qualifications for Medi-Cal, as well as our local hospital's indigent and charity care policy.
Timely billing and collection of receivables from third-party payers and patients is critical to our operating performance. We closely monitor our historical collection rates as well as changes in applicable laws, rules and regulations and contract terms, to assure that provisions for contractual allowances are made using the most accurate information available. Our primary collection risks relate to uninsured patients and the portion of the bill which is the patient's responsibility, primarily co-payments and deductibles. Payments for services may also be denied due to issues over patient eligibility for medical coverage, our ability to demonstrate medical necessity for services rendered and payer authorization for hospitalization. We estimate provisions for doubtful accounts based on general factors such as payer mix, the age of the receivables and historical collection experience. We routinely review accounts receivable balances in conjunction with these factors and other economic conditions which might ultimately affect the collectability of the patient accounts and make adjustments to allowances for contractual discounts and bad debts as warranted.
Medical Group Segment
Operating revenue of our Medical Groups consists primarily of capitation payments for medical services provided by our affiliated physician organizations under contracts with HMOs. Capitation revenue under HMO contracts is prepaid monthly to the affiliated physician organizations based on the number and type of enrollees assigned to physicians in our affiliated physician organizations.
Capitation revenue paid by HMOs is recognized in the month in which the affiliated physician organization is obligated to provide services. Capitation revenue may be subsequently adjusted to reflect changes in enrollment as a result of retroactive terminations or additions. Such retroactive terminations or additions have not had a material effect on capitation revenue.
Variability in capitation revenue exists under Medicare's capitation model referred to as "Risk Adjustment." Under the model, capitation with respect to Medicare enrollees is subject to subsequent adjustment by CMS based on the acuity of the enrollees to whom services were provided. Capitation for the current year is paid based on data submitted for each enrollee for previous periods. Capitation is paid at interim rates during the year and is adjusted in subsequent periods (generally in our fourth fiscal quarter) after the final data has been processed by CMS. Positive or negative capitation
86
adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since we cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated from the health plans, generally in the fourth quarter of the fiscal year to which the adjustments relate. We recorded approximately $4.3 million and $1.6 million in increased capitation revenue in the fourth quarter of fiscal 2009 and 2008, respectively, for risk adjustment factors.
We also earn additional incentive revenue or incur penalties under HMO contracts by sharing in the risk for hospitalization based upon inpatient services utilized. As of September 30, 2009, except for one contract where we are contractually obligated for down-side risk, shared risk deficits are not payable unless and until we generate future risk-sharing surpluses. Risk pools are generally settled in the third or fourth quarter of the following year. Due to the lack of access to timely information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are recorded when such amounts are known. We also receive incentives under "pay-for-performance" programs for quality medical care based on various criteria. Pay-for-performance payments are generally recorded in the third and fourth quarters of our fiscal year when such amounts are known, once we are in receipt of information necessary to reliably estimate these amounts. Risk pool and pay-for-performance incentives are affected by many factors, some of which are beyond our control, and may vary significantly from year to year.
Management fee revenue is earned in the month the services have been performed.
Accrued Medical Claims
Our affiliated physician organizations are responsible for the medical services their contracted or employed physicians provide to an assigned HMO enrollee. The cost of healthcare services is recognized in the period in which it is provided and includes an estimate of the cost of services which have been incurred but not reported. The determination of our claims liability and other healthcare costs payable is particularly important to the determination of our financial position and results of operations and requires the application of significant judgment by our management, and as a result, is subject to an inherent degree of uncertainty.
Our medical care costs include actual historical claims experience and IBNR. We, together with our independent actuaries, estimate medical claims liabilities using actuarial methods based upon historical data, adjusted for payment patterns, cost trends, product mix, utilization of healthcare services and other relevant factors. The estimation methods and the resulting reserves are frequently reviewed and updated, and adjustments, if necessary, are reflected in the period they become known. While we believe our estimates are adequate, it is possible that future events could require us to make significant adjustments or revisions to these estimates. In assessing the adequacy of accruals for medical claims liabilities, we consider our historical experience, the terms of existing contracts, our knowledge of trends in the industry, information provided by our customers and information available from other sources as appropriate.
The most significant estimates involved in determining our claims liability concern the determination of claims payment completion factors and trended per member per month cost estimates.
We consider historical activity for the current month, plus the prior 24 months, in our IBNR calculation. For the fifth month of service prior to the reporting date and earlier, we estimate our outstanding claims liability based upon actual claims paid, adjusted for estimated completion factors. Completion factors seek to measure the cumulative percentage of claims expense that will have been paid for a given month of service as of a date subsequent to that month of service. Completion factors are based upon historical payment patterns. For the four months of service immediately prior to the reporting date, actual claims paid are not a reliable measure of our ultimate liability, given the delay
87
inherent between the patient/physician encounter and the actual submission of a claim for payment. For these months of service we estimate our claims liability based upon trended per member per month ("PMPM") cost estimates. These estimates reflect recent trends in payments and expense, utilization patterns, authorized services and other relevant factors.
The following tables reflect (i) the change in our estimate of claims liability as of September 30, 2009 that would have resulted had we changed our completion factors for all applicable months of service included in our IBNR calculation (i.e., the preceding 5th through 25th months) by the percentages indicated; and (ii) the change in our estimate of claims liability as of September 30, 2009 that would have resulted had we changed trended PMPM factors for all applicable months of service included in our IBNR calculation (i.e., the preceding 1st through 4th months) by the percentages indicated. Changes in estimate of the magnitude indicated in the ranges presented are considered reasonably likely.
Increase (Decrease) in Estimated Completion Factors |
Increase (Decrease) in Accrued Medical Claims Payable |
|||
|---|---|---|---|---|
| |
(in thousands) |
|||
(3)% |
$ | (4,139 | ) | |
(2)% |
$ | (2,759 | ) | |
(1)% |
$ | (1,380 | ) | |
1% |
$ | 1,380 | ||
2% |
$ | 2,759 | ||
3% |
$ | 4,139 | ||
Increase (Decrease) in Trended PMPM Factors |
Increase (Decrease) in Accrued Medical Claims Payable |
|||
|---|---|---|---|---|
| |
(in thousands) |
|||
(3)% |
$ | (735 | ) | |
(2)% |
$ | (490 | ) | |
(1)% |
$ | (245 | ) | |
1% |
$ | 245 | ||
2% |
$ | 490 | ||
3% |
$ | 735 | ||
The following table shows the components of the change in medical claims and benefits payable for the year ended September 30, 2009 and 2008 (in thousands):
| |
Year Ended September 30 | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008(1) | ||||||
IBNR at Beginning of Year |
$ | 20,480 | $ | 21,406 | ||||
Health Care Claims Expense Incurred During the Year: |
||||||||
Related to Current Year |
72,424 | 79,174 | ||||||
Related to Prior Year |
(1,130 | ) | (1,996 | ) | ||||
Total Incurred |
71,294 | 77,178 | ||||||
Health Care Claims Paid During the Year |
||||||||
Related to Current Year |
(56,100 | ) | (59,633 | ) | ||||
Related to Prior Year |
(18,850 | ) | (18,471 | ) | ||||
Total Paid |
(74,950 | ) | (78,104 | ) | ||||
IBNR at End of Year |
$ | 16,824 | $ | 20,480 | ||||
- (1)
- Amounts exclude changes in medical claims and benefits payable related to the AV Entities which are reported in discontinued operations.
88
A negative amount reported for health care claims expense incurred related to prior years, results where claims are ultimately settled for amounts less than originally estimated (a favorable development). A positive amount results from claims ultimately being settled for amounts greater than originally estimated (an unfavorable development). In each of the years ended September 30, 2009 and 2008, we experienced favorable change in estimates related to prior years' claims. The favorable changes reflect provisions for adverse deviation from historical experience, which is consistently maintained.
During the year ended September 30, 2009, $1,130,000 of the total change in estimate related to IBNR as of September 30, 2008, which represented approximately 5.5% of the IBNR balance as of September 30, 2008, approximately 1.5% of fiscal 2008 claims expense, and after consideration of tax effect, approximately 57.6% of net loss from continuing operation for the year then ended.
During the year ended September 30, 2008, $1,996,000 of the total change in estimate related to IBNR as of September 30, 2007, which represented approximately 9.3% of the IBNR balance as of September 30, 2007, approximately 3.2% of fiscal 2007 claims expense and after consideration of tax effect, approximately 8.5% of net loss from continuing operation for the year then ended.
Past fluctuations in the IBNR estimates might also be a useful indicator of the potential magnitude of future changes in these estimates. Quarterly IBNR estimates include provisions for adverse development based on historical volatility. We maintain similar provisions at fiscal year end.
We also regularly evaluate the need to establish premium deficiency reserves for the probability that anticipated future healthcare costs could exceed future capitation payments from the HMOs. To date, we have determined that no premium deficiency reserves have been necessary.
We believe that the amount of our accrued medical claims is adequate to cover our ultimate liability for incurred claims; however, actual claims payments may differ from our estimate. Assuming a hypothetic 1% variance in our estimate of accrued medical claims, our pre-tax profit or loss from continuing operations for the years ended September 30, 2009 and 2008, would increase or decrease by approximately $168,000 and $205,000, respectively.
Goodwill and Intangible Assets
SFAS No. 141, "Business Combinations," requires all business combinations after June 30, 2001 to be accounted for using the purchase method and prohibits the pooling-of-interest method of accounting. ASC 805 also states that acquired intangible assets should be separately recognized upon meeting certain criteria. Such intangible assets include, but are not limited to, trade and service marks, non-compete agreements, customer lists and licenses. SFAS No. 141 is pre-Codification literature. The provisions of ASC 805 (previously issued as SFAS No. 141) are not effective for the Company until October 1, 2009.
ASC 350 (previously issued as SFAS No. 142, "Goodwill and Other Intangible Assets,") requires that goodwill and indefinite life intangible assets not be subject to amortization but be evaluated for impairment on at least an annual basis, or more frequently if certain indicators are present. Such indicators include adverse changes in market value and/or stock price, laws and regulations, profitability, cash flows, our ability to maintain enrollment and renew payer contracts on favorable terms. A two-step impairment test is used to identify potential goodwill impairment and to measure the amount of goodwill impairment loss to be recognized (if any). The first step consists of estimating the fair value of the reporting unit based on recognized valuation techniques, which include a weighted combination of (i) the guideline company method that utilizes revenue or earnings multiples for comparable publicly-traded companies, and (ii) a discounted cash flow model that utilizes future cash flows, the timing of those cash flows, and a discount rate (or weighted average cost of capital which considers the cost of equity and cost of debt financing expected by a representative market participant) representing the time value of money and the inherent risk and uncertainty of the future cash flows. If the estimated fair value of the reporting unit is less than its carrying value, a second step is performed to compute the amount of the impairment by determining the "implied fair value" of the goodwill, which is compared to its corresponding carrying value.
89
Long-lived assets, including property, improvements and equipment and amortizable intangibles, are evaluated for impairment under ASC 360-10-35, (previously issued as SFAS No. 144 "Accounting for the Impairment or Disposal of Long-Lived Assets") whenever events or changes in circumstances indicate that the carrying value of such assets may not be recoverable. We consider assets to be impaired and write them down to fair value if estimated undiscounted cash flows associated with those assets are less than their carrying amounts.
In accordance with ASC 350, we performed our annual goodwill impairment analysis for each reporting unit that constitutes a business for which discrete financial information is produced and reviewed by operating segment management and provides services that are distinct from the other reporting units. For the Hospital Services segment, the reporting unit for the annual goodwill impairment analysis was determined to be at the segment level. For the Medical Group segment, we have determined that ProMed individually and Prospect (which includes all the other affiliated physician organizations) each represent a reporting unit, based on operational characteristics. The ProMed Entities are geographically and managerially their own reporting unit.
Our impairment test at September 30, 2009 resulted in no impairment charges.
The assessment of impairment indicators, measurement of impairment loss, selection of appropriate valuation methodology, assumptions and discount factors, involve significant judgment and requires management to project future results which are inherently uncertain.
Legal and Other Loss Contingencies
We are subject to contingencies, such as legal proceedings and claims arising out of our business. In accordance with ASC 450, "Accounting for Contingencies," we record accruals for such contingencies when it is probable that a liability will be incurred and the amount of loss can be reasonably estimated. A significant amount of management estimation is required in determining when, or if, an accrual should be recorded for a contingent matter and the amount of such accrual, if any.
We are in the process of finalizing certain post-closing matters related to the 2007 ProMed acquisition, including closing balance sheet reconciliations, escrow reconciliations and other matters. We have recorded an estimated settlement amount relating such matters in the accompanying consolidated financial statements.
Recently-Issued Accounting Pronouncements
In December 2007, the FASB issued ("ASC 810"), (previously known as SFAS No. 160, "Noncontrolling Interests in Consolidated Financial Statements—an Amendment of ARB No. 51"). This literature establishes accounting and reporting standards for the noncontrolling interest in a subsidiary and for the deconsolidation of a subsidiary. It clarifies that a noncontrolling minority interest in a subsidiary is an ownership interest in the consolidated entity that should be reported as equity in the accompanying consolidated financial statements separate from the parent company's equity. Net income (loss) attributable to the noncontrolling interest will be included in consolidated net income on the face of the income statement. This standard is effective for fiscal years, and interim periods within those fiscal years, beginning on or after December 15, 2008. It requires retroactive adoption of the presentation and expanded disclosure requirements for existing minority interests. All other requirements of the standard shall be applied prospectively. We will adopt this standard on October 1, 2009 and is currently evaluating the potential impact of such adoption on its consolidated financial statements.
In May 2009, the FASB issued ("ASC 855"), (previously known as SFAS No. 165, "Subsequent Events") which establishes general standards of accounting and disclosure for events that occur after the balance sheet date but before financial statements are issued. This standard was effective for
90
reporting periods ending after June 15, 2009. The adoption of this standard does not impact our consolidated financial position or results of operations, as its requirements are disclosure-only in nature. The consolidated financial statements were available to be issued on December 18, 2009 and we evaluated subsequent events known to management through such date (see Note 18).
In June 2009, the FASB issued SFAS No. 168, "The FASB Accounting Standards Codification and the Hierarchy of Generally Accepted Accounting Principles—a replacement of FASB Statement No. 162". This standard is now included in ASC Topic 105 and established only two levels of GAAP, authoritative and non-authoritative. The FASB Accounting Standards Codification (the "Codification") became the source of authoritative, non-governmental GAAP, except for rules and interpretive releases of the SEC, which are sources of authoritative GAAP for SEC registrants. All other non-grandfathered, non-SEC accounting literature not included in the Codification became non-authoritative. This standard is effective for financial statements for interim or annual reporting periods ending after September 15, 2009. Effective August 1, 2009, we adopted the new guidelines and numbering system prescribed by the Codification when referring to GAAP. The adoption had no impact on our consolidated financial condition, results of operations or cash flows.
In August 2009, the FASB issued Accounting Standards Update ("ASU") No. 2009-05, "Measuring Liabilities at Fair Value," which amends the guidance in ASC 820, Fair Value Measurements and Disclosures, to provide guidance on fair value measurement of liabilities. If a quoted price in an active market is not available for an identical liability, ASU 2009-05 requires companies to compute fair value by using quoted prices for an identical liability when traded as an asset, quoted prices for similar liabilities when traded as an asset or another valuation technique that is consistent with the guidance in ASC 820. ASU 2009-05 will be effective for interim and annual periods beginning after its issuance and is not expected to have a material impact on our consolidated financial position or results of operations.
Acquisitions
Our business has grown through a series of business combinations. These business combinations were all accounted for using the purchase method of accounting, and accordingly, the operating results of each acquisition have been included in our consolidated financial statements since their effective date of acquisition. The purchase price for each business combination was allocated to the assets, including the identifiable intangible assets, and liabilities, based on estimated fair values determined using independent appraisals where appropriate. The excess of purchase price over the net tangible assets acquired was allocated to goodwill and other intangible assets.
We have historically funded our acquisition program with debt, the sale of our common stock, and cash flow from operations. The assets that we and our affiliated physician organizations have acquired have been largely goodwill and intangible assets. The acquisition of physician organizations consists primarily of HMO contracts, primary care and specialist physician contracts and the right to manage each physician organization through a management services agreement. The physician organizations we acquire generally do not have significant tangible net equity; therefore, our acquired assets are predominantly goodwill and other intangible assets. The acquisition of hospital operations consists primarily of trade names, covenants-not-to-compete and property, improvements and equipment.
91
The following table summarizes all business combinations for the three years ended September 30, 2009.
Business Combinations
|
Effective Date | Purchase Price | Location | |||||
|---|---|---|---|---|---|---|---|---|
ProMed Entities |
June 1, 2007 | $ | 48,392,000 | San Bernardino and Los Angeles Counties | ||||
Alta |
August 8, 2007 | $ | 154,935,000 | Los Angeles County | ||||
Brotman (increased investment to a 71.9% interest) |
April 14, 2009 | $ | 2,556,000 | Los Angeles County | ||||
Divestitures
On August 1, 2008, we completed the sale of all of the outstanding stock of the AV Entities for total cash consideration of $8,000,000. As required by ASC 360-10-35, "Accounting for the Impairment or Disposal of Long-Lived Assets," the assets and liabilities of the AV Entities and their operations have been presented in our most recently filed consolidated financial statements as discontinued operations for all periods presented. All references to operating results reflect our ongoing operations, excluding the AV Entities, unless otherwise noted.
Inflation
According to U.S. Bureau of Labor Statistics Data, the national healthcare cost inflation rate has exceeded the general inflation rate for the last four years. We use various strategies to mitigate the negative effects of healthcare cost inflation. Specifically, we try to control physician and hospital costs through contracts with independent providers of healthcare services and close monitoring of cost trends emphasizing preventive healthcare and appropriate use of specialty and hospital services.
While we currently believe our strategies to mitigate healthcare cost inflation will continue to be successful, competitive pressures, new healthcare and pharmaceutical product introductions, demands from healthcare providers and customers, applicable regulations or other factors may affect our ability to control healthcare costs.
Item 7A. Quantitative and Qualitative Disclosures Regarding Market Risk.
Not applicable.
92
Item 8. Financial Statements and Supplementary Data.
The following financial statements and financial statement schedule are included in this report beginning on page F-1:
| |
Page | |
|---|---|---|
Index to Financial Statements and Financial Statement Schedule |
F-1 | |
Report of Independent Registered Public Accounting Firm |
F-2 | |
Consolidated Balance Sheets as of September 30, 2009 and 2008 |
F-3 | |
Consolidated Statements of Operations for the Years Ended September 30, 2009 and 2008 |
F-5 | |
Consolidated Statements of Shareholders' Equity for the Years Ended September 30, 2009 and 2008 |
F-6 | |
Consolidated Statements of Cash Flows for the Years Ended September 30, 2009 and 2008 |
F-7 | |
Notes to Consolidated Financial Statements |
F-9 | |
Schedule II—Valuation and Qualifying Accounts for the Years Ended September 30, 2009 and 2008 |
F-63 |
All other schedules are omitted because they are not required, or the information is included elsewhere in the accompanying Consolidated Financial Statements.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure.
None
Item 9A(T). Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
We carried out an evaluation as of September 30, 2009, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures as defined in Rule 13a-15(e) of the Securities Exchange Act of 1934. Based upon that evaluation, the Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures are effective in timely alerting them to material information relating to us (including our consolidated subsidiaries) required to be disclosed in our reports under the Securities Exchange Act of 1934. In addition based on that evaluation, the Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures were effective in ensuring that information required to be disclosed by us in the reports that we file or submit under the Securities Exchange Act of 1934 is accumulated and communicated to our management, including the Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosures.
Management's Report on Internal Control over Financial Reporting
Our management, under the supervision and with the participation of our Chief Executive Officer and Chief Financial Officer is responsible for establishing and maintaining effective internal control over financial reporting, or Internal Control, as such term is defined in Exchange Act Rule 13a-15(f). Our Internal Control is designed to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of financial statements for external reporting purposes in accordance with U.S. generally accepted accounting principles, or GAAP. PMH's Internal Control includes those policies and procedures that (i) pertain to the maintenance of records that in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of PMH; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with GAAP, and that receipts and expenditures of PMH are being made only
93
in accordance with authorizations of management and directors of PMH; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of PMH's assets that could have a material effect on the financial statements.
Because of inherent limitations in any Internal Control, no matter how well designed, misstatements due to error or fraud may occur and may not be detected. Accordingly, even effective Internal Control can provide only reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with GAAP.
Our management, under the supervision and with the participation of our Chief Executive Officer and Chief Financial Officer, assessed the effectiveness of PMH's Internal Control as of September 30, 2009. The assessment conducted by management excluded a detailed assessment of the Internal Control of Brotman Medical Center "Brotman". Brotman was excluded from management's detailed assessment due to the timing of the Brotman acquisition, April 14, 2009, which did not allow sufficient time to conduct a thorough evaluation. Despite excluding Brotman from management's detailed assessment, management still performed a preliminary evaluation of the Internal Control of Brotman Medical Center. Management's assessment was based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations ("COSO") of the Treadway Commission.
Based upon that assessment which included the evaluation of the material weakness in the financial reporting process at Brotman discussed below, management has concluded that PMH's Internal Control over financial reporting was ineffective as of September 30, 2009.
See below for discussion of material weaknesses in internal control over financial reporting at Brotman, which became a majority-owned subsidiary effective April 14, 2009.
This annual report does not include an attestation report of our registered public accounting firm regarding internal control over financial reporting. Management's report was not subject to attestation by our registered public accounting firm pursuant to temporary rules of the Securities and Exchange Commission that permit us to provide only management's report in this annual report.
Brotman—Material Weakness in Internal Control over Financial Reporting
Summary of Material Weaknesses in Internal Control over Financial Reporting:
As part of our preliminary assessment of internal controls over financial reporting, we identified several deficiencies within the financial reporting process of Brotman. We believe the combination of these deficiencies creates an environment where there is a reasonable possibility that a material misstatement of Brotman's financial statements would not be detected in a timely manner. We have assessed a material weakness in the financial reporting process of Brotman and its related impact on the corporate consolidating financial reporting process. The deficiencies within the financial reporting process are the lack of a formalized month-end close process, limited staff training and financial accounting expertise and a lack of department accounting policies and procedures.
During the financial reporting close for the quarter ended June 30, 2009, Brotman was unable to implement a structured close process which resulted in multiple delays and reiterations of their financial statements. Account reconciliations were not prepared in an accurate or timely manner which resulted in a significant amount of post close adjustments. Also, Brotman's accounting department did not demonstrate a sufficient amount of expertise or training to sufficiently complete the steps needed to execute an accurate or timely close. Additionally, Brotman's accounting department did not utilize or implement policies and procedures to organize or streamline the close process.
As a result of these deficiencies, we are in the process of implementing significant changes in the Brotman accounting department. We added additional resources and personnel with experience in and
94
an understanding of the complexities of the business and a financial reporting process. Additional control processes and oversight procedures have been implemented; however, a longer evaluation period is needed to reasonably validate that such processes and procedures are operating at a level to have fully remediated the material weakness as of September 30, 2009. At Brotman, we continue to expend significant efforts on financial reporting activities, integration of operations and expansion of our disclosure controls and procedures.
Remediation Steps to Address Material Weaknesses:
Based on findings of material weaknesses in our internal control over financial reporting, we have taken steps to strengthen our internal controls within the financial reporting process. We have added to the expertise and depth of personnel within the Brotman accounting department, including the appointment of a new Chief Financial Officer and Controller, with specific and significant expertise in the critical areas identified above. We also added additional resources to assist in the review and preparation of significant account balance reconciliations as well as the implementation of new policies and procedures. Also, senior management has increased its scrutiny and oversight of Brotman's financial statements and has performed significant top-down financial statement analysis to gain additional assurance as to the accuracy of Brotman's financial information. As previously stated, we will continue to work on and improve the financial reporting process of Brotman and its impact on the corporate consolidating financial reporting process. In review, the principal measures that we are in the process of undertaking to remediate the deficiencies are as follows:
- •
- Hired a new Chief Financial Officer and Controller and added additional resources to implement a sound financial reporting
process;
- •
- Enhanced Brotman's accounting and finance policies and implemented robust monitoring control procedures and analytics to
prevent or detect a misstatement on a timely basis;
- •
- Developed a financial reporting responsibility matrix, close calendar and checklist for Brotman, whereby all general
ledger accounts and financial statement line items are specifically assigned to a specific member of the accounting department to perform monthly, quarterly and year-end analysis. The
analysis will be reviewed by senior members of the accounting department team for accuracy and integrity;
- •
- Developing a formal monthly, quarterly and annual reporting package, including specific reporting and information for
identified key risk areas, with formal sign off by the financial executive with specific oversight of each area; and
- •
- Documenting formal accounting policies and procedures with regular compliance reviews of key risk areas to evaluate the
designing and effectiveness of controls.
- •
- Enhancing the corporate financial reporting process oversight of the above mentioned controls and processes.
Changes in Internal Control over Financial Reporting
Except as discussed above, regarding Brotman, there have been no changes in our Internal Control that occurred during the three months ended September 30, 2009 that have materially affected, or are reasonable likely to materially affect, our Internal Control.
Effective December 18, 2009, the Compensation Committee granted a new management bonus arrangement whereby Mr. Heather could be eligible to receive up to 75% of his base salary (currently $350,000) subject to attaining certain criteria, including but not limited to the Company's attainment of certain EBITDA targets set by the Company on an annual basis. On that same date, the Compensation Committee also granted a discretionary executive bonus to Donna Vigil in an amount not to exceed $15,000.
95
Item 10. Directors, Executive Officers and Corporate Governance.
Certain information regarding our directors and our corporate governance will be included in our definitive proxy statement to be filed with the Securities and Exchange Commission not later than 120 days after the end of the fiscal year covered by this Form 10-K, and such information is incorporated herein by reference to the definitive proxy statement. Information concerning our executive officers appears under Part I, Item 1, Business—Executive Officers, of this Form 10-K.
Item 11. Executive Compensation.
Certain information regarding compensation of our executive officers will be included in our definitive proxy statement to be filed with the Securities and Exchange Commission not later than 120 days after the end of the fiscal year covered by this Form 10-K, and such information is incorporated herein by reference to the definitive proxy statement.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related
Stockholder Matters.
Certain information regarding (1) security ownership of certain beneficial owners and management, (2) securities authorized for issuance under equity compensation plans and (3) related stockholder matters will be included in our definitive proxy statement to be filed with the Securities and Exchange Commission not later than 120 days after the end of the fiscal year covered by this Form 10-K, and such information is incorporated herein by reference to the definitive proxy statement.
Item 13. Certain Relationships and Related Transactions, and Director Independence.
Certain information regarding transactions with management and other related parties can be found in Note 7 to the accompanying Consolidated Financial Statements. Additional information on related party transactions and information on director independence will be included in our definitive proxy statement to be filed with the Securities and Exchange Commission not later than 120 days after the end of the fiscal year covered by this Form 10-K, and such information is incorporated herein by reference to the definitive proxy statement.
Item 14. Principal Accounting Fees and Services.
Certain information regarding accounting fees and services will be included in our definitive proxy statement to be filed with the Securities and Exchange Commission not later than 120 days after the end of the fiscal year covered by this Form 10-K, and such information is incorporated herein by reference to the definitive proxy statement.
96
Item 15. Exhibits and Financial Statement Schedules.
The financial statements and financial statement schedule listed under Item 8 are included in this report beginning on page F-1. The following exhibits have been filed with, or are incorporated by reference, in this report:
| 3.1 | Amended and Restated Certificate of Incorporation of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.1 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). | ||
3.2 |
Certificate of Amendment of Amended and Restated Certificate of Incorporation of Prospect Medical Holdings, Inc. dated January 19, 2000 (incorporated by reference to Exhibit 3.2 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
3.3 |
Certificate of Amendment of Amended and Restated Certificate of Incorporation of Prospect Medical Holdings, Inc. dated January 15, 2004 (incorporated by reference to Exhibit 3.3 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
3.4 |
Certificate of Designation of Series A Convertible Preferred Stock of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.4 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
3.5 |
Certificate of Elimination of Series A Convertible Preferred Stock of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.5 to the Registrant's Quarterly Report on Form 10-Q filed on August 20, 2007). |
||
3.6 |
Certificate of Designation of Series B Preferred Stock of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.2 to the Registrant's Current Report on Form 8-K filed on August 10, 2007). |
||
3.7 |
Amended and Restated Bylaws of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.5 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
3.8 |
First Amendment to Amended and Restated Bylaws of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.6 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
3.9 |
Second Amendment to Amended and Restated Bylaws of Prospect Medical Holdings, Inc. (incorporated by reference to Exhibit 3.1 to the Registrant's Current Report on Form 8-K filed on August 10, 2007). |
||
4.1 |
Indenture, dated July 29, 2009, among the Company, certain of its subsidiaries and affiliates (as subsidiary guarantors) and U.S. Bank National Association (as trustee) (incorporated by reference to Exhibit 4.1 to the Registrant's Current Report on Form 8-K filed on July 29, 2009). |
||
4.2 |
Form of 123/4% Senior Secured Notes, Series B, due 2014 (incorporated by reference to Exhibit 4.2 to the Registrant's Registration Statement on Form S-4 filed on September 30, 2009). |
||
4.3 |
Registration Rights Agreement, dated July 29, 2009, among the Company, certain of its subsidiaries and affiliates (as guarantors) and RBC Capital Markets Corporation and Jefferies & Company, Inc. (as the initial purchasers) (incorporated by reference to Exhibit 4.2 to the Registrant's Current Report on Form 8-K filed on July 29, 2009). |
97
| 10.1 | Warrant to Acquire Common Stock between Prospect Medical Holdings, Inc. and Spencer Trask Venture Investment Partners, LLC (incorporated by reference to Exhibit 10.1 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). | ||
10.2 |
Amended and Restated Management Services Agreement, made as of September 15, 1998 and deemed to have been effective as of June 4, 1996, between Prospect Medical Systems, Inc. and Prospect Medical Group, Inc. (incorporated by reference to Exhibit 10.6 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.3 |
Amendment to Management Services Agreement, made as of October 1, 1998, between Prospect Medical Systems, Inc. and Prospect Medical Group, Inc. (incorporated by reference to Exhibit 10.7 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.4 |
Management Agreement dated as of January 1, 2003 between Pinnacle Health Resources Inc. and StarCare Medical Group, Inc. dba Gateway Medical Group, Inc. (incorporated by reference to Exhibit 10.8 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.5 |
Management Agreement dated as of January 1, 2003 between Pinnacle Health Resources Inc. and APAC Medical Group, Inc. dba Gateway Physicians Medical Associates, Inc. (incorporated by reference to Exhibit 10.9 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.6 |
Management Services Agreement, made as of August 1, 1999, between Prospect Medical Systems, Inc. and Nuestra Familia Medical Group (incorporated by reference to Exhibit 10.10 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.7 |
Amendment to Management Services Agreement, made as of January 15, 2009, between Prospect Medical Systems, Inc. and Nuestra Familia Medical Group, Inc. (incorporated by reference to Exhibit 10.3 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
||
10.8 |
Management Services Agreement, made as of July 1, 1999, between Prospect Medical Systems, Inc. and AMVI/Prospect Medical Group (incorporated by reference to Exhibit 10.11 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.9 |
Management Services Agreement dated as of January 1, 2001 between Prospect Medical Systems, Inc. and Prospect Health Source Medical Group, Inc. (incorporated by reference to Exhibit 10.31 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.10 |
Amendment to Management Services Agreement dated as of November 1, 2002 between Prospect Medical Systems, Inc. and Prospect Health Source Medical Group, Inc. (incorporated by reference to Exhibit 10.32 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.11 |
Amendment to Management Services Agreement, made as of January 15, 2009, between Prospect Medical Systems, Inc. and Prospect Health Source Medical Group, Inc. (incorporated by reference to Exhibit 10.4 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
||
10.12 |
Management Services Agreement dated as of October 1, 2003, by and between Prospect Medical Systems, Inc. and Prospect Professional Care Medical Group, Inc. (incorporated by reference to Exhibit 10.33 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
98
| 10.13 | Management Services Agreement dated as of March 1, 2004 by and between Prospect Medical Systems, Inc. and Prospect NWOC Medical Group, Inc. (incorporated by reference to Exhibit 10.34 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). | ||
10.14 |
Employment Agreement made as of April 8, 2004, but effective on April 19, 2004, between Prospect Medical Holdings, Inc. and Mike Heather (incorporated by reference to Exhibit 10.76 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.15 |
First Amendment to Employment Agreement, dated as of February 12, 2009, between Prospect Medical Holdings, Inc. and Mike Heather (incorporated by reference to Exhibit 10.5 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
||
10.16 |
Partnership Agreement dated July 1, 1999 between AMVI/MC Health Network, Inc. and Santa Ana/Tustin Physicians Group (incorporated by reference to Exhibit 10.77 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.17 |
Prospect Medical Holdings, Inc. 1998 Stock Option Plan (incorporated by reference to Exhibit 10.90 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.18 |
First Amendment to Prospect Medical Holdings, Inc. 1998 Stock Option Plan (incorporated by reference to Exhibit 10.91 to the Registrant's Registration Statement on Form 10 filed on May 27, 2004). |
||
10.19 |
Cash Management Agreement among Prospect Medical Systems, Inc., Prospect Medical Holdings, Inc., and Prospect Medical Group, Inc., effective as of June 6, 1996 (incorporated by reference to Exhibit 10.194 to the Registrant's Amendment No. 2 to Registration Statement on Form 10 filed on August 27, 2004). |
||
10.20 |
Second Amendment to Prospect Medical Holdings, Inc. 1998 Stock Option Plan (incorporated by reference to Exhibit 10.195 to the Registrant's Amendment No. 3 to Registration Statement on Form 10 filed on October 21, 2004). |
||
10.21 |
Amendment to Management Agreement, effective as of February 1, 2004 to that certain Management Agreement made and entered into as of January 1, 2003, entered into by and between Pinnacle Health Resources and StarCare Medical Group, Inc. dba Gateway Medical Group, Inc. (incorporated by reference to Exhibit 10.198 to the Registrant's Amendment No. 3 to Registration Statement on Form 10 filed on October 21, 2004). |
||
10.22 |
Amendment to Management Agreement, effective as of February 1, 2004 to that certain Management Agreement made and entered into as of January 1, 2003, entered into by and between Pinnacle Health Resources and APAC Medical Group, Inc. dba Gateway Physicians Medical Associates, Inc. (incorporated by reference to Exhibit 10.199 to the Registrant's Amendment No. 3 to Registration Statement on Form 10 filed on October 21, 2004). |
||
10.23 |
Form of stock option agreement used for incentive stock options granted under the registrant's 1998 Stock Option Plan, as amended (incorporated by reference to Exhibit 99.1 to the Registrant's Current Report on Form 8-K filed on September 20, 2005). |
||
10.24 |
Form of stock option agreement used for non-qualified stock options granted under the registrant's 1998 Stock Option Plan, as amended (incorporated by reference to Exhibit 99.2 to the Registrant's Current Report on Form 8-K filed on September 20, 2005). |
99
| 10.25 | First Lien Credit Agreement dated as of August 8, 2007 among Prospect Medical Holdings, Inc. and Prospect Medical Group, Inc. as the Borrowers, Bank of America, N.A., as Administrative Agent, Swing Line Lender, and L/C Issuer, Cratos Capital Management, LLC, as Syndication Agent, certain other Lenders, and Banc of America Securities LLC, as Sole Lead Arranger and Sole Book Manager (incorporated by reference to Exhibit 10.31 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). | ||
10.26 |
Second Lien Credit Agreement dated as of August 8, 2007 among Prospect Medical Holdings, Inc. and Prospect Medical Group, Inc. as the Borrowers, Bank of America, N.A., as Administrative Agent, certain other Lenders, and Banc of America Securities LLC, as Sole Lead Arranger and Sole Book Manager (incorporated by reference to Exhibit 10.32 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.27 |
Continuing Guaranty (First Lien) dated as of August 8, 2007 by Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and certain of their Subsidiaries as the Guarantor, in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.35 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.28 |
Continuing Guaranty (Second Lien) dated as of August 8, 2007 by Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and certain of their Subsidiaries as the Guarantor, in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.36 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.29 |
Intercreditor Agreement dated as of August 8, 2007 by Prospect Medical Holdings, Inc. and Prospect Medical Group, Inc. as the Borrowers, certain of their Subsidiaries as Guarantors, and Bank of America, N.A., as First Lien Collateral Agent, Second Lien Collateral Agent, and Control Agent (incorporated by reference to Exhibit 10.41 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.30 |
Third Amended and Restated Assignable Option Agreement dated as of August 8, 2007 by Prospect Medical Systems, Inc., Prospect Medical Group, Inc. and Jacob Y. Terner, M.D. (incorporated by reference to Exhibit 10.42 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.31 |
Executive Employment Agreement dated August 8, 2007 between Alta Hospitals System, LLC, and Samuel S. Lee (incorporated by reference to Exhibit 99.4 to Samuel S. Lee's Schedule 13D filed on August 20, 2007). |
||
10.32 |
Amendment to Executive Employment Agreement effective March 19, 2008 by and among Prospect Medical Holdings, Inc., Alta Hospitals System, LLC and Samuel S. Lee (incorporated by reference to Exhibit 7 to the Samuel S. Lee's Schedule 13D/A filed on April 22, 2008). |
||
10.33 |
Second Amendment to Executive Employment Agreement, dated as of July 8, 2008, by and among Prospect Medical Holdings, Inc., Alta Hospitals System, LLC and Samuel S. Lee (incorporated by reference to Exhibit 8 to the Samuel S. Lee's Schedule 13D/A filed on August 15, 2008). |
||
10.34 |
Third Amendment to Executive Employment Agreement, dated as of February 12, 2009, among Prospect Medical Holdings, Inc., Alta Hospitals System, LLC, and Samuel S. Lee (incorporated by reference to Exhibit 10.6 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
100
| 10.35 | Amended and Restated Employment Agreement dated as of May 12, 2009 between Prospect Medical Holdings, Inc. and Samuel S. Lee (incorporated by reference to Exhibit 10.15 to the Registrant's Quarterly Report on Form 10-Q filed on May 15, 2009). | ||
10.36 |
Management Services Agreement between Pomona Valley Medical Group, Inc. and ProMed Health Care Administrators effective October 1, 1998 (incorporated by reference to Exhibit 10.53 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.37 |
Amendment to Management Services Agreement, made as of October 1, 2007, between ProMed Health Care Administrators, Inc. and Pomona Valley Medical Group, Inc. (incorporated by reference to Exhibit 10.1 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
||
10.38 |
Management Services Agreement between Upland Medical Group, A Professional Medical Corporation and ProMed Health Care Administrators effective October 1, 2002 (incorporated by reference to Exhibit 10.54 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.39 |
Amendment to Management Services Agreement, made as of October 1, 2007, between ProMed Health Care Administrators, Inc. and Upland Medical Group, Inc. (incorporated by reference to Exhibit 10.2 to the Registrant's Quarterly Report on Form 10-Q filed on February 17, 2009). |
||
10.40 |
Hospital Inpatient Services Agreement between Alta Los Angeles Hospitals, Inc. and the Department of Health Services, as amended (Certain portions of this Exhibit have been omitted pursuant to an application for confidential treatment filed with the Commission pursuant to Rule 24b-2 under the Securities Exchange Act of 1934) (incorporated by reference to Exhibit 10.55 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.41 |
Amendments Nos. 18 and 19 to Hospital Inpatient Services Agreement between Alta Los Angeles Hospitals, Inc. and the Department of Health Services (Certain portions of this Exhibit have been omitted subject to an application for confidential treatment filed with the Commission pursuant to Rule 24b-2 under the Securities Exchange Act of 1934)(incorporated by reference to Exhibit 10.50 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.42 |
Amendments Nos. 20 and 21 to Hospital Inpatient Services Agreement between Alta Los Angeles Hospitals, Inc. and the Department of Health Services (Certain portions of this Exhibit have been omitted subject to an application for confidential treatment filed with the Commission pursuant to Rule 24b-2 under the Securities Exchange Act of 1934).* |
||
10.43 |
Hospital Inpatient Services Agreement between Alta Hollywood Hospitals, Inc. and the Department of Health Services, as amended (Certain portions of this Exhibit have been omitted pursuant to an application for confidential treatment filed with the Commission pursuant to Rule 24b-2 under the Securities Exchange Act of 1934) (incorporated by reference to Exhibit 10.56 to the Registrant's Annual Report on Form 10-K filed on June 2, 2008). |
||
10.44 |
First Lien Forbearance Agreement dated as of February 13, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.2 to the Registrant's Quarterly Report on Form 10-Q filed on June 16, 2008). |
||
10.45 |
Second Lien Forbearance Agreement dated as of February 13, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.3 to the Registrant's Quarterly Report on Form 10-Q filed on June 16, 2008). |
101
| 10.46 | First Amendment to Forbearance Agreement dated as of March 31, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.4 to the Registrant's Quarterly Report on Form 10-Q filed on June 16, 2008). | ||
10.47 |
Consent Under Second Lien Forbearance Agreement dated as of March 31, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.5 to the Registrant's Quarterly Report on Form 10-Q filed on June 16, 2008). |
||
10.48 |
Amended and Restated Forbearance Agreement dated as of April 10, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.1 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.49 |
Amended and Restated Second Lien Forbearance Agreement dated as of April 10, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.2 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.50 |
Stock Purchase Agreement dated as of April 23, 2008 among Prospect Medical Group, Inc., Prospect Medical Holdings, Inc., Greater Midwest, Sierra Medical Group Holding Company, Inc. and Richard Merkin, M.D. (incorporated by reference to Exhibit 2.1 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.51 |
Amendment No. 1, dated July 3, 2008, to Stock Purchase Agreement dated as of April 23, 2008 among Prospect Medical Group, Inc., Prospect Medical Holdings, Inc., Greater Midwest, Sierra Medical Group Holding Company, Inc. and Richard Merkin, M.D. (incorporated by reference to Exhibit 10.50 to the Registrant's Registration Statement on Form S-4 filed on September 30, 2009). |
||
10.52 |
Amendment No. 2, dated August 1, 2008, to Stock Purchase Agreement dated as of April 23, 2008 among Prospect Medical Group, Inc., Prospect Medical Holdings, Inc., Greater Midwest, Sierra Medical Group Holding Company, Inc. and Richard Merkin, M.D. (incorporated by reference to Exhibit 10.51 to the Registrant's Registration Statement on Form S-4 filed on September 30, 2009). |
||
10.53 |
First Amendment to Amended and Restated Forbearance Agreement dated as of April 30, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.3 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.54 |
First Amendment to Amended and Restated Second Lien Forbearance Agreement dated as of April 30, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.4 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.55 |
Resignation Agreement dated as of May 12, 2008 between Prospect Medical Holdings, Inc. and Jacob Y. Terner, M.D. (incorporated by reference to Exhibit 10.5 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.56 |
Second Amendment to Amended and Restated Forbearance Agreement dated as of May 14, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.6 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
102
| 10.57 | Second Amendment to Amended and Restated Second Lien Forbearance Agreement dated as of May 14, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.7 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). | ||
10.58 |
Second Amendment to First Lien Credit Agreement, Waiver and Consent dated as of May 15, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.8 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.59 |
Second Amendment to Second Lien Credit Agreement, Waiver and Consent dated as of May 15, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., Bank of America, N.A., as Administrative Agent, and the lenders party thereto (incorporated by reference to Exhibit 10.9 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.60 |
Severance and Release Agreement dated as of June 4, 2008 between Prospect Medical Holdings, Inc. and Michael Terner (incorporated by reference to Exhibit 10.10 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.61 |
Third Amendment to First Lien Credit Agreement and First Amendment to Second Amendment to First Lien Credit Agreement, Waiver and Consent dated as of June 30, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.11 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.62 |
Third Amendment to Second Lien Credit Agreement and First Amendment to Second Amendment to Second Lien Credit Agreement, Waiver and Consent dated as of June 30, 2008 by and among Prospect Medical Holdings, Inc., Prospect Medical Group, Inc., and Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.12 to the Registrant's Quarterly Report on Form 10-Q filed on August 12, 2008). |
||
10.63 |
Fourth Amended and Restated Assignable Option Agreement, dated as of August 8, 2008, by and among Prospect Medical Systems, Inc., Prospect Medical Group, Inc. and Osmundo R. Saguil, M.D. (incorporated by reference to Exhibit 10.71 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.64 |
Fifth Amended and Restated Assignable Option Agreement, dated as of November 26, 2008, by and among Prospect Medical Systems, Inc., Prospect Medical Group, Inc. and Arthur Lipper, M.D. (incorporated by reference to Exhibit 10.72 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.65 |
Amendment to Fifth Amended and Restated Assignable Option Agreement, dated July 29, 2009, among Prospect Medical Systems, Inc., Prospect Medical Group, Inc. and Arthur Lipper, M.D. (incorporated by reference to Exhibit 10.11 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
10.66 |
Second Amended and Restated Option Agreement, dated as of August 8, 2008, by and between Prospect Medical Group, Inc. and Osmundo R. Saguil, M.D. (incorporated by reference to Exhibit 10.73 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.67 |
Third Amended and Restated Option Agreement, dated as of November 26, 2008, by and between Prospect Medical Group, Inc. and Arthur Lipper, M.D. (incorporated by reference to Exhibit 10.74 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
103
| 10.68 | Amendment to Third Amended and Restated Option Agreement, dated July 29, 2009, between Prospect Medical Group, Inc. and Arthur Lipper, M.D. (incorporated by reference to Exhibit 10.12 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). | ||
10.69 |
Stock Purchase Agreement, dated as of August 8, 2008, by and among Prospect Medical Systems, Inc., Jacob Y. Terner, M.D., and Osmundo R. Saguil, M.D. (re. Group shares) (incorporated by reference to Exhibit 10.75 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.70 |
Stock Purchase Agreement, dated as of November 26, 2008, by and among Prospect Medical Systems, Inc., Osmundo R. Saguil, M.D., and Arthur Lipper, M.D. (re. Group shares) (incorporated by reference to Exhibit 10.76 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.71 |
Stock Purchase Agreement, dated as of August 8, 2008, by and among Prospect Medical Systems, Inc., Jacob Y. Terner, M.D., and Osmundo R. Saguil, M.D. (re. Nuestra shares) (incorporated by reference to Exhibit 10.77 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.72 |
Stock Purchase Agreement, dated as of November 26, 2008, by and among Prospect Medical Systems, Inc., Osmundo R. Saguil, M.D., and Arthur Lipper, M.D. (re. Nuestra shares) (incorporated by reference to Exhibit 10.78 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.73 |
Amended and Restated First Lien Pledge Agreement, dated as of August 8, 2008, by Osmundo R. Saguil, M.D. in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.79 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.74 |
Second Amended and Restated First Lien Pledge Agreement, dated as of November 26, 2008, by Arthur Lipper, M.D. in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.80 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.75 |
Amended and Restated Second Lien Pledge Agreement, dated as of August 8, 2008, by Osmundo R. Saguil, M.D. in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.81 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.76 |
Second Amended and Restated Second Lien Pledge Agreement, dated as of November 26, 2008, by Arthur Lipper, M.D. in favor of Bank of America, N.A., as Administrative Agent (incorporated by reference to Exhibit 10.82 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.77 |
Form of Indemnification Agreement between Prospect Medical Holdings, Inc. and each of its executive officers and directors (incorporated by reference to Exhibit 10.83 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.78 |
Indemnification Agreement, dated November 26, 2008, by and between Prospect Medical Holdings, Inc. and Arthur Lipper, M.D. (incorporated by reference to Exhibit 10.84 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.79 |
Prospect Medical Holdings, Inc. 2008 Omnibus Equity Incentive Plan (incorporated by reference to Exhibit 10.85 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
104
| 10.80 | Form of Incentive Stock Option Agreement for grant of incentive stock options to participants under our 2008 Omnibus Equity Incentive Plan (incorporated by reference to Exhibit 10.86 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). | ||
10.81 |
Form of Non-Qualified Stock Option Agreement for grant of non-qualified stock options to participants under our 2008 Omnibus Equity Incentive Plan (incorporated by reference to Exhibit 10.87 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.82 |
Non-Qualified Stock Option Agreement between Prospect Medical Holdings, Inc. and Samuel S. Lee, effective as of August 20, 2008 (incorporated by reference to Exhibit 10.88 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.83 |
Restricted Stock Award Agreement for award of restricted stock under our Omnibus Equity Incentive Plan to Mike Heather, dated as of August 15, 2008 (incorporated by reference to Exhibit 10.89 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.84 |
Form of Restricted Stock Award Agreement for award of restricted stock under our Omnibus Equity Incentive Plan to participants, dated as of September 10, 2008 (incorporated by reference to Exhibit 10.90 to the Registrant's Annual Report on Form 10-K filed on December 29, 2008). |
||
10.85 |
Credit Agreement, dated July 29, 2009, among the Company, Royal Bank of Canada (as administrative agent), Jefferies Finance LLC (as syndication agent) and the lenders party thereto (incorporated by reference to Exhibit 10.1 to the Registrant's Current Report on Form 8-K filed on July 29, 2009). |
||
10.86 |
Continuing Guaranty, dated July 29, 2009, in favor of Royal Bank of Canada (as administrative agent), by: Alta Hospitals System, LLC; Alta Hollywood Hospitals, Inc.; Alta Los Angeles Hospitals, Inc.; Genesis Healthcare of Southern California, Inc., a Medical Group; Pomona Valley Medical Group, Inc.; ProMed Health Care Administrators; ProMed Health Services Company; Prospect Hospital Advisory Services, Inc.; Prospect Health Source Medical Group, Inc.; Prospect Medical Group, Inc.; Prospect Medical Systems, Inc.; Prospect NWOC Medical Group, Inc.; Prospect Professional Care Medical Group, Inc.; Starcare Medical Group, Inc.; and Upland Medical Group, a Professional Medical Corporation (incorporated by reference to Exhibit 10.4 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
10.87 |
Intercreditor Agreement, dated July 29, 2009, among Prospect Medical Holdings, Inc. and certain of it subsidiaries from time to time parties thereto, Royal Bank of Canada (as first lien collateral agent), U.S. Bank National Association (as second lien collateral agent) and Royal Bank of Canada (as control agent) (incorporated by reference to Exhibit 10.5 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
10.88 |
Credit Agreement, dated April 14, 2009, between Brotman Medical Center, Inc. (as borrower) and Gemino Healthcare Finance, LLC (as lender) (incorporated by reference to Exhibit 10.6 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
10.89 |
First Amendment to Credit Agreement and Waiver, dated as of December 11, 2009, between Brotman Medical Center, Inc. (as borrower) and Gemino Healthcare Finance, LLC (as lender).* |
||
10.90 |
Loan Agreement, dated July 9, 2008, between Brotman Medical Center, Inc. (as borrower) and JHA West 16, LLC (as lender) (incorporated by reference to Exhibit 10.7 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
105
| 10.91 | Amendment No. 1 to Loan Agreement, dated April 14, 2009, between Brotman Medical Center, Inc. (as borrower) and JHA West 16, LLC (as lender) (incorporated by reference to Exhibit 10.8 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). | ||
10.92 |
Loan Agreement, dated July 9, 2008, between Brotman Medical Center, Inc. (as borrower) and JHA East 7, LLC (as lender) (incorporated by reference to Exhibit 10.9 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
10.93 |
Amendment No. 1 to Loan Agreement, dated April 14, 2009, between Brotman Medical Center, Inc. (as borrower) and JHA East 7, LLC (as lender) (incorporated by reference to Exhibit 10.10 to the Registrant's Quarterly Report on Form 10-Q filed on August 19, 2009). |
||
21.1 |
List of Subsidiaries of Prospect Medical Holdings, Inc.* |
||
23.1 |
Consent of BDO Seidman, LLP.* |
||
31.1 |
Certification of Chief Executive Officer pursuant to Rules 13a-14(a)/15d-14(a) under the Securities Exchange Act of 1934, as amended.* |
||
31.2 |
Certification of Chief Financial Officer pursuant to Rules 13a-14(a)/15d-14(a) under the Securities Exchange Act of 1934, as amended.* |
||
32.1 |
Certification of Chief Executive Officer pursuant to 18 U.S. C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.* |
||
32.2 |
Certification of Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.* |
- *
- Filed herewith.
106
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Los Angeles, State of California, on December 18, 2009.
|
PROSPECT MEDICAL HOLDINGS, INC. (Registrant) |
|||
|
/s/ SAMUEL S. LEE |
|||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature
|
Title
|
Date
|
||
|---|---|---|---|---|
| /s/ SAMUEL S. LEE Samuel S. Lee |
Chairman, Chief Executive Officer and Director (Principal Executive Officer) | December 18, 2009 | ||
/s/ MIKE HEATHER Mike Heather |
Chief Financial Officer (Principal Financial and Accounting Officer) |
December 18, 2009 |
||
/s/ DAVID LEVINSOHN David Levinsohn |
Director |
December 18, 2009 |
||
/s/ KENNETH SCHWARTZ Kenneth Schwartz |
Director |
December 18, 2009 |
||
/s/ JEEREDDI PRASAD Jeereddi Prasad |
Director |
December 18, 2009 |
||
/s/ GLENN R. ROBSON Glenn R. Robson |
Director |
December 18, 2009 |
107
INDEX TO FINANCIAL STATEMENTS AND
FINANCIAL STATEMENT SCHEDULE
F-1
Report of Independent Registered Public Accounting Firm
Board
of Directors and Shareholders
Prospect Medical Holdings, Inc.
Los Angeles, California
We have audited the accompanying consolidated balance sheets of Prospect Medical Holdings, Inc. (the "Company") as of September 30, 2009 and 2008 and the related consolidated statements of operations, shareholders' equity, and cash flows for the years then ended. In connection with our audits of the consolidated financial statements, we have also audited the financial statement schedule listed in the accompanying index. These consolidated financial statements and schedule are the responsibility of the Company's management. Our responsibility is to express an opinion on these consolidated financial statements and schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the consolidated financial position of Prospect Medical Holdings, Inc. as of September 30, 2009 and 2008, and the consolidated results of its operations and its cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
Also, in our opinion, the financial statement schedule listed in the accompanying index, when considered in relation to the basic consolidated financial statements taken as a whole, presents fairly, in all material respects, the information set forth therein for the years ended September 30, 2009 and 2008.
As discussed in Note 16 to the consolidated financial statements, effective October 1, 2008, the Company adopted Financial Accounting Standards Board statement ASC 820-10 (previously issued as Statement of Financial Accounting Standards No. 157, "Fair Value Instruments,") which did not have a material impact on the consolidated financial statements.
/s/ BDO SEIDMAN, LLP
Costa
Mesa, California
December 18, 2009
F-2
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED BALANCE SHEETS
(in thousands, except par value and share amounts)
| |
September 30, 2009 |
September 30, 2008 |
||||||
|---|---|---|---|---|---|---|---|---|
ASSETS |
||||||||
Current assets: |
||||||||
Cash and cash equivalents |
$ | 37,768 | $ | 33,583 | ||||
Restricted cash |
1,395 | — | ||||||
Investments, restricted |
665 | 637 | ||||||
Patient accounts receivable, net of allowance for doubtful accounts of $11,715 and $3,891 at September 30, 2009 and 2008 |
36,806 | 18,314 | ||||||
Government program receivables |
4,852 | 4,365 | ||||||
Risk pool receivables |
— | 338 | ||||||
Other receivables |
1,655 | 2,598 | ||||||
Third party settlements |
1,575 | 216 | ||||||
Notes receivable, current portion |
56 | 224 | ||||||
Refundable income taxes |
1,558 | 2,654 | ||||||
Deferred income taxes, net |
6,644 | 5,788 | ||||||
Inventories |
4,137 | 1,460 | ||||||
Prepaid expenses and other |
5,380 | 2,777 | ||||||
Total current assets |
102,491 | 72,954 | ||||||
Property, improvements and equipment: |
||||||||
Land and land improvements |
31,028 | 18,452 | ||||||
Buildings |
23,665 | 22,233 | ||||||
Leasehold improvements |
2,029 | 1,505 | ||||||
Equipment |
20,255 | 10,628 | ||||||
Furniture and fixtures |
913 | 913 | ||||||
|
77,890 | 53,731 | ||||||
Less accumulated depreciation and amortization |
(14,166 | ) | (7,911 | ) | ||||
Property, improvements and equipment, net |
63,724 | 45,820 | ||||||
Notes receivable, less current portion |
357 | 238 | ||||||
Deposits and other assets |
694 | 778 | ||||||
Deferred financing costs, net |
8,205 | 661 | ||||||
Goodwill |
153,250 | 128,877 | ||||||
Other intangible assets, net |
46,425 | 47,740 | ||||||
Total assets |
$ | 375,146 | $ | 297,068 | ||||
The accompanying notes are an integral part of the consolidated financial statements.
F-3
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED BALANCE SHEETS
(in thousands, except par value and share amounts)
(continued)
| |
September 30, 2009 |
September 30, 2008 |
||||||
|---|---|---|---|---|---|---|---|---|
LIABILITIES AND SHAREHOLDERS' EQUITY |
||||||||
Current liabilities: |
||||||||
Accrued medical claims and other health care costs payable |
$ | 16,824 | $ | 20,480 | ||||
Accounts payable and other accrued liabilities |
31,773 | 16,295 | ||||||
Accrued salaries, wages and benefits |
24,903 | 11,257 | ||||||
Due to government payer |
13,834 | — | ||||||
Current portion of capital leases |
820 | 341 | ||||||
Current portion of long-term debt |
3,805 | 12,100 | ||||||
Other current liabilities |
629 | 107 | ||||||
Total current liabilities |
92,588 | 60,580 | ||||||
Long-term debt, less current portion |
172,539 | 131,921 | ||||||
Deferred income taxes, net |
29,975 | 24,433 | ||||||
Malpractice reserve |
2,824 | 786 | ||||||
Capital leases, net of current portion |
569 | 442 | ||||||
Interest rate swap liability |
— | 6,013 | ||||||
Other long-term liabilities |
162 | — | ||||||
Total liabilities |
298,657 | 224,175 | ||||||
Minority interest |
88 | 81 | ||||||
Commitments, Contingencies and Subsequent Events |
||||||||
Shareholders' equity: |
||||||||
Common stock, $0.01 par value; 40,000,000 shares authorized; 20,619,278 and 20,508,444 shares issued and outstanding at September 30, 2009 and 2008, respectively |
206 | 205 | ||||||
Additional paid-in capital |
94,498 | 93,407 | ||||||
Accumulated other comprehensive loss |
— | (4,917 | ) | |||||
Accumulated deficit |
(18,303 | ) | (15,883 | ) | ||||
Total shareholders' equity |
76,401 | 72,812 | ||||||
Total liabilities and shareholders' equity |
$ | 375,146 | $ | 297,068 | ||||
The accompanying notes are an integral part of the consolidated financial statements.
F-4
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands, except per share amounts)
| |
Year ended September 30 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||||
Revenues: |
|||||||||
Net hospital services revenues |
$ | 205,504 | $ | 126,692 | |||||
Medical group revenues |
196,730 | 202,844 | |||||||
Total revenues |
402,234 | 329,536 | |||||||
Operating expenses: |
|||||||||
Hospital operating expenses |
146,349 | 84,353 | |||||||
Medical group cost of revenues |
151,056 | 158,907 | |||||||
General and administrative |
58,766 | 57,399 | |||||||
Depreciation and amortization |
7,829 | 7,789 | |||||||
Total operating expenses |
364,000 | 308,448 | |||||||
Operating income from unconsolidated joint venture |
2,046 | 2,563 | |||||||
Operating income |
40,280 | 23,651 | |||||||
Other (income) expense: |
|||||||||
Investment income |
(197 | ) | (615 | ) | |||||
Interest expense and amortization of deferred financing costs |
29,161 | 22,341 | |||||||
Loss (gain) on value of interest rate swap arrangements |
5,299 | (3,096 | ) | ||||||
Loss on debt extinguishment |
— | 8,308 | |||||||
Prepayment penalties on debt refinance |
2,588 | — | |||||||
Loss on termination of interest rate swap arrangements |
6,861 | — | |||||||
Total other expense, net |
43,712 | 26,938 | |||||||
Loss from continuing operations before income taxes |
(3,432 | ) | (3,287 | ) | |||||
Income tax benefit |
(1,019 | ) | (1,327 | ) | |||||
Loss from continuing operations before minority interest |
(2,413 | ) | (1,960 | ) | |||||
Minority interest |
7 | 1 | |||||||
Loss from continuing operations |
(2,420 | ) | (1,961 | ) | |||||
Income from discontinued operations, net of tax (Note 4) |
— | 6,169 | |||||||
Net income (loss) before preferred dividends |
(2,420 | ) | 4,208 | ||||||
Dividends to preferred stockholders |
— | (6,760 | ) | ||||||
Net loss attributable to common stockholders |
$ | (2,420 | ) | $ | (2,552 | ) | |||
Per share data: |
|||||||||
Net income (loss) per share attributable to common stockholders: |
|||||||||
Basic and Diluted: |
|||||||||
Continuing operations |
$ | (0.12 | ) | $ | (0.68 | ) | |||
Discontinued operations |
$ | — | $ | 0.48 | |||||
Net income (loss) attributable to common stockholders |
$ | (0.12 | ) | $ | (0.20 | ) | |||
The accompanying notes are an integral part of the consolidated financial statements.
F-5
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF SHAREHOLDERS' EQUITY
(in thousands, except share amounts)
| |
Class A Common Stock Number of Shares |
Common Stock |
Preferred Shares |
Preferred Stock |
Additional Paid-in Capital |
Accumulated Other Comprehensive Income (Loss) |
Retained Earnings (Accumulated Deficit) |
Total, Net | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Balance at September 30, 2007 |
11,402,567 | $ | 114 | 1,672,880 | $ | 17 | $ | 89,751 | $ | (255 | ) | $ | (20,091 | ) | $ | 69,536 | ||||||||||
Accrued dividends on preferred stock |
— | — | — | — | (6,760 | ) | — | — | (6,760 | ) | ||||||||||||||||
Conversion of preferred stock |
8,364,400 | 84 | (1,672,880 | ) | (17 | ) | (67 | ) | — | — | — | |||||||||||||||
Forgiveness of dividends to preferred stockholders |
— | — | — | — | 7,882 | — | — | 7,882 | ||||||||||||||||||
Options exercised |
380,000 | 4 | — | — | 1,196 | — | — | 1,200 | ||||||||||||||||||
Restricted Stock |
30,000 | 0 | — | — | 75 | 75 | ||||||||||||||||||||
Stock-based compensation |
133,333 | 1 | — | — | 1,368 | — | — | 1,369 | ||||||||||||||||||
Warrants exercised |
198,144 | 2 | — | — | (2 | ) | — | — | — | |||||||||||||||||
Sale of the AV Entities |
— | — | — | — | (36 | ) | (36 | ) | ||||||||||||||||||
Comprehensive loss: |
||||||||||||||||||||||||||
Net income before preferred dividends |
— | — | — | — | — | — | 4,208 | 4,208 | ||||||||||||||||||
Unrealized losses on interest rate swaps (net of income tax effect of $3,173) |
— | — | — | — | — | (4,662 | ) | — | (4,662 | ) | ||||||||||||||||
Subtotal—comprehensive loss |
— | — | — | — | — | (4,662 | ) | 4,208 | (454 | ) | ||||||||||||||||
Balance at September 30, 2008 |
20,508,444 | 205 | — | — | 93,407 | (4,917 | ) | (15,883 | ) | 72,812 | ||||||||||||||||
Options exercised |
44,167 | — | — | — | 102 | — | — | 102 | ||||||||||||||||||
Stock-based compensation |
66,667 | 1 | — | — | 989 | — | — | 990 | ||||||||||||||||||
Comprehensive loss: |
||||||||||||||||||||||||||
Net loss before preferred dividends |
— | — | — | — | — | — | (2,420 | ) | (2,420 | ) | ||||||||||||||||
Reversal of unrealized losses upon termination of interest rate swap arrangements (net of income tax effect of $2,677) |
— | — | — | — | — | 4,917 | — | 4,917 | ||||||||||||||||||
Subtotal—comprehensive income |
— | — | — | — | — | 4,917 | (2,420 | ) | 2,497 | |||||||||||||||||
Balance at September 30, 2009 |
20,619,278 | $ | 206 | — | $ | — | $ | 94,498 | $ | — | $ | (18,303 | ) | $ | 76,401 | |||||||||||
The accompanying notes are an integral part of the consolidated financial statements.
F-6
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands)
| |
Year ended September 30, | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||||
Operating activities: |
|||||||||
Net income (loss) before preferred dividends |
$ | (2,420 | ) | $ | 4,208 | ||||
Adjustments to reconcile net income (loss) before preferred dividends to net cash provided by operating activities: |
|||||||||
Depreciation and amortization |
7,829 | 7,789 | |||||||
Amortization of deferred financing costs |
1,189 | 801 | |||||||
Loss on debt extinguishment |
— | 8,308 | |||||||
Provision for bad debts |
17,889 | 5,888 | |||||||
Gain on sale of assets |
34 | 65 | |||||||
Pretax gain on sale of AV Entities |
— | (7,014 | ) | ||||||
Payment-in-kind interest expense |
277 | 220 | |||||||
Amortization of Original Issue Discount |
284 | — | |||||||
Deferred income taxes, net |
(4,108 | ) | (2,992 | ) | |||||
Amortization of other accumulated comprehensive income related to interest swap arrangements |
1,179 | 491 | |||||||
(Gain) loss on interest rate swap arrangements |
12,160 | (3,587 | ) | ||||||
Stock based compensation |
989 | 1,444 | |||||||
Loss from discontinued operations |
— | 431 | |||||||
Changes in assets and liabilities, net of effect of assets acquired and liabilities assumed in purchase transactions: |
|||||||||
Risk pool receivables |
338 | (159 | ) | ||||||
Patient and other receivables |
(12,805 | ) | (9,109 | ) | |||||
Inventory |
180 | (1,460 | ) | ||||||
Prepaid expenses and other current assets |
(470 | ) | 988 | ||||||
Refundable income taxes and taxes payable |
1,096 | 2,388 | |||||||
Deposits and other assets |
(161 | ) | (3 | ) | |||||
Accrued medical claims and other health care costs payable |
(3,656 | ) | (926 | ) | |||||
Accounts payable and other accrued liabilities |
3,742 | 5,040 | |||||||
Net cash used in operating activities from discontinued operations |
— | (546 | ) | ||||||
Net cash provided by operating activities |
23,566 | 12,265 | |||||||
Investing activities: |
|||||||||
Purchase of property, improvements and equipment |
(1,558 | ) | (1,103 | ) | |||||
Decrease in note receivable |
50 | 39 | |||||||
Cash paid for acquisitions, net of cash received |
(2,310 | ) | 326 | ||||||
Capitalized expenses related to acquisitions |
(37 | ) | (81 | ) | |||||
Increase in restricted certificates of deposit |
(27 | ) | (1 | ) | |||||
Other investing activities |
339 | 1 | |||||||
Net cash provided by investing activities from discontinued operations |
— | 5,185 | |||||||
Net cash (used in) provided by investing activities |
(3,543 | ) | 4,366 | ||||||
Financing activities: |
|||||||||
Borrowings from long-term debt |
147,736 | — | |||||||
Cash paid for deferred financing costs |
(7,063 | ) | (730 | ) | |||||
Change in restricted cash |
1,396 | — | |||||||
Borrowings on line of credit, net |
2,888 | 17,750 | |||||||
Repayments on line of credit |
(7,100 | ) | (13,750 | ) | |||||
Repayments of former long-term debt |
(141,837 | ) | (9,219 | ) | |||||
Repayments of capital leases |
(648 | ) | (394 | ) | |||||
Cash paid to terminate interest rate swap arrangements |
(11,312 | ) | — | ||||||
Proceeds from exercises of stock options and warrants |
102 | 1,200 | |||||||
Net cash used in financing activities |
(15,838 | ) | (5,143 | ) | |||||
Net increase in cash and cash equivalents |
4,185 | 11,488 | |||||||
Cash and cash equivalents at beginning of year |
33,583 | 22,095 | |||||||
Cash and cash equivalents at end of year |
$ | 37,768 | $ | 33,583 | |||||
The accompanying notes are an integral part of the consolidated financial statements.
F-7
PROSPECT MEDICAL HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS (Continued)
(in thousands)
| |
Year ended September 30, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
Supplemental disclosure of cash flow information |
||||||||
Details of businesses acquired: |
||||||||
Fair value of assets acquired |
$ | 53,302 | $ | — | ||||
Liabilities assumed or accrued for |
(78,119 | ) | — | |||||
Total net liabilities acquired |
(24,817 | ) | — | |||||
Preliminary goodwill and identifiable intangible recognized |
27,373 | — | ||||||
Cash paid for acquisition |
$ | 2,556 | $ | — | ||||
Less cash acquired |
(209 | ) | ||||||
Net cash paid for acquisition |
$ | 2,347 | ||||||
Equipment acquired under capital lease |
$ | 450 | $ | 177 | ||||
Accrued dividend to preferred shareholders |
$ | — | $ | 6,760 | ||||
Forgiveness of accrued dividend by preferred shareholders |
$ | — | $ | 7,882 | ||||
Interest paid |
$ | 37,110 | $ | 20,194 | ||||
Income taxes paid, net |
$ | 2,067 | $ | 1,300 | ||||
The accompanying notes are an integral part of the consolidated financial statements.
F-8
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Business
Prospect Medical Holdings, Inc. ("Prospect" or the "Company") is a Delaware corporation. Prior to the August 8, 2007 acquisition of Alta Hospitals System, LLC ("Alta"), which was previously known as Alta Healthcare System, Inc., the Company was primarily engaged in providing management services to affiliated physician organizations that operate as independent physician associations ("Medical Groups") or medical clinics. Following the Alta acquisition and acquisition of a majority stake in Brotman Medical Center, Inc., a California corporation ("Brotman") on April 14, 2009 (see Note 3), as of September 30, 2009, the Company owns and operates five community-based hospitals in Southern California, and its operations are organized into three primary reportable segments: Hospital Services, Medical Group, and Corporate as discussed below.
Hospital Services Segment
Alta and Brotman (collectively, the "Hospital Services segment") own and operate in aggregate five hospitals in Los Angeles County, all accredited by the Joint Commission (formerly the Joint Commission on Accreditation of Healthcare Organizations), with a total of approximately 759 licensed beds served by 859 on-staff physicians at September 30, 2009. Alta owns (i) Alta Hollywood Hospitals, Inc., a California corporation dba Hollywood Community Hospital and Van Nuys Community Hospital; and (ii) Alta Los Angeles Hospitals, Inc., a California corporation dba Los Angeles Community Hospital and Norwalk Community Hospital. On April 14, 2009 (the "Acquisition Date"), the Company increased its existing approximately 33.1% ownership stake in Brotman, to approximately 71.9% via an investment of approximately $2.5 million in cash, thereby obtaining a controlling interest. Brotman owns and operates Brotman Medical Center, located in Culver City.
The three community hospitals in Hollywood, Los Angeles and Norwalk offer a comprehensive range of medical and surgical services, including general acute care hospital services, pediatrics, obstetrics and gynecology, pediatric sub-acute care, general surgery, medical-surgical services, orthopedic surgery, and diagnostic, outpatient, skilled nursing and urgent care services. The hospital in Van Nuys provides acute inpatient and outpatient psychiatric services on a voluntary basis. Brotman offers a comprehensive range of inpatient and outpatient services, including general surgery, orthopedic, spine and neurosurgery, cardiology, diagnostic outpatient, rehabilitation, psychiatric and detox services. In addition, Brotman has an active emergency room that plays an integral part in providing emergency services to the West Los Angeles area.
F-9
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Business (Continued)
The table below gives a brief overview of the Company's hospitals and the locations they serve:
Name/Location
|
Primary Service | Number of Beds | ||
|---|---|---|---|---|
Hollywood Community Hospital |
Medical/Surgical | 100 licensed beds/100 staffed beds | ||
Los Angeles Community Hospital |
Medical/Surgical |
130 licensed beds/130 staffed beds |
||
Norwalk Community Hospital |
Medical/Surgical |
50 licensed beds/50 staffed beds |
||
Brotman Medical Center |
Medical/Surgical |
420 licensed beds/240 staffed beds |
||
Van Nuys Community Hospital |
Psychiatric |
59 licensed beds/59 staffed beds |
Admitting physicians are primarily practitioners in the local area. The hospitals have payment arrangements with Medicare, Medi-Cal (the Claifornia version of Medicare) and other third-party payers, including some commercial insurance carriers, health maintenance organizations ("HMOs") and preferred provider organizations ("PPOs").
Medical Group Segment
The Medical Group Management segment is a health care management services organization that provides management services to affiliated physician organizations that operate as independent physician associations ("Medical Groups") or medical clinics. The affiliated physician organizations enter into agreements with health maintenance organizations ("HMOs") to provide enrollees of the HMOs with a full range of medical services in exchange for fixed, prepaid monthly fees known as "capitation" payments. The Medical Group's contract with physicians (primary care and specialist) and other health care providers to provide all of their medical services. As discussed below and in Note 4, effective August 1, 2008, the Company sold the AV Entities to a third party for total consideration of $8 million. Prospect currently manages the provision of prepaid health care services for its affiliated physician organizations in Southern California. The network consists of the following physician organizations as of September 30, 2009 (each, an "Affiliate"):
Prospect
Medical Group, Inc. (PMG)
Santa Ana-Tustin Physicians Group, Inc. (SATPG)
Prospect Health Source Medical Group, Inc. (PHS)
Prospect Professional Care Medical Group
Prospect NWOC Medical Group, Inc. (PNW)
Starcare Medical Group, Inc. (PSC)
F-10
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Business (Continued)
APAC
Medical Group, Inc. (APA) (Inactive)
Nuestra Famila Medical Group, Inc. (Nuestra)
AMVI/Prospect Health Network (AMVI/Prospect)
Genesis HealthCare of Southern California (Genesis)
Pomona Valley Medical Group (PVMG)*
Upland Medical Group (UMG)*
- *
- PVMG and UMG are collectively referred to as ProMed
These Affiliates are managed by the following two medical management company subsidiaries that are wholly-owned by PMH:
Prospect
Medical Systems, Inc. (PMS)
ProMed Health Care Administrators, Inc. (PHCA)
As discussed in Note 4, effective August 1, 2008, the Company sold all of the issued and outstanding stock of Sierra Medical Management, Inc., Sierra Primary Care Medical Group, Antelope Valley Medical Associates, Inc. and Pegasus Medical Group, Inc., (the "AV Entities"). The results of operations of the AV Entities have been classified as discontinued operations for fiscal 2008 and are excluded from the disclosures herein.
All of the Affiliates are wholly-owned by PMG, with the exception of Nuestra, which is 55% owned by PMG, and AMVI/Prospect which is a 50/50 Joint Venture between AMVI and PMG. PMG is owned by a nominee physician shareholder. The results of all of these entities, with the exception of AMVI/Prospect, are consolidated in the accompanying Consolidated Financial Statements.
The AMVI Joint Venture was formed for the sole purpose of combining enrollment in order to meet minimum enrollment levels required for participation in the CalOPTIMA Medicaid (Medi-Cal in California) program in Orange County, California. The joint venture ownership is set at 50/50 to prevent either party from exerting control over the other; however, AMVI and Prospect's businesses are operated autonomously, and enrollees, financial results and cash flows are each separately tracked and recorded. In accordance with the joint venture partnership agreement, profits and losses are not split in accordance with the partnership ownership interest, but rather, are directly tied to the results generated by each separate portion of the business. Separate from any earnings the Company generates from their portion of business within the joint venture, the Company also earns fees for management services they provide to their partner in the joint venture. The Company accounts for their interest in the joint venture partnership using the equity method of accounting. The Company includes in the financial statements only the net results attributable to those enrollees specifically identified as assigned to the Company, together with the management fee that they charge for managing those enrollees specifically assigned to the other joint venture partner. Note 14 contains summarized unaudited financial information for the joint venture.
Prospect Medical Systems, one of the Company's management company subsidiaries ("PMS"), has entered into an assignable option agreement with PMG and the nominee physician shareholder of PMG. Under the assignable option agreement, Prospect acquired an assignable option for a nominal amount from PMG and the nominee shareholder to purchase all or part of PMG's assets (the Asset Option) and the right to designate the purchaser (successor physician) for all or part of PMG's issued and outstanding stock held by the nominee physician shareholder (the Stock Option) in its sole
F-11
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Business (Continued)
discretion. The Company may also assign the assignable option agreement to any person. The assignable option agreement has an initial term of 30 years and is automatically extended for additional terms of 10 years each, as long as the term of the related management services agreement described below (the Management Agreement) is automatically extended. Upon termination of the Management Agreement with PMG, the related Asset Option and Stock Option are automatically and immediately exercised. The Asset and Stock Options may be exercised separately or simultaneously for a purchase price of $1,000 each. Under these nominee shareholder agreements, Prospect has the unilateral right to establish or effect a change of the nominee, at will, and without the consent of the nominee, on an unlimited basis and at nominal cost throughout the term of the Management Agreement. In addition to the Management Agreement with PMG, Prospect, through one of its management company subsidiaries, has a management agreement with each Affiliate. The term of the Management Agreements is generally 30 years. PMG is the nominee shareholder of SATPG, PHS, PPM, PNW, PSC, APA, Genesis, PVMG, and UMG. Dr. Lipper is the nominee shareholder as to the 55% interest in Nuestra.
The Company's Affiliates have each entered into a Management Agreement whereby the Affiliate has agreed to pay a management fee to PMS or PHCA, as applicable (each of which is a wholly-owned subsidiary of Prospect). The fee is based in part on the costs to the management company and on a percentage of revenues the Affiliate receives (i) for the performance of medical services by the Affiliate's employees and independent contractor physicians and physician extenders, (ii) for all other services performed by the Affiliates, and (iii) as proceeds from the sale of assets or the merger or other business combination of the Affiliates. The management fee also includes a fixed percentage fee for marketing and public relations services. The revenue from which this fee is determined includes medical capitation, all sums earned from participation in any risk pools and all fee-for-service revenue earned. Except in the case of Nuestra and AMVI/Prospect, the Management Agreements have initial terms of 30 years, renewable for successive 10-year periods thereafter, unless terminated by either party for cause. In the case of Nuestra, its Management Agreement has an initial 10 year term renewable for successive 1 year terms. In the case of AMVI/Prospect, its Management Agreement has a 1 year term with successive 1 year renewal terms. In return for payment of the management fee, Prospect has agreed to provide financial management, information systems, marketing, advertising, public relations, risk management, and administrative support, including for utilization review and quality of care. The Company has exclusive decision-making authority with respect to the establishment and preparation of operating and capital budgets, and the establishment of policies and procedures for the Affiliates, and makes recommendations for the development of guidelines for selection and hiring of health care professionals, compensation payable to such personnel, scope of services to be provided, patient acceptance policies, pricing of services, and contract negotiation and execution. At its cost, Prospect has assumed the obligations for all facilities, medical and non-medical supplies, and employment of non-physician personnel of its affiliated medical clinics.
The management fee earned by Prospect fluctuates based on the profitability of each wholly-owned Affiliate. Prospect is allocated a 50% residual interest in all profits after the first 8% of the profits or a 50% residual interest in the losses of the Affiliate, after deduction for costs to the management company and physician compensation. The remaining balance is retained by the Affiliates. Supplemental management fees are periodically negotiated where significant incremental efforts and expense have been incurred by Prospect on behalf of the Affiliates.
F-12
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
1. Business (Continued)
The Management Agreements are not terminable by the Affiliates except in the case of gross negligence, fraud or other illegal acts of Prospect, or bankruptcy of the Company. Through the Management Agreements and the Company's relationship with the nominee shareholder of each Affiliate, Prospect has exclusive authority over all decision-making related to the ongoing major or central operations of the physician practices. The Company, however, does not engage in the practice of medicine.
Further, Prospect's rights under the Management Agreements are unilaterally salable or transferable. Based on the provisions of the Management Agreements and the assignable option agreement with PMG, Prospect has determined that it has a controlling financial interest in the Affiliates. Consequently, under applicable accounting principles, Prospect consolidates the revenues and expenses of all the Affiliates except AMVI/Prospect from the respective dates of execution of the Management Agreements. All significant inter-entity balances have been eliminated in consolidation. In the case of AMVI/Prospect, only that portion of the results which are contractually identified as Prospect's are recognized in the financial statements, together with the management fee that the Company charges AMVI for managing AMVI's share of the joint venture operations.
As of September 30, the Prospect Medical Group Management segment manages services to the following number of enrollees under contracts with various health plans:
| |
As of September 30 | ||||||
|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||
Commercial |
135,700 | 144,700 | |||||
Medicare |
21,800 | 21,900 | |||||
Medi-Cal |
19,900 | 27,400 | |||||
Totals |
177,400 | 194,000 | |||||
2. Significant Accounting Policies
Basis of Presentation
The Company consolidates all controlled subsidiaries, which control is effectuated through ownership of voting common stock or by other means. The subsidiaries which have been consolidated under Emerging Issues Task Force No. 97-2, "Application of FASB Statement No. 94 and APB Opinion No. 16 to Physician Practice Management Entities and Certain Other Entities with Contractual Management Agreements" (EITF 97-2), would also be consolidated under the provisions of Interpretation No. 46, "Consolidation of Variable Interest Entities, an interpretation of ARB No. 51" (ASC 810-10). The underlying entities (subsidiaries) have been determined to be variable interest entities due to the existence of a call option under which the Company has the ability to require the holders of all of the voting common stock of the underlying subsidiaries to sell their shares at a fixed nominal price ($1,000) to another designated physician chosen by the Company. This call option agreement represents rights provided through a variable interest other than the equity interest itself that caps the returns that could be earned by the equity holders. In addition, the Company has a management agreement with the subsidiaries and the holders of the voting common stock of the subsidiaries which allows the Company to direct all of the activities of the subsidiaries, retain all of the economic benefits and assume all of the risks associated with ownership of the subsidiaries. In this manner, the Company has
F-13
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
all of the economic benefits and risks associated with the subsidiaries, but has disproportionately few voting rights (based on the terms of the equity). Substantially all of the activities of the subsidiaries are conducted on behalf of the Company and, as such, the subsidiaries are variable interest entities due to the fact that they violate the anti-abuse clause provisions in ASC 810-10. As the Company retains all of the economic benefits and assumes all of the risks associated with ownership of the subsidiaries, the Company is considered to be the primary beneficiary of the activities of the subsidiaries. As a result, the Company must consolidate the underlying subsidiaries under ASC 810-10. All significant intercompany transactions have been eliminated in consolidation.
Discontinued Operations
As discussed in Note 4, effective August 1, 2008, the Company sold all of the issued and outstanding stock of Sierra Medical Management, Sierra Primary Care Medical Group, Antelope Valley Medical Associates, Inc. and Pegasus Medical Group, Inc., (collectively, the "AV Entities") to a third party. As required by the ASC 205-20, the assets and liabilities of the AV Entities and their operations have been presented in the consolidated financial statements as discontinued operations for all periods presented. All prior year amounts have been reclassified in accordance with the provision of ASC 205-20. Unless otherwise noted, all references to operating results reflect the ongoing operations of the Company, excluding the AV Entities.
Revenues and Cost Recognition
Revenues by reportable segment are comprised of the following amounts (in thousands):
| |
Year ended September 30, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
Hospital services |
||||||||
Inpatient |
$ | 186,253 | $ | 118,218 | ||||
Outpatient |
17,560 | 6,668 | ||||||
Other |
1,691 | 1,806 | ||||||
Total revenues: Hospital services |
$ | 205,504 | $ | 126,692 | ||||
Medical Group management |
||||||||
Capitation |
$ | 194,126 | $ | 200,717 | ||||
Management fees |
556 | 553 | ||||||
Other |
2,048 | 1,574 | ||||||
Total revenues: Medical Group management |
$ | 196,730 | $ | 202,844 | ||||
Total revenues |
$ | 402,234 | $ | 329,536 | ||||
The Company presents segment information externally the same way management uses financial data internally to make operating decisions and assess performance. The Company's operations are organized into three reporting segments: (i) Hospital services, (ii) Medical Group management, and (iii) Corporate (see Note 15).
F-14
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
Hospital Services Segment
Net Patient Service Revenues
Operating revenue of the Hospital Services segment consists primarily of net patient service revenue. The Company reports net patient service revenue at the estimated net realizable amounts from patients and third-party payers and others in the period in which services are rendered. The Company has agreements with third-party payers, including Medicare, Medi-Cal, managed care and other insurance programs that provide for payments at amounts different from the Company's established rates. These payment arrangements include prospectively determined rates per discharge, reimbursed costs, discounted charges and per diem payments, as further described below. Estimates of contractual allowances are based upon the payment terms specified in the related contractual agreements. The Company accrues for amounts that it believes may ultimately be due to or from the third party payers. Normal estimation differences between final settlements and amounts accrued in previous years are reported as changes in estimates in the current year. Outstanding receivables, net of allowances for contractual discounts and bad debts, are included in patient accounts receivable in the accompanying balance sheets. A summary of the payment arrangements with major third-party payers follows:
Medicare: Inpatient services rendered to Medicare program beneficiaries are paid at prospectively determined rates per discharge, according to a patient classification system based on clinical, diagnostic, and other factors. Outpatient services are paid based on a blend of prospectively determined rates and cost-reimbursed methodologies. The Company is also reimbursed for various disproportionate share and Medicare bad debt components at tentative rates, with final settlement determined after submission of annual Medicare cost reports and audits thereof by the Medicare fiscal intermediary. Normal estimation differences between final settlements and amounts accrued in previous years are reflected in net patient service revenue in the year of final settlement, which amounts totaled approximately $1,087,000 and $214,000 in fiscal 2009 and 2008 respectively. Cost report settlements are recorded as third-party settlements receivable or payable in the accompanying balance sheets.
Medi-Cal: Inpatient services rendered to Medi-Cal program beneficiaries are paid at contracted per diem rates. The per diem rates are not subject to retrospective adjustment. Outpatient services are paid based on prospectively determined rates per procedure provided. The Alta hospitals are eligible to participate in the State of California Medi-Cal Disproportionate Share ("DSH") programs, under which medical facilities that serve a disproportionate number of low-income patients receive additional reimbursements. Eligibility is determined annually based on prescribed guidelines. The Company accrues a receivable each month based on the expected total annual DSH payments. Differences between the estimated and the actual award (which have not been significant) are recorded in the period known. The Medi-Cal DSH receivable as of September 30, 2009 and 2008 totaled approximately $4,852,000 and $4,365,000, respectively, and were included in government program receivables in the accompanying consolidated balance sheets. For fiscal 2009 and 2008, total Medi-Cal DSH payments received by Alta hospitals were approximately $11,968,000 and $11,276,000, respectively, and total Medi-Cal DSH revenues recorded were approximately $12,245,000 and $11,368,000 respectively.
Managed Care: The Company has also entered into payment agreements with certain commercial insurance carriers, HMOs, and PPOs. The basis for payment under these agreements
F-15
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
includes prospectively determined rates per discharge, per diems and discounts from established charges. Certain agreements also include stop-loss provisions where the Company receives additional reimbursement when charges incurred exceed a predetermined amount. Where the Company provides medical care on a non-contracted basis, it receives standard billed charges or rates negotiated on a case by case basis.
In addition to the aforementioned receivable, Brotman collected $2,000,000 in supplemental payments from the California Medical Assistance Commission ("CMAC") Distressed Hospital Fund in the fourth quarter of fiscal 2009. Of this amount, approximately $1,700,000 was accrued for at the acquisition date of Brotman. The contract between CMAC and Brotman was entered into on September 1, 2005 ("Agreement"). That Agreement has an "evergreen" provision that requires at least 120 days notice for either side to provide the other with termination notice. On June 10, 2009, Brotman entered into an Amendment of this Agreement which extends the earliest termination notice date to July 1, 2010 and, as such, the earliest possible termination to November 1, 2010.
Due to governmental payers and third party settlements
As part of the acquisition of Brotman, the Company recorded a liability to the Centers for Medicare and Medicaid Services ("CMS") arising out of payments for services provided by Brotman to Medicare eligible inpatients for the last four months of calendar 2005, all of calendar 2006, and approximately six weeks of calendar 2007 (ending February 15, 2007).
While Brotman reports financial statements on a fiscal year ending September 30, Medicare cost reports are filed on a calendar year basis. Acute care hospitals receive Medicare reimbursement payments pursuant to a prospective payment methodology based on diagnosis of the patient, but are entitled to receive additional payments, referred to as "outliers" for patients whose treatment is unusually costly. When Brotman acquired the hospital in 2005, CMS provided a ratio of cost to charges (the "RCC") based on the average prevailing market rate in Southern California. This RCC was an interim estimate provided by CMS, subject to final determination upon filing of the hospital's cost reports. Upon filing cost reports, subsequent information called into question whether the interim RCC provided by CMS was supportable, giving rise to a potential claim for return of overpayments. Brotman filed its cost reports with CMS for 2005, 2006 and 2007, respectively, which have been tentatively reviewed by the fiscal intermediary exclusive of any outlier reconciliation to be conducted directly by CMS. CMS has not conducted any outlier reconciliations, has not notified the hospital of any pending reconciliation to be conducted and has not determined the amount of any liability related to possible overpayments. As of September 30, 2009, an estimated liability of $13,834,000 was included in the accompanying consolidated balance sheet related to this matter.
Brotman and Alta have accrued estimated settlement net receivables in the amount of $1,575,000 for filed cost reporting years and estimates for the 12 months ended September 30, 2009. At September 30, 2008, estimated net receivables for cost reports were approximately $216,000.
Charity Care
The Company provides charity care to patients whose income level is below 300% of the Federal Poverty Level. Patients with income levels between 300% and 350% of the Federal Poverty Level qualify to pay a discounted rate under AB774 based on various government program reimbursement
F-16
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
levels. Patients without insurance are offered assistance in applying for Medicaid and other programs they may be eligible for, such as state disability. Patient advocates from the Company's Medical Eligibility Program ("MEP") screen patients in the Hospital and determine potential linkage to financial assistance programs. They also expedite the process of applying for these government programs. Based on the Company's gross charge rates, revenues foregone under the charity policy, including indigent care accounts, were approximately $4.6 million and $1.2 million, for fiscal 2009 and 2008, respectively.
The Company is not aware of any material claims, disputes, or unsettled matters with any payers that would affect revenues that have not been adequately provided for and disclosed in the accompanying financial statements.
Provisions for Contractual Allowances and Doubtful Accounts
Collection of receivables from third-party payers and patients is the Company's primary source of cash and is critical to their operating performance. The Company closely monitors its historical collection rates, as well as changes in applicable laws, rules and regulations and contract terms, to assure that provisions for contractual allowances are made using the most accurate information available. However, due to the complexities involved in these estimations, actual payments from payers may be materially different from the amounts management estimates and records. The Company's primary collection risks relate to uninsured patients and the portion of the bill which is the patient's responsibility, primarily co-payments and deductibles. Payments for services may also be denied due to issues over patient eligibility for medical coverage, the Company's ability to demonstrate medical necessity for services rendered and payer authorization of hospitalization. The Company estimates the provisions for doubtful accounts based on general factors such as payer mix, the age of the receivables and historical collection experience. Management routinely reviews accounts receivable balances in conjunction with these factors and other economic conditions which might ultimately affect the collectibility of the patient accounts, and makes adjustments to the Company's allowances as warranted.
All of our facilities are subject to the Emergency Medical Treatment and Active Labor Act ("EMTALA"). This federal law requires any hospital that participates in the Medicare program to conduct an appropriate medical screening examination of every person who presents to the hospital's emergency department for treatment and, if the patient is suffering from an emergency medical condition, to either stabilize that condition or make an appropriate transfer of the patient to a facility that can handle the condition. The obligation to screen and stabilize emergency medical conditions exists regardless of a patient's ability to pay for treatment. There are severe penalties under EMTALA if a hospital fails to screen or appropriately stabilize or transfer a patient or if the hospital delays appropriate treatment in order to first inquire about the patient's ability to pay. Penalties for violations of EMTALA include civil monetary penalties and exclusion from participation in the Medicare program. In addition, an injured patient, the patient's family or a medical facility that suffers a financial loss as a direct result of another hospital's violation of the law can bring a civil suit against that other hospital. The Company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing that would have a material effect on the Company's financial statements.
See "Concentrations of Credit Risks" below for discussion of revenues received from the Medicare and Medi-Cal programs.
F-17
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
Medical Group Management Segment
Medical Group Revenues
Operating revenue of the Medical Group Management Segment consists primarily of payments for medical services provided by the Affiliates under capitated contracts with various managed care providers including HMOs. Capitation revenue under HMO contracts is prepaid monthly to the Affiliates based on the number of enrollees electing any one of the Affiliates as their health care provider. See "Concentrations of Credit Risks" below for revenues received from the five largest contracted HMOs.
Capitation revenue (net of capitation withheld to fund risk share deficits discussed below) is recognized in the month in which the Affiliates are obligated to provide services. Minor ongoing adjustments to prior months' capitation, primarily arising from contracted HMOs' finalizing of monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to the Company. Additionally, Medicare pays capitation using a "Risk Adjustment model," which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with healthier enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods (generally in our fourth quarter) after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since the Company cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized in the year to which they relate, generally in the fourth quarter, when those changes are communicated by the health plans to the Company. The Company received and recorded as an addition to revenue, approximately $4.3 million and $1.6 million in positive capitation risk adjustments in the fourth quarter of fiscal 2009 and 2008.
HMO contracts also include provisions to share in the risk for hospitalization, whereby the Affiliate can earn additional incentive revenue or incur penalties based upon the utilization of hospital services. Typically, any shared risk deficits are not payable until and unless the Company generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are only recorded when such amounts are known. Risk pools for the prior contract years are generally final settled in the third or fourth quarter of the following fiscal year. In fiscal 2009 and 2008, medical group revenues include approximately $1,228,000 and $472,000, respectively, of additional (reduction in) revenues due to favorable (unfavorable) settlements on prior year risk-sharing arrangements. At September 30, 2009 and 2008, contingent liabilities for carry-forward risk-pool deficits expected to be forgiven, or offset against future surpluses were approximately $6.2 million and $2.6 million, respectively, based on the available information from the health plans.
F-18
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
In addition to risk-sharing revenues, the Company also receives incentives under "pay-for-performance" programs for quality medical care based on various criteria. These incentives, which are included in other revenues, are generally recorded in the third and fourth quarters of the fiscal year and are recorded when such amounts are known.
Management fee revenue is earned in the month the services are rendered. Management fee arrangements provide for compensation ranging from 6% of revenues to 15% of revenues. The Company provides management services to affiliated providers whose results are consolidated in the Company's financial statements under management fee arrangements, which are generally based on a percentage of revenues and a percentage of net income or loss. Revenues and expenses relating to these inter-entity agreements have been eliminated in consolidation.
In connection with providing services to HMO enrollees, the Affiliates are responsible for the medical services their affiliated physicians provide to assigned HMO enrollees.
Medical Group Cost of Revenues
The cost of health care services consists primarily of capitation and claims payments, pharmacy costs and incentive payments to contracted providers. These costs are recognized in the period incurred, or when the services are provided. Claims costs also include an estimate of the cost of services which have been incurred but not yet reported to the Company. The estimate for accrued medical costs is based on projections of costs using historical studies of claims paid and adjusted for seasonality, utilization and cost trends. These estimates are subject to trends in loss severity and frequency. Although considerable variability is inherent in such estimates, management records its best estimate of the amount of medical claims incurred at each reporting period. Estimates are continually monitored and reviewed and, as settlements are made or estimates adjusted, differences are reflected in current operations. See Note 13 for changes in claims estimates during the years ended September 30, 2009 and 2008.
In addition to contractual reimbursements to providers, the Company also makes discretionary incentive payments to physicians, which are in large part based on the pay-for-performance and shared risk revenues and favorable senior capitation risk adjustment payments received by the Company. Since the Company records these revenues generally in the third or fourth quarter of each fiscal year when the incentives and capitation adjustments due from the health plans are known, the Company also finalizes the discretionary physician bonuses in the same period. In fiscal 2009 and 2008, the Company recorded discretionary physician incentives expense totaling approximately $3.4 million and $3.6 million, respectively.
The Company also periodically evaluates the need to establish premium deficiency reserves for the probability that anticipated future health care costs could exceed future capitation payments from HMOs under capitated contracts. To date, management has determined that no significant premium deficiency reserves have been necessary. The Company, for certain matters, maintains stop loss coverage for health care costs that are in excess of set thresholds.
Property, Improvements and Equipment
Property, improvements and equipment are stated on the basis of cost or, in the case of acquisitions, at their acquisition date fair values. Depreciation is provided using the straight-line
F-19
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
method over the estimated useful lives of the assets, and amortization of leasehold improvements is provided using the straight-line basis over the shorter of the remaining lease period or the estimated useful lives of the leasehold improvements. Leasehold improvements are generally depreciated over five to ten years, buildings are depreciated over twenty to twenty-eight years, equipment is depreciated over two to five years and furniture and fixtures are depreciated over two to seven years. Equipment capitalized under capital lease obligations are amortized over the life of the lease. At September 30, 2009 and 2008, the Company had assets under capitalized leases of approximately $6,259,000 and $2,053,000, respectively.
Depreciation expense was approximately $3,514,000 and $3,540,000 for the years ended September 30, 2009 and 2008, respectively.
Goodwill and Other Intangible Assets
Goodwill and other intangible assets totaled approximately $199,675,000 and $176,617,000 at September 30, 2009 and 2008, respectively, and arose as a result of the ProMed, Alta and Brotman business acquisitions. Other intangible assets include customer relationships, covenants not-to-compete, trade names and provider networks. Goodwill represents the excess of the consideration paid and liabilities assumed over the fair value of the assets acquired, including identifiable intangible assets. In conjunction with these acquisitions, management of the Company has reviewed the allocation of the excess of the purchase consideration (including costs incurred related to the acquisitions) over net tangible and intangible assets acquired, and has determined that the goodwill is primarily related to the operating platforms acquired through the addition of the existing renewable HMO contracts in the case of ProMed and new business segments in the case of the Alta and Brotman acquisitions. Acquisitions are discussed further in Note 3 below.
Goodwill Impairment Test
Under ASC 350, "Goodwill and Other Intangible Assets," goodwill and other intangible assets with indefinite useful lives are not amortized; rather they are reviewed annually for impairment for each reporting unit, or more frequently if impairment indicators arise. Impairment is the condition that exists when the carrying amount of goodwill exceeds its implied fair value. A two-step impairment test is used to identify potential goodwill impairment and to measure the amount of goodwill impairment loss to be recognized, if any. As further discussed in Notes 3 and 15, the Company has four operating units, consisting of Alta, Brotman, ProMed and Prospect (which includes all other affiliated physician organizations).
The Company tests for goodwill impairment in the fourth quarter of each year, or sooner if events or changes in circumstances indicate that the carrying amount may exceed the fair value. In evaluating whether indicators of impairment exist, the Company considers adverse changes in market value and/or stock price, laws and regulations, profitability, cash flows, ability to maintain enrollment and renew payer contracts at favorable terms, among other factors. The goodwill impairment test is a two-step process. The first step consists of estimating the fair value of the reporting unit based on a weighted combination of (i) the guideline company method that utilizes revenue or earnings multiples for comparable publicly-traded companies, and (ii) a discounted cash flow model that utilizes expected future cash flows, the timing of those cash flows, and a discount rate (or weighted average cost of capital, which considers the cost of equity and cost of debt financing expected by a typical market
F-20
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
participant) representing the time value of money and the inherent risk and uncertainty of the future cash flows. If the estimated fair value of the reporting unit is less than its carrying value, a second step is performed to compute the amount of the impairment by determining the "implied fair value" of the goodwill, which is compared to its corresponding carrying value (see Note 5). The impairment test at September 30, 2009 resulted in no impairment charge. At September 30, 2009, the remaining goodwill and intangibles related to the Alta, Brotman and ProMed acquisitions (see Notes 3 and 5).
Long-Lived Assets and Amortizable Intangibles
Long-lived assets, including property, improvement and equipment and amortizable intangibles, are evaluated for impairment under ASC 360-10-35, "Accounting for the Impairment or Disposal of Long-Lived Assets." The Company reviews long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying value of such assets may not be recoverable. The Company considers assets to be impaired and writes them down to fair value if estimated undiscounted cash flows associated with those assets are less than their carrying amounts. Fair value is based upon the present value of the associated cash flows. Changes in circumstances (for example, changes in laws or regulations, technological advances or changes in strategies) may also reduce the useful lives from initial estimates. Changes in planned use of intangibles may result from changes in customer base, contractual agreements, or regulatory requirements. In such circumstances, management will revise the useful life of the long-lived asset and amortize the remaining net book value over the adjusted remaining useful life.
Medical Malpractice Liability Insurance
The individual physicians who contract with the Affiliates carry their own medical malpractice insurance. In the Hospital Services segment, Alta and Brotman purchase professional and general liability insurance to cover medical malpractice claims under a claims-made policy. Under the policy, insurance premiums cover only those claims actually reported during the policy term. Should the claims-made policy not be renewed or replaced with equivalent insurance, claims related to occurrences during the policy term but reported subsequent to the policy's termination may be uninsured.
Accounting principles generally accepted in the United States of America require that a health care organization record and disclose the estimated costs of medical malpractice claims in the period of the incident of malpractice, if it is reasonably possible that liabilities may be incurred and losses can be reasonably estimated. The Company has recognized an estimated liability for incurred but not reported claims and the self-insured risks (including deductibles and potential claims in excess of policy limits) based upon an actuarial valuation of the Company's historical claims experience in Alta and Brotman. The claims liability at September 30, 2008 of $786,000 relates to Alta and was estimated using a discount factor of 4.5%. At September 30, 2009, the claims liability of $2,824,000 relating to Alta and Brotman was estimated using a discount factor of 4%.
The claim reserve is based on the best data available to the Company; however, the estimate is subject to a significant degree of inherent variability. The estimate is continually monitored and reviewed, and as the reserve is adjusted, the difference is reflected in current operations. While the ultimate amount of medical malpractice liability is dependent on future developments, management is of the opinion that the associated liabilities recognized in the accompanying consolidated financial statements are adequate to cover such claims. Management is aware of no potential medical
F-21
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
malpractice claims whose settlement, if any, would have a material adverse effect on the Company's consolidated financial position, results of operations or cash flows.
Workers' Compensation Insurance
The workers' compensation coverage provides the statutory benefits required by law and that the employer's liability limits are $1,000,000. The Alta and Prospect workers' compensation coverage for October 1, 2008 through September 30, 2009 had an aggregate loss limit of $2,019,345. The current workers' compensation policy for the period of October 1, 2009 through September 30, 2010 does not have an aggregate loss limitation. Losses within the deductible are funded via a cash loss fund and reconciled annually. Accruals for uninsured claims and claims incurred but not reported of $3,220,000 (relating to Alta and Brotman) and $724,000 (relating to Alta) at September 30, 2009 and 2008, respectively, is estimated based upon an actuarial valuation of the Company's claims experience. Accruals were estimated using a discount factor of 4.5% (2008) and 4% (2009).
The claim reserve is based on the best data available to the Company; however, the estimate is subject to a significant degree of inherent variability. The estimate is regularly monitored and reviewed, and as the reserve is adjusted, the difference is reflected in current operations. While the ultimate amount of the claims liability is dependent on future developments, management is of the opinion that the associated liabilities recognized in the accompanying consolidated financial statements are adequate to cover such claims. Management is aware of no potential claims whose settlement, if any, would have a material adverse effect on the Company's consolidated financial position, results of operations or cash flows.
Earnings per Share
The Company follows ASC 260-10, "Earnings per Share," which established standards regarding the computation of basic and diluted earnings per share ("EPS"). Basic net income per share is calculated by dividing net income attributable to common shareholders by the weighted average number of common shares outstanding. Diluted earnings per share is computed by dividing net income attributable to common shareholders by the weighted average number of common shares outstanding, after giving effect to potentially dilutive shares computed using the treasury stock method. Such shares are excluded if determined to be anti-dilutive.
F-22
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
The calculations of basic and diluted net loss per share for the fiscal years ended September 30 are as follows (in thousands, except per share amounts):
| |
Year ended September 30, | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||||
Basic and Diluted: |
|||||||||
Continuing operations |
$ | (2,420 | ) | $ | (1,961 | ) | |||
Dividends to preferred stockholders |
— | (6,760 | ) | ||||||
|
(2,420 | ) | (8,721 | ) | |||||
Discontinued operations |
— | 6,169 | |||||||
Net loss attributable to common stockholders |
$ | (2,420 | ) | $ | (2,552 | ) | |||
Weighted average number of common shares outstanding |
20,531 | 12,885 | |||||||
Basic and Diluted net loss per share attributable to common stockholders |
|||||||||
Continuing operations |
$ | (0.12 | ) | $ | (0.68 | ) | |||
Discontinued operations |
$ | — | $ | 0.48 | |||||
|
$ | (0.12 | ) | $ | (0.20 | ) | |||
The number of stock options and warrants excluded from the computation of diluted earnings per share due to being anti-dilutive were 4,333,325 and 665,973 in fiscal 2009, respectively, and were 5,087,367 and 665,973 in fiscal 2008, respectively.
Following stockholder approval on August 13, 2008, the holders of all of the outstanding shares of Series B Preferred Stock elected to convert their preferred shares into Common Stock. The former holders also ceased to have any right to receive dividends on the preferred shares, dividends ceased to accrue, and all previously accrued dividends were forgiven and the accrued dividend liability of $7,881,890 was reclassified to additional paid-in capital.
F-23
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
The following proforma basic and diluted earnings per share assume the conversion of preferred shares into common stock at a ratio of 1:5 at the issuance date:
| |
Year Ended September 30, 2008 | ||||
|---|---|---|---|---|---|
| |
(in thousands, except per share amounts) |
||||
Basic and Diluted: |
|||||
Loss from continuing operations |
$ | (1,961 | ) | ||
Income from discontinued operations |
6,169 | ||||
Net income attributable to common stockholders—proforma |
$ | 4,208 | |||
Weighted average number of common shares outstanding—historical |
12,885 | ||||
Add weighted number of preferred shares converted to common shares |
7,264 | ||||
Weighted average number of common shares outstanding—proforma |
20,149 | ||||
Basic net income (loss) per share—proforma |
|||||
Continuing operations |
$ | (0.10 | ) | ||
Discontinued operations |
$ | 0.31 | |||
|
$ | 0.21 | |||
Comprehensive Loss
Comprehensive loss includes net loss, net of taxes, and changes in the fair value of interest rate swaps subject to hedge accounting that are recorded as other comprehensive income. As of April 1, 2008, the swaps ceased to be eligible for hedge accounting under ASC 815. As a result, all further changes in fair value of the swaps were recorded in the consolidated statements of operations and the effective portion of the swaps of approximately $5.4 million, after tax, that was recorded in other comprehensive income through March 31, 2008 continued to be amortized to interest expense, using the effective interest method, over the remaining life of the swaps. The remaining unamortized portion of the interest rate swaps was expensed in July 2009 in connection with the Company's termination of such swaps.
Stock Options
The Company has stock option and restricted stock agreements with certain directors, officers and employees. Stock-based compensation is accounted for ASC 718, "Share-Based Payments," and the supplemental implementation guidance in Staff Accounting Bulletin (SAB) No. 107. ASC 718 requires compensation cost for all share-based payments in exchange for employee services to be measured at fair value. The Company generally issues shared-based awards at or above the market price of the underlying stock.
Compensation costs for option awards are measured and recognized in the financial statements based on their grant date fair value, net of estimated forfeitures over the awards' service period. The fair value of restricted stock and restricted stock unit grants are determined on the date of grant, based on the number of shares granted and the quoted price of the Company's common stock. The Company uses the Black-Scholes option pricing model and a single option award approach to estimate the fair
F-24
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
value of stock options granted. Equity-based compensation is classified within the same line items as cash compensation paid to employees. Cash retained as a result of excess tax benefits relating to share-based payments is presented in the statement of cash flows as a financing cash inflow.
The Company's equity awards vest based on continuous service and currently do not include performance or market vesting conditions. There are no liability awards that may be settled for cash.
Asset Retirement Obligations
The Company recognizes the fair value of a liability for legal obligations associated with asset retirements in the period in which it is incurred, in accordance with ASC 410-20, (previously issued as SFAS No. 143 "Accounting for Asset Retirement Obligations",) if a reasonable estimate of the fair value of the obligation can be made. When the liability is initially recorded, management capitalizes the cost of the asset retirement obligation by increasing the carrying amount of the related long-lived asset. Over time, the liability is accreted to its present value each period, and the capitalized cost associated with the retirement obligation is depreciated over the useful life of the related asset. Upon settlement of the obligation, any difference between the cost to settle the asset retirement obligation and the liability recorded is recognized as a gain or loss in the accompanying consolidated statement of operations.
Cash and Cash Equivalents
Cash equivalents are considered to be all liquid investments with initial maturities of three months or less. At times, cash balances held at financial institutions are in excess of federal depository insurance limits. The Company has not experienced any losses on cash and cash equivalents due to non-performance by financial institutions.
Restricted Cash
At September 30, 2009, restricted cash was established at Brotman pursuant to Brotman's Amended Plan of Reorganization, consisting of contingency reserves, totaling $1,163,000 held in escrow in connection with certain reserves for property taxes, maintenance and emergency room construction required under the JHA loan agreement (see Note 9). Additionally, $232,000 was held in a restricted account pursuant to workers compensation arrangements at September 30, 2009.
Restricted Investments
The Company is required to keep restricted deposits by certain HMOs for the payment of claims. Such restricted deposits are classified as a current asset in the accompanying consolidated balance sheet, as they are restricted for payment of current liabilities.
F-25
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
Deferred Financing Costs
Deferred financing costs are amortized over the period in which the related debt is outstanding using the effective interest method. Deferred financing costs at September 30, 2009 and 2008 are as follows (in thousands):
| |
2009 | 2008 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Gross book value | Accumulated amortization | Net book value | Gross book value | Accumulated amortization | Net book value | |||||||||||||
Deferred financing costs |
$ | 8,732 | $ | 527 | $ | 8,205 | $ | 743 | $ | 82 | $ | 661 | |||||||
Income Taxes
The Company accounts for income taxes under the liability method as required by ASC 740, (previously issued as SFAS No. 109 "Accounting for Income Taxes.") Under the liability method, deferred taxes are determined based on temporary differences between the financial statement and tax basis of assets and liabilities existing at each balance sheet date using enacted tax rates for years in which the related taxes are expected to be paid or recovered. The Company assesses the recoverability of its deferred tax assets and provides a valuation reserve when it is not more-likely-than-not the assets will be recovered. As of September 30, 2009 and 2008, the valuation allowance for deferred tax assets was approximately $23,623,000 and $2,154,000, respectively.
There were no unrecognized tax benefits or interest and penalties recorded on income tax matters as of the date of adoption. In accordance with ASC 740-10, the Company recognized no decrease in deferred tax assets or changes in the valuation allowance. There are no unrecognized tax benefits included in the consolidated balance sheet that would, if recognized, affect the effective tax rate.
The Company's practice is to recognize interest and/or penalties related to income tax matters in income tax expense.
Consolidated and separate income tax returns are filed with the U.S. Federal jurisdiction and in the State of California. The Company's filed tax returns are subject to examination by the IRS for tax year 2007, 2006 and 2005 and the State of California for fiscal years 2007, 2006, 2005 and 2004. Net operating losses that were incurred in prior years may still be adjusted by taxing authorities.
ASC 740-10 did not significantly impact the Company's consolidated financial condition, results of operations or cash flows. At September 30, 2009, the Company had net deferred tax liabilities of approximately $23.3 million.
The net deferred tax liabilities are primarily comprised of temporary differences between book and tax bases for intangible and capital assets acquired and loss carryforwards.
Fair Value of Financial Instruments
The financial instruments reported in the accompanying consolidated balance sheets consist primarily of cash and cash equivalents, investments, patient and other receivables, accounts payable and accrued expenses, medical claims and related liabilities, notes receivable and payable, capital lease obligations, debt, interest rate swaps, and other liabilities. The carrying amounts of current assets and
F-26
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
liabilities approximate their fair value due to the relatively short period of time between the origination of the instruments and their expected realization.
The carrying amounts of notes payable and capital lease obligations approximate their fair value based on the Company's current incremental borrowing rates for similar types of arrangements. Long term debt approximates fair value since the revolving bank loan and bank term loans are variable rate instruments and bear interest at LIBOR plus an applicable margin. Accrued self-insurance liabilities are carried at the estimated present value of such obligations using appropriate discount factors. The interest rate swaps are recorded at fair value.
Interest Rate Swaps
Under ASC 815, (previously issued as SFAS No. 133 "Accounting for Derivative Instruments and Hedging Activities,") and its amendments, the Company recognizes all derivatives on the balance sheet at fair value. Derivatives that are not hedges are adjusted to fair value through income. If the derivative is accounted for as a hedge, depending on the nature of the hedge, changes in its fair value are offset against either the change in fair value of assets, liabilities, or firm commitments through earnings. The Company's derivative instruments comprised two interest rate swap agreements which were entered into on May 16, 2007 in conjunction with the ProMed Acquisition and on September 5, 2007 in conjunction with the Alta Acquisition.
The interest rate swap instruments were designated as cash flow hedges of expected interest payments on the term loans with the hedge effective date of the May 2007 instrument being December 31, 2007 and the hedge effective date of the September 2007 instrument being September 6, 2007. Prior to the hedge effective dates, all mark-to-market adjustments in the value of the swaps were charged to expense. After the hedge effective date, the effective portions of the fair value gains or losses on these cash flow hedges were initially recorded as a component of other comprehensive income, net of taxes, and subsequently reclassified into earnings when the forecasted transaction affected earnings. Effective April 1, 2008, the Company elected to discontinue hedge accounting, and changes in the fair value of the interest rate swaps after March 31, 2008 were recorded as other income or expense. Total net gain (loss) on the interest rate swaps included in earnings for fiscal 2009 and 2008 were approximately $(5.3) million and $3.1 million, respectively. The effective portion of the swaps of approximately $5.4 million, after tax, that was recorded in other comprehensive income through March 31, 2008 and was being amortized as interest expense over the remaining life of the swap instruments.
As discussed in Note 9, concurrent with the offering of the $160 million senior secured notes, effective July 23, 2009, the interest rate swap arrangements were terminated, and the unamortized portion of the swaps, amounting to approximately $4.3 million, was expensed.
Concentrations of Credit Risk
Financial instruments which potentially subject the Company to concentrations of credit risk consist of cash held in financial institutions which exceeds the $250,000 insurance limit of the Federal Deposit Insurance Corporation, receivables due from Medicare, Medi-Cal, patients, health plans and under shared-risk arrangements, and notes receivable.
F-27
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
The Company invests excess cash in liquid securities at institutions with strong credit ratings, following established guidelines relative to diversification and maturities to maintain safety and liquidity. These guidelines are periodically reviewed and modified to take into consideration of trends in yields and interest rates and principal risk. Management attempts to schedule the maturities of the Company's investments to coincide with the Company's expected cash requirements. Credit risk with respect to receivables is limited since amounts are generally due from large HMOs within the Medical Group Management segment and from the Medicare and Medi-Cal programs within the Hospital Services segment. Notes receivable are fully secured by collateral of equal or greater value. Management reviews the financial condition of these institutions on a periodic basis and does not believe the concentration of cash or receivables results in a high level of risk.
The Company was subject to interest rate fluctuation under its floating rate revolving credit facilities and, prior to their termination effective July 23, 2009, interest rate swap agreements.
For the fiscal years ended September 30, 2009 and 2008, the Hospital Services segment received a total of 83% and 94% of their net patient revenues from Medicare and MediCal programs, and the Medical Group Management segment received a total of 77% and 79% of their capitation revenues from it's five largest HMOs, as follows (in thousands):
| |
Revenue Year Ended September 30, 2009 |
% of Total Revenue |
Revenue Year Ended September 30, 2008 |
% of Total Revenue |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Hospital Services |
|||||||||||||
Medicare |
$ | 96,693 | 47 | % | $ | 66,740 | 53 | % | |||||
MediCal |
74,865 | 36 | % | 51,407 | 41 | % | |||||||
Totals |
$ | 171,558 | 83 | % | $ | 118,147 | 94 | % | |||||
Medical Group Management |
|||||||||||||
PacifiCare |
$ | 37,216 | 19 | % | $ | 44,600 | 22 | % | |||||
Health Net |
27,073 | 14 | % | 27,964 | 14 | % | |||||||
Blue Cross |
28,688 | 15 | % | 29,714 | 15 | % | |||||||
Blue Shield |
23,579 | 12 | % | 22,953 | 11 | % | |||||||
Inter Valley Health Plan |
33,556 | 17 | % | 33,733 | 17 | % | |||||||
Totals |
$ | 150,112 | 77 | % | $ | 158,964 | 79 | % | |||||
Approximately 80% of Brotman's employees were covered under collective bargaining agreements as of September 30, 2009. The collective bargaining agreements with the California Nurses Association ("CNA") and Service Employees International Union ("SEIU") will both expire on February 28, 2010.
F-28
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
Use of Estimates
The preparation of financial statements in conformity with U.S. Generally Accepted Accounting Principles requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenues and expenses, and the disclosure of contingent assets and liabilities at the dates, and for the periods, that the financial statements are prepared. Actual results could materially differ from those estimates. Principal areas requiring the use of estimates include third-party cost report settlements, and receivables from, patient and medical related receivables, determination of allowances for contractual discounts and uncollectible accounts, medical claims and accruals, impairment of goodwill, long-lived and intangible assets, valuation of interest rate swaps, share-based payments, professional and general liability claims, reserves for the outcome of litigation, valuation allowances for deferred tax assets and receivables.
Recently-Issued Accounting Pronouncements
In December 2007, the FASB issued ("ASC 810"), (previously known as SFAS No. 160, "Noncontrolling Interests in Consolidated Financial Statements—an Amendment of ARB No. 51"). This literature establishes accounting and reporting standards for the noncontrolling interest in a subsidiary and for the deconsolidation of a subsidiary. It clarifies that a noncontrolling minority interest in a subsidiary is an ownership interest in the consolidated entity that should be reported as equity in the accompanying consolidated financial statements separate from the parent company's equity. Net income (loss) attributable to the noncontrolling interest will be included in consolidated net income on the face of the income statement. This standard is effective for fiscal years, and interim periods within those fiscal years, beginning on or after December 15, 2008. It requires retroactive adoption of the presentation and expanded disclosure requirements for existing minority interests. All other requirements of the standard shall be applied prospectively. The Company will adopt this standard on October 1, 2009 and is currently evaluating the potential impact of such adoption on its consolidated financial statements.
In May 2009, the FASB issued ("ASC 855"), (previously known as SFAS No. 165, "Subsequent Events") which establishes general standards of accounting and disclosure for events that occur after the balance sheet date but before financial statements are issued. This standard was effective for reporting periods ending after June 15, 2009. The adoption of this standard does not impact the Company's financial position or results of operations, as its requirements are disclosure-only in nature. The consolidated financial statements were available to be issued on December 18, 2009 and the Company evaluated subsequent events known to management through such date (see Note 18).
In June 2009, the FASB issued SFAS No. 168, "The FASB Accounting Standards Codification and the Hierarchy of Generally Accepted Accounting Principles—a replacement of FASB Statement No. 162". This standard is now included in ASC Topic 105 and established only two levels of GAAP, authoritative and non-authoritative. The FASB Accounting Standards Codification (the "Codification") became the source of authoritative, non-governmental GAAP, except for rules and interpretive releases of the SEC, which are sources of authoritative GAAP for SEC registrants. All other non-grandfathered, non-SEC accounting literature not included in the Codification became non-authoritative. This standard is effective for financial statements for interim or annual reporting periods ending after September 15, 2009. Effective August 1, 2009, the Company has adopted the new guidelines and numbering system
F-29
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
2. Significant Accounting Policies (Continued)
prescribed by the Codification when referring to GAAP. The adoption had no impact on the Company's financial condition, results of operations or cash flows.
In August 2009, the FASB issued Accounting Standards Update ("ASU") No. 2009-05, "Measuring Liabilities at Fair Value," which amends the guidance in ASC 820, Fair Value Measurements and Disclosures, to provide guidance on fair value measurement of liabilities. If a quoted price in an active market is not available for an identical liability, ASU 2009-05 requires companies to compute fair value by using quoted prices for an identical liability when traded as an asset, quoted prices for similar liabilities when traded as an asset or another valuation technique that is consistent with the guidance in ASC 820. ASU 2009-05 will be effective for interim and annual periods beginning after its issuance and is not expected to have a material impact on the Company's financial position or results of operations.
Reclassifications
Certain prior year amounts have been reclassified to conform to the current year presentation with no impact on the statement of operations.
3. Acquisitions
ProMed Health Services Company
On June 1, 2007, the Company and Prospect Medical Group, Inc. ("PMG"), one of its affiliated physician organizations, acquired ProMed Health Services Company and its subsidiary, ProMed Health Care Administrators ("PHCA") (collectively "ProMed Health Care Administrators"), and two affiliated Medical Groups: Pomona Valley Medical Group, Inc. dba ProMed Health Network ("Pomona Valley Medical Group"), and Upland Medical Group, a Professional Medical Corporation ("Upland Medical Group" and together with Pomona Valley Medical Group, the "ProMed Entities"). PHCA manages the medical care of HMO enrollees served by Pomona Valley Medical Group and Upland Medical Group. Total purchase consideration of $48,000,000 included $41,040,000 of cash and 1,543,237 shares of Prospect Medical Holdings, Inc. common stock valued at $6,960,000, or $4.51 per share. The transaction is referred to as the "ProMed Acquisition."
The ProMed Acquisition, and $392,000 in related transaction costs, was financed by $48 million in borrowings (less $896,000 in debt issuance costs) and $2,379,000 from cash reserves. The debt proceeds and cash reserves were used to fund the cash consideration of $41,040,000 and to repay all existing debt of Prospect Medical Holdings, Inc. ($7,842,000 plus $209,000 of prepayment penalties). The $48 million in borrowings used to finance the acquisition of the ProMed Entities was refinanced in August 2007, using proceeds from the $155 million credit facility entered into in connection with the Alta transaction, described below. The purchase agreements provide for certain post-closing working capital, medical claims reserve and other adjustments, which the Company is currently negotiating.
Alta Hospitals System, LLC
On August 8, 2007, the Company acquired all of the outstanding common shares of Alta Hospitals System, LLC ("Alta"), which was formerly known as Alta Healthcare System, Inc. Alta is a for-profit hospital management company that, through two subsidiary corporations, owns and operates four community-based hospitals—Van Nuys Community Hospital, Hollywood Community Hospital, Los Angeles Community Hospital and Norwalk Community Hospital. These hospitals provide a
F-30
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
3. Acquisitions (Continued)
comprehensive range of medical, surgical and psychiatric services and have a combined 339 licensed beds served by 315 on-staff physicians. Total purchase consideration, including transaction costs, was approximately $154,935,000, comprised of repayment of approximately $41,500,000 of Alta's existing debt, payment of approximately $51,300,000 in cash to the former Alta shareholders, issuance of 1,887,136 shares of Prospect common stock, issuance of 1,672,880 shares of Prospect convertible preferred stock valued, for purposes of the transaction, at $61,030,000, and payment of transaction costs of approximately $1.2 million. Each share of preferred stock was convertible into five common shares upon stockholder approval (which occurred on August 13, 2008). Prior to conversion, each share of preferred stock accrued dividends at 18% per year, compounding annually. Such dividends (amounting to $7,881,890) were canceled upon conversion to common shares on August 13, 2008, and the related liability reclassified to additional paid-in-capital. For purposes of determining the number of shares to be issued in connection with the transaction, Prospect common stock was valued at $5.00 per share and Prospect preferred stock was valued at $25.00 per share. However, for purposes of recording the transaction, (i) the value per share of common stock was estimated at $5.58, based on the average of the stock's closing prices before and after the acquisition announcement date of July 25, 2007, and (ii) the value per share of preferred stock was estimated at $30.19, based on the closing stock price of a common share on the acquisition date, plus a premium for the preference features of the stock. As such, total recorded purchase consideration, exclusive of transaction costs, was approximately $153,772,000.
The Alta Acquisition, the extinguishment of Alta's existing debt and the refinancing of the ProMed Acquisition debt described above were financed by a $155,000,000 senior secured credit facility, comprised of $145 million in term loans and a $10,000,000 revolver, of which $3,000,000 was drawn at closing (see Note 9 for discussion of debt). Net proceeds of $141.1 million (net of issuance discount and financing costs of $6.9 million) were used to repay Alta's existing borrowings of $41.5 million, refinance $47.0 million in outstanding ProMed Acquisition debt, pay the cash portion of the Alta purchase price of $51.3 million and fund approximately $1.2 million in transaction costs. As set forth in Note 9, all amounts owing under the senior secured facility were repaid on July 29, 2009.
Brotman Medical Center, Inc.
On August 31, 2005, the Company invested $1 million for an approximately 33.1% stake in Brotman, a 420-bed licensed and accredited acute care hospital, located in Culver City, California. The Company made the investment with the intention that it, with Brotman, would be able to offer joint contracting to HMOs operating in Brotman's service area. Brotman incurred significant losses before and after the Company's initial investment and, on October 25, 2007 (the "Petition Date"), Brotman filed for bankruptcy protection under Chapter 11 of the U.S. Bankruptcy Code. On the Petition Date, the Company entered into an amendment to its existing consulting services agreement with Brotman, providing for an increased level of service (see Note 7). Additionally, effective April 22, 2008, Samuel S. Lee (Prospect's CEO and Chairman of the Board) was appointed as the Chairman of the Board of Directors of Brotman. On April 14, 2009 (The "Effective Date"), the U.S. Bankruptcy Court confirmed and declared effective the final Chapter 11 Plan of Reorganization (the "Plan") of Brotman whereby, among other things, all of Brotman's outstanding securities were canceled and, in exchange for their pro rata share of the New Value Contribution (as defined in the Plan) totaling $3,500,000, holders of Brotman's securities would receive New Common Stock in Brotman in the same percentage as their pro rata share of the New Value Contribution. Pursuant to the terms of the Plan, the Company made a
F-31
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
3. Acquisitions (Continued)
$1,814,000 investment in Brotman on January 13, 2009 and $705,000 on June 30, 2009, totaling $2,519,000 (net of $37,000 acquisition costs) while the minority shareholders made a total cash investment of $981,000. Based on such contributions, Prospect acquired an additional 38.86% ownership interest in Brotman, effective April 14, 2009, which brought its total ownership interest to 71.96%.
For financial accounting purposes, the additional investment in Brotman was referred to as the "Brotman Acquisition" and in accordance with SFAS No. 141, "Business Combinations", the business combination, which was achieved in stages, provides for recognition of assets at current fair value with respect to the proportion of the Company's incremental ownership interest in Brotman. Under SFAS No. 141, the aggregate cost of the acquired assets, which includes cash paid of $2.5 million and expenses incurred in connection with the acquisition totaling $37,000, were preliminarily allocated to the assets acquired and liabilities assumed. SFAS No. 141 is pre-Codification literature, the provisions of ASC 805 is not effective for the Company until October 1, 2009. The excess of the consideration over the estimated fair value of the assets and liabilities assumed has been allocated to goodwill. Due to negative net book value of assets acquired, goodwill attributable to the minority interest is not recognized. As the non-controlling interest in Brotman exceeds 20%, the accounting basis in the acquired ownership in Brotman have not been pushed-down to the financial statements of Brotman and have been reflected in the Parent Company financial statements. The results of operations of Brotman have been included in the consolidated financial statements since the April 14, 2009 acquisition date. Brotman's operations for the period from April 14, 2009 to September 30, 2009 reflected a net loss of $2,711,000. The Company does not have the intent or ability, including under the terms of its debt agreement, to provide significant financial support to Brotman. A pro rata (approximately 28%) share of net income attributable to Brotman will be included under Minority Interest in the Company's consolidated statement of operations, once the cumulative minority share of such income exceeds their cumulative share of prior losses absorbed by the Company, as its majority interest holder; this would be through the implementation of new relevant accounting literature (see Note 2).
The following is an analysis of the preliminary allocation of asset acquired and liabilities assumed and the preliminary goodwill amount recognized in connection with the Brotman Acquisition, as of April 14, 2009 (in thousands):
Assets acquired |
$ | 53,302 | ||
Liabilities assumed |
(78,119 | ) | ||
Net liabilities assumed |
(24,817 | ) | ||
Total purchase consideration |
(2,556 | ) | ||
Purchase consideration in excess of net liabilities assumed |
(27,373 | ) | ||
Identifiable intangible—trade name |
3,000 | |||
Estimated goodwill |
$ | 24,373 | ||
The assets acquired includes the relative percentage (38.83%) of the step up in basis of the assets acquired to estimated fair value amounting to $10,518,000.
Goodwill from the Brotman Acquisition is primarily related to new capacity for future growth, new geographic coverage, additional types of hospital services and in-place workforce. Through the Brotman Acquisition, the Company expanded into a new service market in the West Los Angeles, California
F-32
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
3. Acquisitions (Continued)
area. As a stock purchase, the goodwill acquired in the Brotman Acquisition is not deductible for income tax purposes. Brotman recorded income related to discharge of debt upon emergence from the Chapter 11 Bankruptcy reorganization (see Note 1). Under Internal Revenue Code 108 ("IRC 108"), an insolvent taxpayer can exclude from its taxable income computation, the income related to discharge of debt to the extent of the insolvency amount. Brotman's tax provision reflects that the entire amount of debt discharge income is qualified for the exclusion under IRC 108. Also, under current tax law, a taxpayer is required to reduce its tax attributes to the extent of the excluded debt discharge income, and this attribute reduction occurs on the first day of the tax year after the debt discharge occurs. In addition, a taxpayer is allowed an election to use alternative tax reduction ordering rules. As of September 30, 2009, management has not completed its analysis and has not concluded on the attribute reduction ordering. The finalization of these tax matters and others (Note 8) may adjust the deferred tax assets or liabilities for which the tax impact will be recognized through purchase accounting.
The following unaudited pro forma financial information for the years ended September 30, 2009 and 2008 gives effect to the acquisition of Brotman as if it had occurred on October 1, 2007. Such unaudited pro forma information is based on historical financial information with respect to the acquisition and does not include synergies or operational or other changes that might have been effected by the Company. Significant proforma adjustments include increased depreciation related to fixed assets acquired.
| |
Year Ended September 30 | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | ||||||
| |
(in thousands, except per share amounts) |
|||||||
Net revenue |
$ | 463,342 | $ | 446,762 | ||||
Net loss attributable to common stockholders |
$ | (5,513 | ) | $ | (1,582 | ) | ||
Net loss per share: |
||||||||
Basic |
$ | (0.27 | ) | $ | (0.12 | ) | ||
Diluted |
$ | (0.27 | ) | $ | (0.12 | ) | ||
Since emergence from bankruptcy, Brotman has continued to incur losses and experience liquidity issues. Additionally, $16 million of the indebtedness due to the Los Angeles Jewish Home for Aging (Note 9) may have to be repaid as early as October 2010. Management is currently implementing operational improvements aimed at returning Brotman to profitability and is evaluating the refinancing of this debt. Prospect has limited ability to fund Brotman's post acquisition operations (Note 9).
Management is currently assessing the Company's ability to utilize the state deferred tax assets, mainly comprised of California net operating loss carryforwards, acquired through the Brotman acquisition. This assessment has however not been completed yet.
4. Divestitures
On August 1, 2008, the Company completed the sale of all of the outstanding stock of Sierra Medical Management, Inc., Sierra Primary Care Medical Group, Antelope Valley Medical Associates, Inc. and Pegasus Medical Group, Inc. (collectively the "AV Entities") pursuant to a Stock
F-33
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
4. Divestitures (Continued)
Purchase Agreement ("SPA"). As part of the sale, the Company also entered into a non-competition agreement in the Antelope Valley region of Los Angeles County.
Total consideration paid by the buyer was $8,000,000, of which $2,000,000 was paid into an escrow account to fund certain AV Entities' liabilities and approximately $815,000 was paid directly to AV Entities' vendors, employees and physicians. Of the remaining amount totaling approximately $5,185,000, $4,219,000 was paid directly to the Company's lenders as required under the modified debt facilities, and approximately $966,000 was paid to the Company.
The Company recorded a gain of approximately $6.6 million in connection with this transaction. The SPA contains certain post-acquisition purchase price adjustment provisions for working capital and claims liabilities which require a final determination of the gain by August 10, 2010. Once the purchase price has been finalized and the net gain on the transaction determined, any adjustment to the gain will be recorded in discontinued operations when known.
The AV Entities have been classified as discontinued operations for all periods presented. As discontinued operations, revenues and expenses of the AV Entities have been aggregated and stated separately from the respective captions of continuing operations in the Consolidated Statements of Operations. Expenses include direct costs of the business that will be eliminated from future operations as a result of the sale. The Company also allocated interest expense associated with the portion of debt required to be repaid for the fiscal years ended September 30, 2008 and 2007 to discontinued operations.
The results of operations of the AV Entities reported as discontinued operations are summarized as follows (in thousands):
| |
Year Ended September 30, 2008 |
||||
|---|---|---|---|---|---|
Medical group revenues |
$ | 14,696 | |||
Operating expenses: |
|||||
Medical group cost of revenues |
9,353 | ||||
General and administrative |
5,425 | ||||
Depreciation and amortization |
46 | ||||
Total operating expenses |
14,824 | ||||
Operating loss |
(128 | ) | |||
Other expense |
339 | ||||
Loss before income taxes |
(467 | ) | |||
Income tax benefit |
(36 | ) | |||
Loss from operations |
(431 | ) | |||
Gain on sale of the AV Entities, net of income taxes of $414 |
6,600 | ||||
Income from discontinued operations |
$ | 6,169 | |||
F-34
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
5. Goodwill and Intangible Assets
In accordance with ASC 350 (previously issued as SFAS No. 142 "Goodwill and Intangible Assets"), the Company performed its annual goodwill impairment analysis for each reporting unit that constitutes a business for which 1) discrete financial information is produced and reviewed by management, and 2) services that are distinct from the other reporting units. For the Medical Group Management reporting segment, the Company has determined that ProMed and other affiliated physician organizations as a group (collectively referred to as Prospect) each constitutes a reporting unit.
While each affiliated physician organization within the Prospect reporting unit earns revenues, incurs expenses and produces discrete financial information (including balance sheets and statements of operations), these entities are similarly organized and operated to provide managed health care services. They share similar characteristics in the enrollees they serve, the nature of services provided and the method by which medical care is rendered. They are centrally managed, sharing assets and resources, including executive management, payer and provider contracting, claims and utilization management, information technology, legal, financial accounting, risk management and human resource support. The entities in the Prospect reporting unit are also subject to similar long-term economic prospects. They form an integrated medical network within a common service area that supports and benefits from each other in delivering care to the Company's patient base. Since goodwill is recoverable from these affiliated physician organizations working in concert, they have been aggregated into a single reporting unit for the purpose of goodwill impairment testing in accordance with ASC 350.
While ProMed is also a physician organization, it is a separate reporting unit in that ProMed has autonomous operations, a separate management team and serves a different market area with different payer contracts from the Prospect reporting unit.
The Company has also determined that all affiliated physician organizations, including ProMed, represent a single reportable segment for financial reporting under ASC 280-10, (previously issued as SFAS No. 131 "Disclosures about Segments of an Enterprise and Related Information") based on the way the chief operating decision maker uses financial data internally to make operating decisions, allocate resources and assess performance.
For the Hospital Services segment, the reporting unit for the annual goodwill impairment analysis is determined to be at the entity level with separate analyses for Brotman and Alta.
As of September 30, 2009 and 2008, all goodwill and intangible assets relate to the Alta, Brotman and ProMed Entities. The Company's impairment test as of September 30, 2009 resulted in no impairment charges.
F-35
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
5. Goodwill and Intangible Assets (Continued)
Identifiable Intangibles at September 30, 2009 and 2008 are compromised of the following (in thousands):
| |
2009 | 2008 | Amortization Period |
|||||
|---|---|---|---|---|---|---|---|---|
HMO membership |
$ | 25,200 | $ | 25,200 | 14 years | |||
Covenants not-to-compete |
3,180 | 3,180 | 4 - 6 years | |||||
Trade names |
23,590 | 23,590 | 15 - 20 years | |||||
Trade name (Brotman hospital) |
3,000 | — | 20 years | |||||
Provider networks |
1,200 | 1,200 | 3 years | |||||
Gross carrying value |
56,170 | 53,170 | ||||||
Accumulated amortization |
(9,745 | ) | (5,430 | ) | ||||
Identifiable intangibles, net |
$ | 46,425 | $ | 47,740 | ||||
Amortization is recognized on a straight-line basis over the respective useful lives and expense for the years ended September 30, 2009 and 2008 was approximately $4,315,000 and $4,249,000, respectively.
Estimated amortization expense for each future fiscal year is as follows (in thousands):
2010 |
$ | 4,270 | ||
2011 |
3,652 | |||
2012 |
3,200 | |||
2013 |
3,119 | |||
2014 |
3,119 | |||
2015 and thereafter |
29,065 | |||
|
$ | 46,425 | ||
6. Notes Receivable
In connection with the April 1, 2004 sale of three medical clinics, the Company received promissory notes in the aggregate amount of approximately $1,068,000. There are three separate notes, each bearing interest at 5% per annum, with varying principal and interest payment requirements. The notes receivable are secured by all of the clinic assets and are personally guaranteed by each of the purchasers.
Current and non-current portions of the notes receivable as of September 30, 2009 were as follows (in thousands):
Total principal outstanding |
$ | 413 | ||
Less current maturities |
(56 | ) | ||
Non-current portion |
$ | 357 | ||
F-36
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
6. Notes Receivable (Continued)
Future minimum payments required under the notes receivable as of September 30, 2009 are as follows (in thousands):
2010 |
$ | 74 | ||
2011 |
74 | |||
2012 |
74 | |||
2013 |
74 | |||
2014 |
74 | |||
2015 and thereafter |
116 | |||
Gross payments |
486 | |||
Amount representing interest |
(73 | ) | ||
Net principal outstanding |
$ | 413 | ||
7. Related Party Transactions
Prospect has a controlling financial interest in the affiliated physician organizations included in its unaudited interim condensed consolidated financial statements which are owned by a nominee physician shareholder designated by the Company. The control is effectuated through assignable option agreements and management services agreements, which provide the Company a unilateral right to establish or effect a change of the nominee shareholder for the affiliated physician organizations at will, and without the consent of the nominee, on an unlimited basis and at nominal cost through the term of the management agreement. Jacob Y. Terner, M.D. was, through August 8, 2008, the sole shareholder, sole director and Chief Executive Officer of Prospect Medical Group, Inc. ("PMG") and was the Chief Executive Officer of most of PMG's subsidiary physician organizations. Dr. Terner also served as the sole shareholder and a director and officer of Nuestra Familia Medical Group, Inc. ("Nuestra"), an affiliated physician organization. Dr. Terner is a shareholder of the Company, and formerly served as its Chairman and Chief Executive Officer through part of fiscal 2008.
The Company had an employment agreement with Dr. Terner that expired on August 1, 2008 and provided for base compensation (most recently $400,000 per year) and further provided that if the Company terminated Dr. Terner's employment without cause, the Company would be required to pay him $12,500 for each month of past service as the Chief Executive Officer, commencing as of July 31, 1996, up to a maximum of $1,237,500. Dr. Terner resigned as the Chief Executive Officer of the Company effective March 19, 2008 and resigned as the chairman of the board of directors effective May 12, 2008. In consideration of Dr. Terner's resignation and other provisions in his resignation agreement, the Company commenced paying to his family trust the sum of $19,361 each month during the twelve-month period ending on April 30, 2009 and the sum of $42,694 each month during the twenty-four month period ending on April 30, 2011, for the total sum of $1,257,000, which amount was recorded as a general and administrative expense in fiscal 2008. In September 2009, the Company ceased making payments to Dr. Terner following its determination that Dr. Terner is not entitled to receive the payments. Subsequently, Dr. Terner filed a complaint against the Company, which seeks restoration of the payments. The parties are currently litigating the matter.
F-37
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
7. Related Party Transactions (Continued)
Dr. Arthur Lipper currently serves as the nominee shareholder of PMG and Nuestra and as the sole director of PMG and its subsidiary physician organizations and the Chief Executive Officer, President and Treasurer of all subsidiary physician organizations, except the ProMed Entities. Dr. Lipper serves as one of two directors of Nuestra, as the sole director of the ProMed Entities, and as a Vice President of Nuestra and the ProMed Entities.
On August 1, 2005 and subsequently amended on October 25, 2007, Prospect Medical Management, Inc. (now known as Prospect Hospital Advisory Services, Inc.), an affiliate of the Company, had entered into a consulting services agreement, to provide administrative, financial and management consulting services to Brotman for a monthly fee of $100,000 plus expenses. The agreement had an initial term of one year and automatically renewed for additional one-year terms unless terminated by either party with 90 days written notice. As discussed in Note 3, Brotman, which filed a voluntary petition for bankruptcy protection under Chapter 11 of the U. S. Bankruptcy Code on October 25, 2007, emerged from the Chapter 11 bankruptcy proceeding on April 14, 2009 (the "Effective Date"). On the Effective Date, the Company increased its approximately 33.1% ownership stake in Brotman, to approximately 71.9% via an incremental investment of approximately $2.5 million. For the year ended September 30, 2008 and for the period October 1, 2008 through April 13, 2009, total fees earned under the agreement were approximately $1,119,000 and $650,000, of which $819,000 and $500,000 was paid, and none of which was compromised pursuant to Brotman's Chapter 11 Plan of Reorganization, respectively. Beginning April 14, 2009, amounts earned under the agreement have been eliminated in consolidation.
PMG, a controlled affiliate of the Company (see description of assignable option agreements and management services agreements above) had entered into a risk pool sharing agreement, dated May 1, 2005, with Brotman. Under the agreement, PMG and Brotman agreed to establish a Hospital Control Program (as defined) to serve HMO enrollees and would earn incentive revenue or incur penalties by sharing in the risk for hospitalization based on inpatient services utilized. Risk pools are generally settled in the following year. For the year ended September 30, 2008, all incentive revenue earned under the agreement was compromised pursuant to Brotman's Chapter 11 Plan of Reorganization. For the period October 1, 2008 through April 13, 2009, no incentive revenue was earned under the agreement. Beginning April 14, 2009, all amounts earned under the agreement have been eliminated in consolidation.
In connection with the above-described risk-sharing agreement, Prospect Medical Systems, Inc. ("PMS") and Brotman entered into an Administrative Services Agreement, dated October 1, 2005, that provides for the administration by PMS of the payment of claims under such risk-sharing arrangement.
On August 31, 2005, PMG, entered into a joint marketing agreement with Brotman. The agreement is for an initial term of 20 years, renewable for successive five-year terms unless terminated by either party with 180 days written notice. During the term, Brotman will contract exclusively with PMG with regard to full risk contracting with HMOs for all lines of business, including Medicare, Medicaid and commercial enrollees. Brotman will not merge into, consolidate with, or sell substantially all of its assets (unless the purchaser or surviving entity expressly assumes these managed care exclusivity arrangements), alter such agreements without the consent of PMG, and agrees to be bound by the exclusivity provision.
F-38
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Income Taxes
The components of the income tax benefit for continuing operations for the years ended September 30, 2009 and 2008 are as follows:
| |
2009 | 2008 | ||||||
|---|---|---|---|---|---|---|---|---|
| |
(in thousands) |
|||||||
Current: |
||||||||
Federal |
$ | 2,577 | $ | 4,200 | ||||
State |
720 | 1,184 | ||||||
|
3,297 | 5,384 | ||||||
Deferred: |
||||||||
Federal |
(2,704 | ) | (5,243 | ) | ||||
State |
(1,612 | ) | (1,468 | ) | ||||
|
(4,316 | ) | (6,711 | ) | ||||
Total: |
||||||||
Federal |
(127 | ) | (1,043 | ) | ||||
State |
(897 | ) | (284 | ) | ||||
|
$ | (1,019 | ) | $ | (1,327 | ) | ||
Temporary differences and carry forward items that result in deferred income tax balances as of September 30 are as follows:
| |
2009 | 2008 | |||||
|---|---|---|---|---|---|---|---|
Deferred tax assets: |
|||||||
State tax benefit |
$ | 1,928 | $ | 1,448 | |||
Deferred Compensation |
1 | 221 | |||||
Allowances for bad debts |
5,115 | 1,667 | |||||
Vacation accrual and other |
4,246 | 1,592 | |||||
Accrued physician bonuses |
4,385 | 2,281 | |||||
Malpractice reserve |
1,369 | 267 | |||||
Deferred rent |
105 | 105 | |||||
Other |
80 | 55 | |||||
Net operating loss |
16,732 | 1,540 | |||||
Unrealized loss on interest rate swaps |
— | 2,644 | |||||
Capital loss carryforward |
2,255 | 2,157 | |||||
Deferred income tax assets |
36,217 | 13,977 | |||||
Valuation allowance |
(23,623 | ) | (2,154 | ) | |||
Net deferred income tax assets |
12,594 | 11,823 | |||||
Deferred tax liabilities: |
|||||||
Intangible assets |
(14,124 | ) | (14,479 | ) | |||
Fixed assets |
(20,430 | ) | (15,699 | ) | |||
Other |
(1,371 | ) | (290 | ) | |||
Deferred income tax liabilities |
(35,925 | ) | (30,468 | ) | |||
Net deferred income tax liability |
$ | (23,331 | ) | $ | (18,645 | ) | |
F-39
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
8. Income Taxes (Continued)
As a result of the ProMed and Alta acquisitions in 2007, the Company recorded approximately $36,226,000 in deferred tax liabilities, principally related to differences in the tax and book basis for intangibles such as customer relationships, trade names, non-compete agreements, provider networks and for property, improvements and equipment, for which deductions are limited to their carryover basis. These deferred tax liabilities were recorded as an increase to goodwill on the respective acquisition dates.
Other deferred income tax assets and liabilities reflect the effect of temporary differences between the assets and liabilities recognized for financial reporting purposes and the amounts recognized for income tax purposes.
Given uncertainty regarding the likelihood of the Company generating sufficient future capital gains to utilize the unrealized capital loss associated with the Brotman investment and the sale of the AV entities, the related deferred tax asset was fully reserved. In 2008 carryover losses related to the sale of the AV entities resulted in an increase in the deferred tax asset of approximately $1,373,000 with a commensurate increase in the valuation allowance.
At September 30, 2009, the Company had federal and state net operating loss carryovers of approximately $39,646,000 and $44,299,000 which, if not utilized, will expire beginning 2027 and 2017, respectively.
Management is currently assessing the Company's ability to utilize the state deferred tax assets, mainly comprised of California net operating loss carryforwards, acquired through the Brotman acquisition. This assessment has however not been completed yet. Due to the lack of positive evidence currently available to support the Company's ability to realize these deferred tax assets, the Company maintains a valuation allowance on these assets for purchase price allocation purposes. On completion of the evaluation, should management conclude it is more likely than not that a portion or all of the acquired state deferred tax assets will be realized by the Company, the income tax benefit associated with these assets will be recorded as a purchase accounting adjustment.
At September 30, 2009, the Company has approximately $416,000 of unrealized excess tax benefits related to employee stock options. This amount is not included in the table of deferred tax assets above and the benefit will be recorded as an increase to additional paid in capital if and when realized.
The differences between the income tax benefit for continuing operations at the federal statutory rate of 34% and that reflected in the accompanying consolidated statements of operations are summarized as follows for the years ended September 30:
| |
2009 | 2008 | |||||
|---|---|---|---|---|---|---|---|
Tax provision at statutory rate |
(34 | )% | (34 | )% | |||
State taxes, net of federal benefit |
(7 | )% | (5 | )% | |||
Change in valuation account |
10 | % | — | % | |||
Other |
1 | % | (1 | )% | |||
|
(30 | )% | (40 | )% | |||
Taxes paid, net of refunds received, totaled approximately $2,067,000 and $1,300,000 for the years ended September 30, 2009 and 2008, respectively.
F-40
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt
Long-term debt consists of the following at September 30 (in thousands):
| |
2009 | 2008 | ||||||
|---|---|---|---|---|---|---|---|---|
Prospect's debt: |
||||||||
New credit facilities |
||||||||
Senior secured notes |
$ | 160,000 | $ | — | ||||
Less original issue discount |
(11,980 | ) | — | |||||
|
148,020 | — | ||||||
Former credit facilities |
||||||||
Term loan—first-lien |
— | 85,443 | ||||||
Term loan—second-lien |
— | 51,478 | ||||||
Revolving credit facility |
— | 7,100 | ||||||
Brotman's debt: |
||||||||
Revolving credit facility |
2,888 | — | ||||||
Term loan-A (net of discount) |
15,655 | — | ||||||
Term loan-B |
6,250 | — | ||||||
Promissory Note—Creditors' Trust |
3,531 | — | ||||||
|
28,324 | 144,021 | ||||||
Less current maturities |
(3,805 | ) | (12,100 | ) | ||||
Long-term portion |
$ | 172,539 | $ | 131,921 | ||||
Prospect's Debt
New Credit Facilities
Senior Secured Notes
On July 29, 2009, the Company closed the offering of $160 million in 12.75% senior secured notes due 2014 (the "Notes") at an issue price of 92.335%. The sale was executed in accordance with Rule 144A under the Securities Act of 1933 and Regulation S under the Securities Act of 1933. Concurrent with the issuance of the Notes, the Company entered into a three-year $15 million revolving credit facility which was undrawn at the closing and is still undrawn, with any future borrowings bearing interest at LIBOR plus 7.00%, with a LIBOR floor of 2.00%.
The Company used the net proceeds from the sale of the Notes to repay all remaining amounts outstanding under its former $155 million senior secured credit facility, plus a prepayment premium of approximately $2.6 million. The Company reflected the repayment premium, together with the write-off of approximately $560,000 of deferred financing related to its former credit facilities, as interest expense. Capitalized deferred financing costs and original issue discount is being amortized over the term of the related debt using the effective interest method.
The terms of the Notes are governed by an indenture among the Company, certain of its subsidiaries and affiliates (as guarantors), and U.S. Bank National Association (as trustee) (the "Indenture"). Interest is payable semi-annually in arrears on January 15 and July 15, commencing on January 15, 2010. The terms of the revolving senior secured credit facility are governed by the Credit Agreement, dated as of July 29, 2009, among the Company, Royal Bank of Canada (as administrative
F-41
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
agent), Jefferies Finance LLC (as syndication agent) and the lenders party thereto (the "Credit Agreement").
The Notes and the revolving senior secured credit facility are jointly and severally guaranteed on a senior secured basis by all of the Company's restricted subsidiaries (as such term is defined in the Indenture) other than Brotman, Nuestra Familia Medical Group, Inc. and certain immaterial subsidiaries. The Notes are secured pari passu with the new revolving credit facility on a first priority basis by liens on substantially all of the Company's assets and the assets of the subsidiary guarantors (other than accounts receivable and proceeds therefrom) including all the mortgages on the Company and its subsidiary guarantors' hospital properties (but excluding a pledge of, or mortgage on, the stock, properties or other assets of Brotman, AMVI/Prospect Health Network and certain immaterial subsidiaries). The lenders under the revolving credit facility have a first priority lien on certain of the accounts receivable of the Company and the subsidiary guarantors and proceeds therefrom while the holders of the Notes have a second priority lien on such collateral.
The Indenture requires the Company to make an offer to repurchase the Notes at 101% of their principal amount in the event of a change of control of the Company and at 100% of the principal amount thereof with certain proceeds of sales of assets. The Indenture also contains certain covenants that, among other things, limit the Company's ability, and the ability of its restricted subsidiaries to: pay dividends or distributions on capital stock or equity interests, prepay subordinated indebtedness or make other restricted payments; incur additional debt; make investments; create liens on assets; enter into transactions with affiliates; engage in other businesses; sell or issue capital stock of restricted subsidiaries; merge or consolidate with another company; transfer and sell assets; create dividend and other payment restrictions affecting subsidiaries; and designate restricted and unrestricted subsidiaries. The Credit Agreement contains a number of customary covenants as well as covenants requiring the Company to maintain a maximum consolidated leverage ratio, minimum fixed charge coverage ratio and a maximum consolidated total leverage ratio. As of September 30, 2009, the Company was in compliance with the financial covenants.
Pursuant to its definitive Prospectus filed with the SEC on September 26, 2009, the Company commenced an offer to exchange up to $160 million of its newly registered 123/4% Senior Secured Notes, Series B, due 2014 (the "Exchange Notes" and together with the Original Notes, the "Notes") for an equal amount of the Original Notes (the "Exchange Offer"). The Exchange Notes are substantially identical to the Original Notes, except that the offer and sale of the Exchange Notes have been registered under the Securities Act of 1933, as amended, and the Exchange Notes do not bear any legend restricting their transfer. The Exchange offer was extended on November 25, 2009 until December 3, 2009, at which time $159 million of the $160 million aggregate principal amount of private notes had been tendered and accepted for exchange. The Company filed the required Form S-4 under the Registration Rights Agreement, on September 30, 2009 and went effective on October 23, 2009.
The Notes will mature on July 15, 2014. Prior to July 15, 2012, the Company may redeem up to 35% of the original principal amount of the Notes at a redemption price equal to 112.75% of the principal amount of the Notes redeemed, plus any accrued and unpaid interest, with the proceeds of certain equity offerings. From July 15, 2012 until July 15, 2013, the Company may redeem all, or any portion, of the Notes at a redemption price equal to 106.375% of the principal amount of the Notes redeemed, plus any accrued and unpaid interest. After July 15, 2013, but before the maturity date of July 15, 2014, the Company may redeem all, or any portion, of the Notes at a redemption price equal to 100% of the principal amount of the Notes redeemed, plus any accrued and unpaid interest.
F-42
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
Effective July 23, 2009, the Company terminated the master swap agreement and the swap arrangements thereunder by payment, on July 29, 2009, of $11.7 million to the swap counterparty in final settlement of all amounts owed under the swap arrangements. All related amounts included in accumulated other comprehensive loss, including related deferred income taxes (of approximately $4.2 million) was recorded as interest expense and to the tax provision, respectively, as of the effective date of the swap terminations.
Former Credit Facilities
Senior Secured Credit Facilities
On August 8, 2007, the Company entered into a $155,000,000 syndicated senior secured credit facility, comprised of a $95,000,000 seven-year first-lien term loan at LIBOR plus 400 basis points, with quarterly principal payments of $1,250,000 and an annual principal payment of 50% of excess cash flow, as defined in the loan agreement; a $50,000,000 seven and one-half year second-lien term loan at LIBOR plus 825 basis points, with all principal due at maturity and a revolving credit facility of $10,000,000 bearing interest at prime plus a margin that ranged from 275 to 300 basis points based on the consolidated leverage ratio.
The Company was subject to certain financial and administrative covenants, cross default provisions and other conditions required by the loan agreements with its prior lenders. While the Company met all debt service requirements timely, it did not comply with certain financial and administrative covenants as of September 30, 2007, December 31, 2007 and March 31, 2008. On May 15, 2008, the credit agreements were formally modified to waive past defaults, amend certain covenant provisions prospectively and make changes to the interest rates and payment terms.
In connection with obtaining forbearance and waivers, during the second and third quarters of fiscal 2008, the Company paid $450,000 in fees to Bank of America, N.A., which was included in general and administrative expenses and $1,525,000 in forbearance fees to the lenders, which was included in interest expense. In addition, the Company incurred $860,000 in legal and consulting fees paid to the lenders' advisors in connection with the forbearance activities, which was included in general and administrative expenses. Pursuant to the amended senior credit facility agreement, the Company was also required to pay an amendment fee of $758,000 in cash and to add 1% to the principal balance of the first and second-lien debt and the revolving line of credit, totaling $1,514,000. The amendment fees were expensed as loss on debt extinguishment in the third quarter of 2008. The Company also began to incur an additional 4% payment-in-kind ("PIK") interest expense on the second-lien debt, which was accrued and added to the principal balance on a monthly basis.
These changes resulted in a substantial modification to the credit facilities, which was accounted for as an extinguishment of the existing debt during the quarter ended June 30, 2008, in accordance with ASC 470-50. In connection with the modifications of the first and second-lien term debt and the revolving line of credit, the Company wrote off the remaining unamortized discount and debt issuance costs of $6,036,000, and expensed as debt extinguishment loss $758,000 in amendment fees paid to lenders and $1,514,000 of PIK interest added to the new debt, resulting in a total charge of $8,308,000 in connection with this debt extinguishment. Additionally, the Company capitalized $327,000 of deferred financing costs related to the new credit agreements, which was being amortized over their remaining terms.
F-43
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
The Company believes that it met all of the May 15, 2008 amended financial covenant provisions for all subsequent reporting periods. However, on March 19, 2009, the Company received notices from its lenders asserting that the Company was in default of a requirement to sell certain assets by a specified date; and on April 17, 2009, the Company received notices from its lenders asserting that the Company's April 14, 2009 increase in ownership of Brotman violated certain provisions of the amended credit agreements. Effective with the first asserted default, the lenders began assessing interest at default rates on all loans. On June 30, 2009, the Company entered into loan amendments whereby, among other things, the lenders waived all alleged events of default, and stopped assessing default interest rates. In connection with these amendments, the Company also entered into an amendment and waiver related to its swap agreements which provided that the alleged events of default under the existing credit facility would not trigger an event of default under the swap agreements. The amendments required the Company to refinance all debt no later than October 31, 2009.
On July 29, 2009, in connection with the offering of the $160 million Notes, the Company repaid all amounts outstanding under the former $155 million senior secured credit facility, plus a prepayment premium of approximately $2.6 million.
Interest Rate Swaps
In connection with the Former Credit Facilities, the Company entered into a $48 million interest rate swap, to effectively convert the variable interest rate (the LIBOR component) of $48 million of borrowings to a fixed rate of 5.3%, and a $97.8 million interest rate swap agreement to effectively convert the variable interest rate (the LIBOR component) of $97.8 million of borrowings to a fixed rate of 5.05%. The notional amounts of these interest rate swaps were structured to decline as the principal balances owing under the term loans declined. Under these swaps, the Company was required to make monthly fixed-rate payments to the swap counterparties calculated on the notional amount of the swaps and the interest rates for the swaps, while the swap counterparties were obligated to make certain monthly floating rate payments to the Company referencing the same notional amounts.
The interest rate swap agreements contained cross-default provisions whereby, in the event the Company was in default under its credit agreements, the Company was also deemed to be in default under the swap agreements.
The interest rate swap agreements were designated as cash flow hedges of expected interest payments on the term loans with the effective date of the $48 million swap being December 31, 2007 and the effective date of the $97.8 million swap being September 6, 2007. Prior to the hedge effective dates, all mark-to-market adjustments in the value of the swaps were charged to expense. After the hedge effective date, the effective portions of the fair value gains or losses on these cash flow hedges were recorded as a component of other comprehensive income, net of tax, to be subsequently reclassified into earnings when the forecasted transaction affects earnings. Effective April 1, 2008, in anticipation of changes to the loan agreements that would impact recording of interest rate swaps, the Company elected to discontinue hedge accounting. Changes in the fair value of the interest rate swaps after March 31, 2008 were recorded as other income or expense. Total net gain (loss) on the interest rate swaps included in earnings for the period October 1, 2008 through July 29, 2009 (see below) and the year ended September 30, 2008 were approximately $(5,299,000) and $3,096,000, respectively. The effective portion of the swaps of approximately $5,400,000 after tax that was recorded in other comprehensive income through March 31, 2008 continued to be amortized as expense over the remaining life of the swaps. Approximately $733,000 and $491,000 was amortized to expense for the
F-44
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
period October 1, 2008 through July 29, 2009 (see below) and six months ended September 30, 2008, respectively.
As set forth above, on July 29, 2009, the Company terminated the interest rate swap arrangements paid $11.7 million in final settlement of all amounts owing under the swap arrangements and expensed all previously unamortized swap fluctuation amounts.
Brotman's Debt
The Brotman entity has debt under a Senior Secured Revolving Credit Facility, Secured Term Loans and Unsecured Promissory Note entered into in conjunction with affecting the Plan of Reorganization described in Note 3. The Company has not guaranteed any portion of Brotman's debt or other obligations. Given the Company's majority ownership in Brotman effective April 14, 2009, all Brotman debt is included in the Company's consolidated financial statements. The Company has no obligation and has limited ability to fund Brotman's operations post acquisition. Under the senior secured notes credit agreement, the Company is permitted to make additional investments in Brotman in an aggregate amount not to exceed $10,000,000, provided that such investments can exceed $10,000,000 if the amounts are funded solely with the proceeds of Equity Interests of the Company (as defined).
Senior Secured Revolving Credit Facility
On April 14, 2009, the Effective Date of the Plan of Reorganization, Brotman obtained a commitment from Gemino Healthcare Finance, LLC ("Gemino") for a three-year, $6.0 million, senior credit facility secured by Brotman's accounts receivable. The facility expires on the earlier of April 14, 2012 and the Los Angeles Jewish Home for Aging ("JHA") loan (see below) maturity date and bears interest at Libor plus 7% per annum (11.0% at September 30, 2009), given a LIBOR floor of 4%. Interest is incurred based on the greater of $2 million or the actual outstanding principal balance. The agreement also includes an unused line fee of 0.5% per annum and a collateral line fee, based on the average outstanding principal balance, of 0.5% per annum. Loan fees associated with the Gemino loan totaling approximately $120,000, were capitalized and have been included as deferred financing costs in the accompanying consolidated balance sheet as of September 30, 2009, with the amount being amortized over the term of the related debt using the effective interest method. The senior credit facility agreement contains customary covenants for facilities of this type including restrictions on the payment of dividends, change in ownership and management, asset sales, incurrence of additional indebtedness, sale-leaseback transactions, and related party transactions. In addition, Brotman must also comply with financial covenants, including a fixed charge coverage ratio of not less than (i) 1.10:1.00 for the fiscal quarter ended June 30, 2009, (ii) 1.15:1.00 originally for the fiscal quarter ended September 30, 2009; and (iii) 1.20:1.00 for each fiscal quarter ending thereafter. As of September 30, 2009, Brotman was not in compliance with the required financial covenants under the Gemino credit agreement. Pursuant to an amendment entered into effective December 11, 2009, the Gemino credit agreement was amended to provide, among other things, a waiver of the specified events of default and the amendment to the definition of fixed charge coverage ratio. Under the amended credit agreement, the fixed charge coverage ratio was amended to require not less than (i) 1.00:1.00 for the fiscal quarters ending December 31, 2009 and March 31, 2010; (ii) 1.05:1.00 for the fiscal quarters ending June 30, 2010 and September 30, 2010, (iii) 1.10:1.00 for the fiscal quarters ending December 31, 2010 and March 31, 2011, and (iv) 1.20:1.00 for the fiscal quarter ending June 30, 2011
F-45
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
and each fiscal quarter ending thereafter. The first calculation of the fixed charge coverage ratio shall be for the quarter ending December 31, 2009.
Secured Credit Facilities Term Loan: A and B
On April 14, 2009, the effective date of the Plan of Reorganization, Brotman consummated the transactions contemplated in the JHA financing and the JHA loan documents. Under the terms of the JHA loan agreements, JHA agreed to provide Brotman with up to $23 million in financing, consisting of two term loans: (i) a Term A loan of $16 million (the "Term A Loan") with a 24-month term and (ii) a Term B loan of up to $7 million, with a term of 36 months (the "Term B Loan"). Subject to the notification requirements set forth in the loan agreements, the term of the Term A Loan can be extended up to 36 months. Interest on the Term A Loan is payable at 10% per annum for the first year of the loan, and 7.5% thereafter. Interest on the Term B Loan is payable at 10% per annum for the term of the loan. The Term A Loan and Term B Loan are secured by certain of Brotman's personal property, and a mortgage on certain Brotman's real property. The proceeds of the JHA loans were used to repay all existing senior secured loans at Brotman as of April 14, 2009. Loan fees associated with the JHA loans totaling approximately $1,549,000, were capitalized and have been included as deferred financing costs in the accompanying consolidated balance sheet as of September 30, 2009, with that amount being amortized over the term of the related debt using the effective interest method.
With respect to the Term A loan, JHA was granted the right ("Put Right") to declare the unpaid loan amount, including remaining interest and any other amounts due and payable under the loan agreements, immediately due and payable at any time following the first twelve months of the Closing Date and prior to the date which is twenty-four months after the Closing Date, subject to JHA providing written notification to Brotman of its exercise of the Put Right at least 180 days in advance. JHA may not however provide notification of its exercise of the Put Right prior to the first anniversary of the April 14, 2009 closing date. As such, the loan is reflected as long-term debt in the consolidated balance sheet.
As part of the JHA financing, Brotman has granted JHA an option to purchase certain Brotman-owned land adjacent to the hospital, where JHA plans to construct a senior living facility, for a purchase price equal to the outstanding principal balance of the Term A Loan plus any prepaid amounts. In connection with JHA's option right, Brotman is required to deposit $130,000 monthly into a reserve account (up to a maximum of $3,120,000), with such funds specifically earmarked for the construction of a new emergency room. Additionally, Brotman is required to deposit $10,000 monthly into a reserve account for capital improvements and a Tax and Insurance Deposit Account to be funded monthly, for purposes of Brotman's annual real estate tax assessments.
In accordance with relevant accounting pronouncements, the Term A Loan, which contains a real estate purchase option, is recorded at its present value, with any excess of the proceeds over that amount recorded as an option deposit liability account. The present value of the loan is estimated using discounted cash flow analyses based on market rates obtained from independent third parties for similar type debt. Based on an estimated market interest rate of 10.0%, the present value of the loan was estimated to be approximately $15,667,000 at inception. The difference of $345,000 between the recorded present value and the carrying value of the loan has been recorded as a discount against the loan and is amortized, using the effective interest rate method, to interest expense, over the term of the loan.
F-46
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
9. Long-Term Debt (Continued)
Subordinated Promissory Note
On April 14, 2009, the Effective Date of the Plan of Reorganization, Brotman executed a $4,000,000 unsecured Class 4 Note, to be held by the Creditor Trust (as defined in the Plan of Reorganization) for the benefit of holders of allowed Class 4 claims (as defined in the Plan of Reorganization) and paid pro rata to holders of allowed Class 4 claims. The Note bears interest at 7.50% per annum and is payable in sixteen equal quarterly installments of principal and accrued interest through February 15, 2013. The Note contains a covenant which, so long as amounts remain outstanding under the Note, restricts Brotman from paying Prospect Medical Holdings, Inc. a consulting fee of more than $100,000 per month, as specified in the consulting services agreement (see Note 7).
Scheduled payments under current and long-term debt are as follows, as of September 30, 2009 (in thousands):
2010 |
$ | 3,805 | ||
2011 |
16,988 | |||
2012 |
7,314 | |||
2013 |
562 | |||
2014 |
160,000 | |||
Total minimum payments |
188,669 | |||
Less debt discounts |
(12,325 | ) | ||
Total, net of discounts |
$ | 176,344 | ||
10. Stockholders' Equity
2008 Omnibus Equity Incentive Plan
On August 13, 2008, the Company's stockholders adopted the 2008 Omnibus Equity Incentive Plan ("2008 Plan"). The 2008 Plan, which replaces the 1998 Plan, permits a variety of equity programs designed to provide flexibility in implementing equity awards, including incentive stock options ("ISO"), non-qualified stock options ("NQSO"), restricted stock grants, stock appreciation rights ("SAR") and performance based awards to employees, directors and outside consultants as determined by the Compensation Committee of the Board of Directors (the "Committee").
The maximum number of shares of Common Stock allocated to the 2008 Plan and reserved to satisfy awards under the 2008 Plan is 4,000,000. The maximum number of shares that may be included in Awards to any participant within a 12 month period is 500,000. Awards may not be granted under the 2008 Plan after the tenth anniversary of the approval of the 2008 Plan, but awards granted prior to such anniversary may extend beyond such date. Once granted, options and stock appreciation rights may not be repriced. Grants of awards to a non-employee member of the Board at the time of grant must be made pursuant to formulas established by the Board before such grant.
Under the terms of the 2008 Plan, the exercise price of an ISO may not be less than 100% of the fair market value of the Company's Common Stock on the date of grant and, if granted to a shareholder owning more than 10% of the Company's Common Stock, then not less than 110%. Stock options granted under the 2008 Plan have a maximum term of 10 years from the grant date, and will be exercisable at such time and upon such terms and conditions as determined by the Committee.
F-47
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Stockholders' Equity (Continued)
The base price, above which any appreciation of the SAR issued under the 2008 Plan is measured, will in no event be less than 100% of the fair market value of the Company's stock on the date of grant of the SAR or, if the SAR is granted in tandem with a stock option, the exercise price under the associated option.
The restrictions imposed on shares granted under a restricted stock award will lapse in accordance with the vesting requirements specified by the Committee in the award agreement. Such vesting requirements may be based on the continued service of the participant with the Company for a specified time or on the attainment of specified performance goals established by the Committee in its discretion. If the vesting requirements of a restricted stock award are not satisfied prior to the termination of the participant's service, the unvested portion of the award will be forfeited and the shares of Common Stock subject to the unvested portion of the award will be returned to the Company.
During fiscal 2009, 642,500 options were issued to various management personnel under the 2008 Plan. During fiscal 2008, 2,001,250 options were issued under the 2008 Plan, of which 500,000 were granted to Samuel S. Lee in connection with his employment as the Chief Executive Officer of the Company and 1,456,250 options outside of the 2008 Plan were granted to Samuel S. Lee. During fiscal 2008, 200,000 shares of restricted stock were issued under the 2008 Plan to Mike Heather in connection with his employment as Chief Financial Officer of the Company. During fiscal 2008, a total of 30,000 shares of restricted stock were issued to outside directors of the Company. As of September 30, 2009, there were 1,461,250 shares available for future grants under the 2008 Plan.
1998 Stock Option Plan
The Company's 1998 Stock Option Plan ("1998 Plan"), as amended, provided for a continuous pool of 2,040,000 shares of the Company's Common Stock for allocation to previously issued and outstanding or exercised stock option awards under the Plan. Options granted under the 1998 Plan could be qualified incentive stock options or non-qualified stock options and each grant is evidenced by a written stock option agreement. The exercise price to be paid for shares upon exercise of each option granted under the 1998 Plan was determined by the Board of Directors at the time the option is granted, but could not be less than the fair market value of the stock, as determined on the date of grant, or have a maximum term in excess of ten years.
An option granted under the 1998 Plan terminates 90 days after the holder ceases to be employed by the Company, except in the case of death or disability. In the case of death or disability, the option may be exercised within twelve months by the holder or the holder's legal representative, executor, administrator, legatee or heirs, as the case may be. The terms of the options granted outside of the 1998 Plan are substantially similar to the terms of the non-qualified options issued under the 1998 Plan, except that 300,000 options were granted to Mike Heather as Chief Financial Officer ("CFO"), provide that if Mr. Heather leaves the employ of the company, he will be able to exercise the options for up to three years after his separation from the Company.
In conjunction with the adoption of the 2008 Plan, effective August 13, 2008, additional equity awards under the 1998 Plan have been discontinued, and all new equity awards are being granted under the 2008 Plan. Remaining authorized shares under the 1998 Plan that were not subject to outstanding awards as of August 13, 2008, were canceled on August 13, 2008. The 1998 Plan will remain in effect as to outstanding equity awards granted under the 1998 Plan prior to August 13, 2008.
F-48
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Stockholders' Equity (Continued)
Outstanding Stock Options and Stock Option Activity
Option Activities
A summary of option activity for the years ended September 30, 2009 and 2008 is as follows:
| |
2009 | 2008 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Options | Weighted Average Exercise Price |
Options | Weighted Average Exercise Price |
||||||||||
Outstanding, beginning of year |
5,087,637 | $ | 3.17 | 2,249,906 | $ | 4.57 | ||||||||
Granted |
642,500 | $ | 3.50 | 3,457,500 | $ | 2.42 | ||||||||
Exercised |
(44,167 | ) | $ | 2.32 | (380,000 | ) | $ | 3.16 | ||||||
Forfeited |
(1,352,635 | ) | $ | 3.90 | (239,769 | ) | $ | 5.54 | ||||||
Expired |
— | — | — | — | ||||||||||
Outstanding, end of year |
4,333,335 | $ | 3.00 | 5,087,637 | $ | 3.17 | ||||||||
Exercisable, end of year |
2,898,546 | $ | 3.04 | 2,180,912 | $ | 3.69 | ||||||||
Range of exercise prices, outstanding options |
$ | 2.25 - $6.45 | $ | 2.40 - $7.15 | ||||||||||
The aggregate intrinsic value of stock options outstanding and exercisable at September 30, 2009 was approximately $6,235,000 and $4,212,000, respectively, and at September 30, 2008 was approximately $323,000 and $126,000, respectively. The aggregate intrinsic value is calculated as the difference between the exercise price of the underlying awards and the quoted price of the Company's common stock for those awards that have an exercise price currently below the quoted market price.
Stock-based compensation expense recognized in fiscal 2009 and 2008 relating to stock options under the fair value method was approximately $989,000 and $1,369,000, respectively. During the years ended September 30, 2009 and 2008, options were exercised for cash proceeds of approximately $102,000 and $1,200,000, respectively. The aggregate intrinsic value of the gross option shares exercised in fiscal 2009 and 2008 was approximately $80,000 and $742,000, respectively. No income tax benefits were recorded for options exercised in 2009 and 2008.
At September 30, 2009, there were 757,479 unvested options. Compensation expense of approximately $637,000 for the unvested options will be recognized ratably over the remaining vesting period. The weighted average remaining contractual life of stock options outstanding at September 30, 2009 was 45 months.
Fair Value Assumptions
The weighted average grant date fair value (determined using Black Scholes option pricing model) of options granted was $1.32 and $0.58 in 2009 and 2008, respectively. Fair value for options granted
F-49
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Stockholders' Equity (Continued)
during the year ended September 30, 2009 and 2008 was estimated with the following weighted average assumptions:
| |
2009 | 2008 | |||||
|---|---|---|---|---|---|---|---|
Market price of the Company's common stock on the date of grant |
$ | 3.50 | $ | 2.40 | |||
Weighted average expected life of the options |
3.17 years | 3.25 years | |||||
Risk-free interest rate |
1.51% | 2.70% | |||||
Weighted average expected volatility |
50.31% | 29.30% | |||||
Dividend yield |
0.00% | 0.00% | |||||
Expected Term—The expected term of options granted represents the period of time that they are expected to be outstanding. The Company has adopted the "simplified method" of determining the expected term for "plain vanilla" options, as allowed under Staff Accounting Bulletin (SAB) No. 107. The "simplified method" states that the expected term is equal to the sum of the vesting term plus the contract term, divided by two. "Plain vanilla" options are defined as those granted at-the-money, having service time vesting as a condition to exercise, providing that non-vested options are forfeited upon termination and that there is a limited time to exercise the vested options after termination of service, usually 90 days, and providing the options are non-transferable and non-hedgeable. We will continue to gather additional information about the exercise behavior of participants and will adjust the expected term of our option awards to reflect the actual exercise experience when such historical experience becomes sufficient.
Expected Volatility—The Company estimates the volatility of the common stock at the date of grant based on the average of the historical volatilities of a group of peer companies. Since the Company's shares did not become publicly traded until May 2005, management believes there is currently not enough historical volatility data available to predict the stock's future volatility. The Company has identified a group of comparable companies to calculate historical volatility from publicly available data for sequential periods approximately equal to the expected terms of the option grants. In selecting comparable companies, management considered several factors including industry, stage of development, size and market capitalization.
Risk-Free Interest Rate—The Company bases the risk-free interest rate on the implied yield in effect at the time of option grant on U.S. Treasury zero-coupon issues with equivalent remaining terms.
Dividends—The Company has never paid any cash dividends on our common stock and does not anticipate paying any cash dividends in the foreseeable future.
Forfeitures—Share based compensation is recognized only for those awards that are ultimately expected to vest. Compensation expense is recorded net of estimated forfeitures. Those estimates are revised in subsequent periods if actual forfeitures differ from those estimates. The Company used historical data since May 2005 to estimate pre-vesting option forfeitures for all our employees on a combined basis.
Restricted Stock Award Activities
On August 15, 2008, upon receipt of stockholder approval, the Company finalized the grant of 200,000 shares of restricted stock under the 2008 Plan to Mike Heather, which grant had been
F-50
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
10. Stockholders' Equity (Continued)
previously committed in connection with his continued employment as the Chief Financial Officer of the Company. Two-thirds of the shares were vested at the time of issuance and the final third vested on June 14, 2009. This resulted in $136,000 and $344,000 of stock based compensation expense for the years ended September 30, 2009 and 2008, respectively.
In conjunction with a March 2004 Private Placement, the Company issued warrants to purchase 659,409 shares of the Company's common stock at $1.00 per share, as a promotional fee. These warrants are exercisable at any time and expire on September 19, 2010. 100,000 and 369,210 of these warrants were exercised on November 3, 2004 and on September 18, 2008, respectively.
In addition to the $1.00 warrants discussed above, the Company also issued warrants to purchase 453,047 shares of common stock at an exercise price of $5.50 to the investors of the Private Placement. These warrants expire in March, 2014.
On June 15, 2004, the Company issued warrants to purchase a total of 22,727 shares of common stock at a price of $5.50 per share for services provided in connection with the March 2004 Private Placement, are exercisable at any time, and expire on June 15, 2011.
11. Commitments and Contingencies
Leases
The Company leases an office facility partly owned by a shareholder of the Company (see Note 7) and various office facilities and equipment from third parties under non-cancelable operating and capital lease arrangements expiring at various dates through 2014. Certain operating leases contain rent escalation clauses and renewal options, which have been factored into determining rent expense on a straight-line bais over the lease terms. Capital leases bear interest at rates ranging from 7%—18% per annum.
The future minimum annual lease payments (net of anticipated sublease income) required under leases in effect at September 30, 2009 are as follows (in thousands):
Years ending September 30,
|
Capital Leases |
Operating Leases |
|||||
|---|---|---|---|---|---|---|---|
2010 |
$ | 820 | $ | 2,666 | |||
2011 |
426 | 1,812 | |||||
2012 |
183 | 1,393 | |||||
2013 |
45 | 1,281 | |||||
2014 and thereafter |
22 | 1,099 | |||||
Total minimum lease payments |
1,496 | $ | 8,251 | ||||
Less amounts representing interest |
(107 | ) | |||||
|
1,389 | ||||||
Less current portion |
(820 | ) | |||||
|
$ | 569 | |||||
Consolidated rent expense for fiscal 2009 and 2008 was approximately $3,765,000 and $3,644,000, respectively. Sublease rental income of approximately $73,000 and $20,000, for fiscal 2009 and 2008, respectively, was recorded as a reduction to rental expense.
F-51
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
11. Commitments and Contingencies (Continued)
Seismic Retrofit
Alta and Brotman are required to comply with the Hospital Seismic Safety Act (SB1953), which regulates the seismic performance of all aspects of hospital facilities in California. SB1953 imposes near-term and long-term compliance deadlines for seismic safety assessment, submission of corrective plans, and the retrofitting or replacement of medical facilities to comply with current seismic standards. These requirements can result in significant operational changes and capital outlays. Management is continuing to assess its options and the methods of financing the required retrofits. Based on management's evaluation, the renovation needs to comply with the California seismic safety standards for its acute-care facilities, including asbestos abatement, are not estimable at this time.
Employee Health Plans
Brotman offers self-insured HMO and PPO plans to employees. Employee health benefits are administered by a local claims Processor, based on plan coverage and eligibility guidelines determined by Brotman, as well as Brotman's collective bargaining agreements. A commercial insurance policy covers losses in excess of $200,000 per occurrence. An actuarially estimated liability of approximately $349,000 and $600,000 for incurred but not reported claims has been included in accrued salaries and benefits as of September 30, 2008 and 2009, respectively.
Regulatory Matters
Laws and regulations governing the Medicare program and health care generally are complex and subject to interpretation. Prospect and its affiliates believe that they are in compliance with all applicable laws and regulations and are not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no such regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation, as well as significant regulatory action, including fines, penalties, and exclusion from the Medicare and Medicaid programs.
The Company's affiliated physician organizations must comply with a minimum working capital requirement, Tangible Net Equity ("TNE") requirement, cash-to-claims ratio and claims payment requirements prescribed by the California Department of Managed Health Care. TNE is defined as net assets, less intangibles and amounts due from affiliates, plus subordinated obligations. At September 30, 2009, the Company and the affiliated physician organizations were in compliance with these regulatory requirements.
Trading Suspension
Following non-timely filing of the Company's Form 10-K for the fiscal year ended September 30, 2007, the American Stock Exchange (now NYSE Amex) suspended trading of the Company's common stock, effective January 16, 2008. Following filing of the Company's Form 10-K and subsequent Forms 10-Q, trading of the Company's shares was resumed, effective June 18, 2008. As of September 30, 2009, the Company's common stock began trading on the NASDAQ Global Market
Litigation
The Company and its affiliated physician organizations and hospitals are parties to various legal actions arising in the ordinary course of business. The Company believes that any potential liability, if any, under these claims will not have a material adverse effect on the consolidated financial position, results of operations, or cash flows.
F-52
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
12. Defined Contribution Plan
Each of the Company's entities—Alta, Brotman, Prospect and ProMed—sponsor a defined contribution plan covering substantially all employees who meet certain eligibility requirements. Under these plans, employees can contribute up to 100% of their compensation up to the IRS deferred annual maximum. There is no company match under the Alta, Prospect and ProMed plans. In fiscal 2009, Brotman suspended the employer match. The Company is currently evaluating alternatives for combining one or more of these plans in fiscal 2010. Total expenses under the plans were approximately $210,000 in 2009 and $200,000 in 2008, respectively.
13. Incurred but Not Reported Medical Group Claims Reserves
The following table presents the roll-forward of incurred but not reported, or IBNR, claims reserves as of and for the periods indicated:
| |
Year ended September 30 | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2009 | 2008(1) | ||||||
| |
(in thousands) |
|||||||
IBNR as of beginning of year |
$ | 20,480 | $ | 21,406 | ||||
Medical group claim expenses incurred during the year: |
||||||||
Related to current year |
72,424 | 79,174 | ||||||
Related to prior year |
(1,130 | ) | (1,996 | ) | ||||
Total incurred |
71,294 | 77,178 | ||||||
Medical group claims paid during the year: |
||||||||
Related to current year |
(56,100 | ) | (59,633 | ) | ||||
Related to prior year |
(18,850 | ) | (18,471 | ) | ||||
Total paid |
(74,950 | ) | (78,104 | ) | ||||
IBNR as of end of year |
$ | 16,824 | $ | 20,480 | ||||
- (1)
- Amounts exclude charges in medical claims and benefits payable related to the AV Entities which are reported in discontinued operations.
Following is a reconciliation of medical group cost of revenues per the consolidated statements of operations to healthcare claims expense reflected in the preceding table:
| |
Consolidated Year ended September 30 | ||||||
|---|---|---|---|---|---|---|---|
| |
2009 | 2008 | |||||
| |
(in thousands) |
||||||
Capitation expense |
$ | 77,640 | $ | 79,121 | |||
Fee-for-service claims expense |
71,294 | 77,178 | |||||
Other physician compensation |
3,159 | 4,546 | |||||
Other cost of revenues |
(1,037 | ) | (1,938 | ) | |||
Total cost of revenues |
$ | 151,056 | $ | 158,907 | |||
F-53
PROSPECT MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)