Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - Encompass Health Corp | form8k-investor111609.htm |

1
Lazard Healthcare Conference
November 17, 2009
November 17, 2009
Exhibit 99.1
Exhibit 99.1
2
Table of Contents

3
Note Regarding Forward-Looking Statements
The information contained in this presentation includes certain estimates, projections and other forward-looking information
that reflect our current views with respect to future events and financial performance. These estimates, projections and other
forward-looking information are based on assumptions that HealthSouth believes, as of the date hereof, are reasonable.
Inevitably, there will be differences between such estimates and actual results, and those differences may be material.
The information contained in this presentation includes certain estimates, projections and other forward-looking information
that reflect our current views with respect to future events and financial performance. These estimates, projections and other
forward-looking information are based on assumptions that HealthSouth believes, as of the date hereof, are reasonable.
Inevitably, there will be differences between such estimates and actual results, and those differences may be material.
There can be no assurance that any estimates, projections or forward-looking information will be realized. All such
estimates, projections and forward-looking information speak only as of the date hereof. HealthSouth undertakes no duty to
publicly update or revise the information contained herein.
estimates, projections and forward-looking information speak only as of the date hereof. HealthSouth undertakes no duty to
publicly update or revise the information contained herein.
This presentation also includes estimates and projections published by the Centers for Medicare and Medicaid Services
(“CMS”). We are not able to verify those estimates or projections or the detailed calculations thereof by CMS which are not
made public. Any changes or errors in those calculations, among other uncertainties such as those referred to below and
changes in CMS’s own rules and policies, could cause actual results to differ materially from CMS’s projections.
Furthermore, we do not believe that CMS numbers are consistent with financial reporting results. CMS data and projections
should not be used as an indication of financial performance.
(“CMS”). We are not able to verify those estimates or projections or the detailed calculations thereof by CMS which are not
made public. Any changes or errors in those calculations, among other uncertainties such as those referred to below and
changes in CMS’s own rules and policies, could cause actual results to differ materially from CMS’s projections.
Furthermore, we do not believe that CMS numbers are consistent with financial reporting results. CMS data and projections
should not be used as an indication of financial performance.
You are cautioned not to place undue reliance on the estimates, projections and other forward-looking information in this
presentation as they are based on current expectations and general assumptions and are subject to various risks,
uncertainties and other factors, including those set forth in our Form 10-K for the year ended December 31, 2008, the Form
10-Q for the quarters ended March 31, 2009, June 30, 2009, and September 30, 2009, and in other documents we
previously filed with the SEC, many of which are beyond our control, that may cause actual results to differ materially from
the views, beliefs and estimates expressed herein.
presentation as they are based on current expectations and general assumptions and are subject to various risks,
uncertainties and other factors, including those set forth in our Form 10-K for the year ended December 31, 2008, the Form
10-Q for the quarters ended March 31, 2009, June 30, 2009, and September 30, 2009, and in other documents we
previously filed with the SEC, many of which are beyond our control, that may cause actual results to differ materially from
the views, beliefs and estimates expressed herein.
Note Regarding Presentation of Non-GAAP Financial Measures
The following presentation includes certain “non-GAAP financial measures” as defined in Regulation G under the Securities
Exchange Act of 1934. The Appendix at the end of this presentation includes reconciliations of the non-GAAP financial
measures found in the following presentation to the most directly comparable financial measures calculated and presented in
accordance with Generally Accepted Accounting Principles in the United States. Our Form 8-K, dated November 16, 2009, to
which the following presentation slides are attached, provides further explanation and disclosure regarding our use of non-
GAAP financial measures and should be read in conjunction with these presentation slides.
The following presentation includes certain “non-GAAP financial measures” as defined in Regulation G under the Securities
Exchange Act of 1934. The Appendix at the end of this presentation includes reconciliations of the non-GAAP financial
measures found in the following presentation to the most directly comparable financial measures calculated and presented in
accordance with Generally Accepted Accounting Principles in the United States. Our Form 8-K, dated November 16, 2009, to
which the following presentation slides are attached, provides further explanation and disclosure regarding our use of non-
GAAP financial measures and should be read in conjunction with these presentation slides.
Cautionary Statements
4
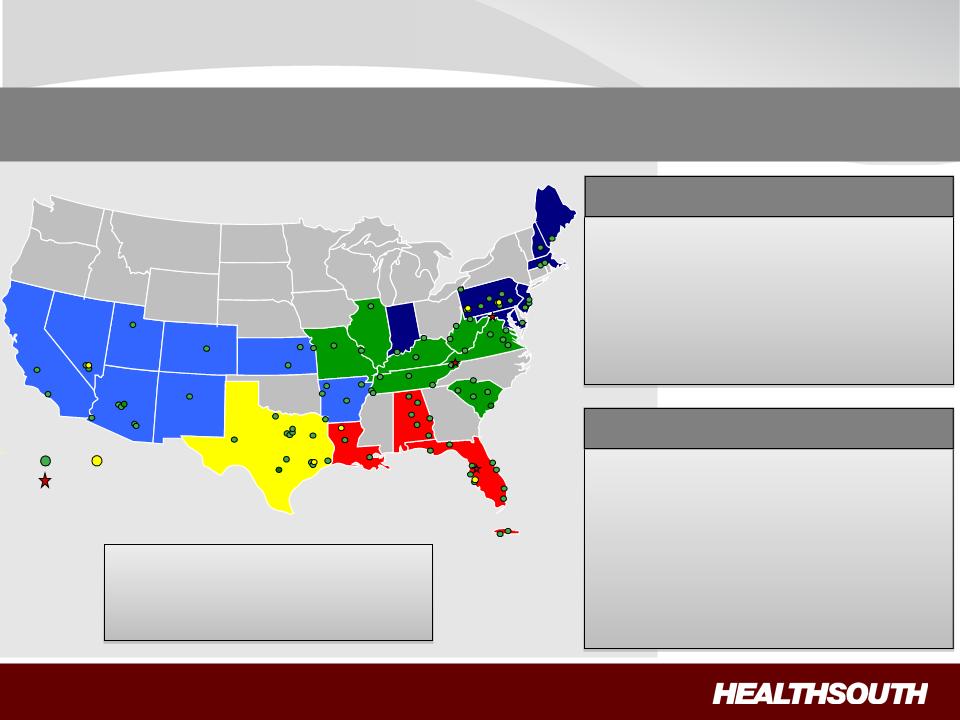
HealthSouth
IRH
LTCH
94 Rehabilitation Hospitals
44 Outpatient Satellites
6 Long-Term
Acute Care Hospitals
25 Hospital-Based Home
Health Agencies
Health Agencies
Operational Components
ü Rehabilitation Nursing
ü Physical Therapy
ü Occupational Therapy
ü Speech-Language Therapy
ü Case Management
ü Specialized Technology
Major Services
Largest Provider of Inpatient Rehabilitative Healthcare Services in the U.S.
Provider of Additional Post-Acute Services
Provider of Additional Post-Acute Services
Development Sites
Employees: ~ 22,000
Corporate Office: Birmingham,
AL
Exchange (Symbol): NYSE (HLS)
5
Near term
To create shareholder value as the preeminent provider of
rehabilitative care in the U.S. by:
rehabilitative care in the U.S. by:
– Driving
organic growth through operational excellence;
– Creating
a strong balance sheet through deleveraging; and
– Pursuing
disciplined, opportunistic growth.
Longer Term
We will pursue acquisitions of complementary, post-acute services
provided they are accretive to HealthSouth. to HealthSouth
provided they are accretive to HealthSouth. to HealthSouth
5-8+% annual Adjusted Consolidated EBITDA growth (1)
15-20+% annual Adjusted EPS growth (1)(2)
(1) For reconciliation to GAAP, see slides 30 through 33. These ranges are based on current assumptions
of external drivers (e.g., healthcare
reform, interest rates) and are subject to change.
reform, interest rates) and are subject to change.
(2) Based on adjusted income from continuing operations per diluted share.
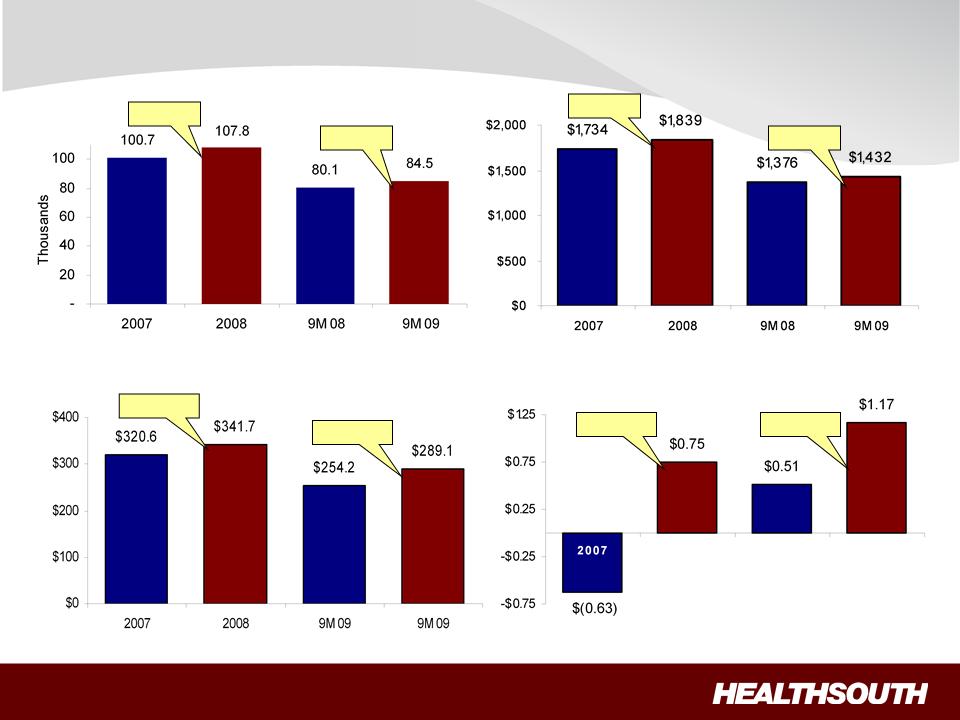
6
Financial Performance
Discharge Volume
Consolidated Net Operating Revenues
($ Millions)
Adjusted Income from Continuing Operations
per Diluted Share(1)
Adjusted Consolidated EBITDA
($ Millions)
+ 4.1%
+ 5.5%
+13.7%
+ 129.4%
+ 7.0%
+ 6.1%
+6.6%
+ 219.0%
(1) Reconciliation to GAAP provided on slides 30 through 33.
2008 9M 08 9M
09
7
“The Basics”: Our Patients
94%
5%
1%
Referral Source
Acute Care Hospitals
Physician Offices
Skilled Nursing Facilities
All patients are referred by a physician:
Most Common Cases
1. Stroke 17.7%
2. Neurological 13.3%
3. Fracture of the lower extremity 11.7%
4. Debility 11.4%
5. Other orthopedic conditions 9.4%
6. LE joint replacement 9.3%
7. Brain injury 7.4%
8. Cardiac conditions 4.7%
9. Spinal cord injury 3.6%
10. All other 11.5%
ü Physicians and Case Managers are key decision-makers.
ü All IRF patients must meet
medical necessity criteria.
ü All IRF patients must be
medically stable and have potential to tolerate
three hours of therapy per day (minimum).
three hours of therapy per day (minimum).
8
“The Basics”: Our Competitors
Competitors
• Other freestanding IRFs
• Inpatient rehab units
• Skilled nursing facilities
• Long-term acute care hospitals
• Home Health agencies
Total Inpatient Rehabilitation
Facilities (IRF): 1,202
Facilities (IRF): 1,202
Hospital-Based Units
983 (82%)
Other
125 (10%)
HealthSouth
94 (8%)
Free-
Standing
Hospitals
Patients
Patients
9
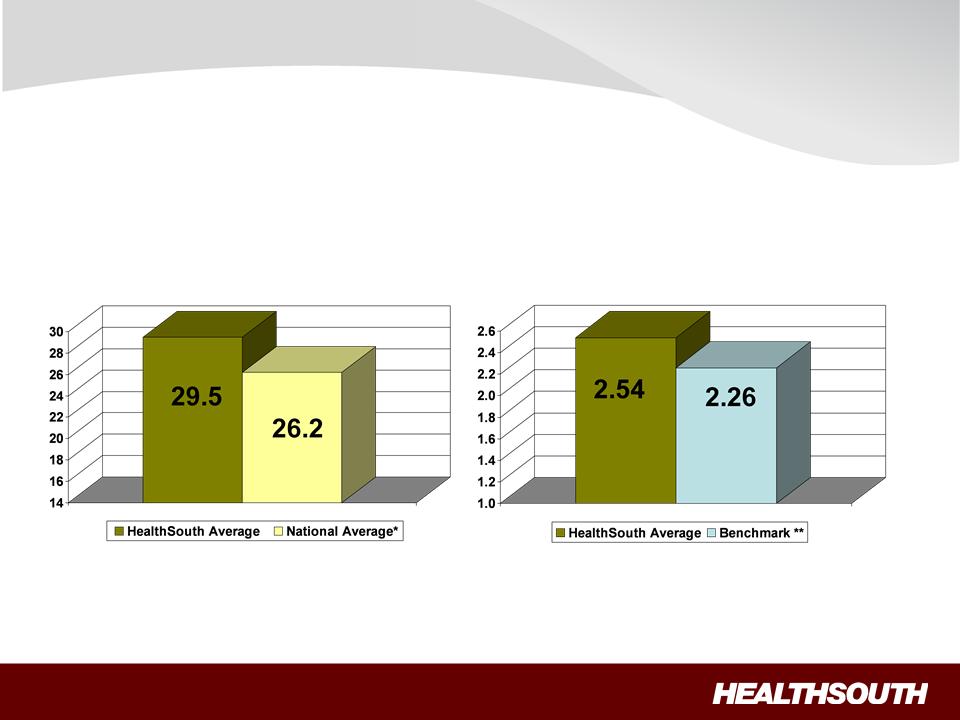
FIM Gain
LOS Efficiency
LOS Efficiency = Functional gain
divided by length of stay
divided by length of stay
Source: UDSmr Database - On Demand
Reports 2008 Year End Report
Reports 2008 Year End Report
FIM Gain = Change in Functional
Independent Measurement (based on
an 18 point assessment) from
Admission to Discharge
Independent Measurement (based on
an 18 point assessment) from
Admission to Discharge
** Benchmark = Expected, Risk Adjusted LOS Efficiency
Operational Excellence = “High-Quality” Care
*Benchmark = Expected Risk Adjusted FIM Change Avg.
10
Operational Excellence = “Cost-Effective” Care
CMS Fiscal Year 2010 IRF Rate Setting File Analysis (1)
|
|
Freestanding (2) |
Units (2) |
Total |
|
HealthSouth |
|
|
Hospitals (2) | ||||
|
Number of IRFs |
228 |
953 |
1,181 |
|
94 |
|
Average # of Discharges per IRF |
649 |
237 |
316 |
|
822 |
|
Outlier Payments as % of Total Payments |
1.32% |
4.08% |
3.00% |
|
0.43% |
|
Average Estimated Total Payment per Discharge for FY 2010 |
$16,452 |
$16,741 |
$16,626 |
|
$15,996 |
|
Average Estimated Cost per Discharge for FY 2010 |
$14,021 |
$17,207 |
$15,945 |
|
$12,633 |
Notes:
(1) All data provided was filtered and compiled from the Centers for Medicare and Medicaid Services (CMS) Fiscal Year 2010 IRF rate setting final
rule file found at http://www.cms.hhs.gov/InpatientRehabFacPPS/07_DataFiles.asp#TopOfPage. The data presented was developed entirely by
CMS and is based on its definitions which are different in form and substance from the criteria HealthSouth uses for external reporting purposes.
Because CMS does not provide its detailed methodology, HealthSouth is not able to reconstruct the CMS projections or the calculation.
rule file found at http://www.cms.hhs.gov/InpatientRehabFacPPS/07_DataFiles.asp#TopOfPage. The data presented was developed entirely by
CMS and is based on its definitions which are different in form and substance from the criteria HealthSouth uses for external reporting purposes.
Because CMS does not provide its detailed methodology, HealthSouth is not able to reconstruct the CMS projections or the calculation.
(2) The CMS file contains data for each of the 1,181 inpatient rehabilitation facilities used to estimate the policy updates for the FY 2010 Final IRF-
PPS Rule. Most of the data represents historical information from the CMS fiscal year 2008 period and does not reflect the same HealthSouth
hospitals in operation today. The data presented was separated into three categories: Freestanding, Units, and HealthSouth. HealthSouth is a
subset of Freestanding and the Total.
PPS Rule. Most of the data represents historical information from the CMS fiscal year 2008 period and does not reflect the same HealthSouth
hospitals in operation today. The data presented was separated into three categories: Freestanding, Units, and HealthSouth. HealthSouth is a
subset of Freestanding and the Total.
11
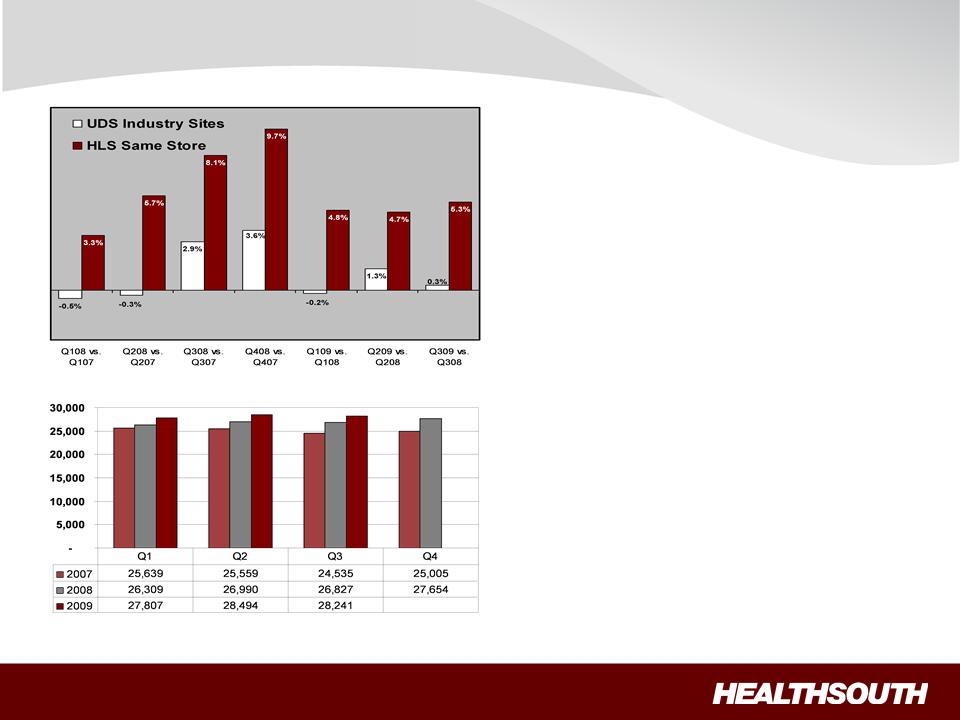
% ∆ Discharges (1)
(1) Data provided by UDSMR, a data gathering and analysis organization for the rehabilitation industry; represents ~ 65-70% of industry, including 90 HealthSouth sites.
(2) Includes 90 consolidated HealthSouth inpatient rehab hospitals and six long-term acute-care hospitals.
(1)
(2)
Operational Excellence: Market Share Gains
HealthSouth vs. Industry
Quarterly Discharges
ü HealthSouth’s volume growth
has outpaced competitors’
has outpaced competitors’
ü TeamWorks = standardized
sales & marketing
sales & marketing
ü Bed expansions will help
facilitate organic growth:
facilitate organic growth:
Ÿ ~ 100 new beds 2009
Ÿ ~ 100 new beds 2010
ü Projected sustainable annual
discharge growth 4+%
discharge growth 4+%
12
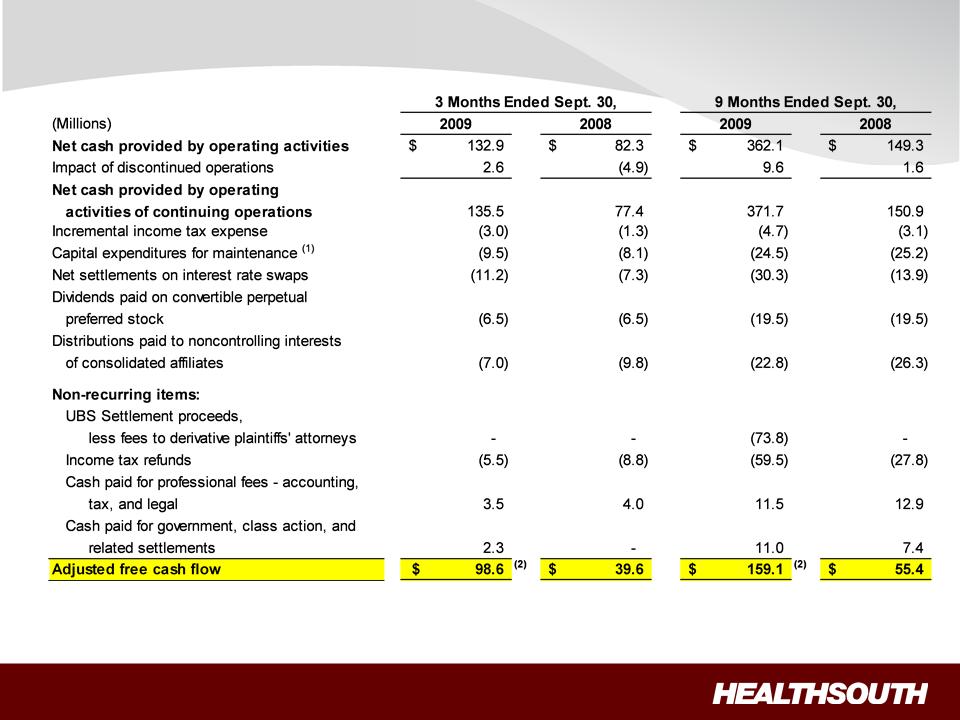
Strong Free Cash Flow
(1) Includes capital expenditures for the hospital refresh program.
(2) Benefited by approximately $19 million for the seasonal effect on working capital related to the interest payment accrual.
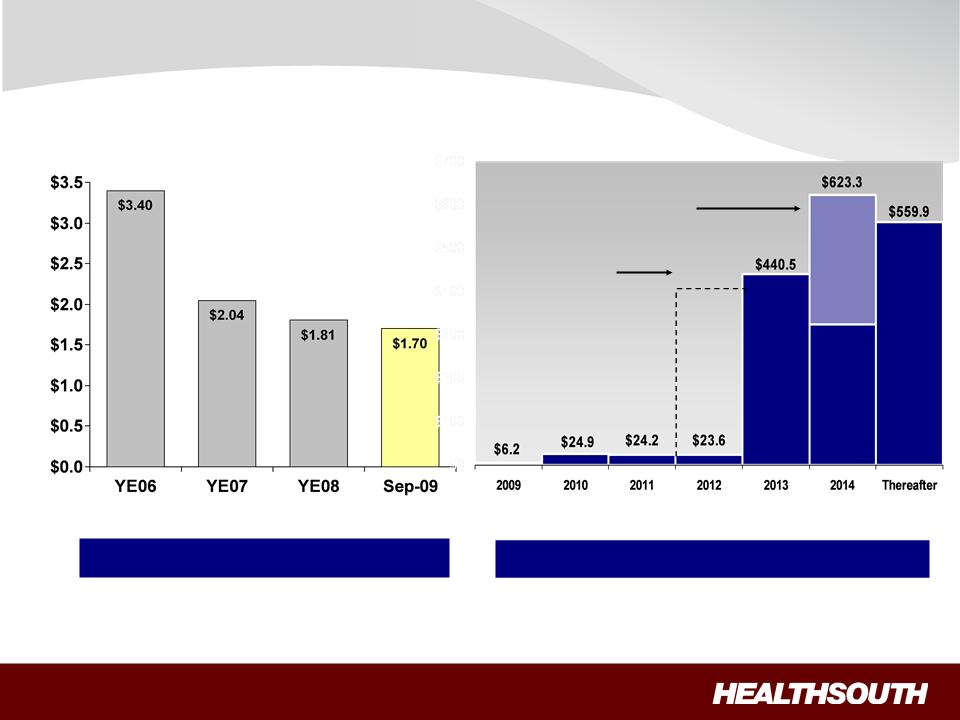
13
(1) October 2009, amendment to the credit agreement increases debt repayment flexibility of non-term loan balances.
(2) Based on four quarter trailing Adjusted Consolidated EBITDA of $376.6 million; see related debt schedule on slide 25, and reconciliation to
GAAP on slides 30 through 33.
GAAP on slides 30 through 33.
6.3x 6.3x 5.3x 4.5x (2)
Year-End 2011 Goal: 3.5x to 4.0x
Successful Deleveraging
Debt to
EBIDTA
Current undrawn
revolver matures
in 2012.
Term loan extendable to Sept.
2015 contingent on the floating
rates notes being refinanced
prior to March 2014.
$400.0
Debt Outstanding (1)
($ Billions)
Current Debt Maturities
($ Millions)
No Near-Term Financing Requirements

14
2009 Guidance
(1) Reconciliation to GAAP provided on slides 30 through 33.
(2) Adjusted income from continuing operations per diluted share.
(3) Lower floating rate interest expense resulted in higher cash payment for the swap.
Key Drivers:
ü Sustainable discharge
growth
growth
ü Market basket update
ü High-quality, cost-effective
patient care
patient care
Adjusted Consolidated EBITDA (1)
Adjusted Earnings per Diluted Share (2)
$375 to $380
Million
$1.45 to $1.50
Per Share
Key Drivers:
ü Increased Adjusted
Consolidated EBITDA
Consolidated EBITDA
ü Deleveraging
ü Lower floating-rate interest
expense (3)
expense (3)
15
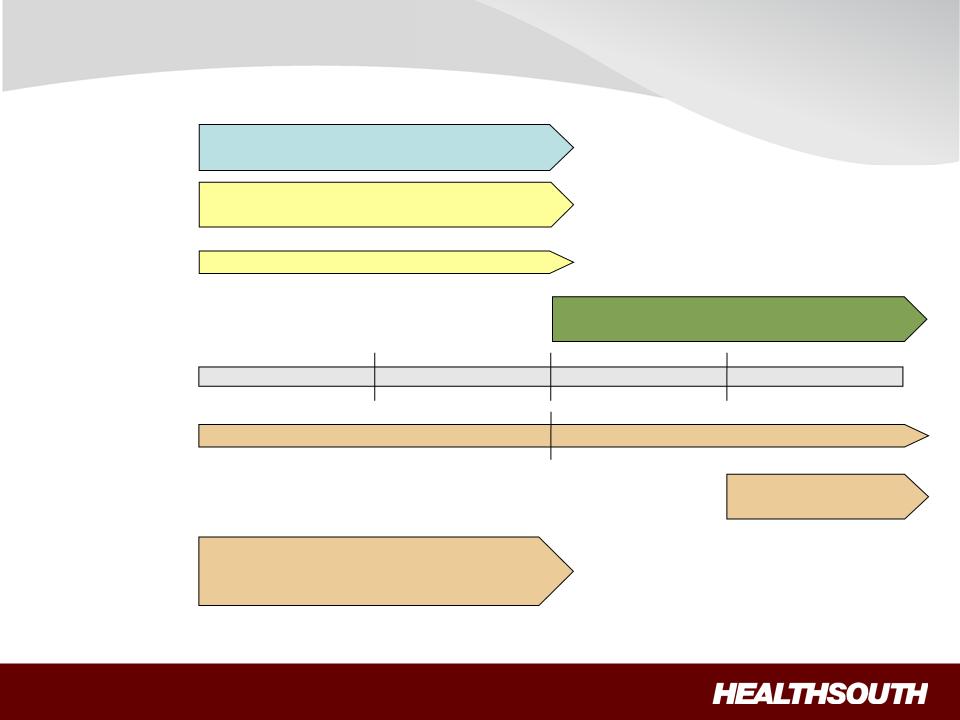
Business Outlook: Deleveraging + Growth
3.5x to 4.0x Debt to EBITDA
(No later than YE 2011)
Organic growth through bed
additions and de novos
additions and de novos
“Tuck-in” IRF acquisitions
DELEVERAGING
GROWTH
2010 2011 2012 2013+
Acquisitions of other,
complementary post-acute services
complementary post-acute services
HEALTHCARE
REFORM
REFORM
1.Market Basket
Update
Update
2.Bundling
- 25 bp - (20bp + “Productivity Adjustments”)
Pilot/Demonstration
Projects
Projects
• LTCH = admission criteria; 25 Rule;
short-stay payment reductions
short-stay payment reductions
• Home Health = reimbursement/outliers
POST-ACUTE
CLARITY
16
Summary
ü Industry Leader: Attractive
industry with good demographics.
ü Strong Cash Flows: Directed
toward debt reduction and growth.
ü Continued Deleveraging: Reduce
leverage to between 3.5x and 4.0x
no later than YE 2011.
no later than YE 2011.
ü Solid Organic Growth: Volume
growth + expense management.
ü Opportunistic, Disciplined Expansion: Bed
expansions and new
hospitals coming online over next three years.
hospitals coming online over next three years.
ü Well Positioned: High-quality
+ cost-effective provider; proven track
record of adapting to regulatory changes.
record of adapting to regulatory changes.
• 4+% annual Discharge growth
• 5-8% annual Adjusted Consolidated EBITDA growth (1)
• 15-20% annual adjusted EPS growth (1) (2)
(1) For reconciliation to GAAP, see slides 30 through 33. These ranges are based on current assumptions
of external drivers (e.g., healthcare
reform, interest rates) and are subject to change.
reform, interest rates) and are subject to change.
(2) Based on adjusted income from continuing operations per diluted share.

17
Appendix and Reconciliations
18
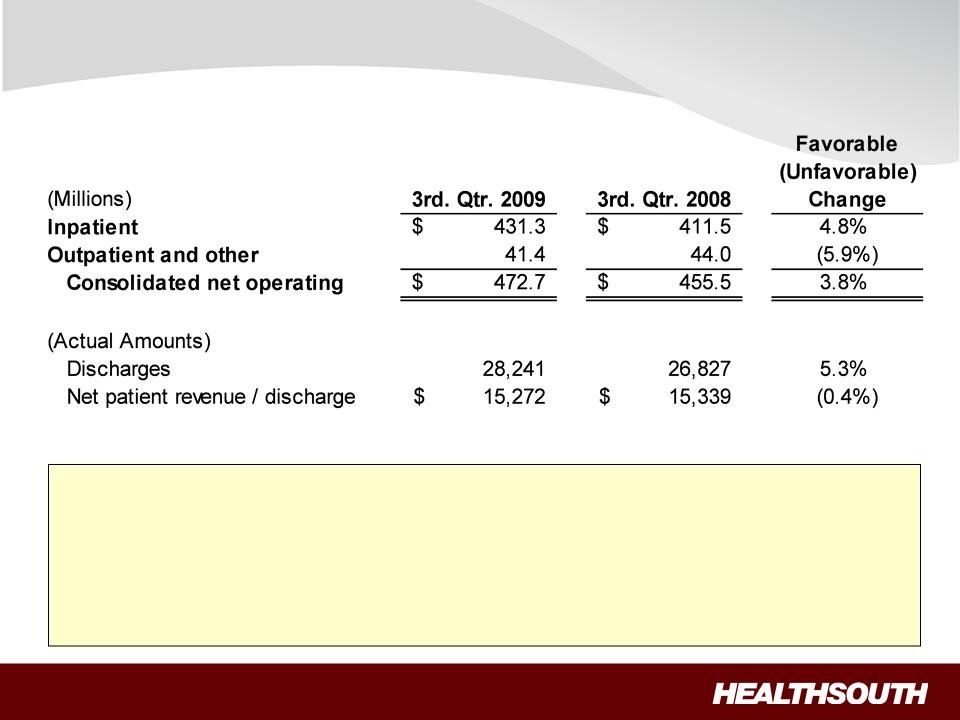
Revenues (Q3 2009 vs. Q3 2008)
• Inpatient revenue growth was driven by strong discharge volumes.
– Volume growth was driven by the sustained sales
and marketing effort.
– Same store discharge growth was 5.3%.
– Pricing essentially flat for the quarter. Q3
2009 marks the end of the Medicare pricing roll-
back.
back.
• Outpatient revenue declined as a result of 11 fewer outpatient
satellites quarter over quarter.
19
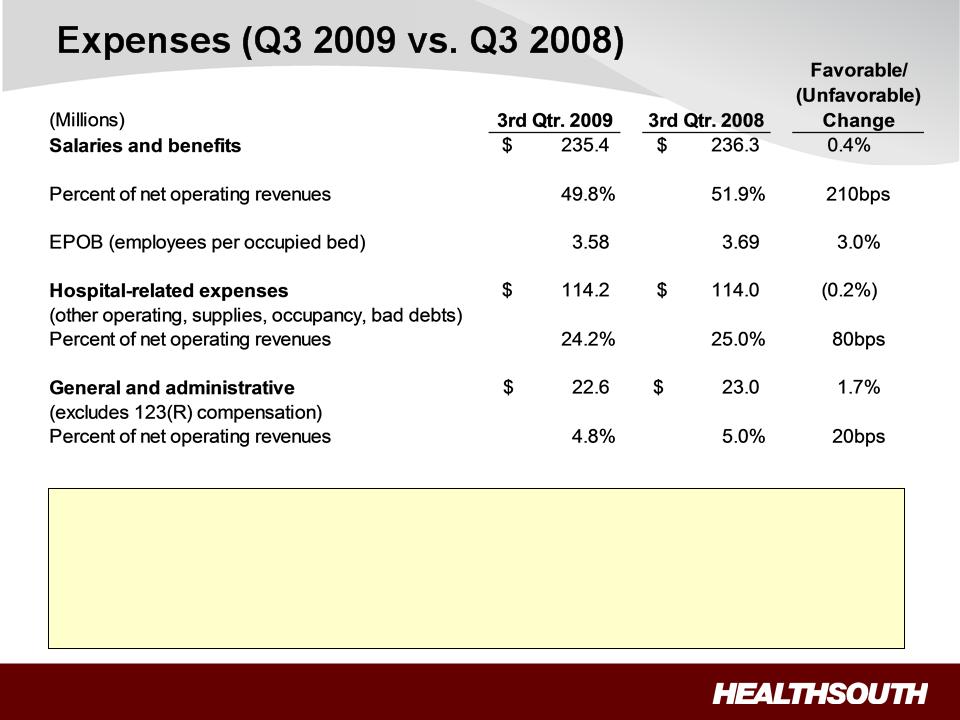
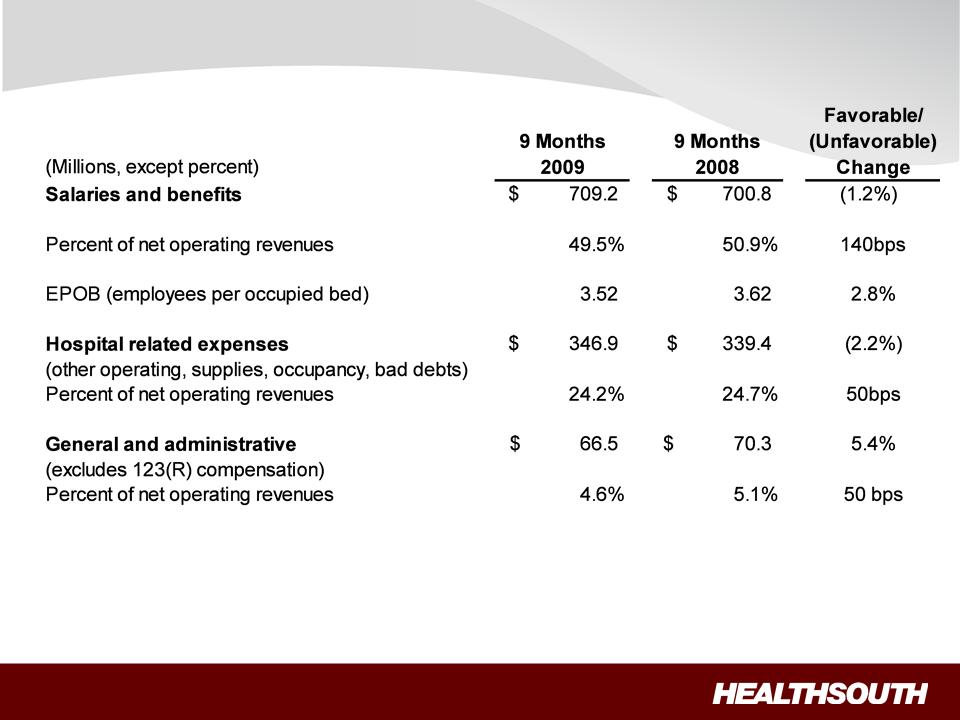
• Continued improvement on labor productivity demonstrated by lower EPOB.
• Hospital-related expenses:
– Despite increased volume, hospital expenses
remained essentially flat producing strong
operating leverage.
operating leverage.
– Increased provision for doubtful accounts to
reflect aging of pending Medicare appeals.
20
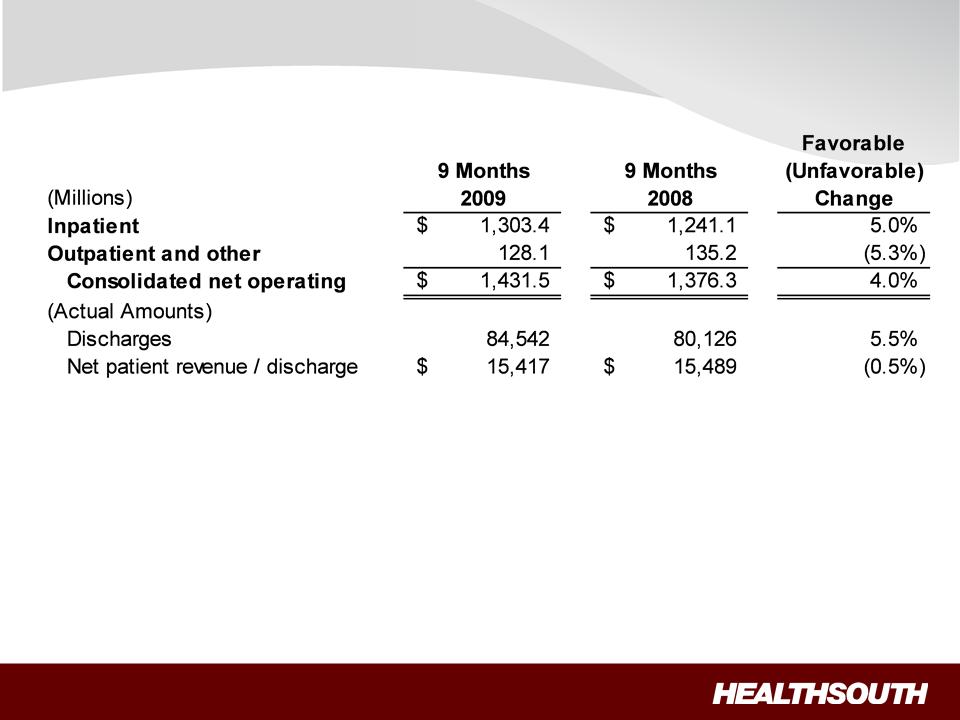
Revenue (9 months)
21
Expenses (9 months)
22
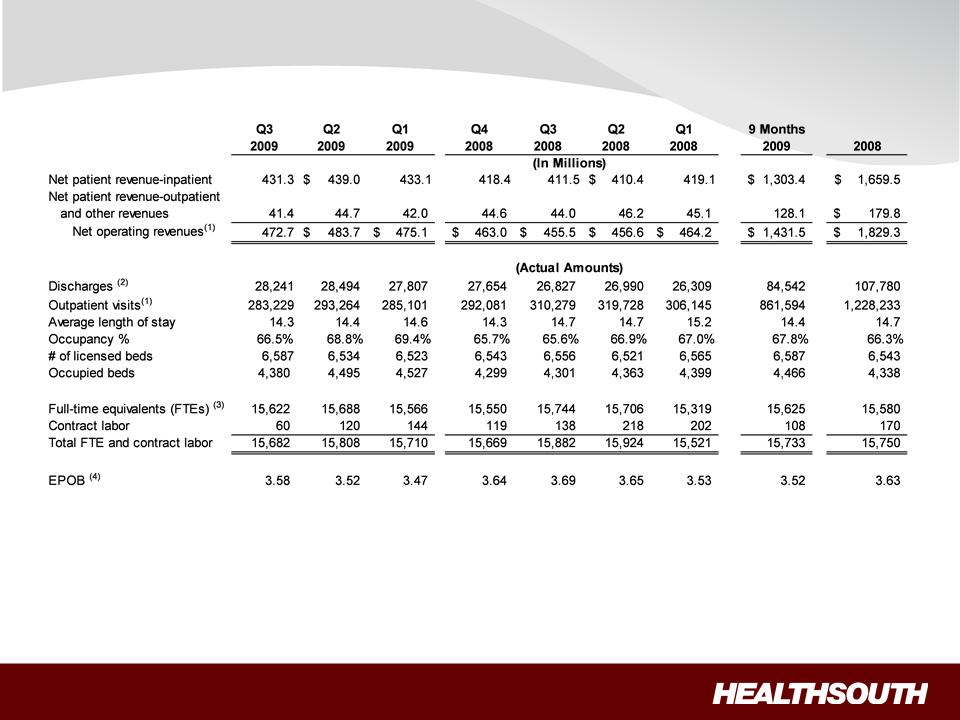
Operational and Labor Metrics
(1) Numbers have been reclassified to reflect current continuing operations.
(2) Represents discharges from HealthSouth’s 91 consolidated hospitals, which includes Mesa, Arizona starting in Q3 2009.
(3) Excludes approx. 400 full-time equivalents, who are considered part of corporate overhead with their salaries and benefits included in general and
administrative expenses in the Company’s condensed consolidated statements of operations. Full-time equivalents included in the above table
represent HealthSouth employees who participate in or support the operations of the Company’s hospitals.
administrative expenses in the Company’s condensed consolidated statements of operations. Full-time equivalents included in the above table
represent HealthSouth employees who participate in or support the operations of the Company’s hospitals.
(4) Employees per occupied bed, or “EPOB,” is calculated by dividing the number of full-time equivalents, including an estimate of full-time equivalents
from the utilization of contract labor, by the number of occupied beds during each period. The number of occupied beds is determined by
multiplying the number of licensed beds by the Company’s occupancy percentage.
from the utilization of contract labor, by the number of occupied beds during each period. The number of occupied beds is determined by
multiplying the number of licensed beds by the Company’s occupancy percentage.
23
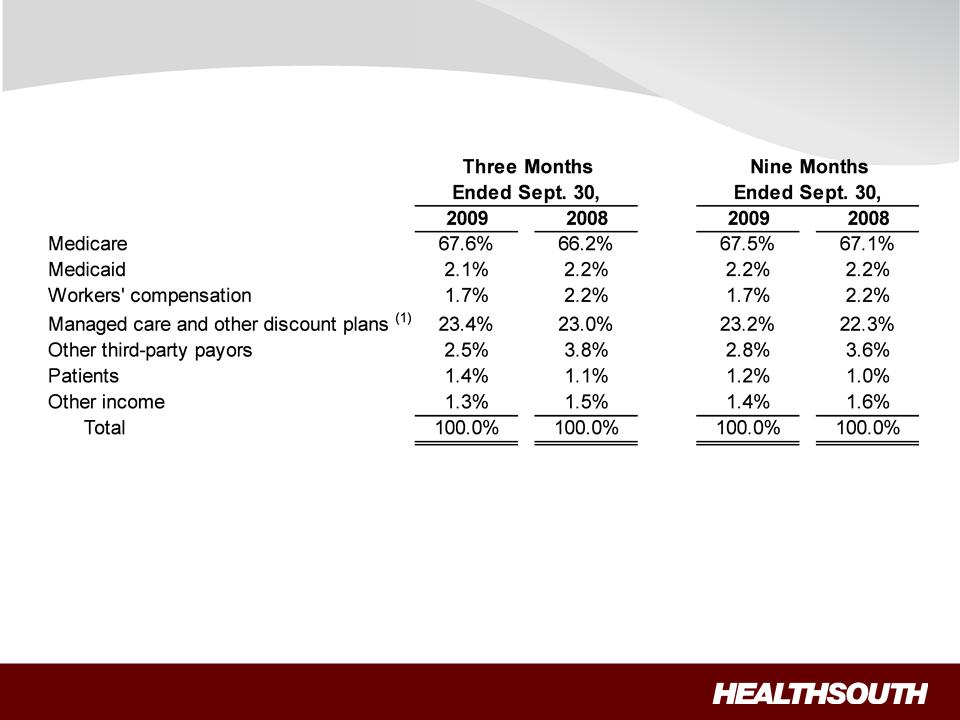
Payment Sources
(1) Managed Medicare revenues represent ~ 8% of total revenues and are included in “Managed care and other discount plans.”
24
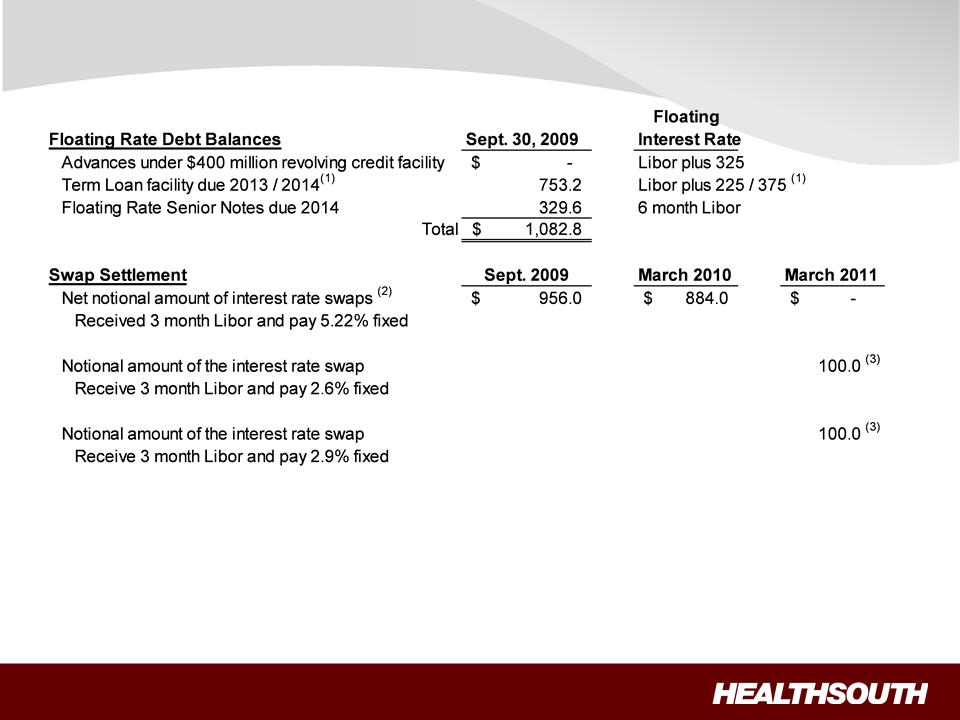
Interest Rate Swaps
(Millions)
(Millions)
(1) In October 2009, the credit agreement was amended. The maturity for $300 million of the term-loan
was extended to 2014, and is
extendable to September 2015, contingent on the floating rate note being refinanced prior to March 2014. The extended portion of the
term loan will bear an interest rate of Libor plus 375.
extendable to September 2015, contingent on the floating rate note being refinanced prior to March 2014. The extended portion of the
term loan will bear an interest rate of Libor plus 375.
(2) In June 2009, we entered into a received-fixed rate swap as a mirror offset to $100.0 million of the $1,056 million interest rate swap.
(3) Forward-starting interest rate swaps (designated as cash flow hedges).
25
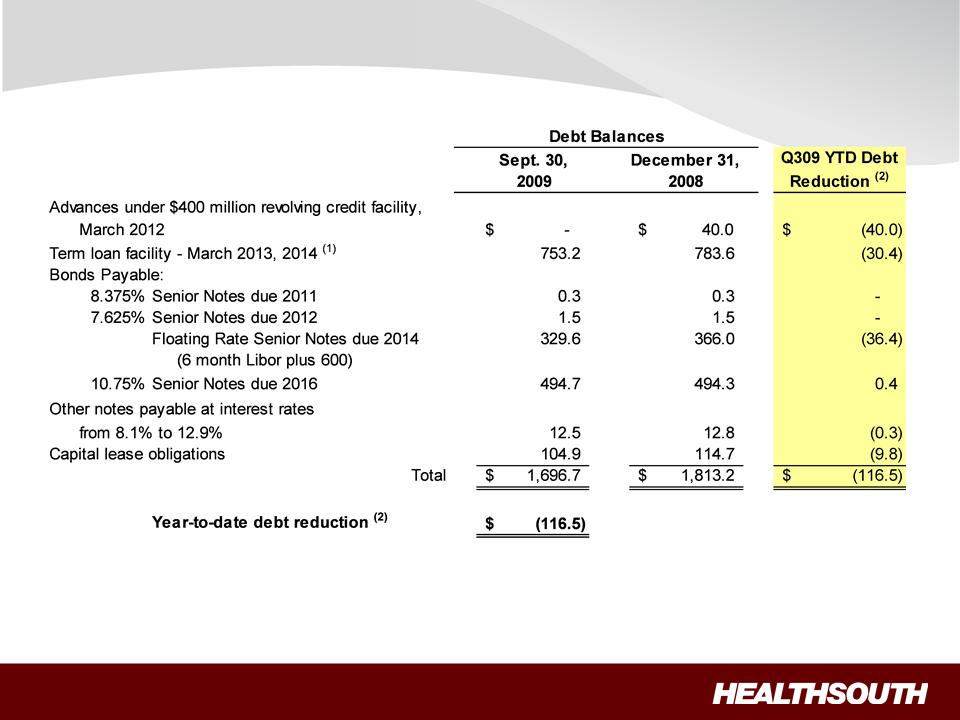
Debt Schedule
(Millions)
(Millions)
(1) October 2009, amendment to the credit agreement increases debt repayment flexibility of non-term loan balances.
(2) The Company had $117.3 million in cash and cash equivalents as of September 30, 2009.

26
Non-Operating Cash/Tax Position
Cash Refunds as of Sept. 30, 2009
• Federal tax recoveries virtually complete.
– Approx. $43 million received.
• State tax refunds in progress.
– Approx. $17 million received.
– Approx. $9 million net receivable on
the balance sheet.
Future Cash Tax Payments
• Expect to pay about $5-7 million per year of
income tax.
income tax.
– State income tax.
– Alternative Minimum Tax (AMT).
• With over $2.5 billion in NOLs and tax
deductions, we do not expect to pay significant
federal income taxes for approximately the next
10-12 years.
deductions, we do not expect to pay significant
federal income taxes for approximately the next
10-12 years.
– At this time, we do not believe the use
of NOLs will be limited before they
expire, however, no assurances can
be provided.
• HealthSouth is not currently subject to an
annual use limitation (AUL) under the Internal
Revenue Code section 382.
annual use limitation (AUL) under the Internal
Revenue Code section 382.
• If we experienced a “change of ownership” as
defined by the Internal Revenue Code section
382, we would be subject to an AUL, which is
equal to the value of the company at the time of
the “change of ownership” multiplied by the long
-term tax exempt rate.
defined by the Internal Revenue Code section
382, we would be subject to an AUL, which is
equal to the value of the company at the time of
the “change of ownership” multiplied by the long
-term tax exempt rate.
GAAP Considerations
• HealthSouth’s balance sheet currently reflects
a valuation allowance for the potential value
of NOLs and future deductions. The valuation
allowance is approximately $1.0 billion.
a valuation allowance for the potential value
of NOLs and future deductions. The valuation
allowance is approximately $1.0 billion.
• GAAP tax rate will net to small amount for
foreseeable future as there will be a reduction
in the valuation allowance when NOLs are
utilized.
foreseeable future as there will be a reduction
in the valuation allowance when NOLs are
utilized.
27
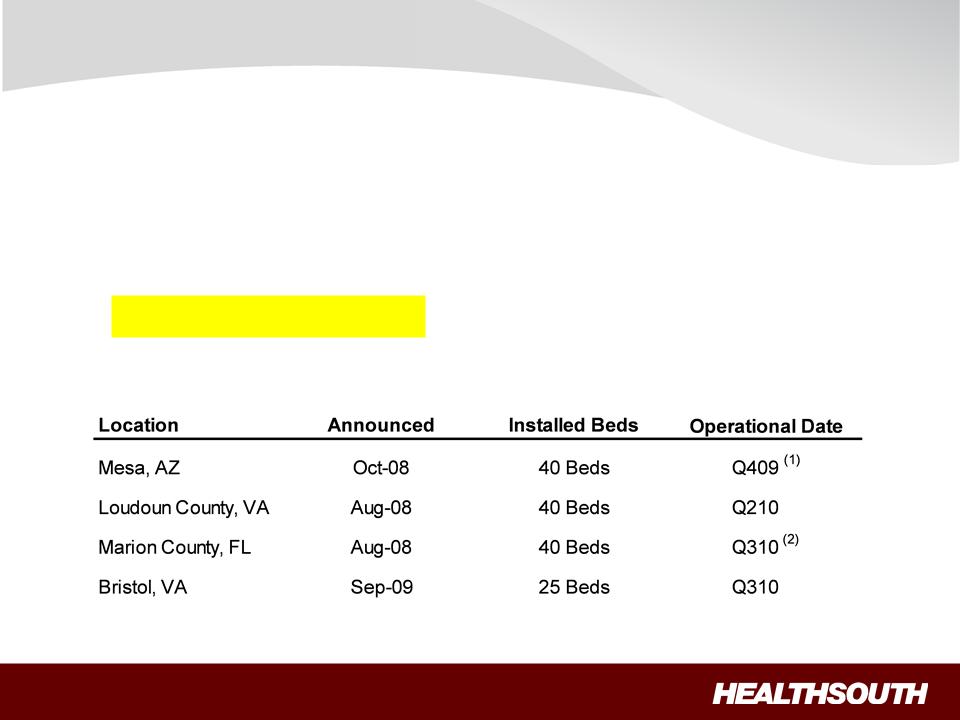
Disciplined Growth - Update
(1) Pending state license survey.
(2) CON is being appealed; operational date may change.
Bed expansions:
• Approximately 100 beds being added in 2009 and
a similar amount
in 2010.
in 2010.
• Average investment per bed:
– Internal renovation = $15 - 45K
– New construction = $100 - 250K
• Cash pay-back: 2
- 3 years
New hospitals:
28
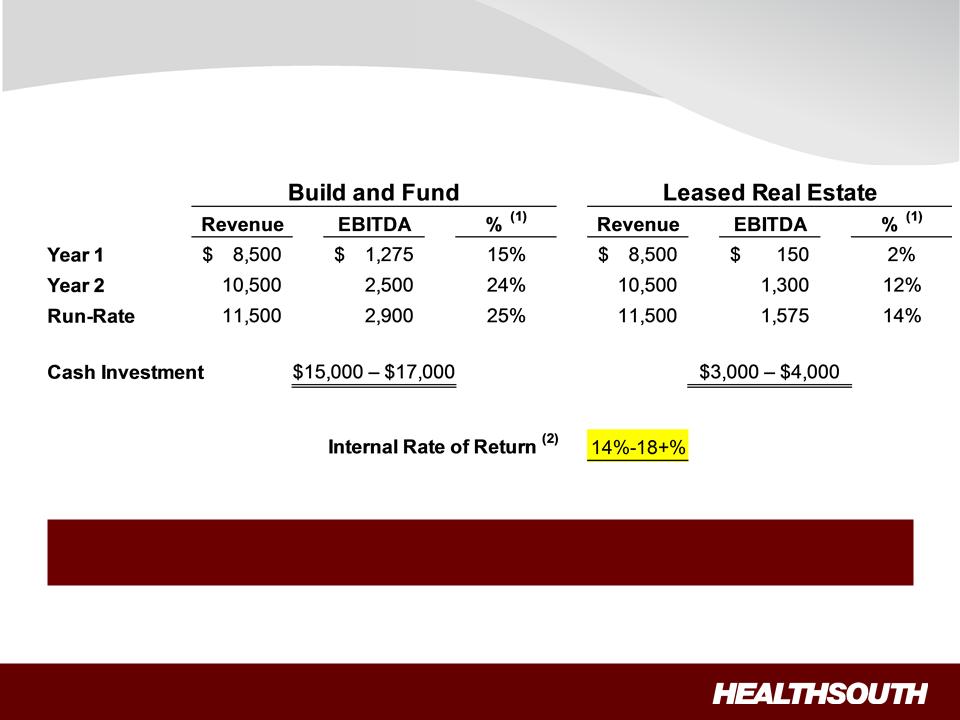
De novo: 40-Bed Proforma Example
(1) Does not include estimated corporate overhead of ~4.75%
of net operating revenues.
(2) Assumes state income taxes only for first five years, then federal and state income taxes.
(2) Assumes state income taxes only for first five years, then federal and state income taxes.
De novo’s attractive for future growth.
We evaluate based on commitment (cash or leased).
29
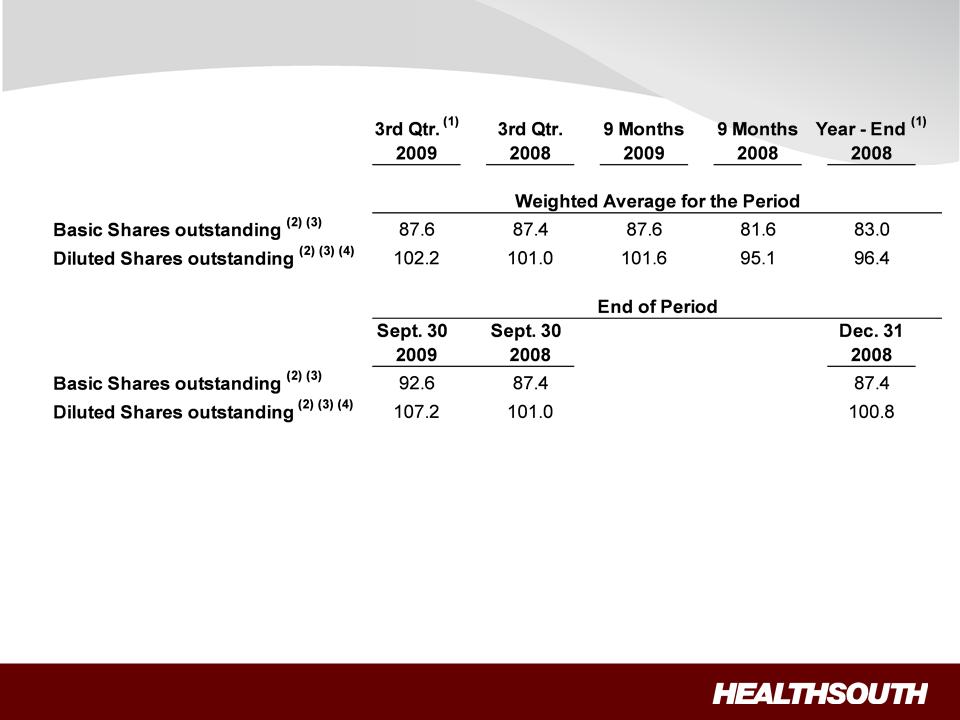
Outstanding Share Summary
(Millions)
(Millions)
Notes:
(1) Completed an equity offering for 8.8 million shares on June 27, 2008.
(2) Does not include 2.0 million warrants issued in connection with a January 2004 loan repaid to Credit Suisse First Boston. In connection with this
transaction, we issued warrants to the lender to purchase two million shares of our common stock. Each warrant has a term of ten years from the
date of issuance and an exercise price of $32.50 per share. The warrants were not assumed exercised for dilutive shares outstanding because
they were antidilutive in the periods presented.
transaction, we issued warrants to the lender to purchase two million shares of our common stock. Each warrant has a term of ten years from the
date of issuance and an exercise price of $32.50 per share. The warrants were not assumed exercised for dilutive shares outstanding because
they were antidilutive in the periods presented.
(3) The agreement to settle our class action securities litigation received final court approval in January 2007. These shares of common stock and
warrants were issued on September 30, 2009. The 5.0 million of common shares are now included in the outstanding shares. The warrants at a
strike price of $41.40 were not assumed exercised for the dilutive shares outstanding because they are anti-dilutive in the periods presented.
warrants were issued on September 30, 2009. The 5.0 million of common shares are now included in the outstanding shares. The warrants at a
strike price of $41.40 were not assumed exercised for the dilutive shares outstanding because they are anti-dilutive in the periods presented.
(4) The difference between the basic and diluted shares outstanding is primarily related to our convertible perpetual preferred stock.
30
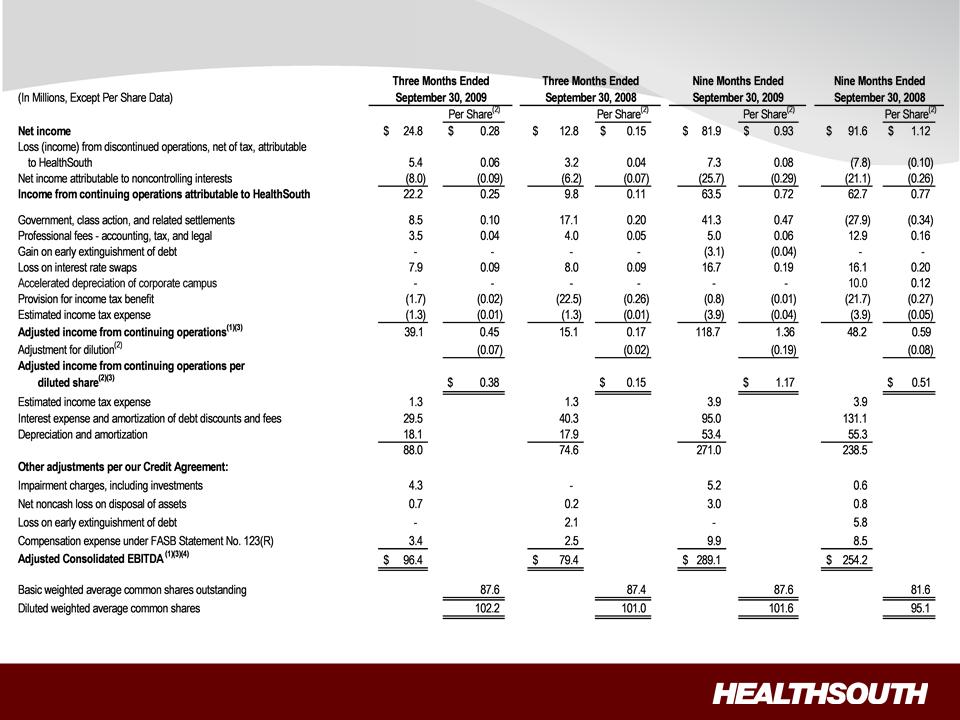
Three & Nine Months Reconciliation of Net Income to Adjusted Income from
Continuing Operations and Adjusted Consolidated EBITDA (1) (3)
Continuing Operations and Adjusted Consolidated EBITDA (1) (3)
(1) (2) (3) (4) - Notes on page 33.
31
32
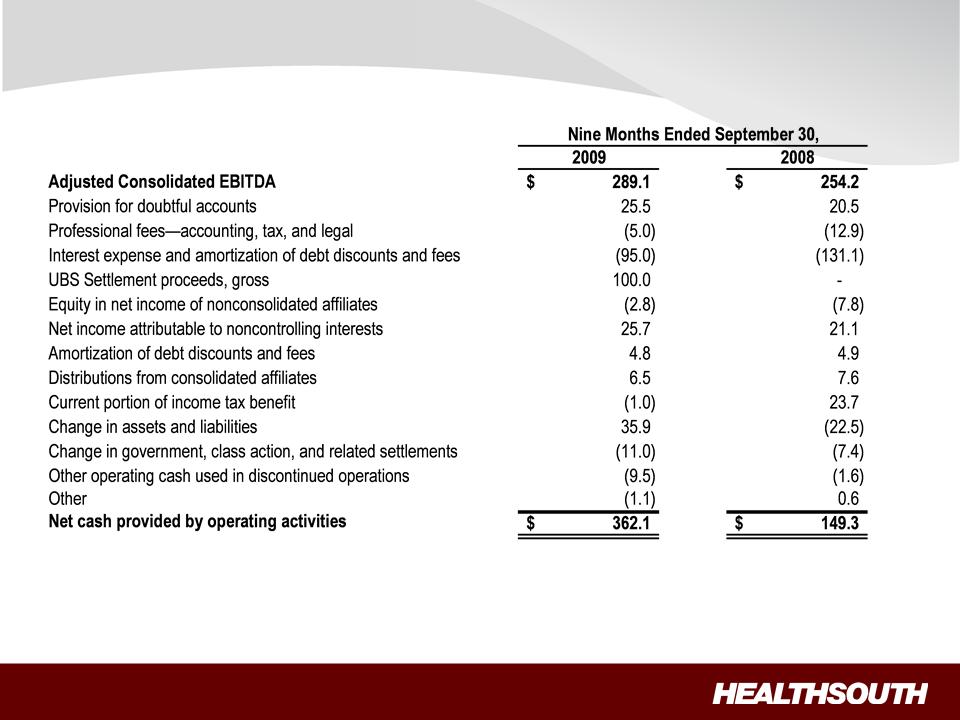
YTD Reconciliation of Adjusted Consolidated EBITDA (1) to Net Cash Provided
by Operating Activities
by Operating Activities
(1) - Notes on page 33.

33
Reconciliation Notes
1. Adjusted income from continuing operations and Adjusted Consolidated EBITDA are
non-GAAP financial measures. The Company’s leverage ratio (Total Consolidated Debt
to Adjusted Consolidated EBITDA for the trailing four quarters) is, likewise, a non-GAAP
financial measure. Management and some members of the investment community
utilize adjusted income from continuing operations as a financial measure and Adjusted
Consolidated EBITDA and leverage ratio as liquidity measures on an ongoing basis.
These measures are not recognized in accordance with GAAP and should not be
viewed as an alternative to GAAP measures of performance or liquidity. In evaluating
these adjusted measures, the reader should be aware that in the future HealthSouth
may incur expenses similar to the adjustments set forth above.
non-GAAP financial measures. The Company’s leverage ratio (Total Consolidated Debt
to Adjusted Consolidated EBITDA for the trailing four quarters) is, likewise, a non-GAAP
financial measure. Management and some members of the investment community
utilize adjusted income from continuing operations as a financial measure and Adjusted
Consolidated EBITDA and leverage ratio as liquidity measures on an ongoing basis.
These measures are not recognized in accordance with GAAP and should not be
viewed as an alternative to GAAP measures of performance or liquidity. In evaluating
these adjusted measures, the reader should be aware that in the future HealthSouth
may incur expenses similar to the adjustments set forth above.
2. Per share amounts for each period presented are based on basic weighted average
common shares outstanding for all amounts except adjusted income from continuing
operations per diluted share, which is based on diluted weighted average shares
outstanding. The difference in shares between the basic and diluted shares outstanding
is primarily related to our convertible perpetual preferred stock.
common shares outstanding for all amounts except adjusted income from continuing
operations per diluted share, which is based on diluted weighted average shares
outstanding. The difference in shares between the basic and diluted shares outstanding
is primarily related to our convertible perpetual preferred stock.
3. Adjusted income from continuing operations per diluted share and Adjusted
Consolidated EBITDA are two components of our guidance.
Consolidated EBITDA are two components of our guidance.
4. The Company’s Credit Agreement allows certain other items to be added to arrive at
Adjusted Consolidated EBITDA, and there may be certain other deductions required.
Adjusted Consolidated EBITDA, and there may be certain other deductions required.